The American Nurses Association - Illinois (ANA-Illinois) is proud to announce that registration is open for “Student Nurse Political Action Day 2022: Empower Yourself –Advocate. Innovate. Find Balance,” to be held on April 5, 2022, in Springfield. Each year, Student Nurse Political Action Day brings together hundreds of nursing students from across the state in Illinois’ capitol for a day of learning, networking and advocacy. We are excited to get back to in person this year.
The health and safety of Student Nurse Political Action Day attendees are always of utmost importance. ANA-Illinois will be adhering to the CDC’s recommendations and local mandates at the time of the event. As the situation evolves, so will our approach to keeping you safe. At this time, COVID-19 vaccination OR a 72-hour negative COVID-19 test will be required to attend the event. Masks are required for all attendees during the event unless eating or drinking. We will be promoting social distancing during the program, encouraging everyone to complete a wellness self-monitoring before the event, and asking participants not to attend if they are feeling ill.
Our 2021 event will:
● feature an exceptional keynote speaker who will inspire and provide concrete lessons on how to weave inclusive thinking into one’s daily life—to be announced in February!
● spark discussion, encourage learning, and foster connection.
● deliver relevant and timely content for the current state of nursing in Illinois.
● energize and fuel the growth of future nurse leaders!
The event is $25 to attend and open to student nurses of all ages. Topics will include public health, school nursing, diversity and inclusion, and legislative issues facing the nursing profession.
For more information or to register visit https://bit.ly/SNPAD2022

Please take a moment today to nominate a nurse deserving of recognition for the work they do.
The Illinois Nurses Foundation is accepting nominations for the 8th Annual 40 Under 40 Emerging Nurse Leader Awards. The awards will recognize 40 Illinois RNs younger than 40 who positively represent their profession by participating in the community as well as professional organizations. Nominations are due April 15, 2022.
Winners will be chosen by their peers based on the following criteria:
Positively represent the nursing profession by actively participating in the community and/or a professional organization.
The award is designed to recognized nurses in Illinois who demonstrate exemplary professional practice along with community engagement and/or advocacy on behalf of the profession and those we serve.
Awards will be presented on September 22, 2022.
Nominate someone today - https://portal4nurses.com/awards/inf/forty-under-forty

Cheryl Anema PhD, RN

Cheryl Anema PhD, RN
Time to check our pulse! Is this a dream, nightmare, or reality? It is hard to believe that this all started in late 2019 and here we are in early 2022 and still dealing with the up and down trends with COVID. It is not over. I work in nursing academia, and we are still making regular decisions surrounding on-campus vs virtual (Zoom) classes, open and closed campus, attendance or live-streaming pinning and graduation, and covering for on-going call-ins for faculty ill with COVID. In addition, we must pay attention to what the departments of public health, state politicians, federal politicians, and our employers are recommending or mandating regarding our practice during the pandemic. Delta is here; Omicron is surging; what may be the next variant?
Faculty and students continue to juggle the demands the pandemic has placed on their lives. Nurses and healthcare workers are still getting sick, all placing more stress on those still working. Some nurses and nursing students are leaving the profession, while others are jumping on board, not always understanding the full impact of the pandemic. I say this to say, nurses will always be needed. We are the lifeline of healthcare. Pandemic or not, the demand for nurses continues, and will continue to increase as skilled nurses are retiring or deciding that the demands today are too great and leaving the profession.
The Illinois Nurses Foundation, along with ANAIL, and other nursing professional associations are here to help support nurses and nursing students. As Spring is upon us, the call for scholarship applications have gone out and a growing number of applicants have been received. It is the time of the year that the INF rejoices in the ability to provide monies to nursing students to support their education. We have been growing our scholarship base with the goal of providing an increasing number of scholarships and dollars. How can we do this, you may ask?
In December 2021, the INF held its first “virtual” Holiday Gala & Fundraiser. We are happy to say we raised over $14,000 through our online Silent Auction, raffles, monetary donations, and Gala ticket purchases. We were not sure how the event would go being 100%

online. It was a success with your support! Thank you. We were entertained with music by the Lakeside Artists Guild & Academy (a strings ensemble), and comedic presentations by comedians with Treuer Laughs Additionally, we presented the Nurse of the Year Award to Kim Cannon and Runner-up award to Betty Van Engen.
The INF Champion for Nursing Award was developed in 2020. Its purpose is to recognize outstanding support and advocacy on behalf of the INF and the nursing profession in Illinois, including, but not limited to, providing support to and participation in programs of the INF, ANA-Illinois, its organizational affiliates, or to Illinois nurses and nursing at large.
During the Gala we recognized the following individuals and organizations as Champions of Nursing. Our first recipient was Laurie Anema for her dedication and role as the INF Holiday & Gala Fundraising Committee co-chair. She donated endless hours in procuring many of our auction and raffle donations. She has also served on our INF Scholarship committee. Our 2nd Champion of Nursing, Mary Ann Tuft, founder, and chair of Tuft & Associates has supported nurses, nursing students and the INF in a multitude of ways. She is a strong financial supporter of the Foundation. Mary Ann was instrumental in helping to establish the first INF Advisory Council. Our final Champion of Nursing award went to the Arthur L. Davis Publishing Agency. The Publishing agency has worked with the INF in the production of the Nursing Voice since 2013. They have also been a financial supporter and have always supported our Foundation events.
We also heard from Monica Terrazas, one of our nursing student scholarship winners, and from one of our grant winners, Dr. Channon Simonovich. Dr. Simonovich shared a very interesting overview of her grant project. It was great to see the outcomes from the Foundation’s investments in nursing education and nursing research.
Of course, the INF Gala would not be the same without our raffles. Raffle tickets were sold online and during the live virtual event; a computer automatically drew the winner for each raffle drawing. It was fun to know your name was spinning around as you sat on the edge of your seat waiting – and then – the computer would say “the winner is…” and your name appeared. Raffle winners were notified, and their winnings were delivered to their homes. The silent auction ended later that night. We had some last-minute auction battles, which brought us to meet our goals for fundraising. From a 7-day trip to Branson, a $400 Dyson hairdryer, and $25 gift cards to Target, we had an array of items and winners. Thank you to all who participated. You will not want to miss this event in December 2022.
Following the Gala, we had a special event arranged with Kendra Scott (jewelry). Kendra Scott donated 20% of all purchases online or in a Kendra Scott store that used our INF special code. We hope to have more of these types of events, please be sure to read the Nursing Voice and follow us on Facebook, Twitter, and our website.
As you can see, the INF is an active Foundation, philanthropic 501C3, that thrives on the support from individuals and companies. We have no membership, just many volunteers. If you would like more information on the INF and opportunities to serve or support the INF, please go to our website www. illinoisnurses.foundation or reach out to our office, Editorial Director, or President.

INF Board of Directors
Officers
Cheryl Anema, PhD, RN
Brandon Hauer, MSN, RN
Karen Egenes, EdD, RN
Directors
Maureen Shekleton, PhD, RN, DPNAP, FAAN
Alma Labunski, PhD, MS, RN
Linda Olson, PhD, RN, NEA-BC
Amanda Buechel, BSN, RN, CCRN
ANA-Illinois Board Rep
Susana Gonzalez, MHA, MSN, RN, CNML
Jeannine Haberman DNP, MBA, RN, CNE
ANA-Illinois Board of Directors
Officers
Elizabeth Aquino, PhD, RN
Monique Reed, PhD, MS, RN
Jeannine Haberman, DNP MBA, RN, CNE
Beth Phelps, DNP, APRN, FNP, ACNP
Directors
Holly Farley, EdD, MS, RN
Susana Gonzalez, MHA, MSN, RN, CNML
Elaine Hardy, PhD, RN
Dorothy Kane, MSN, RN
Zeh Wellington, DNP, MSN, RN, NE-BC
Editorial Committee
Editor Emeritus
Alma Labunski, PhD, MS, RN
Chief Editor
Lisa Anderson-Shaw, DrPH, MA, MSN
Members
Deborah S. Adelman, PhD, RN, NE-BC
Linda Anders, MBA, MSN, RN
Cheryl Anema, PhD, RN
Ellen Bollino RN, MSN, ED, CEN
Kathryn Booth, MSN, RN, CNL, CSRN, NPD-BC
Nancy Brent, RN, MS, JD
Pamela DiVito-Thomas PhD, RN
Amanda Hannan MSN, RN
Phoebe Maholovich MSN, RN
Irene McCarron, MSN, RN, NPD-BC
Linda Olson, PhD, RN, NEA-BC
Lanette Stuckey, PhD, MSN, RN, CNE, CMSRN, CNEcl, NEA-BC
Executive Director
Susan Y. Swart, EdD, MS, RN, CAE
ANA-Illinois/Illinois Nurses Foundation
Article Submission
• Electronic submissions only as a word document attachment using current APA guidelines.
• Email: info@ilnursesfoundation.com
• Subject Line: Nursing Voice Submission: Name of the article
• Must include the name of the author and a title.
• INF reserves the right to pull or edit any article / news submission for space and availability and/or deadlines
• If requested, notification will be given to authors once the final draft of the Nursing Voice has been submitted.
• INF does not accept monetary payment for articles.
Article submissions, deadline information and all other inquiries regarding the Nursing Voice please email: info@ilnursesfoundation.com
Article Submission Dates (submissions by end of the business day) January 15th, April 15th, July 15th, October 15th
Advertising: for advertising rates and information please contact Arthur L. Davis Publishing Agency, Inc., P.O. Box 216, Cedar Falls, Iowa 50613 (800-626-4081), sales@aldpub.com. ANA-Illinois and the Arthur L. Davis Publishing Agency, Inc. reserve the right to reject any advertisement. Responsibility for errors in advertising is limited to corrections in the next issue or refund of price of advertisement.
Acceptance of advertising does not imply endorsement or approval by the ANA-Illinois and Illinois Nurses Foundation of products advertised, the advertisers, or the claims made. Rejection of an advertisement does not imply a product offered for advertising is without merit, or that the manufacturer lacks integrity, or that this association disapproves of the product or its use. ANA-Illinois and the Arthur L. Davis Publishing Agency, Inc. shall not be held liable for any consequences resulting from purchase or use of an advertiser’s product. Articles appearing in this publication express the opinions of the authors; they do not necessarily reflect views of the staff, board, or membership of ANA-Illinois or those of the national or local associations.
Dear Illinois Nurse Colleagues, What the world has learned first-hand over the past two years during the COVID-19 pandemic is something we have always known; nurses are the valuable backbone of the healthcare system. As the shortage of nurses grows while care demands increase, we have seen the unfortunate strain and impact on hospitals’ capacity to provide care.

Together nurses can work to identify solutions that address the issues that contribute to our profession’s shortage. The passage of the Nurse Staffing Improvement Act of 2021 is one solution that aims to help address staffing issues facing Illinois hospitals. We encourage you to visit the new online Nurse Portal to obtain resources, sit on your hospital nursing care committee, and help hold hospitals accountable for supporting the development of nurse-driven staffing plans.
As challenges for our profession continue to evolve and grow, ANA-Illinois will be hosting a Nurse Staffing Summit on March 12, 2022, to discuss current nurse staffing issues and work towards nurse-driven solutions. And as we continue to think of ways to advance and protect our profession, we must prioritize advocacy efforts. Thank you to those who joined us for our annual Nurses Day at the Capitol on February 2, 2022. We look forward to your participation again next year, and if you missed the event, please go to the ANA-Illinois advocacy portal to stay up to date on our advocacy efforts. We need your help to ensure our state and federal elected officials support laws that support the nursing profession.
If you are a student, know a nursing student, or are a nursing faculty member, please encourage nursing students to participate in the annual Student Nurse Political Action Day (SNPAD) on April 5, 2022. We must help plant the advocacy seed in our future generations of nurses; encouraging participation in SNPAD is one way to do just that!
As always, I appreciate you for all you have done and continue to do to advance our profession. I look forward to working with you to transform nursing and healthcare in Illinois.
Wishing you and your families wellness and peace for 2022.
With Gratitude,
President, ANA-Illinois

We would like to recognize and thank the following donors who were instrumental in helping us achieve our goals in 2021. Because of their general support we gave away over $12,000 in scholarships and awarded $10,000 in grants through our grant program.
Lisa Anderson Shaw
Cheryl Anema
Laurie Anema
Grace Ann Garcia
Elizabeth Aquino
Nancy Banash
Mary Barton
Ralph Barzditis
Melissa Bateman
Lindsay Bellows
Baldovino Bessie
Denise Bockwoldt
Mary Bortolotti
Shawn Brown
Pamela Brown
Bridget Buechel
Karen Carroll
Brittany Chimis
Susan Clark
Yalanda Comeaux
Lisa Connolly
Amanda DickensMontgomery
Ethel Doyle
Kimberly Dray
Karen Egnes
Jerry Esker
Raechel Ferry-Rooney
Daniel Fraczkowski
Martha Gano
Susana Gonzalez
Darwyn Hackney
Robin Hannon
Elaine Hardy
Brandon Hauer
Richard Heim
Renata Hornick
Ann Marie Jagiella
Judith Jennrich
Mary Jo Shepard
Susan Johanson-Lentz
Barbara Julion
Dorothy Kane
Karen Kelly
Mary Kelly
Julie Kennedy
Vicki Keough
James Kerridge
Koka Kliora
Alma Labunski
Rick LaGore
Patti Ludwig-Beymer
Kathleen M Lazzara
Anthony Magera
Arlynn Manasse
Mary Ann McDermott
Susan McReynolds
Kim Mettache
Stephanie Meuris
Margaret Miller
Colleen Morley
Monica Najera
Jamie Najera
Catherine Neuman
Emmanuel Olafia
Amanda Oliver
Linda Olson
Diana Ortega
MaryJo Osowski
Ann O’Sullivan
Katherine Pakieser-Reed
Erin Perwoznik
Nancy Possinger
Linda Roberts
Tiffany Saenger
Rocio Sanchez
Ruthann Sanders
Laurel Schaap
Katherine Schilder
Maureen Shekleton
Gloria Simon
Barb Sparks
Cynthia Stetins
Susan Swart
Mildred Taylor
Wayne Taylor
Eric Thomas
Melanie Tomas
Mary Ann Tuft
Yvonne Tumbali
Diane Vander Ploeg
Clint Verhagen
Connie Vincent
Sara Wall
Tiwanna WallaceAgbenyegah
Kristine Walsh
Carol Warfield
Patricia Wienski
Elaine Williams
Lauren Wojtkowski
Arthur L Davis Publishing Walter W. Schultz Agency, Inc
Smits Funeral Homes, LTD
Stepping Stone Financial CarMax
Howard and Geraldine
Knaack Foundation
Philippine Nurses Association of Illinois
Saint Xavier University
Farnsworth Group
Leon J. Witkowski Jr., D.D.S., LTD.
Ann & Robert H. Lurie
Children's Hospital of Chicago
Sarah Bush Lincoln

Kathryn C. Hansen, RN, BSN, STTI
Co-Author: Cynthia Borum, DNP, APRN, FNP-C, NE-BC
Introduction
Nursing is a career filled with an abundance of opportunities that is exciting at the same time is overwhelming and stressful. The new professional nurse must consider their purpose as they grow into their nursing career. The new professional nurse is defined as an individual that is in the initial stages of launching and flourishing within their nursing career. The personality of professional nurses assumes the basic characteristics of compassion and human caring. Finding the right job involves an in-depth appraisal of the organization along with the nursing environment. The professional nurse looks at the organization as a whole and assesses if they align with the mission, values, vision, and beliefs. Additionally, they examine the necessary factors of the nursing environment such as socialization and teamwork amongst coworkers, nursing care provided to patients, and the image of nursing. Mentorship and gaining knowledge about the vast amount of specialty nursing careers will lead them to establishing their career and ultimately their niche.
Mentorship
Success of the new professional nurse developing their career and landing the right job involves a few essential components with mentorship being at the center. The significance of mentorship within the field of nursing has and continues to positively impact nurses in their personal and professional growth. When a mentor and a mentee form a relationship, it is important to recognize that both the mentor and the mentee learn from each other and ultimately influence their career (Marshall, 2021). A well-matched mentorship helps a new professional nurse who is passionate about making a difference in their career lead them in their journey of career development to accomplish their goals. In the article, Mentorship In Nursing: An Interview With Connie Vance (Nickitas, 2014), she addressed the individuals in the field of nursing, “that we can’t and don’t achieve alone; mentors are absolutely essential to our individual and collective success.” (p.68). A new professional nurse experiences a very challenging and rigorous first year out in the field and therefore it is essential that there is support and resources available to help them gain confidence and achieve success in their patient care and overall understanding of their job (Innes & Calleja, 2018). This will in turn affect the overall job satisfaction and decrease the chances of losing outstanding nurses to other professions (Innes & Calleja, 2018). It takes time and effort to find the right individual to create a well-matched mentorship; however, putting in

the work and building connections can only benefit a new professional nurse to grow and develop their career. By doing so, the mentorship has the capacity to be lifelong and create a lasting impact on the new professional nurse to keep striving for excellence within the nursing profession. Ultimately, the mentorship that is formed is significant and creates a lifelong commitment to mentoring and nurturing other professional nurses in the profession.
The customary approach for new nurses seeking employment was in a general medical surgical nursing unit to gain experience with time management and organizational skills and sharpen patient care and nursing skills (Innes & Calleja, 2018). Conversely, today, new professional nurses are taking the non-traditional pathway and pursuing nursing specialty jobs early in their careers. According to Baldwin et al. (2021) greater numbers of new professional nurses are being hired directly into nursing specialty areas. Professional nurses are selecting specialized nursing units for a variety of reasons. New professional nurses are being driven to specialized nursing units to fill the greatest need for staff because of the nursing shortage (Baldwin et al., 2021; Innes & Calleja, 2018). On the other hand, new professional nurses are pursuing specialty nursing jobs to gain respect and earn the badge of honor as a professional nurse. There is a perception that a nurse must work in critical care to be a professional nurse. Professional nursing can be found in many settings such as ambulatory environments, surgery centers, hospitals, and even manufacturing and schools. Moreover, professional nurses are involved with many patient populations that span across the human life cycle from birth to death. Professional nurses take care of infant and pediatrics patients, women’s health needs, adolescents, and geriatrics populations. Consequently, nurses that are competent and have mastered skills for independent nursing practice are professional nurses, regardless of their nursing specialty. Building and strengthening one’s nursing career takes into account the professional nurse's passion for human caring coupled with choosing the right nursing specialty.
Finding a mentor can be as easy as checking mentor programs within your organization, a trusted and admired personal friend, a professor, teacher or even professional organizations such as the American Nurses Association (https://community.ana.org/ pages/mentorprogram?ssopc=1).
Conclusion
Nursing is a special calling and a career for life where professional nurses exemplify the gift of healing and compassion for human caring. A new professional nurse may find themselves in a situation where the job is not a good fit. However, the nurse should not leave the profession of nursing, rather they must explore other opportunities and areas within the nursing field. With the ability to build your career through mentoring and the vast amount of nursing specialty opportunities available, the professional nurse must remain optimistic, and hopeful in successfully landing the right job. Securing the right job will help to avoid the tragedy of losing a new professional nurse to a career outside of nursing.
Although it can be challenging to find the right job, taking the necessary time to explore and gain more knowledge about all the wonderful and rewarding careers within the field of nursing is crucial for the new

Starting to lose sleep, feeling constantly on edge, and arriving way in advance before my shifts to look up my patients was what consumed me throughout my first job as a new professional nurse. Although I felt supported, I was not happy and could no longer enjoy my life outside of work. It was when I started to have panic attacks that I knew I needed to make a switch to another unit. It wasn’t an easy decision— it was tough. I had worked so hard to achieve what I thought was my “dream” job, but my intuition and the physical and emotional toll just wasn’t right. I felt like a failure, and I wanted it to work out so badly. Luckily, through discussions with mentors, I was inspired with confidence, and empowered to search for an area in nursing where I was meant to be. Taking care of yourself is very important and with there being so many opportunities as a nurse, it is okay to not feel okay, however at the same time I realized I can continue mastering skills, sharing my strengths, and ultimately fulfilling my passion and dream as a new professional nurse.
professional nurse. No matter your environment or specialty, the slow or fast work pace, patient acuity, or patient population, you are a professional nurse. You have developed the characteristics that make you qualified for the job. Thus, the new professional nurse must understand that its not, “are you fit for the job,” but “is the job the right fit for you?”
References
Baldwin, K. M., Sleutel, M., Urban, R. W., Wells, J. N., Behan, D., Walsh, J., & Newcomb, P. (2021). An exploration of new graduate nurses transition to specialty practice. Journal for Nurses in Professional Development (37)2, 93-100. https:// doi.org/ 10.1097/NND.0000000000000695
Innes, T., & Calleja, P. (2018). Transition support for new graduate and novice nurses in critical care settings: An integrative review of the literature. Nurse Education in Practice, 30, 62-72. https://doi.org/10.1016/j. nepr.2018.03.001
Marshall, L. S. (2021). Take Charge of Your Nursing Career. Sigma Theta Tau. Nickitas, D. M. (2014). Mentorship in nursing: An interview with Connie Vance. Nursing Economics, 32(2), 65-69. PMID: 24834630
Table 1: Checklist to Identify a Good Mentor
• Admired, trusted, with shared interests and values
• Dyadic Relationship
o Sets goals and mutual expectations
o Invites questions, interactions, ongoing communication
o Advises with active listening and honest feedback
o Inspires confidence
o Encourages professional development and advancement
• Accessible, available, flexible, and responsive
• Willing to share resources, time, and knowledge
• Compatible culture and background





In Honor Donations
Diana Halfer
Isis Reyes
Elizabeth Aquino
Amanda Oliver
Nikki Pano
Kim Cannon
Memorial Donations
Bill O'Sullivan
Kenny Schwerman
Eleanor K Mays
Bill Freckman
Patricia Ann Tanner, RN CCRN
Irene S. McCarron, MSN, RN, NPD-BC Area Director of Education, Chicago Market Kindred Healthcare, Inc. and Deborah S. Adelman, PhD, RN, NE-BC Professor, Graduate Nursing Purdue University Global
A 14-year-old patient and a 76-year-old patient have COVID-19 and both require mechanical ventilation. There is only one ventilator available. They both have an 80% chance of survival if given the ventilator. Who should receive the ventilator? In another hospital, a 12-year-old patient and a 78-year-old patient have COVID-19. They both require mechanical ventilation. The 12-year-old has a 20% chance of survival while the 78-year-old has an 80% chance of survival if given the ventilator. Who should receive the ventilator support?
The most difficult aspect of crisis management are the ethical dilemmas that government and healthcare leaders will face such as those above in deciding who should and should not receive health care in a crisis situation. To apply the best possible interventions in a crisis situation, planning must be done before, not after a crisis strikes, and this led to Crisis Standards of Care (CSC) that were developed to deal with such situations. These are implemented to ensure equitable distribution of resources for the population in a crisis situation, while safely and ethically supporting individual patients when resources are inadequate (Ingram et al., 2021).
Planning for crisis intervention takes into consideration guidance built upon ethical frameworks and limited healthcare resources. Conventionally, deontology takes precedence in a normal medical situation wherein the four basic principles of autonomy, beneficence, non-maleficence, and judgment are applied (IDPH, 2015). In a crisis situation, this ethical framework must shift to meet population needs above the individual patient doing the most good for the greatest number. This leads to a shift in the basic principles to principles that are used during the crisis and can vary by state. The State of Illinois has four principles that guide the provision of care in a crisis situation. The first is solidarity
where interventions must benefit the community by decreasing the morbidity and mortality of the population. Efficacy is the idea that interventions must be scientifically sound, feasible and supported by data. The third principle is that of integrity: the idea that interventions maintain the culture of the community by applying the least destructive alternative, and community stakeholders must endeavor to communicate transparency in all decisions, including ways to enhance community resilience, trust and reciprocity. The last principle is that of dignity which is the notion that interventions must preserve human rights. While crisis situations must prioritize protection for the population, it must not violate human rights, thus, the least restrictive means must be applied (IDPH, 2015).
In Illinois, each principle is used to decide how scare healthcare resources are used during the crisis. Sound planning ensures adequate preparation for any crisis eventuality and public health policies are formulated based on these principles. The Crisis Standards of Care for the State of Illinois lists the following values grounded in these principles (State of Illinois CSC Ethics Subcommittee, 2020):
1. Solidarity: decisions made must benefit the whole community wherein morbidity and mortality are reduced;
2. Individual liberty: individual rights may be suspended as necessary, in a way that is proportional, relevant, least restrictive, and equitable;
3. Protection of the public from harm: may involve restriction of individual liberty but must be communicated openly which includes measures that promote support and compliance, and a mechanism for feedback;
4. Proportionality: restrictions to individuals as well as measures to protect the public from harm should not exceed what is necessary to address the level of risk in the community;
5. Equity: healthcare services may be limited in a way that does not violate the principle of equal human dignity and the distribution of resources must not be based on a person’s gender, race, ethnicity, citizenship, national origin, religious belief, sexual
orientation, pre-existing mental or physical disability, or socioeconomic status, including the ability to pay;
6. Privacy: may be suspended, but in a proportionate way, wherein the only information given is that which is necessary to ensure public health of the community;
7. Duty to provide care: providers weigh the demands of professional roles against own and that of their family and friends;
8. Reciprocity: society is required to support those facing disproportionate burdens such as health care workers, key personnel, and their families;
9. Trust: decision makers must balance the trust of stakeholders while implementing control measures during crisis situations; and
10. Stewardship: those leading crisis interventions must allocate resources so as to achieve patient health and public health in a perceivable fair manner.
Implementing these principles and values is done through the use a crisis intervention toolkit and plan that helps governing bodies formulate methods which can be applied in any crisis event. Crisis interventions involve continuing cooperation, consultation, collaboration, and support from different agencies in the community and each level plays a role in ensuring that those needing the interventions first receive them (Hanfling et al., 2013). In the healthcare and hospital setting, patient survival must include the means of survival and prioritize levels of care for those receiving the interventions. Public health departments prioritize treatment volume and quality of life based on survival and fairness by preserving all generations within the community according to priority (i.e., parents and caregivers, children, pregnant women, and the disabled). The emergency management system and public safety departments prioritize treatment volume and family care, preserving life across generations, and healthcare infrastructure. Another key factor in crisis management at all levels is prioritization of health care for providers.
The emergence of the novel coronavirus (COVID-19) has triggered the activation of CSC and interventions




worldwide including the State of Illinois. The three ethical duties of health care leaders responding to COVID-19 are to plan, safeguard, and guide (Berlinger et al., 2020). These are based on a balanced mix of ethical frameworks focused during the crisis situation where interventions are directed to public-focused care incorporating equality and equity in the distribution of scarce resources. In a crisis, ethical principles are directed toward minimizing morbidity and mortality of the population and limiting or suspending interventions for individual patients to ensure that the needs of the majority are met. This is done to best allocate resources that may become scarce or limited due to the surge, and the decision takes into consideration the provider’s duty to render patient care and the moral equality of persons vs. the equity of distribution of risks and benefits to society. During a crisis, the moral equality of the individual and equity of distribution must take into consideration the least morbidity and mortality possible in providing care to populations (Berlinger et al, 2020). These considerations must be balanced during any crisis and the current COVID-19 crisis is an example where the implementation of CSC has been declared by governors. When planned in advance, CSC interventions are easier to apply and decisions made are efficient, equitable, and fair because they are not based on emotions and tensions but on sound, pre-determined principles and guidelines, and on actual needs for triage decisions in areas of applying appropriate levels of care, initiation of life-sustaining treatment, withdrawal of life-sustaining treatment, and referral to palliative care. This advance planning also provides for provision of alternatives when staffing, space, and supplies become short. The duty to safeguard entails supporting healthcare workers as well as protecting vulnerable populations. For example, in the current COVID-19 pandemic, healthcare workers at heightened risk of occupational hazards amid infectious environments and vulnerable populations have to be considered first. When responders and staff become victims in a crisis, care for all is compromised.
The duty to guide entails contingency levels of care as part of the CSC. In the COVID-19 pandemic, planning for equipment and supplies such as ensuring the availability of ventilators and PPEs is essential to prepare for any surge. When no guidance is available, the quality of care is reduced which can impact population morbidity and mortality as was seen in early 2021, leading to the death
of thousands and further spread of the COVID-19. Other plans in contingency and crisis situations must include infection prevention and the provision for emotional needs when patient visitation is restricted.
Who determines what these plans entail is a multilayered process starting at the institutional level (Berlinger, 2020). In the first scenario mentioned at the onset, based on equal medical status, the ethical principle applied to give the ventilator to the 14-year-old patient is based on the potential years for future life. In the second scenario, the 76-year-old patient should be given the ventilator based on the higher chance of survival which is 80%. When the crisis involves larger geographic areas, city and county public health departments would determine allocation of resources and may issue proclamations that would inform an institution about how to allocate care and resources in the two scenarios.
In the State of Illinois, crisis intervention is guided by the Illinois Emergency Operations Framework which includes the Illinois Emergency Operations Plan (IEOP) and the Emergency Support Function 8 Plan (ESF-8). These plans outline the activation of state resources when hospitals are overburdened and in need of government assistance (idph-crisis-standards_2019. pdf). For the first time, these plans had to be activated during the COVID-19 pandemic and resources from the State or national stockpile were released and aided in the collaboration of stakeholders as well as coalition groups comprised of hospitals, local health departments, and emergency management personnel who provide assistance during the pandemic (State of Illinois Department of Public Health, 2020). These groups coordinate distribution of resources even before crisis levels to try avoiding a move towards CSC.
The IEOP requires that hospitals must have medical disaster preparedness plans and a response plan that includes interventions for catastrophic events such as the surges seen during the COVID-19 pandemic. Hospitals are also required to notify the Illinois Department of Public Health (IDPH) when their disaster response plans have been activated to enable IDPH to effectively guide the allocation of assistance and resources in a larger geographic area. Particular to the COVID-19 pandemic, the State of Illinois developed a tiered system that escalates from conventional to contingency to crisis standards and was used to determine what guidelines had to be followed by the public
and private sectors and what levels. The CSC is implemented when needed to enable hospitals to effectively deliver the best possible care in the crisis to meet the needs of the population as compared to meeting the needs of individuals. During this stage, hospitals may seek governmental intervention, legal and regulatory support, and coordination with other health care providers. When CSC are applied, hospitals are guided by the following:
1. Crisis care should cover strategies that extend or go beyond surge capacity plans where capacity is markedly increased beyond and/or far exceeds normal operating capacity.
2. Crisis care is likely to be activated during long-term events (e.g., the ongoing COVID-19 pandemic) when there is no practical way to obtain critical resources.
3. Crisis care does not allow hospitals to delay care but leads to making immediate decisions related to the critical nature of the necessary minimal health care to sustain population health.
4. The crisis level must gradually revert to contingency or conventional care as additional resources become available such as medication, equipment, and staffing.
5. Crisis care strategies should be updated throughout a crisis as needed, depending on ongoing resource shortages or increases.
6. In addition, ethical principles and crisis standards of care for COVID-19 include the following considerations: a. Non-discrimination in the delivery of care; b. Ethical conservation of scarce resources; c. Distribution of scarce resources; and d. Composition and function of triage teams.
In his most current State address, Illinois Governor Pritzker directed the allocation of emergency services and resources needed to prevent further COVID-19 surge and the prevention of the Omicron variant infection to pandemic proportions. He grounded this in the needs of the State’s citizens based on the CSC established by IDPH and other agencies tasked with the health of the State. Maintaining ethical principles to any crisis situation will help reduce chaos and health care disparities that can lead to negative outcomes. While no state wishes to enact CSC, the COVID-19 pandemic has shown that these work to allocate the best care possible for the greatest number to ensure the lives of the population.
References available upon request

The first COVID-19 vaccination given in the United States was on December 14, 2020. Almost simultaneously came controversy over the vaccine. There was hope for a ‘cure’ to this pandemic so everyone could return to a normal life without masks, and where concerts, theaters, sports events, and family gatherings would go back to the way they were before the COVID-19 epidemic. However, for many people this hope for a cure did not include a vaccine, as the vaccine quickly became a polarizing agent pitting people who refused to get vaccinated against those who were vaccinated.


It is difficult for those who are vaccinated to understand those who refuse or are opposed to vaccination. With cases and hospitalizations rising, health officials have started to make progress in getting some of the unvaccinated people inoculated (Bosman, et.al., 2021). The American Nurses Association (ANA) has had a longstanding position statement that includes mandates that all individuals, including nurses and other health care professionals receive immunizations against vaccine-preventable
diseases according to the current and best scientific evidence, unless there is a medical contraindication that makes a vaccine unadvisable. This statement has now added COVID-19 vaccines (ANA, 2021). Nurses have a professional and ethical obligation to be vaccinated just as we advocate for the public to do the same.
Hesitancy and misinformation are a major stumbling block in increasing the numbers of people getting vaccinated. The National Council of State Boards of Nursing (NCSBN), along with the ANA and other national education, nursing accreditation, and nursing leadership professional nursing organizations, issued and endorsed a policy statement addressing misinformation and misleading COVID-19 information being disseminated by some nurses (Dec. 2, 2021). Misinformation is considered a threat to public health and a public health crisis that can lead to illness and death, as well as prolonging the pandemic. As a trusted profession, nurses have a professional obligation and responsibility for the information they provide to the public. As stated in the policy statement, “nurses are professionally accountable for the information they provide to the public,” and in addition to the potential harm to the public, may also be placing their license at risk (NCSBN, Dec. 2, 2021). The American Medical Association has also adopted a policy aimed at combatting disinformation disseminated by physicians and other health professionals (AMA, 2021). To expect that nurses educate their patients and the public on the evidence available about COVID-19 and its treatment as well as the vaccines, and to not spread misinformation is not the same as saying they should not object to bad practices or to speak out about their needs for providing care that is safe for themselves and their patients (Grace, 2021). In the beginning of the pandemic, there were expressed needs for appropriate resources, such as Personal Protective Equipment (PPE), staffing, and other resources needed to care for patients.
Nurses’ ethical obligation to promote health and wellbeing in individuals and the community, and to provide optimal safe care is expressed in the principles of the Code of Ethics for Nurses (Provision 1, ANA, 2015). Provision 4 addresses nurses’ accountability for their practice and for the nursing care their patients receive, including their responsibilities for teaching, research and administration. In addition, Provision 4.1 states that nurses must adhere to their professional scope and standards of practice and to state nurse practice acts. As role models for their patients and for the public, nurses have been critical to the response to the COVID-19 pandemic. Nurses have an ethical obligation to get
vaccinated in order to maintain their own health so they can safely care for themselves, their patients, their families and their communities (ANA, Sept. 2021; Kearns, 2021)
References
American Medical Association (2021). AMA adopts policy to combat disinformation by health care professionals. Retrieved from: https://www.ama-assn.org/press-center/ press-releases/ama-adopts-policy-combat-disinformationhealth-care-professionals (Nov. 15, 2021).
American Nurses Association (2021). American Nurses Association adds COVID-19 vaccines to longstanding position on immunization. Retrieved from: https://www. nursingworld.org/news/news-releases/2021/americannurses-association-adds-covid-19-vaccines-to-longstandingposition-on-immunization/ (July 8, 2021).
American Nurses Association (Sept. 2021). ANA affirms support for COVID-19 vaccination mandates, promotes safety of vaccines. American Nurse Journal, 16 (9), 39. American Nurses Association (2015) Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: Nursesbooks. org
Bosman, J., Hoffman, J., Sanger-Katz, M., & Arango, T. (2021). Unvaccinated in America? There’s no one answer. New York Times (July 31, 2021, updated Oct. 24, 2021). Retrieved from: (https://www.nytimes.com/2021/07/31/us/virusunvaccinated-americans.html
Grace, P. J. (2021). Nurses spreading misinformation: The ethics of transparency and trust during the COVID crisis. American Journal of Nursing, 121(12), 49-53.
International Council of Nurses (2021). The ICN Code of Ethics for Nurses. Geneva, Switzerland: ICN. https://www.icn.ch/ system/files/2021-10/ICN_Code-of-Ethics_EN_Web_0.pdf Kearns, A.J. (2021). Should nurses take a COVID-19 vaccine? Nursing Outlook, 69(6), 1081-1089.
NCSBN (Dec. 2, 2021). Policy Statement: Dissemination of Non-Scientific and Misleading COVID-19 Information by Nurses. Retrieved from: https://www.ncsbn.org/ PolicyBriefDisseminationofCOVID19Info.pdf
In the December issue, we failed to identify the authors of our Quarterly Ethics Column. We sincerely apologize and thank Dr. Lisa Anderson Shaw and Dr. Linda Olson for their willingness to bring this vital information to the Nursing Voice as a quarterly column.


On November 16, 2021, the National Council of State Boards of Nursing (NCSBN), the American Nurses Association (ANA) and five other nursing professional associations published a Policy Statement, Dissemination of Non-scientific and Misleading COVID-19 Information.

The Policy Statement was published in order to inform all nurse licensees that sharing misinformation about COVID-19 to anyone can be the basis of a disciplinary action by state boards of nursing.
Misinformation in the declaration is defined as “distorted facts, inaccurate or misleading information not grounded in peer-reviewed scientific literature and counter to information being disseminated by the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA).”
US boards of nursing, the profession itself, and the public expect that nurses maintain truthfulness, the principles of the American Nurses Association (ANA) Code of Ethics for Nurses, and highest scientific standards when distributing information about COVID-19 or any other health-related condition or situation. When these standards are not adhered to, the nurse threatens the public’s health.
Disseminating misinformation can take any form, including social media.
The Policy Statement has clear implications for nurse licensees in Illinois. These implications, however obvious at first blush, are even clearer when reviewing certain provisions of the Illinois Nurse Practice Act and its Rules.
The Illinois Nurse Practice Act lists the grounds upon which a nurse licensee, whether an LPN, an RN, or an APRN, can be disciplined.
The Act’s following grounds (225 ICLS 65/70-5) are potentially applicable when disseminating misinformation about COVID-19, depending on the conduct of the nurse licensee:
• (2) Material violations of any provision of the Act
• (5) Knowingly aiding or assisting another person in violating any provision of the Act or rules
• (7) Engaging in dishonorable, unethical or unprofessional conduct likely to deceive, defraud, or harm the public, as defined by rule

• (21) Allowing another person or organization to use the licensee’s license to deceive the public
The Rules to enforce the Act provide further guidance. In detailing dishonorable, unethical or unprofessional conduct listed in the Act’s grounds ((7) above), the Rule states (Administrative Code, Title 68, Part 1300.90a)):
• 1) Engaging in conduct likely to deceive, defraud or harm the public, or demonstrating a willful disregard for the health, welfare or safety of a patient. Actual injury need not be established
• 2) A departure from or failure to conform to the standards of practice as set forth in the Act or this Part. Actual injury to a patient need not be established
• 6) Engaging in activities that constitute a breach of the nurse’s responsibility to a patient
• 7) Engaging in activities that are violative of ethical standards of the profession…..
• 10) Engaging in activities that cause actual harm to any member of the public
Under 1300.90 b) and c), the Code for Nurses with Interpretive Statements (2015) and the Standards of Practice and Educational Competencies of Graduates of Practical/Vocational Nursing Programs (2007) are incorporated by reference to this section.
Last, the Rules list the Standards of Professional Conduct for Registered Professional Nurses and Standards of Professional Conduct for LPNs. Both include that RNs and LPNs must practice in accordance with the Act and their respective listed standards.
How can you, as an Illinois nurse licensee, avoid one or more of these provisions from being the basis of a disciplinary action against you in relation to dispersing misinformation about COVID-19?
The answers are simple.
First, review and conform your nursing practice with the ANA Code of Ethics with Interpretive Statements and the Standards of Practice for Graduates of Practical/ Vocational Nursing Programs. Because these documents are incorporated into the Rules to administer the nurse practice act, a violation of their provisions adds another basis for a professional disciplinary action.
Second, carefully examine your personal beliefs about COVID-19 and its treatment. If you believe what is being recommended by the CDC and the FDA should not be followed, that is your right.
However, these personal beliefs about COVID-19 and its treatment cannot alter your communications with others to whom you provide care or to anyone who asks for your opinion on obtaining vaccinations or seeking unfounded, unscientific treatment.
Remember that nurses are seen by the public as being the most trustworthy health care provider since 1999 by Gallup poles, except for one year when, after 9-11, firefighters were seen as the number one most trustworthy profession.
What you say is taken as truthful and accurate by the public. As a result, the public and/or your patients may delay or reject established care and treatment with potentially disastrous results.
You also have a duty to correct misinformation about COVID-19 and its treatment. Many of your colleagues have done so, not only with patients, but with the public generally, in such modes as webinars, written articles, newspaper interviews, and news programs.
It is essential that you not contribute to more damage to the public’s health and welfare than has already been done by disseminated misinformation about COVID-19.
Do not add to that damage by forfeiting your ability to continue to practice your profession. That, too, would be a great loss.
You can read the entire Position Statement at: https:// www.ncsbn.org/PolicyBriefDisseminationofCOVID19.Info. pdf
The Code of Ethics for Nurses can be found at: https://www.nursingworld.org/practice-policy/nursingexcellence/ethics/code-of-ethics-for-nurses/ LPN Standards are located at: https://www.napnes. org/wordpress2/standards_2009.pdf

Areas: Licensing, Disciplinary Proceedings, Hospital Termination, Nursing Home Proceedings and All Nursing Rights Issues. WE CARE ABOUT NURSES and travel throughout Illinois • Free Consultation
• All Communications Privileged
• All Calls or Emails returned immediately
• Regular office hours in
Contact James B. Goldberg, 312-735-1185
200 Wacker Drive, Suite 3100, Chicago, Illinois 60606
Email: jgoldberg@jbglawfirm.com | Goldberglicensing.com


The Department has received many inquiries regarding 2022 license renewal continuing education requirements for RNs, APRNs, and FPA-APRNs.
• To clarify recent Illinois Continuing Education (CE) requirements for license renewal by May 31, 2022 for Illinois RNs, APRNs, and FPA-APRNs:
o The implicit bias awareness training CE requirement (HB158, Public Act 102004) for Illinois RNs, APRNs, and FPA-APRNs will begin as a license renewal requirement in 2024. Illinois RNs, APRNs, and FPA-APRNs are not required to complete implicit bias awareness training as one of 20 hours of CE required for license renewal in 2022. While the law was passed, the Rules with detail are not yet final.
o Sexual harassment prevention training CE requirement. A law passed in 2019 that went into effect on January 1, 2020 requires individuals with licenses issued by the Division of Professional Regulation (DPR) that require continuing education (CE) to renew their license to also complete one hour of CE on the topic of sexual harassment prevention training. This CE requirement is included in the number of hours already required under the individual Acts and Rules and does not increase the number of hours required to renew a license. One (1) hour of sexual harassment prevention training CE course is intended to fit into the nurse licensee’s regular CE requirements. For example, one of the 20 hours of CE required for RN license renewal must be a sexual harassment prevention training course.
• Beginning with the 2024 RN renewal, Illinois RNs who provide health care services to and have direct patient interaction with adults 26 years of age and older will be required to complete a one-hour course in diagnosis, treatment and care of Alzheimer's disease, along with other dementia types. CE Curriculum will involve how to identify and diagnose Alzheimer's, effective communication strategies and management and care planning. This course may count toward the regular CE requirements (Public Act 1020399, 20 ILCS 2105/2105-365).
• To renew your RN, APRN, or FPA-APRN license, easy access to renewal can be found on the IDFPR Nurses webpage https://www.idfpr.com/profs/nursing.asp On the left side of the page is a calendar icon that says “License Renewals.” This icon wiggles when the renewal site is open. The renewal portal is open will be available 24/7 beginning mid-March 2022 through May 31, 2022. RNs, APRNs, and FPA-APRNs must pay the renewal fee and renew their license by May 31, 2022. Licensees who renew after that date will be required to pay an additional late fee.
• The Illinois Department of Financial and Professional Regulation (IDFPR) is providing renewal assistance for individuals and businesses that are having difficulty with the online renewal process. These steps will help licensees better navigate the account matching process on the Department's updated online portal. For those requiring additional assistance, please email: fpr.lmu@illinois. gov
o Assistance for Individuals: https://bit.ly/3mb8C7U
o Assistance for Businesses: https://bit.ly/3E5Fll8
• To print your license or download an electronic copy to your phone, just head to the IDFPR website.
• On the IDFPR Division of Professional Regulation Nurses webpage, the “Requirements of an Internationally Educated Nurse” document has been updated. Resources on this document now include the names of Board of Nursing approved vendors for items required to apply for an Illinois nurse license. Information includes that endorsing an active license from another state requires: an application by Endorsement. A Credential Evaluation Service (CES) Report is not required if the state of original licensure required a report at the time of original licensure. An English equivalency test is not required as long as the nurse applying for endorsement took and passed the NCLEX® licensure examination.
• The Illinois Department of Financial and Professional Regulation (IDFPR) Resources for Illinois Residents and Licensees Impacted by Coronavirus 2019 Disease (COVID-19) webpage https://www.idfpr.com/COVID-19.asp is still available. This IDFPR webpage has list of resources for Illinois licensees and consumers impacted by the Coronavirus Disease 2019 (COVID-19). This page includes press releases, FAQ sheets, and Executive Orders that affect the professions IDFPR licenses and oversees.
• The list of health care professional temporary practice permits granted in Illinois may be found here: https://www.idfpr.com/Forms/COVID19/Temp%20 Practice%20Permits.pdf
• IDFPR’s Division of Professional Regulation has issued a notice, “Notice that Advice or Treatment Regarding Covid-19 Must conform with Evidence-Based Medicine and Standards of Care,” to remind physicians and other healthcare professionals that any advice or treatment provided to a patient must conform with evidencebased medicine and standards of care and that failure to do so may subject the individual to disciplinary action. Licensed healthcare professionals have an ethical and professional duty to the public and are entrusted to protect the public health and the safety of patients. IDFPR is aware of licensed healthcare professionals providing misinformation regarding COVID-19 mitigations and treatment. https:// www.idfpr.com/Forms/COVID19/IDFPR%20statement-physicians.pdf
• The Health Care Temporary Practice out of state temporary practice permit has been extended through May 31, 2022 or until the expiration of the Gubernatorial COVID-19 Disaster proclamations https://idfpr.com/Renewals/ Apply/Forms/F2398.pdf
• Variance: The Healthcare License Reinstatement Application is specific to the COVID-19 Pandemic and limited to prior State of Illinois licensees who were in good standing, including: Licensed Practical Nurse, Advanced Practice Registered Nurse, and Registered Nurse. The license must have been on an “inactive” status for less than five years. The COVID-19 license will have an expiration date of May 31, 2022 or until the expiration of the Gubernatorial COVID-19 Disaster Proclamations. There is no fee to apply https://idfpr.com/ Renewals/Apply/Forms/F2396.pdf
In 2021, IDFPR’s Military Liaison tripled the number of military service members and spouses assisted compared to 2020. In total, IDFPR received more than 500 applications for licensure from military and military spouse applicants in 2021. The military liaison directly works with service members and their spouses, as well as members of military installations based in Illinois, to expedite and assist their professional licensure process. We wish to thank them for their service for our country! For a copy of the report, 2021 Expedited Licensure Review for Military Service Members and Spouses, use this link https://idfpr.com/Forms/2021%20Annual%20Military%20Report.pdf
The Nursing Education Scholarship Program: annual applications will be accepted from March 1 through April 30, 2022. The goal of the Nursing Education Scholarship Program is to increase the number of nurses available for employment in Illinois by offering scholarships to overcome financial barriers to education. This program has been in place since 1993, with funding from the Nurse Dedicated and Professional Fund, Illinois nurse license renewal fees, since 2016 the annual allocation has been $2million. The program provides financial assistance to qualified individuals pursuing a certificate in practical nursing, an associate degree in nursing, a hospital-based diploma in nursing, a baccalaureate degree in nursing, or a graduate degree in nursing https://dph.illinois. gov/topics-services/life-stages-populations/rural-underserved-populations/nursingeducation-scholarship-program
The State of Illinois Coronavirus Response Site: The COVID-19 Vaccine Plan, up-todate information on what Illinois is doing protecting the health, safety, and well-being of Illinoisans can be found at https://coronavirus.illinois.gov/s/
A complete copy of the Nurse Practice Act and the Rules may be found on the IDFPR website www.idfpr.com or on the Illinois Nursing Workforce Center’s website http:// nursing.illinois.gov/nursepracticeact.asp
Illinois Nurses Foundation is transforming healthcare through the power of nursing. We are problem solving, generating new ideas, creating opportunities for new leaders, and promoting educational opportunities for the profession.
We need your help! Your charitable giving helps us achieve new milestones such as providing scholarships for those interested in the profession as well as for nurses interested in seeking additional degrees, creating new programs like the 40 under 40 Emerging Nurse Leader awards program, providing research and small project grants, and supporting and celebrating the achievements of individual nurses. There are several ways to give. Please scan the QR code below to contribute to the growing mission of the Illinois Nurses Foundation.
Together we will transform healthcare in Illinois.
Register today and Aspire to Trailblaze. It’s not too late, but time is running out. Register today and earn up to 34.25 CEUs during the 2022 ANPD Convention in the historic city of San Antonio, Texas.
This is the perfect time to avail of the latest innovations in nursing professional development thru:
1. Cutting edge NPD Education;
2. Networking and collaboration with NPD practitioners and PD associates; and 3. Earn CEUs that can meet the May 2022 RN* license renewal requirements. For registration information including hotel accommodation and COVID19 requirements, please email us at info@anpd.org or call us at (312) 321-5135.

We need your help !!
Take five minutes after completing license renewal 2022 – share info about you, your nursing specialty and workplace – please participate
RN, APRN and APRN-FPA license renewal will begin mid-March through May 31, 2022. The Illinois Nursing Workforce Center is requesting your help in completion of a short survey. There is a separate survey for each level of licensure; APRNs and APRNFPAs should renew their RN license first. All questions offer multiple-choice response options, with limited spots for comments, which is why RN survey completion time is approximately five minutes.
After completion of payment for Illinois RN , APRN or APRN-FPA individual license renewal, nurses will see the following message:
“We are requesting approximately five minutes (APRN or APRN-FPA will say 10 minutes) of your time. All data will be reported in the aggregate for use in determining nursing workforce projections and needs in Illinois. Individual responses will remain anonymous and confidential. Although this report is not mandatory, your participation is critical, since employees in the field are our best and most reliable real-time source of information available. By participating in this report, you will be helping to ensure that there will be an uninterrupted supply of nurses to meet the increasing future demands in the healthcare industry.” At the end of the message is a link that you will need to click on to reach and participate in the short survey.
Each survey captures data on the demographics, education, state distribution and practice foci of nurses in Illinois. The Nursing Workforce Center goal is to evaluate the impact of changes in the Nurses Practice Act on nursing practice.
Why is data collected with license renewal? Because, according to the U.S. Health Resources and Services Administration (HRSA), state data based on licensure data holds more accurate workforce predictions. Please look for the link to participate after payment of the licensure fee. It is anticipated that there will be some limited changes in the online license renewal process, but request for voluntary participation should occur after license renewal fee payment.
Are there areas in the State where Registered Nurses (RNs), Advanced Practice Registered Nurses (APRNs) or Advanced Practice Registered Nurses with Full-Practice Authority (APRN-FPAs) are concentrated? Where are the greatest needs? Are there popular RN, APRN or APRN-FPA specialties? How would the educational pipeline for RNs be best characterized? Where are the APRN-FPAs seeing patients? We need your help in answering these questions.
Past reports dating back to 1984 are available on the Illinois Nursing Workforce Center website http://nursing.illinois.gov/ResearchData.asp




Nurses want to provide quality care for their patients.
The Nurses Political Action Committee (Nurses- PAC) makes sure Springfield gives them the resources to do that.
Help the Nurses-PAC, help YOU!
So. . . . . . . if you think nurses need more visibility if you think nurses united can speak more effectively in the political arena if you think involvement in the political process is every citizen’s responsibility.
Become a Nurses-PAC contributor TODAY!
❑ I wish to make my contribution via personal check (Make check payable to Nurses-PAC).
❑ I wish to make a monthly contribution to NursesPAC via my checking account. By signing this form, I authorize the charge of the specified amount payable to Nurses-PAC be withdrawn from my account on or after the 15th of each month. (PLEASE INCLUDE A VOIDED CHECK WITH FORM)
❑ I wish to make my monthly Nurses-PAC contribution via credit card. By signing this form, I authorize the charge of the specified contribution to Nurses-PAC on or after the 15th of each month.
❑ I wish to make my annual lump sum Nurses-PAC contribution via a credit or debit card. By signing this form, I authorize ANA-Illinois to charge the specified contribution to Nurses-PAC via a ONE TIME credit/debit card charge.
❑ Mastercard ❑ VISA
Credit card number Expires CVV


The survey was conducted through an email direct request for participation post license renewal. Participation was voluntary, 1,962 of the 16,548 Illinois APRNs completed the survey. The data quantifies the services APRNs provide, the process that is used to bill for these services, and reimbursement for services. Finally, the survey captures the diversity of APRN specialty expertise and the settings where patients receive these specialized services.
Key Findings
• Employment: the majority of APRNs work one job full-time, and 93% provide direct patient care
• Employment setting: slightly more (39%) APRNs work in hospital acute care settings than ambulatory outpatient (35%) settings.
• Diversity: there is more racial and ethnic diversity of APRNs under the age of 45 years in the Illinois workforce.
• Age: approximately 52% of APRNs are over 55 years of age; age cohorts for Illinois APRNs in 2020 are similar to those reported in 2018.
• Education: 89% of APRNs have a masters’ degree, 17% have a doctoral degree.
APRN Workplace Settings
35% Practice in an ambulatory setting – outpatient clinic, private physician practice, etc.
39% Practice in hospital acute care settings, an inpatient unit, the emergency room, etc.
93% Provide direct patient care
Diversity
More APRNs under the age of 55 years are from ethnic and racially diverse backgrounds
Approximately half of Latinx APRNs are under 45years of age
Approximately half of Asian APRNs are under 45years of age
Approximately forty percent of African American or Black APRNs are under 45years of age
APRN Billing/Reimbursement
45% Manage a panel of patients
46% Bill exclusively under their National Provider Identifier (NPI) number Reimbursement for services is split Medicare (34%), Medicaid (24%), Private Insurance (35%)
Summary
Aging APRN workforce, 12% are planning to retire within 10 years
There is an increase in diversity of APRN workforce among younger age groups
Approximately forty percent of APRNs work in an ambulatory setting
Approximately forty percent manage a panel of patients and bill under their NPI number
Reimbursement for services is divided amongst Medicare, Medicaid and Private Insurance
The full report and past reports are available on the Workforce Center website http://nursing.illinois.gov/ResearchData.asp


Notice that Advice or Treatment Regarding Covid-19 Must Conform with Evidence-Based Medicine and Standards of Care
IDFPR is issuing this notice to remind physicians and other healthcare professionals that any advice or treatment provided to a patient must conform with evidence-based medicine and standards of care and that failure to do so may subject the individual to disciplinary action under the Medical Practice Act.
Licensed healthcare professionals have an ethical and professional duty to the public and are entrusted to protect the public health and the safety of their patients. “Engaging in dishonorable, unethical, or unprofessional conduct of a character likely to deceive, defraud or harm the public,” is a violation under the Medical Practice Act at 225 ILCS 60/22(A)(5). The Illinois Department of Financial and Professional Regulation (IDFPR) is aware of licensed healthcare professionals providing misinformation regarding COVID-19 mitigations and treatment.
MASK EXEMPTIONS
Pursuant to various orders and administrative regulations, individuals may be required to wear face coverings in certain environments – such as schools and indoor public places – to prevent the spread of COVID-19. The Centers for Disease Control and Prevention (CDC) has set forth guidelines for wearing masks. Individuals may be exempt from such requirements if wearing such a face covering is medically contraindicated. A physician or other licensed healthcare professional who provides a mask exemption to an individual with whom they do not have a clinician-patient relationship and for whom they have not provided a medical diagnosis that justifies a mask exemption as put forth in the CDC guidelines, is in violation of their respective licensing Act and may be subject to disciplinary action by IDFPR.
Any medication prescribed by a physician or other licensed healthcare professional must be consistent with the standard of care and appropriate clinical indications for each patient. Specifically, Ivermectin is not authorized or approved by the Food and Drug Administration (FDA) for prevention or treatment of COVID-19. Ivermectin is a prescription medication approved by the FDA to treat certain parasitic infections and has no approved use to treat COVID-19. The CDC has issued an official health advisory regarding the reports of severe illness associated with use of products containing Ivermectin to prevent or treat COVID-19. A physician or other licensed healthcare professional who prescribes Ivermectin in a manner inconsistent with the CDC’s recommendations may be subject to discipline.
IDFPR will follow the joint statement released by the American Board of Family Medicine, American Board of Internal Medicine, and American Board of Pediatrics on dissemination of misinformation regarding COVID-19 by board certified physicians. Specifically, the joint statement concluded that “providing misinformation about a lethal disease is unethical, unprofessional and dangerous.” IDFPR also supports the Federation of State Medical Boards’ (FSMB) statement on misinformation relating to COVID-19 and emphasizes that physicians have an ethical and professional duty to practice medicine in the best interests of their patients based on factual and scientifically established information.
Anyone who becomes aware of a licensed health professional’s dissemination of misinformation or practice inconsistent with current state and federal guidelines may file a complaint with the IDFPR.

At Amedisys, we build on skills throughout our careers and provide opportunities for growth with ongoing training and support. Join our family and see how you can step into a new role and make a difference today! Learn more at amedisys.com/careers.


W. Zeh Wellington, DNP, RN, NE-BC; and John Olmstead, MSN, MBA, CNOR, FACHE

In the everchanging and competitive arena of finding qualified applicants, educating personnel for a successful practice in the operating room (OR), and continued onboarding while providing recurrent education; the training and education strategies and approaches that have been used in the past are now proving to be antiquated and out-of-date. In today’s world of reduced applicants and a younger workforce, the tactics, and methods to train the new labor force in the OR must be reexamined, revised and reconsidered. Short training cycles alongside the added pressure to have the new nurses “in the numbers” and the added pressure of the loss of seasoned operating room nurses leads to the push to have nurses trained and ready in a short period is a staggering reality. The wish is to have the nurses hired, trained, and then quickly working competently in the operating room. The team at the Ann & Robert H. Lurie Children’s Hospital of Chicago’s operating room has revamped education to match the modern workforce.
Located in the heart of downtown Chicago, Ann & Robert H. Lurie Children’s Hospital of Chicago is a 360bed facility is ranked among the nation’s top children’s hospitals in the country by U.S. News & World Report. Lurie Children’s Hospital also serves as the pediatric training center for the Northwestern University Feinberg School of Medicine. With more than 1,800 physicians and health professionals in over 70 pediatric specialties, the hospital cared for more than 220,000 children from 48 states and 49 countries in 2020 alone. The Ann & Robert H. Lurie Children’s Hospital of Chicago Operating Room has 22 operating room suites that provide worldrenowned care in the following services: General Surgery, Orthopedics, Trauma, Transplant, Cardiovascular, Fetal, ENT, Plastics, Robotics, Dental, Urology, Ophthalmology, Gastrointestinal and Neurology.
Educating the future nurses in the operating room stretches further than the adage: see one, do one, teach one. We, as nurse educators and leaders, must change our way of thinking to inspire and properly prepare the workforce of today. New challenges have risen, and we must tailor our education strategies to meet the needs of the novice operating room nurses. Being a pediatric hospital, due to the intensive nature of our patients, we immerse the future operating room nurse with all the tools they need to help them develop and mature their successful nursing practice in the operating room. We are proud to highlight various accolades and accomplishments our team has achieved. Lurie Children’s Surgical Services draws patients from across the Midwest. The hospital leads the nation in providing services such as pediatric cochlear implant and laryngotracheal reconstruction. In 2021, Lurie Children’s Hospital performed more pediatric heart transplants than any hospital in the nation.
Pre-hire orientation: Candidates have the opportunity to shadow a day in the OR and meet with a peer/mentor. In this pre-hire shadowing experience, candidates are able to meet and start a bond with their onboarding mentor. At Lurie Children’s Hospital, all of our services are specialty services, which introduces the awardwinning work that is recognized with global excellence. “It is with great confidence that I started my journey in the operating room. I was allowed a day to shadow in the operating room helping me to see first-hand the duties of the circulating nurse and the scrub nurse. I was overwhelmed at first but also very excited to join the team” Annie Cullum, BSN, RN. She went on to add that the orientation was a lot of moving parts and pieces, but everyone was encouraging and as willing to help. She felt supported in her orientation and continues to feel the support of the staff.
Orientation: Our training process stands out for the new orientees because the intensive, self-directed education is a partnership with the new nurse, the educator, the preceptor, surgeons, and the leadership team. (Diagram 1) The physician takes an active role in teaching, educating, and coaching in the operating room. Orientees have the opportunity to master their skills when circulating in the operating room and providing them with an overview of scrubbing the cases. Another factor the orientees face is how to critically think when situations arise that would prove to be a stumbling block. The new nurses are introduced to the sterile processing department and work hand-in-hand with the sister department to understand processing of instruments and instrument substitutions. Coordinators in each service meet once a week to discuss the handoff of the orientees concerning their goals they wish to achieve in the next phase of their orientation. We also offer AORN Periop 101: a core curriculum that is the premier perioperative nurse education program for nurses entering the perioperative specialty. It fully prepares nurses with consistent, current information in the classroom and online, and clinical experience to reinforce what they've learned.
Strategies utilized that have proven positive results are the following: Tailoring the training to match each orientee’s learning style, a strict and meticulous eye on a proper case selection for each orientee, appropriate match with a preceptor, establishing an orientation pathway, emphasis on building resilience to help the new nurse perform their best, developing emotional intelligence, competencies assessments, and building trust and the values of non-threatening and constructive feedback. The nursing professional development nurse maps out the timeframe for education while ensuring everything remains on track including assessment and identification of learning needs. A proven positive result has been the 30/60/90-day meeting with leadership to identify goals, wins and what needs improving.
Our mission for nursing education in the operating room is to ensure OR concepts of the surgical arena while encouraging critical thinking. Weekly huddles and daily debriefing while promoting the magnet model promotes our vision encouraging and stimulating self-directed learning. We are a proud recipient of a 5-time accredited Magnet Hospital by American Nurses' Credentialing Center (ANCC). Magnet hospitals are certified by the ANCC as institutions where nurses are empowered to not only take the lead on patient care but to be the drivers of institutional health care change and innovation.
An important role of a surgical mentor is to help the beginner nurse to identify appropriate resources for continued growth of knowledge. In practice, this means helping the nurse recognize and develop the appropriate resources where the answers will be found, while developing the confidence to find their “nursing voice” – finding the self-assurance to speak-up for the patient. The circulating nurse is the advocate for the patient when the patient cannot speak for themselves. Developing the skill and building confidence is the task at hand when educating the new work force. The support for the front-line nursing staff is assisted with persistent morning, noon and evening management room-to-room rounding, charge nurse rounding, and 2pm staff safety huddles. With all orientation and training, the education and learning never ends with the final day of orientation, the operating room department has a public goal of uncovering at least 2 processes that will be improved each month which is reported to surgeons, staff and administration.
With any successful education program there are lessons to be learned: Motivation improves learning. An enthusiastic surgical mentor and educator who shows their passion about operating room nursing is one of the best motivating factors for a new nurse. Following-up to concerns is key. Our success story has shown drastic improvement in our retention rates of our orientees: 8/2018 – 8/2019: 52% (one year) vs 8/2019 – 8/2021 (two years): 86% .

Unrealistic expectations without the necessary nursing education and appropriate training in operating room nurse’s instruction leads to decreased patient safety, reduced success rates and stress on our workforce. Attention and care must be spent to outline each orientee’s training. Preparing nursing graduates and those who are newly transitioning into perioperative practice to care for patients, is no easy task, but one we all must continually prepare for in today’s changing age.
1:
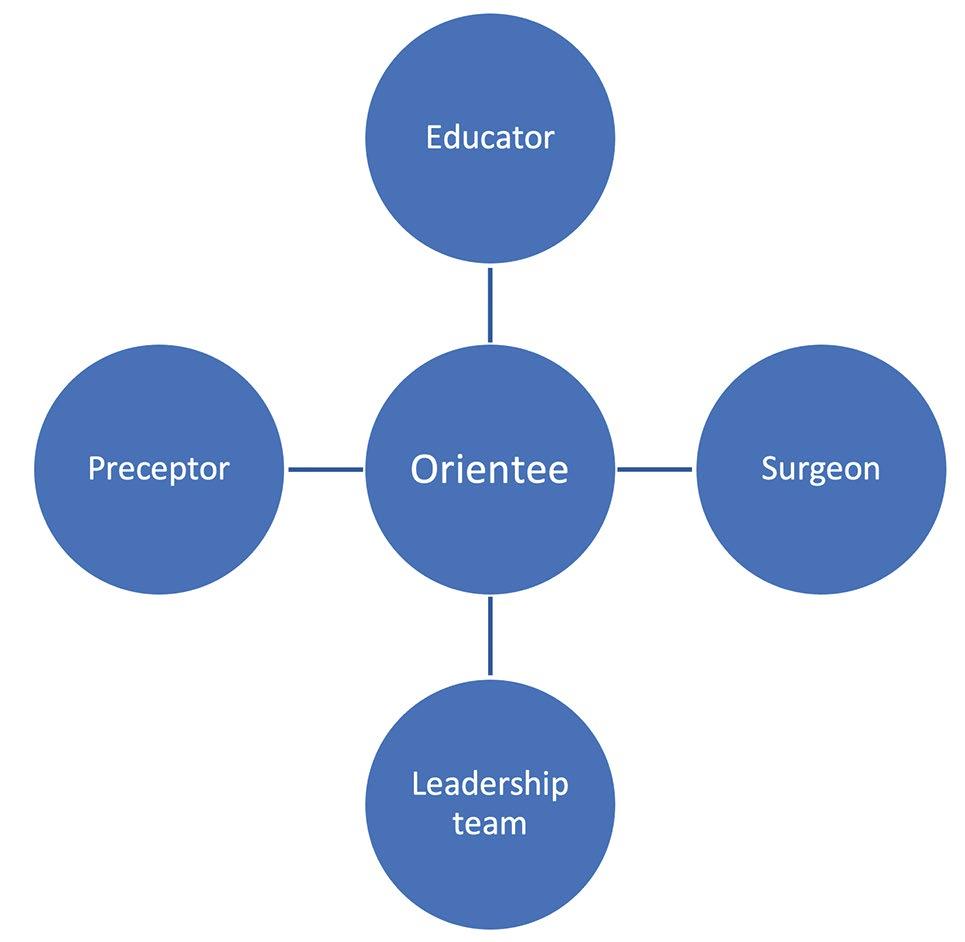
By: Georgia Reiner, MS, CPHRM, Senior Risk Specialist
Nurses Service Organization (NSO) Nurses have grown accustomed to documenting assessment results in the electronic health record (EHR), rapidly clicking responses to assessment checklist questions. However, at times nurses complete these actions without giving enough thought to their documentation because they want to move on to their “real” work: caring for patients.
The danger of this approach is threefold. First, nurses might base their assessment on the checklist not the patient, which can lead to an incomplete assessment, especially if the nurse inadvertently clicks something as being done when it hasn’t. Second, nurses might fail to adequately document a finding if it does not match up with the available options in the checklist. Third, nurses might fail to document assessments when a patient’s condition changes or fail to document practitioner notification of the change.
All three scenarios can leave nurses open to legal action. For example, a harried nurse caring for a patient who had a total hysterectomy clicks “normal” as the result of abdominal auscultation even though she hasn’t completed this assessment and misses the absence of bowel sounds. Soon, however, the patient develops vomiting and severe abdominal pain and is diagnosed with a bowel obstruction. This nurse could be held liable for the delay in treatment.
Dangers of improper documentation
Documentation is a vital nursing responsibility. It’s important for planning patient care, communicating with providers, and demonstrating compliance with federal, state, third-party, and other regulations. But documentation issues can result in professional liability lawsuits or action against a nurse’s license.
NSO and CNA’s Nurse Professional Liability Exposure Claim Report: 4th Edition found that documentation deficiencies are contributing factors in many nurse professional liability claims, and that the average total incurred for claims involving allegations related to documentation was $238,761. The same report also noted that 9.7% of all license protection matters, which involved defending nurses during State Board of Nursing inquiries, were related to documentation. Of these, nearly half (49.6%) involved an allegation of fraudulent or falsified patient care or billing records. Failure to document treatment/care as required by regulatory agencies or facility policy comprised 28.6% of matters related to documentation, followed by documentation that didn’t accurately reflect patient care and services (12.8%), failure to properly correct documentation errors according to facility policy (5.3%), and inadequate or untimely documentation (3.8%). These matters serve as reminders of how nurses need take time ensure they are completing documentation properly.
Benefits of EHRs
Too often nurses view EHRs negatively, feeling they’re cumbersome and take nurses away from the patient. But a well-designed EHR has several benefits, including improved efficiency and quality patient care. For example:
• EHRs provide an excellent mechanism for communicating with a variety of healthcare providers in atimely fashion, thereby improving care coordination.
• EHRs can incorporate guidelines, reminders, and decision support tools that can help providersmake better decisions and deliver better care.
• Electronic documentation eliminates the problem of misinterpretation of handwritten orders.
• EHRs facilitate immediate access to data by multiple people in multiple locations.
EHRs also can protect nurses against lawsuits and actions taken against their licenses. However, to gain the most benefit, nurses need to take full advantage of EHRs. For example, according to NSO and CNA’s Nurse Professional Liability Exposures: 2015 Claim Report Update, 45% of nurses who experienced a liability claim did not use the available EHR, compared with 19.2% of those without a liability claim.
Proper EHR documentation
You can take several steps to ensure you’re documenting assessments and other information correctly in the EHR.
• Follow basic documentation principles. Whether you’re documenting on paper or in an EHR, the same basic principles apply. Document promptly, accurately, and without bias. Don’t interject
opinions about patients or providers. When making a correction to previously recorded information, include the reason for the change. Remember that the EHR provides a date and time for each entry, providing a clear documentation trail.
• Adhere to policies, procedures, regulations, and guidelines. In the event of a legal action, one of the first steps an attorney will take is to determine if you followed your organization’s policies and procedures related to nursing assessments and documentation, as well as any relevant state, federal, or local guidelines, and guidelines from professional associations.
• Copy and paste cautiously. The copy and paste feature in EHRs can be a time saver, but errors, including errors of omission, can easily occur. For example, you copy your note for one patient with a myocardial infarction (MI) into another MI patient’s record but forget to add that you notified the provider of the new S4 you heard on auscultation. If the patient later experiences severe heart failure, you will have no evidence that you notified the provider. Another problem with copy and paste is that errors can rapidly spread as others pick up the same erroneous information. For instance, a nurse copies an assessment for a patient with pneumonia several times, forgetting to update the temperature, which has returned the normal. The patient’s physician reads the note, thinks the patient isn’t responding to treatment, and changes the antibiotic. Subsequently, the patient experiences a significant adverse event from the new antibiotic, which leads to legal action against the hospital, the physician, and the nurse.
A report from the Partnership for Health IT Patient Safety recommends providers “act with volition,” thinking about what is appropriate for copying and pasting and reviewing notes carefully. Ideally, the EHR should have a mechanism for easy identification of material that has been copied and pasted (for example, a different color text), so that providers are reminded to carefully review.
• Beware of autofill and templates. Like copy and paste, the autofill feature can save time by avoiding repetitive entries, but you need to verify that the information automatically filled in is correct. Similarly, templates for regularly occurring events such as the first postoperative visit after a total knee arthroplasty can help save time and ensure needed information is collected, but you still need to be aware of individual patient needs and assessment findings.
• Use notes appropriately. Sometimes what you need to document as an assessment finding isn’t in a checklist or pull-down menu. Don’t choose the “next best” option; doing so can lead to miscommunication and clinical and billing errors. For example, if you select “pressure injury” because “skin tear” isn’t available, legal action would be based on the more serious injury. A better approach is to add a note to the patient’s record. Be sure your note provides vital information in a succinct matter to avoid “note bloat” (also a side effect of inappropriate copy and paste). If an option that you would use frequently isn’t available, talk with your manager or informatics contact about adding it to the EHR.
• Protect patient privacy. Do not share your passwords and change them regularly, according to your facility’s policy. In addition, don’t enter information in view of other patients.
• Don’t ignore alerts. Alerts are there to help you make better decisions when it comes to patient care. For example, when you enter your assessment data, you may receive an alert that a patient could be at risk for sepsis. Your prompt action could save the patient’s life. On the other hand, too many alerts may lessen their efficacy, leading to “alert fatigue”. Talk with your manager or informatics contact to discuss settings.
• Complete an effective assessment. You won’t have the information you need for the EHR unless you perform a quality assessment. Don’t simply consider what a computer checklist tells you to include. Use your critical thinking skills to match the assessment to the patient.
• Document changes in the patient’s condition. Remember to enter changes to the patient’s status into the computer and include if you notified the provider of the change.
A partnership
Rather than having an adversarial relationship with the EHR, nurses should consider the EHR as a care partner. By serving as a repository of data, providing alerts as needed, and facilitating communication, the EHR can help ensure quality patient care—and reduce nurses’ risk of legal action.
Effective use of EHRs
These actions will help you gain the most benefit from the EHR:
• Document promptly and thoroughly. This not only helps protect you from liability but, more importantly, ensures that information is quickly available to other providers.
• Document accurately. Don’t omit key information and don’t try to cover up if you failed to document or take correct action.
• Get involved in EHR selection. Often, nurses don’t use the EHR correctly or take full advantage of its capabilities because the design is poor. Ask to be included on committees tasked with selecting the EHR vendor. Consider which systems best reflect what providers need to document and assess for user interface by checking items such as the font size of screen text.
• Identify opportunities for improvements in EHR function. Instead of engaging in potentially dangerous workarounds, notify leadership where improvements are needed. In some cases, the format of the EHR can be tweaked to make it easier for the user.
• Don’t assume the EHR is always right. The EHR isn’t infallible. If, for example, results of a test don’t seem to match the patient’s symptoms, follow up with the provider – the test may need to be redone.
• Provide education. Consider helping your colleagues learn more about proper documentation in the EHR by providing an education program or suggesting such a program to your professional development department.
• Be patient centered. The ability to document at the patient’s bedside can save time and improve accuracy, but only if you keep your focus on the patient instead of on the computer. Maintain eye contact and consider telling patients what you are entering into the computer, which can help ensure the information is accurate.
RESOURCES Balestra ML. Electronic health records: Patient care and ethical and legal implications for nurse practitioners. J Nurs Pract. 2017;13(2):105-111.
CNA, NSO. Nurse Professional Liability Exposure Claim Report: 4th Edition. 2020. www.nso.com/Learning/Artifacts/ClaimReports/Nurse-Practitioner-Claim-Report-4th-Edition-AGuide-to-Identifying-and-Addressing-Professional-LiabilityExposures
CNA, NSO. Nurse Professional Liability Exposures: 2015 Claim Report Update. 2015. www.cna.com/web/wcm/ connect/e05b5d91-cf38-444d-8727-ab65f25f8f6a/ RC_Health_Nurses_Claim_Report_Update_101615. pdf?MOD=AJPERES&CACHEID=e05b5d91-cf38-444d-8727ab65f25f8f6a
ECRI Institute. Copy/Paste: Prevalence, Problems, and Best Practices. Special Report. 2015. www.ecri.org/Resources/ HIT/CP_Toolkit/CopyPaste_Literature_final.pdf. Kelley T. Electronic Health Records for Quality Nursing and Health Care. Lancaster, PA: DEStech Publications; 2016. Pagulayan J, Eltair S, Faber K. Nurse documentation and the electronic health record. Am Nurs Today. 2018;13(9):48-52, 54.
Partnership for Health IT Patient Safety. Health IT Safe Practices: Toolkit for the Safe Use of Copy and Paste. 2016. https://d84vr99712pyz.cloudfront.net/p/pdf/hitpartnership/copy-paste-toolkit.pdf.
Tsou AY, Lehmann CU, Michel J, et al. Safe practices for copy and paste in the EHR. Appl Clin Inform. 2017;8(1):12-34.
Disclaimer: The information offered within this article reflects general principles only and does not constitute legal advice by Nurses Service Organization (NSO) or establish appropriate or acceptable standards of professional conduct. Readers should consult with an attorney if they have specific concerns. Neither Affinity Insurance Services, Inc. nor NSO assumes any liability for how this information is applied in practice or for the accuracy of this information.
This risk management information was provided by Nurses Service Organization (NSO), the nation's largest provider of nurses’ professional liability insurance coverage for over 550,000 nurses since 1976. The individual professional liability insurance policy administered through NSO is underwritten by American Casualty Company of Reading, Pennsylvania, a CNA company. Reproduction without permission of the publisher is prohibited. For questions, send an e-mail to service@nso.com or call 1-800-247-1500. www.nso.com.
Abstract
Jessica Nuebel Blessing Rieman College of Nursing & Health Sciences
This evidence-based research project implemented a new breast cancer-related lymphedema (BCRL) screening program with the intention of identifying the development of this cancer treatment-related side effect in early stages. When BCRL is diagnosed at stage 0 or 1, it can be treated and reversed, sparing its victims from a lifelong battle with this potentially serious complication. The policy and procedure utilized at the Blessing Breast Center was outdated, requiring literature and equipment research. New equipment was identified, purchased, and implemented, along with an updated policy that includes a new screening protocol and schedule for breast cancer patients. By identifying updated equipment and screening protocols, we aim to reduce the rate of progression to chronic breast cancer-related lymphedema. Educational information has been created to provide to patients before their breast cancer treatment begins so they are aware of what symptoms to report to healthcare providers and steps they can take to reduce their risk of developing lymphedema. Patients with BCRL have a reduced quality of life, making this project worthwhile in improving the care of the community.
Keywords: breast cancer-related lymphedema (BCRL), lymphedema, screening
Breast Cancer-Related Lymphedema Screening
Breast cancer-related lymphedema (BCRL) is a common side effect occurring after cancer treatment and affects approximately 19% of breast cancer patients (Shah et al., 2020). Treatments that have shown to increase the risk of lymphedema include axillary lymph node dissection (ALND), sentinel lymph node biopsy (SLNB), regional lymph node radiation (RLNR), lack of breast reconstruction, and taxane-based chemotherapy (Gillespie et al., 2017). Non-treatment related risk factors for BCRL include high BMI, subclinical edema, and cellulitis infections (Gillespie et al., 2071). BCRL results from a disruption to the lymphatic system, preventing proper drainage of protein-rich lymph fluid from lymphatic vessels. This lymph fluid collects and causes abnormal swelling of the affected upper limb and/or chest wall, resulting in possible arm tightness, heaviness/fullness, pain, and impaired limb function (Gillespie et al., 2017). Not only does this potentially serious side effect cause physical discomfort, but it can also lead to psychological distress as well, reminding patients of their past illness and treatment. Patients’ quality of life can be negatively affected and elevated rates of depression and anxiety have been observed compared to patients without BCRL (Gillespie et al., 2017).
Background of Project
Screening patients for BCRL using circumferential measurements has been the acceptable method; however, screeners must follow identical processes to ensure that proper comparisons are obtained. This has proven to be difficult at the Blessing Breast Center, as there is only one nurse available to perform these screenings,

which has led to missed opportunities to perform screenings. With the creation of new screening equipment, more accurate tools can be utilized by any staff member with minimal training. Screening equipment tools include perometry, bioimpedance spectroscopy, and water displacement. Perometry equipment takes a sizeable room, dedicated to the use of such equipment, and cannot be easily moved. Water displacement can be messy and a patient dissatisfier.
Bioimpedance spectroscopy uses equipment similar to a standing scale, which measures intracellular and extracellular fluid volume in the at-risk limb and compares it to the normal limb. Changes in fluid volume can be detected at the subclinical level, before patients notice any physical signs of developing lymphedema, and proper treatment protocols can be initiated with the intent of halting and even reversing the lymphatic fluid collection. The equipment is easy to use, takes less than 60 seconds to obtain a reading, and can be performed by any staff member after minimal training. Equipment can be used to compare the affected limb to unaffected limb, or in the case of bilateral affected upper limbs-lower limbs are used as the comparison. Screening results are in the form of an L-Dex score and are compared at each screening. When BCRL is identified, patients will be referred to the lymphedema clinic, where treatment will be initiated by a trained lymphedema therapist and close follow-up will be provided.
A literature search was completed using the search engines PubMed and CINAHL. The PICO question was, when monitoring cancer patients for breast cancer-related lymphedema, which method detects lymphedema earlier, manual measurements or use of equipment that performs biometric impedance spectroscopy? The following articles were identified and utilized to guide this research project.
Shah et al. (2016) discussed the data supporting the early detection and treatment of BCRL, a comparison of BCRL diagnostic modalities and data supporting the use of bioimpedance spectroscopy. Clinical practice guidelines were provided to allow for the incorporation of bioimpedance spectroscopy into the management of breast cancer patients before and following therapy. Overall survival of breast cancer patients has increased over the past several decades, which has caused an emphasis on survivorship and diagnosis/management of breast cancer treatment side effects. BCRL has been identified as one of the primary complications of breast cancer treatment which can greatly impact a survivor’s quality of life, as well as increase costs for the patient and healthcare system.
Shah et al. (2020) conducted a meta-analysis which included 50 studies, representing over 67,000 women. The purpose of this meta-analysis was to evaluate how different monitoring techniques identified BCRL and the incidence of chronic BCRL among patients screened with bioimpedance spectroscopy and circumferential measurements. The evidence suggested that utilizing bioimpedance spectroscopy for monitoring allowed for early detection and intervention which drastically decreased the risk of developing chronic BCRL. Monitoring with circumferential measurements did not show a benefit in decreasing the incidence of chronic BCRL. Ultimately, the results showed that bioimpedance spectroscopy should be considered for BCRL screening to detect lymphedema sub clinically and reduce the incidence of chronic BCRL development.
A small study performed by Polat et al. (2017) obtained 245 measurements from 67 study participants, utilizing bioimpedance spectroscopy. Measurements were taken preoperatively and in postoperative months 3, 6, 9, 12, 24, and 36. The findings showed 26.8% of patients were diagnosed with lymphedema and 89% of those patients were diagnosed at stage 0. Risk factors that proved to be statistically significant were axillary lymph node dissection and positivity in three or more lymph nodes. It was concluded that periodic measurements utilizing bioimpedance spectroscopy can be an effective method for early detection of BCRL.
In a retrospective analysis performed by Koelmeyer et al. (2018), data was reviewed from women who underwent bioimpedance spectroscopy measurements from January 1, 2007, to December 31, 2016. Patients were grouped according to when they began screening: preoperatively, within 90 days after surgery, or greater than 90 days postoperative. It was found that women in the early surveillance group received lymphedema therapy much earlier than the women who began screening later, and the women in the latter group had a higher incidence of BCRL diagnosis and at a later clinical stage. It was then concluded that an early surveillance care model utilizing bioimpedance spectroscopy for early detection and management of BCRL was supported.
Each study found that utilizing the bioimpedance spectroscopy method for screening led to earlier detection and intervention of BCRL when compared to other screening modalities. By accomplishing this, the incidence of chronic BCRL was decreased as well as treatment related costs to the patient and healthcare systems. More importantly, breast cancer survivors can benefit from an increased quality of life when BCRL is detected and treated in its earliest stages.





Implementation
A company providing bioimpedance spectroscopy equipment was identified and contacted for product information, pricing, and demonstration. This information was reviewed with the manager of the Breast Center for implementation consideration. Once approval was gained, an equipment demonstration was scheduled to learn about how to add a lymphedema screening program into our day-to-day processes.
Contacts were made to nearby facilities to inquire about their lymphedema screening programs and what successes/failures they had experienced. Many facilities continue to utilize circumferential measurements for lymphedema screening programs, and some do not have a routine follow-up schedule in place. However, a few facilities had successfully implemented bioimpedance spectroscopy equipment with great success.
The decision was made to proceed with the creation of a physician champion group to discuss the proposal of a new lymphedema screening program. Physicians from surgery, medical and radiation oncology, family medicine, OB/GYN, and radiology were asked to join the group, with a radiation oncologist serving as the physician champion. Literature was sent and a virtual demonstration was held for all physicians to learn about the process and equipment utilized in the screening process. All involved physicians were in favor of the proposed program and equipment, without any verbalized concerns.
The next step in the process was to secure funding to purchase the equipment and cover the monthly subscription fee. The cost of the equipment was not so great that it had to be submitted with capital budget but could be purchased anytime. Accessing funds from the Foundation was considered to cover the monthly subscription fee and this was discussed with Fiscal and Compliance departments. However, if a service is provided that can be billed for, the Foundation cannot pay for the equipment or the monthly fees. More discussions were held with Fiscal to determine the service fee that would be charged to patients, keeping in mind that most commercial insurance companies do not cover this service as it is still considered experimental. Lymphedema evaluation with bioimpedance spectroscopy is a Medicare covered service, so the decision was made to use the amount that Medicare
reimburses for the service as the charge amount.
Information technology was consulted to ensure that the technology required to allow the screening equipment to work properly and send data to the cloud was in place and no other considerations were needed before purchasing equipment. Health information management was brought on board to help design an order and create the process for order entry, result retrieval, and charge generation. The financial account services department was consulted to discuss the process of preauthorization and appealing denials. While this took much time and many meetings, a process was agreed upon.
A go-live date was chosen, October 4, 2021, to implement the new equipment and begin screenings. October was chosen as it is Breast Cancer Awareness month and determined to be an ideal time to market this new service. Marketing materials were obtained from the equipment company and sent to the hospital’s marketing department for customization. Information was printed in home mailings, commercials were released, websites were updated, and a lunch and learn session was hosted, to bring awareness and education to hospital staff and community residents. The equipment was purchased and an onsite training and implementation was set.
Screenings would be performed by the Breast Center Navigator, and in the event of her absence, the Breast Center Manager would perform. Screenings will be scheduled to be performed before any treatment, including surgery, chemotherapy, and/or radiation therapy. The next screening will take place two weeks after the conclusion of the final phase of treatment and continue every three months for three years, every six months for years four and five, then annually thereafter. This screening schedule was based on the literature review and the conclusion that the greatest incidence of developing lymphedema occurs in the first three years following treatment. This screening schedule was proposed to the physician champion team and unanimously approved.
The Breast Center Navigator provided education to the office nurses, including indications for screening, the schedule of screenings, and order entry. Patient education materials were obtained from the equipment company and customized for our organization. This
material will be provided to patients at the time of their screening, along with verbal education from the Breast Center Navigator.
The first screening was performed on October 4, 2021, with nearly a dozen screenings since that time. Admittedly, there were a few kinks that needed to be worked through, and they have been successfully resolved. Providers are supportive of this new program and are eager to order the screening for their patients. Several breast cancer survivors, who have been finished with treatment for some time, have contacted the Breast Center, requesting information about screening and question the screening requirements. These patients have been referred to their oncologists or primary care providers to discuss their need for the screenings.
Conclusion
The implementation of the lymphedema screening program is a tremendous win for our health system and community. The availability of this technology to detect lymphedema sub clinically and save breast cancer survivors from a life-long battle with this devastating treatment side effect is tremendous. Data will be collected to track the incidence of lymphedema, the stage at diagnosis, what treatment measures were implemented, and the outcome of treatment measures. When proper education is provided to the patients regarding the possible lasting effects of lymphedema, patients are more than willing to proceed with treatment and so very thankful that this technology is available so close to home.
REFERENCES AVAILABLE UPON REQUEST






Dr. Sandra Martell
Public Health Administrator, Winnebago County Health Department
While much has been published on the role of front-line nurses in the care of individuals with COVID-19 in the hospital acute-care setting, there has been minimal attention focused on the role of nurses in the public health response. School Nurses, Long-term Care Nurses, Correctional Nurses and Public Health Nurses have been critical assets in the public health response viewed from the three (3) core functions –assessment, policy, and assurance.
School Nurses have been the key health team personnel in assuring that schools were safe for in-person learning throughout the pandemic. School Nurses were responsible for assessing students and staff for signs and symptoms of COVID-19, testing for COVID-19, and identifying close contacts to positive cases within the school setting. In partnership with local health departments, ill students and staff were isolated and close contacts were quarantined. School Nurses were responsible for oversight of layered mitigations and enforcing adherence to the sometimes unpopular policies outlined in Executive Orders and endorsed by local school boards. Through their public health efforts, transmission of COVID-19 in school was minimized and schools remained open to address the academic, social, and emotional learning needs of students. The impact of their work while measurable in the short-term with public health metrics around disease rates and secondary cases is not fully measurable or appreciated in the long-term.
Long-term Care Nurses (LTCN) demonstrated extreme tenacity and compassion in caring for individuals in long-term care facilities (LTCF). They were responsible for assuring high level infection control practices to exceptionally vulnerable populations under extreme conditions of shortages of Personal Protective Equipment (PPE) and staff while addressing the social isolation of residents and their families. LTCF nurses were charged with enforcing policy that resulted in visitor restrictions and prolonged separation from loved ones. Levels of care increased within the LTCF to provide for frequent assessments as residents struggled through the viral infection. Death rates among LTCF residents was disproportionately high resulting in significant levels of grief. LTCN stepped up to provide therapeutics routinely administered in hospitals. The impact of their work in protecting the environment and protecting the health of vulnerable and medically fragile individuals minimized the death rate.
Correctional Care Nurses (CCN) were responsible for preventing the transmission of COVID-19 among detained/incarcerated populations. Similar to their LTCN colleagues, these nurses were responsible for the health and safety of vulnerable populations including medically fragile. They, too, administered care under extreme duress without bias and with compassion in a setting where individuals exhibited high levels of anxiety and fear of contracting COVID. Correctional Care Nurses addressed vaccine hesitancy in a population with distrust of governmental systems and provided education around vaccination, administered the vaccine, and provided therapeutics as appropriate.
Public Health Nurses in local health departments have also played a key role in the pandemic response. In many LHDs, Public Health Nurses have applied the nursing process at the population level. They have assessed and analyzed epidemiological data, conducted case investigations and contact tracing, issued isolation and quarantine orders, provided case management and support to individuals infected and/or exposed, planned and implemented mass vaccination efforts, and administered therapeutics. They adapted home visiting strategies to ensure ongoing care to at-risk communities, developed communication campaigns, and addressed vaccine hesitancy. They have served on Boards of Health and been responsible for implementation of often politicized policies to protect the public’s health.
Nurses who have focused on population health have been pivotal in the public health response to COVID-19 at every level of prevention – primary, secondary, and tertiary and protecting health at all levels.