MACOMB COUNTY MEDICAL SOCIETY - June/July/August 2025
July/August/September 2025 | Vol. 33 | No. 3
Cover Photo
Mt. Fuji in Japan
Editor
Narendra D. Gohel, MD
Managing Editor
Heidi L. Leach
Graphic Designer
Lori Krygier
2025 MCMS OFFICERS & DELEGATES
President Narendra D. Gohel, MD
President-Elect
Lawrence F. Handler, MD
Treasurer & Secretary
Daniel M. Ryan, MD
Delegates
Terrence P. Brennan, MD
Narendra D. Gohel, MD
Lawrence F. Handler, MD
Jareer S. Hmoud, MD
Khaled M. Ismail, MD
Carolann Kinner, DO
Cheryl D. Lerchin, MD
Akash R. Sheth, MD
MSMS Region 2 Director
Daniel M. Ryan, MD
Executive Director
Heidi L. Leach
Toll Free 877-264-6592 | E-Mail HLeach@macombcms.org , macombcms@gmail.com Web www.macombcms.org
July/August/September 2025 | Vol. 33 | No. 3
In This Issue
Macomb Medicus Journal is published quarterly by the Macomb County Medical Society. Winter: Jan/Feb/ Mar, Spring: Apr/May/Jun, Summer: Jul/ Aug/Sep, Fall: Oct/Nov/Dec. Subscription to the Macomb Medicus is included in the society’s annual membership dues.
Statements and opinions expressed in articles published in the Macomb Medicus are those of the authors and not necessarily those of the Macomb County Medical Society. Advertisements do not represent approval or recommendation of the Macomb County Medical Society.
Address changes and all communications relative to articles and advertising in the Macomb Medicus should be addressed to: Editor, Macomb County Medical Society, P.O. Box 551, Lexington, Michigan 48450-0551 or email HLeach@macombcms.org.
All material for publication, including advertisements, must reach the Society office no later than the 10th (business) day of the month preceding the date of issue, e.g. December 10 for the Winter issue. Thank you. No portion of the Macomb Medicus may be used for publication elsewhere without permission from the publisher.
"Quality
Quest for Quality & Safety –A Physician’s Perspective
By: Narendra Devisinh Gohel, MD Editor and MCMS President
is not an act, it is a habit." – Aristotle
As physicians, our oath is to do no harm—and in doing so, we inherently commit ourselves to quality and safety. The Oxford Dictionary defines quality as “the standard of something as measured against other things of a similar kind.” But what does that mean in modern clinical practice?
Physicians have historically been strong proponents of selfregulation. We prefer to “police ourselves,” rather than have our clinical practices scrutinized by outside agencies or government regulators. Yet, regulatory oversight is not optional—it’s a condition for participation in key healthcare systems.
The Centers for Medicare & Medicaid Services (CMS) requires hospitals to implement peer review processes as a condition of participation in the Medicare and Medicaid programs. Similarly, The Joint Commission mandates peer review under its Ongoing Professional Practice Evaluation (OPPE) and Focused Professional Practice Evaluation (FPPE) standards as part of hospital accreditation. While both agencies require peer review, they do not prescribe a uniform structure, leaving institutions to tailor these mechanisms to their clinical culture and goals.
Philosophical Roots of Quality
In Zen and the Art of Motorcycle Maintenance, Robert M. Pirsig explores the metaphysical underpinnings of quality. The term, he explains, derives from the ancient Greek concept of aretē, meaning “excellence.” Pirsig proposes two types of quality: Dynamic Quality, which is immediate and experiential, and Static Quality, which encompasses established patterns, values, and institutions.
“Quality… you know what it is, yet you don’t know what it is,” writes Pirsig. His philosophical inquiry reminds us that in healthcare, quality is both a measurable outcome and an aspirational value—shaped by judgment, experience, systems, and evolving standards.
The Harsh Reality of Modern Healthcare
The reality in today’s healthcare system is stark: we face an often-overlooked epidemic of poor-quality care. According to a 2023 paper by Augustine Kumah in Frontiers in Public Health, approximately 10–12% of hospitalized patients in highincome countries experience adverse events annually. 1
Globally, the World Health Organization (WHO) estimates 134 million adverse events occur annually in hospitals in low- and middle-income countries, resulting in 2.6 million deaths. 2 In the United States, a Johns Hopkins study estimated that medical errors contribute to over 250,000 deaths annually, making them the third leading cause of death after heart disease and cancer 3
These errors range from medication mishaps and diagnostic delays to surgical complications and infections. The root causes are multifactorial: system-level inefficiencies, communication breakdowns, cognitive biases, and resource constraints, to name a few.
Patient Safety: A Global Priority
Since its inception in 2019, World Patient Safety Day (celebrated every September 17) has focused attention on pressing safety themes:
• 2023: “Engaging Patients for Patient Safety”
• 2024: “Improving Diagnosis for Patient Safety”
• 2025: “Safe Care for Every Newborn and Every Child”
The WHO emphasizes actionable strategies: strengthening safety protocols, promoting transparency, investing in workforce training, and leveraging digital innovation. These are not abstract concepts; they are practical imperatives for every healthcare organization.
The AI Revolution: Transforming Quality and Safety
Artificial Intelligence (AI) is poised to revolutionize the way we approach quality and safety in healthcare. Far from replacing physicians, AI can act as a powerful assistant, supporting clinical decision-making and reducing errors. Let’s explore key areas where AI can help:
1. Clinical Decision Support
AI can flag abnormal lab trends, potential drug interactions, and alert clinicians to missed diagnoses.
• Example: A machine learning algorithm predicts early signs of sepsis using EHR data, prompting early intervention. 4
2. Peer Benchmarking and Feedback
Real-time dashboards compare a physician’s performance (length of stay, readmissions, complication rates) to benchmarks.
• Result: Transparent data fosters accountability, reflection, and targeted improvement.
continued on page 4
3. Diagnostic Accuracy
AI tools like natural language processing and image recognition enhance radiology and pathology.
• Example: An AI reads a chest X-ray and detects a subtle pulmonary nodule missed in the initial interpretation. ⁵
4. Identifying Practice Gaps
AI can scan thousands of encounters to identify overuse, underuse, or deviations from guidelines.
• Example: An internist receives a monthly report showing suboptimal HbA1c control in their diabetic patients.
5. Reducing Administrative Burden
Voice-enabled AI documentation tools (e.g., Nuance DAX, Suki AI) streamline note-taking and order entry.
• Benefit: Reduced physician burnout, improved accuracy, and more time for patient interaction.⁶
6. AI-Driven Quality Improvement (QI) Dashboards
AI identifies outliers, predicts complications, and informs targeted QI interventions.
• Example: Predictive models flag patients at high risk for readmission, enabling proactive discharge planning.
7. Coaching and Simulation
AI-powered simulators offer real-time feedback for trainees and simulate complex scenarios.
• Example: Emergency physicians practice trauma triage with AI tutors, improving real-world decision-making.
Caution: Not Without Risk
Despite its potential, AI must be approached thoughtfully:
• Bias: Algorithms trained on incomplete or biased datasets can perpetuate disparities.
• Over-Reliance: AI should enhance—not replace—clinical judgment.
• Transparency: Black-box models must be interpretable and auditable for safe clinical use.
Conclusion: Quality as a Collective Responsibility
Healthcare quality is not a fixed destination—it is a continuous journey. While external regulations provide necessary guardrails, it is up to physicians to lead the charge from within.
Let us embrace the tools of today—data, technology, AI—while holding true to our timeless values: excellence, integrity, compassion, and curiosity. As Pirsig writes, “Care and Quality are internal and external aspects of the same thing.”
In the quest for quality and safety, may we remain humble learners and steadfast guardians of our patients’ trust.
References
1. Kumah, A. (2023). Poor quality care in healthcare settings: an overlooked epidemic Front Public Health.
2. World Health Organization. Patient Safety Factsheet
3. Makary, M.A., & Daniel, M. (2016). Medical error—the third leading cause of death in the US. BMJ, 353:i2139.
4. Henry, K.E., et al. (2015). A targeted real-time early warning score (TREWScore) for septic shock. Sci Transl Med, 7(299):299ra122.
5. Rajpurkar, P., et al. (2017). CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning. arXiv preprint arXiv:1711.05225.
6. Downing, N.L., et al. (2021). Evaluating Ambient Voice Technology in the Exam Room. npj Digital Medicine, 4(1), 1–7. F
UNDERSTANDING OUR COMMUNITY THROUGH DATA
• Schools and childcare centers should submit weekly illness data to local health authorities to help monitor and control potential outbreaks.
• All animal bites should be reported immediately to Animal Control to check the risk of rabies.
• Encourage vaccination, as vaccination remains one of the best tools to protect against communicable disease.
The Macomb County Health Department collects, analyzes, and shares a wide range of statistics to better understand and improve the health and wellbeing of Macomb County residents. Providing available health data supports transparency, informs policy and programming, and empowers individuals and organizations to make data-driven decisions. We offer access to a variety of data sources, including:
• Annual reports
• Surveillance data for chronic and communicable diseases
• Trends in births, deaths, car accidents or other unintentional injuries
• Community Health Assessment reports
• Additional community-specific health reports
One especially valuable tool is our Community health profiles, which provide health indicators for individual cities and townships across Macomb County. These profiles are based on responses from the Macomb County Community Survey and help us identify the unique demographics of each community.
Visit our website to view available reports and learn more.
THE MACOMB COUNTY HEALTH DEPARTMENT’S COMMUNICABLE DISEASE SURVEILLANCE PROGRAM
When a healthcare provider in Macomb County identifies a patient with any of the reportable conditions, they are required to report the diagnosis to MCHD to help monitor the health of the community and provide preventive actions as necessary. The cooperation and prompt required reporting by physicians, laboratory scientists, infection preventionists, schools and other providers allows for timely action by local and state public health personnel. Some of the benefits of this teamwork include:
• Identification of outbreaks and epidemics
• Enabling preventive measures and/or education
• Successful targeting of prevention programs, identification of care needs, and efficient use of resources
• Evaluation of the success of long-term control efforts
For more information or to report a disease, contact the Communicable Disease Program at 586-783-8190 or email diseasecontrol@macombgov.org.
WORKING TOGETHER TO HELP PEOPLE LIVE HEALTHIER LIVES
The Communicable Disease Surveillance Program helps protect the community by quickly identifying and responding to communicable diseases and outbreaks. Timely reporting from healthcare providers, schools, and childcare centers is essential to prevent the spread of illnesses such as chickenpox, Hepatitis A, and rabies.
Here’s how you can help
• Healthcare providers and laboratories are required to report diagnosed or suspected cases of communicable diseases to the local health department in a timely manner. Patients should also inform their providers to ensure proper follow-up and reporting.
In 2023, the Macomb County Health Department, along with over 25 partner organizations completed a comprehensive Community Health Assessment (CHA). The CHA was then used to create the 2024-2028 Community Health Improvement Plan (CHIP), which identified three priority areas that would be addressed by the CHIP:
• Behavioral Health & Substance Use
• Social Determinants & Built Environment
• Chronic Disease & Healthy Lifestyle
Workgroups for each priority area were established to help develop local level strategies and activation.
The Chronic Disease and Healthy Lifestyle workgroup includes 11 partners who all share one goal—helping people in Macomb County live healthier lives by:
• Helping people learn about and get access to health screenings which can catch problems early
• Helping people find a doctor they can trust
• Get more people moving by offering fun and helpful exercise programs
continued on page 6
continued from page 5
• Helping people make use of the various parks and recreational sites and trails
If you want to learn more or join the workgroup, please visit the Chronic Disease and Healthy Lifestyle website
FAIR FOOD NETWORK
The Macomb County Health Department is proud to spotlight our partnership with Fair Food Network, a dedicated member of our Healthy Macomb Advisory Committee and an active contributor to our Social Determinants of Health & Built Environment workgroup. Fair Food Network has been instrumental in increasing the number of farmers markets in Macomb County that accept Double Up Food Bucks (DUFB), making it easier for families to access fresh, Michigan-grown produce while supporting local farmers. Currently, DUFB is available at the following Macomb County locations:
Take Charge of Your Mental Health
Achieving and maintaining mental wellness is the foundation for keeping the entire body healthy.
To support that effort, Macomb County Community Mental Health is proud to offer a great on-line, personalized program, My Strength.
“The health club for your mind,” MyStrength provides programs and support for many types of emotional and physical challenges, including:
• Reducing stress • Mindfulness & meditation
• Improving sleep • Balancing intense emotions
• Managing depression
• Managing anxiety
• Dodge Park Farmers Market (Sterling Heights)
• Oakridge Market (Eastpointe)
• Fresh Choice Marketplace (Eastpointe)
Their team has implemented customized onboarding and cashier training at local markets to streamline the DUFB experience and reduce stigma, while also launching community engagement efforts through partnerships with food pantries, senior centers, and local health organizations. They are also piloting innovative enhancements to the Fresh Incentives app such as pre-ordering tools and service referrals to further connect residents with healthy food and supportive resources. Through this multifaceted approach, Fair Food Network continues to strengthen food access and economic opportunity across Macomb County.
To learn more and find additional participating locations, visit doubleupfoodbucks.org
For more information about Fair Food Network please visit fairfoodnetwork.org F
QUARTER 2 REPORTABLE DISEASE UPDATE
The Macomb County Health Department’s 2nd Quarter Reportable Disease Update released July 15th is now available online. The quarterly update identifies communicable disease trends and emerging diseases in Macomb County. Highlights include foodborne illnesses, vaccine-preventable diseases, and vector borne diseases.
• Pregnancy & early parenting
• Managing chronic pain
MyStrength offers daily tips for the mind, body and spirit, and:
• Is Safe, Secure, and Confidential—Your privacy is our top priority, and MyStrength maintains the highest level of security available to create a completely confidential and safe environment.
• Has Proven Resources—based on the latest research and professional advice from best-selling authors.
• Is Packed with Tools — MyStrength offers many resources to improve mental health, with the latest research and professional advice.
It’s easy to get started; Go to mystrength.com and enter access code MCCMHComm and begin your journey to stronger overhall health!
MyStrength has helped many people across the country from the comfort and privacy of their homes.
There is no cost to join, and it is simple to get started. Go to www.mystrength.com. Select “Sign Up” and enter the access code: MCCMHComm. Complete the Wellness Assessment (it takes about ten minutes) and be on your way with personalized tools and supports.
Go Mobile! Using the access code, get the myStrength app for IOS and Android devices at www.mystrength.com/mobile
Macomb County Health Department Reportable Diseases Summary
Diseases Reported in Macomb County Residents*
Cumulative total for previous years, year-to-date total for June 2025 b
producing Escherichia coli per MDHHS; combo of E. coli & Shiga Toxin 1 or 2. ^ Previously reported as "AIDS" b
at this time.
MDHHS ESTABLISHES MANDATORY REPORTING RULE FOR ALS CASES
The Michigan Department of Health and Human Services (MDHHS) has announced the adoption of a new administrative rule requiring mandatory reporting of Amyotrophic Lateral Sclerosis (ALS) cases. ALS is a progressive neurodegenerative disease that affects nerve cells in the brain and spinal cord. It currently has no cure, and slowly impacts diagnosed individuals’ ability to move, speak, eat and breathe.
The rule went into effect on May 15, making Michigan the fifth state in the U.S. to implement mandatory ALS case reporting, which will improve the state’s ability to monitor the disease.
“There are between 4,000 and 6,000 cases of ALS diagnosed across the country annually,” said Dr. Natasha Bagdasarian, chief medical executive. “Mandatory reporting will help provide a better picture of who gets ALS and identify risk factors for the disease. This information will assist with research and could help offer a better future for those with ALS.”
Under the new rule, health care professionals and health care facilities that diagnose and treat individuals with ALS will be required to report cases to MDHHS. These reports will help the department continue to develop a comprehensive registry of chronic diseases and contribute to the broader understanding of chronic disease trends in Michigan.
The rule allows public health officials to track the number of ALS cases and where they occur, offering important insight into the incidence and distribution of the disease across Michigan. Statewide ALS reporting will support trend analysis and epidemiologic understanding that can guide future research and public health actions.
The ALS reporting rule is available online. For questions about the rule or how chronic diseases, including ALS, are tracked in Michigan, contact MDHHS' Chronic Disease Surveillance Team at MDHHS-Chronicle@Michigan.gov.
MICHIGAN BLOOD LEAD TESTING RULES FINALIZED; PHYSICIANS NOW REQUIRED TO ORDER TESTING FOR CHILDREN AT AGES 12 MONTHS AND 24 MONTHS
To help prevent and address lead poisoning of Michigan children as soon as possible, laws requiring physicians provide blood lead testing to all young children in Michigan are now in effect.
In October 2023, Gov. Gretchen Whitmer signed two bills into law requiring blood lead testing for all Michigan children at
ages 12 months and 24 months of age (Public Act 146 of 2023) and that these tests be recorded on the child’s immunization record (Public Act 145 of 2023). This age-based approach to blood lead testing requirements is commonly called “universal testing.”
The MDHHS administrative rules have been finalized and are now in effect. The rules require physicians to test or order a blood lead test for all children at ages 12 months and 24 months, and at other intervals based on lead exposure risk. If there is no record of these tests, children must receive a blood lead test between 24 months and 72 months of age.
Universal blood lead testing will increase the number of children tested in the state. Children with elevated blood lead levels may qualify for nursing case management services with staff trained to visit with families at their homes to discuss ways to help lower blood lead levels.
Children with elevated blood lead levels may also qualify for services provided through the Lead Safe Home Program, which can help eligible families find and fix lead hazards. Eligibility for the program is based on Medicaid or household income status and home location. Eligible families must also submit a completed application.
Families may opt out of universal blood lead testing requirements.
Visit Michigan.gov/MiLeadSafe for more information about lead hazards, blood lead testing and lead services.
Questions and answers for physicians about universal blood lead testing.
MICHIGAN RECORDS LOWEST RATE OF INFANT MORTALITY IN ITS HISTORY; CONTINUES FOCUS ON RESOURCES TO KEEP MOMS, BABIES HEALTHY
Multidisciplinary group of partners gather to advance maternal, infant and family health at 8th annual Maternal Infant Health Summit
As the state marks the lowest recorded infant mortality rate in its history, attendees of the 8th Annual Maternal Infant Health Summit gathered to share ideas on how to continue efforts to improve the health of Michigan moms and babies. The event, hosted by the Michigan Department of Health and Human Services (MDHHS), convened a multidisciplinary group of state and national partners.
continued on page 9
“We are proud of the improvements we are making and will continue to make when it comes to the health of moms and babies,” said Elizabeth Hertel, MDHHS director.
“The dedication of Governor Whitmer and the legislature, quality work conducted by partners across the state and collaboration with Michigan families and communities are key to our current and future success.”
Infant mortality is defined as the death of a live born infant prior to their first birthday; the top three causes are prematurity and low birth weight, congenital anomalies and accidents and adverse outcomes.
In 2023, 607 infants under the age of one died and the state’s infant mortality rate declined to 6.1 infant deaths per 1,000 live births. While there is still work to be done, this is a decrease from 2022’s, 650 deaths and 6.3 deaths per 1,000 live births. Deaths among Black infants fell to 11.9 deaths per 1,000 live births in 2023, also a record low. This is a reduction from 2022’s 14.1 deaths per 1,000 births, however, this rate is still nearly three times the rate of white infant deaths.
MDHHS continues to focus efforts on keeping moms and babies healthy through the Healthy Moms, Healthy Babies initiative that was launched in 2021 to improve health outcomes and reduce disparities. It includes the expansion of postpartum Medicaid coverage to one year after birth and programs designed to assist families through pregnancy, birth and beyond, such as doula services and the Centering Pregnancy model of care.
For more information about programs to improve the health and well-being of women, infants, families and communities, visit MDHHS’ Maternal & Infant Health webpage
Recently, the Health and Human Service (HHS) director issued guidance to change COVID-19 vaccine recommendations for healthy children and pregnant persons. The CDC subsequently issued updated COVID-19 vaccine guidance for children.
The newly restructured Advisory Committee on Immunization Practices (ACIP) also met, and announced two new workgroups, including a review of the current childhood schedule and another to review the safety and effectiveness of vaccines that have not been reviewed for more than seven years.
The Michigan Department of Health and Human Services (MDHHS) continually reviews evidence on new and existing vaccines. This evidence overwhelmingly demonstrates that
vaccines are safe and have saved millions of lives and prevented tens of millions of hospitalizations in the U.S. over the past 30 years.
MDHHS is aware that on May 29, 2025, the CDC made updates to the vaccine schedule on their website
MDHHS continues to recommend COVID-19 vaccination for everyone aged 6 months and older, including those who are pregnant This aligns with longstanding guidance from the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG). Vaccination remains one of the most effective ways to prevent serious illness, hospitalization, and death from COVID-19. Vaccination remains one of the most effective ways to prevent serious illness, hospitalization, and death from COVID-19.
Importantly, COVID-19 vaccination during pregnancy has been shown to protect both the individual and their newborn. Maternal antibodies passed on during pregnancy provide critical early-life protection for infants.
What This Means for Michigan Providers
MDHHS continues to support evidence-based decision-making grounded in thorough safety reviews. The recent changes in CDC guidance were not based on new data, peer-reviewed evidence, or updated medical studies. MDHHS will continue to independently review all federal guidance to ensure alignment with Michigan-specific health priorities and population needs.
We urge providers to stay informed, discuss the benefits of vaccination with patients using shared decision-making practices, and continue offering COVID-19 vaccines as part of routine preventive care, during prenatal visits and pediatric appointments.
If you have questions about this guidance or need additional support, please contact the MDHHS Division of Immunization at checcimms@michigan.gov. F
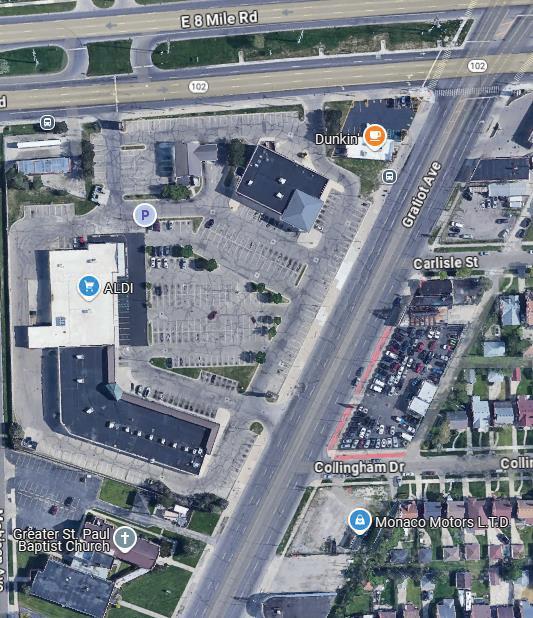
Thursdays from 11am-3pm (parking lot)
Time commitment: One 4-hour shift monthly, bi-monthly or weekly
MICHIGAN STATE UNIVERSITY-
Length of commitment : ≥6 months
medical students. Two students/shift.
COLLEGE OF OSTEOPATHIC MEDICINE PRECEPTING
Medical liability coverage: Full indemnification provided by MSU – letter of proof provided
HARM:LESS
Contact: Dr. Bret Bielawski, bielaws2@msu.edu , (586) 453 9527
students and sign the SOAP note
Michigan State University -College of Osteopathic Medicine Precepting
Scan for a video on Harm:Less / MCSM
The Need: Attending preceptors for Macomb County Street Medicine
Attending preceptors for Macomb County Street Medicine
When: Mondays, Wednesdays and Thursdays from 11am-3pm
Mondays, Wednesdays and Thursdays from 11am-3pm
SW corner 8 -mile/Gratiot (parking lot)
Abscess, soft tissue infections, basic wound care on site antibiotics only phone calls or portal messages
Where: SW corner 8-mile/Gratiot (parking lot) 1st and 2nd year MUC and DMC medical students. Two students/shift.
desire to work with unhoused individuals with SUD
and 2 nd year MUC and DMC medical students. Two students/shift.
monthly, bi-monthly or weekly
Face Addiction Now, HARM:LESS
responsibilities :
Partners: Face Addiction Now, HARM:LESS
Preceptor responsibilities:
• Need to be on site overseeing students and sign the SOAP note
• Urgent care complaints
Need to be on site overseeing students and sign the SOAP note
Urgent care complaints
indemnification provided by MSU – letter of proof provided bielaws2@msu.edu , (586) 453 9527
Partnership!
o Sinusitis, OM, Dental Abscess, soft tissue infections, basic wound care
o Medications dispensed – on site antibiotics only
• No testing, notes to write, patient phone calls or portal messages
o Sinusitis, OM, Dental Abscess, soft tissue infections, basic wound care
o Medications dispensed – on site antibiotics only testing, notes to write, patient phone calls or portal messages
Requirements: Attending physician, desire to work with unhoused individuals with SUD
Requirements : Attending physician, desire to work with unhoused individuals with SUD
Scan for a video on Harm:Less / MCSM
Time commitment: One 4-hour shift monthly, bi-monthly or weekly
commitment: One 4-hour shift monthly, bi-monthly or weekly commitment : ≥6 months
Length of commitment: ≥6 months
Medical liability coverage: Full indemnification provided by MSU – letter of proof provided
liability coverage: Full indemnification provided by MSU – letter of proof provided Dr. Bret Bielawski, bielaws2@msu.edu , (586) 453 9527
Contact: Dr. Bret Bielawski, bielaws2@msu.edu, (586) 453 9527
Scan for a video on Harm:Less / MCSM
Scan for a video on Harm: Less/MCSM
July
Richard Arden, MD
Basivi Baddigam, MD
Mark Bergin, MD
William Carion, MD
Mariann Channell, MD
James Dietz, MD
Lillman Dwarka, MD
Vasilios Gikas, DO
Thomas Graves, MD
John Guest, MD
Jareer Hmoud, MD
Mitchell Hollander, MD
Noori Ibrahim, MD
Carolann Kinner, DO
Linda Lu Kosal, DO
Vijaya Kotha, MD
Donna Kushner, MD
George Kypros, MD
Rakesh Lattupalli, MD
Cheryl Lerchin, MD
Ronald Levin, MD
Richard Lubera, MD
The MCMS would like to wish the following members a very Happy Birthday!
Shyam Moudgil, MD
Anne Nachazel, MD
A. A. Palacio-Chang, MD
Parag Patel, MD
Swarn Rajpal, MD
Naveed Siddique, MD
Naysha Varghese, MD
Mary Veremis-Ley, DO
August
Fadi Al-Qas Hanna, MD
Zeena Al-Rufaie, MD
Jagatbhai Amin, MD
Ramon Aparece, MD
Allen Babcock, MD
Gerald Brueckner, MD
Ricardo Chalela, MD
Amnat Chandra, MD
Genevieve Crandall, MD
Gordhan Diora, MD
Hamsa Gabbara, MD
Stuart Gildenberg, MD
Tristan Guevara, DO
Dorothy Halperin, MD
Theresa Hsu, MD
Danilo Iglesias, MD
Joseph Kinzie, MD
Robert Lechy, MD
Donald Muenk, MD
Ganga Nadarajah, MD
Pradeep Nagaraju, MD
Chakradhar Reddy, MD
Renato Reyes, MD
Kathleen Rheaume, MD
Katie Rosen, DO
Andres Santiviago, MD
Gary Stencel, MD
Philip Tangalos, DO
Salvatore Ventimiglia, MD
Bhavana Vyas, MD
Abdallah Zamaria, MD
September
Ramy Alosachie, MD
Paul Chuba, MD
Mark Decco, MD
We would like to welcome the following New Members!
Stephen Field, MD
Juan Frontera, MD
Narendra Gohel, MD
Brian Guz, MD
Derek Hill, DO
Jane Krasnick, MD
David Law, DO
Amar Majjhoo, MD
Gregory McIntosh, DO
Somsak Metriyakool, MD
Robert Mobley, MD
Eric Neisch, MD
Nwanneka Odumodu, MD
Ashok Reddy, MD
Akash Sheth, MD
Brian Stewart, DO
Alexander Tapper, MD
Steven Thibault, MD
Douglas Verrill, MD
John Vollmer, MD
Sanjay Vora, DO
Sundeep H. Patel, MD
Diagnostic Radiology – Board Certified Medical School: Ross University School of Medicine (FL), 2007. Post Graduate Education: Louisiana State University Health Science Center (LA), completed in 2008; St. Joseph Mercy Oakland, completed in 2012; Beaumont Royal Oak, completed in 2013. Hospital Affiliations: Henry Ford Detroit, Henry Ford Macomb, Henry Ford W. Bloomfield. Currently practicing at Henry Ford Macomb Hospital, 15855 19 Mile Rd., Clinton Twp., MI 48038, ph. 800-653-6568.
Douglas S. Verrill, MD
Physical Medicine & Rehabilitation – Board Certified Medical School: University of Toledo College of Medicine (OH), 2014. Post Graduate Education: Rush University Medical Center (IL), completed in 2015; McGaw Northwestern Medical Center (IL), completed in 2018. Hospital Affiliations: Henry Ford Macomb. Currently practicing at David S. Weingarden MD & Associates, 43555 Dalcoma Dr., Ste. 4, Clinton Twp., MI 48038, ph. 586-228-2882, fx. 586-463-7152, www.dswmd.com.
Tri-County Legislative Committee
Lawmakers want and need to hear from professionals in the field of medicine!
The Tri-County Legislative Committee meets quarterly with legislators from Macomb, Oakland, and Wayne Counties. These meetings provide an open forum for physicians to engage directly with legislators who are often seeking physician input and education on healthcare related legislation.
2025 Meeting Dates
Monday, September 29 –Virtual, 7 pm
Monday, November 17 – Virtual, 7 pm
Anyone interested in joining the Committee please contact Heidi Leach at HLeach@macombcms.org.
Henry Ford Macomb Hospital
EMILY MOORHEAD IS HENRY FORD MACOMB HOSPITAL’S NEW PRESIDENT
Emily became president of Henry Ford Macomb Hospital in 2025. She first joined Henry Ford Health in 2020, serving as Chief Operating Officer and President for the Jackson market, encompassing a nine-county region.
Equipped with a chemistry degree from Michigan State University and an MBA specializing in Strategy and Organizational Development from the University of Michigan, Emily brings a powerful blend of scientific understanding and strategic business insight to her roles. Her extensive experience in senior healthcare leadership includes previous positions as President, Chief Operating Officer, and Chief Strategy Officer.
Emily is highly regarded for achieving strong performance, empowering staff, and cultivating a positive and supportive workplace culture. Her professional passion is centered on advancing prevention and well-being for all individuals at every stage of life.
STEPHANIE GIBSON NAMED CHIEF NURSING OFFICER AT HENRY FORD MACOMB
Stephanie Gibson has been named Vice President of patient care services and Chief Nursing Officer for Henry Ford Macomb Hospital. She had been the interim CNO since May, while continuing her role as director of heart & vascular services and critical care.
Stephanie has been with Henry Ford Health for more than 16 years. She has continued to take on progressive challenges, including her work at our former Mt. Clemens behavioral campus, with grace, operational expertise and an incredible commitment to our patients and team members.
She earned a bachelor’s degrees in psychology and nursing from Oakland University and a master’s in health care administration from Central Michigan University.
MEDICAL RECORDS OF RETIRED PHYSICIANS
Patients looking for their medical records from retired physicians frequently contact the MCMS. If you are retired or will be retiring shortly, please contact the MCMS at 877-264-6592 or email HLeach@macombcms.org and let us know how patients can retrieve their records. If the records have been destroyed, please inform us of that also so we can note our database accordingly. Thank you!
McLaren Macomb Hospital
CONGRATULATIONS, ANNETTE, KELLY, AND LISA! MCLAREN MACOMB DAISY AWARD WINNERS
McLaren Macomb is proud to again recognize members of its care team with the Daisy Award, a nationwide program to recognize outstanding nursing.
Case manager Annette Love, RN, cardiac specialty unit nurse Kelly Frisbee, RN, and endoscopy nurse Lisa Haase, RN, are the latest hospital recipients of the Daisy Award.
“The Daisy Award is a regular and influential reminder that the heart of nursing is the courage, compassion, and commitment nurses bring to their patients each and every day,” said Tricia Haener, McLaren Macomb Chief Nursing Officer. “It is our honor to recognize these nurses, not only for their actions that led to this celebration, but for all nurses who chose this as their profession and calling.”
Annette was nominated by a hospital colleague. Kelly and Lisa were nominated by patients in their care.
MOMENTS OF COURAGE: HONORING BREAST CANCER SURVIVORS AT PINK OUT THE PARK
The spirit of hope and support was palpable at the 13th Annual Pink Out the Park, during the Strike Out Cancer Weekend. The decade-long partnership between the Detroit Tigers, the Barbara Ann Karmanos Cancer Institute and McLaren Health
continued from page 12
Care welcomed thousands of fans, mostly sporting pink, in honor and celebration of the hundreds of attendees who have been affected by breast cancer.
The evening began with the inspiring annual pre-game survivor parade, as hundreds of breast cancer survivors took to the field, joined by the physicians and supportive care team members from Karmanos. Together, they stood in unity offering encouragement to the thousands of individuals diagnosed with breast cancer each year.
These dedicated physicians and support staff stood side by side with survivors, representing the bonds formed through compassionate care and unwavering support. Together, as a team of experts and advocates, they walk every step of the journey with their patients, celebrating victories, offering comfort during challenges, and always fighting for brighter tomorrows.
Breast cancer is the most common cancer among American women, and second only to skin cancer across all genders, according to the American Cancer Society. In fact, about 1 in 8 women in the U.S. will be diagnosed with breast cancer at some point in their lives.
At Karmanos, the Breast Cancer Multidisciplinary Team (MDT) brings together a wide range of experts including surgical oncologists, medical oncologists, radiation oncologists, radiologists, pathologists, plastic surgeons, pharmacists, nurse practitioners, dietitians, social workers, genetic counselors, and patient navigators to support patients during a challenging time in their lives. This team is fully dedicated to breast cancer care, combining their knowledge and experience to design a personalized treatment plan for every patient. F
CME Requirements for Licensure
Every three years physicians are required to complete the following continuing education for license renewal.
150 hr. Continuing Medical Education
75 hr. of which must be Category 1 CME credits for MDs
60 hr. of which must be Category 1 CME credits for DOs
3 hr. Pain & Symptom Management
with 1 hr. Controlled Substance Prescribing 1 hr. Medical Ethics
3 hr. Implicit Bias
Additional Requirements
One time – training for Identifying Human Trafficking Victims
One time – training for Opioids & Controlled Substances Awareness for Prescribers
One time – the Medication Access and Training Expansion (MATE) Act, requires DEA registered prescribers to have 8 hrs. training in opioid use disorders
Greater Macomb Physician Network Empowering Independent Physicians, Elevating Patient Care
Independent physicians often face unique challenges that require more than just support; they require true partnership. That’s where Greater Macomb Physician Network (GMPN) shines. Rooted in the belief that physicians thrive best when empowered, GMPN has become a vital ally for independent practices across the region. At its core, GMPN is committed to delivering an integrated, value-driven, high-performing network that enhances patient health outcomes while sustaining the independence of physicians. By focusing on meaningful collaborations between members and Health Plans, GMPN reinforces the critical physician-patient relationship. As an educator and communications resource, GMPN bridges the gap between complex healthcare systems and practicing physicians—offering the tools, training, and advocacy they need to succeed.
tives to its physicians, rewarding quality and innovation. Their tailored coaching approach has helped raise patient satisfaction scores to an impressive 90% average. The organization has also achieved top-tier performance—reaching the 90th percentile in most preventive health measures across all payers.
Between 2023 and 2024, GMPN’s care management team helped increase primary care visits by 41% and encouraged more appropriate use of specialist visits, leading to a $30 PMPM savings. With their population health tool, Arcadia, GMPN analyzes cost and utilization trends—enabling smart, strategic changes like reducing radiology use by over 1.5%.
The next five years hold continued growth for GMPN, with a strong focus on expanding services that help independent physicians not just survive but thrive—regardless of care model. GMPN will continue to serve as a trusted partner, adapting with agility to healthcare changes and maintaining its commitment to physician independence.
“Our physicians love that we sponsor their membership in the Michigan State Medical Society (MSMS) as it allows them to take education courses that they would have otherwise had to pay for out of pocket. This includes their state mandated CME,” said Angela Vanker, Executive Director, GMPN.
Whether it's daily support or long-term planning, GMPN’s professional team works in tandem with physicians to improve care quality, boost practice efficiency, and navigate Health Plan dynamics. Through close collaboration with practice staff, the network helps identify specific needs, overcome barriers, and adapt to ongoing changes in the healthcare landscape. The goal? To allow physicians to do what they do best—care for patients—with confidence and clarity.
GMPN’s impact is both measurable and meaningful. Each year, the network distributes over $1 million in performance incen-
“We value our partnership with MSMS, it allows us the time to focus on our partnerships with our practices, while MSMS focuses on fixing complex issues at the payer and advocacy level,” said Vanker.
As a fully independent organization—not funded by private equity or owned by a health system, GMPN offers unmatched flexibility, speed, and focus. This independence allows them to make decisions and deploy interventions that are entirely physician-focused and outcome-driven.
In a world where healthcare can feel increasingly multifaceted and corporatized, GMPN remains committed to keeping the physician at the center, championing independence, and delivering results that matter. F
Have you or a MCMS colleague been elected to a position (specialty society, hospital, community based program, etc.) or honored for your volunteer service within the community or abroad? Let us know. We would like to recognize MCMS members in the“Member News” section of the Medicus. Contact Heidi Leach at HLeach@macombcms.org with newsworthy information. Publication is subject to availability of space and the discretion of the Editor.
This Meeting is FREE for MCMS Members and Non-Member Physicians Join Your Colleagues for an Evening of Socializing and Networking
Proactive efforts to promote the value of physicians as the leaders of the health care team and advocates for their patients. Available MSMS resources. PROGRAM HIGHLIGHTS:
Current legislative, regulatory, and payer hot topics. How MSMS is working to improve the lives of Michigan’s physicians
New Scam Letters and Calls Target Medical Practitioners
The Drug Enforcement Administration (DEA) is warning registrants of new fraud schemes in which scammers impersonate DEA personnel and notify registrants that they are under investigation, presumably in an attempt to obtain personal information.
DEA has recently received reports of false letters and phone calls being used to contact both DEA registrants and non-registrants. It is not the DEA’s practice to call registrants regarding investigative matters.
If you are contacted by a person purporting to work for DEA and stating that you are under investigation, please report the incident to the FBI at www.ic3.gov. You may also wish to submit the incident to the Federal Trade Commission, which takes reports at www.ReportFraud.ftc.gov and shares information with more than 3,000 law enforcement agencies. For any victims who have given personally identifiable information like a Social Security number or DEA registration number to a scammer, go to www.identitytheft.gov to learn how to protect against identity theft. Reporting these scams will help authorities find, arrest, and stop the criminals engaged in this fraud.
As a reminder, DEA personnel will never contact registrants or members of the public to demand money or any other form of payment, will never request personal or sensitive information, and will only notify people of a legitimate investigation or legal action in person or by official letter. In fact, federal law enforcement officers are prohibited from demanding cash or gift cards from a member of the public.
The best deterrence against these bad actors is awareness and caution.
Physicians and other healthcare providers are increasingly at risk of being targeted by scams, including impersonation scams where criminals pose as law enforcement or government officials to extort money or steal medical or personal information.
The Macomb County Medical Society (MCMS) recently learned of a new attempt to defraud physicians by scammers claiming to need information as part of a Medicare audit. The Centers for Medicare and Medicaid Services posted the following alert on its Crushing Fraud, Waste, & Abuse website:
CMS has identified a fraud scheme targeting Medicare providers and suppliers. Scammers are impersonating CMS and sending phishing fax requests for medical records and documentation, on CMS letterhead, falsely claiming to be part of a Medicare audit.
Important: CMS does not initiate audits by requesting medical records via fax
Protect your information: If you receive a suspicious request, do not respond. If you think you got a fraudulent or questionable request, work with your Medical Review Contractor to confirm if it is real. F
MSMS Task Force Examines Future Relationship with County Medical Societies
By: Heidi Leach, MCMS Executive Director
Background: Why This Matters
Currently county medical societies, including Macomb County Medical Society (MCMS), are charted components of the Michigan State Medical Society (MSMS) requiring dual membership in both organizations. However, MSMS is considering the "delinking" of county medical societies from MSMS, which could fundamentally change how the MCMS operates, funds itself, and represents its members.
This is the third time in recent memory that MSMS has evaluated a potential separation from county medical societies. The first two attempts were voted down by the House of Delegates (HOD), confirming that members felt the state and county societies were stronger together as unified organizations.
If the MSMS proposal moves forward, it will directly impact the MCMS’ structure, dues model, and long-standing connection to organized medicine at the state level.
Key Resolutions from the 2025 HOD Driving Changes
Three resolutions are prompting the current review:
• Resolution 14-25: Directs MSMS to return to alternating the HOD meeting location between southeast Michigan and Lansing. The resolution was referred to the MSMS Board for further study.
• Resolution 16-25: Creates a task force of county and state leaders to examine history, finances, and bylaws, and recommend a unified path forward for medical societies in Michigan.
• Resolution 47-25: Directs MSMS to study other state medical society structures and bylaws for potential improvements in efficiency and productivity.
MSMS Reorganization Task Force
Following HOD approval, MSMS formed a Reorganization Task Force composed of six MSMS Board members, six county representatives, and one county executive (non-voting). The Task Force will hold three meetings this fall and report final recommendations to the MSMS Board in January 2026. The Task Force is charged with reviewing:
• House of Delegates structure
• Organizational partnerships between MSMS, county medical societies, and specialty societies
• Leadership and governance models for MSMS
The MSMS Board voted at their July meeting to change future HOD meetings to fully virtual with no in-person component beginning in 2026. This is estimated to save MSMS $60,000 annually.
Potential options under consideration by the Task Force include a redefined membership model (delinking MSMS and county medical societies), a smaller MSMS board, longer presidential term of office, revised voting structures, and elimination of the MSMS Judicial Commission and Code of Conduct from MSMS’ Bylaws (due to a lack of authority to perform peer review).
Concerns have been raised about variability among county medical societies in financial management, dues structure, and member benefits offered. Some counties lack functioning boards and/or IRS nonprofit status yet dues are being collected by MSMS on their behalf.
Questions Raised by County Medical Societies County societies are seeking clarity on several issues:
• Structure: What models for state-county relationships are being considered?
• Financial Impact: How will separation affect dues collection and county medical society budgets?
• Representation: Without county medical societies, how will local physicians have a voice at the state level?
• Legal Concerns: Could shared services or reforms strengthen county medical society oversight instead of dismantling unified membership?
• Process: Will there be one or two HOD readings of necessary Bylaw changes, and how will member feedback shape final recommendations?
Your Input Matters
The decisions made over the coming months could significantly impact how Michigan physicians are represented and the future longevity of our county society. MCMS wants to hear your thoughts and concerns regarding a potential separation between MSMS and county medical societies. Please email Heidi Leach, Executive Director, at HLeach@macombcms.org with your feedback. Your input will help guide the MCMS in advocating for what best serves local physicians and the profession statewide. F
By: Daniel M. Ryan, MD, MSMS Region 2 Director
MSMS
ANNOUNCES
NEW LEADERSHIP
FOLLOWING
2025 HOUSE OF DELEGATES ELECTIONS
MSMS is pleased to announce the newly elected officers chosen during the House of Delegates meeting held on Saturday, May 3, 2025. These distinguished leaders will play a vital role in guiding MSMS’s mission to support physicians and advocate for the health of Michigan’s patients and communities.
Immediate Past President Mark C. Komorowski, MD, formally passed the torch of leadership to Amit Ghose, MD, the newly installed President of MSMS. Dr. Komorowski presented the presidential medallion to Dr. Ghose, marking the official transition of presidential duties.
Dr. Ghose operates a private practice at Capital Internal Medicine Associates in Lansing and is a Clinical Professor at Michigan State University’s College of Osteopathic Medicine. He is also part of the Internal Medicine Residency Program faculty at McLaren Greater Lansing. Dr. Ghose previously served as Chief of Staff at Ingham Regional Medical Center and Sparrow Hospital.
In addition to his leadership within MSMS, Dr. Ghose actively contributes to several professional organizations, including the American College of Physicians, the American Medical Association, the British Medical Association, and the Indian Medical Association. He represents Michigan physicians as a liaison to the AMA Senior Physician Section and sits on the Governor’s Council for the Michigan Chapter of the American College of Physicians.
His dedication to excellence in teaching and clinical practice has earned him multiple accolades, including the ACP Michigan Award for Contribution to Private Practice and several honors for clinical teaching.
Phillip G. Wise, MD, of Kent County, was elected President-Elect of MSMS.
Bryan W. Huffman, MD, of Ottawa County, was elected Speaker of the House of Delegates.
Mildred J. Willy, MD, of Saginaw County, was elected Vice Speaker.
Please join MSMS in congratulating Dr. Huffman, Dr. Willy, Dr. Wise, and Dr. Ghose.
MSMS CELEBRATES DOCTOR BOBBY MUKKAMALA’S INAUGURATION AS 180TH AMA PRESIDENT
MSMS proudly congratulates Bobby Mukkamala, MD, a longtime MSMS leader and past president, on his historic inauguration as the 180th president of the American Medical Association (AMA). As a dedicated otolaryngologist from Flint, Dr. Mukkamala brings a powerful blend of clinical expertise and lived experience to the national stage, including a recent personal battle with brain cancer that has deepened his resolve to fight for a more equitable and effective health care system.
In his moving inauguration address, Dr. Mukkamala reflected on the strength of the U.S. health system in saving his life while also calling attention to its inequities, particularly for patients in underserved communities like Flint. His story underscores the urgent need for physician-led advocacy to address rising health care costs, long wait times, physician shortages, and systemic inefficiencies like prior authorization. As AMA president, Dr. Mukkamala pledged to champion reforms that ensure all patients, not just the fortunate few, have access to timely, compassionate, and high-quality care.
MSMS is proud to support Dr. Mukkamala and other Michigan physicians leading change on the national level. His presidency is a testament to the strength of physician leadership in Michigan and the vital role MSMS plays in preparing and empowering those who speak with clarity, urgency, and purpose on behalf of our profession and the patients we serve.
AMA ANNUAL MEETING SUMMARY
On June 11, 2025, the American Medical Association (AMA) Annual Meeting concluded its business having addressed over 60 resolutions and 60 reports from the Board of Trustees and Councils. For Michigan, there was much to celebrate as MSMS past president Bobby Mukkamala, MD, from Flint, was inaugurated as the 180th AMA president. Additionally, MSMS board member, Lou C. Edje, MD, MHPE, FAAFP, was re-elected to the AMA Council on Medical Education, and former MSMS board member, Michael J. Redinger, MD was appointed to the AMA Council on Ethical and Judicial Affairs.
During the Annual Meeting, the Michigan Delegation continued to be a visible and active force within the AMA HOD. Michigan’s Resolution 239, “Ensuring Accessibility and Inclusivity of CDC Resources,” was widely supported. The AMA House of Delegates (HOD) adopted Resolution 239, which advocates for the maintenance of evidence-based public health information and resources on the website of the Centers for Disease Control and Prevention (CDC).
continued on page 19 18 Macomb Medicus | July/August/September 2025
Many timely topics of interest and concern were discussed during the meeting including, but not limited to, Medicaid and Medicare funding, the corporate practice of medicine, artificial intelligence, prior authorization burdens, medical misinformation, and care delivery. The AMA HOD adopted a resolution directing the AMA to elevate Medicaid to an urgent and top legislative advocacy priority alongside Medicare payment reform, as well as a resolution opposing federal action to restrict or eliminate states’ ability to assess provider (hospital and nursing home) and managed care organization taxes to help with Medicaid financing and patient access to care. Additionally, an emergency resolution was introduced and adopted in response to Secretary Kennedy’s removal of all of the members of the Advisory Committee on Immunization Practices (ACIP), which called upon the AMA to initiate public advocacy in support of the ACIP structure, ask for a reversal of the action, and call for an investigation into this action.
For more meeting highlights, click here
KEY FACTS TO KNOW ABOUT MEASLES
The number of confirmed cases of measles in the U.S. continues to rise. Data from the Johns Hopkins University Center for Outbreak Response Innovation shows 1,285 cases as of July 9, 2025. With 18 confirmed cases, Michigan is listed as 7th highest amongst the states and District of Columbia.
The top ten states are as follows: Texas: 792, New Mexico: 95, Kansas: 86, Ohio: 35, North Dakota: 34, Montana: 25, Michigan: 18, California: 17, Oklahoma: 17, Colorado: 16.
Encouraging vaccination is critical to prevent further disease spread. Measles can cause serious health problems like lung infection, brain damage, and even death. While measles cases in Michigan remain relatively low as compared to Texas, New
Mexico, and Kansas, we do not want join those states with major outbreaks. Below are some key messages to share with your patients, family members, and friends:
• The CDC recommends that children receive one dose of the MMR vaccine at 12 to 15 months and a second dose at 4 to 6 years.
• Adults born in 1957 or later who have not received any MMR vaccines or aren’t sure if they have immunity should talk to their health care provider about getting vaccinated. One or two doses are recommended depending on the adult’s risk level.
• If traveling internationally, the Michigan Department of Health and Human Services recommends that adults who have no evidence of immunity and unvaccinated children 12 months and older receive two doses of the MMR vaccine at least four weeks apart before departure.
• Infants ages 6 to 11 months should receive one dose before international travel, but this does not count toward their two-dose series.
• MMR vaccines are available through some health care providers, local health departments, and many pharmacies.
Finally, the Michigan Department of Health and Human Services created this easy to share infographic to highlight what community members need to know about measles. F
BUDGET RECONCILIATION BILL WORSENS ACCESS TO CARE, INCLUDES SIGNIFICANT HEALTH CARE FUNDING CUTS
The One Big Beautiful Bill (OBBB) Act of 2025 (H.R. 1), the massive budget reconciliation bill implementing many of the administration’s top legislative priorities, was signed into law on July 4. The bill includes significant funding cuts and policy changes to Medicaid and the Health Insurance Marketplaces, Medicare physician payment, and medical student loans, among other health care related items:
• Medicaid. The OBBB creates new administrative requirements and conditions on eligibility (including work requirements) for patients seeking to enroll in or maintain Medicaid coverage and restricts states’ ability to use provider taxes to finance their Medicaid programs.
• Access to health insurance coverage through the Affordable Care Act (ACA) marketplaces. The OBBB imposes verification requirements for patients receiving premium tax credits, including pre-enrollment verification requirements that will effectively end automatic re-enrollment for these patients. The OBBB does not address the scheduled expiration of enhanced tax credits at the end of 2025.
• Federal support of medical student loans. The OBBB, in part, removes the ability for medical students to receive Federal Direct Stafford loans and Federal Direct PLUS Loans, caps the amount that can be borrowed for school, and limits federal student loan borrowers to only two repayment options.
• Medicare physician payment reform. The OBBB includes a temporary one-year 2.5% conversion factor update for 2026, replacing the original House bill that called for a 75% MEI inflation update in 2026 followed by annual 10% MEI increase, leaving no permanent, inflation adjusted payment fix.
or costly chronic conditions. That is disappointing, maddening, and unacceptable.”
CMS ANNOUNCES WASTEFUL AND INAPPROPRIATE SERVICE REDUCTION (WISeR) MODEL
CMS recently announced the Wasteful and Inappropriate Service Reduction (WISeR) Model, a new Innovation Center demonstration aimed at reducing Medicare spending on services deemed “low-value” or unnecessary. Beginning in 2026, in selected regions, CMS will use artificial intelligence and machine learning, as well as clinical reviewers to perform pre-payment prior authorization reviews for targeted services, such as electrical nerve stimulator implants, skin and tissue substitutes, and knee arthroscopy procedures. Providers in the selected regions will have the choice to either submit a prior authorization request for these services or instead have claims undergo a pre-payment review. The demonstration will run for six performance years, with participating technology vendors being incentivized to help identify and deny wasteful claims before payment is made. While CMS anticipates savings and more efficient uses of Medicare dollars, the model represents a significant shift in how care is reviewed in Traditional Medicare.
The AMA has serious concerns about WISeR’s potential to increase physicians’ administrative burdens, delay patient care, and shift profit incentives to third-party vendors focused on denials rather than high-quality care. The AMA is especially concerned that this model could further expand prior authorization requirements into Traditional Medicare, by setting a precedent for mandatory programs in the future. The AMA has consistently advocated for clear transparency, fair review standards, real-time processing, and strong protections for both physicians and patients. The AMA is preparing a formal comment letter to CMS and CMMI to share concerns and advocate for improvements that safeguard access to care, reduce unnecessary practice burdens, and urge that all elements of the model (and any future iterations) be truly voluntary.
In a statement issued on July 3, AMA President Bobby Mukkamala, MD, said, “Today is a sad and unnecessarily harmful day for patients and health care across the country, and its impact will reverberate for years. Care will be less accessible, and patients may simply forego seeing their physician because the lifelines of Medicaid and CHIP are severed. This is bad for my patients in Flint, Michigan, and it is devastating for the estimated 11.8 million people who will have no health insurance coverage as a result of this bill. The American Medical Association’s mission is promoting the art and science of medicine and the betterment of public health. This bill moves us in the wrong direction. It will make it harder to access care and make patients sicker. It will make it more likely that acute, treatable illnesses will turn into life-threatening
UPDATES TO THE MEDICARE ADVANTAGE AUDITS
CMS recently announced significant updates to its Risk Adjustment Data Validation (RADV) audit process for Medicare Advantage (MA) plans, aimed at strengthening oversight of MA payments to ensure accurate reflections of enrollees’ health status. Under the updated RADV framework, CMS will now audit all eligible MA contracts (approximately 550) annually. Additionally, CMS aims to increase the number of records audited per plan from 35 to up to 200 per year. CMS has also committed to completing all outstanding audits for payment years 2018-2024 by early 2026. To fulfill these goals, CMS will utilize enhanced technologies and will also increase its team of medical coders from 40 to approximately 2,000 by September 2025.
continued from page 20
The AMA supports efforts to strengthen the integrity of the MA program and reduce improper payments. However, there are concerns about the potential downstream administrative burden placed on physicians. Through these updates, providers are likely to experience increased medical records requests, tighter deadlines for data correction, and potentially heightened demands from MA plans and vendors for repayment. The AMA encourages physicians to track any new audit-related workload challenges, particularly around responding to records requests or coordinating with MA plans under compressed timelines. If you experience any new challenges related to increased RADV audit activity, the AMA encourages you to share your feedback with us to ensure we properly represent your concerns with the administration. F
August 13 ~ Navigating Employee Terminations: Best Practices for Successful Off-Boarding
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75
AMA/PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/ Retired/Life members.
August 13 ~ Best Practice Prescription: Physician Recruitment for Performance & Retention
MSMS Practice Management Series, Live Webinar, 1 pm – 2 pm, 1 AMA/PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/ Retired/Life members.
September 10 ~ Specimen Collection and Test Interpretation in Microbiology: What do you need to know?
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75
AMA/PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/ Retired/Life members.
September 10 ~ Patient Experience in the Age of AI
MSMS Practice Management Series, Live Webinar, 1 pm – 2 pm, 1 AMA/PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/ Retired/Life members.
September 15 ~ Reducing Unconscious Bias - an Imperative (RUBI)
MSMS Monday Night Medicine, Live Webinar, 5:30 pm – 8 pm, 3 AMA/PRA Category 1 CME Credit. Meets LARA’s 3-hr. Implicit Bias requirement. Cost: FREE for Active, Active Emeritus, & Resident members; $140 for Emeritus/Retired/Life members; $190 for non-members.
September 29 ~ Tri-County Legislative Meeting
Virtual meeting, 7 pm. Engage directly with legislators from Macomb, Oakland & Wayne Counties in meaningful dialogue and help guide the future of healthcare policy.. To register email Heidi Leach.
October 8 ~ Steroids in Critical Illness: Focused Updates for Steroid Use
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75 AMA/ PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/Retired/Life members.
October 14 ~ MCMS Annual Membership Meeting
FREE for MCMS Members, 6 pm cocktails, 6:30 pm dinner, 7 pm program, at Ike’s Restaurant in Sterling Heights. Topic: “MSMS: Working For You, With You”, speaker: Stacey Hettiger, Senior Director of MSMS Advocacy & Payor Relations. Registration is required by Oct. 10th. To register email Heidi Leach
November 8 ~ MSMS 29th Annual Conference on Bioethics Hybrid (In-Person and Virtual) Event, 8:30 am – 3:30 pm, at the Double Tree by Hilton in Ann Arbor.
November 12 ~ How to Think Logically and Communicate Clearly in Medicine
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75 AMA/ PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/Retired/Life members.
November 17 ~ Tri-County Legislative Meeting
Virtual meeting, 7 pm. Engage directly with legislators from Macomb, Oakland & Wayne Counties in meaningful dialogue and help guide the future of healthcare policy. To register email Heidi Leach.
December 8 ~ Reimagining Healthcare: A Workshop on Racism, Empathy & Transformation
MSMS Monday Night Medicine, Live Webinar, 5:30 pm – 8 pm, 3 AMA/PRA Category 1 CME Credit. Meets LARA’s 3-hr. Implicit Bias requirement. Cost: FREE for Active, Active Emeritus, & Resident members; $140 for Emeritus/Retired/Life members; $190 for non-members.
December 10 ~ Tired of Being Tired? CPAP Alternatives for the PAP-Intolerant OSA Patient
MSMS Grand Rounds, Live Webinar, 12 pm – 12:45 pm, .75 AMA/ PRA Category 1 CME Credit. Cost: FREE for Active members & office staff; $25 for non-members & Emeritus/Retired/Life members.
Medicaid Changes Ahead & Medical Licensure Bill Progresses in Michigan
Michigan’s healthcare system is facing pivotal changes on two major fronts — federal Medicaid reforms and the state’s potential withdrawal from the Interstate Medical Licensure Compact (IMLC). While the recently passed federal budget reconciliation bill, H.R. 1, threatens to cut Medicaid funding and access, Michigan’s continued participation in the IMLC now depends on the passage of Senate Bill 303.
Medicaid Cuts Loom
Major federal changes to Medicaid are on the horizon after the passage of sweeping federal budget legislation, H.R. 1. While many of the most significant changes don’t take effect immediately, the effects are already being felt across Michigan — from Lansing to the state's most rural corners. Across the state, advocates and Medicaid recipients are sounding the alarm over the looming reductions in eligibility and funding embedded in the new law.
What’s in the Bill? H.R. 1 includes:
• Deep cuts to federal Medicaid funding, pushing more financial responsibility onto states.
• New work and eligibility requirements that will complicate access to care.
• Administrative hurdles that could result in many people losing coverage – even before the official implementation date.
• Though these changes are scheduled for 2027, their influence is already shifting the way Michigan’s healthcare system operates.
How Will This Affect Michigan? Hospitals, physicians, other providers, and state agencies are already bracing for impact:
• Hospitals are postponing major investments, staff recruitment, and expansion plans due to the projected funding shortfall.
• Rural areas, where hospitals are often the largest employers and serve aging, low-income populations, will be hit hardest.
• The Michigan Department of Health and Human Services warns that the state may need to either drastically cut services or find new state revenue to make up for the loss of federal support.
• As eligibility becomes harder to maintain, many people may lose coverage unnecessarily – simply out of confusion or fear.
What Happens Next? While some believe there is still time to revise or soften the bill’s impacts, advocates are urging immediate action:
• The Protect MI Care Coalition, of which MSMS is a member is working to educate the public and prevent premature coverage loss.
• State and local leaders are calling on Congress to revisit the bill’s harshest provisions before implementation begins.
• Healthcare professionals and patients alike are preparing for a more difficult, less secure future. MSMS and MCMS will work to keep members well-informed as implementation of the bill’s various provisions rolls out.
Michigan and the Interstate Medical Licensure Compact
Physicians and healthcare organizations are watching closely as Senate Bill 303 advances through the Legislature — a bill that could determine whether Michigan continues its participation in the Interstate Medical Licensure Compact (IMLC) beyond 2026.
The purpose of the Interstate Medical Licensure Compact is to streamline the process for physicians to become licensed in multiple states, helping them more easily practice across state lines. For physicians holding a State of Principal License (SPL) in Michigan, the compact removes red tape and expands access to patients across the country.
Due to a sunset clause in Michigan law, the state is on track to automatically withdraw from the IMLC on March 28, 2026, unless legislative action is taken. The statute that authorized Michigan’s participation was repealed in March 2025, triggering the formal 12-month withdrawal process.
However, Senate Bill 303 would reverse that course by extending Michigan’s participation in the IMLC. The bill has passed the Michigan Senate and cleared the House Health Policy Committee. It now awaits a vote by the full House of Representatives. If approved by the House, it will be sent to the Governor’s desk for signature — securing Michigan’s continued role in the compact and preserving multi-state licensure pathways for physicians.
In the meantime, Michigan remains an active IMLC member and will continue to participate in IMLC operations through March 28, 2026. MSMS and MCMS will continue to monitor the legislation and keep members informed of its progress. F
MICHIGAN SENATE
Sen. Stephanie Chang (D)
Senate District 3
SenSChang@senate.michigan.gov (517) 373-7346
Sen. Kevin Hertel (D)
Senate District 12
SenKHertel@senate.michigan.gov (517) 373-7315
Sen. Ruth Johnson (R)
Senate District 24
SenRJohnson@senate.michigan.gov (517) 373-1636
Sen. Veronica Klinefelt (D) Senate District 11
SenVKlinefelt@senate.michigan.gov (517) 373-7670
Sen. Daniel Lauwers (R) Senate District 25
SenDLauwers@senate.michigan.gov (517) 373-7708
Sen. Michael Webber (R) Senate District 9 SenMWebber@senate.michigan.gov (517) 373-0994
Sen. Paul Wojno (D) Senate District 10 SenPWojno@senate.michigan.gov (517) 373-8360
COMMITTEES
House – Appropriations
Kimberly Edwards (D), District 12
Thomas Kuhn (R), District 57
Donavan McKinney (D), District 14
House – Appropriations Subcommittee
LARA, Insurance & Financial Services
Donavan McKinney (D), District 14 –
Vice Chair
2025 Macomb County Legislator Contact Guide
MICHIGAN HOUSE
Rep. Joseph Aragona (R) House District 60 JosephAragona@house.mi.gov (517) 373-1785
Rep. Jay DeBoyer (R) House District 63 JayDeBoyer@house.mi.gov (517) 373-1787
Rep. Kimberly Edwards (D) House District 12 KimberlyEdwards@house.mi.gov (517) 373-0852
House – Appropriations Subcommittee
Public Health
Tom Kuhn (R), District 57 - Vice Chair
House – Appropriations Subcommittee
Medcaid & Behavioral Health
Tom Kuhn (R), District 57
House – Families & Veterans
Doug Wozniak (R), District 59
Mai Xiong, (D), District 13
Rep. Jaime Greene (R) House District 65 JaimeGreene@house.mi.gov (517) 373-1775
Rep. Thomas Kuhn (R) House District 57 TomKuhn@house.mi.gov (517) 373-1706
Rep. Mike McFall (D) House District 14 MikeMcFall@house.mi.gov (517) 373-0140
House – Health Policy
Alicia St. Germaine (R), District 62
House – Insurance
Joseph Aragona (R), District 60
Senate – Appropriations
Kevin Hertel (D), District 12
Veronica Klinefelt (D), District 11
Rep. Donavan McKinney (D)
House District 11
DonavanMcKinney@house.mi.gov (517) 373-0849
Rep. Denise Mentzer (D) House District 61
DeniseMentzer@house.mi.gov (517) 373-1774
Rep. Ron Robinson (R) House District 58
RonRobinson@house.mi.gov (517) 373-1794
Rep. Josh Schriver (R) House District 66
JoshSchriver@house.mi.gov (517) 373-0839
Rep. Alicia St. Germaine (R) House District 62
AliciaStGermaine@house.mi.gov (517) 373-0555
Rep. Douglas Wozniak (R) House District 59
DouglasWozniak@house.mi.gov (517) 373-0832
Rep. Mai Xiong (D) House District 13
MaiXiong@house.mi.gov (517) 373-0845
Senate – Health Policy
Kevin Hertel (D), District 12
Veronica Klinefelt (D), District 11
Michael Webber (R), District 9
Paul Wojno (D), District 10
Senate – Regulatory Affairs
Kevin Hertel (D), District 12
Dan Lauwers (R), District 25
Michael Webber (R), District 9
Paul Wojno (D), District 10
Macomb Medicus Journal of the Macomb County Medical Society
The Macomb Medicus is the official quarterly journal of the Macomb County Medical Society. It is a full-color glossy magazine published both electronically and in hard copy format. It is a valued news source for our 600 plus physician members of all specialties and their staff throughout Macomb County. In addition to members the Macomb Medicus is sent to hospital executives, Michigan State Medical Society staff, other county medical society staff, and healthcare related businesses/organizations in Macomb County. The Macomb Medicus is read by an impressive cross section of the healthcare community and is electronically available on our website at www.macombcms.org. FREE Hotlink to Your Website & Free Advertising Design! For advertising rates and information, please contact:
Heidi Leach, Executive Director & Managing Editor Macomb County Medical Society, PO Box 551, 810-712-2546 HLeach@macombcms.org | www.macombcms.org
Macomb County Medical Society
P.O. Box 551
Lexington, Michigan 48450-0551
MSMS Physicians Insurance Agency’s licensed agents can help physicians with all their insurance needs – for business, employees and families. We are ready to assist you in protecting your profession.
Protecting You & Your Team
INDIVIDUAL AND GROUP COVERAGES
• Dental Insurance
• Vision Insurance
Protecting You
LINES
MSMS Physicians Insurance Agency’s licensed agents can help physicians with all their insurance needs – for business, employees and families. We are ready to assist you in protecting your profession.
• Short Term and Long-Term Disability Insurance
• Life Insurance
Protecting You & Your Team
• Accidental Death and Dismemberment MEDICAL COVERAGE OPTIONS
INDIVIDUAL AND GROUP COVERAGES
Insurance
Protecting You
Recreational Vehicles
PERSONAL LINES
• Dental Insurance
• HMO/PPO/POS Health Plans
• Auto Insurance
• Vision Insurance
• Health Savings Accounts (HSAs)
• Health Reimbursement Arrangements (HRAs)
• Short Term and Long-Term Disability Insurance
• Wellness Reward Promoting Healthy Living
• Life Insurance
• Medicare Supplemental
• Homeowners Insurance
Cyber Liability Insurance
• Renters insurance
Workers Compensation Insurance
Business Owners Insurance (BOP)
• Umbrella
Directors and Officers Liability Insurance
• Accidental Death and Dismemberment
• GeoBlue Travel Medical and International Health
• COBRA related services for groups over 20 at no cost to the group
MEDICAL COVERAGE OPTIONS
• Motorcycle
Employment Practices Liability Insurance (EPLI)
Commercial General Liability
Errors and Ommissions (E&O)
• Recreational Vehicles PROTECTING YOUR PRACTICE
• HMO/PPO/POS Health Plans
Protecting your Professional Advice
MEDICAL MALPRACTICE
• Health Savings Accounts (HSAs)
• Exclusive benefits for MSMS members
• Health Reimbursement Arrangements (HRAs)
• Cyber Liability Insurance
• Workers Compensation Insurance
• Business Owners Insurance (BOP)
• Wellness Reward Promoting Healthy Living
• Program discount of 5% for qualified members
• Claims free credit up to 25%
• Medicare Supplemental
• Directors and Officers Liability Insurance
• Employment Practices Liability Insurance (EPLI)
• GeoBlue Travel Medical and International Health
• Tribute Plan recognizes doctors for their loyalty and commitment to the practice of good medicine
• COBRA related services for groups over 20 at no cost to the group