4 minute read
Polodoc: Fractured and Dislocated Shoulder


Dr.med. Andreas Krüger is a Swiss board orthopaedic and trauma surgeon in Zurich, who specialises in knee and shoulder surgery. Andi is a second generation of tournament doctors for equine sports, known as Polodoc since 2013
Fractured and Dislocated Shoulder
Advertisement
Fix it or leave it?
Upper extremity injuries are common and resulting problems are either stiffness or instability. One of the best-known examples is the young Winston Churchill who injured himself while being a Cavalry Officer, “We came alongside of a great stone wall with dripping steps and iron rings for handholds. The boat rose and fell four or five feet with the surges. I put out my hand and grasped at a ring; but before I could get my feet on the steps the boat swung away, giving my right shoulder a sharp and peculiar wrench.” Churchill wrote that this injury was to last him all his life. It would “cripple me at polo… prevent me from ever playing tennis, and [prove] a grave embarrassment in moments of peril, violence and effort.” In fact, as he noted in November 1897, he suffered a total dislocation as he “slipped on a stone stair” prior to competing in the InterRegimental Polo Tournament in Meerut, India in 1899. Despite this handicap, his regimental team won the tournament, Churchill scoring two goals with his right elbow strapped to his torso with a leather harness! All this personal misery is well documented at the international Churchill society. As you can read there – a simple slip can change the whole sporting life of an ambitious polo player. Current advantages in treatment possibilities, with new techniques in shoulder stabilization give far more favourable results with stability and adequate range of motion.
Injury Pattern
A dislocated shoulder is an injury in which the upper arm bone pops out of the cupshaped socket that’s part of the shoulder blade. The shoulder is the body’s most flexible joint, which makes it more likely to dislocate. The anterior shoulder dislocation is the most common injury. Due to the anterior impact the joint capsule and the rim of the shoulder is prone to injury. This happens with falls on an outstretched arm or during the swing when the mallet is stopped by an opponent. When a dislocation happens in a high-speed environment or with an external impact, shoulder fractures may also occur. Nerve or blood vessel damage in or around the shoulder joint may also take place. Shoulders can also become more prone to repeat dislocations, especially if the injury is severe.
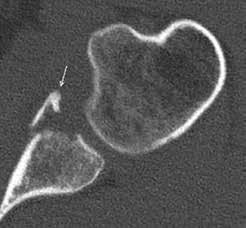
CT picture after dislocation with fracture of the socket rim.

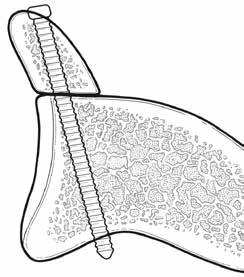
Humerus head with impact and displaced fragment Latarjet bone block fixation with screw fixation


Bone block procedure with screw fixation

MRI picture with soft tissue injury of the capsule
Diagnostics
Initial clinical examination on the field can be difficult due to extraordinary pain. Dislocated shoulder symptoms can include: • A visibly deformed or out-of-place shoulder • Swelling or bruising • Intense pain • Inability to move the joint
Secondary examination follows in the hospital with an X-ray to see whether the shoulder is still dislocated or if it was subluxated without any additional bony injury. To fully assess the soft tissue an additional MRI is needed. If the primary conventional X-ray reveals a suspect bony injury a secondary CT can be helpful to precisely detect the extend.
Treatment
First time dislocations without any bony injury can be treated conservatively. Physiotherapy with muscle stabilisation and a structured return to full motion can be successful when done properly. A bandage with restriction of abduction and external rotation (full swings limited) can be helpful. With recurrent dislocation occurring an operation with soft tissue repair is required. When primary or secondary bone damage is present a more invasive bone block procedure is
MRI picture with impression on the head

Suture of the labrum (soft tissue) with bone anker
needed to achieve stability. When scarring or capsule stiffness occurs, there can be a restriction of the free range in the upper sector or in combination with external rotation, which can be limiting to perform a nice swing.
Recommendation
First time dislocation can be very successfully treated conservatively. Meticulous work up of all dimensions of the injury is recommended to precisely indicate the adequate treatment pathway. Current research shows a lower recrudescence rate when bone block procedures are performed.

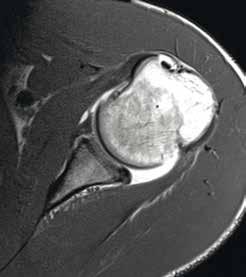
MRI picture with lesion of the capsule and partial bone injury to the lower anterior rim of the cup

Soft tissue repair with Pushlock anker fixation
For more information on Polodoc contact Andreas Krüger at drmedkrueger@gmail.com or www.polodoc.ch
Subscribe now
Why not treat yourself or a friend to Polo Times? Call our friendly subscriptions team: 01452 730 770 or visit www.polotimes.co.uk
iPad