
A TRULY INCLUSIVE MAGAZINE FOR THOSE AFFECTED BY RARE DISEASE, DISABILITY OR CANCER A Same but Different Publication
arity Living your best LIFE ISSUE 5
R

My son Isaac was diagnosed with Moebius syndrome when he was just 11 months old, over the years I could see that people made judgments about who he was based on his appearance, and didn’t always try to get to know him for who really he is. I founded Same but Different to be part of the change I wanted to see, to use the arts to give people the opportunity to see the person behind the rare disease.

To celebrate our first year of Rarity Life we decided to go back to where we started, with children at the heart of this issue. From the science behind the mapping of a new rare disease syndrome to a brilliant list of inclusive children’s book we hope there is something for everyone in this edition. We are so grateful to our contributors, and to you our readers, together we can make a difference.

but Different



ENJOY THE YOUTHFUL ENERGY OF SPRING
IUEG kids domed umbrella, comes in one size with a selection of patterns to choose from.

https://www.amazon.co.uk/IUEG-Umbrella
Yellow kids mackintosh by A2Z 4 kids
https://www.amazon.co.uk/A2Z-Kids®-Jacket

Regatta kids
minnow printed wellies

Availiable on both the Regatta website and on Amazon
https://www.regatta.com/kids-minnowprinted-wellies-maize-yellow-bee/
https://www.amazon.co.uk/RegattaMinnow-Printed-Wellingtons-Yellow



“W here there is love, there is joy.”
Mother Teresa

“H ope is like the sun. When it’s behind the clouds, it’s not gone. You just have to find it.”
Anonymous

“T he things that make me different are the things that make me.”
Piglet (A.A. Milne)
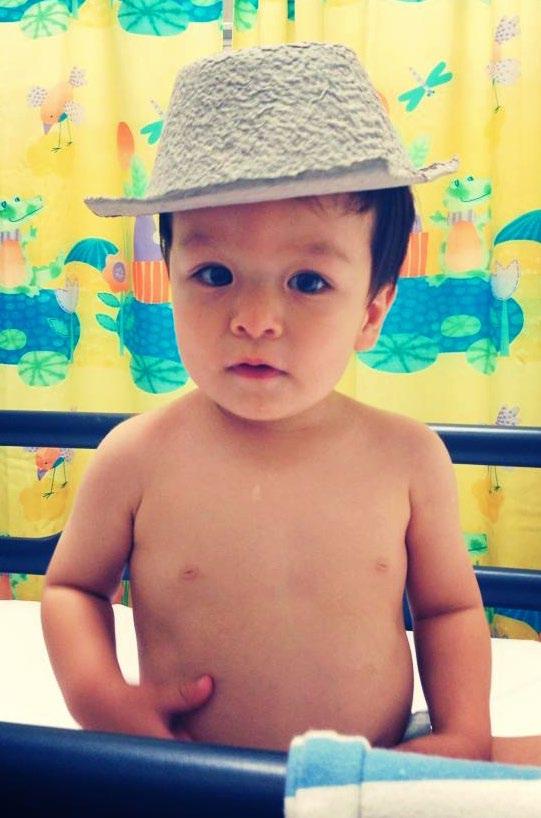
Today is a different story from where we were six years ago. Noah was a healthy baby born weighing in at 8lbs 9oz. We dealt with normal infant illnesses but then when he was 12 months old he caught an infection. We spoke with 111 NHS after he got a fever and became lethargic, and they advised us to take him to Alder Hey Children’s Hospital. We were given all the usual tests on arrival, including a chest X-ray and water sample. The staff gave him ice lollies to help increase his fluids – he absolutely loved that part. Eventually, we were told his X-ray was clear and he had
an infection. The relief as new parents was immense, our first trip to A&E and we were not disillusioned that it may be the last.
Fast forward 2 years. He was growing albeit slowly and living the normal fun life of a newly turned 3-year-old. At bedtime we noticed he would start to cough, not a bad cough, but it was noticeable. It didn’t stop him at all. The cough went on, from days to weeks, so we took him to the GP who organized an X-ray as his chest sounded ‘crackly.’

Noah today is a typical 9-year-old boy, he loves LEGO®sets, gaming and watching YouTubers do silly things.
The new Alder Hey had not long opened so we decided to make the experience as fun as possible. Noah played with the toys in the atrium and we ate lunch before he had his X-ray. Everything went well and they sent us on our way. This didn’t last as we had just set off when we got a call to return to A&E. On arrival we were taken straight through and put into a cubicle, the doctor came in and said that the X-ray wasn't clear and showed us the image. To me, it looked like there was a crumpled-up plastic bag covering the left side where his lung should be. The doctor explained that they believed this to be his intestines, but they needed to do a CT scan. While we waited for the CT scan, more doctors came in to see an ultrasound of his chest. They were all were amazed due to him being a typical 3-yearold, running around having fun, and certainly not showing any issues with his breathing or his lungs. The unbelievable thing was, he was 3-years-old, and it was extremely rare for a diaphragmatic hernia (CDH) to present this late, especially as he had a clear X-ray at 12 months old. Of course, they asked if he had been in any car accidents or had other trauma that could have caused it, which he hadn’t. According to a survey on CDHI’s website, there is only one record
of another child between the ages of 3-5 being diagnosed. Noah needed an emergency operation to correct it and was placed in a ward. We were advised to stay away from Google and that whatever we did come across online would not apply to Noah due to his age. For once, we listened and stayed away from Dr Google – thankfully as it turns out. The respiratory and specialist teams came around and said they would do the operation the following day. Unfortunately due to the number of emergencies that sadly came in that day, all taking precedence over a stable Noah, the operation was postponed for a day or two. That was the plan at least, but he deteriorated as the day went on and he was very uncomfortable by the evening. The surgeon came round as his oxygen had dipped and they decided that he needed the operation straight away and he was taken down that night.

A Congenital diaphragmatic hernia (CDH) is when the diaphragm, the muscle that separates the chest from the abdomen, fails to close during development in pregnancy. This opening allows contents of the abdomen (stomach, intestines and/or liver) to migrate into the chest, impacting the growth and development of the lungs. It is usually diagnosed in utero and happens in approximately 1 in 2500 live births.

Like any parent can imagine it was awful, it was our first time not being with Noah and putting his life in the hands of others, it was daunting and scary. After what seemed like a full day, but in reality it was only approximately 4 hours, Noah was out of recovery and on the HDU ward being monitored, it was 3.30 am and I was allowed to be with him again. In the morning he returned to his room and was closely monitored. However, he did not seem to be improving and his oxygen levels dropped. It was discovered he had a pneumothorax (collapsed lung) on the left side and he was taken back down for emergency surgery. The medical team warned us that he would end up in intensive care as it was a big operation and they didn’t know how his lungs would react.
The surgical team were fantastic and we were allowed into recovery as they were amazed at how quickly his lung had reinflated. Noah was breathing on his own but had chest drains in and needed to be monitored, but he didn’t need intensive care as they had feared nor even HDU, so he was allowed back up to his room. The surgeon thinks that because he had adapted over the previous months or years to only one full lung working, his oxygen level had compensated, so even though his lung collapsed, his body could adapt quickly.
After this emergency surgery, Noah improved daily. His appetite increased, his stats were great, his lung capacity and his heart were good. The medical team believed it would all return to where it should be in time, which it has. They told us nothing about his case was typical, from the age of diagnosis to the complication of the pneumothorax. He was certainly rare.
Due to the possible risk of recurrence, and despite this risk being relatively low for Noah, he has to visit the CDH/Respiratory Clinic yearly to keep a check on his development. Dr Sinha his consultant is fantastic and he is still amazed at the age Noah was diagnosed, especially with his clear X-ray at 12 months and perfect pregnancy. He believes that the spleen possibly blocked the hole in the diaphragm, but as he had grown and developed, the spleen had moved and allowed the bowel to move into the chest cavity.
LINKS
https://alderhey.nhs.uk/
https://cdhuk.org.uk/
https://cdhi.org/cdh-support/

Noah was so young that he doesn’t remember much of his 10-day stay unlike us, but his favourite story, right up to now, is telling everyone his scar is from a shark bite.
Jess Moxham is a writer, an architect, the mother of three children and an avid reader. After a traumatic birth her eldest son Ben was born with cerebral palsy, setting Jess and her family on a path they’d not remotely expected to be on. Over the years she has become more acutely aware of the often invisible world disabled children live in, a world they all too rarely see reflected in the books they read, or the TV shows they might watch. It is “incredibly powerful for kids to see themselves or their families represented in books, and it’s good for all kids to hear those stories and see those characters.”
Opposite is a list of books that Jess has compiled, taken from the books she has read to, or with her children.

El Deafo by Cece Bell

The Secret of Haven Point by Lisette Auton

The Right Way to Rock by Nat Amoore

The Cyborg Cat series by Ade Adepitan
Wonder by RJ Palacio

The Ghost of Grania O’Malley by Micheal
Morpurgo
10 PICTURE BOOKS FOR YOUNGER KIDS



What Happened to YOU?
By James Catchpole & Karen GeorgeMama Zooms
 by Jane Cowen-Fletcher
by Jane Cowen-Fletcher
Can Bears Ski?
By Raymond Antrobus & Polly DunbarWhen Charley Met Emma by
 Amy Webb & Merrilee Liddiard
Amy Webb & Merrilee Liddiard
The Girl Who Thought in Pictures
 by Julia Finley Mosca & Daniel Rieley
by Julia Finley Mosca & Daniel Rieley
Hiya Moriah
by Victoria Nelson & BoddzI am Not a Label
 by Cerrie Burnell & Lauren Baldo
by Cerrie Burnell & Lauren Baldo
The Abilities in Me – series
 by Gemma Keir
by Gemma Keir
We Move Together
 by Kelly Fritsch, Anne McGuire & Eduardo Trejos
by Kelly Fritsch, Anne McGuire & Eduardo Trejos
Susan Laughs
 by Jeanne Willis & Tony Ross
by Jeanne Willis & Tony Ross
In 2021 Jess published her first book, ‘The cracks that let the light in –What I learned from my disabled son.’

‘The Cracks that let the light in’ is a book about the realities of life when your first experiences of motherhood, and of becoming a parent, are nothing like what you had imagined, or hoped for. It is so much more than just a book about life with a child with complex disabilities, it is a book about love and hope. But it’s also a book that gives a clear, unsentimental insight into a life filled with additional responsibilities that most parents do not experience. Available from all good booksellers.
Jess also blogs, you can find her blog here: https://son-stories.com/ or follow her on Instagram at @jessmoxham
 Photographed by Ceridwen Hughes
Photographed by Ceridwen Hughes
Stacy and Jonathan are parents to Lois, a beautiful little girl whose condition makes her truly one of a kind. Lois has an ultra-rare condition, a 5q15-23 deletion.
At Stacy’s routine 20 week pregancy scan a problem with Lois’s heart was identified. After seeing the fetal cardiologist, they found out that her heart was missing the pulmonary valve and that she had a small hole in the bottom two chambers. Due to this her heart was enlarged, and the muscle wall had thickened, so the right chamber was quite small. It was at this point that a few different genetic syndromes were first mentioned as a possible underlying cause, and genetic testing was suggested.
“Because her prognosis was so poor, we didn’t see the point in doing the genetic testing at that time. There was no benefit to doing it then because of the risk of the testing. Then they offered us a termination, saying if she is born, it’ll likely be that palliative care is needed. We decided to go ahead with the pregnancy and look at testing when she was born, if it was needed at that point.” As the pregnancy progressed Stacy was monitored closely with extra scans and when other complications arose, they were handled well. Each milestone in the pregnancy was passed and at 37+5 weeks Lois was born. At this point blood was taken from her umbilical cord and sent off for genetic testing.
“Lois had microarray testing and she was part of the ‘Nextgeneration children’s project,’ which was about doing whole genome sequencing quickly for babies in NICU. It is important to identify children who are poorly in NICU and identify any genetic issues that will impact decisions about what interventions and treatment plans are needed going forward. Our genetic results came back quickly; the letter was dated two weeks after her birth but it wasn’t until she was about 6 weeks old that we got the results. Lois was back in ICU with a respiratory syncytial virus and the genetics team came and said she was not matched to any others on different genetic databases making her unique.”
Having no one else to compare her condition to causes difficulties when planning care. In addition to waiting for heart surgery, Stacy and Jonathan have been advised that she will need screening on her bowel from age 9 or 10. Alongside this, they have been told she will have learning disabilities, but it is unknown how her deletion will really affect her as she grows.
“Probably the most helpful thing we were given initially was an information guide from Unique. Whilst it was for children who had a deletion on 5q22 it has acted as a sort of guide as to things we might expect. On the whole though most of it has been kind of finding things out as we’ve got there.”
Lois’s care involves a considerable amount of communication, coordination and work for the family. They would very much like a more cohesive plan and improved communication between departments. “For instance, the community teams, like physio and speech therapy work on a different database to the hospital, so all those bits of information aren’t shared. When you throw in school and other people it’s quite a complex picture.”
In addition to the coordination, it is difficult to know who to contact when Lois has an issue or is unwell. “There was a point where we were we were going to the GP fairly regularly. Each time we’d go they would do a bit of an assessment and because they just don’t know how she is affected we would then be sent to the hospital. If she was a ‘typical child’ they might have been more confident in treating her. It got to the point where we thought actually maybe we should just bypass the doctor and go straight to hospital.”
Having to explain her condition is time-consuming and even the most knowledgeable of doctors and specialists can’t know every aspect of how it will and does affect her specifically. Not knowing how her condition will impact her in the long term causes the family much anxiety.
“Lois has got a cleft palate, but they don’t want to repair her palate until they can assess her speech, which they can’t do as she’s non-verbal. We don’t know if she will speak in the future, we are kind of stuck in a loop.
There are a few things like that with medical decisions and stuff where we think, well, we don’t know how that’s going to affect you in the future, so is it worth a risky operation? Making medical decisions can be quite hard.”
To help keep track of everything Stacy and Jonathan are organised and believe this has helped them navigate Lois’s care. “I would suggest anyone in a similar position have a good filing system. We had to get all her information together for the DLA application and having everything in one place made it slightly easier. We must have had about 70 or 80 pages of evidence we submitted, it wasn’t easy to do, but it was easier because everything was there, and it was all filed. Without it, trying to find evidence for things would be very tricky.”
Awareness is important to them, more so now than ever. “Since having Lois I have become very aware that each person’s story and experience of a rare disease is completly unique to them. It’s not just saying, ‘you’ve got this syndrome so it must be like this’ but, actually really valuing each person’s uniqueness and their journey. Not having an easily identifiable condition definitely makes things more difficult.”
Even some medical professionals that the family have come across during their journey have struggled with Lois’s diagnosis and how it affects her. Although this is understandable to the family due to the rarity of her condition it still adds to the frustration they feel at times.
One of a kind
They find some professionals make assumptions about how Lois should be because she has similarities to other syndromes, but this isn’t very helpful to the family. “So, we had one professional who was brilliant, and she said to me ‘you are the expert in your child’s condition. I’m not even pretending that I know anything. How do we proceed from here?’ and I thought that was incredibly vulnerable of a very experienced and well qualified consultant to say that. I really valued that. But then we had one medical professional who told me that because her diagnosis

wasn’t named that it wasn’t really a diagnosis and that Lois will probably catch up and I just needed to put a bit more effort in!”
“We celebrate all the small things. Lois is probably her own biggest fan and she likes to celebrate herself. She’ll do something and then she will sit up and clap looking around the room waiting for one of us to join her.
“The best piece of advice I got from someone was just don’t listen to anyone. Just you do you. I carried that with me, from even before Lois was born.”

I think having any child is difficult. It’s still a whole new learning experience. We may be learning more stuff, certainly more medical things, but for us it’s quite important to remember everyone has their own struggles.”
This also leads to the advice and opinions of others, assuming that a ‘one size fits all’ parenting style will work when in reality it’s far from the truth. As parents, we all know how different our children are and how they adapt to life. “The best piece of advice I got from someone was just don’t listen to anyone. Just you do you. I carried that with me, from even before Lois was born.”
Lois attends mainstream school and is adapting to school life well with 1-to-1 support in place. There are obstacles, just like for any child adapting to school, but her parents love watching her friendships blossom, and she is learning makaton to help her communication. This is something her teachers and other pupils are also doing it can only ever be a positive thing, that the children are learning about differences and acceptance from a young age “hopefully they will grow up with a bit more awareness. Hopefully, they ask questions, and the teachers can help them understand difference.”
Since her diagnosis, her parents are learning a lot through her. It has strengthened their relationship and they say everything they do is as a team, leaning on the strengths of the other. “I think the most positive thing for me has been Lois has just taught me so much. I’ve learned so much about the world. Seeing it from her perspective, she’s made me see the world differently and made me probably more of a reflective and critical thinker. I think one of the hardest things is working out what’s going on for her. What’s happening? How do we help that? She’s very rarely upset or angry. If she is, it’s not just your typical temper tantrum she will be like that for a reason.”
“Lois sees the world differently and she's just smiling and happy and content with simple things. Which makes you realise that we should enjoy the simple things in life too.”
A
 by Rob Delaney
by Rob Delaney
published by Coronet, (Hodder & Stoughton Ltd)
It is hard to know what to say first about this beautiful little book. It is both a difficult read and a joyful one, as Rob Delaney writes with true candor about the death of their much-loved son, Henry, at just two years old. It is almost a cliché to point out that whilst a child who loses their parents becomes an orphan there is no name for a bereaved parent, but it bears repeating. Because the loss of a child is simply too great, too hard, too impossible to imagine, to describe, to name. So we often don’t. That is perhaps one of the greatest and kindest things that Rob has done in writing this book, he has given a voice to countless bereaved parents. He gives those of us lucky enough not to have lived through such an immense loss some small insights into a grief we cannot name. It is indeed, ‘the story of what happens when you lose a child, and everything you discover about life in the process.’ It is a book which is truly a gift, but one which should absolutely be approached with caution. I laughed, but I also cried and most importantly it reminded me how lucky we are to enjoy time with those we love.
The Talking Cancer podcast is produced by the charity Macmillan Cancer Support and is available on the usual podcast platforms as well as via the Macmillan website. There have been three series so far, and each episode covers different topics, from diagnosis to life after cancer. Guests include those affected and health experts. Series One and Two were hosted by Magic Radio presenter Emma B and series Three was hosted by Smooth Radio presenter Angie Greaves.
Across the three seasons there are many insightful and informative episodes to listen to, but of particular interest was the episode ‘Talking to children about cancer’ (Series 3, Episode one) in which Angie talks to Toria about her experience of telling her five-year-old twin boys about her cancer, as well as Macmillan professional Azmina Rose who provides some useful guidance for people who need to talk to children about a diagnosis. Not always an easy listen, but an important one!

 directed by Josh Boone
released by 20th Century Fox
directed by Josh Boone
released by 20th Century Fox
In issue 4 of Rarity Life our guest contributor Ella Sinden referenced The Fault in Our Stars in her brilliantly written account of her cancer diagnosis. The book, written by John Green, was first published in 2012 and was an instant bestseller. The subsequent film of the book was also a huge box-office success. Both the stars of the film and the film itself received rave reviews, and at first glance, it’s not hard to see why. A beautifully told, coming-of-age love story centred around two teenage cancer patients who experience both their first love and the agony of loss against the backdrop of Amsterdam and other gorgeously shot locations. Yet there is something a little unsettling about the film because it not only utterly romanticises cancer but in doing so it somehow also diminishes and minimises it. In an early monologue Hazel, the lead character acted with real grace by Shailene Woodley, reflects that “You have a choice in this world, I believe, about how you tell sad stories, you can sugarcoat it – the way they do in movies and romance novels… It’s just not the truth. This is the truth.” But it isn’t the truth. Cancer is infinitely more complex, more messy, more destructive and much more devastating than this, especially if it is terminal as it is for Gus, Hazel’s love
interest in the story. So, whilst at face value, the film is a moving, romantic and at times a well told love story it is also deeply problematic, and misleading. As Ella said, when she found out she had cancer there was a part of her that believed she would have “a ‘The Fault in Our Stars’ moment, where I’d be forever changed by my experience, maybe meet an angsty teen boy and bond over our shared trauma.” Of course, the reality was very different, leaving Ella feeling disillusioned by the Hollywood story we’ve all been sold.

The time from the initial question asked, almost innocently, by my husband during what was expected to be a fairly routine ultrasound scan in the 34th week of my second pregnancy to the subsequent clinical finding of ‘a large fluid-filled cavity is present in the left cerebral hemisphere’ is both crystal clear and hazy. Often the
actual moment in which your life is irrevocably changed is fleeting. But the fear, and shock are deeply seared into your being, the trauma so surprising as to still not feel truly real. Memories that you might revisit often, or try your hardest to bury, but that will always be there, as much part of you now as your name.
When a large porencephalic cyst was found on our baby boy’s brain, a cyst that hadn’t been there at the 20 week scan, no one could really explain why it was there now. Eventually it was decided it was likely ‘just one of those things’ that happens sometimes. But surely even these things

that ‘just happen’ must have happened for a reason? 18 months later we had our answer, our son had an ultrarare mutation in the COL4A2 gene, and was ‘heterozygous for a pathogenic c.1856G>A mutation in exon 25 of the COL4A2 gene.’ But what did that even mean?
First a note on nomenclature, genes are always in italics and proteins are not (in humans).
• Genetics - the scientific study of genes and heredity.
• Genes – a gene is a segment of DNA that contains the instructions for building one or more of the molecules that help our body to work, it is estimated that humans have around 20,000 genes *1
• Genetic mutation - a genetic mutation occurs when there is a change in the sequence of your DNA. If the DNA sequence is in the wrong place, isn’t complete or is damaged you might experience symptoms of a genetic condition.
• Genetic conditions – Genetic conditions are also often referred to as genetic disorders, diseases, or syndromes, however these do describe different functions, listed below *2
• A disease is a pathophysiological response to internal or external factors.
• A disorder is a disruption to regular bodily structure and function.
• A syndrome is a collection of signs and symptoms associated with a specific healthrelated cause.
• Phenotype - In genetics the phenotype is the set of observable characteristics or traits of an organism
• Exons - an exon is a coding region of a gene that contains the information required to encode a protein.
• Transcription factors – In molecular biology a transcription factor is a protein that controls the rate of transcription of genetic information from DNA
Doug Gould grew up on a farm in Consort, a rural farming town with around 600 inhabitants in Eastern Alberta, Canada, before moving to Edmonton to attend the University of Alberta. He thought he might become a teacher, like both his father and grandmother before him, when the decision to take a genetics course changed everything. “I took a genetic course for the first time and was just kind of blown away, that was the first time that there was a real spark there, I took a real interest in it. And so I did a specialization in genetics for my undergraduate degree”

(Some Canadian Universities offer BSc Specialization degrees which provide a more focused education in one area of study).
That summer instead of returning to the farm as he usually did he volunteered in a research lab, where he heard that there was going to be a new Medical Genetics department opening there that year.

“this thing you’ve been observing is potentially bigger and more important than you perhaps initially believed it to be...”Image courtesy of Marco Sanchez, UCSF
“And again, there was just sort of this light switch moment and I realized that my interest in science was underpinning this wider interest in human biology and medicine.” After graduating he went on to join this new department to begin work on his PhD. From there he moved to the Jackson Laboratory in Maine as a postdoctoral fellow, where he worked on using mutagenesis in mice to develop new genetic models of glaucoma (glaucoma is a fairly common eye condition where the optic nerve, which connects the eye to the brain, becomes damaged).
In molecular biology the use of mutagenesis is an important tool where mutations are induced randomly across the genome

to help identify genets that contribute to a particular disease or phonotype (observable physical properties). This approach is then used to understand the normal function of the unmutated version of the gene. It was during the process of studying their findings that Doug observed and began to map something unexpected, mutations in the gene encoding type IV collagen alpha 1 (COL4A1). He still remembers the moment when the realisation hit him that “this thing you’ve been observing is potentially bigger and more important than you perhaps initially believed it to be… I was using a phenotype to map the gene. The way you do this is you figure out what part of
a chromosome the mutation must be on and you look at what genes are in there, then you sequence them. I narrowed the chromosomal interval to a region that contained three or four genes, and two of them are these little transcription factors with very few exons. And then there was type IV collagen alpha 1 and collagen type alpha 2 (COL4A1 and COL4A2) which sit beside each other on the chromosome. And they’re enormous. Or they seemed enormous compared to a three exon transcription factor… and at the time I honestly had zero interest in studying collagens. They just seemed so boring, they are just a scaffold, and the real action, the real biology happens in cells, not in these scaffolds. I was naïve.”
What they were observing in the mice was striking, because they didn’t only have defects in the development of their eyes, they also had lots of other defects, and most notably intercranial cerebral hemorrhages. Following the realisation that in fact a fault, or mutation in the COL4A1 or COL4A2 genes had the potential to be hugely important, and whilst still working in The Jackson Laboratory, Doug shared his findings with a colleague who specialized in brain pathology. On reviewing the brain sections of the mutagenized mice they identified that the cavities they had developed on their brains were very similar to porencephalic cysts found in human brains. After searching through all the published medical science papers on porencephalic cysts he could find to try to understand how this might tie into his research and findings into COL4A1 and COL4A2 he found a paper which documented an ultra-rare familial case of porencephaly. He reached out to the authors and suggested they test for mutations in the families’ gene, and ‘sure enough, they found these mutations.’ Doug presented his groundbreaking findings in the first paper to publish human mutations in COL4A1; Mutations in
COl4A1 Cause Perinatal Cerebral Haemorrhage and Porencephaly by Gould et al. in the journal Science in May 2005.
But porencephaly was not, Doug recalls, ‘the end of the story.’ As COL4A1 and COL4A2 proteins are found in all organs the ways in which an individual can be affected by the mutation are numerous.
“We now know that mutations in COL4A1 and COL4A2 are pleiotropic and genetically complex and lead to a vast spectrum of seemingly unrelated human diseases.”

*3 He secured crucial funding from the Canadian Stroke Network and later moved to the University of California in San Francisco to set up his own lab, The Gould Lab. The central and primary aim of his lab is to continue to research ‘the tissue-specific molecular mechanisms that underlie this multi-system disorder that is caused by mutations in the genes encoding COL4A1 and COL4A2.’
But what does it actually mean if you are told that your loved one has a genetic mutation in COL4A1 or COL4A2 and you receive a genetic report which lists a whole lot of letters and numbers which mean absolutely nothing to the average person? In the identification and mapping of
any new mutation or disease it is typically those most severely impacted that are discovered first. Accordingly, a lot of the early genetic testing done was focused on young children with complex disabilities, children who had for example suffered a perinatal stroke. And so this question of ‘what does this even mean’ was a question that many parents asked when they first began to receive an underlying COL4A1 mutation as a diagnosis for their child. Answers were hard to find, and so over the years, and with the ability to connect via social media parents began to link up online, forming support groups and sharing their experiences. Today there are both a US

And so this question of ‘what does this even mean’ was a question that many parents asked when they first began to receive an underlying COL4a1 mutation as a diagnosis for their child.Photograph: Warren Umoh, Unsplash.
based foundation and a European charity working hard to bring much needed awareness, funding and even recognition to this syndrome. In 2019 the US based support group officially changed the name of the foundation to the Gould Syndrome Foundation, part of a carefully managed campaign to get the National Institute of Health in America to recognise this condition, and to assign it an ICD code (International Classification of Diseases).
In choosing the name Gould Syndrome the foundation carried on the long standing tradition of naming a disease after the person who first identified it, and in this instance who continues to be the main researcher into it. Through being able to engage closely with the patient population the team at Gould Lab have access to the medical histories of a wide range of those individuals with a COL4A1 or COL4A2 mutations, facilitated in large part through the work of the organizations and their linked support groups. And for Doug the experiences of the patients can help to inform the direction and focus of the continued research. As he explains, “the Foundation put together a global registry, where they asked people to self-report and that was
really valuable and helped shape what we do. Seizures were not something that we were directly studying, we’re studying things that might lead to seizures, like the permeability of the blood brain barrier for example, but I hadn’t appreciated that seizures were the biggest concern of patients and their families.” This patient led research focus has, at its heart, the ultimate hope that one day those living with it will have access to ‘mechanismbased therapies that can prevent, reduce or delay disease.’
Today, on receiving the clinical finding that you, or your child, has this seemingly incomprehensible diagnosis of a COL4A1 c.2263G>A p.G755R*4 mutation an initial internet search will give you access to something that makes a little more sense. The Gould Syndrome Foundation website explains that ‘Gould Syndrome is a rare, genetic, multi-system disorder. Gould Syndrome is often characterized by abnormal blood vessels in the brain (cerebral vasculature defects), eye development defects (ocular dysgenesis), muscle disease (myopathy), and kidney abnormalities (renal pathology); however, many other aspects of the syndrome including abnormalities
For more information about Gould syndrome/ COL4A1 and COL4A2 syndrome visit: The Gould Lab at the University of California , San Franciscohttps://ophthalmology.ucsf.edu/ gouldlab/
Associazione Famiglie COL4A1-A2
APShttps://www.col4a1.net/en/
The Gould syndrome Foundationhttps://gouldsyndromefoundation. org/
Gould Talks – Episode 1 is the first in a planned series of virtual discussions looking at COL4a1/a2 which you can find herehttps://www.youtube.com/@ gouldtalks
For support: The Gould syndrome foundation has both a public Facebook page and a private support group page: https://www.facebook.com/ Col4A1Foundation
There is also a private Facebook support group called the Gould Syndrome Family Support Group (Col4a1/Col4a2) which you can find herehttps://www.facebook.com/ groups/col4a1
almost all basal membranes. For this reason, a mutation in the COL4A1 or COL4A2 gene causes a disorder that can affect any organ.’ And, uniquely, what many families who are struggling to understand this new diagnosis also have access to is Doug, someone whose commitment to, and interest in this rare genetic mutation means he truly is the global expert. And whilst he is always sure to point out that he is not a medical doctor, and that he can’t offer a prognosis, or
yet as the number of people with an underlying diagnosis of COL4A1 and COL4A2 grows it is becoming ever more evident that there is a huge breadth and variability in the symptoms experienced. Indeed, Doug explained that the calling card of Gould syndrome seems to be the variability of associated symptoms. Based on the patient data they’ve analysed to date “cerebrovascular disease is the most highly penetrant (so) if you have the mutation, you probably have a cerebrovascular disease…
about 30, or 35%, of people with the mutation have some sort of ocular dysgenesis, then there’s skeletal myopathy in maybe 20% of cases, and then some renal involvement in 15%
Today there are in excess of 500 people who have received a diagnosis for COL4A2 mutation, and for each of those diagnosed there will likely be many, many more who won’t. Interestingly, more recently there are a growing number of adults who are receiving a diagnosis, often after a lifetime of poor health, but some because of the wider familial testing done on behalf of a severely impacted child. So whilst the majority are still ‘de novo’, which means that the mutation happened spontaneously and was not inherited, there are increasing numbers of families that are found to have a hereditary mutation, adding more pieces to the bigger picture. And with each new diagnosis, and through the continued research they are doing, Doug and his team are continuing to ‘put the pieces of the puzzle together’ as they continue to map the genetics of a (relatively) new disease.

FOOTNOTES:
*1 - https://www.nigms.nih.gov/education/fact-sheets/Pages/genetics.aspx
* 2 https://www.healthwriterhub.com/disease-disorder-condition-syndrome-whats-the-difference
*3 Welcome - Douglas Gould Lab - UCSF Department of Ophthalmology
*4 Taken from the presentation in Gould Talks, Episode 1, see ‘Information and Support.’
Eddie is a seven year old boy who has managed to accumulate quite an extensive list of diagnoses, some helpful, some not, and all likely linked to his underlying COL4A2 genetic mutation.

Eddie had a, or several, cerebral infarctions whilst still in utero, resulting in both a large porencephalic cyst that replaces the bulk of the left thalamus (in turn impacting the basal ganglia), and there are also linear foci of gliosis throughout the brain. In terms of what these words actually mean for Eddie, his brilliant paediatrician explained it using the example of a spaghetti junction. If there’s an accident or obstruction on one road the effects are widely felt, resulting in traffic jams and all kinds of related chaos. And so over the first years of his life Eddie received diagnosis after diagnosis; cortical visual impairment (certified blind), right hemiplegia (now changed to cerebral palsy affecting all four limbs), infantile spasms leading to severe, intractable epilepsy, and a global developmental delay which has now been re-assessed as a profound learning disability. Eddie is nonverbal, not independently mobile, has hundreds of seizures daily and needs to be with an adult at all times to ensure he is safe.
Eddie is under the care of multiple different doctors, departments and indeed hospitals, each monitoring and managing a specific diagnosis. When we talk about Eddie we rarely say that he has Gould Syndrome, or a COL4A2 mutation, but we do often explain how his epilepsy has, and continues to have a catastrophic impact on him. Because as Dr Gould explains in his work, ‘the syndrome is really the clinical manifestations and how the patient presents.’ But as his parents we hope that one day he might have access to a centre of excellence where each specialist team can review him over the course of one day, rather than countless appointments scattered throughout
the year at various hospitals. A place where his clinical teams can view his needs holistically, with the broader understanding of how his underlying genetic mutation may affect him over the course of his life. Will he have another stroke? Like all parents we would like answers, we would like to know more, to understand more.
But none of that really tells you who he is. Because he is of course just himself. Irrepressible, loud, vibrant, engaging, opinionated, wild and very loving. An utterly beautiful, and often very cheeky little boy who likes nothing more than a cuddle. Or better still a fight with his dad and big brother! Life isn’t always easy for him, but overall he is thriving, and happy.
And that, that is Eddie.
CEO and founder of arts organization Beyond the Diagnosis, Patricia Weltin, has two daughters with Ehlers Danlos Syndrome. Recently she spoke to us and explained how and why she launched her charity.

Both of Patricia’s daughters presented with differences from a young age. Olivia was sickly from birth and had deformed hands and feet and her other daughter Hana was extremely hypermobile, able to dislocate her shoulder and lick her elbow. They even joked that she should perform it as a trick on the David Letterman show. Finding humour in difficult situations has helped the family cope with uncertainty.
In addition to the hypermobility, both daughters had severe anaphylactic allergies, Olivia to shellfish and Hana to nuts. Olivia
additionally had many issues growing up with ongoing ear infections. These were initially treated by several surgeries whereby tubes were inserted to reduce the fluid build-up. A chance discussion led them to explore the possibility of it being related to allergies.
“I took her to an allergist and they advised she was off the charts for everything. They put her on an allergy regime and she never needed tubes again, but by then she had lost four years of language skills which impacted her speech.”
Olivia was really sporty and an accomplished tennis player. As time went by, she started to experience a number of issues that caused concern, but on their own did not immediately get linked to one specific condition. She started to lose her teeth and had severe pain between her shoulder blades which was so bad that she needed multiple surgeries and was hospitalized. “Olivia never complained. She had a whole team of doctors, yet no one could work out what was happening. Whilst investigating the tooth loss they took a full jaw scan that also included her head. I got a call from the radiologist who told me she had a Chiari malformation. I had previously been to an EDS conference and so knew about it and recognized that a pattern was starting to form. From other parents I was chatting to on EDS Facebook pages I could see that Olivia was ticking quite a few of the boxes.”
“I then asked Hana to do the Beighton scale, which allows you to gauge hypermobility, and she scored nine out of nine. I called up the hospital and told them I thought it was EDS. They regrouped as a team and agreed with my diagnosis. It was crazy that after all this time and so many clinicians involved it was me who identified it.”
What followed was an extremely difficult time for the family. They discovered that both girls had tethered spinal cords and needed brain surgery. There was a point when they were both in wheelchairs and for some time Hana was completely bedridden.
The Beighton score is a popular screening technique for hypermobility. This is a nine–point scale and requires the performance of 5 manoeuvres, four passive bilateral and one active unilateral performance. It was originally introduced for epidemiological studies involving the recognition of hypermobility in populations. Therefore the scale was well suited, being easy and quick to perform with large numbers of people. The criteria of the Beighton score were the first used to recognize hypermobility, and this method has been in use for 30 years. It involves the evaluation of only a few joints and does not include other involved systems.

“There were times when my daughter’s ribs and hips were dislocating and I would need to go into the college to fix them. It was relentless. I started doing everything I could to find a way to ease their symptoms. I was researching autoimmune diseases and found there seemed to be a connection between them and EDS. I read a study that said people who had taken an older style antihistamine were experiencing an improvement in their condition and as they needed to take an antihistamine anyway we swapped it. We immediately saw a huge improvement.

We also adopted the Cusack protocol which recommended a supplements program. My kids were in wheelchairs and recently when we were able to go to the beach, it just hit me and I started crying. I never thought I would see this day. Hana is off at college and Olivia is doing great. There are more surgeries to come but I am not worried about them as things have improved so much.”

“This is the beauty of art. It has a way of reaching so many people.”Images courtesy of Patricia Weltin
Patricia has a degree in finance and was a senior financial analyst for a manufacturing company prior to getting married. She did not have any knowledge of, or qualifications in medicine, however due to her lived experience and desire to learn as much as possible to help her daughters she has recently had an article on tethered spinal cord accepted for publication by the American Journal of Medical Genetics. Having always avoided promoting herself in the past, she now feels it is important to stand up for all those parents who, like her, felt ignored or belittled by a system that often refuses to accept the patient and their carers as partners in care.

“I remember somebody saying to me that people with rare disease often feel like they are on an Island of Misfit Toys and that's stuck with me. I said, we are! We are on an island and slowly more and more people are joining such as pharma companies, support organisations etc., but we're still on the damn Island. We can't get off the island. I want to reach out to the mainstream. Build a bridge off our island.”
Beyond the Diagnosis was originally started as an art exhibition for medical schools and then they were contacted by New England Haemophilia Association who asked to include their exhibition at a conference. Particia explained that they did not have any art included in that specific condition but they did not mind. “This is the beauty of art. It has a way of reaching so many people. It's about educating those people that don't know anything about it.”
Since launching, Beyond the Diagnosis has continued to reach audiences from Harvard Medical Journal to mainstream media. For Rare Disease Day this year she has collaborated with H4B Boston and Havas Health & Me for an exhibition to be displayed on billboards in New York City’s Time Square. Her dream of reaching those who have little or no experience of rare disease is becoming a reality.
Beyond the Diagnosis unites art and science to inspire research and innovation of treatments for people living with rare and neglected diseases. The Beyond the Diagnosis art exhibit’s focus is the rare disease patient. Artists have donated their time and talents to paint rare disease patients for this groundbreaking exhibit. Each portrait represents a single orphan disease. The goal is to put a face to all 10,000 rare diseases. This beautiful exhibit is travelling to medical schools, research institutes and hospitals around the globe encouraging the medical community to look “beyond the diagnosis” to the patient.
Art has been used for thousands of years to successfully convey a message, whether it be a story or a glimpse into the human spirit. At Beyond the Diagnosis, we believe art not only leaves a powerful and lasting visual imprint but creates a unique connection for the viewer.
Visit www.beyondthediagnosis.org
An introduction to the RARE Navigator support service

Same but Different (SbD) was established in 2015 by Ceridwen Hughes, following her experiences of becoming the parent to a child with a rare condition. Isaac, Ceri’s son, was born with a rare syndrome called Moebius, and from the moment he was born she recognised that people made assumptions about him because of the way he looked and behaved. Having met many parents over the years who felt the same frustrations, she decided to use her skills to raise awareness of the people behind the conditions, to show that behind each diagnosis or condition is a person with an important story to share. Through the work she was doing to bring people’s rare stories to focus, Ceri realised that there was a commonly shared experience she was seeing time and time again, a lack of any kind of coordination of care and support. And so in 2019 Same but Different introduced the RARE Navigator service, the first of its kind in the UK;
“Having focussed on building a greater awareness and understanding of the impact of rare disease over the past few years we are now able to support families affected by any rare disease throughout North Wales. We will be working with existing support organisations, healthcare providers and community services to ensure the help is where it is needed when it is needed.”
The Rare Navigator service is open to anyone with a rare disease who is currently living in North Wales, and can be accessed in a number of ways. Individuals and families can self-refer into the service, or be referred by an external organisation or social care provider. Care co-ordination was identified as a key area for improvement in the Rare Disease Framework (2021) and our service helps to address this need and was featured as a case study in the Welsh Cross Party Report on Rare, Genetic and Undiagnosed Conditions (2021).
Through the Rare Navigator service Same but Different offer emotional and practical support and information to individuals, their families and all involved in their care, from the point of diagnosis and beyond. This family-focused care co-ordination and advocacy service aims to ensure that each family is able to access the level of support they require to meet their needs, from access to beneficial services and equipment to the tools and resources that encourage understanding of rare diseases. The Rare Navigator team work closely with national and local health and social care providers to ensure that families are informed and have access to optimum care, treatment and services that can assist daily life and increase opportunities for independence and social interaction.
EC and her family have been supported through Same but Different’s Rare Navigator service over the last few years. EC is a minor, and the initial referral was made on her behalf. The family set up is complex, with other siblings and EC’s father also having additional needs, which means the bulk of the care needs fall to EC’s mother. When Katy first met the family they were at rock bottom. Over the years she has worked closely with the family to repair broken relationships with social services and other involved medical professionals, mediating and liaising with these services to guide outcomes. Katy supports the family in monthly MDT sessions to both support and offer a voice when they feel they can’t, and to drive forward agreed plans to make sure any targets are achieved in a timely fashion.
*Names have been changed
It is important to note that the Rare Navigator doesn’t replace specialist rare disease support organisations, rather we work hand in hand with them but with a local North Wales focus.
We asked Katy, our Rare Navigator, for a little more insight into her role. She explained that “the remit of the role is to help people manage all the different threads of their complex lives better so the remit can be really broad because everyone’s experience is very different. It is a tailored service to the family, which might include liaison, advocacy, communication, and collaboration with all the services involved.”
The support an individual or family needs might include:

An initial home visit or virtual support planning session
Finding and communicating with suitable agencies

Attending medical appointments as an advocate
Advocating in social and education settings
Liaison with and organisation of services, including setting up and chairing multidisciplinary meetings
Prompting agencies involved to review the support offered
The wide-ranging nature of the Rare Navigator role makes it truly inclusive, and able to be reactive to the needs of those using the service. Over the years our Rare Navigator Katy has worked hard at building the role, ensuring that it is both wellused and respected within the local area. The Rare Navigator service is open to children, adults, individuals and families, at its heart however lie those at the start of their rare journey, as it is here that an early, positive experience can really help make a huge difference at what can be a hugely difficult time. “For children with rare diseases, special needs, or disabilities, it is vital to ensure that they have access to available services and interventions which can help them to reach their full potential. I think the Rare Navigator role can be a strong link to ensure this.”
Dr Ali Farah, Consultant Community PaediatricianThe Rare Navigator service has been able to do the work it does thanks to the funding and support from the National Lottery, Steve Morgan Community Foundation and Rejuvo. We are extremely grateful to their support.
Our RAREchatUK closed FaceBook group was launched in March 2021 with the aim of creating a safe and private space for our rare community to connect with one another. RAREchatUK is open to adult individuals and close family members such as parents, foster parents and guardians, grandparents, adult siblings and substantial carers (paid or unpaid). It is a space to network, share success stories, challenges and helpful information. The group is supported by our Rare Navigator or other SbD team members as well as two volunteer peer moderators.
Whilst the reality of a life lived with a rare condition is what unites our community, when it comes to online support many might opt to seek support from groups that pertain specifically to the rare condition/s they live with. The role of RAREchatUK is to be a safe space in which members can drop in for a virtual hug, or check in, and not just for practical advice and support.
If you’d like to join please follow the link below, we’d love to see you there. However do ensure you answer the questions. The privacy and wellbeing of our members is central to the group, so each request to join is carefully reviewed.
As part of our RAREhub service our Rare Navigator team run both a weekly online huddle, and local one to one drop in sessions at a number of different locations.
Our online huddles are kept deliberately small, with typically no more than 5 tickets released, to ensure the space remains a warm, welcoming and safe one for our rare community members. As the huddles are hosted via zoom they are a lovely, friendly and low stress way to grab a coffee with others from the rare community, but all without having to leave the comfort of your own home.
Our one to one drop in sessions are held in Mold, Wrexham and Flintshire and can be pre-booked, though a slot will be allocated on the day if one is available.
Details of both our huddles and drop ins are shared via our Facebook page, links below:
Links:
Support Services — Same but Different (samebutdifferentcic.org.uk)
https://www.facebook.com/groups/rarechatuk/ Same but Different | Facebook


The death of a child is so awful that no word can encompass the horrific and gut-wrenching pain that is felt by a parent. Children become orphans and spouses become widows, but what do we parents become? It is unnatural to lose a child, they should be outliving you. If you know your child’s condition is terminal or not, there is absolutely nothing that can make it easier and no matter how prepared you are or think you are, you will never ever be ready. The fallout will last your entire life – but that’s not to say you still can’t have a full and happy life. I think of life now as covered with a dust of sadness, I will dust and it will go away but it always settles back down waiting for me to dust again.
Arlo died at 20 days old, he had Trisomy 18, also known as Edwards Syndrome. 20 days, that is it. It wasn’t enough time! I could have had him with me for a lifetime and it still would never have been enough time. Our time together was filled with love; that is all our boy ever knew. Love from us, from friends and family and the wonderful hospice staff at Claire House. That was four years ago. It’s only now that I feel brave enough and a little stronger to handle my grief better. Do not misunderstand, the pain – never going anywhere, the loss and the utter helplessness are constant companions. My life is being rebuilt around my grief, but it is no longer all-encompassing.
I often re-live our short time as a family of four and feel guilty for some choices and wish I could change them. Sometimes, the wave of grief comes out of nowhere and I am floored for a while. The ‘what ifs’ and ‘if onlys’ help spur on the grief and longing, and I am now an expert at finding ways to feel guilty. Guilty for not making certain choices, guilty for losing myself in the grief, guilty for being cross with my son or husband, guilty for feeling happy and enjoying life!

I am learning to be kinder to myself. To accept that there are days when I won’t want to face the world. They are less and less as time goes on, but I doubt they will clear completely. Whatever we do we carry Arlo with us. We live now for him also. He is gone from us physically but never ever from our lives. We celebrate his birthday with cake and presents, we talk of him often and he is included in everything we do in life.
So how can you be there for a grieving parent? Sadly, there is no handbook and grief hits everyone personally and differently. I know from my experience and after speaking to other grieving parents the number one thing you can do is talk about a child that has died. Say their name. Remember them together. Mistakenly people think that they will upset grieving parents by bringing up the child or causing them to remember the pain of losing them, but this is so far from the truth. Honestly, a parent knows their child has died, that pain is there constantly, you don’t remind them because I guarantee the parent will have the child in their mind all the time. What you are doing is giving the parent space to talk about their child. By talking about
the child and their life you are acknowledging the grief and the love that is still there. As a parent knowing that you are there and will not shy away from the grief or in fact from them is so important. DO NOT act like the child didn’t exist.
That leads us on to the next thing you can do to support a parent –be there! Personally we found so many people faded from our lives. This can be for many reasons I think, the inability to deal with the grief and emotion from a parent, the inability to deal with their own emotions, not knowing what to do or say etc. Even a simple text, such as just ‘thinking about you today; or ‘do you want to grab a coffee’, can help. There were times when I would sit in front of a TV box set, so as not to have to think, and if I did get a text to go for a coffee etc., 99% of the time I wouldn’t take up the invitation, but knowing that someone had thought about me, my grief and the place I was in, was a little light in my day. I remembered. I appreciated it so much despite me not wanting me to get dressed or face the world.
It seems a little clichéd but the next thing is a meal especially in the first month or two. The ability of a grieving parent to function fully can be difficult. The daily grind of life, the housework, the shopping, the cooking, it all can become overwhelming fast. Not having to think about what to sort out for dinner, especially if there are other children in the home, will be a blessing.
According to the Kübler-Ross grief model, there are 5 stages to grief. These stages can last years. Some people can skip stages and others get stuck on stages. No two people grieve alike, and each of the stages and reactions of the bereaved will be individual to them. Parents grieving the loss of a child will grieve individually to them, despite it being a joint bereavement of a shared child.
The stages are:
Denial - shock, disbelief and numbness. The unwillingness to accept the person has died. It’s our body’s way of dealing with the initial wave of emotions. Anger - looking for blame, angry at doctors or clinicians, anger even at the person for dying. Anger can also manifest in other ways as a focus to direct the grief such as getting angry for little things like the way a person will look at you. It is not always rational.
Bargaining - feelings of guilt of choices made, feelings of being punished, dealing in ‘what if’s’ and ‘if only’s!’ Praying and wishing for different outcomes, despite there being no other way. Depression - this is the stage when loss is really felt. The knowing that the person is not coming back and missing them truly starts. Feeling unable to focus, making decisions are difficult and feelings of hopelessness are common. Changes in well-being such as over or under-eating and disruptive sleep patterns also are normal during this time.
Acceptance - this is not the end of grief or a sudden switch where a person ‘gets over’ the loss in any shape or form. Acceptance is more the realisation of a new reality in which the person is no longer there. Of starting to move forward with this knowledge.
Listen. That’s a huge one. Listen, but do not offer advice or try to ‘fix’ anything. It CAN NOT be fixed, nothing you can do will give the parent their child back or make things different in any way. For me hearing the words ‘I don’t know what to say but I can listen’ was one of the most honest and helpful things. Hearing things like ‘well at least you still have your other child’ infuriated me, and I had to stop myself from asking a parent of two children ‘which child they could live without?’ Others would say ‘time is a healer’ or ‘God only takes the good ones’ The thing for me looking back is I understand that these things were said from a place of goodness, not meant to be hurtful or malicious but at the time it brings little comfort. If a parent gets upset with you for saying the wrong thing, also know that is from grief and if they need to rant let them. I assure you that it will be another thing they will add to the list to beat themselves up over so be kind, do not judge. You don’t have to imagine what the parent is going through as it’s so horrific to contemplate but do try to understand the grief and reactions.
Photographs and videos that you have of the child will be much appreciated, especially over time. I found it difficult to look at any photos and videos for a long time, whereas my husband would sit
for hours looking over them and always wanting to see more, so send any you have over. It may not be immediately acknowledged but they will be wanted.
Take other children in the home out, even just to a local pizza restaurant for dinner or to run around a park. The children are grieving too and as a grieving parent, feeling like you are failing the child or children that are here can exacerbate your feelings of grief, guilt, and failure. It may be hard to do the ‘normal’ family things for a while so offering the parents a lifeline for the other child or children will be a little weight lifted from their shoulders for a little while.
Don’t leave things with ‘if you need me just give me a call’ I never ever once reached out to anyone. I never wanted to bring others down or make them carry my grief and pain with me but having someone reach out to me gave me the opportunity to take that step if I felt I could. That was a gift.
Gather information and share it with the parents. For example, a good grief counsellor or details of a bereaved parent’s group. It may not be that it is right for the parent just yet – or even ever, but you are giving them options that may help them and they may not be in a place to seek out the information themselves just yet.
So how can you be there for a grieving parent? Sadly, there is no handbook and grief hits everyone personally and differently.
Lastly, do not stop the invites. It may be years before a parent wants to accept to do anything again, so just because you have invited them numerous times before and they never attended, to know the option of joining in with friends and family is always there, that you still want their company is meaningful. One day they may be ready to take that step and having the invitation can be immeasurably important to them.
As time moves on, do not fade away or stop talking about the child. Involve the families in everything. Even now four years into our grief, hearing people talk about Arlo, share things about him, and even fundraise in his name is priceless to us. Not having him remembered is the worst feeling and still hurts so much for us all.

Remember that everyone reacts to grief differently. There isn’t a time-limited period, or a one size fits all grief. Take the lead from the parents as much as you can. Ultimately, be there and don’t ever think over time that they should now be done with the grief or over the loss. They never will be.
in children with special educational needs (SEND)
 Contributed by Annie Dewhurst
Contributed by Annie Dewhurst
When I was initially asked to write a piece about managing difficult behaviours in children with SEND, I was really looking forward to writing it…especially given my experiences – both personally and professionally. However, when I began to scribble some ideas down I realised I couldn’t possibly fit everything in.
You see, what’s challenging for me may not be challenging for other parents and vice versa. My poppet may display behaviours that are considered challenging, whereas other children and young people with the same or another rare condition may not display any or all of the behaviours she does. Sometimes behaviours that challenge can happen in particular environments. Sometimes people (like my girl) may use those behaviours for sensory stimulation, when she’s in pain, or happy, or feeling unable to control a situation or unable to express herself, or whatever.
The area of challenging behaviour seems vast, unique to the individual, and sometimes really quite complex. So, I’ll leave the definition alone. What I can do is share a little of our experiences in the hope it may help someone else.
My girl may grind her teeth, bang her head and will often even bite her hands. She used to be a great fan of eating things that weren’t food (still does sometimes) and she’s bitten other people, pulls her own hair and others (especially mine). She has a penchant for throwing things and is completely unaware of her own safety and that of others. She has THE most magnificent pincer grip…hence the reason I always have a tube of arnica cream handy. My arms, regularly, and throughout the years, have been peppered with painful little bruises. The list of behaviours, to be honest, is quite long.
To feel ‘attacked’ can feel quite demoralising. Furthermore, to see my child hurting herself has left me feeling powerless and upset. Over the years however have become more accustomed to it, at times perhaps desensitised to it even. No matter what I do or don’t do, no matter how many strategies I put in place to help her, or how many professionals I’ve sought help from, I know I can’t and won’t ever ‘cure’ her.
Hannah was diagnosed with Cornelia de Lange Syndrome whilst still a baby. CdLS affects between 1 in 10,000 to 30,000 live births and is present at birth. Individuals may display physical, intellectual and behavioural characteristics. However, it can be widely variable and not all people with the condition will show all of the aspects.
For more information visit www.cdlsworld.org which can signpost to the different Foundations. If based in the UK you can find out more at www.cdls.org.uk
The first International consensus statementtreatment and diagnosis protocol is linked here: https://www.cdls.org.uk/ treatment-guidelines/
I can, however, try and make things just that little bit easier.
First off, I observe; read her body language, consider whether there’s a trigger, like the environment – sounds, smells, crowds etc. She’s communicating something with me. What could it be?

I try and stick to a routine, so my girl knows what to expect.
I use pictures and now and next boards. I ask others to use these too.
Given she’s non speaking, I consider whether she’s trying to communicate something to me or others. Is she in pain or anxious or overstimulated?
I keep a diary and look for patterns. Is there a sudden change in behaviour?
I try and de-escalate – taking her away from an environment if necessary or I try to distract her, or encourage her to do something else; for instance, when she’s biting her hands I ask her to squeeze them and demonstrate it myself.
I always try and communicate with others, like school, sharing research papers, professional or personal guidance and any changes in behaviours at homeso that we’re all singing from the same hymn sheet, so to speak. I work at ignoring behaviours so they don’t become cyclical, or praising and rewarding where appropriate.
I am also good now at ignoring other random peoples idiotic comments, those who know absolutely nothing but believe my parenting skills need improvement and their remedy to my child’s behaviour would be the same as what they received i.e. a clip round the earhole because "it didn't do them any harm". Oh sigh. Where to start with that one, eh?
I’ve sought advice and guidance from other parents and professionals too.
I’ve also learned to feel no shame in expressing just how hard navigating this journey, with no compass, can be for me too. Sharing really can be cathartic.
I try to remind myself that I know my child best. Strategies for one child may not be appropriate for another and when she’s directing her attentions at me, whilst it sometimes isn’t very pleasant, I never take it personally and try very hard to keep calm.
I cannot stress this enough, I listen to my gut feeling. I trust it. Intuition has got us out of many a potential scrape.
Behaviours that challenge can be difficult for all concerned. However, there are times when I have been able to reflect and almost/sort of see the funny side - despite (at the time) cringing and wanting the floor to open up and swallow me! Like the time she kicked over a whole table of crockery in a very nice coffee shop. Oh, she thought that MOST amusing.
There was also the time her little jaws latched onto a rather elderly lady’s delicate hand… and wouldn’t let go…whilst we were waiting for the lift in a department store. I had warned the lady that Hannah did have a penchant for biting, however, she chose to dismiss it. Little did she know that the angelic little face looking up at her was looking for a new victim. Thankfully although the lady’s eyes almost popped out of her head Hannah didn’t manage to break the skin and no tetanus was required.. phew! To clarify, the funny side is very relative, and is more about my levels of ‘cringiness’ than Hannah causing destruction or harming others. My child may have profound disabilities, but my goodness, she can be hilarious at times.

So, where can you seek help? Well, for a start, you could talk to a GP, Health Visitor or Paediatrician. They might be able to refer you to someone more specialised. There’s lots of information on the internet too and we’ve included a few great links below.
There will also be social media support groups available, including Same but Different’s RAREchat Facebook group, also linked. Other special parents with lived experiences are often able to provide great hints and tips, and there may even be groups in your local area if you’d like to, or have the time to, meet up with others.
I guess the message I’d most want to convey to parents like me, especially ones that are just starting out on their own journey is that you’re not alone. Please always remember that. Never hesitate in reaching out.
We will catch you!
USEFUL LINKS:
RAREchatUK
RAREchatUK: hosted by Same but Different| Facebook
Contact: https:/ /contact.org.uk/ Here’s a fabulous (in my opinion) factsheet with links to other resources https://cerebra.org.uk/download/factsheetmanaging-challenging-behaviour/ FLACC pain scale https://cerebra.org.uk/ download/flacc-pain-scale-infographic/
Annie writes a brilliant blog on Facebook, which is full of her candid and often humorous insights to their world. You can find her by searching for ‘My kid loves broccoli.’
She has also written, and co-written, books, we’ve included the details below: Cornelia de Lange Syndrome – A Shared Journey: https://www.amazon.co.uk/ Cornelia-Lange-Syndrome-Shared-Journey/dp/ B09MYTK86Z/ref=tmm_pap_ swatch_0?_encoding=UTF8&qid=1639848104&sr=8-1
The (little) Book of Broccoli: https://www.amazon. co.uk/Little-Book-BroccoliDoodles-Journey-ebook/dp/ B092TMFD87
20
ways to awaken in the Spring Season

Get up early, head out to a peaceful location and enjoy the sunrise. Take in the beauty in the light and colour changes around you.
Make a date with a friend and head to a local park for a wander, get lost in conversation and enjoy the company you are in.

It’s bound to rain but don’t let it stop you from enjoying it, wrap up, get some waterproofs and splash in as many puddles as you can find –release your inner child and be in the moment.

Spring is a great time to get out into your garden and plant your summer bulbs and shrubs. Head off to a local garden centre for inspiration, or search #summergardens for some gorgeous photos! Space does not have to be an issue as even pots and planters can transform your environment.
Now is the perfect time to try out a new activity. Pilates and yoga are good for the body and mind or try something a bit more energetic like cycling or Nordic walking.
Spring is also a great time to get creative, or to learn something new – why not have a look at local classes that you would like to do and spend a few hours getting lost in one that appeals to you with like-minded people.

On a dull day, head out to a gallery or museum. Spend a good few hours taking in the beauty and the stories around you.

Have a spring clean! But if the idea of a whole house spring clean is too much, just focus on a small area, sort out a chest of drawers or a wardrobe and focus on that one task and enjoy the sense of achievement.
After your spring clean invest in a new scented candle and curl up with a new book for a while or bring in something into your space to create a cosy atmosphere and sit and enjoy your hard work.
Grab some paper, and some pencils and spend time doodling. You might surprise yourself with your own unique colourful piece of art. Get lost in enjoying the creative process!
Spring is a great season for fresh fruit and vegetables from spring greens to rhubarb. Head out to a local market or farm shop and stock up so you can create a hearty fresh meal to enjoy with loved ones. Try something new.

The nights are slowly starting to get lighter and warmer, and it is a perfect time to enjoy time outdoors. Light a BBQ, wrap up in warm clothes and enjoy eating al fresco for the first time in the new year.
Bring the outdoors in, create a floral arrangement for your home by collecting greenery and spring flowers from your garden or local wild spaces! Or if budgets allow treat yourself to some flowers from a local florist, tulips are a beautiful seasonal flower and bring in some stunning colours.
 Photograph: Blake Cheek, Unsplash.
Photograph: Markus Spiske, Unsplash.
Photograph: Blake Cheek, Unsplash.
Photograph: Markus Spiske, Unsplash.
Easter is just around the corner, spend some time making some easter decorations to use around the house, from felted bunnies to painted eggs, there will be something you will enjoy spending time creating.
Head out to a local café, enjoy a treat and sit back to watch the world go by.
Grab yourself a new notebook and write down your plans and thoughts for the year ahead. Make it as in-depth as you can and look forward to enjoying your upcoming events.
Plan a weekend away, and enjoy looking at locations, places to stay and things you would like to do there. Spring is the perfect time to visit new places.


The weather in spring is never predictable from snow to a heatwave and everything in between. Don’t let this spoil you getting out there, pick something on the day that’s suitable, from building a snowman or heading off to a local beauty spot with a picnic to enjoy some spring sun.
Pick a colour, grab your phone or camera and head off to a place you like to spend time. Capture anything with the colour you have chosen and be creative. Enjoy seeing things you would normally take for granted.
Kick off your shoes and take a barefoot walk across the grass. Along with being enjoyable it also has benefits for your health, from helping circulation, increasing vitamin D to reducing stress.
Visiting Disney World is every child’s (and often adult’s) dream. The memories it creates are treasured all around, watching the joy and awe on a child’s face is pretty priceless. Did you know that there are many Disney Worlds to choose from? Maybe a new bucket list is to do them all – well it is ours.
Disney prides itself on being inclusive for all and its disability services are on hand to help where they can, providing support and information. The website provides a wealth of information to help ensure you can plan the most magical holiday for you. There are also apps that you can use for the parks to help plan your day whilst there.
During Disney holidays there are a range of extras that can make your trip easier such as fast track passes for rides, concierge shopping or photo passes and memory makers. It is always beneficial to check out the options when planning your trip as to what will benefit you.

There are plenty of dining options at all of the Disney resorts worldwide from snack carts to fine dining restaurants and everything in between. Parks usually offer dining packages or meal plans that can help you budget.


Like with all Disney parks around the world, people come for the magic. The chance to meet the famous characters in real life. The wonderful parades through the park and of course the countless rides from gentle to wild, something for everyone from the timid to the thrill seekers. There are also many shows you can see, and each park will have its own time schedule.
We highly recommend seeing the evening parades with the characters and the floats all lit up. Depending on the time of year parks will also put on the most amazing firework displays that some would love.
Every Disneyland Paris hotel offers accessible rooms and there are six to choose from so you will be spoilt for choice. They have a dedicated guest service that will help with bookings and advice.

Transport to the parks is accessible too. Shuttles run from the hotels to the parks. A specially adapted minibus is also available that can be booked via any of the Disney hotel reception desks. It is subject to availability, and it cannot be pre-booked so waiting times may vary.
On offer also are the Access cards at Disneyland Paris. The cards are for guests with disabilities or long-term chronic diseases. A Priority Card or Easy Access Card is for certain activities and services, such as simplified easy access to rides (not immediate access) or booking times. The cards are dependent on the official documents provided by the guest.
Accessibility | Disneyland Paris
Disneyland® Paris (disneylandparis.com)
Accessibility maps for parks
Disneyland® Paris (disneylandparis.com) blue booklet for Autism
This year is the 30th Anniversary of Disneyland Paris. New experiences, special shows, festivities and food all celebrate the anniversary, and it will culminate in a grande finale that will be on 30th September 2023.
 Photograph: Bastien Nvs, Unsplash.
Photograph: Bastien Nvs, Unsplash.
Disneyland is the original Disney Amusement Park, built under the direct supervision of Walt Disney, opening in 1955.

Disney's Grand Californian Hotel & Spa has its own entrance to Disney California Adventure Park and is close to Disneyland Park.
https://disneyland.disney.go.com/guest-services/guests-with-disabilities/
2023 marks 100 years of Disney Animation studios. Disneyland resort is marking the centenary throughout the year, including an all-new light show illuminating main street and Sleeping Beauty’s Castle. Some nights will also include an amazing pyrotechnic show on selected dates. This will be a show to remember bringing more Disney Magic to life.
Here in the Floridian sunshine, you are spoilt for choice with many parks to choose from including Magic Kingdom and Disney’s Blizzard Beach waterpark.

Once again, all the hotels are accessible offering comfort and great locations to stay. Disney’s Budget hotel Art of Animation offers the comfort you need, drawing on its design from the magic of Disney and Pixar films. You can access the skyliner (the aerial gondola) to Epcot direct from the hotel and enjoy a bird’s eye view as you travel. At the other end of the scale, Disney’s Polynesian resort offers luxury in a south pacific style oasis. Direct access to the parks from the resort can be gained via watercraft, monorail or complimentary bus. The hotels all do vary in style and cost so it’s good to look for one within your budget. Complimentary bus shuttles run continuously to the parks and back to the hotels. Disabled Parking is also available at all the parks if you prefer to take your own transport. The auto plazas at the parks will direct you to the specific car parks.
Guests with Disabilities | Walt Disney World® Official Site (disneyholidays.co.uk)
With so many options here in Florida it’s difficult to pin down just one highlight as there is so much to do and see. We really do recommend a visit to Pandora – the world of Avatar. It’s a fully immersive ride and one we are sure you will enjoy.
www.samebutdifferentcic.org.uk

Please share a little background about your rare journey with us:

I had a relatively easy pregnancy until my 34 week growth scan when the sonographer noticed the ventricles in my baby’s brain were slightly enlarged which led to me having an in utero MRI and an amniocentesis. My waters broke early, the placenta started to fail and Isabelle was born at 35+5 weeks by emergency C-section, she weighed 4lb 7oz. Initially she was ok, but started to get tired with her breathing and was taken to PICU to help her breathe and it was here they found that her lactate level was high. She was transferred to Alder Hey Hospital at 4 days old and underwent numerous investigations including an MRI at just over a week old.
The MRI showed Isabelle had significant brain damage and we were told that they were 99 % certain Isabelle had a mitochondrial disorder. The neurologist prepared us that Isabelle would not come off the


ventilator. It was the hardest, saddest day of our lives and we quickly had Isabelle baptised and were able to hold her with all her wires. However, the following day Isabelle came off the ventilator and was breathing for herself and a day later transferred from intensive care to the neuro medical ward. We realised then she is going to be a little fighter.
In April 2012 when Isabelle was 7 months old we got a diagnosis, Pyruvate dehydrogenase deficiency. We felt numb, we had heard the worst news when she was born, but still clung on to a slight hope that ‘they got it wrong’. This confirmed our nightmare was a reality. We were told that Isabelle was at the severe end of the spectrum and the very limited treatments that were available were unlikely to have any impact on her development or life expectancy. We were told she was unlikely to live to the age of 2. But she is 11 now and makes us proud every single day, a true fighter.
What does a typical day in the Gregory household look like?
Day and night often become blurred in our house as Isabelle sleeps very little. Four hours is now considered a good night’s sleep for her (and us) and Isabelle is dependent on us for all her care needs. She is fully tube fed and cannot mobilise, therefore she needs an adult with her at all times. Isabelle needs regular medication, ketone blood testing, feeds making (she’s on a complicated ketogenic diet), changing and monitoring for changes in her condition. We have carers that support Isabelle which is great and gives us some respite but with that comes the awkwardness of having people in your home, which takes some getting used to.
If you could offer any advice to other families on their own rare journeys what would it be?
The support from parents of children with the same condition has been invaluable for us. Although her specific mitochondrial disease is very rare we are lucky that since she was born a charity has been set up for this (see link for the Freya foundation) and we now have an online support group and an annual family meet up. Having parents that are on the same journey is amazing, they are my ‘go to’ experts when things aren’t great. I also find that being one step ahead helps, there are things I know Isabelle will need and everything like adaptions, care, equipment, transport etc takes time so knowing what to expect and starting processes early has helped, I always think if the time comes and we don’t need something it’s better than waiting and doing without when it’s needed.

What do you do for yourself?
I struggle for time for myself, with 2 other children and working full time. Meeting friends for coffee is lovely, and I get a lot of work satisfaction (sad I know!) so often my work is my escape!
What drives you?
After Isabelle was born I set up a local charity to provide support to other parents of children with additional needs, including an accessible play space. This grew out of feeling unsupported after Isabelle was born, and recognising that there were few accessible places we could visit as a family. Sleepless nights and having to give up work to care for her gave me the time and I felt I needed to do something to change the situation for others (and myself!).

Links:
https://spacecheshire.org
https://www.thefreya foundation.co.uk
https://www.thelily foundation.org.uk
Think back to when you were a child. How important and how fun it was to be part of something communal – a bunch of mates from your street, a sports team, a school class –somewhere beyond family where you belonged and thrived.
At Cambridge Rare Disease Network (CamRARE) we recognise that for many kids and young people living with rare diseases (RD), accessing those communities and that sense of belonging can be extra tough.
So, we’ve created our own little RD ‘tribe’ in the Eastern region. We call our ‘gang’ Unique Feet, a community that welcomes all kids and their families, irrespective of their rare condition for friendship, connection, acceptance and support.
We offer regular, super-cool stuff from crafts and dance to horseriding and outdoor pursuits. All activities are fully inclusive and accessible. Unique Feet brings together kids and families who understand each other’s shared challenges but who also know how important it is to celebrate their triumphs. This shared experience empowers them to raise one another up to achieve hopes and dreams that might be so much more difficult to achieve alone. Visit

Supported by:
SPRING SPLASHES
www.amazon.co.uk
www.regatta.com

RARE CHANCE, LUCK & SHARKBITES!
www.alderhey.nhs.uk
www.cdhi.org/cdh-support
www.cdhuk.org.uk
READING TO DREAM
www.son-stories.com
ONE OF A KIND
www.camraredisease.org/uniquefeet
www.rarechromo.org
WHAT WE’RE INTO – REVIEWS
www.macmillan.org.uk
THE SCIENCE OF A RARE DISEASE

www.col4a1.net/en
www.gouldsyndromefoundation.org
www.ophthalmology.ucsf.edu/gouldlab
Kate de Winton Photography in Farndon, England
TRAVEL
www.disneyholidays.co.uk
www.disneylandparis.com
www.samebutdifferentcic.org.uk/raritylife
BEYOND THE DIAGNOSIS
www.beyondthediagnosis.org
www.havashealthandyou.com
www.h4bboston.com
RARE NAVIGATOR SERVICE
www.samebutdifferentcic.org.uk/rarenavigator

SAY THEIR NAME
www.careforthefamily.org.uk
www.childbereavementuk.org
www.tcf.org.uk
www.thegoodgrieftrust.org
www.clairehouse.org.uk
MANAGING BEHAVIOURS
www.cdls.org.uk
www.cerebra.org.uk

www.contact.org.uk
5 QUESTIONS WITH www.thefreyafoundation.co.uk

www.thelilyfoundation.org.uk
www.spacecheshire.org
CAMBRIDGE RARE DISEASE
www.camraredisease.org
We produce powerful films, strong imagery & compelling narrative; creating a visual storytelling experience that allows you to connect more closely with your audience.


We work with organisations, agencies and publications that love to make an impact. We can join as a creative partner and help shape the creative direction into an impactful photography campaign or film, or we can work to your brief.
Helping you connect to your audience with integrity.
Creativity. Collaboration. Empowerment.
Find out more by visiting: www.sbdcreative.co.uk