

2023-2024 Rusty Freeman & Associates, LLC. U.S. Employee Benefits Services Group 245 Landa Street New Braunfels, TX 78130 (830)606-5100 www.usebsg.com www.mybenefitshub.com/hondoisd


Support Contacts Amy Arcos Employee Benefits Office/Benefits Specialist Office: (830) 426-3027 ext. 6007 Email: aarcos@hondoisd.net Tracy Hamel Randi Freeman Senior Account Manager Account Manager Office: (830) 606-5100 Email: Thamel@usebsg.com Rmfreeman@usebsg.com Marlene Freeman Senior Account Manager Office: (830) 606-5100 Email: mfreeman@usebsg.com
Table of Content
Enroll Instructions
Medical – TRS Activecare
Medical Transportation - MASA
Telemedicine – 1800MD
Accident – MetLife
Critical Illness – MetLife
Hospital Indemnity - MetLife
Cancer – Guardian
Disability – The Standard
Dental – Lincoln Financial
Vision – Superior
Group Life – Lincoln Financial

Voluntary Life - Lincoln
Texas Life - Permanent Life
Health Savings Account – HSAbank
Flexible Spending Account - NBS
Omni 403(b) – TPA Services
Benefit Contacts
Page
Benefit Phone Website TRS ACTIVECARE – MEDICAL 1-800-523-2233 www.BCBSTX.COM/TRSACTIVECAREE MASA – MEDICAL TRANSPORT 1-954-334-8261 WWW.MASAMTS.COM 1800MD – TELEMEDICINE 1-800-423-2765 WWW.1800MD.COM METLIFE – ACCIDENT & CRITICAL ILLNESS 1-800-438-6388 WWW.METLIFE.COM/MYBENEFITS METLIFE – HOSPITAL INDEMNITY 1-800-438-6388 WWW.METLIFE.COM/MYBENEFITS GUARDIAN – CANCER 1800-256-8609 WWW.GUARDIANANYTIME.COM THE STANDARD – DISABILITTY 1-800-368-1135 WWW.STANDARD.COM LINCOLN – DENTAL 1-800-423-2765 WWW.LINCOLNFINANCIAL.COM SUPERIOR – VISION 1-800-507-3800 WWW.SUPERIORVISION.COM LINCOLN – GROUP & VOLUNTARY LIFE 1-800-423-2765 WWW.LINCOLNFINANCIAL.COM TEXAS LIFE – PERMANENT LIFE 1-800-283-9233 WWW.TEXASLIFE.COM HSABANK – HEALTH SAVINGS ACCT 1-800-357-6246 WWW.HSABANK.COM NBS – FLEXIBLE SPENDING ACCOUNT 1800-274-0503 WWW.NBSBENEFITS.COM OMNI 403(B) – TPA Services 1-877-544-6664 WWW.OMNI403B.COM 4 - 5 6 7 - 8 9 - 10 11 - 16 17 - 20 21 - 22 23 - 25 26 - 31 32 - 35 36 37 38 - 42 43 - 47 48 - 49 50 - 53 54



4
** Includes a wellness benefit of $200 per covered member, per year.

** Includes a wellness benefit of $50.

3 4 3 4 3 3 2
Wellfleet Accident (NEW)
d 5
2023-24 TRS-ActiveCare Plan Highlights
All TRS-ActiveCare participants have three plan options. Each includes a wide range of wellness benefits.
This plan is closed and not accepting new enrollees. If you’re currently enrolled in TRS-ActiveCare 2, you can remain in this plan. TRS-ActiveCare 2 • Closed to new enrollees • Current enrollees can choose to stay in plan • Lower deductible • Copays for many services and drugs • Nationwide network with out-of-network coverage • No requirement for PCPs or referrals TRS-ActiveCare Primary TRS-ActiveCare Primary+ TRS-ActiveCare HD Plan Summary • Lowest premium of all three plans • Copays for doctor visits before you meet your deductible • Statewide network • Primary Care Provider (PCP) referrals required to see specialists • Not compatible with a Health Savings Account (HSA) • No out-of-network coverage • Lower deductible than the HD and Primary plans • Copays for many services and drugs • Higher premium • Statewide network • PCP referrals required to see specialists • Not compatible with a Health Savings Account (HSA) • No out-of-network coverage • Compatible with a Health Savings Account (HSA) • Nationwide network with out-of-network coverage • No requirement for PCPs or referrals • Must meet your deductible before plan pays for non-preventive care Monthly Premiums Employee Only $376 $ $442 $ $388 $ Employee and Spouse $1,016 $ $1,150 $ $1,048 $ Employee and Children $640 $ $752 $ $660 $ Employee and Family $1,279 $ $1,459 $ $1,320 $ Total Premium Total Premium Total Premium Your Premium Your Premium Your Premium Total Premium Your Premium $1,013 $ $2,402 $ $1,507 $ $2,841 $ How to Calculate Your Monthly Premium Total Monthly Premium Your District and State Contributions Your Premium Ask your Benefits Administrator for your district’s specific premiums. Wellness Benefits at No Extra Cost* Being healthy is easy with: •$0 preventive care •24/7 customer service •One-on-one health coaches •Weight loss programs
programs
pregnancy support
TRS Virtual Health
health benefits
•Nutrition
•OviaTM
•
•Mental
•And much more!
Immediate Care Urgent Care $50 copay $50 copay You pay 30% after deductibleYou pay 50% after deductible Emergency Care You pay 30% after deductible You pay 20% after deductible You pay 30% after deductible TRS Virtual Health-RediMD (TM) $0 per medical consultation $0 per medical consultation $30 per medical consultation TRS Virtual Health-Teladoc® $12 per medical consultation $12 per medical consultation $42 per medical consultation $50 copay You pay 40% after deductible You pay a $250 copay plus 20% after deductible $0 per medical consultation $12 per medical consultation
Sept. 1, 2023 – Aug. 31, 2024 New Rx Benefits!
Express Scripts is your new pharmacy benefits manager! CVS pharmacies and most of your preferred pharmacies and medication are still included.
Certain specialty drugs are still $0 through SaveOnSP. Doctor Visits Primary Care $30 copay $15 copay You pay 30% after deductibleYou pay 50% after deductible Specialist $70 copay $70 copay You pay 30% after deductibleYou pay 50% after deductible $30 copay You pay 40% after deductible $70 copay You pay 40% after deductible Plan Features Type of Coverage In-Network Coverage Only In-Network Coverage Only In-Network Out-of-Network Individual/Family Deductible $2,500/$5,000 $1,200/$2,400 $3,000/$6,000 $5,500/$11,000 Coinsurance You pay 30% after deductible You pay 20% after deductible You pay 30% after deductibleYou pay 50% after deductible Individual/Family Maximum Out of Pocket $7,500/$15,000 $6,900/$13,800 $7,500/$15,000 $20,250/$40,500 Network Statewide Network Statewide Network Nationwide Network PCP Required Yes Yes No In-Network Out-of-Network $1,000/$3,000 $2,000/$6,000 You pay 20% after deductibleYou pay 40% after deductible $7,900/$15,800 $23,700/$47,400 Nationwide Network No Prescription Drugs Drug Deductible Integrated with medical $200 deductible per participant (brand drugs only) Integrated with medical Generics (31-Day Supply/90-Day Supply)$15/$45 copay; $0 copay for certain generics $15/$45 copay You pay 20% after deductible; $0 coinsurance for certain generics Preferred You pay 30% after deductible You pay 25% after deductible You pay 25% after deductible Non-preferred You pay 50% after deductible You pay 50% after deductible You pay 50% after deductible Specialty (31-Day Max) $0 if SaveOnSP eligible; You pay 30% after deductible $0 if SaveOnSP eligible; You pay 30% after deductible You pay 20% after deductible Insulin Out-of-Pocket Costs$25 copay for 31-day supply; $75 for 61-90 day supply$25 copay for 31-day supply; $75 for 61-90 day supply You pay 25% after deductible $200 brand deductible $20/$45 copay You pay 25% after deductible ($40 min/$80 max)/ You pay 25% after deductible ($105 min/$210 max) You pay 50% after deductible ($100 min/$200 max)/ You pay 50% after deductible ($215 min/$430 max) $0 if SaveOnSP eligible; You pay 30% after deductible ($200 min/$900 max)/ No 90-day supply of specialty medications $25 copay for 31-day supply; $75 for 61-90 day supply 6
*Available for all plans. See the benefits guide for more details.
•
•
The Ultimate Peace of Mind for Employees and Their Families
The Harrison’s Story
• Jim and his family were at a local festival when his daughter, Sara, suddenly began experiencing horrible abdominal and back pain, after a fall from earlier in the day.
• His wife, Heather, called 911 and Sara was transported to a local hospital, when it was decided that she needed to be flown to another hospital.
• Upon arrival, Sara underwent multiple procedures and her condition was stabilized.

• After further testing, it was discovered that Sara needed additional specialized treatment at another hospital requiring transport on a non-emergent basis.
Based on a true story. Names were changed to protect identities in compliance with HIPAA.
And then, the Bills came!
Any Ground. Any Air. Anywhere.TM
No matter how comprehensive your local in-network coverage may be, you still have significant exposure to out-of-network emergency transportation. Moreover, when you and your family travel outside your area, there is an 80% chance of being picked up by an out-of-network provider.
A MASA Membership prepares you for the unexpected. ONLY MASA MTS provides you with:

• Coverage ANYWHERE in all 50 states and Canada whether at home or away
• Coverage for BOTH emergent ground ambulance and air ambulance transport REGARDLESS of the provider
• Non-emergent transport services, which are frequently covered inadequately by your insurance, if at all For more information, please contact your local MASA MTS representative or visit www.masamts.com
As a MASA Member If a Non-MASA Member Sara would pay*If In-Network**If Out-of-Network** 911 Ground Ambulance Cost: $1,800 $0$300$1,600 Emergent Air Ambulance Cost: $45,000 $0$4,000$30,000 Non-Emergent Air Transport† Cost: $20,000 $0$20,000$20,000 Total Out-of-Pocket Cost $0$24,300$51,600
*Benefit is dependent on Membership Enrolled. **Out-of-pocket dollars vary dependent on provider, distance, health plan design, current status of deductible and out-of pocket max. These figures are an example of the costs one may incur. †More and more health plans are not covering interfacility transports on a non-emergent basis.
FLYER_COMP_B2B
7
EMERGENCY TRANSPORTATION COSTS
MASA MTS is hereto protect its members andtheir families from the shortcomings of health insurance coverageby providingthem with comprehensivefinancial protectionfor lifesaving emergency transportation services, both at home and away fromhome.

Many American employers and employees believe that their health insurance policies cover most, if notall ambulance expenses

Thetruth is, they DONOT!
Even after insurance payments for emergency transportation, you couldreceive a bill up to $5,000 for ground ambulanceand as high as $70,000 for air ambulance. The financial burdens for medical transportation costs are veryreal.
HOW MASA IS DIFFERENT
Across the US there are thousands of ground ambulance providers and hundreds of air ambulance carriers. ONLYMASA offers comprehensive coverage since MASA is a PAYERand not aPROVIDER!

ONLY MASA provides over 1.6million members with coverage for BOTH ground ambulance and air ambulance transport, REGARDLESS of which provider transports them.

Members are covered ANYWHEREin all50 states andCanada!
Additionally, MASA provides a repatriation benefit: if a member is hospitalized more than 100 miles from home, MASA can arrangeand pay to have them transported to a hospital closer to their place of residence.

Any
BENEFITS
A MASA Membership prepares you for the unexpectedandgives you the peaceof mind to access vital emergency medical transportation no matter where you live, for a minimal monthlyfee.
• Onelow fee for the entire family
• NO deductibles
• NO health questions
• Easy claims process
For more information, pleasecontact Your Broker or MASA Representative
EmergentGround Transportation EmergentAir Transportation Non-EmergentAir Transportation Repatriation U.S./Canada U.S./Canada U.S./Canada U.S./Canada Emergent Plus $14/mo.
EVERY FAMILY DESERVES AMASA MEMBERSHIP OUR
Benefit*
* Please refer to the MSA for a detailed explanation of benefits and eligibility, 8
Ground. Any Air. Anywhere.™
HOW IT WORKS

MEMBER INFORMATION Providing Fast And Convenient Care For Your Medical Needs…
•Access to licensed, board-certified physicians • Little or no time missed from work • No crowded waiting rooms or appointment times • Allergies • Arthritic Pain • Cold & Flu • Tonsillitis • Laryngitis • Pharyngitis • Skin Infections • Gastroenteritis
Ear Infection
Pink Eye
Insect Bites
Minor Burns • Respiratory Infections
Sinusitis
Sprains and Strains
Urinary tract Infection
Consulting for International and Domestic Travel
AND MUCH MORE!
COMMONLY TREATED CONDITIONS
•
•
•
•
•
•
•
•
•
Activate your account online at www.1800MD.com or by calling member services at 1.800.530.8666. Once activated, you will need to setup your member profile and complete your electronic health record. Activate 1 Login to your account online or call member services at 1.800.530.8666 to request a consult anytime 24/7. Request a Consult 2 Receive diagnosis and treatment. 1.800MD provides quality care and peace of mind wherever you are. Receive Care 3 Health and pharmacy information must be completed before requesting a consultation. 9
What is 1.800MD?
1.800MD is a national telehealth company specializing in convenient, quality medical care. With board-certified physicians in all 50 states*, those in need can obtain diagnosis, treatment and a prescription, when necessary, through the convenience of a telephone and digital communications.
*Subjecttostateregulations.
I have a pre-existing condition. Will 1.800MD still accept me?
Absolutely! 1.800MD is not insurance. We do not deny access to quality care because of pre-existing conditions.
Can I get a consultation after hours or on weekends?
Yes. 1.800MD is available 24 hours a day, seven days a week and 365 days a year.
CONVENIENCE
Talk to a doctor any time, day or night, on the weekend or when traveling away from home. No inconvenience or hassle of traveling to the doctor’s office, urgent care or ER and waiting to be seen.
SAVES MONEY
1.800MD reduces unnecessary doctor’s office and emergency room visits. Up to 70 percent of all urgent care and emergency room visits are unneeded, costly and can be handled with a 1.800MD telephone or video consultation.
QUALITY CARE
With an average of 15 years of internal medicine, family practice or pediatrics experience, you can rest assured each physician is properly licensed in your state, board-certified and verified by the National Physician Data Base and the American Medical Association.
CONTINUITY OF CARE
Real-time access to medical records, and the ability to send them to your primary care physi-cian or other providers.
WELLNESS AND PREVENTATIVE HEALTH TOOLS
The 1.800MD member portal contains information and tools to help you make informed health care decisions.
E-PRESCRIPTIONS
If a 1.800MD physician recommends medication as part of your treatment plan, the prescription will be digitally sent to the local pharmacy of your choice.
BENEFITS TO YOU
www.1800md.com CALL 1.800.530.8666 l.800MD does not replace the primary care physician. l800MD does not guarantee that a prescription will be written. l800MD operates subject to State regulations and may not be available in certain States. l800MD does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. l800MD physicians reserve the right to deny care for potentialmisuseofservices. 10

Accident Insurance 11
ScheduleofBenefits&Features
• Unlimitedlifetimemaximumbenefitwithnoage-relatedbenefitreductions
• Benefitspaidbasedonthescheduleofbenefitsprovidedforeachcoveredaccident
• WaiverofPremium:Premiumiswaivedfollowinga60-dayperiodofdisabilityduetoacovered accidentforaslongasthecoveredpersonremainsdisabled.
• Portabilityisincluded.
SpecificInjuryBenefit
Fractures
Closed/Non-SurgicalTreatment
Hip,Thigh(Femur)
Vertebrae,Bodyof(excludingVertebral Process)
Pelvis
Leg(Tibiaand/orFibula)
UpperArm(Humerus) $3,000.00
ShoulderBlade $3,000.00
Collarbone $3,000.00
UpperJaw,Maxilla(exceptAlveolarProcess) $2,500.00
AI-2 MP0000822785
ACCIDENTPLANBENEFITS Custom Accident EmergencyandInitialAccidentTreatmentBenefits Ambulance Ground $200.00 Air $600.00 Water $600.00 EmergencyRoomTreatment $200.00 UrgentCare $75.00 MajorDiagnosticImaging $200.00 X-ray $75.00 HospitalBenefits HospitalAdmission $1,000.00 HospitalConfinement $200.00 Maximumperaccident 365days IntensiveCareAdmission $1,000.00 ICUConfinement $200.00 Maximumperaccident 365days ObservationUnit $100.00
$4,000.00
Skull(exceptBonesofFaceorNose) Depressed
$4,000.00
$4,000.00
$4,000.00
$4,000.00
12
LowerJaw,Mandible(exceptAlveolar Process) $2,500.00 VertebralProcess $1,600.00 Forearm(Ulnaand/orRadius) $1,600.00 Hand,Wrist(exceptFingers) $1,600.00 Kneecap $1,600.00 Foot(exceptToes) $1,600.00 Ankle $1,600.00 Rib $300.00 Coccyx $300.00 Finger,Toe $300.00 EnhancementforOpen/SurgicalReduction 2X ChipFractures 25% Dislocations Closed/Non-SurgicalTreatment Hip $4,000.00 Knee(otherthanKneecap) $2,250.00 Shoulder $2,250.00 Kneecap $1,000.00 Ankleboneorbonesofthefoot $1,000.00 Elbow $1,000.00 Wrist $1,000.00 Boneorbonesofthehand $1,000.00 Jawbone $1,000.00 Collarbone $1,000.00 Onetoeorfinger $300.00 EnhancementforOpen/SurgicalReduction 2X PartialDislocations 25% Lacerations NoRepair $50.00 Repair-upto2inches $50.00 Repair-over2inches,upto6inches $200.00 Repair-over6inches $400.00 Burns 2ndDegreeBurns Atleast1%,butlessthan20%ofskinsurface $100.00 20%orgreaterofskinsurface $500.00 3rdDegreeBurns Lessthan5%ofskinsurface $500.00 Atleast5%,butlessthan20%ofskinsurface $5,000.00 20%orgreaterofskinsurface $10,000.00 SkinGraft DuetoBurns(%ofapplicableBurnbenefit) 50% 13
NotduetoBurns Atleast1%,butlessthan20%ofskinsurface $100.00 20%orgreaterofskinsurface $200.00 ConcussionandOtherBrainInjuries $300.00 DentalBenefit $250.00 EyeInjuryBenefit $200.00 SurgeryBenefits OutpatientSurgeryBenefit FacilitiesotherthanPhysicianOfficeor EmergencyRoom $300.00 PhysicianOfficeorEmergencyRoom $300.00 InternalInjuriesSurgicalBenefits OpenAbdominal&Thoracic $2,000.00 Hernia $200.00 ExploratorywithoutRepair $150.00 Tendon/Ligament/RotatorCuffSurgicalBenefit Single $700.00 Multiple $1,050.00 ExploratorywithoutRepair $150.00 TornKneeCartilageSurgeryBenefit TornwithSurgicalRepair $600.00 ExploratorywithoutRepair $150.00 Diagnosisonlywithnosurgeryorrepair $100.00 RupturedDiscwithSurgicalRepair $600.00 AnesthesiaBenefit GeneralAnesthesia $200.00 EpiduralorRegionalAnesthesia $200.00 MedicalBenefits Blood,Plasma&PlateletsBenefit $500.00 ProstheticDeviceBenefit Oneonly $1,000.00 Twoormore $2,000.00 Appliances $300.00 PainManagementBenefit $200.00 Follow-UpCareandTransportationBenefits PhysicianOfficeVisit $75.00 Maximumnumberofvisits 4 TherapyServicesBenefit(Occupational,Physical, SpeechTherapy) $60.00 Maximumnumberofvisits 12 RehabilitationUnitConfinement $200.00 Maximumnumberofdays 90 14
Residence/VehicleModificationBenefit $1,000.00 Transportation(minimumof100milesfrom residence,upto3roundtrips) $.60/mile Lodging $200.00 Maximumnumberofdays 30 AccidentalDeathBenefits AccidentalDeath Employee $40,000.00 Spouse $20,000.00 Child(ren) $20,000.00 CommonCarrierAccidentalDeath Employee $200,000.00 Spouse $100,000.00 Child(ren) $100,000.00 OrganDonorBenefit $5,000.00 AccidentalDismembermentBenefits Dismemberment LossofBothHands,orLossofBothFeet,orLossof OneHandandOneFoot $40,000.00 LossofOneHandorLossofOneFoot $20,000.00 PartialDismemberment LossofOneorMoreFingersorToes $600.00 PartialAmputationofFingerorToe $200.00 CatastrophicBenefits CatastrophicLoss LossofSightinbotheyesorHearinginbothears $20,000.00 LossofSpeechorSightinoneeyeorHearingin oneear $5,000.00 Coma $20,000.00 Paralysis Paraplegia $15,000.00 Quadriplegia $30,000.00 Riders HealthScreeningBenefitRider: $200.00 Numberofpaymentsperyear,percovered person. 1 Monthly Rates Employee Only Employee & SpouseEmployee & Child(ren)Family Custom Accident $14.00 $24.00 $29.00 $39.00 15
EXCLUSIONS*
Inadditiontoanybenefit-specificexclusion,benefitswillnotbepaidforanylosswhich,directlyorindirectly,in wholeorinpart,iscausedbyorresultsfromanyofthefollowingunlesscoverageisspecificallyprovidedforby nameinthisCertificate:
1.Aninjuryincurredwhileworkingforpayorprofit;
2.Intentionallyself-inflictedinjury,suicide,oranyattemptorthreatwhilesaneorinsane;
3.Participatinginwaroranyactofwarwhetherdeclaredorundeclared;
4.Commissionorattempttocommitafelony;
5.Commissionoforactiveparticipationinariot,insurrection,orterroristactivity;
6.Engaginginanillegalactivityoroccupation;
7.Flightin,boarding,oralightingfromanaircraftoranycraftdesignedtoflyabovetheearth’ssurface,including anytravelbeyondtheearth’satmosphereexceptafare-payingpassengeronaregularlyscheduledcommercial orcharterairline;
8.Practicingfororparticipatinginanysemi-professionalorprofessionalcompetitiveathleticcontest,including officiatingorcoaching,forwhichthecoveredpersonreceivesanycompensationorremuneration;
9.Sickness,exceptforanybacterialinfectionresultingfromanaccidentalexternalcutorwoundoraccidental ingestionofcontaminatedfood;
10.Voluntaryingestionorinhalationofanynarcotic,drug,poison,gasorfumes,unlessprescribedortakenunder thedirectionofaphysicianandtakeninaccordancewiththeprescribeddosage;
11.Operatinganytypeofvehiclewhileundertheinfluenceofalcoholoranydrug,narcoticorotherintoxicant includinganyprescribeddrugforwhichthecoveredpersonhasbeenprovidedawrittenwarningagainst operatingavehiclewhiletakingit.Undertheinfluenceofalcohol,forpurposesofthisexclusion,means intoxicated,asdefinedbythelawoftheStateinwhichthecoveredaccidentoccurred;
12.Carethatisnotrecommendedandapprovedbyaphysician.
16

17
18








19
20
Subcategory Benefit Limits (Applies to Subcategory)

Hospital Indemnity Insurance Plan Summary
Benefit
Admission Benefit 1 time(s) per calendar year
Confinement Benefit
15 days per calendar year
ICU Supplemental Confinement will pay an additional benefit for 15 of those days
Admission
ICU Supplemental Admission (Benefit paid concurrently with the Admission benefit when a Covered Person is admitted to ICU)
Confinement²
ICU Supplemental Confinement (Benefit paid concurrently with the Confinement benefit when a Covered Person is admitted to ICU)
Hondo ISD
ADF# HI1993.18
2 If the Admission Benefit is payable for a Confinement, the Confinement Benefit will begin to be payable the day after Admission.
21
22
www.mybenefits.metlife.com
HONDOINDEPENDENTSCHOOLDISTRICT
GroupNumber: 00574523
ACancerinsuranceplanthroughGuardianprovides:
•Lump-sumcashpaymentsforcertainprocedures,screeningsandtreatmentsrelatedtoacoveredcancerdiagnosis,inaddition towhateveryourmedicalplancovers
•Paymentsaremadedirectlytoyouandcanbeusedforanypurpose
•Abilitytotakethecoveragewithyouifyouchangejobsorretire
•Affordablegrouprates
AboutYourBenefits:
COVERAGE-DETAILSOption1Option2
INITIALDIAGNOSISBENEFIT- BenefitispaidwhenyouarediagnosedwithInternalcancerforthefirsttimewhileinsuredunderthisPlan.
BenefitAmount(s)
BenefitWaitingPeriod- Aspecifiedperiodoftimeafteryour effectivedateduringwhichtheInitialDiagnosisbenefitswillnotbe payable.
CANCERSCREENING
RADIATIONTHERAPYORCHEMOTHERAPY
Benefit
Pre-ExistingConditionsLimitation: Apre-existingcondition includesanyconditionforwhichyou,inthespecifiedtimeperiodprior tocoverageinthisplan,consultedwithaphysician,received treatment,ortookprescribeddrugs.
Portability: AllowsyoutotakeyourCancercoveragewithyouif youterminateemployment.PortedCancerplanterminatesatage70.
Child(ren)AgeLimits
FEATURES
Anti-Nausea
AttendingPhysician
Blood/Plasma/Platelets
$100; $100 for Follow-Up screening
3monthsprior/6months treatmentfree/12monthsafter.
3monthsprior/6months treatmentfree/12monthsafter.
CancerBenefitSummary
CANCER
YourMonthlypremium $18.84$28.10 YouandSpouse $29.78 $43.88 YouandChild(ren) $26.10 $39.56 You,SpouseandChild(ren) $37.04 $55.34
Employee$1,500 Spouse$1,500 Child$1,500
Employee$2,500 Spouse$2,500 Child$2,500
30Days 30Days
$100; $100 for Follow-Up screening
BenefitAmount
.
IncludedIncluded
Childrenagebirthto26yearsChildrenagebirthto26years
$1,500/trip,limit2tripsper hospitalconfinement $1,500/trip,limit2tripsper hospitalconfinement Ambulance $200/trip,limit2tripsperhospital confinement $200/trip,limit2tripsperhospital confinement
25%ofsurgerybenefit 25%ofsurgerybenefit
AirAmbulance
Anesthesia
$50/dayupto$150permonth$50/dayupto$150permonth
$25/daywhilehospitalconfined.
$25/daywhilehospitalconfined. Limit75visits.
Limit75visits.
Benefit information illustrated within this material reflects the plan covered by Guardian as of 04/07/2020 ALL ELIGIBLE EMPLOYEES Benefit Summary The Guardian Life Insurance Company of America, New York, NY 23
FEATURES(Cont.)
BoneMarrow/StemCell
ExperimentalTreatment
Option1
BoneMarrow:$7,500
StemCell:$1,500
50%benefitfor2ndtransplant. $1,000benefitifadonor
Option2
BoneMarrow:$7,500
StemCell:$1,500
50%benefitfor2ndtransplant. $1,000benefitifadonor
$100/dayupto$1,000/month$100/dayupto$1,000/month
ExtendedCareFacility/SkilledNursingcare $ 100/dayupto90daysperyear$100/dayupto90daysperyear
GovernmentorCharityHospital
$300perdayinlieuofallother benefits $300perdayinlieuofallother benefits
HomeHealthCare $50/visitupto30visitsperyear$50/visitupto30visitsperyear
HormoneTherapy $25/treatmentupto12treatments peryear
$25/treatmentupto12treatments peryear
Hospice $50/dayupto100days/lifetime$50/dayupto100days/lifetime
HospitalConfinement $300/dayforfirst30days; $600/dayfor31stdaythereafter perconfinement
$300/dayforfirst30days; $600/dayfor31stdaythereafter perconfinement
$400/dayforfirst30days; $600/dayfor31stdaythereafter perconfinement Immunotherapy
ICUConfinement $400/dayforfirst30days; $600/dayfor31stdaythereafter perconfinement
Outpatientandfamilymemberlodging-Lodgingmustbemorethan 50milesfromyourhome.
OutpatientorAmbulatorySurgicalCenter
PhysicalorSpeechTherapy
Prosthetic
ReconstructiveSurgery
SecondSurgicalOpinion
SkinCancer
$75/day,upto90daysperyear$75/day,upto90daysperyear
$250/day,3daysperprocedure$250/day,3daysperprocedure
$25/visitupto4visitspermonth, $400lifetimemax
SurgicallyImplanted:$2,000/device, $4,000lifetimemax
Non-Surgically:$200/device,$400 lifetimemax
BreastTRAMFlap$2,000
Breastreconstruction$500
BreastSymmetry$250 Facialreconstruction$500
$25/visitupto4visitspermonth, $400lifetimemax
SurgicallyImplanted:$2,000/device, $4,000lifetimemax
Non-Surgically:$200/device,$400 lifetimemax
BreastTRAMFlap$2,000
Breastreconstruction$500
BreastSymmetry$250
Facialreconstruction$500
$200/surgeryprocedure $200/surgeryprocedure
BiopsyOnly:$100
ReconstructiveSurgery:$250
Excisionofaskincancer:$375
Excisionofaskincancerwithflap orgraft:$600
BiopsyOnly:$100
ReconstructiveSurgery:$250
Excisionofaskincancer:$375
Excisionofaskincancerwithflap orgraft:$600
SurgicalBenefit
WaiverofPremium-Ifyoubecomedisabledduetocancerthatis diagnosedaftertheemployee'seffectivedate,andyouremain disabledfor90days,wewillwaivethepremiumdueaftersuch90 daysforaslongasyouremaindisabled.
$0.50/mileupto$1,000perround trip/equalbenefitforcompanion
Scheduleamountupto$4,125Scheduleamountupto$4,125 Transportation/CompanionTransportation-Benefitispaidifyou havetotravelmorethan50milesonewaytoreceivetreatmentfor internalcancer.
$0.50/mileupto$1,000perround trip/equalbenefitforcompanion
TheGuardianLifeInsuranceCompanyofAmerica,NewYork,NY
ALLELIGIBLEEMPLOYEESBenefitSummary
$500permonth,$2500lifetime
$500permonth,$2500lifetime
max
max InpatientSpecialNursing $100/dayupto30daysperyear$100/dayupto30daysperyear MedicalImaging $100/imageupto2peryear$100/imageupto2peryear
Included Included 24
UNDERSTANDINGYOURBENEFITS:
• Cancer –Cancermeansyouhavebeendiagnosedwithadisease manifestedbythepresenceofamalignanttumor characterizedbytheuncontrolledgrowthandspreadofmalignantcellsinanypartofthebody.Thisincludesleukemia, Hodgkin'sdisease,lymphoma,sarcoma,malignanttumorsandmelanoma.Cancerincludescarcinomasin-situ(inthenaturalor normalplace,confinedtothesiteoforigin,withouthavinginvadedneighboringtissue).Pre-malignantconditionsorconditions withmalignantpotential,suchasmyelodyplasticandmyeloproliferativedisorders,carcinoid,leukoplakia,hyperplasia,actinic keratosis,polycythemia,andnonmalignantmelanoma,molesorsimilardiseasesorlesionswillnotbeconsideredcancer. CancermustbediagnosedwhileinsuredundertheGuardiancancerplan.
• ExperimentalTreatment –Benefitswillbepaidforexperimentaltreatmentprescribedbyadoctorforthepurposeof destroyingorchangingabnormaltissue.AlltreatmentmustbeNCIlistedasviableexperimentaltreatmentforInternal Cancer.
ManageYourBenefits:
Gotowww.GuardianAnytime.comto accesssecureinformation aboutyourGuardianbenefits.Youron-lineaccountwillbeset upwithin30daysafteryourplaneffectivedate.
LIMITATIONSANDEXCLUSIONS:
ASUMMARYOFCANCERLIMITATIONSANDEXCLUSIONS:
ConditionalIssueunderwritingisrequiredonthoseenrollingoutsideofthe initialenrollmentperiodorannualopenenrollmentperiod.
Thisplanwillnotpaybenefitsfor:Servicesortreatmentnotincludedinthe Features.Servicesortreatmentprovidedbyafamilymember.Servicesor treatmentrenderedforhospitalconfinementoutsidetheUnitedStates.Any cancerdiagnosedsolelyoutsideoftheUnitedStates.Servicesortreatment providedprimarilyforcosmeticpurposes.Servicesortreatmentfor premalignantconditions.Servicesortreatmentforconditionswithmalignant potential.Servicesortreatmentfornon-cancersicknesses.
NeedAssistance?
CalltheGuardianHelpline(888)600-1600,weekdays,8:00AM to8:30PM,EST.RefertoyourmemberID(socialsecurity number)andyourplannumber:00574523
Cancercausedby,contributedtoby,orresultingfrom:participatinginafelony, riotorinsurrection;intentionallycausingaself-inflictedinjury;committingor attemptingtocommitsuicidewhilesaneorinsane;acoveredperson’smentalor emotionaldisorder,alcoholismordrugaddiction;engaginginanyillegalactivity; orservinginthearmedforcesoranyauxiliaryunitofthearmedforcesofany country.
IfCancerinsurancepremiumispaidforonapretaxbasis,thebenefitmaybetaxable. Pleasecontactyourtaxorlegaladvisorregardingthetaxtreatmentofyourpolicy benefits.
Thisdocumentisasummaryofthemajorfeaturesofthereferencedinsurancecoverage. Itisintendedforillustrativepurposesonlyanddoesnotconstitute acontract.Theinsuranceplandocuments,includingthepolicyandcertificate,comprisethecontractforcoverage.Thefullplandescription,incl udingthe benefitsandallterms,limitationsandexclusionsthatapplywillbecontainedinyourinsurancecertificate.Theplandocumentsarethefinalarbiterof coverage.Coveragetermsmayvarybystateandactualsoldplan.Thepremiumamountsreflectedinthissummaryareanapproximation;ifthereisa discrepancybetweenthisamountandthepremiumactuallybilled,thelatterprevails.
ALLELIGIBLEEMPLOYEESBenefitSummary
TheGuardianLifeInsuranceCompanyofAmerica,NewYork,NY
Contract#GP-1-CAN-IC-12
25

26
27
28
29
30
31
Full-Time Employees of Hondo Independent School District
Benefits At-A-Glance
Dental Insurance
The Lincoln
DentalConnect® PPO Plan:
Covers many preventive, basic, and major dental care services
Also covers orthodontic treatment for children
Features group coverage for Hondo Independent School District employees

Allows you to choose any dentist you wish, though you can lower your out-of-pocket costs by selecting a contracting dentist
Does not make you and your loved ones wait six months between routine cleanings
Calendar (Annual)
Deductible
Contracting Dentists
Individual: $50
Family: $150
Waived for: Preventive
Non-Contracting Dentists
Individual: $50
Family: $150
Waived for: Preventive
Deductibles are combined for basic and major Contracting Dentists’ services. Deductibles are combined for basic and major Non-Contracting Dentists’ services.
Annual Maximum $1,000 $1,000
MaxRewards® lets you and your covered family members roll a portion of unused dental benefits from one year into the next. So you have extra benefit dollars available when you need them most.
$500
$250 per calendar year
$250 per calendar year
$1,000
Lifetime Orthodontic Max $1,000 $1,000
Orthodontic Coverage is available for dependent children.
Waiting Period
This plan includes an additional waiting period if you do not enroll within the defined timeframe when it is first offered to you or within an annual open enrollment period.
12 months for basic services
12 months for major services
12 months for orthodontic services
32
Routine oral exams
Bitewing X-rays
Full-mouth or panoramic X-rays
Other dental X-rays (including periapical films)
Routine cleanings
Fluoride treatments
Space maintainers for children
Problem focused exams
Consultations
Palliative treatment (including emergency relief of dental pain)
Fillings
Prefabricated stainless steel and resin crowns
Simple extractions
Surgical extractions
General anesthesia and
Prosthetic repair
sedation
recementation services
Injections of antibiotics and other therapeutic medications
Oral surgery
Biopsy and examination of oral tissue (including brush biopsy)
Endodontics (including root canal treatment)
Periodontal maintenance procedures
Non-surgical periodontal therapy
Periodontal surgery
Bridges
Full and partial dentures
Denture reline and rebase services
Crowns, inlays, onlays and related services
Build-ups/post & core
To find a contracting dentist near you, visit www.LincolnFinancial.com/FindADentist
This plan lets you choose any dentist you wish. However, your out-of-pocket costs are likely to be lower when you choose a contracting dentist. For example, if you need a crown…
…you pay a deductible (if applicable), then 50% of the remaining discounted fee for PPO members. This is known as a PPO contracted fee.
… you pay a deductible (if applicable), then 50% of the usual and customary fee, which is the maximum expense covered by the plan. You are responsible for the difference between the usual and customary fee and the dentist’s billed charge.
Contracting Dentists Non-Contracting Dentists
Sealants 100% No Deductible 100% No Deductible Contracting Dentists Non-Contracting Dentists
I.V.
80% After Deductible 80% After Deductible Contracting Dentists Non-Contracting Dentists
and
50% After Deductible 50% After Deductible Orthodontics Contracting Dentists Non-Contracting Dentists Orthodontic exams X-rays Extractions Study models Appliances 50% 50% Contracting Dentists/Non-Contracting Dentists Contracting Dentists Non-Contracting Dentists
33
With the Lincoln Dental Mobile App
Find a network dentist near you in minutes
Have an ID card on your phone
Customize the app to get details of your plan
Find out how much your plan covers for checkups and other services
Keep track of your claims
Lincoln DentalConnect® Online Health
Center
Determine the average cost of a dental procedure
Have your questions answered by a licensed dentist
Learn all about dental health for children, from baby’s first tooth to dental emergencies
Evaluate your risk for oral cancer, periodontal disease and tooth decay
Family Members
When you choose coverage for yourself, you can also provide coverage for:
• Your spouse or domestic partner.
• Unmarried dependent children, up to age 26.
Benefit Exclusions
Like any coverage, this dental coverage does have some exclusions. The plan does not cover services started before coverage begins or after it ends. Benefits are limited to appropriate and necessary procedures listed in the summary plan description. Benefits are not payable for duplication of services. Covered expenses will not exceed the summary plan description’s usual and customary allowances. Plan benefits are not payable for a condition that is covered under Workers’ Compensation or a similar law; that occurs during the course of employment or military service or involvement in an illegal occupation, felony, or riot; or that results from a self-inflicted injury. The plan does not cover an orthodontia treatment plan started before coverage begins unless the member was receiving orthodontia benefits from the employer’s previous group dental summary plan description. In this case, Lincoln Financial will continue orthodontia benefits until the combined benefit paid by both policies is equal to this summary plan description’s lifetime orthodontia maximum. Plan benefits are not payable if the orthodontic appliance was installed after the age of 19. In certain situations, there may be more than one method of treating a dental condition. This summary plan description includes an alternative benefits provision that may reduce benefits to the lowestcost, generally effective, and necessary form of treatment. Certain conditions, such as age and frequency limitations, may impact your coverage. See the summary plan description for details.
A complete list of benefit exclusions is included in the summary plan description.
34
Dental
Here’s you pay group rates.
As a Hondo Independent School District employee, you can take advantage of this dental coverage for less than $1.31 a day. Plus, you can add loved ones to the plan for just a little more.
Your estimated cost is itemized below.
Monthly Employee only $39.24 Employee & spouse/domestic partner $76.70 Employee & child/children $70.36 Employee & family $112.02 35
1 -office standard retail lined trifocal amount; member pays difference between progressive and standard retail lined trifocal, plus applicable co-pay
Contact lenses and related professional services (fitting, evaluation and follow-up) are covered in lieu of eyeglass lenses and frames benefit
The Plan discount features are not insurance.
All allowances are retail; the member is responsible for paying the provider directly for all non-covered items and/or any amount over the allowances, minus available discounts. These are not covered by the plan. Discounts are subject to change without notice.
Disclaimer: All final determinations of benefits, administrative duties, anddefinitions are governed by the Certificate of Insurance for your vision plan. Please check with your Human Resources department if you have any questions
36
Full-Time Employees
Term Life and AD&D Insurance
Safeguard the most important people in your life.
Think about what your loved ones may face after you’re gone. Term life insurance can help them in so many ways, like covering everyday expenses, paying off debt, and protecting savings. AD&D provides even more coverage if you die or suffer a covered loss in an accident.
AT A GLANCE:
• A cash benefit of $15,000 to your loved ones in the event of your death, plus a matching cash benefit if you die in an accident
• A cash benefit to you if you suffer a covered loss in an accident, such as losing a limb or your eyesight
• LifeKeys® services, which provide access to counseling, financial, and legal support
• TravelConnect® services, which give you and your family access to emergency medical assistance when you're on a trip 100+ miles from home
You also have the option to increase your cash benefit by securing additional coverage at affordable group rates. See the enclosed life insurance information for details.
ADDITIONAL DETAILS
Conversion: You can convert your group term life coverage to an individual life insurance policy without providing evidence of insurability if you lose coverage due to leaving your job or for another reason outlined in the plan contract. AD&D benefits cannot be converted.
Benefit Reduction: Benefits terminate at retirement. See the plan certificate for details. For complete benefit descriptions, limitations, and exclusions, refer to the certificate of coverage. This is not intended as a complete description of the insurance coverage offered. Controlling provisions are provided in the policy, and this summary does not modify those provisions or the insurance in any way. This is not a binding contract. A certificate of coverage will be made available to you that describes the benefits in greater detail. Refer to your certificate for your maximum benefit amounts. Should there be a difference between this summary and the contract, the contract will govern.
LifeKeys® services are provided by ComPsych® Corporation, Chicago, IL. ComPsych®, EstateGuidance® and GuidanceResources® are registered trademarks of ComPsych® Corporation. TravelConnect® services are provided by On Call International, Salem, NH. ComPsych® and On Call Internationalare not Lincoln Financial Group® companies. Coverage is subject to actual contract language. Each independent company is solely responsible for its own obligations.
Insurance products (policy series GL1101) are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so. Product availability and/or features may vary by state. Limitations and exclusions apply. Lincoln Financial Group is the marketing name for Lincoln National Corporation and its affiliates. Affiliates are separately responsible for their own financial and contractual obligations. Limitations and exclusions apply.
Hondo Independent School District provides this valuable benefit at no cost to you.
37
Voluntary Term Life Insurance
The Lincoln Term Life Insurance Plan:
• Provides a cash benefit to your loved ones in the event of your death
• Features group rates for Hondo Independent School District employees
• Includes LifeKeys® services, which provide access to counseling, financial, and legal support services
• Also includes TravelConnect® services, which give you and your family access to emergency medical assistance when you’re on a trip 100+ miles from home
Full-Time Employees of Hondo Independent School District Benefits
At-A-Glance
Employee
Newly hired employeeguaranteed coverage amount $150,000
Continuing employee guaranteed coverage annual increase amount Choice of $10,000 or $20,000
Maximum coverage amount 5 times your annual salary ($500,000 maximum in increments of $10,000)
Minimum coverage amount $20,000
Spouse / Domestic Partner
Newly hired employee guaranteed coverage amount $50,000
Continuing employee guaranteed coverage annual increase amount Choice of $5,000 or $10,000
Maximum coverage amount 50% of the employee coverage amount ($250,000 maximum in increments of $5,000)
Minimum coverage amount $10,000
Dependent Children
6 months to age 26 guaranteed coverage amount $10,000 Age 14 days to 6 months guaranteed coverage amount $250
38
What your benefits cover
Employee Coverage
Guaranteed Life Insurance Coverage Amount
• Initial Open Enrollment: When you are first offered this coverage, you can choose a coverage amount up to $150,000 without providing evidence of insurability.
Annual Limited Enrollment: If you are a continuing employee, you can increase your coverage amount by $10,000 or $20,000 without providing evidence of insurability . If you submitted evidence of insurability in the past and were declined for medical reasons, you may be required to submit evidence of insurability.
If you decline this coverage now and wish to enroll later, evidence of insurability may be required and may be at your own expense.
You can increase this amount by up to $20,000 during the next limited open enrollment period.
Maximum Life Insurance Coverage Amount
• You can choose a coverage amount up to 5 times your annual salary ($500,000 maximum) with evidence of insurability. See the Evidence of Insurability page for details.
Spouse / Domestic Partner Coverage - You can secure term life insurance for your spouse / domestic partner if you select coverage for yourself.
Guaranteed Life Insurance Coverage Amount
Initial Open Enrollment: When you are first offered this coverage, you can choose a coverage amount up to 50% of your coverage amount ($50,000 maximum) for your spouse / domestic partner without providing evidence of insurability.
Annual Limited Enrollment: If you are a continuing employee, you can increase the coverage amount for your spouse / domestic partner by $5,000 or $10,000 without providing evidence of insurability. If you submitted evidence of insurability in the past and were declined for medical reasons, you may be required to submit evidence of insurability.
If you decline this coverage now and wish to enroll later, evidence of insurability may be required and may be at your own expense.
You can increase this amount by up to $10,000 during the next limited open enrollment period.
Maximum Life Insurance Coverage Amount
You can choose a coverage amount up to 50% of your coverage amount ($250,000 maximum) for your spouse / domestic partner with evidence of insurability.
Dependent Children Coverage - You can secure term life insurance for your dependent children when you choose coverage for yourself.
Guaranteed Life Insurance Coverage Options: $1,000, $5,000, and $10,000.
39
Additional Plan Benefits
Accelerated Death Benefit Included
Premium Waiver Included
Conversion Included
Portability Included
Benefit Exclusions
Like any insurance, this term life insurance policy does have exclusions. A suicide exclusion may apply. A complete list of benefit exclusions is included in the policy. State variations apply.
40
Monthly Voluntary Life Insurance Premium
Here’s how little you pay with group rates.
Group Rates for You
The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $10,000) by the employee age-range premium factor.
$____________ X ___________ = $ coverage amount premium factor monthly premium
Note: Rates are subject to change and can vary over time.
Employee Age Range Life Premium Rate Factor 0 - 24 0.0000300 25 - 29 0.0000500 30 - 34 0.0000800 35 - 39 0.0001000 40 - 44 0.0001600 45 - 49 0.0002100 50 - 54 0.0004200 55 - 59 0.0007800 60 - 64 0.0011400 65 - 69 0.0019200 70 - 74 0.0034600 75 - 79 0.0127100 80 - 99 0.0127100
Employee |Monthly Premiums for Select Life Insurance Coverage Amounts Employee Age Range $20,000 $30,000 $40,000 $50,000 $100,000 $150,000 $200,000 $300,000 $500,000 0 - 24 $0.60 $0.90 $1.20 $1.50 $3.00 $4.50 $6.00 $9.00 $15.00 25 - 29 $1.00 $1.50 $2.00 $2.50 $5.00 $7.50 $10.00 $15.00 $25.00 30 - 34 $1.60 $2.40 $3.20 $4.00 $8.00 $12.00 $16.00 $24.00 $40.00 35 - 39 $2.00 $3.00 $4.00 $5.00 $10.00 $15.00 $20.00 $30.00 $50.00 40 - 44 $3.20 $4.80 $6.40 $8.00 $16.00 $24.00 $32.00 $48.00 $80.00 45 - 49 $4.20 $6.30 $8.40 $10.50 $21.00 $31.50 $42.00 $63.00 $105.00 50 - 54 $8.40 $12.60 $16.80 $21.00 $42.00 $63.00 $84.00 $126.00 $210.00 55 - 59 $15.60 $23.40 $31.20 $39.00 $78.00 $117.00 $156.00 $234.00 $390.00 60 - 64 $22.80 $34.20 $45.60 $57.00 $114.00 $171.00 $228.00 $342.00 $570.00 65 - 69 $38.40 $57.60 $76.80 $96.00 $192.00 $288.00 $384.00 $576.00 $960.00 70 - 74 $69.20 $103.80 $138.40 $173.00 $346.00 $519.00 $692.00 $1038.00 $1730.00 75 - 79 $254.20 $381.30 $508.40 $635.50 $1271.00 $1906.50 $2542.00 $3813.00 $6355.00 80 - 99 $254.20 $381.30 $508.40 $635.50 $1271.00 $1906.50 $2542.00 $3813.00 $6355.00 41
Group Rates for Your Spouse / Domestic Partner
The estimated monthly premium for life insurance is determined by multiplying the desired amount of coverage (in increments of $5,000) by the employee age-range premium factor.
$____________
Note: Rates are subject to change and can vary over time.
Group Rates for Your Dependent Children
One affordable monthly premium covers all of your eligible dependent children.
Note: You must be an active Hondo Independent School District employee to select coverage for a spouse / domestic partner and/or dependent children. To be eligible for coverage, a spouse / domestic partner or dependent child cannot be confined to a health care facility or unable to perform the typical activities of a healthy person of the same age and gender.
Employee Age Range Life Premium Rate Factor 0 - 24 0.0000500 25 - 29 0.0000800 30 - 34 0.0001000 35 - 39 0.0001300 40 - 44 0.0001800 45 - 49 0.0002900 50 - 54 0.0005200 55 - 59 0.0009600 60 - 64 0.0014600 65 - 69 0.0023700 70 - 74 0.0043900 75 - 79 0.0146900 80 - 99 0.0146900
___________ = $ coverage amount premium factor monthly premium
X
Spouse / Domestic Partner | Monthly Premiums for Select Life Insurance Coverage Amounts Employee Age Range $10,000 $25,000 $35,000 $45,000 $50,000 $60,000 $75,000 $150,000 $250,000 0 - 24 $0.50 $1.25 $1.75 $2.25 $2.50 $3.00 $3.75 $7.50 $12.50 25 - 29 $0.80 $2.00 $2.80 $3.60 $4.00 $4.80 $6.00 $12.00 $20.00 30 - 34 $1.00 $2.50 $3.50 $4.50 $5.00 $6.00 $7.50 $15.00 $25.00 35 - 39 $1.30 $3.25 $4.55 $5.85 $6.50 $7.80 $9.75 $19.50 $32.50 40 - 44 $1.80 $4.50 $6.30 $8.10 $9.00 $10.80 $13.50 $27.00 $45.00 45 - 49 $2.90 $7.25 $10.15 $13.05 $14.50 $17.40 $21.75 $43.50 $72.50 50 - 54 $5.20 $13.00 $18.20 $23.40 $26.00 $31.20 $39.00 $78.00 $130.00 55 - 59 $9.60 $24.00 $33.60 $43.20 $48.00 $57.60 $72.00 $144.00 $240.00 60 - 64 $14.60 $36.50 $51.10 $65.70 $73.00 $87.60 $109.50 $219.00 $365.00 65 - 69 $23.70 $59.25 $82.95 $106.65 $118.50 $142.20 $177.75 $355.50 $592.50 70 - 74 $43.90 $109.75 $153.65 $197.55 $219.50 $263.40 $329.25 $658.50 $1097.50 75 - 79 $146.90 $367.25 $514.15 $661.05 $734.50 $881.40 $1101.75 $2203.50 $3672.50 80 - 99 $146.90 $367.25 $514.15 $661.05 $734.50 $881.40 $1101.75 $2203.50 $3672.50 Dependent Children Monthly Premium for Life Insurance Coverage Coverage Amount Monthly Premium $1,000 $0.18 $5,000 $0.90 $10,000 $1.80
42

43

44
45
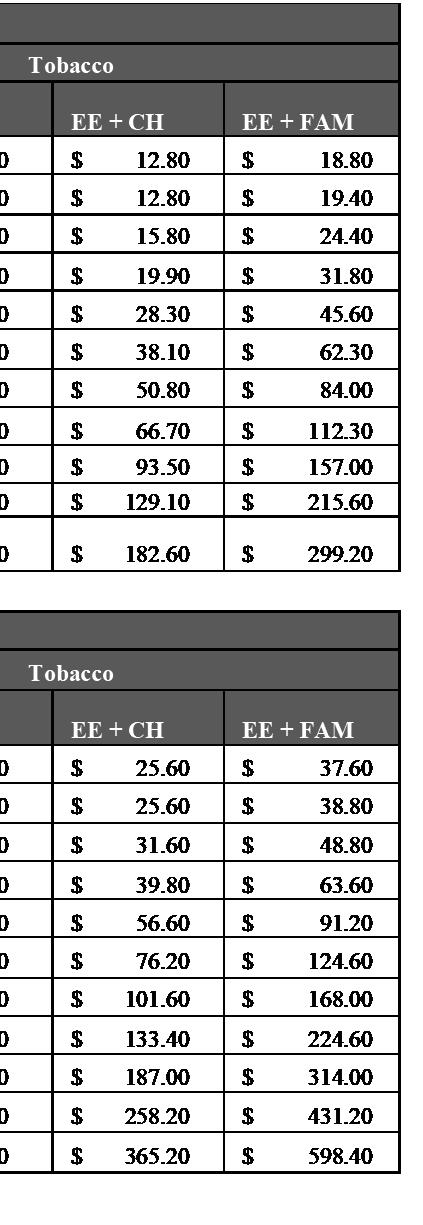
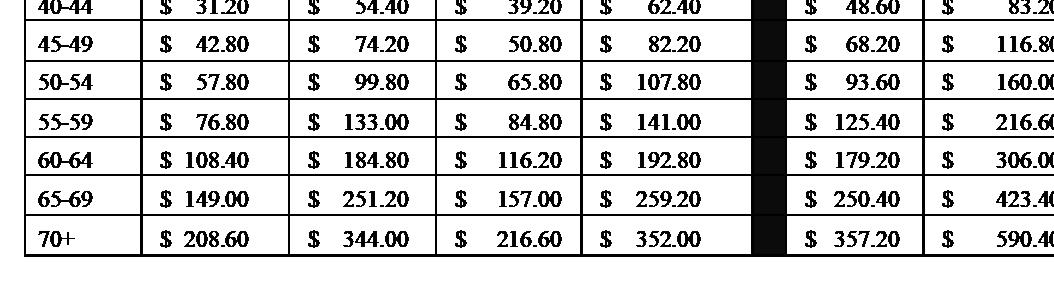
PureLife-plusispermanentlifeinsurancetoAttainedAge121thatcanneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthantheTablePremium.Seethebrochureunder”PermanentCoverage”.
monthlypremiums
ExpressIssue GUARANTEED MonthlyPremiumsforLifeInsuranceFaceAmountsShown PERIOD AgetoWhich Issue Coverageis Age Guaranteedat (ALB) $10,000 $15,000 $25,000 $40,000 $50,000 $75,000 $100,000 $125,000 $150,000 TablePremium 15D-1 9.25 81 2-4 9.50 80 5-8 9.75 79 9-10 10.00 79 11-16 10.25 77 17-20 10.25 15.05 18.25 26.25 34.25 42.25 50.25 75 21-22 10.50 15.45 18.75 27.00 35.25 43.50 51.75 74 23 10.75 15.85 19.25 27.75 36.25 44.75 53.25 75 24-25 11.00 16.25 19.75 28.50 37.25 46.00 54.75 74 26 11.50 17.05 20.75 30.00 39.25 48.50 57.75 75 27-28 11.75 17.45 21.25 30.75 40.25 49.75 59.25 74 29 12.00 17.85 21.75 31.50 41.25 51.00 60.75 74 30-31 12.25 18.25 22.25 32.25 42.25 52.25 62.25 73 32 13.00 19.45 23.75 34.50 45.25 56.00 66.75 74 33 13.50 20.25 24.75 36.00 47.25 58.50 69.75 74 34 14.25 21.45 26.25 38.25 50.25 62.25 74.25 75 35 10.05 15.25 23.05 28.25 41.25 54.25 67.25 80.25 76 36 10.35 15.75 23.85 29.25 42.75 56.25 69.75 83.25 76 37 10.80 16.50 25.05 30.75 45.00 59.25 73.50 87.75 77 38 11.25 17.25 26.25 32.25 47.25 62.25 77.25 92.25 77 39 12.00 18.50 28.25 34.75 51.00 67.25 83.50 99.75 78 40 9.25 12.75 19.75 30.25 37.25 54.75 72.25 89.75 107.25 79 41 9.95 13.80 21.50 33.05 40.75 60.00 79.25 98.50 117.75 80 42 10.75 15.00 23.50 36.25 44.75 66.00 87.25 108.50 129.75 81 43 11.45 16.05 25.25 39.05 48.25 71.25 94.25 117.25 140.25 82 44 12.15 17.10 27.00 41.85 51.75 76.50 101.25 126.00 150.75 83 45 12.85 18.15 28.75 44.65 55.25 81.75 108.25 134.75 161.25 83 46 13.65 19.35 30.75 47.85 59.25 87.75 116.25 144.75 173.25 84 47 14.35 20.40 32.50 50.65 62.75 93.00 123.25 153.50 183.75 84 48 15.05 21.45 34.25 53.45 66.25 98.25 130.25 162.25 194.25 85 49 15.95 22.80 36.50 57.05 70.75 105.00 139.25 173.50 207.75 85 50 16.95 24.30 39.00 61.05 75.75 112.50 86 51 18.15 26.10 42.00 65.85 81.75 121.50 87 52 19.45 28.05 45.25 71.05 88.25 131.25 88 53 20.45 29.55 47.75 75.05 93.25 138.75 88 54 21.45 31.05 50.25 79.05 98.25 146.25 88 55 22.55 32.70 53.00 83.45 103.75 154.50 89 56 23.55 34.20 55.50 87.45 108.75 162.00 89 57 24.75 36.00 58.50 92.25 114.75 171.00 89 58 25.85 37.65 61.25 96.65 120.25 179.25 89 59 27.05 39.45 64.25 101.45 126.25 188.25 89 60 28.55 41.70 68.00 107.45 133.75 199.50 90 61 29.85 43.65 71.25 112.65 140.25 209.25 90 62 31.45 46.05 75.25 119.05 148.25 221.25 90 63 33.05 48.45 79.25 125.45 156.25 233.25 90 64 34.75 51.00 83.50 132.25 164.75 246.00 90 65 36.65 53.85 88.25 139.85 174.25 260.25 90 66 38.75 90 67 41.05 91 68 43.55 91 69 46.05 91 70 48.65 91
Non-Tobacco
PureLife-plus StandardRiskTablePremiums Non-Tobacco
Form:21M013-ICCEXP-A-M-1LO 46
PureLife-plusispermanentlifeinsurancetoAttainedAge121thatcanneverbecancelledaslongasyoupaythenecessarypremiums.Afterthe GuaranteedPeriod,thepremiumscanbelower,thesame,orhigherthantheTablePremium.Seethebrochureunder”PermanentCoverage”.
Tobacco monthlypremiums
GUARANTEED MonthlyPremiumsforLifeInsuranceFaceAmountsShown PERIOD AgetoWhich Issue Coverageis Age Guaranteedat (ALB) $10,000 $15,000 $25,000 $40,000 $50,000 $75,000 $100,000 $125,000 $150,000 TablePremium 15D-1 81 2-4 80 5-8 79 9-10 79 11-16 77 17-20 15.25 23.05 28.25 41.25 54.25 67.25 80.25 71 21-22 16.00 24.25 29.75 43.50 57.25 71.00 84.75 71 23 16.75 25.45 31.25 45.75 60.25 74.75 89.25 72 24-25 17.25 26.25 32.25 47.25 62.25 77.25 92.25 71 26 17.75 27.05 33.25 48.75 64.25 79.75 95.25 72 27-28 18.25 27.85 34.25 50.25 66.25 82.25 98.25 71 29 18.50 28.25 34.75 51.00 67.25 83.50 99.75 71 30-31 21.00 32.25 39.75 58.50 77.25 96.00 114.75 72 32 21.75 33.45 41.25 60.75 80.25 99.75 119.25 72 33 22.00 33.85 41.75 61.50 81.25 101.00 120.75 72 34 22.25 34.25 42.25 62.25 82.25 102.25 122.25 71 35 15.30 24.00 37.05 45.75 67.50 89.25 111.00 132.75 72 36 15.75 24.75 38.25 47.25 69.75 92.25 114.75 137.25 72 37 16.80 26.50 41.05 50.75 75.00 99.25 123.50 147.75 73 38 17.25 27.25 42.25 52.25 77.25 102.25 127.25 152.25 73 39 18.45 29.25 45.45 56.25 83.25 110.25 137.25 164.25 74 40 14.15 20.10 32.00 49.85 61.75 91.50 121.25 151.00 180.75 76 41 15.05 21.45 34.25 53.45 66.25 98.25 130.25 162.25 194.25 77 42 16.15 23.10 37.00 57.85 71.75 106.50 141.25 176.00 210.75 78 43 17.55 25.20 40.50 63.45 78.75 117.00 155.25 193.50 231.75 80 44 18.25 26.25 42.25 66.25 82.25 122.25 162.25 202.25 242.25 80 45 19.25 27.75 44.75 70.25 87.25 129.75 172.25 214.75 257.25 81 46 20.05 28.95 46.75 73.45 91.25 135.75 180.25 224.75 269.25 81 47 21.05 30.45 49.25 77.45 96.25 143.25 190.25 237.25 284.25 82 48 21.95 31.80 51.50 81.05 100.75 150.00 199.25 248.50 297.75 82 49 23.25 33.75 54.75 86.25 107.25 159.75 212.25 264.75 317.25 83 50 24.35 35.40 57.50 90.65 112.75 168.00 83 51 25.45 37.05 60.25 95.05 118.25 176.25 83 52 27.05 39.45 64.25 101.45 126.25 188.25 84 53 28.45 41.55 67.75 107.05 133.25 198.75 85 54 29.75 43.50 71.00 112.25 139.75 208.50 85 55 31.15 45.60 74.50 117.85 146.75 219.00 85 56 32.75 48.00 78.50 124.25 154.75 231.00 85 57 34.35 50.40 82.50 130.65 162.75 243.00 86 58 36.05 52.95 86.75 137.45 171.25 255.75 86 59 37.75 55.50 91.00 144.25 179.75 268.50 86 60 39.55 58.20 95.50 151.45 188.75 282.00 86 61 41.85 61.65 101.25 160.65 200.25 299.25 86 62 44.05 64.95 106.75 169.45 211.25 315.75 87 63 46.25 68.25 112.25 178.25 222.25 332.25 87 64 48.45 71.55 117.75 187.05 233.25 348.75 87 65 50.85 75.15 123.75 196.65 245.25 366.75 87 66 53.45 88 67 56.25 88 68 59.15 88 69 62.25 88 70 65.55 89
PureLife-plus StandardRiskTablePremiums Tobacco ExpressIssue
Form:21M013-ICCEXP-A-M-1LO 47
Health Savings Accounts
Maximize your savings
A Health Savings Account, or HSA, is a tax-advantaged savings account you can use for healthcare expenses. Along with saving you money on taxes, HSAs can help you grow your nest egg for retirement.

How an HSA works:
• Contribute to your HSA by payroll deduction, online banking transfer or personal check.
• Pay for qualified medical expenses for yourself, your spouse and your dependents. Both current and past expenses are covered if they’re from after you opened your HSA.
• Use your HSA Bank Health Benefits Debit Card to pay directly, or pay out of pocket for reimbursement or to grow your HSA funds.
• Roll over any unused funds year to year. It’s your money — for life.
• Invest your HSA funds and potentially grow your savings.¹
What’s covered?
You can use your HSA funds to pay for any IRS-qualified medical expenses, like doctor visits, hospital fees, prescriptions, dental exams, vision appointments, over-the-counter medications and more. Visit hsabank.com/QME for a full list.
Am I eligible for an HSA?
You’re most likely eligible to open an HSA if:
• You have a qualified high-deductible health plan (HDHP).
• You’re not covered by any other non-HSA-compatible health plan, like Medicare Parts A and B.
• You’re not covered by TriCare.
• No one (other than your spouse) claims you as a dependent on their tax return.
48
How much can I contribute?
The IRS limits how much you can contribute to your HSA every year. This includes contributions from your employer, spouse, parents and anyone else.2 Maximum contribution limit
$3,850
Catch-up contributions
You may be eligible to make a $1,000 HSA catch-up contribution if you’re:
• Over 55.
• An HSA accountholder.
• Not enrolled in Medicare (if you enroll mid-year, annual contributions are prorated).
A huge way that HSAs can benefit you is they let you save on taxes in three ways.
1 You don’t pay federal taxes on contributions to your HSA.3
2 Earnings from interest and investments are tax-free.
3
Distributions are tax free when used for qualified medical expenses.
¹ Investment accounts are not FDIC insured, may lose value and are not a deposit or other obligation of, or guarantee by the bank. Investment losses which are replaced are subject to the annual contribution limits of the HSA.
2 HSA contributions in excess of IRS limits are subject to penalty and tax unless the excess and earnings are withdrawn prior to the tax filing deadline as explained in IRS Publication 969.
3 Federal tax savings are available regardless of your state. State tax laws may vary. Consult a tax professional for more information.
© 2022 HSA Bank. HSA Bank is a division of Webster
N.A., Member FDIC. Plan Administrative Services and Benefit Services
Webster Servicing LLC. HSA_Overview_050522
Bank,
are administered by
Triple tax savings
SINGLE PLAN SINGLE PLAN FAMILY PLAN FAMILY PLAN Visit www.hsabank.com
49
Maximum contribution limit
orcallthe numberonthebackofyourdebit cardformoreinformation. $8,300 $4,150 $7,750
2024 2023

What is a Flexible Spending Account (FSA)? Help Make Medical Costs Painless. Visit fsa.nbsbenefits.com for more info or call one of our Benefit Specialists at 800-274-0503 Salt Lake City, UT - Headquarters Dallas, TX | San Diego, CA | Honolulu, HI 800-274-0503 fsa@nbsbenefits.com |www.nbsbenefits.com How Much Can I Save with an FSA? FSA No FSA Annual Taxable Income $24,000 $24,000 Health FSA $1,500 $0 Dependent Care FSA $1,500 $0 Total Pre-tax Contributions -$3,000 $0 Taxable Income after FSA $21,000 $24,000 Income Taxes -$6,300 -$7,200 After-tax Income $14,700 $16,800 After-tax Health and Welfare Expenses $0 -$3,000 Take-home Pay $14,700 $13,800 You Saved $900 $0 50
Flexible Spending Account (FSA)

Partial List of Eligible Expenses:
Medical/Dental/Vision Copays and Deductibles

Prescription Drugs

Physical Therapy
Chiropractor
First-Aid Supplies
Two Types of FSAs
To take advantage of a health FSA, start by choosing an annual election amount. This amount will be available on day one of your plan year for eligible medical expenses.
Payroll deductions will then be made throughout the plan year to fund your account.
A dependent care FSA works differently than a health FSA. Money only becomes available as it is contributed and can only be used for dependent care expenses.
Both are pre-tax benefits your employer offers through a cafeteria plan. Choose one or both — whichever is right for you.
What is a Cafeteria Plan?
A cafeteria plan enables you to save money on group insurance, healthcare expenses, and dependent care expenses. Your contributions are deducted from your paycheck by your employer before taxes are withheld. These deductions lower your taxable income which can save you up to 35% on income taxes!
How to Spend
Spending is easy
Our convenient NBS Smart Card allows you to avoid out-of-pocket expenses, cumbersome claim forms and reimbursement delays. You may also utilize the “pay a provider” option on our web portal.
Lab Fees
Psychiatrist/Psychologist
Vaccinations
Dental Work/Orthodontia

Eye Exams
Laser Eye Surgery
Eyeglasses, Contact Lenses, Lens Solution
Prescribed OTC Medication
Account access is easy
Get account information from our easy-to-use online portal and mobile app. See your account balance, contributions and account history in real time.
Life’s not always flexible, but your money can be.
Enrollment Consideration
After the enrollment period ends, you may increase, decrease, or stop your contribution only when you experience a qualifying “change of status” (e.g. marriage, divorce, employment change, dependent change).
Be conservative in the total amount you elect to avoid forfeiting money at the end of the plan year.
From baby care to pain relief, shop the largest selection of guaranteed FSA-eligible products with zero guesswork at FSA Store. Is your health need FSA-eligible? Find out using our comprehensive Eligibility List.

Get $10 off using code NBS1819.
Shop FSA Store at fsastore.com/nbs
51
What is a Dependent Care Assistance Program (DCAP)?
The Dependent Care Assistance Program (DCAP) allows you to use tax-free dollars to pay for child day care or elder day care expenses that you incur because you and your spouse are both gainfully employed.
To participate, determine the annual amount that you want to deduct from your paycheck before taxes. The maximum amount you can elect depends on your federal tax filing status ($5,000 if you are married and filing a joint return or if you are a single parent, $2,500 if you are married but filing separetely)
Your annual amount will be divided by the number of pay periods in the plan year and that amount will be deducted from each paycheck.
Who is an eligible dependent?
You can use the DCAP for expenses incurred for:
• Your qualifying child who is age twelve or younger for whom you claim a dependency exemption on your income tax return.

• Your qualifying relative (e.g. a child over twelve, your parent, a spouse’s parent) who is physically or mentally incapable of caring for himself or herself and has the same principal place of abode as you for more than half of the year.
• Your spouse who is physically or mentally incapable of caring for himself or herself and has the same principal place of abode as you for more than half of the year.
Special Rule for Parents Who Are Divorced, Separated, or Living Apart
Only the custodial parent can claim expenses from the DCAP. The custodial parent is generally the parent with whom the child resides for the greater number of nights during the calendar year. Additionally, the custodial parent cannot be reimbursed from the DCAP for child-care expenses while the child lives with the non-custodial parent because such expenses are not incurred to enable the custodial parent to be gainfully employed.
What are eligible expenses for the DCAP?
The expenses which are eligible for reimbursement must have been incurred during the plan year and in connection with you and your spouse to remain gainfully employed.
Examples of eligible expenses:
• Before and After School and/or Extended Day Programs
• Daycare in your home or elsewhere so long as the dependent regularly spends at least 8 hours a day in your home.
• Base cost of day camps or similar programs.
Examples of ineligible expenses:
• Schooling for a child in kindergarten or above
• Babysitter while you go to the movies or out to eat
• Cost of overnight camps
Salt Lake City, UT - Headquarters | Dallas, TX | San Diego, CA | Honolulu, HI (800)274-0503 | service@nbsbenefits.com | www.nbsbenefits.com 52
What does it mean to be “gainfully employed”?
This means that you are working and earning an income (i.e. not doing volunteer work). You are not considered gainfully employed during paid vacation time or sick days. Gainful employment is determined on a daily basis.
If you are married, then your spouse would also need to be gainfully employed for your day care expenses to be eligible for reimbursement.

You are also considered gainfully employed if you are unemployed but actively looking for work, you are self-employed, you are physically or mentally not capable of self-care, or you are a full-time student (must attend for the number of hours that the school considers full-time, must have been a student for some part of each of 5 calendar months during the year, cannot be attending school only at night, does not include on-the-job training courses or correspondence schools).
What are some other important IRS regulations?
• You cannot be reimbursed for dependent care expenses that were paid to (1) one of your dependents, (2) your spouse, or (3) one of your children who is under the age of nineteen.
• In the event that you use a day care center that cares for more than six children, the center must be licensed.
• You must provide the day care provider’s Social Security Number/Tax Identification Number (EIN) on form 2441 when you file your taxes.
What are some other important IRS regulations?
The IRS allows you to take a tax credit for your dependent care expenses. The tax credit may provide you with a greater benefit than the DCAP if you are in a lower tax bracket. To determine whether the tax credit or the DCAP is best for you, you will need to review your individual tax circumstances. You cannot use the same expenses for both the tax credit and the DCAP, however, you may be able to coordinate the federal dependent care tax credit with participation in the DCAP for expenses not reimbursed through DCAP.
For more information, please call 1(800) 274-0503
Salt Lake City, UT - Headquarters Dallas, TX | San Diego, CA | Honolulu, HI www.nbsbenefits.com 800-274-0503 service@nbsbenefits.com 53
•American Funds Service Company
•Ameriprise Financial/RiverSource
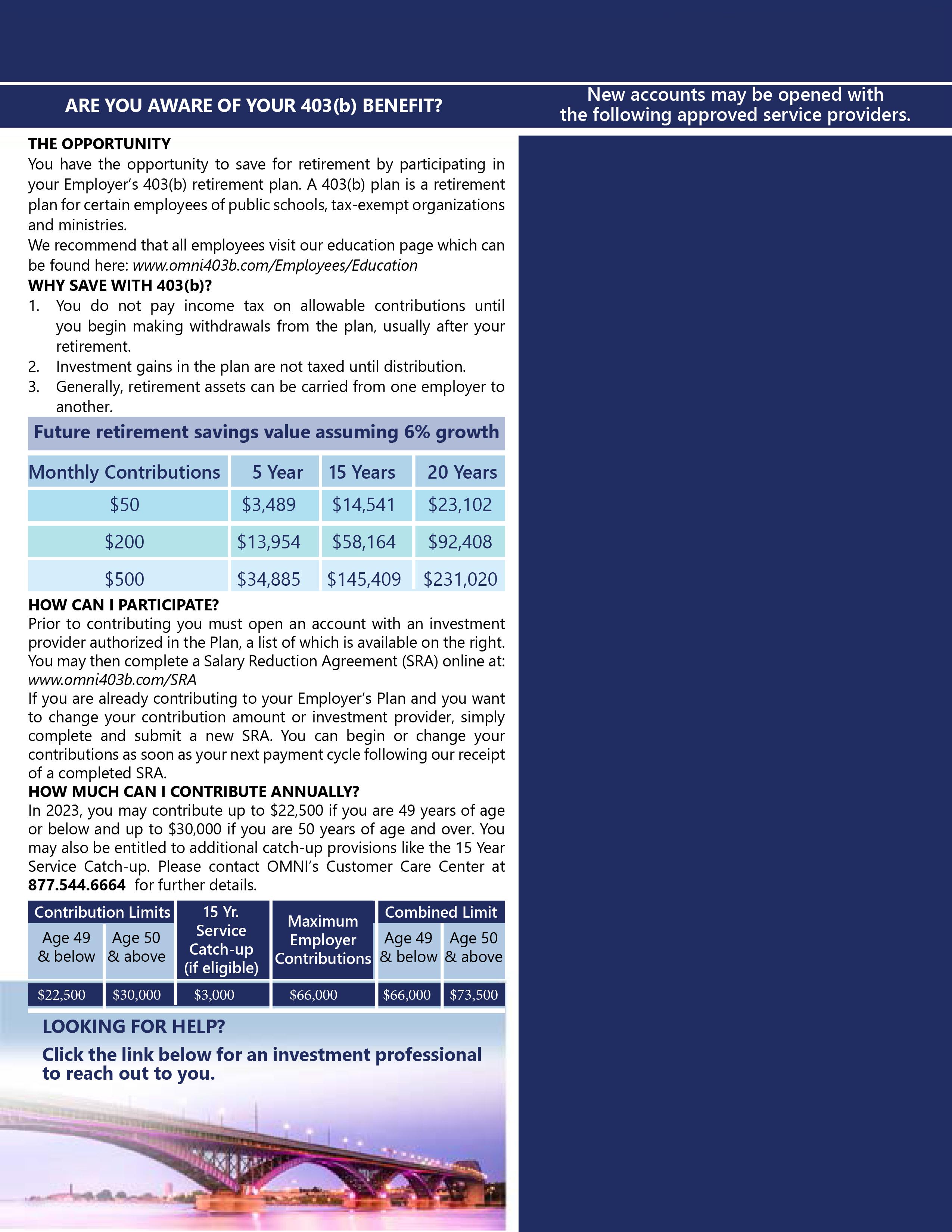
•Athene Annuity and Life (Aviva)
•Conseco Insurance Company
•Equitable (formerly AXA)
•GWN/Employee Deposit Acct
•Jefferson National Life
•National Life Group (LSW)
•PlanMember Services Corp.
•PlanMember Services Corp.
•PlanMember Services Corp.
•ROTH - Equitable (formerly AXA)
•Security Benefit
•The Legend Group, A Lincoln Investment Company
•Thrivent Financial for Lutherans
•TransAmerica
•Voya Financial (Reliastar)
Hondo ISD Plan Detail Page
Hondo ISD
54
50
Notes
