

NEW SERIES!
HEAD CASECHRONICLES
Confessions of a Semi‑Stable Human
Does it sometimes seem like the more letters someone has after their name, the less they seem to remember that you’re a human being too?
I went to a real psychiatrist once. A doctor. She walked in wearing that “I’ve already decided what’s wrong with you”
expression they must teach in medical school. She says she’s going to change my meds.
I tell her, “Hey, I’ve been doing great on this medication—it’s working beautifully. I’d like to keep taking it.” And she looks at me like I just asked her to write me a prescription for
cocaine and a hug.
She said, “So… you’re only here for the drugs?” I said, “Well, I didn’t come for the decor.”
Suddenly she’s typing like I’m a flight risk.
Every click on that keyboard sounded like: ‘He’s lying.’ ‘He’s manipulative.’ ‘He smiled once — suspicious.’
Cold. Condescending. If she had any less warmth, I’d have needed a parka for that appointment.
And I’m thinking: “Lady, if I wanted to get high, I wouldn’t be here trying to renew my prescription. I’d be outside, making new friends.”
I decided that was my last visit with her.
Then came the psychologist. Two-hour drive. Paid him well. He said it was an orientation. It actually turned out to be a a legal briefing in case he ever needed to testify against me.
Every question was like, “Now, if you were to experience emotional distress as a result of this session, that wouldn’t be legally actionable, correct?”
I said, “Buddy, if I wanted a therapy session that starts with a waiver, I could
My name is Joyce Nolin. I have been a resident of Columbia County for more than 60 years. I retired in 2000 from teaching language arts and drama at Evans High School. This is a story of my journey dealing with cancer and why I make and share gnomes.

In 1994, I was scheduled for a bladder tack-up because of severe incontinence. The doctors found a growth in my ovaries. They removed the ovaries and a biopsy confirmed that I had ovarian cancer. After several rounds of chemotherapy, I was declared cancer-free.
We discovered that three of my five daughters and I had the BRACA cancer gene, which is an inherited trait that made us more vulnerable to breast cancer. One daughter developed breast cancer and is a survivor after a mastectomy. Two others had mastectomies as preventive measures. I have lost two brothers, a son-in-law, a daughter-in-law, and a niece to cancer.


In 2002 during a routine colonoscopy, the doctors discovered a mass that they believed to be cancer, and they immediately scheduled surgery. A biopsy revealed that the mass was benign, but they had already removed half my colon. I was very angry at the doctors who made such a mistake. I had a very difficult recovery and stayed in the hospital for several








PARENTHOOD
by Dr. Warren Umansky, PhD
You saw something on Facebook about a class action lawsuit against videogame makers by parents of children who are addicted to gaming. You believe your teen is addicted to gaming. You don’t let him play a lot at homke, but he goes to his grandparents’ home after school each day. He has unrestricted access to games there. He keeps asking you if he can play when he’s home and is unpleasant when you don’t give in. You think you could be a member of the class action suit. What should you do?
A. Your child was in counseling about a year ago before you discontinued it. You think a letter from the counselor might help your case for participation in the lawsuit. You call the counselor and request a letter of support.
B. You contact some of the people who posted the story on Facebook. You discover that many of them have the same experience as you, which motivates you even more to join the lawsuit. You just decide to get the forms from the law firm representing the group and send them in.
C. You realize that the grandparents are enablers of the addiction. You give them the option of enforcing your no electronics rule at their home, or you have to find other caregiving options in the afternoon.
D. If it’s an addiction, it is a losing battle for you to restrict his access to gaming at your house. Restricting access might lead to harming himself out of frustration. You don’t want to be responsible for that.
If you answered:
A. If the counselor is ethical, he or she will decline your request and may suggest that you come in with the grandparents to discuss the role of responsible adults relative to children who want to play videogames all the time.
B. First, the chances of the class action succeeding is very small. Second, the law firms who represent the class are the ones who benefit the most from any monetary settlement. Finally, consider that you might be called as a witness and would have to testify about what you have done to protect your child from playing videogames so much.
C. It is clear that your child’s craving to play videogames is fueled by the unrestricted access provided by adults. Even using an approach like, “Let me see that you have done your homework and then you can play,” and/or “You have to clean up your room at home before you can play games here,” and/or “We need you to help with chores before you can play” will teach your child that time to play games is a privilege that must be earned.
D. If this is your concern, you and your child need to get back into counseling very quickly.
Gaming disorder is not a recognized mental health disorder in the United States, although research is being done in this area. The difficulty is distinguishing between gamers who are passionate about playing and those who tip the scale into an addiction that interferes with life activities.
Keeping children busy in productive activities (school, sports, music, crafts) and surrounding your children with adults who engage with them (eating together, talking, going places, playing games and watching movies) can prevent this problem from occurring.
Dr. Umansky has a child behavioral health practice in Augusta.
THOUGHTS ABOUT THOUGHTS THOUGHTS
“I’LL DO IT TOMORROW” CHRONIC PROCRASTINATION
Editor’s note: Written by local mental healthcare professionals, this series explores how people may think and act when affected by common and not-so-common mental health conditions.
James is a 39-year-old project manager known for being capable, intelligent, and dependable—at least on paper.
In practice, he finds himself staring at his computer late into the evening, heart racing, deadline looming, yet unable to start. He reorganizes his desk, checks emails repeatedly, scrolls his phone, and promises himself he’ll begin “in just a minute.”
This pattern isn’t limited to work. Doctor’s appointments are postponed. Important calls go unanswered. Personal goals remain stuck in the planning phase.
James isn’t lazy or unmotivated. In fact, the stress of unfinished tasks keeps him awake at night.
What he’s experiencing is chronic procrastination—a behavioral pattern driven not by poor time management, but by emotional avoidance.
What is Procrastination?
Procrastination is the voluntary delay of an intended task, despite knowing that the delay will likely result in negative consequences. While occasional procrastination is common, chronic procrastination can significantly impair occupational performance, relationships, mental health, and overall functioning.
In behavioral health, procrastination is increasingly understood as an emotion regulation issue, not a character flaw. Tasks associated with discomfort—such as fear of failure, self-doubt, boredom, or being overwhelmed—are avoided in favor of short-term relief, even when long-term costs are high.
Procrastination frequently co-occurs with:
• Anxiety disorders
• Depression
• Attention-Deficit/Hyperactivity Disorder (ADHD)
• Perfectionism and obsessive traits
• Trauma-related conditions
Signs and Symptoms
Procrastination can present in subtle and pervasive ways, including:
Behavioral Patterns
• Repeatedly delaying tasks despite clear deadlines
• Starting projects but failing to complete them
• Avoiding decision-making
• Filling time with low-priority or distracting activities
Emotional & Cognitive Features
• Anxiety or dread when thinking about a task
• Guilt, shame, or self-criticism after delaying
• Fear of failure or fear of not meeting expectations
• All-or-nothing thinking (“if I can’t do it perfectly, I won’t do it at all”)
Functional Impact
• Missed deadlines or opportunities
• Declining work or academic performance
• Strained relationships
• Increased stress and burnout
What Causes Procrastination?
There is no single cause, but research suggests procrastination develops from a combination of psychological and neurological factors:
• Avoidance of negative emotions such as anxiety, boredom, or inadequacy
• Perfectionism, where high standards make starting feel overwhelming
• Executive functioning difficulties, common in ADHD
• Low distress tolerance, making short-term relief more appealing than longterm goals
• Negative self-beliefs, including fear of judgment or failure
Rather than a time management problem, procrastination is often a way of coping with emotional discomfort.
Common Misconceptions
8 “Procrastinators are just lazy.”
Procrastination often involves high effort—worrying, ruminating, and self-criticizing—without productive action.
8 “They don’t care enough.” In reality, people who procrastinate often care deeply, which increases fear and avoidance.
8 “Better time management fixes it.”
While structure helps, addressing the emotional drivers is essential for lasting change.
Treatment and Management
Effective treatment focuses on both behavior and the emotions underlying avoidance.
Common approaches include:
Cognitive Behavioral Therapy (CBT)
• Helps identify and challenge unhelpful thought patterns, reduce perfectionism, and build task initiation skills
Behavioral Activation
• Encourages small, achievable actions to reduce avoidance and rebuild momentum
from page 1
just talk to my insurance company.”
He never once asked how I was feeling. He was too busy making sure I couldn’t sue him for however I happened to be feeling.
And then he billed me. Full rate. For a conversation that was essentially: “Here’s how you can’t hold me accountable or liable.”
But then... I met someone else. A woman who doesn’t have the right letters after her name. Not an M.D. Not a Ph.D. Just a counselor.
Legally speaking, she can’t diagnose, can’t prescribe, can’t even call herself a “therapist” without risking a strongly worded letter from the State Licensing Board. Some might even say she’s one step up from a fortune cookie.
And yet she’s the one who saved my life.
Because she did the one thing all those other geniuses forgot to do: She listened. She didn’t stare right through me while
THOUGHTS
from page 2
Executive Function Support
• Ta sk chunking, external accountability, and structured planning—especially helpful for ADHD
Treatment of Co-Occurring Conditions
• Addressing anxiety, depression, or ADHD often leads to significant improvement in procrastination symptoms.
• Learning to tolerate discomfort and redefine “progress” rather than “perfection” is a key component of recovery.
Prognosis
With appropriate support, procrastination is highly treatable. Many individuals experience improved productivity, reduced anxiety, and increased self-confidence once the emo -


filling out a form. She didn’t treat me like a liability. She didn’t quote a DSM entry like it was Scripture. She just showed up. Present. Warm. Human.
And somehow, that did more for me than every clinical expert combined.
So here’s what I’ve learned: Apparently the more you pay for a degree, the less you can afford empathy.
The psychiatrist saw me as a walking drug request. The psychologist saw me as a potential lawsuit.
The counselor saw me as a person. And that’s why I’ll take an unlicensed angel over a licensed robot any day of the week.
Because if caring was illegal, she’d be serving life without parole.
Next installment: being treated like El Chapo at the pharmacy.
Editor’s note: this column is written by that highly prolific author, Anonymous, who has no interest in changing his (or her) name.
tional roots of avoidance are addressed. Left unaddressed, chronic procrastination can contribute to long-term stress, occupational impairment, and worsening mental health—making early intervention important. If delaying important tasks has become a persistent source of distress or dysfunction, a behavioral health evaluation can be a meaningful first step toward change.
About Us
IPS provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.




WHAT IS THE STORY BEHIND SUNDAY NIGHT INSOMNIA?
Yes, Sunday Night Insomnia is real; it isn’t just in your head. Well actually, it is in your head, and that’s the problem.
Far from being an imaginary condition, estimates are that as many as 75% of adults experience it. Even the most conservative estimates put the number at 25%.
If you’re one of the few who are unaware, we’re talking about a recurring pattern of difficulty falling asleep on Sunday nights, particularly among people who have no trouble quickly drifting off the other six nights.
Here are a few common causes for this phenomenon:
• sleeping in on Saturdays and Sundays
• altered weekend eating habits
• naps, particularly on Sunday afternoons
• late-day drinking of alcohol or caffeine
• weekend disruption of regular routines
• anticipatory anxiety about Monday and the workweek
Reviewing that list and the ones that may apply to you can mark the pathway to better sleep on Sunday nights.
• wake up at the same time (or near the same time) you do on weekdays. Set your alarm if necessary.
• if you eat out on weekends, consider doing so earlier in the day, or eating light if it’s an evening event.
• try to avoid naps, particularly on Sunday afternoon, but if you do get the drowsies, set a timer for 15 to 30 minutes.
• avoid caffeine or alcohol after noon on Sundays.
• if your M-F job is physical, doing physical chores on the weekend will help maintain the routine that prevents this problem on weeknights.
• if your M-F job is more mental, review the challenges of the week ahead and map out a plan to address them, but do it early in the day on Sunday rather than waiting until bedtime. Once you have reviewed your plan, close the book on it.
• establish a quiet, soothing and restful Sunday night ritual in the final hours before bed. Sleep tight!

www.AugustaRx.com
Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com
AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455
www.AugustaRx.com • E-mail: Dan@AugustaRX.com TM

www.Facebook.com/AugustaRX
1350 WALTON WAY| AUGUSTA
Who is this?

Aword sometimes used to define geniuses — polymath — was practically invented with this man in mind.
The word comes from a blending of two Greek roots: poly-, meaning much or many, and manthanein, meaning “to learn.” True polymaths are pretty rare, since to qualify someone needs to be gifted in multiple fields. One of the foremost examples in American history is Benjamin Franklin, who was a writer, philosopher, diplomat, inventor, scientist, politician and, last but certainly not least, a printer.
The man above, Robert Hooke, was similarly broad in his fields of knowledge: astronomer, architect, geologist, surveyor, meteorologist, and biologist. And that is an abbreviated list.
He lived from 1635 to 1703, so he was a contemporary of another polymath, Isaac Newton (1643-1727). The two were rivals whose work was often expanded upon by the other. In the realm of physics, Hooke first hypothesized elements of planetary motion which became the basis of Newton’s law of universal gravitation.
Although the invention of the microscope is generally attributed to another of Hooke’s contemporaries, Antonie van Leeuwenhoek (1632-1723), it seems Hooke built his microscope about 5 years before van Leeuwenhoek started lensmaking.
If you ever had a microscope in your youth, what did you look at through its lens? It was probably basically a toy, but even so it was probably far more advanced than the one Robert Hooke used. Despite that, guess what he discovered? Cells. The cell. Human cells. In fact, he coined the term “cell” to describe the basic structures he saw in human tissue. At the time, he was still in his twenties. In 1665, at age 30, he published a book entitled Micrographia full of his observations through microscope and telescope lenses, complete with meticulous drawings of tiny structures and creatures revealed through his microscope. As for his telescope, Hooke is credited by some with the discovery of what is known as the Great Red Spot on the planet Jupiter.
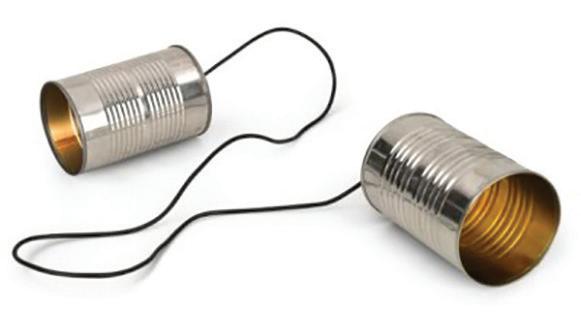
Hooke discovered so many things... why matter expands when heated, that air is composed of invisible particles in constant motion, and yes, in 1667, the tin-can telephone, an invention used for more than 200 years, effective at ranges as great as 3 miles.
Middle Age
BY J.B. COLLUM
Tomorrow we’ll celebrate our 39th wedding anniversary.
That number feels both impressive and slightly unreal. I can still remember when we threw anniversary parties for our parents—big ones, the milestone years. Twenty-five. Forty. Fifty.
Those were the gold standards. The kind of numbers that came with catered food, rented chairs, and speeches that made you realize you were standing on the shoulders of something solid. Lorie’s parents will celebrate their 61st anniversary this year. Sixty-one. Let that sink in for a moment. My parents made it to 56 years before my father passed away, which means that date now carries a strange mix of gratitude and ache. Oddly enough, both sets of our parents were married on the same day, in the same year. What are the odds of that? It’s one of those coincidences that makes you pause, shake your head, and wonder if the universe has a filing system we don’t get to see—or if God has a sense of humor. Spoiler alert: He does. Just watch puppies, monkeys, or penguins waddle around for proof.
magnets.
The problem is, I’m running out of time to treat this like a rehearsal.
This year I’ll hit another chronological milestone, one that now includes discounted camping at Georgia State Parks. Woohoo. Nothing quite drives home the passage of time like saving a few dollars on a campsite because your birth certificate says you’ve earned it.
I am the Michael Jordan of starting.
I also need to start thinking about retirement. I’ll be eligible in two years, though that would mean a smaller monthly check than if I wait a bit longer. And so I find myself doing what any reasonable middle-aged person does when faced with big life questions: outsourcing the existential dread to technology, of course.
As for us, 39 feels like we’re standing just shy of one of those “big” anniversaries. Close enough to look ahead, far enough away to feel uncertain.
With my health being what it is, I’d be lying if I said I don’t sometimes wonder whether I’ll make it to our 50th. After all, I had my first—and so far only—heart attack at 49. My father didn’t have his until the next year, when I was 50. And he was 71! It was one of those topsy-turvy moments life likes to throw at you. There I was, sitting with him in the hospital, reassuring him that everything was going to be fine—that I’d been through it myself and come out the other side, and that he would too.
I was grateful to be there for him then. I just wish the symmetry hadn’t been quite so on-the-nose.
I’ve said this before, and I know I’ll say it again: I really need to get serious—and stay serious—about my health. Starting is easy. I’m excellent at starting. Sticking with it is where I fall apart. Diets, exercise plans, good intentions… I collect them the way some people collect refrigerator
I asked several AI systems how long I might reasonably expect to live. I told them everything—health problems, weight, exercise habits (or lack thereof), family history, the whole messy spreadsheet of my existence. The answers were… not encouraging. What really bothered me was that they were all suspiciously similar. I’m convinced they talked to each other. So now I’m left doing the macabre math— trying to figure out the optimal time to retire, when to slow down, and when to finally take my health seriously. All while celebrating nearly four decades of marriage to a woman who has stood beside me through every version of myself, including the versions that didn’t listen nearly as well as they should have.
Thirty-nine years ago, neither of us was thinking about heart attacks, retirement formulas, or AI-calculated life expectancy. We were just getting started. And maybe that’s the point. Maybe the answer isn’t in the math at all.
Tomorrow, we’ll celebrate 39 years. Not because it guarantees 50. Not because it promises anything beyond today. But because today is still here—and so are we. And for now, that has to be enough.

J.B. Collum, author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com

Special Forces Parenting
There are moments when time doesn’t exactly stop, but it softens. It loses its sharp edges.
That usually happens when Freyja wedges herself between me and the back of the couch.
She’s eight now, athletically built and strong in ways that still surprise me. Like many children on the autism spectrum, she is a pressure seeker. She loves weighted blankets and tight spaces. When she presses herself into that narrow gap behind me, she sometimes makes small sounds that tell me she has found exactly what she was looking for.
Sometimes she reaches forward and rubs her hands across my beard, then presses her cheek against it. Texture matters to her. The coarseness, the scratchiness—it’s grounding. I know all the clinical reasons behind it. I’ve read the explanations, listened to the physicians, and learned
the vocabulary. All of us who care for her have. Her sensory system processes the world differently. Pressure and texture help organize it.
But knowing why doesn’t make the moment any less precious.
I’ll often be on the cusp of getting up to do something. By the way, I’m very good at staying on that cusp, as I am one of the world’s leading procrastinators. Just ask my editor and publisher. Anyway, as I was saying, I’ll be about to get busy doing something important—like trying to finish one of these columns—when she jumps in and throws a monkey wrench into my plans. I’ll think, I should move. I should get back to work. And then I can’t. Because she’s there. Because she chose that spot. Because she feels safe enough to press her whole small self against me, just when I finally worked up the gumption to get started.
For those few minutes, my job description changes. I’m no longer multitasking. I’m furniture. I’m an anchor. I’m the familiar shape that lets her nervous system take a breath.
People sometimes talk about autism and Angelman’s Syndrome in terms of deficits— what’s missing, what’s delayed, what may never come. And yes, Freyja is nonverbal. Yes, her world is different from most. But moments like these are not absences. They are connections. They are communication in a language without words.
She doesn’t say, “I love you.”
She leans.
She presses.
She reaches for my beard and tells me everything she needs to say.
And when she does, whatever else I had planned can wait.

Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
Not counting Nazis, who deserve their own wing in the Hall of Shame, Medical Division, this man is the most prolific serial killer in German history, and possibly world history. That’s saying a lot.
Unfortunately, what enabled Niels Högel to rise to this level of infamy was the phenomenon often abbreviated CYA. Being the kind of quality newspaper we are (Our slogan: Fun for the whole family!), we can’t reveal what that acronym stands for, but here’s an example of it in action:

August 2001: A staff meeting is called at the German hospital where Högel worked to discuss an alarming spike in patient deaths. A physician who suspected that Högel was to blame demanded he be transferred out of his department.
September 2001: The new department Högel was farmed out to (anesthesiology) saw a sudden spike in deaths.
The head physician suspected Högel and confronted him, suggesting he either a.) resign, or b.) move to a department that did not involve direct patient care. Högel chose a.).
October 2001: Högel left with a letter of recommendation lauding his diligence, devotion, cooperative conduct, and concluded with an overall assessment of Högel having completed assigned tasks “to the utmost satisfaction.”



About a month later he was back at it in the employ of another hospital. By 2005, about 75% of the deaths at that hospital were connected to shifts worked by Högel. Of course, that was not discovered until later. In fact, he was discovered tampering with a patient’s medications that year and was arrested, convicted, and given a 5-year sentence.
Subsequent investigations revealed that lone 2005 case was only the tip of the iceberg. When investigators then charged him with three counts of murder and two counts of attempted murder, Högel corrected them: it was more like thirty murders, he volunteered. More investigations led to charges of killing 100 more patients.
Multiple investigations continuously increased Högel’s body count. At minimum, he killed 85 patients and is suspected of killing more than 300 in total.
Why? Boredom was one reason. Högel and his wife had a baby girl in July 2004, and to “sustain his euphoria,” Högel killed a patient during his first shift back at work after the baby’s birth.
As recently as 2022, hospital officials and Högel’s former supervisors were charged with neglecting to take action in order to protect the reputation of their hospitals. The charges were dropped before trial.
+
weeks. Once a code blue was called because my breathing had become so shallow.
I didn’t really start recovering until I let go of my anger, put things in perspective, and decided to be grateful for my very existence. I thought of Dr. Gahamande who, a few years earlier, had performed exploratory surgery on me at midnight because he had the instinct that something was wrong. He discovered two places in my small intestine that were close to rupturing. I probably would have died if he had not acted quickly. I tried to concentrate on my blessings and be grateful for the love and support of friends and family.
I opted to stop getting mammograms when I turned 80 in 2017. I thought there was little chance that I would develop cancer at that age. I still did random selfexams but never expected to find anything wrong.
In October 2022 I noticed a lump in my right breast and mentioned it to Dr.
Rebecca Talley at my annual exam. She ordered a CAT scan which led to a biopsy and confirmation of breast cancer.
I opted to have a double mastectomy in January. I experienced absolutely no pain, my incision healed beautifully, and I was spared from chemotherapy because I have the BRACA II gene. I was told I would have to take an estrogen blocker for the next five years, but I was declared cancer free!
I celebrated my 86th birthday on September 24, 2023, with about 35 children, grandchildren, and great-grandchildren. It was a loud, raucous assembly of the most diverse group you can imagine in one family. It was a happy time that I shall always cherish.
I had no physical health issues when I went to see Dr. Tally for my regular semi-annual checkup that November except a vague down feeling that permeated my mood. I had decided that my family had grown


too large to make individual Christmas gifts as I usually did. I just couldn’t get into the spirit of Christmas.
While sitting in the waiting room in Dr. Tally’s office, I was intrigued by the gnome display on the table near the TV that always played old shows like “I Love Lucy,” “The Honeymooners,” and “Andy Griffith.” When I learned that Dr. Tally’s staff had made the gnomes, I began thinking. I could make gnomes for Christmas gifts for the family!
I found myself planning

how to make the little creatures that would take residence in the homes of my family, and I began to feel excited. I decided to follow one rule: I would use only items and materials I already had.
I’m not sure why gnomes have become so popular recently, but I found their history intriguing. In the 1800s the original gnome was an ugly, gnarled creature with very bad hygiene who lived underground and avoided humans. Over the years they gradually emerged from their tunnels to help humans tend their gardens. Some enjoy playing tricks on humans and are quite mischievous.
Once seen as ugly, dirty, reclusive, and backwards, gnomes are now perceived as responsible, caring, lovable protectors who bring joy to our lives. I certainly felt joy as I made them, and somehow I was able to recapture my love of the season through the ritual of making gifts for those I love. The gnomes were a big hit at our Christmas gathering.
In February 2024 I went to Prompt Care thinking I had bronchitis. Instead, I was told the x-ray revealed a growth in my lungs. Further tests showed the 2020 breast cancer had metastasized to my brain, lungs, and bones. Just a year before I had been declared cancer-free. I could hardly believe it.



Doctors immediately put me on a strong regimen of steroids and chemotherapy. The steroids caused steroid psychosis, and for weeks I felt I was in another dimension, which made it quite difficult for my family to care for me.
As I recovered from the psychosis, I determined that I had to do my part in my recovery. Being a strong believer in the power of positive thinking, I first rallied my family, friends, church family, and strangers I met on the street. I asked them to remember me in whatever way they prayed. I adopted the mantra, “I am not dying of cancer, I am living and thriving with
cancer,” and I have tried to live up to that ideal.
While I was being treated with chemotherapy, I called on my gnomes for help. I even visualized my doctor telling me there was no brain cancer. In May, I had an appointment to discuss the results of my MRI and map out a plan for radiation. The doctor told me, “There is nothing there. You have no brain cancer.” It was just as I envisioned!
The chemo drug did not work on the mass in my lung, so I had a round of radiation. My hair started to fall out, but I never became bald, and my hair grew back in slightly curly. What a price to pay for curly hair! I was delighted.
A full body scan in June showed cancer cells had not spread or grown since my February scan. However, another scan in December revealed that the cancer had spread to my liver. I am starting a new drug that has been developed for patients with the BRACA gene. We are praying that it will be effective.
Early in my treatment I began to expand from family only to giving gnomes to my caregivers to express my appreciation for their care and support. Then I began to share gnomes with other patients in the infusion lab where I received my treatments, as well as to friends and perfect strangers. At this point, I have made and given away about 350 gnomes, which I have come to view as symbolic not only of gratitude and hope, but also the personal connection I share with each recipient. Each one is unique, and each one has a story to tell. They have become a key part of my therapy.
Of course, I know that gnomes do not heal, but they can help us focus on the positive and have hope, which is so important for healing from all afflictions. When I give someone a gnome, I invite them to name it, hug it, cry with it, share it with someone else, or just display it as a reminder that they are loved and appreciated.

TRYTHISDISH
WHITE CHICKEN CHILI
Here’s a warm and flavorful chili recipe that’s perfect for adding a little zest to a cold winter’s day!
The Chicken
• 1-½ tablespoon Salt-free zesty seasoning blend (like Mrs. Dash original)
• 4 cups leftover chicken; shredded OR
• 1-½ pound skinless, boneless chicken breast
The Chili
• 1 Jalapeño Peppers; cut in half and seeds removed
• 1 Poblano Pepper; cut in half and seeds removed
• 4 tomatillos; paper skins removed and cut in half
• ¼ cup cilantro; rough chop
• 1 Large sweet onion, chopped
• 4 Cloves Garlic (minced)
• 1 tablespoon Chili Powder
• 1 large or 2 small zucchini; chopped
• 2 cans reduced sodium Great Northern Beans; drained and rinsed
• 4 cups of reduced sodium Chicken
• Juice of one lime
• Cilantro (optional garnish)

If using raw chicken, trim all visible fat from the chicken and season with spice blend and set aside. Place the peppers, tomatillos, and cilantro in a blender with about 2 tablespoons water. Blend until smooth and set aside. Add the onion to the slow cooker place the seasoned chicken, or leftover shredded chicken plus seasoning, on top of the onions. Add the garlic, chili powder, zucchini, beans, broth and tomatillo sauce. Cook on high for 6 hours or low for 8 hours. Once done, remove the chicken from the slow cooker and shred the chicken (unless you used the leftover already shredded). Add

the chicken back to the slow cooker and combine. Serve with lime juice and cilantro.
Yield: 8 Servings (Serving size: 1 1/3 cups)
Nutrition Breakdown: Calories 180, Fat 3g (0.5g saturated fat), Cholesterol 60mg, Sodium 400mg, Carbohydrate 16g, Fiber 4g, Protein 23g, Potassium 560mg.
Plate Plan: 1 Starch, 3 Lean Meats, ½ Vegetable

NURSING SCHOOL TUTOR

Jacqueline (762) 246-8638
Former Registered Nurse with 19+ years experience in various healthcare specialties offering to tutor nursing students. Will cover documentation, NCLEX questions, and stress-relieving tactics. $40/hr, which includes an initial assessment of knowledge.




Women/non-binary support group
Wanting to start a support group in my home for anyone who has faced childhood experiences in their life such as trauma, bullying, and abuse (emotional/physical) that still affects your life in the present. You may also bring your pet for emotional support. No judgment, just a friend in need of a friend. Please call/text me at (762) 246-8638 anytime day or night. We are here for each other.

Dear Angel, the Money Doctor MD, I just left my life insurance agent’s office and found out that my life insurance—which I thought would carry me for my whole life—was going to run out around age 80 if I didn’t increase the premium or reduce the face amount. What in the world happened? I’ve had this policy since 1989.
Signed, John, “Insured (or Unsure)” Augusta, Georgia
Dear John, Insured (or Unsure),
What you’re describing is extremely common with policies sold in the late 1980s and early 1990s— especially Universal Life (UL) and Variable Universal Life (VUL). You didn’t do anything “wrong.” The policy is doing what it was designed to do; it’s just that the assumptions used decades ago didn’t hold up the way people expected. Here’s what usually happened, in plain English: 1. Your premium was “planned,” not guaranteed. With UL/VUL, the pre-



mium that was illustrated back in 1989 often wasn’t a promise. The policy stays in force only as long as there’s enough cash value to pay the internal monthly charges.
2. The cost of insurance rises as you age. Inside the policy, the insurer charges monthly mortality costs. They’re relatively small at younger ages and increase significantly later in life. If the policy wasn’t funded heavily enough early on, the rising costs can begin draining cash value faster and faster.
3. Interest rates and/or market returns didn’t match the original illustration.
Many older UL illustrations assumed higher crediting rates than what we saw for long stretches. Lower crediting means slower cash growth, which means less “fuel” to cover the rising insurance costs.
(If it’s VUL, weaker market performance can create the same result.)
4. Loans/withdrawals and internal charges can accelerate the run-out date.
Even modest loans or withdrawals can reduce cash value, and that can move the lapse date forward.
What to do next
Ask your agent for an in-force illustration (not the original one) and request it run two ways:
• at current assumptions, and
• at a more conservative assumption (a stress test).
Then ask one clear question:
• “What premium keeps
this policy in force to age 90? 95? 100?”
Also confirm:
• current cash value
• current death benefit option (level vs increasing)
• any outstanding loan balance and loan interest rate
• current crediting rate (or VUL subaccount allocation/ performance)
Your main options (generally speaking):
• Increase premium to carry coverage longer
• Reduce face amount to lower monthly costs
• Restructure (sometimes changing death benefit option helps)
• Consider replacement or ask about a “1035 exchange” (only after careful side-by-side review)
Bottom line: your policy didn’t “go bad”—it just needs a checkup after 30+ years of changing interest rates, rising costs, and aging. Get an updated in-force illustration, stress test it, and then choose the simplest fix that keeps your coverage where you want it without wrecking your budget. If you can answer one question—“What premium holds it to age 95 or 100?”—the path forward usually becomes crystal clear.





---Angel the Money Doctor, MD
This column is for education, not personal tax, legal, or investment advice.
Please consult a qualified advisor who can look at your actual statements, options, and health/ age situation before making a final decision.
Have a question for Money RX: A Prescription for Financial Health?
Send it to info@AugustaRx. com and your question may be featured in a future column. +
SOCIAL MEDIA EPIDEMIC
by Justin White
Part I
In December, Australia passed a law banning children under age 16 from have social media accounts. The new restrictions have been applauded by both parents and child advocacy groups. Australian prime minister Anthony Albanese called it a “proud day” for families, adding that laws like these can curb online harms that have outpaced traditional safeguards.
Naturally, young people and the social media networks themselves oppose the regulation. Even so, TikTok has already deactivated around 200,000 accounts Down
Under, with hundreds of thousands more set to be blocked. An estimated one million children have been affected, with many posting online protests. As with any new and controversial rule, there are attempts to circumvent the laws. However, keeping children and young teens off social media isn’t as easy or as black and white as you might imagine. The responsibility here lies with both the parents and these social media networks themselves.
Australia’s new laws, however, do not restrict children from accessing social media. It simply prevents them from creating accounts. So, on a funda-

mental basis these new laws are not fool-proof: a child might be restricted from joining a network like TikTok or YouTube, but it will not prevent them from viewing content on those sites.
One side effect of the Australian law is that now everyone will be forced to verify their age. The law may specifically target people under the age of 16, but the networks have no way of knowing if a user is 8 or 80.
Another thorny issue surrounds the question of anonymity. With users being forced to provide a legal ID, remaining anonymous on most sites is a thing of the past.
That means networks now have sensitive personal information on users, such as ID numbers and addresses, a potential gold mine for hackers. Social media is not immune to
hackers; all of that data consolidated into one platform makes stealing it that much easier.
To minimize this risk, Australian law requires social media platforms to immediately delete these identity details after verification. However, this doesn’t remove the risk entirely and it puts the networks in an awkward position: Ii the eSafety Commission investigates a platform’s verification standards, the platform that follows the law will have no data to support their claim for having followed the law. But if they do illegally keep these data, then they will have proof of their compliance with these laws.
The biggest issue here, though, is what the law does to free speech; it completely restricts the speech of those under 16.
Another aspect to consider: double standards.
Gaming platforms like Twitch can no longer facilitate engagement with other online gamers, while sports websites, for example, let people, regardless of age, to communicate and engage with others online.
Australia’s laws definitely raise legal questions, and even more are likely to arise from proposed legislation mandating age requirements for using online search engines like Google. A policy such as Australia’s probably wouldn’t fly in the U.S. It would immediately be hit with claims of free speech and First Amendment infringement. While these laws were made with good intentions, they contain fundamental flaws.
Social media’s impact goes far beyond the question of access by minors. It also has a powerful effect on mental health, a topic we will discuss in Part II.
CRASH COURSE

With your permission, we would like to repeat the same couple of introductory paragraphs that appeared here last issue. Why? They are shocking, and even if you read them last time, they bear repeating. If you missed them last time, they deserve a few moments of your attention before we proceed with the rest of the article. Here goes:
Let’s take a fresh look at the title branding of this series above. It’s always there, so it can easily fade into the woodwork and go unnoticed. That would be a tragedy, especially that line below the title. If you haven’t read it recently, take a moment to do so now and meditate on its meaning.
headlights on. Being visible helps keep you from getting hit. In fact, traffic studies reveal a clear pattern: drivers without headlights on in rain were struck more often, especially from the side or rear.
Here’s a question to ponder: why don’t car makers design windshield wipers so that headlights are activated when they’re on?
REMEDIAL EDUCATION II
{ {
The U.S. death toll from the two World Wars is in the neighborhood of 535,000. That is a huge number of lives lost.
But the number of Americans killed in car crashes just since 2000 is even higher.
Considering that traffic experts view the vast majority of crashes (nearly all) to be avoidable (see Crash Course in the Dec. 5 issue for more information) makes the enormous death toll that much more tragic.
So for the remainder of our course time today we’re going to review a few basics of safe driving. Of course, these very same topics are the fundamentals of unsafe driving when they aren’t practiced.
Lights! Action!
Resuming fresh content now, it is rather amazing how many drivers seem to be unaware of a Driving 101 basic: by law, headlights are required to be on when it’s raining. The Georgia statute is a little vague. It mandates lights “any time when visibility is less than 500 feet due to rain, fog, smoke, or other conditions.” That distance could be difficult to estimate and is open to various interpretations. Here’s a handy tip: follow South Carolina’s law whether you live in Georgia or South Carolina. The Palmetto State law is ridiculously simple: “Headlights must be on whenever windshield wipers are in use.”
Why does it matter in broad daylight? Headlights on when it’s raining doesn’t dramatically improve your view of the road, but it does make you dramatically more visible to ther drivers. Some silver and grey cars completely fade into the mist without
Belt drive
Remember the first day of drivers ed? Wearing seat belts on every drive was one of the first things covered. It’s a driving ABC. And yet in 2022, of the 1,797 traffic fatalities in Georgia, fewer than half of the victims (only 47%) were properly restrained. Maybe that proves unbelted drivers are bad drivers, because the overall statewide rate of seat belt use is 87.6%. State estimates are that 657 people are no longer among the living who would still be with us had they been wearing seat belts (numbers for the period 2018-2022).
Another eye-opening figure from CODES (the state’s Crash Outcomes Data Evaluation System): not wearing a seat belt makes a person seven times more likely to be fatally injured in a crash compared to properly restrained occupants.
You can’t drink your problems away
But you can certainly drink your way right into a slew of trouble. No one in their right mind would think that mixing driving and alcohol is a good idea, but that’s just the thing: no one who is drinking (beyond a certain amount) is in their right mind. And the statistics prove it. Example: more than 40% of the alcohol-impaired drivers killed on Georgia roads weren’t even wearing seat belts. Not just duh; double duh. And the problem is getting worse: alcohol-related fatalities in Georgia in 2019: 355; in 2020: 371; in 2021: 469; in 2022: 507. The numbers are going the wrong direction. Are you people sleeping in class?
This installment of Crash Course and the previous class illustrate a profound truth: many highway fatalities, you know, the ones that exceed the death totals in two world wars, are preventable through simple driving habits that even the newest driver should know and be using.
That’s not to much to ask is it? +



I WAS THINKING
by Pat Tante
TENNIS STRATEGY
Of all sports activities, tennis is one of the most healthful. Sometimes called “the total package,” it increases life expectancy by more than nine years. Nine more years of fun! I’m all for that.
These days, when playing with friends and not really expecting to take home a trophy or a sixpack, our games are more relaxed.
I have been a tennis player for thirty years and have always paid attention to how people play their game. While watching pros play, I like to learn something that might enhance my own game. On a local level, here is my observation on the differencea in how men and women preparing for their weekly doubles game.
THE GUYS
1. Arrive at court
2. Greet opponents/partner
3. Open balls
4. Spin for first serve
5. Short warmup
6. Begin play
THE GALS
1. Arrive at court
2. Find a place for tennis bag, purse, water
3. Discuss latest news
4. Apply insect repellent or sunscreen
5. Retrieve sweat bands, visors, etc.
6. Remove/put on glasses/contacts
7. Continue latest news discussions
8. Take two Advil tablets
9. Look at photos from last party
10. Discuss next party (any birthdays?)
11. Speak to folks on next court
12. Retrieve old ball from court
13. Continue news discussion
14. Perform minimal stretching
15. Decide who brought balls
16. Spin for service and court side
17. Begin warm-up
18. Practice net work and long strokes
19. Practice serving
20. Return to sideline and rehydrate
21. Finish news discussion
22. Begin play
You might wonder if we gals get our money’s worth out of our tennis membership. We do!
Yes, absolutely we do.
+






he Examiners


ACROSS
1. DOE site
4. Just a little
7. Totally overused word
14. Negating word
15. Room within a harem
16. Semper Fidelis group
17. Scull power
18. Witches
20. Like some porches
22. Bush Field abbrev.
23. Remnant
24. Patrick Swayze’s mom
26. Phases
28. Edge decorations
30. Exhort
31. 3-cornered forward sail
36. Process starter
37. Slander, old-style
39. Pen prefix
40. Flag signaling system
42. Singles
43. Podiatrist concern
44. Small beard
46. Pays to use or borrow
49. _______ Medicine
51. Gone by
52. Unrealistically optimistic
56. The act of killing a despot
59. Yahoo ISP
60. Effeminate
61. Rep. counterpart
62. How many can play that game
63. Least fresh
64. Social pest
65. Verb preceding Pray and Love DOWN
1. Augusta rarity
2. What an audience or a big truck might do
3. Scheme
by Dan Pearson

CAPTION THIS
Check out our new reader contest on p. 10 Write your most appropriate, clever, or funny caption to the photo shown for a chance to win whatever cool swag we eventually decide to give away! Email your entry to Dan@AugustaRx.com
DEADLINE TO ENTER: 5:00 PM FRIDAY, JAN. 30, 2026 Have fun!
X A M I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
4. Prescribed amount
5. Worships
6. Nobleman
7. The last word in prayers
8. Division of a hospital
9. Before, in poetry
10. Bro’s opposite 11. Beginning 12. Comes together
13. Short literary composition
19. Food rechewed by a ruminant
21. ___ through; scan
24. Cone maker
25. Doc’s org.
26. Plural word with no singular version
27. Love intro
28. Bridgestone product
29. Some nurses
31. Small blemish
32. For each
33. Campus remembered in Neil Young’s Ohio
34. Fencing sword
35. Ascend
37. Big monkeys
38. Third person singular feminine pronoun
41. Toward the stern
42. Cereal plant
44. Food Bank color?
45. Asia
46. Deems
47. Home to Memphis
48. A chain of pots or buckets revolving around a water wheel
49. UGA conf.
50. 1/100th of a rupee
52. B&Bs
53. Eat sparingly
54. State south of Minnesota
55. Blood blocker 57. Knee inj. 58. Born
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
— Robert G. Allen

THEBESTMEDICINE

ha... ha...

Apatient in a mental hospital was known for walking down the hallways with a military clip to his stride, always with his right hand against his chest, tucked unseen into his pajama top.
“Excuse me,” a new staff member asked him one day, “who are you?”
“I am Napoleon Bonaparte,” he replied. Respectfully, the staff member asked, “Who told you that you are Napoleon Bonaparte?”
“God himself,” replied the patient.
“That’s a lie!” a nearby patient said. “I’ve never told you that!”
Joe: I was reading that scientists have developed a car that runs on parsley.
Moe: If only they could make trains that run on thyme.
Moe: So what happened with your first marriage?
Joe: I divorced her because she couldn’t make toast without burning it.
Moe: That seems pretty extreme.
Joe: It isn’t. I have a medical condition. I’m black toast intolerant.
Moe: You did what with your parking ticket???
Joe: I ate it.
Moe: Well, you have always said you love fine dining.
Moe: How do you tell the difference between a walrus and an orange?
Joe: I give. How?
Moe: Take either one and squeeze it as hard as you can. If orange juice doesn’t come out, it’s a walrus.
Joe: What do you call James Bond taking a bath?
Moe: Bubble 07.
Joe: What do you call a woman standing in the middle of a tennis court?
Moe: Annette.
Moe: Have you ever been to a town in Ohio called Engagement?
Joe: Never heard of it. Where is it?
Moe: It’s halfway between Dayton and Marion.
Moe: What has ten toes but isn’t your feet?
Joe: Tell me.
Moe: My feet!
Moe: I got this cool new pen that can write underwater.
Joe: Does it write any other words?
Staring at my phone all day has certainly had no Effect on ME!
By popular demand we’re making at-cost subscriptions available for the convenience
your house!
Choose six months for $26 or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397

Dear Advice Doctor,
The Advice Doctor

I guess this is a love life question if you answer those. I was dating this great girl for almost two years, but a couple weeks ago we broke up over a little argument. I was 100% sure we would get back together, but I had a rude awakening today: I found out she’s already seeing someone else. Do you think she’s just trying to make me jealous, or should I move on?
— Torn at the moment
Dear Torn,
I’m so glad you took the time to write in about this. It’s an important subject that affects more people than most of us would realize. Of course, everyone likes to be awakened gently, but rude awakenings can be especially problematic for people who are sleepwalkers.
There are all kinds of old wives’ tales about what happens when sleepwalkers are awakened, but the simple truth is that sleep walking — technically known as somnambulism — takes place during the deepest phases of sleep. Obviously someone walking around the house or even driving a car is not sleeping lightly. As a result, if they are awakened they can be extremely confused and disoriented, even violent, aggressive and combative.
Because of this, experts with organizations like the National Sleep Foundation recommend the best course of action is to try to gently guide the person back to bed without waking them up, and with minimal physical contact, since that might awaken them. If efforts to return the person to bed are not successful, the next best option is to stay close by to make sure they don’t do anything to endanger themselves. Although the common misconception is that you shouldn’t wake a sleepwalker, it can actually be very dangerous in some situations not to. The person could fall down a flight of stairs, for example.
If you do have to wake up a somnambulist, don’t shake the person. You’re too close to them, and you could be injured by their confused and combative response. Instead, make a loud noise from a safe distance, then gently explain what happened and try to get them back to bed.
I hope this answers your question. Thanks for writing!
Do you have a question for The Advice Doctor about health, life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.


READERS:
CAPTIONTHIS CAPTION THIS
QUOTATION PUZZLE SOLUTION
Many an optimist has become rich by buying out a pessimist
— Robert G. Allen
WORDS BY NUMBER
We behave according to what we can get away with.
— Composer Ned Rorem



PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY


DEVELOPMENTAL PEDIATRICS

Evans Chiropractic Health Center Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

DENTISTRY
Jason H. Lee, DMD 116 Davis Road Augusta 30907
Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901
706-396-0600 www.augustadevelopmentalspecialists.com

Georgia Dermatology & Skin Cancer Center 2283 Wrightsboro Rd. (at Johns Road) Augusta 30904 706-733-3373 www.GaDerm.com SKIN CANCER CENTER Steppingstones to Recovery 2610 Commons Blvd. Augusta 30909 706-733-1935



Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com PHARMACY




706-860-4048 Floss ‘em





study
A clinical research study for people who have or are at risk for heart disease or stroke and have high Lp(a) levels

MOVE-Lp(a) is a clinical research study from Eli Lilly and Company. The MOVE-Lp(a) study will test if an investigational medicine safely lowers Lp(a) levels and reduces the risk for heart disease or stroke.
Can I join the study?
Yes, you may be able to join the study if you:
• are at least 18 years of age
• have a high level of Lp(a) in your blood
• already have heart disease or have had a stroke or are at risk for a first heart attack or stroke
https://e.lilly/3FddF4u or scan the QR code

Lipoprotein(a) is also known as Lp(a). Lp(a) is an important risk factor for heart disease and is largely determined by your genes.
Lp(a) carries cholesterol (a type of fat) in the blood. If you have a high level of Lp(a), you may have a higher risk for heart disease or stroke. You may have a high level of Lp(a) even if you have a healthy lifestyle or are taking other medicine for your cholesterol.
