11 minute read
Benefits of GLP-1 Use in Spine Surgery

With the increasing popularity of drugs such as Ozempic and Mounjaro, glucagon-like peptide-1 (GLP-1) receptor agonists (RAs) have come to the forefront of research and development in the pharmaceutical field. To understand the mechanism of action of these drugs, it is important to understand the natural compounds they mimic. GLP-1 and gastric inhibitory peptide (GIP) are postprandial incretins that are released from the gastrointestinal tract that, among other things, induce insulin secretion and inhibit glucagon secretion. The insulin release concurrently (1) lowers blood sugars by translocating GLUT-4 receptors to adipocyte and myocyte membranes for glucose uptake and (2) acts as an anorexigenic hormone by activating the proopiomelanocortin nucleus in the hypothalamus. Therefore, incretin mimetics such as GLP-1 RAs have quickly become first-line treatment options in type 2 diabetes mellitus and obesity because of their effects in lowering blood sugar and regulating appetite.[1] While these are the main indications for GLP-1 RAs, there are additional effects of GLP-1 RAs on peripheral tissues.
Effects of GLP-1 RAs on Peripheral Tissues
Globally, GLP-1s have been shown to have antioxidant effects by decreasing oxidative stress and inflammatory cytokines.[2,3] GLP-1 RAs increase myocyte synthesis, decrease muscle breakdown, increase microvascular blood flow, and slow gastric, gallbladder, and intestinal emptying.[2,4] Furthermore, GLP-1 RAs exert multiple beneficial effects on cardiovascular health, including reductions in nonfatal myocardial infarction, nonfatal stroke, and death.[5] They can also indirectly impact cardiovascular health because of their effects on blood glucose, obesity, and inflammation.[6] Finally, with regards to osteogenic health, GLP-1 RAs can promote osteogenesis through enhancing osteoblast differentiation, inhibiting osteoclast activity, and reducing fracture risk.[3,7] Specifically, GLP-1 RAs have been shown to enhance lumbar spine and femoral head bone mineral density.[8]
Pathophysiology of Obesity in Spine Pathologies
Obesity is strongly associated with poor bone quality and multiple spine pathologies, including herniated intervertebral discs, spinal stenosis, reduced disc height, and altered spinal alignment.[9-13] Takeuchi et al showed that increased BMI is significantly associated with disc degeneration and Modic changes, as well as the deterioration of paraspinal muscle mass and back extensor strength.[12] Pandya et al found a significant association between increased BMI and decreased spinal canal width. 9 Regarding the biomechanics of the spine, obesity is associated with decreased spinal mobility and increased thoracic kyphosis.[14] Overall, the pathologies associated with obesity can present clinically as low back pain, radicular leg pain, myelopathy, neurogenic claudication, and general functional impairment.[15] Shahi et al found that patients with BMI ≥35 had worse patient-reported outcome measures, lower rates of achieving minimally clinically important difference or patient-acceptable symptom state, and longer postoperative stays and return to driving after minimally invasive transforaminal lumbar interbody fusions.[10] These findings collectively support the consensus that obesity is a modifiable risk factor for the development and progression of degenerative spine pathologies and spinal surgery, and that weight management should be considered as a preventive strategy.
GLP-1 RAs in Spine Surgery
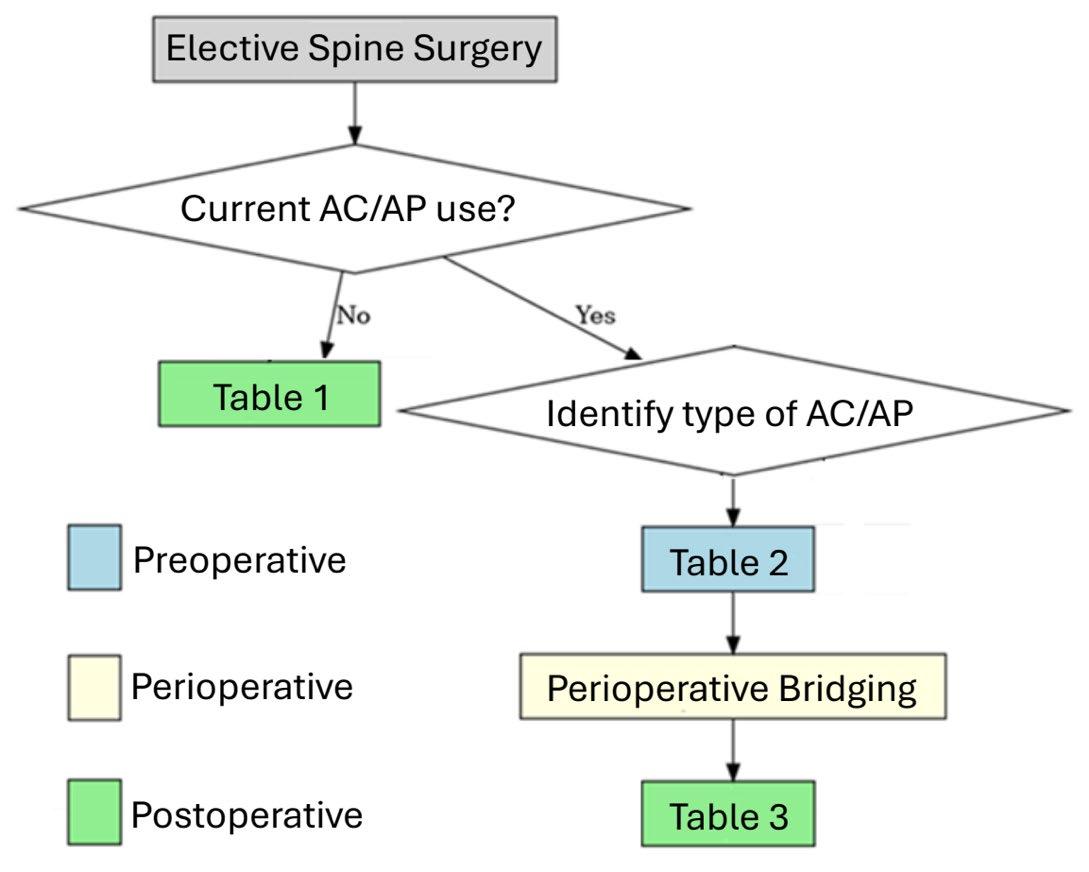
GLP-1 RAs have several reported benefits in spine surgery (Figure 1). They have been reported to decrease perioperative and preoperative complications in spine surgery, specifically among obese and diabetic patients.[16] In a retrospective multicenter study of patients undergoing spine fusion surgery, the use of GLP-1 RAs was shown to be linked to reduced postoperative infection rates, readmission rates, and revisions in both obese and nonobese patient cohorts. In the obese cohort, GLP-1 RAs were linked to markers of improved quality of life such as decreased rates of generalized muscle weakness and mobility abnormalities. In the nonobese cohort, patients using GLP-1 RAs had reduced rates of back pain and mobility abnormalities when compared to nonobese peers who were not taking GLP-1 RAs.[16]

Cervical Spine Surgery
The current literature mostly suggests that GLP-1 RAs are beneficial in procedures concerning the cervical spine. In a large retrospective analysis in patients undergoing anterior cervical discectomy and fusion (ACDF), the incidence of nonfusion was significantly lower in GLP-1 RA users compared to the control cohort at all postoperative timepoints (39% reduction in odds at the 2-year postoperative timepoint). A subgroup comparison of GLP-1 RA users and insulin users showed consistent results with the whole cohort analysis.[17]
Similarly, another retrospective analysis on multilevel cervical fusion demonstrated that patients who used GLP-1 RAs had significantly lower rates of pseudarthrosis in both multilevel ACDF and posterior cervical fusion (PCF). The analysis reported no statistically significant difference in the onset of postoperative infection in either the ACDF or PCF group.[18]
Similarly, another retrospective analysis on multilevel cervical fusion demonstrated that patients who used GLP-1 RAs had significantly lower rates of pseudarthrosis in both multilevel ACDF and posterior cervical fusion (PCF). The analysis reported no statistically significant difference in the onset of postoperative infection in either the ACDF or PCF group.[18]
In contrast, the short-term results from a different database study of patients with type 2 diabetes mellitus undergoing cervical spine decompression and fusion suggests that the usage of GLP-1 RAs have no significant difference in the rates of postoperative surgical complications and 30- and 90-day hospital readmission rates when compared to the control cohort.[19]
Another retrospective study focusing on semaglutide, a class of GLP-1 RAs, showed that postoperative complication rates were generally similar. The rate of cerebrovascular accidents was lower in patients taking semaglutide in comparison to the control (0.88% vs 1.36%). In contrast to other studies including all GLP-1 RAs, the usage of semaglutide was linked to significantly higher rates of pseudarthrosis (13.53% vs 3.31%, p < 0.001) and dysphagia (14.41 vs 7.40%, p < 0.001) 2 years after the operation.[20] Overall, patients undergoing cervical spine surgery received benefit from having been on GLP-1 RAs compared to propensity-matched controls in regard to postoperative complications such as pseudarthrosis and readmission rates.
Lumbar Spine Surgery
More studies have investigated the effect of GLP-1 RAs in lumbar spine surgery on surgical and medical complications. A separate retrospective on the incidence of pseudarthrosis in single-level lumbar fusion procedures found that patients using GLP-1 RAs had significantly reduced rates of pseudarthrosis at all postoperative time points in comparison to nonusers (12.6% vs 17.5%).[21] This finding was further corroborated by an additional retrospective study in a wider range of lumbar spine surgery procedures, including decompression. It was shown that patients using any form of GLP-1 RAs had significantly reduced rates of pseudarthrosis at the 1-year and 3-year postoperative period (8.88% vs 10.77%). There were no significant differences in medical complications in the 90-day postoperative period, including myocardial infarction, deep vein thrombosis (DVT), hospital readmission, and wound dehiscence.[22] Additional retrospective studies focused on thoracic and lumbar fusion surgery for degenerative spine disease showed reduced medical day complications (infection, pneumonia, thromboembolism) in patients taking GLP-1 RAs compared to controls. The 10-year risk of revision surgery, pseudarthrosis, and mechanical failure was reduced in groups using GLP-1 RAs.[23] The data show patients’ benefit from using GLP-1 RAs in comparison to patients who do not. There are lower rates of pseudarthrosis at multiple postoperative timepoints and revision surgery.
Research Opportunities
Current information regarding GLP-1 RA use in spine surgery remains limited by methodology. To date, no prospective studies have examined their perioperative use, and most available data are restricted to obese and diabetic cohorts. Expanding the investigation to nonobese, nondiabetic populations will be critical for understanding whether the observed benefits extend more broadly.
Another unanswered question concerns formulation-specific effects. Agents such as semaglutide, liraglutide, and tirzepatide differ in pharmacokinetics, yet comparative studies evaluating their influence on pseudarthrosis rates, complications, and recovery are lacking. Clarifying whether outcomes vary across drug classes would help guide perioperative decision-making.
Surgical approach also warrants closer study. The relationship between GLP-1 RA use and pseudarthrosis following PCF remains unresolved, with inconsistent findings across current reports.[18,19,20] Focused studies stratified by approach and fusion level could better delineate these risks.
Finally, given their substantial weightloss effects, GLP-1 RAs may play a role in modifying spinal epidural lipomatosis.[24] Evaluating their potential as a nonsurgical alternative to decompression represents another promising avenue for research.
Conclusion
While the data surrounding GLP-1 RAs remains relatively nascent, emerging evidence suggests these agents may offer meaningful benefits in the management of spine pathologies among obese and diabetic patients. Their demonstrated potential to reduce postoperative complications, infection rates, and pseudarthrosis positions GLP-1 RAs as a promising adjunct in perioperative optimization.
Importantly, most existing literature focuses on diabetic and obese cohorts, leaving significant gaps regarding the safety, efficacy, and dosing strategies of GLP-1 RAs in nondiabetic, nonobese patients undergoing spine surgery.
GLP-1 RAs may serve as a valuable tool not only for medical weight management but also as a means of reducing surgical risk and enhancing recovery in spine surgery patients. Integrating these therapies into spine care pathways demands continued clinical investigation, but the potential for GLP-1 RAs to reshape perioperative optimization and postsurgical outcomes is both timely and compelling.
References
1. American Diabetes Association Professional Practice Committee. 8. Obesity and weight management for the prevention and treatment of type 2 diabetes: standards of care in diabetes—2025. Diabetes Care. 2025;48(1 suppl 1):S167–S180.
2. Szekeres Z, Nagy A, Jahner K, Szabados E. Impact of selected glucagon-like peptide-1 receptor agonists on serum lipids, adipose tissue, and muscle metabolism. Int J Mol Sci. 2024;25(15):8214.
3. Zhu S, Hu Y, Wang Z, et al. The mechanism of liraglutide on promoting osteogenesis via macrophage polarization under inflammatory and oxidative stress in osteoporosis. Life Sci. 2025;377:123717.
4. Jalleh RJ, Marathe CS, Rayner CK, et al. Physiology and pharmacology of effects of GLP-1-based therapies on gastric, biliary and intestinal motility. Endocrinology. 2024;166(1):bqae155.
5. Madsbad S, Holst JJ. Cardiovascular effects of incretins: focus on glucagon-like peptide-1 receptor agonists. Cardiovasc Res. 2023;119(4):886–904.
6. Ussher JR, Drucker DJ. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20(7):463–474.
7. Zheng M, Zhao J, Wang Y, et al. Exploring new therapeutic drugs for osteoarthritis and osteoporosis: glucagon-like peptide-1 receptor agonists. Medicine (Baltimore). 2025;104(29):e43239.
8. Li X, Li Y, Lei C. Effects of glucagon-like peptide-1 receptor agonists on bone metabolism in type 2 diabetes mellitus: A systematic review and meta-analysis. Int J Endocrinol. 2024;2024:1785321.
9. Pandya R, Monas A, Chatad D, Bou Monsef J, Razi AE, Ng MK. High body mass index is a predictor of lumbar stenosis: A retrospective MRI study. J Am Acad Orthop Surg. 2025.
10. Shahi P, Subramanian T, Araghi K, et al. Class 2/3 obesity leads to worse outcomes following minimally invasive transforaminal lumbar interbody fusion. Spine J. 2025;25(9):1985–1996.
11. Segar AH, Baroncini A, Urban JPG, Fairbank J, Judge A, McCall I. Obesity increases the odds of intervertebral disc herniation and spinal stenosis; an MRI study of 1634 patients. Eur Spine J. 2024;33(3):915–923.
12. Takeuchi Y, Takahashi S, Ohyama S, et al. Relationship between body mass index and spinal pathology in community-dwelling older adults. Eur Spine J. 2023;32(2):428–435.
13. Urquhart DM, Kurniadi I, Triangto K, et al. Obesity is associated with reduced disc height in the lumbar spine but not at the lumbosacral junction. Spine. 2014;39(16):E962–E966.
14. Bayartai ME, Luomajoki H, Tringali G, De Micheli R, Abbruzzese L, Sartorio A. Differences in spinal posture and mobility between adults with obesity and normal weight individuals. Sci Rep. 2023;13(1):13409.
15. Hasvik E, Haugen AJ, Grøvle L. Symptom descriptors and patterns in lumbar radicular pain caused by disc herniation: a 1-year longitudinal cohort study. BMJ Open. 2022;12(12):e065500.
16. Wiener JM, Sanghvi PA, Vlastaris K, et al. Glucagon-like peptide-1 receptor agonist medications alter outcomes of spine surgery: A study among over 15,000 patients. Spine. 2025;50(13):871–880.
17. Chang Y, Chi KY, Song J, Lin HM. Association between GLP-1 receptor agonists and non-fusion risk after single-level ACDF. Spine J. 2025.
18. Vatsia SK, Levidy MF, Rowe ND, Meister AS, Bible JE. Fusion outcomes of GLP-1 agonist therapy in multilevel cervical spinal fusion: A propensity-matched analysis. Clin Spine Surg. 2025;38(4):213–216.
19. Tao X, Ranganathan S, Van Halm-Lutterodt N, et al. No difference in short-term surgical outcomes from semaglutide treatment after cervical decompression and fusion: a propensity score-matched analysis. Spine. 2025;50(8):515–521.
20. Ng MK, Mastrokostas PG, Mastrokostas LE, et al. Semaglutide use is associated with higher rates of pseudarthrosis and dysphagia in posterior cervical fusion. Spine J. 2025;25(9):1974–1980.
21. Agrawal V, Amasa S, Karabacak M, Margetis K. Perioperative GLP-1 agonist use and rates of pseudarthrosis after single-level lumbar fusion: a retrospective cohort study. Neurosurgery. 2024;97(1):91–97.
22. Tummala S, Gibbs DC, Chavarria J, Alder J, Avramis I, Rizkalla JM. GLP1 receptor agonist use in elective lumbar spine surgery: reduced pseudarthrosis rates and favorable safety profile. J Orthop. 2025;65:227–232.
23. Kishan A, Khela HS, Carayannopoulos NL, Singh M, Cohen L, Chisango Z, et al. Association of glucagon-like peptide-1 receptor agonist use with complications following thoracic and/ or lumbar spinal fusion: a BMI-stratified retrospective study. Spine. Published online September 4, 2025. https://doi. org/10.1097/brs.0000000000005494
24. Barkyoumb D, Muhammad F, Smith ZA, Shakir HJ. Preoperative optimization of obese spine patients with GLP-1 receptor agonists: enhancing surgery and improving outcomes. J Spine Surg. 2025;11(2):339–346.
Contributors:
Raul F. Montes, BS[1,2]
Zora C. Hahn, BA[1]
Anthony R. Lewis, BA[1]
Tomoyuki Asada, MD, PhD[1,3]
Sravisht Iyer, MD[1,2]
From the 1Department of Orthopaedics at the Hospital for Special Surgery in New York City, New York; 2Weill Cornell Medical College in New York City, New York; and 3Department of Orthopedics at the University of Tsukuba Hospital in Tsukuba, Japan.