Your Path to Workplace Health Begins Here






Spring 2023 Edition












 Gregory P. Kolovich, M.D.
Gregory P. Kolovich, M.D.

Neuropathic pain is caused by damage or disease affecting the somatosensory nervous system and is characterized by abnormal sensations or pain created by non-painful stimuli.
Occurrences are usually described as:
• sharp
• burning
• pins and needles
• electrical shocks
• may occur continuously or transiently
Neuropathic pain can be derived from the central nervous system (brain and spinal cord), peripheral nervous system (nerves within the arms or legs), or mixed (central and peripheral). Injuries in the workplace from falls, blunt trauma, and/or heavy lifting can injure the spinal cord while crush injuries, fractures, electrocutions, and/or penetrating damage can cause injuries to the nerves in the limb.
Peripheral nerve injury can be further classified as:

1. stretch-related,
2. lacerated, or
3. compressed

Local stretch injury from a fall or such can cause transient numbness or strength loss as the nerve shuts down from injury. In most cases, these injuries do recover after several weeks; however, more severe traction forces on the nerve can cause permanent damage to the nerve cells leading to chronic neuropathic pain.





Lacerations from penetrating injury can cause partial or complete transection of a peripheral nerve leading to mixed symptoms upon presentation. Partial nerve lacerations may demonstrate partial function of a nerve, whereby some, but not all, strength and sensation are lost. Complete peripheral nerve lacerations demonstrate no nerve-specific strength or sensation distally in the extremity.
Amputations, by definition, cause complete lacerations to peripheral nerves and usually have associated compression and stretch-related injuries to the affected peripheral nerves. Nerve compression can occur from crush injuries or from post-traumatic or post-surgical scar tissue constricting a nerve or adhering to it preventing its normal movement. Chronic compression can restrict blood flow causing reactive swelling and nerve damage.
In more severe or chronic cases, target motor and sensory receptors distal in the extremity suffer as each no longer receives necessary innervation and they start dying off. It is now a race against time, whereby the nerve must recover (through surgical repair, surgical release, or naturally) before a threshold of receptors are permanently lost to make a functional recovery. Typically, a nerve regenerates at a slow rate of one (1) millimeter of growth per day so recovery is dependent on the length and time.
The more proximal or chronic the injury, the longer the recovery or the lower the likelihood of achieving meaningful post-treatment recovery.




Disclosure: Event dates could be postponed, cancelled, or virtual. Please use the following as a guide. If you would like your event added to the Workplace Health magazine calendar of events, please contact Michelle Wilds at michellewilds@selectonenetwork. com. Workplace Health magazine would love to come and cover your event.

April 2023
6 - Workplace Health Symposium –Dublin, GA
12 -14 - Georgia Public Risk
Management Association - Savannah, GA
13 - Atlanta Claims Association
Educational Conference – Atlanta, GA
14 – Georgia State Board of Workers’
Compensation Regional ConferenceTifton, GA
14 - SHRM Legal Summit - Macon, GA
20 - 21 – WCCP - Orlando, FL
24 - 25 – Executive in Workers’
Compensation and Risk Conference –Anaheim, CA
27 - SHRM Jacksonville Annual Conference - Jacksonville, FL
30 - May 3 - National RIMS - Atlanta, GA
May 2023
5 - Georgia State Board of Workers’
Compensation Regional Conference –Alpharetta, GA
8 - 10 – NCCI Annual Issues Conference – Orlando, FL
11 - Atlanta Logistics Golf Tournament - Locust Grove, GA
12 - Georgia State Board of Workers’
Compensation Regional Conference –Cartersville, GA
16 - Physio Emory Symposium –Atlanta, GA
17 - Georgia State Board of Workers’
Compensation Regional Conference –Savannah, GA
22 - 23 – Alabama DOL WC – Perdido
Beach, FL
June 2023
4 - 6 – Georgia Workers’ Compensation Association Spring Conference - Jekyll Island, GA
4 - 7 – National Council of SelfInsurers Annual Conference – Denver, CO
4 - 7 – National PRIMA Conference –Long Beach, CA
5 - 7 – American Association of Safety Professionals Professional Development Conference- San Antonio, TX
8 - Moore Ingram Johnson & Steele Annual Claims Adjuster SeminarAtlanta, GA
11 - 14 – SHRM National Annual Conference - Las Vegas, NV
19 - Atlanta Claims Association Annual Golf Tournament – Atlanta, GA
22 – 23 – Alabama DOL WC –Birmingham, AL
July 2023
13 - 16 – International Workers’ Compensation Foundation Tennessee – Nashville, TN
16 - 19 – Florida Association of SelfInsurers Education Conference –Naples, FL (May change due to hotel renovations from hurricane)
26 - 28 – Florida RIMS – Naples, FL (May change due to hotel renovations from hurricane)
31 – August 4 – SAWCA 75th Annual Convention, Fernandina Beach, FL
August 2023
7 - 9 – Alabama Self Insurers Association Summer Conference –Sandestin, FL
20 - 23 – WCI - Orlando, FL
27 - 30 – Georgia State Board of Workers’ Compensation Annual Conference – Atlanta, GA
September 2023
6 - 8 – Georgia Safety Health and Environmental Annual ConferenceSavannah, GA
13 - Swift Currie Symposium - Atlanta, GA
14 - 15 – Alabama DOL Workers’ Compensation Conference –Huntsville, AL
20 - 22 – National Workers’ Compensation and Disability Conference – Las Vegas, NV
27 - Workers’ Compensation Seminar - Macon, GA
October 2023



4 - 6 – International Workers’ Compensation Foundation North Carolina – Raleigh, NC
11 - 13 – SHRM Georgia State Council Annual Conference – Lake Lanier Lodge, GA
12 - 13 – Alabama DOL Workers’ Compensation Conference –Birmingham, AL
November 2023
2 - 3 – Alabama Workers’ Compensation Organization –Birmingham, AL
5 - 7 – South Carolina WCEA – Myrtle Beach, SC






 Maharsh K. Patel, M.D.
Maharsh K. Patel, M.D.



Carpal tunnel release has an established history as a highly effective procedure. Despite its solid track record, conventional open carpal tunnel release (OCTR) can be plagued with surgical site pain, prologued recovery time, and slow return to productivity. In an effort to minimize morbidity, endoscopic carpal tunnel release (ECTR) was developed.

Carpal tunnel syndrome is one of the most common hand complaints, affecting up to five percent (5%) of the US population and resulting in 500,000 carpal tunnel release surgeries per year. It tends to impact those who have repetitive use of their hands, though other medical conditions—like diabetes and hypothyroidism—can be major contributing factors. At its root, carpal tunnel syndrome is due to increased pressure on the median nerve as it crosses through a defined space at the wrist. The median nerve supplies critical sensation in the thumb, index, middle, and part of the ring finger, as well as the muscle that controls the thumb. Symptoms include numbness, pain, and weakness.

Decreased sensation can make fine motor tasks difficult and uncomfortable tingling can wake people up at night or make them take a break from their work until the symptoms pass. Left untreated, carpal tunnel results in a significantly reduced quality of life and reduced productivity. In the long term, nerve changes can become profound and irreversible.
The goal of carpal tunnel release surgery is to relieve the pressure on the median nerve as it crosses through the carpal canal by dividing the transverse carpal ligament, a ligamentous structure in the heel of the palm. While conceptually simple, the details of this procedure have evolved since it was popularized in the 1950s. Obtaining a complete release of, and avoiding injury to the median nerve remain paramount goals, but secondary goals, like avoiding problematic scarring, palm pain, and reducing the recovery interval have received increased emphasis.
Endoscopic carpal tunnel release has become an accepted alternative to open carpal tunnel release. Here, a small incision (about 1-1.5 cm) is made in the wrist crease and a device with a camera and deployable blade is introduced into the carpal canal. It is designed to displace the nerve and tendons and provide an undersurface view of the transverse carpal ligament, which can then be divided. Advantages to ECTR include excellent visualization and ease of complete release. Further, by avoiding a 3-5 cm incision in the palm required for OCTR, the cutaneous nerves, thick fascia, and muscle in this sensitive location are spared. While it does not eliminate palm pain, it often greatly reduces it.
ECTR has a good safety profile, as well. Initial two-portal techniques and learning curves with the new procedure raised concerns about possible nerve injury. Single portal endoscopic techniques and devices have largely corrected this. In fact, review of the literature has shown OCTR release to have a higher rate of accidental structural damage to the nerve (0.49%) compared to single incision ECTR (0.19%). One downside is ECTR carries with it a learning curve that has to be overcome with additional training. This typically involves an additional year pursuing a hand surgery fellowship.
ECTR has data to support better early results. Several studies show ECTR patients have less post-operative pain, faster return to activities, improved early grip and pinch strength, and higher satisfaction overall. Based on “Quality Adjusted Life Year” modeling, which has become the standard way to compare medical intervention cost versus effect, carpal tunnel release improves quality-of-life at a modest cost. As surgeons, patients, and employers are keenly aware, recovery time after surgery carries a significant cost. Disability costs from lost productivity after carpal tunnel release are estimated to be approximately two thirds of the total costs. Therefore, reduced recovery interval greatly enhances the value of ECTR.
Carpal tunnel release is usually a very satisfying procedure and can greatly improve quality of life and productivity. While open carpal tunnel release remains an excellent and valid alternative, endoscopic carpal tunnel release provides an improved cost benefit by reducing early pain and weakness and returning patients to function sooner.
Maharsh K. Patel, M.D., is a Hand and Upper Extremity Specialist at OrthoGeorgia. A native of Macon, he earned his Bachelor of Science in Microbiology from the University of Georgia in Athens, GA, graduating summa cum laude, and his Doctor of Medicine from the Medical College of Georgia at Augusta University, graduating summa cum laude. Dr. Patel is a member of the American Academy of Orthopaedic Surgeons and the American Society for Surgery of the Hand. He enjoys exercising, traveling, cooking, reading, spending time with his beautiful family, and watching Georgia football games.






What will be the health and safety issues for 2023? Some will focus on layoffs and downsizing while others will focus on the workplace in terms of presence and telecommuting. There will continue to be discussion of “The Great Exodus,” even if that is perhaps fading. The interrelationship between diverse generations and management challenges could be noteworthy.
Companies are focused on downsizing in the face of inflation and uncertainty. Markets are challenged by pandemic, retirements, and global supply issues. The recession impacts demand for products. The buying and equipping during COVID has led to diminished and reworked equipment replacement and upgrade schedules now. Demand is diminished.
The economic downsizing is driving anxiety for those separated. There are also many reports of those separations aggravating the feelings of retained employees. Will they be next? Is the company loyal to them? If so, for how long? Are they valued for the right reasons? Should employees seek other opportunities? Will such efforts undermine their retention if more cuts come? Loyalty is a two-way street.
Is there “generational stress” in the workplace? Company culture may be built by or for one generation, making it the ideal workplace for some and the opposite for others. Do managers understand the differences? Are there distrusts, miscommunications, and misunderstandings? Is the workplace a cohesive and productive team? There are chances in those relationships for distrust, misunderstanding, and anxiety. Some employees may integrate naturally while others may adjust and adapt. There are also those who may suffer hurt feelings, displacement, or worse.
Some businesses have larger issues. There can be bullying in the workplace with coworkers, vendors, customers, and more. Some sense workplace violence is increasingly prevalent. These things can occur in the best of times, but are managers cognizant to the stress employees perceive that may manifest in behavior that can spread or project onto others? Can one be bullied and evolve to bullying?
It is usually difficult to ask for a pay raise. It is harder when the boss just laid-off part of the team. Businesses’ inputs (raw materials, utilities, etc.) are costing more. Can a raise even be discussed? If not, it may challenge employees facing consumer prices in a seemingly incessant upward spiral. Eggs seem to increase in price between the store shelf and the check out. How does one support self and family in such economic challenges?
Modern workplaces present myriad issues that can cause or exacerbate stress. Leading causes of workplace stress include leadership (or lack of it), excessive workload (layoff), job security (layoff), training (turnover/layoff), and feelings of lacking control. As stress increases, there is the potential for sub-par performance, as well as frank psychological and emotional challenges. Any of the stressors might single-handedly be sufficient to interrupt workplace harmony and personal performance. With so many potentials converging in 2023, the risks are increased and magnified.
What will be the health and safety issue for 2023? In a nutshell, it will be a yin and yang of stress and management. There must be careful monitoring and assessment of the workplace, performance, and perceptions. Workers need the understanding and collaboration of leadership to maintain productivity in the difficult months ahead.
Workers and bosses who thrive through these times will be those who recognize stress. Business cannot survive without workers and workers need the jobs; it’s an undeniable interdependence. Those who successfully emerge from this downturn will be the teams striving to maintain the mutual respect and appreciate that brought them together in the first place.
Successful relationships, work or otherwise, are those that include boundaries, healthy responses, communication, work-balance, and mutual respect. Even with those attributes, there will be friction, challenges, and even perhaps a crisis or two. Winners will not be defined by those, but by the manner in which they monitor, appreciate, and respond to the challenges.
Those who both give and expect respect and dignity, empathy, and focus will weather this time splendidly. They will intelligently accept that friction is part of all relationships, and more so in the tough times. They will cooperate, collaborate, and communicate through the friction and deliver. And, they will be better for it.
David W. Langham, has been the Florida Deputy Chief Judge of Compensation Claims since 2006. His legal experience includes workers’ compensation, employment litigation, and medical malpractice. He has delivered hundreds of professional lectures, published over forty articles in professional publications, and has published over 950 blog posts regarding the law, technology, and professionalism. David is a student, a teacher, a critic, a coach, and a leader. He lives in Pensacola, Florida, with his wife, Pamela Langham, Esq.




Clinically proven to effectively restore knee flexion, generally in 60 days or less!


In over 90 percent of 11,000+ patients, Ermi's High-intensity d to avoid secondary surgery. Saving the healthcare system over $ while preventing chronic disability and returning employees to timely manner.



$8,000 per patient, work in a


Info@ermi-motion.com

References: Stinton et al. Journal of Orthopaedic and Research, 2022 & Stephenson et al. Curr Med Res & Opinion, 2011







 David Miklas, P.A.
David Miklas, P.A.
What is the first thing you should do if the Department of Labor (DOL) is investigating your Florida business?
The answer is to contact a reputable Florida labor and employment attorney who has experience with such cases. Going through an investigation without professional guidance is generally not wise; you would not handle an Internal Revenue Service audit on your own, would you?
There are crucial mistakes many Florida businesses make at the beginning of a DOL investigation. When the DOL contacts a Florida company regarding an investigation, they do not tell the business that they should contact a labor and employment lawyer. In fact, many Florida DOL investigators tend to make immediate requests for documents and often provide a short time frame for the business to respond.

Sometimes, the DOL requests for documents be provided within only a couple of days. This can often pose a huge problem for Florida businesses, as they may not even realize they don’t have to give certain documents to the DOL. This is why it’s crucial that a Florida business bring in an employment attorney from the outset.
At times, Florida businesses will allow DOL investigators into the workplace even if they show up out of the blue. This is because most Florida businesses are unaware of their rights. The DOL investigators then to “flash a badge,” which usually results in a business owner being fearful and intimidated. It can give the impression that the DOL is law enforcement and they have to let the investigator into the workplace immediately. This is not correct.
You do not have to stop your business because the DOL wage and hour investigator shows up and asks to inspect the workplace. To clarify, this refers to the standard investigations dealing with wages and hours, not instances of where an investigator from the Occupational Safety and Health (OSHA) investigator may visit due to a work injury or death. Knowing your rights and responsibilities can go a long way.
The Fair Labor Standards Act (FLSA) requires Florida businesses to pay employees a minimum wage and overtime pay. If workers put in more than forty (40) hours in a work week, the employment lawyer should also analyze any independent contractors, freelancers, or vendors the businesses use and issues a 1099 to in order to verify they are properly classified. This is crucial because if the worker is misclassified as an independent contractor, but fails to meet the legal test, then there may be liability for the business due to the misclassification. This is usually caused because the fake business failed to pay overtime when the worker performed work in excess of forty (40) hours in a work week.
Yes, there could be systematic issues if your pay practice extends beyond a single worker at the beginning of a DOL investigation. Your employment lawyer should immediately explain the process and warn the business not to intimidate any workers or make threats pertaining to the DOL investigation. Even if the underlying investigation reveals complete compliance with the law, the business may still violate the law if it is deemed to retaliate against employees.










Yes, both current and former employees of a Florida business may be contacted by the DOL investigator during the investigation. The investigator will usually ask employees various questions about how the business operated and how they were paid. If these witnesses provide testimony inconsistent with what the employer claims, it could create a liability situation for the business. It may be human nature for a business owner to attempt to speak with the current/former employees to “guide” their interview answers. However, this would be a serious mistake and should be avoided at all costs. Always defer to your legal counsel for guidance.


Can my business fire an employer who complained about overtime?
A business should take extreme caution in disciplining any employees during a DOL investigation because it could give the appearance of retaliation. Your attorney will be able to guide you through the appropriate discipline techniques during an investigation. There may be certain times where you can discipline an employee—even during a DOL investigation—but this is risky time to discipline employees. Again, discuss these matters with your attorney.
Every DOL investigation in Florida is unique, but there are certain things you can expect in all investigations that your lawyer should be able to guide you. It’s a detailed process, so get your attorney involved at the onset.
David Miklas has practiced all types of labor and employment law for twenty-four years, exclusively representing Florida employers. A graduate of the University of Florida College of Law, he has written hundreds of employment law articles and is the co-author for the premier legal textbook used by lawyers for Florida employment law. Miklas is a frequent employment law presenter and is a nationally recognized speaker and guest lecturer addressing employment law and human resource issues.
What might be one of the most frustrating issues in Alabama workers’ compensation laws is the question of aggravation versus recurrence within the context of medical causation. These terms come into play when a claimant has previously suffered an accident to the same body part. Differentiating between whether an employee has suffered an aggravation of an injury or a recurrence of one is a fact-based inquiry and can often be a difficult task.



Generally, a court finds a recurrence when the second injury does not contribute even slightly to the causation of the disability. On the other hand, the courts typically find an aggravation of an injury occurs when the subsequent injury contributed independently to the final disability.

Why is this distinction so important? Because if a new injury is classified as a “recurrence,” then a claimant cannot make a new claim for it. However, if a new injury is deemed an “aggravation,” then a claimant can make a claim based on it. Fortunately, there are two recent appellate court decisions that help shed additional light on when a new injury will be designated as an aggravation versus a recurrence:
1.In United-Johnson Bros. of Ala., LLC v. Billups, 350 So. 3d 5 (Ala. Civ. App. 2021), Billups, a delivery-truck driver, injured his lower back in October 2016 while working for the employer. In June 2017, after reaching MMI, Billups returned to a full duty job for the employer, but continued to be treated by his treating physician and regularly complained of back pain. Billups injured his back again on February 12, 2019, when he was lifting a


200-pound lift gate on his delivery truck. On September 3, 2019, Billups filed a complaint against the employer in the trial court. At trial, the issue was whether the February 2019 injury was a recurrence or an aggravation of Billups’s October 2016 injury. The trial court ultimately entered a judgment determining Billups’s February 2019 injury was an aggravation of his October 2016 injury and that the employer was liable for all benefits to which Billups was entitled under the Act for the February 2019 injury, including medical benefits and temporary-total-disability benefits. The employer appealed arguing that the trial court had incorrectly concluded the February 2019 was an aggravation of the October 2016 injury.
The Court of Civil Appeals held that Billups’s subsequent accident resulted in symptoms that were greater in degree than he had suffered since the surgical repair to his back in March 2017. The Court also took into consideration that he was unable to continue working as he had been doing since he had reached maximum medical improvement after the October 2016 injury and his treating physician opined how it was unlikely Billups would return to his baseline condition. Thus, the Court held that it could not conclude Billups had suffered no additional damage to his back from the February 2019 accident or, specifically, that the accident had not at least contributed slightly to the causation of his disability following that accident. Accordingly, the October 2020 judgment finding the injury to be an aggravation was affirmed.
2.A second recent case is Green v. T.R. Miller, 2022 Ala. Civ. App. LEXIS 41. In that case, the employee suffered a right-hand injury while working for BE & K Construction in 1994, and, thereafter, developed reflex sympathetic disorder (“RSD”). In November 2000, while working for another employer, Yother, he fell on his right arm and aggravated his preexisting RSD. In 2020, he sued his employer at the time, T.R. Miller, alleging he had injured his right arm in a December 2019 accident. Yother then filed a motion requesting a hearing to determine its continuing liability to pay for medical treatment based on the last injurious exposure rule. After a hearing to determine who should be liable for any benefits owed, the trial court entered an order determining Green had suffered a recurrence of his 2000 injury. The trial court denied Green’s claim for compensation against T.R. Miller and ordered Yother to continue to provide for medical treatment.
The evidence presented in this case deferred from the Billips case in that Green’s symptoms had actually waxed and waned over the years which permitted him to work for some periods but not others. Also, the symptoms he reported both before and after the December 2019 injury were similar in nature, unlike Billips, whose symptoms were remarkedly worsened. In addition, there was medical testimony that the laceration injury Green sustained in December 2019 would not be expected to cause or contribute to a worsening of his RSD.
In its decision, the Court of Civil Appeals also took the opportunity to clarify that the no-preexisting-injury rule did not apply when determining medical causation, including when deciding if a second injury is a recurrence, an aggravation, or a new injury under the last-injurious-exposure rule. Simply put, there is no hard and fast rule that no preexisting injury exists if the employee was working normally. Also of note, the appellate court pointed out that the trial court was authorized to find certain medical expert testimony more persuasive than the other evidence. The appellate court went on to state they were not permitted to reweigh the evidence because weighing the evidence is solely a function of the trier of fact.
Hopefully, these recent decisions bring more clarity on the issue of recurrence versus aggravation. If you have any questions, feel free to reach out to me at Lauren@esw-law.com.




























As another new year is ushered in, preventing workplace injuries continues to be a focus of organizations. Most organizations strive to create a safety culture in which employees are actively engaged and care for the safety of others. Such a culture can decrease the number of injuries and the costs and resources negatively impacted by workplace claims. However, achieving and sustaining such a culture can be difficult to establish because businesses lack the necessary elements in their safety culture. These elements are: collaboration, communication, and courage.
Collaboration is when individuals work together to achieve a goal or mission. In terms of safety, to get employees to buy-in to the safety goals and mission of the organization, they must be involved in the process. By collaborating with employees at all levels of the organization in the safety process, it gives the employees a sense of ownership over the process and boasts their commitment to the safety culture of the organization because they feel they had a voice in shaping their environment. Thereby, converting some employees to change agents helps to promote and defend the safety culture of the organization through communication with other employees.
Communication is the effective delivery of a message in the proper manner. Unfortunately, most organizations struggle with this element because safety professionals and employees in the organization do not know how to deliver feedback to correct inappropriate safety actions or acknowledge the appropriate safety actions. Most safety departments “police” safety instead of motivating and supporting it.
For example, when sharing safety feedback (supportive or corrective), it should be delivered immediately following the safety behavior. In most instances, this is not the case. Furthermore, some organizations use fear techniques such as a reduction or loss of benefits or scolding employees to try to decrease the number of workplace injuries. However, fear techniques are not effective because they are more likely to make employees hide or not report safety incidents, which can diminish learning opportunities when it comes to safety. Communication is also important because it can lead to trust when information is distributed properly and the organization is transparent with its workforce regarding policies and procedures. Ultimately, building trust creates an environment where team members feel safe enough to display courage.


Courage
Courage is the motivation to take action in frightening or unfavorable situations. In regard to safety, courage is having the competence and confidence to communicate corrective feedback to team members when they are putting themselves or others at risk. Courage entails following the correct safety procedures (with an audience present and when no one is watching) and holding oneself and others accountable for those safety norms. Through training and coaching, employees can develop this tool to assist them in upholding the appropriate safety procedures of the organization, even when challenged by others.
In summary, by incorporating these three “C” elements into the safety culture of your organization, you can create an environment in which employees feel empowered to care for their safety and the safety of others. Additionally, these elements will help create an environment of trust and commitment among employees that will permeate the organization to create a strong or improve the current safety culture.
Christopher Downing, Jr., Ph.D., is an Assistant Professor in the Industrial/Organizational Psychology program at Valdosta State University. His research interests focus on improving the safety and wellbeing of employees in the workplace. Dr. Downing is also an Organizational Development Consultant with consulting experience in an array of industries spanning from retail to health care. He provides various consulting services ranging from safety to workforce development.
Benjamin Martin, Consultant, M.S., ASP, is a Safety and Organizational Development Consultant with over a decade of experience initiating positive behavior change in manufacturing, government, and construction. His specific area of focus uses humanistic behaviorism techniques to motivate a safe working culture by assessing operations gaps and collaborating with clients to develop long term solutions ranging from safe work behaviors to loss control strategies.













 Ben Vinson, Chairman and Chief Appellate Judge
Ben Vinson, Chairman and Chief Appellate Judge



Happy New Year… and how ‘bout them Dawgs?! Wow. Just wow. I am delighted to start off this year by saying congratulations—once again—to our incredible University of Georgia football team for back-to-back national championships. Head coach, Kirby Smart, and quarterback, Stetson Bennett, should be commended for their leadership and perseverance, while the whole team should be credited for tremendous hard work over a long period of time and the key ingredient to this winning season… connectivity.
On behalf of the State Board of Workers’ Compensation, I am pleased to report that we had a successful 2022 with an increase in our proceedings and activities. We look forward to continuing positive results in 2023 and hope to see many of you at our traditional events to focus on connections and progress in the world of worker’s compensation.


Last year, we saw the return to in-person settings for our regional seminars and annual conference, along with several important meetings by other stakeholder groups. Please be on the lookout for details on our 2023 regional seminars and annual conference in the near future. I am grateful to all who participate by sponsoring, exhibiting, speaking, or attending these valuable opportunities to connect with others in the industry and form or bolster the bonds for success.
Speaking of connection, I was delighted to host the annual meeting of the Chairman’s Advisory Council then attend and speak at the State Bar’s Workers’ Compensation Law Institute last fall. Both events provided ample opportunity for subject matter experts to discuss important topics and continue the tradition of gathering together on the coast to seek consensus on issues and maintain stability in our workers’ compensation system. I heard positive reports from each committee and anticipate some activity on the legislative and rules fronts, with particular attention on another increase to the maximum disability amounts and an insurance-based proposal to assist first responders with post-traumatic stress disorder injuries. We will monitor developments on these and any other issues during the 2023 Session of the Georgia General Assembly.
As for Board operations, our Settlement Division is now fully staffed and has worked hard to return to a normal rate of reviewing and approving stipulations filed within the last ten days. Our ADR Division remains busy performing both virtual and in person mediations. Special set mediations are scheduled upon request. The Board is busy working on plans for the Annual Conference to be hosted this August. Hearings in our Trial Division are primarily being conducted in person, but virtual hearings are available when needed and may include the option for hybrid hearings. As a reminder, the Board has peer review for medical disputes and contact information on peer review is located on the Board’s website. If anyone is interested in registering for ICMS and receiving training, please contact Dana Prather at 404-656-2017.
Finally, congratulations to Governor Brian Kemp on his impressive re-election in November and recent swearing in for his second term. Governor Kemp demonstrated steady leadership over the past four years through extremely troubling times and maintained a clear message during his campaign which resonated with millions of Georgia voters. As a loyal Dawg fan, he certainly appreciates and exemplifies the value of hard work and connectivity.
Here’s hoping everyone has a great start to 2023 and I look forward to seeing you at our regional seminars or other events this spring.






 Becky Curtis, NBHWC
Becky Curtis, NBHWC

As the dust cleared and the smell of hot engine oil drifted into my nostrils, I knew that while I had survived the accident, I was now an “injured worker” and my life would be forever changed.
Unable to move from the neck down at the scene, I would soon learn I had a C-4 incomplete spinal cord injury and would develop burning nerve pain from the neck down. I chased all the cures and promises before finally discovering an interdisciplinary recovery program that includes pain education and coaching as the most effective way to help patients get their pain under control.
I have a lifelong empathy for those with chronic pain because I know the challenges firsthand. I also know the best evidence-based approaches to managing pain have more to do with thought patterns, active modalities, and acceptance of pain than with prescriptions and medical procedures.
You don’t feel chronic pain so much as you experience it.
Yes, the experience is painful, but the medications and procedures that work so well for acute pain don’t cut it when it comes to chronic pain. The latest discoveries in neuroscience show chronic pain is more of a learned experience than it is the result of nociception, the sensory nervous system’s process of encoding noxious stimuli. Chronic pain works differently than acute pain; therefore, it should be treated differently, as well.
This is especially true in the early stages of recovery from a catastrophic injury or the sudden onset of chronic pain conditions with unknown causation. If we can prevent the chronic pain experience from developing in the first place, we can “nip it in the bud,” before it gets big enough to take over someone’s life. Sadly, the early use of opioid prescription drugs often ends up robbing the chronic pain patient of their most powerful tool for managing pain: the human brain.
We develop chronic pain by focusing on it. What we focus on, we empower and enlarge. When we focus on pain, we recruit brain cells to experience it and actually end up making it worse in the process.
When I give lectures, I often say, “We know what we focus on we empower and enlarge, so what does someone focus on when they have burning nerve pain from the neck down?” Invariably, someone in the audience cries out, “They focus on the neck up.” That’s exactly right. When we focus on what is right, healthy, and whole, we disempower pain by preventing the formation of neuronal connections that expand the pain experience.

So, how can an injured worker begin implementing a restorative strategy before pain becomes chronic?

By discovering early that small decisions, education, actually help prevent the development of chronic
By discovering early that small decisions, education, and healthy perspectives on pain can give them the upper hand. Interdisciplinary programs that use pain education and coaching strategies work best for empowering those with chronic pain to overcome it. These strategies, when implemented early, can actually help prevent the development of chronic pain.
If we can catch chronic pain before it starts, we can significantly defeat the opioid crisis, as well.
An injured worker herself, Becky Curtis is the founder of an innovative bio-psycho-social approach to pain management called Take Courage Coaching. a telephonic Pain-Management Coaching service to injured workers, which is now part of Override Health. Her passion to help those who share her pain experience drives her incessantly to speak, teach, and write to help further chronic pain education around the world.









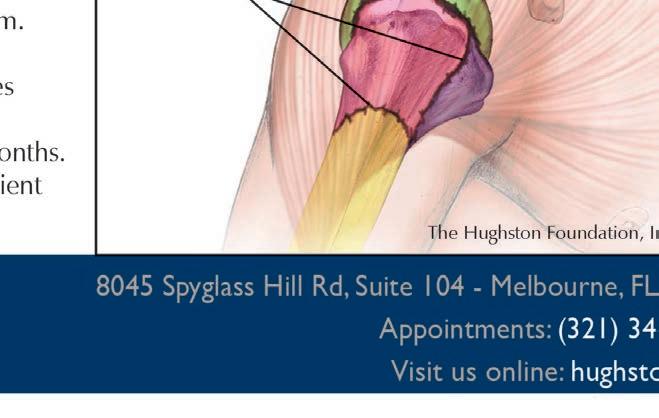
We all know someone who has endured a knee injury or complains about a chronic “bad knee.” You may have experienced a severe knee injury yourself and understand this firsthand. Thankfully, injuries to the knee are better understood now than ever before. Many treatments are available to help those who are injured get back on their feet and remain active. In my practice, I have found that educating patients about their knee condition helps decrease their anxiety. This information can be as important to them as the prescribed treatment.
Knee conditions can be categorized into a few discreet categories based on anatomy. Injuries to the bones include fractures, dislocations, and malalignment. Ligament and tendon conditions consist of many sports injuries, including ACL tears, quadriceps tendon ruptures, and less acute conditions like patellar tendonitis. The meniscus is a structure unique to the knee and can often be implicated in knee problems when torn or displaced. Cartilage difficulties can be confined to one part of the knee, as with osteochondritis dissecans, or throughout the entire knee, as commonly seen in osteoarthritis.
As with any joint, the knee can be affected by infection, tumors, or inflammatory conditions. There are also a few pain syndromes commonly diagnosed despite no objective evidence of any structural damage to the joint, such as patellofemoral syndrome or pain at the front of the knee cap.




History, physical examination, and x-rays provide enough information to diagnose most knee injuries. In some cases, an MRI is helpful to confirm the diagnosis. While general practitioners can address many low-grade knee conditions, consultation with an orthopedic specialist can often clarify the diagnosis and better define the optimal treatment plan. Other than infections and fractures to the bone, most knee injuries benefit from rest, ice, anti-inflammatories, compression, and a course of physical therapy. When necessary, surgical intervention can provide predictable results for many conditions. Surgeries can vary widely from simple arthroscopic procedures (performed through small incisions with a camera and specialized tools) to a complete knee replacement with metal and plastic parts.
An important consideration for knee injuries in the workplace is the question of preexisting knee osteoarthritis. As mentioned above, knee osteoarthritis is primarily a condition of damaged cartilage. Cartilage is the pearly white lining on the surfaces of our joints, and it can degrade over time due to a combination of factors, resulting in inflammation, stiffness, and pain. These factors include the patient’s age, weight, genetics, and prior injuries to the knee.


While a severe knee fracture can directly cause post-traumatic arthritis several years later, this is a rare example of how arthritis could develop from an isolated injury. Normally, arthritis tends to develop and progress over many years, often without the patient even being aware of a problem. An injury more commonly could aggravate osteoarthritis and cause the patient to seek care for the first time. A well-documented visit with an orthopedic specialist and thorough patient education can go a long way to avoid conflicts in this common scenario.
Whatever the situation, many options exist to help those who are injured be restored to an active lifestyle, both at work and home.


















 Eric F. Patten, RN, BSN
Eric F. Patten, RN, BSN


Stress management is an essential aspect of maintaining a healthy work-life balance and ensuring your well-being. Stress can have a significant impact on an individual’s physical and mental health, as well as their productivity and overall work performance. While stress is a natural part of life, it is important to learn how to manage it in a healthy and effective way.
One of the most efficient and effective way to manage stress is to develop a daily routine. In your daily routine, include activities that promote relaxation and well-being such as exercise, meditation, yoga, or deep breathing as tools to assist you. The activities you chose for stress management should be things you like to do and ideally should be conducted at the same time each day to create a sense of consistency and structure.
A key component of stress management is learning how to identify and manage the source(s) of stress. The objectives in learning how to manage stress are knowing how to set boundaries and saying no to unreasonable demands, delegating tasks, and, often, developing better time management skills. Since our lives are stressful, learning how to better manage your thoughts and emotions is key.
The other way to manage stress is to create a healthy work-life balance. This can involve setting limits on the amount of time you spend working and making sure to take regular breaks throughout the day. It also includes scheduling blocks of time on your calendar for leisure activities and spending quality time with loved ones or simply by yourself. The scheduling will help reduce the stress you experience and improve your overall well-being.
Developing a positive and supportive work environment assists in reducing overall stress. This can involve building strong relationships with your colleagues, creating a sense of community and teamwork, and fostering an atmosphere of mutual respect and support. It also involves taking an active role in promoting employee well-being and supporting employee development, such as through training and professional development opportunities.
The last thing to keep in mind is nothing is a one-time solution. The process of stress reduction needs to be continuous, requiring ongoing commitment and effort to maintain a healthy and balanced lifestyle. Ongoing evaluation of your stress levels and adjusting your techniques as necessary will help in maintaining a work-life balance. Seeking additional support, when needed, is important. Utilizing support such as talking to a therapist, counselor, or a human resources representative can also be extremely helpful.
In conclusion, stress management is an essential aspect of maintaining a healthy work-life balance and ensuring the well-being of employees. Developing a daily routine that includes activities promoting relaxation and well-being, identifying and managing sources of stress and creating a healthy work-life balance, lends to a positive and supportive work environment. By implementing stress management techniques into your daily work schedule, you can improve your productivity, performance, and overall well-being.
Eric F. Patten RN, B.S.N., is the Executive Vice President of Operations & Business Strategies for The Kingstree Group, a leader in the Workers’ Compensation industry for over 24 years, utilizes a consultative approach to lead, create and manage clinical product lines for customers. Dustin Thompson
Dustin Thompson
At the outset, an article written by a litigator regarding the benefits of investing in litigation seems self-serving. Well… yes. My firm, partners, and I, along with the remainder of the defense bar, are in the business of litigating cases. You would be hard pressed to find any litigator worth their salt who does not love trying cases. However, knowing when to commit to litigation and developing a reputation for doing so are effective tools for mitigating claim exposure overall.
Committing resources to effectively litigate claims is crucial not only to obtain favorable results at trial, but also serves to outright prevent claims and reach beneficial settlements prior to a hearing for employers and insurers.


From inception, every claim should be handled as if it could eventually reach a hearing. Such mentality is ingrained in the best employers, adjusters, case managers, and attorneys. Of course, handling claims from this standpoint takes more time, effort, and resources. During the pivotal initial investigation, diligence and comprehensiveness are key. The most effective information is obtained when facts are the freshest.
When any accident or injury is reported, it is imperative employers and insurers follow a strict investigative procedure regardless of whether the accident is witnessed or if there are one hundred red flags because when the same protocol is administered for every claim, there is little room for error or inadvertent omissions. Moreover, investing in initial fact-finding endeavors lays the foundation for establishing defenses and ultimately trying cases when needed. Your defense attorney will thank you. Your bottom line will thank you.
As an employer, do you have a fine-tuned post-accident or post-reported accident policy? Hopefully, you do. If not, consider the following:
• require immediate accident reporting;


• utilize a declination of medical treatment statement when treatment is declined;
• provide the panel of physicians and inform the employee they have a choice of with whom to treat from the panel regardless of red flags;
• have the employee and a witness sign and date their panel selection;
• have the employee provided a written statement discussing how the accident occurred, specific body parts injured, and any witnesses to

the incident;
• obtain statements from witnesses;
• identify the employee’s primary care provider and/or recent hospital visits;
• if intoxication is suspected, perform an alcohol screen within three (3) hours or a drug screen within eight (8) hours;
• secure available video footage;
• take photographs of the accident scene; and,
• report the claim to your carrier.
A caveat for employers to remember is every case has good and bad facts. When interviewing employers, I often tell them, “We can work with good facts. We can work with bad facts. We cannot work with facts which are not shared, hidden, or mistruths.” If you want to ensure the best chance to prevail, give your carrier and your counsel all the facts and not just those which benefit you.
As an insurer, do you have a similar checklist when initially investigating claims and obtaining details from your insureds? In addition to the foregoing, the insurers often have the added ability and capacity to take recorded statements of the injured employee, obtain ISO reports, perform medical and pharmacy canvases, request medical records via a WC-207, and obtain prior and subsequent State Board of Workers’ Compensation records via a WC-12 request.
Although adhering to strict investigative policies for each and every reported accident may seem unnecessary, installing such procedures is a front-end costs for long-term gains. Even the most seemingly harmless claim may eventually enter litigation for one reason or another, and you need a solid foundation in place to build your defense and case for hearing.
Once a claim enters litigation, the Georgia Workers’ Compensation Act requires employers and insurers to retain counsel before the first setting of the hearing. From a procedural standpoint, the case will ultimately reach a hearing conducted by one of fifteen administrative law judges (ALJs) depending on where the accident occurred. The case is not typically decided at the hearing, but instead within sixty (60) days of the hearing after parties have submitted post-hearing briefs to the ALJ. In most cases, it is prudent for your attorney to send written discovery which is narrowly tailored to the issues in litigation to the claimant. It is further prudent to allow your attorneys to depose the claimant. Discovery and depositions are fact-finding missions. They help you evaluate both the evidence you have and the evidence you need. They further establish testimony under oath which can be used to impeach a claimant’s credibility at the hearing. It is in only the rarest of circumstances where you would enter a hearing without first knowing what the claimant intends to say. If your litigated issue is medically focused, it may also be worthwhile to depose the claimant’s physicians.
Committing and dedicating resources to discovery, depositions, site visits, witness interviews, and preparing for and trying claims at a hearing not only puts you in the best position to prevail, but also it cements your reputation and stance with employees and the claimant’s bar. When you establish you have the capacity to diligently investigate claims and the commitment to zealously defend them, you are in an overall better posture to decrease meritless cases and mitigate exposure in others. One of the best ways to posture a case for a favorable settlement and evaluate your exposure is to prepare it for a hearing.
Please do not misinterpret this soapbox to state every claim in litigation should be tried at a hearing. Every claim in litigation should not ultimately be tried. The decision to move forward with litigation should be judged on a case-by-case basis as no two claims are the same. The facts you can prove, total exposure, appetite for risk, chances of prevailing, and expenses are just some of the primary factors to be considered when trying cases. However, when you have the right facts and necessary defense foundation from your initial investigation and have invested the means to appropriately prepare the case for hearing through discovery, you will reap the benefits of an effectively litigated case.
Dustin Thompson is a Partner at Swift, Currie, McGhee & Hiers, LLP. He exclusively represents employers and insurers in workers’ compensation claims throughout Georgia. Feel free to contact him at dutsin.thompson@swiftcurrie.com or at 404-888-6214.


Supervisors have direct responsibility for the day-to-day productivity in the workplace. They also have the unique task of balancing production goals while keeping employees safe. Even with a strong safety program accidents unfortunately happen. When an employee is injured, fear can set in. Fear of…
… being fired

… lost wages
… the claim being denied
… reprisal from the supervisor
According to the Workers’ Compensation Research Institute (WCRI), attorney involvement is strongly correlated with an employee’s level of trust in the workplace. When a claim ends up in litigation, a benchmark study from Clara Analytics has shown the average costs can increase as much as 388%. In Georgia, the average number of days of disability on a lost time claim increased from seventy-seven (77) days to 199.6 days when an employee retains an attorney. With so much on the line, it is critical to have a process in place that helps supervisors understand their impact.
Here are some tips to help train your supervisors:



Prevention
When you first hire an employee, we recommend a three-prong new-hire safety orientation. The first two prongs involve a new hire safety video and a checklist of safety standards and employee responsibilities. The third prong requires a supervisor safety walk-through. The walk-through increases accountability with the supervisors and creates a relationship that supports ongoing safety training. If supervisors don’t walk the safety talk, the employees won’t either. If the employee doesn’t trust the supervisor prior to an accident, it will be difficult to build trust afterwards.
If an injury occurs at work, supervisors are usually your first line of communication. Here are four key points that will help your supervisors understand their role if a workplace injury occurs:


Observe, Direct, Document, Communicate
1. Observe: Supervisors must make quick observations at the time of an injury to determine the type of treatment required. These initial observations will ensure the injured employee receives proper care in a timely manner.
2. Direct: Since supervisors are on the front line, they often need to direct the employee to the next steps when they are injured. If they are not properly trained, missteps will increase costs.
3. Document: An accident report is a critical part of the work comp process. Supervisors need to understand how to document the injury and any contributing factors. The observations should be added to the ongoing prevention plan.
4. Communicate: Constant communication and positive reinforcement with injured workers will help to improve morale and keep employees motivated to return to work. The supervisor must continue building trust after the injury by showing respect and not pointing fingers. Supervisor communication is also a key component of the return to work (RTW) process. Lack of communication is cited as another leading cost driver.
My job as an insurance broker is to help my clients reduce costs. That means educating supervisors so they understand their role.
Thomas Musselwhite is a risk and insurance advisor with Sterling Seacrest Pritchard. He is dedicated to helping employers develop risk management solutions that improve safety culture, reduce claims and control insurance costs.



























 Garlana Mathews, Greer Boatright, Phil Boatright- PA for Optim Ortho/Optim Healthcare Dublin/ Sandersville and Michelle Wilds
Garlana Mathews, Greer Boatright, Phil Boatright- PA for Optim Ortho/Optim Healthcare Dublin/ Sandersville and Michelle Wilds
770.400.9460 cstogner@ApolloOH.com

NOW SERVING THE GREATER ATLANTA AREA:



•WORKER’S COMPENSATION TREATMENT
•CORPORATE SERVICES


•ON-SITE SERVICES


•DOT PHYSICALS
•CUSTOM ERGONOMICS PROGRAMS

•TELEMED AND ADVICE LINE
 845 S Carroll RD. Villa Rica, GA 30180
DR. SHOMARI RUFFIN
845 S Carroll RD. Villa Rica, GA 30180
DR. SHOMARI RUFFIN






As more and more seasoned professionals in the Workers' Compensation industry retire after thirty-plus years of service, the industry is facing a crisis in finding qualified and experienced replacements. Companies and medical professionals are struggling to find skilled and knowledgeable professionals to manage their programs, leaving many organizations vulnerable to financial risks and increased workplace injuries. However, mentorship programs offer a viable solution to this crisis.
As more and more seasoned professionals in the Workers' Compensation industry retire after thirty-plus years of service, the industry is facing a crisis in finding qualified and experienced replacements. Companies and medical professionals are struggling to find skilled and knowledgeable professionals to manage their programs, leaving many organizations vulnerable to financial risks and increased workplace injuries. However, mentorship programs offer a viable solution to this crisis.
Mentorship is the practice of providing guidance, support, and expertise to individuals who are new to a field or seeking to develop their skills and knowledge. In the context of the workers’ comp industry, mentorship programs can provide retired professionals with an opportunity to share their expertise and experience with aspiring professionals. By partnering with technical schools, insurance companies, and third-party administrators, the industry can offer training programs for case managers, human resources professionals, safety and risk management professionals, and workers’ comp adjusters.
Mentorship is the practice of providing guidance, support, and expertise to individuals who are new to a field or seeking to develop their skills and knowledge. In the context of the workers’ comp industry, mentorship programs can provide retired professionals with an opportunity to share their expertise and experience with aspiring professionals. By partnering with technical schools, insurance companies, and third-party administrators, the industry can offer training programs for case managers, human resources professionals, safety and risk management professionals, and workers’ comp adjusters.
Mentorship programs have a number of benefits for both mentors and mentees. For mentors, the opportunity to share their knowledge and experience with others can be rewarding and fulfilling. Mentors can also stay connected to the industry and continue to make a meaningful contribution to the field even after retirement. For mentees, mentorship provides an opportunity to learn from experienced professionals, gain valuable insights into the industry, and develop the skills and knowledge needed to succeed in their careers.
Mentorship programs have a number of benefits for both mentors and mentees. For mentors, the opportunity to share their knowledge and experience with others can be rewarding and fulfilling. Mentors can also stay connected to the industry and continue to make a meaningful contribution to the field even after retirement. For mentees, mentorship provides an opportunity to learn from experienced professionals, gain valuable insights into the industry, and develop the skills and knowledge needed to succeed in their careers.
Moreover, mentorship programs can help address the challenges faced by companies and medical professionals in finding qualified professionals. By partnering with technical schools, the industry can provide training programs that offer a mix of classroom instruction and on-the-job training. Retired professionals can serve as mentors and provide guidance and support to students as they navigate the complexities of the industry. This will help ensure that new professionals are well-prepared to enter the workforce and can hit the ground running in their new roles.
Moreover, mentorship programs can help address the challenges faced by companies and medical professionals in finding qualified professionals. By partnering with technical schools, the industry can provide training programs that offer a mix of classroom instruction and on-the-job training. Retired professionals can serve as mentors and provide guidance and support to students as they navigate the complexities of the industry. This will help ensure that new professionals are well-prepared to enter the workforce and can hit the ground running in their new roles.
Best Regards,
Best Regards,






Late on January 26, 2023, the Occupational Safety and Health Administration (OSHA) issued a press release about a significant change in long-standing policy related to instance-by-instance issuance of citations that will become effective in sixty (60) days and radically alter the landscape of certain inspections. The stated purpose of the policy change is “to make [OSHA’s] penalties more effective in stopping employers from repeatedly exposing workers to life-threatening hazards or failing to comply with certain workplace safety and health requirements.”
The press release indicates the impact of the change will be limited to certain conditions where the language of the rule supports a citation for each instance of noncompliance. These conditions and this language include violations such as “lockout/tagout, machine guarding, permit-required confined space, respiratory protection, falls, trenching and for cases with other-than-serious violations specific to recordkeeping,” but related enforcement memoranda suggest this is not how the practice is expected to be utilized.
The practice of issuing citations on an “instance-by-instance” basis (IBI citations) has, since 1990, been limited to “egregious willful citations.” OSHA Instruction CPL 02-00-080, issued on October 21, 1990, states that “[t]he large proposed penalties that accompany violation-by-violation citations are not, therefore, primarily punitive nor exclusively directed at individual sites or workplaces; they serve a public policy purpose; namely, to increase the impact of OSHA’s limited enforcement resources.” The January 26, 2023, press release was issued with the title that stated its purpose: “Department of Labor announces enforcement guidance changes to save lives, target employers who put profit over safety; Seeks to hold employers to greater account for safety, health failures.”
OSHA Instruction CPL 02-00-080 continued and set forth the criteria for application of the policy, which includes:
(1)The employer is found in violation of an OSHA requirement:
(a)Of which she/he has actual knowledge at the time of the violation. Such knowledge may be demonstrated through previous citation history, accident experience, widely publicized agency enforcement, direct evidence of specific recognized jobsite hazards or other appropriate factors; and
(b)Intentionally, through conscious, voluntary action or inaction, having made no reasonable effort to eliminate the known violation.
(2)The violations resulted in worker fatalities, a worksite catastrophe, or a large number of injuries or illnesses.
(3)The violations resulted in persistently high rates of worker injuries or illnesses.
(4)The employer has an extensive history of prior violations of the Act.
(5)The employer has intentionally disregarded its safety and health responsibilities.
(6)The employer’s conduct taken as a whole amounts to clear bad faith in the performance of his/her duties under the Act.
(7)The employer has committed a large number of violations so as to undermine significantly the effectiveness of any safety and health program that might be in place.
As a practical matter, the instance-by-instance citation policy was rarely used. When it was used, it was often limited to cases involving serious injury or death where prior serious injury or death-related inspections were conducted and citations issued. Even more limiting, OSHA often limited this practice to cases where the citations were fully resolved, whether through settlement or adjudication.
The current announcement was tied to an enforcement memorandum that included four (4) factors for determining whether instance-by-instance citations should be issued. The factors to be considered include:
1.The employer has received a willful, repeat, or failure to abate violation within the past five years where that classification is current.
2.The employer has failed to report a fatality, inpatient hospitalization, amputation, or loss of an eye under the requirements of 29 CFR 1904.39.

3.The proposed citations are related to a fatality/catastrophe.
4.The proposed recordkeeping citations are related to injury or illness(es) that occurred because of a serious hazard.
The enforcement memorandum provided the following guidance:
Instance-by-instance citations may be applied when the text of the relevant standard allows (such as, but not limited to, per machine, location, entry, or employee), and when the instances of violation cannot be abated by a single method of abatement. When an inspection may cause instance-by-instance violations, each instance should be documented thoroughly, e.g., type of material being processed, equipment, facility conditions, human factors, personal protective equipment, etc. The case file must contain fully documented justification for IBI citations.
Besides issuing new guidance on when to issue IBI citations, OSHA also issued an enforcement memorandum reminding regional administrators and area directors of their authority not to group violations. The practice of grouping violations typically involves issuing a citation with multiple subparts that carry no penalty but state alternative theories or factual bases to justify the issuance of the citation. Those subparts carry no additional penalty, but they may require abatement of violations beyond the scope of the first listed instance.
That enforcement memorandum set forth the factors that normally are considered when considering when to group citations and then why grouping should not be considered:
Grouping violations should be considered when:

•two or more serious or other-than-serious violations constitute a single hazardous condition that is overall classified by the most serious item
•grouping two or more other-than-serious violations considered together create a substantial probability of death or serious physical harm, or
•grouping two or more other-than-serious violations results in a high gravity other-than serious violation.
Where grouping does not elevate the gravity or classification and resulting penalty, then violations should not be grouped if the evidence allows for separate citations.
Thus, whereas the prior guidance about IBI citations was limited to inspections where egregious willful citations were issued, this guidance would apply the practice to even the lowest level of citable violation: that which is considered other-than-serious.
The enforcement memorandum on grouping violations extends the reach of the program far beyond application of IBI citation issuance to a limited set of other-than-serious recordkeeping violations to many other categories of other-than-serious violation. Whereas the press release of January 26, 2023, suggests that IBI citations will only be issued regarding OSHA recordkeeping citations, the corresponding enforcement memoranda indicate that it could be used for all other-than-serious citations that meet the stated criteria.
What are the takeaways for employers by OSHA? In addition to the significant increase in penalties for OSHA citations that recently became effective, employers are much less likely to see citations grouped—with the consequence of significantly increased penalties multiplied by the number of instances cited. It is fair to assume that the number of cases contested, due to the increased overall penalty exposure, will increase dramatically, depending upon how widespread this practice is utilized and the time to resolution of OSHA citations increased.
Phillip B. Russell and John D. Surma are OSHA attorneys with the law firm Ogletree Deakins Nash Smoak & Stewart PC and members of the workplace safety and health practice group. They have represented employers in hundreds of fatality and other cases nationwide.
It’s a nice, seventy-seven-degree day, as I’m driving south on I-75 from Atlanta headed to a work conference in Savannah. We’re below the gnat’s line when Crystal, one of our company nurses who was riding shotgun, gets a call on her work cell. A typical workday ensues as we navigate in the world of a utility company.
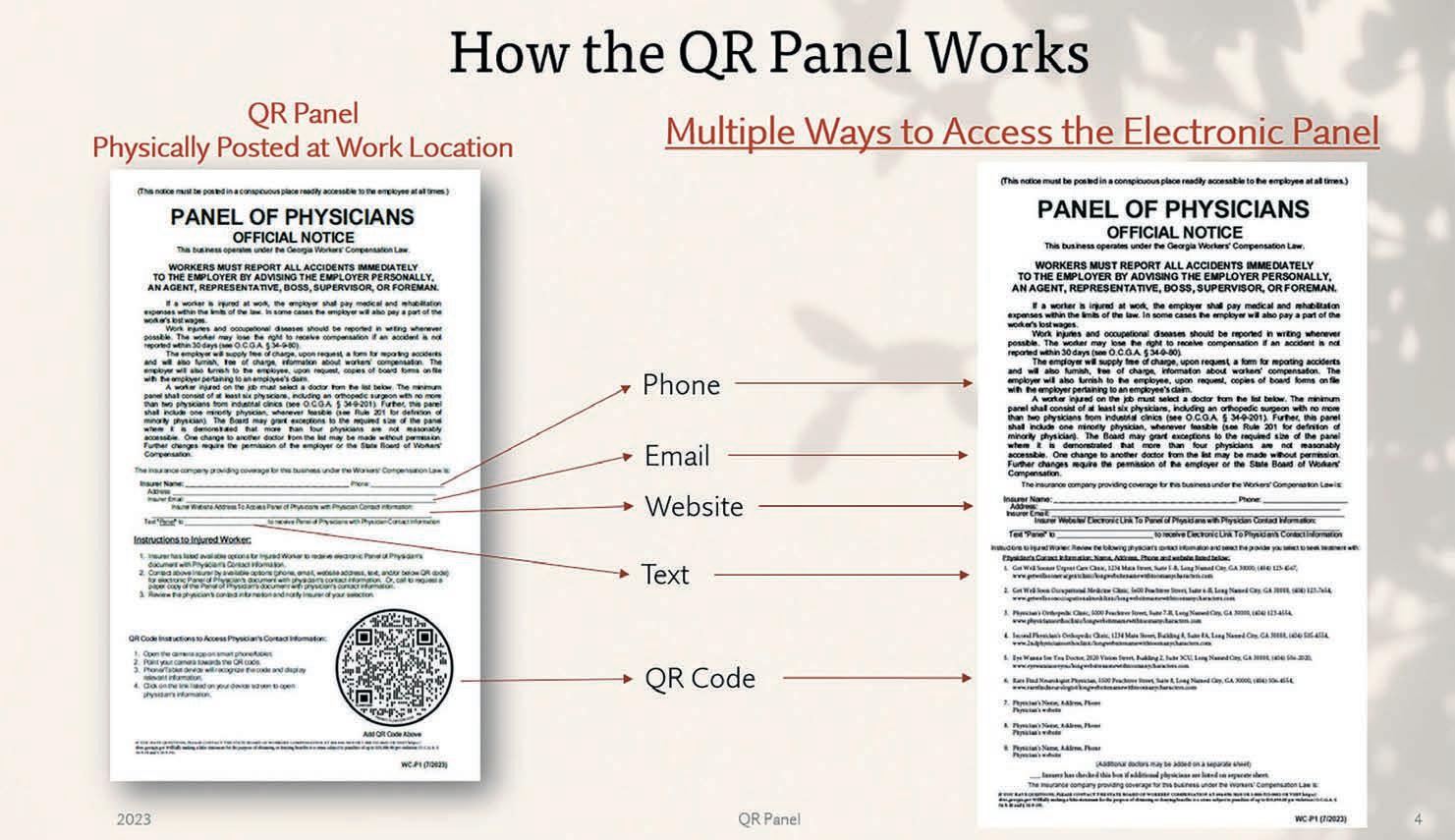
The first call is from Sam, on the distribution line crew, who was working in a neighborhood about an hour-anda-half from his work location when he got injured and needs to see a doctor. Crystal pulls out her laptop, opens the electronic Panel from the Company intranet site, and forwards it to Sam. They review it together, he picks the provider, and she schedules the appointment.
Just as she is finishing up, she gets a call from Simona, a human resources manager (hybrid worker), who is teleworking that day. Simona relays that Stephen, a full-time remote worker, reached out about an accident that happened while working at home. Crystal jots down the details, reaches out to Stephen, and forwards a link to the electronic Panel. Stephen reviews it, makes a selection, and can be seen the same day at the Occupational Medicine Clinic.
Then, Caleb from Safety calls Crystal. Larry, on the Atlanta Distribution construction crew, is on assignment in Dublin (two and a half hours from his work location), had a work accident, and needs immediate medical attention. Crystal locates an urgent care near Dublin for Larry.
Our workforce is as diverse as the locations we work. From in-office jobs to remote workers, from plant workers to line crew, from drone to helicopter pilots, we have a wide variety of jobs and a wide variety of “places” to show up to work. Each of these scenarios is different, but they have the same principle: the need to access an electronic Panel. Our employees use our company intranet site to access all company information, including Panels. Our employees are used to seeing QR codes at work and personally, as well. So, a prototype solution is the QR Panel.
The QR Panel (short for QR Code Panel) would be a secondary option to post at the work location, with five (5) options to automatically link to the electronic panel: 1.Phone
2.website
4.text
The QR code is the quickest of the five options, with an employee going to the camera app on their phone, hovering over the QR code, and clicking the link that shows on their phone screen. It would be a simple, enduser experience for our employees to scan the QR Panel when at a company work location in order to access the electronic Panel.
QR codes aren’t new to our employees – they see them at work and in their personal lives. Federal posters at work already list QR codes, as do flyers, sign-ups, and notifications at work. QR codes are used for attending sports events, concerts, pay-to-park, grocery store ads, food packaging, drive-thru windows, mailers, magazines, billboard ads, and even TV commercials… and that’s not all the places I’ve seen them used lately. There are many reasons why they’re popular, including their functionality of easy access to quickly link to more information.
The QR Panel does the same. It provides on-the-go access, more privacy, and extra technology options since it automatically links to the electronic Panel. An electronic Panel has more versatility than a Paper Panel since it
can list hyperlinks to doctor’s offices, mapping links for phone apps, and phone number hyperlinks to make a quick call. These features help injured employees make informed decisions and get medical care quicker. An electronic Panel also has meta-data in its DNA properties showing the date created or last modified, something a Paper Panel can’t provide. Also, a Paper Panel doesn’t automatically link to the electronic Panel, a missing link to the current process that the QR Panel fixes.

Our workforce has changed where we work, especially post-COVID. It is time to re-evaluate the Panel process and ask questions about what works best for our workforce and the workers’ compensation system. We want our employees to have Panel information with the click of a button, so they can make informed decisions. We value our employees and want this care to shine through.
Go ahead and scan the QR code with your cell phone to take a look at an example electronic Panel – it’s live! The QR Panel would be a secondary option for posting at work locations, if desired. Let’s drive toward the future of electronic Panels together by adding the QR Panel option. We have many more good miles ahead of us on this journey.





Elizabeth Smith is based out of Atlanta, Georgia, working for Georgia Power Company as a Risk Management Supervisor. She holds a bachelor’s degree in English from King University in Bristol, Tennessee. In addition to being Vice Chair of the Georgia Workers’ Compensation Association Board of Directors, she is also a medical committee member on the Advisory Council of the Georgia State Board of Workers’ Compensation.

A manager’s goal is to help workers get their job done and get home safely at the end of their shifts. When driving is an integral part of an employee’s job, whether as a utility provider, delivery driver, or emergency responder, safety concerns can multiply. This is especially true when workforce fleets travel in environments where traffic is heavier and accidents are more common.
The statistics show there’s reasonable cause for concern for workers who spend a lot of time behind the wheel. The National Safety Council reports that the most dangerous part of an employee’s workday is when they are on the road. Motor vehicle crashes remain the leading cause of occupational deaths in the United States, which saw 1,253 workers killed in car crashes on the job in 2021. In total, according to the Bureau of Labor Statistics, car crashes alone represent twenty-four percent (24%) of work-related deaths, far more than workplace violence, exposure to harmful substances, and falls.
On top of the loss of invaluable human life, these events cost employers billions a year. In 2019 alone, the Center for Disease Control (CDC) found that work-related crashes cost employers $39 billion, an average of $75,000 per non-fatal injury and $751,000 per death. The risk of crashes is real. Up to twenty percent (20%) of a fleet will crash annually, with the average crash costing $20,000 in lost wages and downtime, according to Automotive Fleet, not to mention the additional penalty of lawsuits.
Prioritizing road safety should be at the top of the list for managers of even small fleets, given the tremendous costs associated with accidents.
There are multitudes of risk-mitigating solutions available to managers. However, your approach to safety can make a difference in saving lives and should not be taken lightly. In many industries, safety can take a back seat in the organizational planning process. Per OSHA, many business owners would rather take the traditional approach and address mistakes and accidents as they come, focusing instead on productivity and the bottom line. The direct and indirect costs of safety incidents can far outweigh the real and imagined savings of acting only reactively.
In its Recommended Practices for Safety and Health Programs, OSHA details a “proactive approach to managing workplace safety and health,” which aims to:
•Prevent workplace injuries and illnesses
•Improve compliance with laws and regulations
•Reduce costs, including significant reductions in workers’ compensation premiums
•Engage workers
•Enhance their social responsibility goals
•Increase productivity and enhance overall business operations
Based on these goals, a proactive safety policy may not only lead to a safer, more efficient business, but also improve employee retention and promote a more favorable image to the public.
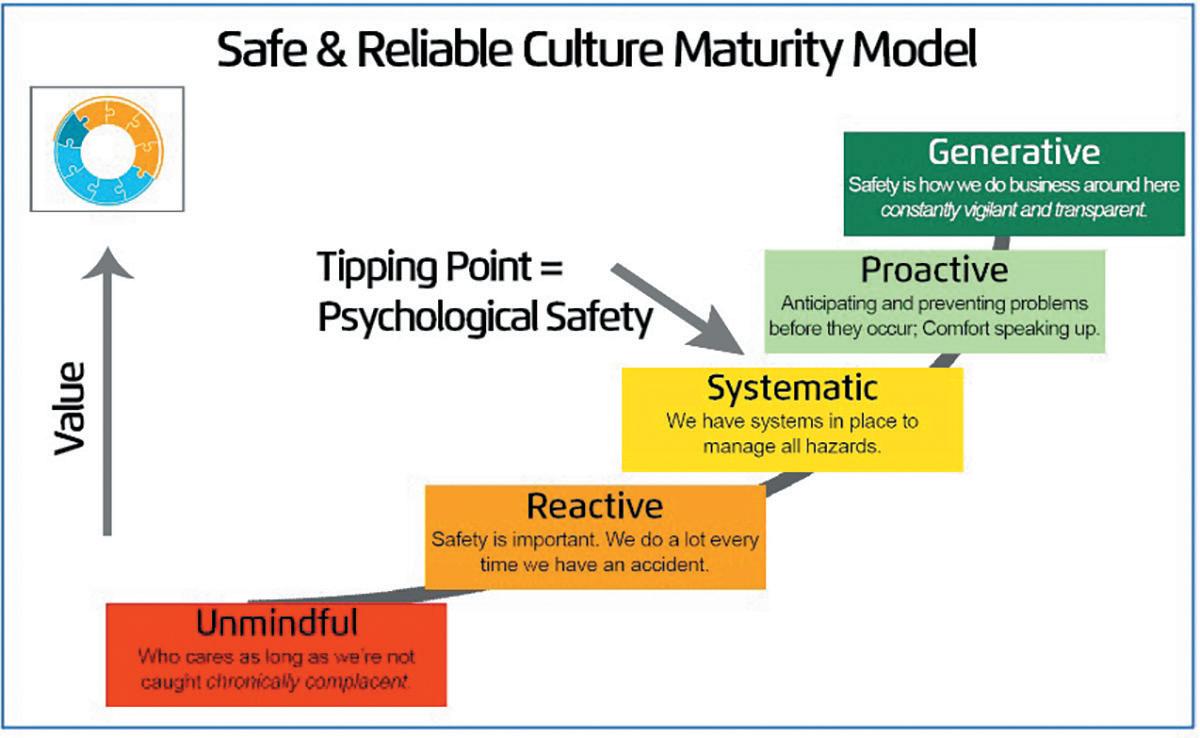
How a person or organization reacts to an accident or emergency can make an enormous difference in the impact of that event. Reactions should be systemized for maximum efficiency through training and procedures in place. However, getting to the point of reaction should be a last resort. Implementing proactive procedures to avoid as many hazards as possible in the first place is a far more effective approach to mitigating risk. Safety management can be viewed along the spectrum of the culture maturity model. According to this model, an organization moves from a lower to higher value safety culture between the extremes of unmindful (lacking any safety procedures) to generative (a complete foundation of safety).
In this model, the tipping point from negative to positive occurs when an institution or company moves past a systematic model of managing risks to a proactive one, in which they anticipate and prevent accidents before they can occur. This is called attaining a level of “psychological safety,” meaning that employees feel both physically and psychologically safe and empowered in their positions to express their safety-related concerns without negative repercussions.



There is no way to mitigate one hundred percent of risk. It’s important to have an efficient process for dealing with accidents after the fact and to identify trends or patterns that lead to safety incidents. Even the best reactive safety measures are no replacement for an enforceable proactive policy, which will save invaluable time, money, and effort.

While learning defensive driving strategies and reviewing the cause of collisions after the fact are important parts of the solution to proactive road safety, it’s not enough to prevent every collision from happening. Advanced Driver Assistance Systems (ADAS) and Collision Avoidance Systems (CAS) are proven, proactive safety tools for fleets and drivers.
Mobileye 8 Connect™ is a retrofit collision avoidance system that helps both prevent collisions and improve driver performance. The system uses advanced vision, acceleration, and velocity sensors to give the driver another “set of eyes” behind the wheel and alert them to hazards, including:


•Pedestrian and Cyclist Collision Warning (PCW)
•Lane Departure Warning (LDW)

•Headway Monitoring and Warning HMW
•Forward Collision Warning
•Speed Limit Indicator

The technology utilizes a revolutionary approach to artificial intelligence to mimic our sight and awareness, allowing it to see potential hazards before we do. Real-time alerts have been proven to reduce collision rates in fleets and vehicles of all sizes, resulting in less downtime for vehicles and drivers and greater savings for businesses.
There is no single solution for safety, and simply relying on short-term or piecemeal reactions when accidents occur is not enough. For an impact to be made, all members of an organization must be empowered to behave safely and trust that there are systems in place to protect them. For fleets, building a safety culture means filling your toolbox with technology, training, and communication.
Eric Royston is a Qualified Safety Sales Professional (QSSP) and Occupational Safety and Health Administration (OSHA) 30 certified Regional Sales Manager, Southeast, at Mobileye, a large electronics company founded in 1999. With a long history in the safety industry, Royston is passionate about providing customized safety solutions to a diverse range of clients. He holds a Bachelor of Science from Western Michigan University.










As with most of the world, the insurance industry is rapidly adjusting to the impact of artificial intelligence (AI) and machine learning which has researchers seeing a rapid transition from a “detect and repair” mentality to a “predict and prevent” one by 2030.
Historically, safety and loss control risk management has generally been reactive—as opposed to proactive— tending to spend more time and resources addressing issues after they are realized. For coverages such as workers’ compensation, this could mean waiting months or years for the true risk of a location to be known before beginning to address said risk. For even one location, this could conservatively mean thousands of dollars in claims leakage.
Two (2) main areas of AI transformation can shift a risk program from reactive to proactive in the safety and loss control sphere:
In the historical approach, a risk management program utilizes the collective experience in their risk careers and even historical data in their program. While the information present is large enough, introducing AI into the picture allows for new relationships and insights between the data sets to be discerned. Further, AI can help digest new datasets significantly quicker than it could a team of risk and data professionals. All of this allows for the true risk propensity of each site and location to be known before claims and issues arise.
To properly address the new aggregate risk profile now in view, it is necessary to reassess the staffing and experience levels therein. While there is a plethora of considerations related to staffing outside the scope of this article, follow-up analysis to complement AI and machine learning can help quantify and suggest not only the number of headcount necessary to handle the exposures and their true risk propensity, but arguably, they can imply the required expertise levels.
For example, lower-risk locations can be paired with more junior staff, while higher-risk locations can be paired with more experienced staff. Additionally, AI and machine learning can help optimize geographic and home office locations to minimize travel and other related costs. While it is not common, especially with the present shortage of experienced risk professionals, it is possible that the transformation of a risk and safety program drives better claims outcomes, as well as lower program costs.
Insurance will always thrive best when there is a balance and coordination of human experience and innovative technology. While AI and machine learning can help address these two fundamental issues in the risk management framework, it is important to involve broker and actuarial partners from the outset such that they quickly help you realize more favorable renewals, procure less costly collateral, connect with higher rated paper, and the like.
Frank Huang, FCAS, MAAA, is the Managing Director and Head of P&C Actuarial Solutions for Davies, formerly Merlinos & Associates. He has twenty years of actuarial experience across consulting firms, an insurance carrier, and a PEO. Frank currently supports self-insureds, insurers, captives, agencies, private equity firms, and PEOs on a broad range of workers’ compensation and other P&C concerns. He lives in Atlanta, Georgia, with his wife and three children.
 Steve Heinen, AAI, CWCP
Steve Heinen, AAI, CWCP

What is the difference between a medical only and a lost time claim?
If a claimant is out of work seven (7) days or less, this is a medical only claim. The claimant will not receive any indemnity (wage replacement) benefit. As long as there are no red flags, the medical bills should be paid and the claim should be closed.

If an employee is out of work for more than seven (7) days, they are entitled to weekly income benefits. This is called an indemnity claim. Their first check should be mailed to the claimant within twenty-one (21) days after the first day of missed work. If the claimant misses more than twenty-one (21) consecutive days, they will be paid for the first week.
Please note: OSHA’s definition of lost time starts on the day after the accident and Georgia’s Workers’ Compensation statutes state a lost time claim is after seven (7) days away from work.
How do they get paid if they are out of work?
They will receive two-thirds of their average weekly wage up to $725/week (as of 7/1/2022) if they do not return to work in any capacity.
What if they cannot return to their full duty job, but you can offer a lower wage job or fewer hours? They will receive a reduced benefit based upon your earnings for a maximum of 350 weeks from the date of injury. This benefit will not exceed $483 per week. The bottom line is employees are not penalized for coming back to work in a restricted capacity working fewer hours or at a lower wage.
For example, if an employee is earning $1,000/week and you bring them back to a transitional duty job earning $500/ a week, they will receive a TPD check from the insurance carrier for $333/week.
Do all injured employees get a settlement?
No, in fact, the statutes do not provide for settlements. This typically occurs when the employee retains an attorney. Forty-two percent (42%) of all lost time claims in Georgia are litigated. The why behind this will be discussed later.
What is a Permanent Partial Disability (PPD) Rating?
If the physician gives the injured employee a disability rating (based upon The American Medical Association’s Guide to the Evaluation of Permanent Impairment, fifth edition), there is a schedule the adjuster must follow, set by the Georgia Legislature.
For instance, if you sustained a fifteen percent (15%) lower extremity impairment rating the rating rates as follows: 225 weeks x .15 (15%) =33.75 weeks. Then, 33.75 weeks is multiplied by your weekly compensation rate to get the amount of PPD owed. So, in the $1,000/ week example above they would get $1,000 x .666 (2/3rds) = 666 x 33.75 weeks = 21,978.

What if the employer does not have a properly posted panel or the did not give the employee choice from the panel?
If the employee retains an attorney and you do not
allow them to choose from a properly posted panel, the claimant attorney will likely get to choose the doctor. This could significantly increase the cost of the claim. Having a proper panel posted and giving the employee choice of physicians from the panel is required by law. Please note there is a second option called the Workers’ Comp Managed Care Network that has its own rules.
Remember there are two (2) requirements with the Posted Panel:
1.You must have no more than two (2) industrial clinics, an orthopedist, and a minority physician. The best practice is to have at least eight (8) doctors and include two (2) orthopedists.
2.The employer must give the employee a choice from the panel. The best practice is to have the employee circle and sign their choice.
If the employee is unhappy with their first selection, they have the right to go back to the panel and select another physician called the one-time change. If the employee refuses treatment (or to be drug tested) you should always get a refusal of treatment form signed.
What are the State Board forms that the employer needs to be familiar with?
•WC-1- First Report of Injury should be completed within twenty-four (24) hours of the injury. It is okay to make a report-only claim. Putting the carrier or TPA on notice quickly will significantly reduce costs.
•WC-207 – Authorization and Consent to Release Information should be part of your injury packet, which should include the panel, the incident analysis form, and the WC-207.
If the claim is a lost time claim, you should be familiar with the following three claim forms:
•WC-6 Wage Statement – The insurer/employer required to calculate the employee’s wage rate using the preceding thirteen (13) weeks of wages. The insurer only has twenty-one (21) days to accept or deny a claim, so they need this form quickly. If the inure pays the wrong rate they could be subject to penalties and interest.
•WC-240 – In the event the employee cannot return back to their regular job and the employer obtains a light duty release from the authorized treating physician, the adjuster may allow you to complete a WC-240. Given Georgia’s high litigation rate and the fact that employees remain out of work significantly longer than most states, understanding the WC-240 process is critical if the employer wants to reduce their work comp costs. Not following the rules regarding the panel are the biggest claims cost driver. Not understanding the WC-240 process is the second biggest cost driver in Georgia claims.
•WC-240a – This form is required to determine if the employee can return to work (RTW). The WC=-240a is a physical analysis of the claimant’s job description. The employer can use your own physical demands form if they have one.
Please note: If you utilize a post-offer health questionnaire, send a copy to the adjuster within seven (7) days of the injury.
What about emergency room treatment?
If an accident warrants the employee going to the emergency room, this is an exception to the panel of physician rules discussed earlier. However, non-emergency visits to the emergency room are generally not going to be authorized. If the employee goes the emergency room and you drug test, you need to be extra vigilant obtaining it as emergency rooms generally don’t like to release drug tests for fear of the claim being denied and not getting paid. Also, once the emergency is over, you should direct them back to the panel for follow-up care.
What about prescription drugs?
Medication can be filled by any pharmacy if the employee has authorization from the insurance carrier. Some insurance carriers issue a pre-filled card.
Steve Heinen, President, Risk Management, Inc., developed the P4 process (now comP4®) in 2002 and it has been utilized by hundreds of organizations to reduce costs. His Work Comp Playbook for Employers has sold over 5,000 copies and his Compass Risk Management System is designed to help organizations implement a proven risk management process.


As a neurosurgeon, I’m often asked what the next procedure might be to revolutionize the treatment of back pain. I believe the Intracept Procedure could be just that.
At Axion Spine & Neurosurgery, we are excited to offer the clinically remarkable Intracept Procedure to our patients. In fact, the physicians at Axion Spine & Neurosurgery, in Alpharetta, were the first in Georgia to offer Intracept commercially and have performed more cases than any group in the Southeast.
The new, minimally invasive Intracept Procedure is unique in that it targets the basivertebral nerve for the relief of chronic vertebrogenic low back pain. The basivertebral nerve lies in the center of the vertebral body and carries pain signals from the vertebral endplates. The procedure involves inserting a probe into the vertebral body that uses radiofrequency heat to destroy the basivertebral nerve, stopping the transmission of the pain signals. The entire procedure takes approximately sixty to ninety (60-90) minutes, does not involve any implants or sutures, and—perhaps most importantly of all—preserves the structure and mobility of the spine. Candidates for Intracept must meet three criteria:
1.Chronic low-back pain for at least six months.
2.Conservative treatments such as physical therapy, medication, or injections have not sufficiently reduced pain.
3.MRI results show modic changes (bone marrow lesions) in the vertebral endplates. This means there is swelling and inflammation that is irritating a nerve in the vertebra.
Before we were introduced to the Intracept Procedure, the primary treatments for those suffering from low back pain have been physical therapy, medications, injections, or invasive surgical options. More recently, research has provided that the vertebral bones above and below a degenerative disc have been shown to be a major pain source. The bad news is that current available treatment options have failed to address these troubling vertebral endplates.
One of the best parts about the Intracept Procedure is that, as opposed to lumbar spine fusion, Intracept has essentially no recovery period. An injured worker can get back to work more quickly than they ever have. The literature supporting Intracept is strong, consistently showing positive outcomes in pain and disability. Approximately seventy percent (70%) of patients have a significant reduction in pain from fifty to one hundred percent (50-100%) relief. One-third of patients are pain-free. About twenty percent (20%) of patients have a more modest pain reduction of twenty-five to fifty percent (25-50%). Average functional disability scores improve from severely disabled to minimally disabled. Pain medication intake is significantly reduced, as well. These results are quite remarkable in the spine field and even more so for such a minimally invasive procedure.
Another benefit is the safety profile. Given the small incisions, lack of implantation, and technical approach that steers clear of neurovascular structures, Intracept is extremely safe. No serious complications have been reported. The non-responder rate—about five to ten percent (5-10%)—is lower than that of most interventional spine procedures. A treatment failure with Intracept does not preclude patients from any other spine intervention, including epidural steroid injections, facet joint injections, facet joint RFA, SI joint procedures, intradiscal procedures, spinal cord stimulation, or even surgery. Conversely, it may be reasonable to start with some of the above less invasive procedures if the diagnosis is not clearly vertebrogenic pain and a more conservative approach is desired.
One of the best parts about the Intracept Procedure is that, as opposed to lumbar spine fusion, Intracept has essentially no recovery period. An injured worker can get back to the job quicker than they ever have. At Axion, we are happy to review any MRI to screen for potential candidates. Come see us in Alpharetta, Atlanta, or Riverdale.
Raymond R. Walkup, M.D., completed his undergraduate degree at Florida State University where he graduated magna cum laude. He completed medical school at the University of Alabama at Birmingham. During his neurosurgical residency at Emory University Hospital in Atlanta, Georgia, Dr. Walkup learned from spine experts in both departments of Neurosurgery and Orthopaedic Surgery where he received training in the latest minimally invasive surgical techniques for spine disorders. With Dr. Christopher Tomaras, Dr. Walkup has built Axion Spine & Neurosurgery, in Alpharetta, Georgia, from the ground up. He is board certified in neurosurgery and continues to publish and contribute to spine research in addition to participating in national education conferences.
With locations in: Louisville, Thomson and Waynesboro Workers' Compensation Coordinator


Beth Benton
Email: bbenton@burkehealth.com
Direct Line: 912.245.7932
PHONE: 912.542.0444
Physicians: Jonathan Le, MD • John S. Sarzier, MD • David Doman, MD
Southern Pain and Spine Associates

With locations in: Gainesville, Jasper, Newnan, and Athens
Director of Workers Compensation
Linda Lee
Email: llee@southernpainandspine.com workcomp@southernpainandspine.com
Workers' Compensation Coordinator
Ashley Jones
Email: ajones@southernpainandspine.com
Direct Line: 678-617-3443
PHONE: 678-971-4167 FAX: (678) 971-5205
Web Address: www.southernpainandspine.com
Physicians: Ankur Patel, DO, RPh • Jordan Tate, MD • Nathan Smith, MD

Email: orders@hearingprovider.com
Web Address: hearingprovider.com

PHONE: 800-598-5300

Steve Heinen
Email: sheinen@pjins.com
Web Address: Managedcomp.net
PHONE: 770-540-3810
Harvard MedTech VR Immersion Therapy
6280 South Valley View Blvd Suite 412 Las Vegas, NV 89118
Contact: Craig Segasser, Senior Vice President
Email: csegasser@harvardmedtech.com
Direct Line: 443-250-6899
Web Address: www.harvardmedtech.com

PHONE: 702-259-1810
Integrity Diagnostics EMG/ NCS

With locations in: Marietta, Snellville, McDonough, Cordele, Columbus, Savannah, Dublin, Cleveland, Augusta, and Macon
Contact: Celia
Email: Referrals@Integrity-DX.Com
Web Address: Integrity-DX.com
PHONE: (470) 809-1581
Caduceus TeleMed
535 North Central Avenue Hapeville, GA 30354
Workers’ Compensation Coordinator

Jackie Martinez
Email: telemed@caduceusoccmed.com
PHONE: 254-TELEMED

Multiple Providers (22 MD/PA/NP)
NuPath
Atlanta, GA
Contact: Patrick Lackey
Email: Patrick@nupathmed.com
Direct Line: 770-776-9417
Web Address: www.nupathmed.com
PHONE: 800-700-6986
10205 Access Rd Ste B Covington, GA. 30014
Contact: Cathy Bowden, MHA, CPC, CPMA, CHISP, CH-CBS
Email: cathy.bowden@pbcpservices.com
Direct Line: 678-218-9522
PHONE: 470-242-7584 ext 101
FAX: 470-443-9230
Team Post-Op
14133 NW 8th Street Sunrise, Florida 33325
Contact: Oscar Salazar
Email: info@teampostop.net
Direct Line: 954-289-8024 ext 104
Web Address: www.teampostop.net

PHONE: 877-252-0968
FAX: 954.541.5561
National RTW Program Resource
Mail drop locations are situated on both the East and West Coasts
Main - Reno, NV • Corporate – Atlanta, GA (Marietta)
Contact: Kerri Butler, Managing Director



Emails: Kerri@Workbridgelink.com Referal@workbridgelink.com
Scheduling@workbridgelink.com
Direct Line: 770-294-5936
Web Address: www.workbridgelink.com
PHONE: 800-890-1620
FAX: 888.530.3222

With locations in: Augusta, GA • Thomson, GA • Waynesboro, GA • Aiken, SC
Workers' Compensation Coordinator
Alisha Bond
PHONE: 706.863.9797 ext 291 FAX: 706.941.5000
Email: alishab@ortho-augusta.com
Web address: www.augustaaikenortho.com
Physicians: John Bojescul, MD • Justin V. Bundy, MD • Nicholas M. Capito, MD
• Ty William Carter, MD • John H. Franklin, MD • David Gallagher, MD
•Justin M. Head, DO • Douglas E. Holford, MD • Jeremy M. Jacobs, MD
•R. Vaughan Massie, MD • Karim Mahmoud, MD • Richard W. Pope, MD
•Physiatrist: Tara Swim, MD • Timothy J. Shannon, MD
With locations in: Alpharetta, Atlanta and Riverdale
Workers' Compensation Coordinator
Crystal Fowler
Direct Line: 470-751-4180
PHONE: 470-579-3962
Email: crystalfowler@axionspine.com
Web address: www.axionspine.com
Physicians: Chris Tomaras, MD • Raymond Walkup, MD
Physiatrist: Shane Mangrum, MD
With locations in: Carrollton, Bremen and Villa Rica
Workers’ Compensation Coordinator
Katie Huckeba
Email: katie.huckeba@carrolltonortho.com
Direct Line: 770-834-0873 ext 225
PHONE: 770-834-0873 FAX: 770-834-6118
Employers/Patients can also text to: 770-830-4136
Web address: www.carrolltonortho.com

Physicians: Taylor B. Cates, MD • Kevin M. Charron, MD • Anthony W. Colpini, MD
•Ralph E. Fleck, Jr., MD • Richard A. Herman, MD
• Bryan P. Kirby, MD • Ki Lin, MD
•Daniel L. Maxwell, MD • E. Franklin Pence, Jr., MD • Brad G. Prybis, MD
•Gregory S. Slappey, MD • Adam M. Sunderland, MD
With locations in: Newnan, Peachtree City, Griffin, Covington and LaGrange
Workers’ Compensation Coordinator
Vickie Calhoun
Direct Line: 770-502-2152
Email: vcalhoun@gbandj.com
PHONE: 770-502-2175 FAX: 770-502-2131
Web address: www.gbandj.com
Physicians: George M. Ballantyne, MD • Michael P. Gruber, MD
•Chad M. Kessler, MD • Michael V. Cushing, MD • Jayson A. McMath, MD
•David J. Heinsch, MD • Trevor W. Turner, MD • Shivam Desai M.D • David Love MD
•Clark Walker MD • Michael A. Webber, MD

With locations in: Jensen Beach, FL • Palm Bay, FL • Fort Pierce, FL • West Palm Beach, FL
•Plantation, FL • Orlando, FL
Workers' Compensation Specialist
Heather Dixon
Direct Line: 800-735-1178 ext.1012
Email: WC@globalneuroandspine.com
PHONE: 800-735-1178 FAX: 772-223-6354
Web address: www.globalneuroandspine.com
Physicians: Michael Slobasky, DO, DABPMR, DABPM
• Ali S. Malik, DO, DAOBPMR, MSBE • Ryan Brooks, DO • Douglas Slaughter, MD Psychiatric Nurse Practitioner: Chantel Rusz, PMHNP-BC
With locations in: Augusta, Evans and Thomson
Workers' Compensation Coordinator
Athena Simpson
Email: workerscomp@legendortho.com
Web address: www.legendortho.com

PHONE: 706.722.3401 ext 172
Physicians: Douglas R. Phillips, MD • Larry W. Carter, MD • Paul J. Herzwurm, MD
•Joseph P. Rectenwald, MD • Randall M. Meredith, MD • Terry L. Arrington, MD
•Matthew Link, MD • Brian E. Abell, DO

210 E DeRenne Avenue Savannah, GA 31405
With locations in: Baxley*, Brunswick*, Claxton, Dublin*, Hawkinsville*, Hinesville*, Macon*, Metter, Milledgeville*, Millen*, Pooler, Reidsville*, Richmond Hill, Rincon, Sandersville*, Statesboro, Sylvania, Vidalia, Waycross* South Carolina locations: Bluffton, Hilton Head Island
Natalie Stephens
Email: workcomp@optimorthopedics.com
PHONE: 912-644-5384
FAX: 912-644-6190
Web Address: www.optimorthopedics.com
Physicians:
Don G. Aaron, MD • Thomas Alexander, MD • Johnathan Christy, MD • Travis Farmer, MD
•Delan Gaines, MD • Jeffrey Goldberg, MD • Patrick Hanson, MD*
•Joseph Hegarty, MD* • Juha Jaakkola, MD • Mark Kamaleson, MD
•Gregory Kolovich, MD • Thomas Lawhorne, MD • John McCormick, II, MD
• Thomas Niemeier, MD • Markus Neiderwanger, MD* • Christopher Nicholson, MD
•David Palmer, MD • Justin Lancaster, MD • David M. Sedory, MD
•Kevin L. Stevenson, MD* • George Sutherland, MD • James Wilson, Jr, MD
•Chad T. Zehms, MD • Michael D. Dykes, MD* • Amir Shahien, MD • Robert Shelley, MD
•Jordan Paynter, MD • Rabindar Bhatti, DO
*Optim Health System works in collaboration with Optim Orthopedics and the physician-owned Optim Medical Center-Tattnall.
With locations in: Macon, Milledgeville, Dublin, Warner Robins and Kathleen
Workers’ Compensation Coordinators
Amanda Mangham (Spine Center)
Email: amangham@orthoga.org
Direct Line: 478-749-1613 FAX: 478-841-3178
Barbara Rodriguez (Warner Robins)
Email: brodriguez@orthoga.org
Direct Line: 478-971-1153 Ext. 701 FAX: 478-971-1174
Rita Boling (Northside, Macon)
Email: rboling@orthoga.org
Direct Line: 478-254-5387 FAX: 478.832.6509
Web Address: www.orthoga.org
Stacy Webb (Macon)
Email: swebb@orthoga.org
Direct Line: 478-254-5302

With locations in: Atlanta and Lawrenceville
Workers' Compensation Manager
Kathy Fuentes
Email: manager@performanceatl.com
Web address: www.performanceatl.com
PHONE: 404.220.7843
Physician: Stephanie Martin, MD