Beyond EDSS: How to monitor disease progression in MS
Prof. Dr Bart Van Wijmeersch
• Define ‘disease progression’ or ‘progressive disease’
– From R(R)MS and SPMS/PPMS, to ‘smoldering disease’
– Clinical visible progression: RAW + PIRA = CDW
– Need for early detection, preferably on the sub-clinical level?
• How to monitor beyond the EDSS, beyond the simple neurological examination
– Clinically
– PRO’s
– Imaging
– Biomarkers
– Neurophysiology (OCT/ Electrophysio)
• Application in clinical practice and on individual level
– ‘monitor chart/ step-based approach’
Defining Progression
No clear criteria exist to determine the conversion from RRMS to SPMS 1,2
Progressive worsening of baseline between relapses signifies transition to SPMS 3
SPMS
Transition from relapsing to progressive course
Clearly defined disease relapses3
Full recovery or recovery with residual deficit3
CNS, central nervous system; CSF, cerebrospinal fluid; RRMS, relapsing–remitting MS; SPMS, secondary progressive MS
1. Lublin FC et al. Neurology 2014; 2. Katz Sand I et al. Mult Scler 2014; 3. Lublin FD, Reingold SC. Neurology 1996; 4. Lassmann H et al. Nat Rev Neurol 2012; 5. Bischof A et al, 2018. Accelerated cord atrophy precedes conversion to secondary progressive disease in relapsing multiple sclerosis
or without relapses
SPMS is generally diagnosed retrospectively based on history of gradual worsening1,2
Available at: https://onlinelibrary.ectrims-congress.eu/ectrims/2018/ectrims-2018/228123/antje.bischof.accelerated.cord.atrophy.precedes.conversion.to.secondary.html. Accessed 08 Nov 2018; 6. Housley WJ et al. Clin Immunol 2015
Research is ongoing to identify imaging and biomarkers (e.g. blood or CSF) for early detection of SPMS 5,6
Progression independent of relapse activity (PIRA)
When does Progression begin?
Preclinical phase Secondary-progressive phase
Clinical disability
Brain volume
Disease burden
CLINICAL TRESHOLD
MRI activity
Adapted from Hersh C, Fox R. 2014. Available from: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/neurology/multiple_sclerosis
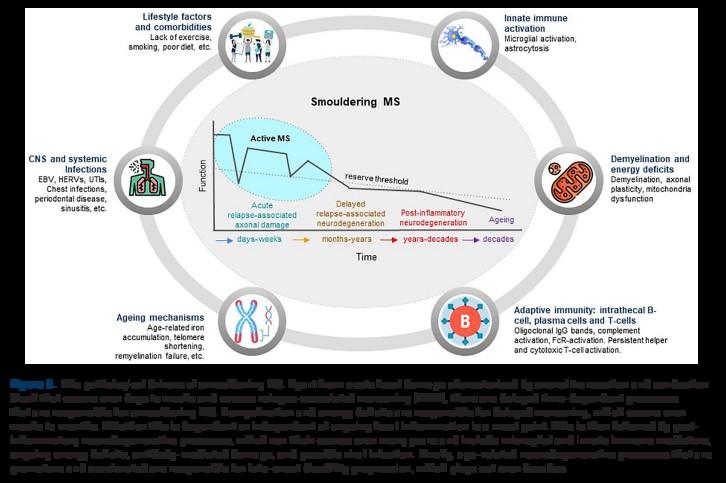
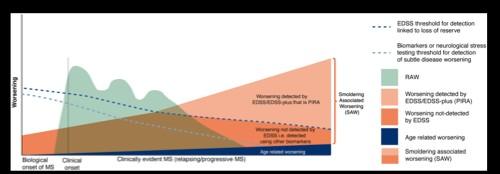
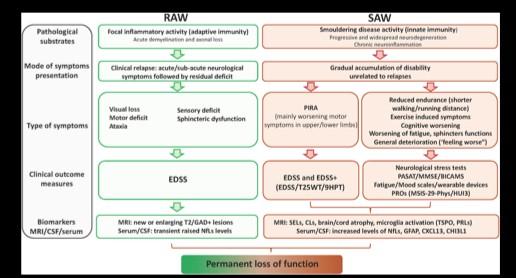
Definitions: ‘smoldering associated worsening’
Definition:
Smouldering disease in MS is an umbrella term characterizing chronic pathobiological processes occurring in the CNS, beyond acute inflammation, associated with neurodegeneration and may manifest clinically as physical worsening, functional deficits and cognitive decline.
A. Scalfari, et al. Ann Neurol. 2024 Jul 25. doi: 10.1002/ana.27034.
Definitions: ‘smoldering associated worsening’
A. Scalfari, et al. Ann Neurol. 2024 Jul 25. doi: 10.1002/ana.27034.
Definitions: ‘smoldering associated worsening’
A. Scalfari, et al. Ann Neurol. 2024 Jul 25. doi: 10.1002/ana.27034.
How to monitor beyond the EDSS Beyond the Neurological examination
Biomarkers
Neurophysiology (OCT/ Electrophysio)
Clinically beyond EDSS
• Cfr Definition of PIRA = EDSS+
– As measured by EDSS or >20% progression in T25 FW or >20% in 9HPT.
Timed 25-Foot Walk (T25FW) measures quantitative mobility and leg function performance
• The patient is directed to one end of a clearly marked 25-foot course and is instructed to walk 25 feet as quickly as possible
• The time from the initiation of the instruction to start to when the patient has reached the 25-foot mark is recorded
• The test is immediately administered again by having the patient walk back the same distance
• Standardized instructions need to be provided and it should be documented whether the test was performed with or without walking aid(s) and, if possible, the same testing condition should be maintained throughout the trial
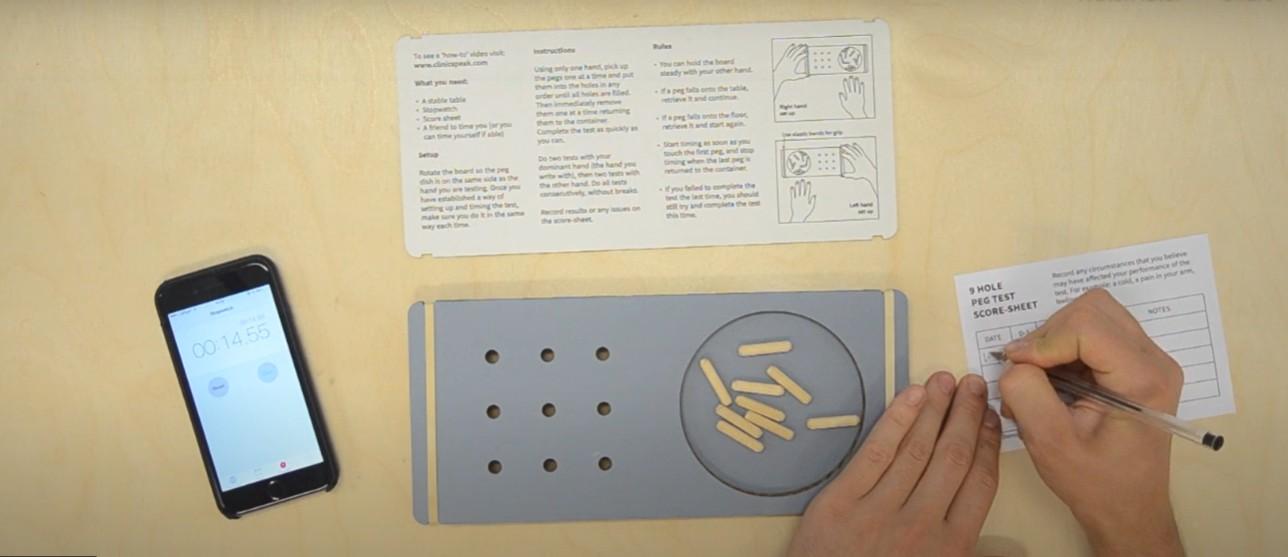
9-HPT
The 9-HPT is a brief, standardized, quantitative test of upper extremity function. It is the second component of the MSFC to be administered at each visit. Both the dominant and non-dominant hands are tested twice. The patient's dominant arm is tested first. Instruct the patient to: o “Pick up the pegs one at a time, using your right (or left) hand only and put them into the holes in any order until the holes are all filled.
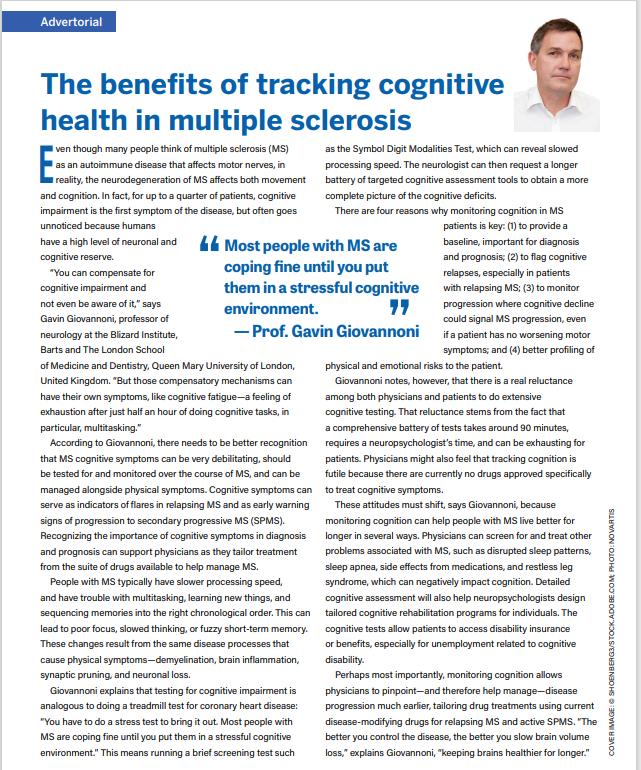
There are four reasons why monitoring cognition in MS patients is key:
(1) to provide a baseline, important for diagnosis and prognosis;
(2) to flag cognitive relapses, especially in patients with relapsing MS;
(3) to monitor progression where cognitive decline could signal MS progression, even if a patient has no worsening motor symptoms;
(4) better profiling of physical and emotional risks to the patient
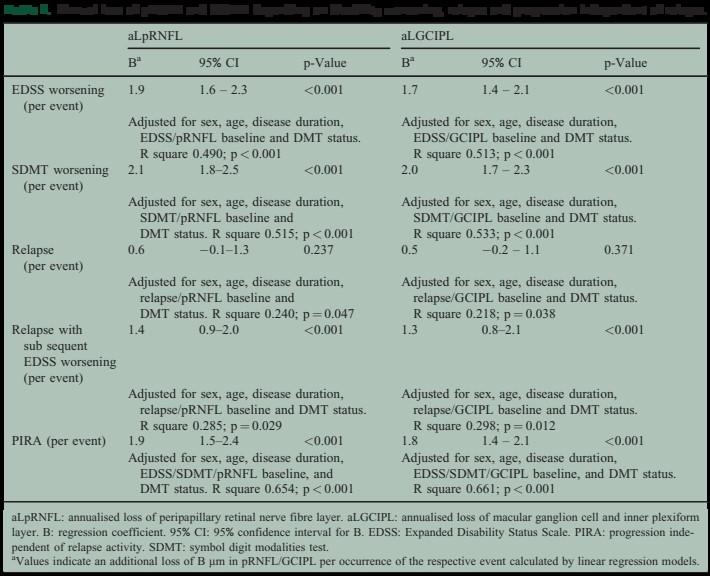
Long-term worsening is common in RRMS patients and is largely independent of relapses or new lesion formation on brain MRI
Typically, these patients have low EDSS scores and are for the most part fully functional
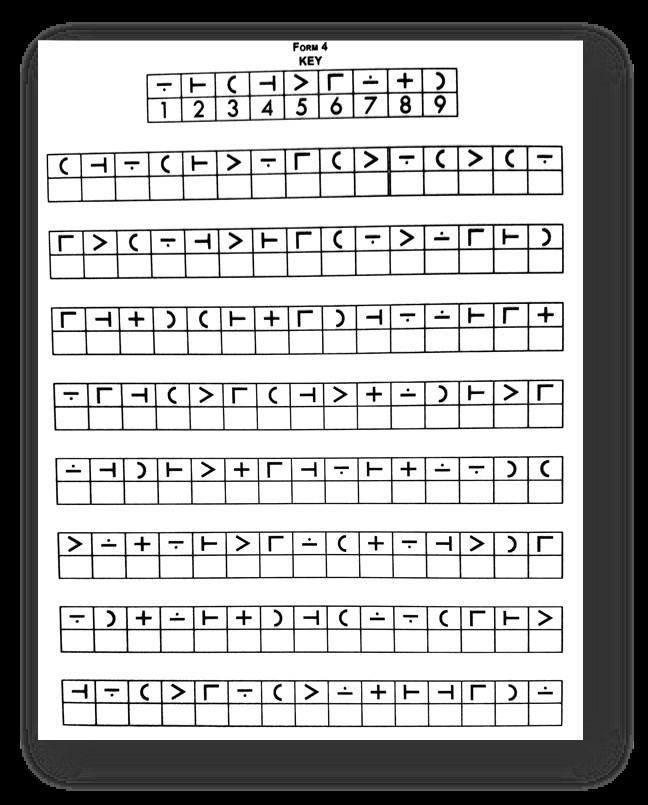
The Symbol Digit Modalities Test (SDMT)
Symbols are paired with the digits 1 to 9; the patient provides the corresponding digit for a given symbol
Tests attention, visuoperceptual processing, working memory, and psychomotor speed
The single most robust predictor of employability and overall ADLs
A raw score change of 4 points is considered clinically meaningful
– Individual level: 8 points change needed!
Not sensitive to self-reported impairment of cognitive function
Test influenced by visual acuity and ocular motor function
Functional testing “stress tests”
• Longer distance walking:
– 2 or 6 minute walking test
• Assessing fatigability
Walking Fatigability
Cognitive Fatigability
• Motor-Cognitive interaction
– Dual Task Cost
• Physically high-challenge measures
– balance and upper extremity coordination
How to monitor beyond the EDSS Beyond the Neurological examination
• Objective versus Subjective measure’s
• Active (Questionaire) vs Passive (Registrations)
• Group vs Individual Results
• Clinically meaningfull change?
• Which PRO’s to use?
Walking
Cognition
QoL
Pain
Bowel & Bladder
How to monitor beyond the EDSS Beyond the Neurological examination
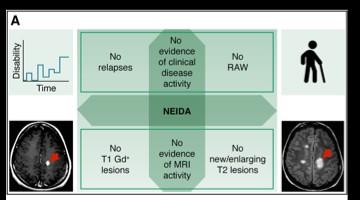
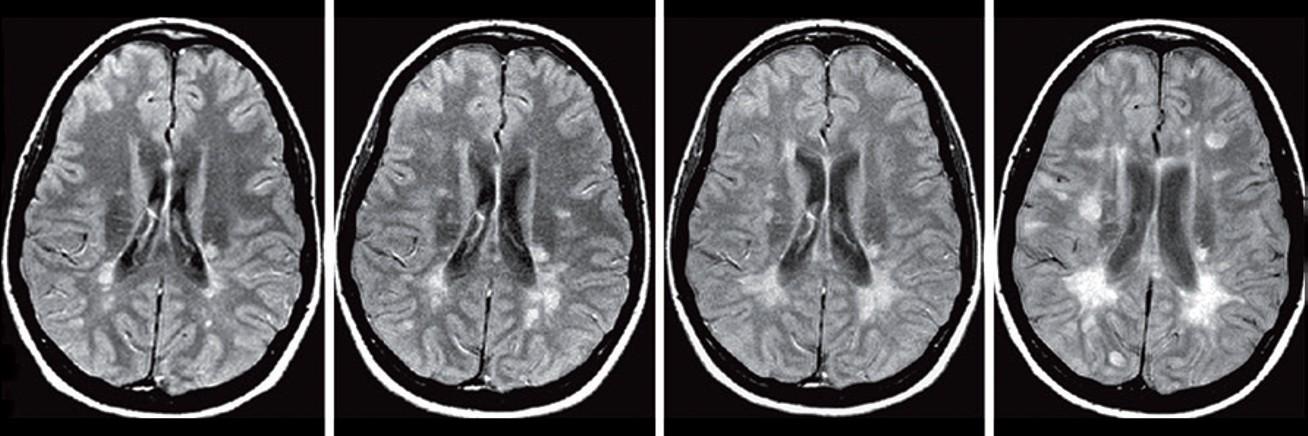
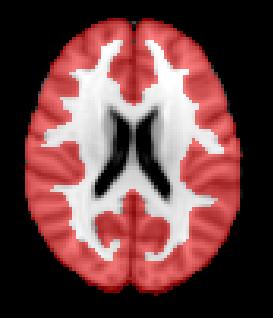
Conventional MRI biomarkers for MS progression
- Slowly Expanding Lesions (SEL’s)
Serial MRI in a patient with relapsing–remitting multiple sclerosis. Proton-density weighted MRI scans obtained at a | baseline, and b | 1 year, c | 2 years and d | 3 years later. Disease progression can clearly be seen in the form of new and enlarging focal lesions over time, shown here as hyperintensities (white spots).
aT2-LV reflects neurodegeneration and has demonstrated sensitivity to MS progression1,2
1. Zivadinov R, et al. Am J Neuroradiol 2019;40:446–452; 2. Dwyer MG, et al. J Neuroimaging 2018;28:490–495; 3. Genovese AV, et al. Radiology 2019;293:424–33.
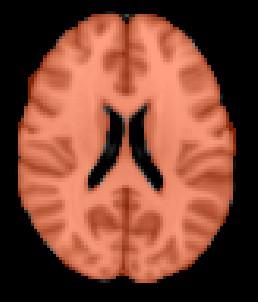
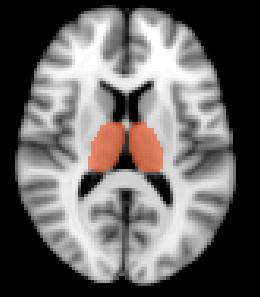
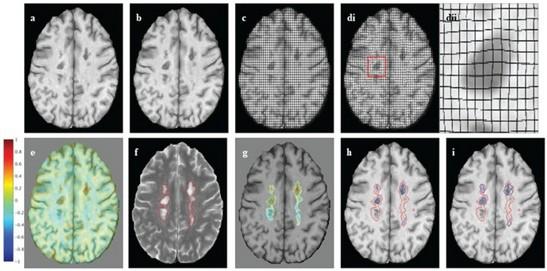
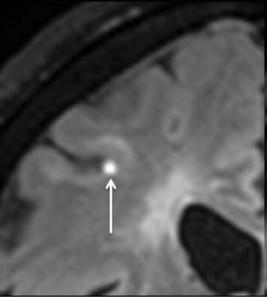
Advanced MRI biomarkers for MS progression
Changes in brainvolume are predictive of clinical and
disability status in CIS, RRMS, and PPMS
Advanced MRI biomarkers for MS progression
Spinal cord atrophy rates in patients with RRMS versus patients who transitioned to SPMS:
mm / year
Patients who developed SPMS showed accelerated spinal cord atrophy rates before conversion compared with their RRMS matches (p<0.0001)
This difference exists at least four years before the conversion to SPMS
Upper cervical cord atrophy, as assessed by MRI, is a predictor of the conversion to SPMS
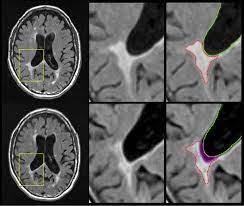
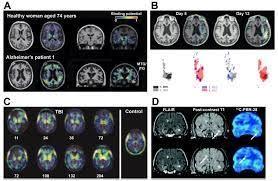
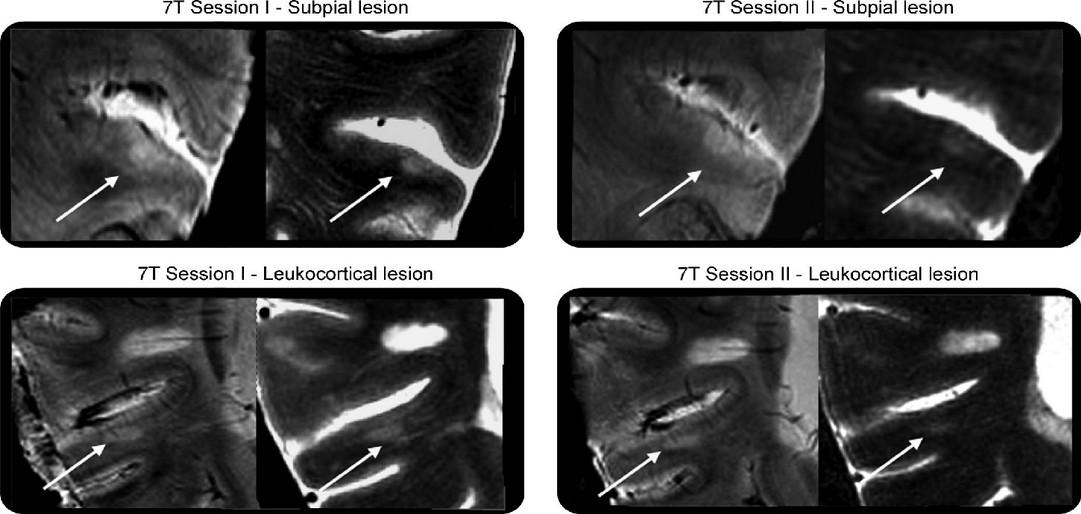
Advanced Imaging biomarkers for MS progression
Chronic pathology within existing lesions slowly expanding/evolving lesions
Microglial activation
transfer ratio1, 7 Tesla MRI2 , Deformation-based (Jacobian) analysis using conventional T2- and T1- weighted images3 , susceptibility-weighted imaging (SWI)4 and quantitative susceptibility mapping (QSM)4
How to monitor beyond the EDSS Beyond the Neurological examination
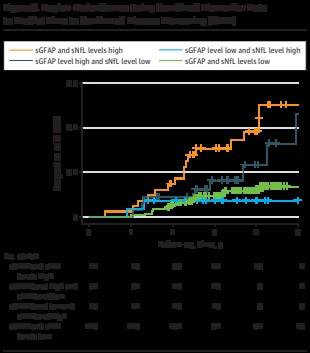
sNFL, sGFAP, sCHI3L1
How to monitor beyond the EDSS Beyond the Neurological examination
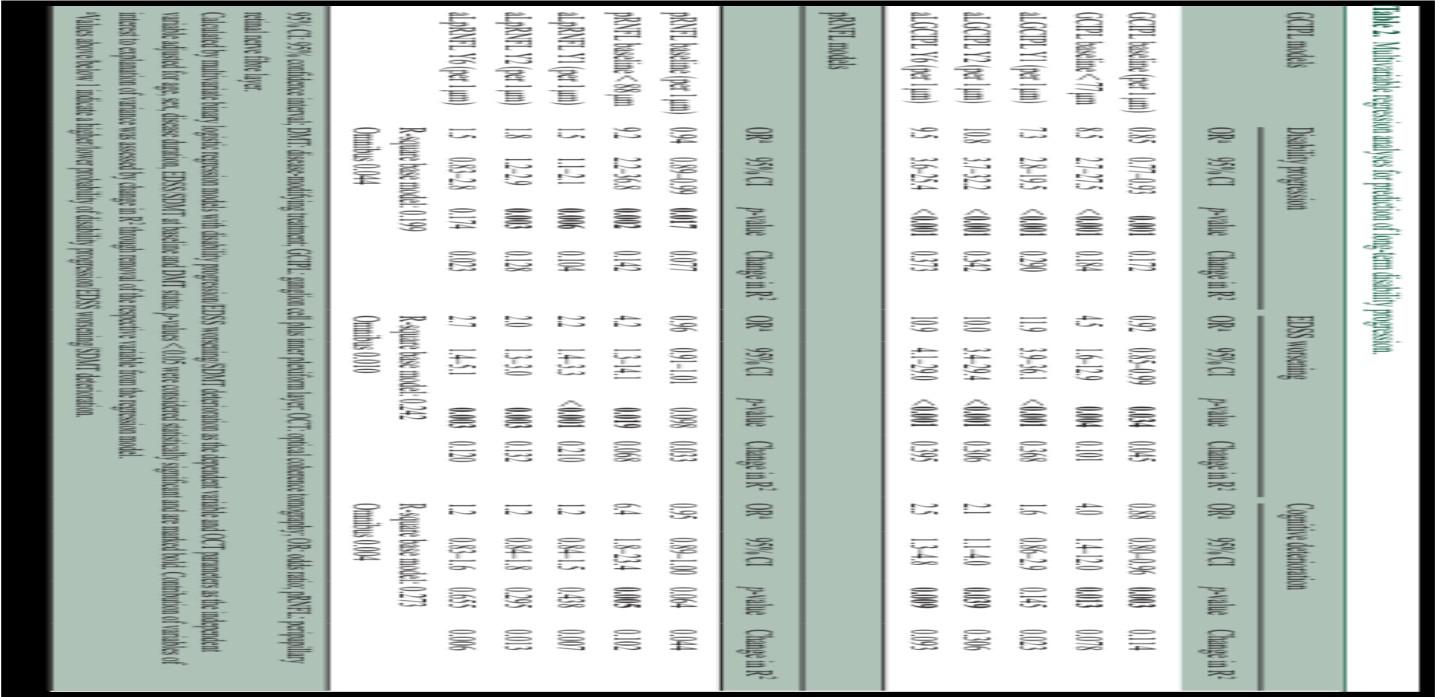
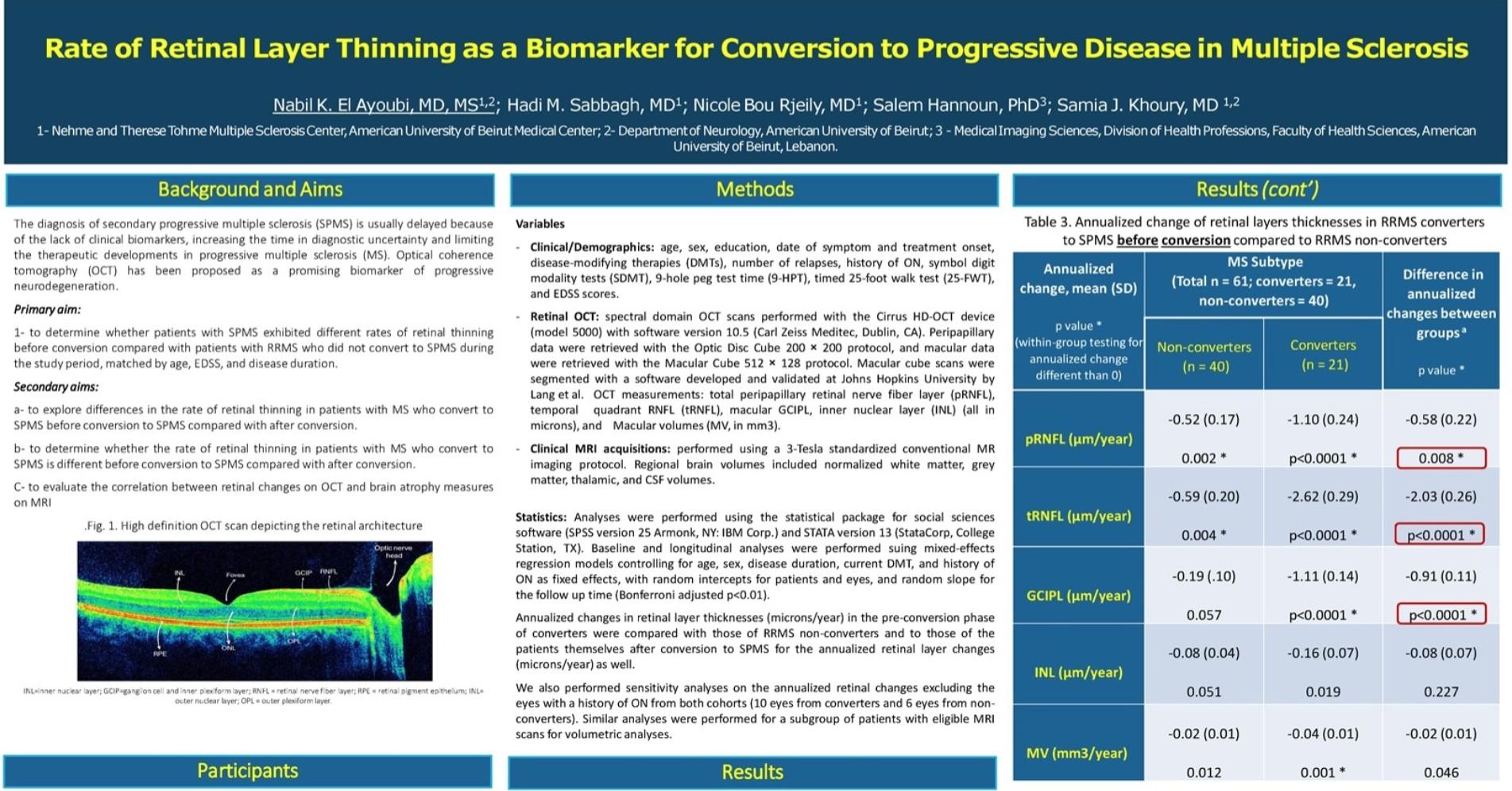
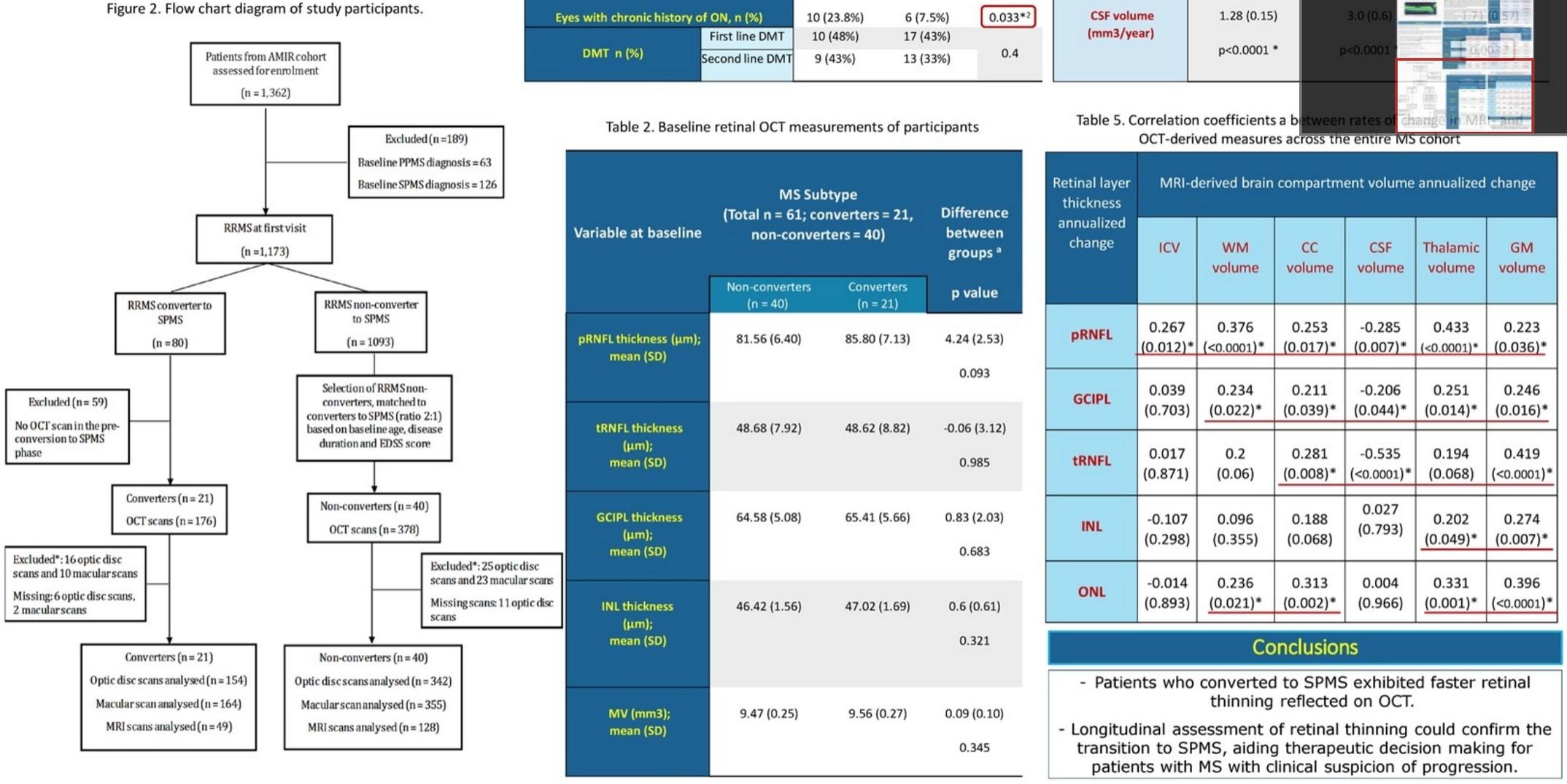
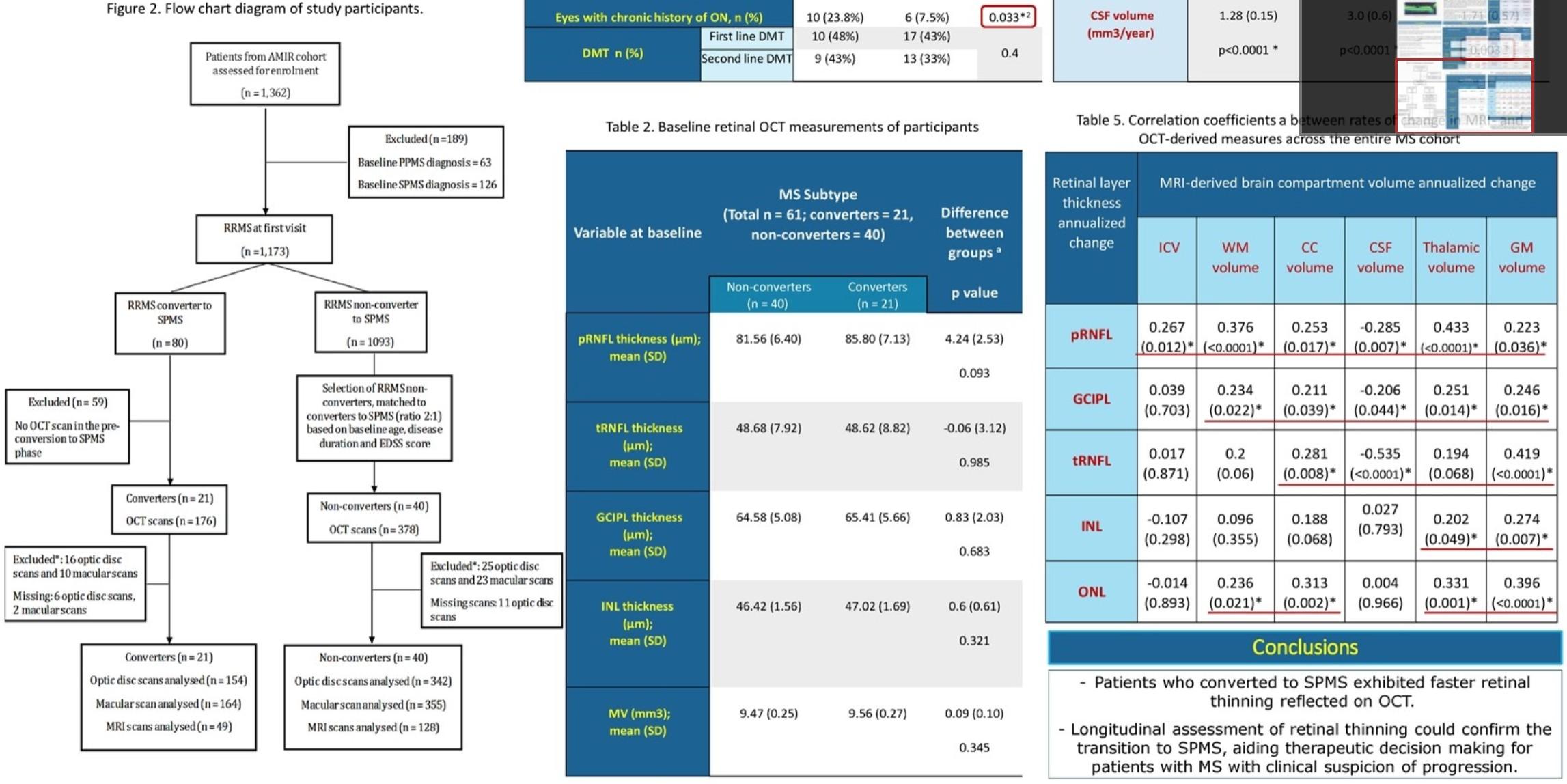
OCT monitoring of neurodegeneration
OCT monitoring of neurodegeneration
Follow-up of neurodegeneration/treatment
EP’s: VEP/SSEP/MEP (TMS)/Multimodal
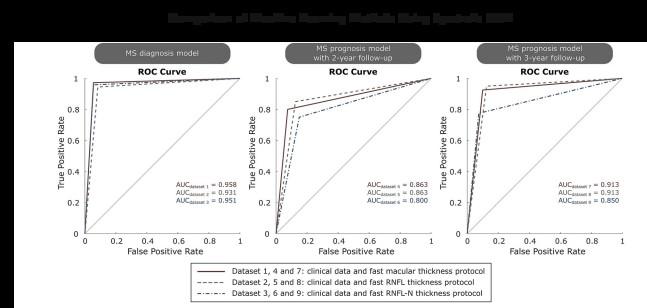
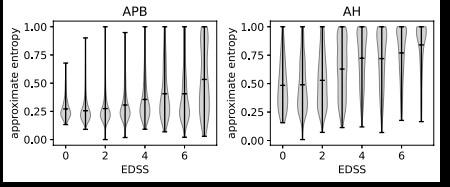
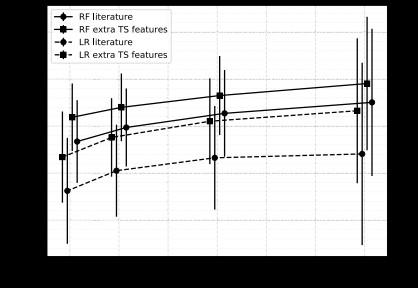
Machine Learning /AI techniques
Machine Learning /AI techniques
Application in clinical practice and on individual level
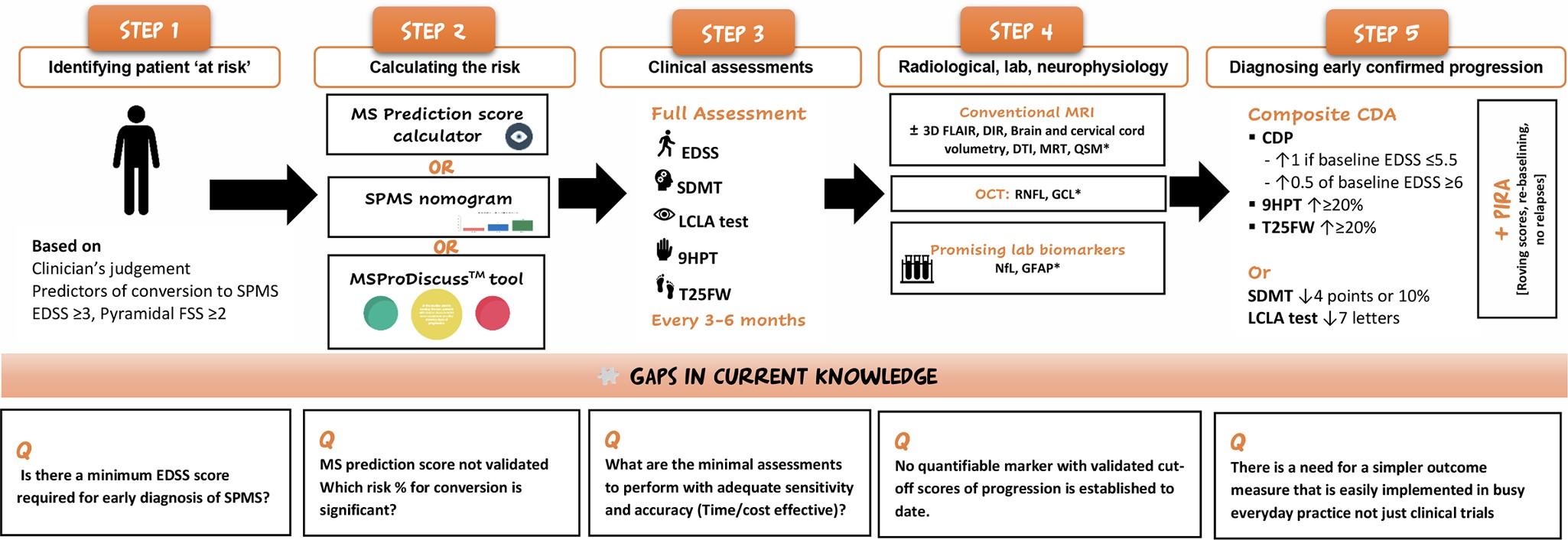
Step 1 & 2: Who is at risk & What is the risk
• Good ‘talk’ (anamnesis) with patient might reveal possible progression
• PRO’s as first level:
– Gap in between consultations
– Devices (passive) vs Questionaires (active)
• Detection of other influences on functionality (co-morbidities, infections, psychosocial factors, disuse, age,…)
• Risk-assesment for SPMS:
– MS predictor score calculator (not validated)
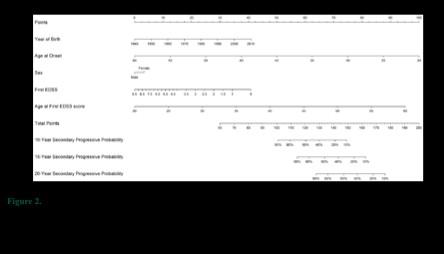
– MS normogram (@RRMS onset)(validated)
– MSProDiscuss tool (validated)
https://msprediction.com/calculator/
https://aliman.shinyapps.io/SPMSnom/
Step 3 & 4: Measures
• Confirmation & Objectivation of Progressive Disease
2. Exclusion of other explanations (co-morbidity & disuse)
3. Confirmed by measures (clinical & technical)
1+2+3 or 2+3 or 3 (subclinical) : red progressive disease, consider R/ adaptation
1+2: orange possible progressive disease, close follow-up vs early R/ adaptation
1 or none: green no progressive disease, continue routine follow-up
• BASIS = good standard multimodal follow-up of patients
• Weakness
- Group (= studies) vs Individual Level of Follow-Up
- Validation studies are often lacking
Thankyou
Prof. Dr Bart Van Wijmeersch
Associate Professor of Neurology at the University of Hasselt
Supporters
Funders support us via Independent Medical Education grants or Sponsorships. When sponsored, we aim for multiple sponsors of a single activity. For each activity we indicate the funding source and contractually agree on the independence of the content we produce.