THE INDEPENDENT VOICE OF PHARMACY
In this issue:
NEWS: First for Pharmacy in new Pilot Project Page 4
MEDICINES: Reforming Pharmaceutical Legislation in Medicines Page 8
FEATURE: Role of the Pharmacist in Smoking Cessation Page 14
CPD: Management of Hay Fever and Allergies Page 20
EDUCATIONAL: Sepsis: A Guide for Pharmacists Page 39
AWARDS: Irish Pharmacy Awards 2023 –Finalists Announced Page 55
TEAM TRAINING: Emergency Contraception Page 94
May 2023 Volume 15 Issue 5
PHARMACYNEWSIRELAND.COM This Publication is for Healthcare Professionals Only
INTRODUCING THE 28 s TABLET PACK
VALUE FOR RECURRENT SUFFERERS
FIND OUT HOW TO SUPPORT YOUR PATIENTS

Product Information: Please consult the Summary of Product Characteristics for full product information. Nexium Control 20 mg gastro-resistant tablets and hard capsules (esomeprazole). Indications: The short term treatment of reflux symptoms (e.g. heartburn and acid regurgitation) in adults. Dosage: The recommended dose is 20 mg esomeprazole (one tablet or capsule) per day. Tablets or capsules may need to be taken for 2-3 consecutive days to achieve symptom improvement. Maximum treatment duration: up to 2 weeks. Contraindications: Hypersensitivity to the active substance, substituted benzimidazoles or to any of the excipients. Esomeprazole must not be used concomitantly with nelfinavir. Precautions: Refer to doctor if patient has: Jaundice or severe liver disease, unintentional weight loss, recurrent vomiting, dysphagia, haematemesis or melaena and when gastric ulcer is suspected or present, malignancy should be excluded as treatment with esomeprazole may alleviate symptoms and delay diagnosis, gastric ulcer or gastrointestinal surgery, continuous treatment of indigestion or heartburn for 4 or more weeks, or is over 55 years old with new or recently changed symptoms. Not suitable for long term use. Treatment with proton pump inhibitors (PPIs) may lead to a slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter and in hospitalised patients, also possibly Clostridium difficile. Consult doctor prior to have an endoscopy or urea breath test. Co administration with atazanavir is not recommended. Interactions with medicinal products metabolised through CYP2C19 should be considered. The use of esomeprazole with clopidogrel should be discouraged. Patients should not take another PPI or H2 antagonist concomitantly. PPI are associated with very infrequent cases of SCLE. If lesions occur, especially in sunexposed areas of the skin, and if accompanied by arthralgia, the patient should seek medical help promptly. Side effects: Common: headache, abdominal pain, constipation, diarrhoea, flatulence, nausea/ vomiting, fundic gland polyps (benign). Uncommon: peripheral oedema, insomnia, dizziness, paraesthesia, somnolence, vertigo, dry mouth, increased liver enzymes, dermatitis, pruritus, rash urticaria. For rare, very rare and other side effects please refer to the SPC for full information. Legal category: Supply through pharmacy only. Product licence number: EU/1/13/860/001; EU/1/13/860/002; EU/1/13/860/003; EU/1/13/860/004 and EU/1/13/860/005. MAH: GlaxoSmithKline Dungarvan Limited, Knockbrack, Dungarvan, County Waterford, Ireland. Additional information is available upon request. Text prepared: June 2022. Contains esomeprazole. Always read the label/leaflet. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-NEX-23-00004

SM4271 2023_Nexium_Irish_Pharmacist_FPA 4 PRESS_READY.indd 1 22/03/2023 15:52







SM4271 2023_Nexium_Irish_Pharmacist_FPA 4 PRESS_READY.indd 1 22/03/2023 15:52
Esomeprazole
Foreword
Page 4: All change for United Drug, LloydsPharmacy and TCP
Page 5: Great Place to Work Accolade for Meaghers

Page 6: All Ireland Pharmacy Conference –Date for the Diary
Page 8: EU announces proposal to reform Pharmaceutical Legislation

Page 14: Smoking Cessation for the Cancer Patient
Page 28: HSE marks Immunisation Week
Page 30: Pharmacies in Ireland embracing sustainability

Page 55: Irish Pharmacy Awards 2023 –The Finalists
PUBLISHER:
IPN Communications
Ireland Ltd.
Clifton House, Fitzwilliam Street Lower, Dublin 2 00353 (01) 6690562
MANAGING DIRECTOR
Natalie Maginnis n-maginnis@btconnect.com
EDITOR
Kelly Jo Eastwood: 00353 (87)737 6308 kelly-jo@ipn.ie
ADVERTISING EXECUTIVE
Amy Evans: amy@ipn.ie
EDITORIAL/ EVENTS & MARKETING EXECUTIVE
Aoife Hunter: aoife@ipn.ie
CONTRIBUTORS
Ruth Morrow | Dr Ailsa Lyons
Gerard Flaherty | Ashley Costello
Damien O’Brien | Aoife Fleming
Sinead Horgan | Lorna Quigley
Denise McCarthy | Rachel Flynn
Professor Patricia Fitzpatrick
Professor Gerald Clarke
Clodagh McCarthy
Aoife McNamara
Michele O’Brien
Professor Frances Dockery
DESIGN DIRECTOR
Ian Stoddart Design
Irish Pharmacy News is circulated to all independent, multiple Pharmacists and academics in Ireland.
All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
An ever increasing and wholly unnecessary administrative burden is detracting from patient care and leading to a shortage of pharmacists the Irish Pharmacy Union (IPU) has warned.

Speaking at an event in Dublin jointly hosted by the IPU and JPA Brenson Lawlor IPU President, Dermot Twomey said many pharmacists are becoming burned out and ultimately leaving the profession as a result of this red tape. Over 100 members of the pharmacy profession attended Community Pharmacy 2023 –The Way Forward.
The event heard from a range of speakers about how best to expand the pharmacy sector and also the importance of ensuring wellbeing and work life balance for those working in community pharmacy. One of the biggest barriers to work life balance and job satisfaction is excessive administration Mr Twomey warned. “Pharmacists are highly trained healthcare professionals, we are not administrators. We have an expertise in medications and are a critical part of our country’s healthcare system. More and more patients are seeing pharmacy as the first port of call for care in the community. Unfortunately, at the same time, health authorities seem content to task this essential frontline profession with endless form filling and bureaucracy.”
The full story is on page 5.
In another of our lead news stories this month, it is revealed that Ireland is once again one of the slowest countries in Western Europe to reimburse and make available new innovative medicines to patients. This is according to figures gathered by data analysts IQVIA for EFPIA, the European pharmaceutical industry body.
The survey of 37 European countries, including 27 in the European Union, covers the full four years between 2018 and 2021 analysing 168 innovative medicines authorised for use by the European Medicines Agency (EMA).
The number of days taken depends both on the timing of companies’ applications and the decision-making processes of health authorities. In Ireland, the figures suggest that between 25% and 30% of the timing is attributable to IPHA member companies’ timing of applications for the reimbursement of a medicine to the HSE after the product has been granted EMA market authorisation.
Turn to page 32 for the full story.
We are delighted to present, within this issue, the Finalists for the 2023 Irish Pharmacy Awards. It might sound cliché, but this year has completely surpassed all previous years in terms of the number of entries received. Feedback from our esteemed judging panel has also demonstrated what a difficult task they faced in shortlisting and selecting the winners. These Awards truly display the enormous amount of ongoing dedication, excellence and service provision being carried out amongst Ireland’s community pharmacy sector.
The Irish Pharmacy Awards take place on Saturday, May 27th and we look forward to seeing you all there. Make sure to watch out for the June issue, which will carry all the details of the night and the winners!




Regulars
CPD: HAY FEVER & ALLERGIES
FEATURE: BOWEL CANCER
P41
P81
FEATURE: OSTEOPOROSIS P86



TEAM TRAINING: EMERGENCY CONTRACEPTION

P94

CLINICAL PR: P96

3 PHARMACYNEWSIRELAND.COM 28
IRISH PHARMACY NEWS 5 30
PHARMACYNEWSIRELAND.COM @Irish_PharmNews IrishPharmacyNews Contents 55 15:52 15:52
All Change with PHX Ireland Group
Exciting times for the teams at United Drug, LloydsPharmacy and TCP with the launch of their new company holding name which changed from McKesson Ireland to PHX Ireland Group Limited on 24th April 2024.

Every day, the PHOENIX group makes an important contribution to comprehensive and safe healthcare in Europe.
Reform Pharmaceutical Legislation
The change to the company holding name is because of the PHOENIX Group acquiring the McKesson Ireland businesses in November 2022 when it concluded a deal to acquire parts of McKesson Europe.
PHX Ireland Group Limited comprises United Drug, Ireland’s leading pharmaceutical wholesaler and distributor; LloydsPharmacy Ireland, a major community pharmacy chain; and TCP Homecare, innovators in clinical home nursing services and direct to patient delivery solutions.
The change in name will not affect how the businesses in Ireland operate. The customers
and suppliers for United Drug, LloydsPharmacy and TCP will continue to have the same points of contact, terms and conditions of trade and other ways of conducting business operations all remain unchanged.
PHX Ireland is part of the PHOENIX group, Europe’s leading healthcare provider. Headquartered in Mannheim, Germany, the PHOENIX group brings together more than 48000 employees from 29 countries, includes 223 pharmaceutical distribution sites, and more than 3200 owned pharmacies and 17000 partner pharmacies. Their mission is to deliver health.
Paul Reilly Chief Executive Officer of PHX Ireland Group Limited stated “We are delighted to be part of the PHOENIX group, Europe’s leading pharmaceutical wholesaler, pharmacy retailer and healthcare service provider. This will further strengthen our leadership position in Ireland and facilitate greater access to additional products, services, and expertise for the Irish market. Our number one priority is to continue to serve our Irish customers and patients providing safe, effective, and futureorientated healthcare solutions that make a difference to customers and patients’ lives every day.”
PHX Ireland Group employs over 1,800 people, operate 5 distribution centres and 88 pharmacies, delivers over 85 million packs to Irish pharmacies and hospitals, and serve 500,000 patients each year.
First for Pharmacy in New Pilot Project
CarePlus Pharmacy is marking World Asthma Day 2023 in Asthma Awareness Week by launching a new service for customers to help assess and manage their condition. The pilot scheme includes the option to have a free FeNO test, in an industry first for Irish retail pharmacy.
Asthma affects over 470,000 people here, and one person is hospitalised due to an asthma attack every four minutes in Ireland*. The new service is being run on a pilot basis at Carrigaline CarePlus Pharmacy in Co. Cork and Woods CarePlus Pharmacy in Mullingar, Co. Westmeath , as staff highlight the importance of managing the condition at the start of Asthma Awareness Week 2023. A FeNO (or exhaled nitric oxide) test helps determine how much lung inflammation is present and how well inhaled steroids are suppressing it in patients with allergic or eosinophilic asthma - which affects up to 70% of sufferers in Ireland. Worryingly, someone with a high FeNO level is four times more at risk of potentially severe exacerbations than someone whose asthma is well managed. Using the test can help to reduce exacerbations by up to 50% in both children and adults.
Owner and Superintendent Pharmacist at Carrigaline CarePlus Pharmacy, Nigel Moloney, says the FeNO test is a vital part of their new service saying, “Knowing your levels can help a patient, doctor and pharmacy team recognise how well your asthma is being controlled and help to avoid asthma episodes. Our new service offers a questionnaire about asthma control, the FeNO test, peak flow measurement and an inhaler technique check. Anyone who wants to know more or is concerned about their asthma can simply pop into our store and ask anyone on the team for more information, we’d be happy to help”.
CarePlus Pharmacy is also encouraging people with asthma to get an Asthma Action Plan if they do not currently have one as this can help along with the results from the Asthma Support Service. Asthma Action Plans
can be downloaded from the Asthma Society of Ireland website asthma.ie. These plans should be reviewed at every available opportunity with a healthcare professional, and will detail asthma medicines, symptoms, triggers, how to know if you are having an asthma emergency and what to do in those situations.
Health and Wellness Manager at CarePlus Pharmacy, Siobhan Kellett, says they’re focused on helping customers manage what can be a worrying condition saying, “Everyone with asthma at some stage can face the risk of an exacerbation. The good news is that these episodes can often be prevented, or the likelihood reduced through good asthma management. This is an aspect of care that CarePlus Pharmacy has always aimed for - helping people manage their own health better, with the support of their community pharmacy team.”
The IPU has welcomed the European Commissions longawaited proposal to reform the EU pharmaceutical legislation in particular the important provisions to improve patients access to medicines regardless of where they live in the EU.
The proposal introduces useful tools to address medicines shortages including earlier notification, monitoring and assessment, and the obligation for marketing authorisation holders to have in place shortages prevention plans for all medicines. These measures will help in mitigating the problem of shortages.
The IPU is concerned, however, that there may be delays in implementation due to the European Parliament elections in 2024, the complexity of the discussions, the different interests at stake, and the fact that the new legislation will be implemented only 18 months after its entry into force.
This means that Irish citizens will have to wait many years to see its impact in real life - and we simply cannot wait that long. We cannot afford to have another crisis such as the one we experienced with the shortage of antibiotics during the winter. Because of this the IPU is calling for short term actions to tackle drug shortages including granting community pharmacists’ greater flexibility in finding alternatives when a medicine is not available, such as therapeutic substitution under a serious shortage protocol.
Commenting on the proposals
Chair of the IPU’s PCC Committee Kathy Maher said, “Given the far-reaching consequences of this legislation for the citizens of Ireland we are once again calling on the Minister for Health to immediately appoint a Chief Pharmaceutical Officer, to lead the constructive dialogue with the co-legislators, the European Parliament, and the Council, during the anticipated long discussions ahead, with a focus on accessibility and affordability of medicines for Irish citizens and our health systems”.
PHARMACYNEWSIRELAND.COM 4 News
Healthy Communities Programme
Cllr Vincent Jackson deputising for Lord Mayor of Dublin Caroline Conroy launched the Cherry Orchard and Ballyfermot Sláintecare Healthy Communities Programme at a community event in the Ballyfermot Civic Officer last month.
Sláintecare Healthy Communities programme will be delivered locally in Cherry Orchard and Ballyfermot in partnership with the HSE, Dublin City Council, Ballyfermot Chapelizod Partnership and other community organisations such as FamiliBase, Ballyfermot Resource Centre and The Orchard Centre.
Cllr Vincent Jackson said, “To make real and lasting change we need to work together to create communities where people can thrive, putting in place the right building blocks for health, stable jobs, good pay, quality housing, good education and accessible amenities that enhance and improve our built environment.”
He continued, “Sláintecare Healthy Communities is a collaborative programme with DCC, the HSE and Ballyfermot Chapelizod Partnership where we all work together to ensure that our communities in greatest need are supported to live longer healthier lives. These are exciting times for the community in Cherry Orchard and Ballyfermot and I look forward to seeing the great progress that has been made.”
Margaret McQuillan, HSE Dublin South, Kildare & West Wicklow Head of Health and Wellbeing spoke next. She highlighted the evidence-based and practical programmes available in the Cherry Orchard and Ballyfermot area as part of the Sláintecare Healthy Communities programme. These include Stop Smoking Service, We Can Quit, Parenting Programmes, Healthy Food Made Easy, Social Prescribing and Making Every Contact Count.
This was further reiterated by Anne Fitzgerald, CEO Ballyfermot Chapelizod Partnership who deliver these programmes in the community. As a well-established community organisation they welcomed the further funding through Sláintecare Healthy Communities Programme which allows them to continue to deliver and expand their services.
Pharmacies strangled by Red Tape
An ever increasing and wholly unnecessary administrative burden is detracting from patient care and leading to a shortage of pharmacists the Irish Pharmacy Union (IPU) has warned. Speaking at an event in Dublin jointly hosted by the IPU and JPA Brenson Lawlor IPU President, Dermot Twomey said many pharmacists are becoming burned out and ultimately leaving the profession as a result of this red tape.
Over 100 members of the pharmacy profession attended Community Pharmacy 2023 – The Way Forward. The event heard from a range of speakers about how best to expand the pharmacy sector and also the importance of ensuring wellbeing and work life balance for those working in community pharmacy.
One of the biggest barriers to work life balance and job satisfaction is excessive administration Mr Twomey warned. “Pharmacists are highly trained healthcare professionals, we are not administrators. We have an expertise in medications and are a critical part of our country’s healthcare system. More and more patients are seeing pharmacy as the first port of call for care in the community. Unfortunately, at the same time, health authorities seem content to task this essential frontline profession with endless form filling and bureaucracy.”
Jason Bradshaw from JPA Brenson Lawlor, leading financial advisors to the sector, stated, “A career in community pharmacy can be very rewarding but the correct work/life balance is a key element in retaining and attracting community pharmacists. We
know pharmacists are leaving the sector and this has been linked to the significant administrative burden thus creating a shortage of community pharmacists.”
According to Mr Twomey, “While community pharmacy practice requires diligent attention to detail, much of the required red tape does nothing for patient care. It is a huge frustration that we are forced to complete multiple boxticking exercises that do nothing to advance clinical safety and which impact on the time available to provide the valuable clinical care for which we are trained.”
Twomey was critical of the HSE for forcing much of the red tape onto pharmacies. “Among the biggest administration burdens is form filling relating to work pharmacists do on behalf of the state such as dispensing medicines to medical card holders. The administration required to get paid for the work we do for the HSE, such as through community drug schemes and the PCRS, is completely unnecessary and adds significantly to the cost of dispensing medicines, a double whammy.”
He said that there were some obvious solutions available that
could be implemented including a national ePrescribing system, reduced administration associated with community drug schemes, better visibility of patient level eligibility for certain medications where restrictions apply and implementation of a Serious Shortage Protocol to support pharmacists in therapeutically substituting medicines in the case of a shortage.
The IPU is now calling on authorities to commit to combatting the problem. “We want to invite relevant parties such as the HSE, HPRA and Pharmaceutical Society of Ireland, to work with us to review and reduce the level of unnecessary bureaucracy imposed on community pharmacists.”
Concluding, Mr Twomey said, “While we jump through hoops patients are left waiting. What is required is a clear commitment to reduce red tape which will empower the sector to deliver the revolution in community care we have been calling for many years. Allowing the problem to continue will exacerbate the shortage of pharmacists, increase the levels of stress for those working in the sector and damage community care.”
Great Place to Work for Pharmacy
Meaghers Pharmacy Group is delighted to announce that it has been named as a Great Place to Work and one of Ireland’s Top 30 medium-sized Great Places to Work for the third consecutive year at the Great Place to Work Ireland Awards.

The prestigious awards, which recognise Meaghers as one of the best workplaces in Ireland, are based on an extensive culture audit and direct feedback from employees, through a trust index employee experience survey which measures the extent to which the organisation is considered to be a great workplace by their people.
As Meaghers continues to grow its team, the pharmacy group consistently maintains that people are its greatest asset and that positive engagement, inclusion and fostering a positive culture and work environment are extremely important.
Oonagh O’Hagan, Managing Director of Meaghers Pharmacy,
said, “It’s such an honour to be named as a Great Place to Work and one of Ireland’s Top 30 medium-sized Great Places to Work for the third year in a row. It is particularly gratifying to know that our people enjoy working for Meaghers. This is in no small part down to our team of managers across the business who put our people at the centre of everything we do and strive to build on our family ethos and culture every day. I have always believed that a happy team makes for happy customers, and I am so proud of our people at Meaghers and the lengths they go to every day to make a true difference in the communities we serve.”
Oonagh O’Hagan, Managing Director of
PHARMACYNEWSIRELAND.COM 5
News
Meaghers Pharmacy
leave with new
Save the Date: 10th All Ireland Pharmacy Conference
The 10th All Ireland Pharmacy Conference (AIPC) will be held at Ballymascanlon House Hotel, Dundalk on 6th and 7th November 2023. The theme for this year’s conference is ‘Creating Momentum & Building Capacity’.

and will involve parallel oral sessions and poster presentations. Further detail on the conference can be found on the IIOP Website under the Courses and Events tab (https://iiop.ie/ content/10th-all-ireland-pharmacyconference-2023).
The day delegate rate for the conference is ¤55 and online registration will be available in midMay through the IIOP website.
Three reasons to register
conference. It is a testament to all those involved in the conference, that despite a hurricane and pandemic it is still here to showcase the work of Pharmacy teams on the island of Ireland.
It is probably the only pharmacy conference that is open to all pharmacy team members that covers research and quality initiatives in the community, hospital academic and regulatory setting.
This conference is jointly coordinated by the Northern Ireland Centre for Pharmacy Learning and Development and the Irish Institute of Pharmacy. Its focus is to share good practice in pharmaceutical care and practice development across the primary and secondary care sectors.
Pharmacists, technicians and qualified assistants are encouraged to exchange ideas for pharmaceutical service development in the Republic of Ireland and Northern Ireland.
Call for Abstracts
The 2023 conference theme is ‘Creating Momentum & Building Capacity’. Abstracts are invited for posters and oral presentations that deal with a broad range of pharmacy practice, including (but not limited to) the following topics:
• Education
• Workforce
• Enhancing Practice
• Leadership
• Policy
Abstracts can be submitted at this link (https://aipc2023.exordo. com/), and further information can be found on the IIOP website, under the Courses and Events tab.
to exchange ideas for Ireland. Abstracts are invited for practice, including (but not further information can for viewing and discussion additional 5 minutes for consideration.
Posters will be on display throughout the conference, with dedicated time for viewing and discussion during the day. Oral
author(s) and whether they wish date for receipt of abstracts fee & accommodation) for
presentations should be 10 minutes in duration with an additional 5 minutes for audience questions. You are welcome to submit multiple abstracts for consideration.
Applicants should clearly indicate the corresponding and presenting author(s) and whether they wish their abstract to be considered for poster or oral presentation. The closing date for receipt of abstracts is Wednesday 31st May 2023.
The organising bodies will cover the conference costs (i.e the day delegate fee & accommodation) for the main presenter of each oral presentation. For those presenting posters, the day delegate fee will be covered.
Conference dates and Registration
On the evening of Monday 6th November, the conference dinner will take place at 8.00pm and provides an opportunity to network with colleagues. The main conference proceedings will start at 9.30am on Tuesday 7th November
Accessibility: It’s very accessible to all practitioners. Sometimes conferences can be quite focused on formal academic research and studies and this makes them feel out of reach for practitioners. At AIPC the focus is on sharing information about initiatives and approaches from practice, and therefore is very applied and accessible to practicing pharmacists and technicians as well as those involved in applied research. You are likely to leave with new ideas for your practice.
Networking: AIPC provides an ideal setting for networking. The diverse range of attendees from both North and South, across all areas of practice, make it a great place to meet new people in pharmacy. The format of short oral and poster presentations, with lots of opportunity for interaction through the dinner and breaks, means it’s very sociable and welcoming experience. You are likely to leave with new connections and friends.
Perspective: It provides a space to consider the Irish profession. The key-note address will provide food for thought on how Irish pharmacy can evolve, and examples of practice from both sides of the border will help to shape thinking over the course of the conference proceedings. You are likely to leave with new ideas about pharmacy’s direction.
We asked one of our previous attendees to share their experience of attending the All Ireland Pharmacy Conference:
‘It is probably 15 years since I went to my first All Ireland Pharmacy
The layout of the event, starting at the dinner the night before, allows for the discussion of information, ideas and resources as well as networking and catching up with old friends.
The posters and oral presentations allow for the sharing of initial ideas and pilots through to larger scale research and practice initiatives. It is always enjoyable to see ideas develop and come to fruition over a number of conferences.
I would recommend the conference to anyone as either an attendee or if you want to share ideas and resources via submission of an abstract. From small acorns mighty oaks grow and the All Ireland Pharmacy conference is a great place to start.’
(Sinead McCool, Hospital Pharmacist, Kilkenny)
In summary, this conference provides a unique opportunity for those working in pharmacy practice, north and south, to consider issues directly relevant to their profession in a friendly and welcoming environment. Don’t miss it.

PHARMACYNEWSIRELAND.COM 6
News
Ballymascanlon House Hotel
We asked one Pharmacy Conference: ‘It is probably all those involved the work of Pharmacy
It is probably the research and quality
The layout of the ideas and resources
I share grow (Sinead
The posters and scale research over a number
In summary, this north and south, environment.
Sinead McCool, Hospital Pharmacist, Kilkenny
“It is probably 15 years since I went to my first All Ireland Pharmacy conference. It is a testament to all those involved in the conference, that despite a hurricane and pandemic it is still here to showcase the work of Pharmacy teams on the island of Ireland”
✓ 100% Preservative Free

✓ Contact lens compatible

















✓ Can be used for up to 6 months from opening












✓ Part of the Heat-CleanseHydrate regimen



Now voted best eye care product, 2 years in a row! It’s no wonder a bottle of HYLO ®-FORTE is sold in Ireland every minute * Do your patients suffer with dry eyes at night? SCOPEIE197 Freephone 1800 816 005 | info@scopeeyecare.com | www.scopeeyecare.com *Data from IQVIA MAT, January 2023. Looking to learn more about our products and grow your eye care category? Find out more about the Scope Pharmacy Partnership Program Try HYLO NIGHT ® for the management of persistent dry eye symptoms at night Scan me 0.2% Sodium Hyaluronate
Proposal to Reform Pharmaceutical LegislationAddressing Medicine Shortages

The IPU has welcomed the European Commissions long-awaited proposal to reform the EU pharmaceutical legislation in particular the important provisions to improve patients access to medicines regardless of where they live in the EU.
market for the State and for Industry, thus facilitating sustainable and affordable access to medicines for patients in Ireland over the next 4 years.
Minister for Health to immediately appoint a Chief Pharmaceutical Officer, to lead the constructive dialogue with the co-legislators, the European Parliament, and the Council, during the anticipated long discussions ahead, with a focus on accessibility and affordability of medicines for Irish citizens and our health systems.” Meanwhile, Concerns around Ireland’s growing medicine shortage crisis were voiced recently during a Dáil Éireann Debate
“Negotiations towards these new Agreements with industry began in May 2021, against a backdrop of a growing annual drugs budget, up from ¤1.95bn in 2016 to almost ¤2.25bn by 2020.”
The Minister outlined the multiannual agreements with the Irish Pharmaceutical Healthcare Association (IPHA) and Medicines for Ireland (MFI) which he said ‘represent an important step in facilitating access to innovative new medicines for patients.’
“Under the terms of the agreement, there is scope for the Department of Health, the HSE, and industry to continue to maintain their engagement throughout the lifetime of the agreement on all matters pertaining to the agreement.
“As of 16th March 2023, there are 25 applications from manufacturers/suppliers currently under review by the HSE, for a pricing increase request related to a claim of increased cost of goods, making continuity of supply to the Irish market and Irish patients unsustainable.
The proposal introduces useful tools to address medicines shortages including earlier notification, monitoring and assessment, and the obligation for marketing authorisation holders to have in place shortages prevention plans for all medicines. These measures will help in mitigating the problem of shortages.
The IPU is concerned, however, that there may be delays in implementation due to the European Parliament elections in 2024, the complexity of the discussions, the different interests at stake, and the fact that the new legislation will be implemented only 18 months after its entry into force. This means that Irish citizens will have to wait many years to see its impact in real life - and we simply cannot wait that long. We cannot afford to have another crisis such as the one we experienced with the shortage of antibiotics during the winter. Because of this the IPU is calling for short term actions to tackle drug shortages including granting community pharmacists’ greater flexibility in finding alternatives when a medicine is not available, such as therapeutic substitution under a serious shortage protocol.
Commenting on the proposals Chair of the IPU’s PCC Committee Kathy Maher said, “Given the far-reaching consequences of this legislation for the citizens of Ireland we are once again calling on the

Deputy Holly Cairns TD asked the Minister for Health, Stephen Donnelly about the steps he is taking to address concerns in relation to the ongoing issue of medicine shortages.
Responding, Minister Donnelly stated that medicine supply issues and their prevention are not unique to Ireland.
He said, “Similar increases in demand and medicines supply issues have been observed in the UK, throughout the EU and across the world at present. In the case of medicines used most often in Ireland, there are typically multiple alternatives available from various sources that remain available to ensure continuity of treatment. Of the products currently in short supply, alternative treatments are available for every single product.
“Management of medicine supply issues necessitates a multi-faceted, multi-stakeholder response to ensure patient safety, continuity of care and protection of public health. To that end, at the request of the Department of Health, the Health Products Regulatory Authority (HPRA) has assumed a coordinating function in Ireland’s response to managing medicine shortages when they occur.
“Two new Framework Agreements on Pricing and Supply of Medicines 2021-2025 were signed in December 2021. These Agreements provide stability to the medicines reimbursement
He added, “There are a number of clauses set out in both agreements in detail, which provide clear pricing rules for applicant companies, that have been agreed between the State and main Pharmaceutical Industry representative groups in Ireland as appropriate and intended to provide a predictable environment for Marketing Authorisation Holders (MAHs) to supply their products (and prevent shortages). These are grossly summarised as:
1. The pricing application form for new medicines is based on a basket of 14 countries (13 EU Member States and the UK). Pricing is permitted to be no more than the average price based on the pricing in these 14 countries.
2. The pricing of non-patented medicines (i.e., generic, biosimilar or hybrid medicine marketed in Ireland) is based on the originator medicine at a specific time point.
In the case of such pricing increase requests the time taken to adjudicate on these is highly variable (on a case-by-case basis) and dependent on a number of factors, that the HSE is required to consider including the number of alternative suppliers for that medicine, the potential alternative therapeutic options, the clinical need for the product, the potential budget impact, and European pricing.
“The HSE also takes an active role at the time of notification, in engaging with manufacturers/ suppliers intending to discontinue priority medicines due to the lack of commercial viability of those products. In many of the cases where this arises as a scenario, the commercial decision relates to global discontinuations and is outside of the control of the HSE i.e., cannot be addressed through pricing increases at a national level.
The Agreements are the product of extensive collaboration between the State, HSE, and Industry. They remain current and appropriate for their purpose since their signing in December 2021.”
PHARMACYNEWSIRELAND.COM 8 Medicine Shortages
Pharmacist Kathy Maher
E45 knows how to support skin
E45 Cream is licensed to treat an extensive range of dry skin conditions including dry/flaky skin, eczema, itchy skin, dry psoriasis, and sunburn. It creates a protective barrier to lock in natural moisture. Helps prevent flare ups and reduces the need for additional treatment.






STRAIGHT UP SKINCARE
Management of Stable and Acute Asthma
2023 marks the 50th anniversary of the Asthma Society of Ireland. Since our inception in 1973 the Asthma Society has been providing services to the 380,000 people in Ireland who suffer from asthma, helping them to live full and symptom free lives. Our mission is to stop asthma deaths and much has been accomplished over the last five decades. As part of our work, we wish to acknowledge the contribution and encouragement given by the Irish pharmacy industry. 2023 is going to be a busy, productive year with plans to mark our 50th anniversary. This starts with Asthma Awareness Week and World Asthma Day in May with a significant media presence highlighting people with asthma, their carers and representatives of the medical profession. Additionally, the Asthma Society will be hosting a webinar on Wednesday 3rd May as part of Asthma Awareness Week. During the year the Asthma Society is also planning some unique events and aims to strengthen our relationships with trusted partners in the pharmacy industry.
Written by Ruth Morrow, Respiratory Nurse Specialist, Asthma Society of Ireland

Test (ACT) and assessing risk factors for poor outcomes. Treatment issues should also be addressed at every visit and should include:
• Review of inhaler technique and adherence
• Asking about side-effects
• Reviewing and updating the patient’s written asthma action plan
• Exploring the patient’s attitudes and goals for their asthma
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation which is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation (GINA, 2022). This article seeks to address the management of asthma in adults both from a stable and an acute perspective.
The key to asthma management is education and empowering patients to manage their asthma as well as the use of appropriate treatment for the patient’s asthma phenotype, symptoms and lifestyle.
Management of Stable Asthma
The goals of asthma management are:
1. Symptom control: to achieve good control of symptoms and maintain normal activity levels
2. Risk reduction: to minimize future risk of exacerbations, fixed airflow limitation and medication side-effects (GINA 2022)
Assessment of asthma control involves assessing symptoms over the previous 4 weeks using the GINA Assessment of Asthma Control and the Asthma Control
The treatment and management of asthma should incorporate the following elements:
Education on the disease process
Management of trigger factors
Medication management – mode of action, inhaler technique, adverse events and adherence
Asthma Action Plan
Management of acute flare-ups of asthma
The goal of asthma management is for the patient to be optimally controlled on the minimum amount of medication. GINA (2022) provides health care professionals with a management approach based on control using a step wise approach. This assists health professionals with the titration of medications using a step down or step up approach in attempt to achieve this goal.
The cornerstone of asthma treatment is inhaled therapy as medications are directly targeted at the airways and therefore, are more effective. This also limits the amount of systemic absorption and reduces adverse events. Patients should be commenced on the appropriate step of the treatment guidelines which is dependent on the severity of their symptoms (GINA, 2022). Each
patient is assigned to one of five treatment steps and patients may move up or down the steps depending on symptoms and the amount of reliever therapy being used. Inhaled glucocorticosteroids (ICS) are the cornerstone of asthma treatment and are the most effective controller medications available. However, there are additional oral medications such as leukotriene receptor antagonists which can be added on and are very useful in patients who have an allergic component to their asthma, experience cold air bronchoconstriction and have exercise induced symptoms. These medications are also licensed for use in allergic rhinitis, a condition which 85% of people with asthma also have. Sublingual immunotherapy is also now recommended at all steps of the guideline depending on the patient’s asthma phenotype.
In 2019, GINA updated their strategy which outlined significant changes to the way asthma is managed in adults and adolescents. The changes recognise a real sea change in the use of short acting bronchodilators (SABA) and the introduction of combination therapy of ICS and long-acting bronchodilators (LABA) as “a needed therapy” at Step 1 and as a maintenance therapy at Step 2. Using a combination therapy as an “asneeded” therapy will require a significant change in the mindset of HCPs given that we have been using SABAs for the last 50 years to relieve asthma symptoms.
Why this change?
Inhaled SABA (Salbutamol, Terbutaline) have been firstline treatment for asthma for 50 years. Traditionally asthma was thought to be a disease of bronchoconstriction with SABA being the drug of choice. Added to this, rapid relief of symptoms, reliance on, patient satisfaction and their low cost have meant that SABAs were widely used, overused and over-relied upon. The perception by patients that their reliever “gives me control
over my asthma”, so much so that they often don’t see the need for other treatment. However, research over the past number of years has shown that regular and frequent use of SABAs decrease bronchoprotection, increase rebound hyperresponsiveness, and decrease bronchodilator response (Hancox, 2000). Patients with apparent mild asthma are at risk of serious adverse events such as near fatal asthma, acute asthma and death from asthma. Regular or frequent use of SABAs is also associated with increased allergic response and increased eosinophilic airway inflammation (Aldridge, AJRCCM 2000). Patients who get 3 or more canisters of SABA per year (average 1.7 puffs/ day) are associated with higher risk of attendance to the emergency department (Stanford, AAAI 2012) and patients who receive 12 or more canisters per year are associated with higher risk of death (Suissa, AJRCCM 1994).
A meta-analysis by Crossingham et al (Cochrane 2021) of four RCTs involving 9,565 patients demonstrated the benefits of LABA/ICS combination therapy showing a 55% reduction in severe exacerbations compared with SABA alone. ED visits or hospitalizations were 65% lower than with SABA alone and 37% lower than with daily ICS.
In their review of the literature, GINA found no evidence to support a Step 1 SABA-only approach. The lack of evidence for SABA-only treatment contrasted with the strong evidence for safety, efficacy and effectiveness of ICS and ICS/LABA. For safety, GINA no longer recommends SABA-only treatment for Step 1. It is now recommended that all adults and adolescents with asthma should receive symptom-driven or regular low dose combination LABA/ICScontaining controller treatment, to reduce the risk of serious exacerbations (GINA, 2022).
Implications for clinical practice
Patients who have symptoms more than twice a month should be
PHARMACYNEWSIRELAND.COM 10 Asthma


















Asthma
prescribed ICS/LABA twice daily (Step 2-5) and patients who have symptoms less than twice a month should use ICS/LABA on “an asneeded basis” (Step1). Daily ICS is no longer listed as a Step 1 option as it has a high probability of poor adherence. It is now replaced by a more feasible as-needed controller option at Step 1.Patients should be offered self-management plans with instructions on how to adjust their medications in response to worsening symptoms and/or worsening PEFR. An example of a self-management plan is available on www.asthmasociety.ie.
In 2019, hmR Ireland worked with 70% of Irish pharmacies conducting research on asthma medication usage trends, using anonymised patient transactional dispensing data. The Health Market Research results found:
• Three in ten use more than twelve reliever inhalers a year, putting them at risk of an asthma-related death
• Seven in ten people are using more than three reliever inhalers a year, putting them at risk of an asthma attack (or some form of asthma exacerbation)
• Within five years of diagnosis, half the asthma population are over-reliant on their reliever inhaler
• In the year after diagnosis, 30% children aged 0-17 are overusing their reliever inhaler
• In the year after diagnosis, 60% people aged 50 or over are overusing their reliever inhaler
Non-pharmacological management
The non-pharmacological management of asthma include management of trigger factors, smoking cessation, management of obesity and gastroesophageal reflux disease. Influenza vaccination is recommended for those with more severe asthma. Gastro-esophageal reflux can worsen asthma symptoms and treatment of reflux may improve asthma symptoms.
Adherence with medication regimes and inhaler technique
One of the biggest challenges in asthma management is adherence to medication as many patients may be asymptomatic and therefore “don’t feel the need to use their medication daily”
Exploring the patient’s beliefs and attitudes can be useful in determining a rationale for non-adherence to medication regime. Saving medication until
it is needed, fear of becoming addicted or the health professional didn’t listen are amongst reasons given by patients in the INCA study (Sulaiman et al, 2014). In the current climate, cost is a significant factor even for the person who has a medical card and should not be overlooked. Two proven ways to address non-adherence are shared decision-making between the health professional and the patient and motivation interviewing. Using motivational interviewing, the health professional can assess the individual’s likelihood to adhere to their medication or to nonpharmacological interventions. Inhaler technique should be checked at every opportunity as errors frequently occur even in patients who are taking inhaled medication for years. Care and maintenance of devices should also be addressed. Inhaler technique videos are available on www.asthma.ie.
Risk factors for poor outcomes
The management of acute asthma includes:
1. Oxygen therapy - 24% delivered by face mask (usually 1L/min) to maintain oxygen saturation 9395%
2. Inhaled short-acting bronchodilator – 4-10 puffs of Salbutamol by spacer, or 5mg by nebulizer, every 20 min for first hour, then reassess severity. If symptoms persist, deteriorate or recur, give an additional 10 puffs per hour and admit to hospital
3. Oral corticosteroids – max 50mgs of oral steroids and continue for 5 -7 days
4. Additional treatments can include - For moderate/severe exacerbations, Ipratropium bromide 80mcg (or 250mcg by nebulizer) every 20 minutes
Criteria for immediate transfer to secondary care include:
Follow-up post exacerbation
All patients should be followed up regularly after an exacerbation, until symptoms and lung function return to normal. Patients are at increased risk during recovery from a further exacerbation. This provides an opportunity to review and update the patient’s asthma action plan, review inhaler technique and adherence and to ascertain if there was a cause ie new trigger factors, for this flare-up which might be helpful in preventing future flare-ups
At follow-up visit(s), the asthma review should include:
• The patient’s understanding of the cause of the flare-up
• Modifiable risk factors, e.g., smoking, weight loss if indicated, addressing new triggers
• Adherence with medications, and understanding of their purpose
• Reliever should be being used as-needed rather than routinely
Patients who experience uncontrolled asthma symptoms, had one or more exacerbations in the previous year, the start of the patient’s usual ‘flare-up’ season (especially if autumn), has major psychological or socio-economic problems, poor adherence with controller medication and/or incorrect inhaler technique are at risk of an exacerbation in the coming months.
1. Features of severe exacerbation at initial or subsequent assessment
• Patient is unable to speak or drink
• Cyanosis
• If controller medication was increased, the increased dose should be maintained for 3 weeks and possibly longer particularly, if flare-up was during the winter or during pollen season
non-adherence are shared decision-making between the health professional and the patient and motivation interviewing. Using motivational interviewing, the health professional can assess the individual’s likelihood to adhere to their medication or to non-pharmacological interventions.
• Inhaler technique skills
• Subcostal retraction
• Oxygen saturation <92% when breathing room air
• Written asthma action plan
Conclusion
Inhaler technique should be checked at every opportunity as errors frequently occur even in patients who are taking inhaled medication for years. Care and maintenance of devices should also be addressed. Inhaler technique videos are available on www.asthma.ie
Assessment and Management of Acute asthma
• Silent chest on auscultation
Risk factors for poor outcomes
Accurate and timely assessment of acute asthma exacerbations should be carried out to ensure a successful outcome. Table 1 differentiates between a mild and severe acute exacerbation.
2. Lack of response to initial bronchodilator treatment
3. Persisting tachypnoea despite 3 administrations of inhaled SABA,
4. Unable to be managed at home
Assessment and Management of Acute asthma
This article has addressed stable and acute asthma management. The rationale for the introduction of LABA/ICS combination therapy has been explored following the changes to the GINA guidelines in 2019.
Patients who experience uncontrolled asthma symptoms, had one or more exacerbations in the previous year, the start of the patient’s usual ‘flare-up’ season (especially if autumn), has major psychological or socio-economic problems, poor adherence with controller medication and/or incorrect inhaler technique are at risk of an exacerbation in the coming months.
References Available on Request
Accurate and timely assessment of acute asthma exacerbations should be carried out to ensure a successful outcome. Table 1 differentiates between a mild and severe acute exacerbation.
Table 1: Assessment of acute exacerbation of asthma (GINA, 2022)
PHARMACYNEWSIRELAND.COM 12
Symptoms Mild Severe Altered consciousness No Agitated, confused or drowsy Oximetry on presentation (SaO2) >95% <92% Speech Sentences Words Pulse rate Peak Flow Pulse rate 100–120 bpm >50% predicted or best <50% of predicted or best Central cyanosis Absent Likely to be present Wheeze intensity Variable Chest may be quiet
Table 1: Assessment of acute exacerbation of asthma (GINA, 2022)
The management of acute asthma includes:
COME RAIN OR SHINE
WE’VE GOT YOU COVERED
Sun Facts
UVA rays can cause skin aging, wrinkles, and pigmentation.

P20 Sensitive Face SPF50+ contains a UVA-PF above 50 which is more than double the amount of UVA protection that is required by EU.
Enlighten yourself at P20.com
P R OT ECT IO N W IT H O U T C O M P RO M I S E
Smoking Cessation for Patients with Cancer –the role of the Pharmacist

Professor Patricia Fitzpatrick and a research team from UCD, the HSE Tobacco Free Ireland Programme, specialist cancer hospitals and patient representatives, conducted a research programme funded by the Irish Cancer Society entitled “Smoking cessation for cancer patients in Ireland: a scoping and feasibility initiative.”
It is well-known that tobacco smoking increases the risk of several cancers. It also has an impact on outcomes for people with cancer who continue to smoke but this is often overlooked. Tobacco smoking is associated with poorer treatment outcomes (including treatment-related complications and toxicities), increased risk of recurrence, the development of second primaries, lower survival, and decreased quality of life among continuing smokers. Notwithstanding the adverse outcomes, a significant number of people who have been diagnosed with cancer continue to smoke.
This research had 6 work packages: a rapid review of smoking cessation interventions in cancer patients; a review of national smoking rates among cancer patients (2014-2018); a national audit of existing smoking cessation services across all adult cancer hospitals; semi-structured interviews with 25 cancer patients
who smoke or quit at diagnosis, semi-structured interviews with 18 cancer healthcare professionals, and a Patient Voice in Cancer Research workshop (www.ucd.ie/ patientvoicecancer) . We selected patients with cancers particularly associated with smoking (head & neck cancer, cervical, lung) and highly prevalent cancers (breast cancer), in addition to other patients attending oncology clinics). The study findings of particular importance for pharmacists are described below. Using Hospital In-Patient Enquiry (HIPE) data we found that during 2014–2017, current smoking on discharge from hospital increased overall in patients with cancer (10.5–11.7%), patients with lung cancer (24.7–27.2%), cervical cancer (11–19.8%) and head and neck cancer (3–12.7%), with small reductions in all in 2018. Smoking rates in patients with breast cancer were stable. These rates are lower than the Irish general population (23–20%) but are increasing or have plateaued, unlike the national figures. It is important to recognise that HIPE data are subject to potential duplicate episodes of care and under-documentation of smoking; patients may also stop smoking in hospital due to a combination of feeling sick and difficulties smoking as an inpatient on smoke-free hospital campuses but revert to smoking on return home. However, trend analysis is useful, as these limitations should be stable.
Qualitative analysis of patient interviews identified key themes as follows: prior to diagnosis, patients were striving but struggling to quit; diagnosis was a shock but also a cue to action with many patients quitting at diagnosis- a reminder of the “teachable moment”; routine
but variable smoking cessation assessment and support was available in hospital; patients felt they needed a well-defined referral system. An important smoking cessation facilitator was support from others (family and healthcare professionals (HCPs)). Patients wanted a sustained, intensive, non-judgmental approach to smoking cessation incorporating pharmacological and behavioural interventions spanning hospital and communitybased settings. Some but not all patients were aware of Nicotine Replacement Therapy (NRT) and other stop smoking medicines like varenicline being free if they have a medical card. Smoking cessation barriers included limited knowledge of smoking cessation support, lack of family support and lack of willpower. Analysis of interviews with Health Care Professionals working in four of nine specialist cancer centres, identified challenges in discussing smoking cessation with patients diagnosed with cancer. While patients expect to be asked about their smoking habit, the timing of the conversation adds a layer of complexity at times when patients are dealing with a new cancer diagnosis, treatment options, disease and treatment-related complications/toxicities. Providing supportive non-judgemental conversations is critical, and pharmacists, using the Make Every Contact Count Framework, specifically Brief Advice and Brief Interventions, are well placed to support patients with cancer on their journey to smoking cessation. Patients are seeking support to quit. Seizing the teachable moment, hospital pharmacists can support the early dispensing of NRT products to patients admitted to smoke-free campus hospitals, as part of either a smoking management approach or a start of smoking cessation Community pharmacists can assist in several ways. Brief advice from pharmacists takes 30 seconds and can double the chance of someone stopping smoking successfully (3 A’s Model - Ask, Advise and Act). Asking about smoking behaviour sets the stage
for support. People who smoke expect to be asked about tobacco use and are surprised when this is not raised with them. Advise people who smoke about the harm it causes and the benefits of quitting. For people with cancer, these harms and benefits are often overlooked. Finally, act by providing or arranging safe, effective, and clinically sound support to stop smoking. If the person with cancer is accompanied by a family member who also smokes, consider extending your advice, as a smoke free home is supportive to smoking cessation. The best chance of successfully stopping smoking is through using behavioural support and stop smoking medicines. Behaviour support is available free of charge across the country through HSE services where patients can be referred (you can find a service near to you here: https://www2.hse.ie/living-well/ quit-smoking/support-services/). Varenicline and combination NRT is recommended in National Stop Smoking Guidelines as the best first-line option where suitable and available. Combination NRT is also a good option, using a long-acting patch and a short acting product like a spray, inhaler lozenge or gum. Pharmacists are well positioned to offer support with over-thecounter medicines and will be able to advise and encourage patients, especially those with cancer who may be on other medicines for comorbidities, on the best options. HSE QUIT services are available on QUIT.ie, Freetext QUIT to 50100, and Freephone 1800201203.
Pharmacists with Healthlink can make a referral using that system, or else a referral can be made by emailing quit@healthmail.ie, which is a safe and secure way to share information. An easy to use onepage resource has been developed by HSE QUIT for pharmacists: https://www.hse.ie/eng/about/who/ tobaccocontrol/national-clinicalguidelines/supporting-peopleto-stop-smoking-advice-forpharmacists.pdf
For further information or to see a list of published outputs please contact Patricia.Fitzpatrick@ucd.ie
References available on request
PHARMACYNEWSIRELAND.COM 14 Pharmacy
Professor Patricia Fitzpatrick
Professor Patricia Fitzpatrick1,2, Dr Paul Kavanagh3, Associate Professor Kate Frazer4, Dr Patricia Fox4, Professor Sinead Brennan5, Dr Ailsa Lyons2, Dr Nancy Bhardwaj1, on behalf of the Research Team
1School of Public Health, Physiotherapy & Sports Science, University College Dublin 2St Vincent’s University Hospital, Dublin 3Health Service Executive Tobacco Free Ireland Programme 4School of Nursing, Midwifery & Health Systems, University College Dublin 5St Luke’s Hospital, Rathgar, Dublin
Quitting is an uphill battle… …support your patients on their quitting journey with Nicotinell


Scan to learn more about Haleon and our brands
Product Information
Please consult the Summary of Product Characteristics for full product information. Nicotinell TTS 10, 7 mg/24 hour Transdermal Patch, Nicotinell TTS 20, 14 mg/24 hour Transdermal Patch, Nicotinell TTS 30, 21 mg/24 hour Transdermal Patch (Nicotine). Indications: Treatment of nicotine dependence, as an aid to smoking cessation. Dosage and administration: Stop smoking completely when starting treatment. For those smoking 20 or more cigarettes a day Nicotinell TTS30 (Step 1) once daily. Those smoking less should start with Nicotinell TTS20 (Step 2) once daily. Different strength patches permit a stepwise reduction in nicotine dose over treatment periods of 3-4 weeks with each strength patch. Maximum recommended treatment period three months (but if abstinence not achieved after three-month period, further treatment may be recommended following a reevaluation of the patient’s motivation by a clinician). Children and young adults: To be used in people under 18 years only on medical advice. Not recommended in children under 12 years. Contra-indications: Known hypersensitivity to nicotine or any of the excipients. Precautions: Use with caution in patients with: cardiovascular disease, history of seizure or those taking anti-convulsant therapy, diabetes mellitus, severe renal and/or hepatic impairment, active oesophagitis, oral and pharyngeal inflammation, gastritis, gastric/ peptic ulcer. Discontinue use if a severe or persistent skin reaction occurs. Nicotinell TTS contains aluminium and should be removed prior to undergoing defibrillation, MRI or cardioversion procedures. Always keep out of the reach and sight of children due to potential poisoning risk. Side effects: See SPC for full details. Certain symptoms such as depression, irritability, nervousness, restlessness, mood lability, anxiety, drowsiness, impaired concentration, and insomnia may be related to withdrawal symptoms associated with smoking cessation. Quitting smoking by any means can lead to asthenia, headache, dizziness, coughing or influenza-like illness. Very common: insomnia, abnormal dreams, nausea, vomiting, application site reactions. Common: agitation, anxiety, nervousness, tremor, palpitations, cough, pharyngitis, dyspnoea, abdominal pain, upper dyspepsia, diarrhoea, dry mouth, constipation, increased sweating, myalgia, application site pain, asthenia, fatigue. Uncommon: hypersensitivity, disturbance in attention, somnolence, affect lability, irritability, depressed mood and confusional state, paraesthesia, dysgeusia, blurred vision, tachycardia, flatulence, hyperhidrosis, arthralgia, malaise, influenza type illness, asthenic conditions, pain and discomfort. Rare: dyspnoea, arrhythmia. Very Rare: anaphylactic reactions, allergic dermatitis, contact dermatitis, photosensitivity. Frequency not known: allergic reactions such as urticaria, rash and pruritus; angioedema and anaphylactoid reaction. PA Number: PA 678/123/001 – 002 – 003. Supply
classification: Supply through general sale. PA holder: Haleon Ireland Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. Further information is available on request. Date of preparation: April 2023.







Contains nicotine. Stop smoking aid. Requires willpower. Always read the label/leaflet. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-NICOT-23-00003

Smoking cessation in 2023
 Written by
Dr Ailsa Lyons, BN, MSc, PhD Head of Preventive Medicine and Health Promotion, St Vincent’s University Hospital, Dublin
Written by
Dr Ailsa Lyons, BN, MSc, PhD Head of Preventive Medicine and Health Promotion, St Vincent’s University Hospital, Dublin


Prof
Patricia
Fitzpatrick,
MD, MPH, FRCPI, FFPHMI
Consultant in Preventative Medicine, St Vincent’s University Hospital, Dublin
Full Professor of Epidemiology and Biomedical Statistics, and Head of Subject for Public Health, University College Dublin
€171m for hospital inpatient admissions, €13m for hospital day case appointments, €15m for hospital outpatient appointments, €10m for hospital Emergency Department attendances and €256m for Primary Care services. Reducing the prevalence of smoking will have a direct positive result on Irish health services.
The Department of Health published the first National Stop Smoking Clinical Guidelines (National Clinical Guidelines No 28) in 2022, following a critical review of the available evidence. These guidelines advise that unsupported quit attempts are less successful than supported quit attempts and recommend the most effective treatment is a combination of stop smoking medications and behavioural support. Behavioural support, either alone or in combination with pharmacological supports, increases the chances of successful quitting and should be recommended to all smokers. Behavioural support can include the initial brief intervention undertaken by a health professional followed by individual or group counselling, telephone support, text messaging support and internet-based support, depending on patient preference. More intensive interventions (e.g. individual or group counselling) are more effective than less intensive (e.g. brief intervention alone) in helping smokers to make a lasting quit.
aerosol the user inhales. Most adults who vape usually either use tobacco simultaneously or are ex-smokers. Smoking tobacco is indisputably harmful to health and is extremely dangerous. Vaping delivers nicotine without many of the toxins in tobacco. Compared to tobacco, vaping may be less harmful, but that does not mean that vaping is harm-free. There is still insufficient evidence about the long-term health impact of vaping and for this reason it is not recommended as a smoking cessation aid. Vaping is banned in all HSE hospitals and buildings. All national stop smoking services in hospitals and the community offer free support and advice to help with nicotine withdrawal, whether a tobacco user or vaper.
Patients worry about the cost of medications. Nicotine Replacement Therapy (NRT) is free under the GMS card and in hospitals and more recently is provided free of charge in community stop smoking clinics, therefore cost should no longer be a deterrent to patients being helped to stop smoking.
Smoking is the leading cause of preventable illness and disease throughout the world; Ireland is no different with tobacco use the leading cause of preventable premature illness and death in Ireland, where almost 6,000 smokers die each year from tobacco related diseases. Smoking related deaths are mainly due to cancers, respiratory and heart disease. Smoking prevalence is Ireland is currently 18% which accounts for both daily smokers (14%) and occasional smokers (4%). There is no safe level of smoking.
The burden of smoking on the Irish health service is substantial. An 2020 Irish study estimated the burden of smoking and secondhand smoke related hospitalisations using smoking prevalence data, hospitalisation data and hospital base cost data from the years 2011 to 2016. The study showed that the number of hospitalisations due to smoking and secondhand smoke exposure increased yearly from 2011 to 2016 in publicly funded hospitals with an approximate total direct cost of €171.5 million and made up 309,117 bed-days. A further 2016 report has estimated the cost of tobacco use to the Irish health service to be
Brief interventions are a range of effective behaviour change interventions that are clientcentred, short in duration and used in a variety of settings by health professionals. There is a national HSE training programme, Making Every Contact Count (MECC), which includes a module on tobacco, available to upskill health professionals in the delivery of effective brief interventions. There is online followed by in-person practical training both of which can be accessed through HSELand: https://www.hseland.ie/dash/Account/Login.
Individual and group counselling offers more intensive support, is free, evidence-based and is available in many hospitals and community settings across the country, with services close to every patient. These can be searched here: https://www2.hse.ie/living-well/quit-smoking/ support-services/. Telephone and internet stop smoking support services are delivered by the national Quit service https://www2.hse.ie/ living-well/quit-smoking/contact/.
Electronic cigarettes, or vapes, are batterypowered devices that heat nicotine mixed with flavourings and other chemicals to create an
To assist patients admitted to smoke-free hospitals there are a number of key steps that can be taken. Stop before the Op is an initiative with surgeons to assist smokers to stop smoking in advance of surgery. While the ideal time to stop smoking pre-operatively is 4-8 weeks before surgery, there are still better outcomes for those patients who stop at any point pre-operatively, compared with those that continue to smoke. It is important that emergency departments and hospital wards can provide NRT quickly to patients to manage their smoking while in hospital, given that all hospitals now have smoke-free campuses. Hospital pharmacists are key to the supply and provision of all recommended products in the new Clinical Guidelines for Smoking Cessation, including NRT, varenicline and bupropion. Community pharmacists are ideally located to deliver brief intervention for tobacco use, advise on over-the-counter stop smoking medications, encourage patients in their quit attempt and encourage them to access, or make a referral for them, to more intensive stop smoking services. HSE QUIT provides information for pharmacists at the following link: https://www.hse.ie/eng/about/who/ tobaccocontrol/national-clinical-guidelines/ supporting-people-to-stop-smoking-advice-forpharmacists.pdf
References available on request
16 | PHARMACYNEWSIRELAND.COM
Dr Ailsa Lyons
Prof Patricia Fitzpatrick




QUIT FOR GOOD WITH NICORETTE IRELAND’S NO.1 BRAND TO QUIT SMOKING * Source: IMS Sales Values & Units MAT December 2022. For verification please contact 1800 22 00 44. NICORETTE® contains Nicotine. ALWAYS READ THE LABEL. NICORETTE® is a stop smoking aid. IE-NI-2300049
Is it Dandruff? A Guide for Pharmacy
Patients approach pharmacists with a host of questions about relatively minor health conditions, and many involve the skin. Dermatologic questions concern allergic dermatitis, dry skin, minor wounds, and numerous other problems.
have lesions on the head, such as the scalp and its margins; on the eyebrows, eyelids, lips, side creases of the nose, nasolabial fold, and forehead; in the inner ear canal; behind the ears; and in the mustache/beard area.
Treatment
Seborrhoeic dermatitis in adults may be very persistent. However, it can generally be kept under control with regular use of antifungal agents and intermittent applications of topical steroids.
Scalp
• Medicated shampoos containing ketoconazole, ciclopirox, selenium sulfide, zinc pyrithione, coal tar, and salicylic acid, used twice weekly for at least a month and if necessary, indefinitely.
• Ketoconazole should be preferred first-choice treatment.
Dandruff and seborrheic dermatitis (SD) are two closely related dermatologic conditions that may be successfully self-treated. However, pharmacists should be aware of the various means by which both are recognised and the possible interventions.

Dandruff
Dandruff is a common condition that affects up to 50% of the population.
Age and sex influence the occurrence of dandruff. Most patients begin to notice dandruff during puberty. Dandruff may continue through middle age and then abate, but some patients will deal with it for their entire lives.
Excess skin oil (sebum) is an underlying contributor to dandruff epidemiology, as illustrated by its preference for males, postpubertal age, and poor hygiene. It is more common in male patients due partly to the influence of androgens but also to the fact that males have larger sebaceous glands on the scalp, especially after puberty.
Their larger glands produce more oil than those of an age-matched set of females. Further, during the onset of puberty, the skin’s sebaceous glands mature into multilobulated configurations, allowing them to produce a heightened amount of sebum, which also leads to acne. Finally, patients who do not bathe or shampoo daily experience an
accumulation of oil on the skin and scalp.
An improper diet may contribute to dandruff, especially if it is low in zinc, B vitamins, or specific types of fats. Dandruff also appears to be more common in patients with compromised immune status or Parkinson’s disease and in those recovering from stress-related situations such as a recent heart attack or stroke.
The hallmark sign of dandruff is excess flaking of the scalp. Normal stratum corneum constantly sheds its upper layer, but the shed skin cells are normally not noticed.
Why is dandruff different?
Dandruff cells have developed an abnormal cohesion, so much so that the resulting scales are visible and unsightly. They are usually white with an oily consistency due to the sebum. Many patients experience scalp itching, perhaps due to irritation from fungal growth residues. Occasionally, the scalp may appear erythematous.
Patients may choose from a wide array of therapeutic shampoos for dandruff.
These products contain zinc pyrithione, selenium sulfide, salicylic acid, coal tar, or keto-conazole.
Seborrheic Dermatitis
SD is a chronic condition marked by remissions and exacerbations. At the present time, no cure is
known. Males are more likely to experience SD. It is more common after puberty, although infants may experience a variant of SD known as cradle cap. SD generally becomes less common as people age, although many experience exacerbations throughout life.
Patients with certain central nervous system disorders may experience increased accumulation of sebum, predisposing them to SD. This includes conditions limiting patient mobility, such as stroke, Parkinson’s disease, head injury, cranial nerve palsies, and major truncal paralyses.
There is an inherited tendency to experience SD, so those with a close relative with SD are at greater risk.
Further, individuals with oily skin, acne, or obesity appear to be predisposed to SD.Those who are stressed or fatigued are at higher risk. Persons who do not bathe or shampoo frequently experience higher rates of SD. Patients who engage in outdoor activities during the summer may find that the condition improves.
SD produces skin scales that are yellowish in colour, oily in consistency, and tend to adhere to the skin. The affected areas of skin are erythematous and pruritic. Plaques may cover large areas of the body, although they are more often found where sebaceous glands are most heavily concentrated. Many patients
• Steroid scalp applications reduce itching, and should be applied daily for a few days every so often.
• Tar cream can be applied to scaling areas and removed several hours later by shampooing.
Advice for Sufferers
• Cleanse the affected skin thoroughly once or twice each day using a non-soap cleanser.
• Apply ketoconazole or ciclopirox cream once daily for 2 to 4 weeks, repeated as necessary.
• 1% Hydrocortisone cream or ointments can also be used, applied up to twice daily for 1 or 2 weeks. Occasionally a more potent topical steroid may be prescribed.
• Topical calcineurin inhibitors such as pimecrolimus cream or tacrolimus ointment may also be useful.
• Severe cases may receive a course of oral antifungal medication or sometimes, ultraviolet radiation.
Cradle cap is a relatively innocuous condition in which a baby’s scalp is covered with thick, crusted, yellow to brown scales. It usually disappears by 1 to 3 years of age. It may be pruritic, causing the baby to scratch the area. Scratching leads to inflammation or infection in some cases. Cradle cap is defined by some authorities as a type of dandruff.
PHARMACYNEWSIRELAND.COM 18 Hair Conditions
ALREADY TRIED EVERYTHING?

1. Peter R.U. & Richarz-Barthauer U. British Journal of Dermatology 1995; 132: 441-445.


ABBREVIATED PRESCRIBING INFORMATION. Nizoral Dandruff 20mg/g Shampoo. Each gram of shampoo contains 20mg of ketoconazole. Presentation: Pink, viscous shampoo. Indications: In the prevention and treatment of infections in which Malassezia (previously called Pityrosporum) infection may be a factor, such as seborrhoea capitis, and seborrhoeic dermatitis of the body. Dosage: Nizoral Dandruff Shampoo is for use in adults and adolescents aged 12 years and over. Seborrhoea capitis: Apply the shampoo to the affected scalp, leave for three minutes, then rinse. Seborrhoeic dermatitis: Wash the affected areas with shampoo and leave for 3 to 5 minutes before rinsing. Treatment should be repeated twice weekly for 2 to 4 weeks. For prophylaxis use once, every 1 to 2 weeks. Method of administration Cutaneous. Usually, a palmful of shampoo suffices for one wash. Contraindications: Use in patients hypersensitive to any of the ingredients. Warnings and precautions: In patients who have been on prolonged treatment with topical corticosteroids, it is recommended that the steroid therapy be gradually withdrawn over a period of 2 to 3 weeks, while using Nizoral Dandruff Shampoo, to prevent any potential rebound effect. Avoid contact with the eyes. If the shampoo should get into the eyes, they should be bathed with water. Interactions: No interaction studies have been performed. Fertility, pregnancy and lactation: There are no known risks associated with the use of Nizoral Shampoo 2% in pregnancy or lactation. Undesirable effects: Dysgeusia, Folliculitis, Eye irritation, Increased lacrimation, Acne, Alopecia, Dermatitis contact, Dry skin, Hair texture abnormal, Rash, Skin burning sensation, Skin disorder, Skin exfoliation, Angioedema, Urticaria, Hair colour changes, Application site erythema, Application site irritation, Application site hypersensitivity, Application site pruritus, Application site pustules, Application site reaction, Hypersensitivity. Refer


to
of Product Characteristics for other adverse effects. Adverse reactions should be reported via HPRA Pharmacovigilance, website: www.hpra.ie. Pack size: bottle containing 60 ml, 100 ml or 120 ml Nizoral Dandruff Shampoo. Not all pack sizes may be marketed. A copy of the Summary of Product Characteristics is available upon request or go to www.clonmelhealthcare.ie. Marketing authorisation holder: Clonmel Healthcare Ltd. Waterford Road, Clonmel, Co. Tipperary. Marketing authorisation number: PA126/315/1. Supply through pharmacies only. Date last revised: January 2023. Nizoral Anti-Dandruff Daily Prevent Shampoo gives ongoing relief for dry, itchy and flaky scalps (cosmetic product). Nizoral Care Scalp Tonic provides protection from itchy and irritated scalp (cosmetic product). Always read the label. 2022/ADV/NIZ/314H. ITCHDAILYRELIEF Nizoral® – Your effective scalp care combination. ON THE GO PROTECTION FROM ITCHY SCALP Fights the cause of dandruff for up to 3 months1 Calms itchy and flaky scalps from the first wash
Summary
Travel Health Considerations for Individuals with Heart DiseaseAdvice for Pharmacists
 Written by Gerard Flaherty, MD, PhD, FRCPI, FFTM, FISTM
Professor of Travel Medicine and International Health, NUI Galway
Written by Gerard Flaherty, MD, PhD, FRCPI, FFTM, FISTM
Professor of Travel Medicine and International Health, NUI Galway
 President-elect International Society of Travel Medicine
Past President Travel Medicine Society of Ireland
President-elect International Society of Travel Medicine
Past President Travel Medicine Society of Ireland
Travel with cardiovascular disease
Community pharmacists are increasingly engaged in the provision of travel health services to their clients. The role of travel pharmacists is particularly well developed in Canada, for example. The International Society of Travel Medicine (ISTM) has an active Pharmacist Professional Group who contribute to research and education in this dynamic field.1 While travel is associated
with well known psychological and physical stressors which may challenge patients with cardiovascular disease (CVD), a previous qualitative study we carried out did not identify significant barriers to international travel in this patient cohort.2 We do not have a clear understanding of the travel patterns and behaviour of travellers with CVD and we cannot be certain of the extent to which heart disease patients attend for pre-travel health counselling and vaccination. We found that 12.8% of travellers attending a specialist travel health clinic in Ireland had a history of CVD or its risk factors, predominantly arterial hypertension.3 As travel medicine practitioners we tend to focus on the health risks of travel, but it is important to recognise that travel also confers mental health benefits and may be an important coping mechanism and ‘release valve’ for a patient living with a chronic illness such as CVD. The Danish author, Hans Christian Andersen, reminds us that “to travel is to live” after all! Patients with CVD have been very careful to reduce their risk of contracting COVID-19 during periods of high community transmission of SARSCoV-2 over the past two years and many will now feel confident again in undertaking international travel, especially if they have received booster doses of a COVID vaccine. There will inevitably be a period of what I have termed ‘Reiseangst’ before travel feels comfortable and routine again.4 These days we are all much more aware of course of how to minimise our carbon footprint and travel responsibly.
This short article will consider some of the more salient points for pharmacists to consider when advising international travellers with heart disease. The reader is referred to standard travel medicine textbooks such as Keystone’s Travel Medicine, the World Health Organization’s travel health information website (https://www.who.int/ travel-advice), or the CDC website https:// wwwnc.cdc.gov/travel) for more information than this overview can provide.
Travel health risks
CVD is the leading cause of death in older international travellers, which of course mirrors the epidemiological situation within most domestic borders. Some people travel overseas to receive medical care more promptly or cost effectively and there are multiple centres of excellence in elective coronary artery bypass surgery tourism around the world, especially in South East Asia. Skiing holidays are popular with older travellers and there have been many well-documented cases of acute coronary syndromes occurring on the slopes, likely the result of a combination of unaccustomed exertion and cold air with its resulting sympathetic activation and surges in blood pressure sufficient to disrupt a vulnerable atherosclerotic plaque. Fitness to fly assessments sometimes arise for travellers with chronic heart failure or following a recent cardiac episode or intervention, but these are beyond the scope of this brief overview of the subject. CVD patients
20 | PHARMACYNEWSIRELAND.COM








Clearing ...to a brighter day Contraindications: Hypersensitivity to the active ingredient, any of the excipients, hydroxyzine or to any piperazine derivatives. Patients with severe renal impairment at less than 10ml/minute creatinine clearance. Medicinal product not subject to medical prescription. A copy of the summary of product characteristics is available upon request. PA 126/267/1-2. PA Holder: Clonmel Healthcare, Waterford Road, Clonmel, Co. Tipperary. Date prepared: February 2022. 2022/ADV/ANT/048H CETIRIZINE DIHYDROCHLORIDE
relief of symptoms of hay fever and other allergic conditions, skin rashes or itchy, watery eyes.
For
with implanted cardiac devices such as pacemakers or cardioverter-defibrillators should be advised to declare the presence of these devices at airport screening stations and carry a manufacturer’s card at all times while abroad.5 Some cardiac medications can give rise to issues during travel, including diuretics in heart failure or hypertension, and anticoagulants in adventure travellers.6
Medications and travel
I advise travellers to obtain a copy of their prescription from their pharmacist and to request double the normal quantities of their regular medications, which should all be carried in hand luggage and ideally split between two bags. All medications should be carried in their original pharmacy-labelled containers or blister packs. Medications should generally be taken at the destination local time to avoid confusion. Specific time zone-related drug adjustment advice is needed for the diabetic traveller who requires insulin. For long-term or expatriate travellers, contact should be made prior to travel with a local English-speaking physician or pharmacist to ensure that an equivalent drug is available in the host jurisdiction. The ISTM global travel clinic directory (https://www.istm. org/AF_CstmClinicDirectory.asp) and the International Association for Medical Assistance to Travellers (https://www.iamat. org/) are excellent resources to recommend to your clients. Some medications will degrade with exposure to sunlight so all drugs should be stored in a cool, dry place. With disruption of the normal daily routine, patient medication adherence may suffer, and the traveller should use day-labelled blister packs to ensure compliance.
Use of warfarin for anticoagulation during longer trips will require access to a reliable INR monitoring clinic or calibrated pointof-care device. Where the INR is unstable prior to prolonged travel, it may be possible for the traveller’s physician to convert the patient to a direct oral anticoagulant to avoid the need for monitoring.7 Anticoagulated patients should be careful not to significantly increase the amount of dietary vitamin K they consume to avoid the risk of developing a sub-therapeutic INR abroad. While transportation of non-psychotropic, non-controlled medications is not likely to present difficulties for the heart disease patient, pharmacists should always remind their travelling clients to check individual country-specific requirements.8
Medical care overseas
Obtaining safe medical care overseas is a perennial concern for travellers with chronic illness. Here, the pharmacist should advise against relying on the availability of medications locally in developing country destinations, given the high rate of counterfeit drugs in circulation. These may have been formulated to appear identical to active agents but be, at the very least, inert and at worst, unsafe. I advise all travellers to carry a comprehensive travel health kit and pharmacists are well positioned to provide the contents of these kits and to
customise them to the needs of individual travellers. They will typically include items such as analgesics, antihistamines, steroid creams, anti-diarrhoeal agents, electrolyte replacement powder sachets, anti-emetics, plasters, bandages, hand sanitiser, a DEET-containing insect repellent, and antiseptics. Do not forget to recommend a high-SPF sun cream for travel to destinations with a high ultraviolet index. Most CVD patients will also be advised to purchase graduated compression stockings at their local pharmacy where their calves can be measured accurately by the pharmacy staff.
Pre-travel health advice
Pharmacists should be familiar with the most important travel-related infectious risks and their geographical distribution and be willing to provide or reinforce key pre-travel health advice regarding food and water consumption, insect bite avoidance, sexual health, and animal bite prevention. Where a traveller is attempting a trek to high altitude, the pharmacist should have a working knowledge of basic high altitude illness prevention advice. No trekker should leave home without a good supply of blister plasters from their local pharmacy. In cases where a traveller has a known drug allergy or is taking drugs such as insulin or corticosteroids, MedicAlert bracelets should be recommended. I am always alarmed at how few of my patients with diabetes ever wore these bracelets. I have never seen a pharmacy that did not stock them.
Travel vaccinations
Some pharmacists will provide pre-travel vaccinations and will be familiar with the precautions to observe when administering vaccine doses intramuscularly in patients taking anticoagulants. My advice around travel vaccines is to follow a personalised approach. Not all vaccines are recommended for all travellers. The choice of vaccines will depend on a detailed travel risk assessment, which takes into account multiple risk factors relating to both traveller and travel itinerary. Apart from the usual routine and recommended vaccines, some travellers to sub-Saharan Africa and parts of South America will be recommended or required to present evidence of yellow fever vaccination. The travel medicine provider will need to be very familiar with the cautions and contraindications that apply to the use of this live attenuated vaccine, especially in older patients. I additionally consider influenza, pneumococcal and hepatitis B vaccines for all travellers with CVD.
Prophylactic medication
For travel to some malaria endemic regions, malaria chemoprophylaxis or possibly emergency self-treatment of malaria may be indicated. The pharmacist will be expert on drug-drug interactions9 and be keenly aware of the importance of avoiding mefloquine in patients with cardiac conduction disturbances, preferring to use atovaquone-proguanil or doxycycline for prevention of falciparum malaria instead. A prescription for an antibiotic to self-treat
moderate to severe travellers’ diarrhoea is common practice in travel medicine, but azithromycin may not be the optimal choice in a traveller with CVD given the association with Q-T prolongation and ventricular tachyarrhythmias and we need to be attentive to the risk of promoting antimicrobial resistance through injudicious use of antibiotics. Chemoprophylaxis of acute mountain sickness is sometimes appropriate if the rate of ascent and maximum altitude warrant it, but the carbonic anhydrase inhibitor acetazolamide must be used with caution, given the risk of causing hypokalaemia. I tend to avoid it if the patient is taking digoxin, for example, and I do not prescribe it if the patient is taking a high dose of aspirin, because of the potential for causing more severe metabolic acidosis.
The ill returned traveller
Our travellers may return unwell and their first port of call may be their community pharmacist or general practitioner. However, a travel history is often not volunteered,10 so pharmacists should be alert to this and routinely ask about travel, especially where the patient presents with fever (malaria?), fever, a rash and arthralgia (dengue, Zika or chikungunya?), persistent abdominal symptoms (intestinal parasite or post-infectious irritable bowel syndrome?). Please also remind your traveller with CVD to bring rapid antigen tests with them for use during their travel and to be mindful of the potential for developing COVID symptoms in the first week of return from abroad. I still perform daily rapid antigen tests on myself for 5 days after returning from travel abroad, even if there is no official public health advice to do so.
Travel insurance
Finally, I believe that all healthcare professionals who encounter departing international travellers should remind them to obtain suitable travel health insurance which includes repatriation coverage and, in the case of the traveller with CVD, to declare all pre-existing medical conditions. Unfortunately, too many of our patients opt not to purchase travel insurance, although the COVID pandemic has highlighted the importance of being adequately insured during travel.
Further educational opportunities
For pharmacists who wish to become more deeply engaged in travel health services or who wish to deepen their knowledge of this fascinating area of practice, I strongly recommend you to consider becoming a member of the Travel Medicine Society of Ireland, the British Global and Travel Health Association or the International Society of Travel Medicine. I am happy to receive enquiries from any pharmacists who wish to collaborate in travel medicine research projects.
References available on request
22 | PHARMACYNEWSIRELAND.COM
Mosquito & Tick Protection For the whole family
Mosquito & Tick Protection For the whole family

NEW DEET FREE VERSION
NEW DEET FREE VERSION
Suitable for children over 3 months old
Suitable for children over 3 months old
30% Naturally Sourced Citriodiol
30% Naturally Sourced Citriodiol
Scan to learn more about our full Insect Repellent range and new Counter Display special offer.
Scan to learn more about our full Insect Repellent range and new Counter Display special offer.

Mosquitoes: 4-6 hours
Ticks: 4-6 hours
Mosquitoes: 4-6 hours
Ticks: 4-6 hours
Freephone: 1800 307777
Freephone: 1800 307777
Common GI Presentations to Pharmacy
Professor Gerard Clarke,

Dyspepsia
What is dyspepsia?
The term dyspepsia refers to a complex of symptoms arising from the upper gastrointestinal tract (GIT) presenting as epigastric pain or discomfort. It is a common condition affecting 20-40% of the world’s population at some point in their lives.1 Affected individuals may complain of postprandial fullness, early satiety, bloating, belching or nausea.2, 3 Dyspepsia has an extensive differential diagnosis. It may occur secondary to organic causes such as Helicobacter pylori infection, peptic ulcer disease (rarely), gastrointestinal malignancies, gastroesophageal reflux disease or may be medication induced. However, up to 80% of patients with dyspepsia will have no explanation for their symptoms at endoscopy; known as functional or idiopathic dyspepsia. The global prevalence of functional dyspepsia is estimated between 5 and 11%.4
What causes it?
While the pathophysiology of functional dyspepsia is not well understood, several mechanisms have been suggested. Disturbances in gastrointestinal motility, impaired gastric accommodation, increased visceral sensitivity, abnormal gut-brain axis and gut microbiota dysbiosis have all been linked to the occurrence of functional dyspepsia. The latter hypothesis is supported by research demonstrating an increased likelihood of dyspepsia following infective gastroenteritis.5-7
Role of pharmacist
Community pharmacists often provide the first line of care for patients with dyspeptic symptoms. According to NICE guidelines,
pharmacists should offer initial and ongoing help to patients presenting with symptoms of dyspepsia. Advice should encompass lifestyle modifications, use of over-the-counter (OTC) medications and highlight when it is appropriate to consult their general practitioner (GP).8 With this in mind, pharmacists should regularly remind themselves of red flag symptoms which should prompt urgent referral to the GP:
- Unintentional weight loss
- Anorexia
- Dyshagia or odynophagia
- Age 55 or over with new onset dyspepsia

- Epigastric mass
Management
1. Non-pharmacological management
Simple lifestyle measures for dyspeptic symptoms include weight loss if appropriate, eating smaller meals, cutting down on caffeine and high fat foods, avoiding late meals, raising the bedhead and adhering to alcohol consumption guidelines. This may also provide an opportunistic consultation for smoking cessation which may also improve symptoms. It may also be appropriate to carry out a medication review to identify any medications that might be causing or worsening symptoms, with one of the most common offenders being nonsteroidal anti-inflammatory (NSAIDs) but can also be caused by corticosteroids, bisphosphonates or iron supplements amongst others.1 However, evidence supporting the use of lifestyle and dietary modifications for symptomatic relief is lacking meaning medical therapy is the mainstay of treatment.2
2. Medication management available OTC
A short interview with the patient can identify the most appropriate course of action. Pharmacists should ask the patient to describe their symptoms in terms of the nature, frequency and severity along with careful screening for the presence of red flag symptoms as mentioned previously. Proton pump inhibitors (PPIs) omeprazole and esomeprazole are available OTC. PPIs inhibit gastric H,K-ATPase thereby inhibiting gastric acid secretion. Due to their short half-life, it takes about 48-72 hours to reach steady state inhibition of acid secretion.9 Alternatively, H2receptor antagonists such as famotidine are also available OTC. This class decreases gastric acid secretion by reversibly binding to histamine H2 receptors on gastric parietal cells thereby reducing acid release. They have a quick onset of action of approximately 60 minutes and provide relief for 4-10 hours.10 However, while these medications can provide relief of symptoms, their OTC indication is for short term use only. Patients who are regularly purchasing these medications s hould be advised to attend their GP for further investigation.
Gastro-oesophageal reflux disease
What is Gastro-oesophageal reflux disease?
Gastro-oesophageal reflux disease (GORD) is a condition that develops when reflux of stomach contents into the oesophagus causes symptoms and/or complications.11, 12
Symptoms
GORD classically presents as heartburn and regurgitation. Heartburn or pyrosis is generally described as retrosternal burning postprandially while regurgitation the upward movement of gastric contents into the mouth or hypopharynx.13 Other symptoms may include chest pain, a feeling of fullness in the throat, hoarseness or a chronic cough.14
What causes it?
The pathophysiology underlying the development of GORD is multifactorial, comprising both physiological and pathological factors. Transient lower oesophageal sphincter (LOS) relaxations, reduced LOS pressure, hiatal hernias, impaired oesophageal acid clearance and delayed gastric emptying are other factors identified in the literature.14, 15 Obesity is a known risk factor for GORD, potentially due to increased intragastric pressure.16, 17 Cigarette smoking is also a risk factor; it reduces pressure across the LOS and increases the time taken to clear acid from the oesophagus.18 Despite an association between certain foods and GORD, evidence linking specific foods with GORD is lacking. Common triggers however, may include fatty foods, spicy foods, coffee, alcohol and fizzy drinks.19-22
How is it treated?
Similar to dyspepsia, the presence of ALARM or red flag symptoms should prompt urgent referral to the GP to rule out possible underlying malignancy.
24 | PHARMACYNEWSIRELAND.COM
Professor Gerard Clarke
Written by
Consultant Gastroenterologist, Portiuncula Hospital and Adjunct Associate Clinical Professor of Medicine, University of Limerick GEMS and Ashley Costello, BPharm, MPharm, Graduate Entry Medical School, University of Limerick
Ashley Costello
Cetrine Allergy 10mg Film-Coated Tablets available in packs of 7s and 30s. Always read the leaflet.


ABBREVIATED PRESCRIBING INFORMATION
Product Name: Cetrine Allergy 10mg lm-coated tablets & 1 mg/ml oral solution. Composition(s): Each tablet contains 10 mg cetirizine dihydrochloride. One ml of the oral solution contains 1 mg cetirizine dihydrochloride. Description(s): White, oblong lm-coated tablets, scored on one side. Can be divided into equal halves. Clear, colourless liquid with banana avour.
Indication(s): Tablets: Adults and paediatric patients 6 years and above. Oral solution: Adults and children 2 years and above. Relief of nasal and ocular symptoms of seasonal and perennial allergic rhinitis (hay fever); relief of symptoms of chronic idiopathic urticaria.

Dosage: Tablets: Adults, elderly and children aged 12 years and over: 10 mg once daily. Children from 6 years to 12 years: 5 mg (half a tablet) twice daily. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. Children under 6 years: Not recommended. Oral solution: Children aged from 2 to 6 years: 2.5 mg twice daily (2.5 ml oral solution twice daily (half a measuring spoon twice daily)). Children aged from 6 to 12 years: 5 mg twice daily (5 ml oral solution (a full measuring spoon twice daily)). Adults and adolescents over 12 years of age: 10 mg once daily (10 ml oral solution (2 full measuring spoons)). Not recommended in children aged less than 2 years. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. In paediatric patients su ering from renal impairment: Adjust dose on an individual basis taking into account the renal clearance of the patient, his age and his body weight. Contraindications: History of hypersensitivity to the active substance, to any of the excipients, piperazine derivatives or hydroxyzine. Severe renal impairment < 10 ml/min creatinine clearance.
Warnings and Precautions for Use: Cetirizine may increase risk of urinary retention, therefore caution in patients with predisposition factors of urinary retention (e.g. spinal cord lesion, prostatic hyperplasia). Caution in epileptic patients and patients at risk of convulsions. Discontinue use of cetirizine three days before allergy testing. Pruritis and/or urticaria may occur when cetirizine is stopped, even if the symptoms were not present before treatment initiation. In some cases, the symptoms may be intense and may require treatment to be restarted. The symptoms should resolve when the treatment is restarted. Tablets contain lactose. Oral solution contains sorbitol, propylene glycol, sodium (essentially ‘sodium free’), methyl - & propyl-parahydroxybenzoate.
Interactions: Caution is advised when taken concomitantly with alcohol or other CNS depressants. Cetirizine does not potentiate the e ect of alcohol (0.5 g/l blood levels). The extent of absorption of cetirizine is not reduced with food, although the rate of absorption is decreased.

Pregnancy and Lactation: Caution during pregnancy and breast-feeding.
Ability to Drive and Use Machinery: Usually non-sedative, patients should take their response to the product into account. In sensitive patients, concurrent use with alcohol or other CNS depressants may cause additional reductions in alertness and impairment of performance.
Undesirable E ects: Cetirizine at the recommended dosage has minor adverse e ects on the CNS, including somnolence, fatigue, dizziness and headache. In some cases, paradoxical CNS stimulation has been reported. Although cetirizine is a selective antagonist of peripheral H1-receptors and is relatively free of anticholinergic activity, isolated cases of micturition di culty, eye accommodation disorders and dry mouth have been reported. Instances of abnormal hepatic function with elevated hepatic enzymes accompanied by elevated bilirubin have been reported which resolves on discontinuation of the drug. Uncommon: Agitation, diarrhoea, pruritus, rash, asthenia, malaise, paraesthesia. See SPC for all adverse reactions.
Marketing Authorisation Holder: Rowex Ltd, Bantry, Co. Cork.
Marketing Authorisation Number: PA0711/075/002-003. Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417
E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription.
Date of Preparation: March 2021
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie

Date of preparation: (04-22) CCF: 24955 Supply status: Supply through pharmacies only.
FAST RELIEF OF ALLERGIES 24hr
1. Non pharmacological management
Non-pharmacological measures should include weight loss where appropriate; weight loss has strong evidence for efficacy and has been shown to have a dose-dependent association with reduction of symptoms.11, 23 Other approaches include elevation of the head of the bed and avoiding large meals close to bedtime.24 Fatty foods, caffeine and alcohol may exacerbate GORD as previously mentioned and should be minimised if known to trigger symptoms. Further, smoking cessation is also recommended.12
2. Pharmacological management available OTC
Antacids are commonly used self-prescribed medications that provide symptomatic relief from the symptoms associated with GORD. They consist of calcium carbonate, sodium bicarbonate and aluminium or magnesium salts in various compounds and combinations. Once dissolved in the stomach, they partially neutralise gastric acid, thus raising gastric pH. This effect also inhibits pepsin activity, thereby reducing its proteolytic activity.25 They are available in both liquid and chewable preparations. Some antacids contain alginate, which have a unique mechanism of action - in the presence of acid, they precipitate into a gel forming a raft that localises to the acid pocket in the stomach.26 Antacids are best taken with food or after meals when symptoms are most likely to occur. For patients taking other medications, it is important to remind patients to avoid taking other medications within 2-4 hours of taking an antacid due to decreased absorption by chelation or adsorption of other drugs.25
It is important to counsel patients that while antacids can provide relief from symptoms, they do not treat the underlying cause and long-term use is not recommended as it may mask disease.

Gastroenteritis
Definition and causative agents
Acute gastroenteritis is defined as diarrhoeal disease that has a rapid onset lasting less than two weeks in duration. It may be accompanied by vomiting, abdominal pain or fever.27, 28 Most cases of acute gastroenteritis are viral with norovirus being the most common offender. Norovirus is also known as the “winter vomiting bug” due to its pronounced peak during the winter months.29 Other common viral pathogens include rotavirus, enteric adenovirus and astrovirus.30, 31
Non-viral causes may include bacteria such as Staphylococcus aureus, Campylobacter jejuni, Shigella spp, Salmonella spp and Escherichia coli. Less commonly, parasites such as Giardia and Cryptosporidium can cause acute gastroenteritis. In light of the current global pandemic, gastrointestinal manifestations of COVID-19 should not be overlooked as a differential diagnosis. Characteristics suggesting viral etiology include an intermediate incubation period (24-60hours), a short duration of symptoms (12-60 hours) and a high frequency of vomiting.32 In terms of duration, Norovirus usually lasts ~2 days, rotavirus lasts between 3-8 days while Campylobacter and Salmonella last approximately 2-7 days.33
Management of symptoms
For most individuals, acute viral gastroenteritis is self-limiting and can be treated at home with supportive measures. Maintaining adequate fluid hydration is the mainstay for the management of acute gastroenteritis and can be achieved with water, sport drinks and oral rehydration solutions which are available OTC. Evidence supporting restriction of certain foods during acute gastroenteritis is weak and so patients should be encouraged to eat as tolerated.34 Anti-emetics such as domperidone may be appropriate for those experiencing nausea and vomiting and pharmacists should refer to the Pharmaceutical society of Ireland (PSI) guidance on the safe and appropriate sale of domperidone taking care to screen for any contraindications to its use.35 The use of anti-diarrhoeal agents such as Loperamide is generally not recommended unless a patient needs to shorten the length of time the diarrhoea lasts. Alarm symptoms and signs identify those who may need referral to the GP or local emergency department and include:
- Severe abdominal pain
- Severe volume depletion/dehydration
- Aged 65 or older
- Comorbidities e.g. immunocompromised
- Prolonged symptoms
- Recent hospitalisation or antibiotic use in the previous 3-6 months
References available on request
26 | PHARMACYNEWSIRELAND.COM
RECOMMEND CONTROL HAY FEVER TOTAL




GETS TO WORK in mins 3
6 in1 R E LI E F


DEFENCE RELIEF
Beconase Hayfever nasal spray 50 micrograms per spray contains beclometasone dipropionate. For the prevention and relief of symptoms of Hayfever and other seasonal allergic conditions. Adults aged 18 and over: 2 sprays into each nostril twice a day. Max 8 applications per day (400 mcg). Seek medical advice if symptoms do not improve after 2 weeks. Do not use continuously for longer than 3 months without consulting a doctor. Do not give to persons under 18 years. Pregnant and breastfeeding mothers should not use without consulting a healthcare professional. Caution: Recent nasal injury or surgery. Side effects: Rare cases of hypersensitivity reactions. Unpleasant taste/smell, dryness/irritation of the nose and throat, raised intraocular pressure, nasal septal perforation. Product not subject to medical prescription. PA 1186/008/001. MAH: Chefaro Ireland DAC, The Sharp Building, Hogan Place, Dublin 2, Ireland. Date of preparation: Feb 2023. SPC https://www.medicines.ie/medicines/beconase-hayfever-31396/spc Becodefence is a medical device. Contraindications: Known hypersensitivity to ingredients or those with a Sesame oil allergy. Date of preparation: 04/2022.

IRE BEC 2023 06
Every Dose counts
HSE marks European Immunisation Week 2023

The HSE has marked the World Health Organization’s (WHO) European Immunisation Week 2023, which takes place each year during the last week of April. The theme for this year is “the big catch-up” and aims to improve vaccination uptake worldwide, especially in younger children who may have missed out on their routine vaccines since the COVID-19 pandemic
Impacting Cancer Treatment

A team of scientists led by those in Trinity has discovered new mechanisms involved in establishing cellular identity, a process that ensures the billions of different cells in our bodies do the correct job.
Vaccines save lives - 75 years of the WHO
On the 75th anniversary of the WHO this European Immunisation Week, we remember how vaccines have been one of the most costeffective health interventions available, saving millions of people from illness, disability and death each year.
Unvaccinated children and young people are most at risk of disease
Many children worldwide are not up to date with their recommended vaccines, making them vulnerable to disease. In the WHO European Region alone, over 1.2 million children have missed out on an MMR vaccine.
Dr Lucy Jessop, HSE Immunisation Lead and Consultant in Public Health Medicine at the National Immunisation Office, outlines, “In Ireland children get two doses of the MMR vaccine so they can be fully protected against measles. However, uptake rates of the first and second doses of the MMR vaccine have dropped below the 95% rate recommended by the WHO to stop measles from spreading.
“Unvaccinated, young children are most at risk of infectious diseases like measles. But if your child has
missed any of their recommended vaccines, it’s not too late to catch up and get protected.”
Young people who are eligible for the Laura Brennan HPV vaccine catch-up programme can get a free HPV vaccine if they missed out on the vaccine when it was offered to them in school. “The more young people vaccinated and women screened the better the spread of HPV infection can be controlled and the more HPV related cancers prevented,” says Dr Jessop.
“Timing matters, so it is important to get vaccinated on time and catch up on any missed doses as soon as possible so your family is protected. We need to act now to catch up on the children who missed out on their vaccines during the pandemic so we can restore immunisation levels to pre-pandemic levels and keep everyone safe,” adds Dr Jessop.
Reflecting on 75 years of the WHO, Dr Éamonn O’Moore Director of National Health Protection, National Health Protection Service of Ireland adds, “We have seen huge milestones in public health and wellbeing over the years thanks to vaccination. The WHO European Region has been free of endemic polio since 2002. The last reported case of polio in Ireland was in 1984.
“In 2000 Europe had over 400,000 cases of tetanus but in 2021 only 43 cases were reported. In Ireland we introduced the tetanus vaccine during the 1940s and saw the last death from tetanus reported in 1967.”
On staying vigilant in the fight against vaccine-preventable diseases, Dr O’Moore, says: “Vaccines have and continue to play a very important role in protecting and saving lives in Ireland and worldwide. But it is important to remember that though the vaccination programmes have been so successful, many of the diseases, with the exception of smallpox, have not entirely gone away. Vaccination remains as important as ever to protect children.”
This new discovery in stem cells – a result so surprising that the team initially believed it to be an error in the lab – has potential translational impacts in cancer biology and associated targeted treatments.
The research focuses on the workings of Polycomb protein complexes, PRC1 and PRC2, which are studied by Professor Adrian Bracken and his team, based in Trinity’s School of Genetics and Microbiology.
PhD student, Ellen Tuck, describes these proteins as “strict librarians” inside cells. “PRC1 and PRC2 block access to certain areas of the genetic library, such that a neuron cell won’t have access to muscle genes, and it doesn’t get confused in its cellular identity.”
A puzzle regarding PRC2 has intrigued the Bracken lab and other scientists in the field for years: two forms (PRC2.1 and PRC2.2) exist in the cell but the Bracken lab previously showed that the two forms of PRC2 target the same regions of DNA and do the same job. So why do we need two versions?
The new discovery from the lab takes an exciting step towards answering this conundrum, as the team found that PRC2.1 and PRC2.2 recruit different forms of the PRC1 complex to DNA, thereby finally explaining why two versions are needed.
Successful PhD graduate of the Bracken lab, Dr Eleanor Glancy, together with Postdoctoral researcher, Dr Cheng Wang, spearheaded the work, with important collaborative support from scientists in Italy and the Netherlands.
This work was funded by Science Foundation Ireland and the Irish Research Council.
PHARMACYNEWSIRELAND.COM 28 News
Dr Lucy Jessop, HSE Immunisation Lead and Consultant in Public Health Medicine at the National Immunisation Office
Click here to register in digital edition
(HERPES ZOSTER VACCINE RECOMBINANT, ADJUVANTED)

IF YOU CAN PREVENT SHINGLES SUFFERING, WHY WOULDN’T YOU?3
SHINGRIX demonstrated >90% efficacy against shingles in all age groups aged 50 years of age or older, based on pooled data from two large, phase 3 randomised control trials.1,2
Shingrix has a clinically acceptable safety profile. This is based on a pooled analysis of data generated in placebo-controlled clinical studies. Local reactions at the injection site may include pain, redness, swelling and itching and systemic reactions may include headache, gastrointestinal distress, muscle and joint pain, fatigue, shivering, fever and malaise.3

SHINGRIX IS NOW AVAILABLE
For more information on SHINGRIX, please scan the QR code.

Shingrix powder and suspension for injection in vials [Herpes Zoster vaccine (recombinant, adjuvanted)].
(Please refer to SmPC before prescribing)
Composition: After reconstitution, one dose (0.5 mL) contains: Varicella Zoster Virus glycoprotein E antigen1,2 50 micrograms. (1adjuvanted with AS01B containing: plant extract Quillaja saponaria Molina, fraction 21 (QS-21) 50 micrograms, 3-O-desacyl-4’-monophosphoryl lipid A (MPL) from Salmonella minnesota 50 micrograms, 2glycoprotein E (gE) produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology).
Therapeutic indications: Prevention of herpes zoster (HZ) and postherpetic neuralgia (PHN) in adults 50 years of age or older and in adults 18 years of age or older at increased risk of HZ. The use of this vaccine should be in accordance with official recommendations. Posology and method of
administration: For intramuscular injection only, preferably in the deltoid muscle. Primary Vaccination: Initial dose of 0.5 ml followed by a second 0.5 ml dose 2 months later. For flexibility the 2nd dose can be administered between 2 and 6 months after the first dose. For subjects who are or might become immunodeficient or immunosuppressed and whom would benefit from a shorter vaccination schedule, the 2nd dose can be given 1 to 2 months after the initial dose. Booster doses: need not established. Contraindications: Hypersensitivity to the active substances or any of the excipients. Special warnings and precautions for use: The name and the batch number of the administered product should be clearly recorded. Appropriate medical treatment and supervision should be readily available in case of an anaphylactic event. Administration of Shingrix should be postponed in subjects suffering from an acute severe febrile illness. However, the presence of a minor infection, such as cold, should not result in deferral. A protective immune response may not be elicited in all vaccinees. Never administer intravascularly or intradermally; subcutaneous administration not recommended as it may lead to an increase in transient local reactions. Caution in individuals with thrombocytopenia or any coagulation disorder since bleeding may occur following intramuscular administration. Syncope can occur following, or before any vaccination as a psychogenic response.
This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia and tonic-clonic limb movements during recovery. It is important that procedures are in place to avoid injury from faints. There are no data to support replacing a dose of Shingrix with another HZ vaccine. There are limited data to support the use of Shingrix in individuals with a history of HZ and in frail individuals including those with multiple comorbidities. The benefits and risks of HZ vaccination should be weighed on an individual basis. Interactions: Shingrix can be given concomitantly with unadjuvanted inactivated seasonal influenza vaccine, 23-valent pneumococcal polysaccharide vaccine (PPV23), 13-valent pneumococcal conjugate vaccine (PCV13) or reduced antigen diphtheria-tetanusacellular pertussis vaccine (dTpa). The vaccines should be administered at different injection sites. Fertility, pregnancy and lactation: There were no effects on male or female fertility in animal studies. It is preferable to avoid the use of Shingrix during pregnancy. The effect on breast-fed infants of administration of Shingrix to their mothers has not been studied. It is unknown whether Shingrix is excreted in human milk. Effects on ability to drive and use machines: Shingrix may have a minor influence on the ability to drive and use machines in the 2-3 days following vaccination. Undesirable effects: Very common (≥1/10): Headache, GIT symptoms, myalgia, injection site reactions, fatigue, chills, fever. Common (≥1/100 to <1/10): injection site pruritus, malaise. Uncommon (≥1/1000 to <1/100): lymphadenopathy, arthralgia. Rare (≥1/1000 to <1/100): Hypersensitivity reactions. Legal Category: POM A. Marketing Authorisation Number: EU/1/18/1272/001
Marketing Authorisation Holder: GlaxoSmithKline Biologicals S.A., Rue de l’institut 89, B-1330 Rixensart, Belgium. Further information is available from GlaxoSmithKline (Ireland) Ltd. 12 Riverwalk, Citywest Business Campus, Dublin 24. Telephone: 01-4955000. Code: PI-7757. Date of preparation: January 2023.
Adverse events should be reported directly to the Health Products Regulatory Authority (HPRA) on their website: www.hpra.ie. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.
of Product Characteristics (SPC), available on https://www.medicines.ie/medicines/shingrix-powder-and-suspe
PM-IE-SGX-JRNA-220001 | Date of Preparation: March 2023 Trade marks are owned by or licensed to the GSK group of companies ©2023 GSK group of companies or its licensor.
neuralgia in the United Kingdom. Epidemiol infecti. 2009 137 38-47. 2. Lal H et al.
adults. N Engl J Med. 2015; 372(22):2087-96. 3. Shingrix, Summary
Last Accessed: March 2023.
References : 1. Gauthier et al. Epidemiology and costs of herpes zoster and postherpetic
Efficacy of an adjuvanted herpes zoster subunit vaccine in older
nsion-for-suspension-for-injectionherpes-zoster-vaccine-recombinant-adjuvanted--35192/spc.
Vaccines are now ordered directly through your usual wholesaler. Wholesalers in Ireland: • United Drug - 01 463 2300 • Uniphar - 01 468 7501 • Galway Drug - 09 156 2728
Pharmacies in Ireland are embracing sustainability
The healthcare sector and the environment
Global greenhouse gas (GHG) emissions have been on the rise in all sectors of the economy the past few decades, and the healthcare industry is no exception, accounting for approximately 4.4% of global emissions ( 1) The following image provides a powerful visual of just how much waste is produced by the healthcare industry. It is an image of the artist Maria Koijck lying among the waste from one single operation. When she asked the operating team save the waste from her operation for an art project, she was astounded when they handed her six refuse bags full of waste from this one operation.
Pharmacies in Ireland are embracing sustainability
‘at the heart of health’ and central to the local community. Having conducted a strategic review this year of both the pharmacy retail sector itself and of our own business within that sector, we felt that there was a real opportunity to build on our current successes and align our retail strategy for growth with a more formalised, sustainable approach and plan”.
How did you go about devising a sustainability strategy?
Can you give an example of what you have implemented to do things more sustainably?
The healthcare sector and the environment
the global population continues to expand, and in the wake of Covid 19, waste generation continuing to grow with no sign of slowing. Every industry is looking at new ways to tackle these issues and minimize waste and emissions, and the pharmacy sector is no exception.
continuing to grow with no sign of slowing. Every industry is looking at new ways to tackle these issues and minimize waste and emissions, and the pharmacy sector is no exception.
Pharmacists across Ireland are starting to look pro-actively at their businesses and ways to do things in a more sustainable, environmentally friendly manner. The Meagher’s pharmacy group has recently introduced a sustainability strategy across their group of 9 pharmacies. The IPN spoke with Oonagh O’Hagan, Managing Director of the Meagher’s group to learn about their new approach to sustainability.
Why did you feel a sustainability strategy was needed?
Global greenhouse gas (GHG) emissions have been on the rise in all sectors of the economy in the past few decades, and the healthcare industry is no exception, accounting for approximately 4.4% of global emissions.1 The image above provides a powerful visual of just how much waste is produced by the healthcare industry. It is an image of the artist Maria Koijck lying among the waste from one single operation. When she asked the operating team to save the waste from her operation for an art project, she was astounded when they handed her six refuse bags full of waste from this one operation.
As the global population continues to expand, and in the wake of Covid 19, waste generation is

Pharmacists across Ireland are starting to look pro-actively at their businesses and ways to do things in a more sustainable, environmentally friendly manner. The Meagher’s pharmacy group has recently introduced a sustainability strategy across their group of 9 pharmacies. The IPN spoke with Oonagh O’Hagan, Managing Director of the Meagher’s group to learn about their new approach to sustainability.


Karliner, J., Slotterback, S., Boyd, R., Ashby, B., Steele, K., Wang, J., 2019. Health Care’s Climate Footprint: The Health Sector Contribution and Opportunities for Action. Available at: https://noharmglobal.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (accessed April 21st 2023)
Why did you feel a sustainability strategy was needed?
“Meagher’s Pharmacy group, is a business that prides itself on being
“We engaged with Pat Kane (Good, Better, Best consultancy) and Sharon Yourell Lawlor (Think, Plan, Do consultancy), two business and sustainability strategists who are on a mission to assist retail businesses on their journey towards a more sustainable future. Our aim was to approach sustainability in a very practical and action orientated way. We started by looking at the key pillars of our overall business strategy, such as supporting our customers, community and staff, delivering operational excellence and strengthening our business through growth. We then focused on all the possible ways we can deliver on these pillars in a much more sustainable manner. For us, it is about embedding sustainable thinking and practices within each of these pillars and across the Meagher’s business, not keeping the sustainability strategy separate. We wanted to develop a sustainability mindset so that everything we do operationally is viewed through a sustainability lens.
“A concrete example is the way we have dealt with disposal of waste from sharps and injections used by patients in the home setting. We partnered with HealthBeacon Plc, an Irish company which develops smart tools to help patients adhere to their medication, and introduced an innovative service to provide a Smart Sharps Bin to our patients on injectable medicines. This technology tracks the patient’s injection history, giving the patient an adherence score and providing personalised reminders. Using this technology, a peer-reviewed study reported improvements in patients’ adherence to medication by up to 26%, across certain therapeutic areas.1 For pharmacists, promoting better health outcomes is our priority, but better adherence also means less medication goes to waste without ever being used. The HealthBeacon solution also safely stores the used injectables so the patient does not have to think about waste disposal. When the sharps bin is almost full, the patient automatically receives an empty one in the post. Their full container is collected and returned to HealthBeacon’s Green Labs facility in Dublin where the used sharps bin is recovered, sterilised and reused, saving plastic, water, and carbon. Before HealthBeacon’s service, this full container would have been sent for incineration or to landfill which is not sustainable at all.
PHARMACYNEWSIRELAND.COM 30 HealthBeacon
Niamh McGrory and Christine Canavan, pharmacists Meagher’s pharmacy Kinvara with Colm Gildea of HealthBeacon
Meagher’s Pharmacy team attend HealthBeacon medication adherence training
Image of the artist Maria Koijck lying among the waste from one single operation
receives an empty one in the post. Their full container is collected and returned to HealthBeacon’s Green Labs facility in Dublin where the used sharps bin is recovered, sterilised and reused, saving plastic, water, and carbon. Before HealthBeacon’s service, this full container would have been sent for incineration or to landfill which is not sustainable at all.
At Meagher’s, we are now on a journey and are committed as a team to taking action and ultimately leading behavioural change and habits amongst our shoppers, our staff and our suppliers. For me personally and for us as a business, we want to play our part to support meaningful change within the pharmacy retail sector, that both protects our planet and supports the people within our communities”.
Reference
1. Karliner, J., Slotterback, S., Boyd, R., Ashby, B., Steele, K., Wang, J., 2019. Health Care’s Climate Footprint: The Health Sector Contribution and Opportunities for Action. Available at: https://noharm-global.org/sites/ default/files/documents-files/5961/ HealthCaresClimateFootprint_092319. pdf (accessed April 21st 2023)
HealthBeacon’s FDA-cleared Smart Sharps Bin

What is the problem that you have solved through this new model?
What is the problem that you have solved through this new model?
to some really passionate, positive discussions on what we can do together to support our patients and our planet”.
How important are partnerships in your sustainability strategy?
Patient education, logistics, end of life options and varied regulations all play a part in the planning and execution of any option that is more sustainable than currently available.
Looking around for potential partnerships and collaborations is needed to drive maximum impact. Collaborations between the private and public sectors, between government regulators and waste handlers, and between an educated public and businesses that can adapt. Only then can we be truly effective in working towards a more sustainable future.
2. Sarhan S, McWhinney S, Shah A, Kelly L. Abstracts of the 25th Annual Meeting of ESPACOMP, the International Society for Medication Adherence, 08–19 November 2021. The HealthBeacon Injection Care Management System shows Improved adherence to Gastrological, Dermatological and Rheumatological Treatments. Int J Clin Pharm 44, 276–299 (2022). https://doi.org/10.1007/ s11096-021-01373-5
“The reality was that before this service, many patients had been disposing of their injection waste in their household refuse. They had the option of collecting their sharps waste together in a sharps bin and then returning the bin either in person or by mail via a
Meagher’s Pharmacy team attend adherence training and tour of HealthBeacon’s Green Labs facility, Dublin

2 Sarhan S., Shah A., Kelly L, McWhinney S. HealthBeacon ICMS: 19% more patients and month 12. (2021) Abstracts from the Ninth Annual National Association of Specialty Pharmacy (NASP) Meeting, Journal of Drug Assessment, 10:sup1, 3-66
“The reality was that before this service, many patients had been disposing of their injection waste in their household refuse. They had the option of collecting their sharps waste together in a sharps bin and then returning the bin either in person or by mail via a collection service. Unfortunately all of these options involved traditional methods of incineration or landfill, which assumes that the earth has an endless supply of resources and an infinite capacity to regenerate. Our challenge was threefold - how did we ensure this waste was retrieved from patients (logistics); what to do with it once it was retrieved (end-of-life); and how to remove as much waste and single use plastics from the system, staying within regulatory boundaries. We are delighted that we have solved this problem by partnering with HealthBeacon”.
Was it difficult to change your old processes and implement change?
“Our team at Meagher’s are always excited about trying new services that can add value for our patients. Our team attended an adherence training program at HealthBeacon and this involved a tour of the Green Labs facility which was an exciting learning experience for our team. It really brought the initiative to life and made our contribution tangible. Our team had the opportunity to meet the people working in the Green Labs facility and ask questions directly. It led
PHARMACYNEWSIRELAND.COM 31
HealthBeacon’s FDA-cleared Smart Sharps Bin
Continued Waits for New Medicines

Ireland is once again one of the slowest countries in Western Europe to reimburse and make available new innovative medicines to patients, according to figures gathered by data analysts IQVIA for EFPIA, the European pharmaceutical industry body.
available faster to patients, as quickly as 102 days, while still managing budgets and doing value for money assessments.
pharmaceutical companies are possible and should become a policy priority in Ireland.
The survey of 37 European countries, including 27 in the European Union, covers the full four years between 2018 and 2021 analysing 168 innovative medicines authorised for use by the European Medicines Agency (EMA). Key points this year are:
• While it takes on average 517 days, post EMA authorisation, to make a new medicine routinely available across European countries, in Ireland it takes 567 days.
• This time has lengthened in Ireland since 2020: up almost
100 days from 477 three years ago. This is despite the welcome allocation of new funds for new medicines by the Government.
• The number of days it takes for new cancer medicines to be made available to patients has increased to 673 post EMA authorisation for Ireland. This wait of nearly two years is far too long for cancer patients as availability of new medicines is a recognised contributor to Ireland’s improved survival rates in cancer. Many other countries can make these medicines
Back-to-back wins for HYLO®-FORTE
• Only six of 37 European countries take longer than Ireland to reimburse orphan medicines for rare diseases, of which 95% do not have a recognised medical treatment. It currently takes on average 877 days from EMA market authorisation of orphan medicines for them to become available to Irish patients. The number of days taken depends both on the timing of companies’ applications and the decision-making processes of health authorities. In Ireland, the figures suggest that between 25% and 30% of the timing is attributable to IPHA member companies’ timing of applications for the reimbursement of a medicine to the HSE after the product has been granted EMA market authorisation. The bulk of the timing is taken by the State’s assessment and decision-making process, which typically includes price negotiations with companies. Longer timelines to availability mean a lower standard of care than could be available for Irish patients, and thus poorer patient outcomes than otherwise could be achieved. The experience of other countries demonstrates that improved partnerships between health authorities and
Oliver O’Connor, Chief Executive of the Irish Pharmaceutical Healthcare Association, said, “Over the past three budgets, the Government has allocated almost ¤100 million to new medicines. The figures released today show how urgent it is now to improve the reimbursement system so that new medicines are available to patients and their doctors faster. Process reform has to go alongside new funding. That’s why we have welcomed the Minister’s new Working Group to build out recommendations from and beyond the Mazars report. We have welcomed the recommendations on transparency already approved by the Minister and look forward to working on further improvements.
“The lengthening timelines demonstrate that there is a significant job to be done to make innovative medicines available faster to Irish patients. In particular, there is a serious issue with the timelines in relation to orphan medicines and medicines for cancer care. We have six months to agree new practical steps and then start implementing. IPHA member companies are ready to collaborate with all stakeholders through the Working Group to ensure this happens sooner rather than later.”
Scope Eyecare is thrilled to announce that HYLO-FORTE® has won ‘Best Eye Care Product of the Year’ award for the second year in a row in the OTC and Retail Pharmacy Product Awards. This award recognises outstanding product quality within the pharmacy eyecare category and given the tough competition, we are extremely proud of these back-to-back wins, having also won this award in 2022. This win would not have been possible without the support of our valued customers, pharmacists, ophthalmologists, optometrists and GPs.
HYLO-FORTE® was praised for its gentle preservative-free formula, as well as the ability to use it for up to 6 months from first opening - making it excellent value for money, with one judge commenting, ‘Great that it is preservative free & phosphate free so it is gentle on sensitive eyes and can be used with content lenses. Also, it lasts for six months after opening which is another great selling point, as I know from personal use of eye drops, you normally throw half a bottle away after 28 days of opening.’
Scope was also recognised for its pharmacy training initiatives which offer support through education on best-practice eyecare management. Other judges’ comments included Scope’s sustainability efforts; ‘Great to see how invested the company are in sustainability and becoming more environmentally friendly. They provide great training and support to pharmacies.’ We pride ourselves on doing our part in preserving the planet and that can be seen with the recent launch of OPTASE® TTO BelphaWipe which are 100% biodegradable eyelid cleansing wipes.
Scope Eyecare is proud to deliver high-quality products that continue to provide both customers and patients with the best possible eyecare solutions.
PHARMACYNEWSIRELAND.COM 32 News




























































For the treatment of the nasal symptoms of allergic rhinitis Nasal Congestion Sneezing and Itching Stuffy or Runny Nose For Adult use only. Not for use in children under 18 years. A copy of the summary of product characteristic is available upon request or alternatively please go to www.clonmelhealthcare.ie. Supply through pharmacies only. PA23180/001/002. PA Holder: Opella Healthcare France SAS T/A Sanofi, 82 Avenue Raspail, 94250 Gentilly, France. Distributed by: Clonmel Healthcare Ltd., Clonmel, Co.Tipperary. Date Prepared: April 2023 2023/ADV/NAS/070H 5 micrograms/dose Nasal Spray Suspension triamcinolone acetonide lle rg y Hayfever
Raising Awareness of Under-Recognised Disease
RCSI University of Medicine and Health Sciences has joined forces with a pioneering patients group to raise awareness of the auto-immune disease, Sjögren’s.

Deirdre Collins who lives with Sjögren’s and is one of the cofounders of the Sjögren’s Ireland patient advocacy group, Dr Sabrina Brennan and Dr Joan Ní GabhannDromgoole, Scientific Lead for the Ocular Immunology Research Group and Senior Lecturer for School of Pharmacy and Biomolecular Sciences
HIQA Consultation on Chickenpox Vaccine
The Health Information and Quality Authority (HIQA) has commenced a public consultation on a draft Health Technology Assessment (HTA) of adding the chickenpox (varicella) vaccine to the routine childhood immunisation schedule.
HIQA undertook this HTA following a request from the Department of Health and the National Immunisation Advisory Committee (NIAC).
often impairing their ability to carry out daily activities and negatively affecting their work and social lives.
Sjögren’s (pronounced ‘SHOWgrins’) is a chronic debilitating autoimmune disease which affects approximately 1 in 200 people worldwide. Up to 1% of the population in Ireland is thought to suffer with the disorder, predominantly women aged between 40-50 years at time of diagnosis.
Academics from RCSI’s Ocular Immunology Research Group have collaborated with the Sjögren’s Ireland patient advocacy group to launch Ireland’s first awareness campaign about Sjögren’s to assist people in receiving an early diagnosis. The campaign will see information posters being displayed in primary care centres such as GP practices, optometrists and dental surgeries throughout the country.
Dr Joan Ní Gabhann-Dromgoole, Scientific Lead for the Ocular Immunology Research Group and Senior Lecturer for School of Pharmacy and Biomolecular Sciences said, “Sjögren’s is as common and as debilitating as other autoimmune diseases such as Crohn’s Disease and ulcerative colitis, but many people mistakenly believe it to be rare and not as serious. This means that, people living with Sjögren’s commonly experience a challenging diagnostic process, limited treatment options, chronic symptoms, and inadequate support.”
In Sjögren’s, the body’s immune system that normally provides
protection from infection, begins to attack parts of the body and in particular the specialised secretory glands called exocrine glands. For those living with Sjögren’s these glands become inflamed and are badly damaged. As a result the glands stop working causing severe dryness of epithelial and mucosal surfaces and leading to dryness of the mouth and eyes. Dryness of the eye surface causes many symptoms ranging from mild discomfort, irritation and vision distortion, to serve damage to the corneal surface. Dryness of the mouth can cause difficulties eating, swallowing and talking. Sjögren’s also often causes damage to other parts of the body including the lungs, kidneys, and nervous system.
People living with Sjögren’s can also experience a wide range of systemic clinical symptoms that can potentially affect any organ system. Systemic extra glandular complications can include profound fatigue, skin rashes, chronic joint and muscle pain, an increased risk of lymphoma, and pulmonary complications ranging from mild reduction in lung function to severe complications such as idiopathic pulmonary fibrosis. At present, there is no way to predict which patients will go on to develop these disease associated complications. Furthermore, treatment options are reactive and limited. Sjögren’s has a considerable impact on the quality of life of those affected,
Dr Ní Gabhann-Dromgoole continued, “Sjögren’s is a very common condition but unfortunately patients experience substantial delays of 5-10 years in diagnosis due to lack of awareness amongst the public and education amongst medical professionals. During the course of our research, we became acutely aware that, for those affected by Sjögren’s, general practitioners, eye, and dental providers often encounter early signs of the disease but do not recognise them. This lack of familiarity with the disease deprives patients of getting a timely diagnosis and proper care and this is what we are aiming to address with our campaign.”
The awareness campaign aims to achieve three core objectives:
• Raise awareness and understanding about Sjögren’s – Educate patients, the public and healthcare professionals by hosting webinars, advertising on social media and creating the first Sjögren’s information leaflet with information from Sjögren’s specialists, including patients.
• Direct research questions –Utilise our annual knowledge exchange events to share research updates and to ask attendees what areas they feel currently need attention to improve their medical care.
• Provide mutual support –Encourage those living with Sjögren’s to stay connected with the Sjögren’s community by joining the Sjögren’s Ireland mailing list and following the Opens in new windowSjögren’s Research Ireland webpage which will have the most up-to-date information on activities and initiatives that are being planned
Chickenpox is an acute, infectious disease most commonly seen in children under 10 years old. The disease is usually mild, although it can lead to serious complications requiring hospitalisation. Anyone who has had chickenpox may develop shingles; this results from reactivation of the virus, and typically occurs in later life.
Dr Conor Teljeur, HIQA’s Chief Scientist, said, “Vaccines against chickenpox have been available for over 30 years. In Ireland, the vaccine is already recommended for non-immune individuals in certain risk groups. Many countries include vaccination against chickenpox in their childhood immunisation schedules; however, the type of vaccine given, the number of doses and the timing of the doses differ.”
The HTA assesses the clinical effectiveness, safety, cost effectiveness, budget impact, ethical and social aspects, and organisational changes associated with expanding the childhood immunisation schedule to include chickenpox vaccination.
Dr Teljeur continued, “From reviewing the evidence, HIQA found that the chickenpox vaccine is safe and effective. Including it in the childhood immunisation programme would reduce the occurrence of chickenpox and would substantially reduce severe disease including hospitalisations. Vaccination is likely to represent a good use of healthcare resources and, when the broader cost to society of chickenpox is taken into account, vaccination is cost saving.”
The report will then be provided as advice to the Minister for Health to inform a decision on whether or not to add the chickenpox (varicella) vaccine to the routine childhood immunisation schedule.
PHARMACYNEWSIRELAND.COM 34 News
SUPER 8
42 Billion Live Bacteria, 8 ‘friendly’ bacterial strains + Vitamin C
Refrigerated in Pharmacies
*Vitamin C contributes to the normal function of the immune system

*IMMUNE
I never compromise when it comes to my health. Super 8 Immune is my No. 1 choice to replenish friendly bacteria and support my immune system.”
Nutritionist and Author
BR Healthcare – Building on a Strong Foundation

BR Healthcare is one of Ireland’s leading healthcare sales, marketing and distribution companies. We recently spoke with Head of Healthcare, Alan Finn to find out more about how their dedicated sales and marketing team offers partners a full suite of trade and consumer marketing services, to grow brand share through effective, efficient sales and distribution.
Established by brothers Michael and William Rochford in 1983, BR Marketing has evolved into a leading distributor of healthcare and grocery brands.
Alan tells us, “BR Healthcare is a division of BR Marketing. The company’s heritage was established in the grocery channel managing brands like Blue Dragon, Pataks and Kühne. Six years ago, the company took the strategic decision to diversify and invest in healthcare distribution and as a result, BR Healthcare has established itself as a leading distributor in the pharmacy channel.”
With 20 years in the healthcare sector Alan has held various sales/ marketing management roles.
He adds, “I have always enjoyed working in the Irish healthcare industry and found pharmacy customers very welcoming and supportive.
“The industry has experienced huge change over this time between deregulation, reduction in the medicine reimbursement scheme and more recently Covid-19. Pharmacies have had to refocus their business model to deal with these challenges.
“The rise in sales from OTC, front of shop and vitamin categories have helped stores generate more footfall and increase sales. BR Healthcare’s range is well positioned to assist stores continue this growth with leading brands in these categories.”
So what key factors sets BR Healthcare apart from their competitors? Alan told us that over the years, the team have strategically partnered with brands and companies to build a comprehensive, yet select, portfolio of brands.
This includes household names such as Olbas, Kalms, Jakemans, Haliborange, Klearvol, Nannycare and Irish nutritional range Somega.
Alan continues, “Having established brands such as Blue Dragon and Patak’s and built them into category leaders, we harnessed this expertise to expand our business into the Irish healthcare sector. We invested in people, technology and systems to support this new division. Our knowledge and

professional staff, along with a fully integrated IT system, allowed us to efficiently capture orders, track deliveries and provide excellent customer service.”
Of course business growth always comes with its own challenges.
Alan explains, “I’m sure like many companies in Ireland Brexit and coming out of Covid 19 has created challenges but also open doors for BR Healthcare. We were lucky that our supply network is strong, and we have a very experienced supply chain team which helped us navigate through these challenges. Looking ahead to the next 12-24 months we need to manage our cost base and ensure that our consumer value offering remains strong. As Irish
PHARMACYNEWSIRELAND.COM 36 Profile
Alan Finn, Head of Healthcare, BR Healthcare
“The industry has experienced huge change over this time between deregulation, reduction in the medicine reimbursement scheme and more recently Covid-19. Pharmacies have had to refocus their business model to deal with these challenges”
consumers deal with rising inflation we need to provide our pharmacy customers with strong product promotions and the supporting materials to ensure they maximise sales during 2023.
“We have an excellent portfolio, and we plan to expand our range, to further deepen and broaden our reach. We want BR Healthcare to be recognised as an innovative company that is continuously bringing new brands to the Irish pharmacy market and is supporting our customers to be more informed about our range.

“Pharmacy staffs’ time is limited in-store so its up to BR Healthcare
to make their jobs easier by providing product information, staff training, supporting materials and promotions to drive sales and customer retention for pharmacy retailers.

“In an evolved healthcare marketplace, where consumers are seeking expert advice, we provide value-added service to our customers through our nutritionally qualified sales team, and we have ambitious plans to grow our presence in the Irish healthcare channel.”
What challenges and opportunities does Alan foresee for pharmacists
moving into 2023? Increased waiting lists may bring about opportunities, he notes.
“As Ireland’s health services continues to struggle with the increasing patient waiting lists, I see the health testing services and advice given by pharmacists expanding. If you have a minor ailment your local pharmacist has the experience to offer advice on treatment options. BR Healthcare’s experienced and nutritional trained sales team are available to provide
detailed product information/ training to assist pharmacists and staff when recommending products in store.
“Our vision for BR Healthcare is to strategically build upon the solid performances of this focused and energetic company, through the tangible cultural values at its core. We have retained William and Michael’s entrepreneurial spirit and can-do attitude but honed this into a more insight driven approach.”
PHARMACYNEWSIRELAND.COM 37
“Our vision for BR Healthcare is to strategically build upon the solid performances of this focused and energetic company, through the tangible cultural values at its core. We have retained William and Michael’s entrepreneurial spirit and can-do attitude but honed this into a more insight driven approach”
check in with the latest diabetes tech from Dexcom

WHAT IS CGM?
Real-time continuous glucose monitoring simplifies diabetes management by taking glucose readings via a sensor worn 24/7. Dexcom systems can be applied on the upper arm or abdomen (age 2+), or upper buttocks (children only †). The data is wirelessly transmitted to the user, their caregiver’s smartphone ‡ or optional receiver, which can then alert them to take action if glucose levels are rapidly rising or falling – all without requiring finger sticks* or scanning.
WHAT ARE THE BENEFITS OF DEXCOM SYSTEMS?
Dexcom rtCGM with smart alerts is clinically proven to help users lower their HbA1c, reduce hyper- and hypoglycaemia, and increase time in range § more than intermittent scanning CGM (isCGM, also known as ‘Flash’)||,1 and self-monitoring of blood glucose (SMBG),¶,2–4 leading to enhanced overall wellbeing and treatment satisfaction. 5–7
Professional societies continue to expand their recommendation of CGM for both adult and paediatric patients, and Dexcom rtCGM systems are included on the long-term illness scheme (LTI) and primary care reimbursement service (PCRS) for people with type 1 diabetes who meet the clinical requirements. 8
WHICH DEXCOM SYSTEMS ARE AVAILABLE IN IRELAND?
Dexcom recently launched the Dexcom G7 rtCGM system in Ireland, which joins the Dexcom G6 rtCGM system that has been available since 2017. Here’s how the two products compare:
BEST FOR
CONNECTIVITY‡
smartphone iOS and android smartwatch receiver
seamless pump integration: can power certain automated insulin delivery (AID) systems#
pump integration coming soon
SENSOR up to 10-day lifespan / water resistance 2.4m – up to 24 hours
2-hour warm up 30-minute warm up
customisable, high and low and urgent low soon
ALERTS
APPS
delay 1st Alert
Dexcom G6 app Dexcom G7 app follow app – circle of support (max 10) / Clarity app – healthcare professionals

WEAR LOCATION back of upper arm / abdomen
upper buttocks (children only 2–17)
upper buttocks (children only 2–6)
DISPOSAL Dexcom recommends that users follow local guidelines for appropriate disposal
Information about the Dexcom G7 real-time continuous glucose monitoring (rtCGM) system launch in Ireland and what you need to know when ordering and dispensing products from the Dexcom rtCGM portfolio.
OUR MOST CONNECTED CGM
OUR SIMPLEST, MOST POWERFUL CGM YET
people with diabetes who use a connected insulin pump people with diabetes, aged 2 and older, who need extra support, such as people who are hypo unaware, pregnant or children
-
For more product information please
visit ie.provider.dexcom.com
separately ‡
Smart devices sold
Smart devices sold separately. ‡
HOW DO I ORDER THESE PRODUCTS FOR MY PHARMACY?
Both Dexcom G6 and Dexcom G7 rtCGM systems are included in the core list for diabetes in the Long-Term Illness (LTI) scheme and are available to order through Uniphar and United Drug. Both systems use sensors that last for 10 days, meaning 3 sensors are needed per month.
Dexcom G6 ordering Dexcom G7 ordering
A funding application form must be completed by a hospital consultant through HSE procurement. Once approved, funding is granted for a 12-month supply. The patient will receive the transmitter every 3 months from Dexcom until the end of the funding period. The prescription for Dexcom G6 sensors is issued by the diabetes healthcare team for dispensing via the pharmacy.
Available items:
3 PACK
GMS Code: 97629
Dexcom G6 Sensor STS-GS-003 3
€225
1 PACK
GMS Code: 97628
Dexcom G6 Sensor STS-GS-002 1
€75
A prescription must be written by a Diabetes Specialist HCP for Dexcom G7. Each patient will then fulfil the prescription via their pharmacy on a monthly basis, requiring 3 sensors per month.
Monthly order:
3X SENSOR 1 PACK
GMS Code: 97631
Dexcom G7 CGM Sensor STP-GT-002 1
€75
Please note, Dexcom G6 uses a separate transmitter in addition to the sensors. Patients will receive Dexcom G6 transmitters direct from Dexcom every 3 months until the end of their annual purchase order. Patient will need to return to their diabetes team to reapply for funding at the end of their annual purchase order.
Sign up for an upcoming Dexcom G7 webinar, access rtCGM training and frequently asked questions at ie.provider.dexcom.com
For product troubleshooting or replacement enquiries, please complete a product support request via the website, or call our helpline 1800 827 603 (Mon–Fri 07.00-18.00, Sat–Sun 08.00-16.30)
*If glucose alerts and readings from the Dexcom CGM do not match symptoms or expectations, use a blood glucose meter to make diabetes treatment decisions. †Ages 2–17 for Dexcom G6 and 2–6 for Dexcom G7. ‡Display devices sold separately. For a list of compatible smart devices, please visit www.dexcom.com/compatibility. §Time in range was defined as 3.9–10.0 mmol/L. ||Average 2hr 48min more time in range after 12 month on Dexcom rtCGM with smart alerts.1 ¶-0.87% reduction in HbA1C in the Multiple Daily Injection group over 3 years.4 #Compatible insulin-delivery device sold separately. **Internet connectivity required for data sharing. Following requires the use of the Follow App. Followers should always confirm readings on the Dexcom App or Receiver before making treatment decisions. 1 Visser MM, et al. Lancet Diabetes Endocrinol. 2023;11:96–108. 2 Beck RW, et al. JAMA. 2017;317(4):371–8. 3 Beck RW et al. Ann Intern Med. 2017;167(6):365–74. 4 Šoupal J, et al. Diabetes Care 2020;43(1):37–43. 5 Lind M, et al. JAMA. 2017;317(4):379–87. 6 Polonsky WH, et al. Diabetes Technol Ther. 2021;23(3):195–202. 7 Polonsky WH, et al. Diabetes Care. 2017;40(6):736-41. 8 Adult type 1 diabetes mellitus. NCG No. 17. https://www.diabetes.ie/wp-content/uploads/2018/06/NCG-No-17-Adult-T1-DM_Web-ready-copy-1.pdf. Dexcom, Dexcom Clarity, Dexcom Follow, Dexcom Share, and any related logos and design marks are either registered trademarks or trademarks of Dexcom, Inc. in the United States and/or other countries. ©2023 Dexcom International Ltd. All rights reserved. Dexcom International Ltd and its affiliated European entities. This product is covered by U.S. patent. dexcom.com | +1.858.200.0200 Dexcom, Inc. 6340 Sequence Drive San Diego, CA 92121 USA | MDSS GmbH Schiffgraben 41 30175 Hannover, Germany. LBL-1002886 Rev001.
Don’t let allergic reactions disrupt your customers’ lives –whether it ’s hayfever, allergic skin rashes or food allergies such as itchy skin, rashes and hives.

Product Information: Piriton 4mg Tablets (Chlorphenamine maleate). Indications: Treatment of acute allergic reactions. Dosage and method of administration: Minimum dosing interval 4 hours. Adults and children 12 years and over: 1 tablet every 4-6 hours (maximum of 6 tablets in 24 hours). The elderly: 1 tablet every 4-6 hours (maximum of 3 tablets in 24 hours). Children 6-12 years: 0.1mg/kg or ½ a tablet every 4-6 hours (maximum of 6 half tablets in 24 hours). Children under 6 years: Not recommended. Contraindications: Hypersensitivity to ingredients. Pre-coma states. Patients who have been on MAOI therapy within previous 14 days. Precautions: May act as cerebral stimulant in children and adults, with children and elderly more likely to experience paradoxical excitation. Use with caution in patients with severe renal or hepatic impairment, epilepsy, severe hypertension and cardiovascular disease, raised intra-ocular pressure, prostatic hypertrophy, bronchitis, thyrotoxicosis, bronchiectasis and bronchial asthma. May cause drowsiness. May seriously a ect ability to drive and operate machinery. Avoid alcohol or concurrent use with sedative drugs. Avoid in elderly with confusion. Should not be used with other anti-histamine containing products. Contains lactose. Keep out of reach and sight of children. Side e ects: Sedation, somnolence, disturbance in attention, abnormal coordination, dizziness, headache, blurred vision, nausea, dry mouth, vomiting, abdominal pain, diarrhea, dyspepsia, fatigue, chest tightness, blood dyscrasias, allergic reactions including anaphylaxis. Neurological anticholinergic e ects, particularly in the young and elderly.

Overdose: Symptoms of overdose likely to be similar to side e ects listed and requires medical attention. Legal category: Pharmacy Only. Product Licence Number: PA 0678/080/001. MAH: GlaxoSmithKline
Consumer Healthcare (Ireland)
c h l o r p h en a m i n e ma l e a t e F ro m 6 y e a r s +
Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. Full product information is available in the SPC. Additional information is available upon request. Text prepared: April 2020. Contains Chlorphenamine maleate. Always read the label/leaflet.
Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-PIRI-21-00004
AUTHOR: Daimen O’Brien, Adrian Dunen Pharmacy, Baldoyle

CPD
60 Second Summary
Hay fever is inflammation of the nasal passage, that occurs when the immune system overreacts to pollen in the air, with approximately 20-30% of the population affected.

This allergic response is due to Immunoglobulin E (IgE) antibodies attaching to pollen, which causes an inflammatory response. Symptoms include sneezing, runny nose, cough, itch and watery eyes.
Diagnosis is usually by examining symptoms and medical history, but allergy testing can be performed. Prevention strategies are vital to reduce symptoms and there are a variety of treatment options.
Second-generation oral antihistamines have been demonstrated to reduce symptoms of hay fever when taken regularly, at the time of maximal symptoms or on pre-exposure to the allergen. Intranasal administration of steroids, antihistamines or a combination of both are effective.
Oral steroids are not as useful due to the potential adverse effects. Eye drops with active ingredients including antihistamines, steroids, mast cell stabilisers and lubricants can provide relief from ocular symptoms.
Leukotriene receptor antagonists can also be used as add-on treatment, particularly if the patient has asthma.
Allergen immunotherapy is an option that can be useful if symptoms are severe, other treatment options have failed or are contraindicated - only under the supervision of a physician with experience treating allergic diseases.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
Introduction and Epidemiology
Hay fever, or seasonal allergic rhinitis, is inflammation of the nasal passage that occurs when the body’s immune system reacts to pollen in the air. Peak pollen season usually occurs from the end of March to September in Ireland. Weather conditions have an impact on the pollen count - with humid, windy and warm weather causing an increase. The Met Eireann website is a very useful resource, providing daily updates on whether the pollen count is low, moderate, high or very high. It also provides a regional breakdown and comments on tree, grass and weed pollen.1, 2 Hay fever is one of the most prevalent conditions in the world. It is difficult to accurately predict the prevalence of hay fever, however some epidemiologic studies predict that 20-30% of European adults are affected. In addition, potentially up to 40% of children suffer from hay fever.3
Symptoms
Hay fever symptoms are generally self-limiting but they can be frustrating for patients and have an impact on their quality of life. The main nasal symptoms are sneezing, coughing, runny or blocked nose, itchy nose and loss of smell. Ocular symptoms including red, itchy and watery
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
eyes are associated with hay fever. Itch in the mouth, headache, earache and fatigue are also common symptoms. Patients with asthma may have additional symptoms including shortness of breath, wheeze and cough.1, 4
There can be some confusion between symptoms of hay fever and respiratory viruses such as the common cold, influenza and Covid-19. However, differences can be observed to aid diagnosis. Symptoms such as fever, body aches and chest discomfort are common in respiratory viruses but almost never present in hay
4 previous
steps, log and record your
fever - although chest discomfort can be observed in patients with asthma and hay fever. Additionally, mucus from a respiratory virus tends to have a yellow or green colour, compared to a clearer mucus that is associated with hay fever. A respiratory virus usually resolves in 1-2 weeks, while hay fever will usually persist for weeks or months.5
Due to the high prevalence of this condition, an excellent understanding of prevention and treatment of symptoms is important. Symptoms often have a negative impact on a patient’s
41 CPD: Allergies
Continuing Professional Development
CPD
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the findings. Published by IPN. Copies can be downloaded from www.irishpharmacytraining.ie Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
Management of Hay Fever and Allergies
Allergies
quality of life. This can lead to reduced sleep quality, poor performance and absenteeism at work or school.6 In patients with severe allergic rhinitis compared to those with mild allergic rhinitis, symptoms such as anxiety, depression and fatigue can be observed to a greater extent.7
Pathophysiology
The underlying mechanism of hay fever involves immunoglobulin E (IgE) antibodies attaching to pollen, which causes the release of histamine, leukotrienes and other inflammatory mediators. These immune reactions are induced by type-2 helper T cells. Inflammation in mucous membranes occurs as the body works to remove the pollen.8 Hay fever should not be considered as an acute response to pollen exposure, but as a complex interaction involving mast cells, T cells, epithelial cells, eosinophils and basophils.9
Diagnosis
Diagnosis of hay fever is often made by a GP, following examination of symptoms and medical history. Time of year, triggers, location and duration of symptoms are all factors to be considered. The patient may also be examined by the GP for nasal polyps - inflammation on the inside of the nose that can be as a result of allergic rhinitis. The GP may initiate treatment with antihistamines. If the patient’s symptoms improve, a diagnosis of hay fever is likely. Commercial allergy testing kits are sometimes used but are not recommended. These testing kits can be unreliable and not of an adequate standard. Laboratory tests can be used to rule out common respiratory viruses.10
Allergy testing may be carried out in some cases, if the cause of the symptoms is unclear. Two main allergy tests are used in diagnosing hay fever. Firstly, a skin prick test can be used where the allergen is placed on the surface of the skin, which is then pricked with a needle to introduce the allergen into the body’s immune system. If the patient is allergic; a small, itchy spot appears on the skin’s surface. A blood test is the second method, which checks for the presence of IgE in the blood. The main drawback of allergy testing is that it is not definitive, with possibilities of both false positive and false negative results.11
It is also possible to be diagnosed with local allergic rhinitis, where systemic diagnosing methods are negative but IgE antibodies are produced in the nose that react with pollen. Symptoms tend to be very similar, with an association of local allergic rhinitis with conjunctivitis and asthma. It is estimated that 25% of patients with allergic rhinitis have local allergic rhinitis.12 This is diagnosed using a nasal allergen provocation test (NAPT).13
Prevention
As with many conditions, prevention is vital in hay fever. There are several prevention strategies and patients should be counselled on these. Staying indoors or reducing time outside during peak pollen season is effective. Using Vaseline around the nostrils and wearing
wraparound sunglasses are very useful as barrier techniques. Keeping windows and doors closed and not allowing animals into the house are also good techniques. Showering and changing clothes after being outside, not drying clothes outside and vacuuming regularly should also be carried out.4
Treatment
The main objective of treating hay fever is symptom relief. A wide variety of therapeutic options for achieving this goal and these include oral antihistamines, oral corticosteroids, intranasal antihistamines, intranasal corticosteroids, leukotriene receptor antagonists (LTRAs) and nasal saline irrigation. Allergen immunotherapy is the sole therapy that is disease-modifying, rather than just symptom relief.
Decongestants can sometimes be used as an add-on treatment option. As hay fever and asthma both contribute to inflamed airways, treatment of asthma is an important consideration in this patient group.11
Oral Antihistamines
Oral antihistamines are first-line treatment for hay fever. In Ireland, they are available both over the counter and on prescription. Pharmacies are often the first port of call for patients to manage symptoms of hay fever. This can allow community pharmacists to assess patient response to treatment and give information that can help in diagnosing and subsequent treatment of hay fever.1
Antihistamines exhibit anti-allergy by being competitive antagonists at the H1 receptors. This reduces the release of histamine that
42 CPD:
Fig 1. Graph showing treatment options available for hay fever Oral Antihistamines Treatment Options Antihistamines Oral Intranasal Eye Drops Leukotriene Receptor Antagonists Allergen Immunotheraoy Decongestants Steroids Oral Intranasal Eye Drops
Fig 1. Graph showing treatment options available for hay fever
causes inflammation in the nasal passage and leads to symptoms such as sneezing and runny or blocked nose. Antihistamines at the H1 receptor are sometimes used to treat different conditions including vertigo, travel sickness or insomnia. Antihistamines that target H2, H3 and H4 receptors don’t have a major role in treating hay fever.14
The older, first-generation antihistamines including diphenhydramine and chlorphenamine are effective in relieving symptoms. However, due to their sedative nature and due to the fact that they can negatively impact functioning and cognition, they are not recommended for first-line treatment of hay fever.11
Second-generation oral antihistamines can reduce symptoms of hay fever when taken regularly, either at the time of maximal symptoms or before exposure to the allergen. They provide relief from symptoms including sneezing, itch, runny nose, red eyes and watery eyes. These second-generation oral antihistamines are therefore first-line treatment for hay fever. Many are available over the counter in Ireland, including cetirizine, fexofenadine and loratadine. Bilastine, levocetirizine and desloratadine are examples of second-generation antihistamines that are available on prescription in Ireland. The below table outlines the availability with supply status, age suitability and maximum licensed doses.11, 15, 16, 17, 18, 19, 20, 21
Second-generation antihistamines selectively bind to peripheral histamine H1 receptors. Due to this selectively, they are generally well tolerated and are not associated with many serious adverse events. They are associated with much less sedation than the firstgeneration antihistamines. They also provide ease of use due
to a possible once-daily dosing schedule.22 There are no major differences in safety and efficacy between the second-generation antihistamines when administered in equivalent doses. Fexofenadine may be the best option in terms of both efficacy and safety, and is therefore suitable as first line therapy for most patients. Cetirizine is the most potent and has been more researched than the other antihistamines.23
The main side effects associated with second-generation antihistamines are headache, fatigue, cough, nausea and vomiting. Some second-generation antihistamines such as ebastine, astemizole and terfenadine can prolong the QT interval, which can result in torsade de pointes. However, these are not licensed for use in Ireland.23 Commonly used second-generation such as loratadine and cetirizine appear to be lower risk for QT prolongation. However, it is best practice to exercise caution in patients who have risk factors for torsades de pointes or are taking some enzyme inhibiting medication.24
Nasal Sprays
Intranasal steroids are a common treatment of hay fever. They act locally by decreasing inflammatory cells and inhibiting the release of cytokines, which reduces inflammation of the nasal mucosa. They have an onset of action within 30 minutes, with maximum effectiveness usually after 2-4 weeks of daily use. Studies have shown that nasal steroids are more effective than both oral and intranasal antihistamines in treating hay fever. Budesonide, beclomethasone, fluticasone, triamcinolone and mometasone are examples of steroids that can be used intranasally. There is limited evidence to suggest which intranasal steroid is superior and consideration should be given to the patient in question. For example, mometasone may be suitable for a younger population and budesonide may be more suitable in pregnancy than other
steroids. Some adverse effects are possible with this delivery method, however it is much less likely to have potential systemic adverse effects such as suppressing the hypothalamic-pituitary axis. Adverse effects are more commonly local effects including nose bleeds, nasal dryness, headache and throat irritation.25 Intranasal antihistamines can deliver a higher concentration of medication to the targeted area compared to oral antihistamines which results in fewer adverse events. Azelastine is the most common antihistamine to be used intranasally. Adverse effects can include nose bleeds, headache and nasal irritation. Their use is limited due to their higher cost compared to oral antihistamines and by their lower efficacy compared to intranasal steroids.25 Combined steroid and antihistamine nasal sprays are also licensed for use in Ireland. If a steroid nasal spray is ineffective, then the combination product can be trialled. It has been shown to be more effective than the individual components, with a very similar safety profile which is useful (26). A combination fluticasone propionate and azelastine hydrochloride is licensed for twice daily use in people over 12. The increase in price is the main drawback with this product.27
Oral Steroids
may be indicated. These cases include where other treatment options have failed or if a patient is intolerant to intranasal options.28
Eye drops
Ocular allergic symptoms can be treated locally using eye drops. Ocular symptoms including itch, watering and redness can reduce quality of life and therefore require treatment.
In comparison with oral antihistamines, topical antihistamines are able to directly target the ocular tissue and have a much quicker onset of actionusually between 3 and 15 minutes. They also have a better safety profile and are better tolerated in general due to less systemic absorption. They are effective in symptom relief but generally only for a short period of time. Additionally, they do not have an effect on other inflammatory mediators such as prostaglandins or leukotrienes. They are more effective in the acute phase and can be used as monotherapy or dual therapy.29 Olopatadine and Ketotifen are two antihistamines that are licensed for twice daily use, in the treatment of ocular symptoms of seasonal allergic conjunctivitis.30, 31
suitability and maximum licensed doses (11) (15) (16) (17) (18) (19) (20) (21).
Steroids have their effect by reducing inflammatory cytokine production, mast cell proliferation and cell mediated immune responses. This reduces inflammation in the nasal passage and is effective in reducing symptoms of hay fever. Despite their effectiveness in treating symptoms of hay fever, the use of oral steroids in treating hay fever is not strongly recommended for use as first-line treatment due to the associated adverse effects. These adverse effects are wideranging and include weight gain, abdominal pain, fluid retention and altered mood. In certain cases, a short course of systemic steroids
Sodium cromoglycate is a mast cell stabilisers that is available both OTC and on prescription in Ireland. It works by inhibiting mast cell degranulation which prevents the release of histamine and other inflammatory mediators. It is most effective when used prophylactically and after a loading period of a few weeks before exposure to the allergen. Lodoxamide tromethamine is another mast cell stabiliser that is sometimes used off-licence in Ireland. They are not often used as monotherapy due to the availability of other treatments that are more effective.32
Steroid eye drops are available for the treatment of steroid-responsive inflammatory conditions of the eye in the short term. They are very effective but are commonly used for short-term therapy only due to increased intraocular pressure and increased risk of cataract development. They can be used as monotherapy or dual therapy, in cases where there is an exacerbation of symptoms.33 Eye drops containing prednisolone and dexamethasone are licensed and commonly used in Ireland.34, 35
antihistamines
in Ireland.
Second-generation antihistamines selectively bind to peripheral histamine H1 receptors. Due to this selectively, they are generally well tolerated and are not associated with many serious adverse events. They are associated with much less sedation than the firstgeneration antihistamines. They also provide ease of use due to a possible once-daily dosing schedule (22). There are no major differences in safety and efficacy between the second-generation antihistamines when administered in equivalent doses. Fexofenadine may be the best option in terms of both efficacy and safety, and is therefore suitable as
43
Antihistamine OTC Prescription Age Max Licensed OTC Dose Max Licensed RX Dose Bilastine No Yes 6 Years N/A 20mg Cetirizine Yes Yes 2 Years 10mg 10mg Desloratidine No Yes 1 Year N/A 5mg Fexofenadine Yes Yes 12 Years 120mg 180mg Levocetirizine No Yes 2 Years N/A 5mg Loratidine Yes Yes 2 Years 10mg 10mg
Fig 2. Table outlining secondgeneration antihistamines on the market in Ireland outlines the availability with supply status, age
Fig 2. Table outlining second-generation
on the market
first line therapy for most patients. Cetirizine is the most potent and has been
44 CPD: Allergies
Ocular NSAID preparations are not regularly used in the treatment of allergic rhinitis but can be useful in some cases, particularly if symptoms are not controlled or the patient can’t use a steroid preparation. NSAIDs block the cyclooxygenase pathway and inhibit production of prostaglandins - which is a mediator of inflammation in IgE mediated allergic responses. After one week of use, topical NSAIDs were found to be effective in significantly reducing symptoms. However, use of NSAIDs is mainly used to treat inflammation in cataract surgery and use in allergic rhinitis would be off-licence. Ketorolac and diclofenac are examples of NSAIDs available as ocular preparations.36 Lubricant eye drops can also be used to dilute and flush the pollen away from the tear film, as well as to treat any dry eyes that may also be present.36
Leukotriene Receptor Antagonists (LTRAs)
LTRAs can be considered for use in treating hay fever when other treatment options are not well tolerated or are not effective in symptom relief. Montelukast is one such LTRA which is particularly useful in patients, where asthma is a comorbidity. Montelukast blocks leukotriene D4 in the airways and therefore leading to decreased inflammation and smooth muscle relaxation.11
Immunotherapy
Immunotherapy is another hay fever treatment option if symptoms are severe.37 Immunotherapy is the only treatment option that modifies the disease, rather than treats the symptoms. Allergen immunotherapy involves the administration of gradually increasing doses of the allergen until a dose is reached that can effectively induce immunological tolerance. Subcutaneous therapy has been shown to be effective in reducing symptoms of hay fever. Immunotherapy is generally reserved for patients that can not tolerate other treatments or symptoms are not controlled after other treatments. This treatment carries the risk of anaphylaxis and should therefore only be prescribed and administered by a physician with adequate training and is properly equipped to manage anaphylactic events. Treatment is typically administered perennially, with weekly dose increases over 6-8 months, followed by monthly
maintenance injections for 3-5 years. Patients tend to have prolonged protection and therapy may be discontinued.11 Apart from the risk of anaphylaxis, allergen immunotherapy has a relatively low risk of serious adverse events.38
Immunotherapy can also be administered sublingually and some treatment options are licensed in Ireland.37 Sublingual immunotherapy involves placing an oral lyophilisate under the tongue until it dissolves. Sublingual treatment offers a better safety profile than subcutaneous treatment. In addition to this, sublingual treatment is generally more acceptable to patients as they can avoid injections and take the medication at home. Most common side effects are local and include throat irritation and oral pruritus. These symptoms usually resolve after one week of treatment. There is a potential risk of a severe systemic allergy and therefore treatment should be initiated by a physician with experience in treating allergic diseases and treating allergic reactions. Treatment should be initiated at least four months prior to the start of the grass pollen season and continue throughout the season. Asthma is a risk factor for systemic allergic reactions, and therefore should be avoided in this patient group.39 Grazax and Oralair are two sublingual allergen immunotherapies used to treatment grass pollen induced rhinitis in adults and children over 5 years. Both Grazax and Oralair are reimbursed under HSE schemes.42
Decongestants
Both oral and topical decongestants can provide relief from nasal congestion associated with hay fever. Pseudoephedrine, phenylephrine and xylometazoline are the most commonly used decongestants. These work by acting on adrenergic receptors, which results in vasoconstriction in the nasal passage and therefore decreasing inflammation. Duration should be limited to short term use due to the risk of rhinitis medicamentosa.43 A combination product containing both cetirizine is licensed for use in Ireland for up to 2-3 weeks. If nasal symptoms are resolved, treatment can be continued with just oral antihistamines.44
Alternative Medicines
Many different complementary or alternative medicines have been investigated for the treatment of
hay fever including homeopathy and acupuncture. However, there no evidence for therapeutic efficacy for any of these therapies.45
Non-pharmacological Treatment
Nasal irrigation with saline involves rinsing the nasal cavity with hypertonic or isotonic saline. It can relieve some symptoms of hay fever in both adults and children. Nasal saline irrigation is available over the counter and can provide a safe and acceptable alternative to pharmacological treatment. It is not unlikely to be associated with adverse effects. It can be used as monotherapy or as an adjunct to other treatments.46
References available on request 5 QUESTIONS AND ANSWERS FOR THE READERS TO ENSURE THEY UNDERSTAND THE ARTICLE
What causes hay fever?
Immunoglobulin E (IgE) antibodies in the body attach to inhaled pollen, which causes the release of histamine, leukotrienes and other inflammatory mediators. These immune reactions are induced by type-2 helper T cells and cause an inflammatory response. Inflammation in mucous membranes then cause symptoms such as itch, sneezing, runny nose, blocked nose, watery eyes and red eyes.
What are the best methods to prevent hay fever?
Prevention is a very important aspect in the management of hay fever. These methods include:
- Staying indoors or reducing time outside during peak pollen season.
- Using Vaseline around the nostrils to block pollen from entering the nasal passage.
- Wearing wraparound sunglasses.
- Keeping windows and doors closed.
- Not allowing animals into the house.
- Showering and changing clothes after being outside.
- Not drying clothes outside.
- Vacuuming regularly.
How can a differential diagnosis be done?
Hay fever can sometimes be confused with common respiratory
viruses such as the common cold, influenza and Covid-19. Symptoms such as fever and body aches are common in respiratory viruses but almost never present in hay fever. Mucus associated with a virus tends to be yellow / green in colour, compared to a clear colour in hay fever. A respiratory virus will usually resolve in one or two weeks, while hay fever will usually persist for weeks or months. Diagnosis of hay fever is often made by a GP following examination of symptoms and medical history. Laboratory tests can be used to test for common respiratory viruses. Allergy testing can be carried out, with a skin prick test or a blood test for the presence of IgE the most common. Which is the preferred steroid treatment option: intranasal steroids or oral steroids?
Steroids work by decreasing inflammation and therefore reducing symptoms of hay fever. Intranasal steroid sprays are among the mainstays of the treatment of hay fever. They act locally to reduce inflammation and reduce symptom severity. They have an onset of action within 30 minutes. Adverse effects are usually local and don’t involve the same systemic adverse effects as oral steroids.
Oral steroids are also very effective in symptom relief. Despite their effectiveness, the use of steroids is not recommended as firstline treatment due to adverse effects including weight gain, abdominal pain, fluid retention and hypopituitarism. They are best used in short-term cases where other treatment options have failed.
Is
immunotherapy useful in the treatment of hay fever?
Allergen immunotherapy is an option that can be useful in hay fever if symptoms are severe, other treatment options have failed or are contraindicated. Immunotherapy is the only treatment option that modifies the disease, rather than treats the symptoms.
Both subcutaneous and sublingual immunotherapy are effective in reducing symptoms of hay fever. Treatment is much more effective if initiated at least four months before exposure to the allergen. Caution must be observed due to the risk of anaphylaxis with immunotherapy.
steroids, particularly if impairment of adrenal function suspected. Systemic effects of nasal corticosteroids may occur, particularly at high doses prescribed for prolonged periods. Visual disturbances may occur with use of topical and systemic steroids. Long-term use may cause oedema of the nasal mucosa. Contains benzalkonium chloride which may cause bronchospasm. Side effects: Dryness and irritation of the nose and throat, nasal ulcers, nasal septal perforation, unpleasant taste and smell, headache and epistaxis. Hypersensitivity reactions including skin rash and oedema of the face or tongue. Eye disorders such as glaucoma and blurred vision. Anaphylaxis/anaphylactic reactions and bronchospasm. See SPC for full details. Legal category: Pharmacy Only. Product

Authorisation Holder: PA0678/095/001. Product Authorisation holder: GlaxoSmithKline Consumer Healthcare (Ireland) Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. Date of last revision: May 2021. Further information available on request. Contains fluticasone propionate. Always read the label/leaflet. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-FLX-23-00001.





















antihistamines, FLIXONASE blocks 6 key inflammatory mediators histamine cytokines leukotrienes chemokines prostaglandins tryptases Don’t let allergies limit your patients’ activities Fluticasone propionate ALLERGY RELIEF / 0.05% NASAL SPRAY / ALLERGY RELIEF 0.05% NASAL SPRAY Product Information: Please consult the summary of product characteristics for full product information. Flixonase Allergy Relief 50 micrograms per dose Nasal Spray (fluticasone propionate 50 micrograms per spray). Uses: Prevention and treatment of allergic rhinitis. Dosage and method of use: Adults: Two sprays into each nostril once or twice a day if required. Maintenance: one spray per nostril once a day if possible. Use lowest possible maintenance dose. Max 4 sprays a day in each nostril. Children under 18 years: Not to be used. Contraindications: Hypersensitivity to ingredients. Precautions: Seek medical advice if inadequate relief after 7 days, or require more than 6 months continuous use. Seek medical advice before use with: concomitant corticosteroid use, fever, nasal/sinus infection, recent nasal injury/surgery, nasal ulceration, pregnancy, breast feeding. Caution with cytochrome P450 3A4 inhibitors like ketoconazole and protease inhibitors, like ritonavir and cobicistat. Caution commencing in those withdrawing from systemic
Unlike
Why Pharmacies are Choosing BOIPA
BOI Payment Acceptance’ s (BOIPA) recent business sentiment survey revealed over 6 in 10 businesses feel the increased use of card payments over cash transactions has had a positive effect on how they run their business.

cash withdrawals. Not only does this limit bank charges, it also cuts down the amount of time pharmacy staff have to spend making trips to their local bank branch, giving time back to staff which can be used to support other tasks.
Financial administration is also simplified with card transactions creating a digital record of payments that can be easily used for reporting and accounting, cutting down the amount of back office time spent on consolidating cash payments. It also supports more routine cash flow into business current accounts with payment service providers like BOIPA guaranteeing next day settlement on all card transactions. The acknowledgement of these advantages have led to a third of businesses saying they would like to go fully cashless on all transactions.
Offering card payments with easy to install card terminals allows pharmacies to accept chip and pin, digital wallet and contactless card transactions within days of signing up to BOIPA.

The advantages for pharmacies accepting card payments has never been clearer with BOIPA continuing to strengthen their foothold as a provider of choice within the Irish market through best-in-class customer service, competitively priced card terminal options and integrations with the leading EPOS solutions pharmacy practices are using in the industry today.
Meet your consumer’s payments preference
The continual increase in noncash transactions began over a decade ago but was undoubtedly accelerated by the pandemic. Consumers started carrying less cash and more businesses began using card terminals for the first time to support quick, frictionless transactions, especially in pharmacies where the need for tap and go, contactless payments was particularly necessary given the heightened risk of contracting Covid-19 in these environments.
According to our 2022 Irish consumer’s attitude to payments
survey, four in five people prefer to use card when paying in a pharmacy. Card transactions are the payment preference of choice with 65% of Irish adults saying they prefer to use card given its convenience and ease of use. Paying through a mobile phone or wearable device is the third most popular payment option and continuing to rise, with customers becoming more aware that they have no contactless limit given their built-in security features. Not only does having card terminals meet your consumers preference but it also affects customer perception with the majority believing businesses offering cash-less payment options are more customer-centric and modern.
How accepting card payments better supports businesses
With running costs highlighted as the key concern for businesses in this year’s survey, it is little surprise to note the high percentage of businesses preferring card payments over cash given their cost effectiveness. Card transactions allow for money to be digitally transferred to pharmacies business bank account without needing to do lodgements or
Why pharmacies are choosing BOIPA
With almost a decade’s experience in the Irish market, BOIPA has fast become a front-runner as a provider of card payments technology. BOIPA’s annual business survey demonstrates continued endorsement for the Irish based company with 2/3 of businesses who had switched provider to BOIPA saying they rate them more highly than their competitors. With no hidden fees and flexible pricing, including Ready Made bundle options, that adapts to suit your business requirements, BOIPA has continued to put the needs of pharmacies at the forefront of what they do. Being an Irish based company with 24/7 business support and on the ground engineers ready to install card terminals amplifies the approach to customer service that has proven to be a key differentiator between BOIPA and other providers. BOIPA’s integration with leading EPOS solutions in the industry today makes accepting card payments easier for your pharmacy by speeding up the transaction time and simplifying administrative duties and reporting.
PHARMACYNEWSIRELAND.COM 46 Advertorial




BOI Payment Acceptance enables pharmacies across the country to accept card payments in-person, over the phone or on the move. We can integrate with all leading EPOS solutions being used by pharmacies today. Looking to start accepting card payments or switch provider? Accept payments anywhere EVO Payments International GmbH, Branch Ireland, trading as BOI Payment Acceptance is registered under Companies Registration Office Ireland number 907681. Further trading name of EVO Payments International GmbH, Branch Ireland, is "BOIPA". EVO Payments International GmbH, Branch Ireland is licenced by the Federal Financial Supervisory Authority BaFin (Bundesanstalt fur Finanzdienstleistungsaufsicht) in Germany (BaFin-ID 50071564 and Bak no. 122963; register available at www.bafin.de) and is regulated by the Central Bank of Ireland for conduct of business rules. EVO Payments International GmbH, Branch Ireland trading as BOI Payment Acceptance is not a member of the Bank of Ireland Group. BOI Payment Acceptance has entered into a marketing alliance with the Bank of Ireland. BOI and the Tree of Life logo are trademarks of The Governor and Company of the Bank of Ireland and are being used under licence by EVO Payments International GmbH, Branch Ireland trading as BOI Payment Acceptance.
Sepsis: a guide for pharmacists
Written by Fleming A1, Horgan S2, Quigley L3, McCarthy D.4
1 Lecturer in Clinical Pharmacy, School of Pharmacy, University College Cork

2
3
Sepsis ADoN South/South Western Hospital Group HSE
Programme Manager, National Clinical Programme for Sepsis
4 Sepsis CNM3 South/South Western Hospital Group HSE
Aoife Fleming

Sepsis claims more lives than lung cancer, and more than breast cancer, bowel cancer and HIV/ AIDs combined.
Sepsis is a time dependent medical emergency where early recognition and prompt treatment is fundamental to increased survival rates and optimal outcome for survivors of sepsis and septic shock. Sepsis is defined as life threatening organ dysfunction caused by a dysregulated host response to infection (Singer et al., 2016). The majority of sepsis is community acquired and approximately 70-80% of patients with sepsis present to the Emergency Department. Sepsis can affect anyone at any age however, 90% of adults and 70% of children who develop sepsis have underlying risk factors (CDC, 2016). Lack of knowledge and awareness can result in late patient presentations and delayed treatment. The infection can occur at any site and be caused by any pathogen – the most common site affected being the respiratory tract followed by the abdomen, then urinary tract. Pregnancy increases vulnerability especially to viral illnesses, while in late pregnancy the genito-urinary tract is the most common site.
Epidemiology
According to the World Health Organisation The Global report on the Epidemiology and Burden of Sepsis 2020, 20% of global deaths are attributed to sepsis (WHO 2020). There were 11,294 cases of sepsis documented in Ireland
in 2020 with an average hospital sepsis-associated mortality rate of 20.1%, 26.5% of which were admitted to a critical care area (HSE 2022). The average crude mortality rate of these patients admitted to a critical care area was 30.8%.
Whilst sepsis incidence increases with age in adults (Figure 1), mortality peaks at the extremes of age. Age > 75years is considered high risk for sepsis mortality, with >20% crude mortality rate. With ageing, co-morbidities are accumulated and the immune system gradually deteriorates leading to increases in both incidence and mortality.
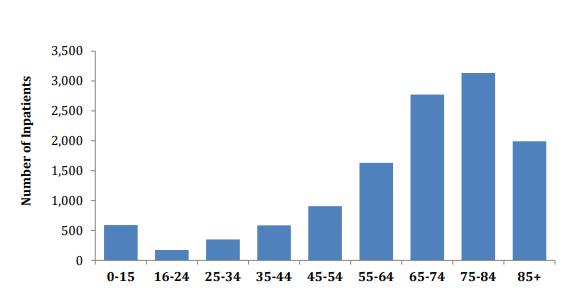
Sepsis Pathway:
The pathology of sepsis involves a complex pathway whereby the normal response to infection is not sufficient to eliminate the local infection. The inflammatory cascade is ramped up and the
signs and symptoms of the Systemic Inflammatory Response (SIRS) manifest i.e. high or low temperature, tachypnoea and tachycardia. The mechanism by which organ dysfunction is triggered is poorly understood. If this process is interrupted with medical intervention (i.e. resuscitation, source control, intravenous antimicrobial therapy) and the infection got under control there can be a rapid return of organ function. Later recognition makes the condition more difficult to treat. A hypo-inflammatory response can then ensue, leading to persistence of infection, secondary infection, worsening organ dysfunction and potentially death.
Screening for Sepsis
Screening for sepsis using a screening tool, as developed by the National Sepsis Programme,
allows for prompt identification of patients with a high-risk presentation e.g. clinically apparent acute organ dysfunction such as acute confusion, respiratory failure or a purpuric rash AND patients who are high risk because of their medical history, e.g. on chemotherapy or having chronic co-morbidities or additional factors such as frailty, age ≥75 and recent trauma or surgery (Figure 2). A further clinical decision support tool, known as the Sepsis Six Bundle, provides guidance on treatment and escalation of care if deterioration.
Community pharmacists are one of the first points of contacts when people present unwell. Therefore, all healthcare professionals need to ask “Could this be sepsis?”. Knowledge of the signs and symptoms of sepsis, prompt diagnosis and early treatment has been shown to improve patient outcomes

(Department of Health, 2021).
How to recognise Sepsis

While the above description presents a picture of a critical illness that requires secondary care admission and medical attention, it is vitally important that all healthcare professionals in all settings are aware of and educated on sepsis. Table 1 below highlights underlying conditions that increase the risk of sepsis in adults and children.
As sepsis is often hard to diagnose in the early stages, it is very important to watch for the signs of sepsis which might develop if
PHARMACYNEWSIRELAND.COM 48 Sepsis
Sinead Horgan
Lorna Quigley
Denise McCarthy
Sepsis Pathway: The
symptoms of the Systemic Inflammatory Response (SIRS) manifest i.e. high or low temperature,
Figure 1. The number of inpatients with a diagnosis of sepsis by age group 2020. (Includes maternity and paediatrics) National Sepsis Outcome Report, Ireland 2020.
pathology of sepsis involves a complex pathway whereby the normal response to infection is not sufficient to eliminate the local infection. The inflammatory cascade is ramped up and the signs and
Figure 1. The number of inpatients with a diagnosis of sepsis by age group 2020. (Includes maternity and paediatrics) National Sepsis Outcome Report, Ireland 2020.









SAME SUPER FORMULA NEW TROPICAL TASTE 1 super supplement with 26 active ingredients including 11 vitamins, 7 minerals and 6 amino acids, all in 1 daily sachet GO TROPICAL THIS SUMMER Telephone: 091 769 803 | Email: customerservice@reviveactive.com or contact your local area representative. † Source: Euromonitor Passport report on Consumer Health National Statistics. Date: September 2022 150mg CoQ10 3,000mg L-Arginine Energy Immune System Heart Fatigue Also available in orange and mango flavour †

and therapy rationalisation then depends on the patient’s clinical response.
By 3 hours from time zero, the patient’s status should be reviewed and care escalated if they are failing to stabilise or deteriorating. By 6 hours of ongoing review and treatment, patients who have failed to stabilise may require pressors and/or critical care input and may now be suffering from septic shock. The latest National Sepsis Outcome Report 2020 is available at: https://www.hse.ie/eng/about/ who/cspd/ncps/sepsis/resources/ national-sepsis-report-2020.pdf.
This report presents data on the burden of sepsis in the acute settings, in terms of the number of cases and associated mortality, and compares the data to previous years.
The role of the pharmacist
the infection is aggressive or is not responding to the initial treatment. Signs and symptoms of sepsis may vary, patients with infection who are deteriorating despite usual care or who develop any signs of acute organ dysfunction (Table 2) need to be reviewed urgently by a doctor. Sepsis is only diagnosed if infection is suspected or proven to be the cause of these signs.
1. Recognition and escalation to medical review
How to recognise Sepsis
Table 2. Signs of new onset organ dysfunction in adults, and sepsis in paediatric patients.
2. Diagnosis and initiation of treatment
healthcare professionals. The National Sepsis Programme provides education aids, posters, presentations and material all available and supported by its website www.hse.ie/sepsis. Sepsis education modules have also been developed and are available on HSELand, the Irish health service national online learning and development portal. It is recommended that all relevant Healthcare Professionals undertake the sepsis eLearning and that it is refreshed on a 3 yearly basis.
Community pharmacists are one of the first points of contacts when people present unwell. Therefore, all healthcare professionals need to ask “Could this be sepsis?”. Knowledge of the signs and symptoms of sepsis, prompt diagnosis and early treatment has been shown to improve patient outcomes (Department of Health, 2021).
Advice is often sought from pharmacists in both the community and hospital settings, with community pharmacists often being the first port of call for patients when they feel unwell. Pharmacists can support sepsis management and improved patient quality of care in the following ways;
1. BE AWARE OF THE RISK FACTORS:
• See Table 1
Management of Sepsis
While the above description presents a picture of a critical illness that requires secondary care admission and medical attention, it is vitally important that all healthcare professionals in all settings are aware of and educated on sepsis. Table 1 below highlights underlying conditions that increase the risk of sepsis in adults and children.

The National Clinical Guideline No.26 Sepsis Management was updated and published in November 2021 by the National Clinical Effectiveness Group (DoH 2021), to standardise management of sepsis in the acute settings. This guideline is pivotal in raising education and awareness of sepsis among medical and nursing professionals as well as among practicing
In terms of active management of sepsis cases two time-dependent processes have been identified as essential for optimal patient care:
1. Recognition and escalation to medical review
2. Diagnosis and initiation of treatment
(time zero), the second time-dependent step is started which is the “Sepsis 6” 1 hour Bundle (Figure 3). The rapid management of sepsis is critical, each hour of delay to antimicrobial administration has been associated with an average decrease in survival of 7.6% in a retrospective cohort study by Kumar et al (2006). Empiric antimicrobial prescribing should be based on locally approved guidelines, the patient’s history of colonisation/infection with antimicrobial resistant organisms, allergy status and the site of infection as determined clinically. Antimicrobials should be reviewed after 24-48 hours by a senior clinician and based on microbiological culture results and clinical response, as per the ‘Start Smart, Then Focus campaign’. (https://www.hpsc. ie/a-z/microbiologyantimicrobialresistance/carebundles/antibioticcarebundle/File,14119,en.pdf.).

Once a diagnosis of sepsis is made, supported by medical review (time zero), the second timedependent step is started which is the “Sepsis 6” 1 hour Bundle (Figure 3). The rapid management of sepsis is critical, each hour of delay to antimicrobial administration has been associated with an average decrease in survival of 7.6% in a retrospective cohort study by Kumar et al (2006). Empiric antimicrobial prescribing should be based on locally approved guidelines, the patient’s history of colonisation/infection with antimicrobial resistant organisms, allergy status and the site of infection as determined clinically. Antimicrobials should be reviewed after 24-48 hours by a senior clinician and based on microbiological culture results and clinical response, as per the ‘Start Smart, Then Focus campaign’ (https://www.hpsc.ie/az/microbiologyantimicrobialresistance/carebundles/antibioticcarebundle/File,14119,en.pdf.).
Once a diagnosis of sepsis is made, supported by medical review
Blood cultures are often negative (in up to 60% of sepsis cases)
• For Community pharmacists, refer patients for urgent medical attention if;
any of the alarm signals (Table 2)
patient has deteriorated while being treated for a systemic infection
patient is unwell without a clear cause
patient presents with deteriorating infection and also immunocompromised
2. SUPPORT PREVENTATIVE MEASURES:
• Infection Prevention and Control: Engage in appropriate infection prevention and control measures – See https://www. hse.ie/eng/about/who/nqpsd/ nirp/ncec-ipc-guideline-2022for-consultation.pdf.
Blood cultures are often negative (in up to 60% of sepsis cases) and therapy rationalisation then depends on the patient’s clinical response.
PHARMACYNEWSIRELAND.COM 51 Sepsis
Figure 2 Sepsis Triage Screening Tool
Figure 2 Sepsis Triage Screening Tool
Figure 3. Sepsis 6, I hour Bundle; Take 3 and Give 3.
By 3 hours from time zero, the patient’s status should be reviewed and care escalated if they are
Figure 3. Sepsis 6, I hour Bundle; Take 3 and Give 3
Sepsis
Table 1. Risk factors for sepsis in adults, paediatrics and maternity Patient group Risk factors
Adults
Age ≥ 75 years
Frailty
Diabetes
Chronic obstructive pulmonary disease
Cancer
Chronic kidney disease
Chronic liver disease
Recent surgery, or wounds/injuries from accidents
HIV/ AIDS
On immunosuppressant medications
- Chemotherapy/radiotherapy
- Anti-rejection medications
- Biological medications
- Corticosteroids
- Methotrexate
Paediatrics Immunocompromised (follow national haematology/oncology guidelines for children with cancer)
Age ≤3 months
Chronic disease
Recent surgery
Break in skin (including chickenpox)
Indwelling line/device
Signs of infection in a wound (including chickenpox)
Incomplete vaccination record
Maternity Pregnancy Related:
Cerclage
Pre-term/prolonged rupture of membranes
Retained products
History pelvic infection
Group A Strep. infection in close contact
Recent amniocentesis
Non Pregnancy Related:
Age > 35 years
Minority ethnic group
Vulnerable socio-economic background
Obesity
Diabetes, including gestational diabetes
Recent surgery
Symptoms of infection in the past week
Immunocompromised e.g. Systemic Lupus
Chronic renal / liver / heart failure
• Vaccination: Encourage and provide vaccination services to ensure that at risk patients are protected from seasonal influenza infection, Covid-19 and pneumococcal pneumonia. Other vaccines are also available for a fee, e.g. chickenpox, shingles. Refer to https://www.hse.ie/eng/health/ immunisation/pubinfo/adult/ pneumo/ for more information. Encourage parents to ensure children are up-to-date with their primary immunisation schedule. https://www.hse.ie/eng/health/ immunisation/pubinfo/.
antimicrobials in all patients and limiting the emergence of antimicrobial resistance. The PAMS-Net has a bank of online resources, discussion fora and links to recorded and upcoming webinars to support appropriate antimicrobial stewardship.
For community pharmacists:
Refer to The HSE Guidelines for Antimicrobial Prescribing in Primary Care (www. antibioticprescribing.ie) when a patient is prescribed an antimicrobial.
Ensure patients are aware of the importance of not missing doses of antimicrobials, and finishing the course.
Stress to patient to contact GP/Pharmacy if troubling side effects to antimicrobial, as alternative may be available.
Stress to patient to re-present to GP/ED if not responding to treatment.
Provide advice when a patient presents with a self-limiting or viral infection and direct them to www.undertheweather.ie.
Manage the expectation of an antimicrobial for a likely viral illness or self-limiting infection, even if the service user may need to see the doctor if unwell.
Remind patients that any unused antimicrobials should be returned to the pharmacy for safe disposal.
For hospital pharmacists:
As sepsis is often hard to diagnose in the early stages, it is very important to watch for the signs of sepsis which might develop if the infection is aggressive or is not responding to the initial treatment. Signs and symptoms of sepsis may vary, patients with infection who are deteriorating despite usual care or who develop any signs of acute organ dysfunction (Table 2) need to be reviewed urgently by a doctor. Sepsis is only diagnosed if infection is suspected or proven to be the cause of these signs.
• Smoking Cessation: See National Clinical Guideline on Smoking Cessation at https://www.gov.ie/en/ publication/4828b-stopsmoking/. Cigarette smoking
has been associated with an increase in the risk of death from sepsis (HR=1.62; 95% CI: 1.11–2.37, p=0.01) (Zhang et al., 2022).
• Management of chronic conditions: Ensuring patients are complying with medications to treat chronic conditions, such as diabetes or kidney disease, so that their condition is well managed. This will reduce the risk of developing sepsis (CDC).
• Appropriate treatment of infection: Engage in active Antimicrobial Stewardship. HSE AMRIC have developed an e-learning module on ‘Antimicrobial Stewardship in Practise’, available on HSEland. They have also developed Guidance on Antimicrobial Stewardship for all healthcare
workers, available at https:// www.hse.ie/eng/services/ list/2/gp/antibiotic-prescribing/ antibicrobial-stewardship-audittools/hse-amric-antimicrobialstewardship-guidance-forall-healthcare-settings-v1published-august-2022.pdf.
• The Irish Institute of Pharmacy have an online CPD programme Antimicrobial Stewardship for Community Pharmacists to outline the concepts of antimicrobial resistance and appropriate use of antimicrobials.
• The Pharmacist Antimicrobial Stewardship Network (PAMSNet), accessed via the IIOP portal, supports pharmacists across all sectors to work towards the common goal of promoting responsible use of
Ensure the patient is prescribed and administered the right antimicrobial therapy for infection or sepsis, in relation to choice, dose, route and duration as guided by local antimicrobial guidelines and specialist input.
Optimisation of antimicrobial prescribing based on microbiological sampling results.
Consider early use of source control – removal of infection devices, catheters, appropriate management of surgery, wound management procedures.
Review of the antimicrobial therapy according to the Start Smart then Focus care bundle at 24-48 hours, and on an ongoing basis. https://www.hse.ie/eng/ services/publications/clinicalstrategy-and-programmes/startsmart-stay-focused.pdf
If on review, sepsis or infection is not diagnosed, stop antibiotics as appropriate.
PHARMACYNEWSIRELAND.COM 52
Table 1. Risk factors for sepsis in adults, paediatrics and maternity
soft capsules


















Paralief 500 mg soft capsules, each capsule contains 500 mg of paracetamol. Pharmaceutical Form: Capsules, soft. Indications: For the short-term treatment of headache, toothache, muscle ache, lumbago, fever and pain with flu and colds. Dosage and administration: Adults and adolescents older than 15 years (> 55 kg body weight): 1 or 2 capsules (500-1,000 mg) at a time, with a maximum of 6 capsules (3,000 mg) within 24 hours. Adults and adolescents older than 15 years (≤ 55 kg body weight): The effective daily dose should not exceed 60 mg/kg/day (up to 2 g/day). Dose adjustment may be required in patients with renal or hepatic impairment. Refer to the SmPC for full dosage guidance. Method of administration: Oral. Swallow capsule with sufficient water. Contraindications: Hypersensitivity to the active substances or to any of the excipients. Warnings and precautions: Long-term or frequent use is not advised. In young people who are treated with 60 mg/kg/day of paracetamol, combination with another antipyretic is not allowed except where there is a lack of efficacy. After the long-term use (> 3 months) of analgesics with intake every other day or more frequently, headache can occur or become worse. In these cases, the use of analgesics must be stopped in consultation with a doctor. The patient should be advised to avoid the simultaneous use of this medicinal product with others containing paracetamol, such as flu or cold medicinal products. If another medicine containing paracetamol is administered, the maximum paracetamol dose of 3,000 mg per day should not be exceeded, taking into account the content of all the medicines used by the patient. Patients diagnosed with impaired liver or kidney function, should seek medical advice before taking this medicinal product. The taking of several daily doses at once can cause severe damage to the liver. Immediate medical help must be sought even if the patient feels well because of the risk of irreversible damage to the liver. Caution is required when administering paracetamol to patients with moderate to severe renal insufficiency, mild to moderate hepatic insufficiency (incl. Gilbert’s syndrome), severe hepatic insufficiency (Child-Pugh > 9), acute hepatitis, the concomitant administration of medicinal products which have an influence on hepatic function, glucose-6-phosphate dehydrogenase deficiency, haemolytic anaemia, alcohol abuse, dehydration and chronic malnutrition. The risk of an overdose is greater in patients with non-cirrhotic alcoholic liver conditions. Caution is required in the case of chronic alcoholism. The daily dose may not exceed 2 grams in this case. No alcohol may be used during treatment with paracetamol. In the case of a high fever, symptoms of secondary infection or the persistence of symptoms, it will be necessary to reconsider the treatment. Caution is required in the case of asthmatic patients who are sensitive to acetylsalicylic acid as mild bronchospasms have been reported as a cross-reaction after the use of paracetamol. Cases of hepatic impairment or liver failure have been reported in patients with glutathione depletion, such as patients with severe malnutrition, anorexia or a low body mass index, or patients who chronically consume too much alcohol. In patients with a condition of glutathione depletion such as sepsis, the use of paracetamol may increase the risk of metabolic acidosis. Caution is advised if paracetamol is administered concomitantly with flucloxacillin due to increased risk of high anion gap metabolic acidosis (HAGMA). Close monitoring, including measurement of urinary 5-oxoproline, is recommended. Paracetamol can have an influence on the urine test with wolfram phosphoric acid as well as the blood sugar test with glucose oxidase peroxidase. Patients with hereditary fructose intolerance (HFI) should not take/be given this medicinal product. Interactions: Paracetamol is metabolised in the liver and can consequently enter into interactions with other medicinal products which follow the same metabolic route or which are able to inhibit or induce the route. In the case of chronic alcohol abuse and the use of drugs, which induce hepatic enzymes such as barbiturates and tricyclic antidepressants, an overdose of paracetamol can take a more severe course as a result of the increased and more rapid formation of toxic metabolites. Caution is required with the concomitant intake of enzymeinducing drugs. In the case of concomitant treatment with probenecid, the dose of paracetamol must be reduced. Paracetamol can cause an increase in the half-life of chloramphenicol. The rate of absorption of paracetamol can be increased by metoclopramide or domperidone and absorption can be reduced by colestyramine. The anticoagulatory effect of warfarin and other coumarins can increase during the long-term, regular use of paracetamol with an increase in the risk of bleeding as a result. With the concomitant chronic use of paracetamol and zidovudine, neutropenia often occurs. Salicylamide can prolong the half-life of paracetamol. Isoniazid ensures a reduction in the clearance of paracetamol, which possibly increases the activity and/or toxicity of paracetamol by preventing metabolism in the liver. The concomitant intake of paracetamol with lamotrigine ensures a reduction in the bioavailability of lamotrigine. Caution should be taken when paracetamol is used concomitantly with flucloxacillin. Fertility, pregnancy and lactation: If clinically needed, paracetamol can be used during pregnancy however, it should be used at the lowest effective dose for the shortest possible time and at the lowest possible frequency. Paralief can be used in therapeutic doses by women who breast-feed. There are no available data on the effect of paracetamol on fertility. Undesirable effects: Agranulocytosis (after long-term use), thrombocytopenia, thrombocytopenic purpura, leukopenia, haemolytic anaemia, Allergies (exclusive of angioedema), Depression, confusion, hallucinations,Tremor, headache,Visual abnormalities, Oedema, Bleeding, abdominal pain, diarrhoea, nausea, vomiting,Abnormal hepatic function, hepatic failure, hepatic necrosis, jaundice, Hepatotoxicity, Sterile pyuria. Refer to the SmPC for a full list of undesirable effects. Adverse reactions should be reported via HPRA Pharmacovigilance, website: www.hpra.ie. Pack size 20 soft capsules. A copy of the Summary of Product Characteristics is available upon request or go to www.clonmelhealthcare.ie Marketing authorisation holder: Clonmel Healthcare Ltd. Waterford Road, Clonmel, Co. Tipperary Marketing authorisation number: PA126/020/7. Supply through pharmacies only. Date last revised: August 2022.

2023/ADV/PAR/028H Date Prepared: March 2023
Table 2. Signs of new onset organ dysfunction in adults, and sepsis in paediatric patients. Adult – Signs of new onset organ dysfunction
Central Nervous System Agitation, confusion, drowsiness
Severe leg pain, unable to weight bear in adolescents
Patients with disabilities may not be functioning at usual level
Respiratory system
Cardiovascular system
Respiratory rate > 30 breaths per minute
Unable to finish sentences in one breath
Cyanosis/hypoxia
Heart rate > 130 beats per minute
Systolic blood pressure < 90 or > 40mmHg drop from usual level.
Unable to palpate radial pulse (by someone who usually can)
Sustained dizziness when upright (so unable to sit up comfortably)
Very pale, cold peripheries with prolonged central capillary refill
Venous lactate ≥ 2mmol/l
Renal system
No urinary output for > 12 hours and no urge to urinate
Very small amounts of very dark urine
In the patient with an indwelling urinary catheter if the urinary output is being measured hourly, a urinary output of < 0.5mls/kg/hr for a minimum of 2 hours
gov.ie/pdf/?file=https://assets. gov.ie/197784/2e897cca-3b574753-b420-c397474dd171. pdf#page=null
Gotts JE, Matthay MA. Sepsis: pathophysiology and clinical management. BMJ 2016;353:i1585 doi:10.1136/bmj.i1585
Centre for Disease Control. CDC Vital Signs. Making Healthcare Safer. Think Sepsis. Time Matters 2016 [Online]. Available: https:// www.cdc.gov/vitalsigns/sepsis/ infographic.html
Coagulation system
Paediatric – Signs of sepsis
Non-blanching rash – this is a new rash that does not disappear when pressed on by glass; it can be petechial or blotchy.
Beware Campbell de Morgan spots/angiomas, which are nonblanching but are not acute
Inappropriate tachycardia (if caused by a fever, pain or fear it should resolve with paracetamol and/or reassurance)
Inappropriate Tachypnoea (if caused by fear or exercise it will settle with reassurance)
Altered mental status (irritability, lethargy, floppiness, difficult to rouse)
Altered functional status
Reduced peripheral perfusion/ prolonged central capillary refill (cold extremities, pallor or cyanosis of extremities, oedema, oliguria)
Non-blanching rash
Health Service Executive, 2022. National Sepsis Outcome Report 2020. Available from: https://www. hse.ie/eng/about/who/cspd/ncps/ sepsis/resources/national-sepsis-report-2020.pdf
Health Service Executive. Guidelines for antimicrobial prescribing in primary care. Available from: https://www.hse.ie/eng/services/ list/2/gp/antibiotic-prescribing/ McPherson D, Griffiths C, Williams M, Baker A, Klodawski A, Jacobson B, Donaldson L. Sepsis-associated mortality in England: an analysis of multiple cause of death data from 2001 to 2010 BMJ Open 2013;3:8.
Management of Sepsis
Evaluate the route of administration and promote early intravenous to oral switch where possible.
Consider patient factors such as interactions, allergies, renal/hepatic impairment, other conditions, age, recent antimicrobial use, or known infection or colonisation with AMR organisms, as they may influence the choice of agent
Liaise promptly with pharmacy procurement when alerted to supply issues in relation to antimicrobials that may cause delays in administration.
how to get better from common infections without the use of antibiotics.
• www.antibioticprescribing.ie for information on infections where antimicrobials have been prescribed.
• Information on vaccination and schedules is available here: https://www.hse.ie/eng/health/ immunisation/pubinfo/
Where appropriate, seek specialist advice from clinical microbiology, infectious diseases, or antimicrobial pharmacist.
The National Clinical Guideline No.26 Sepsis Management was updated and published in November 2021 by the National Clinical Effectiveness Group (DoH 2021), to standardise management of sepsis in the acute settings. This guideline is pivotal in raising education and awareness of sepsis among medical and nursing professionals as well as among practicing healthcare professionals. The National Sepsis Programme provides education aids, posters, presentations and material all available and supported by its website www.hse.ie/sepsis Sepsis education modules have also been developed and are available on HSELand, the Irish health service national online learning and development portal. It is recommended that all relevant Healthcare Professionals undertake the sepsis eLearning and that it is refreshed on a 3 yearly basis
• Consider the need for Infection Prevention and Control awareness in the long term care facility setting in collaboration with nursing and medical colleagues. (Hyperlink to https://www.hpsc.ie/a-z/ respiratory/coronavirus/novelcoronavirus/guidance/ infectionpreventionandcontrolguidance/ residentialcarefacilities/
3. PROVIDE INFORMATION:
• Resources on sepsis, including patient information leaflets, are available at: https://www.hse. ie/eng/about/who/cspd/ncps/ sepsis/resources/
• www.undertheweather.ie, a HSE/ICGP/IPU collaboration that provides information on
Conclusion:
Pharmacists can play a key role in both preventing a patient developing sepsis and improving patient outcomes should it develop. In the community setting, pharmacists can help by educating themselves on sepsis,
and referring patients for urgent assessment if the patient has signs and symptoms. In the hospital setting, pharmacists can ensure optimal antimicrobial stewardship, and compliance with the National Clinical Guideline No 26 in Sepsis Management. Preventative measures in both settings, as well as providing information and education as appropriate will also help to both reduce the burden of sepsis on healthcare in Ireland and improve patient health outcomes. The National Sepsis Programme has developed sepsis patient information leaflets to raise public awareness of the signs and symptoms of sepsis and deterioration which are available on https://www.hse.ie/eng/about/ who/cspd/ncps/sepsis/resources/. The National Programme also strongly recommends that patients with risk factors be vaccinated for preventable infections as a measure to reduce sepsis incidence.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):80110. doi: 10.1001/jama.2016.0287. PMID: 26903338.
World Health Organisation. Global report on the epidemiology and burden of sepsis: current evidence, identifying gaps and future directions. Geneva: World Health Organisation; 2020. CC BY-NC-SA
3.0 IGC. Available from: https:// www.who.int/publications/i/ item/9789240010789
In terms of active management of sepsis cases two time-dependent processes have been identified as essential for optimal patient care:
References
Department of Health (2021). Sepsis management for adults (including maternity). NCEC National Clinical Guideline No. 26. Available at: https://www.
HSE AMRIC AMS Guidance for all Healthcare settings, available at :https://www.hse.ie/eng/services/ list/2/gp/antibiotic-prescribing/antibicrobial-stewardship-audit-tools/ hse-amric-antimicrobial-stewardship-guidance-for-all-healthcare-settings-v1-published-august-2022.pdf.Zhang, N., Liu, Y., Yang, C., Zeng, P., Gong, T., Tao, L., & Li, X. (2022). Association between smoking and risk of death in patients with sepsis: A systematic review and meta-analysis. Tobacco induced diseases, 20.
PHARMACYNEWSIRELAND.COM 54 Sepsis
Table 1. Risk factors for sepsis in adults, paediatrics and maternity
Awards
Irish Pharmacy Awards 2023 –Celebrating Excellence
We are delighted to announce the Finalists for the 2023 Irish Pharmacy Awards across the next 22 pages.
These awards are brought to you by Irish Pharmacy News, Ireland’s best and most influential independent community pharmacy magazine.
The Irish Pharmacy Awards recognise the achievements of individuals and teams working in the community pharmacy sector; their dedication and innovation which positions the profession at the forefront of healthcare, improving the lives of people across the country.
The Irish Pharmacy Awards cross boundaries and foster partnership working and shared learning across community pharmacy all over Ireland.
These Awards represent a unique and high-profile opportunity to celebrate the outstanding accomplishments of Ireland’s pharmacy professionals and reaffirm Irish Pharmacy News’s commitment to the core pursuits of pharmacy: excellence in health and innovation.
They aim to recognise outstanding examples of high standards, best practice, innovation and excellence.

IPN Communications hope that these awards will inspire you to think about your role, that of your team and of the community pharmacy profession in which you operate, as a whole.


The sentiment has been echoed by some of the leading healthcare companies here in Ireland and their support is evident in the most positive way possible with their sponsorship of each of our awards.
We look forward to welcoming you all on Saturday, May 27th for what promises to be an un-rivalled event in the community pharmacy calendar.
Haleon Self-Care Award
United Drug Business Development (Independent) Award





Perrigo Superintendent Pharmacist of the Year
Reckitt Community Pharmacist of the Year


Uniphar Category Development of the Year Award


JPA Brenson Lawlor Young Community Pharmacist of the Year Award
Point of Care Testing Pharmacy of the Year Award
BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award
Viatris Community Pharmacy Team of the Year Award
McLernons Independent Community Pharmacy of the Year Award
Théa Pharma OTC Counter Assistant of the Year Award

TouchStore Community Pharmacy Technician of the Year Award

Easolief DUO Business Development (Chain) Award
Alliance Online Pharmacy Retailer of the Year Award

www.irishpharmacyawards.ie/ Introducing...
2023
The Irish Pharmacy
Finalists Finalists
Point of Care Testing Pharmacy of the Year Award 2023





Health promotion and empowering customers and the community in general to take control of their own health outcomes has long been a goal of the team at Keane’s CarePlus Pharmacy in Edenderry. Promoting this service to customers and promoting the pharmacy team’s availability and knowledge, especially at times when other healthcare professionals may not be available is extremely important. The pharmacy also reaches a portion of the population that will not or may not interact with other medical teams and are a first point of call for many.

The entire team take pride in their ability to be able to take the time to be there for their customers and lead them on a journey to better health and quality of life be that by offering antigen testing so people could travel and see loved ones again or by our health checks that can give patients a starting point in their health journey or piece of mind that they are doing their best to live a long and healthy life.
Mark’s community pharmacy team exemplifies exceptional team spirit and dedication to enhancing patient care at all levels. Working together efficiently and effectively, they create a collaborative and supportive environment, fostering trust and respect among team members and empowering each individual to contribute their unique expertise towards shared goals. Innovation and forward-thinking are central to their operations. The team unites around common objectives. This focused and unified approach to healthcare initiatives has led to numerous successful projects, showcasing our excellence in quality, innovation, productivity, and prevention.
One example of these collaborative efforts is the establishment of point-of-care testing services, such as diabetes screening, to promote prevention, early detection, and disease management. This initiative demonstrates their ability to work together to improve patient access to care through effective and rapid technology.
The pharmacy team at Hickey’s in Gorey jump at every challenge and always have a smile. Their motto in this store is CHOOSE HAPPINESS and the team always try their best to ensure this motto resonates with their customers too.

They provide services to all walks of life and are always there to listen and want to be the friendly ear. The pharmacy prides itself on being a safe place an has helped 12 people between November to the end of January that were suffering with issues ranging from mental health to domestic violence/abuse. More recently they also ran a Blood Pressure event at a local athletics event where there were over 2000 runners in attendance, managing to test over 300 athletes on the night, and raised awareness for blood pressure.

56 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
Mark’s Pharmacy, Ardee
Hickey’s Pharmacy, Gorey
Keane’s CarePlus Pharmacy, Edenderry
Awards
Finalists Finalists
TouchStore Community Pharmacy Technician of the Year Award 2023

Aoife has proven herself over the last number of years from March 2020 at the McCartan’s Pharmacy Portmarnock store, and in her previous roles within the McCartan’s group to have been an extremely valuable asset to the group and her current team. Her dedication, compassion, competence and trusted abilities are roundly recognised within her team and beyond. She has developed deep relationships and friendships with her colleagues, trusted connections with her patients, co-operates and helps co-ordinate patient treatments with the local GP’s and hospitals.




Aoife Marley, Keane’s CarePlus PCC, Mullingar
Aoife Marley is a pharmacy technician with over a decade of experience providing information and care for patients through community pharmacies. She is the dispensary manager and lead technician in Keane’s CarePlus, Mullingar primary care center a position she has held since 2019.
Aoife is a dynamic and driven member of her team. Her work ethic and attention to detail make her an outstanding technician and her compassion, empathy and consideration for her patients make her an integral component of the healthcare team within the pharmacy and the primary care center as a whole. Aoife is a leader within her team. She trains and encourages new members of staff to perform to their full capabilities.
Colette is a very dedicated Pharmacy Technician and a valuable member of Ballisodare Pharmacy Team. Her attention to detail contributes to her high standards of performance. She is meticulous in her approach to all tasks, from creating new working practices, developing relationships with new patients and healthcare teams. Colette would never take shortcuts understanding the importance of risk management.
Colette is a strong team player supporting her fellow technicians when necessary and mentoring their student technician through her course. Her positive attitude and willingness to help have contributed towards a positive and productive work environment that benefits all the team.
Danielle is an integral part of the team at North Road Pharmacy, with an excellent work ethic. She currently works 3 days per week however she easily can cram in 5 days amount of work. There is a team of 5 people on a daily basis comprising of full-timers primarily including a pharmacist and a trainee tech alongside 2 front of shop assistants.
Danielle is always impeccable in her appearance and demeanour, she is always available for consultations on minor ailments, however she also possesses the experience to know when a patient needs to speak to the Pharmacist or if a visit to the GP is necessary. Her knowledge is exemplary and is an intrinsic part of the team.
PHARMACYNEWSIRELAND.COM | 57
Aoife McDevitt, McCartans Pharmacy, Portmarnock
2023 The Irish Pharmacy
Colette Commons, Ballisodare Pharmacy, Sligo
Danielle Murphy, North Road Pharmacy, Drogheda
Awards
Awards
Finalists Finalists
TouchStore Community Pharmacy Technician of the Year Award 2023



Dominika Wikowicz is a Senior Technician in Adrian Dunne Pharmacy Balbriggan. She qualified as an EU Pharmacy Technician in Poland and joined Adrian Dunne group in 2019. In this short period of time she has become the most valuable part of the team. She is hard working and she is totally committed to her job. Her gentle personality has won the hearts of everybody around her in the Pharmacy. The main way Dominika has enhanced the role of the Pharmacy Technician is through her commitment and attention to detail when it comes to stock accuracy. She has achieved the highest live-stock accuracy score in the company.


Liz is a fabulous dispensary manager and pharmacy technician. She has made the role her own since taking it on to cover maternity leave last summer. Liz has introduced procedures that gives her team a task based rota every day which gives a structure to the day and means there’s accountability within the team. The pharmacy joined the Life Pharmacy group in November 2022. The structures and processes for the symbol group have been a challenge for the team on occasion but Liz is always there to reassure staff that change is positive. She is quick to understand changes in supply issues etc and keeps the team involved in decisions ensuring everyone is kept in touch with what’s happening.
Marianna’s standard of work is excellent and her dedication to her role is second to none. Making dispensing errors is a rare event with Marianna, and when she does she learns from it and takes it on board. She treats each prescription as if she is the final check, from putting it through MPS to clinical checks and ensuring to check for any interactions. This gives the pharmacist an enormous peace of mind to have someone as professional as Marianna working alongside them. She without a doubt, really stands out from the crowd when it comes to comparing her with other technicians as an integral part of the pharmacy team and has never shied away from responsibility or challenges.
Meaghers Pharmacy Group prides itself on Being a Great Place to work and this comes from a survey that the staff complete annually, with management listening to what they have to say. This is what differentiates Sarah Cosgrove from others; she really listens, to her patients, her colleagues and customers. She loves pharmacy and fights every day for her patients and to make their life and their health better. She consistently gives her patients and customers 100% She builds on these relationships and these customers come back.
2023
Irish Pharmacy
The
58 | PHARMACYNEWSIRELAND.COM
Dominika Wikowicz, Adrian Dunne Pharmacy, Balbriggan
Elizabeth Moore, Leahys Pharmacy Oakpark, Tralee
Marianna Magiera, Cunningham’s Pharmacy, Athlone
Sarah Cosgrove, Meaghers Pharmacy, Baggot Street Dublin
Introducing...
Finalists Finalists Awards
Haleon Self Care Award 2023
The team at North Road Pharmacy have focused in the last 2 years on achieving a healthy lifestyle through exercise, healthy eating and taking positive steps in self-care, whether that is taking vitamins and supplements, taking up a sport or seeking advice from the local GP if struggling with life in general. This has led patients and customers awareness to alternative ranges they currently stock. The alternative route has been a key focus moving forward and the introduction of a Sports and wellbeing department has been instrumental in the growth of the other areas in the front of shop sales overall as proven from the positive feedback from customers which translated into strong growth in terms of sales in these particular areas.
North Road Pharmacy is now recognised and has the reputation for taking care of all their customers and patients and continually strive to be the best in health care in the local pharmacy community.



Fathimah Kara’s focus on the self-care market has greatly assisted Reidy’s Pharmacy by cementing its place as one of the key healthcare providers in the community complimenting the GP surgeries. Confidence in the pharmacy team and Fathimah has greatly soared and grown phenomenally with patients appreciating the services being provided and the positive impact on their health.
Word of mouth through people who have used the services has increased the uptake in services and also in those using the pharmacy for all their and their families healthcare needs from dispensing of prescriptions to general advice on minor ailments and to help with any concerns they may have.
The identification, implementation, and improvement of services in the pharmacy has greatly helped the local community.
Dunville Pharmacy is an independent pharmacy situated in the leafy suburbs of Dublin 6. The pharmacy team has spent the last seven years developing their self-care offering and in particular their VMS department from one bay in the old shop to one long aisle of supplements and wellness products.
Listening to customer’s needs and requirements helped guide their growth into wellness. By specializing in this health category they have become known for their superior product range and expert advice.
The pharmacy has increased the sales in this area by 250%, over the previous five years, from 3,000 per month to over 10,000 per month and holding steady over the last two years. They have been able to clearly demonstrate how you can grow sales by first becoming an expert in that area.
MGK9299 Haleon Trade Ads.pdf 1 10/08/2022 14:58
Haleon, formerly part of GSK
North Road Pharmacy, Drogheda
Dunville Pharmacy, Dublin
Fathimah Kara, Reidy’s Pharmacy, Rathcoole
2023
PHARMACYNEWSIRELAND.COM | 59
The Irish Pharmacy
The Irish Pharmacy
Finalists Finalists Awards
Théa Pharma Counter Assistant of the Year Award 2023

Geraldine Cooper is the front of house Medicine Counter Assistant Supervisor in the new state of the art greenfield site at Keane’s Careplus Pharmacy in Drumcondra. This shop is a young store, only open since June 2022, with a new “digital over the counter” interface, and a new Keane’s team. Geraldine took the position as over the counter assistant supervisor to lead the front of the shop team in this innovative digital store. Bringing more than 15 years’ experience of working in the local community, Geraldine has supported staff and new customers every step of the way, drawing on her exceptional customer service skills and a wealth of clinical and product knowledge.
Geraldine has consistently delivered with a very high level and quality of professional empathy, and has made the role her own.
Sam
Sam offers a really high level of customer service to the customers of Dunville Pharmacy. His manner and his attitude towards his job, his colleagues and the customers is of such a high level that the pharmacy management regularly receive compliments from customers. Sam has huge empathy. He is confident and polite but also works very hard. He mastered working on the OTC counter within 6 months of starting this new role. His best skill is dealing with the flow of prescriptions from healthmail to the dispensary, helping to organise the workflow and time needed to complete a specific prescription. This in turn takes great pressure from the dispensary and ultimately keeps customers happy.
AnnaLeigh has been ever present in Foynes Pharmacy for the past 7 years. When entering the pharmacy you will always be aware of her presence. Greeted with a warm hello, beautiful smile and on a first name basis.



She is described as someone who is always going over and beyond for her customers, dealing with reps in store and always eager and showing genuine interest in customers.
AnnaLeighs heart and soul goes into what she does daily. Albeit keeping her fellow colleagues in good spirits, looking after her individual customer needs, or simply keeping the store a float.
“AnnaLeigh has a positivity about her that is contagious,” says her pharmacy manager.
60 | PHARMACYNEWSIRELAND.COM
Geraldine Cooper, Keane’s CarePlus Pharmacy, Drumcondra
Harrington, Dunville Pharmacy, Dublin
2023
AnnaLeigh Hanlon, Foynes Pharmacy, Limerick


www.theapharma.ie Europe’s No 1 dry eye drops Hydrates & Lubricates Repairs & Protects Lasts for up to 4 hours Clinically Proven1 to treat symptoms of dry eyes Available on the GMS Action 2 1 Pinto-Bonilla JC et al. Ther. Clin Risk Manag 2015:11;595-603 2 IQVIA MAT September 2022 Ireland Dry Eyes
Finalists Finalists Awards
Théa Pharma Counter Assistant of the Year Award 2023
Edel Cullen, Lannon Late Night Pharmacy, Sligo
Edel has had a considerable impact on her pharmacy team. She is familiar with all regular patients and customers and understands their needs and requirements.
As the pharmacy skincare expert Edel has taken on the promotion of events within the store, identifying brands for promotion and organising these events herself. Edel also liaises with suppliers to identify new products that may do well and introduces them into the pharmacy as a trial. Edel has great communication skills and a warm, friendly demeanour that puts patients at ease and has an ability to listen actively and empathise with people.
Her positive attitude and willingness to help have contributed to a positive working environment within the Pharmacy.
Betty Long, Mocklers Pharmacy, Thurles

Betty is an OTC counter assistant and has worked as part of the team at Mocklers Pharmacy for the past 25 years. Betty brings life and laughter to the pharmacy every day. She has excellent relationships with the customers and knows them all by name. Betty has a vast knowledge of OTC medications and will always have a recommendation for a customer whether it be product information or general advice. Betty always has a friendly and compassionate ear for customers and as a result has built excellent rapport with them. Betty has spearheaded the introduction of many new products and brands sold in the pharmacy over the years and will go above and beyond to ensure nobody is disappointed and ensures the shelves are stocked with products both new and old reliable.
Aoife Bennett, McCabes Pharmacy, Blanchardstown
Aoife Bennett is currently an OTC Sales Advisor and the healthcheck champion at McCabes Pharmacy Blanchardstown. Aoife has worked with McCabes Pharmacy since 2018 and has thrived within her role ever since. She has completed all of the McCabes online OTC training programme and is now one of their Gold standard sales advisors. Aoife plays a major role in supporting the Blanchardstown team in every possible way. Aoife constantly goes above and beyond to support her team and her patients, which includes her voluntarily coming into work on her days off to do healthchecks for her customers who she has built extremely strong bonds and relationships with. Aoife finds so much joy in helping others which is why she happily takes the time out of her days off to ensure that she can help her patients to receive the best possible care. She organises all of the healthchecks within McCabes Pharmacy Blanchardstown which has allowed the team to provide the best service and care to their customers.


62 | PHARMACYNEWSIRELAND.COM
2023
The Irish Pharmacy
Finalists Finalists
Easolief DUO Business Development (Chain) Award 2023
Launched in January 2023 through Boots Pharmacy internal MyHub portal, Boots pharmacists now have access to a new platform to complete the Pharmacy Assessment System (PAS), in a digital, seamless, and user-friendly format. Using the PSI issued templates as a rigid guide, he team behind this business development created a digital mission for each section of the assessment. This gives pharmacists a step by step process to complete the self-audit.
Moving to a digital format provides the Superintendent Pharmacist with complete oversight of the audit process across the pharmacy network. Additionally, the digitisation supports the pharmacist in accurately completing the self-audit. Each section has mandatory fields so nothing can be missed. In addition, the system has digital checks and countdowns to support reporting in line with the PSI requirement of every two months.
CarePlus Pharmacy Network
The introduction of the CarePlus Baby Club has tackled numerous challenges, including brand loyalty and brand differentiation. The creation of the Baby Club, from the free gift to the monthly exclusive offers and e-newsletters, to baby events, to the Care+Conversations podcast and content on social media and website, has provided a safe space and support network for parents within communities to feel as though there is support, not only in their local CarePlus Pharmacy, but beyond that and online.
The CarePlus Pharmacy Network team are continually learning and progressing all the time from customer and member feedback, putting the customer first, while also adapting to market change and sustainability initiatives.




During 2022 Daarwood pharmacy team completed the installation of the new dispensing robot. Every staff member had a role in this implementation to ensure the smooth process of introduction and to build on their knowledge from the initial training that was provided. The entire team got involved in resolving any technical and process errors and this has made the team work closer together as a whole and solidify the robot as a fundamental equipment and irreplaceable in the daily running of the pharmacy. Her name is Roberta! The inclusion of Roberta into the team has led to a reduction in picking errors, more efficient stock management and date checking and it has allowed capacity for prescriptions to grow exponentially.
Stacks Pharmacy Group
Managing Director of Stacks Pharmacy Group, Adrienne Stack has developed Digicare, which is an intelligent workflow solution for medication management in a nursing home/hospital setting for pharmacy teams. The mission is to increase the safety and the efficiency through automating the daily task list, provide live feedback to the users and access to superior analytics.
Digicare deals with the previous lack of live medication administration record for nurses to record patients getting their medication. The mission is to increase the safety and the efficiency through automating the daily task list, provide live feedback to the users and access to superior analytics.

PHARMACYNEWSIRELAND.COM | 63
2023 The Irish Pharmacy
Awards
Daarwood Pharmacy, Newcastle West
Boots Ireland
Finalists Finalists Awards
United Drug Business Development (Independent) Award 2023

The initial key challenge for Higgins Pharmacy was to define their own identity and objectives in order to become known to the Sligo people as kind and trusted professionals, like the Higgins family, who had started the business.

The team had a goal to maintain and then grow the business, whilst facing another challenge of having never run a business without support. One of the most important issues for the owners was to ensure a great team, which they feel is core to running a successful pharmacy business.

All of the business initiatives which they have started have all impacted greatly on the business and the community they serve.
Being accepted onto the ‘Going for Growth’ and ‘Empower’ programmes have really helped in driving their business forward. Their mentorship programmes highlighted areas for improvements and forced the owners to look at areas needing attention.
Mark’s Pharmacy, Ardee
Mark’s community pharmacy team has effectively tackled key challenges through innovative business development initiatives, resulting in exceptional customer service, new business opportunities, and significant achievements. Some of the challenges addressed include expanding their customer base: enhancing customer service: adapting to market trends; developing a skilled workforce and demonstrating strong leadership.

The pharmacy’s innovative approach, rapid growth, and dedication to delighting customers has shown great innovation, with their accomplishments showcasing the power of determination, continuous learning, and passion for delivering exceptional care and service to the community
In order to face new challenges being witnessed by the pharmacy sector as a whole, the team at Village Pharmacy tried to look outside the box in terms of offering something new to their customers and patients and at the same time always being conscious of the fact that their main aim is to get and keep the community healthy and well. What they came up with was unique and different to pharmacies throughout the country, as they opened a Sports Department instore, targeting the individuals who wanted to improve or even begin the road to an active and healthy lifestyle.
Village Sports is a one-of-a-kind department within Village pharmacy which is unique to pharmacy throughout the country and boasts its uniqueness. This initiative works alongside the ethos of pharmacy which provides patients and customers another avenue of selfcare and improved overall wellbeing.
64 | PHARMACYNEWSIRELAND.COM
Higgins Pharmacy, Sligo
Village Pharmacy, Carlingford
2023
The Irish Pharmacy



udwmarketing@united-drug.com United Drug Award Winning Webinar Series 2023 For information regarding all upcoming webinars, please contact UDWMarketing@united-drug.com Free Online webinars to improve Retail Pharmacy offering Hear from the industry’s most influential speakers Exclusive industry insights and trends CPD Learning for your ePortfolio CPD Certificate for all attendees of live event
Awards
Finalists Finalists
BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award 2023
Pharmacy Group

Meaghers Pharmacy are continually evolving to deliver innovative services at the core of their community. The pharmacy team are continuously working on new ideas and services that they can bring to their pharmacies to improve the level of care which is provided to each and every one of their patients. Medication non-adherence is a widespread issue leading to reduced quality of life in patients, increased hospital admissions, premature deaths and increasing healthcare costs. In 2022, Managing Director Oonagh O’Hagan and Superintendent Pharmacist, Elaine Lillis, wanted to highlight the key role pharmacists can play in tackling this issue and so began discussions to identify a new service that they could offer in the pharmacies to set about doing this.
Boots is synonymous with patient care. Caring deeply about not only their patients but their colleagues and the environment in which they work, Every day, the pharmacy team look to see how they can improve the lives of patients and our colleagues. With this innovation, they found a solution that helps both.
The Boots Ireland innovation enables faster and more accurate completion of vital regulator required paperwork. Launched in January 2023 through the internal MyHub portal, Boots pharmacists now have access to a new platform to complete the Pharmacy Assessment System (PAS), in a digital, seamless, and user-friendly format. Using the PSI issued templates as a rigid guide, the team created a digital mission for each section of the assessment. This gives pharmacists a step by step process to complete the self-audit.
In Winter 2022, the HSE alerted healthcare professionals to the significantly lower uptake in children’s flu vaccinations compared to the previous year. To address this issue, Uniphar decided to bring their flu vaccination clinics directly to schools. Uniphar developed a pharmacy led School Vaccination Programme which demonstrated that vaccine uptake can be increased with a school’s programme and that a school’s programme reaches a new patient cohort. This programme can serve as a template for future schools’ programmes and will help the HSE achieve that 40% target.
Uniphar have shown that pharmacy can deliver an efficient schools vaccination programme and the team has provided a template that other pharmacies can follow.



Stacks Pharmacy Group
A dedication to medication management has become a particular interest for Adrienne Stack and the team. Adrienne has launched Digicare, which is an intelligent workflow solution for medication management in a nursing home/hospital setting. The mission is to increase the safety and the efficiency through automating the daily task list, provide live feedback to the users and access to superior analytics.
Digicare is a cloud-based software and has a mission is to dramatically reduce medication errors and the need for investigations. They accomplish this by increasing the safety and time efficiency by automatically updating all stakeholders when a change is made, or a new patient is admitted. It also records all safety related information of patients in one place so at the point of prescribing, administration and dispensing the information is available.
2023 The Irish Pharmacy
Boots Ireland
Uniphar
66 | PHARMACYNEWSIRELAND.COM
Meaghers
Finalists Finalists
Uniphar Category Development of the Year Award 2023
Navi Group saw an education opportunity within the Pain category which accounts for 50% of OTC sales. The team behind the initiative reviewed the category and analysed the different type of pain products for different types of pain and patients and developed detailed training to aid staff in treating customers. CarePlus operate a category management strategy that can leverage the groups spend and maximise value delivered to CarePlus Pharmacies through supplier rationalisation, contract alignment, consistent reporting, robust supplier relationship management, information accessibility and visibility. They regularly carry-out research through exit shoppers and mystery shoppers to see how they perform when categories change and on average score 95% which is excellent achievement for pharmacy teams on the ground.
To develop the probiotic supplement category both in-store and online over the last 12 months, Glengarriff Pharmacy has employed several strategies such as promotions, information, education, and discounts.


To begin with, Glengarriff Pharmacy provided information and education on the benefits of probiotic supplements through various channels. By providing valuable information on the benefits of probiotic supplements, they have positioned themselves as a trusted source of information and have attracted customers who are interested in improving their health. Additionally, Glengarriff Pharmacy ran promotional campaigns that offered discounts or bundle deals on probiotic supplements and offer educational resources, such as brochures and blog posts, in-store and online to help customers understand the different types of probiotic supplements available and which ones may be best suited for their needs.
Dunville Pharmacy has spent the last seven years developing their VMS department from one bay in the old shop to one long aisle of supplements and wellness products. Listening to customer’s needs and requirements helped guide their growth into wellness. The team continue to plan further growth in this area of the business.
They completed a rebrand in 2022 along with an e-commerce website and in-store refit at the end of 2021, all with a new brand identity. This change allowed the pharmacy team to enter 2022 with a new up to date look, communicating exactly who they are and what they stand for.


Navi identified an opportunity in the market to educate female customers on hormonal health and how pharmacies can assist in identifying their specific nutritional needs based on their age and current symptoms.
By arming the pharmacy staff with up-to-date knowledge on women’s health and specific products available, CarePlus pharmacies became an important destination for women’s to get advice and to improve their lives. The key areas focused on were periods, perimenopause and menopause-covering the full female customer base.

PHARMACYNEWSIRELAND.COM | 67
Awards 2023 The Irish Pharmacy
Glengarriff Pharmacy, Glengarriff
Dunville Pharmacy, Dublin
CarePlus Pharmacy Network – Women’s Health Project
CarePlus Pharmacy Network – Pain Project
Finalists Finalists
Alliance Online Pharmacy Retailer of the Year Award 2023



Allcare Pharmacy has an online offering that is unique in comparison to other online pharmacies, remaining available 24 hours a day, always open to support customers with products, advice and service bookings. Allcare Pharmacy gives customers the best online journey using AI tools for personalisation and email segmentation to send customers personalised emails based on demographic information and shopping behaviours.
The team also provide OTC products which is a convenient and accessible service. This supports privacy for customers ordering certain products online with free next day delivery.
This is particularly beneficial for people who do not live close to a pharmacy, the elderly, disabled people, and those who cannot visit their local pharmacy due to opening hours etc.
Whites Pharmacy/Always There Pharmacy
Always There Pharmacy offers a large range of products catering to a wide audience with brands such as La Roche Posay, Vichy, Clarins, Hugo Boss and Marc Jacobs. The team offer nationwide delivery and excellent customer service as standard. Since they launched their website in October 2021, they have expanded the online services to include prescription ordering, live chat, weight management and most recently, have added an online nutritionist service. There is also an online booking system where customers can book in online for instore flu vaccines, covid vaccines and blood pressure monitoring.
As an online pharmacy, Life offers vitamins and supplements, beauty, skincare, fragrance, electrical items, mother & baby care and healthcare services; Medical equipment for assisted living; an Online Doctor service, which is a quick, safe and discreet way to obtain prescriptions and expert blogs written by local pharmacists and healthcare experts.

Life Pharmacy has had exponential growth of app prescription orders due to the convenience and ease of repeat usage and accessibility to in - app history. Benefits of their app include:
Multiple Patient support added to app to enhance convenience.
Inclusion of EHC, Viagra Connect, Online Doctor and Vaccine booking service to app.
Push Notifications to periodically send promotions to patients – instant touchpoint to communicate with channel to drive engagement.
68 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
Life Pharmacy Allcare Pharmacy
The online pharmacy team from Hickey’s, Allcare and Life Pharmacies
Meaghers Pharmacy Group

Meaghers Pharmacy is a well-known Irish pharmacy chain with over 11 locations across the country. In addition to their physical stores, they also have an online store that offers a wide range of health and wellness products, including skincare, vitamins, supplements, beauty products, baby care, and more. The pharmacy team support various health needs such as immune support, energy, and joint health and lead the way in areas such as gut health, pain management, and specialised skincare, with a range of innovative products and knowledge that support patient/customer care. Alongside beauty, lifestyle, and healthcare products, we also offer customers, access to our team of pharmacists, a prescription delivery service, and online sales of OTC medicines. We’re dedicated to providing the same personalised, excellent customer service to our online customers as we do to our in-store customers.
Hickey’s Pharmacy use email segmentation to send customers personalised emails based on demographic information and shopping behaviours and offer the best in class logistics – over the last year the team has updated their warehouse management system, delivering increased efficiency throughout the entire warehousing and distributing processes.
Hickey’s Pharmacy also offer an extended selection of health services alongside online doctor, ask a pharmacist, vaccine bookings and sexual wellness forms and strive to provide a high level of online customer service and support. They have set about achieving this objective by investing in Zendesk customer support software. This allows the team to nurture customer relationships with personalised, responsive support across all channels

Pharmacy Store Ireland

When transferring to online, the Pharmacy Store had one sole purpose to provide the same customer service and journey online as they have been providing instore but using online capabilities to make the process as smooth as possible for customers. They are a community pharmacy that employed e-commerce with a clear focus on innovation with steps to enhance the customer experience and journey the same way online as customers receive in store.
The team focus was to allow local customers and customers nationwide to be able to use the current growth and developed technology to access pharmacy products and services at anytime and anywhere. The Pharmacy Store are thriving to keep stepping up with innovation and new developments in technology to create an even quicker and smoother customer journey.
PHARMACYNEWSIRELAND.COM | 69
Hickey’s Pharmacy
The Irish Pharmacy
Awards
Finalists Finalists
McLernons Independent Community Pharmacy of the Year Award 2023

The team at Rye Pharmacy pride themselves on being a very close-knit one. It can be hard to find a group of people that genuinely enjoy working together and it helps to create a great atmosphere in the pharmacy. The customers definitely notice this atmosphere and feed into it too.

The superintendent and supervising pharmacists work together closely to create an environment that reduces undue stress, enhances workflow and boosts morale which leads to overall improved productivity and a really nice place to work. The ethos is that first and foremost, the team are a part of the community. The Rye Pharmacy has become an integral part of the community in Leixlip for the last 10 years and is continuing to see business grow year on year. Customer service is of utmost importance in an increasingly competitive pharmacy sector.
Says the team, “It is a privilege for us to service the community of Leixlip and we hope to continue to foster this symbiotic relationship for many years to come!”
Reidy’s Pharmacy, Rathcoole

The team at Reidy’s Pharmacy have worked together quite effectively throughout the years of service together. This includes the introduction of new services provided in the pharmacy. This included the 24 BP monitoring and most significantly the vaccination service which has greatly expanded.
The team worked so incredibly hard during the COVID-19 pandemic where they would come in an hour early to work and stay an hour later to finish up all the days tasks at hand. Reidy’s Pharmacy is a family run business serving the needs of the local Four Districts communities for over the past twenty years and continue to go from strength to strength with the quality of healthcare they provide to each and every one of their patients.
The Rye Pharmacy, Leixlip
2023
70 | PHARMACYNEWSIRELAND.COM
Pharmacy Hub has collaborated on a number of projects and initiatives within the community. They recently offered a comprehensive health check for a local business and completed a seasonal flu campaign in local schools. The major annual collaboration is Tallaght Health Awareness Month, which is every October.

Pharmacy Hub opened in 2018 with a vision of creating an independent pharmacy providing a personal customer focus. The team has since then built from 4 to 10 and continue to look forward, embrace change and embed deep roots in their community.


Pharmacy Hub is driven by passion, hard work, dedication, exceptional customer service and innovative thinking. Pharmacy Hub has been recognised and awarded for its attributes within the local community and comprises of a proud team built on traditional core values, considering themselves as a ‘pharmacy family’ within the Hub.
North Road Pharmacy, Drogheda
As a team the togetherness and definition of team-work is defined and unanimously endorsed and proven on a daily basis by the team in North Road Pharmacy. Their flexibility and openness to change and the support of each other is unparalled. From the ordering procedures, the IT involved in inputting orders, the stock control is obviously made easier by the software they use however the time, effort and efficiency of everyone involved to successfully navigate these processes is phenomenal.
“The definition of a community is varied however our belief is it a group of people living together in a larger society. We are part of that environ and a pivotal part of it. We try and help each and everybody in this group,” they say.
Mark’s Pharmacy, Ardee
The team at Mark’s Pharmacy always employ a strategic approach to collaboration and communication, ensuring that every team member is engaged and aligned with the pharmacy objectives.
Mark’s Pharmacy has demonstrated its commitment to excellence in patient care, service delivery, and community engagement. Their dedication to improving public health and enhancing the lives of customers and staff is evident in their numerous achievements and ongoing initiatives. Their proactive approach to improving public health, along with a commitment to staff satisfaction and continuing education, sets them apart as a leading independent community pharmacy.
“We are proud to serve our community and strive to continue making a positive impact on the lives of our customers and staff,” the team states.
PHARMACYNEWSIRELAND.COM | 71
Pharmacy Hub, Tallaght
Eimear, Rita, Julie-Ann, Michelle, Roxana, Mona and Shauna
Finalists Finalists
Perrigo Superintendent Pharmacist of the Year 2023

Tom has a proven track record of consistently delivering high-quality services, fostering a positive working environment for all and contributing to the wider pharmacy industry. He is always looking for new ways of improving and developing the way he works. Outside of his incredibly busy job, Tom is involved with the Pharmacy Contractors Committee with the IPU and the Workforce task group. He is part of the IPU IT steering group. Tom is constantly striving for improvement in pharmacy in Ireland and being directly involved with these committees and steering groups will shape the community pharmacy of the future.
Over the past 12 months, one of Tom’s main focusses has been the re-introduction and improvement of health services provided in pharmacy post pandemic and to launch new and innovative services across the pharmacy network. Under Tom’s skillful guidance, updated SOP’s and training, Health Services such as Blood pressure, Cholesterol and glucose testing have all been successfully reintroduced into all 115 Hickey’s, Allcare and Cara pharmacies.
Working from feedback from his pharmacies, Tom has implemented a pre-prepared system for Healthmail. He has collaborated with the dispensing software provider to utilise and transform the software to best empower the community pharmacist.


The people of Leixlip know Susan and her reputation precedes her as someone who is caring and extremely knowledgeable on a wide range of topics. She is constantly getting involved in community organisations and contributing time and resources when she can. Customers will often go out of their week to seek her opinion and advice.
The major challenges of the past 12 months have included the ongoing Covid 19 pandemic as well as the war in Ukraine. There has been a major impact on all aspects of business with rising costs and widespread product shortages. Susan used her business savvy and her knowledge of the political climate to help her to predict and plan so that the staff could be prepared for any eventuality.
Susan in her role of superintendent pharmacist has successfully guided the pharmacies through the pandemic and unstable political climates to allow her team to continue to deliver impeccable customer service and play a vital role in the community. She has a real vision for what she wants her pharmacies to become in the future and the services she wants to provide in the community.

As which is common in the majority of pharmacies throughout the country, the role of community Pharmacists played a major roll on out the Covid Vaccination programme, This was and continues to be very challenging for all involved and in particular Superintendent pharmacists whom implement safe practice and constantly reviewing the logistical side of ensuring adequate supplies to the stores and ultimately the timetabling of Vaccination Clinics to correspond with the sheer volume enquiring and requesting their vaccine/booster.
As a well respected Pharmacist, John has been exponential due to his approach. He also introduced the 24-hour blood pressure monitoring across his pharmacy stores.
Many believe being a pharmacist is a vocation and not purely a job and John epitomises this belief. His care and patient wellbeing is forefront every day he walks in the door. The forward thinking, he possesses demonstrates the potential and opportunities that pharmacy could benefit from in the future for example the possibility of minor ailments - essential for the future and development of pharmacy.
72 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
Tom Concannon, Hickey’s/Allcare/Life/Cara Pharmacies
Susan Sheehan, The Rye Pharmacy, Leixlip
John McCourt, Millmount Pharmacy, Drogheda
Finalists Finalists
JPA Brenson Lawlor Young Pharmacist of the Year Award
Stephen Lally has made his mark within the community in Swords, particularly with his elderly patients, often dropping prescriptions to their homes to ensure they know how to take the medication. While working in the McCabes Pharmacy Limerick store, Stephen would regularly liaise with the pharmacy department in University Hospital Limerick to supply a High-Tech Medication for regular elderly patient during a prolonged inpatient stay. He would often hand deliver the medicine to the hospital.
Stephen has successfully ran flu and Covid vaccination clinics vaccinating up to 350 patients along with colleagues and has engaged with Instagram live for McCabes Pharmacy with topics such as mental health, diabetes and much more. He is described as an exceptional pharmacist and shows immense qualities that make patients’ lives better every day, his calm demeanour, care for his patients and his professionalism is outstanding.


Lauren has been a pharmacist with Meaghers pharmacy since she qualified in 2020 and since then she has proven to be an excellent, caring and compassionate pharmacy. Her drive to provide the best possible care to patients was evident even as an intern and as a result the team were delighted when Lauren stayed to work with the company after she qualified. Since then, she has excelled in her position as support pharmacist in our Castletymon and Glenview stores. Lauren has been a key figure in the roll out of many public health services with the company since she qualified and her passion for improving the health her patients is evident in her work in these areas.


Daniel’s proactive approach to administering Covid-19 vaccinations and providing flu vaccinations demonstrates his dedication to improving the health and well-being of his community. By offering weekend clinics for children’s flu appointments, he is accommodating busy parents who may have difficulty attending during the week. Furthermore, Daniel’s free blood pressure monitoring service shows his commitment to preventing and managing chronic diseases such as hypertension. Overall, Daniel’s actions show his commitment to providing excellent healthcare services to his community and his willingness to go above and beyond to meet their needs. His efforts will undoubtedly have a positive impact on the health and well-being of those he serves.
Mary is the lead vaccinator in the pharmacy and organizes the service in such a professional manner, with arranging the appointments, maximising the usage of the vials. Her organizational skills have meant that the pharmacy team have been able to provide hundreds of covid and flu vaccines, with little impact on the busy dispensing service.
Mary has also driven the pharmacy blister pack service, working closely with the technicians, she has identified patients who would truly benefit from having their medicines dispensed in blister packs and she has taken the time to explain the benefits of the service and this has demonstrably improved compliance among the patients who need it the most.
Mary has been an extremely strong performing pharmacist within a great team. She has been an integral part of the dispensing team and a leader who stands right up with the very best in the industry.
PHARMACYNEWSIRELAND.COM | 73
2023 The Irish Pharmacy
Awards
Lauren O’Donovan, Meaghers Pharmacy, Dublin
Daniel McCormack. McCauley Health and Beauty Pharmacy, Dungarvan
Mary McCartan, Donaghamede Pharmacy, Donaghmede
Stephen Lally, McCabes Pharmacy, Swords
Finalists Finalists
Reckitt Community Pharmacist of the Year Award 2023

Suzy recently organised the for The Rye Pharmacy to become part of the Safe Pharmacy Initiative to allow the pharmacy consultation room to become a safe space for victims of domestic abuse to call for help. She also provides a compression stocking measurement service and participates in all of the HSE vaccination programs, constantly managing stock levels and appointments as well as administering the vaccines themselves. She is also a tutor pharmacist, a role she thrives with.
Suzy has been described as an excellent worker who is efficient, fast and manages her dispensary extremely well. Despite constant HSE cuts she has managed to increase revenue since she started.
Sheena Mitchell, Milltown totalhealth Pharmacy & Wondercare.ie

Ove the last 12 months, Sheena Mitchell has prioritised the profession of pharmacy over everything else in the name of safe patient care. She has garnered huge support from her equally frustrated pharmacy colleagues and has been humbled by the unity of that support. As an individual it can be difficult to gather the necessary support amongst a profession, but Sheena refused to see that as an obstacle and the impossible became possible.
Sheena has shown dedication to her cause and the pharmacy profession but most importantly to all patients in Ireland. Patients deserve easy access to healthcare and have welcomed Sheena’s motivation to break down historical barriers.

Darragh Kelly, Adrian Dunne Pharmacy, Whitehall


Darragh is described as an outstanding team leader who provides support and care to both patients and his team. He acts as a mentor to both junior technicians and a pre-reg pharmacist, a role he takes very seriously in equipping them with the necessary skills and education required for working in the pharmacy sector. Darragh’s ability to run the pharmacy business, safely dispense medications and lead a team serves as an inspiration to the entire team and in turn makes the pharmacy a more enjoyable place to work.
Giovanni Bonina, Village Green Pharmacy, Tallaght
Giovanni has always offered a top quality customer service by improving people’s experience in his pharmacy. He always takes the time to explain how to take medications and shows care and empathy with every job he undertakes. He has recently started an innovative initiative focused on how to properly inform and educate people about any product they can commonly find on a pharmacy shelf; and has created on the pharmacy social media the hashtag #askourpharmacistjoe.
Giovanni offers a service unlike any other pharmacist in the surrounding areas; he cares about his customers and educates both young and old.
74 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
Suzy Farrell, The Rye Pharmacy, Leixlip
Over the last 12 months, Mark has carried out numerous public health services and initiatives, drawing from his diverse experiences in various pharmacy roles. These services and initiatives showcase his commitment to addressing diverse community healthcare needs. By engaging with local employers and targeting hard-to-reach populations, he demonstrates true dedication to enhancing patient care and expanding pharmacy’s role in the healthcare team.
Mark has an unwavering dedication to improving patient care, expanding pharmacy services, and championing innovation within the industry.
John O`Shaughnessy has been a senior pharmacist for five years in Woods Pharmacy – a Keanes’ CarePlus store –on Mullingar’s main street. He is fully invested in the Keane group’s values in relation to the importance of patient wellbeing, and accordingly leaves no stone unturned to ensure that patients receive the best possible care. During the covid years, he introduced antigen testing, followed by covid vaccinations, showing courage at a time of great uncertainty.

John is totally selfless by nature, and puts others before himself, no matter if they are a patient or a staff member. He may be doing 100 jobs at once - but will drop them all to help anyone with anything, whether that be needing help with a prescription - or taking out the bins from the dispensary.
John has actively engaged with his local community over the last 12 months. Given the location of his pharmacy in the Crescent Shopping Centre, a lot of John’s patients live in local rural communities outside of Limerick and many of the elderly customer base were unable to come into the store to collect their medication during COVID.


John has built up extraordinarily strong relationships with his customers, his level of customer service is second to none and he ensures that he speaks to every customer who comes through the door with a prescription. He has a knack of identifying when a customer has a query or concern that is really bothering them and always displays strong listening skills and empathy to the customer’s needs, ensuring that when they leave the pharmacy, they feel that their concerns have been listened to.
Michelle has been described as someone who continually impresses with her dedication, skills and expertise as a pharmacist. She has always demonstrated a commitment to patient care that goes above and beyond what is expected. Michelle is always willing to go the extra mile to ensure patients receive the medication they need often calling in on her way home with medication if they haven’t been able to attend the Pharmacy.
Michelle is also committed to professional development often discussing recent courses she has completed and highlighting the learning points to the rest of her pharmacy team.

PHARMACYNEWSIRELAND.COM | 75
John O’Shaughnessy, Woods CarePlus Pharmacy, Mullingar
John Myers, McCabes Pharmacy, The Cresecent Dooradoyle
Michelle Dempsey, Ballisodare Pharmacy, Sligo
Mark McPhillips, Mark’s Pharmacy, Ardee
Finalists Finalists
Viatris Community Pharmacy Team of the Year Award 2023
Keane’s CarePlus Pharmacy, Enfield
Positive team dynamics are evident at every touch point that a customer has at Keanes CarePlus in Enfield. A genuine team ethic has increased morale, as well as the efficiency of both the dispensary and the front-of-shop teams. Regular team meetings improve confidence and allow for greater clarity in retail and clinical aspects of the business. Staff feeling empowered to achieve their goals enables them to provide better patient care and, as a result, to continue the growth of the business year after year.
The team at Keane’s CarePlus Enfield have time and time again shown what it means to be a community pharmacy. They truly have embedded themselves into the community that they serve and look forward to providing more of the same excellent service for many years to come.
Mark’s Pharmacy, Ardee
The diverse skillset and responsibilities of each team member at Mark’s Pharmacy contributed to the successful execution of the vaccination service project and the ongoing growth and success of the business. Through collaboration, communication, and a shared commitment to excellence, the team consistently delivers exceptional patient care and service to their community.
This community pharmacy team excels in team spirit and enhancing patient care at all levels. They consistently collaborate and support each other, fostering an environment of trust and respect that allows each member to contribute their unique skills towards shared goals.

Meaghers Pharmacy, Baggot Street
Teamwork is part of the fabric of success in Meaghers Pharmacy Baggot Street; the team of healthcare professionals work together tirelessly to achieve common goals to improve the lives of their customers. Fostering a culture of teamwork among this diverse group of people has revealed new, fresh ideas. And those new ideas are invaluable to the business as a whole and to the customer base of Meaghers Baggot street. The team in Meaghers Baggot street showcase excellence in diligence, commitment and tenacity in delivering initiatives to improve the health and wellbeing of, not only the community in Dublin 4 but the wider community.
Adrian Dunne Pharmacy, Balbriggan
The team at Adrian Dunne Pharmacy in Balbriggan works together to provide the best possible care for their patients.They communicate effectively, share information, and work collaboratively to ensure that patients receive accurate, efficient, and personalised care.



They have consistently demonstrated exceptional commitment, teamwork, and innovation in serving the local community and improving health outcomes with an unwavering commitment to putting the needs of customers and local community first. They regularly go above and beyond to ensure that each customer receives the best possible care and attention, from providing advice on health and wellness to ensuring that they have access to the medications and products they need.
76 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
Empowering people worldwide to live healthier at every stage of life.

With 1,800+ people working across six sites in Ireland, Viatris provides access to medicines, develops innovative solutions and improves healthcare for patients.
Viatris is proud to sponsor The Community Pharmacy Team of the Year Award 2023. Congratulations to pharmacy teams across Ireland for their dedication to consistent patient care.
Job code: NON-2023-3376
Date of preparation: April 2023
Viatris Newenham
Road, Dublin
Dublin, Ireland. Viatris.ie
Court, Malahide
17,
Finalists Finalists
Viatris Community Pharmacy Team of the Year Award 2023
Communication is key to any successful team. There is a strong rapport and chemistry amongst the pharmacy staff at Hickey’s Pharmacy Johnstown. They trust that each team member will consistently and reliably do what they say they will do to benefit the team and their customers.



The team demonstrate the best combination of team spirit, supporting and encouraging each other to enhance patient care at all levels every day. The team know their regular patient’s inside out and go the extra mile for them every day, calling them to let them know their favourite vitamin or skin cream is on offer, reordering repeat prescriptions, going the extra mile delivering prescriptions in their own time when the need arises outside normal delivery times or simply just sharing a joke and getting a smile at the counter.
McCauley Health & Beauty Pharmacy, Enniscorthy

The day to day pace in this pharmacy store is extremely fast moving and co-operation is vital to ensure the business runs well. All staff are trained in multiple disciplines meaning that cover can be provided for any area of the store, no matter the circumstances.
All colleagues work together to support one another in providing a service that appears seamless. It is this level of teamwork that sets them apart from their peers. Even under the most challenging of circumstances, for example, colleague illness or HSE inspection, they will all pull together to share the load and achieve their goals.
The team also takes pride in their ability to diversify. All colleagues are trained in multiple disciplines, from OTC to beauty, from stock management to event planning.
The TCP Homecare Community Pharmacy team is committed to providing high-quality care to their patients. They take pride in their ability to work together seamlessly as an effective, caring, and clinically robust team. This diverse team consists of pharmacists, technicians, customer service representatives, warehouse staff, and delivery drivers who are dedicated to ensuring patients have access to the medications they need.
As an independent community pharmacy, they specialise in dispensing and delivering high- value medicines to patients with rare diseases, managing complex conditions with an approach based on a foundation of clinical excellence, patient care, and teamwork.
Adrian Dunne Pharmacy, Trim
This pharmacy team one of the longest serving teams in the Adrian Dunne Pharmacy Group. Every member has a great passion for their job, they adore their customers and really enjoy working for Adrian Dunne. With long service comes knowledge. They have excellent pharmacists who offer the advice to patients, they really epitomise community pharmacists and offer pharmacist led training to teams twice yearly to ensure all colleagues offer the best advice to patients.
The team are highly engaged and motivated as highlighted in the most recent great place to work survey, where they scored amongst the highest in the group 88% satisfaction score.
78 | PHARMACYNEWSIRELAND.COM
2023 The Irish Pharmacy
Awards
TCP Homecare Pharmacy Team
Hickey’s Pharmacy, Johnstown
Call for papers: make your contribution to Irish Pharmacy News






Articles



Research Papers
Reviews
Programme Descriptions
Reports
Case Reports

Letters to editor
In-depth review articles critique fundamental concepts, issues, and problems that define a field of research or practice and support advanced practitioners as well as aspiring early-year pharmacists.
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients with the aim to improving pharmacy practice.
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions.

Contact: Kelly Jo Eastwood at: kelly-jo@ipn.ie or Aoife Jackson at: aoife@ipn.ie

PHARMACYNEWSIRELAND.COM
Recognising World Hypertension Day
Hypertension (high blood pressure) often goes unnoticed but is among the leading modifiable risk factors for cardiovascular disease and premature death worldwide. The prevalence, consequences, disease risk and associated mortality of hypertension place a considerable burden not only on individuals and but on health service resources.
Written by Clodagh McCarthy, Health Information Manager, Irish Heart Foundation

Foundation is collaborating with the Irish College of General Practitioners (ICGP) and the Irish Pharmacy Union (IPU) on a campaign to raise awareness of the causes and impact of hypertension and motivate people to get their blood pressure checked regularly.
blood pressure through regular checks and small changes to their lifestyle, if needed.
Targeted at undiagnosed adults aged 50 and over, the campaign will run for three years. It will comprise:
• radio and online ads to encourage people to get their blood pressure checked
• a range of health information on understanding and managing hypertension on irishheart.ie
Fieldwork for this research will start in 2024 and results are anticipated to coincide with the final year of the three-year campaign.
Despite being the leading modifiable risk factor for cardiovascular disease and premature death, research has shown that Ireland has one of the lowest rates of awareness, treatment and control of hypertension among 12 highincome countries. Indeed, a review of The Irish Longitudinal Study on Ageing (TILDA) in the Journal of Public Health in 2016 reported that 64% of over-50s had high blood pressure and, worryingly, 45% of those were unaware of their condition. Of those with high blood pressure, 59% were taking medication to reduce it, but almost half of those did not actually have their blood pressure controlled to normal levels.
World Hypertension Day is on 17 May. This year the Irish Heart
The Irish Heart Foundation’s campaign will remind the public that hypertension is a major risk factor for cardiovascular disease (including stroke and heart attack), cognitive decline (including dementia) and kidney disease. It will also inform people of common modifiable risk factors, namely a diet high in salt but low in fruit and vegetables, overweight, high alcohol intake and low physical activity.
Research shows there are significant benefits to hypertension treatment. A major systematic review in the Lancet found that in the populations studied, every 10mmHg reduction in blood pressure resulted in:
• a 17% reduction for coronary heart disease
• a 27% reduction for stroke
• a 28% reduction for heart failure
• a significant 13% reduction in all-cause mortality.
These striking figures point not only to the need for, but also the enormous benefit of, a campaign to help people take control of their
Predicting the ADHD Risk
• posters and flyers, which are being informed by focus groups with underserved communities and will be distributed to community organisations, pharmacies and health centres nationwide.
Another significant element of the campaign will be the availability of free blood pressure checks through the Irish Heart Foundation’s mobile health unit (MHU). The MHU, staffed by nurses, conducts about 10,000 opportunistic blood pressure checks a year in mainly disadvantaged, hard to reach community settings such as men’s sheds, family resource centres and Traveller groups around Ireland. In a three-year period up to 2019, almost one in three (31.6%) health check participants identified with high blood pressure were unaware of having this condition before attending the MHU.
An additional arm of the campaign will be a partnership with The Irish Longitudinal Study on Ageing (TILDA) to assess long-term awareness and behaviour change in relation to hypertension in TILDA’s next wave of research.
Primary care is central to managing hypertension, with multiple opportunities to test and adjust treatment recommendations. Currently, initial blood pressure management and treatment decisions most frequently take place in general practice (involving GPs and wider practice staff), while wider primary care (in particular pharmacy) plays a role supporting adherence to medicines. Recently, there has been a major push to transform healthcare delivery with a focus on achieving better integrated, coordinated, high-value care. The campaign is timely given the recent publication of the HSE’s Second Report of the Structured Chronic Disease Management Programme, which demonstrated reduction in mean population blood pressure readings for those in the programme.
For hypertension in particular, high quality care requires patient awareness of preventive care, regular blood pressure screening, effective communication between healthcare providers and patients and active self-management by patients. The upcoming campaign, led by the Irish Heart Foundation and supported by the ICGP and IPU, presents an opportunity for NGO advocacy, medical expertise and health service engagement to join forces for long-term changes in awareness, behaviours and positive health outcomes.
For more information see www.irishheart.ie
Information available at birth may help to identify children with higher likelihood of developing ADHD, according to new research from RCSI University of Medicine and Health Sciences.
The study, published in Development and Psychopathology, examined data from almost 10,000 children in the United States, showing information about pregnancy and birth may help to help predict the extent of ADHD symptoms in childhood.
The Adolescent Brain Cognitive Development (ABCD) study is an ongoing study of children in the US, born between 2005 and 2009. Children were enrolled to the study at age 9–10 and their parents were asked about aspects of the pregnancy and birth, as well as their child’s current mental health.
The RCSI researchers identified 40 factors that would typically be known by birth, including the sex of the baby, the age of the parents, any complications during the pregnancy or delivery, and the baby’s exposure in the womb to factors such as cigarette smoke. Using machine learning and statistical techniques, the researchers found that 17 of the 40 factors were particularly good at predicting the number of ADHD symptoms in childhood.
PHARMACYNEWSIRELAND.COM 80 Hypertension
Bowel Cancer Awareness at the Irish Cancer Society
April is Bowel Cancer Awareness month and as part of our national awareness campaign, the Irish Cancer Society (the Society) is urging people to be aware of the signs and symptoms of the disease. According to the National Cancer Registry Ireland, nearly 2,600 people in Ireland are diagnosed with bowel cancer each year. Bowel cancer is one of the most common cancers in Ireland; it is the second most common cancer amongst men, and the third most common amongst women.
As with all cancers, the earlier you are diagnosed, the more treatment options available to you and the better your chance of cure. Most recent official data shows that 483 fewer cases of bowel cancers were registered in the first year of the pandemic, compared to what was expected. Clinicians are now seeing more advanced diagnoses, patients that possibly delayed going to their GP during the pandemic.
Early detection is Vital
Due to the embarrassing nature of the signs and symptoms of the disease, delayed diagnosis has unfortunately been a long-standing issue. We are urging the public to go to their GP, if they notice any changes in their bowel habit. Changes including;
• A lasting change in your bowel habit – going more often, looser motions or constipation.
• Blood in your poo or bleeding from your back passage.
• Pain or discomfort in your tummy area or back passage.
• Trapped wind or fullness in your tummy.
• A lump in your tummy area or rectum.
• Feeling you have not emptied your bowel fully after going to the toilet.
• Unexplained weight loss.
• Feeling tired and breathless due to anaemia (fewer red blood cells).
We have developed a bowel online checker tool that can be accessed on www.Cancer.ie/Bowel This tool is designed to help the public assess their bowel health. It can generate a report which can then be brought to their GP and be used as a prompt for a conversation about bowel health.
Bowel cancer is primarily a disease of older people, but the landscape is changing as more and more younger people present with symptoms. It is vital that everyone is bowel aware and acts on signs and symptoms. Separate to symptom awareness, another key part of early detection is engaging in screening. During April, BowelScreen, Ireland’s
national bowel cancer screening programme, is reminding people to complete the simple at-home test that could save their life. BowelScreen offers a free athome test to people aged from 60-69. The test involves taking a small sample of your stool (poo) using a Faecal Immunochemical Test or FIT kit that is sent to your home, and returned to BowelScreen in the post. It’s done in the privacy of your own bathroom. More information is available at: https://www2.hse.ie/ conditions/bowel-screening/
There are risk factors that increase your chance of developing bowel cancer, age, family history of bowel cancer and inherited bowel conditions, obesity, poor diet and excess alcohol. The Irish Cancer Society Freephone Support Line is available on 1800 200 700 for anyone with a cancer-related query or concern.

The research landscape
Through the support of the public and our donors, the Irish Cancer Society is the largest voluntary funder of cancer research in Ireland and we are committed to improving the lives of those impacted by cancer in Ireland through research. In the arena of bowel cancer, we currently fund two exciting studies. Rebecca O’Brien, Irish Cancer Society PhD Researcher of the Year 2023, is a final year PhD Scholar based in Trinity College Dublin. Rebecca’s PhD project investigates the role of immune proteins, called complement proteins, in bowel cancer. Unfortunately, many bowel cancers do not respond to current treatments, and the exact reasons behind this resistance are poorly understood. Rebecca is particularly interested in how these immune proteins and immune cells may affect treatment response in bowel cancer. In addition, Rebecca’s research also looks at whether the amount of these proteins in the blood of bowel cancer patient may help to predict resistance to treatment.
Dr Grainne O’Kane, is a medical oncologist with a wealth of experience in gastrointestinal cancer research, based in Trinity St. James’s Cancer Institute. One of the areas of focus of Grainne’s research is bowel cancer. Grainne
 Written by Aoife McNamara, Education and Engagement Manager, Irish Cancer Society
Written by Aoife McNamara, Education and Engagement Manager, Irish Cancer Society
aims to improve treatment options for bowel cancer patients in Ireland, including providing world class treatment options. Grainne’s research aims to increase the availability of novel clinical trials to patients with bowel cancer in Ireland, to ensure each patient has access to world-class treatment options.
Bowel Cancer
Do you have bloating or trapped wind?
Do you have a lump or pain
in your tummy or back passage?
Does your bowel still feel full
after you go to the toilet?
Are you going to the toilet more?
Do you have diarrhoea or constipation?
Have you lost weight without trying?
Is there blood in your poo?
Is it darker than usual?
PHARMACYNEWSIRELAND.COM 81 Bowel Cancer
Call our Support Line on Freephone 1800 200 700 or email supportline@irishcancer.ie
what to look for
know







Available in sizes: M (10-16) & L (16-22) Liners Few drops or less Light Pads Occasional leakage Pads + Frequent leakage + Underwear Heavy leakage Absorbs bladder leaks & odours in seconds www.prl.ie pgsales@prl.ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park, Rathcoole, Co. Dublin



1 Always Unnoticeable Protection for Incontinence Normal & 1 Always Ultra Long
20 minutes
finishing last
the level of dryness.
www.prl.ie pgsales@prl.ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park, Rathcoole, Co. Dublin
Result of product demonstration consisting of pouring 4x 10ml liquid to
pad.
from
pour, plotting paper pressed on both pads, resulting in measuring
4x drier than sanitary pads
Promoting Awareness of Health
HIQA publishes resources to promote awareness of advocacy in health and social care services
An advocate is a person who protects and promotes people’s human rights, while also respecting their autonomy, privacy, dignity, values, preferences and diversity. Staff in health and social care settings have an important role to play in promoting advocacy services and supporting people to understand and access different types of advocacy.
Written by Rachel Flynn, Director of Health Information and Standards, HIQA

need to be respected and at the forefront of policy.
Advocacy supports person-centred care by placing the person at the centre of any decision-making about their lives and their care. At HIQA, we are committed to promoting person-centred care and supporting staff to uphold a human rights based approach to care. HIQA has now produced a new set of resources on advocacy to help staff incorporate it into their day-to-day work.
All national standards published by HIQA have a focus on advocacy, particularly the National Standards for Adult Safeguarding and the Guidance on a Human Rights-
Based Approach in Health and Social Care. The new online learning course, booklet and educational video on advocacy will help health and social care staff implement national standards and support people using services to have their human rights met. These learning resources were developed in response to a recommendation of the COVID-19 Nursing Homes Expert Panel Report. The report highlighted the ongoing need for advocacy services for nursing home residents, their families and friends during the pandemic.
Several respondents to the Expert Panel emphasised the need to create a new narrative of care for older people incorporating the language of inclusion and empowerment. The final report recommended that HIQA ‘continue to highlight and promote independent advocacy services to residents’, and that the rights of residents – in terms of dignity, freedom, choice and equality –
Yet, knowledge of advocacy is still low in health and social care services. The first National Nursing Home Experience Survey, published in November 2022, found that there was limited awareness of advocacy organisations and how to access advocacy supports among both nursing home residents and their relatives and friends.
In particular, most nursing home residents (77%) said that they did not know how to access advocacy services or organisations that could help them to express their views and wishes, and to help them to assert their rights.
The survey found that 28.9% of relatives and friends said that they did not know how to contact organisations that can support their relative or friend to express their views and wishes, and help them to assert their rights.
HIQA’s resources on The Fundamentals of Advocacy in health and social care are designed to improve knowledge and understanding of advocacy and to support people to have their human rights met.
The resources will help health and social care staff understand their role in advocacy, which includes listening to people and supporting them to have their
voices heard, supporting them to have their will and preferences met, and respecting their autonomy and confidentiality.
HIQA recommends that all health and social care staff complete the one hour online course, read the booklet and watch the video to improve their knowledge and understanding of advocacy and to help them put national standards into practice in their day-to-day work.
We hope that these resources will help ensure that people using health and social care services have their human rights met at all times.
The new resources are available on the HIQA website, and the online learning course is also available on HSeLanD.
At HIQA, we are committed to promoting a person’s human rights, through supporting staff to uphold a human rights based approach to care. If you wish to learn more about advocacy in national standards, you can find the National Standards for Adult Safeguarding and the Guidance on a Human Rights-Based Approach in Health and Social Care on the HIQA website. You can also visit HSeLanD to access our online learning courses; National Standards for Adult Safeguarding, and Applying a Human Rightsbased Approach in Health and Social Care.
Abolition of In-Patient Charges
Abolition of In-Patient Charges
Minister for Health Stephen Donnelly has announced that, with effect from Monday 17 April 2023, public in-patient charges have been abolished in all public hospitals.
Minister for Health Stephen Donnelly has announced that, with effect from Monday 17 April 2023, public in-patient charges have been abolished in all public hospitals.
The Health (Amendment) Act 2023 removes the acute public in-patient charge of ¤80 per day, up to a maximum of ¤800 in a year (including day-case charges) for people accessing care as a public patient in all public hospitals. Following the enactment of the legislation, the Minister for Health signed the Commencement Order providing for the removal of charges from today.
The Health (Amendment) Act 2023 removes the acute public in-patient charge of ¤80 per day, up to a maximum of ¤800 in a year (including day-case charges) for people accessing care as a public patient in all public hospitals. Following the enactment of the legislation, the Minister for Health signed the Commencement Order providing for the removal of charges from today.
Minister Donnelly said, “I am delighted to announce that from today, people will no longer be charged when accessing public inpatient care in our public hospitals.
Minister Donnelly said, "I am delighted to announce that from today, people will no longer be charged when accessing public inpatient care in our public hospitals.
“This legislation removes the existing financial burden of public inpatient charges when accessing care in a public hospital. The removal of these charges, announced as part of Budget 2023, is an important step towards reducing the healthcare costs of patients and families.
“This legislation removes the existing financial burden of public inpatient charges when accessing care in a public hospital. The removal of these charges, announced as part of Budget 2023, is an important step towards reducing the healthcare costs of patients and families.
“This measure builds on the abolition of public in-patient charges for children, which I introduced last year, and is another significant step in ensuring that people have access to affordable healthcare services."
“This measure builds on the abolition of public in-patient charges for children, which I introduced last year, and is another significant step in ensuring that people have access to affordable healthcare services.”
PHARMACYNEWSIRELAND.COM 84 News
RCPI Academy Holds Inaugural Meeting at No. 6 Kildare Street
The meeting brought together over 46 retired or semi-retired consultants across a variety of different specialties, sharing years of experience.
The aim of the group is to assemble these retired members to share their wealth of knowledge, skills and expertise working in healthcare and pass it on in several ways, including through the mentorship of earlystage consultants, examinations, education, college representation and volunteer work.
The Academy is also for those who are interested in connecting and engaging with other Members and Fellows.
Prof Trevor Duffy, Director of Healthcare Leadership at RCPI, highlighted the importance of such a group, sharing its key message: Medicine is an ever-changing landscape where one can continue life-long learning, which certainly does not stop after retirement.

Following Prof Duffy’s address, the group heard from four speakers, who all shared the unique and inspiring ways they are spending their retirement:

Prof Frank Murray shared his experience with the EQUALS Initiative, which seeks to improve healthcare in lowincome countries by working in partnership with less developed
Professor Frank Murray shared his experience with EQUALS Initiative. (via Bobby Studios)
countries and addressing the huge inequality that exists in health globally through:
1. Sourcing and donating good quality equipment which becomes freely available from Irish hospitals to hospitals in Zambia, in response to local need
2. Supporting the training of biomedical engineers
3. Supporting the development of postgraduate medical training for specialist physicians
4. The initiative began in 2013 when Prof Murray received a request from an Irish doctor in Zambia asking to help source an ultrasound machine for Monze Mission Hospital. From here, RCPI and the HSE established the EQUALS Initiative.
5. RCPI is calling for other retired doctors to get involved and join the academy.
6. If you are interested or would like to receive communications about upcoming Academy events, please contact fionamckenna@rcpi.ie
Novel Gene Therapy for Glaucoma
Experts are projecting an increase in those affected to over 110 million by 2040. While topical eye-drops are critical in preventing disease progression, up to 10% of patients become treatment resistant, putting them at risk of permanent vision loss.
The main clinical risk factor for glaucoma is elevated intraocular pressure; dangerous increases in pressure in the globe of the eye can lead to serious damage to the optic nerve head, which transmits light signals to the brain to allow us to see. This elevated pressure is caused by a build-up of unwanted proteins causing a blockage in drainage channels that, over time, can cause fluid to accumulate and pressure to increase.
Here, the team at the Smurfit Institute of Genetics,
in collaboration with the biotechnology company Exhaura Ltd, have shown that a gene therapy-based approach can decrease intraocular pressure in pre-clinical models of glaucoma.
A single injection of a viral vector – essentially a virus the scientists have hijacked with the purpose of using it to deliver specific instructions to cells in the body –can increase the flow of aqueous fluid from the front of the eye and thereby decrease pressure in the eye. The key instructions are for cells to produce an enzyme matrix (metalloproteinase-3, or MMP-3) that helps kick this process into gear.
“This exciting project allowed us to bridge the gap between academia and industry and work very closely with a gene therapy company to
develop a cutting edge therapy that we believe holds immense promise for patients in the future,” said Professor Matthew Campbell, Professor in Genetics at Trinity.
Importantly, the work used multiple models of disease as well as making use of donor human eyes to screen the therapeutic efficacy of the gene therapy approach. This makes the impressive results all the more promising.
From rare to common diseases
Gene therapies have seen a dramatic advance in recent years, with multiple drugs now approved by both the FDA and EMA. However, to date, all of the approved gene therapies are for the treatment of rare or ultra-rare conditions. As our understanding of the underlying mechanism of common diseases is now
becoming more evolved, the concept of using gene therapy for common diseases is now possible. Dr Jeffrey O’Callaghan, Postdoctoral research fellow at Trinity and first author of the study, added, “Our novel approach to treating glaucoma using gene therapy is the culmination of over seven years of research. We are now hopeful that this therapy will pave the way to the development of treatments for other forms of blinding eye diseases.”
A multidisciplinary team of geneticists, ophthalmologists and translational biologists undertook the study. The close collaboration with Exhaura Ltd also allowed the team to direct all experimental outputs towards the translation of the findings to a regulatory focused clinical programme.
PHARMACYNEWSIRELAND.COM 85 News
The Royal College of Physicians held its Inaugural Meeting of the RCPI Academy.
Professor Trevor Duffy welcomes attendees to the RCPI Academy Inaugural Meeting. (via Bobby Studios)
Osteoporosis – Preventing the Silent Killers “Fractures”
The disease Osteoporosis is commonly considered to affect just “Old” women, and many people do not appear to be aware that this disease is preventable and treatable in most people. Women over 65 are the highest risk group for fractures, however it affects all age groups, including our young. Only 19% of people with Osteoporosis are diagnosed, which is why everyone should be checking to see if they have any of the 200 causes of bone loss.
Written by Michele O'Brien, CEO, The Irish Osteoporosis Society

of exercise she was doing to “normal levels”, which resulted in her periods returning, which assisted with her improvement of bone health, as her oestrogen levels returned to normal. She also learned some stress coping techniques that she could use at her office desk, as she had previously increased her running times in an attempt to decrease her stress levels.
the Irish Osteoporosis Society (IOS) would recommend a different form of contraceptive.
Women lose bone leading up to the menopause, going through the menopause and the most significant bone loss occurs in the 10 years post menopause. In general, we can only assume that the more risk factors for bone loss a person has, the higher the bone loss they will experience.
Osteoporosis – Preventing the Silent Killers “Fractures”
An example of this is the DXA scan below (figure 1). It shows the results of a 21 year old female who was diagnosed with severe bone loss at 19 in her spine.
Written by Michele O'Brien CEO
The fact that two of her vertebrae had been eliminated from her DXA scan results, shows that even the young can develop Osteoarthritis, which is why L1 and L3 vertebrae were eliminated. Osteoarthritis can give false higher readings falsely showing the bones are healthier than they are.
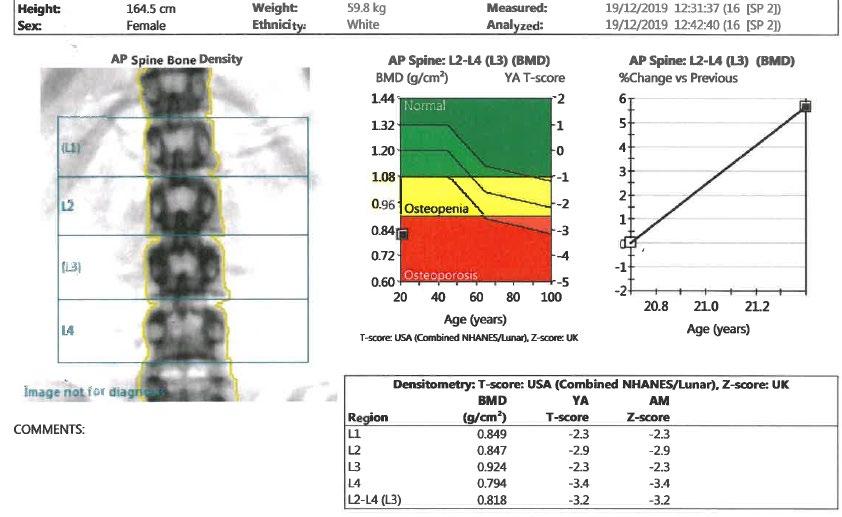 The Irish Osteoporosis Society
The Irish Osteoporosis Society
Her DXA results show she now has marked Osteopenia in L1 and L3, Osteoporosis at L2 and severe bone loss at L4.
Thankfully she was diagnosed, investigated and put on a treatment plan. You can see from the graph named “AP spine: L2-L4 (L3) (BMD) % change vs Previous”, that in two years she has significantly improved her bone health.
This person’s causes of bone loss was due to overexercising, which caused irregular periods and she also had high cortisol levels due to a stressful job. By early intervention occurring the person so far has been able to improve her bone health and prevent vertebral fractures from occurring. Research shows that most fractures occur in the moderate to marked Osteopenia range, which is a T score of -1.5 to -2.49.
After the menopause, the ovaries stop producing oestrogen and the adrenal glands produce the male hormone testosterone, which is then converted into oestrogen by the peripheral fat. When a person is underweight, they do not have enough peripheral fat to assist with this process. Oestrogen is necessary to help protect bone and to also help in the formation of Vitamin D and absorption of calcium. When Vitamin D levels are low, bone loss occurs which increases the person risk of fractures.
1 in 7 women will get breast cancer and there is a breast screening service available. In an ideal world it would be wonderful if DXA scanning would become part of an overall health plan tied into a peri menopause screening, as 1 in 2 women aged 50 will break a bone from Osteoporosis in their lifetime.
The disease Osteoporosis is commonly considered to affect just “Old” women, and many people do not appear to be aware that this disease is preventable and treatable in most people Women over 65 are the highest risk group for fractures, however it affects all age groups, including our young. Only 19% of people with Osteoporosis are diagnosed, which is why everyone should be checking to see if they have any of the 200 causes of bone loss.
It was explained to her the consequences of her lifestyle choices and the effects of what vertebral fractures can do to a person’s quality of life. No one wants to end up disfigured with the possibility of a Dowager’s hump which is not reversable. The individual reduced the amount
The lesson to be learned is that prevention of breaking bones is much cheaper and less painful than just targeting the highest risk group for bone loss.
An example of this is the DXA scan below It shows the results of a 21 year old female who was diagnosed with severe bone loss at 19 in her spine
NOTE Depo Provera has been proven to cause bone loss, therefore unless a young person is very high risk to become pregnant,
Some people are of the belief that DXA scans place a person at high risk of radiation exposure, if you have heard this, it is not accurate. A DXA scan exposes a patient to 10% radiation of a regular Chest X-ray. A person flying from Dublin to New York will be exposed to more radiation than a DXA scan. DXA scanning is what the IOS, the Osteoporosis national experts recommend for the screening, diagnosing and monitoring of bone loss.
Do you want to be the person or a loved one of yours who ends up with multiple fractures which could have been prevented, as research shows that most fractures are preventable?
The Irish Osteoporosis Society believe that focusing on over 65’s is playing “Russian roulette” with people’s lives, especially women’s lives. On the top of page 40 (figure 2) shows why all women should be screened for bone loss. The results also show that when a person has been diagnosed with Osteopenia, which is the early stages of bone loss, they MUST be monitored. The reason monitoring is so important is because bone loss is silent, NO one feels bone loss. There are no signs or symptoms of bone loss and logically all disease’s should
Her DXA results show she now has marked Osteopenia in L1 and L3, Osteoporosis at L2 and severe bone loss at L4
Thankfully she was diagnosed, investigated and put on a treatment plan You can see from the graph named “AP spine: L2-L4 (L3) (BMD) % change vs Previous”, that in two years she
significantly improved her bone health
PHARMACYNEWSIRELAND.COM 86 Osteoporosis
has
Figure 1
and the DXA scan results show the woman’s bone health in her spine had declined by 40% in ten years and 23% in her hips.
Could these fractures have been prevented? No one can say 100% yes. However logically, if she had been regularly monitored and when the initial bone loss occurred in 2018 her causes of bone loss had been investigated and addressed, there is a very high chance, the vertebral fractures could have been prevented.
The woman’s DXA scan results below show that she had a DXA scan done in 2012
Her DXA results (aged 60) from 18 06 2018 show her bone density in her spine had declined 22.8% from her previous DXA scan which was done 6 years prior on 02 08 2012 (aged 54)
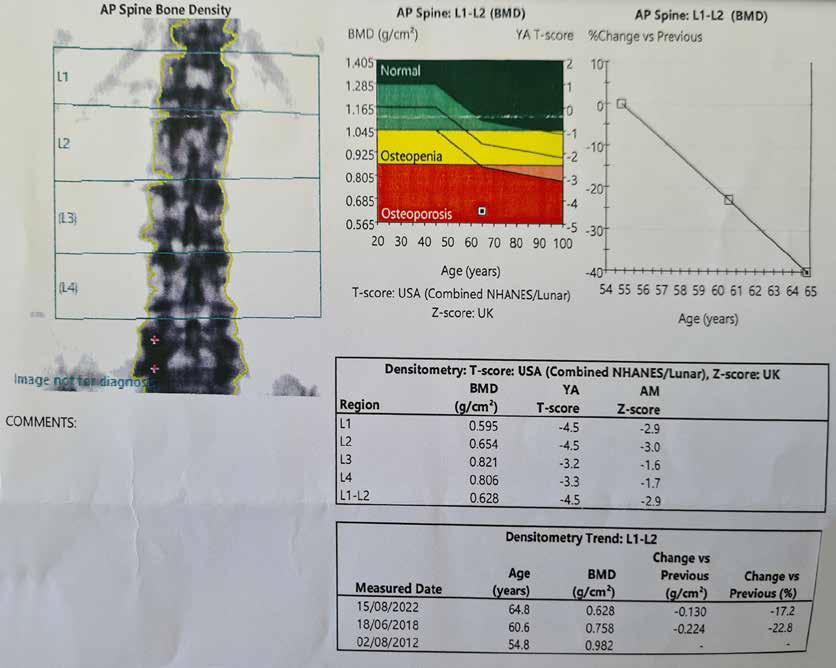
Her latest DXA scan results (aged 64) on 15 08 2022 show her bone density in her spine had declined by 17.2% since 18 06 2018, in 4 years.
Monitoring of bone health is essential, it is common sense. If a person had a heart attack, what cardiologist do you know would say “Come back in 5 years for a check up”. There are those who believe repeat DXA scans should be every 5 years. This woman is a prime example of why if a person has bone loss, they need to be regularly monitored.
be monitored and the DXA scan results show the woman’s bone health in her spine had declined by 40% in ten years and 23% in her hips.
The woman’s DXA scan results below (figure 3) show that she had a DXA scan done in 2012.
Her DXA results (aged 60) from 18 06 2018 show her bone density in her spine had declined 22.8% from
her previous DXA scan which was done 6 years prior on 02 08 2012 (aged 54).
Her latest DXA scan results (aged 64) on 15 08 2022 show her bone density in her spine had declined by 17.2% since 18 06 2018, in 4 years.
The graph in the image on the top of page 41 (figure 4) shows how her BMD (Bone mineral Density) plummeted from age 54 to 64.
Her latest DXA scan results in the image below on 15 08 2022 show her bone density in her hips had declined by a further 9.7% in four years.
The most significant results were from the LVA, which is a Lateral Vertebral Assessment which is a DXA side view of a person’s spine. This woman went through the menopause at 51.
Osteoporosis is not like most other diseases because there are no signs or symptoms prior to someone fracturing. Most people are taking treatments to supress symptoms or slow down the progression of other diseases, Osteoporosis treatments have been proven to reduce fracture risk. It is essential to ensure a person is responding to their treatment and if a decline occurs switching a treatment should not be the first option. Investigating and addressing why their DXA scan results have declined or similar to the case above, investigating why they have fractured is crucial to help keep the person independent.
Her DXA results from 18 06 2018 show her bone density in her hips had declined by 13.3% in 6 years.
The DXA LVA report at the bottom of page 41 (figure 5) shows she now has a T 5 Moderate Biconcavity fracture at T5 and T9 and a severe Biconcavity fracture at L1.
The graph in the image below shows how her BMD (Bone mineral Density) plummeted from age 54 to 64
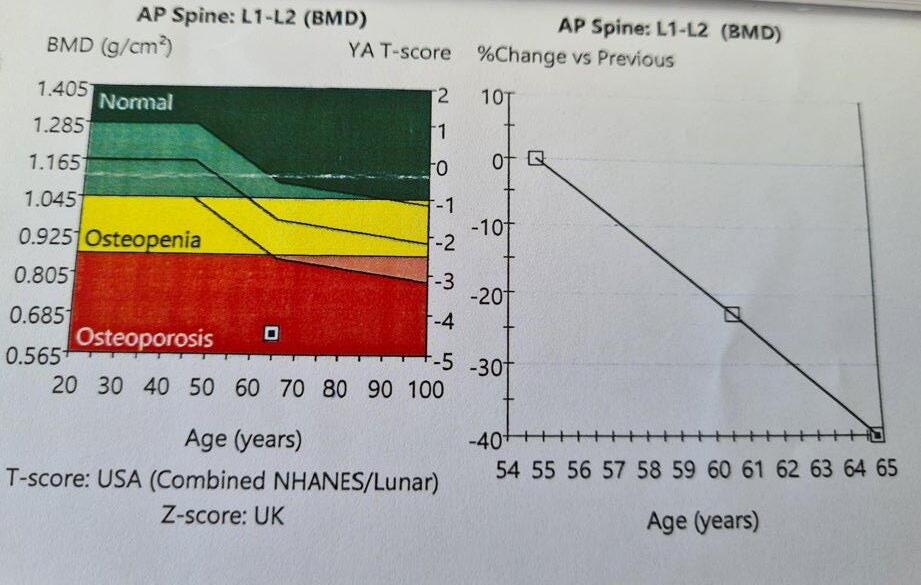
Cancer and Osteoporosis
Anyone who is going to receive chemotherapy or radiation for cancer should have a DXA scan done prior to the initiation of either treatment. If positive or negative for bone loss they should be put on a bone health plan, as both cause significant bone loss. If the person is negative for bone loss prior to the treatment, they need to be placed on an Osteoporosis treatment to prevent bone loss occurring. For a person to fight cancer to stay alive and end up with multiple fractures is not acceptable. Ireland is not a third world country and for any of you or your customers who have had either treatment or are on Medications like Arimidex or aromatase inhibitors, they need to be informed to get a DXA scan done.
Her DXA results from 18 06 2018 show her bone density in her hips had declined by 13.3% in 6 years.
Her latest DXA scan results in the image below on 15 08 2022 show her bone density in her
PHARMACYNEWSIRELAND.COM 87
Figure 2
Figure 3
Diabetes and Osteoporosis
There are two types of Diabetes Mellitus (DM). Type 1 which is a genetic disorder and people are usually diagnosed when they are young due to an insulin deficiency. Type 2 DM usually develops due to a poor dietary intake, and this usually develops over time. People with Type 1 and 2 DM are at risk of fractures due to Osteoporosis.
Menopause and Osteoporosis
When a woman goes through the menopause, it is very important it is not assumed that this is the only cause of her bone loss, as there are approx. 200 other causes of bone loss.
Menopause and Bone Health Tips
• HRT should only be given to those who go through an early menopause before age 45, who do not have contraindications, and those who have menopausal symptoms.
• HRT should not be prescribed just to protect bone health.
• For those who are going through an early menopause HRT should consist of oestrogen and progesterone. Oestrogen only should not be prescribed unless they have had a hysterectomy.
• Premenopausal females who have low oestrogen e.g. due to an eating disorder, can be prescribed either the contraceptive pill, i.e, an oestrogen and a progestogen, or HRT, that contains a different type of oestrogen and progestogen but ensure to tell them that it is not a contraceptive.
• Post-menopausal women who have an early menopause before age 45, if they still have a uterus, should be prescribed HRT consisting of oestrogen and progestogen, because otherwise it can increase the risk of cancer of the body of the uterus.
• Post-menopausal women who have an early menopause before age 45, If they have had their uterus removed they can go on oestrogen only.
Severe bone loss -
A T score of -3.0 or higher on a DXA scan report
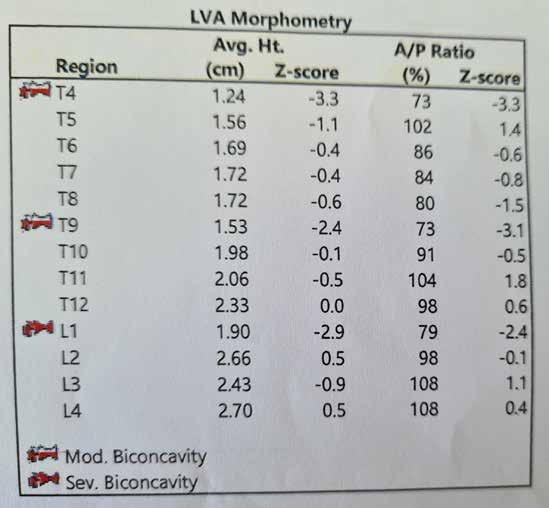
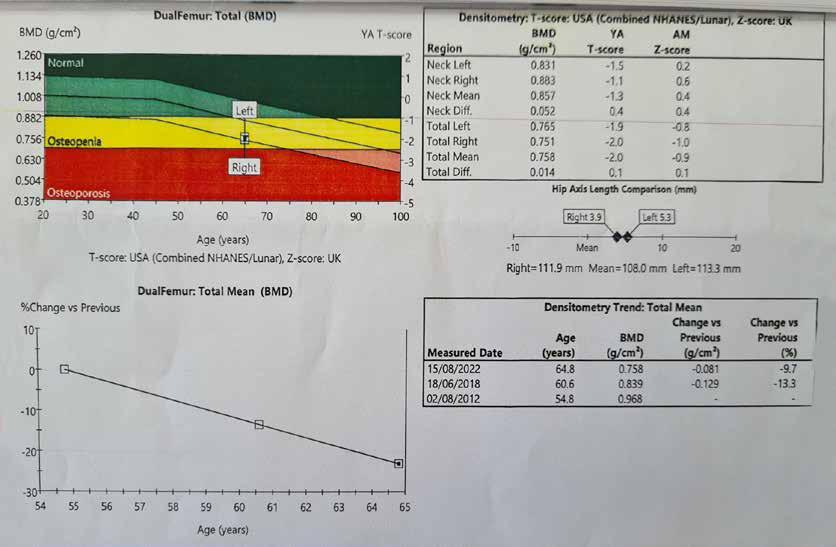
• Avoid when possible, bending forward at your waist with legs straight
• Initially, no lifting anything over 3 pounds
• Put food items in a trolley and only half fill the bags
• Do not use a vacuum, stretch up for items, or twist your body to either side with your feet planted on the ground.
• No stretches or exercise that put stress on the bones in your back such as yoga.
• No lifting of children or pets in and out of a cot, car etc
• Raised garden beds are ideal for those who love gardening
Most people are not aware that fractures should be taken far more seriously, due to the secondary complications which can be life threatening, which are a blood clot, pneumonia or infection. 20% of those who fracture their hip aged 60+ will pass away within 6 to 12 months and 50% will lose their independence. Vertebral fractures significantly impact on activities of daily living, such as washing, dressing and walking.
A person can be diagnosed with Osteopenia and/or Osteoporosis. Osteopenia is the precursor to Osteoporosis, and it is essential that the reasons why a person has lost bone is investigated and addressed, not assumed.
NOTE A calcium and vitamin D supplement is not an Osteoporosis treatment. Calcium, vitamin D and first class proteins when ever possible should be from foods.
Men and Osteoporosis
The diagnosis rate for Osteoporosis in men is very low and the IOS believe it is because of the myth that “Osteoporosis only affects old women”. 1 in 4 men over 50 will break a bone from Osteoporosis in their lifetime. More men pass away from Osteoporosis then get prostate cancer, which is why all men should be checking to see if they have risk factors for bone loss.
Exercise and Bone Health
Appropriate weight bearing exercise is very important for those with bone loss, as well as improving muscle strength and balance. A very common stretch done by people is forward flexion which is shown in the image at the top of page 42 (figure 6). The IOS does not recommend this stretch for anyone other than athletes due to the damage it can inflict on a person. This stretch puts excess compression on the front of the body of the vertebrae and strain on the discs between the vertebrae. This stretch also puts excess strain on your sciatic nerve in your back, that if irritated will cause pain to go down your leg.
PHARMACYNEWSIRELAND.COM 88 Osteoporosis
Figure 4
Figure 5
Signs and symptoms of possible undiagnosed Osteoporosis
• A broken bone caused by a trip and fall from a standing position or less, even if on cement or ice.
• Many people believe that it is normal to lose height as you get older, it can be a red flag for undiagnosed vertebral fractures.
• A person’s head protruding forward from their body or their shoulders becoming rounded or a hump developing on their upper back can be sign that vertebral fractures have occurred.
We do not recommend the following for those with bone loss:
The excess pressure on the vertebrae can cause Vertebral fractures. Professor Moira O’Brien who set up the first Osteoporosis clinic in Ireland as well as being the only Osteoporosis consultant in Ireland, has had patients in their 40’s who fractured vertebrae due to this stretch and the IOS have received helpline calls from people who have also fractured from this forward flexion stretch.
depend on the person’s age, if they have broken any bones yet, their DXA scan results, medical history, causes of bone loss, balance, ability and age.
Walking, but the speed and course need to be altered.
Touching your toes while in the sitting position or when standing bending forward at your waist, doing regular sit ups, exercise on trampolines, excessive weights, yoga, horse riding, skiing, twisting your back with your feet on the ground (golf swing), vibrating machines, high impact exercises such as jumping off boxes or heights or pounding your feet when walking. Jogging and running is not recommended for those who have vertebral fractures
NOTE: Many stretches in Yoga place stress on the bones in the spine, which is why the IOS do not ever recommend yoga for those with and without bone loss.

Walking up and down stairs works the main muscles for walking, is great for your overall health and helps to build up bone in the hip area. So instead of listening to the adverts on TV or watching your partner switch from one station to another during the breaks, why not walk up and down your stairs a couple of times.
Fall Prevention - Balance and coordination including ensuring your home environment is safe. Example – A good pair of walking shoes instead of wearing slippers, as most do not have good support and no one should wear open back shoes as they are a tripping hazard. Incontinence - There have been significant advances in the treatment for incontinence, which can lead to falls, due to people rushing to the bathroom or slipping on urine after having an accident, please contact the Irish Osteoporosis Society for more details.
• A person’s body shape changing, such as a pot belly developing, an increase in clothes size, or the person not being able to reach previously accessible shelves.
• Upper, middle or low back pain should be investigated, and Osteoporosis ruled out, as 75% of people with vertebral fractures have intermittent back pain.
The image below (figure 7) shows the effects of undiagnosed/ untreated bone loss at any age.
Risk Factors for Bone loss
NOTE: The IOS does not recommend anyone with bone loss start an online exercise programme or weights programme, without having been individually assessed by a health care professional, who is up to date on bone loss. Why? To help reduce the risk of people getting hurt. In order for a health professional to put a person with bone loss on a safe and appropriate exercise programme, they must understand DXA scan results. A person can look perfectly fine but have severe bone loss.
We do not recommend the following for those with bone loss:
Summary
People need the causes of their bone loss investigated and addressed
Walking, but the speed and course need to be altered
When it is raining or very windy outside When the weather is very wet and windy, why not stand in front of your favourite TV programme and march on the spot while watching it or while listening to your favourite radio programme or walk around your home, including going up and down your stairs, as every step counts to help keep your independence.
Family history of Osteoporosis or broken bones (as 81% not diagnosed), menopause/ hysterectomy, corticosteroids, Chemotherapy, Radiation, Arimidex, Aromatase inhibitors, Physiological or psychological stress, RA, Protein pump inhibitors, eating disorders & over exercisers, low vitamin D levels, many medications for anxiety and depression.
We DO recommend the following exercises/activities for those with bone loss, but they may not be appropriate for everyone. It will depend on the person’s age, if they have broken any bones yet, their DXA scan results, medical history, causes of bone loss, balance, ability and age.
People need to prevent falls by making their home safe People need to ensure they are doing appropriate exercise People need to ensure their bone health is monitored, as bone loss is silent!
Touching your toes while in the sitting position or when standing bending forward at your waist, doing regular sit ups, exercise on trampolines, excessive weights, yoga, horse riding, skiing, twisting your back with your feet on the ground (golf swing), vibrating machines, high impact exercises such as jumping off boxes or heights or pounding your feet when walking. Jogging and running is not recommended for those who have vertebral fractures.
Dancing, as long as you have good balance, and you are not being swung around.
Walking up and down stairs works the main muscles for walking, is great for your overall health and helps to build up bone in the hip area. So instead of listening to the adverts on TV or watching your partner switch from one station to another during the breaks, why not walk up and down your stairs a couple of times.
NOTE: The IOS does not recommend anyone with bone loss start an online exercise programme or weights programme, without having been individually assessed by a health care professional, who is up to date on bone loss. Why? To help reduce the risk of people getting hurt. In order for a health professional to put a person with bone loss on a safe and appropriate exercise programme, they must understand DXA scan results. A person can look perfectly fine but have severe bone loss.
When it is raining or very windy outside When the weather is very wet and windy, why not stand in front of your favourite TV programme and march on the spot while watching it or while listening to your favourite radio programme or walk around your home, including going up and down your stairs, as every step counts to help keep your independence
Dancing, as long as you have good balance, and you are not being swung around
We DO recommend the following exercises/activities for those with bone loss, but they may not be appropriate for everyone. It will

Strength and conditioning programme, to include core stability. Senior citizens should start out actively exercising their limbs without weights. Light weights should be slowly introduced, as rushing to increase weights and resistance, can place a senior citizen at risk of muscle and joint soreness, which could turn them off exercising, and place those with bone loss at risk of possible fractures.
For those who had previously lifted weights, they should start with low weights and gradually increase.
Exercise in water can help build up muscle strength and endurance, without putting excess stress on joints.
PHARMACYNEWSIRELAND.COM 89
Figure
6
Figure 7
Updates in Ireland’s Fracture Liaison Service

The aim of a Fracture Liaison Service (FLS) is to identify people at risk of fracture, investigate when required, and initiate appropriate bone strengthening medication as indicated.
Written by Professor Frances Dockery, Fracture Liaison Service Database Clinical lead, Consultant Geriatrician, Beaumont Hospital
fracture, to diagnose osteoporosis and identify those most at risk of future falls and more serious fractures such as those of the hip or spine.
FLS uses a consultant led multidisciplinary team approach and is an integrated service between acute and primary care settings. If properly resourced, it has the potential to reduce the number of people with acute, debilitating fractures admitted to the hospital setting. This aligns closely with both Sláintecare and Healthy Ireland principles. Ireland is only the second country globally to develop a national FLS database, with the aim of improving care for these people who sustain a first non-hip fragility fracture.
of recurrent fractures, and for society as a whole in reducing the costs associated with caring for people who lose their ability to live independently as a result of these fractures.
FLS has been adopted globally as real-world data has demonstrated that this model of care has proven benefits in reducing future fracture numbers when investment is made in a high-quality service. Currently, Europe spends an estimated (¤37 billion on managing fragility fractures (¤400 million in Ireland), of which just ¤2 billion is spent on prevention.
A fracture resulting from a simple fall is known as a “fragility fracture”, and usually indicates the presence of osteoporosis. Fractures as a result of osteoporosis are one of the leading healthcare costs across Europe and numbers are rising steeply. A recent Europewide scientific report on fragility fractures predicts that Ireland will see an increase in cases of ~ 58%, the highest of all EU countries
because of ageing demographics (Scope 2021, Kanis). These fragility fractures cause great distress and disability for over 30,000 people annually in Ireland, and can impact survival. Despite highly effective treatments being available to manage osteoporosis and thus reduce the risk of fracture, only a minority receive these.
FLS provides a system for assessing people aged 50 years and over who sustain a fragility
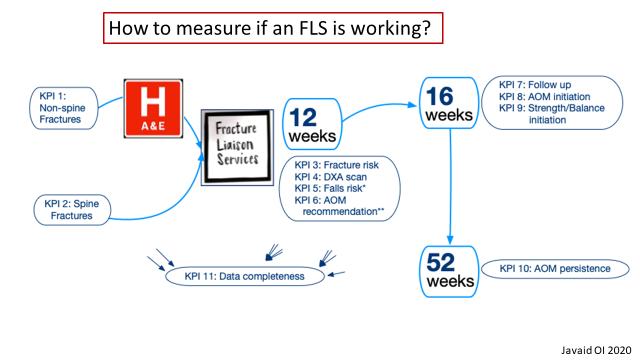
Up to 50% of people who sustain a major fracture (e.g. a hip fracture) would have had a previous nonhip “warning fracture”. Most of these people do not get screened, or treated at that point, for osteoporosis. An assessment of their risk of falling, which might help prevent future fractures, is also seldom carried out at the time of their initial fracture.
Many recent publications in the scientific literature have outlined the benefits that FLS provide, both in reducing the person’s risk
The National Fracture Liaison Service (FLS) Steering Group welcomes the funding of eight advanced nurse practitioner (ANP) posts by the HSE during 2022. These nurses will play a critical role in patient care by proactively identifying and managing the care of patients presenting with fractures. They will ensure screening for, and treatment of osteoporosis and falls risk, with patient education to enable selfmanagement of their bone health. The FLS ANP’s also monitor treated patients for the year ahead to ensure tolerability and adherence with prescribed medication given the very low treatment rates postfracture presently.
PHARMACYNEWSIRELAND.COM 90 Fractures
In October 2022 the first Irish FLS – DB Report was published. This report analysed the secondary preventative management of fragility fractures received by over 2,000
While these ANP posts are welcomed, it is imperative that national implementation with full resourcing occurs in the next two years. This will enable each FLS to address rising fracture numbers, create value for the health service and deliver significant benefits to patients who would otherwise go on to sustain additional fragility fractures.
over 2,000 patients (~ 26% of the expected number) during 2021 in eight out of the sixteen hospitals in Ireland which currently manage patients presenting with fractures. The low proportion of patients identified and treated demonstrates the gaps in service provision within Ireland in adequately managing these patients, in line with international best practice standards.
nurse practitioners for fracture liaison services nationally.”
Prof Frances Dockery, joint clinical lead for the Fracture Liaison Service said: “This report provides a benchmark for future service developments
The current lack of investment in a national Fracture Liaison Service addressed as a matter of urgency so that all 16 hospitals that manage fractures in Ireland can establish a sustainable FLS, which will contribute National FLS Database to monitor the standards of care their patients
The Irish Fracture Liaison Service Database (FLS – DB) was established in 2020 by the National Fracture Liaison Services steering committee under the governance of the National Clinical Programme for Trauma and Orthopaedic Surgery. The FLS – DB is aligned with the International Osteoporosis Foundation’s “Capture the Fracture” initiative which aims to improve access for people to comprehensive Fracture Liaison Services globally.

In October 2022 the first Irish FLS – DB Report was published. This report analysed the secondary preventative management of fragility fractures received by
Mr Paddy Kenny, Joint National Clinical Lead for the National Clinical Programme for Trauma and Orthopaedic Surgery said “The development of a Fracture Liaison Services Database is a key enabler in implementing recommendation 15 of the 2018 HSE report - “A Trauma System for Ireland”. Having Irish data will facilitate policy makers to plan service delivery more effectively and efficiently into the future. I commend the national clinical leads in promoting the work that this group has completed to date and welcome last year’s appointment of eight advanced
Prof Frances Dockery, joint clinical lead for the Fracture Liaison Service Database said: “This report provides a benchmark for future service developments in Ireland. The current lack of investment in a national Fracture Liaison Service needs to be addressed as a matter of urgency so that all 16 hospitals that manage patients with fractures in Ireland can establish a sustainable FLS, which will contribute data to the National FLS Database to monitor the standards of care their patients receive”.
Mr Aaron Glynn, joint clinical lead for the Fracture Liaison Service Database, noted that “Fracture Liaison Services should be considered essential ‘secondary prevention’ services, and as such is an enabler in improving patient health and wellbeing.”

in improving patient health and
The second report of the FLS – Database will be published in October 2023. To find out more about this initiative please contact fls@rcsi.ie
Mr Aaron Glynn, Fracture Liaison Service Database Clinical lead, Consultant Orthopaedic Surgeon, Our Lady of Lourdes Hospital Drogheda, Navan General Hospital
The second report of the FLS – Database will be published in October 2023. To find out more about this initiative please contact fls@rcsi.ie
PHARMACYNEWSIRELAND.COM 91
Mr Aaron Glynn, joint clinical lead for the Fracture Liaison Service D that “Fracture Liaison Services should be considered essential ‘secondary prevention’ services, and as such is an enabler
wellbeing.”
Calls for Asthma Medication to be Free of Charge

The Asthma Society of Ireland has released findings of a new survey of 1,294 men and women living with asthma in Ireland.
Chaithnia
The survey, undertaken as part of Asthma Awareness Week 2023, revealed the stark realities of the impact of the cost of living crisis for those living with asthma in Ireland.
• 96% of those surveyed have been prescribed asthma medications.
• Despite that, 45% of asthma patients have had to forego asthma medications for themselves, or their children, due to financial constraints.
• 48% of households with asthma have been in arrears on mortgage or rental payments; utility bills; hire purchase instalments or other loan payments in the past 12 months.
• 76% also said that their own or their child’s daily activity was limited or severely limited by the disease
• 25% of survey participants described their asthma as bad or very bad.

This survey was undertaken by the Asthma Society ahead of Asthma Awareness Week 2023 which took place from May 1st to 7th. This year is the 50th anniversary of the Asthma Society in Ireland. To mark this milestone, the Asthma Society hosted a virtual conference on May 4thAsthma Care for All.
The conference featured people living with asthma describing their own experiences of being treated for asthma, and the difference
the Asthma Society’s services have made to their lives. The conference was open to people with asthma, their family and caregivers, and the public. Over the past 50 years, the Asthma Society has achieved many successes, including establishing the Asthma Adviceline in 1982 which has helped thousands of families. This free call-back service provides expert advice from respiratory nurse specialists on all aspects of managing asthma, from identifying triggers to creating an Asthma Action Plan. If you, or any member of your family have concerns about your asthma you can call the Adviceline at 1800 44 54 64 or send a message via WhatsApp at 086 059 0132.
The Asthma Society quickly adapted its services during the pandemic, conducting 4,416 nurse appointments through its Adviceline in 2020. In addition to a respiratory crisis, people with asthma are now feeling the weight of the cost of living crisis. A recent survey of 1,294 people with asthma in Ireland revealed concerning figures regarding the affordability of asthma medications. Despite 96% of those surveyed being prescribed asthma medications, 45% have had to forego them in the past three months due to financial constraints.
Asthma Society CEO Eilis Ní Chaithnia said of the survey findings, “These statistics are alarming, considering that 380,000 people in Ireland have asthma, and every four minutes, someone visits the Emergency Department due to asthma. Tragically, each week, a family in Ireland loses a loved one due to the condition.
Therefore, it is crucial to prioritise universal access to asthma medications to ensure that people can manage their condition effectively. The Asthma Society has been advocating for asthma medications to be included free of charge on the Long Term Illness Scheme for years. This is something the organisation urgently calls for, especially since Ireland has the second-highest hospitalisation rate for asthma in the EU.
If people are not using their daily preventer inhaler, they often rely on their reliever inhaler or steroid tablets to treat their worsening symptoms. Overuse of your reliever inhaler or steroid tablets can lead to detrimental side effects. Overuse of your reliever inhaler can lead to fatalities.”
Professor Marcus Butler, Consultant in Respiratory Medicine at St Vincent’s Hospital and Medical Director of the Asthma Society says, “Asthma is a chronic (or long-term) illness and the World Health Organisation considers it to be the most common chronic disease among children, affecting one in every
13 children and adults in Ireland. Chronic illnesses typically persist well beyond six months. 91% of those surveyed by the Society expected their own, or their child’s asthma, to last for six months or longer. 76% also said that their own or their child’s daily activity was limited or severely limited by the disease.1 The tragic deaths we see in asthma are largely preventable with medication.
“What we learned from the survey was very concerning. People with asthma need to take their medication as prescribed as good asthma control is key in preventing asthma attacks, hospitalisations and those asthma deaths.
“It’s important that people know how to use their inhaler properly. If you are in doubt about how best to use asthma medication, you can reach out for free expert advice from our respiratory nurseled Asthma Adviceline or visit your GP for an asthma review. Asthma.ie is also a great resource, providing tips and advice on how to best manage your asthma. It is important to remember that help is available.”
PHARMACYNEWSIRELAND.COM 92 News
Asthma Society CEO, Eilis Ní
“What we learned from the survey was very concerning. People with asthma need to take their medication as prescribed as good asthma control is key in preventing asthma attacks, hospitalisations and those asthma deaths”
Reminder of Precautions to avoid Photosensitivity Reactions with Fastum Gel
A. Menarini Pharmaceuticals Ireland Ltd. wish to remind healthcare professionals of the necessary precautions to avoid the risk of photosensitivity reactions with Fastum Gel.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) undertook a safety review of topical ketoprofencontaining medicines in 2010 and recommended that doctors should strictly follow the contraindications when prescribing topical ketoprofen CHMP also recommended that doctors and pharmacists should inform patients on how to use these medicines appropriately to prevent the occurrence of serious skin photosensitivity reactions. A series of risk minimisation measures for Fastum Gel was agreed with the Health Products Regulatory Authority. The Summary of Product Characteristics and the Patient Information Leaflet were updated accordingly and may be found on www.medicines.ie and www hpra.ie.
Patients should be reminded to wash their hands thoroughly after application of the product and to protect treated areas from sunlight by wearing clothing They should avoid exposing the treated areas to sunlight, even if cloudy, or UVA from sunbeds or solarium during use and for 2 weeks after discontinuation. In addition they should be advised to avoid using Fastum Gel under occlusive bandages and to discontinue Fastum Gel immediately and contact their doctor should any skin reaction develop, including cutaneous reactions after co-application of octocrylene-containing products.
A copy of the patient educational leaflet is available from A. Menarini on 01 284 6744 or 1800 283045 or is available at www.hpra.ie
A. Menarini would like to remind healthcare professionals that any suspected adverse reactions associated with the use of Fastum Gel should be reported to the Health Products Regulatory Authority at www.hpra.ie or by e -mailing medsafety@hpra.ie. A dver se reactions can also be r ep ort ed to A. Menarini’s Pharmacovigilance Department on 01 284 6744.
IR-MEN-203-2021 Date of preparation: October 2021
Topic Team Training – Emergency Contraception
Following on from the April issue Continuing Professional Development on the Pharmacy Role in Emergency Contraception, this 5-Minute Learning Module is designed to enhance the community pharmacy team understanding and ask further questions as to how you can support and advise patients.

After completing this module, you should recognise the different types of emergency contraceptives available, indications and suitability for patients that may present to the pharmacy and appropriate advice and counselling to be given for each.
Emergency contraceptives (EC) are a type of birth control that is used to prevent pregnancy after unprotected sexual intercourse (UPSI) or when other forms of contraception have failed. ECs are sometimes referred to as the “morning-after pill” or the “day-after pill.” There are several different types of ECs available, each with its own method of action and recommended dosages. Since 1st July 2017, medical card holders can get emergency contraception directly from a pharmacy, free of charge, without having to go to their GP for a prescription. Since September 2022, EC has been available for free for women between the ages of 17 and 25 with plans to extend this to 16-30 year olds later this year.
Types of emergency contraception Hormonal methods:
a. Levonorgestrel pill
This pill contains a synthetic form of the hormone progesterone (levonorgestrel). LNG should be taken as soon as possible, preferably within 12 hours after unprotected intercourse, and no longer than 72 hours (3 days) after UPSI.
b. Ulipristal acetate pill (ellaOne®)
This pill is a selective progesterone receptor modulator that prevents or delays ovulation. It is effective up to 120 hours after UPSI but is most effective the sooner it is taken. Ulipristal
Consider:
acetate (ellaOne) has been demonstrated to be more effective than levonorgestrel from 0-120 hours after UPSI so it should be considered first-line oral emergency contraception unless contraindicated.
ellaOne® is highly effective, with a reported efficacy rate of 99.5% when taken as soon as possible after UPSI.
The medication works by delaying ovulation, which means that it prevents the release of an egg from the ovary. This is achieved by inhibiting the production of hormones that trigger ovulation. Non-hormonal methods:
Copper intrauterine device (Cu-IUD) This is a small, T-shaped device that is inserted into the uterus by a healthcare professional. It works by preventing fertilisation or implantation and can be used up to 5 days after unprotected
Reflect on the following in assessing your own knowledge and your team’s training:
Is your knowledge up-to-date on all methods of emergency contraception?
Are you aware of all cases where referral to GP or sexual health clinic are required? Have you an up-to-date SOP implemented?
Do you know what advice should be given to all patients provided with emergency contraception?
Have you details of sources for further support that may be required, either for STIs or crisis situations?
Are you confident explaining the options for ongoing contraception?
sex. It also provides ongoing contraception for up to 10 years. If fertilisation does occur, the copper IUD also makes it difficult for the fertilised egg to implant in the uterus.
Emergency contraception (EC) is generally considered well tolerated and effective. However, like all medications, it may cause side effects. The most common side effects of emergency contraception include: changes to the next period – it can be earlier,
Key Points: Ensure your team understands and is confident explaining the following:
All requests for Emergency Contraception must be referred to the pharmacist
The main aspects of the pharmacist consultation should be explained to the patient if requested
The difference between methods of emergency contraception available from the pharmacy
They have read the appropriate sections of the SOP
All requests for emergency contraception must be treated with utmost confidence
All patient conversations are conducted with discretion, sensitivity, and appropriate tone
later, or more painful than usual; nausea; headache; abdominal pain; fatigue; breast tenderness. Always refer patients to their GP if their symptoms do not go away after a few days or if they think they might be pregnant; the near next period is more than 7 days late; their period is shorter or lighter than usual; they have sudden pain in the lower tummy.
Emergency contraception can be provided by a healthcare professional, including pharmacists, nurse practitioners, and doctors. The choice of method will depend on the individual’s preferences, medical history, and timing.
Women should be advised about all methods of EC available and their effectiveness. They should also be advised that ECs do not provide contraceptive protection for the rest of the cycle, so it is important to avoid sexual intercourse or to use effective contraception after taking them. Women should also be reminded that EC does not protect against sexually transmitted infections (STIs). Pharmacists should advise women that emergency contraception is not 100% effective. If EC fails and a pregnancy would be a crisis, women still have treatment options and there are supports available.
Actions:
Your checklist for Emergency Contraception training should include:
Your own knowledge is up-to-date on methods of EC available from the pharmacy
Refresh your knowledge of contraindications and side-effects
Ensure you know the cases where one method should be provided over the other. The appropriate training has been provided to all team members, and assessed
You have an SOP implemented and followed by all relevant staff
You have a suitable method of carrying out patient consultations, either with a questionnaire or assessment form.
94 | PHARMACYNEWSIRELAND.COM
Advertorial
her morning af ter

PRODUCT INFORMATION ellaOne® 30 mg film-coated tablet (ulipristal acetate). Refer to the SmPC for further information. INDICATION: Emergency contraception (EC) within 120 hours (5 days) of unprotected sexual intercourse or contraceptive failure. DOSAGE: one 30mg tablet taken orally as soon as possible, but no later than 120 hours (5 days) after unprotected intercourse or contraceptive failure. Another tablet should be taken if vomiting occurs within 3 hours of intake. Can be taken at any time during the menstrual cycle. Not recommended for women with severe hepatic impairment. CONTRAINDICATIONS: Hypersensitivity to the active substance or excipients. SPECIAL WARNINGS AND PRECAUTIONS: Occasional use only. Use reliable barrier method after use until next menstrual period. If next menstrual period is delayed >7 days or is abnormal or suggestive symptoms occur then perform pregnancy test. Consider ectopic pregnancy. If pregnancy confirmed, woman should contact their doctor. Concomitant use with EC containing levonorgestrel not recommended. Does not contraindicate the continued use of regular hormonal contraception but reliable barrier method should be used until next menstrual period. Not recommended in severe asthma treated by oral corticosteroids. Concomitant use of CYP3A4 inducers [e.g. barbiturates (including primidone and phenobarbital), phenytoin, fosphenytoin, carbamazepine, oxcarbazepine, herbal medicines containing Hypericum perforatum (St. John’s wort), rifampicin, rifabutin, griseofulvin, efavirenz, nevirapine] not recommended (may decrease efficacy of ellaOne). Long term use of ritonavir not recommended. Not recommended for women who have used enzyme-inducing drugs in the past 4 weeks. Non-hormonal emergency contraception (i.e. a copper intrauterine device (Cu-IUD)) should be considered. Contains lactose. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product. Contains

less than 1 mmol sodium (23 mg) per vial, essentially ‘sodium free’. FERTILITY, PREGNANCY AND LACTATION: Not intended for use during existing or suspected pregnancy. Limited human data does not suggest safety concern. Does not interrupt existing pregnancy. No teratogenic potential was observed; animal data insufficient with regard to reproduction toxicity. Marketing Authorisation Holder maintains a pregnancy registry (www.hra-pregnancy-registry.com) to monitor outcomes of pregnancy in women exposed to ellaOne®. Patients and health care providers are encouraged to report any exposure. Ulipristal acetate is excreted in human breast milk; breastfeeding is not recommended for one week after intake. Breast milk should be expressed and discarded. A rapid return of fertility is likely following ellaOne use; regular contraception should be continued or initiated as soon as possible; subsequent acts of intercourse should be protected by reliable barrier method until next menstrual period.
UNDESIRABLE EFFECTS: Always consult the SmPC before prescribing. Only the most common side effects and those which are rare but may be serious are listed below. Most commonly reported adverse reactions: headache, nausea, abdominal pain and dysmenorrhea. Common (≥ 1/100 to <1/10): mood disorders, dizziness, vomiting, abdominal discomfort, myalgia, back pain, pelvic pain, breast tenderness and fatigue. Rare (≥1/10,000 to <1/1,000): ruptured ovarian cyst.
MARKETING AUTHORISATION HOLDER: Laboratoire HRA Pharma, 200 avenue de Paris 92320 Châtillon - France. MARKETED IN IRELAND BY: Chefaro Ireland DAC, The Sharp Building, 10-12 Hogan Place, Dublin 2, D02 TY74, Ireland MARKETING AUTHORISATION NUMBER(S): EU/1/09/522/003. LEGAL CATEGORY: Medicinal product not subject to medical prescription. Date of last revision of text: March 2023. Unique ID: IE/ELLA/0295.
REFERENCE: 1. Glasier A et al. Lancet 2010; 375 (9714): 555-62.
ellaonepharmacists.ie Be her support and ensure she’s making an informed choice. No other emergency hormonal contraception (EHC) is more ® . 1 It‘s
Adverse events should be reported. Reporting forms can be found at www.hpra.ie or email: medsafety@hpra.ie Adverse events should also be reported to HRA Pharma UK & Ireland limited on Freephone: 1800 812 984 or email med.info.ie@hra-pharma.com Ulipristal acetate film-coated tablet. 30 mg IE/ELLA/0303 Date of preparation: March 2023
Clinical Profiles
ERLEADA®(APALUTAMIDE) APPROVED FOR REIMBURSEMENT IN IRELAND FOR THE TREATMENT OF PATIENTS WITH METASTATIC HORMONE-SENSITIVE PROSTATE CANCER (MHSPC)
Janssen, the Pharmaceutical Companies of Johnson & Johnson, announced that Erleada®(apalutamide) has been granted reimbursement in Ireland for the treatment of adult men with metastatic hormonesensitive prostate cancer (mHSPC) in combination with androgen deprivation therapy (ADT).
Professor Paul Donnellan, Consultant Medical Oncologist, Galway University Hospital, Mayo University Hospital and Galway Clinic said: “For patients with newly-diagnosed metastatic prostate cancer, delaying diseaseprogression and improving survival are paramount. For many years, suppressing androgen production has been the mainstay of treatment. It has been proven that adding an oral agent to this treatment, significantly improves both time to progression and overall survival, without any negative impact on Quality of Life (QoL). This represents a significant advance for all patients with advanced prostate cancer.”
Dr Thorsten Giesecke, General Manager, Commercial Business, Janssen Sciences Ireland UC, said: “Janssen is committed to improving prognosis and outcomes for men across the prostate cancer continuum with a growing portfolio and pipeline of therapeutics spanning all modalities and stages of the disease. Today’s reimbursement of apalutamide for the treatment of mHSPC represents an important, positive step on that journey.”
Data from the Phase III TITAN study assessed the addition of apalutamide to ADT in a broad range of patients with mHSPC, regardless of disease volume, prior treatment with docetaxel or staging at initial diagnosis.1 The dual primary endpoints of the study were overall survival (OS) and radiographic progressionfree survival (rPFS).1,2 Data from the interim analysis2 showed that at 24 months, apalutamide plus ADT significantly improved OS compared to placebo plus ADT with a 33 percent reduction in the risk of death (HR=0.67; 95% CI, 0.51-0.89; p=0.005).2 The interim analysis also revealed that apalutamide plus ADT also significantly improved rPFS compared to placebo plus ADT
with a 52 percent reduction in risk of radiographic progression or death compared to placebo plus ADT (HR=0.48; 95% CI, 0.39-0.60; p<0.001).2
The final analysis of TITAN and its long-term results demonstrate that apalutamide plus ADT consistently provides significant improvements in OS and delays onset of progression.1 The OS rates at 48 months were 65.1% and 51.8% for apalutamide- and placebo-treated patients, respectively.1
The safety profile observed in the TITAN study for apalutamide plus ADT was consistent with that described in previous studies.2,3 In the final analysis, the overall incidence of any treatmentemergent adverse events (TEAEs) was similar between treatment groups and to those reported previously.1 The most common treatment-related AEs (adverse events) related to treatment with apalutamide were rash and fatigue.1 There were no treatmentrelated deaths.1
HSE NATIONAL AMBULANCE SERVICE (NAS) EXPANDS SERVICE
A HSE National Ambulance Service (NAS) led service called Pathfinder, designed to safely keep older people who phone 112/999 in their own home rather than taking them to a hospital
emergency department, has went live in Letterkenny.
Pathfinder improves outcomes for older people by providing safe alternative care at home rather than in hospital and will be provided by National Ambulance Service staff working with colleagues from Letterkenny University Hospital.

Pathfinder has been working as a collaborative service between NAS and Dublin’s Beaumont Hospital Occupational Therapy & Physiotherapy Departments for more than two years and also went live in Limerick, Tallaght and Waterford in October 2022 and last month in Kilkenny and Cork.
Robert Morton, Director of the HSE National Ambulance Service said the expansion of the NAS Pathfinder Model is part of a plan to offer different groups of patients an alternative pathway other than presenting to a busy emergency department.
“The National Ambulance Service is very pleased with the outcomes for individual patients being achieved by this service and we are delighted to be working with Letterkenny University Hospital which has agreed to support the expansion of the Pathfinder model to this part of the country. The NAS Pathfinder model is improving outcomes for older people by
offering safe alternative care pathways for many older people in their own homes who might otherwise have to be conveyed to a busy Emergency Department. Pathfinder is enabling NAS to play an increasing role as an integrator of health service delivery by also connecting 999 patients with the increasing range of community services being developed by the HSE to support the needs of older people.”
Welcoming the introduction of the service to Letterkenny, Sean Murphy, Hospital Manager, Letterkenny University Hospital added: “We are pleased to be able to offer this service to suitable older people in our local communities.
“Through the Pathfinder Model, many older patients can be safely and appropriately managed in their own home rather than being transported to the ED for assessment when they dial 112/999.
“Pathfinder aims to reduce congestion in busy EDs and makes for a better environment for patients and staff on the floor whilst improving overall flow through the ED. The service enables increased ED capacity to care for other patients, by supporting this cohort of complex, frail patients at home,” he added.
JJ McGowan, GM Operations
West with NAS said: “Many patients who present to the emergency department have non-urgent care needs that could be treated elsewhere. Overall, Pathfinder has shown that it is a
PHARMACYNEWSIRELAND.COM 96
Gary Gardiner Advanced Paramedic, Eimear McGlynn Senior Occupational Therapist, Aoife O’Donnell Senior Physiotherapist, Shane Connelly, Advanced Paramedic, Rosaleen Greene Clinical Specialist Occupational Therapist, Martin Conlon Advanced Paramedic
safe and acceptable service for older people who dial 999/112 with low acuity complaints.”
The Pathfinder ‘Rapid Response Team’ respond to 999/112 calls for older people (65 years and older) in their homes. The older person is assessed by both an Advanced Paramedic and Occupational Therapist/Physiotherapist. Where safe, the team supports the older person at home rather than transporting them to emergency department, by linking with a wide range of alternative hospital and community services. Pathfinder also operates a ‘Follow-Up Team’ (Physiotherapy & Occupational Therapy) which provides immediate home-based rehabilitation, equipment provision and casemanagement in the subsequent days following a 999/112 call. On average two thirds of patients seen by Pathfinder following a 999 call have remained at home rather than being brought to the Emergency Department.
CAMPAIGN LAUNCHED FOR VITAL REHABILITATION SERVICES FOR BRAIN INJURY SURVIVORS
A new campaign has been launched to improve rehabilitation services for brain injury survivors in Ireland at a World Congress being hosted in Dublin.

Speaking at the 14th World Congress on Brain Injury organised by the International Brain Injury Association (IBIA) in partnership with Acquired Brain Injury Ireland (ABII), ABII CEO and Co-Founder Barbara O’Connell called for an investment of ¤6 million per annum to meet urgent need.
“19,000 people in Ireland acquire a brain injury each year, and many of these end up unnecessarily in nursing homes long-term. This must end. The slogan of our campaign is ‘Don’t Save Me, Then Leave Me –give me a pathway home’.
“The truth is, in Ireland there is no clear pathway for survivors of brain injury. Once they’re discharged from hospital, their future is in the hands of a geographic lottery – the system is under resourced and under-funded. Assessment Teams and specialist brain injury Case Managers can play a key role in addressing these issues at minimal cost to the State.
“Today at the World Congress on brain injury, ABII is calling for ¤2m to establish a nationwide brain injury Case Management service and ¤4m for three National Assessment Teams for young
survivors living inappropriately in nursing homes.
“This would enable survivors to move much more effectively from acute hospital care, through specialist in-patient rehabilitation if needed, and on to communitybased services. Doing so also avoids delayed discharges from acute hospitals, frees up beds in our National Rehabilitation Hospital, reduces the burden of care on families and creates significant cost savings to the State.
“Too many brain injury survivors are left merely to exist, inappropriately placed in hospitals and nursing homes where they do not belong. We have solutions to help survivors rebuild their lives in their own communities – and we need urgent investment to make it happen.
“It is unfathomable that our Government would not take notice as the World Congress takes place in Ireland this week. Following this Congress, ABII will work closely with the Government and the HSE in order to make this happen,” Ms O’Connell said.
Opening the Congress via video link the Minister of State for Disabilities Anne Rabbitte said:
“It’s very significant for our
country to be hosting the world’s leading experts in brain injury research and rehabilitation for the next three days. In Ireland, we recognise the vital importance of investing in brain health and brain injury treatment at all stages of the neuro rehabilitation pathway, from acute hospital to home. Timely, individualised rehabilitation has the potential to increase independence, maximise ability and enable survivors to participate as active citizens in our communities.
“That’s why Government has committed to addressing the needs of those impacted by brain injury, including through our National Neuro Rehabilitation Strategy. We already have many of the components of an effective brain injury rehabilitation pathway in place to make Ireland a global exemplar in this field. This is a priority for Government and I look forward to working with those involved in the Congress and the sector over the coming months to implement our plans and realise their shared ambition.”
The Congress brings together brain injury professionals from across the world and many different disciplines. Leading Irish rehabilitation physicians,
neurosurgeons, advocates and multidisciplinary practitioners are among the keynotes, panellists and speakers at the Convention Centre in Dublin from Thursday until Saturday.
GLOBAL PATIENT SAFETY AND WELLBEING RESEARCH INITIATIVE INVITES GRANT APPLICATIONS
The MPS Foundation - a global not-for-profit research initiative that aims to shape the future of patient safety – has launched its second grant programme.
Medical Protection Society (MPS) launched The MPS Foundation last year and its first research grant programme received over 150 expressions of interest. 10 applicants were successful in securing funding for their research. This includes a research project in Ireland which will assess the impact of a tailored educational intervention to improve clinical communication involving adults with age-related hearing loss. The Foundation is now inviting new research grant applications from both MPS members and nonmembers. It will invest in research and analysis with a key focus on patient safety and the wellbeing of healthcare professionals and teams, both medical and dental, and applications will again be considered from the jurisdictions where MPS has members. This includes Ireland, Hong Kong, Australia, the UK, New Zealand, South Africa, Singapore, Malaysia, the Caribbean and Bermuda.
PHARMACYNEWSIRELAND.COM 97
Launching a new campaign ‘Don’t Save Me, Then Leave Me – give me a pathway home’ for improved rehabilitation services for brain injury in Ireland was brain injury survivors Niamh Cahill, Des Vallely and Lorraine Duffy together with Acquired Brain Injury Ireland CEO, Barbara O’Connell. The new campaign was launched at the recent World Congress on Brain Injury which took place in Ireland. www.abiireland.ie
Clinical Profiles
Research projects supported by The MPS Foundation need to be academically robust and evidence-based. Available funding will range from EUR 5,694 to EUR 227,767 - the equivalent to £5,000 to £200,000 (subject to currency fluctuations) - depending on the scale, focus and duration of the proposal.
The funding focusses on five main areas:
the impact of human factors on patient safety, outcomes and risk
the impact of processes and delivery models on patient safety, outcomes and risk
the personal and professional wellbeing and development of clinicians
the impact of digital integration and technology on patient safety, outcomes and risk.
the evaluation of the effectiveness of teaching and learning innovations and the impact upon patient care, safety, outcomes and risk.
Dr Graham Stokes, MPS Foundation Chair, said: “Patient safety and the wellbeing of healthcare professionals and teams are more vital today than ever. Until now, funding for research into both has been limited, but this is all set to change with access to research funding through The MPS Foundation. As a global not-forprofit research initiative, we aim to take non-clinical research in a new direction and transform the future of patient safety.
“Our aim is simple: to create sustainable global change through ambitious research that can be used to develop a knowledge base that improves patient safety, enhances the wellbeing of healthcare teams and reduces risks.
“I am delighted with the progress
The MPS Foundation has made and to launch the second grant programme. Our first grant programme saw expressions of interest from all MPS jurisdictions with 10 of those research projects awarded funding. These projects are exciting, diverse and carry great potential.
“All research projects must be academically robust and evidence based. While funding will be available up to £200,000, smaller grants from £5,000 will also be available and I would strongly encourage healthcare professionals to consider applying for support whatever the scale of their proposal.”
Healthcare professionals can register their interest by visiting www.thempsfoundation.org and
entering their details via the online grant portal. Calls for expressions of interest close on 5 May 2023.
The Foundation is part of MPS – the world’s leading protection organisation – which currently supports more than 300,000 doctors, dentists and healthcare professionals, and has almost 130 years of global healthcare experience and expertise.
TWO FITUSIRAN PHASE 3 STUDIES PUBLISHED IN THE LANCET AND THE LANCET HAEMATOLOGY HIGHLIGHT POTENTIAL TO ADDRESS UNMET NEEDS ACROSS ALL TYPES OF HEMOPHILIA
Two studies, published in The Lancet and The Lancet Haematology, evaluating the efficacy and safety of fitusiran, an investigational siRNA therapy for the prophylactic treatment of adults and adolescents with hemophilia A or B, reinforce the potential of this investigational therapy to transform the current standard of care and address unmet needs for all types of hemophilia, regardless of inhibitor status.
Hemophilia A and B are rare congenital lifelong bleeding disorders in which the ability of a person’s blood to clot is impaired, leading to excessive bleeds and spontaneous bleeds into joints that can result in joint damage and chronic pain, and significantly impact quality of life. Fitusiran has the potential to provide prophylaxis for all types of hemophilia, regardless of inhibitor status, with as few as six subcutaneous injections per year.
Dietmar Berger, M.D., Ph.D. Head of Global R&D ad interim and Chief Medical Officer at Sanofi said, “Sanofi is committed to advancing the standard of care for all people with hemophilia through innovative science, providing consistent bleed protection while reducing treatment burden. We are entering a new era in hemophilia where, for the first time, people can choose therapies that meet their personal needs. These published data validate our science and add to a growing body of evidence supporting fitusiran’s potential to transform the treatment landscape. We look forward to sharing additional data on fitusiran later this year.”
Both Phase 3 studies compared once-monthly subcutaneous fitusiran prophylaxis (80mg) with on-demand/episodic use of clotting factor concentrates in the ATLAS-A/B study, and on-demand/ episodic use of bypassing agents in the ATLAS-INH study. Across both clinical studies, prophylactic treatment with fitusiran reduced annualized bleeding rates by
90% (95% CI [84.1%; 93.6%], P <0.0001) compared to the control arms, showing a statistically significant and clinically meaningful improvement in bleeding episodes when compared to on-demand treatments; and showed improvement in quality of life.
In the study ATLAS-INH study published by The Lancet, 66% of participants with inhibitors (25 out of 38) receiving fitusiran 80mg monthly experienced zero bleeding episodes compared to 5% (1 out of 19) receiving an on-demand bypassing agent after nine months of treatment.
The ATLAS A/B study published in The Lancet Haematology showed 51% of participants without inhibitors (40 out of 79) who received fitusiran 80mg monthly prophylaxis experienced zero bleeds compared to 5% (2 out of 40) in the comparator group, receiving on-demand clotting factor concentrates.
Sanofi is currently investigating the efficacy and safety of fitusiran under a revised regimen which includes lower doses and less frequent dosing (as few as six subcutaneous injections per year), maintaining an antithrombin target range of 15-35% in all ongoing studies.
TIZIANA LIFE SCIENCES INITIATES PROGRAM TO DEVELOP INTRANASAL FORALUMAB IN TYPE 1 DIABETES
Tiziana Life Sciences Ltd. (Nasdaq: TLSA) (“Tiziana” or the “Company”), a biotechnology company developing breakthrough immunomodulation therapies via novel routes of drug delivery, has announced that it is initiating a program to develop intranasal foralumab for the treatment or prevention of Type 1 Diabetes.
“With the FDA approval of the humanized anti-CD3 mAb TZIELD™ (teplizumab-mzwv injection) and then its subsequent announced acquisition of Provention Bio by Sanofi for $2.9 billion1, CD3 has emerged as an established and attractive target for Type 1 Diabetes,” commented Gabriele Cerrone, Executive Chairman, Founder and interim Chief Executive Officer of Tiziana. “We believed that having a fully human CD3 antibody may offer benefits to patients across many different chronic disease indications.”
“The potential of not requiring an injection or infusion and having a take-home self-administered nasally delivered therapy would offer additional benefit and convenience to sufferers of Type 1 Diabetes”, stated Matthew W.
Davis, M.D., RPh, Chief Medical Officer of Tiziana. “Although given intranasal, our fully human antiCD3 mAb foralumab has shown to release anti-inflammatory T regulatory cells throughout the body while returning proinflammatory effector T cells to their naïve state.2 We are actively discussing various study designs with our Key Opinion Leaders as well as with an internationally known network of dedicated diabetes physicians. I believe that the data published in PNAS2 shows that the novel immunomodulatory effects of our intranasal fully human anti-CD3 mAb foralumab may have an important role in the diabetes market.”
“MENTAL HEALTH CRISIS AMONG OLDER PEOPLE NOT BEING TALKED ABOUT”:
ALONE, the charity that supports older people, has called for additional focus on mental health difficulties being experienced by older people as the number of interventions to support mental health carried out by ALONE has increased by almost 300% in the past year.
Speaking at the Joint Oireachtas Sub-Committee on Mental Health, ALONE CEO Seán Moynihan said that in Q4 2022, 29% of the 1,926 older people ALONE assessed for their services identified they had issues relating to their mental health, but over half of these had not attended a GP for support. ALONE also cited research from the Irish Longitudinal Study on Ageing (TILDA) which found that 78% of older adults who have evidence of depression, and 85% who have evidence of anxiety, do not have a doctor’s diagnosis.1
“We do not give older age due consideration as a time where mental health difficulties may emerge for the first time. We do not discuss how getting older is associated with age-specific psychosocial risk factors for mental health difficulties, such as living alone, bereavement, physical illness, disability, and cognitive decline,” he said.
“While many older people enjoy positive mental health, there is evidence to suggest that there is a significant mental health crisis among older people which is not being talked about. This has become all the more evident in the aftermath of COVID-19 restrictions. Increasingly, we are working with older people who have completely cut themselves off from their family, friends, community and life in general due to fears around COVID-19 which have not subsided,” Moynihan continued.
PHARMACYNEWSIRELAND.COM
98
The organisation has said that specific mental health policy, evidence-based programmes and research for older people must be committed to, funded, and implemented as part of Sharing the Vision, Ireland’s national mental health policy. ALONE has also said that the action plan to combat loneliness and social isolation must be completed, funded and committed to, including funding for Irish research, and older people must be provided with additional supports to reengage with their communities, in collaboration with experts and the community and voluntary sector.
Moynihan continued, “A Dáil debate took place in April two years ago on COVID-19, mental health, and older people. Many positive ideas were discussed, and not progressed. We believe that significant action on mental health difficulties being experienced by older people is urgently overdue.”
“As a country we put significant effort into telling older people to cocoon and stay inside, and offering them support to do so. We have not done the same to support older people to reengage with their communities. We need to identify and implement precision, research-backed interventions for the loneliness and social isolation which is impacting this group, and all other groups affected by loneliness.”
Moynihan concluded, “We have quoted repeatedly the research which shows that loneliness has been shown to have as severe an impact on our health as smoking.2 Why has it not received the same public health response?”
If you, or an older person you know, requires ALONE’s support please call our National Support and Referral Line at 0818 222 024 from 8am to 8pm.
If you are interested in supporting older people by becoming a volunteer, then you can visit alone. ie/volunteer for more information.
1 https://tilda.tcd.ie/publications/ reports/pdf/w1-key-findings-report/ Chapter6.pdf
2 https://journals.sagepub.com/ doi/10.1177/1745691614568352
INTHELIA THERAPEUTICS
NAMED AS AWARDEE OF BLUE KNIGHT™ QUICKFIRE CHALLENGE
RCSI spin-out company Inthelia Therapeutics has been named as an awardee of the international BLUE KNIGHT™ QuickFire Challenge: Next-Generation Preparedness Solutions related

to the company’s work on nonantibiotic therapies for sepsis.
Blue Knight is a joint initiative between Johnson & Johnson Innovation LLC and the Biomedical Advanced Research and Development Authority (BARDA), part of the Administration for Strategic Preparedness and Response at the U.S. Department of Health and Human Services.
The challenge invited innovators to submit potentially groundbreaking ideas or technologies that aim to enhance preparedness towards future known and unknown disease threats.
Inthelia Therapeutics was recognised for its innovative approach aiming to treat infections by targeting a conserved known host target to which multiple pathogens bind rather than targeting multiple, often evolving, or unknown pathogens. This approach has the potential to uniquely create rapid responses to breakthrough pathogens to better manage or control future pandemics. The award recognises the potential to develop a biomarker-led treatment for early sepsis, a leading cause of hospital deaths. Inthelia’s innovation may also contribute to combating the growing threat of antibiotic resistance.
Inthelia Therapeutics is a spin-out company from RCSI University of Medicine and Health Sciences founded by Professor Steve Kerrigan, RCSI School of Pharmacy and Biomolecular Sciences, and serial entrepreneur, Dr Ivan Coulter.
Professor Steve Kerrigan commented: “Sepsis is a complication caused by the body’s overwhelming and life-threatening response to an infection, which can lead to tissue damage, organ failure, and death. Slow diagnosis and over-dependence on antibiotics1 have resulted in sepsis becoming one of the top three causes of adult hospitalisations and is responsible for half of all hospital deaths globally.”2
“Antibiotics fail in many patients with sepsis, increasing risk of death and antimicrobial resistance. With low success rates, we cannot depend on new antibiotics to solve the growing threats of sepsis and antimicrobial resistance. There is an urgent and significant need for more rapid diagnosis and treatment with novel non-antibiotics or patient targeted therapy in emergency departments.”
“Inthelia Therapeutics is advancing an innovative biomarker-guided, host-targeted therapy towards late-stage clinical trials in early sepsis which has as a goal to have immeasurable impact on human lives especially with the rapid advancement of anti-microbial resistance. We are honoured to be recognised as a Blue Knight QuickFire Challenge awardee for our work to address this significant threat to human health.”
Professor Fergal O’Brien, Deputy Vice Chancellor for Research and
Innovation at RCSI commented: “Congratulations to Professor Steve Kerrigan and the team at Inthelia Therapeutics on their success at the prestigious Blue Knight QuickFire Challenge. This recognition of the work of an RCSI spin-out company on the international stage we feel is a testament to the world-class research at the RCSI School of Pharmacy and Biomolecular Sciences which is being advanced by Inthelia Therapeutics, and will potentially benefit the 49 million people who are impacted by sepsis annually.”
The QuickFire challenge awardees were announced at the 2022 BARDA Industry Day with other awardees being Immunyx, NanoFreeze, and Vaxess Technologies. To help advance their science, the awardees will receive access to the global Johnson & Johnson Innovation – JLABS network through Blue Knight residency with mentorship from experts across the Johnson & Johnson Family of Companies and BARDA. The QuickFire Challenges are managed by Johnson & Johnson Innovation, with the goal to help address today’s greatest healthcare challenges.
RCSI partners with investors and entrepreneurs to support spinout company creation and drive improvements in human health.
PHARMACYNEWSIRELAND.COM 99
Co-founders of RCSI spin-out company Inthelia Therapeutics Professor Steve Kerrigan, RCSI School of Pharmacy and Biomolecular Sciences and Dr Ivan Coulter, CEO, Inthelia

ww w . c o smet i cass o c i at ion.i e 2023 The M ain Hall, RDS, Ballsbridge, Dublin Sund a y 14 th M a y Monday 15 th M a y Tuesday 16 th M a y 10am - 6pm 9am - 8pm 9am - 6pm CHRISTMAS CHRISTMAS Cosmetic & Gift Trade Fair Cosmetic & Gift Trade Fair
