We invite you to join us on the essential journey committed to inclusion, equity, and belonging as we build on the work ANA-Illinois started in 2020. We have created an event that explores our current challenges and teaches us how to be Positively Resilient as we have the difficult discussions and take actions to build a more diverse, equitable, and inclusive profession. We have two keynote presentations that will set the tone for the event.
Morning Keynote – Andrea Dalzell
Andrea Dalzell is the first registered nurse to complete nursing school as a wheelchair user in New York City. She is also a pioneering activist for people with disabilities.
SUMMARY OF PRESENTATION
Afternoon Keynote – Buck Davis
POSITIVELY RESILIENT
Strengthening Essential Skills to Rebound, Recover, & Thrive.
Life and work-life can feel overwhelming at times. Everyday challenges, work-climate changes, mergers and upheavals often come with little or no advance warning. Boring commutes, long
work hours, tight deadlines and constantly increasing demands cause us to have to pivot endlessly. During these nerve-wracking moments, the ability to maintain a good attitude and have some level of optimism while these stressors weigh us down, can be very hard if not seem impossible.
In his dynamic keynote, Positively Resilient, Buck Davis draws from evidence-based research on positive emotions and resiliency while sharing his own insights as to how to remain centered and retain perspective, even when anxiety, burnout, cynicism, self-doubt, and exhaustion threaten to turn motivation on its ear. Through the use of interactive group activities, multi-media visuals, engaging lecture, and storytelling, he delivers a practical and compelling message with insights that can be implemented immediately. Audience members will leave feeling inspired, empowered and reinvigorated — ready to manage the chaos that gets in the way of bringing their most authentic and brilliant selves to work.
You’ll laugh, you’ll think, you’ll weigh in, you’ll collaborate, and you’ll most assuredly be moved. By the end of Positively Resilient, you’ll walk away with a variety of tools and strategies that you can implement right away to become more unabashedly resilient and courageously motivated to complete each day with newfound energy and focus. They say that showing up is half the battle, but at the end of the day you’ll be spurred to do much more than just show up. You’ll have the knowledge, insight and ability to be a more capable and effective leader who is up to the tasks and challenges that await you in your very important role.
- A Critical Connection. The relationship between positive psychology and resilience .
- Mitigating the tendency to DWELL on stressful situations.
- Learning how to pivot with positivity.
- Gaining skills on how to speak to yourself when the hard stuff hits.
- Understanding the importance of prioritizing positivity to buffer the trying times.
- You’ve Got This! Developing your self-efficacy for resilience.
Other Topics Include: Health Literacy
Spiritual Roots in Nursing
Rural Health Care
Role of Nurse Leaders in Dismantling Racism 5.75 hrs CE
Early Bird Rate – ends 9/15
Members & Organizational Affiliate Members $50.00
NonMembers $95.00
Pre-Licensure Student $25.00
Registration Fees after 9/15
Members & Organizational Affiliate Members $65.00 NonMembers $100.00
Pre-Licensure Student $40.00
CE* is jointly provided by the Illinois Nurses Foundation and ANA-Illinois.
The Illinois Nurse Foundation is approved as a provider of nursing continuing professional development by the Ohio Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation. (OBN-001-91).
In our cover article in the June 2021 edition of The Nursing Voice. The name of the school of nursing at Loyola University Chicago was misspelled. The school is the Marcella Niehoff School of Nursing.
We apologize for this error.
INF PRESIDENT'S MES S AGE
The Nursing Voice
INF Board of Directors
Cheryl Anema PhD, RN
The IL Nurses Foundation (INF) has been busy this summer. The work of the Foundation happens with volunteers and a small staff. We have a very dedicated and passionate working Board of Directors. In addition, the majority of the work of the INF occurs in the committees. Even though all of our Directors and Officers serve on multiple committees, we are always looking for additional volunteers to assist us in our work. If interested, please reach out to our Executive Director or to myself with your interest.
In 2021, the Scholarship Taskforce accepted many scholarship applications and were able to distribute thousands of dollars to the scholarship winners. The INF Grant Committee has been busy with Grant applications. The 40 Under 40 Committee members have been planning the Fall 40 Under 40 event. This year will be our second Virtual 40 Under 40 Celebration. We hope our virtual events will be able to return to live in-person events in 2022. The Gala Committee has also been in full swing planning a Virtual Holiday Gala and Fundraising event for Dec. 4th, 2021. We will be having an on-line virtual auction and raffle to help us meet our fundraising goal. Please be sure to mark your calendars.
Another very busy committee is the Editorial Committee. This committee puts together The Nursing Voice – The Official Publication of the Illinois Nurses Foundation distributed quarterly by direct mail to approximately 4,500 RNs and electronically via email to 90,000+ RNs in Illinois. If you know an IL nurse who is not receiving The Nursing Voice, please tell them to contact the INF office and provide a current email.
Additional committee work includes the Finance Committee, which works with the Executive Director to prepare the annual budget and present it for Board approval, as well as monitor the ongoing expenses of the Foundation.
The Covid Stories Publishing Taskforce successfully released their first INF book – Stories from Within: Nurses, Patients, Families, Doctors Share Their Pandemic Experience through Amazon.com in April 2021. It has been selling and providing the Foundation with a steady source of income, as well as the opportunity to share important
stories with the public. The e-version of the book is planned to be released in late Summer 2021.
The INF continues to honor nurses through it’s Honor A Nurse Program and Nurse of the Year. The Nurse of the Year is usually announced at the Annual Gala Fundraising event in December.
The Fund Development Committee is the committee that oversees donations, sponsorships, and fundraising events of the INF. The committee members strategize and initiate efforts to increase donations and sponsorships. As the INF is a philanthropic organization that depends on the donations of others to meet its mission, fund development is foundational for our success, and continuation of support for nurses and the health community in Illinois. One of our ongoing programs is the Illinois License Plate program. A few years ago, the INF collaborated with the State of Illinois to get a Nursing License Plate. When someone goes to the Specialty plate selection on the State of Illinois website, they can choose the Nursing Plate. For each plate purchased, or renewal, the State of Illinois sends the INF $20. I hope you proudly display your Illinois Vehicle INF Nursing License Plate.
In 2020, we added a Board Development Committee. The BOD recognized the need for Orientation and Development of the Board. Some Board members come to the INF with extensive Board experience, and others join us with little to no Board experience. We believe in mentoring and helping nurses grown in their leadership skills in the profession and roles within Nursing Associations and Foundations. This committee has expanded to include support of the entire Board of Directors and the Strategic Planning for the Foundation. Recently, a team of Board members were elected to help in the Strategic Planning for the Foundation, looking at who we are and who we want to be. We look forward to see where the INF will be heading in 2022. We have also contracted with an outside consultant as we look to move the INF to the next level of philanthropic work and promotion of our mission and vision.
As you consider your end of year donations this year, please think of the work of the INF. If you have some available time and would like to be blessed with an opportunity to serve your profession, please reach out to the INF. If you have a few dollars to donate to help celebrate Nurses, Nursing Education, and Healthcare promotion, consider giving to the INF. This is the year you want to be able to say “I Support Nursing!” Honor a Nurse and GIVE TODAY - www.illinoisnurses.foundation
• Electronic submissions only as a word document attachment using current APA guidelines.
• Email: info@ilnursesfoundation.com
• Subject Line: Nursing Voice Submission: Name of the article
• Must include the name of the author and a title.
• INF reserves the right to pull or edit any article / news submission for space and availability and/or deadlines
• If requested, notification will be given to authors once the final draft of the Nursing Voice has been submitted.
• INF does not accept monetary payment for articles.
Rimland Services who supports adults diagnosed with autism is looking for a few nurses to join our dedicated team.
This year Rimland is celebrating our 50th anniversary. Our headquarters are in Evanston, IL. The clients we support are supported through our Residential, Community Day Services and Health and Wellness Program.
We are looking for a part time Registered Nurse to work during the week, three days a week. The Registered Nurse will be conducting medication trainings, monthly medication check in and changeover, body checks and nursing assessments.
We are also looking for a part time Licensed Practical Nurse or Registered Nurse to work on the weekends passing medication in our Residential Program.
Our website is www.rimland.org.
Interested applicants should send their resumes to pwatson@rimland.org
Article submissions, deadline information and all other inquiries regarding the Nursing Voice please email: info@ilnursesfoundation.com
Article Submission Dates (submissions by end of the business day) January 15th, April 15th, July 15th, October 15th
Advertising: for advertising rates and information please contact Arthur L. Davis Publishing Agency, Inc., P.O. Box 216, Cedar Falls, Iowa 50613 (800-626-4081), sales@aldpub.com. ANA-Illinois and the Arthur L. Davis Publishing Agency, Inc. reserve the right to reject any advertisement. Responsibility for errors in advertising is limited to corrections in the next issue or refund of price of advertisement.
Acceptance of advertising does not imply endorsement or approval by the ANA-Illinois and Illinois Nurses Foundation of products advertised, the advertisers, or the claims made. Rejection of an advertisement does not imply a product offered for advertising is without merit, or that the manufacturer lacks integrity, or that this association disapproves of the product or its use. ANA-Illinois and the Arthur L. Davis Publishing Agency, Inc. shall not be held liable for any consequences resulting from purchase or use of an advertiser’s product. Articles appearing in this publication express the opinions of the authors; they do not necessarily reflect views of the staff, board, or membership of ANA-Illinois or those of the national or local associations.
ANA-ILLINOIS PRESIDENT'S MESSAGE
Liz Aquino, PhD, RN
Dear Illinois Nurse Colleagues, ANA-Illinois has been working hard since my last message so I will recap some of our important work over the past few months. The Board of Directors appointed members to two new workgroups: Expert Panel on Nursing Education and Community Service Taskforce. Their work will help guide our association. We started monthly Nursing Hot Topic webinars on a range of exciting topics and will continue to host them and offer CEs for attending. We are always open to special topic ideas, so please reach out if you have a specific interest or would like to present on a topic. The Expert Panel on Diversity, Equity, and Inclusion continues to host quarterly webinars; please go to the ANAIllinois website Expert Panel page to register for future events. The Board of Directors adopted a Diversity, Equity & Inclusion statement and commitments to guide the association. The statement can be found on ana-illinois.org. We are also happy to share that the Nurse Staffing Improvement Act of 2021 was passed during the 2021 legislative session and is awaiting Governor Pritzker’s signature to sign it into law. Now it’s time to make sure the provisions are followed, nurses are part of the solution, and hospitals are held accountable. Visit our advocacy portal to learn more about the provisions of the new law.
Please save the date for the upcoming 40 under 40 Emerging Nurse Leader Virtual Event on September 23rd to celebrate our newest award recipients. The annual Professional Issues Conference will be held virtually on November 6th; we will welcome our newly elected Board of Directors and have essential discussions around resilience and how to take action to strengthen diversity, equity, and inclusion in our profession and healthcare. Make sure to follow ANAIllinois on Facebook, Instagram, and LinkedIn to stay up to date as we continue to introduce new programming and information to engage our members and followers.
As always, I appreciate you for all that you have done and continue to do to advance our profession and look forward to working with you to continue to transform nursing and healthcare.
Sincerely,
Elizabeth (Liz) Aquino, PhD, RN
President, ANA-Illinois
@LatinaPhDRN
ETHICS IN ACTION
Current Challenges in Nursing Education
As a result of the COVID-19 pandemic, the past 18 months have been especially challenging for those in health care related fields. Healthcare workers, first line responders, interdisciplinary health care students - especially nursing students and new nursing professional graduates had their clinical education and experiences drastically changed within days. Nursing programs abruptly interrupted their clinical and in-person nursing education and moved to online teaching platforms. In-person clinical experiences were also abruptly halted due to fear of the COVID-19 virus as well as overwhelmed and often understaffed clinical settings (Michel et al., 2021). Anxiety about clinical work and ongoing education in healthcare settings affected nursing students, new graduate nurses, and all levels of nursing staff.
A recent study found that “nurses reported heightened stress during the COVID-19 outbreak, resulting in substantially higher levels of depression and anxiety” (Serrano et al., 2021, p. 29). This study included all levels of nursing staff.
One of the main ethical challenges for nursing students, instructors, the professional workforce, and nurse administrators during this stressful time was to
continue teaching, taking care of patients and their family members, and, most importantly, taking care of themselves, clinical students and nursing staff. Innovation and simulation ramped up in ways not anticipated in pre-COVID education and work environments. Creative ingenuity produced new ways for communicating with others, especially in helping patients communicate with loved ones when no visitors were allowed into healthcare facilities.
The American Nurses Association (ANA) Code of Ethics with Interpretive Statements, Provision 7 gives homage and direction to clinical nurses during stressful times. Provision 7 states: “The nurse, in all roles and settings, advances the profession through research and scholarly inquiry, professional standards development, and the generation of both nursing and health policy” (ANA, 2015, p. 27).
This provision protects nurses and nursing students and offers guidance during stressful times. The supporting statements of Provision 7 encourages nurses in all roles and settings to contribute to the profession through research and scholarly inquiry, through developing, maintaining, and implementing professional practice standards, and through participating in health policy development.
How can the Code’s provisions be helpful during stressful times such as the ongoing COVID-19 pandemic, public health issues such as gun violence and drug abuse, and the need for professional development and stress management in the workplace?
Provision 7.2 of the ANA Code of Ethics specifies that the Code, as one of the profession’s foundational documents, informs nursing’s scope of practice. Nurse educators are responsible for ensuring that their graduates “possess the knowledge, skills, and moral dispositions that are essential to nursing” (ANA, 2015, p. 28). Some ethical concepts include moral distress,
moral courage, ethical dilemmas, ethical decisionmaking, importance of an ethical work environment, and ethical guidance for everyday ethical issues. The Code, in addition to the recently revised ANA Scope and Standards of Practice, provide guidance on the content in ethics and ethical issues that are addressed.
There are numerous resources for nurse educators on the ANA website (www.nursingworld.org). These include resources developed and disseminated by the ANA Center for Ethics and Human Rights and its Ethics Advisory Board (EAB). The ANA’s Guide to the Code of Ethics for Nurses: Development, Application, and Interpretation Faculty Pak describes ethical concepts and how the Code can be used by nurses to guide clinical decision-making. This resource includes examples of assignments and learning exercises on ethical challenges, sample course PowerPoint slides, and assignment rubrics. Faculty can download the Faculty Pak at no charge.
Other resources include various ethics topics and articles and position statements. One of the ANA publications, OJIN: The Online Journal of Issues in Nursing has articles related to various topics. The January 31, 2021 issue focuses on Nursing Education: Philosophical Perspectives on Current Challenges (http://ojin. nursingworld.org).
There are numerous resources, including ethical considerations and guidelines for nurses during the COVID-19 pandemic and an ANA COVID-19 Resource Center. These resources include coronavirus updates, educational materials, and webinars, as well as results of a series of surveys of nurses used to gather data used to support nurses during the pandemic (https://www. nursingworld.org/practice-policy/work-environment/ health-safety/disaster-preparedness/coronavirus
References available upon request
Lisa Anderson Shaw DrPH, MA, MSN
Linda Olson PhD, RN, NEA-BC
Are You Laughing Yet? Therapeutic benefits of laughter and humor in our practice
Lisa Anderson-Shaw, DrPH, MA, MSN, HEC-C
Try to remember the last time you had a laugh, a real hearty, honest to goodness laugh out loud . . . remember how you felt? Remembering this laugh may also make you smile as you read this because it makes us feel good to smile and laugh.
The past 18 months have been very stressful for most of us, especially our front line healthcare workers. Working extra hours in order to take care of patients during the COVID-19 pandemic were not only stressful for clinical staff, but many times very sad as patients died in hospitals without family or friends near them during their time of need. Though stress on nurses and other health care workers were exacerbated by the pandemic, such stress is often present during non-pandemic times.
Staff shortages at work, family, school, and other responsibilities often make our work/life balance difficult to manage. There are many therapeutic ways we can healthfully relieve anxiety and attempt to re-balance our lives in a healthy manner. One way we can recharge and refresh is through laughter. After all, haven’t we all heard that ‘laughter is the best medicine’?
Recent medical studies on laughter therapy have shown that laughter can “physiologically reduce levels of stress hormones, increase the level of health promotinghormones, and strengthen the immune system by increasing the number of T-lymphocytes through activation of natural killer cells” in the body (Bennett & Lengacher, 2006, p. 188). Laughter can also lower blood pressure as well as lower blood cortisol levels. One of the main health effects of laughter is that it makes us feel better, both physically and emotionally. Laughter helps us reduce the unpleasant feelings related to stress, tension, anxiety, anger, and depression (Bains et al., 2015; Ko & Youn, 2011; Takeda et al., 2010). Laughter can also elevate mood, self-esteem, hope, energy, physical vigor, and improve our overall friendliness, cohesiveness, and quality of life (Yim, 2016, p. 243).
Laughter can be spontaneous, like after you hear a joke or see something funny on TV, a smile or chuckle after seeing a baby smile, or a memory that makes you feel happy from a vacation or event you recently had. Laughter can also be a therapeutic session with a laughter coach! Yes, laughter therapy is real and a rather recent form of therapy. According to The United States National Cancer Institute, laughter therapy is a type of therapy that uses humor to help relieve pain and stress and improve a person’s sense of well-being. It may be used to help people cope with a serious disease, such as cancer. Laughter therapy may include laughter exercises, clowns, and comedy movies, books, games, and puzzles. It is a type of complementary therapy, also called humor therapy (https://www.cancer.gov/publications/ dictionaries/cancer-terms/def/laughter-therapy).
A recent study in the Journal of Clinical Nursing (Fang et al., (2019) showed that humor therapy decreased feelings of helplessness, fear, and anxiety and concluded from their data that “administrators pay attention to the cultivation of nursing staff’s humor, such as providing nurses with musical CD’s or humorous books” (p. 3691) as a way to of providing stress management and humor training to nurses. The study conclusion recommends cultivating nurses ‘humor competency’ to help alleviate work stress.
So . . . what is "humor training?" To find this out I spoke with a laughter leader/wellness coach, Jacci Andersen, who provides laughter therapy sessions through her company Andersen Wellness. Jacci explained that her role as a laughter leader and wellness coach is to “focus on improving the human condition by exploring the scientifically proven benefits of laughter, humor and mirth (amusement often expressed in laughter).
Laughter leaders provide programs for individuals, organizations, and communities that are uplifting, simple, and therapeutic. I work with people through a systematic exposure to laughter in a supportive environment along with laughter exercises with a multi-step process for attitudinal changes. Laughter is natural, organic, and innate" (J. Andersen, personal communication, July 8, 2021). She further explained that stress-related illnesses often come from a loss of emotional balance that can affect the chemistry in our brain.
Jacci was inspired to become a laughter coach after many years working in leadership roles in financial sales and retail management. She was inspired to go back to her roots of laughter, play, and life balance to become a certified laughter leader and national trainer/joyologist through World Laughter Tour. She continued her training with Patch Adams, MD, while on a mission trip to Costa Rica, where her group provided comedic relief for those experiencing tragedy, illness, and loss in their lives. Jacci states, “One of the most important purposes in my life is to work with people and organizations to change their perspective and ‘find the funny’ in everyday life struggles and stress”.
She encouraged people who work in stressful jobs, such as nurses and others in the medical professions, to look for humor in their work. She states, “It is okay to laugh with your co-workers, and even your patients”. She offers some helpful hints to keep humor in your day (J. Andersen, personal communication, July 8, 2021):
• Start your day off positive – before you get out of bed put a big smile on your face and think of five things you are grateful for
• Be aware of your stress level throughout your day when you feel stress coming on, take a deep breath and breath in and out for 4 seconds, hold for 7 seconds, and breath out for 8 seconds
• Bring a clown nose to work and wear it when you think appropriate – it will make others laugh and also make you laugh
• Create a laughter library for your unit – this can be a collection of books, cartoons, audio and video tapes – whatever makes you laugh will likely make others laugh as well
• Create a basket of humor supplies – clown noses, goofy hats, Groucho glasses, rubber chicken, joke medicine bottles, use when appropriate with co-workers and patients (always ensure a safe environment and focus on reactions – stop when necessary)
• Organize quarterly laughter/humor event on your unit as part of your staff wellness program and Nurses Week activities
“A day without laughter …is a day wasted” (Charlie Chaplin)
For more information on laughter therapy go to Andersen-Wellness.com, email Jacci @ jacci.andersen@ gmail.com, cal 708-655-5113, or look for Andersen Wellness on Facebook, Instagram, and Linked In. References available upon request
Table 1
Laughter @ Work: Nearly 34% of waking adult life is spent at work.
In today’s world, employees are….
83% Stressed Out
70% Disengaged
47% Struggling To Be Happy
Causing the U.S. Economy to lose nearly $1 trillion per year
• $500B in lost productivity
• $300B in health care costs
• $11B in employee turnover
Source: Humor that Works, Andrew Tarvin, https:// www.humorthatworks.com/book/
Table 2
The Benefits of Laughter @ Work:
• Increased productivity: employees who have a good time together are more productive
• Recruit talent: the best employees want to thrive in a ‘jovial humorous’ environment.
• Improved communication: nothing bonds employees more than laughing at the same thing.
Source: Brian Volk-Weiss, CEO of Comedy Dynamics. https://www.cnbc.com/2017/05/19/here-are-3-reasonsyou-need-to-laugh-at-work.html
Table 3
10 Scientific ways to be happy:
• Go outside – experience nature
• Connect with family & friends
• Plan a vacation, even if you don’t take it
• Meditate – rewire your brain
• Practice smiling
• Sleep more
• Practice gratitude
• Help others (up to 2 hours a week)
• Exercise (at least 7-10 minutes a day)
• Move closer to work – if your commute is too long
Source: Jeff Harden, https://www.inc.com/jeffhaden/10-scientifically-proven-ways-to-be-incrediblyhappy-wed.html
Local Leader Re-Elected to ANA Board of Directors
The American Nurses Association (ANA) announced the results of its annual leadership elections. The voting representatives of ANA’s Membership Assembly elected leaders to serve on the board of directors and nominations and elections committee. Voting took place from Friday, June 18th until Thursday, June 24th at 11:59 EST. All terms of office begin on January 1, 2022.
ANA’s Membership Assembly elected the following members to serve two-year terms on the 9-member board of directors:
Treasurer Joan Widmer, MS, MSBA, RN, CEN, of the New Hampshire Nurses Association; Director-at-Large Amy McCarthy, MSN, RNC-MNN, NE-BC, of the Texas Nurses Association.
Vice President Susan Swart, EdD, MS, RN, CAE of ANAIllinois, and Director-at-Large, Recent Graduate Marcus Henderson, MSN, RN, of the Pennsylvania State Nurses Association were re-elected to their positions on the board of directors.
Those continuing their terms on the ANA board in 2022 are: President Ernest Grant, PhD, RN, FAAN, of the North Carolina Nurses Association; Secretary Stephanie Pierce, PhD, MN, RN, CNE, of the Louisiana State Nurses Association; Director-at-Large, Staff Nurse Amanda Buechel, of ANA-Illinois; BSN, RN Director-at-Large Jennifer Gil, BSN, RN, of ANA-Massachusetts; Director-atLarge Brienne Sandow, MSN, RN, NEA-BC of ANA-Idaho. Elected to serve on the Nominations and Elections Committee are: Gayle Peterson, RN-BC of ANAMassachusetts; Larlene Dunsmuir, DNP, FNP, ANP-C of the Oregon Nurses Association; Nelson Tuazon, DNP, DBA, RN, NEA-BC, CENP, CPHQ, CPPS, CPHQ, FANP, FACHE, FAAN of the Texas Nurses Association and Linda Taft, RN of ANAMichigan.
New Continuing Education (CE) requirement for Illinois LPN, RN and APRN license renewal beginning in 2022
The implicit bias awareness training is required of all persons who hold a professional license issued by the Division of Professional Regulation and are subject to a continuing education (CE) requirement (HB158, Public Act 102-004). These licensees shall complete a one-hour CE course on implicit bias awareness training. Any training on implicit bias awareness applied to meet any other State licensure requirement, professional accreditation or certification requirement, or health care institutional practice agreement may count toward the 1-hour implicit bias awareness training requirement. This requirement shall become effective for all applicable license renewals occurring on or after January 1, 2022.
How many hours of Continuing Education (CE) will I need for 2022 license renewal?
This 1 hour of implicit bias awareness training CE course is intended to fit into the licensee’s regular CE requirements. RNs will be renewing their licenses in 2022, 1 of the 20 hours of required CE must be an implicit bias awareness training course; 1 of the 20 hours of required CE must be sexual harassment prevention training. APRNs will be renewing their licenses in 2022, 1 of the 80 hours of required CE must be an implicit bias awareness training course; 1 of the 20 hours of required CE must be sexual harassment prevention training. LPNs will begin renewing their licenses in late fall 2022, and 1 of the 20 hours of required CE must be an implicit bias awareness training course; 1 of the 20 hours must be a sexual harassment prevention training course.
What are the CE Rules for Illinois LPNs, RNs and APRNs renewing their licenses in 2022?
The Rules regarding CE requirements indicate that courses shall only be provided by existing Division-approved continuing education providers or sponsors or by persons or entities who become Division-approved continuing education sponsors.
How do I know if the sponsor is approved or licensed? Is there a list of approved CE Sponsors and Programs for Illinois nurse license renewal in 2022?
CE sponsors must either be pre-approved per Rule 1300.130 or must have a CE sponsor license. The list of preapproved CE Sponsors and Programs is in the Rules for the Administration of the Nurse Practice Act, Section 1300.130: http://nursing.illinois.gov/NursingCE.asp
c) Pre-Approved CE Sponsors and Programs
1) Sponsor, as used in this Section, shall mean:
A) Approved providers of recognized certification bodies as outlined in Section 1300.400(a).
B) Any conference that provides approved Continuing Medical Education (CME) as authorized by the Illinois Medical Practice Act.
C) American Nurses Credentialing Center (ANCC) accredited or approved providers.
D) Illinois Society for Advanced Practice Nursing (ISAPN).
E) American Academy of Nurse Practitioners.
F) Nurse Practitioner Association for Continuing Education (NPACE).
G) American Association of Nurse Anesthetists, or National Board of Certification and Recertification for Nurse Anesthetists.
H) National Association of Clinical Nurse Specialists (NACNS).
I) American College of Nurse Midwives.
J) Illinois Nurses Association or its affiliates
K) Providers approved by another state's board of nursing
L) Nursing education programs approved under Section 1300.230 or 1300.340 wishing to offer CE courses or programs.
M) Employees licensed under the Hospital Licensing Act (210 ILCS 85) or the Ambulatory Surgical
Treatment Center Act (210 ILCS 5)
N) Any other accredited school, college or university, or State agency that provides CE in a form & manner consistent with this Section.
Please note that this is not a complete list. In addition, organizations may obtain CE sponsor licenses issued by the Department.
License Look Up: type in: Nurse CE Sponsor: https://www. idfpr.com/LicenseLookUp/LicenseLookup.asp
This is my first time renewing my Illinois LPN, RN or APRN license – do I need to complete the 1 hour of implicit bias awareness training CE prior to license renewal in 2022?
No, a renewal applicant shall not be required to complete 1 hour of implicit bias awareness training prior to the first renewal of an Illinois LPN, RN or APRN license.
How long is the implicit bias awareness training course?
The implicit bias awareness training course must be at least one hour or 60 minutes, which is 1 CE.
Are there any other new CE requirements for this renewal cycle?
No, however, SB677 provides that beginning January 1, 2023, a health care professional who has continuing education requirements must complete at least a one-hour course in training on the diagnosis, treatment, and care of individuals with Alzheimer's disease and other dementias per renewal period. This requirement shall only apply to health care professionals who provide health care services to, and have direct patient interactions with adult populations age 26 or older in the practice of their profession. Details available at a later date.
What is the fee for Illinois LPN, RN or APRN license renewal in 2022?
The fee for the Illinois RN or APRN license renewal in 2022 shall be calculated at the rate of $40 per year, or $80 at the time of renewal. For Illinois LPNs, whose license renewal begins in late fall 2022 and ends January 31, 2023, the fee for the renewal shall be calculated at the rate of $40 per year, or $80 at the time of renewal.
Additional Continuing Nursing Education information, including a FAQ sheet and a list of pre-approved CE sponsors is available on the Illinois Nursing Workforce Center Website http://nursing.illinois.gov/NursingCE.asp
Joan Widmer
Susan Swart
Amy McCarthy
Marcus Henderson
Alert Systems Online? Yes!
Laura Kay Wood, DNP,
RN,
CMCN, Professor, Graduate Nursing Programs, Purdue University Global School of Nursing
Deborah S. Adelman, PhD, RN, NE-BC, Professor, Graduate Nursing Programs, Purdue University Global School of Nursing
Working online exclusively for over 20 years, we have learned about alert systems at our university as a part of new faculty orientation. Neither of us thought we would use the system, but that changed in the last few years and made us rethink the value of these systems, especially now that most if not all nursing programs have gone online for at least a year in response to COVID-19.
Alert systems are systems that anyone at a college or university can use to start a specified series of steps to deal with an impending or actual disaster or emergency. When teaching on ground, we have found that this system seemed unnecessary since one could call the local EMS. Even online, when the university, staff, faculty, and students were all in the same geographic location, it seemed that having an internal alert system would not be of real value. Two events have changed our thinking on this.
The first event happened about 10 years ago when one of us worked online for an on-ground university in another state that had no alert system. Being the only faculty member there who had online experience, the chairperson of the nursing program called to ask about covering for an online faculty member who lived 1400 miles away. The adjunct faculty member had not been in class for two weeks. The chairperson was annoyed. She wanted coverage for the course and also wanted to fire the adjunct faculty member. When the faculty member who had online experience advised the chairperson to call 911 in the adjunct’s city, the chairperson was hesitant but did so.
The police department in the adjunct’s suburban location responded by doing a wellness visit. When the adjunct did not answer the door, the police broke into the house and found her at the bottom of the basement stairs. She had been laying there for at least a week and a half. Had the chairperson not called the police department, it might have possibly been weeks longer before anyone checked on her. Fast forward about five years later to an online university that had an alert system in place. A student who had been in one of our classes two terms previously wrote an email stating he was a bit down and wanted to just say hi and missed the instructor. Feeling something was not right about the email, the instructor wrote back and asked if he felt okay. He replied that things were not okay, and voices were telling him to kill himself and others.
The instructor was unsure if this situation was a Code Red or a Code Yellow condition. She corresponded promptly with the chairperson by way of the internal
chat program. The chairperson subsequently continued correspondence throughout the entire duration of communications between the student and the instructor. The chairperson contacted several higher administrators who contacted the fire department in the student’s city.
In the end, the student received the help he needed, and the alert system saved his life. Numerous individuals at the university, working with the student’s local EMS, came together in a coordinated manner to deal with the emergency through proper use of the alert system.
An alert system usually consists of two tiers: Code Red and Code Yellow. These alerts are a means of ensuring that matters critical to students, campus operations, and the college or university can be reported promptly to ensure management responds in a timely manner. The alerts are discerned by threat level.
A Code Red signifies a threat is happening, such as imminent harm to person or property, and must be set in motion within 60 minutes of anyone becoming aware of a perceived threat, emergency, or disaster.
A Code Yellow would be described as any non-life-threatening, but serious issue, such as precautionary instructions in lieu of a possible emergency situation. The yellow alert must be activated within 24 hours of anyone becoming aware of a potential threat, emergency, or disaster.
To understand how these codes work, we will go back to the two case studies presented above. The primary need for alert systems can produce appropriate responses equal to the level of an existing or perceived threat. Questions that can help determine the type of alert needed should be a part of human resource training and include:
• Do college or university staff, faculty, and students need to be aware of and prepared for a possible situation or disaster? This would be a Code Yellow situation.
• Does one need to take immediate action? This would be a Code Red situation.
The alert systems represent a commitment to address the health and safety of students, faculty, staff, and the university. Alert systems inform us, provide direction, prepare and mitigate coming threats, and most importantly, save lives. Both of the events described earlier depict Code Red situations.
The most important consideration is would you know what to do and does your college or university have a plan, in case a faculty member or student is experiencing an actual or impending emergency situation.
Challenges in the Nursing Workforce, Graduate Nursing Education, and Future of Nursing
Georgianna Thomas, D.Ed., MSN, RN
Somi Nagaraj, DNP, MSN, RN, CSSGB, CONTL
The healthcare sector is an intricate, albeit fundamental, part of ancient and modern societies. It comprises a long list of agents, from the individual seeking healthcare services to the medical staff and nurses, all operating within a legal framework involving providers, consumers, insurance companies, government, medical schools, nursing schools, and regulatory institutions (Amorim Lopes et al., 2015).
The healthcare market is always composed of both suppliers of health services and patients demanding their services. On the one side is the workforce of physicians, nurses, and remaining clinical staff educated according to standards and criteria, ready to assist those in need. On the other side stand the forces that drive the demand for medical services, strongly related to demographic, socioeconomic, and epidemiological factors. Analyzing these two market forces is a critical step in assessing whether the available health care human resources are enough in quantity and skills to meet the current and future demand in due time and may lay solid foundations for further research, considering perhaps changes to the existing health policy framework (Amorim Lopes et al., 2015).
A high degree and extent of uncertainty affect supply and demand: asymmetric information between physicians, nurses, and patients, restrictions on competition, an aging workforce in all areas, strong government interference, and supply-induced demand are some of the most glaring differences that can be pinpointed. These may be relevant when assessing the impact of any policy involving Healthcare Human Resource [HHR] planning (Amorim Lopes et al., 2015).
Supply
Supplying human capital with the appropriate expertise to enable workers to perform and satisfy the demand for health care is no simple task. The time and effort required to equip HHR, especially physicians and advanced nurse practitioners, exceeds most other professions. In some particular healthcare professions, the set of necessary skills to qualify for medical practice is acquired through extensive academic learning, which involves enrollment in long courses that may take up decades to complete due to a strict licensing process. The analysis of the medical and nurse education process is relevant but may be insufficient, as several other factors may affect the efficiency and effectiveness of the care services delivered (Amorim Lopes et al., 2015).
Despite the limitations, some measures to overcome imbalances in the quantity (number) of physicians and nurses have already been identified in the health policy literature (Chopra et al., 2008), namely the following: increasing the number of domestic- and foreign-trained medical graduates or increasing the number of medical and nursing schools and classroom sizes; increasing the enrollment limits; reducing the requirements for entry to medical and nursing schools; raising the wages of the medical and nursing staff, as well as the perspectives for their future career path; or reducing the costs of attending medical and nursing school,
which may encourage potential students to enroll. These proposals are short-term measures to alleviate the immediate stress put on the healthcare system triggered by an undersupply of personnel and may not be suitable for tackling long-term imbalances due to huge shortages or surpluses of medical and nursing staff (Amorim Lopes et al., 2015).
Demand
Demand for health care is a derived demand (Grossman, 1972), which means that people do not seek health care services as a final good for consumption but as an intermediate service allowing them to be healthy and to improve their stock of health capital (well-being). They want to improve their health, and to do so; they seek healthcare services (Amorim Lopes et al., 2015).
The concept of needs in health care is not consensual in the health literature, with a semantic confusion arising from its use in health economics (Hall & Mejia, 2009). While the economic or effective demand translates the actual, observed demand, usually measured in terms of service utilization ratios such as bed occupancy rates, number of inpatients, the needs component tries to fully encompass the epidemiological conditions that characterize a given population, measured through morbidity and mortality rates or by the opinion of a panel of experts, and how that may translate into a given quantity of required healthcare services. Therefore, we see that the classical concept of economic demand may not reflect the biological needs of the population, as it may leave out the necessities of the population regardless of their ability to pay (Amorim Lopes et al., 2015).
An integrated approach uses a dynamic, system-level perspective covering key drivers of supply and demand that includes manpower planning and workforce development is critical to overcoming such challenges (Stordeur et al., 2010). The importance of paying attention to needs is also continuously stressed, as changes in the health patterns of the populations take place (Tomblin et al., 2009). The impact of microeconomic and organizational changes in productivity and the skill mix, of the evolution of demand for healthcare services, and also of the evolution of health diseases and its potential impact on the health system. The given quantity of workers may provide more or less healthcare services depending on their productivity and skill mix, influencing the conversion from headcounts to full-time equivalents (FTEs). Such conversion is critical to properly assess the healthcare workforce, as a significant number of physicians and nurses work part-time only. For this reason, FTE is a more accurate measure as it normalizes headcounts. On the demand side, economic (effective) demand can be initially measured by analyzing utilization indicators. How this demand will evolve in the future will then be subject to typical economic factors such as demography and the growth of the income/GDP (Amorim Lopes et al., 2015).
In parallel, potential needs can be assessed by incorporating the incidence and prevalence of diseases and then mapping a given disease to an estimate of FTE requirements. Whether future supply forecasts should tackle all of the estimated needs is a decision left to the consideration of the policymaker, as the analysis does not incorporate financial constraints. Despite the abundance of approaches and techniques to determine supply and need for professionals, none of the methodologies has ultimately proved to be superior (Ricketts, 2011).
Recent studies testing current forecasting models show that there is still plenty of room for improvement given the gap between projected and actual results (Greuningen et al., 2013). It becomes even clearer that workforce planning should be accurate and performed in due time, given the attritions and the delays in enacting policies in the healthcare sector. Adapting medical and nursing schools, altering legislation, and changing roles is an effort that may take years to bring forth. Therefore, planning has to target a long enough time horizon to be useful and applicable and has to be done pre-emptively (Amorim Lopes et al., 2015).
Accurate HHR planning requires an approach that is both integrated and flexible, featuring supply and demand (potential and effective) and incorporating less tangible factors, such as skill mix and productivity (Amorim Lopes et. al., 2015).
Academia
Looking at the area of academia, there are many issues at hand that present challenges for nursing education at the doctoral level. Having enough faculty to provide quality education to those interested in pursuing a doctoral degree in nursing relies on competent individuals. Presently there are two types of doctoral degrees one can earn, both are terminal degrees, and both allow nurses to continue to practice in the clinical field. The Doctor of Nursing Practice (DNP) has a clinical focus that allows the nurse to possess expert knowledge to influence healthcare outcomes across direct patient care, advocating for healthcare policy implementation, and collaborating with organizational leadership (Leveck, 2020, Chism 2010). The Doctor of Philosophy (PhD) focuses on research in advancing the nursing profession and change the quality of patient care and outcomes in the field. PhD nurses also teach and mentor nurses at the college and university level, growing the next cohorts of professional nurses. There is a difference between these two degrees in their primary foci and length of education (registerednursing.com). However, the DNP degree has become the more soughtafter degree, and individuals who have earned it are considered equal at many institutions in academia in relation to tenure attainment and administrative positions. It was more common to see the individual with a PhD in the academic setting. However, individuals seeking this degree are decreasing in number, and some individuals are having difficulty completing their dissertation. This adds to the faculty shortage we continue to experience in the profession. There is a distinction between the two degrees and needs to be recognized and valued in advancing new nurses, however, the DNP graduate is more prepared for the clinical arena.
According to Drs. Di Fang and Karen Kesten, one-third of the current nursing faculty workforce in all levels of education are expected to retire by 2025 (ANA Fact Sheet, 2020). This will certainly have an effect on the numbers of students who will be accepted when they apply for nursing education overall.
Continuous changes in the nursing and medical fields have been rapidly evolving because of technology and studies such as the genome project. Graduate student feedback to courses and discussions with clinical affiliates to the college/university are two ways that information can be ascertained in relation to curricular issues for content. Accreditation standard revisions and the recently adopted Essentials with emphasis on outcomes and competencies in learning have also added to many of the changes schools are making to revise overall curriculums (AACN, 2021). Learning theories are used to expose students to various learning experiences. Online teaching, simulation, inter-professional learning, case studies, and other teaching formats take much time to prepare and grade and may not all be familiar for present faculty to fulfill.
Interdisciplinary education (IPE) among the various healthcare providers is expected to be utilized in schools. This type of education provides shared experiences that allow for better understanding, improved engagement, and clearer insight into cooperation in the work
environment and quality patient care. This activity in schools with major medical affiliations has an edge in providing this type of learning while many smaller colleges and universities struggle to gain this opportunity. Many IPE opportunities that do exist are noted through simulation-enhanced activity (Fawaz, 2018). Although simulation is helpful, real-time situations may affect the learner differently when exposed.
Technology has become more influential in our lives, especially after the past year and a half of pandemic experiences. However, online education is not a new concept in education. Use of learning platforms, Zoom meetings, Wiki’s, Google docs, social media, Electronic Health Records, and so on have not been mastered by all in education, faculty, or student. Many students like the idea behind online learning in that they can study at their own pace often or at a time that is most convenient for them. This strategy for education allows for flexibility to view course material in both an asynchronous and, at times, synchronous format. Faculty find this learning takes more time in their schedule for preparation and grading than when classes met traditionally. Class size is not always capped. Lack of support staff with course development and difficulty managing technological changes have been identified as barriers to distance education (Iwasiw et al., 2020). This becomes frustrating to both teacher and student in that the partnership that develops in learning is not fully developed.
Future of Nursing
The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity, study sponsored by Robert Wood Johnson Foundation identified, that a nation cannot thrive fully until everyone can live their healthiest possible life, and helping people live their healthiest life is and has always been the essential role of nurses. The ultimate goal is to achieve health equity in the United States built on strengthened nursing capacity and expertise (National Academies of Sciences, Engineering, and Medicine, 2021).
The committee developed a framework identifying the key areas for strengthening the nursing profession to meet the challenges of the decade ahead. These areas include the nursing workforce, leadership, nursing education, nurse wellbeing, and emergency preparedness and response, as well as responsibilities of nursing with respect to structural and individual determinants of health (National Academies of Sciences, Engineering, and Medicine, 2021).
In 1998 the Pew Health Professions Commission, a group of healthcare leaders charged with assisting health policymakers and educators teaching health professionals to meet the changing needs of healthcare systems, completed a report listing competencies healthcare providers of the future would need. The competencies are listed in the Fourth Report of the Pew Health Professions Commission (O’Neal & Pew Health Professions Commission, 1998).
The book To Err Is Human: Building a Safer Health System (Kohn, Corrigan, & Donaldson, 1999) brought national attention to the issue of patient safety by discussing the number of people who die each year from medical errors. This, in turn, sharpened the focus of patient safety in nursing education (Scheckel, 2008).
Despite the practice setting in which students learn nursing care, it will include using various technologies and knowledge of informatics to assist with patient care. These technologies can include but are not limited to medical devices patients will use to provide self-care, as well as information retrieval, clinical information management, and documentation technologies (Scheckel, 2008). Students’ use of these devices has important implications for improving their clinical judgment (Newman & Howse, 2007). Nurses are also being exposed to the use of variety of clinical management systems, like patient surveillance systems many of which have implications for ensuring quality and safety.
A significant movement that accompanied the curriculum revolution involved using pedagogies to ensure students could think critically in clinical practice. Traditionally, students who learned the nursing process were thought to be learning critical thinking. During the past few decades, the nursing process has been challenged as the best approach to developing students’ critical thinking (Scheckel, 2008). However, current research in nursing education suggests that students also need to engage in thinking processes that promote reflective thinking, where they build practical knowledge, embodied thinking, where they learn the importance of intuition and pluralistic thinking, where they consider a clinical situation using many perspectives (Scheckel & Ironside, 2006).
Innovations
As nurses assume increasing responsibility for patient care in primary care settings, the combination of increased clinical and systems knowledge, as well as the capability to apply and evaluate evidence to practice innovations, can only have
a positive impact. The presence of DNP-prepared APRNs in primary care will expand educational opportunities. In the short term, the DNP-prepared APRNs can mentor the MSNprepared APRNs within the system. Equally important is the opportunity for enhanced preceptor education for nursing students in primary care (Dunbar-Jacob et al., 2013). Indeed, the preparation of the DNP will influence the perception of health care systems regarding the added value of DNP education. If graduates of such programs bring an increased depth of knowledge and skill to the clinical arena, the DNP will likely flourish. If graduates bring little more than what is offered by master’s-level education, the DNP will not be an attractive addition to the clinical arena. Thus, the quality of the preparation of the DNP will influence the adoption of the DNP practitioner and administrator by health care systems (Dunbar-Jacob et al., 2013).
Conclusion
Challenges in building DNP programs include the identification of qualified faculty for each specialty, qualified capstone advisors, and qualified clinical preceptors. A further challenge is the simultaneous education of master’s cohorts and DNP cohorts. The challenges by requiring faculty to obtain a doctoral degree, developing critical academic–service partnerships in mentoring students for practicum and capstone projects, and discontinuing MSN advanced practice specialty programs while focusing on the BSN-toDNP and MSN-to-DNP programs. High-quality DNP academics and DNP clinicians are crucial to help meet these challenges. Each educational program must assess its challenges and strategies for addressing those challenges. How we proceed will determine the impact of our programs on the future of the health care system (Dunbar-Jacob, Nativio, & Khalil, 2013).
In academia, both the PhD and DNP prepared nurses can work together to ensure quality education for our nursing students. Both need an educational foundation to be learned to be successful educators. The distinction of the PhD concentrating on teaching theory and research to assist nursing to maintain its scientific foundation and the DNP concentrating on the clinical skills and acting as preceptor/ clinical educator at any level of nursing appear to be the ideal partnership to develop. Both nurses can assist academia and the clinical arena in staying current and developing innovative care measures to provide quality care to clients. When looking at the definitions noted at the beginning of this work, this collaboration in teaching nurses fits what was noted.
PRACTICE CORNER
Illinois
Law & Nursing Practice
Question:
A nursing faculty member teaching nursing students in their clinical rotation was told that students are practicing nursing under her Illinois professional nursing license. She is very concerned that her potential liability for professional negligence and/or a disciplinary action by the state board of nursing is increased. She wants to know if the statement is correct and what legal liability she has as a faculty member.
Answer: The statement is not correct.
The Illinois Nurse Practice Act provides guidance for the nursing faculty member. It is true that the Act clearly states that no one can practice professional, or any other type of nursing, without being licensed under the Act. The only individual who can legally practice nursing with a license is the person whose name is on the license.
However, the Act does not prohibit the practice of nursing which is included in a program of study by students enrolled in programs of nursing. This is one of the exceptions to the requirement that anyone who practices any kind of nursing in Illinois be properly licensed to do so. The student nurse, then, does not practice under anyone’s license because a license is not required.
A faculty member’s potential liability can be based on the Illinois Nurse Practice Act and Rules. If the nursing
faculty member violates a provision of the Act or its rules in his or her personal capacity as a nursing faculty member, he or she can face a professional disciplinary action by the Illinois Board of Nursing.
An example of this potential liability is not following the Illinois Nursing Act’s mandates for nursing education programs. One rule governing nursing education programs states that in the clinical area, if faculty are directly supervising students, the ratio of students to faculty cannot exceed 10.1. If this ratio is exceeded, liability for the faculty member and the nursing education program is real, whether or not a patient injury is alleged.
A nursing faculty member can also be named in a professional negligence suit in his or her personal capacity as a nursing faculty member. The law of professional negligence requires nursing faculty to be accountable and responsible for their own decisions and actions. The standard of care for the faculty member is what ordinary, reasonable, and prudent nursing faculty members would have done in the same or similar circumstances in the same or similar community.
There are several theories of liability in the law for nursing faculty in their personal capacity as a faculty member. As stated earlier, one is for his or her own negligent acts. For instance, suppose the faculty member does not correctly teach and demonstrate to a student how to give an injection or start an IV. If the student follows the faculty member’s instructions and injures a patient, the faculty member can be named in the patient’s lawsuit.
Another theory of liability for nursing faculty is negligent supervision. The faculty member has a duty to continually evaluate students in the clinical area and ensure they have completed patient care safely and have responded to any changes in the patient’s condition.
Standardizing Patient Education: Challenges
Marla Long, MS, RN
Total Joint Replacement Coordinator
Nurses have a powerful role in patient preoperative education related to key selfcare measures that drive high-quality patient outcomes (Giardina et al., 2020; Smith et al., 2021). Nurses who provide preoperative education to the patient and caregiver can effectively help them navigate the postoperative course and prepare them for self-care measures needed in the postoperative home.
Vital teaching topics include prevention and recognition of postoperative complications, safe self-management of postoperative pain and preparation and maintenance of the surgical home. (Smith et al., 2021). In addition, nurses provide one-on-one patient-centered teaching allowing the assessment of the patient’s and caregiver’s understanding. Increased understanding improves the postoperative course and also improves outcomes, reduces patient and caregiver anxiety and decreases overall costs (Krause et al., 2018).
Within the joint replacement patient population the directive is for decreased length of stay without an increase in readmissions (Pelt et al., 2018). This requires coordinated preoperative patient teaching to prepare the patient and caregiver for a confident and safe discharge to the surgical home. Patient preoperative education spans the clinic, joint replacement class, pre-anesthesia, and the postoperative unit.
Experience in a tertiary hospital system has shown that unless the education script is coordinated, the patient leaves the hospital with conflicting information regarding surgical dressing, therapy, mobility, infection prevention, and DVT prophylaxis. The outcomes are lack of patient and caregiver discharge confidence, increased complication related readmissions and increased costs.
Nurses have a unique approach to patient education and often have access to multiple resources; however, it is vital that the education message provided is standardized within the interdisciplinary team (Gallegos et al., 2019). Elimination of variation in a process can improve system efficiency and overall quality (Langley et al., 2009).
A study by Pelt et al. (2018) showed the importance of incorporating a comprehensive standardized interdisciplinary preoperative program for total hip and knee replacement patients. This study showed the result of standardized patient messaging through the preoperative and postoperative patient education videos, preoperative joint replacement class (taught by a team including nursing leadership), inpatient nursing team, preoperative and postoperative patient calls with the providers. The results were a decrease in the number of discharges to postoperative acute care centers and the number of readmissions.
Nurses have a critical role in developing programs and resources to decrease interdisciplinary patient education variation and positively affect patient outcomes. (Smith et al., 2021)
References available upon request
Part of the potential liability under a negligent supervision theory is of the faculty member negligently determined the assignment of the student to care for a particular patient. The student must be competent to provide the care the patient requires.
These theories are not all of the potential theories of liability for nurse faculty. Even so, they do provide implications for this nursing faculty member and for you, if your role requires teaching students in clinical rotations. They include:
* Maintain one’s own clinical competency
* Be present and accessible to students in the clinical area
* Carefully and continually evaluate students in one’s clinical group
* Properly assign students for patient care assignments based on your evaluations
* Comply with the Illinois Nurse Practice Act and Rules
* Maintain one’s own and students’ scope of practice parameters based on the Illinois Nurse Practice Act and Rules
* Document student care with anecdotal notes, not only for evaluation purposes but also in the event a suit is filed alleging some form of negligence against a student or you
* Maintain a professional liability insurance policy that covers your roles as a faculty member
You can read the entire Nurse Practice Act and its Rules by going to the Illinois Nursing Workforce Center at: nursing.illinois.gov/nurspracticeact.asp and click on the Act and its Rules.
Education Evolution to Professional Development
Submitted by Kimberly Chant, MSN, RN
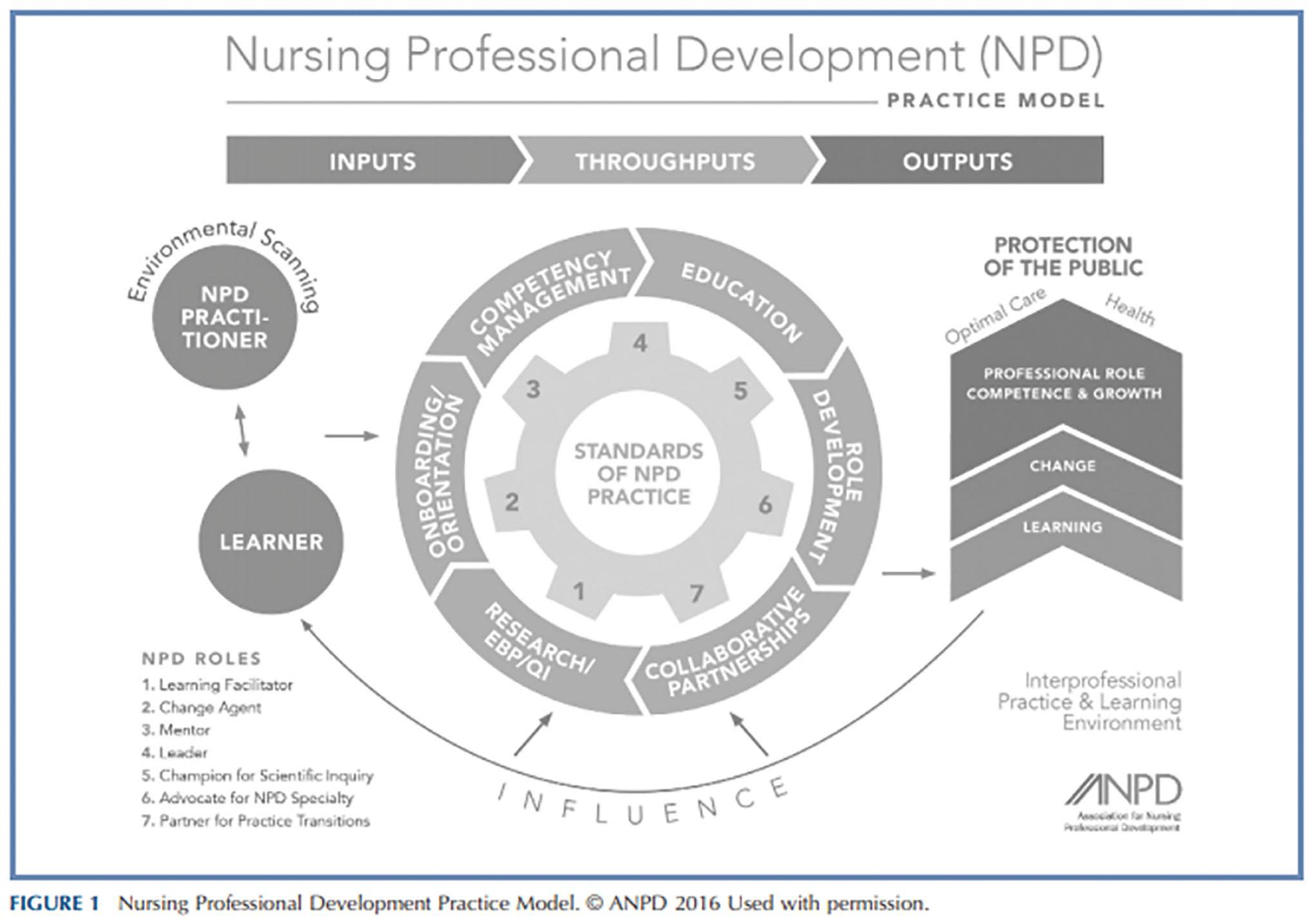
Clinical education fulfills a core necessity at UnityPoint Health Trinity. Over time, the department has transitioned through various reporting structures to meet changing needs of the organization. In September 2019, clinical education transitioned to Clinical Professional Development (CPD). Evidence-based practices and national trends revealed the Nursing Professional Development (NPD) Model could provide the structure needed to support the hospital in improving patient outcomes.
The first few months were spent defining relationships, a purpose statement and framework. Just as CPD was ready to “go live”, we experienced the eruption of COVID-19 pandemic. One year later, we begin again, seeking to help our organization understand how CPD is a part of this change management.
The Nursing Professional Development (NPD) practice model defines the Standards of NPD Practice and Performance. These are essential to how the NPD Practitioner influences the practice environment, including professional competence and growth (Harper, 2016). The NPD Practitioner utilizes various inputs to identify learning gaps in clinical performance and facilitates learning through specific clinical partnerships and influences. This disciplined approach provides clarity to the work of Clinical Professional Development and its impact on change management to improve patient outcomes.
References available upon request
Diagram: (Reingans, 2016).
Nancy J. Brent, MS, JD, RN
IACN - Resiliency in Nursing
According to Merriam-Webster Dictionary (2021), “resilience” is defined as “an ability to recover from or adjust easily to misfortune or change.” For nurses, resiliency is an especially important quality. Even before the COVID-19 pandemic, nurses often juggle inconsistent schedules, excessive work hours, and adjustments in the workplace. Many also choose to add the challenges of returning to school to advance their nursing education.
“To me, resiliency is the ability to continue your practice as an educator/clinician in light of the many challenges that are faced. There is constant change, expectations from students and employers, educational requirements, and increased use of technology that adds to all of the existing requirements as an educator/ clinician,” said Pam Ferguson, Dean of Nursing at Methodist College.
Read on for some of the challenges that nurses face, as well as the ways that many in the profession show resilience.
Resiliency Against Burnout in Nursing
The variety of stresses involved with nursing can culminate in something called burnout. Burnout is widespread and exemplified by “a reduction in nurses’ energy that manifests in emotional exhaustion, lack of motivation, and feelings of frustration” (Mudallal et al., 2017).
Unfortunately, our members are too familiar with burnout. “We need more nurses,” said Holly Farley, Chair of the School of Nursing at Eastern Illinois University. “Too many organizations are working with minimum staff. This creates constant stress and eventually burnout.” Our nurses are also well versed in how to combat burnout. Judy Shackelford, Dean of Academic Affairs
at St. John’s College said, “Nurses should practice self-care first before caring for others. You need to know your inner strength and that it is not defined by circumstances.”
Loneliness in Nursing
While burnout is typically thought of as simply being overworked, lack of community and loneliness are also key parts. In regard to loneliness in nursing, Pam Ferguson said, “The development of a supportive workplace environment can assist individuals who are stressed, for any reason. This is difficult to manage during a hectic workday and before or after shifts. Nurses also need supportive families and friends who can comfort them as needed. The comfort of a work mentor would also provide some added relief as needed.”
Judy Neubrander, Dean of Illinois State University’s Mennonite College of Nursing, agrees. “Mentorship is a critical part of ensuring that new nurses are successful, and that talented young nurses step up into leadership positions—something healthcare desperately needs. Our Nurses On Boards initiative is starting to work on tackling that issue in McLean County.”
Resilience in Nursing
At the Illinois Association of Colleges of Nursing, we know that times are tough for nurses. We want you to know that we are here for you. If you are a nurse, we encourage you to reach out to us for help and advice. You can contact us at http://illinoiscollegesofnursing.org/ contact-us/.
Lastly, we offer this piece of wisdom from Judy Shackelford on how to stay resilient: “Practice self-care by doing things that nurture your spirit. Set boundaries for downtime and rejuvenation. And also, eat right, get enough sleep, and exercise.”
References available upon request
ANA-Illinois appoints members to serve on a Community Service Task force
ANA-Illinois has been approached by members seeking opportunities to volunteer, spend time together at a volunteer activity, or meet people via group volunteering. The Board of Directors recently appointed nurses from around the state to assist in developing such a program. The task force's charge is to explore how ANA-Illinois can facilitate this work and bring recommendations to the board on the resources necessary to launch such a program successfully.
Taskforce members include –
• Carissa Heise, BSN, RN – Waterloo
• Kim Seggebruch, MSN, RN, CNOR – Onarga
• Toni L Oats, RN – Chicago
• Jana Rich, MSN, RN – Hanover Park
• Margaret C Miller, MSN, RN – Waterloo
• Maggie Smith, DNP, MSN/Ed, RN, OCN - Frankfort
• Gloria E. Barrera, MSN, RN, PEL-CSN – Orland Park
• Debra (Debbi) Waters, MSN, RN, MJ, CHCPlainview
• Minnette Willard Scott, BSN RN PMGT-BC - Aurora
• Jennifer Kane, MSN, BSN RN - Chicago
• Renee C. Brown, RN – Loves Park
• Jacinta Staples, MSN, RN - Lynwood
Nurses want to provide quality care for their patients.
The Nurses Political Action Committee (Nurses- PAC) makes sure Springfield gives them the resources to do that.
Help the Nurses-PAC, help YOU!
So. . . . . . . if you think nurses need more visibility if you think nurses united can speak more effectively in the political arena if you think involvement in the political process is every citizen’s responsibility.
Become a Nurses-PAC contributor TODAY!
❑ I wish to make my contribution via personal check (Make check payable to Nurses-PAC).
❑ I wish to make a monthly contribution to NursesPAC via my checking account. By signing this form, I authorize the charge of the specified amount payable to Nurses-PAC be withdrawn from my account on or after the 15th of each month. (PLEASE INCLUDE A VOIDED CHECK WITH FORM)
❑ I wish to make my monthly Nurses-PAC contribution via credit card. By signing this form, I authorize the charge of the specified contribution to Nurses-PAC on or after the 15th of each month.
❑ I wish to make my annual lump sum Nurses-PAC contribution via a credit or debit card. By signing this form, I authorize ANA-Illinois to charge the specified contribution to Nurses-PAC via a ONE TIME credit/debit card charge.
❑ Mastercard ❑ VISA
Credit card number Expires CVV
Signature:
Please mail completed form & check to:
HONOR A NURSE – NOMINATE SOMEONE FOR THE 2021 NURSE OF THE YEAR
Each generation has its heroes. We grow up hearing stories of superheroes – the caped crusaders who leap tall buildings and use their powers in extraordinary feats. Heroes make things look easy. Nurses are some of the hardest working individuals in the healthcare industry. In 2020, the world recognized the important work that nurses do for those we serve. We are no longer the unsung heroes. Nurses are the steadfast heroes among us, and the Illinois Nurses Foundation knows they deserve to be celebrated.
Nurses have the most interesting stories - they witness pain and heartache one moment alongside joy and triumph the next- Nurses make the world a better place for the patients, families, and profession.
The Honor a Nurse / Nurse of the Year award is a program that gives friends, family, and colleagues a way to share the story of a nurse who has made a difference. Make a $25 donation and honor a nurse who has inspired you, mentored you, fought for the advancement
of the profession, stood by you, or who deserves recognition for their commitment to their patients and the work nurses do every day. Don’t forget to submit the story that makes them your hero!
The Honoree will be listed on the INF website, in the December issue of the Nursing Voice and will also be entered as a nominee for the “Nurse of the Year” award* which will be awarded during the Illinois Nurses Foundation December Virtual Holiday Gala and Fundraiser.
*A story detailing the impact and contributions of the honoree must be submitted to be eligible for the Illinois Nurse of the Year.
In Honor donations can be made on the Illinois Nurses Foundation website www.illinoisnurses.foundation and https://bit.ly/HONOR_A_NURSE or using the QR Code
Nursing Career Path
At Amedisys, we build on skills throughout our careers and provide opportunities for growth with ongoing training and support. Join our family and see how you can step into a new role and make a difference today! Learn more at amedisys.com/careers.
THINK OUTSIDE THE HOSPITAL
To access electronic copies of The Nursing Voice, please visit http://www.NursingALD.com/publications
• Located in Chicago - relocation assistance available!
• Sponsorship assistance available!
2021 ANA-ILLINOIS CANDIDATES ANNOUNCED
The election for the ANA-Illinois Officers and Directors will be held online September 17th thru October 1st The election will be conducted electronically. Watch your email and the ANA-Illinois website www.ana-illinois. org for the additional details. Candidates are listed in alphabetical order according to position.
A Candidate’s Forum will occur on September 8th at 6:30p via Zoom. Watch for additional details and registration information.
All terms are for two years.
CANDIDATES FOR PRESIDENT
CANDIDATES FOR SECRETARY
CANDIDATES FOR DIRECTOR (2 to be elected)
CANDIDATES FOR NOMINATING COMMITTEE (2 to be elected)
CANDIDATES FOR ANA REPRESENTATIVE (2
be elected)
Elizabeth Aquino, PhD, RN DePaul University, School of Nursing Associate Professor
Beth Phelps, DNP, APRN-FNP, ACNP Springfield Clinic & University of Illinois Chicago College of Nursing, APRN – Full Practice Authority | Assistant Clinical Professor
Susana Gonzalez, MSN, MHA, RN, CNML ASI Home Care, DePaul University & Morton College Nurse Educator | Adjunct Faculty
Elaine Hardy, PhD, RN University of Illinois Chicago College of Nursing Clinical Assistant Professor
Beth Phelps, DNP, APRN-FNP, ACNP Springfield Clinic & University of Illinois Chicago College of Nursing, APRN – Full Practice Authority | Assistant Clinical Professor
Renae Denise Hale, DNP, RN, MHN-BC University of Illinois College of Nursing Visiting Clinical Instructor
to
Elaine Hardy, PhD, RN University of Illinois Chicago College of Nursing Clinical Assistant Professor
Susan Hovey, PhD, RN University of Illinois College of Nursing Springfield Campus, Clinical Assistant Professor, Associate Director
Casey Ketchum, BSN, RN, CCRN University of Chicago Medicine Clinical Nurse Associate
2020 Nurse Educator Fellow Recipients
The IDFPR/Illinois Nursing Workforce Center (INWC) Advisory Board and the Illinois Board of Higher Education (IBHE) are proud to acknowledge the 2020 Nurse Educator Fellow recipients, each of whom is awarded $10,000 to help promote excellence in nursing education. Sixteen educators were selected from 38 nominations from 24 institutions in FY21 and were awarded the Fellowships through the Illinois Board of Higher Education (IBHE).
“As we enter Phase 5 of Illinois Restored, we can look back on the role the pandemic has and continues to have in exposing the inequities in healthcare,” said Cecilia Abundis, Acting Director Division of Professional Regulation. “It has forced us to look at teaching modalities and at community partnerships in the racial, ethnic minority and the LGBTQ communities. We want to thank nursing education for leading the way, with the creative education modalities used to prepare students to graduate and for licensure.”
Several fellows are pursuing master’s and doctorate degrees or certifications, learning new teaching techniques for student nurses, and preparing to present research findings on the national level.
The Fellows completed a short survey, with the final survey question about how educating nurses post COVID-19 pandemic might change elicited comments in four areas: the transition to online teaching; the future to include continued flexibility with didactic and online teaching; clinical settings will broaden to include more non acute care, community settings; and the need to include educating students regarding self-care.
The fellows were recognized at a virtual ceremony on June 16, 2021 hosted by the Illinois Nursing Workforce Center (INWC) Advisory Board.
Alisha Betka, DNP, MSN/Ed, RN, CHSE University of Illinois Chicago
Cynthia D. Young, MSN, RN, CMSRN Morton College
Lynnann B Murphy, MN, RN University of Saint Francis
Sheri ComptonMcBride, DNP,RN Southern Illinois University Edwardsville
Angela Gilbreth, MSN, RN, CLS Southwestern Illinois College
Michele Shropshire, PhD, MSN, RN Illinois State University
Monica E. Hall, PhD, RN Illinois Wesleyan University
Tamara Boll, MSN, MBA, RN-BC Trinity Christian College
Lindsay A. White, MSN, RN, CNE, SANE Western Illinois University
Jorgia B. Connor, PhD, RN Loyola University of Chicago
Cristan Sabio, PhD, MSN, RN Northern Illinois University
Kara Richardson, MSN/Ed, RN Heartland Community College
Sara McPherson, PhD, RN,CNE University of Illinois Chicago in Springfield
Therese Gallagher, DNP, APRN, FNP-BC, CNL Rush University
A Blended Approach to Nurse Preceptor Training
Jennifer Elliott, BSN, RN
Many virtual learning opportunities have emerged, but UnityPoint Health-Trinity Quad Cities also felt it was important to keep the in-person component for our Nurse Preceptor Training. Typically, we have nurses who precept others attend a four-hour class every two years to receive training.
For 2021 we decided to do a blended learning approach. Nurses attend a two-hour in-person class led by a Clinical Professional Development Specialist. The classroom learning is enhanced with short activities, scenarios for group discussion, and a video that reminds the nurses why we are in this profession: because we care. They also complete a virtual learning “Escape Room” scenario done through Google forms.
There are many resources online describing how to do this, and the possibilities are endless. The participants unlock codes as they review important issues specific to our hospital as well as concepts important to precepting. Content is also correlated with the classroom topics.
This virtual piece is sent to their email to be completed within 30 days to be considered in compliance to receive preceptor pay. We hope by utilizing this blended approach, we can facilitate meaningful learning while decreasing class time.
Expert Panel on Nursing Education Appointed
ANA-Illinois is pleased to announce the selections for the Expert Panel on Nursing Education
The ANA-Illinois Board of Directors has chosen the following individuals to serve as the steering committee.
Carol Alexander, DNP, APRN, ACNS/NP-BC - CAAN Academy of Nursing
Julie Bowen, MSN, RN, CPHQ - Gibson Area Hospital & Health Services
Yolanda Coleman, PhD, MS, RN, FACHE, NEA-BC - CTCA Chicago
Jeannine Haberman, DNP, MBA, MSN, CNE – Oak Point University
Nadja James, PhD, MSN, MHA, RN, CNE - National Council of State Boards of Nursing
Joan Libner, EdD, MSN, FRE, RN-BC, CNE - Benedictine University
Judy Neubrander, EdD, APRN, FNP - Illinois State University
Julio Santiago, RN, DNP, CCRN, VA-BC - Joliet Junior College
Additionally, 19 other individuals have been appointed to serve on the advisory group. The advisory group will help with workgroups, provide feedback on processes, and give input on the recommendations developed by the steering committee. The advisory group members include -
Anne Kowalczyk, MS, RN-BC, CPN - DePaul University
Melinda Wildermuth, DNP RN - Trinity College of Nursing & Health Sciences
Julia Koklys, DNP, APRN, FNP-BC - Lewis University
Julie Kennedy, PhD, RN, CMSRN - Millikin University
Barbara Meagher, DNP, MSN, MAPS, CNM, RDMS, RN - University of Illinois Chicago
Vanessa DeBiase, MSN, MEd, RN, NPD-BC - Northwestern Medicine
Jennifer Maffucci, EdD, RN, ACNS-BC - University of Illinois at Chicago
Michelle Dawn Metzger, DNP, MBA, RN - Froedtert South Pleasant Prairie
Linda F Samson, PhD, RN, BC, NEA, BC - Governors State University
Sheila M Auer, RN MDS Coordinator - Sharon Healthcare Elms
George Velianoff, PhD, RN
Janet Thorlton, Ph.D., M.S., R.N. - University of Illinois Chicago
Lovey Reynolds, MSN, RN, CPN - Malcolm X College (Nursing Adj at DePaul Univ)
Christina Haag, MSN, RN, NPD-BC - Gibson Area Hospital
Deborah S. Adelman, PhD, RN, NE-BC - Purdue University Global
Melissa A Bateman, BA,RN - Humana, Inc
Ann M. O'Sullivan, MSN, RN, CNE, NE-BC, ANEF - Illinois College
Gretchen LaCivita, DNP, MPH, RN, CNE, CPN – Oak Point University
Nurses must be better prepared to work in the evolving health care environment with a nursing workforce representative of the population being served. The panel will look at the current state of nursing education in Illinois and make recommendations to the Board on how ANA-Illinois and our partners can proactively address the education, regulation, and practice of nursing to better prepare individuals interested in entering the profession.
ANA-Illinois Board of Directors issued the call for expert panel members who will guide the association in proactively addressing nursing education issues that limit our ability to address the supply of nurses and the level of health care services needed in Illinois. The expert panel will meet primarily by conference call and via e-mail starting in late August 2020. Thank you to everyone who promoted this application opportunity. The successful outcome and caliber of the applicants are a testament to your efforts. We will certainly keep the nursing community apprised as this work moves forward.
Congratulations to the Illinois Nurses Foundation 2021 Scholarship Winners
One of the primary functions of the Illinois Nurses Foundation is to provide scholarships to students who have decided to major in nursing or to nurses who are looking to continue their education. Eleven individuals were awarded scholarships totaling $13,500.
2021 Scholarship Awards
Centennial Scholarship
Centennial Scholarship
Centennial Scholarship
Centennial Scholarship
Arthur L. Davis Scholarship
D2 Scholarship
D21 Scholarship
Isabella Albertoni, Chamberlain University
Barbara Gaydasch, Chamberlain University
Monica Terrazas, DePaul University
Rylee Camp, Illinois State University
Tamara Boll, University of Nevada
Bryanna Gueness, University of St. Francis
Jocelyn Carbajal, Chamberlain University
North Suburban Scholarship Alexandria Epperson, Northern Illinois University
South Suburban Scholarship
Joanna Sieczka, St Xaviers University
Wendy Burgess Memorial Scholarship Noell Carrillo, Elmhurst University
Sonne Scholarship
Erin Bateman, Malcolm X College
The
Illinois Department of Financial and Professional Regulation (IDFPR) home page for your online nurse resources
The IDFPR home page (https://idfpr.com/) has a direct link to the following:
• To print your license or download an electronic copy to your phone: use the icon under the blue middle section of the IDFPR homepage. www.idfpr.com
• Address update: Please note that all IDFPR correspondence are now delivered electronically, including renewal reminders (in lieu of the paper postcard sent by U. S. Mail). Licensees are strongly encouraged to visit IDFPR’s online address change webpage (https://www.idfpr.com/applications/LicenseReprint/) to provide a current email address and ensure contact information is up-to-date and accurate.
• Name change: Change of name CANNOT be completed via this online process. If your name has changed, you must submit a written notice to the Department and include documentation of the name change (marriage license, court order, or divorce decree) For a copy of the written notice, please use this link https://www.idfpr.com/Forms/DPR/ DPRCOAnamechange.pdf
The Illinois Nurse Practice Act Rules were finalized on January 4, 2021. A copy is available at this link: https://nursing.illinois.gov/nursepracticeact.asp
The State of Illinois Coronavirus Response Site: The COVID-19 Vaccine Plan, up-to-date information on what Illinois is doing protecting the health, safety, and well-being of Illinoisans can be found at https://coronavirus.illinois.gov/s/
The Illinois Nursing Workforce Center (http://nursing.illinois.gov/)
Education: Post-licensure Illinois nursing education programs are separated between baccalaureate degree completion and graduate education opportunities. The graduate education page includes a grid of which practice specialty each graduate program includes. http://nursing. illinois.gov/Gradeducation.asp
Continuing Education Resource: Re-licensure continuing education FAQs are available for LPNs, RNs, APRNs, APRN-FPA’s http://nursing.illinois.gov/NursingCE.asp
Reports: the 2020 RN survey results highlighting data collected during online license renewal are now available at http://nursing.illinois.gov/ResearchData.asp There are also supply and demand reports of Illinois nurses dating back to 2007.
The NCLEX exam, or the National Council Licensure Examination, is a standardized test that every state regulatory board uses to determine if a candidate meets eligibility requirements to become licensed as a nurse. Administered by the National Council of State Boards of Nursing, there are two levels of NCLEX exams, and which test you take depends on the pre-licensure program from which you graduated.
Graduates of practical nursing programs sit for the NCLEX-PN. In several states, such as California, practical nursing programs are known as vocational programs. Those who have graduated from a pre-licensure program for registered nursing; whether an Associate Degree Program in a community college, a Baccalaureate Degree Program in a 4-year college or university, or a Master’s Entry Level Program; are eligible to sit for the NCLEX-RN.
As to be expected, the COVID-19 pandemic has had an effect both on how well potential nurses were able to prepare for the NCLEX and the outcomes of the exam. The challenges to complete one’s last semester of nursing courses and comprehensive exit exams in a learning environment that quickly changed to virtual, select a review course and implement a study plan, schedule taking the NCLEX with changes in availability of testing sites, and meet ongoing employment and personal responsibilities were exacerbated by the onset of the pandemic in March 2020.
Illinois NCLEX Scores
The results of Illinois’s Nursing Program NCLEX scores can be found here. NCLEX results are reported by program and exam type by the Illinois Department of Financial and Professional Regulation (IDFPR). The NCLEX score averages changed in the following ways in Illinois:
● Master’s Entry Level Programs, MSN: the NCLEX-RN pass percentage average declined by 3.3 percent from 2019 to 2020.
● Baccalaureate Degree Programs, BSN: the NCLEX-RN pass percentage average declined by 0.45 percent from 2019 to 2020.
IACN: How COVID Affected NCLEX Scores
● Associate Degree Nursing Programs, AAS in Nursing: the NCLEX-RN pass percentage average declined by 4.93 percent from 2019 to 2020.
● Practical Nursing Programs, PN Certificate: the NCLEX-PN pass percentage average declined by 2.23 percent from 2019 to 2020.
The nursing program NCLEX pass rate for first time testtakers required by the Illinois Nurse Practice Act is 75%. Program outcomes in Illinois in 2020 compared to 2019 were:
● MSN Entry Level Programs: 100% of programs achieved an NCLEX-RN program pass rate of 75% or greater in 2019 and 2020.
● BSN Programs: 94% of programs achieved an NCLEXRN program pass rate of 75% or greater in 2019 and 90% did so in 2020.
● AD Nursing Programs: 93% of programs achieved an NCLEX-RN program pass rate of 75% or greater in 2019 and 86% did so in 2020.
● PN Programs: 87% of programs achieved an NCLEXPN program pass rate of 75% or greater in 2019 and 84% did so in 2020.
Illinois NCLEX Score Analysis
As shown above, there was a drop in the percentage of nursing students who passed the NCLEX in all categories for 2020 as compared to 2019. While overall, the drop of 0.45% was not statistically significant, Illinois programs realized a decline in the NCLEX pass rates in 2020, and it was the resilience, creativity, and innovation demonstrated by all Illinois nursing programs during the pandemic that was significant. This article from nurse.org provides some insight for the lower pass rates, including having student clinicals delayed or canceled. Beyond the changes made to many nursing programs as a result of COVID, the article also outlines some changes that were made to formatting and scheduling NCLEX.
Apart from all nursing and NCLEX-related factors, the last factor to consider is that the COVID-19 pandemic
has been stressful for many people. The high degree of external stress is another potential contributing cause.
Confidence in our Illinois Colleges and Universities
Despite the drop in the percentage of students who passed, IACN has confidence in both our nursing students and in our colleges. A significant piece of data is that the pass rate of Illinois candidates who sit for the NCLEX is consistently higher than the national average. In 2020, 88% of Illinois candidates passed the NCLEX-RN while 87% did so nationally. For the NCLEX-PN, 87% of Illinois candidates passed the NCLEX-PN while the national pass rate was 83%. We have much to be proud of relative to the commitment of Illinois nursing graduates and programs. Illinois nursing faculty continue to promote strategic innovation and sensitivity to their students to facilitate success as graduates. Learn more about how IACN institutions have adapted in the face of the COVID-19 pandemic here.
CONTINUING E D U C AT ION OFFERING
Being Nimble: Adjusting to the Pandemic in the Academic Setting
Author: Linda Anders, MBA, MSN, RN, CSRN, NPD-BC
Purpose: To aid in the education of nurses in Illinois about the struggles of nursing education, both faculty and students during the recent pandemic while attempting to recover and establish a new normal.
Objectives: Upon completion of this reading, the participants will:
1. Recall the background of nursing education and what nursing education looks like today
2. State various ways nursing students struggled throughout their academic career during the pandemic
3. Describe how faculty and nursing students can be supported as healthcare moves forward after the pandemic
Nurses are in virtually every space and place, in every corner of each community. There is so much more that nurses bring to our society than what is acknowledged or seen on a daily basis. An essential component of the profession of nursing that often gets overlooked is aiding in the development of nursing students and new nurses. With surging of the Coronavirus, elimination of nursing students in the hospital setting, and challenges with faculty, the last year has been nothing short of a challenge. Students and faculty struggled to be nimble and change with the evolving situation. There are many aspects to unpacked and explore in relation to the academia side of nursing and the new difficulties that have developed.
History of Nursing Education
“Formal nursing education began at the end of the 19th century when events such as the Civil War and the Industrial Revolution emphasized the need for well-trained nurses” (Ervin, 2017, p. 5). In America, the Civil War can be coined the start of the formalized nursing education. Many soldiers died due to the women who transitioned from being at home to the battlefield to help without proper training or education, lack of resources, and lack of adequate hygiene (Ervin). As soldiers were dying, it was very apparent that nurses needed a structured, formal education.
With the development of formal education, the Nightingale educational model was embraced. This model allowed and encouraged nursing education to be autonomous, meaning not necessarily reliant on the hospitals. The Nightingale educational model focused on education and not just the nurses providing a free service to the hospitals (Ervin, 2017). This approach was radical at the time and challenged the status quo as they knew
it. Unfortunately, this educational model eventually was no longer the standard. In the early 20th century, the foundational pieces of the Nightingale educational model were discarded, and service became the first priority of nursing school with education as a second priority (Ervin). It was not until the 1950s that schools of nursing were moved to the university setting to allow for nurses a more comprehensive education to be able to provide competent care to more complex patients with “incurable” conditions (Nurse.com, 2012).
Current Educational State
As the years have progressed, so has the acuity of the patients that nurses are required to provide care for. Increasing acuity of patients makes both bedside nursing a bigger challenge and complicates what nursing education and clinicals look like today. Factoring in complex disease processes, the current formal nursing education provides dense course work in relatively short periods of time. This short timeline results in challenges for retaining the content and applying such with critical thinking. A few written interviews were conducted to gain insight to the perspectives of what truly is the current educational state from the view of a faculty member and a nursing student.
Clinical Aspect
One associate professor of nursing at Trinity College of Nursing and Health Sciences described the current state:
“Last fall, we experienced a surge of COVID-19 in our area and reached the point where there were no patients to take care of because all patients were either COVID positive or pending. We used case studies that were peer reviewed and validated for clinical hours, but there is nothing like real clinical experience to apply theory to practice” (M. Wildermuth, personal communication, May 22, 2021). The clinical experience is essential to take the content and theory taught and learned in the classroom and apply in real life practice situations while critically thinking through complex situations within the context of the health care system (Woodley, 2018).
The lack of clinical experience was also identified by the nursing students themselves. One nursing student, Rumler (personal communication, June 10, 2021) who is attending an associate degree program in nursing in Illinois stated that she had to swiftly pivot in the spring 2020 because she was, “quite literally stuck teaching myself how to be a
nurse”. Rumler (personal communication, June 10, 2021) goes on to expound on her experience by saying, “The inhospital clinicals help the most. I just know that my hours are not near enough of what they would have been. I missed out on so many opportunities to practice skills. I, to this day, have never: started an IV, inserted a catheter, inserted a NG tube, tested glucose, or given any sort of injection”.
Virtual Classroom
In additional to the lack on-site clinical practice, classes transitioned from in-person to online causing additional stress to both the students and the faculty. As the written interview continued, Wildermuth (personal communication, May 22, 2021) discussed the current situation with faculty: “Faculty burnout is detrimental to both faculty and students, and once again it is important for leadership to recognize the need for support and adequate resources so that faculty can achieve work-life balance and in turn bring their best selves to the classroom and clinical”. Work-life balance became ever more important while trying to navigate the pandemic and trying to ensure students were staying on track to meet their educational milestones in a virtual setting.
Rumler (personal communication, June 10, 2021) mentioned the fact that she saw her classmates that had children and worked as superheroes. “I still tell them every day that they are superheroes for going through nursing school, with children in a pandemic. Some of them worked, taught themselves, and their children”. The mandatory virtual classroom placed additional strain on the already stressed nursing student.
Online Classroom Incivility
One unforeseen situation that came to light with the virtual classroom was the persistent accusations from professors of students cheating. Rumler (personal communication, June 10, 2021) expressed that the accusations of online cheating was mentally exhausting and frustrating. Various news outlets began to highlight increasing numbers of academic cheating during the pandemic when classes were entirely virtual. One article published by CBC News stated that contract cheating had increased almost 10 times during the pandemic (Rossiter, 2020). As faculty had a basis to be concerned, which was amplified in the media, Rumler (personal communication, June 10, 2021)made mention that it was a challenge when accused of cheating since she put the hard work and dedication in to learn the material while she felt the instructors were mostly unavailable to her.
The online environment is also prone to bullying and students being uncivil towards each other. The expectation for the virtual classroom is the same as if in-person where individuals are expected to be respectful of each other. The evidence, however, has shown that the online learning environment is more vulnerable to bullying and incivility (De Gagne, 2018). If the virtual environment was not fostered to be a safe space for learning, the effects lead to detrimental issues in our future nursing workforce.
Providing Support
The pandemic created a space of uncertainty in everyone’s lives which made providing support even more challenging. Students and faculty not only had to transition the way that they taught and learned, but inevitably everyone shifted their place on Maslow’s hierarchy of needs which changes the way the support needs to be provided. The daily thought processes of individuals transitioned from being complex and critically thinking through processes and problems to basic needs and concerns for safety of themselves and their families.
The Maslow Shift
“According to Maslow, during emergencies emotions may refer mainly to the first three levels of the pyramid of needs: physiological, safety, love and (social) belongingness” (Cerbara et al., 2020, p. 7156). In addition to emotions, one could argue that all aspects during an emergency such as a global pandemic transition back to the base levels of the pyramid. With the review of the pyramid and the surging of COVID-19, it appears that everything except the things associated with survival of persons and family are less important (Cerbara et al.).
This change was extremely evident at the very beginning of the pandemic as we saw Americans mass purchasing essential items like toilet paper, paper towels, and antibacterial wipes. Instead of being mindful and conscious of the fact that the pandemic did not cause any extreme gastrointestinal concerns, many purchased packages and packages of toilet paper leaving some without access. This painted a clear picture of individuals and their shift in the pyramid from Maslow’s hierarchy of needs as they acted out of concern for their safety.
Social Learning Theory
A crucial component of support for both faculty and students includes the social aspect of the academic setting. As we know, humans are social beings. The social learning theory explains that learning takes place through social interactions. Learning is not only behavioral but also cognitive where the learner is not a passive recipient of content and information, but rather cognition, environment, and behavior all influence each other (Power & Warren, 2021).
In identifying ways to support students and faculty, it is important to keep the social learning theory concepts in mind. The pandemic enforced isolation which made learning and teaching much harder. Rumler (personal communication, June 10, 2021) expressed that she struggled as she no longer had fellow students to bounce ideas off, but rather had to attempt to critically think in a one-bedroom apartment completely isolated. Rumler went on to explain the questions she struggled with during the pandemic in relation to her learning: Am I good enough to do this? Am I supposed to be a nurse? Will this ever get easier? These questions about the educational journey and career pathway were coupled with the constant battle of wanting to blame instructors for “not being there”.
Moving Forward
The pandemic propelled nursing into this new, unprecedented area for both faculty and nursing students. This area of resilience is like none other which requires support from everyone moving forward. The pandemic is not over just yet with protocols, policies, and roles continuing to evolve as we adjust to this new way of life and are starting to see different variants of the virus surfacing. Blake (2021) said it best when describing building a new normal by stating there are five requests of nurses that should be taken into consideration: hear me (feedback), protect me (adequate supplies), prepare me (training), support me (physical needs), and care for me (holistic support).
Support and Getting Through This Together
Teamwork is a foundational building block for an effective nursing team, but through the pandemic working together now seems to mean something different. “Going forward, know that you’re not alone in any challenge you face. You’re stronger as an involved and committed member of your team” (Gelinas, 2021, p. 5). As nurses were banning together across the globe, their voices were being heard. This ability to be heard offered a sense of strength and support.
The concept of getting through something traumatic and devasting as the pandemic applies to all: the bedside
nurses, faculty, and the student nurses. The weight of the events that the nurses have been through is felt at all levels. Nurses at the bedside experienced constant inadequate staffing, frequent deaths of patients, and less than appropriate personal protective equipment. As students have begun to filter back into the bedside nurses’ space, the bedside nurses have been perceived as irritable. This perceived agitation with students can be associated to feelings of instability related to moral distress as well as feelings of anger, frustration, and anxiety (Cacchione, 2020). As with students and faculty, the bedside nursing profession has not had the adequate time to decompress, debrief, or work through the emotional, physical, and mental hardships that the global pandemic inflicted upon them. One key component is for faculty and students to support each other and the bedside nurse to ensure that the student nurse gets a safe educational experience.
Seeking Help
For many years there has been a stigma associated with mental illness. Nursing is not immune to this stigma. In a literature review performed by de Jacq, Norful, and Larson (2016), there is evidence that nurses had negative thoughts and perceptions of individuals with mental illness and are more negative about mental illness than physicians. With these preconceived ideas and negative perceptions of mental illness, it is challenging to openly seek help. “During the pandemic, rates of depression and anxiety tripled with healthcare workers being at higher risk for experiencing depression and anxiety. The COVID-19 pandemic has highlighted a gap in mental health needs of nurses during extended high-intensity conditions” (Serrano et al., 2021, p. 31).
During the height of the pandemic, many facilities offered employee assistance program (EAP) counseling to help employees process through their situations and emotions. However, in many situations, the EAP counseling did not apply to students. Without access to EAP, students experienced a gap in mental healthcare as compared to the hospital-based nurses. However, it is important to note that in addition to EAP opportunities, cognitive behavioral therapy (CBT) is a great option. CBT can be done virtually or in an office setting with a trained therapist. Cognitive behavioral therapy has been shown to significantly aid in the treatment of mental health disorders such as anxiety and depression and is a great avenue to process thoughts, feelings, and emotions in a safe space.
Self-Care
Self-care has been a buzz word even before the pandemic. There are many beliefs about what self-care is varying from things like taking a bath to getting a pedicure to treating yourself to a delicious coffee drink. Self-care can be anything from individual habits, customs, or a set of beliefs (da Silva Junior et al., 2020). It is essential for each nurse, no matter what their role, to identify what it means to care for themselves, to rejuvenate and recharge.
Some suggestions for self-care would include journaling daily to process thoughts and feelings, yoga and mindful meditation, going on walks, or even a soothing bubble bath. By embracing various self-care habits and incorporating them into the nurses’ daily lives, they show up as better people. Understanding how to perform selfcare techniques helps to facilitate growth of nurses both personally and professionally which could lead to better learning environments for students and better teaching environments for faculty (da Silva Junior et al., 2020).
Embracing Innovation
The last way for the profession to move forward would be through embracing of innovation. The pandemic has propelled nurses into waters that were unchartered before with innovation in almost every conversation. However, it is worth noting that nurses have been innovating since the beginning of the profession, but this has just been deemed as ‘part of the job’. “Because nursing is a knowledgeintensive profession, nurses have a deep understanding of clinical needs and can identify and communicate ideas and opportunities for improvement” (Sensmeier, 2021, p. 15).
Innovation at the bedside is essential, but innovation for students and faculty is just as important. As faculty pivot to make adjustments to each class, students need to embrace being nimble and willing to adjust accordingly. Students and faculty can also be somewhat of an incubation hub stepping into the clinical space for short periods of time seeing care from a different lens as the bedside nurse and offering innovative ways to perform care. “New generations of nurses are entering the workforce more comfortable with technology-driven innovation and embracing a creative spirit” (Sensmeier, 2021, p. 16).
Conclusion
The pandemic has brought numerous struggles to the nursing profession. Faculty and students were not exempt from these struggles. The pandemic propelled the nursing academia to pivot quickly to embrace a new way
of learning and teaching. Nursing faculty and students alike experienced unique difficulties but were able to be agile and changed to embrace the restrictions placed upon them all while embracing innovative ways to learn and grow. As we begin to establish the “new normal”, it is important to take care of oneself and support one another no matter what the role in the nursing profession is.
References available upon request
CE Offering
1.0 Contact Hours
This offering expires in 2 years: September 09, 2023
Learner Outcome:
80% of those reading the article and completing the post-test will self-report increased knowledge of the struggles faced by nursing students during the pandemic and support efforts for students and faculty post-pandemic.
HOW TO EARN
CONTINUING EDUCATION CREDIT
This course is 1.0 Contact Hours
1. Read the Continuing Education Article 2. Go to https://www.surveymonkey.com/r/ SelfStudy09-2021 to complete the test and evaluation. This link is also available on the INF website www.illinoisnurses.foundation under programs.
3. Submit payment online.
4. After the test is graded, the CE certificate will be emailed to you.
HARD COPY TEST MAY BE DOWNLOADED via the INF website www.illinoisnurses.foundation under programs
DEADLINE
TEST AND EVALUATION MUST BE COMPLETED BY SEPTEMBER 09, 2023
Complete online payment of processing fee as follows: ANA-Illinois members- $8.00 Nonmembers- $15.00
ACHIEVEMENT
To earn 1.0 contact hours of continuing education, you must achieve a score of 80%
If you do not pass the test, you may take it again at no additional charge
Certificates indicating successful completion of this offering will be emailed to you.
The planners and faculty have declared no conflict of interest.
ACCREDITATION
Illinois Nurses Foundation is approved as a provider of nursing continuing professional development by Ohio Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation. (OBN-001-91)
CE quiz, evaluation, and payment are available online at https://www.surveymonkey.com/r/ SelfStudy09-2021 or via the INF website www. illinoisnurses.foundation under programs.