



Jordan Faulkner and Dr Marcus Geyer consider anatomy and injection techniques

• Results seen as early as 7 days, lasting up to 4 months in upper facial lines1
• A well characterised safety profile1
• Convenient – no refrigeration needed prior to reconstitution1



Scan the QR code to access BOCOUTURE UK and Ireland Prescribing Information
1.BOCOUTURE Summary of Product Characteristics. Merz Pharmaceuticals GmbH: https://www.medicines.org.uk/emc/product/600/smpc (Last accessed July 2025).

Merz Aesthetics Exchange (MAX) is a promotional website developed and funded by Merz Aesthetics UK & Ireland.
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at https://yellowcard.mhra.gov.uk/. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/reportan-issue. Adverse events should also be reported to Merz Aesthetics UK Ltd by emailing UKdrugsafety@merz.com or calling +44 (0) 333 200 4143.



08 News
The latest product and specialty news
16 News Special: UK Government Announces New Licensing Scheme to Regulate Cosmetic Procedures
Aesthetics explores the Government’s plans to regulate the field and the community’s response
18 Experience the Future of Medical Aesthetics
CCR returns to London this month
25 Special Feature: Improving the Gut Microbiome
Three professionals explore the gut-skin axis
29 Aesthetica: A Trusted Supplier
Aesthetica Solutions provides reliable service, ethical values and a forward-thinking approach
31 CPD: Chin Augmentation with Dermal Fillers
Dr Jordan Faulkner and Dr Marcus Geyer consider anatomy and injection techniques
36 Understanding How Fasting Helps Metabolic Stability
Dr Vix Manning and Dr Charlotte Woodward explore FMD protocols
39 Exploring Emerging Treatment Approaches for AGA
Dr Selina Ahmed provides an introduction to treatment approaches for AGA in men
43 Exploring the Possibilities of Treatment Layering
Dr Ifeoma Ejikeme examines same-day treatment stacking
46 Combining Topical Therapies and Skincare for Rosacea
Dr Sonakshi Khorana discusses combination therapies for rosacea
51 Spotlight On: EXOMIND
A new brain stimulation therapy used to support mental wellbeing
52 Exosomes and the Power of Bio-Pulsing: A New Era in Regenerative Aesthetics
Redefining skin regeneration with precision exosome therapy and advanced bio-pulsing delivery
53 Abstracts
A round-up and summary of useful clinical papers
57 Practising Strategic Leadership to Boost Clinic Success
Marcus Haycock shares how leading strategically boosts clinic success
60 Navigating Patient Dissatisfaction in Aesthetic Practice
Tanya Khan presents strategies on challenging patient interactions
62 Understanding the Lifetime Value in Medical Aesthetics
Rick O’Neill discusses building sustainable growth through patient-centric strategies
65 In Profile: Dr MJ Rowland-Warmann
Dr MJ Rowland-Warmann shares insights into her dental background and recent US innovations
66 The Last Word: Vulvo-Vaginal Treatments
Dr Shirin Lakhani debates specialty progression with vulvo-vaginal treatments

News Special: UK Government Announces New Licensing Scheme
Page 16

Special Feature:
Improving the Gut Microbiome to Transform Aesthetic Outcomes
Page 25







Dr Jordan Faulkner is a cosmetic physician, clinical educator at Interface Aesthetics, brand ambassador for Revanesse and faculty member at DermaFocus. At The Aesthetics Awards 2025, he was the specialty speaker and Rising Star of the Year Winner.
Dr Marcus Geyer is founder of Dr Marc Aesthetics in London, specialises in regenerative, full-face treatments that support skin health, longevity and natural outcomes, integrating evidence-based techniques with lifestyle strategies for sustainable, patient-centered results.
Dr Selina Ahmed is a GP with an extended role in dermatology. As founder and medical director of Dr Selina Clinics in London, she specialises in advanced injectable treatments, regenerative therapies and skin health optimisation, delivering safe, natural results.
Dr Ifeoma Ejikeme graduated from Bristol University and trained at the Imperial College Trust Hospitals in London, before completing a fellowship in head and neck surgery at the University of Columbia.
Dr Vix Manning has clinical experience over general practice and medical aesthetics. Having prescribed GLP-1 and GIP medications for over three and a half years, she has extensive experience managing post-treatment metabolic challenges.
Dr Charlotte Woodward ventured into the world of aesthetics over 20 years ago and now works exclusively in the aesthetics sector. She is the co-founder of River Aesthetics, has been involved in various clinical research and is a trainer/KOL for Sinclair, Mint PDO Threads, Desirial and Vaginal Revolution.
Dr Sonakshi Khorana is a GP specialising in medical and cosmetic dermatology. She is the non-surgical services lead at Kat&Co in Birmingham. She holds memberships at the Royal College of GPs, British Medical Laser Association and Aesthetic Complications Expert (ACE) Group World.

for further information please scan QR code Discover the combined power of: Non-Crosslinked hyaluronic acid (HA) & Glycerol

www.cromapharma.com/uk Info.uk@cromapharma.com Croma Pharma UK cromapharmauk
1) Instructions for use 2) Sulovsky M, Müller D, Prinz V, Moellhoff N, Cajkovsky M, Duschek N, Frank K. A prospective
multicentre study evaluating
tissue filler in the correction of lateral canthal and perioral lines. J Cosmet Dermatol. 2022 Jan;21(1):191-198. doi: 10.1111/jocd.14460. Epub 2021 Sep 24. PMID: 34559948 3) Succi, I. B., Da Silva, R. T. & Orofino-Costa, R. 2012. Rejuvenation of periorbital area:
based
Dermatol Surg,
Data on file

Shannon Kilgariff Editor & Event Director @shannonkilgariff
This month marks a big moment for medical aesthetics in England. After many years of individuals, associations and companies in our sector voicing serious concerns around safety and botched jobs, we finally have clarity from the Department of Health and Social Care that there will be regulation! Our News Special this month runs through all the key updates, with the most notable being that clinics administering fillers and toxin will need to meet strict standards to obtain a licence. Alongside this, only suitably qualified healthcare professionals will be able to deliver high-risk procedures such as Brazilian butt lifts. Read more on p.16, where you can also read about the medical aesthetic community’s response to the latest Government announcement.
From my personal perspective, this response feels long overdue. When I first joined the Aesthetics Journal as a journalist 10 years ago, we were constantly referring back to the 2013 Keogh Review, which warned that “dermal fillers are a crisis waiting to happen.” Sadly, that
concern remains relevant today. While this latest update is certainly a step forward, there are still many questions left unanswered. A further public consultation is expected in early 2026 to determine exactly which procedures will fall under the licensing scheme, so the conversation is far from over.
At CCR this month, regulation and future-proofing the field will take centre stage. Alongside live talks and updates from the JCCP, BAMAN, BCAM and the MHRA, the JCCP will also be hosting a Stakeholder Round Table Meeting (invite only – please contact the JCCP for details). This important discussion will help shape the future of licensing, safety, and next steps in our profession. You can register free for CCR on p.21
Beyond regulation, the September issue of the Journal dives into our Medical Longevity & Wellness theme, with a Special Feature on gut health and its impact on skin, articles on fasting for metabolic stability and the exciting potential of combining exosomes with microneedling for hair loss in men. Don’t miss our inserted Agenda at a Glance and CCR preview inside, including what’s in store at the Medical Longevity Summit on September 25-26.
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Sharon Bennett is the former chair of the British Association of Medical Aesthetic Nurses (BAMAN), UK lead of the BSI committee for aesthetic non-surgical standards and member of the Clinical Advisory Group for the JCCP. She is a trainer and a registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Sharon Bennett, Clinical Lead



Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS, and is an examiner and fellow of the Royal College of Ophthalmologists.
Mr Adrian Richards is a plastic and cosmetic surgeon with over 30 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
PORTFOLIO MANAGEMENT
Shannon Kilgariff • Editor & Event Director
T: 0203 196 4351 | M: 07557 359 257 shannon.kilgariff@easyfairs.com
EDITORIAL
Holly Carver • Deputy Editor & Content Manager
T: 0203 196 4427 | holly.carver@easyfairs.com
Amer Saleh • Journalist | T: 020 3196 4270 amer.saleh@easyfairs.com
Mia Sawyer • Content Writer | T: 020 3196 4242 mia.sawyer@easyfairs.com
Sophia-Fai Roche • Journalist sophia-fai.roche@easyfairs.com
DESIGN
Aimee Bish
• Senior Graphic Designer
Callum Benyon • Junior Graphic Designer



Dr Mayoni Gooneratne (MBBS, BSc, MRCS, MBCAM, AFMCP) was an NHS surgeon before establishing The Clinic by Dr Mayoni and founding Human Health – an initiative combining lifestyle with traditional and functional medicine to provide a ‘cell-up’ regenerative approach to aesthetics. She is also the co-founder of The British College of Functional Medicine.
Jackie Partridge is an independent nurse prescriber. She is the clinical director and owner of Dermal Clinic in Edinburgh and a KOL for Galderma. She holds an MSc in Non-surgical Aesthetic Practice and a BSc in Dermatology. Partridge is a stakeholder group member with Scottish Government/HIS, Honorary BACN member and JCCP Fitness to Practice Nurse.
Dr Souphi Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.
ADVERTISING & SPONSORSHIP
Judith Nowell • Head of Sales
T: 0203 196 4352 | M: 07765 407629
judith.nowell@easyfairs.com
Charlotte Norville • Senior Sales Executive
T: 020 3196 4418 | Charlotte.norville@easyfairs.com
MARKETING
Susana Burguera • Senior Marketing Manager
T: 020 3196 4281 | susana.burguera@easyfairs.com
Ella Carey • Marketing Executive T: 020 3196 4410 | ella.carey@easyfairs.com
Isabell Wise • Marketing Executive T: 020 3793 5845 | isabell.wise@easyfairs.com
If you are interested in contributing to the journal, get in touch...
Email: editorial@aestheticsjournal.com

Dr Sophie Shotter is the founder & medical director of Illuminate Skin Clinic in Kent and Harley Street, London. Her passion is for natural treatments delivered with utmost attention to safety. She works closely with Allergan as part of their UK and International Faculty.

Dr Anjali Mahto is one of the UK’s leading consultant dermatologists. She is a Fellow of the Royal College of Physicians, member of the Royal Society of Medicine and a spokesperson for The British Skin Foundation. In 2023 Dr Mahto opened Self London, a dermatology and lifestyle clinic aimed at managing skin conditions holistically.

Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please email, contact@aestheticsjournal.com
© Copyright 2025 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Follow us on Instagram @aestheticsjournaluk
#Publication
Dr Victoria Manning BM MBCAM
@drvix.manning
Yesterday was a dream come true with the launch of my new book, Busting the Code to Ageing: How to Win the Inflammation Game. I’m thrilled for what lies ahead!

#Training FILLMED UK
@fillmeduk
#Anniversary
British Association of Medical Aesthetic Nurses @bamanurses
Celebrating one year of BAMAN! One year on from our name change, we’re proud to reflect on the progress we’ve made across the medical aesthetics nursing community!
Our first Juvelook & Lenisna training at Church Pharmacy is complete! It’s been brilliant to see so many professionals eager to explore this next -generation approach to collagen biostimulation.

#Socialising
Khatra Paterson
@kp_aesthetics_clinic
A wonderful social event to celebrate the launch of The Nurses Network’s new app, the TNN App!

#Event
Julie Scott @nursejuliescott
An evening of heartfelt conversations, celebrating skin health and collaboration. Congratulations to The Skin Diary team!

Peterborough City Council is investigating ongoing potential botulism cases after individuals have been admitted to hospital with complications.
A small number of people have reportedly experienced difficulty swallowing, blurred or double vision, slurred speech and breathing difficulties, after receiving cosmetic procedures involving botulinum toxin. The investigation follows 38 previously reported botulism cases in the East of England and East Midlands, where patients experienced similar complications after receiving what they believed was botulinum toxin.
Investigations are ongoing; however, the incidents are suspected to involve unlicensed botulinum toxin-like products and are believed to be linked to private practitioners working in their own or patients’ homes, according to the city council.
Andrew Rankin, trustee of the Joint Council for Cosmetic Practitioners (JCCP), said, “The JCCP has made recommendations designed to mitigate risks like these, ranging from supervision requirements by accountable prescribing professionals, to audit requirements in order to evidence the medicine trail from prescription through pharmacy supply to administration and disposal.”
The UK Health Security Agency (UKHSA) and the NHS are working with the council to stop the practitioners linked to the cases from carrying out further procedures.
Social Media
The UK Government has partnered with social media platform TikTok in a bid to tackle the risks of overseas cosmetic procedures.
The campaign is centred around medical influencers, such as midwife Marley Henry and oncology specialst registrar Dr Talvinder Bhogal, making trustworthy online content which raises awareness of potential risks.
Prospective patients are being encouraged via TikTok to speak to a UK doctor before travelling abroad for a procedure, to invest in travel insurance and to avoid package holidays that bundle in procedures. The Foreign, Commonwealth and Development Office has updated its online travel guidance, advising people on how to stay safe when traveling abroad for medical or cosmetic reasons.
Ms Nora Nugent, consultant plastic surgeon and president of the British Association of Aesthetic Plastic Surgeons (BAAPS), said, “Many people research cosmetic surgery via social media particularly Instagram and TikTok nowadays. But it can be difficult to distinguish between glossy marketing and quality information. Medically-focused educational content on the risks of cosmetic tourism can only be a positive step forward.”
The UK’s largest medical aesthetics event, the Clinical Cosmetic Regenerative Congress (CCR), returns to the Excel, London on September 25-26.
The two-day event will focus on evidence-based treatment approaches, emerging technologies and clinical best practices across the specialty.
This year’s congress welcomes a broader portfolio of sponsors, reflecting the sector’s continued growth and continued momentum. BTL Aesthetics has been announced as Registration Sponsor, focusing on its new innovation EXOMIND.
Dermalux will support the Aesthetics Mentoring initiative, aimed at helping professionals build specialty connections. HYPO21 has been confirmed as the official Skin Prep Partner, and Initial Medical returns as Clinical Waste Partner. Aesthetic Complications Expert (ACE) Group World will once again serve as Complications Partner, providing guidance on patient safety, and Quantificare will supply 3D imaging and clinical documentation throughout the venue.
Harley Academy also joins this year as the Getting Started in Aesthetics Partner.
A major addition to this year’s event is the inclusion of the Regenerative Aesthetic Surgery Symposium (RASS), a new agenda stream focused on the latest scientific developments in regenerative and medical aesthetics. InMode has been confirmed as the Lead Sponsor of RASS.
Shannon Kilgariff, editor and event director at Aesthetics, commented, “CCR continues to evolve in step with the specialty it serves. This year, we are not only expanding the content but sharpening its focus. With the inclusion of RASS, we’re aiming to provide a space where meaningful conversations can happen – grounded in research, innovation and real-world practice.”
Turn to p.19 to register for free now.
Healthcare professionals in Scotland have raised concerns about the rising number of men seeking injectable penile rejuvenation procedures.
According to reports from STV News, there has been an increase in unregulated pop-up clinics offering injectable treatments marketed for erectile dysfunction and perceived concerns around size.
The Royal Alexandra Hospital in Paisley has reportedly seen a rise in cases linked to unsafe cosmetic procedures in recent months, according to a source quoted by the Daily Record. One NHS insider described an incident in which a patient was rushed to A&E after a Vaseline-like substance had been injected into his penis, resulting in serious complications. According to The Mirror, the severity of the side effects ultimately required amputation. Healthcare Improvement Scotland (HIS) has confirmed it is reviewing the regulatory framework surrounding these types of procedures. All private aesthetic clinics in Scotland are currently required to be registered with HIS, with more than 500 clinics now listed.
A spokesperson for HIS stated, “Having a cosmetic treatment is a serious undertaking that should only be entered into with due consideration to the very real risks to an individual’s health and safety.”
A recent ITV investigation revealed that half of women who have undergone non-surgical cosmetic procedures required medical assistance afterwards (ITV, 2025)
Out of 2,002 women in the UK, 61% say their self-esteem has been affected by hair loss, but only 13% consulted a trichologist
(Philip Kingsley, 2025)
Intense pulsed light was the UK’s most searched for cosmetic treatment, with more than 2.5 million searches from June 2024-2025
(The Devonshire Clinic, 2025)
5.2 million men in the UK are considering a dermal filler treatment, with the leading age group being 26 34-year-olds (Teoxane, 2025)
Out of 2,007 people across the UK, 31% of respondents admitted they “couldn’t be bothered” to apply sunscreen, while 25% confessed to overexposing themselves in pursuit of a tan
(British Skin Foundation, 2025)
Only 42% of 2,000 women surveyed in the UK feel that their age group is well represented in the skincare specialty (Face The Future, 2025)
18th-19th September 2025
The BAMAN Autumn Conference
25th-26th September 2025
CCR 2025
11th October 2025
BCAM Conference
22nd November 2025
Interface Expo
29th-31st January 2026
IMCAS World Congress
13th-14th March
ACE & Aesthetics Awards
The Advertising Standards Authority (ASA) has released rulings on multiple slimming and supplement adverts.
In August, the ASA upheld five rulings against companies for making unauthorised claims involving GLP-1 production and comparisons with prescription weight-loss drugs. These cases, identified through the ASA’s AI-powered Active Ad Monitoring system, form part of a broader investigation into online food supplement advertising.
In February 2025, supplement company Arrae was among the brands cited in the rulings. Two paid Meta ads for its product described it as an “all-natural Faux-Zempic” and claimed it could reduce body fat, boost metabolism, curb cravings and regulate blood sugar and cholesterol. One video featured testimonials praising weight loss results and appetite suppression, including the claim “It helped quiet food noise for me.”
Isabel Dharmasiri, media relations officer at the ASA, commented, “These rulings make clear that ads must not make unauthorised health, medical or weight-loss claims. Ads can’t claim or imply that a food supplement can impact GLP-1 production or provide other effects associated with prescription-only weight loss medicines.”
Aesthetics reached out to Arrae for a comment but received no response.
Device
Sharon Bennett discusses new Government licensing on LBC Radio
Sharon Bennett, nurse practitioner and clinical lead of the Aesthetics Clinical Advisory Board, appeared on LBC Radio. Following the Government’s announcement proposing a new licensing scheme for non-surgical cosmetic procedures, Bennett stated, “It has been a long time coming. It is a free-for-all when it comes to who can inject and buy in the UK.” She emphasised that in most developed countries, clear legislation already regulates who may administer aesthetic treatments, with Australia’s regulatory update providing a recent example.
Loose Women panel debuts health-focused episode
ITV’s Loose Women aired a themed episode, Loose Doctors, featuring GPs discussing a range of health topics, placing particular emphasis on women’s health. Dr Amir Khan highlighted the importance of vulva health awareness, noting many women delay visiting their GP due to embarrassment. He said, “There is nothing embarrassing about your vulva. Particularly after menopause, any changes must always be checked by your doctor.” Dr Khan, along with Dr Zoe Williams and Dr Nighat Arif, demonstrated how to perform vulva self-examinations, while Dr Hilary Jones encouraged women to feel empowered to seek help.
Aesthetic device company BTL Aesthetics has announced the launch of its EXOMIND device debuting at the Clinical Cosmetic Regenerative Congress (CCR).
The company describes EXOMIND as a non-invasive device, designed to support and improve mental wellbeing. By stimulating key areas of the brain linked to emotional regulation, cognitive function and self-control, EXOMIND aims to enhance neural connectivity and promote overall psychological wellness.
Zbyněk Pišťák, regional manager of BTL Aesthetics UK&I, Baltics & Finland and Jamaica & Malta, commented, “Around 50% of aesthetic patients experience challenges with their mental wellbeing. As a specialty, we’re beginning to recognise the connection between mental health and physical appearance, and the need to support both equally. While most treatments focus purely on the physical, EXOMIND offers a science-backed way to support emotional balance.”Turn to p.51 to read more about EXOMIND.
BTL Aesthetics is exhibiting at CCR this month. Turn to p.19 to register for free now.
Medical Tourism
Cosmetic surgery provider Longevita has published a white paper advocating for the regulation of international medical tourism.
The company claims that many clinics abroad operate without any legal requirements to conduct pre-admission screening, obtain informed consent, perform risk assessments or ensure staff accreditation. The company is calling for the establishment of an independent UK Medical Tourism Accreditation Association to oversee and accredit international providers treating UK patients. Other recommendations in the white paper include mandatory medical tourism insurance, tighter advertising regulations and the development of integrated aftercare pathways within the UK. Kagan Seymenoglu, CEO of Longevita, said, “We cannot continue to let patients be misled into thinking overseas surgery is safe and risk-free. Our proposals will ensure safety, transparency and accountability for patients choosing to go abroad.”
The Aesthetics Awards

Entries are now open for The Aesthetics Awards 2026 – your chance to gain recognition at the most prestigious event in medical aesthetics.
Known as the ‘Oscars of Aesthetics’, The Aesthetics Awards has earned its place as the leading accolade for excellence across the specialty.
The glamorous evening is a unique celebration of innovation, safety and outstanding practice, offering an unparalleled opportunity for practitioners, clinics, teams, companies and service providers to showcase their achievements. With a stringent judging process accredited by an Advanced Trust Mark from the Independent Awards Standards Council, the ceremony highlights only the very best the aesthetics field has to offer.
The Aesthetics Awards is open to both new and established professionals, companies and clinics looking to elevate their profile and stand out in a competitive field. Entries are £190 +VAT and Elite members of Aesthetics can submit entries to as many applicable categories as they wish for free.
Finalists will be announced on January 2, 2026, followed by public voting from January 5 through to February 2. Winners will be revealed during the highly anticipated ceremony on Saturday, March 14, 2026.
Shannon Kilgariff, editor and event director at Aesthetics, commented, “Each year, The Aesthetics Awards continues to raise the bar for excellence in our specialty. It’s more than just a celebration – it’s a powerful platform to recognise those truly driving innovation, safety and ethical practice in medical aesthetics. I can’t wait to see the inspiring entries that come through for 2026.”
Turn to p.19 to read more.
Health and social care secretary Wes Streeting has initiated the annual pay review for doctors in a letter to the Doctors and Dentists Review Body (DDRB).
Mr Streeting outlined in the letter, which was published on July 22, that the Government remains committed to bringing the 2026 to 2027 pay announcements forward, in line with the broader goal of ensuring more timely annual pay processes. This comes two months after the Government backed the DDRB’s advice to award a 4% pay increase for doctors in 2025 to 2026.
In response to the pay increase, the chair of the British Medical Association (BMA) council, Professor Philip Banfield, said, “4% is below the rate of the Retail Price Index inflation – the measure of inflation that reflects real life costs like housing and food – and this means on the current trajectory, most consultants in England will never see their pay fully restored to where it should be, in their working lives.”
The BMA believes the 4% pay award for general practice is “woefully inadequate,” as they believe it has failed to redress historic losses of pay; however, according to digital publication GP Online, doctors’ leaders are expected to welcome the earlier start to the pay review process.
Mr Streeting said, “Public sector workers delivering our vital public services deserve timely pay awards. That is why we are launching this pay round two months earlier than the previous pay round. All pay must be funded from departmental budgets, and there will be no additional funding available for pay settlements.”
A round-up of the latest news and events from the British Association of Medical Aesthetic Nurses
BAMAN AUTUMN
AESTHETIC CONFERENCE
More than 350 nurses will be uniting at the BAMAN Autumn Aesthetics Conference on September 18-19 for two inspiring days of learning, networking and connection. This year’s programme features 24 specialist speakers – including 17 nurses – covering everything from biostimulators and regenerative medicine to intimate health, anatomy, menopause, skincare, lasers and business growth.
We’re thrilled to welcome key stakeholders such as the Nursing and Midwifery Council (NMC) and the Association for Prescribers, along with nine sector-leading sponsors, including our 2025 Headline Sponsor, pharmaceutical company Evolus UK. Alongside live sessions and demonstrations, delegates can explore more than 40 handpicked exhibitors in our biggest-ever exhibition hall, showcasing the latest products and services in the specialism. We truly can’t wait to be back together at the UK’s largest event for medical aesthetic nurses once again. There are only a handful of tickets remaining, so get yours now on the BAMAN events page or scan the QR code below.
Shortly after the Autumn Aesthetic Conference closes, our attention will turn to another major organisation milestone, The BAMAN Awards. Taking place alongside the BAMAN Christmas party on November 14, the Awards will recognise the exceptional contributions being made within our profession, from clinical innovation and patient safety initiatives, to education, mentoring and community engagement.
Open to all BAMAN members, the nomination process has now closed, and the next exciting phase is underway – judging! Our independent panel will be reviewing all submissions over the coming weeks to select our shortlist. The shortlist will be announced in September.
The evening will be an opportunity to celebrate as a community, with a black-tie dinner, canapés, live entertainment and the chance to acknowledge those who have made a significant impact in medical aesthetic nursing this year. The evening is a free event, and exclusive to BAMAN nurses. We can’t wait to see you there.
This column is written and supported by BAMAN

14 March 2026, Hilton Park Lane
Over the last 12 months, have you created incredible results, worked hard at improving patient outcomes and experiences, or contributed to the growth of the aesthetics specialty through research? The Aesthetics Awards 2026 is the perfect opportunity to showcase your achievements and celebrate the best of medical aesthetics.

With entries open now, Winner of the Crown Aesthetics Award for Best Non-surgical Result, Michelle Mclean, provides her advice for getting the most out of the awards. How did winning last year benefit you and your clinic?
The benefits of winning were immediate. Firstly, the recognition brought with it a strong sense of credibility and validation among peers. But more importantly, it allowed my work to reach a wider audience. I’ve since been able to connect with and treat many facial palsy patients who might not have found me otherwise. Colleagues also began reaching out to learning more about treating facial palsy what to consider and when it’s appropriate to treat.
What tips do you have for writing a successful entry?
Speaking as both a past applicant and a judge for The Aesthetics Awards, I can honestly say that preparation is key. My biggest tip would be to start early, don’t leave it to the last minute. Start with a Word document and write down anything and everything that comes to mind for each question – achievements, milestones, team development, patient feedback, case studies, innovation, etc. Make sure that you include supporting documents as it makes a huge difference and gives weight to your entry.
Also, don’t forget to humanise your story. Judges connect with purpose, passion and impact, not just numbers and statistics. Let your values and team ethos shine through!
Why are the Awards so important for the specialty?
Aesthetics can sometimes feel like an isolated journey. It feels like we’re heads down, focused on treating patients and managing a business. The Aesthetics Awards provide an opportunity to pause, reflect and celebrate the collective progress we’re making as a specialty.
From a team perspective, it’s brilliant for morale. Whether you’re shortlisted or you win, just being part of the event gives everyone a sense of pride and community.
Entries to The Aesthetics Awards close on October 20 – head to the website to enter.
The Joint Council for Cosmetic Practitioners (JCCP) and the British Association of Aesthetic Plastic Surgeons (BAAPS) has announced a collaboration aiming to enhance patient safety.
The JCCP outlined its plans to collaborate with BAAPS to codesign and improve practice standards and guidance for invasive non-surgical procedures. These include complex clinical techniques such as intravenous lines, minor surgical interventions and guided ultrasound.
Professor David Sines, executive chair of the JCCP, commented, “The JCCP is delighted and privileged to be working in formal partnership with BAAPS to codesign evidence-based standards of clinical excellence in both the surgical and non-surgical aesthetic sectors in the UK. We very much look forward to working together to inform best practice standards as part of the UK and Scottish Government’s forthcoming regulatory and licensing schemes.”
The JCCP is hosting a regulation roundtable at CCR this month, by invite only. Contact the JCCP for more details.
Wellness Programme
Healthcare platform MAP Health is launching at the Medical Longevity Summit (MLS), part of the Clinical Cosmetic Regenerative Congress (CCR).
MAP Health is a data-focused platform designed to help clinics deliver personalised, holistic skin health solutions to their patients. By integrating genetic insights, blood tests and lifestyle data, it creates tailored action plans covering skincare, nutrition, supplements, sleep and lifestyle, the company shares. Andrew Melton, co-founder of MAP Health and managing director of Glow Strategy Group, commented, “We believe the UK medical aesthetics specialty is ready to grow beyond injectables and skincare, and into a new era of wellness and longevity. MAP Health allows clinics to launch their own medical wellness programme.”
MAP Health is exhibiting at CCR this month. Turn to p.19 to register for free now.
Medicine Authenticator
The Medicines and Healthcare products Regulatory Agency (MHRA) has released a new function called the Medicines Website Checker (MWC). The new feature allows the public to access a searchable database that lists fraudulent websites known to be selling, or offering to sell, medicines illegally. Among the listed sites are those offering authentic products without adhering to legal requirements, such as selling prescription-only medicines without a valid prescription.
Andy Morling, head of the MHRA’s Criminal Enforcement Unit, said, “MWC is a new public service designed to help people stay safe when buying medicines online. The service also links directly to a new e-reporting tool, and signposts to resources like the MHRA’s long-running Fake Meds campaign. This phased launch ensures the MWC is tested, refined and fully effective before being more widely promoted.”
The MHRA is exhibiting at CCR this month. Turn to p.19 to register

Skincare company Medik8 has launched a new Advanced Pro Collagen+ Peptide Cream.
Available through aesthetic distributor Healthxchange, Medik8 shares that key ingredients include sh-Oligopeptide-1, Nicotinamide Adenine Dinucleotide and Carnosine. The company explains that the formulation of these ingredients aims to improve the skin’s structure, delay visible signs of ageing and boost collagen, elastin and hyaluronic acid levels.
Daniel Isaacs, Medik8’s chief product officer and founding partner, said, “We engineered this formula for multi-faceted support to help enhance and preserve collagen reserves, promoting an environment where collagen in the skin thrives; for a naturally rejuvenated and healthy looking complexion with less visible lines and wrinkles.”
Healthxchange is exhibiting at CCR this month. Turn to p.19 to register for free now.
Laser Device

Aesthetic device company Sciton has unveiled a new laser hair removal device.
According to the company, the OMNI contains 5,000W of power and has multiple wavelength options, including 760 nm, an 810/940 nm blend and 1060 nm, along with various spot sizes and treatment modes.
Sciton adds that the device also includes integrated contact cooling that helps to maintain patient comfort.
Sciton key opinion leader and physician Dr Dianne Quibell, said, “OMNI by Sciton allows us to choose the right wavelength for the skin types and tones we treat, with so many customisable options. With two handpieces connected at once, we can easily switch between small and large spot sizes, making treatments not only fast and effective but also efficient.”
Sciton is exhibiting at CCR this month. Turn to p.19 to register for free now.
Portfolio Growth
Aesthetic distributor Eden Aesthetics has announced the expansion of its JetPeel range with the introduction of JetCare Med.

According to the company, the range is a series of osmolyte-enriched infusions for in-clinic use. The collection comprises four targeted treatments and one booster, each containing over 5.5% osmolytes, aiming to support collagen and elastin production. Delivered via JetPeel’s MDJet handpiece in pre-filled 5ml syringes, the range addresses skin concerns including firmness, elasticity and radiance, the company shares. Key ingredients include betaine, xylitol, inositol and propanediol, selected for their potential roles in supporting hydration, barrier-strengthening and rejuvenating properties.
Lindsay Gray, managing director at Eden Aesthetics, commented, “We’re excited to offer JetCare Med to our practitioners as an extension of the JetPeel range. The range of infusions allow practitioners to target specific skin concerns, while also invigorating collagen and elastin.”
Digital Platform
Collaborative organisation The Nurses Network (TNN) has launched a membership-based app for the medical aesthetics specialty.
The UK-based app reportedly offers tailored support for prospective members at every stage of their aesthetics career. According to TNN, the platform provides users with access to on-demand learning, business training, exclusive resources and discounts, all available 24/7.
Reportedly, one standout feature of the app is its comprehensive calendar, which displays all major events in the aesthetics field, alongside TNN-hosted events. Another popular element among members is the built-in leadership points system – a gamified feature that rewards users for active learning and engagement within the app, TNN shares.
Nurse prescriber Kate Monteith-Ross, said, “TNN is a fully inclusive hub for medical injectors, a supportive community across the UK, regardless of experience. For just £35 a month, members can gain access to training, events, business mentorship and direct guidance from our directors whilst even being rewarded for their learning on our new app. Together, we’ll navigate the specialty, ensuring safety, competency and growth for every injector whilst having fun on the way.”
The Nurses Network is exhibiting at CCR this month. Turn to p.19 to register now.


Skincare company AlumierMD has released its new HydraRescue Biocellulose Face Mask.
The company shares that the mask is made with ultrafine cellulose fibres, and powered by sodium hyaluronate, niacinamide and AlumierMD’s biocellulose technology. It is reportedly soaked in a concentrated serum comprising sodium hyaluronate, pyrococcus extract, bisabolol and a microalgae.
Mr Ash Soni, plastic surgeon and global key opinion leader for AlumierMD, commented, “The mask forms a gel-like texture when you place it on your face, which really feels almost like a second skin. I tried the mask for the first time during a flight and was really impressed by its performance. It’s absolutely incredible; even after 15 minutes, it still had so much more to give.”
UK training provider Harley Academy Limited has attained SkinViva Training Academy in Manchester.
The campus is expected to be fully operational from October 2025, offering aesthetics courses that include an Ofqual-regulated qualification, a Level 7 Diploma in cosmetic injectables and cosmetic dermatology programmes.
Dr Tristan Mehta, founder and CEO of Harley Academy, commented, “SkinViva Training Academy has played an important role in the development of aesthetic practitioners in the North. We’re excited to build on that foundation by bringing Harley Academy’s fully JCCP-approved, Level 7 Diploma aesthetics courses and more to the region.”
Getting Started in Aesthetics Partner Harley Academy is exhibiting at CCR this month. Turn to p.19 to register for free now.
A round up of the latest aesthetic clinics opening across the UK
Aesthetic practitioner Dr Adaugo Onyeador officially opened Line & Lift Aesthetic Clinic in Soho, London on July 18. The clinic offers botulinum toxin, skin consultations and polynucleotide treatments. Dr Onyeador commented, “I’m super excited to be using my surgical
Aesthetic manufacturer mesoestetic UK has appointed Wendy Rogers as the new head of training.
The company shares that Rogers has more than 30 years of experience, spanning clinical education, practitioner development and leadership of national training programmes, as well as a specialist understanding of the hyaluronic acid filler market.
Stephen Schofield, commercial director at mesoestetic UK, added, “Rogers’ appointment reflects mesoestetic UK’s continued investment in excellence, education and innovation within medical aesthetics. With the recent launch of our first two mesofiller nexha dermal fillers, Rogers will be pivotal in delivering the high-quality training and support we’re committed to providing our customers.”
Pharmaceutical company Galderma has released data from a clinical trial evaluating the effectiveness of injectable treatments for facial volume loss.
Galderma investigated the aesthetic outcomes and appearance of Restylane Lyft or Volyme in combination with Sculptra for cheek or jawline augmentation, and correction of contour deficiencies in patients experiencing facial volume loss associated with medication-driven weight loss. The nine-month phase IV clinical trial consisted of 41 participants, 39 female, aged 32 to 79 – with 35 completing the full trial. The trial used the SHAPE Up Holistic Individualised Treatment (HIT) and improvements were measured using bioinstrumentation tools, including a corneometer.
According to Galderma, Restylane was found to improve skin hydration by a peak of 41.52% at month five, with a significant improvement of 32.9% maintained at month nine. Sculptra was observed improving skin radiance by a peak of 16.65% at month seven, sustaining a significant 15.85% improvement at month nine. Clinical trial investigator and plastic surgeon Mr Paul Lorenc said, “The improvements we observed with Sculptra and Restylane at nine months are hugely encouraging and represent a meaningful step forward in addressing the most predominant aesthetic concerns of patients along their weight loss journey.”
Galderma is exhibiting as Headline Sponsor at CCR this month. Turn to p.19 to register for free now.
experience and specialty knowledge to provide aesthetic services for patients in Soho.”
General practitioner Dr Libby Artingstall and Rob Artingstall, head physiotherapist at England Rugby League, are set to open Projuvenate this September in Manchester. The clinic will debut the newly launched BTL EXOMIND, offering a combination of non-invasive aesthetic wellness treatments, physiotherapy
services and science-backed health optimisation therapies.
Independent nurse prescriber Leah Cooke has announced the launch of a new clinic, Glowing by Leah, located in Stroud, Gloucestershire. The clinic opened on August 19 and offers services such as botulinum toxin, dermal fillers, polynucleotides and skin boosters.
If you’re opening a new UK clinic soon, let us know at editorial@aestheticsjournal.com

Skincare company The Skin Diary invited press and practitioners to celebrate the launch of the Age Defence Moisturising Day Cream at Jeru, Mayfair. Guests gathered for a drinks reception and a sit-down dinner, chaired by independent nurse prescriber and strategic advisor for The Skin Diary, Julie Scott, who also serves as the brand’s key opinion leader.
Presentations were delivered from Dr Clare Kiely, consultant dermatologist and co-founder of The Skin Diary, and Dr Tamara Griffiths, consultant dermatologist and head of product innovation at The Skin Diary. Dr Beibei Du-Harpur, consultant dermatologist and lead science educator, then shared insights into skin ageing and The Skin Diary’s gene expression research.
Dr Kiely commented, “The launch event was an opportunity to bring together specialty colleagues to share the rigorous research that shaped this formulation. Our aim was to take guests on the full journey from the molecular pathways of skin ageing, to the formulation decisions that make Age Defence unique. The evening sparked valuable conversations, deepened understanding of DNA repair and epigenetic science and reinforced our commitment to creating products that are truly proven by science.”
Intelligence
Patient booking software company Zenoti has introduced its latest digital platform, HyperConnect.
According to Zenoti, the system uses artificial intelligence technology to capture details from patient interactions and present them on a central dashboard, helping staff personalise care, track service history and respond quickly to patient needs.
Geraldine Fusciardi, Zenoti senior vice president for Europe, commented, “Designed to slot effortlessly into any business, HyperConnect makes every interaction feel personal, remembered and effortless. With AI-powered insights, smart automation and a complete view of each patient’s journey, your team can anticipate needs, create moments of delight and turn every visit into a lasting relationship.”
Zenoti is exhibiting at CCR this month. Turn to p.19 to register now.
Product Launch
Skincare solution brand CACI has launched the Infusion Atomiser handset and the Skin Revive Infusion Serum with plant polydeoxyribonucleotide (PDRN).
According to the company, the handset and infusion serum work in tandem to optimise product penetration, without the use of a needle, to improve skin quality and enhance skin regeneration and repair.
CACI shares that the Infusion Atomiser handset combines electro infusion, ultrasonic atomisation and LED therapy. Electro infusion delivers short, high-voltage electrical pulses; ultrasonic atomisation breaks the serum into nano-sized molecules; and LED therapy offers a choice of red, blue, or dual red/blue high-powered LEDs to stimulate and rejuvenate skin cells, according to the company.
CACI’s managing director, Dean Nathanson, said, “By integrating advanced transdermal delivery technology with a powerful, vegan-friendly regenerative serum, this new system delivers results comparable to injectable polynucleotides – without the needles or downtime. It’s a game-changer for patients seeking clinical-grade skin repair, hydration and antiageing benefits in a comfortable, bespoke treatment.”
The British College of Aesthetic Medicine (BCAM) has published a new mission statement. According to BCAM, the update reflects the company’s commitment to supporting medical professionals, driving the highest standards of practice and safeguarding the wellbeing of patients across the UK. BCAM’s board of trustees said, “Our refreshed mission statement reaffirms our promise to champion clinical excellence, raise specialty benchmarks and place patient safety at the heart of everything we do.”
Sensilis unveils new retinol product
Skincare company and manufacturer Sensilis has launched the Retinol Body Treatment. The company shares that the new lotion, designed for sensitive skin, contains 1.65% retinyl palmitate, encapsulated in lipsomes, which reportedly provides better absorption. The lotion works deep within the skin to stimulate collagen and elastin, helping to improve firmness, elasticity and overall skin resilience, according to Sensilis.
AestheticSource names KOL trainers for SuneKOS
Aesthetic distribution company
AestheticSource has announced general practitioner Dr Raj Dhillon and aesthetic practitioner Dr Javed Hussain as key opinion leader trainers for SuneKOS. Dr Dhillon and Dr Hussain will oversee clinical education and certification for SuneKOS injectable treatments, deliver hands-on training and ensure regulatory compliance. Lorna Bowes, CEO of AestheticSource, said, “Their expertise and passion for patient safety, teaching and mentoring will be invaluable in supporting practitioners and representing the SuneKOS brand.”
REVIV announces IV therapy memberships
Global wellness provider REVIV has introduced IV therapy memberships to the UK. The memberships offer a range of monthly treatments that include HELIIX, Miniboost and Vitaglow drips and a variety of intramuscular injections (IM) of vitamins. Luke Mills, global collaboration and partnerships director at REVIV, said, “Our patients are no longer looking for one-off treatments, they want a long-term wellness plan. Memberships are our answer, offering structure, value and consistency in a fast-growing longevity space. It’s how REVIV evolves from a treatment provider into a true partner in our customers’ proactive, personalised health journeys.”
Aesthetics explores the Government’s plans to regulate the field and the community’s response
The Department of Health and Social Care (DHSC) has confirmed plans to introduce a national licensing scheme for non-surgical cosmetic procedures in England.1,2
Announced on August 7, 2025, the aim is to establish consistent standards across the aesthetics sector and improve patient safety across England.1,2 The Government notes that the new regulations will be subject to public consultation and parliamentary scrutiny before being introduced.1,2
This announcement follows a comprehensive public consultation conducted in 2023, which garnered nearly 12,000 responses from a wide range of stakeholders, including members of the public, specialty professionals and regulatory bodies.1,3 The consultation revealed overwhelming support for tighter regulation within the aesthetics sector, reflecting widespread concerns over patient safety, unregulated and unlicensed practitioners and inconsistent standards of care.1,3
Professionals within the field believe a significant factor influencing the regulatory update was the death of Alice Webb in September 2024.1,4 The 33-year-old mother of five passed away at Gloucestershire Royal Hospital after undergoing a non-surgical Brazilian butt lift (BBL) procedure performed by a non-healthcare professional (HCP).4 Webb’s death led to new guidelines issued by the Joint Council for Cosmetic Practitioners (JCCP), the Chartered Institute of Environmental Health (CIEH) and the British Beauty Council, but further measures were called for to enhance patient protection and safety.5 Currently, there are no mandatory licensing requirements for individuals offering procedures such as botulinum toxin, dermal fillers or other aesthetic treatments, unless the treatment involves a surgical procedure or is carried out by a HCP in a regulated setting.1,2 This has led to variation in practitioner qualifications and oversight, particularly for higher-risk procedures.
This regulatory update follows the Scottish Government’s recent proposals in June 2025, following the December 2024 consultation.6 Key developments following the consultation include plans to introduce a licensing regime for higher-risk procedures delivered by non-HCPs in England.6
The proposed framework would mandate that practitioners offering high-risk procedures, such as the non-surgical BBL, thread lifting procedures and hair restoration surgery, will need to be qualified HCPs operating from Care Quality Commission (CQC)-registered premises.1
The initial consultation outlined a traffic-light tiered system: green-light procedures, such as microneedling and non-ablative laser hair removal; amber-light procedures, including botulinum toxin injections and dermal fillers; and red-light procedures involving augmentation of the breast, genitals or buttocks, as well as hair restoration surgery.1 The recent Government announcement specified lower-risk treatments, including botulinum toxin, lip filler and facial dermal fillers, will come under stricter oversight through a new local authority licensing scheme, requiring practitioners to be licensed by local authorities and meet strict hygiene, training and insurance standards.1
Once regulations are introduced, practitioners who breach the rules on the highest risk procedures will be subject to CQC enforcement and financial penalties.1
The Government has not mandated that lower-risk cosmetic procedures be performed exclusively by HCPs; under the new licensing scheme, such treatments may still be carried out by licensed non-HCPs, subject to defined standards and, for certain procedures, oversight requirements.1
According to the Government, priority will be given to introducing regulations to restrict the highest-risk procedures first – such as the injection of fillers into the breasts and genitals.1 A public consultation will be published early next
year to gather views on the range of procedures that should be included in these restrictions.1
The legislation will also introduce age restrictions for certain procedures for individuals under the age of 18, unless authorised by a HCP, and grant enforcement powers to local authorities and the CQC.1 Providers who fail to comply may face penalties or be banned from practising.1
Discussing the new regulatory update, Amy Bird, nurse prescriber and chair of the British Association of Medical Aesthetic Nurses (BAMAN), points out the benefit the new scheme may have for patient safety. She says, “For patients, it would mean greater transparency – clear evidence of a practitioner’s qualifications, regulatory status and adherence to safety protocols –so they can make safe, informed choices.”
Acknowledging the serious consequences of insufficient regulation, Professor David Sines, executive chair of the JCCP, explains, “The number of new practitioners entering the field has increased, with many lacking adequate training. This has resulted in high-profile cases in which patients have suffered physical and psychological harm due to a lack of training.” Professor Sines elaborates, “While such cases are not representative of the sector as a whole, they underscore the need to eliminate unwarranted variation and ensure consistently safe, effective clinical experiences for the public.”
The Irish College of Aesthetic Medicine (ICAM) also demonstrates support, stating, “ICAM welcomes any progress towards stronger regulation of the aesthetics sector. We commend the hard work and determination of our sister organisation, the British College of Aesthetic Medicine (BCAM), and urge the Irish Government and relevant regulatory bodies to go beyond incremental change and move toward comprehensive reform.”
Having practiced aesthetics for more than 30 years across England and Ireland, aesthetic practitioner Dr Patrick Treacy views it as an opportunity to elevate standards. He explains, “The proposed licensing scheme has the potential to elevate standards by mandating practitioner qualifications, hygiene protocols and indemnity insurance, addressing the current lack of oversight in England’s aesthetics sector.”
While greater regulation within the specialty is widely recognised as beneficial, the new Government licensing
“We believe that the Government’s decision will not only help to bring the clarity, protection and regulation that we have been campaigning for, but will reassure patients navigating our specialty. In recent years, the lack of regulation has resulted in patients being exposed to unnecessary risk and danger when booking procedures of this nature, and we hope that what follows in legislation will help to mitigate those risks.”
Lesley Blair, CEO and chair of The British Association of Beauty Therapy and Cosmetology (BABTAC)
scheme has been met with caution by the wider community. Nurse prescriber and clinical lead of the Aesthetics Clinical Advisory Board Sharon Bennett comments, “This legislation is not, and should not be, focused solely on preventing non-medical practitioners from performing injectable BBLs, despite the media emphasis on this point.” Bennett continues, “The consultation and subsequent response suggest that the Government has not yet developed a nuanced understanding of medical aesthetics, continuing to categorise treatments as purely ‘cosmetic’ rather than recognising their clinical or medical dimensions. This gap in knowledge is concerning, and could negatively impact the final legislative outcome.” Bennett concludes, “Once legislation is enacted, it becomes difficult to amend and carries the risk of being expedited without informed consideration. Frequent ministerial changes, budgetary constraints and limited specialist insight further exacerbate this concern.”
After sharing his views on social media, aesthetic practitioner Dr Steven Land told Aesthetics he sees the proposals as a “holding pattern.” He says, “The Government has been forced to make a statement through Webb’s death, alongside the cases of iatrogenic botulism in the East of England. The update contained nothing we did not already know. They have only now released the feedback from the first consultation, 18 months overdue, and are merely proposing another consultation to take place in no less than six months’ time.”
Dr Treacy also voices concerns in regard to the Government timelines, suggesting it’s a delay tactic. He explains, “While the announcement signals intent to address the ‘Wild West’ of aesthetics, it feels more like a political delay tactic than a robust reform. The Health and Care Act 2022 empowered the Government to regulate non-surgical procedures, yet three years later, the scheme remains in consultation, with implementation delayed until 2026-2027.” 1
Dr Catherine Fairris, aesthetic practitioner and president of BCAM, notes that while public pressure has prompted Government action, there remains reluctance to fully address non-HCPs. She says, “Financial considerations play a role, as the initial public consultation noted the sector’s significant economic value, over £20 billion annually, creating tension between protecting the public and supporting specialty growth. Consequently, the Government has limited only the most visibly high-risk procedures, falling short of measures that would most effectively safeguard public safety.”
Supporting safe practice
Considering the final legislation and the potential impact on the field, Dr Fairris suggests, “The Government should require that any injectable procedure involving a prescription medication, or one that may require a prescription medication to address complications, be carried out only on CQC-regulated premises, under the direct supervision of a qualified HCP present during the procedure.” Dr Fairris continues, “As the Government has shown
no appetite to restrict these procedures exclusively to HCPs, this approach represents the most realistic means of ensuring the highest level of public protection within the current limitations.”
Bird advises that sector stakeholders should use the period leading up to the 2026 consultation to act proactively and in coordination. This includes, “Gathering robust evidence on patient harm and complication management, and presenting a unified position on key safety issues – in particular, advocating for a ban on non-HCPs performing injectable treatments and ensuring that all complications are reported through the Medicines and Healthcare products Regulatory Agency’s Yellow Card Scheme,” says Bird.7
Similarly, Professor Sines encourages practitioners to start aligning themselves with the introduced measures. He comments, “Practitioners should operate from safe, infection-free premises, hold appropriate medical indemnity and work within their professional scope. They should also engage with professional associations and follow progress updates over the next 12 months as Government licensing proposals develop.”
“The British Association of Aesthetic Plastic Surgeons (BAAPS) welcomes the Government’s proposals to regulate the non-surgical aesthetic sector. We look forward to further details on which HCPs are covered by the regulations and who will be authorised to perform higher-risk procedures. We also look forward to working with the Government to help achieve a safe, qualified environment in medical aesthetics that benefits patient safety.”
Ms Nora Nugent, consultant plastic surgeon and president of the British Association of Aesthetic Plastic Surgeons (BAAPS)
Following the announcement on August 7, the Government’s forthcoming public consultation on non-surgical cosmetic procedures, scheduled for early 2026, will focus on finalising the scope of procedures to be regulated under the new licensing scheme.1 Practitioners working within the field are advised to follow the latest updates relating to the proposed legislation, and ensure they operate within safe and professional scopes and present a united stance on patient safety.
To join the regulation attend the Clinical Cosmetic Regenerative Congress debate (CCR) this month. Here’s what’s on:
· Thursday, September 25: Understanding the New Government Licensing Scheme: Implications for the Aesthetics Sector at the In Practice Theatre – 10:25-11:00
· Friday, September 26: The Illegal Market for Aesthetic and Cosmetic Pharmaceuticals at the In Practice Theatre –15:30-16:00
· Friday, September 26: JCCP Stakeholder’s Meeting: Working Together to Shape the Future of Aesthetic Regulation, Licensing and Next Steps. Gallery Hall – 9:30 Invite only. Email the JCCP for more info

















The Clinical Cosmetic Regenerative Congress (CCR) returns to London this month


· New Networking Trail sponsored by Healthxchange
New In Practice Zone
· New panel discussing the proposed UK Government Licensing Scheme
· New Regenerative Aesthetic Surgery Symposium partnership
· New British Skin Foundation charity partner
· New VIP enhanced offering
As the field of medical aesthetics continues to evolve, staying informed, connected and inspired has never been more vital. Whether you’re striving to elevate your clinical skills, expand into regenerative or longevity medicine or strengthen the business foundations of your practice, bringing together multidisciplinary expertise can ignite the kind of change that benefits not only individual practitioners but the specialty as a whole.
By exploring emerging treatments, ethical approaches and evidence-based strategies, professionals have the opportunity to drive standards forward, refine patient outcomes and foster a more collaborative and future-facing aesthetic community.
This is where the Clinical Cosmetic Regenerative Congress (CCR) comes in. Acting as a hub for clinical excellence, innovation and shared learning, CCR offers a space for aesthetic professionals to engage with the latest developments, challenge current thinking and invest in their ongoing growth – ultimately helping to shape the future of medical aesthetics.
Understanding the New Government Licensing Scheme: Implications for the Aesthetics Sector
Following the announcement of the recent Government licensing scheme for aesthetic practice, CCR is bringing together key specialty leaders to discuss its implications for the sector. This session, taking place at the In Practice Theatre at 10:25 on Day 1, will provide an overview of the new regulatory framework and explore what it means for practitioners, patients and the future of medical aesthetics in the UK. Experts from across the field will share their insights, concerns and expectations as the field prepares to adapt to this significant legislative development.
New to CCR 2025, the Regenerative Aesthetic Surgery Symposium (RASS) aims to bring together global pioneers, innovators and thought leaders in regenerative surgery to share groundbreaking techniques,
· New Aesthetics Awards Hall of Fame Feature
· New experience levels for content – easily find out what content suits your level
· Enhanced Mentoring Speed Dating themes with more events than ever, sponsored by Dermalux
· Galderma and CCR Blimp streaming event highlights onto the theatres
· Bigger Medical Longevity Summit with new women’s health theme
technologies and research which is redefining the future of cosmetic, aesthetic and reconstructive surgery.
The day will be led by a distinguished scientific committee including Mr Tunc Tiryaki, Mr George Christopoulos and Dr Steven Cohen; and will cover cellular treatments, subcellular treatments, surgical treatments and non-surgical treatments.
Head to our website to purchase your ticket now, as spaces are limited.
Curated in collaboration with Dr Mayoni Gooneratne, founder of Human Health Professionals, in association with the Women’s Integrative Health Collective, the Medical Longevity Summit is a hub of insights and evidence-based strategies to support patients through integrative, regenerative and lifestyle treatments.
Alongside a packed educational programme, the dedicated exhibition area will showcase the latest products, services and technologies in health and preventative medicine. From hormone optimisation and sexual wellness to diagnostics, supplements and advanced skincare, visitors can discover innovative solutions designed to enhance clinical outcomes and expand their wellness offering in this fast-growing field.
Sessions will include:
· Oestrogen and the Brain: Effects on Mood and Cognition with Dr Felice Gersh
· Cardiometabolic Risk in Women
– Missed Signs, Better Solutions with Dr Wendy Denning
· Why is Bone Health Central to Female Longevity? with Dr Rory Melville
· Sexual Longevity – Health Benefits for Maintaining Sexual Vitality in the Menopause and Andropause with Dr Michael L. Krychman
· Mitochondria, Movement & Muscle – Why Women Must Train Differently with Dr Nichola Conlon
While clinical skills are essential, running a successful aesthetics practice requires much more than hands-on expertise. The dedicated In Practice Zone, sponsored by Dermis AI, offers practical, actionable advice to help bridge that gap – supporting professionals in building sustainable, ethical and profitable clinics.
Sessions at the theatre include:
· How ChatGPT Can Accelerate Business Growth and Streamline Clinic Scaling with Ashley and Sheena Mckenna
· A Look Into The Latest Trends In The Medical Aesthetics Specialty with Ben Pask. This session will also see the launch of the Annual Trends and Product Launches Report. Attendees can grab a free copy to explore everything that has gone on over the past year and discover the latest CCR Innovation Trail products.
· Understanding and Embracing Neurodiversity Among Aesthetic Practitioners with Dr Aryan Ala’Aldeen
· Meet the Press: Elevating Your Profile in the Aesthetic Space with Alice Hart-Davis, Victoria Woodhall, Francesca Ogiermann-White, chaired by Mr Adrian Richards
Outside the theatre is a hub of all the service and solution providers you need to help elevate your clinic.
CCR offers even more opportunities to boost your learning and professional development, with three more dedicated educational theatres running across both days of the event. By attending a range of expert-led sessions, you can earn up to 16 CPD points. At the Aesthetics Journal Arena, brought to you by the team behind Aesthetics, you’ll gain practical insights through inspiring talks and live demonstrations. Learn from leading voices in the specialty as they explore the latest scientific research, clinical innovations, and evidence-based techniques to help you improve outcomes, make informed decisions and elevate patient care. Returning as Headline Sponsor, Galderma will once again showcase its pioneering science and forward-thinking developments on this stage,
presenting on treating the effects of rapid weight loss and launching a new innovation.
The Innovation Forum sponsored by SkinCeuticals, is the place to discover fresh ideas for developing your clinic offering. Through bite-sized workshops you’ll explore the newest products, treatment protocols and technologies from some of the most forward-thinking skincare and device brands in the specialty.
In the Aesthetics Mastery Theatre sponsored by DermaFocus, brands will present in-depth treatment demonstrations led by top KOLs. Over the two days, you’ll see the latest techniques in action, helping you enhance your skills, build confidence and deliver safe, high-quality aesthetic results. Don’t miss the Aesthetics Challenge on Day 2 – a two-hour session exploring the art and precision of dermal filler application. Watch as experts share their critiques and guidance during live treatments, offering valuable learning moments throughout.
New Networking Trail, sponsored by Healthxchange
This year, we’re thrilled to launch the CCR Networking Trail – your official guide to the unmissable networking opportunities across the show floor. Whether you’re a practitioner, clinic owner, specialty supplier or medical professional, the trail connects you with the right people, in the right places, at the right time.
With designated networking hours, dedicated lounges and drinks receptions, the Networking Trail gives you a clear path to build your community, strengthen relationships and share ideas with peers across the aesthetics space.
Here’s what you can expect to experience as part of the official trail:
Doctors and Dentists Networking Hour
Where: BCAM Stand
When: Day 1 at 11am
A dedicated hour for medical doctors and dentist to meet peers and share experiences over some light refreshments.
Nurses Networking Hour
Where: BAMAN Stand
When: Day 2 at 11am
A relaxed session for nurses working in medical aesthetics to connect, learn from one another and celebrate their role in the specialty. Light refreshments supplied.
VIP Networking Hours
Where: VIP Lounge
When: 2:30pm daily
Join fellow VIPs for a relaxed drink and conversation each afternoon, perfect for connecting with high-level practitioners and business owners in an exclusive setting (open to VIPs only).
Official CCR Networking Event
Where: Networking Lounge
When: Day 1 at 5:00-7:00pm
The key social moment of CCR! This lively evening drinks reception brings together practitioners, speakers, exhibitors and press for a celebratory toast at the heart of the show.
Aesthetics Members & Clinical Advisory Board Networking Drinks
Where: Aesthetics Members Lounge
When: 3:30pm daily
A chance for Aesthetics Members, the Aesthetics Clinical Advisory Board, and Aesthetics Reviewing Panel to meet, network and share ideas in a relaxed lounge environment.
Aesthetics Industry Drinks
Where: Aesthetics Lounge
When: Day 1 at 4:00pm
Open to suppliers, exhibitors and anyone interested in collaborating with the Aesthetics brand. Come meet the Aesthetics team and fellow specialty leaders over drinks.
How to follow the trail:
· Pick up your printed Agenda at a Glance highlighting the trail map at registration
· Look for the Networking Trail icon on the You Are Here boards
· Use the event app to add networking moments to your personal agenda
· Visit designated trail points and connect!
Bringing The Aesthetics Awards Winners to you
Brand new for this year is the Hall of Fame, featuring all product and device Winners from this year’s Aesthetics Awards. You can get up close and personal with the innovations and ask the companies any questions you might have.
The feature will include:
· AviClear, Winner of The DigitRx by Church Pharmacy Award for Best New Innovative Product
· DP Dynamis NX, Winner of Device of the Year
· Obagi Medical, Winner of Skin Product/ Range of the Year
· Plinest by Mastelli, Winner of The TSK Laboratory UK Award for Injectable Product of the Year
· Evolus, Winner of Manufacturer of the Year
· Church Pharmacy, Winner of the CCR Award for Distributor of the Year
Entries for The Aesthetics Awards 2026 are open now – head to p.11 to find out more.
25 & 26 September 2025 Excel, London

Taking place on September 25-26 at the Excel, London, there’s only a few weeks left to register for CCR. Scan the QR code now to register for free and be part of the conference shaping the future of medical aesthetics.
chance to register





















Counterfeit devices put your patients, and your reputation, at risk. Alma is buying back fake and outdated systems at unbeatable value so you can afford to upgrade.















READY TO SEE WHAT YOUR TRADE-IN IS WORTH? SCAN THE QR TO FIND OUT. You might be just one click away from boosting your clinics revenue.




























UNLOCK









































































Nutri Complex purasomes NC150+
Stimulates fibroblasts to repair skin damage, boosting collagen production and improving skin elasticity.3
Skin Glow Complex purasomes SGC100+
Reduces oxidative stress and improves the appearance of scars, dull and hyperpigmented skin.
Purasomes + Microneedling Book Training Now
Hair & Scalp Complex purasomes HSC50+
Restores hair follicle function for a healthier scalp and thicker, strong hair.4
Manufactured by Dermoaroma Italy. Exclusively distributed in the UK by DermaFocus. Purasomes products are not medical devices and are not intended to be injected. Please refer to the IFU for face, scalp and body.
References 1. J.Chenau et al., Secretome: Definitions and biomedical interest 2. Han, G. et al., 2022. The Potential of Bovine Colostrum-Derived Exosomes to Repair Aged and Damaged Skin Cells. 3. Privitera, A. et al., 2024. Nutri Complex 150+: A New and Effective Approach to Facial Rejuvenation. 4. Ferruggia, G. et al., 2024. Effectiveness of a Novel Compound Hair & Scalp Complex on Hair Follicle Regeneration.
The gut microbiome is now recognised as a fundamental regulator of human physiology, with wide-ranging effects on immunity, inflammation and tissue repair.1 Far beyond its role in digestion, the gut microbiome is a dynamic ecosystem that influences systemic health through immune modulation, metabolic signalling and cross-talk with the nervous and endocrine systems. 2,3 Its impact extends directly to the skin, where microbial balance helps determine barrier integrity, inflammatory responses and resilience to environmental stressors.4
For aesthetic practitioners, this raises an important consideration: supporting gut health may not only improve skin quality but could also enhance outcomes from clinical interventions. We talk to three professionals to get their perspectives on how this can be achieved successfully.
The gut microbiome comprises trillions of microbes – including bacteria and fungi – that vastly outnumber human cells.5,6
Aesthetic practitioner Dr Mayoni Gooneratne describes it as, “Really like an organ in its own right. These microbes don’t just digest food – they produce metabolites that talk to the rest of the body, including the skin.”
This microbial community educates and regulates the immune system, helping the body distinguish between friend and foe.7 It generates vitamins and neurotransmitters, influences energy metabolism, and modulates stress responses through the gut-brain axis.8 Neuro-immunologist Neil Bindemann explains, “The microbiome doesn’t sit in isolation. It is in constant dialogue with the immune, endocrine and nervous systems. If that communication is disrupted, you see ripple effects across the whole body.”
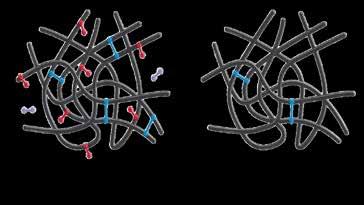
Inflammation is one of the clearest examples. When balanced, microbes produce short-chain fatty acids (SCFAs) that dampen inflammatory pathways.9 When diversity is reduced – through things like diet, antibiotics, or chronic stress – the barrier weakens, inflammatory molecules leak into circulation, and systemic low-grade inflammation develops.9 Consultant ophthalmic and oculoplastic surgeon Miss Rachna Murthy notes, “If inflammation starts in the gut, it doesn’t just stay there – it shows up everywhere else in the body, including the skin.”
The microbiome also influences hormone regulation.
Dr Gooneratne highlights the estrobolome, the group of gut bacteria involved in metabolising oestrogens. She says, “If the estrobolome isn’t working well, oestrogen metabolism is thrown off, which can affect everything from menstrual symptoms to bone health – and of course, the skin.” 10
By acting as a hub for immune, metabolic and hormonal regulation, the gut microbiome is increasingly understood as a cornerstone of systemic health, with direct implications for the skin.
The gut-skin axis refers to the bidirectional communication between the intestinal microbiome and the skin. Dysbiosis – microbial imbalance – can disrupt systemic inflammation, barrier function and immune responses that directly affect skin health.11
Miss Murthy explains, “When one becomes unbalanced, the other often shows signs of stress.” She notes that in practice, this often presents as patients with rosacea, eczema or sensitive skin who also describe gut symptoms such as bloating or irregular bowel habits.11
Dr Gooneratne highlights how this connection plays out in aesthetic consultations, noting, “Patients may come in asking about dullness, pigmentation or breakouts, but when you start asking about their diet, digestion or even stress, you often uncover an underlying gut imbalance. That becomes part of the conversation about what might be driving their skin changes.” Mechanistically, gut microbes shape immune signalling. SCFAs support barrier integrity and reduce pro-inflammatory cytokines, while dysbiosis can trigger mediators of acne, eczema or rosacea.9 Bindemann explains, “You can’t separate immune health from gut health. Around 70% of the immune system sits in the gut, and that constant crosstalk is what ultimately shows up in the skin.” 12
Research has linked small intestinal bacterial overgrowth (SIBO) with rosacea,13 shown altered microbiota compositions in patients with acne and eczema,14,15 and identified gut microbial signatures associated with psoriasis.16 Together, these findings illustrate that the gut-skin axis is not just theoretical, but clinically relevant. As Miss Murthy summarises, “When you treat the skin in isolation, you’re only dealing with the surface expression. If you also consider the gut, you’re addressing one of the roots of the problem.”
Optimising gut health can enhance outcomes across aesthetic treatments, as many depend on skin resilience, immune balance and wound-healing capacity.17
“The microbiome doesn’t sit in isolation. It’s in constant dialogue with the immune, endocrine and nervous systems. If that communication is disrupted, you see ripple effects across the whole body”
Neil Bindemann
Dr Gooneratne explains, “So much of what we do in aesthetics relies on how well the skin repairs and remodels. If the gut is inflamed or the microbiome is disrupted, the patient’s ability to respond to treatment can be compromised. You may still get results but, in my experience, they won’t be as good, and sometimes the downtime is longer.”
Injectables such as dermal fillers and botulinum toxin may be indirectly affected, since chronic inflammation can impair tissue quality, collagen stability and vascular function, potentially reducing the longevity of results.18
Skin rejuvenation procedures – including chemical peels, microneedling and energy-based devices – may be particularly dependent on underlying microbiome balance.17 Miss Murthy observes, “Patients with an imbalanced gut often present with more reactive skin. In my experience, when you treat those patients, they can be more prone to erythema or slower healing. If you can support the gut first, the skin barrier tends to behave better, and you see more predictable outcomes.”
Bindemann adds, “Healing is not just about the skin cells; it’s about the immune signals that coordinate repair. Since most of those signals are trained in the gut, it makes sense that patients with a healthy microbiome recover more efficiently from aesthetic interventions.”2
How
If the gut microbiome influences immune function, inflammation and skin repair, the key question is: how can it be improved?
Dr Gooneratne explains, “We can’t prescribe a ‘perfect’ microbiome, but we can help patients create the conditions for it to thrive. That means focusing on the basics – fibre, hydration, reducing ultra-processed foods and managing stress.”
Dietary strategies
A high-fibre diet improves microbial diversity by feeding beneficial bacteria that produce SCFAs.19 Miss Murthy notes, “When patients increase fibre, they often come back saying their skin feels calmer and more hydrated. You’re not just feeding the gut, you’re feeding the skin as well.”
Dietary diversity is equally important: plant-based foods encourage microbial diversity, processed foods reduce it.20
Fermented foods such as kefir, kimchi, and yoghurt have been shown to increase diversity and lower systemic inflammation.21 Mediterranean-style diets also support diversity and lower inflammatory burden, with benefits for skin ageing and inflammatory conditions.22,23
“If the gut is inflamed or the microbiome is disrupted, the patient’s ability to respond to treatment can be compromised”
Dr Mayoni Gooneratne
Polyphenol-rich foods, including berries, green tea and cocoa, appear to promote the growth of beneficial bacteria such as Lactobacillus and Bifidobacterium.24 Omega-3 fatty acids, found in oily fish, chia and flaxseed, promote beneficial bacteria and anti-inflammatory metabolites.25 Bindemann highlights how simple this can be in practice, noting, “Even something as small as adding a handful of seeds each day can make a difference.”
Conversely, diets high in refined sugar and low in fibre are associated with dysbiosis.26
Dr Gooneratne often frames this in practical terms for patients. She explains, “One of the first things I talk about is cutting back on ultra-processed foods and sugar. Patients may not realise how much that constant low-level inflammation from diet is affecting their skin. Once they make that shift, they often notice they respond better to treatments.”
Probiotics and supplementation
Trials suggest probiotics can improve skin barrier function,27 reduce acne lesions28 and shorten recovery from dermatological interventions.29 Certain strains, such as Lactobacillus rhamnosus GG and Bifidobacterium breve, show benefits in eczema and acne.30
The professionals caution, however, that probiotics should not be seen as a quick fix. Dr Gooneratne says, “Supplements can help, but they’re not a substitute for a healthy diet.”
Bindemann takes a pragmatic view on supplementation. He notes, “It can feel overwhelming for patients to overhaul their diet all at once. For some, a good probiotic is a manageable first step while they start building better habits. If it helps them feel improvement, that can be motivating.”
The professionals agree that large-scale, long-term studies are still needed to clarify which strains are most effective in different contexts.
Lifestyle factors
Sleep, stress, exercise and medication use all shape microbial balance.31-37 Stress reduces microbial diversity, increases gut permeability and fuels inflammation.33 Sleep disruption is linked to dysbiosis and impaired immune regulation,34 while exercise promotes diversity and anti-inflammatory microbes.35 Antibiotics, though sometimes essential, can disrupt microbial communities for months.36,37
Hormonal pathways also play a role. Microbes regulate neurotransmitters including oxytocin, melatonin and serotonin.38-40 As Miss Murthy notes, “About 80% of serotonin is produced in the gut.40 So by looking after your gut, you improve not only your skin but your serotonin levels – it’s all connected.”
She highlights the importance of addressing this with patients. She says, “We often forget to ask about stress in consultations, yet it has such a visible effect on the skin. Patients who are anxious or burned out frequently show more inflammatory skin responses.”
Miss Murthy also considers antibiotic use in treatment planning. She says, “If a patient has recently had a course of antibiotics. Their microbiome may be depleted, so their recovery could take longer.”37
Furthermore, Bindemann points out that exercise doesn’t need to be extreme, advising, “You don’t have to be running marathons. Even daily walking helps the microbiome and, in turn, helps the immune system.”
Clinically, these adjustments can make a tangible difference. Dr Gooneratne notes, “I find very quickly that patients see huge responses, particularly if they’ve been suffering with rosacea or acne. Their skin becomes more stable – they notice less irritability, more glow and sometimes even say their makeup sits better. Conversely, they may see how alcohol or stress makes things flare. Importantly,
once the gut is supported, I consistently see better outcomes from the in-clinic treatments we deliver.”
Integrating gut health into aesthetic practice
Having discussed the evidence linking the gut microbiome with skin health, inflammation and treatment recovery, the next step is how practitioners can apply this knowledge in day-to-day practice. The professionals each highlight ways in which gut health can be meaningfully incorporated without overwhelming patients or detracting from core aesthetic care.
Consultation and assessment
Miss Murthy advises raising gut health early. She says, “I ask about diet, stress and digestion in the first consultation. Patients are often surprised, but once you explain the link to recovery and outcomes, they engage.” Simple questions – about dietary diversity, antibiotic use or gut symptoms – can flag imbalances and add depth to the assessment. Bindemann notes, “When you ask about lifestyle, patients feel you’re looking at them as a whole person, not just their skin.”
Patient advice and education
Advice should be simple and achievable. Dr Gooneratne says, “Patients don’t need a lecture on microbiology – they need two or three things they can do straight away, like adding a fermented food, cutting back on sugar or going for a walk.”
Miss Murthy adds, “If patients understand the connection between gut and skin, they’re more likely to follow advice around pre- and post-treatment care.”
“About 80% of serotonin is produced in the gut. So by looking after your gut, you improve not only your skin but your serotonin levels”
Miss Rachna Murthy
Treatment planning and aftercare
Gut health can inform treatment timing and expectations. Patients recovering from antibiotics, or showing signs of systemic inflammation, may benefit from supporting the microbiome before undergoing intensive procedures. Dr Gooneratne reflects, “Sometimes the best thing you can do for a good aesthetic result is delay a procedure until the patient is in a better place systemically – that way the result is safer and longer-lasting.”
Follow-up and long-term engagement
Follow-up appointments are an opportunity to reinforce advice and track progress. Bindemann observes, “Patients are motivated when they see how small changes improve their recovery. That creates a positive feedback loop where they keep making better choices.” For practices, he emphasises that this also builds
longer-term relationships and positions the clinician as a partner in holistic wellbeing.

Figure 1: Patient before and four weeks after following Miss Murthy’s Microbial Mantle trademarked protocol. This involves Purifeyes hypochlorous spray before and after treatment as well as daily application, daily oral intake of The Skin Biotic nutraceutical, combined with twice-daily application of The Gentle Cleaner and The Active Cream from AWvi. Results show an improvement in redness and rosacea. Images courtesy of Miss Rachna Murthy.
Integrating testing
Bindermann notes the importance of testing patients for conclusive results. “For me, lab-verified testing – such as that by Test-Based Nutrition – is a vital and valuable service. Through this type of testing, we can uncover more personalised ways to strengthen the gut-skin connection and improve overall health. Our collaboration with the Lifestyle Health Foundation and the Person-Centred Neurosciences Society has shown that personalised therapeutic approaches deliver clear benefits – including visible improvements to skin health within just two to four weeks,” he says.
Dr Gooneratne adds that it’s important to remember aesthetic practitioners are not qualified, and are not expected to be experts, in nutrition/diet. “It’s always important to collaborate or refer to a suitably trained professional in this area,” she says.
The gut microbiome is a key regulator of systemic health, with direct influence on skin function, inflammation, and treatment recovery. Recognising this connection allows practitioners to optimise outcomes not only through treatment but by guiding patients towards healthier habits.
As Miss Murthy observes, “When you address gut health, you’re not just improving recovery, you’re helping patients build a healthier foundation for everything else they do.” Dr Gooneratne agrees, highlighting that, “Simple, practical advice empowers patients to take an active role in their results.” Bindemann concludes, “It doesn’t need to be complicated – small, sustainable changes are often the ones patients actually stick with, and those can have meaningful impacts over time.”
Dr Gooneratne is the content curator of the Medical Longevity Summit at CCR, taking place on September 25-26.
Educational sessions will cover factors contributing to women’s health including gut health, hormone health, the skin microbiome and more. Turn to p.19 to register now.
Lead sponsor: Sponsor: 25 & 26 SEPTEMBER


New to CCR 2025, The Regenerative Aesthetic Surgery Symposium (RASS) aims to bring together global pioneers, innovators and thought leaders in regenerative surgery to share groundbreaking techniques, technologies and research which is redefining the future of cosmetic, aesthetic and reconstructive surgery.


















Solutions supports UK cosmetic clinics with reliable service, ethical values, and a forward-thinking approach
Aesthetica Solutions is a leading supplier to UK’s cosmetic clinics. They’re trusted by many practices as a competitive online pharmacy service committed to their core values. As well as making ethically-conscious choices, Aesthetica Solutions is dedicated to always putting the customers first. They constantly strive to understand and anticipate their customers’ needs and deliver a smooth and efficient service. As a pioneering supplier, they’re at the forefront of innovations in the industry and enjoy sharing their insights into valued products with customers.
OUYE the exclusive dermal filler range from Aesthetica Solutions
The OUYE dermal filler range, now exclusively offered by Aesthetica Solutions, provides the ideal balance of a superior volume effect combined with long-lasting performance. OUYE is made up of three unique formulas, all containing lidocaine for a virtually pain-free treatment.
Appearance No impurities, transparent and colourless
Syringe volume 1.1ml (1.0ml HA +0.1ml lidocaine)
Recommended indication Superficial dermis Superficial dermis Middle layer of subcutis Middle to deep layer of subcutis
Needle size Two 30G x 1/2” UTW (ultra thin wall)
Two 27G x 1/2” UTW (ultra thin wall)
Storage 2-25 degrees C
Product Information
Two 25G x 1/2” UTW (ultra thin wall)
Key benefits include:
· Less complications
· Less inflammation
· Less irritation
· Less swelling
OUYE is a transparent, colourless gel consisting of highly pure levels of HA. Throughout the entire production process, from base material to final product, the OUYE range is produced according to the most rigorous quality control systems and regulations such as KCMPISO13485 and ISO9001.
When testing this product for its purity, one of the key results to account for is the BDDE 1.4 Butanediol Diglycidyl Ether residue levels. This chemical cross-linking agent produces HA into a gel form, and its residue should not exceed 2ppm, a standard which not all fillers manage to meet. In the testing of OUYE fillers however, the BDDE
If you’re looking for a dermal filler range with 100% purity to offer excellent results, pleasing your clients, look no further than OUYE. As the exclusive OUYE supplier, Aesthetica Solutions will be happy to discuss your needs further.
The OUYE dermal filler range is an excellent choice when you’re looking to smooth wrinkles, enhance contours and restore volume for youthful radiance. OUYE offers significant advantages over other filler brands due to its 100% purity. It means less inflammation and irritation, helping to avoid the facial puffiness that long-term use of facial fillers can bring. This is naturally very attractive to your clients.
residue was undetectable, making it one of the safest and most reliable products in the market, as it ensures a significant reduction in adverse side effects, such as allergic reactions or swelling.
The HY-BRID technology used in the OUYE range enables the production of highly dense and uniform filler particles in the treatment area, ensuring volume maintenance for at least six months before the dissolution process begins.


Figure 1: Uniform particle size and dissolution rate How it works:

1. Injection of the OUYE filler into the treatment site.
2. Due to its uniform particle size, OUYE yields a natural-looking volume.
3. OUYE maintains the same dissolution rate and is naturally dissolved and absorbed uniformly in the body.


scan to find out more
Discover a new generation of hyaluronic acid fillers which combines hyaluronic acid and succinic acid to enhance cellular regeneration without causing inflammation. The advanced dual release technology allows the immediate and progressive release of active ingredients, exceeding the expectations of a conventional filler and promoting cell regeneration that rejuvenates and revitalises the skin from within.
Pioneering technology, exclusive production and clinically proven efficacy position neostimulation as the future of medical-aesthetic solutions.
Dr Jordan Faulkner and Dr Marcus Geyer discuss key anatomical considerations and injection techniques for safe and effective chin enhancement
The chin plays a pivotal role in defining the lower third of the face and is essential for overall facial symmetry and aesthetic balance. A recessed or underdeveloped chin can create a sense of disproportion, disrupting the harmony of the facial profile. Although surgical genioplasty remains a viable solution for structural correction, non-surgical chin augmentation using dermal fillers presents a safe, effective and customisable alternative that significantly reduces patient downtime.1-3
Continued advancements in filler technology, combined with a deepened understanding of facial anatomy, have broadened the applications of non-surgical chin augmentation. This modality now allows clinicians to enhance projection, elongate the lower third of the face, address asymmetries and refine contour. When executed with anatomical precision, these procedures can produce natural and predictable results.2,3
A comprehensive understanding of chin anatomy is essential for aesthetic success and risk mitigation. The chin constitutes a distinct anatomical unit, delineated superiorly by the mentolabial groove, laterally by the labiomandibular grooves and inferiorly by the submental ligaments.¹ It is anatomically separate from adjacent compartments such as the jowls and submental region.1
The overlying skin is relatively thick and supported by dense subcutaneous fat that is closely adherent to both the dermis and underlying musculature. Muscular structures in this region include the depressor anguli oris (DAO), depressor labii inferioris (DLI) and the central mentalis muscles, with fibres from the DAO and DLI blending with the platysma.1 Structurally, the anterior mandible forms the osseous foundation, making it the principal target for projection and elongation techniques.1
Osteologically, the chin derives its prominence from several key landmarks. The mental protuberance forms a triangular midline prominence at the mandibular base, flanked by the mental tubercles which contribute to the chin’s width and contour. The pogonion represents the most anterior point on the sagittal profile, while the gnathion is identified as the most inferior midline point of the mandibular symphysis. Just below this lies the menton, which marks the lowest point on the symphysis in the vertical dimension. These landmarks are unified by the mandibular symphysis, the developmental fusion line of the two mandibular halves.1-3
The region’s vascular supply is both variable and rich in anastomoses. The mental arteries, branches of the inferior alveolar artery, emerge near the second premolar along the mid-pupillary line.
The ascending mental artery, a submental artery terminal branch, courses within the muscular plane approximately 6mm lateral to the midline and 4mm beneath the skin surface. This vessel is particularly relevant during paramedian injections. The submental artery also contributes to regional perfusion by traversing the mylohyoid muscle.1 Midline supraperiosteal injections are considered the safest due to lower vascular density. In contrast, the paramedian region is riskier and better approached using a blunt-tipped cannula.¹ Sensory innervation is provided by the mental nerve, which exits through the mental foramen between the first and second premolars and supplies the lower lip and chin. Motor innervation is derived from the marginal mandibular branch of the facial nerve.²
Median perforating
Median perforating canal
A thorough full-face assessment is crucial in chin augmentation.4 This includes analysis of facial proportions, symmetry and the relationship between the chin and adjacent landmarks such as the lips, nose and jawline.4 The chin plays a foundational role as one of the structural “anchors” of facial contour, alongside the cheeks.4 Its shape, projection, and definition significantly influence overall facial balance, harmony and emotional expression.4 Chin enhancement can improve the appearance of surrounding areas – such as the jawline and neck – and contribute to a more youthful, proportionate and gender-aligned facial shape.4
Two primary assessment tools are particularly useful:
1. Ricketts’ E-Line, drawn from the nasal tip to the pogonion, serves as a reference for profile harmony. Ideally, the upper lip should rest approximately 4mm behind this line and the lower lip about 2mm behind.2,6 Although this measurement is often used in Caucasian female profiles, preferred lip positions vary with ethnicity and sex and should therefore be considered in the initial aesthetic evaluation.4
2. The Zero Meridian, or the vertical plane aligned with the Frankfort horizontal plane, offers insight into chin retrusion. A chin positioned less than 1cm behind this plane is classified as Grade I retrognathia; 1-2cm as Grade II; and over 2cm as Grade III, which may necessitate surgical intervention.2,5
Non-surgical chin augmentation is indicated for mild-to-moderate chin retrusion, vertical shortening of the lower face, congenital or acquired asymmetries and patients seeking improved contour and lower facial balance.2,4 Additionally, chin augmentation often forms part of holistic facial balancing, helping achieve ideal proportions such as a heart-shaped face in females or a squarer, more angular appearance in males.2,4
Contraindications include pregnancy, breastfeeding, active infection at the injection site, prior adverse filler reactions, hypersensitivity to filler components or hyaluronidase and unrealistic aesthetic expectations.11
Another study evaluated Ricketts’ E-line and examined how observer and patient sex and race/ethnicity affect preferences for lip profile aesthetics.15 It found that both judge and patient demographics significantly influenced what was considered attractive.15 African judges preferred more protrusive lips compared to Japanese and Hispanic American judges.15
Although there are general and published ideals, practitioners should not assume individual patients relate to these and a thorough educational consultation is necessary to identify their preferred aesthetic.
Choosing the appropriate filler is central to treatment success. Products with high G-prime values offer the structural resilience required for maintaining projection and shape against dynamic facial forces.⁹ High-density HA fillers are particularly effective for deep placement in the chin, offering support and durability. Injection technique should be customised to the patient’s anatomy and aesthetic goals. Needles are preferred for accurate supraperiosteal delivery, especially in the midline where structural support is critical.⁸ Cannulas are often used in the paramedian or lateral chin zones to minimise vascular injury risk posed by arteries such as the ascending mental artery.⁸
Non-surgical chin augmentation is indicated for mild-to-moderate chin retrusion, vertical shortening of the lower face, congenital or acquired asymmetries, and patients seeking improved contour
Aesthetic ideals for chin and lower facial proportions are influenced by gender, ethnicity and cultural norms. Typically, feminine faces feature high, full cheeks with lateral apices tapering to a narrow chin, forming a heart-shaped aesthetic. Masculine faces, conversely, tend to exhibit flatter cheeks, a broader jaw and a square chin, producing a flatter ogee curve.⁴ As the face ages, fat redistribution, mid-facial volume loss and tissue descent result in diminished cheek projection and jawline definition. These changes invert the youthful facial triangle and accentuate features such as the nasolabial fold and jowls.⁴
Facial evaluation should incorporate gender-specific proportional ideals, particularly the bigonial-to-bizygomatic width ratio.² In men, a squarer lower face results from a ratio between 0.80 and 0.95, while women tend to have a softer, tapered profile with ratios between 0.70 and 0.80.² Important skeletal landmarks in chin assessment include the pogonion, menton and gonion. The intergonial width should ideally align with nasal alae in women and the modiolus in men.4
Ethnic preferences play an important role in facial aesthetics. In a study conducted in China with 596 female patients, over half preferred a narrow lower face with a pointy chin (51.93%), followed by a round chin (36.52%), while a square lower face was least favoured (0.17%).18
The optimal plane for projection and elongation is supraperiosteal, providing structural lift. Subcutaneous injection may be used for contour blending and refinement.1,8 Initial filler volumes typically range from 0.5 to 1.0ml and should be incrementally layered based on reassessment.² Overfilling, particularly in female patients, can result in an undesirable bulky or masculine appearance.²
Best practices include slow deposition of small product aliquots, cannula use in high-risk zones and careful avoidance of the mental foramen to prevent nerve injury.¹ The role of aspiration before injection is a highly contentious point in medical aesthetics, however both authors advocate for its use. A meticulous approach ensures aesthetic quality and reduces risk.
Chin augmentation techniques are versatile and can be applied to address projection, vertical elongation, asymmetry and contour refinement.
Enhancing projection involves supraperiosteal bolus placement at the pogonion, with smaller boluses along the midline as needed for symmetry. Chin position should be aligned with Ricketts’ E-line to optimise profile balance.1,2 Vertical elongation is achieved by placing filler at the lower border of the mandibular symphysis.1,2 For asymmetry correction, microboluses or subcutaneous cannula injections may be used to restore balance.1,2 Tailored photographic and dynamic assessments guide precise product placement. Masculinisation involves augmenting chin width, projection and angularity using high G-prime filler placed over the lateral mental tubercles and mandibular borders, often with larger volumes and combined jawline contouring.
Chin filler treatment may also provide functional benefits through myomodulation.⁵ Injecting into specific muscular regions has been shown to regulate muscular overactivity, helping correct imbalances associated with structural deficiencies or volume loss.1,5
A case series looking at 144 patient images demonstrated that targeted filler placement at the labiomental angle and chin apex normalised mentalis activity, improved contour and eliminated dynamic wrinkling.⁵ These interventions preserved natural expression while enhancing muscular coordination, suggesting both aesthetic and therapeutic potential.1,5
Though generally safe, dermal filler use in the chin carries potential complications. Common immediate effects include erythema, oedema, bruising, pain and discomfort.¹¹
Vascular compromise is among the most serious risks and often results from inadvertent intravascular injection into the ascending mental or submental arteries.³ This can be mitigated by midline needling, aspiration, slow injection and cannula use in lateral zones.1,17 Aesthetic Complications Expert (ACE) Group World guidelines recommended prompt intervention includes administration of hyaluronidase, warm compresses, massage and escalation to a full vascular occlusion protocol when necessary.17
Capillary refill time (CRT) helps guide management. If CRT exceeds three seconds or symptoms persist, high-dose pulsed hyaluronidase should be administered.3,17 Antiplatelet agents such as aspirin may be used to prevent thrombus formation.¹⁷ In rare instances, vascular occlusion may lead to tissue necrosis, requiring antibiotics, wound care, antivirals (if indicated), debridement and specialist referral.17
A particularly rare but severe complication is tongue necrosis resulting from embolisation or compression of the submental and lingual arteries.⁸ Thanasarnaksorn et al. describe such cases, emphasising early detection and aggressive management, including hyaluronidase, anticoagulants, vasodilators and hyperbaric oxygen therapy.⁸
Sterile technique and appropriate antiseptic preparation reduce infection risk.¹² Excessive filler or misjudged facial proportions can result in unnatural outcomes, such as a ‘witch’s chin’ or unintended masculinisation in females.3,4 Staged treatments and conservative dosing help mitigate these issues.
Hypersensitivity reactions may range from irritation to angioedema.16 According to ACE Group World guidelines, treatment options include antihistamines, corticosteroids and nonsteroidal anti-inflammatory drugs. Anaphylaxis, though exceedingly rare, remains a theoretical risk.16 Delayed nodules and granulomas can be treated with antibiotics, hyaluronidase or immunosuppressants.16 Filler migration or palpable nodules typically result from superficial placement or poor technique.3
An effective method for augmentation
Chin augmentation with dermal fillers is a safe and effective method to enhance lower facial aesthetics when performed by trained practitioners. Success depends on comprehensive anatomical understanding, detailed patient evaluation, appropriate product selection and meticulous technique. Complications, while rare, require prompt recognition and management. When incorporated into broader facial rejuvenation strategies, chin augmentation contributes meaningfully to facial harmony and patient satisfaction.2,4

Dr Jordan Faulkner is a full-time cosmetic physician and founding director of Allo Aesthetics. Founder and lead mentor at Unite Aesthetics Initiative. Clinical educator at Interface Aesthetics, Brand Ambassador for Revanesse and faculty member at DermaFocus. ‘Rising Star of the Year’ Winner, Aesthetics Awards 2025.
Qual: BMedSci, BMBS, PGDip(AesMed)

Dr Marcus Geyer is the founder of Dr Marc Aesthetics in North West London, is an aesthetic physician with over a decade of medical experience. He specialises in regenerative, full-face treatments that support skin health, longevity, and natural outcomes, integrating evidencebased techniques with lifestyle strategies for sustainable, patientcentered results.
Qual: MB BCh

Complete the multiple-choice questions and email memberships@aestheticsjournal.com to receive your CPD certificate!
1. Which anatomical landmark represents the most anterior point on the sagittal profile of the chin?
2. The ascending mental artery is most relevant during paramedian injections because it lies approximately:
3. According to Ricketts’ E-Line, the ideal position for the lower lip is approximately:
4. Which of the following patients would be unsuitable for non-surgical chin augmentation with dermal fillers?
5. In the event of suspected vascular compromise with capillary refill time >three seconds, the recommended immediate intervention includes:
a. Gnathion
b. Pogonion
c. Menton
d. Mental protuberance
a. 2mm lateral to the midline and 6mm beneath the skin
b. 6mm lateral to the midline and 4mm beneath the skin
c. 4mm lateral to the midline and 6mm beneath the skin
d. 1cm lateral to the midline and 3mm beneath the skin
a. 2mm in front of the line
b. 4mm behind the line
c. 2mm behind the line
d. Flush with the line
a. A 32-year-old with mild chin retrusion and good skin quality
b. A 45-year-old seeking improved jawline contour after midface volume loss
c. A 28-year-old currently breastfeeding
d. A 50-year-old with mild asymmetry and realistic expectations
a. Apply ice packs and observe
b. High-dose pulsed hyaluronidase
c. Administer corticosteroids immediately
d. Aspirate the filler and re-inject elsewhere
Answers: B, B, C, C, B













Woodward examine how medically supervised FMD protocols address post-GLP-1 metabolic
The landscape of metabolic medicine has been revolutionised by GLP-1 and GIP receptor agonists, with remarkable success in achieving rapid weight loss and glycaemic control. However, a growing clinical challenge is emerging: what happens when patients experience metabolic ‘wobbles’ during or after these treatments? In the UK, the metabolic health crisis continues to escalate. According to NHS England data from 2024, 29% of adults are classified as obese, with 64% overweight or obese.¹
Type 2 diabetes prevalence reached 7% of the population by March 2024,² while cases among under-40s have risen alarmingly, with almost 168,000 now affected an increase of over 47,000 since 2016-17.³ These statistics underscore the urgent need for innovative therapeutic interventions addressing metabolic dysfunction at its cellular foundation.
A Fasting Mimicking Diet (FMD) offers a scientifically validated intervention originally developed for type 2 diabetes management, but now showing particular promise for patients experiencing post-GLP-1 metabolic instability.
Data suggests that FMD protocols involving five consecutive days of fasting per month over a six to 12 month period, conducted under medical supervision, with clinical trials demonstrating diabetes reversal rates of 40-50% in selected patients.³ Emerging data also suggests additional benefits including restoration of hyposmia (reduced sense of smell) with patients reporting return of normal smell function after six cycles.⁴
For aesthetic practitioners, particularly those with a special interest treating patients with inflammatory skin conditions, understanding FMD represents more than academic interest. The intimate connection between metabolic health and skin appearance means that interventions addressing systemic inflammation and cellular renewal directly impact aesthetic outcomes.
The science of fasting mimicking diets
FMD operates through interconnected biological pathways that distinguish it from simple caloric restriction. The protocol
involves five consecutive days of reduced caloric intake (approximately 750-1,100 calories on day one, reducing to 480-800 calories on subsequent days) while maintaining specific macronutrient ratios designed to trigger beneficial cellular responses.5
Ketosis and autophagy: Within 48-72 hours, the body shifts from glucose-dependent metabolism to ketone utilisation, activating adenosine monophosphate-activated protein kinase (AMPK), the body’s ‘master metabolic switch’.⁵ This triggers autophagy – the cellular ‘housekeeping’ process whereby damaged organelles and misfolded proteins are recycled. Research demonstrates FMD protocols can significantly increase autophagy markers, with research having shown two to three fold increases in LC3-II flux and other autophagy indicators compared to baseline.6
Inflammatory modulation: FMD protocols demonstrate remarkable anti-inflammatory effects, with studies showing significant reductions in C-reactive protein (CRP), interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α).4,6-8 This occurs through reduction in visceral adipose tissue, enhanced cellular stress resistance and improved gut microbiome diversity.
While the post-GLP-1 applications are emerging, FMD’s foundation lies in its established efficacy for type 2 diabetes management.
The potential for FMD to reverse type 2 diabetes lies in its ability to address fundamental pathophysiological mechanisms rather than merely managing symptoms. Clinical trials have demonstrated significant outcomes, with studies showing significant improvements in diabetes markers and pancreatic function in carefully selected patients.9-11
Beta cell regeneration: Animal studies suggest FMD can promote pancreatic beta cell regeneration through activation of stem cell populations and reduction of inflammatory beta cell destruction.5,12,13 While human data remains limited, preliminary evidence suggests similar regenerative potential.
Insulin sensitivity restoration: FMD protocols consistently demonstrate improved insulin sensitivity, with one study showing 20-30% improvements in HOMA-IR scores within three months of intervention.14 This improvement appears to persist for three to six months post-intervention, suggesting durable metabolic reprogramming.
Hepatic fat reduction: Non-alcoholic fatty liver disease, present in up to 70% of type 2 diabetics, responds dramatically to FMD interventions. Research has shown 20-40% reductions in hepatic fat content, directly correlating with improved glucose homeostasis.15
The aesthetic benefits of FMD extend beyond weight loss to encompass fundamental improvements in skin health. Autophagy activation clears damaged collagen while simultaneously upregulating new collagen synthesis through growth hormone pathway activation.15 In my experience I have also found patients often report improved skin texture and reduced fine lines within four to six weeks of FMD completion. The anti-inflammatory effects of FMD can significantly improve conditions such as acne, rosacea and eczema, with emerging case reports suggesting benefits in inflammatory skin conditions following FMD protocols.16 By reducing glucose exposure and enhancing cellular antioxidant capacity, FMD helps prevent and potentially reverse glycation-induced skin damage – a major contributor to premature ageing.
Ideal candidates for FMD following GLP-1/GIP therapy include patients experiencing weight loss plateaus after six or more months of treatment, those planning medication discontinuation for cost or side effects, patients with recurrent appetite dysregulation despite continued therapy and individuals seeking to reduce medication dependence while maintaining metabolic benefits.
Multiple FMD options are now available, ranging from the research-based USC protocol and ProLon system to newer entrants like Fastic, Zero and various telehealth platforms offering supervised programmes. Traditional weight management companies and wellness clinics have also developed their own fasting-mimicking protocols.
A more recent FMD protocol is from L-Nutra, which addresses root causes of metabolic dysfunction through monthly five day fasting cycles that trigger autophagy and cellular regeneration, potentially providing more durable metabolic improvements than pharmaceutical appetite suppression alone. Patients develop confidence in managing metabolism without continuous medication, reducing psychological dependence.
Example protocol
The recent UK launch of L-Nutra for type 2 diabetes management provides a structured framework for implementing FMD in clinical practice, following established clinical protocols for medically supervised fasting interventions.17
Month one to six: Monthly five day FMD cycles under close medical supervision with regular monitoring of glucose, ketones and metabolic markers.
Month seven to 12: Continued monthly cycles with reduced supervision frequency as patients become more experienced with the protocol.
Post-12 months: Individualised maintenance schedules, potentially quarterly or bi-annual cycles based on metabolic stability and patient preference.
The protocol’s design recognises that metabolic reprogramming requires time and repetition. Unlike acute pharmaceutical interventions, FMD works through cumulative cellular renewal that builds metabolic resilience over months rather than days.
Early UK clinical observations
While formal data collection is ongoing, early anecdotal observations from UK practitioners implementing L-Nutra protocols suggest several promising patterns. However, these observations are preliminary and not yet published in peer-reviewed literature.
Successful transitions: Patients who complete six or more cycles appear better to be able to maintain weight loss post-GLP-1 cessation compared to those attempting microdose approaches alone.
Psychological benefits: Many patients report increased confidence in their ability to manage appetite and cravings independently.
Metabolic stability: Monthly monitoring suggests more stable glucose patterns and reduced insulin resistance compared to microdosing strategies.
Unexpected benefits: The hyposmia improvement noted in clinical trials is being replicated in UK patients, often dramatically improving quality of life and relationship with food.
While FMD protocols demonstrate significant therapeutic potential, careful patient selection remains paramount. Absolute contraindications include active eating disorders, pregnancy, breastfeeding, type 1 diabetes and severe cardiovascular or hepatic disease.18 Particular caution is warranted in patients over 75 years and those with mental health comorbidities, where enhanced psychological screening becomes essential.19 Clinical experience suggests that structured fasting may inadvertently trigger restrictive eating patterns in vulnerable individuals, necessitating ongoing monitoring for obsessive behaviours around food restriction and social withdrawal from meal-based activities. 20 Practitioners should remain vigilant for emerging psychological distress, with protocols discontinued immediately if disordered eating patterns develop. The intimate relationship between metabolic interventions and psychological wellbeing underscores the importance of holistic patient assessment before FMD initiation. 21
Medically supervised FMD represent a paradigm shift in metabolic medicine, particularly relevant given the growing availability of structured FMD protocols for type 2 diabetes management and post weight loss medication.
For aesthetic practitioners, this is particularly relevant as patients increasingly seek holistic approaches addressing both metabolic health and appearance goals. The unexpected benefits of FMD, including restoration of smell function, highlight systemic effects extending far beyond weight management. As practitioners gain experience with FMD protocols, evidence suggests structured fasting may offer superior long-term outcomes compared to indefinite pharmaceutical management, providing patients a pathway to genuine health transformation rather than continuous medication dependence.
25 & 26 September 2025 Excel, London

Dr Vix Manning has clinical experience over general practice and medical aesthetics. She has a particular special interest in reducing inflammation and its impact on ageing. Having prescribed GLP-1 and GIP medications for over three and a half years, she has extensive experience managing post-treatment metabolic challenges. She is the author of Busting The Code to Ageing: How to Win The Inflammation Game.
Qual: BM, DFFP, MBCAM

Dr Charlotte Woodward is co-founder of River Aesthetics with over 20 years of clinical experience spanning general practice and medical aesthetics. She specialises in thread lifts and collagen stimulation treatments.
Qual: MBCHB, MRCGP, MBCAM


Dr Selina Ahmed provides an introduction to treatment approaches for AGA in men, focusing on regenerative methods
Hair loss can have a considerable psychological impact, even in otherwise healthy individuals. In men, androgenetic alopecia (AGA) is the most common cause of hair loss.1,2 It often begins with thinning at the temples and vertex and progresses gradually.
While pharmacological options such as minoxidil and finasteride remain widely used, many patients are reluctant to commit to long-term daily medications or are concerned about potential side effects. In recent years, an increasing number of men have pursued hair transplant procedures abroad, often drawn by lower costs and aggressive marketing. Hair transplant procedures in Asia, Australia and the Middle East has surged, with the largest group being male patients aged between 30-39 years old. 3 While transplants can offer dramatic results, they are not without risk, including over harvesting of donor areas, unnatural hairlines and variability in clinical standards. 3
For those seeking alternatives, regenerative options like exosomes, platelet-rich plasma (PRP) or combination protocols provide a middle ground and minimally invasive interventions with no donor site trauma and natural, progressive outcomes. Among these, exosomes are emerging as part of the broader field of regenerative medicine, drawing growing interest worldwide.4
In the highlighted case, a non-surgical microneedling-based treatment was used to address early to moderate hair thinning in a 40-year-old male.
Causes and effects of AGA
AGA, commonly known as male pattern hair loss (MPHL), is the most prevalent form of hair loss, affecting up to 80% of men by the age of 70, with incidence increasing with age.5 This condition is characterised by the progressive conversion of terminal hairs into intermediate and vellus hairs, driven by shortened anagen (growth) and a prolonged telogen (resting) phase.5 Over time, affected follicles may shrink to the point where they cease producing hair altogether.
Hair loss in men can occur at any age after puberty. It results from a combination of genetic predisposition and hormonal influences, particularly the action of dihydrotestosterone (DHT) on scalp hair follicles. DHT triggers a process called ‘miniaturisation’, in which affected follicles produce progressively finer, lighter hairs until the follicles shrink entirely and cease hair production. 2 AGA is hereditary and may be inherited from either or both parents, with more than 190 genes identified as contributing factors. 2
This genetic complexity explains why the condition varies in severity and onset among family members. In AGA there are no physical scalp symptoms, although patients may occasionally report some itching.1,2
There are several treatment options that can be considered for treating MPHL, such as topical minoxidil, oral minoxidil, 5-alpha reductase inhibitors and more.
Topical minoxidil
Topical minoxidil is approved by the Medicines and Healthcare products Regulatory Agency (MHRA) to treat AGA in the UK. It was first approved in 1988 for men with mild-to-moderate AGA by the US Food and Drug Administration. (FDA).5 Originally developed in the 1960s as an oral medication for high blood pressure, it was later reformulated for topical use after hair growth was noticed as a side effect. Minoxidil is available over the counter in 2% and 5% foam or liquid, with stronger concentrations sometimes made by compounding pharmacies. It works best at the vertex and frontal scalp, helping to slow hair loss and encourage regrowth by prolonging the growth phase and increasing hair thickness.5
Around 40% of users may see improvement in hair density and thickness, so it’s not effective for everyone.6 Side effects are usually mild and may include scalp itching, irritation or unwanted facial hair, especially with higher strengths. Consistent application is essential, minoxidil must be applied once or twice daily. Results usually start to become visible after four to eight months, with the best outcome seen around 12 to 18 months. However, if treatment is stopped, hair loss often resumes within 12 to 24 weeks. 2 Hair can also shed in the first four to six weeks of starting minoxidil before new hairs start to come through. 2
Oral minoxidil
Oral minoxidil, while not FDA-approved and less commonly used than finasteride, has been studied as a treatment for MPHL.5 In men, higher doses (around 5mg daily) have produced significant improvement, though side effects are more common.5 Reported benefits include increased hair growth and density, but side effects, such as unwanted body hair growth (hypertrichosis), tachycardia, fluid retention, weight gain and peripheral oedema can occur.5 These effects are generally dose-dependent and reversible when the medication is stopped. While oral minoxidil may be more convenient than topical application, its potential for systemic side effects often makes it a second-line option.5
5-alpha reductase inhibitors in male patients
5-alpha reductase inhibitors are a well-established therapeutic option for AGA in men. Dutasteride, at a dose of 0.5mg daily, is generally considered the most effective, with research showing significant increases in total hair count and noticeable improvements on serial photographic assessment.6 Finasteride, taken at 1mg daily, is a widely used alternative. Emerging evidence suggests that a single 5mg dose taken once weekly may offer comparable efficacy at a lower cost. Increasing the finasteride dose beyond these levels does not confer additional benefit.6
In clinical practice, up to 90% of appropriately selected male patients respond favourably to finasteride.6 However, continued use is required to maintain therapeutic gains, as discontinuation is typically followed by gradual loss of regrown hair.6
Prior to initiation, patients should be counselled on potential adverse effects, which include a small risk of reduced libido, erectile dysfunction and ejaculatory disorders. In some cases, these effects may persist after discontinuation. Both finasteride and dutasteride reduce serum prostate-specific antigen (PSA) concentrations, typically halving the measured result. This is important to consider during prostate cancer screening and monitoring.⁶
Low-level laser therapy (LLLT) was first identified in the 1960s, when researchers observed that low-intensity red light could stimulate hair growth in mice.5 Since then, decades of research have since established LLLT as a commercially available treatment option for AGA. FDA-cleared devices such as the Capillus laser cap and Hairmax Lasercomb or Laserband are now available for home use in the form of caps, helmets or combs.
AGA, commonly known as male pattern hair loss, is the most prevalent form of hair loss, affecting up to 80% of men, with incidence increasing with age
Although the precise mechanism is not fully understood, it is thought that red light absorption by mitochondrial cytochrome c oxidase leads to the release of nitric oxide, enhanced ATP production, modulation of reactive oxygen species and activation of transcription factors.5 These changes promote protein synthesis, improve scalp blood flow and may reduce follicular inflammation.5 More research is required to ascertain the effectiveness on hair density in humans. 2
PRP therapy is an autologous treatment for hair loss that uses the patient’s own blood to stimulate hair follicle activity. A small volume of blood is drawn and centrifuged to isolate the platelet-rich fraction, which contains a high concentration of growth factors such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF) and insulin-like growth factor-1 (IGF-1). This is then injected into the scalp.5 These bioactive molecules promote angiogenesis, enhance nutrient delivery, activate dermal papilla and stem cells and support the transition of follicles from the resting (telogen) to growth (anagen) phase.5
PRP is most effective in early-stage AGA, when follicles are still viable and can increase hair density, thickness and overall scalp coverage. Typically, one PRP treatment is recommended each month for three to six months, followed by a maintenance session every six months to sustain the results. Outcomes depend on the patient’s own physiological health and cellular health, and there can be significant variability in response due to differences in PRP quality between patients.
Hair transplantation is a surgical treatment for advanced or irreversible hair loss, involving the relocation of hair follicles from a donor site, typically the back or sides of the scalp, to areas affected by thinning or balding. The procedure is performed under local anaesthesia in an outpatient setting. It can be carried out via strip excision (ellipse), which yields a high number of grafts but leaves a linear scar, or follicular unit excision (FUE), which removes small follicular groupings with fine punches to avoid a visible linear scar. 3,5 Hair transplant surgery does not prevent further loss of existing non-transplanted hair, may require combination with medical therapy for optimal long-term results and carries potential risks such as scarring, suboptimal density or patient dissatisfaction with the cosmetic outcome. 3,7
Exosomes are nanosized extracellular vesicles, typically 30 -150 nm in diameter, that facilitate intercellular communication. 8 They possess a phospholipid bilayer enriched with specific surface markers and carry a range of bioactive cargos, such as cytokines, growth factors and regulatory microRNAs (miRNAs), which influence cell signalling and gene expression. 8
Although their precise mechanism of action in hair regeneration is not fully understood, it is thought that exosomes modulate paracrine signalling, enabling communication between epithelial and mesenchymal cells during the hair growth cycle. 8 For instance, exosomes derived from dermal papilla cells (DPC-Exos) have been shown to activate the Wnt/β-catenin pathway in outer root sheath cells (ORSCs), thereby promoting the transition from telogen to anagen in mice. 8
Patient consultation and assessment
A 40-year-old male presented with gradual hair thinning affecting the bilateral temples and vertex. He reported no significant past medical history, was not taking any medications and had no known drug allergies. He was a non-smoker and a social drinker, consuming less than 14 U of alcohol per week. The patient had not previously used topical or oral treatments for hair loss and expressed interest in exploring non-pharmaceutical options.
On examination, the patient exhibited signs of early AGA, with noticeable follicular miniaturisation along the temporal regions and reduced hair density at the vertex. He was classified as Hamilton-Norwood Scale grade 4. The patient was seeking a minimally invasive option. Options discussed were injectable polynucleotides, PRP, medical therapy and exosomes. As long as there is hair present, exosome treatments can help to thicken and elongate existing hairs.
There was no signs of scarring alopecia, inflammation or seborrhoeic dermatitis. A recent blood test, conducted as part of a Well-Man screen (a routine health check offered to all patients at age 40 in primary care),9 returned within normal limits and showed no evidence of nutritional deficiencies. There was also no family history of autoimmune disease.
The patient’s goals were to slow the progression of hair thinning, stimulate regrowth in affected areas and improve overall scalp condition. After discussing various approaches including minoxidil, finasteride, PRP, hair transplants or the option of no treatment, he opted for a regenerative approach using microneedling combined with Purasomes HSC50+. Purasomes HSC50+ contains 20 billion exosomes per 5ml vial and is derived from bovine colostrum, a nutrient-rich secretion harvested within the first few hours postpartum. Bovine colostrum is known to contain high levels of biologically active compounds including immunoglobulins, growth factors and antioxidants, making it an optimal treatment option.10
The exosomes in this formulation are not isolated from stem cells but from bovine secretome, a complex mix that includes exosomes, proteins, cytokines and signalling molecules.10 These vesicles interact with dermal papilla cells in the scalp, which play a key role in regulating the hair cycle.10 By enhancing cellular signalling and promoting an anti-inflammatory, growth-conducive environment, the formulation aims to support the restoration of hair follicle function and overall scalp health.10
Unlike PRP which depends on individual variability and requires venepuncture, exosomes offer a standardised, cell-free approach that avoids the need for patient blood and delivers a consistent concentration of active components, with some studies showing more favourable outcomes with exosome based treatments, compared to PRP.11
The treatment was explained in full, and consent was obtained for a course of six sessions spaced four weeks apart, as part of the recommended protocol.10
The patient was advised on the importance of a balanced, nutritional diet and was recommended supplements where appropriate. Focus was placed on vitamins known to support hair and scalp health, including biotin, vitamin D, vitamin C, B-complex vitamins (such as B3, B5, B6 and B12) and zinc, all of which contribute to cellular repair, follicular function and keratin production.13 Sleep hygiene, stress reduction and general wellbeing were also discussed, as these systemic factors can influence hormonal balance and the hair growth cycle.
The patient underwent a total of six monthly treatments using the Derma FNS microneedling pen from SkinMed, with needle depth set between 0.5-1mm.10 The needle depth can vary between patients depending on the thickness of the skin. The aim is to create tiny micro channels for the exosomes, and this can be gauged when then skin turns pink.
Each session began with thorough cleansing of the scalp. A topical anaesthetic LMX cream was applied during the first two treatments to manage discomfort, but was not required for the subsequent sessions, as the patient found the procedure tolerable at the chosen depth. The solution was applied immediately after microneedling to the bilateral temples and vertex and used as a glide during the procedure. Microneedling was performed in a uniform, linear technique over areas of visible thinning. Each session lasted approximately 30 minutes. The patient was advised to avoid washing the scalp for 24 hours and refrain from strenuous exercise or sun exposure for 48 hours post treatment.10 No additional topicals were used between treatments.
Hair thickness, density, darkening of the hair and elongation of the vellous hairs was gradual and progressive. Four weeks following the first session, the patient reported a notable reduction in hair shedding, which had previously been one of his main concerns. Four weeks after the second treatment, he began to notice early signs of hair thickening, particularly along the temporal regions. Three months into his treatment plan, after three completed sessions, a significant visible improvement was observed. Density at the vertex had improved, with a more uniform appearance and emerging terminal hairs visible along the hairline. Coverage over the crown was notably enhanced, and the temples had continued to fill in.
The patient expressed high satisfaction with the result. While we do not currently use trichoscopy to quantify changes, photographic documentation and the patient’s self-assessment both indicated a meaningful clinical response. A maintenance treatment every six months was recommended to help preserve results.
Practitioners should make sure they are adequately insured for the use of microneedling in conjunction with topical products, particularly those marketed as cosmetics. According to MHRA guidance, the method of application and intended purpose can influence whether a product is regulated as a medicine. The act of microneedling a cosmetic product, especially one containing biologically active ingredients like exosomes, may be interpreted as administering it for a medicinal purpose, potentially reclassifying the treatment under medicinal use.15
Practitioners should also consider important ethical aspects related to the sourcing of exosomes. In the UK, the use of human-derived exosomes in aesthetic treatments is strictly regulated and generally prohibited without appropriate licensing. Practitioners are advised to ensure full compliance with relevant local regulations and to exercise careful clinical judgment.16
Exosome therapy using bovine colostrum-derived secretomes, when paired with microneedling, may offer a safe and effective option for hair restoration in males with early to moderate AGA. While further research and controlled trials are needed, case-based outcomes like this provide encouraging support for their role in future treatment pathways.5,11,14 Human exosomes are illegal in the UK and exosomes are not permitted to be injected deep into the skin, nor are they FDA approved. Bovine colostrum based exosomes are a safer option due to their higher biocompatibility and stability during the manufacturing process.14

Dr Selina Ahmed is a GP with an extended role in dermatology and has more than seven years of experience in medical aesthetics. As founder and medical director of Dr Selina Clinics in South Woodford, London, she specialises in advanced injectable treatments, regenerative therapies and skin health optimisation, delivering safe, natural results grounded in evidence-based practice.
Qual: MBChB, MRCGP, DCH, PGDipDerm, PGCertMenopause

Join Lynton at CCR on 25-26 September, stand F40, for our external, expert-led talks.
Join our interactive talks; discover ideas, unlock techniques and take the next steps in your CO2 journey.

Scan for agenda
Call one of our experts today on 01477 536 970 or visit lynton.co.uk


In partnership with DEKA

her
In today’s busy world, patients are demanding prompt results, and in recent years, a rising trend has emerged – the practice of combining multiple aesthetic treatments into a single session. Reports indicate that patients and providers see combination therapies as a strategic way to accelerate outcomes compared to single treatments. In fact, over 70% of clinicians surveyed noted that their patients specifically request combined procedures because they deliver faster, more noticeable improvements.1 Combining treatments also offers greater convenience for patients, as delivering multiple treatments in one appointment means they can minimise disruption to their daily routine. They can spare themselves the hassle of scheduling multiple visits to a clinic, while also limiting the time spent out of action post treatment due to erythema, bruising or swelling.
Energy-based devices such as lasers, intense pulsed light (IPL), high-intensity focused ultrasound (HIFU) and microneedling are just some of the treatments that can be used to optimise a number of aesthetic treatments, such as skin rejuvenation, pigment reduction and scar improvement.2-4
This article will present a case study demonstrating how a combination of CO2 lasers, picosecond lasers, light emitting-diode (LED), platelet-rich plasma (PRP), chemical peels and exosomes can be effectively utilised to improve skin tone and texture in a patient with Fitzpatrick Skin Type VI.
Combining multiple aesthetic treatments can lead to synergistic effects, enhancing the overall outcomes. As early as 2004, the botulinum toxin pioneers Drs Jean and Alastair Carruthers noted that the rejuvenating effects of IPL treatment could be enhanced by the use of botulinum toxin.5 They noted that IPL alone led to a remarkable improvement in facial telangiectasias, lentigines and skin texture, however, the improvement increased by 15% in all categories when the treatment was combined with toxin injections prior to a course of IPL treatments.5 They suggested that the combined treatments act synergistically to produce optimal clinical effects, due to the broader effect of toxin on the presynaptic network and other autonomic systems involved in facial ageing, in particular, the vascular system.
Moreover, researchers Cuerda-Galindo et al. performed a review of 15 studies which combined lasers, IPL, radiofrequency (RF), toxin and fillers for rejuvenation on the same day.6 These studies reported clinical improvement in various features of photodamaged skin, no increase of adverse effects and no decrease in efficacy of the substances injected.6
Laser and light sources have also been shown to work well with chemical peels. A review by Effron et al. summarises the findings following a dermatologist roundtable, and states that superficial chemical exfoliation prepares the skin by removing surface debris and the stratum corneum, thereby improving the penetration and uniformity of energy-based device treatments.7 This synergistic approach has demonstrated superior improvements in skin tone, pigmentation irregularities and texture, and has been applied
effectively in the management of photodamage, melasma, acne scarring and fine lines.7
It’s not just injectable and peel treatments that can be combined with lasers and light sources. Preliminary results of studies are emerging which combine various technologies including IPL and fractional ablative lasers,8 alongside HIFU and RF microneedling in the same treatment session.9,10 In a study by Byun et al. it was shown that combining HIFU with bipolar RF synergistically improves skin rejuvenation, including pore reduction, periorbital wrinkle improvement, skin elasticity and skin moisturisation.9
In recent years, exosomes have also been used in combination with energy-based devices. In a 2025 study, researchers Fusco et al. evaluated the efficacy of applying a collagen-boosting serum containing exosomes immediately following fractional CO2 laser treatment, using forearm skin samples from a healthy adult.11 Optical coherence tomography (OCT) was used to monitor skin vascularisation and healing dynamics. The treated areas receiving both the CO2 laser and exosomes demonstrated faster crust expulsion and an accelerated healing process compared to skin treated with the CO2 laser alone. Additionally, zones treated with the exosome-enhanced protocol exhibited reduced vascularisation during healing, suggesting potentially less inflammation or erythema.11
Patient background
The patient, a 58-year-old woman, led a healthy lifestyle characterised by regular exercise and a balanced diet. Her nutrition was rich in fruits, vegetables and protein, with low carbohydrate intake and no sugar. She slept six to seven hours a night and maintained an overall healthy regimen.
Her skin history included a past battle with acne, although at the time of treatment she was only experiencing occasional spots. Menopause, which began approximately four years ago, may have been a contributing factor to the resurgence of minor acne flare-ups.
Initial concerns and conditions
When the patient first sought treatment, her primary concerns included:
· Active acne Acne scars
· Post-inflammatory hyperpigmentation (PIH)
· Hyperpigmentation on her lower face, around the mouth and forehead
· Enlarged pores
· Facial skin that appeared darker than the rest of her body
· General tiredness and visible eye bags
Her skin’s uneven tone, pigmentation issues and textural concerns were of particular concern. Additionally, the presence of varicosities, enlarged pores and signs of fatigue around the eyes added to her dissatisfaction with her appearance.
The following treatment combination was prescribed to target the patient's specific skin concerns. The treatments were spaced four weeks apart and compromised of:
· Full face fractional skin rejuvenation using Lynton's DEKA SmartPICO: Eight sessions to target the patient’s pigmentation, acne scars and general skin texture.
· CO2 full face treatment using Lynton’s DEKA SmartXide Punto: Three sessions to promote deeper skin resurfacing and tightening.
· Chemical peels by VI Peel: Four sessions to exfoliate and



Comprehensive skin purifying treatment to cleanse, smooth, and illuminate skin for glass-like clarity
• Hydrodermabrasion: Gently cleanses, exfoliates, and replenishes1,2
• Dual-Mode Cupping Massage: Facilitates lymphatic circulation and sculpted appearance*1,2
• LED Treatment with Biocellulose Mesh Mask: Protects and boosts radiance1,2




brighten the skin, addressing pigmentation and pore size.
· Exosome face treatment by EXO|E: Eight sessions to accelerate skin healing, regenerate healthy skin cells and improve overall skin quality.
· PRP by RegenPRP: Six sessions to enhance skin healing and rejuvenation.
· LED therapy by ZKIN: Administered after every DEKA SmartPICO and CO2 session to calm the skin, reduce inflammation and encourage faster recovery.
SmartPICO and CO2 laser treatments were sequenced to balance efficacy with tolerability, managing the patient’s concerns without overwhelming the skin. Adjunctive therapies – including LED therapy, exosomes and PRP – were layered between sessions to support dermal regeneration, reduce inflammation and optimise wound healing. Chemical peels were introduced to target pigmentation and acne breakouts without interrupting the progress of the concurrent laser work. As with all patients of Fitzpatrick Type IV-VI, PIH was a risk, and care was taken to mitigate this through adjusting laser fluence, increasing the intervals between high-intensity treatments and the use of pigment-regulating topicals.
This multimodal, patient-responsive approach allowed for safe treatment intensification while preserving skin integrity.
Results and patient satisfaction
The patient is extremely pleased with her progress and the results achieved through the treatment plan (Figure 1). Her skin’s texture has significantly improved, appearing much smoother and brighter. Hyperpigmentation, which was a primary concern, has been addressed with notable success, particularly around the lower face and forehead.
The acne scarring has diminished considerably, and the overall appearance of her skin is more youthful and revitalised. The patient has also observed a reduction in tiredness, with her eye bags becoming less prominent. Her skin now looks healthier, more even-toned and better matches the rest of her body.




Even with cost savings, combination packages may still feel financially out of reach for some patients. By continuing to offer single treatment plans it ensures broader accessibility, or you can offer flexible payment options to help accommodate varying budgets. Each practitioner must assess the range of patients and suitability for combination treatments to ensure the requirement is there. For example, medical history, skin type and treatment goals of their patient demographics.
This multimodal, patient-responsive approach allowed for safe treatment intensification while preserving skin integrity
Communication with the patient around the benefits of combination treatments needs to be done ahead of moving to this approach. Otherwise you risk overwhelming or intimidating current patients. Above all, it is important that safety always remains paramount when undergoing aesthetic treatments. It’s essential that prior to devising a combined treatment regimen, practitioners consult with their device and product suppliers to ensure that appropriate, science-based treatment protocols are followed, as there will be some treatment combinations that will be unsuitable for combination on the same day. In general, consideration should be made of the depths of skin being targeted, and generally the deepest layers of the skin should be treated first. For example, if combining RF microneedling with HIFU, start with the deepest HIFU settings and then ensure that the needle depth used for microneedling is less than the depth of the HIFU treatment. If in doubt, or when treating reactive or sensitive skin, or skin prone to PIH, then it’s generally best to avoid stacking treatments on the same day, and instead schedule them at two to four weekly intervals.
The practice of combining aesthetic treatments in a single session offers patients a streamlined, efficient path to visible results with minimal disruption to their daily lives. This approach not only reduces downtime but also enhances outcomes through the synergistic effect of complementary modalities. It allows for comprehensive rejuvenation by addressing multiple concerns simultaneously – whether texture or tone. When performed safely and strategically, same-day treatment stacking delivers transformative results that deliver both patient satisfaction and clinic success.

Dr Ifeoma Ejikeme is the founder of Adonia Medical Clinic. She graduated from Bristol University and trained at the Imperial College Trust Hospitals in London, before completing a fellowship in head and neck surgery at the University of Columbia. Dr Ejikeme also gained board certification in internal medicine at New York Medical College.
Qual: MD, MBChB, BSc, MSc Aesthetic Medicine
Dr Sonakshi Khorana discusses the role of topical therapies and medical-grade skincare in the effective management of rosacea
Rosacea is a chronic, non-contagious, inflammatory skin condition that manifests in various clinical subtypes and severities.1,2 Rosacea affects about 5% of the global population, including one in 20 UK patients.3,4 It causes facial flushing, erythema, papules, pustules and sometimes ocular symptoms.5-9 More common in women and fair skin types, it requires an individualised, multifaceted approach due to varied triggers, severity and presentations.10-17
Causes of rosacea
The pathophysiology of rosacea is complex and not fully understood.5,7 Proposed mechanisms include ultraviolet radiation-induced dermal damage triggering inflammation, and increased neural sensitivity leading to neurogenic inflammation, which may explain burning or stinging sensations.5,7,18 Elevated levels of the antimicrobial peptide cathelicidin also suggest a role for innate immune dysregulation.5,7
Microbial dysbiosis, both cutaneous and gastrointestinal, appears to contribute.19 On the skin, patients often show increased Demodex mite density, particularly D. folliculorum and D. brevis, which correlates with severity.19 While not proven causal, these mites may promote inflammation by disrupting follicles and activating immune pathways.19
Gut dysbiosis is increasingly recognised as a factor in rosacea.19 Altered intestinal microbiota have been linked to gastrointestinal conditions such as Helicobacter pylori infection, small intestinal bacterial overgrowth (SIBO) and irritable bowel syndrome (IBS), all more frequent in rosacea patients. Dysbiosis in the gut may trigger systemic inflammation that affects the skin’s immune response and vascular function, potentially exacerbating or initiating rosacea flares.19,20-22 Some studies report improvements in skin symptoms following treatment of gut conditions like SIBO, and interest is growing in probiotics and dietary modulation as adjunctive therapies.23,24 While further research is needed to clarify causality, these findings support a more holistic, systems-based approach to rosacea management that includes gut health optimisation as part of broader wellness strategies.
Rosacea is often underdiagnosed in individuals with skin of colour (Fitzpatrick types IV-VI) due to reduced clinical awareness and subtler visual cues.5,25,26 Typical features, such as central facial erythema, flushing and telangiectasia, are more evident on lighter skin, while in darker skin they may appear as hyperpigmentation, warmth or textural change, sometimes accompanied by post-inflammatory hyperpigmentation (PIH) or scarring.27,28 Traditional dermatology training has historically underrepresented skin of colour, contributing to delayed or missed diagnoses.29,30
Rosacea has traditionally been categorised into clinical subtypes based on predominant features observed at presentation.5,7,9 The most widely used classification, originally outlined by the National Rosacea Society (NRS) Expert Committee, identifies four principal subtypes – erythematotelangiectatic, papulopustular, phymatous and ocular – but this system does not account for overlapping or evolving presentations.5,9 In response, the global ROSacea COnsensus (ROSCO) panel proposed a phenotype-based approach, focusing on specific clinical features rather than rigid subtypes, which allows for more individualised management.5,9,31-33
Diagnosis relies on comprehensive history, examination and exclusion of differential diagnoses. While validated grading tools such as the Rosacea Area and Severity Index (RASI) can assess severity, they do not capture psychological burden, an important consideration given the condition’s impact on quality of life.31,34,35
Key clinical features:
· Persistent central facial redness (erythema) Non-comedonal papules and pustules
· Flushing or episodes of warmth
· Visible telangiectasia
· Skin sensitivity, including burning or stinging
· Ocular symptoms such as dryness, grittiness or irritation
To assess broader impact, patient-reported outcome measures such as the Rosacea-specific Quality of Life index and
the Dermatology Life Quality Index can be valuable.32,36
Topical therapies for rosacea management
Topical agents are the mainstay for mild to moderate rosacea, especially in patients with inflammatory papules, pustules and persistent erythema.37-38
The four most widely used options are metronidazole, azelaic acid, ivermectin and brimonidine.
Metronidazole (0.75% cream or gel) has anti-inflammatory and antioxidant effects, reducing erythema and lesion counts.39 It is generally well tolerated and suitable for long-term use, though alcohol-based formulations may be less tolerable in dry or sensitive skin.13,40 Often used for milder disease or in combination therapy.41
Azelaic acid (15% gel) offers anti-inflammatory, antimicrobial and anti-keratinising actions, improving both lesions and erythema.42 It is particularly useful in sensitive skin or PIH.42 Transient stinging or burning may occur, but usually subsides.43 Recognised in European and US guidelines as a first-line option for mild to moderate, especially papulopustular, disease.44
Ivermectin (1% cream) combines antiparasitic and anti-inflammatory effects, and has shown greater efficacy than metronidazole in reducing lesion counts.45 Well tolerated with a good safety profile, it suits moderate to severe papulopustular rosacea.46 Initial irritation may occur, so gradual introduction with barrier-supportive skincare is recommended.46
Brimonidine (0.5% gel) is an alpha-adrenergic agonist that treats persistent erythema via vasoconstriction, acting within 30 minutes for up to 12 hours.47 Patients should be advised of possible rebound erythema, flushing or irritation, particularly with overuse.48 It is best reserved as an adjunct for significant background erythema alongside other therapies.49,50 Selecting agents should be guided by symptom profile, skin sensitivity and patient preference, often combining treatments for optimal results.
Implementing topicals into clinical practice For patients with sensitive skin or mild disease, a skincare-led approach is often preferred.14 Some may avoid pharmacological treatments, focusing instead on barrier repair, inflammation control and trigger avoidance.51,52 However, combining topical pharmacological agents with medical-grade skincare often achieves a more comprehensive effect.53
Medical-grade skincare for rosacea
Medical-grade skincare for rosacea focuses on formulations that support the skin barrier, reduce inflammation and prevent flare-ups. Key beneficial ingredients include:
· Niacinamide (vitamin B3): An anti-inflammatory and barrier-restoring ingredient that improves hydration and regulates sebum, typically used at 2-5% concentrations in products for sensitive or redness-prone skin.54-58
· Ceramides: Reinforce the lipid barrier and benefit patients with impaired skin barrier function common in rosacea.56
· Hyaluronic acid: A potent humectant that supports hydration and barrier repair; formulations combining multiple molecular weights tend to be better tolerated.54,56,59
· Glycerine and panthenol: Hydrating and soothing agents that promote barrier support and skin healing, useful during flare-ups or post procedure.60-62
· Green tea extracts: Provide antioxidant and anti-inflammatory effects, reducing erythema and oxidative stress, often included in calming gels or serums.7,60,63
· Titanium dioxide: A mineral sunscreen filter offering broad-spectrum UV protection with low irritation risk, ideal in SPF 30+ tinted sunscreens for sensitive skin.54,64,65
· Aloe: Extracted from the aloe vera plant, soothing aloe contains amino acids, vitamins and minerals.51,53,54
· Poria cocos extract: Recognised as a widely used herb in traditional Chinese medicinal formulations, this extract has soothing properties, excellent for redness and blemish-prone skin.54,66
· Hinokitiol: Extracted from the oils of the western red cedar tree, hinokitiol has antioxidant and brightening properties.54,67
A recent study in Journal of Drugs in Dermatology validated a rosacea-specific skincare regimen featuring AlumierMD’s Calm-R Serum, HydraCalm Moisturiser and Clear Shield Broad Spectrum SPF 30.51,53-59,66-67 In 30 subjects aged 35-65 with fair skin, eight weeks of use resulted in a 27% reduction in erythema, 37% improvement in radiance, 26% better overall appearance and 28% increased hydration – with no reported tolerability issues.54
Medical-grade products differ from over-the-counter options by offering higher active ingredient concentrations, enhanced stability and evidence-based delivery systems.68,69 These formulations complement prescription treatments by targeting inflammation, dysbiosis and vascular reactivity, helping improve long-term control and skin barrier restoration in rosacea.53
Topical treatments for rosacea are generally safe but may cause side effects such as dryness, peeling, irritation and contact dermatitis, particularly with azelaic acid, ivermectin, metronidazole and brimonidine.70 These effects are usually transient but can be worsened by overuse or compromised skin barriers. Rebound erythema may occur with brimonidine, especially in patients with reactive skin.70
Brimonidine should be used cautiously in individuals with cerebral insufficiency or severe cardiovascular disease due to its vasoconstrictive effects, despite minimal systemic absorption.70-71 Clinicians should review cardiovascular history before prescribing.45,71 Other topicals like ivermectin and azelaic acid do not share this vascular risk.
Azelaic acid can transiently lower skin pH and increase transepidermal water loss, potentially causing irritation, especially in sensitive skin, typically during the initial weeks of treatment.72,73
To minimise adverse effects, integrating medical-grade skincare that supports barrier repair and soothes inflammation – containing ingredients like ceramides, niacinamide, glycerine and panthenol – is essential.74 Daily use of broad-spectrum mineral sunscreen (e.g. titanium dioxide) is critical to protect against UV-triggered flares.44,75
Gradual introduction of topical agents and early clinical follow-up (within four to six weeks) helps optimise tolerability and adherence, allowing adjustments in treatment frequency and reinforcing skincare education.76,77
In patients with severe or treatment-resistant rosacea, oral therapies are often introduced. For papulopustular rosacea, first-line treatment typically includes tetracycline antibiotics (contraindicated in pregnancy).37 Options include doxycycline 40mg daily, which reduces antibiotic resistance risk, and lymecycline 408mg or doxycycline 100mg daily, which can be taken with or without food.38,78 When tetracyclines are contraindicated, erythromycin or clarithromycin (250–500mg twice daily) may be used.78 Treatment courses usually last around three months but can be adjusted based on response.
For flushing and erythema, beta-blockers such as carvedilol (6.25mg twice daily) or propranolol may be prescribed for three to six months.79-80 Clonidine (50mcg twice daily) is another option, particularly for women with pronounced flushing.80
Laser and light-based therapies, including pulsed dye laser and intense pulsed light, are effective for fixed erythema
and telangiectasia.81
Emerging treatments include botulinum toxin injections to reduce redness and sebum production, AI tools for diagnosis and monitoring and exosome-based skincare to aid healing and inflammation control.82-85
While research is ongoing, exosomes are being explored as a potential therapeutic approach for rosacea and other sensitive skin conditions. Research suggests exosomes can reduce redness, calm inflammation and improve skin barrier function.84,86,87
Other areas of interest include microencapsulated benzoyl peroxide, microbiome-supportive topical and oral therapies, LED phototherapy and minocycline 1.5% foam for inflammatory lesions.88-91
Rosacea is variable and relapsing, so I assess both clinical and patient-reported outcomes.5,31
My evaluation includes reduced stinging, burning, itching, flushing, erythema and lesions; improved skin comfort, hydration and product tolerance; increased confidence (e.g. going makeup-free); and less frequent or severe flares.14,92
While RASI is helpful, regular patient follow-ups should be prioritised.35 An initial check at six weeks can assess tolerability, another at 12 weeks to evaluate effectiveness and maintenance reviews every three to six months.
Rosacea management demands flexibility, empathy and an understanding of both the medical and emotional dimensions of the condition.1,5-7,11,31-32,36-38 Tailoring treatment by rosacea subtype, severity and skin tolerance – combining pharmacological and supportive skincare – provides effective relief and long-term skin health.1-2,5,7,9,14-17,53

Dr Sonakshi Khorana is a GP specialising in medical and cosmetic dermatology. She is the non-surgical services lead at Kat&Co in Birmingham, and holds memberships at the Royal College of GPs, British Medical Laser Association and Aesthetic Complications Expert (ACE) Group World. Qual: MBChB, MRCGP, PGDip Clinical Dermatology
Not an actual patient. For healthcare professionals who are eligible to prescribe neuromodulators. Relfydess™ is indicated for the temporary improvement in the appearance of moderate-to-severe glabellar lines (GLs) at maximum frown and moderate-to-severe lateral canthal lines (LCLs) at maximum smile alone or in combination, in adult patients under 65 years, when the severity of these lines has an important psychological impact on the patient.1
1. Galderma. Relfydess™ Summary of Product Characteristics. 2024.
This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions.

Join us and step into the future

18 & 19 September 2025

BAMAN: Relfydess™ Symposium
MARY IRVING RGN INP
Thursday 18th September
9:40am - 10:00am
The Eastside Rooms, Birmingham

25 & 26 September 2025 Excel, London
DR. MJ ROWLAND-WARMANN BSc BDS MSc Aes.Med. PGDip Endod. PGCert MJDF RCS
Thursday 25th September
12:00pm - 12:30pm
Aesthetics Journal Arena, Excel, London
Gold sponsors of BAMAN 2025
QR code to prescribing information and adverse event reporting.
Headline sponsors of CCR 2025 Visit us at stand F50
Galderma portfolio available at our distribution partners

Introducing Aura, the 3D imaging solution redefining workflow and results in aesthetic practice.
Capture the entire face and neck in one seamless shot, with full visual reconstruction and analysis completed in under a minute. It’s quick to use, easy to learn, and delivers instant, high-definition imaging backed by real-time skin, structure, and volume insights.
Built for aesthetic professionals, Aura streamlines your consultations with:
· Speed that fits your schedule
· Ease of use that fits your team
· Consistent, high-quality visuals that build patient trust




Discover Aura and the future of facial analysis.




















Request your demo.





aestheticsource.com
info@aestheticsource.com

Mental wellness has been identified as the number one health concern among adults, surpassing cancer and obesity.1 It has also been found that 50% of aesthetic patients are struggling with their mental health.2
To help combat this, a new device, EXOMIND, has recently been introduced by BTL Aesthetics into some UK aesthetic and regenerative clinics. With more aesthetic clinics onboarding more wellness, health and longevity services, this new approach is well suited to many clinics.
Transcranial magnetic stimulation (TMS) has been used in psychiatric medicine for more than four decades as a non-invasive treatment for certain mental health conditions such as depression and anxiety.3
TMS received US FDA clearance in 2008 for depression and has an extensive safety record in psychiatric use.4 Using this technology, EXOMIND has been US FDA-cleared for depression and CE-marked in Europe for depression, anxiety, obsessive-compulsive disorder (OCD) and binge eating.5
During treatment, the patient reclines while the EXOMIND device’s integrated coil is positioned on the left side of the head. The coil delivers controlled electromagnetic pulses to stimulate the targeted brain areas. Each session lasts around 25 minutes, is painless and does not require anaesthesia or downtime.5
The stimulation aims to restore optimal activity in neural circuits that influence mood
and cognition. Studies on TMS more broadly have shown that repeated stimulation over a course of sessions can encourage the brain to adapt its signalling patterns – a process known as neuroplasticity – which may contribute to sustained improvements in emotional wellbeing.6,7
A typical course of EXOMIND begins with a detailed consultation and wellbeing questionnaire to assess the patient’s mental health, treatment goals and suitability for TMS-based intervention. The recommended programme consists of six sessions, spaced five to 10 days apart.5
Reported benefits may last between six and 12 months, after which a maintenance session schedule may be considered.5
According to manufacturer BTL Aesthetics, there are currently four clinical studies available (though these are not yet published), with a total of 115 patients across all studies. Results indicated:5
· 90% reported improvements in well being
· 74% felt less stressed
· 71% slept better
· 87% improved self control over food cravings
· Patients seeking weight loss lost 2.3kg on average
Independent research is ongoing, with further data expected to be published later in 2025.
Treatment costs vary depending on the clinic but typically start from around £500 per session.5

Aesthetic practitioner
Miss Sherina Balaratnam has been offering EXOMIND in her clinic since December 2024, one of the first practitioners in the UK to offer the device, after being drawn to the science-driven innovation behind the device and its potential to complement her holistic approach to patient care. “As medical practitioners, we take a holistic view of patients, and this offers another unique way to support them,” she says.
She notes that over the years many of her patients have experienced anxiety, decision fatigue, poor quality sleep – particularly peri- and post-menopausal women – and increasingly sedentary lifestyles. “EXOMIND improves emotional wellbeing by restoring balance to our patients’ emotions by improving neuroplasticity. I have found this treatment is helping them optimise their lifestyle organically,” she explains.
The protocol in her clinic follows the recommended six treatments spaced across three to six weeks, with outcomes tracked via mental health questionnaires and video diaries. According to Miss Balaratnam, results can be rapid. “Patients tell me they feel lighter, their minds are clearer and they’re ready to get back on track,” she notes. She recalls one bereaved patient with severe social anxiety and panic attacks who, after three weeks of EXOMIND, was “socialising again, playing tennis and engaging with life. I have never seen anything work like this before.”
Miss Balaratnam also observes aesthetic improvements alongside wellbeing benefits, which she attributes to the brain-skin axis – the bidirectional communication between the nervous system and skin. “Since incorporating the device into my practice I have been conducting a study to see the difference the results of this device can have on the skin , muscle and connective tissue. It appears by treating the brain, there is a degree of neuromodulation occurring. I have found that when patients are more relaxed mentally, there are reductions in inflammation, breakouts, redness and even skin laxity,” she says.
Miss Balaratnam has also found it helpful for patients transitioning off GLP-1 medications, supporting emotional balance during what can be a challenging period, but notes more research is needed in this area.
While medical aesthetics has traditionally focused on improving physical appearance, there is increasing awareness of the role mental wellbeing plays in patient satisfaction and treatment outcomes.
Incorporating technologies such as EXOMIND reflects a broader trend towards holistic care, where physical and psychological health are addressed together.
The official UK launch of EXOMIND will take place at CCR on September 25-26. Turn to p.19 to register.
Redefining skin regeneration with precision exosome therapy and advanced bio-pulsing delivery
In the dynamic field of regenerative and medical aesthetics, few innovations have generated as much interest as exosomes. These nanoscale extracellular vesicles (EVs), secreted by cells to facilitate intercellular communication, offer unprecedented therapeutic potential thanks to their ability to modulate inflammation, stimulate tissue repair and support skin and hair regeneration.
Yet not all exosomes are created equal. Through its patented Bio-Pulsed technology, AM Biotech has transformed the production and delivery of exosome-based treatments, enhancing their biological activity, clinical reliability and regulatory readiness. In this article, we delve into the science behind exosomes, how Bio-Pulsing optimises their performance and what the latest research reveals about their use in aesthetic and regenerative practice.

Exosomes are extracellular vesicles ranging in size from 30 to 150 nm, secreted by numerous cell types, including mesenchymal stem cells (MSCs). They carry a potent biological cargo of proteins, mRNAs, microRNAs (miRNAs) and lipids, components that are capable of influencing the behaviour of the recipient cell. Their naturally low immunogenicity and ability to cross physiological barriers have made them ideal vectors for regenerative medicine, from wound healing and scar repair to antiageing and hair restoration therapies.1-3
In dermatology and aesthetics, exosomes are being investigated for their ability to:
· Promote dermal fibroblast proliferation
· Boost collagen and elastin production
· Regulate pigmentation and inflammation
· Stimulate hair follicle activity
Despite this promise, conventional exosome therapies face limitations in yield, purity and batch-to-batch consistency, issues that Bio-Pulsed technology seeks to solve.
The challenge: limitations of conventional exosome production
Traditional methods of isolating exosomes from mammalian cells typically yield small quantities with inconsistent molecular content. Purification processes often leave behind residual proteins, cell debris, or microvesicles, which can compromise safety and efficacy. Additionally, most commercial exosomes are unstable at room temperature and require cold-chain storage, which increases the cost and logistical complexity for clinical use.3
Bio-pulsing: a scientific leap forward
Bio-Pulsing is AM Biotech’s patented preconditioning process designed to radically enhance exosome production, purity and bioactivity. This is achieved by stimulating non-human stem cells, specifically, pathogen-free chicken embryo-derived MSCs, with botanical cues such as Polygonum multiflorum extract.
This biochemical stimulation induces a surge in exosome secretion, up to 93 times higher than baseline, and enriches their cargo with regenerative proteins and miRNAs.4 Preclinical findings confirm this: Biopulsed cells upregulate RAB27A (a key exosome-release gene), leading to superior EV output and quality.
Critically, these exosomes are then ultra-purified to greater than 99.99% purity, offering a shelf life of up to 3 years at room temperature. This eliminates the need for cold-chain storage while enhancing clinical versatility.
Clinical results: what the data says AM Biotech’s lead product, ExoGiov® and its brand LA EXO has been extensively validated in both laboratory and
clinical settings:
In Vitro Efficacy:
· Fibroblast proliferation: +113% with ExoGiov® vs. +87% with minoxidil
· Collagen Type I production: ↑ up to 389%
· Collagen Type III production: ↑ up to 340%
· Elastin expression: ↑ up to 390%
· Hair follicle dermal papilla cell growth: ↑ 127%
· Cytokine suppression (TNF-α, IL-6): ↓ up to 50%
These metrics strongly support the use of Bio-Pulsed exosomes in facial rejuvenation, scar repair and hair restoration applications.
Clinical trials highlights
A 2025 IRB-approved clinical study involving 60 human participants using topical Bio-Pulsed AMSC-sEV formulations (LA EXO® ampoule and essence) reported:
· Wrinkle depth: ↓ 7.3%
· Collagen density: ↑ 18.2%
· Hair A/T ratio (anagen/telogen): ↑ 48.7%
· Hair shedding: ↓ 46.5%
· No adverse events or sensitivity reported5 These outcomes were achieved using standardized trichoscopy, ultrasound and molecular assays such as qPCR and miRNA profiling, reinforcing the translational potential of this cell-free therapy.
Final thoughts
For clinicians seeking cutting-edge, non-cellular regenerative therapies, Bio-Pulsed exosomes provide an elegant solution supported by both scientific evidence and clinical data. Whether used post-laser, in conjunction with microneedling, or as part of a bespoke facial or hair treatment protocol, these biologically active vesicles are setting a new standard in results-driven aesthetics.
With a robust safety profile, regulatory clearance and strong clinical support, Bio-pulsed exosomes represent a pivotal advance in regenerative medicine, offering a needle-free approach that eliminates the need for stem cells and systemic risks.

Title: Rheological Properties of Hyaluronic Acid Fillers for Lip Volumization
Authors: Patricia Miranda Sousa Nogueira, et al.
Published: Aesthetic Plastic Surgery, August 2025
Keywords: Dermal filler, Hyaluronic acid, Volumization
Hyaluronic acid (HA) is widely used for facial rejuvenation and soft tissue volumization, with lip augmentation being one of its primary applications. The rheological properties of HA fillers are essential to ensure the efficacy and safety of procedures, directly influencing the aesthetic outcome and material longevity. This study aims to evaluate the rheological properties of three hyaluronic acid-based fillers indicated for lip volumization: Belotero Intense (Merz), Kysse (Galderma), and Volift (Allergan). Twenty-four syringes of fillers were analyzed, with 8 samples from each brand. The rheological properties investigated included storage modulus (G’), loss modulus (G’’), complex modulus (G*), phase angle (Tan(delta)), and cohesiveness. Measurements were conducted using the Kinexus PRO rheometer with parallel plate geometry. The results revealed significant differences among the three fillers. Volift exhibited higher resistance to deformation, reflected by the higher G* values, while Kysse stood out for its greater cohesiveness. These rheological variations suggest that each filler may be more suitable for different clinical applications, such as lip augmentation or deeper tissue filling.
Title: Skin Rejuvenation with Hyaluronic Acid and Sirtuin-1 Activa-tors (Nicotinamide Adenine Dinucleotide and Resveratrol): A Comparative Clinical Study of Microneedling and Injection Delivery
Authors: Dr Keiron Lord and Dr Arash Khademi
Published: Journal of Aesthetic and Regenerative Medicine, July 2025
Keywords: Skin rejuvenation, Hyaluronic acid, Microneedling
A novel skincare formulation has been developed to address these changes using five syner-gistic components: dual molecular weight hyaluronic acid (HA), Nicotinamide Adenine Dinucleotide (NAD+), liposomal resveratrol, biomimetic peptides, and mannitol. These actives collectively target hydration, oxidative stress, col-lagen synthesis, and mitochondrial function. Central to the formulation is the activation of Sirtuin-1 (SIRT1), a longevity-associated gene involved in DNA repair and cellular resilience (1), enhanced through the synergistic action of NAD+ and resveratrol. This clinical study was randomized and evaluated the efficacy of the formulation delivered through two methods: microneedling, consistent with the product’s authorized cosmetic use, and a five-point injection technique, representing an off-label application, in a total of 20 patients. The off-label administration was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and received prior approval from an ethics committee. Results showed a 55% increase in hydration and a 42% improvement in elasticity for the injection group, compared to 38% and 25%, respectively, for the microneedling group.
Title: Correction of Facial Asymmetry Using Dermal Fillers: Understanding the Role of Facial Rotation
Authors: Erik Koppert, et al.
Published: The Journal of Craniofacial Surgery, August 2025
Keywords: Asymmetry, Dermal filler, Rotational dynamics
Facial asymmetry is a common challenge in esthetic medicine, requiring a comprehensive understanding of three-dimensional rotation patterns-X, Y, and Z axes-that significantly influence treatment outcomes. Traditional correction methods often overlook these rotational dynamics. This manuscript presents a case study of a 38-year-old Asian male patient with facial asymmetry, treated with hyaluronic acid (HA) fillers using a novel approach incorporating facial rotation concepts. By identifying the patient’s clockwise facial rotation pattern and applying targeted, asymmetric filler placement, a significant improvement in facial harmony was achieved. The rheological properties of the MaiLi Extreme (Sinclair) were particularly suited for structural correction. This approach highlights the importance of rotation-based assessment and personalised treatment planning in achieving optimal esthetic outcomes.
Title: Thirty Years of Autologous Platelet Concentrates: From Platelet-Rich Plasma to Platelet-Rich Fibrin
Authors: Richard J Miron, et al.
Published: Journal of Periodontal Research, August 2025
Keywords: Growth factors, Platelet-rich fibrin, Platelet-rich plasma
Nearly three decades have passed since autologous platelet concentrates (APCs) were introduced into clinical practice. Harnessing the body’s natural healing capacity, platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) emerged to concentrate growth factors and cells at supra-physiological levels. Professor Robert Marx first demonstrated that PRP-obtained via centrifugation of whole blood with anti-coagulants-could accelerate healing across various indications. Later, eliminating anti-coagulants led to PRF, promoting a more natural and efficient healing process. In dentistry, APCs have consistently accelerated soft and hard tissue healing, either alone or with biomaterials. PRF has shown benefits in root coverage, periodontal regeneration, ridge preservation, third molar healing, sinus grafting, guided bone regeneration, and peri-implant soft tissue healing. Beyond dentistry, PRF improves outcomes in treating diabetic ulcers, managing joint pain, and enhancing esthetic procedures. This review highlights APC evolution, focusing on clinical applications and recent advancements such as horizontal centrifugation, concentrated PRF (C-PRF), and extended-PRF (e-PRF) membranes. These albumin-based membranes degrade over months and are now used as alternatives to collagen membranes in routine dental procedures.
Take your aesthetic expertise to the next level with guidance from the Merz Aesthetics Faculty. Whether you're refining your skills or expanding your knowledge, this programme is your next step toward becoming a toxin expert.

M-BOC-UKI-0658
Scan the QR code to access BOCOUTURE UK & Ireland
Prescribing Information
Date of Preparation: July 2025
Register your interest today

Scan the QR code to get in touch with one of our Aesthetic Account Managers
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at https://yellowcard.mhra.gov.uk/. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/reportan-issue. Adverse events should also be reported to Merz Aesthetics UK Ltd by emailing UKdrugsafety@merz.com or calling +44 (0) 333 200 4143.

Leadership coach Marcus Haycock shares how embracing the practice of leading strategically can boost your clinic success
The medical aesthetics field is evolving at an extraordinary pace, and with this expansion comes a range of challenges for clinic owners and practice managers. Practices today must manage economic pressures, stricter regulations and rising patient expectations, all while competing in an increasingly crowded market. Yet, one of the most overlooked hurdles is the underinvestment in staff training and leadership development. When clinics neglect structured leadership training, teams become disengaged, turnover rates climb, operations become inefficient and business growth stalls.
Over my two decades of experience within the aesthetics specialty, I have calculated that the top-performing 5% of clinics consistently place leadership development, staff training and team empowerment at the heart of their success. These practices weather market disruptions and flourish by building strong, value-driven teams that support their strategic goals.
What strategic leadership really means
Strategic leadership focuses on long-term planning and having a clear vision for the future.1 It involves leaders using creative problem-solving and strategic thinking to help their teams and organisations reach their goals.1 At its core, strategic leadership is more than just a style, it’s a mindset. It requires understanding the current situation, analysing data and planning ahead to achieve both current and future goals. Leaders who use this approach do well in changing environments, especially when facing competition or rapid market changes.
Through a medical aesthetics lens, this can be demonstrated by a clinic owner facing rising patient complaints. Instead of quick fixes, they review the clinic’s long-term direction, address cultural and procedural issues, introduce targeted training and embed shared values into daily operations – aligning purpose with practice. This future-focused approach improved patient experience, team cohesion and created sustainable change.
Set a clear vision for your clinic’s future by defining where you want to be in three to five years. Clearly articulate your mission and values so they’re evident in daily work. Establish a few measurable long-term goals to track progress and celebrate achievements.
In my experience of engaging with hundreds of teams and practices, it is common for clinic leaders to confuse management with leadership and vice versa. Management focuses on operational efficiency and task completion, while leadership emphasises inspiration, direction, team development and empowerment. The best leaders know this and balance task management with the motivational alignment of staff, ensuring operations run smoothly while creating that important environment, where creativity and growth can flourish.
A hallmark of strategic leadership is helping teams prioritise their high pay-off activities – the tasks that directly contribute to achieving long-term goals. Without this focus, teams can get bogged down by low-priority work and distractions, and business performance suffers. Effective leaders give their teams the support and resources to stay focused and productive. Ultimately, a practice owner’s role is to lead the clinic toward sustainable success by empowering every team member to achieve their full potential.
Within a clinic setting, a manager fixes delays by reshuffling the schedule – keeping operations on track. A leader addresses recurring delays by involving the team in finding solutions, inspiring ownership and improving processes for lasting results and greater staff engagement.
Clinic leaders should regularly review key performance indicators such as patient satisfaction, rebooking rates and revenue. Weekly, they can identify and address operational bottlenecks with the team. Additionally, allocating dedicated time for long-term planning and conducting monthly team meetings helps maintain focus and drive continuous improvement.
One of the most rewarding lessons from my career is that leadership can be developed and nurtured. Great leaders are made, not born, despite the myth often peddled online. With the proper training, practice owners and managers can elevate their effectiveness and bring out the best in their teams.
Empowered leadership can deliver remarkable results, such as reduced turnover, improved collaboration, higher patient satisfaction and a more cohesive workplace. When teams feel supported and connected to a shared purpose, the impact on patient outcomes is significant. Happy teams create exceptional patient experiences. This connection is rooted in empowered leadership. When managers prioritise strategic thinking and empower their teams, they cultivate a high-trust culture, one where people feel valued, prepared and psychologically safe.
An interesting study published in the Harvard Business Review highlights the tangible impact of this approach.2 Employees in high-trust organisations report 74% less stress, 106% more energy and 50% greater productivity.2 They also take fewer sick days, experience less burnout and report significantly higher engagement and life satisfaction.2
Developing leadership skills in aesthetics requires intentional effort and ongoing growth. The following roadmap outlines practical steps to foster leadership within your team.
1. Schedule leadership and communication workshops annually to build essential skills.
2. Establish mentorship pairings by matching senior practitioners with newer team members.
3. Conduct quarterly peer-feedback sessions to encourage constructive dialogue and development.
4. Rotate staff through small leadership projects, such as managing social media campaigns or improving the patient journey, to cultivate hands-on experience.
Monitor key metrics like patient satisfaction, treatment quality and retention closely. Conduct quarterly reviews focused on progress, not pressure. Remain flexible, adjusting plans as market trends, regulations or patient needs evolve to ensure continued clinic success.
Bringing purpose, vision and values to practice
Why does your clinic exist? What inspires your team to come to work every day? Answering these questions is central to strategic leadership. When team members connect with a practice’s mission, their work takes on greater meaning and motivation becomes



intrinsic, sustaining engagement even through challenges. Strategic leaders keep purpose front of mind by tapping into intrinsic motivation. Simple habits, like sharing the week’s most meaningful patient testimonials or reflecting as a team on what brings fulfilment, reinforce why the work matters.
Many clinic owners start their businesses with a clear vision and strong values. But as the practice grows, these guiding principles can become diluted and the vision can become clouded. I’ve worked with leaders who display their values prominently in their clinics but fail to embed them in day-to-day operations. When values remain surface-level, they lose their power and effectiveness. As clinics expand, core values can fade. Embedding them in daily decisions, recognising real examples in performance reviews and sharing ‘values in action’ stories during huddles keeps them alive – ensuring patient care, compassion and integrity remain the driving force behind every choice and interaction. Embedding values in documentation is not enough, they must be consistently demonstrated. Regular coaching conversations between managers and staff help uncover what motivates individuals. Questions like “What are you most proud of this week?” reveal whether core values, such as care and service, are truly shared. If responses focus solely on financial gain, it may indicate a cultural misalignment. In service-led practices, patient care must remain a lived and collective priority to preserve the integrity of the culture.
Successful clinics I’ve worked with have transformed performance by embedding core values, such as teamwork, empathy and respectful communication, into staff evaluations. These values are clearly defined for each role, guiding behaviours like supporting colleagues and caring for anxious patients. Common pitfalls include vague definitions, inconsistent scoring and leaders failing to model values, which undermine fairness and credibility. Rather than focusing on results, effective clinics also assess how goals are achieved, ensuring work aligns with agreed values. This fosters accountability, pride and ownership across the team while reinforcing the clinic’s true culture.
To embed clinic values, implement a ‘Values in Action’ board or a 10-minute weekly team huddle. Agenda items can include sharing a patient success story, recognising a team member living the clinic’s values and highlighting upcoming challenges aligned with the clinic’s mission.
Six critical questions to uncover leadership gaps
If a practice’s mission is to deliver five-star patient care, practitioners support this by providing consistently patient-centred consultations.
1. Is your practice’s mission and vision clearly defined, and does every team member understand their role in achieving it? During onboarding, provide staff with clear role descriptions linked to the practice’s mission and values. Supply a concise induction pack outlining the clinic’s vision. Ensure performance management frameworks evaluate both values-based behaviours and operational goals.
2. Are your values embedded in daily operations, and can your team members articulate and live by them? Staff can show compassion and teamwork by supporting patients and coordinating care, like a nurse calming a patient while working with colleagues.
3. Do you and any other managers you work with understand the difference between leadership and management? Are you all equipped to empower your teams, or is further strategic brainstorming required?
4. Is your team aligned around shared goals, focusing on high-payoff activities that support strategic objectives? Leaders can guide self-focused staff by aligning personal goals with team objectives, using empathy, clear expectations, feedback and celebrating collaborative progress.
5. Do you have structured training programmes in place to create embed leadership skills and enhanced collaboration?
6. Is your practice culture built on trust, open communication, continuous feedback and psychological safety? Embedding continuous feedback and supportive leadership promotes inclusion, empowerment and ongoing improvement – ensuring every team member feels valued, heard and motivated.
costs of underinvesting in leadership
Lack of structured leadership development can lead to some serious setbacks:
High staff turnover: Talented employees without growth opportunities will often seek positions elsewhere, creating more business disruption, extra workloads and potentially lower morale.3
· Disengaged teams: When staff lack a clear purpose, do not set meaningful goals and do not strive to achieve them, motivation will often wane, and consequently, practice performance will also take a hit.4
· Operational inefficiencies: Managers who focus solely on task completion to drive efficiency may completely miss human opportunities to connect, delegate, innovate, develop and empower their teams.
The positive news is that all these issues can be relatively easily addressed with commitment to professional management and leadership development.
Adopting a strategic leadership approach, if done well, will often deliver the following results:
· Stronger collaboration: Shared goals often inspire increased accountability and greater teamwork.
· Lower staff turnover: A culture that values and supports employees, making them want to stay.
Higher patient satisfaction: Engaged staff deliver exceptional service and care.
· Greater resilience: A clear sense of purpose helps teams remain motivated during challenging times.
Now is the time to act
The challenges facing the medical aesthetics specialty are real, but so are the opportunities. By investing in strategic leadership development, you can create a thriving, purpose-driven practice where your values come to life, your team excels and your patients receive exceptional patient experience.

Marcus Haycock, a leadership development coach, has more than 22 years of expertise in medical aesthetics. He founded Transformational Leadership Consulting Ltd, and partners with Leadership Management International (LMI), supporting its Total Leader programme.
Within the medical aesthetics specialty, where treatments are widely accessible and expectations high, patient dissatisfaction is inevitable. Managing it is one of the most complex and emotionally challenging parts of practice.
Patient dissatisfaction may stem from unmet clinical outcomes, unrealistic expectations shaped by social media or psychological factors like anxiety, body image issues, recent trauma or undiagnosed Body Dysmorphic Disorder (BDD). Regardless of the cause, its effects extend far beyond the individual consultation, influencing the clinic’s reputation, team morale and the practitioner’s own sense of professional fulfilment and wellbeing.1-5
Understanding the roots of patient dissatisfaction
Often, a patient’s unhappiness isn’t a direct reflection of the clinical outcome, especially when the procedure has technically gone to plan. Persistent complaints, like asymmetry, subtle results or unmet internal ideals, can arise despite objectively good outcomes. Understanding why is key to effective management.1,4
expectations
Unreasonable standards remain a primary driver of patient dissatisfaction, often fuelled by mass media and celebrity culture. Patients may seek flawless or surgical-level results from non-surgical treatments, often reinforced by idealised marketing.
To avoid this, practitioners should use real, unedited patient images (with consent) and ensure all marketing reflects achievable outcomes, in line with the Advertising Standards Authority (ASA) and Committee of Advertising Practice (CAP) guidelines, prohibiting exaggerated claims or edited imagery to protect patients and build trust.6 Referencing edited images in consultations can help manage expectations and guide patients toward realistic, informed goals.
It’s essential to clearly explain what a treatment can and can’t achieve – under-eye filler, for instance, won’t address skin laxity or pigmentation, which may require additional procedures. Set realistic timelines, as results from toxins take days to weeks, while skin treatments often require multiple sessions. Be transparent about common side effects like swelling or redness and mention rare but serious risks such as vascular occlusion.
Always discuss limitations openly, emphasise that combination treatments may be needed and ensure the patient fully understands the process. 2,4 Providing this information in writing, via consent forms, pre-treatment leaflets or post-consultation emails, helps reinforce patient understanding and ensures informed consent.
Aesthetic concerns often reflect deeper psychological issues. While BDD affects about 1.9% of the general population, rates rise to 13-20% in cosmetic settings, especially for procedures like rhinoplasty.1,5 Individuals with BDD often seek cosmetic treatment
to resolve internal distress but typically report low satisfaction post-procedure.6 UK guidelines recommend referring suspected BDD cases for mental health assessment before treatment. 3 Other factors – like anxiety, perfectionism, past trauma or personality disorders, can also lead to dissatisfaction. Red flags include excessive focus on minor flaws, conflict with past providers or disproportionate emotional reactions. Ethical practice requires assessing psychological needs and referring when necessary. 3,4
Routine screening should include observing behaviour, using tools like the Body Dysmorphic Disorder Questionnaire (BDDQ) or Dysmorphic Concern Questionnaire (DCQ) and documenting mood and attitude.7-9
Clinics must have referral pathways and train staff to recognise and escalate issues. Treatment should be declined if expectations are unrealistic, distress is excessive or motivations seem psychological. This decision must be explained, documented and follow guidance from the General Medical Council (GMC), Nursing and Midwifery Council (NMC), General Dental Council (GDC) and the Joint Council for Cosmetic Practitioners (JCCP). 3,4,10-13
Communication breakdowns
Seeds of dissatisfaction are often sown early due to rushed consultations, limited listening and failure to explore patient motivations. Clear, honest and empathetic communication is essential – not just to build trust and manage expectations, but also to prevent negative reviews, complaints or legal issues.1,4
Practical strategies to reduce these risks include:
· Using layman’s language: Avoiding clinical jargon wherever possible.
· Supporting explanations: Use visual aids such as standardised before-and-after photos or anatomical diagrams.
· Implementing structured communication protocols: Post-consultation summaries, written aftercare instructions and follow-up calls or emails to ensure patient understanding.
· Encouraging open-ended questions: Check comprehension and clarify uncertainties.
Communication is a team effort. Front-of-house staff should be trained in empathy and active listening to support positive interactions and detect early concerns. A 2022 review shows empathy training improves communication, satisfaction and outcomes.8
Technology enhances the patient journey by streamlining information gathering, personalising follow-ups and supporting care between visits. When used well, it boosts clarity, consistency and engagement.1,4
Despite best efforts, complaints happen. A structured, calm approach reflecting professional standards is essential.4
The review meeting is crucial for addressing dissatisfaction by reviewing records, listening actively and validating patient concerns in a supportive setting.
· Preparation: Thoroughly review the patient’s records, including consultation notes, consent forms, alongside pre- and post-treatment photographs before the meeting.
· Setting: Ensure a private, unhurried environment for an open discussion. While initial contact may be by phone or email, a face-to-face review is recommended to fully assess the issue and show commitment to resolution. 2
· Listen first: Allow the patient to express their concerns fully and without interruption. Employ active listening techniques,
such as nodding, maintaining eye contact, paraphrasing their concerns (‘So what I’m hearing is that you felt…’) and asking clarifying questions (‘Can you tell me more about what you expected?’), to show you understand their perspective and are taking their experience seriously.
· Validate feelings: Acknowledge the patient’s expressed feelings (e.g. ‘I understand that you feel disappointed or concerned’) without prematurely admitting clinical error when the outcome falls within expected parameters.4
Use evidence: Refer to clinical photos and the documented discussion points regarding expected outcomes and potential risks from the initial consultation and consent process.
· Reiterate realism: Gently, but clearly, restate the realistic outcomes and limitations discussed pre-treatment, using the documented information for support.
Communication strategies
Use reflective listening (e.g., “If I understand you correctly…”) to validate concerns and build understanding. Focus on 'I' statements based on clinical assessment rather than potentially confrontational 'you' statements. Stay calm, use professional body language and speak in plain, non-medical terms. Be honest and transparent when delivering difficult news to build trust and defuse tension.1,4
Declining further treatment
If further treatment is inappropriate or unlikely to help, especially due to unrealistic expectations or psychological factors, practitioners must be ready to decline. Frame this around patient safety and clinical integrity.1,4 Use a calm, empathetic tone with clear reasoning, such as, “Given your response so far, further treatment is unlikely to help and may increase risk.” Reinforce that this decision follows best practice and ethical standards. Offer alternatives, such as a future review or mental health referral if needed, and document the rationale clearly.1,2,4
Second opinions and formal complaints
When appropriate, offer a second opinion from a trusted, qualified colleague, ideally within a recognised register or peer network.1 If dissatisfaction persists, clearly explain your clinic’s formal complaints process. This should follow the standards of the GMC, NMC, GDC and the Professional Standards Authority for Health and Social Care (PSA), with a written policy outlining steps, timelines and escalation options.4,12,13 Walk the patient through the process with empathy and transparency, reinforcing your commitment to professional care and resolution.1,2
Managing online fallout
Professional standards apply equally online.4 Respond to negative reviews calmly and respectfully, avoiding defensive language.1,4 Acknowledge feedback while safeguarding patient confidentiality, never disclose clinical or personal details.1,4 Where possible, move the conversation offline via phone, email or a follow-up appointment to address concerns directly. For example:
“Thank you for your feedback. We’re sorry your experience did not meet expectations. While we cannot discuss individual cases publicly, we welcome the chance to speak directly. Please contact us at [email] or call [number].”
This approach reflects GMC, Aesthetic Complications Expert (ACE) Group World, NMC and GDC guidance on handling complaints professionally. 2,4,12,13
Refunding a patient when there’s no clinical failure is complex and often feels unjust. However, it can sometimes be a pragmatic
decision based on a holistic assessment of the situation. Consider the total ‘cost’ beyond financial matters, such as the emotional energy, time investment, potential team stress and risk of protracted conflict or formal complaint escalation. Ask yourself, is the dissatisfaction primarily emotional or psychological? Is further dialogue unlikely to yield resolution? Is a refund the most efficient way to achieve closure and de-escalate?
In the UK, refunds are not legally required if services meet agreed standards and consent. However, under the Consumer Rights Act 2015, patients may seek redress if services fail to meet promises or professional standards.12,14
There’s no one-size-fits-all answer, but decisions about refunds should not be driven by guilt. If issuing a refund, do so with a carefully worded letter, preferably reviewed by your indemnity provider. In the UK, valid professional indemnity cover is a legal requirement for all healthcare and aesthetic practitioners.10 Be empathetic, avoid admitting liability and, if appropriate, confirm the outcome was within expected standards.1,4
Be mindful of repeat refund requests or complaints, as patterns of entitlement or manipulation may emerge. Maintain clear communication, detailed records and firm boundaries. Where appropriate, advise that further treatment is not in the patient’s best interest and decline future services in writing.12
Managing patient dissatisfaction can be emotionally draining, making practitioner and team wellbeing vital for safe, ethical and sustainable care.
· Set boundaries: Clearly communicate work hours and contact methods. Avoid using personal devices and learn to say ‘no’ when needed.
· Prevent burnout: Medical aesthetics carries high stress. Watch for signs like exhaustion or detachment and prioritise selfcare and peer support.
· Support the team: Train all staff to handle early signs of dissatisfaction and have clear protocols for escalation. Foster open communication and debrief after difficult cases.
Clinic owners should respond to team complaints supportively and professionally. Review the case together, checking records, communications and photo evidence. Avoid blame, focus on facts and reassure practitioners, especially those early in their careers. Use the incident as a learning opportunity, document outcomes, address system gaps, reinforce protocols and seek indemnity advice if required.1,4,12
Managing dissatisfied aesthetic patients requires empathy, clear communication, confidence and ethical practice. Though challenging, these situations offer valuable learning opportunities. Our priority is to provide safe, evidence-based care while addressing concerns respectfully, without needing to resolve every emotional response.1,4

Tanya Khan is an independent nurse prescriber with more than 16 years of experience in medical aesthetics, specialising in theatre nursing and ophthalmology surgery. A Level 7 qualified injector and lead representative for Northern Ireland at the British Association of Medical Aesthetic Nurses (BAMAN), she advocates for patient safety, ethical practices and stricter regulations in cosmetic treatments.
Qual: RGN, INP, PgCert, PgDip Level 7
Digital marketing consultant Rick O’Neill shares insights on building sustainable growth through patient-centric strategies
The specialty is filled with promises of quick results, such as ‘30 new patients a week. Guaranteed!’ Unfortunately, the reality is far more complex. A 2025 sociological study based on interviews with aesthetic surgery patients found that trust develops over multiple encounters, including institutional, interpersonal and in-clinic interactions.1 People don’t rush into treatments, they build confidence over time, especially with elective procedures. The truth is that most new patients spend between three to 18 months researching treatments before making a booking. 2 This delay is especially true for high-value procedures like body contouring or higher budget combination treatment plans. Clinics that expect instant conversions will struggle to see sustainable growth. Instead, success lies in understanding the patient journey and providing the right content and engagement at each stage. This article highlights the challenges and best practices for converting leads in medical aesthetics.
The myth of instant conversions
It is tempting to think that someone will see an ad, click and book straight away. But in medical aesthetics, most people need multiple interactions before taking that step. Studies suggest that a prospective patient may need six to 12 touchpoints before they feel confident enough to make an enquiry. One such study was the ZMOT study, by Google. Zero Moment of Truth (ZMOT) model highlights that for 88% of consumers, decisions are made long before any direct contact. On average, they consult around 10 sources when researching treatments. Especially in elective fields like medical aesthetics, that online research phase is key: it’s where potential patients form impressions, weigh risks and only gradually arrive at booking intent. 3,4
During this time, potential patients are silently engaging with your brand, following your social media, reading reviews and searching for information. Many will Google questions like “How long does Botox last?” or “Best skin clinic near me?” long before they ever reach out. This is why simply generating leads is not
enough. Clinics must have strategies in place to nurture and guide those leads towards booking a treatment.
role of the front-of-house team
Effective lead conversion is not just a marketing function; it requires a clinic-wide approach. Front-of-house teams, treatment providers and reception staff all play a crucial role.
Some key best practices include:
· Pre-booking future treatments: Encourage patients to plan their next visit before they leave the clinic.
· Understanding patient timelines: When a new enquiry comes in, ask when they are hoping to proceed. If they are not ready yet, schedule a follow-up.
· Using WhatsApp for follow-ups: Many people feel self-conscious about treatments, making unexpected calls intrusive. A quick message first can improve response rates.5 Remember, to comply with General Data Protection Regulation (GDPR), you do need the patient’s consent to continue any WhatsApp conversation, long before any direct contact.
For example: “Hi Jenny, this is Rick from LTF Clinic. Thank you for your enquiry about full facial rejuvenation. I just wanted to check if you’d like me to share some further information or arrange a time for a chat. No rush at all, I’ll work around what suits you best.”
· Accurate lead tracking: Ensure that patient records reflect their actual journey. Someone who originally found the clinic via Google but booked after an email campaign represents two key touchpoints that should be logged.6
Mapping the patient journey
In order to grow sustainably, you need to meet patients where they are.
Awareness stage (zero to six months) At this stage, potential patients have just discovered your clinic. This could be
through an ad, a social media post or a friend’s recommendation.
What works best:
· Quick Instagram Reels showcasing treatment results or debunking myths.
· Behind-the-scenes content showing the team and treatment processes
· Non-pushy, educational ads that inform rather than sell
Consideration stage (three to 12 months)
Now, they are researching and comparing clinics. They might be reading reviews, asking for recommendations or looking up common treatment concerns.
Effective strategies, with content repurposed across all platforms and channels ideally:
· Blog posts or carousel posts answering “Is Profhilo right for me?”
Patient journey content in video and written form that shows real experiences
· Interactive quizzes on your website such as “Which treatment is right for me?” or “Tell us your skin type by answering these five questions” (this data can then be used to customise future email campaigns)
· Email sequences covering FAQs and treatment benefits
Decision stage (one to six months)
They have filled out a form, sent a DM or even called, but they still hesitate before committing.
Ways to encourage conversion:
· Warm WhatsApp follow-ups providing clear next steps
· Detailed consultation availability and preparation guides
· Videos explaining what happens during a first visit
· Case studies showcasing patient investment and long-term results
Booking and first visit
The patient has committed to their first appointment. This is where retention efforts should begin.
Best practices:
· Structured consultations that map out long-term plans
· Automated reminders and pre-treatment advice
· Starter product bundles or aftercare packages
Retention and loyalty
Long-term success in aesthetics depends on retention. A single treatment is just the beginning.
Retention strategies:
· Monthly 'Skin Club' in-person check-ins or tweakment reviews as part of a membership offering
· Loyalty rewards or referral perks
· Before-and-after comparisons to track progress and reinforce treatment value
Effective digital marketing tactics for lead conversion
Turning interest into action requires the right mix of strategy, timing and tools.
Email marketing that nurtures
Aesthetic clinics benefit from structured email campaigns that educate and build trust over time.7 These can include:
· Informational content about popular treatments
· Real patient stories and case studies
· Special consultation invitations or seasonal treatment reminders
Smart lead management systems
Many enquiries do not convert immediately, but with proper tracking, they can be re-engaged when the time is right. Effective systems include:
· Customer relationship management (CRM), such as Beamy, Zenoti or Pabau 2, tools to track where each patient is in their journey
Automated but personalised follow-ups for older leads
· Pipeline visibility to help front-of-house teams prioritise outreach
Targeted paid campaigns
Not all potential patients respond to the same type of messaging. Tailored ads should match where a person is in their journey:
· Awareness stage: Educational content and brand introduction
· Consideration stage: Case studies and detailed FAQs
· Decision stage: Invitation to book a consultation if the patient feels ready
SEO-driven content
Many potential patients begin their journey with Google searches. Well-optimised content can help clinics rank for key questions such as:
· “How long does laser hair removal last?”8
· “What is the difference between skin boosters and Profhilo?”
Some of the most competitive keyword terms for aesthetic clinics include “Dermal filler treatments near me” or “Aesthetic clinic near me,” and it’s important to create content and meta data across your website that includes such terms, along with educational content that will show Google you are the expert in these areas.
This type of content establishes credibility and attracts warm leads who are already in research mode.
Building sustainable patient relationships
Medical aesthetics is not about instant sales; it is about building trust over time. Clinics that prioritise patient education, follow-ups and relationship-building will always outperform those chasing quick wins.
Every potential patient represents long-term value. Treating them accordingly, by respecting their research timeline and supporting them with the right content, ensures steady, sustainable growth for any aesthetic practice.
I worked with a London-based clinic that struggled with high website traffic but low conversions. Instead of increasing ad spend, we refined their lead nurturing approach by implementing:
· A structured email sequence for educational follow-ups
· Warm, conversational WhatsApp messages to previous enquirers
· Regular social proof via patient testimonials and before-and-after imagery
Six week email sequence:
We built a six-week automated email journey designed to educate and reassure, not push.
Week 1: Welcome and orientation
Subject: “What to expect on your treatment journey”
Content: A simple thank-you, an outline of available treatments, and a link to a “Your First Consultation” guide
Weeks two and three: Educational spotlight emails
· One per week focusing on a common concern
· Example: “Are dermal fillers safe? What every patient should know”
· Language used: “You’ve probably heard mixed messages online. Let’s clear up the facts…”
Weeks four and five: Social proof and storytelling
· Patient testimonials and before -and-after imagery with consent
· Example: “Meet Sarah, who wanted a subtle refresh before her wedding. Here’s her experience…”
Week six: Consultation prompt
A gentle nudge: “Whenever you’re ready, we’d love to welcome you. Click here to book your consultation at a time that suits you”
Timing:
First message within 48 hours of their initial enquiry
Second message seven days later if no reply
· Final courtesy check-in after three weeks
Sample messages:
· “Hi Emma, thanks again for reaching out to [Clinic Name]. I just wanted to check if you’d like more details on the [treatment name] you enquired about. No pressure, happy to share whenever you’re ready.”
· “Morning Emma, I thought you might find this helpful: a quick before -and-after from someone with similar goals to yours. Would you like me to send it across?”
This approach worked well because patients often felt more comfortable replying to a message than answering a phone call. According to Cognism’s 2025 data, the average live answer rate now stands at only 2.3%, nearly half the rate seen in 2024.9 That underlines why clinics need a nurturing sequence rather than relying on phone-first contact.

Rick O’Neill is a digital marketing consultant with 26 years of experience. O'Neill is a digital consultant to the medical aesthetics, cosmetic surgery and pharma sectors and is founder of LTF Digital – an agency dedicated to the aesthetics market.




“Aesthetics is a fast moving field, and you can never really anticipate what's around the corner”
Dr MJ Rowland-Warmann shares insights into her dental background and recent US innovations

Raised in Germany, dentist and aesthetic practitioner Dr MJ Rowland-Warmann was raised in a family deeply rooted in medicine. With a mother who is a doctor, and several relatives working as doctors and dentists, healthcare was a constant topic of conversation at home. This environment naturally sparked her lifelong interest in the field.
At age 11, she moved to England for secondary education, intending to pursue a career in medicine. However, in 2000, very few universities accepted students under 18 into medical programmes. Having completed her A-levels at 16, Dr Rowland-Warmann’s options were limited, and she did not achieve the grades required for medical school. Instead, she chose to study biomedical sciences at Manchester University – a decision she now describes as a “wonderful occurrence.”
Studying biomedical sciences opened up a new path for Dr Rowland-Warmann, as she developed a growing interest in dentistry. She was drawn to its blend of hands-on skill, patient interaction and scientific knowledge. This led her to apply for dentistry at Manchester University, where she completed the programme and qualified in 2009. Reflecting on her academic journey, Dr Rowland-Warmann shares, “I loved every minute of it. The path I chose made me a much more mentally sophisticated student. I viewed my degree in biomedical sciences as a bit of a dry run for maturity and adulthood, helping me develop the focus and discipline to study effectively.”
After qualifying in 2009, Dr Rowland-Warmann began taking her first aesthetic training courses and quickly developed an interest in the field. She explains, “My mom practiced aesthetics since the early 2000s, so I had always had it on my radar and it was one of the things that I really wanted to get into. She advised me to do it as soon as I could.”
Dr Rowland-Warmann established her own practice in 2013, alongside her now husband, with the vision of integrating dental and aesthetic services. She initially opened a modest aesthetic clinic in Liverpool, consisting of just one treatment room and a reception area, but the clinic grew steadily over time and within a year of opening, dental services were introduced. In 2014, she began her masters degree in medical aesthetics at Queen Mary University, graduating with Distinction in 2016. Dr Rowland-Warmann’s dissertation focused on the management of vascular occlusions, as she describes this as a subject that was “largely overlooked” in the specialty at that time. By 2016 the clinic had doubled in size, and by 2018 it expanded again into a multi-room facility offering comprehensive aesthetic
and dental services. Just before the COVID-19 pandemic, it developed into an aesthetic hub with six treatment rooms, dental surgeries and a lecture space for training.
Dr Rowland-Warmann shares, “As a dentist and injector, I have always felt that toxins, fillers and managing complications are a natural extension of my skill set – areas where I feel confident, highly competent and genuinely enjoy working.” She adds that introducing ultrasound technology into her practice five years ago was a transformative milestone, significantly enhancing safety, precision and her ability to manage complications effectively.
Reflecting on the progression of treatments within the specialty, Dr Rowland-Warmann discusses the use on cannulas in practice. “I entered the field when cannulas weren’t really a thing. At the Clinical Cosmetic Regenerative Congress (CCR), back in 2012, I saw Dr Kate Goldie injecting on stage with a cannula.” She elaborates, “The audience around me were saying this was never going to catch on, and how wrong were we!”
She describes the clinic’s current routine as a balance of injectables, complication management and an expanding portfolio of skin and laser treatments. Each team member is encouraged to deliver the highest standard of care, while Dr Rowland-Warmann retains her role as the leading authority on injectables and ultrasound-guided procedures. She stresses that it is better to master a select number of treatments with precision and safety than to offer a broad range that cannot be delivered to the same standard.
Her commitment to innovation is evident in her interest in regenerative treatments. She is particularly excited by products emerging in the US, such as platelet-derived growth factor (PDGF) for the under-eye area, alongside injectable fat regeneration treatments, which show for delicate areas like the neck and hands. She explains, “I've seen some very promising results from my colleagues in the US, and I'm hoping that soon we will have that available in the UK market.”
Beyond her clinic, Dr Rowland-Warmann’s serves as a key opinion leader for Galderma, teaching practitioners across the globe. She speaks at conferences, delivers masterclasses on Sculptra and demonstrates innovative techniques, including the use of the new neurotoxin, Relfydess. Reflecting on her passion for teaching, Dr Rowland-Warmann concludes, “It provides me with insight into how other practitioners operate, and you get to meet new people. It can be daunting, standing in front of people and teaching with authority, but it’s also rewarding.”
What is your favourite holiday destination?
I go to the US a lot because that's where I fly. So I guess I'd have to say my favourite holiday destination is the sky!
What is your best career advice?
If you don’t like your career, change it. I converted to aesthetics full time and haven’t looked back!
Who is your role model, in the specialty or outside of it?
My role models in the world are all the female pilots out there.
Dr MJ Rowland-Warmann will be speaking at the Aesthetics Journal Arena at CCR on Thursday September 25 at 12:00pm. Turn to p.19 to register for free now.
Dr Shirin Lakhani debates whether the specialty has come far enough in its approach to vulvo-vaginal treatments
When I first began offering vulvo-vaginal treatments, such as platelet-rich plasma (PRP) and radiofrequency, it was very clear that there was a lack of awareness and education around this area – both among patients and practitioners. Women simply didn’t know the options available to them, and those who did often felt embarrassed or ashamed to ask. There has long been a taboo surrounding intimate health. It was often referred to as ‘designer vagina’ implying the treatments were purely aimed at improving the aesthetic appearance of the vulva, rather than providing real life-changing functional improvements. Even in clinic settings, the topic wasn’t openly discussed.
In recent years, we’ve seen real progress. The technology has advanced significantly, and we’re finally starting to have more open, honest conversations – both in clinic and in the media – about what women go through and what can be done to help. But despite all of that, I still believe we have a long way to go.
A changing landscape
In 2017, I went on daytime TV show This Morning to talk about vaginal health. The press went crazy. There were multiple articles with a lot of negative comments from the public. The majority of people weren’t ready to hear it. There was a lot of awkwardness, and I think it made people feel uncomfortable.
However, when I went on the same show earlier this year, the response was completely different. The press did what they usually do, however the public response to the articles was very different. Instead of trying to shame women and perpetuate the taboos, the comments instead focussed on reprimanding the media for trying to sensationalise medical treatments. Women were messaging to say thank you, saying they finally understood that there were options out there. A subject that used to be completely taboo is now being received well, helping to normalise the conversation.
The technology has also come such a long way. When I first started offering these treatments, the devices were more limited – you had to really manage patient expectations. But now, we have far more advanced systems with better energy delivery, more safety data and protocols that can be tailored to different concerns, whether it's laxity, dryness or urinary incontinence. Newer devices such as the Empower RF from InMode combine multiple treatment modalities in one platform allowing a customisable approach to intimate treatments. The results are much more predictable, and patients are seeing real changes, not just physically but emotionally too.
Interestingly, I’ve found that once a woman has had a positive experience with vaginal treatments, she will tell her friends. These patients are becoming advocates – not just for the treatment itself, but for breaking the silence. Word-of-mouth is still the most powerful tool we have in normalising this area of care.
What’s missing is practitioner confidence. That’s why I spend a lot of time encouraging other professionals to explore this area – not just as a business opportunity, but as a chance to really transform lives.
We’re not there yet
Despite this progress, we’re still not where we need to be. The landscape is changing, yes, but the shift has been slow. The stigma hasn’t completely gone – it’s just become more subtle. Even now, many patients will say things like, “I’m really sorry to talk about this,” or “I’ve never mentioned this to anyone before.” They’ll lower their voice or look uncomfortable. And I get it – they’ve never been given permission to speak openly about these concerns. The embarrassment, the hesitation, the idea that these concerns are somehow ‘less important’ than other treatments is all still there, just beneath the surface.
That’s why it’s so important to create a safe, open space where these conversations can happen without shame. From the moment a patient walks through the door, they need to feel that this is a normal, valid and treatable issue. We shouldn’t be relying on patients to carry the responsibility of spreading awareness. The medical aesthetics specialty has to step up too.
As the scope of the NHS shrinks, medical aesthetics clinics can help fill the void. It is clear that we have access to safe, effective treatments that are unlikely to be available on the NHS, but we have a responsibility and a duty of care, to ensure the treatments we offer have a suitable evidence base behind them for safety and efficacy, and have the appropriate certification.
What we need is more visibility around these treatments. They should be featured more heavily in conferences, discussed in training programmes and represented in medical journals and the consumer media – not hidden in the background. We should be seeing case studies, best practice guidelines and a clear message that vulvo-vaginal health is just as important as anything else we treat. It’s time to stop seeing it as a niche service and start recognising it as a fundamental part of holistic patient care. We need to model what it looks like to speak about vaginal health openly, professionally and compassionately. That’s how we build trust – not just with patients, but across the specialty.
Of course, it should be emphasised that these treatments should absolutely be done by people who are properly trained, people who understand the anatomy, the indications and how to approach the conversation sensitively. I firmly believe that female intimate health treatments should be carried out by doctors with gynaecology qualifications (MRCOG, DRCOG) or under their supervision.
So yes, the landscape is changing, and that’s encouraging. But we’ve not come far enough. There’s still work to be done to remove the stigma, increase accessibility and make vaginal treatments a standard part of aesthetic care. Until every woman feels comfortable talking about her intimate health – and confident that she can find effective, respectful treatment – our job isn’t finished. The conversation has started. Now it’s up to us to keep it going.

Dr Shirin Lakhani is a cosmetic practitioner specialising in advanced aesthetic treatments, intimate health and HRT for men and women. Dr Lakhani appears regularly on television and in the press, as well as contributing to articles and speaking at conferences both in the UK and internationally.
Qual: MBBS, DRCOG, MRCGP
