7 minute read
Advances in Atraumatic Bone Removal in Spine Surgery

Bone removal remains an important part of nearly all spine operations. Whether done for the purposes of decompression, osteotomy, or instrumentation, resection of bone within the spine is technically demanding given the immediate proximity of neural structures, hollow organs, and blood vessels. Bone removal must be carried out precisely to achieve the goals of surgery while avoiding iatrogenic instability. Despite improvements in visualization, navigation, and neuromonitoring, the inherent risks of neurological, vascular and visceral injury remain a challenge for spine surgeons. Rotary burrs may chatter, skip, or wrap delicate structures, while Kerrison and pituitary rongeurs can tear dura during ligamentum flavum resection. These limitations have driven the development of devices designed to make bony work more precise and less traumatic. Ultrasonic bone scalpels and oscillatory burrs are 2 of the most recent options now commercially available.
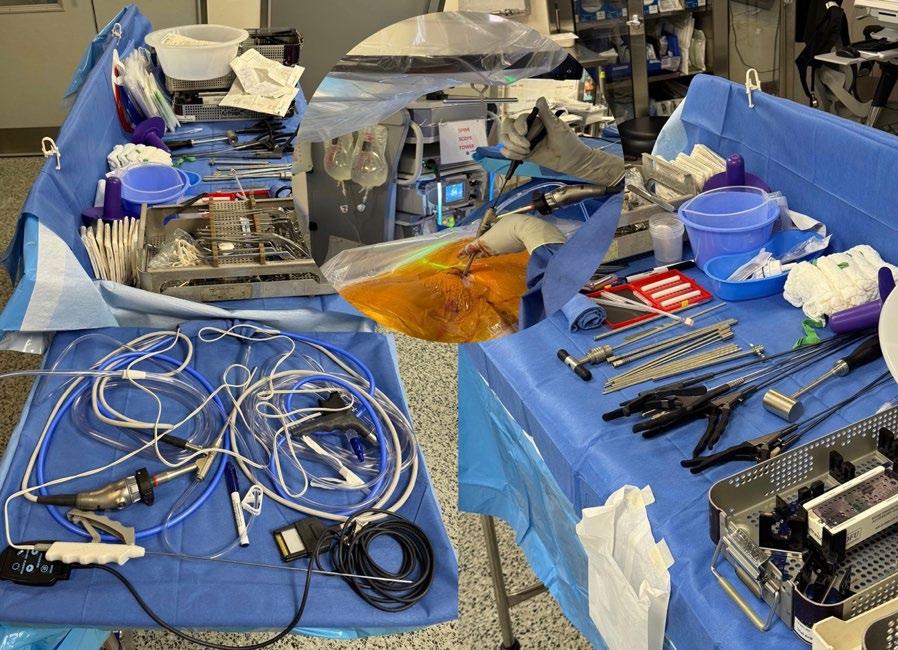
Ultrasonic bone removal (UBR) tools (Stryker’s Sonopet and Misonix’s BoneScalpel; Figure 1) use high-frequency vibration to preferentially cut mineralized tissue while sparing adjacent soft tissue. Rigid bone microscopically fractures in response to high frequency vibration, whereas elastic structures such as dura and nerve roots deform without shearing. This selectivity makes ultrasonic devices increasingly attractive in spine surgery, allowing bone removal without risk of durotomy or nerve injury. Both devices are coupled with continuous irrigation to mitigate thermal injury.
The technology is built on piezoelectric transduction, which converts electrical energy into oscillatory motion at ultrasonic frequencies (typically 20–35 kHz). At these frequencies, mineralized bone cannot absorb and dissipate the vibrational energy, leading to microfracture and fragmentation. In contrast, soft tissues deflect under the same load, dispersing energy without permanent deformation. The constant irrigation serves a dual purpose: cooling the cutting edge to prevent thermal necrosis and flushing away bone slurry to preserve visualization. Unlike a rotary burr, which generates constant frictional heat, the intermittent contact of ultrasonic vibration tends to produce lower peak temperatures at the cutting surface. This physical selectivity allows ultrasonic scalpels to be placed confidently at the bone–dura interface.


A review by Renjith et al summarized the application of UBR in decompression, laminoplasty, anterior cervical discectomy and fusion (ACDF), and osteotomies, concluding that the instruments are both safe and effective, with the primary barriers being cost and the learning curve.[1] Steinle et al compared lumbar laminectomies performed with UBR to conventional instruments and reported a durotomy rate of 0% with UBR compared to 12.5% with traditional tools.[2] Matthes et al evaluated thermal effects, showing that ultrasonic devices generated significantly less heat than high-speed drills, reducing the risk of thermal injury.[3]
Several randomized studies have demonstrated the safety and efficacy of ultrasonic bone removal tools when compared with traditional burrs. Rittipoldech et al found that thoracolumbar decompressions performed with UBR resulted in shorter laminectomy times and reduced intraoperative blood loss without increasing complications.[4] In ACDF, Yao et al demonstrated that UBR reduced operative time and blood loss compared with high-speed drills, with no dural or neurological injuries in the ultrasonic group.[5] Endoscopic applications have also been described. Tsai et al reported that UBR facilitated precise decompression in unilateral biportal endoscopic spine surgery with minimal blood loss and no durotomies.[6] Most recently, Segerlind et al found that high-frequency ultrasonic osteotomy shortened operative time and hospital stay while maintaining safety during spinal tumor removal.[7]
Oscillating burrs represent another newer option for atraumatic bone removal during spine surgery. Rather than rotating a continuous 360 degrees, these burrs utilize a back-and-forth motion, rotating 180 degrees prior to reversing direction. Similar to ultrasonic tools, oscillating drills offer a potentially safer means of bone removal near critical structures due to the distinct mechanical responses of bone and soft tissue to oscillatory motion. Oscillation produces rapid back-and-forth displacement over a limited arc, which efficiently fractures the mineralized matrix of bone while leaving compliant tissues such as dura and nerves more likely to deform and displace rather than shear. Because the tip does not rotate continuously, there is less opportunity for tissue wrapping or entanglement, and the intermittent contact reduces the buildup of thermal energy that can occur with highspeed rotary drilling. The restricted motion path also limits skiving across cortical bone, improving control in confined anatomical spaces. These devices are new to the US device market, with DuraPro (Globus Medical) being the only widely distributed device currently available.
Oscillating drills blend the precision of hand instruments with the efficiency of powered devices. The oscillatory action does not transmit the same torsional force back into the surgeon’s hand as a high-speed burr, which may reduce fatigue during long decompressions or multilevel procedures. In addition, the motion produces a distinctive tactile and auditory feedback that differs from rotary instruments, which can be helpful in gauging the depth and density of bone being removed. Because oscillating motion tends to follow a stable trajectory, these tools are useful adjuncts to navigation. When preparing pedicle entry points or working through narrow minimally invasive retractors, the reduced tendency to “walk” across cortical bone may improve accuracy. In revision cases where scar tissue or prior instrumentation complicates the use of conventional burrs, oscillating drills may provide a wider margin of safety.
Ultrasonic bone scalpels and oscillating drill systems are promising alternatives for atraumatic bone removal during spine surgery. Ultrasonic instruments already have substantial clinical evidence demonstrating reductions in durotomy rates, blood loss, and operative time in both open and minimally invasive contexts. Oscillating systems offer a mechanical solution that may reduce soft tissue wrapping and provide improved trajectory control, potentially at lower cost. As newer generations of these devices evolve, additional studies will be needed to define optimal indications as well as quantify their impact on complication rates, operative efficiency, and overall cost-effectiveness. Currently, ultrasonic scalpels are supported by a significant body of evidence demonstrating their utility. Oscillating drills are at an earlier stage of adoption but show theoretical advantages grounded in tissue biomechanics. Together, these technologies reflect ongoing efforts to improve safety and efficiency of bone removal during spine surgery.
References
1. Renjith KR, Eamani NK, Raja DC, et al. Ultrasonic bone scalpel in spine surgery. J Orthop. 2023;41:1–7.
2. Steinle AM, Chen JW, O’Brien A, et al. Efficacy and safety of the ultrasonic bone scalpel in lumbar laminectomies. Spine Surg Relat Res. 2022;7:242–248.
3. Matthes M, Pillich DT, El Refaee E, et al. Heat generation during bony decompression of lumbar spinal stenosis using a high-speed diamond drill with or without automated irrigation and an ultrasonic bone-cutting knife: a single-blinded prospective randomized controlled study. World Neurosurg. 2018;111:e72–e81.
4. Rittipoldech CA, Limsomwong P, Thamrongskulsiri N. Ultrasonic bone scalpel versus conventional technique for thoracolumbar spinal decompression: a prospective randomized controlled trial. Rev Bras Ortop (Sao Paulo). 2023;58:706–711.
5. Yao Z, Zhang S, Liu W, et al. The efficacy and safety of ultrasonic bone scalpel for removing retrovertebral osteophytes in anterior cervical discectomy and fusion: a retrospective study. Sci Rep. 2024;14(1):80.
6. Tsai SHL, Chang CW, Lin TY, et al. The use of ultrasonic gone scalpel (UBS) in unilateral biportal endoscopic spine surgery (UBESS): technical notes and outcomes. J Clin Med. 2023;12(3):1180.
7. Segerlind JP, Staartjes VE, El-Hajj VG, et al. High-frequency ultrasonic osteotomy in the treatment of intradural spinal tumors: matched cohort study. Eur Spine J. 2025;34(8):3570-3577.
Contributor:
Brandon P. Hirsch, MD
From DISC Sports and Spine Centers in Newport Beach, California.