22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: info@residerm.com
TEL: + 91 22 2345 1404
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“Residerm ” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of April -2025
RESIDERM: A RESIDENT’S PATH IN DERMATOLOGY & EMPOWERING THE FUTURE
Dermatology continues to hold its place as one of the most competitive and sought-after medical specialties. With such a strong academic foundation, dermatology residents are among the brightest, most skillful, and competent minds in medicine today. Their journey, however, begins with curiosity—and at times, confusion.
Recognizing the need for a dedicated platform that supports and encourages young dermatologists, “RESIDERM” was created to empower residents to express, explore, and evolve. Here, residents are given the freedom to share their experiences, showcase clinical insights, and find guidance from those who’ve walked the path before them.
Starting out in dermatology can feel overwhelming. From mastering complex diagnoses to finding one’s niche, it’s a journey of continuous growth. This platform aims to offer the right support—whether it’s helping residents make career-shaping decisions or enhancing their role in the broader learning ecosystem that includes peers, students, and institutions.
In this issue, we spotlight important areas within medical dermatology. The case report on Dowling-Degos Disease highlights a rare genodermatosis, emphasizing its clinical presentation, diagnostic challenges, and histopathological findings—shedding light on a condition often overlooked in routine practice. Additionally, we explore the psychosocial burden of acne through a study on the Dermatology Life Quality Index in adult acne vulgaris, underlining the importance of holistic assessment in managing chronic inflammatory skin disorders.
We’re sure you’ll find value in the perspectives shared. We also invite you to be a part of this growing community. Share your experiences, your cases, your questions— your voice matters.
Hope you have a great read!
We are looking forward to your contributions for the next issue.
Thanks & Cheers!
- Dom Daniel Executive Editor & Publisher
Dowling-Degos Disease: A Case Report
Dr. Adhishree Agarwal
2nd Year Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dr. Manan Gulati
3rd Year Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR,New Delhi
Dr. Ipshita Bhattacharya
Senior Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dr. Paschal Dsouza
MD, Dermatology
Professor & Head of Department
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
Dr. Tejas S Naik
MBBS, MD (3rd Year Resident)
Department of MD Dermatology, Venerology and Leprosy Goa Medical College and Hospital, Bambolim, Goa
Dr. Raghuvir Alias Tanmay M Kane
MBBS, MD (Senior Resident)
Department of MD Dermatology, Venerology and Leprosy Goa Medical College and Hospital, Bambolim, Goa
Dr. Varadraj V Pai
MD
Assistant Professor
Department of MD Dermatology, Venerology and Leprosy Goa Medical College and Hospital, Bambolim, Goa
Dr. P. Shukla
MD
Professor & Head of Department
Department of MD Dermatology, Venerology and Leprosy Goa Medical College and Hospital, Bambolim, Goa
Dowling-Degos Disease: A Case Report
Dr. Adhishree Agarwal
2nd Year Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dr. Manan Gulati
3rd Year Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dr. Ipshita Bhattacharya
Senior Resident
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Dr. Paschal Dsouza
MD
Professor & Head of Department
Department of Dermatology, Venereology and Leprosy
ESI-PGIMSR, New Delhi
Introduction
Dowling-Degos disease (DDD) is a rare, benign, autosomal dominant genodermatosis that usually
develop during adulthood around the age of 30-40 years.1 It is also referred to as 'Dark Dot Disease' and affects predominantly
women in a ratio of 2:1 and has no race predilection.2
Mutations in different genes like KRT5, POFUT1, POGLUT1 and, most recently, PSENEN are responsible for the clinical manifestation by affecting melanosome transfer, and melanocyte and keratinocyte differentiation.1 While mutations in the keratin 5 (KRT5) gene, which is responsible for cell adhesion and transfer of melanosomes, favor a reticular distribution pattern, mutations in the POGLUT1 gene lead to a disseminated, papular clinical picture.3
This disease falls within the category of classical Reticulate Pigmentary Disorders of the skin, which include presentations with “net-like,” “sieve-like,” or “chicken wire” configuration of the skin lesions, which vary in size and pigmentary content.
DDD is characterized by acquired reticulate hyperpigmentation over the flexures, comedonelike follicular papules, and pitted perioral scars.1 The hyperpigmentation begins in the armpits, groin and later spreads to other skin folds and can uncommonly affect the wrist, the antecubital and popliteal hollow, the
face, scalp, scrotum and vulva. These lesions do not change with sun exposure and can be associated with pruritus. Comedo-type black lesions on the neck and back, along with perioral cribriform scars in patients with no history of acne, can help the diagnosis. Other features may be present such as mental retardation and pillar cyst.2
The disease has been associated with Hidradenitis Suppurativa (HS), and multiple keratoacanthomas, perhaps because DDD causes a defect in the pilosebaceous epithelial proliferation.2
The histopathology of the skin biopsy shows dilated follicular, fingerlike projections called rete ridges (dermal pegs), with thinning of the suprapapillary plates, resulting in an "antler-like" pattern and increased pigmentation of the basal layer.2
Case Report
We report a case of a 34-year-old female who presented to the Dermatology OPD with symmetrically located dark brown to black lesions over the body since adolescence. The lesions were asymptomatic, gradually progressive
with the eruption starting over the face and slowly spreading to involve the flexures including the axilla, trunk and inframammary folds. She also had eruption of small, pinhead sized skin coloured- brownish black raised lesions over the face, buttock and trunk and multiple depressed lesions over the face.
There was no history of flushing over the face. There was no significant past medical or surgical history. She was born out of a nonconsanguineous marriage and her father, sister and two sons were affected by the same disease.
Her general physical and systemic examination were normal.
Cutaneous examination revealed multiple hyperpigmented macules 2-4 mm in diameter arranged in a reticular pattern over the face, bilateral axilla, trunk and bilateral inframammary folds. (Figure 1-3). Few hyperpigmented hyperkeratotic papules were present over the chest. (Figure 4). Multiple comedo like openings were present over the buttocks and few over the axilla (Figure 5-6) and multiple 1-3 mm pits present around the perioral area. (Figure 7)
Palms and soles were spared. Examination of the mucosa, hair and nails was within normal limits.
1: Hyperpigmented macules over
Figure 2
Figure (2 & 3) : Hyperpigmented macules over bilateral axilla, trunk and bilateral inframammary folds. Figure 3
Figure 4: Hyperpigmented hyperkeratotic papules over the chest.
5
6 : comedo like openings over the axilla.
On investigation, complete hemogram, liver and kidney function test and lipid profile were all within normal limits.
Thus based on the above clinical findings, a diagnosis of Dowling-Degos disease was made and the patient was started on topical retinoids which gave an unsatisfactory response. Hence the patient has now been planned for isotretinoin.
Discussion
Dowling Degos disease usually appears and/or worsens after puberty. Although sporadic cases are reported, most cases are familial as seen in our patient.
The differential diagnosis that we considered in this patient included Familial Dyskeratotic Comedones, other reticulate pigmentary disorders including Dyschromatosis Universalis
Hereditaria (DSH), Reticulate acropigmentation of kitamura (RAPK) and Haber Syndrome.
Since in our patient, there were distinctive black comedones, follicular pits and reticulate pigmentation and there was family history suggestive of autosomal dominant inheritance, the diagnosis of Familial
Figure
the face
Figure
: Multiple comedo like openings over the buttocks.
Figure
Figure 7 : Multiple 1-3 mm pits present around the perioral area.
Dowling-Degos
Disease: A Case Report
Since in our patient, there were distinctive black comedones, follicular pits and reticulate pigmentation and there was family history suggestive of autosomal dominant inheritance, the diagnosis of Familial Dyskeratotic comedones was ruled out. RAPK is characterized by atrophic pigmented spots on the back of the hands and feet and palmar pits.4 These lesions may or may not be observed in patients with DDD as were not seen in our patient.
Dyskeratotic comedones was ruled out.
RAPK is characterized by atrophic pigmented spots on the back of the hands and feet and palmar pits.4 These lesions may or may not be observed in patients with DDD as were not seen in our patient.
DUH (a generalized disorder) and DSH (a localized disorder) are characterized by diffuse symmetrically distributed hypopigmented macules or papules mixed with hyperpigmentation. In DSH, the pigmentary changes are confined to the back aspects of the hands and feet.4
DUH (a generalized disorder) and DSH (a localized disorder) are characterized by diffuse symmetrically distributed hypopigmented macules or papules mixed with hyperpigmentation. In DSH, the pigmentary changes are confined to the back aspects of the hands and feet.4
Patients with Haber syndrome develop a photosensitive rosacea like eruption over the face during adolescence which was also not seen in our patient.
Other less common entities which should be ruled out include Acanthosis Nigricans which can be easily differentiated clinically be the presence of velvety plaques and histologically by less pronounced elongatoion of rete ridges.
Other less common entities which should be ruled out include Acanthosis Nigricans which can be easily differentiated clinically be the presence of velvety plaques and histologically by less pronounced elongatoion of rete ridges.
Patients with Haber syndrome develop a photosensitive rosacea like eruption over the face during adolescence which was also not seen in our patient.
Patients with neurofibromatosis 1 develop freckles in the axilla and groin and should be Differentiated from DDD.
Patients with neurofibromatosis 1 develop freckles in the axilla and groin and should be Differentiated from DDD.
Disease
Dowling Degos disease
Dyschromatosis Universalis
Hereditaria
Dyschromatosis Symmetrica
Hereditaria
Clinical Features
Progressive reticular pigmentation distributed in flexures, genital areas, brown papules with variable hyperkeratosis, comedo like lesions, perioral pitted scars. Hair and nails are not involved.
Hypo and hyperpigmented lesions mainly located on the trunk, dorsa of the hands, palms and soles may be involved but there is sparing of the mucosae, hair and nail may be involved.
Multiple freckle like macules over the face. Small hyper and hypopigmented macules on the dorsa of hands, feet, sparing
Histopathology
Increased basal layer pigmentation with finger like rete ridges with suprapapillary thinning giving an antler like pattern.
Focal increase and decrease in the melanin content in the basal layer in the hyperpigmented and hypopigmented macules respectively.
Increased melanin in the basal keratinocytes in the hyperpigmented macules, decreased DOPA positive melanocytes in hypopigmented ones. the palms, soles and mucosae.
Reticulate acropigmentation of Kitamura Reticulate hyperpigmented atrophic macules on the hands which darken and spread
Epidermal thinning with elongation of rete ridges with increased pigmentation at their tips.
Table 1: Differential diagnosis of Dowling Degos Disease
Dowling-Degos Disease: A Case Report the palms, soles and mucosae.
Reticulate acropigmentation of Kitamura
Naegeli-Franceschetti-Jodasson Syndrome
Reticulate hyperpigmented atrophic macules on the hands which darken and spread proximally on extensors of limbs, face and trunk.
Reticular cutaneous pigmentation starting in early life (by 2 years) and lightening during adolescence . Intolerance to heat with hypohidrosis poor dentition, palmoplantar hyperkeratosis
Epidermal thinning with elongation of rete ridges with increased pigmentation at their tips.
Pigmentary incontinence of melanophages in hyperpigmentary lesions
Treatment options include topical treatments like hydroquinone, tretinoin, adapalene, corticosteroids. Oral retinoids like isotretinoin have also been tried. Improvement following treatment with Erbium:YAG laser has also been reported.
Conclusion
Treatment options include topical treatments like hydroquinone, tretinoin, adapalene, corticosteroids. Oral retinoids like isotretinoin have also been tried.
Improvement following treatment with Erbium:YAG laser has also been reported.
development of new treatment modalities is warranted.
References
1. Stephan C, Kurban M, Abbas O. Dowling Degos disease: a review. International Journal of Dermatology. 2021 Aug;60(8):944-50.
Oct 31. PMID: 36314591.
4. Wititsuwannakul J, Noppakun N. Generalized dowling-degos disease. Annals of Dermatology. 2013 Aug;25(3):360.
Dowling Degos disease is a rare disease that predominantly affects women with limited cases reported. Hence it should always be considered in a patient presenting with hyperpigmented lesions of flexural sites, not only in women but also in men. Also, as there is no known definitive treatment and the available treatment modalities are limited, development of new treatment modalities is warranted.
Conclusion
REFERENCES
1. Stephan C, Kurban M, Abbas O. Dowling‐Degos disease: a review. International Journal of Dermatology. 2021 Aug;60(8):944-50.
Dowling Degos disease is a rare disease that predominantly affects women with limited cases reported. Hence it should always be considered in a patient presenting with hyperpigmented lesions of flexural sites, not only in women but also in men. Also, as there is no known definitive treatment and the available treatment modalities are limited,
3. Papadopoulou K, Karsai S, Böer-Auer A. Disseminated papular variant of DowlingDegos disease: Histopathological features in POGLUT1 mutation. J Dtsch Dermatol Ges. 2022 Nov;20(11):1423-1429. doi: 10.1111/ddg.14897. Epub 2022
3. Papadopoulou K, Karsai S, Böer-Auer A. Disseminated papular variant of Dowling-Degos disease: Histopathological features in POGLUT1 mutation. J Dtsch Dermatol Ges. 2022 Nov;20(11):1423-1429. doi: 10.1111/ddg.14897. Epub 2022 Oct 31. PMID: 36314591.
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
Dr. Tejas S Naik
MBBS, MD (3rd Year Resident)
Department of MD Dermatology, Venerology and Leprosy
Goa Medical College and Hospital, Bambolim, Goa
Dr. Raghuvir Alias Tanmay M Kane
MBBS, MD (Senior Resident)
Department of MD Dermatology, Venerology and Leprosy
Goa Medical College and Hospital, Bambolim, Goa
Dr.
Varadraj V Pai
MD
Assistant Professor
Department of MD Dermatology, Venerology and Leprosy
Goa Medical College and Hospital, Bambolim, Goa
Dr.
P. Shukla
MD
Professor & Head of Department
Department of MD Dermatology, Venerology and Leprosy
Goa Medical College and Hospital, Bambolim, Goa
Abstract
Background: Acne vulgaris is a common chronic skin condition characterised by inflammation of the
pilosebaceous units, with varied clinical presentation some of which are difficult to treat. Acne affects the
majority of teens; however, it can last until adulthood. Acne can have a negative impact on a patient's quality of life due to skin changes, acne scars, and post-acne pigmentation.
Aims: The goal of this study was to determine the dermatology life quality index in acne vulgaris in patients attending tertiary care centre in Goa.
Methods: A 3-month time bound observational cross-sectional study with Dermatological Life Quality Index (DLQI) Questionnaire was done on 59 acne vulgaris patients 18 years and above, in a tertiary care hospital in Goa. Interpretation and impact on quality of life (QoL) was done and graded as no effect, small effect, moderate effect, very large effect and extremely large effect.
Results: Females made up 39 (62.71%) of the 59 acne vulgaris cases. The majority of patients had grade 2 acne (40.68 percent), followed by grade 1 acne (37.29 percent), and grade 4 acne (less than 5%), (8.47 percent). Acne DLQI scores revealed that 15.25 percent had a very large effect, 45.76 percent had a little effect, and 10.17 percent of patients had no effect.
Limitations: Limited sample size due to COVID pandemic and time bound nature of study.
Conclusion: Acne patients' quality of life (QoL) should be assessed in conjunction with early acne treatment to enhance patients' QoL. Moderate acne, whether with or without scarring, can result in psychosocial morbidity.
Introduction
Acne is one of the most frequent skin condition dermatologists encounter in their clinical setting. It is a common chronic skin condition of the pilosebaceous unit that manifests as papules, pustules, nodules, cysts, and comedones and can be inflammatory or noninflammatory.
Face, upper chest, and upper back are the most prevalent areas. Follicular hyperkeratinization, ,,,,,,,,, seborrhoea, inflammation, and Propionibacterium acnes colonisation are all part of the acne aetiology. Acne accounts for approximately 3% of the total and 16% of the global dermatologic disease burden. Acne appears during puberty, peaking between the ages of 14 and 17 for females and 16 and 19 for males.(1)
Patients with facial acne may develop substantial emotional and mental disorder since the face reflects essential components of one's opinion of body image. Due to skin changes, post-acne scarring, and hyperpigmentation, acne creates erroneous selfperception.(2)
Patients’ psychological wellbeing is affected by postacne alterations, particularly in adolescents who strongly associate beauty with appearance. Patients frequently feel unimportant and unaccepted, leading to humiliation, social and professional retreat, melancholy, rage, and anxiety.(3)
Quality of life (QoL) is a critical word that encompasses all aspects of a patient's well-being in relation to an illness. WHO defines QoL as an individual's view of their situation in relation to their objectives, expectations, standards, and concerns in the context of the culture and value systems in which they live.(4) Several QoL surveys have been developed to better evaluate the impact of acne on patients' daily lives and to aid clinicians in determining the efficacy of treatment. The Dermatological Life Quality Index (DLQI), established by
Finlay and Khan, is one such questionnaire that can be used in research studies and ordinary clinical practise to detect changes in QoL.(5) The purpose of this study was to determine quality of life in patients with various grades of acne vulgaris attending a tertiary care centre in Goa.
Methods
A three-month time bound hospital-based observational cross-sectional study on 59 acne patients in the Outpatient Department of tertiary care centre, using the Dermatological Life Quality Index (DLQI) questionnaire after approval of institutional ethical committee. After obtaining informed written agreement, educated (minimal qualification of matriculate) adult patients aged 18 to 35 years who were clinically diagnosed with acne vulgaris and had lesions on their face solely were included in the study. Patients with a personal or family history of mental illness, as well as nonconsenting patients, were excluded from the study. A thorough medical history of the patient, including the presenting complaint, the age at which the acne began, the duration of the acne, personal history, any aggravating factors, the presence of a medical
ailment, and treatment history.
Acne was graded based on clinical features and split into four severity levels: Grade 1 with comedones and few papules, Grade 2 with mostly papules and a few pustules, Grade 3 with predominantly pustules, nodules and abscess, and Grade 4 with nodulocystic acne.(6) Acne scars were graded into mild:< 5 scars, moderate: 5-10 scars and severe: >10 scars.(7) The DLQI questionnaire was given to the patients along with the instructions for filling it out.
The DLQI questionnaire consists of 10 questions encompassing various domains which includes cutaneous symptoms like itching, burning or stinging, degree of embarrassment or self-consciousness, interference with daily activities, influence over the choice of clothing, interference with leisure and social activities, difficulty in performing sporting activities, interference with work or study, difficulty in interpersonal relationships, sexual difficulty and problems due to treatment of the condition.
Each domain includes four possible responses ranging
from 0 to 3, with a total possible score of 30 (0-not at all, 1-little, 2-lot, 3-very much). The influence on QoL is assessed as no effect (01), little effect (2-5), moderate effect (6-10), very big effect (11-20), and extremely large effect (21-30) depending on the final score (21-30).(8)
Patients were instructed to complete the DLQI questionnaire on their own. The clinician's judgement of acne severity was strongly associated with the patient's response to the questionnaire.
MS Excel was used for data entry, and SPSS 26 was used for data analysis. Data was analysed by means of percentages and chisquare test to compare each variable with DLQI.
Results
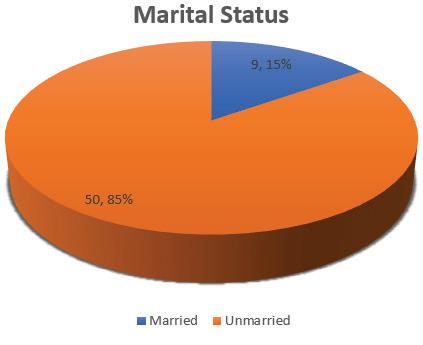
Out of 59 acne vulgaris patients, 37 (62.71%) were females and 22 (37.29%) were men, indicating a female preponderance. The majority of the patients were between the ages of 20 and 35, with 33 (55.93%) belonging to the 20-25 age group and 7 (11.86%) belonging to the 30-35 age group. Only 9 people (15.25 percent) were married, with the rest being single (Figure 1).
Figure 1 : Distribution of acne based on marital status.
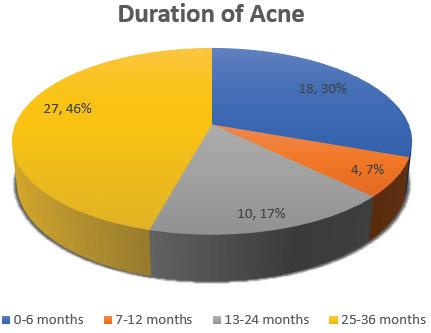
In our study, the majority of patients experienced symptoms for 25–36 months, whereas those with symptoms for 7–12 months had the shortest duration (Figure 2).
Figure 2: Distribution of acne based on duration of symptoms.
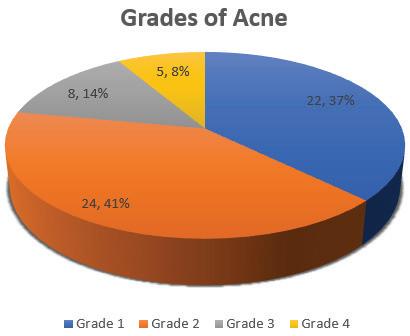
Grade 2 Acne was seen in majority of patients 24 (40.68%) followed by grade 1: 22 (37.29%) while grade 4 was least 5 (8.47%) (Figure 3).
Figure 3 : Grading of acne in patients with acne vulgaris.
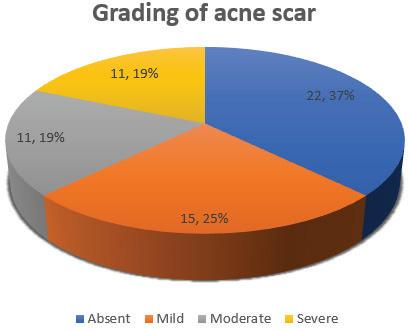
Scarring from acne was absent in the majority of patients 22 (25.42%), whereas severe and mild scarring were seen in the smallest number of patients (Figure 4).
Figure 4: Grading of acne scars in patients with acne vulgaris.
After acne, 45 patients (76.27 percent) exhibited hyperpigmentation/erythema, while 14 patients (23.73 percent) had none.
Acne had no effect in 6 (10.17 percent) of patients, a little effect in 27 (45.76 percent) of patients, a moderate effect in 17 (28.81
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
percent) of patients, and a very big effect in 9 (15.25 percent) of patients, according to DLQI scores.
Twelve of the twenty-four cases of grade II acne and five of the eight cases of grade III acne had a minor impact on the patient's life (Figure 5).
Figure 5: Distribution of Dermatological Quality of Life (DLQI) based on grades of acne.
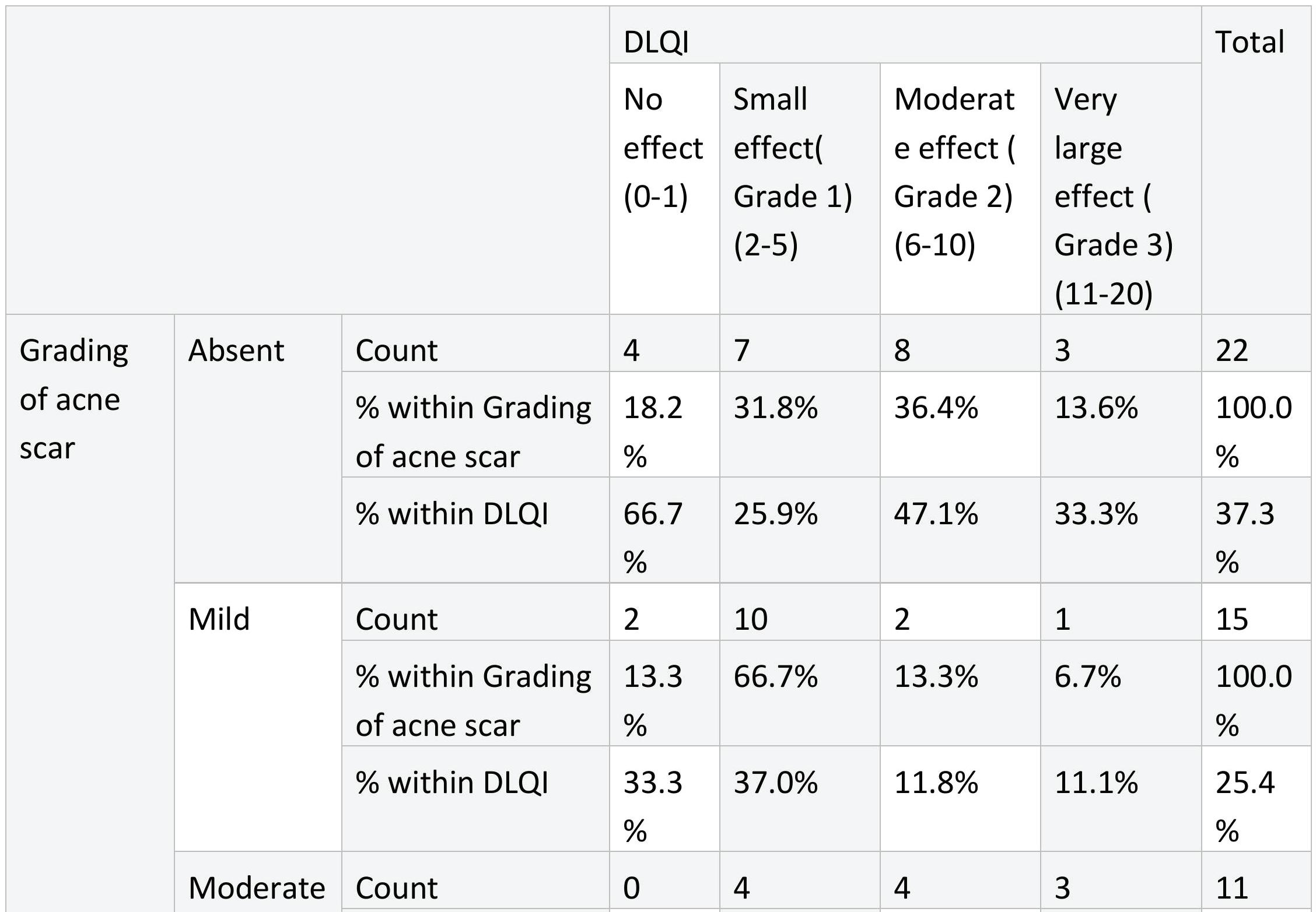
Patients with no acne scars (7/22) had a minor impact on their lives, whereas 3 out of 11 patients with moderate scars and 2 out of 11 patients with severe acne scars had a significant impact (Table 1).
Table 1: Distribution of Dermatological Life Quality Index (DLQI) based on grading of acne scar.
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
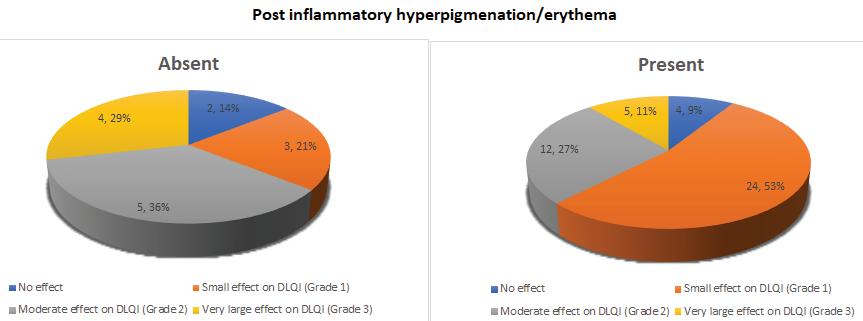
A DLQI score of 2-5 was found in 24 of 45 cases with post-acne hyperpigmentation/ erythema, indicating a minor effect (Table 2).
Table 2: Distribution of Dermatological Life Quality Index (DLQI) based on post acne hyperpigmentation/erythema.
Table 2: Distribution of Dermatological Life Quality Index (DLQI) based on post acne hyperpigmentation/erythema. hyperpigmentation/erythema, indicating a minor effect (Table 2).
Dermatology Life Quality Index in Adult Acne Vulgaris in Tertiary Care Centre in Goa- A Cross-Sectional Study
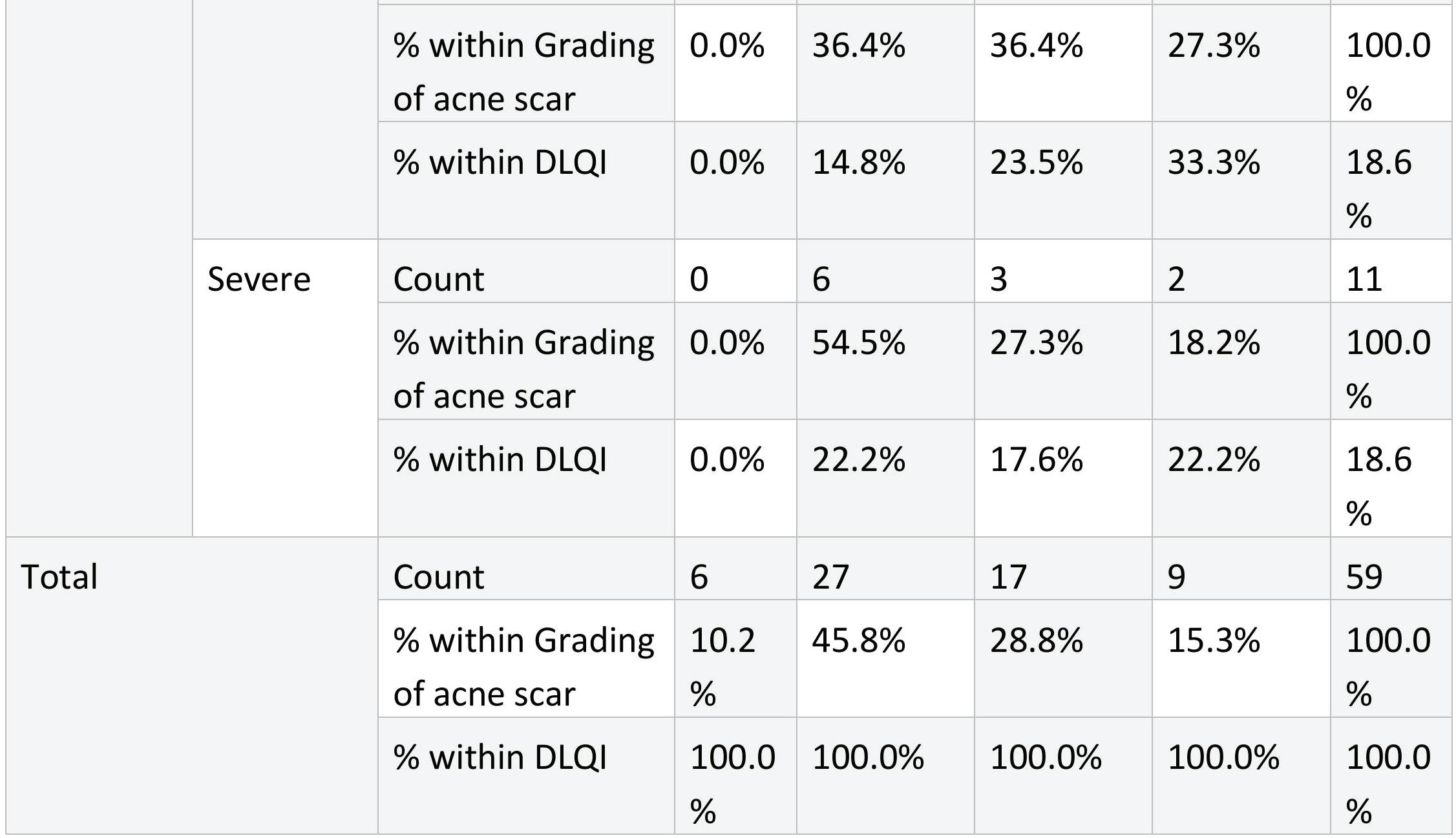
The DLQI interpretation of minor effect was seen in 17 of 37 female patients and 10 of 22 male patients (Figure 6).
Figure 6: Distribution of Dermatological Quality of Life (DLQI) based on gender.
Figure 7: Distribution of Dermatological Quality of Life (DLQI) based on age group.
Dermatology
Figure 8: Distribution of Dermatological Quality of Life (DLQI) based on duration of acne symptoms.
9: Distribution of Dermatological Quality of Life (DLQI) based on grade of acne scar.
Figure 10: Distribution of Dermatological Quality of Life (DLQI based on post inflammatory hyperpigmentation/erythema.
As a result, we discovered that patients with grade 2 acne vulgaris, no scars, and postacne hyper-pigmentation/erythema had the highest DLQI ratings in the range of 2-5 (Small effect).
Discussion
Acne on the face has a psychological influence on patients, affecting their motivation as well as how they perceive their look. The term "self-esteem" is used to describe a person's total feeling of self-worth, personal value, and self-image. Self-image, on the other hand, relates to one's opinion of one's own look. Both self-esteem and self-image have an impact
Figure
on one's quality of life.(9)
Acne affects the majority of young individuals due to hormone imbalances, lifestyle changes, stress, food, and other indirect or direct reasons. Patients with facial acne may experience substantial emotional and psychological repercussions. There are research analysing the influence of acne on QoL from various nations, however there are few studies on Indian patients. (10) A total of 59 participants were enrolled in our study. Out of 59 patients, 37 (62.71 percent) were females and 22 (37.29 percent) were men, indicating a female preponderance. Similarly, in their study, Rapp DA et al. discovered that the prevalence of acne was 64 percent in women and 36 percent in men, correlating with our findings of a female preponderance.(11) In their research, Tasoula E et al. and Jankovic S et al. both found a female preponderance in acne vulgaris patients.(8,12) In our study, the majority of patients with facial acne were between the ages of 20 and 25, with 33 individuals in total (55.93 percent ). Acne lesions appear at the age of 15 and can last far into the thirties and forties. Maximum numbers were found among
the population of 11–19 years old, according to Tasoula et al.(8) The majority of the patients, 50 (84.7%), were single. Acne can have a detrimental influence on mood, self-esteem, and interpersonal connections, as well as contribute to depression and suicide ideation among unmarried females and males.(13) Hazarika et al., showed that the bulk (42%)(14) in their study had acne for <6 months however patients in our study had duration of symptoms ranging from 24-36 months probably considering ours is a hospital based study with bulk of patients presenting for regular follow ups as well as being a tertiary care centre patients were referred from periphery institutions for treatment of same.
Out of 59 participants in our study, 24 (40.68 percent) had grade II acne. Hazarika et al. found the highest frequency of grade II acne (67.5%), whereas Durai and Nair found the highest prevalence of comedones (95%) in their research.(14,15) Twenty-two patients (25.42%) had no acne scars in our study, while the majority of patients had grade II acne, and 18.6 percent of cases had moderate to severe acne scars. In a research, Kane
A found that 40.2 percent of people had acne scars, whereas Hayashi et al. found that 90.8 percent of people had acne scars.(16,17)
Patients' QoL may be negatively impacted by postacne hyperpigmentation/ erythema. In our study, 45 individuals (76.27 percent) had post-acne hyperpigmentation/ erythema. According to a research by Hazarika et al., 75.4 percent of people had post-acne pigmentation, which is consistent with our findings.(14)
Our DLQI values were increased in 53 of our 59 individuals. The majority of those impacted had a little impact (45.6 percent), followed by a moderate impact (28.81 percent), and a significant impact (15.25 percent), with no one having a severely negative impact on their quality of life. These findings matched those of Hazarika et al.(14)
In our study, acne had an impact on the QoL in both males and females. Nearly 38% of females had moderate effect and nearly 14% of males had moderate effect on QoL. Nearly 8% of females had very large effect and nearly 27% of males had very large effect. The above findings of our study
corroborated with the study done by Hazarika et al. and Durai et al.(14,15) A study done by Sivaramakrishnan et al. showed that acne had a greater impact on QoL in females which was not the case in our study(18) wherein we found greater impact on QoL in males, indicating that even males may have higher self-consciousness about facial perception compared to females.
The study by Hazarika et al showed a greater impact on QoL with increasing age in contrast to the study done by Sivaramakrishnan which showed a lesser impact on QoL with age.(14,18) Our study showed that 10% of patients in the age group 18-20 years and nearly 24% of patients in the age group 20-25 years had very large effect on QoL, where as none of the patients above 25 years had very large effect on QoL. Nearly half of the patients above 25years had moderate effect on QoL. Our study neither showed a greater impact nor a lesser impact on QoL with increasing age.
The marital status of an individual affects the QoL due to the cosmetic appearance. Individual relationships and thus appearance has significant weight age in married people. The study
done by Durai et al. in acne patients showed statistically significant association between marital status and impact on QoL(15). Nearly 67% of married patients had moderate effect on QoL, where as 22% of unmarried patients had moderate effect. None of the married patients had very large effect where as 18% of unmarried patients had very large effect on QoL. Less number of married patients enrolled in the study may be the reason behind this finding. Therefore, we propose QoL to be affected irrespective of marital status in patients with acne.
In our study, 27.8% patients who had acne for less than 6 months had very large effect on QoL. About 11 percent patients who had acne for 25-36 months had very large effect on QoL. The DLQI values were not proportionately high in patients with long duration of acne. Twelve out of 24 cases with grade II acne and 5/8 grade III acne had a small effect on patient's life. Two out of 5 cases (40%) with grade IV acne had very large effect. Duration of acne and severity of acne did not have a statistically significant relationship with QoL. Durai et al. and Sivaramakrishnan et al. observed that the
DLQI values correlated with severity of acne and the scores worsened with increasing severity.(15,18)
Patients having no acne scars (3/22) had very large effect on their life while 2 patients out of 11 with severe acne scars had very large effect. It was found in our study that some cases with mild scar had elevated DLQI scores which implied that even mild scars can pose a cosmetic problem to some patients, diminishing their QoL. Similar finding was observed in the study conducted by Hazarika et al. They also reported greater mean DLQI scores in patients with severe acne scars when compared with patients having low grades of acne scar.(14) Our study did not show an increasing impact on the quality of life with severity of acne scars.
Limitations
A major limitation of our study is sample size as it was a 3-month time bound study and also owing to COVID 19 pandemic patients avoided visiting hospitals for conditions like Acne Vulgaris. Another limitation being including follow up pre diagnosed cases which lead to majority of patients having symptom duration in range of 24-36 months. We found DLQI values higher in
Dermatology Life Quality Index in Adult Acne Vulgaris
male then in female patients, also DLQI values in married individuals were higher which needs to be tested by further studies.
Conclusion
Quality of life is a multifaceted notion that encompasses a person's subjective physical, psychological, emotional, mental, social, and spiritual well-being. Facial acne primarily affects young individuals and has a negative influence on their quality of life. Our research found that even moderate acne, whether with or without scarring, and/or post-acne pigmentation/erythema, can result in psychosocial morbidity. Young acne sufferers have expressed feelings of embarrassment and frustration, which can lead to anxiety and despair. As a result, assessing QoL in acne patients should be addressed in conjunction with early acne treatment to avoid disease progression and enhance patients' QoL by lowering illnessrelated psychosocial consequences.
Source(s) of support: Nil
Presentation at a meeting: Nil
Organisation: Not Applicable
Place: Not Applicable
Date: Not Applicable
Conflicting Interest (If present,
give more details): Nil.
Acknowledgement (if any): None
Sample Size was not calculated as we have done a 3 month time bound study.
References
1. Karimkhani C, Dellavalle RP, Coffeng LE, Flohr C, Hay RJ, Langan SM, et al. Global Skin Disease Morbidity and Mortality: An Update From the Global Burden of Disease Study 2013. JAMA Dermatol. 2017 May 1;153(5):406–12.
2. Koo JY, Smith LL. Psychologic aspects of acne. Pediatr Dermatol. 1991 Sep;8(3):185–8.
3. Aktan S, Ozmen E, Sanli B. Anxiety, depression, and nature of acne vulgaris in adolescents. Int J Dermatol. 2000 May;39(5):354–7.
4. The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med 1982. 1995 Nov;41(10):1403–9.
5. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994 May;19(3):210–6.
6. Adityan B, Kumari R, Thappa DM. Scoring systems in acne vulgaris. Indian J Dermatol Venereol Leprol. 2009 Jun;75(3):323–6.
7. Kulthanan K, Jiamton S, Kittisarapong R. Dermatology Life Quality Index in Thai Patients with Acne. Siriraj Med J. 2006;58(12):3–7.
8. Tasoula E, Gregoriou S, Chalikias J, Lazarou D, Danopoulou I, Katsambas A, et al. The impact of acne vulgaris on quality of life and psychic health in young adolescents in Greece. Results of a population survey. An Bras Dermatol. 2012 Dec;87(6):862–9.
9. Oliveira WA de. Quality of
life, facial appearance and selfesteem in patients with orthodontic treatment. Rev Mex Ortod. 2017 Aug 21;5(3):138–9.
10. Chowdary NK, Shenoi SD, Nayak SUK, Prabhu SS. Quality of life in acne patients: A clinical and dermatology life quality index (DLQI) based cross-sectional study. J Pak Assoc Dermatol. 2018 Jan 1;28(4):415–9.
11. Rapp DA, Brenes GA, Feldman SR, Fleischer AB, Graham GF, Dailey M, et al. Anger and acne: implications for quality of life, patient satisfaction and clinical care. Br J Dermatol. 2004 Jul;151(1):183–9.
12. Jankovic S, Vukicevic J, Djordjevic S, Jankovic J, Marinkovic J. Quality of life among schoolchildren with acne: results of a cross-sectional study. Indian J Dermatol Venereol Leprol. 2012 Aug;78(4):454–8.
13. Fried RG, Wechsler A. Psychological problems in the acne patient. Dermatol Ther. 2006 Aug;19(4):237–40.
14. Hazarika N, Rajaprabha RK. Assessment of Life Quality Index Among Patients with Acne Vulgaris in a Suburban Population. Indian J Dermatol. 2016 Apr;61(2):163–8.
15. Durai PCT, Nair DG. Acne vulgaris and quality of life among young adults in South India. Indian J Dermatol. 2015 Feb;60(1):33–40.
16. Kane A, Niang SO, Diagne AC, Ly F, Ndiaye B. Epidemiologic, clinical, and therapeutic features of acne in Dakar, Senegal. Int J Dermatol. 2007 Oct;46 Suppl 1:36–8.
17. Hayashi N, Miyachi Y, Kawashima M. Prevalence of scars and “miniscars”, and their impact on quality of life in Japanese patients with acne. J Dermatol. 2015 Jul;42(7):690–6.
18. Sivaramakrishnan S, Jayakar T. A study on the dermatology life quality index in patients with acne vulgaris. Int J Res Dermatol 2019;5:774-8.
MUMBAI 202
MUMBAI 2025
1 Day Conference, Hands on Workshop and Exhibition
AESTHETICCON Mumbai 2025 is just the event for you with practical insights shared in the Conference, tips while training in the Hands on workshop and interaction
AESTHETICCON Mumbai 2025 is just the event for you with practical insights shared in the Conference, tips while training in the Hands on workshop and interaction with product manufacturers.
Spend the day catching up and meeting with your fellow Dermatologists colleagues.