HYPERTENSION
Definitions
• Hypertension is defined as a systolic BP (SBP) 130 mmHg and/or a BP (DBP) 80 mmHg in persons not taking antihypertensive medication. Those with a 120-129 mmHg systolic and < 80 mmHg diastolic are classified as elevated BP. These patients have increased risk of cardiovascular events by 1.1-1.5 fold compared with a normal BP mmHg) and have annual rate of developing hypertension of> 15%. The positive correlation between BP and cardiovascular morbidity and mortality is continuous and stronger for SBP than for DBP. Aging is associated with a progressive increase in SBP, a reduction in DBP a widening of pulse pressure. This is related to reduction in the compliance or stiffening the large conduit arteries.
• Isolated systolic hypertension (ISH) is defined as SBP 130 mmHg in the presence of DBP of :::; 80 mmHg. It is the predominant form of hypertension in the elderly. The accuracy of diagnosis and staging of hypertension is markedly improved by using SBP rather than DBP as the dominant criterion.
"' Essential (primary or idiopathic) hypertension is defined as high BP due to neither secondary cause nor a monogenic (mendalian) disorder. It accounts for 90% of all cases.
• Secondary hypertension is high BP caused by an identifiable and potentially curable disorder.
• Resistant hypertension is defined as BP 130/80 mmHg despite adequate doses of 3 or more antihypertensive drugs including a diuretic given for at least one month, or hypertension requi1ing 4 or more drugs regardless of blood pressure level achieved.
"' Spurious hypertension (or pseudohypertension) is artefactually elevated BP by indirect cuff measurement over a rigid, often calcified brachial artery.
• White coat hypertension. This term describes patients whose BP is > mmHg in an office or clinic setting, with a normal daytime ambulatory BP (<120/80 This is a relatively benign condition with low risk of morbid events. However, the risk may increase with long term follow up 6 years).
• Masked hypertension is a mirror image of white coat hypertension. The clinic is normal but ambulatory or home measurements are high and associated with high risk. It occurs 6% of the normotensive population.
• Hypertensive crises encompass both hypertensive emergencies and hypertensive urgencies. Hypertensive emergencies are defined as elevation in SBP and/or DBP 80 mmHg and/or> 120 mmHg respectively) associated with impending or progressive target organ damage such as major neurological changes, hypertensive encephalopathy, cerebral infarction, intracranial haemorrhage, acute LV failure, acute pulmonary oedema, aortic dissection, renal failure or eclampsia. Hypertensive urgencies denote isolated BP elevation of systolic and/or BP> 180 and/or 120 mmHg respectively without target organ damage.
• Accelerated hypertension is a hypertensive emergency associated with retinal haemorrhage and exudates.
• Malignant hypertension is a hypertensive emergency associated with papilloedema.
Prevalence
The global prevalence of hypertension in adults aged 25 years and above is 40%. The prevalence increases with age, so that well over half of the population above the age 55 have hypertension and in the 75+ age group, the prevalence is 70-80%. SBP in the population increases with advancing age throughout life whereas DBP tends to plateau or fall after age Consequently, the prevalence ofISH is much greater in the elderly than in middle-aged and younger individuals.
A higher percentage of men than women have hypertension until age 45. From age 45-54, the percentages men and women with hypertension are similar and after age 55, a much higher percentage of women have hypertension than do men.
The lifetime of developing hypertension is about 90% for men and women who were not hypertensive at 55-65 years old and survived to age 80-85.
In both sexes, hypertension is associated with higher body mass index (BMI) and black race.
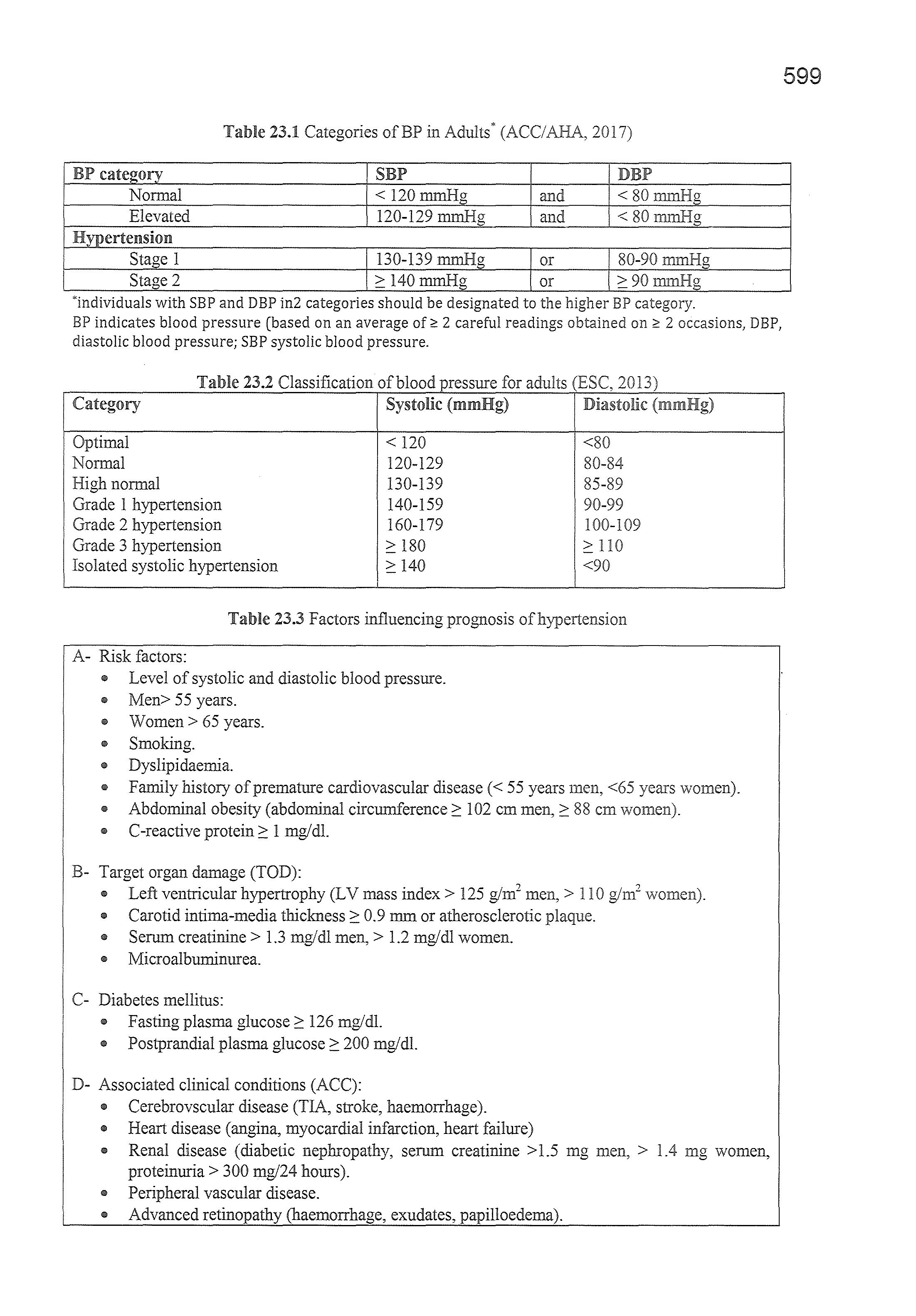
An updated classification of hypertension in adults> 18 years of age is given in table 23.1. The classification is based on the mean of two or more properly measured seated blood pressure readings on two or more office visits. Normal BP is defined as levels below 120/80 mmHg. Hypertension is defined as systolic BP 2: 130 or diastolic BP 2: 80 mmHg. Systolic BP of 120-129 or diastolic BP < 80 mmHg is classified as elevated BP. These patients are at increased risk for progression to hypertension.
Hypertension is divided into 2 stages:
- Stage 1 includes patients with systolic BP 130-139 or diastolic BP 80-89 mmHg.
- Stage 2 includes with systolic BP 2: 140 or diastolic BP 2: 90 mmHg.
A more elaborate classification of blood pressure is provided by the European Society of hypertension (ESH) and the European Society of Cardiology (ESC) (Table 23.2).
The continuous relationship between the level of blood pressure and cardiovascular risk makes any numerical definition and classification of hypertension arbitrary. Blood pressure should be measured on at least 2 occasions. If the hypertension is stage 1, measurement should be made within l month of each other. If stage 2, within a week and if more severe, immediate action is necessary. Patients should be clearly informed that a single elevated reading does not constitute a diagnosis of hypertension but is a sign that further observations are required.
risk
e The between BP and cardiovascular disease mortality is positive, strong and continuous. Death from ischaemic heart disease increases continuously and linearly from BP levels as low as 115 mmHg systolic and 75 mmHg diastolic upward.
e An increment of 20 mmHg in SPB or 10 mmHg in DPB in middle aged and elderly persons is associated with a twofold increase in cardiovascular disease (both ischaemic heart disease and stroke) the entire range BP. Likewise a decrease of 20 mmHg in SBP or 0 mmHg DBP halves cardiovascular mortality.
e Individuals with a BP in the elevated BP range (SBP 120-129 mmHg or DBP < 80 mmHg) also have a significantly greater risk of developing a cardiovascular event than those \vith a normal BP (<120/80 -
Total cardiovascular
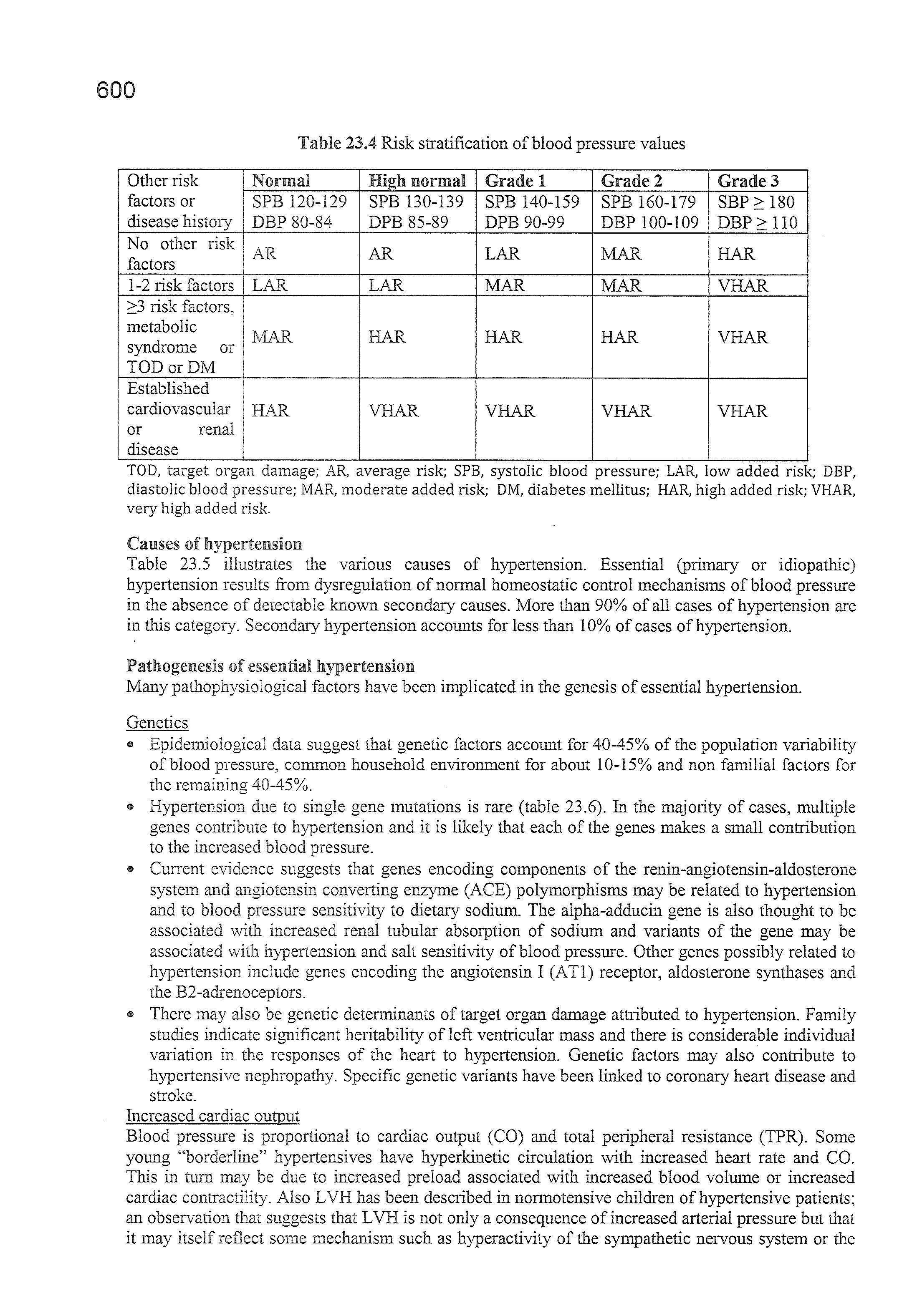
The presence of other cardiovascular risk factors particularly diabetes mellitus, target organ damage (TOD) and associated cardiovascular and renal disease substantially increase the risk of hypertension regardless of its level. The level of risk is used to determine the threshold and type of therapeutic intervention. Table 23.3 indicates the most common risk factors, target organ damage and associated clinical conditions which are used to stratify risk On the basis of such association, the ESH/ESC proposed a classification of the level of added risk associated with different values of blood pressure (Table 23.4).
The terms low, moderate high and very high added risk are calibrated to indicate an approximate 10years risk of cardiovascular disease of <15%, 15-20%, 20-30% and >30% respectively or an approximate absolute risk of fatal cardiovascular disease of <4%, 4-5%, 5-8% and >8% respectively.
Table 23.1 Categories of BP in Adults*
BP category
Normal < 120mmHg and <80mmHg
Elevated 120-129 mmHg and <80mmHg
Hypertension
Stage 1
130-139 mmHg or 80-90mmHg
Stage 2 :::: 140mmHg or ::'.:90mmHg
*individuals with SEP and DBP in2 categories should be designated to the higher BP category.
BP indicates blood pressure (based on an average 2 careful readings obtained 2 occasions, DBP, diastolic blood pressure; SBP systolic blood pressure.
Table 23.2 Classification of blood ressure for adults (ESC, Category
Optimal < 120 <80
Normal 120-129 80-84
High normal 130-139 85-89
Grade 1 hypertension 140-159 90-99
Grade 2 hypertension 160-179 l 00-109
Grade 3 hypertension :::: 180 :::: lO
Isolated systolic hypertension :::: 140 <90
Table 23.3 Factors influencing prognosis ofhypertension
A- Risk factors:
" Level of systolic and diastolic blood pressure.
" Men> 55 years
., Women > 65 years.
e Smoking.
• Dyslipidaemia.
" Family history of premature cardiovascular disease(< 55 years men, <65 years
• Abdominal obesity (abdominal circumference:::: 102 cm men,:::: 88 cm
• C-reactive protein:::: l mg/dl.
B- Target organ damage (TOD):
" Left ventricular hypertrophy (LV mass index > 125 g/m2 men, > l 0 glm2
• Carotid intima-media thickness:::: 0.9 mm or atherosclerotic plaque.
e Serum creatinine > 1.3 mg/dl men,> 1.2 mg/dl women.
" Microalbuminurea.
C- Diabetes mellitus:
" Fasting plasma glucose:::: 126 mg/dl.
" Postprandial plasma glucose:::: 200 mg/dl.
D- Associated clinical conditions (ACC):
" Cerebrovscular disease (TIA, stroke, haemorrhage).
• Heart disease (angina, myocardial infarction, heart failure)
" Renal disease (diabetic nephropathy, serum creatinine > 1.5 mg men, > .4 mg women, proteinuria > 300 mg/24 hours).
• Peripheral vascular disease.
• Advanced retinopathy (haemorrhage, exudates, papilloedema).
Table 23.4 Risk stratification of blood pressure values
Other risk Normal High normal Grade 1
Grade 2 Grade 3 factors or SPB 120-129 SPB 130-139 SPB 140-159 SPB 160-179 SBP 180 disease history DBP 80-84 DPB 85-89 DPB 90-99 DBP 100-109 110
No other risk AR AR LAR MAR HAR factors
1-2 risk factors LAR LAR MAR MAR VHAR risk factors, metabolic MAR HAR HAR HAR VHAR syndrome or TODorDM
Established cardiovascular HAR VHAR VHAR VHAR VHAR or renal disease
TOD, target organ damage; AR, average risk; SPB, systolic blood pressure; LAR, low added risk; DBP, diastolic blood pressure; MAR, moderate added risk; DM, diabetes mellitus; HAR, high added risk; VHAR, very high added risk.
Causes of hv1oer·te11sum
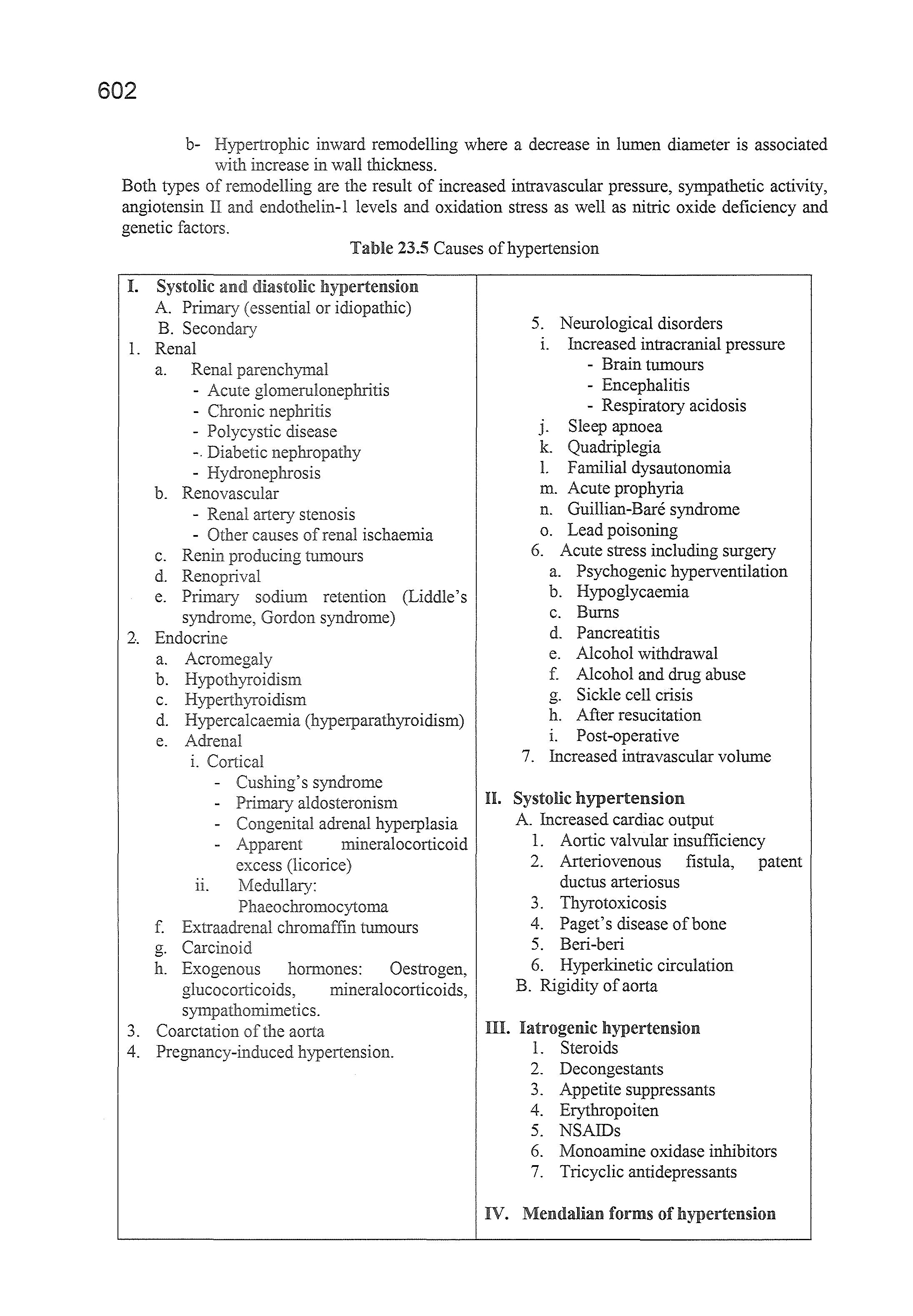
Table 23.5 illustrates the various causes of hypertension. Essential (primary or idiopathic) hypertension results from dysregulation of normal homeostatic control mechanisms of blood pressure in the absence of detectable known secondary causes. More than 90% of all cases of hypertension are in this category. Secondary hypertension accounts for less than 10% of cases of hypertension.
Pathogenesis of essential hypertension
Many pathophysiological factors have been implicated in the genesis of essential hypertension.
Genetics
" Epidemiological data suggest that genetic factors account for 40-45% of the population variability of blood pressure, common household environment for about 10-15% and non familial factors for the remaining 40-45%.
" Hypertension due to single gene mutations is rare (table 23.6). In the majority of cases, multiple genes contribute to hypertension and it is likely that each of the genes makes a small contribution to the increased blood pressure.
" Current evidence suggests that genes encoding components of the renin-angiotensin-aldosterone system and angiotensin converting enzyme (ACE) polymorphisms may be related to hypertension and to blood pressure sensitivity to dietary sodium. The alpha-adducin gene is also thought to be associated with increased renal tubular absorption of sodium and variants of the gene may be associated with hypertension and salt sensitivity of blood pressure. Other genes possibly related to hypertension include genes encoding the angiotensin I (ATl) receptor, aldosterone synthases and the B2-adrenoceptors.
" There may also be genetic determinants of target organ damage attributed to hypertension. Family studies indicate significant heritability of left ventricular mass and there is considerable individual variation in the responses of the heart to hypertension. Genetic factors may also contribute to hypertensive nephropathy. Specific genetic variants have been linked to coronary heart disease and stroke.
Increased cardiac output
Blood pressure is proportional to cardiac output (CO) and total peripheral resistance (TPR). Some young "borderline" hypertensives have hyperkinetic circulation with increased heart rate and CO. This in turn may be due to increased preload associated with increased blood volume or increased cardiac contractility. Also LVH has been described in normotensive children of hypertensive patients; an observation that suggests that LVH is not only a consequence of increased arterial pressure but that it may itself reflect some mechanism such as hyperactivity of the sympathetic nervous system or the
renin-angiotensin system that causes both LVH and hypertension. In mature primary hypertension, the CO is normal and TPR elevated. The switch from elevated CO to elevated TPR may be due to autoregulatory vasoconstriction in response to organ hyperperfusion. Thereafter, hypertension becomes self sustaining due to the accelerated arteriosclerosis. Plasma volume is usually normal or slightly lower than normal in established primary hypertension. However it may still be higher than it should be given the elevated blood pressure.
Sodium and potassium
" For each 50 mmoV day increase in sodium intake, BP increases by about 5/3 and if sodium intake is lowered, BP generally falls.
" Low potassium diets also predispose to hypertension and inclusion of potassium rich foods in the diet lowers BP.
" The main consequence of sodium retention and potassium depletion is an increase in the vascular tone. Sodium excess activates some pressor mechanisms (such as increases of intracellular calcium and plasma catecholamines and upregulation of angiotensin II type I receptors) and it increases insulin resistance. About half of hypertensive patients are particularly salt sensitive (as defined by the blood pressure rise induced by sodium loading) as compared with about a quarter of normotensive controls. The mechanism of sodium sensitivity may be renal sodium retention. This may be related to 4 mechanisms:
Rightward shift of the renal pressure-natriuresis curve.
Secretion of a sodium pump inhibitor (endogenous ouabain) by the adrenal cortex. Inhibition of the sodium pump increases intracellular sodium which subsequently increases intracellular calcium (and vascular tone) by sodium-calcium exchange.
Inappropriately high renin levels.
Reduced nephron number.
Sympathetic nervous system
" Increased sympathetic activity and/or reduced parasympathetic activity, increase heart rate, stroke volume, cardiac output, peripheral resistance, norepinephrine and epinephrine secretion by the adrenal medulla and renin secretion by activation of the beta-adrenergic receptors on the juxtaglomerular apparatus of the kidney. All of these effects raise BP.
" The normal response to an elevated BP is activation of baroreceptors to reflexly lower the pressure. There is evidence that in hypertensive individuals, baroreceptor sensitivity is reduced, blunting the normal response to an elevated BP and allowing for the maintenance of the hypertension.
" Renal sympathetic nerve stimulation is increased in hypertensive patients, inducing renal tubular sodium and water reabsorption resulting in intravascular volume expansion and increased BP.
" Chronic sympathetic stimulation induces vascular remodelling and left ventricular hypertrophy presumably by action of norepinephrine on its receptors as well as on release of various trophic factors including transforming growth factor-beta, insulin-like growth factor 1 and fibroblast growth factors.
Vascular reactivity
" Hypertensive patients manifest greater vasoconstrictor responses to infused norepinephrine than normotensive controls. The expected downregulation of noradrenergic receptors in response to increased circulating norepinephrine dose not occur in hypertensive patients. This may be genetic in origin.
" Exposure to stress increases sympathetic outflow and repeated stress induced vasoconstriction may result in vascular hypertrophy leading to increased peripheral vascular resistance and BP.
Vascular remodelling
" There are two types of arterial remodelling in hypertension: a- Eutrophic inward remodelling in which there is decease in lumen diameter without a change in arterial wall thickness.
b- inward remodelling where a decrease in lumen diameter is associated with increase in wall thiclrness.
Both types of remodelling are the result of increased intravascular pressure, sympathetic activity, angiotensin ll and endothelin-1 levels and oxidation stress as well as nitric oxide deficiency and genetic factors.
Table 23.5 Causes of hypertension
I. Systolic and diastolic hypertension
A. Primary (essential or idiopathic)
B. Secondary
1. Renal
a. Renal parenchymal
- Acute glomerulonephritis
- Chronic
- Polycystic disease
-. Diabetic nephropathy
- Hydronephrosis
b. Renovascular
- Renal artery stenosis
- Other causes of renal ischaernia
c. Renin tumours
d. Renoprival
e. Primary sodium retention (Liddle' s syndrome, Gordon syndrome)
2. Endocrine
a. Acromegaly
b.
C.
d. Hypercalcaernia (hyperparathyroidism)
e. Adrenal
i. Cortical
- Cushing' s syndrome
- Primary aldosteronism '-"V""'"'"''"'.u adrenal hyperplasia
- Apparent mineralocorticoid excess (licorice)
IL Medullary: Phaeochro1nocytoma
f. Extraadrenal chromaffin tumours
g. Carcinoid
h. Exogenous hormones: Oestrogen, glucocorticoids, rnineralocorticoids, sympathornimetics.
3. Coarctation of the aorta
4. Pregnancy-induced hypertension.
5. Neurological disorders
i. Increased intracranial pressure
- Brain tumours
- Encephalitis
- Respiratory acidosis
J. Sleep apnoea
k. Quadriplegia
L Farnilial dysautonornia
m. Acute prophyria
n. Guillian-Bare syndrome
o. Lead poisoning
6. Acute stress including surgery
a. Psychogenic hyperventilation
b. Hypoglycaemia
c. Burns
d. Pancreatitis
e. Alcohol withdrawal
f. Alcohol and drug abuse
g. Sickle cell crisis
h. After resucitation
i. Post-operative
7. Increased intravascular volume
II. Systolic hypertension
A. Increased cardiac output
1. Aortic valvular insufficiency
2. Arteriovenous fistula, patent ductus arteriosus
3. Thyrotoxicosis
4. Paget's disease of bone
5. Beri-beri
6. Hyperkinetic circulation
B. Rigidity of aorta
ID. Iatrogenic hypertension
1. Steroids
2. Decongestants
3. Appetite suppressants
4. Erythropoiten
5. NSAIDs
6. Monoamine oxidase inhibitors
7. Tricyclic antidepressants
IV. Mendalian forms of hypertension
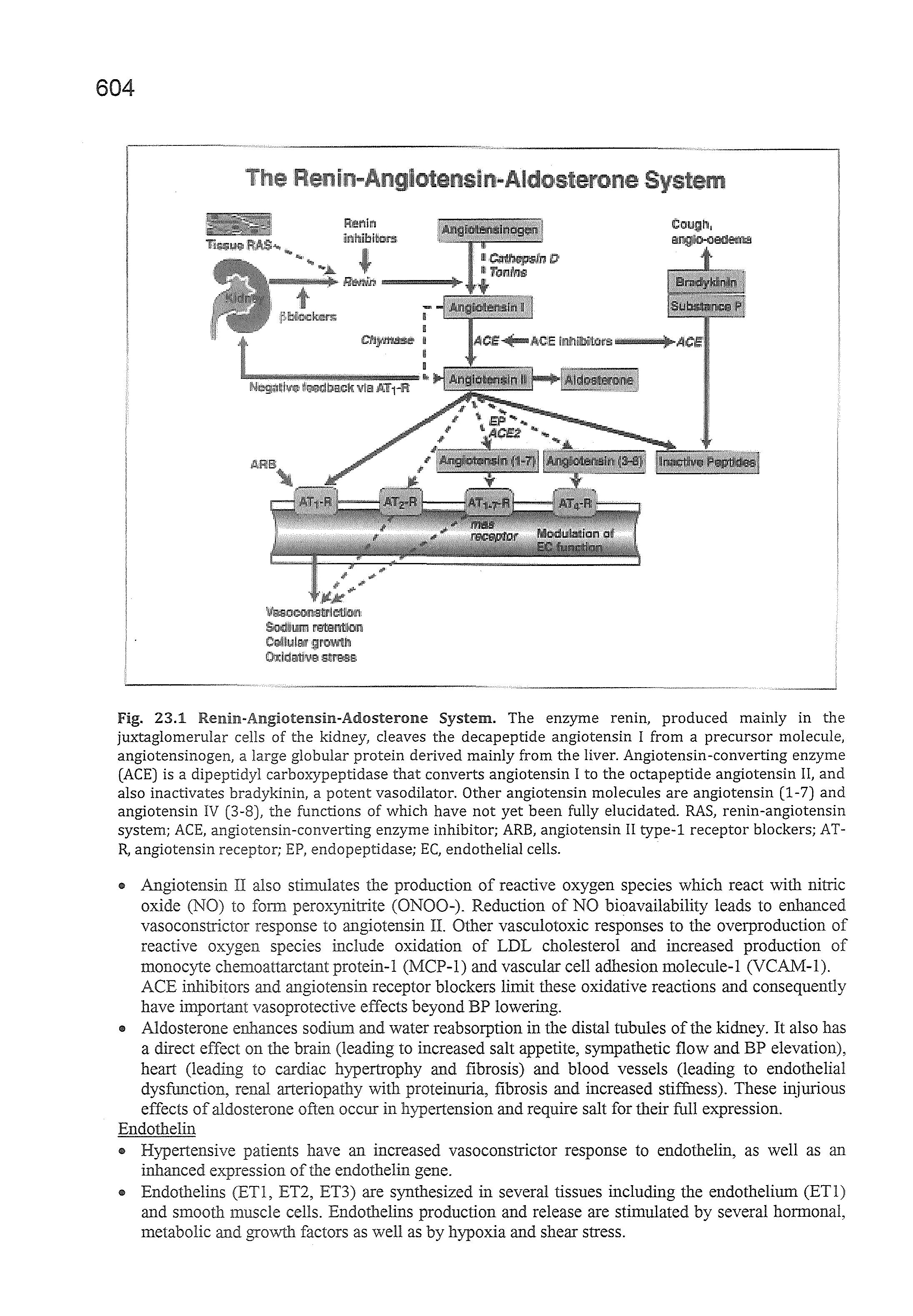
Fig. 23.1 Renin-Angi.otensin-Adosterone System. The enzyme renin, produced mainly in the juxtaglomerular cells of the kidney, deaves the decapeptide angiotensin I from a precursor molecule, angiotensinogen, a large globular protein derived mainly from the liver. Angiotensin-converting enzyme (ACE) is a dipeptidyl carboxypeptidase that converts angiotensin I to the octapeptide angiotensin II, and also inactivates bradykinin, a potent vasodilator. Other angiotensin molecules are angiotensin (1-7) and angiotensin IV (3-8), the functions of which have not yet been fully elucidated. RAS, renin-angiotensin system; ACE, angiotensin-converting enzyme inhibitor; ARB, angiotensin II type-1 receptor blockers; ATR, angiotensin receptor; EP, endopeptidase; EC, endothelial cells.
• Angiotensin II also stimulates the production of reactive oxygen species which react with nitric oxide (NO) to form peroxynitrite (ONOO-). Reduction of NO bioavailability leads to enhanced vasoconstrictor response to angiotensin II. Other vasculotoxic responses to the overproduction of reactive oxygen species include oxidation of LDL cholesterol and increased production of monocyte chemoattarctant protein- I (MCP-1) and vascular cell adhesion molecule- I (VCAM-1 ). ACE inhibitors and angiotensin receptor blockers limit these oxidative reactions and consequently have important vasoprotective effects beyond BP lowering.
• Aldosterone enhances sodium and water reabsorption in the distal tubules of the kidney. It also has a direct effect on the brain (leading to increased salt appetite, sympathetic flow and BP elevation), heart (leading to cardiac hypertrophy and fibrosis) and blood vessels (leading to endothelial dysfunction, renal arteriopathy with proteinuria, fibrosis and increased stiffness). These injurious effects of aldosterone often occur in hypertension and require salt for their full expression.
Endothelin
e Hypertensive patients have an increased vasoconstrictor response to endothelin, as well as an inhanced expression of the endothelin gene.
e Endothelins ET2, ET3) are synthesized in several tissues including the endothelium (ETl) and smooth muscle cells. Endothelins production and release are stimulated by several hormonal, metabolic and growth factors as well as by hypoxia and shear stress.
e This may be related to congenital oligo-nephropathy, a reduced number of nephrons at birth that leads to both systemic and glomerular hypertension.
e Regardless of how low birth weight predisposes to hypertension (as well as diabetes and coronary heart disease), the prevention of low birth weight may be an effective way to prevent hypertension. Low birth weight is usually associated with teenage pregnancy, short intervals between pregnancies, inadequate nutrition and familial aggregation.
Diagnosis of hvioe1rtensJ1on
Uncomplicated hypertension is usually asymptomatic and many of the symptoms often attributed to hypertension such as headache, tinnitus, dizziness and fainting are probably psychogenic in origin. They may reflect hyperventilation induced by anxiety over the diagnosis of a life long disease, which threatens well-being and survival. However, recent data indicate that surprisingly a person's general sense of well-being often improves during initiation of medical treatment of hypertension. These new data suggest that hypertension may not be as asymptomatic as was previously assumed. Even if not totally asymptomatic, hypertension can go unrecognised for years because overt symptoms and signs generally coincide with the onset of target organ damage.
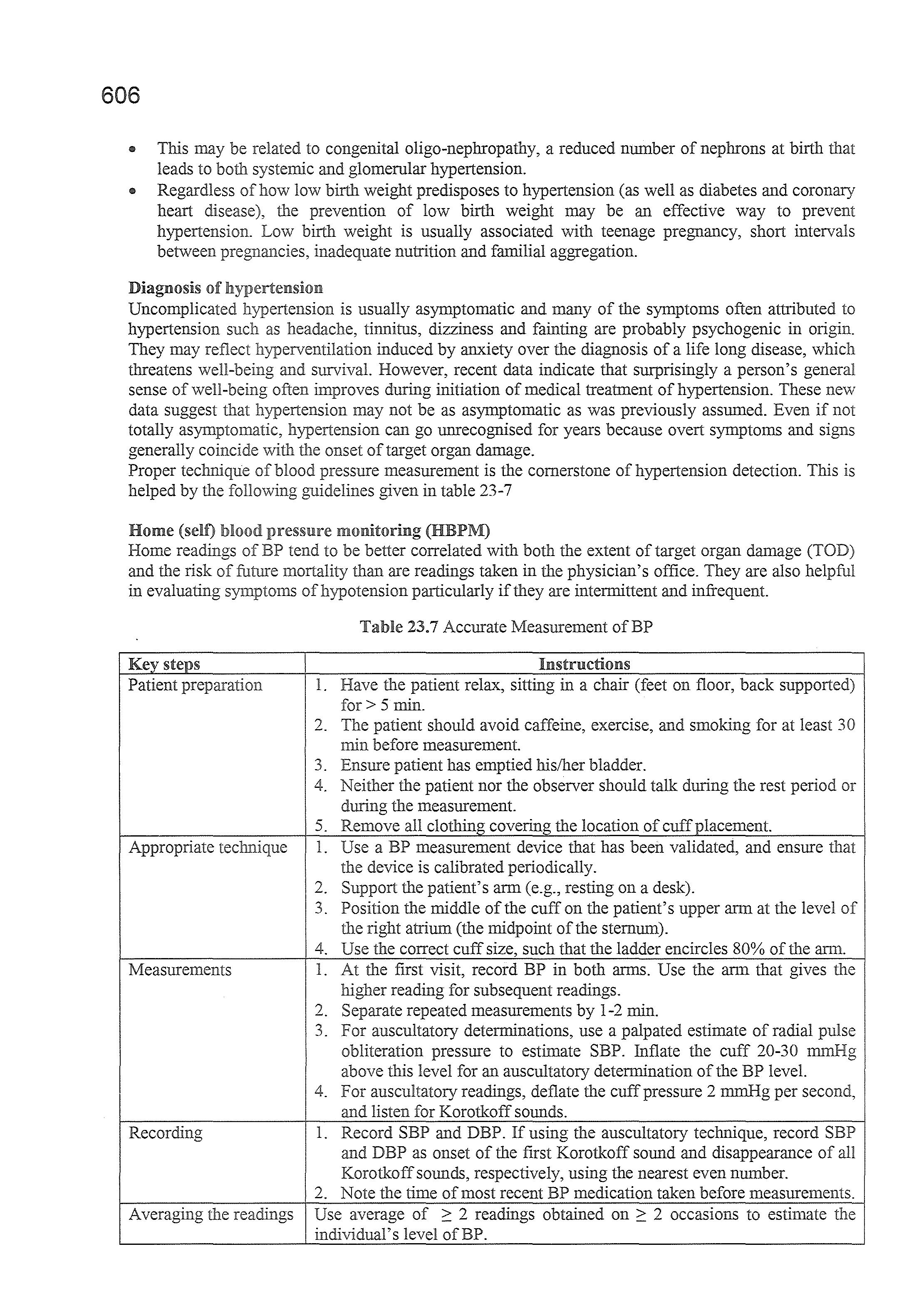
Proper technique of blood pressure measurement is the cornerstone of hypertension detection. This is helped by the guidelines given in table 23-7
Home (self) blood pressure monitoring (HBPM)
Home readings of BP tend to be better correlated with both the extent of target organ damage (TOD) and the risk of future mortality than are readings taken in the physician's office. They are also helpful in evaluating symptoms ofhypotension particularly if they are intermittent and infrequent.
Table 23.7 Accurate Measurement of BP
Key steps Instructions
Patient prP:p::.miti()n
1. Have the patient relax, sitting in a chair (feet on floor, back supported) for> 5 min.
2. The patient should avoid caffeine, exercise, and smoking for at least 30 min before measurement.
3. Ensure patient has emptied his/her bladder.
4. Neither the patient nor the observer should talk during the rest period or during the measurement.
5. Remove all clothing covering the location of cuff placement. Appropriate tPrhnir;.""
1. Use a BP measurement device that has been validated, and ensure that the device is calibrated periodically.
2. Support the patient's arm (e.g., resting on a desk).
3. Position the middle of the cuff on the patient's upper arm at the level of the right atrium (the midpoint of the sternum).
4. Use the correct cuff size, such that the ladder encircles 80% of the arm.
Measurements
Recording
1. At the first visit, record BP in both arms. Use the arm that gives the higher reading for subsequent readings.
2. Separate repeated measurements by 1-2 min.
3. For auscultatory determinations, use a palpated estimate of radial pulse obliteration pressure to estimate SBP. Inflate the cuff 20-30 above this level for an auscultatory determination of the BP level.
4. For auscultatory readings, deflate the cuff pressure 2 mmHg per second, and listen for Korotkoff sounds.
1. Record SBP and DBP. If using the auscultatory technique, record SBP and DBP as onset of the first Korotkoff sound and disappearance of all Korotkoff sounds, respectively, using the nearest even number.
2. Note the time of most recent BP medication taken before measurements. Averaging the readings Use average of 2: 2 readings obtained on 2: 2 occasions to estimate the individual's level of BP.
Lifestyle changes and a close follow up should be implemented in all patients with isolated office hypertension. Drug treatment is instituted when there is evidence of organ damage or high cardiovascular risk profile.
A less frequent phenomenon is masked hypertension or "reverse of isolated office hypertension". This refers to individuals with normal office blood pressure (<130/80 mmHg) but elevated ambulatory blood pressure values (isolated ambulatory hypertension). These individuals display a greater than normal prevalence of target organ damage and both their BP and their concomitant risk factors should be managed aggressively.
• Refractory hypertension. This may be the result of a genuinely resistant hypertension, noncompliance or an exaggerated white coat hypertension. The best clue to this exaggerated white coat effect is a persistently elevated office pressure in the absence of target organ damage. Such patients can be evaluated either with ABPM or initially with home monitoring. Another cause of refractory hypertension is the sleep apnoea syndrome. A clue to this may be that although the average BP level and heart rate fall during night, their variability increases.
e Intermittent symptoms possibly related to blood pressure. Episodes of light headedness, particularly in patients who are on antihypertensive medication, may be a manifestation of transient hypotension. This can potentially be detected by ABPM.
• Episodic hypertension. Episodic symptoms accompanied by transient elevation in BP may occur in a variety of conditions including phaeochromocytoma and panic attacks.
• Episodic hypotension.
- ABPM may be helpful in cases of idiopathic orthostatic hypotension because many patients who are orthostatic during the day are hypertensives during the night. There are huge swings of BP during the day, depending to a large extent on changes of posture and physical activity and relatively stable but high pressure at night when the patient is supine. In contrast, the heart rate is relatively constant throughout day and night.
- Autonomic neuropathy is common in type l diabetes and has been related to interruption of both vagal and sympathetic control of the circulation. The former is manifested by a relatively fixed heart rate and the latter by orthostatic hypotension. In common with patients with idiopathic orthostatic hypotension, BP remains high at night.
Compared with casual BP measurements, ABPM measurements are better predictor of LVH, cardiac function and overall scores summing optic, carotid, renal and peripheral vascular damage resulting from elevated BP. Most normotensive patients and perhaps 80% of hypertensives have at least 10% drop in BP during sleep compared with daytime average. There is about 3-fold increased risk of cardiovascular events among those with non dipping BP.
Technique and precautions
When measuring 24-hour blood pressure, care should be taken to:
e Use only devices validated by international standardized protocols.
• Use cuffs of appropriate size and compare the initial values with those from a sphygmornanometer to check that the differences are not greater than ± 5 mmHg.
• Set the automatic readings at no more than 30 minutes intervals and have most hours represented if some readings are rejected because of artefacts.
• Instruct the patients to engage in normal activities but to refrain from strenuous exercise and to keep the arm extended and still at the time of measurement.
• Ask the patient to provide information in a diary on unusual events and on duration and quality of night sleep. There is evidence that subjects in whom nocturnal hypotension is blunted and thus exhibit a relatively high night blood pressure may have an unfavourable prognosis.
• Obtain another ambulatory blood pressure monitoring if the first examination has less than 70% of the expected values because of a high number of artefacts.
• Normal 24-hour ambulatory BP is <115/75 mmHg with a mean of< 120/80 mmHg during the day and< 100/65 mmHg at night. Blood pressure usually falls about 15% at night, during sleep, to rise to daytime levels 1-2 hours before awakening. Blood pressure usually peaks in the late afternoon and evening. Some patients (called non-dippers) have a smaller fall of blood pressure during sleep, sometimes none. These patients are at greater risk for cardiovascular disease, a more rapid
• Previous antihypertensive therapy:
Drugs used efficacy and adverse effects.
• Personal, family and environmental factors that may influence blood pressure, cardiovascular risk as well the course and outcome of therapy.
Physical examination
In addition to methodological blood pressure measurement (see earlier), physical examination should search for the following manifestations:
• Signs suggesting secondary hypertension:
Features of Cushing syndrome.
Skin stigmata ofneurofibromatosis (phaeochromocytoma).
Diminished and delayed femoral pulse and reduced femoral blood pressure (aortic coarctation, aortic disease).
Palpation of enlarged kidneys (polycystic kidney)
Ausculatation ofprecordial or back murmurs (aortic coarctation or aortic disease or abdominal murmurs (renovascular hypertension).
• Signs of target organ damage:
Brain: murmurs over neck arteries, motor or sensory defects.
Retina: fundoscopic abnormalities.
Heart: cardiac enlargement, arrhythmias, gallop sounds, pulmonary crackles, dependent oedema.
Peripheral arteries: absence, reduction, or asymmetry of pulses, cold extremities, ischaemic skin lesions.
Laboratory investigations
These should be directed at providing evidence of additional risk factors, searching for secondary hypertension and assessing presence or absence of target organ damage. They include routine tests, recommended tests (based on recent studies) and specific tests for extended evaluation of hypertensive complications and causes of secondary hypertension.
• Routine tests: Electrocardiogram.
Plasma glucose (preferably fasting).
Serum total cholesterol.
Serum high-density lipoprotein (HDL)cholesterol.
Fasting serum triglycerides.
Serum uric acid.
Serum creatinine.
Serum potassium.
Haemoglobin and haematocrit.
Urinalysis (dipstick test and urinary sediment examination).
• Recommended tests: Echocardiogram
Carotid (and femoral) ultrasound.
C-reactive protein.
Microalburninuria (essential in diabetics).
Quantitative proteinuria (if dipstick is positive).
Fundoscopy (in severe hypertension).
• Extended evaluation:
Complicated hypertension: tests of cerebral, cardiac and renal function. Search for secondary hypertension: measurement of renin, aldosterone, corticosteroids, catecholamines, arteriography, renal and adrenal ultrasound, computed tomography (CT) and magnetic resonance imaging (MRI).
Target organ damage (TOD)
Hypertensive cardiac damage is identified by the following features
velocity measurement and the augmentation index measurement device (Sphygmocor which measures the boost given to the peak systolic pressure waveform by the reflected wave that arrives back at the aorta). Both are of interest particularly in view of the claim that aortic blood pressure (and therefore the pressure exe1ted on the heart and brain) may be different from that which is usually measured at the arm, may be better predictive of outcomes and may be differently affected by different antihypertensive drugs.
e Detecting endothelial dysfunction:
Endothelial dysfunction or damage is an early marker of cardiovascular damage. Current studies on circulating markers of endothelial damage may soon provide simpler tests of endothelial dysfunction. Such markers include nitric oxide and its metabolites, endothelins, cytokines and adhesion molecules.
Pseudo-hypertension
This term refers to the rare situation where BP measurements by the usual indirect sphygmomanometry are much higher than direct intravascular measurements. These differences are usually attributed to very stiff and calcified arteries that are nearly impossible to compress with the bladder in the usual BP cuff. The Osler manoeuvre (palpating the walls of the brachial artery when blood flow has been interrupted by inflating the cuff higher than systolic pressure) has been recommended as a simple but neither sensitive nor specific measure to diagnose the condition. More precise methods involve intra-arterial measurements and perhaps an infusion of an intravenous antihypertensive agent to calibrate the difference between direct and indirect BP measurements. The benefit of lowering BP in older patients with stiff arteries is well established.
Hypertensive renal damage is identified by the following features
• Blood urea nitrogen (BUN), serum creatinine, serum electrolytes and urinalysis (particularly for proteinuria) are the only measures of renal function that are currently routinely recommended for evaluation of all hypertensive patients. However, these are very insensitive indicators of the onset and progression of hypertensive nephrosclerosis. The presence of chronic kidney disease (CKD) is confirmed by renal biopsy or glomerular filtration rate (GFR) of <60 ml/minute/ l. 73 m 2 for longer than 3 months. The clinical associations are serum creatinine of 2:: 1.2 mg/dl in women and 2:: 1.4 mg/dl in men and microalbuminuria (30-300 mg/ day) or albuminuria (> 300 mg/ day). A slight increase in serum creatinine and urate may sometimes occur when antihypertensive therapy is instituted or intensified but this should not be taken as a sign of progressive renal deterioration. Hyperuricaemia, defined as serum urate level above 7 mg/dl is frequently seen in untreated hypertensives and has also been shown to correlate with the existence of nephrosclerosis.
" Microalbuminuria occurs in 5-40% of nondiabetic persons with essential hypertension and is a marker of BP control. BP control with all agents (except dihydropyridine calcium channel blockers and central or peripheral sympathetic blockers) reduces albuminuria. The amount of MA is proportional to the severity of systolic, diastolic and mean BP elevation. Moreover, MA predicts the development of ischaemic cardiovascular events related to the development of atherosclerosis. It is an indicator of increased vascular permeability and hence altered barrier function of the endothelium. When albumin leaks into the interstitial space, cellular injury occurs secondary to free radical and cytokine production enhanced by the presence of albumin. Subjects with MA and type 2 diabetes mellitus have approximately total mortality of 8% and cardiovascular mortality of 4% annually. These values are up to 4 times higher than those of patients without MA. Similar increases in cardiovascular mortality are also present in people with MA and without diabetes. Routine assessment of MA in diabetic patients is well advised, but in hypertensives without diabetes mellitus its value is still debatable. Perhaps all hypertensives with trace proteinuria (300500 µg/day) when measured by conventional dipsticks could have a spot urine measurement of the albumin/creatinine ratio. A ratio of 30-200 mg albumin/ creatinine signifies microalbuminuria and >200 signifies CKD.
e Hypertension is both a cause and complication of CKD and lowering BP slows the progression of renal disease. The systolic BP goal in patients with CKD is <130 mmHg, with monitoring of the estimated filtration rate.
Renal. Parenchymal disease
This is the most common cause of secondary hypertension in adults. It accounts for 2-4% of cases of hypertension. The renal parenchymal disease can be acute or chronic, unilateral or bilateral and does not have to be associated vvith renal insufficiency. Almost all forms of renal parenchymal disease may lead to These include the glomerulonephritides, diabetic nephropathy, chronic pyelonephritis, analgesic nephropathy and adult polycystic kidney disease. Chronic renal disease is defined as a reduction in the golmerular filtration rate to <60 ml/min/ 1.73 rn2 or persistent albuminuria of>300 mg/day for >3 months.
Several mechanisms have been proposed for elevated BP in renal parenchymal disease: Inability of the reduced renal mass to excrete salt and water is the most important mechanism. Activation of renin-angiotensin-aldosterone system.
Activation of sympathetic nervous system
Increased secretion of an endogenous oubain-like natriuretic factor that inhibits the Na+-K+ATPase pump.
Increased production of an endogenous asymmetrical dimethylarginine (ADMA), a nitric oxide synthase inhibitor.
Secondary
Investigations
Assessing the presence of protein, erythrocytes and leucocytes in the urine as well as measuring serum creatinine concentration are the appropriate functional screening tests. Creatinine clearance should be calculated with the Cockcroft-Gault, the modification of diet in renal disease (MDRD) or the chronic kidney disease epidemiology collaboration (CKD-EPI) equations. If these tests are positive, a detailed work-up for kidney disease should follow. Renal parenchymal disease may be excluded and serum creatinine concentration are repeatedly normal. Renal ultrasound has now almost completely replaced intravenous urography in the anatomical exploration of the kidney. It provides all the necessary anatomical data about kidney size and shape, cortical thickness, urinary tract obstruction and renal masses.
Acute renal disease
e Hypertension may appear with any sudden severe insult to the kidneys that markedly impair excretion of salt and water or reduces renal blood flow (e.g. cholesterol emboli).
e Nonsteroidal anti-inflammatory drugs (NSAIDs) and ACEis or ARBs may suddenly worsen renal function in with pre-existing renal disease. NSAIDs block the synthesis of prostaglandins which act as renal vasodilators and both ACEis and ARBs release the compensatory renal efferent arteriolar vasoconstriction in patients with bilateral renovascular disease thus sharply reduce the golmerular filtration rate.
Chronic renal disease
@ All chronic renal diseases are associated with a higher prevalence of hypertension and hypertension accelerates the progression of renal damage. Control of hypertension can slow or stop progression of renal disease and of its cardiovascular sequelae. In patients with diabetes, control of hypertension is more cost-effective than intensive glycemic control or reduction in hypercholesterolaernia.
Haemodialysis patients
In patients with end-stage renal disease who are on dialysis, hypertension is a significant risk factor for mortality. Elevated BP tends to fall progressively after dialysis is complete, remains depressed during the remainder of the first 24 hours and rises again during the second day as a consequence of excessive fluid retention. achieving dry weight with 8-hour haemodialysis can BP be controlled.
Renal transplantation
Although renal may cure essential hypertension, various problems can result in hypertension in about 50% of patients within one year. These include stenosis of the renal artery at the
Investigations
e Morning plasma aldosterone concentration (in ng/dl) to plasma renin activity (in ng/ ml/hour) ratio >20 with plasma aldosterone concenation at least 12 ng/dl, should prompt confirmatory testing. A ratio >70 with a plasma aldosterone concentration ?J5 ng/dl and plasma renin activity :Sl ng/ml/hour is diagnostic of primary aldosteronism.
e If the screening test is positive, the next step is an aldosterone suppression test. After hypokalaemia is corrected, patients are given a high sodium diet (4-6 g/day as tablets) for 3 days. On day 3, a 24 hour urine specimen is collected for measurement of aldosterone, sodium and potassium. A 24 hour urinary sodium excretion >200 mg is considered adequate documentation of sodium repletion. Urinary aldosterone excretion> 12 mecq/ 24 hour is diagnostic of aldosteronism. Imaging studies to detect adenomata include CT and MRI. All adenomata ;::LO cm in diameter can be located accurately.
e Adrenal venous aldosterone levels should be measured when the biochemical findings are highly suggestive of an adenoma but the adrenal CT or MRI is ambiguous.
Treatment
e Medical therapy is indicated in patients with adrenal hyperplasia, bilateral adrenal adenomas and those who are poor surgical risks. A combination of a diuretic with either spironolactone 100-200 mg/day or eplerenone 50-100 mg/day corrects the hypokalaemia and normalizes the BP within 2-4 weeks.
e Laparoscopic adrenalectomy is indicated for unilateral aldosterone producing adenomas. Preoperative drug treatment is needed to correct BP and hypokalaemia for at least 8-10 weeks. When an adenoma is resected, about half the patients will be normotensive whereas the others although improved remain hypertensive from pre-existing essential hypertension or complicating ·renal damage.
Cushing's syndrome
Spontaneous Cushing's syndrome may be classified into:
e Corticotrophin-dependent: due to pituitary tumour (70-80%) or ectopic ACTH syndrome
e Corticotrophin-independent: usually due to unilateral cortisol producing adenoma or carcinoma. Rarely, the condition is due to bilateral adrenal hyperplasia
Hypertension occurs in about 80% of patients with Cushing's syndrome. The excess cortisol production may overwhelm the ability of the renal 11 dehydrogenase to convert active cortisol into an inactive cortisone at the renal mineralocorticoid receptor level, so that cortisol persists and stimulates the mineralocorticoid receptors to retain sodium and expand the extracellular fluid volume. Cortisol also stimulates the synthesis of renin substrate and the expression of angiotensin II receptors and also potentiates the response of vascular smooth muscle to vasoconstrictor agents. Additionally, in Cushing syndrome, the ACTH excess may stimulate production and release of endogenous mineralocorticoids especially 11-deoxycorticosterone.
Investigations
'" 24 h urinary free cortisol (UFC) or overnight dexamethasone suppression test is the initial screening test. A 24 h UFC >40 µg or serum cortisol >5 µg/dl in a blood sample withdrawn at 8:00 am after giving .0 mg of dexamethasone at 11 :00 pm the night before suggests the diagnosis. This should measurement of plasma ACTH at 8:00 am.
e Plasma ACTH
a- A low plasma ACTH level is suggestive of an adrenal tumour or hyperplasia and should be evaluated further by abdominal CT.
b- A high ACTH level in excess of 200 pg/ml is suggestive of ectopic ACTH-production and should prompt a search for ACTH-producing tumours such as small cell bronchial carcinoma or carcinoid tumours.
c- A high plasma ACTH level but less than 200 pg/ml suggests the diagnosis of either a pituitary tumour or ectopic ACTH production. Differentiation can be made by low-dose and high-dose
e The three most common symptoms are headache, palpitation, and sweating. Many other symptoms may occur anxiety, weakness and tremor. When norepinephrine is the primary hormone produced, usually occurs but if substantial amounts of epinephrine are produced, flushing develops.
e Episodic hypertension develops as a result of catecholamine release from the tumour and the sympathetic nerves. Although some BP readings may be normal, most measurements are in the hypertension range but with wide variability.
Investigations
e 24 h excretion of metanephrines is the most reliable screening procedure. Since any single hormone may or may not be elevated, an array of these substances should be measured. Urinary creatinine should also be measured to verify that collection represents the 24-h excretion. To reduce the incidence of false positive results, the patient should be in a non-stressful situation when the sample is obtained. Newer chromographic techniques usually obviate the need for dietary restncuons, some drug (e.g. labetalol and tricyclic antidepressents) interferences remain.
e Plasma catecholamines (norepinephrine plus epinephrine) are measured when the urinary assays are borderline. If the levels exceed 2000 pg/ml in the basal state, the presence of phaeochromocytoma is likely. If the levels are less than 600 pg/ml, the diagnosis is very unlikely. In patients with plasma catecholamine levels between 600 and 2000 pg/ml, the clonidine suppression test may be useful. Elevated serum dopamine implies the possibility of malignant transformation which in turn suggests the possibility that the tumour may arise in an extra-adrenal site.
e Clonidine suppression test. Plasma catecholamine levels are obtained at baseline and hourly for 3 hours after 0.3 mg of clonidine is given orally. The normal response to clonidine is suppression of plasma catecholamine level by at least 50% from baseline to below 500 pg/ml. Non-suppression of elevated catecholamines by clonidine is strongly suggestive ofphaeochromocytoma.
e Glucagon stimulation test.
Plasma catecholamine level <1000 pg/ml in a patient with clinical features suggestive of phaeochromocytoma is about the only indication for this test. Plasma catecholamine levels are obtained at baseline and 3 minutes after intravenous injection of 2 mg glucagon. A positive result is indicated 3-fold increase in plasma catecholamine levels or an absolute level >2000 pg/ml. A blood pressure iise of at least 20/15 mm.Hg is desirable but not essential to confirm the diagnosis. The test is dangerous and rarely indicated. Phentolamine 5 mg intravenous bolus after a 0.5 mg test dose should be readily available to terminate a life-threatening pressor response.
e CT and MRI of the abdomen are used to localize the tumour after the diagnosis is established by the above tests. Patients with biochemical diagnosis and negative localization studies should have m I metaiodobenzylguanidine (MIBG) total body scan to provide both anatomical localization and functional characterization of extra-adrenal phaeochromocytomas and metastases. The agent undergoes active concentration in the sympathoadrenal tissues by the catecholamine reuptake mechanism, so drugs block catecholamine reuptake (e.g. tricyclic antidepressant, cocaine) may result in false-negative results.
Treatment
e Phaeochromocytomas should be resected. Endoscopic procedures are now the standard. Preoperative usually includes several weeks of alpha blockers (especially phenoxybenzamine) and rehydration to avoid abrupt hypotension from withdrawal of the elevated catecholamines once the tumour pedicle is clamped. Beta-blockers can control arrhythmias during the perioperative period but should be administered only in conjunction with a-blockers to avoid unopposed agonist influence. After tumour resection, patients should be followed up at least on annual basis to screen for recurrence or the development of a second pheochromocytoma.
e It the tumour is unresectable, chronic medical therapy can be used with the alpha blocker phenoxybenzamine or the inhibitor of catechol synthases a-methyl-tyrosine.
Pharmacological causes of hypertension
Drugs, which cause hypertension, are divided into 3 categories:
@ Vasoconstrictors: Phenylephrine, pseudoephedrine, 0-agonist boronchodilators, anti-adrenergic agent withdrawal, monoamine oxidase inhibitor co-adrninisteration with tyramine containing foods or medications, alcohol excess.
@ Volume expanders: glucocorticoids, oestrogens (oral contraceptives), nonsteroidal antiinflammatory agents (NSAIDs).
@ Miscellaneous: Psychotropic drugs that interfere with antihypertensive agents, cyclosporin, tarcolimus, erythropoietin.
Oral contraceptive pills cause hypertension in 5% of their users over 5 years. The likelihood of developing hypertension increases among those over age 35, obese, those who drink large quantities of alcohol or have hypertension during a prior pregnancy. Hypertension is usually mild but it may be severe and may persist after the drug has been discontinued. Possible mechanisms of producing hypertension include renin-angiotensin-aldosterone mediated volume expansion, sodium retention and induction of insulin resistance and hyperinsulinaemia.
Women given the pill should have their blood pressure monitored. If it rises, an alternative contraceptive should be offered. If the pill remains the only acceptable contraceptive, the elevated BP should be reduced with appropriate therapy. In view of the possible role of aldosterone, use of a diuretic-spironolactone combination seems appropriate. Those who stop taking the drug should be evaluated for secondary hypertension after at least 3 months have elapsed to allow for the changes in renin-angiotensin-aldosterone system to remit.
Postmenopausal oestrogen use does not appear to induce hypertension.
The immunomodulating drugs cyclosporine and tarcolimus can cause hypertension in over 50% of instances. Possible mechanisms of hypertension include direct nephrotoxicity, production of renal vasoconstrictor eicosanoids, failure of vasodilator prostaglandin synthesis, interference with endothelial-derived relaxing factor or increased renal sympathetic activity. Because of cyclosporine' s binding to the intracellular calcium binding protein cyclophilin, the resulting hypertension is particularly sensitive to treatment with dihydropyridines e.g. nifedipine. In contrast. ACE inhibitor may worsen their renal :function and diuretic may exacerbate the hypomagnesaemia induced by this drug.
The intake of large amounts of alcohol has also been associated with secondary hypertension presumably because of increased sympathetic activity and inhibition of sodium transport across cell membrane with consequent increase in intracellular Ca2+ concentration.
Hypertension during pregnancy
Hypertension during pregnancy is defined as BP > 130/80 mmHg on two measurements at least 4 h apart, or a diastolic BP> 110 mmHg at any time during pregnancy or up to 6 weeks postpartum. It affects about 10% of pregnancies.
Classification
Hypertension in pregnancy is classified into five categories:
Chronic hypertension. This refers to hypertension appearing prior to pregnancy or before 20 weeks of gestation. It persists for more than 12 weeks postpartum.
@ Pre-eclampsia. This denotes hypertension associated with proteinuria (>300 mg/24 hours) developing after 20 weeks gestation. It is more common in nulliparas multiple gestations, women with hypertension for 4 years or more, presence of family history of pre-eclampsia, hypertension in previous pregnancy and renal disease. It may progress to eclampsia (seizures).
<11 Chronic hypertension with superimposed pre-eclampsia. This is recognized new onset of proteinuria after 20 weeks gestation in a woman with hypertension. In a woman with hypertension and proteinuria prior to 20 weeks gestation, it is recognized by sudden 2 to 3 fold increase in proteinuria or the development ofthrombocytopenia or elevated alanin aminotransferase (ALT) or aspartate aminotransferase (AST).
* Gestational hypertension. This is characterized by the development of hypertension without proteinuria after 20 weeks gestation. It may represent pre-proteinuric phase of pre-eclampsia or recurrence of chronic hypertension abated in mid-pregnancy and may evolve into pre-eclampsia.
converting enzyme inhibitors and angiotensin II receptor antagonists are contraindicated in pregnancy because of reported fetal renal effects and death.
@ In pre-eclampsia, if delivery is imminent (in less than 48 hours), parenteral antihypertensive agents are practical and effective. Intravenous labetalol is the first choice. Rarely sodium nitroprusside is needed for resistant cases with due attention to the development of fetal cyanide poisoning if drug infusion is needed for more than 4 hours.
Treatment of hypertension
Goals of therapy
The ultimate goal of treatment of the hypertensive patient is to achieve the maximum reduction in the long term total risk of cardiovascular morbidity and mortality. This requires:
@ Treatment of all reversible risk factors identified including smoking, dyslipidaemia and diabetes mellitus.
e Appropriate management of associated clinical conditions such as congestive heart failure, coronary artery disease, peripheral vascular disease and transient ischaemic attacks.
@ For adults with confirmed hypertension, a BP target ofless than 130/80 is recommended. Clinical decision making is based on the average of BP measurements on 2 or more occasions. Some patients will benefit from systolic BP treatment goal below 120 mm.Hg especially those with high risk of cardiovascular disease.
e Concerns continued to be raised over dangers of lowering blood pressure too to a level below which adequate perfusion of vital organs can be maintained, particularly when atherosclerotic vascular disease, already impairs blood supply. This phenomenon is called a "Jcurve" i.e. a falling mortality as blood pressure is lowered down to a nadir beyond which mortality rises.
Almost all evidence for a J-curve has been seen with reduction in diastolic blood pressure. The myocardium may be uniquely susceptible to reduced perfusion from lower diastolic levels for multiple reasons. All large coronary artery flow occurs during diastole, the myocardium usually hypertrophies in hypertension and needs more blood flow, whereas, the brain and kidney often shrink in size. Unlike the brain and kidneys, with increased demands, the heart cannot extract any more oxygen than under basal conditions; and the atherosclerotic coronary vessels may not be able to vasodilate to increase blood flow when perfusion pressure falls, i.e. poor autoregulation. Therefore caution remains advisable in reducing diastolic blood pressure to below 60 mm.Hg particularly in those in whom unrecognized coronary heart disease is likely.
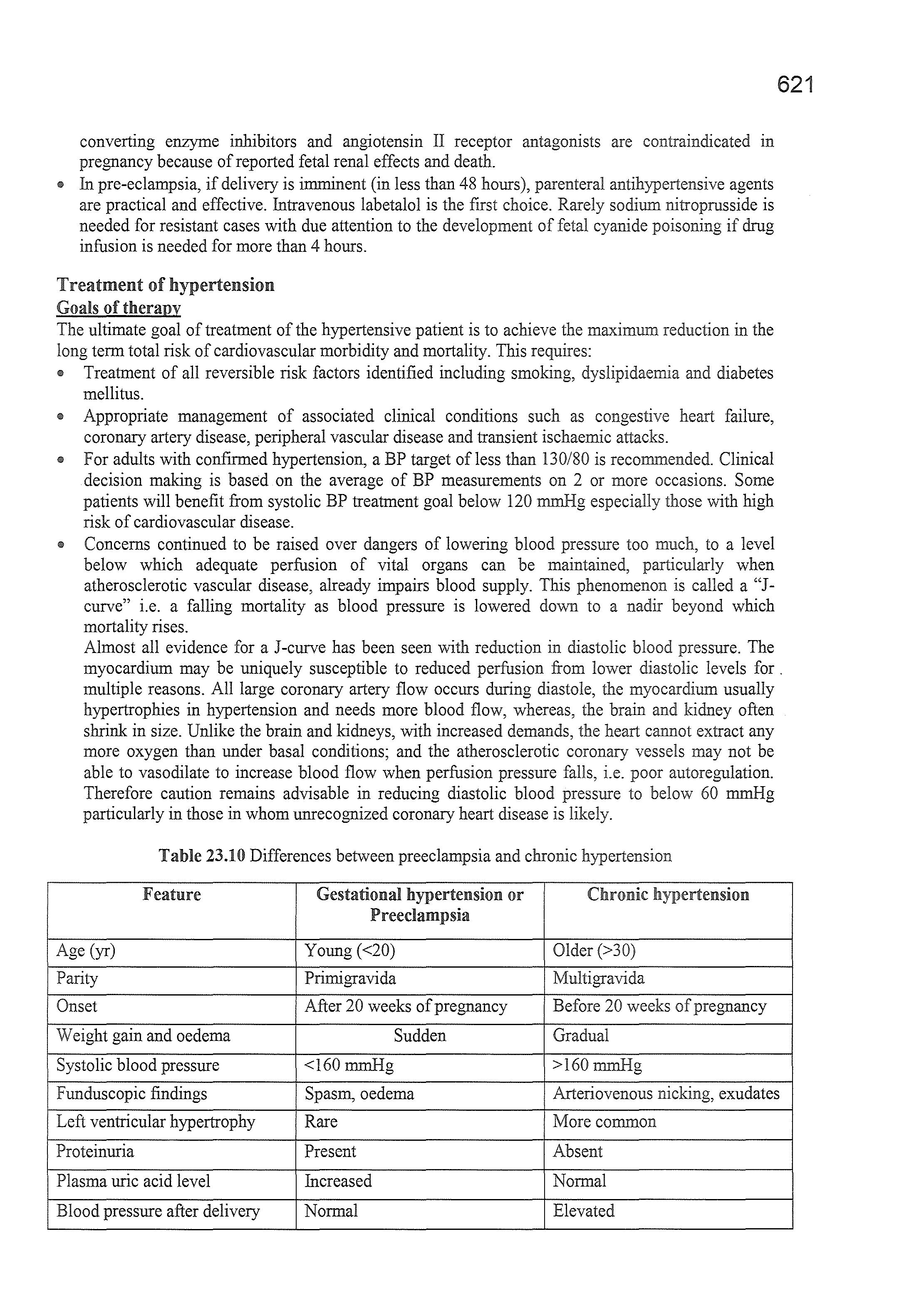
Table 23.10 Differences between preeclampsia and chronic hypertension
Feature
Age (yr)
Parity
Onset
Gestational hypertension or Chronic hypertension
Preedampsia
Young (<20)
Primigravida
After 20 weeks of pregnancy
Older(>30)
Multigravida
Before 20 weeks of pregnancy
Weight gain and oedema Sudden Gradual
Systolic blood pressure
Funduscopic :findings
<160mm.Hg
Spasm, oedema
Left ventricular hypertrophy Rare
Proteinuria Present
Plasma uric acid level
Increased
Blood pressure after delivery Normal
>160 mm.Hg
Arteriovenous nicking, exudates
More common
Absent
Normal
Elevated
In the elderly with isolated systolic hypertension and "naturally" occurring low diastolic pressure, an increase in stroke rate has been noted when diastolic pressure is reduced to below 65 mmHg with antihypertensive therapy, so caution seems appropriate in these patients as well. Clinical judgement, patient preference and a team-based approach to assess risk/benefit is reasonable for decisions regarding intensity of BP lowering and choice of antihypertensive drugs in older adults (:'.::65 years of age).
Lifestyle modifications
Lifestyle modifications listed in table 23.11 are often the only therapy indicated for patients with elevated BP mmHg) and low risk stage l hypertension (130-139/80-89 mmHg), and they are always indicated along with drug therapy for the remainder.
11 Cessation of
This is the single most powerful lifestyle measure for the prevention of noncardiovascular and cardiovascular diseases including stroke and coronary heart disease. Each cigarette raises blood pressure acutely and 20 or more cigarettes a day keeps the blood pressure higher the times the patient is awake and over time causes arterial stiffuess. Each cigarette activates the sympathetic nervous system raising the BP by 10-15 mmHg for 30-45 min. Smoking is also an important cause of masked hypertension and it is essential that the smoker measures the BP while smoking and the physician should use that BP to guide therapy. In addition smoking may interfere with the beneficial effects of some antihypertensive agents such as betaadrenergic blockers. When necessary nicotine replacement or bupropion (central adrenergic and serotoninergic receptor inhibitor) or varenicline (partial nicotin cholinergic receptor agonist) therapy should be considered since they appear to be safe in hypertension and to facilitate smoking cessation.
11 Weight reduction and exercise.
Weight reduction reduces blood pressure in overweight patients and has beneficial effects on associated risk factors such as insulin resistance, diabetes, hyperlipidaemia and left ventricular hypertrophy. Attainment ideal body weight is by no means necessary to produce lower blood pressure. Blood pressure is lowered by 1.6/l.l mmHg for every kilogram of weight loss. Many hypertensive patients have much more than l 0 kg of excess adiposity and many of them would no longer be hypertensive if they lose this amount of body fat. The blood pressure lowering effect of weight reduction may be enhanced by a simultaneous increase in physical exercise. Thus sedentary should be advised to take up modest levels of aerobic exercise on regular basis such as at least 30 minutes per day, most days of the week. Resistance training is also recommended. However, isometric exercise such as heavy weight-lifting can have pressor effect and should be avoided. If hypertension is poorly controlled and in severe hypertension, heavy exercise be discouraged or postponed until appropriate drug treatment has been instituted and to be effective. Body mass index (BMI) should be maintained between 18.5 and 24.9 kg/m2 • Appetite suppressants that contain substances known ton raise BP should be avoided. Bariatric surgery has become widely used clearly with metabolic and cardiovascular benefits that extend as long as 15 years.
• Reduction salt intake and other dietary changes.
Reducing dietary intake to <1500 mg/day is the the optimal goal but at least reduction of l 000 mg/day be in most adults. There is considerable heterogenicity in BP response to salt intake. Salt sensitivity (excessive rise of BP in response to salt loading) may be due to genetic factors or renal damage and it increases the risk of target organ damage. Patients should be advised to avoid added salt, to avoid obviously salted food particularly processed foods and to eat more meals cooked directly from natural ingredients containing more potassium. Hypertensive patients should also be advised to eat more fruit and vegetables, to eat more fish and to reduce their intake of saturated and cholesterol. This is well achieved by adoption of the Dietary to Stop Hypertension (DASH) eating plan.
The diet is rich in fruits, vegetables, low fat dietary foods, whole grains, poultry, fish and nuts and is reduced in fats, red meat, sweets and sugar-containing beverages. It contains reduced amounts of total and saturated fat and cholesterol and increased vegetables and nuts which are
responsible for at least half of the total effect of the DASH diet the DASH diet is reasonably low in cost The DASH diet can be approximated by taking 4 servings of fruit, 4 servings of vegetables and 3 servings of low fat dairy products per day. The combined effects on blood pressure of low sodium intake and the DASH diet are greater than the effects of either alone and are substantial. Additional benefits of reducing sodium intake include diureticinduced hypokalaemia, greater ease of BP control with diuretic therapy, from osteoporosis and fractures (by reducing calcium excretion) and favourable effects on left ventricular hypertrophy. However, the evidence that sodium restriction can reduce cardiovascular events is sparse.
Enhanced potassium intake aiming for 3500-5000 mg/day is recommended preferably by consumption of a diet rich in potassium.
111 Moderation of alcohol consumption.
There is a linear relationship between alcohol consumption, blood pressure levels and prevalence of hypertension in populations. High levels of alcohol consumption are associated with a high risk of stroke particularly so for binge drinking. Additionally alcohol attenuates the effects of antihypertensive drug therapy. Heavy drinkers may also experience a rise of blood pressure after acute alcohol withdrawal. Accordingly hypertensive patients who be advised to limit their consumption to no more than 30 ml of ethanol (the equivalent of two drinks per day) in men and no more than 15 ml of ethanol (one drink) per day in women and weight men. This is because women absorb alcohol more rapidly and metabolize alcohol more strongly than men and the effects of alcohol are inversely proportional to body mass.
111 Caffeine consumption has no long-term effect on blood pressure but may increase blood pressure acutely particularly in hypertensives and smokers.
Pharmacological
therapy (Fig. 23-2)
111 There are five first-line antihypertensive drug classes which have been shown to prevent cardiovascular disease. These include diuretics, ACE inhibitors, ARBs, calcium channel blockers· and Bblockers. blockers are less effective than calcium channel blockers and thiazide diuretics in preventing stroke. ACE inhibitors are less effective in preventing heart failure and stroke compared with calcium channel blockers in black patients. Thus thiazide diuretics (especially chlorothalidone) or calcium channel blockers are the best initial choice for single therapy in this population.
111 For stage 1 hypertension without evidence of atherosclerotic cardiovascular disease and estimated 10 year risk:::; 10% (by the ACC/AHA Pooled Cohort Equation), non pharmacological therapy is initiated. BP response should be assessed in 3-6 months. BP lowering medications are started in these patients if BP remains:'.:: 130/80 mmHg. Stage l patients with atherosclerotic cardiovascular disease or 10 year risk > 10% should be initiated on combined non pharmacological and BP lowering medications simultaneously and the results are assessed in l month. If blood pressure remains:::: 130/80, adherence to therapy is assessed and intensification of therapy is considered.
111 For stage 2 hypertension non pharmacological therapy and BP lowering are initiated simultaneously and the results are assessed in 1 month with assessment of adherence and intensification of therapy if BP remains:::: 130/80.
111 Simultaneous use of ACE inhibitors, ARBs and/or renin inhibitor is harmful and is not recommended.
111 Beta-blockers are the least cost effective treatment for hypertension and less effective than the recommended first line drugs. They are significantly worse at preventing stroke than other drugs. Beta-blockers-thiazide combination should be avoided in patients with impaired fasting glucose, since they increase the risk of new-onset diabetes. However beta-blockers are clearly indicated for hypertensive patients with coronary heart disease or heart failure.
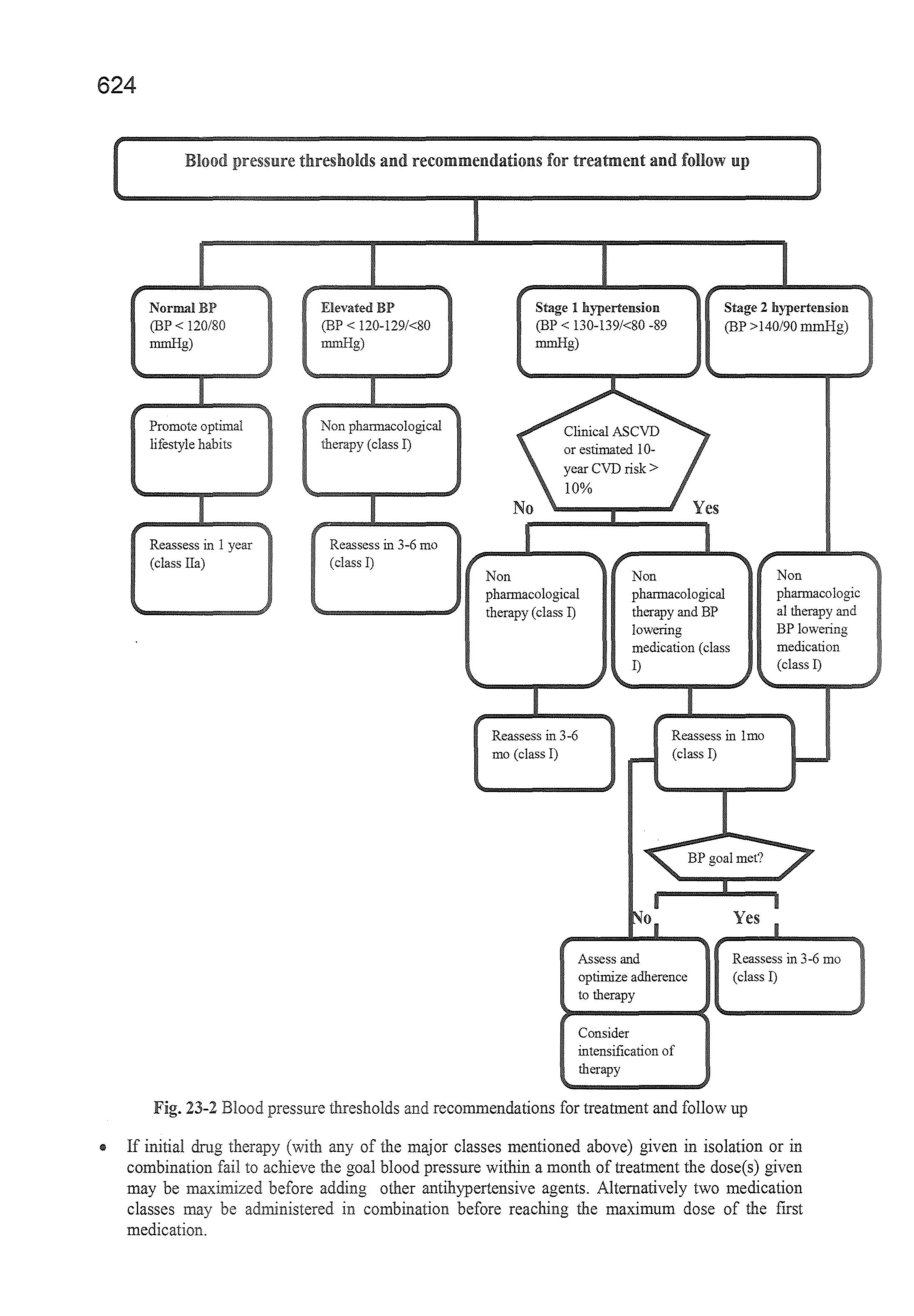
Blood pressure thresholds and recommendations for treatment and follow up
Normal BP (BP< 120/80 mmHg)
Promote optimal lifestyle habits
Elevated BP (BP< 120-129/<80 mmHg) Non pharmacological therapy (class I)
Stage 1 hypertension (BP< 130-139/<80 -89 mmHg)
Stage 2 hypertension (BP > 140/90 mmHg)
Reassess in 1 year (class Ila)
Reassess in 3-6 mo (class I)
Non phannacological therapy (class I)
Non pharmacological therapy and BP lowering medication (class I)
Reassess in 3-6 mo (class I)
Reassess in lmo (class I)
Non pharmacologic al therapy and BP lowering medication (class I)
0
Assess and optimize adherence to therapy
Consider intensification of therapy
Yes
Reassess in 3-6 mo (class I)
Fig. 23-2 Blood pressure thresholds and recommendations for treatment and follow up
• If initial drug therapy (with any of the major classes mentioned above) given in isolation or in combination fail to achieve the goal blood pressure within a month of treatment the dose(s) given may be maximized before adding other antihypertensive agents. Alternatively two medication classes may be administered in combination before reaching the maximum dose of the first medication.