Act now to avoid losing your documents and records
STAY SUPPORTED AND CONNECTED
There’s still time to renew your Osteopathy Australia membership
MANAGING PERSISTENT POST-CONCUSSION SYMPTOMS AN OSTEOPATHIC APPROACH INTRODUCTION
We offer a full range of products for your practice, from treatment tables and assessment tools to rehabilitation aids, pain management products, braces, orthotics, and massage essentials. Whether you're setting up a new clinic or stocking up on essentials, we've got you covered!
PRESIDENT’S MESSAGE
A WARM WELCOME TO THE JULY EDITION OF OSTEO LIFE
As we reach the middle of 2025, it’s a great time to reflect on what’s been achieved so far and to get excited about what’s to come.
In May, our Board came together over election weekend in Sydney for a face-to-face meeting. These sessions are always a highlight, not just for the strategic discussions, but for the chance to connect in person with the incredible staff team at Osteopathy Australia. They shared updates on the many projects they’re working on, all focused on making a real difference for members. It was energising to see the passion behind their work and the positive impact it’s having across the profession.
One of the biggest things we’re looking forward to in the second half of the year is the launch of a brand-new member database and website. We know the current system hasn’t always been the easiest to navigate, so we’re really excited to bring you a more user-friendly experience.
The new website will be fresh, simpler, and much easier to use. These upgrades will allow us to start rethinking and enhancing our membership offerings as the profession continues to grow and diversify.
We’re also gearing up for our Member Town Halls, which will be happening in every state and territory later in the year, as well as
online. These sessions are a great way for members to ask questions, share feedback, and hear directly from the association about what’s happening behind the scenes. We really value these opportunities to stay connected and listen to what’s important to you. I would encourage you all to make the effort to come along to your state and territory night, the feedback we receive is incredibly important.
A big part of the association’s strength is our Board, and I want to take a moment to recognise two members who’ve recently completed their terms: Don Hunter and Julia Biernaki. Don and Julia have both made significant contributions during their time on the Board, bringing insight, care, and dedication to their roles. We’re incredibly grateful for all they’ve done and thank them sincerely for their time and energy. Julia was our first ever young career osteopathic director; this role was a new addition to the board only two years ago and Julia has done a remarkable job in making it an incredibly valuable addition to the board.
We’re also excited to welcome some new faces. Heath Williams joins the Board with a strong background in occupational health and innovation, and Molly McCarthy as our new early-career osteopath who’ll bring a valuable fresh perspective to our leadership team. It’s great to see a mix of experience and new energy coming through, something that really reflects the direction of the profession.
Thanks again to all of you for your ongoing support, feedback, and involvement. There’s lots on the go, and we’re looking forward to continuing to build a stronger, more connected future for osteopathy in Australia.
Yours in health,
MATT COOPER President
mcooper.director@osteopathy.org.au
Osteopathy Australia
T (02) 9410 0099
E info@osteopathy.org.au W www.osteopathy.org.au osteopathyaustralia osteopathyau osteopathyaustralia
OSTEO LIFE is a magazine for Osteopathy Australia members.
For enquiries, feedback, or to contribute, contact
Communications on 02 9410 0099 or comms@osteopathy.org.au
For advertising enquires, email info@osteopathy.org.au
Communications and Marketing
Working Group Tara Bain, Toby Barker, Adam Nicholson, Rebekka Thompson-Jones
Chief Executive Antony Nicholas
Editor Rebekka Thompson-Jones
Designer Stephanie Goh
Advertising info@osteopathy.org.au
Individually, we can achieve great things. But when you belong to a community swarming towards a common goal, that’s when we form our strongest line of defence, and the sky’s the limit.
Guild Insurance and Osteopathy Australia have partnered for over 20 years now
to protect the future of your profession. With us, you’ll be shielded by a policy created from unmatched insight into your profession, access to risk management materials to help you reduce the risk of a claim, backing from the industry body that stands up for Australian osteopaths, and so much more.
Together, we form the network that ensures Australian osteopaths don’t have to fly solo. Get the full picture of how you can be part of something bigger by visiting guildinsurance.com.au/osteopaths or calling 1800 810 213 today.
Don’t go it alone
OSTEOPATHY AUSTRALIA NEWS
Osteopathy Australia aims to support, enhance and promote the profession. Here’s a quick recap of everything osteo from the past few months.
NOTES FROM THE ASSOCIATION
What do you want, what do we need to change, what do we need to improve?
As always, that is something we listen to and think about. This year, as with past years, we have some core projects to improve our services and make your life easier.
Having great clinic management software makes your life and your patients’ lives easier. It is no different for us. A modern CRM (customer relationship management) system and website are essential for us to form the backbone of a seamless, user-friendly experience for you. Over the second half of 2025 we will begin the process of migrating to a new system to make your lives and our lives easier.
The new system will allow greater choice, easier access, better automation of CPD records, tailored communications, events and a more efficient renewals process – all in one place. When paired with the newer intuitive website, it ensures you can register for events, access CPD and find resources easily, plus update your details without frustration. In today’s digital-first world, we are aiming for a smooth online member experience. As anyone who has migrated databases systems also understands, it may come with hiccups and headaches, but we will keep you informed so you hardly notice what happens behind the scenes.
What’s of value to you? Over the last few months, we have been engaging an expert to look at our user experiences, what you value and what you think about us. This included independently ) with a range of osteopaths across the career span and roles, plus some non-members on why not. Along with the focus groups we conducted on CPD late last year, will help us model our services, what we offer and potentially the things you don’t value to drop. If you have great ideas let us know.
“Renew today and keep the support flowing – because when you back us, we can better back you.”
Finally, it’s that time of year with membership renewal in full swing. Thank you to the thousands of osteopaths who have already renewed. For those still deciding – why is it important to be a member?
To have a voice that matters. Osteopathy Australia is the only organisation advocating solely for osteopaths – pushing for fair policies, better funding, and greater recognition. When we stand together, we’re stronger. Your membership directly funds this vital work.
To boost your credibility and career advancement. Need advice on regulations, complaints, HR, or practice management? We’ve got your back – with practical tools, templates, and expert guidance to save you time and reduce stress. It’s a mark of professionalism that sets you apart.
Ease of access to help, tools and support to make life easier. You can always reach out to us for help. Whether regulatory, practice, complaints, HR advice or business templates and clinical resources, we provide practical tools that save you time and reduce stress.
Stay sharp and up to date. From free webinars to low-cost training and the latest research, we help you stay ahead –clinically, professionally, and in step with healthcare changes. Build your community. Join a network of peers who understand your world. Share ideas, ask questions, and build relationships that lead to mentorship, collaboration, and opportunity.
Renew today and keep the support flowing – because when you back us, we can better back you.
ANTONY NICHOLAS Chief Executive ceo@osteopathy.org.au
RENEWED? THANK YOU. NOT YET?
THERE’S STILL TIME.
Awarm thank you to all our members who’ve renewed their Osteopathy Australia membership for the 2025–26 year – your commitment helps strengthen your profession and allows us to lobby and advocate on your behalf. And, you continue to have access to all the cost-saving benefits, career and professional development.
If you haven’t yet renewed, your access to member benefits ceased on 30 June including access to professional support services, CPD tracking, legal and HR advice and exclusive member benefits.
BUT THERE’S GOOD NEWS: THERE’S STILL TIME.
You can reactivate your membership before 31 July and avoid paying the rejoin fee, which comes into effect on 1 August. It’s quick to renew and restores your full benefits instantly.
Your membership is more than a transaction – it’s a powerful show of unity and a practical investment in your professional standing.
Let’s continue building a strong, connected osteopathy community together.
RENEW NOW. STAY SUPPORTED. STAY CONNECTED.
“My membership gives me the backing I need –professionally, legally, and personally. I wouldn’t practise without it.”
WELCOMING OUR NEWEST TEAM MEMBER:
ALEX NORDEN
his month, we’re delighted to welcome Alex Norden to the Osteopathy Australia team. Alex brings with him six years of operational management and stakeholder engagement experience from the arts sector, along with a strong commitment to community health. He has volunteered with Independent Community Living Australia, Results Australia, and Cancer Council NSW, sharpening his administration and advocacy skills within the health sector.
Recently completing a Master of Public Health at the University of Sydney, Alex stepped into the professional association space during his studies, developing his skills in membership engagement. Now, he’s focused on growing his expertise in policy and advocacy, working closely with stakeholders across the health and allied health sectors to help raise the profile of osteopathy and amplify the voice of our profession. You can contact Alex via policy@osteopathy.org.au
We’re thrilled to have him on board.
WE ALSO HAVE SOME EXCITING NEWS!
Our Policy and Advocacy Manager, Stephanie Santos, will be going on maternity leave in mid-June 2025 and will be returning in 2026. We extend our congratulations to Natasha Owens who will be stepping into the Policy and Advocacy Manager role. Please contact Natasha Owens queries going osteopathy.
MEET THE PAEDIATRICS ADVANCED
AND EXTENDED PRACTICE RECOGNITION OSTEOPATHS
Supporting the health and wellbeing of babies, children, and young people is a specialised and rewarding area of osteopathy. Our Paediatrics Advanced and Extended Practice osteopaths bring a high level of clinical skill, knowledge, and dedication to helping young patients and their families navigate complex developmental and health challenges through a whole-body approach.
Whether it’s feeding difficulties in infancy, musculoskeletal concerns, or ongoing developmental issues, these osteopaths combine evidence-informed techniques with a compassionate, family-centred approach to care.
WHAT IS ADVANCED AND EXTENDED PRACTICE RECOGNITION IN PAEDIATRICS?
The Advanced and Extended Practice Recognition program acknowledges osteopaths who have pursued focused professional development and experience in a particular clinical area – in this case, paediatrics. These practitioners are equipped with deep expertise, enabling them to provide care that complements and enhances general osteopathic practice.
• Advanced Practice Recognition is awarded to members who have completed tertiary qualifications or demonstrated extensive clinical experience in paediatric care. This includes rigorous assessment by a multidisciplinary panel, peer-reviewed case studies, and evidence of ongoing professional development.
• Extended Practice Recognition is for osteopaths progressing along the paediatric pathway, completing shorter accredited training, mentorships, or structured clinical placements. It formally recognises their evolving skill set in this area.
WHY THIS MATTERS
This recognition is more than a title. It offers reassurance to parents and carers that their osteopath is working within a framework of enhanced competence and accountability. For practitioners, it opens new opportunities in interdisciplinary practice, research and community health programs. Only osteopaths formally awarded these titles by Osteopathy Australia may use them.
THINKING OF ADVANCING YOUR PAEDIATRIC EXPERTISE?
Whether you’re passionate about treating babies, children, or adolescents, there’s a place for you in the Paediatrics Advanced and Extended Practice Recognition programs. You’ll gain formal recognition, grow your clinical confidence, and join a network of peers committed to delivering excellent care to the next generation. If you are thinking of applying, make sure you keep any relevant CPD records even if they are older than what’s needed under the registration standards! Find out more information on page 16.
Find out how to get started and take your osteopathic career further.
ADVANCED PRACTICE
Anna Walton Benjamin Lai
Betsy Foskett Carly Broadbent
Emily Jones
WHY NOT JOIN US?
Advanced Practice Recognition can be gained in the following areas:
EXTENDED PRACTICE
• Paediatrics
• Sports Management
• Exercise-based Rehabilitation
• Occupational Health
• Pain Management
Kara Rosker
Kate Burke
Kelly Marie Flaherty Kirsty Greenwood
Melinda Banks
Melissa McDougall
Reena Murray
Rosemarie Tomolo
Kristin Guley
Kylie McWhirter
Lauren Collins Marnie Norfolk
Anita Biddle
Tink Gee
Zoe Freshwater
FROM SOLO LEAP TO BUSTLING HEALTH HUB:
HOW A YOUNG OSTEOPATH IS TRANSFORMING CARE IN DARWIN
Seven years into her osteopathic career, Bek Hitchens reflects on the nerve-wracking decision that would change not just her own path, but the way healthcare is delivered in one of Australia’s most remote urban centres.
After completing her studies in Melbourne – a city known for its saturated healthcare market and fast-paced rhythm –she craved something different. Drawn by a desire to make a meaningful impact and contribute to regional health equity, she packed up and moved to Darwin. “It was a mix of needing a change and really wanting to support communities where access to care can be limited,” she says.
Like many in the allied health space, she initially faced the expected challenges: isolation, uncertainty, and the weight of starting a practice from scratch. But the biggest risk she took wasn’t just geographical – it was philosophical.
“Clinically, I felt a tension. There’s often a pressure in private practice to focus on retention – to keep patients coming back indefinitely. But I found real professional satisfaction in getting someone to the point where I could sign off and say, ‘You’re good. You don’t need me anymore, I’ll be here when you do.’ That felt like a win,” she explains.
“Darwin is small enough that if you do right by people, the community really backs you.”
Trusting her instincts, she set out solo. The early days were quiet, but word began to spread – rapidly. “Darwin is small enough that if you do right by people, the community really backs you.”
That groundswell of support turned her one-woman operation into a thriving, multidisciplinary clinic that now includes osteopaths, remedial massage therapists, a chiropractor, a naturopath, clinical pilates trained instructors, and a Pilates studio. The team serves a diverse and growing patient base – from FIFO workers and tradies to new mums and retirees. The ethos remains unchanged: help people get better, not just keep them coming back.
Now, the clinic is bursting at the seams. New patient bookings are constant, and the waitlist grows by the week. “We’re always on the lookout for another osteopath – or two – who want to join the team, embrace this lifestyle, and really contribute to something that feels bigger than a business.”
And lifestyle is no small part of the draw. “Darwin’s always sunny, the pace is slower, and the people are genuine. You can leave work, go for a swim, and be on a deck watching the sunset with friends by 6:00. It’s a different rhythm – and one that suits me.” Fortunately, if you are willing to work hard the financial benefits come also.
In an industry where burnout is common and values can get blurry, Reform Osteopathy and Pilates has allowed something refreshingly aligned. A clinic powered by purpose, sustained by word-of-mouth, and grounded in care that’s genuinely patient-first.
If you are wanting a tropical change please reach out to Bek at bek@reformosteopathyandpilates.com.au.
As an osteo, you know your athletes need more than an adjustmentthey need a robust return-to-play plan, load management strategies, and collaboration with performance coaches who push the limits.
The WESTERN BULLDOGS ATHLETIC PERFORMANCE SUMMIT is your chance to learn directly from the sharpest minds in strength & conditioning, athletic rehab, and high-performance sport. Walk away with strategies you can apply immediately in the clinic on Monday.
BRETT BARTHOLOMEW
Performance Coach & Author of Conscious Coaching How to Harness Conflict, Navigate Hard Conversations & Build a Stronger Team
RESEARCH TO PRACTICE:
HANNAH MOORE
Researcher & AFLW
Strength & Conditioning Coach, Western Bulldogs
Coaching the Diverse Needs of Female Athletes to Optimise Wellbeing and Performance
KEYNOTE PRESENTATIONS:
ANDREW RUSSELL
Former Director of High-Performance, Carlton & Hawthorn Football Club Systems for Success: Adaptive Programming for Performance
RETURN TO PLAY CASE STUDY:
SCOTT HULM & NICK STONE
Rehab Physiotherapists, Western Bulldogs
T-Junction Hamstring Rehabilitation
SIMON HARRIES
Head of Strength & Conditioning at the NSW Institute of Sport Unpacking On-field Rehabilitation to Optimise Return to Play
MORE THAN JUST TALKS…
• Facilitated HighPerformance Q&A giving you the chance to ask the questions you really want to know
• 90-Minute Networking session to grow your referral network (Drinks Package & Canapés Included)
• Tour the Clubs HighPerformance Facilities
• Catered Lunch, Coffee, Tea & Refreshments
OSTEOPATHY AUSTRALIA LAUNCHES $100K TARGETED RESEARCH GRANT
As part of our commitment to advancing evidence-informed care, we’re launching a Targeted Call for Research into osteopathy for musculoskeletal conditions.
Musculoskeletal conditions are among the leading causes of disability in Australia. Osteopathy is an integral part of the primary health landscape for supporting sufferers of complex and chronic musculoskeletal conditions, yet evidence gaps remain for high-quality research that showcases the benefits of osteopathy-based practice in improving the health and wellbeing of these patients.
The Osteopathy Australia board has allocated $100 000 towards a one-time partnership grant opportunity to foster
multi-sector partnerships and attract research proposals that are strategically relevant to Osteopathy Australia’s objectives. Osteopathy Australia intends to select and partner with one applicant for their submission to a Category 1 funding scheme such as, but not limited to, ARC Linkage or NHMRC Partnership.
The objectives behind Osteopathy Australia’s Targeted Call to Research are:
• Inform healthcare providers and funders about the effectiveness and value of osteopathy-based practice in managing musculoskeletal conditions;
• Ensure that research funding translates directly into impactful results – benefiting patients, practitioners and the wider healthcare system;
• Generate evidence that will support our advocacy and lobbying efforts for the profession.
This TCR has a two-stage application process – Stage 1 expressions of interest are currently open and closing on 1 October 2025. Applicants will be shortlisted and selected applicants invited to complete a full application by the end of 2025.
For more information: including forms, guidelines, and timelines, visit: www.osteopathy.org.au/article/targeted-
A wonderland of winter savings!
As a member of Osteopathy Australia, you have access to great o ers from Member Advantage, bringing you savings when you travel, shop or dine out.
savings at restaurants in Australia with discounted eGi cards.
up to 60% over retail with negotiated corporate rates at leading car hire providers.
pricing with The Good Guys and JB HiFi!
on savings at Coles and Woolworths, saving you money on every shop.
EARLY CAREER SPOTLIGHT MAX CHAMINGS
Where did you study and when did you graduate? RMIT and graduated in 2021.
Where did you land your first job after university? Where are you now? Coast Osteopathy in Adelaide! I have now started my own practice – CONNECT Osteopathy & Performance. I have loved being able to create something for myself.
What’s something you learned in university you still remember and/or use now? I still remember all that I was taught in relation to common conditions, physiology, anatomy and apply this understanding with every one of my clients.
What’s something you learned being in private practice? That communication and connection is essential for what we do. ‘Change happens at the speed of trust.’
What’s your favourite part of the job? Meeting people from all walks of life, hearing multiple different perspectives and learning from my clients. My clients are what makes osteopathy rewarding and enjoyable for me.
What’s something you’d change about working in private practice? More ways for osteopathy to be accessible to the general public. For example, if CDM plans were extended to 10 visits, or if there were government/workplace incentives for getting our population healthier (and osteopathy was a part of those incentives).
What’s something you’d tell a new osteopathy student and/or new graduate? That after 24 hours, 80 per cent of what you tell a client will be forgotten, and 50 per cent of the remaining will be misinterpreted. So, with all that in mind, I get clients to focus on one key takeaway and ask them at the end of the session to tell me (in their words) what that takeaway was. I make sure to get that one message across and build from there. Small hinges open big doors.
What’s something you’ve found helpful from your Osteopathy Australia membership?
The CPD resources are great for learning and having the Members’ Facebook Forum as a place for discussion and for questions relating to practice. Both are great resources.
LEARNING: HOW YOUR FEEDBACK IS REIMAGINING CPD AT OSTEOPATHY AUSTRALIA
BY DOMINIC BUCHTA
You spoke. We listened. Now we’re making changes. Late last year, Osteopathy Australia commissioned a national review of our continuing professional development (CPD) program. The aim was clear: to make sure our CPD reflects the way osteopaths practise – now and into the future.
Conducted by Advanica Consulting, the review included a national member survey, insights from funders like NDIS and DVA, focus groups with members and our CPD Working Group, and a scan of national education and health policy trends. Nearly 100 osteopaths took part in the survey, offering a rich cross-section of experiences and priorities.
This wasn’t just about what’s popular or trending. It was about finding out what really matters – clinically, professionally, and practically – for the people delivering care every day.
WHAT YOU TOLD US
What stood out above all were five areas which were identified for skill development over the next 1–2 years. You identified that chronic pain (39 per cent of respondents), neurology (35 per cent), paediatrics (29 per cent), musculoskeletal shoulder conditions (28 per cent), and women’s health (26 per cent) were conditions showing up every week in your clinics, and that you want more confidence and current evidence in managing them.
“This wasn’t just about what’s popular or trending. It was about finding out what really matters – clinically, professionally, and practically – for the people delivering care every day.”
But the feedback also went beyond clinical conditions. Many members shared a desire to grow in areas not always covered in formal CPD – things like business and leadership (particularly at mid-career), ethical decision-making, communication, report-writing, and cultural capability. For those working with funding schemes, understanding rules, reporting requirements and outcome measures was described as essential.
There’s a growing sense that CPD should reflect the full reality of practice – not just manual technique, but the broader skills osteopaths need to thrive in complex systems and changing patient landscapes.
HOW YOU WANT TO LEARN
The format of CPD matters just as much as the content. Most osteopaths said they prefer short, flexible options. Self-paced online modules (65 per cent) and webinars (64 per cent) remain popular, especially for theory or introductory content. But more than half of respondents (57 per cent) still value in-person learning – particularly for practical skills.
Half-day sessions were strongly favoured over full-day or weekend formats. Evening and weekday options were preferred to minimise disruption to clinical practice. Many members described blended learning as ideal: start online, then come together in person for hands-on application and discussion.
What also came through clearly was a desire for connection. Members want CPD to be social as well as educational. Case discussions, peer learning sessions, journal clubs and small group workshops - in clinics, cafes or university rooms – were all popular suggestions. For many, CPD isn’t just about content; it’s about community. That means greater interaction and engagement from members during webinars.
WHAT GETS IN THE WAY
Time pressures, cost and geography remain common barriers to accessing CPD – especially for those in rural or regional areas. Some members said they weren’t always sure which sessions were most relevant to their learning needs or aligned with expectations from funders. Others noted the lack of a clear development pathway between generalist and advanced practice and called for greater oversight of CPD quality and credibility.
WHAT FUNDERS SAID
It’s not just members who want CPD to evolve. Funding bodies including those overseeing NDIS, DVA and other compensable schemes told us they need osteopaths who can work confidently in multidisciplinary teams, communicate outcomes clearly and manage complex care presentations with both clinical and administrative skill.
Importantly, all funders involved said they’re open to collaborating with Osteopathy Australia to design training that
WHAT YOU ASKED FOR IN SKILL DEVELOPMENT
Chronic pain
Neurology
Paediatrics
Musculoskeletal shoulder conditions
meets these expectations. That’s a strong endorsement and an opportunity we intend to pursue.
WHAT HAPPENS NEXT
We are customising CPD to align with your needs, including relaunching podcasts as an immediate response. Your feedback has already been implemented, influencing CPD offerings since the review findings were published in 2024.
As shown in the table below, we have been – and continue to – develop CPD content that supports the top five skill development areas you identified.
Further to tailoring content to your needs, formats will shift too, with a focus on short, blended learning that gets to the point without taking you away from practice unnecessarily.
Behind the scenes, we’re building a new CPD platform and a refreshed website to make finding CPD offerings simpler and faster.
BE PART OF THE NEXT CHAPTER
This is only the beginning. In June, we invited members to express their interest in shaping the future of CPD by joining the CPD Working Group. This dynamic group will collaborate with Osteopathy Australia’s Learning and Development Officer to guide and refine CPD offerings, ensuring they remain relevant, engaging, and in demand.
Together, we’re creating a CPD environment that’s responsive, evidence-informed and future-focused designed not just for learning, but for growth.
HOW WE ARE SUPPORTING YOUR NEEDS
• We organised The Perrin Technique workshops in Brisbane, Melbourne, Perth and Sydney.
• We produced the Osteo Talk podcast The pain perspective: research, relief and resilience with Alison Sim and Angie Bruce.
• We organised Frank Willard’s The lateral cranial nerves seminar.
• We produced the Osteo Talk podcast Beyond the headache: the science and personal struggles of migraines with Beth Yule and Rachel Lee.
• We produced eLearning modules 6–7 years and 8–9 years (full sets).
• We produced the Osteo Talk podcast Early childhood paediatrics: a guide for the first two years with Betsy Foskett and Steph Kellett
• We held a Mastering shoulders workshop in Melbourne.
• We held a Mastering shoulders workshop in Brisbane.
Women’s health
• We produced the Osteo Talk podcast 101 on women’s health with Elizabeth Howard and Lorrae Griffiths (parts one and two).
YOUR CPD RECORDS AND COURSES – ACT NOW!
As this issue of Osteo Life reaches you, we’ll be just weeks away from launching our new website. While we’re thrilled about the fresh look and enhanced experience, there are a few important steps you’ll need to take.
Unfortunately, when we move to our new website, we won’t be able to transfer any CPD attachments, such as certificates, you have previously uploaded. Therefore, it is up to you to export all your CPD attachments and any CPD summaries pre-2019.
WHAT HAPPENS IF YOU IGNORE THIS ACTION REQUEST?
You will lose:
• Uploaded attachments, such as certificates; • Pre-2019 CPD summaries.
EXPORTING YOUR CPD SUMMARIES AND DOWNLOADING CPD ATTACHMENTS
COMPLETE THIS BEFORE 17 SEPTEMBER 2025
This involves a two-step and then a three-step process. See How-to-videos link here
Downloading CPD attachments
STEP 1: Enter the website via your dashboard and click on My CPD Activities
STEP 2: Scroll down the page to the section titled Your CPD activity and certificates.Here, you must click on EVERY SINGLE LINK in the Documents column.
Each link represents a document you have uploaded to our platform.
How to export your CPD summaries
STEP 1: Click on the My CPD Activities button
STEP 2: Scroll down to Select CPD cycle and select the CPD year you need to extract your CPD summaries from.
STEP 3: Once the year has been selected, click on the Export CPD Summary button
“While we’re thrilled about the fresh look and enhanced experience, there are a few important steps you’ll need to take.”
COMPLETING YOUR COURSES (WEBINARS AND eLEARNING)
COMPLETE THIS BEFORE 31 AUGUST 2025
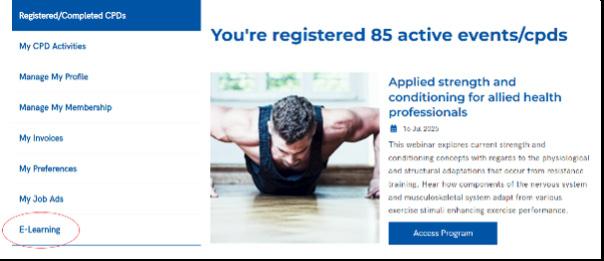
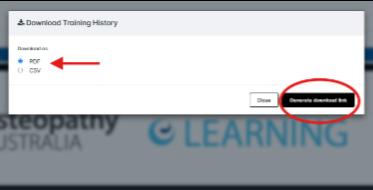
STEP 1: Go to eLearning in your dashboard.
STEP 2: Start and complete any enrolled courses. If you’ve enrolled but haven’t started a course, it must be finished by 31 August 2025.
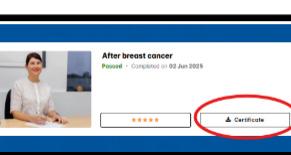
STEP 4: Click on Certificate to access the certificate relating to each completed course.
STEP 5: Click on Training history on the top right-hand side of the screen
STEP 3: Download any completed course certificates you want to keep.
Go to Completed Courses in your eLearning dashboard.
STEP 6: Click on the Generate download link. The defaulted export format is PDF.
Note: New registrations for eLearning and on-demand webinars will be closing soon. Only register if you’re sure you can complete the course by 31 August 2025.
ALL ABOUT WORK HEALTH AND SAFETY
Ensuring the safety and wellbeing of workers is a fundamental responsibility for every employer. Work, Health and Safety (WHS) laws exist to protect workers from harm, promote safe workplaces, and ensure businesses meet their legal obligations. While WHS compliance may seem like just another regulatory requirement, a strong WHS framework can deliver significant benefits, from reduced costs to better staff retention.
This article provides an overview of WHS responsibilities, the risks of non-compliance, and practical steps employers can take to create a safe and compliant work environment.
THE IMPORTANCE OF A STRONG WHS FRAMEWORK
A proactive, well-maintained WHS system helps businesses meet legal obligations while supporting a safer, more productive workplace. It reduces the risk of penalties, legal claims, and regulatory action, while also showing that employee wellbeing is a priority – building trust, lowering injury risks, and fostering a culture of care.
In turn, fewer workplace incidents mean less downtime, fewer operational disruptions, and lower costs associated with injury management. Beyond internal benefits, businesses that take safety seriously are more likely to build a strong reputation, retain skilled staff, and earn the trust of clients, customers, and industry partners.
RISKS OF POOR WHS PRACTICES
Neglecting WHS can lead to serious consequences. These include:
• Workplace injuries and illnesses – which may result in lost workdays, compensation claims, and long-term impacts on affected workers;
• Legal and financial repercussions – such as enforcement actions, or even fines;
• Low staff morale and high turnover – as employees are less likely to stay in a workplace they perceive as unsafe or poorly managed.
The cost of non-compliance can far outweigh the investment in preventative safety measures.
Practical steps to improve WHS compliance
For employers looking to strengthen their WHS approach, the following steps are a practical starting point:
1. Develop and implement a WHS policy
A clear, accessible WHS policy sets expectations for all staff and outlines how risks will be managed in your organisation. Members can access the SharePoint HR Portal for our template WHS Manual and implementation guide.
2. Conduct regular risk assessments and safety audits
Walk through your workplace to identify hazards. Review incident reports and consult with workers to get their perspective. Prioritise any high-risk areas for immediate action.
EXAMPLES OF POOR WHS PRACTICES
• Failing to identify or act on known hazards;
• Not providing adequate safety training or induction for new staff;
• Poor maintenance of equipment or lack of safety checks;
• Allowing or expecting excessive overtime, leading to fatigue and increased risk of incidents.
WHS RESPONSIBILITIES FOR EMPLOYERS
Under the Model Work Health and Safety Act, employers (or ‘persons conducting a business or undertaking’ –PCBUs) must take reasonable steps to protect the health and safety of their workers. This includes:
• Providing a safe work environment – Ensure workspaces, equipment, and systems of work do not pose risks to health or safety.
• Managing risks and hazards – Identify potential hazards and assess, control, and monitor risks on an ongoing basis.
• Providing information, training and instruction –Workers must know how to perform their jobs safely and be aware of workplace procedures.
• Consulting with workers – Employers must involve employees in discussions and decisions about safety, including proposed changes to the workplace.
• Maintaining records – Report notifiable incidents to the relevant WHS authority and keep records of incidents, hazards, and actions taken. These responsibilities apply not only to employees but also to contractors, apprentices, and other people at the workplace.
WHS AND INDUSTRY-SPECIFIC CONSIDERATIONS
WHS obligations apply to all workplaces, but the risks and how they’re managed vary by industry, environment, and tasks. High-risk settings may need stricter controls for equipment and manual handling, while others may focus on infection control, ergonomics, or psychosocial risks like stress and bullying.
In addition, remote and hybrid work arrangements bring their own set of considerations, including home office safety,
3. Provide training and refresher sessions
Safety training shouldn’t be limited to induction. Schedule regular sessions to update employees on policies, procedures, and emergency response protocols.
4. Foster a culture of open communication
Encourage employees to report hazards, near misses, or safety concerns without fear of blame. Make it easy for them to speak up and ensure concerns are acted on promptly.
5. Maintain proper documentation
Keep records of incidents, risk assessments, training sessions, and WHS meetings. Good documentation not only helps track progress - it’s also essential in the event of a regulatory inspection or claim.
Practical Tips for Businesses
• Create or update your WHS policy to ensure it reflects current legislation and operational realities.
• Invest in training that is role-specific and easy to understand. Visual or hands-on learning can be especially useful for high-risk tasks.
• Encourage employee participation in safety planning and toolbox talks. A shared commitment to safety builds trust and accountability.
• Ask for help – if you’re unsure, seek expert WHS advice to ensure your policies and practices are fit for purpose.
communication practices, and mental wellbeing. Regardless of the industry, it’s essential for employers to assess the specific risks relevant to their workplace and implement tailored strategies to ensure the safety and health of all workers.
CONCLUSION
Work Health and Safety is more than a box to tick – it’s a critical component of running a responsible and successful business. By creating a safe and compliant workplace, employers not only meet their legal obligations but also lay the foundation for a more engaged, productive, and resilient workforce.
If you have any questions about this article, please contact the Osteopathy Australia HR Service on 1300 143 602, or via email at HRHotline@osteopathy.org.au
MITIGATING FLOOD DAMAGE RISKS
Floods are an unfortunate part of life for many people and businesses in Australia and the devastation they cause can be catastrophic. Sadly, the recovery from flood damage is often not as quick as people would hope and this can have significant consequences for businesses.
We can’t prevent a flood from occurring, but we can take steps to reduce the impact of a flood. The tips below will assist business owners and their staff to be better prepared for a flood and better able to prevent or reduce impacts to the business. They’ll help you get back on your feet and trading again sooner.
For the purpose of this article, the definition of Flood is as per your Product Disclosure Statement (PDS), which is: Flood means the covering of normally dry land by water that has escaped or been released from the normal confines of any of the following:
• a lake (whether or not it has been altered or modified);
• a river (whether or not it has been altered or modified);
• a creek (whether or not it has been altered or modified);
• another natural watercourse (whether or not it has been altered or modified);
• a reservoir;
• a canal; or
• a dam.
PRE-FLOOD PLANNING
• Make yourself aware of the flood rating and likelihood for the location you’re in. If new to an area, engage with others who live and work there to understand the flood history of that area.
• When fitting out your business, consider using materials which are less susceptible to damage when wet, therefore limiting the potential need for replacement after a flood. If you’re part of a larger organisation and don’t have complete ownership or control over the fit out of your business, have a conversation with your organisation to raise their awareness of this need. This isn’t always obvious to those who live outside of flood risk areas.
• Have an evacuation plan and ensure all staff are familiar with this. It should include details on the likely warning timeframes and cover not just leaving the premises, but also the area if people need to move to higher ground. Again, engage with others in the area to assist in creating a safe plan.
• Have a plan for moving stock, electronic equipment, and other moveable equipment and furniture where possible. This might be to a higher level of the building or to another premises/location less likely to be impacted by flooding.
If you’re part of a larger organisation and don’t have complete ownership or control over the fit out of your business, have a conversation with your organisation to raise their awareness of this need. This isn’t always obvious to those who live outside of flood risk areas.
• Have a plan for sandbagging both outside the premises as well as inside over floor drains and toilets. There are sandfree sandbags available which are worth considering.
• Prepare an emergency kit that allows access to important information, equipment or tools. There’ll be occasions where the damage to a building is so great that it can’t be safely entered. Therefore, business owners must consider what they’ll need to access to both deal with the damage caused (such as insurance details and an asset register) and maintain business operations as much as is possible.
• Have your data and any business information which is stored electronically backed up in a way that can be accessed off site. This is important if the premises can’t be accessed or if information has been lost due to power shortages. Alternatively, consider cloud hosted storage solutions to protect your data.
• Ensure your business’ asset register is up to date. A detailed asset register means the process of an insurance claim is much faster and hassle free.
Contact your Guild Insurance Account
Manager or insurance adviser as soon as is possible to notify them of the event and any losses suffered.
• Discuss insurance cover, including business interruption, and its cost with your Guild Insurance Account Manager or insurance adviser and ensure you understand the financial protection afforded to you in the event of a flood.
• Have a maintenance program in place so your building and fit out is in an ideal condition. A building which has been allowed to deteriorate or has been poorly maintained may suffer more damage during a flood.
• If there are maintenance issues with your building and you lease the premises, engage with your landlord as soon as possible to discuss a plan and the necessary action.
• Develop a business continuity plan that will detail how you’ll manage your customer needs as well as your business and financial needs immediately after a catastrophic event. Thinking about this before an event can make the immediate impact and stress more manageable.
• Given there’ll likely be high demand for many services and trades, it would be wise to create a list of local services before there’s an urgent need. Utilise the knowledge of your local real estate agents; they can be a great support for putting you in touch with local trades and services.
PLANNING WHEN A FLOOD IS IMMINENT
• Don’t be complacent when there are flood warnings. Floods not only cause significant damage to buildings and other material possessions, but sadly they can lead to loss of life. Listen to all local advice and ensure you don’t delay implementing your flood preparation plan in a safe way, given time available before floodwaters are forecast to inundate your property.
• Have a plan for where and how you’ll access local and current advice when a flood is approaching, to be sure you can make the most appropriate decisions regarding when to move furniture and equipment and when to evacuate.
• When there are warnings that a flood appears likely, bring inside any outdoor furniture, equipment or other items where possible. This not only prevents them from being damaged by heavy rain and rising water levels, but also stops them from being washed away.
• When evacuating a building due to a flood, where possible turn off the gas and electricity supply. Be sure you know how to do this ahead of time. Post-flood response
• Contact your Guild Insurance Account Manager or insurance adviser as soon as is possible to notify them of the event and any losses suffered.
• If you begin the clean-up yourself and wish to dispose of any damaged and unsalvageable items, ensure you take a photo of these items first, and keep a list of what’s been thrown out, to assist with your insurance claim.
• If you aren’t fully insured and are therefore managing aspects of the clean up and recovery yourself, it’s advisable to begin by prioritising what needs to be done and determining how you’ll do this and whose assistance you’ll need. There are restoration services available that can assist with this.
• Following natural disasters, there’s often government support available to assist in the recovery. Be sure to stay up to date on what’s available from your local, state and federal governments.
CPD
MANAGING PERSISTENT POST-CONCUSSION SYMPTOMS: AN OSTEOPATHIC APPROACH INTRODUCTION
BY CLIFF BUTLER
Concussion, a form of mild traumatic brain injury (mTBI), is common in sport and daily life. While most concussions resolve within days to a few weeks, a significant subset of patients experience symptoms that linger well beyond the typical recovery period.1
These persistent post-concussion symptoms (PPCS) –previously known as post-concussion syndrome – can affect up to 30 per cent of individuals after mTBI.2 PPCS can be frustrating and life-altering, impacting patients’ ability to work, study, or enjoy daily activities.
Osteopaths, with their whole-body approach and patientcentred approach, are well placed to help manage PPCS. By considering the wide range of factors that may contribute to lingering symptoms – from musculoskeletal issues in the cervical spine to autonomic nervous system imbalance and even gut-brain interactions – osteopaths can formulate comprehensive treatment plans. This article provides a detailed look at how osteopathic manual therapy (OMT), including structural, visceral, and cranial techniques, alongside adjunctive therapies like graded exercise and nutritional support, can assist patients with PPCS.
WHAT ARE PERSISTENT POST-CONCUSSION SYMPTOMS (PPCS)?
PPCS refers to a collection of concussion-related symptoms that persist beyond the expected time frame of recovery from the initial head injury. There is some variation in definitions: some criteria define “persistent” as beyond 10–14 days in adults (and >4 weeks in children), 3 whereas other guidelines (including recent consensus) simply consider symptoms lasting longer than four weeks in any age group as persisting.4
In practice, any concussion symptoms that are not improving or that continue beyond the normal healing period (generally a few weeks) can be considered PPCS.1
Importantly, these symptoms might not be solely due to the brain injury itself – they can result from a combination of factors triggered by the injury.
Common symptoms: Patients with PPCS can present with a wide array of symptoms affecting multiple domains. Typical complaints include:
To formally diagnose post-concussion syndrome, historical definitions like the ICD-10 required at least three of these symptoms persisting after the injury.6
Regardless of definitions, what matters in practice is recognising that the patient is still suffering ongoing symptoms beyond the usual recovery window, warranting further evaluation and care.
It’s also crucial to reassure patients (and us as practitioners) that “persistent” does not mean “permanent.” Many patients with PPCS do improve over time, especially with appropriate active rehabilitation. With that optimistic outlook, osteopaths can play a key role in identifying the factors contributing to each patient’s PPCS and addressing them through a multifaceted treatment approach.
“Regardless of definitions, what matters in practice is recognising that the patient is still suffering ongoing symptoms beyond the usual recovery window, warranting further evaluation and care.”
WHY DO SYMPTOMS PERSIST? – KEY CAUSES OF PPCS
Persistent post-concussion symptoms are usually multi-factorial in origin, the initial brain injury sets off a cascade of physiological events, but prolonged symptoms often involve more than just the acute concussion pathology. Here we explore a few key contributors to PPCS that osteopaths should consider:
CERVICAL SPINE INVOLVEMENT IN CONCUSSION
Given the close anatomical and biomechanical relationship between the head and neck, it’s perhaps unsurprising that cervical spine dysfunction can be a significant (and treatable) contributor to PPCS.7
A concussion often results from acceleration-deceleration forces to the head; these forces are very similar to those that cause whiplash injuries to the neck. Even relatively minor neck trauma (as low as 4.5 g of acceleration) can injure cervical soft tissues – a much lower threshold than the 60–100+ g forces that typically cause concussions. In other words, most concussions likely involve a simultaneous mild whiplash injury. Indeed, one study found 100% of examined athletes with concussion had signs of cervical strain as well.7
The symptoms of cervical injury (often termed whiplashassociated disorder, WAD) can closely mirror concussion symptoms. Table 1 of Marshall et al. (2015) neatly illustrated that headache, dizziness, balance problems, nausea, visual disturbances, concentration difficulty, and fatigue –common in concussion – are also frequently reported after whiplash neck injuries.7
The overlap is so striking that patients with WAD can exhibit “cognitive” symptoms like concentration and memory issues, possibly due to pain and sensorimotor disturbances from the neck.6 This overlap means a patient’s persistent “post-concussion” headache or dizziness may actually be largely cervicogenic in origin, or at least compounded by neck dysfunction.
“Recognising cervical involvement is critical, because it represents a treatable cause of persistent symptoms.”
Key cervical issues in PPCS include:
• Cervicogenic headache: Injury to upper cervical joints (e.g. C0-C3) or muscles (suboccipital, upper trapezius, sternocleidomastoid, etc.) can refer pain into the head. Patients may have occipital or temporal headaches linked to neck position or muscle tension. Osteopathic evaluation often finds segmental restrictions or tender points in the upper neck corresponding to the headache pattern. For example, a restriction or tenderness at C2-3 with associated trigger points in suboccipital muscles might reproduce a patient’s frontal-temporal headache.7
• Cervicogenic dizziness: Proprioceptive dysfunction from the cervical spine can cause dizziness and balance issues (sometimes called cervical vertigo). If vestibular testing is normal in a PPCS patient with dizziness, the neck is a likely culprit. Suboccipital muscle tension and upper cervical joint dysfunction can disrupt normal input to the vestibular nuclei, leading to a sense of disequilibrium. Patients might describe feeling “off-balance” or lightheaded, especially with quick head movements, which can be mistaken for persistent vestibular concussion symptoms.
• Restricted cervical mobility and soft tissue dysfunction: Many PPCS patients have guarded, stiff neck posture after the injury, either from pain or instinctive protection. Reduced cervical range of motion (especially rotation and extension) is common and correlates with headaches and dizziness severity. Palpation often reveals localised segmental joint dysfunctions and myofascial tightness or trigger points in neck and shoulder girdle muscles. Recognising cervical involvement is critical, because it represents a treatable cause of persistent symptoms
Marshall et al. reported on a case series where five patients with long-standing PCS (five weeks to 31 months post-injury) received treatments aimed at restoring cervical function – all five had very favourable outcomes.
In fact, one randomised trial found that weekly manual therapy focused on the neck (combined with vestibular rehab) led to 73 per cent of chronic concussion patients becoming asymptomatic, versus only 7 per cent who recovered in a control group without this therapy.
These findings underscore that for many PPCS patients, “it’s the neck!” – or at least a big part of it. As osteopaths, we should always assess and, if needed, treat the cervical spine in post-concussion cases.7
AUTONOMIC NERVOUS SYSTEM
DYSREGULATION AND VAGAL TONE
Beyond structural injuries, concussion can disturb the autonomic nervous system (ANS), leading to dysregulation of sympathetic and parasympathetic balance. Patients with PPCS often report symptoms suggestive of autonomic imbalance: for example, heart rate and blood pressure
irregularities, dizziness upon standing (orthostatic intolerance), temperature dysregulation, or simply feeling “on edge” with anxiety and poor stress tolerance. Low vagal tone is often a feature of this dysregulation.
A useful objective marker for autonomic function is heart rate variability (HRV). Research shows that concussion can lead to lowered HRV, indicating a shift toward sympathetic dominance or reduced vagal input.8
A recent systematic review (2024) confirmed that even after clinical recovery, individuals with a history of concussion may have persistently reduced time-domain HRV measures, consistent with lingering ANS changes.8
In simpler terms, a concussion can leave the patient’s “fight or flight” sympathetic system more active and the “rest and digest” parasympathetic influence relatively diminished. This ANS imbalance might contribute to symptoms such as rapid heart rate, anxiety, poor digestive function, and delayed recovery.
The vagus nerve is of particular interest. The vagus exits the skull at the jugular foramen and innervates much of the thoracic and abdominal organs. Concussive head trauma could affect vagal function through central mechanisms (brainstem concussion effects) or peripheral mechanisms (upper cervical/jugular foramen strain). Reduced vagal activity has downstream effects: diminished vagal tone can impair regulation of heart rate (leading to decreased HRV) 9 and lessen the vagus’ normal antiinflammatory influence.10
SIGNS AND SYMPTOMS OF CONCUSSION SIGNS AND SYMPTOMS OF WAD
• Headache
• Pressure in head
• Neck pain
• Nausea/vomiting
• Dizziness
• Blurred vision
• Balance problems
• Sensivity to light
• Sensivity to noise
• Feeling slowed down
• Feeling like ‘in a fog’
• ‘Don’t feel right’
• Difficulty concentrating
• Difficulty remembering
• Fatigue or low energy
• Confusion
• Drowsiness
• Trouble falling asleep
• More emotional
• Irritable
• Sadness
• Nervous or anxious
• Neck/shoulder pain
• Reduced/painful neck movements
• Headache
• Reduced/painful jaw movements
• Numbness, tingling or pain in arm or hand
• Numbness, tingling or pain in leg or foot
• Dizziness/unsteadiness
• Nausea/vomiting
• Difficulty swallowing
• Ringing in ears
• Memory problems
• Problem concentrating
• Vision problems
• Lower back pain
Table 1 A comparison of signs and symptoms of concussion, from the post-concussion symptom score of the Sideline Concussion Assessment Tool version 3 (SCAT3) [3], and whiplash associated disorder (WAD, from the WAD Form C of the Quebec Task Force for Whiplash Associated Disorder [19].7
Clinically, signs of autonomic dysregulation in PPCS can include:
• Exercise intolerance (exaggerated symptom increase with physical exertion, often due to abnormal heart rate/ BP responses);
• Orthostatic symptoms (light-headedness on standing due to autonomic cardiovascular control issues);
• Headaches or flushing triggered by autonomic stimuli;
• Gastrointestinal changes (since vagus influences gut motility and secretion).
Being attuned to these signs is important for osteopaths, as improving autonomic balance – especially increasing vagal tone – can be an important treatment goal in PPCS. Techniques that stimulate the vagus nerve or normalise autonomic function may help break the cycle of dysregulation.
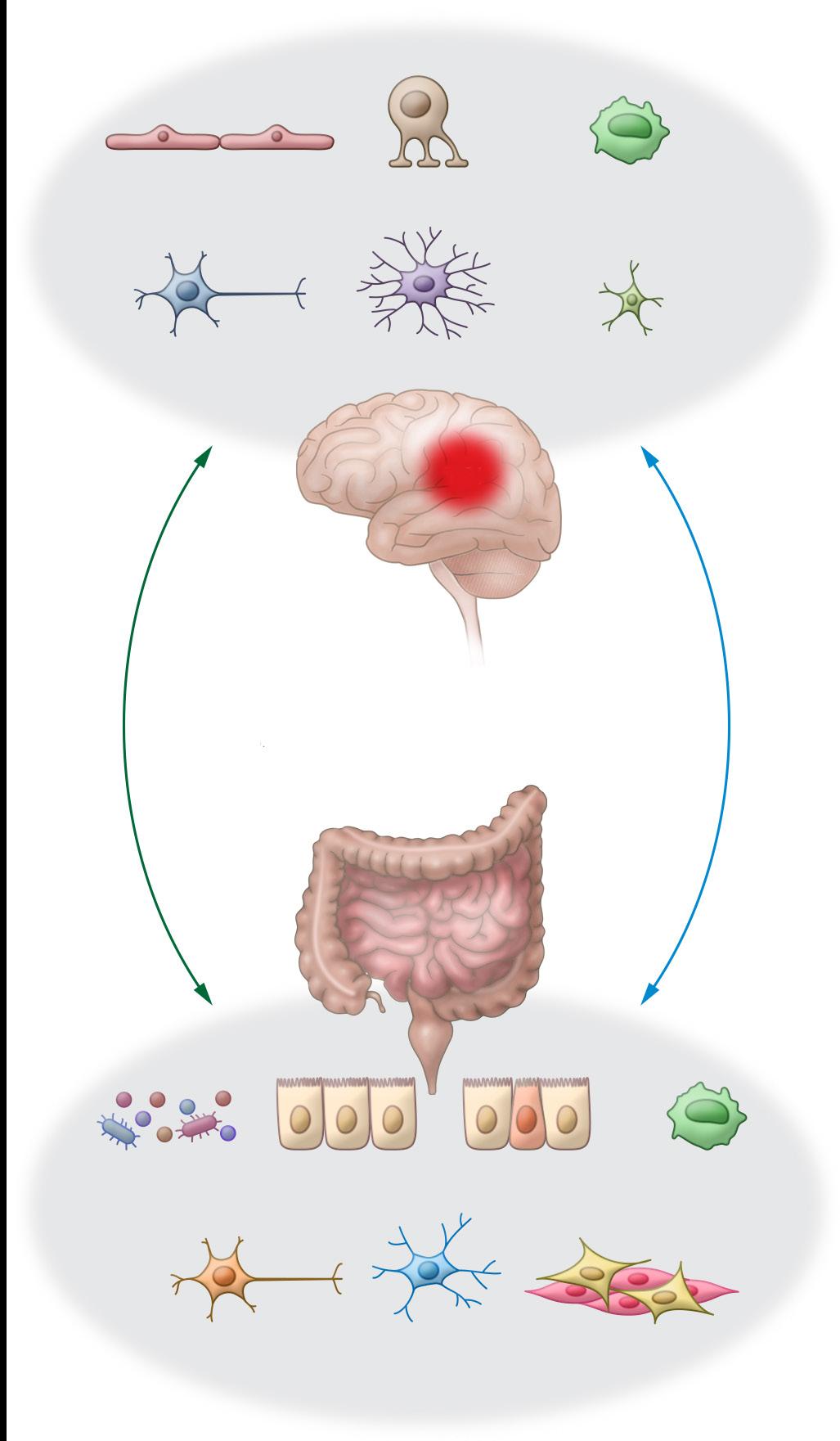
GUT-BRAIN AXIS, VAGAL TONE AND NEUROINFLAMMATION
The impact of concussion is not confined to the head – it can have body-wide effects, including on the gut. There is growing recognition of a gut-brain axis dysfunction in traumatic brain injury, even in milder forms. The bidirectional communication between the brain and gastrointestinal system (through neural pathways like the vagus and through hormonal/immune pathways) means a concussion can lead to gastrointestinal changes, and vice versa.10
After a brain injury, studies have shown neuroinflammation and autonomic dysfunction can alter gut function, leading to issues such as slowed motility and increased intestinal permeability (“leaky gut”). 10
In turn, a disturbed gut can send pro-inflammatory signals back to the brain. For example, a more permeable gut lining can allow bacterial endotoxins (like LPS) into circulation, which provoke inflammation that can worsen neuroinflammation in the brain. This creates a vicious cycle: brain injury triggers gut dysfunction, which triggers further inflammation that may prolong neurological symptoms.10
The vagus nerve is a key player in this gut-brain link. Normally, vagal efferent activity helps maintain gut barrier integrity and modulate intestinal inflammation (via the anti-inflammatory reflex). Vagal afferents constantly inform the brain about the state of the gut and can even signal the presence of inflammation or microbial metabolites to the central nervous system.
If vagal tone is compromised post-concussion, the gut may be more prone to dysfunction and inflammation. Conversely, gut inflammation can reduce vagal signalling.10
In practical terms, some patients with PPCS might exhibit gastrointestinal symptoms that were not present pre-injury: for instance, new onset of irritable bowel syndrome-like symptoms, changes in appetite, bloating, or altered bowel habits.
Furthermore, systemic markers of inflammation (like certain cytokines) can remain elevated in patients with prolonged concussion symptoms, hinting at ongoing immune activation possibly fed by gut issues.11
Addressing the gut-brain axis can therefore be another avenue to help PPCS patients. By improving vagal tone and gut health, we may reduce systemic and central inflammation, helping to calm the persistent symptoms. This could involve manual techniques aimed at the vagus and abdominal viscera, as well as nutritional interventions. The concept of treating the “whole person” is fitting here: an osteopath might work on a patient’s neck and consider their digestive function and diet in the same treatment plan – a truly whole-body approach that can yield better outcomes.
Endothelial cells (BBB)
Systemic: Immune cells
Cytokines/chemokines HPA axis
Microbiome
“After a brain injury, studies have shown neuroinflammation and autonomic dysfunction can alter gut function, leading to issues such as slowed motility and increased intestinal permeability (‘leaky gut’).”
Figure 1 Bidirectional interactions of the gut brain axis and therapeutic targets10
ANS: Sympathetic Vagus
“The evidence for structural OMT in PPCS comes mostly from case reports and related research on neck treatment in concussion.”
OSTEOPATHIC MANUAL THERAPY TECHNIQUES FOR PPCS
Osteopathic manual therapy (OMT) offers a toolkit of techniques that can be tailored to address the multifactorial issues in PPCS. It’s worth noting that evidence in this specific area (OMT for concussion/PPCS) is still emerging; however, related research and clinical experience provide support for the approaches described.
STRUCTURAL OMT FOR THE CERVICAL SPINE AND MUSCULOSKELETAL FACTORS
Key techniques and their application include:
• Soft tissue techniques and myofascial release: Gentle stretching, pressure, and inhibition techniques can help relieve hypertonicity in the cervical and upper thoracic musculature. For example, suboccipital muscle release can reduce tension in the suboccipital triangle muscles, often alleviating associated headaches, enhancing vagal function, improving cervical range of motion, and reducing dizziness triggered by cervical proprioceptors.
• High-velocity, low-amplitude (HVLA) manipulation: If no contraindications, osteopathic thrust techniques to address specific cervical joint dysfunctions can be very effective. Restoring motion at a segment like C1 (atlas) or C2 can alleviate pressure on associated nerves and improve local biomechanics. Some PPCS patients have upper cervical joint dysfunction that, when released, leads to notable improvement in headache frequency and intensity.7
• Muscle energy technique (MET): MET is useful for gently improving cervical segmental motion and relaxing tight muscles. For instance, if an osteopath finds a restricted rotation at C1 on the right, they might employ MET by having the patient gently turn their head right against resistance, then relax, to encourage increased left rotation of C1 (the atlas) on C2. This can reduce positional asymmetry that might be contributing to dizziness or headache. MET can also be applied to suboccipital muscles or scalene muscles to ease any neurovascular compression in the neck.
• Articulation and functional techniques: Rhythmic articulation of the cervical joints or functional balancing techniques can help if the patient is too acute or anxious for HVLA. These techniques gently coax the spine toward
better function and can modulate neurological tone. For example, gentle OA joint (occiput-atlas) articulation can free up the area around the jugular foramen, potentially easing vagus nerve passage and improving parasympathetic output.12
• Addressing other regions: Osteopaths will also look at the whole body. Pelvic or lower limb dysfunction from the injury (say, if it was a fall) could affect gait and posture, indirectly impacting head and neck symptoms. The thoracic diaphragm’s mobility influences breathing and venous/lymphatic return from the brain. Thus, structural treatment might include balancing the thoracolumbar junction, rib cage, or other areas to optimise the patient’s overall biomechanics and physiology.
The evidence for structural OMT in PPCS comes mostly from case reports and related research on neck treatment in concussion. As noted, Marshall et al. described cases where targeted cervical soft tissue therapy, spinal manipulation, and exercise led to resolution of persistent symptoms in a matter of weeks.7
In one case, a 25-year-old with four months of PPCS (daily headaches, dizziness, noise sensitivity) was found to have a C2/3 dysfunction and trigger points reproducing his headache pattern. He underwent a course of OMT: soft tissue release (including Active Release Technique) to sub occipitals and neck muscles, spinal manipulative therapy to the restricted cervical joint, and home exercises for deep neck flexors. After three treatments he had significant symptom reduction, and after eight treatments he had full resolution of symptoms.7
This is a powerful example of how structural OMT can directly target a root cause of PPCS.
VISCERAL OMT TO INFLUENCE AUTONOMIC AND GUT FUNCTION
Visceral osteopathic techniques are an important part of the whole-body approach when considering the autonomic and inflammatory factors at play. The goals of visceral OMT in PPCS are often to normalise vagal nerve function, improve
circulation (blood and lymphatic) to abdominal organs, and relieve any restrictions affecting the diaphragm or vagus nerve pathway. This in turn can help rebalance the autonomic nervous system and support the gut-brain axis in recovery. Specific visceral and related techniques that may be applied include:
• Suboccipital decompression (OA release): This technique aims to profoundly influence the vagus nerve. By gently lifting the occiput and massaging the suboccipital region, an osteopath can reduce tension around the jugular foramen, where cranial nerves IX, X, and XI exit.12
Improved vagal tone can mean better regulation of heart rate and blood pressure, calmer mood, and stimulation of digestive activity – aligning with our goals for ANS rebalance.
• Diaphragm release and rib mobilisation: The thoracic diaphragm is innervated by the phrenic nerve (C3–5) and closely related to vagal function (the vagus nerve passes through the diaphragm at the oesophageal hiatus). Tension or restriction in the diaphragm can impair breathing mechanics and vagal nerve signalling to the abdominal organs. Osteopaths often use myofascial release on the diaphragm (for example, stretching the lower rib cage or applying a technique directly to the central tendon area) to improve its motion. Better diaphragmatic motion enhances respiratory function and promotes venous/ lymphatic return, aiding clearance of inflammatory waste from the brain and gut. It may also indirectly stimulate the vagus nerve – deep diaphragmatic breathing is known to activate vagal pathways, so restoring the diaphragm’s full excursion can facilitate that natural vagal stimulation.
• Abdominal visceral manipulation: Gentle palpation and mobilisation of organs like the stomach, liver, intestines, and mesenteries can help relieve areas of congestion or hypertonicity in the visceral fascia. For example, a concussion patient under a lot of stress might develop a tight solar plexus region (celiac region) or a stomach with restricted mobility (sometimes felt as epigastric tightness). Techniques such as the celiac plexus release
(pressing gently just below the xiphoid to release tension around the celiac ganglia) or colonic massage can encourage normal gut peristalsis and function. Visceral manipulation may also help to improve blood supply to the gut and drainage of lymph. By improving gut function, we aim to reduce any ongoing gut-derived inflammation. In theory, if the patient’s bowels are moving regularly and the gut lining is healthier (better perfused and less leaky), there will be fewer inflammatory cytokines and toxins entering circulation to aggravate the brain, Visceral OMT practitioners often report that treating the abdomen can also produce a general relaxation response in patients, again reflecting an autonomic shift towards parasympathetic activity.
• Addressing the sympathetic chain influence: While vagal tone is one side of the coin, an overactive sympathetic nervous system (fight/flight) is the other. Osteopathic treatment can target areas where sympathetic outflow to the head and gut can be influenced. For instance, the upper thoracic spine (T1–T4) houses sympathetic nerves to the head/neck – treating dysfunctions there might reduce sympathetically mediated symptoms like lingering light sensitivity or vascular headaches. Similarly, the mid-back (T5–T9) covers sympathetic supply to the upper abdominal organs; tension or facilitation in these segments could affect the gut. Techniques like rib raising or paraspinal inhibition in the thoracolumbar region can help calm down an overactive sympathetic nervous system. This complements the increase in parasympathetic tone we seek, aiming for a balanced ANS state.
W hile formal research directly on visceral OMT for concussion is scant, we can extrapolate from related findings. We know vagus nerve stimulation in medical contexts can reduce intestinal inflammation and even brain inflammation.11
“Visceral OMT practitioners often report that treating the abdomen can also produce a general relaxation response in patients, again reflecting an autonomic shift towards parasympathetic activity.”
“A small pilot study in 2018 found that a single session of osteopathic cranial treatment in patients with concussion resulted in improvement in symptoms for most participants, and the approach was deemed safe and well-tolerated.”
OMT isn’t electrical stimulation, but by mechanically stimulating vagal pathways (like condylar decompression or visceral manipulations that stretch vagal fibers), we may achieve a milder form of vagal activation. Additionally, there is evidence that OMT can modulate immune function; one study on osteopathic treatment noted changes in inflammatory markers and proposed that OMT’s beneficial effects might be partly via the autonomic and immune systems.9
In summary, visceral OMT in PPCS is about restoring internal balance: freeing the diaphragm, calming the nerves of the digestive tract, and stimulating that all-important vagus nerve. It’s a wonderful example of how an osteopath treats the whole person – we might work on a patient’s head and neck, and also spend time gently working on their abdomen, knowing that the impact of concussion is far from just “in the head.”
CRANIAL OSTEOPATHY (OSTEOPATHY IN THE CRANIAL FIELD)
For patients with persistent post-concussion symptoms, cranial techniques are a popular and often effective addition to treatment.
Rationale: A concussion can create subtle (or not-so-subtle) strains in the cranial bones, membranes (like the dura mater and glymphatic system), and associated structures. Patients may have compressive lesions at sutures (e.g. a side-impact head injury causing a strain at the spheno-basilar synchondrosis, or compression of the occipitomastoid suture affecting the jugular foramen). By applying delicate corrective pressure, the practitioner aims to release cranial suture restrictions, normalise cranial bone motion, and improve circulation of cerebrospinal fluid (CSF). This can relieve headaches, reduce pressure sensations, and improve cognitive clarity.13
Techniques: Cranial techniques relevant to PPCS include:
• Sutural spreading and decompression: Gently disengaging impacted sutures like the occipitomastoid suture (to free the passage of CN IX, X, XI) or frontal bone releases (which can ease frontal headaches and sinus congestion). In concussion, common patterns like SBS compression (the base of skull) can be treated with techniques to encourage flexion-extension mobility of the sphenoid and occiput.
• Venous sinus drainage techniques: These involve gently pressing on specific cranial sutures overlying venous sinuses (like the transverse sinus, occipital sinus, etc.) to enhance venous blood drainage from the brain. This can reduce any venous congestion which might be contributing to post-traumatic headaches or fogginess.
• CV4 (Compression of the fourth ventricle): A classic osteopathic cranial technique where the practitioner holds the occiput in a way that encourages a still point in the cranial rhythm, purportedly improving the fluctuation of CSF. CV4 is often used for its general calming effect on the autonomic nervous system and to help reboot the body’s self-healing rhythms. Patients often report feeling profoundly relaxed after CV4, and it may help with sleep and anxiety in PPCS.
• Balanced membranous tension: Gently balancing the tension in the dural membranes (falx cerebri, tentorium cerebelli) can alleviate strange post-concussive sensations and vertigo. Concussions can cause these membranes to strain (imagine jostling the brain like jelly in a mould – the meninges can get tugged). By subtle movements, the osteopath can help the membranes “unwind” to a more neutral tension.
Evidence and safety: A small pilot study in 2018 found that a single session of osteopathic cranial treatment in patients with concussion resulted in improvement in symptoms for most participants, and the approach was deemed safe and well-tolerated.14
In summary, cranial osteopathy offers a gentle yet powerful means to address the lingering effects of concussion at their source – the head. By releasing cranial strains and improving fluid dynamics, it can alleviate headaches, cognitive clouding, and other central symptoms. For osteopaths experienced in this modality, it is a highly recommended component of PPCS treatment. For those less familiar, even basic cranial holds and suboccipital releases can be incorporated to good effect.
ADJUNCTIVE THERAPIES TO COMPLEMENT OMT
While OMT is central to the osteopathic approach, optimal management of PPCS is typically multidisciplinary. Osteopaths should be aware of and, where appropriate, recommend or incorporate adjunctive therapies that have evidence for aiding concussion recovery. Two key adjuncts are graded exercise and nutritional supplementation. These can synergise with manual therapy: exercise helps reintegrate neurological and cardiovascular function, and nutrition helps restore the biochemical environment needed for healing.
GRADED EXERCISE AND REHABILITATION
Gone are the days when prolonged rest was the only advice for concussion. Research now strongly supports the use of controlled, gradual aerobic exercise in patients with persistent concussion symptoms – provided it’s done below the threshold that provokes a worsening of symptoms. This is often referred to as sub-symptom threshold exercise Rather than worsening the condition, carefully dosed exercise
can help recalibrate the brain’s autonomic control, improve cerebral blood flow regulation, and reduce deconditioning and anxiety associated with inactivity.15
Besides aerobic exercise, vestibular and ocular rehabilitation exercises (gaze stability drills, balance exercises) might be indicated if those specific systems are affected. While usually guided by specialised therapists, an osteopath should be aware of these and refer if outside their scope of practice.
As osteopaths, we should champion a balanced approach of rest and activity: typically, after the initial days of rest, most patients benefit from gradually resuming physical (and cognitive) activity at a tolerable pace.
NUTRITIONAL SUPPORT AND SUPPLEMENTATION
Nutrition plays an important role in brain recovery and in modulating inflammation. Following a concussion, the brain is in a metabolically compromised state, often with increased oxidative stress and a need for certain nutrients to aid neural repair. Additionally, as discussed, if gut function is altered, ensuring proper nutrition and possibly adding supplements can help to restore systemic balance. Osteopaths can offer general advice on this or work in conjunction with nutritionists.
Nutrients that support neuroplasticity, reduce inflammation, and repair neural tissue include:
• Omega-3 fatty acids: Support neural repair and reduce neuroinflammation;16,17
• Magnesium: Alleviates symptoms and supports neurotransmitter balance;18
• Vitamin D and B vitamins: Support immune modulation and neural function;19
• Probiotics: May help restore gut microbiota balance and reduce systemic inflammation;
• Creatine monohydrate: supports ATP production to assist with energy production and neurotransmitter balance.20
About Cliff Butler
Cliff Butler is a Melbourne osteopath with extensive training in concussion, headache and migraine management. Twenty years’ experience, and further study into headache and concussion management, allows Cliff to assist patients who may be struggling with ongoing head and neck pain and sporting/collision injuries.
TREATMENT TIMELINES, OUTCOMES, AND EXAMPLE TREATMENT PLANS
Managing PPCS often requires patience and a staged approach. Every patient’s timeline will differ based on the severity of their concussion symptoms, how long symptoms have persisted, and which factors are most dominant (cervical vs vestibular vs autonomic, etc.).
Generally, an osteopath can outline a plan that spans several weeks to a few months, with regular reassessments and modifications along the way.
We also emphasise that improvement is rarely strictly linear – there can be good days and bad days, and sometimes as patients become more active, they might feel a temporary uptick in symptoms (which can be part of the adjustment process).
A reasonable expectation to set is that meaningful improvement (such as better tolerance for mental or physical activity, reduction in symptom severity) often occurs by about 6–8 weeks into a comprehensive treatment program. Many patients will feel significantly better by the three-month mark with consistent therapy, even if a few mild symptoms linger. Of course, there are cases that resolve faster (some within a few treatments, if their main issue – like a cervical fixable lesion –is addressed quickly) and unfortunately some that take longer (very chronic cases can take 6+ months for full recovery, but even those usually see incremental gains earlier).2
CONCLUSION
Patients with PPCS are often relieved to find a practitioner who understands the breadth of their condition – that their persistent symptoms are real, have identifiable causes, and can be addressed on multiple fronts. With a relaxed yet confident approach, the osteopath can educate and empower the patient: explaining how a whiplash injury might be causing their ongoing headaches, or how stimulating the vagus nerve might ease both their gut issues and anxiety.
This reassurance and active treatment approach instils hope, which is therapeutic given how demoralising prolonged concussion symptoms can be.
Persistent post-concussion syndrome requires a phased, goal-oriented rehabilitation strategy that mobilises the expertise of multiple allied health professionals. Osteopathic management of PPCS exemplifies the principle of treating the person, not just the disease. By addressing cervical biomechanics, calming the autonomic nervous system, supporting visceral health, and promoting healthy lifestyle changes, osteopaths can significantly assist patients in regaining their health after a concussion. Coupled with a multidisciplinary approach, including occupational therapy for functional reintegration, psychology for mental health support, and dietetics for recovery nutrition, osteopaths can help restore normal daily function, with PPCS symptoms either resolved or effectively self-managed. The osteopathic profession’s unique blend of manual skill and holistic outlook is ideally suited to guide patients on this path to recovery.
Scan for references
To find the full list of references for this article, scan the QR code here.
BEYOND BENDY: UNDERSTANDING HYPERMOBILITY AND THE ROLE OF OSTEOPATHY IN SUPPORTING PEOPLE LIVING WITH HSD AND HEDS
BY ASHTON WILSON | OSTEOPATH | DIRECTOR OF ALPHA SPORTS MEDICINE
Hypermobility is so much more than just being “flexible”.
For some people, joint hypermobility may be an incidental finding, it may be asymptomatic, have no other associated complications and may be even an asset for athletes like dancers, gymnasts and swimmers. But for some, joint hypermobility can be one of the first signs of a much more complex, systemic condition that affects widespread connective tissue, proprioception, and overall quality of life. Hypermobility Spectrum Disorders (HSD) and hypermobile Ehlers-Danlos Syndrome (hEDS) are still considered rare and remain underdiagnosed and misunderstood. On average, it takes a person living with hEDS/HSD 10 years to reach a diagnosis.1 As osteopaths, we have an incredible opportunity to offer a whole-body, integrative approach to patients presenting with hypermobility, we just need to be more aware of what to look for, what questions to ask and how to utilise our skillset.
UNDERSTANDING HYPERMOBILITY AND ITS SPECTRUM
There are 13 subtypes of Ehlers-Danlos Syndrome (EDS), 12 of which have a genetic marker. Hypermobile Ehlers-Danlos Syndrome (hEDS), which is considered the most common of the EDS subtypes, does not, nor does Hypermobility Spectrum Disorder (HSD). The overall prevalence of Ehlers-Danlos syndromes (EDS) is recognised as 1 in 5000, 2 which is why it is considered to be rare. However this statistic includes all 13 subtypes, 12 of which are extremely rare, so it is now believed that these figures underestimate the prevalence of hEDS and HSD in the community which is thought to be 1 in 500.3 While many individuals with hypermobile joints experience no pain or dysfunction, others live with persistent musculoskeletal pain, fatigue,
and instability that impact daily function which is why we desperately need to better understand it.
In 2017 international classification has clarified the differentiation between hEDS and HSD, which was previously referred to as Benign Joint Hypermobility. A HSD diagnosis is made when a patient does not meet the hEDS criteria, which seems simple, and yet many patients continue to experience delay in diagnosis and confusion among their healthcare team. A diagnosis of hEDS is currently a clinical diagnosis, based on a combination of clinical history, Beighton scoring, multiple systemic features, the presence of co-morbidities and the exclusion of other EDS subtypes, autoimmune conditions and connective tissue disorders.4
CLINICAL PRESENTATION AND COMMON CO-MORBIDITIES
People with HSD and hEDS will often present with a multitude of symptoms that go beyond joint hypermobility.
• Bladder and Bowel Dysfunction (incontinence, urgency);
• Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Post Exertional Malaise (PEM).
Anywhere there is connective tissue can be impacted.1
THE ROLE OF OSTEOPATHY IN THE MANAGEMENT OF HEDS/HSD
Osteopaths have an ability to play a vital role when it comes to supporting patients with hEDS and HSD and here’s why. Osteopaths are trained to be holistic, to look at the body as a whole, which is essential when working with a person presenting with hypermobility. Osteopaths have the capacity to be integrative practitioners, and can combine the many skills like biomechanics knowledge, manual therapy, exercise rehab and health education into developing a customised treatment plan to cater to individual needs.
Osteopaths have a range of hands-on techniques that can be beneficial for helping manage pain including gentle soft
tissue techniques, muscle energy techniques and myofascial techniques can help modulate pain, improve proprioceptive feedback, and reduce muscle guarding. Manual therapy alone is not enough to help a person comprehensively manage their hEDS/HSD symptoms, so this is where we have to really apply our whole-body treatment approach.
EDUCATION
Education is power for a hypermobile person who may not know much about hEDS/HSD. Helping them understand what is happening in their body and why they are experiencing their symptoms is not only validating to the patient but incredibly empowering. It takes on average 10 years to reach a diagnosis, so you can imagine how liberating it would feel to understand your body. Education is also important because there is no cure for hEDS/HSD, but there are management strategies available. Helping hypermobile clients understand that management of their symptoms isn’t just about their pain, it should involve management of their other co-morbidities as well.
“While many individuals with hypermobile joints experience no pain or dysfunction, others live with persistent musculoskeletal pain, fatigue, and instability that impact daily function which is why we desperately need to better understand it.”
“Assisting a hypermobile person to become aware of how to move their body is essential, and we should place an emphasis on control of joint range, energy pacing, and gradual progression to avoid flare ups of symptoms.”
MOVEMENT BASED THERAPY
It’s true, strong muscles will make for strong joints, but for hypermobile people, it’s not as simple as “just get stronger”. Movement and exercise prescription will look different for everyone, there’s no blueprint. Helping a hypermobile person stand with their joints away from end range is often a good starting point, helping them understand how to stack their posture under gravity without having to lock their joints at end range or clench through their muscles, this is often very challenging both physically and mentally. Assisting a hypermobile person to become aware of how to move their body is essential, and we should place an emphasis on control of joint range, energy pacing, and gradual progression to avoid flare ups of symptoms.5
CREATE A TREATMENT TEAM
With the multi-system nature of EDS/HSD, creating a support system for hypermobile clients is crucial for their success. When there are multiple systems involved, you have to address all of the contributing factors, so knowing who to refer to for management of existing co-morbidities can ensure your patient is getting the whole-body care they need. Starting communication channels amongst the treating practitioners and fitness professionals can add extra support for the client, but also for us as practitioners.
About Ashton Wilson
Ashton Wilson is an osteopath who has a keen interest in rehabilitation and strength training, particularly for those from sporting backgrounds.
BE CURIOUS, BE AN ADVOCATE
Unfortunately, patients with hypermobility disorders often experience medical gaslighting, diagnostic fatigue or clinician associated trauma.7 Osteopaths have an opportunity to play an important role in validating experiences, explaining the nature of connective tissue conditions, and coordinating referrals to relevant specialists. It’s also important to remember that you don’t need to be the expert in everything to do with EDS/HSD, but before you dismiss something you don’t understand, be curious to learn more, ask questions, do some research, talk about it with your colleagues.
WHAT’S NEXT FOR THE FIELD?
This is a field that is constantly changing and evolving, however the research into EDS and HSD is still limited. The 2017 EDS International Classification acknowledged the need for genetic markers for hEDS and HSD, there are some promising signs, but as of now, there is still no definitive genetic marker.4
Promising directions include:
• Research into potential genetic markers for hEDS;8
• Development of standardised clinical diagnostic testing; 9
• The advancement of the Beighton Score to include more specificity and sensitivity to include joints through the Upper Limb Hypermobility Assessment Tool10 and the Lower Limb Assessment Score;11
• Greater inclusion in allied health research;
• Interdisciplinary education and awareness campaigns. Osteopaths should advocate for inclusion of hypermobility-related disorders at university level and in continuing education programs. Osteopaths should also advocate for more recognition in the EDS community as being able to play a vital role in the practitioner care team for people living with hypermobility.
CONCLUSION
EDS and HSD are complex conditions, but they don’t have to be complicated. Once you know what to look for, you just have to listen to the patient’s needs and customise your treatment plan. Osteopaths are uniquely equipped as holistically trained practitioners to provide whole-person care that integrates manual therapy, movement, education, and advocacy. As awareness for hypermobility grows, our profession has the opportunity to be the leaders in the development of best practice frameworks for hypermobility care.
By staying curious, being informed, and always, remaining patient-centred, we can help improve long term outcomes for this often-misunderstood population.
Scan for references
To find the full list of references for this article, scan the QR code here.
CPD CALENDAR
Key dates for your diary throughout the coming months.
WORKSHOPS
22 AUGUST 2025
Athletic performance summit, Western Bulldogs
Presenters: The line up of presenters can be found here
• Hypermobility for healthcare and fitness professionals, Queensland OSTEO TALK PODCASTS
• Early childhood paediatrics: a guide for the first two years
• The pain perspective: research, relief, and resilience
• From burnout to balance, clinicians reclaiming work-life harmony
• Sleep matters and its role in repair, recovery and restoration of the body
3-DAY WORKSHOP
ENHANCE YOUR OSTEOPATHIC SKILLS WITH THE PERRIN TECHNIQUE TM
A structured approach to assessing and managing ME/CFS and fibromyalgia
M
any people living with myalgic encephalomyelitis and chronic fatigue syndrome (ME/CFS) face ongoing barriers to appropriate care, despite the increasing need for long-term support. This November, our Perrin Technique workshop offers you the chance to support these patients.
The osteopathic based technique is designed specifically to support people with ME/CFS, fibromyalgia and similar complex conditions. For osteopaths, it’s a pathway to deliver help to a marginalised patient group - one that all too often is searching for practitioners who understand their needs.
• What it’s like treating people with ME/CFS in clinic
• Practical insights and lessons they’ve learned over two years
• How you can maximise professional opportunities, while helping patients
• Why this patient cohort has brought some of the most meaningful work of their careers
“To give you a real-world view of what’s possible, the latest podcast episode of Osteo Talk features Amanda Oosterweghel and Ray Power, early adopters of the Perrin Technique.”
Don’t wait too long, there are limited spaces. Find out more and register by clicking here.
FlexEze Heat Wraps deliver evidence-based, continuous low-level heat - promoting movement in line with the Australian Low Back Pain Clinical Care Standard
As temperatures drop, FlexEze Hand Warmers provide gentle, targeted warmth to improve blood flow and relieve cold hand stiffness, helping your patients keep comfortable and Moving with Eze
The most innovative sleep system designed by health experts for spinal alignment and quality rest.
Following five years of research and development and a further two years of real-time trials in an osteopathic clinical setting, our DrRest experts have created a mattress that health professionals can confidently recommend to patients. A sleep system that complements and supports the care that osteopathic practitioners provide.
Learn more about becoming a DrRest referrer or partner at drrest.com.au/join
ENDORSED BY*
Patented design, Australian owned and made.
Victor Compression Legs Kit
The Victor Compression Legs Kit is a pneumatic compression system which uses dynamic air compression to create a massaging effect to help increase circulation, reduce swelling and muscle soreness for a faster recovery. Perfect for sports recovery use.
Features and Benefits:
» Advanced Compression Technology: Dynamic air compression to help increase blood circulation, reduce muscle soreness & swelling and assist recovery.
» Overlapping Chambers: 6 chamber sleeves with overlapping sections for uniform compression.
» Customizable Settings: Easily adjustable pressure levels and timing settings to suit your personal needs and preferences.
» Durable and Comfortable: Made from premium materials to ensure long-lasting durability and comfortable fit.
» Portable Design: Lightweight and easy to carry, perfect for use at home, in the gym, or on the go. VCOMPLEGSKIT
Comes with a stylish bag to easily store and carry the compression boots & controller. VICTOR
SPECIFICATIONS:
Pressure Settings: 80 - 260mmHg
Massage Modes: 6
Treatment Time Settings: 10 - 90mins
Operation: LED Touch Screen
Input Voltage: AC100 - 240V
Rated Power: 49W
Output: DC12.6V, 4A
Power Supply: Rechargeable 5200mAh Li Battery
Air Chamber: 6 Chambers (Air Bags)
6 Selective Chamber Controls: Target or skip specific chambers
Materials: Unit - ABS Sleeves - TPU
Size: 21 x 13 x 8.6 cm
Weight: 2.5kg
Warranty: 12 Months
EXERCISE PRODUCTS
66fit Weighted Hula Hoop
Designed to boost core muscle strength, tone abdominals, trim your waistline and aid weight loss. Burn up to 300 calories per hula hooping session. Available in three different colour coded weights for different level users.
1.2KG
66fit Goniometer – Plastic
Designed to accurately measure the axis and range of motion in a particular joint. 360 degrees. Metric and Imperial.
66fit Pilates Soft Balls – Set of 2
Ideal tool for strength and rehabilitation exercise programmes.
66fit Spiky Muscle Roller Stick
Designed to help relieve muscle pain and discomfort with the application of pressure.
66fit Spikey Massage Ball 9cm – Individual
Effective self -massaging tool, providing deep tissue massage to tight or knotted muscles.
66fit Wooden Balance Board – PVC Surface – 40cm
Designed to help regain your sense of balance and coordination post-injury.
66fit Four Way Massager
A self-massage tool designed to eliminate deep rooted knots and trigger points.
66fit EPP Foam Roller – 15cm x 90cm
The 66fit High Density Foam Roller is designed to target specific trigger point areas to help relieve muscular aches and tension.
66fit Ankle Wrist & Dumbbell
Cuff Weight Set – 4kg
Perfect companion to your existing exercise regime enabling you to up the ante and go that extra mile.
Barrier Mask – Reusable
AllCare Super Stretcher
Designed to assist with many stretching exercises. Made from a strong elastic strap.
66fit Height Adjustable Aerobic Step
Height adjustable stepper perfect for all types of aerobic workout. Designed to help improve cardiovascular strength and stamina.
Offers protection for up to 50 washes. Can be worn for up to 4 hours at a time (must be washed after each use). Filtration efficiency for 3 micron particles.
66fit Super Stretcher
Strong elasticated stretching band. Lightweight & portable so you can stretch anywhere, anytime. Assists stretching most muscle groups.
TUBULAR BANDAGES
Victor Pro Compband Elasticated
Benefits of Compband:
» Provides comfortable pressure to joints and limbs
» Clinically proven to provide extra support
» Available in six different sizes
» Reusable and washable
» Frays less
Material Composition:
95% Cotton, 5% Spandex.
Colour:
Sizes & Applications:
Size B: 6cm x 10m
Applications: Small Wrists
Size C: 6.7cm x 10m
Applications: Medium Wrists, Small Elbows
Size D: 7cm x 10m
Applications: Large Wrists, Medium Elbows, Small/Medium Ankles, Small Knees
Size E: 8.5cm x 10m
Applications: Large Elbows, Medium Knees, Medium/Large Ankles
Size F: 9.5cm x 10m
Applications: Large Knee, Small Thigh
Size G: 11cm x 10m
Applications: Extra Large Knee, Medium Thigh
Price quoted exclude GST and delivery fees. Special for Compband ends 31 July, 2025. Prices subject to change without notice.