Johannesburg Office: Woodlands Office Park, Building 13, Ground Floor, Woodlands Drive, Woodmead, Sandton 2191
Postal Address: PO Box 784698, Sandton, Johannesburg, 2146 T +27(0)11 877 6111 F +27(0)11 713 9024 www.medicalacademic.co.za
Printed by Novus Print, Cape Town COVER PRICE Specialist Forum per issue R80,00 VAT Incl. ISSN: 2218-8282
Published by Media24 (Pty) Ltd
Disclaimer: Please take note that the products featured in this journal are available in South Africa. Products may be marketed under a different name or might not be registered in your country. For more information, contact your local representative. All content in Specialist Forum is sourced independently and under no circumstances should articles be considered promotional unless specified with a postscript.
Articles are created with the assistance of artificial intelligence (AI) tools to aid in research and drafting. The content has been reviewed and edited by a human expert for quality and reliability.
Please note that all advertising is intended for healthcare professionals only.
April: No fooling around –It is a BIG month for medicine
April is not just about autumn’s arrival – it is packed with key healthcare awareness days. From World Parkinson’s Day and World Haemophilia Day to World Malaria Day and World Irritable Bowel Syndrome Awareness Day, this month highlights a broad spectrum of medical conditions. Professional societies like the Faculty of Consulting Physicians, the Neurological Association of South Africa, and Pain SA are also actively contributing to discussions and advancements in patient care.
Our CPD articles this month explore pressing clinical topics that impact daily practice. These include infection risks and vaccine strategies in individuals infected with HIV, the challenge of differentiating between seasonal illnesses and allergic rhinitis, and the complexities of managing anticoagulation therapy. By completing these CPD activities, you can earn six (6) CPD points. If you missed our CPD-accredited webinars, which offer two general points and one ethics point, check the back of the magazine for instructions on how to claim your points.
Beyond CPD, this issue covers a range of critical healthcare discussions, from evolving treatment approaches to ethical considerations in practice. With insights on disease prevention, innovative therapies, and best practices in patient management, there is plenty to keep you informed and engaged.
Whether you are here to enhance your clinical knowledge, stay on top of emerging trends, or earn CPD points, this issue offers valuable insights. So, grab a coffee, dive in, and make the most of April’s must-know medical updates!
Enjoy the read!
René and team
Cultural conflicts and
informed consent
Researchers Dr Hilde Miniggio and Lesego Masha from Sefako Makgatho Health Sciences University, South Africa describe a unique study funded by The Medical Protection Society (MPS) Foundation into the issue of informed consent within African culture in oral healthcare.
Respect for autonomy and the doctrine of informed consent are considered fundamental pillars of healthcare provision all over the world. However, in the African context, this approach has been criticised for failing to give due attention to traditional values and beliefs.1,2,3
To investigate this issue, a study has been funded by The MPS Foundation, to explore the compatibility of informed consent and autonomy with African traditional values and beliefs in the context of oral healthcare. There are currently no empirical studies that explore the experiences, views, and opinions of patients from African communities regarding this compatibility in the context of oral healthcare provision. Hence there is an important gap in the knowledge on this topic which consequently impacts healthcare professionals and their patients.
This project aims to explore the influence of African traditional values and viewpoints on patients’ decision-making process, as well as its influence on the communication between health practitioners and patients. This will assist in establishing culturally sensitive informed consent practices that consider the wishes and the needs of patients from African communities, and that are compatible with their communal values and belief systems.
Legal requirement
The doctrine of informed consent is an ethical and legal requirement in healthcare in South Africa, as mandated by the Health Professions Council of South Africa. However, the challenges of relying on such individualism in the process of informed consent when treating patients from African communities are underexplored and may adversely affect the communication between healthcare practitioners and patients, as well as negatively impact patients’ decision-making process. This can, in turn, compromise the quality of care that patients receive. The question then arises, how can autonomy be accommodated in consent processes in oral healthcare provision without overlooking the significance of communal norms and communal relationships in the African context?
Cultural context
The applicability of the principle of respect for autonomy in different cultural contexts has been criticised by several authors.2,3,4 The principle is rooted in notions of selfhood and individualism which, although significant in Western culture, may not be harmonious with African tradition. As Behrens writes, ‘on many African accounts this notion of autonomy is problematic’.3
‘A pervasive notion is that it is central to the worldview of most Africans that community is prized and that individuals are bound up with their communities. Decisions about one’s body and life
are, therefore, not to be taken by individuals acting alone, but in engagement with their families and communities’. Behrens suggests that the principle of autonomy should be replaced by the principle of ‘respect for persons’ initially advanced in the Belmont Report, as it is better suited in acknowledging both self-governance as well as social and cultural aspects which are important in the individual’s life and decision-making. In this way, the principle of ‘respect for persons’ is broad enough to allow for the inclusion of a patient’s family members or various other members of the patient’s community in the decision-making process if it is of cultural significance to the patient. Furthermore, Behrens argues that respecting a patient’s relationships is a way of respecting the patient’s autonomy, particularly when that patient’s autonomy is reflected in their community.3
Ubuntu philosophy
Lastly, the principle of ‘respect for persons’, is considered to be more fitting with the Ubuntu philosophy prevalent in southern African communities, which underscores the importance of interconnectedness of the community members. The Ubuntu philosophy highlights the significance of shared decision-making and communal care in considering issues related to health and disease. In these African contexts, connection with fellow community members and harmony within the community hold such significance that individualism is perceived in the contexts of the community.3,5
This interconnectedness, harmony, care, and involvement that underpins Ubuntu comes to light when a community member is dealing with an illness. It is common practice that the family and community members closest to the patient become involved in assisting the patient to make decisions about the choice of treatment, including advising on the choice of healthcare providers or traditional healers.3
The care and involvement of the community in dealing with illness underpins the Ubuntu philosophy and belief of interrelatedness best described by this quote from Desmond Tutu: ‘[Ubuntu] speaks to the very essence of being human, it means my humanity is caught up, is inextricably bound up, in theirs’. We belong in a bundle of life…. Harmony, friendliness, community are great goods. Social harmony is for us… the greatest good’.6 Further details and updates about the project can be found at www.thempsfoundation.org
The MPS Foundation is a part of MPS – South Africa’s leading protection organisation for doctors, dentists and healthcare professionals – and invests in research, analysis, education and training to help MPS members provide better care for their patients and improve their own wellbeing.
References are available on request. SF
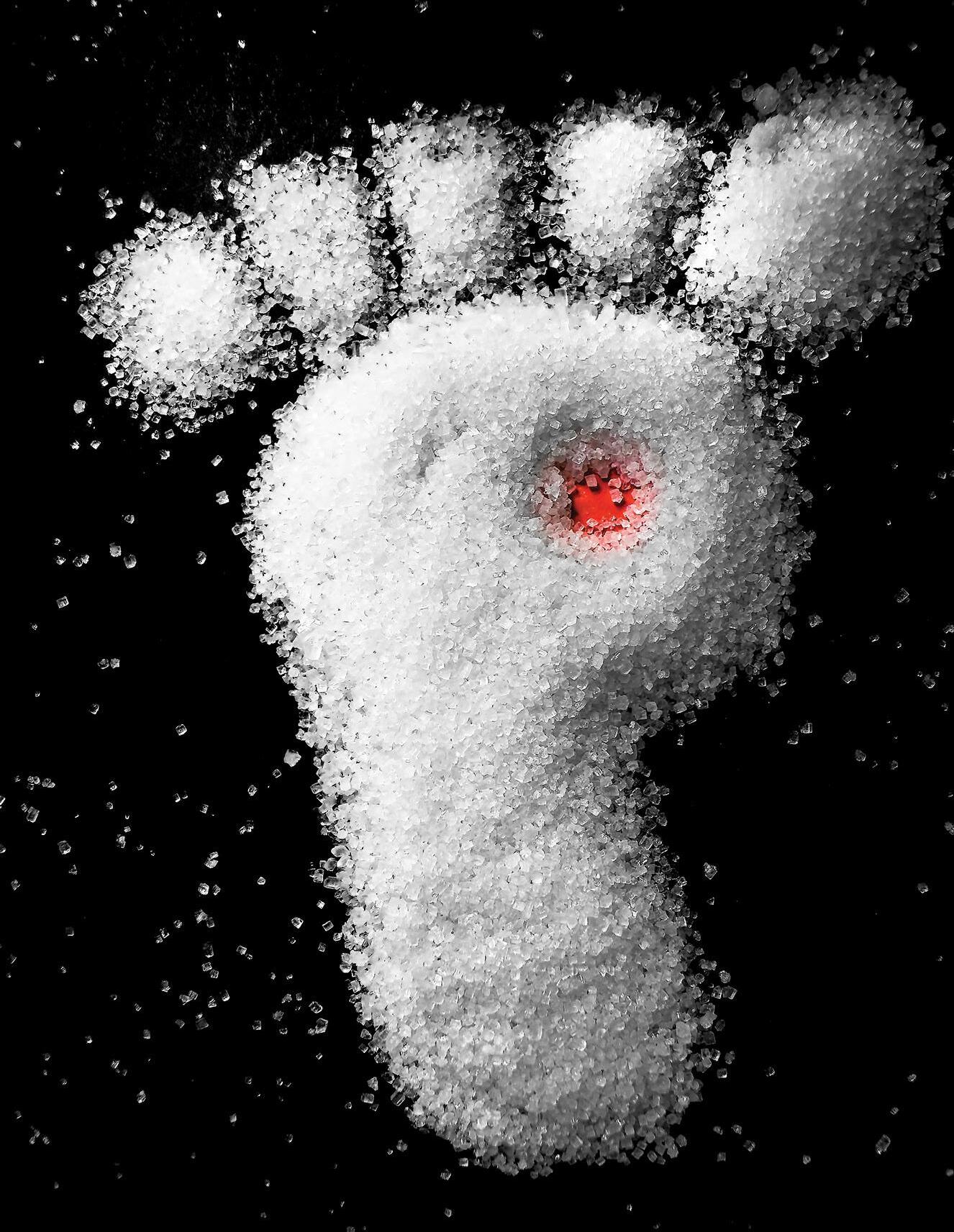
ADT is the gold standard for advanced prostate cancer
5,6
* levels of < 20 ng/dl maintained, current standard of < 50 ng/dl. 1,2 † treatment of locally advanced or metastatic, hormone-dependent.
References: 1. Shim M , Bang W J, Oh CY, et al. Effectiveness of three different luteinizing hormone-releasing hormone agonists in the chemical castration of patients with prostate cancer: goserelin versus triptorelin versus leuprolide. Investig Clin Urol 2019;60(4):244–250. doi: 10.4111/icu.2019.60.4.244. 2. Breul J, Lundstrom E, Purcea D, Venetz WP, Cabri P, Dutailly P, et al. Efficacy of testosterone suppression with sustained-release triptorelin in advanced prostate cancer. Adv Ther 2017;34(2):513–523. doi: 10.1007/s12325-016-0466-7. 3. Heyns CF, Simonin M-P, Grosgurin P, Schall R, Porchet HC. Comparative efficacy of triptorelin pamoate and leuprolide acetate in men with advanced prostate cancer. BJU Int 2003;92(3):226–31. doi: 10.1046/j.1464-410x.2003.04308.x. 4. Klotz L, Tat T. Testosterone nadir and clinical outcomes in patients with advanced prostate cancer: Post hoc analysis of triptorelin pamoate Phase III studies. BJUI Compass 2024:10;5(3):392–402. doi: 10.1002/bco2.318. 5. Crawford ED, Heidenreich A, Lawrentschuk N, Tombal B, Pompeo ACL, Mendoza-Valdes A, et al. Androgen-targeted therapy in men with prostate cancer: evolving practice and future considerations. Prostate Cancer Prostatic Dis 2019;22(1):24–38. doi: 10.1038/s41391-018-0079-0. 6. Gil T, Aoun F, Cabri P, Perrot V, Van Velthoven R. Triptorelin for the relief of lower urinary tract symptoms in men with advanced prostate cancer: results of a prospective, observational, grouped-analysis study. Ther Adv Urol 2017;9(7):179–190. doi: 10.1177/1756287217712379.
Achieves and sustains castrate levels of testosterone beyond current standards* 1-4 S4 TRELSTAR LA 3,75 mg (powder for prolonged-release suspension for injection). Reg. No.: 52/21.12/0034. Each vial contains triptorelin embonate equivalent to 3,75 mg triptorelin. S4 TRELSTAR
How practice management and portals
boost engagement
Patient engagement has become a critical factor in improving health outcomes and enhancing the overall patient experience. Digital health tools, such as practice management solutions and patient portals, play a vital role in empowering patients, increasing their participation in their own healthcare, and ultimately improving retention and satisfaction. As medical practices and healthcare organisations adopt these tools, they witness significant advancements in patient interaction, adherence to treatment plans, and overall well-being.
Practice management solutions streamline administrative processes, enhance communication, and improve the overall patient experience. These systems integrate various functionalities, such as scheduling, billing, and medical record management, to ensure a seamless healthcare experience for both providers and patients.
in medical practices significantly enhances patient retention and satisfaction by offering convenience, personalised care, and improved health outcomes.
S Personalised patient experience: Digital tools cater to individual needs, offering customised health recommendations, tailored treatment plans, and interactive wellness programmes.
1. Appointment scheduling and reminders: Automated scheduling systems reduce no-show rates by sending timely reminders, helping patients stay on track with their healthcare appointments.
2. Billing and claims processing: Digital billing solutions simplify payment processing and provide patients with transparency regarding their healthcare expenses and medical scheme coverage.
3. Telehealth integration: Many practice management platforms support virtual consultations, offering patients convenient access to healthcare services.
4. Data management and analytics: These solutions enable healthcare providers to track patient interactions, treatment adherence, and satisfaction levels, leading to improved care strategies.
Patient portals: A gateway to enhanced healthcare access
Patient portals are secure online platforms that provide patients with access to their medical records, test results, and direct communication with healthcare providers. These tools enhance transparency, empower patients with knowledge, and improve healthcare coordination.
1. Access to medical records: Patients can review their lab results, imaging reports, and visit summaries, ensuring they are well informed about their health status.
2. Secure messaging with providers: Patient portals enable secure communication between patients and healthcare teams, allowing for quick clarifications, medication adjustments, and follow-ups.
3. Prescription management: Many portals offer electronic prescription information, serving as reminders of previously prescribed medications.
4. Billing and payment management: Patients can view their medical bills, understand medical scheme coverage, and make payments online, simplifying administrative tasks and reducing billingrelated confusion.
Improving patient retention and satisfaction
The integration of practice management solutions and patient portals
S Reduced wait times and improved efficiency: Online scheduling and automated workflows streamline the patient experience, reducing long waiting periods and administrative burdens.
S Empowerment and education: With access to health data and educational resources, patients become more engaged in their care, leading to better treatment adherence and self-management.
S Stronger doctor-patient relationships: Continuous interaction through digital platforms fosters trust, improving overall satisfaction and encouraging patients to remain loyal to their healthcare providers.
Challenges and considerations
While digital health tools offer numerous benefits, some challenges must be addressed to maximise their effectiveness:
1. Data privacy and security: Protecting patient data is crucial to maintaining trust and complying with laws such as POPIA.
2. Technology accessibility and digital literacy: Not all patients are tech-savvy or have access to the internet, necessitating alternative engagement strategies.
3. Integration with existing healthcare systems: Seamless integration of digital tools with electronic health records (EHRs) is necessary to avoid information silos and inefficiencies.
4. User experience and adoption: Healthcare providers must ensure that digital platforms are user-friendly and provide adequate training for patients and staff.
Conclusion
The rise of practice management solutions and patient portals has revolutionised patient engagement, offering more accessible, efficient, and personalised healthcare experiences. These digital tools empower patients to take charge of their health, improve provider communication, and enhance overall satisfaction. As healthcare continues to evolve, medical practices that embrace and optimise these digital tools will improve patient outcomes and foster long-term patient loyalty and success in an increasingly digital world. SF
HIV and pneumococcal risk
Vaccinate to protect
Invasive pneumococcal disease (IPD) remains a major cause of morbidity and mortality in individuals infected with HIV, even in the era of antiretroviral therapy (ART). The incidence of IPD is up to 100 times higher in this group than in the general population, with streptococcus pneumoniae being the most common cause of bacteraemic pneumonia. IPD also includes meningitis, sinusitis, and otitis media, with recurrent infections occurring in ~25% of cases within a year.
RThere is an Increased Risk of Pneumococcal Disease in Older Adults.
isk factors for severe disease include low CD4 counts, prior pneumonia, chronic illnesses, and smoking. Additional risk factors include age >60, hepatitis C co-infection, and high HIV RNA levels. ART and pneumococcal vaccination provide protection.
HIV weakens the immune system, increasing susceptibility to S. pneumoniae infection. Individuals infected with HIV are more frequently affected by serotypes common in children and show higher rates of penicillin resistance. In South Africa, serotype 8 is most prevalent, with high case fatality rates (CFRs) observed for serotypes 6A, 11A, and 22F.
Vaccination strategies differ globally. The British HIV Association recommends PCV13 for all infected adults, followed by PPV23 for those qualifying under immunisation programmes. South African guidelines recommend a prime-boost strategy, starting with PCV13 followed by PPV23.
Studies confirm PCV13’s efficacy, with a 40% reduction in vaccine-type IPD. A Malawian study found 74% efficacy in preventing recurrent IPD. Prime-boost strategies further enhance immunity, and PCV13 is superior to PPV23 in immune response. Despite variations in response due to CD4 levels, PCV13 remains essential in reducing pneumococcal disease burden in HIV-infected individuals. Safety studies show no negative effects on immune stability, making PCV13 a critical intervention for this population. Click here to read the full article and access the quiz.
Transitioning to holistic diabetes management with Ozempic®
What got us here won’t get us there
Diabetes is a chronic, progressive cardiometabolic disorder that affects 10.5% of adults worldwide. In 2021, diabetes contributed to >6.7 million deaths. Around 90% of affected individuals have type 2 diabetes (T2DM). Over the past decade, diabetes management has evolved from a primarily glucose-centric focus on lowering HbA1c levels to a more holistic approach. This approach incorporates complications- and pathogenesis-centric strategies.1,2
Apathogenesis-centric strategy targets the underlying metabolic dysfunction – particularly excess adiposity – that drives the development and progression of T2DM, while a complications-centric strategy prioritises the prevention of both short- and long-term complications.1
What is a holistic person-centred
approach?
The American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) consensus report emphasises the importance of a structured, person-centred approach for T2DM management, ensuring that plans are specific, measurable, achievable, realistic, and time-bound.2 This approach involves timely therapy, continuous monitoring, and adjustments based on ongoing assessments to meet evolving needs. The goal is to prevent or delay complications while maintaining quality of life (QoL), which includes managing blood glucose (BG), weight, cardiovascular (CV) risk factors, comorbidities, and complications.2
Key interventions involve lifestyle changes such as dietary modifications, physical activity, and behavioural support, with weight management playing a crucial role in improving glycaemic control and reducing cardiometabolic risks.2
The ADA/EASD report also stresses the importance of individualised management, considering factors like personal preferences, behaviours, clinical data (eg HbA1c, BMI, hypoglycaemia risk), and broader health considerations such as CV and renal status, mental health, and social determinants of health.2
Pharmacological treatments should be chosen based on cost, accessibility, and ease of use, with shared decision-making central to developing a collaborative, patient-focused management plan.2
Ten key principles for managing T2DM effectively
The latest American Association of Clinical Endocrinology consensus statement outlines nine key principles for managing T2DM effectively: 3
1. Lifestyle modifications form the foundation of all therapy.
2. Achieving and maintaining optimal weight is essential for better glycaemic control and overall health.
4. Ease of use and accessibility should be factored into treatment choices.
5. Optimal HbA1c should be ≤6.5% or as close to normal as is safe and achievable for most patients. A less stringent HbA1c target (eg 7%-8%) can be considered in individuals who have limited life expectancy, a history of severe hypoglycaemia, hypoglycaemia unawareness, advanced renal disease, other severe comorbid conditions with a high risk for CVD events, long T2DM disease duration with difficulty to attain an HbA1c goal and those with prohibitive cognitive and/or psychological status.
6. Glycaemic targets should be individualised, considering HbA1c, glucose management indicator, time in range, fasting BG, and postprandial glucose.
7. Timely intervention is crucial – treatment adjustments should be made within three months if targets are not met.
8. Hypoglycaemia should be avoided to ensure affected individuals’ safety.
9. Continuous glucose monitoring is strongly recommended to help affected individuals achieve their glycaemic goals safely.
10. Managing comorbidities, like hypertension and dyslipidaemia, is crucial in T2DM care. Effective glycaemic control should be combined with treatment of these conditions to reduce the risk of cardiovascular disease and retinopathy.
Managing individuals with CV risk factors
CV events in individuals living with T2DM are a leading contributor to the increased risk of premature mortality and have emerged as a growing global health concern. The primary CVDs linked to T2DM include ASCVDs such as HF, stroke, coronary artery disease, and peripheral artery disease. These complications account for at ~50% of deaths among individuals with T2DM. As a result, CVDs play a critical role in the progression and prognosis of T2DM.4
Recent clinical trials highlight that glucagon-like peptide 1 receptor agonists (GLP1-RAs) or sodium-glucose cotransporter-2 (SGLT-2) inhibitors not only lower HbA1c effectively but also reduce the risks of CVD and mortality.1
For individuals with a history of CVD or at high CV risk, the
2. Increased hepatic glucose production
The eight components of the ominous octet:5
ADA/EASD consensus report recommends GLP1-RAs, or SGLT-2 inhibitors, which play key roles in reducing these risks – improving patient outcomes.2
Pathogenesis-centric approach: Targeting the ominous octet in T2DM
The ominous octet is a concept introduced by Dr Ralph DeFronzo in 2009 to describe the eight key pathophysiological defects that contribute to the development and progression of T2DM, which impact treatment decisions.5
The eight components of the ominous octet:5
1. Decreased insulin secretion from beta-cells
2. Increased hepatic glucose production
3. Increased lipolysis
4. Impaired appetite regulation
5. Increased glucagon secretion by islet alpha cells
6. Decreased incretin effect
7. Increased glucose reabsorption
8. Decreased glucose uptake
According to DeFronzo, GLP-1 RAs effectively target six of the eight components of the ominous octet in T2DM. Their actions include: 6
S Enhancing insulin secretion: GLP-1 RAs stimulate insulin release in response to glucose
S Inhibiting glucagon secretion: By reducing glucagon levels, GLP-1 RAs help regulate hepatic glucose production
S Reducing hepatic glucose production: Inhibition of glucagon secretion leads to a decrease in liver glucose output
1. Decreased insulin secretion from betacells
8. Decreased glucose uptake
7. Increased glucose reabsorption
6. Decreased incretin effect
5. Increased glucagon secretion by islet alpha cells
4. Impaired appetite regulation
3. Increased lipolysis
OZEMPIC® - A once-weekly GLP-1 RA for the treatment of patients with uncontrolled Type 2 Diabetes1
PROVEN CV RISK REDUCTION2-6*
PROVEN WEIGHT LOSS BENEFIT2-6*
In patients with Type 2 Diabetes with established CVD, Ozempic® reduced the risk of MACE (CV death, non-fatal, MI and non-fatal stroke)7
26 %
CV EVENT RISK REDUCTION WHEN ADDED TO STANDARD OF CARE* VS. PLACEBO7
[HR=0.74
39 %
SIGNIFICANT DECREASE IN STROKE BY VS. PLACEBO7*
[HR=0.61 (95 % CI, 0.38-0.99; P=0.04)]
NON-SIGNIFICANT DECREASE IN NON-FATAL MYOCARDIAL INFARCTION BY
*Results apply to Ozempic® across SUSTAIN trials, which included placebo, sitagliptin, dulaglutide, exenatide and insulin glargine.3-6
References: 1. Ozempic® Approved Professional Information, 17 February 2023. 2. Pratley RE, Aroda VR, Lingvay I, et al ; SUSTAIN 7 Investigators. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. LancetDiabetesEndocrinol.2018;6(4):275-286. 3. Aroda VR, Bain SC, Cariou B, etal.Efficacy and safety of onceweekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. LancetDiabetesEndocrinol.2017;5(5):355-366. 4. Ahren B, Masmiquel L, Kumar H, etal . Efficacy and safety of onceweekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. LancetDiabetesEndocrinol.2017;5(5):341-354. 5. Rodbard HW, Lingvay I, Reed J, etal . Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. JClinEndocrinolMetab.2018;103(6)(suppl 1):1-28. 6. Ahmann AJ, Capehorn M, Charpentier G, etal. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): a 56-week, open-label, randomized clinical trial. DiabetesCare.2018;41:258-266. 7. Marso SP, Bain SC, Consoli A, et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. NEnglJMed.2016;375(19):1834-1844.
Novo Nordisk (Pty) Ltd.
ZA24OZM00174 January 2025.
SCAN THE QR CODE FOR API
Patient Portrayal.
S Correcting the gastrointestinal incretin defect: GLP-1 RAs provide a pharmacologic dose of GLP-1, compensating for the natural incretin deficiency in T2DM
S Suppressing appetite and promoting weight-loss: GLP-1 RAs exert a central effect on the brain, leading to appetite suppression and promoting weight reduction
S Improving insulin sensitivity: The weight loss induced by GLP-1 RAs indirectly enhances insulin sensitivity in muscle and liver tissue.
How can a complications-centric strategy improve T2DM management?
As mentioned, a complications-centric strategy prioritises the prevention of both short- and longterm complications. Acute complications include diabetic ketoacidosis, a medical emergency characterised by dehydration, Kussmaul breathing, abdominal pain, and potential coma. Prompt treatment reverses the condition.1,7
Hypoglycaemia, caused by excessive insulin, missed meals, or intense exercise, leads to sweating, dizziness, confusion, and, if severe, unconsciousness. Immediate glucose intake is required. Hyperglycaemia results from insufficient insulin, leading to serious complications if untreated.7
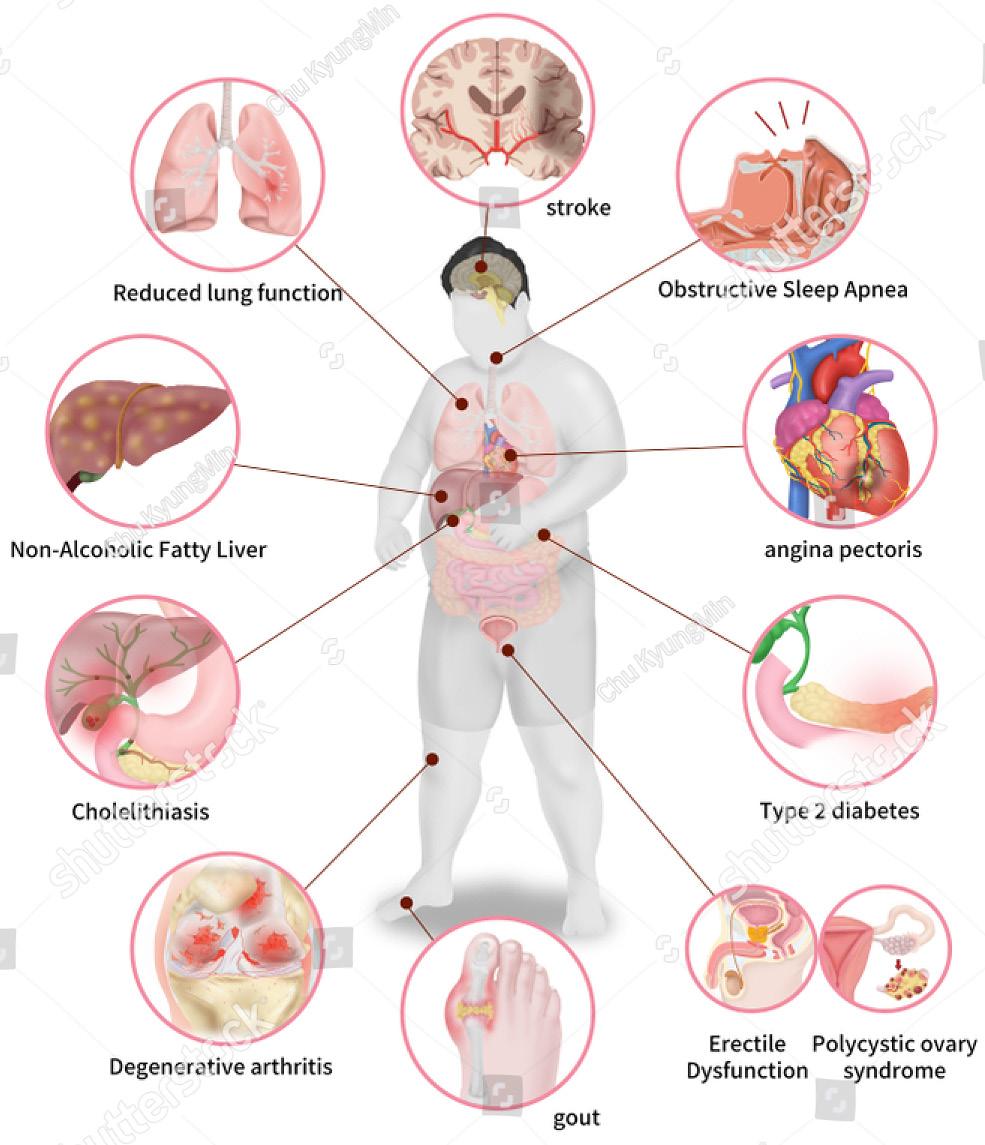
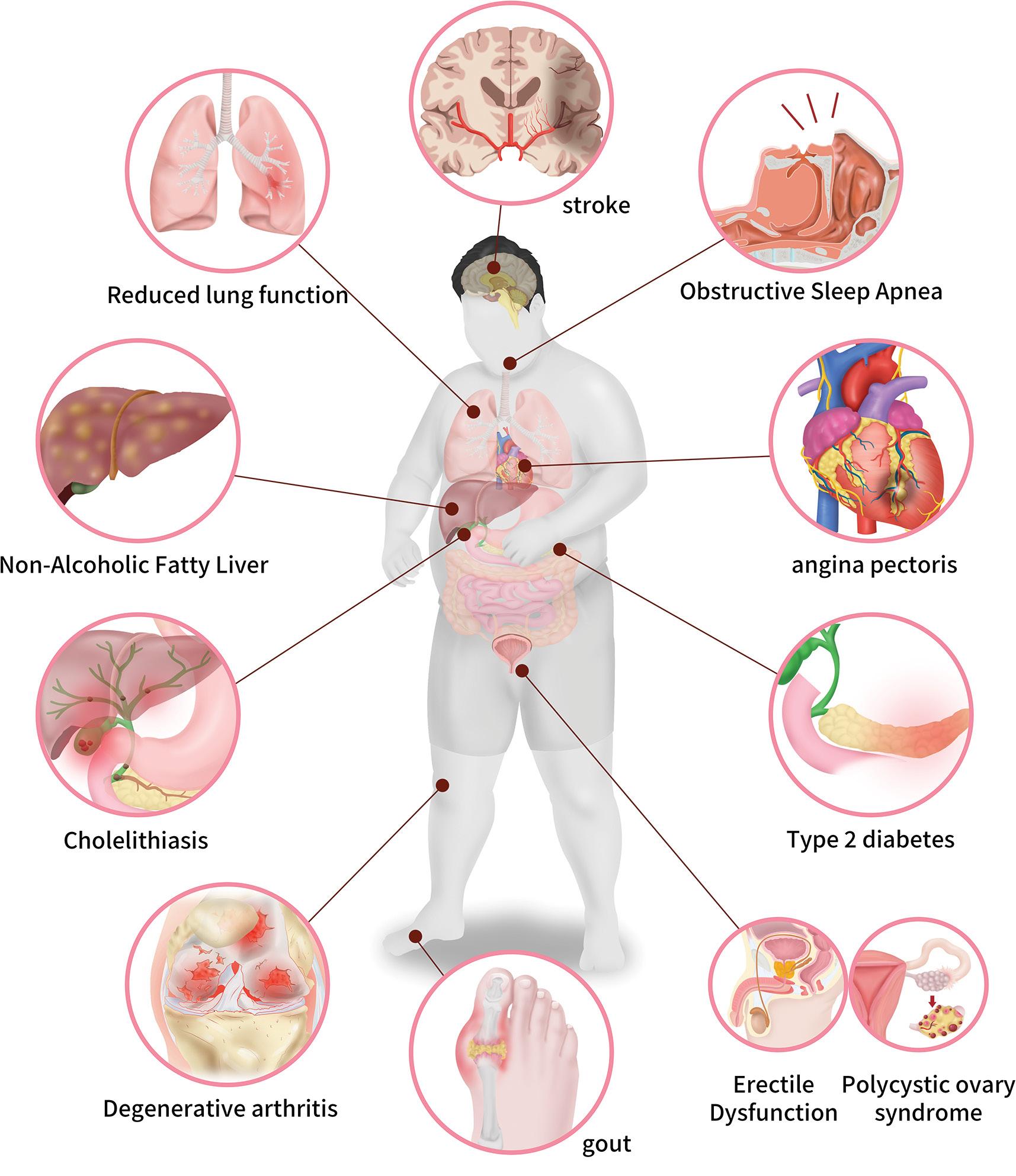
T2DM affects multiple organs over time. Long-term complications include macroangiopathy, which leads to ASCVDs, and erectile dysfunction. Microvascular complications include retinopathy (vision loss), nephropathy (renal failure), neuropathy (sensory issues and pain), and diabetic foot (ulcers and amputations). Diabetes also increases the risks of infection and osteoporosis and damages the liver.7
reduction in multiple trials. The SUSTAIN™ studies show in addition to improving glycaemic control, Ozempic ® led to greater weight loss compared to liraglutide, sitagliptin, exenatide, and insulin glargine. Furthermore, a higher proportion of participants met key health targets, showcasing its potential as an effective therapy for managing T2DM with added weight management benefits. These findings emphasise its broad therapeutic advantages.9-17
The Efficacy and Safety of Semaglutide Once-weekly Versus Placebo in Drug-naïve Subjects With Type 2 Diabetes (SUSTAIN™ 1) trial, found that Ozempic ® (0.5mg and 1mg) significantly reduced HbA1c by 1.45% and 1.55%, respectively, compared to placebo (0.02%). Body weight decreased by 3.73kg and 4.53kg with Ozempic ® versus 0.98kg with placebo by week 30.9
The ADA and EASD consensus highlights a structured, person-centred approach to T2DM management, ensuring treatment plans are specific, measurable, achievable, realistic, and time-bound for optimal outcomes
T2DM doubles the risk of myocardial infarction (MI) and significantly increases HF and hypertension risks. CV autonomic neuropathy affects heart rate regulation, increasing the likelihood of arrhythmias and sudden cardiac death. Diabetes is also linked to atrial fibrillation, exacerbated by comorbid conditions like ASCVD and hypertension.7
The Ozempic® Tri-Zone: Balancing CV risk reduction and glycaemic control
In our previous issues, we have extensively covered the findings of the Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes (SUSTAIN™ 6). In short – SUSTAIN 6 evaluated the CV effects of Ozempic ® in individuals living with T2DM at high CV risk. A total of 83.0% of participants had established CVD, CKD or both. The primary outcome (CV death, non-fatal MI, or stroke) occurred in 6.6% of the Ozempic ® group vs 8.9% in placebo. Non-fatal stroke risk was significantly lower (39% relative risk reduction). Non-fatal MI occurred in 2.9% of participants receiving Ozempic ® and in 3.9% of those receiving placebo and the rates of new or worsening nephropathy were lower in the Ozempic ® group.8
Ozempic ® has demonstrated benefits beyond HbA1c risk
The Efficacy and Safety of Semaglutide Onceweekly Versus Sitagliptin Once-daily as add-on to Metformin and/or TZD in Subjects With Type 2 Diabetes (SUSTAIN™ 2) study showed Ozempic ® (0.5mg and 1mg) reduced HbA1c by 1.3% and 1.6%, respectively, and weight by 4.3kg and 6.1kg, compared to sitagliptin (1.9kg).10
The Efficacy and Safety of Semaglutide Onceweekly Versus Exenatide ER 2.0 mg Once-weekly as add-on to 1-2 Oral Antidiabetic Drugs in Subjects With Type 2 Diabetes (SUSTAIN™ 3) study found that Ozempic ® (1mg) reduced HbA1c by 1.5% and body weight by 5.6kg, superior to exenatide, which reduced HbA1c by 0.9% and weight by 1.9kg.11
The Efficacy and Safety of Semaglutide Once Weekly Versus Insulin Glargine Once Daily as add-on to Metformin With or Without Sulphonylurea in Insulin-naïve Subjects With Type 2 Diabetes (SUSTAIN™ 4) trial showed Ozempic ® (0.5mg and 1mg) reduced HbA1c by 1.21% and 1.64%, respectively, and weight by 3.47kg and 5.17kg, compared to insulin glargine, which caused a 1.15kg weight gain. Hypoglycaemia rates were lower with Ozempic ® 12
The Semaglutide Added to Basal Insulin in Type 2 Diabetes (SUSTAIN™ 5) study found that Ozempic ® (0.5mg and 1mg) reduced HbA1c by 1.4% and 1.8%, respectively, and body weight by 3.7kg and 6.4kg, compared to 0.1% and 1.4kg with placebo.13
The Efficacy and Safety of Semaglutide Versus Dulaglutide as add-on to Metformin in Subjects With Type 2 Diabetes (SUSTAIN™ 7) trial demonstrated that Ozempic ® (0.5mg and 1mg) outperformed dulaglutide in reducing HbA1c (1.5% and 1.8% vs 1.1% and 1.4%) and weight (4.6kg and 6.5kg vs 2.3kg and 3kg).14
In the Efficacy and Safety of Semaglutide Versus Canagliflozin as add-on to Metformin in Subjects With Type 2 Diabetes (SUSTAIN 8) study, the primary endpoint was change from baseline in HbA, and the confirmatory secondary endpoint was change from baseline in bodyweight, both at week 52. From overall baseline, participants receiving Ozempic® had significantly greater reductions in HbA1c and bodyweight than those receiving canagliflozin, an SGLT2 inhibitor, HbA1c estimated treatment difference was -0.49 percentage points, and bodyweight estimated treatment difference was -1.06kg.15
The endpoints in the Efficacy and Safety of Semaglutide Onceweekly Versus Placebo as add-on to SGLT-2i in Subjects With Type 2 Diabetes Mellitus (SUSTAIN 9) were change in HbA1c from baseline at week 30 (primary) and change in bodyweight from baseline to
week 3 (secondary). Participants in the Ozempic ® group had greater reductions in HbA1c (estimated treatment difference −1·42%) and bodyweight (−3·81kg versus those randomised to placebo).16
Finally, the Efficacy and safety of once-weekly semaglutide1.0mg vs once-daily liraglutide 1.2mg as add-on to 1-3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10) showed that the mean HbA1c (baseline 8.2%) decreased by 1.7% with Ozempic ® and 1% with liraglutide. The mean body weight (baseline 96.9kg) decreased by 5.8kg with Ozempic ® and 1.9kg with liraglutide. Ozempic ® also showed greater proportions of participants achieving glycaemic targets and weight loss milestones.17
Conclusion
Ozempic ® has demonstrated consistent efficacy across diverse patient populations living with T2DM, including those with varying comorbidities and treatment backgrounds. The SUSTAIN™ studies highlight its robust ability to reduce HbA1c and body weight, outperforming other treatments like liraglutide, exenatide, and insulin glargine. Notably, Ozempic ® provides additional benefits in managing CV risk, CKD, and weight loss, making it a versatile and effective option for individuals with complex health needs. Its broad therapeutic advantages, combined with its safety profile, reinforce its role in personalised, holistic diabetes management strategies for optimising patient outcomes.
References
1. Galindo RJ, et al. Advances in the management of type 2 diabetes in adults. BMJ Med, 2023.
2. Davies MJ, et al Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care, 2022.
3. Samson SL, et al American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm – 2023 Update. Endocr Pract, 2023.
4. Ma CX, et al Cardiovascular disease in type 2 diabetes mellitus: progress toward personalized management. Cardiovasc Diabetol, 2022.
5. DeFronzo RA. From the Triumvirate to the Ominous Octet: A New Paradigm for the Treatment of Type 2 Diabetes Mellitus. Diabetes, 2009.
6. DeFronzo RA. Combination therapy with GLP-1 receptor agonist and SGLT2 inhibitor. Diabetes Obes Metab, 2017.
7. Farmaki P, et al Complications of the Type 2 Diabetes Mellitus. Curr Cardiol Rev, 2020.
8. Marso SP, et al. SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med, 2016.
9. Sorli C, et al Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol, 2017.
10. Ahrén B, et al Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol, 2017.
11. Ahmann AJ, et al Efficacy and Safety of Once-Weekly Semaglutide Versus Exenatide ER in Subjects With Type 2 Diabetes (SUSTAIN 3): A 56-Week, Open-Label, Randomized Clinical Trial. Diabetes Care, 2018.
12. Aroda VR, et al Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol, 2017.
13. Rodbard HW, et al Semaglutide Added to Basal Insulin in Type 2 Diabetes (SUSTAIN 5): A Randomized, Controlled Trial. J Clin Endocrinol Metab, 2018.
14. Pratley RE, et al SUSTAIN 7 investigators. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol, 2018.
15. Lingvay I, et al. Efficacy and safety of once-weekly semaglutide versus daily canagliflozin as add-on to metformin in patients with type 2 diabetes (SUSTAIN 8): a double-blind, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol, 2019.
16. Zinman B, et al. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): a randomised, placebo-controlled trial. Lancet Diabetes Endocrinol, 2019.
17. Capehorn MS, et al Efficacy and safety of once-weekly semaglutide 1.0mg vs oncedaily liraglutide 1.2mg as add-on to 1-3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab, 2020. SF
Abbreviated Professional Information
Ozempic Professional Information February 2023 (v1.0)
Scheduling status: S4 Name of the medicine: Ozempic ® Qualitative and quantitative composition: Semaglutide 1,34 mg/ml Therapeutic indication: Ozempic ® is indicated: a) for the treatment of adults with insufficiently controlled type 2 diabetes mellitus as an adjunct to diet and exercise • as monotherapy when metformin is considered inappropriate due to intolerance or contraindications. • as combination therapy with oral anti-diabetic medicines (metformin, thiazoledinediones, sulphonylurea), basal insulin with or without metformin and pre-mix insulin. b) to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction or non-fatal stroke) in adults with type 2 diabetes mellitus and established cardiovascular disease. Posology and method of administration: Ozempic ® starting dose is 0,25 mg once weekly. After 4 weeks, the dose should be increased to 0,5 mg once weekly. After at least 4 weeks with a dose of 0,5 mg once weekly, the dose can be increased to 1 mg once weekly to further improve glycaemic control. Ozempic ® is to be administered once weekly at any time of the day, with or without meals. Ozempic ® is to be injected subcutaneously in the abdomen, in the thigh or in the upper arm. The injection site can be changed without dose adjustment. Ozempic ® should not be administered intravenously or intramuscularly. The day of weekly administration can be changed if necessary as long as the time between two doses is at least 2 days (>48 hours). When Ozempic ® is added to existing sodiumglucose cotransporter 2 (SGLT2) inhibitor therapy, the current dose of SGLT2 inhibitor can be continued unchanged. Contraindications: Hypersensitivity to semaglutide or to any of the excipients, a personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), pregnancy and lactation. Special warnings and precautions for use: Ozempic ® should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis. Ozempic ® is not a substitute for insulin. Acute pancreatitis has been observed with the use of Ozempic ® Patients should be informed of the characteristic symptoms of acute pancreatitis. If pancreatitis is suspected, Ozempic ® should be discontinued; if confirmed, Ozempic ® should not be restarted. Patients treated with Ozempic ® in combination with a sulfonylurea or insulin may have an increased risk of hypoglycaemia. The risk of hypoglycaemia can be lowered by reducing the dose of sulfonylurea or insulin when initiating treatment with Ozempic ®. Risk of Thyroid C-cell Tumours: Cases of MTC in patients treated with liraglutide, another GLP-1 receptor agonist have been reported in the post marketing period; the data in these reports are insufficient to establish or exclude a causal relationship between MTC and GLP-1 receptor agonist use in humans. Interaction with other medicines and other forms of interaction: In vitro studies have shown very low potential for Ozempic ® to inhibit or induce CYP enzymes and to inhibit drug transporters. The delay of gastric emptying with Ozempic ® may influence the absorption of concomitantly administered oral medicines. The potential effect of Ozempic ® on the absorption of co-administered oral medicines was studied in trials at Ozempic ® 1 mg steady state exposure. Fertility, pregnancy and lactation: Ozempic ® is contraindicated during pregnancy and lactation. Undesirable effects: The most frequently reported adverse reactions with Ozempic ® in clinical trials were gastrointestinal disorders, including nausea, diarrhoea and vomiting. Adverse reactions by system organ class and absolute frequencies identified in all phase 3a trials listed here as Very common (>1/ 10): Hypoglycaemia when used with insulin or sulfonylurea, nausea, diarrhoea; Common (>1/100 to <1/10): Hypoglycaemia when used with other OADs, decreased appetite, dizziness, diabetic retinopathy complications, vomiting, abdominal pain, abdominal distension, constipation, dyspepsia, gastritis, gastrooesophageal reflux disease, eructation, flatulence, cholelithiasis, fatigue, increased lipase, increased amylase, weight decreased; Uncommon (>1/1,000 to <1/100): hypersensitivity, dysgeusia, increased heart rate, injection site reactions, hypersensitivity, acute pancreatitis; Rare (>1/10,000 to <1/1,000): anaphylactic reaction; Frequency unknown: angioedema. Overdose: There is no specific antidote for overdose with Ozempic ®. In the event of overdose, appropriate supportive treatment should be initiated according to the patient’s clinical signs and symptoms. A prolonged period of observation and treatment for these symptoms may be necessary, taking into account the long half-life of Ozempic ® of approximately 1 week. Reg. No.: 53/21.13/0497. For full prescribing information, refer to the Professional Information approved by the Regulatory Authority. Novo Nordisk (Pty) Ltd. Reg. No.: 1959/000833/07. 150 Rivonia Road, 10 Marion Street Office Park, Building C1, Sandton, Johannesburg, 2196, South Africa. Tel: (011) 202 0500. Fax: (011) 807 7989. www.novonordisk.com. ZA25OZM0004
Scan QR code for abbreviated PI
Weight loss key to
joint and bone health
Overweight and obesity have become a global health crisis, affecting ~60% of adults. By 2030, obesity is projected to affect one billion people – equivalent to one in five women and one in seven men – further escalating this global health crisis. A 2024 study by the Human Sciences Research Council found that 67.9% of South African women are either overweight or obese. Obesity not only increases the risk of metabolic diseases but also contributes to musculoskeletal disorders, a leading cause of pain and disability worldwide. These issues arise from mechanical strain and physiological changes, intensifying the health burden of obesity and impacting overall well-being.1,2,3
Summary
Obesity affects ~60% of adults globally and is projected to impact one billion people by 2030. Beyond metabolic diseases, it contributes to musculoskeletal disorders like sarcopenic obesity, osteoporosis, and osteoarthritis, leading to pain, disability, and reduced QoL. Joint stress, inflammation, and reduced mobility as a result of obesity worsen these conditions. Studies show that modest weight loss can alleviate symptoms. Effective interventions include lifestyle changes, pharmacotherapy, and bariatric surgery. AOMs such as phentermine, orlistat, and liraglutide support weight loss but remain underutilised. A combined approach integrating weight loss strategies such as lifestyle modification, pharmaco- and psychological therapies, can significantly improve musculoskeletal health and well-being.
Increased joint forces from higher body mass, reduced range of motion, cardiovascular (CV) strain, early fatigue, and neuromuscular deficiencies all contribute to injury risk. A high body mass index (BMI) alters lifting mechanics, affecting trunk inclination and acceleration, further increasing musculoskeletal injury risk.1
Calenzani et al found the most affected sites in individuals living with obesity were the ankles/feet (87.80%), lumbar region (68.29%), and knees (68.29%), with activity limitations most linked to ankle/ foot (46.34%), knee (43.90%), and lower back (41.46%) pain.4
Common obesity-related musculoskeletal diseases include sarcopenic obesity, osteoporosis, tendinopathy, and osteoarthritis, leading to disability. Low-level systemic inflammation is a key driver of tissue degeneration, pain, and impaired recovery in these conditions.5
Sequalae of obesity and musculoskeletal diseases
Obesity and musculoskeletal conditions significantly reduce quality of life (QoL) by causing chronic pain, limiting mobility, and affecting social and emotional well-being. These conditions make daily activities more challenging, reducing independence, interfering with work performance, affecting relationships, and overall well-being.4
Pain caused by musculoskeletal diseases leads to a 7.8% decline
Lite
*Studies were conducted on the HCl formulation. Duromine is available as sustained action ion exchange resinate granules in capsules containing phentermine 15 mg or 30 mg. Duromine should be used in conjunction with an exercise, diet and behaviour modification program. Patients require medical review after a defined course of treatment, which ideally should not exceed 3 months.
References: 1. Duromine® approved professional information, October 2020. 2. Moldovan CP, Weldon AJ, Daher NS, Schneider LE, Bellinger DL, Berk LS, et al. Effects of a Meal Replacement System Alone or in Combination with Phentermine on Weight Loss and Food Cravings. Obesity 2016; 24:2344-2350. 3. Munro JF, Maccuish A. C, Wilson EM, Duncan LJP. Comparison of Continuous and Intermittent Anorectic Therapy in Obesity. Br Med J 1968;1:352-354. 4. Based on internal analysis by iNova Pharmaceuticals (Pty) Ltd using data from the following source: IQVIA Rx_OTC Dec 2024, ATC3- A8A, Brands measured in Dispensed Units, reflecting estimates of real-world activity.
IQVIA. All rights reserved.
in physical function, making daily tasks harder. It also contributes to an 11% reduction in the ability to work and perform daily responsibilities. Long-term activity restrictions further intensify these challenges, making it 17.5% harder for individuals to maintain employment and complete essential tasks.4
As mentioned, chronic pain plays a major role in reduced QoL, accounting for a 9.7% decline over a 12-month period, while more recent (in the past week) pain episodes have an even greater impact (22.6%). Mobility restrictions worsen this issue, contributing to a 20.7% reduction in QoL, reinforcing the cycle of pain and movement limitations.4
Pain in the past week led to a 4% decline in social functioning, while mobility limitations make social engagement 10.2% more difficult. Activity limitations also contribute to emotional distress, accounting for 13.3% of role-emotional difficulties.4
Can weight-loss improve/reverse musculoskeletal diseases?
As demonstrated in the study by Calenzani et al the most commonly affected anatomical sites in individuals living with obesity include the ankles/feet, lumbar region, and knees. According to Vincent et al weight loss can improve musculoskeletal pain, particularly in weight-bearing joints.4,6
As weight loss occurs, the compressive forces through joints are dramatically reduced, with some studies indicating a reduction by fourfold. This reduction in load can significantly alleviate pain and may also decrease the fear of movement associated with joint discomfort.
6
In individuals living with obesity, even a modest weight loss of ~5% can help relieve some joint pain. However, more substantial weight loss – around 10% of body weight – is associated with moderate to large clinical improvements in joint pain. This suggests that a greater reduction in body weight may provide more significant relief for individuals suffering from musculoskeletal pain.6
What does the updated NICE guidance recommend?
The 2025 National Institute of Health Care and Excellence (NICE) guidance (excluding individuals from African descent) classifies overweight and obesity as:7
S Overweight: BMI 25kg/m² to 29.9kg/m²
S Obesity class 1: BMI 30kg/m² to 34.9kg/m²
S Obesity class 2: BMI 35kg/m² to 39.9kg/m²
S Obesity class 3: ≥BMI 40kg/m²
NICE does caution that clinical judgment should be used when interpreting the healthy weight category (BMI 18.5kg/m² to 24.9kg/ m²), as individuals in this range may still have central adiposity.7
According to the NICE guidance, individuals from African descent are more prone to central adiposity and may face an increased cardiometabolic risk at lower BMIs. For this groups, the following BMI thresholds should be used as practical measures of overweight and obesity:7
S Overweight: BMI 23kg/m² to 27.4kg/m²
S Obesity: BMI ≥27.5kg/m²
NICE emphasises developing a tailored plan to meet individual needs, regularly reviewing the individual’s health and progress towards meeting their goals (including weight loss), psychological counselling to address the effect of weight stigma, increased
physical activity, following dietary interventions to achieve nutritional balance while reducing energy intake, and encouraging adherence to behavioural management interventions.7
NICE recommends increasing physical activity for its health benefits, even without weight loss. To prevent obesity, most individuals should engage in 45-60 minutes of moderate-intensity exercise daily, especially if they do not reduce calorie intake. Those maintaining weight loss after obesity may need 60-90 minutes per day.7
Dietary improvements are also encouraged for benefits such as better lipid profiles and reduced risk of type 2 diabetes and CV disease. Effective weight management requires maintaining an energy deficit through approaches like low-fat or low-carbohydrate diets or other methods to reduce overall calorie intake.7
NICE recommends that pharmacotherapy for weight management should be considered after dietary, exercise, and behavioural approaches have been tried and evaluated in adults living with overweight or obesity. All pharmacotherapy options should be used in conjunction with a reduced-calorie diet and increased physical activity.7
Bariatric surgery is recommended for individuals with a BMI of ≥40kg/m², or those with a BMI between 35kg/m² and 39.9kg/m² who have a significant health condition that could improve with weight loss. The individual must also agree to the required longterm follow-up, including lifelong annual reviews after the surgery.7
AOMs: Lending a helping hand
According to Coutinho and Halpern, weight loss is more complex than often portrayed. An extensive population study reveals that only one in 210 males and one in 124 females with a BMI between 30kg/m² and 35kg/m² achieve normal weight without bariatric surgery. For those with a BMI >40kg/m², the figures are even lower, with only one in 1220 males and one in 677 females achieving normal weight.8
Lifestyle changes alone typically result in <5% reduction in body weight over the long term. A meta-analysis of 14 intervention trials on diet and exercise for weight management found that most patients regain much of the weight lost within four- to seven-years of follow-up.8
Studies show that treatment with anti-obesity medications (AOMs) typically leads to greater weight loss compared to lifestyle changes alone. A key requirement for the approval of any AOM is its proven effectiveness in maintaining long-term weight loss. However, AOMs are often underutilised, primarily due to the stigma surrounding these medications, which discourages their prescription, noted Coutinho and Halpern.8
Phentermine, one of the oldest and most widely used obesity treatments, was approved in the United States in 1959. As a Schedule 5 medicine it has recognised medical benefits with a low potential for abuse. Phentermine is an atypical amphetamine analogue that works by inhibiting appetite through norepinephrine agonism in the central nervous system. It is approved for shortterm use (up to 12 weeks) for obesity treatment, primarily due to a lack of long-term studies, according to Coutinho and Halpern. However, real-world data suggests that it can be a useful option for long-term use. Caution is advised with longer-term use, and individuals should consult their treating physician at least every 12-weeks.8,9
In South Africa, phentermine is recommended as a short-term adjunct to a medically supervised comprehensive weight reduction programme, which should include exercise, diet (caloric/kilojoule restriction), and behaviour modification.10
The recommendation is particularly applicable to individuals living with obesity, who to do not have a satisfactory clinical response with a suitable weight reduction programme on its own. Phentermine is not recommended for children <12-years.10
Phentermine treatment may be considered for individuals with a lower BMI when the risk of morbidity from other medical conditions is high. Individuals with the following comorbidities may qualify for medical weight reduction assistance, even if their BMI is ≤30kg/m².11
S Sleep apnoea
S Insulin-resistant diabetes
S Pre-diabetes or impaired glucose tolerance linked to obesity
S High cardiovascular risk due to obesity.
How effective is phentermine?
Numerous studies have investigated the efficacy of phentermine for weight reduction. Weintraub et al explored obesity treatment with a combination of low-dose phentermine and fenfluramine. The study compared different regimens: phentermine resin (30mg), fenfluramine hydrochloride (20mg three times a day), a combination of phentermine (15mg) and fenfluramine (30mg), and a placebo. Phentermine monotherapy (10kg) and fenfluramine (7.5kg) led to greater weight loss compared to placebo (4.4kg), with combination therapy resulting in the most significant weight loss.12
Kim et al assessed phentermine’s effects on weight reduction and safety in healthy individuals with obesity (BMI ≥25kg/m²). Participants were randomised to either phentermine or placebo daily, along with behavioural therapy. The phentermine group lost significantly more weight (7kg) and reduced waist circumference (3.5cm) compared to placebo (2- 3kg). A higher
percentage of the phentermine group achieved >5% weight loss (85.7% vs 16%) and >10% weight loss (50% vs 8.3%).13
Kang et al found significant weight loss (8.1kg) and waist circumference reduction (0.5cm) with phentermine diffusecontrolled release, along with improved lipid profiles. The study concluded that short-term DCR treatment resulted in weight reduction and metabolic improvement without severe adverse events. Kim et al reported that 45.6% of participants achieved ≥5% weight loss, with an average of 4kg lost.14,15
Conclusion
Obesity presents significant health challenges, particularly due to its strong link to musculoskeletal disorders and the resulting impact on quality of life. Weight loss, especially through a combination of diet, exercise, and behavioural changes, can alleviate musculoskeletal pain and improve mobility. Phentermine is approved for short-term use. This medication may offer a valuable tool for individuals struggling with obesity, particularly when other weight reduction methods fail. References are available on request. SF
Obesity complications
Lower back pain
Best practices
The global burden of low back pain (LBP), the leading cause of disability worldwide, continues to increase. LBP is characterised by pain, muscle tension, or stiffness located between the costal margin and the inferior gluteal folds, with or without radiating leg pain (sciatica). In 2020, it affected ~619 million people – nearly 10% of the world’s population. By 2050, this number is expected to reach ~843 million.1,2
Summary
LBP is the leading cause of disability worldwide. In 2020, LBP affected ~619 million people, with projections reaching ~843 million by 2050. In Africa, the lifetime prevalence is 47%, with significant economic and societal burdens. Chronic LBP contributes to depression, reduced mobility, comorbidities and loss of productivity. LBP risk factors include obesity, smoking, and occupational strain. Management strategies emphasise NSAIDs, physiotherapy, and lifestyle modifications, with limited efficacy for opioids and muscle relaxants. Emerging therapies, including fluoroscopic interventions, show promise but require further investigation.
Asystematic review of population-based studies conducted in Africa found that the lifetime prevalence of LBP was 47%, with an annual prevalence of 57% and a point prevalence of 39%. A hospital-based, cross-sectional study examining LBP prevalence among nurses in KwaZulu-Natal, reported a point prevalence of 59%, with bending, prolonged postures, and patient transfers identified as key contributing factors.2
Another population-based study in KwaZulu-Natal found an LBP prevalence of 45% among individuals of Indian descent, and 32.6% among People of Colour, highlighting factors such as multiple pregnancies or children, lower education levels, and long-distance driving as significant predictors. Similarly, a crosssectional study on LBP management in South African primary
care settings reported a lifetime prevalence of 73.2%, with 26.3% of individuals experiencing chronic LBP. In primary care, ~50% of LBP cases involve fluctuating pain of low-to-moderate intensity. Most LBP cases resolve within two- to six-weeks, with only a small percentage (9%) of individuals developing chronic, disabling pain.2
The societal and economic impact
However >90% of the socioeconomic burden of LBP is attributed to this small group of individuals. Most of them will not make a full recovery and will experience regular flare-ups and recurrent symptoms.2 LBP not only impacts affected individuals’ daily lives but also imposes a heavy social burden and economic cost. For example, in the United Kingdom, it costs the National Health Service ~R9.9m annually from general practitioner appointments alone. In the United States, the expenditure for LBP and neck pain was ~R1.9bn in 2016.1,3 LBP – most prevalent among working-age individuals – leads to increased absenteeism, reduced productivity, and early retirement. For example, in Brazil, LBP resulted in 100 days of work absence per person annually between 2012 and 2016, with productivity losses amounting to about R32bn.1
A 2022 South African study conducted in KwaZulu-Natal estimated the total annual direct medical costs for acute LBP, defined as lasting <12-months, in the province at ~R17m, with a cost of ~R1861 per patient. Pain medications, particularly opioids (tramadol) and non-steroidal anti-inflammatory drugs (NSAIDs) such as diclofenac and celecoxib, made up 83% of the total cost (~R14m), or ~R1505 per patient. Other expenses included rehabilitation (~R951 067, 5.4%) and opioids (~R2.5m).3
For chronic LBP, defined as lasting >12-weeks, the total annual direct medical cost was ~R84m, with an average cost per patient of ~R28 535. The elderly had the highest costs, with females averaging ~R41 114 and males ~R35 867.29. Inpatient care accounted for the largest portion of the cost (46.31%), followed by outpatient care (26.5%). Medication made up 79.6% of outpatient costs (R15m), with NSAIDs (R10m) and opioids (R4m) being the key contributors. Overall, the total annual cost for both acute LBP and chronic LBP was R102m.3
Consequences of LBP
LBP has significant effects on psychological health. Chronic LBP is linked to increased depression, which in turn correlates with greater disability and poorer recovery outcomes.1,2 Chronic LBP is also
strongly associated with reduced sexual activity and is frequently linked to insomnia. Some studies suggest that chronic LBP may contribute to earlier mortality, as it often leads to significant disability and activity limitations due to fear-avoidance behaviour.2 Over time, this can exacerbate existing comorbidities like hypertension, diabetes, hypercholesterolemia, and other systemic conditions, especially when compounded by weight gain from reduced physical activity.2
Mechanisms of LBP
LBP can be classified into three main types: Axial, radicular, and spinal stenosis. This classification helps identify the underlying cause of the pain, allowing for targeted treatment.4
S Axial LBP: Is more common in women, older individuals, and those with higher baseline pain. It is often associated with acute trauma or chronic conditions like degenerative diseases. The pathophysiology involves complex interactions between ligaments, spinal discs, muscles, and the brain, leading to muscle contractions and nociceptive pain. In most cases, axial LBP resolves within 12 months with appropriate treatment, but 28% of patients may experience pain beyond this period. Axial LBP is subdivided into include:
Í Discogenic pain (40%): Typically has an inciting event, such as trauma, but can also have an insidious onset. Symptoms include pain felt over the midline, occasionally radiating to the upper thigh or knee. Aggravating factors include activities that load the spine, prolonged sitting.
Í Facet joint pain (15%-30%): Often has an insidious onset, with inciting events present in 50% of cases. Signs are typically localised to the lumbosacral region, often overlying the affected facet. Pain may radiate to the groin or knee. Aggravating factors include prolonged standing and transitional movements.
Í Sacroiliac joint pain (15%-30%): Symptoms are often related to strenuous, repetitive movements, or trauma. Pain is often delayed by 12 days. Symptoms are typically localised to the paraspinal and gluteal regions. Rarely radiates beyond the lumbosacral area. Aggravating factors include transitional movements, and palpation of the paraspinal muscles.
Í Paraspinal muscle pain: Caused by trauma or strain. Symptoms are localised to the paraspinal muscles, sometimes radiating to the glutes. Aggravating factors include rapid or strenuous movements, palpation of the paraspinal muscles.
S Radicular pain: Results from nerve root pathology, often due to mechanical causes like herniated discs, infections, or degenerative diseases. The pain can be accompanied by numbness or tingling, a condition called radiculopathy. Conservative treatment shows good results in many cases, but up to 40% of patients may experience prolonged symptoms >3-months. The primary symptom to consider for radicular LBP is pain that follows a lumbar dermatomal distribution. The most common causes include:
Í Herniated intervertebral discs at L4-L5 or L5-S1, which account for 90% of cases
Í Foraminal stenosis due to severe disc herniation, responsible for 10% of cases.
Patients typically report aggravation of pain when bending, coughing, or sneezing, with relief when lying down. A clinical examination should focus on a neurological assessment, including testing pain and temperature sensation in the lumbar dermatomes. Mapping these dermatomes helps localise the pain to specific
vertebral levels. Additional diagnostic tests for radicular LBP include the passive straight leg raise test, which has a sensitivity of 91% and specificity of 26%. An important cause of radicular pain is cauda equina syndrome, which results from significant disc herniation or mass effect compressing the cauda equina. This condition is a red flag and requires urgent surgical intervention, as it can cause radicular pain, loss of bowel and bladder function, and perineal numbness or loss of sensation.
S Lumbar spinal stenosis (LSS): Age (especially >65-years), previous spine surgery, and conditions like osteoarthritis or inflammatory arthritis contribute to the risk of developing chronic stenosis. It shares similarities with radicular pain but is distinguished by neurogenic claudication symptoms. LSS results from anatomical changes, including disc herniation, facet hypertrophy, and other conditions that narrow the spinal canal. Over time, untreated stenosis can lead to chronic neuropathic pain. The key characteristic of lumbar spinal stenosis is neurogenic claudication, which involves increased radicular pain when standing or walking, with rapid relief upon sitting. The pain typically radiates to the gluteal region and legs in a dermatomal pattern. Motor weakness is commonly present, and a negative straight leg test helps rule out facet joint pathology. The pain arises when the spinal canal’s crosssectional area narrows, leading to nerve compression or pressure on specific spinal tracts, such as during lumbar extension. Relief is usually achieved by lumbar flexion.
Red flags for serious conditions
Certain symptoms or red flags may indicate non-musculoskeletal causes of LBP, such as cancer, infections, or vascular issues. These include:4
S Urinary or faecal incontinence
S Saddle paraesthesia
S Severe tenderness
S Unexplained weight loss or acute pain onset. Although red flags are often present, they only correlate with serious pathology in a small percentage of cases (~1%). Thus, red flags always warrant further investigation by specialists.4
Global review of guidelines
Distinguishing between acute and chronic LBP helps in understanding the cause and guiding treatment. Risk factors, clinical presentations, and the presence of red flags are essential in managing and diagnosing LBP effectively.5
A recent 2024 global comparison of clinical practice guidelines for managing LBP identified several key therapeutic recommendations across various types of LBP, including education, psychological therapy, exercise therapy, electrotherapy, manual therapy, and medication.5
For acute LBP, most guidelines recommended non-steroidal
24th South African Spine Society Congress 22-24 March
Century City Conference Centre, Cape Town
anti-inflammatory drugs (NSAIDs), exercise, staying active, spinal manipulation, opioids, heat therapy, massage, acupuncture, and muscle relaxants. Common options include:
S Non-selective NSAIDs: Ibuprofen, naproxen
S Selective NSAIDs: Cyclooxygenase enzymes-2 (COX-2) inhibitors: Etoricoxib, celecoxib. NSAIDs exert their effects by inhibiting the COX enzyme, which converts arachidonic acid into thromboxanes, prostaglandins, and prostacyclins. The therapeutic benefits of NSAIDs stem from the suppression of these eicosanoids. Thromboxanes facilitate platelet adhesion, prostaglandins contribute to vasodilation and fever regulation, and prostacyclins play a role in pain modulation.6
Two COX isoenzymes exist: COX-1, which is constitutively expressed and supports gastrointestinal protection, kidney function, and platelet aggregation, and COX-2, which is inducibly expressed during inflammation. Non-selective NSAIDs inhibit both, while COX-2 selective NSAIDs primarily target inflammation with fewer GI side effects.6
Other treatments included self-management, paracetamol, and therapies such as cognitive behavioural therapy (CBT) and laser therapy.4,5
For subacute LBP, NSAIDs, staying active, therapeutic exercise, spinal manipulation, massage, muscle relaxants, and heat therapy were frequently recommended. Other approaches included spinal mobilisation, acupuncture, and CBT. Muscle relaxants are helpful for non-specific LBP, especially when a myofascial component is involved. While not recommended as first-line treatment, they can be considered for short-term use under supervision. Long-term use should be monitored by a pain specialist. Types of muscle relaxants include:4,5
2025 PainSA Congress
Date: 16th - 18th May
Venue: Century City Conference Centre, Cape Town
Registrations Open
S Benzodiazepines: Lack sufficient evidence for efficacy and are not recommended due to risks like sedation and addiction
S Antispasmodics: Agents like baclofen are better tolerated, acting as gamma-aminobutyric acid-B antagonists in the spinal cord to reduce pain transmission.
For LBP of unspecified duration, guidelines generally advised staying active, self-management, NSAIDs, therapeutic exercise, spinal manipulation, spinal mobilisation, and CBT. Multidisciplinary treatment and returning to work were also frequently mentioned.5
Other options and their efficacy
S Opioids are controversial due to inconsistent evidence and the risk of addiction and misuse. While commonly prescribed, their use is not generally recommended for LBP, particularly because high-quality evidence is lacking.4
S Anti-epileptics have shown no benefit for chronic LBP, even when neuropathic pain is present, and their use is not recommended unless supervised by a pain specialist.4
S Serotonin-norepinephrine reuptake inhibitors may help in managing chronic LBP when considering the biopsychosocial model of pain, addressing both psychological and biological components.4
S Topical agents are frequently used by LBP patients, but evidence for their effectiveness is limited. While agents like arnica show no significant benefit, topical cayenne has been shown to reduce pain scores effectively.4
S Therapeutic injections and fluoroscopically guided procedures have become more popular, though they have not significantly reduced surgery or disability rates. All injections should be performed under the supervision of a pain specialist. Epidural steroid injections are the most commonly used interventional technique, providing well-established pain relief for radicular pain, often lasting for six weeks or more. The transforaminal approach tends to offer better pain relief compared to interlaminar approaches. However, psychosocial factors and concurrent opioid use can reduce the effectiveness of these injections.4
S Fluoroscopically guided radiofrequency ablation can be effective for patients who benefit from diagnostic blocks. Options include continuous and pulsed radiofrequency. Continuous radiofrequency ablation uses thermal injury to the dorsal root to prevent pain transmission but may damage surrounding structures. Pulsed radiofrequency ablation, which avoids nerve coagulation, is more promising as it causes changes in the dorsal root nerve structures, leading to decreased nociceptive transmission without harming surrounding tissues.4
Conclusion
LBP remains a major global health challenge, with rising prevalence and significant economic and social burdens. In South Africa, the high costs of treatment, particularly for chronic cases, highlight the need for costeffective management strategies. While NSAIDs, physiotherapy, and lifestyle changes remain first-line treatments, emerging interventions such as fluoroscopic-guided procedures offer potential benefits. Addressing psychosocial factors, improving workplace ergonomics, and promoting early intervention may help reduce long-term disability. Future research should focus on optimising treatment pathways, preventing chronicity, and reducing the financial strain on healthcare systems while improving patient outcomes. References are available on request. SF
Summary
BV is one of the most common causes of VDS among women of reproductive age, with a prevalence ranging from 5% to 70%. While ~30% of cases resolve spontaneously, recurrence rates are high, with up to 80% of women experiencing a relapse within nine months. BV is caused by an imbalance in vaginal microbiota, leading to overgrowth of harmful bacteria. Symptoms may include a fishy odour and vaginal discharge, though many women remain asymptomatic. Treatment options include metronidazole and clindamycin, with oral or intravaginal formulations. Prolonged treatments and adjunct therapies like boric acid or probiotics may help reduce recurrence. Despite effective treatment options, BV remains a challenging condition due to its high recurrence rate, emphasising the need for improved diagnostic and therapeutic strategies.
BV battles
Treatment options and recurrence risks
Bacterial vaginosis (BV) is one of the most common forms of vaginal discharge syndromes (VDS) among females of reproductive age, with prevalence estimates ranging from 5% to 70%. While ~30% of cases resolve spontaneously, recurrence rates are high, with up to 80% of women experiencing a relapse within nine months of treatment.1
BV is particularly widespread in parts of Africa and is characterised by an imbalance in the normal vaginal flora, leading to an overgrowth of certain bacteria. Beyond its immediate symptoms, BV is associated with an increased risk of various gynaecological and obstetric complications, including preterm delivery, spontaneous abortion, early pregnancy loss in in vitro fertilisation, and increased susceptibility to acquiring and transmitting HIV and other sexually transmitted infections (STIs).1,2
More than just an odour: Diagnosing bacterial vaginosis with precision
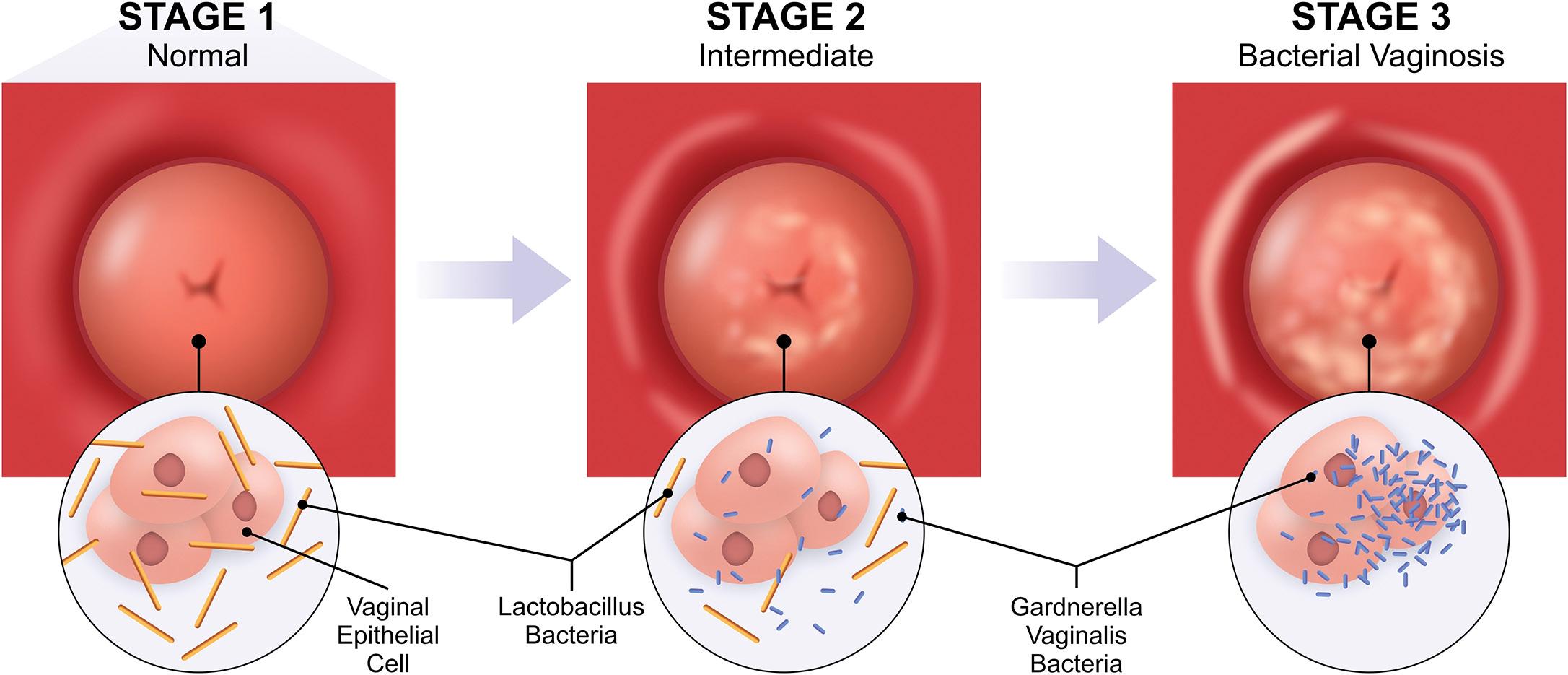
Current evidence suggests that BV is a polymicrobial syndrome marked by a shift in vaginal microbiota from an ‘optimal’ to a ‘non-optimal’ state. This imbalance is characterised by a decline in protective lactobacilli and an increase in bacterial diversity, including facultative and strict anaerobes such as Gardnerella species, Atopobium vaginae, Prevotella species, and other BVassociated bacteria. While the exact causative pathogens are still under debate, a recent conceptual model proposes that virulent strains of Gardnerella, along with Prevotella bivia and Atopobium vaginae, play a key role in BV development.2
BV is typically diagnosed clinically and confirmed through laboratory testing. Up to 50% of BV-affected women do not experience symptoms. In symptomatic women, BV often presents with a malodorous vaginal discharge, which may worsen after
sexual intercourse. Other symptoms can include dysuria, dyspareunia, and vaginal itching, though many individuals remain asymptomatic. Clinicians should assess risk factors such as vaginal douching, multiple sexual partners, recent antibiotic use, smoking, and intrauterine device use. A thorough history of previous BV infections is also crucial.1,2
A pelvic examination helps distinguish BV from other infections like vaginal candidiasis, chlamydia, gonorrhoea, trichomoniasis, and herpes simplex virus. Additionally, BV increases the risk of pelvic inflammatory disease, HIV, and other STIs. Clinicians should assess for fever, pelvic pain, and STI history to rule out more serious conditions. Cervical swabs for chlamydia and gonorrhoea may be necessary, as well as evaluating for cervical motion tenderness. Self-collected swabs and pap smears are unreliable for diagnosing BV.1
Diagnosis involves obtaining a vaginal swab, assessing pH levels, and performing a wet mount microscopy. A vaginal pH >4.5, the presence of clue cells – epithelial cells coated with bacteria –and a positive whiff test (a fishy odour after adding potassium hydroxide) suggest BV. If vaginal discharge is present, two of these criteria suffice for diagnosis, if absent, all three are required.1
The Amsel criteria are commonly used in clinical practice, requiring at least three of four findings:1
S A thin, homogeneous vaginal discharge
S Clue cells on microscopy, pH >4.5
S A positive whiff test.
A modified version considers only two criteria and has shown similar diagnostic accuracy. The Amsel criteria have a sensitivity of 70% and specificity of 94%. Alternatively, the Nugent scoring system, primarily used in research, relies on a gram stain of vaginal fluid to quantify bacterial presence. This method has a sensitivity
of 89% and specificity of 83%. While molecular diagnostic assays offer higher sensitivity (90.5%-96.7%) and specificity (85.8%-95%), their cost limits routine use. Point-of-care testing is also uncommon due to expense, but newer methods, such as Gardnerella strain isolation, continue to improve BV detection.1
What drives recurrence?
Recurrent BV is defined as ≥3 confirmed episodes of BV within a 12-month period. Despite initial improvement after treatment, about one in three women will experience a recurrence of BV symptoms within three months, and >50% will have a recurrence within 12 months.3
Recurrences may be due to a new infection or a relapse of the original infection. Factors contributing to recurrence include the persistence of a BV-associated biofilm, failure to restore lactobacilli dominance, reinfection from an untreated partner, potential host genetic or immune factors, if treatment is discontinued prematurely, medications are not used correctly, or the infection was not fully treated.2,3
Furthermore, recent studies have shown that the presence of an intrauterine device (IUD) is linked to an increased risk of prevalent BV, particularly with copper IUDs, a non-hormonal form of contraception. In a prospective study involving asymptomatic women, the prevalence of BV increased in those who initiated copper IUDs, rising from 27% at baseline to 35% at 30 days, 40% at 90 days, and 49% at 180 days. In contrast, women initiating hormonal contraception had no change in BV prevalence.4
The recurrence of BV not only prolongs symptoms but also increases distress and frustration for women, often leading to repeated visits to healthcare providers or the use of unproven home remedies.2
Bacterial vaginosis
Symptoms
Risk factors
E M P O W E
RIN
G W O M E N
*CDC - Centers for Disease Control and Prevention; #Associated with BV; † Vs. single 500mg oral dose of metronidazole
References: 1. Metrogel Approved package insert 31 August 2021. 2. Kingsburgh C, Strydom K-A. The aetiology, diagnosis and management of the vaginal discharge syndrome. AmpathChat 2020;66:1-4. 3 Pirotta, M, Fethers K, Bradshaw C. Bacterial vaginosis more questions than answers. Australian Family Physician June 2009; Vol. 38, No. 6. 4 Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2015. MMWR / June 5, 2015 / Vol. 64 / No. 3. 5. Beigi R, Austin M, Meyn L, et al. Antimicrobial resistance associated with the treatment of bacterial vaginosis. Am J Obstet Gynecol 2004;191:1124-1129. 6 Weir CB, Le JK. Metronidazole [online] May 2019 [cited 27 May 2020]; Available from URL: https://www.ncbi.nlm.nih.gov/books/NBK539728/. 7 Agnew KJ, Hillier SL. The E ect of Treatment Regimens for Vaginitis and Cervicitis on Vaginal Colonization by Lactobacilli. Sex Transm Dis 1995;22(5): 269-273. 8. Austin MN, Beigi RH, Meyn LA, et al. Microbiologic Response to Treatment of Bacterial Vaginosis with Topical Clindamycin or Metronidazole. J Clin Microbiol 2005;43(9):4492–4497. 9 Wain AM. Metronidazole Vaginal Gel 0.75% (MetroGeI-Vaginal®) A Brief Review. Infect Dis Obstet Gynecol1998;6:3-7.
How to treat BV
Antibiotics are the first line treatment for BV. The recommended therapeutic regimens include oral, intravaginal metronidazole or intravaginal clindamycin. A comprehensive review by Muzny et al recommends treatment for all symptomatic women to alleviate vaginal symptoms. Therapies such as metronidazole 500mg (oral) for seven days, metronidazole (gel 0.75%) for five days, or clindamycin (vaginal cream 2%) for seven days, as there is no new evidence to suggest alternative treatments.4,5
The World Health Organization recommends treatment with metronidazole combined with lifestyle modifications. It is important to recommend that women avoid excessive vaginal cleansing, douching, and intravaginal practices. Other treatments include metronidazole gel, tinidazole, and clindamycin (oral and topical). Women presenting with vaginal discharge should be treated for BV, candidiasis, and trichomoniasis. Metronidazole covers both BV and trichomoniasis, while antifungals can be used to treat candidiasis. Metronidazole can be administered orally, intravenously, or topically. It comes in capsule, tablet, topical and intravenous forms. It comes in capsule, tablet, topical and intravenous forms.6,7
According to the American Society for Academic Specialists in General Obstetrics (SASGOG) and Gynecology, metronidazole (oral or vaginal) or clindamycin (vaginal) cures acute BV in 80% to 90% of cases.8
How is recurrent BV treated?
SASGOG notes that there is no standardised treatment for recurrent BV.8 However, some experts recommend an extended course of metronidazole (500mg twice daily for 10-14 days).9
In a randomised trial of by Wawalka et al, participants were treated with povidone iodine suppositories or lactobacilli capsules. Both treatments improved clinical symptoms and secretion condition. By day 15, povidone iodine showed a trend towards better efficacy, particularly in acute BV patients, and more effectively reduced pathogenic bacteria. lactobacilli counts decreased in the povidone iodine group initially but increased later, suggesting no need for additional lactobacilli supplementation after antiseptic treatment.10
The Centers for Disease Control and Prevention concurs.
Another regimen involves metronidazole (oral) 500mg twice daily for seven days, followed by 600mg of intravaginal boric acid daily for 21 days. Additionally, a monthly treatment regimen includes metronidazole (oral) 2g along with 150mg of oral fluconazole.1
Improving adherence to treatment to prevent recurrence
As previously mentioned, two key factors contributing to BV recurrence are premature treatment discontinuation and incorrect medication use. To improve adherence, it is crucial to consider patient preference and tolerability alongside treatment efficacy when prescribing BV treatments.2,3,11
Given the high recurrence rates, there is a clear need for advancements in diagnosis, treatment, and overall management. A significant challenge in this area is the unresolved question of BV’s exact cause, which remains a barrier to progress.11
According to Munzy et al, until the aetiology of BV is fully understood, this challenge will persist. Research into combining antibiotics, biofilm-disrupting agents, and/or probiotics may improve treatment outcomes, restore normal vaginal microbiota, and reduce recurrence.11
The recent introduction of single-dose oral and intravaginal therapies offers more convenient alternatives for individuals who prefer not to follow multidose regimens. However, no studies have shown that single-dose therapies are more effective than traditional multidose regimens for BV. Ultimately, healthcare providers should consider the patient’s preferences to enhance adherence and improve clinical outcomes.11
Conclusion
Metronidazole is one of the cornerstones of treatment for BV, with both oral and intravaginal formulations being highly effective. Its use in various regimens, such as metronidazole (oral or gel) has demonstrated significant efficacy in resolving symptoms and reducing the risk of complications. Despite its efficacy, BV recurrence is common, highlighting the need for effective treatment strategies to enhance outcomes. Ultimately, metronidazole continues to be a reliable first-line treatment, but further research is needed to optimise long-term management and prevent recurrence.
References are available on request. SF
ABalancing bleeds and beats: AFib anticoagulation
Atrial fibrillation (AFib) is the most common cardiac arrhythmia, significantly increasing the risk of cardiovascular events such as stroke, systemic embolism, and heart failure. To prevent stroke in AFib patients, oral anticoagulants (OACs), including vitamin K antagonists (VKAs) and non-VKA oral anticoagulants (NOACs), are used. However, NOACs are now preferred due to their superior efficacy and safety.
ll OACs, including NOACs such as apixaban, dabigatran, and rivaroxaban, carry a risk of gastrointestinal (GI) bleeding, which can lead to major morbidity and mortality. Major GI bleeding, defined by significant blood loss or the need for a transfusion, can result in complications such as hospitalisation, ICU admission, and blood transfusion. Studies show that NOACs vary in their GI bleeding risk depending on the drug and patient factors. For instance, apixaban and rivaroxaban are associated with higher rates of upper GI bleeding, while dabigatran leads to less GI involvement. Risk factors for GI bleeding with NOACs include patient age, renal impairment, and comorbidities like chronic kidney disease (CKD). Furthermore, the twice-daily dosing regimen of NOACs, such as apixaban, may present a safer option compared to
once-daily regimens due to lower peak drug concentrations, reducing bleeding risks.
Management of GI bleeding involves prompt discontinuation of OACs and supportive care. Specific reversal agents, such as idarucizumab for dabigatran, may be used for life-threatening bleeds. The decision to resume anticoagulation therapy after a major GI bleed should be based on the balance between thromboembolic risk and bleeding risk, with resumption offering substantial benefits for stroke prevention.
Click here to read the full article and access the quiz. SF
Haemophilia A
X-linked, rare, clotting chaos
Haemophilia A is a rare genetic disorder caused by a deficiency in clotting factor VIII, preventing normal blood clotting and leading to prolonged bleeding. While typically inherited, it can also arise from spontaneous mutations. This disorder primarily affects males due to its X-linked recessive inheritance pattern, though females can be carriers and occasionally exhibit symptoms.
Haemophilia A varies in severity based on factor VIII activity levels:
S Mild (5%-40% activity): Occasional prolonged bleeding, usually after surgery or trauma.
S Moderate (1%-5%): Frequent prolonged bleeding, occasional spontaneous bleeding.
S Severe (<1%): Spontaneous bleeding, especially into joints and muscles, leading to chronic pain and potential disability. Without treatment, severe cases may experience recurrent joint damage and life-threatening internal bleeding.
on the X chromosome. Around 70% of cases are inherited, while 30% arise from new mutations. Since males have only one X chromosome, they are more likely to be affected. Carrier females may have mild symptoms due to X chromosome inactivation.
Diagnosis
Diagnosis includes:
S Medical history and physical examination: Assessing bleeding tendencies and family history.
S Blood tests: Activated Partial Thromboplastin Time: Prolonged in haemophilia A.
S Factor VIII clotting activity test: Confirms diagnosis and severity.
S Genetic testing: Identifies mutations and detects carriers.
Treatment
While haemophilia A has no cure, modern therapies significantly improve quality of life. Treatment options include:
S Recombinant factor VIII (preferred due to lower infection risk).
S Plasma-derived factor VIII (sourced from blood donors).
S On-demand therapy (used to treat bleeding episodes in mild/ moderate cases).
S Prophylactic therapy (regular infusions to prevent severe bleeding).
S Desmopressin: Stimulates temporary factor VIII production for mild cases.
S Antifibrinolytics: Help prevent clot breakdown.
S Gene therapy (emerging treatment): Research is ongoing to correct the F8 gene.
Complications: Inhibitors
Around 30% of individuals with severe haemophilia A develop inhibitors-antibodies that neutralise replacement factor VIII. Management includes:
S Immune tolerance induction: Gradual desensitisation to factor VIII.
S Bypassing agents: alternative clotting factors to manage bleeding episodes.
Conclusion
Early diagnosis and proper management allow individuals with haemophilia A to lead active lives. Specialised haemophilia treatment centres provide comprehensive care, and ongoing advancements, including gene therapy, offer promising future treatment options. Reference available on request. SF
Pre-winter sniffles
Don’t confuse AR with the common cold or flu
Allergic rhinitis (AR), commonly known as hay fever, is a chronic inflammatory condition triggered by immunoglobulin E (IgE) in response to inhaled allergens. It affects 20%-30% of adults and 40% of children, with a strong link to asthma –50%-80% of individuals with asthma also have AR.
AR symptoms include nasal itching, sneezing, congestion, and rhinorrhoea, along with red, swollen eyes and itching in the eyes, palate, and ears. Triggers range from outdoor pollens and house dust mites to pet dander and mould. Rising global temperatures have intensified pollen seasons, worsening allergic reactions.
AR is classified as intermittent or persistent. Seasonal AR is more common in children, while perennial AR is prevalent in adults. Symptoms can range from mild to severe, potentially leading to sleep disturbances, fatigue, and headaches. Poorly managed AR may increase the risk of sinus infections, recurrent ear infections, and asthma exacerbations.
Diagnosis relies on clinical history, symptom response to corticosteroids, and allergy testing. Skin testing offers immediate
results, while serum IgE testing is convenient but less sensitive. Misdiagnosis is common, as AR symptoms overlap with colds, flu, and other conditions like vasomotor rhinitis.
Treatment focuses on allergen avoidance, pharmacotherapy, and immunotherapy. Intranasal corticosteroids (INCS) are the first-line treatment, with second-generation antihistamines providing symptom relief.
Combination therapy, such as fluticasone propionate/azelastine hydrochloride, offers faster and more effective symptom control than monotherapy.
Click here to read the full article and access the quiz. SF
Malaria ends with us
Malaria is a deadly parasitic disease spread by Anopheles mosquitoes, impacting millions worldwide. It triggers recurring fevers, chills, and severe complications such as cerebral malaria and anaemia. Rapid diagnosis and treatment are essential to prevent deaths. Every two minutes, a child succumbs to malaria, emphasising the critical need for prevention and treatment. The theme of this year’s World Malaria Day (25 April) is: Malaria Ends
With Us: Reinvest, Reimagine, Reignite
.
Deaths: Malaria cases and deaths have significantly declined over the past two decades, yet the disease still claims >600 000 lives annually, with children <5-years accounting for ~80% of fatalities.
Highrisk areas: >90 countries are malaria-endemic, with the highest burden in sub-Saharan Africa. Travellers to these regions are also at risk.
Incubation period: Symptoms appear eightto 40-days after infection, depending on the Plasmodium species.
Treatment: Antimalarial drugs include chloroquine, artemisinin-based combination therapy, atovaquone-proguanil, and quinine, depending on the species and resistance patterns. Common symptoms: Fever, chills, sweating, headache, muscle aches, nausea, and vomiting. Severe cases may cause anaemia, seizures, coma, or organ failure.
Reference Buck E, Finnigan NA. Malaria. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551711/ SF
Classic malarial cycle: Cyclic fevers – chills followed by fever, sweating, and a return to normal temperature – often occur every 48- to 72-hours.
Severe malaria: Can cause cerebral malaria, kidney failure, respiratory distress, and death, especially in children and pregnant women.
Diagnosis: Blood smears, rapid diagnostic tests, and PCR detect malaria parasites and their species.
Prevention: Mosquito nets, insect repellents, antimalarial prophylaxis for travellers, and indoor spraying reduce infection risks.
Future challenges: Climate change and drug resistance threaten malaria control, making vaccines and global efforts critical for eradication.
World Malaria Day
25 April
Photo credit: Shutterstock.com
Managing wound infection in diabetic foot ulcers
Diabetic foot complications are often underestimated, and many healthcare professionals fail to consider the potential for diabetic foot ulcers (DFUs) when treating individuals living with diabetes. A holistic approach is necessary to detect early-stage problems that could lead to severe complications, such as amputations. These individuals frequently present with unnoticed wounds or issues that require careful examination, including the removal of shoes during clinical visits to inspect for ulcers.
Emergency room staff, nurses, and general practitioners are in an ideal position to detect these issues early, as affected individuals often visit these settings when they first notice problems or perceive potential concerns. This gives healthcare professionals a chance to prevent the worsening of these conditions through early intervention and appropriate management.
Globally, the scale of the issue is alarming. There are currently >537 million adults living with diabetes, with a significant portion (three in four) residing in low-income countries such as South Africa.
Every five seconds, an individual dies from diabetes-related complications, and the statistic for limb loss has worsened, with an individual losing a limb every 20 seconds – an improvement over the previous statistic of every 32 seconds. In Africa, the situation is even more dire, with one in 22 adults diagnosed with diabetes, though half of these cases go undiagnosed.
In South Africa, about one in nine adults live with diabetes, a statistic compounded by an increasing prevalence of the disease. Risk factors for diabetes, such as poor lifestyle choices and socioeconomic challenges, contribute to rising obesity rates, which in turn increase the risk of developing diabetes. Despite this, South Africa spends a fraction of the global budget on diabetes care and prevention, highlighting a lack of resources to tackle the issue.
A 2024 South African study revealed that 28% of individuals living with diabetes present at primary healthcare clinics with diabetic foot ulcers, many of which are already in advanced stages. The study also found that ~50% of these individuals were never given proper preventive education.
Common comorbidities such as hypertension, dyslipidaemia,
and peripheral neuropathy contribute to the severity of these ulcers. Additionally, polypharmacy – where patients are prescribed multiple medications –often leads to poor management and increased complications due to drug interactions.
In clinical practice, healthcare providers must prioritise inspecting the feet of diabetic patients regularly, even if they’re not presenting for foot-related issues. Many patients with diabetic foot ulcers may not be aware of the severity of their condition, and early detection can prevent longterm disability. Simple actions, like asking patients to remove their shoes during check-ups, could potentially save limbs and lives.
To watch a replay of the webinar, click here or scan the QR code. SF This webinar was sponsored by Smith + Nephew and is accredited for one (1) ethics CPD point. Once you have watched the replay, send an e-mail to john.woodford@newmedia.co.za and request to have your CPD point allocated to your profile on the HPCSA database. Include the webinar names and your HPCSA number in your e-mail. Please note, it may take up to four weeks for your point to be reflected on your portfolio and points are allocated at the discretion of the HPCSA.
Dr Ethel Andrews
BPH: The dual action of solifenacin and tamsulosin for
improved patient outcomes
Combination therapy with tamsulosin (a selective alpha blocker) and solifenacin (antimuscarinic), addresses both obstructive symptoms of benign prostatic hyperplasia (BPH) and irritative symptoms of overactive bladder (OAB), which often coexist.
BPH is a common condition in ageing men, characterised by an enlarged prostate that obstructs urine flow, leading to symptoms like slow urinary flow, hesitancy, and intermittent stream. These mechanical issues result from difficulty in the bladder exerting enough pressure to push urine out past the prostate. Additionally, storage symptoms such as urgency, frequency, nocturia, and urge incontinence often coexist, causing significant distress for patients. While obstructive symptoms are common, irritative symptoms are typically more bothersome to patients, affecting their quality of life.
The initial approach to managing BPH focuses on using alpha blockers, which relax the smooth muscle of the prostate and alleviate obstructive symptoms by improving urine flow. However, up to 30% of patients may still experience irritative symptoms, necessitating the use of combination therapy.
Tamsulosin helps alleviate obstructive symptoms by relaxing the smooth muscle in the prostate and bladder neck. However, when patients continue to experience irritative symptoms like urgency and frequency, antimuscarinics such as solifenacin are introduced. Solifenacin works by inhibiting the muscarinic receptors in the bladder, decreasing bladder contractility and reducing symptoms of urgency and frequency.
Historically, urologists have been cautious about using antimuscarinics alongside alpha blockers due to concerns about urinary retention. However, clinical trials have demonstrated that when carefully dosed, these drugs can be used together without significant worsening of urinary flow or obstruction. Solifenacin, at a dose of 6mg, has shown good efficacy with a relatively mild side-effect profile compared to higher doses, which can cause dry mouth, constipation, and other anticholinergic effects.
The two-in-one combination therapy of tamsulosin (0.4mg) and solifenacin (6mg) offers several potential advantages. It simplifies treatment by reducing the pill burden, which can improve patient adherence. Additionally, if the combination drug is more cost-effective than using both medications separately, it
provides a practical benefit. However, one significant disadvantage is that if the patient experiences adverse effects, both drugs must be stopped simultaneously. This contrasts with the flexibility of using the two drugs separately, where the dose of one drug can be adjusted or replaced without discontinuing the other.
While this fixed-dose combination may appeal to some patients, it is not recommended as a first-line treatment.
Dr David Smart
Physicians should start with monotherapy, typically an alpha blocker, and only introduce the second agent if symptoms persist. A conservative approach allows for careful monitoring of side effects, and if needed, switching to combination therapy.
The decision to combine these agents should be made after assessing the individual patient’s response to monotherapy. Additionally, clinicians should be cautious when prescribing anticholinergics, as they have side effects, including cognitive impairments, particularly in older patients.
To watch a replay of the webinar, click here or scan the QR code. SF
This webinar was sponsored by Cipla and is accredited for one (1) CPD point. Once you have watched the replay, send an e-mail to john.woodford@newmedia.co.za and request to have your CPD point allocated to your profile on the HPCSA database. Include the webinar names and your HPCSA number in your e-mail. Please note, it may take up to four weeks for your point to be reflected on your portfolio and points are allocated at the discretion of the HPCSA.
treatment: Balancing autonomy and intervention Ethical dilemmas in addiction
In South Africa, the misuse of prescription drugs, particularly opioids like codeine-based products and benzodiazepines, is contributing to a growing addiction crisis. Initially prescribed for legitimate medical conditions, such as managing pain, these medications can quickly lead to dependency. Systemic issues, including inconsistent healthcare access and socioeconomic disparities, exacerbate the problem, creating a cycle of misuse and addiction.
Healthcare providers face a significant ethical dilemma in prescribing pain medications. Over-prescribing can lead to addiction, overdose, or misuse, while under-prescribing can result in unnecessary suffering and diminished quality of life for patients. Striking the right balance between alleviating pain and avoiding harm is essential, especially as addiction to prescription drugs, including opioids, continues to rise.
Addiction is not solely about the substance but also about what it represents – an escape, numbness, or relief from life’s struggles. Opioids, often prescribed by healthcare professionals, are perceived as less dangerous, creating an additional ethical responsibility for those prescribing them. As addiction rates rise, there is an urgent need to improve access to healthcare, education, and support systems for those struggling with addiction.
While statistics on prescription drug addiction in South Africa are scarce, it is estimated that ~15% of the population experiences some form of drug addiction, with a growing portion linked to prescription medications. Codeine-containing products, tramadol with paracetamol, and sedative tranquilisers like alprazolam are commonly misused. The increase of behaviours such as patients frequently requesting prescription replacements, altering medication for alternative use, and consulting multiple doctors highlights the need for tighter control in prescribing practices.
The increasing prevalence of online pharmacies and virtual consultations adds new ethical challenges, making it harder to prevent misuse. Healthcare providers must adhere to legal guidelines such as the Prevention of and Treatment of Substance Abuse Act (2008) and the Medicines and Related Substances Act.
These laws emphasise the importance of informing patients about the risks, benefits, and consequences of treatment options. The National Health Act also requires that patients be fully informed of their treatment choices, complicating decision-making, especially with the growing demand for painkillers driven by self-diagnosis through online resources.
In this complex landscape, healthcare providers must balance patient autonomy with their legal and ethical duty to prevent harm, particularly when managing patients with addiction. Referring patients to specialists or withdrawing treatment may be necessary, but abandoning patients is ethically unacceptable. Prescription drug misuse has become a public health issue in South Africa, and addressing it requires collaboration among healthcare providers, policymakers, insurance companies, and law enforcement.
General practitioners (GPs) are particularly affected by these ethical dilemmas, as they must balance competence, altruism, and accountability while managing expectations from various stakeholders. Pain management involves weighing beneficence (doing good) with non-malfeasance (avoiding harm), especially when prescribing medications that may contribute to addiction. Socioeconomic factors also influence addiction, with lower-income groups being more susceptible to painkiller abuse.
GPs must navigate their legal and moral responsibilities as gatekeepers to medications and specialist services, ensuring fair access to care while adhering to guidelines. In cases of ethical dilemmas, medical professionals must assess the situation from both clinical and ethical perspectives, consulting authoritative sources, evaluating options, and considering the consequences.
The ethical responsibility of healthcare providers extends to addressing the pharmaceutical industry’s role in promoting addictive substances. A collective approach is required to ensure responsible prescribing and tackle the opioid crisis in South Africa.
In conclusion, the practice of medicine is not merely a trade but a calling, one that requires both head and heart. As Sir William Osler once said, the best part of a doctor’s work often lies in the exercise of moral influence on patients. Ethical decision-making in pain management, especially regarding prescription drugs, is a challenging but necessary aspect of the profession.
To watch a replay of the webinar, click here or scan the QR code. SF
This webinar was sponsored by Zydus and is accredited for one (1) ethics CPD point. Once you have watched the replay, send an e-mail to john.woodford@newmedia.co.za and request to have your CPD point allocated to your profile on the HPCSA database. Include the webinar names and your HPCSA number in your e-mail. Please note, it may take up to four weeks for your point to be reflected on your portfolio and points are allocated at the discretion of the HPCSA.
Dr Shafrudeen Amod
Don’t gamble with neuropathic pain
is indicated for the treatment of adult patients with neuropathic pain due to herpes zoster infection and diabetes
According to Dejager S et. al., Vildagliptin has shown e cacy1:
• as monotherapy
• in combination with other antidiabetic medicines or insulin
• in elderly patients
VILDAGLIPTIN HAS A LOW RISK OF HYPOGLYCAEMIA AND WEIGHT GAIN1