In one of our lead news stories this month, it is revealed that medicines in short supply in Ireland currently include 344 products, with 72% of participants in a new nationwide poll of pharmacists, published by Azure Pharmaceuticals, stating that they dispense unlicensed drugs one to ten times per day due to shortages, while 47% of pharmacists have expressed some level of discomfort at dispensing unlicensed drugs.
124 of these medicines in short supply have no alternative, therefore requiring the prescription of unlicensed medicines or a change in therapy. 98% of pharmacists dispense unlicensed drugs every day, with 43% stating they dispense them one to five times per day, 29% six to ten times per day, 18% eleven to twenty times per day and 8% say they dispense unlicensed drugs over twenty times per day.
Additionally, 86% of pharmacists surveyed have stated that they would like to see patient leaflets for unlicensed drugs to be translated into English in order to prevent errors and inadequate outcomes, alongside a database which verifies the origin of the product.
58% of pharmacists believe that the medicines regulator should be responsible for verifying the origins of these products. You can read more about this on page 5.
Irish Pharmacy News is circulated to all independent, multiple Pharmacists and academics in Ireland. All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
In other news, Medicines for Europe recently hosted their European conference in Dublin, marking 30 years of delivering more equitable access to off-patent medicines. Commenting ahead of the conference, President of Medicines for Europe, Elisabeth Stampa said: “Our 30th anniversary is not just a celebration of our past achievements but a testament to our unwavering commitment to the future of healthcare in Europe. We are proud of the role we have played so far, but our journey is far from over and we are dedicated to continuing our work towards delivering solutions to tackle medicines shortages, clearer laws to allow access to generic and biosimilar medicines and incentives for value-added medicines.” The full coverage is available on page 20.
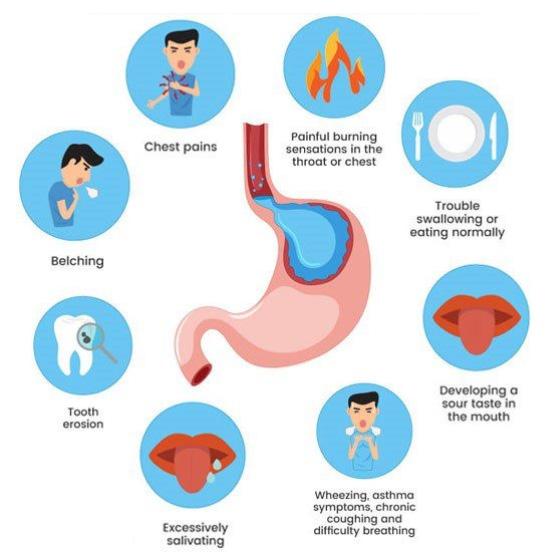
While it may only be the start of the summer, community pharmacies will soon be setting up their merchandising for the Back to School market. Our special section this month carries a number of articles designed to keep your pharmacy staff educated on some of the more common ailments and conditions parent will be seeking advice for. Whilst our CPD for July focuses on the pharmacy role in managing Gastrooesophageal Reflux Disease on page 41.
I hope you enjoy the issue.
McCabes Pharmacy & LloydsPharmacy Deal Completes
The competition authority has approved the takeover of McCabes Pharmacy chain by LloydsPharmacy subject to a commitment to sell two stores in Lucan in Dublin.
The combined group will operate 112 pharmacies across Ireland, including the 32 McCabes pharmacies located predominantly in the greater Dublin area, and Sharon McCabe will serve as CEO of the new retail entity.
Sharon McCabe
LloydsPharmacy owner PHX
Ireland has completed its acquisition of McCabes Pharmacy after receiving CCPC approval. Terms of the deal have not been disclosed.
The combined group will operate 112 pharmacies across Ireland, including the 32 McCabes pharmacies located predominantly in the greater Dublin area, and Sharon McCabe will serve as CEO of the new retail entity.
“By joining the PHX Ireland family, we will integrate the McCabes Way of patient care and doing business in more communities across Ireland," said McCabe, CEO of McCabes Pharmacy.
"We remain committed to improving the level of care and support offered to Irish patients and their families. On a personal level, I am honoured to lead the next chapter of the McCabes Pharmacy story, which will now operate over 110+ pharmacies throughout the country.
"I am confident that our expanded team has the skills, passion and
Pharmacy Consultation on CPD
dedication to deliver the highest standards of service and care for patients and customers.”
The proposed deal was renotified to the CCPC in February 2024 after the first notification received in October 2023 was declared invalid (see CCPC rejects notification). A preliminary investigation was established to look at how the deal would affect levels of competition between pharmacies, including potential consequences for consumers.
During the investigation, the CCPC had particular concerns about how levels of competition in the Lucan area of Dublin would be affected by the deal. To address these concerns, LloydsPharmacy agreed to sell two pharmacies in Lucan (McCabes Pharmacy Finnstown and McCabes Pharmacy Griffeen Centre) to a buyer who will be approved by the CCPC. In order to allow time in this case to finalise the commitments, a full investigation was opened.
LloydsPharmacy also agreed not to do anything which could negatively impact on the pharmacies before their sale, and not to buy these pharmacies back for at least 10 years.
The Pharmaceutical Society of Ireland (PSI) is seeking feedback on seven proposed themes that will assist and guide pharmaceutical assistants when self-reflecting on their practice as part of their CPD requirements.
These themes have been developed in consultation with the Pharmaceutical Assistants Association (PAA) and are intended to be reflective of pharmaceutical assistants’ practice.
The public consultation is open from Thursday, 20 June 2024 to 6pm on Thursday, 18 July 2024. This is your opportunity to provide feedback on the proposed CPD themes.
Pharmaceutical assistants may work in conjunction with a pharmacist in the sale and supply of medicines, or carry out the activities of a pharmacist during their temporary absence from the pharmacy. Pharmaceutical assistants must be registered with
the PSI in order to practise in Ireland.
The Regulated Professions (Health and Social Care) (Amendment) Act 2020 introduces a new requirement for PSI to ensure that pharmaceutical assistants undertake appropriate Continuing Professional Development CPD. In response, the PSI committed to the development of a CPD model for pharmaceutical assistants as part of their Corporate Strategy 2021-2024.
To assist in identifying an appropriate model of CPD, they sought external expertise. The consultants, Mazars, were appointed and their report, Report to Support the Development of a Continuing Professional
Johnson & Johnson Ireland
Johnson & Johnson has announced its pharmaceutical business segment will adopt the Johnson & Johnson brand name in Ireland. Janssen, its pharmaceutical segment, will become Johnson & Johnson Innovative Medicine, and the medical technology segment will continue to be named Johnson & Johnson MedTech.
The announcement marks the next era for Johnson & Johnson in Ireland, which is leveraging its expertise in innovative medicine and medical technology to prevent and treat complex diseases and introduce solutions that are smarter, less invasive, and more personalised.
Johnson & Johnson has a long heritage in Ireland since 1935, and a large footprint with a workforce of more than 6,000 people[i]. Its Irish operations which comprise both the Innovative Medicine and MedTech segments, make a significant contribution to the company’s global success with ten sites located in five counties (Cork, Dublin, Limerick, Galway and Mayo) spanning research and development, manufacturing, shared services and country commercial businesses.
These changes are part of a global rollout of the new Johnson & Johnson brand that was announced in September 2023. The updated brand will be applied to all company materials, product packaging, and branding assets over time.
Development CPD Model for Pharmaceutical Assistants makes recommendations for a proposed CPD model. The report, and the recommended CPD model, were approved by the Council of PSI at its meeting of 22 June 2023. The recommended CPD model, is a bespoke CPD model that draws on elements from the CPD model for pharmacists, and that utilises the infrastructure (ePortfolio) already in place.
One recommendation included in the Report, is that the PSI develop guidelines / standards or ‘themes’ that will provide direction and guidance for pharmaceutical assistants to conduct and manage their CPD learning activities within the new CPD model.
The new Johnson & Johnson brand identity builds on the Company’s legacy, while also modernising key elements to showcase healthcare innovation in a way that is inclusive and demonstrates the Company’s ability to tackle the world’s toughest health challenges. Johnson & Johnson Innovative Medicine applies rigorous science with compassion to confidently address the most complex diseases in the areas of oncology, immunology, neuroscience, cardiopulmonary and specialty ophthalmology to develop the potential medicines of tomorrow.
There will be no change to the company names and/or legal status of our Johnson & Johnson Innovative Medicine or MedTech companies in Ireland.
Budget 2025
The Irish Cancer Society has launched its Budget 2025 Submission, urging Government to stop underfunding the National Cancer Strategy. This call for investment in the National Cancer Strategy is supported by the two main representative bodies for cancer doctors in Ireland, the Irish Society of Medical Oncologists (ISMO) and the Irish Society of Radiation Oncologists (ISRO).
According to the HSE, the National Cancer Control Programme’s annual budget for implementation of the National Cancer Strategy should have increased incrementally over the past 8 years to be ¤110m higher in 2024 than in 2016. The actual incremental increase has only been ¤65m. As a result, the cumulative loss of investment in cancer services from 2017 to 2024 is almost ¤180m.
Due to this underfunding:
• screening has not been expanded as planned;
• target waiting times for cancer are not being met;
• cancer surgeries are frequently delayed;
• investment in infrastructure is lacking;
• radiotherapy services are operating below capacity;
• clinical trials are falling far short of target; and
• access to new medicines is much slower in Ireland than in other European countries.
CEO, Averil Power said, "Budget 2025 must prioritise the National Cancer Strategy, with ringfenced new recurrent development funding for the National Cancer Control Programme of at least ¤20 million. It should also include a commitment to multiannual funding for the Strategy going forward, to enable effective planning for improvements in the coming years.”
The Irish Cancer Society is also urging the Government to address the cost of cancer for cancer patients in Budget 2025, which requires action from several government departments. Recommendations include: the abolition of hospital parking fees, an automatic entitlement to the medical card, enhanced access to the domiciliary care allowance, and a statutory ‘right to be forgotten’ for cancer survivors.
Irish Pharmacist Clare Fitzell elected as PGEU President 2025
At a recent General Assembly meeting, the Pharmaceutical Group of the European Union (PGEU) has elected Clare Fitzell from the Irish Pharmacy Union (IPU) as PGEU President for 2025 and Claude Hostert-Pfeiffer from the Union of Luxembourg Pharmacists (SPL) as PGEU Vice-President. They will start their mandate from 1st January 2025.
In her acceptance speech Clare Fitzell stressed, "I am truly honoured to have been elected to serve as PGEU President. 2025 will be a crucial year to determine the course of the European Union action on health matters. The upcoming mandates of the newly elected European Parliament and the next European Commission present an unparalleled opportunity to continue working to keep health at the top of the EU political agenda and to build a strong European Health Union. I will work hard to ensure that community pharmacists’ voices are heard by the EU policymakers, especially during the negotiations on the reform of the EU pharmaceutical legislation that will continue over the next year. We need to ensure a regulatory framework that recognises the role of community pharmacists in the healthcare system and brings real benefits to patients by improving access to medicines and mitigating shortages. Supported
by the valuable cooperation of PGEU members, I am determined to work for shaping the future of our profession”.
Clare Fitzell is a qualified pharmacist with over 24 years of experience in community-based practice. A graduate of Trinity College Dublin, she has served both as a community pharmacist and a community pharmacy manager. Throughout her career, Clare has undertaken a wide array of roles, gaining extensive experience in pharmacy service delivery, regulatory affairs, and
quality management in pharmacy practice. Currently, Clare holds the position as the Head of Strategic Policy at the Irish Pharmacy Union (IPU).
Pharmacy Survey on Medicine Shortages
Medicines in short supply in Ireland currently include 344 products, with 72% of participants in a new nationwide poll of pharmacists, published by Azure Pharmaceuticals, stating that they dispense unlicensed drugs one to ten times per day due to shortages, while 47% of pharmacists have expressed some level of discomfort at dispensing unlicensed drugs.
124 of these medicines in short supply have no alternative, therefore requiring the prescription of unlicensed medicines or a change in therapy. 98% of pharmacists dispense unlicensed drugs every day, with 43% stating they dispense them one to five times per day, 29% six to ten times per day, 18% eleven to twenty times per day and 8% say they dispense unlicensed drugs over twenty times per day. Additionally, 86% of pharmacists surveyed have stated that they would like to see patient leaflets for unlicensed drugs to be translated into English in order to prevent errors and inadequate outcomes, alongside a database which verifies the origin of the product.
58% of pharmacists believe that the medicines regulator should be responsible for verifying the origins of these products.
Azure Pharmaceuticals Managing Director, Sandra Gannon, stated in response to the results of the research, “That 47% of pharmacists are uncomfortable with the level of dispensing of unlicensed medicines is very notable. They, like patients, need solutions. Over half of pharmacists surveyed want the regulator to be responsible for unlicensed medicines oversight, with 86% wanting the patient leaflets translated into English to prevent medicine errors. These are among the types of measures we need to move on.”
Drug shortages have persisted throughout the last two years in Ireland, with many crucial drugs in short supply or simply unavailable, including products such as antibiotics or those used to treat Alzheimer's, Cancer, anxiety, depression and high blood pressure.
She went on to say, “The level of concern among pharmacists is clear. Faced with continued shortages, their options are narrowing, leaving them with little choice but to increasingly dispense unlicensed medicines. It’s tangible proof of the consequences of not addressing medicine shortages and flies in the face of recent, highly expensive EU-wide reforms.”
Clare Fitzell, IPU, President, PGEU
CarePlus Pharmacy welcome three new franchise members
CarePlus Pharmacy (part of Navi Group) enables independent pharmacy owners to maintain their name and is flexible when adapting the existing pharmacy fitout, tailoring owner needs to accelerate business success.
The goal of CarePlus is maximum turnover and margin return for your pharmacy. Three pharmacy owners who have recently come on board are Eugene & Róisín Daly, of Dooradoyle CarePlus Pharmacy; Bernardo Viana of Pophams Road CarePlus Pharmacy, Cork and Ronan O’Farrell of College Road CarePlus Pharmacy, Cork.
Eugene and Róisín Daly are also the proud owners of Keating’s CarePlus Pharmacy in Dooradoyle, Limerick and Mahers CarePlus Pharmacy in Thurles, Co. Tipperary. Their new franchise store, Dooradoyle CarePlus Pharmacy, is in a prime location, directly beside University Hospital Limerick.
Ronan O’Farrell is new to the franchise group, with College Road CarePlus Pharmacy located right next to UCC on College Road, Cork. Ronan is due to open another CarePlus Pharmacy in the coming months.
Bernardo Viana is also new to the group, recently purchasing Pophams Road Pharmacy in Farranree, Co. Cork, and re-branding the store as a CarePlus Pharmacy.
We are thrilled to welcome three new owners to the franchise and are excited to see their stores thrive.
Expanding the Role of Pharmacy
As Irish Pharmacy News was going to press, the public consultation to gather views about expanding the role of pharmacists in Ireland was closing.
On 24 July 2023, the Minister for Health Stephen Donnelly established an Expert Taskforce to create polices that will enable the expansion of the role of pharmacists in Ireland. The aims of expanding the role of pharmacists are to:
• improve access to healthcare for people
• reduce the workload for doctors in general practice
• increase the healthcare services which pharmacists can provide for people
The Taskforce has identified pharmacists prescribing some medications as a potential expansion of the role of pharmacists. For example, pharmacists prescribing under a Common Conditions Scheme. Under such a scheme, pharmacists would be able to prescribe and supply some prescription-only medicines for uncomplicated conditions, without the need for a doctor’s visit. Pharmacists prescribing has been done in other countries for common conditions such as, sore throat, uncomplicated urinary tract infections, common skin infections such as impetigo.
The Taskforce conducted a Public Consultation to gather views about a Common Conditions Scheme and about the expansion of the role of pharmacists generally. The results will help the Pharmacy Taskforce develop recommendations about expanding the role of pharmacists in Ireland. We will carry full details of the outcome and next steps in the August issue.
RSV Pathfinder Programme
Minister for Health, Stephen Donnelly has received Government approval for an infant Respiratory Syncytial Virus (RSV) Immunisation Pathfinder Programme.
The programme, which will run between September 2024 and February 2025, aims to ease the burden that RSV places on the healthcare service by reducing the number of illnesses and hospitalisations among young children.
It follows advice from the National Immunisation Advisory Committee (NIAC) recommending the use of monoclonal antibody immunisation for the 2024/2025 season. The vaccine will be offered to an estimated 28,000 infants during this period.
Based on evidence from a similar programme implemented in Spain, it’s estimated that the infant RSV programme in Ireland will lead to the avoidance of up to 453 hospitalisations and up to 48 ICU admissions.
Minister Donnelly said, “Last winter, we saw the significant impact of RSV on our health service, particularly in paediatric hospitals. We saw the highest ever number of RSV hospitalisations among children, with babies under one year being the most affected.
“I’m delighted to have secured Government approval today for this programme that directly and swiftly responds to this issue and will hopefully deliver an immediate impact by reducing illness and minimising the burden on our healthcare resources over the winter.
“This Pathfinder programme will also help to inform the development of future RSV programmes aimed at reducing incidences of illnesses and hospitalisation among the population.”
The Pathfinder programme is being implemented by the Health Service Executive (HSE) as a temporary measure for the 2024/2025 RSV season and may be modified following the outcome of Health Technology Assessments (HTAs) on RSV immunisation currently being undertaken by the Health Information and Quality Authority (HIQA).
FAST ACTING PAIN RELIEF
Expansion of our Panadol ActiFast range with a new USP of a lemon flavouring in a soluble format.
• 24 tablets – Pharmacy Only
• Made in Ireland (Dungarvan)
• MRSP* €8.50
• Trade Price €5.67
*price is at the sole discretion of the retailer.
In-store activation material available
Please ask your Haleon Rep. ATL & BTL support including TV, Digital & OOH Campaign.
The HSE and the Irish Pharmaceutical Healthcare Association (IPHA) wishes to improve Ireland’s clinical trial footprint and recently they announced a significant development to achieve that aim – the CRO-mCTA.
Including patients in clinical trials is critical in developing new innovative treatments and ultimately in improving the nation’s health. There is clear published evidence that by including patients in clinical trials their health will improve substantially.
Both institutions are of the view that Ireland can play a leading role in the provision of clinical trials in Europe. There is no doubt that Ireland’s decision to join the European Clinical Research Infrastructure Network has the potential to widen our access to clinical research networks in Europe.
There are practical steps we can take here at home to speed up and improve our performance in relation to clinical trials. These include the use of a standardised site contract (the Clinical Trial Agreement [CTA]) for clinical trials
Dr Rebecca Cramp, Director of Code and Regulatory Affairs, IPHA
that involve Contract Research Organisations (CROs), that is convention in a number of other EU countries.
Until now, there have been various slightly different versions of those CRO CTAs, each of which underwent review, costing hospitals money and delaying clinical trial start-up. Provision of a single standard CRO CTA for Ireland will reduce delays in hospitals, reduce costs for hospitals and companies, increase efficiencies, enable more trials to set up on time in Ireland and thus, importantly and ultimately, improve patient outcomes.
To that end HSE&IPHA has agreed a standard (model) CRO CTA for use between the Site, the CRO and the Sponsor. The HSE & IPHA CRO model CTA (CRO-mCTA) has been reviewed extensively
by a subgroup of CROs, IPHA member companies, the HSE and other stakeholders dedicated to developing a fair and balanced standardised document. The key to the success of the new CRO-mCTA is that it is standard and it is the standardisation itself that will speed up the process by reducing the number of rounds of discussion and review for this contract. This will in turn reduce the administrative and financial burden for the hospitals, CROs and companies. However, critically it will reduce the time taken to start up clinical trials in Ireland thus improving clinical trial competitiveness and most importantly improving individual patient health.
The CRO-mCTA is standardised and therefore changes to the standard text in the document are not permissible. It must be used for any mCTA contract negotiations with CROs commenced after 20.05.24. However, if discussions have already commenced on a CTA before 20.05.24 then the CROmCTA will not be mandatory.
Dr Rebecca Cramp, Director of Code and Regulatory Affairs at IPHA stated, “We are pleased to announce the removal of a significant roadblock that negatively affected the conduct of clinical trials in Ireland. Today’s announcement represents the result of forward thinking by our government, close collaboration between IPHA and the HSE and dedication by all to a difficult to achieve outcome. Today’s roll out of the CRO-mCTA will reduce costs, decrease the administrative burden on hospitals and significantly increase the speed at which patients can get lifesaving interventions.”
Engaging Pharmacy in Smoking Cessation
In a statement issued recently, the International Pharmaceutical Federation (FIP) and the World Health Organisation (WHO) urge national tobacco control programmes and pharmacy associations to develop and implement plans to engage more pharmacists in advancing tobacco cessation.
The statement sets out a number of ways to work towards this goal. “This statement builds on our federation’s previous collaboration with the WHO on engaging pharmacists in tobacco cessation, including in the development of tobacco cessation tools. “In response to the urgent need to help the over 1.25 billion global tobacco users quit all nicotine and tobacco products, this statement calls for a collaborative effort among healthcare professionals," said Vinayak Prasad, head of the No Tobacco Unit at the WHO.
"Specifically, it advocates for national action to empower all pharmacists to routinely provide tobacco cessation support. If every pharmacist identifies and advises just one tobacco user to quit each day, this collective action could reach over 4 million users in a single day,” Dr Prasad added.
FIP has also published a new global intelligence report on pharmacist-led tobacco cessation services. The report presents the findings of a literature review and a survey of FIP member organisations in 78 countries, shedding light on service availability, scope, funding mechanisms, remuneration models and regulatory frameworks.
The literature review suggests that tobacco cessation services or interventions provided by pharmacists are strongly correlated with health outcomes, economic savings, increased health system efficiency and reduced burden on other healthcare sectors through interprofessional collaborations.
The data collected indicate that while most countries support the implementation of tobacco cessation services, the scope of professional standards and policies, the remuneration frameworks and the public advocacy of the role of pharmacists in tobacco cessation varies greatly amongst countries.
Not all topical diclofenac products are the same. Formulation Matters.1
Voltarol Emulgel Extra Strength Gel is clinically proven to demonstrate deep tissue penetration into the joint 2
For all-day relief from joint pain†
Learn more about the formulation of Voltarol Emulgel Extra Strength Gel
† apply once, morning & evening
References: 1. Derry S et al. Cochrane Database Syst Rev 2015; 6: CD007402. 2. Seefried et al. Ther Adv Musculoskel Dis (2020) Vol 12: 1-13.
Product Information: Please consult the Summary of Product Characteristics for full product information.
Voltarol Emulgel 1% w/w Gel (diclofenac) and Voltarol Emulgel Extra Strength 2% w/w Gel (diclofenac). Indications: For the local symptomatic relief of pain and inflammation in trauma of tendons, ligaments, muscles and joints, localised forms of soft tissue rheumatism. Dosage: Adults and adolescents 14 years and over: Voltarol Emulgel 1% w/w Gel: 2-4g of gel, applied topically 3-4 times daily. Maximum treatment duration is 7 days. Voltarol Emulgel Extra Strength 2% w/w Gel: 2-4g of gel, applied topically 2 times daily – morning and evening. Maximum treatment duration is 14 days. All gels: Patients should consult their doctor if the condition does not improve within 7 days, or worsens. Contraindications: Patients with or without chronic asthma in whom asthma, angioedema, urticaria or acute rhinitis are precipitated by aspirin or other non-steroidal anti-inflammatory agents. Hypersensitivity to diclofenac, acetylsalicylic acid, other non-steroidal anti-inflammatory drugs, or any other ingredient in the gel. Use in third trimester of pregnancy. Use in children and adolescents aged less than 14 years. Warnings and precautions: Apply only to intact, non-diseased skin and not to skin wounds or open injuries. Do not smoke and avoid naked flames. It should not be used with occlusion, allowed to come into contact with the eyes or mucous membranes or ingested. Application over extensive areas for prolonged periods or application in excess of recommended dosage may give rise to systemic effects. Discontinue if rash develops. Use with caution in patients with a history of peptic ulcers, gastrointestinal bleeding, hepatic or renal insufficiency, or bleeding diathesis, or intestinal inflammation. Voltarol Emulgel 1% w/w Gel: Contains propylene glycol and benzyl benzoate, which may cause skin irritation. Voltarol Emulgel Extra Strength 2% w/w Gel: Contains propylene glycol and butylhydroxytoluene which may cause skin reactions or irritations, and fragrance limonene and linalool which may cause allergic reactions. Side effects: Very rare: rash pustular, hypersensitivity (including urticaria), angioedema, asthma, photosensitivity reaction. Rare: Dermatitis bullous. Common: Dermatitis (including contact dermatitis), rash, erythema, eczema, pruritus. MA Holder: Haleon Ireland Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. MA Number: Voltarol 1% w/w Gel: PA 678/140/2. Voltarol 2% w/w Gel: PA 678/140/3. Legal Category: 1%: GSL, 2%: Pharmacy only. Text revised: July 2023. Further information available on request. Contains diclofenac diethylammonium. Always read the label/leaflet. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-VOLT-23-00025.
Diclofenac diethylammonium
Celebrating a Decade of Growth
Tanaiste Micheál Martin joined Cork company, PrecisionBiotics to mark a decade of success for their flagship product, Alflorex. The event was held at the Glucksman Gallery in UCC last month, to celebrate Alflorex which was launched in 2014 and is now sold in 22 countries worldwide.
Developed by scientists and gastroenterologists at PrecisionBiotics in collaboration with the APC Microbiome Institute at University College Cork, Alflorex features the exclusive live culture, 35624®, which has undergone rigorous clinical testing and research spanning over 15 years. Alflorex is an award winning supplement and the leading overthe-counter probiotic among Irish pharmacists. Since its inception, Alflorex has been at the forefront
of probiotic innovation, delivering clinically proven results.
Commenting on the milestone, Minister Martin said, “It’s wonderful to see the success of an outstanding Cork company like PrecisionBiotics as it continues on its journey of innovation. The future is bright for the scientists and industry leaders who continue to create top quality and global products at its Irish base. This morning’s event was a celebration of the past ten years, and I have no
Managing Hayfever Season
Cormac Kearney, CEO Pamex Limited; Dr Eileen Murphy, Head of Global Portfolio Science and Exploration with Novonesis; Alison Winger, General Manager Novonesis Ireland; Tánaiste Micheál Martin, and Head of Ireland PrecisionBiotics, Colm O’Sullivan pictured at The Glucksman Gallery, UCC for a celebration of Cork company PrecisionBiotics. The event marked 10 years of PrecisionBiotics' flagship product, Alflorex. Photo: Darragh Kane
Pharmacy Cancer Support
The Irish Cancer Society is reminding healthcare professionals about the vast range of information and support services it provides, which could benefit some of the 42,000 people diagnosed with cancer every year.
The Society is the biggest producer of cancer information in Ireland. It has 100 publications, almost 800 webpages and six patient education programmes in video format. Throughout 2024, it will run cancer awareness campaigns promoting symptom awareness and early detection at community events, in its hospital-based Daffodil Centres and across its social media channels.
doubt PrecisionBiotics will continue to flourish in the years to come.”
Alison Winger, Ireland’s General Manager of Novonesis said, "As we celebrate a decade of Alflorex in Ireland, we reflect on the profound impact it has had on individuals seeking treatment for gut conditions. Our commitment to delivering effective and scientifically validated solutions remains unwavering. Alflorex continues to redefine standards in gut health, providing relief to those in need. It was fitting to celebrate this milestone with an event at The Glucksman in UCC, where research for Alflorex started.”
The Covid pandemic had a devastating impact on the diagnosis and management of cancer in Ireland, the results of which are still being felt today. Preliminary data* on the impact of the pandemic indicates that the number of cancer cases diagnosed in 2021 was down 1,665 cases or 6% lower than projected. In 2020, it was 10%. The combined number of missed cancers from 2020 and 2021 tells us that 1 in 12 expected cancers were not detected over the first 2 years of the pandemic.
As we approached a period of high pollen on the June Bank Holiday weekend, the Asthma Society of Ireland issued urgent advice on managing asthma and hay fever. Hay fever affects a significant portion of the population: Over 450,000 people in Ireland are living with asthma, and 80% of those also experience hay fever. Proper management techniques can significantly improve quality of life, especially when wanting to enjoy the outdoors.
In a recent survey conducted by the organisation of over 1,200 people living with asthma and/or hay fever, 76% of people with hay fever (727) said that it limits their or their child's daily activities and has a disruptive effect on their lives. Almost four in five (78%) revealed that during the hay fever season (March to September), their or their child's participation in sports or activities is disrupted due to hay fever.
Typical symptoms of seasonal hay fever and perennial allergic rhinitis
are not limited to just a few, but can include a number of the following:
• Sneezing, as well as an itchy, blocked, or runny nose
• Red, itchy, or watery eyes
• An itchy throat, inner ear, or mouth
• A post-nasal drip
• A diminished sense of taste and smell
• Headaches, reduced concentration, and a general feeling of unwellness
Ruth Morrow, a Respiratory Nurse Specialist at the Asthma Society, emphasises the importance of proper management techniques. "For individuals impacted by hay fever during sports or outdoor activities, planning ahead is essential. This includes taking antihistamines as prescribed, using nasal sprays to alleviate congestion, wearing wraparound sunglasses to protect the eyes from pollen, and splashing your eyes with cold water to flush out pollen and soothe them.”
“We don’t yet have the full picture of whether these cancers were diagnosed at a more advanced stage, but what we do know is that the later the stage of diagnosis, the more complex, more costly, and more invasive cancer is to treat. These patients need more support and more information,” commented Aoife McNamara, Head of Education and Engagement with the Society.
All of the Society’s information is available free of charge. Copies of print publications can be ordered for hospitals at: www. cancer.ie/about-us/cancerresources-and-publications
As well as cancer information, the Irish Cancer Society also provides a range of services for people affected by cancer including its Support Line, which is staffed by specialist cancer nurses, Monday – Friday, 9am –5pm. Freephone 1800 200 700.
55 micrograms/dose
Nasal Spray Suspension triamcinolone acetonide
For Adult use only. Not for use in children under 18 years. A copy of the summary of product characteristics is available upon request or alternatively please go to www.clonmelhealthcare.ie. Product not subject to medical prescription. Supply through pharmacies only. PA23180/001/002. PA Holder: Opella Healthcare France SAS, 157 avenue Charles de Gaulle, 92200 Neuilly-sur-Seine, France. Distributed by: Clonmel Healthcare Ltd., Clonmel, Co.Tipperary. Date Prepared: February 2024
2024/ADV/NAS/063H
For the treatment of the nasal symptoms of seasonal allergic rhinitis
Nasal Congestion
Sneezing and Itching
Clinical Updates in Eye Health at ICO Conference
The Irish College of Ophthalmologists hosted their Annual Conference 2024 at the Knockranny House Hotel in Westport, Co Mayo from Wednesday 15th to Friday 17th May. Over 200 ophthalmologists gathered for the three-day scientific conference to hear the latest clinical and scientific developments in the specialty from eye experts at home and abroad.
Key symposia at this year's conference focused on Vision and Strabismus, Orbit and Socket, and Sustainability in Ophthalmology
Among the keynote guest speakers, the College was delighted to welcome Mr Ian Marsh, Consultant Ophthalmic Surgeon at the Liverpool University Hospital NHS Trust and Dr Arvind Chandna, Senior Clinician Scientist at Smith Kettlewell Eye Research Institute, San Francisco to present at the Vision and Strabismus symposium on the opening morning of the conference (Wednesday, 15th May), alongside Ms Kathryn McCreery, Children’s Health Ireland at Crumlin Hospital.
Ms McCreery discussed difficult paediatric ophthalmology and strabismus consultations including drop administration in children, evaluation of the child with autism and delivering bad news. The management of strabismus surgery complications and the informed consent process in paediatric and adult strabismus surgery were also discussed, with an emphasis on effective communication with children, their parents and adults in advance of undergoing strabismus surgery.
Mr Ian Marsh currently runs a comprehensive strabismus service mainly for adults but also including more complex squint in children at Liverpool University Hospital NHS Trust in Liverpool and spoke to delegates about decoding the process of strabismus management. Recent
developments have included the introduction of Bupivacaine injections to permanently straighten eyes, the use of inferior medial rectus plication in near exotropia and since the Covid pandemic, a regular video clinic and a monthly local anaesthetic squint list.
Dr Arvind Chandna is a Senior Clinician Scientist at Smith Kettlewell Eye Research Institute (SKERI) conducting research programmes dealing with significant gaps in clinical and scientific knowledge of common childhood eye conditions with poor management outcomes, and investigating them in collaboration with SKERI’s vision scientists.
He is a Consultant Paediatric Ophthalmologist, Alder Hey Children’s Hospital, Liverpool and gave a comprehensive presentation at the ICO Annual Conference on Cerebral Visual Impairment and a structured approach to managing the condition beyond visual acuity. His talk outlined this investigation of visual brain neuroscience and oculomotor behavior using eye tracking, photorefraction, psychophysics and visually evoked brain potentials in childhood eye disease.
Mr Manoj Parulekar, Consultant Ophthalmic Surgeon at the Birmingham Women's and Children's NHS Foundation Trust and Oxford University Hospitals NHS Trust and Professor Geoffrey Rose, Consultant Orbital, Lacrimal and Plastic Reconstructive Surgeon at Moorfields Eye Hospital, London were guest speakers at the Orbit
Keynote speakers at the Vision and Strabismus symposium (Wednesday, 15th May); (L-r) Ms Kathryn McCreery, Consultant Ophthalmic Surgeon, Children's Health Ireland at Crumlin Hospital, Dublin, Dr Arvind Chandna, Senior Clinician Scientist, Smith Kettlewell Eye Research Institute San Francisco and Consultant Paediatric Ophthalmologist, Alder Hey Children’s Hospital, Liverpool, session chair Mr Sean Chen, Consultant Ophthalmic Surgeon, Blackrock Health Galway Clinic and Mr Ian Marsh, Consultant Ophthalmic Surgeon, Liverpool University Hospital NHS Trust, Liverpool
and Socket symposium. Mr Tim Fulcher, Consultant Ophthalmic Surgeon at the Mater Misericordiae University Hospital Dublin chaired and presented on the management of socket complications at this session.
Mr Parulekar outlined the clinical assessment, differential diagnosis and management of benign and malignant lesions of the paediatric orbit. He contributes to the paediatric ophthalmology service at the Birmingham Women’s and Children’s Hospital, the largest women’s and children’s hospitals in Europe, where he treats a wide range of childhood eye conditions including strabismus, paediatric cataracts and glaucoma, oculoplastics and neuroophthalmology, ocular oncology, and external eye diseases. He has special expertise in the treatment of eye cancers in children and is Consultant Ophthalmologist to the Birmingham National Retinoblastoma Unit, the largest nationally designated retinoblastoma center in the UK. Mr Parulekar contributes to the ocular motility service (squints and complex eye movement disorders), and the neuro-ophthalmology service at the Oxford University Hospital where he provides a supra-regional service to Oxfordshire, Buckinghamshire, Berkshire and Wiltshire.
Prof Geoffrey E. Rose, Honorary Consultant Ophthalmic Surgeon, Moorfields Eye Hospital, and Senior Research Fellow of the Biomedical Research Centre at the Institute of Ophthalmology,
London, gave a detailed presentation on 'Managing the Removal of an Eye' at the Orbit and Socket symposium. In his talk, he discussed the problems that can occur with socket management and the alternatives to eye removal, the patient consent process and challenges which can occur as a result of "over promise" by the physician. Prof Rose addressed the mechanics of eye removal and how to manage (largely by prevention) the volume deficiency that would otherwise arise from removal of the globe.
It was a great honour for the College to invite Professor Rose to deliver the Annual Mooney Lecture at the 2024 ICO Conference, which he presented on the evening of Wednesday 15th May.
Prof Rose's lecture entitled "Trends in rehabilitation of patients with thyroid eye disease" considered what thyroid eye disease means, in practical terms, to the patient and the mechanism of the disease in terms of the underlying inflammatory mechanism, and the biomechanics of the condition.
A fascinating lecture outlining the historical treatment of thyroid eye disease in patients, up to modern day advances and the changes in treatment approaches.
Four decades ago, changes in treatment were largely directed to improving surgical techniques to allow a better restoration of function and appearance, with less injury to neighbouring tissues, Prof Rose explained. From the 1990s, it was widely recognised that the final functional deficit and aesthetic disturbance could be reduced considerably by shortening the inflammatory phase of TED. Early immunosuppressive regimes were based on various regimes for systemic corticosteroids, either oral or intravenous (and occasionally intraorbital administration). These early regimes were modified by adjunctive use of steroid-sparing agents and, in some cases, use of low-dose orbital radiotherapy. More recently, the immune response has been mollified with monoclonal antibodies directed against the inflammatory mediators or cells. Over the last 20 years, it has been shown that changes of TED appear to be
References:1)*Countries: Europe (Austria, Belgium, Bulgaria, Croatia, Czech Republic, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Netherlands, Norway, Poland, Portugal, Romania, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, UK) Source: Based on internal analysis by Laboratoires Théa using quarterly data from the following source: IQVIA Consumer Health Customized Insights for the period 2023, volume and value sales in Euros MNF, limited to CHC 07A3, reflecting estimates of real-world activity in these countries: Austria, Belgium, Bulgaria, Croatia, Czech Republic, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Netherlands, Norway, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, UK. Copyright IQVIA. All rights reserved. 2) Pinto-Bonilla JC et al. Ther. Clin Risk Manag 2015:11;595-603 3) Schmidl D et al. Cornea 2015;34(4):421-6 TP24032
& Protects
Suitable for all dry eye sufferers including contact lens wearers A single drop Lasts for up to 4 hours3 Clinically Proven2 to treat symptoms of dry eyes
www.theapharma.ie
Conference
produced through an immune activation of the TSH-receptor and IGF1-receptors. With the recent proliferation of biological therapeutics, the treatment of TED is now very much directed towards blocking activation of the TSH and IGF1 receptor pathway. Early biological agents directed against IGF-1 receptors have shown an excellent effect on the active phase of TED, and also some activity in the apparently ‘burnt-out’ phase of the condition; usage of these drugs can, however, have some major side-effects, Prof Rose noted.
On the final day of the conference, a dedicated symposium on Sustainability in Ophthalmology welcomed national and international experts to share their knowledge on ways to minimise the carbon footprint of the specialty and plan for the future from both an environmental and sustainable practice perspective.. Healthcare is a notable contributor to greenhouse gas emissions, accounting for an estimated 5% of total emissions globally. The ophthalmic field, like many others in healthcare, has a significant environmental footprint. Cataract surgery is the number one surgical procedure in Ireland carried out by volume, and utilises a high amount of consumables and energy, and generates significant waste.
Miss Radhika Rampat, Consultant Ophthalmic Surgeon at the Royal Free London NHS Trust outlined the sustainability in ophthalmology journey so far of the American European Congress Of Ophthalmic surgery - Green Working Group, examining “how can I act locally and share globally”. She examined what has been achieved to date in eye clinics and theatres locally and internationally in the efforts to
Keynote speakers at the Sustainability in Ophthalmology symposium (Friday, 17th May) are (l-r): Dr Philip Crowley, National Director of Strategy and Research, HSE and National Lead for Climate Strategy, Dr Emilie Mahon, Ophthalmology Clinical Tutor, Royal College of Surgeons in Ireland, Dublin and Mr Arthur Cummings, Consultant Ophthalmic Surgeon, Wellington Eye Clinic, Dublin
reduce the carbon footprint in the specialty. Miss Rampat is the co-chair of AECOS Green Working Group.
Ireland is among the major healthcare emitters per capita internationally. The ICO welcomed Dr Philip Crowley, National Director of Strategy and Research and HSE National Lead for Climate Change who spoke to delegates about the HSE Climate Action Strategy 2023-2050 being adopted to reduce emissions and protect population health in the Irish healthcare system.
The strategy is one of the first national health service climate strategies globally, and Dr Crowley outlined the progress on implementation in its target to achieve net-zero emissions for the HSE by 2050, the relevant actions for ophthalmology practice and the work to mobilise health service staff.
Dr Emilie Mahon, RCSI
Ophthalmology Clinical Tutor at the Royal Victoria Eye and Ear Hospital, outlined the findings of her research on the ecological impact of phacoemulsification
cataract surgery where she examined the single-use items consumption and the results concerning the carbon footprint of cataract surgery in the Eye and Ear Hospital.
Mr Arthur Cummings, Consultant Ophthalmologist at the Wellington Eye Clinic in Dublin looked at the practice side of sustainability in ophthalmology in light of the growing burden of ophthalmic needs building globally while the number of ophthalmologists is decreasing.
Mr Cummings highlighted the need for the specialty to become more efficient and effective while the shortage of ophthalmologists is addressed. His talk reviewed three areas that can help achieve greater efficacy and efficiency, namely system design, artificial intelligence and maximising the role of the allied health professional team.
Workshop sessions, paper and poster presentations and the European Society of Ophthalmology (SOE) Lecture 2024 presented by Mr Michéal O'Rourke, Royal Victoria Eye and Ear Hospital, St James's Hospital and Children's Health Ireland at Crumlin, Dublin on the topic of Paediatric Oculoplastics
also featured on the three day conference programme.
The Barbara Knox Medal for Best Paper was awarded to Dr Shane O'Regan for his paper entitled "Eyes on Spina Bifida: A TwoDecade Retrospective Exploration of Ophthalmic Manifestations in Paediatric Patients at Temple Street Children’s University Hospital, Dublin".
The William Wilde Medal for Best Poster was awarded to Dr Patrick Murtagh for his poster "Uveal Melanoma Patients Treated with Iodine Plaque versus Ruthenium Plaque versus Proton Beam Radiation: A Ten-Year Review."
Dr Murtagh was presented with his medal by Professor Brendan Kelly, Consultant Psychiatrist, Tallaght University Hospital, Dublin and Professor of Psychiatry at Trinity College Dublin who shared with the audience his insights on human behaviours and reactions to perceived challenges in his fascinating talk on "Pandemics in Ireland, and Lessons Learned from Covid (If Any)"
Prof Kelly's recently published book 'Resilience: Lessons from Sir William Wilde on Life After Covid' reflects on the pandemic in Ireland and what we might learn as a society and as individuals from the experience.
Professor Geoffrey Rose (right), Consultant Orbital, Lacrimal and Plastic Reconstructive Surgeon, Moorfields Eye Hospital, London, who delivered the Mooney Lecture at the ICO Annual Conference 2024 is pictured with Mr John Doris (centre), President, Irish College of Ophthalmologists and Mr Tim Fulcher, Consultant Ophthalmic Surgeon, Mater Misericordiae University Hospital, Dublin
The ICO announced the publication of its Annual Report for 2023 at the conference in Westport. The ICO is a registered Irish charity. The organisation is committed to the advancement and improvement of eye health and patient safety and works to protect, enhance and promote the highest standards in the delivery of eye care.
The Annual Report 2023 outlines the activities undertaken by the College and finances for that year.
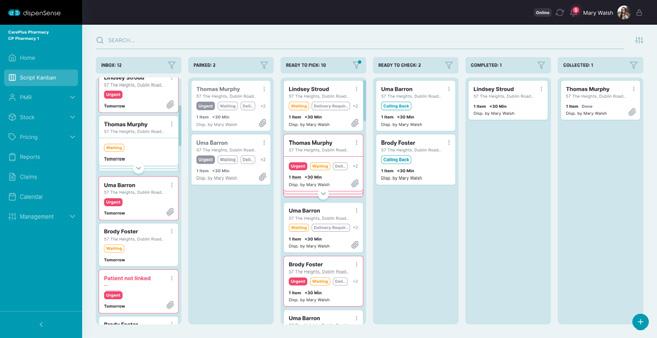
Using the latest, cutting-edge technologies to make dispensing to your patients reliable, safe & e cient.
Heathmail integration now live
Nursing Home module now available
• Unique intervention logging
• IHI (Individual Health Identifier) number now recorded
To learn more or book a demo, get in touch on info@navi.ie or check out our website, navi.ie.
The Role of the Pharmacist in HPV Vaccination
United Drug Webinar Series returns with insightful talk on HPV Vaccination and the role of the Pharmacist
As part of their added value Knowledge Hub and CPD learning programme, United Drug recently hosted an informative webinar on the topic of HPV Vaccination. The webinar specifically focussed on the role of the pharmacist in the vaccination process, leading to a reduction in Cervical Cancer.
Some key points covered on the night were:
• The role of the pharmacist in the vaccination process
• Understanding the scheduling and dosage of vaccination in various cohorts
• Increasing the uptake of HPV Vaccination and how the pharmacist can assist with this
• Scope of the vaccine going onto Schedule 8 and how the pharmacist will play a role in this.
Hosted by Clinical Governance Pharmacist at LloydsPharmacy Ireland Martin Hynes, the webinar was designed as a Q&A for Pharmacists to have readily available access to an expert speaker on HPV and Cervical Cancer prevention.
Sinéad Cleary, Advanced Nurse Practitioner and Colposcopy Nurse in Tallaght University Hospital began the webinar with an educational and informative overview of HPV, the progression to Cervical Cancer and the importance of HPV Vaccination and screening in the eradication of Cervical Cancer.
All United Drug webinars are held with the patient in mind and
aim to equip the Pharmacist to better assist in the community. If this sounds like something you’d be interested in, please don’t hesitate to contact United Drug for information on future webinar topics along with access to previous webinar content.
Don’t forget, this and all webinars by United Drug can be considered in your CPD portfolio. All attendees are issued with a certificate of attendance.
For more information, please contact UDWMarketing@united-drug.com
Pharmacists Discuss Solutions to Medicine Shortages
The Standing Committee of European Doctors (CPME) and the Pharmaceutical Group of the European Union (PGEU) recently met to exchange views on solutions for shortages of medicines, medical devices and healthcare professionals in a joint event with policymakers, academics and professionals.
Pharmacists and doctors are concerned about the rise of medicine shortages across Europe, affecting the quality of care of patients.
PGEU President Aris Prins said, “Doctors and pharmacists need earlier notifications of shortages. The security of supply could be further improved by ensuring that pharmaceutical companies have robust shortages prevention and mitigation plans in place and introducing progressive requirements for rolling buffer stocks. In the next EU mandate, the ongoing revision of the general pharmaceutical legislation and a possible Critical Medicines
Act provide opportunities to offer solutions.”
Professionals are also concerned about shortages of some essential medical devices becoming increasingly common, with no alternatives available in many cases. CPME President Dr Christiaan Keijzer said, “We need long-term solutions that address the inadequate implementation of the new medical device and in-vitro diagnostics regulations and notified bodies capacity, to ensure that patient safety is preserved.
“Special attention should be paid to the availability of orphan medical devices and there
should be a prudent system of incentives that avoids the artificial ‘orphanisation’ of devices to exploit the system.”
Finally, pharmacists and doctors reaffirm how the shortages of healthcare professionals are threatening the foundations of the entire health sector. CPME and PGEU urge member states and the European Commission to implement a coordinated EU Health Workforce strategy that prioritises retention and recruitment by safeguarding minimum training requirements and lawful practice conditions, as well as investing in workforce planning.
Emerging Drug Trend Laboratory
A new state-of-the-art HSE Emerging Drug Trend laboratory opened recently at the National Drug Treatment Centre (NDTC), Dublin. The laboratory will analyse drug contents, purity and potency, enhancing the HSE’s ability to monitor and respond to new drug trends and market changes to protect and support the health of people who may choose to use drugs.
The new lab utilises the latest forensic techniques and technology including:
• a gas chromatography-mass spectrometer used to analyse different substances within a sample
• a mobile FT-IR spectrometer to identify the composition of samples, ensuring precise and reliable testing results
Gas chromatography–mass spectrometry (GC–MS) is an analytical method that combines the features of gas-chromatography and mass spectrometry to identify different substances within a sample. It produces a mass spectrum of the compound the fragmentation pattern of which (the mass spectrum) is specific to that compound.
Fourier-transform infrared spectroscopy (FTIR) is a technique used to obtain an infrared spectrum of a substance. The spectrum obtained is like a fingerprint for the compound analysed. This technique lends itself to portability and is used in the field by various types of organisations including customs, police and in festival drug checking.
The mobile FT-IR technology has already been successfully used by the National Drug Treatment Centre laboratory as part of the HSE Safer Nightlife programme to identify harmful high strength substances through the ‘back of house’ drug checking service at festivals.
Officially opening the new laboratory, Colm Burke TD., Minister of State with special responsibility for Public Health, Wellbeing and the National Drugs Strategy said, “The landscape of drug use in Ireland and Europe is rapidly evolving, presenting new challenges to public health. It is vital that we increase our preparedness to identify and react to these new threats.”
Diabetes
Diabetes Technology Network Arrives in Ireland
For the first time ever in Ireland a conference focusing on diabetes technologies was held recently in Dublin and a new healthcare professional (HCP) group “Diabetes Technology Network Ireland (DTN IRL)” was launched.
The conference for HCPs was developed by Consultant Endocrinologists Tomás Griffin, Hannah Forde and Una Graham who co-operated to bring the UK-based “Diabetes Technology Network” to Ireland. Supported by Diabetes Ireland, 160 healthcare professional delegates took part in the inaugural conference to hear about plans to develop a DTN Ireland network and learn from a range of national and international experts in diabetes technology.
Delegates learned from international speakers Professor Partha Kar, Consultant in Diabetes and Endocrinology from Portsmouth who shared his inspirational thoughts on how to begin to improve access to diabetes technology for people with diabetes, highlighting his UK experience as Type 1 Diabetes & Technology lead for NHS England, and Professor Rob Andrews (University of Exeter), well-known expert in exercise and diabetes, who presented on managing type 1 diabetes and exercise with hybrid closed loop technology.
Ms Sonya Browne, Diabetes Nurse Specialist, Beaumont Hospital, Dublin, shared very practical tips on how to expand diabetes technology and insulin pump services in a very busy diabetes clinic and Mr Ken Barclay, a person living with type 1 diabetes and huge technology enthusiast shared his perspective on how technology can change individual’s lives.
Professor Orla Neylon, Consultant Paediatric Endocrinologist, University Hospital Limerick shared her expertise with adolescents and young adults providing tips for using technology in transition services, Dr Tomás Griffin, University of Galway, explained how to interpret the data provided by automated insulin delivery systems, and Dr Christine Newman, Consultant Endocrinologist, Galway University Hospital, explained how to manage diabetes with technology during pregnancy.
Dr Kevin Moore, Consultant Endocrinologist from Tallaght University Hospital and Naas General Hospital who led the group developing Type 1 Diabetes clinical recommendations in Ireland, outlined the most important aspects of this newly launched guideline https://www.diabetes.ie/newupdated-recommendations-forimproving-access-quality-andsafety-of-care-for-adults-withdiabetes-have-been-launched/) and expressed his hopes for implementation of the guidelines which would significantly improve access to care for people with diabetes.
Attendees also availed of a hands-on experience during a technology speed-dating session with companies showcasing their products to delegates.
It was acknowledged that the landscape of technology, in particular in managing type 1 diabetes is changing at an unprecedented pace. Dr Tomás Griffin said, “We have come a long way in a short period of time from having limited access to Continuous Glucose Monitoring (CGM) to today where there is an unprecedented expansion and uptake in Hybrid Closed Loop therapy.”
However, there are not many opportunities in Ireland to learn about them and the goal of DTN Ireland is to enhance access to technology for people living with diabetes. The primary goals of the diabetes technology network Ireland are to develop a network to:
• Learn together from best international guidance and expertise;
• Share best practice through guidance documents and pathways on diabetes technology development;
• Support healthcare professionals in the delivery of technologies by delivering practical education on diabetes technology utilisation;
• Be a voice to advocate for better diabetes technology utilisation and uptake for people with diabetes in Ireland;
• Work with relevant stakeholders to increase access to diabetes technologies in Ireland.
Dr Kate Gajewska, Diabetes Ireland manager for Advocacy and Research, said, “Knowing how challenging for some people living with diabetes it is to access diabetes technologies, mainly insulin pumps and hybrid closed loop systems, and that a postcode lottery exists in Ireland due to various reasons such as lack of resources, work-overload, but also lack of training and experience with pumps and CGMs, we are thrilled to see so many people willing to learn and improve their knowledge. We are sure that the DTN IRL launch will help the diabetes community access the best available treatments based on their needs.”
Dr Tomás Griffinn continued, “We were delighted with the positivity shown by delegates towards the development of a DTN Ireland Network and we received a lot of feedback from them on areas we need to address to support the many diabetes teams around the country. We will taking all of the feedback on board and developing a plan to support our colleagues in delivering access to the most appropriate technology to people with diabetes.”
Dr Kevin Moore, Dr Christine Newman, Dr Orla Neylon, Dr Tomás Griffin
L-R Dr Tomás Griffin, Dr Kevin Moore, Dr Kate Gajewska, Prof. Partha Kar and Prof. Rob Andrews
Marking 30 Years of Equitable Off-Patent Medicines Access
Medicines for Europe marks 30 years of delivering more equitable access to off-patent medicines as it opens its annual European conference in Dublin, in partnership with Medicines for Ireland.
The off-patent medicines industry supplies 70% of essential medicines in Europe, including treatments for cancer, autoimmune diseases, diabetes, cardiovascular disease, and others. Generic medicines represent over 90% of the EU critical medicines list, positioning the industry as a key enabler of a strong European health system.
Producers of off-patent medicines are also central to addressing health challenges across Europe and, as such, Medicines for Europe has built strong partnerships within the European Union and with key decision makers to drive policy
change. The review of European pharmaceutical legislation should deliver EU-wide solutions to tackle medicines shortages, clearer laws to allow patients to access generic and biosimilar medicines after patent expiry, and strong incentives for affordable value added medicines innovation and repurposing. For the secure supply of medicines, a future EU Critical Medicines Act should encourage more investment in essential medicines and active pharmaceutical ingredient (API) manufacturing and implement security of supply criteria into procurement and other market policies.
Keith Moore, Programme Coordinator, Sustainable Healthcare Coalition, UK, Maja Anette Flønes Monsen, Norwegian Hospital Procurement Fund, Skyehusinnkop, Courtney Soulsby, Global Director for the Healthcare and Life Sciences Sector Team, BSI, Ines Windisch, Member of the Sustainability Steering Committee, Medicines for Europe and Head of Communications, Corporate Affairs & Sustainability, Zentiva Group and Silke Oeschger-Delautre, Corporate Communication Lead, Europe, Dr. Reddy’s Laboratories
Commenting ahead of the annual conference, President of Medicines for Europe, Elisabeth Stampa said: “Our 30th anniversary is not just a celebration of our past achievements but a testament to our unwavering commitment to the future of healthcare in Europe. We are proud of the role we have played so far, but our journey is far from over and we are dedicated to continuing our work towards delivering solutions to tackle medicines shortages, clearer laws to allow access to generic and biosimilar medicines and incentives for value-added medicines. In this regard, we strongly encourage the new EU leadership to prioritise a Critical Medicines Act and the adoption of the new pharmaceutical legislation in the first 100 days in office.”
Also commenting, Chair of Medicines for Ireland, Paul Neill said: “We are delighted to be co-hosting this year’s European annual conference in partnership with our European association. While it is important to celebrate the successes of our advocacy efforts over the past three decades, it is vital that Medicines for Europe and its member national associations remain focused on delivering greater access to essential generic, biosimilar and value-added medicines in Ireland
and across the continent. It’s very encouraging to see increasing penetration of generic medicines in Ireland in recent years, however several influencing factors are causing Ireland to still lag behind our European counterparts, and these must be addressed. To fully realise the potential of enhanced patient access and affordability through increased penetration, it is pivotal that Ireland fosters a market ecosystem that promotes fair competition and the availability of essential medicines into the future.
“By fostering competition, reforming EU pharmaceutical laws, and implementing dynamic policies, we believe we can ensure access, affordability, and availability of essential medicines. As we face formidable challenges in Ireland’s healthcare system, the role of a resilient and sustainable medicines industry cannot be overstated. I truly believe that Ireland’s situation is a good example of the challenges we all face in making sure medicines are readily available and accessible across Europe. By encouraging the use of generic, biosimilar, and value-added medicines, we can alleviate the strain on our healthcare system and ensure that every patient has access to the medicines they need when they need them.”
Professor Michael Barry, National Clinical Lead, Medicines Management Programme for Ireland during the Panel Discussion
Philippe Drechsle, Vice President EU Portfolio, Teva & Member of the Medicines for Europe Executive Committee
Hosted in partnership with Medicines for Ireland (MFI) the diverse conference programme explores the:
• Value proposition of off-patent medicines and their importance in providing cost-effective treatment options.
• Evolution of the off-patent sector, and the major challenges and potential solutions in promoting the use of generic medicines in healthcare.
• Future supply chain security for critical medicines and the role that robust European regulation and policy can play.
• Opportunities to improve existing treatments through value-added medicines and the positive
impact evolving innovation can have on the sustainability of health systems.
• Merging of environmental sustainability with improved access to medicines, looking at best practices, and initiatives within the off-patent medicines industry.
• Future of the off-patent pharmaceutical industry in Europe including emerging trends, technologies, and market dynamics shaping the industry landscape.
• Value proposition of off-patent medicines and their importance in providing cost-effective treatment options.
• Evolution of the off-patent sector, and the major challenges and potential solutions in promoting the use of generic medicines in healthcare.
• Future supply chain security for critical medicines and the role that robust European regulation and policy can play.
• Opportunities to improve existing treatments through value-added medicines and the positive impact evolving innovation can have on the sustainability of health systems.
• Merging of environmental sustainability with improved access to medicines, looking at best practices, and initiatives within the off-patent medicines industry.
• Future of the off-patent pharmaceutical industry in Europe including emerging trends, technologies, and market dynamics shaping the industry landscape.
President of Medicines for Europe, Elisabeth Stampa
Deirdre Kelly, Country Manager, Ireland and Malta with Consilient Health; Vice Chairperson, Medicines for Ireland with Moderator Maja Graf, Associate Director Policy & Market Access, Medicines for Europe
Olivier Girard, Head of Unit for Medical Counter Measures in the Health Emergency Preparedness and Response Authority (HERA) of the European Union, European Commission
Chair of Medicines for Ireland Paul Neill
Max Newton, Engagement Manager, IQVIA
Infectious-Disease Stigma Research
A new survey from RCSI University of Medicine and Health Sciences reveals the urgent need for greater education about HIV stigma for healthcare workers and students. The survey was carried out during the development of a new online module on HIV stigma by the RISE project, based at RCSI’s Department of International Health and Tropical Medicine.
75% of those surveyed say they have witnessed stigmatising or prejudiced comments from a colleague about a person living with an infectious disease. Respondents shared examples of the stigma they witnessed, including unnecessary double gloving and the overuse or unnecessary use of personal protective equipment. They also reported witnessing the stereotyping of patients living with HIV as “intravenous drug users” and/or as “sexually promiscuous”.
Participants identified a lack of knowledge among healthcare workers about HIV transmission and risk factors, with just 42% of healthcare workers and 27% of healthcare students saying they received education on HIV stigma and discrimination.
45% of the healthcare workers surveyed say they have completed further training or CPD related to HIV since their qualification. Of those who have not engaged with CPD on HIV, 68% say they would if it was available.
Across all concepts tested in the survey, healthcare workers show better understanding than students. Across both cohorts, the
most poorly understood concept is ‘treatment as prevention’ which refers to the taking of HIV medication to prevent sexual transmission of the infection.
RISE project
The survey findings were shared today during the launch of a new project aimed at providing education to healthcare professionals and students on HIV stigma and its impact on the patient population.
The RISE (Redefining Institutional Stigma Education) project aims to bridge the gap in stigma education and enhance service providers’ understanding of the barriers to testing, treatment, and prevention by placing those impacted by HIV at the centre of an interactive online learning module. The innovative online learning module has been designed for healthcare professionals and students to address the challenges created by stigma.
Dr Eoghan de Barra, consultant in infectious diseases at Beaumont Hospital and senior lecturer at RCSI, said: “According to the Health Protection Surveillance Centre, there was 68% marked
increase in total number of people diagnosed with HIV in Ireland in 2022. This highlights that even with increased effective prevention tools, those working within the health system will encounter more and more people living with HIV, highlighting the importance of ensuring all health care providers, regardless of role, are able to create a stigma-free environment for their patients.”
Dr Amir K. Bachari, RISE project lead, noted that: “Despite remarkable strides in HIV treatment development and accessibility to antiretroviral therapy, the enduring toll of HIV stigma persists within our communities.
“The RISE module represents a collaborative effort to empower healthcare professionals with the knowledge and skills necessary to combat stigma effectively. By equipping our healthcare workforce with comprehensive education on HIV stigma, RISE endeavours to foster a more inclusive and compassionate healthcare environment for people living with HIV.”
L-R: Dr Amir K. Bachari, Dr Eoghan de Barra, former Taoiseach Dr Leo Varadkar, Michael O’Dea and Ellen Conlon at the launch of the RISE (Redefining Institutional Stigma Education) project report, RCSI University of Medicine and Health Sciences
Speaking at today’s launch, Aoife Cummins, who is a registered nurse and a person living with HIV, reflected on the potential impact of RISE and said: “As a woman living with HIV I think it’s important that our voices are included in the education of healthcare students and workers going forward so we are no longer stigmatised in a setting where we should feel most understood.”
The survey, carried out between June and November 2023, was aimed at both healthcare workers and healthcare students in Ireland. The survey had 117 responses –67 healthcare workers, 30 students and 20 'other'.
RISE is supported by Gilead Sciences Fellowship Grant and through resources made available by RCSI, including the Student Engagement and Partnership (StEP) fund.
Healthcare workers and students who are interested in accessing the module can find out more via the project’s Instagram @riseproject_ie.
Former Taoiseach Dr Leo Varadkar
Call for papers: make your contribution to Irish Pharmacy News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to editor
In-depth review articles critique fundamental concepts, issues, and problems that define a field of research or practice and support advanced practitioners as well as aspiring early-year pharmacists.
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients with the aim to improving pharmacy practice.
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions.
24 Back2School - Vaccines
Know your Role in Childhood Vaccinations
The role of pharmacists in immunisation and vaccination varies across the world; in some countries pharmacists are primarily involved in ensuring the safe supply and dispensing of vaccines, as well as advocating for immunisation, while in other countries they are empowered to play a more active role, as they are legally authorised organise vaccinations activities and campaigns.
It is estimated that ten million lives per year could be saved by increasing access to medicines and vaccinations. Community pharmacists are therefore in a strong position to provide a major contribution to public health due to their accessibility, distribution and available medicines expertise.
Vaccines being Offered:
During the school year
• Children in Junior Infants will be offered 4 in 1 and MMR vaccines
• Students in first year of secondary school will be offered HPV, Tdap and MenACWY
These vaccines are also available to students who are in special schools or are home schooled in the same age group.
Meningococcal Disease
Meningococcal disease is caused by infection with Neisseria meningitidis and presents as bacterial meningitis (15 per cent of cases), septicaemia (25 per cent of cases), or a combination of the two. It is the leading infective cause of death in early childhood.
There are several strains or ‘groups’ of meningococcal bacteria (A, B, C, W, X and Y). In the past
50 years, most meningococcal disease in the UK and Ireland has been due to group B (MenB) and group C (MenC), although the MenC vaccine introduced in 1999 has now successfully reduced cases to just a handful each year. Currently MenB accounts for the vast majority of meningococcal disease although we have recently seen an alarming rise in a particularly deadly strain of meningococcal W meningitis and septicaemia.
There are five main groups that commonly cause disease - MenA, MenB, MenC, MenW, MenY.
MenB causes the majority of the disease.
How it is caused:
• Around 10% of the population carries meningococcal bacteria in the back of their throats at any given time. This is usually healthy carriage and helps develop immunity
• Occasionally the bacteria defeat the body’s defences and cause infection
• The bacteria are passed from person to person by coughing, sneezing and intimate kissing
• The bacteria break through the lining at the back of the throat and pass into the bloodstream
• They can travel in the bloodstream to infect the meninges, causing meningitis, or while in the bloodstream they can cause septicaemia
From September 2021, secondary school children in first-year are offered a meningococcal ACWY booster vaccination.
The Meningococcal ACWY vaccine will boost children’s protection against group C meningococcal disease. It will also provide additional protection against meningococcal groups A, W and Y. In addition, this vaccine also reduces the risk of carrying the disease so can help protect other people too.
MenACWY being used in Ireland is Nimenrix. This is a conjugate vaccine containing Group A, C, W and Y polysaccharides conjugated to tetanus toxoid carrier protein. The vaccine protects against N. meningitidis Groups A, C, W and Y invasive disease.
Since 2015 more cases of invasive meningococcal serogroups W and Y disease have been seen in Ireland. Prior to 2015 the annual number of both serogroups was low. Between 1999 and 2014 there was an average of two cases for both serogroups reported per year.
Between 2015 and 2018, a total of 36 serogroup W and 20 serogroup Y cases were reported, giving an average annual notification rate 9 cases per year of serogroup W and for 5 cases per year of serogroup Y.
In view of the emergence of meningococcal serogroups W and Y, the National Immunisation Advisory Committee (NIAC) recommended that one dose of MenACWY vaccine should be given to all students in 1st year of second level education replacing the MenC vaccine in 2019.
Meningococcal disease can start very suddenly. Symptoms include fever, stiff neck, headache, joint pains and a rash.
Meningococcal disease can occur at any age, but the highest rate occurs in children under 5 years of age, especially children under 1 year old. The next high-risk group are young people aged 15-19 years.
Importantly for community pharmacists to be aware, they might have school children and/ or their parents presenting to the pharmacy with associated after effects. Some students can have an area of soreness, swelling and redness in their arm where the injection was given. This usually passes after a day or two.
Some students may get a headache, feel sick in their tummy or run a slight temperature. If this happens, paracetamol or ibuprofen will help.
HPV vaccine for girls and boys
The HPV vaccine has been offered to girls in their first year of secondary school since 2010. This is because the most common cancer caused by the HPV virus is cervical cancer which only affects women.
Since September 2019, boys have also been offered the HPV vaccine. This is because HPV can cause cancers and genital warts in boys too.
Conditions caused by HPV infection
In girls, HPV infection can cause cancer of the:
• cervix
• vulva (the area surrounding the opening of the vagina)
• vagina
• anus
• oropharynx (part of the throat at the back of the mouth)
In boys, HPV infection can cause cancer of the:
• anus
• oropharynx (part of the throat at the back of the mouth)
• penis
HPV infection can also cause genital warts in both girls and boys.
Back2School - Vitamins
Vitamin Supplements in Children
To supplement or not to supplement? That is the question
Vitamins and minerals are important for healthy growth and development in children. Children who eat a well-balanced diet usually do not need a vitamin or mineral supplement. However, some children are at risk for deficiencies and may need a supplement.
When to Supplement
Children who follow vegetarian or vegan diets may need to supplement with vitamin B12 since it's only found in animal-based foods. Children who have coeliac disease are at a higher risk for nutritional deficiencies and may need supplements. Additionally, children who have a poor appetite, drink a lot of sugar-sweetened beverages, take certain medications or have chronic medical conditions that interfere with intake may need a supplement.
Important Considerations
Parents should strive for a wellrounded diet to ensure their child meets the daily recommended vitamin and mineral intakes. A balanced diet includes dairy or dairy alternatives, fruits and vegetables, whole grains and protein foods such as poultry, fish, eggs, nuts and legumes including beans and lentils. While all vitamins and minerals are important for growth and development, some are especially critical for children.
Vitamins, minerals and supplements (VMS) have always been an important category in the pharmacy with various benefits for not only adults but children of all ages from birth right up to the elderly.
It is generally recommended that all children aged 6 months to 5 years are given vitamin
supplements containing vitamins A, C and D every day. Babies who are having more than 500ml (about a pint) of infant formula a day should not be given vitamin supplements. This is because formula is fortified with vitamins A, C and D and other nutrients.
Babies who are being breastfed should be given a daily vitamin D supplement from birth, whether or not mum is taking a supplement containing vitamin D herself.
Vitamin D
Babies need vitamin D for healthy growth and development. It helps them build strong, healthy bones and teeth.
Babies who don’t get enough vitamin D are said to have a deficiency. If the levels are low enough, they are at risk of getting rickets, a disease that affects the way bones grow and develop.
The recent re-emergence of rickets (a severe form of vitamin D deficiency causing deformity of the bones) amongst infants in Ireland indicated the widespread low levels of vitamin D in the Irish population. FSAI recommendations
The recommendations are as follows:
1. All babies living in Ireland should be given a vitamin D only supplement providing 5µg Vitamin D from birth. This is
necessary because babies aged 0-12 months are at high risk of vitamin D deficiency, due to their rapid growth rates during this period.
2. Supplements that provide only vitamin D and are in a suitable form to be given to infants should be used to supplement infants in Ireland. The daily amount of vitamin D provided by such supplements should be 5µg per day.
3. Health professionals and parents need to be made aware that vitamin D deficiency is prevalent in Ireland, particularly among dark-skinned infants and young children.
Vitamin A is important for babies and young children, and some may not be getting enough.
It's needed for a healthy immune system, can help their vision in dim light, and keeps skin healthy.
Good sources of vitamin A include:
• dairy products
• fortified fat spreads
• carrots, sweet potatoes, swede and mangoes
• dark green vegetables, such as spinach, cabbage and broccoli
Vitamin C
Vitamin C is important for child's general health and immune
system. It can also help their body absorb iron.
Good sources of vitamin C include:
• oranges
• kiwi fruit
• strawberries
• broccoli
• tomatoes
• peppers
Calcium helps build strong bones as a child grows. Good sources include milk, cheese, yogurt, tofu, and calcium-fortified orange juice.
Iron builds muscle and is essential to healthy red blood cells. Iron deficiency is a risk in adolescence, especially for girls once they begin to menstruate. Good sources include beef and other red meats, turkey, pork, spinach, beans, and prunes.
Megavitamins - large doses of vitamins - aren't a good idea for children. The fat-soluble vitamins (vitamins A, D, E, and K) can be toxic if kids get too much of them. The same goes with iron.
For children and teens with highly selective diets, such as vegetarianism or a dairy-free diet, and for children with erratic eating patterns, you can recommend a daily supplement. Over-thecounter vitamin supplements are typically safe and come in chewable forms in case a child has difficulty swallowing.
Remember, however, that higherthan recommended dosages of supplements can cause problems. For example, giving high doses of vitamin C in hopes of preventing colds and the flu can cause a child to have nausea, diarrhea, and cramps.
Children’s vitamins and supplements may come in fun colours and shapes, but they are not candy. Make sure parents are able to communicate with their child that vitamins are a kind of medicine—not a snack. They should also always follow label instructions about serving size and dosage instructions.
Back2School - Allergies
Educating on Allergies
As summer comes to a close, there is always a lot to be done to get kids ready to go back to school.
As children re-integrate with their peers and continue with their lifelong learning, there is a critical role pharmacy teams can play in providing effective health education to help reduce the risk of illness and advance public health.
Providing customers with easy to navigate back-to-school sections in community pharmacy, with relevant point of sale and prominent window displays during August and September, will help remind parents and carers that preparation is key when it comes to the management of back-toschool self-treatable conditions.
In addition, many parents worry about whether they should keep their children at home or send them to school when they are ill. Pharmacy teams should be prepared to ask appropriate questions and offer advice to help them to make that decision. For example, does the child seem well enough to carry out the usual day-to-day activities they would at school, or is their condition serious or contagious enough to be passed on to classmates or teachers? Helping people to make such decisions will add to their self care skills and knowledge for managing coughs and colds.
Managing Allergies
The sun may still be out, and September historically sees some of our sunniest weather, so children will be out playing sports during school. This
increases the risk of not only sports-related injuries but also exposure to allergens.
Nasal allergy in children, if unrecognised or badly managed, can have a significant toll on emotional as well as physical well-being.
Kids allergies can leave sufferers incredibly troubled when it comes to getting through the school day.
Itchy eczematous skin, snuffly and irritable noses and wheezy chests, carry a significant burden of ill health. Dr Paul Carson of the Slievemore Clinic Ireland says, “If the nasal allergy is especially troublesome the child may get intermittent hearing loss. One day he’s bright and alert in class, inter-reacting and co-operating. Next day he seems distant and detached, ignoring questions or not fully grasping what’s going on. The teachers are at a loss to explain these variations in attentiveness and the boy’s parents can’t quite understand the situation either. It’s not uncommon for these children to be labelled ‘difficult’.
“Nasal allergy also provokes intense fatigue. If an affected child is not treated he misses out on ordinary children’s activities and can be isolated and ignored.
“The term Allergic Irritability Syndrome (ARS) has been coined to explain the many unpleasant symptoms and features children with untreated nasal allergy show.”
Children with un-recognised ARS have:
• A significantly impaired quality of life.
• Significant learning difficulties.
• A lower ability to achieve different types of knowledge (factual, conceptual and knowledge application) compared with healthy children.
• May cause impaired hearing if fluid collects in the inner ear (medical term: serous otitis media).
• Nasal blockage and irritation (sneezing, rubbing at the nose to relieve itch); dark circles around the eyes with puffiness of the lower lids.
• Poor concentration; disruptive behaviour and unexplained mood swings.
Below are the common effects of persisting nasal allergy in children.
Nasal Congestion
Sometimes a child’s nose is congested (obstructed) to the point that he or she breathes through the mouth, especially while sleeping.
If the congestion is left untreated this forces air currents through the mouth. The strength of the air changes the way the soft bones of the face grow. The features may become abnormally elongated in a pattern called ‘adenoidal face’. This causes the teeth to come in at an improper angle as well as creating an overbite. Braces or other dental treatments may be necessary to correct these problems.
Nasal allergy and ear infections
Nasal allergy can lead to inflammation in the ear and may cause fluid accumulation which in turn can trigger ear infections and decreased hearing. If this happens when the child is learning to talk, poor speech development may result. Hayfever can also cause earaches and ear itching, popping and fullness (‘stuffed up ears’).
Nasal allergy while at school
Nasal allergy can last throughout the school year. For some kids this means absences due to allergy flares. Here are some of
the problems to look out for so that the condition can be properly diagnosed and treated, as well as several suggestions for helping the allergic child.
• Dust irritation: reducing dust in the home will be helpful to most allergic family members. At school, children with allergy problems should sit away from the blackboards to avoid irritation from chalk dust.
• School pets: furry animals in school may cause problems for allergic children. If your child has more problems while at school, it could be the class pet.
• Asthma and physical education: sports are a big part of the school day. Having asthma does not mean eliminating these activities. Often medication administered by using an inhaler is prescribed before exercise to control their symptoms. Children with asthma and other allergic diseases should be able to participate in any sport the child chooses – provided the doctor’s advice is followed.
• Dry air: with the onset of cold weather using a humidifier to accompany forced air heating systems may be helpful in some regions of the country. Adding a small amount of moisture to dry air makes breathing easier for most people. However, care should be taken not to allow the humidity above 40%, which promotes the growth of dust mites and mould.
• Change in behaviour: children cannot always vocalise their annoying or painful symptoms. Their discomfort may manifest as behaviour problems. Be on the alert for possible allergies if your child has bouts of irritability, temper tantrums or decreased ability to concentrate in school. These may be signs of ‘allergic irritability syndrome’ caused by nose and ear symptoms in allergic children. Sometimes allergic children are badly behaved and have short attention spans. Needless to say their schoolwork suffers. When a child’s allergies are properly treated, his symptoms, behaviour and school performance can improve dramatically.
FAST RELIEF OF ALLERGIES 24hr
Cetrine Allergy 10mg Film-Coated Tablets available in packs of 7s and 30s. Always read the leaflet.
Composition(s): Each tablet contains 10 mg cetirizine dihydrochloride. One ml of the oral solution contains 1 mg cetirizine dihydrochloride. Description(s): White, oblong lm-coated tablets, scored on one side. Can be divided into equal halves. Clear, colourless liquid with banana avour.
Indication(s): Tablets: Adults and paediatric patients 6 years and above. Oral solution: Adults and children 2 years and above. Relief of nasal and ocular symptoms of seasonal and perennial allergic rhinitis (hay fever); relief of symptoms of chronic idiopathic urticaria.
Dosage: Tablets: Adults, elderly and children aged 12 years and over: 10 mg once daily. Children from 6 years to 12 years: 5 mg (half a tablet) twice daily. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. Children under 6 years: Not recommended. Oral solution: Children aged from 2 to 6 years: 2.5 mg twice daily (2.5 ml oral solution twice daily (half a measuring spoon twice daily)). Children aged from 6 to 12 years: 5 mg twice daily (5 ml oral solution (a full measuring spoon twice daily)). Adults and adolescents over 12 years of age: 10 mg once daily (10 ml oral solution (2 full measuring spoons)). Not recommended in children aged less than 2 years. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. In paediatric patients su ering from renal impairment: Adjust dose on an individual basis taking into account the renal clearance of the patient, his age and his body weight. Contraindications: History of hypersensitivity to the active substance, to any of the excipients, piperazine derivatives or hydroxyzine. Severe renal impairment < 10 ml/min creatinine clearance.
Warnings and Precautions for Use: Cetirizine may increase risk of urinary retention, therefore caution in patients with predisposition factors of urinary retention (e.g. spinal cord lesion, prostatic hyperplasia). Caution in epileptic patients and patients at risk of convulsions. Discontinue use of cetirizine three days before allergy testing. Pruritis and/or urticaria may occur when cetirizine is stopped, even if the symptoms were not present before treatment initiation. In some cases, the symptoms may be intense and may require treatment to be restarted. The symptoms should resolve when the treatment is restarted. Tablets contain lactose. Oral solution contains sorbitol, propylene glycol, sodium (essentially ‘sodium free’), methyl - & propyl-parahydroxybenzoate.
Interactions: Caution is advised when taken concomitantly with alcohol or other CNS depressants. Cetirizine does not potentiate the e ect of alcohol (0.5 g/l blood levels). The extent of absorption of cetirizine is not reduced with food, although the rate of absorption is decreased.
Pregnancy and Lactation: Caution during pregnancy and breast-feeding.
Ability to Drive and Use Machinery: Usually non-sedative, patients should take their response to the product into account. In sensitive patients, concurrent use with alcohol or other CNS depressants may cause additional reductions in alertness and impairment of performance.
Undesirable E ects: Cetirizine at the recommended dosage has minor adverse e ects on the CNS, including somnolence, fatigue, dizziness and headache. In some cases, paradoxical CNS stimulation has been reported. Although cetirizine is a selective antagonist of peripheral H1-receptors and is relatively free of anticholinergic activity, isolated cases of micturition di culty, eye accommodation disorders and dry mouth have been reported. Instances of abnormal hepatic function with elevated hepatic enzymes accompanied by elevated bilirubin have been reported which resolves on discontinuation of the drug. Uncommon: Agitation, diarrhoea, pruritus, rash, asthenia, malaise, paraesthesia. See SPC for all adverse reactions.
Marketing Authorisation Number: PA0711/075/002-003. Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription.
Date of Preparation: March 2021
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
Back2School - Pain in Children
Pain in Children
It can be a challenge to recognise the symptoms of pain in children. Are they really hurting, or are is the parent overreacting? Pain is a highly individual and complex experience. Here we take a look at reading the symptoms of pain in children.
Symptoms of Pain in Babies
Unlike with older children, crying isn't always a reliable pain indicator in babies. That's because crying is a baby's way of expressing a whole host of needs. Here are signs that a baby may be in pain.
Changes in crying patterns. A baby's distressed cry sometimes, but not always, sounds different from ordinary crying. Changes in a baby's behavior can also be a tip-off. For example, crying that can't be soothed with a bottle, diaper change, or cuddling could signal pain. Also, a calm baby who becomes unusually fussy could be in pain.
Crying while nursing. The baby who cries while nursing could very well have a painful ear infection. Prolonged, intense crying, often at the same time each day. This behavior is common with colic. It often starts at the age of 2
weeks, peaks at 6 weeks, and then gradually declines.
Crying and drawing the legs up to the abdomen. The baby could have colic or a serious medical condition.
Withdrawing. Chronic pain can sap a baby's energy, causing him or her to become still, quiet, and to avoid eye contact.
Symptoms of Pain in Toddlers
Fortunately, at this age, children in pain can talk. They will often also clutch the part that hurts. Pulling or rubbing the ear is common in toddlers and although it can sometimes indicate ear pain, it may be habit. Suspect an ear infection if the child has had cold symptoms or a fever and begins to tug at the ear suddenly.
Symptoms of Pain in Children and Adolescents
Chronic or recurrent pain is common in children and adolescents. Research has shown
that as many as 30% to 40% complain of pain at least once a week.
Acute abdominal pain. Pain that comes on suddenly can be caused by viral infections or by something more serious like appendicitis. If a child’s pain seems to be localised to the right of the belly button and is accompanied by nausea, vomiting, and desire to stay very still, they should be evaluated for appendicitis.
Recurrent stomach aches and headaches. A stomach ache that goes away after a bowel movement could signal a problem with constipation or, less often, inflammatory bowel disease. Daily abdominal pain without nausea, vomiting, or diarrhea could be a special form of migraine, or could fall under the category of chronic recurrent abdominal pain, a common but frustrating complaint in children.
Communicating with and involving children in taking their medications will have a significant impact on their adherence. Children take responsibility for their medications at different ages. Children are often not present when their parents collect their medications from the pharmacy and, therefore, this prevents them from receiving support and advice from community pharmacists so ensure parents are well educated on the symptoms, medications and side effects.
Communication
• Check parents understand what the medication is for and supplement knowledge if needed;
• Ensure parents are aware of the most common adverse effects and what to do if these occur;
• Explain what to do if their child misses a dose;
• Explain anything relevant to the particular medication (e.g. to take phenoxymethylpenicillin on an empty stomach);
• Check parents understand how to administer the medication to their child;
Discomfort during a febrile illness is often due to associated
pain; e.g. myalgia, sore throat, headache. Ibuprofen and paracetamol may be considered to improve comfort (with accompanying improvements in feeding activity and irritability), because they may also provide relief from pain and may reduce the risk of dehydration. They should be used to make the child more comfortable and not used routinely with the sole aim of reducing the temperature. The use of antipyretic medication and attention to the fever must not detract from monitoring the child’s activity and level of consciousness (as an indicator of worsening illness) and paying attention to adequate hydration.
Both paracetamol and ibuprofen are safe and effective for shortterm use in children. The practices of combining or alternating paracetamol and ibuprofen have limited value and are not recommended. Dose of antipyretic medication in children should be accurately based on body weight and should not merely be estimated. For accurate dosing, liquid medicines should be administered with a syringe. The use of NSAIDs has been associated with an elevated risk of severe skin and soft-tissue infections in patients with varicella zoster virus infection. Therefore, paracetamol is recommended as the antipyretic of choice in children with chicken pox. Medicines containing combinations of NSAID(s), paracetamol, codeine and/or antihistamines should not be used in children.
Nonpharmacological measures can be used as an adjunct therapy in the management of pain in both adults and children. Nonpharmacological strategies such as physical and psychological comfort measures are useful in conjunction with pharmacological options to help lower levels of anxiety, distress and pain. Some physical comfort measures include the use of massage or heat and/or cold compresses, applying pressure or vibration and repositioning. Psychological comfort measures include use of imagery, distraction and relaxation techniques.
Back2School - Asthma
Back to School Checklist for Children with Asthma
Asthma is the most common chronic condition among children, affecting 1 in 10 children and adolescents under 18. Children with the condition miss on average five days of school each year, making it one of the leading causes of absenteeism.
There is a dramatic rise in the number of children admitted to hospital for their asthma in September each year known as the “September spike”. Triggers which are commonly found in schools include:
• Chemical fumes
• Perfumes
• Aerosols
• Chalk dust
In addition, changes in weather, an increase in fungal spores, moulds and in an increase in circulating viruses such as RSV all contribute to an increase in asthma symptoms at this time of year.
Advice for parents:
This checklist should help you control your child’s asthma during September and into the winter months.
• Have your child’s asthma reviewed by your GP in August/ September
• Ensure your child has an Asthma Action Plan and it is up to date
• Use the inhaler technique videos on asthma.ie to help your child take their inhaler properly
• Make sure your child carries their reliever inhaler (usually blue) at all times
Written by Ruth Morrow, Respiratory Nurse Specialist, Asthma Society of Ireland
Asthma Policy for Schools
The Asthma Society of Ireland recommends that all schools have an Asthma Policy in place that is reviewed regularly. As part of their Asthma Policy, it is also recommends that schools create an asthma record sheet for all students with asthma. The Asthma Society is warning teachers to be vigilant for asthma triggers at this dangerous time of year and to talk to parents to ensure you are aware of any students with asthma in your class.
Students with Asthma – advice for teachers
Once you know what triggers the child’s asthma, you can take practical steps to reduce their impact.
• Damp dust chalkboard and classrooms regularly to get rid of dust mites and pollen
• Don’t keep furry or feathery pets in the classroom.
• Try to avoid fumes in science and art classes.
• Rigorously enforce a nonsmoking policy on school grounds.
• Check that they take their medication every day with a fridge planner
• Leave a spare reliever inhaler and spacer in the school, with their name clearly labelled
• If your child is participating in PE or other activities, place a reliever inhaler and spacer in their bag
• Never send a sick child to school
• Show them how to wash their hands correctly and explain why this is important
• An older child/teenager often require extra supervision and cannot be relied on to selfmedicate independently - put systems in place as they may avoid taking their medication
• Visit the school and make sure your child’s teacher is aware that they have asthma
• Explain what their triggers are and what to do if your child has an asthma attack
• Check if there is a School Asthma Policy in place
• If your child is starting a new school, speak to teachers about your child’s asthma, even if they are well right now
When a student with asthma joins your class, there are a number of steps can be taken to ensure they are supported as much as possible which include:
• Familiarise yourself with the school’s Asthma Policy
• Always ensure that students with asthma have access to their reliever inhaler including during school trips, sports and PE. Relievers should never be locked away.
• Tell parents when their child has an attack or needs their reliever inhaler in school and encourage older students to tell you or another staff member if they use their reliever.
• Speak to parents about concerns over missed days, tiredness in class due to night-time symptoms or lack of concentration due to asthma. Students with severe or poorly controlled asthma may require extra support due to missed school days.
• Monitor students with asthma to ensure they don’t feel excluded or experience bullying.
• Provide opportunities for all students to learn about asthma in class.
• Think about requesting resources from the Asthma Society of Ireland to ensure the school is well informed about asthma and how to manage the condition.
• Make sure the school is cleaned regularly.
• Heating and ventilation systems should be well maintained.
• Air classrooms to avoid mould and condensation.
• Avoid plants that give off high amounts of pollen
• Use non-latex gloves.
• Make sure that play areas and sports fields are free of autumn leaves as they are full of mould and fungal spores.
• Avoid mowing sports fields or grassy areas during school hours.
• Make sure changing rooms and bathrooms are well ventilated.
• Avoid opening windows and allow students with pollen allergies to stay indoors when pollen is high, such as during and after thunderstorms.
P.E. and Sports
Exercise improves lung function and is an important part of a healthy lifestyle. Asthma symptoms shouldn't stop children from taking part in sport and PE, provided that certain precautions are taken.
This article has addressed managing asthma in schools at a time of year when asthma can be increasingly problematic. Strategies for children, parents and teachers were discussed.
For pharmacists only
Helping patients forget the itchy rash of chicken pox...
skin conditions. It now also can be used to relieve the itchy rash of chicken pox - helping little ones get back to being themselves again.
Product Information
Piriton 4mg Tablets (Chlorphenamine maleate) Indications: Symptomatic control of allergic conditions Also, for symptomatic relief of itch associated with chicken pox Dosage and method of administration: Minimum dosing interval 4 hours Adults and children 12 years and over: 1 tablet every 4 - 6 hours (maximum of 6 tablets in 24 hours) Elderly: 1 tablet every 4 - 6 hours (maximum of 3 tablets in 24 hours) Children 6 - 12 years: 0 1mg/kg or 1/2 a tablet every 4 - 6 hours (maximum of 6 half tablets in 24 hours) Children under 6 years: Not recommended Do not use for more than 2 weeks without consulting a doctor Contraindications: Hypersensitivity to ingredients Pre-coma states Patients who have been on MAOI therapy within previous 14 days Precautions: May act as cerebral stimulant in children and adults, or hepatic impairment, epilepsy, severe hypertension and cardiovascular disease, raised intra-ocular pressure, prostatic hypertrophy, bronchitis, thyrotoxicosis, operate machinery Avoid alcohol and seek advice before using concurrently with sedative drugs Avoid in elderly with confusion Should not be used with other antihistamine containing products Contains lactose Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine Sedation, somnolence, disturbance in attention, abnormal coordination, dizziness, headache, blurred vision, nausea, dry mouth, vomiting, abdominal pain, diarrhoea, dyspepsia, fatigue, chest tightness, blood dyscrasias, hepatitis including jaundice, allergic reactions including anaphylaxis, angioedema, anorexia Legal category: Pharmacy Only Product Authorisation Number: PA 0678/080/001 Marketing Authorisation Holder: Haleon Ireland Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland Full product information is available in the SPC Additional information is available upon request Text prepared: June 2023
Trade marks are owned by or licensed to the Haleon group of companies
Back2School - Dental Health
Scoring High in Dental Health
Tooth decay is a common disease affecting up to 90% of children worldwide and remains the single most common disease of childhood. It impacts on quality of life and can be the reason for thousands of children needing dental treatment under general anaesthetic in hospital.
However, it can easily be prevented by good oral health habits such as brushing teeth regularly with toothpaste that contains fluoride and cutting down on sugary food and drinks. If left undisturbed, the unhelpful bacteria in the mouth- which cause decay- multiply and stick to the surfaces of teeth producing a sticky film. Then when sugar is eaten or drank, the bad bacteria in the film make acid resulting in tooth decay.
Children are losing crucial days of their education each year due to rotting teeth, as well as suffering pain, sleepless nights and missing out on doing the things they enjoy the most - which is being a child!
Promoting oral health in the early years is essential to protecting young teeth and establishing good habits. Children need to form good oral habits from an early age to help avoid tooth decay.
There are three main themes in good dental health:
• Limit frequency of and keep sugary and acidic food and drinks to mealtimes
• Brush teeth at least twice a day with a fluoride toothpaste
Written by Dr Madelaine Jackson, Dentist, New Life Teeth
@DoctorMadelaine
• Visit the dentist regularly
If appropriate measures are applied early enough, it is possible to prevent dental disease.
Dental caries
Enamel is made up of calcium and phosphorus minerals. When the mouth becomes too acidic, it begins to pull these minerals out of the teeth. This process is called ‘demineralisation’. Tooth demineralisation is caused by acids excreted by bacteria as a product of their metabolism of sugar or acidic foods. A diet high in sugars supports an acidic environment promoting demineralisation of dental enamel; if this continues deeper into the tooth it can eventually lead to a cavity (dental caries).
Saliva acts as a natural buffer; it contains calcium and phosphorus and bathes our teeth to replace these lost minerals. This process is called ‘remineralisation’. Early cavities that are just beginning to form can be reversed through remineralisation.
Onset of dental caries
By the age of 12 months, infants begin to establish an oral environment that places them at risk of dental caries. Breastfeeding up to 12 months of age is associated with a decreased risk of tooth decay, whilst prolonged bottle feeding, can provide an oral environment ideal for decay producing bacteria to proliferate. Streptococcus mutans, implicated as the principal bacteria responsible for the initiation of dental caries, is acquired by infants primarily from their mother.
Fluoride
Fluoride acts to bring calcium and phosphate ions together, making the teeth resistant to demineralisation, at the same time enhancing enamel remineralisation.
Topical fluoride in toothpastes, mouthwash and professionally applied varnish are highly effective in increasing resistance of children’s teeth to dental caries.
Special care needs
Children with special care may have special dental needs. They have a higher susceptibility to gum disease, dental caries, and oral trauma. Extra care and support must be taken to
prevent dental caries, infection, and other problems among these children.
Promoting good oral care at home
Oral health and nutrition are essential for the proper growth and development of children. Parents and caregivers often receive little guidance about oral health care and prevention, including fluoride and nutrition.
To promote good oral health in infancy caregivers should provide the correct amounts of fluoride alongside a healthy diet. It important to limit amount and frequency of sugary foods and drinks and avoid sugar-containing foods and drinks at bedtime when saliva flow is reduced, and buffering capacity is reduced.
To reduce the incidence of dental caries, parents and other caregivers should be educated about proper feeding practices during infancy and the preschool years. Preventative oral strategies and education should begin with the mother before birth and continue throughout infancy and childhood. Support mothers who breastfeed, to do so exclusively for the first 6 months, breastfed babies experience less tooth decay. For parents and carers feeding babies by bottle only breastmilk, formula or cooled boiled water should be given in a bottle. Babies should be introduced to drinking from a free flow cup at 6 months of age and bottles discouraged from 1 year. Specific recommendations include elimination of a bottle in bed, early use of soft bristled toothbrushes with parental supervision and limitation of sugar after the teeth have been brushed.
Toothbrushing should begin when the first tooth erupts, with a soft bristled toothbrush and a tiny amount of fluoride toothpaste. Brush last thing at night and one other time of day. Children 3-6 years should apply a pea size amount. Toothbrushing should be supervised until at least 7 years of age. Each child should attend the dentist by no later than 12 months of age.
In early infancy 0-6 months, although the teeth have yet to erupt, the teeth and jaw are developing rapidly. Thumb sucking and pacifiers may cause problems with tooth alignment and jaw development at this stage.
Future and new possibilities include xylitol wipes, antibacterial against streptococcus mutans, tested for cleaning babies’ gums and erupting teeth, show some promise as an intervention in preventing caries.
Finally, there are still some inconsistencies and grey areas to be resolved in defining, labelling, and marketing ‘no added sugar’ food and drinks, containing concentrated amounts of natural and free sugars that adversely impact children’s’ teeth.
step by step
Jordan Step by Step
Children have different needs as they grow older. Step by Step is a unique kids range that follows the children's development and offers tailored design with different features to make brushing easy and effective at every age. The handle, head size, bristles and design are all tailor made to help you establish good dental care habits from the first tooth. Choose the one that fits your child.
Back2School - Injuries
Checklist on Injuries
With the return to school looming, now is the perfect time for an important check on first aid in schools. Trips, falls and slips in school are only natural and some of the most common injuries we see come from the playground.
Sports-related injuries will also be common and so ensure your pharmacy is stocked with a ready supply of external analgesics and hot and cold treatments. First aid is easy to learn, easy to remember and easy to do. Pharmacists have the opportunity not only to demonstrate how easy first aid is, but also to advocate for the public to learn more themselves.
Cuts, scrapes, and bruises are among the most common injuries, and no family member is safe from minor accidents. Fortunately, these injuries usually can be treated at home without a doctor visit. Pharmacists need to be able to advise patients on how to treat these injuries if medical attention is not necessary, as well as to counsel patients as to when they should seek medical attention.
Scrapes (or abrasions) are wounds in which layers of skin are scraped or torn. The most common sites for scrapes are the hands, elbows, and knees. These injuries often are the result of a fall. Although the scrapes may ooze blood, bleeding does not always occur. Objects
penetrating the skin cause cuts (or lacerations). Depending on the depth, cuts often will bleed.
Bruises are the result of hard contact with a person or an object. The impact causes an injury to the tissue beneath the skin, and blood from the injury settles near the skin. Bruises usually start out looking red, then within a few hours turn blue or purple, and finally appear yellow as they fade.
Treating Cuts and Scrapes
Minor scrapes and cuts are easily treated at home with basic wound-care or first-aid supplies. Because cuts can happen at any time, every home should have tweezers, gauze pads, bandages, and antibiotic ointment.
Here are some steps that pharmacists should tell patients to follow in treating cuts at home:
• Rinse a cut with cool water
• Wash around the cut with soap; avoid getting soap into the wound
• Remove dirt and debris from the wound with tweezers; clean the tweezers with rubbing alcohol before using them
• Apply direct pressure with a clean gauze pad to a bleeding cut
• Treat the cut with antibiotic ointment
• Cover the cut with a bandage (deeper cuts may require a butterfly bandage)
• Do not pick at a scab while a cut is healing
Treating Bruises
Although bruises can be painful, treatment is limited. The best care for bruises involves rest and ice. Ice stops blood flow to the injury site, thus limiting the size of the bruise. Rest allows the site to heal.
Here are some further guidelines for patients for treating bruises at home:
• Apply ice packs or cold compresses as soon as possible
• Reapply ice packs every hour for 10-15 minutes during the first day, if needed
• With bruised legs or feet, elevate the legs as much as possible during the first day
• Take acetaminophen, if needed, for pain; do not take aspirin
• With large bruises, limit activity during the first day
• Use heat packs after 48 hours to promote healing
Here are some signs that bruises need medical attention:
• The bruise swells
• The bruise does not start to fade within a week
• The bruise occurs easily or for no obvious reason
Burns and scalds
A burn is caused by dry heat, such as fire or an iron, while a scald is caused by wet heat, such as boiling water.
Treatment and advice
• Remove any clothing or jewellery near the burnt area of skin, but not if it is stuck to the skin
• Cool the burn with cool running water for 20-30 minutes – don’t use ice, iced water or creams
• After cooling the burn, cover it with a layer of cling film
• Recommend an analgesic
• Raise the affected area to reduce swelling.
When to refer
• Large burns bigger than the size of the patient’s hand
• Deep burns
• Any burn on the face, neck, hands, feet, joints or genitals
• All chemical and electrical burns
• Any sign of shock
• Children under 10 years of age
• Anyone with a medical condition, such as heart, lung or liver disease, or diabetes
• Anyone with a compromised immune system.
Vivio Junior Masterclass
Vivio Junior Held held their fussy eating Masterclass with Clinical Nutritionist Eva Hamilton and Fussy Eating Expert/ Celebrity Chef Louise Lennox in the Exploruim in Dublin.
The evening was a huge success and had a variety of 40 guests such as journalists from Irish country Magazine, influencers like Rosalind Lipsett and parents.
Both Eva and Louise explained tips and tricks to help fussy eaters with:
• Practical strategies to encourage adventurous eating habits.
• Creative ways to introduce new foods.
• Tips for maintaining a positive mealtime environment.
• Expert advice on understanding and addressing picky eating behavior.
• As well as the importance of including a multivitamin and probiotic into children’s diet. Each guest got their very own goodie bag with our Vivio products as well as family pass for the Exploruim in Dublin. The event was a huge success and had lots of positive engagement online.
Eva Hill Hamilton and Louise Lennox
Jessica Mattimoe Sandra Niland with Sarah Ussher
Caitriona Eves and Joyce Mcdonagh Roz Lipsett
My First Skincare Routine: Preparing Young Skin for the School Year Ahead
As the summer winds down and the buzz of the back-to-school season picks up, young people and their parents are gearing up for the year ahead with new routines and fresh starts. Among the essentials for a successful school year is the foundation of a good skincare routine, especially important during the teenage years. This is where Bare Addiction steps in as the ideal ally for young skin, offering a blend of the best of nature and science that makes it a standout choice for pharmacies to feature in their back-to-school displays.
Understanding Young Skin’s Needs
Teenage skin is particularly prone to hormonal changes that can lead to increased oil production and breakouts. It's a critical time to establish a skincare routine that is not only effective but also gentle enough to cater to young, sensitive skin. Bare Addiction’s product line is crafted with this delicate balance in mind, ensuring that each product supports the skin's natural barrier while tackling common concerns like acne, oiliness, and sensitivity.
Why Choose Bare Addiction for a First Skincare Routine?
The inception of a first skincare routine is a pivotal moment for many young people, symbolising a step towards independence and self-care. Bare Addiction offers an accessible, straightforward approach to skincare that demystifies the often overwhelming array of choices in the skincare aisle. Our products are free from harsh chemicals like SLSs, parabens, and irritating alcohols, which are often found in more aggressive acne treatments that can strip and damage young skin.
Back to School with Bare Addiction
As students prepare to return to school, they seek confidence and comfort in their own skin. Bare Addiction's routines are designed to be simple yet effective, perfect for busy school mornings. Products like the Daily Foaming Gel Cleanser and the Daily Defence Moisturiser SPF30 provide a quick, effective routine that keeps skin clear and protected throughout the school day. The inclusion of SPF in our day moisturiser is particularly crucial for young people in Ireland, where despite the climate, UV protection is essential year-round. It also has a blue light guard, which helps protect young skin from exposure to artificial light from screens.
The Bare Addiction for Pharmacies
For pharmacies, offering Bare Addiction is more than just selling products; it’s about guiding young customers and their parents towards establishing a lifelong healthy skin routine. Stocking Bare Addiction aligns your pharmacy with a brand that values efficacy, safety, and
environmental consciousness. Our packaging is eco-friendly, using materials such as postconsumer recycled plastics, which appeals to the growing market of environmentally aware consumers.
Bare Addiction stands out in the skincare market with its dedication to young skin health, making it an ideal choice for anyone's first skincare routine. Developed by award-winning dermatologists, our products are formulated with a high percentage of natural ingredients, ensuring safety and efficacy.
Designedtoprovide a complete introduction to essential skincare, the Bare Addiction trial kit also serves as a compact, travel-friendly companion to maintain a consistent skincare regimenanywhere.
Bare Addiction strikes the perfect balance between nature and science, creating effective, safe, and naturally-based skincare tailored for the challenges faced by tweens, teens, and young adults. Here’s what sets Bare Addiction apart:
• Nature Meets Science: Emphasises the combination of natural ingredients with scientifically-proven actives for gentle yet effective skincare.
• Expert Formulation: Developed by renowned cosmetic scientists and dermatologists in London, ensuring top-quality and effective formulations.
• Ethical and Sustainable Practices: Commitment
to ethical sourcing and environmental consciousness, utilising Post-Consumer Recycled (PCR) plastic and aiming for fully recyclable packaging.
• Focused on Young Skin: Products specifically designed to tackle the core concerns of young skin, such as acne and sensitivity, without harsh chemicals.
• Safe and Clean: Free from irritating elements, drying alcohols, essential oils, phthalates, SLSs, and parabens.
• Community and Well-being: 10% of profits supports mental health initiatives, reflecting a commitment to the well-being of young users.
• Cruelty-Free and Vegan: No animal testing and vegan friendly formulations.
Bare Addiction is proudly distributed in Ireland by BR Healthcare. For more information on the Bare Addiction range please contact your local BR Healthcare representative or our office on 01-885 0800.
West Coast: Tanya Marum / tanya.marum@brmark.ie / 0860331614
East Coast: Bernadette Denning / bdenning@brmark.ie / 0861278639
before use with any other medication. Antacids may interact with certain medications. Patients with renal or hepatic impairment should consult a physician before using Pepcid Duo Chewable Tablets. In case of renal failure, monitoring of serum magnesium and calcium should be undertaken. Pepcid Duo is contraindicated in patients with severe renal failure. As some serious underlying conditions can have symptoms in common with simple indigestion, it is recommended patients seek medical advice in case of: indigestion symptoms accompanied by unintentional weight loss, difficulty swallowing, persistent abdominal discomfort, heartburn occurring for the first
AUTHOR: Fergal Garvey MPharm, MPSI
Fergal Garvey graduated with a first-class honours degree in Pharmacy from Queen’s University, Belfast in 2009. Following successful completion of pre-registration training in Northern Ireland, Fergal joined Bradlon Pharmacy Group in Drogheda where he has worked for almost 15 years. To date in his career, Fergal has worked as support pharmacist, supervising pharmacist and superintendent pharmacist for the group, and has supported dispensary colleagues in their training. His passion in pharmacy is to improve patient outcomes through health promotion and education.
60 Second Summary
• Gastro-oesophageal reflux disease (GORD) is often a chronic condition involving the reflux of gastric contents back into the oesophagus, causing symptoms of heartburn and regurgitation.
• The incidence of GORD is increasing, with 25% of people reporting heartburn once a month, 12% at least once per week and 5% with daily symptoms.
Pharmacy Management of Gastro-oesophageal Reflux Disease CPD
• Genetics and lifestyle factors such as pregnancy, smoking, obesity, and diet are all involved in the development of GORD, the main mechanism being inappropriate relaxation of the lower oesophageal sphincter.
• GORD causes a variety of oesophageal and extraoesophageal symptoms, and important complications such as stricture, haemorrhage, Barrett’s oesophagus, and carcinoma.
• The aim of treatment is to relieve the symptoms of GORD and reduce the risk of recurrence and associated complications of GORD.
• Initial management of GORD involves lifestyle modifications and OTC medications including alginates and proton pump inhibitors (PPIs).
• Current guidelines advise a “treat first, endoscope later” approach.
• Following endoscopy, GORD can be classified as either: endoscopy negative reflux disease (ENRD) - when a person has symptoms of GORD but the endoscopy is normal, or reflux oesophagitis – where there is evidence of inflammation and mucosal erosions.
• Further investigation is reserved for patients who fail to respond to acid suppression, rapidly relapse on stopping therapy or have alarm features.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
Introduction
The occasional reflux of stomach contents into the oesophagus is a normal physiological occurrence, which relates to the transient relaxation of the lower oesophageal sphincter and gives us the ability to belch.1 Small volumes of ingested food and gastric acid may pass into the oesophagus when this occurs and is not usually a cause for concern. However, when the reflux of stomach contents is persistent, or causes troublesome symptoms and/or complications for the patient, it is known as gastro-oesophageal reflux disease (GORD).2
Epidemiology
GORD was originally thought to be a problem of the western world, with the prevalence of GORD in Europe estimated to be between 8% and 26%.3 A review of symptoms in the community indicates that 25% of people in western populations report having GORD symptoms at least once a month, 12% report symptoms at least once weekly, and 5% describe daily GORD symptoms.4 However, this trend is now occurring worldwide, with a recent systematic review estimating that 1.03 billion people suffer from the condition globally,5 linking it to the obesity epidemic and an ageing population.6
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
by HPN.
can be downloaded from
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
The exact relationship between age and prevalence of reflux symptoms is unclear, but there is evidence that prevalence increases with age.7 Interestingly, studies have shown that although there is a slightly higher prevalence of GORD in women, men are more likely to experience complications of GORD (e.g. Barrett’s Oesophagus or Oesophageal cancer).8
Prevalence has also been found to be higher in smokers, nonsteroidal anti-inflammatory drug (NSAID)/aspirin users and patients with a raised BMI.9
Clinical features
The typical clinical symptoms of GORD are heartburn and regurgitation. Heartburn is a burning sensation in the chest, which is usually intermittent, and can be exacerbated by eating, bending, or lying down. GORD can also present with a variety of atypical symptoms such as dysphagia (difficulty swallowing); odynophagia (painful swallow); belching; epigastric pain; water brash (excessive salivation in the mouth caused by the presence of acid); and nausea.10 Patients with GORD may also experience extra-oesophageal symptoms such as chronic cough; nonatopic asthma; halitosis (bad breath); dental erosions; laryngitis; and hoarseness.2,11,12
Symptoms of GORD can have a significant negative impact on patient well-being and quality of life, through reduced enjoyment of food and physical activities involving bending, such as gardening or sport. Sleep disturbance can also occur, affecting concentration at work and resulting in reduced productivity. GORD has a significant economic burden globally, with studies estimating the cost to be approximately £760m per year in the UK alone.5
Complications of GORD
Extra-Oesophageal symptoms: GORD is a common noninfectious contributor to bronchitis, non-atopic asthma, laryngitis, hoarseness, and pneumonia.14 Due to the sensitivity of the lungs, pharynx and larynx to acid and their slow healing, traditional management of extraoesophageal GORD involved treatment with high dose proton pump inhibitors (PPIs) for prolonged periods. However, recent studies have cast doubt on the benefit of long-term, high-dose acid suppression in these patients.15
Oesophageal strictures: Oesophageal strictures occur in approximately 0.1% of cases and are associated with white males, increasing age, and a long history of GORD.16 There is good evidence
that sustained acid suppression reduces the need for repeated dilatations of the stricture.17
Oesophageal ulcers: Reflux commonly causes superficial erosions of the oesophagus, however a small percentage of these progress to deeper ulceration involving the muscular layers of the oesophagus. Oesophageal ulcers have a prevalence of approximately 0.05% and are also associated with white males and increasing age.16
Haemorrhage: Erosive oesophagitis has been implicated as a cause of bleeding in patients with GORD.18 Although it has been proposed that oesophagitis may be responsible for a significant percentage of upper gastrointestinal (GI) bleeding cases,19 bleeding from erosive oesophagitis is a relatively uncommon cause for acute presentation to the hospital, but rather is more likely to present as chronic iron deficiency anaemia.20
Barrett’s oesophagus: Barrett’s oesophagus occurs in response to prolonged GORD where the normal squamous cells of the oesophagus undergo metaplasia to columnar cells which resemble the intestinal mucosa. Approximately 10–15% of patients who have GORD will go on to develop Barrett’s oesophagus, however it is uncommon in those younger than 50 years old.21 Barrett’s oesophagus increases the risk of oesophageal adenocarcinoma.
Oesophageal adenocarcinoma: Since the 1980s the incidence of oesophageal adenocarcinoma has increased sixfold and is one of the most rapidly increasing cancers in the Western world.22 It is estimated that 1–10% of those diagnosed with Barrett’s oesophagus will go on to develop oesophageal adenocarcinoma within 10–20 years.23
Aetiology
The cause of GORD is likely multifactorial, encompassing a range of genetic, lifestyle and/or environmental factors.
Genetics: Genetic factors possibly contribute 18-31% to the cause of GORD,24 with evidence that reflux symptoms often affect members of the same family.5 Identical twins have been found to have a higher concordance of GORD symptoms than that of non-identical twins.26
Lifestyle: Lifestyle factors also contribute to GORD. Obesity, especially central adiposity, independent of BMI has been linked to higher incidences of GORD and related complications such as Barrett’s oesophagus and oesophageal adenocarcinoma.27 This is likely due to increased intra-abdominal pressure and mechanical pressure on the diaphragm increasing transient relaxation of the sphincter and increasing the risk of developing a hiatus hernia. Poor posture, tight fitting clothing and pregnancy can
also cause GORD due to these increased pressures.
Smoking, alcohol, caffeine, chocolate, and spicy foods can reduce the tone of the gastrooesophageal sphincter.28 Eating fatty foods can also delay gastric emptying, leading to GORD.29
Environmental: The relationship between Helicobacter pylori (H. pylori) infection and GORD is complex and not yet fully elucidated. Some studies indicate that there is a negative correlation between patients who are H. pylori-positive and GORD.30 The hypothesis is that atrophic gastritis associated with H. pylori infection can reduce gastric acid secretion and offer protection against GORD. However, other review articles state that concomitant infection with H. pylori does not alter symptom severity or treatment efficacy in those with GORD symptoms.31 Due to the strong association between H. pylori infection, peptic ulcer disease and gastric adenocarcinoma, guidance continues to recommend eradication of H. pylori whenever present.32
Medication-induced: Medicines that can cause GORD, or make the symptoms worse, include alpha-blockers, anticholinergics, benzodiazepines, beta-agonists, beta blockers, bisphosphonates, calcium channel blockers, corticosteroids, nitrates, nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives and tricyclic antidepressants.32
Pathophysiology
The pathophysiology of GORD is multifactorial, involving transient lower oesophageal sphincter relaxations and lower oesophageal sphincter pressure abnormalities. Other associated factors include hiatal hernia, impaired oesophageal clearance, delayed gastric emptying and impaired mucosal defence mechanisms. Together, these lead to the reflux of stomach acid, bile, pepsin, and pancreatic enzymes, resulting in oesophageal mucosal injury.23
GORD can be subdivided into:
Reflux oesophagitis: these patients will suffer from typical reflux symptoms, such as acid
regurgitation and heartburn. Those with reflux oesophagitis often respond well to acid suppression and show healing of mucosal erosions.22
Endoscopy-negative reflux disease (ENRD): ENRD is the most common manifestation of GORD and shows no evidence of injury to the oesophageal mucosa. Patients often have severe and atypical symptoms, and an incomplete response to acidsuppressing drugs.22
The role of the community pharmacist
Community pharmacists often provide the first point of easily accessible contact for patients and are well-placed to offer initial and ongoing help for people suffering with symptoms of GORD. This involves offering lifestyle advice, using appropriate OTC medication; highlighting prescribed medications that may be an issue,33 and advice about when to refer to GP.
History taking
GORD can often be diagnosed using the symptoms described by the patient alone and therefore, a detailed history should be obtained from the patient.2 Information gathered should cover pain location, frequency, severity, timing (day or night) and duration of symptoms, as well as any specific triggers (e.g. food, on bending or lying down), and medicines that they take.
When to refer
When questioning patients with GORD symptoms it is important to recognise signs and symptoms that may require referral to their GP. Red-flag symptoms include:
• >55 years of age with unexplained treatment-resistant GORD for more than 4 weeks duration.
• Pain described as severe, debilitating or wakes the patient in the night.
• Progressive difficulty swallowing
• Persistent vomiting
• Progressive unintentional weight loss
• Jaundice
• GI bleeding (haematemesis and/ or melena)
• Iron deficiency anaemia
Fig 1. Common symptoms of GORD13
* If symptoms recur after successful treatment, advise patient to step down PPI therapy to the lowest
dose to control symptoms, or promote the 'as needed' use of PPIs instead.
These red flag symptoms may be signs of serious pathologies e.g.: upper GI malignancy, peptic ulcer disease, coeliac disease, pancreatitis, inflammatory bowel disease and coronary artery disease.22
Initial management of GORD Lifestyle advice
Simple lifestyle measures can aid symptom control.23 Smoking cessation, drinking less alcohol, and weight-loss have all been shown to help. In fact, a decrease in BMI as little as 3.5 kg/m2 leads
to a nearly 40% reduction in risk of GORD, even among women with a normal BMI.34
Other lifestyle modifications that can be advised include reducing caffeine intake, having small, regular meals, taking regular exercise, and avoiding eating in the three-to-four hours before bed. GORD patients may report a trigger for symptoms such as spicy foods, citrus fruits, tomatoes, onions, chocolate and fizzy drinks. Therefore, keeping a food diary with avoidance of trigger foods may be beneficial.35
GORD symptoms can also be managed by raising the head of the bed by around 10-20cm.23 This can be achieved by placing blocks under the head of the bed or by placing a wedge underneath the mattress. Additional pillows should not be used as this tends to compress the stomach, worsening symptoms.32
There is an association between anxiety and GORD.23 Therefore, a discussion on stress and anxiety levels can be useful along with the encouragement of relaxation strategies.
Fig 2. Management algorithm for patients with GORD. Adapted from NICE guideline [CG184]32
Medicines known to cause or exacerbate symptoms of GORD should be reviewed, reduced, and discontinued if appropriate. This will require an appropriate consultation between the patient and GP.
OTC management
Initial management of GORD can often be achieved with antacids and/or alginates; however, longterm, continuous use of these is not recommended.33 Antacids and alginates can affect the absorption of other medications and therefore they should not be taken within one to two hours of other medicines.36
Antacids: Antacids work by neutralising the stomach acid. Their efficacy depends on the metal salt used in its composition. Sodium and potassium salts are highly soluble which make them fast acting, but with a short duration of action. Magnesium and aluminium salts have a slower onset and longer duration of action, whereas calcium salts are fast acting but also have a prolonged duration of action.37 It should be noted that calcium and aluminium salts may cause constipation and magnesium salts can cause diarrhoea.38 They are best given after food as gastric emptying is delayed in the presence of food, giving the antacid more time to work. Antacid therapy should ideally not be continued beyond 2 weeks. If symptoms have not resolved, another product should be tried, or patients should be referred to their GP.
Alginates: Alginate preparations, on contact with gastric acid, form a viscous matrix barrier over gastric contents and prevent reflux of stomach contents. They demonstrate superior symptom control to antacids. They are best given after each meal and at bedtime, or on an as-required basis.39
Proton Pump Inhibitors (PPIs): PPIs decrease acid secretion in the stomach by blocking the H+/ K+ ATPase enzyme (proton pump) within the parietal cells of the stomach. This enzyme is the final step of acid secretion into the stomach.
44 CPD: GORD
Patients with persisting symptoms of GORD, in the absence of red flag symptoms, should be started on a four-week trial of a PPI once daily as a way of confirming the diagnosis.32 PPIs should be taken 30 minutes before food, to provide optimal control of gastric pH. Acid suppression with a PPI provides effective relief of symptoms for most patients with GORD. The recommended doses of PPIs for the management of GORD are detailed in Table 1 below.
According to The Medicines Management Programme,40 pantoprazole is the preferred PPI for the management of GORD. This is due to the favourable adverse drug reaction and drug interaction profiles of pantoprazole. Pantoprazole also has a favourable cost profile in both available strengths.
NICE Guidance32 suggests that people with GORD should be offered
• A full-dose PPI for 4 weeks (or 8 weeks if they have endoscopyproven severe oesophagitis).
• If symptoms recur after successful treatment, patients should be advised to step down PPI therapy to the lowest daily dose to control symptoms. ‘Asneeded’ use of PPIs should also be discussed.
• If there is an inadequate response to a PPI, a H2 receptor antagonist (H2RA) may be offered instead (Fig. 2).
Contraindications and cautions
of PPIs
PPIs are often well tolerated, with a relatively low incidence of side-effects during short term use. Adverse effects may include headache, diarrhoea, nausea, vomiting, abdominal pain, constipation, and dizziness. Very rarely PPIs can cause subacute cutaneous lupus erythematosus, severe cutaneous adverse reactions, liver dysfunction and blood dyscrasias.33
Long term suppression of gastric acidity has been linked to the reduced absorption of vitamins and minerals. As a result, PPIs should be prescribed with caution to those at risk of hypomagnesaemia (i.e. patients already receiving digoxin and/ or diuretics) and magnesium concentrations monitored. Patients at risk of osteoporotic fracture (e.g. post-menopausal women) should be advised to maintain adequate intake of calcium and vitamin D as long term use of PPIs is associated with an increased risk of fracture, especially when used in high doses for over a year. The reduced acidity of the stomach caused by PPIs permits bacterial colonisation of the upper GI tract and can lead to Clostridium difficile (C. difficile) infection, which can be particularly harmful in clinically vulnerable patients. Rebound acid hypersecretion may occur on stopping PPIs, resulting in an increase in reflux symptoms. To reduce this risk, PPI therapy should be tapered to a lower dose and then taken as required. Patients should be counselled about the risk and advised to manage symptoms with antacid and/or alginate use.40
To minimise the risk of sideeffects associated with long-term PPI use, prescribers should only prescribe PPIs when indicated, at the lowest possible dose, and for the minimum duration of time.41 Patients who require long-term PPI therapy, should be reviewed on an annual basis at a minimum.41
Patients with red flag symptoms should not be prescribed PPIs before endoscopy, as PPIs may mask the symptoms of upper GI malignancy. If the patient is currently taking a PPI and subsequently needs endoscopy, the PPI should be stopped at least two weeks before the procedure.23
Interactions
PPIs have possible interactions with a range of medications.33 These include, but are not limited to:
• Clopidogrel: omeprazole and esomeprazole can significantly reduce the antiplatelet effect of clopidogrel, and they should be avoided. Pantoprazole and rabeprazole have lowest risk.
• Citalopram and escitalopram: omeprazole or esomeprazole can lead to higher levels of citalopram and escitalopram. Dose may need to be adjusted.
• Digoxin: may cause small rise in serum digoxin levels.
• Warfarin: Monitor International normalised ratio as PPIs can enhance warfarin effects.
• Methotrexate: excretion possibly reduced leading to increased risk of toxicity.
H2 Receptor Antagonists (H2RAs)
H2RAs reversibly bind to histamine (H2) receptors on gastric parietal cells, acting as a competitive
antagonist, thereby decreasing gastric acid secretion.42 They can be used as needed for heartburn/ GORD or taken prophylactically 30-60 minutes before known triggers, or if taken once daily, at night is best.42
Further Management of GORD If reflux symptoms fail to respond to full dose acid suppression or symptoms rapidly relapse on stopping treatment, investigations should be carried out to confirm the diagnosis of GORD.32 H.pylori testing should be considered in patients who have no red-flag symptoms, and have failed to respond to lifestyle changes, antacids and a four-week trial of PPI therapy. Other diagnostic tests performed in secondary care include upper GI endoscopy, barium swallow and ambulatory pH monitoring.
Surgery may be used in the management of medicationresistant GORD and for those unable to tolerate PPIs. The most common surgical procedure is the Nissen fundoplication, which involves wrapping a portion of the gastric fundus around the lower oesophagus. However, approximately 50% of patients managed by surgery, report the use of PPIs at 5-10 years' followup. Consequently, long term medical therapy with PPIs may be more cost effective.43
Special considerations: GORD in pregnancy
Heartburn in pregnancy is common and triggered by hormonal changes, the enlarged uterus causing increased intraabdominal pressure, and relaxing of the lower oesophageal sphincter. Complications are rare due to the short-term nature of reflux, which usually resolves after giving birth.44
Diet and lifestyle changes along with the use of antacids/alginates should be recommended as first line. However, if a woman is taking iron supplements, antacids will interfere with their absorption, and therefore the antacid should be taken two hours before or after the iron supplement.33
Women whose GORD remains uncontrolled despite these measures may be prescribed acid suppression with PPIs. Omeprazole is clinically appropriate for pregnant women with severe or complicated reflux disease.33
References available on request
*Off-label dose for GORD
*Off-label dose for GORD
According to The Medicines Management Programme40, pantoprazole is the preferred PPI for the management of GORD. This is due to the favourable adverse drug reaction and drug interaction profiles of pantoprazole. Pantoprazole also has a favourable cost profile in both available strengths.
Table 1. PPI doses for management of GORD
Table 1. PPI doses for management of GORD.
Customer Service Training in Pharmacy
So, what is customer service? It is providing assisting and advising a customer. Everybody does this in a pharmacy setting. What is good customer service? It is when you leave an amazing lasting impression on a customer and hope they tell all their friends. How can we provide this? Read on!
How to sell with confidence and lead with integrity and value
So firstly confidence. Do you know the product ranges inside out? If not start reading the information leaflets contained on the pack or go to the medicines.ie website and have a look at two of the medicines leaflets per day until you feel confident about selling products. I remember I felt out of my depth when I started working in a pharmacy, so many medications interact with over the counter products and it is important to sell the correct item. If in ANY doubt always check with a pharmacist and don’t wing it!
Secondly integrity and value. So maybe a customer has a medical card and you know they have recently become unemployed. It is important to give the customer the best product at the best price. Maybe you have been taking Vitamin D (I have!) and have worked out what Vitamin D product is the best value for money. It is okay to pass this onto a customer. EVERYONE likes to feel they have come out with a great deal after leaving a shop.
As a manager in a shop the first thing to do is to look at your staff. Are they happy? Are they willing to go the extra mile for the customer? All of us have troubles. Are your staff able to put their worries aside and give the best customer service all day every day? Your manager can’t mend a broken heart or fix a money issue. They can give you a bit of leeway but to practice good customer service means that YOU are responsible for your own mood.
Written by Jean Dunphy, Allcare Cara Pharmacy, Dun Laoighaire
So, it is a Monday morning. The kids didn’t get up in time because you didn’t set your alarm correctly. It is lashing rain and you are running late. You come into the workplace late and you are in fowl form. You are in the negative mode. You walk in and talk about the morning to your colleagues. You bring your colleagues down by doing so. The first customer of the day comes in. Do you think that you are going to be able to give them a good customer experience in this mood?
Now the same scenario, rain, late for work, kids didn’t make it to school on time and you walk into the workplace. But this time you leave your mood at the door. You apologise for being late. You laugh and you start your day. What will be that customers experience be like if you put your feelings about the morning to the back of your mind?
So, someone is in the shop! You are halfway there. Now how to approach them. Do you smile at them from afar? Do you approach them and ask them if they need help? So, nobody is going to see you smile. You must approach the customer. I personally don’t like being approached as soon as I enter a shop. Let the customer browse the shelves for a minute. Hover nearby fixing a shelf and smile. It won’t work. Instead of saying “HI there can I help you”, try saying “Hi there, how are you”. Yes, it is a small difference. It is not rude, it is not too pushy, you are letting a person know you are there if they need you.
You are busy putting stock on shelves, you have been told that the shop needs to be date checked and you don’t have time to approach customers, you have too many boxes to put out on the shelves. NO!!!! You make time for each customer, you should make the time to approach them.
So, they approach you. You ACTIVELY listen to their question. What is active listening? It is hearing what they are saying. It is comprehending their need. It is fulfilling the need. And maybe going beyond their need.
In a pharmacy setting you see someone approach you. You say
heh there how are you, they tell you their son has a cold. You ask them the age of the child. You sell them a product with pseudoephedrine. Say thanks and complete the transaction. The customer leaves.
Now is this going to be a memorable visit for the customer? No! Will they come back to the shop? Maybe. Now go back. A customer enters a shop, their son has a cold. You actively listen to the customer using the 2WHAM method. What are their symptoms, what medications have been tried already, how long symptoms have been present etc. By actively listening you concentrate on what is being said by the customer. Saying yes, hmmmn and nodding of your head indicate to the customer that you understand what they are being asked. By now you have a better idea of a product to sell. Which leads onto what is best for a customer. Maybe a product with pseudoephedrine isn’t suitable. How many products can you sell to the customer? Tissues, olbas oil, vicks vaporub, a cough bottle, strepsils, vitamin C, echinacea. The list of link sales with the Sudafed is endless.
Now how do you translate the link sale products with the main product. I say “I take vitamin C
every day”. By now the customer has built up a rapport and trusts you. By saying studies have shown that Vitamin C can boost your immune system can also influence the sale.
Now it is time to close the sale. A customer has been given a list of products and you have made the sale of Vitamin C. Great! But just before you take the money and give them their change, did you ever say to a customer “Is there anything else you need”? They can’t be rude back to this question I have never had anyone say how dare you ask me this. Sometimes it works and a customer buys a third item. You haven’t been pushy (Irish people don’t like that), you have just done your job to the best of your ability.
So, in the above scenario things worked out fine and the customer left satisfied. Another thing you can do is to ask the customer to let you know how it all went and this lets them know that you care about the customer and if there is anything else we can do give us a call or pop into the shop another day. If a customer is happy with the service they have been given they will be more likely to come back to you.
Let’s say there are 2 pharmacies on the street. They both sell the
same products for colds and flus and are the same price. There is a chance they will come back to you because they are happy with the service, they got from you the last time they were in. Maybe you seemed kind, knowledgeable and helpful. We need repeat business to sustain the company.
How to deal with the irate angry customer. But sometimes when people are ill, they take it out on you and sometimes no matter what advice you tell them or what you say they are still angry. So how to deal with them? I often think it says more about them as a person and you are just the person that they are taking it out on. I would love to tell you that it is okay to let the person leave, or throw them out of the shop, but it isn’t. Here are a few scenarios. Woman comes back demanding her money back on a product. She was told by another colleague that due to COVID that she wouldn’t be able to return the product. She chances her arm anyway and demands her money back. It has been three weeks ago, and she tells you that she hasn’t had a chance to come in until today. You check and the product – it has obviously been opened and tried. Firstly, you reiterate what your colleague said. She denies it but you remember a note in the diary about this woman the colleague was new and had left a message.
She knew there may be trouble ahead of time. Luckily in this instance there is a manager present.
She tells you to give the woman credit and she purchases other things. You feel a bit undermined.
HOWEVER do you know that for every bad customer service experience that a customer has they tell 7 people. For every good experience the customer tells no-one and for every excellent experience a person tells three people. And in the age of social media do you want your business slammed by this irate customer. NO!! The customer has left satisfied and although she was angry with you at the start, she has had her need met and leaves reasonably satisfied.
A customer comes to pay for a product and argues that the price on the shelf is ¤3 more than it should be, she has seen on the internet that it is a certain price. She acts very peculiar and is very sharp with you. She is angry from the start of the transaction and tells you that you don’t know your special offers and why the SEL is wrong. You are having a busy day and a member of staff is sick. You have a line of customers behind her. You check the Instagram post. The product is similar to the one shown in the Instagram post but not the same. She is also giving out about the cost of another product she is buying. You are having difficulty with this person and can feel yourself getting angry back at her.
She is speaking loudly and is making everyone wait. If you feel you can’t deal with her anymore, get another colleague to deal with her. It is okay to ask for help. It is
fine to go to another person and ask their advice and get them to deal with the angry customer. Sometimes when they perceive you as being incompetent the best thing to do is to get another person to deal with them. In this scenario the customer did get their ¤3 off the cost of the product. Again, remember the customer can tell 7 of their friends about their bad experience and that could be 7 people less that will walk into the shop.
Some extra tips on sales. Make sure to be informed on the latest services that the pharmacy is using. Mention to the customer about Covid vaccination programme. Let the person know that cholesterol testing is done. Tell them that we can deliver to their home.
Another trick is to come from behind the counter and hand a customer the link sale product. A customer is way more likely to buy a product if they feel the item and hold it.
Another thing to note is some people only want a box of paracetamol. They don’t want to be bombarded with take tissues, olbas oil and strepsils. Some people just want a product and leave. You can tell by body language. With these customers just let them come into the shop and leave, be polite and let them go back to the office after lunch, collect the children from school or whatever. Some people will be more receptive to information. That is fine too! You must use your own judgement with each person and decide
how to approach each of them. You must relate genuinely to the needs of others and use emotional intelligence and have genuine authentic empathy with people.
Dealing with change is the only thing that is constant. Who would have thought we would be dealing with a pandemic? Business models all over the world have had to adapt to the new normal.
EMPATHY
Show empathy for the customers plight. Emotions can be central to making decisions – they will feel heard and you will have information to help them.
MIRRORING
Not just copying what mannerisms on screen but take the last three words hey say and speak it back to them. When people hear the last 3 words, they day you are showing active listening and using words with empathy “It seems like” for example makes you seem more empathetic. Follow up with silence – let a customer talk and explain to you.
And just remember if you can keep most people happy most of the time, then you are doing a good job. You’ll never keep everyone happy all the time. Be kind, have empathy and showing you care about your customer are important to sustaining the business.
Credit to Hickeys Pharmacy, Virgin Cinemas and their Customer Service document; Alf Dunbar’s book - Just Looking Thanks! The Straight-Forward Guide to Creating Brilliant Customer Service
When Menopause gets Complicated
Background: As a person begins to experience ovarian hormone disruption (perimenopause) through to and beyond their final menstrual period (post menopause) they may be affected by a variety of symptoms.
The most commonly mentioned symptoms include vasomotor flushing and/or sweating, mood changes (low mood, irritability, feeling overwhelmed), joint aches & pains, fatigue, etc. Urogenital symptoms like vaginal dryness; which might in turn cause discomfort (particularly during exercise or intercourse) can be a problem at this time. Some (peri) menopausal people suffer a worsening in their pre-existing GU problems such as frequency of urination or more frequent UTI’s. These and the more than 50 additional complaints attributed to menopause may have a severe impact on the patients’ quality of life, conversely there are some lucky people who notice very little disruption at this time. It is very hard to predict who will have a rough time in menopause and who won’t but as clinicians we are trained to offer a sympathetic ear and try to help where we can.
For many decades offering menopause support in the form of Hormone Replacement Therapy (HRT) tablets was common practice. But, in 2002, after the publication of an editorial discussing early results of the Women’s Health Initiative (WHI) trial in the USA, concerns were raised about that trial’s use of equine estrogen tablets blended with the synthetic progestagen ‘medroxy provera acetate’ (MPA) and raised risk of breast cancer as well as thrombotic events including CVA and MI.
During the following 10-15 years many clinicians feared prescribing
HRT and a lot of patients weren’t too keen on having to use it. Demand fell, interest in training in menopause waned and patients were left with very few options. Things did slowly improve after the shock waves of the WHI subsided a little. It was known back then but subsequent studies have now affirmed that not all HRT is the same.
Concerns that were raised about the connection with HRT use and breast cancer were somewhat offset by analysis of the absolute risk vs the relative risk. The WHI data showed an increased risk of breast cancer diagnosis with use of oral equine estrogen +MPA HRT use in the order of 1.27. This is about the same risk attached to drinking 2 units of alcohol a day and much lower than the risk attached to being overweight/ obese. So this does not dismiss risk - there is an association - but helps put risk into perspective. Roehm E. A Reappraisal of Women's Health Initiative Estrogen-Alone Trial: Long-Term Outcomes in Women 50-59 Years of Age. Obstet Gynecol Int. 2015; 2015:713295. doi: 10.1155/2015/713295. Epub 2015 Jan 1. PMID: 25685151; PMCID: PMC4313058
Other information from more recent trials on HRT use and breast cancer risk data examined the effect of the choice of HRT progestagen on risk. It is thought that more modern, less androgenic progestagens particularly micronised progesterone and dydrogesterone, seem to have
Written by Dr Deirdre Lundy Specialist in Women’s Health and Menopause at The National Maternity Hospital
less of an impact on breast cancer risk than the powerful MPA used exclusively in the WHI study. Fournier A, Berrino F, ClavelChapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat. 2008;107(1):103-111. doi:10.1007/s10549-007-9523-x
Concerns we had about orally ingested estrogen (e.g. the COCP or oral HRT) do not appear to apply to the low dose, transdermal 17 beta estradiol - the type typically used in modern transdermal HRT. Orally administered estrogen affects the thrombin system and can increase the risk of VTE but modest doses of TD 17 beta estradiol have a neutral effect on clotting.
So in recent years, not only is the fear of HRT use abating, we are seeing the demand for menopause consultations and HRT products outstripping supply. Hamoda H, Panay N, Pedder H, Arya R, Savvas M. The British Menopause Society & Women’s Health Concern 2020 recommendations on hormone replacement therapy in menopausal women. Post Reprod Health. 2020;26(4):181-209. doi:10.1177/2053369120957514
This has been challenging. Clinicians have not always kept up their confidence surrounding menopause guidelines so may be worried about offering up to date advice. Even for general practitioners with expertise,
advising on menopause management options and prescribing HRT (and alternatives) is not really supported in primary care. There are no special considerations for what can be a lengthy and nuanced consultation and perhaps ‘first menopause/ perimenopause visit’ should be added to the chronic disease payment schedule. Added frustration for prescribers is ongoing as the demand for high quality TD estrogens and the more ‘breast friendly’ progestagens has been so high, many patients find that they cannot reliably access their HRT in Irish pharmacies. www.hse.ie/eng/about/who/cspd/ ncps/medicines-management/ guidance-on-shortages/mmpguidance-for-prescribers-on-hrtshortages-september-2022.pdf
Typical Menopause vs ‘Complex’ Menopause
When a person develops symptoms that may be attributable to (peri) menopause there are many well established therapies available. There is no single, best answer when it comes to maintaining wellbeing and improving symptoms in menopause, but the fact remains HRT has been proven most effective for vasomotor symptoms caused by hormonal fluctuations at this transitional time. Maclennan AH. Evidence-based review of therapies at the menopause. Int J Evid Based Health. 2009 Jun;7(2):112-23. doi: 10.1111/ j.1744-1609.2009.00133. x. PMID: 21631851
But what about prescribing HRT to people with underlying medical conditions? What are the rules?
Well, that’s a little tricky.
Research on (peri) menopause and HRT and their impact on serious medical conditions is staggeringly poor. We are only beginning to see female biological variables being taken into consideration as part of mainstream health research & pharmaceutical studies. Yakerson, A. Women in clinical trials: a review of policy development and health equity in the Canadian context. Int J Equity Health 18, 56 (2019). https://doi.org/10.1186/s12939019-0954-x
Studies on using HRT in groups of people with serious underlying
FOR HRT THAT IS AS INDIVIDUAL AS SHE IS
Oestrogel is indicated for:
Hormone replacement therapy (HRT) for oestrogen deficiency symptoms in postmenopausal women.2 Prevention of osteoporosis in postmenopausal women at high risk of future fractures who are intolerant of, or contraindicated for, other medicinal products approved for the prevention of osteoporosis.
BODY IDENTICAL HRT 2,3
Prescribing Information Oestrogel (estradiol) Pump-Pack. For full prescribing information, including side effects, precautions and contraindications, please consult the Summary of Product Characteristics (SPC). Presentation: Transdermal gel containing Estradiol as (hemihydrate) 0.06% w/w. Each pump actuation is 1.25 g of Oestrogel, which contains 0.75mg of Estradiol. This medicine contains 0.5 g alcohol (ethanol) in each dose of 1.25 g gel. Indication: 1: Hormone Replacement Therapy (HRT) for oestrogen deficiency symptoms in postmenopausal women. 2: Prevention of osteoporosis in postmenopausal women at high risk of future fractures who are intolerant of, or contraindicated for, other medicinal products approved for the prevention of osteoporosis. The experience treating women older than 65 years is limited. Dosage and Administration: Oestrogel is an oestrogen-only product to be administered daily on a continuous basis for women without a uterus. In women with an intact uterus, a progestogen should be added for at least 12 days each month. The pump pack will require priming before using a new pump pack for the first time. The first dose dispensed should be discarded. The gel should be applied to at least 750 cm2 of clean, dry, intact areas of skin (e.g. arms, shoulders, inner thighs). It should not be applied on or near the breasts or on the vulval region. The patient should apply the gel herself and avoid skin contact with others, particularly a male partner, for at least 1 hour after application. Patients should be informed that children should not come in contact with the area of the body where Oestrogel was applied on Menopausal and postmenopausal symptoms: The usual starting dose is 2 pumps (2.5 g containing 1.5 mg 17β-estradiol) once daily. If effective relief is not obtained after one month’s treatment, this may be increased to a maximum of 4 pumps (5 g containing 3.0 mg estradiol) daily. For initiation and continuation of treatment, the lowest effective dose for the shortest duration should be used. Prevention of postmenopausal osteoporosis: The minimum effective dose is 2.5 g Oestrogel once daily. For full details of usage please refer to the SPC. Contraindications: Hypersensitivity to estradiol or any of the excipients; known, past or suspected breast cancer; known or suspected oestrogen-dependent malignant tumours (e.g. endometrial cancer); undiagnosed genital bleeding; untreated endometrial hyperplasia; previous or current venous thromboembolism (deep vein thrombosis, pulmonary embolism), known thrombophilic disorders, active or recent arterial thromboembolic disease (e.g. angina, myocardial infarction); acute liver disease or history of liver disease whilst liver function tests are abnormal; porphyria. Warnings and Precautions: HRT should only be initiated for symptoms that adversely affect quality of life. The risks and benefits should be reviewed annually and HRT only continued as long as the benefit outweighs the risk. A personal and family medical history should be taken before initiating or reinstituting HRT. Periodic check-ups are recommended during treatment. Physical examination and investigations including appropriate imaging tools should be carried out according to the clinical needs of the patient. Patients should be closely supervised if any of the following conditions are present, have occurred previously and/or have been aggravated during pregnancy or previous hormone treatment since they may recur or be aggravated during treatment with Oestrogel: leiomyoma (uterine fibroids) or endometriosis; risk factors for thromboembolic disorders; risk factors for oestrogen-dependent tumours; hypertension; liver disorders; diabetes mellitus with or without vascular involvement; cholelithiasis; migraine or severe headache; systemic lupus erythematosus; history of endometrial hyperplasia; epilepsy; asthma and otosclerosis. Oestrogel should be discontinued if a contraindication is discovered or the following occur: jaundice or deterioration in liver function; significant increase in blood pressure; new onset of migraine-type headache; pregnancy. In women with an intact uterus the risk of endometrial hyperplasia and carcinoma is increased when oestrogens are administered for prolonged periods of time. Break through bleeding and spotting may occur during the first months of treatment but if they occur after some time on therapy or continue after treatment has been discontinued the reason should be investigated. Unopposed oestrogen stimulation may lead to premalignant or malignant transformation in the residual foci of endometriosis. Evidence shows an increased risk of breast cancer in women taking combined oestrogen-progestogen or oestrogen-only HRT that is dependent on the duration of taking HRT. HRT increases the density of mammographic images which may adversely affect the radiological detection of breast cancer. Evidence suggests a slight increased risk of ovarian cancer in women taking oestrogen-only or combined oestrogenprogestogen HRT. HRT is associated with a 1.3 to 3-fold risk of developing venous thromboembolism (i.e. deep vein thrombosis or pulmonary embolism) especially in the first year of use. HRT should be stopped 4 to 6 weeks prior to elective surgery if prolonged immobilisation is to follow. The benefit-risk of HRT should be considered in women already on chronic anticoagulant treatment. If venous thromboembolism occurs during treatment, HRT should be discontinued. Patients should contact their doctors immediately if they have potential thromboembolic symptoms (painful swelling of a leg, sudden chest pain or dyspnoea). Combined oestrogenprogestogen and oestrogen-only therapy are associated with up to a 1.5-fold increase in risk of ischaemic stroke. The risk increases with age. Care should be taken with women with cardiac or renal dysfunction since oestrogens may cause fluid retention. Women with pre-existing hypertriglyceridaemia should be followed closely during oestrogen replacement or HRT since pancreatitis can result from rare cases of large increases in plasma triglycerides. Oestrogens increase binding proteins such as thyroid, corticoid and sexhormone binding globulins leading to increased circulating hormones. There is some evidence of increased risk of probable dementia in women who start HRT after the age of 65. It may cause burning sensation on damaged skin. This product is flammable until dry. FOR THE FULL LIST OF WARNINGS AND PRECAUTIONS PLEASE CONSULT SECTION 4.4 OF THE FULL SPC. Interactions: Patients should avoid strong skin cleaners and detergents, skin products of high alcoholic content (e.g. astringents, sunscreens) and keratolytics which may alter the barrier structure or function of the skin. Also, any skin medication which alters skin production (e.g. cytotoxic drugs) should be avoided. The metabolism of oestrogens may be increased, (leading to a decreased effect and changes in the uterine bleeding profile) by enzyme-inducing products (e.g. phenobarbital, phenytoin, carbamazepine, rifampicin, rifabutin, nevirapine, efavirenz). Ritonavir, nelfinavir and St John’s wort may also induce the metabolism of oestrogens. As transdermal administration avoids the first pass effect in the liver, transdermally applied oestrogens may be less affected by enzyme inducers than oral hormones. Hormone contraceptives containing oestrogens shown to significantly decrease plasma concentrations of lamotrigine when co-administered. This may reduce seizure control. Pregnancy and breastfeeding: Oestrogel is not indicated in pregnancy or during breastfeeding. If pregnancy occurs during medication with Oestrogel, the treatment should be withdrawn immediately. Undesirable effects: The following commonly (≥1/100; ≤1/10) occur with HRT: headache, nausea, abdominal pain, breast swelling/ pain, breast enlargement, dysmenorrhoea, menorrhagia, metrorrhagia, leucorrhoea, endometrial hyperplasia, weight change (increase or decrease), water retention with peripheral oedema. The following uncommonly (≥1/1,000; <1/100) occur with HRT: depression, mood swings, vertigo, migraine, venous thromboembolic disease, flatulence, vomiting, pruritus, benign breast neoplasm, increased volume of uterine, leiomyoma, vaginitis/vaginal candidiasis, asthenia. The following risks apply in relation to systemic oestrogen/progestogen treatment: breast cancer; endometrial cancer; ovarian cancer; venous thromboembolism; coronary artery disease; ischaemic stroke. For further information on side effects and risk estimates, please consult the SPC. Overdose: Symptoms may include breast pain, nausea, and withdrawal bleeding. There are no specific antidotes and treatment should be symptomatic. Legal category: POM. Marketing Authorisation number: PA 1054/004/001. Marketing Authorisation Holder : Laboratoires Besins International, 3 rue du Bourg L’Abbé, 75003 Paris, France. Date of preparation of Prescribing Information: January 2024 OES/2024/002-ROI Further information is available upon request or in the SmPC.
Utrogestan 100mg is indicated for: Adjunctive use with oestrogen in post-menopausal women with an intact uterus, as hormone replacement therapy (HRT).3
Prescribing Information Utrogestan (micronised progesterone) 100 mg capsule, soft. For full product information, including side effects, precautions and contraindications, please consult the Summary of Product Characteristics (SmPC). Presentation: Each capsules contains 100 mg progesterone (micronised). Indication: adjunctive use with estrogen in post- menopausal women with an intact uterus, as hormone replacement therapy (HRT) Posology and method of administration: Recommended dose is 200 mg daily at bedtime for 12 days in the last half of each therapeutic cycle (beginning on Day 15 of the cycle and ending on Day 26). Withdrawal bleeding may occur in the following week. Alternatively, 100 mg can be given at bedtime from Day 1 to Day 25 of each therapeutic cycle, withdrawal bleeding being less with this treatment schedule. Dose for elderly is the same. Not indicated in the paediatric population. Oral capsules should not be taken with food. Contraindications: When used in conjunction with estrogens, Utrogestan should not be used in patients with the following conditions: known hypersensitivity to the active substances, soya lecithin, peanut or to any of the excipients, known past or suspected breast cancer; known or suspected estrogen-dependent malignant tumours (e.g genital tract carcinoma) undiagnosed genital bleeding; previous or current thromboembolism disorders (e.g. deep venous thrombosis, pulmonary embolism) or thrombophlebitis; known thrombophilic disorders; acute liver disease or history of liver disease as long as liver function tests have failed to return to normal; porphyria; cerebral haemorrhage; breast-feeding. Warnings and Precautions: For the treatment of postmenopausal symptoms, HRT should only be initiated for symptoms that adversely affect quality of life. Careful appraisal of the risks and benefits should be undertaken at least annually. Utrogestan is not suitable; in confirmed pregnancy; in the treatment of premature labour, or as a contraceptive. Before initiating or reinstituting HRT, a complete personal and family medical history should be taken. Women should be encouraged to be aware of their breasts and report any changes to their doctor or nurse. Investigations, including appropriate imaging tools, e.g. mammography, should be carried out in accordance with currently accepted screening practices, modified to the clinical needs of the individual. Patients with a current or any past history of the following should be closely supervised due to the possibility of recurrence or aggravation during treatment with Utrogestan; leiomyoma (uterine fibroids) or endometriosis; risk factors for thromboembolic disorders, risk factors for oestrogen dependent tumours (e.g. 1st degree heredity for breast cancer), hypertension, liver disorders (e.g. liver adenoma); diabetes mellitus with or without vascular involvement; cholelithiasis; migraine or severe headache; systemic lupus erythematosus; a history of endometrial hyperplasia; epilepsy; asthma; otosclerosis; depression; photosensitivity. Therapy should be immediately discontinued in case a contraindication is discovered and in the following situations: jaundice or deterioration in liver function, significant increase in blood pressure, new onset of migraine- type headache, pregnancy, sudden or gradual, partial or complete loss of vision; proptosis or diplopia, papilloedema, retinal vascular lesions. Evidence suggests an increased risk of breast cancer in women taking combined estrogen-progestogen and possibly also estrogen-only HRT, dependent on the duration of taking HRT. HRT, especially estrogen-progestogen combined treatment, increases the density of mammographic images which may adversely affect the radiological detection of breast cancer. Slightly Increased risk of ovarian cancer in women taking estrogen-only or combined estrogen- progestogen HRT, which becomes apparent within 5 years of use and diminishes over time after stopping. HRT is associated with a 1.3-3-fold risk of developing venous thromboembolism (VTE). The occurrence of such an event is more likely in the first year of HRT than later. If VTE develops after initiating therapy, the drug should be discontinued. Patients should be told to contact their doctors immediately when they are aware of a potential thromboembolic symptom. The relative risk of coronary artery disease during use of combined estrogen + progestogen HRT is slightly increased. Combined estrogen-progestogen and estrogen-only therapy are associated with an up to 1.5-fold increase in risk of ischaemic stroke. HRT use does not improve cognitive function. There is some evidence of increased risk of probable dementia in women who start using continuous combined or estrogen-only HRT after the age of 65. Utrogestan contain soybean lecithin and may cause hypersensitivity reactions (urticarial and anaphylactic shock in hypersensitive patients). There is a possible relationship between allergy to soya and peanut, patients with peanut allergy should avoid using Utrogestan. Interactions: Drugs known to induce the hepatic CYP450-3A4 (such as barbiturates, anti-epileptic agents (phenytoin, carbamazepine), rifampicin, phenylbutazone, bromocriptine, spironolactone, griseofulvin, some antibiotics (ampicillins, tetracyclines) and herbal products containing St. John’s wort, may increase metabolism and the elimination of progesterone. Ketokonazole and other inhibitors of CYP450-3A4 such as ritonavir and nelfinavir may increase bioavailability of progesterone. Utrogestan may raise the plasma concentration of ciclosporin, diazepam, tizanidine. Aminogluthethimide markedly reduces plasma concentrations of medroxyprogesterone acetate and megestrol. Progesterone may enhance or reduce the anticoagulant effect of coumarins. Progesterone antagonises the anticoagulant effect of phenindione. Use of ulipristal acetate may result in reduced efficacy of progesterone. An adjustment in anti-diabetic dosage may be required. Breakthrough bleeding may occur when using terbinafine with progesterone. Progesterone may also affect the laboratory tests of hepatic and/or endocrine functions. Pregnancy and lactation: If pregnancy occurs during medication, Utrogestan should be withdrawn immediately. Data relating to inadvertent foetal exposure to combinations of estrogens + progesterone indicate no teratogenic or foetotoxic effect. Prescription of progesterone beyond the first trimester may reveal gravidic cholestasis. Utrogestan is not indicated during breast-feeding. Progesterone is distributed into breast milk. Effects on ability to drive and use machines: Utrogestan may cause drowsiness and/or dizziness; therefore, care should be taken when driving or using machines. Undesirable effects: Frequency unknown; Primarily from oral administration of progesterone: abdominal pain, nausea, fatigue, headache, somnolence, dizziness, vaginal haemorrhage, pruritus. Following risks apply in relation to systemic oestrogen/progestogen treatment: breast cancer; endometrial cancer; ovarian cancer; venous thromboembolism; coronary artery disease; ischaemic stroke. Adverse reactions with systemic estrogen/progestogen treatment include: rash, urticaria, chloasma/melasma, pyrexia, insomnia, alopecia, irregular menstruation, amenorrhoea, breast pain/ mastodynia, fluid retention/oedema, weight changes, changes in libido, depression, gall bladder disease, probable dementia in over 65 years of age, skin and subcutaneous disorders (erythema multiforme, erythema nodosum, vascular purpura). Overdose: Symptoms may include drowsiness, somnolence, dizziness, or fatigue. Treatment of overdosage consists of discontinuation of Utrogestan together with institution of appropriate symptomatic and supportive care. Legal Category: POM Marketing Authorisation Number: PA 1054/003/001 Marketing Authorisation Holder: Laboratoires Besins International, 3 rue du bourg L’Abbé, 75003 Paris, France Date of Preparation: February 2024, UTO/2024/002-ROI Further information is available upon request or in the SmPC. Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Besins Healthcare (UK) Ltd, Drug Safety on 01- 4004466 or Email: pharmacovigilance@besins-healthcare.com References 1. Data on file (REF-OES-00104) Oestrogel is the N°1 global leader in transdermal estradiol products in volume. 2. Oestrogel Pump-Pack
50 Menopause
medical conditions are very few and far between. In the absence of actual data, experts look to see what (if any) impact menstruation, pregnancy and use of hormonal contraceptives might have on specific medical conditionsthen try to work out what impact menopausal changes and HRT use might be gleaned from this information. Not ideal and often unhelpful.
So what do we know about use of HRT for females with menopausal symptoms who have background medical issues? There are some guidelines when it comes to chronic manageable conditions as well as the more serious situations where if at all possible referral to a colleague with specific menopause training is advised. The British Menopause Society is generally regarded as the ‘go-to’ resource for up to date guidance and advice in Ireland. They have been enormously supportive of colleagues both in Britain and Ireland. www.bms.org.uk
They advise that expert advice should be sought in a variety of situations including women with complex medical backgrounds (such as women with breast cancer, personal history of venous thrombosis or personal history of stroke, ischemic heart disease, etc.).
Menopause itself is often triggered by medical intervention for serious disease and its treatments. People with female hormonesensitive cancers may undergo oophorectomy on medical advice which can cause sometimes very troublesome menopausal symptoms and if done before 40 yrs. of age could go on the undermine future health outcomes. ESHRE guideline group. ESHRE Guideline: management of women with premature ovarian insufficiency. Hum Reprod. 2016 May;31(5):926–37
Pelvic radiotherapy and certain forms of chemotherapy can cause temporary or even permanent ovarian failure. Anti-endocrine therapies are often prescribed for females with estrogen sensitive malignancies - most commonly but not exclusively, breast cancer. These medicines improve cancer outcomes but (depending on the patient) the side effects and the menopausal symptoms they can trigger disimprove quality of life and often limit compliance with the prescribed therapy. Meade E, et.al. Survivorship care for postmenopausal breast cancer
women in Ireland: What do women want? Eur J Oncol Nurs. 2017 Jun;28:69–76.
Being diagnosed with cancer when already using HRT may become a problem and oncologists might sometimes advise discontinuation of the HRT leading to a rapid return of menopausal symptoms.
Menopausal symptoms can be managed with hormonal, nonhormonal and non-pharmacological therapies. MHT is the most effective method of managing menopausal symptoms but may not be suitable for all after a cancer diagnosis as the role of hormone receptors in many types of cancer and their treatment may complicate the discussion about when MHT should or should not be used.
There is a growing list of therapies and medications that have been shown to be useful in relieving some of the symptoms of menopause for women who are either on anti- estrogen therapies or who have been advised to avoid standard HRT. The British Menopause Society offers guidelines on their “Tools for Clinicians” webpage. Interestingly one of the management options with the best range of meno symptoms relief is Cognitive Behavioural Therapy which has been shown to be effective over placebo in helping with vasomotor flushing and sweating, fatigue, weight gain, musculoskeletal (MSK) pain and sexual function
Franzoi MA, et al Evidence-based approaches for the management of side-effects of adjuvant endocrine therapy in patients with breast cancer. Lancet Oncol. 2021 July
but access to one on one CBT is limited and so some people may be directed to on online therapy and/ or smart phone apps to seek relief. Other strategies that have been shown to be helpful include:
- SSRI’s & SNRI’s which may help some people with vasomotor symptoms, mood and MSK issues
- Anticonvulsants like gabapentin may help with vasomotor flushing
- Antispasmodics like Oxybutynin can also help with both vasomotor flushing and urinary issues
- Antihistamines with sedating properties may help with sleep disruption
Other options that have shown benefit include yoga and acupuncture, gently physical activity and exercise and hypnosis. Franzoi MA, et al Evidence-based approaches for the management of side-effects of adjuvant endocrine therapy in patients with breast cancer
New medical therapies designed to reduce vasomotor flushing specifically for people with a breast cancer diagnosis are being launched to market in Europe in 2024. The root cause of VMS appears to be linked to heightened signalling of certain neurotransmitters (particularly neurokinin B & its receptor (neurokinin 3 & 4 receptors) - these affect the autonomic thermoregulatory pathway. A group of drugs known as the NK3R antagonists can block NK3R related VMS seemingly as
effectively as HRT. The Oasis 4 trial is helping to explore one of these NK antagonist drugs. They are recruiting here in Ireland at time of writing. https://findoasisnow.com/ gb-en/hcp
Applying the research
In our Complex Menopause Clinic at The National Maternity Hospital we aim to offer patients time to discuss the symptoms of menopause that are affecting people with comorbidities or a past diagnosis that might limit typical menopause options. This is a new service funded by the HSE’s National Infant and Women’s Health Program. We are one of six clinics operating around the republic of Ireland.
We try to validate the patients’ individual experience (as some people sadly seem to have been given little forewarning about what the menopausal effects of procedures and treatments for cancers). We explore lifestyle issues and offer support there where we can. We take them through the varied non-HRT strategies that could bring them some relief and allow them improve their QoL. We prescribe where appropriate and review them after 3 months to see if there is any improvement - if they are still struggling we try something else. Some of our patients never really regain their optimal QoL- some we barely help at all I worry - but most patients have expressed a gratitude for having been given a safe space to be listened to, to discuss their symptoms and worries and to be offered treatments wherever we have them.
Pharmacy Report Card on Men’s Health
During International Men's Health Week 2024, everyone was, once again, being asked to ‘Know Your Numbers’ - but, this time, these are numbers that could save your life.
Men’s Health Week (Monday 10th June to Sunday 16th June 2024) offered an ideal opportunity to raise awareness of preventable health problems, support men and boys to live healthier lives, and encourage them to seek help or treatment at an early stage. The platform provides the perfect time for everyone to commit to simple, practical and realistic actions to improve their health and live a longer life.
Ireland’s Pharmacists are encouraging men and boys to take time this week to inform themselves about their health. The Irish Pharmacy Union (IPU) is advising men to visit their local pharmacy for advice and support on measuring and improving health and wellbeing.
Sinead McCool the IPU’s Head of Professional Services said, “Men often shy away from discussing their health or undergoing regular checkups. Certain metrics can provide a key indication of a man’s health, such as blood pressure, weight, BMI, heart rate and cholesterol. This Men’s Health Week we are encouraging men to ‘know their numbers’ and learn vital health information to plan for a healthy future.
“Many pharmacies nationwide can provide blood pressure checks, heart rate checks and measure BMI. A quick visit to your pharmacy can help to inform all men about their health and raise certain issues. Pharmacies can also provide advice on managing health such as smoking cessation, weight loss and managing stress.
“Pharmacy staff are also experienced at advising men about their health needs, which can happen in a discrete and private manner.
This could be the difference between a problem being identified early and actionable or only after a serious problem arises.
“We want all men to understand that ignoring concerns and problems is not necessary. Getting regular checks and dealing with problems as early as possible is the best step any of us can take. Pharmacies can function as a first point of contact between men and the health service and we encourage all men to do so this week.” Concluded Ms McCool.
The Irish Pharmacy Union encouraged men to use the convenience of their local pharmacy during Men’s Health Week 2024.
Men's Health Week this year focused upon three types of numbers:
Statistics on the state of men's health that policy makers and service providers need to know if they are to address the issues facing men and boys.
Key numbers that men, themselves, need to know, to take control over some elements of their own health.
Contact numbers for help and support services that everyone needs to know at times of difficulty or crisis.
To support and inform the week, the Men’s Health Forum in Ireland launched a number of new publications:
Two ‘Men’s Health Report Cards’ - one focusing upon the Republic of Ireland and one upon Northern Ireland. These shine a light upon the ‘big picture’ of men’s health on the island of Ireland, and offer easy-to-understand key statistics in an infographic format.
A ‘Do You Know Your Numbers’ z-card for men themselves, which highlights a range of key numbers that all men need to be aware of in relation to their personal health.
Colin Fowler, Director of Operations for the Men’s Health Forum in Ireland said, “The statistics in the Report Cards provide some cause for optimism, along with some grounds for concern. So, there is still room for improvement.
“The four main causes of death among local males continue to be neoplasms, circulatory system diseases, respiratory system diseases, and external causes of injury and poisoning. That said, it is important to note that death rates from these have often been reduced due to factors such as the adoption of healthier lifestyles, the uptake of screening programmes, better diagnostic tools, improvements in health literacy and help seeking behaviours, availability of support services, and more effective treatments.
“Yet, excessive alcohol use remains high. Too many males are overweight. The number of males diagnosed with gonorrhoea has increased. Many boys under-achieve in education. At the same time, the mortality rate for all invasive cancers (excluding NMSC) has fallen and the survival rate has increased. There are fewer male smokers. The number of male suicides has fallen. Healthy life expectancy for males has increased.”
Yet, overall, the numbers show that local men suffer a disproportionate burden of ill health and:
They continue to die younger than women do.
Poor lifestyles (including smoking, drinking, diet and lack of physical activity) are responsible for a large proportion of chronic diseases.
Males have higher death rates than women for almost all of the leading causes of death, and at all ages.
Men’s mental health needs are often under the radar and remain unmet.
Late presentation to health services can lead to a number of problems becoming untreatable in the future.
But this is not a lost cause, and much can be done to change this situation. To support men, an updated ‘Action Man’ Manual has been produced - in both hard copy and as an online download.
Finian Murray, Senior Health Promotion and Improvement Officer in the HSE, and one of the authors of the Man Manual, explains, “The ten top tips put men into the driving seat, and give them the tools and DIY instructions to make positive changes - if they choose to be their own ‘Action Man’. It starts with a clear warning: reading this booklet could seriously improve your health. During Men’s Health Week 2024, everyone is being asked to ‘Know Your Numbers’ because men’s health counts.”
First line prescribed treatments for Osteoporosis To treat or not to treat this Silent Killer
Written by Michele O’Brien, CEO of the Irish Osteoporosis Society and Professor Moira O’Brien, Osteoporosis Consultant, Affidea Dundrum, Dublin
You could ask many people who treat patients with Osteoporosis/ Osteopenia what they think should be the first line to treat those with bone loss and they would all give different answers. Every patient should be individually assessed to see which is the most appropriate treatment for them, as there are so many causes of this Silent disease. If you asked who should be treated for bone loss you will also get different answers. Those who want to be proactive about their bone health are now being discouraged. Most people who have experienced fragility fractures, or watched their loved ones suffer horrendously from untreated bone loss, are much more proactive about their bone health.
Have you ever heard of people being discouraged of ensuring that they do not develop or have a disease that has no signs or symptoms, that is known worldwide as the “Silent Killer” and is preventable in most people?
Have you ever heard of a patient under 60 with cancer not be given a first round, never mind a second round of Chemotherapy or Radiation, or not referred for a bone scan to screen for cancer due to the horrendous side effects from these treatments or radiation exposure?
The answer we would assume is NO. Why? It would be considered by many to be unethical. With bone loss, not to treat a person with a treatable disease, leaves them at risk of becoming disfigured, loss of their independence and dying prematurely. Like all medications the long term use of them legally have to be monitored and those
who do not fit the typical older Osteoporosis patient profile should not be discarded and refused treatment, as this will increase their cortisol levels, which will further increase their fracture risk.
NOTE: Research shows that most fractures happen in the moderate to marked Osteopenia range, which is why the IOS (Irish Osteoporosis Society) still use these terms, as there is a significant difference in risk of fracture from a person having mild Osteopenia versus marked Osteopenia. Osteopenia is the early stage of osteoporosis, and a bone health plan should be initiated right away.
There are not many treatments for bone loss, but we all know the long term effects if a person is continually on steroids. This is why it is essential that no matter what age a person is (children are not included in this statement), they should be put on a bone health plan to prevent fractures occurring or recurring in the first place.
What we do know is that if we do not treat those with bone loss pre 60 years, these patients are at risk for the horrific secondary consequences of fractures, which lead to disfigurement, loss of independence and premature death. A woman in Ireland committed suicide and left a note saying that she could no longer live with the pain of multiple fractures. We are not a third world country, and no one should ever be placed in a position like this ever again.
A survey done last year by Athena pharmaceuticals of Irish men and women aged 40 to 90 years of age, found that 1 in 5 adults have
fractured a bone since turning 40 years of age. Over one third of those surveyed reported they had fragility fractures, and the rate of fragility fractures was highest among the 40–54-year-old age group, which would have been expected in the older age groups.
Vertebral wedge fractures result in a dowager’s hump, leaving a person disfigured and in pain and will significantly affect a person’s quality of life. Most lose the ability to be intimate with their partners, have low self-esteem, their ability to eat and drink can be affected, depending on how far forward their head is protruding, their ability to wash and dress themselves and actually live independently is taken away from them. It also leaves them at risk for mental health issues such as depression, anxiety and usually leads to isolation as they are embarrassed that they no longer look “normal”.
The significant damage to their vertebrae and rib cage, puts pressure on the intestines and bladder, leading to incontinence. The dowagers hump alters their centre of gravity, which places them at high risk of falling and encountering further fractures. They have difficulty buying clothing as their body shape has changed, and most women no longer can wear a bra. The rib cage is in contact with the pelvis; therefore, they have trouble reaching items higher than shoulder height or below hip level from kitchen cupboards etc.
We believe that not investigating and treating those under 60 who have had fragility fractures or are high risk for them, is playing “Russian roulette” with their lives, due to the secondary effects of fractures, many may not survive till 60 to be treated.
Unlike most treatments for other diseases, which people are taking to slow down the progression of the disease or to calm down the symptoms of the disease, Osteoporosis treatments have been proven to reduce fracture risk.
Those with a Dowager’s hump due to undiagnosed osteoporotic fractures are easily identifiable. It is those who have multiple risk factors for bone loss and undiagnosed bone loss who have not fractured yet, who should be
referred for DXA scans to prevent them ending up disfigured and a burden on the health system.
A person can look perfectly healthy on the outside and have severe bone loss on the inside and the most cost-efficient way of knowing, is by getting a base line DXA scan, which costs approximately ¤120. A misconception is that a DXA scan has very high amounts of radiation, when it has 10% radiation of a regular chest X-ray. If a person has flown from Dublin to New York, they will have been exposed to more radiation than having a DXA scan done.
Bone markers are a way of checking to see how much bone is being lost and how much bone is being formed, however these tests are not cheap, and many GPS do not have access to request them, which is why a DXA scan, which is the world standard for measuring bone density should be one of the tools used to screen and diagnose people.
Considering 50% of women and 25% of men will develop bone loss, there should be a screening programme in Ireland for women and access for men at high risk to fracture, but it should not be based on age. It should be based on clinical judgment by the treating physician/s. We are all aware that women over 65 are the highest risk group for bone loss, due to having smaller bones and having gone through the menopause, however more men die from the complications of Osteoporotic fractures than develop prostate cancer.
There are some individuals who believe that due to the limited number of prescribed treatments for bone loss, treatment initiation to prevent fractures should not be initiated in younger age groups, unless they have had multiple fractures. Lately a prescription for vitamin D appears to be the most common treatment they are offered. The issue with this is, that sadly many of them will possibly end up in agony, lose their independence and not actually survive to be put on an Osteoporosis treatment.
Bone loss occurs leading up to the menopause, during the menopause, and significant bone
Michele O’Brien Professor Moira O’Brien
loss can occur up to ten years post menopause. In an ideal world, every woman should have a DXA scan when they start to lose their periods heading into the menopause. This way if it shows the person already has lost bone, they can be put on a bone health plan, to build up their bone strength to help protect themselves, whilst going through the menopause. If they have good bone density, a plan can be put in place to help prevent bone loss.
NOTE: This type of strategy could save our health service a fortune long term as the cost of treating fractures in Ireland (those diagnosed) are shocking. The inpatient cost of just treating hip fractures in Ireland from 2014 to 2020 was ¤296 million and its rising.
Some women lose up to 30% of the overall bone in their body, when going through the menopause. This is why if a person has risk factors for bone loss, no matter what age, they should be referred for a DXA scan, as prevention is much cheaper and less painful, than treating fractures. It would be prudent to think about a national screening programme for women, similar to breast check considering 1 in 2 women will develop this Silent killer. 1 in 7 women will get breast cancer and all women are offered this screening service. Women have smaller bones and experience more changes in hormone levels, especially following menopause which is why they are more at risk than men.
Mammograms contain a similar amount of radiation as DXA scans, yet no one is talking about cancelling the National Breast Screening programme. The HSE initiated a DXA scan referral for GP’s, which should be encouraged, as DXA scanning is the world standard for screening/ diagnosing bone loss. With breast cancer, thankfully in many cases, symptoms such as lumps etc develop, but with Osteoporosis, there are no signs or symptoms until the person fractures.
Osteoporosis is one of the commonest diseases worldwide and hospital inpatient bed days, secondary to fractures are increasing. Research has shown that most fractures are preventable, which is why prevention of fractures in the first place, should be a major, logical priority. The fact a patient in their 30’s with severe Osteoporosis in their spine was told by a consultant, when the patient raised concerns that his bone density was continuing to decline on his DXA reports “Come back to me
when you fracture” is shocking, but sadly is becoming more common. Would they allow their loved ones to fracture? For every 1 standard deviation decrease in BMD, the relative risk of fracture is significantly increased.
Those who have fought to survive cancer, should not end up disfigured, have loss of self-esteem and the secondary effects that occur from becoming deformed, because they are not 60+. It is much cheaper to prevent fractures occurring in the first place, than to treat the consequences of fractures, which are not only physical but also psychological traumatic.
Menopause can occur at any age, the average is 51, but it can occur in the 20 and 30’s. The most common cause of bone loss in women is low levels of the sex hormone oestrogen, which keeps bones healthy and strong, and it naturally declines during menopause. If women are also under a lot of stress, which dealing with the menopause itself is very stressful, this will also lower their oestrogen levels. As a result, they lose even more bone and the majority of people who contact the IOS have a minimum of 3 risk factors contributing to their bone loss.
Osteoporosis is unlike many diseases, in that it is linked to so many other conditions or diseases, treatments and medications, as well as poor lifestyle choices, which is one of the reasons why many who contact the IOS have 3 to 6 risk factors for bone loss.
Why prevention of bone loss is essential
Osteoporosis medications can help to reduce fracture risk by up to 70%.
Ireland has the 6th highest hip fracture rate in the world.
A women’s risk of fracture is greater than her combined risk of cardiovascular disease and breast cancer.
More women die from the complications of osteoporosis fractures than the combined deaths from cancer of the ovaries, uterus and cervix.
Approximately 48,000 fractures occur in Ireland annually. In 2022, 72,852 acute hospital bed days were occupied by hip fracture patients. That same year the cost of one hip fracture was ¤12,425 with 3,909 hip fractures occurring at a cost of ¤45,569,325. 69% were women, 84% were admitted from their homes, with 49% having a high function ability mobility score prior to fracturing.
20% of people aged 60+ who fracture their hip will die within six -12 months, 50% will lose the ability to wash and dress themselves, and to walk across a room unaided.
It is the secondary consequences of a fracture that can cause death, such as pneumonia, blood clot, or infection.
The life expectancy in 1995 was 75 years and by 2030 the estimated life expectancy is 84. We already
have a bone health crisis and with our population aging there is going to be a bone health tsunami, therefore preventing those at risk not only makes ethical sense but also monetary.
Many vertebral fractures are not diagnosed and are asymptomatic, with only one third of all vertebral fractures clinically diagnosed. There is an increased mortality and morbidity rate similar to hip fractures, however obvious associations with specific causes of death have so far not been reported. Increased mortality has also been found in some studies to be independently associated with low bone mineral density without fractures.
A lateral thoracic Xray is the first line for diagnosing vertebral fractures, however a DXA is necessary to monitor the bone loss and the patient’s response to treatment.
FRAX: There are approximately 200 causes of bone loss, and unfortunately FRAX only lists 12. Vitamin D deficiency, increased bone turnover, frailty and falls are not included on it. For those who do not deal with many Osteoporosis patients, it is a helpful tool. A detailed questionnaire is more through and will pick up on additional risk factors, which is available from the IOS info@irishosteoporosis.ie
The images below show the horrific, irreversible skeletal damage that occur at any age due to vertebral fractures.
Reduce pain and disability associated with fractures
Reduce risk of losing independence
Reduce risk of premature death
• Refer to chartered physiotherapist for a safe and appropriate weight bearing and core strengthening exercise programme
NOTE: A person may have a T score of -1.8 but if they have had a major fragility fracture, they should be considered to have Osteoporosis, unless proven otherwise and prevention of further fractures is crucial.
Treatments
What treatment a person is put on should depend on
• Clinical judgement of the treating physician
• The causes of their bone loss which should be investigated and addressed, not assumed. Examples menopause or steroids.
• If they have fractured already
• Their DXA scan results of their spine and hips
• The patient’s ability to swallow tablets or ability to self-inject
• Contraindications to any of the treatments
• The patient’s cognitive ability
• Results from blood tests, Vitamin D being one of the most crucial
• Their medical history
• Their age
Osteoporosis medications should always be used in combination with:
• Calcium and vitamin D, preferably through food
• A well-balanced diet with adequate calories including first class proteins
• Adequate Fluid (preferably water) intake at least one and half to 2 litres a day
• Stopping smoking
• Reducing excessive caffeine, alcohol and fibre intake
• 30 minutes of safe and appropriate weight bearing exercise daily for adults, 60 minutes for children, suitable for their age, ability and DXA results.
• Reducing stress levels
NOTE: The concept of yoga is wonderful, but it was developed without the knowledge we now have and the IOS do not recommend it for anyone with and without bone loss.
NOTE: Reducing stress is essential, as stress can affect sex hormone levels which will cause bone loss.
Patients who have not sustained a fracture
• Investigate and address cause/s of bone loss
• Prevent further bone loss and reduce the risk of fracture by putting a bone health plan in action
• Treating those who are high risk preventatively
• Refer to chartered physiotherapist for a safe and appropriate weight bearing and core strengthening exercise programme
Patients who have sustained a fracture
• Investigate and address cause/s of bone loss
• Prevent further bone loss
• Reduce the risk of further fractures
There are two main types of medications, antiresorptive and anabolic.
Antiresorptive medications
These slow down the formation of osteoclasts, the cells that break down bone, these include the Bisphosphonates, Denosumab, SERMS (selective oestrogen receptor modulators) and to a lesser extent HRT.
Anabolic medication
These stimulate the osteoblasts cells that build up new bone. Treating patients with fractures or very low bone density with anabolic medication and antiresorptive drugs will achieve higher bone mineral density earlier, which reduces their risk of further fractures very quickly.
Bisphosphonates
There are several forms of Antiresorptive medications
1) Weekly tablets
2) Monthly tablets
3) By IV once a year
Bloods measuring PTH, vitamin D, calcium, renal function and ideally bone turnover markers should be done. Ideally the vitamin D levels should be 70 up to 125nmol/L, with a normal level of PTH, as high PTH levels cause bone loss.
Bisphosphonates are nonhormonal drugs that have to be incorporated into bone and can help to reduce the risk of fractures in the spine and hips in postmenopausal women and men.
Bisphosphonates have their place in treating patients but unfortunately, they are poorly absorbed, and they form mosaic bone, not normal bone. It is essential that they are taken with the person upright or standing/ walking. One of the issues is that over the last several years the amount of people contacting the
IOS saying they are unable to tolerate them has drastically risen to approximately 70%, which significantly affects compliance. Approximately 20% are put on protein pump inhibitors to counteract the stomach issues they developed taking them, which is counterproductive because they cause bone loss.
Oral bisphosphonates should not be given to patients who have any of the following
Absorption issues, Hiatus hernia, Oesophageal abnormalities such as reflux, Barrett’s Oesophagus, impaired renal function or ulcers.
NOTE: Currently it is recommended that you do not take bisphosphonates for more than a total of 5 years, not 5 years on each one. Consideration should be taken for those who may be able to d/c Prolia by keeping 1 of these 5 years to close off the action of Prolia.
Denosumab (Prolia) is an antiresorptive medication. It is a Monoclonal antibody which binds to RANK Ligand inhibiting the maturation of osteoclasts, thus protecting the bone from degradation, preventing bone loss and osteoporosis. It does not have to be incorporated into bone, which is why It forms normal bone.
Prolia reduces the risk of vertebral, non-vertebral and hip fractures.
It is given as a Subcutaneous injection 60mg, given 6-monthly. It is approved for postmenopausal women at high risk to fracture and men and women who are undergoing chemotherapy, radiation and sex hormone ablation therapy, to prevent bone loss.
Bloods measuring PTH, vitamin D, calcium, renal function and ideally bone turnover markers should be done before each injection. Ideally the vitamin D levels should be 70 up to 125nmol/L, with a normal level of PTH.
NOTE: It is essential that the patient drinks adequate fluids to prevent urinary tract infections.
Prof O’Brien stated “Hypocalcaemia is a contraindication and Prolia is suspended in a lactose solution. Patients who were very allergic to lactose may have a reaction to Prolia. I have only had a couple of patients who are extremely sensitive to lactose that were not able to tolerate it”.
Patients on Prolia should take it preferably six months to the day of their last injection. The maximum delay after the due date for the injection should be four weeks to prevent the rebound increase in bone loss, which can result in spontaneous vertebral
fractures. Pharmacists can assist by noting the dates the injection was picked up.
NOTE: An antiresorptive medication e.g. an IV bisphosphonate must be prescribed if Prolia is being discontinued to close off the action of Prolia on bone, to prevent an increase in bone loss, which would result in vertebral fractures. The marked increase in Bone marker CTX1 will reflect this risk. No patient should ever be put on a Prolia drug holiday.
Teriparatide (Parathyroid hormone) is an anabolic bone forming agent, that stimulates the formation of new bone. It can only be prescribed by a consultant, as it is a High-Tech drug for severe osteoporosis. It is given as a daily 20mcg, subcutaneous injection in the thigh or abdomen for 12/24 months. Teriparatide is usually recommended for those with spinal fractures and/or very low bone density. It also helps to prevent bone loss for people on corticosteroids and reduces vertebral and nonvertebral fractures in women.
Prof O’Brien stated “Teriparatide was not developed to decrease pain but 95% of my patients experience a significant decline in vertebral fracture pain after several weeks on the treatment. Many of these patients would have been put on morphine patches prior to seeing me, which 85% would have reported no decline in their fracture pain level from morphine”.
It is contraindicated in patients who have had radiation, have multiple myeloma, Paget’s disease, are pregnant or breast feeding. It is essential that the patient has normal vitamin D, Parathyroid hormone levels, normal calcium, liver and kidney function.
HRT - Hormone replacement therapy or the contraceptive pill
Oestrogen/progesterone hormone therapy Sex hormones play a vital role in determining the onset of osteoporosis. Both testosterone in males and female hormone oestrogen have a protective effect on bones and help prevent the breakdown of bone.
The normal age of menopause (no periods for one year) is usually in the early 50s, if it occurs below 45 years it is considered an early menopause.
Menopause is a major cause of osteoporosis due to oestrogen deficiency, which causes many women to develop symptoms such as hot flushes, difficulty with sleep, vaginal dryness, sweats, mood changes and brain fog. This usually increases stress levels (cortisol levels), which causes further bone loss.
HRT is usually recommended for postmenopausal symptoms to help improve the person’s quality of life and their families! Patients should be informed of the benefits and negative effects of HRT treatment, and they should be monitored.
HRT is usually the first choice for treatment of menopausal symptoms provided there are no contraindications. It is usually not recommended just for the prevention and treatment of osteoporosis, unless the person has an early menopause.
HRT is not suitable for people who have a family history of breast cancer, particularly if there is a history of deep vein thrombosis.
Prof O’Brien stated “Teenagers with eating disorders may not have started having periods or will have lost their periods and have very low oestrogen and progesterone levels. Those I have treated with severe bone loss have Z scores of -3.5 to -5.5, on a DXA machine using special paediatric software. Example: I have 18 year olds with vertebral fractures. For optimal results, any male or female with an eating disorder should be referred for a DXA scan urgently.
HRT Oestrogen on its own is available in many forms including tablets, skin patches and gels but is usually combined with a progestogen, a synthetic version
of the hormone progesterone and this may be in the form of a coil. Oestrogen on its own should only be used by women who have had a hysterectomy.
It may be used as a sequential combined therapy; oestrogen is taken every day and progestogen for approximately 12 days which should result in menstrual bleeding. Continuous combined therapy is when both oestrogen and progestogen are taken every day as a result there are no periods, this should not be started until they have had no periods for a year.
Selective Oestrogen Receptor Modulators (SERMS)
SERMS: Tamoxifen, Raloxifene, they are not oestrogen but have some similar to oestrogen increasing oestrogen levels in bone and preventing osteoporosis mainly in the spine.
Tamoxifen is also used in the treatment of ER positive breast cancers.
Raloxifene is usually prescribed for postmenopausal women provided they have no contraindications, particularly a history of deep vein thrombosis and pulmonary loss.
It is 60 mg tablet taken once a day.
NOTE: It should not be given to women who are experiencing hot flushes as it will increase them or to pregnant women.
Romosozumab (EVINITY)
NOTE: It is a High-Tech drug which is available in the US and Europe and hopefully will be available soon in the Republic of Ireland.
It is another type of antiresorptive drug which is a monoclonal antibody against Sclerostin, this is the first anabolic medication that increases bone formation and decreases bone resorption.
It is licensed for postmenopausal women who have had osteoporotic fractures or are at high risk of fractures. it is a monthly subcutaneous injection that is given in 2 separate injections for one year. Contraindications in those with hypocalcaemia, a history of stroke or myocardial infarction or sensitivity to the substance.
Summary
All patients need to be monitored as bone loss is silent and currently DXA scanning is the most efficient way.
Osteoporosis is treatable and fractures are preventable, but one low trauma fracture increases the risk significantly of a second fracture in the next year if not diagnosed and treated.
Postmenopausal white women are the highest risk group affected, but it can occur at any age in both males and females, and all races. Effective treatments have been available for more than a decade; however, research shows that most people who fracture, or are at risk of fracture, are never assessed or treated for their underlying osteoporosis, and they go on to have additional fractures and the associated morbidity.
All medications have possible side effects but the benefits to bone health by preventing future fractures, skeletal deformities, loss of independence and possibly premature death, usually far outweigh the risk of a side effect.
Please make bone health a major priority in Ireland and help the IOS to ensure that people age with their dignity intact and fracture free, in order that they can actually enjoy their retirement.
Osteoporosis Bone Section
Faro - Experience the Ultimate Salon-Quality Blow-Dry at Home with Faro Hair Care Products
Recognised as a MULTI AWARD winning range of hair care products. Faro aims to arm everyone with a hairbrush that offers a salon-quality blow-dry at home.
Faro celebrated its success at an exclusive luncheon hosted by the brand's founder, Mairead Ronan, in the heart of Dublin. The event brought together industry insiders, including hairstylists, pharmacy's, and influencers. Attendees were treated to a vibrant display of Faro's award-winning hair care products, set in the
delightful ambiance of Lennans Yard. The venue was adorned with stunning summer colours and floral arrangements, perfectly complementing the essence of the Faro brand.
The luncheon commenced with an engaging drinks reception, where guests had the opportunity to experience the results of Faro's hairbrushes at the style bar, in collaboration with Peter Mark salon and the talented hairstylist Katie Judge from Peter Mark, Bray. Amidst the convivial atmosphere, Nuala-Anne Curley, Head of Marketing at Pharmed Ireland, welcomed the guests and shared the fruitful journey of Faro products under Pharmed's distribution.
The highlight of the event was undoubtedly Mairead Ronan's insightful narrative of her journey in television to creating the Faro range. Her dedication, along with her business partner
together to heat and dry your hair in record time. Faro barrel brushes come in a sizes ranging from 53mm, 32mm and 25mm suitable for all hair types and styles.
One undeniable favourite that was repeated around the room was the One Minute Hair Mask! Developed in Faros earlier years, FARO's One Minute Hydration Hair Mask is designed to give you healthy, glossy & resilient hair, the mask hydrates and reconstructs the hair. It is especially effective on coloured hair and yes! you can see results in as little as one minute being left in damp hair.
The product is also Vegan friendly and Sulphate & Paraben Free.
Debbie Lawless, in developing the Faro range of brushes resonated with the audience, emphasising the brand's commitment to providing everyone with the tools to achieve a professional salon look at home.
One exciting topic of the evening was sharing new product development. Coming from one of Faros most popular products, The Glide, came the idea to create a compact version of the very same
product and aptly named “The Mini Glide”. – perfect for traveling or popping into your handbag, gym bag or holiday bag. The Glide brushes are perfect for detangling/ brushing after a shower and are the perfect compliment to the range of Faro barrel brushes.
Why Choose Faro barrel brushes
The superior barrel brushes feature cushioned ergonomic handles and a lightweight design for a comfortable grip. The unique temperature-controlled cap allows you to safely turn the brush as you style your hair, while the extra-large vents and ionic-coated barrel work
Trisha & Chara with Karen KosterWards Pharmacy, Longford
The luncheon concluded with lively conversations about hair and brushes, accompanied by a sumptuous three-course lunch, as attendees were immersed in the world of Faro's exceptional hair care products.
Confidence Created by Faro
Mairead Ronan, brand founder
Elaine K Dunne, Pharmed and Katie Judge, Peter Marks.
Jennifer Zamparelli & Bernadette Byrnes - HairPeople Salon
Shauna O’ Rourke - Uniphar
Kristine - Your Local Pharmacy
Topic Team Training – Headlice
A community pharmacy environment that fosters teamwork ensured high levels of consumer satisfaction. This series of articles is designed for you to use as guide to assist your team in focusing on meeting ongoing CPD targets and to identify any training needs in order to keep the knowledge and skills of you and your team up to date.
The below information, considerations and checklist provides support to enable you to run a team training session and identify opportunities for learning within the topic of Head Lice.
Head lice are grey or brown insects that live close to the scalp on human heads. They are 1mm to 3mm long. They can be white, yellow or brown.
The main symptom is itching, but only about 1 in 3 children with head lice have an itch. It is estimated that 1 in 10 children suffer from head lice at any one time, with 80% of head lice infestations occurring in children between the ages of four and 16. According to the Irish Pharmacy Union (IPU) all children should be screened for head lice once a week when they return to school. Head lice are spread via direct contact with the hair from an infected person so they cannot hop or fly. Those at greatest risk have had head to head contact or comes close to an infected individual. Whilst uncommon, sharing clothing is also a risk such as hats, scarves, coats, combs, brushes, or towels used by an infected person. Lice
Consider:
cannot live more than 24 hours off the scalp, but there is a high probability of catching an infection.
Head lice mostly proliferate in the school and educational activity settings, due to the greater number of children concentrated in each classroom or playground and the longer contact time. Head lice can become a cause of bullying or harassment in school, since the population erroneously associates this condition with a hygiene problem or social class. It is generally agreed that in children head lice are not related to hygiene, however it might be in adults.
Adults and children who do not attend a school setting may also be infected in other situations, especially throughout the global family. In general, it can be stated that the household - understood as the group of people that constitute a family group - is the maintenance of the disease and the school is the propagation medium.
Clinically, head lice can be asymptomatic. The pruritus is the most common symptom. Furthermore, this can sometimes prove to be so intense that, when scratched, it causes erosions in
Can I explain the life cycle of head lice to my pharmacy team and how they can apply this knowledge to treatment?
Can I/my team explain to a parent how to detect head lice? Can we teach the technique of detection combing?
Can I do more to liaise with school nurses, head teachers, local general practices, health visitors and infection control nurses to ensure we are all giving the same information to patients and we can refer to one another as appropriate?
Can I explain the correct use of head lice preparations?
Do I know what to recommend if a customer returns saying the treatment has not worked?
the skin and subsequent bacterial infections. In this situation, the scalp is suffering and in need of treatment. Fundamentally, the control of the pediculosis is the healing of each infected individual that is part of the affected social group, through the total elimination of all living phases of lice. This is achieved by treating individually using chemical pediculicides or other extraction and disposal techniques.
Pediculosis is a widespread social problem in all human populations. Although at family level it is often a reason for anguish, your assessment should not be alarmist about the consequences and meaning of the illness.
However, the eradication or elimination of local outbreaks and therefore of possible epidemics, requires measures that are more complex. The health and care information as to how to do this is freely made available through the education and awareness of schoolchildren, parents and educators. A child infected with lice scratches their head and when parents start getting alerts from the school informing them that it has been diagnosed, some of their classmates often panic. This can causes tremendous disruption within the household as parents must, every night, check everyone’s hair including their own, meticulously combing and treating. This can take up to 2-3 hours per night.
Key Points:
Check your pharmacy team are aware and understand the following key points:
Misconceptions around head lice – how they spread and how to treat them
How to check for the presence of live head lice; the importance and technique of detection combing
Scalp itching is not always caused by head lice; the itch develops if the person is allergic to lice
When to recommend an appropriate treatment and how to use it
The role of preventive products such as repellents
In addition, those within the household who also suffer from other conditions may find it additionally stressful. Parents must take the risk that once their child’s headlice has cleared up, there is a high risk of re-infection once they return to school and so in this regard, head lice are a common, repetitive cause for concern.
Currently there are many products, such as shampoos, lotions and creams, designed specifically to combat lice. However, it must be borne in mind that they are products with an insecticidal action and they must be used scrupulously following the instructions on the package insert for them to be effective. If the lice are still resist treatment, it is possible to resort to oral treatments.
At the end of any treatment, it will be necessary to remove the remaining nits with a fine-toothed comb and maintain the use of the antiparasitic shampoo or lotion for some time. For children under two years of age, this type of product should not be used and it is best to remove nits and lice by hand, combing through wet hair with a fine-toothed pin. It will be necessary to repeat the operation, with intervals of two or three days, for at least for two weeks after having seen the last louse.
Actions:
Include POS with associated condition treatments such as other areas associated with school and going back to school
Ensure efficient sign posting to further help and advice or reputable sources for head lice treatment
Ensure there is a discreet area in which staff can assist with advice and product selection
Keep products merchandised together, along with related products to help build sales
Ensure the team are able to communicate lifestyle advice on treating head lice
Train the team to meet all the above considerations
Staying SunSmart
The HSE National Cancer Control Programme (NCCP), Healthy Ireland and partners have launched a SunSmart campaign, supporting people in the simple ways in which they can enjoy the sun safely, while protecting themselves and their family.
With more people spending time outdoors as summer approaches, whether in the garden, exercising locally or enjoying a runaround in the park with the children, it’s important to protect they protect their and their children’s skin.
Pharmacists are also advising parents to be sun smart and protect their children’s skin when they are outside enjoying the fine weather, as children’s skin is very sensitive to the sun’s rays.
Who is at risk of skin cancer?
Anyone can get skin cancer so everyone needs to protect their skin from UV light. But some people are more at risk than others.
Children and adolescents are more at risk.
Some people may also be more at risk if they:
• have fair skin - burns easily and tans poorly
• work outdoors
• do outdoor sport and activities
• sunbed use
The SunSmart campaign, an action in the National Skin Cancer Prevention Plan, is supporting people to build skin cancer awareness into their everyday wellbeing routine.
All Ireland Schools of Pharmacy Conference 2024
The All-Ireland Schools of Pharmacy Annual Research Conference 2024, a showcase of the most innovative and impactful research carried out in pharmacy schools in Ireland will be held this year from August 27-28th at RCSI Dublin.
This year's event will adopt a conference-style format, offering you a chance to network with peers from schools of pharmacy throughout Ireland. The conference will host four keynote speakers, covering topics on AI in pharmacy education, translational therapeutics, clinical pharmacy/practice, and innovations in drug delivery.
Additionally, early-career/postdoctoral researchers, PhD/MSc students, and undergraduate students will have opportunities to showcase their research through oral presentations or moderated poster sessions. Prizes will be awarded for the best presentations.
• Please note: Registration for this event will open in early June 2024
The simple SunSmart code messages are the 5 S’s:
1. Slip on clothing that covers your skin, such as long sleeves, collared t-shirts
2. Slop on sunscreen on exposed areas, using factor 50+ for children
3. Slap on a wide-brimmed hat
4. Seek shade - especially if outdoors between 11am and 3pm - and always use a sunshade on a child’s buggy
5. Slide on sunglasses to protect your eyes.
Professor Anne-Marie Tobin, Consultant Dermatologist at Tallaght University Hospital, says, “Exposure causing sunburn is the most damaging to skin, but frequent non-burning exposures also significantly increase the risk of skin cancer. By adopting the SunSmart 5 S’s the majority of skin cancers caused by UV sun exposure could be prevented. “Children and young people are particularly vulnerable. UV exposure during the first 10–15 years of life makes a disproportionately large contribution to lifetime risk of skin cancer. Children have lower concentrations of the protective skin pigment melanin and thinner skin, therefore are more susceptible to the dangers of UV. Greater than three instances of severe sunburn during childhood
doubles the risk of developing melanoma in later life. Protect yourself and your children today and your skin will thank you for the rest of your life.”
The National Skin Cancer Prevention Plan 2023-2026 provides information about how they are working to reduce skin cancer in Ireland. Find the Healthy Ireland SunSmart resources below for use to reduce the risk of skin cancer.
Posters and information leaflets on SunSmart are available to download or order printed resources at www. healthpromotion.ie Choose 'cancer' from the drop down menu. Children resources
Most resources are now available to download and order on www.healthpromotion.ie. Choose 'cancer' from the drop down menu.
• Sample sun protection policy on outdoor play for Early Learning Centres (PDF, size 2.9MB, 8 pages)
• Let's Go Summer Camps Games Manual (PDF, size 3,304KB, 12 pages)
o Let's Go Summer Camps Games Manual cards for relay races(PDF, size 4,104KB, 30pages)
o Let's Go Summer Camps Games Manual poster (PDF, size 1,190KB, 1 page)
Crohn’s & Colitis Ireland Releases Survey Results of 1,400 People with IBD
Ahead of World Inflammatory Bowel Disease (IBD) Day which took place on May 19, Crohn’s and Colitis Ireland has released the results of a survey of almost 1,400 people with IBD.
There are approximately 40,000 people living with IBD in Ireland, with the two most common types being Crohn’s disease and ulcerative colitis. IBD causes inflammation, swelling and ulceration of the intestines, with the most common symptoms being urgent and frequent bowel motions, sometimes with blood, diarrhoea, and stomach cramps.
On World IBD Day (May 19), Crohn’s and Colitis Ireland celebrated their 40th anniversary by hosted a conference in the Kingsley Hotel, Cork city, with talks on dating and relationships, and on eating well with IBD.
Comprehensive Survey
The research survey of people with IBD was undertaken by Crohn’s and Colitis Ireland between February and March 2024. Amongst the key findings were:
• Getting diagnosed. One in seven (14%) had to wait more than a year between being referred to hospital and getting diagnosed. Separately, almost half (47%) had to go to A&E with symptoms before being diagnosed with IBD
• Symptoms. When it comes to the worst symptom of IBD, a quarter of respondents (28%) noted abdominal pain and cramping, followed by a similar number for diarrhoea (26%), and one in five (20%) identifying fatigue and tiredness. On their worst day, one in two (50%)
would visit the bathroom more than ten times, while two in five (45%) had found it hard to cope with IBD over the past year on a consistent basis
• Flare-ups. One in two (52%) had experienced a flare of their IBD in the previous 12 months, with three-quarters (75%) of these having two or more flares. A substantial number had to attend hospital because of their flare
• Stigma. One in three (35%) had experienced stigma or unfair treatment because of their IBD in the past 12 months
• Facilities. An overwhelming majority of respondents (86%) believe shops/public spaces should do more to support people with IBD, with access to a toilet top of the list
• Costs. One in two (53%) respondents estimated the annual cost of medications, GP and hospital visits to be in excess of ¤1,000, with three in five (62%) saying the cost of treating their IBD is a financial burden in their life. It is worth noting that IBD is not currently covered under the Long-Term Illness Scheme
Two-thirds (65%) of those surveyed were in full or parttime employment. Of these respondents, the following findings were noted:
• Disclosing a diagnosis. Almost four in five (77%) say their boss knows about their IBD
Pictured is Amy Kelly, COO and Bruno Lucas Board Chair Celebrating the 40th anniversary of Crohn’s and Colitis Ireland
diagnosis, while one in four (23%) had not disclosed their diagnosis. Four in five (82%) had also disclosed their diagnosis to colleagues
Disappointing Findings
For Professor Aoibhlinn O’Toole, consultant gastroenterologist at Beaumont Hospital, much work needs to be done to enhance access to diagnostics, improve symptom control and provide proper financial supports to patients.
She said, “The survey findings around delays in diagnosis, as well as emergency presentation to access diagnostics, are very disappointing. Specifically, 47 per cent were diagnosed following attendance at the ED, with symptoms likely reflecting patients with more severe disease that can present as a medical emergency, such as acute severe colitis, bowel obstruction or a peri-anal abscess. However, I suspect also that for some patients, there was no alternative to access care except via the emergency room. The figure of 14 per cent waiting for more than a year to get diagnosed is also unsatisfactory and we must strive to improve referral pathways and access to diagnostics such as imaging, endoscopy and calprotectin stool tests for patients with suspected IBD.
“Almost half (45 per cent) reported difficulty coping with symptoms, which points to a significant number of patients struggling with disease control and poor quality of life, and this needs to be addressed. Overall, these results highlight massive delays in accessing care, a large cohort of patients living with poorly controlled symptoms, as well as having to deal with stigma, financial and occupational stress.
Clearly much work needs to be undertaken to improve disease control and quality of life for patients living with IBD in Ireland, as well as recognising IBD as a long-term illness in terms of State financial support.”
Unnecessary Stress
Amy Kelly, Chief Operations Officer at Crohn’s & Colitis Ireland added, "People living with inflammatory bowel disease, also known as IBD, know only too well that it is more than just managing physical symptoms; it's about navigating a plethora of emotional and financial challenges too. Our survey shows that patients are shouldering a heavy financial burden, with many spending over ¤1,000 annually on medications, GP visits, and hospital care. This financial strain adds an additional layer of stress to an already very difficult situation. We know that IBD is a long-term illness but, inexplicably, it continues to be excluded from the Long-Term Illness Scheme. This needs to change urgently so that patients receive the financial support that they desperately need.
“The survey also showed the challenges faced by people with IBD in getting diagnosed, coping with distressing symptoms and flare-ups, and experiencing stigma. We need to ensure uniformity of access to specialised healthcare professionals such as dietitians and psychologists in addressing the needs of people with IBD. These professionals offer invaluable guidance in navigating dietary restrictions, managing flare-ups, and coping with the psychological impact of chronic illness. We need to see more compassion and support for those grappling with the challenges of IBD but, most of all, we need to see action.”
There is currently no cure for IBD, but early diagnosis and treatment can help to stabilise the disease and provide a normal quality of life. For more information on the supports and services offered by Crohn’s and Colitis Ireland, call the Support Line on 01 531 2983 (Mon/Wed/Fri, 9.30am to 12.30pm) or visit www.crohnscolitis.ie.
Fighting Blindness Conference held in Dublin
Paralympians Orla Comerford and Greta Streimikyte officially launched the 2024 Retina International World Congress hosted by Fighting Blindness in Dublin.
One of the biggest global gatherings of eye experts this year, the congress brought together scientists and clinicians leading advancements in eye research from around the world. The conference welcomed over 500 delegates from 23 countries including the USA, Australia and Brazil.
As part of the event at the Dublin Royal Convention Centre, a public engagement day aimed at the sight loss community took place on Saturday June 8. The day offers a rare opportunity for people who are blind or who have a vision impairment, along with their families, to hear about the latest cutting-edge research developments taking place and to ask questions of eye experts.
Their sights firmly set on the Paris Paralympics in August of this year, Fighting Blindness ambassadors Orla Comerford and Greta Streimikyte, have both experienced what it is to live with sight loss. Orla was just a child when she was diagnosed with Stargardt’s, an inherited retinal degeneration which impacts central vision.
Genetic Eye Specialist and Consultant Ophthalmologist, Professor David Keegan, addressed the challenges facing clinicians and patients in getting new medicines approved.
He said, “With the Target 5,000 programme funded by Fighting Blindness, we are playing our part in providing people who have an inherited vision impairment with a genetic diagnosis. Without that piece of knowledge, people won’t be able to access the sight-saving gene therapies that are coming down the tracks. We are now able
to access and deliver diseasechanging clinical trials and provide in-country approved therapies with the approved centre for advanced medicinal product delivery at the Mater Hospital.
“We also acknowledge the changes Government are making to match that ambition with an overhaul of the approval and reimbursement process. This should help avoid the delays we, in Ireland, experienced on approval of the world’s first gene therapy for inherited sight loss, Luxturna. We are also appealing to our global regulators to recognise the importance for patients of stabilising vision and optimising residual visual function, as much as restoring vision.
“In addition, one of the trials that I’m involved with at the moment is for dry AMD (age-related macular degeneration) which has no current approved treatment in Europe. It involves the placement of an intraocular telescope device in the eye to enhance vision and visual performance. With more structure and resource, we could scale up meaningful interventional clinical trial activity in the field of retinal disease and other ocular conditions such as glaucoma and optic neuropathies. The Clinical Trial Networks, National Registers and European Reference Network membership are great first steps.”
The principal sponsor of the Retina International World Congress is Johnson & Johnson Innovative Medicine. Among the other companies lending their support are AbbVie, Astellas, Boehringer Ingelheim, Roche, Fountain, and MeiraGTx.
World Haemochromatosis Awareness Week
It is estimated that 20,000 people in Ireland are living with undiagnosed cases of haemochromatosis or ‘iron overload’. Haemochromatosis is the nation’s most common genetic condition yet still remains one of the lesser known amongst the population.
In Ireland, 1 in 5 people are carriers, equating to a massive 20% of the population, and 1 in 83 people are predisposed to develop it. Ireland has the highest rates of this genetic disorder in the world, giving it the nickname ‘the Celtic Gene’.
Haemochromatosis is a genetic disorder where large amounts of iron are absorbed from the diet into vital organs, in other words ‘iron
overload’. Early diagnosis is vital and if left untreated, iron overload can lead to organ damage or even premature death.
To mark World Haemochromatosis Awareness Week 2024, which took place from 1st – 7th June, the Irish Haemochromatosis Association aims to raise awareness of the condition and
is urging people to ‘Get Checked for Haemochromatosis’ and understand the symptoms in order to save lives – symptoms that range from chronic tiredness and joint pain, to abdominal pain and irregular heartbeat.
Professor Suzanne Norris, Consultant in Hepatology and Gastroenterology at St. James’s Hospital says, “Early diagnosis of
haemochromatosis is vital, which is why serious complications as a result of haemochromatosis can be avoided if a patient is diagnosed as early as possible. The work of the Irish Haemochromatosis Association has helped to increase awareness of Ireland's most common genetic disorder and educate the public on identifying symptoms and seeking treatment.”
(L-R) Dr Shannon Lee and Jessica Karuntu
(L-R) Avril Daly, Alena Reznichenko, Adrianna Montague and Finbarr Roche
The Irish Network for Gynaecological Oncology: Giving a Voice to Gynaecological Cancers in Ireland
New research carried out in April 2024 amongst adult women in Ireland, has highlighted that four out of five are not confident to recognise the symptoms of ovarian cancer.
The study was commissioned by the Irish Network for Gynaecological Oncology (INGO) (https://isgo.ie/irish-networkfor-gynaecological-oncology/) to mark World Ovarian Cancer Day on Wednesday 8th May 2024. The INGO is a voluntary group of over thirty of Ireland’s foremost gynaecological cancer campaigners, researchers and patient advocates whose aim is to raise awareness of gynaecological cancers across the Island of Ireland. The group are part of an international effort for 2 major awareness events annually; World Ovarian Cancer Day on May 8th and World Gynaecological Oncology Day on September 20th.
Unfortunately, more than three quarters of patients with ovarian cancer are diagnosed when the disease is at a late stage. This is partly due to the vagueness of symptoms and similarity with other conditions such as irritable bowel syndrome, and in some cases, symptoms may not always be obvious or present at all.
The INGO run an annual campaign to raise awareness of the symptoms of ovarian cancer and encourage women to contact and explain their symptoms to their GP if they are worried, as early diagnosis can save lives. The campaign emphasises the BEAT symptoms:
• Bloating that is persistent and doesn’t come and go
• Eating less and feeling full more quickly
• Abdominal and pelvic pain you feel most days
• Toilet changes in urination or bowel habits
The clear message is that if a woman experiences any of these symptoms for three weeks or more, she should contact her GP.
The INGO partnered with Brazilian street artist Brutto who created an impressive mural on Grafton Street on May 4th 2024 depicting BEAT messaging, which was widely shared on social media and educated passersby on ovarian cancer symptoms.
Several notable landmarks across the country lit up in teal, World Ovarian Cancer Day’s official colour, on the 8th of May, including Leinster House in Dublin, the Titanic Museum Belfast and City Hall in Cork.
Annually, approximately 400 women are diagnosed with ovarian cancer, and almost 300 women die from this disease in the Republic of Ireland (National Cancer Registry Ireland). In Northern Ireland, almost 300 are diagnosed and 128 women die (Northern Ireland Cancer Registry). Ovarian cancer is the fourth leading cause of cancer death in women in Ireland, after lung, breast, and colorectal cancer.
Written by Dr Sharon O’Toole, Trinity College Dublin and Co-ordinator of the INGO, on behalf of the Irish Network for Gynaecological Oncology
There is no standard screening test to pick up ovarian cancer in women who don’t have symptoms. Early diagnosis can significantly improve survival – 88% of patients diagnosed with stage one ovarian cancer are alive five years after diagnosis compared to 17% with stage four ovarian cancer.
The campaign also sought to dispel the myth that cervical screening detects ovarian cancer. The research showed that one in three mistakenly believe that CervicalCheck Screening Programme checks for all five gynaecological cancers (ovarian, cervical, uterine, vulva and vaginal). It is important for women to understand that cervical screening only checks whether a woman is at risk of having cervical cancer and no other cancer type.
The INGO will continue to highlight gynaecological cancers and are working with key stakeholders in an effort to improve on the current low awareness levels of symptoms.
On September 20th, World Gynaecological Oncology Day, the INGO will focus their message on all five gynaecological cancers.
The Irish Network for Gynaecological Oncology (INGO) Members
ARC Cancer Support Centres, Dublin; Answers for Cancer Podcast team; Breakthrough Cancer Research; Cancer Care West; Cancer Trials Ireland; CERVIVA; Circle of Friends Cancer Support Centre; Coombe Hospital, Dublin; Cork ARC Cancer Support; Cork Cancer Care Centre; East Galway and Midlands Cancer Support Centre; Emer Casey Foundation; Irish Cancer Society; Irish Society of Gynaecological Oncology; Karen Fenton Ovarian Cancer Fund; Lynch Syndrome Ireland; Marie Keating Foundation; Mater Hospital Dublin; National Cancer Control Programme; National Immunisation Office; National Women’s Council of Ireland; OvaCare; Hive Cancer Support, Derry; Purple House Cancer Support; Queens, Belfast; Sláinte an Chláir; Sligo Cancer Support; SOCK; Swell Fermanagh Cancer Survivorship Group; St. James’s Hospital Foundation (GynaeCancerCare); Trinity College Dublin; Trinity St. James’s Cancer Institute; University College Cork; University College Dublin School of Medicine; University College Dublin Gynaecological Oncology Group and 221+ CervicalCheck Patient Support Group.
For more information, please visit: www.thisisGO.ie | www.isgo.ie
New Revive Active Manufacturing Facility
Revive Active, Ireland’s No1 VMS brand, recently announced the opening of its second state-of-the-art manufacturing facility in Mullingar, Westmeath. The new 10,000 sq. ft facility was officially opened by The Minister for Enterprise, Trade and Employment, Mr. Peter Burke T.D. on Monday 17th June. This new factory comes on the back of Revive Active’s extraordinary growth over the last number of years.
Revive Active has become the largest VMS brand in Ireland, sold through an extensive network of 1500 pharmacies and health food stores across the county.
The additional 10,000 sq. ft. of manufacturing and warehousing space underpins the company’s international expansion, out of which they will service customers in the Middle East, Europe and Africa, amongst others. With this second site now operational, Revive Active has created over 40 jobs for the local area and has 75 employees nationwide.
The multi-award-winning Irish supplement brand is also a proud member of Guaranteed Irish and Love Irish Food. Celebrating its 13th year in business next month, Revive Active has cemented its reputation as Ireland’s number-one supplement range, and continues to stand out from its competitors due to its powerful formulation, only using the best
active ingredients that significantly impact your health and well-being.
Enterprise Ireland has been fundamental to the success story having provided mentoring and financial support from the initial set up in the early days. This funding has ensured growth within the Irish and International markets and was pivotal pre-Brexit when founder Daithi ‘O Connor made a decision to move production from an outsourced facility in the UK to Mullingar. The first plant was opened in 2018 attended by Minister Burke and today’s opening of the 2nd facility marks a fundamental part of the international growth journey for the business.
wish to congratulate Revive Active on their new state-of-the-art facility here in Mullingar and commend the global ambition of this indigenous company to compete at the highest level, supplying to some of the largest retailers across Ireland, the UK and the Eurozone. Enterprise Ireland is committed to supporting companies like Revive Active to increase their level of innovation, improve their competitiveness and expand their global footprint, with the ultimate goal of delivering export growth and jobs in Ireland and we look forward to continuing to work with the company in the future.”
Most recently Revive Active has internationally launched into Celerio Group in Portugal, which will see the full product range on
Minister for Enterprise, Trade and Employment, Mr. Peter Burke T.D. Opens 10,000 sq ft State-Of-The-Art Revive Active Manufacturing Facility In The Heart Of Mullingar
the shelves of a prestigious health store group throughout the country. Further expansion will come through Nordics and UAE markets in 2024 with European growth forecast in 2025
Colm Horton, Operations Director, Revive Active Comments: “We are delighted to welcome Minister Burke to officially open our 2nd plant in Mullingar today. It doesn’t seem like it 5 years ago when Minister Burke attended the opening of our first factory in Lough Sheever Park, Mullingar. Our goal at that time was to provide employment to 10 people in the locality and it is a very proud moment for the entire company to see growth over the last five years that has seen our team grow to 40 people.”
The multi-award-winning Irish supplement brand is also a proud member of Guaranteed Irish and Love Irish Food. Celebrating its 13th year in business next month, Revive Active has cemented its reputation as Ireland’s number-one supplement range and continues to stand out from its competitors due to its powerful formulation, only using the best active ingredients that significantly impact your health and well-being. As the number 1 VMS brand in Ireland, thousands of people wake up to a sachet of Revive Active each morning and the brand’s mission is for Revive Active to become a morning routine for a global audience. The new production facility in Mullingar will allow for further international expansion in the coming years.
Exploring career choices of pharmacy graduates over 15 years: A
cross-sectional
evaluation
Written by Katie L. Fitzpatrick, Evin A. Allen, Brendan T. Griffin, Joseph P. O'Shea, Kieran Dalton, Harriet Bennett-Lenane University
College Cork, Cavanagh Pharmacy Building, College Road, Cork, Ireland
The pharmacy profession has evolved over time and continually adapted to the needs of society and the everchanging healthcare system. 1,2 Within clinical settings, this has comprised a more patient-centred, rather than a product-orientated role, as provision of patient counselling, drug monitoring, and advanced practices have led to improved treatment outcomes for patients.1,3 In 1997, the World Health Organisation (WHO) introduced the concept of the ‘7-star pharmacist’2,4,5, which detailed the roles which pharmacists should perform – namely: ‘caregiver’, ‘communicator’, ‘decision-maker’, ‘manager’, ‘teacher’, ‘lifelong learner’, and ‘leader’. Later, three additional roles were added, including ‘researcher’, ‘entrepreneur’, and ‘agent of positive change’, resulting in the ‘ten-star pharmacist’.6,7 Owing to the diversity and transferability of many of these roles, pharmacy graduates, now more than ever, appear fully equipped to work in multidisciplinary roles across both patient and non-patientfacing settings.
Increased recognition of the highly educated pharmacy graduate workforce across the wider employment landscape has significantly expanded graduate career prospects. The broad set of technical skills and expertise obtained through a pharmacy degree enables graduates to thrive professionally within both an integrated healthcare sector and the global employment marketplace.8 Typically, careers outside of the clinically focused or “patientfacing” settings of community or hospital pharmacy have been associated with a career within pharmaceutical manufacturing. However, increasingly diverse employment opportunities are now also arising in other nonconventional “non-patient facing” settings, such as drug regulatory authorities, academia, public bodies, consulting, and beyond. This has resulted in an increase in varied employment prospects for pharmacy graduates in different areas like never before - thus providing a golden opportunity for pharmacists to diversify their career paths and professional aspirations.
While these nonconventional opportunities are certainly welcomed, the increasing numbers of pharmacists employed in nonpatient facing sectors has meant a decrease in the proportion of pharmacy graduates choosing employment in patient-facing roles, of which pharmacists are the only healthcare professionals licensed to hold. This has resulted in an increased global demand and significant international pressures on the patient-facing pharmacy workforce worldwide. A 2021 report by the International Pharmaceutical Federation (FIP) raised concerns over access to pharmacists,9 while their 2018 report also anticipated increasing capacity challenges in the future, predicting a 40% growth of the global pharmacy workforce over the next 15 years.10,11 Similarly, the World Health Organisation estimates a projected shortfall of 10 million health workers by 2030.12 Therefore, considering continued pressures on the patient-facing workforce and the ever-evolving pharmacy landscape, it appears pertinent to create more accurate predictors of where pharmacy graduates are working. In doing so, helping to create increasingly accurate projections of workforce capacity to inform pharmacy workforce models.
Numerous international studies have examined career intentions or aspirations of pharmacy students, including countries such as Australia,13 Jordan,14 Malaysia,15 Northern Ireland,16 Nigeria,17 Qatar,18 S audi Arabia,19,20 Sudan,2 and the United States of America (USA).21, 22, 23, 24, 25 While a previous study did examine the career choices of pharmacy graduates in the early career stage (<3 years post-graduation) in Japan,26 the authors believe the present study is novel as it provides the first cross-sectional analysis of pharmacy graduate career paths over a 15-year time frame. Furthermore, given the current landscape of patientfacing workforce capacity problems internationally, the everwidening graduate employment opportunities, and apparent paucity of robust European data, this study presents a timely opportunity to investigate the career paths of graduates from a pharmacy training programme in Ireland.
Using an online survey and publicly accessible Linkedin® profile data, this study primarily aimed to provide an overview of the career paths of pharmacy graduates from University College Cork (UCC) School of Pharmacy since its establishment in 2004. Secondary aims included identifying the proportions of graduates per employment sector across both patient-facing and non-patient-facing roles, those who have completed post-graduate education, along with graduate satisfaction with the pharmacy programme and their chosen career paths. This research should help inform key stakeholders of trends in Irish trained pharmacy graduate employment over the past fifteen years, guide strategic development of pharmacy programmes and future policy-making, while also informing current pharmacy students of potential employment opportunities through data-driven analysis of graduate career paths
Methods
Study context
First established in 2024, UCC School of Pharmacy is currently one of only three schools in the Republic of Ireland (ROI) accredited by the Pharmaceutical Society of Ireland (PSI) and entry to the UCC undergraduate pharmacy programme is competitive. A pharmacy degree is unique in delivering both a healthcare and pharmaceutical science curriculum, providing students with a strong education in the main areas of pharmaceutical chemistry, biochemistry, pharmaceutics, sterile manufacturing, microbiology, pharmacology, and clinical pharmacy practice.
Prior to 2015, ROI pharmacy students undertook a ‘4 year plus 1 year’ pharmacy programme: a 4 years Bachelor’s degree in UCC plus a 1 year Masters. The final year comprised a 1-year work placement (with a minimum of 6 months in a patient-facing setting) and academic modules completed via the Royal College of Surgeons in Ireland. Since 2015, all incoming pharmacy students undertake an integrated five-year Master of Pharmacy (MPharm) degree, all completed with UCC. Students undertake a 4-month
experiential work placement in the fourth year in either a patient-facing setting or a non-patient facing (such as in pharmaceutical industry, academia, or a public body etc.).
Study design and participants
The population eligible for inclusion were graduates of UCC pharmacy programmes (BPharm and MPharm) from 2007 to 2022 (n = 798). As student contact email information becomes inaccessible upon graduation from UCC, this study utilised two approaches to collect data on graduates’ career paths: an online survey and analysis of publicly accessible information from Linkedin® profiles. Ethics approval for this study was granted by UCC›s Social Research Ethics Committee. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement was used to guide study reporting.27
Data collection
Survey design
The survey (Supplementary Material 1) was created based on previous literature2,3,13,14,22 by the research team, consisting of pharmacist academics based in UCC, some of whom are current students or previously graduated from UCC›s pharmacy programme. The survey used a combination of multiple-choice questions, yes/no questions, and Likert-scale ratings. Participant names and year of graduation were required to avoid duplication of graduates during the crosscheck process described below. An information sheet preceding the survey highlighted that any identifying information would be removed prior to data analysis
Survey distribution
School of Pharmacy staff contacted one class representative from each graduating year from 2007 to 2022 with whom they had a professional or personal connection via email, phone, or social media between the 15th of May and 25th of June 2023 (date of survey closure). To ensure consistency representatives were contacted using a pre-determined body of text containing the study aims. They were also provided with
a participant information sheet and asked to distribute the online survey link via email, phone, or social media. The survey link was also posted to the “UCC Pharmacy Alumni” Linkedin® page on the 9th of June. Participation was voluntary and participants could withdraw from the survey up until the point of data submission. Efforts to maximise the response rate involved a reminder message sent to the class representatives two weeks after initial contact. Data was extracted from the survey platform (Microsoft® Forms, Microsoft Office, 2016).
LinkedIn® profiles and PSI register
Publicly accessible LinkedIn® profile information of graduates was searched online. Information like that obtained from the online survey was collected (current role, employment sector, and postgraduate training enrolment/ completion). Graduates who were currently undertaking postgraduate education were classified similarly to those who had completed postgraduate education. Finally, the PSI register of registered pharmacists was used to attain graduates’ registration status (which is required to legally practise as a pharmacist in ROI).
Data analysis
A valid survey response was achieved when a participant clicked ‘submit’ at the end of the survey. Three duplicate responses from one participant were identified, deemed invalid, and removed. All survey questions were answered by all respondents (i.e., no incomplete surveys). Graduate
LinkedIn® profile information was cross-checked with the survey responses to avoid any duplication. The final information was imputed into a master Microsoft® Excel (Microsoft Office 2016) spreadsheet. Any discrepancies between LinkedIn® information and survey answers were resolved on a case-by-case basis.
Data remediation was performed both manually and using Microsoft® Excel (Microsoft Office 2016) functions to reduce the chance of human error, and thereafter analysed using descriptive and inferential statistics in Statistical Package for Social Sciences (SPSS), Version 27. Chi-squared (χ2) tests were conducted to examine the association between graduate demographics and their responses. As part of the analysis on time since graduation, the year groups were categorised into 2007–2011, 2012–2016, and 2017–2022 cohorts representing those 0–5, 6–10, and 11–15 years after graduation. Post-hoc analysis was conducted using the z-test to compare column proportions; adjustment for multiple testing using the Bonferroni method was also performed.
Results
Since the inception of the school of pharmacy, there have been 798 graduates over a 15-year period; in this study, data from 556 of these were obtained (69.7%). This included 203 valid survey responses (25.4%), 148 of whom had a corresponding LinkedIn® profile (18.6%), with data from LinkedIn® only from 353 graduates (44.2%) (Supplementary Material 2). Over 90% (92.1%) of graduates are cur-
rently named on the PSI pharmacy regulator list of registered pharmacists. Entering on this register and maintaining registration to practice as a pharmacist in Ireland was more commonly observed (χ2 = 9.59, df = 2, p < 0.05) for those who graduated in the last 5 years (2017–2022) at 96.6% versus those from the years 2012–2016 (90.1%) and 2007–2011 (88.5%) - highlighting an attrition rate of deregistering as time from pharmacy graduation increases.
Patient-facing versus non-patient-facing roles
Approximately two thirds (n = 362; 65.4%) of graduates were working primarily in pharmacy-based patient-facing roles at the time of the study i.e., in community or hospital pharmacy settings (Fig. 1). The percentage working in patient-facing settings ranged from 79.5% for 2022 graduates to 36.7% for 2010 graduates (Fig. 2). Factors which appeared to affect differences in patient-facing employment prevalence are seen in Table 1 (year of graduation, PSI registration status).
Women were significantly more likely to be working in a hospital pharmacy setting compared to men (20.9% versus 10.2%; p < 0.05), whereas a significantly higher proportion of men were working in academia (12% versus 3.6%; p < 0.05).
Patient-facing roles
A higher proportion (χ2 = 18.94, df = 2, p < 0.05) of 2017–2022 graduates were primarily employed in community pharmacy (59.4%) versus 2012–2016 (41.1%) and 2007–2011 (39.5%) graduates
(Fig. 3). Table 2 shows that the variety of community pharmacy roles included pharmacy owner, superintendent pharmacist, supervising pharmacist, support pharmacist, locum pharmacist, and pharmacy manager. Practising as a locum pharmacist was more prevalent among the 2017–2022 cohort of community pharmacists (25.2%) versus those in the 2012–2016 (12.8%) and 2007–2011 (6.5%) groups (χ2 = 11.66, df = 2, p < 0.05). Of those not primarily working in community pharmacy at the time of the study, 61.1% had previously worked full time as a pharmacist in community pharmacy.
At the time of the study, 17.7% of graduates were primarily working in hospital pharmacy, where roles included basic grade hospital pharmacist, senior hospital pharmacist, and chief hospital pharmacist; these roles refer to different grades of pharmacist within the ROI hospital system. Of these graduates working in hospital pharmacy, 65.2% had previously worked full time as a pharmacist in community pharmacy.
Non-patient-facing roles
Of the 192 graduates (34.7%) working in non-patient-facing pharmacy roles, the highest proportion (62.2%) worked in the pharmaceutical industry (21.5% of total). There were a wide variety of roles in industry-based graduates, as displayed in Table 2. A higher proportion of 2012–2016 graduates (29.2%) were employed in the pharmaceutical industry versus the 2007–2011 (20.7%) and 2017–2022 (15.5%) respectively (χ2 = 12.06, df = 2, p < 0.05).
Fig. 1. Total percentage of pharmacy graduates per employment sector (n = 554).
Most graduates in pharmaceutical industry were PSI registered (85.7%). Working primarily in academia, a public body, or another workplace collectively accounted for the remaining 13.1% of graduates. Of graduates primarily working in academia, 81.8% were working in ROI.
Postgraduate education
Postgraduate education uptake and related demographics (including year of graduation and
PSI registration status) are shown in Table 1 and Fig. 4. Over twofifths (43.1%) of graduates had either completed a postgraduate degree since their pharmacy graduation or were undertaking one at the time of the study. Of these, 38.4% undertook a postgraduate degree in UCC. Over one fifth of these have undertaken a Doctor of Philosophy (PhD) (n = 49; 22.0%).
Other than a PhD, the range of postgraduate degrees undertaken by graduates included: Master of
Science (38.1%), Postgraduate Diploma (17.5%), Postgraduate Certificate (8.7%), Postgraduate Entry Medicine (7.6%) Master of Business Administration (2.2%). Of those who undertook a Master of Science programme, 41.2% did so in clinical pharmacy or hospital pharmacy. No substantial difference was seen between men (45.8%) and women (41.9%) in undertaking postgraduate degrees (Table 1). Graduates not PSI registered displayed a higher prefer-
Fig. 2. Percentage of pharmacy graduates per employment sector in each graduating year from 2007 to 2022. Blue shades represent patient-facing pharmacy roles, whereas red shades represent non-patient-facing roles (n = 554)
ence (χ2 = 9.31, df = 1, p < 0.05) to undertake postgraduate degrees (65.1%) versus PSI-registered graduates (41.1%). Higher numbers of graduates primarily in non-patient-facing roles (χ2 = 67.62, df = 1, p < 0.05) had undertaken a postgraduate degree (66.5%) versus those primarily in patient-facing roles (29.3%).
Within patient-facing roles, a higher proportion (χ2 = 95.89, df = 1, p < 0.05) of graduates working in hospital pharmacy
Fig. 3. Visual representation of the grouped analysis of graduate career sectors (i.e. 2007–2011, 2012–2016, and 2017–2022).
2017–2022 graduates were significantly more likely (p < 0.05) to be in a patient-facing role versus 2007–2011 and 2012–2016 graduates (n = 554).
have undertaken postgraduate degrees (68.1%) versus graduates in community pharmacy (13.7%).
As seen in Fig. 4, graduates primarily working in community pharmacy represented the lowest rate in undertaking postgraduate degrees, which was lower (χ2 = 150.22, df = 1, p < 0.05) than graduates primarily working in other sectors (65.2%).
Graduates primarily working in hospital pharmacy (68.1%) (χ2 = 29.94, df = 1, p < 0.05) or the pharmaceutical industry (53.0%) (χ2 = 6.01, df = 1, p < 0.05) displayed a higher prevalence for completing/ undertaking a postgraduate degree compared to others.
Discussion
The study findings provide a unique insight into trends in career pathways of pharmacy graduates over a 15-year period. Results will be of interest to pharmacy educators, potential employers, policymakers, and prospective students alike. While international pharmacy education structures may differ from Ireland, the roles filled by pharmacists are often generalisable across regions. Thus, this research provides a universal mechanism to track career progression and may be used to inform improved methods of pharmacy workforce capacity prediction. Considering the diverse employment opportunities increasingly available to pharmacy graduates, rebalanced workforce analyses which account for nonconventional and emerging pharmacy career paths will provide
a truer representation of the workforce available to the patient-facing pharmacy sector. The timing of future pharmacy workforce planning analyses by educators or regulators is also significant according to results obtained in this study. Here, approximately twothirds of graduates (65.4%) were primarily working in patient-facing settings (community or hospital pharmacy). However, differences in preferences for patient-facing versus non-patient facing settings, as well as likelihood of registration with the Irish pharmacist regulator, between graduates when grouped ≤5 years graduated versus graduated >5 years were identified. In line with previous findings that the median time for pharmacists to change their primary practice setting is seven years post qualification,28 this study suggests to obtain a more reflective estimate of long-term practice setting choices, future pharmacy workforce analyses involving data collection from graduates should be undertaken >5 years post-graduation. By this period, it is more likely that graduates will have chosen their long-term practice setting, thereby providing educators and regulators with increasingly accurate patientfacing workforce data to fulfil the global demand.
Within patient-facing settings, nearly half of the graduates (47.7%) worked in community pharmacy at the time of the study. A career as a community pharmacist is considered a respected career choice in Ireland, as ‘local pharmacists’ have been
4. Percentage of graduates per employment sector who have completed/are completing postgraduate training versus those who have not undertaken any postgraduate training (n = 518)
found the most trusted group of professionals by the Irish public.29 During their pharmacy education, it is common for students to be heavily exposed to community practice due to weekend work or experiential placement, which may influence career choices.30 Accordingly, this higher preference for community pharmacy seen in this study is in line with previous studies of pharmacy students› career intentions and preferences where higher preferences for this sector were also seen in Australia (50.42%),13 Northern Ireland (57%),16 and USA (50.9%).23 However, despite this prevalence rate, trends of decreased preference for working primarily in community pharmacy as time post-graduation progressed were observed in this study. Our findings also highlighted the greater appeal of locum community pharmacist positions for newer graduates. Within the Irish pharmacy context, these results align with a previous workforce survey finding that preference for locum work decreases with age, as 52% of pharmacists surveyed aged <35 years had worked as locum pharmacists, while this dropped to 25% in those >46 years.28 Such positions offer perceived advantages like less responsibility, improved remuneration, and flexible hours, while the wide availability of locum positions upon graduation may be attractive to newer graduates.28 In comparison, further from graduation, those in community roles appear to have switched to more classical fixed
roles of supervising pharmacist, superintendent pharmacist, or pharmacy owner.31
This apparent trend of graduates beginning their careers in community pharmacy but migrating away from this sector over time is reinforced by our finding that 61.1% of graduates not primarily working in community pharmacy had previously held a full-time community pharmacy role. This aligns to previous findings that 1 in 5 pharmacists in Ireland have changed their primary practice area since registration, where the biggest reason for changing was ‘looking for enhanced professional satisfaction’.28 A recent Irish qualitative study of pharmacists identified six categories affecting community pharmacy retention in Ireland based on the views of 23 interviewees. These included working conditions, limited career fulfilment, and professional progression opportunities.31 Similar themes were also highlighted in a similar Northern Irish qualitative study,32 as well as in a recent Irish workforce survey of 1272 PSI registered pharmacists (September 2023). There, 70% of respondents in community pharmacy strongly agreed that job stress is a feature of the role and 73% had experienced burnout.33 Within the Irish pharmacy context, these reports arise in the backdrop of significant workforce capacity shortages in the community pharmacy sector. Previous research in 2022 found that 57% of pharmacist respondents were ‘concerned’ or ‘extremely concerned’ about the patient-facing workforce capacity issues28, where a heavy reliance on the transient locum pharmacist workforce and high prevalence of vacancies nationwide were also highlighted. Meanwhile, a 2023 PSI workforce survey has worryingly revealed that over one quarter of respondents (27%) intend to leave the profession.33
Fig.
Reasoning why almost two thirds of those in hospital pharmacy previously worked in community pharmacy is likely multifaceted related to the factors negatively affecting community retention in addition to a combination of skill utilisation, specialisation potential, and job security factors.8,12,27 More broadly speaking, factors influencing primary practice choice setting by pharmacists are varied and have also previous been explored internationally.15,23,34, 35, 36 In relation to community pharmacy however, while graduates in community expressed lower career path satisfaction ratings versus those in other sectors, it must be remembered that overall satisfaction in the sector was still very positive (78.8%). Furthermore, the ability of students to move career sector can also be seen as a positive reflection of the wide applicability of the skillset attained through a degree in pharmacy. Recommendations recently highlighted by the Irish pharmacy regulator and beyond33,37 aim to initiate the process of addressing concerns among community pharmacists and incentivise more graduates to remain in community pharmacy settings long-term.
In this study, the proportion of graduates primarily in non-patient-facing settings lies at greater than one third (34.6%), where almost 20% of these have relinquished their ability to be named on the PSI register of registered pharmacists. This substantial proportion of graduates occupying non-patient facing roles, highlights the significant current underestimation of the non-patient-facing cohort according to Irish pharmacy regulator statistics, which stand at only 10.4% (i.e., three times lower, as of November 2023). Therefore, our findings highlight discrepancies associated with the use of this register as a predictor of pharmacist career paths, most definitely in this cohort of graduates. In reality, the present study’s results are more comparable to statistics from Scandinavia, where the percentage of pharmacists in non-patient-facing roles in Sweden and Denmark have risen to 50% or more.30,38 While multifaceted, one reason for this increase could be due to higher career path satisfaction, as found in this study. Furthermore, as previously mentioned, Irish pharmacy students are now also being exposed to more non-patientfacing placement opportunities at an earlier stage in their education. Over one fifth of Irish pharmacy graduates (21.5%) were primarily working in the pharmaceutical industry at the time of the study. This may have been aided by
the fact that Ireland represents one of the leading locations for pharmaceutical industry in Europe.39 The proximity of many pharmaceutical employment may in some way account for the large proportion of pharmacy graduates working in this sector, while the pharmacy degree also remains sole degree which meets all criteria to act as a ‘Qualified Person’ in the European pharmaceutical industry.40 Furthermore, pharmacy represents a clinical and pharmaceutical science degree, and as a result pharmacy graduates represent a unique cohort of students, attractive to potential industry employers and equipped with real world communication skills developed through clinical practice. This draw to the pharmaceutical industry for Irish graduates can be contrasted to other countries, such as Saudi Arabia,19 Sudan2 and Malaysia15 where the percentage of undergraduate pharmacy students that wished to pursue a role in industry ranged from 7%19 to 17.8%15. The importance of proximity to pharmaceutical companies was also previously highlighted in a Nigerian study, where a significantly higher percentage of students in a Nigerian university situated in a highly industrialised environment (36.5%) chose industry as their career preference versus other Nigerian universities (22.5% and 20% respectively)17
In terms of postgraduate education, completion or undertaking of such was less prevalent among those in patientfacing versus non-patient-facing roles. However, stark differences were seen in undertaking a postgraduate degree between those in community (13.1%) and hospital pharmacy (68.1%). These differences were echoed in a workforce survey where 34% of respondents in community had undertaken additional formal higher education compared to 86% of respondents in hospital.33 Such differences could be linked to the fact that experiential learning and standard continuous professional development (CPD) are more commonly crucial elements of community pharmacy skills enhancement, while no postgraduate education is required to progress to more senior roles in the sector. The relevance of micro-credentials versus traditional postgraduate qualifications may also need to be considered. Comparatively, undertaking a clinical pharmacy master›s degree is a common desirable criterion of progression for hospital-based pharmacists in Ireland (albeit
not essential), and is at times even funded by the employer. For non-patient-facing roles, a possible explanation behind the high rates of postgraduate study uptake may be that these graduates are competing with non-pharmacists for employment. Depending on the sector, they may either require a postgraduate qualification or perhaps be financially supported by an employer to undertake studies to upskill and aid progression to more senior positions. This in turn may aid pharmacist retention within these sectors due to clear career progression opportunities. This is further supported by 2018 research which revealed that nearly half (45%) of pharmacists in industry roles believed that postgraduate education is essential for such roles.30 It was suggested that responses may have been influenced by the individual›s own entry pathway to pharmaceutical industry, as 22% of those respondents entered nonpatient-facing settings following a postgraduate qualification.
Along with overall high career path satisfaction, high satisfaction rates with the pharmacy training programme among graduates from all career sectors highlights the applicability of the programme to support varied career pathways over a 15-year period since the school’s inception. The variance in career sectors across all graduating years also suggests that changes to the MPharm degree have not limited nor dissuaded Irish Pharmacy graduates from taking up employment across varied sectors. Moving forward, this study provides capacity to inform potential strategic adjustments to the delivery of the pharmacy programme to meet the needs and skillsets of the graduates’ prospective employment sectors, while also providing useful information to prospective and current pharmacy students and associated employers. The advantages of more precise mechanisms for maintaining contact with graduates and tracking career progression by universities was also highlighted.
Regarding study strengths and limitations, it is recognised that 30% of graduates were not accounted for in this study and data is representative of one pharmacy training programme. Secondly, at the time of data collection, graduates who were currently undertaking postgraduate education were classified similarly to those who had completed postgraduate education, as exact timing of programme completion was not available from LinkedIn® profiles. It is recognised
that this method of data collection does not facilitate a quantitative comparison of those undertaking versus those who have completed a postgraduate degree. It is also not possible to say that all LinkedIn® data was up to date, as some users may have been more frequent users of the platform than others. While the use of two data collection methods allowed for a greater number of graduate data to be identified, this meant the survey was not anonymous and may have influenced answers provided. It is also acknowledged that this study is limited by providing p-values above or below the 0.05 level, rather than reporting specific values. However, this study provides an impetus for potential further research comparing results to those obtained both internationally and across other pharmacy training programmes in Ireland.
Conclusion
This study has successfully analysed career paths of pharmacy graduates from a school of pharmacy over a 15-year period. Impacts of this research include the revelation that although nearly two thirds of graduates currently occupy patient-facing roles, this proportion has decreased as time from graduation increased. Consequently, future workforce capacity data collection initiatives may be optimised by considering the growing non-patient-facing pharmacy workforce and undertaking analyses of graduate career choice at least >5 years post-graduation. Then, a more precise estimate of graduates occupying the patient-facing workforce in the long term will likely be achieved. In this study graduates in non-patient facing roles were shown to display a higher degree of career path satisfaction along with higher rates of postgraduate degrees versus graduates in community pharmacy. This study indicates that future research should more closely examine the motivators for pharmacy graduates in choosing a given career sector. Given the increasingly multimorbid ageing population, while the increasingly diverse professional opportunities for pharmacists are welcomed, it is vital that we have sufficient pharmacists in patient-facing roles to provide pharmaceutical care. The present study demonstrates the importance of evaluating pharmacist career paths and represents a springboard for further research to inform future pharmacist workforce planning worldwide to avoid potentially significant implications of shortages in patient-facing pharmacy workforce.
Brain Research
Advancing Brain Research and Treatment: FutureNeuro's Vision to Change the Patient Journey
Written by Prof David Henshall, Bridget Doyle, and Fiona McLoone
Brain disease is one of the biggest challenges for public health, society and the economy in Ireland. With one in three individuals affected over their lifetime, the annual burden on healthcare and welfare systems amounts to an estimated ¤30 billion. In Ireland alone, more than 800,000 people grapple with conditions impacting the brain and central nervous system, ranging from epilepsy and Amyotrophic lateral sclerosis (ALS) to Parkinson's disease, Multiple Sclerosis (MS), and acquired brain injury. More than 30% of people affected will also contend with psychiatric disorders, adding complexity to their care.
FutureNeuro, an Ireland-based interdisciplinary research centre, is committed to alleviating this burden by accelerating progress and translating innovations into real-world solutions. With a focus on improving diagnosis, developing targeted treatments, and advancing healthcare management, the Centre is committed to making tangible differences to patient outcomes. Already, FutureNeuro's research has led to transformative
interventions, including genetic testing to identify patients most suitable for life-changing therapies.
Navigating the Path Forward: FutureNeuro's Vision for the Future
As FutureNeuro embarks on its second phase, fuelled by remarkable achievements since it launched in 2017, its vision for the future remains clear - to change the patient journey. However, the
reality is that most brain diseases still lack effective treatments and diagnosis remains a prolonged process for many. Recognising the scale of the challenge ahead, the Centre has brought together the very best scientists, clinicians, and academic and industry partners. Together they will work on an integrated research programme to progress the Centre’s ambition to become a world-leading research institute that directly connects with the needs of patients and their clinicians.
An electroencephalography - or EEG cap monitoring electrical activity in the brain
Expanding the Team
FutureNeuro's integrated academic and clinical research network
To realise transformative advances, FutureNeuro, led by David Henshall, Centre Director and Professor of Molecular Physiology and Neuroscience at RCSI University of Medicine and Health Sciences, is scaling up its operations and integrating new science, talent, and expertise in brain research from prestigious institutions across Ireland, including RCSI University of Medicine and Health Sciences, Trinity College Dublin, Dublin City University, University College Dublin, University of Galway, University College Cork, Maynooth University and South
David Henshall, Centre Director
Bridget Doyle, Centre Manager
Fiona McLoone, Communications Lead
East Technological University. Most importantly, the Centre is integrated with a researchengaged national clinical network who collectively inform the research questions and ensure valuable access to patients and their data in order to make the research relevant and translational.
While maintaining a strong focus on epilepsy and Motor Neuron Disease (MND), FutureNeuro is broadening its impact to include neurodevelopmental disorders, multiple sclerosis, Parkinson's disease, traumatic brain injury, and their intersections with psychosis and mental health. FutureNeuro has grown their network to over thirty research leaders, their dedicated teams and new enabling infrastructure. This collective expertise will further our understanding of the mechanism of action of the brain and brain disease, enable the identification of new molecular diagnostics, neurogenetics, noncoding RNA biology, and gene therapies.
Moreover, FutureNeuro recognises the invaluable potential in cross-pollinating discoveries across different disease areas. By leveraging insights gleaned from one condition to inform research and treatments for others, the Centre aims to maximize impact and efficiency, ultimately accelerating progress towards addressing the broader spectrum of brain diseases.
New Research Frontiers: From Diagnostics to Therapy and Beyond
FutureNeuro’s research is built on three connected themes –diagnosis, therapy and digital health. The Centre is rolling out an integrated programme of work across their eight academic partners which will be complemented by collaborative projects with world-leading industry partners.
Diagnosis
This strand of the programme concentrates on discovering
genes that cause brain disease or influence how people respond to treatments. The Diagnostics Team is examining the chemistry of the blood and fluid that surrounds the brain to look for answers to causes and prognosis, recognising that errors in DNA may not always be the sole cause.
By analysing the chemistry outside brain cells, researchers can create a molecular fingerprint or profile specific to a particular brain condition. These are known as biomarkers. When combined with brain imaging, artificial intelligence, and recordings of brain activity, these biomarkers enable increasingly accurate predictions of how a brain disease will develop in an individual overtime.
Genomics is transforming the diagnosis of neurological diseases, paving the way for the emergence of precision medicine. FutureNeuro has been instrumental in incorporating genomics into clinical practice, leading to faster and more
The eight academic partner institutions
accurate diagnoses. Currently, FutureNeuro Deputy Director, Prof Gianpiero Cavalleri is co-leading an Irish consortium of partners to contribute to the ¤20M Digital Europe Call “Federated European infrastructure for genomics data”. This initiative is geared towards advancing the European 1+ Million Genomes Initiative, aiming to realise a unified platform for genomic data across Europe.
Therapeutics
FutureNeuro’s therapeutics research is organised as a pipeline, drawing on the insights from their diagnostics teams to identify to identify potential targets for future medications. A ground-breaking capability lies in the ability to generate human brain cells in the lab, allowing safer and more effective drugs to be screened for. But, to fully capitalise on the promise of genetics, however, requires gene therapy. Encouragingly, remarkable progress has been achieved; Clinical investigator Prof Orla Hardiman is trialling a number of pioneering gene therapy-based treatments for ALS in collaboration with world-leading pharmaceutical companies.
The Centre is also looking at how to safely deliver genes to precise areas of the brain, to control their activation via on/off switches and minimise potential side effects. Research extends to areas such as small noncoding RNAs and the biology of the blood-brain barrier. With a sharpened focus on accelerating clinical development and understanding the intricacies of the human brain, FutureNeuro is charting a course towards neurotherapeutics of the future.
Digital Health
In the rapidly evolving landscape of digital health, innovations are fundamentally reshaping healthcare delivery, access, and system operations. FutureNeuro's research program stands at the forefront, driven by the insights of clinicians and patients alike. Leveraging a rich data environment and cuttingedge digital technologies, they are co-designing solutions for proactive, personalised, and costeffective healthcare.
A researcher carefully uses a pipette in the lab
72 Brain Research
The Centre is laying the groundwork for a learning health system. This involves ethically integrating diverse datasets, including electronic health records and passive data from connected devices in homes. Furthermore, responsible artificial intelligence (AI) solutions aim to extract valuable insights from data, aiding clinical decision-making and continually improving patient care.
In tandem, FutureNeuro is pioneering a smartphone appbased digital therapeutic. Tailored to capture lifestyle data, it provides personalised interventions for mental well-being. Moreover, through strategic industry partnerships nurtured by programs like SFI SPOKE (EMPOWER and Precision ALS), they are advancing next-phase projects focused on health data analytics and building trust in the secondary use of data, alongside the utilisation and adoption of technologies such as artificial intelligence.
Mental Health
Mental health research is threaded throughout the new programme. In diagnostics, a significant new study is underway to look for changes in blood chemistry, aiming to identify people at risk earlier than is currently possible. In the drug development programme, researchers are targeting genes associated with psychosis while incorporating assessments for depression, anxiety, and psychosis across all drug development projects. This approach not only enhances drug efficacy but also provides insights into addressing the underlying mechanisms of mental health disorders. In the digital therapeutics program, efforts are focused on leading advancements in technologies that not only monitor but also positively intervene in brain health. This includes digital therapeutics that offer individuals greater control and continuity of care.
Rare Diseases
The Irish Government is committed to addressing rare diseases, with plans underway to create a National Rare Diseases Plan and a National Genetics and Genomics Medicine Network. FutureNeuro clinical researchers are developing patient registers for rare genomic diseases in order to stratify patients for clinical trials and be ready to implement advances in genomic medicine. Additionally, promising treatments are emerging at pre-clinical stage for epilepsy, including those for conditions like Dravet syndrome.
FutureNeuro will prioritize these often-overlooked conditions, aiming to drive progress and improve patient outcomes.
New Research Projects
FutureNeuro is already working on some remarkable projects that are taking a deep dive into the workings of the human brain. One such project involves recording patterns of electrical activity of brain cells, essentially eavesdropping on neurons and listening for when they misfire. This is possible because sometimes doctors will implant electrodes into the brains of people with treatment-resistant epilepsy to pinpoint the source of their seizures. The researchers have found a way to measure gene activity at the site of those recordings. This is helping to discover new genes that influence brain function and could hold promise for clinical decisionmaking. Like so much of the Centre’s work, this research relies on specialised scientific skills and collaboration with their dedicated clinical partners. This is only made possible by the robust framework upon which FutureNeuro is built.
Another exciting study aims to understand how to repair leaky blood vessels in the brain. In a healthy brain, blood vessels are tightly sealed, but in many neurological diseases, they become permeable. This hallmark is also associated with psychosis. By reapplying the genetic 'glue' responsible for maintaining the blood-brain barrier, researchers hope to open the doors to a completely new type of treatment.
Education, Public and Patient Engagement
A further evolution within FutureNeuro is the deeper
integration of patients within the Centre. They contribute to identifying research priorities, evaluating progress, and aid in communication with the public, funders, and policymakers, ensuring that research aligns closely with patient needs. Their Patient Panel played a key role in preparing the research strategy for FutureNeuro. The Centre is now actively developing diseasespecific patient panels that will be embedded across all areas of their research, including Parkinson's disease and MS.
Education and public engagement is another key component of their mission. The Brain Health webinar series, developed in partnership with Epilepsy Ireland, is just one example of the strategic collaborations they have undertaken to help break down barriers and make epilepsy research accessible to all. The team will also raise awareness of brain health and wellness with the wider community through an innovative education and engagement campaign called ‘My Moving Brain’, co-delivered across Ireland with patient advocacy groups and local sports partnerships as part of an SFI Discover Award. This initiative will build on their highly successful ‘Cell Explorers’ school programme that will continue to inspire the next generation of life scientists.
With over 350 engagement activities undertaken, including collaborative events with charitable organizations, enlightening workshops in schools, thoughtprovoking discussions at the Pint of Science festival, the creation of informative blogs for wider audiences, and valuable contributions to national policy, the Centre will continue to raise awareness and capture the
public's imagination, supported by a dedicated Education and Public and Patient Engagement Lead. Industry
Collaborating with industry is fundamental to the success of FutureNeuro. To date, the Leadership Team have undertaken more than 30 collaborative research projects, including partnerships with Roche, UCB, IQVIA, Novartis, Janssen, and Congenica. These include bringing new diagnostic supports to market, advancing a pipeline of new drugs through development and testing, and expanding digital health solutions to enable patients and their clinicians to co-monitor their health better than ever before. In FutureNeuro, the team will expand engagement with industry with a collective aim to advance new therapeutics and precision medicines, identify faster and more precise diagnostics tools, leverage the power of AI to accelerate discoveries based on clinical data and promote Ireland as a preferred location for early-stage clinical trials.
As FutureNeuro embarks on its mission to revolutionize brain research and treatment in Ireland, it commits not only to unravelling the complexities of brain diseases but also to leading the charge in translating these findings, paving the way for improved patient outcomes and transformative strides in healthcare.
For more information on the work of FutureNeuro go to www.futureneurocentre.ie
Over the Counter Preventative Supplements for Joint Health
Written by Hazel Windsor-Aubrey & Orla Walsh, Orla Walsh Nutrition
‘Supple’ and ‘pain free’ is how we would all like to be able to describe the way in which our body moves. The absence of joint stiffness or pain is something many may have once taken for granted. Reality can instead be filled with stiffness and discomfort which can significantly take from quality of life. When a person’s body doesn’t function as they wish, the psychological impact can be profound.
When we think of joint issues and loss of fluidity of movement we may immediately think of commonly discussed and afflicted joints such as our hips, knees and elbows. However, this is just the tip of the iceberg! The human body has an impressive 360 joints! That’s 360 potential problems if joint health is neglected or not prioritised.
As we age, a certain amount of wear and tear on joints is expected but joint issues can vary widely, spanning the odd painful niggle to very painful and debilitating chronic conditions such as osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, bunions and gout. These diseases affect not only the joint itself but also the bones, ligaments, tendons, muscle and cartilage surrounding it.
With regards to prevention of joint problems, we know that inflammation plays a role in their onset and progression so reducing the amount of inflammation inflicted is the number one preventative measure. The research confirms that for specific conditions such as osteoarthritis, obesity is a modifiable risk factor, meaning we can do something to change the trajectory. With excess body fat comes associated inflammation1,2 and increased pressure on weight-bearing joints such as knees and hips.
While prevention of joint issues should be a focus, more often action is taken in reaction to joint complaints. Treatment options come with side-effects and practitioners also need to consider person-preference, cost, availability and time. Therefore, it’s none too surprising that many people consider using supplements in a bid to experience some pros without the
Hazel Windsor-Aubrey
cons. Supplements are often also considered in conjunction with the pharmacological or surgical route, in a bid to enhance the body’s response and help manage potential pitfalls of the disease or treatment.
Commonly recommended over-the- counter supplements for joint health and the research
1. Omega 3 fats. Fish oils have been shown to reduce inflammation and may be beneficial with regards to joint health. Research has suggested that fish oil-based supplements may help reduce pain in those with rheumatoid arthritis,3,4 while a randomised controlled trial (RCT) which ran over two years found that a low dose fish oil was more beneficial at improving pain, stiffness and physical function when compared to a high dose in those with OA.6 So, more is not always more.
2. Antioxidants vitamins A, C and E. While a 2007 Systematic Review declared the quality of the studies available was low and therefore no conclusive recommendations could be drawn, another study in 2012 found that vitamin E may be helpful for knee pain.7 Adding more nuts and seeds, which are rich in vitamin E, to the daily diet may provide more benefits.
3. Vitamin D. The evidence specifically for joint health isn’t strong due to inconsistencies in findings and quality of research.
However, vitamin D is linked with lowering inflammation and cytokine synthesis8 as well as increased muscle strength,9 which is vital to protect muscles from excessive wear and tear. A study showed that for people with knee OA, those that had adequate serum vitamin D levels (>50nmol/l) had significantly improved structural and functional outcomes compared with those who had insufficient status.10 Currently, the Irish Osteoporosis Society advises 70nmol/l as an adequate vitamin D level. Current HSE guidance on 15mcg per day for adults in Ireland remains best practice.
4. Collagen. A 2021 systematic review looked at the effects of Type II collagen supplementation on joint function and recovery from joint injuries and found that in all five studies collagen was successful in reducing joint pain, joint function, length of pain free strenuous exertion and reducing the need for alternative therapies especially when combined with a structured exercise programme.11
5. Turmeric. A 2021 systematic review that looked at the safety and efficacy of Curcuma Longa (turmeric extract) and curcumin on OA found that it was successful at relieving pain, joint stiffness and improving joint function. They advised at least 12 weeks use.12
6. Glucosamine and chondroitin. A systematic review that looked
at supplements specifically for treating OA found that the most commonly used supplements for joint health, glucosamine and chondroitin were not clinically effective in reducing pain or improving physical function, even in the short term for people with OA.13
A food-first approach is always advised. Food is more than the sum of its parts. Supplements can never recreate the complexity of whole foods and dietary patterns. Changing what people eat, and when they eat it is likely to have a bigger impact that any one supplement. Our focus isn’t just on an anti-inflammatory dietary pattern but also a lifestyle that works in tandem. Supplements are likely to exhibit a greater response if used to supplement a holistic approach than a tool to help people dig upwards.
Furthermore, supplements may be considered in response to medications consumed by those with joint pain. For example, ongoing inflammation in the body can lead to iron deficiency. So, iron supplementation may need to be considered if that occurs. Additionally, steroids may be used as part of treatment. If that is the case, calcium-rich foods as well as other nutrients important for bone health like protein and vitamin K as well as vitamin D and magnesium need to be a focus.
References available on request
Key Trends in Irish Community Pharmacy
Summary Q1 2024
Irish Economy
Value of sales
Fitzgerald Power regularly update community pharmacy across Ireland as to the latest trends affecting the sector.
The latest Central Bank quarterly report for Q1 2024 expects the domestic economy to grow at a moderate pace; 2.2% in 2024, 1.9% in 2025 and 2% in 2026.
Their quarterly reports offer valuable insight and expert analysis into how the Pharmacy and SME markets are performing.
Inflation
Every three months the team look at the key trends of certain sectors, and provide thorough breakdowns to help you get members get their heads around the numbers.
The below is a summary of the latest analysis of the key trends in the Irish Community Pharmacy sector, prepared on a quarterly basis.
Inflation in the Eurozone was 2.4% in March 2024, a decrease from 2.6% in February. A year earlier the rate was 6.9%. Energy prices, which had increased last year as a result of Russia’s invasion of Ukraine, continued to reduce, with the rate of deflation moving from -3.7% to -1.8%.
Global Economy
Revenue Pulse
The global economy is poised for a second consecutive year of slower growth, largely attributed to high interest rates. The Q1 2024 baseline forecast maintains a global real GDP growth projection for 2024 at 2.7%, consistent with Q4 2023, with a forecast of 3.1% growth in 2025.
Value of sales
2024 moderate 2024, a the rate last year as a to reduce, -1.8%. consecutive interest global real consistent with though labour long-run remains economic average 4.5% 300
The value of sales, as measured by the CSO, increased by 0.2% in March 2024 against the same period last year. Value of Sales:
The value of sales, as measured by the CSO, increased by 0.2% in March 2024 against the same period last year.
Labour Market
The value of sales, as measured by the CSO, increased by 0.2% in March 2024 against the same period last year.
SOURCE: CSO
SOURCE: CSO IQVIA data has found RX classes are up 7% in value and 2% in volume vs the same period last year.
SOURCE: CSO
Rx Tracker
The labour market remains near full capacity, though employment growth has decelerated, and overall labour force expansion is anticipated to be below the long-run average. Despite this, the unemployment rate remains near historic lows. Given projections for modest economic growth, the unemployment rate is forecast to average 4.5% through 2026.
Medicine Shortages
data has found RX classes are up 7% in value and 2% in volume vs the same period last year. SOURCE: IQVIA
Top RX Classes by Growth
There is a current shortage of approximately 300 medicines in Ireland, placing “phenomenal pressure” on pharmacists nationwide according to the President of the Irish Pharmacy Union (IPU). The IPU has warned that most pharmacists fear it will become an even bigger issue over the coming year.
Summary
SOURCE: IQVIA
The value of sales, as measured by the CSO, increased by 0.2% in March 2024 against the same period last year.
Irish Economy - The latest Central Bank quarterly report for Q1 2024 expects the domestic economy to grow at a moderate pace; 2.2% in 2024, 1.9% in 2025 and 2% in 2026.
Revenue Pulse Rx Tracker
Inflation - Inflation in the Eurozone was 2.4% in March 2024, a decrease from 2.6% in February. A year earlier the rate was 6.9%. Energy prices, which had increased last year as a result of Russia’s invasion of Ukraine, continued to reduce, with the rate of deflation moving from -3.7% to -1.8%.
SOURCE: CSO IQVIA data has found RX classes are up 7% in value and
Global Economy - The global economy is poised for a second consecutive year of slower growth, largely attributed to high interest rates. The Q1 2024 baseline forecast maintains a global real GDP growth projection for 2024 at 2.7%, consistent with Q4 2023, with a forecast of 3.1% growth in 2025.
Labour Market - The labour market remains near full capacity, though employment growth has decelerated, and overall labour force expansion is anticipated to be below the long-run average. Despite this, the unemployment rate remains near historic lows. Given projections for modest economic growth, the unemployment rate is forecast to average 4.5% through 2026.
Medicine Shortages - There is a current shortage of approximately 300 medicines in Ireland, placing “phenomenal pressure” on pharmacists nationwide according to the President of the Irish Pharmacy Union (IPU). The IPU has warned that most pharmacists fear it will become an even bigger issue over the coming year.
OTC Tracker
IQVIA data shows OTC classes are up 2% in value, but down 4% in volume, as against the same period last year.
Market Pulse
Market Pulse
It was another strong quarter for sales, with Fitzgerald Power estimating 8 transactions completed in the 1st Quarter of 2024.
Market Pulse
OTC Tracker
SOURCE:
Benchmark Pulse
Benchmark Pulse
The Irish Pharmacy
Irish Pharmacy AwardsThe Best of Pharmacy Awards
Over 650 pharmacy and industry professionals were in attendance as winners across 13 categories were announced at the annual Irish Pharmacy Awards.
Each year Irish Pharmacy News, Ireland’s only independent monthly publication for community pharmacy, celebrates and acknowledges the achievements of teams and individuals within the pharmacy profession.
The 13th annual Irish Pharmacy Awards took place on Saturday, May 25th 2024. Hosted by Marty Whelan, the awards ceremony took place in the Clayton Hotel, Burlington Road, Dublin.
The Irish Pharmacy Awards recognise the achievements of individuals and teams working in the community pharmacy sector; their dedication and innovation which positions the profession at the forefront of healthcare, improving the lives of people across the country.
Pictured are some of those who attended.
1. Emma Keane, Kirsty Keogh and Clara Cobelo, Chemist Warehouse 2. The team from Finnegan's Pharmacy, Gillian Daisy, Mark MacMahon, Cherry McKilinery, Nuala Anne Curley and Elaine Curley, Pharmed 3. The pharmacy team from Ryan’s Pharmacy with Shane Ryan (middle) 4. All smiles for the camera at the 2024 Irish Pharmacy Awards 5. Ian Healy, Liz O’Hagan, Dan Whelan, Lisa Coffey and pharmacy team from Meaghers Pharmacy Group 6. The team from LloydsPharmacy
1. Fiona Curran,Leighan Weston, Linda Morrissey, Mary Butler, Laura Manley, Christine Peters and Juste Lileikyte, Pharmacy O'Regan, Moorefields, Newbridge
2. Michelle Higgins and Jessica Carroll, McCartans Donnelly’s Pharmacy 3. Denis O’Driscoll and Hillary Collins with team
4. The girls from Bradlon Ltd, Millmount Pharmacy, Village Pharmacy and North Road
Pictured
1. Jane Taylor and Sarah Mackessy, Boots Ireland 2. The pharmacy team from Adrian Dunne Pharmacy, Rush 3. Lisa Coffey, Aisling Gallen, Ian Healy, Daisy O’Shea and Renee Flynn, Meaghers Pharmacy Group 4. Andra Rooney with Maria Leonte, and Rosemary Conway, Athlone Pharmaceuticals 5. Jennifer Fitzgerald and Aisling Canavan, Uniphar 6. David Beggs with the team from Pure Pharmacy
1: Jenny Percival and team from Ryan’s Pharmacy 2. The team from GSK 3. Brian Battles, Pharmacy Success with Ciara Murphy, Nicola Talos and Lucian Talos, McCabes Pharmacy 4. Anne Morrissey, Lorraine O’Dwyer, Ciaran Sheehy, Ann Browne and Eve Brennan, Newpark Life Pharmacy 5. Rachel Dungan and Padraig O’Neill 6. The pharmacy team from Ryan’s Pharmacy
Clinical Profiles
CROÍ UNVEILS AMBITIOUS THREE-YEAR STRATEGY TO ENHANCE CARDIOVASCULAR HEALTH
Croí, the Heart and Stroke Charity, officially launched its comprehensive three-year strategy at a well-attended event at Croí Heart and Stroke Centre in Galway. The strategy, which outlines the charity’s goals and objectives from 2024 to 2027, aims to significantly improve cardiovascular health outcomes across more communities through widened geographical reach and increased service capacity.
The launch event featured contributions from Croí Chief Executive Mark O'Donnell, Croí Chairman Mark Gantly, former CEO of Croí and Executive Director of Global Heart Hub Neil Johnson, Croí's Medical Director, Professor Jim Crowley, volunteer Mary Lillis and Dr. Lisa Hynes, Croí’s Head of Health Programmes / Health Psychologist. The event was attended by a diverse group of stakeholders, including invited guests, volunteers, service users, and supporters.
Croí's vision is "an end to premature death or disability from cardiovascular disease in Ireland." To achieve this, the foundation's mission focuses on preventing heart disease and stroke, saving lives, and empowering people, families, and communities to take control of their health and well-being.
The cornerstone of the new strategy is to extend Croí's reach and capacity, while committing to a clear set of actions and targets. The charity aims to deliver better cardiovascular health outcomes by increasing access to prevention, support, and advocacy services across the region.
Dr Lisa Hynes, Croí’s Head of Health Programmes / Health Psychologist, Croí Chairman Mark Gantly, volunteer Mary Lillis, Croí Chief Executive Mark O'Donnell and Professor Jim Crowley
Strategic Objectives
The strategy outlines eight key strategic objectives, each supported by specific metrics and actions designed to ensure measurable progress:
1. Prevention: Increase access to early detection and support for managing risk factors.
2. Support: Provide comprehensive care and support to individuals and families affected by heart disease and stroke.
3. Patient Empowerment and Advocacy: Empower patients through education and advocacy efforts.
4. Community: Prioritise serving the communities with the greatest unmet need, with an expanded focus on the region.
5. People: Focus on the development of Croí's team, Board & volunteers
6. Financial Sustainability: Ensure long-term financial health and sustainability.
7. Communication: Enhance communication strategies to raise awareness and engage with stakeholders.
8. Governance: Maintain best practices in governance to ensure transparency and accountability.
Key Actions and Initiatives
• Targeted Prevention Programmes: Deliver programmes and campaigns based on risk factor management.
• Psychological Support Services: Develop multi-tiered support services for those impacted by cardiovascular diseases.
• Stroke Hub: Operationalise the new Stroke Hub at Croí House by 2025.
• Advocacy and Policy Change: Actively campaign for the development of a National Cardiovascular Health Plan.
• Community: Expand Croí’s regional footprint with a particular emphasis on counties Galway, Mayo, Clare, Leitrim, Roscommon, Sligo and Donegal.
Mark Gantly, Croí Chairman, emphasised the importance of community support in achieving these ambitious goals. "We are grateful for the exceptionally generous legacy donation from the Joe and Helen O’Toole Charitable Trust, which has been a catalyst for our strategic planning. Together, we can make a real difference in the health of our community," he said.
DARZALEX ® (DARATUMUMAB) SUBCUTANEOUS (SC) FORMULATION BECOMES THE FIRST TREATMENT FOR NEWLY DIAGNOSED SYSTEMIC LIGHT CHAIN AMYLOIDOSIS TO BE APPROVED FOR REIMBURSEMENT IN IRELAND
The Janssen Pharmaceutical Companies of Johnson & Johnson has announced the reimbursement of DARZALEX® (daratumumab) subcutaneous (SC) formulation in combination with bortezomib, cyclophosphamide and dexamethasone (D-VCd) for the treatment of adults with newly diagnosed systemic light chain (AL) amyloidosis. The announcement follows EC approval of daratumumab for this indication, based on positive results from the Phase 3 ANDROMEDA study, presented at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting and at the 26th European Haematology Association (EHA) Congress.1,2
AL amyloidosis is a rare and incurable blood disorder that is potentially life-threatening, caused by a build-up of amyloid, an insoluble protein, in tissues and organs.3,4 This eventually causes organ deterioration, most commonly in the heart, kidneys and liver.5
Dr Vitaliy Mykytiv, Consultant Haematologist, Cork University Hospital said “Today’s announcement marks significant progress for Irish patients living with Light Chain (AL) amyloidosis who face particularly high unmet medical need due to a lack of approved treatment options. This unmet need is further compounded by the fact that the disorder is rare and can be extremely hard to diagnose. It is very encouraging to see the results of the Phase 3 ANDROMEDA study and the deep responses this treatment regimen has seen from patients.”
Dr Brid Seoighe, Medical Director, Janssen Sciences Ireland UC, said: “At Janssen, our goal is to improve and prolong patients’ lives as we continue our work to advance research and ultimately deliver cures. This reimbursement marks an important milestone as the first treatment for this group of patients and will help to reduce symptom burden and improve quality of life for those living with this disease. We are delighted that newly diagnosed systemic AL amyloidosis patients in Ireland can now access this combination treatment.”
The Phase 3 ANDROMEDA study evaluated D-VCd compared with VCd alone, a common treatment regimen used in adult patients with newly diagnosed AL amyloidosis. Patients receiving treatment with daratumumab experienced a significantly higher haematologic complete response rate (hCR) compared to patients receiving VCd alone (60 percent vs. 19 percent; p<0.0001).6
Furthermore, at 25.8 months median follow up, more patients achieved a very good partial response or better (≥VGPR) (D-VCd vs VCd, 79% vs 50%; P<0.0001).6
References available on request
PROFESSOR DEBORAH MCNAMARA ELECTED AS NEW PRESIDENT OF RCSI
RCSI (Royal College of Surgeons in Ireland) has announced the election of Professor Deborah McNamara as the new President of the College.
Professor McNamara takes up office following the College’s biennial Council Elections. A consultant general and colorectal surgeon, she has built a deep experience of the healthcare system as co-lead of the National Clinical Programme for Surgery and as a national healthcare quality improvement leader.
Professor Michael Kerin, consultant general surgeon at Galway University Hospital, has been elected Vice-President.
Speaking on her appointment, Professor Deborah McNamara said: “I feel incredibly honoured to have been elected President of this College, which for over 240 years has been to the forefront of improving surgical care for patients, safeguarding standards of practice and providing leadership in the field of surgery.
A key focus of my work as President will be to support the younger generation of surgeons who are dealing with considerable challenges. It is incumbent on us all, but particularly those within leadership roles in our community,
to support this generation. I am also committed to continuing RCSI’s engagement with policymakers, regulators, service providers and patients, particularly on issues related to access to surgical care and patient safety.”
Following her appointment as a consultant general and colorectal surgeon at Beaumont Hospital in 2003, Professor McNamara was appointed clinical director for surgery at the hospital, where she has led the development of its colorectal cancer biobank and contributed to research collaborations between Beaumont clinicians and RCSI-affiliated scientists. She founded the betterbeaumont quality improvement learning collaborative in 2014 to support a range of hospital-based improvement activities.
Among her many roles in leadership and teaching, she has guided the Rectal Cancer Lead Clinician Group of the Health Service Executive National Cancer Control Programme. Through her work with the National Clinical Programme for Surgery, she has helped colleagues in all surgical specialties to publish implementable evidence-based policies and care pathways that will improve the delivery of surgical care in Ireland.
Since her election to the Council of RCSI in 2014, Professor McNamara has contributed as a member and chair of several RCSI and national committees. She has served as Chair of the Committee for Surgical Affairs, Faculty President of the RCSI Surgical Society and the Clinical Lead of the HSE/RCSI Transforming Theatre Healthcare Quality Improvement Programme.
Her outstanding contributions have been recognised with numerous national and international distinctions with highlights including Honorary Fellowship of the American College of Surgeons, the AWS Olga Jonasson Distinguished Member Award for outstanding mentorship and the Patey Prize. She delivered the 2019 Freyer State of the Art Lecture and the 2022 Robert Smith Lecture at the Association of Surgeons of Great Britain and Ireland.
Professor Michael Kerin is a Consultant General Surgeon at Galway University Hospital with a special interest in breast and endocrine cancer. He is deeply committed to the integration of academic surgery into healthcare delivery and clinical practice which he drives through his leadership roles including Professor and Head of the Department of Surgery at University of Galway and Director of the Cancer Managed Clinical Academic Network for Saolta University Health Care Group.
RYBREVANT® (AMIVANTAMAB) PLUS LAZERTINIB SHOWS LONGER PROGRESSIONFREE SURVIVAL VERSUS OSIMERTINIB IN THE FIRSTLINE TREATMENT OF PATIENTS WITH HIGH-RISK EGFRMUTATED NON-SMALL CELL LUNG CANCER
Janssen-Cilag International NV, a Johnson & Johnson company, have announced new data from the Phase 3 MARIPOSA study demonstrating the efficacy of firstline treatment with RYBREVANT® (amivantamab) in combination with lazertinib in patients with highrisk disease or clinical features, which occur in nearly 85 percent of patients with non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) mutations.1,2 Results from the new analysis show the amivantamabcombination consistently and significantly improved progression free survival (PFS) compared to
osimertinib in patients with NSCLC with EGFR exon 19 deletion (ex19del) or L858R mutations.1
These data were presented at the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting (Abstract #8504) taking place in Chicago, Illinois from 31 May – 4 June 2024.1
“These new data demonstrate the efficacy of amivantamab plus lazertinib, showing a significant reduction in the risk of disease progression or death compared to osimertinib in several high-risk subgroups of patients with EGFRmutated NSCLC,” said Byoung Chul Cho, M.D., Ph.D, medical oncologist and professor in the Division of Medical Oncology at Yonsei Cancer Center, Yonsei University College of Medicine in Seoul, Republic of Korea, and the study author.* “These findings support the potential of this combination as an important firstline option for these patients who face significant unmet needs.”
The MARIPOSA study enrolled treatment-naïve patients with EGFR-mutant (ex19del or L858R) advanced NSCLC.1 Overall, results showed amivantamab plus lazertinib resulted in a significant reduction in the risk of disease progression or death compared to osimertinib as previously reported.1 High-risk features, such as liver or brain metastases, baseline TP53 co-mutations, and circulating tumour DNA (ctDNA) shedding are common in patients with EGFR-mutated advanced NSCLC and associated with poor prognoses.3,4,5,6 In the study, 89 percent of enrolled patients had one or more of these high-risk disease or clinical features at baseline. Specifically, 41 percent had brain metastases, 16 percent had liver metastases, 54 percent had TP53 co-mutations, 70 percent had ctDNA present at baseline and 15 percent continued to shed ctDNA after two cycles of treatment.1
Results from the analysis showed treatment with amivantamab plus lazertinib significantly reduced the risk of disease progression or death consistently across all highrisk subgroups:1
• 31 percent compared to osimertinib in patients with a history of brain metastases (18.3 vs 13.0 months; hazard ratio [HR], 0.69; [95 percent confidence interval [CI], 0.530.92]; P=0.010)
• 42 percent compared to osimertinib in patients with liver metastases at baseline (18.2 vs 11.0 months; HR, 0.58 [95 percent CI, 0.37-0.91]; P=0.017)
• 35 percent compared to osimertinib among patients with
• 32 percent compared to osimertinib in patients with detectable ctDNA at baseline (20.3 vs 14.8 months; HR, 0.68 [95 percent CI, 0.53-0.86]; P=0.002)
• 51 percent compared to osimertinib in patients without cleared ctDNA at C3D1 (16.5 vs 9.1 months; HR, 0.49 [95 percent CI, 0.27-0.87]; P=0.015)
“High-risk features are incredibly prevalent in first-line EGFRmutated non-small-cell lung cancer and are associated with a poor prognosis,” said Henar Hevia, Ph.D, Senior Director, EMEA Therapeutic Area Lead, Oncology, Johnson & Johnson Innovative Medicine. "The encouraging findings from this study, demonstrating improved progression-free survival in this critical patient subgroup treated with amivantamab and lazertinib, highlight our commitment to pioneering precision medicine and establishing new standards of care for one of the largest lung cancer patient populations."
As reported at the European Society for Medical Oncology (ESMO) 2023 Congress, the safety profile of the combination of amivantamab and lazertinib was consistent with the safety profiles of the individual treatments, with mostly Grade 1 or 2 adverse events (AEs) reported.7 Toxicity was largely manageable with dose interruptions and reductions, along with supportive care measures commonly used in the treatment of patients with NSCLC.7 The most common Grade 3 or higher treatment-related AEs were rash and paronychia.7 Amivantamab plus lazertinib had higher rates of EGFR and MET-related AEs (hypoalbuminemia and peripheral oedema) and venous thromboembolism compared to osimertinib, with higher rates of diarrhoea being observed with osimertinib.7 The rate of discontinuation of all study treatments due to treatmentrelated AEs for the amivantamab combination was 10 percent.7 The rate of interstitial lung disease (including pneumonitis) was less than three percent in both arms.7
“With the majority of patients with EGFR-mutated lung cancer having high-risk disease and clinical features, ensuring that all patients receive the most appropriate treatment in the first-line setting is critical. The results presented at ASCO suggest amivantamab plus lazertinib may offer a new standard of care in this patient population,” said Craig Tendler, M.D., Vice
New President of RCSI, Professor Deborah McNamara
Clinical Profiles
President, Late Development and Global Medical Affairs, Johnson & Johnson Innovative Medicine.
“These new findings continue to demonstrate how amivantamabbased regimens are transforming treatment for patients with EGFR-mutated non-small cell lung cancer and add to the growing body of evidence that supports the potential promise of this chemotherapy-free approach.”
References available on request HELIUM ARTS GOES NATIONWIDE WITH LAUNCH OF ITS CREATIVE HEALTH PROGRAMME IN HOSPITALS AND IN THE COMMUNITY IN DUBLIN
Helium Arts – the children’s charity committed to improving the wellbeing of children and young people living with lifelong physical health conditions – has today (11.06.24) announced the expansion of its Creative Health programme to hospital and community settings in Dublin.
The programme provides free, artist-led creative workshops in hospital paediatric outpatient clinics to children and young people living with lifelong physical health conditions. Following the hospital-based workshops, participants can be referred to Helium Arts’ community and online programmes, which include free workshops and camps
Pictured at an event in the Naughton Institute at Trinity College Dublin on 11th June to announce the launch of Helium Arts’ Creative Health programme in Dublin were: Helene Hugel, CEO, Helium Arts, Dr Pamela O’Connor, Consultant Neonatologist Paediatrician working in Children’s Health Ireland (CHI) at Crumlin and The Coombe Women and Infants University Hospital, Dublin, and Dr Judith Meehan, Dean of the Faculty of Paediatrics, Royal College of Physicians in Ireland.
Photo: Julien Behal
during school holidays and weekends. These workshops, led by professional artists, provide on-site medical support and are accessible to participants with a variety of needs.
Supported conditions include diabetes, epilepsy, cystic fibrosis, cerebral palsy, allergies, heart conditions, asthma, spina bifida, juvenile arthritis, rare or complex conditions and many more.
In Dublin, the programme is initially being rolled out at Children’s Health Ireland (CHI) at Connolly in Blanchardstown and Children’s Health Ireland (CHI) at Tallaght, in partnership with the CHI Arts in Health Programme.
The expansion to Dublin signifies a milestone in the growth of Helium Arts, marking the programme’s first five years delivering impactful, creative and transformative partnerships, and establishing the Mullingar-based charity as a nationwide organisation.
According to Helium Arts’ latest impact report for 2023 published today, 2,881 children and young people took part in its programmes last year. The programme has already been running in hospital and community settings in Cork, Limerick, the Mid West, Galway and the West, and is also offered online, allowing children to participate no matter where they are.
Announcing the launch of the programme in Dublin, CEO of Helium Arts, Helene Hugel, said: “As we celebrate five years of our Creative Health programme, we’re excited to expand the reach of our hospital-based programmes to Dublin. In Ireland, 156,437 or 12% of all children and teenagers live with the effects of illness or disability every day. This key step in our national growth means that even more children can have improved outcomes in health, wellbeing, social connection and creative expression.
“Our new partnership with the CHI Arts in Health Programme in Dublin is a testament to the strength of community and collaboration that drives us forward to improve access to creative opportunities for more children living with chronic health conditions.”
Also commenting on the launch, Fiona Smith, Arts in Health Programme Curator for CHI, said: “It’s widely recognised that engaging with art and creativity can play an important role in promoting health and wellbeing, and sustainable arts programmes based on excellence can improve the quality of the patient experience in paediatric healthcare. By working closely with established arts in health practitioners such as Helium Arts, we can give children and young people the opportunity to explore a range of age-appropriate creative activities that can positively impact their healthcare experience.”
ASCO: SARCLISA IS FIRST ANTI-CD38 TO SIGNIFICANTLY IMPROVE PROGRESSION-FREE SURVIVAL IN COMBINATION WITH VRD FOR NEWLY DIAGNOSED TRANSPLANTINELIGIBLE MULTIPLE MYELOMA IN PHASE 3
Data from the IMROZ phase 3 study demonstrated Sarclisa (isatuximab) in combination with standard-of-care bortezomib, lenalidomide and dexamethasone (VRd) followed by Sarclisa-Rd (the IMROZ regimen) significantly reduced the risk of disease progression or death by 40%, compared to VRd followed by Rd in patients with newly diagnosed multiple myeloma (NDMM) not eligible for transplant. IMROZ is the first global phase 3 study of an anti-CD38 monoclonal antibody in combination with standard-of-care VRd to significantly improve PFS and show deep responses in this patient population who often have poor prognoses. The results were shared in an oral presentation at the American Society of Clinical Oncology (ASCO) annual meeting and simultaneously published in the New England Journal of Medicine (NEJM).
The use of Sarclisa in combination with VRd in transplant-ineligible NDMM is investigational and has not been fully evaluated by any regulatory authority.
Thierry Facon, MD - Professor of Haematology in the Department of Haematology, Lille University Hospital, Lille, France, member of French Academy of Medicine and IMROZ Principal Investigator
“The significant progression-free survival benefit observed with Sarclisa combination therapy
compared to VRd is important and encouraging for patients with newly diagnosed multiple myeloma. Effective frontline therapy has the potential to modify the course of the disease, which is a key outcome for transplant-ineligible patients who often face high rates of attrition in later lines of therapy. The IMROZ results demonstrate the promise of Sarclisa as a backbone to frontline therapy, which may improve long-term outcomes for this incurable disease.”
Key Results
IMROZ is a global, randomized, multi-center, open-label study. At the data cut-off of September 26, 2023, through the median followup of 59.7 months, the following were observed for Sarclisa-VRd compared to VRd:
Primary endpoint
• 40% reduction in the risk of disease progression or death for patients treated with SarclisaVRd versus VRd (HR 0.596; 98.5% CI: 0.406 to 0.876; p=0.0005). At the median followup of 59.7 months, the median PFS with the Sarclisa-VRd combination was not reached versus 54.3 months with VRd.
• The estimated PFS at 60 months was 63.2% for patients treated with Sarclisa-VRd versus 45.2% for VRd.
Secondary endpoints
• Approximately three-quarters (74.7%) of patients treated with Sarclisa-VRd achieved a complete response (CR) compared to 64.1% of patients taking VRd (OR 1.7; 95% CI: 1.097-2.5; p=0.008).
• More than half (55.5%) of patients treated with SarclisaVRd achieved MRD negative CR compared to 40.9% of patients taking VRd (OR 1.8; 95% CI: 1.229-2.646; p=0.0013).
• MRD was sustained for at least 12 months among nearly half (46.8%) of patients in the Sarclisa-VRd arm compared to less than one-quarter (24.3%) of patients taking VRd (OR 2.7; 95% CI: 1.799-4.141).
At the date of data cut-off, 47.2% of patients (125/263) treated with Sarclisa-VRd and 24.3% of patients (44/181) treated with VRd were still on treatment. The median treatment duration for the SarclisaVRd combination was 53.2 months vs. 31.3 months for VRd.
The safety and tolerability of Sarclisa observed in this study was consistent with the established safety profile of Sarclisa-VRd with no new safety signals observed.
Grade ≥3 treatment-emergent adverse events (TEAE) occurred in 91.6% of patients taking SarclisaVRd and 84% of patients taking VRd. Treatment-emergent events (TAE) of any grade led to treatment discontinuation in 22.8% of patients taking Sarclisa-VRd and 26% of patients taking VRd.
FULBRIGHT IRISH AWARDEES FORGE LINKS IN THE USA
The Department of Foreign Affairs, Department of Tourism, Culture, Arts, Gaeltacht, Sport and Media, and the Embassy of the United States of America in Dublin are pleased to announce 21 Fulbright Irish Awardees for 2024-2025. Recipients were presented with Awards at a ceremony in Iveagh House last night.
The Fulbright bilateral exchange programme has facilitated academic and cultural exchanges and strengthened IrelandU.S. relations since 1957. The programme has a reputation for selecting exceptional candidates from across Ireland to study and work in disciplines ranging from health, science, technology and business to culture, the arts and the Irish language. Academics, professionals, students and scholars will research, study, teach and collaborate with experts at leading U.S. institutions. Their innovative research will have lasting impacts for society.
From August 2024 to August 2025, Fulbright Irish Scholars, Students and Professionals will attend diverse institutions ranging from the University of Puerto Rico, New York University and the University of Maine to the University of Colorado Denver, The New School and the National Renewable Energy Laboratory. Awardees will research an exciting range of fields including urban
studies, literature, information science, public health, fine arts, political science, engineering, physics, pharmacology, journalism, and genetics. Fulbright Foreign Language Teaching Assistants (FLTAs) will teach the Irish language at such universities as Davidson-Davie Community College, Catholic University of America, the University of Montana, and the University of Notre Dame to name a few.
Irish awardees will serve as cultural ambassadors in the U.S. and share their knowledge, ideas and experience when they return home. Inspired by the mission and ethos of the Fulbright Commission, they will strengthen connections between the U.S. and Ireland and contribute to creating a global culture of understanding that is vital in today’s ever more polarised world.
The Fulbright Irish Awards will open on 29th August, 2024. Interested candidates should visit www.fulbright.ie for more information.
Chair of the Fulbright Commission Ireland Board, Professor Paul
Donnelly, said, “As Chair of the Fulbright Ireland Board, I am delighted to congratulate the recipients of the 2024-2025 Fulbright Irish Awards. In a year that saw the Commission award Fulbright Public Service Awards to Speaker Emerita Nancy Pelosi and Dr. Anthony Fauci, so too do Fulbright awardees represent the core Fulbright values of meticulous, innovative and highquality research and teaching in service to the public good. As they begin their cultural and educational exchanges in the U.S., awardees join a distinguished global network of Fulbright alumni, experts, peers and colleagues who have achieved success and accolades in all disciplines. I wish the new awardees an enjoyable and fruitful experience in the United States.”
ITEOS AND GSK INITIATE GALAXIES LUNG-301 PHASE 3 STUDY, ASSESSING BELRESTOTUG AND DOSTARLIMAB IN PREVIOUSLY UNTREATED, UNRESECTABLE LOCALLY ADVANCED / METASTATIC PD-L1 SELECTED NON-SMALL CELL LUNG CANCER
iTeos Therapeutics, Inc. (Nasdaq: ITOS) (“iTeos”), a clinical-stage biopharmaceutical company pioneering the discovery and development of a new generation of immuno-oncology therapeutics for patients, and its development partner GSK, have initiated the first, global Phase 3 registration study of belrestotug + dostarlimab doublet versus placebo + pembrolizumab in patients with previously untreated, unresectable, locally advanced or metastatic PD-L1 selected non-small cell lung cancer (NSCLC).
“With the initiation of the first Phase 3 study for belrestotug, we are entering a monumental stage in our journey to develop a worldleading oncology company. Nearly 70% of patients with first-line PDL1 high non-small cell lung cancer rely upon a chemotherapy-free regimen. We believe belrestotug + dostarlimab are poised to potentially advance the therapeutic regimen in this setting and establish new benchmarks,” said Michel Detheux, Ph.D., president and chief executive officer of iTeos.
“Based on our high-quality doublet exceeding its pre-defined efficacy criteria for clinically relevant activity in an interim assessment from the Phase 2 GALAXIES Lung201 study, we believe initiating the Phase 3 program with this patient population will serve as the foundation to our broader strategy and marks our first step in building a franchise.”
The randomised, double-blind, placebo-controlled, multicenter
trial will enroll approximately 1,000 patients with previously untreated, unresectable, locally advanced or metastatic PDL1 selected NSCLC in North America, South America, Europe and Asia. The primary endpoints of the trial are progression free survival and overall survival. In the GALAXIES Lung-301 trial, patients will be randomized 1:1 to either an intravenous infusion of the belrestotug + dostarlimab doublet or placebo + pembrolizumab.
In May 2024, iTeos announced an interim assessment of the Phase 2 GALAXIES Lung-201 study of the belrestotug + dostarlimab doublet in previously untreated, locally advanced, or metastatic PD-L1 selected NSCLC exceeded pre-defined efficacy criteria for clinically relevant activity and showed an acceptable safety profile in line with the TIGIT:PD-1 class. Clinically meaningful tumor reduction was observed at every belrestotug + dostarlimab dose vs dostarlimab monotherapy.
About iTeos Therapeutics, Inc. iTeos Therapeutics is a clinicalstage biopharmaceutical company pioneering the discovery and development of a new generation of immuno-oncology therapeutics for patients. iTeos Therapeutics leverages its deep understanding of tumor immunology and immunosuppressive pathways to design novel product candidates with the potential to restore the immune response against cancer. The Company’s innovative pipeline includes three clinicalstage programs targeting novel, validated immunosuppressive pathways designed with optimized pharmacologic properties for improved clinical outcomes, including the TIGIT/CD226 axis and the adenosine pathway. iTeos Therapeutics is headquartered in Watertown, MA with a research center in Gosselies, Belgium.
JOB: SUPERVISING PHARMACIST REQUIRED IN LOUTH, FOR FURTHER DETAILS