MACOMB COUNTY MEDICAL SOCIETY October/November/December 2025
18 36
Editor Narendra D. Gohel, MD
Managing Editor
Heidi L. Leach
Graphic Designer
Lori Krygier
2025 MCMS OFFICERS & DELEGATES
President Narendra D. Gohel, MD
President-Elect
Lawrence F. Handler, MD
Treasurer & Secretary
Daniel M. Ryan, MD
Delegates
Terrence P. Brennan, MD
Narendra D. Gohel, MD
Lawrence F. Handler, MD
Jareer S. Hmoud, MD
Khaled M. Ismail, MD
Carolann Kinner, DO
Cheryl D. Lerchin, MD
Akash R. Sheth, MD
MSMS Region 2 Director
Daniel M. Ryan, MD
Executive Director
Heidi L. Leach
Toll Free 877-264-6592 | E-Mail HLeach@macombcms.org , macombcms@gmail.com Web www.macombcms.org
October/November/December | Vol. 33 | No. 4
Macomb Medicus Journal is published quarterly by the Macomb County Medical Society. Winter: Jan/Feb/ Mar, Spring: Apr/May/Jun, Summer: Jul/ Aug/Sep, Fall: Oct/Nov/Dec. Subscription to the Macomb Medicus is included in the society’s annual membership dues.
Statements and opinions expressed in articles published in the Macomb Medicus are those of the authors and not necessarily those of the Macomb County Medical Society. Advertisements do not represent approval or recommendation of the Macomb County Medical Society.
Address changes and all communications relative to articles and advertising in the Macomb Medicus should be addressed to: Editor, Macomb County Medical Society, P.O. Box 551, Lexington, Michigan 48450-0551 or email HLeach@macombcms.org.
All material for publication, including advertisements, must reach the Society office no later than the 10th (business) day of the month preceding the date of issue, e.g. December 10 for the Winter issue. Thank you. No portion of the Macomb Medicus may be used for publication elsewhere without permission from the publisher.
Ernest Amory Codman, MD and His End Result Idea
By: Narendra Devisinh Gohel, MD Editor and MCMS President
“The Idea is so simple as to seem childlike… We believe that the general acceptance of a system of hospital organization based on the truthful record of the answers to these questions means the beginning of True Clinical Science.”
— Ernest Amory Codman, Surgery, Gynecology & Obstetrics, January
Ernest Amory Codman, MD (1869–1940) was a visionary Boston surgeon whose ideas anticipated the modern quality improvement and patient safety movements by nearly a century. Although he made significant contributions in multiple areas— including anesthesiology, radiology, duodenal ulcer surgery, orthopedic oncology, and shoulder surgery—his greatest and most enduring legacy is his “End Result Idea.”
Codman’s concept was elegantly straightforward: hospitals should track every patient treated, follow them long enough to determine the outcome, identify errors or failures, learn from those failures, and use the findings to improve future care. While this may sound self-evident today, Codman’s call for transparency and accountability was considered radical—and threatening—in the early 20th century.
Codman was born into a prominent Boston Brahmin family, educated at The Fay School and St. Mark’s, and graduated from Harvard Medical School. After joining the surgical staff at Massachusetts General Hospital (MGH), he became an innovator in clinical practice and medical education. He introduced the first morbidity and mortality (M&M) conferences, collaborated with Harvey Cushing in advancing diagnostic radiology, and emphasized outcome measurement before it became mainstream.
When he proposed systematic tracking of surgeon performance, however, his hospital rejected the plan. In 1914, Codman lost his staff privileges at MGH, a defining moment that underscored the resistance to transparency and accountability in that era.
Undeterred, Codman established his own End Result Hospital, where he meticulously tracked patients on index cards—his original “End Result Cards.” Each card documented basic demographics, diagnosis, treatment, and one-year outcomes. Between 1911 and 1916, Codman publicly reported 123 errors among 337 patients treated at his hospital.
References
1914
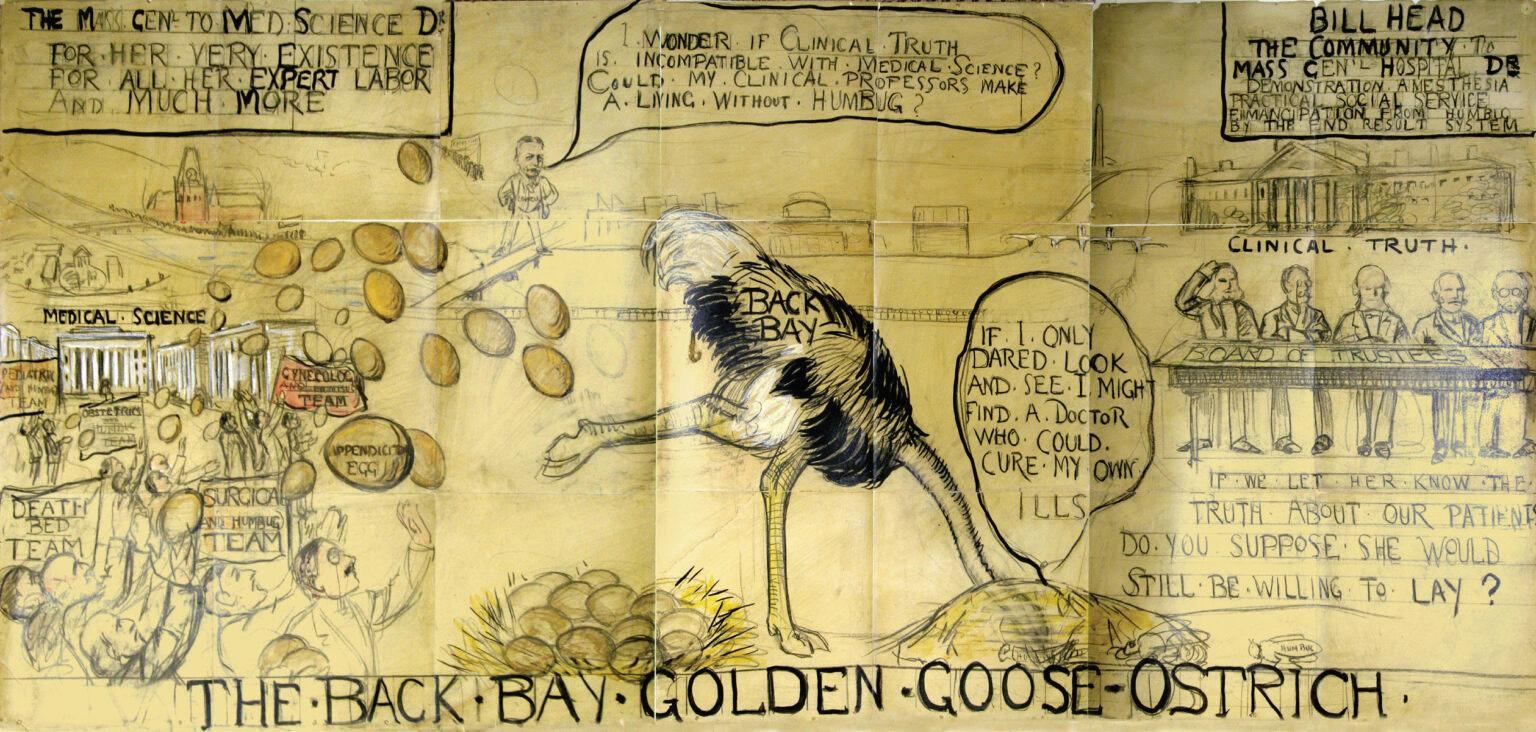
In a now-famous eight-foot cartoon titled 'The Back Bay Golden Goose–Ostrich', Codman depicted Boston’s wealthy elite as an ostrich with its head buried in a “hill of humbug,” while golden eggs flowed to physicians uninterested in clinical truth. The cartoon, rather than endearing him to the medical establishment, further alienated him, but it has since become a historic symbol of the early struggle for transparency in medicine.
Although Codman’s ideas were initially dismissed, they laid the foundation for modern quality assurance. His work inspired the American College of Surgeons’ Hospital Standardization Program in 1918, which eventually evolved into The Joint Commission (founded in 1951 as JCAH).
Codman’s later years were marked by hardship. Diagnosed with melanoma, he sold off personal assets to support himself and his work. He asked that his ashes be stored in a family mausoleum to avoid the cost of a burial plot. Decades after his death, the American College of Surgeons, The Joint Commission, and the American Shoulder and Elbow Surgeons honored his legacy with a bronze memorial at Mount Auburn Cemetery.
Codman’s legacy is now woven into the fabric of healthcare quality and safety: transparency, accountability, continuous improvement, and courage to speak truth to power. F
Codman EA. The Product of a Hospital: Its End Results. Boston Medical and Surgical Journal. 1913.
Codman EA. A Study in Hospital Efficiency. Privately Published, Boston, 1916.
Donabedian A. The Quality of Care: How Can It Be Assessed? JAMA. 1988;260(12):1743–1748. DOI: 10.1001/jama.260.12.1743. Berwick DM. Measuring and Improving Quality in Health Care NEJM. 1989;320:53–56. DOI: 10.1056/NEJM198901053200110.
Neuhauser D. Ernest Amory Codman MD. Qual Saf Health Care. 2002;11(1):104–105. DOI: 10.1136/qhc.11.1.104. Chun J. Background and History of Quality Measurement. PMCID: PMC3926916.
MACOMB COUNTY CHILDREN’S SPECIAL HEALTH CARE SERVICES (CSHCS)
The Macomb County Health Department’s CSHCS program serves more than 4,000 clients with over 2,700 qualifying diagnoses, from birth through age 26, with lifetime coverage for certain chronic conditions like cystic fibrosis, sickle cell disease, and hemophilia. The program improves health outcomes for children and youth with special health care needs through coordinated care, financial help, and family support.
CSHCS assists families with applications, medical bills, insurance coordination, transportation to appointments, and access to specialists. It is open to all income levels, with fees based on household size and income, and waived for Medicaid, MIChild, foster care, or court guardianship. CSHCS supplements primary insurance to cover eligible specialist care and related costs. In 2025, eligibility expanded to age 26, allowing more young adults to stay enrolled.
Families can connect with the Macomb County CSHCS Program by calling 586-466-6855 or the CSHCS Family Phone Line at 1-800-359-3722.
PARTNER SPOTLIGHT: URBAN SEED
Some ways you can get involved include:
• Visit Urban Seed’s volunteer section online to learn how to get involved
• Donate funds or give gently used gardening materials
• Share their story and impact with your community
Whether it's lending a hand in the garden, donating resources, or simply helping spread the word, there are many ways to support their mission.
Learn more about Urban Seed and how to get involved with their organization through volunteer opportunities, making a donation, or sharing their story with your community.
THE MACOMB COUNTY HEALTH DEPARTMENT’S COMMUNICABLE DISEASE SURVEILLANCE PROGRAM
The Communicable Disease Surveillance Program helps protect the community by quickly identifying and responding to communicable diseases and outbreaks. Timely reporting from healthcare providers, schools, and childcare centers is essential to prevent the spread of illnesses such as chickenpox, Hepatitis A, measles, and rabies.
For over a decade Urban Seed has been transforming vacant land into vibrant community gardens that fight food insecurity and bring neighbors together. Their Eastpointe garden has donated over 1,600 pounds of fresh produce last year alone. An impact that has then inspired their expansion into South Warren. Located at 13690 Toepfer Road, the South Warren Community Garden is planting the seeds of opportunity, equity, and connection among neighbors.
Through the Macomb County’s Health Department’s SNAPEd program, we supported this expansion by providing tools and materials like mulch, shovels, tomato cages, and more. This partnership is part of our work to expand access to fresh, healthy food while creating opportunities for residents to connect, learn, and give back.
When a healthcare provider in Macomb County identifies a patient with any of the reportable conditions, they are required to report the diagnosis to Macomb County Health Department to help monitor the health of the community and provide preventive actions as necessary.
The cooperation and prompt required reporting by physicians, laboratory scientists, infection preventionists, schools and other providers allows for timely action by local and state public health personnel. Some of the benefits of this teamwork include:
• Identification of outbreaks and epidemics
• Enabling preventive measures and/or education
• Successful targeting of prevention programs, identification of care needs, and efficient use of resources
• Evaluation of the success of long-term control efforts
For more information or to report a disease, contact the Communicable Disease Program at 586-783-8190 or email diseasecontrol@macombgov.org. F
Macomb County Health Department Reportable Diseases Summary
Diseases Reported in Macomb County Residents*
Cumulative total for previous years, year-to-date total for September 2025 b
**Shiga-toxin producing Escherichia coli per MDHHS; combo of E. coli & Shiga Toxin 1 or 2. ^ Previously reported as "AIDS" b 2025 total is tentative at this time.
The MCMS held its Annual Membership Meeting on October 14, 2025 at Ike’s Restaurant in Sterling Heights. It was a smaller group this year, but it was nice to see some new faces along with some of our longtime members.
Our guest speaker was Stacey Hettiger, Senior Director of the Michigan State Medical Society’s Advocacy and Payor Relations Department. She gave a fantastic presentation on how MSMS is working for members and with members. Some highlights of the program included: MSMS joining the federal lawsuit against MultiPlan and serval payors including Aetna, BCBS, Cigna and UnitedHealth for allegedly engaging in a price-fixing conspiracy to systematically underpay out of network healthcare providers; MSMS urging Cigna to rescind its new downcoding of certain higher level E/M codes that began Oct. 1; MSMS using a $ 50,000 grant to place billboards in Lansing to oppose HB 4399, that would allow Nurse Practitioners to practice without physician supervision; new legislation that MSMS hopes to have introduced soon to lower Michigan’s CME requirements from 150 hours (one of the highest in the nation) to roughly 75 hours.
Also during the meeting, members approved the proposed amendments to the MCMS Bylaws. F
• Firearm Safety
• Sustainable Growth Rate (SGR)
• Smoke-free Michigan
• Seat belt law
• Medical expansion
• Common drug formula for contracted Medicaid health plans
• Tort reform
• ACA provisions
• Scope of practice
• MIPS recognition of PGIP PCMH
• Primary care and OBGYN Medicaid uplifts
• Pre-diabetes prevention program
• Prior authorization reform
• Physician-Payer Quality Collaborative
• Rescinding EO2020-17
• Modifier 25
Multi Plan
• Processed out of network claims for commercial insurance companies
• Used pooled pricing data to fix prices and lower payments
• MultiPlan and the payors profited from underpaying for services
The Plaintiffs
• Seek compensation for underpayment
• Damages x3
• MSMS/AMA seek injunctive relief from anti-competive practices
Physician-led Care = Stronger Teams and Safer Patients No on HB 4399
2025-2026
Legislative Session
• Challenges and opportunities
• Examples of priority topics
- Scope of practice
- Reducing burdensome CME requirements
- Promoting physician-led, team based care
- Medicare and Medicaid reimbursement
The plaintiffs seek monetary damages and injunctive relief, arguing that the MultiPlan (recently rebranded as Claritev) cartel resulted in billions of dollars in underpayment to providers.
Recent Developments
In April 2025, the U.S. Department of Justice filed a statement of Interest supporting the plaintiffs' legal theory-reinforcing that coordination among competitors through third-party intermediaries, like Multiplan, can violate antitrust law. In June 2025, Judge Kennelly denied the defendant's' motion to dismiss, and the case is proceeding to discovery.
NP Scope
MSMS Key Victories
MSMS Legislative Advocacy
COVID -19 VACCINE UPDATE AND STANDING RECOMMENDATION FROM MICHIGAN’S CHIEF MEDICAL EXECUTIVE DOCTOR NATASHA BAGDASARIAN
In response to Gov. Gretchen Whitmer’s Executive Directive to state agencies to ensure Michigan families can access COVID-19 vaccines, the state’s Chief Medical Executive Dr. Natasha Bagdasarian has issued a Standing Recommendation for the COVID-19 vaccine. The Michigan Department of Health and Human Services (MDHHS) continues to recommend the COVID-19 vaccine in alignment with the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Obstetricians and Gynecologists. “National medical organizations and scientific experts continue to recommend routine COVID-19 vaccination for those at high risk, but also recommend vaccines be made available for all those who want them, ages six months and older,” said Bagdasarian. “COVID-19 vaccines have been proven to reduce the likelihood of emergency department or urgent care visits, as well as hospitalizations and severe outcomes. They are one of our best defenses against the virus. As the state’s chief medical executive, it is my duty to protect and promote public health, and everyone deserves the opportunity to access COVID-19 vaccine if they desire one. This Standing Recommendation will help to protect vaccine accessibility and availability in our state.”
On Wednesday, Aug. 27, the U.S. Food and Drug Administration (FDA) approved the 2025-2026 vaccine for those 65 years of age and older and those ages 5 through 64 years with at least one underlying condition that puts them at high risk for severe outcomes from COVID-19. However, the FDA did not define the list of underlying conditions. The Centers for Disease Control and Prevention’s list includes conditions such as obesity and physical inactivity and states it is “not exhaustive” and “should not be used to exclude people with underlying conditions from recommended measures for prevention or treatment of COVID-19.”
In her recommendation, Bagdasarian stated, “Any person over the age of six months without contraindication who has not received a dose of a FDA -approved or -authorized 2025-2026 COVID-19 vaccine may be considered to have an underlying condition that puts them at high risk for severe outcomes from COVID-19 and is thus eligible to receive an age-appropriate dose.”
MDHHS has several resources available that provide up to date information on vaccines and other health care topics. Visit the MDHHS Division of Immunization page for updates and
information on vaccines, statistics and access to the Michigan Care Improvement Registry(MCIR). Immunize.org offers education for healthcare providers and advocates to remove barriers for immunizations for all. On Infodemiology.com you’ll find live dashboards that track trending online health conversations, practical trainings, and the latest resources.
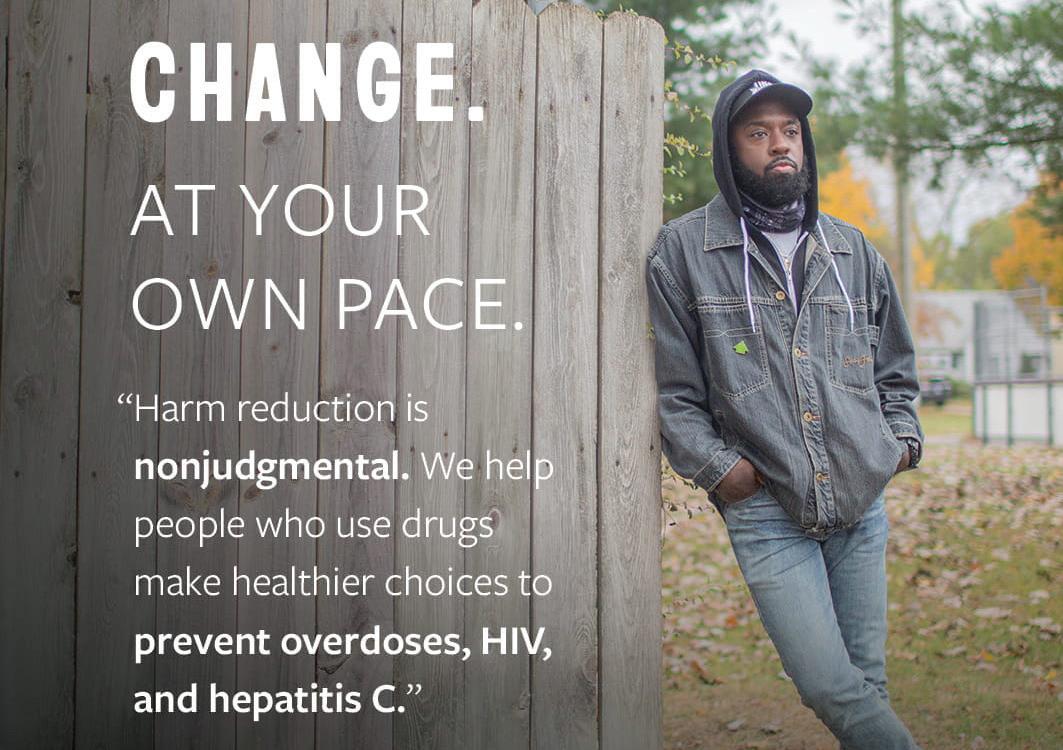
MDHHS STUDY FINDS HARM REDUCTION EFFORTS MAKE SIGNIFICANT IMPACTS ON OVERDOSE DEATHS, HOSPITALIZATIONS, CASES OF HEPATITIS C
Harm reduction programs have saved lives, reduced hospitalizations and emergency department (ED) visits and prevented hepatitis C (HCV) cases, according to a new modeling study by the MDHHS.
Harm reduction programs provide life-saving tools like naloxone, which can reverse the effects of opioids and prevent overdose deaths. These programs also help to stop the spread of HIV and HCV. Since 2018, MDHHS has been integral in developing Michigan’s robust harm reduction infrastructure, currently comprised of 37 harm reduction agencies (HRAs) with more than 100 locations.
“Harm reduction is a key component of our opioids response in Michigan, and it is working,” said Elizabeth Hertel, MDHHS director. “According to the most recent year of data, Michigan ranked in the top five states in the country for greatest reduction in overdose deaths.”
“Our modeling shows that the more we increased investments in harm reduction programming the more lives we saved, with more than 550 Michigan lives saved in 2024 alone with naloxone,” said Dr. Natasha Bagdasarian, chief medical executive. “These are not just statistics, they are our neighbors, our family members and our friends.”
Analysis of provisional data from earlier in 2025 indicates a 36% reduction in overdose deaths from 2,931 deaths in 2023 to a provisional 1,877 in 2024. A recent MDHHS modeling analysis has examined the impact of Michigan’s expansion in harm reduction efforts from 2017 to 2024 and estimated:
continued on page 8
• More than 1,650 deaths prevented due to increased access to naloxone.
- An increase from 135 deaths prevented in 2019 to 569 deaths prevented in 2024.
• More than 13,000 hospitalizations due to injection drug use prevented between 2018 and 2024.
- An increase from 323 hospitalizations prevented in 2018 to 2,800 hospitalizations prevented in 2024.
• Approximately 13,200 ED visits prevented between 2018 and 2023.
- An increase from 2,521 ED visits prevented in 2021 to 5,300 ED visits prevented in 2024.
• More than 4,000 HCV cases avoided through the impacts of Medicaid treatment initiatives like We Treat Hep C and the expansion of HRAs.
- An increase from 211 HCV cases averted in 2018 to more than 1,000 cases of HCV prevented in 2024.
The analysis was funded through the State of Michigan Opioid Healing and Recovery Fund, which is receiving payments from the nationwide settlement with the three largest pharmaceutical distributors, as well as opioid manufacturer, Johnson and Johnson. Michigan is slated to receive nearly $1.6 billion from the settlement by 2040 with half being distributed to the state’s fund and the other half being distributed directly to county, city and township governments. Over the last several years, MDHHS has been authorized by the Michigan Legislature to invest these funds in the state strategy addressing prevention, harm reduction, treatment and recovery.
Key harm reduction programs
The outcomes shown in the modeling analysis reflect the result of sustained, community-based work made possible through ongoing MDHHS investment in HRAs. These local agencies serve as trusted frontline partners, delivering crucial prevention and care services across the state – producing results that have reduced strain on EDs, prevented community outbreaks and saved lives from overdose.
• Overdose prevention: Through the launch of Michigan’s Naloxone Direct Portal, more than 1.3 million free naloxone kits have been distributed statewide and there have been nearly 34,000 reported uses to reverse overdoses and help save lives. In 2024, HRAs ordered more naloxone from the portal than any other agency type.
• Infectious disease testing and linkage to care: To reduce the risk of transmission and outbreaks, HRAs and syringe service programs have expanded access to infectious disease prevention. Today, more than 100 community-based sites – up from just 29 in 2019 – offer tools to prevent thez spread of HIV, HCV and other bloodborne infections. Fromz 2018 to 2024, HRAs provided more than 9,000 HIV and HCV tests and connected people living with these infections to social services, medical care and treatment.
• Substance use disorder (SUD) treatment and referrals: People who engage with HRAs are five times more likely to access SUD treatment and recovery services, and three times more likely to reduce or stop substance use. From 2018 to 2024, HRAs made more than 8,000 referrals to SUD treatment, supporting recovery for thousands of Michigan residents.
• Data-driven innovation and early warning tools: State funding has also supported early detection of emerging contaminants in the drug supply and the development of data tools that inform both local and statewide response strategies, ensuring a responsive, evidence-based approach to public health.
“Harm reduction agencies are making a measurable, life-saving impact across Michigan, and MDHHS remains deeply committed to supporting these agencies and the communities they serve,” said Bagdasarian.
To learn more about harm reduction and treatment programs, visit Find Help at Michigan.gov/SUD.
To find an HRA, visit Michigan.gov/SSP
More information about programming and resources can be found on the SUD Resources website.
MDHHS LAUNCHES MI OPTIONS CALL CENTER TO SUPPORT MEDICARE NEEDS, LONG-TERM CARE
Free service empowers Michigan residents to navigate health care supports MDHHS has launched a statewide MI Options system, offering free and comprehensive person-centered options counseling for adults looking for long-term care services and supports.
continued on page 9
Medicare counseling is also offered through the State Health Insurance Assistance Program and Medicare Improvements for Patients and Providers Act program for those navigating enrollment or reenrollment.
“MDHHS is excited to launch this statewide platform to increase the understanding and awareness of long-term care supports and services, including home and community-based options,” said Elizabeth Hertel, MDHHS director.
Michigan residents can call 800-803-7174, 8 am to 8 pm, Monday through Friday, to speak with an agent who can then schedule an appointment or provide a referral to a trained, certified counselor in their community. There is no cost to the individual or caregiver for this service. The new MI Options system supports older adults and people with disabilities, providing information to help individuals make informed decisions and exercise control over their long-term care needs by incorporating their personal goals and preferences.
Person-centered options counseling can help with:
• Exploring long-term care and support options for adults, including home and community-based services.
• Identifying next steps after a major life event to better understand what services and supports are available.
• Building actionable steps for pursuing options that align with an individual’s preferences and values.
Medicare counseling can help with:
• Medicare enrollment assistance.
• Medicare and Medicaid coordination.
• Discussions on cost savings, including low-income subsidies.
• Prescription drug coverage options.
• Billing questions.
• Benefits explanation.
The 2024 Home and Community Preferences Survey from the AARP indicates that at least 75% of Americans age 50+ would like to live in their current homes as long as possible. MI Options counseling can assist individuals in identifying the steps and resources needed to stay happily and safely in their homes and communities longer.
To reach a MI Options counselor or to find out more information about the MI Options program in Michigan, call 800-803-7174 or visit Michigan.gov/MDHHSMIOptions.
MDHHS, GETSETUP CELEBRATE FIVE YEARS OF DELIVERING INNOVATIVE AGING PROGRAMMING
Partnership provides virtual resources to older adults across Michigan
The MDHHS is proud to celebrate five years of partnership with GetSetUp, a community-driven service that transforms the lives of older Michigan residents through virtual resources. Having reached more than half a million residents so far with more than 1.5 million virtual class attendees, GetSetUp is helping residents stay healthy, connected and informed across all 83 Michigan counties.
Since 2020, this innovative collaboration has addressed some of the state’s most urgent aging challenges — including digital literacy, social isolation, economic security and equitable access to health resources — by leveraging the power of peer-to-peer virtual learning.
GetSetUp’s programming mirrors the goals of the Michigan State Plan on Aging by addressing topics that include:
• Affordable housing and aging in place – virtual classes on budgeting, mobility and health empower older adults to thrive safely at home.
• Health and well-being – mindfulness, fitness and disease prevention classes support healthier lifestyles.
• Caregiver support – sessions on dementia, stress management and community tools provide meaningful relief and guidance.
• Access to services and bridging the digital divide – tech tutorials and state program resources ensure older adults know how and where to get help.
• Social inclusion – with daily social sessions on topics ranging from coffee chats, creative groups and interest circles, participants are able to receive the positive benefits of community connection and regular social interactions.
The MDHHS-GetSetUp model is cost-effective and adaptable, reaching an audience of millions over the last two years alone. By reaching those in assisted living communities and rural homes, the platform has expanded partnerships with Area Agencies on Aging (AAA), the Michigan Veterans Affairs Agency and more across the state.
Looking ahead, MDHHS and GetSetUp will continue to expand the initiative, enhance culturally inclusive programming and offer new courses on artificial intelligence, entrepreneurship and fraud prevention.
GetSetUp classes are taught in English, Spanish, Hindi and Mandarin. Learn more at GetSetUp and follow the program on LinkedIn F
Reach your audience with a print and digital publication. Your digital ad will be hyperlinked to your website. Contact Heidi Leach at HLeach@macombcms.org for more information
The Split That Could Reshape Medicine in Michigan
MSMS Restructuring Sparks Debate on the Future of Physician Representation
Physician advocacy in Michigan is at a crossroads. The Michigan State Medical Society (MSMS) is evaluating structural changes that could lead to de-unification between the state organization and County Medical Societies. These potential shifts could dramatically reshape how physicians connect, collaborate, and advocate for their profession.
For decades, Michigan’s state and local medical societies have operated under a unified structure– physicians joining both their county and state societies through a single, connected membership model. This alignment ensures seamless advocacy from the exam room to the state legislature.
But in recent years, MSMS has faced challenges in funding, membership retention, and perceived value, prompting their leadership to re-examine this model. For the third time in recent memory, MSMS is evaluating a potential de-unification from County Medical Societies. The 2017, 2018 and 2019 House of Delegates (HOD) strongly opposed these attempts.
Resolutions adopted at the 2025 HOD directed MSMS leaders to explore structure and partnerships:
Resolution 16-25: Creates a task force of county and state leaders to examine history, finances, and bylaws, and recommend a unified path forward for medical societies in Michigan.
Resolution 47-25: Directs MSMS to study other state medical society structures and bylaws for potential improvements in efficiency and productivity.
MSMS leadership has utilized these directives to form a Reorganization Task Force to focus on major, structural and bylaws changes. This task force is comprised of six MSMS leaders and six County Medical Society Leaders (determined by and invited by MSMS leadership versus being chosen by the County Medical Societies to equally represent them) and a single County Medical Society executive director to serve as a non-voting advisor (also chosen by MSMS leadership).
This task force is only scheduled to meet for three, 90-minute sessions in order to review bylaws and consider restructuring the long-standing, MSMS-County Medical Society unified membership.
At this writing, MSMS leadership has only reached out to County Medical Society leadership once– a 90minute meeting set by MSMS in July where the agenda was largely focused on MSMS leaders presenting proposed Task Force recommendations prior to the Task Force being named or having met:
· Revisiting how county and state memberships are linked.
· Exploring alternative membership models.
· Restructuring bylaws to allow more flexibility in future decision-making.
County Medical Society leaders had to digest this information in real time and had to work within the time constraints to provide on-the-spot feedback.
County Medical Societies and the physicians they represent face uncertain but important decisions about the future of organized medicine in Michigan. These decisions must be made with equal state and County Medical Society input and must be communicated transparently with our unified membership to receive robust feedback prior to adoption. The question isn’t just about structure – it’s about ensuring physicians have a strong and coordinated voice.
Task Force Members
Brian Stork, MD– MSMS/Muskegon
Paul Bozyk, MD– MSMS/Oakland
Mark Komorowski, MD– MSMS/Bay
Eric Larson, MD– MSMS/Kent
Brad Uren, MD– MSMS/Washtenaw
John Waters, MD– MSMS/Genesee
Nick Fletcher, MD– Wayne/Resident
Gary Sarafa, MD– Oakland
Richard Schultz, MD– Grand Traverse
Salim Siddiqui, MD– Wayne/MSMS President 2023 -2024
David Whalen, MD– Kent
Claudia Zacharek, MD– Saginaw
Romy Shubitowski– Oakland County Medical Society Executive Director
What Happens Next & How to Stay Involved
Proposed Changes & Potential Pitfalls
With major structural changes to the future of physician representation in Michigan being considered in such a limited time frame, the County Medical Societies are still seeking clarity on several issues:
Structure: What models for membership and the statecounty relationship are being considered? Will there be a an effort to solicit robust, widespread member feedback to help shape final recommendations? Are innovative membership ideas being investigated or has de-unification already been recognized as the goal with task force activities focused on the ramifications and implementation?
Financial Impact: How could de-unification affect dues collection and County Medical Society budgets?
Representation: If de-unification goes forward, how will physicians joining only their County Medical Society have a voice at the state level? How will MSMS provide a local voice for their members who don’t join their County Medical Society?
Legal Concerns: Could shared services or reforms strengthen MSMS and County Medical Society structures instead of dismantling unified membership?
Implementation Process:
The MSMS Board approved just this July to move the 2026 HOD to a virtual platform vs. an in-person meeting, citing cost containment.
· Will there be one or two HOD readings to approve changes to the MSMS bylaws?
· Will the final recommendations be presented at the next regular HOD meeting or will the MSMS speaker and Board call special meetings of the House?
This time presents an opportunity for physicians across Michigan to weigh in on how they prefer to advocate for their patients and their profession. Whether unified or de-unified, the future of organized medicine in Michigan will depend on physicians making their voices heard now.
MSMS has stated that the task force will present its final recommendations in early 2026. Any structural changes, including de-unification, would ultimately be decided by HOD delegates through the amendment process. A proposed amendment is typically laid on the table until the next session, unless 75 percent of delegates present agree to waive the waiting period for an immediate vote.
Stay informed: Follow updates from County Medical Society and MSMS newsletters.
Engage in task force surveys: Direct input will shape the recommendations moving forward.
Attend forums and information sessions: Counties will host discussions for members to share feedback.
Contact your delegates: Submit written feedback to your County Medical Society to ensure your concerns and ideas are represented at the HOD.
Membership in one requires membership in the other Separate, distinct memberships for County Medical Society (CMS) and MSMS
Shared funding and administrative support
Sharing of programs and member services reduces duplicative staff time and cost for both MSMS and CMS
Strong, collective advocacy at the state and local levels
CMS bill their own dues separately from MSMS – CMS will have more autonomy to set their own rates but may face financial uncertainty if they are reliant on bundled dues
Opportunity for CMS to offer more tailored programs and member services
Potential for CMS to attract physicians who feel disconnected from state-level advocacy but reduced unified lobbying strength could lead to fragmentation of physician voice at either the state or local level or both
Key Milestones in Michigan’s Physician Advocacy Structure
Key Milestones in Michigan’s Physician Advocacy Structure
1819- Michigan Medical Society formed under Territorial laws. This original society limited itself largely to the execution of state laws regulating the practice of medicine.
1819- Michigan Medical Society formed under Territorial laws. This original society limited itself largely to the execution of state laws regulating the practice of medicine.
Licensed physicians in any county were granted the right to form a local, county medical society which, within the limits of the county, had the same rights as the territorial society:
Licensed physicians in any county were granted the right to form a local, county medical society which, within the limits of the county, had the same rights as the territorial society:
June 1827- Washtenaw County
June 1827- Washtenaw County
June 1831- Oakland County
June 1831- Oakland County
July 1835- St. Joseph County
July 1835- St. Joseph County
January 1836- Macomb County & Monroe County
January 1836- Macomb County & Monroe County
June 1837- Branch County
June 1837- Branch County
April 1849- Wayne County
April 1849- Wayne County
March 1853- March 1860- Peninsular Medical Society formed to advance medical science, promote the AMA code of ethics, publish the Peninsular Medical Journal, and help the University of Michigan medical department improve its scholastic program.
March 1853- March 1860- Peninsular Medical Society formed to advance medical science, promote the AMA code of ethics, publish the Peninsular Medical Journal, and help the University of Michigan medical department improve its scholastic program.
1866- Michigan State Medical Society formed.
1866- Michigan State Medical Society formed.
1889– Kent County Medical Society formed.
1889– Kent County Medical Society formed.
1902- MSMS reorganized along the lines of a delegate body.
1902- MSMS reorganized along the lines of a delegate body.
1969-1970– MSMS begins offering management services to specialty groups and, later, County Medical Societies.
1969-1970– MSMS begins offering management services to specialty groups and, later, County Medical Societies.
1974– MSMS begins to collect dues for county medical societies (optional at first but later became mandatory).
1974– MSMS begins to collect dues for county medical societies (optional at first but later became mandatory).
1994– The County Medical Society Executives group formed to address issues similarly affecting all county medical societies.
1994– The County Medical Society Executives group formed to address issues similarly affecting all county medical societies.
Over the years, MSMS convened a series of task forces to examine membership structure and governance:
Over the years, MSMS convened a series of task forces to examine membership structure and governance:
1981– Taskforce on MSMS Structure
1981– Taskforce on MSMS Structure
1997– Governance Task Force
1997– Governance Task Force
2002– Task Force on Regionalization of County Medical Societies
2002– Task Force on Regionalization of County Medical Societies
2003– Task Force on Regionalization of County Medical Societies in West Michigan
2003– Task Force on Regionalization of County Medical Societies in West Michigan
2006– Task Force on Federation Issues
2006– Task Force on Federation Issues
2011: Governance Task Force
2011: Governance Task Force
2015– MSMS ceases association management services to specialty and county medical societies.
2015– MSMS ceases association management services to specialty and county medical societies.
2017-2019– MSMS works with consulting groups to study membership structure and governance. Delegates at the in-person 2017, 2018 and 2019 House of Delegates meetings strongly oppose de-unification.
2017-2019– MSMS works with consulting groups to study membership structure and governance. Delegates at the in-person 2017, 2018 and 2019 House of Delegates meetings strongly oppose de-unification.
2019– Changes to MSMS Board of Directors governance approved
2019– Changes to MSMS Board of Directors governance approved.
2025- Task Force on Membership and Sustainability created to explore future options for membership and governance structures.
2025- Task Force on Membership and Sustainability created to explore future options for membership and governance structures.
2025– MSMS Board of Directors vote to make 2026 House of Delegates Virtual.
2025– MSMS Board of Directors vote to make 2026 House of Delegates Virtual.
Your Voice, Your Future
This is your chance to voice your preference in how MSMS and the County Medical Societies continue to advocate for patients and the profession. Whether unified or de-unified, the future of organized medicine in Michigan will depend on physicians making their voices heard now.
This is your chance to voice your preference in how MSMS and the County Medical Societies continue to advocate for patients unified, the future of organized medicine in Michigan will depend on physicians or
Please contact the MCMS office at HLeach@macombcms.org or 810-712-2546 to share your suggestions and concerns.
The MCMS would like to wish the following members a very Happy Birthday!
October
Howard Adelson, DO
Roberto Barretto, MD
Kenneth Cervone, MD
Randall Colvin, MD
Victor Corondan, MD
Jay Eastman, MD
Robert Fishman, MD
Steven Fite, MD
Amit Garg, MD
James Giliberto, DO
John Habicht, MD
Bijaya Hans, MD
Timothy Horrigan, MD
Syed Husain, MD
Khaled Ismail, MD
Steven Kotsonis, DO
Jeanette Marchand-Mateyak, MD
Robert Mendelson, MD
Mark Mishack, MD
Gerald Mullan, MD
Adam Rubin, MD
Milton Simmons, MD
Graciano Singson, MD
Cheryl Sobocinski, MD
Anil Thomas, MD
Kenneth Tucker, MD
Isaac Turner, MD
November
Wassim Bazzi, MD
Yousef Bishai, MD
Jeffrey Budzyn, MD
Amy Cardellio, DO
David Coviak, DDS, MD
Eddie El-Yussif, DO
Allison Engel, MD
Michael Fozo, MD
Gunateet Goswami, MD
Miguel Herrera-Martinez, MD
Mouhammed Joumaa, MD
Joseph Kaiser, DO
Stacey Ker, DO
Akhila Lattupally, MD
Christopher Lee, MD
Candice Mansoor, MD
November 4 ~ Vaccine Update from MDHHS Chief Medical Executive Natasha Bagdasarian, MD
MI's Public Health Webinar Series, 12 pm – 12:45 pm, .75 AMA/PRA Category 1 CME Credit. Cost: FREE for Active members, office staff & Residents; $25 for non-members & Emeritus/Retired/Life members.
November 7 ~ A Day of Board of Medicine Renewal Requirements
MSMS In-Person Meeting, 8:30 am – 4:45 pm, the Double Tree by Hilton in Ann Arbor. This conference fulfills: 3-hrs Pain Management, 1-hr. Controlled Substances, 3-hrs DEA MATE Act, 1-hr Medical Ethics, 3-hrs Implicit Bias. 7 AMA/PRA Category 1 CME Credits. Cost: FREE for Active, Active Emeritus, & Resident members; $180 Retired/Emeritus/Life members; $350 for non-members.
November 8 ~ MSMS 29th Annual Conference on Bioethics –Cases that Haunt Us
Hybrid (In-Person and Virtual) Event, 8:30 am – 3:30 pm, at the Double Tree by Hilton in Ann Arbor. 5.5 AMA/PRA Category 1 CME Credits. Cost: FREE for Active, Active Emeritus, & Resident members; $50 for Emeritus/Retired/Life members; $100 for non-members.
November 12 ~ How to Think Logically and Communicate Clearly in Medicine
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75 AMA/PRA Category 1 CME Credit. Cost: FREE for Active, Active Emeritus, & Resident members; $25 for non-members & Emeritus/Retired/Life members.
November 12 ~ HIPAA Update
MSMS Practice Managements Series, Live Webinar, 1 pm – 2 pm, 1 AMA/PRA Category 1 CME Credit. Cost: FREE for Active, Active Emeritus, & Resident members; $25 for non-members & Emeritus/Retired/Life members.
November 17 ~ Tri-County Legislative Meeting
Virtual meeting, 7 pm. Engage directly with legislators from Macomb, Oakland & Wayne Counties in meaningful dialogue and help guide the future of healthcare policy in Michigan. To register email Heidi Leach
Shiva Maralani, MD
Gregory Oldford, MD
Thomas O'Neil, DO
Heather Orkwis, DO
Malati Patel, MD
Sundeep Patel, MD
Susan Radtke, MD
Chada Reddy, MD
Jerome Seid, MD
Brian Seifman, MD
Jack Shartsis, MD
Gail Soo Hoo-Williams, MD
Sevak Valijan, MD
Kenneth Weinberger, MD
Stanley Wolfe, MD
December
Kootaybah Al Sheikhly, MD
David Altman, MD
Lenise Banse, MD
James Bookout, MD
Terrence Brennan, MD
Bruce Carl, MD
Matthew Edwards, DO
Jessica Ezell, DO
Sheldon Gonte, MD
Eileen Hopman, MD
A. Joseph Hoski, MD
Syed Husain, MD
Ghaith Ibrahim, MD
Ajith Kadakol, MD
Christina Leo, DO
Nada Macaron, MD
Daniel Macek, MD
Daniel Malach, MD
Vittorio Morreale, MD
Rajika Munasinghe, MD
Andrew Ogawa, MD
Alan Parent, MD
Benedict Pellerito, MD
S. Bhimsen Rao, MD
Mouhamad Rihawi, MD
Adam Rourke, DO
Paul Sweda, MD
Ethel Villanueva, MD
David Weingarden, MD
November 19 ~ Addressing the “Why” Behind Health: SDOH Screening in Action
GMP Network webinar open to physicians, nurses, pharmacists, care managers and practice staff. Cost $20 per participant. For your convenience the webinar will be offered at two times 12 pm – 1 pm and 6 pm – 7 pm.
December 8 ~ Reimagining Healthcare: A Workshop on Racism, Empathy & Transformation
MSMS Monday Night Medicine, Live Webinar, 5:30 pm – 8 pm, 3 AMA/ PRA Category 1 CME Credit. Meets LARA’s 3-hr. Implicit Bias requirement. Cost: FREE for Active, Active Emeritus, & Resident members; $140 for Emeritus/Retired/Life members; $190 for non-members.
December 10 ~ Tired of Being Tired? CPAP Alternatives for the PAP-Intolerant OSA Patient
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75 AMA/PRA Category 1 CME Credit. Cost: FREE for Active, Active Emeritus, & Resident members; $25 for non-members & Emeritus/Retired/Life members.
December 10 ~ CPT Updates for 2026
MSMS Practice Managements Series, Live Webinar, 1 pm – 2 pm, 1 AMA/PRA Category 1 CME Credit. Cost: FREE for Active, Active Emeritus, & Resident members; $25 for non-members & Emeritus/ Retired/Life members.
December 17 ~ From Reactive to Proactive: Elevating Chronic Disease Management
GMP Network webinar open to physicians, nurses, pharmacists, care managers and practice staff. Cost $20 per participant. For your convenience the webinar will be offered at two times 12 pm – 1 pm and 6 pm – 7 pm.
January 20 ~ MSMS History of Medicine Series – Dr. Alexander Loudin Turner, Detroit’s First Black Surgeon FREE Live Webinar, 7 pm – 8 pm.
We would like to welcome the following New Members!
Eugene J. Agnone, MD
Medical Oncology – Board Certified, Internal Medicine –Board Certified
Medical School: Wayne State University School of Medicine, 1975. Post Graduate Education: St. John Hospital, completed in 1980. Hospital Affiliations: Corewell Beaumont Grosse Pointe, Henry Ford St. John, Henry Ford Warren. Currently practicing at The Cancer & Hematology Centers – MI Cancer Specialists, 18223 E. 10 Mile Rd., Ste. 100, Roseville, MI 48066, ph. 586-778-5880, fx. 586-778-4362, www.thechc.com.
Daniel W. Cole, MD
Dermatology – Board Certified, Dermatopathology
Medical School: Wayne State University School of Medicine, 2020. Post Graduate Education: Trinity Health Ann Arbor, completed in 2021; University of Michigan, completed in 2025. Currently practicing at Hamzavi Dermatology, 43151 Dalcoma Dr., Ste. 1, Clinton Twp., MI 48038, ph. 586-286-8720, www.hamzaviderm.com.
Jessica Ezell, DO
Pediatrics – 1st year of practice
Medical School: Lincoln Memorial University Debusk College of Osteopathic Medicine, 2022. Post Graduate Education: DMC - Children’s Hospital of MI, completed in 2025. Currently practicing at Shelby Pediatric Associates, 15125 22 Mile Rd., Shelby Twp., MI 48315, ph. 586-532-0599, www.shelbypediatricassociates.com.
Vera Maranci, MD
Hematology – Board Certified, Medical Oncology –Board Certified, Internal Medicine – Board Certified Medical School: Wayne State University School of Medicine, 2004. Post Graduate Education: Detroit Medical Center, completed in 2007; University of MI Health System, completed in 2010. Hospital Affiliations: Corewell Beaumont Grosse Pointe, Henry Ford Macomb, Henry Ford St. John, Henry Ford Warren. Currently practicing at The Cancer & Hematology Centers – MI Cancer Specialists, 18223 E. 10 Mile Rd., Ste. 100, Roseville, MI 48066, ph. 586-778-5880, fx. 586-778-4362, www.thechc.com.
Lokesh Nagori, MD
Hematology – Board Certified, Medical Oncology –Board Certified, Internal Medicine – Board Certified Medical School: Ravindra Nath Tagore Medical College (India), 1999. Post Graduate Education: University of Texas Health Science Center at San Antonio, completed 2001-2007. Hospital Affiliations: Corewell Beaumont Grosse Pointe. Currently practicing at The Cancer & Hematology Centers – MI Cancer Specialists, 18223 E. 10 Mile Rd., Ste. 100, Roseville, MI 48066, ph. 586-778-5880, fx. 586-778-4362, www.thechc.com.
Adli Yakan, MD
Hematology – Board Certified, Medical Oncology –Board Certified, Internal Medicine – Board Certified Medical School: University of Aleppo Faculty of Medicine (Syria), 1997. Post Graduate Education: Ascension Providence Hospital, completed 2001-2007. Hospital Affiliations: Corewell Beaumont Grosse Pointe, Henry Ford Macomb, Henry Ford St. John, Henry Ford Warren. Currently practicing at The Cancer & Hematology Centers – MI Cancer Specialists, 18223 E. 10 Mile Rd., Ste. 100, Roseville, MI 48066, ph. 586-778-5880, fx. 586-778-4362, www.thechc.com
Jenny Yang, DO
Pediatrics – 1st year of practice
Medical School: Kansas City University College of Osteopathic Medicine, 2022. Post Graduate Education: DMC - Children’s Hospital of MI, completed in 2025. Currently practicing at Shelby Pediatric Associates, 15125 22 Mile Rd., Shelby Twp., MI 48315, ph. 586-532-0599, www.shelbypediatricassociates.com F
Please contact Heidi Leach at HLeach@macombcms.org
Tri-County Legislative Committee
Lawmakers want and need to hear from professionals in the field of medicine! The Tri-County Legislative Committee meets quarterly with legislators from Macomb, Oakland, and Wayne Counties. These meetings provide an open forum for physicians to engage directly with legislators who are often seeking physician input and education on healthcare related legislation.
continued on page 12
Upcoming Meeting
Monday, November 17 – Virtual, 7 pm
Anyone interested in joining the Committee please contact Heidi Leach at HLeach@macombcms.org.
Macomb County Medical Society Foundation ’s 2025 Holiday Sharing Card Project
Dear Macomb County Medical Society Members,
For this year’s Holiday Sharing Card Project we are giving you the option of contributing to either or both of the following local charities. With all of the recent cuts to safety net programs the need in Macomb County has never been greater and we hope that you will help those that are less fortunate in our community. The Macomb County Medical Society Foundation is a 501(c)(3) non-profit charitable organization, as it pays for all costs associated with this project; your donation is 100% tax deductible The Macomb County Medical Society FDN’s Tax ID number is 38-3180176.
Macomb Food Program serves people in need of food through its 50 pantry distribution sites and its “Fresh to You” Mobile Pantry Last year the Macomb Food Program served 148,388 households, a 15% increase from the previous year, (a 40% increase since 2021) and the need continues to grow. Every dollar donated stays in Macomb County and is used to feed hungry families, children, veterans, the elderly, and the disabled throughout the County.
Turning Point Shelter
is Macomb County’s only comprehensive agency supporting survivors of domestic violence, sexual assault, and human trafficking. They provide a 24-hour crisis hotline, emergency shelter, Forensic Nurse Examiner Program, legal advocacy, prevention education, support groups and counseling services that help thousands of women and their children.
We will be sending holiday cards to all Macomb County Medical Society members with a list of this year’s Holiday Sharing Card donors inside . If you would like to have your name included as a donor, please complete the form below and return it along with your check to the Macomb County Medical Society office no later than December 5, 2025.
If you have any questions, please contact the MCMS office at HLeach@macombcms.org or call 810-712-2546
Form and payment must be returned by December 5th
Name(s) to appear on holiday card
The Macomb County Medical Society FDN is a 501(c)(3) non-profit charitable organization sponsored by the Macomb County Medical Society. As the Foundation pays for all costs associated with this project, your donation is 100% tax deductible Macomb County Medical Society FDN Tax ID # 38-3180176. $ Contribution to Food Program
Contribution to Turning Point
Please make check payable to: Macomb County Medical S ociety FDN Return to: Macomb County Medical Society FDN, PO Box 551, Lexington, MI 48450-0551
Henry Ford Macomb Hospital
HENRY FORD HEALTH LEADING THE WAY IN SAFER APPROACH TO HEART PROCEDURES
Henry Ford Health is outpacing a national trend toward a safer, less invasive approach for opening blocked heart arteries, giving patients a more comfortable experience.
More than 75% of the health system’s percutaneous coronary interventions (PCI) are performed using radial access — threading a catheter through the wrist instead of the groin — compared to a national average of 57.5% in 2022, according to research published in the European Heart Journal
FACT-CHECK: DEBUNKING THE TOP MYTHS AROUND VIRAL “VACCINE STUDY”
Henry Ford Health condemns the spread of dangerous disinformation connected to a “documentary” that falsely claims our nationally recognized academic medical center and research institute suppressed a draft of a research study because of its results.
The purposeful twisting of information in the “documentary” poses a direct public threat. We implore anyone who comes across these myths to read the facts below.
Myth #1: “The study proves vaccinated children are 2.5x more likely to develop chronic health conditions than unvaccinated children.”
FACT: This draft did not prove anything. The very first internal review revealed serious flaws in the data and methodology, and the paper was abandoned. Anyone who conducts public health research would agree that comparing vastly different sample sizes over different time periods with inconsistent demographic foundations is problematic.
Myth #2: “The study wasn’t published due to political reasons – or because of its results.”
The study, which analyzed more than 6.6 million PCIs performed in the United States between 2013 and 2022, found radial access cases rose sharply from 20.3% in 2013 to 57.5% in 2022, overtaking the traditional femoral approach, which enters through the groin.
“As the study shows, we believe that patients do better with this approach,” said Dr. Herb Aronow, an interventional cardiologist and Medical Director of Heart and Vascular Services at Henry Ford Health. “Well designed studies have convincingly demonstrated that bleeding complications occur less frequently with a radial than a femoral approach, and among patients who are in the throes of a heart attack, the radial approach is also associated with better survival.”
Radial access often means patients can sit up and move sooner after the procedure, have less discomfort, and face a lower risk of bleeding. The radial access approach has long been the standard in many other countries, but U.S. hospitals have been slower to adopt it.
Henry Ford Health’s high adoption rate reflects a commitment to investment in training, technology, and process improvement in its cardiac catheterization labs.
The analysis showed that radial access was linked to:
• Fewer other major vascular complications (– 0.21%)
The study did note a slightly higher risk of ischemic stroke (+ 0.05%), but the overall benefits were clear.
FACT: The draft wasn’t submitted for publication or shared with the public because the data and analyses were flawed, and it’s irresponsible to share scientifically flawed studies with the public.
Myth #3: “The study was hidden from the public.”
FACT: Reputable academic medical research institutions like Henry Ford Health subject research papers to stringent, internal, and scientific scrutiny that often points out issues with data, methodology or other flaws. It’s rare that a paper makes it to the scientific journal submission phase, and even rarer that papers get published. This wasn’t hidden; it was simply rejected for scientific lapses.
Myth #4: “This is the ‘most important vaccine study ever.’”
FACT: Dr. Jake Scott, an infectious disease physician from Stanford who testified on Capitol Hill, wrote “…this flawed analysis reveals how thoroughly political theater has replaced scientific literacy in our public discourse.” The first internal reviewers determined the paper wasn’t scientifically sound— and it never made it past draft status.
Myth #5: “The ‘documentary’ proves the health system is withholding the study.”
FACT: The film proved nothing except that we have rigorous scientific standards in place for a reason: to ensure the only studies we submit for publication come from research rooted in sound, infallible data that have passed our stringent review processes. We do not bend to pressure from those with special interests and will never compromise the standards that have helped make us a world-renowned academic medical research institution. Read more on our perspective in this Detroit Free Press article. F
McLaren Macomb Hospital
MCLAREN
MACOMB EXPANDS BREAST CARE CAPABILITIES WITH ADDITION OF ADVANCED TECHNOLOGY
McLaren Macomb, part of statewide Karmanos Cancer Institute and a regional leader in cancer care and screening procedures, has enhanced its capabilities to assess patients’ risk for developing breast and other common cancers with the addition of Volpara® Risk Pathways.
An industry-leading software program, Volpara determines patients’ individual and unique risk for cancers and manages their care to ensure they receive the appropriate level of timely care.
Volpara will be available to patients through the McLaren Macomb Breast Centers at its four locations throughout Macomb County.
“The importance of early cancer detection cannot be overstated,” said Pat Keigher, McLaren Macomb Regional Director of Cancer Services. “It is not only about finding this disease early, but it’s also about giving the patient a fighting chance for hope, and makes recovery a true possibility. Adding Volpara gives our patients and providers greater ability to identify patients most at-risk for breast cancer and connecting them with the level of care their condition needs.”
Patients serve a crucial role in their risk assessment by providing details about personal and family history. Volpara uses an easyto-access digital health questionnaire for patients to complete in their homes at their convenience. Using the information provided, clinical teams can identify high-risk patients with the application of risk models and clinical guidelines, and those patients can be directed to follow-up care, such as mammograms, ultrasounds, and breast MRIs.
During their lifetime, one in eight women will be diagnosed with breast cancer, making it critical for women to receive not only regular mammography screenings but also to discuss their personal risk for developing breast cancer with their provider, who may recommend additional screenings or care.
Volpara also facilitates convenient integration with leading genetic labs. If the need for genetic testing or other follow-up care has been determined, the software allows providers to track patients’ progress, update their risk profiles, and generate additional communications, including educational and medical necessity materials.
Learn more about the cancer care capabilities at the Karmanos Cancer Institute at McLaren Macomb at www.mclaren.org/ macombcancer
MCLAREN STROKE NETWORK AGAIN EARNS NATIONAL RECOGNITIONS FOR PROFICIENCY OF CARE
The McLaren Stroke Network, which provides timely and potentially lifesaving care in the midst of the medical emergency, has again earned national honors for the exceptional level of care provided at its network hospital sites.
The American Heart Associated/American Stroke Association recognized several McLaren hospitals with its Get With Guidelines® – Stroke distinctions, a sign that those hospital-based stroke programs consistently adhere to the latest care guidelines while achieving improved patient outcomes.
Get With The Guidelines from the AHA/ASA help ensure patient care is aligned with the latest research- and evidence-based guidelines. Get With The Guidelines - Stroke is an in-hospital program for improving stroke care by promoting consistent adherence to these guidelines, which can minimize the longterm effects of a stroke and even prevent death.
Target: Stroke are additional honors earned for program’s proficiency in aspects of care associated with the treatment of stroke. Each year, program participants qualify for the award by demonstrating how their organization has committed to providing quality care for stroke patients. In addition to following treatment guidelines, Get With The Guidelines participants also educate patients to help them manage their health and recovery at home.
“Beginning with the development of the McLaren Stroke Network in 2015, we have worked hard to establish a fantastic team throughout the state who share a dedication to be the frontline of stroke care and provide patients with advanced stroke care right when they need it,” said Dr. Aniel Majjhoo, interventional neurologist and medical director of the McLaren Stroke Network. “These recognitions validate their effort in the service they provide, truly making them assets to their communities.”
McLaren Macomb
Get With Guidelines® – Stroke SILVER PLUS
Target: Stroke Honor Roll Elite Plus
Target: Type 2 Diabetes Honor Roll
Advanced Therapy
Strokes are the fifth leading cause of death in the United States— globally, it is the second leading cause of death—and the leading cause of adult disability. There are approximately 800,000 strokes annually in the US, with more than 600,000 of those being firsttime strokes.
To view the locations and learn the capabilities of the McLaren Stroke Network, visit www.mclaren.org/stroke F
Aniel Majjhoo, MD Interventional Neurologist & Medical Director of the McLaren Stroke Network.
Join Us for Our Webinars
• The Power of Prevention: Enhancing Annual Wellness Visit Impact
• Addressing the “Why” Behind Health: SDOH Screening in Action
• From Reactive to Proactive: Elevating Chronic Disease Management
Webinars for Physicians and Your Staff
GMP Network (GMPN) is presenting a series of webinars on topics for medical professions. These webinars will be beneficial to physicians, behavioral health specialists, pharmacists, nurses, care managers/coordinators, practice managers, and other practice staff. All webinars are $20.00 per participant and offer two times for your convenience, 12pm – 1pm and 6pm – 7pm. GMP Network is a non-profit physician organization who has provided timely and useful education to physicians for over 30 years.
Webinar Dates
October 15th
The Power of Prevention: Enhancing Annual Wellness Visit Impact
November 19th
Addressing the “Why” Behind Health: SDOH Screening in Action
December 17th
From Reactive to Proactive: Elevating Chronic Disease Management
Please scan the QR code or click the button below to join us for these valuable learning opportunities!
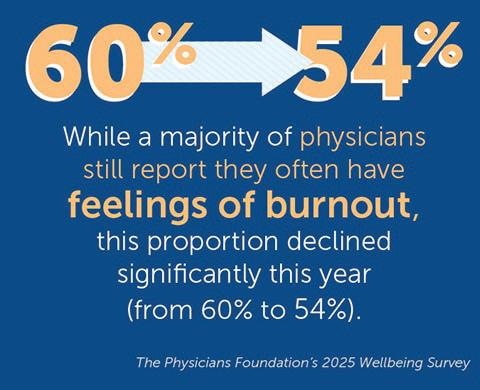
The Physicians Foundation Releases 2025 Wellbeing Survey: Stress and Anxiety Surge During a Tumultuous Year in Medicine
As anger and stress increase to pandemic levels, there is an urgent need to ensure physicians have the support to address mental health
On September 17th The Physicians Foundation announced findings from its 2025 Wellbeing Survey of America’s Physicians, revealing a troubling paradox: while reported burnout has declined from last year, physicians’ stress and anxiety have risen to levels not seen since the height of the pandemic. The Foundation’s latest version of its survey, 2025 Survey of America’s Physicians, also showed that physicians continue to face mounting challenges that exacerbate burnout, including stigma and structural barriers surrounding mental health care access. In recognition of National Physician Suicide Awareness Day (NPSA Day), The Physicians Foundation and The Dr. Lorna Breen Heroes’ Foundation continue their call for systemic change through Vital Signs: The Campaign to Prevent Physician Suicide.
Throughout 2025, the U.S. healthcare landscape has been reshaped by significant changes: ongoing consolidation in healthcare, evolving reimbursement models, the widespread rise of mis- and disinformation, and major leadership and policy shifts within agencies, such as HHS, CDC, and NIH, affecting physicians’ ability to deliver cost-effective, high-quality care and transforming how physicians practice and engage with their patients. The Foundation’s latest survey on physician wellbeing showcases the impact on physicians.
Key Survey Findings:
• 57% of physicians felt inappropriate anger, tearfulness or anxiety in the past year—levels similar to 2021–2022.
• 46% withdrew from family, friends or co-workers, up from 38% last year.
• 34% felt hopeless or without purpose, up from ~30% last year and consistent with rates in 2023 and earlier (34–35%).
• More than half of physicians have felt levels of debilitating stress (55%).
• While a majority of physicians still report they often have feelings of burnout, this proportion declined significantly this year (from 60% to 54%).
• More than 7 in 10 (73%) agree that there is stigma surrounding mental health and seeking mental health care among physicians, declining from 8 in 10 reporter last year.
“This year has been filled with substantial shakeups to the healthcare community and we are seeing the impact on the wellbeing of our physicians,” said Dr. Gary Price, president of The Physicians Foundation. “Even as burnout shows signs of easing, the rising tide of stress and anxiety we’re hearing from physicians is deeply concerning. This isn’t just about clinician morale—it’s about patient access, care quality and the longterm stability of our healthcare system. Physicians are navigating relentless administrative burdens, staffing shortages and mounting complexity in care delivery, all of which erode the time and energy they can dedicate to patients.”
The path forward begins with proactive, system-level efforts to strengthen physician wellbeing, reduce the risk of tragic outcomes and sustain a healthy, effective workforce. The Physicians Foundation and the Dr. Lorna Breen Hereos’ Foundation urge healthcare stakeholders to prioritize systemic solutions that reduce administrative burden, support mental health access without punitive repercussions and establish cultures where physicians can seek care without stigma.
“Physicians are beginning to feel the impact of changes designed to support their mental health, and it’s encouraging to see signs that burnout is easing,” said Dr. Stefanie Simmons, chief medical officer at the Dr. Lorna Breen Heroes Foundation. “At the same time, the surge in stress and anxiety to near-pandemic levels this year is an urgent warning: we must double down on systemic reforms that reduce administrative burden, ensure confidential, stigma-free access to mental health care and foster practice environments that truly prioritize clinician wellbeing. When we sustain these changes, we not only protect our physicians—we strengthen patient access and improve the quality of care across our healthcare system.”
Read the full survey results and methodology here. Learn more and access the resources and solutions mentioned at NPSADay.org.
This information is intended for educational purposes only. If you or someone you know may be in a crisis, call or text 988 or chat 988lifeline.org. F
SHARE YOUR NEWSWORTHY ITEMS!
Have you or a MCMS colleague been elected to a position (specialty society, hospital, community based program, etc.) or honored for your volunteer service within the community or abroad?
Let us know. We would like to recognize MCMS members in the “Member News” section of the Medicus.
Contact Heidi Leach at HLeach@macombcms.org with newsworthy information.
Publication is subject to availability of space and the discretion of the Editor.
CME Requirements for Licensure
Every three years physicians are required to complete the following continuing education for license renewal.
150 hr. Continuing Medical Education
75 hr. of which must be Category 1 CME credits for MDs
60 hr. of which must be Category 1 CME credits for DOs
3 hr. Pain & Symptom Management
with 1 hr. Controlled Substance Prescribing 1 hr. Medical Ethics
3 hr. Implicit Bias
Additional Requirements
One time – training for Identifying Human Trafficking Victims
One time – training for Opioids & Controlled Substances Awareness for Prescribers
One time – the Medication Access and Training Expansion (MATE) Act, requires DEA registered prescribers to have 8 hrs. training in opioid use disorders
Macomb County Offers the Lowest Dues Rates in Southeast Michigan!
Why Membership Matters
Whether you’re a solo practitioner, member of a group practice, or employed by a health care system, the Macomb County Medical Society is focused exclusively on advocating for our local physician members, across a wide-range of specialties. From federal legislative and regulatory issues, to state and local ordinances, to payor relations and public health concerns, external forces are continuously impacting your practice and your patients. We recognize there is strength in numbers and we provide a unified voice for physicians.
There are three easy ways to renew:
1. Online at www.msms.org/renew
2. Call your MSMS Account Specialist, Christina Spitzley, at 517-336-5762
3. Print the invoice from your account record and fax it to 517-336-5716
As a member, your concerns are addressed and your voice is amplified! Together we are stronger and we need your support!
By: Daniel M. Ryan, MD, MSMS Region 2 Director
MSMS HOUSE OF DELEGATES IS GOING FULLY VIRTUAL IN 2026!
The MSMS House of Delegates will be fully virtual and online in 2026. The general session to act on the Reference Committee recommendations (the Blue Report) will be held Saturday, April 18, 2026, starting at 8:00 am. It will work similarly to the online Reference Committees with live testimony, as well as live voting by delegates. The change is intended to allow more physicians to participate in the policy making process and to reduce expenses of an in person meeting. More information on the Reference Committee schedule, officer speeches and voting instructions will be coming soon. The deadline for resolutions is Monday, February 23, 2026. For questions regarding the House of Delegates, please contact Rebecca Blake at rblake@msms.org or 517-336-5729.
ACT NOW! CONTACT CIGNA ABOUT NEW DOWNCODING POLICY
Starting October 1, 2025, Cigna began to adjust certain higherlevel evaluation and management (E/M) codes to a lower level – a practice also known as downcoding. Downcoding occurs when the payer determines the encounter criteria in the claim does not rise to the complexity required for the E/M code in the submitted claim. Cigna’s policy will apply to codes 99204-99205; 99214-99215; and 99244-99245, which represent professional claims for level 4 and 5 E/M services and indicate moderate or high-level complexity visits for new and established patients.
In a letter to Cigna, MSMS urged the payer to rescind the policy. Regarding MSMS’s opposition to this new policy, MSMS President Amit Ghose, MD, stated the following:
“We request that Cigna immediately rescind this policy, as it conflicts with current E/M coding guidelines and threatens our physician members with unfair, unwarranted payment reductions at a time when physicians face unprecedented financial challenges.
This approach creates unnecessary friction with physician practices, undermines trust between providers and health plans, and makes it even more difficult to deliver high-quality care in an already resource-limited environment.”
Cigna maintains the policy is intended to place additional scrutiny only on claims billed by providers their records indicate as having a consistent pattern of coding at a higher E/M level compared to their peers. They have indicated that they will identify which physicians will continue to undergo the downcoding policy based on a review of claims submitted over a 12-month period, with a focus on those who consistently bill diagnosis codes and higher-level E/M codes not typically associated with complex cases requiring additional decision-making time.
Next steps for physicians: MSMS encourages physicians and medical groups to continue voicing their concerns until the policy is formally withdrawn. When contacting Cigna, physicians should emphasize that:
• The policy lacks transparency and fails to disclose claims adjudication criteria.
• It conflicts with AMA and CMS E/M coding guidelines.
• It will increase administrative burdens and costs for both practices and the insurer.
Please contact Cigna Customer Service at 1-800-88-CIGNA (1-800-882-4462) or via the provider portal and request that the company rescind the R49 downcoding policy.
LEGAL ALERT: HIPAA REPRODUCTIVE HEALTH RULE VACATED NATIONALLY—UPDATED HIPAA GUIDE
On September 10, 2025, the U.S. Court of Appeals for the Fifth Circuit dismissed an appeal of a June 2025 federal district court ruling in Purl et al. v. Department of Health & Human Services vacating new HIPAA Privacy Rule protections for uses and disclosures of information related to lawful reproductive health care. Although Covered Entities no longer need to comply with the new Privacy Rule provisions addressing reproductive health care, the federal court ruling did not disturb the new Privacy Rule requirements addressing substance use disorder treatment records covered under 42 CFR Part 2. Accordingly, medical practices and other continued on page 22
continued from page 21
Covered Entities must still update their HIPAA Notice of Privacy Practices by February 16, 2026 to address limitations on the use and disclosure of substance use disorder treatment records covered under Part 2.
MSMS is working on updates to its HIPAA Guide to reflect these latest regulatory changes.
MSMS JOINS FEDERAL LAWSUIT AGAINST MULTIPLAN
MSMS recently became a co-plaintiff in the federal MultiPlan lawsuit, filed in US District Court in Chicago. The suit alleges that MultiPlan, a company that provides out-of-network claims processing for insurance companies, violated federal antitrust laws by using billing information from its client companies to drive down payments for medical services over a ten-year period.
MSMS has joined the suit on behalf of its member physicians to seek injunctive relief to end to these unfair practices. Medical practices throughout Michigan may have been unwit ting victims of the MultiPlan scheme and could be entitled to compensation for underpaid claims and other damages. Physicians should consider joining the suit as co-plaintiffs.
Medical practices will not share in any settlement unless they register as plaintiffs. Plaintiffs’ attorneys are working on a contingency fee basis, which means there are no out-of-pocket costs.
For more information, please click here. To watch MSMS’ Oct.1 webinar where members to heard directly from MSMS CEO, Tom George, MD, and the plaintiff attorneys click here. F
ACTIVATE YOUR POLITICAL VOICE
The Michigan Doctors’ Political Action Committee (MDPAC) is the political arm of the Michigan State Medical Society. MDPAC supports pro-medicine candidates running for the State legislature, Michigan Supreme Court and other statewide positions. Join today!
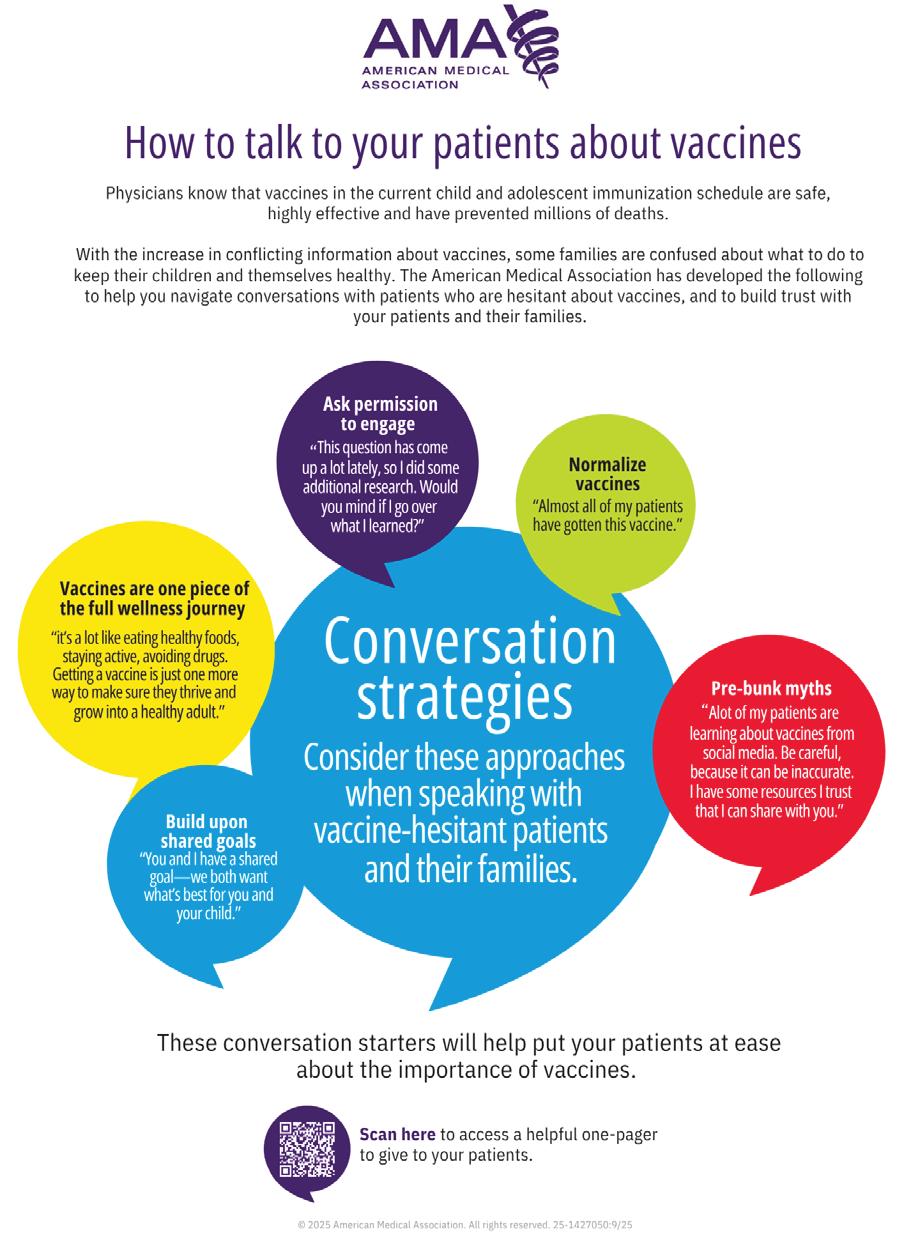
AMA LAUNCHES VACCINE INFOGRAPHICS FOR PATIENTS AND PHYSICIANS
The AMA has released new tools to help patients and physicians cut through the confusion around vaccines and have open, honest conversations with each other. An infographic for patients (PDF) explains why vaccines are an important part of staying healthy and encourages them to talk with their doctor if they have questions. A second infographic for physicians (PDF) includes sample conversation starters they can use when speaking with patients who may be unsure about vaccines—helping to build trust and understanding.
“Many people are confused about vaccines or unsure where to turn for evidence-based answers,” said AMA President Bobby Mukkamala, MD. “Doctors know vaccines are one of the most effective ways to protect our health. We want to make sure patients have clear, up-to-date information on everything from the public health measures to prevent the spread of illness to the benefits of getting vaccinated, including reducing the risk of serious illness, hospitalization and death for themselves and the community around them. Our goal is to cut through misleading information, facilitate informed conversations between patients and physicians, and build trust.”
The AMA is committed to serving as a trusted resource on vaccines and will soon launch additional evidence-based tools and information for patients and physicians.
AMA SEEKS PHYSICIAN EXEMPTION FROM H-1B VISA PROCLAMATION
The AMA led a sign-on letter with 57 national medical specialty societies to Secretary of Homeland Security, Kristi Noem, concerning the Proclamation entitled, “Restriction on Entry of Certain Nonimmigrant Workers.” This Proclamation implements a $100,000 fee, to be paid by the prospective employer, upon initial application for an H-1B visa beginning on Sept. 21, 2025. The letter urged Secretary Noem to issue clarifying guidance stating that H-1B physicians’ entry into the U.S. is in the national interest of the country, thereby exempting them from the Proclamation and the $100,000 fee.
In addition, the AMA has had multiple meetings with members of Congress to discuss this issue and explain why physicians should be exempt from this Proclamation. If you would like to reach out to your members of Congress, the AMA has also created a grassroots campaign on this issue. More information on this grassroots campaign can be found at: Be Heard | Physicians Grassroots Network.
NEW, UPDATED PHYSICIAN SECURITY RISK ASSESSMENT TOOL AVAILABLE FOR DOWNLOAD
The Assistant Secretary for Technology Policy/Office of the National Coordinator for Health Information Technology (ASTP/ ONC), in collaboration with the Department of Health and Human Services (HHS) Office for Civil Rights (OCR), developed an updated downloadable Security Risk Assessment (SRA) Tool to help guide small and medium-sized physician practices through conducting a risk assessment of their organizations.
The Health Insurance Portability and Accountability Act (HIPAA) Security Rule requires that covered entities and business associates conduct a risk assessment to ensure compliance with HIPAA’s administrative, physical, and technical safeguards. It is important to emphasize that covered entities are required to ensure the confidentiality, integrity, and availability of all electronic protected health information (ePHI) that they create, receive, maintain or transmit. Organizations can use information from their assessments to inform decisions regarding security measure implementation and determine which policies and procedures may need to be created or improved to protect ePHI.
The updated tool is a desktop application that walks users through the security risk assessment process using a simple, wizard-based approach. There are multiple-choice questions focused on threat and vulnerability assessments and asset and vendor management, as well as references and additional guidance given throughout the course of the assessment.
PHYSICIAN PARTICIPATION IN ALTERNATIVE PAYMENT AND DELIVERY MODELS
A new report by the AMA examines the recent trends in participation in care delivery models as well as the use of fee-for-service (FFS) and alternative payment models (APMs). continued on page 24
In addition, it describes how participation in care delivery models varies across practice characteristics.
The analysis finds that:
• Participation in ACOs has grown over the past decade, with more than half of physicians (53.5%) reporting that their practice participated in at least one ACO type (commercial, Medicare, or Medicaid) in 2024. Still, although long term participation was up, there was evidence of a stagnation in trend between 2022 to 2024.
• Participation in ACOs and medical homes was higher among physicians in practices with primary care physicians (PCPs), multi-specialty practices, and hospital-owned practices than among physicians in practices without PCPs, solo practices, and physician-owned practices, respectively.
• FFS remained the most prominent payment method as in prior years, with 82.8% of physicians reporting that their practice received at least some payment from this method in 2024.
• The use of APMs has also become more prevalent, as 62.4% of physicians were in practices that received at least some payment from one of the four APMs asked about in the survey (capitation, bundled payments, pay-for-performance, and shared savings), up from 59.0% in 2014.
• In 2024, for every $100 in practice revenue received, $32.30 was from APMs (with the remainder from FFS), up from just $28.10 in 2014.
The rise in ACO participation highlights how more providers are embracing patient-centered, coordinated care designed to improve quality of care while controlling costs. It signals some shifts toward value-based care, as evidenced by a gradual move away from complete dependence on FFS and toward greater use of APMs. Nonetheless, FFS remains a significant and stable source of revenue partly because many APMs are “built off” FFS payments.
WHITE HOUSE ANNOUNCES NEW ACTIONS ON DIRECT-TO-CONSUMER DRUG ADVERTISING
President Trump issued a presidential memorandum directing the HHS secretary and the Food and Drug Administration (FDA) to take new actions to regulate direct-to-consumer (DTC) prescription drug advertising. The memorandum directs HHS to mandate more significant and detailed disclosures from drug manufacturers regarding any safety risks associated with the drug being advertised. The memorandum further directs FDA, who is tasked with regulated DTC drug advertising, to take enforcement action against any advertising it finds misleading.
Following the issuance of the memorandum, HHS announced that FDA’s enforcement would be “aggressive” and that the agency would move to close regulatory loopholes that have “allowed companies to withhold vital safety information.” The Department also announced that enforcement actions would span all platforms including digital platforms and
that enforcement actions would include individuals such as influencers and on AI-generated content and chatbot interactions. AMA will be monitoring HHS and FDA’s action in this space. AMA policy has long opposed DTC drug advertising.
HHS TO INCREASE RESOURCES DEDICATED TO INFORMATION BLOCKING ENFORCEMENT
The Department of Health and Human Services (HHS) announced that it will take a more active enforcement stance against health care entities that are restricting the flow of information to patients and other entities and interfering with the access, exchange or use of electronic health information (EHI).
To be clear, HHS did not announce new policy on information blocking but rather declared a renewed interest in enforcing the existing information blocking rules. Currently, information blocking claims can be submitted online through the Assistant Secretary for Technology Policy/Office of the National Coordinator for Health IT (ASTP/ONC) Report Information Blocking Portal. Through Aug. 31, 2025, there have been over 1,300 possible claims of information blocking reported through the portal.
The AMA encourages physicians to take advantage of ASTP/ONC’s educational resources related to information blocking, as well as additional information from the AMA, including a summary of the June 2024 Final Rule (PDF) that implemented disincentives for providers participating in specific Medicare programs.
Further information blocking resources are included in the AMA Patient Access Playbook. Physicians can also find a twopart explanation of the basics of information blocking (PDF) to help them understand what information blocking is, when information can be withheld, and how they can comply with information blocking regulations (PDF).
In instances where physicians believe an electronic health record (EHR) developer, or a health information exchange (HIE)/health information network (HIN) is blocking information unnecessarily or using legal or financial roadblocks to prevent access to patients’ medical records, those actors may be information blockers and subject to civil money penalties. Such instances should be reported through the ASTP/ONC portal. F
New State Budget has Major Health Funding Changes
Michigan’s new state budget was signed in October, and one of the biggest shifts is in the Department of Health and Human Services (MDHHS). The Department’s $30 billion budget marks a 20% drop in overall funding, largely because of federal changes in H.R. 1, which includes eligibility changes and cuts off billions in Medicaid dollars over the next ten years.
To soften the blow, the state is increasing its General Fund contribution by 6.2%, but the loss of federal support still leaves a major gap. Much of the reduction stems from new federal limits on “provider taxes” — fees hospitals and insurers pay that help draw in federal matching funds.
In response, Michigan has moved several programs into “contingency funds,” essentially placeholders totaling over $9 billion, while the state works to secure a waiver from federal health officials that would allow these funds to be released.
Additionally, the budget preserves approximately $6.4 million in funding for the MIDOCS program. While advocates had hoped that last year’s one time infusion of $4.6 million for a total allocation of $11 million this fiscal year would be continued, this continued investment will still allow MIDOCS to sustain its mission of expanding residency opportunities and bringing expert medical care to underserved communities across Michigan.
Action Needed on House Bill 4399 – Oppose NP Scope Expansion
With the budget now complete, many expect lawmakers to pivot their attention to remaining priorities before the end of session. Among those is House Bill 4399, which would allow nurse practitioners to practice medicine without physician supervision.
The MCMS and MSMS, along with our coalition partners, have actively opposed this dangerous legislation since its introduction. Despite strong advocacy, the bill remains a real possibility—and your voice can make a difference. For information on the bill, click here.
The most effective way to express your position is by contacting your legislators directly. Sending a brief email to share your concerns is a simple but powerful step. Attending local events— such as coffee hours or office hours—is another excellent way to engage face-to-face with your representatives and share your perspective. We have heard from reliable sources that nurse practitioners are consistently showing up to such events and working hard to counter the concerns we’ve identified in testimony, public messaging, and legislator visits.
Check your legislators’ websites or social media pages for information on their upcoming local events. F
MACOMB FOOD PROGRAM
Provides immediate relief to those in need of food through a network of more than 70 pantry sites, hunger relief organizations, and the Fresh To You Mobile Pantry. The program supplies food at no cost to income eligible seniors and families with children throughout Macomb County. For more information visit the Macomb Food Program website or call (586) 469-6004.
RENT AND MORTGAGE ASSISTANCE
Income-eligible Macomb County residents facing eviction, foreclosure, or homelessness may be assisted in resolving their emergency. Eligibility and guidelines will vary based on available programs. For more information contact your local Community Action Center at (586) 469-6964. For residents of Warren, Roseville, Eastpointe or Centerline call (586) 759-9150.
UTILITY ASSISTANCE - ELECTRICITY, GAS
Income eligible Macomb County residents facing utility shut off may be assisted in resolving their emergency. Utility assistance may be available for electric service, natural gas service, and deliverable fuels used to heat the home. Eligibility and guidelines will vary based on available programs. For more information contact your local Community Action Center at (586) 469-6964. For residents of Warren, Roseville, Eastpointe or Centerline call (586) 759-9150.
WATER RESIDENTIAL ASSISTANCE PROGRAM (WRAP)
Eligible households are offered credits on their water and sewer bills so that they pay no more than 3% of their household's annual income for up to two years. Eligible seniors and permanently disabled persons can obtain bill credit assistance without an expiration date.
To qualify for WRAP, households must be in a community in the service area, have a combined income at or below 200% of the federal poverty level, be primarily responsible for the water or sewer bill and have to reside in the home they rent or own. For more information and to apply visit the Macomb Community Action’s website or call (586) 469-6464.
TRANSPORTATION ASSISTANCE
This department provides transportation to essential medical appointments and other specific locations for eligible Macomb County residents. For more information visit Macomb Community Action’s website or call (586) 469-5225.
MYRIDE2 - CONNECTING SENIORS & ADULTS WITH DISABILITIES TO RIDES
AgeWays (formerly Area Agency on Aging) MyRide2 service can help find transportation options for seniors and adults with disabilities – helping them get to the store, to doctor’s appointments, or out to visit friends and family. Myride2 is a transportation concierge service that arranges transportation from start to finish. There is no charge for arranging transportation through myride2, but there may be a cost for any transportation services they use. Payments are made directly to transportation providers. For more information visit MyRide2 website or call (855) 679-4332.
Macomb County Assistance Programs for Your Patients
In this tough economy many of your patients may be struggling to meet their basic needs as well as those of their families.
There are programs available to help. Below are some resources you can direct your patients to for assistance.
HOME INJURY PREVENTION
The Home Injury Prevention Program installs devices to ensure safety and prevent falls in the homes of eligible Macomb County seniors. A home assessment determines which safety devices will be installed. Services are free but contributions are appreciated. For more information visit Macomb Community Action’s website or call (586) 469-6329.
HOUSING REHABILITATION
The Housing Rehabilitation Program provides assistance to eligible homeowners to repair their homes to achieve decent, safe and sanitary housing. Assistance is provided in the form of a no-interest loan. For more information visit Macomb Community Action’s website or call (586) 466-6256.
WEATHERIZATION ASSISTANCE
The Weatherization Assistance Program performs the installation of energy efficient items to conserve energy in Macomb County homes. These improvements reduce energy use and can save an average of 30% on heat and utility bills. A home energy audit determines which items will be installed. Services are free for income-eligible residents. For more information visit Macomb Community Action’s website or call (586) 469-6329.
WARMING & COOLING CENTERS
There are places across Macomb County where individuals can find respite from the extreme heat and cold. For a full list visit Macomb Community Action’s website
DIRECT CARE PROGRAMS – TO HELP SENIORS
STAY LIVING AT HOME
Home care services help seniors and people with disabilities continue to live safely in a home setting. These services provide assistance with daily activities a senior might have trouble doing for themselves – things like bathing, dressing, meal preparation or housekeeping. AgeWays (formerly the Area Agency on Aging) has several programs that offer direct care for Southeast Michigan families. For more information visit the AgeWays website or call (800) 852-7795.
PROGRAMS OFFERED SPECIFICALLY FOR SENIOR THROUGH MACOMB COUNTY SENIOR SERVICES
The following programs are offered to Macomb County residents age 60 or older. For more information on any of these services visit the Macomb County Senior Services website or call (586) 469-5228.
ADULT DAY CENTER
Provides daytime assistance for aging adults in need of structured activities, exercise, and supervision. The credentialed center can provide caregivers with a needed break while giving older adults a chance to socialize with their peers and remedy the isolation and loneliness many experience. For more information call (586) 469-5580.
FRIENDLY CALLER
Program volunteers reach out over the phone to connect with seniors interested in a friendly social conversation. It’s an informal social call that can last anywhere from 10 minutes to 30 minutes depending on interest and natural flow of conversation.
HANDY HELPERS
Provides assistance with household maintenance tasks such as replacing light bulbs or faucets, washing windows and walls, repairing furniture, pest control, yard clean up, leaf raking, weatherizing, and more.
RESOURCE ADVOCACY
Provides consultation for seniors to assess needs, recommend services and assist with tax credits, Medicare Part D enrollment, Medicaid application process, community resources, and more.
NUTRITION ASSISTANCE
DINING SENIOR STYLE
A daily lunch program for seniors at 24 locations throughout Macomb County. Seniors are provided a well-balanced meal while also socializing with their peers.
MEALS ON WHEELS
Delivers a ready to eat meal to homebound residents no longer able to leave their homes on a regular basis without assistance or able to prepare meals.
ENSURE PLUS PROGRAM
Meals on Wheels offers cans of Ensure Plus as a supplement for Macomb County’s most vulnerable homebound seniors with a prescription from their physician for Ensure Plus.
HOLIDAY MEALS ON WHEELS
Holiday meals are available for seniors who would be otherwise home alone on the holiday. A special hot lunch is freshly prepared that day, including many traditional favorites. Meal delivery is available for Easter, Thanksgiving, and Christmas.
SENIOR PROJECT FRESH COUPONS
Offers income-eligible seniors the chance to purchase fresh produce such as carrots, tomatoes, melon, and even honey. Seniors who participate will receive a $20 coupon book to use at local farmers' markets and stands.
MICHIGAN SENATE
Sen. Stephanie Chang (D)
Senate District 3
SenSChang@senate.michigan.gov (517) 373-7346
Sen. Kevin Hertel (D)
Senate District 12
SenKHertel@senate.michigan.gov (517) 373-7315
Sen. Ruth Johnson (R)
Senate District 24
SenRJohnson@senate.michigan.gov (517) 373-1636
Sen. Veronica Klinefelt (D) Senate District 11
SenVKlinefelt@senate.michigan.gov (517) 373-7670
Sen. Daniel Lauwers (R) Senate District 25
SenDLauwers@senate.michigan.gov (517) 373-7708
Sen. Michael Webber (R) Senate District 9 SenMWebber@senate.michigan.gov (517) 373-0994
Sen. Paul Wojno (D) Senate District 10
SenPWojno@senate.michigan.gov (517) 373-8360
COMMITTEES
House – Appropriations
Kimberly Edwards (D), District 12
Thomas Kuhn (R), District 57
Donavan McKinney (D), District 14
House – Appropriations Subcommittee
LARA, Insurance & Financial Services
Donavan McKinney (D), District 14 –
Vice Chair
2025 Macomb County Legislator Contact Guide
MICHIGAN HOUSE
Rep. Joseph Aragona (R) House District 60
JosephAragona@house.mi.gov (517) 373-1785
Rep. Jay DeBoyer (R) House District 63
JayDeBoyer@house.mi.gov (517) 373-1787
Rep. Kimberly Edwards (D) House District 12
KimberlyEdwards@house.mi.gov (517) 373-0852
House – Appropriations Subcommittee
Public Health
Tom Kuhn (R), District 57 - Vice Chair
House – Appropriations Subcommittee
Medcaid & Behavioral Health
Tom Kuhn (R), District 57
House – Families & Veterans
Doug Wozniak (R), District 59
Mai Xiong, (D), District 13
Rep. Jaime Greene (R) House District 65 JaimeGreene@house.mi.gov (517) 373-1775
Rep. Thomas Kuhn (R) House District 57 TomKuhn@house.mi.gov (517) 373-1706
Rep. Mike McFall (D) House District 14 MikeMcFall@house.mi.gov (517) 373-0140
House – Health Policy
Alicia St. Germaine (R), District 62
House – Insurance
Joseph Aragona (R), District 60
Senate – Appropriations
Kevin Hertel (D), District 12
Veronica Klinefelt (D), District 11
Rep. Donavan McKinney (D)
House District 11
DonavanMcKinney@house.mi.gov (517) 373-0849
Rep. Denise Mentzer (D) House District 61
DeniseMentzer@house.mi.gov (517) 373-1774
Rep. Ron Robinson (R) House District 58
RonRobinson@house.mi.gov (517) 373-1794
Rep. Josh Schriver (R) House District 66
JoshSchriver@house.mi.gov (517) 373-0839
Rep. Alicia St. Germaine (R) House District 62
AliciaStGermaine@house.mi.gov (517) 373-0555
Rep. Douglas Wozniak (R) House District 59
DouglasWozniak@house.mi.gov (517) 373-0832
Rep. Mai Xiong (D) House District 13
MaiXiong@house.mi.gov (517) 373-0845
Senate – Health Policy
Kevin Hertel (D), District 12
Veronica Klinefelt (D), District 11
Michael Webber (R), District 9
Paul Wojno (D), District 10
Senate – Regulatory Affairs
Kevin Hertel (D), District 12
Dan Lauwers (R), District 25
Michael Webber (R), District 9
Paul Wojno (D), District 10
Macomb Medicus Journal of the Macomb County Medical Society
The Macomb Medicus is the official quarterly journal of the Macomb County Medical Society. It is a full-color glossy magazine published both electronically and in hard copy format. It is a valued news source for our 600 plus physician members of all specialties and their staff throughout Macomb County. In addition to members the Macomb Medicus is sent to hospital executives, Michigan State Medical Society staff, other county medical society staff, and healthcare related businesses/organizations in Macomb County. The Macomb Medicus is read by an impressive cross section of the healthcare community and is electronically available on our website at www.macombcms.org.
FREE Hotlink to Your Website & Free Advertising Design! For advertising rates and information, please contact:
Heidi Leach, Executive Director & Managing Editor Macomb County Medical Society, PO Box 551, 810-712-2546 HLeach@macombcms.org | www.macombcms.org
Where Physicians and Patients Come First
The Surgery Center of Michigan (SCM) is a fully accredited ambulatory surgery center offering physicians a modern, efficient, and patient-focused environment.
• Two State-of-the-Art ORs + Procedure Suite
• Carl Zeiss Microscopes & Bausch & Lomb Stellaris Systems
• Femto Laser & ORA Systems
• Vaser & Renuvion for Advanced Body Sculpting
• Lumenis CO2 Laser for Skin Rejunevation
• Staffed CRNAs
• AAAHC Accreditation
• Favorable Block Time Availability
• Streamlined Scheduling & Lower Overhead than Hospitals
• Convenient Sterling Heights Location
Join a growing group of physicians who are not only optimizing their surgical practice but also building long-term value.
• Attractive entry for ophthalmologists, plastic & cosmetic surgeons, and other specialists
• Flexible ownership structures designed for physician success
• A chance to invest in your future and your patients’ experience