According to the latest estimates, more than 90% of uninsured people living with a mental, neurological or substance use condition in South Africa do not have access to evidence-based mental health care (Docrat, Besada, et al., 2019). Even though there have been some advances in service delivery, research and policy, the mental health gap is unacceptably high and the quality of care is often inadequate. In this chapter we highlight the various successes in the mental health sector for the period 2015–2020, but also raise areas of concern that require urgent attention. We call attention to system failures and other challenges, which are imperative for government decision-makers and the mental health community to address.
This chapter embraces a dimensional approach to mental health, i.e. that mental health exists on a continuum from severe disability to well-being, as defined in the Lancet Commission on Global Mental Health (Patel et al., 2018). The chapter covers five areas. We begin with two recent crises in South African mental health, namely, the Life Esidimeni tragedy and the COVID-19 pandemic. These crises were moments when radical changes could have been implemented to expand and improve mental health services. The second section addresses service organisation. We highlight the importance of making optimal use of scarce resources and bring into focus the need for a comprehensive approach to service provision, including mental health promotion and prevention.
Third, we address concerns related to human resources in the context of the inequitable distribution of specialist mental health professionals and facilities across the country. We discuss the merits of task-sharing in the context of a resource-constrained environment and identify issues that should be considered to ensure the success of such an approach.
Fourth, we focus on the depth of research on public mental health conducted in South Africa. It is fortunate that the country has a highly trained and committed cadre of researchers in public mental health. We showcase some of the pioneering work that has been conducted on low-cost intervention delivery methods for mental health. Finally, we address the issue of mental health service costs and needed investments in the context of the National Health Insurance (NHI) transition and the post-pandemic fiscal climate.
Two major crises have been enormously destructive to the mental health of individuals and to the system of service provision in South Africa. These are the Life Esidimedi tragedy of 2016/17 and the COVID-19 pandemic of 2020/21.
The LE tragedy involved the death of 144 persons with mental health conditions in 2016. To conserve costs, the Gauteng Department of Health terminated a contract with Life Esidimeni, which resulted in 1 711 patients being transferred to the care of their families, NGOs and other institutions. The NGOs were not capacitated to provide the necessary specialised care to service users and 144 died due to starvation and neglect. At the LE Arbitration in 2017, former Deputy Chief Justice Dikgang Moseneke referred to the ‘inhumane treatment and torture of mental health care users’ that led to these deaths (Durojaye & Agaba, 2018).
Opposition parties, the media and members of the public sought to hold decision-makers and public servants accountable. They campaigned for compensation, mainly for family members (rather than those who survived the experience) and discussed how similar disasters could be prevented in the future. However, the fundamental questions of where and how people with severe and long-term psychosocial disabilities should be cared for, and how this tragedy could influence potential improvements in mental health care, were not addressed. The human rights of people with psychosocial disabilities, such as the right to liberty and to live in a community, rather than in institutional care, were given very low prominence.
The response of the Health Minister, Dr Aaron Motsoaledi, was to get every person who had been transferred out of the LE institutions back into facilities where they would be safe and where their basic and health care needs would be met. Unfortunately, this approach meant returning to a largely discredited status quo. Instead, what was required in the short term was investment in developing and supporting community-based services and facilitating access to specialist support in the District Health Services (DHS). The Department’s Mental Health Policy Framework states that there is currently an over-reliance on psychiatric hospitals and that community mental health services should be scaled up (Department of Health, 2013). Thus, simply getting people back into institutions was retrogressive. The LE crisis would have been the perfect opportunity to start adequately resourcing and training community facilities and thereby give persons with psychosocial disabilities more humane and more normal lives than is currently the case. Importantly, service users were returned to institutions without
consultation. The state was prepared to pay for institutional care, and in fact increased the daily amount from prior to the crisis (M. Freeman, personal communication, 20 October 2021). However, it was not prepared to invest the same amount for care provision within the community.
Following the LE tragedy, the South African Human Rights Commission held hearings in 2017 into the status of mental health care in South Africa and recommended improvements in services and legislation (SAHRC, 2017). The National Department of Health (NDoH) is currently working on how best to implement these recommendations that include, inter alia, reduced reliance on institutions and building community mental health care. However, thus far progress has been minimal, and the opportunity created by the huge public interest in mental health following the tragedy appears to have been squandered. It is critical that every effort is made to move rapidly to strengthen community mental health services.
The COVID-19 pandemic of 2020 and 2021 brought the realities of poor mental health and the need for mental health promotion and care into focus for millions of South Africans and people globally. A Lancet review of mental health effects of COVID-19 in low- and middle-income countries (LMICs) showed an increased prevalence of psychological distress and mental disorders (Kola et al., 2021). These may be attributed, inter alia, to continued uncertainties about the spread of the disease, the consequences of containment strategies, bereavement, and uncertainty about when and how everyday life would return to normal. The lockdown, aimed at mitigating the spread of COVID-19, has increased peoples’ isolation and has had huge negative economic impacts such as job loss and business closures, which in turn have impacted mental health. Family violence including gender-based violence has also increased (Clark, 2020). In South Africa the volume of calls to the South African Depression and Anxiety Group helpline doubled during the pandemic. An average of 1 400 people reached out every day, reflecting the added mental health burden from COVID-19 (Pijoos, 2021). In March 2021 the results of an innovative methodology to assess the impact of the pandemic on mental well-being across diverse global settings demonstrated that South Africa and the United Kingdom scored the lowest in terms of mental well-being. South Africans were estimated to be facing the highest levels of financial distress due to COVID-19, with the impact experienced mainly by younger people (Newson et al., 2021).
Vulnerable groups, such as persons in psychiatric hospitals or social care homes, people with disabilities, and women experiencing domestic violence or abuse, have been at even greater risk of psychological distress, because pre-existing failures in human rights protection have worsened. Persons living with mental health conditions (as well as other health conditions) were afraid or unable, for example, due to lack of transport, to receive ongoing treatment. Further fuelling the risk of widespread relapse and the need for inpatient care, between April and June 2020, medications for mental health conditions represented 3% of the stock-out reports received by the Stop Stockouts Project. By August, this figure increased to nearly 30% (Lopez Gonzalez, 2020).
The pandemic has also had significant effects on health care workers, who were already at high risk of burnout and psychological distress prior to the COVID-19 pandemic (Liebenberg et al., 2018; Roomaney et al., 2017). Witnessing large
numbers of COVID-19-related deaths has likely added to already high levels of trauma and burnout among health workers (Johnson et al., 2020), resulting in the development of trauma and stress-related mental disorders. The pandemic has brought into focus the need for attention to employee well-being more broadly.
The NDoH has been cognisant of the mental health impacts of COVID-19 and has introduced important interventions and guidelines. For example, a toolkit was developed and distributed aimed at helping people cope with emotional distress and to enhance well-being during COVID-19. The toolkit focussed on topics such as managing stress, identifying mental health symptoms, advising people on the need to keep in touch with others and continue with psychiatric medication, and assisting children during COVID-19. Guidelines were also developed on how to respond to COVID-19 in mental health facilities. Fortunately, and unlike several other countries, these facilities were not scaled down to make way for the hospital treatment of COVID-19 service users. However, the initiatives introduced fell short of using the opportunity to implement the recommendations of the WHO to invest in mental health services.
The United Nations has indicated that humanitarian crises such as natural disasters and conflict situations are opportunities to develop sustainable mental health services (Guterres, 2020). The COVID-19 pandemic has also been such an opportunity. There has been a clear need for government to step up services and assist people with mental health conditions or those in psychological distress. Such an initiative would have filled the gap between the existing need and actual services. If mental health was truly perceived as integral to health, then funding would have been found for these services, particular at the community and primary care level. All age groups, all disorders, and all levels of the health system require strengthening, which is what the investment case aims to do.
The COVID-19 pandemic has yielded the benefit of expanding the use of telemedicine. The ethical rules of the Health Professions Council of South Africa (HPCSA) have changed to allow the use of remote methods of providing mental health care. This approach can provide specialist mental health support to rural districts where it is not possible to attract suitably trained professionals. However, such services should include a large component of training and supervision of less qualified providers, as well as a consultation service for people with complicated conditions. Budgeting for information technology, including budgeting for data costs, is integral to making this approach a workable solution to providing access to specialist care. Simple infrastructure constraints (i.e. working telephones) in government facilities and a lack of digital infrastructure development have resulted in rural communities benefitting the least from such innovations (Wooyoung Kim, 2020). Some shifts such as the drafting of the Gauteng Province Mental Health Strategy and Action Plan 2019 – 2023 (Robertson et al., 2021) and the responses to COVID-19 outlined above have resulted from the LE and COVID-19 crises and from the opportunities for change presented by them. However, neither crisis has thus far sparked fundamental and long-lasting reform in the mental health system.
In the democratic era, South Africa has advanced considerably in policy and legislation aimed at transforming the mental health system and improving access, equity and quality of mental health services. Before 1994 under the Mental Health Act of 1973, mental health services were largely custodial, followed a medical and paternalistic approach, were vertically organised, and were largely not aligned with human rights principles. The thread of the improvements can be traced back from the White Paper on the Transformation of the Health System in South Africa which was adopted in 1997 to the promulgation of the Mental Health Care Act, Act No 17 of 2002 in 2004 and subsequently to the adoption of the National Mental Health Policy Framework and Strategic Plan 2013–2020.
The National Mental Health Policy Framework and Strategic Plan (2013–2020) (NDoH, 2020) and the Framework and Strategy for Disability and Rehabilitation Services in South Africa (NDoH, 2016) promote a comprehensive approach to mental health. This comprehensive approach should include the promotion of mental health, the prevention of mental health conditions and disability, early identification of disorders, and interventions with a disability-inclusive recovery-oriented approach. These services are to be implemented in a community-based framework, with task-sharing as a strategy for addressing the scarcity and maldistribution of resources.
The National Mental Health Policy Framework and Strategic Plan 2013–2020 recommends the establishment of District Mental Health Specialist teams. These teams are intended to plan services in each district in a way that makes use of local resources and provides access to care through the primary health care (PHC) system. The South African Mental Health legislation is regarded as one of the most progressive internationally.
However, weaknesses are experienced at implementation level (SAHRC, 2017). The clauses of the mental health legislation dealing with the promotion of community care, and the mental health policy framework that similarly emphasises community care, have hardly been implemented within provinces, which is where service delivery takes place. Both the mental health legislation and policy are now in need of updating due to developments such as the adoption of the Convention on the Rights of Persons with disabilities. It is unfortunate that the guidance provided in these documents, that should have resulted in a community-based approach to mental health, have largely been ignored.
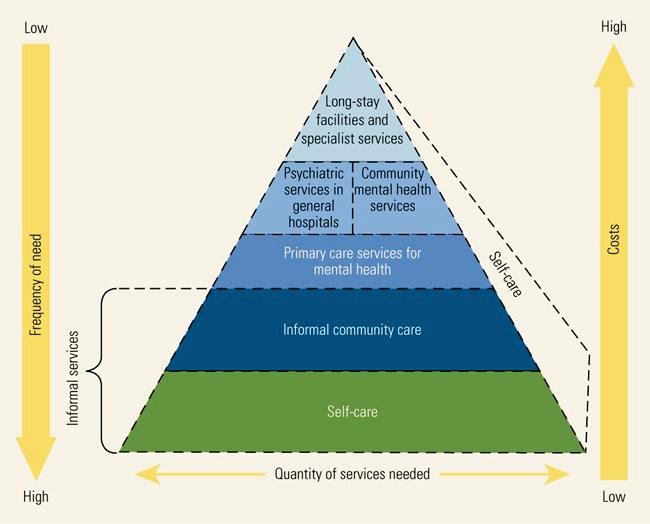
The Mental Health Care Act of 2002 and Mental Health Policy Framework (2013–2020) prescribe how the mental health system should be organised, in keeping with the WHO optimal mix of services model. Currently, mental health services are provided through PHC, community-based mental health services, mental health services in general hospitals, specialised psychiatric hospitals, and care and rehabilitation centres in the public, private and not-for-profit organisations. Mental health services are also provided in a range of other sectors, including the South African Police Services, the South African Military Health Services, Correctional Health Services, Employee Health and Wellness Programmes in workplaces, and in Basic Education and Higher Education.
However, in the current model, resources remain largely concentrated in inpatient care and in psychiatric hospitals, with relatively under-developed primary care and community-based services (Docrat, Besada, et al., 2019). There is also an inequitable distribution of mental health services, with most specialised services being unevenly distributed across provinces and concentrated in urban areas, and with little or no access to specialised care in peri-urban and rural areas.
Figure 10.1 displays the organisation of publicly funded mental health services in South Africa. Figure 10.2 displays the organisation of privately funded mental health system, and Figure 10.3 shows the WHO optimal mix of services model.
All PHC facilities in South Africa are mandated to provide basic mental health services, including screening, detection, treatment and/or referral for mental disorders, and dispensing and management of psychotropic medication for those on long-term medication. School health nurses are expected to conduct screening for mental health as part of the school health services. Again, implementation appears to be uneven given the shortage of nurses and is difficult to assess due to lack of data. Unfortunately, existing District Health Information System (DHIS) indicators for monitoring service utilisation of mental health care in the country are not disaggregated at the patient level. Only the total number of outpatient visits and inpatient admissions are enumerated for a given time period. For example, 75% of overall outpatient visits for mental health clients in 2016/17 took place at the PHC level. However, in the absence of data that reflect the number of visits per client for mental, neurological and substance use (MNS) disorders as well as patient-level outcomes, coverage cannot be determined (Docrat, Besada, et al., 2019).
The PHC re-engineering project of the NDoH includes the integration of mental health care into chronic disease management. This inclusion has been a major step forward in terms of making mental health care accessible to people with common mental disorders as well as those with severe mental illness. However, primary care providers need the support of specialist mental health professionals to be able to deliver an acceptable level and quality of service. The package also does not address the acute need for appropriate services for children and adolescents.
Specialised community mental health services are key to ensuring that specialist support is funded by and provided by the DHS. The establishment of District Mental Health Specialist Teams (who plan and organise services and provide a
specialist consultation/intervention service and a supportive/mentoring/teaching role for generalist primary care providers) is included in the policy document and strategic plan. Only 11 teams have been appointed in four of the nine provinces. Budgetary constraints have been cited for this state of affairs. If these services could be established as envisaged in the policy document and strategic plan, it is likely that at least some inpatient admissions could be prevented, in particular, readmissions (which are a proxy for relapse and are unacceptably high in South Africa) (Dreyer & Viljoen, 2019).
The latest available data indicate that there are 355 community-based mental health services that are licensed in terms of Regulation 43 of the Mental Health Care Act, 2002 Regulations. Of these, 261 are residential and 94 are day care facilities. These are largely run by non-governmental organisations with subsidies from the provincial departments of health and social development. Little has been published on their capacity, costs per patient, and subsidies received from government.
Forty general hospitals in South Africa have a psychiatric unit attached, with a total of 1 665 beds. The units attached to district and regional hospitals are largely run by medical officers with support provided by psychiatrists from specialised psychiatric hospitals. Units attached to tertiary and central hospitals have psychiatrists and other members of the multidisciplinary team providing mental health services. These hospitals are mandated to provide services by mental health care practitioners such as psychologists, social workers, psychiatric nurses and occupational therapists. All other general hospitals that are without dedicated units attached are also mandated to provide outpatient and inpatient mental health services for less complex mental health problems and emergency cases. However, the implementation of these mandates is uneven across provinces. The latest information submitted by provinces in terms of the Regulation 12 of the Mental Health Care Act 2002 General Regulations as amended indicate that there are 188 general hospitals designated to conduct 72-hour assessment of involuntary mental health care users. A national study released in 2019 showed that most of these facilities do not meet the required specifications outlined by the Mental Health Care Act (2002). For example, 62% of designated district hospitals sampled across the country indicated that adult mental health inpatients are kept in general wards with other service users. There is a dearth of facilities for adolescents requiring inpatient care and they are usually admitted to general adult medical wards. Similar to medicines for physical health, lack of access to psychotropic medications has also been reported and rural provinces often bear the brunt of stock-outs and a limited range of available medications (Sunkel & Viljoen, 2017).
There are 25 specialised psychiatric hospitals and care and rehabilitation centres in South Africa with a total of 10 732 beds. These hospitals are unevenly distributed among provinces with one province, Mpumalanga, having no specialised psychiatric hospital and KwaZulu-Natal and the Western Cape having as many as five. The role of these facilities includes:
• Provision of inpatient and limited outpatient care
• Provision of sub-specialist services
• Provision of ongoing routine training and supervision of secondary and primary health care services.
The South African Police Service and the South African Military Health Service subsidise mental health services for their members through membership of medical insurance. Most universities provide some form of mental health services to students through their student counselling programmes. However, services are inadequately provided to those in other higher education institutions such as technical and vocational training institutions, which approximately half of all post-school students attend. These health services are currently being transformed to provide comprehensive health services under Higher Health, a non-government organisation working closely with the Department of Higher Education and Training.
Data from the NDoH indicate that there are 41 private hospitals licensed to provide inpatient mental health services in terms of Regulation 42 of the Mental Health Care Act, 2002 General Regulations, with a total of 755 beds. Most psychiatrists and inpatient beds are concentrated in urban areas at the expense of rural regions. In the private sector, of 270 conditions that form the prescribed minimum benefits (PMBs), only two are explicitly psychiatric conditions. These are major affective disorders, including unipolar and bipolar depression, and schizophrenia. The PMBs include a range of other conditions including epilepsy, sexual abuse/rape (counselling), HIV counselling and testing, acute stress disorder, and attempted suicide. Many of these conditions are treated in hospital. Most mental health admissions are due to mood disorders, even though it is possible to treat these patients out of hospital. Funding by private health insurance (i.e. medical aids) for schizophrenia is limited to inpatient treatment only, and therefore individuals and families incur significant out-of-pocket expenses in order to receive appropriate ambulatory care. This arrangement encourages costly, hospital-centric care and most often members incur large co-payments for out-of-pocket medication. An unpublished South African Society of Psychiatrists (SASOP) study has called attention to the uneven distribution of psychiatrists and the need for the involvement of professionals such as nurses, occupational therapists, social workers and others in delivering mental health services (SASOP, 2020).
According to data obtained from Discovery Health which dominates the medical aid market, based on the number of claiming members in 2019 and 2020, depression claims were among their top 10 disease spends (Quantium, 2021). This figure
represents a prevalence of 8.5% and contributes 52% of Discovery’s overall psychosocial spend in 2020. Pharmaceutical claims for mental health increased by 3.5% in 2020, with claims for antidepressants in particular exceeding 6.5% of claims in 2020. Of the 29 000 Discovery Health members who were admitted for inpatient care as at December 2020, those without specified comorbidities stayed in hospital for an average of 6.6 days whilst those with depression spent an average of 9.3 days as an inpatient (Quantium, 2021). During the trajectory of the COVID-19 pandemic, critical mental health services were suspended in tandem with a higher demand than ever for these very services across all segments of the South African population (Docrat, Besada, et al., 2019).
The lifespan of the Mental Health Policy Framework and Strategic Plan (NMHPF) 2013–2020 (the Policy) ended in 2020. It is apparent that most aspects of the Policy were either poorly implemented or not implemented at all in some provinces due to a lack of dedicated resources and technical capacity to develop costed implementation plans (Docrat, Lund, et al., 2019). This state of affairs has been heightened by weak information systems to support service planning. However, the content of the Policy remains relevant, and its proper implementation and resourcing will improve the quality of and access to mental health services. The NDoH is undertaking an update of this policy, taking into account recent developments such as the COVID-19 pandemic and the need for specific targets to justify the allocation of resources.
The South African mental health system is organised in a manner that facilitates integration of mental health into the general health services environment as prescribed by the Mental Health Care Act of 2002. It is necessary that the barriers that have impeded the implementation of the NMHPF are identified as part of the development of the post-2020 follow-up policy to the NMHPF, the phased implementation of the NHI scheme, and the post-pandemic response. We are at a critical juncture in which to seize the opportunity to leverage existing government efforts to integrate mental health in the post-pandemic response whilst concurrently solidifying its comprehensive inclusion in the South African NHI agenda. Part of the challenge is service organisation that ensures maximum reach to the widest range of the population.
An important barrier to improving the quality of mental health services in under-served areas in South Africa is the lack of measurable indicators. Indicators which would be helpful to monitor services include the following:
• Number of district mental health specialist teams established in each province
• Indicators of evidence-based mental health promotion and prevention activities in each district
• Service utilisation of inpatient and outpatient mental health care services disaggregated by MNS disorder
• Number of people attending primary care clinics identified with an MNS disorder per district
• Post-hospitalisation PHC utilisation
• Monitoring of stock-outs of antidepressant, antipsychotic and anti-epileptic drugs.
Human resources are a critical instrument for the delivery of mental health care, and therefore are a crucial consideration in planning mental health services in South Africa. Opportunities for collaboration among health care workers should be actively sought, with a view to expanding opportunities for service provision. Funding for positions for counsellors, including lay counsellors, along with training, infrastructure, and ongoing supervision are of considerable importance if services are to be made available to all who require them.
Transformation to redress historical injustices in the helping professions is a challenge facing South African society following decades of apartheid education, when Black students and those with disabilities had limited training opportunities. Transforming the mental health professions is rooted in the transformation of training at institutions of higher education. Universities have made strenuous efforts to recruit, train and graduate Black students (Meela et al., 2021). However, enrolment of Black students in graduate training in psychology, psychiatry and other mental health professions is uneven. The cadre of mental health professionals still does not reflect that of the South African population. Further, decolonised pedagogical transformation reflecting African values, cultures and literacy need to be incorporated into our largely Westernised biomedical mental health curricula.
There is an inequitable distribution of specialist mental health professionals and facilities across the country. Most specialists in all mental health professions work in urban and private settings. To illustrate this, the national ratio of public sector psychiatrists to the population was 0.31 per 100 000 (ranging from 0.08 in Mpumalanga to 0.89 in the Western Cape) (Docrat, Besada, et al., 2019). It is estimated that at least 1.9 psychiatrists per 100 000 population will be required in sub-Saharan Africa by 2050 (Charlson et al., 2014). To achieve this number in rural areas and for people who are not members of a medical aid scheme, a redistribution of personnel will be essential.
The South African Society of Psychiatrists reported that in October 2020, 785 psychiatrists were registered with the HPCSA (SASOP, 2020). However, not all of these are active practitioners. Over 84% of psychiatrists are based in three provinces: Gauteng (302), Western Cape (251) and KwaZulu-Natal (209) and 73% of psychiatrists work in the private sector (Miric & Thom, 2021). While the inequitable distribution of psychiatrists is a key consideration, by drawing on psychiatrists in the public and private sectors, this combined workforce would result in an estimated ratio of psychiatrists to population of 1.3 psychiatrists per 100 000 – a significant step closer to the 2050 target. Similar shortages and disparities exist for other specialist mental health professionals including psychologists, registered counsellors and mental health nurses. It is vital that they are prioritised alongside psychiatrists to build multidisciplinary teams. There is also inefficient utilisation of human resources. Most specialist mental health professionals in the public sector work in inpatient units, resulting in insufficient community-based specialist mental health professionals.
Task-sharing, also referred to as task-shifting, refers to the delivery of mental health services by non-specialist health care providers, who are trained and supervised by a mental health specialist. We prefer the term ‘task-sharing’, as it implies a collaborative approach between specialists and non-specialists and is more than just shifting tasks. Task-sharing provides an opportunity for psychologists and counsellors to collaborate in ways that may expand the range and scope of mental health services. As a strategy, task-sharing has been widely endorsed, including by the WHO’s flagship mhGAP programme, as a means of narrowing the treatment gap for mental health conditions (WHO, 2010).
The rationale for task-sharing is the need for an integrated care approach, in addition to limited numbers of highly trained mental health specialists to provide care to all those in need at a population level. Task-sharing represents an opportunity to use available resources efficiently and increase the coverage of mental health care. Typical settings for task-sharing include primary care clinics and community settings, where non-specialist health care staff should be available and can provide care that is accessible and close to the places where most people live and work.
The approach of task-sharing has been endorsed in the National Mental Health Policy and Strategic Plan (2013–2020) (Department of Health, 2013) which strongly advocates for the training of non-specialist primary care and community health workers in basic mental health care. Unfortunately, during the course of the policy’s implementation period, there has been little evidence of systematic scaling up of task-sharing approaches in South Africa.
The main arena in which task-sharing has been implemented and evaluated during the 2015–2020 period has been in research through initiatives such as the Programme for Improving Mental Healthcare (PRIME) (Lund et al., 2015; Petersen et al., 2016), the Mental Health Integration (MhINT) programme (Reiss-Brennan, 2014), Project MIND (Myers et al., 2018), the Africa Focus on Intervention Research for Mental Health (AFFIRM) (Lund et al., 2015) and the Health Systems Strengthening in Sub-Saharan Africa (ASSET) study (Boisits et al., 2021), described in more detail below.
These studies have identified the following challenges in implementing tasksharing. First, training needs to be carefully tailored to the skills and competencies of the non-specialist providers and should be scheduled at a time that fits in with providers’ already busy clinical work. Second, it is vital that systems of ongoing supervision and support for non-specialists are established following training. Staff require ongoing supervision and support as they are likely to face service users with challenging issues. Without this supervision and support, knowledge and skills are frequently forgotten and the quality of service deteriorates. In addition, with rapid turnover of staff in primary care settings, training of new staff is often required. Third, there are several implementation challenges. As existing staff are frequently very busy with their current workload, they may not be motivated to take on additional mental
health tasks, and new referral pathways frequently need to be established to manage complex patients and provide the right level of care. Fourthly, and finally, there are several regulatory challenges associated with task-sharing. For example, scope of practice guidelines may need to be modified by the Health Professions Council of South Africa, the South African Nursing Council, and the South African Pharmacy Council, both to allow specialists to provide supervision, and to allow non-specialists to take on certain tasks, such as psychological counselling and prescription of psychotropic medication. Nonetheless, some important breakthroughs have been demonstrated in task-sharing approaches, which have been shown to be effective in improving care and clinical outcomes. For example, in the PRIME study, primary care nurses were able to achieve a significant improvement in detection of depression (from 5.8% to 16.4%) and alcohol use disorders (from 0% to 13.8%), and 55.2% of people with depression showed a clinically significant improvement, compared to 23.4% in the control group when supported by trained primary care nurses (Petersen et al., 2019). Three strategies have been key to these successes. First, training and supervision materials that are tailored to the relevant non-specialists need to be developed. Second, roles and scope of practice need to be carefully developed. Third, overall health systems strengthening strategies such as continuous quality improvement and establishing referral pathways are essential.
The Academy of Science of South Africa consensus study report (Academy of Science of South Africa, 2021) has made specific recommendations for providing core competencies that will allow for improved mental health care. These include: (1) training of community health workers in screening for mental disorders and managing chronic mental disorders; (2) integrating traditional healers into the health care system so that they may collaborate more formally with the formal health care system; (3) including mental health into the nursing curriculum so that nurses can have greater competencies in mental health service provision; (4) addressing concerns related to scopes of practice, legal issues of accountability, requisite training and the need for ongoing supervision of community health workers; (5) training existing mental health professionals in mentoring persons with less specialised skills; and (6) scaling up prevention and management of substance use disorders by combining medical and psychosocial interventions. Implementing these recommendations will play an important role in increasing task-sharing opportunities in the provision of mental health care.
Task-sharing holds enormous potential as a means of narrowing the treatment gap for mental health conditions in South Africa. However, it is a complex undertaking, requiring careful planning and consideration of the research evidence. In the context of resource constraints, good data on the efficacy and effectiveness of interventions, including task-sharing approaches, are necessary.
Several studies over the past few years have focused on delivering low-cost, high-quality evidence-based interventions in resource-constrained settings. The Programme for Improving Mental Health Care (PRIME, 2011–2019) studied the integration of mental health services into primary care settings, by developing and implementing district mental health care plans in five countries: Ethiopia, India, Nepal, South Africa and Uganda (Lund et al., 2012). The South African district site was located in the Dr Kenneth Kaunda district in the North West province. Researchers worked closely with the Department of Health at district, provincial and national levels to develop and implement a district mental health care plan focusing on integrating care for depression and alcohol use disorders into primary care for chronic health conditions (Petersen et al., 2016). Significant improvements were shown in both detection and clinical outcomes for depression and alcohol disorders (Petersen et al., 2019).
The Mental Health Integration programme (MhINT), building on the experience of PRIME, sought to develop the model further and replicate it in districts in Mpumalanga and KwaZulu-Natal (Reiss-Brennan, 2014). The work has emphasised the importance of health systems strengthening and continuous quality improvement as cornerstones of integrating mental health into general health care systems. It has focused on providing care for depression comorbid with chronic health conditions such as diabetes, hypertension, HIV and TB.
Project MIND has focused its work on urban and rural areas of the Western Cape in a large cluster randomised controlled trial, led by researchers at the Medical Research Council and the University of Cape Town, in partnership with the Western Cape Department of Health and numerous non-profit organisations (Myers et al., 2018). The study focused on comparing two models of integrating mental health into primary care for depression and alcohol use disorders comorbid with HIV and diabetes. The trial included 24 primary care clinics, eight for each model and eight for a control condition (Myers et al., 2018).
The Africa Focus on Intervention Research for Mental Health (AFFIRM, 2011–2016) study evaluated a task-sharing psychological counselling intervention for maternal depression in Khayelitsha, Cape Town (Lund et al., 2014). The study was an individual-level randomised controlled trial, which compared psychological counselling delivered by community health workers to enhanced usual care (supportive telephone calls to study participants). While the study did not show a significant improvement in the primary outcome of clinical depression, it found a significant reduction in psychological distress in the treatment arm compared to the control arm (Lund et al., 2020). The study showed the need for ongoing sustained supervision and support for non-specialist community health workers.
It is vital that research is conducted in close collaboration with public sector services, chiefly the NDoH, as well as relevant non-profit organisations. This will allow findings to be taken up in routine practice, at scale, to benefit the many thousands of South Africans who currently have no access to care. Currently, although the NDoH has been very involved in these studies, translation into practice has not yet occurred.
Furthermore, researchers involved in these studies do not have clear communication channels with clinicians working in the private and public sectors, nor are these findings being actively taken up by universities involved in the training of psychiatrists and psychologists in the country. For example, many universities involved in the training of clinical psychologists continue to teach highly individualised long-term psychodynamic psychotherapies, which are both expensive and do not make use of the evidence from task-sharing approaches. Such approaches have the potential to meet the needs of many thousands more people living with mental health conditions. The integration of research findings into training curricula for mental health professionals is a matter that requires continuous programme renewal based on a scientist–practitioner model of professional training. To enhance success in this regard, clinical training programmes in psychology, nursing, psychiatry, social work and counselling will need to place a greater emphasis on evidence-based practice including research methodology, statistics and systematic reviews in the context of population health. This will increase the likelihood of lecturers and clinicians being research literate and thus being more amenable than at present to adapt training curricula in response to research findings.
Despite ongoing research, there remain areas that require investigation. First, there is an enormous gap in research on interventions for children and adolescents, taking low-cost models of service provision to scale. Second, health systems need to be strengthened to create the capacity for integrating mental health into existing primary care and community health systems. Third, while important strides have been made in evaluating mental health interventions, there are still large gaps in our knowledge about interventions that address the social determinants of mental health in South Africa, including poverty and gender-based violence. Rural mental health, a largely neglected area, is a further issue that requires investigation.
The 2018 Lancet Commission on Global Mental Health and Sustainable Development Goals emphasised the inclusion of mental health care in the universal health coverage (UHC) agenda (Patel et al., 2018). Both the WHO and World Bank endorsed investments in mental health as humanitarian and development priorities (Mnookin, 2016). It has been estimated that US$5–17 trillion in lost output is expected by 2030 without significant investment in the treatment of mental disorders. Promisingly, a growing body of evidence for cost-effective options to reduce the burden of mental disorders and improve outcomes for physical health problems, particularly in LMICs, is emerging. One analysis estimates that for every $1 invested in the treatment of depression and anxiety a return of $3–5 can be expected through improved productivity and instrumental benefits of improved mental health over the 15 years of the Sustainable Development Goals (Chisholm et al., 2016).
An explicit pledge to transform mental health services was outlined in the South African National Mental Health Policy Framework and Strategic Plan 2013–2020 (MHPF) (Department of Health, 2013). However, barriers to implementation of the MHPF include weak health information systems to understand the local burden of illness, uneven patterns of service access, inadequate human and financial resources for mental health, as well as a lack of technical capacity to generate costed and budgeted strategic plans for mental health services in all provinces (Docrat & Lund, 2018; SAHRC, 2017). Financial incentives to increase efficiency or resource allocation for mental health services in provinces are minimal (Bateman, 2015). Hence, the struggle to actively fund existing services continues.
In pursuit of UHC, financial protection and health system efficiency, the South African government has committed to the phased implementation of an NHI system (South African National Department of Health, 2017). However, evidence from the NHI pilot districts has raised concerns that mental health priorities have not been explicitly addressed and reflected in the policies and activities supporting its overall implementation. This omission is likely to make future prospects for the South African mental health system uncertain (Schneider et al., 2016).
Until recently, there has been inadequate information about existing resources for mental health care, taking into account the variability across districts and provinces, the degree of policy implementation, and availability and existing uptake of services for mental health at all levels of the health system (Docrat, Besada, et al., 2019). The NDoH has acknowledged these concerns and in 2017 supported a study to evaluate the full costs of mental health services and programmes. Findings revealed that South Africa’s public mental health expenditure fell in the lower recommended bound of 5% of the total public health budget, that the treatment gap was approximately 92%, and that under 1% of the uninsured population were receiving inpatient care (Docrat & Lund, 2018). One reason for the treatment gap was that most expenditure occurred at the inpatient and specialised hospital levels. In 2016/17, 86% of mental health care expenditure was on inpatient care, 50% of which was directed at the psychiatric hospital level. Furthermore, readmission rates of nearly 25% consumed 18% of overall mental health expenditure, indicating a lack of service provision following discharge from hospitals (Docrat & Lund, 2018). Understanding the current inequities in resources, access to services, and inefficiencies in the use of resources provides the foundational tools to promote the redistribution of budgets towards more cost-effective responses to mental health needs.
It has been suggested that UHC should involve the explicit inclusion of mental health services within reimbursement and mandatory insurance schemes as a standard, not as a complementary option (Patel et al., 2018). The NHI is an opportunity rather than a threat to the improvement of mental health services, but its success depends on how the system is managed. If mental health professionals are brought on board collaboratively and adequately remunerated for their work, then NHI could be an opportunity to improve services. The South African government is currently moving towards developing and defining the mechanisms by which the NHI fund will operate. A significant opportunity exists to generate the economic evidence to support decision-making regarding the mental health service benefits for all South Africans, as well as the complementary system reforms and capacity-building efforts that will be needed to realise successful implementation and scale-up. Beyond raising the global profile of mental well-being, with all sectors of society recognising its importance, the COVID-19 response has brought best practices that may be leveraged to improve mental health outcomes for all South Africans under the future NHI. As evidenced by collaborative efforts to respond to the COVID-19 pandemic, a culture of data-sharing (integrating utilisation and clinical records) and standardised treatment approaches grounded in public (mental) health care paradigms and broader reciprocity and alignment across the public and private sectors serves as an opportunity to automate systems for integrating utilisation and clinical records delivered through all facilities in the country, towards NHI-led purchasing mechanisms that incentivise quality of care and integration in broader NCD service packages.
In 2019, an Investment Case for Mental Health was commissioned by the NDoH which indicated its intentions to strengthen financing for mental health services (Besada, Docrat, & Lund, 2021). Such an exercise aimed to provide a clear quantification of and integrated case for investments to transform mental health services in line with international and local evidence by estimating the expected return-on-investment (ROI) over a 15-year period from scaling-up interventions targeting anxiety, depression (including perinatal depression), psychosis, bipolar disorder, epilepsy, idiopathic developmental intellectual disability, behavioural disorders, dementia and alcohol and substance-use (opioid and non-opioid) disorders. Further, in acknowledgement of the need for preventative efforts, the ROI associated with (1) early interventions for those exhibiting risky alcohol and substance-use behaviours and (2) the development and roll-out of social-emotional learning programmes delivered in schools to learners (aged 12–17 years) represented a key component of the initiative.
Building on global guidelines, and driven by insights from the NDoH, the approach to this work innovatively introduced methodology that reflects the importance of engagement with multisectoral, national and sub-national structures, clinicians, academic experts, and service-user organisations in addition to the National Treasury throughout the modelling process. Decisions of clinical, policy and systems interventions that were prioritised and modelled reflected the diverse perspectives and priorities of a variety of stakeholders, beyond only those responsible for the existing and future allocation and prioritisation of funds and resources.
Return on investment can change significantly due to systems constraints. The approach goes a step beyond global guidelines for examining the costs and benefits of scaling up packages of interventions for priority MNS disorders, by quantifying the infrastructural (capital), human resource and programmatic requirements that must be complementary for the achievement of mental health service scale-up. This means that
services delivered under the future NHI will adhere to requirements for quality and humane mental health care. The key financing streams, roles and responsibilities of sectors beyond health will thus be leveraged.
Released in October 2021, the South African Mental Health Investment Case provides practical methodologies for LMICs, particularly those transitioning to mandatory health financing mechanisms to improve the likelihood that cases for investment in mental health translate into committed bridge and long-term, sustainable mental health care financing. The Investment Case provides a synthesis of the increasing burden imposed by MNS disorders and quantifies the significant cost of inaction on the economy and population well-being. It provides an explicit treatment package to be provided at each level of care to address population needs, thereby serving as a tool for which the NHI benefits package can draw on (Besada, Docrat, & Lund, 2021). Ultimately, beyond the positive returns on investment demonstrated by the Investment Case, the initiative has unequivocally shown that the cost of inaction to the South African economy far outweighs the cost of investing in the mental health of our country. Even when accounting for existing rates of unemployment and labour force participation, lost workforce productivity due to unaddressed mental health well-being translates into an annual economic loss of R161 billion annually (approximately 4% of the country’s gross domestic product per year). In contrast, the projected needed spend for a paced, rational approach to service scale-up and progressive decentralisation across all sectors is estimated in the region of R26 billion per year, though this average does not account for the gradual increase in coverage and associated investments. For example, in the first year of scale-up, the costs associated with direct service provision, training, supervision, governance and behaviour change campaigns, falling within the mandate of the NDoH, would translate to an amount of R6.74 billion; in comparison, currently estimated expenditure on mental health services amounts to R8.12 billion. For the modelled community-based service platform, the Department of Social Development is mandated to provide subsidies for individuals living with mild to moderate intellectual disability, in addition to the provision of substance-use rehabilitation. Together, these investments would assume a marginal 0.02% of the Department of Social Development’s current resource envelope. It is expected that the Department of Basic Education will finance the social and emotional learning programmes modelled in the Investment Case, translating to only 1% of its allocated budget of R28.59 billion in the 2022/23 period. Finally, in light of the mandate of the Department of Human Settlements to provide housing needs for vulnerable populations, capital costs estimated for the establishment of community-based residential units would amount to just under 3% of its allocated budget.
Many of these aggregates include upfront investments related to infrastructure development for rehabilitation, recovery, and prevention of disability through a community-based residential and day-care service platform and for revitalising dilapidated hospital infrastructure for mental health. These represent a long-term investment and are not anticipated to contribute to recurrent costs.
Due to research and return on investment calculations, a great deal is known about what needs to be done to strengthen mental health services in South Africa, and much of this has in fact been included in the current legislation and policy. As a consequence of Life Esidimeni and the COVID-19 pandemic there have also been several opportunities to introduce changes and reforms. However, implementation, especially by the provinces has been slow. Even without additional resources, or with some transitional funding, much can be accomplished with sufficient buy-in and prioritisation of mental health care. While greater investment is required, in the current economic climate, few resources will go into mental health unless it is part of the current crisis response or part of ‘building back better’. The last five years have shown us a great deal about what can be done, but the next five will have to show more in terms of real changes in systems and services. Moves towards greater emphasis on community care will be essential. Moreover, though not dealt with in any detail in this chapter, reducing the social and economic determinants of mental health, giving greater emphasis to prevention and promotion programmes, and working across sectors will need to be prioritised if population mental health is to truly change.
Academy of Science of South Africa. (2021). Provider core competencies for improved Mental health care of the nation. https://doi.org/http://dx.doi.org/10.17159/ assaf.2019/0067
Bateman C. Mental health under-budgeting undermining SA’s economy. SAMJ: South African Medical Journal. 2015;105(1): 7–8.
Besada D, Docrat S, Lund C. Mental Health Investment Case for South Africa. Final Report of the Mental Health Investment Case Task Team. 2021.
Boisits S, Abrahams Z, Schneider M, Honikman S, Kaminer D, Lund C. Developing a task-sharing psychological intervention to treat mild to moderate symptoms of perinatal depression and anxiety in South Africa: a mixed-method formative study. International Journal of Mental Health Systems. 2021;15(1): 1–14.
Charlson FJ, Diminic S, Lund C, Degenhardt L, Whiteford HA. Mental and substance use disorders in sub-Saharan Africa: predictions of epidemiological changes and mental health workforce requirements for the next 40 years. PloS One. 2014;9(10): e110208.
Chisholm D, Sweeny K, Sheehan P, Rasmussen B, Smit F, Cuijpers P, Saxena S. Scaling-up treatment of depression and anxiety: a global return on investment analysis. The Lancet Psychiatry. 2016;3(5): 415–424.
Clark B. Gender-based Violence and COVID-19 in South Africa The Clash of Pandemics. 2020. file:///C:/Users/skagee/OneDrive - Stellenbosch University/ Desktop/LN_ROL_CAFE_White_Paper_20201202.pdf
Department of Health. (2013). National Mental Health Policy Framework and Strategic Plan.
Department of Health. (2016). Framework and Strategy for Disability and Rehabilitation Services in South Africa. Department of Health. (2020). NATIONAL MENTAL HEALTH POLICY FRAMEWORK AND STRATEGIC PLAN (2013-2020). file:///C:/Users/ skagee/OneDrive - Stellenbosch University/aaaAshrafs Manuscripts II/2017/ a-Manuscripts in preparation/SA Health Reforms Book chapter/National-MentalHealth-Policy-Framework-and-Strategic-Plan-2013-2020 (1).pdf
Docrat S, Lund C. Evaluation of the Health System Costs of Mental Health Services and Programmes in South Africa 2016/17 Financial Year. 2018.
Docrat S, Besada D, Cleary S, Daviaud E, Lund C. Mental health system costs, resources and constraints in South Africa: a national survey. Health Policy and Planning. 2019;34(9): 706–719.
Docrat S, Lund C, Chisholm D. Sustainable financing options for mental health care in South Africa: Findings from a situation analysis and key informant interviews. International Journal of Mental Health Systems. 2019;13(1): 1–11. https:// doi.org/10.1186/s13033-019-0260-4
Dreyer R, Viljoen AJ. Evaluation of factors and patterns influencing the 30-day readmission rate at a tertiary-level hospital in a resourceconstrained setting in Cape Town, South Africa. South African Medical Journal. 2019;109(3): 164–168.
Durojaye E, Agaba DK. Contribution of the Health Ombud to accountability: The life Esidimeni tragedy in South Africa. Health and Human Rights. 2018;20(2): 161.
Guterres A. Launch of the policy brief on COVID-19 and mental health. 2020. https:// www.un.org/en/coronavirus/mental-health-services-are-essential-part-allgovernment-responses-covid-19
Johnson SU, Ebrahimi OV, Hoffart A. PTSD symptoms among health workers and public service providers during the COVID-19 outbreak. PloS One. 2020;15(10): e0241032.
Kola L, Kohrt BA, Hanlon C, Naslund JA, Sikander S, Balaji M, Benjet C, Cheung EYL, Eaton J, Gonsalves P, et al. COVID-19 mental health impact and responses in low-income and middle-income countries: Reimagining global mental health. The Lancet Psychiatry. 2021.
Liebenberg AR, Coetzee JFJ, Conradie HH, Coetzee JF. Burnout among rural hospital doctors in the Western Cape: Comparison with previous South African studies. African Journal of Primary Health Care & Family Medicine. 2018;10(1): 1–7.
Lopez Gonzalez L. Mental health: are medicine shortages fuelling a shadow epidemic? Mental Health Matters. 2020;7(4): 26–29.
Lund C, Alem A, Schneider M, Hanlon C, Ahrens J, Bandawe C, Bass J, Bhana A, Burns J, Chibanda D, Cowan F, Davies T, Dewey M, Fekadu A, Freeman M, Honikman S, Joska J, Kagee A, Mayston R, … Susser E. Generating evidence to narrow the treatment gap for mental disorders in sub-Saharan Africa: Rationale, overview and methods of AFFIRM. Epidemiology and Psychiatric Sciences. 2015;24(3). https://doi.org/10.1017/S2045796015000281
Lund C, Schneider M, Davies T, Nyatsanza M, Honikman S, Bhana A, Bass J, Bolton P, Dewey M, Joska J, Kagee A, Myer L, Petersen I, Prince M, Stein DJ, Thornicroft G, Tomlinson M, Alem A, Susser E. Task sharing of a psychological intervention for maternal depression in Khayelitsha, South Africa: study protocol for a randomized controlled trial. Trials. 2014;15. https://doi.org/10.1186/17456215-15-457
Lund C, Schneider M, Garman EC, Davies T, Munodawafa M, Honikman S, Bhana A, Bass J, Bolton P, Dewey M, et al. Task-sharing of psychological treatment for antenatal depression in Khayelitsha, South Africa: Effects on antenatal and postnatal outcomes in an individual randomised controlled trial. Behaviour Research and Therapy. 2020;130: 103466.
Lund C, Tomlinson M, De Silva M, Fekadu A, Shidhaye R, Jordans M, Petersen I, Bhana A, Kigozi F, Prince M, et al. PRIME: a programme to reduce the treatment gap for mental disorders in five low-and middle-income countries. PLoS Med. 2012;9(12): e1001359.
Meela MM, Libhaber E, Kramer B. Transformation of a health sciences postgraduate population (2008-2017) at a higher education institution in South Africa: has this occurred? South African Journal of Higher Education. 2021;35(1): 209–230.
Miric A, Thom R. Unpublished report prepared for the South African Society of Psychiatrists. 2020.
Mnookin S. Out of the shadows: Making mental health a global developmental priority. 2016. http://documents1.worldbank.org/curated/ en/270131468187759113/pdf/105052-WP-PUBLIC-wb-background-paper. pdf
Myers B, Lund C, Lombard C, Joska J, Levitt N, Butler C, Cleary S, Naledi T, Milligan P, Stein DJ, et al. Comparing dedicated and designated models of integrating mental health into chronic disease care: study protocol for a cluster randomized controlled trial. Trials. 2018;19(1): 1–13.
Newson J, Pastukh V, Sukhoi O, Taylor JTT. The Mental State Of The World Report. 2021.
Patel V, Saxena S, Lund C, Thornicroft G, Baingana F, Bolton P, Chisholm D, Collins PY, Cooper JL, Eaton J, Herrman H, Herzallah MM, Huang Y, Jordans MJD, Kleinman A, Medina-Mora ME, Morgan E, Niaz U, Omigbodun O, … UnÜtzer Jü. The Lancet Commission on global mental health and sustainable development. The Lancet. 2018;392(10157): 1553–1598. https://doi. org/10.1016/S0140-6736(18)31612-X
Petersen I, Bhana A, Fairall LR, Selohilwe O, Kathree T, Baron EC, Rathod SD, Lund C. Evaluation of a collaborative care model for integrated primary care of common mental disorders comorbid with chronic conditions in South Africa. BMC Psychiatry. 2019;19(1): 107.
Petersen I, Fairall L, Bhana A, Kathree T, Selohilwe O, Brooke-Sumner C, Faris G, Breuer E, Sibanyoni N, Lund C. et al. Integrating mental health into chronic care in South Africa: the development of a district mental healthcare plan. The British Journal of Psychiatry. 2016;208(s56): s29–s39.
Petersen I, Lund C, Bhana A, Flisher AJ, Health M, Consortium PRP. A task shifting approach to primary mental health care for adults in South Africa: human resource requirements and costs for rural settings. Health Policy and Planning. 2011;27(1): 42–51.
Pijoos I. Help! Lockdown sees calls to SA Anxiety and Depression Group double. Times Live. 2021. https://www.timeslive.co.za/news/south-africa/2021-03-24-helplockdown-sees-calls-to-sa-anxiety-and-depression-group-double/ Quantium. (2021). Insights from the Discovery Health data.
Reiss-Brennan B. Mental Health Integration Programme. Journal of Primary Care & Community Health. 2014;5(1): 55–60. https://doi. org/10.1177/2150131913508983
Robertson LJ, Moosa MYH, Jeenah FY. Strengthening of district mental health services in Gauteng Province, South Africa. South African Medical Journal 2021;111(6): 538–543.
Roomaney R, Steenkamp J, Kagee A. Predictors of burnout among HIV nurses in the Western Cape. Curationis. 2017;40(1): 1–9. https://doi.org/10.4102/curationis. v40i1.1695
SAHRC. Report of the National Investigative hearing into the status of mental health care in South Africa. 2017.
SASOP. Equality in mental health hampered by lack of access, lack of investment. 2020. https://www.sasop.co.za/equality-in-mental-health-hampered
Schneider M, Baron E, Breuer E, Docrat S, Honikman S, Onah M, Sorsdahl K, der Westhuizen C, Lund C, Kagee A, et al. Integrating mental health into South Africa’s health system: current status and way forward. South African Health Review. 2016;2016(1): 153–163.
South African National Department of Health. (2017). Government Notices - National Health Insurance Policy. Government Gazette, 7(40955): 1–70. https://www.gov. za/sites/default/files/gcis_document/201707/40955gon627.pdf
Sunkel C, Viljoen M. Shortage of psychiatric medications in South Africa. The Lancet Psychiatry. 2017;1(4): 15–16.
Wooyoung Kim A. Is it time to rethink how we deliver mental healthcare services? Mental Health Matters. 2020;7(3): 30–32.
World Health Organization. (2010). mhGAP Intervention guide for mental, neurological and substance use disorders in non-specialized health settings: version 2.0. https://doi.org/10.1590/0047-2085000000206
World Health Organization. (2003). Organization of services for mental health. World Health Organization.