

THE WORLD’S FIRST FUNKY OPHTHALMOLOGY MAGAZINE Cover Story Ophthalmologists Discuss Important Topics in Vitreoretina with the PIE Radio Show p16 THE RADIO SHOW ISSUE June/July 2020 piemagazine.org 14
nAMD DME RVO
EYLEA® is indicated for adults for the treatment of neovascular (wet) age-related macular degeneration (AMD), visual impairment due to macular edema secondary to retinal vein occlusion (branch RVO or central RVO), visual impairment due to diabetic macular edema (DME), and visual impairment due to myopic choroidal neovascularization (myopic CNV).



REFERENCES: 1 EYLEA® approved package insert Singapore March 2019, Bayer (South East Asia) Pte Ltd. 2. Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab or ranibizumab for diabetic macular edema: two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology. 2016;123:1351-1359 3 Korobelnik JF, Do DV, Schmidt-Erfurth U et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology 2014;121:2247-2254. 4 Eleftheriadou M, Gemenetzi M, Lukic M, et al. Three-year outcomes of aflibercept treatment for neovascular age-related macular degeneration: evidence from a clinical setting. Ophthalmol Ther. 2018;7:361-368. 5 Pielen A, Clark WL, Boyer DS, et al. Integrated results from the COPERNICUS and GALILEO studies. Clin Ophthalmol. 2017;11:1533-1540.
ABBREVIATED PRESCRIBING INFORMATION
EYLEA SOLUTION FOR INJECTION IN VIAL 2MG. Approved name(s) of the active ingredient(s) One ml solution for injection contains 40 mg aflibercept. Each vial provides a usable amount to deliver a single dose of 50 µl containing 2 mg aflibercept. Indication EYLEA is indicated for the treatment of neovascular (wet) age-related macular degeneration (AMD), macular edema secondary to retinal vein occlusion (branch RVO or central RVO), diabetic macular edema (DME) and myopic choroidal neovascularization (myopic CNV). Dosage Regimen wAMD: The recommended dose for EYLEA is 2 mg aflibercept, equivalent to 50 µl. EYLEA treatment is initiated with one injection per month for three consecutive doses, followed by one injection every two months. Based on the physician’s judgement of visual and/or anatomic outcomes, the treatment interval may be maintained at two months or further extended, such as with a treat-and-extend dosing regimen, where treatment intervals are increased in 2- or 4- weekly increments to maintain stable visual and/or anatomic outcomes. If visual and/or anatomic outcomes deteriorate, the treatment interval should be shortened accordingly to a minimum of two months during the first 12 months of treatment. There is no requirement for monitoring between injections. Based on the physician’s judgement the schedule of monitoring visits may be more frequent than the injection visits. Treatment interval greater than 4 months between injections have not been studied. Branch RVO or central RVO: The recommended dose for EYLEA is 2 mg aflibercept, equivalent to 50 microliters. After the initial injection, treatment is given monthly until visual and/or anatomic outcomes are stable. Three or more consecutive, monthly injections may be needed. The interval between two doses should not be shorter than one month. If there is no improvement in visual and anatomic outcomes over the course of the first three injections, continued treatment is not recommended. If necessary, treatment may be continued and the interval may be extended based on visual and/or anatomic outcomes (treat and extend regimen). Usually, monitoring should be done at the injection visits. During treatment interval extension through to completion of therapy, the monitoring schedule should be determined by the treating physician based on the individual patient’s response and may be more frequent than the schedule of injections. DME: The recommended dose for EYLEA is 2 mg aflibercept, equivalent to 50 microliters. EYLEA treatment is initiated with one injection per month for five consecutive doses followed by one injection every two months. There is no requirement for monitoring between injections. After the first 12 months of treatment with EYLEA, and based on visual and/or anatomic outcomes, the treatment interval may be extended, such as with a treat-and-extend dosing regimen, where the treatment intervals are gradually increased to maintain stable visual and/or anatomic outcomes; however there are insufficient data to conclude on the length of these intervals. If visual and/or anatomic outcomes deteriorate, the treatment interval should be shortened accordingly. The schedule for monitoring should therefore be determined by the treating physician and may be more frequent than the schedule of injections. If visual and anatomic outcomes indicate that the patient is not benefiting from continued treatment, EYLEA should be discontinued. Myopic CNV: The recommended dose for EYLEA is a single intravitreal injection of 2 mg aflibercept, equivalent to 50 microliters. Additional doses should be administered only if visual and anatomic outcomes indicate that the disease persists. Recurrences are treated like a new manifestation of the disease. The monitoring schedule should be determined by the treating physician based on the individual patient’s response. The interval between two doses should not be shorter than one month. Method of administration Intravitreal injections must be carried out according to medical standards and applicable guidelines by a qualified physician experienced in administering intravitreal injections. Following intravitreal injection patients should be instructed to report any symptoms suggestive of endophthalmitis (e.g., eye pain, redness of the eye, photophobia, blurring of vision) without delay. Each vial should only be used for the treatment of a single eye. Contraindications Hypersensitivity to the active substance aflibercept or to any of the excipients, active or suspected ocular or periocular infection, active severe intraocular inflammation. Special warnings and special precautions for use Endophthalmitis, increase in intraocular pressure, immunogenicity, systemic adverse events including non-ocular haemorrhages and arterial thromboembolic events. As with other intravitreal anti-VEGF treatments for AMD, the safety and efficacy of Eylea therapy administered to both eyes concurrently have not been systematically studied. When initiating Eylea therapy, caution should be used in patients with risk factors for retinal pigment epithelial tears. The dose should be withheld and treatment should not be resumed earlier than the next scheduled treatment in the event of: a decrease in best-corrected visual acuity (BCVA) of ≥30 letters compared with the last assessment of visual acuity; a subretinal haemorrhage involving the centre of the fovea, or, if the size of the haemorrhage is ≥50%, of the total lesion area. The dose should be withheld within the previous or next 28 days in the event of a performed or planned intraocular surgery. EYLEA should not be used in pregnancy unless the potential benefit outweighs the potential risk to the foetus. Women of childbearing potential have to use effective contraception during treatment and for at least 3 months after the last injection of aflibercept. Undesirable effects Very Common: Conjunctival hemorrhage, eye pain. Common: Retinal pigment epithelial tear, detachment of the retinal pigment epithelium, retinal degeneration, vitreous haemorrhage, cataract (cortical, nuclear, subcapsular), corneal erosion, corneal abrasion, intraocular pressure increased, vision blurred, vitreous floaters or detachment, injection site pain, foreign body sensation in eyes, lacrimation increased, eyelid edema, injection site hemorrhage, punctate keratitis, conjunctival hyperemia, ocular hyperemia. For a full listing of precautions and undesirable effects, please refer to the full product insert. For further prescribing information, please contact: Bayer (South East Asia)Pte Ltd. 2 Tanjong Katong Road #07-01 Paya Lebar Quarter 3 Singapore 437161. Date of revision of text March 2019.
Bayer (South East Asia) Pte Ltd
2, Tanjong Katong Road #07-01, Paya Lebar Quarter 3, Singapore 437161. Tel: +65 496 1888 Fax: +65 6496 1491 Website: www.bayer.com
PP-EYL-SG-0054-1(09/19)
ded dosing1–5
TRE A T W I T H Achieve uns
COVID-19


Coronavirus





Treatment

22 36 CEO & Publisher Robert Anderson Media Director Hannah Nguyen Production & Circulation Manager Gloria D. Gamat Chief Editor Brooke Herron Editor Ruchi Mahajan Ranga Project Manager Writers Andrew Sweeney April Ingram Chow Ee-Tan Joanna Lee Hazlin Hassan Konstantin Yakimchuk Khor Hui-Min Olawale Salami Sam McCommon Tan Sher Lynn Graphic Designer Maricel Salvador Media MICE Pte. Ltd. 6001 Beach Road, #19-06 Golden Mile Tower, Singapore 199589 Tel: +65 8186 7677 Fax: +65 6298 6316 Email: enquiry@mediamice.com www.mediaMICE.com Published by Society Friends Asia-Pacific Vitreo-retina Society Vitreo-Retinal Society - India All India Ophthalmological Society IN THIS ISSUE... We are looking for eye docs who can contribute articles to PIE magazine. Interested? Let's talk! Send us an email at enquiry@mediamice.com. To place an advertisement, advertorial, symposium highlight, video, email blast, or other promotion in PIE magazine contact CEO Matt Young at matt@mediamice.com. Beovu: What’s the latest with the ophthalmic community’s concerns? Options Abound for Jim Mazzo’s Future Pediatric Retina Why Early Screening and Diagnosis is Crucial The Future Role of Telemedicine From Diagnostic to Therapeutic? Posterior Segment Enlightenment 26 28 A New Era in the Treatment of Hereditary Optic Neuropathies Ophthalmic Patient Resources in the Time of COVID-19 Experience Greater Control with CONSTELLATION Combined with ULTRAVIT
Ramifications in Ophthalmic Business
Side Effects
Regimens and Missed AntiVEGF Injections Prof. Anat Loewenstein On Keeping Family and Professional Life in Harmony Asian Markets Require Adaptability due to Coronavirus Ophthalmologists Discuss the “New Normal” APTOS Launches Bi-Weekly Telemedicine Webinar Q&A from Quarantine Highlights from the Low Point Innovation Conference Highlights 14 12 08 07 22 24 30 32 38 40 34 16 Cover Story
Discuss Important Topics in Vitreoretina m a g a z i n e p os terior s e gment nnovation en ightenment with the PIE Radio Show Ophthalmology Innovation Summit
Ophthalmologists
Radio Still Symbolically Matters… Even in Ophthalmology
As a young boy, I grew up in a home with radios on all floors –basement, first, second and third. Often they would be tuned to the same talk radio station, blaring a voice that you could not escape no matter which floor you were on.
Talk radio was often the alarm clock – an annoying beep replaced by a cacophonous on-air voice.
Family cars never started to the tune of melodious FM music. The drives always began with AM radio shows.
Radio, therefore to me, was something omnipresent, which is fitting for the theme this time as we are Media Partner for the World Ophthalmology Congress (WOC) Virtual, which takes place both for the world and technically everywhere.
You just need a wifi or data connection to register, log in and explore more than 2,000 talks from world experts in ophthalmology.
Obviously, we are now well beyond the age of radio, and yet the radio host still conveys timelessly a powerful presence – which I aspire to do as an interviewer at the time of WOC. Through some combination of charisma, questions, entertainment, and an uncanny ability to partner with your morning coffee to get the day going, radio hosts through mere voice alone make groggy mornings hospitable, dreaded commutes tolerable, and brains everywhere a little more knowledgeable.
Paying tribute to on-air talent during WOC, we can do so nowadays with a variety of multimedia. Sure, there’s the voice element, but there’s also video now. There’s the ability to be in a fantastic on-air studio broadcasting to the world, but also show ourselves and our interviewees – and especially important notion to feel connected while coronavirus still wreaks havoc on the world with lockdowns and forcing at least some degree of isolation and social distancing.
Video itself isn’t only for TVs anymore. No, we’ll be infusing even our e-blasts to the world with our video interviews, posting multimedia on our new PIE and CAKE websites, and turning more conventional A4-size publications into digital ones that are enhanced by our “Radio Show” video capabilities.
What does all this mean for the field of ophthalmology?
It means that while South Africans have been saddened that the world of ophthalmology could not come and learn and network on its fantastic land due to COVID-19, it can rest assured that its messages will be broadcast worldwide. It means that the rest of the world will be sure to interact at the WOC with each other, including ophthalmologists from all over Africa and beyond.
are willing to undergo a bit of “jetless lag,” as we called it based on our time covering ASCRS Virtual from Asia (in other words, a short-lived interruption of the body’s typical biological rhythms after self-imposed sleep changes, in order to be present virtually across many time zones – at least as defined by us at Media MICE).
All-in-all, the WOC will indeed be on air. So will we both thematically and as Media Partner to WOC, helping to broadcast important ophthalmic messages worldwide.
Provided you’re willing to tune-in, ophthalmology has never been more omnipresent. And that, despite the circumstances, is a fantastic development in our industry’s history.

Matt Young
Never before could ophthalmologists from, say, Cambodia, so easily access the education of a world-class ophthalmology meeting, provided they CEO & Publisher Media MICE, PIE and CAKE magazines
C M Y CM MY CY CMY K LETTER TO READERS
| June/July 2020 4
Providing Solutions for Subretinal Injection



jections are challenging. Let make it easier with our wide etinal injection cannulas so the one that is best for each t that with our MicroDose give you precision and total the injection process. Having ls can make the job easier.

nstellation®, Bausch & Lomb Stellaris® and DORC Eva® with David M. Brown, MD, Houston, TX Kit includes preassembled adapter and syringe 3275 MicroDose™ Injection Kit
Control + Precision with our MicroDose™ Injection Kit and Subretinal Cannulas M ed On e Surg i cal, I n c. ● TEL : 9 41 .3 59 3 1 2 9 6 7 0 T a ll e v a st Ro ad, S a r a s o t a, F L 34 24 3 U S A ww w M e d On e com ● M ed O n e@ M e d O ne. c o m
Dr. Cheung currently serves as deputy head and senior consultant of the medial retina service for Singapore National Eye Centre (SNEC), as well as senior clinician investigator for the Singapore Eye Research Institute (SERI). Her research interests include the study of risk factors and clinical features of macular diseases that may be unique in Asian populations.

Dr. Cheung has published more than 150 articles, mostly regarding age-related macular degeneration, including polypoidal choroidal vasculopathy, and conducted several clinical trials in anti-vascular endothelial growth factor therapies. Dr. Cheung has also been actively involved in training and education, and has served as an instructor on Asia-Pacific Academy
of Ophthalmology (APAO) and American Academy of Ophthalmology (AAO) courses and many other educational programmes. In addition, she is also a volunteer faculty member for the ORBIS Flying Eye Hospital Programme.
Dr. Cheung has received a number of prestigious awards, including the Macula Society Young Investigator Award (2017), APAO achievement award (2017), APAO Nakajima Award (2014), APAO Outstanding Service in Prevention of Blindness Award (2013), the Bayer Global Ophthalmology Research Award (2012), the Roper-Hall Medal (2005) and the Elizabeth Hunt Medal (Royal College of Ophthalmologists, UK).
gemmy.cheung.c.m@singhealth.com.sg
Prof. Gillies presently holds a number of positions including: director of research and director of the Macula Research Group for the Save Sight Institute; foundation fellow for the Sydney Medical School; professor in the Department of Clinical Ophthalmology at the University of Sydney; head of the Medical Retina Unit at the Sydney Eye Hospital; deputy chair for the Ophthalmic Research Institute of Australia; and director of Eye Associates in Sydney.
Prof. Gillies has served as a principal investigator or associate investigator in more than 70 clinical trials, and his research regarding macular degeneration and drug safety and efficacy has been published in 188 journals. He has also received a number of grants to study treatments for age-related macular degeneration, retinal disease and Muller cell dysfunction
– among other treatments and studies. Prof. Gillies has also appeared in national media on numerous occasions, including the evening news of all major networks, on ABC radio as a local expert, as well as in print media.

His dedication and research has resulted in multiple awards. Most recently, he received Gerard Crock trophies for the best papers at the Royal Australian and New Zealand College of Ophthalmologists (RANZCO) Annual Scientific Meeting (2013 and 2015), an achievement award from the Asia-Pacific Academy of Ophthalmology (APAO) in 2014, and an achievement award from the American Academy of Ophthalmology (AAO) in 2015.
mark.gillies@sydney.edu.au
Dr. Gupta currently serves as a professor of ophthalmology at Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh in India. Throughout her career, she has completed original work in the fields of intraocular tuberculosis, optical coherence tomography, diabetic retinopathy, and fungal endophthalmitis. In addition, she is actively studying vitreoretina and uveitis diseases.

She has been published in 65 per-reviewed journals, and has authored 17 book chapters and four complete books. Dr. Gupta also holds a US patent for the development of
multiplex PCR for uveitis. In addition, she is a sought after speaker, and has made more than 350 presentations in various national and international meetings.
Dr. Gupta has received several awards for her work, including the first JN Pahwa award from the Vitreo Retinal Society of India, the first NA Rao Award from the Uveitis Society of India, and the first NA Rao award from All India Ophthalmological Society (AIOS).
vishalisara@yahoo.co.in
| June/July 2020 6
Dr. Gemmy Cheung
Prof. Mark Gillies
ADVISORY BOARD MEMBERS
Experience Greater Control with
CONSTELLATION Combined with ULTRAVIT
by Brooke Herron
The CONSTELLATION Vision System from Alcon offers a new level of control in the OT. Combined with ULTRAVIT High Speed Vitrectomy Probes with duty cycle control – and features like integrated pressurized infusion and IOP compensation, advanced xenon illumination and more –CONSTELLATION is considered to be a pioneering vision system, delivering consistent results, safely and efficiently.
Unveiling CONSTELLATION features
Various features of CONSTELLATION target IOP. This includes its closed loop IOP system, which adjusts infusion pressure to match flow; while the ‘fluidair exchange to IOP control transition’ mitigates the transition from an airfilled to a fluid-filled eye.
Customization of the duty cycle is useful for surgeons who want lower cut rates; while its 435nm UV filtered xenon light source has dramatic effects on safety calculations.
For an undiluted vitreous sample, another useful feature is skip prime, where the cassette is primed, but no fluid is run through the aspiration line. Other features include: proportional reflux using the foot pedal, reflux autoreplenish mode, proportional diathermy and a max flow adaptor for silicone oil removal.
‘Probing’ into ULTRAVIT


What makes one cutter better than another?
According to Dr. Pear Pongsachareonnont, from Chulalongkorn
University & King Chulalongkorn Memorial Hospital in Thailand, the ULTRAVIT 10K cutter can be used as a multifunctional tool in many situations, and in both the anterior and posterior chambers.
For example, when entering via the anterior with a small-gauge cutter for silicone oil removal, the small port can go through the angle – and because of CONSTELLATION’s IOP control, the vacuum can be increased, without causing the anterior chamber to collapse. The IOP control also allows PFCL to be injected into the retina smoothly, without big bubbles, and is less likely to have small bubbles, which can migrate into the subretinal space.
Other instances showed a cutter removing a cataract, as well as retrieving fragments that drifted to the posterior.

She also demonstrated using the cutter to trim around a vitreous retina break. A video showed how the tip of the port in the ULTRAVIT probe is shorter – so it can easily go close to the retina –which allowed to her grasp the opposing hyaloid and lift it.
“With the ULTRAVIT cutter, you can use it to peel off the epiretinal membrane with suction, grabbing and trimming the membrane to cut it down closer to the retina, to release the traction in the periphery area,” explained Dr. Pongsachareonnont.
Overall, Dr. Pongsachareonnont says that the ULTRAVIT 10k cutter can do almost anything a surgeon needs, except laser: “It causes less traction in the retina, minimizes turbulence, can be used for suction and cutting, and reduces the time needed to exchange instruments, thus improving efficiency and patient safety.”
Getting closer to the retinal surface
Dr. Shu Yen Lee, from the Singapore
National Eye Centre, looked at complex diabetic cases using the ULTRAVIT 10K Beveled High Speed Vitrectomy Probe.

For her, the ULTRAVIT’s most important feature is that the port is at the bottom, which allows it to get closer to the retinal surface. To illustrate this point, Dr. Shu Yen’s first video showed her clearing a vitreous hemorrhage. In the example, the beveled tip was clearly visible, and she said that the larger port size made it very efficient: “Dense blood can be cleared quite easily, without feeling that the gauge size has been reduced and that the surgery might be prolonged.”
In the case of a diabetic tractional detachment, the same efficient removal was demonstrated. Dr. Shu Yen was also able to dissect the membranes of the retinal surface and remove the posterior hyaloid nicely, using only the cutter.
She demonstrated the same ease of getting onto the retinal surface in other cases, including a buckle vitrectomy detachment and a complicated cataract surgery/retinal detachment.
These cases, as demonstrated by Drs. Shu Yen and Pongsachareonnont, serve as prime examples of the ULTRAVIT’s advantages. In fact, Dr. Shu Yen concluded: “Once surgeons start using the Ultravit® 10K, they won’t want to use their original cutter anymore.”
Reporting for this story took place at amplifEYE, an Alconsponsored event to share user experience, in Hong Kong on March 4, 2019.
| June/July 2020 7
POSTERIOR SEGMENT OPHTHALMIC TOOL
Note:
Editor’s
Ophthalmic Patient Resources in the Time of COVID-19
by April Ingram
Ensuring that patients are wellinformed is key to treatment adherence, optimal outcomes and safety. In ophthalmology, a significant proportion of the patient encounter is spent in deep conversation, describing, explaining and assuring . . . and explaining and assuring again. As COVID-19 enveloped the globe, eye care practices have had to adapt, modifying usual clinic behavior and triage practices — and importantly, educating patients on how these changes could affect their care.
Unfortunately, if we are not providing patients with current and accurate information, they will seek it elsewhere — likely online where sources may not be based on science or fact (Hello, Dr. Google?). Studies have shown that over 70% of people go online to search for medical or healthrelated information, and it has been reported that the Internet, rather than physicians, is the first source of
information for many people. It is no secret that misinformation can lead to misdiagnosis, delayed diagnosis, untreated and undertreated ocular disease, resulting in non-optimized care and poor outcomes for patients.

Additionally, in this COVID-19 era, physicians have seen patients that are too fearful to attend appointments — thus, risking their vision — while others defiantly visit the clinic, hiding or misrepresenting symptoms, because they decided that they “need” the appointment.
There is no argument: The safety and well-being of patients are of the utmost importance. The impact of a recurring treatment schedule during this pandemic, where there are severe restrictions on clinical services and social distancing measures, are critical aspects that physicians and practices need to address.
Guidelines serve patients and physicians alike
Prof. Jean-François Korobelnik and Prof. Anat Loewenstein of the Vision Academy, with support from Bayer, recognized the critical importance of providing guidance for physicians, practices, staff and patients. They assessed international retinal practices and noted a lack of consistent evidence-based guidelines (or readily available information) for clinicians to communicate to their patients on how their clinics are adapting in response to COVID-19.
“Early on, we saw the extensive impact that COVID-19 was having across our ophthalmology practices with a growing decrease in clinic attendance and immediate measures needed to be put in place to reduce risk of exposure to patients and clinic staff,” Prof. Loewenstein explained. They jumped into action and published clinical
| June/July 2020 8
Like skydiving, returning to regular clinic visits is a scary prospect for some seniors.
TREATMENT GUIDELINES POSTERIOR SEGMENT
recommendations on how to effectively adapt clinic practices to minimize risk of COVID-19 exposure to medical staff and patients, including prioritization of those with the greatest treatment need.
The Letter to Editor, “Communicating with patients with nAMD and their families during the COVID-19 pandemic” was published in Graefes Archives of Clinical and Experimental Ophthalmology in June 2020.* We all know that publishing in a highly impactful peer-reviewed journal can take considerable time, so to ensure the timely availability of these resources to the ophthalmology community, they gained consensus from contributing authors and developed a suite of resources to be published . . . in record time!
The Vision Academy comprises an international group of more than 80 experts worldwide. “Through our collective expertise, the Vision Academy seeks to provide guidance for best clinical practice in the management of retinal disease, particularly in areas with insufficient conclusive evidence,” described Prof. Loewenstein. They not only compiled guidance for clinicians on how to adapt clinic practices in light of COVID-19 to minimize risk of exposure of both patients and medical staff, they also developed patient facing materials to support clinicians in their proactive communication with their patients.
In developing these recommendations, Profs. Korobelnik and Loewenstein had in-depth discussion with colleagues from across the world. “We identified a critical gap of available guidance for clinicians to communicate with their patients, especially those with nAMD, and their families about how we were adapting our clinical practice to help minimize their risk of exposure to COVID-19 and to acknowledge the importance for them to continue receiving these essential treatments to preserve their vision,” explained Prof. Loewenstein. “This pre-communication step is critical in order to alleviate their anxiety as best we can and prepare them for how to engage during the appointment itself. We know now that there was a substantial number of patients that did not come for timely treatment and lost vision due to disease progression, sometimes with massive
subretinal hemorrhage with irreversible vision loss,” she added.
As a priority, they identified that providing a clear explanation of infection prevention protocols and safeguards of each clinic, including what to expect before, during and after the appointment may help to alleviate concerns.
Prof. Loewenstein shared why they focused on nAMD patients: “Our patients are elderly and may have other conditions that put them in the at-risk population. Understandably, patients with conditions such as nAMD were anxious about attending their regular appointments, due to the risk of exposure to COVID-19.”

“One of the most important aspects of achieving this is communicating with the patient ahead of time to reassure that specific measures have been put in place to minimize their risk, and that of our staff and to prompt them on what to expect when they arrive at their appointment. Even preparing them that the conversation will be limited and their caregiver will be asked to wait outside, could already prepare them and avoid further explanation when arriving at the clinic,” she added.
The team from Vision Academy recognized that circumstances differ around the world and developed these resources to adapt to local regulations and standards. Maybe most importantly, these resources include a communication template that can be used as a proactive tool, to be sent via email or text message, to patients and their families ahead of appointments to reassure them that their safety and eye health remains a priority.
Prof. Loewenstein described the care taken in the development of these patient facing materials: “We aimed to develop materials that are easily accessible, simple and adaptable by ophthalmologists to prepare patients and their families for their upcoming appointment. The template letters, for instance, can be easily adapted to local regulations and standards, deleting sections or adding as necessary, and shared with patients ahead of their appointments. Along
with this, we also developed engaging infographics and videos to support these communications, which can be shared ahead of time or used in clinic. To ensure ease of access, we have translated all of these resources into multiple languages and they are available on the Vision Academy website to ensure local applicability and quick adaptation.”
Online materials include an educational slide deck, a “Dear nAMD Patient & Family” template, a “Dear Patient & Family” treatment postponement template, patient guidance infographic and patient information video. Visit the Vision Academy website for access to the resources.
* Korobelnik J-F, Loewenstein A. Communicating with patients with nAMD and their families during the COVID-19 pandemic. Graefes Arch Clin Exp Ophthalmol. 2020; 258(6): 1335–1337.
Contributing Doctor
Anat Loewenstein , MD, is a professor of ophthalmology, vice dean of the Faculty of Medicine, and Sidney Fox Chair of Ophthalmology at the Sackler Faculty of Medicine at Tel Aviv University, and the chairman of the Division of Ophthalmology at Tel Aviv Medical Center. Prof. Loewenstein’s main field of interest is the investigation of drug administration and toxicity to the retina, early detection of macular degeneration and home monitoring of disease. Prof. Loewenstein is frequently an invited speaker at international meetings, has published 400 papers in peer reviewed journals, and contributed multiple chapters to ophthalmology textbooks. She currently serves as the general secretary of EURETINA, and serves on the Editorial Boards of numerous prestigious ophthalmic journals. Prof. Loewenstein is a proud mother to her three children, a physician, a data scientist, a financial business developer with Roche, and has three granddaughters. In addition to her extremely active clinical and research activities, Prof. Loewenstein enjoys reading and spends two hours each day doing fitness activities such as running, swimming, yoga or strength training.
| June/July 2020 9
anatl@tlvmc.gov.il
Guidance for patients with neovascular age-related macular degeneration (nAMD) and their families during the COVID-19 pandemic
Adapting clinic practice:
Patients with urgent needs and those requiring frequent management are being seen at this time.
Non-urgent appointments are being rescheduled.
Information regarding your upcoming appointment:
Planning:
• Before your appointment, your doctor’s office may reach out to you regarding your current health status.
• Scheduling will be adapted to ensure minimal patients are in the waiting room.
During your visit:
• To reduce your time in clinic, you may not receive your regular visual acuity test, or eye scan.
• Your ophthalmologist may wear a mask with a plastic shield over their eyes and limit conversation during the examination.
• Your doctor’s office may defer scheduling of your next appointment via phone.
Ways you can reduce the risk of exposure during your visit:
If you’ve had direct exposure to a person who is COVID-19 positive or have a cough or fever, it is essential to let your doctor’s office know ahead of time.
If you arrive at the appointment and are unwell, you may be asked to reschedule.
If you anticipate a cough or sneeze, kindly cover your face with your bent elbow or a tissue and dispose of any used tissues immediately. Wash your hands with soap and water or disinfectant immediately.
| June/July 2020 10
MA-PFM-OPHT-ALL-0154-1 | April 2020
Ways you can reduce the risk of exposure during your visit:
Please limit to one person accompanying you to your appointment.
The clinic may ask you, or the person accompanying you, to wait outside, to maintain social distancing.
While in the waiting room, maintain a distance of at least 1.5 to 2 meters (5-6 feet) between yourself and others.*
You may, or may not, be given a mask to wear during the treatment.
If you are unable to attend your visit: Your doctor’s office will only ask patients for whom treatment is crucial to attend appointments and will take all measures to minimize risk. Risk cannot however be completely eliminated, and your doctor will understand if you choose to cancel a visit at any time.
Please contact the clinic as soon as able to cancel your appointment and schedule a replacement appointment.
In the lead up to your next appointment, regularly monitor your vision, such as with an Amsler Grid test.
If you do notice a change in your vision, please contact your doctor to assess if an emergency visit is needed.
For more information on ways to limit your exposure to COVID-19 and reduce your risk, please visit: https://www.who.int/emergencies/diseases/novelcoronavirus-2019/advice-for-public
The Vision Academy comprises an international group of more than 80 experts worldwide. Through their collective expertise, the Vision Academy seeks to provide guidance for best clinical practice in the management of retinal disease, particularly in areas with insufficient conclusive evidence. The Vision Academy is supported by Bayer.
| June/July 2020 11
Sources: World Health Organization MA-PFM-OPHT-ALL-0154-1 | April 2020
*Please refer to your local government’s guidance on social distancing measures.
A New Era in the Treatment of Hereditary Optic Neuropathies
Should these treatments prove to be effective and safe, they will radically transform the treatment approach to patients at risk of visual loss. Gene therapies are emerging for several inherited retinal diseases as well. These recent scientific and clinical developments may represent the beginning of an era of approved gene therapies for a wider range of neurologic diseases.
Retinal degenerative diseases are a leading cause of irreversible blindness. The central pathology in many of these conditions is retinal death, induced by a mix of genetic and environmental factors. Inherited conditions are increasingly recognized as an important component of the neuro-ophthalmic differential diagnosis of sub-acute vision loss. For these blinding conditions, innovations in gene and cell therapy approaches offer therapeutic intervention at various disease stages.
A recent review by Dr. Tatiana Bakaeva et.al from Harvard Medical School, Boston sheds light on hereditary optic neuropathies.1
A journey in discovery
For experts in the field, it’s been a long journey towards understanding the pathophysiological pathways that underlie degenerative retinal diseases how these insights translate into the development of novel treatments. The investigators reported that: “To date, many promising treatments have been showing disappointing results in human trials. However, newer insights into the genetic basis, natural history and phenotypic heterogeneity of these conditions have set the stage for targeted therapies that are moving into clinical trials.”
by Olawale Salami
Leber’s hereditary optic neuropathy (LHON) is an important example, in which visual loss can be severe and permanent. It is associated with three primary pathogenic mitochondrial DNA mutations, with varying degrees of penetrance, suggesting additional environmental factors. A variety of treatments have been tried in the past including systemic steroids, hydroxycobalamin and cyanide antagonists, vitamin C and riboflavin. The results were disappointing. However, a new class of drugs has shown promising results in clinical studies. These are known as CoQ10 analogues, or mitochondrial “cocktails,” They interact with the mitochondrial electron transport chain to facilitate mitochondrial electron flux and bypass complex within this class, Idebenone and EPI-743 have appeared to be the most promising judging by early results from clinical trials showing a trend toward preserved acuity and RNFL thickness. However, as reported by Dr. Bakaeva and colleagues, data from larger studies are needed to validate these results.
Bridging the genetic gap
Given the unspecific nature of existing therapies for LHON Experts in the field have evaluated gene therapy as a targeted therapy that could effectively and safely prevent visual loss in highrisk but pre-symptomatic patients. The past decade has brought an exciting set of advances in gene therapy for this condition. Using genetically engineered vectors, most commonly the adenovirus2 experts have assembled replacement genes, like the human ND4 gene, that hopefully will be efficiently expressed by the vectors and carried into the mitochondria, to replace deficient genes in the eye tissue of patients, and restore vision. Impressive results in in-vivo
animal studies have led to early phase human studies at various stages of completion.
In other inherited retinal conditions, research and development in new therapeutic strategies have progressed much further. Leber’s congenital amaurosis (LCA) is a spectrum of inherited retinal disorders, characterized by severe visual impairment presenting at birth or within the first few months of life, usually accompanied by roving eye movements or nystagmus, poor pupillary responses, and severely abnormal full field electroretinogram (ERG).3 At present, there are 24 known gene mutations and the most common mutation occurs in the RPE65 gene, which accounts for approximately 16% of cases. Until recently, management of most forms of LCA has been symptomatic, but the previous decade has brought major scientific advances leading to a major breakthrough in the treatment of the specific form associated with mutations in the RPE65 gene.4 Gene therapy for RPE65-associated retinopathy is commercially available, but prohibitively expensive, beyond the reach of many patients.5
Choroideremia is a rare disease characterized by progressive degeneration of the choroid, retinal pigment epithelium (RPE), and photoreceptors, starting with night childhood blindness that ultimately progresses to severe blindness. It has an X-linked recessive inheritance pattern caused by a loss of function mutation in the CHM gene that encodes REP1 (Rab escort protein 1). In other hereditary and nonhereditary retinal diseases in which gene therapy is being explored include achromatopsia, retinitis pigmentosa, X-linked retinoschisis, Usher’s syndrome, Stargardt’s disease, and age-related
| June/July 2020 12 RETINOPATHIES POSTERIOR SEGMENT
macular degeneration, clinical studies of novel gene therapy-based treatments offer the promise of long lasting restoration of vision.
What about stem cell therapy?
Stem cell therapies are being explored extensively as treatments for degenerative eye diseases, either for replacing lost neurons, restoring neural circuits or, based on more recent evidence, as paracrine-mediated therapies in which stem cell-derived trophic factors protect compromised endogenous retinal neurons from death and induce the growth of new connections.6 Stem cell therapy may offer an opportunity for restoring vision for patients in whom the extent of structural damage is too severe for effective gene therapy. These conditions can include chronic LHON and other acquired optic neuropathies, as well as most inherited retinal degenerations including retinitis pigmentosa.
Unlike gene therapy that is intended to enhance the function of poorly functioning existent cells, the goal of stem cell therapies is to regenerate dysfunctional tissue and restore lost cells. There have been many promising animal and preclinical studies over the past 20 years that involve the use of embryonic induced pluripotent and bone marrow–derived stem cells for retinal and neurologic diseases. Ongoing research is focused on optimizing techniques that allow safe delivery of an adequate number of cells to the recipient eye with the appropriate development of tissue structure. Several clinical trials are focused on treatment of age-related macular degeneration and
References:
other inherited retinal degenerations.
In contrast to progress being made in rigorous, well-conducted studies, patients and clinicians should be aware of an alarming trend of commercially advertised stem cell treatments that are not regulated, with substantial risk of poor outcomes including endophthalmitis, cataract progression, fibrous proliferation and tractional retinal detachment, and retinal artery occlusion following subretinal, intravitreal, and/or periocular injections of bone marrow–derived stem cells.7
Translation to clinical setting
LHON and other genetic causes of visual loss are important clinical entities that can cause profound visual loss. To date, therapeutic options have been quite limited. Insights into the genetic basis of these diseases and advances in the ability to deliver effective and safe gene therapy have opened the door for new therapeutics that may revolutionize the approach to treating these conditions.
While carefully conducted, controlled studies are keys to understanding the effects of these potential treatments and defining the optimal treatment populations, how do all these translate to real-world clinical setting? More importantly, the crucial first step is diagnosis. “In trying to arrive at the diagnosis, it would be helpful to examine parents and/or siblings, as many genetic conditions, though may have variable penetrance and expressivity, may have some detectable clinical manifestations,” shared Dr. Manoharan Shunmugan, vitreoretina
1 Bakaeva T, Mallery R, Prasad S. Emerging Treatments for Leber’s Hereditary Optic Neuropathy and Other Genetic Causes of Visual Loss. Semin Neurol. 2019;39(6):732-738.
2 Dalkara D, Byrne LC, Klimczak RR, et al. In vivo-directed evolution of a new adeno-associated virus for therapeutic outer retinal gene delivery from the vitreous. Sci Transl Med. 2013;5(189):189ra76.
3 Fazzi E, Signorini SG, Scelsa B, et al. Leber’s congenital amaurosis: An update. Eur J Paediatr Neurol. 2003;7(1):13-22.
4 Bainbridge JWB, Smith AJ, Barker SS, et al. Effect of gene therapy on visual function in Leber’s congenital amaurosis. N Engl J Med. 2008;358(21):2231-9.
5 Apte RS. Gene Therapy for Retinal Degeneration. Cell. 2018;173(1):5.
6 Mead B, Berry M, Logan A, et al. Stem Cell Treatment of Degenerative Eye Disease. Stem Cell Res. 2015;14(3):243-57.
7 Herberts CA, Kwa MSG, Hermsen HPH. Risk Factors in the Development of Stem Cell Therapy. J Transl Med. 2011;9:29.
specialist in Kuala Lumpur, Malaysia.
Having a special interest in hereditary degenerative neuropathies, Dr. Shunmugam highlighted critical points on this subject matter, including genetic counseling. “For patients with hereditary conditions it is imperative that the parents receive genetic counseling so that they are aware of the possibilities of these conditions affecting any other children. It would also be prudent to ensure siblings or extended families have a routine eye examination,” he explained. Furthermore, a thorough social and dietary history is necessary, according to Dr. Shunmugam. “Some modern dietary restrictions have been shown to have an impact on even normal individuals let alone those with underlying genetic conditions,” he added.
Contributing Doctor
Dr. Manoharan Shunmugam is a consultant ophthalmologist, adult and pediatric vitreoretinal surgeon who trained in the United Kingdom and returned to Malaysia in 2012. He has a keen interest in research with publications in a wide-range of highimpact journals and has been invited to many international conferences as a speaker. He is also a contributing author of two book chapters in vitreoretinal reference textbooks. He graduated in Scotland and subsequently undertook his Ophthalmic Specialist Training and VR Fellowship in London. En route, he further honed his skills with a Pediatric VR fellowship at L.V. Prasad Eye Institute, Hyderabad, India –making him one of the few pediatric VR surgeons serving the Asia-Pacific region. Today, he continues to serve at Hospital Kuala Lumpur, Pantai KL & Assunta Hospital. He is also the Hon. Secretary of the Malaysian Society of Ophthalmology (MSO), and is a member of the Asia-Pacific Vitreoretinal Society (APVRS) and the American Society of Retinal Specialists (ASRS).
manoshun@gmail.com

| June/July 2020 13
Beovu: What’s the latest with the ophthalmic community’s concerns?
by Sam McCommon
Reports and opinions keep pouring in about Novartis’ Beovu® (brolucizumab), meant to treat wet or neovascular age-related macular degeneration (nAMD). In February, the American Society of Retina Specialists (ASRS) noted a risk of intraocular inflammation and retinal vasculitis associated with the drug; more concerning was that 11 of the 14 cases of vasculitis were occlusive retinal vasculitis, which can lead to vision loss. The drug’s main appeal is that it reduces the rate of injection to once a quarter following the initiation of treatment.
Novartis backed these findings in April, noting a “confirmed safety signal of rare adverse events of retinal vasculitis and/ or retinal vascular occlusion that may result in severe vision loss.” Novartis’ safety review committee (SRC) noted a 3.3% rate of retinal vasculitis in study patients who had been treated with Beovu. Most of the patients
(74%) experienced symptoms within six months of the treatment, though some (12%) experienced it as late as 12-18 months afterwards. According to an ASRS report, the earlier events were associated more frequently with moderate or severe vision loss.
Fast forward to May, and an editorial in the American Journal of Ophthalmology asked if this was a 737 MAX moment for brolucizumab, drawing a connection between the drug and Boeing’s flawed flyer. Authors Philip J. Rosenfeld and David J. Browning asserted that, as there are other drugs currently available to treat wet AMD, there is no reason to subject patients to the risks associated with Beovu. They argued that previous warnings hadn’t gone far enough: While announcements from the ASRS and Novartis did note the risks associated with the drug, they didn’t call for stopping its use. These authors took that stop and called for its halt.
“In the face of the known risk, its use is unwarranted,” they wrote. “We praise the post-marketing surveillance of the vitreoretinal community in identifying these never-events, but now we need the ASRS, the Retina Society, the Macular Society, the AAO and the FDA to make official what many retina specialists have already implemented — a moratorium on its use until the results of further investigations are concluded and remedies are implemented.”
Other drugs currently on the market have not been associated with the same levels of intraocular inflammation (IOI). As the authors said, “The retinal community had not reported this type of vision-threatening occlusive retinal vasculitis after intravitreal injections of other commonly used anti-VEGF drugs, such as aflibercept (Eylea; Bayer, Leverkusen, Germany), bevacizumab (Avastin; Genentech, California, USA), and ranibizumab (Lucentis; Genentech, California, USA). Retinal specialists
| June/July 2020 14
ANTI-VEGF
POSTERIOR SEGMENT
TREATMENT
started sharing this brolucizumab information with each other through social media, at meetings and through published reports.”
So the new kid on the block has raised a few eyebrows. Where are we now?
To get a clearer view of the picture, we reached out to Dr. Kenneth Fong, president of the Malaysian Society of Ophthalmology.
Doctor’s orders
Dr. Fong acknowledged the concerns brought up by the ASRS and confirmed by the SRC. “These reports of retinal vasculitis in patients receiving brolucizumab are very concerning as such side effects have not been observed in millions of patients treated with the current choices of anti-VEGF agents: bevacizumab, ranibizumab or aflibercept,” he said.
“Patients receiving brolucizumab should be informed of this potentially serious side effect before treatment,” he added. Doctors who administer the drug should be aware of the current findings, and pass the information along to their patients.
Dr. Fong noted that he has only used Beovu for a small number of patients as part of a study that compares the drug to aflibercept for diabetic macular edema (DME).
Is it any use at all?
Despite the calls for the drug’s use to be halted by the authors of the AJO op-ed, there may still be some use for Beovu. However, it may not be the go-to, frontline drug for nAMD that Novartis had previously planned.
“In my practice, brolucizumab is a potential second line agent for patients that have not responded to the current line of anti-VEGF agents available, which all have excellent long-term visual acuity gain and safety profiles,” said Dr. Fong. “Despite the fact that it is FDA approved for wet AMD, it would be hard to recommend it as a first line agent until the safety issues have been clarified further.”
Dr. Fong further pointed out that the risk of serious vision loss — a loss of more than 15 letters — was at 0.7% according to the current studies. So, while upwards of 99 out of 100 patients do not suffer severe vision loss, the risk is still there. Nobody wants to be that one in 100.
To Novartis’ credit, they’ve received praise from the ophthalmic community for their transparency and quick action regarding the drug. Once the risks are better understood, the drug could come roaring back and be that frontline player it was meant to be. The company defended the drug’s value as a treatment and reaffirmed their commitment to transparency.
As a company spokesman said, “Novartis believes that Beovu continues to represent an important treatment option for patients with wet AMD, with an overall favorable benefit-risk profile. We are committed to collaborating with the scientific community to better understand the causes, potential risk factors and management of these events.”
What’s next for Beovu?
The drug is being investigated, as the reason behind its link to IOI is still unknown. The drug is still on the market, and its use will have to be decided at each doctor’s discretion. As the ASRS’s ReST committee noted, “With all therapeutics, the risk of adverse events and their visual consequences need to be balanced with potential benefits. The ReST Committee believes that this riskbenefit assessment at the individual patient level is best determined by the judgment of the treating provider.”
As to the cause? We don’t yet know, but Dr. Fong has a theory.
“The reason for retinal vasculitis is unclear,” he said, “but it is probably an immune mediated reaction to the drug and that is the possible reason for delayed appearance of this side effect after 6 months.”
One interesting note the ReST committee pointed to is that brolucizumab and aflibercept share roughly the same risk of vision loss over time: 7.4% and 7.7%, respectively. The ASRS report does not indicate what causes said vision loss; just that it occurs.
Novartis stock took a significant hit in February and into March, though the drop was concurrent with wider market trends. It has since clawed back around half of its losses and share prices have been essentially steady between April and June, as of this writing.
With millions of patients being treated for wet AMD, doctors will need to take note of any updated information regarding Beovu. Retinal vasculitis has not been reported as a result of the other current, popular drugs, so their use will likely continue. Patients who were hoping for a reduced injection regimen may have to put up with the current rate of injections — unless they and their doctor decide going off the reservation is worth the risk.
Contributing Doctor
Consultant Vitreoretinal Surgeon Dr. Kenneth Fong , MA MB BChir (Cambridge), FRCOphth (UK), FRANZCO (Aust), CCT (UK), AM (Mal), is recognized as an ophthalmologist in the UK, Australia and Malaysia. He graduated with a medical degree from the University of Cambridge in 1998 and trained to be an eye surgeon in London. Dr. Fong then spent two more years training in the UK and at the Royal Perth Hospital in Australia to subspecialize in retina. After 18 years of working in the UK and Australia, he returned to Malaysia in 2009 to serve as associate professor and consultant ophthalmologist and retinal surgeon at the University of Malaya in Kuala Lumpur. He is currently the managing director of OasisEye Specialists in Kuala Lumpur. Dr. Fong is the president of the Malaysian Society of Ophthalmology and serves as a council member for the Asia Pacific Vitreoretinal Society.
kcsfong@gmail.com

| June/July 2020 15
with the PIE Radio Show
Ophthalmologists Discuss Important Topics in Vitreoretina
by Brooke Herron
At PIE, we’re sometimes known as the “shock jocks” of ophthalmic publishing — thanks to our funky style (in both fashion and medical reporting). So, we decided to try on those radio show shoes, with a segment of our own: the PIE Radio Show.
We asked renowned surgeons from around the world to chime in on some of the most important topics in ophthalmology today — from COVID-19’s impacts, to business decisions and innovations in medical and surgical retina. So, sit back, relax and don’t touch that dial . . . the PIE Radio Show is ON AIR!

Dr. Diva Kant Misra
Lucknow, India
Vitreoretinal Consultant at Eye-Q Super Speciality Eye Hospital
Song Request: “Believer” by Imagine Dragons
Dr. Anil Arora Sydney, Australia Ophthalmic Surgeon for Central Coast Eye Specialists and Medical Director of the Laser Vision Clinic Central Coast


Song Request: “I Can See Clearly Now” by Johnny Mathis
That’s enough, COVID-19
I don’t know about you, but we have coronavirus fatigue here at PIE. Unfortunately, until a vaccine is developed or the virus is somehow contained, it’s going to be hanging around — like an uninvited dinner guest. Worldwide, we are learning to live with it: People are making lifestyle changes to ensure their safety and that of others.
Dr. Kenneth Fong

Kuala Lumpur, Malaysia Consultant Vitreoretinal Surgeon and Managing Director of OasisEye Specialists
Dr. Gemmy Cheung

Singapore, Singapore Deputy Head and Senior Consultant of Medical Retina at Singapore National Eye Centre (SNEC)
Dr. Chirag Shah
Boston, USA
Vitreoretinal Surgeon at Ophthalmic Consultants of Boston and Co-Director of the Tufts/OCB Vitreoretinal Surgery Fellowship
And not to sound like a broken record, but COVID-19 has undoubtedly affected ophthalmology — including patients, doctors, staff, clinics, hospitals, equipment and device companies . . . the list goes on. So, what’s happening now that practices are reopening and doctors are seeing patients again?
PIE: Have you noticed any patients with vision loss or disease progression
following reopening from the pandemic due to missed treatment?
Dr. Diva Kant Misra: Yes, a lot of patients could not get immediate care for urgent retinal conditions like retinal detachment. In such patients, even minor delays can lead to a poorer visual prognosis. A few of my patients from other cities were able to reach me after considerable hardship and delay. Thankfully we were able to salvage
COVER STORY
| June/July 2020 16
these eyes, but I had a CRAO (central retinal artery occlusion) patient who came to me after one month, and by that time it was too late for him.
Dr. Anil Arora: I have, unfortunately, had four or five patients who have had worsening of their exudative macular degeneration because they have not kept their appointment for intravitreal anti-VEGF injections. Some patients have been too frightened to come out and some patients (who were residents of nursing homes) were told that if they left their premises, they would have to self-isolate for two weeks upon returning and they did not want to go through that. Fortunately, the decline in vision was not marked in any of these patients and hopefully vision will recover with resumption of regular treatment.
Dr. Kenneth Fong: Yes, there have been a few patients with AMD (agerelated macular degeneration) who lost vision due to the lockdown as they were unable to attend the clinic for their usual injections.
Dr. Gemmy Cheung: During the month of May 2020, about 25% of patients who have active disease in our unit did not attend their appointments. When our team called up this group of patients, about 40% reported that the main reason for not attending their appointment was fear of getting infected. About 90% of patients reported their subjective vision is stable. For the 10% who reported subjective worsening, they agreed to attend the urgent appointment which we re-scheduled to evaluate their condition and reinstate their injections if indicated.
Dr. Chirag Shah: Unfortunately, two patients developed significant submacular hemorrhages and associated visual loss due to missed intravitreal anti-VEGF injections. Further, delayed macular hole surgeries resulted in larger macular holes and reduced visual potential after repair.
PIE: It’s unfortunate to hear that some patients have lost vision during lockdown. Do you think anything in ophthalmology will permanently change as a result of coronavirus?
Dr. Fong: The levels of hygiene will improve significantly in all health care institutions and this will benefit staff and patients in reducing the risk of infectious diseases. Within a few months, the whole world will be used to the idea of universal mask use and social distancing.
PIE: Right, so moving forward it seems like there will be extra caution . . . with everything.
Dr. Misra: We are switching to telemedicine, practicing social distancing — and most of all; we see and meet patients from behind the mask. This definitely is going to hamper the patient-doctor connection. It’s ironic that you may not even know the face of the person you trust your eye with. But such are the times, and such is life. We have to do the best with what we have.
Dr. Shah: Coronavirus will likely have many lasting effects on our field. Prior to coronavirus, private equity was spreading throughout ophthalmology practices in the United States, benefitting senior partners at the expense of junior and all future partners. What a stark contrast to the effects of our current pandemic. Now, with uncertainties in revenue and profitability of ophthalmology practices, as well as with volatility in public markets, we may witness a regression of private equity takeovers.
PIE: You’re right, the virus hasn’t only created safety concerns — it’s hit all aspects of the business . . .
Dr. Shah: Yes, and with regard to changes in individual practice, it is possible that those who can work remotely, like administrative assistants and call center staff will continue to do so. Telehealth might also become part of the fabric, particularly for external disease. Sadly, I think many of us will have to retire our tie collection, as ties can serve as a fomite for infectious diseases. Same goes for white coats.
Dr. Anil Arora: I don’t think that anything will change permanently. There will be temporary changes, as are already taking place, which will continue — such as the wearing of masks and goggles; having shields and
screens over slit-lamps; reducing clinic bookings; reducing the number of chairs in the waiting room (to keep waiting rooms less crowded); and sanitizing hands and equipment between patients. As restrictions ease, and hopefully as the disease is contained, I think there will be a tendency for things to return to how they were pre-coronavirus.
PIE: These are all valid points — and it will be interesting to see how the lasting effects of COVID-19 play out in ophthalmology. Speaking of the pandemic, are there any questions about it that you’re tired of answering?
Dr. Fong: None, as the situation seems to change weekly, my answers to the same questions are also changing weekly. For example: risk of infection spread caused by aerosolization during cataract surgery; the PPE requirements are not clear yet so I am wearing an N95 mask for all my surgeries, but I do not use a face shield or cover the surgical field excessively.
Dr. Misra: People keep asking about the “new normal.” I am as clueless as anyone else. These are unprecedented times and it will be very difficult to predict how the situation will further develop.
Dr. Shah: None.
Dr. Arora: There is one question and one comment that I have heard frequently that has become a little tiresome. The question is: “When will there be a vaccine for coronavirus?” Everyone seems to have an opinion on this, with projections ranging from later this year to never. I have no idea when there will be a vaccine. There is still no vaccine for HIV or hepatitis-C, so it may be that there will never be a vaccine for COVID-19.
The comment that is tiring after some time is: “Things will never be the same again.” I think that there is always a tendency for people to return to old habits and once restrictions ease — and particularly as domestic and international travel resumes — things will be the same as they were before.
The two things that the coronavirus restrictions have taught me is that we can all do with less than we think, and
| June/July 2020 17
that we need to respect Mother Nature. I tend to view viral pandemics as nature’s way of trying to restore the balance when one species becomes too powerful and disrupts that balance. I hope that I and others will continue to remember this as life returns to normal.
Show me the money: Business decisions
In addition to affecting patients and individual practices, the pandemic has also hit the industry’s ophthalmic device and equipment companies — many of whom, like small and medium-sized enterprises (SMEs), may be struggling to stay afloat as demand dries up.
PIE: Are you, or is your clinic/ hospital planning to purchase any new equipment or devices in 2020? In 2021? And if so, what?
Dr. Misra: All planned purchases have been stalled for the moment. We are evaluating the rapidly changing scenario and will reconsider those purchase decisions after everything stabilizes.
Dr. Arora: We have recently upgraded to the ZEISS CIRRUS 6000 model of optical coherence tomography (OCT). We have purchased two of these and are particularly enjoying the rapid image acquisition speed, along with several other new features. We are also
looking at purchasing the CLARUS widefield fundus imaging system (from ZEISS) in the coming year.
Dr. Fong: No, due to a reduction in workload caused by the pandemic and lack of budget.
Dr. Shah: My practice bought scrubs for all of the staff in an effort to provide clothing that would be washed after a day of work to minimize the spread of coronavirus. They also plan to buy an intense pulsed light (IPL) laser for dry eye treatment.
Vitreoretinal hits: What’s topping the charts?
Moving on, technology and treatments for posterior segment conditions are constantly evolving. Let’s talk about that. . .
PIE: Are there any innovations in the development pipeline that you’re following closely in surgical? In medical?
Dr. Misra: I am closely observing the developments in the field of bionic eyes and related research.
Dr. Fong: 3D visualization systems will be helpful as they will not require surgeons to be so close to the surgical field — and they could also potentially reduce occupational related neck and back pain.
Dr. Arora: In medical, I am looking forward to seeing the introduction of brolucizumab (Beovu; Novartis, Basel, Switzerland) in Australia for the treatment of exudative age-related macular degeneration (AMD). I have not used it myself, but if it can reduce the frequency of intravitreal injections from monthly — as is typically the case now — to every three to four months as the company claims, it will greatly reduce the burden of treatment for ophthalmologists . . . and hopefully, reduce the massive cost that intravitreal injections have on the health system in
many countries.
I am aware of reports and concerns about it [Beovu] producing occlusive retinal vasculitis. These have occurred in the U.S. following approval of the drug for wet AMD and were not present (or at least not with anywhere near the same frequency) in the clinical trials preceding approval. There may be an immune response and apparently some treatment naive patients have antibodies to Beovu. The company is addressing these concerns and hopefully, if they are resolved, we will have a new medication in our arsenal to manage AMD more effectively.
In surgical, having become comfortable with 25-gauge vitrectomy for almost all vitreoretinal procedures, I look forward to making the transition to 27-gauge vitreoretinal surgery in the near future. It is amazing to think that we can do vitreoretinal surgery and procedures such as laser photocoagulation, silicone oil injection and membrane peeling, through openings that are the same size as a needle used by diabetics to administer insulin.
Dr. Shah: Stem cell transplantation for atrophic AMD is always an intriguing topic to help stabilize — or even restore some vision — in patients with a presently blinding condition. If approved, I do wonder how operating rooms will be able to accommodate the surgical volume if transplantation requires vitrectomy with subretinal delivery.
PIE: Indeed, these new treatments and devices certainly sound both interesting and promising. Building on that, what do you think is the most important topic in vitreoretina today? Or is there a topic that you feel deserves more attention?
Dr. Arora: I’m not sure I can single out one topic as being the most important. I think if you ask 10 different ophthalmologists you may get 10 different answers. Perhaps the condition that is most in need of a treatment is dry (or atrophic) AMD. While we now have a variety of intravitreal agents for wet AMD, there are still no really good answers for the dry form.

COVER STORY | June/July 2020 18
Dr. Fong: We need longer acting drugs or depot devices to deliver treatments for AMD, diabetic macular edema (DME) and retinal vein occlusion (RVO). The pandemic has shown that we need to reduce our retina patient visits without compromising on their vision. Current anti-VEGF agents only allow, at most, three monthly intervals between visits for a small number of patients. Most patients still need to come back monthly.
Dr. Misra: I feel the role of artificial intelligence in battling diabetic retinopathy blindness will be a game changer in a country like India.
Dr. Shah: At the moment, it is most imperative to keep our elderly, the most vulnerable patients, safe in our offices. This requires careful consideration of all the steps patients take during a typical office visit so that we can maximize the efficiency of the visit to minimize risks associated with patients congregating in the waiting room. This may also require a reevaluation of the patient scheduling, possibly stretching out the day and reducing the number of patients per hour.
PIE: It sounds promising that there are some devices and treatments in the R&D pipeline to address some of these sight-threatening retinal diseases. Furthermore, as the pandemic continues, it’s clear that continued vigilance will be required to not only keep patients safe, but to keep businesses running.
Well, looks like we’re out of time . . . we appreciate all the “callers” who “phoned-in” to the inaugural PIE Radio Show. Until next time…
Editor’s Note:
Answers to these questions were submitted via email by the surgeons interviewed. Responses have been edited for length and clarity, and edited into a Radio Show transcript. And while the PIE Radio Show did not occur in real time, the answers are real.
Contributing Doctors
Dr. Diva Kant Misra completed his vitreoretinal surgery fellowship from Sri Sankaradeva Nethralaya. He holds the post of general secretary for the Young Ophthalmologists Society of India and chief editor for the Young Ophthalmologists Times. He is the recipient of various Ophthalmic awards like the APAO Achievement Award, Bangkok 2019; Best of IJO Award 2017-18; Ophthalmic Hero of India 2017 & 2018; KOS International Travel Grant 2019, Busan; the Yasuo Tano Award from Asia Pacific Academy of Ophthalmology, Singapore 2017; and the APVRS Tano Award 2018, Malaysia; and other national & state level awards. He has published extensively (26 publications and book chapters) and has presented in conferences held at various international and national forums and has been an invited faculty in international forums like EURETINA, APAO and AAO.
divakant@gmail.com
Dr. Kenneth Fong is recognized as an ophthalmologist in the U.K. ,Australia and Malaysia. He graduated with a medical degree from the University of Cambridge in 1998 and trained to be an eye surgeon in London. Dr. Fong then spent two more years training in the UK and at the Royal Perth Hospital in Australia to subspecialize in retina. After 18 years of working in the UK and Australia, he returned to Malaysia in 2009 to serve as associate professor and consultant ophthalmologist and retinal surgeon at the University of Malaya in Kuala Lumpur. He is currently the managing director of OasisEye Specialists in Kuala Lumpur. Dr. Fong is the president of the Malaysian Society of Ophthalmology and serves as a council member for the Asia Pacific Vitreo-retinal Society.
kcsfong@gmail.com
Dr. Anil Arora is an ophthalmologist practicing in the Central Coast and in Sydney since 1998. He completed his medical degree through the University of Sydney in 1985 and after carrying out his internship and residency training at Royal North Shore, Westmead and Royal Prince Alfred Hospitals, he embarked on a career in ophthalmology. He is a Fellow of the Royal Australian and New Zealand College of Ophthalmologists (RANZCO), American Academy of Ophthalmology (AAO) and American Society of Cataract and Refractive Surgery (ASCRS). Clinical interests include cataract surgery, particularly with multifocal
intraocular lenses, retinal diseases and surgery, and laser refractive surgery. He also has an interest in ophthalmology in developing countries and in charity work: Dr. Arora sponsors 60 children in all parts of the world through World Vision and has been a member of Amnesty International for over 10 years.
anilarora1@hotmail.com
Dr. Chirag Shah is a vitreoretinal surgeon at Ophthalmic Consultants of Boston and codDirector of the Tufts/OCB Vitreoretinal Surgery Fellowship. He is the section editor of the Clinical Trials section of Retina Times, and serves as a sub-investigator on numerous clinical trials. He recently co-authored Financial Freedom Rx: The Physician’s Guide to Financial Independence, which should be in press in 2021.
cpshah@eyeboston.com
Dr. Gemmy Cheung currently serves as deputy head and senior consultant of the medial retina service for Singapore National Eye Centre (SNEC), as well as senior clinician investigator for the Singapore Eye Research Institute (SERI). Her research interests include the study of risk factors and clinical features of macular diseases that may be unique in Asian populations. Dr. Cheung has published more than 150 articles, mostly regarding age-related macular degeneration, including polypoidal choroidal vasculopathy, and conducted several clinical trials in anti-vascular endothelial growth factor therapies. Dr. Cheung has also been actively involved in training and education, and has served as an instructor on Asia-Pacific Academy of Ophthalmology (APAO) and American Academy of Ophthalmology (AAO) courses and many other educational programs. In addition, she is also a volunteer faculty member for the ORBIS Flying Eye Hospital Programme. Dr. Cheung has received a number of prestigious awards, including the Macula Society Young Investigator Award (2017), APAO achievement award (2017), APAO Nakajima Award (2014), APAO Outstanding Service in Prevention of Blindness Award (2013), the Bayer Global Ophthalmology Research Award (2012), the Roper-Hall Medal (2005) and the Elizabeth Hunt Medal (Royal College of Ophthalmologists, UK).
gemmy.cheung.c.m@singhealth. com.sg
| June/July 2020 19
From Da Nang, Vietnam to the World
Q&A from Quarantine
As the coronavirus traversed the globe, countries around the world imposed social distancing and shelter-in-place orders (with various levels of restrictions) on their citizens. During this time, all but essential services came to a standstill, including non-emergency and elective ophthalmic procedures. How did surgeons and industry professionals cope — and continue to learn, network and share information — during the pandemic?
To learn more — and as part of PIE and CAKE magazines’ continuing coverage of the COVID-19 pandemic and its impact on ophthalmology — CEO Matt Young, in Da Nang, Vietnam interviewed KOLs from around the world. Here are some of those connections . . .
Be sure to check out all the videos in the video section of our new websites cakemagazine.org and piemagazine.org
EUROPE >>>
1 5 6
2 7
4
9
3 8
| June/July 2020 20
Dr. Mario Romano Director of the Ophthalmology Department at Humanitas Gavazenn Bergamo, Italy
Dr. Luis Diaz-Santana Head of Ophthalmology at Cambridge Consultants Cambridge, United Kingdom
Mr. Adel Bencheikh Director, Eye Care Division at Canon Medical Systems Europe B. V. Zoetermeer, The Netherlands
Mr. Frederic Giulj Export Manager at Moria SA Montrouge, Île-de-France, France
Mr. Alessio David Business Development Manager, Alfa Intes Industria Terapeutica Splendore Napoli, Italy
Dr. Paisan Ruamviboonsuk Assistant Director of the Centre of Medical Excellence at Rajavithi Hospital Bangkok, Thailand
Dr. Kenneth Fong Managing Director of OasisEye Specialists, Congress President, The 36th Congress of APAO (APAO 2021) Kuala Lumpur, Malaysia
Dr. Rafiq Hasan Former Vice-President and Global Head of Ophthalmology at Bayer Basel, Switzerland
Dr. Arun Sethi Arunodaya Deseret Eye Hospital Gurugram, India
| June/July 2020 21
Dr. Igor Kozak Vitreoretinal Surgeon at Moorfields Eye Hospital Center Abu Dhabi, United Arab Emirates (UAE)
Mr. Armond Dantino Senior Vice President of International Sales for MacuLogix Pensacola, Florida, USA
Dr. Adrienne Graves Corporate Board member; Independent Director; Chair of Compensation and Governance Committees North Carolina, USA
Mr. Franck Morand Vice President for Asia-Pacific at Quantel Medical Chiang Mai, Thailand
13 15 14 11 10 12
Mr. Thomas Dunlap Ophthalmic Medical Device Consultant Orange County, California, USA
Mr. Alex Bergoudian Vice President of Sales at Katalyst Surgical St. Louis, Missouri, USA
16
Mr. Jim Mazzo Adviser and Consultant for Carl Zeiss Meditec Dublin, California, USA
COVID-19
Ramifications in Ophthalmic Business
by Brooke Herron
As the coronavirus continues, so does PIE magazine’s Q&A from Quarantine interview series. And now, as business worldwide begins to resume, the ramifications of the pandemic are starting to emerge. So, how has ophthalmology practice and business changed (perhaps indefinitely)?
Thirty-year industry veteran Thomas Dunlap, an ophthalmic medical device consultant based in Orange County, California, has personal experience and insight on this matter. Below, he discusses ophthalmology’s way forward with PIE magazine CEO Matt Young.
Testing out the new normal
We’ve heard a lot about the “new normal” — but what does it actually look like in practice? In a word? It’s different. The rise of telemedicine and enhanced safety protocols are perhaps two of the biggest changes borne from the pandemic.
Mr. Dunlap said that there’s no question that telemedicine is going to play a role.
“How big of a role? I think that’s yet-tobe-determined,” he shared. “Patients like to sit across the table from their physician — particularly if they’re going to have surgery.”
Meanwhile, patients returning to clinics will likely see some big changes. “I was in a practice recently . . . and with social distancing, it’s different. Before we’d sit shoulder-to-shoulder with 20 people and now there’s only five people in the waiting room.”
During his visit, Mr. Dunlap said his temperature was taken before entering and then again once he was inside. He noted that the clinic was practicing
social distancing in the waiting room: “There were stickers on each of the chairs: ‘Don’t sit here, don’t sit here, this is where you sit.’”
Everyone in the clinic wore a mask and any areas patients’ touched (like chairs) were cleaned between each person. This shows patients that every precaution is being taken, which will help increase their comfort level, added Mr. Dunlap.

Marketing matters: Mind your brand
According to Mr. Dunlap, there are certain industries that are making safety and social distance accommodations better than others. He uses a popular American airline carrier as an example: “They’re filling up the plane to 80 percent or more, there’s no masks, no temperature taken and people are shoulder-to-shoulder like the old days,” he said. “That is an example of what I wouldn’t want to see as a patient [in a medical practice], and I don’t want to experience that on a flight yet either.
“Therefore, practices have to rethink
what they want to be — and think about that patient experience — more than ever before,” continued Mr. Dunlap. “The patient experience, getting the patients comfortable in the office environment, and then making that commitment to a surgery.”
These types of considerations will be especially important for cataract surgeons, who primarily deal with older or elderly patients, who will likely be more timid to return for elective procedures. “It’s going to start
• Patients’ comfort level and perception of safety can influence brand metrics.
• Lack of funding could slow down progress in R&D and ophthalmic innovation.
• Education remains key as in-person meetings are replaced with virtual interactions.
• Experts keep a keen eye on AsiaPacific as a growing market over Europe and the United States.
COVID-19 SPECIAL REPORT INNOVATION
| June/July 2020 22
happening, but not fast . . people have to be comfortable — but the last thing we want is to return to the old days, like some airlines are doing,” said Mr. Dunlap.
And not only does ignoring things like safety procedures endanger people, it can also hurt the company or clinic’s brand.
“Think about your practice: What does it stand for? What do you want to communicate to patients?” said Mr. Dunlap, further adding to the airline example: “All of the airlines are in trouble, but I think they’re making a big strategic mistake that is going to affect their brands.
“Everything that consumers are experiencing right now is going to affect their thinking about certain companies or brands,” he continued. Refunds — and the hoops customer’s must jump through to get them — will also affect their future brand perception. Therefore, companies can either emerge from the pandemic in a positive way or with a potentially damaged brand.
Pandemic pounds the R&D pipeline
Another potential casualty of COVID-19? Young, entrepreneurial ophthalmic companies.
“So much innovation in ophthalmology comes from these young companies,” said Mr. Dunlap, adding that the biggest industry companies have built a lot of their portfolio by acquiring these younger start-ups.
So, what are these younger companies experiencing? Cash flow is one likely issue: Where will they get the money to fund new innovations? The bigger companies are trying to figure out their model for moving forward, so investing in smaller companies may not be feasible in the near-term, said Mr. Dunlap. In turn, lack of investment could slow down new technology in the R&D pipeline.
In the short-term, he said that young companies that need cash to continue their operations will be in a precarious position. Meanwhile, the long-term
impacts are more uncertain as larger companies rethink their business model and reallocate funds elsewhere.
Unfortunately, many of these young businesses are big players in the ophthalmology R&D pipeline. “There is so much innovation in ophthalmology, but will there be enough resources for those companies to continue operations? Before, business was moving along nicely for everyone and now it’s kind of falling off a cliff in terms of funding. Over a period of time, that will come back,” said Mr. Dunlap. “So, this will delay innovations for ophthalmology in the R&D pipeline . . . ultimately, some won’t make it. There’s just not enough resources.”
Rebooting the marketplace with education
While the commercial landscape has shifted, one thing remains static: The need for continued education, especially as ophthalmic business begins to return.
“Marketing and commercialization is going to be very different and I think everyone in the industry has to find a way forward, but education is going to be at the center of that,” said Mr. Dunlap. “I envision that there will be an explosion of educational forums . . . and video conferencing will play an enormous role.
Webinars have been around for years — some companies embraced them and some didn’t.
“Now, everybody is forced to really embrace them . . . and you can come up with creative ways to get people excited about participating in some kind of educational venue. This education will be important for both consumers and practices,” he continued. “I think it’s different, but it’s an opportunity.”
Rethinking marketing strategies is a key component of this: In a traditional exhibition, for example, medical devices rely on push marketing. Now, Mr. Dunlap is thinking differently: “It’s more of pull marketing that the push efforts we’re accustomed to.”
Eyeing Asia-Pacific
While markets worldwide remain in flux, China’s markets are beginning to reopen. This is good news for both ophthalmic companies and patients in the region — and according to Mr. Dunlap, Asia-Pacific is red hot for ophthalmic investments and technologies.
One reason? It’s a much shorter path to commercialization. “The traditional ways (the United States’s FDA and Europe’s CE mark) are pretty slow and costly,” he explained. “Right now, there’s a lot of money in China and a high interest in bringing in more technology. It’s a pretty strategic move on the part of China, so we might see more of those things occurring.”
In addition, he shared that for many bigger companies, growth in AsiaPacific is outpacing that in the United States or Europe. This is why Mr. Dunlap, who is also the former CEO for Hoya, set up the company’s global headquarters in Singapore.
“The growth was substantial in AsiaPacific and it was a long-term strategic decision to play in those markets,” he said of Hoya’s headquarters. “If you look at growth in Japan, in the United States and in Western Europe, it’s relatively slow — in the single digits, less than 5 percent. But in Asia-Pacific, it’s in the double digits — so there’s significant opportunities for companies to make that investment [there].”
Editor’s Note:
This story is part of the ‘ Q&A from Quarantine’ series of PIE Talks, where Matt Young (CEO of Media MICE and Publisher of PIE and CAKE magazines), during the time of COVID-19 lockdown, reached out to KOLs and industry friends to evaluate and discuss the impact of this pandemic to the ophthalmic world. A version of this story was first published on piemagazine.org
| June/July 2020 23
Coronavirus Side Effects Treatment Regimens and Missed
Anti-VEGF Injections
by Brooke Herron
At this point, nearly everyone is feeling the pandemic’s effects in some form or another. Families have lost loved ones, many have lost jobs, and uncertainty seems to lurk around every corner.
In ophthalmology, clinics and hospitals have been shuttered, except for emergencies. As a result, some patients may experience vision loss due to delayed treatment.
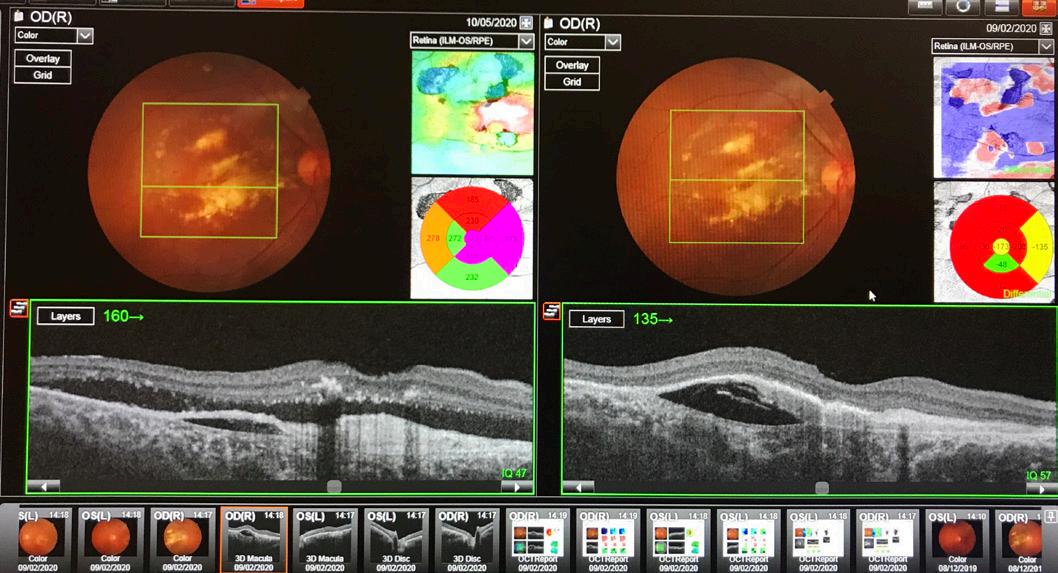
Dr. Paisan Ruamviboonsuk, former president of the Royal College of Ophthalmologists of Thailand and assistant director of the Centre of Medical Excellence at Rajavithi Hospital, in Bangkok, Thailand, is witnessing this first-hand. He’s recently returned to the clinic and is seeing patients again. Dr. Ruamviboonsuk shared details from one case: “I saw
a patient yesterday who had received more than 40 anti-VEGF injections at this point. Recently, we’ve been able to extend his injections to every eight to 10 weeks — however, any longer than that, and a small amount of subretinal fluid would return.”
The patient’s last injections were in early February; he was due for his next treatment in mid-April. “Somehow, the appointment was postponed due to the pandemic,” he continued. “Now, about 12 weeks after the last injection, there is a tremendous amount of subretinal fluid.
“The patient was injected yesterday, but we need to see him again in four weeks, instead of 10 weeks like the last time,” said Dr. Ruamviboonsuk, adding that he expects to see more cases like this in the next few months.
Guidelines aim to preserve sight and safety
For patients with neovascular (or wet) age-related macular degeneration (nAMD), maintaining a regimen of intravitreal anti-VEGF injections is crucial to slowing the progression of the disease. Currently, there is no cut-anddry regimen: Injections can be given monthly, every two or three months (extended-fixed), or as needed (pro re nata, PRN). More recently treat-andextend (T&E) is being used, where treatment intervals are extended as long as there are no signs of disease progression.1
However, in the midst of the pandemic, expert organizations and physicians have come together to set treatment guidelines for these patients. The Vision Academy, supported by Bayer, is an international group of retina physicians working together to provide recommendations where the literature is inconclusive. Together, they have devised a set of anti-VEGF guidelines2 for ophthalmologists to follow, noting that the “practicality and risk–benefit of a treatment approach should be carefully considered to minimize patient exposure and preserve sight.”
For example, they recommend that patients with nAMD (especially those in the first two years of treatment)
| June/July 2020 24 TREATMENT REGIMEN INNOVATION
ANTI-VEGF TREATMENT
OCT from February versus May: Delayed treatment has resulted in an increase of subretinal fluid and an increased treatment and monitoring regimen. [Photo credit: Dr. Paisan Ruamviboonsuk]
should be a priority, and their treatment schedules should be maintained. On the other hand, patients with diabetic macular edema (DME) or branch retinal vein occlusion (BRVO) are less likely to permanently lose sight and could be postponed.
Similarly, the Royal College of Ophthalmologists (RCOphth) have also announced guidelines for nAMD patients. Specifically, those patients should maintain anti-VEGF therapy every eight weeks with no clinic review, unless there is a significant drop in vision. They recommend DME patients postpone anti-VEGF injections and review in the clinic after four months.
The Vision Academy also recommends fixed dosing schedules or T&E over PRN approaches at this time: “Under normal circumstances, T&E regimens are highly beneficial to reduce the number of intravitreal injections a patient requires. However, with PRN the additional monitoring appointments that this regimen often requires may make it unsuitable during this unprecedented time, where there is a need to limit patient exposure and free up resources . . . therefore, fixed dosing intervals with reduced monitoring should be considered.”
Changing tides of treatment
Certainly, the coronavirus has disrupted . . . well, everything. But it’s also offered an opportunity for reflection and improvement.
Dr. Rafiq Hasan, former vice president and global head of ophthalmology at Bayer (Basel, Switzerland) said that there has been greater interest in T&E over the past two years . . . and he expects that to be the case as we move out of the pandemic. Treat-and-extend has been favored by some ophthalmologists for its benefits of fewer patient visits and fewer injections, while maintaining visual outcomes.
“I think, over time, certain countries are moving toward the treat-and-extend approach, but as we come out of this pandemic episode, there will be even greater emphasis on that,” explained Dr. Hasan.
“There is a difference of opinion about what treat-and-extend means . . . for example, what criteria do you use to extend intervals,” continued Dr. Hasan. “Some level of consistency and consensus around how you do that I think would be helpful. As we come out of this, I think our desire to protect our patients and minimize the number of injections, while optimizing the outcome, will be important.”
Dr. Hasan explained that the T&E approach has evolved over time, and was generated through both randomized control trials and real-world experience. “As we know, real world evidence is becoming more and more of an important issue in our environment, as we all accept that randomized control trials are very important but also have some limitations.”
Drive-through injections
As each country wages its own battle with the coronavirus, people around the world are in different stages of lockdown: Some areas are in total lockdown, some are lowering restrictive measures, and in some places things are nearly back to normal. When each country or region returns to a semblance of normalcy will differ, but the patients’ need for treatment will not, unfortunately.
Therefore, finding new ways of monitoring and treating patients is important. Dr. Hasan has one impressive example of this: A drivein anti-VEGF clinic in Southampton, U.K. There, the patients are driven to the door of the clinic where they have a health assessment (checking temperature and for coronavirus symptoms). “If they are okay, they will walk into the clinic and into the injection suite; after the injection, they walk back to the car,” shared Dr. Hasan.
“With these types of solutions, they are making sure that the patient gets treated — along with minimizing the time in the [clinic],” he said, adding that he expects to see more innovations like this in the future.
He also relayed the importance of
remote monitoring and assessment for patients with nAMD or diabetic eye disease. “[This] will become more important to minimize the time spent in clinics and hospitals . . . and it also minimizes the risk.”
The Vision Academy also recommends using telemedicine where appropriate, specifically to monitor patients who are at less risk of irreversible vision loss — but with the caveat that it should not extend beyond four months.
One positive of being forced inside and online is that it’s spurred innovation by leaps and bounds. “We have been getting feedback that historically, health systems have been very slow to innovate because of processes and other issues — but at this time of crisis, suddenly the speed of innovation has really increased,” said Dr. Hasan.
“We need to be ready in case there is a second wave or a future virus. The lessons learned from this experience will be very valuable . . . the guidelines in place and how to deal with future pandemics — and we will get even better at measuring these types of situations.”
References:
1 Li E, Donati S, Lindsley KB, et al. Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. Cochrane Database Syst Rev. 2020;5:CD012208.
2 Korobelnik J, Loewenstein A, Eldem B, et al. Guidance for anti-VEGF intravitreal injections during the COVID-19 pandemic. Graefes Arch Clin Exp Ophthalmol. 2020;23: 1–8.
Editor’s Note:
This story is part of the ‘ Q&A from Quarantine’ series of PIE Talks, where Matt Young (CEO of Media MICE and Publisher of PIE and CAKE magazines), during the time of COVID-19 lockdown, reached out to KOLs and industry friends to evaluate and discuss the impact of this pandemic to the ophthalmic world. A version of this story was first published on piemagazine.org .
| June/July 2020 25
Options Abound for Jim Mazzo’s Future
by Sam McCommon
As CAKE magazine reported back in March, ophthalmic industry titan Jim Mazzo stepped down from his position as global president of ophthalmic devices at Carl Zeiss Meditec (Jena, Germany) in May. He has been succeeded by Euan S. Thomson, President of Carl Zeiss Meditec Ophthalmic Devices and Head of Carl Zeiss Meditec Digital Business Unit.
In a recent interview with PIE magazine’s intrepid publisher Matt Young, Mr. Mazzo explained his current position as a consultant at ZEISS, as well as his thoughts on the state of the industry.
Jim Mazzo and ZEISS
Mr. Mazzo has been at ZEISS for the past three-and-a-half years and has witnessed the company make some significant leaps. “My goal has been to work with great people in ZEISS to take ZEISS back to where it should be. Over those three years, we accomplished a
lot with the help of people like yourself (Matt), moving from number four to number two. There were a lot of positive new introductions, new acquisitions, new team members . . . so really it was all in the works that I had committed in three years,” he said.


Mr. Mazzo noted that he’ll remain an important advisor to ZEISS until September 2020, and subsequently will remain a full-time advisor with the company until October 2021.
How will COVID-19 impact ophthalmology?
It’s not often the world witnesses a sea change in operations in one of its key sectors. Mr. Mazzo compared the changes we’d witness in ophthalmology to the changes witnessed in aviation and travel after 9/11.
“There is no way the waiting room is going to have the patient and three or four family members,” he said. “There are going to be a lot of pre-checks.
There is going to be a lot of remote testing as they are not going to have time to meet with the patient. Surgeries are going to be spaced out a little more because of the disinfection of the surgeries. So, the practices are going to be a lot different and you will see a different methodology.”
Not only will ophthalmic practices change for the foreseeable future, but ophthalmic instrument manufacturers will as well. Notably, reusable equipment, especially of the low-cost variety, may go the way of the dodo to allay concerns of virus transmission. “Reusable is probably going to be tough to sell now,” said Mr. Mazzo. “It is going to be a lot of disposable. Why run the risk; just dispose of the tubing.”
What is ZEISS doing to help doctors and patients?
ZEISS is certainly not missing this opportunity to help doctors and patients. Their changes include both the equipment they’re manufacturing as
INDUSTRY LEADER ENLIGHTENMENT
| June/July 2020 26
well as their training methods.
“At ZEISS, we will be providing face shields for the doctors, as well as the technicians, because of the proximity between them and the patients, and proper disinfection modes and how to disinfect the equipment.” He continued: “[The] transformation of ZEISS is going to be in the diagnostic arena right now, which we are doing, helping the interface. The products we introduce post-COVID would be much easier to ‘disinfect’ and easier to transmit between operating rooms.”
Much of their training has been made remote, and there’s a good chance it’ll stay that way in the future. “Thinking about other practices, there is going to be a need for a lot of virtual training,” he said. “We used virtual training during the downtime and we are going to continue to do that. This actually has become a part of the norm. Even if they [physicians] had the time, they would appreciate that they can do some of the training virtually and they don’t have to go to a meeting.”
What about the meetings — and the future of the industry?

Speaking of meetings — what will happen to important industry conferences? Mr. Mazzo noted that the big conferences would still be there — but the smaller ones may not make it. Instead, he suggests that the industry
will see greater specialization within the meetings, and within the industry itself.
“I think the large meetings will continue to be there, as people will use those for networking, however, they are going to be framed differently,” he said. “If you look at all the academy, ASCRS, and ESCRS, the greatest penetration is in the speciality days. It is in the mind of the doctors that they want speciality. So, I think you are still going to see the speciality days. The small meetings, which have been proliferating over the past years, they are just not going to be able to continue. Financially, doctors can go, some companies can survive and change dramatically.”
In an ever-evolving industry, there is always room for surprises and for greater specialization. As he put it, “People thought refractive was dead, then SMILE comes in and completely transforms the industry. My point here is — why broaden, when we still have (a) virtual unknown landscape?”
He recommended specializing in different sections of the retina. He further noted that glaucoma and dry eye, for example, are diseases with no known cure.
Jim Mazzo’s future in the industry
The industry certainly seems resilient, despite the knocks it may have taken. Mr. Mazzo will remain a big player for some time. In addition to remaining an advisor at ZEISS, Mr. Mazzo will remain an executive chairman of Neurotech, a retina implant company, as well as take on an important role at another company which he plans to announce soon. As he puts it, “I will still be involved heavily in ophthalmology and optometry, just more behind the scenes working with ZEISSs.”
Editor’s Note:
This story is part of the ‘ Q&A from Quarantine’ series of PIE Talks, where Matt Young (CEO of Media MICE and Publisher of PIE and CAKE magazines), during the time of COVID-19 lockdown, reached out to KOLs and industry friends to evaluate and discuss the impact of this pandemic to the ophthalmic world. A version of this story was first published on piemagazine.org
Which way is forward?

| June/July 2020 27
The Future Role of Telemedicine
We’d all like to be beside the sea . . . we’d all like to be exiting the lockdowns caused by the pandemic . . . you get the picture. It would be pretty fantastic if we could all get back to normal.
Lockdowns are still in place in most countries — so, sadly, for most of us, songs about the seaside are as close as we’re going to get to beaches and waves. Many also desperately want to get back to their clinics and resume regular ophthalmology. This at least is becoming easier to facilitate thanks to an increase in telemedicine uptake.
Telemedicine has emerged as a hero during the coronavirus pandemic. Uptake has increased exponentially since the crisis began and the technology is now

having a beneficial impact in several sectors of ophthalmology — mainly in primary patient care. According to one recent study, telemedicine could allow clinicians to screen patients and continue routine treatments1 in high volume environments like emergency rooms. The lessons learned are increasingly being applied to ophthalmology.
From Diagnostic to Therapeutic?
by Andrew Sweeney
Lessons from the desert
The ophthalmology industry is abuzz with discussion about telemedicine. The consensus is that while telemedicine cannot replace surgery, it does offer considerable efficacy in a number of areas. What’s more, developments in telemedicine technology made during the coronavirus crisis may facilitate its growth into areas like surgery in the future.
Dr. Igor Kozak is a consultant ophthalmologist and a specialist in vitreoretinal surgery and uveitis. Working at Moorfield Eye Hospital’s satellite facility in Abu Dhabi, United Arab Emirates (UAE), Dr. Kozak has witnessed sweeping changes brought about by the coronavirus. While the UAE is a global travel hub, it has seen relatively few cases of the virus, which allows for interesting observations.
The UAE is currently reporting between 200-400 new cases of the virus per day, primarily among the country’s vast number of guest workers, who mostly live in squalid labor compounds. A strong testing regime is in place and hospitals have been re-focused
| June/July 2020 28 TELEMEDICINE UPDATE ENLIGHTENMENT
entirely on coronavirus. Similar to other countries, most elective and non-urgent ophthalmic surgeries are cancelled.
Dr. Kozak reports that telemedicine is experiencing a major upsurge in interest in the UAE. Going beyond primary care, telemedicine is being used in a variety of areas, including to facilitate discussion on what procedures can and cannot continue. This discussion is international in scope and involves doctors across the region.
“Yesterday we had a webinar with representatives from Bahrain and Kuwait about what is elective . . . What was urgent before COVID-19 is also urgent now,” Dr. Kozak said.
“The patients with macular degeneration, acute glaucoma, retinal detachment should be treated. However, regarding cosmetic procedures like refractive surgery, I would just wait and see,” he said.
From triage to laser treatment

The buzz about telemedicine in the Middle East is perhaps unsurprising. Uptake was already higher than in other global regions, with interest in the technology encouraged by governments and businesses alike. Telemedicine’s improved applicability during coronavirus, combined with an already receptive environment, makes it likely to be a permanent fixture of ophthalmology in the Middle East.
While recognizing that its primary role is diagnostic and not therapeutic, Dr. Kozak argues that telemedicine could have a therapeutic role in the future. He points to the results of study he co-authored in 2017 that concluded that it was safe and feasible to use telemedicine to perform navigated retinal laser treatments.2
“If a patient appears with conjunctivitis and they want to come in for follow-up, it can be done using telemedicine. This would be helpful for somebody with a sty or somebody using glaucoma eye drops,” Dr. Kozak said.
He expects the UAE to weather the coronavirus storm comfortably and that
telemedicine will become a permanent, post-coronavirus. He expects this to alter triage methods and how insurance companies interact with clinics and patients. Dr. Kozak also believes that patients will welcome this development.
“Once the crisis is over, all those patients whose appointments were delayed will flock back, there will be a huge influx. According to one study in California,3 when offered the option, 80% of patients prefer telemedicine”, Dr Kozak said. “We have home monitoring devices for retinal diseases, which can check vision distortion. All of this is possible.”
Given the enthusiasm that is emerging for telemedicine, its long-term uptake is a welcome thing to look forward to, just like dreams of sitting by the seaside once again. While at the moment, we may continue to have a bleak outlook, there will be sunnier times ahead — in both ophthalmology and wider society — and not all of the changes we make will be negative.
References:
1 Rademacher NJ, Cole G, Psoter K, et al. Use of Telemedicine to Screen Patients in the Emergency Department: Matched Cohort Study Evaluating Efficiency and Patient Safety of Telemedicine. JMIR Med Inform. 2019;7(2):e11233.
2 Kozak I, Payne JF, Schatz P, et al. Teleophthalmology Image-Based Navigated Retinal Laser Therapy for Diabetic Macular Edema: A Concept of Retinal Telephotocoagulation. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1509-1513.
3 Schallhorn SC, Hannan SJ, Teenan D, et al. Informed Consent in Refractive Surgery: In-Person vs Telemedicine Approach. Clin Ophthalmol. 2018;12:2459-2470.
Editor’s Note:
This story is part of the ‘ Q&A from Quarantine’ series of PIE Talks, where Matt Young (CEO of Media MICE and Publisher of PIE and CAKE magazines), during the time of COVID-19 lockdown, reached out to KOLs and industry friends to evaluate and discuss the impact of this pandemic to the ophthalmic world. A version of this story was first published on piemagazine.org
| June/July 2020 29
can be used for more than nightclubs.
Lasers
Prof. Anat Loewenstein On Keeping Family and Professional Life in Harmony
by April Ingram
At PIE magazine we take great pleasure in profiling ophthalmologists who are doing exceptional work and providing leadership within the specialty. We particularly enjoy sharing stories of women in these roles and so here we consider it a privilege to introduce our readers to Professor Anat Loewenstein – although we’re certain that no introduction is necessary.
It’s all in the family
Anat Loewenstein, MD is a Professor of Ophthalmology, Vice Dean of the Faculty of Medicine, and Sidney Fox Chair of Ophthalmology at the Sackler Faculty of Medicine at the Tel Aviv University, and the Chairman of the Division of Ophthalmology at the Tel Aviv Medical Center. Prof. Loewenstein has really always known that she would be a physician; it is kind of the family business.
“In my family everyone was a physician: my mother was a cardiologist, my grandfather was an internist, my father, a dentist, my aunt, a gynaecologist, and my brother is a surgeon. So, it was absolutely obvious that this is my direction too. I always thought that being a physician is a profession that I can excel in by working hard,” she explained. Simply stating that Prof. Loewenstein works hard feels like a tremendous understatement, which you will see as we delve into her numerous accomplishments.
Prof. Loewenstein studied medicine at the Hebrew University in Jerusalem,
which was followed by four years serving in the Israeli Navy. She made the decision to go into ophthalmology during her internship, choosing it over internal medicine. “I realized that in this profession I can be very good at because I thought it was more limited than internal medicine (which it is not) and that I could find a niche in it where I can really know everything,” she shared. Prof. Loewenstein completed her residency in the Department of Ophthalmology at the Tel Aviv Medical Center.
When asked, why she specialized in retina, Prof. Loewenstein replied, “At that time, in my department there was no fellowship trained retina specialist and I thought that becoming a retina specialist will secure my position in the department.” Adding that it was also a bit of a team decision, “In addition, my husband, a very astute business man, convinced me that in the area of retina there will be many new developments (and he was right!).” He certainly was! Prof. Loewenstein completed a fellowship in retina vascular diseases and vitreoretinal surgery unit at the Wilmer Institute, at Johns Hopkins University Hospital in Baltimore, Maryland. Next, she returned to Israel and after holding the position as Head of the Vitreoretina Unit for two years, Prof. Loewenstein became the Chairman of the Department of Ophthalmology at the Tel Aviv Medical Center. When others may sit back, relax and admire all that they have accomplished, Prof. Loewenstein also completed her Master of Health
Triumph over cultural concepts
For someone so accomplished and a leader in retinal disease, we asked Prof. Loewenstein if she feels that there have been unique challenges because she is a woman in ophthalmology. She shared her insight, “Being a woman brings along challenges resulting from cultural concepts. For example: when I did my vitreoretinal fellowship at the Wilmer Institute, my husband had to quit his work and he, our three children and my mother-in-law moved to the United States for more than two years. The concept of a husband leaving his job for his wife’s career, while in my family it was acceptable, created challenges both social and economical.”
Prof. Loewenstein describes two people that had important roles in inspiring some of her key decisions, “My mother who taught me that whatever I do, I have to be the best in, and my husband who so clearly inspired me to see where the best chances were to make real changes are.”
“People may be surprised to learn just how much my husband thoughts and feelings and satisfaction are important for me,” she added. Sounds like a perfect team.
| June/July 2020 30 ENLIGHTENMENT WOMEN IN OPHTHALMOLOGY
Administration degree at the Tel Aviv University Business School.
Research is a fundamental part of Prof. Loewenstein’s work, with her main interests being in the investigation of drug administration and toxicity to the retina, early detection of macular degeneration and home monitoring of disease. “I enjoy novel technologies very much, providing the clinical support to start up and novel ideas,” she said.
She has been integral to the development of multiple innovative efforts, leading the efforts toward the development of novel technology for early detection of macular degeneration, automated technology for detection of retinal disease activity and augmented virtual reality to replace the operating microscope, as well as, development of home OCT.
Prof. Anat Loewenstein’s work appears in over 400 peer-reviewed journal articles and sharing her expertise by her contributions to multiple chapters in ophthalmology textbooks. She also serves as the Editor-in-Chief of the Journal Case Reports in Ophthalmology, is an associate editor of the European Journal of Ophthalmology and Ophthalmologica.
A global leader in retina
You can catch Prof. Loewenstein presenting at retina conferences around the world, frequently as an invited speaker, or serving her multiple roles in the most prominent retina societies. Her favorite part of attending these large, international conferences, “Mainly the peer discussion and to enjoy the friendship I have made with people, all with the same aims as myself, from all over the world.” She currently serves on the International committee of the Macula Society and is the General Secretary of the EURETINA. In Israel, she is the President of the Israeli Ophthalmological Society and Chair of the Ministry of Health’s ethics committee. In addition, she is a member of the National Council of Surgery and anesthesia.
Prof. Loewenstein’s work has been honored with numerous international awards, including the “Rosenthal” award, and the Patz medal of the Macula Society, as well as the

Michelson Award of the Macula Society, and the Silver Fellow Medal of ARVO.
Mentorship of young ophthalmologists and retina specialists is important to Prof. Loewenstein, as she is a leader in mentorship educational programs in partnership with ARVO, EURETINA and mentorship programs supported by the ophthalmic industry.
A proud (tireless) mom
One might be exhausted simply reading about all of these accomplishments, and extremely active clinical and research activities, but there is far more to Prof. Loewenstein. She is a proud mother to her three children, a physician, a data scientist and a financial business developer with Roche. It would seem that perhaps they also had a mother that inspired them to work hard and be the best at whatever they did. She also has three granddaughters.
Prof. Loewenstein is an avid reader and found it challenging to narrow down a favorite book. “Oh, I have many favorites! Just to name a few: A Tale for the Time Being by Ruth Ozeki, about two strong Japanese ladies in two different time periods, The Island of Sea Women by Lisa See about Jeju island in South Korea, where women of all ages support for their families by fishing, and The Professor and The Madman by Simon Winchester about the writing of the Oxford dictionary.
We may wonder where Prof. Loewenstein finds all her energy to
fit so much into her days, she shares her dedication to fitness and sport, spending two early morning hours each day doing sports or fitness activities such as running, swimming, yoga or strength training.

We asked if she could offer any words of wisdom for women just beginning their careers in ophthalmology, or perhaps those considering this career path. “I think that ophthalmology is the best profession, for men and women alike. Specifically for women I think ophthalmology is great because it is a profession which opens multiple doors from which you can chose one or more: you can go to academics, to being a leader, to pharmaceutical industry, to clinical work, to basic research, whichever is right for you at a specific time. I would tell women just beginning their careers that family work balance is essential. Harmony between these parts of our life is the only way to be able to free your mind to really enjoy and succeed in your professional life.”
Editor’s Note:
PIE magazine is grateful and honored to have Prof. Loewenstein as one of our contributors in this issue.
| June/July 2020 31
Prof. Loewenstein with her grandchildren (left) and husband (right).
due to Coronavirus Asian Markets Require Adaptability
by Andrew Sweeney
China is ground zero of the global coronavirus pandemic and as a recent spike in infections centered on Beijing demonstrates, the country is not out of the woods yet. Markets have responded to the pandemic and many multinational companies operating in Asia are adopting a pillarized approach. This is to split the region into two groups; Mainland China and the rest of East Asia.
This approach is required due to the pandemic more than government red tape. The virus is subsiding in most East Asian countries like Japan and South Korea, whereas the situation in China remains unpredictable. There are also different requirements for products in different countries, with glaucoma treatment being high in demand in mainland China, for example.
Franck Morand, the Vice President for Asia and the Pacific at Quantel Medical (Cournon-d’Auvergne, France), is optimistic about his company’s future in both the Chinese and the general East Asian market. One of the leading manufacturers of ophthalmological equipment in the world, Quantel Medical has remained buoyant during the coronavirus crisis. This is despite slowdowns in some global regions.
Dual approach for China and Asia
Mr. Morand makes the point that while business may have slowed down it has not stalled. There will always be a need for medical equipment and services. The only variance is demand in different countries and the financial capability of healthcare providers to be able to purchase medical products.
“Our business has not stalled as one might expect, like it has in Europe for instance. What I’m referring to is all
the public tenders which were going on and were postponed, for instance in Thailand, will be held later this year,” Mr. Morand said.
“This is good news, though I need to speak about China separately because China itself is a different market and an altogether different situation because coronavirus started from there. The rest of Southeast Asia has been slow in the first quarter, I won’t deny that,” explained Mr. Morand.

Mr. Morand is confident that despite market slowdowns normal business momentum will resume by the end of Q2, with the third and fourth quarters likely to see even more activity. The key will be successfully identifying which countries are more promising, and conversely, which are least promising. Mr. Morand points to Australia and New Zealand as offering more potential than other countries in his purview.
“China is definitely not going to catch up with the first two months of the year. The country is likely to be pretty hectic,” Mr. Moran said.
“Bangladesh is also in my area and it’s been hit pretty hard, so right now it’s quiet,” he added.
Promising outlook for Q3 and Q4
Mr. Morand also praised the response of the Taiwanese government to the coronavirus crisis as it moved rapidly to close the country and contain the virus’ spread. China’s ongoing crisis will make opportunity difficult to find but not impossible. Discussion is ongoing about conferences being held later this year in China, the issue will be adapting to increased localization as the Chinese market draws inward.
Echoing the sentiments of many working in ophthalmology Mr. Morand believes there is considerable room for optimism. This applies to both the industry in general and to his purview of China, Asia and the Pacific. The key will be embracing change and looking for new opportunities.
“I’m an optimistic person, I think now it’s really reasonable to say that we are looking at a much brighter future. This applies to this quarter [Q2] and especially in quarters three and four,” Mr. Morand said.
Editor’s Note:
This story is part of the ‘ Q&A from Quarantine ’ series of PIE Talks, where Matt Young (CEO of Media MICE and Publisher of PIE and CAKE magazines), during the time of COVID-19 lockdown, reached out to KOLs and industry friends to evaluate and discuss the impact of this pandemic to the ophthalmic world.
Contributor
Franck Morand is Quantel Medical’s Vice President for the Asia-Pacific region, and is based in Chiang Mai, Thailand. He manages a sales and marketing network of distributors, from the Subcontinent to Australasia and the Pacific Islands. He holds a master’s degree in English and Economics and Applied Languages, from Universite of Clermont-Ferrand, as well as International Business from the CEFRI Institute in Paris. He spent four years overseas after completing his initial studies, travelling around the world and teaching in New Zealand, which turned out to be a classic car paradise, and spent another two years teaching in Tunisia, North Africa, for his National Service. He is an avid classic cars enthusiast and a member of the Classic Cars of Lanna group which gathers old car fans in the Chiang Mai and Northern Thailand area. Mr. Morand speaks French, English, Spanish, and can get by in the Thai spoken language.
franckmgv8@gmail.com
| June/July 2020 32 ENLIGHTENMENT OPHTHALMIC BUSINESS

| June/July 2020 33
Q&A from Quarantine Highlights from the Low Point
by Brooke Herron
When our very own PIE magazine CEO and Publisher Matt Young came down with COVID-19, the pandemic really hit home. As countries around the world locked down, and Matt emerged healthy from quarantine, we knew that a shift was occurring — and hence, Q&A from Quarantine was born. This online video series (on www. piemagazine.org) features interviews with key opinion and thought leaders in ophthalmology, with discussions centering on COVID-19’s impact in ophthalmology.
Below, we share some highlights from Q&A from Quarantine…
Adrienne Graves, Ph.D., North Carolina, USA
Dr. Adrienne Graves is a corporate board member and visual scientist with experience in pharmaceutical and medical device sectors. She spoke with Matt shortly after his COVID-19 recovery from her home in the mountains of North Carolina (USA).

As a board member for numerous companies, Dr. Graves is uniquely positioned to take the pulse of the industry. As the coronavirus really began to spread worldwide earlier this year, she explained that things certainly had changed: clinical trials stopped and industry companies began to reassess their finances. She noted that most of the companies she works with are wellcapitalized, however some companies will likely have cash flow problems.
She lamented the loss of corneal transplants during COVID-19 as devastating, although she was encouraged by the uptick in telemedicine and believes there will be opportunities for new innovation once the pandemic abates.
Throughout the interview, she expressed her gratitude to the healthcare workers serving on the frontlines. And for leaders, Dr. Graves said listening to others is the most important thing you can do.
| June/July 2020 34 ENLIGHTENMENT COVID-19 SPECIAL REPORT
On patients and telemedicine: “Once the crisis is over, all those patients whose appointments were delayed will flock back, there will be a huge influx. According to one study in California, when offered the option, 80% of patients prefer telemedicine.”

On anti-VEGF injection regimens: “I think, over time, certain countries are moving toward the treat-and-extend approach, but as we come out of this pandemic episode, there will be even greater emphasis on that.”

On telemedicine: “What is it that you can do to help monitor their eye health from home? What devices can you make that would help? I think there are a lot of things in between taking a selfie and sending it to your doctor, to having something that can monitor your eye health in clever ways by using good data.”


On emerging from the pandemic: “Marketing and commercialization is going to be very different and I think everyone in the industry has to find a way forward, but education is going to be at the center of that,” said Mr. Dunlap. “I envision that there will be an explosion of educational forums . . . and video conferencing will play an enormous role.”

On reopening: “There are going to be a lot of prechecks. There is going to be a lot of remote testing as they are not going to have time to meet with the patient. Surgeries are going to be spaced out a little more because of the disinfection of the surgeries. So, the practices are going to be a lot different and you will see a different methodology.”
On safety: “What I want to really share is the problem of COVID-19 is not the eyes, it’s ophthalmology itself, because we’re very close to the patients during examination. So the main problem is not conjuntivitis — we can find the eye disease. But the problem is our safety and the safety of the patients that we are in contact with, because we are visiting mostly old people — so a high risk population.”
| June/July 2020 35
Dr. Igor Kozak, Moorfields Eye Hospital Centre, Abu Dhabi, UAE
Dr. Luis Diaz-Santana, Cambridge Consultants, United Kingdom
Mr. Jim Mazzo, Adviser and Consultant for Carl Zeiss Meditec
Dr. Rafiq Hasan, former Vice President and Global Head of Ophthalmology, Bayer, Switzerland
Mr. Thomas Dunlap, Ophthalmic Medical Device Consultant, California, USA
Dr. Mario Romano, Director of the Ophthalmology Department at Humanitas Gavazenn, Bergamo, Italy
Pediatric Retina

Why Early Screening and Diagnosis is Crucial
by Khor Hui-Min
Control of childhood blindness is a priority for the World Health Organization. Therefore, a panel of experts presented multidisciplinary approaches to curtail pediatric retinal disorders at the 13th Asia-Pacific Vitreoretina Society Congress (APVRS 2019), held last November in Shanghai, China.
Retinopathy of prematurity
Retinopathy of prematurity (ROP) occurs in premature babies when retinal blood vessels do not develop properly before birth. It’s one of the top causes of preventable childhood blindness in middle-income countries and occurs mostly in infants of low birth weight and low gestational age at birth.1
Studies show that a multidisciplinary approach with close collaboration among stakeholders (including

physicians, nurses, other caregivers, hospital administrators, and parents) could make a positive impact on ROP.2
“ROP screening should be an essential part of modern neonatal care, as more and more low birth weight and preterm babies are surviving,” said Professor Emeritus Rajvardhan Azad, M.D., chairman of the University Service Commission in Bihar, India, and president of the Indian ROP Society.
“The mean period to develop treatable ROP is variable across the world and Asia-Pacific region and screening guidelines vary from country to country,” said Professor Azad. “The majority of developed nations use a lower gestational age or birth weight cut-off, while developing nations recommend screening larger babies. The current international screening guidelines need to be modified to suit local scenarios.”
Familial exudative vitreoretinopathy
Another disease affecting infants is familial exudative vitreoretinopathy (FEVR), an inherited disorder of retinal blood vessel development that results in incomplete vascularization of the retina and poor vascular differentiation.
Regarding genetic heterogeneity, Dr. Peiquan Zhao from Xin Hua Hospital in Shanghai, China, said that the same phenotype can be caused by the mutations of different genes, such as ZNF408 and Wnt Pathway (NDP, FZD4, LRP5, TSPAN12). He added that recently, other suspected genes causing FEVR include KIF11, JAG1 and CTNNB1.
“LRP5 and FZD4 were found to be of the highest frequency and tend to cause asymmetric FEVR. NDP causes the
| June/July 2020 36
APVRS 2019 COVERAGE
CONFERENCE HIGHLIGHTS
most severe manifestations, usually in both eyes. FEVR caused by a TSPAN12 mutation is less severe and more consistent between contralateral eyes. Digenic mutations may cause more severe phenotypes and mutations in some genes (NDP, LRP5, KIF11, etc.) can cause special lesions,” said Dr. Zhao.
Ocular trauma
Ocular trauma is another cause of visual disability in children. And because childhood is the key stage of visual development, delayed treatment of ocular could result in permanent vision loss. In children, open globe injury occurs more frequently than closed globe injury. Anterior segment ocular trauma is also more common than posterior segment ocular trauma.
Accidents are a common cause of ocular trauma — mostly injury by sharp objects, such as pencils, scissors, sticks, iron wires, needles, injectors and branches. This is followed by injury caused by blunt objects (like balls, tools, bullets and catapults) and others, including: blast injuries (by fireworks, detonator or lighter); car crashes; chemical burns; and injury by animals.
“In the emergency management of ocular trauma, we have to first identify any potentially life-threatening problems and give prior treatment. For patients with open globe injury, we have to ensure adequate tetanus immunization. For eyes with chemical burns, we need to provide emergent copious irrigation. Do not squeeze the ruptured or perforated eyes. Do not cover the eye for a long time, which will result in amblyopia,” said Dr. Huan Yan from Tianjin Medical University General Hospital in Heping, China.
Pediatric endophthalmitis
In pediatric endophthalmitis, early detection is critical. Symptoms include decreased visual acuity, pain and photophobia — while the tell-tale signs are conjunctival congestion; purulent discharge; corneal edema/infiltration; endothelial deposits; hypopyon; fibrin in the anterior chamber; vitritis; retinitis; loss of fundal glow; lid edema;
restricted extraocular muscle (EOM); and proptosis.
“The signs are more important than the symptoms. Streptococcal species and Haemophilus influenza are two common organisms that cause endophthalmitis in children. Another cause is fungus. In adults, Staphylococcus epidermidis and Bacillus species are the most common pathogens that cause endophthalmitis,” said Professor Dipak Kumar Nag, M.D., from the National Institute of Ophthalmology and Hospital, Sher-E-Bangla Nagar, Dhaka, Bangladesh.
“Treatment should commence once the diagnosis of suspected endophthalmitis is made. Oral antibiotics and steroids can be prescribed. Topical antibiotics, steroids and mydriatics, as well as intravenous antibiotics, can also be used,” explained Professor Dr. Nag.
“In surgical treatment, intravitreal antibiotics (IVAB)/steroids/pars plana vitrectomy (PPV) can be used once there is access to a sterile environment and general aesthesia. PPV should be used if there is no response to IVAB in 24 hours,” he added.
Hereditary retinal disorders
Retinal dystrophies are hereditary diseases that alter the anatomy and/ or function of the retina, resulting in progressive and severe loss of vision. The first type are diffuse photoreceptor dystrophies, which include retinitis pigmentosa, Leber congenital amaurosis and cone dystrophies. The second type are macular dystrophies, including Stargardt disease, vitelliform dystrophy, familial drusen, pattern dystrophy and Sorsby macular dystrophy.
“Genotyping is the key to developing possible gene-based therapies. With many gene therapies in the pipeline, there is hope for patients. Recombinant adeno-associated virus (AAV) and lentivirus can be engineered specifically as a vector,” said Dr. S. Natarajan, president of All Ocular Trauma Societies.
Toxocariasis and toxoplasmosis in children
Toxocariasis is caused by Toxocara canis and less frequently, Toxocara catis, which are intestinal nematodes (roundworms) found in dogs and cats, respectively. Humans are incidental hosts, and the invasive larvae will migrate for months through different organs, until they are overcome by the human inflammatory reaction and die.
Ocular toxoplasmosis is the most common cause of eye inflammation in the world, and is an infection caused by the parasite called Toxoplasma gondii. Toxoplasmosis can be acquired or present at birth — this is known as congenital toxoplasmosis. The infection will cross the placenta from the newly infected mother to the baby.
“Ocular toxocariasis and toxoplasmosis are macular locations which result in severe vision loss in children; suspected in those with history of contact with pets. When other organs are affected, then systemic involvement workups are needed. Early diagnosis and treatment are crucial to restore macular sequelae,” concluded Dr. Atchara Amphonphruet, from Rajavithi Hospital and College of Medicine, Queen Sirikit National Institute of Child Health, Rangsit University, Bangkok, Thailand.
Editor’s Note:
The 13th Asia-Pacific Vitreo-retina Society Congress (APVRS 2019) was held in Shanghai, China, on November 22-24, 2019. Media
MICE Pte Ltd, PIE magazine’s parent company was the Official Media Partner at APVRS 2019. Reporting for this story also took place at APVRS 2019.
References:
1 Gilbert C. Retinopathy of prematurity: a global perspective of the epidemics, population of babies at risk and implications for control. Early Hum Dev. 2008;84(2):77-82.
2 Graham E Quinn. Retinopathy of prematurity blindness worldwide: phenotypes in the third epidemic. Eye Brain. 2016 (8): 31-36.
| June/July 2020 37
Ophthalmologists Discuss the “New Normal”
by Brooke Herron
consultations. This first step begins over the phone to determine that the patient does not have COVID-19 or symptoms of the virus before visiting the clinic.
It’s safe to say that the pandemic has resulted in one clear trend: Webinars are now more popular than ever before. Prior to social distancing and COVID-19, these technologies — although available — were not fully embraced by many in the business or medical community.
And not only are webinars popular now — in ophthalmology, they are crucial for continued education. In addition, these virtual meetings are also providing crucial COVID-19 information to surgeons — which is especially critical as ophthalmology clinics and hospitals slowly begin to reopen for elective procedures.
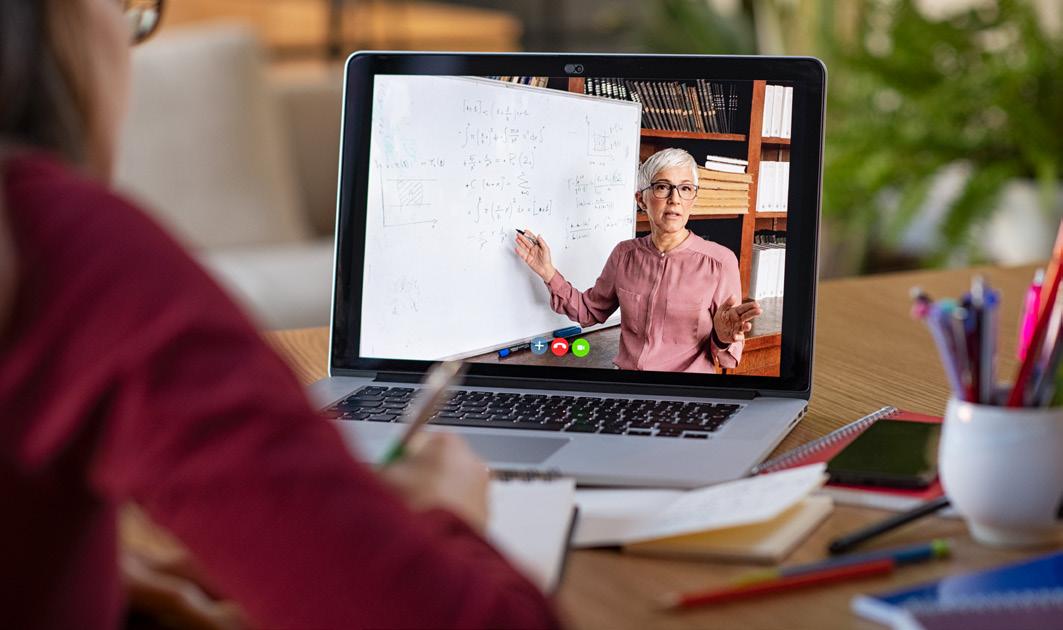
One such webinar was hosted by Arunodaya Deseret Eye Hospital
(ADEH), Gurugram, Haryana, India, and Team Arunodaya, including Drs. Arun Sethi, Reena Sethi, Vaibhav Sethi, Sahebaan Sethi and Aditya Sethi. Called “Surviving the Storm: An International Perspective on COVID-19 and the Future Of Ophthalmic Practice,” this webinar featured discussions on how the pandemic has impacted career direction and finances, along with insights into the “new normal.”
Reopening safely is the main priority
Dr. Barbara Parolini, an ophthalmologist in northern Italy, closed her private practice on March 2; it reopened in mid-April with new protocols for
“The second selection [for consultations] is on-site with a questionnaire, their temperature is measured and gloves and masks are offered,” she explained. Patient bookings have changed too: “I used to see three patients per hour, but now I am seeing two and they are never overlapping in the waiting room.”
In addition, after each patient, she said they disinfect everything, including door handles, chairs and instrumentation. “Still, we are not using puff or air tonometry, only single-use tonometers,” added Dr. Parolini.
Waiting for the new normal
“In my local area, the case fatality [from COVID-19] is somewhere around 10 percent,” said Dr. Cathleen McCabe, an ophthalmologist based in Sarasota, Florida, United States.Even so, the state is reopened for elective procedures back on May 4.
“In our facility, we are restricting
| June/July 2020 38 WEBINAR COVERAGE CONFERENCE HIGHLIGHTS
volume, so we can maintain social distancing and do all of the things that keep people safe,” she said. In addition, they are limiting surgeries for patients over age 75 and for those with serious comorbidities.
“The old days are gone,” she continued, adding that the “new normal” is not going to look like our previous normal. “My top concern is safety for the patients, staff and doctors . . . and we need to do that while maintaining some level of efficiency.” Dr. McCabe said that this will change the workflow, as well as local and international outreach.
“In the U.S., we don’t have rapid or accurate COVID-19 testing — it would be wonderful if we did — a lot of our phase 1 and 2 reopenings are around that, and it’s not practical because it’s not available, at least in my area,” she continued.
To stay safe, in addition to implementing social distancing measures, Dr. McCabe said they’ve invested in telemedicine. “Our practice, as a whole, just did its 1,000th telehealth call.”
She said that some doctors are embracing telemedicine more than others, and that there are some limits on what can be done virtually. “Certainly you can do a lot of the patient consultation and education,” she explained, adding that it’s also good for triaging the urgency of an in-person
visit, avoiding patient trips to crowded ERs, establishing and reinforcing relationships, and for follow-up visits. They are also looking at hybrid visits with telemedicine, home monitoring for IOP and home OCT, and drive-through testing.

Hit the share button
Along with ophthalmologists from around the world, PIE magazine CEO and Publisher Matt Young joined the panel for this timely webinar. During his presentation, Mr. Young explained his personal experience with COVID-19 and described how it’s changed the way we communicate in the industry.
One thing he’s noticed? That most ophthalmic media moved from very high production value to very low production value. Therefore, Mr. Young encouraged ophthalmologists to record their own personal videos and submit them to industry media.
“For the ophthalmologists who want to get their news out, start taking those selfie videos and recording your webinars and submitting them (if interesting) to ophthalmology media companies,” he shared.
“Ophthalmologists are out there on the front lines and things are happening to you, consider not only sharing the clinical aspect of what’s going on, but also the personal aspect.
“Engage your media partners around the world, whether it’s us or other companies, because we are adept at telling stories and getting those important stories out there,” he concluded.
Editor’s Note:
The “Surviving the Storm: An International Perspective on COVID-19 and the Future of Ophthalmic Practice” webinar occurred on May 2 from 5-7p.m. (IST). A version of this story was first published on piemagazine.org. PIE magazine parent company Media MICE was the Official Media Partner of the webinar
DOUBLE Lutein Blue™

Non toxic intraocular dye for ILM and ERM staining
(Pure benzyl-Brilliant Blue)
LUTEIN based intraocular dyes
| June/July 2020 39
INNOVATIVE
AN
RECENTLY DEVELOPED NEW BLUE DYE PATENTED PATENTED PBB ®
APTOS Launches Bi-Weekly Telemedicine Webinar
by Andrew Sweeney
Ophthalmology has a new webinar series to keep our intellectual whistles whetted. On Friday, June 12, the Asia Pacific TeleOphthalmology Society (APTOS) launched its first webinar seminar on telemedicine. Gathering a wide array of ophthalmologists from around the world the webinar was detailed and concise.
The APTOS seminar, Telemedicine and COVID-19, was only one hour long; however it managed to pack in oodles of information and shared experience of telemedicine in ophthalmology. The webinar was introduced by Dr. Alarcos Cieza, World Health Organization (WHO) coordinator for blindness and deafness prevention, disability and rehabilitation, who emphasized the importance of ensuring patients are able to access care again after the coronavirus crisis abates.
Primarily a lecture by Professor Tien-Yin Wong (medical director of the Singapore National Eye Centre) the webinar also included open discussion and contribution by attendee ophthalmologists. Prof. Wong is a
specialist in medical retina and has a research focus on diabetic retinopathy. He pointed to previous efforts to utilize telemedicine in this field as being prescient for the coronavirus crisis.
Ophthalmology needs to plan for a new normal
Prof. Wong believes that ophthalmological telemedicine must be governed by the ‘three improves’: improving availability of expertise, improving access to care, and improving the efficiency of health systems. The best testing grounds for the ‘three improves’ policy are very densely populated countries like Singapore.
Telemedicine might be that new normal.

3. Business impact - Increased operational costs and reduced revenue. These are both immediate (surgery cancellations) and long-term (repeated lockdowns).
• The Asia Pacific TeleOphthalmology Society has launched a new seminar on telemedicine in ophthalmology.
• The seminar will be held twice a month and is scheduled to bring together ophthalmologists from around the world.
• The first seminar focused on the importance of adapting to the new coronavirus normal and the growing importance of telemedicine.
Sharing screenshots of patients in clinics pre-coronavirus, during the lockdown and now, Prof. Wong drew the viewers’ attention to how clinics can plan to reopen in the last six months of this year. Clearly, due to social distancing guidelines the old rules cannot apply. The professor argues a new normal will need to be accepted in ophthalmology.
He lists the following key considerations in this new normal that apply to all ophthalmology businesses and practices;
1. Patient and staff safety - Concern about elderly patients with comorbidities and difficulty in screening asymptomatic cases.
2. Infrastructure - New safe distancing norms in clinics and infection control measures.
The parameters of this new normal mean that there will be fewer face to face visits and increased uptake of telemedicine. It will also cut time and touch points in clinics, and shift vision assessment and investigations towards the community. More staff will work from home, and tests and EMR will become increasingly digitized.
AI and VR represent major opportunity for ophthalmology
The webinar’s participants generally concurred that if telemedicine is to successfully enjoy widespread community uptake it requires an understanding of patient concern and technological innovation. Dr. Robert Chang of Stanford University pointed to the success of drive through testing
APTOS 2020 COVERAGE CONFERENCE HIGHLIGHTS
| June/July 2020 40
centers as an example. In his view, ophthalmology should be looking for a balanced approach towards telemedicine.
This approach needs to look for a sweet spot. Ideally, this spot should sit at the nexus of ease of access and comfort of use. Dr. Chang believes patients want telemedicine solutions that provide quick answers therefore at home testing should be a priority, for which he is studying the application of VR technology.
The importance of embracing technological innovations like VR and AI in conjunction with telemedicine was also emphasized. Pointing to the Chinese word for crisis (comprised of the words for danger and opportunity), Prof. Wong says there is huge potential in AI. Despite, in his own words decades of disappointment in this field, telemedicine is synergistic with AI.
INDUSTRY UPDATE
Coronavirus offers an opportunity to synchronize these technologies and create new, profitable models for patient care. Nearly 30% growth is expected in telemedicine in the U.S. alone over the next five years and according to Prof. Wong, AI will account for a significant share of this figure. Several of the webinar’s participants agreed, emphasizing new technology needs to be practical and profitable.
“It’s telemedicine, you have to make sure that someone is paying for it, nobody will do it for free, it’s so hard to maintain if it’s free,’’ said Dr. Ming He of the University of Melbourne. His comments sparked a response from Prof. Wong.
“People are always asking who’s going to pay for it and we need to think really carefully about this,” Prof. Wong said.
“People are willing to pay $30-40 for food delivery and for other online stuff. This is something all of us in ophthalmology should see as an inference as healthcare is now the foundation of the economy,” he added.
Editor’s Note:
Launched on June 12, 2020, the Asia Pacific Tele-Ophthalmology Society (APTOS) Webinar Series will be made a recurrent event on the second Friday of every month. Visit asiateleophth.org/webinars for more information. A version of this story was first published on piemagazine.org
SNEC & SERI Launch Heroes Fund to Strengthen Defense Against Future Epidemics
It’s clear that COVID-19 has had devastating consequences worldwide — industries across every sector have been impacted, including ophthalmology. Therefore, in an effort to deal with the ongoing crisis, and strengthen Singapore’s defense against future epidemics, the Singapore National Eye Centre (SNEC) and the Singapore Eye Research Institute (SERI) have launched the Heroes Fund. This campaign aims to raise $1 million by January 31, 2021.
The campaign is named for SNEC and SERI’s frontline medical workers; funds will support the Centre’s healthcare workforce by providing them with the latest training, tools, innovation and methods of care in ophthalmology. This includes redefining clinical care to meet the urgent needs of patients; driving cutting-edge research to keep COVID-19 at bay; and maximizing healthcare knowledge for a future-ready frontline workforce.
“We recognize the urgency to meet the
evolving needs of our patients, health care providers and research teams, especially during this period of enormous change and uncertainty,” said Adjunct Associate Professor Ho Ching Lin, Director of Philanthropy, SNEC. “While COVID-19 remains, there are many patients who are also suffering from eye diseases that may lead to vision loss. This is why it is critical that we focus on new ways to approach the crisis and with better preparedness. The funds will greatly enable us to improve on our clinical care processes and to develop cutting-edge research as we move forward.”
New models of care, like using technology to conduct tele-consultations for glaucoma patients, are already in place at SNEC. The Centre has also implemented a home monitoring service in an effort to decrease non-essential visits and proactively detect those who may experience severe visual symptoms and prevent blindness.
Funds raised will also help to develop e-learning programs to facilitate undisrupted
training and upgrading of skills — ensuring that these healthcare heroes can complete their training and acquire the skills needed to treat increasingly complex eye diseases, and thus giving patients a better quality of life.
Speaking on the Heroes Fund, Professor Wong Tien Yin, Medical Director at SNEC said: “We must continue to be forwardlooking and future ready. COVID-19 has presented us with an opportunity to innovate and better equip ourselves to face what is ahead of us. Therefore, it is imperative to continue to channel our efforts to upgrade our existing model of care, develop cost-effective treatments and create breakthroughs in the research for COVID-19.”
The Heroes Fund is part of the VisionSave campaign, a philanthropic drive spearheaded by SNEC and SERI. Corporate, personal, or anonymous donations can be made to the Heroes Fund by visiting the online campaign website at www.giving.sg/shf-snec-fund/ heroes-fund.
| June/July 2020 41


APVRS 2021 Taipei December 10 -12, 2021 nd The 62 Annual Meeting of TOS http://2021.apvrs.org/



| June/July 2020 43 6001 Beach Road, #19-06 Golden Mile Tower, Singapore 199589 Phone: +65 8186 7677 | U.S.: +1 302 261 5379 E-mail: enquiry@mediamice.com Web: www.mediamice.com www.piemagazine.org www.cakemagazine.org magazine posterior segment innovation enlightenment CONTENT MARKETING + ADVERTISING + MEDICAL WRITING












2 18 November 2022 | Issue #1 SHOW DAILY by DIGITAL MARKETING + ADVERTISING + VIDEO PRODUCTION + MEDICAL WRITING + EVENTS Request our 2023 Media Kit Now! Write enquiry@mediamice.com for a copy HQ Office: 6001 Beach Road, #09-09 Golden Mile Tower, Singapore 199589 Phone: +65 8186 7677 Satellite Office: 2 Nuoc Man 2 Street, Da Nang City, Vietnam 50506 Phone: +84 868 063 773 E-mail: enquiry@mediamice.com Web: www.mediamice.com
