PIH in Darker Skin CPD




































































Dr Abirami Pararajasingam and Dr Sandeep Cliff explore treatment for PIH

Special Feature: Post-Procedure Makeup

Practitioners discuss using makeup following aesthetic treatment










Male Toxin Treatments
Mrs Aggie Zatonska details techniques for toxin injections in male patients

Successful Media Interviews
Julia Kendrick shares her top 10 media training tips













































VOLUME 6/ISSUE 6 - MAY 2019
AESTHETICSENTRYAWARDSNOWOPEN!
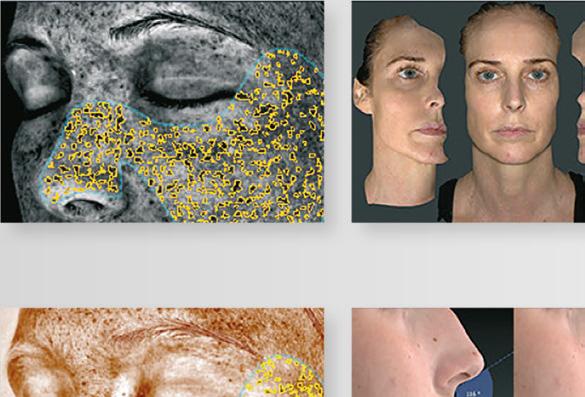
Surface Imaging Solutions is the exclusive distributor partner in the UK and Ireland for Canfield Scientific (www.canfieldsci. com) , the market leader in healthcare imaging solutions. Our rich portfolio includes Aesthetic Systems such as the VISIA® complexion analysis system, the VECTRA®3D range and IntelliStudio® and in Medical Dermatology the VECTRA®3D WB360, VECTRA®3D H1 XP, IntelliStudio® and VEOS® products and DermaGraphix® application software. As a market leader in healthcare imaging solutions, we deliver outstanding photographic systems, software applications, consultancy and support services to consultant surgeons, physicians and practitioners in Aesthetic, Cosmetic, Plastic and Reconstructive Surgery across the NHS and Private practices and Aesthetic Clinics in our market space.




SIS ensure all healthcare professionals are provided the tools to offer the best services to their patients improving communication, planning and managing treatment outcomes across the continuum of care, combined with methods and services to support them in today’s regulatory environment.
Ready to Try?
Experience the latest 3D imaging technology that will enable your patients to clearly express, visualise and document their aesthetic desires. Using our FREE VectraView® 3D application, you have full camera and rotation control of your patients’ 3D data capture, right in your consulting room.


Ready to Buy?
ViewMyConsult®




 Lease VISIA or VECTRA H1 from £95 / week. Full warranty over lease purchase term
Lease VISIA or VECTRA H1 from £95 / week. Full warranty over lease purchase term
SU R FA C E I M AG I NG SOLUTIONS +44 (0) 77 7480 2409 surfaceimaging.co.uk
We offer a wide range of purchase options and support packages to help grow your practice, including the
patient
Increase patient satisfaction Differentiate your practice Communicate the possibilities
portal.
Clinical Contributors
Find your category and make 2019 your year!
Mrs Aggie Zatonska describes toxin injections in male patients
Advertorial: Innovative Skin Systems from Skinceuticals Targeting Ageing and Blemish Prone Skin
Dr Fiona McCarthy details how radiotherapy affects the skin


Miss Jennifer Doyle explores using topical skincare in the periorbital area


for Skincare Penetration Dr Ifeoma Ejikeme outlines procedures that increase skincare penetration

Dr Sandeep Cliff is a consultant dermatologist at a university hospital. He has lectured extensively on various non-invasive techniques for facial rejuvenation, including lasers, dermal fillers and toxins. He is a clinical sub-dean at Brighton and Sussex Medical School.

Miriam Martinez Callejas is the chief pharmacist at Roseway Labs and specialises in formulating and compounding medications for skin, hair and hormones and she has more than 10 years of experience in compounding.

Professor Bob Khanna is a cosmetic and reconstructive dental surgeon, with 23 years’ experience in facial aesthetics. He runs the DRBK clinic and the Dr Bob Khanna Training Institute for all aspects of cosmetic and surgical dentistry and facial aesthetics.
Mrs Aggie Zatonska is an aesthetic practitioner with 10 years’ experience in facial aesthetics. She is a specialist ENT surgeon and holds a post-graduate degree in aesthetic and antiageing medicine accredited by the L’Union Internationale de Medecine Esthetique.
Dr Fiona McCarthy is a consultant medical oncologist in the NHS in addition to running her aesthetic clinic. Dr McCarthy was awarded a PhD from the University of London in 2017 for her research on the links between inflammation and cancer.

Miss Jennifer Doyle has a Bachelor of Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She is currently a lead trainer at Harley Academy.
Dr Ifeoma Ejikeme is a board-certified NHS medical consultant. Dr Ejikeme is a senior lecturer in aesthetic medicine at Queen Mary’s University and the medical director of Adonia Medical Clinic.
Dr Xavier Goodarzian discusses his pathway into the aesthetics specialty
Aesthetic nurse Bethany Hall explores using social media forums when seeking professional guidance in the event of a complication

Entry for the Aesthetics Awards 2019 is now open! Contents • May 2019 Subscribe Free to Aesthetics Subscribe to Aesthetics, the UK’s leading free-of-charge journal for medical aesthetic professionals. Visit aestheticsjournal.com or call 0203 096 1228 Special Feature Makeup Post Procedure Page 21
Dr Abirami Pararajasingam has completed a Bachelor of Medicine and a Bachelor of Surgery with Honours, as well as a Bachelor of Science in neuroscience. She is a core medical trainee at East Surrey Hospital and has a keen interest in dermatology.
NEXT MONTH • IN FOCUS: Lower Face • Blepharoplasty • Rebranding Your Website 06 News The latest product and industry news 15 On the Scene Out and about in aesthetics 16 News Special: Millennials and Aesthetic Treatment Aesthetics investigates non-surgical treatments in the younger generation 18 Advertorial: Meet the Trainer AestheticSource shares its training opportunities for practitioners CLINICAL PRACTICE 21 Special Feature: Makeup Post Procedure Practitioners discuss dangers of patients using makeup following injectables 26 CPD: Post-inflammatory Hyperpigmentation in Darker Skin
and Dr
Cliff explore treatment for PIH in individuals with Fitzpatrick skin types III-VI 30 Topicals for Hair Loss
discusses treating hair loss with topicals 35 Advertorial: Anti-senescence Activity of Salvia Haenkei Nurse
outlines the use of Profhilo® Haenkenium® 36 Profile Assessment Professor Bob Khanna shares tips for assessing the patient profile 38 The Aesthetics Awards Entry is Open
Dr Abirami Pararajasingam
Sandeep
Pharmacist Miriam Martinez Callejas
prescriber Anna Baker
43 Male-specific Approach to Toxin Treatment
46
49 Radiotherapy on the Skin
53 Periorbital Skincare
56
61
IN
62 ROI
64 Successful
67 Recommending
71
Enhancing Delivery
Abstracts A round-up and summary of useful clinical papers
PRACTICE
and Digital Marketing Business analyst Ed Challinor details how to calculate return on investment
Media Interviews PR consultant Julia Kendrick provides advice for media training
Skincare Clinical educator Victoria Hiscock shares her tips for skincare retailing
In Profile: Dr Xavier Goodarzian
72
The Last Word
SUNSCREEN
SELF TAN
•
BRONZER
• Contains a light natural bronze colour to give instant glow
HYDRATING
• Luxurious Lotion nourishes and repairs the skin with silky finish
TANCREAM™ ABOUT THE INGREDIENTS
TANCREAM™ is formulated to allow skin to breathe, therefore pores do not get blocked, it leaves a silky smooth finish and also helps avoid prickly heat and skin irritations.
• Troxerutin is anti-oxidant and anti-ageing with antiinflammatory properties. It is a free radical scavenger and also accelerates the DHA* tanning process. The skin is protected from any damage caused by DHA on application

• High UVA and UVB protection also reduces free radical formation and is a photostable broad spectrum SPF system
• The sun protection is a blend of organic sunscreens with added ingredients to form the five star UVA protection
• Glycerin is part of the preservative system and is a well known extremely safe moisturiser.
*According to the American Academy of Dermatology, the most effective sunless tanning products contain dihydroxyacetone (DHA) as the active ingredient. DHA is a colorless chemical (it is derived from glycerin) that interacts with the amino acids in dead skin cells to produce a brown colour change.

The World’s First SPF 50 UVA Ultra Sun Protection with Gradual Self Tan & Instant Bronzer Luxury Lotion Protect. Hydrate. Glow
Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 info@aestheticsource.com www.aestheticsource.com
Ultra sun protection from blended organic ingredients
• SPF50 UVA/UVB
Gradual daily self tan for face and body that’s odour and streak free
ANTI-AGEING PARABEN FREE | | | | ANTI-OXIDANT CRUELTY FREE DERMATOLOGIST ENDORSED SCIENTIFICALLY PROVEN Look Healthy, Stay Healthy. Stay Safe all Year Round SUN AWARENESS WEEK May 6th-12th 5* UVA PROTECTION FOR FACE & BODY UVA ULTRA SPECIAL OFFER £20 + VAT Thoughout May
Amanda Cameron Editor


Welcome to the May issue of our superb journal! The start of May means the 2019 Aesthetics Awards entry has opened! The Awards celebrates everything this wonderful specialty is about, and is open to those established and new to aesthetics across a variety of fields. See this year’s categories on p.38. Now, the clocks have moved forward an hour thank goodness, so there is a feeling that the warm weather may be on its way, which means that more people will be starting to expose more flesh! Time for body treatments and great skin to be in focus. On this note, our theme this month is topicals. ‘What can you apply to the skin and does it work?’ is probably something you get asked on a daily basis. How about the questions about post-procedure makeup? ‘Can I wear makeup after my treatment? When should I apply makeup? What sort of makeup should I use?’ If you want some help and consistency with answering these questions, turn to p.21. The skin is a barrier – designed to keep
things out – but how do we let the good ingredients in?! What are the innovative mechanisms being used to enhance transcutaneous delivery? Dr Ifeoma Ejikeme provides a valuable overview on p.56 And it’s not just skincare we are talking about when it comes to topicals this month – ever thought about topical treatments for hair loss? Pharmacist Miriam Martinez Callejas takes us through the different types and pathology of hair loss with some interesting topical solutions on p.30. Sadly an issue that is necessary but rarely considered is the effects of radiotherapy on the skin. Many patients we will see in aesthetic clinics will have undergone radiotherapy treatment after a cancer diagnosis, so what specific skincare considerations do we need to make? Consultant oncologist and aesthetic practitioner Dr Fiona McCarthy advises on p.49 Finally, who dreads the thought of having to ‘sell’ your skincare to your patients? This can be daunting for some, especially those from an NHS background, so education specialist Victoria Hiscock shares her approach to achieving sales and retaining patients on p.67 So are you ready to read? Let’s go!
Editorial advisory board
Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with over 20 years’ experience. He is an international presenter, as well as the medical director and lead tutor of Medicos Rx.
Mr Humzah also runs the multi-award winning Dalvi Humzah Aesthetic Training courses. He is a founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow.



Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic non-surgical medical standards. She is a registered university mentor in cosmetic medicine and currently a second year student on the Northumbria University Masters course in non-surgical cosmetic interventions. Bennett has been developing her practice in aesthetics for 25 years.


Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons (BAPRAS) and the British Association of Aesthetic Plastic Surgeons (BAAPS).

Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Christopher Rowland Payne is a consultant dermatologist and internationally recognised expert in cosmetic dermatology. As well as being a co-founder of the European Society for Cosmetic and Aesthetic Dermatology (ESCAD), he was also the founding editor of the Journal of Cosmetic Dermatology and has authored numerous scientific papers and studies.

Aesthetics
Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years' experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer in the cosmetic use of botulinum toxin and dermal fillers.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine and ensures that along with day-to-day clinic work he also attends and speaks at numerous conferences.
Dr Maria Gonzalez has worked in the field of dermatology for the past 22 years, dividing her time between academic work at Cardiff University and clinical work at the University Hospital of Wales. Dr Gonzalez’s areas of special interest include acne, dermatologic and laser surgery, pigmentary disorders and the treatment of skin cancers.

Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multiaward winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts. Dr Williams is also author of Amazon-No-1 Bestseller ‘Look great, not done’.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University. Dr Samizadeh frequently presents at international conferences and is passionate about raising industry standards.

Editor’s letter
We are honoured that a number of leading figures from the medical aesthetic community have joined the Aesthetics journal’s editorial advisory board to help steer the direction of our educational, clinical and business content
© Copyright 2019 Aesthetics. All rights reserved. Aesthetics Journal is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184 DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final. ABC accredited publication PUBLISHED BY PORTFOLIO MANAGEMENT Chris Edmonds • Chairman T: 0203 096 1228 chris@aestheticsjournal.com Suzy Allinson • Brand Director T: 0207 148 1292 | M: 07500 007 013 suzy@aestheticsjournal.com Jenny Claridge • Commercial Director T: 0203 096 1228 | jenny@aestheticsjournal.com ADVERTISING & SPONSORSHIP Judith Nowell • Business Development Manager T: 0203 740 3886 | M: 07494 179535 judith@aestheticsjournal.com EDITORIAL Amanda Cameron • Editor T: 0207 148 1292 | M:
•
ARTICLE PDFs AND REPRO Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
07810 758 401 mandy@aestheticsjournal.com Chloé Gronow
Deputy Editor & Communications Manager T: 0207 148 1292 | M: 07788 712 615 chloe@aestheticsjournal.com
Shannon Kilgariff • Senior Journalist
T: 0207 148 1292 shannon@aestheticsjournal.com Megan Close • Journalist T: 0207 148 1292 megan@aestheticsjournal.com Sophie Thompson • Content Executive T: 0207 148 1292 sophie@aestheticsjournal.com
CUSTOMER LIAISON
FOLLOW US Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Chloe Carville • Customer Liaison Executive T: 0203 096 1228 | contact@aestheticsjournal.com Lian Graham • Customer Liaison Executive T: 0203 096 1228 contact@aestheticsjournal.com EVENTS Kirsty Shanks • Events Manager T: 0203 096 1228 | kirsty@aestheticsjournal.com DESIGN Peter Johnson • Senior Designer T: 0203 096 1228 | peter@aestheticsjournal.com Chiara Mariani • Designer T: 0203 096 1228 | chiara@aestheticsjournal.com
Talk #Aesthetics
#Regulation
Jackie Partidge
@mrsjackiepartridge
Working with Scottish Government to improve patient safety. Representing BACN (British Association of Cosmetic Nurses)

#PatientSafety #TeamWork
#ClinicOpening

Mr Benji Dhillon
@drbenjidhillon
It’s official! @defineclinic is now open! We truly appreciate all those that attended.
@drmarkhughes @slainesmiles and myself gave an insight into our values and what we would like people to experience when walking into the building. But most importantly everyone seemed like they had fun on the night!

#ReconstructiveSurgery
BFIRST
@BFIRSTraining
We’re getting the #FridayFeeling knowing the vital impact our work can make to those less fortunate overseas. A huge thank you to all who continue to support the work of #BFIRST around the world.
#Monaco
Dr. Kathryn Taylor-Barnes
@RealYouClinic
Dr Kathryn delivered her talk in Monaco today, on her original university master’s research regarding ultrasound and botulinum toxin and modernising injecting methods. It went really well and it’s a brilliant conference! #AMWC2019
#DreamTeam
Dr Dev Patel @drdevpatel1
Always good coming back to my clinic and incredible team. This man (also my dear friend) coordinates my dream team and ensures I can focus on what I am doing wherever I may be in the world, without worrying about our patients or other clinic matters #Friends #Loyalty @perfect_skinsolutions

Dermal filler
Allergan launches Juvéderm
VOLUX
Global pharmaceutical company Allergan has launched Juvéderm VOLUX, a hyaluronic acid injectable gel that uses the existing VYCROSS patented technology. The CE-marked product is design to be used to sculpt the chin and jaw area, giving facial definition that can last for up to 24 months, the company claims. In a clinical trial where the primary goal was to evaluate the mean change in facial angle from baseline compared with a control group of 85 patients, 95% reported that they were satisfied with the results three months’ post treatment. At 18 months, 62% of patients still felt results were positive. Allergan explains that this product also contains lidocaine to aid with comfortable treatment experience. Marc Princen, executive vice president and president of international commercial for Allergan said, “As the global leader in medical aesthetics we’re constantly looking to evolve our portfolio of products and technologies, and now, with Juvéderm VOLUX, men and women around the world can achieve the defined and contoured lower face that they’re looking for.”
Regulation
JCCP introduces fast track assessment for cosmetic practitioners
The Joint Council for Cosmetic Practitioners (JCCP) has introduced a new process for practitioners who are already registered with a professional statutory regulatory body, like the GMC or GDC for example, to join the voluntary register. The JCCP explains that it recognises there are many existing practitioners who have developed and acquired knowledge through a wide range of experiential and formal learning who may not wish to undertake a regulated qualification, which is required for others wanting to join the register. With this in mind, the organisation has created a process called fast track assessment (FTA) for those who wish to demonstrate that they have an equivalent level of knowledge, skill and competence. Practitioners must provide information to support their existing FTA application, such as certificates, clinical placements and testimonials. They must then pass a knowledge test under time-constrained examination conditions and a test of competence through an appropriate clinical assessment. The JCCP Trustee Board has approved this new assessment process and is currently seeking consultative feedback from practitioners and stakeholders, with the intention of implementing an agreed process by the end of June 2019.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Follow us on Twitter @aestheticsgroup and Instagram @aestheticsjournaluk
Calecim Professional adds fourth product to its portfolio
Singapore-based biotech company CellResearch Corporation, the owner of cord-lining stem cellbased cosmeceutical Calecim Professional, has added a fourth product to its portfolio, the Recovery Night Complex. The new product is a gel formulation that the company explains is rich in stem cell proteins (50%), as well as other cooling, calming and hydrating factors such as aloe vera, niacinamide and calmosensine, a lipopeptide. According to the company, it provides a breathable gel barrier on sensitised skin, aiding comfort with numbing peptides, while keeping skin moist and protected. The Recovery Night Complex provides relief for skin in distress and is designed to be applied after the Professional Serum, or on its own on the evening of a treatment. It is to be worn throughout the night and washed off the next morning.
Vital Statistics
32% of 14,457 patients worldwide are currently considering a facial injectable treatment (Allergan, 2019)
In a survey of more than 300 aesthetic doctors and dentists, only 4% did not offer toxin treatments in their practice (BCAM, 2018)
Awards
Entry for the Aesthetics Awards 2019 is now open
Practitioners, clinics, suppliers, distributors and other aesthetic companies now have the opportunity to be recognised for their excellence at the leading awards event in the specialty, the Aesthetics Awards 2019. With 26 categories available to enter, all of those who want to participate in the unmissable event are encouraged to turn to p.38 for more information on each specific award and requirements. Aesthetics journal editor Amanda Cameron commented, “I’m so excited that entry is now open for another year! We have made updates to many categories this year and as always, the calibre of entries is expected to be extremely high. I would advise all of those in this specialty to enter early and make sure that you include as much evidence and supporting information as you can. Good luck to you all!” New sponsors have also been confirmed including pharmaceutical company Sinclair Pharma who will be supporting the Best Independent Training Provider, Healthxchange Group, who will sponsor the Award for Sales Representative of the year, and aesthetic skincare company AestheticSource, who will be sponsoring the award for the Best New Clinic, UK and Ireland. Entry for the Aesthetics Awards closes June 28 and finalists will be announced on September 2.

43% of 1,030 patients in the UK said they were considering cosmetic treatments in order to improve self confidence (RealSelf, 2018)
In 2018, 53% of 300 UK aesthetic practitioners who experienced a complication did not report it (Hamilton Fraser Cosmetic Insurance, 2019)
According to 1,329 plastic surgeons, male patients account for 14% of the demand for cosmetic surgery procedures worldwide (ISAPS, 2018)
50% of patients admit they look to celebrities to define beauty (Allergan, 2019)
As of January 2019, there are currently 45 million active social media users in the UK (Hootsuite, 2019)
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Stem cells
Events diary
8th-10th May 2019
37th Annual Conference of the British Medical Laser Association, London www.bmla.co.uk/bmla-conference-2019
14th May 2019
British Association of Sclerotherapists Annual Conference, Windsor www.bassclerotherapy.com
5th-8th June 2019
Vegas Cosmetic Surgery and Aesthetic Dermatology Conference www.vegascosmeticsurgery.info
21st September 2019
British College of Aesthetic Medicine Conference www.bcam.ac.uk
Dermal filler
Merz launches Belotero Revive
Aesthetic manufacturer Merz is set to launch a new dermal filler containing a combination of hyaluronic acid and glycerol, called Belotero Revive, into the UK in 2020. The product is already available in selected countries in Europe and Latin America. Merz explains that Belotero Revive is designed to improve hydration, elasticity and firmness of the skin to address the appearance of fine lines. The product was clinically assessed in a study involving 24 patients, where it was injected into the lower cheek area and results were evaluated over an observation period of 36 weeks. It was reported that 100% of patients showed improved aesthetic results at week 12, more than 80% were satisfied with the treatment at week 24 and 90% would recommend it to friends. Merz has also launched a Belotero Revive campaign, which encourages patients to ‘show off the best version of themselves without a filter’. The company explains that it is also designed to appeal to all age groups, while encouraging women to make choices that bring out their own individuality and natural beauty.
7th December
The Aesthetics Awards 2019 www.aestheticsawards.com
Education
Dr Tapan Patel introduces Ignite training
Aesthetic practitioner Dr Tapan Patel will be launching a new learning experience called Ignite, designed for beginner and novice practitioners. The first workshop will be held on May 24 in London and will cover a number of topics including anatomy, botulinum toxin treatment, dermal filler techniques, consultation advice, assessment strategy and tips for enhancing reputation, amongst others. Dr Patel said, “The course is designed for doctors, dentists and nurses of any experience and even those with no experience at all. I understand that at the beginning of your career it can be difficult to find the right training, hence my decision to start Ignite. This will run in addition to my online training e-MASTR and will offer a multifaceted approach to all of my existing and new delegates.”
iS Clinical adds exfoliating mask to portfolio
Skincare company iS Clinical has released the Tri-Active Exfoliating Masque, designed to smooth and polish the skin whilst simultaneously helping to minimise pore size and reduce the signs of ageing, the company explains. It is made up of seven ingredients; cellulose and vitamin B ecofriendly microbeads, Brazilian blood orange extract, salicylic acid 1.5%, copper PCA 1%, papain (papaya) enzymes 0.25%, and bromelain (pineapple) enzymes 0.25%. Alana Chalmers, founder of Harpar Grace International, the exclusive UK distributor of iS Clinical, commented, “The Tri-Active Masque will be a popular product for those suffering from acne-prone skin seeking an effective but not invasive prevention therapy, as well as those with ageing skin that seek to provide an extra phase of renewal. It is recommended as a bi-monthly treatment and can be left on from 20 minutes to overnight.”

Conference
Cosmetic Courses to hold conference in June
Aesthetic training provide Cosmetic Courses will hold its third annual conference on June 8 at the Royal Society of Medicine. The day is aimed towards practitioners who are new to the aesthetics specialty and will include interactive workshops on recognising and managing complications, dealing with complaints and claims, business building, a JCCP update, an overview of preventative ageing and a question and answer session. Two live demonstrations will also take place; these include lip augmentation and full face contouring with dermal fillers.
Those interested in attending should visit the Cosmetic Courses website.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Skincare
Venus Concept appoints new Northern-based sales manager


Manufacturer of non-invasive aesthetic devices
Venus Concept has appointed Julie Henderson as its new aesthetic sales manager for the north. The company has confirmed that she will be responsible for sales growth in the North of England and Scotland, as well as supporting existing customers. Henderson has previously worked for aesthetic device company Lumenis and prior to this, worked within the medical device and pharmaceutical sectors. She commented, “Having met all of the Venus Concept team, I feel privileged to be a part of a dynamic, customer focused and dedicated company. I hope to work in partnership with new and existing customers by demonstrating how they can improve their profitability with our cutting-edge technologies, our marketing and educational programmes, and practice enhancement strategies.”
Device
InMode releases a radiofrequency microneedling device
Medical device manufacturer InMode Aesthetic Solutions has released the Morpheus8, a radiofrequency device with combined microneedling, designed for use on the face and body. The device features 24 silicone-coated pins that penetrate into the sub-dermal tissue, while the bipolar radiofrequency technology is delivered at 200, 300 and 400 microns, which allows the needles to reach the deeper subcutaneous layers of the skin. According to the company, this tightens fat and contracts connective tissue, which can improve fine lines, wrinkles and acne scars. Aesthetic practitioner Dr Ash Dutta, who has been trialing the device, commented, “I have been using the Morpheus8 for the face and body, and my patients are delighted with the results. One of the main advantages is that it can be combined with other non-surgical or surgical treatments.”

Partnership
Transform practitioners set to join JCCP register
Clinic operator Transform, part of the Transform Hospital Group, has confirmed that all of its healthcare professionals delivering non-surgical aesthetic treatments will be required to join the Joint Council for Cosmetic Practitioners (JCCP) register, as part of a new partnership between the two parties. All registrants from Transform will need to meet the JCCP and Cosmetic Practice Standards Authority (CPSA) standards and Transform will cover the cost for each individual registrant. Tony Veverka, CEO of Transform, commented, “We are taking a leading role alongside the JCCP to drive up standards across the industry so all patients can start their treatment journey with confidence in the practitioner, the clinic and the standard of care being delivered.” Professor David Sines, chair of the JCCP commented, “The JCCP is delighted to announce its first major partnership with a national chain of clinics/hospitals providing non-surgical treatments, Transform. We both share the primary aim of enhancing public protection and patient safety.”
Lou Sommereux, aesthetic nurse
prescriber
How long have you been working in aesthetics?
My nursing career started at the Middlesex Hospital in London and Addenbrooke’s Hospital in Cambridge, before I specialised in community mental health nursing at Fulbourn Hospital in Cambridge. I really enjoyed working with autonomy in the community and this paved the way for my initial autonomy as an aesthetic nurse. My aesthetic career spiralled from an opportunity to be a model for botulinum toxin treatment and a visit to the inaugural IMCAS conference. I trained with a plastic surgeon and in 2002 I founded the Cosmex Clinic. During the last 17 years my competency, expertise and knowledge have grown and developed. The clinic has a loyal and expanding database and we recently coined the phrase ‘The Cambridge Look’, which refers to natural enhancements to boost confidence and positivity.
What’s your biggest passion?
I was one of the original founders of the BACN and I’m passionate about the importance of education, developing accredited training, appropriate regulations and safeguarding patients. I feel strongly that, as practitioners, it is important to select evidence-based products. I look for robust clinical trial evidence and data, patient satisfaction and results which are reproducible. My patients want repeat treatments with reliability that bring similar results. I would not risk my reputation by administering a product with scanty clinical evidence, which I do not trust implicitly.
What matters to you when choosing a toxin or a dermal filler?
My patients like to see results quickly so it’s important to me to use a toxin that has a fast onset and has reliable data for longevity. I use the same product because I understand its science and understand the field of effect, plus it continues to give me predictable and reproducible results, even on the third or fourth retreatment. For fillers I choose from the Restylane Portfolio. I like the broad product range and the scope for injecting in the correct dermal plane and supporting tissues that the OBT and NASHA range give me, so with an artistic eye I can rejuvenate, sculpt and restore facial volume loss with minimal downtime.
OTH19-04-0127 DoP: March 2019
This column is sponsored by Galderma.
60
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Recruitment
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses

BACN WEBSITE
A major upgrade of the BACN website is taking place throughout May, with a launch date scheduled for the end of the month. After listening to feedback, the members’ area of the website will be streamlined and made as accessible as possible, along with a dedicated CPD area for revalidation purposes, more resources, webinars, complications support, and an updated practitioner finder. There will be a number of other benefits added to the members’ area, and the BACN website will be fully optimised for mobile use. Members will be provided with online tutorials for how to use the new website, with a website roadshow being rolled out at the Autumn regional meetings.
BACN EVENTS
It was great to see so many members attend the first round of regional meetings in April, with Cardiff, Belfast and Glasgow having strong attendance, and with provoking and supportive peer networking. The foundation of what the BACN is all about is support, and the regional meetings are an ideal place to get the latest updates from BACN partners, along with meeting other members in the region. Throughout May, Tara Glover, events manager, will be travelling the country to meet members and work with BACN Regional Leaders to run events with a whole host of exciting agendas. Meetings are still available to book onto via the BACN Events page.
RENEWALS
Members have renewed their membership in record time this year, and it is exciting to see so many nurses who wish to remain part of the largest professional association for aesthetic nurses in the UK. Last reminders will be sent out throughout the month, along with calls to gain feedback about the year with the BACN and as a final push for any members who need to renew!
This column is written and supported by the BACN
Association
BCAM obtains charity status

The British College of Aesthetic Medicine (BCAM) has been awarded registered charitable status in England and Wales by the Charity Commission under the Charities Act. President of BCAM, Dr Paul Charlson, said he was thrilled with the announcement, commenting, “The awarding of charitable status to BCAM is another step on the journey to becoming the leading organisation for the setting of standards and delivery of safe, effective and appropriate aesthetic treatments to the public by qualified and trained doctors and dentists.” In a statement released by BCAM, it was noted that the association aims to promote health and safety in the field of aesthetic medicine and advancing practitioner education. The organisation hopes to achieve this by promoting and encouraging the study of this specialty, conducting research, encouraging training standards, as well as promoting the prevention, diagnosis and treatment of diseases, disorders and conditions associated with the practice of aesthetic medicine.
Device
Thermal fractional skin rejuvenation system launches

Aesthetic distribution company AZTEC Services has launched a new version of the Tixel device, called Tixel 2. Launched at the Aesthetics Conference and Exhibition this year, the device was created by the Israel-based manufacturer Novoxel, and is a thermal fractional skin rejuvenation system that has both an ablative and non-ablative mode with two handpieces instead of one. According to AZTEC, this gives practitioners the ability to quickly switch from a facial treatment to a periorbital treatment at the touch of a button, as it can accommodate both handpieces at the same time. The company adds that the Tixel 2 employs a 400°C metallic tip consisting of 81 small pyramids to the skin. This creates craters 100320mm wide with a thermal zone 100-170mm deep, stimulating the skin’s recovery mechanisms and promoting cell renewal. Anthony Zacharek, general manager for AZTEC Services, said, “With Tixel 2, both the facial and periorbital handpieces are connected at the same time, eliminating the need to swap handpieces during treatments, therefore saving time and making the treatment experience smoother.”
Milestone
Allergan reaches 100 million milestone for Botox
Global pharmaceutical company Allergan has manufactured the 100 millionth vial of botulinum toxin type A Botox, which the company has said is a ‘significant milestone in the history of the brand’. Allergan explains that it is currently used in 97 countries for aesthetic and therapeutic use in 35 different indications and has been subject to 148 clinical trials. According to the company, it is continuing to collaborate with researchers, scientists and academic bodies to find new uses for botulinum toxin. Mitchell Brin, senior vice president global drug development and chief scientific officer said, “After 30 years of studying this drug, we have a large safety database and we are now moving into other disorders that I would say two decades ago I would have not had anticipated going into.”
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Campaign Government launches patient safety campaign
The Department of Health and Social Care will launch a media awareness campaign on May 13 to highlight the potential dangers and safety issues around surgical and non-surgical aesthetic treatments in the UK, targeted towards the younger generation.
In a survey conducted by pharmaceutical company Allergan, 98% of 21 to 35 year olds said they would consider professional treatment at some point in their lives. Another recent survey of 1,033 UK women aged between 18 and 30, carried out by Deltapoll and commissioned by the BBC, suggests that 48% believe that having a cosmetic procedure is a lot like having a haircut.
At the time of print, further details about the campaign are yet to be disclosed, however aesthetic nurse prescriber Sharon Bennett, who has been working with the DHSC, said, “Some of the key messages are for patients to search for practitioners on the Save Face and the Joint Council for Cosmetic Procedures (JCCP) voluntary registers, make sure they choose a practitioner who has the correct insurance and training and is competent in their procedures, don’t be pressured into making decisions and have time to reflect, don’t be tempted with time-limited offers and deals, and be careful of cosmetic procedures abroad.”
Bennett added that aesthetic practitioners should take note of the Government’s campaign, and familiarise themselves with its recommendations.
“We need to affirm that what we are doing is right and correlates with the Government’s recommendations. We can also use it to determine how we are perhaps lacking in some areas, or could improve in others. For example, if the Government is recommending that patients should not have their treatment at home and practitioners are doing this, perhaps they should consider working with other peers in a purpose-built clinic and becoming a member of an organisation,” she said.
Professor David Sines, chair of the JCCP, added, “The JCCP is working closely with the DHSC in support of their forthcoming media awareness campaign and has inaugurated a new Communications and Marketing Committee to engage with members of the public and raise the profile of the key safety issues that affect the sector. Focus should not only be on practitioner services but also on the use of genuine safe products. The JCCP will seek to bring key suppliers together to collaborate in the interests of public protection/safety.”
Murad releases Night Fix Enzyme Treatment

Skincare company Murad has launched the Night Fix Enzyme Treatment, an overnight skin treatment that the company explains works with the body’s circadian rhythm to treat the signs of sleep deprivation including dryness, dullness, dehydration and fine lines. The product includes chronopeptide, a peptide that aims to specifically support natural repair for renewed skin vibrancy, as well as tri-enzyme technology, which is purified from red and green microalgae and aims to provide potent antioxidant protection and detoxification to reduce visible signs of premature ageing. Lastly, the product includes violet, cedarwood and lemon aromas, all of which are designed to enhance sleep quality. According to Murad, the treatment is safe for sensitive skin and should be massaged over the face and neck after applying its night moisturiser.
Devices
PureSkin introduces new laser device

Aesthetic equipment manufacturer and distributor PureSkin has introduced a new device, the SyrioQS. Manufactured in Italy, the device can be used for a range of treatments, including, tattoo removal, skin rejuvenation, carbon peeling, acne treatment and treating pigmented lesions, the company claims. The SyrioQS is a Nd:YAG device, and is supplied with three interchangeable tips, 1.5mm, 2mm and 3mm, for treating different sized areas of the skin. The device works with two wavelengths, 1064 nm and 532 nm. A potassium titanyl phosphate (KTP) crystal doubles the frequency of pulsed Nd:YAG laser energy to a 532 nm wavelength, the company claims. PureSkin explains that by reducing the wavelength leads to a different interaction between laser beam and skin, resulting in faster skin healing. Founder of PureSkin, Jayne Mitchell, said, “We’re delighted to bring the SyrioQS to market as it delivers fast, effective treatments with greatly reduced pain. Having spent time with therapists and aestheticians, we understand the issues they face in the treatment room and we can finally offer a laser which helps them to serve their clients to their optimum ability.”
Breast Implants
Q Medical confirmed as UK distributor for B-Lite
Distributor Q Medical has become the exclusive UK distributor for the B-Lite breast implants. B-Lite is a lightweight silicone gel breast implant that contains high-purity hollow borosilicate microscopic spheres that aim to reduce the implant’s mass, whilst maintaining its volume. The spheres are spatially fixed within the cohesive silicone gel of the implant, ensuring no migration and a natural feel, the company says.
Q Medical also states that the B-Lite implants are 30% lighter than regular silicone implants, which lessens the stress on the connective tissue in the breast and helps to preserve its shape and appearance.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Antiageing
Skin of colour
Suncare campaign for darker skin types launches
The online resource for patients with skin of colour, Black Skin Directory, will be launching a Sun Awareness Campaign on Monday May 6, aiming to increase awareness of sun damage in darker skin types. According to the Black Skin Directory, it has partnered with Swiss suncare brand, Ultrasun, to launch a campaign that directly speaks to an audience with darker skin. The campaign will include a video advert, a billboard and a pop-up e-shop on the Black Skin Directory website, including a selection of suncare products suitable for darker skin tones. Founder of Ultrasun, Abi Cleeve said, “I’m absolutely delighted that the team at Black Skin Directory has opened a serious fact-based dialogue on the concerning ratio of lower risk to higher mortality rates in skin cancer among those with darker skin tones.”
AQ Skin Solutions releases hormonebalancing serum
Skincare company, AQ Skin Solutions, has launched the Endo-Test, a solution that aims to restore hormonal balance and increase the body’s energy levels. The product uses a peptidespecific signaling technology, which the company claims activates the proteins involved in testosterone production, boosting the body’s natural production of free testosterone. When the body has replenished its testosterone levels using the Endo-Test, the signaling technology will ensure no excess formula boosts the hormone levels, as the body no longer needs testosterone replenishment, according to the company. AQ Skin Solutions explains that men are safe to use the product daily, whilst women are advised to take one month of rest after one months’ use.

Candela brings new pulsed-dye laser device to the UK
Medical Aesthetic device company, Candela has officially launched the Vbeam Prima in the UK. The device is a pulsed dye laser (PDL) with two wavelengths, 595 nm and 1064 nm, and offers a zoom handpiece that allows practitioners to treat areas between 0.5-12mm. According to Candela, Vbeam Prima can be used to treat a number of indications, including leg veins, vascular lesions, stretch marks, rosacea, warts and wrinkles. Consultant dermatologist Dr Firas Al-Niaimi was the first in the UK to receive the device, and said, “The ability to choose contact cooling enables me to get an effective, comfortable treatment of surface pigment, and in the same treatment session I can now combine 595 nm PDL with 1064 nm Nd:YAG laser system, allowing me to treat superficial vessels and deeper vessels effectively.” VBeam Prima was launched globally in July 2018, and is now available to purchase by medical aesthetic practitioners in the UK and Ireland through Candela.

Distribution
Harpar Grace secures global distribution rights for Déesse Pro
Aesthetic distributor Harpar Grace has secured the exclusive global distribution rights for Déesse Pro LED technology. Previously the exclusive distributor for the UK and Ireland, Alana Chalmers, founder and director of Harpar Grace, said she is thrilled to take on the new rights, “Securing the exclusive global distribution rights to the Déesse brand is exciting for Harpar Grace as I believe the Déesse brand has led the way in LED mask technology arena. We are able to take our experience and expertise of building a brand in the UK and apply this on a global level whilst taking on the nuances of each particular international territory.”
Technology
Cutitronics introduces skincare analyser and dispenser
Skincare technology company, Cutitronics, has launched a prototype of a small portable device that can analyse skin on the go, and dispense the recommended amount of product, called the CutiTron. According to the company, the device can detect the hydration of a patient’s skin and draw on a wide range of external information, such as their location, the outside temperature and the humidity in the air. It has an accompanying smartphone app that can be tailored to suit any skincare brand, allowing companies the ability to create a bespoke package to suit each patient’s needs, the company states. The brand’s formulation is then kept in a capsule inside the device. Once the device has analysed the skin, the correct amount of product is automatically dispensed. Dr David Heath, founder and chief executive at Cutitronics, explained, “The system is tailored to what patients’ skin needs.” He added, “It can then dispense the right amount of product to get the best results for their skin.”
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
UK distribution
Hormones
3D-Lipo Ltd appoints ISO co-ordinator

Aesthetic device manufacturer 3D-Lipo Ltd has appointed Aimee Downing as its new International Organization for Standardization (ISO) coordinator Downing’s role will involve developing a comprehensive management system, which meets the requirements of the medical device regulations and ISO 13485:2016, supporting 3D-lipo Ltd as it aims to be certified under this standard by the end of 2019. Downing is an ISO lead auditor and practitioner certified by the Chartered Quality Institute, with a strong background in engineering with rail companies management systems. Marketing director of 3D-lipo Ltd, Phoebe Cowley, said, “The introduction of ISO 13485 and the medical device regulations will ensure that 3D-lipo Ltd remains a robust organisation, cementing the company’s position as a market leader in the aesthetics industry. Aimee is excited to be part of the company’s evolution, bringing the team at 3D together to achieve this.”
Conference
5-Continent-Congress 2019 dates confirmed
The 11th annual 5-Continent-Congress (5CC) will take place from August 29 to September 1 this year in Barcelona. The conference is open to physicians, practitioners, students, distributors and industry representatives with an interest in aesthetic medicine. The four-day event will feature a free four-hour full facial filler masterclass with aesthetic practitioner Dr Tapan Patel, as well as a full-day expert panel session on business advice and social media with aesthetic business consultant Wendy Lewis. Dr Michael Gold, the congress president, commented, “Barcelona has been home to the 5CC for the past several years and we are thankful to more than 150 incredible international faculty members and nearly 2,000 delegates for taking part. For those truly interested in learning from the best of the best, the 5CC is an educational experience not to be missed.” To find out more about this conference and the agenda, visit the 5CC website.
Deleo adds small applicator to CRISTAL range
French device manufacturer Deleo has added a small area applicator kit to its CRISTAL Cryolipolysis device range, called the A2 and A3 CRISTAL. According to the company, the two new smaller applicators allow practitioners to treat areas previously harder to reach with the standard applicators, such as the submental area, jawline, knee area and arms. The A3 applicator is larger than the A2 applicator, allowing practitioners to treat a range of smaller areas. Aesthetic practitioner, Dr Worapon Sukeewattana, said, “The new small area applicator kit allows for the refining and reduction of bulges in areas that are impossible to treat with the standard applicators on the first-generation machines. These mini applicators are almost painless in the treatment of pseudo gynaecomastia in men compared to the previous generation applicators.”
News in Brief
Allergan to launch support website
Global pharmaceutical company Allergan will launch a website called Allergan Spark in mid-May to support healthcare professionals working within medical aesthetics. According to the company, the website aims to provide ongoing clinical and business support for new and experienced healthcare professionals, through their aesthetic journey. Features of the site will include access to a knowledge hub, real-time support and advice, information about Spark Events and details of local training providers.
Phototherapy course for hair loss launches
Medical device company TheradomeInc has launched a new online course that aims to educate medical and aesthetic practitioners in laser phototherapy for the treatment of hair loss. The course will cover topics including the history of lasers, how and why lasers assist hair growth, the benefits of laser phototherapy technologies and an overview of the causes of hair loss in men and women, amongst others. Trichologist SallyAnn Tarver, UK distributor for Theradome, said, “It’s one of the first courses of its kind available and will be paramount in educating individuals on the scientific benefits of laser phototherapy treatment.”
Dr Mayoni Gooneratne recognised as top entrepreneur

Aesthetic practitioner Dr Mayoni Gooneratne has been listed as one of 2019’s top female entrepreneurs by campaign f:Entrepreneur. The campaign is designed to recognise the dynamic and inspirational businesses led by women in the UK. Dr Gooneratne said, “I am delighted to be listed as one of the f:Entrepreneur’s top 100 female entrepreneurs in the UK and am thrilled to have created my company. It’s so important to recognise individuals within small independent businesses and this campaign does that perfectly.”
Clinisept+ Prep & Procedure now available in larger bottle
UK aesthetic distributor AestheticSource has introduced the Clinisept+ Prep & Procedure in a new 500ml pump bottle. The bottle also features a 4ml measured pump aimed to deliver a more accurate application.
Marketing manager at AestheticSource, Vikki Baker, explained, “The increase from a 400ml to 500ml has not affected the price, which remains the same, and based on the calculation of product required per treatment to patient, this new larger size will last one month for approximately 35 patients.”
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Staff recruitment
Cryolipolysis



AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
On the Scene
Epionce Symposium with Dr Carl Thornfeldt, London
Out and about in the specialty Dr Rasha Mayfair Clinic Opening, London
A new aesthetic clinic was launched on April 11 at Mayfair’s Shepherd Market in London. The clinic is owned and run by aesthetic practitioner Dr Rasha Rakhshani
On April 3, more than 80 delegates attended a training event hosted by skincare company Epionce and its official UK aesthetic distributor and training provider, Eden Aesthetics. The founder of Epionce, Dr Carl Thornfeldt, who had flown from the US specifically for the event, introduced the agenda for the day, discussing the brand’s philosophy for skin health and clinical results. There was also a focus on adult acne, which related to the recently-launched Epionce Purifying Acne Duo. The symposium drew to a close with a question and answer session. Dr Thornfeldt said that he felt the day was a huge success, “One of the things that I have liked about today is that people seem to be extremely engaged and they had very thoughtful questions at the end.” He added, “What we are trying to teach is not only how Epionce is different to any other product in the market, but also to help delegates think differently about what causes the conditions that they see.” Carly Poore, marketing manager at Eden Aesthetics, added, “Historically we have hosted one event in one location when Dr Carl Thronfeldt visits the UK. This time, we have hosted events in London, Manchester, Belfast and Dublin. This demonstrates how much the Epionce brand has grown over the years.”


Moghadam, who was born in Kuwait and attended medical school at Kuwait University, before moving to the UK to practise general medicine in 2015. At her launch event, she shared her passion for aesthetics with friends, family and patients, who enjoyed canapés and drinks alongside demonstrations of clinic offerings such as the VISIA machine and Skinade tasters. Dr Rasha said she was thrilled to finally have the chance to open her clinic and share it with the public. “It took me nine months to find the perfect location and I am thrilled to be in Mayfair. The event was amazing, there were so many people here to support me. It was great to have the opportunity to talk about all the difference procedures we have available, such as facial mapping, Obagi Medical, ZO Skin Health, and Dr Levy Switzerland, INTRAcel, the M22 device, the Envy Facial, as well as our signature facial which combines different treatment modalities,” she said.
JCCP-CPSA Stakeholder Meeting, London
On April 4, the Joint Council for Cosmetic Practitioners (JCCP) and Cosmetic Practice Standards Authority (CPSA) held a meeting with stakeholders in London to discuss how to successfully raise public awareness of the risks associated with non-surgical procedures and encourage the public to seek qualified practitioners.
Following a brief introduction and update from the JCCP and CPSA, a panel of speakers provided their recommendations on how to move forward, followed by suggestions from attendees. Journalist Vivienne Parry, who also served as a member of the Keogh Review Team, highlighted that the current messaging within the sector has focused on negative experiences, so more positivity is required to promote public confidence in best practice. Healthcare marketing agency director Olly Caporn also emphasised the need for the JCCP to utilise social media to promote its message, while recommending that stakeholders work together to improve and increase the data available on patient demographics and rates of complications. From a patient perspective, Dawn Knight, who has previously suffered a complication from treatment, outlined
what she believed could be done to improve public awareness. She focused on the importance of showing the public what good practice looks like, mapping out what could and should happen if things go wrong, liaising with the Advertising Standards Authority on stopping misleading advertising, engaging with social media platforms to challenge inappropriate posts, and encouraging everyone within aesthetics to support the JCCP in order to bring all parties together in the interest of public protection and safety. Stakeholders also contributed their recommendations and suggested that messaging should highlight the cost to the NHS of ‘botched’ and unsafe treatments, as well as placing focus on practitioners who use genuine, safe products. Professor David Sines, chair of the JCCP, informed attendees that all suggestions would contribute to an action plan moving forward, as well as being shared with the Department of Health and Social Care, which has recently launched a national public awareness campaign. He concluded that all participants are encouraged to report any issues around misleading advertising and the inappropriate use of social media to the JCCP.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Millennials & Aesthetic Treatment Aesthetics
Have you seen a growth in patients aged under 35 visiting your clinic for treatment? While aesthetic practitioners will be more than familiar with the lip filler trend, particularly amongst those in their early to mid-twenties, new figures released by global pharmaceutical company Allergan suggest that the demand for aesthetic treatment in general is growing amongst millennials aged 21 to 35.
The Allergan 360° Aesthetics Report surveyed 14,584 adults from 18 countries, who selfidentified as ‘interested in looking better and willing to spend money on it’. More than 1,300 practitioners from across the globe also contributed to the report, sharing their views and experiences of providing non-surgical aesthetic treatments.1
Results suggest that 98% of millennials would consider professional treatment at some point in their lives, while the age group is more likely than any other to consider treatment as soon as they notice a concern; 39% of those aged 21-35 said they were likely to consider treatment at the age they are now, compared to 32% of 36-55 year olds and 21% of those aged 56-65. In addition, 82% of the millennials surveyed believe injectable treatments are socially acceptable and 63% said they feel appearance impacts how successful they are in life.1
Aesthetic surgeon Miss Jonquille Chantrey participated and supported the research for this report, launching it at the Aesthetic and Anti-Aging Medicine World Congress in Monaco last month. She says, “I wasn’t that shocked by the statistics; we’re seeing that millennials are more aware and open to treatments than they were five years ago and it’s becoming more of a norm for that generation to consider their appearance. My own patient group are very well educated and generally have a healthy mindset, carefully considering their diet and fitness.”
As a result, Miss Chantrey was not surprised by other statistics in the report, which suggest that millennials are more likely to consider preventative injectable treatment than older cohorts, with 33% aged 21-35 citing they would, compared to 24% of 36 to 55-year-olds and
just 13% of those aged between 56 and 65. This aligns with US-based figures collated in 2018 which indicate that since 2010, the number of botulinum toxin procedures performed on 20 to 29-year-olds has increased by 28%, while enquiries for antiwrinkle treatments have increased by more than 50% year on year.2
From a practitioner perspective, the majority of those surveyed believe that the demand from the younger generation is positive, with 53% agreeing they should start seeing females in their 20s. For men, 38% of the practitioners surveyed said they should start seeing them in their 20s too, even if only for skincare advice.1
From Miss Chantrey’s point of view, this approach to preventative ageing can be beneficial, however notes that it should be considered from an overall health perspective. “This is what I’m doing at my clinic; we work on patients’ mental and emotional wellbeing as well,” she explains, adding, “People are seeking better lifestyles and want to be happier in general; it’s not just about what you look like. I think there will be a bigger movement towards this, especially with the younger generation.”
The statistics from the Allergan 360° Aesthetics Report also suggest that millennials are heavily influenced by social media when considering aesthetic treatment. While results indicate that 37% of consumers worldwide search online for treatment and 32% use social media to search about specific problem areas or treatments, the figures for the millennial generation are particularly notable.
According to the report, the percentage of US-based 21-35-year-olds using Facebook as a leading source of information is 93%, while 82% use Instagram and 56% use Snapchat. In addition, 20% of consumers across the globe said they follow a practitioner on social media.1
Miss Chantrey said these high percentages are definitely reflected in the UK too. “While some of the stats suggest consumers are influenced by friends and family, social media is the main source of influence,” she says, highlighting, “And it’s not just social media that has a big impact, it’s media in general as well. The rise in celebrity culture and daily coverage of how celebrities look being reported online and in print is far more of a phenomenon than ever before.” While of course there are benefits to the ease in which consumers can find information and trustworthy practitioners on social media,

Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 93% of 21-35-year-olds use Facebook as a leading source of information
investigates the growth of non-surgical procedures amongst the younger generation
98% of millennials would consider professional treatment at some point in their lives
figures from a survey conducted by the Journal of the American Medical Association (JAMA) Facial Plastic Surgery in 2018 suggest that there has been an upsurge in requests for preventative ageing in order to emulate the ‘flawless’ image projected by photo filters.3 This is supported by the 360° report, which found that 34% of USbased consumers always use apps to modify or erase something on their face before posting a photo on social media.1 “It’s important that practitioners are really responsible on social media,” says Miss Chantrey, who emphasises that there is a difference between educating patients and advertising to them. She encourages practitioners to use evidenced-based products and quantities when promoting and administering treatments, especially to millennials. “Social media is not real education. Education is direct face-to-face contact with good practitioners. These are really young people who may be on their way to having treatment for decades. Please refrain from over injecting; it’s more about minimal


preventative action rather than constantly keeping up with trends.” Miss Chantrey also notes that while millennials are a generally welleducated group, that’s not always the case for some patients. “They may be convinced about what treatment they should have because they’ve seen so much of it on social media,” she says, “Don’t be swayed into doing something, just because a patient has asked for it. Base your treatment approach on appropriate assessment and good medical principles. Additionally, she highlights the fact that the younger generation can be a potentially more vulnerable, sensitive group, advising, “You don’t want to encourage concerns about how they look. It may be that there is a clinical need for treatment, however it’s about giving a gentle, supportive introduction to that.” According to Allergan, similar surveys will continue to be conducted, with the aim of aiding better understanding across aesthetics as a whole. Miss Chantrey concludes by saying that her only hope for practitioners treating the millennial generation is that it is done in a ‘truly authentic way, for the right reasons, not just because they can sell more syringes’.
REFERENCES
1. Allergan, Allergan 360 Aesthetics Report (2019) <https://1zlw9r3t73l23y8qa315nqg1-wpengine. netdna-ssl.com/wp-content/uploads/2019/04/Allergan-360-Report-1.pdf>
2. Valenti, L and Atkins, C. Preventative Botox in Your 20s is Real – But it Could Be Aging You. (Vogue, August 2018) <www.vogue.com/article/preventative-botox-injections-twenty-somethings-expertguide-wrinkles-fine-lines-eyes-lips-forehead>
3. Rajanala, S et al, Selfies—Living in the Era of Filtered Photographs, JAMA Facial Plast Surg. 2018;20(6):443-444 <www.jamanetwork.com/journals/jamafacialplasticsurgery/articleabstract/2688763>
Unique Oxygenating Foundations and Moisturisers
that work like a virtual breathable second skin
Oxygenating Foundation I SPF 25+
Containing the patented Ceravitae™ Complex it stimulates skin cell production and helps the healing process following most procedures. Soothes, heals and protects damaged skin thanks to its oxygen-enriched, natural components making it virtually a second skin. Available in 14 shades.

Oxygenating Foundation Acne Control I SPF 25+


This unique and revolutionary formula was three years in the making! tarted working hard to create the perfect acne control foundation that is also an oxygenating treatment foundation developed to simultaneously clear and conceal the frustrating conditions of acne.
NEW Oxygenating Hydro-Matrix


Much more than a simple moisturiser, this hydrating and healing post-treatment behaves like a ‘second skin’, containing Oxygenetix’s patent formula Ceravitae™, that allows oxygen to penetrate the skin and reinforce the natural healing process. It also beautifully primes the skin ready for the application of the Oxygenetix Oxygenating Foundation. Available in 30ml, 50ml and 100ml.
breathable liquid foundations.
Exclusive to
Exclusive to
e: info@magroup t: 02380 676733 www.magroup.co.uk
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Tell us about the training opportunities at AestheticSource. What makes your company unique?
Education is at the heart of the AestheticSource business. Lorna McDonnell-Bowes, CoFounder of AestheticSource has been training in the industry since the early 1990s and is dedicated to furthering the understanding of skin and aesthetic possibilities for Aesthetic Practitioners. Since launching AestheticSource over seven years ago, Lorna with the help of a brilliant team of experts, provide a comprehensive theoretical and practical learning experience for customers and those new to skin fitness. The multi-disciplinary team of qualified professionals deliver the specific brand training covering skincare, peels from very superficial to deep, mesotherapy and injectable products. AestheticSource Training is designed to ensure our delegates are confident in the use of our ranges, covering all aspects from marketing to assessment, products and protocols, to successful outcomes including managing adverse events. We have carefully chosen experienced practitioners for our training team. AestheticSource is frequently approached by professionals wishing to join our training team and we expect our trainers to be passionate about the brands they train on. AestheticSource has a strong belief that we have chosen the best clinically proven options for clinics in the UK, and our trainers share this passion.
Who would benefit most from attending your training sessions?
Our evidence-based training courses are designed for specific target audiences such as aesthetic therapists and aesthetic medical practitioners. Depending on their experience and qualification level, there are multiple course options available. The registration process


includes careful verification of appropriate qualifications in line with Health Education England, and manufacturer guidelines, which are stricter.
How is a typical training day structured?
AestheticSource courses all follow a similar format:
• A full or half day CPD-approved training on the chosen course – NeoStrata, Exuviance®, Skin Tech® or RRS®
• Pre-training reading one, two or three chapters with multiple choice questions to be completed prior to the training day
• Comprehensive training manuals
• Training day verification of prior learning then theory in the morning; a demonstration of relevant techniques being taught and practical hands-on learning throughout the afternoon
• Follow-up support and optional refresher courses are available free of charge
What support do you offer once a practitioner’s training has been completed?
Taking on one of our brands is a journey and not just a one-day course. As well as the pre-course reading and core training modules, our team follow up with course attendees and offer in-clinic assistance as and when required. We also have a clinical member of staff available 24/7 for any adverse events or concerns. All delegates are welcome to attend refresher courses free of charge, with the opportunity to revisit the theory and have the opportunity to watch live demonstrations. The training pack the delegate receives is a comprehensive tool kit that provides them with protocols, FAQs, consent and medical history forms, marketing material, including direct-to-consumer advertising including social media assets and print materials, sachets of the skincare appropriate for posttreatment use, a USB with all relevant PDFs and in-clinic collateral.
What are the measurable outcomes for trainees and how are they assessed?
Depending on the course attended/ completed, delegates will receive CPD points for their development, as well as
certification Future training dates Course Title Date Venue NeoStrata May 2 Harley Academy Exuviance May 14 Harley Academy RRS– Injectable Biorevitalisation May 16 Harley Academy Exuviance June 4 RSM NeoStrata June 11 Harley Academy Skin Tech – Advanced June 12 Church Pharmacy Training Room Skin Tech June 17 RSM RRS – Injectable Biorevitalisation June 25 Harley Academy
the Trainer AestheticSource outlines the value of its training courses and opportunities for practitioners @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2019 18 Meet the Trainer AestheticSource
Meet
to state that they have completed the course and are trained in the given course. For example, the NeoStrata Products and Peels training attracts nine CPD points with the combination of pre-course reading and the one-day theory and practical course. The certificate is given at the end of the day once the trainer has confirmed that the delegate is competent. The NeoStrata Products and Peels one-day training course is preceded by three chapters of in-depth reading on skin anatomy and physiology, as well as terminology pertaining to skin and skin treatments. Each chapter is followed by a series of multiple-choice questions (MCQs). We ask delegates to complete the MCQs prior to the course, and to come armed with questions raised during the learning process. We send delegates a 10-day prepeel prep pack so that they can bring their own model to the training, prepped and ready for a peel. This allows the delegate to follow up with their training model to observe the peeling process and create their own case study following the course.
How do you ensure your training is kept up-to-date?
Both we and our delegates benefit that our brands that we work with are all equally passionate about on-going development and training. Updated training materials are delivered to us at European and International Distributor Meetings, as well as when new products are launched, changes in the legal framework require updates or when a new treatment protocol is launched; ensuring we have the latest materials and all EU specific updates. Our training team, supported by the directors, and in conjunction with the manufacturers, ensure that all products adhere to current law, for example the EU Cosmetics Directive 1223/2009.
OUR KEY TRAINERS
ANNA BAKER – Clinical Lead & Lead Trainer for Skin Tech and NeoStrata


Courses
Anna Baker is a cosmetic and dermatology nurse practitioner with a keen interest in facial anatomy. Baker holds a post-graduate certificate in Applied Clinical Anatomy, specialising in head and neck anatomy, and won Aesthetic Nurse Practitioner of the Year at the 2017 Aesthetics Awards. She is part of the Editorial Board for the Journal of Aesthetic Nursing and a Specialist Nurse Advisor for PMFA News.
“AestheticSource has a broad portfolio of brands for treating a wide variety of skin concerns for the face and body; from skin preparation, to synergistic formulations – a treatment option for most patient needs and budgets. Their award-winning brands are backed by clinical evidence, which is increasingly important for discerning patients.”
DR MAYONI GOONERATNE – RRS Trainer

Dr Mayoni Gooneratne is a London-based general surgeon with over 18 years of medical and surgical experience. She began her career in surgery after graduating from St George’s Hospital Medical School in London and has been a member of the Royal College of Surgeons since 2002.
“It’s incredible to have a skincare portfolio that actually works and covers all aspects of skin ageing. AestheticSource has done its homework so you don’t have to worry. There is a full range of treatments and retail products with fabulous training and sales aftercare.”
DR AMIEE VYAS – NeoStrata Trainer

Dr Amie Vyas undertook her medical training at King’s College London and the University Hospitals of Leicester before moving into private practice. Dr Vyas developed a particular interest in skin during medical school, where she was appointed a member of the British Association of Dermatologists DermSchool subcommittee. She has since taken an active role in teaching and training for other healthcare professionals.
“AestheticSource is a perfect match for me as we both believe in the importance of robust evidence-based technologies and real results when it comes to skincare… through training I aim to create clinicians who are well versed in their treatments and responsible with their service. AestheticSource is a name that I can trust and therefore I am confident that my trainees will have the all support they require once they go back to clinic.”
Due to increased demand and growth, our Training Manager, Nikki Jones will be building and growing our team of AestheticSource Trainers.
We will also be running our first AestheticSource Symposium in September this year with an exciting agenda with a multitude of industry experts from the UK and overseas, sharing their knowledge and experience of diagnosis, treatment and maintenance for pigmentation.
HIGHLY COMMENDED 2018 BEST SUPPLIER TRAINING PROVIDER To find out more and book an
130 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2019 19 Meet the Trainer AestheticSource This advertorial is written and supported by
AestheticSource training course: Email kacey@aestheticsource.com Call 01234 313

Makeup Post Procedure
As you wave goodbye to your happy patient following another successful non-surgical aesthetic procedure, it is a fact that you have no control over what they do next. It might be that they head straight to the gym, even though you have said that exercise might cause irritation after a chemical peel. Or, because it’s a Friday, they might consume alcohol after their toxin treatment, which you have told them can worsen bruising. Perhaps they may get straight into their car, or onto local transport, and whip out their concealer or foundation to cover up that tiny red mark left by your dermal filler entry point.
There are numerous studies that highlight the importance of makeup application to a woman’s life, which emphasise how hard it can be to get some patients to comply to your recommendations of avoidance. One survey of 3,000 women suggests that a third wouldn’t leave the house without wearing makeup,1 while more recent research indicates that of 2,200 women, 60% wear makeup on a weekly basis, a further 26% put it on at least twice a week and 28% use it every day. The reasons behind use were to feel good when dressing up for a special occasion (78%), to boost confidence (63%), hide blemishes (47%) and to accentuate or highlight certain features (32%).2 A separate survey of 1,500 women found that one in four even admit to sleeping with makeup on, despite the fact that doing so has negative effects on skin.3
But why is makeup application following a medical aesthetic procedure a problem? And how can you maintain control of your patients’ makeup application even after you have said your goodbyes?
The dangers of makeup following aesthetic procedures
There are limited studies that highlight the potential impact of makeup use following aesthetic procedures. However, some practitioners interviewed for this article have experienced complications which they believe were associated with posttreatment makeup application (Case studies 1 & 2).
Dermatologist Dr Harryono Judodihardjo suggests that there are risks associated with makeup application after any aesthetic procedure that has reduced the barrier function of the skin, such as injectables, chemical peels, dermarollers and ablative lasers, among others. “When the skin’s barrier function is compromised then chemicals, bacteria, fungus and viruses that are normally blocked by the skin will be able to enter. This can lead to allergic reactions or infections. The chances of problems occurring will depend on the treatment and what affect it has on the barrier function of the skin. For example, you’re most likely to get infection or allergic reactions if you apply foundation after a CO2 laser resurfacing treatment,” Dr Judodihardjo explains. Although practitioners note that complications following makeup application are rare in their experience, they believe practitioners should be mindful of the risks and how to prevent them.
Infection
Unfortunately, it is very unlikely that the makeup that a patient applies, and the applicator that they use to apply it following an aesthetic procedure, is sterile. This is essential, aesthetic practitioner Dr Zunaid Alli explains, saying, “Unless it’s sterile, anything that goes on the skin after a procedure, which damages the barrier, poses a risk of causing infection.” Makeup is particularly problematic, practitioners note, because patients often transport their makeup around, have it lying at the bottom of a handbag or car for example, use it out of date, or even share it. There are several studies that highlight the dangers of pathogens in makeup, as well as their applicators. One small study of 44 participants indicated that women tend to continue to use makeup far beyond the expiry date (70.5%) and that these products have a high level of contamination with pathogenic microorganisms which are associated with infections (S. aureus in 79% and P. aeruginosa in 13% of mascara samples).4
Another study looked at the contamination of 100 samples of beauty salon tools including a blusher brush and face sponge. All the samples were examined microbiologically for the contamination of S. aureus, P. aeruginosa, yeast and fungus. It was observed that S. aureus was present in 100% of sponges and brushes, P. aeruginosa
Case study 1: Dr Zunaid Alli’s dermal
filler complication
Following consultation for filler treatment, I cleaned the area around the patient’s nasolabial folds with chlorhexidine 2% and injected a thick filler, indicated for that location, using a needle. There was minimal bleeding, no bruising and the patient was given my usual aftercare instructions verbally, which included not touching the face or applying any makeup for at least four hours after the procedure. The patient was discharged at about 4pm, however the next morning I received a message saying that the area was a bit painful, throbbing slightly, and quite warm to the touch (Figure 1).
Figure 1: Infection likely due to makeup application.

I arranged for an emergency appointment and upon examination, I observed blanching and redness about 6mm above the entry point, which indicated to me that it was the start of a bacterial skin infection. To determine the cause of the infection, I asked the patient exactly what she did following treatment. The patient said that she had touched-up her foundation after the procedure because she was going back to work. I therefore established that using occlusive makeup, or the application of this makeup with a non-sterile brush to recently injected skin, was the likely reason for the problem.
I prescribed clarithromycin 500mg twice a day for seven days, and 24 hours later there was a good clinical response. The infected area had already started to become smaller and there was no pain at the day-two examination. After the completion of the antibiotics the issue was completely resolved and there were no more problems following. My main learning point from this experience was that aftercare instructions must be given both verbally as well as written and handed to the patient.
Practitioners discuss the dangers of patients using makeup following treatment and provide advice on management
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com





TEOSYAL RHA ® AVAILABLE FROM CHURCH PHARMACY WELCOME TO THE ERA OF DYNAMIC AESTHETICS /ChurchPharmacyUK www.churchpharmacy.co.uk info@churchpharmacy.co.uk @ChurchPharmacy +44 (0)1509 357 300
one stop shop for all your medical aesthetic and clinic supplies.
| Online
2018 Wholesaler of the Year
2016 Best Customer Service
The
London | Loughborough
WINNER
WINNER
Case study 2: Dr Beatriz Molina’s dermal filler complication
A patient came to me to address some facial acne scarring. Due to the nature of the scars I thought a dermal filler would achieve the best results for the patient. I performed several injections on the face and immediately following the procedure the patient appeared to be fine. However, when she left she applied makeup to cover the redness caused by the entry points. Soon thereafter she developed a superficial infection on the skin, which was limited to the forehead and was not present elsewhere. As I employed appropriate injection practice before and after injection, which included cleansing the skin, followed by hypochlorous for disinfectant, I believe that the infection was likely due to the unsterile brush the makeup was applied with. I prescribed antibiotics and the infection was gone two days later. This complication highlighted to me the importance of making sure the patients are aware of the risks associated with makeup application, and if they
was present in 69.6% of face sponges and 81.8% in brushes, and counts obtained for fungus were 51.5% in sponges and 30.3% in brushes. It was observed that the major cause of contamination of salon tools is repetitive usage on all customers without considering the hygienic conditions.5
Inflammation and sensitivity
Practitioners also suggests that it is not only the sterility of the makeup and applicators, but the components and formulation of the products themselves. Aesthetic practitioner Dr Julia Sevi explains, “Other issues besides infection are the inflammatory processes of the skin; following treatment the skin is more sensitive so anything a patient uses that contains perfume, preservatives, fragrances and parabens, for example, means there is a higher risk of reaction because it is more fragile.” Aesthetic practitioner Dr Beatriz Molina adds, “One of the problems with people applying makeup immediately post procedure is that they may have bought their makeup from the high street and many, if not most, will have some form of chemicals or perfumes, which can cause irritation or reactions to the skin post procedure.”6 Dr Molina says that although it’s not usually formulated specifically for use after medical aesthetic procedures, 100% mineral-based makeup can help to avoid irritation because it does not contain man-made unnatural additives.7 She adds, “Pure mineral makeup also contains vitamins which have natural anti-inflammatory properties and they usually also have SPF, which is good.”
Dr Judodihardjo adds, “Makeup that has small chemical molecules are riskier as they’re easier to penetrate the broken skin. Minerals are large elements and usually do not enter the skin so it should be safer.” However, he notes, “Not every so-called ‘mineral makeup’ is made from 100% minerals, as most do add chemicals. There’s currently no law that stipulates the percentage of minerals needed before a makeup can be called ‘mineral makeup’.”8,9
When can makeup be applied following treatment?

Aesthetics contacted several injectable companies to learn their manufacturer recommendations of makeup application following treatment – most that responded recommend at least 12 hours (Figure 3). The Aesthetic Complications Expert Group also advises 12 hours.10 However, practitioners acknowledge that realistically, the amount of time one would advise patients to wait would very much
are absolutely going to apply, educate them on what is better to use. Following this complication, I now suggest to apply light 100% mineral makeup or specially-formulated aftercare makeup to my patients’ skin using a sterile brush in clinic so that they do not do so themselves.
depend on the type of procedure, and the technique employed. Dr Sevi explains, “If you are using a 35 gauge needle, for example, and are doing tiny micro punctures the injection holes will be very small and will likely seal within half an hour, whereas a 22 gauge cannula introduced by a 21 gauge needle will probably take several hours, depending on the age of the patient. So, I suspect the advice to wait at least 12 hours is because that covers every possible eventuality for the skin to heal.” However, knowing how important makeup is to many patients’ lives, is it realistic to expect them not to put makeup on following an aesthetic procedure?
Dr Sevi and Dr Molina believes it isn’t. “It’s really hard for a lot of patients – women who are working or have a busy schedule in particular – not to wear makeup straight after a procedure to hide any treatment marks, such as filler entry points, bruising or redness. As many procedures take time for the skin to settle, it’s unrealistic to assume that patients won’t just put makeup on straight away, and certainly not for the suggested time following the procedure,” Dr Molina says. So how can practitioners lower the risk of makeup infection and skin irritation post procedure?
Practitioner advice
Although Dr Alli advises patients use a post-procedure makeup product, he prefers to focus heavily on patient education and
Allergan: recommends that the patient does not use any makeup during the 12 hours following the injection treatment. IBSA Farmaceutici Italia: doesn’t recommend use of any makeup after aesthetic procedures except its own sterile Viscoderm Cover Up. Timing would very much depend on the clinical decision of the practitioner treating the patient and procedure – anything between 12 to 24 hours.
Sinclair Pharma: recommends no makeup for 24 hours following dermal filler and thread treatments to allow the exit and entry points to heal and to minimise massage/movement of the face. Teoxane: no makeup recommended within 12 hours after injection.11
Figure 3: Some of the manufacturers that Aesthetics contacted which provided guidelines for makeup application following treatment.
Figure 2: Infection following makeup application.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com

The original LED mask, re-engineered for maximum efficacy & performance 6 Treatment Modes 4 Wavelengths THE GLOBAL LEADER PRO EDITION Features for post injectable treatment TRI WAVE MODE •Global brand awareness •Marketing support •Free Training •Unrivalled A list PR •Low investment / high return JOIN the world leaders in LED mask technology Make your money back in 12 days! SPECIAL Launch Offer £1200 REJUVENATION | PROBLEMATIC SKIN | INFLAMMATION | POST PROCEDURE ENQUIRE NOW CONTACT US NOW FOR MORE INFORMATION & A VIRTUAL DEMO T: +44 2038 686 242 | E: ENQUIRIES@HARPARGRACE.COM | W: DEESSEPRO.COM INTEGRATE INTO YOUR TREATMENT MENU TODAY + Vat
instructs patients to wait his recommended timeframe. “Applying a post-procedure antibiotic cream or ointment over the area may work to deter the patient from putting makeup on so soon after procedures. Also consider the time of day your patient is coming in for treatment – if it’s towards the end they are more likely to go home rather than back to work,” he says. Dr Molina and Dr Sevi believe that although manufacturers may recommend a certain number of hours, the only way to help guarantee that patients will not apply their own makeup is to do it for them before they leave clinic, employing strict protocols to avoid possible contamination and complications.
Dr Molina will either choose to use a makeup product that is specially formulated for post-procedure coverage that doesn’t have any ingredients that may irritate the skin, promotes skin healing and allows it to breath, or 100% mineral powder. She says, “We find that if we don’t apply the makeup for them, people will just go into their car and apply makeup themselves, which is unsterile and their makeup is also likely to contain harmful chemicals. We apply makeup post treatment for almost all procedures and we use
Makeup marketed for post-procedure application
The below are some examples of the products available that can be used as foundation, which are developed and marketed for concealing and covering treatment areas following medical aesthetic procedures.
Oxygenetix
Oxygenetix is a foundation that, according to the manufacturer, provides anti-bacterial qualities, promotes collagen cell production and connective tissue growth and removes dead surface cells. It has been developed to be used post-aesthetic treatment, allowing for improved healing and breathability, according to the company. It also contains SPF 30.12

Viscoderm Cover Up
According to the manufacturer, Viscoderm Cover Up is a sterile, paraben free cosmeceutical formulation that comes in two colours, offering hydration, anti-inflammatory relief and cell stimulation immediately following aesthetic treatments. The manufacturer recommends use following a range of aesthetic procedures.13
a brush that’s been cleaned and is sterile.” Dr Sevi says that she always applies specially formulated postprocedure makeup to patients and doesn’t use powdered mineral makeup because she believes it is difficult to fully sterilise applicators such as brushes, as you must get deep into the bristles. Her protocol is firstly to disinfect the skin following the procedure with hypochlorous or chlorhexidine, then apply a sealant product over the top, such as Opsite or DermaSeal, to ensure product can’t get into the skin. “The only time we don’t do this is if the patient absolutely swears that they’re going home, not seeing anyone and just going to bed. I believe this step is part of our duty of care – they leave looking great and the products we use also promote healing and reduces inflammation,” Dr Sevi explains. She adds, “We also have a policy of how we deal with our makeup application in clinic. Our makeup is in an airless pump which is never opened and we discard if it is. The bottles are sterilised with alcohol wipes every day; inside the lid and on the pump. We also expel the first bit of makeup out of the pump and discard it so it hasn’t been in contact with air, and is clean. We will apply the makeup with gloved hands that have been sterilised – at all times we are trying to reduce the possibility of pathogens being in or around the makeup.” Dr Sevi will then provide the patient with a post-procedure care pack, which includes advice on makeup considerations, as well as a small vile of makeup that they can use to reapply later in the day if they need it, using their finger that has ideally been cleaned with disinfectant.
Summary
All practitioners highlight that makeup application is one of several important factors for appropriate aftercare instructions to achieve safe and successful results, and must be communicated clearly and effectively to patients. Dr Molina concludes, “Make sure patients are aware of the dangers, give written aftercare instructions, ask what type of makeup they use, and if you think they might not be compliant to your instructions, I advise to put the makeup on for them in clinic using sterile applicators.”
REFERENCES
1. Eleanor Harding, My make-up’s a must! One in three women won’t leave the house without a full face on, Mail Online, 2011. <https://www.dailymail.co.uk/femail/article-1346530/Make-agoraphobiaA-women-wouldn-t-dare-outside-make-on.html>
2. Victoria Waldersee, One in six women wear makeup at the gym, YouGov, 2019. <https://yougov. co.uk/topics/lifestyle/articles-reports/2019/03/14/one-six-women-wear-makeup-gym>
3. Katie Winter, Insecure Brits: A quarter of women wear make-up to go to BED in a bid to impress their partner, Mail Online, 2013. <https://www.dailymail.co.uk/femail/article-2353772/A-quarterwomen-wear-make-to-BED-bid-impress-partner.html>
4. CB Giacomel, G Dartora, HS Dienfethaeler and SE Haas, Investigation on the use of expired makeup and microbiological contamination of mascaras, International Journal of Cosmetic Science, 2013, 35, 375–380.
5. S Naz, M Iqtedar, Q ul Ain, K Aftab, Incidence of Human Skin Pathogens from Cosmetic Tools used in Beauty Saloons from Different Areas of Lahore, Pakistan, Journal of Scientific Research, 2012.
6. Sarah Barker, Using Make-up Post-Procedure, Aesthetics, 2015. <https://aestheticsjournal.com/ feature/using-make-up-post-procedure>
7. Riku Campo, Best in Beauty: An Ultimate Guide to Makeup and Skincare Techniques, Tools, and Products, Simon and Schuster,31 Aug 2010.
8. Julia Layton, Is mineral makeup really natural? Mineral Makeup Marketing Claims, How Stuff Works. <https://health.howstuffworks.com/skin-care/beauty/skin-and-makeup/mineral-makeup1.htm>
9. Shannon Romanowski, How is Mineral Make-Up Different Than Traditional Make-Up?, Self, 2011. <https://www.self.com/story/is-mineral-makeup-better-than>
Image Skincare I Conceal

The manufacturer claims the I Conceal foundation increases oxygen uptake in cells to increase wound healing, hyaluronic acid and collagen production, while also soothing irritation and regenerating the skin. The product is marketed as suitable for postaesthetic procedures and is SPF 30.14
10. ACE Group, Management of acute skin infections in non-surgical aesthetic practice, 2018. <http:// acegroup.online/wp-content/uploads/2018/08/ACE-Group-Acute-Infection-v2.1.pdf>
11. Statements obtained directly from manufacturers. References on file. April 2019.
12. Oxygenetix, Products. <http://www.oxygenetix.com/products>
13. IBSA, Viscoderm Cover Up. <https://www.ibsaderma.com/en/viscoderm_coverup.htm>
14. Image Skincare, I BEAUTY - I CONCEAL flawless foundation SPF 30 – Natura. <https:// imageskincare.com/catalog/product/view/id/872/s/flawless-foundation-natural/category/1010/>

Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
PIH in Dark Skin
Dr Abirami Pararajasingam and Dr Sandeep Cliff explore treatment for post-inflammatory hyperpigmentation in individuals with Fitzpatrick skin types III-VI
What is post-inflammatory hyperpigmentation?
Post-inflammatory hyperpigmentation (PIH) is an acquired hypermelanosis which occurs in all skin types, but it is more prevalent among individuals of darker skin, defined as Fitzpatrick type III-VI.1 Dyschromias, of which PIH comprise a significant proportion, are among the most common reasons for African and Asian patients to seek the care of a dermatologist.2-4 PIH can have a significant psychosocial impact on this cohort of patients as lesions often occur more frequently and persist for a longer duration, with greater severity.5 The condition typically arises following inflammation to the skin (for example with acne, psoriasis or atopic dermatitis), but can also occur after cutaneous injury including aesthetic interventions such as dermabrasion, laser and epilation, to name a few.6-9 When there is inflammation or injury to the epidermis, melanocytes are triggered to produce excessive melanin, which is then distributed to surrounding keratinocytes. Although the exact mechanism is unknown, the increase in melanocytic activity has been shown to be stimulated by prostanoids, cytokines, chemokines and other inflammatory mediators as well as reactive oxygen species.10-13 The excessive melanin manifests as dyschromic macules or patches, which in darker individuals can range in colour from red/purple to brown/black depending on baseline skin tone and depth of discolouration.14 If the basal layer is involved, melanin pigment is released and subsequently engulfed by macrophages in the papillary dermis. This can give the skin a blue-grey appearance and lesions may be exacerbated by exposure to sunlight. PIH may remain at the site of inflammation/injury long after the initial wound has recovered, typically resolving after many months to years.15 Management of the condition is challenging and therapeutic strategies often produce variable outcomes. Note that many of the studies mentioned below do not specify the exact Fitzpatrick type of the participants, so patients’ skin colour has been referred to using the same terminology as the study.
Management options for PIH in darker skin
As with other medical conditions, prevention of PIH is better than cure. The importance of controlling the underlying source of cutaneous inflammation or injury must be emphasised. Shah et al showed that early and efficacious treatment of acne in patients with darker skin helps minimise hyperpigmentation.16 This, of course, can be challenging in severe cases. For severe or persistent lesions, which often occur in darker-skinned individuals, there is a wide range of safe and effective treatment strategies which include topical agents, chemical peels, laser therapy and intense pulse light (IPL).
There are also treatments that aim to conceal hyperpigmented lesions, remove the excessive pigment or regulate melanin production, or a combination.
Topical formulations
There are several topical treatments which can help regulate melanogenesis by targeting the enzyme tyrosinase, which converts dihydroxyphenylalanine (DOPA) to melanin (Figure 1). The amino acid
tyrosine undergoes hydroxylation to produce DOPA and subsequently oxidation to produce DOPAquinone; both reactions are catalysed by the enzyme tyrosinase.17 The addition of cysteine to DOPAquinone leads to the formation of eumelanin. In the absence of cysteine, DOPAquinone undergoes conversion to DOPAchrome, which leads to the formation of eumelanin.18
Hydroquinone
Hydroquinone is an agent which acts on this pathway and continues to play an important role in the treatment of hyperpigmentation disorders. A concentration of 2-5% hydroquinone is commonly used for this indication for all skin types.19,20 It can be used as a monotherapy, or in formulation with other agents including corticosteroids and retinoids. Hydroquinone formulations including cortiscosteroid allows treatment of co-existent inflammation. In one study, hydroquinone combined with retinol 4% and 0.15% micro-sponge in patients with Fitzpatrick II-VI skin showed mean improvement in PIH of 39%, 77%, and 77% from baseline to weeks four, eight, and 12, respectively.21 Similarly in another study microencapsulated hydroquinone 4% and retinol 0.15% with antioxidants demonstrated 75% overall improvement in pigmentation at week 12 in 63% of subjects.22 Hydroquinone is currently only available on prescription and commercial use is highly regulated because of the recognised complications, which include contact dermatitis, permanent leukoderma and exogenous onchronosis; these are true for all skin types. Carcinogenicity of hydroquinone has been reported in animals, but there is no established increased risk of cancer in humans.23
Retinoids
Another group of topical agents are the retinoids, which are structural and functional analogues of vitamin A. In a randomised controlled trial with 54 black patients, topical tretinoin cream 0.1% applied once daily for 40 weeks was more effective than placebo at lightening PIH lesions.24 However, 50% of patients developed dermatitis, which is an important consideration and advocates titrating retinoid concentrations
Figure 1: Schematic of melanin synthesis.18 DOPAquinone DOPA Tyrosine -cysteine (Brown to black) (Yellow to Red) +cysteine DOPAchrome Eumelanin Pheomelanin Cysteinyl-DOPA Tyrosinase Tyrosinase Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 1 oint
and usage with time.24,25 Newer generation retinoids, which include adapalene and tazarotene, have also been shown to be efficacious in the treatment of dyschromias in people with a dark skin tone 26,27 In one open label study of 65 African patients with acne associated with PIH, the severity of PIH significantly improved with 0.1% adapalene gel at four, eight and 12 weeks.38 Similarly, in a randomised controlled trial involving 74 dark-skinned patients with acne, 0.1% tazarotene cream was found to be effective against PIH in terms of overall disease severity.39 The oral form of retinoid, isotretinoin, is invaluable in the treatment of severe acne and in one report its use was successful in the treatment of PIH in an Asian patient.28
Other topicals
Other topical treatments have also been implemented in the management of PIH, although evidence is limited. Azelaic acid is produced by malassezia furfur, an anthropophilic fungus which forms part of our natural skin flora. Its mechanism of action is complex and poorly understood, but its efficacy and safety in the treatment of PIH in individuals with a dark complexion has been demonstrated.29-32 One randomised vehicle-controlled double-blind trial of 52 patients (skin types IV-VI) with facial hyperpigmentation treated PIH with topical azelaic acid 20%. It demonstrated greater improvement in hyperpigmentation after 24 weeks of treatment versus vehicle, as measured by the investigator’s subjective scale and chromometric analysis. Side effects were mild and transient.33 Similar results were reported in a 16-week study looking at 15% azelaic acid in the treatment of acne-related PIH in 20 individuals with Fitzpatrick skin type IV-VI.34 Soybean is a legume that is native to East Asia and is a substance which has emerged as an effective skin-bleaching agent with promising results in the treatment of PIH. In a double-blind, placebo-controlled clinical study of African-American, Hispanic, and Asian patients with Fitzpatrick skin types III-V who had acneinduced PIH there was a significant improvement in PIH in patients using over the counter anti-acne medications containing soy compared to those without soy.35
Cysteamine (2-mercaptoethylamine) hydrochloride has been known to have depigmenting effects for decades, although exact mechanism remains unclear. Two randomised controlled trials showed positive outcomes in patients (skin types III-V) with melasma using a cream containing cysteamine compared to controls (Figure 2,3,4).36,37 Patients showed positive results after they were instructed to wash their face in the evening using a prescribed syndet bar and then apply a thin layer of the cream (placebo or cysteamine 5% w/w) to their lesions 30 min later.22 Although the exact pathophysiology underlying melasma and PIH are distinct, they are both considered disorders of hypermelanosis, thus further studies may reveal benefit of topical cysteamine in PIH patients.
Other examples of depigmenting agents which have shown promising results in the treatment of dyschromias include vitamin C cream (or ascorbic acid), kojic acid (a potent inhibitor of tyrosinase by chelating copper at the active site of the enzyme), liquorice extract, niacinamide (physiologically active derivative of vitamin B3 or niacin), N-acetyl glucosamine (an amino sugar that is a precursor to hyaluronic acid), and arbutin.38-40 Evidence surrounding the efficacy of these products in PIH of all skin types is limited and further studies are required.
Concealment
Skin camouflage is described as the application of pigmented creams that are designed specifically to mask skin discolouration or scarring.41 The pigment-rich products are matched to the patient’s normal skin
Before Before
Figure 2: A 37-year-old woman with a five-year history of melasma, before and after four months of treatment with topical cysteamine cream. Fitzpatrick type not specified, however only those with Fitzpatrick skin types III, IV and V were recruited to the study.36


Images courtesy of Scientis Pharma SA, Geneva, Switzerland.
Figure 3: Another 37-year-old woman with a five-year history of melasma, before and after four months of application of cysteamine cream.36 Images courtesy of Scientis Pharma SA, Geneva, Switzerland.



Before
After After After
Figure 4: A 36-year-old woman
Images courtesy of Scientis Pharma SA, Geneva, Switzerland.
colour for a natural appearance. Products are usually waterproof, non-comedogenic and long-lasting. As camouflage is non-invasive and avoids trauma to the skin, there is a favourable safety profile, particularly for individuals with a darker skin tone who are inherently more prone to developing PIH.42
Chemical peels
Chemical peels, which involve the application of acid to remove dead skin cells, are one of the most common non-surgical cosmetic procedures performed in the UK.43 Most chemical peels are brief procedures that require little recovery time, although multiple treatments are usually necessary to achieve best results. There is a long-standing myth that chemical peels are not safe to use in
with a three-year history of melasma, before and after four months of treatment with topical cysteamine.36
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
For severe or persistent lesions, which often occur in darker-skinned individuals, there are a wide range of safe and effective treatment strategies
darker-skinned individuals due to risks of pigmentation disorders;44 however, careful selection of the type and strength of peel can help avoid this potential complication and achieve positive results. Options include glycolic acid, salicylic acid, mandelic acid and trichloroacetic acid peels. Glycolic acid peels, in combination with tretinoin 0.05%, hydroquinone 2%, and hydrocortisone 1% have been shown to produce more rapid reduction in pigmentation compared to topical treatment alone for PIH in dark-complexioned individuals.45,46
Light therapies
Lasers have been described to treat skin conditions for more than 40 years. Although topical agents remain first line for treatment of PIH, laser and light therapies may serve as useful adjuncts. Melaninspecific high energy Q-switch laser systems can successfully lighten or eradicate pigmented lesions in all skin types.47 The short pulse laser systems effectively treat lesions by confining their energy to the melanosome (tiny granules within pigment cells which contain melanin). The results of the laser treatment depend on the depth of the melanin and the colour of the lesion and is, to some degree, unpredictable. Typically, energy from short wavelength lasers is more efficiently absorbed by superficial or epidermal melanin, while longer wavelengths penetrate deeper with more selective absorption by dermal targets. A greater safety margin can be achieved using longer pulse durations and cooling devices, while still maintaining efficacy in darker-skinned individuals.48 In one study, the 1064 nm Q-switched Nd:YAG laser with low-fluence was shown to be effective in the treatment of PIH caused by procedures such as laser surgery and chemical peeling in five Asian patients.49,50 A pulse-in-pulse mode IPL worked well for facial PIH in 25 Korean patients, with 23 patients showing more than 50% improvement.51 Use of the picosecond 755 nm Alexandrite laser produced similar results in three Korean patients (skin type IV) with melasma or PIH.52 Combined therapy using Q-switched ruby laser and cutaneous bleaching with tretinoin and hydroquinone was used in 18 Japanese patients with 38.9% and 44.4% showing excellent or good clearing of periorbital hyper pigmentation, highlighting a potential role for combined strategies in selected patients.53
Discussion
With the treatment options discussed, particularly chemical peels and laser therapy, it is important to recognise that treatment itself may exacerbate or cause PIH particularly in darker-skinned individuals.54 Patients should be counselled appropriately prior to commencing interventions. Furthermore, although not considered as a treatment of PIH, sun protection also plays an integral role in management. In one study, regular use of sunscreen in 89 African-American and Hispanic patients (types IV-VI) for eight weeks showed an improvement in dyschromia and skin darkening as measured by colourimetry, which is a device used to test the concentration of a solution by measuring its absorbance of a specific wavelength of light.55 Daily use of broad spectrum sunscreen (SPF 30 or more) and sun-protective measures should be advised to patients in order to minimise the darkening of lesions of PIH.56,57 This must be emphasised to darker-skinned individuals with PIH as sun protection measures are often used less frequently by this cohort of patients.58
Conclusion
PIH is common among those with darker skin and can cause a significant psychological burden. Understanding available treatment options are important to allow physicians to tailor an approach that is
most acceptable and efficacious for the patient. There are currently a wide range of safe and effective therapies for this condition which we have discussed here. Although some options like hydroquinone and laser therapy are well-established treatments, others have less evidence underpinning their usage, highlighting a need for more research in this area. Regardless of the chosen approach, it is important to initiate treatment early, including the use of regular sun protection and controlling the underlying inflammatory dermatosis.
Dr Abirami Pararajasingam has completed a Bachelor of Medicine and a Bachelor of Surgery with Honours at the University of Liverpool, as well as a Bachelor of Science in Neuroscience at University College London. She is a core medical trainee at East Surrey Hospital and has a keen interest in dermatology as well as teaching and research. Her special interests include inflammatory dermatoses and skin cancer.

Dr Sandeep Cliff is a consultant dermatologist at a university hospital and has a particular interest in skin cancer and inflammatory dermatosis. He has lectured and demonstrated extensively throughout the world on various non-invasive techniques for facial rejuvenation, including lasers, dermal fillers and toxins. He has been principal investigator for over six clinical research trials and is a clinical subdean at Brighton and Sussex Medical School.

REFERENCES
1. Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of colour: a comparative practice survey. Cutis. 2007;80:387–394
2. Taylor S, Grimes P, Lim J, Im S, Lui H. Postinflammatory hyperpigmentation. J Cutan Med Surg. 2009;13(4):183–91
3. Halder RM, Nootheti PK. Ethnic skin disorders overview. J Am Acad Dermatol. 2003;48(6 Suppl):S143–8.
4. Sofen B, Prado G, Emer J. Melasma and Post Inflammatory Hyperpigmentation: Management Update and Expert Opinion. Skin Therapy Lett. 2016 Jan;21(1):1-7.
5. Park JH, Kim JI, Kim WS. Treatment of persistent facial postinflammatory hyperpigmentation with novel pulse-in-pulse mode intense pulsed light. Dermatol Surg. 2016;42(2):218–24.
6. Epstein JH. Postinflammatory hyperpigmentation. Clin Derma- tol. 1989;7(2):55–65.
7. El-Essawi D, Musial JL, Hammad A, Lim HW. A survey of skin disease and skin-related issues in Arab Americans. J Am Acad Dermatol. 2007;56(6):933–8.
8. Sanchez MR. Cutaneous diseases in Latinos. Dermatol Clin. 2003;21(4):689–97.
9. Dunwell P, Rose A. Study of the skin disease spectrum occur- ring in an Afro-Caribbean population. Int J Dermatol. 2003;42(4):287–9.
10. Chang MW. Disorders of hyperpigmentation. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology. 2nd ed. Elsevier Mosby; 2009. pp. 333–389.
11. Taylor SC, Grimes PE, Lim J, et al. Postinflammatory Hyperpigmentation. J Cutan Med Surg. 2009;13:183–191.
12. Ortonne J. Retinoic acid and pigment cells: a review of in-vitro and in-vivo studies. Br J Dermatol. 1992;127(Suppl 41):43–47
13. Nordlund JJ, Abdel-Malek ZA. Mechanisms for post-inflammatory hyperpigmentation and hypopigmentation. In: Bagnara JT, editor. Advances in Pigment Cell Research: Proceedings of Symposia and Lectures from the Thirteenth International Pigment Cell Conference. New York, NY: Liss; 1988. pp. 219–239. Tucson, AZ; October 5–9 1986
14. Pandya AG, Guevara IL. Disorders of hyperpigmentation. Dermatol Clin. 2000;18(1):91–98.
15. Park JH, Kim JI, Kim WS. Treatment of persistent facial postinflammatory hyperpigmentation with novel pulse-in-pulse mode intense pulsed light. Dermatol Surg. 2016;42(2):218–24.
16. Shah SK, Alexis AF. Acne in skin of color: practical approaches to treatment. J Dermatolog Treat. 2010 May. 21(3):206-11
17. Chaowattanapanit et al. Postinflammatory hyper pigmentation a comprehensive overview. American Academy of Dermatology 2017.
18. S A. N. D’Mello, G J. Finlay, Bruce C. Baguley, M E. Askarian-Amiri Signaling Pathways in Melanogenesis. Int J Mol Sci. 2016 Jul; 17(7): 1144.
19. Grimes PE. Management of hyperpigmentation in darker racial ethnic groups. Semin Cutan Med Surg. 2009;28:77-85.
20. Spencer MC. Topical use of hydroquinone for depigmentation. JAMA. 1965;194:962-964
21. Grimes PE. A microsponge formulation of hydroquinone 4% and retinol 0.15% in the treatment of melasma and postinflam- matory hyperpigmentation. Cutis. 2004;74(6):362–8.
22. Cook-Bolden FE, Hamilton SF. An open-label study of the efficacy and tolerability of microencapsulated hydroquinone 4% and retinol 0.15% with antioxidants for the treatment of hyperpigmentation. Cutis. 2008;81(4):365–71.
23. Nordlund JJ, Grimes PE, Ortonne JP. The safety of hydroquinone. J Eur Acad Dermatol Venereol. 2006;20:781-787.
24. Bulengo-Ransby SM, Griffiths CE, Kimbrough-Green CK, et al. Topical tretinoin (retinoic acid) therapy for hyperpigmented lesions caused by inflammation of the skin in black patients. N Engl J Med. 1993;328:1438-1443.
25. Callender VD. Acne in ethnic skin: special considerations for therapy. Dermatol Ther. 2004;17:184–195.
26. Jacyk WK, Mpofu P. Adapalene gel 0.1% for topical treatment of acne vulgaris in African patients. Cutis. 2001;68(4 suppl): 48-54. 16. Kligman AM, Willis I.
27. Grimes P, Callender V. Tazarotene cream for postinflammatory hyperpigmentation and acne vulgaris in darker skin: a double-blind, randomized, vehicle-controlled study. Cutis. 2006 Jan. 77(1):45-50.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
28. Smit N, Vicanova J, Pavel S. The hunt for natural skin whitening agents. Int J Mol Sci. 2009 Dec 10. 10(12):5326-49.
29. Woolery-Lloyd HC, Keri J, Doig S. Retinoids and azelaic acid to treat acne and hyperpigmentation in skin of color. J Drugs Dermatol. 2013 Apr. 12(4):434-7.

30. Balina LM, Graupe K. The treatment of melasma: 20% azelaic acid versus 4% hydroquinone cream. Int J Dermatol. 1991;30:893–895.
31. Sarkar R, Bhalla M, Kanwar KJ. A comparative study of 20% azelaic acid cream monotherapy versus a sequential therapy in the treatment of melasma in dark-skinned patients. Dermatology. 2002;205:249–254.
32. Verallo-Rowell VM, Verallo V, Graupe K, et al. Double-blind comparison of azelaic acid and hydroquinone in the treatment of melasma. Acta Derm Venereol Suppl (Stockh) 1989;143:58–61.
33. Lowe NJ, Rizk D, Grimes P, et al. Azelaic acid 20% cream in the treatment of facial hyperpigmentation in darker-skinned patients. Clin Ther. 1998;20:945–959.
34. Kircik LH. Efficacy and safety of azelaic acid (AzA) gel 15% in the treatment of post-inflammatory hyperpigmentation and acne: a 16-week, baseline-controlled study. J Drugs Dermatol. 2011;10:586590.
35. Sah A, Stephens TJ, Kurtz ES. Topical acne treatment improves postacne postinflammatory hyperpigmentation (PIH) in skin of color [Poster] J Am Acad Dermatol.
36. Mansouri P, Farshi S, Hashemi Z, Kasraee B. Evaluation of the efficacy of cysteamine 5% cream in the treatment of epidermal melasma: a randomized double-blind placebo-controlled trial. Br J Dermatol. 2015 Jul;173(1):209-17.
37. Farshi S, Mansouri P, Kasraee B. Efficacy of cysteamine cream in the treatment of epidermal melasma, evaluating by Dermacatch as a new measurement method: a randomized double blind placebo controlled studym J Dermatolog Treat. 2018 Mar;29(2):182-189.
38. Callender VD, St Surin-Lord S, Davis EC, Maclin M. Postin- flammatory hyperpigmentation: etiologic and therapeutic con- siderations. Am J Clin Dermatol. 2011;12(2):87–99.
39. Alexis AF, Blackcloud P. Natural ingredients for darker skin types: growing options for hyperpigmentation. J Drugs Derma- tol. 2013;12(9 Suppl):s123–7.


40. Nestor M, Bucay V, Callender V, Cohen JL, Sadick N, Waldorf H. Polypodium leucotomos as an adjunct treatment of pigmen- tary disorders. J Clin Aesthet Dermatol. 2014;7(3):13–7.
41. Antoniou C, Stefanaki C. Cosmetic camouflage. J Cosmet Dermatol. 2006;5:297–301.
42. Kayama et al. Camouflage Therapy for Post-Inflammatory Hyperpigmentation on the Face Caused by Fixed Drug Eruption. Journal of Cosmetics, Dermatological Sciences and Applications, 2013, 3, 8-10 Leyden J, Wallo W. The mechanism of action and clinical benefits of soy for the treatment of hyperpigmentation. Int J Dermatol. 2011 Apr. 50(4):470-7.
43. Cosmetics UK, Non-Surgical Treatments Statistics, 2015. <https://www.cosmedics.co.uk/nonsurgical-treatments-statistics/>
44. Castillo DE1, Keri JE Chemical peels in the treatment of acne: patient selection and perspectives. Clin Cosmet Investig Dermatol. 2018 Jul 16;11:365-372.
45. Burns RL, Prevost-Blank PL, Lawry MA, Lawry TB, Faria DT, Fivenson DP. Glycolic acid peels for



postinflammatory hyperpigmentation in black patients. A comparative study. Dermatol Surg. 1997 Mar. 23(3):171-4; discussion 175.
46. Sarkar R, Parmar NV, Kapoor S. Treatment of Postinflammatory Hyperpigmentation With a Combination of Glycolic Acid Peels and a Topical Regimen in Dark-Skinned Patients: A Comparative Study. Dermatol Surg. 2017 Apr. 43 (4):566-573.
47. DermNet NZ, Lasers in dermatology, 2014. <https://www.dermnetnz.org/topics/lasers-indermatology/>

48. AF Alexis. Lasers and light-based therapies in ethnic skin: treatment options and recommendations for Fitzpatrick skin types V and VI. Br J Dermatol. 2013 Oct;169 Suppl 3:91-7.
49. Kim S, Cho KH. Treatment of procedure-related postinflam- matory hyperpigmentation using 1064nm Q-switched Nd: YAG laser with low fluence in Asian patients: report of five cases. J Cosmet Dermatol. 2010;9:302-306 .
50. Rokhsar CK, Ciocon DH. Fractional photothermolysis for the treatment of postinflammatory hyperpigmentation after carbon dioxide laser resurfacing. Dermatol Surg. 2009 Mar. 35(3):535-7.
51. Park JH, Kim JI, Kim WS. Treatment of Persistent Facial Postinflammatory Hyperpigmentation With Novel Pulse-in-Pulse Mode Intense Pulsed Light. Dermatol Surg. 2016 Feb. 42 (2):218-24.
52. Lee YJ, Shin HJ, Noh TK, Choi KH, Chang SE. Treatment of Melasma and Post-Inflammatory Hyperpigmentation by a Picosecond 755-nm Alexandrite Laser in Asian Patients. Ann Dermatol. 2017 Dec. 29 (6):779-781
53. Momosawa A1, Kurita M, Ozaki M, Miyamoto S, Kobayashi Y, Ban I, Harii K.Combined therapy using Q-switched ruby laser and bleaching treatment with tretinoin and hydroquinone for periorbital skin hyperpigmentation in Asians. Plast Reconstr Surg. 2008 Jan;121(1):282-8.

54. Halder R, Munhutu M, Foltis P, Battie C, Verschoore M, Ore- sajo C. Evaluation and effectiveness of photoprotection com- position (sunscreen) on subjects of skin of color (abstract). J Am Acad Dermatol. 2015;72(5 Suppl):AB215.
55. Halder R, Rodney I, Munhutu M, et al. Evaluation and effectiveness of a photoprotection composition (sunscreen) on subjects of skin of color [abstract]. J Am Acad Dermatol. 2015;72(5 suppl):AB215.
56. Ruiz-Maldonado R, Orozco-Covarrubias ML. Postinflammatory hypopigmentation and hyperpigmentation. Semin Cutan Med Surg. 1997;16(1):36–43.
57. Imokawa G, Yada Y, Miyagishi M. Endothelins secreted from human keratinocytes are intrinsic mitogens for human melano- cytes. J Biol Chem. 1992;267(34):24675–80.
58. Maymone MBC, Neamah HH, Wirya SA, Patzelt NM, Zanca- naro PQ, Vashi NA. Sun-protective behaviors in patients with cutaneous hyperpigmentation: a cross-sectional study. J Am Acad Dermatol. 2017;76(5):841–846.e2.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 info@aestheticsource.com www.aestheticsource.com Pigmentation Hyper
you are treating PIH, melasma or photoageing, our portfolio of skin brightening products help protect,
you
sun, medication, hormones or
our
gives you
flexibility
your
out more today by contacting AestheticSource • Cysteamine® • NeoStrata® Enlighten Range • Skinbetter® Even Tone and Alpharet® • Skin Tech Blending and Bleach & AD Aclarance® • NeoStrata® Pro System Peels • Skin Tech Peels • Skin Tech Bene Bellum® coming soon • RRS® Whitening INJECTABLE CHEMICAL PEELS TOPICAL
Whether
prevent and target hyper-pigmentation. Whatever pigment issue
are addressing, the
inflammation,
comprehensive portfolio
the
to tailor
patient’s treatment plan to their needs and budget. Find
Topicals for Hair Loss

Different types of alopecia
Causes of alopecia, specifically androgenic alopecia, can be down to a number of factors including seasonal variation, ageing, nutritional factors, hormone imbalances, autoimmune hair disorders, mutation of the hairless gene, inflammatory hair loss and psychological factors. Seasonal variations such as length of day, and even jet lag, invoke changes in the level of certain hormones, while lower levels of melatonin and prolactin will lead to shorter hair.3 As well as this, ageing leads to a reduction in density and decreased growth rate of anagen hairs, which typically begins around 30 years old but it might begin before, depending on the type of alopecia.4 There are three main types of alopecia that might be treated with the below topical ingredients:
More than 30% of the population suffers from alopecia1 and there are a number of treatments available on the market for this. Some of the most popular include hormone rebalancing, vitamins and supplements, antifungals and antiparasitic, prostaglandin analogues and antihypertensive vasodilators and 5-alpha-reductase (5AR) inhibitors. Other treatments such as hair implants, infrared devices and corticosteroid injections are also an option. I believe that despite the treatment approach, all should be supported with the use of topical solutions. It is important to note, however that topicals shouldn’t be used when the skin is broken, such as during hair transplant surgery. In this article, I explore the topical treatments available to attain the best results for common causes of hair loss.
Understanding the hair cycle
Hair growth occurs in a series of stages, starting with the anagen phase. During this period, cell division in the matrix of the hair bulb, which forms the base of the hair follicle, produces keratinocytes and these form the various layers of the individual hair shaft. Melanocytes in the hair bulb provide the keratinocyte with pigment. After the hair reaches a certain length, which varies depending on the body region, it enters the catagen phase, when cell division and pigmentation cease.2 During the telogen phase, a new follicle appears below the original follicle, the hair shaft grows back into the original follicle, and the previous hair shaft is shed. It is the dysfunctions during the telogen and anagen stages that appear to result in hair loss.2
Androgenic alopecia: a common cosmetic hair disorder, resulting from interplay of genetic, endocrine, and ageing factors leading to a patterned follicular miniaturisation. Microinflammation seems to be a potential active player in this process.5
Alopecia areata: most investigators agree that, although there are hardly any reported symptoms of inflammation, microscopic inflammatory changes seem to play an important role in alopecia areata. Hair loss of an isolated, asymptomatic area seems to be because of a circumscribed plaque (a lesion), usually on the scalp. Progress is often very unpredictable in many patients and the patch can expand or regrow in a few months.6 This benign form of plaque may develop gradually into more severe ones, eventuating sometimes in universal alopecia.6
Telogen effluvium: may begin at any age with a sudden increase in hair loss and maintenance of the frontal hair density. Surgery, fever, childbirth, iron deficiency, stress, chronic diseases, and dietary changes are factors commonly associated with the disorder.7 A time interval of two to three months between the triggering factor and the onset of the disorder is most commonly observed, and it lasts from four to six months in its acute forms. It is suggested that early entrance in the telogen phase is triggered by the inciting event, causing the habitual asynchrony in normal hair loss to go through a synchronic shedding period.7
Diagnosis
Although the aetiology for the condition is complex, there is much one can do to seek improvement. The first step in the process is to go through a complete assessment.
Figure 1: The hair growth cycle2
Pharmacist Miriam Martinez Callejas discusses suitable topical applications for patients experiencing hair loss Anagen Phase (Growing Phase) Catagen Phase (Transition Phase) Telogen Phase (Resting Phase) Telogen Phase (Exogen) (Shedding Phase) Early Anagen Phase (Growing Phase) Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
In this step, photographs to document progression can be useful. The second step is to determine whether immediate medical evaluation is necessary, which could include alopecia associated with redness and inflamed skin. Biopsies for evaluation of inflammation, bacterial, fungal or parasitic infections is essential to eradicate any serious underlying medical conditions.8,9 If none of the causes seem to be related, then hormonal imbalance and nutritional deficits should be ruled out and wider health examinations and behavioural observations undertaken, being cognisant that hair loss can result from several causative factors working together.
Topical solutions
Alopecia areata and androgenic can be treated using topical application of certain medication such as hormones, spironolactone, finasteride, latanoprost, and minoxidil, amongst others. Research has shown the efficacy of oestradiol and progesterone when applied topically on the scalp, discussed in more detail below.9,10 Working with physiological doses and local application reduces risks associated with treatments. It is also believed that when applied topically using the right vehicle, the below ingredients might have a reduced systemic absorption,11 thus reducing the amount of side effects from the ingredients but having a more desired localised effect. As noted below, there is little research on the use of topicals and many of the studies are either conducted on very small sample sizes or more than ten years old. It is therefore fair to say that more research needs to be done in this area. How long each topical should be applied for is generally dependent on each individual product and patient using it. Commonly, each topical discussed treats androgenic alopecia and areata.
Oestradiol
Oestradiol inhibits the conversion of testosterone to the metabolite dihydrotestosterone (DHT) by suppressing 5AR activity.12 In addition, by inhibiting 17β-dehydrogenase, it impedes the conversion process of androstenedione to testosterone, resulting in a reduction in the synthesis of testosterone and DHT.12 DHT is believed to be the main cause of pattern hair loss in both men and women. As well as this, it accelerates the conversion of testosterone to oestradiol by stimulating aromatase, decreasing the level of testosterone and leading to a reduction in DHT. The drug has been reported to stimulate the generation
of hair follicular matrix cells.12 One study conducted in 2012 showed positive effects on 53 women with female pattern hair loss. Subjects applied the topical for eight months and results showed a significant result in hair count and diameter.13 I have found that the most common topical oestradiol is 0.025%.
Progesterone
Progesterone is a natural inhibitor of 5AR,14 which is an enzyme that converts testosterone into DHT. Without the presence of progesterone (or with not enough), 5AR can perform its converting activities. This means more DHT is produced, triggering further hair thinning and loss in those with androgenic alopecia. For example, a study conducted in 1987 saw 10 male patients suffering with androgenetic alopecia treated over one year with a lotion containing 1% hydroxyprogesterone. After treatment, patients saw an increase in the number and mean hair shaft diameter of anagen hair roots.11 In my experience, the most common strength of progesterone to be applied topically is around 2%.
Spironolactone
Spironolactone acts as an androgen antagonist by competitively blocking androgen receptors, as well as inhibiting ovarian androgen production.15,16 One particular study conducted in 1988 saw six healthy male patients use a topical spironolactone to a well-defined skin area. It concluded that the product worked to a local effect without much systemic absorption.17 However, as this was such a small sample size, I think that it is fair to say that much more research is needed. I have found that the most common strength used is between 1-3%.
Finasteride
Finasteride works by inhibiting 5AR II enzyme, which is responsible for catalysing the conversion of testosterone to the much more
active chemical DHT.14 A study of 24 healthy males conducted in 2014 evaluated a newly developed finasteride 0.25% topical solution, in comparison to the marketed finasteride 1mg tablet, looking at the movement of drugs within the body and suppressive effects on plasma DHT. It concluded that a strong and similar inhibition of plasma DHT was found after one week of treatment with both the topical and tablet, albeit finasteride plasma exposure was significantly lower with the topical than with the oral product.18 As oral finasteride is associated with a number of risks and side effects, this study suggests that use of topical finasteride could be particularly beneficial.
Latanoprost
In 2012, a double-blind scientific study found that latanoprost, a drug that mimics naturally-derived compound molecules called prostaglandins, significantly increases hair density (by 22%) on the scalp after 24 weeks of treatment in young men with mild hair loss.19 While the sample size of the study was small (only 16 subjects), the researchers found that 50% of the subjects had significant differences in hair density in regards to increased hair pigmentation and thickness. Another interesting finding is that the proportion of hairs in the anagen phase versus the telogen phase remained stable. The strength used, and generally most common in my experience, is 0.005%. Latanoprost has also been used to treat eyelash alopecia at 0.005%.20
Minoxidil
Minoxidil topical hair loss treatment has been used since the 1990s to treat baldness in men and women. The mechanism of action is complicated, but its role is known as a vasodilator, increasing the blood flow and nutrient uptake for the hair follicles causing follicles in the telogen phase to shed, which, as discussed above, are then replaced by thicker hairs in a new anagen phase. It is
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
I believe that despite the treatment approach, all should be supported with the use of topical solutions
a recognised safe and effective treatment by itself if used during the early onset of alopecia.21 It was reported in one study that topical minoxidil normalises hair follicles and increases blood flow to the scalp, although clinical trial results are varied.22 In my experience, the most common strengths of minoxidil used are 2% and 5%.
Considerations
Practitioners should be treating hair loss like any other condition, diagnosing and treating in a professional manner. Once the diagnose has been established, the treatment must be chosen carefully considering contraindications, cautions, interactions, side effects, allergies and medical history. Oestradiol or any hormone must be avoided when there is a family history of cancer, if the patient has been treated for cancer, or if they have had cancer.23,24 Hormones should be used with caution in male patients since there is a risk of gynaecomastia from scalp inunction of estradiol.25 Spironolactone has been shown to be safe when applied topically however the potential for oestrogen-dependent malignancies when taken orally remains controversial, with possible links to certain types of cancer.26 However, many believe there is not sufficient evidence to suggest spironolactone has a direct causal link to the development of breast cancer.26,27 There is not enough evidence to claim the safety of topical finasteride and within existing studies, side effects haven’t been discussed. There are a number of side effects reported through the use of oral finasteride including depression, erectile dysfunction and headaches however as we can see from the above study, the topical use appeared to be just as effective as the oral and could indicate promising however further research would need to be done.28 Latanoprost applied topically (or on the eyelashes) has
no reported side effects, but it is advisable to avoid this treatment when glaucoma and herpes simplex keratitis is suspected.20 Lastly, it’s reported that topical minoxidil is contraindicated in pheochromocytoma and may cause a dry and flaky scalp with use. Although systemic effect is rare through topical application, this can be compromised if the skin is irritated or sunburnt.29
Conclusion
Topical solutions, especially when used in combination with other treatments, can be effective when treating different types of alopecia, especially androgenic alopecia and areata. It is important to take a full medical history to ensure that there are no underlying medical conditions resulting in hair loss, however knowledge of topical ingredients for this concern is useful to be aware of for a condition that affects so many.
Miriam Martinez Callejas is the chief pharmacist at Roseway Labs and specialises in formulating and compounding medications for skin, hair and hormones. She has more than 10 years of experience in compounding and has a passion for helping others using her experience and knowledge of medicines.

REFERENCES
1. Salman K, Altunay I et al., Frequency, severity and related factors of androgenetic alopecia in dermatology outpatient clinic, Journal of Brazilian Annals of Dermatology, January 2017 < https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312176/>
2. Martel, J, Badri, T Anatomy, Hair Follicle, StatPearls, January 2019 <https://www.ncbi.nlm.nih.gov/books/NBK470321/>
3. Mahoney M, Shift work, Jet Lag and Female Reproduction, International journal of Endocrinology, October 2009 <https:// www.hindawi.com/journals/ije/2010/813764/>
4. Trüeb R, Oxidative stress in ageing of hair, International journal of Trichology, January 2009, <https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC2929555/>
5. Bergeld W, Alopecia: histologic changes, Advances in dermatology and allergology, < https://www.ncbi.nlm.nih.gov/ pubmed/2701796>
6. Muller S A, Winkleman R K, Alopecia Areata, JAMA Dermatology September 1963, <https://jamanetwork.com/ journals/jamadermatology/article-abstract/528193>
7. British Association of Dermatologists, Telogen Effluvium, December 2016 <http://www.bad.org.uk/shared/get-file. ashx?id=132&itemtype=document>
8. El-Domyati M, Attia S, Androgenetic alopecia in males: a
histopathological and ultrastructural study, Journal of Cosmetic Dermatology, June 2009 <https://europepmc.org/abstract/ med/19527330>
9. Chanda S, Robinette L et al., 17β-Estradiol and ICI-182780 regulate the hair follicle cycle in mice through an estrogen receptor-α pathway, American Physiological Society, February 2000 <https://doi.org/10.1152/ajpendo.2000.278.2.E202>
10. Kiesewetter F, Arai A, Schell H, Sex hormones and antiandrogens influencein vitrogrowth of dermal papilla cells and outer root sheath keratinocytes of human hair follicles, Journal of Investigative Dermatology, July 1993 < https://www. ncbi.nlm.nih.gov/pubmed/8326159>
11. Van Der Willigen AH, Peereboom-Wynia JD et al., A preliminary study of the effect of 11a-hydroxyprogesterone on the hair growth in men suffering from androgenetic alopecia, Acta Dermato-Venereologica, 1987 <https://www.ncbi.nlm.nih.gov/ pubmed/2436423>
12. Blume-Peytavi U, Whiting D et al., Hair growth and disorders, Springer Books, 2008 < https://books.google. co.uk/books?id=pHrX2-huQCoC&pg=PA368&redir_ esc=y#v=onepage&q&f=false>
13. Jae-Hong K, Sung Yul L, et al., The Efficacy and Safety of 17a-Estradiol (Ell-Cranell alpha 0.025%) solution on female pattern hair loss: single center, open-label, non-comparatve, phase IV study, Annals of Dermatology, August 2012 < https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC3412238/>
14. Hairguard, Best Natural 5 alpha Reductase Inhibitors <https:// www.hairguard.com/best-natural-5-alpha-reductase-inhibitors/>
15. WebMD, Hairloss in Women: Treatments <webmd.com/skinproblems-and-treatments/hair-loss/hair-loss-treatments#3-5>
16. Struthers A, Krum H, Williams GH, A comparison of the aldosterone-blocking agents eplerenone and spironolactone, Clinical Cardiology, April 2008 <https://www.ncbi.nlm.nih.gov/ pubmed/18404673>
17. Rey FO, Valterio C et al., Lack of endocrine systemic side effects after topical application of spironolactone in man, Journal of Endocrinological Investigation, April 1988 < https://www.ncbi.nlm. nih.gov/pubmed/3411088>
18. Caserini M, Radicioni M et al., Effects of a novel finasteride 0.25% topical solution on scalp and serum dihydrotestosterone in healthy men with androgenetic alopecia, International journal of clinical pharmacology therapy, January 2014 <https://www. ncbi.nlm.nih.gov/pubmed/?term=finasteride+0.25%25+topical+solution+in+comparison+to+the+marketed+finasteride+1mg+tablet>
19. Blume-Peytavi U Lönnfors S Hillmann K Garcia Bartels N A randomized double-blind placebo-controlled pilot study to assess the efficacy of a 24-week topical treatment by latanoprost 0.1% on hair growth and pigmentation in healthy volunteers with androgenetic alopecia, Journal of the American Academy of Dermatology, May 2012 <https://www.ncbi.nlm.nih. gov/pubmed/21875758>
20. Coronel-Perez IM, Rodriguez-Rey EM, Camacho-Martinez FM, Lantroprost in the treatment of eyelash alopecia in alopecia areata universalis, Journal of the European Academy of Dermatology and Venereology, April 2010 <https://www.ncbi. nlm.nih.gov/pubmed/20028444>
21. Rumsfield JA, West DP, Fielder-Weiss VC, Topical minoxidil therapy for hair regrowth, Clinical Pharmacology, May 1987 <https://www.ncbi.nlm.nih.gov/pubmed/3311578>
22. Fielder-Weiss VC, Topical minoxidil solution (1% and 5%) in the treatment of alopecia areata, Journal of the American Academy of Dermatology, 1987 <https://www.ncbi.nlm.nih.gov/ pubmed/3549811> WAS 12
23. Levy L, Emer J, Female pattern alopecia: current perspectives, International journal of womens health, August 2013 <https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC3769411/>
24. ScienceDirect, Breast cancer and hormone-replacement therapy in the Million Women Study, The Lancet, August 2003 <https://www.sciencedirect.com/science/article/pii/ S0140673603140652>
25. Swerdloff R, Ng J, Gynecomastia: Etiology, Diagnosis and Treatment, Endotest, August 2015 <https://www.ncbi.nlm.nih. gov/books/NBK279105/>
26. Mackenzie I, Morant S V et al., Spironolactone use and risk of incicent cancers: a retrospective, matched cohort study, British Journal of Clinical Pharmacology, March 2017 <https://www.ncbi. nlm.nih.gov/pmc/articles/PMC5306481/>
27. Biggar RJ, Andersen EW et al., Spironolactone use and the risk of breast and gynecologic cancers, Cancer Epidemiology Journal, December 2013 <https://www.ncbi.nlm.nih.gov/ pubmed/24189467>
28. Blayne W, McArthur E, Ordon M et al., Association of Suicidality and Depression With 5α-Reductase Inhibitors, JAMA Network, May 2017 < https://jamanetwork.com/journals/ jamainternalmedicine/fullarticle/2610105>
29. Prescribers Digital Reference, Minoxidil Drug Summary, <https:// www.pdr.net/drug-summary/Minoxidil-minoxidil-774>
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Practitioners should be treating hair loss like any other condition, diagnosing and treating in a professional manner
Find out why medical professionals love


“Gives the effect of a CO2 laser, but without the downtime... its safety profile is excellent. I cannot begin to say how Tixel has changed my practice and increased my patient footfall”

















 Sabrina
Sabrina
Shah-Desai Consultant ocular plastic surgeon, Perfect Eyes Ltd








“I have been using Tixel for the past year and a half, one of the best devices I ever bought, particularly for peri-orbital rejuvenation, fantastic results for scarring and general skin sundamage”



 Dr
Dr



Tapan Patel – PHI Clinic London









EXCLUSIVELY to
AZTEC Services supply Tixel
doctors and nurses
For further information or to arrange a demo contact AZTEC Services at: az@aztecservices.uk.com | 01494 956644 | www.aztecservices.uk.com After 3 Tixel treatments
Before Tixel.indd 1 01/04/2019 14:33






FROM THE NATURAL ESSENCE OF SALVIA HAENKEI TO THE FORMULA THAT NOURISHES THE SKIN Exclusive UK & Ireland distributor / training provider of IBSA’s aesthetic products GENTLY POWERFUL Enhancing & maintaining skin cellular vitality Improves skin elasticity & firmness Advanced complex combining high & low molecular weight of hyaluronic acid & Haenkenium® MULTI-ACTION ANTIOXIDANT FORMULA
Anti-senescence activity of Salvia Haenkei
Anna Baker BN RGN INP PGCert (App. Clin. Anat.) PGCert (Clin. Ed.) details the science behind Profhilo® Haenkenium® from IBSA Italia
Profhilo® Haenkenium® is a unique and innovative topical formulation which deeply nourishes the skin at a cellular level. This advanced hyaluronic acid complex utilises a patented botanical extract of Salvia Haenkei (0.25%), also known as Prawn Sage, which originates from Bolivia with proven anti-ageing properties. An integrated senescence-screening assay conducted by Matic et al., (2016) outlines findings from more than 3,000 chemical and natural compounds to demonstrate that Salvia Haenkei decreased replicative and UV-mediated senescence in human primary fibroblasts, as well as in a model of in vitro reconstructed human epidermis. Furthermore, the authors report pre-clinical and clinical testing of this extract by performing toxicity and irritability evaluation in vitro to demonstrate the safety of Salvia Haenkei extract for use as a safe and effective antiageing skin treatment. In addition, phosphatase and tensin homolog protein (PTEN) is a key cellular senescent regulator (Childs et al., 2015), and data from Matic et al., (2016) demonstrate that Salvia Haenkei is a strong inhibitor of senescence driven by depletion of PTEN, decreasing senescence of 50% when compared to untreated control, and by-passing the growth arrest promoted by PTEN loss.
Whilst it is acknowledged that reactive oxygen species (ROS) are produced as a product of normal cellular functioning, excessive amounts can cause detrimental effects (Liochev, 2013). Furthermore, oxidative stress also promotes cellular senescence and premature ageing to the skin (Polefka et al., 2012). Further findings from Matic et al., (2016) describe in-vitro testing of human dermal fibroblasts exposed to hydrogen peroxide, which is a potent inducer of ROS, with the antioxidant activity of Salvia Haenkei assayed immediately after the exposure. The effect of Salvia Haenkei within these cells was similar to N-acetylcysteine (NAC), a known antioxidant compound tested and used to prevent the accumulation of ROS in different inflammatory conditions (Kang et al., 2003). These cumulative data findings from Matic et al., (2016) demonstrate the intracellular levels of ROS, and positive effects of Salvia Haenkei, supporting its efficacy in preventing different types of senescence.
Cocetta et al., (2016) concur that Salvia Haenkei proved to be capable of modulating ROS production in conditions of oxidative stress and that it was able to prevent the increase of Nrf-2 gene expression induced by UVB exposure. The Nrf-2 signalling pathway is a key defence mechanism that is triggered by cells in response to oxidative stress. In addition, the authors noted a protective role of Salvia Haenkei against cellular stress. Cocetta et al., (2016) and Matic et al., (2016) conclude that Salvia Haenkei acts as a gerosuppressant agent, providing protection from free radicals, a cause of oxidative stress and premature cellular senescence, combined with the protective strength of an anti-oxidant. By contrast, the anti-ageing efficacy of Profhilo® Haenkenium® extrapolated from in vivo data demonstrated statistically significant improvements in redness, wrinkle depth, elasticity and antioxidant potential at day 84 from baseline parameters. Specifically, a reported
9.2% increase in elasticity, as well as a 55.3% increase in antioxidant potential at day 84 from baseline, demonstrating the ability to visibly reduce signs of ageing through improved skin firmness, elasticity and tone.
In addition, Profhilo® Haenkenium® contains a 0.2% hyaluronic acid complex, harnessing the power of different molecular weights to stimulate specific biological functions and responses within the skin (D’Agostino et al., 2017). The high molecular weight hyaluronic acid gives a characteristic protective benefit to the skin, specifically helping to restore and maintain the integrity of the hydrolipidic film (H-HA 800kDA). The low molecular weight hyaluronic acid facilitates optimal skin hydration and hygroscopic properties (L-HA 300kDA). The formulation also contains IBSA’s ultrapure hyaluronic acid, produced with a patented biofermentation process of Streptococcus Zooepidemicus which is ranked worldwide as top highquality owing to its safety and purity (D’Agostino et al., 2015).
Profhilo® Haenkenium® is available in a 50ml airless pump bottle and is suitable for use immediately after Profhilo® injectable treatment as well as daily use alongside as a treatment to sustain the injectable bioremodelling effects of the patented stabilised hybrid cooperative complexes (NAHYCO™). Ideal for the face, neck and décolletage. HA-Derma is the exclusive distributor of IBSA’s aesthetic portfolio in the UK and Ireland.
Before After After
Figure 1: Before and five weeks after twice daily use of Profhilo® Haenkenium®. Images courtesy of Anna Baker, Anna Baker Aesthetics.

Before After
Figure 2: Before and two weeks after twice daily use of Profhilo® Haenkenium® (blue represents wrinkle depth/crow’s feet). Images courtesy of IBSA Italia.
REFERENCES
1. Childs B.G., Durik M., Baker D.J. van Deursen J.M. (2015) Cellular senescence in aging and agerelated disease: from mechanisms to therapy Nat. Med. 21:1424-1435.

2. Cocetta V., Catanzaro D., Miolo G., Cadau J., Ragazzi E., Alimonti A., Montopoli M. (2016) Antisenescence activity of Slavia Haenkei on a skin cellular model AMWC Monaco Poster Presentation.
3. D’Agostino A., Stellavato A., Corsuto L., Diana P., Filosa R., La Gatta A., De Rosa M., Schiraldi C. (2017) Is molecular size a discriminating factor in hyaluronan interaction with human cells? Carbohydrate Polymers 157(10):21-30.
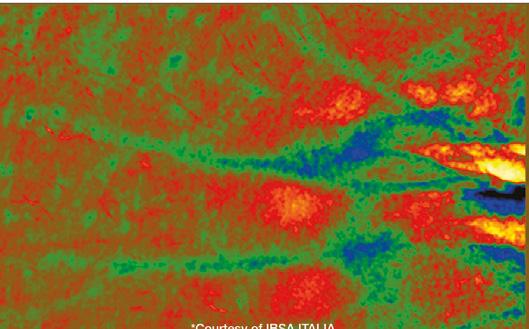
4. D’Agostino A., Stellavato A., Busico T., Papa A., Tirino V., Papaccio G., La Gatta A., De Rosa M., Schiraldi C. (2015) In vitro analysis of the effects on wound healing of high and low molecular weight chains of hyaluronan and their hybrid H-HA/L-HA complexes BMC Cell Biology 16:19 DOI 10.1186/ s12860-015-0064-6.
5. Kang S., Chung J.H., Lee J.H., Fisher G.J., Wan Y.S., Duell E.A., Voorhees J.J. (2003) Topical N-Acetyl Cysteine and Genistein Prevent Ultraviolet-Light-Induced Signalling That Leads to Photoaging in Human Skin in vivo 120(5): 835-841.
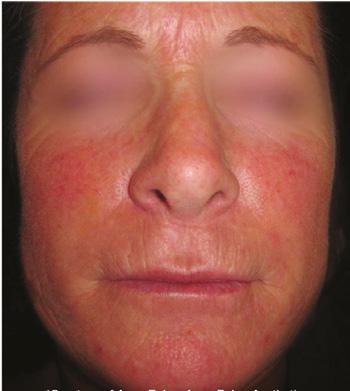
6. Liochev S.I. (2013) Reactive oxygen species and the free radical theory of aging Free Radical Biology and Medicine 60:1-4.
7. Matic I., Revandkar A., Chen J., Bisio A., Dall’Acqua S., Cocetta V., Brun P., Mancino G., Milanese M., Mattei M., Montopoli M., Alimonti A. (2016) Identification of Salvia haenkei as gerosuppressant agent by using an integrated senescence-screening assay Aging 8:1-17.
8. Polefka T.G., Meyer T.A., Agin P.P., Bianchini R.J. (2012) Cutaneous oxidative stress J Cosmet Dermatol 11(1): 55.

Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Profile Assessment
When I would assess patients for facial aesthetic procedures back in 1996, like my peers of that era, I performed an extensive evaluation of primarily the frontal view. Back then, the most common treatments were botulinum toxin to the upper facial region and dermal filler injections to the lips and nasolabial lines. In this article, I will show you that it’s in fact the profile (side view) that sets the tone for 3D facial aesthetics, and why it should be your primary consideration in every facial assessment. I will also explore my trademarked BK P-Line system for profile assessment and how you can utilise this to set yourself up for treatment success.


Importance of the profile view
Up until around 2007, I was examining every patient from the frontal facial view to begin with, before incorporating the other views. Based on my experience of training aesthetic practitioners from all over the world, I believe that this is still what the majority of practitioners are doing, especially those new to aesthetics, as it seems to be the natural way to approach an assessment. Of course, the patient assessment should never just include one view but should incorporate the information obtained from a comprehensive three-dimensional approach. In this way, a thorough diagnosis can take place, leading to appropriate treatment options and results for our patients. Based on 27 years of clinical practice, I have noticed that people with aesthetic profiles tend to have the most aesthetically-pleasing faces It is important to appreciate the differences between all types of patients and adopt an ‘individualised’ approach. I am often seeing male patients being feminised and females being almost ‘dehumanised’ by
Before After
treatments. The mid-face and perioral areas are typical regions which are vulnerable to such anomalies in both sexes. Equally, we must consider what is appropriate for different ethnicities; for example, I find it’s generally rare for you to see a male in the Far East to have an angular, European jawline as they typically have more of a heart-shaped face and it may look very odd if you create one.1 A full discussion of the differences between genders and ethnicities, along with appropriate treatment approaches, is beyond the scope of this article, but there are a number of resources that explore these considerations.2,3,4
Patient assessment using my BK P-Line system
To help with my initial assessment, I endeavour to take good quality photographs. These provide vital discussion aids with the patient to facilitate a truly co-diagnostic exercise. I will then use my BK P-1 to BK P-3 parameters to identify the relationship of the forehead, nose, lips, chin and jawline to ascertain where the discrepancies lie and which areas need to be considered for treatment (Figure 2). Tying in all of my parameters will give me a good understanding as to whether or not I need to augment the forehead, nose, lips and/ or chin and, importantly, to what extent. My BK Ps are not the only parameters, of course, but are an excellent way to get you thinking about the right way for profile assessment.
BK P-0
The BK P-0 Line is a horizontal straight line that runs from the midtragus to the mid-alar and will help set your horizontal determinant for a successful assessment. To ensure you take accurate and standardised before/after photographs, the line needs to be completely straight and parallel to the floor. I use this concept instead of the Frankfort plane, which is a line that intersects both porions and the left orbitale, and is commonly used to orient the head so that the plane is horizontal.5 In my opinion, the Frankfort plane is not as reproducible as using soft tissue landmarks.
BK P-1
The BK P-1 line falls vertically through the most anterior point of the upper lip. Once you have identified this line, observe the soft tissue regions associated with the glabella (the most anterior position on the profile view of the patient’s forehead, which lies between the eyebrows), nasion, (the deepest part of the frontonasal sulcus) and pogonion (the most anterior point of the chin). Taking into account males, females and people from differing ethnic backgrounds I have developed a range in millimetres for each parameter. This will help the practitioner determine the precise amount of augmentation required.
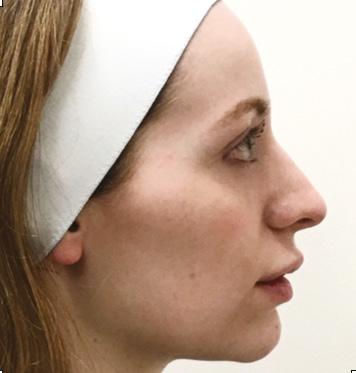
BK P-2
The BK P-2 line runs from the most anterior point on the tip of the nose to the pogonion, allowing us to observe the projection of the lips. This will identify how much room is available for augmentation and subsequent projection. The BK P-2 line is similar to the traditional Ricketts’ line, which is a line drawn from nose tip to chin.6 Ricketts is based on cephalometric assessment, which in my view is limited and outdated when looking at current facial aesthetic procedures. According to Ricketts, the upper lip lies around 4mm behind the line, while the lower lip lies 2mm behind;6 however, this is based on Caucasians and doesn’t take into account racial differences. In fact,
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Professor Bob Khanna shares his key concepts for assessing the patient profile to achieve successful facial rejuvenation
Figure 1: Apart from the lack of volume in the mid-face justifying possible treatment, it is not possible to assess the lack of lower facial support (mandibular) in the before image without assessing the profile correctly. The after image is following chin and jawline augmentation (the patient’s main area of concern).
Photography
There is nothing worse than a bad before and after image. I understand that as medical professionals we are not photographers, however I believe that it’s something that is seriously lacking in our field and all practitioners need to have more of a focus on improving this. Exceptional before and after photographs not only allow for great marketing resources (with the correct consent of course), but it also provides clear proof of how the patient was before treatment, should you ever find yourself in the instance of an unhappy patient.10
My best advice for taking photographs is consistency and reproducibility. The head and body position, lighting, camera settings such as angles and zoom, and device are all factors to consider, among others.10 Patient expression should also be kept as consistent as possible; however, I understand that this is difficult to replicate especially as many patients are much happier following their treatment. I use a DSLR camera in my clinic rather than a phone or tablet as I find it takes better quality images, and I also have several staff members trained in its use. We also take the images at one designated location in clinic, which always has the same background and lighting.10 When taking images, ensure to follow General Data Protection Regulation (GDPR) and know the legal and regulatory issues surrounding their use.10,11
Other views
As discussed, the profile should not be assessed in isolation and the other views are also very important, such as the three quarter profile view, revealing both eyes and to some extent the characteristics of the profile,8 and frontal facial view. From these views, I can determine key measurements (angles, lengths and widths) to ascertain to what extent I need to augment in terms of facial proportions – facial thirds and facial fifths.9
most people with an African descent will actually violate that line – this doesn’t make them un-aesthetic, it just means that it is normal for their racial background.7 In certain cases, it is appropriate for the patient’s upper and lower lip to touch the BK P-2 line. If the lips touch BK P-2 pretreatment, I would be reluctant to augment a patient’s lips and if I were to treat, it would be for a rejuvenation, hydration effect with very little volumisation. This is because volumising will risk causing the infamous ‘trout-pout’ and could easily ‘dehumanise’ your patient. In such cases, it would be appropriate to facilitate this by adjusting BK P-2 by careful chin augmentation, making sure the BK P-1 line is respected.
BK P-3
The BK P-3 line allows you to reference the mid-face in relation to the eyes. It is a vertical line that is perpendicular to BK P-0, and crosses the anterior part of the cornea of the eye. This will help determine to what extent we can project the anterior section of the mid-face. The mid-face is actually really important for the profile view because by correcting mid-facial projection, particularly the antero-medial portion of the cheek, you can make the nose look less projected.
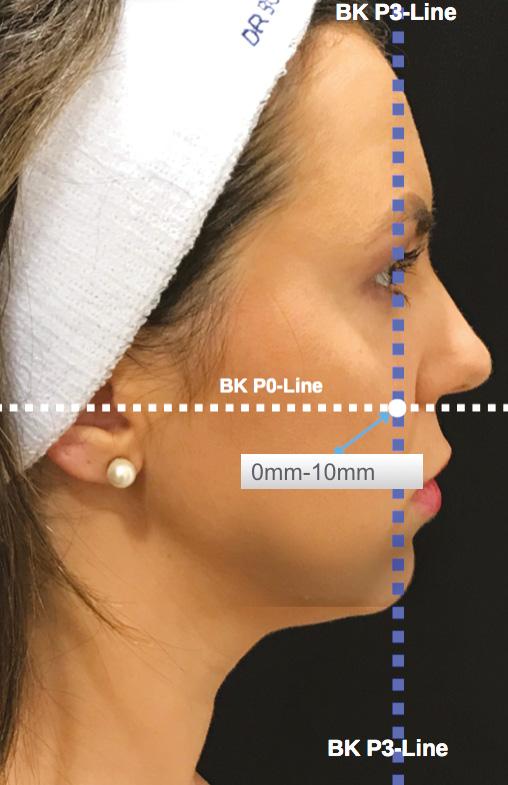
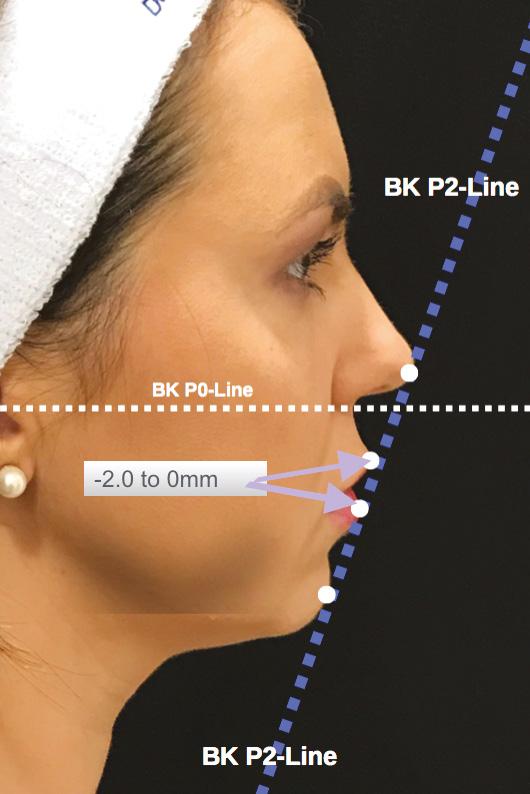
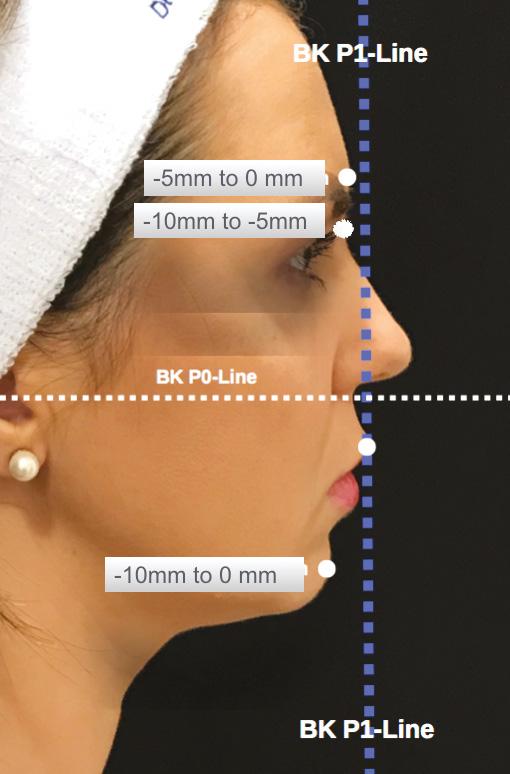
Figure 3: A 26-year-old patient treated using my BK P-Line system for analysis. Areas treated with dermal filler were the nose, mid-face, lips and chin.

Treatment considerations
I usually conduct most of my treatments over at least two sessions. Should the patient require it, I will firstly craft the forehead convexity, then I’ll look at the nasal frontal sulcus, the nose, the mid-face –including the tear troughs and the cheeks – and then I will move down to the chin and the jawline, and finally the lips. When treating patients, my general rule is that the lips are ‘the icing on the cake’, so I will always do these last as they will complement all the other features.

Summary
By assessing the patient’s profile first, followed by a three-dimensional analysis of the full face from all angles, you will be well positioned to understand the areas that require treatment and tailor your approach to each patient, regardless of age, gender and racial background.
Professor Bob Khanna is cosmetic and reconstructive dental surgeon, with more than 23 years’ experience in facial aesthetics. He is an international lecturer and key opinion leader, and is invited to speak at many global aesthetic conferences. Practitioners and patients travel from around the globe to visit DRBK clinic and the Dr Bob Khanna Training Institute for all aspects of cosmetic and surgical dentistry and facial aesthetic procedures.
REFERENCES
and Age Groups, Ann Occup Hyg.2010 Jun;54(4):391-402.
3. de Maio, M. Ethnic and Gender Considerations in the Use of Facial Injectables: Male Patients. Plastic and Reconstructive Surgery. November Supplement, Volume 136, Number 5S 2015.

4. Andrew F. Alexis, and Jasmine O. Obioha, Ethnicity and Aging Skin, Journal of Drugs in Dermatology, 2017.
5. Santos RMGD, De Martino JM, ‘Influence of different setups of the Frankfort horizontal plane on 3-dimensional cephalometric measurements.’ Am J Orthod Dentofacial Orthop. 2017 Aug;152(2):242-249.
6. Robert MurrayRickett, A foundation of cephalometric communication, American Journal of Orthodontics, 1960, 46(5):330-357.
7. Vinay V Umale, Kamlesh Singh, et al., Evaluation of Horizontal Lip Position in Adults with Different Skeletal Patterns: A Cephalometric Study, Journal of Oral Health and Craniofacial Science, 2017.

8. J. Powell, & R.K. Rayson,‘The Profile in Facial Aesthetics’, British Journal of Orthodontics,Vol 3,No 4, pp.207-215.
9. Jovana Milutinovic, Ksenija Zelic, & Nenad Nedeljkovic,Evaluation of Facial Beauty Using Anthropometric Proportions, The Scientific World Journal, 2014.
10. Chloé Gronow, Special Feature: Managing Patient Photography, Aesthetics journal, <https:// aestheticsjournal.com/feature/special-feature-managing-patient-photography>
11. Martin Swann, Patient Photography and Data, 2018. <https://aestheticsjournal.com/feature/patientphotography-and-data>
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
1. Future Lear, Identifying the ethnicity of a skull, Forensic Facial Reconstruction, The University of Sheffield. <https://www.futurelearn.com/courses/forensic-facial-reconstruction/0/steps/25658> 2. Zhuang Z,Landsittel D,Benson S,Roberge R,Shaffer R, Facial Anthropometric Differences among Gender, Ethnicity,
Figure 2: The trademarked BK P-Line system for profile assessment.
Before After
Make 2019 Your Year!
Get the recognition you deserve at the most prestigious awards ceremony in aesthetics

Following the spectacular success of 2018, the Aesthetics Awards is back and ready to reward the best of the best in the non-surgical aesthetic specialty.


Winning, or even being shortlisted as a finalist, is a prestigious endorsement of your achievements within the specialism, helping to raise your profile and increase marketing and PR opportunities. It also allows you to demonstrate to patients and clients why they should put their trust in you and your brand, and choose you over your competitors. Covering all aspects of the non-surgical aesthetic field, the Aesthetics Awards recognises clinics, medical practitioners, products, manufacturers, distributors and other companies in the aesthetics specialty in 26 categories.
Taking place on December 7 at the dazzling Park Plaza Westminster Bridge Hotel in central London, the glamorous ceremony is set to host more than 800 guests, providing another remarkable evening full of entertainment, unlimited networking opportunities, and acknowledgement of the hardest working individuals in the field.
You could be presented with an esteemed award for Commended, Highly Commended or even crowned a Winner in front of hundreds of like-minded peers and dance the night away in celebration of another glorious year in the specialty.
ENTRIES OPEN MAY 1 ENTRIES CLOSE JUNE 28 FINALISTS ANNOUNCED AND VOTING OPENS SEPTEMBER 2 VOTING AND JUDGING CLOSES OCTOBER 31 WINNERS ANNOUNCED AT THE AESTHETICS AWARDS CEREMONY DECEMBER 7 1 2 3 4 5 KEY DATES Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
AESTHETIC NURSE PRACTITIONER OF THE YEAR
Aesthetic nurses who continue to deliver exceptional care and clinical expertise will get the recognition they deserve with this esteemed accolade. Finalists selected will demonstrate an outstanding commitment to patient safety, continued professional development and illustrate actions to demonstrate how they are making a difference in the aesthetics specialty.
MEDICAL AESTHETIC PRACTITIONER OF THE YEAR
Doctors, dentists and surgeons are invited to demonstrate their contribution to the profession, as well as how they have been dedicated to providing outstanding care and treatment to their patients in the last 12 months. Applicants must also validate how they have worked hard to continue their professional development as well as display an unprecedented commitment to patient safety.
This prestigious trophy will be awarded to an individual with a distinguished career in aesthetics who has made a significant contribution to the profession. There will be no finalists for this category and the winner will be selected from within the profession by Aesthetics Media. Readers are invited to share their suggestions by emailing contact@aestheticsjournal.com
TEAM OF THE YEAR
Did you open your very own clinic after January 1 2018? Show your current and potential patients that your new clinic is something to be proud to be associated with. Finalists should demonstrate initiatives designed to promote growth, commitment to
BEST CLINIC GROUP, U K & IRELAND @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The reception staff are the face of your business, and it’s time your fabulous team members were recognised for their hard work. If you can provide evidence of outstanding customer service, a continuous training programme, strong practitioner support and effective teamwork, then you need to enter your team into this category.
(3 CLINICS OR MORE) BEST CLINIC GROUP, UK & IRELAND (10 CLINICS OR MORE)
ACHIEVEMENT
OUTSTANDING
IN MEDICAL AESTHETICS
BEST CLINIC NORTH ENGLAND BEST CLINIC MIDLANDS & WALES BEST CLINIC SOUTH ENGLAND BEST CLINIC SCOTLAND BEST CLINIC IRELAND BEST CLINIC LONDON CLINIC FINALISTS IN EACH REGION ACROSS THE UK WILL BE RECOGNISED FOR THEIR COMMITMENT TO EXCELLENCE IN PATIENT CARE AND SAFETY, CUSTOMER SERVICE AND EVIDENCE OF GOOD FEEDBACK FROM THEIR PATIENTS. ENTER NOW TO PUT YOUR MARK ON THE MAP! THE AESTHETICSOURCE AWARD FOR BEST NEW CLINIC, UK AND IRELAND
CATEGORIES CLINICS
CLINIC RECEPTION
customer service, patient care and safety, as well as good feedback from patients.
The categories to the right are open to clinic groups in the UK and Ireland with either more than three clinics (but less than 10) or 10 clinics or more. The group will be judged as a whole on their obligation to excellence in the service they provide, patient care and safety, and exceptional feedback. FIND YOUR CATEGORY BELOW! WHETHER YOU ARE A WINNER OR A FINALIST , YOUR HARD WORK SHOULD BE SOMETHING TO SHOUT ABOUT PROFESSIONALS Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019
PRODUCTS
PRODUCT INNOVATION OF THE YEAR
The Aesthetics Awards will celebrate the products that have truly revolutionised the market in 2019. The judges will look for widelyused products displaying genuine innovation leading to treatment for new indications, quicker or more straightforward results and enhanced patient safety, all backed by sound evidence.


INJECTABLE PRODUCT OF THE YEAR
Manufacturers or UK distributors of injectable products for the UK aesthetics market are invited to enter this category. Highlight why your product stands out from the crowd by showcasing evidence of good safety and efficacy, optimum duration and tangible benefits over similar products on the market.
ENERGY DEVICE OF THE YEAR
If you are a supplier or manufacturer of an energy device, then now is the chance to prove why yours is the best in the UK. Your device must demonstrate a wide range of indications, optimum duration and tangible benefits over similar treatments on the market and most importantly, evidence of good safety and efficacy.
TOPICAL SKIN PRODUCT/RANGE OF THE YEAR
With an abundance of topical skincare on the market, it can be challenging for practitioners to select which ones to adopt in their clinic. This award will be given to the manufacturer or exclusive UK distributor who can demonstrate that their topical skin product/range is effective, safe and easy to use.
CLINIC, COMPANY OR ORGANISATION
PROFESSIONAL INITIATIVE OF THE YEAR
Have you, your company or association launched a patient-focused and professional campaign within the last year or made significant developments to an existing initiative? The judges will look for evidence of activity designed to benefit the industry as a whole, along with tangible outcomes, rewarding the promotion of consumer education and patient safety.
TRAINING PROVIDERS
THE SINCLAIR PHARMA AWARD FOR BEST INDEPENDENT TRAINING PROVIDER
Judges will look for the independent training provider who offers a programme with engaging methods of delivery, a high-quality continued development strategy and achievement of measurable outcomes.
BEST SUPPLIER TRAINING PROVIDER
Do you offer excellent training events or programmes to clients who stock your products or services? This award will look for engaging methods of delivery, a high-quality, relevant programme and achievement of measurable outcomes.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
INDUSTRY
PHARMACY DISTRIBUTOR OF THE YEAR
Brand new to 2019, this award acknowledges the vital role played by UK pharmaceutical distributors who bring new, international pharmaceutical products and treatments to the UK medical aesthetic market. Finalists will be selected on the basis of their product representation, customer service, and ongoing support to practitioners.
AESTHETIC PRODUCT DISTRIBUTOR OF THE YEAR
If you offer a range of products at competitive prices, then this is the category for you. Aesthetic distributors that have demonstrated exceptional customer service, product representation and ongoing support to practitioners will be recognised with this award.
BEST MANUFACTURER IN THE UK
Are you a UK-based skincare or equipment manufacturer that offers excellent customer support and the latest range of products? Prove to your clients that your product developments and support for practitioners is superior and enter this category.
BEST UK SUBSIDIARY OF A GLOBAL MANUFACTURER
If your company manufactures an up-to-date range of products or equipment and is owned by more than 50% of an international parent company, then this is the category for you. This award will recognise the excellent service provided to clients by subsidiaries of global manufacturers.
THE HEALTHXCHANGE GROUP AWARD FOR SALES REPRESENTATIVE OF THE YEAR
What do you do to offer unsurpassed levels of customer service to your clients? Those chosen will be able to show outstanding levels of support for their customers, a strong commitment to their industry and a proven ability to assist clinics in supporting patients and growing sales of their product and/or services.
BEST CLINIC SUPPORT PARTNER
Does your company offer outstanding support to medical aesthetic clinics in the specialty? Those who enter will offer business services tailored to the aesthetics market such as CRM, clinic software, PR, advertising, marketing, financial support, legal advice and insurance.
HOW TO ENTER
All entries must be made via aestheticsawards.com
You can enter as many categories as you wish, but you may only enter yourself, a company you work for, an employee who works for your company or a product made that is distributed by your company. Entries made on behalf of a third party will not be accepted. You may only enter each category once. All entries must be accompanied by the supporting evidence requested in the entry form.
YOUR ENTRY
You are encouraged to keep your entry concise and clear; use bullet points and take advantage of formatting options such as bold, underlines and italics to ensure your entry is easy to digest for judges. Please note that formatting cannot be copied and pasted from Word documents, so you should only add these when submitting your entry on the website. A strict word limit is enforced for each question and you must not exceed this; however, your entry does not have to meet it.
THE JUDGING PROCESS
After the entry closing date of June 28, a list of finalists will be selected in each category, which will be published in the September issue of the Aesthetics journal and on the website on September 2. Users registered on the Aesthetics website are able to vote for a winner in the designated categories, which will also be evaluated by an expert judging panel. Other categories will be assessed solely by the judging panel, which will be carefully selected to avoid conflicts of interest.
OUR TOP TIP!
What makes you stand out from the crowd?! Your entry should not only be supported by evidence, but judges will be looking for new and exciting developments, so be sure to highlight what makes you different from the rest!
Group ENTER TODAY Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com

THE INViSIBLE NEEDLE 14% THINNER THAN 33G Near painless. Minimal bleeding. Low dead space hub design. www.tsklab.com
Male-specific Approach to Toxin Treatment
Mrs Aggie Zatonska describes her approach to botulinum toxin injections in male patients
Men are the fastest growing segment of patients in aesthetic In the US, they represent approximately 10% of consumers of injectable cosmetic treatments and this number has grown 355%
It is estimated that there were approximately half a million male patients treated with botulinum toxin (BoNT-A) in and between 2010 and 2014 the use of BoNT-A in
Typically, men tend to seek mostly minimally-invasive procedures and those with minimum or no downtime, such as BoNT-A, dermal fillers and intense pulsed light treatments, as opposed to surgical procedures that require downtime and may result in some recent increased social acceptability and greater perception of safety and efficacy of BoNT-A procedures encourages 2,4
It is important for practitioners to recognise physiological and anatomical differences between male and female faces (known as sexual dimorphism) to avoid over-feminising a male face. As there are also differences in expectations driven by what primarily appears to be a desire to improve men’s competitiveness in the workplace, detailed below, male patients require a gender-specific approach when using BoNT-A injections. The male-tailored approach includes consultation, injection technique and the consent process.1 In this article, I outline what I believe to be the motivations behind male toxin treatments, discuss my preferred technique and provide an
Why do male patients consider BoNT-A treatments?
In 2016, the Department of Dermatology at the University of California conducted an online study with 600 men aged between 30-65. They asked how concerned they were by the appearance of 15 age-related facial features. The results of the survey indicated that 60% of men were concerned about the appearance of their glabellar There are underlying anatomical and physiological reasons of why a male forehead is more susceptible to wrinkling. For example, the skin is markedly thicker, facial musculature is stronger and sunprotective habits are less common than in females.3,6
Angry vs. approachable
I have found that one of the main reasons that men consider BoNT-A treatments does not appear to be related to visible improvement of facial appearance, but rather to achieving a more ‘relaxed’, youthful and less angry look. I have found that this is particularly relevant for my patients that work in customer-facing roles. Interestingly, results from a questionnaire conducted by 107 members of the American Academy of Facial Plastic and Reconstructive Surgery suggested that both men and women want cosmetic treatment so that they can look younger, particularly women. However, members noted that men are more likely than women to cite a work-related reason and competitive reasons as their motivation for treatment.2 When asked during their initial consultations why men might be reluctant to undergo cosmetic procedures, the main reason for hesitation noted by those surveyed
was fear of appearing feminised.7 Some might have experienced this undesirable appearance after receiving BoNT-A treatments that did not include a gender-specific approach. Men tend to be aware of sexual dimorphism of facial features and typically wish to maintain or enhance traditionally masculine features.8
Treatment technique
Prior to treatment it is important to remember key characteristics of the male face. There are differences in the facial skeleton (male skulls are larger and differently shaped), and they have greater glabellar projection. Men tend to have more prominent supraorbital ridges (they provide a good landmark for eyebrow position), their eyebrows are flatter and positioned lower on the orbital rim. For comparison, in women, the eyebrow is typically positioned just above the supraorbital ridge with the arches peaking in the lateral third of the face.4 Forehead height and width are also greater in men, with a greater backward slope.4 Presence of androgenic alopecia further optically increases the height of the forehead.2 In women, forehead contour is higher, smoother, and rounder to the point of forward protrusion. Female orbits are proportionally larger in relation to the size of the skull. In the lower face, males tend to have a wider and larger chin with more significant forward prominence, and a prominent flexure of the mandible.2,4
Consultation
Physical examination should include assessment of frontal and oblique view, at rest and on animation, identification of baseline asymmetries, static and dynamic rhytides and estimation of facial muscle mass.2 Prior to consenting, educating the patient on the procedure, informing them of adverse events and establishing expectations from treatment should take place, as with all treatments. Patients should be made aware that satisfaction rate increases with continued treatments. Typically, dynamic lines improve first, while static lines can improve with repeated treatments. Common side effects include swelling, bruising and erythema. Men are also more prone to develop ecchymosis due to greater density of microvasculature.4 As for every patient, appropriate selection, individually adjusted dosing and placement of injections is key to achieving desired outcomes. Treatments with neurotoxins in male patients should aim to preserve lower position of the brows and flatter arches.9,10
Treatment example: forehead
To my knowledge, the only multi-centre, randomised, doubleblinded, placebo-controlled study that adjusted BoNT-A dosing for different sexes was published in 2009.11 Results suggested that men are less responsive to the doses used. Due to larger muscle mass and men having more severe rhytides than women, larger doses of BoNT-A are typically recommended in male patients. The author suggests doses higher than 20 units, however it greatly depends on the individual, muscle strength and expectations.12 Softening of the horizontal lines while still allowing movement is often preferred in men. The position and shape of the brow is also very important as an arched brow will usually feminise the face.2 Improperly administered BoNT-A can cause brow ptosis, sensation of heaviness, and make male patients look older, as well as potentially impacting their vision. A consensus for treating the face and neck was published in the Plastic and Reconstructive Surgery journal
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
which detailed the following recommendations for treatment of the frontalis muscle:13
• 8-25 units of BoNT-A across four to eight injection points
• Injection to be performed intramuscularly in horizontal rows with purposeful lateral injection to prevent arching of the brow.2,13 Some panelists within the consensus group recommend using a lower volume of toxin in the dermis in the lateral frontalis, as they believe it can improve rhytides on the lower forehead without causing brow descend
• Lowest injection points should ideally be located at least 1cm above the orbital rims
• Injection points on the frontal scalp in men with alopecia should be higher and an extra dose might be required below receding hair line to prevent unnatural lines in this area2,13
The consensus shows the trend towards neuromodulation rather than paralysis, including lower dosing of the upper face, more frequent
Case study
A 55-year-old male patient presented in my clinic with primary concerns regarding appearance of his forehead and periorbital rhytides. He felt that this made him look tired and unhappy. He had his first and only BoNT-A treatment in the forehead and



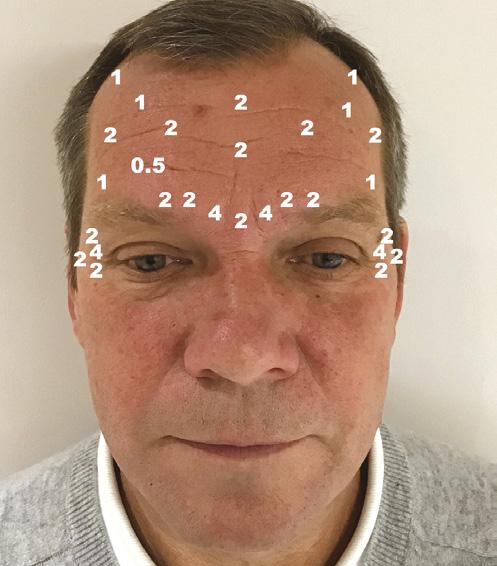

Before Before
combination treatments with hyaluronic acid fillers and intracutaneous injections where indicated to limit depth and degree of action.13
Treatment example: glabella
Men tend to have deeper furrows in the glabella.2 Softening of those lines can decrease appearance of aggressiveness and make the overall face appear more youthful. Relaxing glabellar muscles shouldn’t result in their immobilisation. This will create an unnatural look and can additionally result in lifting of the lateral brow. Therefore, while treating the glabella in men I recommend treating the forehead laterally. In my practice, typical treatment will include:
• 12-40 units of BoNT-A injected across three to seven injection points
• While injecting into corrugators (presence of dimpling), ensure you stay approximately 1cm above the orbital rim in order to prevent diffusion to the levator palpebral superioris. Bloom et al.14 recommend identifying the most lateral aspect of the corrugator
Treatment
Before
glabellar lines 18 months ago in my clinic. He was previously very satisfied with the result, stating that he achieved a very natural result that made him look younger and more relaxed. His concerns and expectations were discussed in detail during the first consultation. The patient’s main concern was the risks of elevating the eyebrow and ‘looking feminine’. During his second consultation he specifically asked for the same results as before. Figure 1 and 2 shows the patient before the second treatment took place. The upper face was reassessed, and we discussed the risks, down-time and possible side effects. The before and after photographs were taken and the patient had the opportunity to ask questions and to consider alternative treatments prior to signing the consent forms.
I used a 0.3ml Becton Dickinson syringe with a 31 gauge, 8mm needle for injection. BoNT-A was used, injected intramuscularly into the central glabella, and very superficially (subcutaneously) in the lateral part of the glabella, frontalis and orbicularis oculi muscle. I use the on-label recommendation for reconstitution volume of 2.5ml of 0.9% saline with preservative (benzoic acid) for 100 units vial of BoNT-A (4U/0.1ml), of which my preferred product of choice was Botox.15 The numbers shown in Figure 3 represent the location of injection and corresponding numbers of international units of BoNT-A used. Please note that due to natural facial asymmetry, there is a small imbalance in the location and number of units injected on each side of the face. Additional injections were made into the frontotemporal hairline, where the hairline recedes. The patient was followed up two weeks later and was extremely satisfied with the achieved results. Figure 4 and 5 show results of the treatment upon frowning and at rest, respectively. Note a minimal brow elevation on the right-hand side, despite additional correction for asymmetry in the primary treatment that was not noticed before by the patient. He was offered an additional one unit of BoNT-A into the lateral frontalis muscle on the right-hand side with a satisfactory outcome. No further follow-ups were required.
After After
Figure 3: The location of injection and corresponding numbers of international units of botulinum toxin type A used
Figure 1 and 2: Patient’s front and profile, at frown and rest retrospectively before treatment
Figure 4 and 5: Patient’s front and profile, at frown and rest, retrospectively, two weeks after treatment
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
and placing the lateral injections just medial to this insertion point
• Injections placed too superiorly in the mid-glabella may also affect medial frontalis and will likely result in elevation of lateral brow2
• Avoid injecting into the glabella alone to prevent elevation of the brow. Men often prefer horizontal brows. If the glabella is treated, forehead will require adjustments as well14

Conclusion
Men are becoming more aware of the cosmetic use of BoNT-A and are more frequently seeking those treatments. They require a different approach, beginning from the initial consultation. Male patients should be assured that the treating practitioner is aware of the sexual dimorphism. For optimal results muscle movement will be preserved to achieve a natural look. Currently there is limited amount of data on using BoNT-A in men and I believe that this growing area of aesthetic practice requires further studies.
Mrs Aggie Zatonska is an aesthetic practitioner with over 10 years’ experience in facial aesthetics. She is a specialist ENT surgeon and holds a post-graduate degree in Aesthetic and Anti-Ageing Medicine accredited by the L’Union Internationale de Medecine Esthetique. Mrs Zatonska is the founder and director of Atelier Clinic in Egham, Surrey.

REFERENCES
1. Frucht CS, Ortiz AE. Nonsurgical Cosmetic Procedures for Men:Trends and Technique Considerations. J Clin Aesthet Dermatol 2016;9(12):33-43
2. Jones IT, Fabi SG. The Use of Neurotoxins in Male Face. Dermatol Clin 2018; 36: 29-42.
3. Sadick NS. The Pathophysiology of the Male Ageing Face and Body. Dermatol Clin 2018; 36: 1-4
4. Keaney TC, Alster TS. Botulinum Toxin in Men: Review of Relevant Anatomy and Clinical Trial Data. Dermatol Surg 2013; 39:1434-1443
5. Jagdeo J, Keany T, Narurkar V, et al. Facial treatment preferences among aesthetically oriented men. Dermatol Sure 2016;42(10): 1155-63
6. Thieden E, Philipsen PA, Sandby-Moller J, et al. Sunscreen use related to UV exposure, age, sex and occupation based on personal dosimeter readings and sun-exposure behaviour diaries. Arch Dermatol 2005; 141(8):967-73
7. Sadick NS. Cosmentic Dermatology for Men. Preface. Dermatol Clin 2018; 36:ix-x
8. Keaney T., Male Aesthetics. Skin Therapy Lett 2015;20(2):5-7
9. Burgess CM. Soft tissue augmentation in skin of color: market growth, available fillers, and successful techniques. J Drug Dermatol 2007; 6:51-5



10. Carruthers JD, Carruthers A. Botulinum A exotoxin in clinical ophthalmology. Can J Ophtalmol 1996; 31:389-400
11. Kane MAC, Brandt F, Rohrich RJ, Narins RS, et al. Evaluation of Variable-dose Treatment With a New use of Botulinum Toxin Type A(Dyspott) for Correction of Moderate to Severe Glabellar Lines. Phase 3, randomised, double-blind, placebo-controlled study. Plast Reconstr Surg 2009;124:1619-29
12. Jones D., Gentlemen, Relax. Commentary on Botulinum Toxin in Men: A review of relevant anatomy and clinical trial data. Dermatol Surg 2013;39:1444-1445.
13. Sundaram H, Liw S, Signiorini M, et al. Global Aesthetics Consensus: botulinum toxin type A evidence based review, emerging concepts, and consensus recommendations for aesthetic use, including updates on complications. Plat Reconstr Surg 2016; 137(3): 518e-29e

14. Bloom JD, Green JB, Bowe W, et al. Cosmetic use of abobotulinum toxin A in men: considerations regarding anatomical differences and product characteristics. J Drugs Dermatol 2016; 15(9):1056-62

15. Botox Medical, Botox Reconstitution and dilution procedures, <https://www.botoxmedical.com/ Common/Assets/APC15WD15_Recon_Dilution_Instructions.pdf>
FURTHER READING
Handler MZ, Goldberg DJ. Cosmetic Concerns Among Men. Dermatol Clin 2018; 36: 5-10
• Henry, M. Cosmetic Concerns Among Ethnic Men. Dermatol Clin 2018; 36: 11-16 Harman SM, Metter EJ, Tobin JD, et al. Longitudinal effects of ageing on serum total and free testosterone levels in healthy men. Baltimore longitudinal study of ageing. J Clin Endocrinol Metab 2001;86(2):724-31
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
“I cannot believe the improvements in my skin after the Morpheus8 treatment. I went out the next day, with no problems! Right away I noticed improvements to the deeper lines around my mouth and nose, and my skin feels so much smoother.”
- ROSE, PATIENT
R A DIAN T & B E AU TI F U L C ON T OUR S
VPOMO0918 UN COV E R N ATUR A L AN D YOUTH F U L CON TOUR S INFO@INMODEMD.CO.UK WWW.INMODEMD.CO.UK +44 (0) 208 965 2594 Before After COMBINATION TREATMENT - MORPHEUS8 & FACETITE PHOTOS COURTESY OF PIER PAOLO ROVATTI MD Before After PHOTOS COURTESY OF JUDITH HELLMAN MD C M Y CM MY CY CMY K Morpheus8_PO_0918 copy.pdf 1 15/04/2019 16:15
F R A C T I O N A L RF T R E A T M E N T
INNOVATIVE SKIN SYSTEMS FROM SKINCEUTICALS

Targeting ageing and blemish prone skin
SkinCeuticals strives to improve the appearance of skin and promote long term skin health through research, education and innovation. The results-driven skincare brand has now developed two exciting new retail kits delivering high quality, proven formulations that reflect and enhance the care you provide to your patients in your clinic. The kits reflect SkinCeuticals scientific approach to skincare and the development of effective topical regimens designed to address the needs of two common skin concerns frequently seen in clinics: ageing skin on the one hand and ageing, blemish prone skin on the other.
AGE RENEWAL SYSTEM
The Age Renewal System is suitable for patients who wish to tackle loss of elasticity and diminish the signs of photodamage caused by Atmospheric Skin Ageing. It comprises three high performance products that improve the appearance of fine lines, wrinkles and skin tone whilst safeguarding it against further damage.


Dr Fiona McCarthy welcomes the new SkinCeuticals Skin Systems. Dr McCarthy initially embarked on a career within the NHS. Today she continues to work part time as a consultant oncologist, specialising in dermatological cancers, whilst heading up her own skin clinic and pursuing her interest in a holistic and preventative approach to ageing. She says: “I am excited to be able to offer my patients the Age Renewal Skin System as an introduction to evidence-based anti-ageing skincare. This kit combines three of my favourite products in the SkinCeuticals range and the ones I recommend the most to my patients. The powerful protective antioxidant effect of C E Ferulic, the collagen stimulation and reduction of fine lines and wrinkles by Retinol 0.3 and the hydrating and plumping action of H.A. Intensifier ensures that patients will see a visible anti-ageing effect with the introduction of these products.”
• C E Ferulic 30ml is a patented triple antioxidant serum that fights Atmospheric Skin Ageing to deliver firmer, fresher and radiant skin. The combination of vitamins C and E combined with ferulic acid delivers eight times the skin’s natural protection again environmental aggressors1. It is formulated to provide not only cosmetic benefits, but also to prevent future skin damage by protecting against UVA, UVB, IRA, and ozone pollution all of which slow down the skin ageing process.

• H.A. Intensifier 30ml is a fast-absorbing serum that boosts the skin’s hyaluronic acid levels by +30% to support the skin’s matrix, resulting in improved firmness and plumpness2. Additionally, it delivers surface hydration which makes the skin feel smoother and more supple immediately after use. Recently indicated also for use in periorbital and perioral areas, H.A. Intensifier is clinically proven to improve the appearance of fine lines, wrinkles and skin texture in four weeks3

• Retinol 0.3 30ml is a potent night cream featuring 0.3% pure retinol enhanced with the latest stabilisation and delivery technologies to ensure a steady, even release with minimal irritation. Its benefits include improving the appearance of fine lines, wrinkles and dark spots, as well as minimising pores by accelerating cellular turnover and enhancing collagen production. Retinol 0.3 is a good first introduction to using retinol as part of an anti-ageing skincare regimen.

Aesthetics | May 2019 46 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial SkinCeuticals
CLARIFYING SKIN SYSTEM


The Clarifying Skin System has been specifically designed for patients experiencing signs of problematic skin and ageing simultaneously, acting on blemishes while providing targeted exfoliation – tackling concerns such as inflammation, along with key signs of ageing such as hyperpigmentation and fine lines.
The kit includes three clinically effective products to help with the unique set of ageing concerns experienced by patients with imperfections; as oil glands enlarge with age, pores increase in size and skin’s texture becomes rough.

Dr Benji Dhillon, well-renowned facial aesthetics doctor and co-founder of the new Define clinic in Beaconsfield, says: “There aren’t a great deal of kits available for newcomers to cosmeceutical skincare that deliver results. The new SkinCeuticals Clarifying Skin System is one of the first kits to provide first timers an effective, easy to follow morning regimen to manage their blemish prone, ageing skin. The kit features three products that work together to help promote cell turnover, whilst improving blemishes and
• Blemish + Age Cleanser Gel 240ml thoroughly cleanses skin removing impurities and excess oils. It contains salicylic acid which promotes desquamation and glycolic acid that acts as an effective exfoliant. Together they accelerate exfoliation to decongest pores, reduce imperfections and deliver a more even skin tone.

• Blemish + Age Defense 30ml is a powerful lightweight corrective serum clinically proven to help prevent the formation of blemishes and clogged pores whilst improving the appearance of fine lines, wrinkles and uneven skin tone4. Key ingredients include dioic acid, which helps to regulate sebum production and discolouration, plus salicylic acid, glycolic acid and citric acid. The serum has been shown to be as effective as tretinoin (0.0025%), demonstrating significantly better results in specific criteria such as improving skin tone, blotchiness and reducing total lesions5
• Phyto Corrective 30ml is a lightweight oil-free moisturising serum to soothe reactive skin. Enriched with botanical extracts, it hydrates the skin for a clearer, fresher looking complexion whilst also calming irritated skin to reduce the appearance of redness and give a fresher looking complexion.

The kits present you, as skincare experts, with opportunities to discuss effective management of ageing skin with your patients and so introduce them to evidence-based cosmeceutical skincare. Your patients will find that the three step daily regimens are very userfriendly, thus making the move to advanced skincare feel a logical and progressive next step in taking a long-term approach to the care of their skin.
For further information
Email: contact@skinceuticals.co.uk
REFERENCES
1. J Invest Dermatol.125:826-832,2005 2. DOF: A 4-week study on 12 females, ages 45 – 65. Hyaluronic acid localisation was visualised using a biotinylated hyaluronic acid binding protein and streptaviden-conjugated horse radish peroxidase 3. DOF: An 8-week, single-centre clinical study was conducted on 50 females, ages 35-60, Fitzpatrick I-VI, with mild to moderate under eye hollows and thin lips. H.A. Intensifier was applied twice a day. Efficacy evaluations were conducted at baseline and weeks 4 and 8. 4. DOF: Dermatologist controlled study of 50 multi-ethnic subjects aged 25-50 with blemish prone skin for 4 weeks 5. Kircik L., Dahl A., Yatskayer M et al. Safety and Efficacy of Anti-Acne / Anti-Ageing Treatments in Subjects with Photodamaged Skin and Mild to Moderate Acne Vulgaris. J Drugs Derm 2012: 11 (6) 737-740
Aesthetics | May 2019 47 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial SkinCeuticals
Radiotherapy and Skin

Consultant oncologist Dr Fiona McCarthy details how radiotherapy affects the skin and considerations for treatment
Radiotherapy (RT) is a lynchpin of oncological treatment worldwide and can be used alone or in combination with chemotherapy and surgery to maximise tumour control, reduce tumour burden and improve quality of life. Since its advent over a century ago, considerable advances have been made to improve the efficacy of radiotherapy, as well as minimising its toxicities. The most common manifestations of radiation toxicity are acute and chronic skin reactions, commonly described as ‘radiation dermatitis’. Despite the advent of intensity-modulated radiotherapy (IMRT) and other new technologies which reduce the dose intensity of radiotherapy on the skin, radiation dermatitis remains the most common side effect of RT in both the acute and chronic setting.1,2 These reactions can cause serious functional impairment as well as cosmetic disfigurement, which may result in a significant impact on the patient and their quality of life, both physically and
Other considerations of RT
psychologically. An increasing incidence of cancer in the general population, as well as improved survival rates,3 makes it highly probable that all aesthetic practitioners will, at some point, manage patients who have undergone RT, and indeed, may be asked to help improve the aesthetic appearance of cutaneous toxicities. Therefore, it is essential that aesthetic practitioners have an understanding of the effects of radiotherapy on the skin, what complications are likely to arise, and how best to manage them.
Factors affecting skin reactions to radiotherapy
The dermatological side effects experienced by patients during or after a course of RT are wide-ranging and dependent on a multitude of variables. Site of disease, radiation dose, technique, and frequency of treatment can impact on the potential for skin toxicities with patients treated with RT.2 Breast, lung, and head and neck cancers are more likely to develop cutaneous complications due to the higher radiation dose administered to the dermal layers.1 Other risk factors for developing skin toxicity include obesity, advanced age, female gender, chronic sun exposure, diabetes and smoking.1,4-7 Concurrent diagnoses of connective tissue diseases such as systemic lupus erythematosus (SLE) and scleroderma, also increases the risk of developing cutaneous side effects.8 Cutaneous reactions to RT can be categorised into acute or chronic reactions, depending on timing of onset of clinical signs.
Acute RT reaction
Acute skin toxicity usually develops within three months of commencing RT. The acute reaction ranges from a transient erythema (which is self-limiting) to a more severe dry desquamation, which is characterised by hyperpigmented, dry, flaky skin. The most severe acute reaction is moist desquamation, where the skin barrier dysfunction results in a leakage of serous fluid and associated ulceration and necrosis.2 Due to the impaired epidermal barrier in moist desquamation, there is a significant risk of superadded infection so the affected area should be protected from extremes of temperature as well as sunlight, allergens and other potential sources of irritation to avoid further tissue injury.1 Acute radiotherapyrelated skin reactions should only ever be managed by a consultant oncologist in the hospital setting with specialist dermatology input if required. As such, any patient requesting aesthetic input or advice with any of the clinical signs described above within three months of radiotherapy should be referred to their treating oncologist immediately for review.
Chronic RT reaction
Chronic radiation-induced skin reactions (RISRs) can occur as early as three months following completion of treatment to many years later.9,10 Chronic RISRs may have a significant impact on patients’ quality of life due to the often irreversible nature of the damage. Chronic RISRs may occur in patients who experienced only minimal acute radiation dermatitis and therefore can develop on skin that appears normal. This significant cosmetic disfigurement caused by chronic RISRs may lead to patients’ seeking aesthetic treatments to improve the appearance of the skin.9,10
A well-known effect of RT is the carcinogenic potential of ionising radiation. Patients treated with RT are at risk of radiation-induced secondary malignancies (RISM) and, in particular, secondary cutaneous malignancies such as basal cell carcinomas (BCCs) in the irradiated field. This risk is lifelong, increases with time and is dose-related.21,22 The BCCs that present in the field of radiation often follow a more aggressive and unusual course than expected. Patients who have undergone RT for breast cancer have a 9% rate of local recurrence of their original disease reported with a median follow-up of 17.2 years.1
Clinical manifestations of chronic RISRs
Chronic RISRs are characterised by dermal fibrosis or atrophy with associated alterations in skin
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
pigment.5,11 Post-inflammatory hyperpigmentation is particularly common and this may either resolve very slowly or worsen with time depending on the Fitzpatrick skin type of the patient and the severity of the skin reaction.1 Skin over the affected area may become xerotic and hyperkeratotic. Significant cutaneous toxicity is characterised by persistent dyspigmentation, dermal atrophy, and telangiectasia with the potential for permanent loss of nails and skin as well as absence of hair follicles resulting in alopecia.1,12 Radiation-induced telangiectasia are particularly common in chronic RISRs and are thought to occur in up to 13% of patients.2 Telangiectasia are vascular lesions which result from the dilatation of poorly supported vasculature in the skin and, due to their appearance, are associated with a poor body image following RT.13
Radiation-induced fibrosis
Radiation-induced fibrosis (RIF) of the skin and subcutaneous tissues is often considered the most severe of all chronic RISRs and the most difficult to treat. RIF may potentially develop at any RT treatment site, however patients who have undergone RT for breast cancer are most commonly affected. This is because the site of RT treatment has often also previously undergone surgical intervention creating distortion of the skin architecture and making it more susceptible to RIF.1 However, in general, the risk for developing RIF is low following the introduction of skin sparing radiotherapy techniques in breast cancer. Signs and symptoms of RIF include skin retraction, pain, necrosis and ulceration.14 Chest wall RIF may result in restricted arm and neck movement, lymphoedema, and brachial or cervical plexopathy.15 RIF is mediated by inflammation which occurs immediately after RT and may continue for months and years. The pro-inflammatory cytokines tumour necrosis factor alpha (TNF-α), Interleukin 6 (IL-6) and IL-1 promote this response with concurrent fibroblast activity, enhanced by transforming growth factor beta (TGF-β) and platelet-derived growth factor (PDGF).9,16-18 These changes, in addition to radiation-induced alterations of the vascular system, contribute significantly to development of late cutaneous toxicities related to RT.19
Pathophysiology of chronic RISRs
Pro-inflammatory and pro-fibrotic cytokines are overexpressed in chronic RISR tissue. TNF-α, TGF-β, IL-6 and IL-1 as well as (PDGF) are present immediately after RT and may persist for months to years.1
TNF-α, IL-6, and IL-1 are responsible for persistent inflammation, whereas TGF-β and PDGF promote fibrosis by activating fibroblasts and are involved in synthesis of extracellular matrix proteins and matrix metalloproteinases.1,9,17,20 The combination of impaired vascular perfusion to the skin due to RT, along with activated fibroblasts and pro-inflammatory cytokines, can exacerbate the fibrotic process.19
Management of chronic RISRs
Recommendations available on management of chronic RISRs suggest both topical and oral treatments.4,19 A number of small case studies have suggested that using the xanthine derivative Pentoxifylline in combination with vitamin E for more than three years may help with the symptoms experienced with RIF. However, controversy remains regarding both the optimal treatment dose and duration of Pentoxifylline, as well as the importance of the addition of vitamin E.23,24 From my experience, the management of telangiectasia and dyspigmentation are the clinical signs that are most likely to present to aesthetic practitioners.
Laser
Laser treatment of vascular lesions including telangiectasia are well established. The presence of telangiectasia may be psychologically distressing for the patient and pose as a constant reminder of their cancer. Pulsed dye laser (PDL) has been shown to be superior in terms of vessel clearance and patient satisfaction to intense pulsed light (IPL) for post-radiotherapy-induced telangiectasia, as demonstrated in a randomised split-lesion trial of 40 patients by Nymann et al.25 More recently, a small cohort of eight breast cancer patients with radiation-induced telangiectasia were treated with PDL at Memorial Sloan Kettering Cancer Centre (MSKCC) in New York.26 Outcomes were measured based on patients’ wellbeing and satisfaction with results, with all patients reporting a significant clinical improvement from baseline after an average of four sessions. Although PDL has demonstrated a clinical improvement in the above studies, larger randomised control trials are required to better define the risk of using PDL on irradiated skin and the long-term effects of the laser treatment on vessel recurrence. A further case report involving three patients described the use of an alexandrite laser in the treatment of radiation-induced hyperpigmentation. These patients had previously been treated with RT for BCCs more than 15 years previously. A good aesthetic result was reported by both patients and doctors after four to five weeks of treatment.27
Advances in laser therapy have led to the use of fractional laser treatment (FLT) to treat fibrosis associated with hypertrophic scars and morphea, leading to tissue repair and, ultimately, scar remodelling. There is a hypothesis that FLT can normalise the fibrotic process and induce normal scar remodelling in patients affected by chronic radiation injury. Understanding and correcting this underlying fibrotic process can help restore normal skin functions in patients affected with chronic radiation dermatitis (RD) and other debilitating fibrotic diseases in dermatology, such as scleroderma, morphea, or nephrogenic systemic fibrosis.28 A pilot study on the effect of laser on reversing chronic radiation injury is currently taking place on 22 patients with significant RIF to test this hypothesis. Each patient will receive FLT using the Lumenis Ultrapulse Carbon Dioxide (CO2) laser as well as a control no-treatment area randomised to site. Patient age, type of cancer, method and dosage of radiation, latency between radiation treatment and start of study as well as
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The most common manifestations of radiation toxicity are acute and chronic skin reactions
characteristics of skin changes will be recorded. Assessments will be conducted immediately before and after each treatment and at regular intervals up to 12 months after the last treatment.28
Discussions for patient management
Patients may present to aesthetic practitioners for assistance with scarring, dyspigmentation and telangiectasia following RT. From a unique position as a consultant oncologist as well as an aesthetic practitioner, I would urge great caution in treating areas of chronic RISRS, or indeed any area previously treated with radiotherapy. Secondary skin malignancies are relatively common in the site of previous radiotherapy, even many years later.29 For patients with breast cancer, recurrence of the tumour can occur on the chest wall in sites of previous radiotherapy or surgical scars. Distorting the architecture of the skin purely for a cosmetic result may have an impact on diagnosing a recurrent or de novo malignancy in this area. The small cohort of studies described above focus on successful cosmetic results with intervention using laser therapy but do not consider the longer-term oncological complications that may occur. Prior to advising the widespread use of laser/light therapy to treat chronic RISRs, good quality randomised clinical trials are required. In short, in the best interest of the long-term health of the patient, I strongly advocate avoiding cosmetic procedures or intervention in areas of RISRs or RIF.
REFERENCES
1. Hymes SR, Strom EA, Fife C, Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006, J Am Acad Dermatol. 2006 Jan;54(1):28-46.
2. Leventhal J, Young MR, Radiation dermatisis: recognition, prevention, and management, Oncology Williston Park N.Y, 2017
3. National Cancer Institute <https://www.cancer.gov/>
4. Bray FN et al., ‘Acute and Chronic Cutaneous Reactions to Ionizing Radiation Therapy’, Dermatology and Therapy, 2016.
5. Brown KR & and Rzucidlo E, ‘Acute and Chronic Radiation Injury’, Journal of Vascular Surgery, 2011.
6. Ryan JL, ‘Ionizing Radiation: The Good, the Bad, and the Ugly’, Journal of Investigative Dermatology 2012.
7. Meyer F et al., ‘Predictors of Severe Acute and Late Toxicities in Patients with Localized Head-andNeck Cancer Treated with Radiation Therapy’, International Journal of Radiation Oncology Biology Physics, 2012
8. Lin A, Abu-Isa E et al., Toxicity of radiotherapy in patients with collagen vascular disease, American Cancer Society, 2008
9. Michèle Martin, Jean Louis Lefaix, & Sylvie Delanian, ‘TGF-Β1 and Radiation Fibrosis: A Master Switch and a Specific Therapeutic Target?’, International Journal of Radiation Oncology Biology Physics, 2000.
10. N. Salvo and others, ‘Prophylaxis and Management of Acute Radiation-Induced Skin Reactions: A Systematic Review of the Literature’, Current Oncology, 2010.
11. Felicia A. Mendelsohn and others, ‘Wound Care after Radiation Therapy.’, Advances in Skin & Wound Care, 2002.
12. JW Denham & M Hauer-Jensen, ‘The Radiotherapeutic Injury - A Complex “Wound”’, Radiotherapy and Oncology, 2002.
13. Richard Payne, Eduardo Medina, & James W Hampton, ‘Quality of Life Concerns in Patients with Breast Cancer: Evidence for Disparity of Outcomes and Experiences in Pain Management and Palliative Care among African-American Women.’, Cancer, 2003.
14. Frassica DA, Bajaj GK, Tsangaris TN, Treatment of complications after breast-conservation therapy, Oncology Williston Park N.Y, 2003
15. Sylvie Delanian et al., ‘Kinetics of Response to Long-Term Treatment Combining Pentoxifylline and Tocopherol in Patients with Superficial Radiation-Induced Fibrosis’, Journal of Clinical Oncology, 2005.
16. Oliver Haase & HP Rodemann, ‘Fibrosis and Cytokine Mechanisms: Relevant in Hadron Therapy?’, in Radiotherapy and Oncology, 2004.
17. SM Bentzen, ‘Preventing or Reducing Late Side Effects of Radiation Therapy: Radiobiology Meets Molecular Pathology’, Nature Reviews Cancer, 2006.
18. Amir Abdollahi et al., ‘Inhibition of Platelet-Derived Growth Factor Signaling Attenuates Pulmonary Fibrosis’, The Journal of Experimental Medicine, 2005.
19. Spalek M, Chronic radiation-induced dermatitis: challenges and solution, Clinical, Cosmetic and Investigational Dermatology, 2016
20. Dirk Pohlers et al., ‘TGF-Beta and Fibrosis in Different Organs - Molecular Pathway Imprints’, Biochimica et Biophysica Acta - Molecular Basis of Disease, 2009.
21. Roy E. Shore, ‘Radiation-Induced Skin Cancer in Humans’, in Medical and Pediatric Oncology, 2001.
22. Joanna L. Perkins at al., ‘Nonmelanoma Skin Cancer in Survivors of Childhood and Adolescent Cancer: A Report from the Childhood Cancer Survivor Study’, Journal of Clinical Oncology, 2005.

23. Magnusson M, Höglund P, et al., ‘Pentoxifylline and vitamin E treatment for prevention of radiationinduced side-effects in women with breast cancer: a phase two, double-blind, placebo-controlled randomised clinical trial (Ptx-5)’, Eur J Cancer. 2009 Sep;45(14):2488-95.
24. Jacobson G1, Bhatia S et al., ‘Randomized trial of pentoxifylline and vitamin E vs standard follow-up after breast irradiation to prevent breast fibrosis, evaluated by tissue compliance meter.’, Int J Radiat Oncol Biol Phys. 2013 Mar 1;85(3):604-8.
25. Nymann P, Hedelund L, Haedersdal M, Long-pulsed dye laser vs. intense pulsed light for the treatment of facial telangiectasias: a randomized controlled trial, J Eur Acad Dermatol Venereol. 2010 Feb;24(2):143-6.
26. Rossi AM, Nehal KS, Lee EH, Radiation-induced Breast Telangiectasias Treated with the Pulsed Dye Laser, J Clin Aesthet Dermatol. 2014 Dec;7(12):34-7.
27. Santos-Juanes J, Coto-Segura P, et al., ‘Treatment of hyperpigmentation component in chronic radiodermatitis with alexandrite epilation laser.’, Br J Dermatol. 2009 Jan;160(1):210-1.
28. ClincalTrials.gov, Pilot Study of the Effect of Laser on Reversing Chronic Radiation Injury, Massachusetts General Hospital. <https://clinicaltrials.gov/ct2/show/NCT01910818>
29. Dracham CB, Shankar A, Madan R, Radiation induced secondary malignancies: a review article, Radiation Oncology Article, 2018
I would urge great caution in treating areas of chronic RISRS, or indeed any area previously treated with radiotherapy
Dr Fiona McCarthy is a consultant medical oncologist in the NHS, as well as running her aesthetic clinic on the King’s Road, Chelsea. As well as her medical qualifications, Dr McCarthy was also awarded a PhD from the University of London in 2017 for her research on the links between inflammation and cancer.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com ENTER TODAY FLICK BACK TO P.38 FOR THE CATEGORIES OVERVIEW!


A recognized leader in vascular treatments, Syneron Candela now brings you the latest pulsed-dye laser with more enhancements than ever before. Technology You Trust Innovation You Need SPTL-1 First FDA-cleared PDL Vbeam Classic Proprietary 595 nm wavelength Vbeam Perfecta 8 micropulses Vbeam Prima* § Dual wavelength § Dual cooling § More user-friendly features § Better treatment experience © 2019 Candela Corporation. This material contains registered trademarks, trade-names and brand names of Candela Corporation and its affiliates, including Syneron, Candela, DCD, Dynamic Cooling Device, EverCool, ScleroPlus, Vbeam, and Vbeam Perfecta. All other trademarks are the property of their respective owners. All rights reserved. PB99071EN Contact us now: 0845.5210698 | ukinfo@syneron-candela.com candelamedical.com/uk
Periorbital Skincare
eye area
Audrey Hepburn had it right when she highlighted the cosmetic importance of the periorbital area. One of her famous quotes said, “The beauty of a woman must be seen from in her eyes, because that is the doorway to her heart, the place where love resides.” This is reflected in the fact that blepharoplasty (eyelid surgery to remove excess skin/fat) is one of the most common surgical cosmetic procedures performed worldwide.1 Being one of the thinnest areas of skin found on the body, the periorbita is one of the first to show signs of ageing.2 This article explores how we should tailor our patient’s topical skincare to address the specific concerns of this delicate area.
Why periorbital skin needs care
The periorbital area is often one of the top areas patients will want to rejuvenate. Whilst there is a variety of modalities at an aesthetic practitioner’s disposal, from anti-wrinkle injections and dermal fillers to laser resurfacing or platelet-rich plasma (PRP), it is important for any practitioner to know what topical agents are available to stave off further ageing changes, or that can be used to augment the result of more invasive treatments.
Applying topical skincare around the eye

In general, the areas of concern tend to be the under-eye area and the lateral canthal (crow’s feet) area. As such, I would advise patients to concentrate their topical treatments on these areas. Applying product directly to the eyelid is not necessary in my opinion as the lids themselves are rarely the area of concern, and it also enhances the risk of product entering the eye. The periocular area is
When we think about aesthetic concerns in the periorbital area, the most common things that our patients complain about include dark circles, puffiness and fine lines and wrinkles. The appearance of this area can influence how others perceive your wellness or mood, so it’s no wonder this is a top area for concern.5
Whichever cosmeceutical skincare ranges you use in your clinic, you will notice that many formulate a line of products that specifically target the periorbital area. Why is this the case? Is it just a marketing gimmick? The periorbital skin is delicate, with eyelid skin being the thinnest found in the body, measuring on average 0.2mm in thickness.3 For comparison, the skin on the tip of the nose is typically 3.3 times thicker than the upper eyelid skin, and the skin of the brow/ forehead is 2.8 times thicker.4 Its delicate nature, along with its proximity to the eye itself, means that caution must be used when applying topical agents. When we think about the periorbital area, there is a variety of active products found in medical-grade skincare that can help to rejuvenate the area.
I firstly always recommend starting by ensuring that your patient is aware of the impact of ultraviolet (UV) exposure on skin ageing and is taking appropriate steps to protect their skin. Protecting the periocular skin from UV radiation follows the same principles as protecting the rest of the skin, however it is often neglected. This is evident in the burden of skin malignancies seen in this region.7 Many sunscreens may advise against use around the periocular region, especially avoiding contact with the eyes and eyelids for risk of irritation, should the product enter the eye. So, what are our other options and do they work? Over the years, we have become more conscious of protecting our eyes against UV exposure with sunglasses, but do they protect the periocular skin as well? Whilst conclusive evidence standardise what UV protection is advised for eyes,8 in general UV protection sunglasses do provide some protection to the periocular area.9,10 However, the amount of protection will depend on the size of the lens, distance from the face, as well as any reflection or scattered UV. Interestingly, antireflective coatings increase reflection of UV radiation to the eye and periocular skin.8 Advising patients if they are outside in sunny conditions to supplement this protection with other methods such as sunhats can add further protection. I will now explore how products including retinoids, antioxidants, caffeine, growth factors and peptides can be used to actively rejuvenate the area.
small and delicate, so advising patients to apply their product sparingly and gently so as not to stretch the skin too aggressively is key. Repetitive rubbing of the eyelids can damage the thin skin and further reduce its elasticity, leading to excess laxity and wrinkles.6 You will often hear people recommending that patients apply their eye cream with their ring finger; whilst there is no clinical evidence regarding this specifically, the general principle is logical. Applying with your ring finger can limit the amount of
pressure applied and ensure that the area is handled gently. Applying products sparingly will also help prevent excess from entering the eye. Remembering how thin the skin is in this area is also important as you will not need much product to penetrate the skin. Skincare ranges often aim to take into account the small and delicate nature of the periocular skin, producing products in smaller volumes and often with lower concentrations of active products that can cause irritation.
Ophthalmologist Miss Jennifer Doyle explores how to tailor topical skincare to achieve the best results in the delicate
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Retinoids
It has long been known that retinoids can help improve fine lines, wrinkles and photoaged skin.11 A recent prospective study by Park et al. in 2016 looked at the efficacy at treating periorbital wrinkles specifically.12 Participants (n=19) applied 0.1% tretinoin cream each night to the right periorbital area for three months. Outcomes were assessed using digital photography, and blinded evaluation of these were carried out by five independent dermatologists, which found that wrinkles decreased by 21% after 12 weeks. The study compared the improvement in wrinkles from tretinoin use to fractional Er:YAG laser and intense pulsed light (IPL) therapy (treated to the left periorbital area for comparison), and found they all resulted in a similar degree of wrinkle improvement. Participants, when surveyed, indicated that they preferred the tretinoin as it was the most minimally invasive and convenient to use. Interestingly, this is in spite of the fact that seven out of 19 of the participants experienced adverse effects from the tretinoin; including erythema, burning sensation, peeling and pruritis. These symptoms were classed as mild in severity in all and did decrease towards the end of the treatment period.12
With more than 30% experiencing adverse effects from the tretinoin application, this highlights how delicate the skin is in the periorbital area. Studies such as this have contributed to many cosmeceutical companies developing retinoids of a lower strength, such as 0.1%, specifically marketed for use in the periocular area. One can also counsel your patients that as your skin becomes more accustomed to using the retinoid, the adverse effects are less likely;12 gradually increasing the usage of the retinoid can therefore help to minimise adverse effects. It is also important to advise patients to not get any of the product in the eye itself, as retinoids can cause damage to the surface of the eye.13,14
Antioxidants
Vitamin C is an antioxidant that has been shown to not only reduce the appearance of fine lines and wrinkles by promoting collagen formation and scavenging free radicals, but also has a brightening effect on the skin by inhibiting melanogenesis.15 Skin tightness can also be improved, which could be useful with the under-eye area where increased laxity of the skin can lead to a baggy appearance.6 Other antioxidants include vitamin E, vitamin B3 (niacinamide) and green tea, all of which have an antiageing effect by scavenging free radicals. Whilst they are safe to use in the periocular area, dermatitis is a potential side effect, of which the patient should be warned.3
Caffeine
A range of cosmetic, as well as cosmeceutical eye products, contain caffeine but it is rarely found as the main sole ingredient. Have you ever wondered why? It is often claimed that caffeine can reduce puffiness of the under-eye bags. Boaventura et al. reviewed the supporting evidence and found that the clinical studies that evaluated the efficacy of caffeine in the periorbital area were often tested in conjunction with other ingredients (e.g. antioxidants).16 It is therefore difficult to evaluate what effect caffeine alone has on the area and calls for further research to be done to fully evaluate the benefit of topical application to the skin.
Growth factors
There is a wealth of evidence suggesting that growth factors and cytokines have a rejuvenating effect in improving wrinkles and repairing photodamaged skin.17-19 Hussain et al. evaluated their use
in the periorbital area in 2008 and found that periorbital wrinkles improved by 33% on average over a six-month treatment period. They also carried out histological evaluation, which revealed an increased thickness of the epidermis, increased fibrocytes and fibroblasts, and a reduction in elastosis.20 Many other studies support that the use of growth factors in the periorbital area can improve the appearance of wrinkles in the periorbital area.21,22,23 Growth factors have also been used following blepharoplasty and shown to improve the incision scar appearance; this is thought to be due to the role they play in wound healing.24 Mild adverse events, including itching and redness of the skin, have been noted and patients should be warned about this on commencing treatment; these symptoms were found to resolve after discontinuation of the product.14 Ocular irritation has occurred if the cream inadvertently entered the eye, but no long term serious adverse effects have been found.21
Peptides
Topical application of peptides has been shown to rejuvenate the skin by stimulating collagen and elastin production.3 They have even been advocated as a stand-alone treatment for the rejuvenation of the periocular skin.25 Reivitis et al. carried out a prospective study that specifically looked at the periocolar area in 2013, which evaluated the use of a topical treatment containing tripeptide and hexapeptide on 10 patients, twice daily over a 12week period. They carried out evaluations using photography as well as patient questionnaires. After 12 weeks, they found a 41% improvement in periocular wrinkles, a 29% improvement in the under-eye hollows, 48% improvement on the under-eye bags and 39% improvement in dark circles. All patient questionnaires also noted an improvement in skin quality.25 You will note the small number of patients involved in this study, and this is not unusual. Peptide technology is relatively new and as interest grows, more research with larger study numbers are anticipated.
Conclusion
In summary, the periocular skin is delicate and is often one of the first areas to show the signs of ageing. Always ensure that your patients are aware of the impact of UV exposure and are taking appropriate measures to protect their periocular area, as it is often neglected. There is some evidence for the beneficial effect of active products including retinoids, antioxidants, caffeine, growth factors and peptides, but interest and research into the use of these products is always growing. Skincare ranges often have dedicated lines for topical treatments to the eye area, reflecting the different nature of the skin in this area. In general, advising patients to apply products sparingly to the periocular area given its small size and the thinness of the skin is advisable. Being aware that adverse effects may be accentuated in this area due to the delicacy of the skin and advising your patients of such is key. When thinking about active products like retinoids for example, you may find them in a lower strength, and can also advise your patients to gradually increase the frequency of their use to minimise adverse effects. Whichever of these products you choose to recommend to your patients, be aware that they can cause local irritation to the skin, or to the eye itself should it inadvertently enter the eye, and warn your patients of the above. Most adverse effects in the literature are limited to mild irritation, and reversed upon ceasing use of the product, which is also reassuring.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Miss Jennifer Doyle has Bachelor in Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She has complete the Level 7 in Injectables and is a lead trainer at Harley Academy. Miss Doyle currently works as an NHS registrar in ophthalmology, as well as leading her clinic Oxford Aesthetics.
REFERENCES
1. M.G.Neimkin,J.B.Holds Evaluation of eyelid function and aesthetics Facial Plast Surg Clin N Am,24(2016), pp.97-106
2. Chopra K, Calva D, Sosin M et al, (2015) A comprehensive examination of topographic thickness of skin in the human face. Aesthet Surg J Nov;35(8):1007-13
3. Bucay VW, Day D Adjunctive skin care of the brow and periorbital region. Clin Plast Surg. 2013 Jan; 40(1):225-36.
4. Ha RY, Nojima K, Adams WP Jr, Brown SA. Analysis of facial skin thickness: defining the relative thickness index. Plast Reconstr Surg. 2005 May; 115(6):1769-73
5. Looking tired or angry may have more to do with facial aesthetic than how you feel (US: ScienceDaily, 2008) <https://www.sciencedaily.com/releases/2008/05/080528102900.htm>
6. Greco M, Vitagliano T, Fiorillo MA, Ciriaco AG. A new technique of upper eyelid blepharoplasty using the orbicularis muscle flap. Aesthetic Plastic Surgery February 2012, Volume 36, Issue 1, pp 18-22
7. Behar-Cohen F, Baillet G, de Ayguavives T, et al. Ultraviolet damage to the eye revisited: eyesun protection factor (E-SPF®), a new ultraviolet protection label for eyewear.Clin Ophthalmol. 2013;8:87-104.

8. Krutmann J, Behar-Cohen F, Baillet G, de Ayguavives T, Garcia PO, Pena-Garcia P, Reme C, Wolffsohn J. Towards standardisation of UV eye protection: what can be learned from photodermatology. Photodermatology, Photoimmunology & Photomedicine/ Volume 30, Issue 2-3, 08 November 2013
9. Rosenthal, FS,Bakalian, AE,Lou, CQ,Taylor, HR.The effect of sunglasses on ocular exposure to ultraviolet radiation.Am J Public Health1988;78:72–74.
10. Citek, K.Anti reflective coatings reflect ultraviolet radiation.Optometry2008;79:143–148
11. Hubbard B, Unger J, Rohrich R. Reversal of skin aging with topical retinoids. Plast Reconstr Surg 2014;133:4:481e-490e.
12. Park SE, Kim SS, Kim CW, Her Y. A Prospective Split-Face Comparative Study of Periorbital Wrinkle Treatments: Fractional Erbium-Doped Yttrium Aluminum Garnet Laser, Intense Pulsed Light, and Topical 0.1% Tretinoin Cream.Ann Dermatol. 2016;28(5):650-652.
13. Fraunfelder FW. Corneal toxicity from topical ocular and systemic medications. Cornea. 2006 Dec;25(10):1133-8
14. Mukherjee S, Date A, Patravale V, Korting HC, Roeder A, Weindl G. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety.Clin Interv Aging. 2006;1(4):327-48.
15. Pullar JM, Carr AC, Vissers MCM. The Roles of Vitamin C in Skin Health.Nutrients. 2017;9(8):866. Published 2017 Aug 12. doi:10.3390/nu9080866
16. Boaventura, G. Krause L, Queiroz N, Granados C. Cosmetics with caffeine: real benefits versus marketing claims. Cosmetica em Foco, Rio de Janeiro, RJ, Brasil. 2013. <https://s3.amazonaws. com/academia.edu.documents/32227569/254pt.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53 UL3A&Expires=1552338007&Signature=s07HH68WM%2F7hn%2FO2acv0bb3Zopc%3D&resp onse-content-disposition=inline%3B%20filename%3DCosmetics_with_caffeine_real_benefits_ ve.pdf>


17. Fitzpatrick RE, Rostan EF. Reversal of photodamage with topical growth factors: a pilot study.J Cosmet Laser Ther. 2003;5(1):25–34.
18. Ehrlich M, Rao J, Pabby A, Goldman MP. Improvement in the appearance of wrinkles with topical transforming growth factor beta(1) and l-ascorbic acid.Dermatol Surg. 2006;32(5):618–625
19. Werner S, Grose R. Regulation of wound healing by growth factors and cytokines.Physiol Rev. 2003;83(3):835–870.
20. Hussain M, Phelps R, Goldberg DJ. Clinical, histologic, and ultrastructural changes after use of human growth factor and cytokine skin cream for the treatment of skin rejuvenation.J Cosmet Laser Ther. 2008;10(2):104–109.
21. Gold MH, Goldman MP, Biron J. Human growth factor and cytokine skin cream for facial skin rejuvenation as assessed by 3D in vivo optical skin imaging. J Drugs Dermatol. 2007 Oct; 6(10):1018-23.
22. Lupo ML, Cohen JL, Rendon MI. Novel eye cream containing a mixture of human growth factors and cytokines for periorbital skin rejuvenation. Journal of Drugs in Dermatology. 01 Jul 2007, 6(7):725-729
23. Gold MH, Goldman MP, Biron J. Efficacy of novel skin cream containing mixture of human growth factors and cytokines for skin rejuvenation. Journal of drugs in Dermatology. February 2007. Volume 6. Issue 2.
24. Murdock J, Sayed MS, Tavakoli M, Portaliou DM, Lee WW. Safety and efficacy of a growth factor and cytokine-containing topical product in wound healing and incision scar management after upper eyelid blepharoplasty: a prospective split-face study.Clin Ophthalmol. 2016;10:1223-8. Published 2016 Jun 30. doi:10.2147/OPTH.S109517
25. Reivitis A, Karimi K, Griffiths C, Banayan A. A single-center, pilot study evaluating a novel TriHex peptide- and botanical-containing eye treatment compared to baseline. J Cosmet Dermatol 2018 Jun;17(3):467-470.
AESTHETICSJOURNAL.COM VISIT WWW.AESTHETICSJOURNAL.COM TO JOIN FREE TODAY Keep up-to-date with the latest aesthetics developments and best practice guidance on your desktop, tablet or phone Search our Library for a huge range of categorised content and tools relating to your specialism and interests Add training to your personal Training Record for easy reference Complete accredited CPD articles and receive digital certification Advertise and search for job opportunities and clinic equipment for sale in the Marketplace Explore the Aesthetics website
Enhancing Delivery for Skincare Penetration
however, the stratum corneum acts as a rate-limiting step, preventing further penetration.4,9 Once the stratum corneum is crossed, molecules are then able to pass through the layers of the epidermis into the dermis with much greater ease.10
Therapeutic medication and effective cosmeceuticals have been shown to penetrate to deeper layers through two distinct routes:4
The skin is the largest organ in the body and acts as a barrier to chemical, thermal, physical and, at times, biological agents. The skin’s functions include synthesis of vitamins, preventing loss of vital nutrients, excretion of waste products, thermoregulation and an aesthetic evolutionary role.1
Cosmetic procedures that improve the complexion of the skin are highly sought after in aesthetic practices, particularly procedures that improve hydration, pigmentation or reduce erythema, in my experience. The skin is designed to act as a barrier to prevent the movement of molecules from the environment into the body, so pharmaceutical and cosmeceutical products are continually being innovated to improve delivery of the active ingredients through this barrier. It is not only important what active ingredient is delivered into the skin, but how it is delivered and there are a plethora of mechanisms used in the manufacture of cosmeceutical products to improve the concentration below the stratum corneum.2 The use of nanoemulsions, liposomes, nanosomes and nanospheres are just a handful of ways active ingredients are packaged to improve the penetration of products through the skin.3 However, in aesthetic practice, other treatment modalities can be utilised to further increase this skin penetration, with the goal of gaining greater therapeutic effect.4
The epidermis
The epidermis is composed of a stratified squamous epithelium. It contains a number of different cell types, each with specialised barrier functions:
• Langerhans cells have an immune function1,5,6
• Melanocytes produce pigment and reduce the harm of ultraviolet radiation1,4,6
• Merkel cells have a sensory function and form part of the thermoreceptors on the skin, alerting against extremes in temperature, which enables an appropriate somatic and humeral response5
• Keratinocytes are the most popular cell type and contribute to approximately 80% of the epidermis. These cells have the primary function of regenerating the epidermis and their keratin composition aims to maintain the integrity of the epithelium1,7
The epidermis is subdivided into distinct layers, each layer showing progressive patterns of keratinocyte differentiation. The layers of the epidermis from superficial to deep are described in Figure 1 Note that the stratum lucidum is only seen in thick skin such as the hands and feet.6 Whilst each of the layers play an important role in the barrier function, the most significant is the stratum corneum as it is the outermost layer. Some topically-applied solutions can penetrate into deeper layers of the epidermis due to their formulation, such as the use of lipsomes for a delivery system. This enables transport of active ingredients across the stratum corneum.7 For most large molecules,
1. Transappendageal pathways, via the hair follicles and sweat glands
2. Transepidermal through intracellular and intercellular pathways
The dermis is split into two parts: the papillary dermis and the reticular dermis. The dermis houses a network of nerve fibres, blood vessel and connective cells such as fibroblast, elastin and collagen fibres. For cosmeceuticals to have a significant or therapeutic effect, they would need to reach certain end points in the skin. Intrinsic and extrinsic ageing of the skin are multi-factorial processes and all elements of the skin are affected in some way. The central aspect of ageing includes induction of matrix metalloproteinases and production of reactive oxygen species. Cosmeceuticals that are able to overcome these aspects at the epidermal and dermal layers of the skin can be beneficial.11 In 2015, Ali et al. described five mechanisms to enhance penetration of drugs through the skin. The authors classified the methods as follows:10
• Chemical enhancement
• Physical enhancement
• Biochemical enhancement
• Supersaturation enhancement
• Bioconvertable prodrug
In medical aesthetics, whilst there can be a benefit in delivering selected products to deeper layers of the skin, the goal would be to retain product in the skin and to limit systemic delivery and potential side effects of the product. This is the likely reason most aesthetic techniques focus on physical and chemical enhancement. There are a number of procedures that can improve the delivery of topical products deeper into the skin: dermabrasion, lasers, chemical peels, microneedling, and plasma. Note that there are limited studies available on the use of each system for delivering skincare formulations and much of the literature discusses pharmaceutical penetration.
Dr Ifeoma Ejikeme explores the procedures that increase skincare penetration to enhance
Figure 1: The distinct layers of the epidermis6 Keratinocytes Tactile epithelial cell (Merkel cell) Dendritic cell Sensory nerve ending Melanocyte Dermis Stratum basale Stratum spinosum Stratum granulosum Stratum lucidum Stratum corneum Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
results























































































































Follow us:
by
Physical ablation: dermabrasion
Dermabrasion is the process of mechanically exfoliating the skin. The degree of exfoliation would depend on the device used and the force applied, but removal of the entire dermis can be achieved through this method. Microdermabrasion is a modified procedure leading to superficial resurfacing with the resultant reduction or removal of the stratum corneum.12 There are few studies looking at the effectiveness of microdermabrasion as a delivery system. In one small study done by Kim et al in 2016 (p=13), the authors suggested dermabrasion may lead to increased skin permeability via the transappendageal pathway.13 One could hypothesise that if this is effective, it could lead to increased uptake of a topicallyapplied substance. Care must be taken with this approach as there can be deeper epidermal and dermal layers inadvertently removed, leading to complications such as scarring, hyperpigmentation and infection.12 Loesch M. et al describes the use of hydradermabrasion, which has the same indications as microdermabrasion. The authors describe hydradermabrasion may be particularly useful when treating darker skin types and sensitivity in those with dry or mature skin. Hydradermabrasion may overcome the risks of pigmentation and increased sensitivity in mature and sensitive skin.4 A study by Freedman shows hydradermabrasion was used to increase the penetration of antioxidants into the skin in 20 women aged between 34 and 56 years. They were randomised into two groups and had treatments over six weeks. Group A had hydrabermabraion and a polyphenolic antioxidant serum every seven to 10 days. Group B had the serum alone. The results showed Group A had an increase in papillary dermal thickness, epidermal thickness and increase in polyphenolic antioxidant levels in the skin (P<0.01). Group B showed no change in the structure of the skin or antioxidant levels.14
Physical ablation: ablative lasers
Use of ablative lasers has steadily increased over the last 40 years and fractional ablative laser (FAL) has enabled a wider proportion of patients to tolerate this procedure as it is associated with less risks and downtime.4 Ablative fractional laser utilises micro-thermal treatment zones (MTZ) in a grid-like pattern, which penetrate through the epidermis and dermis, while the undamaged adjacent zones enable rapid healing.4 This procedure has been combined with topical treatments to improve and increase drug delivery to the skin, utilising the MTZ to bypass the stratum corneum.4,9 A clinical study by Togsverd-Bo K et al. was done to assess the effectiveness of FAL in increasing the effect of methyl-5-aminolevulinate photodynamic therapy (PDT) on the management of actinic keratosis.11 Patients with actinic keratosis were randomly assigned to receive FAL-PDT or PDT alone. The combined FAL-PDT showed fewer residual actinic keratosis lesions.4 FAL treatment can be augmented to determine the depth of delivery of topical agents by changing the laser settings. Care must be taken as thermal energy generation causes an increase in vascularity and this increases the risk of transdermal drug delivery to the systemic circulation – this should be minimised to reduce the risk of unwanted systemic side effects.4,9 Settings must be carefully monitored, as well as the substance used to reduce risks of systemic effects of the topical agent. When starting out, I advise that aesthetic practitioners opt for mild abrasion and progress with training to more ablative techniques and devices such as FAL. It is important to note that many cosmeceutical preparations are not developed for penetration beyond the stratum corneum, thus preparations must be specifically formulated for use at the intended layer and have appropriate regulatory standards of safety.
Chemical ablation: peels
Chemical peels are one of the most common non-invasive aesthetic procedures. This is a form of chemical exfoliation, leading to a desired layer of cutaneous ablation.15 Historically peels have been classified as:15
• Superficial – epidermal
• Medium – full thickness epidermis into the papillary dermis
• Deep – full thickness epidermis, papillary dermis and mid-reticular dermis
Application of different agents such as glycolic, salicylic, mandelic, trichloroacetic (TCA) peels can be used to partially or fully ablate a specific layer of the skin. This overcomes the uneven ablation of mechanical exfoliation with dermabrasion and carries less downtime than laser ablation. Specific peels can, therefore, be chosen based on indication, patient skin type and patient tolerance.15 Re-epithelialisation takes three to 14 days depending on the depth of the peel.16 As the stratum corneum has been breached, there will be increased permeability of topicals applied post peel.13,15 In my experience, it’s best to wait for re-epithelialisation prior to resuming active products as this procedure does carry a number of risks, including infection and post-inflammatory hyperpigmentation, amongst others.8,16 A chemical peel predictably causes increased skin permeability;10 this allows the practitioner to choose a product that can target the condition causing concern. This carries a caution as a greater percentage of an agent is able to pass through the skin, for example it’s been suggested that 80% of hydrocortisone is able to pass through skin with a disrupted barrier compared to 1% in skin with an intact barrier.10 The practitioner would therefore need to use a product indicated for use below the barrier surface of the skin at the appropriate percentage.
Physical ablation: microneedling
Microneedling has been used to physically bypass the stratum corneum to deliver medicaments to the dermis and the subcutis.16 It has been used as a method to breach the barrier function of the skin and to increase skin permeability.2,17 The literature shows limited, but promising evidence of the use of microneedling as a delivery method for topicals through the skin.2,17 In 2013 Dhurat et al demonstrated the use of microneedling as a drug delivery system for minoxidil in patients with androgenic hair loss.18 The study was a comparative evaluator blinded 12-week study of 100 patients with mild to moderate androgenic hair loss who were randomised to two groups. The treatment group had weekly microneedling with 5% minoxidil placed 24 hours after needling. The control group had minoxidil 5% alone. The results showed a hair count of 91.4 per cm2 in the treatment group compared to 22.2 in the control group (p=0.039). The evaluators and participants also felt greater satisfaction with hair growth in the treatment group.17,18 In 2016 Farid et al. demonstrated the use of microneedling as a delivery system for platelet-rich plasma (PRP) in the management of hair loss in women.2 More studies are needed on which ingredients work effectively with microneedling, as well as a reproducible protocol on how many treatments should be done, needling length for different aesthetic indications, and a protocol for maintenance.
Plasma
Plasma has been described as the fourth state of matter and has been extensively studied for medical applications such as sterilisation and wound healing,8,19,20 as well as being used as a drug delivery system for conditions such as Alzheimer’s disease for improved drug delivery.8
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The use of a plasma jet can ablate parts of the stratum corneum and its use has been extended for non-surgical rejuvenation.8 In cosmetic medicine, further studies are needed to fully assess the ability to maintain topical concentration in the skin and reduce systemic absorption.







Conclusion


The barrier function of the skin is vitally important in maintaining homeostasis, immunity and thermoregulation. When breaching the barrier function of the skin, the most important step is penetration or ablation of the stratum corneum. Whilst treatments to improve the concentration of topical ingredients within the skin can be beneficial, care must be taken by practitioners to ensure the treatment does not increase delivery of the topical product into the systemic circulation which may lead to unwanted side effects. More studies would be welcome in this area to explore the effective penetration of certain skincare formulations with each delivery system.




Dr Ifeoma Ejikeme is a board-certified NHS medical consultant. She trained at Bristol University, and holds a post-doctoral fellowship in head and neck surgery from Columbia University. She has a master’s degree with distinction in aesthetic medicine. Dr Ejikeme is a senior lecturer in aesthetic medicine at Queen Mary’s University and the medical director of Adonia Medical Clinic.

REFERENCES
1. Mackenzie IC. Retroviral transduction of murine epidermal stem cells demonstrates clonal units of epidermal structure. J Invest Dermatol 1997;109; 377–383.

2. Fertig R.M., Gamret A.C., Tosti J.C.A., ‘Microneedling for the treatment of hairloss’ JEADV 2018 (32):564569.

3. Hougeir F.G., Kircik L., ‘A review if deliver systems in cosmetics’ Dermatologic Therapy, 2012 25); 234-237

























4. Loesch M. M., Somani A., et al ‘Skin resurfacing procedures: new and emerging options’ Clinical, Cosmetic and investigational dermatology. 2014 (7): 231-241






5. Irving G. The role of the skin in peripheral neuropathic pain. European Journal of Pain Supplements, 2010:4(2): 157–160








6. Losquadro WD. Anatomy of the Skin and the Pathogenesis of Nonmelanoma Skin Cancer.Facial Plast Surg Clin North Am.2017 Aug;25(3):283-289.

7. MyersS, Navsaria H, Sanders R, Green C, Leigh I.Transplantation of keratinocytes in the treatment of wounds. Am J Surg. 1995:170(1):75–83 8. Shimizu K., Kristof J., ‘Enhancement of percutaneous absorption on skin by plasma drug delivery method’ IntechOpen 2017 (6): 111-136 9. Levin K.M., Juhasz M.L., Maemur E.S., ‘An update on combination treatments with fractional resurfacing lasers’ Curr Derm Rep. 2016 (5): 191-199 10. Ali S., Shabbir M., et al ‘T he Structure of Skin and Transdermal Drug Delivery System- A Review’ Research J. Pharm and Tech 2015 (2): 103-109
11. Kohl, E., Steinbauer J., Landthaler M., ‘Skin Ageing’ J Eur Acad Dermatol Venereol.2011 Aug;25(8):873-84. 12. El-Domyati M., Hosam W., et al ‘Microdermabrasion: a clinical, histometric and histopathological study’ JCD 2016 (15): 4: 503-513 13. Kim S.J., Kang I. J., et al ‘Impact of chemical peeling combined with negative pressure on human skin’ International journal of cosmetic science, 2016 (38):440-443

14. Freedman B.M., ‘Hydradermabrasion: an innovative modality for nonablative facial rejuvenation.’ J Cosmet Dermatol 2008 (7):4: 275-280










15. Soleymani T., Lanoue J., Rahman Z., ‘ A Practical Approach to Chemical Peels’ J Clin Aesthet Dermatol’ 2018 (8): 21-28
16. O’Conner A.A., Lowe P.M., Shumack S., Lim A., ‘Chemical Peels: A review of current Practice’ Australasian Journal of Dermatology 2018 (59) 171-181
17. Kelly Y, Blanco A, Tosti A. ‘Androgenic Alopecia: An update of treatment options Drugs’ 2016 (76): 13491364


18. Dhurat R., Sukesh M. S., Avhad G., et al ‘A randomised Evaluator blinded study of effect of microneedling in androgenic alopecia: A pilot Study’ Int J Trichology 2013:5(1) 6-11

19. Fridman G, Friedman G, Gutsol A, Shekhter A B, Vasilets V N and Fridman A. Applied plasma medicine. Plasma Process. Polym. 2008;5:503–533. DOI: 10.1002/ppap.200700154
20. Ishaq M, Evans M M and Ostrikov K K. Effect of atmospheric gas plasmas on cancer cell signaling. Int. J. Cancer. 2014;134:1517–1528. DOI: 10.1002/ijc.28323
































































































Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
with Juvéderm® VOLUX 1,*
INT/0654/2018. Juvéderm® VOLUX final clinical study report & clinical evaluation report – efficacy and duration data. Oct 2018. 4. Allergan. Data on File. INT/0074/2019. Juvéderm® VOLUX final clinical evaluation report, July 2018. Jan 2019. 5. Raspaldo H etal.JCosmetDermatol. 2010;9:11–15. ©2019 Allergan. All rights reserved. Material developed and produced by Allergan. UK/0203/2019 Date of preparation: April 2019
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk Adverse events should also be reported to Allergan Ltd. UK_Medinfo@allergan.com or 01628 494026.

When you want to define the lower face, there’s a new, structural gel that allows you to
the
and jaw
Juvéderm® VOLUX can restore and create facial volume 1,† in the chin and jaw area for 18–24 months.3,4,‡ Model treated with JUVÉDERM®. Results may vary. * Juvéderm® VOLUX contains lidocaine.1 The addition of lidocaine does not alter the physical properties of JUVÉDERM® products.5 † No available controlled clinical data on the effectiveness and tolerance of Juvéderm® VOLUX injection into anatomic regions other than the chin and jawline. ‡ Based on comparative preclinical testing and results from repeat treatment data, added to Juvéderm® VOLUX clinical study showing duration beyond 18 months after initial treatment or initial + top-up treatment in the chin and jaw, and based on clinical results for Juvéderm® VOLUMA with lidocaine showing 24 month duration in the mid-face establishes Juvéderm® VOLUX as having an
situ
months.4 1. Juvéderm® VOLUX DFU. 72778JR10. Revision 2018-07-26. 2. Allergan. Data on File. INT/0663/2018. Juvéderm® VOLUX final clinical evaluation report. Oct 2018. 3. Allergan. Data on File.
focus on
chin
area.1–3
in
duration of 18–24
A summary of the latest clinical studies
Title: Fractional CO2 Laser Versus Combined Platelet-Rich Plasma and Fractional CO2 Laser in Treatment of Acne Scars
Authors: Galal O, Tawfik AA, et al.
Published: Journal of Cosmetic Dermatology, April 2019
Keywords: CO2 laser, acne, PRP
Abstract: Fractional CO2 laser and platelet-rich plasma (PRP) treatments have been used in the treatment of acne scars. Thirty patients with atrophic acne scar lesions were included in this study. Patients were randomized to receive fractional CO2 laser therapy to one side of the face while the other side of the face was treated with fractional CO2 laser followed by intradermal PRP injection. Follow-up using the skin analysis camera system and photography was done for three months. A dramatic improvement was observed in the scar depth on both sides of the face. However, the combined fractional CO2 laser and PRP showed more significant improvement. Although 70% of our patients were of a dark skin type, no hyperpigmentation was reported. The combined use of fractional CO2 laser and PRP achieved better results. It reduced the downtime of the fractional CO2 laser. The use of the skin analysis camera provided an objective assessment of the results.
Title: The Use of HIFEM Technology in the Treatment of Pelvic Floor Muscles as a Cause of Female Sexual Dysfunction
Authors: Hlavinka TC, Turčan P, and Bader A
Published: Journal of Women’s Health Care, March 2019
Keywords: Pelvic floor, menopause, HIFEM
Abstract: Pelvic Floor Muscles (PFM) supports the pelvic floor organs, control continence and is crucial for adequate genital arousal and attainment of an orgasm. Due to the aging process, post-delivery condition or menopause, the PFM weaken. Therefore, they do not provide sufficient support to pelvic organs, bladder control, and they may negatively affect intimate satisfaction. We aimed to investigate the High-Intensity Focused Electromagnetic (HIFEM) technology for strengthening of PFM in women with impeded sexual functioning. 30 women (average age 36.41 ± 5.62) with limited arousal, ability to achieve orgasm and painful intercourse participated in the study. Patients underwent 6 treatments (28 minutes each) scheduled twice a week. Standardized Female Sexual Function Index (FSFI) questionnaire was used pre-, post-treatment, and at the 3 month follow-up visit. FSFI scores were statistically evaluated through student´s t-test (ɑ=0.05). Subsequently, Pearson correlation coefficient was calculated for sections arousal/lubrication, lubrication/orgasm, orgasm/satisfaction, and pain/desire. The average total FSFI score significantly (p<0.001) increased from 20.06 ± 6.55 to 30.69 ± 7.55 posttreatment and to 30.29 ± 7.37 during the 3-month follow-up. A significant improvement was observed in all FSFI sections. The most significant change at the 3-month follow-up was observed in desire (76%), satisfaction (76%) and orgasm (60%) items. The overall FSFI score was improved in 93% (n=28) of patients post-treatment. All patients (n=30; 100%) showed improvement during the 3-month follow-up. Our initial experience shows that HIFEM technology is a promising method in addressing women’s decreased sexual satisfaction through the strengthening of PFM.
Title: The Efficacy of Ultrasound-guided Selective Botulinum Toxin Type A Therapy for Finger Spasticity Following Stroke
Authors: Furukawa T, Kurihara Y, Masakado Y
Published: The Tokai Journal of Experimental and Clinical Medicine, April 2019
Keywords: Botulinum toxin, spasticity
Abstract: A 64-year-old man had spasticity of digits 3 and 4 of the right hand for 22 years following a stroke. Activities of daily living (ADL) were impaired due to the disuse of the right arm. The flexor digitorum superficialis and flexor digitorum profundus muscles of digits 3 and 4 of the patient’s right forearm were identified using ultrasound guidance, and botulinum toxin type A was selectively injected into those sites. Furthermore, following the injections, occupational therapy was performed for the right arm and fingers, and spasticity was assessed after 2 weeks and at 1, 2, 3, 4, and 5 months. The patient showed improvement in all the evaluations (the Modified Ashworth Scale, Disability Assessment Scale, functional independence measure, active range of motion angle, and movement of holding a cup), and function was maintained throughout the evaluation period. Performing botulinum toxin type A injection under ultrasound guidance to selectively identify the flexor digitorum superficialis and flexor digitorum profundus muscles involved in finger spasticity helped restore finger functioning and improve ADL.
Title: Adjustable Depth Fractional Radiofrequency Combined with Bipolar Radiofrequency: A Minimally Invasive Combination Treatment for Skin Laxity
Authors: Dayan E, Chia C, et al.
Published: Aesthetic Surgery Journal, April 2019
Keywords: Radiofrequency, microneedling Abstract: Increasingly, patients are seeking minimally invasive methods to tighten skin and remodel adipose tissue. A large treatment gap exists among 3 types of patients: (1) the younger demographic, who increasingly desire soft tissue tightening without traditional operations, scars, and downtime; (2) patients with soft tissue laxity who are not “severe enough” to justify an excisional procedure, but not “mild enough” to rely on liposuction with soft tissue contraction alone; and (3) those with recurrent laxity who already underwent traditional excisional procedures. In these populations, plastic surgeons risk under- or overtreating with traditional methods. The purpose of this supplement is to describe the utility of radiofrequency (RF) microneedling (Fractora modified to Morpheus8 InMode Aesthetic Solutions, Lake Forest, CA) in combination with bipolar RF (FaceTite/BodyTite, InMode Aesthetic Solutions). By combining these procedures, the aforementioned treatment gap can be addressed. The RF microneedling allows for subdermal adipose remodeling and skin tightening. Addition of bipolar RF also tightens the skin by contraction of the underlaying fibroseptal network in addition to induction of neocollagenesis, elastogenesis, and angiogenesis at skin surface temperatures of 40° to 50°C. In our experience, these technologies have been effective and safe in these patient populations.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Digital marketing is a huge part of any clinic’s marketing plan and it is estimated that 70-80% of consumers research companies online before visiting or making a purchase.1 But how do you know if your strategy is working? And how would you calculate your return on investment (ROI) effectively? The key word here is ‘investment’. In your personal life you don’t make investments lightly, you do research, speak to lawyers and find people who can help you evaluate risks and predict ROI. So, why then are some so blasé when it comes to investing in marketing? I believe that ROI is one of the most misunderstood metrics in business – which is surprising since it’s a pretty simple ratio. Within this article, I share the approach that I use in my clinic and explain why I believe this is beneficial to implement into other aesthetic settings too.
What is profit?
Profit means net profit. That’s a better measure than gross profit because sometimes in an aesthetic business the overheads can be substantial. Profit does not mean revenue! Revenue is income; the amount you make when you sell something. Gross profit is that number minus the price of the box of filler or the service you’re providing. Net profit is the important number because it includes the overheads such as staff wages, electricity, computers and insurance. And what is left is what you (usually) get to take home. While many digital marketing platforms offer analysis on your gross profit as a result of your investment in their technology, I strongly advise that you do not rely on these for an accurate reflection of your financial position. Instead, I recommend the following approach:
• Get financial clarity and work out your profits for each product. Financial clarity just means understanding how to read a balance sheet and profit and loss statement in order to understand the margins and profits that you make on each thing you sell.
• Verify the figures with your own calculations from your accountant or bookkeeper. I have found that some marketing platforms inflate the figures by giving you gross profit. It’s tricky for them to give a net profit figure because they don’t know all of your costs. From this, I would advise using the gross profit figures from marketing platforms and then calculate what your net profit is by considering your fixed costs, in order to figure out whether that campaign is delivering ROI.
You need to first know how much revenue is required to turn a profit before you can determine how much it should cost you to acquire an asset or a customer. This is called the contribution margin and represents a ‘sweet spot’ revenue level where you begin to make serious inroads into your costs’ base and start making a decent profit.2
Once you have an understanding of your figures, you can better understand what products and treatments are making you money and, as a result, will offer you a better ROI from your digital marketing. You can then make decisions on whether to discontinue or promote certain treatment offerings.
A guide to calculating
I often get asked whether I use a third-party to calculate my ROI in digital marketing or whether I do this in house. At my clinic, we don’t have an accountant prepare our management accounts. I run them off our software, Xero, each month after the bookkeeper has finished reconciling them. The benefit of this is it’s cheaper and quicker so you can have management over accounts every month. I don’t think that there’s any use waiting for your end of year accounts to come in to determine whether campaigns have been profitable; they can sometimes be 12 or 18 months after the event. Speed and agility are key when making marketing decisions. I also look at marketing metrics daily as I believe this allows me to monitor what is and isn’t working well very closely; however, if you are unable to do this daily, or have someone who can, I would say once a week would suffice. I measure the ROI of different
profit
customer Calculating Return on Investment Business analyst Ed Challinor shares his advice on effectively calculating your return on investment in digital marketing Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
You need to first know how much
revenue is required to turn a
before you can determine how much it should cost you to acquire an asset or a
treatment offerings such as botulinum toxin, fillers and energy-based treatments, and analyse the data to find where the optimum levels of performance are. Now onto the calculations, first of all it is essential that you always use net profit in the calculation, as previously discussed. Our framework for calculations is customised to our business but can be adapted for any aesthetics business.
these numbers in excel by just multiplying or dividing the numbers.3 Note, however, how I needed to know important things like conversion rates at booking and during consultation. Without these numbers, a good or bad CPM means nothing. I then use this to forecast future results. I overlay my presumptions about what the market’s doing to overlay a ‘demand’ metric and get a relevant number that forms the basis of our monthly targets. The demand metrics are taken from forecasting based on what happened in previous years and any data I can get from a wide variety of sources.
Understanding the challenges
So, each product category has the below data points assigned to it:
• Net profit margin metric (net profit divided by the investment x 100)
• Referrals metric: the number of referrals that are generated from these treatments. For example, we see lots of lip augmentation patients who like to talk to their friends about their results, so the referral numbers are huge.
• Customer lifetime value: this is how long the patient keeps coming back to the practice. Do you have loyal customers or one-time patients trying you out and then moving onto the next?
• Average cost per acquisition (CPA) from each platform: this means the average cost per acquisition of a patient from each platform. So X amount of people click the ad, X amount visit the website, X amount book an appointment and X amount have the treatment.
I find the more you break things down and the more numbers you look at, the more control you have and things will improve.
I like to take all the verified data points and make them into a simple algorithm in a Microsoft Excel document. So let’s say 10,000 people click on an ad. The clickthrough rate is 1.0% which means that 100 people visit your website. Of those 100 people, 10% call the practice. That’s 10 people. Our front-of-house team book about 50% of the people who call the practice so that’s five appointments. Our clinicians convert 50% of their appointments into treatments so that’s about 2.5 people going ahead and paying. So, it takes 10,000 views to make 2.5 patients. That’s 4,000 impressions of an ad to make a patient. You can get the cost per thousand impressions (CPM) number from any marketing platform and create your forecasting algorithm from
Utilising the tools
I use a range of tools including competitive analysis software like SEM Rush, Alexa (the original Alexa not Amazon’s talking box) and Google Analytics. I also track our calls and web-forms and get heat maps with Hotjar to improve the user experience; all things that impact ROI. I use these products because I find that they are the best for a business of our size, however many others are available. For cold advertising (advertising to people who’ve never heard of you) and re-targeting (advertising to people who’ve recently interacted with your brand), I use landing page builders like Leadpages. This is an app that creates mobile-friendly landing pages to convert patients who are closer to their ZMOT (known as the zero moment of truth; the point in the buying cycle when the consumer researches a product often before the seller knows they exist)4 and are more likely to book treatments. You can build the landing page yourself or choose from pre-made and pre-tested landing pages that have been designed and tested to get leads, convert patients or get the phone ringing. Then you can install a plugin to incorporate them into your website or have them hosted locally by the landing page builder. For example, the URL might be https://www.yoursite.com/ landing-page-botox with the plugin of https:// www.leadpages.yourpage.com/botoxlanding-page

For top-of-funnel users (people who are thinking about products but don’t know what or where they want it) I find that its content and information marketing techniques that work best. While these tools are useful, I think it’s important to note that people can become over-reliant on software, when traditional critical analysis makes the difference for us. Employing someone who is experienced in this field or even investing in some basic training yourself will make a huge difference to your business.
Channels change so we need to change with them. We have a marketing mix at my clinic that includes organic (appearing on page of Google), local (appearing on maps) and paid search (paying for adverts on Google) at the top of the funnel, social retargeting in the middle and then good old-fashioned phone, emails and real-world offline channels at the bottom-of-the funnel. However, there can, of course, be gaps in the data. For example, issues such as anomalies in the data and inexplicable trends can throw you off track. I think these problems can be fixed with experience-based guesswork and extrapolation. If you’re measuring an action from three different angles and one fails, it’s not the end of the world. I get a report every night from the front-of-house team detailing how many patients are booked, whether they were ‘call-ins’ (where the patient calls us) or ‘outbounds’ (where the front-of-house team chase leads by calling people who’ve interacted with our ads). My front-of-house team are an invaluable data source.
Conclusion
To summarise, my key tips for anyone looking to improve how they calculate ROI in digital marketing would be to first of all get financial clarity; without understanding the profit and loss statement and balance sheet of your business you cannot calculate ROI. Then you will be able to design your own system divided into categories and channels based on how much money marketing makes for your business and break it down from there. I believe that digital marketing is going to continue to thrive for small businesses so gaining a clear understanding of exactly what’s working and what’s not will help you to be your most successful yet.
Ed Challinor studied LLB Law at Exeter University and for an LLM Master’s in Corporate Law, being accepted to the Bar in 2006. After six years, he decided to have a career change and founded Smileworks in Liverpool, where he oversees the business, management and marketing. Challinor was shortlisted for the UK Search Awards in 2018 and is a Certified Digital Marketing Professional.
REFERENCES
1. Bluecornona.com, Small Business Digital Marketing Statistics <https://www.bluecorona.com/blog/29-small-business-digitalmarketing-statistics>
2. Acconting tools, Contribution margin, June 2018 <https://www. accountingtools.com/articles/2017/5/16/contribution-margin>
3. Ashe-Edmunds S, What does CPM stand for in advertising?, Small Business Chron < https://smallbusiness.chron.com/cpmstand-advertising-20847.html>
4. Pardot.com, The Zero Moment of Truth: What is it & Why should you care? <https://www.pardot.com/blog/moment-truth-care/>
Profit Investment x100 Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Many practitioners regard media interviews with a sense of dread – there is often a fear of being misquoted or ‘tripped up’ by unforeseen or difficult questions. However, when handled correctly, press interviews can be a key building block of your professional profile, helping boost visibility, showcase your credentials and pave the way to future success. Media training is a critical tool in your arsenal and with some simple preparation you can mitigate the risks of press interviews and build your confidence.
1. Do your homework
Much of the ‘fear factor’ of press interviews revolves around the unknown – what is the journalist going to ask? What if they ask something you’re not prepared for? The key is to mitigate as much of this in advance as possible – preparation and practising your techniques will give you confidence. Don’t be afraid to ask the journalist key information in advance:
• What do they want to talk to you about? Get as much detail as possible on what they’re looking for and what information they already have
• What questions do they plan to ask you? Ask for these on an email so you have a written record and can plan out your responses
• Are they speaking to anyone else? If so, research their backgrounds and anticipate what their angles/points of view might be
• What is the broader context for the interview? It’s always essential to know the broader context within which your opinion is being framed
• What format will the interview take and how long will it be?
Bear in mind, while you can always ask in advance for the planned interview questions, these are unlikely to be ‘set in stone’ and you should expect that the interviewer may take a different approach, or include some different questions on the day. See this as a base to build from and do your prep work around it – rather than relying on a rigid blueprint of what the conversation will entail.
2. Know your audience
Research the publication’s audience demographic so you can adapt your style and make responses relevant. For example, an interview with a journalist who works for a trade
publication will want you to answer using your regular medical terminology, but a consumer magazine journalist will prefer layman’s terms. Consider: what is this audience likely to think and care about or understand? By putting yourself in the audience’s shoes, you will be able to map out additional questions or situations that may emerge during the interview and thereby prepare yourself more effectively, rather than being ‘caught out’ by an unexpected question or angle from the journalist.
3. Hone your messages
There is a critical misconception that you are simply there just to answer questions – but this is not the case! You are there to put across YOUR messages at the same time. As the interviewee, you must ensure you are crystal clear on what your key messages and desired outputs of the interview are. Ask yourself – what do you want the audience to know, understand, remember or do?
For example, this could be educating the audience on the main symptom they should look out for if they are experiencing a certain filler complication, perhaps visit a specific website for more information, or sign up to support a charitable campaign. Keep your key messages short, relevant and repeated – no more than three per interview (irrespective of the interview length) and aim to repeat each message three times (3x3). This technique is far more effective for audience retention than five to 10 individual messages, which only get
interviewee,
interview
Successful Media Interviews PR and communications consultant Julia Kendrick provides her top 10 tips for successful media interviews Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
As the
you must ensure you are crystal clear on what your key messages and desired outputs of the
are
mentioned once and are likely to be forgotten instantly. Equally, I find the journalist is more likely to include your key messages if they are clear and repeated.
4. Master bridging technique
This is the critical tool to get from what you’ve been asked, to what you want to say. This is something usually covered in proper training where you learn to use various ‘bridging phrases’ to move the conversation on from an unhelpful or irrelevant question and allow you to introduce or restate your key messages.1 However, be warned, this does not mean you should ignore a journalist’s question! The key to success is to answer the question factually and briefly – yes or no – then quickly BRIDGE to steer the conversation back to the points you want to make (i.e. your key messages).
Examples of bridging phrases include:
• What’s important to understand here is that…
• The key issue is…
• Let me tell you the facts…
• What really matters to [insert audience] is…
• What we do know is…
• What I can tell you is….
• What my patients tell me is that…
• From my own experience, I can say….
5. Keep calm
During your interview, try to relax. Be confident in yourself and your expertise – this is why you are being interviewed in the first place. Breathe deeply and take your time to answer to the questions – this also helps avoid ‘umming and aahing’. Be aware of your tone – if discussing a contentious issue, or receiving ‘negative’ questions, make sure you respond with a calm, considered approach. Make sure to stop once you’ve answered the question/ delivered your message – silence or ‘dead air’ is the cue for the journalist to ask more questions, don’t feel you have to fill the gap!
6. Body language
This applies regardless of interview format –TV, radio, face-to-face or telephone. Be aware of your body posture, hand movements and facial expressions. You need to portray confidence and authority – so sit comfortably. Remember BBC – bottom in back of chair – and keep movement to a minimum; no jiggling hands or feet! Hand gestures can help you make a point, but don’t overdo it. If you tend to ‘talk with your hands’, try folding
them in your lap as otherwise this can look distracting on camera. Make the interview work for you – try standing up on telephone interviews to feel more confident and help you focus.
7. What not to wear
When undergoing a video interview, try to avoid wearing fussy patterns or small prints such as dog tooth or geometric shapes as these play havoc with the TV cameras. You should avoid green if there is a green screen involved, as the colours will get picked up on the camera and your body will morph into the background. Instead, wear bright singular colours that ‘pop’, or complementary colour tones – avoid black or white as these may drain colour from your face. Make sure your clothes are comfortable as you need to feel confident and smartly turned out. If on camera, avoid bulky or excessive jewellery/ accessories as they will be distracting in regards to the sound, and of course don’t wear anything too short (skirts or trouser legs) – as you may be sat on a low sofa or seat. Make sure your hair isn’t hanging over your face – it will distract you, and the viewers.
8. Getting into your comfort zone
Being comfortable in yourself and your surroundings will help boost your confidence and make for a successful interview experience. To help establish your comfort zone:
• Bring a change of clothing in case of any last-minute accidents
• Get to the studio/venue early to familiarise yourself with the area and calm your nerves
• Don’t forget time needed for hair and makeup on a TV set (even the men)
• Don’t be afraid to ask silly questions – like where the toilets are!
• Make sure you have a glass of water on hand just in case
9. Managing pitfalls
So, what should you do if there is a negative or aggressive question? Remain in control and remember what you are there to talk about and revert back to your three key messages. Keep to your bridging technique – deal with the question quickly – yes or no – then bridge to what you want to say. A key mistake is to repeat negative language, even to disagree, for example:
Journalist: “Is this a disaster?”
Interviewee: “No this isn’t a disaster” All the audience remembers is the word ‘disaster’. Instead, counter by saying, “No I
don’t agree”, “That isn’t accurate” or “That is untrue.”
Importantly, don’t get drawn into speculation as you will likely end up getting tangled. Don’t be afraid to say you don’t know or aren’t able to comment on something as it is not within your area of expertise. Simply bridge to a factual overview such as, “Let me give you the facts...” or “Here’s what I DO know.” Never say, “No comment.” This is a cliché and is likely to make you look evasive or uncooperative.
You should also remember that there’s no such thing as ‘off the record’ and remain focused after the interview ends. The microphones may still be live and you wouldn’t want an unguarded comment to be picked up.
10. Keeping it credible
Lying (whether intentional or not) is the quickest way to destroy your reputation and be blacklisted by press. No journalist will risk their professional integrity if they can’t rely on you – if you make a mistake or speak an untruth, correct it quickly and clearly. Remember your goal – to get your messages across and to make this a success to pave the way for future coverage opportunities!
Conclusion
Press interviews can be a huge opportunity to build your profile and visibility, with potential future successes in terms of clinic revenue and additional media engagements. By taking the time to prepare and mastering some key techniques, such as bridging and key messages, you should be able to handle media interviews competently and confidently.
Julia Kendrick is an awardwinning PR, communications and business strategy consultant with more than 14 years’ experience. She owns Kendrick PR, which recently acquired consumer PR agency EBWPR and she now offers both trade and consumer PR for the beauty, wellbeing and aesthetic medicine industries. Kendrick also created the E.L.I.T.E. Reputation Programme – the industry’s first online PR and marketing training developed specifically for medical aesthetic practitioners.

REFERENCES
1. Brad Phillips, Media Interview Bridging: An Introduction, Mr Media Training, <http://www.mrmediatraining.com/2015/10/19/ media-interview-bridging-an-introduction/>
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
BREAKTHROUGH INNOVATION
Menopause causes accelerated collagen loss and significantly ages the skin. Clinical studies show that low collagen levels result in up to 30% loss of skin’s collagen in the first 5 years of menopause1


Emepelle® featuring MEP Technology® is a new class of cosmeceutical which safely and effectively rejuvenates, restores and rebalances skin affected by menopause. Clinically proven to significantly improve2,3: •

to target accelerated collagen loss and skin ageing caused by menopause.
LAXITY
LINES AND WRINKLES Find out how you can empower your clients to confidently and effectively manage the ageing process of their skin with Emepelle® aestheticare.co.uk/emepelle 0800 0195 322 info@aestheticare.co.uk
DRYNESS • DULLNESS •
•
“At only
weeks over
of participants said that the products alleviated
the skin issues
FEMALE, AGE 60 BEFORE WEEK 8 REFERENCES 1. Archer DF. Postmenopausal skin and oestrogen. Gynecol Endocrinol. 2012;28(suppl 2): 2-6.
2. Draelos ZD. A double-blind randomized pilot study evaluating the safety and efficacy of topical MEP in the facial appearance Improvement of oestrogen deficient females. Drugs
Data on file.
Emepelle Joel Cohen, MD, Board Certified Dermatologist USA, commented:
8
90%
some or all of
associated with menopause3.”
doi:10.3109/09513590.2012.705392.
Dermatol. 2018;17(11):1032-1035. 3.
Recommending Skincare
Hiscock
Clinical modalities can offer outstanding outcomes towards skin health and rejuvenation,1,2 but if patients use non-active skincare in-between visits to your practice, will they ever truly reach their full aesthetic potential? Corrective adjunctive skincare containing retinoids, acids and antioxidants for use at home can contribute significantly to long-term patient outcomes.3,4,5 A dentist wouldn’t advise their patients to avoid brushing in-between biannual check-ups any more than a personal trainer would advise their clients to eat fast food in-between workouts. As skincare professionals, I believe we must be advising our patients to use medical-grade skincare to maintain and gain upon the results we are achieving in-clinic. However, I am regularly hearing that medical professionals find the process of selling skincare awkward, uncomfortable and sometimes even intimidating.
Doctors, nurses and dentists leaving the NHS often report to me that they find it difficult to ask for money in the private sector of medical aesthetics, especially in exchange for skincare. Fear of losing patient trust and professional credibility are among the reasons given, as are ideas that skincare is rather ‘fluffy’. In my experience, common objections to recommending skincare to patients include, “My patients don’t want to be sold to, they just want their toxins” or, “I like my patients so I find it hard to suddenly try and sell to them.”
This article explores how to change your mindset around selling to help your patients achieve their skin goals and to help you build your business potential.

Your patients want skincare
Research indicates that while the global facial injectables market size is valued at USD £6.5 billion,6 skincare sales generated as much as $121 billion.7 Beauty e-commerce generated about $3.8 billion in sales in the US in the past year and in a survey conducted by AT Keary, 28% of 502 shoppers actively researched information online and carried that knowledge with them to stores where it is used to make more informed purchases.8
This shows that patients are seeking advice, so don’t you want to help them? Not only do these figures represent wide-spread desire and need for effective skincare, but also lost opportunities to your business if you are not stocking skincare or optimising your skincare sales. Alongside this, healthcare professionals have a duty of care. It is estimated that there
are 15,400 new cases of melanoma in the UK each year,9 and in 2019 there will be around 96,480 new cases in the US;10 so we need to be promoting daily application of broad-spectrum UVA and UVB sunscreen as a bare minimum. I find that although patients want skincare, they don’t want to be sold to because they feel like they’ve heard it all before. Consumerism is saturated with skincare companies claiming to be ‘antiageing’, ‘clinically proven’ or ‘backed by science’ and many patients are under the impression that they have tried everything, and none of it works. They have no reason to believe that we, or the skincare we are recommending, are any different. This can make patients a little defensive and the consultation process a little challenging. For this very reason, it is no longer powerful enough to simply promote a skincare product as ‘antiageing’ or ‘scientifically backed’ and hope we get ‘lucky’ with a sale. We must sympathise with our patients’ frustration in not seeing the results they were promised and offer them in-depth information about the differences between well marketed high-street skincare and medical-grade topical solutions, which include differing percentages of active ingredients, molecule size, pH and the inclusion of delivery systems, to name but a few.
In the muddled mindfield of information available, it’s our duty to offer patients correct, and more importantly, personalised skincare education. By 2024, the global skincare market is estimated to be worth US $180 billion.8 To avoid the majority of that money being spent on non-active skincare offering nothing more than a pleasant experience, rather than medical-grade topical solutions provided via licensed skin and healthcare professionals, we must act together to give our patients the education they deserve. Let us not be salespeople, but a united information service for the public. Forget sales, get used to educating.
How to ‘educate’ rather than ‘sell’ Firstly, it is vital that you know the value of what you are selling or recommending to your patients and are able to explain it thoroughly, in layman’s terms. You can’t teach what you don’t know intimately, so start learning. Anatomy of healthy skin and the pathology behind common skin conditions such as acne, hyperpigmentation and rosacea should be at the forefront of your mind. There are bountiful books and courses available to deepen your knowledge on
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Clinical educator Victoria
addresses the challenges of skincare retailing and how practitioners can change their mentality around recommending products
PRIMARY QUESTION FIRST FOLLOW-UP QUESTIONS SECOND FOLLOW-UP QUESTIONS
Q 1. When did you first notice your skin condition?
A When I was 25
Q 1.1. Were there any significant changes at that time, pregnancy/ relocation/stress?
A I relocated to England
Q 1.2. What time of year was it?
A December
Q 1.3. Did your skin condition come on quickly or slowly get worse?
A. It got worse over time
Q 2. What skincare do you use in the morning?
A Vitamin C serum
Q 2.1. What is the texture like?
A: Quite creamy
Q 2.2. Do you know the percentage?
A. I think it’s 10%
Q 2.3. Have you noticed it working for you?
A I’m not sure, I don’t really notice it having an effect
cosmetic dermatology if it’s not currently your area of expertise.11,12
If you are already working in partnership with a skincare company, start revising the products and the mechanism of action of their hero ingredients or contact the company for additional education. If you are still looking for the perfect brand for your business, start researching companies and scrutinising their formulas. In either scenario, pick molecules that spark your interest and search Google scholar, NCBI and PubMed for credible clinical studies backing up their efficacy. Through this method of research, you will build knowledge in your products and a portfolio that you believe in and, more importantly, see the value in.
The consultation
Following a structured consultation will keep you on track and guide you through asking the right questions for personalised and effective skincare recommendations in a timely fashion. Don’t enter your consultation with only the pressure to remember all the clinical knowledge and convince your patient to believe your claims. Take in a list of questions, textbooks and medical illustrations, clinical evidence and before and afters. Let the science do the talking for you. You can break down your consultation into three parts: interested investigation, generous education, and comprehensive recommendations.
Part 1: Interested investigation
To avoid feeling like a used car salesperson pushing something our patient doesn’t want or need, we must care about their desires and offer solutions they are willing and
Q 1.1.1. Where did you live before?
A Australia; it was a much sunnier, drier climate
Q 1.1.2. How long did you live there?
A All my life, so 24 years
Q 1.1.3. How soon after your relocation did you notice the changes?
A. Straight away, but it gradually got worse and I became more concerned about it
Q 2.1.1. Do you like the creamy texture?
A. I don’t mind it
Q 2.1.2. Do you like hydrating skincare?
A. Yes, I find that my skin becomes quite dry
Q 2.1.3. Have you tried any other vitamin C products?
A No I haven’t, what should I be looking for?
excited to incorporate into their daily lives. Ask your patients as many questions as you can about their complaints, current routine and lifestyle. This will help you suggest the right products specifically for them. Try and ask three questions for every answer you get until you feel you have gathered adequate information for your assessment (see Table 1 for examples). Not only will this allow you to identify potential causes of skin conditions, it will help you build a picture of what products they like and have time to use. This, in the short-term, allows them to feel heard, and in the long-term ensures patient compliance.
Part 2: Generous education
This education includes general anatomy of healthy skin and the pathology of their skin condition. Educate your patient about the appearance of the visible presentations that they may see on their skin; these might include pustules, hyperpigmentation, redness and telangiectasias. Then talk them through skin physiology; this might mean talking about the sebaceous gland, melanocytes or the demodex mite; again use layman’s terms. At this point, general lifestyle tips are a useful way to help your patients get results. You might talk about cleaning makeup brushes regularly to remove bacteria, staying out of the sun to avoid pigmentation getting worse, or reducing flushing by avoiding hot to cold environments. There are certain ingredients that target these conditions universally, meaning you can offer unbiased information about ingredients like salicylic acid,13 arbutin14 or vitamin C15 without trying to sell a single product.
Once the patient understands what is happening to their skin and what ingredients they need to look out for and avoid, you can then ask them, “Would you like me to talk you through the products I would recommend which contain the correct percentages of these ingredients?” The patient then has the power to say yes, or no. If they say no, don’t take it personally, you have empowered them with the knowledge and any decision they make for their skin moving forward will be an educated one. A comment such as, “I understand, but know that I will be happy to explain this to you if you change your mind in the future,” is a great way to leave the door open.
Part 3: Comprehensive recommendations
If they say yes, you have full permission to move onto part three, during which you can explain individual products in detail, comfortable with the knowledge the patient WANTS the information. At this point, it is important that you are completely selfless with your knowledge. The choice is theirs, not yours. Recommending just one or two products to not seem pushy will only give your patient the option to buy one or two products. Instead, give patients the ability to choose a full programme, rather than potentially limiting their results. A patient using powerful antioxidant15 and broadspectrum sun protection16 in the morning and regenerative retinol17 and acids18 in the evening is more likely to see results than their peer only using a cleanser and one serum. Give the full extent of your recommendation, informing your patient that although a streamlined, budget-focused option is always available, the full programme will yield
Table 1: Examples of potential questions to ask your patient to understand their skincare needs and their hypothetical answers.
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
quicker, measurable results. Explain the cost and its breakdown thoroughly, including initial payment, length of use, and subsequent monthly, weekly and even daily cost. Sometimes a full programme of medical-grade skincare can work out at just £3 per day, so this is a good way to make it viable for the patient.
Don’t talk yourself out of a sale
Every patient has a different skin type, condition, income, willingness to spend and desperation to see change. Stop grouping your patients into one bundle and thinking, ‘they never buy’ and ‘my patient doesn’t want homecare’ and treat each patient like a true individual by taking the time to get to know their history with skincare. You don’t know that your patient isn’t already spending £300+ on a serum, or why they might be spending £2.99 on a supermarket cream. In my experience, patients’ lack of education is guiding their spend, and often they are not making well-educated decisions that optimise their skin health, or will complement the results of in-clinic treatments. Give patients as much information as you can, then let them make an informed, empowered and welleducated decision for themselves.
Victoria Hiscock has been teaching advanced skincare to dermatologists and aesthetic doctors for almost 15 years. She completed her NVQ in beauty therapy 16 years ago, specialising in skin health. She has a passion for cosmetic science and is currently clinical educator and brand spokesperson at skincare company AlumierMD.

REFERENCES
1 Landau M. Chemical Peels. Clinics in Dermatology 2008;26(2):200-208.
2 Laser treatment of photodamaged skin: Rostan EF: Facial Plast Surg.2005 May;21(2):99-109.
3 Kafi R, et al., Improvement of naturally aged skin with vitamin A (retinol). Archives of Dermatology, May 2007;143(5):606-12.
4 Telang PS, Vitamin C in dermatology. Indian Dermatol Online J 2013 Apr-Jun;4(2):143-6.
5 Devasagayam TPA, Tilak JC et al., Free radicals and antioxidants in human health: current status and future prospects..= Journal of Association of Physicians of India 2004;52:794–804.
6 Grand View Research, Facial Injectables Market Analysis By Product (Collagen, Hyaluronic Acid, Botulinum Toxin Type A, Calcium Hydroxylapatite, Polymer Fillers), By Application (Aesthetics, Therapeutics), By Region, And Segment Forecasts, 2018 – 2025. Published 2017.
<https://www.grandviewresearch.com/industry-analysis/facial-injectables-industry>

7 Statista, Size of the Global Skin Care Market from 2012 to 2024. <https://www.statista.com/ statistics/254612/global-skin-care-market-size/>
8 ATKearney, Beauty And The E-Commerce Beast 2017. <https://www.atkearney.com/ communications-media-technology/beauty-and-the-e-commerce-beast>
9 Cancer Research UK, 2015, <https://www.cancerresearchuk.org/health-professional/cancerstatistics/statistics-by-cancer-type/melanoma-skin-cancer#heading-Zero>
10 American Cancer Society. “Cancer Facts and Figures 2018”. Atlanta: American Cancer Society; 2019.
11 M. G. Rubin, N. Y. SchüRer, L. G. Wiest, U. Gout, Illustrated Guide To Chemical Peels, 2014.
12 Leslie Baumann, Cosmetic Dermatology, second edition, 2009.
13 Tasleem Arif, Salicylic acid as a peeling agent: a comprehensive review, Clin Cosmet Investig Dermatol. 2015; 8: 455–461
14 Rashmi Sarkar,Pooja Arora,1andK Vijay Garg, Cosmeceuticals for Hyperpigmentation: What is Available?, J Cutan Aesthet Surg. 2013 Jan-Mar; 6(1): 4–11
15 Rock CL, Jacob RA, Bowen PE, Update on biological characteristics of the antioxidant micronutrient, Vitamin C, Vitamin E and the carotenoids, J Am Diet Assoc. 1996;96:693–702.
16 Reena Rai,Sekar C Shanmuga,andCR Srinivas, Update on Photoprotection. Indian J Dermatol. 2012 Sep-Oct; 57(5): 335–342.
17 Mukherjee S, Date A et al. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging December 2006;1(4)327-48.
18 Smith WP.J, Epidermal and dermal effects of topical lactic acid, Am Acad Dermatol.1996 Sep;35(3 Pt 1):388-9
A Revolution in Skin Bio-revitalisation
IMPORTANT NOTICE
PRX-T33 is a formula protected by Patent manufactured and distributed worldwide by GPQ Srl of Italy, owner of the WiQo and PRX-T33 brands.

In each country we appoint rigorously qualified exclusive distributors who fully understand how to train in the use, store and transport our products.
As the benefits of our products have been quickly recognised we regret that they are being offered by unauthorised traders in several territories. Our Exclusive distributor for the United Kingdom and Ireland is Medical Aesthetic Supplies Ltd. When you order from them you can be sure that you are receiving our product correctly stored and transported. They will also fully support clinics post sale.
Supplies offered from ANY other source may not have been properly acquired, stored or shipped which will affect the efficacy of the product.
GPQ Srl will take vigorous legal action against all non-authorised traders.
GPQ Srl Legal Department
For information about PRX-T33 please contact Medical Aesthetic Group: Unit 3 Compass Point, Ensign Way Hamble, Southampton, Hampshire SO31 4RA
Telephone: 02380 676733 Email: info@magroup.co.uk www.magroup.co.uk
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com PRX-T Half Page Horizontal Aesthetics Journal April 2019 33 % TCA H202
PATENTED
Personalized Body Sculpting: The Next Evolution
Revolutionize your practice with truSculpt® iD, the powerful, noninvasive, body sculpting platform that tailors to patients’ individual needs. Regardless of body or skin type, fat cells are permanently destroyed in as little as one comfortable 15-minute treatment.


More than 10 years into his aesthetics career, it’s fair to say that Dr Xavier Goodarzian has achieved a lot. Whether he is lecturing or training delegates all over the globe or running his aesthetic practice in Southampton, there is one thing that’s clear when talking to this Belgium-born practitioner; he has always had a keen interest and passion for all things skin and topical treatments.
Dr Xavier Goodarzian begins his interview with Aesthetics by emphasising, “Topicals are the baseline; the foundation of great skin and skin health. You can do a lot of toxin and filler treatments, but if the surface of the skin doesn’t look great then that’s the first thing that everyone is going to notice.”
His interest in topical treatments and formulations really started when he studied dermatology during his medical degree, which originally made him consider a career in cosmetic production. That, however, was soon eliminated when Dr Goodarzian realised his love for helping patients.
“I’m a really sociable person and I love making others feel good. Being able to help my patients through the use of aesthetic treatments and skincare is so rewarding. Seeing patients flourish and become confident because of the work I have done is just amazing.”
Dr Goodarzian completed his degree in medicine at the University of Louvain in 2000 and then decided to move to the UK where he undertook his post-graduate degree in clinical dermatology at Queen Mary University of London. It was later that year that Dr Goodarzian attended his first botulinum toxin training course with MediZen and spent the next five years attending several courses and aesthetics-focused conferences, alongside working full-time in general practice. In 2005 he decided to set up his clinic, Xavier G. Clinic in Southampton. A year later he left the NHS and began working in aesthetics full time. Now, teaching and lecturing other practitioners is something that Dr Goodarzian is particularly passionate about. He says, “The first time I started teaching was in 2006 and

I absolutely love this element of my work. When you teach someone it’s great revision for yourself. It’s essential to update and educate yourself constantly, no matter how long you have been in a sector.”
When asked how he incorporates topicals into patients’ treatment protocols, Dr Goodarzian notes that one of the biggest challenges is actually getting patients to recognise their importance, “I always talk to my patients about topicals in their initial consultation and ask what their current routine is at home and how they feel about their skin. It can be a challenge to sell regimes to your patients, but by doing this I am able to understand their needs and advise accordingly. I will begin by introducing one or two key ingredients until they are ready to commit to something a bit stronger,” he explains.
Dr Goodarzian declares that he is no stranger to trying treatments himself; in fact, he encourages all practitioners to undergo aesthetic treatments to help understand the patient journey and experience. He says, “When you are treating patients, you should have some personal experience with not only the products, but the treatments too. I’m not saying that every practitioner should have everything done, but I think you should at least have had botulinum toxin once, know how a filler feels when its injected in the skin so you
can empathise with the pain, or try a chemical peel if you are offering them in your clinic; having first-hand experience of the necessary downtime and how it affects your daily life will benefit your communication with patients.”
Dr Goodarzian believes in this so much that he provides a booklet in the reception area of his clinic featuring images of himself and his staff detailing exactly what procedures they have had and how they make them feel. He says, “I’ve always been very open about everything I’ve had done. In this field, your face is your marketing and you are a walking advertisement for the work that you do. For example, you wouldn’t go to an obese personal trainer or nutritionist, would you? I believe that if you can’t look after yourself, how can people expect you to look after them? As an absolute minimum, you should be looking after your skin.”
Despite his extensive experience, Dr Goodarzian still remains humble when sharing his biggest achievements to date; he says, “Although I have lots of professional achievements, the one thing that mainly sticks out to me is a lot more personal. I came to the UK with £800 and wanted to make something of myself, I wanted to be different. I am comfortable with my own capabilities and knowing that I have achieved what I wanted to achieve is priceless.”
What’s the best piece of career advice that you have ever been given?
A friend of mine, Dr Mark Palmer, who I met on my very first botulinum toxin course said to me, “Stay connected and do not become isolated.” He was also the reason I decided to become a member of the British College of Aesthetic Medicine.
What treatment do you enjoy giving the most?
A full facial volumisation treatment. And of course, chemical peels – that’s my domain!
Do you have a motto that you live by?
To always provide exceptional customer experience. My business partner, Martin MacKenzie, comes from a background in customer service and he has helped to implement extremely high standards within my clinic.
What aspects of your work do you enjoy most?
I love socialising and meeting existing and new friends. Places like the Aesthetics Conference and Exhibition and the Aesthetics Awards, which I attend annually, are perfect places to do this!
“When you teach someone, it’s great revision for yourself”
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Xavier Goodarzian discusses his pathway into the aesthetics specialty and shares his passion for topical products and treatments
The Last Word
Recent figures suggest that for Facebook alone, there are more than 2.32 billion active users per month.1 In a world of smartphones and unwavering WiFi connections, would it be silly not to utilise this 24/7 support network for our own business?
As someone who embraces the power of social media from a personal and business perspective, I have recently observed that the popular forums available to aesthetic practitioners like myself, have lately stopped being a place to share best practice and points for debate. Rather, I believe that for some, they have become somewhat of an emergency helpline.
This article aims to unpick whether social media platforms such as Facebook are an appropriate place to seek advice and guidance in the event of a live clinical emergency; or if the forums are better used as a reflective tool, post-event.
Why use forums?
I fully support the use of forums in a retrospective, reflective way. They are somewhere to share best practice, offer words of support and perhaps consider and debate different approaches for the future. These are all the things you may discuss in a ‘normal’ team environment. Much of the despair associated with the rise of the aesthetic industry does relate to
lone working. As healthcare professionals, we often go from working in relatively large teams – with a variable skill mix – to working alone. It is reasonable to suggest that perhaps this is very detrimental to patient outcomes, especially in an instance where a complication occurs.
As aesthetic practitioners often work in isolation, situations where we do need to ‘bounce’ ideas off one another (as you would in any other role) are missed, which is disheartening, especially in a panic-ridden situation. Further to this, it is sometimes years before even an ‘advanced’ practitioner can experience a ‘true’ complication. For example, many posts on social media forums are regarding severe bruises/ haematomas but the practitioner has worried
that they are a ‘true’ complication such as a vascular occlusion and upon further assessment/advice it is not. Although an advanced practitioner may have a wealth of clinical experience, anyone’s first experience of managing a complication will likely bring doubt, fear and panic. So, would a live, constantly updating forum not be the ideal place to seek immediate reassurance? While the use of forums to ask urgent questions, such as, ‘Can anyone help?
Potential vascular occlusion?’ may ultimately lead to a successful outcome for the patient, is it worth considering whether a practitioner frantically seeking advice from a Facebook forum can lead to a lack of faith and trust in a patient’s chosen practitioner and thus, any future treatment? Additionally, the advice provided on the forums may quite possibly be coming from those who are still relatively inexperienced, or their advice may not be entirely evidence based. Similarly, there is the risk of being given conflicting information from different professionals within the same thread. So, the injector who has originally posted for support and clinical advice may still indeed be left without the information they are seeking.
The argument
Independent accreditation body Save Face recently published its 2017/18 Consumer Complaints Report.2 It found that 934 of 939 total patient complaints and concerns were related to practitioners who were not registered with the body, and 83% of treatments were carried out by nonmedical professionals. I am someone who feels strongly regarding the progression of medical aesthetics to a specialism of its own. I also feel it is perhaps fair to say that any practitioner, regardless of whether or not they are held accountable by a regulating body, should absolutely not be undertaking any treatment where there has not been a sufficient demonstration of practical and
Aesthetic nurse Bethany Hall explores the use of social media forums for seeking professional guidance in the event of a clinical complication
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Is it worth considering whether a practitioner frantically seeking advice from a Facebook forum can lead to a lack of faith and trust in a patient’s chosen practitioner and thus, any future treatment?
theoretical competency in complications management as a part of their professional training. If done effectively – and these skills are maintained – this should enable all injectors to be wholly competent in managing complications, regardless of the outcome. There are also resources available, such as the British Association of Cosmetic Nurses’ (BACN) competency framework that supports practitioners to identify and develop their skills in relation to all aspects of aesthetic nursing.3 Able, knowledgeable, skillful and efficient are all adjectives that often accompany the term ‘competent’. So, the argument is, should someone who considers themselves a ‘competent practitioner’ be able to see all procedures through, despite the outcome, as we would in any other area of nursing or medicine? Is it safe, efficient, and fair to seek advice from (potential) strangers in the event of a problem via a social media forum? I say – no. As stated, I do not condemn the use of social media forums. I do believe that they fit very well into the modern, technology-driven world we have curated. However, there is a specific time and place for their use. Ultimately, this is not during a live clinical complication.
The solution
Preparation. Nobody necessarily wants to be faced with managing any complication, but by ensuring we are adequately prepared and trained in managing adverse events may help stop the requirement for panicked, rushed messages via a Facebook forum. The Aesthetic Complications Expert Group (ACE) has a range of evidencedbased protocols and algorithms for all members to view, and download from its website/forum if desired.4-7 ACE members have access to robust guidance relating to a multitude of events; such as acute infections, oedema and ptosis. These protocols and algorithms also state what to include in any emergency kit, of which every practitioner should have to hand in clinic if relevant to the treatments offered. In recent months, ACE has also developed an emergency helpline, further emphasising the fact that their Facebook forum is not the place for emergency guidance.8 The helpline is for practitioners who need assistance in the management of a complication in progress, who may not have experienced a complication before, or who perhaps usually work alone. This helpline is manned by aesthetic experts, with extensive knowledge and experience in managing a variety of complications.
I believe this is a more appropriate avenue to pursue should you need help managing a complication, rather than a social media forum. Although the protocols and the helpline can be utilised as a great support in a complication situation; it is imperative that this guidance, and others like it, is not solely relied upon as a way of managing complications or as a means of replacing specialist training. They are simply an extra tool in the box, and should be used proactively. There are also other professional groups, such as the BACN9 and the British College of Aesthetic Medicine (BCAM),10 which have resources and services available to help and support their members. The BACN, for example, has local groups that can be utilised to find a local ‘buddy’ that practitioners can seek for assistance with complications. I believe a fellow practitioner who one could call upon to share expertise and knowledge at a time of potential panic is much more useful and appropriate than an unknown practitioner on a social media forum. There are also conferences that you can attend that specifically look at complications, such as the International Association for Prevention of Complications in Aesthetic Medicine (IAPCAM), which is where you can meet and learn from experts who are experienced in managing complications and seek their guidance. Notably, the importance of competent complications management is also being actively encouraged by many leading training companies, pharmacies and aesthetic practitioners – raising awareness and promoting best practice.
As stated, we can continue to utilise social media forums in a reflective manner; encouraging innovative and practical discussion around individual experiences. It is wonderful to see practitioners sharing complication management case studies within the group – in retrospect of the event. It is useful to see how this was managed, what support the practitioner may or may not have sought – and perhaps what they might do differently should a similar situation occur again. This information sharing not only allows the practitioner involved to reflect on their individual practice; it may also encourage other members of the group to identify certain areas within their own skills et that they need to develop further. This professional information sharing is something we can all participate in, and perhaps this proactive type of development is what will ultimately allow us to feel more competent in the eventuality of the live complication.
Summary
Anyone undertaking aesthetic procedures should be sufficiently prepared with evidencebased knowledge and a sufficient stock of the necessary emergency medications to deal with any adverse event. It is not fair on the patient to witness their practitioner seeking advice that is (potentially) not evidence based on a social media forum at a time when they are relying on their practitioner’s professionalism and medical training. We must not rely on these platforms as a safety net for any complication that may arise in our clinic. We must, as registered, accountable practitioners, ensure we are fully prepared with the right training, right support network, right protocols, right medication and right expectations (of our patient). We must do this not only to ensure that our patient is safe, and outcomes are as optimal as can be; but to maintain the credibility of our skill set, our duty of care and ultimately, our medical training.
Bethany Hall is an aesthetic nurse and community prescriber and owns a skincare clinic in Saltaire, West Yorkshire. Hall’s special interest in dermatology has led to previous journal publications on a variety of topics. She is especially interested in preventative and proactive treatment approaches. Hall is an active member of both the BACN and ACE Group.
REFERENCES
1. The Top 20 Valuable Facebook Statistics – Updated January 2019 (Florida: Zephoria, 2019) <https://zephoria.com/top-15valuable-facebook-statistics/>
2. Complaints Report (UK: Save Face, 2019) < https://www. saveface.co.uk/complaints- report/>
3. Benefits (UK: ACE Group, 2019) <http://acegroup.online/ benefits/>
4. An Integrated Career and Competency Framework for Nurses in Aesthetic Medicine, BACN, 2014. <http://www.bacn.org.uk/ content/550fe6a64c2ba0.60466002.pdf>
5. M King & E Davies, 2018, Management of Acute Skin Infections in non-surgical aesthetic practice, ACE Group Guidelines,available to members only.

6. M King, Management of Oedema in non-surgical aesthetic practice, 2018, ACE Group Guidelines,available to members only.
7. M King, Management of Ptosis, ACE Group Guidelines,available to members only.
8. ACE Group launches emergency helpline, Aesthetics, December 2018. <https://aestheticsjournal.com/news/acegroup-launches-emergency-helpline?authed>
9. BACN, Membership benefits, 2019. <https://www.bacn.org.uk/ become-a-member/membership-benefits/>
10. BCAM, Why be a member? 2019. <https://bcam.ac.uk/ membership/why-be-a-member/ >
Reproduced from Aesthetics | Volume 6/Issue 6 - May 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com



M U LTI- AWARD WINNING TRE ATM E N T F OR A WIDE RANG E O F S KIN C O NC E RN S Aesthetic Technology Limited T: 0845 689 1789 E: info@dermaluxled.com derma l ux l ed . co m Contact us for more information or to arrange a free demonstration of our systems AWARD WINNING MANUFACTURER Five-time Winner of Best Treatment at the Aesthetics Awards S t a y Connecte d GLOBAL BEST-SELLING SYSTEM UNIQUE TRI-WAVE TECHNOLOGY POWERFUL STANDA RESU WORLD LEADERS IN LED PHOTOTHERAPY MULTI-AWARD TREATMENT FOR RANGE OF SKIN CONCERNS Aesthetic dermaluxled.com Treatment at the Aesthetic Awards Stay Connected THE MOST ADVANCED PORTABLE LED PHOTOTHERAPY SYSTEM IN THE WORLD CLINICALLY PROVEN WAVELENGTHS MULTIPLE PROTOCOLS CERTIFIED TRAINING STANDALONE RESULTS
‘ABOBOTULINUM TOXIN IN ACTION: KEY PRINCIPLES & TREATMENT FOR GLABELLAR LINES’

IT WILL BE HELD ON MONDAY JUNE 17 AT 7PM.
How do I guarantee my place on ‘Abobotulinum toxin in Action: Key Principles & Treatment for Glabellar Lines’ Webinar’?
1. Visit www.aestheticsjournal.com/ Webinar_GaldermaJune2019
2. Login OR join as a member for free
3. You will then be prompted to use your DocCheck* password to confirm that you are a Doctor, Nurse or Dentist and able to access this webinar (if you registered for the last Aesthetics webinar, your DocCheck account will be valid)
4. Tick the box to confirm that you would like to sign up for the webinar. You’ll then receive reminder emails for the event closer to the time to ensure you don’t miss out!
*What if I don’t have a DocCheck login?
Register with DocCheck for free www.doccheck.com/register
Please note that you will need to provide the following when you have registered your contact details:
- A PDF of your record on the register downloaded from the GMC/NMC/GDC website as appropriate AND proof of ID (passport or driving licence)
- OR your personal certificate from your medical qualification
Your information will be checked and once it has been verified you can then visit the Aesthetics webinar page, use your DocCheck password and confirm you would like to sign up for the webinar by ticking the box. If you have any issues with your DocCheck verification please contact cream@doccheck.com
IMPORTANT: You will need to register and provide proof of your medical qualification to DocCheck by Thursday June 13 in order to guarantee that your registration will be processed in time for access to the webinar
PLEASE LOOK OUT FOR THE NEXT GALDERMA WEBINAR...
Botulinum toxin
are different
on the
Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: In individuals with hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Injections at more frequent intervals/higher doses can increase the risk of antibody formation. Avoid administering different botulinum neurotoxins during the course of treatment with Azzalure. To be used for one single patient treatment only during a single session. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the
ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Lactation & Fertility: Not to be used during pregnancy or lactation. There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies. Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally treatment/injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Eye movement disorder. Rare (≥ 1/10,000 to < 1/1,000): Urticaria. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site disorders (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases). Prescribers should consult the summary of product characteristics in relation to other side effects. Packaging Quantities & Cost: UK 1 Vial Pack (1 x 125u) £64.00 (RRP), 2 Vial Pack (2 x 125u) £128.00 (RRP), IRE 1 Vial Pack (1 x 125u) €93.50, 2 Vial Pack (2 x 125u) €187.05 (RRP) Marketing Authorisation Number: PL 06958/0031 (UK), PA 1613/001/001 (IRE) Legal Category: POM Further Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 Clarendon Road, Watford, Herts. WD17 1DS, UK. Tel: +44 (0) 1923 208950 Fax: +44 (0) 1923 208998 Date of Revision: September 2018
Adverse events should be reported.
For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie. Adverse events should also be reported to Galderma
Ltd.
Date of Preparation: April 2019 Job code: AZZ19-04-0034e
(UK)
Azzalure Prescribing Information (UK & IRE) Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units of reconstituted solution (powder for solution for injection) Indications: Temporary improvement in appearance of moderate to severe: • Glabellar lines seen at maximum frown, and/or • lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient. Dosage & Administration: Azzalure should only be administered by physicians with appropriate qualifications and expertise in this treatment and having the required equipment.
units
depending
medicinal products.
WEBINAR
HEALTHCARE PROFESSIONALS
AESTHETICS
THE NEXT
FOR
HOSTED BY
JOURNAL IN ASSOCIATION WITH GALDERMA WILL BE