Relfydess™ provides a natural, revitalised look that patients are satisfied with and would recommend1-5
~90% were satisfied after 1 month and satisfaction remained high through 6 months*2,3
Up to 98%
would return for treatment and recommend Relfydess™ after 1 month, with up to 90% agreeing through 6 months†4,5 71% preferred Relfydess™ compared to previous neuromodulators they’d been treated with after 1 month‡6
Relfydess™ is indicated for the temporary improvement in the appearance of moderate-tosevere glabellar lines (GLs) at maximum frown and moderate-to-severe lateral canthal lines (LCLs) at maximum smile alone or in combination, in adult patients under 65 years, when the severity of these lines has an important psychological impact on the patient
FLTSQ, Facial Lines Treatment Satisfaction Questionnaire; GL, glabellar line; ITT, intention-to-treat; LCL, lateral canthal line.
* Based on the Facial Lines Treatment Satisfaction Questionnaire (FLTSQ) completed by all ITT patients treated with Relfydess in the READY-1 and -2 studies. 94% (GLs, n=218) and 87% (LCLs, n=226) of patients at Month 1 and 77% (GLs, n=210) and 71% (LCLs, n=223) at Month 6 were satisfied or very satisfied with their treatment.2,3
† Based on the FLTSQ completed by all ITT patients treated with Relfydess in the READY-1 and -2 studies. 98% (GLs, n=218) and 93% (LCLs, n=226) of patients at Month 1 and 90% (GLs, n=210) and 86% (LCLs, n=223) at Month 6 agreed or strongly agreed with the statement ‘I would have this treatment done again’. 98% (GLs) and 93% (LCLs) of patients at Month 1 and 90% (GLs) and 88% (LCLs) at Month 6 agreed or strongly agreed with the statement ‘I would recommend this treatment to others’.4,5
‡ Based on the Subject Treatment Questionnaire completed by all ITT patients treated with Relfydess in the RELAX study (n=99). Patients agreed or strongly agreed with the statement ‘I prefer to be treated with this study product than with other neuromodulators I received in previous treatments’.6
References: 1.Galderma. Relfydess Summary of Product Characteristics. July 2024. 2. Galderma Laboratories. MA-47072. Clinical Study Report for Protocol 43QM1602: READY-1. Fort Worth, TX: 2021. 3. Galderma Laboratories. MA-47073. Clinical Study Report for Protocol 43QM1901: READY-2. Fort Worth, TX: 2021. 4. Galderma Laboratories. MA-47073. Clinical Study Report for Protocol 43QM1901: READY-2. Tables 14.2.12.4 and 14.2.13.2. Fort Worth, TX: 2021. 5. Galderma Laboratories. MA-47072. Clinical Study Report for Protocol 43QM1602: READY-1. Tables 14.02.11.04 and 14.02.12.02. Fort Worth, TX: 2021. 6. Galderma Laboratories. MA-59692. Clinical Study Report for Protocol 43QM2106: RELAX. Fort Worth, TX: 2023.
This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions.









Transformative results with advanced RF microneedling, enhanced by professional skincare.


Clinically Proven Results
Synergistic Skincare Support
Growth for Every Clinic

Discover how Gentlo and PCA Skin can work together in your clinic.

08 News
The latest product and specialty news
17 News Special: CQC Launches Autumn Consultation to Refine Regulatory Framework
Aesthetics examines the upcoming CQC autumn consultation, reflecting on past regulatory failings and a sector-specific inspection model
18 Event Report: Shaping the Future of Medical Aesthetics
CCR returned to London for another year of networking and education
23 Special Feature: Combining Modalities to Rejuvenate the Periorbital Area
Three leading practitioners share approaches to rejuvenating the eye area
29 CPD: Combining PRP and PRF with other Aesthetic Modalities
Dr Edward Robinson discusses a combination approach using PRP/PRF
34 Case Study: Addressing Facial Palsy with Toxin
Michelle McLean demonstrates using botulinum toxin for facial palsy
39 Mitigating Hyperpigmentation Risk in Higher Fitzpatrick Skin Types
Kate Monteith-Ross explores exosomes and energy-based devices
43 Aesthetica – A Trusted Supplier
Aesthetica Solutions supports UK clinics with reliability, ethical values and forward-thinking
44 Microtoxin for the Management of Acne
Dr Lisa Dinley discusses microtoxin therapy in the management of acne
46 Performance Beauty
It’s a mindset. A mission. A movement.
48 Combination Treatments for Fitzpatrick IV-VI Skin Types
Dana Beiki demonstrates strategies for treating varied skin types
52 Introducing Tor-bac
Alison Stevenson introduces the new single-dose bacteriostatic saline solution
53 Abstracts
A round-up and summary of useful clinical papers
54 Curating Successful In-Clinic Events
Michael Guberti offers guidance on planning in-clinic events
56 Managing Neurodiversity in Clinical Practice
Dr Aryan Ala’Aldeen explores neurodiversity within clinical practice
58 Optimising Personalisation for Patient Retention
Donna Ofsofke outlines strategies to optimise patient relationships
60 In The Life Of: Dr Anna Hemming
Dr Anna Hemming shares a day in her life as she balances running a busy and providing personalised care to her patients
62 The Last Word: Questioning Regenerative Culture
Julie Scott examines the shift from enhancement to antiageing

News Special: CQC Launches Autumn Consultation Page 17

Special Feature: Combining Modalities to Rejuvenate the Periorbital Area Page 23





Dr Edward Robinson is a cosmetic physician and NHS anaesthetics doctor, specialising in skin and hair rejuvenation and treating the male face. He is also an associate member of the British College of Aesthetic Medicine (BCAM).
Michelle McLean is the founder and medical lead of Aesthetically You. She is also a KOL for Galderma and BTL Aesthetics. In addition, McLean founded The Facial Palsy Association (FPA).
Kate Monteith-Ross is the owner and founder of La Ross Aesthetics and The Clinic by La Ross. Monteith-Ross is also the co-founder of The Nurses Network, an organisation focused on supporting medical practitioners navigate their business.
Dr Lisa Dinley is a dental surgeon, aesthetic practitioner and owner of The Castle Clinic in Nottingham. She is also a clinical trainer for Laboratoires Fillmed UK. She is also a member of the Elsevier advisory board.
Dana Beiki is a pharmacist specialising in dermatological research and medical aesthetics. His work focuses on translating research into structured care models that prioritise patient-centred outcomes and evidence-based treatment pathways.
Reveal more visibly refined facial geometry and improved V-shape in 12 weeks.
saw visibly youngerlooking facial geometry
84% 86%
saw a visible improvement in facial hollow areas
92%
saw a reduction in the appearance of fine lines
Commit to Your Skin™

Subjects demonstrated a visible improvement in facial V-shape including a more defined jawline and tapered chin resulting in a more sculpted appearance.
An advanced peptide serum clinically shown to complement the visible effects of injectables and deliver measurable results as a standalone solution. Powered by four cutting-edge peptide technologies, this innovative formula visibly smooths lines and wrinkles and improves the appearance of facial elasticity, volume, and lift—leading to a more structured appearance and refined-looking facial geometry in just 12 weeks.

Shannon Kilgariff Editor & Event Director @shannonkilgariff
We have just returned from an incredible two days at the Clinical Cosmetic Regenerative Congress (CCR), and wow – what an event! Personally, my highlight was catching up with so many familiar faces after a busy summer and seeing all the latest and greatest innovations coming to the fore in aesthetics. Events like these are vital for staying connected as a community, and it was fantastic to see everyone sharing knowledge, experiences and ideas in person. A heartfelt thank you to everyone who helped make this event such a success, and to all of you who took time away from clinic to prioritise your involvement in our incredible field of medical aesthetics. In this issue of the Aesthetics Journal, you’ll find our full CCR event write-up, covering the standout moments, key presentations and exciting innovations that were on display. And don’t forget to mark your diary for our next event, ACE, coming up on March 13-14. It promises to be another unmissable opportunity to learn and connect with the aesthetics community.
This month, our theme is combination treatments, highlighting the increasing sophistication of multi-modality approaches in aesthetic practice – a big focus at CCR actually! Our Special Feature (p.23) explores combining treatments for periorbital rejuvenation, while other articles cover combining exosomes with energy-based devices to treat hyperpigmentation, and strategies for combination treatments in high Fitzpatrick skin types. In addition, our CPD article examines the integration of PRP and PRF with other aesthetic modalities, providing practical guidance for safely and effectively combining these treatments in clinic.
Don’t forget… entry for The Aesthetics Awards 2026 is still open! In this issue, we feature some of last year’s winners, including Dr Anna Hemming and Michelle McLean, whose achievements continue to inspire the community. If you’d like to be part of this year’s event, make sure you submit your entries by the October 20 deadline. And if you need any assistance – whether it’s choosing a category, understanding the process or just some gentle encouragement – please get in touch with our team. We’re always happy to support you and help you showcase the incredible work being done in aesthetics.
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Sharon Bennett is the former chair of the British Association of Medical Aesthetic Nurses (BAMAN), UK lead of the BSI committee for aesthetic non-surgical standards and member of the Clinical Advisory Group for the JCCP. She is a trainer and a registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Sharon Bennett, Clinical Lead



Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS, and is an examiner and fellow of the Royal College of Ophthalmologists.
Mr Adrian Richards is a plastic and cosmetic surgeon with over 30 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
PORTFOLIO MANAGEMENT
Shannon Kilgariff • Editor & Event Director
T: 0203 196 4351 | M: 07557 359 257 shannon.kilgariff@easyfairs.com
EDITORIAL
Holly Carver • Deputy Editor & Content Manager
T: 0203 196 4427 | holly.carver@easyfairs.com
Amer Saleh • Journalist | T: 020 3196 4270 amer.saleh@easyfairs.com
Mia Sawyer • Content Writer | T: 020 3196 4242 mia.sawyer@easyfairs.com
Sophia-Fai Roche • Journalist sophia-fai.roche@easyfairs.com
DESIGN
Aimee Bish
• Senior Graphic Designer
Callum Benyon • Junior Graphic Designer



Dr Mayoni Gooneratne (MBBS, BSc, MRCS, MBCAM, AFMCP) was an NHS surgeon before establishing The Clinic by Dr Mayoni and founding Human Health – an initiative combining lifestyle with traditional and functional medicine to provide a ‘cell-up’ regenerative approach to aesthetics. She is also the co-founder of The British College of Functional Medicine.
Jackie Partridge is an independent nurse prescriber. She is the clinical director and owner of Dermal Clinic in Edinburgh and a KOL for Galderma. She holds an MSc in Non-surgical Aesthetic Practice and a BSc in Dermatology. Partridge is a stakeholder group member with Scottish Government/HIS, Honorary BACN member and JCCP Fitness to Practice Nurse.
Dr Souphi Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.
ADVERTISING & SPONSORSHIP
Judith Nowell • Head of Sales
T: 0203 196 4352 | M: 07765 407629
judith.nowell@easyfairs.com
Charlotte Norville • Senior Sales Executive
T: 020 3196 4418 | Charlotte.norville@easyfairs.com
MARKETING
Susana Burguera • Senior Marketing Manager T: 020 3196 4281 | susana.burguera@easyfairs.com
Ella Carey • Marketing Executive T: 020 3196 4410 | ella.carey@easyfairs.com
Isabell Wise • Marketing Executive T: 020 3793 5845 | isabell.wise@easyfairs.com
If you are interested in contributing to the journal, get in touch...
Email: editorial@aestheticsjournal.com

Dr Sophie Shotter is the founder & medical director of Illuminate Skin Clinic in Kent and Harley Street, London. Her passion is for natural treatments delivered with utmost attention to safety. She works closely with Allergan as part of their UK and International Faculty.

Dr Anjali Mahto is one of the UK’s leading consultant dermatologists. She is a Fellow of the Royal College of Physicians, member of the Royal Society of Medicine and a spokesperson for The British Skin Foundation. In 2023 Dr Mahto opened Self London, a dermatology and lifestyle clinic aimed at managing skin conditions holistically.

Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please email, contact@aestheticsjournal.com
© Copyright 2025 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Follow us on Instagram @aestheticsjournaluk
#Parliament
British Association of Medical Aesthetic Nurses
@bamannurses
Following the parliamentary debate on non-surgical cosmetic treatment regulations, we went to the Houses of Parliament, alongside BCAM, to champion patient safety!

#Summit
InMode UK & Ireland
@inmodeuk
From world-class innovation to connection, collaboration and inspiration. What an experience!

#Lecture
Alessandra Haddad
@clinicaalessandrahaddad

#Connection
Kate Monteith-Ross @kate_laros
It is a huge honor to be part of the NeoGen Plasma global family, pictured here at their Global Summit 2025!

#Launch KLIRA
@Kliraworld
We celebrated the launch of The Dayscript in style at Sachi Restaurant, with Dr Emma Craythorne revealing all the exciting details!
I had the honour of participating in GAIN LATAM and it was a truly enriching experience!

MPs gathered in Westminster Hall to address the urgent need for the regulation of non-surgical cosmetic treatments.
The debate, which took place on September 11, was brought forward by Nicky Robinson, independent nurse prescriber and the British Association of Medical Aesthetic Nurses (BAMAN) regional leader for the West Midlands, and was led by Bradley Thomas Conservative MP for Bromsgrove. Thomas, expressed growing concern that the aesthetic specialty remains largely unregulated and called the lack of regulation a “public health crisis.”
He continued, “Each year, more people undergo these treatments, and each year, more are left vulnerable to devastating complications because of a systematic failure in our legal system. The statistics paint an indisputable picture. Without raising the baseline minimum level of clinical standards, millions across the country will continue to suffer, and some will pay with their lives.”
Thomas called for stronger regulations with greater protections in place for young people and clearer rules to prevent the public from being misled. One solution mentioned was to require all images and videos used in advertising across all platforms to display a clear symbol indicating if they have been digitally altered or enhanced, an idea originally put forward by Conservative MP for Hinckley and Bosworth Dr Luke Evans in a private Member’s Bill.
An idea that was brought forward by Thomas was to amend the health and social care legislation, expanding the powers of the Secretary of State to introduce regulations on operations and making “surgeon” a protected title.
Also in attendance was Democratic Unionist Party MP for Strangford Jim Shannon, who echoed calls for reform. Shannon questioned why in Northern Ireland a child requires parental consent for a filling at the dentist, but under-18s are allowed to access non-surgical procedures. He said, “It seems idiotic. This simply has to stop.”
Minister of State at the Department of Health and Social Care (DHSC), Karin Smyth, responded to the questions raised in the debate, saying, “For too long the sector has been left with little in the way of safeguards, and we need to balance the priority of public safety without stifling creativity and innovation.”
The minister explained that the Government plans to prioritise developing legal restrictions on the high-risk cosmetic procedures, as outlined last August, in which the DHSC confirmed plans to introduce a licensing scheme for non-surgical cosmetic procedures in England.
Smyth said, “We will come down on providers who flout these rules like a ton of bricks with tough enforcement from the Care Quality Commission. It’s currently far too easy for someone with minimal or no training to set themselves up as a practitioner.”
Robinson, who initially brought this issue to Thomas’ attention, was in attendance at the debate alongside BAMAN chair Amy Bird and chief operating officer Gareth Lewis.
Members of the British College of Aesthetic Medicine (BCAM) also attended Westminster for the debate. BCAM president Dr Sophie Shotter commented, “There is a lot of work to be done on this before we have a framework that delivers the patient safety we all so desperately need. BCAM is very clear – we will continue to use our voice to push for enforceable legislation that improves patient safety.”

Entries are closing on October 20 for the most prestigious and longstanding awards ceremony in the UK medical aesthetics specialty, The Aesthetics Awards.
The ceremony celebrates clinical excellence, innovation and outstanding achievement across the profession. Open to both new and established professionals, companies and clinics, the 2026 Awards provide a platform for entrants to elevate their profile and stand out in a competitive field.
Elite members can submit entries in as many applicable categories as they wish, ensuring every area of excellence has the chance to shine.
Shannon Kilgariff, editor and event director at Aesthetics, commented, “The Aesthetics Awards are the benchmark of excellence within our specialty. Each year, we are proud to showcase the incredible work, innovation and dedication of individuals and teams who are helping to shape the future of medical aesthetics. We encourage all those contributing to the specialty to put themselves forward this year.”
The Medicines and Healthcare products Regulatory Agency (MHRA) has issued an official warning on the illicit trade in unlicensed botulinum toxin products.
Released on August 30, 2025, the MHRA’s Criminal Enforcement Unit shares that this warning comes in response to 41 confirmed cases of botulism reported between June 4 and August 6. Affected regions include the North East, East Midlands, North West and Yorkshire.
According to the MHRA’s Criminal Enforcement Unit, unlicensed botulinum toxin products are being illegally obtained by a number of sellers and practitioners, then administered in informal and unregulated environments, including domestic kitchens and hair salons. The unit noted that these procedures are often promoted via social media platforms, where individuals are drawn in by adverts promising quick results at low cost. The Criminal Enforcement Unit is currently investigating these illegal operations. Under the Human Medicines Regulations 2012, those found guilty of selling or supplying unlicensed botulinum toxin may face up to two years in prison and unlimited fines. This action forms part of the MHRA’s broader campaign to combat the illegal supply of botulinum toxin. Since May 2023, the agency has seized more than 4,700 vials of unlicensed products, the majority of which originated from South Korea. These include brands not authorised for sale in the UK, such as Botulax, Innotox, reNTox and Toxpia.
Andy Morling, head of the MHRA’s Criminal Enforcement Unit, commented, “Criminals are exploiting the popularity of cosmetic treatments by peddling dangerous, unlicensed products, putting profit before safety. We are working across the country to identify those responsible, seize illegal products and bring cases to court. We use the full range of our enforcement powers and techniques to shut down these operations and bring offenders to justice.”
Out of 2,000 women in the UK aged between 40-60, 61% agree that many age targeted skincare products do not fully address the specific needs of menopausal skin (Face the Future, 2025)
In 2024, the UK exported £4.3 billion worth of beauty and personal care products, accounting for 1.3% of total UK goods exports (The British Beauty Council, 2025)
A recent survey of 8,000 UK adults found that 40% of 16-24 year olds feel lonely or socially isolated when working remotely (Bupa, 2025)
UK job vacancies fell by 5.8% between May and July 2025 with vacancies now 16.8% lower than a year ago
(Office for National Statistics, 2025)
more than 2,408 patients have been waiting more than four years for a first plastic surgery outpatient appointment
(Department of Health Northern Ireland, 2025)
1 in 3 doctors feel unable to progress in their education, training or career as they’d like to
(General Medical Council, 2025)
11th October 2025
BCAM Conference
8th November 2025
Interface Expo
22nd November 2025
IAAFA Conference
29th-31st January 2026
IMCAS World Congress
13th-14th March 2026
Aesthetics Conference & Exhibition (ACE)
14th March 2026
The Aesthetics Awards
Lorraine discusses the use of weight-loss injections on children
ITV’s Lorraine aired a segment featuring GP Dr Amir Khan, who discussed whether children should use weight-loss injections. The discussion comes after a review indicated that using weight-loss injections on children aged six to 17 was effective in lowering blood sugar levels and helping with weight loss. Dr Khan strongly opposed the idea, saying, “We’ve got to tackle the root cause, we should not be medicating these children against something that we can change at the root.” Host Lorraine Kelly agreed with Dr Khan, adding that children’s weight is the responsibility of the parents.
Alice Hart-Davis discusses aesthetic trends
Appearing on Beauty x Medicine, a new video series hosted by pharmaceutical company Galderma, beauty journalist and author Alice Hart-Davis discussed aesthetic trends. Sharing her thoughts with CEO of Galderma Flemming Ørnskov, Hart-Davis predicted that regenerative procedures, from biostimulators onwards, will become increasingly popular, explaining, “Patients love the idea of being able to renovate their skin from within.”
She also highlighted the rising shift of longevity within aesthetics, noting, “Practitioners are realising it’s not just about improving a patients face – it’s about supporting overall lifestyle changes.”
Revised Pricing
Pharmaceutical company Eli Lilly increased the price of the weight loss injection tirzepatide as of September 1.
In a statement, Eli Lilly shared that the price adjustment reflects the company’s efforts to fairly share the costs of medical research across developed countries. The company stated it is working with Governments to aimfully ensure patient access, including an agreement with the UK to raise the price of tirzepatide while maintaining availability for NHS patients.
Prior to the price change, a temporary order freeze was enforced from August 27 until September 1, to enable the company to complete previous orders placed. At the time, Eli Lilly reiterated that there are legal protections in place, enforced by the Medicines and Healthcare products Regulatory Agency (MHRA), to prevent “inappropriate stockpiling of medicine”.
Aesthetics reached out to Eli Lilly regarding the price change, and the company commented, “We are working with private providers on commercial arrangements to maintain affordability and expect these to be passed onto patients. We are already seeing providers respond in different ways to the list price change, with a range of options available for eligible patients. We also want to work in partnership with the Government to expand NHS access for eligible patients, building on the commitments in the Government’s 10 Year Plan.”
Surgical Research
Research published in September by the British Association of Aesthetic Plastic Surgeons (BAAPS) highlighted the broader benefits of aesthetic procedures.
Published in the Aesthetic Surgery Journal, the research highlighted consistent improvements across physical, functional and psychosocial outcomes. Breast reduction surgery provided pain relief, improved posture and greater ease in daily life. Body contouring after weight loss alleviated skin irritation, mobility limitations and boosted self-esteem. Facial cosmetic surgery was linked to reduced anxiety, improved social confidence and a healthier self-image.
Ms Nora Nugent, consultant plastic surgeon and president of BAAPS, commented, “This research aims to inform surgeons and their patients about the genuine health benefits of aesthetic plastic surgery, while addressing misconceptions that reduce it to purely superficial motivations. The positive health impacts of aesthetic plastic surgery are frequently overlooked and understated.” Podcast
The British Skin Foundation (BSF) debuted its new four-part podcast series, Skin, Unfiltered, this September.
The programme is hosted by presenter and BSF ambassador, Lex Gillies, and according to the company, forms part of the BSF’s ongoing mission to fund life-changing research into disease, and improve quality of life for the 60% of people in the UK who will experience a skin condition in their lifetime.
Guests include TV presenter Coleen Nolan, broadcaster Gail Porter, former Apprentice contestant Saira Khan and content creator Kadeeja Khan, who share personal experiences with conditions such as skin cancer, alopecia and acne.
Consultant dermatologists Dr Emma Wedgeworth, Dr Derrick Phillips, Dr Adil Sheraz and Dr Angela Tewari also contribute specialist perspectives, addressing misinformation and answering listener questions.
Gillies commented, “I’m absolutely thrilled to be the host of the Skin, Unfiltered podcast. I’ve spent two decades learning how to love my skin (rosacea and all!) and I could talk about skin, confidence and appearance all day. So, getting the opportunity to chat to some incredible guests about their own skin journeys has been such a joy.”
Aesthetics launched its 2025 Trends & Product Launches Report at the Clinical Cosmetic Regenerative Congress (CCR) on September 25.
The report integrates the latest trends and product launches in the specialty from the past 12 months, serving as a definitive guide to the most significant developments shaping the field.
Compiled in partnership with healthcare data and research company Rare: it draws on insights from thousands of aesthetic clinics and distributors across the UK. Key themes include injectables, longevity and regulation. The findings highlight the most in-demand treatments, emerging treatment categories and areas of declining popularity, while also illustrating regulatory shifts. The publication also highlights all major product launches in the specialty, organised into five categories namely devices, skincare and injectables. This overview offers a clear snapshot of the most influential techniques, ingredients and treatment approaches introduced during the year by leading companies.
Shannon Kilgariff, editor and event director at Aesthetics, commented, “This year has brought remarkable momentum to the aesthetics field, one of the most rapidly advancing areas in modern medicine. From innovations in regenerative therapies to cutting-edge skincare and wellness supplements, new developments are transforming how we approach patient care. Within our annual report, we take a closer look at the breakthroughs, trends and emerging products poised to shape the future of the field.”
An in-person training programme, founded by consultant ophthalmologist and vitreoretinal surgeon Mr James Neffendorf and founding director of the Complications in Medical Aesthetic Collaborative (CMAC) Gillian Murray, has debuted.
The course reportedly equips clinicians with the skills to assess and identify concerning symptoms of vision loss following dermal filler. In addition to the teaching, clinicians receive resources, including template wording for filler consent, a hyaluronidase consent form, a step-by-step emergency management protocol, a retrospective documentation template and guidance on developing local referral pathways.
Mr Neffendorf said, “Aesthetic Ocular Safety course equips clinicians with the confidence and assurance that they have done everything possible to secure the best outcome, guided by the expertise of ophthalmologists and senior aestheticians.”
Regulatory support provider BAXCQC has announced a new Care Quality Commission (CQC) compliance platform.
The BAXCQC Compliance Platform is an online system that supports healthcare providers to self-assess and manage their compliance against the 34 Quality Statements within the CQC’s Single Assessment Framework. Robin Naudi, director at Baxendale, which encompasses BAXCQC, said, “This launch is about reducing last-minute panic and replacing it with a calm, proactive grip on compliance. The BAXCQC Compliance Platform helps teams demonstrate against the Assessment Framework, visualise progress and manage tasks."
A round-up of the latest news and events from the British Association of Medical Aesthetic Nurses
BAMAN AUTUMN
AESTHETIC CONFERENCE
On September 18-19, the 2025 BAMAN Autumn Aesthetic Conference returned to Birmingham, once again hosting the UK’s largest gathering of medical aesthetic nurses. With more than 350 attendees, it was our biggest conference to date and a testament to the commitment and engagement that underpin our growing community.
Across two packed days, we welcomed 25 specialist speakers, more than 40 exhibitors and a broad range of voices from across the field. We were also proud to welcome key stakeholders, including representatives from the Nursing and Midwifery Council and the Association for Prescribers, who shared valuable updates directly with attendees.
The atmosphere throughout was warm, energising and supportive, and we can’t thank every delegate, speaker, sponsor and exhibitor enough for joining us and contributing to our favourite event of the year.
Just a week later, on September 25-26, BAMAN exhibited at the Clinical Cosmetic Regenerative Congress (CCR) at Excel, London. It was a pleasure to connect with so many of you, welcome new members, introduce new team faces and keep the momentum going after such a brilliant month for medical aesthetic nursing.
This autumn, BAMAN is bringing in-person regional meetings to Newcastle, London, Dundee and Manchester, with hands-on learning, peer reviews, optional basic life support training and time to reconnect. All sessions are CPD-accredited and free for members. Book your place today via the QR code below. Meanwhile, member voting is open until October 3 for the first-ever BAMAN Awards, celebrating nurses driving innovation, mentorship and community impact. Winners will be announced at our black-tie Awards Ceremony on November 14 – BAMAN’s biggest event of the year.
This column is written and supported by BAMAN

The Aesthetics Conference and Exhibition (ACE) returns in 2026

Following the success of the Clinical Cosmetic Regenerative Congress (CCR), it’s time to look ahead to your next must-attend event – the Aesthetics Conference and Exhibition (ACE). Taking place on March 13-14 at the Business Design Centre, ACE is dedicated to empowering the medical aesthetics community with world-class education, unparalleled networking and access to the specialty’s most trusted manufacturers, suppliers and brands.
But don’t just take our word for it… Community perspective
“ACE is a fantastic weekend providing opportunities to learn and network all under one roof. The diverse talks and treatment demonstrations meant I could easily pick relevant ones to my practice and I was able to speak to lots of different companies about a potential device purchase for my clinic.”
Dr Bethany Rossington, Aesthetic Practitioner
“ACE is fresh and exciting, with plenty of new things to discover. I kept bumping into friends and meeting new people – it had such a fantastic buzz!”
Professor Brian Franks, Aesthetic Practitioner
“The ACE conference was an outstanding experience from start to finish. The quality of presentations was top-tier, delivering valuable insights, while the sheer variety and volume of suppliers were second to none.”
Sheena McKenna, Founder of EQUALS3
Scan the QR code below to register your interest for ACE 2026 and join your community in advancing the medical aesthetics specialty.
Don’t forget, The Aesthetics Awards take place after the second day of ACE at the Hilton Park Lane. Tickets are on sale now – secure yours soon to take advantage of the early bird rate!
Appointment

The British College of Aesthetic Medicine (BCAM) has introduced former president elect, aesthetic practitioner and Aesthetics Clinical Advisory Board member Dr Sophie Shotter as its new president. This leadership change follows the departure of Dr Catherine Fairris, aesthetic practitioner and outgoing president of BCAM as the organisation expressed its gratitude for Dr Fairris’ contributions. BCAM further noted that Dr Shotter brings extensive clinical experience, a background in education and a commitment to advancing standards of practice in medical aesthetics.
Discussing her new role with Aesthetics, Dr Shotter commented, “Over the coming months, I aim to continue conversations with colleagues and stakeholders to shape BCAM’s future direction, whilst continually improving patient safety.”
Educational Platform
Aesthetic distributor DermaFocus has launched the Regenerative Innovation and Scientific Education (RISE) training programme. According to the company, RISE includes a range of training modules, such as injection technique videos demonstrating polynucleotide protocols, alongside specialty-led webinars. Notable sessions include Perioral Regeneration, presented by plastic surgeon Mr George Christopoulos and aesthetic practitioner Dr Raquel Amado.
Dr Kam Lally, aesthetic practitioner and faculty scientific and education lead at DermaFocus, commented, “RISE represents far more than another education hub – it’s a movement to change the way we approach regenerative aesthetics. For the first time, practitioners will have access to not only evidence-based clinical training and live demonstrations, but also the business strategies and peer support needed to implement regenerative treatments in practice.”
Annual Summit
Aesthetic device company InMode held its annual 2025 summit in Gran Canaria on September 11-14.
The four-day event gathered 600 specialists, including 40 delegates from the UK, along with 36 international speakers. Notable among them were InMode co-founder and plastic and reconstructive surgeon Mr Stephen Mulholland, maxillofacial and plastic surgeon Mr Alfredo Hoyos and urogynaecologist and pelvic surgeon Mr Mickey Karram.
The agenda featured lectures, workshops and demonstrations covering developments in aesthetics, dermatology, gynaecology, ophthalmology and plastic surgery. Victoria Voysey, managing director at InMode UK&I, commented, “The 2025 InMode summit united world-class practitioners, educators and innovators. The event reflected InMode’s commitment to education, collaboration and advancing excellence in the sector worldwide.”
Skincare

Skincare company ZO Skin Health introduced the Peptide Facial Refining Concentrate at the Clinical Cosmetic Regenerative Congress (CCR).
According to the company, the serum contains peptides such as acetyl octapeptide-3 and acetyl hexapeptide-8, which are designed to target expression lines and deeper wrinkles. It also includes the ZPOLY complex, a plant derived polysaccharide designed to minimise signs of premature ageing.
Additional ingredients include a refining peptide complex, which aims to contribute to more refined facial geometry, and a volumising tripeptide which aids hyaluronic acid activity for enhanced fullness, shares ZO Skin Health.
Lauren Gibson, director of education and training EMEA at ZO Skin Health, commented, “We have developed the Peptide Facial Refining Concentrate to amplify the benefits of in-clinic injectables into the daily skincare routine at home. While professional treatments sculpt and volumise, this formula works between visits to refine facial geometry, which allows for enhancing contours, improving skin density and supporting structural harmony.”
LED Mask
Aesthetic practitioner Dr Ifeoma Ejikeme has launched the ZKIN LED Mask.
The ZKIN mask features four wavelengths, blue light (460 nm), red light (630 nm and 660 nm) and near infrared light (850 nm), targeting concerns like fine lines, acne, circulation, collagen production and overall skin rejuvenation. According to Dr Ejikeme, the mask uses medical grade silicone, aiming to create a lightweight, flexible structure that adapts to the contours of the face.
Dr Ejikeme comments, “In my day-to-day work, I hear countless concerns about reducing fine lines, managing blemishes and improving overall skin health. My answer has consistently been light therapy. With ZKIN, I’ve worked to provide a more effective, comfortable and easy solution for at-home LED therapy. I’m so excited to bring this advancement in face mask technology to the market.”
Educational Summit
Skincare company SkinCeuticals gathered aesthetic practitioners at the St Pancras Renaissance Hotel for its annual educational summit.

Hosted on September 11, the programme began with talks from Caroline O’Neil, managing director of L’Oréal Dermatological Beauty UK&I, the division that encompasses SkinCeuticals. Alongside O’Neil was Patricia Brieva, vice president of global medical affairs at SkinCeuticals and professor Giuseppe Valacchi, a professor of regenerative medicine at North Carolina State University.
Other specialty speakers included aesthetic surgeon Miss Jonquille Chantrey, dermatologist Dr Ariel Haus and NHS consultant plastic surgeon Miss Rebecca Rollett. These speakers led sessions exploring ethical aesthetics, multi-modality treatments, future market trends and the role of SkinCeuticals’ innovations, including the Advanced RGN-6.
Oliver Pearce, medical events and communications manager at SkinCeuticals, commented, “This year’s Master Physician event was a powerful testament of our commitment to our medical partners. Seeing the incredible learning and networking unfold, and the genuine inspiration in the room, confirmed we truly delivered on our promise to support their growth and, ultimately, the best patient outcomes.”
Training
Nurse practitioner Tracey Dennison has unveiled the Menopause Advocacy Training course for healthcare professionals.
According to Dennison the one-day course provides a broad, generalist approach to menopause education, equipping clinicians with the knowledge and tools to recognise hormonal symptoms, support patients in their care and signpost appropriately.
She commented, “By addressing medical, lifestyle, workplace and legal perspectives, we are building a network of advocates who can make a real difference in everyday care.”

Aesthetics attended the British Association of Medical Aesthetic Nurses (BAMAN) Autumn Aesthetic Conference on September 18-19.
Hosted at The Eastside Rooms in Birmingham, the conference presented engaging sessions on regenerative approaches, intimate health and psychological assessment – alongside regulatory updates from the Nursing and Midwifery Council (NMC) and Association for Prescribers (AfP).
The BAMAN board of directors also featured on stage, with chair and nurse prescriber Amy Bird opening both day one and day two, alongside vice-chair and nurse prescriber Alex Mills showcasing a live lips and perioral combination treatment demonstration. The conference also incorporated an evening network drinks reception, providing attendees with an opportunity to network.
Gareth Lewis, chief operating officer at BAMAN, commented, “Networking and the sharing of best practices to improve patient safety were at the heart of this event. We were thrilled with the incredible response from both delegates and exhibitors – the largest attendance we’ve ever had. It was especially rewarding to see so many nurses on stage, a representation of something BAMAN is truly passionate about.”
Skin Mist

Skincare company Esse Skincare has unveiled the Esse Live Probiotic Mist.
The company states that the product is intended to support hyaluronic acid production, reinforce the skin barrier and help maintain microbiome balance. Containing live Bacillus coagulans, the formulation is reported to increase hydration by 66% in a single use. Esse Skincare adds that the product is designed to retain moisture, reduce transepidermal water loss and support beneficial skin microbes.
Trevor Steyn, founder of Esse Skincare, commented, “We can finally deliver live probiotics in a water-based format without compromising potency or shelf life. The two-part activation system ensures 10 million viable cells per application, giving professionals and patients a proven way to improve hydration, barrier function and microbiome balance.”
A round up of the latest aesthetic clinics opening across the UK
Aesthetic practitioner Dr Sally McCluskey has co-founded the Facial Aesthetics Centre in West Sussex with oral surgeons Mr Bill Schaeffer and Mr Guy Barwell. The new clinic which opened on September 15 offers medical grade skincare including AlumierMD, Klira and SkinPen, as well as injectables, mole checks and minor
Skincare company Revision Skincare has launched its Triple-Action Exfoliator.
Available through aesthetic distributor AestheticSource, Revision Skincare shares that the product is designed to address dead skin cells across surface and deeper layers. The company adds that micro-fine particles aim to polish the skin, while alpha- and beta-hydroxy acids attempt to promote cellular turnover. Natural enzymes further aid in supporting smoother skin, according to the company.
Lorna Bowes, CEO of AestheticSource, commented, “The new Triple-Action Exfoliator combines physical, chemical and enzymatic exfoliants to offer a safe, effective approach to at-home skin renewal. We’re delighted to share a solution that provides instant and long-term results without compromising skin health, also making it ideal for those wanting to maintain smooth, radiant skin between in-clinic treatments.”
The Body Dysmorphic Disorder (BDD) Foundation has confirmed the appointment of nurse prescriber Julie Scott as ambassador for safer medical aesthetic practice.
Scott shares that the role involves acting as a patient advocate and providing guidance on psychological screening and risk assessment, while also delivering educational content through webinars and publications. She will additionally contribute to discussions on regulatory frameworks to ensure that mental health safeguarding is fully embedded within aesthetic practice.

Scott commented, “I’m incredibly humbled to represent the BDD Foundation as ambassador for safer medical aesthetic practice. This role is about bringing psychological awareness into the heart of medical aesthetics, supporting practitioners, protecting vulnerable patients and raising awareness across the specialty.”
surgical procedures. Dr McCluskey said, “The great thing about this opportunity is that I finally have the chance to run an entire clinic and introduce other team members in order to offer a 360-degree service to any patient who walks through our doors.”
Aesthetic practitioner Dr David Jack has partnered with Liberty London to launch his first in-store clinic, opening on October 13. The clinic will offer advanced
aesthetic treatments, from injectables such as botulinum toxin and dermal fillers, regenerative therapies including polynucleotides and exosomes as well as facials and laser treatments. Dr Jack said, “For me, this launch is about making evidence-based aesthetics more accessible within a retail setting but without losing the precision, safety and artistry that define our clinics.”
If you’re opening a new UK clinic soon, let us know at editorial@aestheticsjournal.com
On The Scene
Skincare brand Klira welcomed press at PR launch and specialist guests to an evening at the SACHI rooftop restaurant in London to debut The Dayscript. The evening began with a speech from Klira’s founder and consultant dermatologist Dr Emma Craythorne, who discussed the brand, the launch of The Dayscript and the accompanied evening treatment, The Klira Special. In attendance, alongside Dr Craythorne, was co-founder and CEO Sophie Kerbegian, as well as medical directors at Klira and consultant dermatologists Dr Ellie Rashid, Dr Cristina Psomadakis and Dr Rhonda Meys.
Dr Craythorne commented, “It was a pleasure to welcome our guests and partners to the launch of The Dayscript, our new seven-in-one daytime formula. Designed to work alongside The Klira Special, these two formulations provide a simple, comprehensive routine that opens access to bespoke dermatology and helps everyone achieve their best skin health.”
Event Report
Aesthetic device company Cutera invited press and practitioners to the Cutera University Clinical Forum (CUCF) at the De Vere Beaumont Estate on September 13.
The Laser and Light Summit hosted 20 sessions, with topics including Prioritising Patient Care While Driving Business Success, Treating Hyperpigmentation in Skin of Colour with Lasers, Unlocking Elite Results with Excel V+ and more.
Guests were also able to attend panel discussions and Q&As, as well as a roundtable featuring consultant dermatologists Dr Ryan De Cruz and Dr Matthias Wahn, aesthetic practitioners Dr Nestor Demosthenous, Dr Tatiana Mandavia, Dr Anna Hemming, Dr Manav Bawa and ENT surgeon Mr Rishi Mandavia.
Dr De Cruz, a visiting Cutera KOL from Australia, commented, “CUCF 2025 UK&I was such a well-run, engaging and truly educational experience. I felt honoured to be part of it alongside such talented and passionate clinicians and educators. The organisation was seamless, and the sense of community created by the Cutera team was inspiring.”
On The Scene
Skincare company AQ Skin Solutions invited practitioners to a masterclass at the Royal Society of Medicine in London.
The event, organised by aesthetic manufacturer Smart Group Medical, offered UK practitioners the opportunity to learn directly from Professor Ahmed Al-Qahtani, immunologist and founder of AQ Skin Solutions.
The day began with a welcome from CEO of Smart Group Medical Joshua Yardley. This was followed by a keynote lecture by Dr Al-Qahtani, a Q&A session, networking over refreshments and live demonstration videos of the AQ portfolio. The company shares that the masterclass focused on educating attendees about AQ’s growth factor technology, its clinical applications and its role in skin and hair rejuvenation. Yardley commented, “We were delighted to welcome practitioners to this exclusive masterclass with Professor Dr Al-Qahtani. The day provided a rare opportunity to learn directly from the founder of AQ Skin Solutions and to explore the science and results behind growth factor technology. The feedback has been incredibly positive, with attendees excited to take this knowledge back to their clinics and offer their patients the benefits of AQ’s award-winning range.”
Dr Patrick Treacy receives accolade Aesthetic practitioner Dr Patrick Treacy was honoured with the World Regenerative Medicine Innovation Award at the World Scientific Conference at Kings College. The award celebrated Dr Treacy’s contributions, particularly his development of non-surgical hair growth techniques using platelet-rich plasma (PRP) and stem cells. A conference spokesperson said, “Dr Treacy’s contributions are reshaping how we approach hair restoration and beyond, offering hope through cutting-edge, non-invasive solutions.”
PLIM upgrades platform with concierge service
Fintech payment platform PLIM has been upgraded to include a new concierge service. According to the company, this new feature is designed to help users focus solely on treatments, with PLIM team members assisting practitioners with administrative tasks and supporting patients with clinic research, bookings and payment plans. Nada Ali Redha, founder and CEO of PLIM, said, “Launching a concierge service transforms everyday interactions into luxurious experiences, inspiring loyalty, delighting discerning patients and elevating our partner clinics’ business.”
iS Clinical announces new partner accounts
Skincare company iS Clinical has expanded its UK network by appointing two new partner accounts. The new additions are Rebecca Walker, a facialist and founder of The Rebecca Walker Technique, and Caroline Hall, an independent nurse prescriber and founder of R&R Aesthetics Clinic. Head of engagement and relations at Harpar Grace International distributor of iS Clinical, Katie Hughes-Dawkins commented, “We are delighted to welcome both Walker and Hall to their passion for skin health makes them the perfect partners.”
HydroPeptide introduces new moisturiser and serum
Skincare company HydroPeptide has launched The ReActivate RX Moisturiser and ReActive RX Serum. The moisturiser is an evening cream that includes NIMNI Technology, a blend of vitamin C (BV-OSC), tocopherol and other antioxidants. The serum combines NIMNI Technology, Micellular CellRenew-16, a NAD precursor and antioxidants like vitamin C, designed to provide comprehensive, visible antiageing results.

for further information please scan QR code Discover the combined power of: Non-Crosslinked hyaluronic acid (HA) & Glycerol

www.cromapharma.com/uk Info.uk@cromapharma.com Croma Pharma UK cromapharmauk
1) Instructions for use 2) Sulovsky M, Müller D, Prinz V, Moellhoff N, Cajkovsky M, Duschek N, Frank K. A prospective
multicentre study evaluating
tissue filler in the correction of lateral canthal and perioral lines. J Cosmet Dermatol. 2022 Jan;21(1):191-198. doi: 10.1111/jocd.14460. Epub 2021 Sep 24. PMID: 34559948 3) Succi, I. B., Da Silva, R. T. & Orofino-Costa, R. 2012. Rejuvenation of periorbital area:
based
Dermatol Surg,
Data on file
Aesthetics examines the upcoming CQC autumn consultation, reflecting on past regulatory failings and a sector-specific inspection model
England’s independent regulator for health and social care service, the Care Quality Commission (CQC) is launching a formal public consultation this autumn as part of its efforts to rebuild its regulatory framework following last year’s widely reported organisational failings.1,2
The healthcare regulator has shared that the consultation will invite providers, stakeholders and the wider public to give their views on the proposals that have been developed. This is to ensure the new regulatory system is evidence-informed, inclusive and geared towards continuous improvement.3
The consultation follows two major reviews of the CQC in 2024 by chair of the NHS Dr Penny Dash as well as oncologist and chair of the CQC, Professor Sir Mike Richards. Dr Dash’s review uncovered “significant failings” within the regulators internal workings, with issues ranging from unclear rating methodologies to a loss of sector expertise.4 In October 2024 Dr Dash made seven recommendations for the CQC, which included rebuilding expertise, clarifying rating calculations, increasing transparency and rapidly addressing operational performance.4
Under current guidelines, the CQC regulates providers of non-surgical and surgical cosmetic treatments carried out by a registered healthcare professional (HCP) that involve surgical procedures or non-surgical medical approaches. Some of these include cosmetic surgery, liposuction, thread lifting, treatment with prescription medication for a medical condition such as hyperhidrosis, bruxism, acne and rosacea or weight loss support.5,6
Aesthetic practitioner Dr Olivia McCabe-Robinson who has a clinic in Glossop, Derbyshire, faced challenges during her CQC application process, including the loss of her online application following a system change. This resulted in Dr McCabe-Robinson having to resubmit in paper format which she says caused the process to take over a year to complete, due to what she agrees are “failures in the system.”
Nurse practitioner and regulation consultant at Inspire to Outstand, Tracey Jones, believes there is a need for a clear and consistent set of requirements, adding, “The duration of registration interviews significantly vary depending on the inspector, and the timeline for these interviews can span anywhere from four to six months.” She reflects on past instances where inspectors have requested clinics to stock emergency medications that are not aligned with the specific patient demographic or clinical risk profile of the service. Jones believes this suggests a limited understanding that not all services operate in the same way or serve the same population.
Sector-specific approaches
A series of regional roadshows organised by the CQC earlier this year aimed to help the regulator listen and co-design the future of regulation with the people who live it every day.1 A key theme raised was the idea of sector-specific inspection approaches that reflect how different services operate.1
Dr McCabe-Robinson believes a sector-specific model for CQC inspections would be hugely beneficial for medical aesthetics, explaining it would help move the conversation away from a one-size-fits-all approach and towards a model that genuinely supports high standards. She argues the broad and generic framework that was originally designed with GP surgeries or hospitals in mind doesn’t always reflect how aesthetic clinics actually operate.
Dr McCabe-Robinson notes, “Issues like product procurement and storage, traceability, managing complications and ensuring patients truly understand consent are at the heart of safe practice. These are often overshadowed when the inspection criteria are geared towards bigger healthcare settings with very different systems and pathways.”
Jones believes that a sector-sensitive approach will help ensure inspectors have specialist knowledge. She says, “This ensures a more informed, fair and relevant assessment of the specific service being reviewed.”
CQC’s involvement with aesthetic regulation
The urgent need for the regulation of non-surgical cosmetic treatments was discussed during a Westminster Hall debate on September 11.7 Minister of State at the Department of Health and Social Care (DHSC), Karin Smyth, explained that the CQC will have a clear role in the Government’s plans to prioritise developing legal restrictions on high-risk cosmetic procedures such as the non-surgical Brazilian butt lift. This was previously announced in August 2025, when the DHSC confirmed plans to introduce a licensing scheme for non-surgical cosmetic procedures in England.8
Smyth says, “Bringing the restricted high-risk procedures into the CQC’s scope of registration will mean procedures being performed only by suitably qualified, regulated HCPs working for providers who are registered with the CQC. We will come down like a ton of bricks on providers who flout the rules, with tough enforcement from the CQC.”
Jones explains that implementing a more robust CQC framework alongside the proposed licensing scheme will help prevent unregulated practice. She adds, “Ensuring that HCPs understand the necessity of CQC registration will reduce the risk of individuals working outside their professional scope, thereby, protecting both patient safety and their own professional registration.”
Jones also believes that the proposed licensing scheme may lead to more treatments being brought under the CQC’s scope of registration, which would strengthen public safety while also requiring a greater number of HCPs to consider CQC registration.
Director of engagement at the CQC Chris Day shared that following the autumn consultation, the new assessment approach will begin to roll out.3 Day says, “We will continue working together, learning from what’s working, adjusting what isn’t and keeping pace with a changing care sector.”
Dr McCabe-Robinson encourages all aesthetic practitioners to submit their responses to the consultation when it opens, noting, “This is everybody’s problem who works in the aesthetic sector, so make sure you have your say otherwise nothing will get better for our patients.”


CCR returned to London for another year of networking and education


The UK’s largest medical aesthetics conference, Clinical Cosmetic Regenerative Congress (CCR), welcomed 3,849 attendees to the Excel, London on September 25-26. This year, CCR was a dedicated space to connect all facets of the medical aesthetics specialty through knowledge sharing, debates, networking and collaboration.
The event hosted 150 exhibitors and 183 speakers across the two days, and all attendees were welcomed by Registration Sponsor BTL Aesthetics.
Shannon Kilgariff, event director and editor of the Aesthetics
portfolio, commented, “It was incredible to welcome so many aesthetic professionals and companies to CCR 2025. This year, the standard of scientific, clinical and business education, along with the exhibition and breadth of participating organisations, was truly outstanding. A huge thank you to our speakers for sharing their expertise, research and live demonstrations, particularly our international keynote speaker aesthetics nurse practitioner, Dan Julien. I’m also deeply grateful to our sponsors, exhibitors, partners and the Aesthetics Clinical Advisory Board for their continued support in driving CCR forward year after year. I look forward to seeing everyone again at our next event, ACE, in March!”
Galderma
Pharmaceutical company Galderma returned as CCR Headline Sponsor. Rapid weight loss can leave patients with significant facial volume loss and an aged appearance, affecting confidence and wellbeing. In response to this, Galderma explored how Sculptra and Restylane can be combined to restore natural facial contours through collagen stimulation and targeted hyaluronic acid volumisation. Speakers Dr Munir Somji and Dr Ana Mansouri delivered practical strategies, patient selection tips and safe injection techniques to help patients reclaim a healthy, refreshed look after weight loss. CCR also saw the launch of Galderma’s latest innovation, with Dr MJ Rowland Warmann introducing a the new Relfydess advancement in the company’s portfolio.
Galderma also hosted the CCR Networking Lounge across the two days, providing delegates with refreshments in between talks and the space to create vital new connections.
Dr Wojciech Konczalik, head of marketing UK&I at Galderma, commented, “Galderma was proud to serve as Headline Sponsor for the UK’s largest event of its kind. The opportunity to showcase our innovative portfolio significantly enhanced brand equity and visibility. Our symposia and booth sessions were exceptionally well attended, sparking high-quality engagement with healthcare professionals throughout. It was a must-attend event that truly delivered impact.”
Bringing the Aesthetics Journal to life, this Arena was the go-to place for the latest scientific research and innovative techniques. International keynote speaker Dan Julien shared his proven strategies for success in medical aesthetics, presenting his theoretical framework through patient assessment and injection demonstration. He explored a wide range of techniques, offering insights into how to approach each patient as an individual and achieve natural, harmonious outcomes.
Other highlights included a Full-face Masterclass with live demonstration by speakers Mr James Olding, Julie Scott, Mr Felix Kast and Dr Yousrah Ahmed; as well as Non-Surgical and Lifestyle Interventions in Aesthetic Medicine, in association with the Royal Society of Medicine.
Crucial Updates in Regenerative Aesthetic Medicine were presented by Amy Bird, Claudia Mcgloin, Dr Raquel Amado, Dr Ifran Mian, Kate Monteith Ross and Dr Mannish Mittal.
CCR’s charity partner the British Skin Foundation also took to the stage, with speaker Dr Derrick Phillips discussing psychodermatology.
Top brands showcased their latest techniques through live treatment demonstrations at the Aesthetics Mastery Theatre featuring leading KOLs.
The stage saw the return of the Aesthetics Challenge, chaired by Dr Ayad Harb and Sharon Bennett. The sessions allowed delegates to discover the power of precision through an engaging live demonstration where three top injectors (Dr Yusra Al-Muktar, Dr Thuba Jabbar and Mohammed Harb) pushed the boundaries of artistry using hyaluronic acid dermal filler to treat the nose. Bennett and Dr Harb assessed the outcomes in real time, providing in-depth critiques and before-and-after comparisons.
Other companies who took to the Mastery stage included:
· ACE Group World
· Beautyform
· BNC Global
· DermaFocus
· Dermapenworld
· Fotona
· Genefill
· Klira
· Needle Concept
· Promoitalia
Across the two days, theatre sponsor DermaFocus hosted lunchtime takeovers with Dr Bibi Ghalei, Dr Kam Lally, Mr Ash Soni, Dr Yusra Al-Mukhtar, Dr Xavier Goodarzian, Dr Raquel Amado, Caroline Hall and Dr Edward Robinson, discussing exosomes and polynucleotides.
Running a successful medical aesthetic practice takes more than just clinical skills and techniques – it takes acute business acumen.
This year, the In Practice Zone, sponsored by Dermis AI, served as a dedicated space for the services, products and solutions designed to improve clinic processes, as well as hosting the In Practice Theatre, where key speakers shared their insights into business success.
Following the announcement of the recent Government licensing scheme for aesthetic practice, Aesthetics has brought together key specialty leaders to discuss its implications for the sector. This session provided an overview of the new regulatory framework and explored what it means for practitioners, patients and the future of medical aesthetics in the UK. The panel session with Andrew Rankin, Amy Bird and Dr Catherine Fairris highlighted how the field can prepare to adapt to this significant legislative development.
Other highlights included a session hosted by Ben Pask on the latest trends in the medical aesthetics specialty where the annual Aesthetics Trends and Product Launches Report was launched to delegates. Compiled in partnership with healthcare data and research company Rare:, the report draws on insights gathered from thousands of aesthetic clinics and distributors across the UK. Key trends highlighted include injectables, longevity and regulation. The report presents data on the most in-demand treatments, emerging treatment categories and areas experiencing a decline in popularity. It also illustrates regulatory shifts – such as the rise in oversight within clinics and the discontinuation of treatments in unregulated settings.
The Getting Started in Aesthetics Partner, Harley Academy, also took to the stage with an agenda designed to help aesthetic professionals kick start and stand out in their aesthetics career.
The stage saw several discussion panels throughout the two days including a Women in Business panel, a Gloves Off ‘Trendy or Timeless’ panel and a press panel discussing how practitioners can elevate their profile.
Sponsors of the theatre included The Cosmetic Consultants, Dermis AI, Phorest, Hygeia Digital Healthcare and InMode.
The Innovation Forum, supported by theatre sponsor SkinCeuticals, provided attendees with in-depth guidance for developing their clinic offerings through 30-minute workshops.
Key opinion leaders took the stage to represent companies including:
· Acclaro Medical
· BTL Aesthetics
· Cure Medical
· Cutera
· Esse Skincare
· Hydrafacial
· InMode
· Korea Meditech
· Med&Skin SRL
· Novus Medical
· Sciton
· SkinCeuticals
· Sofwave
· ZO Skin Health
Curated in collaboration with Dr Mayoni Gooneratne, founder of Human Health Professionals, in association with the Women’s Integrative Health Collective, the Medical Longevity Summit was a hub of insights and evidence-based strategies to support patients through integrative, regenerative and lifestyle treatments.
The content this year focused on women’s health in particular, looking at topics such as the effects of oestrogen and the brain, the impact of the skin microbiome, why bone health is central to female longevity and a look at how PCOS, endometriosis, infertility affect women in the workplace.
Alongside a packed educational programme, the dedicated exhibition area showcased the latest products, services and technologies in health and regenerative medicine.
Sponsors at the Summit this year included Associate Sponsor Roseway Labs, Halo IV, L-NUTRA, Minerva Research Lab, Nuchido, Totally Derma, Uberlube, and Yotsuba Japan.
On the success of the summit, Dr Gooneratne commented, “It was another incredible two days bringing together the brightest minds globally in the wellness space, along with some of the newsest brands. It was great to launch the WIHC and have support from our amazing partners and sponsors. We are already excited for next year to be even bigger and better!”


On Thursday 25 September, the Regenerative Aesthetic Surgery Symposium (RASS), sponsored by InMode, launched as a brand-new surgical stream at CCR 2025, delivering a full day of CPD-accredited education dedicated to advancing regenerative approaches in aesthetic and reconstructive surgery. The programme was led by the distinguished Scientific Committee – Mr Tunc Tiryaki, Dr George Christopoulos and Dr Steven Cohen – who curated an international faculty of leading experts to share pioneering research, clinical experience and future directions in the field.
Across the day, delegates heard from renowned speakers including Dr Kai-Uwe Schlaudraff, Professor Ali Ghanem, Dr Pietro Gentile, Dr Olivas Menayo, Dr Francisco Bravo and many more. Sessions explored cutting-edge topics such as stromal vascular fraction (SVF), exosomes, nanofat, enriched fat grafting and hybrid stem cell facelifts, as well as nonsurgical regenerative applications. Through expert lectures, panel discussions and case-based presentations, the symposium highlighted the transformative potential of regenerative strategies to reshape standards of practice in both cosmetic and reconstructive surgery, while fostering collaboration across specialties.

Recognising excellence through CCR’s award winners
· Best Stand – Galderma
· Best Marketing Campaign – Cosmetic Courses
Most Innovative Launch – EXOMIND by BTL
· Best Visitor Experience – Healthxchange
As well as unmissable education, CCR offered delegates the opportunity to network and discover with hundreds of specialty brands on the exhibition show floor.
CCR brought delegates the latest products, services and solutions through the easily accessible Innovations Trail. The trail provided a simple and direct way to discover the latest and most influential products on the UK market. The products in the trail included:
· Ameela Exosomes – Amedica
· AutologIX – Beautyeurope.eu
· Cellu M6 Infinity – LPG Systems UK
· EXOMIND – BTL Aesthetics
· Peptide Facial Refining Concentrate – ZO Skin Health Relfydess – Galderma
· Glace Treatment – Candela
· IRÄYE Reusable Eye Patches – IRÄYE
· MAP Health – MAP Health
· PUA Exosome Matrix Drink – Yotsuba Japan
· SkinCeuticals Advanced RGN-6 – SkinCeuticals
· Vol.U.Lift – Wigmore Medical
Delegates also had the opportunity to get up close and personal with product winner’s from the 2025 Aesthetics Awards, at the Hall of Fame feature.
The Korea Zone, delivered in partnership with IBITA, was a key feature of CCR 2025, dedicated to showcasing the latest innovations in Korean medical aesthetics. The pavilion offered delegates the opportunity to discover advanced technologies and products preparing to launch in the UK market. It provided an ideal platform for exhibitors to present new solutions, forge partnerships, and highlight Korea’s reputation as a global leader in medical aesthetics.
As well as educational learning, CCR helped delegates to expand their professional community through the introduction of the new networking trail sponsored by Healthxchange.
Throughout the two days, delegates experienced:
· Doctors & Dentists Networking with BCAM
· Nurses Networking with BAMAN
· VIP Networking Hour
· Members & Clinical Advisory Board Drinks
· Aesthetics Industry Networking Drinks
· Official Healthxchange Networking Drinks
Jackie Tuzee, CMO at Healthxchange, said, “Attending CCR this year was a proud milestone for Healthxchange, as we celebrated 25 years at the forefront of aesthetics. Sponsoring the networking reception was more than an honour, it was a moment to reflect on our journey as a trusted partner in delivering excellence across the UK and Ireland. For a quarter of a century, we’ve championed premium products, world-class education, and enduring partnerships that elevate the standards of aesthetic practice. CCR was the perfect stage to mark this legacy with our colleagues, peers, and customers.”
The VIP lounge was sponsored by Sofwave, where VIPs enjoyed access to dedicated networking drinks, a private lounge to relax and recharge, and a comfortable space to catch up with colleagues or hold conversations away from the busy show floor.
Attendees also had the chance to meet top practitioners in the specialty at the brand-new Aesthetics Mentoring initiative, supported by Dermalux.
Now that CCR 2025 has concluded, it’s time to start looking forward to your next event in medical aesthetics. Aesthetics Conference and Exhibition (ACE) 2026 will be taking place on March 13-14 at the Business Design Centre in London. Scan the QR code below to register your interest and keep updated with all the latest information.
And that’s not all! The Aesthetics Awards will be back with a bang after the second day of the conference. Entries are open until October 20 and Finalists for the event will be announced in our January issue. Tickets are on sale now! Make sure to purchase your tickets before December 31 to receive the early bird rate.
We can’t wait to see you all again soon!





































Three leading practitioners share their approaches to rejuvenating the delicate eye area through combination protocols
The periorbital region is often the first area to reveal signs of ageing. Fine lines, hollows, pigmentation and puffiness can make patients appear tired or older than they feel, with a significant impact on confidence and wellbeing. Demand for safe, effective rejuvenation around the eyes continues to grow, but this region poses unique anatomical and technical challenges.1-3
Increasingly, practitioners are turning to combined treatment protocols – blending injectables, biostimulators, lasers, radiofrequency and advanced skincare and more – to address multiple facets of ageing simultaneously. In this feature, independent nurse prescriber Dan Lowrie, along with aesthetic practitioners Dr Amy Law and Dr Rita Rakus, share how they approach periorbital concerns, with insights into consultation, product choice, protocols and the advice they offer both patients and colleagues.
The eyes are a focal point of facial expression and identity, and the practitioners highlight how patients frequently present with concerns that belie their age. As Lowrie explains, presentations span decades. He says, “I start seeing people from their mid-20s right through to their 80s. The most common issues are dark circles and hollowing tear troughs, often caused by volume loss, thinning skin, and changes in fat distribution with age.1-3 However, patients are often unsure what’s happening and need education about the ageing process.”
Dr Law highlights that the delicate eyelid skin is the thinnest on the body, making it particularly vulnerable. She explains, “Fine lines and wrinkles are common, often from the 30s onwards, due to repeated blinking, UV damage and poor protection. Darkness and shadowing are also key concerns, and while fillers may help with hollows, they cannot address pigmentation or poor skin quality.”
For Dr Rakus, patient motivations range from subtle prevention to correction. She notes, “Patients in their late 20s often want crow’s feet softened or hooding improved so they can apply makeup better, while older patients may present with eye bags or laxity that ultimately require surgical referral.”
The psychological impact of periorbital ageing is significant. As Lowrie notes, “Even mild changes can undermine confidence. Patients seek solutions not just for appearance, but for how they feel about themselves.”
Research highlights that periorbital changes such as hooding, laxity and hollowing not only alter physical appearance but also create an impression of fatigue or sadness, with direct consequences for self-esteem and social perception.4 Similarly, blepharoplasty research has indicated that surgical correction of eyelid ageing can lead to significant improvements in psychological wellbeing and quality of life, underscoring the emotional impact of this small anatomical region.5
and assessment
Each practitioner emphasises that outcomes depend on a thorough, individualised consultation. Lowrie assesses psychological drivers as well as anatomy. He explains, “We talk through the range of solutions, but also how patients feel before and after treatment. Restoring confidence is as important as restoring volume.”
Dr Rakus underscores realistic goal-setting. She says, “We provide patients with all the options – from botulinum toxin to energy devices to surgery – so they can make informed decisions. Especially around the eyes, it’s vital to know when non-surgical approaches won’t be sufficient.”
Dr Law adds that careful mapping of periorbital anatomy is essential at this stage, particularly the retaining ligaments that define tear troughs and mid-face grooves. By combining this anatomical assessment with an understanding of patient expectations and lifestyle, she ensures treatment plans are both safe and sustainable.
Precise knowledge of periorbital anatomy underpins both safety and efficacy in treatment. Age-related changes involve interplay between skin, ligaments, muscles, fat compartments and vascular structures.1-3 With time, attenuation of the orbital septum and descent of mid-face fat pads expose ligamentous boundaries, creating visible depressions such as the tear trough and palpebromalar groove. Altered lymphatic function contributes to oedema and the development of malar mounds. 3,4
Dr Law highlights how these changes shape treatment planning. She explains, “Retaining ligaments such as the tear trough ligament and zygomatic cutaneous ligament define the grooves patients perceive as hollows. The infraorbital fat pad, lymphatic drainage and malar mounds all influence outcomes and swelling risk.” 1-4
Dr Rakus stresses the need for technical precision, emphasising, “Proper depth and correct placement are essential to patient safety.”
Periorbital ageing is often multifactorial, and a single modality may not address every presentation. The practitioners agree that it’s essential to begin by identifying the principal driver – hollowing, laxity/crepiness, wrinkles, pigmentation or a combination – then layer modalities and sequence them for safety, synergy
scan to find out more

The new mesofiller nexha range are the first fillers in the world to combine cross-linked hyaluronic acid with succinic acid leading to enhanced cellular regeneration without causing inflammation.
The advanced dual release™ technology allows the immediate and progressive release of active ingredients, exceeding the expectations of a conventional filler and promoting cell regeneration that rejuvenates and revitalises the skin from within.
Pioneering technology, exclusive production and clinically proven efficacy position neostimulation as the future of medical-aesthetic solutions.
and realistic downtime and budget. The following protocols show how product choice, technique and scheduling come together to deliver predictable outcomes.


Patients most often ask Lowrie to address dark circles and hollowing, and his starting point is a conservative hyaluronic acid (HA) approach to the tear trough. He favours Revanesse Revise+ for this indication, citing a softer gel feel in use and a tendency to behave predictably under thin periorbital skin.6 He says, “Because the skin around the eyes is so thin, other fillers with higher HA contents typically swell. This has a significantly lower swell factor.”6 He also points out the practical benefit of the 1.2ml syringe for bilateral work and touch - ups.
Lowrie explains that maintenance typically requires re-treatment every nine to 18 months depending on individual metabolism and aesthetic goals, with minor touch-ups helping to preserve a natural result. While generally safe in experienced hands, potential adverse events include bruising, swelling, contour irregularities, Tyndall effect, and in rare cases vascular occlusion.7
Lowrie uses a cannula in the tear trough to reduce intravascular risk and bruising, placing small aliquots in a deep, controlled plane. This approach is widely recommended to reduce the likelihood of intravascular entry in high - risk zones such as along the angular and infraorbital arteries, though it does not eliminate risk.7
He prefers under- correction at the first session, inviting patients back once any early oedema has settled. “I under-treat rather than over-treat and review later,” he says. This staged strategy, together with a cannula -first plan, is intended to minimise issues such as overfill, Tyndall, or the need for reversal.7 Where appropriate, he advises that results can remain satisfactory for around a year, and sometimes longer, acknowledging ongoing skeletal and soft-tissue change over time.8
Lowrie rarely treats volume in isolation. To improve texture and elasticity and to blend the refreshed under- eye with adjacent tissues, he integrates a short series on Harmony XL Pro using the ‘BioBoost’ protocol alongside active, science - led skincare. BioBoost stacks non -ablative ClearLift with fractional ablative iPixel in a single session to stimulate neocollagenesis at multiple depths with minimal downtime, making it suitable alongside injectables or as a primer before volumisation.9,10
Harmony XL Pro is a multi -application platform that includes Q -switched 1064/532 nm and fractional resurfacing technologies; ClearLift is a non -ablative, fractional Q -switched Nd:YAG modality that drives photoacoustic dermal remodelling at selectable depths; iPixel is a fractional ablative 2940 nm Er:YAG handpiece used for texture and fine rhytides.11-14
Lowrie’s standard protocol comprises three sessions roughly a month apart, with a booster at six months, and he emphasises maintaining the rest of the face so that rejuvenated eyes do not appear discordant. He highlights, “If patients have beautifully re -volumised eyes then we need to make sure the rest of the face keeps up.”
Lowrie continues to explain, “I typically use laser to prime the skin – in my experience, thicker, more elastic skin tolerates filler better. I often alternate treatments: laser first, fillers about two weeks later, then further laser sessions to maintain skin quality.”
To maintain results and improve dermal quality, Lowrie places patients on active, science - led skincare rather than volume alone. This typically includes retinoids/retinol for collagen remodelling and fine - line reduction, topical vitamin C for photodamage and dyschromia, and niacinamide for barrier support and pigment irregularity – underpinned by daily broad -spectrum SPF to slow photoageing.15-18 He has developed his own skincare line – Skin at 28 – comprising these formulations.
From a safety perspective for laser sessions, patients are counselled about transient erythema and oedema with non -ablative passes and several days of roughness/peeling after fractional ablative resurfacing.10-12,19 He also cautions budget- conscious patients against seeking cheaper, inexperienced providers, noting that complications are costlier and slower to correct.
“Fine lines and wrinkles are common, often from the 30s onwards, due to repeated blinking, UV damage and poor protection. Darkness and shadowing are also key concerns”
Dr Amy Law
Polynucleotides and targeted skin boosters
Dr Law prioritises polynucleotides for fine lines, laxity and early periorbital change. She explains, “My first protocol is always a course of three sessions of polynucleotides about three to four weeks apart.” She sequences Plinest Eye (7.5mg/ml) for minimal downtime in sensitive patients, then steps up to Plinest (20 mg/ml) where greater biostimulation is desired, depending on swelling tolerance and clinical response. 20,21 Dr Law highlights, “If someone wants the least downtime, Plinest Eye is really good. Plinest is



Nutri Complex purasomes NC150+
Stimulates fibroblasts to repair skin damage, boosting collagen production and improving skin elasticity.3
Skin Glow Complex purasomes SGC100+
Reduces oxidative stress and improves the appearance of scars, dull and hyperpigmented skin.
Purasomes + Microneedling Book Training Now
Hair & Scalp Complex purasomes HSC50+
Restores hair follicle function for a healthier scalp and thicker, strong hair.4
Manufactured by Dermoaroma Italy. Exclusively distributed in the UK by DermaFocus. Purasomes products are not medical devices and are not intended to be injected. Please refer to the IFU for face, scalp and body.
References 1. J.Chenau et al., Secretome: Definitions and biomedical interest 2. Han, G. et al., 2022. The Potential of Bovine Colostrum-Derived Exosomes to Repair Aged and Damaged Skin Cells. 3. Privitera, A. et al., 2024. Nutri Complex 150+: A New and Effective Approach to Facial Rejuvenation. 4. Ferruggia, G. et al., 2024. Effectiveness of a Novel Compound Hair & Scalp Complex on Hair Follicle Regeneration.
more viscous, you’ll see bumps for a couple of days, but you get more power.”
For pigmentation-predominant dark circles, Dr Law layers a poly-revitalising HA skin booster – FILLMED NCTF 135HA – adjacent to the blebs from polynucleotides treatment in the same sitting. She avoids HA skin boosters in patients with a tendency to periorbital puffiness and cautions that, in her experience, recent tear-trough filler may prolong swelling after polynucleotides.8 “As long as I’ve managed expectations, patients are usually happy to go ahead,” she explains.


Dr Law spaces polynucleotides at three-to-four-week intervals for three sessions, then considers maintenance at approximately three months, particularly in pigment-prone patients. When combining with NCTF, she treats in the same appointment, polynucleotides first, then micro-bleb the booster between polynucleotide deposits. Dr Law summarises, “Polynucleotides do improve pigment, but combining them with the glutathione-rich skin booster gives a ‘double-whammy’ effect – it works really well and results generally last six to nine months.”20,21
Radiofrequency and injectables
Dr Rakus employs Thermage FLX for non-invasive tightening of the upper and lower eyelids, crow’s feet and periorbital crepiness, including treatments directly over the lids with appropriate intra-ocular shields. “Thermage FLX gives an excellent eye lift,” she says, explaining, “It can also treat the crepiness on the actual eyelid, but you have to use a shield.” Thermage FLX is a fourth-generation, non-invasive monopolar radiofrequency system indicated for the treatment of periorbital rhytids including upper and lower eyelids. It delivers bulk dermal heating while actively cooling the epidermis; clinical effect builds gradually over two to six months as neocollagenesis occurs.22-24 A dedicated Eye Tip 0.25cm² (450 REP) facilitates precise treatment on the lids when corneoscleral shields are in place.25
Dr Rakus typically combines Thermage with injectables to address similar concerns. She pairs treatment with small doses of botulinum toxin to relax the crow’s feet muscles, so the skin-tightening can work more effectively.26
Where dermal quality needs further support, she layers polynucleotides (PolyPhil) periorbitally either before or after Thermage depending on each patient’s availability and tolerance for transient swelling (Figure 1). Dr Rakus explains “Polynucleotides are a game-changer for the eye area, consistently delivers brighter, firmer skin with minimal downtime.”
If etched rhytides or textural change persist after tightening, she stages fractional laser resurfacing – typically using the UltraClear platform – tailoring depth and density to the patient’s downtime tolerance. Dr Rakus explains that she selects UltraClear for its controllable fractional ablation and its ability to deliver meaningful texture and rhytide improvement with predictable recovery in the periorbital region.27 According to the manufacturer, the cold fibre laser technology of UltraClear minimises unwanted thermal damage, allowing safe use across all skin types, including those previously considered higher risk (Fitzpatrick III and above).²⁷
Nevertheless, Dr Rakus advises caution in patients with a history of post-inflammatory hyperpigmentation, keloid or hypertrophic scarring, recent isotretinoin use, active infection, photosensitivity or impaired wound healing.27
Dr Rakus also advises that, in her professional experience, some presentations such as significant herniated fat or advanced dermatochalasis will likely be better served by blepharoplasty, with energy devices used before or after surgery to optimise skin quality and maintain results.28 Of course, she adds that it’s essential to refer to a surgical colleague in these cases.
Each professional offers guidance for colleagues entering this field. Lowrie urges comprehensive training, emphasising, “Learn from oculoplastic surgeons and build your armoury slowly – from fillers to lasers to regenerative medicine.”
Dr Rakus recommends starting with botulinum toxin, energy-based treatments and polynucleotides. “These are effective, safe, and versatile entry points,” she says, advising, “Leave tear trough filler until you have significant expertise.”
Dr Law highlights the value of building case studies. She notes, “Before-and-after photos build confidence for both practitioner and patient and help manage expectations.”
“I typically use laser to prime the skin – in my experience, thicker, more elastic skin tolerates filler better”
Dan Lowrie
Periorbital rejuvenation requires a nuanced approach, balancing anatomical sensitivity with a growing toolkit of injectables, biostimulators, and energy devices. By combining modalities, practitioners can address the multifactorial nature of ageing around the eyes, restoring both appearance and confidence. As Dr Rakus concludes, “The eyes are delicate and special. Patients deserve the safest, most comprehensive consultation and treatment plan we can provide.”



Dr Edward Robinson discusses a combination approach to regenerative aesthetics using PRP and PRF in synergy with other aesthetic treatments
Regenerative treatments have emerged as a leading focus of medical aesthetics in recent years.1-4 An increasing patient demand for long-lasting, natural results that work with the body’s own healing mechanisms rather than against them,5 combined with the widespread adoption of treatments such as polynucleotides (PNs)6-8 and exosomes,9,10 has been driving market growth.5
In addition, there is a rising demand for multi-modal, combination approaches,11 with combination treatments, also referred to as ‘treatment stacking’12 offering patients more personalised and holistic solutions alongside optimised outcomes.11,13
Recent innovations bring both of these concepts together by allowing us to combine tissue regenerative therapies such as platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) with modalities such as microneedling, lasers, PNs and biomodulators.14,15
While regenerative aesthetics (RA) may be seen as a relatively new subsection of cosmetic practice,5 tissue regenerative therapies such as PRP5,16-18 and PRF19,20 have been clinically validated and established as a treatment concept in a variety of medical disciplines, including orthopaedics, sports injuries and regenerative medicine (RM) for many years.21-27
These autologous treatments harness growth factors to promote collagen synthesis, angiogenesis and tissue healing,16-28 providing a rationale for their use in aesthetic indications such as hair loss15,29-31 and skin rejuvenation.14,27,28,32,33
The terms PRP and PRF are often used interchangeably, but it is important to understand the distinction.34-36
PRP
PRP is prepared by drawing a sample of the patient’s blood and processing it in a centrifuge to separate its components.14,18,30-32,37,38 This process removes most red blood cells and produces a golden-yellow plasma enriched with platelets.37 These platelets contain dense bodies (serotonin, ADP, calcium) and alpha granules, which release more than 300 growth factors and cytokines when activated.39 Among the most important are platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF) and transforming growth factor beta (TGF-β), which play key roles in angiogenesis, fibroblast stimulation, collagen synthesis and tissue repair.32,39,40 The resulting concentrated plasma is therefore widely used in regenerative treatments.32
PRF
PRF, the second-generation product,41 is obtained via lower-speed centrifugation without anticoagulant, yielding a fibrin-rich matrix that entraps platelets, leukocytes and growth factors.41,42 This matrix enables a sustained release, theoretically enhancing regenerative capacity and reducing inflammation.42 PRF can be prepared in liquid form43 or as a gel, with liquid PRF particularly suited to injectable and microneedling applications.43-45
In clinical practice I use a form of liquid PRF known as Autologous Conditioned Plasma (ACP).43 ACP refers to an autologous plasma with a concentrated number of platelets, in which the erythrocytes and leukocytes have been separated out to the greatest extent.43 This is important as both can trigger inflammatory reactions.46-50 In addition, studies indicate that liquid PRF may outperform PRP in
inducing collagen formation.33,44,45
In a study by Wang et al., skin fibroblasts migrated over 350% more in fluid-PRF when compared to control and PRP (200% increase). Fluid-PRF also significantly induced greater cell proliferation at five days. While both PRP and fluid-PRF induced significantly elevated cell mRNA levels of PDGF, it was observed that TGF-beta, collagen 1, and fibronectin mRNA levels were all significantly highest in the fluid-PRF group. Lastly, fluid-PRF demonstrated a significantly greater ability to induce collagen matrix synthesis when compared to PRP.45
Despite their autologous nature, not all PRP and PRF preparations are equivalent. Several variables can significantly influence clinical outcomes.51-54
The method used to prepare PRP is a critical determinant of its quality.51–54 While blood spun in a simple diagnostic tube and a basic centrifuge will produce a plasma fraction, this does not guarantee an optimal concentration of platelets, nor the effective separation of pro-inflammatory cells such as red blood cells and leukocytes.37,55 Commercial PRP systems are designed to enhance platelet yield while reducing unwanted cellular contaminants, but they differ considerably in performance.18-37-56,57
Systems may be open or closed:18-37-56,57
· Open systems require transferring blood between containers during processing, which increases the risk of contamination.18-37-56,57
· Closed systems maintain sterility throughout, minimising exposure to air and reducing handling steps.18-37-56,57
The choice of system also affects whether anticoagulants or separation gels are used, which can alter the biological profile of the final product. A closed system may be preferable (Arthrex ACP double syringe) because the PRP does not come into contact with a separation gel or anticoagulants.58,59 Other commercially available brands include Cellenis, EmCyte, PRP Pure and RegenLab.
Other factors
Centrifugation protocols: Speed, time and technique (horizontal vs. vertical spin) alter platelet concentration, leukocyte content and fibrin structure.18,37,60,61
Cellular composition: High concentrations of neutrophils or red blood cells can impair efficacy.47-50 Neutrophils release proteases and reactive oxygen species that damage tissues,62 while red blood cells degrade to release inflammatory by-products.63 Leukocyte-poor, fibrin-rich preparations are often preferred in aesthetic applications because they minimise inflammatory side effects.48,49,64-67 This is important so as not to create inflammation.
Patient factors: Hydration, smoking, nutrition, alcohol intake and medications (e.g. nonsteroidal anti-inflammatory drugs, anticoagulants, antiplatelet drugs) all influence platelet yield and functionality.68-69 Older patients with comorbidities may generate plasma with reduced regenerative potential.70
Delivery method: Direct injection, microneedling or combination with devices (e.g. radiofrequency, laser) changes bioavailability and depth of action.64,71 Topical application after ablative treatments can enhance penetration.72
Avoidance of local anaesthetics: Co-injection of lidocaine or other local anaesthetics can reduce platelet activity; topical numbing cream is acceptable, but direct mixing with PRP/PRF should be avoided.73
Skin rejuvenation
Treatment with PRP or PRF can improve skin texture and quality by addressing pore size, wrinkles, pigmented spots, crepiness, laxity, loss of collagen density and skin thinning.14,27,28,32
It can also be used for scar revision (including acne scars).33 In addition to the skin of the face, the literature also describes successful treatment results around the eyes, on the hands, on the neck and decolletage and for stretch marks.58,74,75
Redaelli et al. reported outcomes in 23 consecutively treated patients who underwent full-face and neck revitalisation with PRP. The study found consistent improvements in skin texture, fine wrinkles, and luminosity, with high patient satisfaction. In addition, Lin et al. documented benefits for pore size, wrinkles, pigmentation and laxity, as well as applications for periocular, hand and neck or decolletage rejuvenation.75
Hair restoration
PRP/PRF injected into the scalp is a treatment option for hair loss (androgenetic alopecia and alopecia areata). Mild to moderate diffuse hair loss responds best to non-surgical treatments.15,29-31,77,78
The growth factor vascular endothelial growth factor triggers neoangiogenesis and stimulates the blood supply to the hair follicles, increasing the diameter and thickness of the hair.79,80 In addition, the dormant hair follicles are stimulated by the growth factors released.79,80 Treatment is particularly effective in female pattern hair loss, which tends to be more diffuse and responsive to non-surgical modalities.81,82
PRP/PRF can also be effectively employed preoperatively, intraoperatively and postoperatively to improve the overall clinical result in the case of hair transplants and density of the hair follicles.83-86
The logic of combining therapies is deeply rooted in medical practice. In anaesthesia, the use of balanced or multimodal approaches – where multiple agents are administered at lower individual doses – has long been the standard, optimising desired effects while minimising adverse ones.87
This principle directly translates to medical aesthetics and regenerative combination treatments. Pairing PRP/PRF with other treatment modalities allows the simultaneous activation of multiple regenerative pathways, often leading to synergistic outcomes that are more impactful than standalone interventions.87,88 When used alongside device-based treatments such as microneedling, lasers or radiofrequency (RF), or in conjunction with agents like PNs and biostimulators, these platelet-derived concentrates can enhance treatment outcomes by accelerating healing, reducing inflammation and amplifying collagen remodelling.14,15
For patients, these combination regimens also often translate into less recovery time, meeting demand for effective, minimally disruptive treatments64,89,90 and increased satisfaction.91,92
Microneedling
PRP is most commonly combined with microneedling, often referred to as the ‘vampire facial’. Multiple studies have demonstrated that this combination achieves superior clinical results and higher patient satisfaction compared with microneedling alone.71,76,93-98 The rationale lies in the creation of controlled micro-channels that not only stimulate a wound-healing response but also facilitate the direct delivery of platelet-derived growth factors into the dermis, enhancing collagen synthesis and skin remodelling.71,76,93-98
PRP can be combined with either mechanical microneedling (pen devices) or RF microneedling. Mechanical microneedling provides controlled micro-injury that promotes neocollagenesis,71,76,93-98 while RF microneedling penetrates deeper dermal layers and delivers thermal energy to stimulate collagen remodelling and skin tightening.99 When used together with PRP or PRF, these modalities act synergistically; the device creates an optimal environment for tissue repair, while platelet concentrates accelerate recovery, reduce inflammation and amplify regenerative outcomes.71,76,93-99
Li et al. compared PRP alone, PRP with microneedling and PRP with RF microneedling for the treatment of neck wrinkles.99 15 female participants with a neck Lemperle Wrinkle Assessment Scale (WAS) score of 3-4 were enrolled in the randomised clinical trial. The subjects were randomly assigned to three treatment groups: PRP injection, MN and PRP topical PRP application and RF and PRP injection. They received treatment once a month for three consecutive months, and a clinical outcome evaluation was performed at one and six months after the final treatment.
The WAS scores and global aesthetic improvement score (GAIS) demonstrated a notably greater number of participants experiencing improved outcomes in the RF and PRP group six months post-treatment.99
A growing body of evidence indicates that combining PRP or PRF with laser and light-based treatments produces superior outcomes compared with these modalities used alone.100-106 Clinical studies have demonstrated that platelet concentrates applied after laser resurfacing can promote fibroblast proliferation, accelerate re-epithelialisation, reduce transepidermal water loss (TEWL) and enhance overall healing. Patients have also reported higher satisfaction and improved cosmetic outcomes when PRP was included as an adjunct.102-106
PRP or PRF may be used as supportive therapies following both ablative and non-ablative fractional laser procedures.101-106 Fractional lasers and intense pulsed light devices, such as BroadBand Light (BBL), can generate significant inflammation as part of their mechanism of action. The addition of PRP or PRF helps to counteract this response by supplying anti-inflammatory cytokines and regenerative growth factors, thereby reducing post-procedure erythema and downtime.102–106
PRP and PRF may also be used in combination with biostimulators such as hyper-diluted calcium hydroxylapatite (CaHA).107-109 CaHA, when diluted with saline, acts primarily as a collagen stimulator rather than a volumising filler. CaHA microspheres, which act as a scaffold for fibroblasts, initiating a cellular response that results in the body producing new collagen and elastin through a variety of cellular mechanisms, including mechanotransduction.108-109
In clinical practice, a proportion of the diluent can be replaced with PRF, creating an injectable solution that delivers both the mechanical stimulation of CaHA microspheres and the regenerative benefits of
platelet-derived growth factors, to target further regenerative cellular pathways, optimising outcomes for skin rejuvenation.108-109
Polynucleotides
PNs demonstrate efficacy in improving skin texture, elasticity and wrinkle reduction.6-8 Early evidence suggests PNs may complement platelet-derived therapies by enhancing collagen synthesis and providing antioxidant and anti-inflammatory effects.110
Their mechanisms of action are multifaceted: they stimulate adenosine A2A receptors, activating intracellular pathways that promote growth factor release and exert anti-inflammatory effects.111,112 The use of PNs has been reported to stimulate collagen production, improve skin elasticity and reduce inflammation.6,113 Additionally, they have been shown to promote hair growth114 and improve the appearance of scars.115
Importantly, PNs target distinct biological pathways compared with PRP and PRF. Whereas platelet-derived preparations primarily release platelet growth factors to stimulate collagen synthesis and tissue repair, PNs activate separate receptor-mediated processes, supporting vascularisation and antioxidative protection.6,110-116
The ideal candidate for PRP/PRF combination treatments is:64
· Healthy, non-smoker, well-hydrated and not on medications that impair platelet function.
· Experiencing early-to-moderate changes – whether skin ageing or hair thinning – rather than advanced pathology.
· Willing to commit to a course of treatments and realistic about gradual improvement over months, not days.
· Unsuitable candidates/contraindications include those with advanced hair follicle miniaturisation, active systemic illness, anticoagulant therapy, chemotherapy, infection risks or unrealistic expectations.64
Safety and practical considerations
PRP and PRF are generally regarded as safe autologous treatments, with minimal risk of adverse events when prepared and administered correctly.117 Reported side effects are uncommon and usually limited to transient bruising, swelling, or infection related to the injection technique rather than the product itself.117-118 The greatest risk is often a lack of response, which may be influenced by patient-specific factors such as platelet quality and overall health.
When combining PRP or PRF with other modalities, clinicians should be aware of a few key points. Importantly, PRF is inactivated by lidocaine; therefore, co-injection with anaesthetic agents should be avoided to preserve its regenerative potential.73 In practice, platelet concentrates can be safely combined with most injectables and energy-based devices, with no evidence of major contraindications.93-106 However, combinations with biostimulators require greater caution, as these agents carry a higher risk of inflammatory complications such as nodules or granulomas.107-109
Treatment protocols and outcome expectations
Regenerative protocols typically consist of three to six sessions, spaced at four- to six-week intervals, with maintenance treatments often recommended every three to six months for indications such as hair restoration.44,101,119 Results develop gradually, with visible improvements usually becoming apparent after four to six weeks.44,101,119
Combination treatments involving PRP and PRF represent an important evolution in regenerative aesthetics.12-15 By harnessing the biological potential of autologous platelet concentrates alongside device-based or injectable modalities, clinicians can
stimulate multiple pathways simultaneously, achieving results that are greater than the sum of their parts.87-92 Evidence suggests that such multimodal strategies can enhance efficacy, reduce downtime and improve patient satisfaction.87-92
However, outcomes are highly dependent on factors such as preparation system, centrifugation protocol, cellular composition, patient selection, and treatment delivery.51-73 Standardisation of protocols and further high-quality clinical trials remain essential to validate long-term benefits and optimise reproducibility.

Test your knowledge!
Complete the multiple-choice questions and email memberships@aestheticsjournal.com to receive your CPD certificate!
1. Which of the following best explains the key difference between PRP and PRF?
2. What is a primary advantage of using a closed PRP system compared with an open system?
3. Why are leukocyte-poor, fibrin-rich preparations often preferred in aesthetic practice?
4. What is the main rationale for combining PRP/PRF with microneedling or laser therapy?
5. Which patient would be the most suitable candidate for PRP/PRF combination treatments?

a. PRP contains more red blood cells than PRF
b. PRF is prepared with anticoagulants to prolong platelet activity
c. PRF forms a fibrin matrix that allows sustained release of growth factors
d. PRP contains no leukocytes, while PRF is leukocyte-rich
a. It always produces a higher platelet concentration
b. It removes the need for centrifugation
c. It reduces the risk of contamination by limiting exposure to air
d. It requires fewer tubes, making it cheaper
a. Leukocytes increase fibroblast activity
b. Neutrophils and red blood cells can promote inflammation
c. Red blood cells release additional growth factors
d. Fibrin decreases platelet concentration
a. To reduce the number of platelets needed
b. To increase dermal thickness by mechanical stretching alone
c. To activate multiple regenerative pathways for synergistic effects
d. To replace the need for topical anaesthesia
a. A smoker with advanced alopecia and poorly controlled diabetes
b. A healthy, well-hydrated patient with early signs of skin ageing
c. A patient on long-term anticoagulant therapy
d. A patient expecting immediate volumisation after one session
Answers: C,C,B,C,B
Dr Edward Robinson is an NHS anaesthetics doctor based in Cheshire. He specialises in skin and hair rejuvenation treatments and treating the male face. He is an associate member of BCAM, and a key opinion leader for Arthrex and Sciton.
Qual: MBBS, BSc
(Hons)

Headline Sponsor:


Nurse prescriber Michelle McLean shares her approach to using botulinum toxin in the treatment of facial palsy
In aesthetic practice, it has been seen that long-term facial palsy significantly impacts the aesthetic, functional and psychosocial wellbeing of patients.1,2
The condition can be derived from multiple aetiology such as Ramsay Hunt syndrome, infection, trauma, neurological conditions or tumours.3 It presents as a unilateral peripheral facial nerve palsy, which leads to involuntary static and dynamic variations of facial expression.3
The imbalance resulting from this muscular paralysis can significantly affect everyday tasks we take for granted, such as eating, drinking and articulation. Functional consequences can vary from difficulties with speech resulting from perioral synkinesis, to impaired vision from ocular synkinesis.4 Emotional expression is vastly affected due to these factors. Furthermore, when we consider the aesthetic appearance, most facial palsy patients feel unaccepted in society due to their asymmetry, and this has a pronounced, profound psychological effect on their wellbeing, self-esteem, anxiety, social isolation and depression.1,2
Several treatment pathways are available to manage the effects of facial palsy, including medication, surgery, physical therapy and facial aesthetic treatments.5
This article will explore the use of botulinum toxin (BoNT-A) in combination with high-intensity facial electromagnetic stimulation (HIFES) technology in particular.
Clinical presentation
Flaccid palsy
In this flaccid variety of facial palsy, patients present with an absence of wrinkling to the forehead on the paralysed side, and brow and facial ptosis may be evident with severe facial atrophy. Furthermore, these patients can also present with scleral show, an effaced nasolabial fold, labial commissure descent and a lack of animation on the affected side.6
On the unaffected side, patients can present with compensatory muscular hypertonicity and hypercontraction, whether static or dynamic, resulting in an elevation of the brow, exacerbated wrinkling and attraction of the labial commissure region.6
In the non-flaccid variation, the paralysed side of the face is affected by the presence of spasticity, overactive and involuntary facial muscle movement; meanwhile, the unaffected side may also be affected, although less evidently than in flaccid paralysis. With age, facial asymmetry becomes exacerbated and wrinkling increases on the unaffected/healthy side, and over time, synkinesis can emerge which is deemed responsible for a worsening of facial palsy asymmetry.6
Synkinesis
Synkinesis arises when involuntary concomitant muscle contractions occur, where a single muscle or muscle group contracts, despite the patient wishing to move another. This typically develops three to six months following facial paralysis or nerve trauma during the period of neuronal repair and is evident during spontaneous facial movement. Oro-ocular and oculo-oral synkinesis are the most commonly encountered.7
A comprehensive patient assessment is pivotal to determine the time-course of the facial paralysis, as it is deemed controversial to treat facial paralysis within six months of its onset due to the risk of worsening synkinesis.8 The majority of Bell’s palsy and other idiopathic lower motor neuron palsies will experience some degree of spontaneous recovery within three to six months and early use of botulinum toxin could interfere with the natural return of function thus making it harder to assess genuine recovery.8,9
In the absence of a confirmed diagnosis of facial palsy, the clinician must refrain from treatment and refer the patient back to their GP for further investigation as the responsibility of diagnosis lies solely with the GP or secondary care.
When tailoring treatment for patients with facial paralysis, it is essential that the clinician is both highly trained and experienced. If a clinician lacks sufficient experience in managing facial palsy, or a severe
facial paralysis presents or the condition continues to worsen despite intervention, it is advisable to refer on to an appropriate specialist service or back through their NHS care pathway.
Muscles need to be carefully examined at rest and on animation, with standardised images monitored at baseline and throughout the patient journey to evaluate effectiveness of treatment. This includes observing the face at rest, and during brow elevation, pouting, puckering, grinning, nose wrinkling, complete eye closure and lowering of the lower lip.10 These movements are also observed for synkinesis triggers.
From this, an individualised toxin treatment plan can be developed with consideration to target the frontalis, glabellar, orbicularis oculi, pre-tarsal, levator labii superioris, levator labii superioris alaeque nasi, depressor anguli oris, depressor labii inferioris, platysma bands and major and minor zygomatic muscles,11 with the primary objective to create balance and facial harmony without overtreating.
Botulinum toxin approach in facial palsy
BoNT-A has been used since 1987 in the non-paralysed side of the face for the treatment of facial palsy and asymmetry presentation.7,8 It has the capacity to produce significant results, reducing involuntary muscle contractions, improving facial asymmetry and quality of life.6 However, despite its widespread use, no standardised recommendations for its use in treatment of this condition exist.
Practitioners must formulate protocols based on an individualised patient consultation, assessment, presenting complaint and their experience of treating this complex group. Clinicians must have a sound underpinning knowledge and understanding of agonist and antagonist muscle groups,12 as elevators and depressors work in opposition for symmetry and facial harmony or expression. BoNT-A is administered to the unaffected side to reduce hyperkinesis (excessive movement of facial muscles) which, in the case of effective treatment, results in an improvement to symmetry and facial harmony at rest and during animation.8 To treat synkinesis, BoNT-A is administered into specific muscles to eliminate or diminish involuntary muscle action.8
The objective when treating the upper third of the face is to ensure a natural appearance and create balance and harmony between the synkinesis and the affected side. On the unaffected/healthy side we often see hyperactivity of the frontalis, exacerbating the widening of the palpebral slit opening, and because of this, a higher dose of BoNT-A is required in the frontalis and brow
depressors.13 It is imperative to palpate and observe the muscles during contraction to determine the dosage required.
The mid and lower face are the most challenging areas for clinicians to treat because an over-correction in this area can result in oral incompetence, lack of functioning of the smile, a further paralysed appearance and exacerbation of facial asymmetry.3 Conservative doses (dependent on area treated, below case study details conservative dose related to individual presentation) of BoNT-A are therefore recommended when targeting the zygomaticus major muscle, alaeque nasi muscle, depressor anguli oris, depressor labii inferioris and platysma bands to reduce the likelihood of an adverse effect, and to minimise functional discomfort.14
Consideration for precise injection location, depth and angle of treatment is pivotal, as incorrect injection points can cause unnecessary side effects and exacerbate facial asymmetry. This could cause speech abnormalities, oral incompetence, ptosis, diplopia and a worsening of psychosocial wellbeing for this vulnerable patient group. To help minimise risks, under-correction is essential in the initial treatment plan, as additional injections can be made during subsequent review appointments, allowing for a better understanding of the patient’s toxin requirements.
A 38-year-old female presented with Bell’s palsy, first diagnosed in January 2023, with unilateral flaccid paralysis of the lower third of the left side of the face, accompanied by compensatory hypertonicity of the right mentalis muscle. Her self-esteem and confidence had been significantly impacted, leading her to be referred to the charity Facial Palsy UK for local support.
A facial assessment was conducted, including examination of ocular and perioral musculature. Findings included reduced brow elevation, flattening of the left nasolabial fold, asymmetry of the smile with reduced oral commissure lift and compensatory hypertonicity of the right mentalis. These findings were consistent with an incomplete recovery and associated synkinesis, and the presentation was graded as House–Brackmann (HB) Grade III (Moderate Dysfunction). The HB scale is one of the most widely used clinician grading scales for facial nerve palsy.6
The patient underwent four sessions of EMFACE scheduled at one-week intervals. The treatment aimed to improve facial symmetry, with a focus on tightening and strengthening the elevator muscles of the face. EMFACE settings were adjusted individually to stimulate the appropriate muscles, with assessments performed
prior to each setting. The device delivers synchronised radiofrequency and high-intensity facial electrical stimulation (HIFES), primarily affecting the frontalis, zygomaticus major and minor and risorius muscles. In addition to muscle activation, the radiofrequency component generates tissue warming, which may support increased local blood flow and circulation.15
Subsequently, four weeks following completion of a course of EMFACE an individualised botulinum toxin treatment plan using BoNT-A (Azzalure) was delivered.16
1. Orbicularis oculi: Three injection points per side; 10 Speywood Units (s.U) per point administered via superficial intramuscular injection.
2. Procerus: One central injection point; 10 s.U delivered as a deep intramuscular injection.
3. Corrugator supercilia: Two injection points on each side; 10 s.U per point. Injections placed approximately 1cm above the orbital rim to minimise the risk of diffusion into adjacent muscles.
1. Levator labii superioris: One injection point, 5 s.U administered laterally to bony nasal prominence.
2. Levator labii superioris alaeque nasi: One injection point 5 s.U. targeting the superior point of the nasal ala.
3. Mentalis: One injection point 5 s.U administered deeply (full needle length, perpendicular to the skin) on the chin prominence. Injection positioned close to the midline to support symmetry and optimise facial harmony by reducing unwanted tension/hyperactivity, thus improving symmetrical function.
Four weeks following completion of the EMFACE course, a significant lift in the mid-face was observed, with evidence of muscle tightening and strengthening. A lifting effect was noted in the brow and eye area, with improved symmetry, balance and enhanced skin quality.
Two weeks after administration of the strategically placed BoNT-A, improvement in mentalis synkinesis was observed, alongside a more symmetrical smile and enhanced eye apertures during animation, further restoring facial balance and harmony.
There was a tangible improvement in smile dynamics, which the patient described as “life-changing,” noting improved social interactions, increased confidence and enhanced self-esteem. Additionally, she reported greater facial muscle mobility and reduced facial tension. Improvement in overall skin texture and quality was also noted (Figure 1&2).


The patient was scheduled for a follow-up assessment after four months for ongoing toxin management. While results from EMFACE can typically be maintained for up to two years, reassessment will be required at six-month to yearly intervals to evaluate facial symmetry and treatment maintenance.
Botulinum toxin injection is an effective treatment for improving symmetry, restoring balance and/or harmony and improving synkinesis in facial palsy patients. However, combining this with facial electromagnetic stimulation technology offers a complementary approach, supporting neuromuscular re-education, enhancing facial tone and contributing to more natural and sustained outcomes. A bespoke, individualised treatment injection plan following facial assessment with examination of ocular or perioral musculature is key to reduce the likelihood of an adverse event and optimise patient efficacy and satisfaction.

Michelle McLean is the founder and medical lead of Aesthetically You. She is a KOL for Galderma and BTL Aesthetics. In addition, McLean founded The Facial Palsy Association (FPA). She was the Winner of the Crown Aesthetics Award for Best NonSurgical Result at the 2025 Aesthetics Awards. Qual: RGN INP, MSc, BSc, PGCert, DIP/HE
INJECTABLES | SKINCARE | DEVICES NO.1 DISTRIBUTOR IN THE UK & IREL AND*


















Aesthetic nurse Kate Monteith-Ross discusses the role of exosomes and energy-based devices for treating hyperpigmentation
Hyperpigmentation and hypopigmentation are significant dermatological concerns that can arise as complications following various therapeutic interventions, including the use of energy-based device treatments. These dyschromias not only affect cosmetic outcomes but may also impact patient satisfaction and quality of life, making effective management and prevention critical aspects of post-treatment care.1
In recent years, the application of exosomes in dermatology has gained traction as an innovative and promising approach to enhancing skin recovery and mitigating pigmentation irregularities. Recent research underscores the potential of exosomes as an innovative tool in dermatology for skin recovery and the regulation of pigmentation. Exosomes, extracellular vesicles released by various cell types, are rich in bioactive molecules like proteins, lipids and genetic material, enabling them to mediate cell communication and regeneration.2 Their therapeutic applications have been explored in areas such as reducing wrinkles, improving skin texture, mitigating inflammation and managing pigmentation disorders like hyperpigmentation and vitiligo.3 It has been shown that exosomes can influence melanocyte activity, modulating melanin production to reduce pigmentation irregularities. Additionally, their ability to enhance tissue repair has shown promise for accelerating skin recovery and rejuvenation.4
This review aims to explore the benefits of integrating exosome therapy to address risks of hyperpigmentation.
Hyperpigmentation refers to the darkening of the skin due to increased melanin production or deposition, often triggered by inflammation, injury, or therapeutic interventions. In contrast, hypopigmentation denotes a reduction or loss of normal skin pigment, arising from melanocyte dysfunction or destruction, and is typically more challenging to reverse.5
Patients with higher Fitzpatrick skin types (FST) IV-VI present unique challenges in aesthetic dermatology due to their increased risk of post-inflammatory hyperpigmentation (PIH), keloid formation and prolonged erythema following invasive or ablative procedures. Melanocytes in darker skin are more reactive to trauma and inflammation, which limits the suitability of certain resurfacing technologies such as ablative lasers or medium-depth chemical peels. As a result, treatment strategies must be carefully selected to minimise melanocyte disruption while still achieving visible skin rejuvenation outcomes.5
For individuals with FST IV-VI, safer and more targeted modalities are preferred to minimise pigmentary complications.
Lasers
Fractional non-ablative lasers, such as 1,550 nm erbium-doped devices, create controlled dermal micro-injuries while sparing the epidermis, which significantly reduces the risk of PIH. It has been reported at as low as a 4% incidence, with most cases resolving within two months when combined with pre- and post-treatment hydroquinone 4%.6 This study is specific to FST IV and beyond but wider studies may still be needed. A broader systematic review confirms that non-ablative energy-based treatments generally produce only mild to moderate adverse events in darker skin types, making them substantially safer than ablative alternatives.7
Chemical peels
Superficial chemical peels, such as glycolic acid (20-70%), salicylic acid (20-30%), lactic acid and Jessner’s solution, target the stratum corneum to exfoliate and refresh the skin with a relatively low complication profile. A retrospective analysis of FST III-VI patients found only a 3.8% overall complication rate, primarily crusting, PIH (1.9%) and erythema (1.9%); all of which resolved within eight months. However, type VI individuals had a higher likelihood of adverse events (odds ratio 5.14).8
Platelet-rich plasma (PRP) offers a regenerative adjunct through intradermal injections, delivering growth factors such as TGF-β, PDGF and EGF, which help to downregulate melanogenesis and support extracellular matrix remodelling. A systematic review and meta-analysis found PRP to be both safe and effective in treating melasma, significantly improving Melasma Area and Severity Index (MASI) scores without serious adverse effects. The study does not explicitly state which FST I-VI are involved, so further research may be required.9
Nitrogen plasma technology has emerged as a non-ablative energy-based approach for skin rejuvenation, offering controlled dermal remodelling with epidermal preservation.10 Devices utilising this modality convert nitrogen gas into plasma – a high-energy, ionized form of matter – which is delivered to the skin in precisely controlled pulses. This energy induces targeted thermal effects within the epidermis and dermis without immediately disrupting the skin’s surface integrity.
Mechanisms of action:10
1. Thermal stimulation: The delivered plasma energy generates a uniform increase in skin temperature, inducing controlled thermal injury at selected depths. This activates dermal fibroblasts and promotes neocollagenesis and elastin production.
2. Resurfacing with epidermal integrity: The stratum corneum remains intact during treatment, serving as a biological dressing that facilitates healing while minimising risk of infection. Over time, this outer layer naturally exfoliates to reveal newly regenerated skin.
3. Collagen remodelling and tissue contraction: Immediate tightening effects result from thermal contraction of collagen fibres, with progressive remodelling contributing to long-term improvement in skin tone, texture and laxity.
4. Energy modulation for individualised care: Treatment parameters can be adjusted to address specific clinical indications, including photoageing, pigmentary disorders, acne scarring and laxity. Lower fluences are typically employed for patients with higher FST to reduce the risk of PIH.
Nitrogen plasma has been shown to be effective across a range of dermatologic concerns and is considered versatile enough for use in diverse skin types. However, when treating higher FST, careful energy modulation and adjunctive therapies may enhance outcomes and mitigate risks
associated with pigmentary alteration.11 According to a secondary meta-analysis, one study focused on patients with FST IV and V. Results were promising and around 90% of participants reported positive outcomes.11
Exosomes
Bovine colostrum has garnered increasing attention in biomedical research due to its rich content of bioactive compounds, including extracellular vesicles such as exosomes. A systematic review by Guberti et al. highlights the presence of numerous immunologically active components within bovine colostrum that exert immunomodulatory, antimicrobial and anti-inflammatory effects. Among these, exosomes are of particular interest for their role in intercellular communication. These nanosized vesicles carry functional proteins, lipids and nucleic acids that contribute to immune regulation and tissue regeneration processes.12
Further investigation into the dermatologic potential of bovine colostrum-derived exosomes was undertaken by Han et al., who examined their reparative effects on various human skin cell types. In keratinocytes, these exosomes demonstrated a protective effect against ultraviolet (UV)-induced oxidative stress by reducing intracellular reactive oxygen species (ROS).13 In melanocytes, they attenuated melanin synthesis following UV stimulation, suggesting a modulatory role in pigment regulation. In dermal fibroblasts, exosomes were shown to downregulate matrix metalloproteinases – enzymes implicated in collagen degradation – while simultaneously enhancing collagen synthesis and cellular proliferation. These findings support the potential utility of colostrum-derived exosomes in therapeutic strategies targeting skin ageing and photo-induced damage.13
The adjunctive use of exosome-based therapies following energy-based dermatologic procedures is increasingly being explored for their regenerative and protective properties.14 In the context of nitrogen plasma resurfacing, post-procedural integration of exosomes may offer specific benefits related to inflammation control, melanocyte regulation and tissue repair, particularly in patients with higher FST (III-VI), who are at elevated risk of PIH.14
Plasma treatments operate via controlled thermal injury to the dermis and epidermis, which initiates a cascade of inflammatory and oxidative stress responses crucial to wound healing and tissue remodelling.15 However, in melanin-rich skin, this inflammatory response can also inadvertently lead to melanocyte hyperactivation and pigmentary alterations.16 The potential for exosomes – especially those derived from bovine colostrum – to counteract these risks is supported by emerging evidence on their bioactive capabilities. Key mechanisms supporting the use of exosomes:
1. Attenuation of oxidative stress: Plasma-induced ROS can trigger prolonged inflammation and oxidative injury, both of which are implicated in the development of PIH. Exosomes exhibit intrinsic antioxidant properties through cargo molecules such as catalase, glutathione peroxidase and miRNAs that modulate oxidative stress pathways.17
2. Melanocyte modulation: Inflammatory cytokines released during skin injury – such as IL-1 and TNF-α – can upregulate melanogenesis via cAMP/PKA signalling in melanocytes.18 Han et al. found that colostrum-derived exosomes inhibit melanin synthesis in melanocytes subjected to UV-induced stress, indicating their potential to modulate pigmentary response following procedural inflammation.15
3. Enhanced tissue repair and reduced inflammatory duration: Accelerated wound healing reduces the duration of inflammatory mediator exposure, thereby minimising pigmentary complications. Exosomes support fibroblast activity, matrix remodelling and re-epithelialization through paracrine delivery of growth factors and miRNAs (e.g. miR-21, miR-146a), expediting tissue repair.19
Taken together, these findings support a theoretical and evidence-based rationale for integrating exosome therapy in post-procedural care following nitrogen plasma resurfacing. By counterbalancing oxidative and inflammatory stressors while enhancing regenerative pathways, exosomes may lower the risk of PIH and optimise outcomes, particularly in patients predisposed to pigmentary sequelae.
More studies are needed in this area to validate hypothesis and anecdotical findings.
This case study presents the treatment of a 54-year-old female patient of Italian descent with FST III-IV, who sought intervention for longstanding facial pigmentation irregularities. The patient had a history of pigmentary sensitivity, raising concern for PIH, particularly in response to energy-based therapies.
The rationale for combining high-energy nitrogen plasma with exosome therapy in this case was to optimise post-procedural healing dynamics while minimising adverse pigmentary outcomes. The below products and protocol preferred are based on personal experience, and more studies are needed in this area. In my practice it has been found that this approach may be particularly advantageous for patients with intermediate-to-higher FST undergoing resurfacing procedures.
Given her desire for overall skin rejuvenation and improvement in tone and texture, a single high-energy nitrogen plasma treatment was selected using the NeoGen system at 1.7 Joules, a setting aimed at achieving dermal remodelling through controlled thermal injury while preserving the epidermal barrier.
The application of Purasomes post-NeoGen treatment was used for plasma-induced permeabilisation, resulting in improved exosome absorption and enhanced therapeutic outcomes.20,21



The patient underwent a single treatment with two consecutive passes of nitrogen plasma treatment using the NeoGen device, each delivered at an energy setting of 1.7 Joules. Following the procedure 1.5ml of Purasomes was applied topically to the treated area to support post-procedural skin repair and mitigate the risk of pigmentary alterations. We chose this energy – which is considered a medium to high energy treatment – as this would provide a deeper penetration into the tissue and create more of an architectural change to the skin quality, as well as a resurfacing result.
Clinical photographic documentation was obtained at baseline (pre-treatment), as well as at five days and 30 days post-treatment (Figure 1). The sequential imaging demonstrated progressive improvements in
skin. In the first couple of days the patient had darkened patches surrounding previous pigmentation which then shed in the latter period of the downtime.
Post-procedural aftercare is an essential
Treatment
Emerging treatment options
This case study illustrates the potential efficacy of combining high-energy nitrogen plasma resurfacing with adjunctive application of bovine colostrum-derived
Unlock light’s regenerative and healing powers. No pain, no downtime.
Low-overhead, high-prof it, award-winning technology.1
INTRODUCING THE TRI-WAVE MD
Medical device CE class IIa-certified and FDA class II-cleared.
Indications include: acne, psoriasis, pigmentation, healing, redness, inflammation, rejuvenation, pain and more.2




Previous issues of Aesthetics Journal offer valuable clinical insights, trend analysis, expert advice, and educational content that remain essential resources for staying informed and inspired. The monthly resource for medical aesthetics professionals
Discover the archive
Aesthetica Solutions supports UK cosmetic clinics with reliable service, ethical values, and a forward-thinking approach
Aesthetica supporting UK cosmetic clinics
Have you already worked with Aesthetica Solutions? They’re proud to be a primary supplier to the UK’s leading cosmetic clinics. As a competitive online pharmacy service committed to their core values and ethically-conscious practices, they are the first choice for many. This integrity carries through to customer service; Aesthetica Solutions are dedicated to always putting the customer first. They create a relationship with their customers, helping them to understand their business and consequently anticipate and meet their needs. As a pioneering supplier, they’re at the forefront of innovations in the industry and enjoy sharing their insights into valued products with customers.
Have you heard of Plenhyage?
Plenhyage is a type of regenerative medicine that is the modern way to treat facial ageing. Plenhyage contains polynucleotides – powerful wound healing polymers that help repair tissues by repairing cell damage and deeply nourishing fibroblasts – which are an important type of skin cell in your skin. Fibroblasts are powerful agents for repairing, revitalising and regenerating facial tissue.
Our Plenyhage is sourced to minimise side effects
Our raw material comes from royal alaskan wild salmon sperm DNA, and because it originates from a non-human source, it minimises immunological side effects. Salmon sperm contains the protamine sulphate, a basic protein with high arginine content, that is isolated from salmon sperm, which has a powerful regenerative effect on the skin.
The purification process is highly rigorous. Once the raw DNA has been extracted, it goes through ultra purification, final sterilisation giving pure Plenyhage with no attached peptides, proteins or lipids.
How Plenyhage works
The polynucleotides in Plenyhage work by
scavenging free radicals. Free radicals build up due to external factors like UV radiation and stress and wreak havoc on skin cells, leading to cell damage, dehydration and skin elasticity reduction. The moisturising action and anti-free radical activity of Plenyhage helps to create an optimal environment for the growth of fibroblasts, helping to restore the elasticity of the tissues.
Key benefits:1
· Boosts fibroblast production
· Induces tissue repair processes
· Reduces inflammatory process
· Regulates melanogenesis (creation of pigment in the skin)
· Promotes hydration
· Promote myofibroblast
When to use Plenyhage
· Young or mature or damaged skin
· Acne, strophic scars and imperfections of the face
· Androgenetic alopecia, hair loss and thinning
· Before and after trichological (hair transplant) surgery






Plenyhage can be injected via a needle or a cannula.
Using a needle for the face, neck, decollete, hands, abdomen, flank, scalp, intimate areas to an intradermal depth means the mechanical action of the needle helps by inducing activation of the natural tissue repair processes. There is the possibility of bruising with this method.
Using a cannula for the face, neck, decollete, hands, abdomen, flank to an intradermal depth has the benefit of a temporary lifting effect that’s painless, with a reduced risk of bruising. Absorption is more gradual with this technique, however.
Excellent when used in combination
For optimal results, consider combining Plenhyage treatments with complementary skincare products. Look for products containing hyaluronic acid, stem cells and other ingredients that support tissue regeneration and skin hydration. Combining Plenyhage XL with Jalucomplex (hyaluronic acid) improves skin texture and has an anti-aging plumping and lifting effect. Combining fractional microneedling and Plenyhage XL improves severe skin laxity.
Plenyhage is available in two strengths (Strong: 50mg/2ml and Medium: 40mg/2ml)
If you’re looking for regenerative medicine that will delight your clients, look no further than Plenyhage. As a trusted supplier of products with sustainable sourcing, Aesthetica Solutions will be happy to help you.
This advertorial was written and supplied by Please visit aestheticcasolutions.co.uk to find out more about Plenyhage and other high grade aesthetic products.

Dr Lisa Dinley discusses the clinical rationale, mechanisms of action and practical application of microtoxin therapy in
Acne vulgaris (AV) is a multifactorial, chronic inflammatory condition of the pilosebaceous unit, driven by sebaceous hyperactivity, follicular hyperkeratinisation, Cutibacterium acnes (C. acnes) colonisation and inflammation.1 It is thought to affect 9.4% of people globally, ranking it as the eighth most common skin disease.1 Acne sufferers have a profoundly reduced quality of life, with a significantly increased likelihood of developing psychiatric conditions including depression and anxiety, as well as an increased risk of self-injury and suicide.2
These consequences highlight the need for effective therapies that address the underlying pathogenetic mechanisms of AV. Current treatment options include topical retinoids, oral antibiotics, hormonal therapy and isotretinoin, alongside a range of adjunctive modalities such as laser and light-based therapies, novel topical retinoid and antibiotic formulations, systemic agents (e.g. oral probiotics and biologics) and combinations approaches.2 While effective, these treatments are often limited by factors such as antibiotic resistance, systemic side effects and issues with patient adherence.¹
These issues have prompted the need for novel interventions, such as microtoxin (MT) – an expanded, off-license, diluted intradermal form of botulinum toxin type A (BoNT-A) as a promising treatment for managing AV with added aesthetic benefits.4,6 MT was first popularised by Mr Woffles Wu, a plastic surgeon from Singapore, who first started sharing his technique in 2001.3 The dermatological application of BoNT-A has expanded beyond the inhibition of acetylcholine at the neuromuscular junction due to discovery of its effects on fibroblasts, sebocytes, mast cells and collagenesis.4 Unlike conventional BoNT-A treatments aimed at reducing muscle activity, MT has been reported to decrease pore size, erythema, and sebum production, relax superficial rhytides and improve overall skin quality.⁴
This article will examine the effectiveness of BoNT-A in the management of AV.
Pathogenesis of AV
Four major factors are involved in the pathogenesis of AV:5
1. Increased sebum production (with altered lipid composition)
2. Abnormal follicular keratinisation leading to comedogenesis
3. C. acnes biofilm formation (due to metagenomic modifications of the bacterial microbiome)
4. Inflammatory cytokine secretion and inflammatory infiltrate into the perifollicular dermis
It is thought that alterations within the sebaceous gland (SG) and seborrhoea influences the other three factors responsible for AV pathogenesis, as SGs and sebaceous follicles are larger in AV prone individuals.5 Early, non-inflammatory AV lesions (comedones) develop when the infundibulum is filled with excessive sebum, and the pore is plugged by follicular keratinocytes (Figure 1).
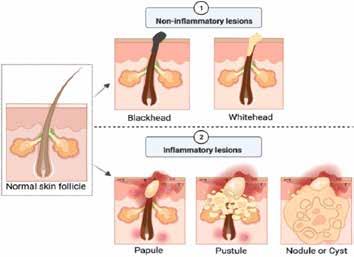
Figure 1: Highlights non-inflammatory and inflammatory AV lesions1 AV demonstrates an altered cholinergic response of the pilosebaceous unit and exacerbation of AV results from a stress response via cholinergic signalling.5 As BoNT-A has an inhibitory action on acetylcholine, it can be considered in the treatment for AV, along with the current and emerging treatment methods highlighted previously.2,5 The mechanisms of action of BoNT-A, specific to acne relates to the four major AV pathogenic factors.6-9
Sebaceous control and keratinisation
Sebum excretion rates correlate with the severity of AV, therefore, reducing sebum production and release in turn reduces AV.6 SGs and the follicular epithelium are controlled by the cholinergic system. Acetylcholine acts via the muscarinic and nicotinic receptors of the cells of the SGs and play a role in sebocyte differentiation and sebum production. Acetylcholine also drives keratinocyte adhesion, migration, differentiation and apoptosis.7 This implies that BoNT-A can downregulate sebum production as well as inhibiting adhesion of keratinocytes withing the infundibulum preventing comedone formation.6
In addition to reducing sebum production, BoNT-A paralysis arrector pili muscle, preventing contraction of the SG and sebum release.8
C. acnes control
AV severity correlates to increased emotional stress due to release of catecholamines. This in turn triggers an increase in sebum production as well as an increase in biofilm formation of C. acnes. BoNT-A has an inhibitory effect on secretion of catecholamines and in turn, a reduction in C. acnes.6
An increase in neuropeptide secretion in AV sufferers occurs in response to emotional stress leading to inflammation. Of these, Substance P (SP) has been shown to initiate and exacerbate inflammation associated with AV lesions. SP has also been shown to stimulate sebum production in SGs of AV patients, proliferation of C. acnes and inflammatory reactions.6 BoNT-A prevents release of SP providing anti-inflammatory properties.6
Arachidonic acid (AA) is an inflammatory mediator crucial in acne pathogenesis and BoNT-A has been shown to lower intradermal AA levels.6 Cyclooxgenase-2, an enzyme that plays a key role in cytokine-mediated acne inflammation, is also inhibited by BoNT-A. Mast cell number and activity is increased in inflammatory acne lesions in SGs. BoNT-A by cleaving the SNARE (soluble
N-ethylmaleimide-sensitive-factor attachment protein receptor) proteins within the mast cells preventing their degranulation. BoNT-A also inhibits TRPV1 transient receptor potential vanilloid subtype 1 (TRPV1) a regulator of sebocyte activity and pathogenesis of AV.6 In addition to the direct effects on the pathogenesis of acne and seborrhoea, BoNT-A also improves skin texture by minimising pore size, erythema, surface oiliness and tone, offering a dual therapeutic-aesthetic benefit.9
Delivery techniques and injection approaches
MT can be delivered by a variety of techniques, including, but not limited to:
1. Intradermal mesotherapy injection: Administered in a grid-like pattern approximately 1cm apart, raising a bleb at the injection site to ensure superficial placement3
2. Microneedling10
3. Stamping devices (e.g. AquaGold or WOW fusion)11
Among these, intradermal injections have been shown to be more effective, have a higher patient satisfaction and longer duration of results.10
Technique and protocol
MT has been reported to improve sebum control and acne severity, with younger patients with oily skin or mild to moderate AV appearing to respond particularly well (especially where oil-related or inflammatory types).9 MT may be considered in patients where systemic therapies are contraindicated, or as an adjunctive option alongside conventional treatments.4,9
MT involves diluting the chosen brand of BoNT-A in a ratio of 1:2.5 to 1:5, based on standard reconstitution protocols. In the UK, the current licenced BoNT-A brands include Alluzience, Azzalure, Bocouture, Botox, Letybo, Nuceiva and Relfdyess.
For the treatment of acne and seborrhoea, a dilution of 1:3 is commonly employed, with injections focused on the T-zone, cheeks and other areas of seborrhoea and AV involvement.12 intradermal injections are administered and to ensure accurate delivery depth, clinicians may utilise devices designed to inject at 0.6mm. Options include stamping devices, as mentioned or the NANOSOFT needle (a latex free CE marked micro-needle technology with three silicon needle of 0.6mm). This approach has been described as facilitating controlled intradermal delivery of MT.12
MT treatment can be repeated every three to four months depending on AV flare-ups and sebum output, but other therapies can be employed to prolong treatment intervals, such as laser and light based treatments, chemical peels, medical-grade skincare and mesotherapy treatments.6-9,13-15
In clinical practice, MT treatments typically are a combination of BoNT-A and a polyrevitalising solution, rich in non-cross linked hyaluronic acid, vitamins, amino acids and coenzymes, such as NCTF 135 HA in a 1:3 ratio.13,14
Some studies suggest that combining BoNT-A with polyrevitalising solutions may provide synergistic effects.13,14 Vitamin B3 also aids in inhibiting sebum production, improving the epidermal barrier and reducing transepidermal water loss, evening skin tone and texture, providing an anti-inflammatory environment as well as anti-microbial activity, to name but a few.15
To improve skin quality further and to prolong results, additional treatments of NCTF 135 HA can be administered following MT at four-week intervals as needed.
A 33-year-old otherwise healthy female patient presented with an acute flare of AV. The patient was fit and well with no significant medical history. She was experiencing considerable psychological distress due to the visibility of her lesions, particularly given her upcoming role as a bridesmaid in two weeks’ time.
Given the limited timeframe to achieve clinical improvement, a treatment strategy was selected to target both immediate skin quality and underlying inflammatory activity. A MT treatment was selected, utilising Nuceiva 50 IU, reconstituted with 3ml of NCTF 135 HA. Treatment was delivered via intradermal injections using a NANOSOFT needle. Post-treatment care included use of Skin Perfusion B3 recovery cream to help soothe the skin further.


Clinical limitations
It must be noted that this treatment is an off-label use of BoNT-A and patients need to be fully informed and have consented to this. Contraindications include pregnancy or breastfeeding, neuromuscular disorders and BoNT-A allergies.16 Whilst MT is an effective and promising treatment with minimal downtime, typically limited to mild redness, there is a reduced risk of bruising when using devices to facilitate administration. However, it should be noted that long-term data is lacking. Furthermore, as BoNT-A is delivered intradermally – where there are more dendritic cells compared to intramuscular injections – there is a theoretical risk that MT could be more immunogenic.16 It is also important to ensure correct depth of placement in the superficial dermis to maximise effects and minimise unwanted side effects such as paralysis of underlying musculature.3,9,16
Future directions
MT provides a promising quick acting adjunctive or alternative therapy for acne management, especially in aesthetic clinic settings where patients value both therapeutic and cosmetic improvement. This technique enables practitioners to deliver safe, effective treatments with a high degree of patient satisfaction.

Dr Lisa Dinley is a dental surgeon, aesthetic practitioner and owner of The Castle Clinic in Nottingham. She is also a clinical trainer for Laboratoires Fillmed UK. She has completed three master’s degrees and is a member of the Elsevier advisory board. She has been a dentist for 28 years and practising aesthetic treatments for 18 years, and is particularly interested in regenerative aesthetic treatments.
Qual: MClinDent Pros, MSc and MSc
We’re Evolus, a Performance Beauty company intent on doing things differently. So, what is Performance Beauty? It’s a mindset. A mission. A movement to reshape the way people express their beauty.
We know the modern beauty consumer sees aesthetics as part of their beauty routine. That’s why we are merging art and science to deliver experiences that are accessible, delightful and modern.
We’re building a brand that looks, feels and sounds like the beauty world — because that’s where our customers live, and what consumers want. Beauty brands are great at capturing trends and creating memorable, aspirational experiences. The healthcare sector is great at developing treatments that perform. We believe in the power of blending the two, grounded in clinical excellence, but designed to feel joyful and modern.
At Evolus, we think, speak and do business differently.
We’re Performance Beauty pioneers dedicated to delivering the precise results customers trust and beauty consumers love. Regardless of age, these beauty lovers possess a millennial mindset – one that values authenticity, transparency and experiences over tradition.
Millennials and those with a millennial mindset are the future of aesthetic treatments, with a preference for brands that are digital-savvy and aligned with their lifestyle. They’re evolving beauty standards, favoring a natural-yet-refreshed look over drastic transformations. We strive to deliver delightful experiences to customers that feel unapologetically millennial. That’s why our fun, edgy brand aesthetic looks, feels and sounds like a beauty brand.
At Evolus, everything starts with our commitment to evolution:
· Exclusive Focus On Aesthetics
Unlike other companies, we’re 100% dedicated to aesthetics
· Next Generation Manufacturing1
Our products are manufactured for consistency, quality and performance
· Tech Forward Customer Experience
We’re focused on creating a digital-first, seamless customer experience.
· Disrupting The Status Quo Shaped by boldness, backed by science, we’re on a mission to challenge the status quo of what’s expected in our industry.
As a Performance Beauty brand, safety is our #1 priority - for ourselves, our customers and their patients. That’s why we focus on delivering high-quality, innovative solutions while maintaining the highest standards of safety, efficacy and compliance.

Please refer to the Nuceiva® SmPC for full Prescribing Information including: indication, dosage, side effects, contraindications, warnings and precautions. The Nuceiva® PRESCRIBING INFORMATION can be accessed by scanning the QR code below.

Legal Classification: POM
List price: 50 units powder for solution for injection per vial: £75.50
This advertorial was commissioned, written and edited by Evolus for UK healthcare professionals only. Sept 2025 GB-P-2500070


Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov. uk/yellowcard or search MHRA Yellow Card in the Google Play or Apple App store. Adverse events should also be reported to Evolus International Ltd at medicalinformation@evolus.com or 08000541302.
| October 2025
We are deeply committed to understanding the safety and quality of our products through:
· Rigorous Clinical Testing
· FDA & Global Regulatory Approvals including in Europe and the UK
· State-of-the-Art Manufacturing
· Post-Market Monitoring
Our flagship product Nuceiva (prabotulinumtoxinA) is a modern1 aesthetic neurotoxin delivering fast onset, strong effect, and long-lasting results. 2,3 With over 1 million treatments since 2019,4 it’s not hard to understand why we are shaking things up as the fastest growing toxin in the US.4 Connect with our team to find out more.
Practitioner perspectives


"Working with Evolus has been a breathe of fresh air, bold, inspiring and helping me think differently. I’d say that’s evolution." Frances Turner Traill, FTT Skin Clinics, Glasgow, Hamilton and Inverness
"Performance Beauty is here and now – I see it in my patients who are both beauty consumers and a driving force in aesthetic medicine. They see treatments like Nuceiva as part of their overall beauty routine and they want a different type of experience as a result" Dr Steven Land, Novellus Aesthetics, Newcastle-Upon-Tyne.
References
1. Daewoong Method for production of botulinum toxin. Accessed May 2024. https://patents.google.com/patent/US9512418B2/en
2. Nuceiva® SmPC (Accessed Sept 2025)
3. Rzany B, et al. Aesthet Surg J. 2020;40(4):413-429
4. Data on file.




Pharmacist Dana Beiki shares strategies for safely and effectively treating varied skin types
Contemporary aesthetic practice increasingly serves diverse populations, where variations in skin physiology, facial structure and pigmentation render standardised approaches insufficient. Fitzpatrick skin types (FST) IV–VI face higher risks of pigmentary complications, hypertrophic scarring, keloids, melasma, post-inflammatory hyperpigmentation (PIH) and atrophic scarring compared with lighter phototypes.1-3 Beyond biology, cultural identity strongly shapes treatment goals.
FST IV–VI encompass individuals with darker skin tones, including but not limited to people of African, Afro-Caribbean, South Asian, Middle Eastern and certain Latin American or Indigenous backgrounds.4-9
Approaching cultural and aesthetic preferences
Beauty is interpreted through cultural context. While FST I-II, such as Scottish, Irish and Russian patients, may often emphasise facial shape, African patients may prioritise skin tone and reflectance.10 Morphometric studies highlight how ideals of proportion differ across populations. Asian, Caucasian and African groups show distinct preferences in nasal width, inner canthal distance and jawline definition.11,12 East Asian patients may value larger eyes, narrower noses and sharply pointed chins, whereas Western patients may prioritise redder lips, higher malar projection and a balanced profile.13
Ageing trajectories also differ, as Asian patients develop pigmentary changes earlier but wrinkle later than Caucasians, while African Americans show less photoageing, yet greater mid-facial volume loss.14,15
These variations highlight that aesthetic goals cannot be generalised. Increasingly, patients seek refinement rather than erasure of ethnic traits, underscoring the importance of culturally sensitive, identity-affirming care. Within this framework, combination treatments, integrating injectables, energy-based devices and topical therapies, offer versatile, safe and natural outcomes.16
Anatomical and physiological differences
Personalised, complication-free outcomes rely on recognising how anatomy and physiology vary across skin types. In FST IV–VI, these differences extend beyond pigmentation to include dermal structure, barrier dynamics, pigmentation behaviour, scarring tendencies and vascular architecture, all of which influence treatment planning. Integrating these anatomical and physiological insights allows practitioners to tailor combination treatments to each patient’s skin type, maximising safety, efficacy and aesthetic harmony.
Dermal structure
FST IV–VI skin demonstrates melanin extension into the papillary dermis, altering dermal – epidermal junction morphology and fibroblast–melanocyte signalling, heightening the risk of PIH.17-19
Treatment implications: Fillers should be placed subdermally to reduce potential disruption at the dermal-epidermal interface.20 In laser therapies, safety can be enhanced by lowering fluence,
extending pulse duration, and favouring 1064 nm Nd:YAG wavelengths to minimise epidermal injury.21,22 In clinical practice, treatments are typically spaced at four to six-week intervals to allow subclinical inflammation to resolve and to reduce cumulative trauma.22
Barrier function and sebum
Darker skin is not inherently more resilient. Transepidermal water loss (TEWL) is consistently higher in FST IV–VI than in lighter phototypes, indicating altered barrier function.23 Sebum composition also varies, with African and South Asian skin showing higher triglyceride and free fatty acid level.24 Lower ceramide levels in Black skin further predispose to lipid imbalance, xerosis and barrier dysfunction.25
Treatment implication: Pre- and post-procedure use of a moisturiser, ideally with niacinamide, to restore barrier support, reduce TEWL and improve tolerance to peels, topicals and microneedling.26
Pigmentation dynamics
Although melanin protects against UV-induced DNA damage, it absorbs visible light (400-700 nm), increasing PIH risk. Enhanced melanocyte reactivity further amplifies this risk following epidermal injury.27,28
Treatment implication: Low-fluence Q-switched lasers minimise epidermal injury while effectively targeting melanin.29 Superficial glycolic or lactic acid peels are safer than medium or deep options.30 Hydroquinone, tranexamic acid and niacinamide can suppress melanogenesis and promote pigment clearance.31,32
Scarring propensity
Hypertrophic and keloid scars occur in 4.5-16% of patients with FST IV–VI, compared with much lower rates in lighter phototypes (FST I-III).33 A Brazilian study of 146 patients found that higher phototypes were associated with greater risk of keloid and mixed scar formation, with the highest prevalence observed in FST III–VI.34 These differences are attributed to fibroblast hyperactivity, melanocyte-driven inflammation and genetic predisposition.35
Treatment implications: Aggressive ablative resurfacing should be avoided, as a systematic review reported PIH rates of 8.1%.36 Instead, a staged approach is recommended – beginning with superficial peels to promote turnover, followed by low-density fractional lasers – to minimise injury and reduce fibroblast overactivation.36
Fat morphology
Ethnic variations extend to fat distribution, which can affect filler distribution and contouring outcomes.37
Treatment implications: Ultrasound-guided injections with blunt cannulas help navigate variable vascular anatomy, reduce intravascular risk and optimise contouring precision.38
Treatment modalities
Achieving safe, natural-looking outcomes requires more than technical skill; it demands thoughtful adaptation of injectables, energy-based devices and topical therapies to match each patient’s anatomy, pigment biology and cultural preferences.
Facial morphology varies widely across ethnic groups, necessitating tailored injection strategies.11-13 East and South East Asian patients often present with limited mid-face projection, broader facial width and flatter nasal bridges.11-13 In such cases, balance is restored through targeted supraperiosteal injections at the premaxillary, pyriform and premental regions, corresponding to the anterior nasal spine, pyriform aperture margins and chin prominence, to enhance central projection without adding excessive lateral volume.39,40
By contrast, Caucasian patients usually show stronger nasal projection and deeper orbital rims.14 Their aesthetic priorities often benefit from lateral cheek and malar augmentation, while thinner dermis and earlier rhytide onset make superficial placement more suitable for fine line correction.14,15
African populations demonstrate distinct structural characteristics, including significantly longer dermal-epidermal junction with enhanced papillary fibroblast activity.41 For these populations, calcium hydroxylapatite (Radiesse) has demonstrated excellent safety and effectiveness profiles in terms of keloids, hypertrophic scarring or pigmentation changes.42 In contrast, low-viscosity fillers such as those – including Belotero Balance, Juvéderm Volbella and Restylane Kysse – are preferable for delicate regions such as the lips, temples and periorbital areas, where they help minimise the risk of the Tyndall effect.43
Injection safety is equally variable. In South Asians, the angular artery runs more superficially, making on-bone placement essential.44 In the temple, deep cannula techniques reduce the risk of injuring the superficial temporal artery.44 Given the wide variability in arterial depth, particularly in East Asian faces, real-time ultrasound guidance is increasingly recommended to confirm appropriate planes and reduce intravascular injection risk.44
Energy-based devices
While protective against UV damage, epidermal melanin complicates laser use due to strong absorption of shorter wavelengths. Segment selection is critical because absorption decreases at longer wavelengths.44,45 Given the thermal relaxation time of melanosomes, nanosecond pulses are necessary for selective targeting without collateral injury.45
Key wavelengths include:
· 1064 nm long-pulsed Nd:YAG: Considered first-line for FST IV–VI skin types, this wavelength penetrates deeply with minimal epidermal absorption, making it preferable for vascular, hair reduction and rejuvenation treatments. One study reported clearance rates exceeding 50% with minimal adverse effects when conservative parameters were applied, specifically fluences of 30-50 J/cm² and pulse durations of 15-30 ms.45
· 1550 nm fractional non-ablative: This erbium fibre laser targets dermal water while sparing the epidermis. It achieves texture remodelling and improvement in acne scarring, with PIH rates as low as 4% in darker phototypes. The risk is further reduced when low-density protocols are applied.46
· Ablative CO2 (10,600 nm) and Er:YAG (2940 nm): By contrast, these lasers carry substantially higher risks of PIH and scarring in FST IV-VI compared with 1550 nm lasers and should be used typically in select cases, such as acne or traumatic scars, with extreme caution.2,47
Chemical peels and topicals
Superficial chemical peels are safe and effective in darker skin types when preceded by two to four weeks of skin priming with topical depigmenting agents.48 Glycolic acid peels significantly improve melasma severity, while salicylic and mandelic acid combinations offer superior tolerability and anti-inflammatory benefits, particularly in Indian cohorts.48-50 Hydroquinone 2-4% remains the most effective priming agent for reducing PIH risk, with alternatives such as kojic acid or low-concentration glycolic acid.51,52
By contrast, medium depth trichloroacetic acid (TCA) peels carry substantially higher PIH risk due to unpredictable penetration depth and poor clinical endpoint visualisation in darker skin.35 Sequential glycolic acid TCA protocols may help reduce melasma recurrence, but PIH risk persists and evidence for long-term benefit is limited.30,53
Topical therapy remains foundational, with hydroquinone long regarded as standard, yet azelaic acid offers comparable efficacy, with additional anti-inflammatory properties and better tolerability.31,52 Combination regimens, such as glycolic acid peels paired with hydroquinone, consistently outperform monotherapy.31,53
Finally, photoprotection is indispensable. Visible light (415-455 nm) stimulates melanogenesis through opsin-3 activation, a pathway blocked only by iron oxide-containing sunscreens.27,54 These outperform standard UV-only formulations and reduce relapse rates in darker phototypes.27,47
Contraindications must also be tailored.20 FST IV patients should avoid deep peels and use hydroquinone priming, whilst FST V patients should avoid medium and deep peels without prophylaxis and must ensure rigorous photoprotection.55 FST VI patients, having the highest susceptibility to PIH, require triple-agent priming, corticosteroid prophylaxis and lifelong use of iron oxide sunscreen.55
A structured, four-phase approach – priming, injectables, energy-based treatments and conservative resurfacing – provides a safe, personalised framework for managing FST IV–VI skin. Not all patients require every phase, but careful sequencing minimises risk while optimising outcomes.
Priming begins with two to four weeks of topical agents, typically 2-4% hydroquinone for melasma or kojic acid for general lightening.50,51 While not required for injectables alone, priming downregulates melanocyte activity, reduces baseline pigmentation and lowers the risk of post-inflammatory hyperpigmentation.50 It may also benefit subsequent chemical peels and energy-based therapies.55
Injectables such as hyaluronic acid fillers can be placed subdermally to restore volume.20 Treatments should be staged at least two weeks prior to energy-based procedures, allowing subclinical inflammation to resolve and potentially reducing the risk of filler migration.56-58
Energy-based therapies, including non-ablative fractional lasers or long-pulsed 1064 nm Nd:YAG, are typically performed one to two weeks after injectables (or post-priming if injectables are omitted).56 Conservative parameters, such as reduced fluence, longer pulse durations and epidermal cooling, help protect against PIH.40,56
Conservative resurfacing, such as 20% glycolic acid peels or microneedling, is reserved for texture refinement once erythema subsides, usually after four to six weeks.47 If resurfacing is unnecessary, patients continue with maintenance topicals and strict photoprotection.47
As aesthetic demographics diversify, personalised care becomes a clinical necessity. Recognising variations in skin biology and cultural aesthetics is imperative for achieving safe and successful outcomes, while honouring and validating identity.

Dana Beiki is a pharmacist specialising in dermatological research and medical aesthetics. His work focuses on translating research into structured care models that prioritise patient-centred outcomes, long-term skin health and evidence-based treatment pathways. He advocates for standardised, ethically grounded frameworks that integrate scientific rigor with clinical practice.
Qual: MPharm, PhD, IPres, DipEd(Derm), L7 DipCAIT
Take your aesthetic expertise to the next level with guidance from the Merz Aesthetics Faculty. Whether you're refining your skills or expanding your knowledge, this programme is your next step toward becoming a toxin expert.

M-BOC-UKI-0658
Scan the QR code to access BOCOUTURE UK & Ireland
Prescribing Information
Date of Preparation: July 2025
Register your interest today

Scan the QR code to get in touch with one of our Aesthetic Account Managers
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at https://yellowcard.mhra.gov.uk/. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/reportan-issue. Adverse events should also be reported to Merz Aesthetics UK Ltd by emailing UKdrugsafety@merz.com or calling +44 (0) 333 200 4143.
Alison Stevenson, managing director of
manufacturer Tor Generics Ltd, introduces the new single-dose bacteriostatic saline solution
Practitioners offering injectable procedures are familiar with using bacteriostatic saline to reconstitute medicinal products for intramuscular or intradermal injection. Tor-bac, a preserved saline solution, contains sodium chloride 9mg with 0.9% (9mg/ml) benzyl alcohol, which provides both bacteriostatic protection and reduced injection-site pain compared to ordinary saline.
Traditionally, however, bacteriostatic saline solution has only been available in 30ml vials. Until now. Tor-bac can be purchased in convenient single-use 5ml ampoules. In addition, they are easier to administer and compliant with both single-use botulinum toxin and hyaluronidase applications. With Tor-bac, there’s no risk of cross contamination and the single-use doses means they are cost effective too!1
Evidence supports the use of preserved saline for periocular injections, including botulinum A and local anaesthesia. Since 1928, more than 60 studies have reported significantly lower pain scores when using benzyl alcohol containing saline.2
Benzyl alcohol itself is a naturally occurring aromatic alcohol found in plants such as jasmine and present in foods and cosmetics. It has both anaesthetic and bacteriostatic qualities, contributing to its effectiveness in reducing pain and maintaining sterility during injectable procedures.

Aesthetic nurse prescriber Emma Davies says, “Since a single patient treatment rarely requires more than 2.5ml of saline to reconstitute a single vial of toxin, either practitioners are wasting a great deal of product, or they are in breach of regulations, by reusing a 30ml multi-dose vial for multiple patients. As such, the new 5ml vials offer a valuable solution!”


Alison Stevenson started Tor generics in 2002, from pound-zero. The business started initially to re-wholesale unusual markets products, but very quickly moved into its own tor-licenced specialised products in unusual niche market areas.
Tor prides itself on unusual, first-to-market, novel preparations; Tor-Bac being one of those. Originally, the product came to market in 2018, and has built a solid following from both aesthetic and full-line wholesalers since then.

This advertorial was written and supplied by

Please visit tor-generics.com to find out more about Tor-bac and other high grade aesthetic products.

Title: Differences in Antibody Responses of Intradermal and Intramuscular Injections of Botulinum Toxin Type A
Authors: Yuttana Srinoulprasert, et al.
Published: Dermatol Ther (Heidelb), September 2025
Keywords: Botulinum toxin type A, Complexing protein, Route of injection
This pilot study evaluated antibody responses following intradermal versus intramuscular injection of six BoNT/A formulations: incobotulinumtoxinA, onabotulinumtoxinA, abobotulinumtoxinA, letibotulinumtoxinA1, letibotulinumtoxinA2, and prabotulinumtoxinA. A total of 120 subjects were divided into intradermal and intramuscular groups, with equal distribution across toxin types. Blood samples were collected and analyzed using ELISA to quantify human IgG (hIgG) targeting whole BoNT/A molecules, functional domains, and complexing proteins. Intradermal injections consistently induced higher BoNT/A-specific hIgG levels than intramuscular injections, except with letibotulinumtoxinA. Anti-functional domain hIgG levels peaked at day 30 and declined thereafter, aligning with the 90-day retreatment interval commonly recommended. Anti-complexing protein hIgG levels remained relatively stable across time points. Notably, all antibody levels remained below thresholds associated with clinical nonresponse. Intradermal injection of BoNT/A appears to elicit a stronger immunogenic response than intramuscular administration, although antibody levels did not reach clinically significant thresholds.
Authors: Mohammad Khatib, et al.
Published: Aesthetic Plastic Surgery, September 2025
Keywords: Complications, Hair transplantation surgery, Safety Hair transplant surgery is often tended to as a last resort for different types of alopecia. An electronic search was performed on databases: PubMed, Scopus, MedRxiv, and Google Scholar. Articles were subjected to data extraction through a specialized data extraction form. Data was then analyzed qualitatively and quantitatively. This review included 45 articles that were divided under two categories: 24 case reports describing 27 cases and 21 observational studies. Mean age of included patients was 40.46 ± 13.5 years in cases and 40.31 years for non-case studies. In cases, 20 (74%) patients reported donor-site complications early after surgery, and 25 (92.6%) late complications. At the recipient site, 6 (22.2%) patients reported complication early, and 8 (29.6%) patients reported delayed complications. In observational studies, 442 patients reported complications out of 2353 included in reviewed studies. Pain and discomfort were the most reported complications. In cases, 6 (22.2%, p = 0.32) patients reported pain at the donor area and observational studies included 281 (63.57%) pain-complaining patients. Arteriovenous fistulas (AVFs) were reported in 11 patients (40.7%, p = 0.073) and were associated with the use of punch graft technique for FUE.
Authors: Elizabeth Kream, et al.
Published: J Cosmet Dermatol, September 2025
Keywords: Longevity, Skin health, Aging
The aim of this comprehensive review is to illuminate “skinspan” as a framework for guiding long-term skin health. The authors review the molecular drivers of skin aging along with appraise current evidence-based interventions and synthesize evidence into an algorithm to expand skin span. A comprehensive literature review was conducted to examine the molecular hallmarks of skin aging: genomic instability, mitochondrial dysfunction, cellular senescence, and proteostasis decline, and how they are targeted by lifestyle modifications, pharmacologic agents, and aesthetic procedures. Proactive interventions, including lifestyle interventions, topical agents, systemic therapies, and noninvasive procedures, show promise in mitigating aging mechanisms and preserving skin health. To expand skinspan based on current evidence, we recommend a first-line approach of sun protection, topical retinoids, and antioxidants. Second-line interventions include procedures such as laser and energy-based devices. Clinicians may also consider emerging therapies-including stem cell-based treatments, sirtuins, nicotinamide, and natural SIRT activators-as adjunctive third-line add-ons, while continuing to monitor the evolving evidence base. A need exists for more randomized controlled trial studies to strengthen the evidence base.
Title: Anatomical-Based Diagnosis and Filler Injection Techniques: Nasolabial Folds
Authors: Gi-Woong Hong, et al.
Published: J Craniofac Surg, September 2025
Keywords: Dermal Fillers, Facial anatomy, Injection techniques
The dermal filler used in this study is Maili hyaluronic acid filler (Sinclair Pharma), derived from a novel proprietary manufacturing technology known as OxiFree™ technology (Kylane Laboratoires , Switzerland). The study analyzes various injection techniques, including needle-based and cannula-based approaches, with emphasis on safe and effective practices such as the Fern leaf and Duck walk techniques. A layered injection approach addressing both superficial and deep tissue planes is examined. Three distinct types of nasolabial folds are identified: those caused by volume deficiency, tissue laxity, and muscular attachments. Each type requires a tailored treatment approach. It is not uncommon to find a combination of 2 of the types together in one person. The study highlights the importance of understanding anatomic variations, particularly the course of the facial artery in the Korean population, for safe injection practices. A thorough understanding of nasolabial fold anatomy and appropriate treatment strategies is crucial for achieving optimal outcomes in aesthetic medicine. This is especially important for the nasolabial folds, which are highly mobile, and could easily cause misplaced dermal fillers to migrate. Future research on combination intervention techniques, including botulinum toxin, lipolytic agents, and thread-lifting, may further enhance overall treatment efficacy.
Clinics can use in-person events to engage with current patients and attract new ones. Events can take many forms – patient appreciation nights, open houses, workshops, treatment demos, grand openings or holiday celebrations. These in-person experiences create lasting positive memories, strengthen rapport and build the ‘know, like and trust’ factor that’s essential for long-term loyalty.
Hosting in-clinic events provides a platform to promote products and treatment packages, increase revenue, collaborate with complementary businesses and generate positive publicity through online content. This article will explore the key elements to consider when planning a successful in-clinic event that leaves a lasting impression on your patients.
When planning an event, consider the who, what, where, when, how and why.
Most clinics host on-site, showcasing their environment to new patients and welcoming existing ones. Attendance must align with clinic size and local regulations. In the UK, this means following Health and Safety Executive guidelines, Care Quality Commission (CQC) standards for regulated activities and licensing under the Health and Care Act for non-surgical procedures. Clinics must also meet fire safety, occupancy, hygiene, training, insurance and noise requirements.1
Budgets of £750-£1,500 are typical, with Thursday evenings (6pm-8pm) being most successful. This timing suits professionals’ schedules and avoids family conflicts. UK clinics should consider local factors like public transportation availability and cultural preferences, but the timing has proven successful in similar markets.
Live treatment demonstrations – such as laser services, lip injections or body sculpting – offer engaging, educational experiences. Demonstrations typically occur in treatment rooms, where staff can highlight benefits, explain processes and provide pre- and post-care guidance. Complementary hors d’oeuvres, cocktails and custom-branded cookies elevate the guest experience.
Since summer travel often reduces attendance, fall is an ideal season for in-clinic events. Patients return to routines, and seasonal décor, like foliage or pumpkins, creates a welcoming atmosphere. A branded step-and-repeat backdrop can also elevate the experience, providing professional photo opportunities for social media sharing.
• Patient appreciation evenings: Social gatherings to thank loyal patients, featuring canapés, mini treatment tasters and giveaways.
• Open houses or launch events: Ideal for new clinics, relocations or unveiling new treatments/devices.
• Educational workshops: Specialist talks or Q&As on skincare and aesthetics, building authority.
• Live treatment demonstrations: Real-time procedures to inform and reassure.
• Themed or seasonal events: Timed to holidays or trends.
• Collaborative wellness events: Partnering with lifestyle specialists.
• VIP or exclusive events: Invite-only for press, high-value patients or influencers.
Tailoring themes to your audience also enhances impact. Younger patients (18-35) respond well to trendy, interactive setups such as Instagram-worthy décor, neon lights, photo booths, wellness influencers or tech demos. Mature patients (40+) may prefer sophisticated experiences, from specialist panels and longevity discussions to elegant décor, wine tastings and networking opportunities. These emphasise personalisation, trust and education over glamour.
With thoughtful planning, your event becomes more than a gathering – it delivers memorable experiences that strengthen relationships, foster loyalty and encourage repeat visits and referrals.
Generate excitement with prizes and offers
Raffles and prize draws generate excitement and can be linked to purchases or automatic entry, with prizes showcasing premium offerings like broadband light or body-contouring treatments. A ‘golden ticket’ strategy – rewarding the first 10-20 attendees with redeemable discounts or pre-purchased packages – boosts punctuality and secures advance revenue. Goody bags, offered as early arrival perks or raffle prizes, can include branded items, skincare samples, vouchers or small gifts, with their value emphasised to enhance perceived benefit and extend engagement beyond the event. Prizes and exclusive offers increase attendance and participation. Including discount codes or vouchers ensures all attendees feel rewarded, for example, “15% off any treatment booked within 30 days.” Messaging that highlights both the event and tangible perks drives attendance and encourages future bookings.
Additionally, clinics may provide concise skin assessments and individualised treatment plan consultations during events to demonstrate their team’s expertise and promote subsequent appointments. It is crucial to remember that in the UK, some aesthetic treatments cannot be offered as prizes or discounted promotions in accordance with Advertising Standards Authority (ASA) guidelines.2,3 Cosmetic surgery cannot be promoted in a time-limited offer such as a competition prize or discount period because it can trivialise the decision patients need to make to undergo such a procedure.2 Moreover, prescription-only medicines such as botulinum toxin and weight loss injections cannot be promoted to the public in any capacity, including as a competition prize.3
In the UK, clinic events are often complimentary for select guests such as social media influencers, specialty representatives or loyal patients. Influencers should be carefully chosen to reflect the clinic’s target demographic, such as aesthetic or wellness audiences, with proven engagement, authentic content and a record of positive collaborations. It is also important to consider that the ASA states UK influencers must disclose any monetary or in-kind compensation received at the event.2 Vet candidates by reviewing past posts,
audience demographics, external reviews and mutual connections.
When properly selected, influencers can enhance attendance through targeted shares, increase visibility via broader reach and media mentions as well as drive future bookings by leveraging follower trust. In exchange, they may highlight treatments, adding an educational dimension, while the clinic simultaneously acknowledges and rewards patient loyalty.
Inviting press and media partners further amplifies visibility. Outreach may include local lifestyle journalists, health and beauty editors or radio and podcast hosts covering community events. Clinics can also pitch TV segments, newspaper features or radio contests to build awareness. All contacts should be vetted and provided with photos and videos to maximise post-event coverage.
Because of the high-value prizes, education, refreshments and other festivities, some clinics choose to charge a fee for event attendance. For example, one aesthetic practice I worked with charged approximately £37 per person, communicating the value by highlighting that attendees could walk away with prizes and services worth thousands. This approach reflects a price juxtaposition strategy, positioning the modest entrance fee against the potential for substantial rewards and reinforcing the event’s value to patients.4
For an invite-only event, define your guest list, prioritising loyal patients, high-value patients or local influencers. Send personalised invitations via text, email or print, emphasising exclusivity. This approach strengthens relationships, encourages attendance and enhances the perceived value of your clinic’s services.
You can also work with other local businesses and integrate them into your event. For example, if you collaborate with a functional medicine specialist, fitness trainer, microblading professional or another business, ask them if they want to have a table or speaking slot at your event in exchange for offering one of their services or products. Ask them to promote your event to their social media followers and email subscribers, but still expect to do the bulk of the marketing yourself. If you get a positive turnout for your event, your promotional partners will receive exposure and may get new patients as well.
Clinics may invite representatives from the aesthetic companies they partner with to attend events. These reps can explain the benefits of their products and technologies, providing further value to attendees. Contact
sales reps for the devices, skincare or treatments you offer, and ask them to bring samples, brochures or educational materials. Many companies budget for promotional support, so this is often feasible. Encourage reps to arrive early, set up at a table or walk around to engage with attendees. If they are active on social media, ask them to post about the event and tag your clinic for added exposure.
Adding a philanthropic element can also make your event more impactful. For example, one clinic hosted a raffle with proceeds benefiting St Jude Children’s Research Hospital, while another supported a local dog rescue. Inviting a charity representative to speak briefly at your event can help inspire donations and build community goodwill.
Once your event theme, time, location, offers, prizes and itinerary are set, it’s time to start promoting. Begin about two months in advance to give your community time to check schedules and mark their calendars. Use email, text and social media to spread the word. Email marketing tools like Mailchimp can estimate the best send times, while Instagram and Facebook provide insights on when your audience is most active. For text communications, it is advisable to conduct testing within specific timeframes, such as between 11am-1pm, or at approximately 5:30pm. However, the optimal timing should ultimately be determined by the habits and work schedules of the target audience. Track email and social post success by monitoring bookings. Many practices see increased inquiries and ticket sales after targeted promotions, revealing valuable insights into marketing effectiveness.
If you already send weekly emails, start including event promotions there. Send roughly four to six text messages in the two months leading up to the event, adjusting frequency based on responses. Always mention your clinic name and include the event’s date, time and a clear call to action. Social media is key. Post highlight reels from prior events, behind-the-scenes prep and staff interactions to build excitement and give a sense of exclusivity. Hiring a photographer or videographer can help, but staff can also capture images if budget is tight. Paid Instagram ads can target existing and prospective patients, typically with a budget up to £1,500. Finally, leverage in-person promotion – ask staff to mention the event during appointments and display posters or signage in your clinic.
Strategic follow-ups after your in-clinic event are key to maximising impact, reinforcing
messages and driving sales and loyalty. Within 24-48 hours, send a personalised thank-you email, “Thank you for joining us at our Patient Appreciation Event! We loved seeing you enjoy the cocktails, demos and prizes”.
Share the recap video on social media, tagging attendees, partners and product representatives, with a caption highlighting your brand, “What a fun night! Thanks to our amazing patients for celebrating with us, check out the highlights!” About a week later, send a second email or text with a stronger promotional push, featuring treatments or products from the event and special offers. Gather feedback through a short survey to learn what worked and what can improve. Track bookings, redemptions and survey responses. Aim for two to three post-event touchpoints over two weeks to maintain engagement without overwhelming attendees. Timely thank-you messages, recap content and targeted promotions reinforce your brand, drive sales and strengthen patient loyalty.
Hosting in-clinic events can strengthen patient loyalty but requires careful evaluation of financial and operational trade-offs. Well-attended events may offset costs by generating substantial follow-up bookings and delivering a positive return on investment, especially when services or packages are sold during the event.
However, staff strain is a notable concern, as events demand significant time for planning, delivery and post-event review. Practices should prioritise quality over quantity, hosting fewer but better-promoted events. Finally, return on investment should be monitored by tracking bookings and assessing financial outcomes to guide future event strategies.
In-clinic events build loyalty and trust, creating memorable experiences that keep your clinic top-of-mind. Consistently delivering value at events cultivates a growing, engaged patient base and supports long-term practice success.

Michael Guberti is a digital marketing strategist, specialising in services for plastic surgeons, aesthetic practitioners, functional medicine specialists and related professionals. He earned his marketing degree from Fordham University in 2018 and is currently based in Greenwich, Connecticut.
Qual: BC-HHP, B.S. Marketing Magna Cum Laude
Neurodiversity refers to the inherent and important diversity in neurocognitive functions, including variations in cognition, perception, learning, sensory processing and communication.1 It serves as an umbrella term that encompasses a range of specific learning and developmental differences, including Attention Deficit Hyperactivity Disorder (ADHD), autism, dyspraxia, dyslexia and dyscalculia.2
Neurodiversity is gaining increasing recognition within the medical aesthetics field, yet many practitioners continue to work without sufficient understanding or support. Globally, an estimated 15-22% of the population is thought to be neurodivergent, with figures suggesting that more than 15% of people in the UK fall within this group.3,4
In aesthetics, we work at the intersection of science and sensitivity – a space that is both deeply human and highly technical. For neurodivergent practitioners, this creates a distinctive combination of opportunities and challenges.
The concept of neurodiversity, first introduced in the 1990s, describes the natural variations in the way individuals think, learn and perceive the world around them.2 Common neurodivergent traits include sensory processing differences, anxiety-related conditions, executive functioning challenges, emotional regulation difficulties and co-occurring mental health concerns like mood disorders.1
In healthcare environments, these traits are not rare. Many professionals experience sensory sensitivities or mental health disorders; however, the prevalence among healthcare professionals is considerably higher than in many other fields due to high-stress environments, emotional demand and exposure to trauma.5
A systematic review of 38 studies including 53,784 participants reported burnout in 46% of individuals, with rates of depression, anxiety and post-traumatic stress disorder varying widely and reaching over 80% in high-pressure roles.6
Executive dysfunction, including difficulties with planning, organisation and time management, is a common challenge faced by neurodivergent practitioners.7 Additionally, anxiety, emotional dysregulation and sensory sensitivities can intensify stress, increasing the risk of fatigue and burnout.7
Managing multiple roles simultaneously can quickly become overwhelming. Balancing the demands of a busy clinic alongside other commitments, such as teaching or training, can stretch practitioners thin. Dividing attention across too many areas may reduce effectiveness and increase stress.
Recognising these challenges and adjusting commitments – through measures such as reducing clinic hours, introducing flexible work arrangements or creating personalised work plans with digital tools like Notion or Trello that allow tasks to be prioritised, tracked and adapted to individual needs – can enhance work quality. This approach enables greater focus and energy for each task, encourages thoughtful preparation and reduces the risk of burnout.
Creating sensory-friendly environments is vital, as overstimulating spaces can cause distress or anxiety.8 Options like quiet areas, adjustable lighting and noise-controlled spaces help neurodivergent colleagues and patients stay calm, focused and emotionally regulated.8
Benefits of an inclusive practice
Neurodivergence can bring notable advantages, such as:
Attention to detail: Practitioners may observe subtle asymmetries, variations in skin tone or nuanced muscle movements that necessitate precise, individualised procedural techniques to optimise care quality.9,10
· Empathy and sensory awareness: Attentiveness to patient cues, such as subtle facial expressions, changes in tone and body language, can foster trust and enhance the patient experience through careful dialogue and tailored procedural adjustments.11,12
· Hyperfocus: The ability to maintain deep concentration and consistently approach treatment planning and procedural tasks with accuracy helps minimise treatment errors.9
· Creative problem solving: The ability to customise treatment plans, integrate multiple techniques and adapt standard protocols to optimise patient outcomes fosters innovation in treatment planning.9
Pattern recognition and visual thinking: Identifying recurring procedural challenges, such as difficulty achieving symmetry in injections, variation in product uptake or complications in healing, allows continuous improvement and quality assurance in practice.9
Innovative learning and multimodal thinking: Innovative learning needs multimodal thinking, yet rigid formats, time pressures and sensory-heavy environments hinder growth. Visual, practical and experiential training fosters creativity, diverse learning and professional development.9,10,13
· Patient retention and satisfaction: Thoughtful, precise treatments and clear, effective communication foster patient loyalty and encourage repeat visits.11
Reduced practitioner burnout: Inclusive workplace practices improve job satisfaction, engagement and staff retention.9
Enhanced productivity: Focused attention, meticulousness and innovative problem-solving drive more efficient and higher-quality outcomes.6
Supporting neurodivergence in clinical practice becomes more effective with the right strategies. Four key areas often requiring attention are time management, communication, environmental adaptations and self-care, as these can present particular challenges for neurodivergent individuals.
Time management is vital in clinical practice, yet neurodivergent practitioners may face challenges due to executive functioning differences. These can include underestimating task duration, difficulty breaking projects into steps or hyper-focus on one task. Sensory sensitivities, fatigue or anxiety may further hinder schedules, deadlines and multitasking in busy settings.14,15
Effective time management is essential for sustaining focus and mitigating stress. Practitioners may benefit from using visual planning tools – such as calendars, whiteboards or digital apps like visual planner Tiimo, to organise daily and weekly tasks.
Setting reminders for appointments, follow-ups and documentation helps ensure that key actions are not overlooked. Additionally, speech-to-text or text-to-speech software (e.g. Jamie or Apple Dictation) can reduce demands on literacy and handwriting skills when documenting. Structured workflows, such as task batching and time blocking, help practitioners focus on one activity at a time, reducing cognitive load and improving the manageability of complex projects.
Communication
Neurodivergent practitioners, particularly those with autism or ADHD, may face communication challenges linked to social cognition, language processing and sensory perception.15 This can make it difficult to voice concerns about time management, sensory overload or executive dysfunction. Sustained focus during consultations or conversations with colleagues may also be more challenging, particularly in high-stimulation or unpredictable environments. Strategies such as visual notes, scripting responses or structured agendas can help maintain attention and manage cognitive load. Practitioners can strengthen communication by scheduling one-on-one meetings to discuss workload, preparing discussion points in advance or setting clear signals and boundaries to request support. Partnering with a trusted colleague or mentor can further aid advocacy, improve workload management and enhance team
interactions, promoting both efficiency and wellbeing.
Environmental adaptations
A hallmark of neurodiversity is variation in sensory perception, meaning noisy, unpredictable or high-pressure environments can cause fatigue, communication difficulties or reduced efficiency.15
Creating sensory-friendly environments is essential, as chaotic or overstimulating spaces can trigger overload when the brain struggles to filter lights, sounds or smells, leading to distress or anxiety. Strategies to support focus and emotional regulation include private quiet areas, temporary ‘quiet zones,’ adjustable lighting and noise-controlled spaces or headphones.8 In treatment rooms, checklists or shared-space agreements help maintain organisation and reduce clutter. Designating specific areas for particular tasks, such as quiet rooms for high-intensity procedures and low-stimulation spaces for staff decompression, further supports focus, efficiency and wellbeing for neurodivergent colleagues and patients.15
These adaptations not only enhance practitioner wellbeing but also foster calmer, more controlled environments.
Self-care and pacing
Self-care is essential for neurodivergent practitioners who may be more prone to sensory overload, fatigue and burnout. Scheduling recovery periods, pacing workloads and recognising early warning signs of burnout, such as mood changes or insomnia, helps maintain focus and reduce errors.16 Recovery periods should be scheduled according to individual needs, ranging from short daily pauses to extended breaks following periods of intense workload.
Incorporating mindfulness practices such as breathing and centring techniques, journaling and reflections, along with brief physical activity or structured downtime between appointments, can help sustain focus and energy.
By recognising limits and planning, practitioners sustain empathy, precision, consistency, reducing errors and emotional exhaustion.
Supportive workplace environments are vital for practitioner wellbeing and patient care. Inclusivity can be strengthened through open communication about workload, structured guidance for complex tasks, flexible scheduling and access to sensory-friendly spaces. Predictable routines – supported by shared calendars or visual
aids outlining appointments, administrative blocks and breaks – help with planning and prioritisation. Using multiple communication channels, including written, verbal and visual formats such as checklists, flowcharts, team briefings, infographics or task boards, further ensures clarity and minimises cognitive overload.
Disclosure of neurodiversity should always remain voluntary. When supported appropriately, however, it can improve collaboration and outcomes. Incorporating neurodiversity training into team meetings or professional development fosters awareness, highlights strengths and challenges and promotes inclusive practices without compromising confidentiality.17 Training should cover communication strategies, environmental adjustments and management approaches, delivered through comprehensive induction, regular refreshers, annual updates and integration into onboarding.
Normalising these discussions reduces stigma, fosters psychological safety for disclosure and strengthens team cohesion.
Neurodivergent practitioners may face financial challenges affecting growth and sustainability, often linked to time management, task initiation and attention. Administrative tasks like scheduling and billing can divert focus from clinical work.18 Self-employed practitioners may benefit from support, virtual assistants or software such as QuickBooks or Zoho Books. Clear budgeting, expense tracking and specialist financial advice can reduce stress and support long-term stability.
Neurodiversity should be recognised, supported and celebrated. Inclusive policies, training and mentorship strengthen teams, reduce burnout and enhance care. Embracing diverse cognitive styles enriches skill and connection, while inclusive environments allow both practitioners to thrive professionally and neurodivergent patients to feel understood, respected and better cared for.

Dr Aryan Ala’Aldeen is a GP and director of The Cosmederm Clinic. She holds a master’s degree in medical aesthetics and postgraduate diplomas in Aesthetic Injectables and Clinical Dermatology. Qual: MUDr, MScAesMed, PgDipAes, MRCGP, PgDipDerm
Business strategist Donna Ofsofke outlines practical strategies to optimise the potential of CRM in aesthetic clinics
At first glance, your customer relationship management (CRM) may appear to be functioning effectively – organising patient details, sending occasional newsletters and automating birthday promotions are expected. However, beneath this surface-level efficiency lies a common but overlooked issue: generic, non-segmented communication is quietly limiting your clinic’s revenue potential.
A successful CRM centralises patient data, and enables clinics to deliver timely, personalised and relevant experiences across the patient journey.
According to Campaign Monitor, segmented email campaigns generate up to 760% more revenue than non-segmented ones.1 And yet, many aesthetic clinics continue to send generic, one-size-fits all messages to their entire database – often without seeing the results they’re hoping for.
In aesthetics, where trust, professionalism and long-term relationships are vital, a CRM should act as the bridge between clinical care and business success. The aesthetics field has become increasingly crowded and fast-moving. Clinics compete not only on clinical results, but also on experience, service and brand perception. Standing out in this environment requires more than good treatments – it requires building loyalty, trust and consistent engagement.
Personalisation in aesthetics isn’t just a marketing technique – it’s a psychological signal of care, trust and relevance. Patients
who feel recognised are more likely to return to invest in additional treatments and recommend the clinic.
Generic blasts, by contrast, make patients feel invisible and replaceable – and in such a competitive market, that’s a fast track to churn.
In aesthetics, patient loyalty is built on three essential pillars: personalisation, trust and relevance.
Personalisation
Patients expect communications that recognise their history, preferences and treatment cycles. A CRM enables clinics to move beyond one-size-fits-all messages by sending tailored reminders, educational content and offers aligned with each patient’s journey. Personalisation is about who the patient is. It is the detail that makes them feel recognised and valued – their name, their birthday, their treatment history. It tells them you see them as an individual, not a number in a database.
A CRM is only as effective as the strategy guiding it. If your clinic is sending the same post-treatment offer to a 24-year-old first time botulinum toxin patient and a 52-year-old Morpheus8 regular, that’s not personalisation – it’s broadcasting. And broadcasting doesn’t build trust. It doesn’t encourage loyalty. And it rarely converts. Here is what non-segmented communication silently erodes in your clinic: 1. Rebooking rates: A patient who is unsure about next steps won’t respond to a vague “10% off this month” email. They need confidence, education and timely nudges such as segmented e-shots.
2. Lifetime value: Patients offered irrelevant services that don’t align with their own history, needs or goals, stop engaging. Your CRM stops becoming a patient communication channel and starts looking like spam.
3. Open rates: Generic subject lines such as ‘Discover What’s New at (Clinic Name) or Enhance Your Natural Beauty with Our Latest Treatments’, lose appeal fast. Once patients ignore your emails, re-engagement becomes an uphill battle.
4. Team efficiency: When automation lacks precision, staff are left handling avoidable queries or following up with patients who should have already been re-engaged through targeted communication.
Aesthetic treatments are intimate and high-stakes; patients need to believe their clinic knows them and has their best interests at heart. Thoughtful, relevant communication signals professionalism, consistency and care. Over time, repeated positive touchpoints build trust, which is the strongest driver of patient retention.
Relevance is about what you are saying. It ensures every message is timely, useful and aligned to their interests. Patients are more likely to engage when the message speaks directly to their needs, goals or timing. For example, promoting skincare to skincare buyers, highlighting body treatments to patients who’ve shown interest or inviting the right audience to an EMSculpt event. Relevant communication feels like helpful guidance – “It’s time for your skin review” – rather than pushy sales – “15% off everything!” Relevance drives action, whether that’s rebooking, trying a new service or recommending the clinic.
When clinics align their CRM strategy around these three pillars – personalisation, trust and relevance – they reduce churn, increase patient retention and unlock long-term revenue growth.
During a recent audit, we identified a common pitfall in patient re-engagement strategies. One clinic had been sending a generic message – “We miss you! Come back for 15% off” – to all patients who had not engaged for 90 days. This approach yielded minimal response.
We redesigned their reactivation workflow using segmentation based on service history, spending behaviour and prior engagement. Within the first month of launching the tailored automations, the clinic saw a 38% increase in rebooking rates.2
1. Audit: Reviewed and identified weaknesses in timing, targeting and compliance
2. Segmentation: Created patient groups by treatment type and responsiveness to past campaigns
3. Automation journeys: Designed separate email or SMS flows
4. Personalisation: Added patient names, referenced last treatment dates and used clinic voice to build trust
5. Optimisation: Triggered automations at key intervals with staggered nudges, monitored results and refined subject lines and timing
It is essential that aesthetic clinics ensure all promotional activity complies with Advertising Standards Authority (ASA) guidelines. Non-compliant marketing not only risks reputational damage but can also result in formal investigations and penalties. While discounts are permitted, clinics must take particular care with how they are presented. Pressure-based tactics – such as “today only” botulinum toxin offers –are frequently considered irresponsible within the aesthetics sector, as they may encourage patients to make rushed medical decisions without sufficient time for reflection.
In line with best practice and ethical standards, patients should always be given adequate time to consider treatment options before proceeding. The general ASA rules on discounts – that they must be transparent, genuine and not misleading – remain applicable. However, in medical aesthetics, additional caution is required. Promotional strategies common in retail, such as flash sales or daily deals, may be deemed inappropriate in this context due to the healthcare implications involved.3
What segmentation looks like in a clinic setting
Segmentation isn’t just a technical concept – it’s a strategic mindset. It enables clinics to create a more personalised experience tailored to the patient before they even step in the door. In practice, effective segmentation might include:
· Sending a six month post-lip filler check-in to encourage maintenance treatments
· Inviting female patients over 45 to targeted menopause skincare webinars Offering high-value patients priority access to premium services
· Triggering an educational nurture sequence for first-time toxin consultations When implemented thoughtfully, segmentation can reduce no-shows, increase spend per visit and fosters deeper brand loyalty.
A London-based aesthetic clinic approached us seeking support after experiencing a decline in patient engagement. While their CRM system was technically functional, marketing performance had stagnated – promotions were underperforming, and consultation conversions had dropped significantly.
Despite having a patient database of more than 9,000 individuals, there was no segmentation in place; every campaign was sent to the entire list, regardless of patient behaviour or profile. We conducted a comprehensive CRM audit and implemented a segmentation strategy based on the following criteria:
· First time vs. returning patients
· Age groups (under 30, 30-45, 45+)
· Treatment categories (injectables, skin, body)
· Inactivity periods (three, sixth or nine months)
Within 60 days of implementation: Email open rates increased from 11% to 34%4
· Click-through rates tripled5
· Bookings from dormant patients rose by 42%6
Importantly, the clinic did not alter their offers – rather, they refined who received them, when and how.
Consider the following approach:
1. Audit your database: Tag patients by treatment type, date of last visit and service frequency.
2. Build profiles: Identify your regular patients and those who have lapsed.
3. Segment campaigns: Test targeted messaging – for example, send a skincare promotion exclusively to patients who have booked facials in the last six months.
4. Create pathways: Develop tailored nurture flows for new patients, dormant patients and high-spenders.
5. Measure and adapt: Monitor key metrics such as open rates, rebooking rates and unsubscribes by segment. Segmentation does not have to be complex – it just needs to be intentional.
Segmentation doesn’t have to be complex or resource heavy. Start small, prove the value and build confidence. Even basic segmentation (like dormant vs. active patients) delivers better results than blanket blasts.
Here are some ways to overcome the common pitfalls:
1. Data quality issues: Poor records equates to poor targeting. Clean up your database and make updating patient details part of the clinic routine.
2. Resistance from staff or management: Automation can feel like extra work or a threat. Show how it reduces admin and share early wins to build buy-in.
3. Overcomplicating segmentation: Too many micro-groups create overwhelm. Start with three to four core segments (e.g. injectables, skincare, devices and dormant patients).
Leading clinics are increasingly adopting AI-driven segmentation, where patient behaviour informs and anticipates the next communication before manual intervention is needed. Some advanced CRMs such as Pabau and Phorest offer features such as:
· Predictive booking prompts based on individual patient habits
· Dynamic content blocks that automatically customise messaging for each recipient
· AI-assisted churn risk alerts can flag patients who are at risk of disengaging (e.g. those who haven’t rebooked within their usual cycle, or whose treatment plans have lapsed). With this insight, clinics can take proactive steps, such as sending a personalised reminder, offering a follow-up consultation or re-engaging them with a relevant promotion before they drift away4
Harnessing the power of AI-driven segmentation equips your clinic to scale growth efficiently and strategically.
Most aesthetic CRMs are fully capable of segmentation – they are simply not being utilised to their full potential. If your CRM isn’t delivering the right message to the right patient at the right time, then it isn’t functioning as a true CRM, but rather as a static database – and that limits both patient engagement and growth.

Donna Ofsofke is the founder of AesthetiCore and author of Doctors Can’t Sell. She is a qualified laser and skin specialist with over two decades of handson aesthetic experience across the UK, Europe and US.

A typical working day...
No two days are quite the same, but most of my days begin around 6am – depending on how late I have been working the night before. With two young children, my mornings are lively: getting them up, organising school bags, prepping snacks and juggling the endless list of little things they need for their activities.
We then cycle to school as I gave up using public transport back in 2009, when I was working in Buckingham Palace. It had snowed, and there were no buses, trains or tubes running, so I decided to walk. Later, when I moved to Twickenham, I swapped walking for cycling – and I haven’t looked back since. It’s saved me a fortune!
I then head to the clinic, park my bike and set off for a run along the river to Richmond and back. That 25 to 30 minutes is the calmest, most peaceful part of my day – a rare pocket of tranquillity just for me. After a quick shower, I’m into my scrubs ready to start work.
I usually arrive at the clinic between 9 to 9.30am, and from then on, it's back-to-back appointments. We are a result-driven patient-focused clinic and my days vary, from new consultations to treatments and follow-ups with existing patients.
What I love most about my job is seeing the difference these treatments make to my patients – the results can be truly transformative. That said, I also genuinely enjoy the technical side, especially needlework. One of my signature treatments is the Thames Uplift which is a specific treatment replacing lost fat in key areas of the face – including the temples, cheeks, jawline and chin.
In between appointments, I handle emails, oversee the smooth running of the clinic and respond to requests from press releases, journalists or partner companies. Admin never really stops – there are presentations to prepare, conferences to attend such as the Clinical Cosmetic Regenerative Congress (CCR) or the Aesthetics Conference and Exhibition (ACE) and content to write – but I try not to let it take too much time away from patients.
Lunch is usually a casual affair. I start my day with a breakfast smoothie that keeps me going for hours. My favourite blend includes half a banana, frozen blueberries, cherries, a small spoonful of yogurt, water, sometimes half a kiwi and, if I want it chunkier, a handful of ice. Occasionally I add kale or spinach for an extra boost. During the day I might nibble on ham, tomatoes or sugar snap peas, but I rarely have time to stop for a proper meal.
After work, it's back on my bike to collect my children, and once we’re home, the evening is dedicated entirely to them. We eat, play, bounce on the trampoline, read and laugh together. Somewhere between it all, I squeeze in tidying up and household jobs, but really, that time is theirs.
Once they have gone to sleep – usually around 9:30pm though it is becoming increasingly later – I switch back to work mode. This is when I tackle the business side of my job, accounts, admin, writing, updating the website, responding to queries and supporting colleagues. That is if I don’t fall asleep with them, which happens occasionally!
These tasks often keep me busy until 11pm, though in the early days of running the clinic, I’d work until 2 or 3am before starting all over again at 6am!
Over the course of my career, I have delivered numerous national and international presentations across a wide range of topics, including skin physiology, developing in-clinic services, business building, treatments for acne, rosacea and pigmentation.
As a long-standing key opinion leader (KOL) for ZO Skin Health, I have launched new product ranges, and presented on recognising and treating rosacea at the ZO Symposium. Most recently, I delivered a presentation on integrating skincare into clinics and building patient-focused service models.
I am also a global KOL and ambassador for Cutera. This role entails leading international webinars on rosacea, and sharing insights on selecting the right clinical partners and services to optimise patient outcomes.
Alongside these commitments, I serve as KOL for EXO|E, where I have conducted studies, trained practitioners and educated on exosome therapy. I have also produced educational content for the British Associates for Hair Restoration Surgery on incorporating exosomes into hair restoration clinics.
Beyond clinical and specialty work, I am passionate about mentoring. I support practitioners joining my clinic, guide students through career decision-making via school outreach programmes and regularly contribute to initiatives such as the Breakfast Bites series, introducing young people to medical and aesthetic career pathways. When the opportunity arises I also mentor GCSE and A-level students, offering exam preparation advice, stress management strategies and encouragement. Unfortunately, there is not a huge amount of time in between my other commitments to give to this, but I am sure it will expand in the future.
Most memorable moment in your career…
After losing my dad, I made a promise to myself that the remaining and following year would be good. Since then, I have won five national awards including The DermaFocus Award for Best Injectable Result at The Aesthetics Awards 2025.
Who has been the biggest supporters in your aesthetics journey?
David Hicks, who met me at the start of my career and believed in me, and Lorna Bowes.
If you could choose a career outside the medical field, what would it be?
I would have been a goldsmith, jewellery designer or gem and diamond dealer as this is what I wanted to be when I was 16.
What career advice would you give to other practitioners?
Have the courage to listen to what you truly need — you only get this time once. Get to know yourself and learn what genuinely makes you happy.

Entries are now open for The Aesthetics Awards 2026. Submit your application by October 20 for your chance to gain recognition at the most prestigious event in medical aesthetics.





With recent developments in the medical aesthetics specialty, it is widely accepted that a holistic antiageing treatment plan maximises the preventative potential of regenerative medicine. The argument that treatments focused on prevention and preservation help patients navigate the ageing process at their own pace is a compelling one. As this has become increasingly possible, it could be argued that the specialty’s focus has shifted from enhancement to antiageing. This is a shift that invites both opportunity and ethical concern, particularly around the risk of medicalising the natural ageing process and creating unrealistic expectations of perpetual youth.
It prompts an important debate: should we continue down this path of prevention, or pause to consider whether aesthetics is beginning to promise too much? Should they progress at different rates, a widening gap between them could make it increasingly difficult to determine how best to deliver the patient-centred care our specialty aims to make standard practice? 1,2
The ethical implications of early
The adoption of a preventative, rather than enhancing, approach to medical aesthetic treatments extends the patient demographic beyond those already demonstrating signs of ageing. Therefore, a discussion must be had about how early is too early to begin treating. It is no longer sufficient to have a blanket policy of not treating anybody who is under 18 years old. While regenerative medicine is rooted in restoring optimal function, not all patients who appear suitable for preventative treatment are, upon closer assessment, appropriate candidates.
Should a patient present in their early twenties seeking preventative treatment, there are a plethora of modalities which could be employed. Exosomes may be utilised to maintain skin brightness and integrated with microneedling to increase stimulation and begin collagen banking.3,4
Yet at this point in a patient’s life they have not begun to age visibly, and their collagen production is still maximal – while it might be preventative, is it possible to deem these treatments truly necessary?5 The qualitative nature of a preventative approach makes it incredibly difficult to determine its results and efficacy, and harder still to draw a line. I believe it is vital that the long-term implications of this are fully considered, alongside a careful assessment of whether the treatment is truly necessary or appropriate for the individual patient.
With medical aesthetic practitioners perpetuating new lines of thought, it follows that patients with differential psychology may also appear. For those predisposed to anxiety, low mood or other emotional vulnerabilities, this preventative push could be interpreted as a fear of ageing.
Foil to the ‘positive ageing’ archetype, the emergence of ‘negative ageing’ patients – young people experiencing unnecessary levels of concern about preventing ageing – is a likely unfortunate side effect of the shift to antiageing that is communicated with anything but the utmost care.
Screening tools such as the PHQ-9 and GAD-7 can be useful in indicating patients who are likely to be susceptible to negative self-esteem or who may not be in the right mindset to undergo aesthetic treatment.6 At all steps on the patient journey, consideration of the mental wellbeing and emotional landscape of the patient must be prioritised.
The creation of patients obsessed over constant improvement, serves neither patient nor practitioner in the long-term. Fear-based marketing is not the way forward and real thought must be given to how we communicate these new treatments to patients. An anxious mind can be very powerful and can easily distort well-intended messages to fit an internal narrative of worry.
A sentiment as simple as ‘this treatment focuses on preservation, like collagen banking’ could give an anxious patient the message ‘if I don’t do this, I’ll be depleted and age quicker’. Stressing that these treatments are and will always be optional could not be more important. Though we may be moving away from visual enhancement, an enhanced quality of life should always be an outcome of aesthetic treatments, not a maintenance of concern. This is especially true as with preventative treatments becoming more widely adopted, the public perception and acceptance of the normal signs of ageing could be forgotten.
To continue to foster healthy expectations in patients, an ‘educate, not manipulate’ approach is vital to ensure patients’ understanding grows in line with the technology available to them. Though we increasingly have the technology to lessen visible ageing, we must remember that ageing is not only normal – it is inevitable.
The shift from enhancement to antiageing brings powerful new tools to aesthetic practice, but also introduces complex ethical considerations. While regenerative medicine holds great potential to support the body's natural reparative functions, its use must be carefully balanced with patient need, psychological safety and responsible communication.
Preventative treatments may offer exciting possibilities, but the long-term implications and necessity of early intervention must always be questioned. As we navigate this evolving landscape, practitioners must ensure that ambition does not outpace ethics, and that ageing is not portrayed as something to fear but to understand and support.

Julie Scott is an independent nurse prescriber, Level 7 qualified aesthetic injector and trainer with more than 30 years of experience in the field of plastics and skin rejuvenation. She is an aesthetic mentor and international speaker, who has won The Aesthetics Awards ‘Aesthetic Nurse Practitioner of the Year’ in both 2022 & 2024, and ‘Best Clinic South of England’ 2023 awards.
Qual: RGN, NIP, PGDip(Aes)
“The imedpen® is great – reliable, efficient, and constantly being used in my clinics. The customer support is exemplary.”

Dr. Munir Somji Dr Medispa
Globally-recognised as one of the leading doctors in aesthetics, with over 133K followers on social media