Patients eligible for case management services are those with needs that may affect their health care, including women at any age with a high-risk pregnancy. Case managers help patients access medical, non-medical, dental, behavioral health and other services.
HERITAGE AND HEALTH
Rural Surgical Deserts All fingers are not equal: Addressing surgical inequity
Izi Obokhare, MD, FACS, FICS, Professor of Surgery TTUHSC Amarillo; and Muhammad Haris Nazim, MD, FACS, FICS, MEHP, Professor of Surgery TTUHSC Amarillo
Beyond Symptoms: Integrating culture into mental health treatment
Sounding the Alarm: Hearing loss is an underrecognized and undertreated burden that demands more attention in clinical practice
We Must Protect our Firefighters from Cancer By Rachelle Hamblin, MD,
Lessons Learned Rehabbing a Nursing Home in San José, Costa Rica By Arya Bietz; Gabriel Bietz, MD; and Amita Kumar,
PUBLISHED BY: Traveling Blender, LLC. 10036 Saxet Boerne, TX 78006
PUBLISHER: Louis Doucette louis@travelingblender.com
BUSINESS MANAGER: Vicki Schroder vicki@travelingblender.com
GRAPHIC DESIGNER: Jennifer Nelson jennifer@travelingblender.com ADVERTISING
Sandy Weatherford sandy@travelingblender.com
Gerry Lair gerrylair@yahoo.com For
San Antonio Medicine is the official publication of Bexar County Medical Society (BCMS). All expressions of opinions and statements of supposed facts are published on the authority of the writer, and cannot be regarded as expressing the views of BCMS. Advertisements do not imply sponsorship of or endorsement by BCMS
EDITORIAL CORRESPONDENCE:
Bexar County Medical Society 4334 N Loop 1604 W, Ste. 200 San Antonio, TX 78249
Email: editor@bcms.org
MAGAZINE ADDRESS CHANGES: Call (210) 301-4391 or Email: membership@bcms.org
SUBSCRIPTION RATES: $30 per year or $4 per individual issue
ADVERTISING CORRESPONDENCE: Louis Doucette, President Traveling Blender, LLC.
A Publication Management Firm 10036 Saxet, Boerne, TX 78006 www.travelingblender.com
For advertising rates and information Call (210) 410-0014
Email: louis@travelingblender.com
SAN ANTONIO MEDICINE is published by SmithPrint, Inc. (Publisher) on behalf of the Bexar County Medical Society (BCMS). Reproduction in any manner in whole or part is prohibited without the express written consent of Bexar County Medical Society. Material contained herein does not necessarily reflect the opinion of BCMS, its members, or its staff. SAN ANTONIO MEDICINE the Publisher and BCMS reserves the right to edit all material for clarity and space and assumes no responsibility for accuracy, errors or omissions. San Antonio Medicine does not knowingly accept false or misleading advertisements or editorial nor does the Publisher or BCMS assume responsibility should such advertising or editorial appear. Articles and photos are welcome and may be submitted to our office to be used subject to the discretion and review of the Publisher and BCMS. All real estate advertising is subject to the Federal Fair Housing Act of 1968, which makes it illegal to advertise “any preference limitation or discrimination based on race, color, religion, sex, handicap, familial status or national origin, or an intention to make such preference limitation or discrimination.
SmithPrint, Inc. is a family-owned and operated San Antonio-based printing and publishing company that has been in business since 1995. We are specialists in turn-key operations and offer our clients a wide variety of capabilities to ensure their projects are printed and delivered on schedule while consistently exceeding their quality expectations. We bring this work ethic and commitment to customers along with our personal service and attention to our clients’ printing and marketing needs to San Antonio Medicine magazine with each issue.
We call this Insurance For Good because it shows up for you and your community every day.
Unlike most insurers, we don’t answer to shareholders—we answer to our TMA members. So when there’s a surplus, those funds stay right here in Texas.
That means your premiums (with no hidden costs or inflated rates) help provide resources physicians genuinely rely on.
It’s when a colleague shares how emergency relief helped them through a crisis. Or when you discover your insurance provider funded your CME course. Or when a resident you mentor opens up about receiving free, confidential counseling, made possible not through their employer, but through the physician community itself.
And this fall, your coverage can do even more.
We’ve already helped over eight hundred practices across Texas access group PPO coverage, even those without employees. This Open Enrollment season, we’re working with members to review their health insurance options, from updating coverage to looking for potential savings and exploring new choices for their families or practices.
We’re ready to help you discover just how much your insurance can do.
Whether you practice solo, with a partner, or lead a team, you may still qualify for group PPO coverage even just for yourself and your family. See what’s possible. Call 800-880-8181, Monday through Friday, 8:00AM-5:00PM CST, or visit tmait.org to get started. SCAN TO CALL
BCMS BOARD OF DIRECTORS
ELECTED OFFICERS
John Shepherd, MD, President
Lyssa Ochoa, MD, Vice President
Jennifer R. Rushton, MD, President-Elect
Lubna Naeem, MD, Treasurer
Lauren Tarbox, MD, Secretary
Ezequiel “Zeke” Silva, III, MD, Immediate Past President
DIRECTORS
Woodson “Scott” Jones, Member
John Lim, MD, Member
Sumeru “Sam” G. Mehta, MD, Member
M. “Hamed” Reza Mizani, MD, Member
Priti Mody-Bailey, MD, Member
Dan Powell, MD, Member
Saqib Z. Syed, MD, Member
Nancy Vacca, MD, Member
Col Joseph J. Hudak, MD, MMAS, Military Representative
Jayesh Shah, MD, TMA Board of Trustees Representative
John Pham, DO, UIW Medical School Representative
Robert Leverence, MD, UT Health Medical School Representative
Cynthia Cantu, DO, UT Health Medical School Representative
Lori Kels, MD, UIW Medical School Representative
Ronald Rodriguez, MD, UT Health Medical School Representative
Alice Gong, MD, Board of Ethics Representative
Melody Newsom, BCMS CEO/Executive Director
George F. “Rick” Evans, Jr., General Counsel
BCMS SENIOR STAFF
Melody Newsom, CEO/Executive Director
Brissa Vela, Chief Membership & Development Officer
Yvonne Nino, Controller
Betty Fernandez, BCVI Director of Operations
Phil Hornbeak, Auto Program Director
Al Ortiz, Chief Information Officer
Jacob Hernandez, Advocacy and Public Health Specialist
PUBLICATIONS COMMITTEE
Jennifer C. Seger MD, Chair
Timothy C. Hlavinka, MD, Member
John Robert Holcomb, MD, Member
Soma S. S. Jyothula, MD, Member
George-Thomas Martin Pugh, MD, Member
Adam Ratner, MD, Member
Rajam Ramamurthy, MD, Member
Patrick Reeves, MD, Member
John Joseph Seidenfeld, MD, Member
Amith Skandhan, MD, Member
Francis Vu Tran, MD, Member
Subhashini Valavalkar, MD, Member
Louis Doucette, Consultant
Brissa Vela, Staff Liaison
Gabriella Bradberry, Staff Liaison
Trisha Doucette, Editor
Ayomide Akinsooto, Student
Gabrielle Holliefield, Student
Rita Espinoza, DrPH, Volunteer
Melissa Rosales, Volunteer
Ramaswamy Sharma, MS, PhD, Volunteer
Andrea Wazir, Volunteer
11 days after appendectomy, tests for acute abdominal pain revealed a
retained object
left inside the patient.
Surgical miscounts are considered never events because they are usually preventable by following established procedures.
ProAssurance offers risk assessments designed to help practices minimize errors by establishing and evaluating safety procedures and communication protocols.
With reliable procedures in place, our insureds are more likely to reduce errors in their medical practice, avoid claims, and make claims more defensible if they do occur.
The Heritage of Military Medicine in San Antonio
By John Shepherd, MD, President, Bexar County Medical Society
While other medical students were worrying about the Krebs cycle and how the kidneys really work on their first day of school, I was getting my first high-and-tight haircut and learning how to march with a platoon in the sweltering San Antonio summer heat at Fort Sam Houston. In those weeks, I learned more than anatomy, and eventually I took away lessons that went far beyond a medical degree.
Basic training in San Antonio was just the beginning. What started with blisters on my feet and the sound of cadence calls soon carried me to Airborne School, and eventually to a special operations aviation unit. Along the way, I discovered that medicine in uniform isn’t only about sutures or stethoscopes — it’s about resilience, teamwork and showing up for one another in moments of chaos and crisis. And for me, it was also about pride. Pride in serving soldiers who had dedicated themselves to serving their country, and pride in knowing that every sick call, every splint, every interaction mattered in a larger story of sacrifice and service.
A Legacy of Innovation
San Antonio has long stood at the crossroads of healing and service.
Brooke Army Medical Center (BAMC) traces its roots back to 1879, when it began as the Post Hospital at Fort Sam Houston. Today, it is the oldest continually operating hospital in the Army and the only Level I trauma center in the Department of Defense. Over its long history, BAMC has grown into a hub where battlefield lessons become bedside practices, serving both military families and the civilian community of South Texas.
Also at Fort Sam Houston is the U.S. Army Institute of Surgical Research , home to the renowned Army Burn Center. This facility is one of the most advanced in the world, pioneering treatments and protocols that have transformed burn care for soldiers and civilians alike. Its innovations — ranging from fluid resuscitation to skin grafting techniques — continue to set the standard for burn care across the globe.
Across town, Wilford Hall — once the largest Air Force medical center in the world — remains a symbol of military medical excellence. Though its inpatient services were consolidated at BAMC in 2011, Wilford Hall continues today as a premier ambulatory surgical and outpatient center, carrying forward its legacy of Air Force medicine.
And then there is the Center for the Intrepid, a world-class rehabilitation facility built in 2007 for wounded warriors who have sustained severe injuries in combat. More than bricks and mortar, it is a place where innovation meets the indomitable human spirit. With advanced prosthetics labs, computer-assisted therapy and virtual reality systems, the Center has given thousands of service members
not only the ability to walk again, but also the chance to run, climb, compete, and reclaim their lives. Every visit there is a reminder of resilience at its purest.
Together, these institutions have created a medical ecosystem where innovation and compassion intertwine.
A Spirit Beyond Science
What strikes me most about the heritage of military medicine is not just the science — it’s the spirit. That spirit of service shows up in the way military medicine approaches every challenge. Whether it’s treating a soldier injured in combat, preparing for a humanitarian mission overseas, or responding to a local disaster here at home, the mission is clear: be ready, and do what it takes to save lives.
In that environment, medicine becomes more than a profession — it becomes a calling, shaped by discipline, adaptability and a deep sense of responsibility. The culture of readiness doesn’t just prepare us for the battlefield; it filters into every patient encounter, every training exercise and every moment of care. It reminds us that the work we do matters beyond the walls of any single clinic or hospital.
Even for those of us in civilian practice, the military’s influence is woven into our daily work. Trauma protocols at University Hospital? Built on lessons from battlefield medicine. Burn care standards across the nation? Advanced right here in San Antonio. The helicopter that lifts a car-crash victim from I-35 to a trauma center? That life-saving chain of care traces directly back to combat evacuation strategies.
This blend of science, spirit and readiness doesn’t just shape individual providers — it shapes the identity of San Antonio itself. Our community has grown alongside these institutions, and together they’ve built a medical heritage that extends far beyond military bases.
Airborne jump from a Chinook helicopter.
A Heritage That Shapes a City
San Antonio is sometimes called “Military City, USA,” but that phrase doesn’t capture the depth of what military medicine means to our community. These hospitals and research centers employ thousands of military and civilian personnel. They train the next generation of doctors, nurses and allied health professionals. They connect San Antonio to missions around the world, from humanitarian disaster relief to peacekeeping operations.
Our city’s reputation as a hub for trauma research, critical care, rehabilitation and prosthetics is inseparable from this military heritage. When the world looks for expertise on how to save lives in impossible conditions, it often looks to San Antonio. And for those of us who have worn the uniform, there is a quiet but enduring pride: to have stood beside soldiers who serve their country, and to have had the privilege of serving them in return.
Lessons for Today
Military medicine also challenges us to look forward. It reminds us that healthcare must be prepared for extremes — mass casualty events, pandemics, humanitarian crises. It insists that teamwork across specialties is not optional but essential. And it teaches us that health is not just about the patient in front of us, but about the community we serve and protect together.
As we celebrate diversity and heritage this month, let us honor San Antonio’s unique role in shaping the story of medicine. Ours is a city where courage meets innovation, where sacrifice meets science and where lessons learned under duress have been transformed into healing for all.
So, for me, military life that began with a haircut and marching in step under the San Antonio sun, ended up giving me lessons no textbook could have taught. It gave me a profound sense of pride: pride in wearing the uniform, pride in serving those who served their country, and pride in carrying forward a tradition of military medicine — through BAMC, Wilford Hall, the Burn Center and the Center for the Intrepid — that continues to shape our city, our profession and our patients today.
John Shepherd, MD, 2025 President of the Bexar County Medical Society and TEXPAC Chair, is a proud graduate of the Uniformed Services University of the Health Sciences, Class of 1987. He served in the United States Army for 18 years, jumping out of planes with the 101st Airborne Division, flying around in helicopters with the 160th Special Operations Aviation Regiment and, above all, feeling honored to care for the men and women who chose to serve their country.
Pre-Airborne training at USUHS medical school.
Empty Nesters: Still soaring
By Danielle Henkes
“If the nest is truly empty, who owns all this junk?” Erma Bombeck
Those of us who have found ourselves in a suddenly quiet, empty home may have pondered this exact irony. And just as likely been asking ourselves, “What now?” Even though we plan for children to venture out on their own or our transition into retirement, it’s always a shock when reality sets in. It’s a loss, and tremendously so if our later years bring the death of a spouse. We find ourselves an “Empty Nester.”
Our Bexar County Medical Society Alliance mission statement states, “We are families supporting families from training to retirement.” To fully embody this mission, we created our Empty Nesters group to reach out to and re-engage with members in mid-to-later stages of their medical family journey. Beginning with a kick-off luncheon last September, the group has attracted a vibrant group of physician spouses. Our members range in age from 40 to 80+ and are parents to teens (soon to leave the nest), true empty nesters, grandparents and widows. Some are still working, others are retired or their spouse has retired. We count 14 BCMS Alliance Past Presidents and 3 TMAA Past Presidents among our members. A diverse group with many talents and interests, we come together seeking camaraderie, new experiences and a connectedness to the family of medicine. Over 35% of all BCMS Alliance members have opted-in to be added to our Empty Nesters contact list.
At our initial planning meeting, it was decided that Empty Nesters would meet bi-monthly and that members would team up and take turns planning the activities. This flexibility allows the planners to
choose the activity and plan it for a day and time that is convenient to them. Past events included:
• September 2024 – Kick-Off Luncheon to plan our focus and future, hosted by Danielle Henkes
• December 2024 –Holiday Dutch Treat Lunch at Los Barrios, organized by Louise Chumley
• February 2025 –Alliance Projects Work Session making Doctor’s Day Cards at the BCMS office, orchestrated by Mary Jo Dotson
• April 2025 – Connect & Create event to assemble AllMed centerpieces and goodie bags, hosted by Mary Jo Dotson and Katrina Theis
• June 2025 – Off for Summer Travel
• August 2025 – Museum and Lunch outing to The Witte Museum followed by lunch at The Hayden, organized by Danielle Henkes and Lisa Trevino
To learn more about BCMS Alliance Empty Nesters, contact Danielle at bcmsalliance@bcms-alliance.org.
Danielle Henkes is the 2020 BCMSA Past President and current Steering Committee Member. She and husband, David Henkes, MD, became empty nesters in 2020. They’ve since filled their home with three stray cats.
August 2025, The Witte Museum. L-R: Katrina Theis, Dena Frolichstein
August 2025, The Witte Museum. L-R: Dena Frolichstein, Danielle Henkes, Victoria Kohler-Webb, Katrina Theis
April 2025, Connect & Create for AllMed. L-R: Rebecca Waller, Katrina Theis, Virginia Profenna, Jenny Shepherd
February 2025, Doctor’s Day Cards at BCMS. L-R: Rebecca Waller, Katrina Theis, Cheri Schilling, Sue Bernstein, Mary Jo Dotson
August 2025, Lunch at The Hayden. L-R: Seated - Lisa Trevino, Dena Frolichstein, Standing - Victoria Kohler-Webb, Danielle Henkes
December 2024, Los Barrios Holiday Lunch. L-R: Dena Frohlichstein, Dionne Fortenberry, Louise Chumley, Michelle Richardson, Victoria Kohler-Webb, Danielle Henkes, Mary Jo Dotson
Science in Motion: How tai chi and other traditional therapies are changing healthcare
By Claire Kowalick
People may picture tai chi as graceful, slow-motion movements practiced in parks or community centers. But Wei Liu, PhD, research director of the Human Performance and Rehabilitation Research Lab and associate professor in the Department of Physical Therapy at The University of Texas at San Antonio Health Science Center School of Health Professions, sees tai chi as more than cultural tradition or gentle exercise. His research shows tai chi is a quantifiable, therapeutic tool that merges Chinese medicine with the rigor of Western science. “There was a gap in knowledge. People were using tai chi in interventions without a clear scientific rationale,” Liu said. “We didn’t know what forms worked best, or for whom.”
Motion to Medicine
Liu began his career in biomechanics and biomedical engineering, analyzing movement with high-tech, motion-tracking systems. In his lab, reflective markers attached to points on the body show the biomechanics of tai chi, revealing how each form alters joint load, balance and coordination.
His early studies discovered that not all tai chi forms have the same benefits. For older adults or people with knee osteoarthritis, some movements improve mobility while others instead risk increased joint stress. “Not every form has a benefit for every individual, so we pick what is best,” Liu said. “We found we could reduce 24 forms to just four while still achieving the same clinical outcomes.”
By optimizing the process, Liu said it’s possible to transform tai chi from a “one-size-fits-all” intervention into something far more precise and clinically effective.
Integrative Medicine: Where tradition meets evidence
Liu’s work fits within the broader field of integrative medicine, which blends conventional care with evidence-based complementary therapies. Ancient traditional practices like yoga, acupuncture and meditation have all shown measurable benefits in areas ranging from chronic pain to mental health. “These are called nonpharmacologic approaches. They are low-cost, safe, and can often reduce reliance on medications,” said Liu.
In a time of rising healthcare costs and growing concern about over-medication in aging populations, this alternative approach is gaining traction. By offering strategies that may improve mobility, relieve pain, and boost cognitive resilience, integrative therapies show promise for complementing traditional care, not replacing it.
Tai chi, like yoga, trains both the body and the mind. Its squatbased postures build leg strength while its sequences challenge coordination and memory, stimulating cognitive networks. Acupuncture, likewise, has been integrated into pain clinics and oncology care, where it has been shown to ease symptoms without drug interactions. Mindfulness meditation is increasingly “prescribed” along with behavioral therapy for stress and insomnia. “The practice of medicine is not
only about prescribing a pill,” Liu said. “It is ultimately about helping people connect with their body and mind in ways that support longterm health.”
Mind-body Connection in Dementia Care
One of Liu’s most promising areas of research involves using tai chi to diminish fall risks for older adults with dementia. Tai chi, with its emphasis on balance and mindful movement, is well-suited for this approach. “When you’re practicing tai chi, it is a challenge to your dynamic balance,” Liu said. “That means you’re using your brain, connecting your muscles, then making the whole thing work. Our hypothesis is that if people with dementia learn to handle those balance challenges, they’ll be less likely to fall in daily life.”
What sets his approach apart is the focus on both mobility and cognition. Where most dementia studies concentrate on memory, Liu’s team investigates how movement training can simultaneously sharpen executive function. “It’s not like walking, which can become automatic,” he said. “With tai chi, you must plan, remember sequences, and coordinate the motions. That takes continuous engagement in the brain.”
Ancient to AI: The frontier ahead
Liu’s lab is also pioneering artificial intelligence tools that can provide personalized tai chi interventions. By inputting motion data, demographics, medication history and fall records into machine-learn-
SHOULDN’T YOU BENEFIT
ing models, his team is building a predictive system to match patients with the right tai chi regimen. “AI helps us personalize intervention, which can save time for providers and maximize benefit for patients,” Liu said.
His lab hopes to create a mobile app that can integrate with electronic health records, provides at-home instruction, and even helps insurers stratify fall risk to reduce emergency room costs.
Integrative, Affordable, Empowering
Liu’s tai chi research is a model of what integrative medicine can offer — affordable, accessible therapies that enhance, without replacing, Western treatments. “It’s a win-win-win,” he said. “Providers can reduce medication burden, patients feel empowered and insurers save money on preventable injuries.”
Claire Kowalick is a science writer and senior public relations specialist with The University of Texas at San Antonio Health Science Center. She is a graduate of the University of North Texas. As a science writer, she combines her passion for writing with a deep appreciation of biomedical science to tell people about the groundbreaking research and novel discoveries happening at South Texas’ largest academic research institution.
Rural Surgical Deserts
All fingers are not equal: Addressing surgical inequity
By Izi Obokhare, MD, FACS, FICS, Professor of Surgery TTUHSC Amarillo; and Muhammad Haris Nazim, MD, FACS, FICS, MEHP, Professor of Surgery TTUHSC Amarillo
The following article was adapted with permission from the fall 2025 issue of Panhandle Health, the journal of the Potter-Randall
County Medical Society.
Surgical deserts refer to underserved rural and urban geographical areas with absent or limited access to surgical care. These geographical areas either lack surgical facilities, surgical equipment or well-trained healthcare providers, resulting in limited access to lifesaving procedures.1 Rural surgical deserts are plagued with increased morbidity and mortality as well as increased cost due to delay in care and transportation needed to receive care. For example, a patient with a common bile duct stone in a surgical desert presenting with symptoms of fever, right upper quadrant abdominal pain and jaundice will often require a general surgeon and a gastroenterologist for a laparoscopic or robotic cholecystectomy and endoscopic retrograde pancreatography for stone extraction. In a surgical desert, this patient will encounter a delay in care and may progress to cholangitis if not treated expeditiously; they will need to be transported either by vehicle or by air to the nearest facility with a gastroenterologist and surgeon with the adequate expertise to remedy this situation. If the patient is diabetic or immuno-compromised, even with the right antibiotic coverage, the mortality rate increases significantly when there is a delay in care.
A substantial portion of our country can be characterized as surgically underserved, despite several programs designed to provide healthcare services in underserved communities through enhanced reimbursement.2 The prevalence of surgical deserts is due to multiple factors, which are difficult to surmount. These factors can be broken up into several major reasons such as geographical, insufficient human resources, economic barriers (limited facilities) and, finally, cultural/ linguistic challenges.
Geographical Isolation
Due to geographical isolation, patients must travel long distances to reach a specialist or subspecialist in that field. Patients in rural Texas typically travel over 100 miles for a doctor's visit.
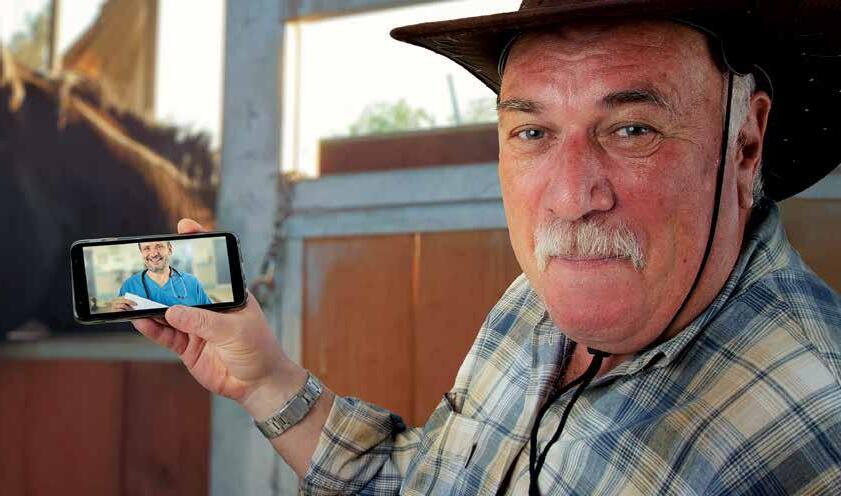
The growth of telemedicine has made a positive impact on rural access; unfortunately, invasive surgical procedures cannot be practiced via telemedicine. Examples include procedures ranging from preventive and screening services such as upper and lower endoscopies to life-saving emergency situations like blunt and penetrating trauma.
Insufficient Human Resources
Delivery and continuation of healthcare are made possible by having an adequate level of human resources. Efficiently running a surgical hospital or healthcare facility requires surgical staff ranging from the central supply manager, surgical instrument cleaners, OR nurses, first assistants, certified nurse anesthetists, anesthesiologists, cardiac perfusionists and surgeons. If any member of the team is absent or poorly trained, the volume and quality of healthcare delivered suffers. According to the analysis by Uribe-Leitz et al, a surgical desert with minimal access to surgical care has a benchmark of less than six general surgeons, six orthopedists and eight anesthesiologists per 100,0000 people per county. Despite increased technology, without the human factor providing interaction with the patients, the delivery of healthcare is impossible.3
Limited Facilities
One hallmark of surgical deserts is the absence or limited number of healthcare facilities. While the expansion of Medicare and Medicaid coverage has been a lifeline to rural patients needing medical services, these benefits don’t always extend to surgical services. In addition, medical facilities in surgical deserts depend on the availability of government support to remain financially viable. Recently the Big, Beautiful Bill was passed, but its impact on surgical deserts remains unknown. Keeping Critical Access Hospitals open will have a positive impact on morbidity and mortality of surgical patients. For a patient
involved in a motor vehicle accident, local first responders will need to take the patient to the nearest trauma facility during the “golden hour,” when more than 80% of the mortality after trauma can be prevented by arresting life-threatening bleeding. The term “golden hour” was coined by Professor Richard Cowley after his observations in Baltimore and in the Second World War. He concluded that the vast majority of deaths within the first hour after polytrauma are due to massive head injury or exsanguination. The presence of a facility with healthcare professionals trained in conducting the Advanced Trauma Life Support (ATLS) primary survey significantly reduces mortality by arresting life-threatening bleeding. First responders and local hospitals need to be familiar with the management of these five crucial steps: Airway, Breathing, Circulation, Disability and Exposure (ABCDE).4
Economic Barriers
The impact of economic barriers can be felt from the standpoint of the patient, healthcare provider and the facility. Lack of insurance coverage or inadequate coverage can result in patients waiting until the last minute to receive medical care. End-stage surgical disease is not only costly financially due to the need for prolonged recovery periods and surgical intensive unit care, it often requires surgical subspeciality care. An example is a patient with a symptomatic ventral hernia who waits until the last minute to seek medical care and presents with gangrene of the bowel and a necrotizing soft tissue infection. Typically, hernia repairs are performed as a same-day procedure, but this patient will require a prolonged stay in the hospital, multiple surgical procedures and perhaps many days on the ventilator. This causes a strain on the already limited hospital resources. Ultimately, that patient may need to be transported to a tertiary medical facility for multidisciplinary care. At the end, the final hospital bill may be over a million dollars to be covered via taxpayers’ contribution (or not covered at all). Patients with adequate insurance coverage and the financial ability to seek care often seek specialized care and do so early, before such devastating complications can arise.
Cultural and Linguistic Barriers
Language barriers and cultural differences commonly seen in our rural patients can also pose an obstacle to the delivery of timely and well-informed healthcare. Patients are more likely to be compliant with screening and preventive services if they understand the need for the service. Compliance with therapy and patient outcomes are closely related. In surgical deserts, an adequate number and sufficient diversity of the medical staff is crucial to improving the outcome of the patient. Several complex factors often interact to lead to racial or cultural disparities in the delivery of healthcare; however, at the core of this issue are language and educational barriers. According to Haider et al, systemic factors (low volume hospital, low capacity, large minority population with limited access) and patient factors (underinsured or uninsured patients with advanced presentation, greater disease burden and increased comorbidity), coupled with provider factors (low volume surgeon, bottom decile surgeon and few specialist referrals), contribute to worse outcomes in these populations.3 Lack of culturally competent providers can hinder or delay access to adequate surgical care for these diverse populations in surgical deserts.
Impact of Surgical Deserts
In short, the presence of surgical deserts has deleterious consequences for the health and well-being of rural residents by increasing morbidity and mortality through the delay of surgical intervention in patients with urgent and chronic conditions. Surgical deserts also aggravate health disparities by disproportionately affecting vulnerable populations, such as low-income individuals, minorities and those with chronic health conditions. The major financial impact of surgical deserts is strain on the healthcare system and increased cost of access to timely and appropriate surgical care, often leading to prolonged care or traveling long distances for treatment.
Interview with Dr. Jay Blasingame from Perryton, Texas
(Jay Blasingame, MD, is an American Board of Surgery Certified Surgeon born and raised in Perryton, trained at Methodist Health System in Dallas, Texas and practicing as a general surgeon in Perryton, Texas.)
IO: What is the impact on the community?
JB: Patients living in surgical deserts often lose faith and confidence in the medical care they receive, especially if there is lack of continuity of care after a referral is made. They may have to jump through many hurdles such as financial and geographical ones to get care at a tertiary center.
IO: What difficulties and challenges have you faced as a surgeon in a surgical desert?
JB: There are many difficulties one would face out here. A good example was during the COVID-19 pandemic, when transferring complicated surgical patients out was very difficult due to the lack of beds in other hospitals. At one time, I had to perform a complex operation with makeshift surgical abdominal wall retractors and an assistant who passed out during the procedure because that was her first time assisting in a complex procedure. The patient needed ICU care and there were no beds available.
IO: What potential solution or advice would you give to a surgeon working in a surgical desert?
JB: I would recommend developing an alliance or a network/support system locally and regionally. So, there is someone you can call right away if you need a specialist in a higher level of care center. It takes a team to get a sick patient well again. More importantly, as a surgeon, you have to know your limitations. Some patients would be best served at a facility with more resources. Identify those and send them as soon as possible.
IO: Looking ahead where do you see the future of caring for patients in surgical deserts and the impact of the Big, Beautiful Bill?
JB: Facilities with reduced financial backing will face some difficulties and may close down, but facilities with a good financial foundation will thrive as safety net hospitals. Facilities in surgical deserts can bring in specialists and subspecialists on a weekly or monthly basis so patients can receive quality care in their own back yards. We can do a better job educating the patient on the need to seek medical care early to avoid requiring emergency surgical procedures.
Potential Solutions to Address the Unique Needs of Surgical Deserts
Addressing the profound impact of a surgical desert on patient care and patient outcomes requires a multifaceted approach involving policy changes, workforce optimization and deployment and innovative customized solutions.
Potential Solutions for Surgical Deserts
Policy changes
Workforce optimization
Training providers
Financial support
Cultural and language training
Leveraging tech
Strengthening relationships
Incentivizing practitioners: Surgical deserts face extreme difficulty recruiting and retaining talented practitioners. Retaining physicians and practitioners can be achieved by offering financial incentives such as higher pay, sign-on bonuses, loan forgiveness programs and housing support in order to encourage practitioners to relocate to underserved areas. In addition, specialists from surrounding urban centers can be hired to visit on a periodic basis, either weekly or monthly. An example is having an orthopedic surgeon or colorectal surgeon visit a surgical desert twice a month to provide service at that facility, so the patient does not have to travel many miles to get the same level of care. This may provide major benefits to the hospitals, the patients and the community.
Expanding training programs: Increasing residency training spots for surgeons with a focus on rural surgery is an excellent way to increase the number of surgeons equipped and mentored to practice in surgical deserts. According to an AAMC survey, about 66% of residents trained in Texas remain in the same area after training. Recently, the Accreditation Council for Graduate Medical Education (ACGME) approved 14 new training spots for general surgery residency in Amarillo. The residents will have elective rotations in rural towns such as Hereford and Perryton to encourage graduates to practice in rural areas after graduation. The old mantra of train and retain is a proven strategy to build and sustain a robust workforce in surgical deserts.
Leveraging technology: Utilizing telemedicine and robotic assisted surgery has been a pipeline dream and is gradually becoming a reality. Used in combination, it will be a valuable tool to mentor, provide expert consultation, and even perform remote surgery, potentially expanding access to surgical care in remote areas.
Strengthening existing resources: Financial support of existing critical access healthcare facilities in rural areas can improve the capacity to provide excellent surgical care particularly for emergency and preventative care. Developing and nurturing relationships with higher level centers can facilitate rapid transfer of patients through resource sharing.
Ultimately, addressing the unique needs of surgical deserts and fighting for surgical care equity requires collaboration among policymakers, healthcare organizations, professional associations and local communities to ensure equitable access to essential surgical care for all individuals, regardless of their geographic location or socioeconomic status. State and national legislatures, organizations like the ACGME and the American College of Surgeons and surgical subspecialty organizations need to redouble their efforts if we are to bring life to these surgical deserts.
References:
1. Brînzac, M.G., Kuhlmann, E., Dussault, G., Ungureanu, M.I., Cherecheș, R.M., Baba, C.O. Defining medical deserts—an international consensus-building exercise. European Journal of Public Health. October 2023;33(5):785–788
2. Belsky, D., Ricketts, T., Poley, S., Gaul, K. Surgical deserts in the US Counties without surgeons. Bulletin of the American College of Surgeons. Sept 2010:32-35
3. Uribe-Leitz, T., Esquivel, M.M., Garland, N.Y., Staudenmayer, K.L., Spain, D.A., Weiser, T.G. Surgical deserts in California: an analysis of access to surgical care. J Surg Res. 2018 Mar;223:102-108. doi: 10.1016/j.jss.2017.10.014. Epub 2017 Nov 15. PMID: 29433860
4. Marsden, N.J., Tuma, F. The polytraumatized patient. 2023 Jul 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan
5. Haider, A.H., Scott, V.K., Rehman, K.A., Velopulos, C., Bentley, J.M., Cornwell, E.E. 3rd, Al-Refaie, W. Racial disparities in surgical care and outcomes in the United States: a comprehensive review of patient, provider, and systemic factors. J Am Coll Surg. 2013 Mar;216(3):48292.e12. doi: 10.1016/j.jamcollsurg.2012.11.014. Epub 2013 Jan 11
Izi Obokhare, MD, FACS, FICS, is a board-certified General Surgeon with fellowship training in Colorectal Surgery. He has practiced in Amarillo for over a decade and is currently the Program Director of the new General Surgery residency program, the Associate Dean for Faculty Development at TTUHSC Amarillo and the Principal Investigator of a five-million-dollar colorectal cancer education and screening grant through CPRIT. He is married to Dr. Joy Obokhare, an Otolaryngologist and Facial Plastics Surgeon, and they have three wonderful kids. He is focused on training the next generation of skilled, emotionally balanced and empathetic surgeons equipped to practice in rural communities.
Muhammad Haris Nazim, MD, FACS, FICS, FACCWS, CWSP, MEHP, is the Dr. William and Sue Hale Distinguished Professor of Surgery, Regional Chair of Surgery and Regional Assistant Dean for Quality Improvement at Texas Tech University Health Sciences Center in Amarillo. With more than a decade of experience in clinical care, surgical education and public health, he has led transformative initiatives in rural and underserved regions of the Texas Panhandle, including launching new subspecialty services and securing ACGME accreditation for TTUHSC’s General Surgery Residency Program on its first attempt. Dr. Nazim has directed major trauma system advancements at multiple hospitals, expanded cancer screening programs across 30+ counties, and published extensively on trauma, wound care and rural health systems.
Beyond Symptoms: Integrating culture into mental health treatment
By Ruba Krichati, OMS-III; Mahima Parappurath, OMS-II; Phoebe Lay, OMS-II; and Ramaswamy Sharma, MS, PhD
There is a growing body of literature that reports an increase in the incidence of mental disorders after the COVID-19 pandemic. The World Health Organization (WHO) states that mental health is “a state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community.” While the definition does not explicitly include cultural beliefs, their crucial role in influencing mental health is well-known. In several non-Western cultures, mental illness symptoms are framed through spiritual, moral or social beliefs in addition to the biological context. Global mental health efforts must, therefore, be grounded in local cultural paradigms. Since definitions of mental health and illness are constructed based on social and cultural perceptions of what is normal or abnormal, it is important to integrate these beliefs and perspectives in the diagnosis and treatment of mental health for providing effective and contextually appropriate care.
Cultural Beliefs and Stigma
Cultural beliefs influence how an illness is perceived and experienced; importantly, they also extend to making decisions regarding care. In terms of mental health, cultural influences may lead to patients delaying seeking help or avoiding treatment altogether for a multitude of reasons such as stigma, fear of being judged, or the notion that emotional distress should be managed privately. A recent study showed that Latinos with limited English proficiency and low health literacy may not fully understand depression as mental illness due to cultural barriers; they preferred to seek help from faith, family or community-based informal support systems and were skeptical of psychiatric treatment. Stigma can be (i) structural, involving laws, policies or practices related to access and quality of mental healthcare, (ii) affiliative, as experienced by family members or friends of patients with mental illness, (iii) public, demonstrated by the negative attitudes and beliefs held by the general population toward patients with mental illness due to lack of knowledge as well as beliefs based on culture, or (iv) self, wherein patients internalize public stigma and believe the negative stereotypes about themselves. All of the above types of stigma have been identified as major themes within minority ethnic groups. In addition, specific cultural themes, such as the Latin-American misconception of antidepressants as addictive and harmful, also highlight the importance of
considering cultural beliefs for treatment. Importantly, demographic and cultural factors work in conjunction to shape mental health disparities; foreign-born individuals exhibit a lower lifetime prevalence of mental disorders as compared to their counterparts in the United States, suggesting that sociocultural influences tied to the country of origin play a protective role in determining mental health outcomes.
In addition to racial and ethnic inequities in mental healthcare, language differences also affect communication with physicians. Patients struggle to communicate with their physicians, resulting in underutilization of psychiatric care. Moreover, only 10% of psychiatrists in the U.S. come from underrepresented backgrounds, which can lead to a lack of trust in healthcare institutions, miscommunication aand poor understanding of mental health conditions among marginalized populations.
Incorporating Cultural Competency in Diagnosis and Care
As Bexar County continues to grow in diversity and cultural plurality, our healthcare systems must evolve to cater to the needs of all communities. Tackling mental health disparities in culturally diverse populations requires a multipronged approach that involves addressing the systemic and cultural factors that shape mental health perceptions, reducing language barriers, and improving cultural competency.
Collaborating with community leaders and faith-based organizations to provide culturally sensitive education can help bridge gaps in trust and accessibility and reduce stigma associated with mental illness.
Effective communication is vital for delivering culturally competent care. Physicians must be trained to decode culturally distinct verbal and nonverbal cues. The importance of using open-ended dialogue to invite patients to share their perspectives and active listening to uncover nuanced beliefs, normalize conversations around mental health, and foster mutual understanding and trust must be emphasized. Healthcare institutions can prioritize hiring multicultural staff who are well-versed in the local language, reflecting the diversity of the populations they serve. They can also provide interpreter services to ensure complete and accurate communication.
Cultural competency in mental health treatment involves understanding and respecting the cultural identities, beliefs and values of patients, and integrating them into diagnostic and therapeutic processes. Physi-
cians and other healthcare providers must be mindful of how cultural identity impacts willingness or reluctance to seek treatment for mental health disorders; they should be ready to adapt their clinical practices to align with the cultural, linguistic and psychosocial expectations of their patients who may come from varied backgrounds. This approach helps improve the accuracy of their diagnosis and enhances their therapeutic alliance with the patient. For example, somatization, which involves expressing psychological distress through physical symptoms, is more common in some Asian and Latin American populations. It is easy to misinterpret these presentations in the absence of cultural awareness, leading to misdiagnosis or inappropriate treatment. Trauma-informed care, which integrates the patient’s experiences with their cultural background, can help guide the selection of the most appropriate and effective therapeutic approach. Culturally competent care also requires clinicians to use validated screening tools and avoid assumptions based on stereotypes. Self-awareness that includes reflecting on one’s own biases and engaging in ongoing education is essential for physicians striving to provide culturally competent care. It allows patients to define their experiences and explain their perception of the illness — what they believe to be the cause, course and treatment of their condition.
Conclusion
By building care teams that reflect the local culture, and by fostering inclusive conversations that normalize the discussion of mental health, physicians and other healthcare providers can enhance trust and promote better healing. Training programs in cultural competence promote better physician-patient interactions and improve treatment adherence as well as perceived quality of care, resulting in overall patient satisfaction. Cultural competency is, therefore, a clinical necessity for providing mental healthcare.
References:
1. Alvarez, K., Fillbrunn, M., Green, J.G., Jackson, J.S., Kessler, R.C., McLaughlin, K.A., Sadikova, E., Sampson, N.A., & Alegría, M. (2019). Race/ethnicity, nativity, and lifetime risk of mental disorders in US adults. Social Psychiatry and Psychiatric Epidemiology, 54(5), 553–565. https://doi.org/10.1007/s00127-018-1644-5
2. Cabassa, L.J., Molina, G.B., & Baron, M. (2010). Depression fotonovela: Development of a depression literacy tool for Latinos with limited English proficiency. Health Promotion Practice, 13(6), 747–754. https://doi.org/10.1177/1524839910367578
3. Campinha-Bacote, J. (2002). The process of cultural competence in the delivery of healthcare services: A model of care. Journal of Transcultural Nursing, 13(3), 181–184. https://doi. org/10.1177/10459602013003003
4. Dragano, N., Reuter, M., & Berger, K. (2022). Increase in mental disorders during the COVID-19 pandemic—the role of occupational and financial strains. an analysis of the German National Cohort (Nako) study. Deutsches Ärzteblatt International. https://doi. org/10.3238/arztebl.m2022.0133
5. Gary, F.A. (2005). Stigma: Barrier to mental health care among ethnic minorities. Issues in Mental Health Nursing, 26(10), 979–999. https://doi.org/10.1080/01612840500280638
6. Henderson, S., Horne, M., Hills, R., & Kendall, E. (2018). Cultural competence in healthcare in the community: A concept analysis. Health; Social Care in the Community, 26(4), 590–603. https:// doi.org/10.1111/hsc.12556
7. Hook, J.N., Davis, D.E., Owen, J., Worthington, E.L., & Utsey, S.O. (2013). Cultural humility: Measuring openness to culturally diverse clients. Journal of Counseling Psychology, 60(3), 353–366. https:// doi.org/10.1037/a0032595
8. Kirmayer, L.J., & Young, A. (1998). Culture and somatization: Clinical, epidemiological, and ethnographic perspectives. Psychosomatic Medicine, 60(4), 420–430. https://doi.org/10.1097/00006842199807000-00006
9. Kleinman, A. (1980). Patients and healers in the context of culture: An exploration of the borderland between anthropology, medicine, and psychiatry. University of California Press
10. Misra, S., Jackson, V.W., Chong, J., Choe, K., Tay, C., Wong, J., & Yang, L.H. (2021). Systematic review of cultural aspects of stigma and mental illness among racial and ethnic minority groups in the United States: Implications for interventions. American Journal of Community Psychology, 68(3–4), 486–512. https://doi. org/10.1002/ajcp.12516
11. Ogundare, T. (2020). Culture and mental health: Towards cultural competence in mental health delivery. Journal of Health and Social Sciences, 5(1), 23–34. https://doi.org/10.19204/2019/cltr6
12. Thomeer, M.B., Moody, M.D., & Yahirun, J. (2022). Racial and ethnic disparities in mental health and mental health care during the COVID-19 pandemic. Journal of Racial and Ethnic Health Disparities, 10(2), 961–976. https://doi.org/10.1007/s40615-022-01284-9
13. Ohtani, A., Suzuki, T., Takeuchi, H., & Uchida, H. (2015). Language barriers and access to psychiatric care: A systematic review. Psychiatric Services, 66(8), 798–805. https://doi.org/10.1176/appi. ps.201400351
14. Sue, S., Cheng, J.K.Y., Saad, C.S., & Chu, J.P. (2012). Asian American mental health: A call to action. American Psychologist, 67(7), 532–544. https://doi.org/10.1037/a0028900
Ruba Krichati, OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027. Her interests include internal medicine, health advocacy and healthcare policy. She is dedicated to improving health equity, addressing systemic disparities in underserved communities, and advancing patient-centered care through leadership, community engagement and evidence-based practice.
Mahima Parappurath, OMS-II, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2028. She is interested in pursuing a career in Anesthesiology and is committed to giving back to communities with limited access to medical care.
Phoebe Lay, OMS-II, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2028. She is interested in pursuing a career in Pathology. She is passionate about community engagement, public health and pathology, finds joy in mentoring others and in playing pickleball.
Ramaswamy Sharma, MS, PhD, is a Professor of Histology and Pathology at the University of the Incarnate Word School of Osteopathic Medicine. He is interested in delineating the multiple molecular and cellular roles of melatonin in maintaining our quality of life. Dr. Sharma serves on the BCMS Publications Committee.
During Health Literacy Month, Health Confianza Shines a Light on Plain Language
By Sandra Zaragoza, MA, and Melanie Stone, DrPH, MEd
Health communications are an ever-present part of our daily lives — a flyer at a health fair, an in-take document at the doctor’s office, a wellness TikTok, an infographic or a written follow-up we receive from our health provider. While health communications are around in different forms, they may be filled with medical jargon, complex sentences and hard-to-follow guidance. In short, they may not be written in plain language.
Plain language is defined as communication with clear wording, structure and design for the intended audience to easily:
• Find what they need
• Understand what they find
• Use that information
Increasingly, the healthcare and nonprofit communities are recognizing the important role of plain language in removing barriers to healthcare, enhancing patient safety and increasing the patient’s ability to make informed health decisions. At the same time, training in plain language communication is not a part of standard education for healthcare providers, which means plain language must be intentional. Fortunately, we are beginning to see more health providers, communi-
ty health workers and health communicators learning plain language skills and making this a communication priority in their organizational policies and practices.
Spotting the Mistakes
One of the easiest ways to start employing plain language is to be able to spot when it doesn’t meet the standards. To that end, the Institute for Healthcare Advancement (IHA) created a list of the 10 most common errors that health providers make when communicating with patients.
IHA points out that health providers tend to create prescription instructions “that are written at an 11th grade reading level or higher, rather than 5th grade reading level at which the majority of the country’s population reads.”
Another common error, according to IHA, is handing out reading material that is printed in a font size too small for the patient, particularly seniors. The type should be at least 12-point font with adequate space between lines.
Additionally, the power of graphics to explain complex topics is often overlooked when creating materials. IHA points out that simple visuals for medical instruction can enhance patient understanding, but
Communication is only effective if the receiver actually comprehends the message sent. I often remind healthcare professionals, ‘What’s the point of your medical knowledge if you cannot convey it to the person who needs it? I challenge our trainees with the quote from Albert Einstein, ‘If you can’t explain it simply, you don’t understand it well enough.’ Plain language helps ensure people understand what you are saying the first time you say it.
-Dr. Melanie Stone
they warn that graphics should demonstrate and explain concepts in the text and should never be abstract or for decorative purposes only.
Overburdening patients with numeracy skills is another area to be mindful. Providing context for numbers (use 1 in 5 versus 20%), removing the need for the reader to perform calculations, and using appropriate visuals can help improve plain language numeracy.
Unfortunately, mistakes in health communications come with both a human and financial impact, with an estimated $236 billion in unnecessary healthcare expenses annually due to the inability of patients to understand what medical providers are communicating to them, according to a 2008 article in Nurse Educator.
The good news is that there is guidance, techniques and tools that encourage the use of plain language.
History of Plain Language
The Plain Writing Act of 2010 requires federal agencies to train staff to use plain language when they communicate with the public. As part of that act, the federal government offers plain language guidance.
Among the most common techniques for achieving plain language:
• Reader-centered organization
• “You” and other pronouns
• Active voice, not passive
• Short sentences and paragraphs
• Common, everyday words
• Easy-to-follow design features (lists, headers, tables)
Additionally, The Center for Plain Language offers 5 Steps to Plain Language that each include more detailed information:
1. Identify and describe the target audience
2. Structure the content to guide the reader through it
3. Write the content in plain language — keep it short and to the point
4. Use information design to help readers see and understand
5. Work with the target user group to test the design and content
Dr. Melanie Stone, co-director of Health Confianza, recommends that health professionals initially introduce the medical term that the patient will encounter (e.g. myocardial infarction), immediately followed by the plain language version (e.g. heart attack). This will help the patient connect the terms. She also recommends using analogies your patient may be familiar with to help make your medical concept clearer, such as the mechanics of a car representing your cardiovascular system.
How to Check if it’s Plain Language
There are paid and free tools that can help a health communications professional review and assess adherence to plain language principles.
Some examples are:
Free Resource: The National Library of Medicine’s Health Education Materials Assessment Tool (HEMAT)
XPaid Resource: Health Literacy Innovation’s Health Literacy Advisor (HLA) — software that assesses and improves the readability of your documents using plain language principles
There still must be an understanding of the principle of plain language and, at least at this time, AI requires a human editor to make sure that it doesn’t insert errors or misunderstandings.
While technology can be a useful tool to enhance plain language (e.g. using a chatbot to write your information in a conversational tone), a human editor is still needed to check for accuracy, potential misunderstandings and overall use of plain language principles.
Keeping Plain Language Top of Mind
One way to keep an organization or team thinking in terms of health literacy and plain language is to make sure they have access to trainings, refresher courses and webinars.
The U.S. Centers for Disease Control & Prevention, the Center for Plain Language and Health Confianza are just some of the organizations that offer affordable health literacy education.
Sandra Zaragoza, MA, is a Senior Marketing and Communications Specialist with Health Confianza, located at UT San Antonio Health Science Center. She has decades of experience as a communicator with specializations in media relations, science writing and health communications.
Melanie Stone, DrPH, MEd, is an Assistant Professor of Family & Community Medicine at Long School of Medicine at The University of Texas at San Antonio Health Science Center and the Director of Community Engaged Learning (CEL) at the Cheever Center for Medical Humanities & Ethics. A public health expert, her passion is health literacy. She serves as Co-Director of the innovative Health Confianza community education and training initiative.
Healing Through Heritage: The impact of Filipino cultural values on healthcare
By Camille Irene Hulipas, OMS-III; Alyssa Francesca Ahorro, OMS-III; and Ramaswamy Sharma, MS, PhD
Filipino American History Month is recognized each October. Filipinos are the third largest Asian ethnic group in the United States today, with vibrant communities thriving in California (40%), Hawaii (9%) and Texas (5%). According to the 2020 census data, Texas is home to approximately 232,000 Filipino Americans, with 1% of those calling Bexar County home. As a minority group, they often suffer from higher rates of chronic diseases and related complications than white Americans. It is important to respond to minority patients in a culturally sensitive manner because culture, oftentimes at an unconscious level, shapes beliefs about health, illness and treatment. It is essential for healthcare providers to acknowledge, respect, and incorporate the cultural values of their patients into care plans. Culturally competent care does not have a standardized protocol; rather, it demands for the provider to respond in a way that first addresses a patient’s personhood — as a whole person with values, beliefs, fears and a cultural background. Healthcare delivery with this focus in mind can range from offering interpreter services at each visit, recognizing medical pluralism, and providing spiritual support. This article offers a nuanced understanding of how to engage with Filipino immigrants and members of the diaspora in culturally responsive ways.
Filipino culture, like many other Asian cultures, emphasizes collectivism, social harmony and balance. While Filipino psychology (Sikolohiyang Pilipino), a philosophy that was borne in response to the colonial history of the Philippines, encompasses a wide range of named cultural values, they are ultimately anchored around the core concept of kapwa, which describes an interconnectedness to a person’s inner self. It recognizes that the self is never isolated but exists in relation to others. Kapwa has two subcategories that translate
loosely to “outsider,” referring to someone who is not part of one’s inner social circle and with whom interactions are formal, and “oneof-us,” referring to family, close friends or trusted community. Filipino psychology also categorizes behaviors as accommodative surface values and confrontative surface values. The former category includes hiya (“shyness” or “sense of propriety”) and pakikisama (“conformity”). The latter includes bahala na, which can be understood as fatalism or a willingness to take risks. These cultural values reflect why Filipinos and Filipino Americans, as opposed to other Asian demographics, interface with the healthcare system in the ways that they do.
As a previous United States colony, many Filipinos today are familiar with American traditions and are proficient in English. English is included as one of the Philippines’ official languages. Therefore, Filipinos, especially those who are less accultured, may feel reluctant to admit limited English proficiency. This behavior may also be related to the accommodative surface values, hiya and pakikisama. Hiya, although more nuanced, can be simplified to shame. Being able to speak English as a Filipino immigrant is a point of pride because it reflects a certain level of education in the Philippines. Pakikisama, which emphasizes smooth interpersonal relationships, is generally a positive value; however, it can convey a false sense of understanding to a healthcare provider. For example, a patient may be reluctant to ask deeper questions about their health because it could be seen as pushing back and questioning the thought process of a presumed expert. This same interaction could also be seen as creating shame because the patient is admitting to a knowledge gap out loud. Clear communication may be sacrificed to save face and preserve social harmony. Trust and communication are paramount in any patient-provider relationship.
However, this may be more difficult if the patient, harkening back to the subcategory of kapwa, that notates “outsiders,” does not see their provider as someone with their best interest in mind. Since there is already an inherent power imbalance, culturally competent providers should seek to foster relationships that dissolve such strict stringency and create community without causing embarrassment.
Filipino culture also emphasizes harmony and balance amongst the self and inanimate. Superstitious beliefs abound and touch every aspect of life. Some may view illness as retribution for some kind of offense, a sort of divine intervention to settle a score. Psychiatric diseases and other culture-bound syndromes have been attributed to inherent imbalances in a person’s constitution. Behavior discordant to moral values can create or even exacerbate illness behavior. Folk healers and faith healers are still utilized today. Part of this engagement may be due to unmet healthcare needs and a desire to not burden their families, financially or socially. The latter is further complicated because being ill could itself be seen as shameful or be read as a personal shortcoming. Certain conditions such as diabetes could also preclude Filipinos from participating in the community since food has ritualistic significance and declining to eat when offered could be seen as a social snub. Recommendations for lifestyle modifications should be culturally sensitive. Filipinos, although comparatively understudied, have also been shown to engage in traditional, complementary and alternative medicine practices to better incorporate a holistic view of health and grant more autonomy to the patient. However, this plurality could delay care and result in poor health outcomes.
It is widely acknowledged that racial and ethnic minorities experience lower rates of preventive medical screening, perhaps due to their fatalistic attitude. The confrontative surface value of bahala na supposedly endorses this worldview. While some Filipinos subscribe to this attitude, bahala na is better understood as a willingness to embrace risk in the face of adversity. Such an outlook acknowledges a greater force at hand but also empowers the individual and encourages personal responsibility. At the same time, Filipino culture, like many other Asian cultures, is still collectivist. Ancestor worship and filial piety shape behavior, and healthcare should be tendered in a way that acknowledges the family as a collective when appropriate. Research shows that culturally competent healthcare leads to greater patient engagement, improved understanding of treatment plans, and better health outcomes, which may reduce health disparities among marginalized populations.
References:
1. Afable-Munsuz, A., Pasick, R., Nguyen, K.H., & PeÂ, E.J. (2011). Understanding Filipina women's health orientation and the implications for colorectal cancer screening. Diversity and Equality in Health and Care, 8(3)
2. Anderson, J.N. (1983). Health and illness in Pilipino immigrants. Western Journal of Medicine, 139(6), 811
3. Becker, G. (2003). Cultural expressions of bodily awareness among chronically ill Filipino Americans. The Annals of Family Medicine, 1(2), 113-118
4. Cervantes, C.L. (2023). Deep Ecology, Nature Spirits, and the Filipino Transpersonal Worldview. International Journal of Transpersonal Studies, 42(1), 4
5. David, E.J.R., & Nadal, K.L. (2013). The colonial context of Filipino American immigrants’ psychological experiences. Cultural Diversity & Ethnic Minority Psychology, 19(3), 298
6. Estrellado, J.E., Felipe, L.C.S., & Celestial, J.E. (2022). Colonial mentality and psychological flexibility among Filipinx Americans. Asian American Journal of Psychology, 13(1), 8
7. Finucane, M.L., & McMullen, C.K. (2008). Making diabetes self-management education culturally relevant for Filipino Americans in Hawaii. The Diabetes Educator, 34(5), 841-853
8. Hong, Y. (2020). Powerlessness and a social imaginary in the Philippines: A case study on Bahala Na. The Asbury Journal, 75(1), 9
9. Jiro, M.C., Sigua, M., Dio, M., Hennein, L., & Cocohoba, J. (2024). Experiences of older adult Filipino-Americans surrounding eye surgery and factors in health decision-making: a qualitative study. BMC Health Services Research, 24(1), 1599
10. Jose, C.G., Lucy, R., Parker, A.M., Clere, J., Montecillo, L., & Cole, A.M. (2024). Pakikisama: Filipino patient perspectives on health care access and utilization. The Journal of the American Board of Family Medicine, 37(2), 242-250Khalil, C., Chaplin, A., Esmundo, S., Crochetiere, A., & Almario, C. V. (2022). Filipinos’ attitudes, barriers, and enablers on colorectal cancer screening: Insights from a qualitative research study. Cancer treatment and research communications, 33, 100657
11. Leake, A.R., Bermudo, V.C., Jacob, J., Jacob, M.R., & Inouye, J. (2012). Health is wealth: methods to improve attendance in a lifestyle intervention for a largely immigrant Filipino-American sample. Journal of Immigrant and Minority Health, 14, 475-480
12. Sanchez, F., & Gaw, A. (2007). Mental health care of Filipino Americans. Psychiatric services, 58(6), 810-815
13. Tolentino, D.A., Roca III, R.P.E., Yang, J., Itchon, J., & Byrnes, M.E. (2023). Experiences of Filipino Americans with type 2 diabetes during COVID-19: A qualitative study. Western journal of nursing research, 45(6), 562-570
14. Villero, O., Macaerag, I., & Burke, N.J. (2014). Pakikisama: lessons learned in partnership building with Filipinas with breast cancer for culturally meaningful support. Global health promotion, 21(1), 68-72
Camille Irene Hulipas, OMS-III, is a medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027.
Alyssa Francesca Ahorro, OMS-III, is a Filipino-American medical student at the University of the Incarnate Word School of Osteopathic Medicine, Class of 2027. She is currently pursuing her interests in surgery and oncology while also completing a Master of Public Health.
Ramaswamy Sharma, MS, PhD, is a Professor of Histology and Pathology at the University of the Incarnate Word School of Osteopathic Medicine. He is interested in delineating the multiple molecular and cellular roles of melatonin in maintaining our quality of life. Dr. Sharma is a member of the BCMS Publications Committee.
Sounding the Alarm: Hearing loss is an underrecognized and undertreated burden that demands more attention in clinical practice
By Lance Jackson, MD, FACS
Hearing loss (HL) is a very prevalent neurologic and sensory disorder. According to the World Health Organization (WHO), approximately 1.5 billion people (over 20% of the global population) live with some degree of HL. 1 Individuals within the United States are not spared but rather commonly affected. According to the National Institute on Deafness and Other Communication Disorders (NIDCD), about 15% of U.S. adults report some trouble hearing.2 Based upon U.S. population in 2025, the Hearing Loss Association of America (HLAA) estimated that more than 50 million Americans suffer from HL.3 The prevalence of HL sharply increases with age; 25% of adults aged 65-74 have objective disabling hearing loss, and 50% of adults aged 75+ have disabling hearing loss in the U.S.2 However, children are not spared,
with nearly 2% of children aged 3-17 (roughly 1.1 million) having some degree of hearing loss.
Unfortunately, HL is frequently not appreciated by the effected patient, and even when noticed by the patient and/or family, the patient often denies the presence of HL. Correspondingly, considering that the patient often does not complain of HL, medical providers frequently miss the opportunity to assist their patients in this area. It is estimated that 80% or more of HL cases in the U.S. are not adequately addressed by medical providers, resulting in non-diagnosis and frequently lack of treatment.3,4 HL not only affects quality of life, but can be costly. The WHO has estimated that unaddressed HL costs the global economy ~U.S. $980 billion annually, which includes healthcare costs, educational support, productivity losses and societal costs.5
Morbidity of Hearing Loss
Hearing loss can have significant effects on a person's health and quality of life. Many studies outline the negative consequences of HL, which spans physical, psychological and social domains:
Cognitive decline and dementia: HL increases dementia risk by 1.9-fold.6 Studies have also shown that HL is the number one modifiable risk factor regarding cognitive decline, contributing to 8% of dementia cases.6 Increasing research indicates that treating HL can reduce progression and possibly even reverse cognitive decline.7,8 Depression and mental health: HL raises depression risk by 1.4fold.9 Impaired communication leads to reduced social engagement and loneliness, and 70-80% without hearing aids face higher mental health burden.10
Falls and physical safety: HL increases fall risk by 2.4-fold.11 This can lead to fractures, head trauma, hospitalizations and death, with falls being the number one cause of injury-related death among individuals 65+.
Social Isolation: HL reduces social participation, with around half of 65+ with HL reporting isolation.12 Reduced quality of life is reported, with ~60% of untreated HL patients reporting lower life satisfaction.3 Economic and functional burden: HL reduces work productivity and independence. Adults 50-64 suffering HL have 2-fold higher unemployment rates.13 Untreated HL adds annual healthcare costs of ~$15,000 per person.14 Of patients 65+ with HL, ~30% report functional limitations, such as difficulty with daily activities.15 Associated comorbidities: HL is linked to cardiovascular disease (possibly via shared vascular pathology), diabetes and Parkinson’s disease.
Screening for Hearing Loss
Considering the prevalence of HL, which commonly goes undiagnosed and untreated, the American Academy of Otolaryngology— Head and Neck Surgery Foundation in 2024 released clinical practice guidelines for managing age-related HL.4 The recommendation was that all patients aged 50 and above should be screened for HL, because detecting HL early and taking appropriate steps can help minimize the negative effects associated with untreated HL. It would be ideal for all medical providers to do their best to recognize HL and refer for evaluation and treatment accordingly. This would include clinicians, like primary care providers, to perform hearing screenings on patients 50+ in their office; screening options include:
• Inquiring from patient if they have difficulty hearing
• Questionnaires regarding HL, such as the Hearing Handicap Inventory for the Elderly (HHIE-S being the shorter version, a 10-item questionnaire)
• Use of a handheld tone emitting otoscope
• Testing hearing with whispered voice, finger rub, and/or watch tick test
• Use of various audiometry screening tools available on the market, such as tablet or smartphone-based hearing screening apps
In the event of signs of HL, a person should be referred to a clinician who can obtain an audiogram. When appropriate, referral should be made to a clinician that can address potential issues like asymmetry in hearing (important to rule-out conditions such as skull base tumor) or recoverable forms of HL, like cerumen impaction or tympanic membrane perforation.
Treatment of Hearing Loss
As a practicing neurotologist (specializing in the ear, balance and skull base disorders), I tell patients that almost all forms of HL can be treated in some way. The treatment recommended can depend on the type and severity of HL. Conductive hearing loss (CHL) is caused by conditions that prevent sound from reaching the inner ear, such as cerumen impaction, middle ear fluid as seen with otitis media, perforated tympanic membrane, and ossicular abnormalities such as otosclerosis. Fortunately, most forms of CHL have the potential to be recovered, such as with the use of medicines or surgery. Sensorineural hearing loss (SNHL) is most often caused by aging, noise exposure and/or genetic predisposition, and is generally not reversible (unless it is of sudden onset and recent occurrence, making it an otologic emergency to have the patient rapidly evaluated audiometrically and treated accordingly). Mixed hearing loss (MHL) is a combination of both CHL and SNHL in the same ear.
SNHL is by far the most common type of HL seen in adults, accounting for ~80-90% of HL cases per NIDCD.16 It is typically progressive with age. Although it is generally not reversible, treatment can still be offered, with options including: Avoidance of noise exposure: Important for prevention of HL, including use of hearing protection in situations like a noisy workplace, around firearms, or at live music performances.
Assistive listening devices: Includes FM systems and TV streamers. Aural rehabilitation: Includes counseling and communication strategies.
Hearing aids (HAs): The landmark ACHIEVE study, a randomized controlled trial investigating the effects of hearing interventions in elders, suggests that HAs can slow cognitive decline by 48-62% in high-risk groups.17
Cochlear implants (CIs): A 2024 meta-analysis found that CI users age 60+ with severe-profound HL had a 30-50% slower cognitive decline over five years than untreated peers.18
In an effort to encourage treatment of HL, U.S. Congress passed the Over-the-Counter Hearing Aid Act of 2017, which became effective in October 2022, which allows adults 18+ with perceived mild/ moderate HL to buy OTC HAs without a prescription, exam or professional fitting.19 While the legislation has improved awareness of HL, there are limitations, including that a large percentage of individuals purchasing over-the-counter HA's today have advanced HL, a category not covered by the FDA's rule. Fortunately, when individuals come to recognize their HL and realize that treatment is needed, it is common that they discover over-the-counter hearing aids do not provide adequate benefit and then seek more specialized care.
Summary
Hearing loss is a very prominent condition, frequently not diagnosed, and inadequately treated 80+% of the time. Untreated HL has significant morbidity, reduction in quality of life and societal costs. Fortunately, it is almost always treatable. It is advisable for all clinicians to perform hearing screening and then refer patients with suspected HL to providers that can provide the appropriate care, whether it be medical or surgical treatment, HAs or cochlear implantation. Let's work together to make sure these patients with HL are identified, diagnosed, and treated, so that we can do our part to help these 80+% of HL patients inadequately treated, allowing us to decrease the morbidity of HL and improve our patients’ overall health and quality of life.
References:
1. World Health Organization. Deafness and hearing loss. Published February 7, 2023. Accessed July 1, 2025. https://www. who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss
2. National Institute on Deafness and Other Communication Disorders (NIDCD). Quick statistics about hearing. Updated March 25, 2021. Accessed July 1, 2025. https://www.nidcd.nih. gov/health/statistics/quick-statistics-hearing
3. Hearing Loss Association of America (HLAA). Hearing loss facts and statistics. Published 2023. Accessed July 18, 2025. https://www.hearingloss.org/understanding-hearing-loss/hearing-loss-101/hearing-loss-by-the-numbers/
4. American Academy of Otolaryngology–Head and Neck Surgery Foundation (AAO-HNSF). Clinical practice guideline: Age-related hearing loss. Published 2024. Accessed July 1, 2025. https://www.entnet.org/quality-practice/quality-products/clinical-practice-guidelines/age-related-hearing-loss/
5. World Health Organization. Global costs of unaddressed hearing loss and cost-effectiveness of interventions: A WHO paper, 2017. Accessed July 1, 2025. http://iris.who.int/handle/10665/254659
6. Livingston, G., Huntley, J., Sommerlad, A., et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413-446. doi:10.1016/ S0140-6736(20)30367-6
7. Bucholc, M., McClean, P.L., Bauermeister, S., et al. Association of hearing loss with dementia: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2021;147(5):410-419. doi:10.1001/jamaoto.2020.5367
8. Jiang, F., Mishra, S.R., Shrestha, N., et al. Association between hearing aid use and cognitive decline among community-dwelling older adults with hearing loss. J Am Geriatr Soc. 2021;69(9):2482-2490. doi:10.1111/jgs.17264
9. Redd, S.C., Lin, F.R., Huang, A.R., et al. Hearing loss and depressive symptoms in older adults: A systematic review and meta-analysis. J Gerontol B Psychol Sci Soc Sci. 2021;77(2):356366. doi:10.1093/geronb/gbab153
10. Reed, N.S., Altan, A., Deal, J.A., Lin, F.R. Hearing loss and mental health: A review of the evidence. JAMA Otolaryngol Head Neck Surg. 2021;147(5):456-464. doi: 10.1001/jamaoto.2020.5678
11. Jiam, N.T., Li, D., Lin, F.R. Hearing loss and falls: A systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. 2016;71(11):1467-1474. doi:10.1093/gerona/glw070
12. AARP. Social isolation and hearing loss: The connection. Published 2020. Accessed July 1, 2025. https://www.aarp.org/health/ conditions-treatments/info-2020/hearing-loss-social-isolation. html
13. Hearing Industries Association (HIA). Hearing loss and employment: A report. Published 2019. Accessed July 1, 2025. https:// www.hia.org/reports/hearing-loss-employment
14. Reed, N.S., Altan, A., Deal, J.A., et al. Economic burden of untreated hearing loss in older adults. JAMA Otolaryngol Head Neck Surg. 2021;147(12):1041-1048. doi:10.1001/jamaoto.2021.2872
15. National Health and Nutrition Examination Survey (NHANES). Hearing loss and functional limitations: Data from 2015-2020. Centers for Disease Control and Prevention. Accessed July 1, 2025. https://www.cdc.gov/nchs/nhanes/index. htm
16. National Institute on Deafness and Other Communication Disorders. Quick Statistics About Hearing, Balance, & Dizziness. National Institutes of Health. Updated July 2022. Accessed July 20, 2025. https://www.nidcd.nih.gov/health/statistics/quick-statistics-hearing
17. Lin, F.R., Deal, J.A., Reed, N.S., et al. Effect of Hearing Aids on Cognitive Decline in Older Adults With Hearing Loss: A Randomized Clinical Trial. JAMA. 2023;330(14):1345–1354. doi:10.1001/jama.2023.17060
18. Yeo, B.S.Y., Song, H.J.J.M.D., Toh, E.M.S., et al. Cochlear implantation and cognitive decline in older adults: A meta-analysis. JAMA Otolaryngol Head Neck Surg. 2024;150(2):113-122. doi:10.1001/jamaoto.2023.4055
19. U.S. Food and Drug Administration. Over-the-counter hearing aids: Final rule. Published October 17, 2022. Accessed July 1, 2025. https://www.fda.gov/medical-devices/hearing-aids/overcounter-hearing-aids
Lance Jackson, MD, FACS, is an Otologist/Neurotologist board certified in Otolaryngology—Head and Neck Surgery with subspecialty certification in Neurotology. He practices with the Ear Institute of Texas. He cares for patients with ear-related disorders, including hearing loss, dizziness and skull base tumors. A prime focus of his practice is cochlear implantation, which can have a dramatic positive impact on a recipient’s life. He is an executive board member for the nonprofit organization Aid The Silent, which helps to provide help to deaf and hard-of-hearing children. He has a passion for addressing hearing loss in San Antonio and surrounding areas, with hopes to minimize the negative effects of nontreatment, including cognitive decline, dementia, withdrawal and depression. Dr. Jackson is a member of the Bexar County Medical Society.
COMMUNICATING WITH CONFIANZA — A HEALTH LITERACY ECHO
TOGETHER, WE CAN IMPROVE COMMUNICATION AND HEALTH LITERACY SKILLS
Join us for a free online learning series designed to empower health professionals with health literacy education, resources and knowledge-sharing tools. The series is presented by Health Confianza, an award-winning health literacy nonprofit funded by Bexar County and housed at The University of Texas Health Science Center at San Antonio.
Who is this for? Health professionals, including physicians, nurses, community health workers, social workers and pharmacists.
Join our expert team the first and third Friday of each month
TOPICS:
• Acknowledging perspectives
• Shame/stigma; Creating a shame-free environment
• Plain language
• Shared decision-making
• Teach Back
WHAT: Free, six-part series
DATE/TIME: Sept. 5th - Nov. 21, 1st and 3rd Fridays of the month, 12:00-1:00 p.m.
REGISTER: bit.ly/Communicatingwith Confianza CE credits are available
We Must Protect our Firefighters from Cancer
By Rachelle Hamblin, MD, MPH; Amelie Ramirez, DrPH, MPH; and Ramon Cancino, MD, MBA, MS, FAAFP
As of 2022, firefighting has been designated a known Group 1 human carcinogen by the International Agency of Research on Cancer (IARC). Firefighting is a risk factor for the following cancers: bladder, brain, breast, cervical, colon, esophageal, kidney, prostate, multiple myeloma, non-Hodgkin's lymphoma, testicular, thyroid, leukemia, mesothelioma and melanoma.1–3
Unfortunately, cancer remains the leading cause of death in firefighters, surpassing heart disease and mental health, with 75% of line of duty deaths caused by cancer. Compared to the general population, firefighters are at a 9% greater risk of getting cancer and a 14% greater risk of dying from cancer.4 Moreover, firefighters are at a greater risk of getting multiple types of cancer, getting certain cancers at a younger age of diagnosis, and getting more aggressive cancers.5
The reason for these outcomes may be due in part to the hazardous materials that firefighters are exposed to during and after firefighting. The IARC found there are over 40 known, probable and possible human carcinogens in fires and their by-products of combustion that are from every day materials such as plastics, furniture and electronics. MicroRNAs play a prominent role in carcinogenesis. Exposure to just one structure fire caused microRNA expression within new firefighter recruits.2
The full answer is complex and multi-factorial, extending beyond the fire scene to encompass other risk factors including behavior, other environmental exposures, poor nutrition, lack of physical activity, interrupted and limited sleep, tobacco use, lack of education on occupational cancer both for firefighters and healthcare providers, lower utilization of primary care and preventative services, and limited research on occupational cancer in the fire service.
That is where Mays Cancer Center at The University of Texas at San Antonio Health Science Center and UT San Antonio Health Science Center come in.
In April 2025, Mays Cancer Center and UT San Antonio partnered with University of Miami’s Sylvester Comprehensive Cancer Center’s Firefighter Cancer Initiative to answer the San Antonio Fire Department’s (SAFD’s) call for help and formed the San Antonio Firefighters Cancer Prevention Program.
The San Antonio Firefighters Cancer Prevention Program aims to better understand and reduce the burden of cancer among local first responders. To accomplish this, the program leaders aim to:
• Explore the opportunity to launch an annual cancer risk assessment study based on the national firefighter annual cancer cohort study of Sylvester Comprehensive Cancer Center
• Tailor Miami’s Firefighter Cancer Initiative educational resources for San Antonio firefighters and host educational sessions with the SAFD
• Develop an additional referral and navigation system to connect SAFD firefighters to UT San Antonio and the Mays Cancer Center providers for early cancer screening, diagnosis and survivorship programs
• Connect SAFD firefighters to cancer clinical trials and research studies at Mays Cancer Center
• Identify opportunities to advise the National Institute for Occupational Safety and Health (NIOSH) and other relevant stakeholders on a strategy to collect Firefighter Cancer Registry data
• Collaborate with SAFD leaders to train UT San Antonio primary care providers on the unique screening needs and potential occupational or environmental exposures relevant to firefighters or emergency service personnel
The effort has already demonstrated an impact.
San Antonio Firefighters Cancer Prevention Program leaders, along with the SAFD Occupational Cancer Committee, have helped to open the conversation about relevant research that would be high impact to the SAFD and the wider fire department community, including partnership on ongoing research with the Sylvester Comprehensive Cancer Center.
Multiple UT San Antonio team members shared health materials and opportunities to participate in research programs with hundreds of local firefighters and emergency service personnel at the recent SAFD Wellness and Cancer Prevention Fair, including health education (through the Institute for Health Promotion Research at UT San Antonio), primary care and dermatology. The program has also initiated an immediate response system with the Mays Cancer Cen-
ter to provide cancer care referrals to firefighters who receive a cancer diagnosis. Multiple firefighters have used the group as a resource for questions or even guidance about treatment. Finally, a large group of primary care clinicians were educated on the higher cancer risks in this patient population.
Firefighter teams are essential to the health and safety of our community. With the San Antonio Firefighters Cancer Prevention Program, efforts are being made to drive down the burden of cancer in this group and to educate the community of physicians about their increased cancer risk.
Resource List:
• Letter to PCP - Dr.-Hamrock-Letter-to-Health-Care-Providers.pdf,
o https://connecticutfirechiefs.com/wp-content/ uploads/2021/02/Dr.-Hamrock-Letter-to-Health-CareProviders.pdf
• Letter to Firefighters - FDIC 2011 EXTINGUISHING CANCER IN FIREFIGHTERS PRESENTATION
o https://www.iaff.org/wp-content/uploads/Firefighter_Pre_ Physical_Prep_Guide.pdf
• Provider’s Guide to Firefighter Medical Evaluations - Healthcare Providers Guide-FINAL_7-29; Providers-Guide.pdf
o https://www.iafc.org/docs/default-source/1safehealthshs/ healthcareprovidersguide.pdf
• NFPA 1582 Guidelines (Occupational Health Screenings for Firefighters) - NFPA 1582 Standard Development; NFPA_Form_1582_-_Firefighter_Physical.pdf
o https://www.nfpa.org/codes-and-standards/ nfpa-1582-standard-development/1582
o https://core-docs.s3.amazonaws.com/documents/asset/ uploaded_file/1192719/NFPA_Form_1582_-_Firefighter_Physical.pdf
• NFPA 1582 Guidelines for Firefighters SummaryFRC31260_Firefighter_Physical_NFPA1582_Brochure_ v3.indd
o https://www.iafc.org/docs/default-source/1safehealthshs/ nfpa1582_physicalguidebrochure.pdf?sfvrsn=146d6b0c_0
• Firefighter Cancer Initiative – University of Miami and Sylvester Cancer Center - Firefighter Cancer Initiative | Sylvester Comprehensive Cancer Center | University of Miami Health System
o https://umiamihealth.org/sylvester-comprehensive-cancer-center/research/firefighter-cancer-initiative
• UT Health/Mays Cancer Center San Antonio Firefighters Cancer Prevention Program - With Male and Female Firefighter Cancer Screening Guidelines
o https://ihpr.uthscsa.edu/firefighters/
References:
1. Calabrò, P. et al. Lipid-Lowering Therapy in Patients With Coronary Demers PA, DeMarini DM, Fent KW, Glass DC, Hansen J, Adetona O, Andersen MH, Freeman LEB, Caban-Martinez AJ, Daniels RD, Driscoll TR, Goodrich JM, Graber JM, Kirkham TL, Kjaerheim K, Kriebel D, Long AS, Main LC, Oliveira M, Peters S, Teras LR, Watkins ER, Burgess JL, Stec AA, White PA, DeBono NL, Benbrahim-Tallaa L, Conti A de, Ghissassi FE, Grosse Y, Stayner LT, Suonio E, Viegas S, Wedekind R, Boucheron P, Hosseini B, Kim J, Zahed H, Mattock H, Madia F, Schubauer-Berigan MK. Carcinogenicity of occupational exposure as a firefighter. The Lancet Oncology. 2022;23(8):985-986. doi:10.1016/S1470-2045(22)00390-4
2. Jeong KS, Zhou J, Griffin SC, Jacobs ET, Dearmon-Moore D, Zhai J, Littau SR, Gulotta J, Moore P, Peate WF, Richt CM, Burgess JL. MicroRNA Changes in Firefighters. J Occup Environ Med. 2018;60(5):469-474. doi:10.1097/JOM.0000000000001307
3. IARC Working Group on the Identification of Carcinogenic Hazards to Humans. Occupational Exposure as a Firefighter. International Agency for Research on Cancer; 2023. Accessed August 23, 2025. http://www.ncbi. nlm.nih.gov/books/NBK597253/
4. Firefighter Cancer Rates: The Facts from NIOSH Research | Blogs | CDC. May 10, 2017. Accessed August 23, 2025. https://blogs.cdc. gov/niosh-science-blog/2017/05/10/ff-cancer-facts/
5. Landgren O, Zeig-Owens R, Giricz O, Goldfarb D, Murata K, Thoren K, Ramanathan L, Hultcrantz M, Dogan A, Nwankwo G, Steidl U, Pradhan K, Hall CB, Cohen HW, Jaber N, Schwartz T, Crowley L, Crane M, Irby S, Webber MP, Verma A, Prezant DJ. Multiple Myeloma and Its Precursor Disease Among Firefighters Exposed to the World Trade Center Disaster. JAMA Oncol. 2018;4(6):821-827. doi:10.1001/jamaoncol.2018.0509
Rachelle Hamblin, MD, MPH, is a family medicine physician at Health by Design, the Retiree Police and Firefighter Clinic. Dr. Hamblin volunteers with the SAFD Occupational Cancer Committee; teaches at the Fire Training Academy; and has also completed the Citizen's Fire Training Academy.
Amelie G. Ramirez, DrPH, MPH, is chair and professor of Population Health Sciences at UT San Antonio, where she also is founding director of the Institute for Health Promotion Research and associate director of cancer outreach and engagement at the Mays Cancer Center at The University of Texas at San Antonio Health Science Center.
Ramon Cancino, MD, MBA, MS, FAAFP, is a Professor/ Clinical in the Department of Family & Community Medicine at UT San Antonio, Executive Director of the UT Health San Antonio Primary Care Center, Senior Medical Director of Medical Management, and Co-Chair of the UT Health San Antonio MD Anderson Cancer Center/UT Health San Antonio Joint Cancer Prevention and Screening Committee. Dr. Cancino is a member of the Bexar County Medical Society.
Healing Together: Patients, families and community at heart of UT San Antonio’s Center for Brain Health
Courtesy of The University of Texas at San Antonio Health Science Center
After nearly a decade of planning, The University of Texas at San Antonio Health Science Center will open the doors of its innovative Center for Brain Health in December 2025. The $100 million, 103,000-square-foot facility brings together clinical care, research and caregiver support — all under one roof — and promises to change how we understand and treat diseases of the brain.
Vision Years in the Making
The vision began more than seven years ago when Sudha Seshadri, MD, DM, professor of neurology and founding director of the Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases, sought to create a dedicated space for research and patient care. “My hope is that we can make Alzheimer’s a condition people live with and manage, like diabetes or high blood pressure,” Seshadri said. “That’s the kind of hope we’re working to bring to every patient.”
That hope resonates with Carlayne Jackson, MD, FAAN, chair of the Department of Neurology and professor of neurology and otolaryngology. “When I was an early neurology resident, there were no treatments and nothing we could do for these devastating conditions,” she said. “The Center for Brain Health is a place of hope and innovation where we can diagnose, manage symptoms, optimize function, and support patients and families for the journey ahead.”
State-of-the-Art Design, Location
A unique aspect of this project is that Seshadri, Jackson, and other faculty members worked side-by-side with architects and designers throughout the planning period. “The architects didn’t just hand us a draft of the blueprints. We were there every step of the way,” Jackson said. With input from the community, the team created a welcoming space where patients and their families are invited to work in tandem with healthcare professionals for treatment of these devastating brain diseases.
Located adjacent to the Medical Arts and Research Center and near the new UT Health San Antonio Multispecialty and Research Hospital, the center will foster collaboration across clinical and research teams.
“This center is the culmination of years of effort to build a space that not only meets the care needs of patients and families, but also expands our research capacity,” said Seshadri. “A diagnosis doesn’t define a person, and it certainly doesn’t stop their story.”
Integration of Research, Patient Care
Jackson said what excites her most about the center is the integration of patient care and research. “Many of the disorders we treat don’t yet have therapies that stop or even slow progression,” she said. “Being able to manage patients in the same space where research and clinical trials are happening is something we’ve never had before.”
The center will treat conditions such as Alzheimer’s disease and other dementias, stroke, amyotrophic lateral sclerosis (ALS) and Parkinson’s disease with multidisciplinary teams of neurologists, therapists, counselors and support staff — reducing the need for multiple appointments in different locations. It will feature 75 exam rooms, 12 infusion chairs for new and investigational treatments, and specialty areas for therapy, diagnostics and wellness.
Jackson has long championed this model of care. She developed the department’s first multidisciplinary ALS clinic in 1996 and dreamed of expanding the approach to all neurological conditions. “We just didn’t have the space, capacity or funding to do it, and now we do,” she said.
Other services will include geriatric psychiatry, neuropsychology, genetic counseling, nutrition, physical therapy and mental health support. A physical therapy gym will allow comprehensive assessments on-site. Community spaces will host support groups and educational programs for families. The center will also house Texas’ first 7-Tesla Terra.X magnetic resonance imaging scanner, providing ultra-high-resolution brain scans for early diagnosis and novel research.
Personal Journey Behind the Mission
For Jackson, the mission is also personal. As a resident, she navigated the healthcare system for her son with a neurological disorder, coordinating therapy and medical visits across multiple locations. “The burden of handling his medical care was more overwhelming than the fact that I had a handicapped child,” she said. “I always believed there had to be a better model of care, and that belief guided how we set this facility up.”
Meeting the Neurodegeneration Challenge
“As our country and state get older, we’re facing an epidemic of neurodegeneration,” Jackson said. “We’ve been effective at treating cancer and diabetes, but if we don’t take this next bold step now, we’ll be facing a public health crisis with no effective treatments.”
Ultimately, both leaders say, the center is designed to instill confidence. “Being diagnosed with any brain disorder can feel devastating and isolating,” Jackson said. “I want patients to know they are receiving the best, most comprehensive care possible from a team that truly cares.”
“The Center for Brain Health represents hope — a place where care and discovery come together to preserve brain health, ensure early diagnosis and help people keep doing what they love for as long as possible,” Seshadri said.
For more information about the new center, visit uthscsa.edu/physicians/center-brain-health.
Lessons Learned Rehabbing a Nursing Home in San José, Costa Rica
By Arya Bietz; Gabriel Bietz, MD; and Amita Kumar, MD
In 2013, Máximo Nivel, a company specializing in community service in Latin American countries, was founded. This company grew to thrive in three different countries across the Americas by introducing volunteers to a new environment and providing them with the opportunity to impact the area around them. Fast forward to June of 2025, when my family and I decided to explore Máximo Nivel and make an impact in a place of need. The establishment in Costa Rica was welcoming, knowledgeable and ready to help. A local family who partnered with Máximo Nivel provided housing for me, my parents and my younger brother. The local family has been hosting volunteer workers for 38 years and has welcomed over 20,000 volunteers during that time.
On the first day, we were given our assignment: an old nursing home, established in 1972, needed internal demolition of one of the existing buildings, as well as a remodel. Our goal was to help transform the old bathroom space into a livable environment that could house
more citizens of Costa Rica. This building would eventually house another 23 residents.
A local foreman, Oscar, explained the changes that needed to be made to the building to meet Costa Rican standards. He works with Máximo Nivel, helping to run their construction community service program and the projects that are conducted in San José. Although our time working in Costa Rica was only a week long, a definite impact was made. Those seemingly little actions will create a bright new future for the nursing facility.
At first glance, the decaying building seemed to have little worth. Inside the structure were walled-off bedrooms covered in molding paint and grime that needed to be scraped or pressure-washed off the walls. Some rooms required complete demolition and removal of large walls, including two bathrooms and shower areas, which were lined with thick tiles. After clearing the dust and cobwebs, I began to explore the space with an open mind. This allowed the true beauty of the archi-
tectural structure to reveal itself. Most walls were not load-bearing; however, they were eight inches thick and made of solid concrete and cinder block, which would take time to break down without the right tools. We were provided with three hammers, a miniature sledgehammer, a handheld jackhammer and several extension cords to provide power. Oscar informed our team that the first step was to remove all debris from the inside of the building, including old clothes and furniture from past residents. Once we were able to complete this task, demolition could begin in the common area.
Prior to any physical work, our team ensured that all water and electricity had been disconnected from the building in order to prevent damage or injury. Containment measures, such as closing doors and opening windows, were also taken to minimize the spread of dust and debris during demolition. These protocols ensured that residents of the nursing facility would not be affected or harmed in any way by the work that was being done.
Once safety measures were in place and all members of our small team of eight men and women were equipped with gloves, eye protection and masks, the project began. At first, progress was slow as we encountered many new obstacles that were not easily crossable.
After numerous attempts at using different angles with the handheld jackhammer, we discovered weak points in the walls that could be easily knocked out, creating a point of leverage. We learned how to listen for weak points and know if an area was hollow or solid concrete based on how it felt after hitting it with the sledgehammer. This was an incredible learning experience that taught me that construction is possible with the proper knowledge, not just the newest and/or best tools.
A few days into the project, my parents noticed some residents with health issues across the nursing home. They decided to volunteer their medical services to help those who needed them. Both of my parents are physicians and actively practice in San Antonio, Texas. Dr. Gabriel Bietz is a vascular surgeon, and Dr. Amita Kumar practices internal medicine, specializing in outpatient primary care. They both reviewed medical records and helped the elderly. Healthcare facilities like nursing homes are not simply structures — they’re places of recovery. They require special amenities, such as ADA-accessible ramps, additional plumbing and emergency generators. Similar to Costa Rican compliance, Texas facilities are subject to 25 Texas Administrative Code 133. These structures should not be located near hazards such as gas pipes or flood zones, and they must have broad corridors, sprinklers and red electrical receptacles for emergencies in operating rooms and ICUs.
One week of demolition marked the start of a significant change that will benefit many new senior citizen residents to come. This demonstrates that even a few days of dedicated effort can have a lasting impact and positively transform a community.
Costa Rica showed me what construction can be and how it changes societies for the better. I want to study construction science and earn a degree in the field, with a specialization in healthcare buildings, such as hospitals and nursing homes. Although it was only a few days, the week was filled with inspiration. I learned that ADA compliance was not just about regulations but also dignity. Large, open doorways allow residents to move freely without worrying about their wheelchairs, walkers or other mobility aids. Although healthcare facility construction is complex, it is beyond fulfilling for the soul. Máximo Nivel has done and will continue to do a considerable service to communities across Latin America.
Reference:
1. Texas Administrative Code, Title 25, Part 1, Chapter 133, Subchapter I: Physical Plant and Construction Requirements (Sections 161–165). Justia/State repository
Arya Bietz, a junior at Alamo Heights High School, has won numerous journalism contests sponsored by the University Interscholastic League. After high school graduation, she aspires to pursue a degree in construction science with a sub-specialty in healthcare facility development.
Gabriel Bietz, MD, is a board-certified Vascular Surgeon and Chairman of the Board for San Antonio Surgical Center of Excellence. He is a partner at Texas Cardiac and Vascular Institute, serving patients across San Antonio, Seguin and Corpus Christi. He is recognized for his expertise in both open and endovascular procedures, along with his leadership in advancing patientcentered vascular care. In addition to his medical career, Dr. Bietz is a serial entrepreneur with ventures spanning healthcare and private investments, and is a member of the Bexar County Medical Society.
Amita Kumar, MD, is a board-certified Internal Medicine physician whose clinical practice emphasizes preventive medicine and patient education. In 2022, she expanded her work by completing coach training at the Health Coach Institute. She also serves on the boards of Planned Parenthood South Texas and The Patient Institute, mentors medical students at UIW, and coaches fellow physicians. Dr. Kumar is a member of the Bexar County Medical Society.
Healthcare Professionals Are Key to Preventing Domestic Violence
By Erica Haller-Stevenson, MPH
Domestic violence can impact anyone regardless of economic class, race, sex or gender; no person is immune. But healthcare professionals can help stop the cycle of violence.
Domestic violence has many forms and may be perpetrated as economic, physical, sexual, emotional and psychological abuse. Women are most affected, however, males are also victimized. Domestic violence is multigenerational. Children are impacted directly by abuse or by what they see, causing adverse childhood events (ACEs), leading to a higher risk of perpetuating the cycle of violence in adulthood. The stress of domestic violence is also associated with chronic diseases, such as hypertension.
Domestic violence is underreported nationwide due to stigma and fear.1 Although it is underreported, it continues to be pervasive. Just in Bexar County, there were 58,554 calls to law enforcement for assistance in 2024 and over 17,000 people received support services during the same year. Sometimes, domestic violence results in mortalities. There were 30 lives lost in the Bexar County area in 2024, including 16 women, 11 men, and 3 children.2
Healthcare professionals have an opportunity to intervene in domestic violence. Through patient interviews and examinations, they may identify signs of abuse, or a patient may disclose their experience. Short, validated tools such as the Danger Assessment-5 (DA-5)3 can be used in a medical practice for screening.
When a patient, family member or friend seems open to help, healthcare professionals need a place to refer people to resources. Family Violence Prevention Services operates the local shelter and provides extensive services for the Bexar County area. The Bexar County and City of San Antonio governments have programs that work in partnership with local law enforcement to provide crisis support and case management. Making a law enforcement report is not a requirement to receive services from any of these organizations. However, people should always be encouraged to call 911 for emergencies.
Healthcare offices can also display brochures and posters or signs that direct people to these resources. The sticker featured here is available at no cost through the City of San Antonio. Visit sa.gov/DVsigns for more information.
Healthcare providers are in a unique position to identify domestic violence and serve as a trusted resource. Learn more about applying the practice of medicine to identify and intervene in domestic violence through a continuing education article available from the National Library of Medicine.4
City of San Antonio Metropolitan Health District SA.gov/directory/departments/SAMHD
Assistance is available through the following places:
• Family Violence Prevention Services, fvps.org, or call the 24/7 hotline at 210-733-8810
• Bexar County through the Sheriff’s Office non-emergency line at 210-335-6000
• City of San Antonio through the Police Department’s non-emergency line at 210-207-SAPD
References:
1. Piquero, A.R. and Wheeler, A. (Oct. 2024). Toward a better estimate of domestic violence in America. Council on Criminal Justice. https://counciloncj.org/toward-a-better-estimate-of-domestic-violence-in-america/
3. Messing, J. T., Campbell, J. C., Snider, C. (Dec. 2017). Validation and adaptation of the danger assessment-5: A brief intimate partner violence risk assessment. Journal of Advanced Nursing, 73(12):3220-3230. doi: 10.1111/jan.13459
4. Huecker, M. R., King, K. C., Jordan, G. A., and Smock W. (Apr. 2023). Domestic violence. StatPearls Publishing. https://www. ncbi.nlm.nih.gov/books/NBK499891/
Erica Haller-Stevenson, MPH, is the Violence Prevention Administrator for the City of San Antonio Metropolitan Health District. She oversees several programs focused on serving the community and preventing violence. She was trained as a health educator and received an MPH degree from Emory University.
An Immigrant’s Story
Artist’s Note: An Immigrant'sStory is a print of a mother and her child in a foreign city for the first time. The background is abstract to capture the overwhelming essence of landing in a city like New York for the first time. The mother is sitting in an "Asian squat" as she looks after her child, who poses in a stance indicating that more children are on the way. They are outside the frame of the city to emphasize their new home.
Medium: Intaglio Print on Copper Plate
Long School of Medicine at The University of Texas at San Antonio Health Science Center Class of 2027
Zainah Siddiqi
In the Letter I Write to My Future Son
My dear child, I just want to say I’m sorry, For deciding the future of our little family. Your house is no longer whole and may lack the warmth it had, A change that I fear will make you sad.
Countless nights, I’ve wrestled my heart, Wondering if tearing us apart Was the right choice — I cannot know. Forgive me, my child, for the seeds I sow.
I’m flawed, A man who still stumbles, no map to follow. My steps, like a child’s, leave prints as I roam, Seeking a better self, though far from home.
The day that I signed and turned away, I felt your gaze as bright as day. Within those eyes, so pure and clear, I saw myself as a child, my dear, With gray hair, with colors dimmed, Lost in layers of light grown thin.
I’m sorry for shaping a world for you that seems strange, For crafting a new “normal” you didn’t arrange, You’ve yet to know what another might mean. But trust, my son, life is more than it seems.
Somewhere, I think, in a universe wide, There’s another boy, with my name on his jacket, Who wears the same shoes as you, and walks a path where love pulls him through.
We may not share the same closeness we had, But whenever you call, know I’m your dad. A friend, a protector, who longs for your smile— Let me be your hero, if just for a while.
When you read this, you’ll have grown strong, A person of beauty, where you belong. Your future will flourish, your family bloom, Bringing new light to dispel the gloom.
Raise your child, teach him with care, Show him the strength that you now bear. And I will fade to a smaller frame, A fleeting part of a picture’s flame.
An ordinary man in life’s great scheme, But one who lived his liveliest dream. For since I met you, my world’s been anew, And forever, my son — know I love you.
Linh Nguyen
University of the Incarnate Word School of Osteopathic Medicine Class of 2027
Shop Businesses Who Support BCMS
BCMS Business Directory
As a BCMS member, you can find exclusive discounts on premium products and services that you and your practice use every day.
ACCOUNTING FIRMS
Sol Schwartz & Associates P.C. (HHH Gold Sponsor)
Sol Schwartz & Associates is the premier accounting firm for San Antonio-area medical practices and specializes in helping physicians and their management teams maximize their financial effectiveness.
Christopher Davis, CPA 210-384-8000, ext. 118 cbd@ssacpa.com www.ssacpa.com
“Dedicated to working with physicians and physician groups.”
CLA - CliftonLarsonAllen LLP (HH Silver Sponsor)
Transform complexity into opportunities. Work with professionals who understand the specific financial, operational, clinical, and strategic needs of physician practices and medical groups. Our team is made up of knowledgeable, accessible, and responsive individuals devoted to the health care industry.
Bryan Garcia
210-298-7924
Bryan.Garcia@CLAconnect.com CLAconnect.com
"We'll get you there."
ASSET WEALTH MANAGEMENT
Aspect Wealth Management (HHH Gold Sponsor)
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Atlas Retirement Strategies LLC is a comprehensive financial planning firm dedicated to serving the unique needs of the medical community. We offer customized strategies in business planning, retirement planning, risk management, wealth preservation, estate planning, and wealth transfer – empowering healthcare professionals to achieve long-term financial security, clarity, and peace of mind.
David M. Webb, Ph.D., MSM, CLF, CLTC, LACP
Founder & Principal
210-281-4400
David@atlas-plans.com www.atlas-plans.com
BANKING
Broadway Bank (HHH Gold Sponsor)
Healthcare banking experts with a private banking team committed to supporting the medical community.
Thomas M. Duran
SVP, Private Banking Team Lead 210-283-6640
TDuran@broadway.bank www.broadwaybank.com
“We’re here for good.”
Texas Partners Banks (HHH Gold Sponsor)
Our private banking team specializes in healthcare banking and will work with you to craft and seamlessly integrate financial solutions for you and your practice, including practice loans, lines of credit and custom local lockbox solutions headquartered in San Antonio.
Established in 1983, Lone Star National Bank has provided banking services to communities in South Texas for the past 41 years. LSNB is an independent and locally owned bank subsidiary of Lone Star National Bancshares-Texas, Inc with consolidated assets of $3 billion (12/31/23) and 36 full-service banking centers throughout Starr, Hidalgo, Cameron and Bexar counties. Aside from personal and business banking, LSNB offers investments, wealth management & trust along with property and casualty insurance, health insurance and supplemental coverage.
“We do what the Little Banks can’t, and the Big Banks won’t!”
Amegy Bank of Texas (HH Silver Sponsor)
We believe that any great relationship starts with five core values: Attention, Accountability, Appreciation, Adaptability and Attainability. We work hard and together with our clients to accomplish great things.
Robert Lindley
SVP | Private Banking Team Lead 210-343-4526
Robert.Lindley@amegybank.com
Denise Smith
Vice President | Private Banking 210-343-4502
Denise.C.Smith@amegybank.com
Scott Gonzales
Assistant Vice President | Private Banking 210-343-4494
Looking for low loan rates for mortgages and vehicles? We've got them for you. We provide a full suite of digital and traditional financial products, designed to help physicians get the banking services they need.
Synergy FCU Member Services 210-750-8333 info@synergyfcu.org www.synergyfcu.org
“Once a member, always a member. Join today!”
CREDENTIALS VERIFICATION ORGANIZATION
Bexar Credentials Verification, Inc. (HHHH 10K Platinum Sponsor)
Bexar Credentials Verification Inc. provides primary source verification of credentials data that meets The Joint Commission (TJC) and the National Committee for Quality Assurance (NCQA) standards for healthcare entities.
Betty Fernandez Director of Operations 210-582-6355
Betty.Fernandez@bexarcv.com www.bexarcv.com
“Proudly serving the medical community since 1998”
FINANCIAL ADVISORS
Avid Wealth Partners (*** Gold Sponsor)
For over 15 years, Avid Wealth Partners has been the trusted financial partner for local physician specialists and practice owners. We specialize in physician-focused financial advising, offering proactive tax planning, customized investment strategies, and comprehensive risk management solutions. Our approach addresses every aspect of your financial life, protecting your hardearned assets and building lasting wealth. With a team of credentialed specialists, we simplify complexity so you can focus on what you do best— caring for patients
Elizabeth Olney with Edward Jones (HHH Gold Sponsor)
We learn your individual needs so we can develop a strategy to help you achieve your financial goals. Join the nearly 7 million investors who know. Contact me to develop an investment strategy that makes sense for you.
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Michael Clark President 210-268-1520
MClark@aspectwealth.com www.aspectwealth.com
“Your wealth. . .All aspects”
Hancock Whitney (HH Silver Sponsor)
Since the late 1800s, Hancock Whitney has embodied core values of Honor & Integrity, Strength & Stability, Commitment to Service, Teamwork and Personal Responsibility. Hancock Whitney offices and financial centers in Mississippi, Alabama, Florida, Louisiana and Texas offer comprehensive financial products and services, including traditional and online banking; commercial, treasury management, and small business banking; private banking; trust; healthcare banking; and mortgage services.
John Riquelme
San Antonio Market President 210-273-0989
John.Riquelme@hancockwhitney.com
Serina Perez
San Antonio Business Banking 210-507-9636
Serina.Perez@hancockwhitney.com
GERIATRICS/PRIMARY CARE
UT Health San Antonio
MD Anderson Cancer Center
(HHH Gold Sponsor)
UT Health provides our region with the most comprehensive care through expert, compassionate providers treating patients in more than 140 medical specialties at locations throughout San Antonio and the Hill Country.
UT Health San Antonio Physicians
Regina Delgado Business Development Manager 210-450-3713
DelgadoR4@uthscsa.edu
UT Health San Antonio
MD Anderson Mays Cancer Center
Laura Kouba Business Development Manager 210-265-7662
NorrisKouba@uthscsa.edu
Appointments: 210-450-1000
UT Health San Antonio
7979 Wurzbach Road San Antonio, TX 78229
HOSPITALS/PRACTICE SERVICES
Golden Billing & Benefits (HHH Gold Sponsor)
Golden Billing is owned and operated for over 20 years in Houston, TX. The owner, Marcus Yi, is focused on creating a partnership with clients. We are dedicated to optimizing the small business doctor’s productivity and maximizing practice cash flow by accurate claims coding and timely processing. Call today for a free consultation. If you don’t want to use us at lease maybe we can help you fine tune your decision.
Marcus Yi 713-263-0054
MYi@goldenbilling.com www.goldenbilling.com
Genuine Health Group (HHH Gold Sponsor)
Genuine Health Group partners with primary care providers to help them successfully adopt value-based payment models and demonstrate better health outcomes. Providers choose us for our proven expertise and consistency both for their patients enrolled in Medicare Advantage plans and for their patients with traditional Medicare who can align with one of ACOs. We have a track record of effectively reducing the cost of care while simultaneously improving care quality.
Equality Health deploys a wholeperson care model that helps independent practices adopt and deliver value-based care for diverse communities. Our model offers technology, care coordination and hands-on support to optimize practice performance for Medicaid patients in Texas.
Cristian Leos
Network Development Manager 210-608-4205
CLeos@equalityhealth.com www.equalityhealth.com
“Reimagining the New Frontier of Value-Based Care.”
SpeedEz’s (** Silver Sponsor)
For over three decades, SpeedE’z has been Bexar County’s truly local partner for answering service, contact center and courier solutions. R.N. owned and family-led, we combine compassionate care with professional expertise. Our HIPAA Certification, SOC 2 Type II Compliance and Woman-Owned HUB status reflect our commitment to integrity and security. Ranked Top Ten nationally in the ATSI Award of Excellence, our team delivers results that stand out – rooted right here in San Antonio!
Lauren Garza 210-615-0964
Lauren@speedez.com https://speedez.com
DialOPS
(H Bronze Sponsor)
Dialops is a trusted U.S.-based medical answering service and virtual receptionist solution designed specifically for healthcare practices. We provide 24/7 live call handling, HIPAA-compliant messaging, appointment scheduling, and reliable after-hours and overflow support. Our medically trained agents answer every call with professionalism and care— just like your in-office staff—ensuring your patients always feel heard and supported. From solo providers to busy clinics, Dialops helps reduce missed calls, ease front desk overload, and improve the patient experience—all at a fraction of the cost of hiring in-house. Rachel Caero Rachel@dialops.net
877-2-DIALOPS/210-699-7198 www.dialops.net
INSURANCE
TMA Insurance Trust (HHHH 10K Platinum Sponsor)
TMA Insurance Trust is a full-service insurance agency offering a full line of products – some with exclusive member discounts and staffed by professional advisors with years of experience. Call today for a complimentary insurance review. It will be our privilege to serve you.
“We offer BCMS members a free insurance portfolio review.”
INSURANCE/MEDICAL MALPRACTICE
Texas Medical Liability Trust (HHHH 10K Platinum Sponsor)
With more than 20,000 healthcare professionals in its care, Texas Medical Liability Trust (TMLT) provides malpractice insurance and related products to physicians. Our purpose is to make a positive impact on the quality of healthcare for patients by educating, protecting and defending physicians.
Patty Spann Director of Sales and Business Development 512-425-5932
Patty-Spann@tmlt.org www.tmlt.org
“Recommended partner of the Bexar County Medical Society”
INSURANCE/MEDICAL MALPRACTICE
The Bank of San Antonio Insurance Group, Inc. (HHH Gold Sponsor)
We specialize in insurance and banking products for physician groups and individual physicians. Our local insurance professionals are some of the few agents in the state who specialize in medical malpractice and all lines of insurance for the medical community.
Katy Brooks, CIC 210-807-5593
Katy.Brooks@bosainsurance.com www.thebankofsa.com
“Serving the medical community.”
MedPro Group (HH Silver Sponsor)
Rated A++ by A.M. Best, MedPro Group has been offering customized insurance, claims and risk solutions to the healthcare community since 1899.
Visit MedPro to learn more.
Kirsten Baze, RPLU, ARM
AVP Market Manager, SW Division 512-658-0262
Fax: 844-293-6355
Kirsten.Baze@medpro.com www.medpro.com Continued on page
BCMS Business Directory
IT-TELEMEDICINE SERVICES
LASO Health Telemedicine and Rx App (HH Silver Sponsor)
LASO Health is the industry’s only solution that makes healthcare services accessible, cost-transparent and convenient. Its mission is to reinvent “healthcare” in the United States by empowering every individual and employer, insured or uninsured to have easy, timely, predictable, cost-effective care. LASO combines an intuitive, mobile superapp with a marketplace of virtual and in-person health services to give customers a one-touch, onestop-shop, comprehensive health solution.
Ruby Garza, MBA 210-212-2622
RGarza@texaskidneycare.com www.lasohealth.com
MICROPRACTICE SERVICES
Parvus Medical Suites (HHHH 10K Platinum Sponsor)
Parvus Medical Suites offers a new way to start your own private clinical practice, either full-time or part-time, at a much lower cost than a traditional clinic. We take care of providing well-qualified employees, so that you can focus solely on delivering high-quality patient care. Our turn-key practice spaces in San Antonio and New Braunfels are available for short- and long-term lease options, and come complete with all amenities. Micropractice medicine is revolutionizing independent clinical care.
John Rodriguez, MD Chief Medical Officer 210-632-3411
DrJohn@parvussuites.com www.parvussuites.com
MEDICAL SUPPLIES AND EQUIPMENT
Henry Schein Medical (HH Silver Sponsor)
From alcohol pads and bandages to EKGs and ultrasounds, we are the largest worldwide distributor of medical supplies, equipment, vaccines and pharmaceuticals serving officebased practitioners in 20 countries. Recognized as one of the world’s most ethical companies by Ethisphere.
Kelly Emmon
Field Sales Consultant
210-279-6544
Kelly.Emmon@henryschein.com www.henryschein.com
“BCMS members receive GPO discounts of 15 to 50 percent.”
Empowering physicians for a Balanced Future. Our virtual health associates alleviate administrative burdens in the evolving healthcare landscape, combatting burnout. Join us in transforming healthcare delivery, prioritizing your wellbeing and patient care.
D.Rodriguez@eleosvhs.com www.equalityhealth.com “Reimagining the New Frontier of Value-Based Care”
PHYSICIAN ORGANIZATIONS
Methodist Physician Practices (HH Silver Sponsor)
Methodist Physician Practices is committed to providing exceptional care for patients in greater San Antonio and South Texas. As part of Methodist Healthcare, we are dedicated to raising the standards of performance excellence while advancing the health and well-being of the communities we serve. Our extensive network of highly-skilled primary care physicians, specialists and surgical care providers ensures patients receive comprehensive, coordinated and compassionate care. As part of the Methodist Healthcare System, our physicians are committed to delivering personalized, high-quality services that meet the diverse needs of our patients. At Methodist Physician Practices, we go beyond healthcare — providing hope, healing and unwavering support for each individual we serve.
Erin Fitzgerald Methodist Healthcare I Methodist Physician Practices M:281-673-7350 methodistphysicianpractices.com
PROFESSIONAL ORGANIZATIONS
The Health Cell (HH Silver Sponsor)
“Our Focus is People” Our mission is to support the people who propel the healthcare and bioscience industry in San Antonio. Industry, academia, military, nonprofit, R&D, healthcare delivery, professional services and more!
Kevin Barber President 210-308-7907 (Direct) KBarber@bdo.com
Valerie Rogler Program Coordinator 210-904-5404 Valerie@thehealthcell.org www.thehealthcell.org
“Where San Antonio’s Healthcare Leaders Meet”
San Antonio Medical Group Management Association (SAMGMA) (HH Silver Sponsor)
SAMGMA is a professional nonprofit association with a mission to provide educational programs and networking opportunities to medical practice managers and support charitable fundraising.
Jeannine Ruffner President info4@samgma.org www.samgma.org
Serving the Texas healthcare community since 1981, Favorite Healthcare Staffing is proud to be the exclusive provider of staffing services for the BCMS. In addition to traditional staffing solutions, Favorite offers a comprehensive range of staffing services to help members improve cost control, increase efficiency and protect their revenue cycle.
San Antonio Office 210-301-4362 www.favoritestaffing.com
“Favorite Healthcare Staffing offers preferred pricing for BCMS members.”
2025 Audi Q6 e-tron
Courtesy of Audi Dominion
The arrival of the Audi Q6 e-tron marks the beginning of the second-generation of Audi electric vehicles and is the next technological leap in premium electric mobility for its customers. Epitomizing the brand’s philosophy of Vorsprung durch Technik — or “progress through technology” — the Q6 e-tron incorporates thoughtful improvements to motor construction and battery technology, both of which advance the efficiency and performance of the new model over the first generation of Audi EVs, and make this the brand’s most advanced electric powertrain yet.
The Premium Platform Electric (PPE) was developed jointly with Porsche at Audi headquarters in Ingolstadt, and will underpin several important future new models from Audi, as the brand expands its global range of e-mobility products across key market segments by 2027. Audi has announced it will introduce more than 20 new or significantly redesigned models, half of them fully electric, over the next two years as part of its most robust portfolio refresh in brand history.
With a striking blend of futuristic design and classic Audi elegance, the Q6 e-tron features a sleek, aerodynamic profile with a coupe-like roofline. The upright front of the car is immediately recognizable with the brand’s e-tron characteristic closed Singleframe grille — reimagined for the EV era and masked in either selenite silver or gloss black, and flanked by ultra-slim matrix LED headlights with customizable digital light signatures. New to the Q6 e-tron are a pair of highly positioned digital daytime
running lights above the optional LED headlights, marking the first-time a quad headlight design has found its way into an Audi product and lending the model a more distinctive and independent appearance.
In the case of the available second-generation digital OLED taillights, six panels can generate a new image every ten milliseconds using a specially developed algorithm. This active signature creates an impression that the car is alive and awake — making the Q6 e-tron appear more intelligent than ever before. The individual light segments “shimmer" and interact in such a way that the total light intensity of the light signature does not vary. Customers can personalize their Q6 e-tron at the touch of a finger to select among the eight front and rear light signature designs to their liking through the new Audi Multi-Media Interface (MMI) and via the myAudi app.
Audi Q6 e-tron’s interior is a tech-savvy sanctuary that blends luxury, sustainability and innovative design. Generous legroom and headroom for all passengers, with supportive seats in premium yet sustainable materials, are designed for long-haul comfort. Or upgrade to fine Nappa leather with diamond stitching, sweetgum or birch wood trim, and brushed aluminum accents for a more traditional luxury vibe. Go from 18.6 cubic feet to 54 cubic feet of cargo capacity when the rear seats are folded.
The Q6 e-tron model family also has an all-new, fully connected digital interior comprised of an 11.9-inch Audi OLED virtual cock-
pit in front of the driver and a 14.5-inch center touch OLED display, both integrated as one slim, free-standing, curved panoramic design element oriented toward the driver. At night, sleekly integrated ambient lighting makes the Curved Display seem to float above the dashboard.
For the first time in an Audi, the Q6 e-tron offers an optional 10.9-inch MMI passenger LCD display. The front passenger display features Active Privacy Mode, which integrates active shuttering technology to prevent it from distracting the driver. This allows the front passenger to stream films or other video content, assist with navigation, or help find a charging station.
The Audi infotainment system is available with two different Bang & Olufsen Premium sound systems, and uses the Android Automotive operating system for the first time. The latest Audi connect services and enhanced e-tron route planner come standard. Apps such as YouTube, Spotify and Zoom are available via the Audi App store and can be integrated directly into the MMI without the use of a smartphone.
The Audi Digital Stage can be further extended with an available second-generation Augmented Reality (AR) Head-up Display (HuD) available in both Premium Plus and Prestige trimlines. It reflects an image on the windshield towards the driver, showing relevant information such as speed, traffic signs, assistance and navigation symbols overlaid on the road ahead, and may be perceived up to 650 feet down the road. To the driver, the display
appears to float in front of the vehicle as if projected on an 88-inch display. This prevents the driver from having to shift focus back and forth between the dashboard displays and what’s happening on the road.
To help owners access all the new functionalities of the Q6 e-tron, Audi has integrated a new self-learning voice-activated system called Audi Assistant. Deeply integrated into the vehicle, Audi Assistant activity is displayed using an avatar in the central touch display of the MMI, as well as in the Augmented Reality Head-up Display. The new voice assistant controls more than 800 functions, with more than 100 voice commands each possible, and has the ability to understand 23 different languages.
For long-distance driving, both the range and charging times have been improved over the previous generation e-tron for a maximum of 321 miles with DC fast charging capability of 10-80% in 22 minutes using Electrify America stations. Recently named a 2025 Top Safety Pick Plus from Insurance Institute for Highway Safety, the new Audi Q6 e-tron was introduced with a more attractive price point, starting at $63,800 for the standard design and $69,600 for the sportback model.
For more information or to test drive a new Audi Q6 e-tron, reach out to Anthony Garcia at 210-681-3399 or visit AudiDominion.com.
11911 IH 10 West San Antonio, TX 78230
Coby Allen 210.725.5447
Northside Honda 9100 San Pedro Ave. San Antonio, TX 78216
Daniel Garcia 210-988-9644
Audi Dominion 21105 West IH 10 San Antonio, TX 78257
Rick Cavender 888-901-8483
Northside Chevrolet 9400 San Pedro Ave. San Antonio, TX 78216
Emilio Gonzalez 210-341-3311
Bluebonnet Chrysler
Dodge Ram 547 S. Seguin Ave. New Braunfels, TX 78130
Don Bartholomew 830-606-3463
Mercedes Benz of Boerne 31445 IH 10 West Boerne, TX 78006
William Taylor 830-981-6000
14610 IH 10 West San Antonio, TX 78249
Mark Hennigan 210-941-4556
Mercedes Benz of San Antonio 9600 San Pedro San Antonio, TX 78216
James Godkin 210-366-9600
North Park Lexus 611 Lockhill Selma San Antonio, TX 78216
Jose Contreras 210-308-8900
9455 IH 10 West San Antonio, TX 78230
Jordan Trevino 210-738-3499
North Park Lexus at Dominion 25131 IH 10 W Dominion San Antonio, TX 78257
James Cole 210-816-6000
Northside Ford 12300 San Pedro San Antonio, TX 78216
David Starnes 210-319-5684
North Park Lincoln 9207 San Pedro San Antonio, TX 78216
Sandy Small 210-341-8841
North Park Subaru 9807 San Pedro San Antonio, TX 78216
Steven Markham 726-226-0028
Cavender Toyota 5730 NW Loop 410 San Antonio, TX 78238
Spencer Herrera 210-862-9769
North Park Toyota 10703 SW Loop 410 San Antonio, TX 78211
Justin Boone 833-669-2401
North Park Subaru at Dominion 21415 IH 10 West San Antonio, TX 78257
Phil Larson 888-718-9510
Kahlig Auto Group
Kahlig Auto Group
Kahlig Auto Group
Kahlig Auto Group
Kahlig Auto Group
Kahlig Auto Group
Kahlig Auto Group
Providing Timely Patient Care
American Health Imaging reduces friction points in the care continuum with easy patient referrals and fast prior authorizations for no-hassle scheduling, along with prompt delivery of standard reports within hours – not days.