(Ebook)PainMedicine:ACaseBasedLearning Series:TheChestWallandAbdomenbyStevenD. Waldman,MD,JDISBN9780323846882,0323846882
https://ebooknice.com/product/pain-medicine-a-case-basedlearning-series-the-chest-wall-and-abdomen-53914588
Start reading on any device today!
(Ebook) The Chest Wall and Abdomen: Pain Medicine: A Case Based Learning Series by Waldman MD JD, Steven D. ISBN 9780323846882, 0323846882
https://ebooknice.com/product/the-chest-wall-and-abdomen-pain-medicine-a-casebased-learning-series-53998588
ebooknice.com
(Ebook) The Wrist and Hand: Pain Medicine: A Case-Based Learning Series by Waldman MD JD, Steven D. ISBN 9780323834537, 0323834531
https://ebooknice.com/product/the-wrist-and-hand-pain-medicine-a-case-basedlearning-series-53998474
ebooknice.com
(Ebook) Headache and Facial Pain Pain Medicine-A Case-Based Learning Series (Mar 25, 2022)_(0323834566)_(Elsevier) by Waldman MD JD, Steven D. ISBN 9780323834568, 0323834566
https://ebooknice.com/product/headache-and-facial-pain-pain-medicine-a-casebased-learning-series-mar-25-2022-0323834566-elsevier-53908714
ebooknice.com
(Ebook) The Spine: Pain The Spine Pain Medicine-A Case-Based Learning Series by Waldman MD, Steven D. ISBN 9780323756365, 0323756360
https://ebooknice.com/product/the-spine-pain-the-spine-pain-medicine-a-casebased-learning-series-53908736
ebooknice.com
Elsevier 1600JohnF.KennedyBlvd. Ste1800 Philadelphia,PA19103-2899
PAINMEDICINE:ACASE-BASEDLEARNINGSERIES THECHESTWALLANDABDOMEN Copyright © 2023byElsevier,Inc.Allrightsreserved
ISBN:978-0-323-84688-2
Allunnumberedfiguresare ©ShutterstockCh1#1313408291,Ch2#1170763714,Ch3#1813998932, Ch4#118647259,Ch5#1246458301,Ch6#1450389707,Ch7#354598628,Ch8#1419717965, Ch9#1536469760,Ch10#56680288,Ch11#1442971682,Ch12#1112390603,Ch13#1788595244, Ch14#568200667,Ch15#1657365622
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans, electronicormechanical,includingphotocopying,recording,oranyinformationstorageand retrievalsystem,withoutpermissioninwritingfromthepublisher.Detailsonhowtoseek permission,furtherinformationaboutthePublisher’spermissionspoliciesandourarrangements withorganizationssuchastheCopyrightClearanceCenterandtheCopyrightLicensingAgency, canbefoundatourwebsite: www.elsevier.com/permissions
Thisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythe Publisher(otherthanasmaybenotedherein).
Notice Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgein evaluatingandusinganyinformation,methods,compoundsorexperimentsdescribedherein. Becauseofrapidadvancesinthemedicalsciences,inparticular,independentverificationof diagnosesanddrugdosagesshouldbemade.Tothefullestextentofthelaw,noresponsibility isassumedbyElsevier,authors,editorsorcontributorsforanyinjuryand/ordamageto personsorpropertyasamatterofproductsliability,negligenceorotherwise,orfromanyuseor operationofanymethods,products,instructions,orideascontainedinthematerialherein.
ExecutiveContentStrategist: MichaelHouston
ContentDevelopmentSpecialist: JeannineCarrado/LauraKlein
Director,ContentDevelopment: EllenWurm-Cutter
PublishingServicesManager: ShereenJameel
SeniorProjectManager: KarthikeyanMurthy
DesignDirection: AmyBuxton
PrintedinIndia.
Lastdigitistheprintnumber: 987654321
InternationalSpaceStation.Justsaveyourbreath;itmakesabsolutelynosenseto yourstudents.Yes,theywanttoplease,sotheywillmemorizetheelementsofthe ReviewofSystems,butthatisaboutasfarasitgoes.Ontheotherhand,ifyoupresentthecaseofJannettePatton,a28-year-oldfirst-yearmedicalresidentwithafever andheadache,youcanseethelightsstarttocomeon.Bytheway,thisiswhat Jannettelookslike,andasyoucansee,Jannetteissickerthanadog.This,atitsmost basiclevel,iswhat Case-BasedLearning isallabout.
Iwouldliketotell youthat,smartguy thatIam,Iimmediatelysawthelight andbecameaconvert to Case-BasedLearning. Buttruthbetold,it wasCOVID-19that reallygotmethinkingabout Case-Based Learning.Beforethe COVID-19pandemic, Icouldjustdragthestudentsdowntothemed/surgwardsandwalkintoa patientroomandriff.Everyonewasawinner.Forthemostpart,thepatients lovedtoplayalongandthoughtitwascool.ThepatientandthebedsidewasallI neededtoprovidethecontextthatwasnecessarytoillustratewhatIwastrying toteach the “whyheadacheandfeverdon’tmix” kindofstuff.HadCOVID-19 notrudelydisruptedmyabilitytoteachatthebedside,Isuspectthatyouwould notbereadingthis Preface,asIwouldnothavehadtowriteit.Withinaveryfew daysaftertheCOVID-19pandemichit,mydaysofbedsideteachingdisappeared,butmystudentsstillneededcontext.Thisgotmefocusedonhowto providethecontexttheyneeded.Theanswerwas,ofcourse, Case-BasedLearning. Whatstartedasadesiretoprovidecontext becauseitreallywas harderthan itlooked ledmetobeginworkonthiseight-volume Case-BasedLearning textbookseries.Whatyouwillfindwithinthesevolumesareabunchoffun,real-life casesthathelpmakeeachpatientcomealiveforthestudent.Thesecasesprovide thecontextualteachingpointsthatmakeiteasyfortheteachertoexplainwhy, whenJannette’schiefcomplaintis, “MyheadiskillingmeandI’vegotafever,” itis abigdeal.
Havefun!
StevenD.Waldman,MD,JD
Spring2021
Averyspecialthankstomyeditors,MichaelHouston,PhD,JeannineCarrado, andKarthikeyanMurthy,foralltheirhardworkandperseveranceintheface ofdisaster.GreateditorssuchasMichael,Jeannine,andKarthikeyanmaketheir authorslookgreat,fortheynotonlyunderstandhowtobringtheThreeCsof greatwriting...Clarity 1 Consistency 1 Conciseness ...totheauthor’swork,but unlikeme,theycanactuallypunctuateandspell!
StevenD.Waldman,MD,JD
P.S. ...Sorryforalltheellipses,guys!
1 ThomasWang A28-Year-OldStockbrokerWith SevereAnteriorChestPain LEARNINGOBJECTIVES • Learnthecommoncausesofchestwallpain.
• Developanunderstandingoftheuniqueanatomyofthechestwall.
• Developanunderstandingofthecausesofcostosternaljointpain.
• Developanunderstandingofjointinjury.
• Learntheclinicalpresentationofcostosternalsyndrome.
• Learnhowtousephysicalexaminationtoidentifypathologyofthecostosternal joint.
• Developanunderstandingofthetreatmentoptionsforcostosternaljointpain.
ThomasWang ThomasWangisa28-year-oldstockbrokerwiththechiefcomplaintof, “Mychestiskillingme.” Thomas statedthatabout1weekago,hewas involvedinamotorvehicleaccident whendrivinghomefromaparty. “ A dogranoutofnowhereandstartled me,andthenextthingIrememberis wakingupaftercrashingintoatree. ThegoodnewsisIdidn ’ thitthedog; thebadnewsisIgotaDUI.Ihada coupleofglassesofwinewithmyfriends,butthoughtIwasokaytodrive home. ” Iaskedifhewaswearinghisseatbeltandhegavemean “areyoukiddingme? ” lookasheansweredthatheal wayswearshisseatbelt. “Doctor,I don ’ tknowwhetheritwastheseatbeltortheairbagthatgotmychest,butit hurtswheneverItakeadeepbreathorreachforanything.Ihadtobuysome go-cupsbecauseIcan’ tgetmycoffeemugsoutofthecabinet!Ithoughtit wouldgetbetter,butitreallyhasn’t. ” Iresponded, “I’ mhappytohearyou werewearingyourseatbelt. So,didyouhityourhead? ” Hesaidhedidn’tthink so,thathethoughthejustfellasleepafterhehitthetree.Theytookhimtothe emergencyroom,andthescanofhisheaddidn ’tshowanything. “Doctor,I reallyscreweduphere.IhopeIdon ’tlosemylicenseforthislittlestunt.My bloodalcoholwasoffthecharts!Ican ’ tfigureitout;itwasonlyacoupleof glassesofwine.Ireallybungedupmychest.Theysaidnothingwasbroken,so whydoesithurtsomuch? ”
IaskedThomasifhehadanythinglikethishappenbefore.Heshookhis headandresponded, “ Never.Ineverdrinkanddrive.IusuallytakeanUber, buttheywereonpricesurge,andthati sjustarip-off.IwassureIwasgoodto drive. ”“ WhatImeant,Thomas,washaveyoueverpassedoutorlostconsciousness? ”“ No, ” heresponded. “Thathasneverhappened.Iamverycareful withthedistracteddrivingandall youknowwhatImean?Whatworriesme isthatmychestjustisn’ tgettingbetter,anditismakingitreallyhardtositata computermonitorallday.Itfeelslik esomethingisbrokeninthefrontofmy chest.Iamevenhavingahardtimereachinguptowashmyhairandtoshave.”
IaskedThomasaboutanypreviousproblemswithalcohol,passingout, DUIs,orforgettingwherehewas,andheshookhisheadno. “Doc,Iwasnever muchofadrinker,justacoupleglassesofwinewithdinner.Ireallyenjoythe Californiareds.” IaskedThomaswhathetriedtorelievehischestpain,andhe saidthathehadtriedsomeAdvilandTylenol,buttheydidn’tdomuch.Hewent ontosaythataheatingpadseemedtohelpalittlebit.IaskedThomaswhat
madehispainworse,andhesaid, “AnytimeIusemyarmstoreachforanything ortakeadeepbreath.IhateitwhenIhavetocoughorsneezebecausethatreally hurts.” Thomaswentontosaythatwhenhereachedup,hefeltpaininthefront ofhischestaroundhisbreastbone.Iaskedhowhewassleeping,andheshook hisheadandsaid, “Doc,I’llbetthispainwakesmeup100timesanight.Iusually sleeponmyleftside,butsinceIhadthewreckIcan’tdothat,soItrytosleepon myrightside.EverytimeIrollovertomyleftside,thepainwakesmeup.”
IaskedThomastopointwithonefingertoshowmewhereithurtthemost. Hepointedtoeachsideofhissternumandsaid, “Doc,it’srightherewhere somethingiswrong.Itfeelslikesomethingisbroken.Ikeepthinkingthere shouldbeabruiseorsomething,butit’sdowndeep.” Iaskedifhehadanyfever orchills,andheshookhisheadno.
Onphysicalexamination,Thomaswasafebrile.Hisrespirationswere16and hispulsewas68andregular.Hisbloodpressurewas112/70.Hishead,eyes, ears,nose,throat(HEENT)examwasnormal,withnoscleralicterus.Hiscardiopulmonaryexaminationwasunremarkable.Histhyroidwasnormal.His abdominalexaminationrevealednoabnormalmassororganomegaly;specifically,Iwasunabletodetectanyhepatomegaly.Therewasnocostovertebral angle(CVA)tendernessorperipheraledema.Hislowbackexaminationwas unremarkable.Visualinspectionofthechestwallwasunremarkable;specifically,therewasnoobviousbonydeformityorinfection.InotedthatThomas wassplintinghisshouldersalittleforwardtoavoidmovinghischestwall. PalpationofthecostosternaljointsexacerbatedThomas’spain(Fig.1.1).Idid notappreciateanyobviousseparationofthecostosternaljoint.Iperformedthe shoulderretractiontestforcostosternalsyndrome,whichwaspositivebilaterally(Fig.1.2).Examinationofthejointsofthehandsandothermajorjoints revealednoevidenceofinflammatoryarthritis.Acarefulneurologicexaminationoftheupperextremitiesrevealednoevidenceofperipheralorentrapment neuropathy,andthedeeptendonreflexeswerenormal.Thomas’smentalstatus examinationwasnormal.
KeyClinicalPoints—
THEHISTORY ’ Ahistoryofacutetraumatothechestwallfromanairbagandseatbelt
’ Ahistoryofmotorvehicleaccident
’ Historyofdrivingwhileintoxicated
’ Historyofdailyalcoholintake
’ Nohistoryofprevioussignificantchestwallpain
’ Nofeverorchills
Fig.1.2 Toelicitashoulderretractiontestinpatientswhoaresuspectedofsufferingfromcostosternalsyndrome,thepatientisplacedinthestandingpositionwiththeshouldersinneutralposition,facingtheexaminer.Thepatientisthenaskedtoretracttheshouldervigorously.Theshoulderretraction testisconsideredpositiveiftheretractionmaneuverreproducesthepatient’santeriorchestwallpain. (FromWaldmanS. PhysicalDiagnosisofPain:AnAtlasofSignsandSymptoms.ed.4.Philadelphia: Elsevier;2021[Fig.143-1].)
WhatTestsWouldYouLiketoOrder? Thefollowingtestswereordered:
’ Plainradiographsofthechestwall
’ Completebloodcount
’ Comprehensivechemistrypanel,includingliverenzymes
TESTRESULTS Theplainradiographsofthesternumandcostosternaljointsrevealednofracturesordislocations.
Thecompletebloodcountrevealednomegaloblasticanemia.
Thecomprehensivechemistrypanelwaswithinnormallimitswithnoelevationofliverenzymes.
ClinicalCorrelation—PuttingitallTogether Whatisthediagnosis? ’ Costosternalsyndromesecondarytoacutetraumaticinjury
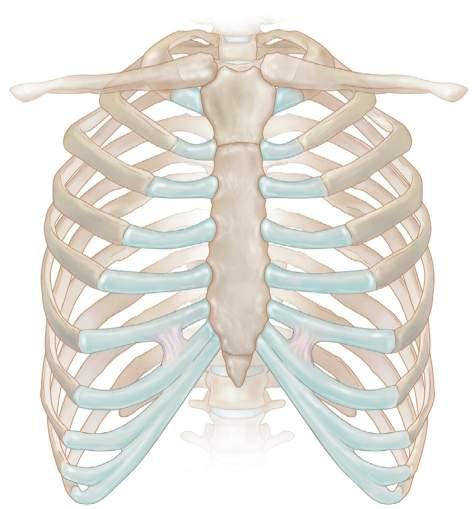
TheScienceBehindtheDiagnosis ANATOMYOFTHECOSTOSTERNALJOINTS Thecartilageofthetrueribsarticulateswiththesternumviathecostosternal joints(Fig.1.3).Thecartilageofthefirstribarticulatesdirectlywiththemanubriumofthesternumandisasynarthrodialjointthatallowsalimitedgliding movement.Thecartilageofthesecondthroughsixthribsarticulateswiththe bodyofthesternumviatruearthrodialjoints.Thesejointsaresurroundedbya thinarticularcapsule.Thecostosternaljointsarestrengthenedbyligamentsbut
Fig.1.3 Theanatomyofthechestwall.(FromWaldmanS. AtlasofPainManagementInjection Techniques.ed.4.St.Louis:Elsevier;2017[Fig.99-3].)
Clavicle
Costal cartilage
Costosternal joint
Costochondral joint Jugular notch of sternum
canbesubluxedordislocatedbyblunttraumatotheanteriorchest.Posteriorto thecostosternaljointarethestructuresofthemediastinum.Thesestructuresare susceptibletoneedle-inducedtraumaiftheneedleisplacedtoodeeply.The pleuralspacemaybeenterediftheneedleisplacedtoodeeplyandlaterally,and pneumothoraxmayresult.
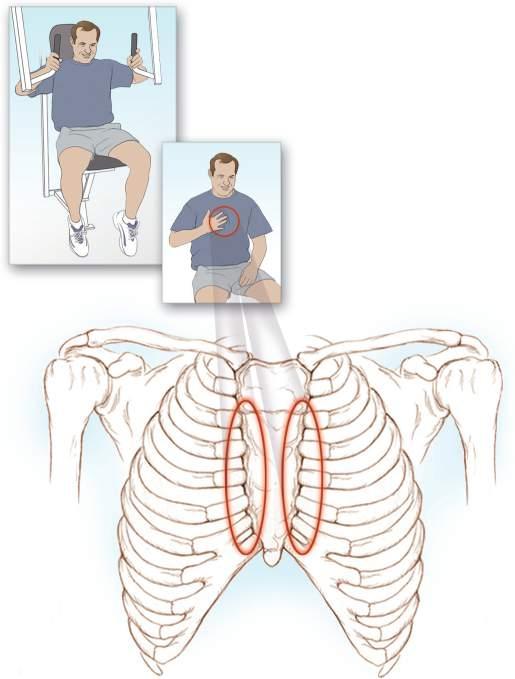
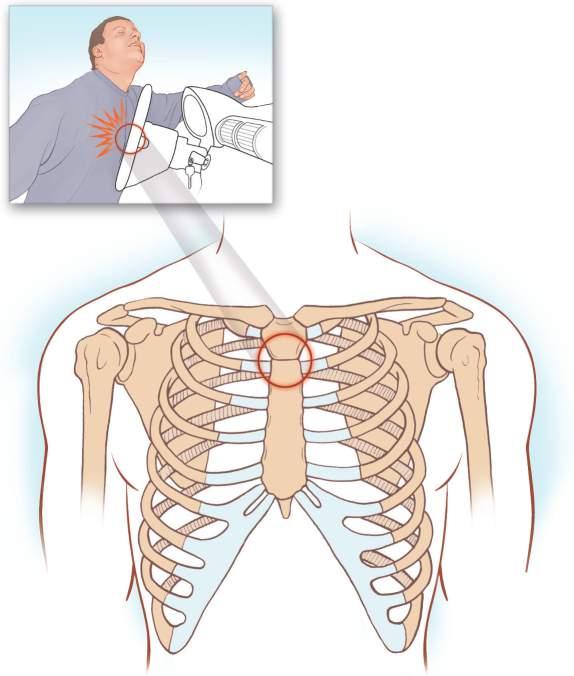
CLINICALSYNDROME Manypatientswithnoncardiogenicchestpainsufferfromcostosternaljointpain. Mostcommonly,thecostosternaljointsbecomepainfulinresponsetoinflammationasaresultofoveruseormisuse,orinresponsetotraumasecondaryto acceleration-decelerationinjuriesorblunttraumatothechestwall(Fig.1.4).With severetrauma,thejointsmaysubluxateordislocate.Thecostosternaljointsare
Sternum Costosternal joints
Fig.1.4 Irritationofthecostosternaljointsfromoveruseofexerciseequipmentcancausecostosternal syndrome.(FromWaldmanS. AtlasofCommonPainSyndromes.ed.4.Philadelphia:Elsevier;2019 [Fig.61-1].)
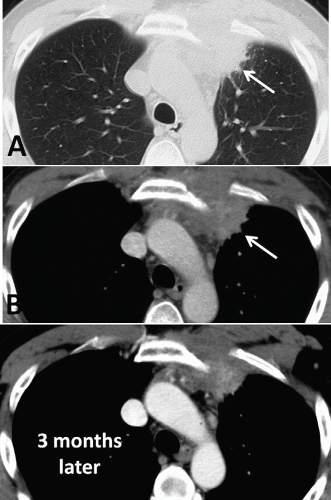
CFig.1.6 Computedtomography(CT)scanofapatientwithanteriorchestwallpain.CTscanningof anterioruppermediastinalmassafteriodinatedcontrastadministration.Lungwindow(A). Mediastinumwindow(B)showsinhomogeneouscontrastenhancementofthemass.Enhanced multidetectorCTfollow-upafter3months(C)showsdecreaseinvolumeofmediastinalmass. (FromDeFilippoM,AlbiniA,CastaldiV,etal.MRIfindingsofTietze ’ssyndromemimickingmediastinalmalignancyonMDCT. EurJRadiolExtra .2008;65(1):33 35[Fig.1].ISSN1571-4675, https:// doi.org/10.1016/j.ejrex.2007.10.006, http://www.sciencedirect.com/science/article/pii/S1571467 507000892.)
sustainedtraumatotheanteriorchestwall.Thecostosternaljointsandadjacent intercostalmusclesmaybetendertopalpation.Thepatientmayalsocomplain ofaclickingsensationwithjointmovement.
TESTING Plainradiographsareindicatedforall patientswhopresentwithpainthatis thoughttobeemanatingfromthecostosternaljointstoruleoutoccultbony disorders,includingtumor( Fig.1.5 ).Iftraumaispresent,radionuclidebone scanningmaybeusefultoexcludeoccultfracturesoftheribsorsternum. Basedonthepatient ’ sclinicalpresentation,addi tionaltestingmaybeindicated,includingacompletebloodcount,pr ostate-specificantigenlevel,erythrocytesedimentationrate,andantin uclearantibodytesting.Laboratory evaluationforcollagenvasculardiseaseisindicatedinpatientssufferingfrom costosternaljointpainifotherjoin tsareinvolved.Computedtomography
(CT)scanning,magneticresonanceimag ing(MRI),andultrasoundimagingof thejointsareindicatedifjointinstabilityoroccultmassissuspected,ortoelucidatethecauseofthepainfurther( Figs.1.6,1.7 ,and 1.8 ).Injectionofthe costosternaljointcanserveasbothadi agnosticandatherapeuticmaneuver ( Figs.1.9 and 1.10 ).
DIFFERENTIALDIAGNOSIS Asmentioned,thepainofcostosternals yndromeisoftenmistakenforpainof cardiacorigin,anditleadstovisitsto theemergencydepartmentandunnecessarycardiacworkups.Iftraumahasoccurred,costosternalsyndromemay coexistwithfracturedribsorfracturesofthesternumitself,whichcanbe missedonplainradiographsandmayrequireCTorradionuclidebonescanningforproperidentification( Fig.1.11 ).Tietzesyndrome,whichispainful enlargementoftheuppercostochondral cartilageassociatedwithviralinfection,maybeconfusedwithcostosternalsyndrome( Box1.1 ).
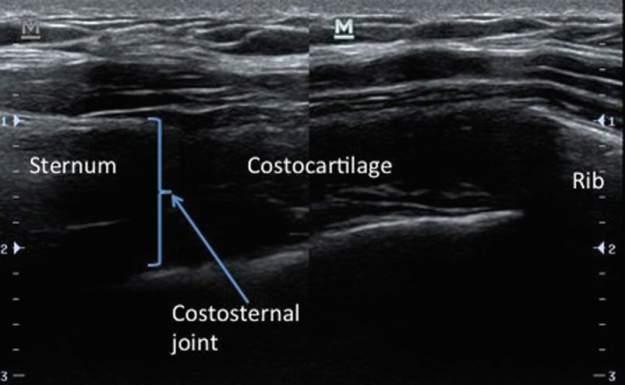
Neuropathicpaininvolvingthechest wallmayalsobeconfusedorcoexist withcostosternalsyndrome.Example sofsuchneuropathicpainsyndromes includediabeticpolyneuropathiesand acuteherpeszosterinvolvingthethoracicnerves.Diseasesofthestructuresofthemediastinumandchestwallmay Fig.1.7 Properplacementofthehigh-frequencylinearultrasoundprobeforultrasoundevaluationof thecostosternaljoint.
Transverseultrasoundimageofthecostosternaljoint.
Third costochondral junction
Fig.1.9 Injectionofthecostosternaljoint.(FromWaldmanS. PainReview.2nd.ed.Philadelphia: Elsevier;2017:9780323448895[Fig.286-1].)
Carrico & Shavell
Fig.1.8
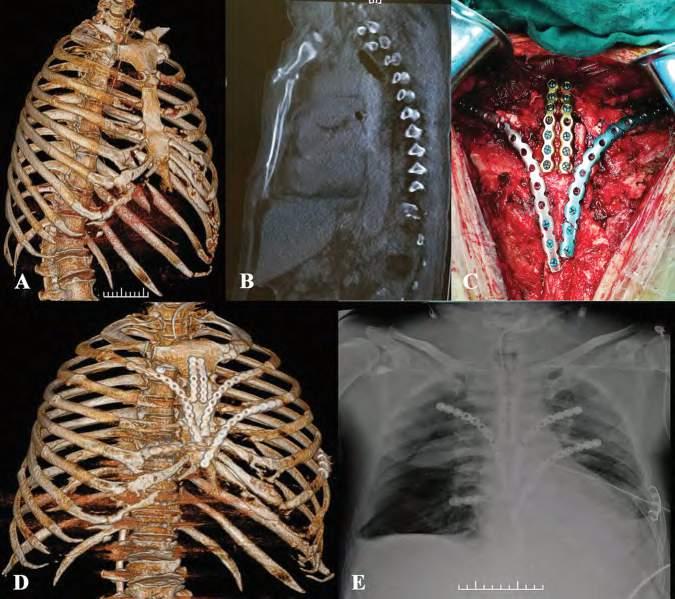
Fig.1.11 Crushinjuryofthechestwithmassivechestwalltrauma.(A)Computedtomographic(CT) three-dimensionalreconstructionimageofthechestwallonadmission.(B)CTimageofthesternum.(C) Surgicalprocedure:fixationofsternalandmultiplecostalcartilagefractures.(D)CTthree-dimensional reconstructionimageofthechestwallafteroperation.(E)Chestfilmobtained4daysafteroperation. (FromGaoE,LiY,ZhaoT,etal.Simultaneoussurgicaltreatmentofsternumandcostalcartilagefractures. AnnThoracSurg.2019;107(2):e119 e120[Fig.1].ISSN0003-4975, https://doi.org/10.1016/j. athoracsur.2018.06.044, http://www.sciencedirect.com/science/article/pii/S0003497518310488.)
Strainofthecostosternaljoint ’ Manubriosternalarthritis ’ Tietzesyndrome
’ Costochondritis ’ Xiphodynia
’ Costovertebraljointdisorders
Septicarthritis
Ribtrauma
’ Ribfracture
’ Primaryandmetastaticneoplasmoftheribinfection
’ Slippingribsyndrome
PainArisingFromtheSoftTissues
’ Myositis
’ Musclestrain
’ Fibromyalgia
’ Myofascialpain
MiscellaneousSourcesofPain
’ Precordialcatchsyndrome
’ Acuteherpeszoster
’ Zostersineherpete
’ Somatiformdisorders
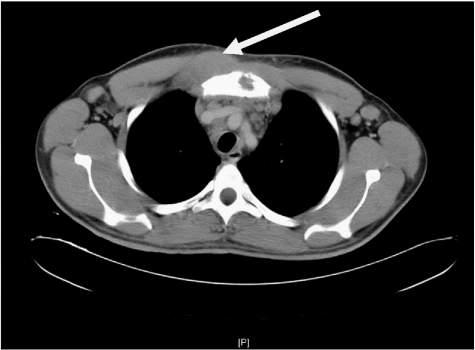
Fig.1.12 Computedtomographyscanofapatientcomplainingofrightcostosternalpainrevealinga rightchestwallmassatthelevelofthesecondrib (arrow).(FromRichBS,McEvoyMP,Honeyman JN,etal.Hodgkinlymphomapresentingwithchestwallinvolvement:acaseseries. JPediatrSurg 2011;46(9):1835 1837[Fig.2].ISSN0022-3468, https://doi.org/10.1016/j.jpedsurg.2011.05.015, http://www.sciencedirect.com/science/article/pii/S0022346811004428.)
COMPLICATIONSANDPITFALLS Becausemanypathologicprocessescanmimicthepainofcostosternalsyndrome,theclinicianmustcarefullyruleoutunderlyingcardiacdiseaseanddiseasesofthelungandstructuresofthemediastinum.Failuretodosocouldlead todisastrousresults.Themajorcomplicationoftheinjectiontechniqueispneumothoraxiftheneedleisplacedtoolaterallyordeeplyandinvadesthepleural space.Infection,althoughrare,canoccurifstrictaseptictechniqueisnot
followed.Traumatothecontentsofthemediastinumisalsoapossibility.The riskofthiscomplicationcanbegreatlydecreasedwiththeuseofultrasound guidanceforneedleplacement.
HIGH-YIELDTAKEAWAYS • Thepatientisafebrile,makinganacuteinfectiousetiology(e.g.,septicarthritis) unlikely.
• Thepatient’ssymptomatologyistheresultofacutetrauma,andphysical examinationandtestingshouldfocusontheidentificationofotherpathologic processesthatmaymimictheclinicalpresentationofcostosternalsyndrome.
• Thepatient’spainislocalizedtothecostosternaljoints.
• Thepatient’ssymptomsinvolveonlythecostovertebraljoints,whichismore suggestiveofalocalprocessthanasystemicpolyarthropathy.
• Sleepdisturbanceiscommonandmustbeaddressedconcurrentlywiththe patient’spainsymptomatology.
• Plainradiographswillprovidehigh-yieldinformationregardingthebony contentsofthecostovertebraljoints,butCTscanning,ultrasoundimaging,and MRIwillbemoreusefulinidentifyingsofttissuepathology.
SuggestedReadings AylooA,CvengrosT,MarellaS.Evaluationandtreatmentofmusculoskeletalchest pain. PrimCare.2013;40(4):863 887.
HillenTJ,WessellDE.MultidetectorCTscanintheevaluationofchestpainofnontraumaticmusculoskeletalorigin. ThoracSurgClin.2010;20(1):167 173.
LuCH,HsiehSC,LiKJ.Tophiinanteriorchestwall. JointBoneSpine.2014;81(4):366.
StochkendahlMJ,ChristensenHW.Chestpaininfocalmusculoskeletaldisorders. Med ClinNorthAm.2010;94(2):259 273.
WaldmanSD.Arthritisandotherabnormalitiesofthecostosternaljoint.In: Waldman’ s ComprehensiveAtlasofDiagnosticUltrasoundofPainfulConditions.ed.2.Philadelphia: WoltersKluwer;2016:513 518.
WaldmanSD.Costosternaljointinjection.In: PainReview.ed.2.Philadelphia:Elsevier; 2017:462 463.
WaldmanSD.CostosternaljointinjectiontechniqueforTietzesyndrome.In: Atlasof PainManagementInjectionTechniques.ed.4.Philadelphia:Elsevier;2017:349 351.
WaldmanSD.Ultrasound-guidedinjectiontechniqueforcostosternaljointpain. In: Waldman’sComprehensiveAtlasofUltrasoundGuidedPainManagementInjection Techniques.ed.2.Philadelphia:WoltersKluwer;2020:591 594.
PeteWilder PeteWilderisa23-year-oldprinter withthechiefcomplaintof, “Every timeItakeadeepbreath,itfeelslike somebodyisstabbingmeinthechest withaknife.” Petestatedthathe stoppedtohelpawomaninaminivanfullofkidswhowastryingto changeatire.Thenextthingheknew, hewokeupintheintensivecareunit oftheuniversitymedicalcenter.
“Doctor,IguessIwastryingtoliftthespareupontothewheelwhenaguyina pickuptruckcameoverthehillandknockedmeintonextweek.Abystander decidedIdidn’thaveapulseandstartedCPR.Hemusthavereallypumpedthe helloutofmychestbecausenowmybreastboneclickswitheverybreath.The ICUdoctorsaidIhadadislocationorsomething.”
“Doctor,Iconsidermyselfaprettytoughguy youknow,Ijoinedthe Marinesrightoutofhighschool butanytimeIcoughorsneeze,thepainisso badIjustwanttoscream.Itreally,reallyhurts.”
IaskedPeteifhehadexperiencedanypainorhadanypreviousinjuryorsurgeryofthechestwallbeforeallthisstarted,andheshookhisheadnoand replied, “Iamashealthyasahorse.Iguessnogooddeedgoesunpunished. IguessIamluckythatIdidn’tgetkilledtryingtohelpthatlady.Ireallydon’t remembergettinghitbythecarorgettingmychestpoundedon.Iguessthat’ sa goodthing ornot!?” Iasked, “Howisyoursleep?” Petereplied, “I’msleeping inmyreclinerbecauseitkeepsmefromrollingover,whichreallyhurts.Even then,Ibetthepainwakesmeup50timesanight.Mybosshasbeenprettynice aboutthewholething,butprintingisaprettyphysicalactivity.”
IaskedPetetoshowmethelocationofthepain,andhepointedtothecenter ofhissternum. “Ithurtsrighthere.It’srighthere,andthisiswheretheclicking comesfrom,righthere.” IaskedPeteaboutanyfever,chills,orotherconstitutionalsymptomssuchasweightlossornightsweats,andheshookhisheadno. Hedeniedanyothermusculoskeletalorsystemicsymptoms.
Onphysicalexamination,Petewasafe brile.Hisrespirationswere18,his pulsewas74andregular,andhisbloodpressurewas124/76.Pete’ shead, eyes,ears,nose,throat(HEENT)examwasnormal,aswashisthyroidexam. Auscultationofhiscarotidsrevealednobruits,andthepulsesinallfour extremitieswerenormal.Hehadaregularrhythmwithoutabnormalbeats. Hiscardiacexamwasotherwiseunremarkable.Hisabdominalexamination revealednoabnormalmassororganomegaly.Therewasnoperipheraledema. Hislowbackexaminationwasunremarkable,althoughflexionofthelumbar
Fig.2.1 Photographshowinganobviousstep-offinthemanubriosternaljointfollowingdislocation. (FromLyonsI,SahaS,ArulampalamT.Manubriosternaljointdislocation:anunusualriskoftrampolining. JEmergMed.2010;39:596 598.)
spinecausedsomepainintherightbuttocks.Therewasnocostovertebral angle(CVA)tenderness.VisualinspectionofPete’santeriorchestwallwas unremarkable.Therewasnoevidenceofecchymosisorobviousswelling. PressureonthesternumcausedPetetocryoutinpain.Therewasanobvious bonydeformitywithaclearlydefinedst ep-offofthemanubriosternaljoint, suggestiveofamanubriosternaldislocation( Fig.2.1 ).Petesaid, “I’ vehad aboutallthefunwiththepokingaroundthatIcanstand.Areyouabout done? ”“ Sorry,Pete,Ijustwanttofigureoutwhatweneedtodotogetyoubetter.Weareaboutdonehere. ” Carefulneurologicexaminationsofboththe upperandlowerextremitieswerenormal.Deeptendonreflexeswerephysiologicthroughout. “IamprettysureIknowwhatiscausingthepain,andwe shouldbeabletogetyoubetter.”
KeyClinicalPoints—What’sImportantandWhat’sNot
THEHISTORY ’ HistoryofseveremidsternalpainafterreceivingCPR
’ Painmadeworsewithpressureonthemanubriosternaljoint
’ Nohistoryofpreviouschestorchestwallpain
’ Nofeverorchills
’ Significantsleepdisturbance
TESTRESULTS X-rayofthesternumwasunremarkablewithnofractureorbonyabnormality. Ultrasoundofthemanubriosternaljointwasreportedasnormal(Fig.2.3).
ClinicalCorrelation—PuttingItAllTogether
Whatisthediagnosis?
’ Manubriosternaljointpain
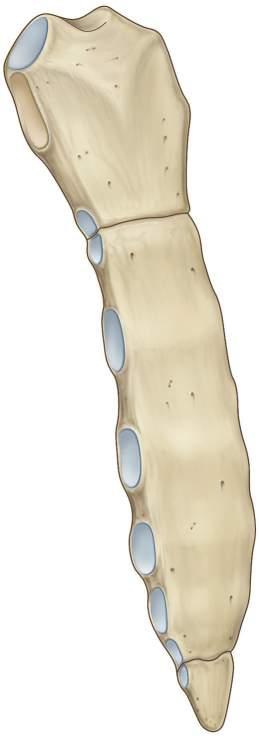
TheScienceBehindtheDiagnosis ANATOMY Themanubriumarticulateswiththebodyofthesternumviathemanubriosternaljoint.ThejointarticulatesatananglecalledtheangleofLouis,whichallows foreasyidentification(Fig.2.4).Thejointisafibrocartilaginousjointorsynchondrosis,whichlacksatruejointcavity.Themanubriosternaljointallowsprotractionandretractionofthethorax.Above,themanubriumarticulateswiththe sternalendoftheclavicleandthecartilageofthefirstrib.Below,thebodyofthe sternumarticulateswiththexiphoidprocess.Posteriortothemanubriosternal jointarethestructuresofthemediastinum.Thesestructuresaresusceptibleto needle-inducedtraumaiftheneedleisplacedtoodeeply.Thepleuralspacemay beenterediftheneedleisplacedtoodeeplyandlaterally,andpneumothorax mayresult.
CLINICALSYNDROME Painoriginatingfromthemanubriosternaljointcanmimicpainofcardiacorigin.Themanubriosternaljointissusceptibletothedevelopmentofosteoarthritis,rheumatoidarthritis,ankylosingspondylitis,Reitersyndrome,and psoriaticarthritis.Thejointcanalso betraumatizedduringaccelerationdecelerationinjuriesandblunttraumatothechest(Figs.2.5 and 2.6 ).With severetrauma,thejointmaysubluxateordislocate,withthedislocationclassifiedonthebasisofthepositionofthesternumrelativetothemanubrium ( Fig.2.7 ).Overuseormisusecanresultinacuteinflammationofthemanubriosternaljoint,whichcanbequitedebilitating.Thejointisalsosubjecttoinvasion bytumorfromprimarymalignanttumors,includingthymoma,orfrommetastaticdisease.Rarely,septicarthritisofthemanubriosternaljointcanoccur ( Fig.2.8 ).
Articular site for clavicle
Attachment site for rib I
Articular demifacets for rib II
Articular facets for ribs III–VI
Articular facets for rib VII
Jugular notch
Manubrium of sternum
Sternal angle (manubriosternal joint)
Transverse ridges
Body of sternum
Xiphoid process
Fig.2.4 Theanatomyofthesternum.(FromDrakeR,VoglW,MitchellA. Gray’sAnatomyfor Students.ed.4.Philadelphia:ChurchillLivingstone;2020[Fig.3-23].)
collagenvasculardiseaseisindicatedin patientssufferingfrommanubriosternaljointpainifotherjointsareinvolv ed.Magneticresonanceimaging(MRI), ultrasoundimaging,and/orcomputed tomography(CT)ofthejointisindicatedifjointinstability,infection,oroccultmassissuspected,ortofurtherelucidatethecauseofthepain(Figs.2.10 and 2.11 ).TheuseofmultidetectorCT forpatientspresentingtotheemergencydepartmentwithacutechestpainhas ledtomorerapidandaccuratediagnosi sofchestwallpainsyndromes(see Fig.2.6 ).Theinjectiontechniquedescribed laterservesasbothadiagnosticand atherapeuticmaneuver(Fig.2.12 ).
Manubriosternal joint
Fig.2.5 Themanubriosternaljointissusceptibletothedevelopmentofarthritis.Itisoftentraumatized duringacceleration-decelerationinjuriesandblunttraumatothechest.(FromWaldmanS. Atlasof CommonPainSyndromes.ed.4.Philadelphia:Elsevier;2019[Fig.62-1].)
DIFFERENTIALDIAGNOSIS Asmentioned,thepainofmanubriosternalsyndromeisoftenmistakenforpain ofcardiacorigin,anditleadstovisitstotheemergencydepartmentandunnecessarycardiacworkups.Iftraumahasoccurred,manubriosternalsyndromemay coexistwithfracturedribsorfracturesofthesternumitself,whichcanbemissed onplainradiographsandmayrequireradionuclidebonescanningforproper identification.Tietzesyndrome,whichispainfulenlargementoftheuppercostochondralcartilageassociatedwithviralinfection,maybeconfusedwithmanubriosternalsyndrome.
Neuropathicpaininvolvingtheche stwallmayalsobeconfusedormay coexistwithmanubriosternalsyndrome.Examplesofsuchneuropathic painsyndromesincludediabeticpolyneuropathiesandacuteherpeszoster
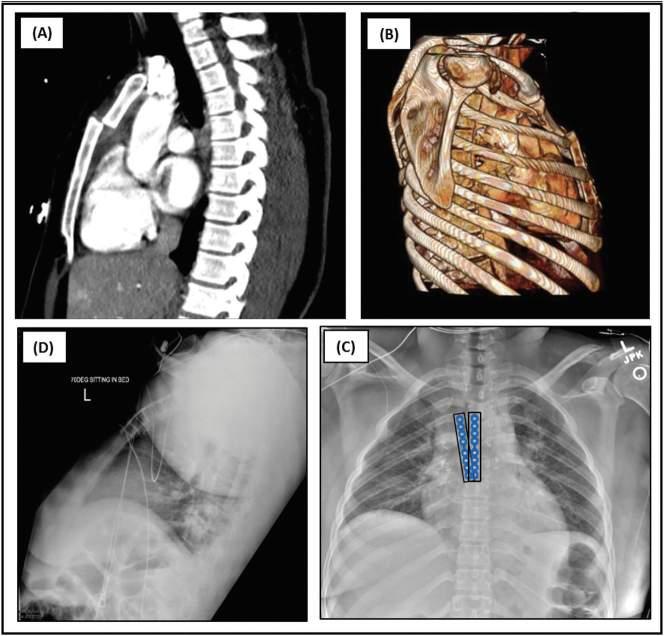
Manubrium
Body of sternum
Xiphoid process
Fig.2.6 (A)Preoperativesagittalcomputedtomographyofchestrevealingaposteriordislocationofthe sternalbodyonthemanubrium.(B)Preoperativesagittalthree-dimensionalreconstructionofchest. (C)Postoperativechestroentgenogramwithsternalfixationplatesandscrews (blue).(D)Postoperative lateralchestroentgenogramrevealingstablesternumwithfixationplateandscrews.(FromSarkeshik AA,JamalA,PerryPA.Manubriosternaljointdislocationduetobluntforcetrauma. TraumaCaseRep 2019;21:100187[Fig.1].ISSN2352-6440, https://doi.org/10.1016/j.tcr.2019.100187, http://www. sciencedirect.com/science/article/pii/S2352644019300214.)
involvingthethoracicnerves.Diseasesofthestructuresofthemediastinumare possibleandcanbedifficulttodiagnose.Pathologicprocessesthatinflamethe pleura,suchaspulmonaryembolus,infe ction,andBornholmdisease,mayalso confusethediagnosisandcomplicatetreatment,asmayundiagnosedsystemic diseasesthataffectthemanubriosternaljoint( Fig.2.13 ).
TREATMENT Initialtreatmentofthepainandfunctionaldisabilityassociatedwithmanubriosternalsyndromeincludesacombinationofnonsteroidal
Fig.2.8 Primarysepticarthritisofthemanubriosternaljoint.Enhancedcomputedtomographyaxial imageofthemass;noteismadeofthepresenceofsmallairbubblesrelatedtosuppurativesofttissue involvement (arrows).(FromCarnevaleA,RighiR,ManiscalcoP,etal.Primarysepticarthritisofthe manubriosternaljointinanimmunocompetentyoungpatient:acasereport. RadiolCaseRep. 2017;12(4):682 685[Fig.3].ISSN1930-0433, https://doi.org/10.1016/j.radcr.2017.08.006, http:// www.sciencedirect.com/science/article/pii/S1930043317302613.)
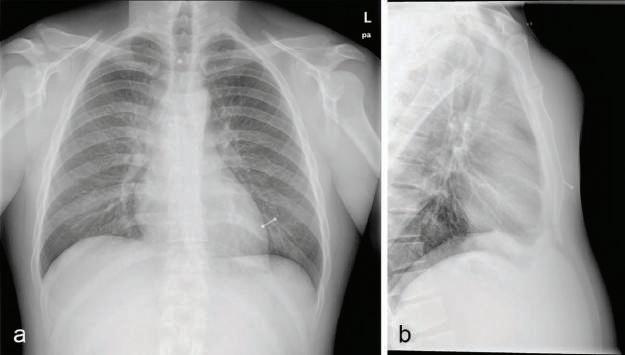
Fig.2.9 Septicarthritisofthemanubriosternaljoint.(a)Posterior-anterior(PA)chestroentgenogramand (b)lateral (L) viewofthesternum,showingasofttissueswellingoverthemanubriosternalregion;mild jointspacewideningandarticularsurfacesirregularityarenoted.(FromCarnevaleA,RighiR,Maniscalco P,etal.Primarysepticarthritisofthemanubriosternaljointinanimmunocompetentyoungpatient:a casereport. RadiolCaseRep.2017;12(4):682 685[Fig.1].ISSN1930-0433, https://doi.org/10.1016/j. radcr.2017.08.006, http://www.sciencedirect.com/science/article/pii/S1930043317302613.)
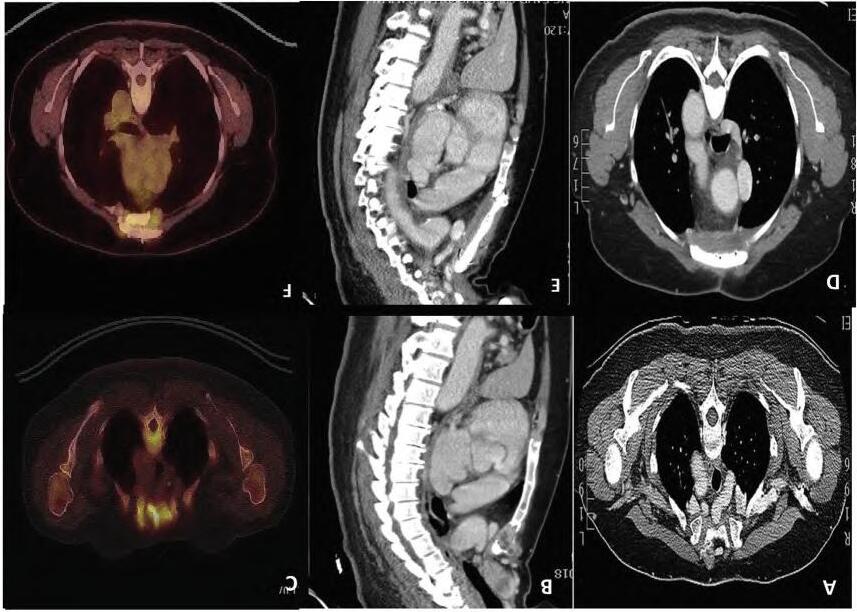
Fig.2.10 (A,B)Computedtomography(CT)scanofthethorax,axialandsagittalviews,showingmanubrialmetastasis.(C)Preoperativepositronemission tomography(PET)scanofthethoraxshowingmetastasis.(D,E)PostoperativeCTscanshowingreconstructionofthemanubriumsterniiwithanMMSplate.(F) PETscanofthethoraxafter2yearsshowingthemethylmethacrylatemarlexmeshplate(MMS)plateingoodpositionandnorecurrence.(FromChaudhryIUH, CheemaA,AqeelC,etal.Radicalresectionandimprovisedmanubriosternalreconstructiontechniqueforsolitarymanubriosternalmetastasisfrom papillarythyroidcancer. IntJSurgCaseRep.2020;76:278 281[Fig.2].ISSN2210-2612, https://doi.org/10.1016/j.ijscr.2020.09.201, http://www.sciencedirect.com/science/article/pii/S2210261220308749.)
Fig.2.11 Softtissueultrasonography,longitudinalplane,demonstratingalobulatedheterogeneouslyhypoechoicmass (straightarrows) overthemanubriosternaljoint (curvedarrow).(From CarnevaleA,RighiR,ManiscalcoP,etal.Primarysepticarthritisofthemanubriosternaljointinan immunocompetentyoungpatient:acasereport. RadiolCaseRep.2017;12(4):682 685[Fig.2]. ISSN1930-0433, https://doi.org/10.1016/j.radcr.2017.08.006 , http://www.sciencedirect.com/science/article/pii/S1930043317302613.)
Fig.2.12 Properneedleplacementforout-of-planeultrasound-guidedinjectionofthemanubriosternal joint.