*Guided by the World Health Organization’s National Assessment Tool on integrated antimicrobial stewardship programs

Jakarta, Indonesia November 2023





Pillar 1.
Pillar 2.
Pillar 3.
Pillar 4.
Pillar 5.
Conclusions
Establish and develop national coordination mechanisms for antimicrobial stewardship and develop guidelines
Ensure access to and regulation of antimicrobials
Improve awareness, education and training
Strengthen water, sanitation and hygiene, and infection prevention and control Surveillance, monitoring and evaluation
Pillar 1. Establish and develop national coordination mechanisms for antimicrobial stewardship and develop guidelines
Domain 1. Establish and maintain a national coordinating mechanism for AMS that is functional at national, subnational and district levels
Item 1.1. Is there a national policy on integrated AMS?
Item 1.2. Is there a central national coordination unit at the ministry of health or designated agency or institution focused on AMS?
Item 1.3. Has the central national coordination unit established a national coordination mechanism for integrated AMS activities with diverse membership, including civil society and the private sector?
Item 1.4. Have similar coordination mechanisms with diverse members, including from civil society and the private sector, been established at subnational and district levels?
Item 1.5. Are there clear reporting lines and feedback mechanisms from subnational mechanisms to the national coordination mechanism on integrated AMS activities?
Item 1.6. Is there funding allocated for the national coordinating unit and the national, subnational and district coordination mechanisms?
Item 1.7. Does the national coordination unit have clear terms of reference (TOR)?
Item 1.8. Is there a linkage to other relevant stakeholders e.g. from tuberculosis (TB), infection protection and control (IPC), water, sanitation and hygiene (WASH) or universal health coverage (UHC)?
Item 1.9. Is there a monitoring and evaluation (M&E) framework and have national targets been set for AMS activities based on nationally and internationally agreed indicators?
Item 1.10. Have other programmes, such as IPC, WASH, TB, malaria, HIV, UHC and primary health care (PHC), integrated AMS activities within their action plans?
Domain 2. Develop national treatment and stewardship guidelines, standards and implementation tools
Item 2.1. Have the national treatment guidelines for the management of infections been updated within the last 3–5 years?
Item 2.2. Do the national treatment guidelines include AMS principles?
Item 2.3. Is there monitoring of implementation and compliance to treatment guidelines?
Item 2.4. Is there coordinated guidance and interventions to improve availability and appropriate use of diagnostics to guide therapeutic decisions?
Item 2.5. Are there specific standard operating procedures for AMS activities in health-care facilities and in community settings?
Item 2.6. Are there mechanisms and activities for the dissemination of guidelines, standards and implementation tools on AMS activities?
Pillar 2. Ensure access to and regulation of antimicrobials
Domain 3. Improve access to essential, quality-assured, safe, effective and affordable antimicrobials
Item 3.1. Has the WHO Model List of Essential Medicines (EML) and Access, Watch, Reserve (AWaRe) system been incorporated into the national EML formulary and health-care facility treatment guidelines?
Item 3.2. Is there a system in place to monitor access to essential, quality-assured, safe, effective and affordable antimicrobials?
Item 3.3. Is there a system to periodically identify availability of affordable antibiotics at health-care facilities?
Item 3.4. Is there a mechanism in place to report shortages and stock-outs of antibiotics in the country?
Item 3.5. Is there a mechanism to report the antibiotics used by patients?
Item 3.6. Is there a process to report the antibiotics used in the AWaRe system?
Domain 4. Regulate social triggers and remuneration policies that promote responsible antimicrobial prescription and dispensing behaviors
Item 4.1. Are health worker behavioral change principles incorporated into policies addressing diagnosis, prescription, dispensing and administration of antimicrobials?
Domain 5. Legislate and regulate responsible and appropriate use and disposal of antimicrobials
Item 5.1. Is there a regulation on prescription-only sale/ dispensing of antibiotics?
Item 5.2. Are regulations on dispensing antibiotics by prescription only being enforced (where access is not an issue)?
Item 5.3. Is there an enforceable regulatory mechanism to prohibit sale of substandard and falsified drugs?
Item 5.4. Are there standards and criteria for responsible manufacturing and disposal of antimicrobial agents?
Pillar 3. Improve awareness, education and training
Domain 6. Improve awareness and engagement to support behavioral change of antimicrobials use
Item 6.1. Have studies on determinants of behavior in health professionals and other stakeholders, including the general public, been completed to support design of awareness campaigns?
Item 6.2. Does the country hold World Antimicrobial Awareness Week (WAAW) activities annually?
Item 6.3. Does the country have regular public awareness campaigns on the responsible and appropriate use of antibiotics?
Item 6.4. Are tailored AMS messages integrated into broader health promotion, prevention, treatment and rehabilitation services and initiatives such as World Water Day, World Toilet Day, World Children’s Day, immunization campaigns, World AIDS Day, World TB Day, World Malaria Day and World Nutrition Week for sustained action?
Oxford University Clinical Research Unit
Item 6.5. Is regular assessment/evaluation of the impact of education and awareness campaigns on knowledge attitudes and behaviors of health workers and the public conducted?
Domain 7. Strengthen health worker capacity through the provision of tailored education and training packages according to health worker roles and functions
Item 7.1. Are AMS principles and strategies included in the educational curriculum of pre-service healthcare professionals?
Item 7.2. Is there access to in-service training, including continuous professional development (CPD) on antimicrobial prescribing and AMS for all healthcare professional groups in the country?
Item 7.3. Are AMS concepts and principles incorporated within the curriculum of other complementary disciplines e.g. the curriculum for IPC professionals
Pillar 4. Strengthen water, sanitation and hygiene and infection prevention and control
Domain 8. Enhance WASH in health facilities and communities
Item 8.1. Is there representation of the AMS coordinating unit on the WASH programmes and vice versa?
Item 8.2. Is the WHO WASH Facility Improvement Tool (FIT) being promoted to assess WASH in healthcare facilities?
Domain 9. Implement IPC core components in health facilities
Item 9.1. Is there representation of the AMS coordinating unit on the IPC programmes and vice versa?
Item 9.2. Are there systems linking the monitoring and reporting of healthcare-associated infections (HAIs), antimicrobial use, AMR, patient outcomes and quality of care?
Pillar 5. Surveillance, monitoring and evaluation
Domain 10. Surveillance of antimicrobial use and consumption
Item 10.1. Is there a national surveillance programme for antimicrobial resistance, use and consumption with defined structures, governance and work objectives (i.e. data collection, validation, analysis, reporting and data sharing with all stakeholders)?
Item 10.2. Are there guidelines/standard operating procedures for the use of (a) antimicrobial medicines use (AMU), (b) antimicrobial medicines consumption (AMC), and c) AMR data to inform action for national and institutional decision-making to inform action for national and institutional decision-making?
Domain 11. Surveillance of AMR
Item 11.1. Is there a plan to strengthen laboratory capacity to support accurate diagnosis for decision-making?
Domain 12. Monitoring and evaluation of AMS activities
Item 12.1. Is there a national M&E framework, including internationally and locally agreed key performance indicators for integrated AMS interventions and activities in human health?
Item 12.2. Is there an accountability mechanism put in place at the local level which includes positive feedback and recognition of local leadership?
Antimicrobial resistance (AMR) is a public health problem that jeopardizes progress in health outcomes. The inappropriate use of antimicrobial agents contributes to the emergence of AMR and diminishes the efficacy of commonly used antimicrobials in treating infections. Antimicrobial stewardship (AMS) is one of the key strategies in the global and national action plans to control AMR. In response to the Global Action Plan (GAP) and the increasing burden of AMR, Indonesia developed its first National Action Plan (NAP) on AMR in 2017 for the period of 2017–2019, followed by the current NAP on AMR for the period of 2020–2024. In parallel, the Indonesian Ministry of Health (MoH)and the Indonesian Food and Drug Authority (Badan Pengawas Obat dan Makanan, BPOM) developed and released policies to support AMR control and integrated AMS activities in hospitals or healthcare facilities and the community.
The implementation of AMS requires a comprehensive and integrated approach, involving all relevant stakeholders, the commitment to steward its execution through the formulation and enforcement of policies and guidelines, the integration with all relevant programs, and structural, financial, and human resource support. As part of a regional project initiated by the US CDC, we performed a national assessment of the current progress, challenges, and areas for improvement in AMS implementation in Indonesia based on insights from national-level stakeholders and a review of relevant documents. In this analysis, we used the World Health Organization (WHO)’s national assessment tool from the WHO policy guidance on integrated antimicrobial stewardship activities to evaluate AMS implementation at the national level with 5 (five) pillars, 12 domains and 44 items (Figure 1). The 12 domains represent 12 packages of interventions and activities that need to be considered and implemented to create a strong backbone for an integrated AMS approach to preserve antimicrobials. The policy guidance also seeks synergy and efficiency for the implementation of comprehensive interventions across key sectors and at all levels.

AMR
AMS
AWaRe
BPOM
CDC
EML
FAO
GAP
GLASS
IPC
JKN
KPRA
MoH
NAP
NRL
PHC
TB
TOR
UHC
WAAW
WASH FIT
WHO
Assessment report of AMS implementation at the national level Acronyms
: Antimicrobial Resistance
: Antimicrobial Stewardship
: Access - Watch - Reserve
: “Badan Pengawas Obat dan Makanan” or the Indonesian Food and Drug Authority
: Centers for Disease Control and Prevention
: Essential Medicines List
: Food and Agriculture Organization
: Global Action Plan
: Global Antimicrobial Resistance and Use Surveillance Survey
: Infection Prevention and Control
: “Jaminan Kesehatan Nasional” or the National Health Insurance
: “Komite Pengendalian Resistensi Antimikroba” or the Committee on Antimicrobial Resistance Control
: Ministry of Health
: National Action Plan
PHCPrimary Health Care
SOPStandard Operating Procedure
TB Tuberculosis
TORTerms of Reference
UHCUniversal Health Coverage
World Antimicrobial Awareness Week
Water and Sanitation for Health Facility Improvement Tool
World Health Organization

Establish and develop national coordination mechanisms for antimicrobial stewardship and develop guidelines
The national policies on integrated AMS activities for human health are issued by the MoH and BPOM. These policies are aimed at regulating and guiding AMS implementation in hospitals or healthcare facilities and in the community, e.g., the national formulary, guidelines of antibiotic use that was updated in 2021, national guideline on AMS implementation in hospitals that was released in 2021, the smart community movement in using drugs regulation and guideline, and standards of pharmacy services in hospitals and pharmacies.
To support integrated activities in AMR control in healthcare facilities, the MoH established a national coordinating body called the Committee on AMR Control (Komite Pengendalian Resistensi Antimikroba, KPRA) with a clear terms of reference (ToR). This committee operates as an independent agency under the MoH and comprises experts and consultants from the MoH, hospitals, health professional organizations, and civil society. The KPRA has five working groups, including AMS and infection prevention and control (IPC). Furthermore, the support for integrated AMS activities was demonstrated by the national government through the allocated budget for 2020–2024, aiming for AMR control, including AMS implementation.
This report identified three gaps that require further improvement under this pillar. First, a policy on AMS implementation in the primary healthcare (PHC) is currently lacking, while PHC serves as the initial point of contact between the patient and the healthcare facility. Inappropriate antimicrobial use in this setting will have repercussions for subsequent antimicrobial use and AMS implementation in hospitals. Second, there are no well-defined integrated reporting lines or feedback mechanisms from the subnational levels (province and district) to the national level concerning AMS activities and impact. Third, there is limited coordination between AMS implementation and other relevant programs, such as water sanitation and hygiene (WASH) and universal health coverage (UHC). Tuberculosis, HIV, malaria, and IPC programs have been integrated into the AMS implementation at different degrees.
The Government of Indonesia has issued a number of guidance documents to ensure the supply of essential antimicrobials with high quality, safety, effectiveness, and affordable prices. The list of essential medicines (EML) and the WHO Access, Watch, Reserve (AWaRe) systems have been integrated into the national formulary, the national antibiotic guidelines, and the guidelines for implementing AMS within hospital settings. However, there is currently no system at the national level to perform direct monitoring on AMS implementation at the hospital level related to antibiotic prescribing practices beyond the national formulary, tracking antibiotic stockouts in hospitals, and tracking antibiotic use as reported by patients.
Standards and criteria for responsible manufacturing and disposal of antimicrobial agents have also been established. Existing policy and regulatory structures also apply to antimicrobials, regulating the acts of trading in pharmaceuticals, including counterfeit drugs, ingredients for making counterfeit drugs, substandard medicinal ingredients, and substandard drugs, under the responsibility of the BPOM. Regulations on the sale and dispensing of prescription-only antibiotics are in place in registered pharmacies and healthcare facilities. However, enforcement remains weak, and dispensing over-the-counter medicines, including antimicrobials that require prescription by physicians, is widespread. Greater regulatory measures are needed to reduce inappropriate antibiotic use in community settings.
Strategies to instigate behavioral changes among health workers regarding antimicrobial prescribing, dispensing, and administration have been incorporated into various policies in healthcare facilities and the community.
Strategies aimed at improving awareness and promoting behavioral change in antimicrobial use have been implemented to varying extents. Public awareness campaigns on responsible and appropriate antibiotic use and World Antimicrobial Awareness Week (WAAW) are regularly conducted. However, studies focusing on the determinants of behavior among health professionals are not yet fully integrated into these public awareness campaigns. In addition, the assessment of the impact of education and awareness campaigns on the knowledge, attitudes, and behaviors of both health workers and the public remains inconsistent.
Nationwide AMS training for healthcare professionals has been conducted, and participants are rewarded with continuous medical education credit points. However, strategies to strengthen the capacity of healthcare providers by incorporating AMS principles and strategies into the pre-service education curriculum for healthcare professionals are currently limited.
The integration between AMS, IPC, and WASH programs is still limited in Indonesia. WASH programs have been implemented in primary healthcare and community settings in Indonesia using the WHO WASH Facility Improvement Tool (WASH FIT). However, WASH is currently not available in hospitals, nor is AMS in PHC. Therefore, there is a gap in the representation of the AMS coordinating unit within the WASH programs, and vice versa. IPC procedures and implementation have been integrated into the guidelines for the implementation of the AMS program in healthcare facilities. The guidelines state the inclusion of IPC staff roles in the membership representation of the AMS team. Hospitals submit reports on antimicrobial use to the MoH for synthesis and monitoring, although these are not linked to AMR, patient outcomes, or quality of care.
A national surveillance program on AMR and antimicrobial use and consumption has been implemented at a limited number of healthcare facilities. Indonesia’s participation in the Global Antimicrobial Resistance and Use Surveillance System (GLASS) has enhanced the capacity of National Reference Laboratories (NRL), including the implementation of external quality assessments and the enforcement of infection diagnostic capacities at the hospital level. Nevertheless, only a limited number of hospitals are included in GLASS. A nationwide database for collection, reporting, monitoring, and evaluation (M&E) of AMR, antimicrobial use and consumption, and AMS metrics remains unavailable.
In conclusion, Indonesia has achieved a number of significant milestones and achievements in establishing an integrated national framework for AMS, aiming to ensure the responsible use of antimicrobials and contribute to managing the burden of AMR. These include the available regulatory and coordination structures in most required domains needed for the initial setup, administration, and operation of AMS programs in hospitals, the linkages with IPC practices in hospitals, and the establishment of an early AMR surveillance network to monitor and track resistance over time for timely actions. Implementation of AMS programs is influenced by various contextual elements, and AMS activities should be conducted in an integrated manner to optimize antimicrobial prescribing and ensure patient and public safety. However, this national assessment also identified several gaps in the implementation of integrated AMS activities, which limit the effectiveness of AMS program implementation. These gaps pinpoint the following main areas for improvement:
Establish an AMS policy for PHC that is relevant to different PHC settings and integrated into existing PHC programs, such as WASH, health promotion, infectious disease prevention and treatment, maternal and child health, and sexual and reproductive health. Increase effective coordination mechanisms between the national and subnational governments through a collaboration framework that integrates AMS activities into policy, relevant programs, and budgeting at the provincial and district levels. The national and subnational governments should populate and sustain a national-level database accessible to all healthcare facilities for reporting AMS activities and outcome indicators.
Coordinate with the relevant stakeholders responsible for the development and implementation of the curriculum for medical and allied health professionals, e.g., the Ministry of Education, Culture, Research, and Technology and the Indonesian Medical Council, to include AMS principles as part of competency-based pre-service education training.
Develop and strengthen effective enforcement mechanisms for the implementation of integrated AMS policy at all levels through the establishment of a national-level online system accessible to healthcare providers and the community to report the findings of prescription-only sale and dispensing of antibiotics and the sale of substandard and falsified drugs.
Develop integrated M&E and surveillance mechanisms at the national level and in healthcare facilities based on the nationally agreed indicators through the establishment of a national-level database to collect data on AMS outcome indicators (e.g., antimicrobial use and consumption, etc.). This approach can simplify national-level AMS program data collection, assessment, reporting, and feedback at a potentially lower cost. Further, the WAAW and AMR campaigns have to be followed up with regular M&E relevant to the promoted behavioral change activities.
AMR has emerged as a global public health concern that threatens progress in health outcomes and the attainment of sustainable development goals [1]. Global data suggested that AMR was responsible for 1.27 million deaths and contributed to 4.95 million in 2019 [2]. The overuse and misuse of antimicrobial drugs have accelerated the development of AMR, rendering many commonly used antimicrobials ineffective against once-treatable infections [3]. AMR incurs clinical consequences, such as treatment and prophylaxis failure, prolonged infections, increased morbidity and mortality [4,5] as well as increased economic burdens for patients and health systems [6–8]. Therefore, the implementation of effective AMS programs has become paramount to curbing AMR, optimizing antimicrobial use, and improving patient outcomes.
Indonesia is a populous and diverse middle-income country in Southeast Asia, with an estimated population of 278 million people in 2023 [9], vulnerable to AMR due to a number of factors, including persistently high infectious disease burdens, unequal access to quality healthcare, and inadequately enforced antibiotic policies [10,11]. Indonesia is facing an alarming increase in many antimicrobial-resistant bacteria that are important for human health, with reported resistance rates among the highest in Asia and the world. Indonesia has launched several initiatives to curb AMR through various schemes, including AMS policies and programs targeting healthcare facilities and the community, and antibiotic use control in the One Health context. AMS programs in Indonesian healthcare facilities, primarily implemented in hospitals, were initiated in the early 2000s, but their implementation has been inconsistent for the first 15 years [12,13]. Following the Global Action Plan (GAP) agenda [14], in 2017, Indonesia developed a National Action Plan (NAP) on AMR for the years 2017–2019 [15], followed by an updated plan for the period 2020–2024 [16], with the objectives of minimizing the emergence and spread of resistant pathogens, ensuring the availability of safe, effective, quality, and affordable antimicrobials, as well as the prudent and responsible use of antimicrobials [16]. Since 2018, all hospitals have been mandated to establish an AMS team and implement an AMS program under hospital accreditation [17].
To date, there has been no national report on the state and outcomes of AMS implementation in Indonesia, yet recent studies have uncovered several challenges in AMS execution. The decentralized health governance system challenges AMS implementation in hospitals, especially prior to mandatory hospital accreditation [13]. Most hospitals are under the authority of subnational governments (province and district), while local AMS policies at these levels are lacking [13]. Furthermore, hospitals have been struggling to deliver effective AMS programs due to a lack of adequate dedicated funding to run the program, suboptimal or unsustainable leadership support from hospital executives, limited reimbursement for infection diagnostic tests under the national health insurance scheme, and minimal funding flow to ensure optimal operations of infection diagnostic infrastructure [13,18].
The successful implementation of integrated AMS interventions and activities requires a systematic approach grounded in public health principles. Integrating IPC, and water, sanitation, and hygiene (WASH) practices into AMS implementation is crucial for the comprehensive and efficient management of AMR [19]. In this project, our objective was to evaluate the accomplishments, challenges, and areas for improvement in AMS implementation in Indonesia. To conduct the assessment, we followed the WHO policy guidance on integrated AMS activities in the human health sector [19]. This report presents an evaluation of the current progress in AMS implementation, based on insights from national-level stakeholders and a review of pertinent published documents.
We used the national assessment tool of the WHO policy guidance on integrated AMS activities to review current AMS implementation at the national level [19] using the specific questions categorized in the below five (5) pillars to guide our data collection, analysis, and synthesis of the results:
A. Establish and develop national coordination mechanisms for AMS and develop guidelines.
B. Ensure access to and regulation of antimicrobials.
C. Improve awareness, education, and training.
D. Strengthen water, sanitation, hygiene, and infection prevention and control.
E. Surveillance, monitoring, and evaluation
These 5 (five) pillars consist of 12 domains and 44 question items. For each question item, a rating of the current state of AMS implementation items was chosen, along with justifications given for the response as well as an elaboration on the contextual factors that have contributed to the achievements and challenges. Following are the 5 (five) options of response for each question, the responders were instructed to select one of these options as the final response to each question during the data collection process:
1= No or Not implementing;
2= No, but a priority;
3= Planned but not started;
4= Partially implemented;
5= Fully implemented.
To review current AMS implementation at the national level, we conducted interviews with key stakeholders at the national level and performed a document review. The interviews were conducted from March to April 2022 with three key stakeholders. These stakeholders were purposively selected based on their knowledge regarding nationwide implementation of AMS programs and their roles in the development of national-level AMR and AMS policies and guidelines, antibiotic guidelines, and national formulary. The participants interviewed included:
A representative from the AMS coordinating unit at the national level or the Committee on Antimicrobial Resistance Control (Komite Pengendalian Resistensi Antimikroba, KPRA);
A member of the infection prevention and control (IPC) working group in the KPRA who was also a stakeholder in the Indonesian Society of Infection Control (Perkumpulan Pengendalian Infeksi Indonesia, PERDALIN);
A consultant for the Indonesian Food and Drug Authority (Badan Pengawas Obat dan Makanan, BPOM) involved in the formulation of the national formulary.


We also conducted a comprehensive review of policies, guidelines, and news related to AMR and AMS to re-evaluate the scoring and track the progress made within the past year. The search for published documents was performed by exploring the websites of relevant ministries involved in national AMS implementation, including the Ministry of Health of Indonesia and BPOM. We also searched for relevant publications by international organizations and funders such as the WHO, the Centers for Disease Control and Prevention (CDC), the United Nations Children's Fund (UNICEF), and the Fleming Fund. A snowballing approach was employed to identify relevant publications and documents focusing on AMR, antimicrobial use, and AMS in Indonesia. We combined and adjusted the item scores based on the cumulative scores from the participants and the review of documents on the progress of AMR control and AMS implementation activities.

Establish and develop national coordination mechanisms for antimicrobial stewardship and develop guidelines
Establish
Current status:
Partially implemented
As guided by the Global Action Plan (GAP) [14] in 2017, the Ministry of Health (MoH) of Indonesia, in collaboration with the World Health Organization (WHO), developed and issued a National Action Plan (NAP) on AMR control for 2017–2019 [15] Despite progress, there were challenges in effectively incorporating AMS activities and approaches within the broader One Health framework, including coordination with other relevant ministries. Consequently, the NAP for the period 2020–2024 was introduced under Regulation Number 7 of 2021 by the coordinating minister for Human Development and Cultural Affairs [16], with the objective of addressing this issue.
The national policies on integrated AMS activities for human health, which encompass regulations, guidelines, and strategies, are issued by the MoH and the Indonesian Food and Drug Authority (Badan Pengawas Obat dan Makanan, BPOM). These policies are aimed at regulating and guiding AMS implementation in hospitals or healthcare facilities and in the community. However, to date, there is no specific national-level policy on integrated AMS activities in primary healthcare (PHC) settings [20].
a. Policy of the Ministry of Health
* Policy on national coordination on integrated AMS implementation and AMR control and surveillance:
The National Institute of Health Research and Development (Badan Penelitian dan Pengembangan Kesehatan, Balitbangkes), was appointed Center for the National Coordination of the National Surveillance System of AMR under the Decree of the Minister of Health Number HK.01.07/MENKES/722/2019 [16]; National Reference Laboratory (NRL) and sentinel sites were designated for the Implementation of Global Antimicrobial Resistance and Use Surveillance System (GLASS) under the Decree of the Director General of Health Services Number HK.05.07/2020[16];
Decree of the Minister of Health Number HK.01.07/MENKES/6460/2021 on the establishment of the Committee on Antimicrobial Resistance Control (Komite Pengendalian Resistensi Antimikroba, KPRA) [21];
Item 1.1.
* Policy on integrated AMS activities in hospitals or healthcare facilities
Regulation of the MoH Number 2406 of 2011 on Guidelines of Antibiotic Use, aiming to guide prescribers in antibiotic decision-making [22];
Regulation of the MoH Number 58 of 2014 on Standards of Pharmacy Services in Hospitals, delineating the regulations on standardized hospital pharmacy services; management of pharmaceutical preparations, equipment, and consumables; and monitoring of drug safety and efficacy [23];
Regulation of the MoH Number 8 of 2015 on AMR Control Program in Hospitals, aiming to guide hospitals in the development and implementation of hospital AMS programs, the formation of hospital AMS teams or committees, and monitoring and evaluation of hospital AMS programs [24];
Regulation of the MoH Number 27 of 2017 on Guidelines on the Prevention and Control of Infections in Healthcare Facilities, with the goals to ensure patient safety and to prevent healthcare-associated infections through IPC implementation, surveillance, monitoring, and prudent use of antimicrobial agents [25];
Regulation of the MoH Number 5 of 2019 on Planning and Procurement of Drugs Based on Electronic Catalogs, aiming to track, monitor, and evaluate the purchase, access, and availability of drugs in healthcare facilities through the electronic catalog system [26];
Regulation of the MoH Number 28 of 2021 on Guidelines on Antibiotic Use, aiming to guide prescribers in antibiotic decision-making [27];
Decree of the MoH of the Republic of Indonesia Number HK.01.07/MENKES/1970/2022 on the Amendment to MoH Decree number HK.01.07/MENKES/6485/2021 on the National Formulary [28];
Regulation of the MoH Number HK.01.07/MENKES/1128/2022 on Hospital Accreditation requires hospitals to form an AMS team and implement AMS programs [29]
* Guidelines on integrated AMS activities in hospitals or healthcare facilities
The National Guideline on AMS Implementation in Hospitals, First Edition, was released in 2021 by the Directorate General Health Services of the MoH in collaboration with the WHO [30]
The Guideline for Managing Damaged and Expired Medicines in Healthcare Facilities and Households was released in 2020 by the MoH to guide the handling and disposal of drugs in health facilities and households [31]
* Policy on integrated AMS activities in the community
Regulation of the MoH Number 35 of 2014 on Standards of Pharmacy Services in Pharmacies, delineating the regulations on standardized pharmacy services (including home pharmacy care); management of pharmaceutical preparations, equipment, and consumables; monitoring of drug safety and efficacy; and access to medicine [32]
Regulation of the MoH Number HK 02.02/MENKES/427/2015 on Smart Community Movement in Using Drugs (Gerakan Masyarakat Cerdas Minum Obat, GeMa CerMat), aiming for prudent selection, use, storage, and disposal of medicine in the community through education for the community [33]
Item 1.1. (con’t)
GeMa CerMat Program Implementation Guideline was released in 2020 by the MoH to guide the implementation of the program, including the coordination mechanisms, intervention strategies, monitoring and evaluation, and standardized tools and indicators to assess program outcomes [34]
The Guideline for Managing Damaged and Expired Medicines in Healthcare Facilities and Households was released in 2020 but the MoH to guide the handling and disposal of drugs in health facilities and households [31]
Regulation of the Food and Drug Authority Number 34 of 2018 on Guidelines for Good Medicine Manufacturing, which delineates the standardized criteria for good drug manufacturing, quality assurance, product quality assessment, quality risk management, supervisory mechanisms, and procedures for imposed sanctions.35Following this regulation, in 2018, BPOM released the Guideline on Good Manufacturing Practice (updated from the 2012 Guideline) [36]
Regulation of the Food and Drug Authority Number 4 of 2018 on Management Supervision of Drugs, Remedies, Narcotics, Psychotropics, and Pharmaceutical Precursors in Pharmaceutical Service Facilities, which stipulates that prescription drugs are only available on prescription [37]
Regulation of the Food and Drug Authority Number 8 of 2023 on the Guidelines Assessing Efficacy and Safety of Antibacterial Drugs [38]
Item 1.2.
Current status:
Fully implemented
Is there a central national coordination unit at the Ministry of Health or designated agency or institution focused on AMS?
The management of national coordination for AMS in healthcare facilities is currently overseen by the Committee on Antimicrobial Resistance Control (Komite Pengendalian Resistensi Antimikroba, KPRA). KPRA was established in 2021 under the Decree of the Minister of Health Number HK.01.07/MENKES/6460/2021.21 This committee operates as an independent agency under the MoH and comprises various experts and consultants from both internal and external entities of the MoH. There are five working groups in the committee, including one designated for AMS:
1. Awareness;
2. Surveillance and research;
3. Infection prevention and control;
4. Antimicrobial stewardship;
5. Innovation and investment.
The roles of KPRA are described in item 1.7, the terms of reference (ToR) of KPRA.
Item 1.3.
Current status:
Partially implemented
Has the central national coordination unit established a national coordination mechanism for integrated AMS activities with diverse membership, including civil society and the private sector?
Indonesia has established a multisectoral central national coordination unit for AMR control, including in the One Health framework. However, the coordination mechanism for integrated AMS activities in all sectors of human health has not yet been integrated at the national level, despite the existing collaboration between diverse groups. For example, the MoH collaborated with Pfizer and IQVIA (private sectors), the Clinical Microbiology Professional Association (a professional organization), and the WHO (a non-governmental organization, NGO) in developing the first edition of the national AMS guideline published in 2021 and training hospitals on the implementation of this guideline. Another example is the collaboration between Yayasan Orang Tua Peduli, YOP (a civil society), Pfizer (private sector), hospitals, and pharmacies initiated in 2021, called the “Victory program” through the 2T movement: Tuntas menentukan (complete assessment) and Tuntas menggunakan (complete use) [39].
“Complete assessment” focuses on healthcare professionals to perform a complete assessment to determine diagnosis in order to support AMS implementation in their respective hospitals. The program activity includes a series of virtual educational workshops to help strengthen the capacity of the hospital AMS team. “Complete use” focuses on patients, aiming for patients to take a complete dose of antibiotics based on their doctor's recommendations. Pfizer offers assistance for patients who need antibiotics but cannot afford them, so they are able to consume the full dose of antibiotics. This program engaged 20 partner pharmacies in 17 cities in Indonesia [39].
Item 1.4.
Current status:
Partially implemented
Have similar coordination mechanisms with diverse members, including from civil society and the private sector, been established at subnational and district levels?
To date, the AMS coordination mechanisms aiming for AMS implementation in hospitals are mainly available at the national level and not yet at the subnational (provincial and district) levels. At the community level, there is a community-based program initiated in 2015, called GeMa CerMat (see item 1.1 for the relevant policy on GeMa CerMat). The primary objective of this program is to increase awareness and promote behavioral changes in the community, encouraging them to make informed decisions regarding the selection, obtaining, usage, storage, and disposal of medicine [33,34]. Despite the primary objective of this program does not specify the term “antimicrobial stewardship,” in the rising awareness and attention to AMR, AMS-related behavior change has become one of the main focuses of its implementation. At the ground level, an essential aspect of GeMa CerMat is the active participation of community pharmacists as agents of change who play a pivotal role in educating the community and improving their awareness and practices regarding the selection, use, storage, and disposal of medicine, including antimicrobial agents [33,34]. At the higher level, in its implementation, GeMa CerMat involves stakeholders from different government levels (MoH in collaboration with provincial and district governments) and sectors, including health professional organizations (e.g., the Indonesian Pharmacists Association), universities, religious leaders, community leaders, the media, and other community elements.
Item 1.5.
Current status: No
Are there clear reporting lines and feedback mechanisms from subnational mechanisms to the national coordination mechanism on integrated AMS activities?
To date, there are no well-defined integrated reporting lines or feedback mechanisms from the subnational levels (provincial and district) to the national level concerning AMS activities.
Item 1.6.
Current status:
Partially implemented
Is there funding allocated for the national coordinating unit and the national, subnational and district coordination mechanisms?
In the past, AMS implementation at the national level faced challenges due to the limited funding allocated for such activities, and consequently mainly relied on international donors. For example, in 2019, the KPRA conducted monitoring and evaluation in hospitals, but these activities had to be discontinued due to budget constraints. Despite the availability of international funding like the Fleming Fund and Captiva, these schemes only covered specific AMS-related activities, such as AMS trainings, AMR surveillance, the development of information and technology (IT) systems and enhancing the capacity of the National Reference Laboratory (NRL) and sentinel sites.
Over the past three years, notable progress has been made in regard to the allocation of funding for AMR control and integrated AMS activities. At the national scale, a cumulative budget of USD 12,615,225 (with an exchange rate of 1 USD to IDR 15,000) has been designated for AMR control within the One Health framework across four ministries and one agency for the years 2020 to 2024 [16]. Under this budget allocation, in regard to integrated AMS implementation for human health, USD 4,794,878 was allocated to the MoH and USD 416,877 to BPOM. However, a mechanism for coordinating budget allocations for AMS activities at the subnational levels (provincial and district) is currently absent.
Current status: Fully implemented
Yes. The ToR for the national coordination unit, or KPRA, is delineated in the Decree of the Minister of Health Number HK.01.07/MENKES/6460/2021.21
1. The roles of KPRA are to:
Developing a strategic and action plan for national AMR control programs. Providing recommendations to the MoH regarding the framework of AMR control policies in healthcare facilities, including hospitals, community health centers (Puskesmas), clinics, laboratories, etc.
Providing recommendations to the MoH regarding the AMR control programs in the community.
Assisting the AMR control program manager in the program’s implementation. Providing expertise to support the improvement in human resource management and technical capabilities of the implementers of the AMR control programs.
Providing recommendations regarding the advanced action plan for further development and expansion of the AMR control programs and research, AMR surveillance, and prudent antimicrobial use.
Performing an evaluation of the national AMR control program’s achievements as recommendations for program improvement. Submitting regular reports to the MoH.
2. In carrying out the tasks outlined above, KPRA can coordinate with relevant ministries/agencies and cross-sectors and form an ad hoc team as needed.
3. Funding that arises as a result of carrying out KPRA tasks is borne by the Budget Implementation Entry List of the Directorate General of Health Services and/or other sources of funds that are not binding in accordance with the provisions of laws and regulations.
4. The working period of the current KPRA membership is valid from 20 January, 2020, until 31 December, 2024.
Item 1.8.
Current status:
Partially implemented
Item 1.9.
Current status:
Partially implemented
Is there a linkage to other relevant stakeholders e.g. from tuberculosis (TB), infection protection and control (IPC), water, sanitation and hygiene (WASH) or universal health coverage (UHC)?
The linkage between AMS and IPC stakeholders is evident from the involvement of IPC stakeholders from relevant subdirectories within the MoH engaging in IPC and from the Indonesian Society of Infection Control in the IPC working group of the KPRA [40]. Nevertheless, the linkage with stakeholders from WASH, UHC (or Jaminan Kesehatan Nasional, JKN—the UHC scheme in Indonesia), malaria, TB, and HIV was limited to providing expertise based on demand. There has been ongoing discussion with the JKN stakeholders related to diagnostic stewardship, AMU and restrictions, and payment schemes for certain infectious diseases. Nevertheless, hospitals are accountable for the technical components of JKN implementation on the ground. Therefore, stakeholders at the national level cannot dictate the implementation of these technical components.
Is there a monitoring and evaluation (M&E) framework and have national targets been set for AMS activities based on nationally and internationally agreed indicators?
The NAP for years 2020 to 2024 outlines the nationally agreed M&E framework and indicators to assess the achievements of activities based on the NAP objectives, including to minimize the emergence and spread of resistance microbes; to ensure the availability of safe, effective, high-quality, and affordable antimicrobial agents; and to ensure prudent and responsible use of antimicrobials [16]. For human health, the targets and indicators for 2024 are:
To decrease the prevalence of Extended Spectrum Beta-Lactamase (ESBL) by 10% (from the current prevalence of 62%);
To maintain the prevalence of qualified antimicrobials in circulation (98%);
To decrease the prevalence of antimicrobial use at first-level healthcare facilities for non-pneumonia acute respiratory (from 21.28% to ≤ 20%) and non-specific diarrhea (from 18.27% to ≤ 8%).16
Furthermore, to monitor and evaluate AMS implementation in hospitals, the MoH released the National Guideline on AMS Implementation in Hospitals, First Edition, in 2021 [30]. This guideline includes the AMS framework, assessment tool, and indicators. Furthermore, the assessment tool and indicators in this guideline follow the “Hospital Antimicrobial Stewardship Program Assessment Checklist,” developed between 2016 and 2017 by a panel consisting of experts in infectious diseases, researchers, and leaders from Asian countries [41]. The questions included in the checklist are consistent with the Transatlantic Taskforce on Antimicrobial Resistance (TATFAR) set of core and supplementary indicators for hospital AMS programs [42,43], and with the US CDC checklist for core elements of hospital AMS programs [44]. The assessment of the compliance of this AMS guideline has not taken place yet, but it is regarded as a priority.
Item 1.9.
(con’t)
To date, there is no policy or guidelines for AMS in PHC, hence, the M&E framework in this context remains absent. At the community level, the guidelines for GeMa CerMat program implementation (see item 1.4 for an elaboration on GeMa CerMat) has not yet included indicators to assess behavior changes specific to antimicrobial use.
Item 1.10.
Current status:
No,but a priority
Have other programmes, such as IPC, WASH, TB, malaria, HIV, UHC and primary health care (PHC), integrated AMS activities within their action plans?
The AMS activities are not currently integrated with WASH or UHC, and partially integrated with IPC. Integrated AMS activities for tuberculosis,45 malaria,46 and HIV47 programs are limited to the provision of treatment guidelines for these three syndromes. AMS is currently not available in PHC. There is, however, a proposal to formulate AMS regulations for PHC settings.
Item 2.1.
Current status: Fully implemented
Have the national treatment guidelines for the management of infections been updated within the last 3–5 years?
The 2011 national guidelines for antibiotic treatment applicable for healthcare facilities have been updated in 2021 [27].
Item 2.2.
Current status:
Fully implemented
Item 2.3.
Current status: No, but a priority
Do the national treatment guidelines include AMS principles?
The 2021 national guidelines for antibiotic use [27] have incorporated the AMS principles, including antibiotic categorization based on the WHO AWaRe (Access, Watch, Reserve) classification.
Item 2.4.
Current status: Planned but not started
Is there monitoring of implementation and compliance to treatment guidelines?
Currently, there is no established integrated national-level mechanism to oversee the implementation and adherence to treatment guidelines. However, according to Regulation of the MoH Number HK.01.07/MENKES/1128/2022 on Hospital Accreditation,29 hospitals are obligated to implement AMS programs and monitor compliance with antibiotic guidelines. As a result, some hospitals have conducted evaluations of antibiotic use and adherence to guidelines at the hospital level, as indicated in a systematic review and metaanalysis of studies conducted in Indonesia between 2000 and 2021 [12].
Is there coordinated guidance and interventions to improve availability and appropriate use of diagnostics to guide therapeutic decisions?
At the national level, there is no such mechanism yet. However, as described in item 1.8, there has been ongoing discussion with the JKN stakeholders related to diagnostic stewardship to ensure the availability and use of infection diagnostics under the JKN scheme.
Item 2.5.
Current status: Partially implemented
Are there specific standard operating procedures for AMS activities in health-care facilities and in community settings?
At the national level, guidelines have been established for implementing integrated AMS programs in healthcare facilities (specifically hospitals) and community settings. However, as described in item 1.1, there is currently no specific policy, or guideline, or SOP for AMS activities in PHC [20]. According to the regulation of the Minister of Health Number HK.01.07/MENKES/1128/2022 on Hospital Accreditation [29], hospitals are required to develop their own AMS strategies and SOPs. Some healthcare facilities with active AMS programs have developed their own facility-specific SOPs developed locally for specific activities and interventions, such as auditfeedback of antimicrobial prescriptions and guidelines on assessing the risks of infection with antibiotic-resistant microorganisms.
In the community, the MoH released Regulation of the Minister of Health Number HK 02.02/MENKES/427/2015 on Smart Community Movement in Using Drugs (GeMa CerMat, Gerakan Masyarakat Cerdas Minum Obat) in 2015 [33]. Subsequently, the MoH launched a guideline covering the SOPs for the GeMa CerMat program’s planning, implementation, and coordination, as well as the tools and indicators for monitoring and evaluation [34].
Item 2.6.
Current status: Partially implemented
Are there mechanisms and activities for the dissemination of guidelines, standards & implementation tools on AMS activities?
The AMS guidelines and tools have been widely distributed through a range of activities, such as uploading them to pertinent websites, organizing seminars, and collaborating with professional organizations or groups. Nevertheless, there is no mechanism yet to assess whether all hospitals and healthcare professionals have accessed these guidelines.

Item 3.1.
Improve access to essential, quality-assured, safe, effective and affordable antimicrobials
Has the WHO Model List of Essential Medicines (EML) and Access, Watch, Reserve (AWaRe) system been incorporated into the national EML formulary and health-care facility treatment guidelines?
Current status:
Partially implemented
The WHO EML has been integrated into the national formulary based on the Decree of the Minister of Health of the Republic of Indonesia Number HK.01.07/MENKES/1970/2022 on the Amendment to Minister of Health Decree number HK.01.07/MENKES/6485/2021 on the National Formulary [28]. The AWaRe classification has been incorporated into the recent Guidelines on Antibiotic Use under the Regulation of the Minister of Health Number 28 of 2021 [27] and the National Guideline on AMS Implementation in Hospitals, First Edition, released in 2021 [30]. Hospitals that cater to patients under the JKN scheme are required to adhere to the national formulary. However, there is no system at the national level to track whether all healthcare facilities, including hospitals and PHCs, in Indonesia have incorporated the EML and AWaRe systems into the antibiotic guidelines at the facility level.
Item 3.2.
Is there a system in place to monitor access to essential, quality- assured, safe, effective and affordable antimicrobials?
Current status: Partially implemented
As elaborated in item 1.1, the MoH and BPOM released the regulations and guidelines to ensure and monitor access to essential, quality-assured, safe, effective, and affordable antimicrobials:
Regulation of the MoH Number 5 of 2019 on Planning and Procurement of Drugs Based on Electronic Catalogs, aiming to track, monitor, and evaluate the purchase, access, and availability of drugs in healthcare facilities through the electronic catalog system [26];
1. The Regulation of the Food and Drug Authority Number 34 of 2018 on Guidelines for Good Medicine Manufacturing, which delineates the standardized criteria for good drug manufacturing, quality assurance, product quality assessment, quality risk management, supervisory mechanisms, and procedures for imposed sanctions [35];
2. The Regulation of the Food and Drug Authority Number 8 of 2023 on the Guidelines Assessing Efficacy and Safety of Antibacterial Drugs [38];
4.
3. HCFs, including hospitals and PHCs, implementing the JKN scheme are required to order drugs through the e-catalog provided by the Government Purchasing Goods/Services Policy Authority (Lembaga Kebijakan Pengadaan Barang/Jasa Pemerintah, LKPP). The monitoring of access to drugs, including antimicrobial agents, is performed electronically through the drug purchased through the e-catalog [26], including the drug order, distribution, and payment. Besides, hospitals are required to send a monthly report to the MoH regarding the drug supply, including antimicrobials, in the respective hospitals. The antimicrobial supply list from the hospitals has to match the list in the national formulary. In addition, the MoH imposes a certain target for hospitals to meet the antimicrobial availability based on the national formulary. However, the MoH cannot monitor if hospitals or prescribers prescribe antibiotics outside the reported list or unnecessary antibiotics to patients. Furthermore, the existing JKN payment system incorporates a ceiling mechanism that does not consider the various components of payment, including antibiotic prescriptions. Consequently, it becomes challenging to evaluate the appropriateness of antibiotic prescribing and identify any instances of unnecessary antibiotic prescriptions. The MoH is currently engaged in efforts to consolidate and analyze data at the national level, with the aim of evaluating the appropriateness of prescription practices in the near future.
Item 3.3.
Current status:
No
Item 3.4.
Current status: No
Item 3.5.
Current status: No, but a priority
Item 3.6.
Current status:
Partially implemented
Pillar 2
Is there a system to periodically identify availability of affordable antibiotics at health-care facilities?
There is currently no system in place at the national level to periodically identify the availability of affordable antibiotics at healthcare facilities to allow for prompt intervening actions when required. The data are exclusively accessible within individual hospitals, posing challenges for the government to monitor the availability of affordable antibiotics. The hospital pharmacy department typically seeks alternative drug supplies autonomously in the event of stockouts, often resorting to utilizing drugs from different brands or patented alternatives.
Is there a mechanism in place to report shortages and stock-outs of antibiotics in the country?
There is currently no established reporting mechanism in place for hospitals to periodically monitor and notify the government in the event of a shortage or stockout of antibiotics and promptly have solutions when required.
Is there a mechanism to report the antibiotics used by patients?
There is no nationwide system to monitor antibiotics used by patients in healthcare facilities or in community settings, and this is a priority for the government at the moment.
Is there a process to report the antibiotics used in the AWaRe system?
The AWaRe classification has been integrated into the 2021 Guidelines on ABU in the categorization of antibiotics [27] and the first edition of the National Guideline on AMS Implementation in Hospitals released in 2021 [30] as indicators in assessing antibiotic use. Consequently, the MoH has begun the process of reporting antibiotic use based on the AWaRe classification.
Item 4.1.
Current status: Partially implemented
Assessment report of AMS implementation at the national level
Are health worker behavioral change principles incorporated into policies addressing diagnosis, prescription, dispensing and administration of antimicrobials?
In the context of hospitals, the following national-level policies and guidelines have incorporated various mechanisms to support behavioral change in addressing diagnosis, prescription, dispensing, and administration of antimicrobials in hospitals:
Regulation of the MoH Number 58 of 2014 on Standards of Pharmacy Services in Hospitals [23]
Regulation of the MoH Number 8 of 2015 on AMR Control Program in Hospitals [48]
Regulation of the MoH Number 27 of 2017 on Guidelines on the Prevention and Control of Infections in Healthcare Facilities [25]
Regulation of the MoH Number 28 of 2021 on Guidelines on Antibiotic Use [27]
The National Guideline on AMS Implementation in Hospitals, First Edition, released in 2021 by the Directorate General Health Services of the MoH [30]
Regulation of the MoH Number HK.01.07/MENKES/1128/2022 on Hospital Accreditation [29]
The hospital AMS team has to work in conjunction with the hospital pharmacy and therapeutics committee, the IPC committee, and the quality and patient safety committee. In this instance, the pharmacy and therapeutics committee have the role of supervising the dispensing of antimicrobial drugs. The IPC committee is involved in preventing and controlling the spread of resistant microorganisms. The quality and patient safety committee is responsible for addressing issues related to the quality of patient care and ensuring their safety. The National Guideline on AMS Implementation in Hospitals outlines the specific responsibilities of the AMS team, which encompass conducting prospective reviews and offering feedback to prescribers, as well as providing consultation and recommendations pertaining to the diagnosis and management of infectious diseases and antimicrobial prescriptions [30]. Hospitals have implemented clinical pathway guidelines, integrating patient safety and practices for prudent drug use. Additionally, all hospitals are required to implement the specified policies and guidelines concerning AMR, AMS, and IPC, as mentioned earlier.
Item 4.1. In the context of community pharmacies, the behavioral change principles were incorporated in Regulation of the Minister of Health Number 35 of 2014, delineating the standardized pharmacy services, including home pharmacy care, dispensing of drugs, and correct administration of drugs.32 Regulation of the Minister of Health Number HK 02.02/MENKES/427/2015 on Smart Community Movement in Using Drugs (GeMa CerMat) describes the roles and activities of community pharmacies as educators and agents of change to educate the communities about the selection, use, storage, and disposal of drugs.(33)
In the context of PHC, Regulation of the Minister of Health Number 27 of 2017 on Guidelines on the Prevention and Control of Infections in Healthcare Facilities25 and Regulation of the Minister of Health Number 28 of 2021 on Guidelines on Antibiotic Use27 are also applicable in this context. However, there is currently no policy addressing behavioral change principles related to AMS implementation in the PHC context.
Furthermore, the similar aforementioned policies at the subnational levels (provincial and district) remain unknown.

Item 5.1.
Current status: Fully implemented
Is there a regulation on prescription-only sale/ dispensing of antibiotics?
Concerning antimicrobial prescribing and dispensing at the community level, the Regulation of the Food and Drug Authority Number 4 of 2018 imposes restrictions on the dispensation of antibiotics [37]. Only licensed pharmacists are authorized to dispense antibiotics upon verification of a valid prescription. Conversely, drug stores are strictly prohibited from selling any form of restricted drug, including antibiotics, regardless of the circumstances. Moreover, pharmacies are required to have a licensed pharmacist present, while drug stores must have a pharmacy technician overseeing the process of drug dispensing [37]. In healthcare facilities, Regulation of the Minister of Health Number 28 of 2021 defines the authority and procedures for antibiotic prescribing and dispensing [27].
Item 5.2. Are regulations on dispensing antibiotics by prescription only being enforced (where access is not an issue)?
Current status: Partially implemented
Regulations on dispensing antibiotics by prescription only are in effect and are in place in all registered pharmacies and healthcare facilities (as described in item 5.1). However, the enforcement of antimicrobial dispensing has not been consistently and uniformly applied in all settings. A study carried out in 2019, encompassing urban and rural areas of Indonesia, revealed that the dispensing of antibiotics without prescriptions remained prevalent in both pharmacies (76%) and drug stores (50.4%) [49]. Moreover, dispensing over-the-counter medicines that require prescription by physicians is common (according to the results of several small-scale community studies), and greater regulatory measures are needed to reduce inappropriate antibiotic use in community settings.
Current status:
Fully implemented
Assessment report of AMS implementation at the national level
The BPOM issued Regulation of the Food and Drug Authority Number 34 of 2018 on Guidelines for Good Medicine Manufacturing, which delineates the standardized criteria for good drug manufacturing, quality assurance, product quality assessment, quality risk management, supervisory mechanisms, and procedures for imposed sanctions [35]. Following this regulation, BPOM released the Guideline on Good Manufacturing Practice (updated from the 2012 Guideline) [36]. Furthermore, BPOM oversees the monitoring of pharmaceutical products through the issuance of dissemination permits. This process involves the sampling of drugs to be distributed to health facilities. In the case of substandard drugs, the respective companies responsible will be subject to varying degrees of reprimand. This involves a scenario wherein a company is requested to rectify the pharmaceutical products. During this process, the company is rendered ineligible to distribute the drugs until they have successfully undergone tests by BPOM. The BPOM will ask the pharmacies to provide details regarding the specific batch and brand name of the substandard products and request the return of the respective drugs to the supplier. In the case of counterfeit or falsified drugs, the illicit drugs will be confiscated, and the implicated company will face penalties.
However, a study conducted between 2017 and 2018 reported challenges related to the manufacturing of substandard and falsified drugs [50], which has implications for the sale of these drugs. The quality of drugs was influenced by market forces, such as government pressure to lower medicine prices to help achieve UHC and incentives for healthcare providers. The pressure to lower medicine prices had the implication of substandard drug manufacturing because revenues could not cover the cost of quality-assured production and legitimate manufacturers did not get a fair profit [50]. Consequently, despite the regulations and oversight mechanisms imposed by BPOM to restrict the sale of substandard and falsified drugs, there were contradictory mechanisms that hindered these efforts and prevented effective enforcement of regulations.
Current status:
Fully implemented
These following policies, released by the MoH and BPOM, delineate the standards and criteria for responsible manufacturing and disposal of medicine, including antimicrobial agents:
The Regulation of the Food and Drug Authority Number 34 of 2018 on Guidelines for Good Medicine Manufacturing, which delineates the standardized criteria for good drug manufacturing, quality assurance, product quality assessment, quality risk management, supervisory mechanisms, and procedures for imposed sanctions [35]
The Guideline on Good Manufacturing Practice issued by BPOM in 2018 [36]
The Guideline for Managing Damaged and Expired Medicines in HCFs and Households issued by the MoH in 2020 to guide the handling and disposal of drugs in health facilities and households [31]
In practice, BPOM works with the pharmacy department in healthcare facilities and community pharmacies to handle expired or spoiled drugs.

Item 6.1.
Current status:
Partially implemented
Have studies on determinants of behavior in health professionals and other stakeholders, including the general public, been completed to support design of awareness campaigns?
There have been small-scale studies in communities and healthcare facilities on knowledge, attitudes, and practices (KAP), as well as associated factors of health workers’ and community behaviors in antimicrobial prescription, antimicrobial use, and AMR. Most of these studies were carried out by research institutes, NGOs, and healthcare facilities [13,49,51,52]. Hence, systematic surveillance of KAP and related factors is needed in order to increase representativeness and track indicators over time, providing evidence for the planning and evaluation of the effectiveness of antibiotic awareness, and AMR interventions. The findings of the studies to date have been limited in their reach, primarily reaching specific audiences, for example, academics and clinical staff engaged in AMS programs, and only limited study results have been used to design AMR awareness-raising activities and behavioral change programs, which include campaigns targeted at the general public.
Item 6.2.
Current status:
Fully implemented
Does the country hold World Antimicrobial Awareness Week (WAAW) activities annually?
The WAAW events have been regularly organized and conducted by the national government and various institutions, such as universities, hospitals, professional groups, and non-government organizations.
Item 6.3.
Current status: Fully implemented
Does the country have regular public awareness campaigns on the responsible and appropriate use of antibiotics?
Multiple strategies have been implemented to enhance public awareness concerning appropriate antibiotic use. One such approach involves the availability of YouTube videos and podcasts presented by experts in AMR and infectious diseases, which serve to educate the public about proper antibiotic use. GeMa CerMat implementation involves various stakeholders from different sectors, including health professional organizations, universities, religious leaders, community leaders, the media, and other community elements. An essential aspect of the program involves the active participation of community pharmacists, who play a pivotal role in educating the community and improving their awareness and practices regarding drug use, including antimicrobials [33,34]. Additionally, professional groups such as “The Indonesian Pharmacists Association” and civil society organizations like Yayasan Orang Tua Peduli have initiated various programs and activities to boost public literacy and prudent drug usage. These efforts involve training and educational programs, consultations with pharmacists, doctors, or other healthcare providers, as well as the provision and distribution of relevant posters, leaflets, and brochures [53,54].
Item 6.4.
Current status: Partially implemented
Are tailored AMS messages integrated into broader health promotion, prevention, treatment and rehabilitation services and initiatives such as World Water Day, World Toilet Day, World Children’s Day, immunization campaigns, World AIDS Day, World TB Day, World Malaria Day and World Nutrition Week for sustained action?
Tailored AMS messages have been integrated into World TB Day but not yet into other broader health promotion, prevention, treatment, and rehabilitation services and initiatives.
Item 6.5.
Current status: Partially implemented
Is regular assessment/evaluation of the impact of education and awareness campaigns on knowledge attitudes and behaviors of health workers and the public conducted?
There are published reports on the GeMa CerMat program’s outputs from several sites or districts [55,56]. However, to date, there is no report showing whether the evaluations of the effectiveness of training and awareness campaigns on the KAP of health workers and communities throughout the country are regularly performed.
Item 7.1.
Current status:
No, but a priority
Strengthen health worker capacity through the provision of tailored education and training packages according to health worker roles and functions
Are AMS principles and strategies included in the educational curriculum of pre-service healthcare professionals?
Medical students have been exposed to the principles of prudent antibiotic usage, which are based on evidence of disease-causing microorganisms, through pre-clinical subjects like clinical microbiology, pharmacology, and internal medicine. However, to date, the AMS program has not been incorporated as a standalone subject in the pre-clinical curriculums for healthcare professionals, including doctors, nurses, midwives, and relevant allied health professionals. Nevertheless, the KPRA has actively participated in discussions with public universities, advocating for the integration of AMS principles into the medical curriculum.
Item 7.2.
Current status: Partially implemented
Is there access to in-service training, including continuous professional development (CPD) on antimicrobial prescribing and AMS for all healthcare professional groups in the country?
The MoH, the KPRA, health professional organizations, NGOs, hospitals, universities, and pharmaceutical companies (in collaboration or independently) have organized trainings for healthcare professionals regarding antimicrobial prescribing and AMS programs in various formats. Attendees of these trainings were also rewarded with continuous medical education (CME) credit points. Healthcare workers are encouraged and supported to take part and receive CME credit points. However, depending on the actual conditions in their healthcare facilities and on appropriate professional contents, these trainings have not been able to reach every healthcare professional nationwide, and the access and quality of such training initiatives remain inconsistent.
Item 7.3.
Current status: No
Are AMS concepts and principles incorporated within the curriculum of other complementary disciplines e.g. the curriculum for IPC professionals?
Currently, AMS concepts and principles have not been included in the curricula of other complementary disciplines.

Item 8.1.
Current status: No
Is there representation of the AMS coordinating unit on the WASH programmes and vice versa?
As described in item 1.1, there is currently no national policy in place that makes it mandatory for PHC facilities to implement AMS programs. Consequently, there is currently no representation of the AMS coordinating unit on the WASH programs, and vice versa.
Item 8.2.
Current status: Partially implemented
Is the WHO WASH Facility Improvement Tool (FIT) being promoted to assess WASH in healthcare facilities?
The WHO WASH Improvement Tool (FIT) is currently focused on PHC settings and has not been used in hospital settings. In 2020, the collaboration between the national government, WHO, and UNICEF led to the initiation of WASH FIT in 185 Puskesmas (PHC) across five provinces in Indonesia [57].
Item 9.1.
Current status: Partially implemented
Is there representation of the AMS coordinating unit on the IPC programmes and vice versa?
In the hospital context, AMS is integrated with IPC program implementation as part of the activity. IPC procedures and implementation are integrated into the National Guideline on AMS Implementation in Hospitals [30]. Under this guideline, the subcommittee on monitoring of antimicrobial use and monitoring of AMR of microorganisms (which is part of the Drug and Therapeutics Committee) in collaboration with the hospital’s AMS team, and the Drug and Therapeutics Committee in collaboration with the Infection Prevention and Control Department should aim to develop an AMS program and organize its implementation in each hospital. In this process, the head or staff in charge of infection prevention and control is one of the members of the AMS Team.
However, as mentioned earlier, nationwide AMS implementation has not yet included PHC. Therefore, the above arrangements in hospitals have not yet occurred in PHC.
Item 9.2.
Current status: Partially implemented
Are there systems linking the monitoring and reporting of healthcare-associated infections (HAIs), antimicrobial use, AMR, patient outcomes and quality of care?
Systems for monitoring and reporting antimicrobial use are currently in place at the facility and national levels. There are currently no linkages to connect those data with AMR, patient outcomes, or quality of care.

Item 10.1.
Current status:
Partially implemented
Is there a national surveillance programme for antimicrobial resistance, use and consumption with defined structures, governance and work objectives (i.e. data collection, validation, analysis, reporting and data sharing with all stakeholders)?
Currently, Indonesia is in the process of establishing a national surveillance program for AMR. To this end, Indonesia officially joined the WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS) in 2019 [58], which has resulted in enhanced laboratory capacity in the NRL, the implementation of external quality assessment, and the enhancement of infection diagnostic capabilities at the hospital level, all aimed at meeting international standards for AMR surveillance.
In order to achieve this, Indonesia has set up 20 AMR surveillance sites, 16 of which consistently contribute data to GLASS [59]. The MoH has developed a database to report AMR surveillance in hospitals. However, there is no official system to monitor antimicrobial use and consumption. Data on surveillance of antimicrobial use and consumption is not currently shared with stakeholders.
Item 10.2.
Current status: No
Are there guidelines/standard operating procedures for the use of (a) antimicrobial medicines use (AMU), (b) antimicrobial medicines consumption (AMC), and c) AMR data to inform action for national and institutional decision-making to inform action for national and institutional decision-making?
There are no guidelines or standard operating procedures for the use of AMU, AMC, and AMR data to inform action for decision-making at the national and healthcare levels.
Item 11.1.
Current status:
Partially implemented
Is there a plan to strengthen laboratory capacity to support accurate diagnosis for decision-making?
At the national level, efforts have been made to strengthen laboratory capacity by setting up NRL and sentinel sites following Indonesia's participation in GLASS. This initiative is supported by the Fleming Fund. However, progress is still limited, with only a small fraction (40 out of more than 3000 hospitals) being included in GLASS as part of the national plan to enhance laboratory capacity support. These laboratories are required to ensure quality standards according to the GLASS standards.
Item 12.1.
Is there a national M&E framework, including internationally and locally agreed key performance indicators for integrated AMS interventions and activities in human health?
Current status:
Partially implemented
Item 12.2.
Current status:
No
The National Guideline on AMS Implementation in Hospitals, released in 2021, includes a description of the key performance indicators for M&E of AMS interventions in hospitals [30]. While the current priority lies in providing AMS training for hospitals, funding for M&E AMS programs and activities has been allocated for the years 2022, 2023, and 2024, as outlined in the NAP for years 2020–2024 [16]. In 2019, a limited number of 70 hospitals underwent an assessment to evaluate the availability of AMS core elements, funded by Pfizer, although sustainable funding for the continuation of activities has been lacking. However, as described above, the policies and guidelines for AMS implementation in PHC are currently unavailable, and so is the M&E framework in this context.
At the community level, the GeMa CerMat Program Implementation Guideline includes the M&E components, including the nationally agreed standardized tools and indicators to assess program outcomes [34].
Is there an accountability mechanism put in place at the local level which includes positive feedback and recognition of local leadership?
There is currently no specific accountability mechanism related to the implementation of AMS programs at the local level.
The objective of the WHO policy guidance on integrated AMS activities is to provide a set of evidence-based and pragmatic recommendations to drive comprehensive and integrated AMS activities under the oversight of a central national coordination unit or other equivalent national authorities [19]. The guiding principles of this policy guidance are to take into account the national and local contexts and structures of health systems when implementing AMS, to give priority to the AMS activities that are most likely to provide the most benefits based on national and facility need assessments, to strengthen the national and subnational mechanisms for coordinating the implementation of AMS, and to have effective linkages and synergies with AMR-related areas and programs at all levels, including infection prevention and control, WASH, HIV, tuberculosis, malaria, and the UHC agenda [19].
Indonesia developed its first NAP on AMR in 2017 for the period of 2017–2019 [15], which has been extended for another four years, from 2020 to 2024 [16] in response to the GAP and increasing burden of AMR. Consequently, there is substantial progress in the implementation of integrated AMS activities, as reflected in the following key aspects.
The issue of national-level policies aimed at supporting AMS implementation in hospitals or HCFs and the community. These policies include regulations and guidelines to guide AMU in HCFs, enforce hospitals to develop and implement AMS programs, ensure access to quality-assured antimicrobials, regulate antimicrobial dispensing, and prohibit the sale of substandard and falsified drugs. Behavioral change principles have also been incorporated into policies addressing the diagnosis, prescription, dispensing, and administration of antimicrobials.
The establishment of a national-level coordinating unit for AMR control that includes a working group for AMS implementation consisting of stakeholders from the national government and experts in infectious diseases from hospitals, health professional organizations, and civil society.
The national antibiotic guidelines and the national formulary have integrated the WHO EML and AWaRe classification.
The public awareness education and campaign on the responsible and appropriate use of antibiotics are regularly conducted through regular WAAW and a community-based program (GeMa CerMat) initiated by the national government, in collaboration with provincial and district governments, health professional organizations, and civil society.
The integration between AMS and IPC programs, including the representation of IPC stakeholders and experts in the national-level coordinating unit (KPRA) and AMS team in hospitals.
The WHO WASH FIT has been promoted and implemented in PHC settings.
The national M&E framework for AMS implementation in hospitals has included internationally and locally agreed key performance indicators, respectively.
However, this national assessment also identified several gaps in the implementation of integrated AMS activities, which limit the effectiveness of AMS program implementation. Therefore, based on the following gaps, we propose several recommendations to optimize the implementation and outcomes of integrated AMS activities in Indonesia (Table 1).
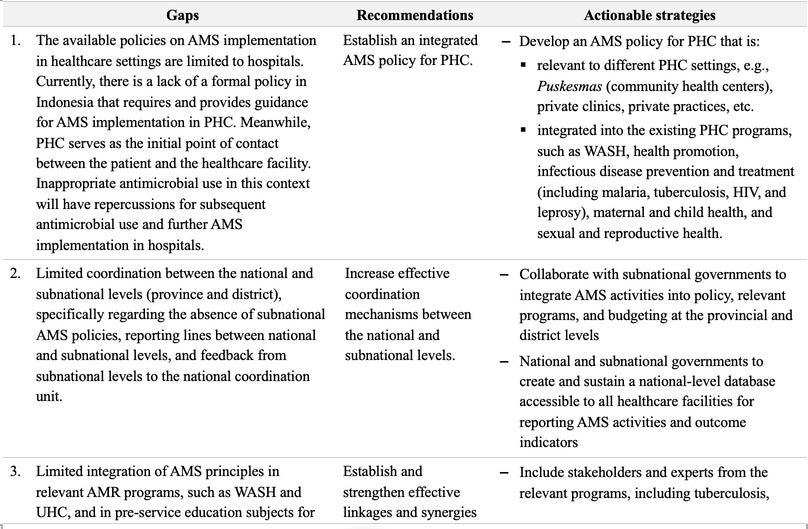
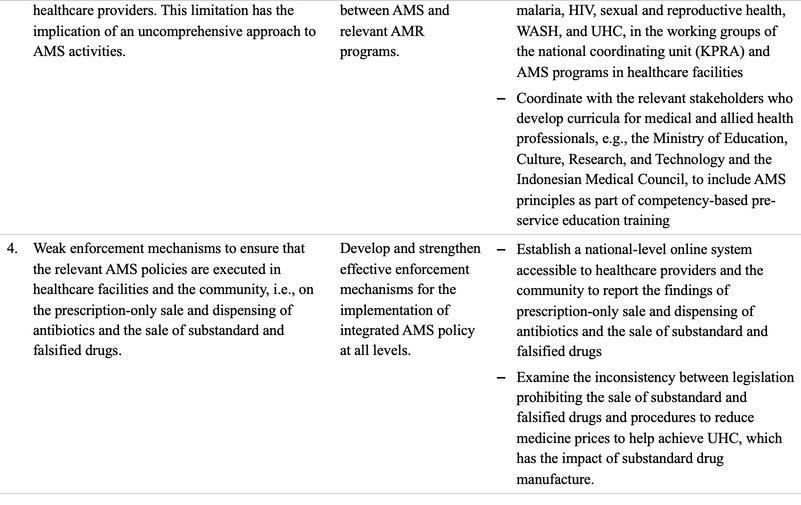
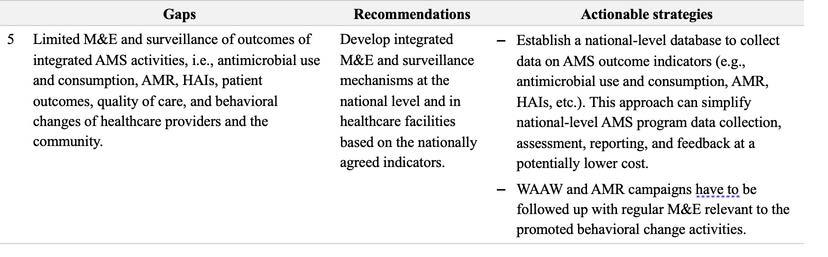
In conclusion, Indonesia has achieved a number of significant milestones and achievements in establishing an integrated national framework for AMS, aiming to ensure the responsible use of antimicrobials and contribute to managing the burden of AMR. Implementation of AMS programs are influenced by various contextual elements, and AMS activities should be conducted in an integrated manner to optimize antimicrobial prescribing and ensure patient and public safety. The AMS coordination unit at the national level must take a leadership role by strengthening collaboration with stakeholders at the subnational levels in strategic policy formulation, planning, and enforcement. This collaboration will determine priorities for AMS implementation as well as oversee policy enforcement and monitor the progress of AMS programs, all aimed at achieving the formulated target indicators.
World Health Organization Regional Office for Europe. Fact sheet on Sustainable Development Goals (SDGs): health targets. Antimicrobial resistance. Copenhagen, 2017 www.euro.who.int/sdgs (accessed July 13, 2023).
Murray CJL, Ikuta KS, Sharara F, Swetschinski L, Aguilar GR, Gray A et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet 2022; 6736. https://doi.org/10.1016/S0140-6736(21)02724-0.
Laxminarayan R, Duse A, Wattal C, et al. Antibiotic resistance—the need for global solutions. Lancet Infect Dis 2013; 13: 1057–98.
Friedman ND, Temkin E, Carmeli Y. The negative impact of antibiotic resistance. Clinical Microbiology and Infection 2016; 22: 416–22.
Naylor NR, Atun R, Zhu N, et al. Estimating the burden of antimicrobial resistance: a systematic literature review. Antimicrob Resist Infect Control 2018; 7: 58.
Wozniak TM, Barnsbee L, Lee XJ, Pacella RE. Using the best available data to estimate the cost of antimicrobial resistance: A systematic review. Antimicrob Resist Infect Control 2019; 8: 1–12.
Macvane SH, Tuttle LO, Nicolau DP. Impact of extended-spectrum β -lactamase-producing organisms on clinical and economic outcomes in patients with urinary tract infection. J Hosp Med 2014; 9: 232–8.
Alsan M, Schoemaker L, Eggleston K, Kammili N, Kolli P, Bhattacharya J. Out-of-pocket health expenditures and antimicrobial resistance in low-income and middle-income countries: An economic analysis. Lancet Infect Dis 2015; 15: 1203–10.
Badan Pusat Statistik Indonesia. Jumlah Penduduk Pertengahan Tahun (Ribu Jiwa), 2021-2023. 2023.
https://www.bps.go.id/indicator/12/1975/1/jumlah-penduduk-pertengahan-tahun.html (accessed July 13, 2023).
Mboi N, Murty Surbakti I, Trihandini I, et al. On the road to universal health care in Indonesia, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet 2018; 392: 581–91.
Parathon H, Kuntaman K, Widiastoety TH, et al. Progress towards antimicrobial resistance containment and control in Indonesia. BMJ (Online) 2017; 358: 31–5.
Limato R, Lazarus G, Dernison P, et al. Optimizing antibiotic use in Indonesia: a systematic review and synthesis of current evidence to inform opportunities for intervention. The Lancet Regional - Southeast Asia 2022; 2. DOI:https://doi.org/10.1016/j.lansea.2022.05.002.
Limato R, Broom A, Nelwan EJ, Hamers RL. A qualitative study of barriers to antimicrobial stewardship in Indonesian hospitals: governance, competing interests, cost, and structural vulnerability. Antimicrob Resist Infect Control 2022; 11: 1–10.
WHO. Global action plan on antimicrobial resistance. Geneva: WHO Document Production Services, 2015 https://apps.who.int/iris/handle/10665/193736.
Kementerian Kesehatan Republik Indonesia. National action plan on antimicrobial resistance Indonesia 20172019. Jakarta, Indonesia, 2017 https://www.who.int/publications/m/item/indonesia-national-action-planon-antimicrobial-resistance-indonesia-2017-2019.
Kementerian Koordinator Bidang Pembangunan Manusia dan Kebudayaan Republik Indonesia. Peraturan Menteri Koordinator Bidang Pembangunan Manusia dan Kebudayaan Republik Indonesia Nomor 7 Tahun 2021 Tentang Rencana Aksi Nasional Pengendalian Resistensi Antimikroba Tahun 2020-2024. Indonesia, 2021.
Komisi Akreditasi Rumah Sakit. Standar Nasional Akreditasi Rumah Sakit Edisi 1. 2017.
Herawati F, Ananta SC, Parwitha IAA, et al. Interview-based cross-sectional needs assessment to advance the implementation of an effective antibiotic stewardship program in Indonesian hospitals. Health Policy Open 2020; 1: 100002.
WHO. WHO Policy Guidance on Integrated Antimicrobial Stewardship Activities. Geneva, 2021.
Ayu Octavi Anjani. Pendekatan One Health untuk Atasi Resistensi Antimikroba. Kompas. 2023; published online May 27. https://www.kompas.id/baca/humaniora/2023/05/27/masih-sulitnya-menanggulangi-resistensiantimikroba (accessed July 21, 2023).
Kementerian Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor Hk.01.07/Menkes/6460/2021 Tentang Komite Pengendalian Resistensi Antimikroba. 2021.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 2406/MENKES/PER/XII/2011 Tentang Pedoman Umum Penggunaan Antibiotik. 2011. https://persi.or.id/wp-content/uploads/2020/11/pmk24062011.pdf.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 58 Tahun 2014 Tentang Standar Pelayanan Kefarmasian di Rumah Sakit. 2014 http://binfar.kemkes.go.id.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesian Nomor 8 Tahun 2015 Tentang Program Pengendalian Resistensi Antimikroba di Rumah Sakit. 2015.
25.
Menteri Kesehatan Republik indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 27 Tahun
2017 Tentang Pedoman Pencegahan dan Pengendalian Infeksi di Fasilitas Pelayanan Kesehatan. Indonesia, 2017.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 5 Tahun 2019
Tentang Perencanaan dan Pengadaan Obat Berdasarkan Katalog Elektronik. 2019.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 28 Tahun 2021 tentang Pedoman Penggunaan Antibiotik. Indonesia, 2021.
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor
HK.01.07/MENKES/1970/2022 Tentang Perubahan Atas Keputusan Menteri Kesehatan Nomor
HK.01.07/MENKES/6485/2021 Tentang Formularium Nasional. 2022.
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor
HK.01.07/MENKES/1128/2022 Tentang Standar Akreditasi Rumah Sakit. 2022.
Direktorat Pelayanan Kesehatan Rujukan, Direktorat Jendral Pelayanan Kesehatan KKR. Panduan Penatagunaan Antimikroba di Rumah Sakit Edisi 1. 2021.
Kementerian Kesehatan Republik Indonesia. Pedoman Pengelolaan Obat Rusak dan Kadaluwarsa di Fasilitas
Pelayanan Kesehatan dan Rumah Tangga. 2021.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 35 Tahun
2014 Tentang Standar Pelayanan Kefarmasian di Apotek. 2014.
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor HK.
02.02/MENKES/427/2015 Tentang Gerakan Masyarakat Cerdas Menggunakan Obat. 2015.
Kementerian Kesehatan Republik Indonesia. Direktorat Jendral Kefarmasian dan Alat Kesehatan. Pedoman
Pelaksanaan Program Gerakan Masyarakat Cerdas Menggunakan Obat (GeMa CerMat). Jakarta, 2020.
Badan Pengawas Obat dan Makanan. Peraturan Badan Pengawas Obat dan Makanan Nomor 34 Tahun 2018
Tentang Pedoman Cara Pembuatan Obat yang Baik. 2018.
Badan Pengawas Obat dan Makanan. Pedoman Cara Pembuatan Obat yang Baik. 2018.
Kepala Badan Pengawas Obat dan Makanan. Peraturan Badan Pengawas Obat dan Makanan Nomor 4 Tahun
2018 Tentang Pengawasan Pengelolaan Obat, Bahan Obat, Narkotika, Psikotropika, dan Prekursor Farmasi di Fasilitas Pelayanan Kefarmasian. 2018.
38.
39. 40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
Kepala Badan Pengawas Obat dan Makanan. Peraturan Badan Pengawas Obat dan Makanan Nomor 8 Tahun 2023 Tentang Pedoman Penilaian Khasiat dan Keamanan Obat Antibakteri. 2023.
PT. Pfizer Indonesia. Kemitraan Sektor Swasta dan Peran Masyarakat Diperlukan dalam Mempromosikan Penggunaan Antibiotik Secara Rasional dan Tuntas. 2021; published online June 21.
https://www.pfizer.co.id/news/kemitraan-sektor-swasta-dan-peran-masyarakat-diperlukan-dalammempromosikan-penggunaan-antibiotik-secara-rasional-dan-tuntas (accessed Aug 14, 2023).
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor
HK.01.07/Menkes/55/2020 Tentang Komite Pengendalian Resistensi Antimikroba. 2020.
Apisarnthanarak A, Kwa ALH, Chiu CH, et al. Antimicrobial stewardship for acute-care hospitals: An Asian perspective. Infect Control Hosp Epidemiol 2018; 39: 1237–45.
Pollack LA, Plachouras D, Sinkowitz-Cochran R, Gruhler H, Monnet DL, Weber JT. A concise set of structure and process indicators to assess and compare antimicrobial stewardship programs among EU and US Hospitals: Results from a multinational expert panel. Infect Control Hosp Epidemiol 2016; 37: 1201–11.
Pollack LA, Plachouras D, Gruhler H, et al. Transatlantic Taskforce on Antimicrobial Resistance (TATFAR)
Summary the modified Delphi process for common structure and process indicators for hospital antimicrobial stewardship programs. 2015.
CDC. Core elements of hospital antibiotic stewardship programs. Atlanta, GA, 2019 https://www.cdc.gov/antibiotic-use/core-elements/hospital.html.
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor HK.01.07/MENKES/755/2019 Tentang Pedoman Nasional Pelayanan Kedokteran Tata Laksana Tuberkulosis. 2019.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia Nomor 22 Tahun 2022 Tentang Penanggulangan Malaria. 2022 www.peraturan.go.id.
Menteri Kesehatan Republik Indonesia. Keputusan Menteri Kesehatan Republik Indonesia Nomor HK.01.07/MENKES/90/2019 Tentang Pedoman Nasional Pelayanan Kedokteran Tata Laksana HIV. 2019.
Menteri Kesehatan Republik Indonesia. Peraturan Menteri Kesehatan Republik Indonesia nomor 8 tahun 2015 tentang program pengendalian resistensi antimikroba di rumah sakit. 2015.
Wulandari LPL, Khan M, Liverani M, et al. Prevalence and determinants of inappropriate antibiotic dispensing at private drug retail outlets in urban and rural areas of Indonesia: A mixed methods study. BMJ Glob Health 2021; 6. DOI:10.1136/bmjgh-2021-004993.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
Hasnida A, Kok MO, Pisani E. Challenges in maintaining medicine quality while aiming for universal health coverage: a qualitative analysis from Indonesia. BMJ Glob Health 2021; 6: 1–11.
Limato R, Nelwan EJ, Mudia M, et al. A multicentre point prevalence survey of patterns and quality of antibiotic prescribing in Indonesian hospitals. JAC Antimicrob Resist 2021; 3. DOI:10.1093/jacamr/dlab047.
Limato R, Nelwan EJ, Mudia M, et al. Perceptions, views and practices regarding antibiotic prescribing and stewardship among hospital physicians in Jakarta, Indonesia: a questionnaire-based survey. BMJ Open 2022; 12: e054768.
Yayasan Orang Tua Peduli. Waspadai Pandemik Berikut: Ketika Antibiotik Tak Lagi Jadi Penyelamat Jiwa. 2021. https://milissehatyop.org/waspadai-pandemik-berikut-ketika-antibiotik-tak-lagi-jadi-penyelamat-jiwa/ (accessed July 20, 2023).
Hermansyah A, Sainsbury E, Krass I. Multiple policy approaches in improving community pharmacy practice: The case in Indonesia. BMC Health Serv Res 2018; 18. DOI:10.1186/s12913-018-3258-8.
Adji Prayitno Setiadi. Edukasi Kesehatan Berbasis Masyarakat: Model Pengawalan GeMa CerMat oleh Apoteker. 2019.
Hardiyanto Soegiantoro D, Rhema Soegiantoro H, Hope Soegiantoro G. Evaluation of GeMa CerMat Program during the Peak of COVID-19 Pandemic in Indonesia. Jurnal Manajemen Kesehatan Yayasan RS Dr Soetomo 2022; 8.
WHO Indonesia and UNICEF. Learning Note: Improving water, sanitation and hygiene in primary care health facilities during the COVID-19 pandemic in Indonesia. 2020.
WHO. GLASS Report: Early Implementation 2020. Geneva, 2020 https://www.who.int/publications/i/item/9789240005587.
WHO. Indonesia: WHO Monitoring and Supporting Progress to Combat Antimicrobial Resistance in Indonesia. WHO. https://www.who.int/about/accountability/results/who-results-report-2020-mtr/countrystory/2020/indonisia-amr (accessed July 21, 2023).


The Oxford University Clinical Research Unit (OUCRU) is a large-scale clinical and public health research unit with site offices in Viet Nam, Indonesia, and Nepal.
Part of the Centre for Tropical Medicine and Global Health at the University of Oxford (UK), OUCRU was first established in Ho Chi Minh City in 1991, hosted by the Hospital for Tropical Diseases (HTD), Viet Nam.
In 2003, OUCRU Nepal was established in Kathmandu, Nepal, hosted by Patan Hospital and the Patan Academy of Health Sciences.
OUCRU Ha Noi was established in 2006 in partnership with the National Hospital of Tropical Diseases (NHTD), Viet Nam.
In 2008, OUCRU Indonesia was established in Jakarta, Indonesia, in partnership with the Faculty of Medicine University of Indonesia.
Our vision is to have a local, regional and global impact on health by leading a locally-driven research programme on infectious diseases in Southeast Asia.
Our research programme covers clinical and laboratory research with hospital and community-based patient populations, including epidemiology, immunology, host and pathogen genetics, molecular biology, microbiology and virology, mathematical modelling, bioinformatics, biostatistics, and social science. This work is supported by an extensive clinical trials unit and data management centre compliant with national and international regulations and comprehensive management, finance, public engagement, and administrative support offices.
OUCRU receives considerable support from Wellcome as part of the Africa and Asia Programmes. Together with our partners, we have led a highly successful effort in enhancing the infrastructure and capacity to perform clinical trials and basic scientific research in Viet Nam, Indonesia, and Nepal.
Website: www.oucru.org
OUCRU-NP
Kathmandu, Nepal
OUCRU Indonesia
Jakarta, Indonesia
Assessment
OUCRU Hanoi
Viet Nam
OUCRU Ho Chi Minh City
Oxford University Clinical Research Unit
Website: oucru.org
For more information, contact us at: communications@oucru.org