U-M Health Neurosurgery INNOVATE Newsletter Fall 2024
Wajd Al-Holou
Battling brain tumor resistance
Toshiro Hara
Manipulating cellular environments
Maria Castro
Taking the fight to glioblastoma
Todd Hollon
AI meets diagnostics
Kevin Chen
Illuminating neural circuit dysregulation
Suresh Magge
Department of Neurosurgery, University of Michigan Health 4 10 6 12 8 14
Advancing care for pediatric patients
Ann Arbor, Michigan
DEAR COLLEAGUES,
The University of Michigan Health Department of Neurosurgery aims to provide the highest quality comprehensive neurosurgical care. We recognize the immense need and opportunity to contribute to science and innovation in creating a better tomorrow for our patient population. With that in mind, it gives me great pleasure to introduce our inaugural publication “Michigan Neurosurgery Innovates to Contribute to a Better Tomorrow,” which highlights some of our faculty and their teams who are innovating in the neurosciences. Our goal is to highlight our most innovative and impactful contributions through this biannual publication. This inaugural issue covers new work in brain tumor heterogeneity, brain tumor metabolomics, AI use in neurosurgery, and advances in pediatric brain tumor care. As a department, we take pride in advancing the understanding of neurological pathologies and pioneering the development of minimally invasive therapies. The team science featured in this issue, and in those to come, exemplify our dedication and passion to improve patient outcomes and experiences. I hope you enjoy the issue.
Sincerely,
Aditya S. Pandey, MD
Julian T. Hoff Professor and Chair Department of Neurosurgery
University of Michigan Health adityap@med.umich.edu
Innovate: The Latest Research at The University of Michigan, Department of Neurosurgery
BATTLING BRAIN
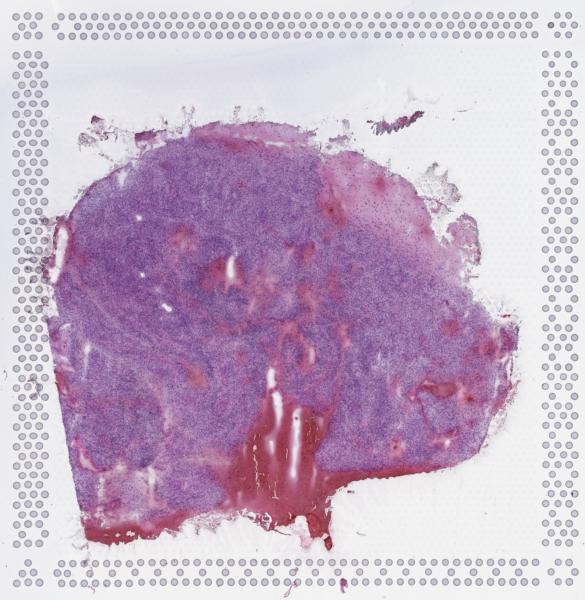
In our Brain Tumor Microenvironment Laboratory, we work at the intersection of spatial biology, genetics, cutting-edge therapeutics, and patient care. Our commitment is to identify new treatments to enhance the survival and outcomes of patients with brain tumors.
The primary question we are attempting to address is why brain tumors are so aggressive and seemingly resistant to current treatments.
We aim to understand how brain cancer stem cells interact with normal brain cells and immune cells in the brain tumor microenvironment. By studying these complex interactions, we can uncover the mechanisms driving aggressive tumor behavior and identify potential vulnerabilities. This information could be pivotal in developing novel, groundbreaking treatments for these life-threatening neoplasms.
For the first time, we have identified rare stem cells within the original tumor that survive initial chemotherapy and radiation, leading to rapid relapse due to interactions with normal cells in the brain.
We are now focused on determining how to target these highly resistant cells by studying their interactions within the tumor micrenvironment. By targeting these interactions, we hope to discover new cures for brain tumors.
We also work closely with other brain tumor researchers at the University of Michigan Health to develop clinical trials aimed at addressing other ways that brain tumors become resistant.
In the future, we hope to identify a vulnerability in these brain cancer stem cells and attack that vulnerability with new drugs. This could lead to new clinical treatments that improve survival and outcomes for our patients.
The advanced sequencing technology utilized in the Brain Tumor Microenvironment Laboratory has uncovered the highly variable microscopic genetic features of brain tumors, providing insights into how tumor cells interact with their microenvironment to drive aggressive behavior.
TUMOR RESISTANCE with
“For the first time, we have identified that there are rare stem cells that survive initial chemotherapy and radiation and lead to rapid relapse.”
Dr. Wajd Al-Holou, M.D.
Dr. Wajd Al-Holou
Innovate: The Latest Research from the Department of Neurosurgery, University of Michigan Health
TAKING THE FIGHT TO GLIOBLASTOMA
with Dr. Maria Castro, Ph.D.
IDH1-R132H acts as a tumor suppressor in glioma via epigenetic up-regulating the DNA damage response.
Patients with glioma, whose tumors carry a mutation in isocitrate dehydrogenase 1 (IDH1R132H), are typically diagnosed at a younger age and live longer. These IDH1 mutations co-occur with other molecular lesions, such as 1p/19q codeletion, inactivating mutations in the tumor suppressor protein 53 (TP53), gene, and loss-of-function mutations in alpha thalassemia/mental retardation syndrome X-linked gene (ATRX). We developed a genetically engineered mouse model harboring IDH1R132H, TP53, and ATRX inactivating mutations. Through studies using our mouse model and primary patient-derived glioma cultures, we discovered that IDH1R132H expression (1) increases median survival in the absence of treatment, (2) enhances DNA damage response (DDR) via epigenetic up-regulation of the homologous recombination DNA repair mechanism, and (3) elicits tumor radioresistance. Accordingly, pharmacological inhibition of cell cycle checkpoint kinases 1 and 2, essential kinases in the DDR, restored the tumors’ radiosensitivity. Applying these findings to patients with IDH1132H glioma harboring TP53 and ATRX loss could improve the therapeutic efficacy of radiotherapy and, consequently, patient survival.
Inhibition of 2-hydroxyglutarate (D-2HG) causes metabolic reprogram-
ming and enhances immunity against IDH1 gliomas.
The role of D-2HG within the tumor microenvironment of mIDH1 gliomas remains unexplored. However, inhibiting D-2HG, when used as monotherapy or in combination with radiation and temozolomide (IR/TMZ), increased the median survival (MS) of mIDH1 glioma-bearing mice. Also, D-2HG inhibition elicited anti-mIDH1 glioma immunological memory. In response to D-2HG inhibition, PD-L1 expression levels on mIDH1-glioma cells increased to similar levels as observed in WT-IDH gliomas. Thus, we combined D-2HG inhibition/IR/TMZ with anti-PDL1 immune checkpoint blockade and observed complete tumor regression in 60% of mIDH1 glioma-bearing mice. This combination strategy reduced T cell exhaustion and favored the generation of memory CD8+ T cells. Our findings demonstrate that metabolic reprogramming elicits anti-mIDH1 glioma immunity, leading to increased MS and immunological memory. Our preclinical data support the testing of IDH-R132H inhibitors in combination with IR/TMZ and anti-PDL1 as targeted therapy for mIDH1 glioma patients.
H3.3-G34R mutation-mediated epigenetic reprogramming increases the effectiveness of immune-stimulatory gene therapy in pediatric high-grade gliomas.
Pediatric high-grade gliomas (pHGGs) are diffuse, highly aggressive brain tumors with a 5-year overall survival rate of less
than 20%. What’s more, they are currently incurable. To this end, we studied pHGGs harboring the H3.3-G34R mutation. H3.3-G34R pHGGs are restricted to the cerebral hemispheres and are found predominantly in adolescents. Our analysis of H3.3-G34R pHGGs by RNA-sequencing and ChIP-sequencing revealed alterations in the molecular landscape associated to H3.3-G34R expression. In particular, the expression of H3.3-G34R modifies the histone marks deposited at the regulatory elements of genes belonging to mediating immune responses, leading to an immune permissive tumor immune microenvironment. Consequently, this tumor subtype is more susceptible to TK/Flt3L immune-stimulatory gene therapy. Implementing this gene therapy increased the median survival of H3.3-G34R tumor-bearing animals and stimulated the development of anti-tumor immune response and immunological memory. Our data suggest that the proposed gene therapy has potential for clinical application in treating patients with H3.3-G34R high-grade gliomas.
Another significant study we conducted was a phase 1, first-in-human clinical trial combining cytotoxic and immune-stimulatory gene therapy for adult patients with high-grade glioma. High-grade gliomas have a poor prognosis and do not respond well to conventional treatment. Effective cancer immune responses depend on functional immune cells, which are typically absent from the brain.
Our trial aimed to evaluate the safety and activity of two adenoviral vectors expressing HSV1-TK (Ad-TK) and Flt3L (Ad-Flt3L) in patients with high-grade glioma.
The trial is registered with ClinicalTrials.gov under the identifier NCT01811992. Between April 8, 2014, and March 13, 2019, we evaluated patients for eligibility, enrolling 18 patients with highgrade glioma. The treatment was
well-tolerated by patients, with no dose-limiting toxicity observed and the maximum tolerated dose unreached. No treatment-related deaths occurred during the study. The median overall survival was 21.3 months (95% CI 11·1- 26·1). The combination of two adenoviral vectors demonstrated both safety and feasibility in these patients. We are now working on implementing a novel phase 1b/2 clinical trial based on these findings.
Epigenetic reprogramming in adult and pediatric gliomas.
Drs. Castro & Lowenstein in their laboratory at Michigan Medicine.
“Our
goal is to manipulate adult stem cells toward a treatment for neurodegenerative disease that can restore lost function.”
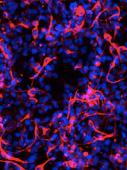
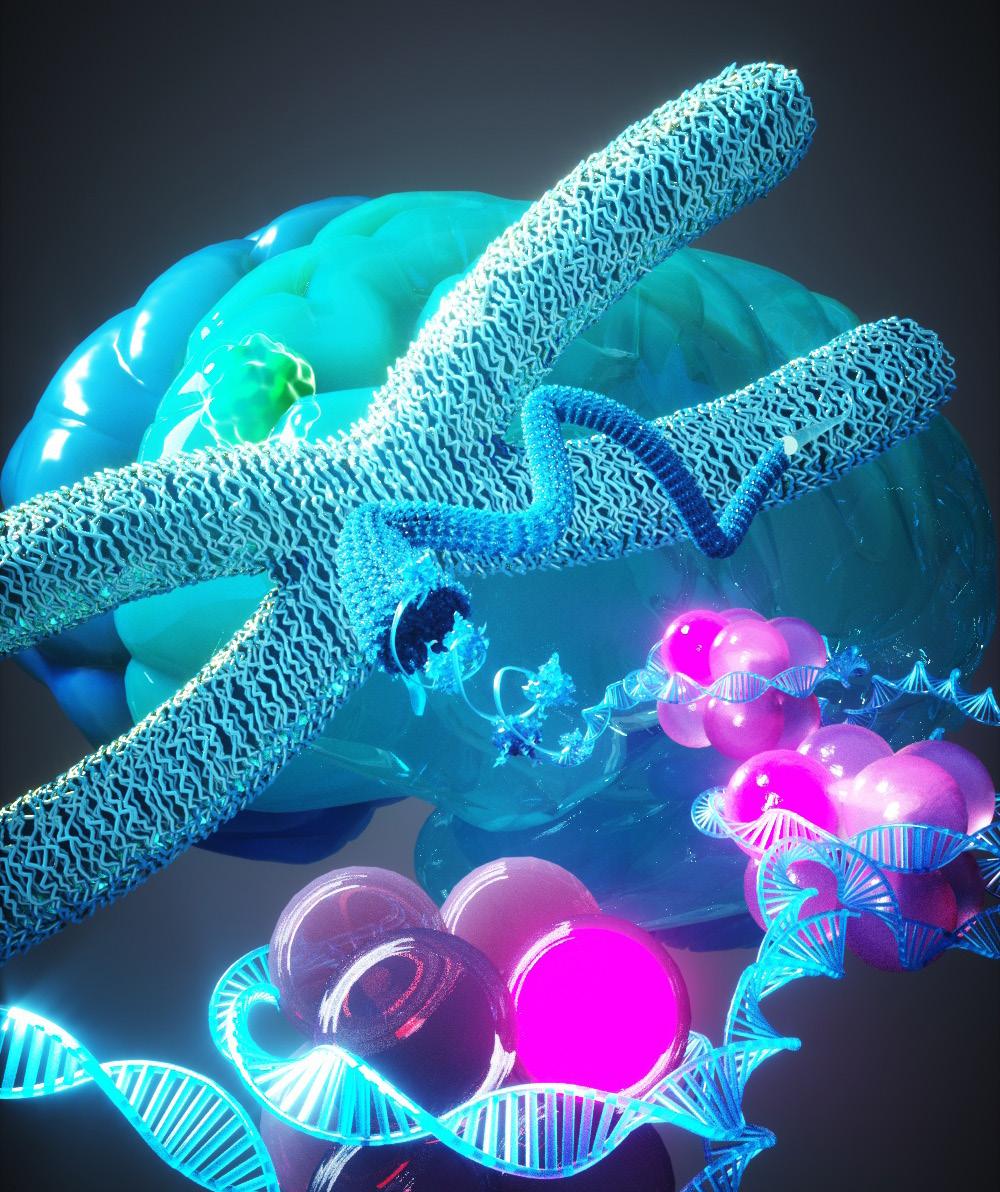
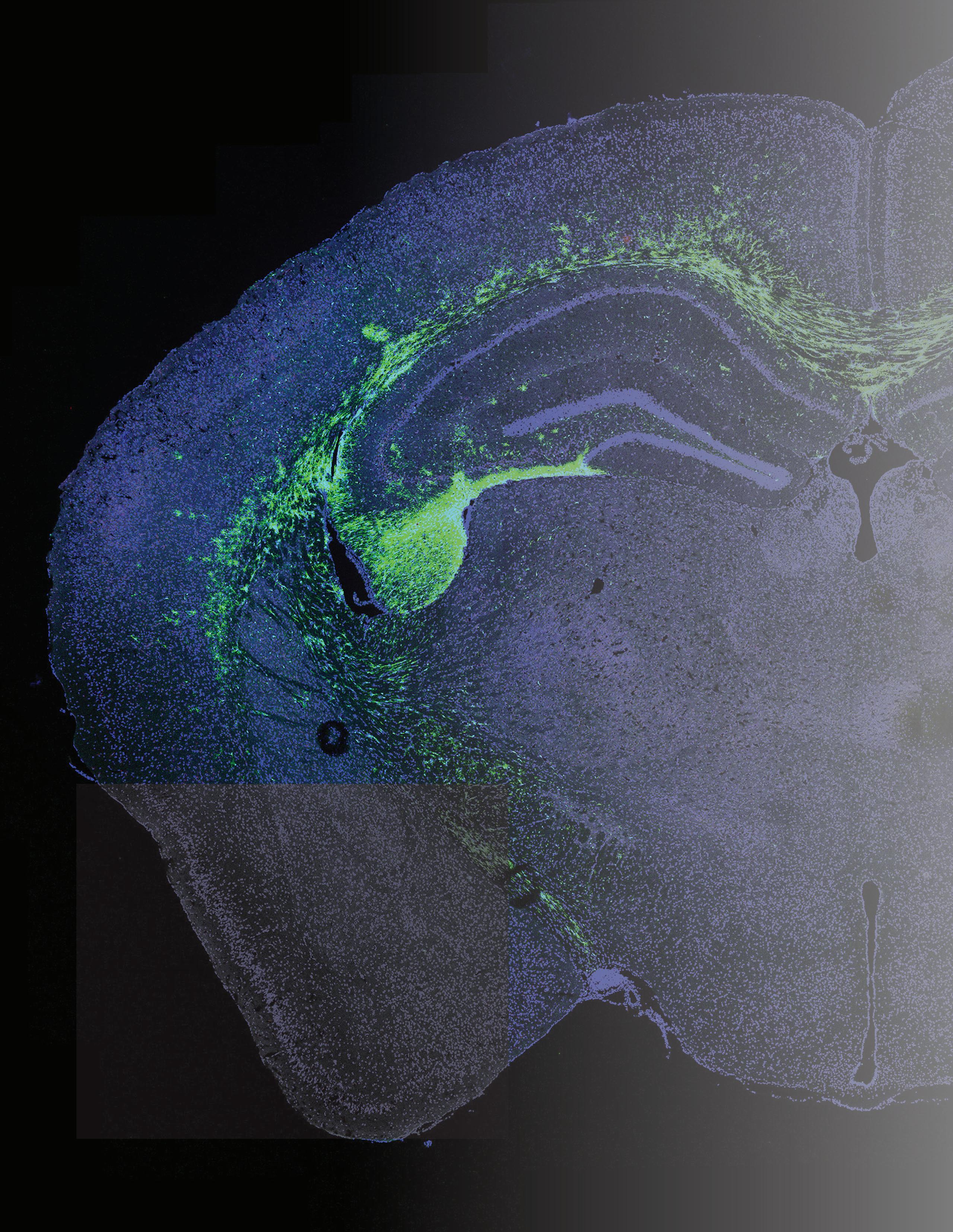
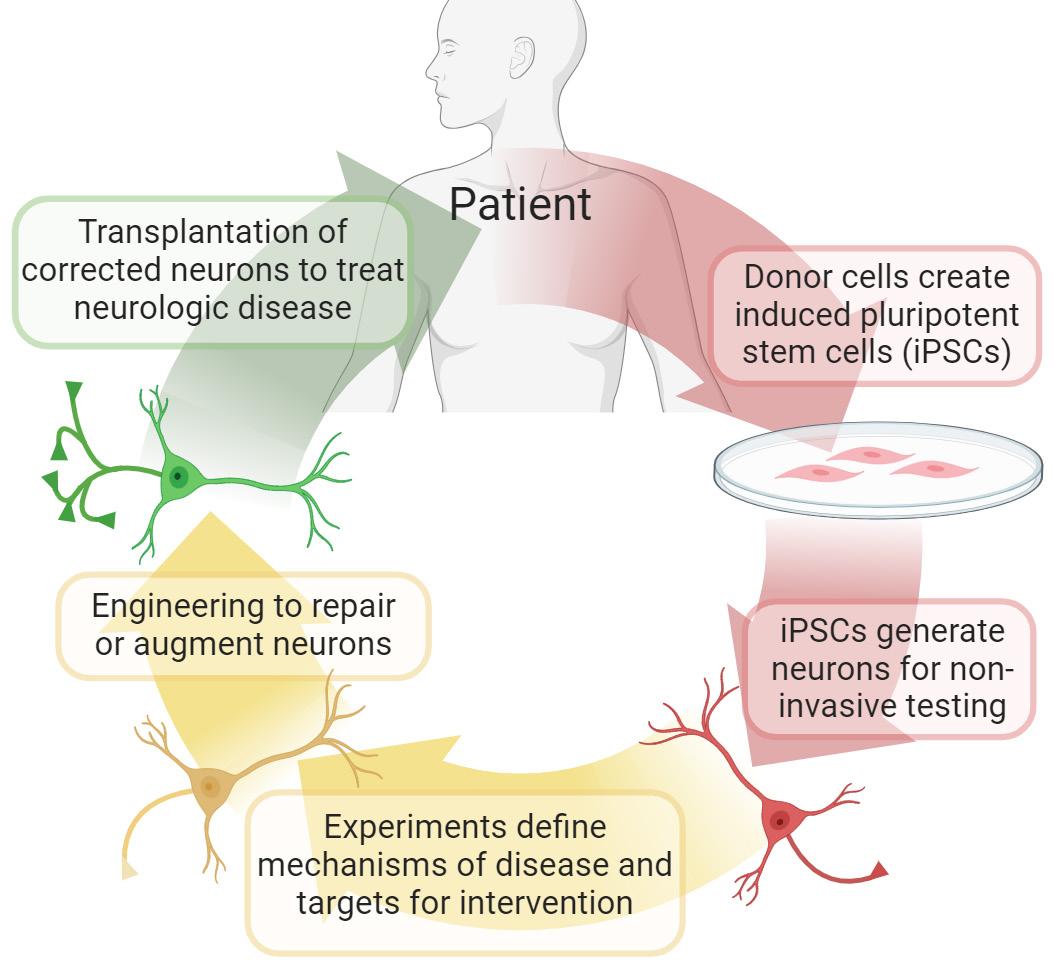
This page: Fluorescent-labeled neural stem cells (green) are transplanted into the memory centers of a mouse brain with Alzheimer’s disease (blue). Dr. Chen is investigating the mechanisms by which stem cells may improve memory and cognition.
Facing page: Dr. Chen’s research uses adult patient-donated cells (e.g., skin cells) that are reprogrammed in the lab to create induced pluripotent stem cells and eventually neurons. This allows for controlled experiments to define disease mechanisms. A future goal is to “repair” these neurons and transplant them back to patients, enabling a patient-specific treatment for neurodegenerative disease.
ILLUMINATING NEURAL CIRCUIT DYSREGULATION
with Dr. Kevin Chen, M.D.
I am interested in understanding how neural circuits become dysregulated in neurodegenerative diseases like Alzheimer’s disease and amyotrophic lateral sclerosis (ALS). Increasing evidence shows that in these diseases, neuronal activity becomes overactive and hyper-synchronized – like a car with the gas pedal stuck down – leading to abnormal signaling, neuronal exhaustion, and cell death. The cause may be due to issues with inhibitory interneurons, which are local short-range neurons that typically regulate and “brake” neural activity. We are investigating potential causes of interneuron dysfunction and finding ways to reverse these abnormalities through methods based on induced pluripotent stem cells (iPSCs). Essentially, we are investigating a therapy to restore proper interneuron regulation of neural circuits by generating iPSCs from an adult donor’s cells (e.g., skin cells) and transforming them into “corrected” interneurons to be transplanted back into the same patient.
We have published multiple papers demonstrating that stem cell therapy improves cognitive function in animal models of Alzheimer’s disease. Our findings suggest that the stem cells act by normalizing signaling from inflammatory cells in the brain. Additionally, we have optimized the immunosuppression regimen used in these stem cell transplant experiments to improve cell survival while minimizing animal stress and side effects.
Currently, we are establishing an in vitro model of interneurons using iPSCs from Alzheimer’s disease and ALS donors. This model would allow us to study how interneurons degenerate in a controlled experimental manner, avoiding the invasiveness of direct animal or human studies. By identifying key pathways that go awry in diseased interneurons, we can target these pathways for pharmacologic treatment or gene therapy. For example, we have observed significant disruption in genes related to mitochondrial function and energy production within diseased interneurons. Therefore, we may be able to use existing drug compounds to restore mitochondrial energy function and normalize proper neural circuit regulation in neurodegenerative diseases.
Innovate: The Latest Research from the Department of Neurosurgery, University of Michigan Health
MANIPULATING CELLULAR MICROENVIRONMENTS
“Our goal is to develop therapeutics to perturb glioblastoma gene expression.”
with Dr. Toshi Hara, Ph.D.
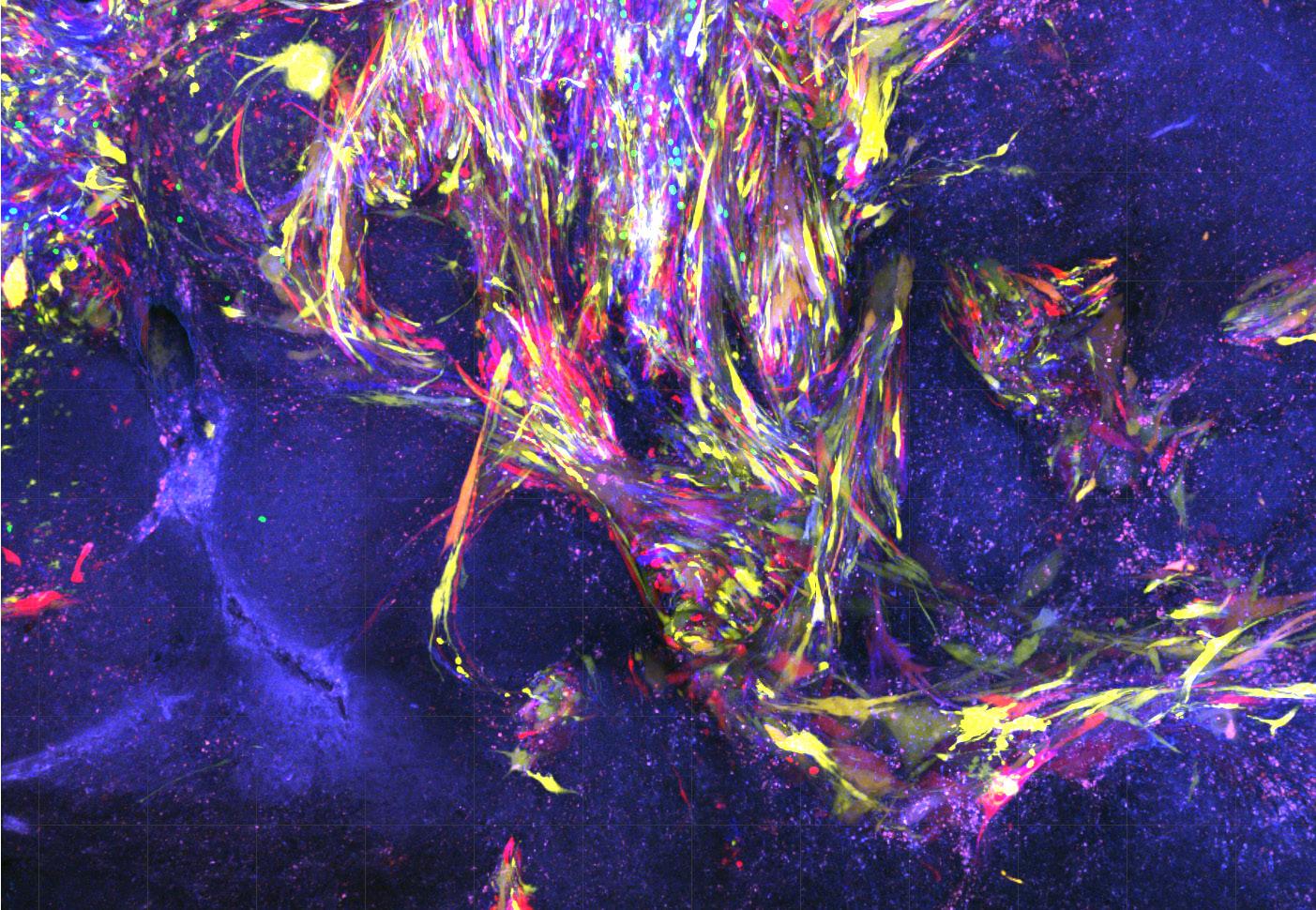
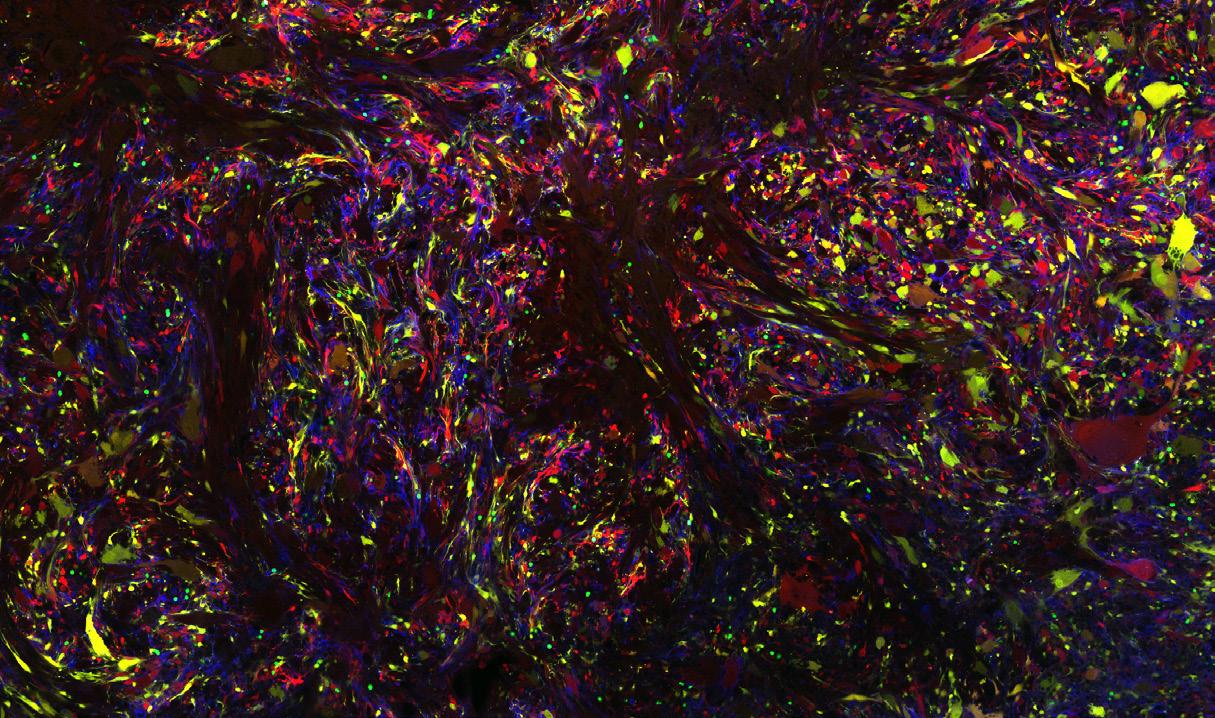
Glioblastoma is an incurable form of primary brain tumor. It consists of a diverse community of tumor cells that coexist in the brain, engaging in various forms of cellular communication, from tumor-immune to tumor-brain cell interactions. Understanding its intricacies could pave the way for improved therapies and better patient outcomes. To measure gene expression of individual tumor cells, including those that invade and hide in the brain, we use a technology called single-cell RNA sequencing (scRNA-seq). This approach reveals that tumor cells switch their gene expression identities, turning genes on and off based on their location. We hypothesize that signals from the surrounding environment are recognized by tumor cells and help determine their identities and functions. By controlling these environmental signals, we aim to disrupt the gene expression of glioblastoma cells, thereby hindering their abnormal behavior. Our goal is to develop new strategies that could significantly increase recurrence-free survival for glioblastoma patients, a feat currently unattainable.
In my previous research, I collaborated with clinical fellows and computational scientists and performed scRNA-seq on a cohort of 28 glioblastoma patients. We found that malignant cells in glioblastoma exist in four distinct cellular states. To explore the potential for cells to transition between these states, I developed an integrative approach by combining mouse models of glioblastoma, a DNA-barcode system, and scRNA-seq. This approach demonstrated the plasticity be-
Members of the Hara Laboratory.
Glioblastoma is an incurable brain cancer. The diversity of glioblastoma cells, illustrated as rainbow colored cells in these images, is a major impediment for successful therapy. By using sc-RNA-seq, a new way of measuring the cells, we found that the diverse malignant cells converge to a limited set of four cellular states. My current goal is to make glioblastoma cells homogenous to develop effective therapy.
tween states and revealed that a single cell could reconstruct all four states. More recently, I established both in vivo (mouse) and in vitro (spheroid) models for the heterogeneity of cellular states in glioblastoma. Using these models, we demonstrated the role of macrophages in driving glioblastoma cells toward a mesenchymal-like (MES-like) state, one of the four recurrent states. We also leveraged functional approaches to uncover a ligand-receptor mechanism causing state transitions toward the MES-like state. Importantly, our results indicated that induced MES-like states are vulnerable to T cell-mediated cytotoxicity, suggesting potential implications for immunotherapy. These findings provide a clear example of the impact of studying cell-to-cell interactions within the tumor ecosystem and offer novel insights to address the challenges posed by cellular diversity in cancers. Our study, which was the first comprehensive study to apply scRNA-seq to glioblastoma, is featured on the cover of the WHO Classification of Tumors of the Central Nervous System, a textbook on brain cancer pathology.
Our goal for the next few years is to deepen our understanding of cell-to-cell communication in brain cancers. We will continue to develop new therapeutic tools that can alter the course of the disease and collaborate with colleagues in the Department of Neurosurgery. We believe these efforts will lead to improved clinical outcomes for patients treated at the University of Michigan Health and around the world. We are also committed to sharing our innovations with the broader community and to training and supporting our students, residents, and fellows, who represent the next generation of leaders in neurosurgery and neuro-oncology.
USING AI TO DETECT GLIOMA MUTATIONS
with Dr. Todd Hollon, M.D.
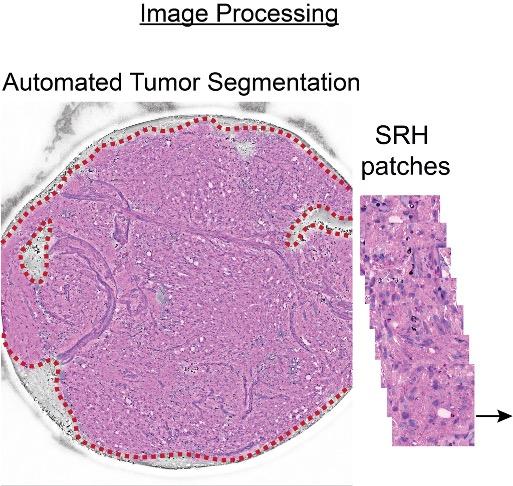
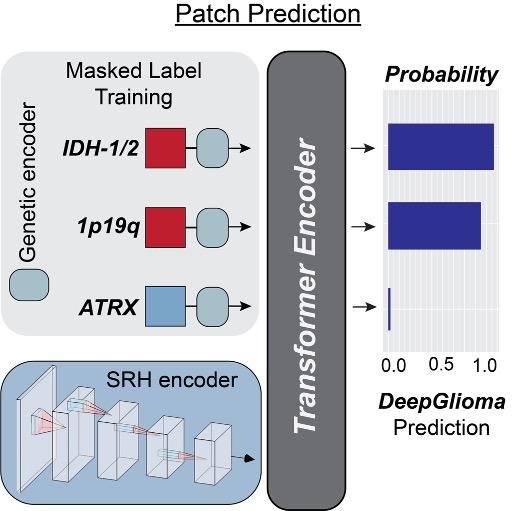
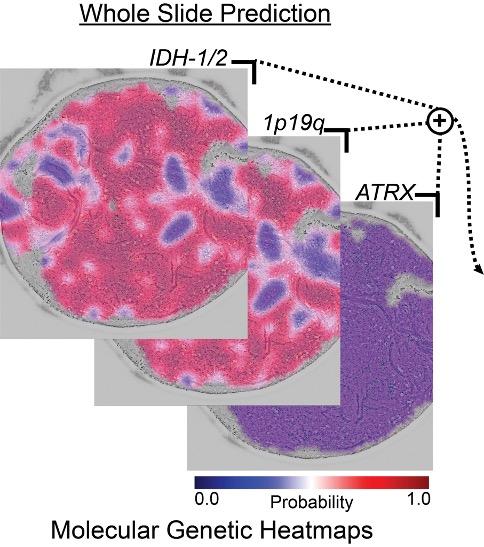
Achieving timely and accurate molecular diagnosis of brain tumors is critical for guiding treatment decisions, but current methods often face delays and limitations. To address this, my team and I have developed DeepGlioma, an artificial intelligence-based system designed to streamline molecular classification of diffuse gliomas. This cutting-edge model leverages stimulated Raman histology (SRH), a label-free optical imaging technique, to achieve rapid (<90 seconds) molecular classification in the operating room.
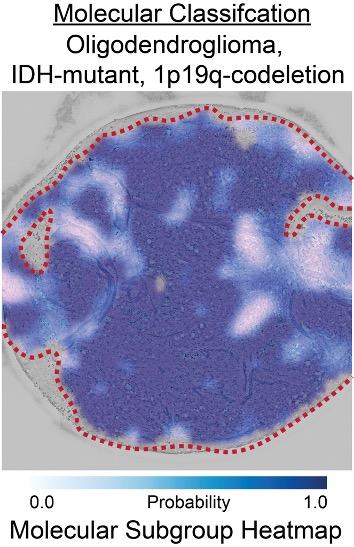
DeepGlioma uses multimodal data from SRH images and public genomic datasets to identify key molecular alterations, such as IDH mutations, 1p19q co-deletion, and ATRX mutation, all of which define the most clinically significant subgroups of diffuse glioma according to the World Health Organization’s classification system. In a prospective, multicenter cohort study of 153 patients, DeepGlioma demonstrated an impressive molecular classification accuracy of 93.3 ± 1.6%, with consistent performance across diverse medical centers and patient populations.
By providing real-time, intraoperative molecular classification, DeepGlioma represents a significant advancement in the treatment of glioma, enabling more precise surgical strategies and potentially improving early enrollment in clinical trials. This technology underscores the growing role of artificial intelligence (AI) in enhancing cancer diagnostics and patient care.
The workflow of DeepGlioma (left to right): An AIbased molecular classification of diffuse gliomas.
At the Machine Learning in Neurosurgery Lab (MLiNS), our research focuses on integrating AI, machine learning, and computer vision into neurosurgery to enhance the diagnosis and treatment of neurological diseases. We aim to improve patient outcomes through innovative techniques like automated tumor localization, molecular classification of brain tumors, and intraoperative pathology augmentation.
In the coming years, we intend to further advance AI integration in clinical settings, enhance precision in neurosurgical procedures, and expand our research to cover more neurological conditions. Our goal is for these innovations to be widely adopted in clinical practice, significantly improving patient care and outcomes.
Some of our key achievements include:
• Introducing HiDisc, a hierarchical discriminative learning AI method for biomedical microscopy and intraoperative pathology, which we presented at the 2023 Computer Vision and Pattern Recognition Conference.
• Creating OpenSRH to optimize brain tumor surgery using intraoperative stimulated Raman histology. We showcased this work at the 2022 Conference on Neural Information Processing Systems.
“We hope to see our innovations widely adopted in clinical practice, significantly improving patient care and outcomes.”
Members of the MLiNS Laboratory.
Innovate: The Latest Research from the Department of Neurosurgery, University of Michigan Health
ADVANCING CARE FOR
”I’m very hopeful that this work will bring about better outcomes for these children.”
As the Surgical Director of the pediatric brain tumor program, I collaborate with neuro-oncologists like Drs. Koschmann, Franson, Upadhyaya, Presner, and Robertson, and the neuropathology team, on a variety of clinical projects and trials aimed at different types of pediatric brain tumors.
I have a particular interest in finding better treatments for diffuse intrinsic pontine glioma (DIPG), which is a type of invasive pediatric brain tumor with no cure. For decades, there was little advancement in DIPG treatment because invasive biopsies were avoided due to associated risks, which led to a lack of tissue for study and stagnated research. However, through several studies, we have shown that needle biopsies can be performed safely, allowing us to obtain tissue to study tumor genetics. This has significantly advanced our understanding of DIPG over the past decade, and we are now on the cusp of developing better treatments.
While we are able to perform biopsies, my goal is to develop a less invasive liquid biopsy technique, where we can sample spinal fluid
from children, instead of performing invasive biopsies, to identify tumor cells and track tumor burden over time. This approach involves the use of Ommaya reservoirs – catheters implanted in the brain with a small reservoir under the skin. This system provides a less invasive way to sample spinal fluid over time, avoiding the need for lumbar punctures, which can be traumatic for children. By using this method, we can obtain repeated samples without extensive procedures.
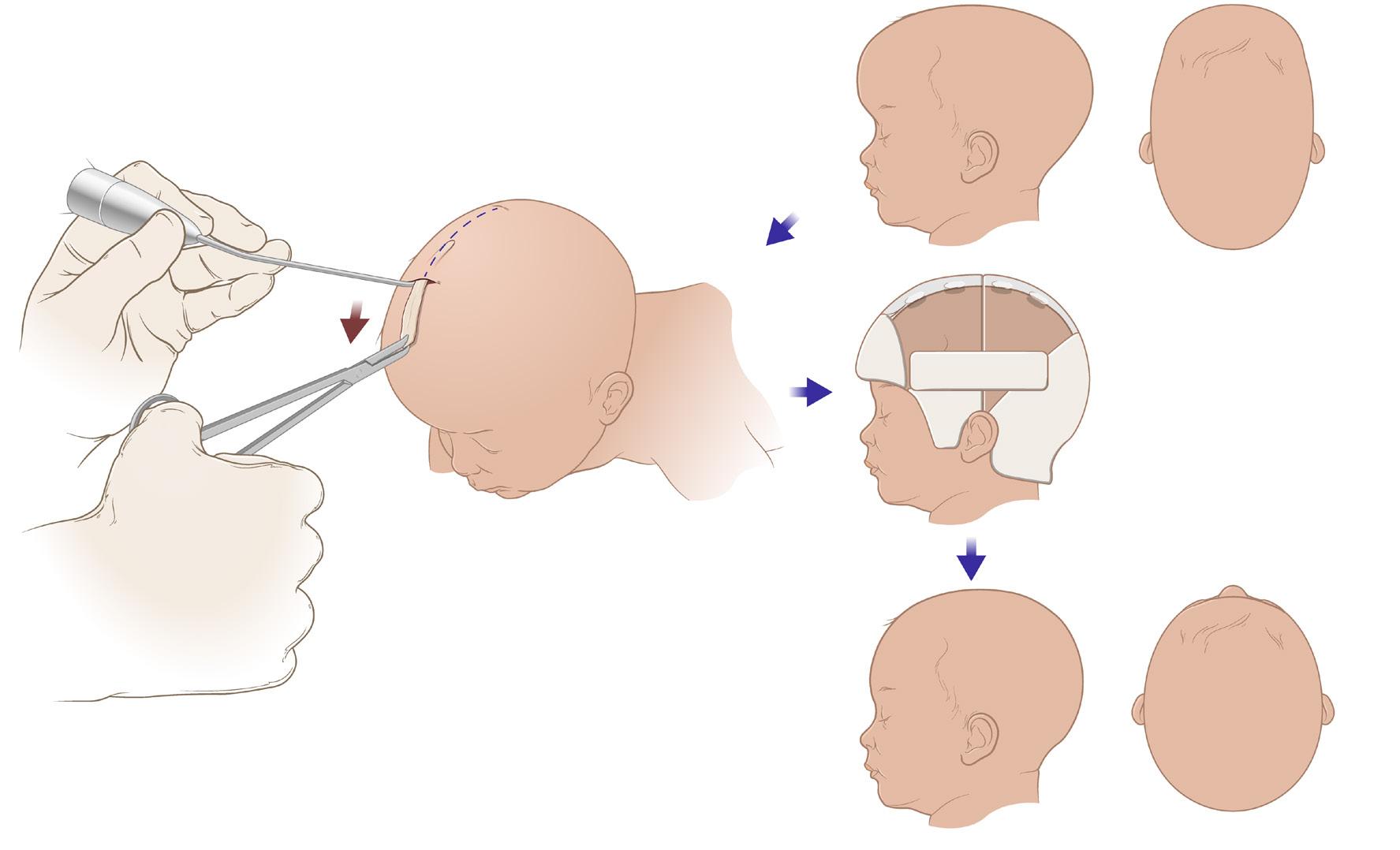
In addition to my work on DIPG, I have a strong interest in craniosynostosis. This condition is caused by early fusion of the skull and causes skull deformities in newborns. In collaboration with Dr. Vercler and the plastic surgery department, we recently joined SynRG, which is a multicenter collaborative to advance research and establish best practices for craniosynostosis surgery. While I perform both traditional open surgery and minimally invasive endoscopic surgery, my research has focused on understanding the best techniques for endoscopic surgery. We recently published a multicenter study in JAMA Network Open comparing long-term outcomes of traditional and endoscopic surgeries in children with craniosynostosis, examining aesthetic and cognitive outcomes. I also have an interest in pediatric neurovascular diseases like arteriovenous malformations and Moyamoya Disease, with ongoing research in these areas.
I am inspired by the tremendous research done at Michigan Health, including dedicated work in the labs of Drs. Maria Castro and Pedro Lowenstein, and the support from the Chad Carr Foundation.
PEDIATRIC PATIENTS
with Dr. Suresh Magge, M.D.
In my role as Surgical Director of the Pediatric Brain Tumor Program, I aim to foster robust collaboration between neurosurgery, neuro-oncology, neuropathology, radiation oncology, neuroradiology, and other providers involved in pediatric brain tumor care. My focus is on initiating more surgical trials and advancing treatment options for pediatric brain tumors and beyond. Through these efforts, I am hopeful that we will achieve better outcomes for children facing these challenging conditions.
Endoscopic (minimally invasive) surgery for craniosynostosis and its outcome in pediatric patients.
MICHIGAN MEDICINE LEADERSHIP
Marschall S. Runge, MD, PhD, Executive Vice President for Medical Affairs University of Michigan, Dean, U-M Medical School, CEO, Michigan Medicine
David C. Miller, MD, MPH, Executive Vice Dean for Clinical Affairs, President U-M Health
Eric Barritt, Senior Associate Vice President and Chief Development Officer
David Brown, MD, Associate Vice President and Associate Dean for Health Equity and Inclusion
Amy Cohn, PhD, AB, Chief Transformation Officer
Matthew C. Comstock, MBA, MHSA, Chief Operating Officer, Medical School
T. Anthony Denton, JD, MHA, Senior Vice President and Chief Environmental, Social, and Governance Officer, U-M Health
Keith Dickey, PhD, AB, Chief Strategy Officer
Rose M. Glenn, Chief Communications and Marketing Officer
Keith Gran, CPA, MBA, Chief Patient Experience Officer
Elizabeth Harry, MD, Chief Well-Being Officer
Jovita Thomas-Williams, MBA, MILR, Chief Human Resources Officer
Steven L. Kunkel, Executive Vice Dean for Research and Chief Scientific Officer
Kara Morgenstern, JD, MPH, Associate Vice President and Deputy General Counsel, University of Michigan