13 minute read
Venous Thromboembolism Prophylaxis After Elective Spine Surgery

A Narrative Review
Venous thromboembolism (VTE), which includes deep venous thrombosis and pulmonary embolism, is an uncommon but serious and preventable complication following spine surgery.[1,2] Reported incidence varies markedly, from 0.3% to 31%, reflecting heterogeneity in patient populations, surgical indications, and prophylactic strategies.[1,3-5] With an aging population and a growing prevalence of comorbidities, increasing numbers of patients are undergoing elective spine surgery while already receiving anticoagulant or antiplatelet (AC/AP) therapy.[6] Although the overall incidence of VTE in elective spine procedures is relatively low (1.1–3.2%) compared with trauma or oncology cases, associated morbidity and mortality remain clinically significant.[2,7-11] Conversely, postoperative bleeding, particularly epidural hematoma (EDH), is reported in only 0–0.7% of cases, and it poses a major concern given its potential for irreversible neurological injury.[2,12-15] The balance between preventing VTE and avoiding hemorrhagic complications therefore remains a central perioperative challenge in spine surgery.
In contrast to joint replacement, where well-defined guidelines for VTE prophylaxis exist and are widely implemented,[16] spine surgery lacks universally accepted protocols. Current recommendations are inconsistent, and no consensus has been firmly established. In 2009, the North American Spine Society concluded that evidence was insufficient to support routine chemoprophylaxis in elective spine surgery.[7] Later, in 2012, the American College of Chest Physicians recommended mechanical prophylaxis over chemoprophylaxis or no prophylaxis, with pharmacologic prophylaxis reserved for moderate- to high-risk patients (eg, combined anterior–posterior surgery, paralysis, multiple traumas, malignancy, spinal cord injury, or hypercoagulable states), unless there was high bleeding risk.[17]
Over the past 2 decades, mechanical and pharmacologic strategies have been extensively evaluated. Nonpharmacologic measures such as early mobilization, thromboembolic deterrent stockings, and sequential compression devices are consistently recommended due to their noninvasiveness, efficacy, and low complication rates.[2,7,12,13,15,18,19] These devices enhance venous return by compressing the superficial venous system, thereby increasing venous flow and promoting fibrinolysis.[20] In contrast, pharmacologic prophylaxis—including low-molecular-weight heparin (LMWH), unfractionated heparin, direct oral anticoagulants (DOACs), and aspirin—remains debated because of variable efficacy and the risk of wound complications or EDH.[1,14,21,22]
Practice patterns differ considerably among institutions and regions. Retrospective series, randomized trials, and consensus statements all demonstrate variation in the timing, choice, and stratification of prophylaxis.[1,8,13] Recent reviews and meta-analyses further suggest no significant difference in thromboembolic or hemorrhagic events among low-risk patients with or without chemoprophylaxis[2,9,13] while also pointing to potential benefits of earlier initiation in carefully selected high-risk groups, highlighting the importance of individualized assessment.[10,23]
Given these persistent uncertainties, a synthesis of current evidence is needed. This narrative review consolidates recommendations from major guidelines and consensus statements—including the 2023 Delphi guideline,[8] the 2020 AO Spine global survey,[1] and the 2009 North American Spine Society guideline[7]—together with recent literature on elective spine surgery and proposes an evidence-informed framework to guide spine surgeons toward safer, more standardized perioperative practice.
Algorithm
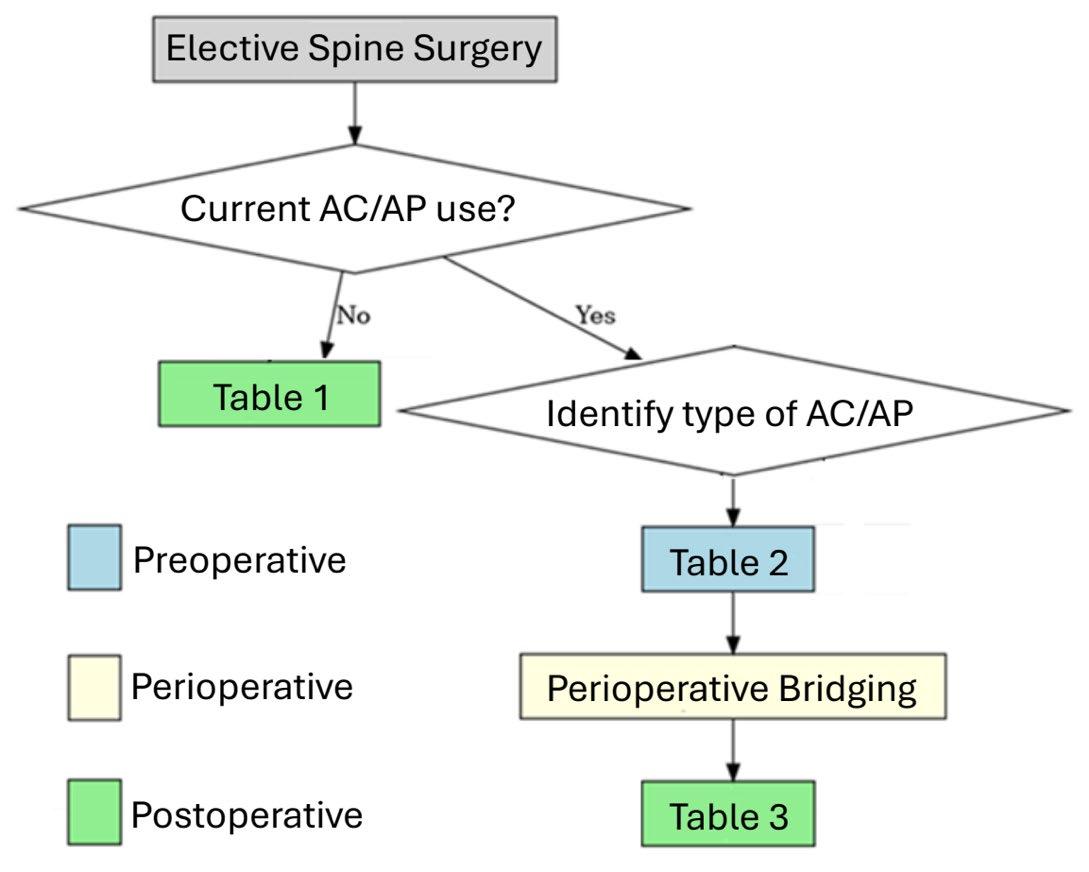
For patients undergoing elective spine surgery, the first step is to establish whether there is current or prior use of AC/AP therapy, as well as to evaluate risk factors for VTE. This assessment forms the basis of perioperative planning. The proposed algorithm (Figure 1) guides clinicians through subsequent decision-making by linking to the relevant risk stratification tables (Table 1–3). These tables provide a structured framework for assigning risk scores based on patient-specific characteristics, thereby categorizing individuals into low-, medium-, or high-risk groups for both thromboembolic and bleeding complications. A stepwise application of this approach allows AC/AP management and VTE prophylaxis to be individualized according to each patient’s clinical profile.

Postoperative Initiation of AC/AP in Patients Not on Baseline AC/AP Therapy
In 2 institutional protocols, anticoagulation was initiated 24 hours after surgery with either enoxaparin or rivaroxaban.[12,24] In an international cross-sectional survey,most surgeons reported mobilization and mechanical prophylaxis beginning on postoperative day (POD) 0–1, while LMWH was either not used or was started within the same timeframe.[1] Consensus recommendations emphasized the use of risk stratification tools, such as the guideline proposed by Zuckerman et al, which introduced a structured scoring system.[8]
On the basis of these data and consensus statements, the evidence was consolidated into Table 1, which stratifies patients according to risk factors such as prior VTE, cardiac intervention, malignancy, oral contraceptive or hormone use,[8] and surgical complexity or approach.[7] Importantly, the guideline distinguishes a true anterior abdominal approach—where iliac vessels are mobilized—from prepsoas or transpsoas approaches, in which vascular manipulation is minimal or absent. For clarity, POD 1 is defined as the morning following surgery, regardless of the finishing time. Accordingly, the timing of postoperative initiation of AC/AP therapy is determined by the cumulative risk score, and careful neurological monitoring is advised once chemoprophylaxis is introduced. A standardized regimen of enoxaparin, 40 mg once daily, is preferred over weight-based dosing.[8]

Preoperative Cessation of AC/AP in Patients on Chronic AC/AP Therapy
Compared with VTE prophylaxis, perioperative AC/AP management remains relatively underexplored.[25,26] Based on drug half-life and reversibility, current guidance suggests discontinuing DOACs 2 days before surgery, warfarin 5 days prior, and all other AC/AP agents, including aspirin, 7 days prior.[7,8] These recommendations are summarized in Table 2, which also includes available reversal agents for each AC/AP drug, to serve as a practical reference for perioperative decision-making.[27]

Perioperative Bridging Method in Patients on Chronic AC/AP Therapy
To our knowledge, no clear consensus has been established on the optimal strategy for perioperative bridging. In patients discontinuing warfarin, intravenous heparin may be considered as a bridging option and should ideally be guided by specialist consultation, given its greater controllability and predictability compared with LMWH. Nevertheless, LMWH, most commonly enoxaparin, is also regarded as a reasonable alternative.[7,8]
Postoperative Resumption of AC/AP After Elective Spine Surgery
In the 2020 international survey, the timing of AC/AP resumption in patients on chronic therapy showed a bimodal pattern worldwide, with most providers restarting on either POD 0–1 or POD 5–6.[1] Subsequent consensus recommended resumption at POD 7 for low-risk, POD 5 for medium-risk, and POD 2 for high-risk patients (Table 3).[8] It should be emphasized that recommendations from internists, hematologists, or cardiologists should be prioritized when available, as these supersede general consensus guidance. This recommendation is particularly relevant in nonacademic or community settings, where spine surgeons may lack timely access to specialist consultation.

Prophylaxis for High-Risk Thromboembolism Patients
Beyond the elective risk categories outlined in Table 1, certain patient groups are recognized as having an intrinsically higher risk of postoperative VTE. These include individuals with polytrauma and associated spinal fractures, patients with spinal cord injury, and those with spinal tumors.[8,23,28,29]
Unlike routine elective cases where risk stratification determines timing, these populations are generally recommended to start chemical prophylaxis as early as POD 1–2 in conjunction with mechanical methods. Evidence indicates that such early intervention reduces VTE incidence without increasing major bleeding or overall mortality, and this benefit extends to nonoperative spinal trauma or spinal cord injury patients.[13,23,31,32]
Complication Balance
While VTE incidence after spine surgery varies widely, elective cases generally fall within a lower range (1.1%–3.2%),[2,7,8,10] whereas rates are higher in patients with elevated baseline risk.[5,12] In contrast, EDH occurs in less than 1% of cases, with pooled analyses estimating an incidence of approximately 0.4% (range 0%–0.7%) and showing no significant difference between patients who did and those who did not receive chemoprophylaxis.[12,13,23]
Regional and Practice Variation
International surveys have demonstrated marked regional variability in perioperative VTE prophylaxis, particularly in the timing of AC/AP initiation, cessation, and resumption.[1] In general, 70.3% of surgeons reported routinely performing anticoagulation risk stratification, regardless of location. Moreover, most providers implemented early mobilization, LMWH, and mechanical prophylaxis irrespective of patient history. By contrast, one area of relative uniformity has been the management of acute spinal cord injury, where global practice has consistently adhered to established prophylactic protocols, reflecting both the exceptionally high VTE risk in this population and the availability of well-validated guidelines.[33-35]
Conclusion and Future Directions
VTE remains an uncommon but serious complication after spine surgery, with incidence influenced by patient risk profile, surgical complexity, and perioperative management. Mechanical prophylaxis is consistently supported as safe and effective, whereas the role of chemoprophylaxis remains debated due to the competing risk of EDH. Recent consensus statements, international surveys, and systematic reviews highlight the need for individualized, risk-stratified approaches—summarized in this narrative review—to guide perioperative management of AC/AP initiation, cessation, resumption, and bridging. These findings emphasize the persistent challenge of balancing thromboembolic prevention against bleeding risk and reinforce the importance of developing evidence-informed, standardized protocols for spine surgery. The absence of statistical significance in current studies should be interpreted with caution, and future large-scale, multicenter prospective trials with consistent inclusion criteria, standardized surgical classifications, and uniform outcome measures are warranted. Such investigations, specifically designed to assess both thromboembolic and hemorrhagic endpoints, will be essential to validate risk-stratification tools and to establish standardized management of preoperative AC/AP therapy and VTE chemoprophylaxis in adult elective spine surgery.
References
1. Louie P, Harada G, Harrop J, et.al. Perioperative anticoagulation management in spine surgery: initial findings from the AO Spine anticoagulation global survey. Global Spine J. 2020;10(5):512-527.
2. Muralidharan A, Gong DC, Baumann AN, et al. Venous thromboembolism chemoprophylaxis is not supported following elective spine surgery: a systematic review and meta-analysis of randomized controlled trials. J Spine Surg. 2025;11(2):242-255.
3. Glotzbecker MP, Bono CM, Wood KB, Harris MB. Thromboembolic disease in spinal surgery: a systematic review. Spine (Phila Pa 1976). 2009;34(3):291-303.
4. Rockson HB, DiPaola CP, Connolly PJ, Stauff MP. Venous thromboembolism prophylaxis for patients having elective spine surgery: when, why, and how much. J Bone Joint Surg Am. 2019;101(13):1220-1229.
5. Schulte LM, O’Brien JR, Bean MC, Pierce TP, Yu WD, Meals C. Deep vein thrombosis and pulmonary embolism after spine surgery: incidence and patient risk factors. Am J Orthop (Belle Mead NJ). 2013;42(6):267-270.
6. O’Lynnger TM, Zuckerman SL, Morone PJ, Dewan MC, Vasquez-Castellanos RA, Cheng JS. Trends for spine surgery for the elderly: implications for access to healthcare in North America. Neurosurgery. 2015;77(suppl 4):S136-S141.
7. Bono CM, Watters WC 3rd, Heggeness MH, et al. An evidence-based clinical guideline for the use of antithrombotic therapies in spine surgery. Spine J. 2009;9(12):1046-51.
8. Zuckerman SL, Berven S, Streiff MB, et al. Management of anticoagulation/antiplatelet medication and venous thromboembolism prophylaxis in elective spine surgery: concise clinical recommendations based on a modified Delphi process. Spine (Phila Pa 1976). 2023;48(5):301-309.
9. Ellenbogen Y, Power RG, Martyniuk A, Engels PT, Sharma SV, Kasper EM. Pharmacoprophylaxis for venous thromboembolism in spinal surgery: a systematic review and meta-analysis. World Neurosurg. 2021;150:e144-e154.
10. Sansone JM, del Rio AM, Anderson PA. The prevalence of and specific risk factors for venous thromboembolic disease following elective spine surgery. J Bone Joint Surg Am. 2010;92(2):304-13.
11. Piper K, Algattas H, DeAndrea-Lazarus IA, et al. Risk factors associated with venous thromboembolism in patients undergoing spine surgery. J Neurosurg Spine. 2017;26(1):90-96.
12. Aljohani H, Alashkar AH, Alkafarnah GK, Almeshigeh MM, Alsadoon AA, Alfakhouri A. A protocol for venous thromboembolism prophylaxis in elective spine surgery: a retrospective evaluation of a single-center experience. Cureus. 2025;17(6):e85297.
13. Rahmani R, Eaddy S, Stegelmann SD, Skrobot G, Andreshak T. Chemical prophylaxis and venous thromboembolism following elective spinal surgery: a systematic review and meta-analysis. N Am Spine Soc J. 2023;17:100295.
14. Glotzbecker MP, Bono CM, Wood KB, Harris MB. Postoperative spinal epidural hematoma: a systematic review. Spine (Phila Pa 1976). 2010;35(10):E413-20.
15. Kepler CK, McKenzie J, Kreitz T, Vaccaro A. Venous thromboembolism prophylaxis in spine surgery. J Am Acad Orthop Surg. 2018;26(14):489-500.
16. Lieberman JR, Heckmann N. Venous thromboembolism prophylaxis in total hip arthroplasty and total knee arthroplasty patients: from guidelines to practice. J Am Acad Orthop Surg. 2017;25(12):789-798.
17. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 suppl):e227S-e277S.
18. Epstein NE. Intermittent pneumatic compression stocking prophylaxis against deep venous thrombosis in anterior cervical spinal surgery: a prospective efficacy study in 200 patients and literature review. Spine (Phila Pa 1976). 2005;30(22):2538-2543.
19. Sachdeva A, Dalton M, Lees T. Graduated compression stockings for prevention of deep vein thrombosis. Cochrane Database Syst Rev. 2018;11(11):CD001484.
20. Comerota AJ, Chouhan V, Harada RN, et al. The fibrinolytic effects of intermittent pneumatic compression: mechanism of enhanced fibrinolysis. Ann Surg 1997;226(3):306-313; discussion 313-4.
21. Schroeder GD, Hilibrand AS, Arnold PM, et al. Epidural hematoma following cervical spine surgery. Global Spine J. 2017;7(1 suppl):120S-126S.
22. Kou J, Fischgrund J, Biddinger A, Herkowitz H. Risk factors for spinal epidural hematoma after spinal surgery. Spine (Phila Pa 1976). 2002;27(15):1670-1673.
23. Mohanty S, von Riegen H, Akodu M, et al. Timing of chemical anticoagulant administration in spine trauma and its impact on VTE, bleeding, and mortality: a systematic review and meta-analysis. Global Spine J. Published online July 6, 2025. https:// doi.org/10.1177/21925682251353138
24. Shafiei M, Sabouri M, Aminmansour B, et al. Comparison between rivaroxaban versus enoxaparin for venous thromboembolism prophylaxis following spine surgeries, a randomized clinical trial. J Clin Neurosci. 2022;105:51-57.
25. Epstein NE. When to stop anticoagulation, anti-platelet aggregates, and non-steroidal anti-inflammatories (NSAIDs) prior to spine surgery. Surg Neurol Int. 2019;10:45.
26. Cuellar JM, Petrizzo A, Vaswani R, Goldstein JA, Bendo JA. Does aspirin administration increase perioperative morbidity in patients with cardiac stents undergoing spinal surgery? Spine (Phila Pa 1976). 2015;40(9):629-635.
27. Yee J, Kaide CG. Emergency reversal of anticoagulation. West J Emerg Med. 2019;20(5):770-783.
28. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 suppl):338S-400S.
29. Ghobrial GM, Maulucci CM, Maltenfort M, et al. Operative and nonoperative adverse events in the management of traumatic fractures of the thoracolumbar spine: a systematic review. Neurosurg Focus. 2014;37(1):E8.
30. Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuünemann HJ; American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel. Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 suppl):7S-47S.
31. Dornbush C, Maly C, Bartschat N, et al. Chemoprophylaxis timing is not associated with postoperative bleeding after spinal trauma surgery. Clin Neurol Neurosurg. 2023;225:107590.
32. Lambrechts MJ, Toci GR, Issa TZ, et al. Immediate vs delayed venous thromboembolism prophylaxis following spine surgery: increased rate of unplanned reoperation for postoperative hematoma with immediate prophylaxis. Spine J. 2024;24(11):2019-2025.
33. Eichinger S, Eischer L, Sinkovec H, et al. Risk of venous thromboembolism during rehabilitation of patients with spinal cord injury. PLoS One. 2018;13(3):e0193735.
34. Matsumoto S, Suda K, Iimoto S, et al. Prospective study of deep vein thrombosis in patients with spinal cord injury not receiving anticoagulant therapy. Spinal Cord. 2015;53(4):306-9.
35. Teasell RW, Hsieh JT, Aubut JA, Eng JJ, Krassioukov A, Tu L; Spinal Cord Injury Rehabilitation Evidence Review Research Team. Venous thromboembolism after spinal cord injury. Arch Phys Med Rehabil. 2009;90(2):232-45.
Contributors:
Kuan-Po Chen, MD
Po-Hsin Chou, MD, PhD
Yuan-Kun Tu, MD, PhD
Nathan J. Lee, MD
From the Department of Orthopedic Surgery at Midwest Orthopedics at Rush in Chicago, Illinois.