ABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics before prescribing. PRESENTATION KEYTRUDA 25 mg/mL:
One vial of 4 mL of concentrate contains 100 mg of pembrolizumab. INDICATIONS • KEYTRUDA as monotherapy is indicated for the treatment of adults and adolescents aged 12 years and older with advanced (unresectable or metastatic) melanoma. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults and adolescents aged 12 years and older with Stage IIB, IIC or III melanoma and who have undergone complete resection. • KEYTRUDA, in combination with platinum-containing chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment, is indicated for the treatment of resectable non-small cell lung carcinoma at high risk of recurrence in adults. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults with non-small cell lung carcinoma who are at high risk of recurrence following complete resection and platinum-based chemotherapy. • KEYTRUDA as monotherapy is indicated for the first-line treatment of metastatic non-small cell lung carcinoma (NSCLC) in adults whose tumours express PD-L1 with a ≥50% tumour proportion score (TPS) with no EGFR or ALK positive tumour mutations. • KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of metastatic non-squamous NSCLC in adults whose tumours have no EGFR or ALK positive mutations. • KEYTRUDA, in combination with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of metastatic squamous NSCLC in adults. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic NSCLC in adults whose tumours express PD-L1 with a ≥1% TPS and who have received at least one prior chemotherapy regimen. Patients with EGFR or ALK positive tumour mutations should also have received targeted therapy before receiving KEYTRUDA. • KEYTRUDA as monotherapy is indicated for the treatment of adult and paediatric patients aged 3 years and older with relapsed or refractory classical Hodgkin lymphoma (cHL) who have failed autologous stem cell transplant (ASCT) or following at least two prior therapies when ASCT is not a treatment option. • KEYTRUDA, in combination with enfortumab vedotin, is indicated for the first-line treatment of unresectable or metastatic urothelial carcinoma in adults. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic urothelial carcinoma in adults who have received prior platinum-containing chemotherapy. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic urothelial carcinoma in adults who are not eligible for cisplatin-containing chemotherapy and whose tumours express PD L1 with a combined positive score (CPS) ≥ 10. • KEYTRUDA as monotherapy or in combination with platinum and 5-fluorouracil (5-FU) chemotherapy, is indicated for the first-line treatment of metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC) in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA as monotherapy is indicated for the treatment of recurrent or metastatic HNSCC in adults whose tumours express PD-L1 with a ≥ 50% TPS and progressing on or after platinum-containing chemotherapy. • KEYTRUDA, in combination with axitinib, is indicated for the first-line treatment of advanced renal cell carcinoma (RCC) in adults. • KEYTRUDA, in combination with lenvatinib, is indicated for the first line treatment of advanced renal cell carcinoma in adults. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults with renal cell carcinoma at increased risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions. Microsatellite instability high (MSI-H) or mismatch repair deficient (dMMR) cancers Colorectal cancer (CRC) • KEYTRUDA as monotherapy is indicated for adults with MSI-H or dMMR colorectal cancer in the following settings: – first line treatment of metastatic colorectal cancer – treatment of unresectable or metastatic colorectal cancer after previous fluoropyrimidine-based combination therapy. Non-colorectal cancers • KEYTRUDA as monotherapy is indicated for the treatment of the following MSI-H or dMMR tumours in adults with (a) advanced or recurrent endometrial carcinoma, who have disease progression on or following prior treatment with a platinum-containing therapy in any setting and who are not candidates for curative surgery or radiation, (b) unresectable or metastatic gastric, small intestine, or biliary cancer, who have disease progression on or following at least one prior therapy. • KEYTRUDA, in combination with platinum and fluoropyrimidine based chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic carcinoma of the oesophagus in adults whose tumours express PD-L1 with a CPS ≥ 10. • KEYTRUDA, in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery, is indicated for the treatment of adults with locally advanced, or early-stage triple-negative breast cancer at high risk of recurrence. • KEYTRUDA, in combination with chemotherapy, is indicated for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumours express PD-L1 with a CPS ≥ 10 and who have not received prior chemotherapy for metastatic disease. • KEYTRUDA, in combination with lenvatinib, is indicated for the treatment of advanced or recurrent endometrial carcinoma in adults who have disease progression on or following prior treatment with a platinum containing therapy in any setting and who are not candidates for curative surgery or radiation. • KEYTRUDA, in combination with chemotherapy with or without bevacizumab, is indicated for the treatment of persistent, recurrent, or metastatic cervical cancer in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with trastuzumab, fluoropyrimidine and platinum-containing chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic HER2-positive gastric or gastro-oesophageal junction adenocarcinoma in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with fluoropyrimidine and platinum-containing chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic HER2-negative gastric or gastro-oesophageal junction adenocarcinoma in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with gemcitabine and cisplatin, is indicated for the first-line treatment of locally advanced unresectable or metastatic biliary tract carcinoma in adults. DOSAGE AND ADMINISTRATION See SmPC for full details. Therapy must be initiated and supervised by specialist physicians experienced in the treatment of cancer. The recommended dose of KEYTRUDA in adults is either 200 mg every 3 weeks or 400 mg every 6 weeks administered as an intravenous infusion over 30 minutes. The recommended dose of KEYTRUDA as monotherapy in paediatric patients aged 3 years and older with cHL or patients aged 12 years and older with melanoma is 2 mg/kg bodyweight (up to a maximum of 200 mg), every 3 weeks administered as an intravenous infusion over 30 minutes. For use in combination, see the Summary of Product Characteristics (SmPC) for the concomitant therapies. KEYTRUDA must not be administered as an intravenous push or bolus injection. When administering KEYTRUDA as part of a combination with intravenous chemotherapy, KEYTRUDA should be administered first. When administering KEYTRUDA as part of a combination with enfortumab vedotin, KEYTRUDA should be administered after enfortumab vedotin when given on the same day. Treat patients until disease progression or unacceptable toxicity (and up to maximum duration of therapy if specified for an indication). For the adjuvant treatment of melanoma, NSCLC, or RCC, KEYTRUDA should be administered until disease recurrence, unacceptable toxicity, or for a duration of up to one year. Refer to the SmPC for dosing in neoadjuvant and adjuvant treatment of resectable NSCLC and neoadjuvant and adjuvant treatment of locally advanced, or early stage triple-negative breast cancer at high risk of recurrence. KEYTRUDA, as monotherapy or as combination therapy, should be permanently discontinued (a) For Grade 4 toxicity except for: endocrinopathies that are controlled with replacement hormones; or haematological toxicity, only in patients with cHL in which KEYTRUDA should be withheld until adverse reactions recover to Grade 0-1; (b) If corticosteroid dosing cannot be reduced to ≤10 mg prednisone or equivalent per day within 12 weeks; (c) If a treatment-related toxicity does not resolve to Grade 0-1 within 12 weeks after last dose of KEYTRUDA; (d) If any event occurs a second time at Grade ≥ 3 severity. Patients must be given the Patient Card and be informed about the risks of KEYTRUDA. Special populations Elderly: No dose adjustment necessary. Renal impairment: No dose adjustment needed for mild or moderate renal impairment. No studies in severe renal impairment. Hepatic impairment: No dose adjustment needed for mild or moderate hepatic impairment. No studies in severe hepatic impairment. Paediatric population: Safety and efficacy in children below 18 years of age not established except in paediatric patients with melanoma or cHL. CONTRAINDICATIONS Hypersensitivity to the active substance or to any excipients. PRECAUTIONS AND WARNINGS
than one body system can occur simultaneously. Immune-mediated adverse reactions are immune-mediated pneumonitis, immune-mediated colitis, immune-mediated hepatitis, immune-mediated nephritis, immune-mediated endocrinopathies (including adrenal insufficiency, hypophysitis, type 1 diabetes mellitus, diabetic ketoacidosis, hypothyroidism, and hyperthyroidism), immune-mediated skin adverse reactions (also including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN)). Refer to SmPC for more information and management of immune-mediated adverse reactions. Complications of allogeneic Haematopoietic Stem Cell Transplant (HSCT): Cases of graft-versus-host-disease (GVHD) and hepatic veno-occlusive disease (VOD) have been observed in patients with classical Hodgkin lymphoma undergoing allogeneic HSCT after previous exposure to pembrolizumab. Infusion-related reactions: Grades 1, 2, 3 or 4 infusion reactions including hypersensitivity and anaphylaxis, could be seen with pembrolizumab treatment. Refer to SmPC for more information and management of infusion-related reactions. Patients with Biliary tract carcinoma (especially those with biliary stents) should be closely monitored for development of cholangitis or biliary tract infections before initiation of treatment and, regularly, thereafter. Overdose: There is no information on overdose with pembrolizumab. In case of overdose, monitor closely for signs or symptoms of adverse reactions and treat appropriately. INTERACTIONS No formal pharmacokinetic drug interaction studies have been conducted with pembrolizumab. No metabolic drug-drug interactions are expected. The use of systemic corticosteroids or immunosuppressants before starting pembrolizumab should be avoided because of their potential interference with the pharmacodynamic activity and efficacy of pembrolizumab. Corticosteroids can be used as premedication, when pembrolizumab is used in combination with chemotherapy, as antiemetic prophylaxis and/or to alleviate chemotherapy-related adverse reactions. FERTILITY, PREGNANCY AND LACTATION Women of childbearing potential Women of childbearing potential should use effective contraception during treatment with pembrolizumab and for at least 4 months after the last dose of pembrolizumab. Pregnancy No data on use in pregnant women. Do not use during pregnancy unless the clinical condition of the woman requires treatment with pembrolizumab. Breast-feeding It is unknown whether pembrolizumab is secreted in human milk. A risk to newborns/ infants cannot be excluded. Fertility No clinical data available. SIDE EFFECTS Refer to SmPC for complete information on side effects. Pembrolizumab is most commonly associated with immune-mediated adverse reactions. Most of these reactions resolved with appropriate medical treatment or withdrawal of pembrolizumab. The most serious adverse reactions were immune-mediated and infusion-related adverse reactions. When pembrolizumab is administered in combination with axitinib or lenvatinib, refer to the SmPC for axitinib or lenvatinib prior to initiation of treatment. For additional lenvatinib safety information related to advanced RCC see the SmPC for Kisplyx and for advanced EC see the SmPC for Lenvima. When pembrolizumab is administered in combination with enfortumab vedotin, refer to the SmPC for enfortumab vedotin prior to initiation of treatment. For additional enfortumab vedotin safety information related to advanced UC see the SmPC for Padcev. Monotherapy: Very Common: anaemia, hypothyroidism, decreased appetite, headache, dyspnea, cough, abdominal pain, nausea, vomiting, constipation, musculoskeletal pain, arthralgia, asthenia, oedema, pyrexia, diarrhoea, pruritus, rash, fatigue. Common: pneumonia, thrombocytopenia, neutropenia, lymphopenia, hyponatraemia, hypokalaemia, hypocalcaemia, insomnia, neuropathy peripheral, lethargy, dry eye, cardiac arrhythmia (including atrial fibrillation), hypertension, hyperthyroidism, dizziness, dysgeusia, pneumonitis, colitis, dry mouth, hepatitis, severe skin reactions, vitiligo, dry skin, eczema, alopecia, dermatitis acneiform, erythema, dermatitis, myositis, pain in extremity, arthritis, influenza like illness, chills, AST and ALT increases, increase in blood alkaline phosphatase, hypercalcaemia, blood bilirubin increased, blood creatinine increased, infusion related reaction. In combination with chemotherapy: Very Common: Anaemia, neutropenia, thrombocytopenia, hypothyroidism, hypokalaemia, decreased appetite, insomnia, neuropathy peripheral, headache, dyspnoea, cough, diarrhoea, vomiting, nausea, abdominal pain, constipation, alopecia, pruritus, rash, musculoskeletal pain, arthralgia, pyrexia, fatigue, asthenia, ALT increase, AST increased. Common: pneumonia, febrile neutropenia, leukopenia, lymphopenia, infusion related reaction, adrenal insufficiency, thyroiditis, hyperthyroidism, hyponatraemia, hypocalcaemia, lethargy, dizziness, dysgeusia, dry eye, cardiac arrhythmia (including atrial fibrillation), hypertension, pneumonitis, colitis, gastritis, dry mouth, hepatitis, severe skin reactions, erythema, dermatitis, dry skin, dermatitis acneiform, eczema, myositis, pain in extremity, arthritis, acute kidney injury, oedema, influenza-like illness, chills, blood bilirubin increased, blood alkaline phosphatase increased, blood creatinine increased, hypercalcaemia. In combination with axitinib or lenvatinib: Very Common: urinary tract infection, anaemia, hypothyroidism, decreased appetite, headache, dysgeusia, hypertension, dyspnoea, cough, diarrhoea, abdominal pain, nausea, vomiting, constipation, rash, pruritus, arthralgia, musculoskeletal pain, myositis, pain in extremity, fatigue, asthenia, oedema, pyrexia, lipase increased, alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Common: pneumonia, neutropenia, thrombocytopenia, lymphopenia, leukopenia, infusion-related reaction, adrenal insufficiency, hyperthyroidism, thyroiditis, hyponatraemia, hypokalaemia, hypocalcaemia, insomnia, dizziness, neuropathy peripheral, lethargy, dry eye, cardiac arrhythmia (including atrial fibrillation), pneumonitis, colitis, pancreatitis, gastritis, dry mouth, hepatitis, severe skin reactions, dermatitis, dry skin, erythema, dermatitis acneiform, alopecia, arthritis, nephritis, influenza like illness, chills, amylase increased, blood bilirubin increased, blood alkaline phosphatase increased, hypercalcaemia. PACKAGE
Scan the QR code with your phone to view the KEYTRUDA SPC on medicines.ie
Oak North, South County Business Park, Leopardstown, Dublin D18 X5K7, Ireland.
Contents Foreword
First Use of New Biological Aortic Heart Valve P5
Beacon Hospital unveils new Aseptic Compounding Unit P7
Irish Medical Council makes statement of scope and practice of Physician Associates P8
Marie Keating Foundation highlights achievements of 2024 P16
Achievements and Challenges for Thrombosis Ireland P26
HPN reflects on a year gone past P36
Viatris support the Irish Wheelchair Association P40
Professional 100 2023 P46
REGULARS
Feature: Physiologic Pacing P28
Feature: Bladder Cancer P34
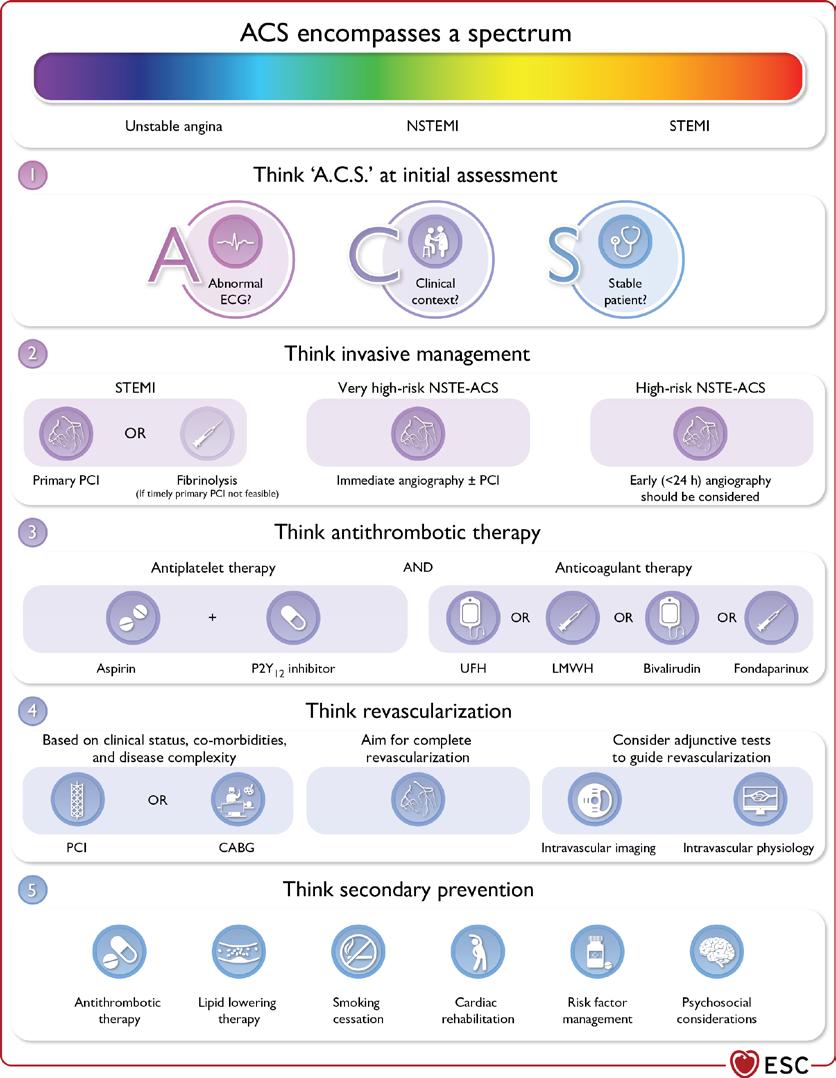
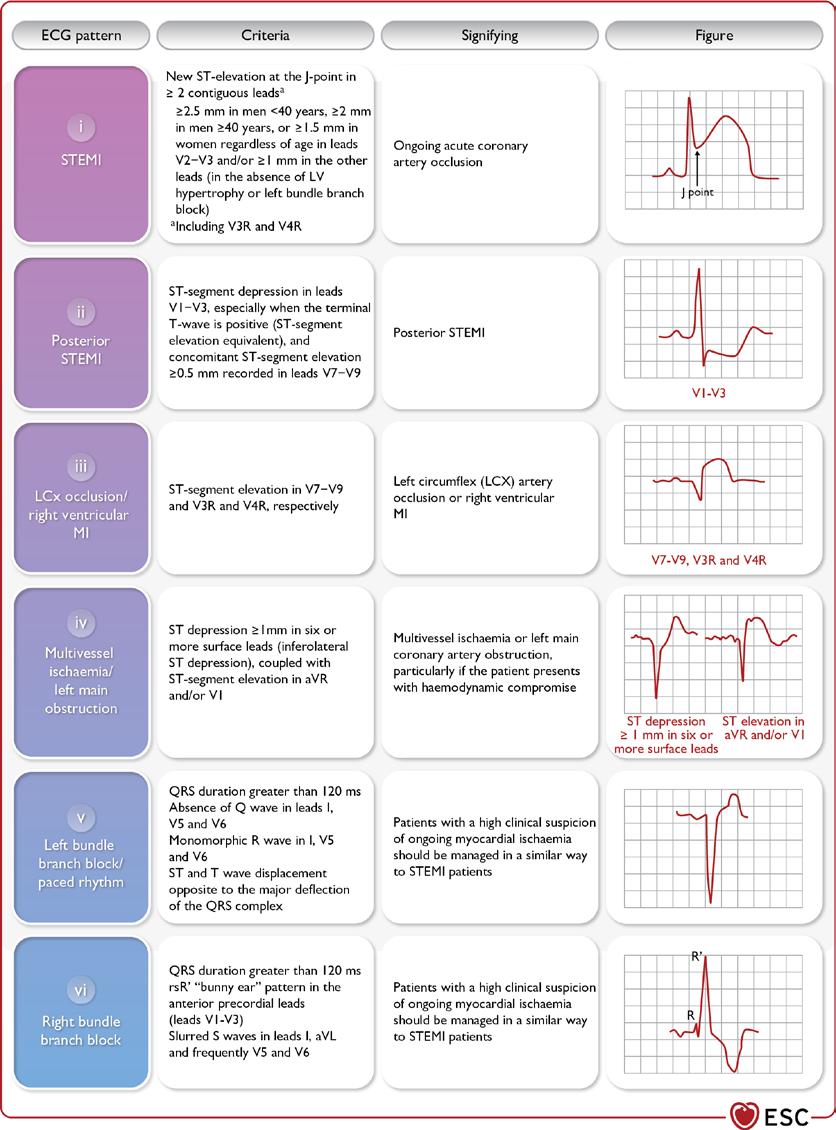
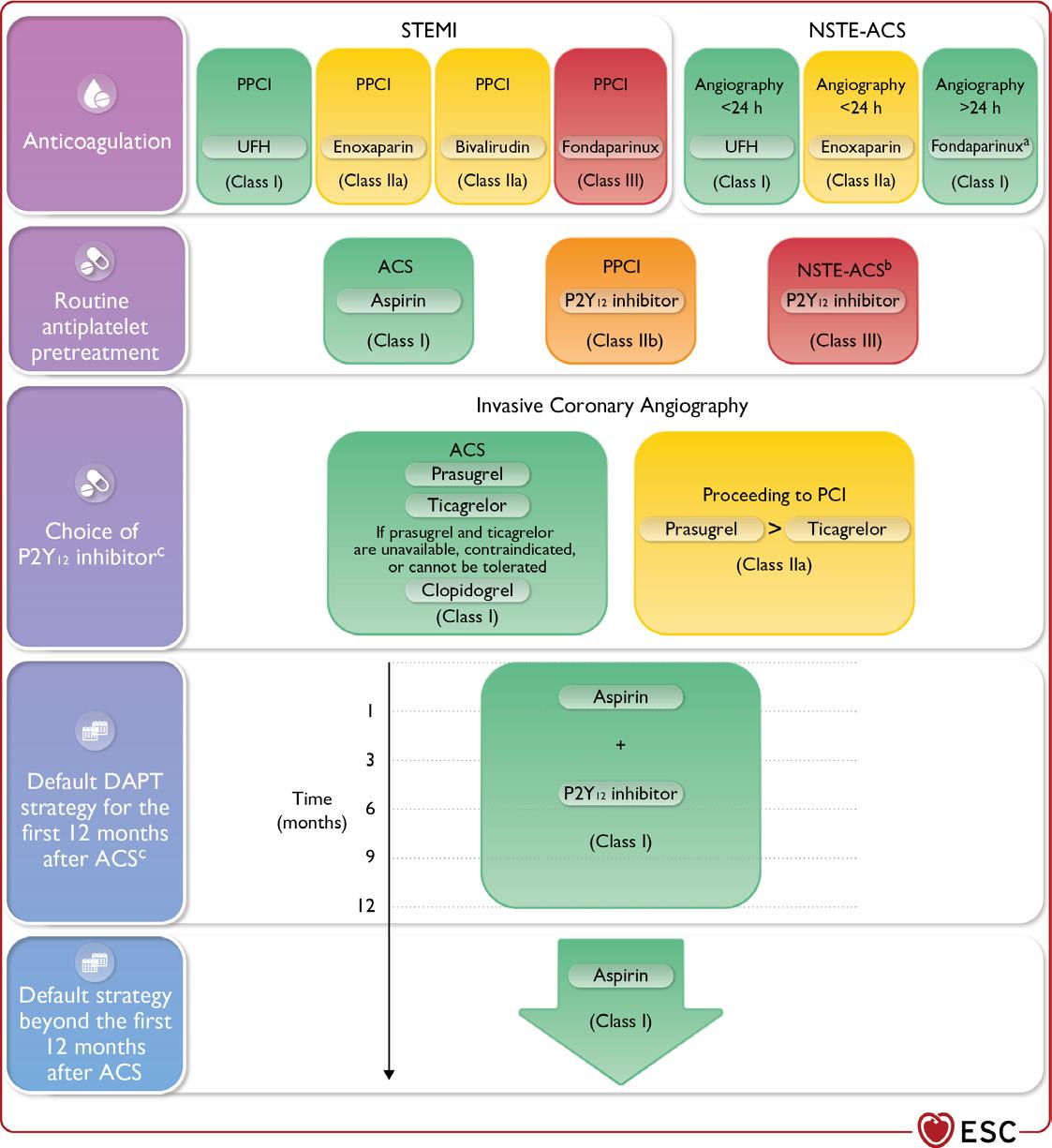
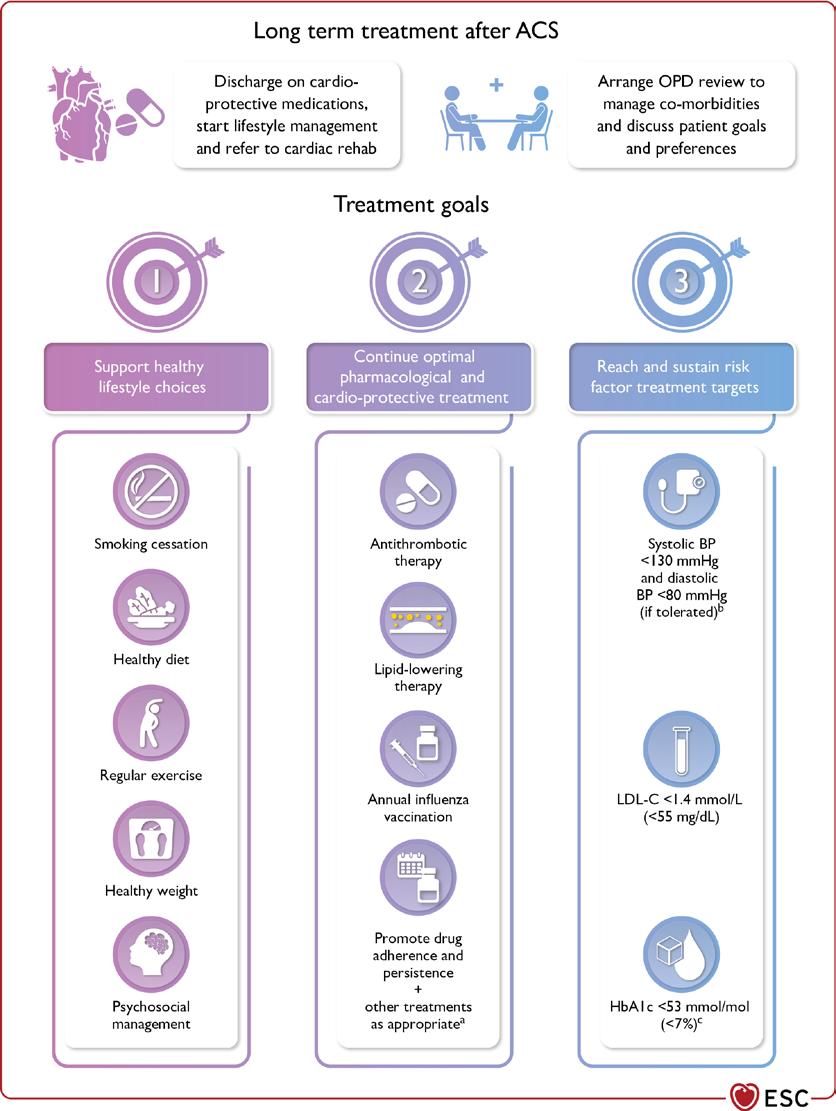
CPD: Acute Coronary Syndromes P41
Clinical R&D: P96
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
In one of our lead news stories this issue, we detail the results of the 2024 National Inpatient Experience Survey have been published today, highlighting the experiences of patients in public acute hospitals across Ireland. This year, 12,367 patients took part in the survey, sharing feedback on their experience of care in Irish hospitals. The survey revealed that the majority of respondents (85%) rated their hospital care experience positively, with 58% rating their care as “very good” and 27% as “good”.
Compared to 2022 survey findings, the 2024 results show that patients’ rating of their overall care experiences have improved, particularly regarding being discharged from hospital, which had consistently received the lowest scores in previous surveys.
You can read more about this on page 4.
The December End of Year Review section carries a plethora of contributed articles from Irish Societies and Associations, including The Irish Cancer Society (page 10) for whom 2024 was a year of great success; The Irish Osteoporosis Society (page 14) who talk of their vision and hopes going forward and The Irish Heart Foundation (page 19) who note that 2024 was a ‘landmark year.’
“In some ways 2024 was a landmark year for the cause of cardiovascular health in Ireland. But many concerns and frustrations also remain over the lack of priority given to minimising preventable death and disability from heart disease and stroke in Ireland,” says Chris Macey, Director of Advocacy and Patient Support.
Page 34 carries an in-depth discussion with Dr Michelle Roche, , Associate Professor in Physiology, Co-Director of the Centre for Pain Research at the University of Galway, and President of the Irish Pain Society. Dr Roche recently spoke at the Chronic Pain Ireland and University of Galway ‘Day of the Girl’ event.
In our interview, Dr Roche discusses developing guidelines and an agenda for research on sex and gender as variables in pain.
Of course no December issue would be complete without our annual Professional 100 – detailing those innovative and dedicated professionals making their mark on the sector. It is fair to say the dedication, passion and innovation behind the hospital profession is never lacking.
Finally, may I take this opportunity on behalf of the entire HPN team to wish all our readers and supporters a very Merry Christmas, and a prosperous New Year. See you in 2025!
76% of Consultants in ‘Firefighting Mode’
A new survey commissioned by the Irish Hospital Consultants Association (IHCA) has found that 56% of consultants believe
their working environment rarely or never reflects a culture of mutual support, cohesion, or trust, with 76% saying that
IHCA President, Professor Gabrielle Colleran
they are very often or always in ‘firefighting mode’.
The Association published the results in advance of its Annual Conference in Kilkenny which focused on the theme of compassionate leadership. Among the speakers attending the conference was the Minister for Health and international healthcare leadership experts, Professor Michael West and Professor Helen Thomas.
When exploring the theme of compassionate leadership, 56% say that their workplace rarely or never reflects a culture of mutual support, cohesion and trust. This is despite 72% of consultants believing in collaborative leadership, yet only 16% feel that management seeks their input in decision-making.
More than six in 10 (63%) consultants report a lack of access to necessary capacity and resources. Just 9% of the over 650 consultants who responded to the survey believe they have adequate time to forward plan in their roles.
Despite these challenges consistently being faced by consultants operating in difficult circumstances, almost threequarters (72%) state they feel they are making a valuable contribution to patient care, research and teaching.
Close to two-thirds (63%) of consultants feel a sense of worth in their work, while almost 70% say their work is very or completely meaningful to them. Overall, 70% stated that they find satisfaction in their roles, day to day.
Commenting, IHCA President, Professor Gabrielle Colleran said, “Healthcare can often feel consumed by contention and confrontation. Healthy debate has its place, but it should not define us.
“The path forward requires a new mindset—a shift towards collaborative and compassionate leadership. We all must play our part. We must foster a culture of connection, trust, and respect, because only through collective effort can we overcome the challenges ahead.”
National Survey Highlights Areas for Improvement in Irish Hospitals
Results of the 2024 National Inpatient Experience Survey have been published recently, highlighting the experiences of patients in public acute hospitals across Ireland. This year, 12,367 patients took part in the survey, sharing feedback on their experience of care in Irish hospitals.
The survey revealed that the majority of respondents (85%) rated their hospital care experience positively, with 58% rating their care as “very good” and 27% as “good”.
Compared to 2022 survey findings, the 2024 results show that patients’ rating of their overall care experiences have improved, particularly regarding being
discharged from hospital, which had consistently received the lowest scores in previous surveys.
In 2024, patients indicated positive interactions with healthcare staff, with:
83.8% reporting they always felt treated with respect and dignity
79.1% always had confidence and trust in hospital staff
78.7% reporting adequate pain management
79% feeling fully confident in the safety of their treatment and care.
Despite overall positive feedback, patients identified a number of key areas to be improved, and highlighted long waiting times in the emergency department:
19.7% said they were unable to find staff to discuss their worries
15.3% reported not receiving enough information on managing their condition post-discharge
13.4% said their family did not have enough opportunities to talk to a doctor
72.6% reported waiting longer than six hours before being admitted to a ward, with 1,078 people (13.4%) waiting more than 24 hours.
Responding to the survey findings, Minister for Health Stephen Donnelly, said: “The National Inpatient Experience Survey is a valuable resource that provides patients with a voice and helps
the health service in responding to their needs.
This year, the survey included five new questions relating to patient safety, and the responses indicated a largely positive experience. This indicates that people feel confident in the safety of their treatment and care, with good communication about their care and treatment between doctors, nurses and other hospital staff.
The results of this survey highlight improvements in many areas compared to 2022 and I would like to acknowledge the hard work of our many healthcare professionals who have contributed to this. I particularly wish to thank all the participants for giving generously of their time in completing the survey."
First Use of New Biological Aortic Heart Valve
University Hospital Galway is the first hospital in the country to use a new biological aortic heart valve, putting it at the forefront of valvular heart surgery.
Surgical aortic valve replacement is a surgical procedure in which a diseased aortic valve is removed and replaced with a new tissuebased or mechanical valve. This takes over the original valve’s function to enable oxygen-rich blood to flow efficiently out of the heart.
Medtronic's Avalus Ultra valve, a new ground-breaking innovation
University Hospital Galway, the first hospital in the country to use a new biological aortic valve in patients with severe aortic stenosis, while also being the first hospital in Ireland and the UK to implant the new Avalus Ultra biological valve. From left, Luke woods, Perfusionist, UHG; Leah Johnston, Trainee Perfusionist, UHG; Rachel Hambelton, Perfusionist, UHG; Dave Ceely, Business Manager, Medtronic; Professor Alan Soo, Consultant Cardiothoracic Surgeon, UHG; Ryan Scott, Territory Manager, Medtronic; Trudy Hodkinson, Territory Manager, Medtronic and Michelle Hanniffy, Marketing Manager Western Europe, Medtronic
in biological aortic valves, was specifically designed to provide simplicity of use at implant while also empowering cardiac patients to improve their quality of life.
Aortic valve disease causes the valve to narrow, making the heart work harder to pump blood through the body, causing the heart to weaken and function poorly. Patients with aortic valve disease, either stenosis (blocked) or regurgitant (leaky), often require valve replacement.
Noel O'Brien of Tynagh in County Galway who was the first patient to undergo the Avalus Ultra valve implant surgery on 22 October, led by Professor Alan Soo and his surgical team at University Hospital Galway stated, "I was always an active person, but in the last year or so I'd noticed that even after doing a small amount of work, I felt tired and breathless.
Speaking about the new innovation, Professor Alan Soo, Consultant Cardiothoracic Surgeon said, “The
Commitment to Medicines Welcomed
Medicines for Ireland (MFI) has welcomed the inclusion of several of its key priorities in the manifestos and policy papers of Fine Gael, Sinn Féin, and Labour, all of which have committed to promoting the use of generic and biosimilar medicines.
As an organisation, MFI’s core objective is to improve how Ireland procures and supplies medicines to expand patient access to affordable, lifesaving, and lifeenhancing treatment. While there are obstacles to achieving that objective, MFI believes they can be overcome through cooperation with political stakeholders.
Earlier this month, MFI launched its General Election Manifesto, calling on all political parties to prioritise investing in generic, biosimilar, and value-added medicines and the systems that deliver value for patients and the State. MFI has been actively engaging with political stakeholders to highlight the critical importance of a resilient and sustainable generics, biosimilars, and value-added medicines industry, especially considering rising medicine costs, an ageing population, and the increasing burden of chronic diseases.
Noting the policy commitments, MFI Chair Paul Neill commented,
“We are encouraged to see our calls reflected in political manifestos, demonstrating a clear commitment to improving the accessibility and sustainability of generic and biosimilar medicines. We know that Ireland is behind our EU counterparts when it comes to the availability of offpatent medicines to patients. There are many reasons for that lag, including the relatively unfavourable local environment for early generic launch, reduced price entry point, downward-only pricing structures, and lengthy timelines for price uplifts for unviable products. These factors have an overall impact on the
new Avalus Ultra valve represents a significant advancement to our current generation of surgical biological valves.
“It has long-term durability based on a decade of clinical experience and will benefit patients significantly who have aortic valve disease.
“We are delighted to be the first hospital in the country to offer this innovation to our patients, while also being the first hospital in Ireland and the UK to implant the new Avalus Ultra valve.”
attractiveness of the Irish market for manufacturers and lead to less competition and availability of medicines within the market. It is timely to have these discussions ahead of the negotiations on the new Framework Agreement that will allow us to address many of these challenges.”
Paul concluded, “We are encouraged to see that the majority of political parties want to see increased use of offpatent medicines, and we are committed to working with them to deliver better value for patients and the State while ensuring the healthcare system is equipped to meet future challenges.”
Profiling Gene Activity
A groundbreaking method to profile gene activity in the living human brain has been developed by researchers at FutureNeuro, the Research Ireland Centre for Translational Brain Science and RCSI University of Medicine and Health Sciences, in collaboration with international partners.
This innovative approach opens new avenues for understanding and treating neurological conditions like epilepsy.
Studying gene activity in the brain without requiring invasive tissue samples from surgery or post-mortem donation has been a long-standing challenge in neuroscience. By analysing molecular traces – specifically RNA and DNA – collected from electrodes implanted in the brains of patients with epilepsy and linking these with electrical recordings from the brain, the researchers were able to take a
Professor David Henshall, Director of FutureNeuro and Professor of Molecular Physiology and Neuroscience, RCSI
of the brain’s seizure networks, potentially improving the precision of epilepsy surgeries.
Professor David Henshall, Director of FutureNeuro and Professor of Molecular Physiology and Neuroscience at RCSI, said, "This study represents a significant advancement in epilepsy research, providing a method to detect active genes within the living brain of individuals with epilepsy. This technology has the potential to complement traditional brain imaging and EEG tests that measure electrical activity in the brain, offering valuable insights to guide surgical decision-making in the treatment of those with epilepsy."
‘snapshot’ of gene activity in the living brain.
These electrodes, clinically used to pinpoint seizure activity in patients enabling surgical interventions, provide a unique opportunity to link brain activity to the genes being switched on or off in specific regions. The study demonstrates how integrating molecular data with electrical recordings of seizures can enhance our understanding
IPHA Announces New Website
The Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the research-based biopharmaceutical industry in Ireland, has launched new features on the IPHA website which further highlight our commitment to transparency and compliance.
Knowledge of the IPHA Codes of Practice and the medicine advertising legislation is essential for ensuring compliance and promoting high standards of conduct within the pharmaceutical industry. To meet diverse needs, IPHA are delighted to offer three tailored training options. Each of these options are designed to equip participants with the knowledge and skills needed to adhere to the IPHA Codes effectively and ensure those working within the sector remain compliant with industry standards.
Details of each of these options, and how to book training, are now available in a ‘one-stop-shop’ on the IPHA website and are listed below:
• A comprehensive online training module, which offers flexibility to learn at your own pace and is accessible anytime via the IPHA Code website. This can be accessed for free by IPHA members and IPHA Affiliates. There is a small fee for nonmembers.
• In-Person Training, which is conducted annually, is an extremely popular option providing a deep dive into the IPHA Codes in an interactive setting. This is exclusively for IPHA members and affiliates, and booking is required.
• Tailored training sessions are also available to suit an individual organisation’s specific needs. These sessions are in
a customisable format and are designed to address unique challenges and scenarios. These are available to all and incur a small fee.
IPHA members are expected to act with integrity, to keep patients at the heart of what they do and to have high levels of transparency about their actions. To help enhance this transparency a robust complaints system is in place. All alleged breaches of IPHA Code of Practice for the Pharmaceutical Industry or the IPHA Self-Care Advertising Code are taken very seriously. Aligned with this, IPHA has recently launched a new online complaints section on its website, the aim of which is to encourage members, stakeholders and the public to report any concerns about IPHA members’ activities.
Commenting on these new features Director of Code and Regulatory Affairs Dr. Rebecca Cramp said:
Epilepsy affects approximately 40,000 people in Ireland, with one in three people unable to control seizures through medication. For these individuals, surgical intervention is often the best option, but its success hinges on accurately mapping the regions responsible for seizure activity. Beyond epilepsy, the study lays the groundwork for broader applications, including research into Alzheimer’s, Parkinson’s, and schizophrenia, where understanding molecular processes in the living brain is vital.
“At IPHA, we are committed to requiring our members to maintain the highest ethical and compliance standards. We expect that our companies continuously comply with our Codes and that IPHA and its members work to uphold and develop the standards within our Codes.
“These new features on the IPHA website offer an enhanced user experience and better support for members and non-members. We are delighted to offer varied options for Code training, as it is important to be cognisant of individual needs to enable higher levels of participation. We also wish to encourage the reporting of complaints. Thus, should any individuals have concerns about the action of any of our members, they are encouraged to report it immediately. This new reporting feature on the website should make the complaints process more visible, streamlined and effective.”
New Aseptic Compounding Unit at Beacon News
Last month the team at Beacon Hospital celebrated another milestone as they gathered for the official opening of the new Aseptic Compounding Unit.
The expansion of this new hightech Aseptic Compounding Unit future proofs Beacon Hospital Pharmacy’s in-house supply of individually tailored chemotherapy and biological treatments as we expand their Cancer Services.
This new facility will benefit cancer patients and will also support the future delivery of new Cancer Clinical Trials here at Beacon Hospital.
A tremendous amount of effort has gone into this project over the past few months. The official opening is a fitting recognition of everyone’s hard work.
Congratulations to the entire Aseptic Pharmacy team, facilities team, projects team and all involved on their hard work and dedication.
Medical Council launches CAREhub
The Medical Council has launched CAREhub, an independent, confidential service operated by Lyra Health International. The service provides wellbeing support to medical students, doctors, and members of the public who are engaging with the Medical Council’s regulatory processes.
CAREhub was launched at the Medical Council’s offices at Kingram House, Dublin 2, at a stakeholder briefing with representatives from patient advocacy groups, doctors, medical universities and other professional regulators invited to attend.
CAREhub provides independent mental health support to doctors, medical students, and members of the public who are engaging
with the Medical Council’s regulatory processes. This service offers confidential, impartial, and empathetic guidance to those interacting with the Medical Council’s regulatory processes, such as education, training, complaints, investigations, and fitness to practise procedures.
With CAREhub, individuals will have immediate access to trained counsellors who are equipped to provide a supportive, understanding environment. This initiative reflects the Medical Council’s dedication to prioritising mental wellbeing and aligning with global best practices, ensuring that emotional support is readily available to all those affected by the regulatory process.
Speaking at CAREhub’s launch, Dr Suzanne Crowe, President of the Medical Council said, “CAREhub is a new initiative designed to enhance wellbeing of doctors and members of the public who are engaging with a regulatory process. The Medical Council’s regulatory role spans the entire lifecycle of a doctor’s career, ensuring the highest standards of care from education through to retirement.
“We hope that those engaging with the Medical Council will utilise this service if they need it, and that it will help doctors, medical students and members of the public to feel supported. It’s worth highlighting that only a very
Cutting the ribbon at the new Aseptic Compounding Unit at Beacon Hospital
small percentage of all doctors are subject to complaints during the course of their career.”
Paul Byrne, Executive Director of Regulatory Operations and Support Services at the Medical Council welcomed the new initiative: “As a key strand of our new Liaison and Support Services framework, CAREhub strengthens the Medical Council’s mission to support a healthcare system where the health and wellbeing of our key stakeholders - doctors, medical students, and the public - is of utmost importance. By embedding kindness and empathy into our regulatory processes, we hope to provide a more compassionate and effective regulatory environment.”
Statement on Scope of Physician Associates
“Physician Associates support doctors by working under the supervision of a named consultant or GP, and their level of tasks and oversight can vary……The Medical Council’s Regulatory Policy Department has set out key considerations in establishing our position on the regulation of PAs in the future.”
The Medical Council has published a statement articulating its position on the scope of practice and regulation of physician associates (PAs) in the Irish health care sector. As the independent statutory body which regulates doctors in Ireland, the Medical Council is of the opinion that it is not the appropriate regulatory body for PAs. The Medical Practitioners Act 2007, (as amended in 2020 and 2023) has no provision to regulate health professionals other than doctors.
The Medical Council’s primary purpose is to protect the public by setting high standards of professional conduct, education, training, and competence among doctors.
The Medical Council is aware that PAs are being trained and employed in the Irish health care system, working under the supervision of doctors to support the provision of health care, contribute to patient management, and improve healthcare access. It considers it essential that these PA roles are defined with respect to their scope of practice.
Commenting on the position statement, President of the
Medical Council, Dr Suzanne Crowe said, “Physician Associates support doctors by working under the supervision of a named consultant or GP, and their level of tasks and oversight can vary.
“The RCSI, which oversees the training of Physician Associates in Ireland, states that the PA’s role is to ‘support doctors and surgeons in the diagnosis and management of patients and are trained to perform several roles, including taking medical histories, performing examinations, making diagnoses and analysing test results.’
“The Medical Council’s Regulatory Policy Department has set out key considerations in establishing our position on the regulation of PAs in the future.
“We welcome the timely production of a framework by the Department of Health to guide future decisionmaking on the regulation of health and social care professionals, which was used to support the drafting of the Statement.”
Fiona McVeigh, Head of Regulatory Policy at the Medical Council, added, “As the regulator of doctors in Ireland, it is important that the Medical Council engages in policy discussions.
Dr Suzanne Crowe, President, Irish Medical Council
“Our research paper and position statement have set out key details around the training, titles and scope of PAs. We have given extensive consideration into how PAs integrate into the health system now and in the future; and have highlighted concerns to be considered going forward related to scope, understanding and role titles.
“We aim to ensure that patient safety remains paramount, the scope of PA practice is clearly defined, and the integrity of the medical profession is upheld.”
The Irish Hospital Consultants Association (IHCA) welcomed the publication stating that the Association agrees fully with the Medical Council’s view that it is essential that the PA role is defined with respect to scope of practice, and that PAs cannot be seen as a substitute for doctors.
The Association added, “We are also in agreement that the Medical Council is not the appropriate regulatory body to oversee PAs. In its submission to the HSE on this matter in September, the IHCA made clear that a logical and structured approach must be followed and that this would firstly necessitate an appropriate audit and scoping exercise to be undertaken at national level to identify skill deficits in the health service and the most appropriate healthcare staff required to address them.
“The purpose of the exercise should be to establish the risks and benefits of introducing a PA role. The next logical step would be to formulate and define the PA’s scope of practice, not just for “day one” but specifically by reference to the role in the particular specialty or clinical setting in which the PA will practise.”
The IHCA has submitted that the professional title of ‘Physician Assistant’ should instead be used in order to reflect their role within clinical teams. To do otherwise would unhelpfully blur the distinction between doctors and nonmedically qualified professionals. The Association will continue to engage with the HSE and the Medical Council on this important issue.
The School of Medicine at the Royal College of Surgeons in Ireland offers the only MSc in
Physician Associate Studies programme in the Republic of Ireland and RCSI has been advocating for a regulator since the role was first introduced in 2016, to regulate and set a scope of practice. A regulator that ensures a streamlined process for monitoring physicians associates and their supervising consultants, while protecting the public, is the overarching goal that RCSI has been advocating for.
The RCSI also welcomed the statement adding, “Physician associates are not replacements for doctors, but they increase the productivity of the medical or surgical team by enhancing access to care for patients and complement the roles of medical or surgical trainees, as directed by their consultant supervisor.
“The proportion of the Irish population aged over 65 is expected to grow from 15% currently, to 18% by 2030 and towards 30% by the 2050s. As we age and our population grows, the demand for healthcare will increase. By 2030, demand for inpatient bed days could increase by up to 37%. Demand for emergency department care could increase to somewhere between 16% and 26%. Demand for GP visits is expected to increase by between 20% and 27%.
“Without significant change in our health service, the future demand for healthcare is unsustainable and we will face a public healthcare crisis that will see many more of us unable to access the care we need. Worldwide there is broad agreement that the most promising model for a sustainable healthcare system is one that increases productivity by extending the scope of practice of existing healthcare professionals and creates new professional groups, in line with calls from the World Health Organisation (WHO) to innovate medical workforces.
“To that end, RCSI introduced prescribing for nurses in 2007, is a strong advocate for advanced nurse practitioners, is supportive of prescribing rights for pharmacists and has successfully completed a pilot that allowed integration of physician associates into the Irish health workforce.
“RCSI’s introduction of the Physician Associate Studies programme underpins our commitment to supporting an increased capacity in the Irish healthcare system to provide safe and quality patient care.”
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
End of Year Review
Irish Cancer Society2024 A Year of Many Successes
The Irish Cancer Society’s ‘Your Health Matters’ Roadshows kicked off in January and carried on throughout the year. The roadshows cover the length of breadth of the country and bring cancer nurses into every community in Ireland to raise awareness of and talk to people about cancer. The roadshows promote positive lifestyle changes, increase awareness of cancer symptoms, and they aim to improve early detection.
Shortly after the start of this year, the Irish Cancer Society announced an investment of €400,000 for the Julie Wren Complementary Therapy Service, with the ambition to support 1,000 families with over 5,500 complementary therapy sessions over five years.
The Julie Wren Complementary Therapy Service is located in St John’s Ward in Children’s Health Ireland (CHI) at Crumlin. It provides complementary therapies to children and their families while receiving cancer treatment in hospital as part of their plan of care.
In February, researchers from around the country were honoured at the Irish Cancer Society Research Awards. People involved in ground-breaking research projects around the country were honoured at the awards ceremony in Trinity College Dublin. The preliminary results of an Irish Cancer Society-funded project
centred on reducing cancerrelated lymphoedema at University Hospital Limerick were published in March. It found that the project, which aims to detect and prevent cancer-related lymphoedema, was improving patient outcomes.
Of 294 breast patients seen in the first 19 months, 43 showed early signs of lymphoedema. Of these, 30 resolved with treatment with 13 continuing to undergo treatment to reverse or reduce the swelling.
Corrinne Hasson, Director of Services at the Irish Cancer Society, said: “We are thrilled to see the incredible impact of this pilot project. Not only have we witnessed an improved experience and outcomes for patients involved, but we have also seen an improved quality of care for people already living with cancer-related lymphoedema.”
March featured Daffodil Day, a highlight in the Irish Cancer Society’s fundraising calendar, which this year raised over ¤5 million. People across Ireland went all in against cancer, raising vital funds for cancer patients and their families.
In April, the Irish Cancer Society worked with 20 leading cancer doctors and researchers highlighting issues with patient waiting times, surgery delays and the need for proper funding for the National Cancer Strategy. Averil Power, CEO of the Irish Cancer Society, said: “The Irish Cancer Society has been warning for
some time that Irish patients are not being given that chance due to lack of Government investment in cancer services and research. That has now been backed up by over 20 of the top cancer doctors and researchers in the country.”
A report from the European Cancer Organisation (ECO) and the Irish Cancer Society that was published in April highlighted the state of cancer care in Ireland and the specific areas that require urgent attention from policymakers, with a particular emphasis on tackling cancer inequalities.
Speaking at the launch of the report, Averil Power, CEO of the Irish Cancer Society, said: “We know that people across the country do not have equal access to cancer care and services in Ireland. Inequality between public and private patients is growing, particularly in terms of access to new medicines.
“The lack of Government investment in Ireland’s current National Cancer Strategy means target waiting times for cancer tests are consistently being exceeded. Those who cannot afford to go private are too often left languishing on long waiting lists, getting more anxious with each day that passes.
“We need to ensure that every Irish person, regardless of their background or income, has the best possible chance of surviving cancer. Without proper multiannual funding for the National Cancer Strategy, not only are Ireland’s cancer outcomes unlikely to improve but we are at serious risk of going backwards.”
During the summer, the Irish Cancer Society announced funding of ¤300,000 for research to improve psychosocial knowledge and support for those with a high hereditary cancer risk. This project, to understand psychosocial needs and pilot a service to patients with an increased hereditary cancer risk, is led by St Vincent’s University Hospital (SVUH) Psychology Department in collaboration with the UCD School of Psychology. It is made possible by the funding from the Irish Cancer Society.
The project team will explore the complex relationship between
the risk of hereditary cancer and psychosocial wellbeing, recognising that living with an increased risk of cancer due to hereditary factors can be a profound emotional and psychological experience, impacting people’s emotional wellbeing and their quality of life.
In June, the Irish Cancer Society lodged its pre-Budget submission calling on the Government to stop underfunding the National Cancer Strategy. This call for investment in the National Cancer Strategy was supported by the two main representative bodies for cancer doctors in Ireland, the Irish Society of Medical Oncologists (ISMO) and the Irish Society of Radiation Oncologists (ISRO).
Preliminary results from a clinical trials scoping analysis undertaken by Forvis Mazars using clincialtrials.gov were published in September and highlighted that over a six-year period (2018-2023) there were, on average, three times the number of interventional cancer clinical trials started annually in Denmark, when compared to Ireland.
When the results were published, the Irish Cancer Society warned that the Government’s underinvestment in clinical trials was just one of the many ways that cancer patients in Ireland were being left behind.
New funding for the National Cancer Strategy was announced in Budget 2025, and the Irish Cancer Society shared its hope that Budget 2025 signalled a new approach to cancer funding. The new funding of ¤33m will be used for cancer services in 2025, rising to ¤46m in 2026.
Averil Power, CEO of the Irish Cancer Society, said: “The Irish Cancer Society welcomes the priority given to people affected by cancer in Budget 2025. The investment provided for in this Budget will benefit people with cancer and their families all over the country. It will enable improvements in prevention, screening, diagnostics, treatment, psychological supports and community-based services.
“It will help cancer patients avoid Emergency Departments if they need urgent medical help between
their scheduled appointments. It will improve access to new cancer medicines. And it will provide increased support to women who need post-mastectomy products such as specialised bras after breast cancer treatment.”
October was Breast Cancer Awareness Month and saw people up and down the country host Big Pink Breakfasts in their houses, workplaces and colleges. The breakfasts helped to fund vital Irish Cancer Society services like free transport to treatment, night nursing care, counselling sessions, and the Support Line, to ensure they are available to those who need them most.
A major milestone was reached towards the end of the year, when a landmark legislative win was achieved for new mothers undergoing cancer treatment. Legislation was passed to allow women to defer maternity leave in cases of serious illness, and this change came about two years
after the Irish Cancer Society’s #LeaveOurLeave campaign, calling for the legislative change, began. #LeaveOurLeave was spearheaded by three women: Erica Tierney, Mary Canavan and Emma McGuinness, who all underwent cancer treatment whilst on maternity leave.
A groundbreaking ¤4.9 million lung cancer research programme, funded by the Irish Cancer Society, was launched in October. The research programme is a partnership between the Irish Cancer Society and Beaumont RCSI Cancer Centre. The pioneering initiative aims to transform lung cancer care and research in Ireland. In collaboration with specific GP practices in North Dublin and the Northeast region, it will invite high-risk individuals to attend community-based mobile scanning units for lung health checks.
The initiative also includes the use of rapid blood tests to
determine the best treatment options for newly diagnosed lung cancer patients, and the use of immunotherapy to treat patients with a type of lung cancer called KARS-mutant, which is common in Ireland but particularly difficult to treat. The Beaumont RCSI Cancer Centre will also work closely with GPs to improve lung cancer detection, diagnostics and survivorship pathways.
The Irish Cancer Society’s campaign highlighting the cost of cancer and delays to cancer treatment, and the damaging impact it has on cancer patients, kicked into full swing when the General Election was called in November. The Irish Cancer Society is calling on the next government to ensure that cancer patients receive the care they need quickly and without being burdened by financial costs for things like treatment, medication, parking fees, and travelling to and from appointments.
2024 was a year of many successes for the Irish Cancer Society, with the launch of a lung cancer research programme marking the largest single investment in lung cancer in the history of State and the passing of legislation prompted by the #LeaveOurLeave campaign. However, providing services for cancer patients when they need them is an integral part of our work that carries on every day. Every night, Night Nurses go into the homes of cancer patients across the country and provide care to them when it’s most needed, the Cancer Nurses on our Support Line and in our Daffodil Centres offer advice and support to people affected by cancer, and our Transport Service bring patients to and from their treatment.
All of the Irish Cancer Society’s vital free services and supports are fuelled by fundraising. None of which would be possible without the incredible generosity of the public. To find out more about the Irish Cancer Society visit cancer.ie.
National Cancer Registry of Ireland Annual Report
In anticipation of the full implementation of the six new health regions in early 2025, the NCRI annual report on national cancer statistics has, for the first time, examined cancer incidence and survival across these six geographies for the four most common cancers in Ireland: lung, bowel (colorectal), breast and prostate cancer. This data are presented alongside national statistics providing an annual update on the status of cancer in Ireland.
In Ireland as a whole, an average of 44,000 tumours were diagnosed each year during 2020-2022. Professor Deirdre Murray, Director of NCRI, and Professor of Epidemiology at University College Cork, noted that the majority of these (24,200) were potentially life-changing invasive cancers
requiring extensive treatment. On average 9,800 people died each year from cancer during 20202022. One in five deaths were due to lung cancer.
Considering the six new health regions, the majority (60%) of all invasive cancers diagnosed during 2020-2022 occurred in the three eastern geographical areas (Dublin and North East, Dublin and Midlands, and Dublin and South East). Compared to the national average, the lung cancer incidence rate was higher in Dublin and Midlands, and lower in Dublin and South East. By contrast, the rate of prostate cancer was higher in Dublin and South East, but lower in Dublin and North East.
The proportion of people diagnosed during 2009-2018 and surviving at 5-years following
diagnosis was lower than the national average for those living in the Mid West for colorectal, lung, and female breast cancer. Fiveyear survival for prostate cancer was also lower than the national average for people resident in the Dublin and North East region at the time of their diagnosis.
The report also found that, in Ireland as a whole, the number of people living with and beyond cancer continues to grow with an estimated 220,700 people who had been diagnosed with cancer still alive at the end of 2022 (about 1 in 23 of the Irish population).
Professor Murray, said, “One of the core functions of the NCRI is to provide data for cancer service planning, evaluation and policymaking. While geographic variation must always be
interpreted with care these data can point to important opportunities for improvement across cancer care from prevention, early diagnosis, and screening, to access to services and treatment.”
Chair of the NCRI Board, Dr Robert O’Connor added: “This report provides a comprehensive overview of cancer statistics as our country began to recover from the COVID-19 pandemic. The data reveal critical insights into regional health outcome differences and emerging trends in cancer survival rates. The findings underscore the continued need for targeted, strategic investments in cancer research, prevention, treatment, and post-treatment care to equitably maximise patient outcomes and community health.”
End of Year Review
Parkinson’s Ireland - Our Achievements and Challenges
Written by Shane O’Brien, CEO, Parkinson’s Ireland
Parkinson’s Disease (Parkinson’s) is the fastest growing neurological condition and is the second most common neurodegenerative disease after Alzheimer’s.
Parkinson’s is a progressive neurological disorder, and is classified as a Movement Disorder, as it primarily affects movement. It is variable in its progression, i.e. some people progress more slowly than others, and the symptoms can be effectively controlled with medication for many years. Parkinson’s disease is caused by a loss of a chemical called dopamine.
Although Parkinson’s is a movement disorder, there are both motor and non-motor (e.g anxiety, issues with sleep etc.) symptoms associated with it.
Parkinson’s Ireland (PI) is the main charity for people with Parkinson’s and their loved ones. PI has been in existence since 1987 and provides a range of services both locally and nationally. The current activities of PI include:
• Parkinson’s nurse freephone helpline – currently staffed by two Parkinson’s Nurse Specialists and a dietitian.
• Weekly nurse clinics.
• Newly diagnosed programmes, which are run by our Parkinson’s nurses.
• Online classes, including Exercise, Yoga, Singalong and Wellness.
• Local services which are provided by our 20 local branches. These include exercise classes, physiotherapy, speech therapy, dancing, choir and social support groups.
• Holding education webinars throughout the year on a range of relevant topics.
• Provision of information on Parkinson’s by way of information booklets and online resources.
• Investing in research and partnering with research bodies such as the Parkinson’s Disease Research Cluster in UCC.
• Raising awareness of Parkinson’s Disease among the general public.
• Advocacy on a range of different issues which are relevant to people with Parkinson’s and their loved ones; such as additional community services, access to neurologists, medication shortages etc.
Achievements
Although there has been challenges in 2024, overall, it has been a very successful year for PI.
Nursing
We have hired two additional nurses in the past 12 months to meet the demand for our services. This brings our total number of employees to 6. We were granted additional funding by the HSE in July 2024 in respect of our nursing services.
Awareness
We ran a very successful awareness campaign during Parkinson’s Awareness Month in April 2024. Titled ‘Different For Everyone’, the campaign highlighted that there are over 40 different symptoms in Parkinson’s and that everyone experiences Parkinson’s differently. This campaign reached a huge number of people over national radio, national print media, Spotify, outdoor advertising and digital media. The campaign has been shortlisted for Education Project of the Year at the Irish Healthcare Awards.
Branches
We set up two new branches in 2024: Wicklow and Monaghan. This means additional local services in these counties.
Education
Our Parkinson’s nurses have started working with the Irish Medication Safety Network. This work includes working with the IMSN on updating the safety alerts for Parkinson’s. We will also have a stand at the upcoming 1st All-Island Medication Safety Conference. One of our nurse specialists Lisa Wynne will be speaking at the event about Parkinson’s Disease.
Information Services
We updated our information leaflets which contain information on various aspects of Parkinson’s. We also designed a new booklet for people who are newly diagnosed and are working on a new diet booklet. We are a trusted provider of information, and this remains an important part of our work.
Fundraising
We held our new flagship fundraiser in 2024: ‘A Walk in The Park for Parkinson’s’. This walk took place in September at various locations around Ireland. In addition to raising vital funds, the event was very successful in raising awareness of Parkinson’s and our services. This event has huge potential to grow in the coming years. We are delighted to have Home Instead as the title sponsor and major supporter of the event.
We also had some very successful voluntary fundraising initiatives. Our presence in the areas of Wills is increasing and this is becoming an important source of funding for us.
Advocacy
We welcomed the announcement of ¤2m investment in regional
neurology services in 5 hospitals in the recent budget. We campaigned on this issue with our colleagues in the Neurological Alliance of Ireland. Although the investment is welcome, it is vital that the posts associated with this investment are advertised as soon as possible. We continued to highlight the relatively small amount of government funding that we receive (see below) across the local and national media.
Challenges
Funding
The need for increased funding and certainty on income levels, remains the biggest challenge for PI and most other small charities in Ireland. The fundraising environment remains volatile and unpredictable after the COVID pandemic, although there has been an improvement in 2024. We have also had to respond to the challenges associated with people carrying less cash and a move towards more online events.
As Parkinson’s is the fastest growing neurological condition and is projected to double by 2040, it is crucial that the government provides increased HSE section 39 funding to our charity. In 2023 we only received ¤70,000 from
the government. This figure is tiny and there is a need for major increases over the coming years. The new government will need to recognise the challenge that neurodegenerative diseases will bring over the coming years, with the increase in life expectancy.
Need for improvements to services in the HSE
We jointly launched a major national audit report with UCC on the quality of care received by people with Parkinson’s across Ireland. The report identifies significant areas of improvement across a range of different areas including waiting lists, lack of nurse specialists and the lack of allied health professional (such as dietitians, counsellors, speech therapist).
Plans for 2025
We have ambitious plans to continue to expand our nursing services and the services that our local branches provide in the community. However, this is dependent on receiving additional government funding.
We will be continuing our focus on raising awareness and in expanding our flagship fundraiser: ‘A Walk in the Park for Parkinson’s’.
We aim to increase our membership by 10% in 2025. A key part of this will be to ensure
that neurologists provide our ‘newly diagnosed packs’ to patients in the clinic.
Subject to funding, we also hope to increase our research footprint and invest in a major research project in 2025.
All of the work that we do is made possible by people who fundraise for us or make a donation, however small; the hard work of my team of staff, and our team of volunteers across the country. Inspired by this goodwill and the courage that people with Parkinson’s and their loved ones have in dealing with the condition, we are excited by our future plans and are ready to meet the inevitable challenges that we will face along the way.
Pictured during the ‘A Walk in the Park for Parkinson's’
The ‘A Walk in the Park for Parkinson's’ T-Shirts
End of Year Review
Fractures ARE Preventable in most people
Our vision in the Irish Osteoporosis Society is for the amount of people affected by bone loss to dramatically decrease. The charity is committed to increasing the awareness of this Silent disease, which is preventable in the majority of people. Prevention should start in schools with physical education being made mandatory, which long term will not only reduce the risk of bone loss in later life but also multiple other conditions such as obesity, diabetes, heart disease etc.
In order for our vision to be successful, we need your support to spread awareness of this disease and the charity itself. www.irishosteoporosis.ie This disease has no signs or symptoms warning a person they are losing bone; and it is causing pain, disability and premature death, daily in Ireland.
2024 for the Irish Osteoporosis Society was spent increasing awareness of the many myths regarding this disease, which has always been one of our major challenges. It is quite shocking, the fact that we are not a 3rd world country, yet so much misinformation is in the public and health care domain regarding this disease.
The following are the main messages that the charity highlighted throughout this past year
• Yoga/forward flexion should not be done by anyone with bone loss.
• Calcium and Vitamin D supplements are not treatments.
• Anyone who has broken a bone from a trip and fall or less should be assumed to have Osteoporosis unless proven otherwise.
• Osteopenia should not be considered a “touch of bone loss”.
• Why monitoring of bone loss is essential.
• Why Bone loss is different to most diseases.
• The importance of normal vitamin D levels.
Written by Michele O’Brien, Irish Osteoporosis Society
• A survey in 2023 showed 1 in 5 adults have fractured since turning 40. Over 1/3 reported to have had a fragility fracture, which is a broken bone from a trip and fall or less, which if a person had healthy bones, they would not have fractured. The rate of fragility fractures was highest amongst 40 to 54 year olds.
• Research does show that most broken bones (fractures) occur within a T score of -1. 5 to -2.49, which is the moderate to marked Osteopenia range.
• More men pass away from Osteoporosis than get prostate cancer, which is why it is essential for men to see if they have risk factors for this silent disease.
• Osteoporosis is preventable and treatable in the majority of people; we have 80+ year olds who have improved their bone health. Check out Kays videos on the Irish Osteoporosis Society Facebook page.
• Women over 65 (Caucasian and Asian) are the highest risk group, however Osteoporosis effects 50% of women and 25% of men 50+, and all age groups can be affected.
• More women pass away from Osteoporosis than from the combined deaths of cancer of the ovaries, uterus and cervix. Lung cancer is the only cancer that supersedes Osteoporosis in deaths, which is why all women should be making their bone health a major priority for 2025.
• Anyone with bone loss needs their bone health monitored closely due to the fact that there are NO signs or symptoms of bone loss occurring or improving. Why the Irish Osteoporosis Society does not recommend Yoga
Touching your toes while in the sitting position or standing position, excessive bells, yoga, jumping off boxes, stopping your feet when walking, trampolines
• Anyone who is on any medication or treatment for other diseases such as Chemotherapy, Radiation, Arimidex, Aromatase inhibitors, proton pump inhibitors, Depo-Provera, progesterone only contraceptives and corticosteroids, are high risk.
The concept of yoga is wonderful, but the reality is that it is not appropriate for most people, especially senior citizens. The reasons are that many of the stretches contain excessive flexion of the spine which puts excessive stress on the anterior aspect of the vertebrae, as well as the discs between them and the sciatic nerve. Stress on the vertebrae, when a person has bone loss, can and has caused vertebral fractures. Excessive stress on the discs and sciatic nerve can cause a herniated disc/s which causes radiating pain down a person’s leg.
Written by Michele O'Brien, CEO,
World Osteoporosis Day – Time for a Check
With World Osteoporosis having Society are asking everyone to Why prevention of Fractures
Written by Michele O'Brien CEO, Irish Osteoporosis Society
of appropriate monitoring will place people at risk of fracturing. The Irish Osteoporosis Society have never heard of a diabetic patient been told “Come back in 5 years”, so why this trend is occurring is baffling.
Vitamin D can cause aches and pains, which mimic the symptoms of Fibromyalgia.
Worldwide, up to 37 million fragility equivalent of 70 fractures per minute. that if the persons bones were
What level should my Vitamin D be for bone health?
having taken place on 20th October, the Irish Society are asking everyone to check to see if they have risk factors for
With Cardiac issues a patient will usually develop signs or symptoms that there is an issue, the same with Diabetes. With bone loss being silent and having no signs or symptoms, the only signs will be of people fracturing, leaving many losing their independence and others facing premature death.
Some labs consider a “normal” Vitamin D level of 30 or 50nmol/L to 125nmol/L.
The Irish Osteoporosis Society recommend a Vitamin D level of between 70 to 125nmol/L for bone health.
Why prevention of Fractures is common sense as well as economical
Normal bone Image
Worldwide, up to 37 million fragility fractures occur annually in people over equivalent of 70 fractures per minute. A fragility fracture is a broken bone that if the persons bones were healthy, the fracture would not have occurred.
The Irish Osteoporosis Society (IOS) does not recommend yoga/ chair yoga for anyone, as many of the stretches contain excessive forward flexion stretches.
Normal bone Image
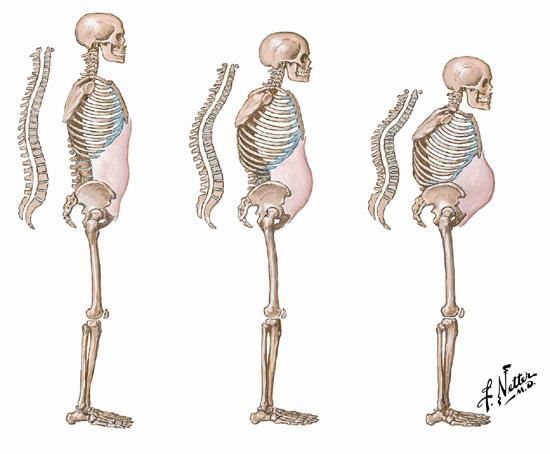
The images show the positions those with bone loss and senior citizens should avoid, as many senior citizens have undiagnosed vertebral fractures and bone loss.
Unfortunately the Irish Osteoporosis Society receives a significant number of calls from people who have developed disc and sciatic nerve problems, as well as fractured vertebrae doing forward flexion stretches.
Did you know that calcium and vitamin D supplements are not “Osteoporosis treatments”?
Answer: Taking the daily recommended amounts of Calcium and Vitamin D are very important but they are not actual Osteoporosis treatments. There appears to be a small amount of people who do need a calcium and Vitamin D supplement, due to not liking milk etc. Both should be taken preferable through food, if this is not possible, then through a supplement. Many just need a Vitamin D supplement, in conjunction with a bone health plan to prevent fractures or a prescribed Osteoporosis medication if the person has fractured or is very high risk to fracture.
important is to ensure that you are taking enough of both but also to check that you are not taking too much of either of them.
Did you know that research shows that the majority of fractures (broken bones) occur in the moderate to marked Osteopenia range?
Most people are not aware that Osteopenia should not be considered a “touch of bone loss”. Research shows that most broken bones occur in the Moderate to marked Osteopenia range, which is a T score of -1.5 to -2.49. It is essential that when a person is diagnosed with bone loss that a plan to prevent further bone loss is put in place and the causes of their bone loss are investigated and addressed.
Did you know that Osteoporosis is a Silent disease
People are encouraged to prevent Diabetes and cancer to name a few but with bone loss those who are proactive are now being discouraged, it makes absolutely no sense.
Most hospitals, due to patient volume have difficulty accessing initial and repeat DXA scans, which is why our health service should invest in more DXA scans for hospital settings, as prevention of fractures have been proven to be cost effective.
Do you know why treating Osteopenia or Osteoporosis is very different to treating other diseases out there?
With most diseases people are taking a medication to slow down the progression of the disease or to help with relieving symptoms of it. With Osteoporosis treatments, the prescribed medication/ treatments help to either slow down bone loss or increase bone formation which improves bone quality and helps to reduce the risk of fractures.
Bone image with bone
Bone image with bone loss
1 in 2 women over age 50 will experience 50, even though research shows A recent survey in Ireland showed experienced a fragility fracture. expected/assumed by most people
The importance of Vitamin D, especially in the winter months
With winter arriving and especially since we really did not have a sunny summer, it is essential that people protect not only their bone health but their overall health.
The Irish Osteoporosis Society depends significantly on donations to help achieve its goals. Could you, your friends or coworkers help raise funds for this small (2 employees to cover Ireland!) but dedicated charity? Could you consider Payroll giving, which is an easy and efficient way for people to donate to our work directly from their monthly salary?
1 in 2 women over age 50 will experience osteoporosis fractures, and 1 50, even though research shows that most fractures are preventable. A recent survey in Ireland showed that over one third of Irish adults over experienced a fragility fracture. The level of fractures in the survey would expected/assumed by most people to be amongst the older age groups.
The fact is no one feels bone loss. It is essential that a person’s response to their Osteoporosis treatment is monitored. A person’s bone health may be declining without anyone’s knowledge, which is why it is essential their repeat DXA scans are performed to monitor their status.
Did you know that the Irish Osteoporosis Society, who are the national experts in bone loss, do not ever recommend a person wait 5 years to be rescanned?
Why not email info@irishosteoporosis.ie for a copy of our Vitamin D and calcium calculator. The reason this is so
Currently there is a new trend regarding DXA scanning. Some DXA clinics are now recommending rescanning every 5 years. Lack
There are some in Ireland who older, as they are the highest risk survey was highest amongst 40 common sense, but financially living in Ireland. This is to help independence and their care costing
Vitamin D is essential for the absorption of calcium from food, as well as assisting the immune system. The bones are the depository for calcium. In the event someone cannot absorb calcium, the body is programmed to take it from the bones, resulting in bone weakening.
NOTE: Those diagnosed with Fibromyalgia should have their Vitamin D levels checked, as a person may be taking it but not fully absorbing it. Low levels of
Our hope for 2025 is that all of you reading this piece will make a conscious effort to help to increase awareness of this Silent disease. You can request to be emailed fact sheets, as well as female and male questionnaires that help find causes of bone loss from the charity by emailing info@irishosteoporosis.ie OR by just passing on the National helpline phone number 01 637 5050 would make a significant difference in helping to reduce the amount of people suffering from this treatable disease.
There are some in Ireland who believe that DXA scans should only be older, as they are the highest risk group. Considering the rate of fragility survey was highest amongst 40 to 54-year-olds shows that prevention common sense, but financially for our health service and for the overall living in Ireland. This is to help prevent people at high risk ending up disfigured, independence and their care costing far more than the €120 to do a DXA
The Irish Osteoporosis Society a person who is high risk to fracture member who suffered from Osteoporosis health. There was a person in Ireland left, the person said that they could We are not a third world country situation should never occur.
The Irish Osteoporosis Society who are the National experts in Osteoporosis
Normal bone Image
End of Year Review
Marie Keating FoundationContinuing Impact across Ireland
Looking back on 2024, there are so many highlights to be celebrated and recognition that despite many challenges, the Marie Keating Foundation has continued to have a tremendous impact in communities around Ireland. I am immensely proud of how our team has again risen to meet the challenge of ever-growing cancer diagnoses.
1 in 2 of us will get cancer at some point in our lives and cancer is now the leading cause of death in Ireland. Cancer has become more prevalent in Ireland over the last two decades, with more than 43,000 people diagnosed with cancer in Ireland annually. The incidence of cancer is expected to increase substantially by 2045 if current rates continue.
That is why our mission ‘to make cancer less frightening by enlightening and our vision ‘to create a world free from the fear of cancer’ is even more important today.
Over the course of 2024, our specialist cancer nurses engaged with more than 21,000 people throughout Ireland bringing the allimportant message of early cancer detection to communities, schools and workplaces at venues all around the country. By providing all our cancer awareness and support activities free of charge and focussing particularly on disadvantaged and marginalised communities, the Foundation ensures we are providing our
Written by Liz Yeates, CEO, Marie Keating Foundation
to whether Ireland’s colorectal cancer screening programme should be extended to 50-54.
In June, our Early Detection of Cancer show garden at Bord Bia Bloom saw the Marie Keating Foundation team and volunteers engage with thousands of visitors about cancer awareness. As part of our Bloom activity, we also launched our Supporting Early Cancer Detection policy report which outlined the Marie Keating Foundation’s actionable policy recommendations urging the Government to prioritise early cancer detection through several measures, including:
services to those who need us most and where we will have greatest impact.
We seek to highlight and break through the most prominent barriers to early cancer diagnosis. Lack of sign and symptom awareness, poor health literacy, an overcrowded health system, long waiting lists to access healthcare, inequalities in access to treatment, poor uptake of existing screening services and lack of other screening programmes are all significant contributory factors as to why patients from disadvantaged groups have disproportionately poorer outcomes compared with those from more advantaged areas.
This is why the Marie Keating Foundation puts a special focus on our partnerships with underserved access to appropriate information and support, in order to educate, advise, and eliminate the fear and lack of knowledge that may prevent people seeking support.
Our April Bowel Cancer Awareness Campaign, No Regrets made a call on the government to reduce screening age in recognition of the increase in diagnoses of Bowel Cancer in under 50’s. In Ireland 1 in 10 diagnoses of Bowel Cancer are to people under 50, with screening age starting at 59, too many people are being diagnosed at a later stage due to an assumption that Bowel Cancer is a disease of older age. Our campaign aligned with patient group Bowel Cancer Ireland, strives to change this perception and through our petition and increased awareness led to the Health Information and Quality Authority conducting a review as
• Commit to multi-annual funding of the National Cancer Strategy.
• Improve awareness of early cancer symptoms.
• Provide funding to promote higher uptake of all existing screening programmes.
• Lower the age limit for breast cancer screening to 45 years.
• Expand the screening age for Bowel Cancer from 59 - 69 to 50 – 74.
• Establish a lung cancer screening pilot programme targeting high-risk people.
• Invest in improving access to cancer diagnostics.
• Fund and Implement the NCCP Early Diagnosis of Symptomatic Cancer Plan 2022-2025.
Innovation and collaboration remain at the heart of what we do at the Marie Keating Foundation, and we were delighted to receive a nomination for the second time at the All-Ireland Marketing Award in the Innovation and Creativity category for our November lung cancer awareness campaign. This multichannel campaign saw the introduction of an AR filter on Snapchat and Instagram highlighting the important signs and symptoms of lung cancer, Ireland’s deadliest cancer.
Other notable highlights during 2024 were achieving the Triple Lock of Good Governance in the charity sector for the ninth year, continuing our commitment to the highest levels of transparency and accountability and also being one of four Finalists of the Good Governance Awards 2024 for charity organisations in our category.
While 2024 was largely a positive year for the Marie Keating Foundation, it was not without its challenges as a charity. Over the past year, fundraising for the Marie Keating Foundation has been both rewarding and challenging. With less than 5% of our total income coming from statutory sources, our charity relies heavily on donations from the public and corporate supporters as well as our own fundraising efforts to secure funds towards our cancer awareness and support services. In 2024, this vulnerability was further amplified due to external factors of the cost-of-living crisis, rising inflation, war in Ukraine, and conflict in the Middle East.
Increasing demands on our services with a small, dedicated team meant that navigating this was challenging. We are team of just 23 people, meaning that while demand for our services is increasing, our capacity and financial resources are limited.
Sadly, we saw significant loss within our patient groups and ambassadors particularly in our Bowel Cancer Awareness patient advocates, further steadfasting our mission to pursue change when it comes to screening in Ireland and promoting early detection, and also ensuring that our support services for those living with and beyond cancer continue to grow and develop.
Ultimately, the Marie Keating Foundation is all about people. It is about ensuring that we are with the cancer community, patients and families, at every step of the way.
May I take this opportunity to pass on our thanks to all of those who make our work possible including our Board members, the Keating family, volunteers, supporters and patient ambassadors who give their time and expertise freely, and particularly to the entire Marie Keating Foundation team for their extraordinary passion, dedication and commitment. Together we are achieving our mission of ‘making cancer less frightening by enlightening’ and our vision of a ’world free from the fear of cancer’ making a real difference for families and communities affected by cancer throughout Ireland.
As we reflect on 2024, Crohn’s & Colitis Ireland (CCI) celebrated it’s 40th anniversary and has continued to support and empower individuals living with Inflammatory Bowel Disease (IBD), building on our mission to improve daily life and foster resilience. This year has been one of both challenges and remarkable achievements, from gaining critical insights through our IBD Patient Survey to launching impactful initiatives that reached thousands of people. In November 2024, we proudly launched our 200 page IBD Diet Information & Recipe Book.
IBD Patient Survey 2024 –A Window into the Lived Experience of IBD
One of our most significant undertakings this year was the IBD Patient Survey, which ran from February to March 2024. With over 1,500 responses, the survey provided invaluable insight into the lived experience of those with Crohn’s disease and ulcerative colitis. The data revealed startling statistics that underscore the pressing need for more comprehensive and accessible care for IBD patients in Ireland:
• 47% of patients waited over a year before seeking medical help.
• 33% went to A&E once or more before receiving a diagnosis.
• A staggering 85% reported that their mental health was not addressed in clinical settings.
• 68% lacked access to diet and nutrition support.
• 68% were never asked about non-gut complications of IBD.
• 62% of respondents said IBD care placed a financial burden on them.
• 35% experienced stigma or unfair treatment.
• 44% stated that IBD impacts their daily tasks, and 69% weren’t asked about fatigue.
• Over 50% of patients reported not having regular care reviews.
• 70% shared that they have struggled to cope with their IBD in the past year.
The full report is available on our website, where it serves as a valuable resource for policymakers, healthcare professionals, and the public. The survey has also reinforced the need for CCI’s continued advocacy for better services, as we strive to ensure that the voices
End of Year Review
Crohn’s & Colitis Ireland
of those living with IBD are heard and acted upon.
Helpline and Support Services
This year, our helpline saw a 47% increase in demand compared to 2023, illustrating the growing need for our support services. We have remained committed to providing practical and emotional support through various channels, including online support meetings, four patient days in Dublin, Cork, Carlow, and Sligo, and speaking at three medical student events. We also delivered two webinars: one focused on diet and IBD, and another on living with an ostomy.
World IBD Day Media Campaign – Raising Awareness
Our World IBD Day (19th of May) campaign, themed “It Takes Guts,” showcased the courage and resilience of people living with IBD. The campaign garnered significant media attention, with coverage from over 120 outlets, including national and local radio, TV, print, and digital platforms. The widespread exposure helped raise awareness and destigmatise IBD, encouraging empathy and understanding.
Partnership with Cork Airport
This year, we collaborated with Cork Airport to address an issue that has been a growing concern for many IBD patients: the detection of stomas by airport scanners. In partnership with the airport, we are training security staff to handle passengers with stomas with dignity and respect. We are also creating educational content to help passengers understand the process and know what they can request for a more comfortable journey. We are excited to expand this initiative to Dublin, Shannon, Knock, and Kerry airports in the near future, further improving the travel experience for IBD patients.
Gutcast – Empowering Through Stories
Our award-winning podcast Gutcast continues to be an essential platform for sharing lived experiences and expert advice. This year, the episode featuring patient advocates Victoria Spillane and Ciarán Davis, along with IBD nurse Angela Mullen, provided listeners with personal insights into life with IBD and the evolution of care over the past 40 years. With over 30,000 listens, Gutcast remains a vital resource for patients and
Written by Amy Kelly, COO, Crohn’s & Colitis Ireland
healthcare professionals alike, offering practical advice, emotional support, and an open dialogue on the challenges faced by those living with IBD.
We introduced a new service in 2024, the Clinical Referral Programme, which aims to provide timely support for those newly diagnosed with Crohn’s or colitis. In collaboration with the Mercy Hospital, the IBD nurse team referred patients to our service, providing them with tailored information, time to answers all their questions, and an introduction to the full range of CCI’s services. This bespoke service empowers patients by offering them the tools and support they need to manage their condition from the outset.
Boo4Poo – Engaging the Next Generation
In response to the concerning rise in paediatric IBD diagnoses, CCI launched the Boo4Poo campaign, a Halloween-themed colouring competition aimed at educating and engaging primary school students about IBD. The campaign not only raised awareness but also fostered empathy for children living with the condition. With over 100 entries, Boo4Poo has proven to be a highly successful initiative, and we look forward to expanding it in 2025.
IBD Diet Information &
Recipe Book – A New Resource for Patients
In November 2024, we proudly launched the IBD Diet Information & Recipe Book, a comprehensive resource designed to help individuals with IBD manage their diet and improve their overall health. According to our 2024 patient survey, 68% of respondents reported a lack of access to specialised diet and nutrition support, highlighting the need for this resource. The book, written by dietitian Lorraine Cooney and reviewed by a panel of experts, contains over 60 IBD-friendly recipes and expert advice. It
covers a range of topics, from managing flare-ups and remission to navigating social events and dining out.
Looking Ahead to 2025 –Continued Progress and Advocacy
As we look toward 2025, CCI remains committed to building on the momentum of 2024. Our advocacy efforts will continue to focus on raising awareness and effecting systemic change, particularly in light of the upcoming general election. We aim to ensure that IBD patients’ voices are heard in the new government, advocating for policies that address the gaps in care and support revealed by our patient survey.
We will also expand our network of support services, working closely with healthcare providers to ensure that IBD patients have access to the care, support, and information they need to live well. Through initiatives like our helpline, patient days, and online support meetings, we will continue to provide a vital safety net for those navigating the complexities of living with IBD.
In addition, we are excited about the continued development of our collaborations with airports and other organisations to improve the quality of life for IBD patients. The success of the Boo4Poo campaign and the IBD Diet Information & Recipe Book demonstrates the power of education and empowerment, and we look forward to creating more resources that support IBD patients in the year ahead.
2025 promises to be another year of progress, and we are deeply grateful for the unwavering support of our members, partners, and supporters. We will continue to fight for better care, increased awareness, and an improved quality of life for all those diagnosed with Crohn’s disease and ulcerative colitis in Ireland.
End of Year Review
Medicines for Ireland unveils General Election Manifesto
Chairperson of Medicines for Ireland
Paul Neill
2. Access to essential and affordable medicines: Guarantee the availability of vital
Chairperson of MFI, Paul Neill said, “As we approach a critical juncture in Ireland’s healthcare landscape, we must prioritise the accessibility and affordability of essential medicines. Our manifesto outlines a clear path to achieving this by addressing the barriers to early market entry for generics and biosimilars. By implementing these
the manifesto, Ireland can ensure a healthier future for all its citizens.
Vice-Chair of MFI, Deirdre Kelly says, “The future of healthcare in Ireland lies in embracing sustainability and digital innovation. Our manifesto calls for a collaborative approach to integrating green practices and
Medicines for Ireland’s priorities
Medicines for Ireland’s priorities
Medicines for Ireland’s priorities
Medicines for Ireland’s priorities
Patent reform to ensure fair competition
Patent reform to ensure fair competition
Address the barriers to early market entry for off-patent companies caused by the current and developing legal landscape favouring originator pharmaceutical companies, leading to significant overspending by the Irish State and delayed access to cost-effective generics.
Address the barriers to early market entry for off-patent companies caused by the current and developing legal landscape favouring originator pharmaceutical companies, leading to significant overspending by the Irish State and delayed access to cost-effective generics.
Patent reform to ensure fair competition
Patent reform to ensure fair competition
Address the barriers to early market entry for off-patent companies caused by the current and developing legal landscape favouring originator pharmaceutical companies, leading to significant overspending by the Irish State and delayed access to cost-effective generics.
Address the barriers to early market entry for off-patent companies caused by the current and developing legal landscape favouring originator pharmaceutical companies, leading to significant overspending by the Irish State and delayed access to cost-effective generics.
Access to essential and affordable medicines
Access to essential and affordable medicines
Guarantee the availability of vital medicines at prices that are accessible to all, supporting public health and delivering value to patients and the healthcare system.
Guarantee the availability of vital medicines at prices that are accessible to all, supporting public health and delivering value to patients and the healthcare system.
Access to essential and affordable medicines
Guarantee the availability of vital medicines at prices that are accessible to all, supporting public health and delivering value to patients and the healthcare system.
Access to essential and affordable medicines
Guarantee the availability of vital medicines at prices that are accessible to all, supporting public health and delivering value to patients and the healthcare system.
An industry fit for the green, digital era
An industry fit for the green, digital era
The future of healthcare lies in embracing sustainability and digital innovation. We urge political parties to actively engage with the off-patent industry to avoid any unintended consequences when supporting initiatives that drive environmental responsibility. MFI calls on political representatives to accelerate the use of technologies to improve efficiency, reduce waste, and enhance patient care.
An industry fit for the green, digital era
The future of healthcare lies in embracing sustainability and digital innovation. We urge political parties to actively engage with the off-patent industry to avoid any unintended consequences when supporting initiatives that drive environmental responsibility. MFI calls on political representatives to accelerate the use of technologies to improve efficiency, reduce waste, and enhance patient care.
The future of healthcare lies in embracing sustainability and digital innovation. We urge political parties to actively engage with the off-patent industry to avoid any unintended consequences when supporting initiatives that drive environmental responsibility. MFI calls on political representatives to accelerate the use of technologies to improve efficiency, reduce waste, and enhance patient care.
In some ways 2024 was a landmark year for the cause of cardiovascular health in Ireland. But many concerns and frustrations also remain over the lack of priority given to minimising preventable death and disability from heart disease and stroke in Ireland.
In terms of the Irish Heart Foundation’s agenda, the highlights were the first ever national funding for community support services for stroke survivors and heart patients in Ireland, along with the restoration of Ireland’s credentials as a world leader in tobacco control.
On the downside, another year passed without publication of the National Review of Specialist Cardiac Services and without an overarching National Cardiovascular Health policy. This represents not so much a gaping hole as a chasm in Ireland’s health services given that cardiovascular disease is responsible for almost 30% of all-cause mortality here. It has to be recognised, however, that funding provided in the recent Budget for the Irish Heart Foundation’s national stroke and heart support services will have a life-changing impact on many thousands of patients in every corner of the country.
Cardiovascular patients represent a huge portion of Ireland’s population, in the region of 600,000 people. And there are as many as 80,000 discharges of heart and stroke patients from Irish hospitals each year – the equivalent of one every seven minutes.
When the pandemic struck, the Irish Heart Foundation set up a phone-based check-in service in collaboration with the national heart and stroke programmes to support patients who couldn’t attend hospital appointments or were being discharged home earlier than usual to free up space for Covid patients.
This provided the basis for the development of a pathway of phone, online and face to face services that support patients almost literally from the hospital gates for as long as they need us. A great many describe these practical, social and emotional supports as their lifeline.
They are changing a deep sense of abandonment among stroke survivors caused by the chronic dearth of community rehabilitation. They are also helping to tackle
End of Year Review A Landmark Year for Cardiovascular Health
the revolving door syndrome of a 90 day hospital readmission rate among heart failure patients that has been estimated at 30%, often for the want of basic information and support.
Over one in three stroke survivors returning home nationally are being referred in to the services, which also support thousands more patients across a broad range of cardiac conditions. And the recurrent funding championed by Minister for Health Stephen Donnelly provides the basis for long term sustainability for support that can continue to grow in scale and depth in line with stroke survivor needs.
Until recently Ireland had lost its way in terms of tobacco and nicotine addiction. Youth smoking rates had risen for the first time in a generation; we were one of the last countries in Europe to ban the sale of vapes to under 18s; and we remained around half a million smokers short of reaching the Tobacco Free Ireland target of a 5% smoking rate by 2025.
However, the Irish Heart Foundation-led campaign for legislation to make Ireland the first EU country to increase the legal age of sale of tobacco to 21 has breathed new life into tobacco control in Ireland. We know this measure will be effective from its success in the US where it was made federal law by President Donald Trump in 2019. And through our own experience when the age of sale in Ireland was increased here from 16-18, reducing smoking in that age group by 30%.
Perhaps most importantly it sets Ireland on a path to the total phasing out of legal tobacco sales, as is in train in the UK –a move supported by 83% of the Irish public in a poll for the HSE. Unlike in the UK, this must be accompanied by a gradual process of denicotinisation of cigarettes to reduce their addictive nature and therefore demand for them over time.
In addition to the ¤1 budget increase on a pack of cigarettes, the imposition of a specific tax on e-cigarette liquid imposed for the first time will act as a deterrent to young people taking up vaping. And whilst legislation to protect young people from nicotine addiction following the explosion in youth vaping could not be passed
Written by Chris Macey, Director of Advocacy and Patient Support, Irish Heart Foundation
before the general election, there is broad cross-party consensus that tough action is needed.
But nor can the negative impact of the absence of a national plan for cardiovascular disease since the previous policy expired in 2019. The absence of a policy framework for the prevention, detection and treatment of cardiovascular disease, along with services and supports that maximise patients’ health and wellbeing in the community is preventing the development of lifesaving services. This is resulting in preventable death, disability and loss of quality of life on a significant scale.
It should be acknowledged that there was some funding in the Budget for implementation of the National Stroke Strategy and for the development of a new cardiovascular plan.
However, this is against the background of a lack of comprehensive national cardiac registries providing health planners with vital real-time data; restricted access to cardiac diagnostics is resulting in long waiting lists; and an urgent need for investment in cardiac imaging, including echocardiography, cardiac CT and cardiac MRI. The incoming President of the Irish Cardiac Society, Prof Brendan McAdam said at a recent hearing of the Oireachtas Health Committee that due to such deficits the cardiovascular community was currently unable to deliver care at a level consistent with international guidelines.
The incoming Government should urgently publish the National Cardiac Services Review with a robust and fully funded implementation plan, and prioritise the publication of a new National Cardiovascular Policy and Strategy, also with a commitment to full multi-annual funding.
Our other priorities include:
- Full implementation of the National Stroke Strategy 20222027 with an overall investment of ¤36 million and a subsequent plan with guaranteed multiannual funding that places a far greater emphasis on the community services and supports that enable survivors to make the most of life after stroke.
- Priority for implementing the model of care for cardiac rehabilitation, which can reduce deaths from heart disease by at least a fifth. Services in many parts of the country are at crisis point with staffing down 63% since 2009 in the face of a major population increase and waiting times in some instances in excess of two years.
- We need a firm commitment on legislation to tackle Ireland’s obesity crisis, including protection for children from junk food marketing – with teenagers seeing around three ads for unhealthy food and beverages every ten minutes they are online. This saturation level of exposure is a key driver of Ireland’s childhood obesity crisis which the State’s own research predicts will cause the premature deaths of 85,000 of this generation of children in Ireland.
- We should also build on the success of the Sugar Sweetened Drinks Tax, which reduced sugar intake from soft drinks by a quarter in its first year by incentivising product reformulation. A tax on high sugar food products, coupled with programmes to increase consumption of fruit and vegetables, would reduce the national waistline and promote healthier diets.
- Other crucial evidence-based measures to tackle childhood obesity include no fry zones near schools and restrictions of price promotions and in store marketing.
- Completion of legislation to protect children from vaping put forward by the outgoing Government.
End of Year Review
Advocating for those with Asthma
The Asthma Society of Ireland advocates for the well-being of the 450,000 people in Ireland currently with asthma and the 890,000 affected at some point in life. Its vision is for all individuals with asthma to live symptomfree, with a mission to reduce asthma deaths and improve lives. The Society empowers patients, raises awareness, influences policy, and collaborates with healthcare, research, and education professionals. It actively supports all levels of care, working closely with the National Clinical Programme Respiratory (NCPR).
Achievements
In 2024 the Asthma Society has been working hard to advocate, care, inform and educate those with asthma, their carers and health care professionals. Our patient services consist of Asthma/COPD Adviceline, and the WhatsApp nurse messaging service part of which is the webinar series. We also support healthcare professionals with resources in the form of written and electronic resources. In addition, the website is very often the first port of call for clients seeking information on their condition.
Patient Services
WhatsApp Nurse messaging Service: 086 059 0132
The WhatsApp nurse messaging service supported 395 new patients in 2023, surpassing that number by mid-November 2024. Each new admission has approximately 10 interventions. Over 4,000 interventions are
Written by Ruth Morrow, Respiratory Nurse Specialist, Asthma Society of Ireland
nurse followed by a Q&A session. Subjects this year included: Smoking & Vaping, Women & Asthma, Allergic Rhinitis & Asthma, Back2School for parents, carers, teachers and SNAs and Winter Wellness. Between 200 and 300 people registered for each webinar and on average 130 attended. People can avail of webinar recordings to watch back on our website and through our monthly e-zine communication.
E referral
expected by year-end. This nurse-led service enables asthma and COPD patients, their families, and carers to confidentially message respiratory nurses for disease management advice, access health tools, and receive referrals. Insights show the service is effective for one-time use but has greater impact with repeated engagement.
Asthma Adviceline: 1800 44 54 64
By mid-November 2024, the Asthma/COPD Adviceline surpassed 2023 figures with over 4,000 consults. This free call back service offers 30-minute consultations with asthma nurses, providing education, self-management support, and healthcare signposting, with follow-ups as needed. In partnership with COPD Support Ireland, the COPD Adviceline helps patients understand and manage their condition while connecting them to COPDSI services and support groups.
Webinars
Webinars are held regularly to support self-management and provide education to patients, carers and healthcare professionals. Expert speakers present on topical subjects alongside an ASI respiratory
An e referral for health care professionals to refer their patients to the Adviceline has been developed. Patients can also self-refer. The referral is available on the website. Simply fill in the referral form and submit. The administrative staff will then contact the client and give them an appointment at a time that suits. This e referral has become popular with integrated hubs and GP practices. We welcome referrals from all health care professionals who feel their patients would benefit from the Asthma society augmenting their care
Resources
The Asthma Society provides vital patient education, distributing over 10,000 resources annually. Updated booklets, such as Asthma and Allergy, Take Control of Your Asthma, Asthma and your Child
and Asthma and Pregnancy are now more literacy-friendly, featuring larger fonts, fewer words, and more graphics, approved by the Medical Advisory Group. New infographics are also available for the WhatsApp service, social media, and the website. A key 2024 resource, developed with the HSE National Clinical Programme Respiratory, is the MART Asthma Action Plan for patients using Maintenance and Reliever Therapy, accessible on the website.
Campaigns and Communication
In 2024 the ASI ran a number of successful campaigns throughout the year. Campaigns aim to raise awareness amongst key stakeholder groups about the seriousness of asthma or hayfever and encourage people and their carers to take action towards proactive disease management
Asthma Awareness Week
Asthma Awareness Week took place during the first week of May. The focus this year was ‘Asthma Education Empowers’ which aimed to empower people with asthma with the appropriate education to manage their disease, and to recognise when to seek medical help when their asthma worsens.
Hayfever Campaign
This year the Asthma Society conducted a very successful
Hayfever campaign. Every opportunity was taken to share expert advice on managing this condition. A top tips release with practical tips was shared with key broadcast, print and online media. Numerous national and regional interviews took place with Respiratory Nurse Specialist Ruth Morrow and Prof Marcus Butler as well as sharing the personal stories of patients with asthma who experience severe hayfever symptoms. The campaign continued throughout the summer months.
Asthma Safe School Programme
The aim of this program is to train one teacher per school in PHECC (Pre Hospital Emergency Care Council) approved and certified basic life support and administration of Salbutamol for emergency treatment of adults and children with an acute asthma attack.
This program enables school staff to identify what to do in the case of an acute asthma attack, to encourage schools to provide a supportive environment for students with asthma, to create better public awareness of the 5 Step Rule and how to recognize and manage an asthma attack. Part of the programme included an Asthma Safe School webinar, free for all principals, teachers and SNAs in September.
Oral Corticosteroid Tablet use
This campaign was based on research conducted by IQVIA and Irish company specialising in analytics and clinical research services to the life sciences industry. Longitudinal retail pharmacy prescription data was used and then reviewed by the Asthma Society of Ireland’s Medical Advisory Group. The research showed that almost 1 in 5 patients were dispensed multiple courses of steroid tablets within a 12 month period. Steroid tablets are associated with significant adverse side effects and should be prescribed at the lowest possible dose for the shortest possible time. This media relations campaign addressed the concerns surrounding the overuse of oral steroids in asthma management while highlighting best practices for treatment
Training days on the safe schools programme
Advocacy and research
Towards Optimal Severe Asthma Care report
During 2024, the Asthma Society of Ireland undertook research to examine the standards of care for severe asthma in Ireland. Following a literature review a survey was conducted of patients with severe asthma that revealed new insights on the existing gaps in the Irish healthcare system. This was explored in further detail with a focus group of patients and carers of children living with severe asthma. Both research projects showed inconsistencies in care standards, diagnostic hurdles, significant financial strain on patients and a lack of understanding and awareness from healthcare professionals, employers and the general public. These findings were then presented at a roundtable of experts who were in agreement with the challenges and potential solutions raised by patients. The experts underlined the need for government to allocate funding to support the introduction and maintenance of a severe asthma registry.
Tobacco 21 Alliance
We wholeheartedly welcome the Public Health (Tobacco) (Amendment) Bill 2024, which will raise the legal age of the sale of tobacco products from 18 to 21. Once officially passed, the Tobacco 21 Alliance, of which we are an active member, will issue a short statement welcoming the bill and showing our support for it to reduce smoking among young people. The Act will come into operation on 1 February 2028.
Other important groups the Asthma Society is a member of include;
• Climate change and air pollution working group
• The HSE inhalers action group
• Irish lung health alliance and the International Respiratory Coalition
• Physical activity for chronic conditions working group
• Tobacco stakeholders group
Challenges
The Asthma Society faces challenges on behalf of those it represents. Asthma severity is often underestimated, delaying diagnosis and treatment. Socioeconomic and geographic disparities hinder access to care, medications, and diagnostic tools. Educating patients on medication adherence and trigger avoidance remains a persistent issue. Funding is needed for research to address care gaps, raise climate change awareness, and advocate for supportive health policies.
Winter illnesses like flu, COVID-19, and RSV exacerbate difficulties for respiratory patients, as reported via WhatsApp and Adviceline services. Additional challenges include inflation, GP access issues, and financial constraints forcing patients to skip GP visits or asthma medications. The cost-of-living crisis also affects those requiring oxygen or nebulised medication.
Looking to 2025
The Asthma Society looks forward to planning growth within the organisation in 2025. We will endeavor to measure our impact using data that reflects what we do and allows us to review our activities.
A new website will be launched in the New Year that will have a new architecture and be easier to navigate. Information will be updated on an ongoing basis for the website and for all educational resources.
The ASI strategy 2020 -2025 is complete next year. A project to develop a new strategy will begin.
A research proposal to review the impact of the ASI patient services activities has been developed and funding dependent this research will be carried out in 2025.
We have a number of campaigns, events and webinars in the plan for next year so follow us on social media, print media and broadcasting media or go onto our website and join our emailing list to keep updated.
We strive to reach out further to those who need our services and build relationships with stakeholders. Along with patient services, the Asthma Society will build on its advocacy and research work to meet the needs of people with asthma.
Acknowledgments
The author would like to acknowledge the help of Mary McDonald, Patient Services Manager and Caroline Reilly, Patient Services Coordinator for their assistance with this article.
End of Year Review
Migraine Ireland
Written by Naomi Oziel, Individual Giving, Donor and Grants Development Officer, Migraine Association of Ireland
“Next year, in 2025, we intend to add and highlight our schools programme, our Healthcare professional Guide for GPs and Pharmacists, and will continue to bring interesting speaker from all over the world to give as much insight into migraine as possible”
With 2024 being Migraine Ireland’s 30th Anniversary, the team has worked incredibly hard on making it a year to be remembered. Arguably our biggest year yet, Migraine Ireland has received national recognition through its nomination for the Irish Healthcare Awards. The project entitled, “In Their Words” was a first-of-itskind video series dedicated to exploring migraine through the lived experiences of migraineurs themselves. It’s the stories such as theirs that drive this team of five to continue its mission of advocacy, education and patient support.
Rewinding to the beginning of the year, Migraine Ireland presented a talk at Trinity College Dublin to an audience of doctors and nurses on the effectiveness of Compassion Focused
Therapy (CFT) for migraine. This informative session presented collaborative findings of Migraine Ireland, Sláintecare and the Department of Psychology of Beaumont’s 6-week trial of CFT and found that most patients cited moderate to significant improvements in their migraine management as a result of their participation. Delivering this news to a large audience of PhDs in such an esteemed academic establishment helps to further validate and advocate for migraineurs across the nation.
Mid-year saw the introduction of a brand-new role in Migraine Ireland through the hiring of an Individual Giving, Donor and Grants Development Officer, marking a continued period of growth in the organisation. Around
the same time, the team travelled to LinkedIn headquarters here in Ireland to provide an in-person workplace talk on migraine and how to manage it in the office. Opening with an articulate explanation of the phases of migraine, the presenters later shift into exploring small yet effective adjustments that employers could make in their workplaces to help their employees who live with migraine. This talk marked a large step towards migraine education on a larger scale corporate level.
Moving into the final quarter, Migraine Ireland launched fundraising events of which the funds go right back into providing services for the migraine community. The positive impact which results from these events is what drives this organisation continue organising ones such as the Autumn Cycle Challenge and the current Winter Lapland Quest, which is still live through Dec 31st. The teams look forward to the year ahead and bringing our best to the team and to you!
Next year, in 2025, we intend to add and highlight our schools programme, our Healthcare professional Guide for GPs and
Pharmacists, and will continue to bring interesting speaker from all over the world to give as much insight into migraine as possible. Throughout the year, as all these talks and events take place, Migraine Ireland does significant work which may be lost in the noise of its more outwardly ambitious activities. Our membership management and communication is key to engaging with our support base. Migraine Ireland has logged over 200 contacts with its Infoline service users to date. These interactions are so important to the organisation and represents the voice of the person living with migraine in Ireland on a daily basis. Listening to and being trusted with the stories of people living and fighting every day with migraine is what informs our work and our objectives.
Over the year we have had our biweekly group conversations. This informal peer to peer support represents the beauty of people who understand each other supporting each other. Often people living with migraine face stigma, misunderstanding and social isolation. Being present at those conversations is a privilege and an inspiration.
Migraine Ireland has been on the same mission for its thirty-year lifespan and while this mission will never change, we are constantly exploring new paths and avenues to achieve it. This year has been one of change, creativity and recognition for us and as we look to the year ahead, we hope that our efforts will continue to pay off as we increase the visibility of migraineurs in Ireland.
Over 600,000 people in Ireland live with Migraine, and as the only not-for-profit organisation in the country dedicated to migraine and other primary headache disorders we are really privileged and proud to represent their interests. We can be contacted via email on info@migraine.ie or see out website at www.migraine,ie
PREVENT
THE DISRUPTION OF MIGRAINE1
The only oral once-daily calcitonin gene-related peptide (CGRP) receptor antagonist for both episodic and chronic migraine patients1,2
Tablet not actual size.
Typical characteristics of migraine are headache of unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and phonophobia.3
ABBREVIATED PRESCRIBING INFORMATION. AQUIPTA®▼ (atogepant) 10 mg tablets; 60 mg tablets. Please refer to the Summary of Product Characteristics (SmPC) before prescribing.
PRESENTATION: Each tablet contains: 10 mg atogepant in 10 mg tablet, 60 mg atogepant in 60 mg tablet. INDICATION: Prophylaxis of migraine in adults who have at least 4 migraine days per month. DOSAGE AND ADMINISTRATION: The recommended dose is 60 mg taken orally once daily with or without meals; swallowed whole and not split, crushed or chewed. Missed dose to be taken as soon as it is remembered. If forgotten for an entire day, missed dose to be skipped and next dose taken as scheduled. Dose Modification: The recommended dosage of atogepant with concomitant use of strong CYP3A4 inhibitors or strong OATP inhibitors is 10 mg once daily. Special Populations: Elderly (≥65 years): No dose adjustment of atogepant is needed in elderly patients. Renal impairment: In patients with severe renal impairment (creatinine clearance [CLcr] 15-29 mL/ min), and in patients with end-stage renal disease (ESRD) (CLcr <15 mL/min), the recommended dosage of atogepant is 10 mg once daily. For patients with ESRD undergoing intermittent dialysis, atogepant should preferably be taken after dialysis. No dose adjustment is recommended for patients with mild or moderate renal impairment. Hepatic impairment: Avoid use of atogepant in patients with severe hepatic impairment. No dose adjustment is recommended for patients with mild or moderate hepatic impairment. Paediatric Population: The safety and efficacy of atogepant in children (< 18 years of age) have not yet been established. CONTRAINDICATIONS: Hypersensitivity to active substance or any of the excipients. SPECIAL WARNINGS AND PRECAUTIONS: Atogepant 60 mg tablets contain 31.5 mg sodium per tablet; this is equivalent to 1.6% of the WHO recommended maximum daily intake of 2 g sodium for an adult. Atogepant 10 mg tablets contain less than 1 mmol sodium (23 mg) per dose, that is to say essentially ‘sodium-free’. Atogepant has no or negligible influence on the ability to drive and use machines. However, if affected by somnolence, patients should exercise caution before driving or using machinery. FERTILITY, PREGNANCY AND LACTATION: Pregnancy: Atogepant is not recommended during pregnancy and in women of childbearing
potential not using contraception. Breast-feeding: It is unknown whether atogepant is excreted in human milk. A decision must be made whether to discontinue breast-feeding or to discontinue/ abstain from therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Fertility: No human data on the effect of atogepant on fertility are available. Animal studies showed no impact on female and male fertility with atogepant treatment. UNDESIRABLE EFFECTS: Common (≥ 1/100 to <1/10): Decreased appetite, nausea, constipation, fatigue/somnolence, weight decreased. Refer to Section 4.8 of the SmPC for details of other side effects, and for further information.
▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie.
LEGAL CATEGORY: POM (S1B). MARKETING AUTHORISATION NUMBERS: EU/1/23/1750/001 AQUIPTA 10 mg tablets in blisters, in cartons of 28 tablets; EU/1/23/1750/003 AQUIPTA 60 mg tablets in blisters, in cartons of 28 tablets. MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany. Further information is available on request from: AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24. DATE OF REVISION: October 2023. PI/1750/001.
References: 1. AQUIPTA® Summary of Product Characteristics, available at www.medicines.ie. 2. Morena-Ajona D, et al. J Clin Med. 2022;11(6):1656. 3. Ferrari MD, et al. Nat Rev Dis Primers. 2022;8(1):2.
End of Year Review
Thrombosis
Ireland
Written by Fionnuala Ní Áinle, Siobhán Ní Bhriain, Michael O’Connor
(1) HSE National Clinical Lead, National Clinical Programme in VTE
(2) HSE National Clinical Director Integrated Care, Office Chief Clinical Officer
(3) HSE National Clinical Advisor and Group Lead, Access and Integration
The National Clinical Programme in VTE and the Launch of “Eve’s Protocol” in Memory of Eve Cleary
Introduction
Venous thromboembolism (VTE, comprising deep vein thrombosis and pulmonary embolism) represents a major healthcare risk throughout the world. In the community, it is a common disease affecting 1 in 12 people overall during their lives and symptoms and signs can be overlooked. VTE is a leading cause of hospital-associated morbidity and mortality and is the leading cause of maternal death overall in the UK and Ireland. Of all survivors, at least half will have long-term sequelae including post-thrombotic syndrome of the lower limbs, post-pulmonary embolism dyspnoea, chronic thromboembolic pulmonary hypertension, anxiety and posttraumatic stress disorder.
Despite the incidence, mortality and long-term health impact of VTE, awareness of this condition in the general population is very poor. A US survey reported that 75% of respondents had never heard of DVT and fewer than 1 in 10 had an awareness of DVT symptoms. This is a major clinical and societal risk that must be urgently addressed, given the missed opportunities to prevent death and long-term disability.
VTE is a major burden for health care systems worldwide. For example, VTE costs EU health systems ¤1.5-2.2 billion per year in direct costs. However, the effects of chronic disability and loss of productive life years due to thromboembolic diseases can cause indirect costs, that in Europe have been estimated to be as high as 13.2 billion per year (source: International Society on Thrombosis and Haemostasis).
Despite the fact that VTE is so prevalent and avoidable, it often lacks the prioritisation it deserves in many countries. In a transformative step towards raising VTE awareness and driving systemic improvements in VTE
prevention and care, the HSE launched the National Clinical Programme in VTE (NCP-VTE) in October 2022. The programme aims to establish national standards for the prevention, diagnosis and management of VTE and for a post-VTE recovery programme, integrated in the community. Under the mandate of Dr Colm Henry, Chief Clinical Officer, HSE, and with the strong advocacy of Melanie SheehanCleary, who tragically lost her beloved daughter, Eve Cleary, due to a pulmonary embolism (PE), the NCP-VTE has been commissioned to form a taskforce to write “Eve’s Protocol”— a first national guideline intended to guide multidisciplinary care providers in the community and in hospitals in managing VTE across the patient journey and to raise VTE awareness among the public.
Establishing the National VTE Programme: A Milestone in VTE Care
The role of the NCP-VTE is to develop guidance and advice for the healthcare system on the prevention, diagnosis, management, and long-term care of VTE through an integrated care approach across the community (including primary and prehospital care) and hospitals. Since its inception, the NCP has built a robust governance structure at both national and regional levels, aiming to establish a streamlined, standardised approach to the implementation of the recommendations for patient safety in VTE. This governance structure includes a VTE Clinical Advisory Group with extensive multidisciplinary clinical representation from all healthcare regions. Moreover, the NCP-VTE has been extremely fortunate to include amongst its working team a range of multidisciplinary leadership from around the country, including nursing, advance nurse practitioner, psychology, physiotherapy and clinical colleague which has led to
the formation of very active VTE working groups focussing on the highest priority issues facing VTE.
The NCP-VTE team, working with active and committed colleagues throughout the country, has made significant advances to date since its inception in 2022. A key performance indicator (KPI) estimating suspected hospitalacquired thrombosis rates is collected and reviewed, with feedback provided to support local assessment and to drive quality improvement. The programme’s strategic alignment with the 2024 National Service Plan and the anticipated resource approvals from the Department of Health demonstrate the prioritisation of VTE care in Ireland. Resources have been dedicated particularly in the context of unscheduled emergency care and women’s healthcare—two areas where VTE risk and management needs are especially high.
Eve’s Protocol: A National Guideline for a Safer Future
At the centre of the NCP-VTE mission is the development of a National Guideline for the prevention, diagnosis and management of VTE and supporting evidence-based strategies supporting VTE recovery. The Guideline taskforce is honoured to name this “Eve’s Protocol”, in memory of Eve Cleary. Eve’s Protocol is intended as a living legacy to the lessons learned from Eve’s passing and her mother Melanie SheehanCleary’s determined advocacy. This protocol will commemorate all those who died from VTE. In July 2024, the National Clinical Director for Integrated Care commissioned the development of the protocol, highlighting the protocol’s importance to improving patient safety and quality of care in Ireland. The commissioning is a clear mandate from the highest levels of the HSE, with support from HSE CEO.
The Protocol will be built on evidence and an understanding of the patient experience and patient and family representatives will serve on the guideline task force along. This patient i involvement is deeply appreciated and serves as an important reminder of the need for a patient-centered approach to healthcare policy and guideline creation. This will ensure that the voices of those directly affected by VTE remain central to the NCP-VTE mission. This mission is enshrined in one of the most important of the draft protocol’s recommendations highlighting the need to improve awareness of VTE signs and symptoms in the community and for patients who have been hospitalised. A truly collaborative approach to improving VTE awareness was exemplified by the development of a “Blood Clot Alert Card” by the HSE Quality and Patient Safety directorate in 2018 working closely with the patient organisation Thrombosis Ireland (Figure 1). The Protocol will include the messaging included in this valuable resource and will also promote alternative strategies aimed at a wider audience, including videos suitable for dissemination on social media and a wide range of patient information leaflets. The blood alert card will undergo further review to update it.
Multidisciplinary Collaboration: A Foundation of the National VTE Programme
The day to day work of the NCP-VTE is characterised by a strong multidisciplinary approach, including perspectives from many varied professionals, which will ensure that recommendations are reflective of different healthcare settings. The development othe Protocol will further benefit from this strong professional collaboration. This collaborative approach is particularly important, given the broad spectrum of VTE’s impact across patient demographics and clinical scenarios.
BLOOD CLOT ALERT CARD
WHAT IS A BLOOD CLOT?
This is the formation of a clot inside a blood vessel, usually in the leg, which may break off and go to the lungs. This can be fatal.
60%of clots happen in HOSPITAL or in the 90 DAYS following admission.
Blood clots can be very serious - but there are effective treatments to deal with them and help prevent them
SIGNS AND SYMPTOMS OF A BLOOD CLOT
Swelling or pain in one leg or arm
Warmth or redness in the leg or arm
➢Short of breath or rapid breathing
Chest pain
(particularly when breathing deeply)
Coughing or coughing up blood
If you have one or more of these, you may have a clot and need urgent treatment
BLOOD CLOT ALERT CARD Am I at risk?
WHAT CAN I DO TO HELP MYSELF?
Ask for your risk of blood clots to be assessed, especially if you are in one of the higher risk groups listed opposite
➢Walk and move as much as possible
➢Drink plenty of fluids
➢If directed to use stockings or medication to prevent or treat a clot follow instructions exactly
Remember, a blood clot in the veins is more likely up to 90 days after being in hospital
If you have any signs or symptoms of a clot, take immediate action to seek medical help
Data-Driven Improvement: The Role of Performance Metrics
A key pillar of the NCP-VTE’s emerging strategy has been its focus on data and performance metrics. The programme already advises in the HSE’s measurement of the rate of suspected hospitalassociated VTE and assists in data interpretation. Through this work, opportunities are identified for quality improvement and valuable feedback is provided to key stakeholders with responsibility for quality improvement. This data-driven approach fosters accountability and transparency, with the goal of reducing the incidence of preventable VTE and enhancing the quality of VTE care nationwide. The NCP-VTE’s vision is that similarly, the implementation of the Protocol recommendations
will also be driven by formal Quality Improvement strategies.
Moving Forward: The Future of VTE Care in Ireland
The NCP-VTE started its work in 2023 and is now progressing with the Protocol which is scheduled to complete in early 2025. The programme plans to make recommendations on the standardisation of VTE prevention, diagnosis, and management through implementation of this protocol. As the NCP-VTE continues to evolve, its objectives will continue to reflect the core values of safety, quality, and patient-centered care.
As the NCP-VTE’s work moves forward, the collaborative efforts of multidisciplinary colleagues and patient advocates will
YOU MAY BE AT HIGHER RISK IF YOU: are admitted to hospital and for 90 days after you go home have active cancer or receiving cancer treatment are pregnant or have had a baby less than 6 weeks ago become immobile (more than 3 days in bed / travel non-stop more than 6 hours / in a leg cast)
RISK MAY INCREASE FURTHER IF: you or a close relative had a blood clot you had surgery in the last 90 days you have thrombophilia (tendency to clot) you are on the oral contraceptive pill or HRT you have heart, lung or inflammatory disease you are over 60 years of age or are overweight you have varicose veins that become red and sore
always stay vital to its success. Each healthcare provider has a role to play in preventing VTE and safeguarding patients from its potentially life-threatening complications. With the Protocol as a guide, the NCP-VTE will advise and guide in the creation of a safer healthcare environment for all Irish patients and to establish Ireland as a leader in comprehensive VTE care.
Conclusion
The establishment of the National VTE Programme and the drafting of Eve’s Protocol mark a major step forward in Ireland’s approach to VTE. Through leadership, multidisciplinary collaboration, and a strong commitment to patient-centred care, the NCPVTE is committed to advise on
card)
the implementation of strategies that will potentially improve VTE outcomes and reduce preventable VTE incidents. We wish to see a safer future. For all involved in the implementation journey— clinicians, patient advocates, and healthcare professionals across Ireland—this initiative will honour the memory of Eve and others who died from VTE by driving lasting changes in VTE care.
Figure 1: Thrombosis Ireland/NCPVTE Blood Clot Alert Card (Upper panel: Front of card; Lower panel: Back of
Treatment of Acute Coronary Syndrome1
2.5 mg
Product subject to medical prescription which may not be renewed (A)
fondaparinux sodium
The Only Selective & Synthetic Factor Xa Inhibitor Injectable Anticoagulant Licensed for Use in Adults1
Reference: 1. Arixtra® 2.5 mg/0.5 ml solution for injection, pre-filled syringe. Summary of Product Characteristics (SmPC). Available at: www.medicines.ie. Last accessed: August 2024.
ABBREVIATED PRESCRIBING INFORMATION
Arixtra (fondaparinux sodium) 2.5 mg/0.5 ml solution for injection, pre-filled syringe
Please refer to Summary of Product Characteristics (SmPC) before prescribing Indications, Dosage and Administration:
Indications:
Prevention of Venous Thromboembolic Events (VTE) in adults undergoing major orthopaedic surgery of the lower limbs such as hip fracture, major knee surgery or hip replacement surgery. Prevention of Venous Thromboembolic Events (VTE) in adults undergoing abdominal surgery who are judged to be at high risk of thromboembolic complications, such as patients undergoing abdominal cancer surgery. Prevention of Venous Thromboembolic Events (VTE) in adult medical patients who are judged to be at high risk for VTE and who are immobilised due to acute illness such as cardiac insu ciency and/or acute respiratory disorders, and/or acute infectious or inflammatory disease.
Treatment of unstable angina or non-ST segment elevation myocardial infarction (UA/NSTEMI) in adults for whom urgent (<120 mins) invasive management (PCI) is not indicated. Treatment of ST segment elevation myocardial infarction (STEMI) in adults who are managed with thrombolytics or who initially are to receive no other form of reperfusion therapy. Treatment of adults with acute symptomatic spontaneous superficial-vein thrombosis of the lower limbs without concomitant deep-vein thrombosis.
Dosage
Patients undergoing major orthopaedic or abdominal surgery: The recommended dose of fondaparinux is 2.5 mg once daily administered post-operatively by subcutaneous injection. The initial dose should be given 6 hours following surgical closure provided that haemostasis has been established. Treatment should be continued until the risk of venous thromboembolism has diminished, usually until the patient is ambulant, at least 5 to 9 days after surgery.
Medical patients who are at high risk for thromboembolic complications based on an individual risk assessment: The recommended dose of fondaparinux is 2.5 mg once daily administered by subcutaneous injection. A treatment duration of 6-14 days has been clinically studied in medical patients.
Treatment of unstable angina/non-ST segment elevation myocardial infarction (UA/NSTEMI): The recommended dose of fondaparinux is 2.5 mg once daily, administered by subcutaneous injection. Treatment should be initiated as soon as possible following diagnosis and continued for up to a maximum of 8 days or until hospital discharge if that occurs earlier. If a patient is to undergo percutaneous coronary intervention (PCI), unfractionated heparin (UFH) as per standard practice should be administered during PCI, taking into account the
patient’s potential risk of bleeding, including the time since the last dose of fondaparinux, the timing of restarting subcutaneous fondaparinux after sheath removal should be based on clinical judgment. In the pivotal UA/NSTEMI clinical trial, treatment with fondaparinux was restarted no earlier than 2 hours after sheath removal.
Treatment of ST segment elevation myocardial infarction (STEMI): The recommended dose of fondaparinux is 2.5 mg once daily. The first dose of fondaparinux is administered intravenously and subsequent doses are administered by subcutaneous injection. Treatment should be initiated as soon as possible following diagnosis and continued for up to a maximum of 8 days or until hospital discharge if that occurs earlier. If a patient is to undergo non-primary PCI, unfractionated heparin (UFH) as per standard practice should be administered during PCI, taking into account the patient’s potential risk of bleeding, including the time since the last dose of fondaparinux. The timing of restarting subcutaneous fondaparinux after sheath removal should be based on clinical judgment. In the pivotal STEMI clinical trial, treatment with fondaparinux was restarted no earlier than 3 hours after sheath removal.
Patients who are to undergo coronary artery bypass graft (CABG) surgery: In STEMI or UA/NSTEMI patients who are to undergo coronary artery bypass graft (CABG) surgery, fondaparinux where possible, should not be given during the 24 hours before surgery and may be restarted 48 hours post-operatively.
Treatment of superficial-vein thrombosis: The recommended dose of fondaparinux is 2.5 mg once daily, administered by subcutaneous injection. Patients eligible for fondaparinux 2.5 mg treatment should have acute, symptomatic, isolated, spontaneous superficial-vein thrombosis of the lower limbs, at least 5 cm long and documented by ultrasonographic investigation or other objective methods. Treatment should be initiated as soon as possible following diagnosis and after exclusion of concomitant DVT or superficial-vein thrombosis within 3 cm from the sapheno-femoral junction. Treatment should be continued for a minimum of 30 days and up to a maximum of 45 days in patients at high risk of thromboembolic complications. Patients could be recommended to self-inject the product when they are judged willing and able to do so. Physicians should provide clear instructions for self-injection. Patients who are to undergo surgery or other invasive procedures: In superficial vein thrombosis patients who are to undergo surgery or other invasive procedures, fondaparinux, where possible, should not be given during the 24 hours before surgery. Fondaparinux may be restarted at least 6 hours post-operatively provided haemostasis has been achieved.
Special populations: Prevention of VTE following Surgery: In patients undergoing surgery, timing of the first fondaparinux injection requires strict adherence in patients ≥75 years, and/or with body weight <50 kg and/or with renal impairment with creatinine clearance ranging between 20 to 50 ml/min. The first fondaparinux administration should be given not earlier than 6 hours following surgical closure. The injection should not be given unless haemostasis has been established.
Renal impairment:
Prophylaxis of VTE - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min. No dosage reduction is required for patients with mild renal impairment (creatinine clearance >50 ml/min). Treatment of UA/NSTEMI and STEMI - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. No dosage reduction is required for patients with creatinine clearance >20 ml/min.
Treatment of superficial-vein thrombosis - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min. No dosage reduction is required for patients with mild renal impairment (creatinine clearance >50 ml/min).
Hepatic impairment:
Prevention of VTE and Treatment of UA/NSTEMI and STEMI - No dosing adjustment is necessary in patients with either mild or moderate hepatic impairment. In patients with severe hepatic impairment, fondaparinux should be used with care as this patient group has not been studied. Treatment of superficial-vein thrombosis - The safety and e cacy of fondaparinux in patients with severe hepatic impairment has not been studied, therefore fondaparinux is not recommended for use in these patients.
Paediatric population - Fondaparinux is not recommended for use in children below 17 years of age due to a lack of data on safety and e cacy.
Low body weight: Prevention of VTE and Treatment of UA/NSTEMI and STEMIPatients with body weight <50 kg are at increased risk of bleeding. Elimination of fondaparinux decreases with weight. Fondaparinux should be used with caution in these patients. Treatment of superficial-vein thrombosis - The safety and e cacy of fondaparinux in patients with body weight less than 50 kg has not been studied, therefore fondaparinux is not recommended for use in these patients.
Administration
Subcutaneous administration: Fondaparinux is administered by deep subcutaneous injection while the patient is lying down. Sites of administration should alternate between the left and the right anterolateral and left and right posterolateral abdominal wall. To avoid the loss of medicinal product when using the pre-filled syringe do not expel the air bubble from the syringe before the injection. The whole length of the needle should be inserted perpendicularly into a skin fold held between the thumb and the forefinger; the skin fold should be held throughout the injection.
Intravenous administration (first dose in patients with STEMI only) Intravenous administration should be through an existing intravenous line either directly or using a small volume (25 or 50 ml) 0.9% saline minibag. To avoid the loss of medicinal product when using the pre-filled syringe do not expel the air bubble from the syringe before the injection. The intravenous tubing should be well flushed with saline after injection to ensure that all of the medicinal product is administered. If administered via a minibag, the infusion should be given over 1 to 2 minutes.
Presentation: Solution for injection
Contraindications:
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Active clinically significant bleeding.
Acute bacterial endocarditis.
Severe renal impairment defined by creatinine clearance < 20 ml/min.
Warnings and precautions: Fondaparinux is intended for subcutaneous use only. Do not administer intramuscularly.
There is limited experience from treatment with fondaparinux in haemodynamically unstable patients and no experience in patients requiring thrombolysis, embolectomy or insertion of a vena cava filter.
Haemorrhage: Fondaparinux should be used with caution in patients who have an increased risk of haemorrhage, such as those with congenital or acquired bleeding disorders (e.g. platelet count <50,000/mm3), active ulcerative gastrointestinal disease and recent intracranial haemorrhage or shortly after brain, spinal or ophthalmic surgery and in special patient groups. As for other anticoagulants, fondaparinux should be used with caution in patients who have undergone recent surgery (<3 days) and only once surgical haemostasis has been established.
(For prevention of VTE) Agents that may enhance the risk of haemorrhage should not be administered concomitantly with fondaparinux. These agents include desirudin, fibrinolytic agents, GP IIb/IIIa receptor antagonists, heparin, heparinoids, or Low Molecular Weight Heparin (LMWH). When required, concomitant therapy with vitamin K antagonist should be administered. Other antiplatelet medicinal products (acetylsalicylic acid, dipyridamole, sulfinpyrazone, ticlopidine or clopidogrel), and NSAIDs should be used with caution. If co-administration is essential, close monitoring is necessary.
For treatment of UA/NSTEMI, STEMI and superficial-vein thrombosis: Fondaparinux should be used with caution in patients who are being treated concomitantly with other agents that increase the risk of haemorrhage (such as GPIIb/IIIa inhibitors or thrombolytics).
PCI and risk of guiding catheter thrombus: In STEMI patients undergoing primary PCI, the use of fondaparinux prior to and during PCI is not recommended. Similarly, in UA/NSTEMI patients with life threatening conditions that require urgent revascularisation, the use of fondaparinux prior to and during PCI is not recommended. These are patients with refractory or recurrent angina associated with dynamic ST deviation, heart failure, life-threatening arrhythmias or haemodynamic instability.
In UA/NSTEMI and STEMI patients undergoing non-primary PCI: the use of fondaparinux as the sole anticoagulant during PCI is not recommended due to an increased risk of guiding catheter thrombus. Therefore adjunctive UFH should be used during non-primary PCI according to standard practice.
Patients with superficial-vein thrombosis: Presence of superficial-vein thrombosis greater than 3 cm from the sapheno-femoral junction should be confirmed and concomitant DVT should be excluded by compression ultrasound or objective methods prior to initiating treatment of fondaparinux.
Spinal/Epidural anaesthesia:
In patients undergoing major orthopaedic surgery, epidural or spinal haematomas that may result in long-term or permanent paralysis cannot be excluded with the concurrent use of fondaparinux and spinal/epidural
anaesthesia or spinal puncture. The risk of these rare events may be higher with post-operative use of indwelling epidural catheters or the concomitant use of other medicinal products a ecting haemostasis.
Elderly patients: The elderly population is at increased risk of bleeding. As renal function is generally decreasing with age, elderly patients may show reduced elimination and increased exposure of fondaparinux. Fondaparinux should be used with caution in elderly patients.
Low body weight: Prevention of VTE and Treatment of UA/NSTEMI and STEMI - Patients with body weight <50 kg are at increased risk of bleeding. Fondaparinux should be used with caution at a daily dose of 5 mg in this population. Elimination of fondaparinux decreases with weight. Fondaparinux should be used with caution in these patients.
Treatment of superficial-vein thrombosis - Fondaparinux is not recommended for treatment of superficial-vein thrombosis in patients with body weight less than 50 kg.
Renal impairment: Fondaparinux is known to be mainly excreted by the kidney. Prophylaxis of VTE - Patients with creatinine clearance <50 ml/min are at increased risk of bleeding and VTE and should be treated with caution. For the treatment of UA/NSTEMI and STEMI- there are limited clinical data available on the use of fondaparinux 2.5 mg once daily in patients with creatinine between 20 and 30 ml/min. Therefore, the physician should determine if the benefit of treatment outweighs the risk. For treatment of superficial-vein thrombosis - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min.
Severe hepatic impairment: Prevention of VTE and Treatment of UA/NSTEMI and STEMI - Dosing adjustment of fondaparinux is not necessary. However, the use of fondaparinux should be considered with caution because of an increased risk of bleeding due to a deficiency of coagulation factors in patients with severe hepatic impairment.
Treatment of superficial-vein thrombosis - Fondaparinux is not recommended for the treatment of superficial-vein thrombosis in these patients.
Heparin Induced Thrombocytopenia: Fondaparinux should be used with caution in patients with a history of HIT.
Latex Allergy: The needle shield of the pre-filled syringe may contain dry natural latex rubber that has the potential to cause allergic reactions in latex sensitive individuals.
Interactions with other medicinal products and other forms of interaction: Bleeding risk is increased with concomitant administration of fondaparinux and agents that may enhance the risk of haemorrhage. In clinical studies performed with fondaparinux, oral anticoagulants (warfarin) did not interact with the pharmacokinetics of fondaparinux; at the 10 mg dose used in the interaction studies, fondaparinux did not influence the anticoagulation monitoring (INR) activity of warfarin. Platelet inhibitors (acetylsalicylic acid), NSAIDs (piroxicam) and digoxin did not interact with the pharmacokinetics of fondaparinux. At the 10 mg dose used in the interaction studies, fondaparinux did not influence the bleeding time under acetylsalicylic acid or piroxicam treatment, nor the pharmacokinetics of digoxin at steady state.
If follow-up treatment is to be initiated with heparin or LMWH, the first injection should, as a general rule, be given one day after the last fondaparinux injection. If follow up treatment with a Vitamin K antagonist is required, treatment with fondaparinux should be continued until the target INR value has been reached.
Fertility, pregnancy and lactation:
Pregnancy: No clinical data on exposed pregnancies are available. Animal studies are insu cient with respect to e ects on pregnancy, embryo/foetal development, parturition and postnatal development because of limited exposure. Fondaparinux should not be prescribed to pregnant women unless clearly necessary.
Breast-feeding: Fondaparinux is excreted in rat milk but it is not known whether fondaparinux is excreted in human milk. Breast-feeding is not recommended during treatment with fondaparinux. Oral absorption by the child is however unlikely.
Fertility: There are no data available on the e ect of fondaparinux on human fertility. Animal studies do not show any e ect on fertility.
Undesirable effects:
Serious adverse reactions reported with fondaparinux are bleeding complications (various sites including rare cases of intracranial/intracerebral and retroperitoneal bleedings). Fondaparinux should be used with caution in patients who have an increased risk of haemorrhage.
Very common (≥1/10): None. Common (≥1/100, <1/10): anaemia, post-operative haemorrhage, uterovaginal haemorrhage, haemoptysis, haematuria, haematoma, gingival bleeding, purpura, epistaxis, gastrointestinal bleeding, hemarthrosis, ocular bleeding, bruise.
For details of uncommon, rare and very rarely reported adverse events and those of unknown frequency, see SmPC.
Reporting of adverse reactions:
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Website: www.hpra.ie. Adverse reactions/events should also be reported to the marketing authorisation holder at the email address: pv.ireland@viatris.com or phone 0044(0)8001218267.
Legal Category: Product subject to prescription which may not be renewed (A).
Full prescribing information available on request from: Viatris, Dublin 17. Email: enquiry.ire@viatris.com
Date of Revision of Abbreviated Prescribing Information: 27 Feb 2024
Reference Number: IE--AbPI-Arixtra-2.5mg-v003
fondaparinux sodium
Cardiac Pacing
Advances in Physiologic Pacing ; New Era of Novel Left Bundle Branch Pacing
Written by Dr. Luke Kelly, Dr. Arifa Salim, Professor Usama Boles Cardiology Department, Tipperary University Hospital, Clonmel, Ireland. Limerick University, School of Medicine and Life Science
Introduction
Cardiac pacing is a well established safe and effective therapy for a variety of indications including many bradyarrhythmia’s and a subclass of heart failure.1,2,3
Traditional pacing involved right ventricular apical pacing were effective though crude, their non-physiologic pacing resulting in both electrical and mechanical dyssynchrony with the associated complications of dyssynchrony –induced cardiomyopathy and heart failure in a good proportion of patients who become pacemaker dependent.1-3
Advances in pacing technology, procedural technique and precision have introduced the possibility of physiologic pacing via the native conduction system of the heart1. Left ventricular lead placement epicardially commonly referred to as cardiac resynchronisation therapy (CRT) and the innovative Left Bundle Branch Pacing (LBBP)1. This method has many theoretical benefits most notably reducing electrical and mechanical dyssnchrony, through physiologic pacing in LBB, and their associated complications. In this article we review indications and techniques of LBBP, an innovative and promising pacing modality.
Left Bundle Pacing ; Criteria and rationale
Left bundle pacing is an innovative pacing modality wherby pacing
is achieved via capture of the left bundle branch.
To achieve left bundle capture the ventricular lead is inserted into the interventricular septum distal to the bundle of His. Lead advancement in PA and LAO X ray projections with various captures threshold (i.e. current threshold to capture LBB) to identify the ideal LBBP location. This is to be confirmed by contrast (i.e. dye)
injections locally at leads tip as well as other parameters of ECG as described in details in table 1.
Left bundle pacing is formally described based on a number of electrophysiological criteria used to confirm left bundle capture. This includes analysis of QRS morphology and duration and peak left ventricular activation time (pLVAT).1
LBBP paced QRS morphology in left bundle pacing demonstrates a right bundle branch pattern in lead V1(predominantly negative QRS).1 Peak left ventricular activation time (pLVAT) is a measure of the time from onset of pacing spike to the peak of the R wave in leads V5 –V61. It is an indirect measure of the speed of LV activation, ideally <80ms1
Current implantation techniques in left bundle pacing
Venous access is required to pass the pacing lead into the right ventricle1. Once in the right ventricle key anatomical landmarks are identified under fluoroscopic guidance, notably the tricuspid valve annulus.1,2 The interventricular septum can then be mapped physiologically to determine the site of the left bundle branch through a specifically designed delivery sheath.1,2
Once the site of the left bundle has been determined, the pacing lead can be screwed into the interventricular septum until it has
Figure 1 : A – Graphic representation of LBBP with illustration of native conduction system. Location of the HBP lead and LBBP leads in the right anterior oblique. Background of Chest radiograph post left bundle branch pacing. Pacing lead can be seen in septal area – red arrow. Reproduced from case in Mater private hospital, Dublin, Ireland. C– 1 ECG before left bundle pacing. Slow atrial fibrillation with expectation of high pacemaker dependency. C – 2 ECG post left bundle pacing demonstrating left bundle capture criteria listed in table 1 - RBBB in V1, ascending notch “Sr” on V1, LVAT 65 ms, QRS duration 126 ms. Reproduced from case in Mater Private Hospital. AVN = atrioventricular node, HB = His Bundle, RBB = right bundle branch, LBB = left bundle branch, IVS = interventricular septum
Dr. Luke Kelly
Dr. Arifa Salim
Professor Usama Boles
Criterion for left bundle branch area pacing
Abrupt shortening of RWPT or LVAT in V6 > 10 ms at high output during septal position with subsequent short and constant LVAT at low output with further advancement of lead V6 RWPT < 74 ms in non-LBBB and < 80 ms in LBBB (i.e. interval between beginning of Q wave to R wave peak “or ventricular activation time” in ms)
Gradient “difference” between V6 & V1 interpeak interval >44 ms (i.e from LBB conduction to full myocardial activation and RBB conduction)
Difference in LBB to V6 RWPT in sinus versus paced rhythm < 10 ms
Stimulus to V6 RWPT + 10 ms < (intrinsicoid deflection time – transseptal conduction time in LBBB)
Programmed deep septal stimulation demonstrating differential capture (i.e. high and low threshold) with associated change in paced morphology
Difference in V6 RWPT between (corrective) HBP and LBBP > 8 ms in LBBB
Table 1 : Simplified Criteria for left bundle area pacing4. CT = computerized tomography; HBP = His bundle pacing; LBB = left bundle branch; LBBB = left bundle branch block; LBBP = left bundle branch pacing; LBBAP = left bundle branch block area pacing; LV = left ventricle; LVAT = left ventricular activation time; RWPT = R – wave peak time;’ V6 RWPT = R wave peak time in lead V64.
advanced to such a depth as to have reached the left ventricular subendocardium.1 A number of electrophysiologic criteria exist for confirming left bundle capture outlined in Table 1.1,2 Some operators inject contrast through the delivery sheath to confirm tip placement at the septum and ensure the anatomy.
Left bundle capture : optimum lead position is determined electrophysiologically by a pLVAT of < 80 ms and QRS morphology of qR or RSR in V1.1,2 The depth within the septum should be approximately 1.4 cm +- 0.23cm, however variation in septal size means that this should be
measured radiographically prior to lead placement.1,3
Echocardiogam is well established in clinical practice to ensure synchronous LV contractility and preserved LV ejection fraction. From the same example above (ECG and CXR), we analysed
global longitudinal strains to confirm reasonable and acceptable LBBP parameters (Fig 2)
Role of LBBP in Current Practice – Evidence and Guidelines
In the wake of several recent studies demonstrating the safety and efficacy of physiologic pacing
2:
post left bundle pacing – global peak longitudinal strain with speckle tracking. Superior image demonstrating diastole. Inferior image demonstrating
Mechanical synchrony achieved with left bundle pacing showing reasonable synchronous LV wall contractions and relaxation
Fig
Echocardiogram
systole.
Cardiac Pacing
via the left bundle branch both the American and European cardiology communities have issued updated guidelines to advise on its indications.4,5,7-14 We summarise the most important of these studies in a table (Table 2). Their findings indicate that LBBP is a safe and effective alternative to traditional pacing modalities with reduced electrical and mechanical dyssynchrony. They also identified a lack of evidence about long term outcomes as an area for future research.
Recent guidelines from the American heart rhythm society emphasise the significance of physiological pacing, particularly for patients who are likely to require substantial ventricular pacing, especially those with an ejection fraction ranging from 36% to 50% (class 2a recommendation).5
Physiological pacing is critical as it facilitates more synchronous contractions of the ventricles, thereby enhancing cardiac output and mitigating the risk of pacinginduced cardiomyopathy.
The guidelines endorse LBBP for patients with a normal ejection fraction who are expected to be dependent on a pacemaker.
In this patient population, LBBP may improve ventricular function, thereby preventing the progression of heart failure and promoting hemodynamic stability through a more physiological conduction system. For example, LBBP is recommended for patients with persistent atrial fibrillation and bradycardia who require pacing. This technique has been associated with enhanced functional capacity, increased exercise tolerance, and improvements in ejection fraction, ultimately leading to a reduction in heart failure symptoms.5
In contrast, cardiac resynchronisation therapy continues to be the preferred pacing modality for patients with heart failure characterized by an ejection fraction of less than 35%, left bundle branch block, a QRS duration exceeding 150 ms, and New York Heart Association (NYHA) class II to IV symptoms despite guideline-directed medical therapy.5
For patients who are non responders for CRT due to anatomical challenges, scar, arrhythmia induction with LV pacing; LBBP presents a valuable alternative, with the potential to improve clinical outcomes and overall quality of life. (class 2c recommendation).5
Future research and .knowledge gaps
Left bundle pacing has been demonstrated as an effective modality of physiologic pacing, however, many questions remain about it’s long-term safety outcomes and optimum patient selection.6
It has emerged as an alternative to biventricular pacing in heart failure patients, however, it is not yet known which patients are best suited to left bundle pacing despite of HRS recommendations as class IIa in most indications as a replacement to conventional CRT.5 Many studies and expert opinion are placing this technique as first choice.4 Further studies will better describe the degree to which the theoretical benefits of physiologic pacing are translated into improved patient outcomes and identify the
patient cohorts in which this is the optimum pacing modality.5
However, overall LBBP emerges as higher lead stability, less percentages of non responders, easier procedure techniques and finally more synchronous LV contractility.
Conclusion
Physiologic pacing and in particular left bundle branch pacing is of great importance due to its technical feasibility and benefits of reduced electrical and mechanical dyssnchrony with a paced narrow QRS complex. Several important studies demonstrate its safety and efficacy and it has emerged as the pacing modality of choice for a great variety of indications.
The future of LBBP pacing is promising and upskilling the knowledge and techniques as led by electrophysiologists will undoubtedly benefit a large cohort of heart failure patients and lead to improved clinical outcomes including cardiac morbidity and mortality with an associated positive impact on the healthcare financial burden.
Figure 3: Algorithm for pacing strategies for patient with bradyarrhymthmia – adapted with minor modifications from AHRS guidelines5. LVEF = left ventricular ejection fraction, CRT with BiV pacing = Cardiac resynchronisation with biventricular pacing: HBP = His bundle pacing; LBBAP = Left bundle branch area pacing; LBBB = left bundle branch block; RV = right ventricle
Table 2 : Summary of several recent important trials on physiologic and left bundle branch pacing Study/Year Aim
(Parlavecchio et al 2023)
Left bundle versus biventricular pacing for cardiac resynchronisation therapy: A systematic review and meta-analysis
(LI et al 2024)
Long-term efficacy of left bundle branch and biventricular pacing in patients with heart failure complicated with left bundle branch block
(MAREK et al 2022)
Left bundle branch area pacing outcomes : the multicentre European MELOS study.
Compare LBBP-CRT versus BVP-CRT in HF patients.
Compare long-term efficacy of left bundle branch pacing (LBBP) vs. biventricular pacing (BiVP) in heart failure (HF) patients with complete left bundle branch block (CLBBB), focusing on LVEF, LVEDD, and clinical outcomes.
Evaluate outcomes of left bundle branch area pacing (LBBAP) for bradyarrhythmia and heart failure in a multicentre European study
Patient randomisation
Meta-analysis and systematic review of ten studies enrolling 1063 patients comparing LBBPCRT versus BVP-CRT in heart failure patients
(PONNUSAMY et al 2021)
Feasibility, safety and outcomes of left bundle branch pacing in octogenarians
(WANG et al 2021)
Randomized trial of left bundle branch vs biventricular pacing for cardiac resynchronization therapy
Assess the feasibility, safety, and outcomes of left bundle branch pacing (LBBP) in octogenarians (≥80 years).
120 HF patients with CLBBB (LVEF ≤ 35%) undergoing CRT, divided into two groups: 60 received LBBP, 60 received BiVP.
Exclusions: RBBB, atrial fibrillation, pre-existing pacemakers, or age under 18. Median follow-up: 37 ± 19 months
2,533 patients (mean age: 73.9 years, 57.6% female, 27.5% with heart failure) from 14 European centers. Observational, registrybased, non-randomized study.
Results
LBBP-CRT led to significant reduction in HF hospitalization [7.9% vs.14.5%; RR: 0.60 (95%CI: 0.39-0.93); p = .02], QRSd [MD: 30.26 ms (95%CI: 26.68-33.84); p < .00001] and pacing threshold. LBBP-CRT improved LVEF, the rate of responder and superresponder patients and the NYHA class compared to BVP-CRT.
LVEF improvement: LBBP (14.8%) vs. BiVP (10.7%) (P = 0.02).
Super response rate (LVEF ≥15%): LBBP (65%) vs. BiVP (45%) (P = 0.02).
All-cause mortality: LBBP (1.7%) vs. BiVP (10%) (P = 0.11).
LBBAP lead implantation success: 89.6% overall (92.4% for bradyarrhythmia, 82.2% for heart failure).
Success rate plateaued after 250 cases.
Complication rate: 11.7% overall; 8.3% related to ventricular transseptal lead.
Capture types: Left bundle fascicular (69.5%), Left ventricular septal (21.5%), Proximal left bundle branch (9%).
Average follow-up: 6.4 months.
11 patients (mean age: 82.1 ± 2.5 years) with indications for pacing: AV block (5), LBBB with low EF (4), sinus node dysfunction (1). Nonrandomized.
Compare the efficacy of left bundle branch pacing (LBBP) vs. biventricular pacing (BiVP) for cardiac resynchronization therapy (CRT) in heart failure patients with left bundle branch block (LBBB).
40 patients with nonischemic cardiomyopathy (NICM), LBBB, and LVEF ≤40%, aged 18-80 years, randomized 1:1 to LBBPCRT (n=20) or BiVP-CRT (n=20). Crossovers: 10% (LBBP) and 20% (BiVP).
LBBP success: 91% (10 out of 11 patients).
QRS duration reduced from 145.9 ms to 107.1 ms (p=0.00001).
LVEF improved from 47.6% to 58.4% (p=0.017).
Stable pacing parameters over 7.7 months.
No acute complications.
LBBP-CRT showed a greater LVEF improvement at 6 months (mean difference: 5.6%, p=0.039) compared to BiVP-CRT. LBBP resulted in larger reductions in left ventricular end-systolic volume (-24.97 mL) and NTproBNP (-1,071.80 pg/mL). Both groups had similar improvements in functional class, QRS duration, and 6-minute walk distance.
Conclusion
In HF patients, LBBP-CRT was superior to BVP-CRT in reducing HF hospitalization. Further significant benefits occurred within the LBBP-CRT group in terms of QRSd, LVEF, pacing thresholds, NYHA class and the rate of responder and super-responder patients
LBBP showed better long-term outcomes in LVEF, LVEDD, and super response rate. Mortality and hospitalization rates were similar, but LBBP demonstrated overall superior efficacy and could be a firstline therapy.
LBBAP is feasible for bradyarrhythmia and heart failure, though randomized trials are needed to confirm long-term outcomes. Improvements are needed for heart failure success rates and safety.
(LIANG et al 2022)
Left bundle branch pacing versus biventricular pacing for acute cardiac resynchronization in patients with heart failure
(SHUNMUGA et al 2020)
Left bundle branch review: A comprehensive review
Compare left bundle branch pacing (LBBP) vs. biventricular pacing (BVP) for cardiac resynchronization therapy (CRT) in heart failure patients with left bundle branch block (LBBB).
Provide a comprehensive review of left bundle branch pacing (LBBP), covering implantation techniques, troubleshooting, clinical implications, and outcomes from the literature.
21 heart failure patients with LBBB (mean age 67 ± 10 years, 48% male), randomized in a crossover fashion to receive LBBP and BVP during CRT implantation.
A review of multiple LBBP studies, summarizing success rates, thresholds, and clinical outcomes across cohorts.
LBBP provided greater reductions in QRS duration (-11 ms, p=0.003) and QRS area (-85 µVs, p<0.001) compared to BVP. LBBP improved intraventricular synchrony (Ts-SD reduced by -14 ms, p=0.001) and left ventricular dP/dtmax (6% higher than BVP, p=0.002).
LBBP showed high procedural success rates (80.5%-97%) across studies.
It significantly improved QRS duration, left ventricular function, and lead stability compared to conventional pacing methods.
LBBP is safe and effective in elderly patients, showing significant improvements in QRS duration and LVEF. Further trials are needed to confirm these findings.
LBBP-CRT provided superior LVEF improvement and comparable results in other measures to BiVP-CRT, suggesting it as an effective alternative for CRT in heart failure patients with LBBB
LBBP produced superior electrical and mechanical resynchronization, along with better acute hemodynamic improvements than BVP, making it a promising alternative for CRT in heart failure patients with LBBB.
LBBP is a promising alternative to His bundle and biventricular pacing, offering physiological pacing with stable, low thresholds. Further large-scale trials are needed to confirm its long-term safety and efficacy.
Cardiac Pacing
References
1 Liu P, Wang Q, Sun H, Qin X, Zheng Q. Left Bundle Branch Pacing: Current Knowledge and Future Prospects. Frontiers in Cardiovascular Medicine [Internet]. 2021 Mar 23;8. Available from: https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC8021709.
2 : Slotwiner DJ, Raitt MH, DelCarpio Munoz F, Mulpuru SK, Nasser N, Peterson PN. Impact of Physiologic Pacing Versus Right Ventricular Pacing Among Patients With Left Ventricular Ejection Fraction Greater Than 35%: A Systematic Review for the 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay. Journal of the American College of Cardiology. 2019 Aug;74(7): 988–1008.
3 : Lamas GA, Lee KL, Sweeney MO, Silverman R, Leon A, Yee R, et al. Ventricular Pacing or Dual-Chamber Pacing for SinusNode Dysfunction. New England Journal of Medicine. 2002 Jun 13;346(24):1854–62.
Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA). 2022 May 1;75(5):430–0.
5 : Chung MK, Patton KK, Lau CP, R.J A, Al-Khatib SM, Arora V, et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm Society. 2023 May 1;20(9).
6 : Burri H, Jastrzebski M, Cano Ó, Čurila K, Jan de Pooter, Huang W, et al. EHRA clinical consensus statement on conduction system pacing implantation: endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS). 2023 Apr 15;25(4): 1208–36.
Appendix 1. - References for papers summarized in Table 2
7 : Parlavecchio A, Vetta
G, Caminiti R, Coluccia G, Magnocavallo M, Ajello M, et al. Left bundle branch pacing versus biventricular pacing for cardiac resynchronization therapy: A systematic review and metaanalysis. Pacing and clinical electrophysiology : PACE [Internet]. 2023 May;46(5):432–9. Available from: https://pubmed.ncbi.nlm.nih. gov/37036831/
8 : Li J, Yi H, Han J, Han H, Su X. Long-term efficacy of left bundle branch pacing and biventricular pacing in patients with heart failure complicated with left bundle branch block. Frontiers in cardiovascular medicine [Internet]. 2024;11:1363020. Available from: https://pubmed.ncbi.nlm.nih. gov/38486707/
9 : Jastrzębski M, Kiełbasa G, Cano O, Curila K, Heckman L, De Pooter J, et al. Left bundle branch area pacing outcomes: the multicentre European MELOS study. European Heart Journal [Internet]. 2022 Oct 21 [cited 2023 Feb 26];43(40):4161–73. Available from: https://pubmed.ncbi.nlm.nih. gov/35979843/.
Some 20% of adults in Ireland would tell no one if they were experiencing suicidal thoughts, St Patrick’s Mental Health Services’ 2024 annual Attitudes to Mental Health and Stigma Survey has revealed. The survey also found a significant 49% of people who have experienced mental health difficulties have not sought treatment due to stigma or embarrassment. In light of these findings, St Patrick’s Mental Health Services is urging everyone to check in on their own and their loved ones’ mental health and wellbeing, particularly during the Christmas period when the pressures of the season can often take over, and to seek support if needed.
For over 10 years, St Patrick’s Mental Health Services has commissioned this annual survey to track changing attitudes towards mental health and stigma. While there have been improvements in attitudes, the 2024 findings highlighted that stigma is still a significant barrier to seeking help, with shame or
embarrassment often impacting willingness to disclose mental health difficulties and to engage in treatment. For example, this year’s survey, which polled a nationally representative of over 1,000 adults in the Republic of Ireland, found:
53% of respondents have experienced a mental health difficulty, yet more than one-third (34%) did not seek treatment, with the main reason for not doing so cited as shame.
23% of people would consider it a sign of weakness if they sought help for a mental health difficulty. At the same time, 11% would consider it a sign of weakness if a friend or loved one sought help, indicating the prevalence of self-stigma.
Speaking about the findings, Paul Gilligan, CEO of St Patrick’s Mental Health Services said, “While attitudes towards mental health are improving in many ways, as reflected year-on-year in our annual survey findings, one concerning area that has seen little change is in the disclosure
Feasibility, safety and outcomes of left bundle branch pacing in octogenarians. Indian Heart Journal. 2021 Jan;73(1):117–20.
11 : Ponnusamy SS, Arora V, Namboodiri N, Kumar V, Kapoor A, Vijayaraman P. Left bundle branch pacing: A comprehensive review. Journal of Cardiovascular Electrophysiology. 2020 Jul 30;31(9):2462–73.
12 Wang Y, Zhu H, Hou X, Wang Z, Zou F, Qian Z, et al. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. Journal of the American College of Cardiology. 2022 Sep;80(13):1205–16.
13 : Liang Y, Wang J, Gong X, Lu HY, Yu Z, Zhang L, et al. Left Bundle Branch Pacing Versus Biventricular Pacing for Acute Cardiac Resynchronization in Patients With Heart Failure. Circulation-arrhythmia and Electrophysiology. 2022 Oct 28;15(11).
14 : Zhang S, Zhou X, Gold MR. Left Bundle Branch Pacing. Journal of the American College of Cardiology. 2019 Dec;74(24):3039–49.
of suicidal thoughts and the idea that it’s a sign of weakness to seek help for your mental health.
“In the busyness of the holiday season, it’s important to remember that the most important thing we
can do with our time is to connect with our emotional selves and to check in on how we, and others, are really feeling. If we ourselves, or someone we love, is struggling, don’t let stigma stand in the way of seeking support.”
Deteriorating Mental Wellbeing of Doctors
Almost two thirds (64%) of doctors in Ireland say they are frequently burnt out and exhausted and 1 in 5 (19%) describe their mental wellbeing as “of concern”, according to a recent survey by the Medical Protection Society (MPS).
In the MPS survey of 548 doctors, 60% also said the Government does not do enough to ensure mental health services for doctors are properly funded.
MPS, which represents the professional interests of over 16,000 healthcare professionals in Ireland, says that as soon as the new government has formed, it should take a fresh look at what needs to be done to tackle the deteriorating mental wellbeing of healthcare professionals, to avoid greater numbers leaving the profession due to wellbeing issues.
Professor Gozie Offiah, MPS Council member said, “A significant and concerning number of healthcare professionals are burnt out, disillusioned and their mental wellbeing is deteriorating.
“We see firsthand how poor mental wellbeing affects doctors personally, and how it can impact on patient care. Without early support, mental wellbeing issues can also result in doctors needing extended time off work or leaving the healthcare profession altogether.
“We hope the new Government will work with the HSE and private healthcare providers to ensure healthcare professionals are in supportive environments with
Professor Gozie Offiah, MPS Council member
resources such as counselling, peer support networks and specialist support available as standard. This would help to tackle issues early on, avert crises down the line, and ultimately enable healthcare professionals to continue to care for patients safely.
“Independent mental wellbeing services, such as the Practitioner Health Matters Programme, are also vital and can provide a lifeline for many who are struggling to cope, but they often rely on donations. The Government should help to ensure they are properly funded and safeguarded, so healthcare professionals are always able to access confidential, specialist help outside of their place of work, without fear of repercussions from their employers.
“The provision of adequate mental wellbeing support is crucial to retaining our healthcare workforce. While we recognise that the new Government will face a range of pressing issues affecting doctors and patients when it has formed, we hope it will take a fresh look at this issue and understand the need for long-term thinking.”
Anonymous comments from doctors who took part in the MPS survey:
“No one truly understands the internal struggles individuals face, both physically and mentally. Colleagues, management, patients, and even family members often cannot see what you’re going through. Medical practice in Ireland is evolving, with increasing patient loads, more complex cases, shifting demographics, more demanding patients, unrealistic key performance indicators, limited resources, and a more litigious environment, all of which contribute to the mental burden on healthcare professionals.”
“Chronic under resourcing of team, constant fear of being blamed along with unrealistic patient, family, other service expectations has resulted in me feeling high levels of stress and frustration on daily basis. Feel like I’m shouting into a vacuum.”
Perindopril Arginine Clonmel
Clonmel Healthcare is delighted to announce the launch of Perindopril Arginine Clonmel 5mg, 10mg film-coated tablets.
Perindopril Arginine Clonmel is indicated for;
• Treatment of hypertension
• Treatment of symptomatic heart failure
• Reduction of risk of cardiac events in patients with a history of myocardial infarction and/or evascularisation
Full prescribing information is available on request or alternatively please go to www.clonmel-health.ie. Medicinal product subject to medical prescription.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information.
PA 126/366/001-002. PA Holder: Clonmel Healthcare Ltd., Clonmel, Co. Tipperary. Date prepared: December 2024. 2024/ADV/PER/286H
Bridging the Gap: Addressing Sex and Gender Disparities in Chronic Pain Research
“My hope would be that by considering sex and gender as variables in pain research would allow for more personalised treatments and care to be provided to individuals with chronic pain. For example, current data suggests that cox inhibitors and glucocorticoids elicit greater analgesia with reduced side effects in males, while CGRP based treatments and cognitive based therapies may be more effective in females”
In October, Chronic Pain Ireland and the University of Galway hosted a pivotal event marking the ‘Day of the Girl.’ The hybrid event, entitled Exploring Sex and Gender Disparities in Chronic Pain, brought together researchers, clinicians, and patients to shed light on the profound
differences in how chronic pain is experienced and managed across sexes and genders. The program examined groundbreaking findings, including the influence of the latest PAINDIFF research, and their implications for diagnosis, treatment outcomes, and health policies.
Dr Michelle Roche
Among the event’s key voices was Dr Michelle Roche, Associate Professor in Physiology, CoDirector of the Centre for Pain Research at the University of Galway, and President of the Irish Pain Society. Dr. Roche’s keynote address, Developing Guidelines and an Agenda for Research on Sex and Gender as Variables in Pain, highlighted the urgent need to address these disparities. In a follow-up interview, she elaborated on her work and vision for the future of pain research.
Can you tell us about your background and what inspired your interest in sex and gender as variables in pain research?
Dr Roche’s career has focused on the neurobiology underlying mood disorders, chronic pain, and their interactions. She noted a glaring disparity in previous research, much of which focused predominantly on males, despite the higher prevalence of these conditions among females.
She says, “I am an Associate Professor in Physiology with a research focus on understanding the neurobiology underlying mood disorders, such as depression and anxiety; pain and their interactions. Both mood disorders and chronic pain are more prevalent in females compared with males, however up until relatively recently the majority of research conducted in these
fields was conducted in males only. This disparity could account, at least in part, for the failure of several clinical trials and lack of new treatment strategies for these conditions, thereby reduce quality of life for individuals experiencing such conditions.
“As a consequence, research in our lab examines the biological mechanisms that underlie sex differences in the comorbidity between mood-disorders and chronic pain. Ultimately, we hope to identify new sexspecific therapeutic targets and management strategies for these conditions, bringing us one step closer to personalised medicine. While research examining the influence of sex on pain has expanded over the past decade, the influence of gender on pain is less well understood, with research in this area is only in its infancy.” How would you describe the current state of research on sex and gender in pain research? What gaps do you see?
Increased awareness and funding requirements have catalysed a surge in studies examining sex and gender differences across biomedical sciences, including pain. However, Dr Roche identified critical gaps.
She continued, “Increased awareness of the importance of sex and gender as key contributors to health and disease, together with requirements of funding agencies, has resulted in profound increases in the number of studies investigating sex and/ or gender differences across the biomedical sciences including pain. This welcome development has resulted in mounting evidence for genetic, molecular, cellular, systems-level, social and psychological differences in the pathophysiology and experience of pain between and across sexes and genders.
“However, many gaps still remain which we hope will be addressed into the future. For example, there are a lack of studies examining the interaction between biopsychosocial factors and as mentioned, the study of gender as a variable in pain has largely been overlooked. Furthermore, inconsistency in research findings
across and between research groups is widely recognised, and as such there is a pressing need for guidelines on how best to incorporate sex and gender as variables into pain research.”
What are some common misconceptions about sex and gender differences in pain and how can we prevent these misconceptions?
A common misconception in pain research is the conflation of sex and gender, often treated interchangeably and limited to binary categories (male/ female, man/woman). Dr Roche stressed the importance of recognizing sex and gender as distinct, fluid, and dynamic variables that extend beyond binaries. Misunderstandings also persist about the causes of sex differences in pain, often attributed solely to hormonal changes.
“One common misconception is that sex is all that matters, and that gender does not impact on pain experience or management,” she highlighted.
“As such until recently the terms sex and gender were used interchangeably and only on a binary level (male: female and/or, man:women) in both research and clinical settings which has lead to confusion and inconsistencies. It is important that researchers, clinicians and allied health professions are aware of the definitions of sex and gender, acknowledge that this extends beyond the binary, and is fluid and may change over the life course of an individual. As such it is critical that information on both sex and gender is collected where possible to enable fully understanding of the influence of these variables on pain.
“Other misconceptions include that increased pain responding and pain experience reported in females is primarily due to changes in hormone levels, despite multiple lines of evidence demonstrating a wealth of biological, psychological and social factors that underlie the effects of sex on pain. Recognition of the interactions between biopsychosocial factors that underlie the effects of sex and gender is important in dispelling such misconceptions.”
What are your primary objectives for developing guidelines on sex and gender as variables in pain research?
At this time of rapid acceleration in the number and scope of
studies examining sex and gender as variables in pain, it is essential that the researchers adopt consistent research approaches in order to maximize progress in this critically important area. With this in mind, with the support of ERA-NET NEURON and the Irish Health Research Board (HRB), we established an international group of 32 interdisciplinary experts, including leading senior scientists, early career researchers and patient advocates, from 22 different institutes across 8 countries, termed the PAINDIFF Network.
The aim of this network are to (1) identify areas of methodological consensus and best practice, (2) identify gaps in the knowledge or inconsistencies in the application and (3) develop a set of consensus recommendations on how best to study sex and gender as variables in pain research To achieve this we have conducted an extensive review of the literature, completed an comprehensive international survey of the pain research community on current methodological practices and opinions, and following extensive discussion and consensus, have developed a set of guidelines and recommendations for the best practice study in this area.
Can you outline the main components that you think should be included in these guidelines?
Dr Roche envisions these guidelines being widely adopted in clinical, research, and hospital settings. Beyond pain research, they hold relevance for neuroscience and other disciplines studying sex and gender variables. Implementation could lead to better reproducibility, personalized treatments, and improved outcomes for diverse patient populations.
“The PAINDIFF guidelines and recommendations will focus on experimental design, methodological approaches, data analysis, presentation and reporting when conducting pain research with sex and/or gender as variables. Furthermore, specific recommendations pertaining to key stakeholders including researchers, ethics boards, journal editors and funding bodies will be highlighted.”
How do you envision these guidelines being implemented in clinical and research settings as well as in hospital settings?
“Adoption and implementation of these recommendations
will reduce variability and lack of reproducibility between laboratories, and improve the translatability of research findings, ultimately leading to better outcomes for people living with chronic pain. Furthermore, much of the content and recommendations will have general relevance beyond pain research specifically, to many different areas of neuroscience research where sex and gender are studied as variables,” she added.
How can researchers be encouraged to incorporate sex and gender considerations into their studies?
“Due to the increased awareness of the importance of including sex and gender into research, and requirements from funding agencies, there has been a steady increase in the number of studies including all sexes and/or genders in their design. However, data from our survey and published data demonstrate that the majority of studies choose not to analyse or report on sex specific effects, and rarely examine effects of gender.
“We propose that by analysing and reporting on the effects of sex and/or gender in their studies, researchers will yield additional rich source of data, understanding and insight, into sex and gender specific pain management and treatment options. In studies were sex and gender are not the primary outcome variable, analysis and reporting will enable future researchers to use and combine data across studies to provide greater understanding of pain perception and management across a diverse sex and gender population.
“However, there also needs to be widespread recognition and acknowledgement by funding agencies, journal editors, journal and grant reviewers, regulatory authorities, institutional ethics committees, facilities management and researchers themselves, that greater resources are required to study sex and gender as variables in pain research, including but not limited to financial resources, infrastructural resources, time, and human resources.”
Looking ahead, what are your hopes for the future of pain research as it relates to sex a nd gender?
Dr Roche’s hopes for the future of pain research are rooted in the promise of personalized medicine. For example, certain treatments like COX inhibitors and glucocorticoids may work
better in males, while CGRPbased therapies and cognitive interventions could be more effective for females. By deepening our understanding of sex and gender in pain, researchers can tailor treatments to individual needs.
Emerging technologies such as machine learning and AI also offer exciting possibilities for integrating sex and gender considerations into research design.
“My hope would be that by considering sex and gender as variables in pain research would allow for more personalised treatments and care to be provided to individuals with chronic pain. For example, current data suggests that cox inhibitors and glucocorticoids elicit greater analgesia with reduced side effects in males, while CGRPbased treatments and cognitive based therapies may be more effective in females. Thus, expanding our understanding of the influence of sex and gender in pain will ultimately result in better pain treatment and management for all.”
Are there any emerging trends or technologies that you believe could enhance our understanding of sex and gender in pain?
Dr Roche adds, “There are many trends and technologies that will enable and facilitate the incorporation of sex and gender into research practice, including machine learning and AI. Multi-and inter-disciplinary research from basic science through to clinical practice and back, is critical to further our understanding in this field. However at the outset, researchers need to consider these variables in their research design and analysis and the PAINDIFF guidelines will provide them with a framework on how to undertake such studies.”
She concluded, “Integrating sex and gender specific approaches into pain research and clinical practice will improve development of novel therapeutic strategies (pharmacological and non-pharmacological) for all. However, collaboration between researchers, healthcare professionals, funders and policymakers will be crucial in addressing sex and gender disparities in pain care and management.”
2024 YEAR END REVIEW
JANUARY
The National Hospital Pharmacy Technicians Association of Ireland launched their Statutory Campaign for Hospital Pharmacy Technicians at Forsa Headquarters.
St. Vincent's Healthcare Group and UCD School Of Medicine has proudly unveiled the St. Vincent’s UCD Cancer Centre.
At an Oireachtas briefing session held TDs and Senators heard of the human impact of delayed access to new, innovative medicines and the consequences for patients of no dedicated funding.
93% of doctors in Ireland believe staff shortages present ‘a significant threat’ to patient safety, and nearly 2 in 5 (38%) say the impact on patients is affecting their mental health, according to a survey by the Medical Protection Society (MPS).
Blackrock Health hosted a Cardiac Arrhythmia Symposium. The event focused on new advances in the treatment of arrhythmias and was a forum to discuss the exchange of knowledge and best practice techniques.
FEBRUARY
The Minister for Health Stephen Donnelly announced that 1,548 consultants signed the new contract since it was launched last March.
High waiting lists for cancer diagnosis and treatment could be significantly reduced by the use of teledermatology technology, but only six out of 13 national dermatology departments are currently using the HSE approved service, a major new report revealed.
A new partnership between RCSI and Irish diagnostics company Serosep Ltd is set to personalise treatment for ulcerative colitis, it was revealed.
HPN launched the 2024 Hospital Professional Honours.
Our ‘Ask the Expert’ series for February featured an exclusive discussion with Professor Seamus O’Reilly of Clinical Cancer Trials Ireland.
Viatris employees joined the Irish Wheelchair Association in the Sport Ireland Campus for a fast-paced charity fundraiser which raised over £6,000.
MARCH
The European Commission published the first Union list of critical medicines, together with the European Medicines Agency (EMA) and the Member States' Heads of Medicines Agencies (HMA).
The Guaranteed Irish Pharmaceutical Forum, sponsored by MSD, took place recently where insights were shared around the theme of "Innovation in the Community – Positioning Ireland to Deliver Best Patient Care".
Osteoporosis, antimicrobial resistant infections and several types of cancer were among the ailments that will be tackled by seven drugs newly approved by the HSE.
Clinical Guidance for Surgical Hubs was published by the Elective Surgical Hubs Clinical Design Group. The guidance is aimed at supporting the timely implementation of the six new surgical hubs which are intended to reduce waiting lists for scheduled surgical care.
ONOURS
Hospital Professional 2024
2024 YEAR END REVIEW
APRIL
Professor of Innovation at Maynooth University, Professor Martin Curley, stated that Ireland is in a prime position to develop the most advanced electronic health record system in the world if the appropriate strategy and funding is forthcoming from Government.
In a ground-breaking study, scientists from Trinity and Princeton and Harvard Medical School shared newly uncovered secrets to suppress appetite control, which offer promise in the battle against obesity and type-2 diabetes.
It was revealed that women would soon have the power to tackle devastating menopause symptoms at the touch of a button through the launch of a new app by the Menopause Hub.
Leading diabetes researcher and Acting Director of the Institute for Clinical Trials at University, Professor Fidelma Dunne, was recognised by the largest global diabetes research and educational organisation in the world – the American Diabetes Association.
MAY
The Irish Medical Organisation (IMO) warned that the Department of Health risks repeating the same “regressive” mistakes of the austerity years if it plans to move away from health service investment in order to prioritise savings.
A new cross-border report – Buying All-island in Healthcare –North and South - found common barriers for smaller vendors in healthcare and urged an all-island shift to innovation procurement to enable SMEs and Start-ups to thrive in domestic health tech markets.
In the presence of Mayor of Clonmel Borough District, Cllr Richie Molloy, Clonmel Healthcare, popular consumer health brand, has announced the completion of the construction of a brand new ¤3 million euro warehouse facility in Clonmel.
The Trinity St James’s Cancer Institute (TSJCI) announced the roll-out of ‘My Gynaecology Patient Passport,’ a resource for patients diagnosed with, or undergoing investigation for, gynaecological cancer which will be carried by patients throughout their cancer journey.
JUNE
Recognising their crucial role of Hospital Pharmacists, the European Association of Hospital Pharmacists (EAHP) released its 2024 European Parliament Elections Manifesto, highlighting five critical topics for the upcoming legislative cycle.
Ireland is attracting fewer clinical trials than some European countries with similar populations and economic performances, according to a report by the Irish Pharmaceutical Healthcare Association (IPHA).
Increased penetration of generic, biosimilar, and value-added medicines will be critical to enhancing treatment accessibility for patients, while managing the healthcare spend of EU member states. That was the message from Medicines for Ireland (MFI) to European election candidates in its ‘Manifesto for Europe’ setting out the association’s key European policy asks.
A major National Conference on Stroke, hosted by the South Tipperary Stroke Communication Group, took place at the Cashel Palace Hotel, Cashel. The Conference heard from professionals and stroke survivors and included demonstrations on developments in the area of innovations for persons with spinal cord injury, stroke, multiple sclerosis and other neurological conditions.
2024 YEAR END REVIEW
JULY
Professor Deborah McNamara as elected as the new President of the Royal College of Surgeons Ireland. Professor McNamara took up office following the College’s biennial Council Elections.
Medicines for Europe marked 30 years of delivering more equitable access to off-patent medicines as it opened its annual European conference in Dublin, in partnership with Medicines for Ireland.
Professor Robert Byrne welcomed everyone to the inaugural Mater Private Network Heart Summit, a symposium organised by Mater Private, in collaboration with the RCSI University and the Cardiovascular Research Institute, with support from the Irish Cardiac Society.
The 2024 ASCO Annual Meeting was held in Chicago, IL, from May 31-June 4, and was a unique opportunity for clinicians and researchers to come together and share the latest innovations in cancer care and research. This issue carried a full round-up of the key talks.
AUGUST
Mahreen Khosa, Senior Pharmacist at Mater Private Network in Dublin recently won the first prize for her poster at the Hospital Pharmacists Associa Conference in Dublin for her poster entitled 'Planning the Implementation of a New Oncology Compounding Information System in an Aseptic Compounding Unit: A Mixed Methods Study'.
The latest figures from the National Treatment Purchase Fund (NTPF) show a significant increase of almost 328,000 in the number of people waiting for care compared with May 2017 at the launch of Sláintecare.
The Health Products Regulatory Authority (HPRA) reported a sharp increase in the volume of illegal medicines detained in the first half of 2024 compared to the same period last year.
We published a report authored by Ciara Ni Dhubhlaing, Chief I Pharmacist, St Patrick’s Mental Health Services which detailed the role of hospital pharmacists and pharmacy teams in Ireland, where they have got and where they are going.
SEPTEMBER
The Medical Council published its 2023 Medical Workforce Intelligence Report.
New figures published by the National Treatment Purchase Fund (NTPF) confirmed that targets to reduce waiting lists by 6% this year are increasingly unlikely to be met, according to the Irish Hospital Consultants Association (IHCA).
The European Society of Cardiology (ESC) released updated guidelines on the management of elevated blood pressure and hypertension to better identify people at risk of heart attack and stroke. The guidelines were produced by an international panel of experts, including co-chairpersons, Professor Bill McEvoy of University of Galway.
A research team at RCSI University of Medicine and Health Sciences developed a new implant that conveys electrical signals and may have the potential to encourage nerve cell (neuron) repair after spinal cord injury.
2024 YEAR END REVIEW
OCTOBER
The Irish Medical Organisation (IMO) warned that a consistent failure to properly fund and resource the health system has left it at a “critical juncture” and facing a number of persistent and worsening crises in medical staffing, bed capacity and infrastructure.
The Board of the Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the research-based biopharmaceutical industry in Ireland, announced Shane Ryan as its new President.
A new ¤32 million Education and Research Centre (ERC) at Connolly Hospital was officially opened by RCSI University of Medicine and Health Sciences.
A research team at RCSI University of Medicine and Health Sciences developed a new implant that conveys electrical signals and may have the potential to encourage nerve cell (neuron) repair after spinal cord injury.
This issue featured full coverage of the 2024 Hospital Professional Honours, and the winners across 15 categories.
NOVEMBER
A new survey commissioned by the Irish Hospital Consultants Association (IHCA) found that 56% of consultants believe their working environment rarely or never reflects a culture of mutual support, cohesion, or trust, with 76% saying that they are very often or always in ‘firefighting mode’.
The Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the research-based biopharmaceutical industry in Ireland, welcomed the allocation of ¤30 million for new medicines in Budget 2025.
A new research paper titled “The Top Ten Priorities in Adults Living with Type 1 Diabetes in Ireland and the United Kingdom – A James Lind Alliance Priority Setting Partnership” was published, shedding light on the most pressing concerns and priorities of adults living with Type 1 diabetes.
The annual Eye Care in Focus Conference, hosted by the Irish College of Ophthalmologists, took place on Tuesday, 1st October at The Gibson Hotel, Dublin.
As a participating member of Medicines for Ireland (MFI), Donagh O’Leary, Managing Director at Clonmel Healthcare along with John Donnelly had the pleasure to meet with MEP Barry Andrews in conjunction with Paul Neill, Chairperson of MFI and Eimear O’Leary, Director of Communications and Advocacy at the Irish Pharmaceutical Healthcare Association (IPHA).
Viatris Team Showcase Court Skills
Viatris colleagues demonstrate their court and team skills, while supporting Irish Wheelchair Association
Viatris Inc. (NASDAQ: VTRS) colleagues in Ireland joined the Irish Wheelchair Association last month in the Sport Ireland Campus, Blanchardstown, Dublin, for a fast-paced and entertaining wheelchair basketball event. The experience raised over ¤10,000 for the registered charity, which runs corporate team building days with the underlying aims of changing attitudes, facilitating access to sports, and supporting facilities for people with disabilities. The event is part of a pan-European #BuildingHealthierCommunities initiative at Viatris, a global healthcare company, which aims to engage employees and local healthcare communities across Europe to support social and environmental projects. The unique, fun-filled experience was enjoyed by over 100 employees from Ireland and across Europe, including members of Viatris’ Leadership team.
Enis Otuk, Country Manager - Ireland, explained, “We’re honoured to join Irish Wheelchair Association today to experience adapted physical activity through wheelchair basketball. At Viatris, we believe diverse perspectives drive innovation and our ability to make an impact in the world. Today’s event is a celebration of diversity and inclusion.” Enis went on to say, “In Ireland we support approximately 30 Irish charities and organisations each year, nominated and chosen by
our employees. We aim for these partnership efforts to make a real difference in the local community. These collaborations also influence our employees, helping them not only understand the challenges of the communities we live and work in but also embrace our many differences and realise our own potential. I am proud to be part of an organisation that has community and diversity in mind. As the Viatris motto goes, we are ‘Stronger Together’.”
Ann-Marie O'Grady, Chief Executive Officer, Irish Wheelchair Association added, "We are incredibly grateful for Viatris' continued partnership - now in its second year - and their generous donation of ¤10,000 euro towards, and participation in, this unique Corporate Wheelchair Basketball
Enis Otuk, Country ManagerIreland, Viatris and Paul Ryan, Irish Wheelchair Association Sports National Operations Manger
event. This is the second time we've had the pleasure of working with Viatris on this fantastic initiative, hosted at Sports Campus Ireland, and their support is truly making a difference. These events are a wonderful way for colleagues to come together to raise vital funds for Irish Wheelchair Association’s work across Ireland.
“Viatris' donation will help sustain our IWA Multi Sports Clubs across the country, as well as our vital work in IWA Community Centres keeping our members active and
engaged through sports like boccia and other community activities. For people with disabilities, these services are more than just recreational—they're a lifeline. They help combat loneliness and isolation, empowering our members to stay connected, active and involved in their communities and support their physical and mental wellbeing.
“Together with partners like Viatris, we can continue to make a lasting impact on the lives of people with disabilities, ensuring they can live the life they choose."
Viatris Ireland employees and employees from the Irish Wheelchair Association
Enis Otuk, Country ManagerIreland and Ann-Marie O’Grady Chief Executive Officer, Irish Wheelchair Association
AUTHORS: JJ Coughlan1,2, Robert A. Byrne1,2
Author affiliations:
1. Cardiovascular Research Institute, Mater Private Network, Eccles Street 73, Dublin 7, D07 WKW8, Ireland
2. School of Pharmacy and Biomolecular Sciences, RCSI University of Medicine and Health Sciences, Dublin, Ireland
60 Second Summary
Acute coronary syndromes (ACS) encompass a spectrum of conditions that include patients presenting with recent changes in clinical symptoms or signs, with or without changes on 12-lead electrocardiogram (ECG) and with or without acute elevations in cardiac troponin (cTn) concentrations. ACS can be subdivided into unstable angina (UA), non-ST segment elevation myocardial infarction (NSTEMI) and ST segment elevation myocardial infarction (STEMI).
In this article, we highlight some of the most important aspects of the management of patients with ACS, from the initial diagnosis and risk stratification to invasive assessment, revascularisation and discharge.
We finish the article by focusing on the secondary prevention measures recommended for ACS patients. The aim of the article is to provide readers
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings. Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. Viatris has no editorial oversight of the CPD programmes included in these modules
Acute Coronary Syndromes
Introduction
Acute coronary syndromes (ACS) encompass a spectrum of conditions that include patients presenting with recent changes in clinical symptoms or signs, with or without changes on 12-lead electrocardiogram (ECG) and with or without acute elevations in cardiac troponin (cTn) concentrations. ACS can be subdivided into unstable angina (UA), non-ST segment elevation myocardial infarction (NSTEMI) and ST segment elevation myocardial infarction (STEMI). In this article, we try to highlight the most important aspects of the management of patients with ACS from the 2023 European Society for Cardiology (ESC) ACS guidelines, which combined the
journey, from initial presentation through to discharge and secondary prevention measures.
Initial assessment
Patients are generally suspected to have ACS based on clinical symptoms, most commonly chest pain. However, this acute chest ‘pain’ may be described as discomfort, pressure, tightness, heaviness, or burning. Chest pain descriptors should be classified as cardiac, possibly cardiac, and likely non-cardiac. The use of the descriptor ‘atypical’ should be avoided. Chest pain-equivalent symptoms can include dyspnoea, epigastric pain, and pain in the left or right arm or neck/jaw. Any of these symptoms should prompt consideration of the
should take a focused history and clinical examination and obtain a 12 lead ECG. This will provide all the information required to decide on the need for emergent invasive management, which is the next step in the management algorithm for patients with ACS.
Invasive management
One of the most critical and time sensitive decisions when managing a patient with ACS is deciding upon the need for immediate invasive assessment with emergent coronary angiography. Patients with ST segment elevation (or equivalents) and very highrisk patients NSTEACS patients without ST segment elevation on ECG are the two groups of patients who should be stratified
Robert A. Byrne
JJ Coughlan
42 CPD 114: ACUTE CORONARY SYNDROMES
Figure 1. Central Illustration summarising the most important steps when managing a patient presenting with an acute coronary syndrome
mechanical complications and/or recurrent dynamic ECG changes suggestive of ischaemia. These patients should be transferred to the cardiac catheterisation laboratory as soon as possible.
Anti-thrombotic therapy
All patients with ACS will require treatment with antithrombotic therapy, consisting of antiplatelet therapy and anticoagulation. The default recommended antithrombotic treatment regimens for patients with ACS are summarised in Figure 3. All patients with ACS are recommended to receive parenteral anticoagulation at the time of diagnosis. For ACS patients without a separate indication for anticoagulation (i.e., atrial fibrillation), anticoagulation does not need to be continued beyond the acute phase (i.e., the inpatient hopsitalisation). Conversely, all patients with ACS should be treated with antiplatelet therapy, which will continue beyond the acute hospitalisation stage. Aspirin is recommended for all patients without contraindications at an initial oral loading dose (LD) of 150–300 mg (or 75–250 mg intravenously [i.v.]) and a subsequent maintenance dose (MD) of 75–100 mg once daily (o.d.) for long-term treatment. In all ACS patients, a P2Y12 receptor inhibitor (prasugrel, ticagrelor or clopidogrel) is recommended in addition to aspirin, given as an initial oral LD followed by an MD for 12 months unless there is high bleeding risk (HBR). A proton pump inhibitor in combination with DAPT is recommended in patients at high
Figure 2. Electrocardiographic abnormalities in patients with STEMI and ECG findings that, if present, may prompt triage for immediate reperfusion therapy
this is most commonly performed via percutaneous coronary intervention (PCI). Coronary artery bypass grafting (CABG) represents an alternative revascularisation modality, although this is less commonly performed than PCI for patients with ACS. The decision on whether PCI or CABG is most appropriate is based on clinical presentation, patient comorbidities and coronary artery disease complexity. Regardless of the revascularisation modality and clinical presentation (STEMI, NSTEMI, UA), complete revascularisation (i.e., treatment of all significant lesions in major epicardial coronary arteries) should be the goal for all patients. Intravascular imaging (intravascular ultrasound or optical coherence tomography) and intracoronary physiology (i.e., fractional flow reserve testing) can be used to help guide revascularisation decisions. The use of drug eluting stents is generally recommended in patients undergoing PCI. Secondary prevention
As soon as an ACS event is diagnosed, secondary prevention begins. The long-term treatment plan and recommended goals for patients with ACS are summarised in Figure 4. All patients with ACS should be discharged on cardioprotective medications (antiplatelet therapy, lipid lowering therapy), with information on lifestyle management and a referral to cardiac rehabilitation. Healthcare providers should aim to help support patients in making healthy lifestyle choices. This includes smoking cessation, adopting a healthy
44 CPD 114: ACUTE CORONARY SYNDROMES
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Website: www.hpra.ie. Adverse reactions/events should also be reported to the marketing authorisation holder at email address: pv.ireland@viatris.com or phone 0044(0)8001218267
fondaparinux
Figure 4. Long-term management after an acute coronary syndrome
possibly cardiac, and likely noncardiac. The use of the descriptor ‘atypical’ should be avoided.
True/False Statement 2: If a patient is diagnosed with ACS, the decision to treat with parenteral anticoagulation should be made based on the ischemic and bleeding risk of the patient.
Answer: False
Explainer: All patients with ACS should be treated with parenteral anticoagulation at the time of diagnosis.
True/False Statement 3: All patients suspected to have a diagnosis of NSTEACS (unstable angina or NSTEMI) should receive pretreatment with a P2Y12 inhibitor immediately.
Answer: False
Explainer: Routine pretreatment with a P2Y12 inhibitor is not recommended in patients with NSTEACS in whom coronary anatomy is not known and early invasive management (<24 h) is planned.
True/False Statement 4: Patients should be allowed time to recover from their ACS episode before intensifying cardioprotective medical therapies, including lipid lowering therapies.
Answer: False
Explainer: Patients should be discharged on cardioprotective medications, with information on lifestyle advice and a referral to cardiac rehabilitation. It is recommended that high-dose statin therapy is initiated or continued as early as possible, regardless of initial LDL-C values.
True/False Statement 5: For ACS
Hospital Professional
As we look ahead into 2025, now is the time to reflect on those who have been, and who will be, empowering others moving into the future.
We’re marking the end of 2024 with our unique HPN Professional Top 100 – a prestigious annual list which celebrates Ireland’s top hospital and healthcare achievers.
The HPN Top Professional Top 100 is a carefully constructed network of the most influential hospital professionals across a range of disciplines, both in the healthcare and pharma industries, who act as ambassadors and role models for their peers and colleagues.
Over the past many months, our team of writers has reached out to pharmacists, consultants, clinical specialists, representative bodies and organisations throughout the sector and encouraged them to put forward those colleagues they feel are redrawing the landscape for the future.
Those who have made our final list have displayed motivating behaviour and inspirational leadership affecting the development of hospital services across Ireland.
Professional 100
Dr Richard Armstrong, Blackrock Health
During 2024, Dr Armstrong was raising awareness of the most commonly experienced heart health conditions. Data has shown that the top reasons why people seek heart health investigations are chest pain at 51%, palpitations caused by possible heart arrhythmia at 30% and heart failure at 10%, according to 2023 admission data from Blackrock Health’s Rapid Cardiac Care Service which is available at Blackrock Clinic, Galway Clinic and Hermitage Clinic. Further research conducted by Blackrock Health last year also showed that 77% of people have experienced one of the symptoms associated with one of these conditions yet almost 20% of people did not take any action regarding their symptoms.
On the back of this data, Consultant Cardiologist Dr Richard Armstrong at Blackrock Health is striving to drive awareness of the most commonly experienced heart health conditions and importantly when to seek medical attention. Dr Armstrong is a Consultant Interventional and General Cardiologist.
Professor Elizabeth Barrett, Children’s Health Ireland/University College Dublin
Professor Barrett is a Consultant in Child and Adolescent Liaison Psychiatry (Psychological Medicine) and Associate Professor of Psychiatry. She is Chair of the College of Psychiatrist’s Academic Faculty and has served on national and international model of care, guideline, and review groups for Liaison Psychiatry, Paediatric Medicine, Training, and Eating Disorders.
She has a clinical and research interest in the interface between Medical and Psychiatric co-morbidity, with interests including Liaison psychiatry, Eating disorders, Somatic Symptoms in medicine, Anxiety, Neuropsychiatry, and with Medical Education projects. She sees training and inter-professional education as crucial to early detection and intervention, and to longer term improved health outcomes, for children. She holds a masters in Medical Education and a postgraduate diploma in Innovation.
Dr Peter Barrett, St Finbarr’s Hospital Cork
Dr Barrett and his team won the 2024 GSK Viiv Infectious Diseases Project of the Year at the annual Hospital Professional Honours. The team recognised that their internal and external communication mechanisms needed to become more robust and streamlined; most new cases and outbreaks of infectious diseases were being notified electronically to the Department, rather than via the more traditional mechanisms of paper/postage.
An Acute Health Protection Duty Room was developed at the end of 2022 to provide a more robust model of delivering the acute public health response to new cases and outbreaks of infectious disease.
In 2023, Dr Barrett became the first public health physician to be awarded a HRB Clinician Scientist Fellowship.
Mr Fabio Bartolozzi, University Hospital Galway
Mr. Bartolozzi is a senior cardiothoracic surgeon. Mr. Bartolozzi is the part of minimally invasive cardiac surgery team who have successfully completed 100 minimally invasive cardiac surgeries, making University Hospital Galway the pioneers in minimally invasive cardiac surgeries in the country and the only public sector hospital in the country to perform such procedures. Mr. Bartolozzi and the team are doing minimal invasive aortic valve replacement and mitral valve repair and replacement successfully in University Hospital Galway. Minimally invasive cardiac procedures prevents cutting the sternum, which causes post operative pain and is prone to wound infections in cardiac surgery patients. Patients are discharged home early and return to their daily activities sooner compare to the conventional cardiac surgery patients.
Dr Harriett Bennett-Lenane, University College Cork
In October of the year, Dr Bennett-Lenane and colleagues received a grant to use modern computational methods to develop critical medicines for improving global health and equality.
Their project, "Advancing Global Health Drug Formulation Development Using ML and AI," aims to develop artificial intelligence (AI) and machine lear ning (ML) tools that can accelerate the creation of medicines for conditions that disproportionately affect those in developing countries, such as malaria and other tropical diseases.
The tools they are building will be made freely accessible via an open-source, webbased platform, ensuring that this technology can be leveraged worldwide. This ambitious project aligns to the UCC Futures thematic areas of Future Medicines and AI & Data Analytics. Dr Harriett Bennett-Lenane is currently a lecturer in Clinical Pharmaceutics at the School of Pharmacy in University College Cork.
Patrick Boland, Mater Misericordiae University Hospital/ University College Dublin
Patrick recently won the Royal College of Surgeons in Ireland National Research Medal at the annual RCSI Millin Meeting.
Patrick is a CLASSICA project Research Fellow with the UCD Centre for Precision Surgery University College Dublin Mater Misericordiae University Hospital. He presented his work titled, Intratumoural Variability of Fluorescent Signals May Accurately Classify Rectal Neoplasia. The RCSI National Surgical Research Medal is awarded to the best oral presentation, with presentations judged by an international panel of surgeons.
Professional 100
Dr David Breen, Galway University Hospital
Professor Ann Marie Brady, Tallaght University Hospital
Professor Anne-Marie Brady has been appointed the new Chair of the Tallaght University Hospital Board, taking over from the outgoing Chair Mr. Liam Dowdall. Professor Brady has served on the Hospital Board since 2018 and was until recently the Vice Chair of the Board. She had also previously served as Chair of the Quality, Safety & Risk Management Committee.
Professor Anne-Marie Brady is Chair of Nursing & Chronic Illness in the School of Nursing & Midwifery and Director of Trinity Centre for Practice & Healthcare Innovation at Trinity College Dublin. She previously served as Head of School (2017-20); Director of the Trinity Centre for Practice & Healthcare Innovation (2014-17) and as Director of Teaching & Learning (Postgraduate) (2010-2014). She is a Registered General Nurse and Registered Nurse Tutor with over 35 years of clinical practice, management, education, and research experience in healthcare innovation.
Dr David Breen is currently a Respiratory Consultant/ Interventional Pulmonologist and also the Lung Cancer Lead based in Galway University Hospital. He was appointed in 2010 and from there developed the Rapid Access Lung Clinic for the West of Ireland. The RALC service was established to streamline the diagnostic pathway for those patients whose presentation was highly suspicious of cancer, with the aim that any new patient referred to the RALC would be offered a clinic appointment within 10 working days, and from there, appropriate cases could be prioritised for urgent diagnostic work-up. Thanks to David and his team, this service has currently seen 888 patients this year. David continued his passion to ensure cancer patients were treated efficiently and timely by developing the Joint Thoracic Clinic, which is an MDT clinic where patients receive their diagnosis, but also start their treatment plan with the collaboration of Surgeons, Medical Oncologist or Radiation Oncologist. This is a unique service to the West of Ireland, founded on David’s personal belief that “service users deserve nothing less than our best” This clinic celebrates 10 years this year.
In addition, David leads the pleural service in Galway University Hospital, which provides diagnostic and long-term management of pleural disease for all of the West of Ireland.
Claire Boles, SSPC SFI Reseatch Centre for Pharmaceuticals, University College Dublin
Claire Boles, a PhD student at the SSPC SFI Research Centre for Pharmaceuticals, based at University College Dublin, joined Ireland’s Women’s Rugby Sevens team at the 2024 Olympic Games in Paris, France this year. Claire works under the supervision of Dr Jessica Whelan and Dr Roderick Jones, researching the development of a Process Analytical Technology (PAT) method, using a PharmaFlow system for real-time monitoring and control of manufacturing processes that improve efficiency, accuracy, and consistency in pharmaceuticals products.
Her particular focus is on the application of the technology to cell culture media preparation to facilitate biopharmaceutical production. Dr Whelan said, “Claire’s participation in the Olympics is a testament to her exceptional skills and the support of her academic and athletic communities.”
Jennifer Brown, Mater Misericordiae University
Hospital
Pharmacy Head of Operations, Jennifer and her pharmacy team were shortlisted as Finalists for the Hospital Professional Honours 2024 Athlone Pharmaceuticals Hospital Pharmacy Team of the Year.
The Mater Misericordiae University Hospital (MMUH) pharmacy team is a dynamic, ambitious and supportive team who strive to deliver the hospital’s mission to care for the sick with compassion and professionalism at all times, respect the dignity of human life, and to promote excellence, quality and accountability through their activities. The MMUH Pharmacy delivers a number of critical clinical services to hospital patients including dispensary, clinical pharmacy, aseptic compounding, medicines information, infectious diseases, antimicrobial stewardship, heart lung transplantation, pulmonary hypertension and drug safety services.
The large pharmacy team support each other to perform to the highest standards while ensuring staff are ongoing development and motivation in all aspects of their role. This is achieved from their first day of service in the MMUH Pharmacy with the dedicated onboarding process that includes an assigned mentors and dedicated training programmes for all new staff.
Professor Conor Buckley, AMBER
Professor Buckley, principal investigator in AMBER, the SFI Centre for Advanced Materials and BioEngineering Research, and Professor in Biomedical Engineering in Trinity’s School of Engineering, has secured the ¤150,000 funding for iDISC.
Professor Buckley is also affiliated with the Trinity Centre for Biomedical Engineering, and the Trinity Biomedical Sciences Institute, and is an Honorary Associate Professor in RCSI. He will develop injectable biomimetic hydrogel systems for the lower back that aim to halt degeneration and restore natural biomechanical function through minimally invasive spine treatment strategies.
Emma Burke, Galway University Hospital/Integrated Care/HSE
Emma has set up a COPD (Chronic Obstructive Pulmonary Disease) Virtual Care Ward taking significant initiative and leadership in Galway University Hospital. She is an inspirational leader in her dynamic thinking by identifying the need for a Virtual Care Ward. She saw an opportunity to improve patient care for those with COPD, particularly in an era where telemedicine is becoming increasingly vital.
Emmas’ focus was a commitment to enhancing the patients experience when presenting with acute exacerbation of their COPD.
The COPD-VW has provided 50 care episodes since launching- April 2024. The average length of stay (LOS) is 7.3 days, 35.5% improvement on LOS compared to the national average. The HIPE data report (2024) estimates costings ¤8179 per COPD hospital stay. This pilot to date has saved 370.4 days an estimated ¤408,000.
Professional 100
Rose Cafferkey, Mayo University Hospital
Louise
Byrne,
Tallaght University Hospital
Louise was shortlisted as a Finalist for the 2024 Pharmasource Hospital Pharmacist of the Year Honour. Louise Byrne is the pharmacy aseptic unit manager and a pharmacy management team member in Tallaght University Hospital (TUH) since 2001. Over the last 26 years she has presented and supported the development of over 30 posters which have been submitted to Irish and International Conferences such as HPAI, NAHPT, EAHP, IPHOS, QAPs annual conferences since 2000. Her commitment to the evolvement of aseptic unit services in Ireland and the advancement of the profession has been unparalleled.
Rose has over 20 years of experience in hospital pharmacy and currently serves as a Senior Antimicrobial Stewardship (AMS) Pharmacist at Mayo University Hospital. Over her career, she has held diverse roles, including being instrumental in establishing the hospital’s aseptic unit. Rose has been a leader in AMS, becoming one of the first AMS Pharmacists in Ireland when the position was established in 2008. She was instrumental in setting up the AMS committee and program at Mayo University Hospital.
Alongside her colleague Marie Ronan, Rose recently won the HPN Excellence in Patient Safety Honour for her work on penicillin allergy delabelling. She was also recognized at the 2019 HPN Awards, receiving the GSK Infectious Disease Project of the Year award for her work on CPE and contributing as a key member of the Consultant-Led Hospital Team of the Year.
Mr Ronan Cahill, Mater Misercordiae University Hospital/University College Dublin
Mr Cahill has completed ten years in his role as Consultant Surgeon and Professor of Surgery at the Mater/UCD. Most recently, the UCD Centre of Precision Surgery (which he leads) has completed project team work on the RCSI’s Working Group Report “New Technology for Future of Surgery in Ireland” and convened a successful Health Research Board (HRB) conference “AI & Computer Aided Surgery” with a registered attendance of nearly 200 people from clinical, academic and industry backgrounds over two days and an international faculty of surgical experts in the field including input regarding regulatory, legal and clinical trial perspectives.
The Centre continues a high academic output with an average of 26 peer reviewed publications a year for the past five years. The centre has also completed its field-leading Disruptive Technologies and Innovation Funded consortium award “Future of Colorectal Cancer Surgery” and Horizon 2020 consortium “Protecting Operating Room Staff against Aerosolised Viruses) and continues its leadership of the Horizon Europe consortium award “CLASSICA- Validating AI in classifying cancer in realtime during surgery” which is entering clinical deployment stage of AI software during endoscopic surgery for colorectal cancer and large polyps. The Clinical Anatomy Centre and Surgical Training Unit at the Mater hospital continues as the only in-hospital training site with access to highest level fidelity models for surgical training including team based lear ning and deep specialisation at consultant level with courses and practice enhancement regarding innovation and new medical devices across every surgical specialty with industry collaboration. Ronan is also now a three-term member of council at RCSI.
Angela Clayton-Lea, Cancer Trials Ireland
Angela has made a significant impact at Cancer Trials Ireland (CTI) since joining as Chief Operations Officer (COO) in October 2023. With over 20 years of experience in healthcare, including a clinical background as a Research Radiation Therapist and senior roles in operations management, Angela has brought a wealth of expertise and vision to CTI. Her leadership has been pivotal in shaping the organisation’s operational strategy, enhancing efficiency, and driving forward key initiatives.
Angela’s influence at CTI can be seen in her leadership of a substantial organisational restructure, which has included the establishment of a new Start-Up Team. This team, designed to expedite the start-up phase of cancer clinical trials, is a response to the ongoing challenge of reducing the "time to first patient" (TTFP).
Sinead Cobbe, University Hospital Limerick
Sinead and her team won the Excellence in Oncology Honour 2024 at the recent Hospital Professional Honours. T Breast cancer Related Lymphoedema (BCLR) is a well-known side effect of breast cancer treatments including surgery, chemotherapy, radiation therapy and endocrine therapies. Damage or overload to the lymphatics predisposes high-risk cohorts to the development of arm lymphoedema.
The aim of this project is “to introduce a lymphoedema early detection service in UHL oncology unit for all breast and gynae patients who have had surgery and/or radiation to reduce the incidence and impact of lymphoedema in Ireland. The findings from the pilot will be used to support future funding for similar services in all oncology centres.”
Professor Gabrielle Colleran, National Maternity Hospital
Earlier this year Professor Colleran was appointed President of the Irish Hospital Consultants Association.
Professor Colleran will shape the IHCA’s agenda by focusing on the need for additional clinical capacity and emphasising the importance of the green transition in healthcare.
Professor Colleran is a distinguished Clinical Associate Professor in Paediatrics at Trinity College Dublin and Assistant Clinical Professor in Women’s and Children’s Health at the University College Dublin School of Medicine. She leads the radiology department at the National Maternity Hospital and is the Radiology Lead for the national fetal MRI programme.
Professional 100
Elaine Condon, Managing Director, TCP Homecare
Elaine Condon, Managing Director of TCP Homecare, Ireland's largest private Clinical homecare provider of ‘direct to patient services.’ Part of the country board for PHX Ireland.
TCP Homecare was first established in 2000 as a logistics company to deliver temperature sensitive pharmaceutical products to hospitals, GPs and patient homes in a patented fleet of temperature controlled vans. As Managing Director of TCP, which is part of PHX Ireland group, Elaine Condron has led the rapid expansion of TCP over this time to a position today where they employ 215 experienced healthcare professionals, who uniquely provide the dispensing and distribution of pharmaceutical products, an extensive range of homecare nursing services and sharps waste management and facilitate a unique turnkey solution for the delivery of hospital care in the patient’s home.
TCP provides services 365 days a year and plays a pivotal role in local communities as they facilitate the transition of care from Hospitals to the local community and homes. Elaines dedication and commitment helped build and develop this highly successful team that collectively focus on delivering high quality care while always keeping patients at the centre of what they do.
Some of the unique and innovative services offered by TCP include:
1) Service for home distribution in Ireland of Clotting Factor Concentrates to haemophilia patients is still recognised as a global first
2) TCP Homecare provide serialised GS1 Bar Code labelling for real time Track ‘n Trace of individual products to enable (if needed) a rapid product recall
3) Electronic Patient Management System is a first of its kind; allowing real time patient evaluation reports to be sent to the referring team
4) TCP Homecare established the first out-of-hospital infusion centre in Ireland
Dr Niamh Connolly, Royal College of Surgeons in Ireland
Dr Connolly is one of the partners on a newly announced project known as the 4DPD-Omics project, which hopes to enhance understanding of the neurodegenerative disorder Parkinson’s disease through advanced analysis techniques.
The project will explore how specific genes and proteins behave across different cell types and disease stages. Focusing on the abnormal protein deposits known as α-synuclein that are characteristic of Parkinson’s, the researchers are aiming to find new targets for future treatments. Dr Connolly is an electronic engineer turned systems biologist/neuroscientist who loves the complexity of the brain. She is passionate about doing things the right way, and is eager to better understand the intricacy of brain function so that better biomarkers, diagnostics, and therapies can be designed.
Chief 2 Pharmacist and Cancer Services Clinical Pharmacy Lead at Cork University Hospital, Katie’s exceptionally leadership skills, patient-centred focus and commitment and devotion to her role and the hospital cancer Directorate are exemplar. She continues to be involved in almost every initiative ongoing in the hospital that involved SACT and the Aseptic Compounding Unit – she is always in the thick of it, being innovative, and out-of-the-box thinker and ultimately impossibly thoughtful, kind and empathetic. She has been described as a credit and a blessing to the CUH hospital and the Hospital Pharmacy Service nationally and internationally.
Katie was a Finalist for the 2024 Pharmasource Hospital Pharmacist of the Year Honour.
Katie Cooke, Cork University Hospital
Emer Cronin, University Hospital Waterford
Emer Cronin is a Hospital Pharmacist in University Hospital Waterford (UHW). UHW is a model 4 hospital and the regional cancer centre for the HSE South East Cancer group. Emer graduated from University College Cork with a masters in pharmacy in 2019 and completed her MSc in Clinical Pharmacy in University College Cork in 2023.
She has worked in a number of areas but has worked as an acting senior pharmacist in the area of oncology/haematology for the past year and a half. Emer has been an excellent addition to the hospital pharmacy department in UHW, excelling in every area, and rapidly showing competency befitting an early ascension into an acting senior role.
Emer was shortlisted as a Finalist for the 2024 Young Hospital Pharmacist of the Year Honour.
Dr Suzanne Crowe, Children’s Health Ireland/University College Dublin
Dr Crowe is President of the Irish Medical Council. She works in children’s health as a Paediatric Intensivist at Children’s Health Ireland, Crumlin Hospital, Dublin.
She is Associate Clinical Professor in UCD School of Medicine in Women and Children’s Health. Dr Crowe is a board trustee for three charities – the Down Syndrome Centre, Cheshire Ireland, and LGBT Ireland. She advocates for doctors’ wellbeing, diversity, equity and inclusion, and medical ethics; and regularly speaks and writes on these topics.
In 2024, the Medical Council launched ‘CAREhub’, an external mental health support for doctors, medical students and members of the public who are engaged with the Council’s regulatory functions.
Professor Sally-Ann Cryan, Professor of Drug Delivery and Pharmacoengineering, School of Pharmacy and Biomolecular Sciences, RCSI
Professor Cryan is part of a team of pharmacy researchers who this year have investigated the potential for a specific host-directed therapy to stimulate the immune system to eliminate tuberculosis (TB), while minimising harmful inflammation as one way to help bypass antibiotic resistance and complement existing treatments.
RCSI researchers used a technique called ‘microfluidics’ to manufacture inhalable biodegradable nanoparticles (NPs), containing the vitamin A derivative ATRA, that are small enough to be used in a nebuliser and reach the alveoli in the lung. The research shows that despite their susceptibility to TB infection, alveolar epithelial cell defences can be boosted by ATRA to efficiently eliminate the bacteria. The results are promising for future research into ATRA-loaded NP formulations as inhaled host-directed therapies for TB.
Dr Kieran Dalton, University College Cork
Dr Dalton, Lecturer in Clinical Pharmacy, won the Best Poster Presentation Award for the Hospital Pharmacy section at the FIP World Congress held in Cape Town, South Africa on September 1st-4th 2024. The 82nd FIP World Congress of Pharmacy and Pharmaceutical Sciences took place in Cape Town, South Africa from the 1st to 4th of September 2024. Dr Dalton won the Best Poster Presentation Award for the Hospital Pharmacy section at this conference for a study that involved pharmacist-led medication optimisation for palliative care patients.
This poster was selected as the winner from 128 posters in this category, and Kieran was presenting this study on behalf of the research team, which included Ciarán McAdam and Eimear O’Dwyer – both of whom are pharmacists working in Our Lady's Hospice & Care Services.
Dr Dalton is a Senior Lecturer in Clinical Pharmacy, and has worked as a lecturer in UCC's School of Pharmacy since January 2019.
Professional 100
Dr Theresa Donnelly, Midland Regional Hospital Tullamore
Dr Donelly and colleagues won the 2024 Galapagos Multidisciplinary Team of the Year. Dr Donnelly is a Consultant Geriatrician at Midland Regional Hospital in Tullamore.
The RAFT (Rapid Access Frailty Team) at Midland Regional Hospital, Tullamore is a team of healthcare professionals specialising in the care of older people in the Emergency Dept (ED). The team focus on people with frailty over the age of 75 years attending the ED.
The RAFT initiative was set up in 2016 as a joint initiative with ED and the Geriatric department at MRHT to address the increasing presentations of frail patients to the ED. The primary goal was enhanced frailty assessments in ED with discharge to Community Reablement teams. Following a success pilot in 2016, a business application followed and the team has evolved since then.
Professor Eilís Dowd
Professor Dowd is the lead Neuroscientist on a project funded by The Michael J. Fox Foundation for Parkinson’s Research (MJFF) and Science Foundation Ireland, which shows that transplanting the immature cells in a collagen hydrogel dramatically improves both their survival and maturation in the brain. The discovery could revolutionise stem cell-based brain repair therapy for Parkinson’s disease. The new research aims to understand how the immune system in the brain reacts when cells are transplanted alone versus when they are transplanted in combination with the hydrogel.
The research will continue to be led by Professor Dowd, in collaboration with colleagues from CÚRAM - the Science Foundation Ireland Research Centre for Medical Devices based at University of Galway, the University of Edinburgh and the University of Melbourne.
Jane Ensor, Mater Misericordiae University Hospital
In September 2024, Jane was appointed into the Acting Cancer Services Clinical Pharmacy Lead (Chief II), which has afforded the opportunity to continue working in the ACU, alongside offering pharmacy support to the MMUH Cancer Directorate. Jane completed the UCC MSc. in Clinical Pharmacy in 2024 that included a research project on microbial contamination monitoring practices and results trending within the MMUH ACU.
Jane is the Aseptic Compounding Unit (ACU) Deputy Services Manager, leading the day-to-day functioning of the unit and ensuring consistent and safe provision of Systemic Anti-Cancer Therapy (SACT) and other sterile manufacturing services for MMUH patients. The role requires management of the ACU pharmacists & pharmacy technician team, including their specialist training, validation and support to ensure the continuity of ACU service provision. Jane is also involved in the provision of clinical trial drug services for oncology / haematology patients and, in 2024, in the preparation of the first Luxturna® treatment dose in Ireland.
Ita Fitzgerald, St Patrick’s Mental Health Services/ University College Cork
Ita is a Senior Psychiatric Pharmacist in St Patrick’s Mental Health Services, currently working in research and clinical practice. Ita also teaches undergraduate and postgraduate pharmacy students and holds an adjunct clinical lectureship with the School of Pharmacy in UCC. Ita also recently completed advanced specialist credentialing with the College of Mental Health Pharmacy in the UK.
More recently, Ita has convened a research group focussing on use of novel implementation science methodology to increase patient autonomy and shared decision-making within psychosis management. Ita has published her research within Q1 peer-reviewed journals in psychiatry, has been involved in national obesity management guideline development in Ireland and has presented at research conferences both nationally and internationally.
Mr Gerard Fitzmaurice, St James’s Hospital Dublin
Recently, Mr Fitzmaurice was appointed to the Staging and Prognostic Factors Group (SPFG) of the International Association for the Study of Lung Cancer. This is the first time that surgical patients in Ireland will contribute to the IASLC’s international lung cancer staging project signifying Ireland’s growing role in advancing global cancer care
The centralisation of complex lung cancer care has enabled St James’s to develop a unique cross-specialty team of dedicated healthcare professionals who are focused on the provision of optimal international standard thoracic surgical oncology care. This has been recognised by their recent accreditation by the European Society of Thoracic Surgeons (ESTS). They are the first European Accredited Thoracic Surgical Oncology Centre in Ireland, a key performance metric recognising excellence in the provision of thoracic surgical oncology care to Irish lung cancer patients.
Mr Fitzmaurice and his team were Finalists in the 2024 Consultant-Led Team of the Year Honour.
Patrick Foley, Blackrock Health Hermitage Clinic
The Medication Safety team at Blackrock Health Hermitage Clinic led by the Medication Safety Pharmacist Patrick Foley is one of the most comprehensive in the country. Based on publicly available HIQA inspection data, they record more data than the majority of hospitals in Ireland regardless of size or bed capacity. The medication safety programme itself is comprised of doctors, nurses and pharmacists within the hospital. The improvements to the medication safety processes at the Hermitage now mean they have one of the most comprehensive systems in the country. One of the most impressive components of the process was the introduction of Qlik App software for analysis of the data. In tandem with the IT department, they have built a dedicated piece of software that extracts data so that it can be presented in an extremely user-friendly manner.
Patrick and his team were Finalists for the 2024 Excellence in Patient Safety Honour.
Professional 100
Mr Jonathan Gallagher, Beaumont Hospital
Beaumont Hospital’s Cardiology Department won the Viatris Excellence in Cardiovascular Initiative at the 2024 Hospital Professional Honours. Mr Gallagher, Senior Psychologist and his team provide cardiac patients with the most comprehensive Cardiac Rehabilitation (CR) programme in Ireland. As well as delivering the largest annual throughput of patients, the department is internationally recognised as a centre of excellence for CR. Beaumont Hospital is the first and only CR centre in Ireland and the UK to achieve international accreditation in CR and secondary prevention.
Patients are provided with an exceptionally high concentration of multi-disciplinary expertise overseen by an actively involved Medical Director (Consultant Cardiologist), and each member of the multi-disciplinary team (MDT) has recognised expertise in their respective field. This seamless CR service benefits from close cooperation and communication between MDT members, allowing patients to achieve optimal health.
Jack Gleeson, Cork University Hospital/University College Cork
Professor Gleeson is a Medical Oncologist in the Cork University Hospital/University College Cork (CUH/UCC) Cancer Centre. He is a Principal Investigator (PI) on the Irish Cancer Society funded LIAM Mc cancer survivorship trial for men with genitourinary cancers. The LIAM Mc trial involves a 12-week intensive multidisciplinary interventional programme for patients with advanced cancer diagnoses, to provide them with the tools and supports to live well with and beyond their cancer diagnosis, and to help researchers learn how best to integrate these services into routine cancer care for all patients. The feedback to date on this initiative shows how the research study has significantly improved the lives of many patients, and it has been shortlisted for a number of awards and commendations.
Professor Gleeson is also the PI for the IMPROVE TMZ study, an observational brain tumour research study, investigating the causes of haematological toxicity in patients undergoing treatment with a chemotherapy called temozolomide (TMZ) for their brain tumours, with a view to developing a predictive model for patients in future.
Profeesor Brendan Griffin, University College Cork
Professor Griffin has been leading research into using computational methods to develop critical medicines for improving global health and equality. In October of 2024 he and his team received ¤950,000 in funding from the Bill & Melinda Gates Foundation to use artificial intelligence (AI) and machine learning (ML) to accelerate the development of medicines for conditions that impact those in developing countries.
Professor Griffin is a Senior Lecturer in Pharmaceutics and represents the School of Pharmacy on the College of Medicine and Health Graduate Studies Committee. The School of Pharmacy offers taught MSc programmes and also MSc and PhD research programmes. He is course director for the MSc in Pharmaceutical Technology and Quality Systems, an online masters course designed to train graduates working in the pharmaceutical industry to become a Qualified Person (QP). Prof Griffin has extensive experience in supervising and examining research students from across Ireland and other countries.
Gerry Hanna, Cancer Trials Ireland
Professor Gerry Hanna has made significant contributions to cancer care and research in Ireland and internationally. His recent appointment as Vice-Clinical Lead for Cancer Trials Ireland highlights his commitment to advancing oncology services and fostering collaboration across institutions. In this role, he will help shape the future of cancer trials in Ireland, building on his extensive experience in clinical leadership and research.
As the Marie Curie Chair of Clinical Oncology at Trinity College Dublin, the Trinity St James’s Cancer Institute, and the St Luke’s Radiation Oncology Network (SLRON), Professor Hanna has played a key role in improving cancer services and integrating research into clinical practice. His work is closely aligned with the National Cancer Strategy 2017–2026, contributing to advancements in radiation oncology and enhancing patient outcomes.
Dr Lucia Hartigan, Regional Hub for Women’s Health, Nenagh Hospital
Thanks to the work of Dr Hartigan and team, fertility investigations and treatments are available to public patients for the first time through the development of regional hubs such as the one at Nenagh Hospital.
The regional Fertility Hub services of the UL Hospitals Group launched in September 2023. Dr Hartigan and her team provide comprehensive fertility investigations for couples across the Mid West. Assessment and treatment requires specialised, skilled care by a team of doctors, an andrologist, specialist nurses and clinical specialist radiographer sonographers.
Professor Ann Marie Healy, School of Pharmacy, Trinity College Dublin
Professor Healy’s mentorship has resulted in the successful graduation of 23 PhD students and the guidance of 27 postdoctoral researchers to date. She has over 25 years’ experience in pharmaceutics, pharmaceutical technology and drug delivery research. Her research is focused on obtaining an increased understanding of the physicochemical properties of active and excipient materials used in a variety of different dosage forms, and on harnessing that knowledge to improve product design in terms of in vitro and subsequently in vivo performance. This research objective is achieved through collaborative efforts and interdisciplinary research with both academic and industry partners.
Through the EPSRC-SFI Centre for Doctoral Training in Transformative Pharmaceutical Technologies, which is co-funded by the Engineering and Physical Science Research Council (EPSRC) of the UK and SFI, Professor Healy has worked with colleagues in Univeristy College Cork, University College Dublin, the University of Nottingham, and University College London to develop a unique, multidisciplinary training programme for PhD students.
The programme is designed to prepare strategic-thinking scientists for high achieving careers in the pharmaceutical and healthcare sectors and will train 75 PhD students between the UK and Ireland over an eight-year period (2019-2027). As Co-Director, Professor Healy has a pivotal role in ensuring the successful delivery of a comprehensive scientific and soft-skills training curriculum, that aligns with PhD students’ needs and interests.
Bernadette Hayes, University Hospital Limerick
Bernadette was shortlisted as a Finalist for the Young Hospital Pharmacist of the Year accolade this year. She is a Senior Pharmacist at University Hospital Limerick and has worked as a valued member of the Aseptic Compounding Unit team within the Pharmacy Department for the past two years. Bernadette is highly motivated and demonstrates a true passion for her work, embodying dedication and expertise in her role. Bernadette was one of the primary drivers of the recent innovation project of semi-automated compounding which has been implemented successfully into work practices within the Aseptic Compounding Unit, thereby increasing capacity within the unit for chemotherapy compounding all the while ensuring both patient and staff safety were at the forefront.
Professional 100
Professor Nuala Healy, Royal College of Surgeons in Ireland
Professor Nuala Healy has been appointed Chair of Radiology at RCSI University of Medicine and Health Sciences. In her role, Professor Healy will lead RCSI’s academic Department of Radiology while providing patient care as a consultant radiologist at Beaumont Hospital.
Professor Healy completed her undergraduate medical training at University of Galway. Following basic surgical training, she undertook a lab-based MD and was awarded a Molecular Medicine Ireland Clinician Scientist Fellowship, and she also completed a master's in clinical education at the University of Galway
Professor Dominic Hegarty, Mater
Private Hospital Cork
The 7th Interventional Pain Congress was held in Istanbul and Prof. Dominic Hegarty was invited as president of World Institute of Pain (WIP) to attend the 3 day conference in Istanbul. Professor Hegarty opened the meeting and was honoured to preside over the 3 day event organised by the WIP Turkish Registered sections. He instructed on the workshop and was an examiner. He gave a key note lecture specifically on the new advance in Orofacial pain and updated the congress on the present best practice and what the future might be.
Professor Hegarty and his team were Finalists for the 2024 Grunenthal Advancing the Standard of Care in Pain Management Honour.
The team’s post-implant pathway was based on the traditional principal of “face-to-face” clinical interactions. Several steps of the pathway were labour intensive, time restricted and an expensive use of clinical resources. The Mater Private Hospital, Cork and Medtronic collaborated on a pilot programme to deploy Get Ready®, a digital remote patient management solution for truly connected care that aims to optimise the entire care pathway. This platform has shown to have a potential and significant role in providing quality the aftercare without impacting negatively on the patient outcome.
Professor David Henshall, SFI FutureNeuro Research Centre
Professor David Henshall, Professor of Molecular Physiology and Neuroscience at RCSI and Director of the SFI FutureNeuro Research Centre, has been elected as a Member of the Royal Irish Academy (MRIA), Ireland’s foremost body of experts in the sciences and humanities, at a ceremony held in the Academy’s headquarters in Dublin.
Professor David Henshall’s research focus is on the causes and treatment of the neurological condition epilepsy. Some of his major research projects are examining the patho-mechanisms underlying epilepsy development following brain injury, in particular the role of epigenetics and non-coding RNAs and using the discoveries to develop new therapies for epilepsy and exploring for this disease.
Alice won the 2024 MedFind Solutions Innovation and Service Development Honour at the Hospital Professional Honours held this year.
A Community Midwife in The National Maternity Hospital (NMH), upon recognising the impact of spoken affirmations for women during labour, designed a set of positive affirmation cards for pregnancy, labour and the postnatal period. She successfully pitched for funding from The NMH foundation who award small grants twice a year.
Over 800 sets of cards were distributed nationally over a six-month period in 2023. This demonstrates the transfer ability of this project not only nationally but internationally. This project was largely successfully through the deep commitment and passion for women centred midwifery care by the team. A collective leadership style was adopted. Each team member is driven by a mutual purpose and shared vision namely to provide maternity service users with support tools to assist in a positive journey into parenthood.
Alice Hoffmeister, National Maternity Hospital
Ellen Holmes, Mater Misericordiae University Hospital
Ellen was instrumental in co-ordinating the logistics for several significant pharmacy projects in 2024 including the automated dispensing system replacement that involved decommissioning of the previous robots, new robot installation, commissioning and go-live. Ellen managed the dispensary services for the down time including drug storage planning and dispensing to minimise drug supply disruptions; a hugely impressive feat, considering the scale of the project.
Ellen was also the project lead for the installation of a new pharmacy cloud based temperature monitoring system. The project involved coordinating new system installation of new system, migration from the previous system, troubleshooting, staff training and associated policy updates.
Gráinne Johnston, Mater Misericordiae University Hospital
Throughout her career, Gráinne has consistently demonstrated her passion for hospital pharmacy and her genuine concern for the well-being of patients. Her approach to her work is characterised by a relentless pursuit of excellence and always striving to deliver the highest standard of care to all patients who cross her path. What truly sets Gráinne apart, however, is her deep commitment to advancing healthcare in Ireland and pushing past the current status quo.
One of Gráinne's most remarkable achievements is her pivotal role in the establishment of START, Ireland's first dedicated phase 1 oncology clinical trials unit. This ground-breaking endeavour represents a significant milestone in cancer care in Ireland. Gráinne's vision, leadership, and tireless efforts were instrumental in aiding to bring this project to fruition, demonstrating her leadership, innovative spirit and commitment to driving forward cancer care in Ireland.
Olaitan J Jeremiah, Mater Misericordiae University Hospital
Olaitan joined the Mater Misericordiae University Hospital (MMUH) as a clinical Pharmacist in July 2023, having previously worked as a lecturer and research scientist. Olaitan took up the Pharmacy Education and Training Coordinator role in January 2024 and is a senior member of the MMUH clinical pharmacy team. Olaitan is very passionate about patient care and at ward level, demonstrates compassion and professionalism while providing clinical input on medication use. Her clinical interventions afford patients the best possible treatment outcomes. Olaitan is involved in the training of new clinical pharmacists, helping them to settle into a challenging & expanding clinical environment.
Since taking up the Pharmacy Education role, Olaitan has coordinated several clinical placements in the hospital, involving both pharmacy students and pharmacy technician students.
Professor Brendan Kelly, Trinity College Dublin/Tallaght University Hospital/HSE
Brendan Kelly is Professor of Psychiatry at Trinity College Dublin, Consultant Psychiatrist at Tallaght University Hospital, Dublin, and Visiting Full Professor at the School of Medicine at University College Dublin, Ireland.
Professor Kelly has authored and co-authored over 300 publications in peer-reviewed journals, over 700 non-peer-reviewed publications, 26 book chapters and book contributions, and 20 books (including 13 as sole author).
He also features regularly on radio and in print media, discussing topics relating to mental health, psychiatry, and society.
Brendan’s recent books include ‘Asylum: Inside Grangegorman’ (Royal Irish Academy, 2023), and ‘The Modern Psychiatrist’s Guide to Contemporary Practice: Discussion, Dissent, and Debate in Mental Health Care’ (Routledge, 2024).
Professional 100
Deirdre Kelly, Country Manager, Consilient Health – Ireland and Malta/Vice-Chair, Medicines for Ireland
In 2024, Deirdre and the team at Medicines for Ireland published its new five-year vision Looking forward: Building the framework for a sustainable generic, biosimilar and value-added medicines industry in Ireland. The vision sets out MFI’s approach to address current and emerging market challenges, including demographic shifts, access to medicines, and inflationary pressures.
Established in 2016, MFI is the leading voice for the generic, biosimilar, and value-added medicines industry with its members supplying the majority of medicines to the HSE and patients directly. Generic companies play an essential role in the supply of prescription medicines in Ireland, with eight of the top 10 companies in the total prescription market (based on volume of units) supplying generic medicines.
Deirdre joined Consilient Health in 2014 to set up the Irish business unit. Since then, Deirdre and the Irish team have successfully launched a range of medicines across CH’s key therapeutic areas in both the secondary and primary care settings with new launches in Malta from 2021.
Prior to joining Consilient Health, Deirdre spent 13 years at Eli Lilly, most recently as business unit manager responsible for the Osteoporosis, Cardiology, Oncology and Primary Care product portfolios. At Novo Nordisk, she was the lead marketer for growth hormone in the UK & Ireland territories. Deirdre started her career at Nutricia where she held a number of management positions.
Deirdre has a BSc (Hons) in Nutrition & Dietetics from Trinity College, Dublin with post graduate qualifications in marketing, health economics and a Diploma from the Institute Of Directors. Deirdre is also a board member of Medicines For Ireland trade association, Irish Medicines Verification Organisation and is completing her term as President of the Irish Pharmaceutical Managers Institute (2022 / 2023).
Professor Helena Kelly, Head of the School of Pharmacy, RCSI
Professor Kelly was appointed earlier this year and succeeds Professor Tracy Robson, who was recently appointed Deputy Vice-Chancellor for Academic Affairs at the university. She will lead the School of Pharmacy and Biomolecular Sciences in its ambition to be recognised internationally as a leading centre for pharmacy education, research and innovation.
A registered pharmacist, Professor Kelly undertook her PhD in the area of stimuliresponsive hydrogels and sustained drug delivery. She spent eight years in the pharmaceutical and biopharmaceutical industry before returning to academia in 2008. In March 2022 she was appointed as Deputy Head (Programmes Innovation) in the School of Pharmacy and Biomolecular Sciences with responsibility for the implementation of two new programmes, an MSc in Technologies and Analytics in Precision Medicine and a BSc in Advanced Therapeutic Technologies.
Professor Kelly’s research focuses on the use of delivery platforms in translational research applications.
Ronan Kelly, University Hospital Galway
Mr Ronan Kelly is a Cardiothoracic Surgeon in University Hospital Galway. Mr. Kelly is the part of minimally invasive cardiac surgery team who have successfully completed 100 minimally invasive cardiac surgeries, making University Hospital Galway the pioneers in minimally invasive cardiac surgeries in the country and the only public sector hospital in the country to perform such procedures. Mr. Kelly and the team are doing minimal invasive aortic valve replacement and mitral valve repair and replacement successfully in University Hospital Galway. Minimally invasive cardiac procedures prevents cutting the sternum, which causes post operative pain and is prone to wound infections in cardiac surgery patients. Patients are discharged home early and return to their daily activities sooner compare to the conventional cardiac surgery patients. Mr. Kelly is also an experienced minimally invasive thoracic surgeon.
Professor Steve Kerrigan, Cardiovascular Infection Research Group/Royal College of Surgeons in Ireland
Founded by Professor Steve Kerrigan, his RCSI spin-out Inthelia Therapeutics was awarded the 2024 Innovation Award at the Future Health Summit. The award recognises Professor Kerrigan’s contribution as a founder of Inthelia Therapeutics, an RCSI spin-out clinical-stage pharmaceutical company that aims to develop personalised therapeutic approaches to treat patients with sepsis. Sepsis is the leading cause of death worldwide, causing over 11 million deaths globally per year.
Since his faculty appointment, he has published over 90 articles in leading peer-reviewed international journals and filed 11 patent/disclosures and supervised 22 doctoral candidates to completion as primary supervisor. He has a current h-index of 36 (almost 6,000 citations). Prof. Kerrigan's work has won awards such as Research: Science Foundation Ireland Commercialization Award (2023); Innovation: International Future Health Summit Innovation Award (2024); Education: The Council for Advancement and Support of Education Europe Region Award (2024).
Mariosa is the Clinical Pharmacy Service Manager at MMUH, and together with the team, was shortlisted for the 2024 Athlone Pharmaceuticals Hospital Pharmacy Team of the Year.
The Mater Misericordiae University Hospital (MMUH) pharmacy team is a dynamic, ambitious and supportive team who strive to deliver the hospital’s mission to care for the sick with compassion and professionalism at all times, respect the dignity of human life, and to promote excellence, quality and accountability through their activities. The MMUH Pharmacy delivers a number of critical clinical services to hospital patients including dispensary, clinical pharmacy, aseptic compounding, medicines information, infectious diseases, antimicrobial stewardship, heart lung transplantation, pulmonary hypertension and drug safety services.
The large pharmacy team support each other to perform to the highest standards while ensuring staff are ongoing development and motivation in all aspects of their role. This is achieved from their first day of service in the MMUH Pharmacy with the dedicated onboarding process that includes an assigned mentors and dedicated training programmes for all new staff.
Anna Marie Kiernan, Pain Management Centre, Croom Orthopaedic Hospital
As an Advanced Nurse Practitioner (ANP) in pain medicine, Anna Marie has integrated clinical expertise with a passion for innovation to advance patient care. This combination has allowed her to become a role model and ambassador for peers, fostering collaboration and inspiring change within the healthcare system through cutting-edge approaches and continuous professional development.
She strives to exemplify leadership in vision, strategy, innovation, collaboration and patient-centred care. By modelling these qualities in everyday life, she aims to lead with purpose with a focus on delivering sustainable, measurable outcomes. Through her collaboration and leadership at the intersection of healthcare and innovation she works towards a vision of a better future for healthcare and also actively drives the transformation necessary to achieve it.
Marios Kieran, Mater Misericordiae University Hospital
Professional 100
Professor Mary McCarron, Trinity College Dublin
Professor McCarron has won an HRCI Research Impact Award this year. Professor McCarron was presented with the award for her work on transforming dementia care for people with intellectual disabilities.
The award recognised Professor McCarron’s research - co-funded by The Alzheimer Society of Ireland and the Health Research Board (HRB) - that has reshaped care practices and policy for the many people with intellectual disabilities who live with dementia and improving care for this often neglected group.
People with intellectual disability have an extremely high risk of developing dementia and may also develop dementia earlier and experience significant impacts on their independence from relatively small changes. Despite this they have been largely over-looked.
Ireland
Until April of 2024, Mairead McCaul was Managing Director of MSD Ireland (Human Health) before taking up her new position as Managing Director of MSD Animal Health Benelux. She is also Head of the MSD Ireland Country Leadership Team which includes representatives from MSD’s six sites in Ireland and key business areas.
Prior to her appointment to her current role, Mairead was Business Unit Director, Oncology and Market Access, MSD Ireland (Human Health) and has a wealth of experience in senior roles across Sales Management, Marketing and Commercial Operations since joining MSD Ireland in 2007.
Earlier in 2024, Mairead was part of the Pharmaceutical Forum 2024 Panel at the Guaranteed Irish Pharmaceutical Forum. During this event, insights were shared around the theme of "Innovation in the Community – Positioning Ireland to Deliver Best Patient Care". The importance of data being at the centre for digital healthcare improvements was discussed. Progress in digital data technology will allow more innovation and access for patients to make informed choices with healthcare professionals.
She is a passionate advocate of diversity and inclusion and has led many programmes of activities to support this area, previously co-leading the MSD Women’s Network in Europe and most recently acting as an ambassador for MSD’s 2021 Neighbour of Choice partnership with Teen-Turn.
Prior to joining MSD, Mairead worked for eight years within the laboratory diagnostics sector. She qualified in nursing and midwifery and holds a BA (Hons) in Business Management from Dublin Business School. Mairead is an active member of a number of working groups within the Irish Pharmaceutical Healthcare Association and was recently appointed to the Board of Guaranteed Irish.
Therese McGlacken, HSE
Therese is an exceptional healthcare professional whose work exemplifies inspirational leadership and advocacy. With a career spanning public health medicine and general practice, she has significantly enhanced services for underserved populations, particularly women and marginalised groups.
Her commitment to addressing health inequities and driving systemic improvements is evident in her leadership of transformative initiatives, such as the evaluation and enhancement of the HSE Women’s Health Service (WHS) and the Anti-Human Trafficking Team. These efforts have expanded healthcare access for vulnerable women while highlighting the importance of culturally sensitive and trauma-informed care. Additionally, Therese conducted a qualitative review with sex workers, providing insights that informed clinical and social care delivery and set a standard for multidisciplinary healthcare approaches.
Through her advocacy and policy development, Therese has become a campaigner for women’s rights in underserved communities. Her lead developing the National Health Improvement Strategic and Operational Plan (2024–2025), focused on health inequalities, demonstrates her strategic vision and leadership. Her contributions to the National Screening Service and CervicalCheck include research on cervical screening self-sampling and evaluation projects, ensuring Ireland’s services remain evidence-based.
Therese has recently commenced work as a forensic medical examiner for the Sexual Assault and Treatment Unit (SATU) in the West of Ireland, which provides specialised care in sexual assault cases, further expanding her impact on public health and the protection of vulnerable individuals.
Jason McGrath, Royal College of Surgeons in Ireland
A second-year postdoctoral researcher, Jason was shortlisted as a Finalist for the 2024 MSD Excellence in Oncology Honour at the Hospital Professional Honours. He is deeply committed to understanding the complexities of breast cancer brain metastases (BCBM) and exploring new ways to improve outcomes for patients with this devastating condition.
His work is focused on deciphering how breast cancer cells metastasize to the brain, why they colonize specific areas, and how switching hormonal receptor statuses, such as estrogen receptor (ER) activation or deactivation might create opportunities for new treatments.
His research investigates the therapeutic potential of PARP inhibitors (PARPi), particularly in triple-negative breast cancer (TNBC) cases, which lack targeted therapies.
Mairead McCaul, Managing Director, MSD
Olivia McLoughlin, Cancer Trials Ireland
Olivia McLoughlin’s dedication and leadership in clinical trials make a significant impact on the work of Cancer Trials Ireland. Her recent appointment as Head of Start-Up marks a new challenge in her career, which spans nearly two decades with the organisation and a total of 30 years in clinical research. In her new role, Olivia is spearheading efforts to streamline trial activation processes, a critical area in improving access to cutting-edge treatments for patients across Ireland.
The establishment of a dedicated Start-Up Team with Olivia as the head, is a strategic initiative designed to reduce the time to first patient (TTFP) and ensure trials are activated swiftly and effectively. The work of this new team will focus on the initial stages of clinical trials, from site selection and ethics submissions to contract negotiation and regulatory approvals. These early stages are often the most resource-intensive, and Olivia’s leadership is essential in identifying and addressing bottlenecks to accelerate timelines.
Dr Rosa McNamara, St Vincent’s University Hospital
Dr Rosa McNamara has been appointed as HSE’s Clinical Lead for the National Clinical Programme (NCP) for Emergency Medicine.
Dr McNamara is a consultant in emergency medicine, working with the St Vincent’s University Hospital. She is Associate Clinical Professor at University College Dublin and Chair of the Geriatric Emergency Medicine Special Interest Group at the International Federation for Emergency Medicine.
The National Clinical Programme for Emergency Medicine is within the portfolio of NCPs that are under the governance of Dr Mike O’Connor, the HSE’s National Clinical Advisor and Group Lead for Acutes (NCAGL Acutes).
Caroline Monahan, Tallaght University Hospital
Caroline won the Medisource Hospital Pharmacy Technician of the Year Honour for 2024.
Caroline Monahan is a hard-working, reliable and enthusiastic team player who strives for excellence in all her endeavours. As a Senior Pharmaceutical Technician and Medicine Management Technician Supervisor, Caroline has spent the last 20 years championing the expanding role of the hospital technician and has demonstrated exceptional leadership in rolling out innovative technician services in Tallaght University Hospital (TUH).
Professional 100
Dr Carla Moran, Beacon Hospital/St Vincent’s University Hospital/University College Dublin
Dr Moran is an exceptional leader in the field of thyroid disease, whose pioneering work, clinical expertise, and significant contributions to research have had a lasting impact both in Ireland and internationally. Dr Moran completed her Thyroid Fellowship and PhD at the University of Cambridge in 2014, where she developed a deep and broad understanding of thyroid physiology and disease. This world-class training provided her with the foundation to become a leader in the field. Following her fellowship, Dr Moran led the Thyroid Service at Addenbrooke’s Hospital in Cambridge and served as the co-director of a National Rare Thyroid Disease Service in the UK for five years. Dr Moran's contributions extend well beyond clinical practice. She was awarded the Van Meter Award from the Am erican Thyroid Association in 2024, one of the most prestigious recognitions in endocrinology, making her the first person from Ireland to receive this honour.
Dr Tanya Mulcahy, Director of Health Innovation Hub Ireland
Dr Mulcahy is the Director of Health Innovation Hub Ireland (HIHI). In this role she is responsible for leading HIHI. Just last month she was selected as an expert advisor for the World Health Organisation technicial Advisory Group on Public Health Innovation.
Her key priority is to ensure that the objectives of HIHI; supporting companies as they navigate the healthcare system, supporting healthcare innovators to assess and develop their ideas and delivering education programmes to encourage innovation; are achieved across all partner sites of HIHI.
Eibhlin Mulroe, Cancer Trials Ireland
Under Eibhlin’s leadership, Cancer Trials Ireland has seen considerable growth, with the organisation’s staff doubling in size. A notable achievement during her tenure has been the establishment of the new biometrics division, enhancing the efficiency and quality of clinical trials in Ireland.
Earlier this year, Eibhlin led the publication of a report on the challenges posed by GDPR regulations for clinical trials, which affect every hospital in Ireland. Her advocacy on this issue highlighted the need for regulatory changes and prompted discussions with government and regulators, aiming for improvements that would benefit both patients and researchers.
Eibhlin has also worked hard to raise the profile of clinical trials within the political sphere. In the run up to the 2024 General Election, she organised a hustings event to question political representatives on their support for clinical trials and has continually worked to ensure that clinical research remains a priority in public policy. Through her efforts, she has demonstrated how effective advocacy can lead to positive change in the healthcare system.
Professor Jarushka Naidoo, Beaumont Hospital, Dublin
Professor Naidoo is a Thoracic Oncologist at the Beaumont Hospital Dublin (Ireland), Professor in RCSI and Adjunct Professor of Oncology at Johns Hopkins University. She currently serves as national lung cancer lead for Cancer Trials Ireland.
She serves on several international guideline panels including ASCO and SITC (Society of Immunotherapy for Cancer), and is an experienced clinical trialist- having developed and completed several investigator-initiated, industry-funded and cooperative group clinical trials.
She has received a number of grants including a young investigator award from the International Association for the Study of Lung Cancer (IASLC), Lung Cancer Foundation of America (LCFA), and a career development award from the National Institutes of Health (NIH) KL2-program. She is the IASLC Communications Committee Chair.
Sadhbh Ni Cheallaigh, Beaumont Hospital
Paul Neill, Country Manager, Teva/Chairperson, Medicines for Ireland
Medicines for Ireland is the leading representative body for the generic, biosimilar, and value-added medicines industry. Paul and the team at MFI recently highlighted the urgent need for action to address the increasing medicine shortages affecting the Irish population. He has identified a multifaceted approach to address these shortages including implementing dynamic pricing policies that encourage competition and evolving the best-value biologics process.
Under Paul’s leadership, Medicines for Ireland co-hosted the European annual conference in Dublin this year, which marked saw the organisation marking 30 years of delivering more equitable access to off-patent medicines. Paul is the Country Manager for Teva Pharmaceuticals Ireland, the largest supplier of prescription medicines to the State. Paul brings with him a wealth of practical experience gained from almost twenty years in various commercial roles in the Pharmaceutical Market – ten of these in leadership roles in Teva.
Sadhbh is a Senior Pharmacist at Beaumont Hospital and alongside her team, won the 2024 Viatris Excellence in Cardiovascular Initiative.
Beaumont Hospital’s Cardiology Department provides cardiac patients with the most comprehensive Cardiac Rehabilitation (CR) programme in Ireland. As well as delivering the largest annual throughput of patients, the department is internationally recognised as a centre of excellence for CR. Beaumont Hospital is the first and only CR centre in Ireland and the UK to achieve international accreditation in CR and secondary prevention.
Patients are provided with an exceptionally high concentration of multi-disciplinary expertise overseen by an actively involved Medical Director (Consultant Cardiologist), and each member of the multi-disciplinary team (MDT) has recognised expertise in their respective field. This seamless CR service benefits from close cooperation and communication between MDT members, allowing patients to achieve optimal health.
Professional 100
Ciara Ni Dhubhlaing, St Patrick’s University Hospital
Ciara is a Chief Pharmacist at St Patrick’s Mental Health Services. A newly announced strategic partnership between the School of Pharmacy at University College Cork (UCC) and the Pharmacy Department at St Patrick’s Mental Health Services (SPMHS) based in Dublin will see the two organisations come together over the coming five years to advance research and clinical training in mental health pharmacy.
Ciara and her team were also shortlisted as a Finalist for the MedFind Innovation and Service Development Honour 2024.
St. Patrick’s Mental Health Services (SPMHS) is the largest independent provider of acute mental health services in Ireland. The relatively small team of 20 staff including pharmacists, technicians and support staff provides pharmacy services to inpatients, homecare patients, and outpatients. The team works together to deliver high quality, effective, patient-centred care; and to ensure the safe and appropriate use of medication to support our service users (SUs) in their recovery.
There was a change in practice in SPMHS whereby the day on which SUs were admitted for planned maintenance Electroconvulsive Therapy (mECT) changed from a Tuesday to a Monday. SUs were now being admitted on a Sunday when the SPMHS pharmacy is closed. This meant that a supply of medication was not readily available and there was potential for a patient safety risk due to missed doses of medication.
Pharmacy Technicians identified this potential risk and looked at how best to supply medication to ensure it was available on the ward for SU’s admitted for mECT on a Sunday. The mECT medication supply project has had a positive impact in reducing errors of omission measured as reducing from 0.9 omissions per SU to 0.2 omissions per SU over the same time period before and after implementation.
Kathy Nugent, University Hospital Limerick
Kathy and her team won the 2024 Excellence in Oncology Honour at the Hospital Professional Honours. Breast cancer Related Lymphoedema (BCLR) is a well-known side effect of breast cancer treatments including surgery, chemotherapy, radiation therapy and endocrine therapies. Damage or overload to the lymphatics predisposes high-risk cohorts to the development of arm lymphoedema.
The aim of this project is “to introduce a lymphoedema early detection service in UHL oncology unit for all breast and gynae patients who have had surgery and/or radiation to reduce the incidence and impact of lymphoedema in Ireland. The findings from the pilot will be used to support future funding for similar services in all oncology centres.”
Grainne O’Brien, Mater Misericordiae University Hospital
Grainne started working in hospital pharmacy services in the Mater Misericordiae University Hospital in 2023 after 9 years in community pharmacy. Utilising her previous professional achievements and exceptional work ethic, Grainne quickly embedded into MMUH clinical pharmacy services provision including service leadership, education and training.
In addition to this, Grainne took up post as Deputy Clinical Pharmacy Service Manager in September 2024, where she has been further supporting staff within the Clinical Pharmacy team. Tasks undertaken include rostering, managing performance of the clinical daily audit, assisting in general clinical pharmacy service management and training and education of new staff members.
Joanne O’Brien, Beaumont Hospital
Joanne is an Advanced Nurse Practitioner in Pain Management at Beaumont Hospital. She is past president of the Irish Pain Society and past Irish Councillor to the European Pain Federation, EFIC, successfully bidding for Ireland to host the European Pain Congress in 2022 for the first time. In 2023 the Pain Team in Beaumont secured Slaintecare funding to develop an Integrated Community Based Pain Service, the first of its kind in Ireland, with a specific focus on developing pathways for the assessment and management of low back pain, radicular pain and fibromyalgia. Joanne, together with her colleagues David Moore (Pain Medicine), Roisin Ormond (Physiotherapy), Komal Hamid (Psychology) and Tanya Clarke (Administration) were delighted to be awarded the Grunenthal ‘Advancing the Standard of Care in Pain Management’ Honour at the 2024 Hospital Professional Honours for developing the iPainCentre and reaching out into the community to reform the way chronic pain is being managed.
Louise O’Brien, St James’s Hospital
Louise was a Finalist this year for the Pharmasource Hospital Pharmacist of the Year Honour.
Louise is the Senior Cardiothoracic Pharmacist in St. James’s Hospital, where they carry out over 300 cardiac operations a year and over 500 thoracic surgeries, primarily for lung cancer.
Louise is involved in the care of the patient throughout their journey, she reviews their medications in the Pre Assessment Clinic, ensures appropriate medications are stopped, then during their hospital stay she continues to communicate with the patients and explains medications they are prescribed.
In the HSE, James has been a leading ambassador for healthy places for people to grow, live, work and age. Through his work, James has been a role model for how we in the health service can work with all sectors of society to help create healthy places. As a Specialist Registrar in Public Health Medicine, his practice, advocacy work, research and contributions to service development in the HSE can demonstrate this.
As an advocate, James has worked hard to develop a compelling argument for healthy places that emphasised their important in supporting a healthy population to ensure our ageing society and economy are sustainable in an uncertain future. James successfully communicated this on the radio, in the local print media (making front page news on the Galway City Tribune), online, at local authority meetings, at national and international scientific conferences and in a dedicated webinar he organised for professionals working across the public sector.
Professor P. Ronan O’Connell, St Vincent’s University Hospital
Former President of RCSI Professor O’Connell has been made an Honorary Fellow of the American College of Surgeons in recognition of the significant contribution he has made to the practice of surgery throughout his career.
Professor P. Ronan O’ Connell is Emeritus Professor of Surgery UCD and Consultant Surgeon at St Vincent’s University Hospital. An international leader in the field of colorectal surgery, Professor O’Connell was President of RCSI from 2020 to 2022. He has also served as President of the European Surgical Association.
Professor O’Connell was RCSI President during the COVID-19 pandemic. His leadership ensured that the College continued to deliver excellence in surgical training throughout the lockdowns and that it supported surgeons in practice who endeavored to continue to provide surgical care in incredibly challenging circumstances.
James O’Connell, HSE
Professional 100
Dr Cathal O’Connor, Fellow, Great Ormond Street Hospital for Sick Children/Cork University Hospital
Dr O’Connor has been chosen as a ‘Future Leader’ of both the European Society of Dermatological Research and the European Society of Paediatric Dermatology. This year Cathal won the RCPI William Stokes award and the British Association of Paediatric and Adolescent Dermatology award for his research into sleep and early neurodevelopmental outcomes in atopic dermatitis (eczema). He also won the prestigious Royal Academy of Medicine in Ireland (RAMI) research award for his publication on early emollient bathing and atopic dermatitis outcomes.
He is recipient of the 2024 International Fellowship Award from the Irish Association of Dermatology and the 2024 Ainsworth scholarship from University College Cork. Cathal is the programme lead for the RCPI’s postgraduate diploma in dermatology, delivering teaching to doctors, nurses, and other healthcare workers all over the world.
Fiona O’Connor, Mater Misericordiae University Hospital
Fiona commenced the role of Medicines Information (MI) Service Manager in August 2024 after working as a senior MI pharmacist for over 3 years. Fiona works diligently to consistently deliver a high-quality MI service in the Mater Misericordiae University Hospital (MMUH).
Fiona is currently a member of the pharmacy team developing & implementing a MMUH Medication app.
Fiona’s research project titled ‘Clinical audit to evaluate Intravenous Iron Therapy in MMUH’, conducted as part of a MSc in Advanced Clinical Pharmacy Practice, was highly commended among her peers. Through the provision of a new guideline on the management of Iron Deficiency Anaemia and a multifaceted education drive, Fiona significantly improved the appropriate use of IV iron, and showed a potential annual cost saving of over ¤194,000 by avoiding the inappropriate use of IV iron.
Professor Tom O’Connor, Royal College of Surgeons Ireland
Professor O’Connor has been appointed President Elect of the European Pressure Ulcer Advisory Panel (EPUAP) for 2025. Professor O’Connor will be the Panel’s President in 2026.
Professor O’Connor is a Lead Researcher in the Skin Wounds and Trauma (SWaT) Research Centre, based at RCSI’s School of Nursing and Midwifery. He is widely published in the field of skin wounds and trauma and has recently focused on early indicators of pressure and diabetic foot ulcers, evaluation of pressure ulcer prevention education programmes and physiological differences in response to injury depending on skin tone.
The EPUAP provides a platform for clinicians, researchers, educators, policy makers, industry and the public to collaboratively work on improved health outcomes for those at risk or suffering from pressure ulcers.
Cillian O’Donovan, Tallaght University Hospital
Cillian has been a valued member of the Tallaght University Hospital (TUH) pharmacy team since completing his pre-registration training there in 2019. In his current role, Cillian works as a senior pharmacist in the discipline of pharmacy informatics. Currently, Cillian is an active member of the hospital’s electronic patient record (EPR) clinical advisory group and project steering group; whereby he represents the pharmacy department’s viewpoint on any ongoing and upcoming EPR developments.
As part of this role, Cillian has been responsible for working closely with the EPR Programme Manager, the Chief Clinical Information Officer and the EPR vendor to develop safer and more efficient medication management functionality on the EPR platform at transitions of care, including electronic transmission of discharge summaries to the patient’s primary care provider.
Professor Caitriona O’Driscoll, Chair of Pharmaceutics in the School of Pharmacy, and Director of UCC Futures - Future Medicines
In May of this year, Professor O’Driscoll was elected as a member of the prestigious Royal Irish Academy (RIA). She was among 28 new members admitted Friday 24 May 2024 for their exceptional contributions to the sciences, humanities, and social science, as well as to public service.
Recognised globally for her research in non-viral delivery of RNA therapeutics, Professor O'Driscoll has helped build an internationally recognised team in the field of RNA medicines within the School of Pharmacy. Her work focuses on developing innovative drug delivery systems to improve the effectiveness and safety of RNA-based therapies.
Dr Patrick O’Dwyer (UCC), St James’s Hospital
Dr O’Dwyer and colleagues at University College Cork School of Pharmacy have recently won a grant to accelerate medicine delivery to developing countries. Access to life-saving medicines in developing countries is often fraught with obstacles. For major pharmaceutical companies, the financial incentive to develop treatments for smaller, under-served populations simply isn’t there. Local manufacturers, meanwhile, often grapple with a lack of technical expertise and resources needed to navigate the rigorous process of bringing a drug to market. The challenges are compounded by inadequate infrastructure and harsh climatic conditions, making the path to accessible medicines even steeper.
Addressing this issue, a team from University College Cork’s School of Pharmacy - led by Professor Brendan Griffin, Dr Patrick O’Dwyer, and Dr Harriet Bennett-Lenane - is driving forward the "Advancing Global Health Drug Formulation Development Using ML and AI" project.
Dr O'Dwyer completed his PhD at the National and Kapodistrian University of Athens, supervised by Prof. Christos Reppas. His PhD was part of the PEARRL project, a European Training Network funded under the EU Horizon 2020 research and innovation programme.
Professional 100
Dr Catherine O’Gorman, St James’s Hospital Dublin
Dr O’Gorman and her team were behind the launch of the My Gynaecology Patient Passport’ project which will see patients of St James’s Hospital be given the document, which they can carry throughout their cancer journey.
The passport, which is filled in collaboratively by patients and their clinicians at the Trinity St James’s Cancer Institute, will include important information and visual aids related to the patient’s diagnosis and care plan, and will provide helpful resources to support patients both before and after treatment.
The passport will be provided to patients being treated for ovarian, uterine, cervical, vaginal and vulval cancers during their first visit with the St James’s Hospital gynaecology team.
Professor Grainne O’Kane, St Vincent’s University Hospital
Professor O’Kane has been appointed as the Pat Smullen Chair in pancreatic Cancer at University College Dublin. The new position will anchor expertise in pancreatic research in Ireland, with the ambition of creating a global centre of excellence for the treatment and research of this form of cancer, which has one of the poorest outcomes.
The role will allow Professor O’Kane to divide her time between clinical work as a treating physician at St Vincent’s University Hospital (the national surgical centre for pancreatic cancer) and research work at UCD School of Medicine, where she will work to identify, attract, and open new pancreatic cancer trials, train the next generation of specialists in pancreatic cancer, and work to integrate care for pancreatic patients on the island of Ireland.
Donagh O’Leary, Clonmel Healthcare
Donagh O’Leary is the Managing Director of Clonmel Healthcare who, earlier this year, announced the completion of the construction of a brand new ¤3 million euro warehouse facility in Clonmel. The 1650 square metre build, comes after a previous extension of 1,800 square metre in 2017, and will see the increase in production potential of STADA AG pharmaceutical products through this additional distribution capacity for specialised medical products supplied to pharmacists and medical professionals across Ireland.
Further, as a participating member of Medicines for Ireland (MFI), Donagh recently had the pleasure to meet with MEP Barry Andrews in conjunction with Paul Neill, Chairperson of MFI and Eimear O’Leary, Director of Communications and Advocacy at the Irish Pharmaceutical Healthcare Association (IPHA). The meeting was held at the new European Parliament office in Dublin where they discussed the Urban Wastewater Treatment Directive (UWWTD), the impact on the pharmaceutical sector and what we believe to be the potential negative implications the Directive will have if introduced in Ireland for the industry.
Professor Seamus O’Reilly, Cancer Trials Ireland
Professor O’Reilly has demonstrated exceptional leadership and dedication since taking over as Clinical Lead at Cancer Trials Ireland in January this year. In 2024 Cancer Trials Ireland has seen a steady increase in trial activations and patient accruals, even in the face of challenging conditions, and there are currently 25 new trials in development for 2025 across various cancer types, including breast, gynaecological, and genitourinary cancers.
Professor O’Reilly has also been a key advocate for improving the broader infrastructure surrounding clinical trials in Ireland. His leadership in engaging with the National Clinical Trials Oversight Group and addressing challenges such as GDPR compliance demonstrates his ability to tackle systemic barriers and promote sustainable growth in cancer research.
Beyond his work with Cancer Trials Ireland, Professor O’Reilly is a respected consultant medical oncologist at Cork University Hospital, Cork-Mercy and South Infirmary Victoria University Hospitals. He brings a wealth of experience from his training at Johns Hopkins Hospital, where he also served as Assistant Professor and completed a PhD in Clinical Investigation with a focus on cancer pharmacology.
Emer O’Sullivan, Bantry General Hospital
Emer won the 2024 Haematology Project of the Year Honour. Local rates of hospital acquired VTE had exceeded the national rates. National HA-VTE rates were approximately 8 per 1000 while local HA-VTE rates are at an average of 32.2 per 1000 for 2022. The hospital group introduced VTE risk assessments on the medication charts but this failed to reduce rates. Emer and Carol Walsh undertook a Postgraduate Certificate in Quality Improvement Leadership in Healthcare in the RCPI with the goal of using the skills gained during the course to find a solution to this problem and improve care for patients attending Bantry General Hospital. The overall aim of the project was to reduce the rate of HA-VTE to zero for patients admitted to Bantry General Hospital.
Sharon O’Toole, St James’s Cancer Institute/Trinity College Dublin
Sharon co-ordinates the Irish Network for Gynaecological Oncology (INGO) which comprises over 30 of Ireland’s foremost gynaecological cancer campaigners, researchers and patient advocates. It is a voluntary network dedicated to raising awareness of gynaecological cancers across the Island of Ireland. With external sponsors and public relations firm, The Reputations Agency, INGO have been giving ovarian cancer a voice in Ireland on World Ovarian Cancer Day, May 8th.
Sharon and her team developed an All-Ireland media relations approach to the campaign ensuring all key media correspondents were briefed on the campaign, experts and case studies, and all campaign materials were syndicated, and interviews were pitched and generated with all key outlets. On behalf of the INGO, Sharon accepted the Patient Organisation Project of the Year from the Irish Healthcare Awards this month.
Professional 100
Professor Eamonn Rogers, Saolta University Health Care Group
Professor Rogers has been appointed co-lead of the National Clinical Programme for Surgery (NCPS) IN 2024.
Professor Rogers is a Consultant Urologist working with the Saolta University Health Care Group and Chairman of the Patient Office of the European Association of Urology. He served as National Clinical Advisor for Urology for the NCPS for the past nine years, leading the development and publication of a model of care for the specialty. The aim of the National Clinical Programme for Surgery is to provide a framework for the delivery of safer, timely, accessible, more cost-effective and efficient care for all surgical patients.
Marie Ronan, Mayo University Hospital
Marie has over 15 years of experience in hospital pharmacy and currently serves as a Senior Antimicrobial Stewardship (AMS) Pharmacist at Mayo University Hospital. Marie, alongside her colleague Rose Cafferkey, recently received the HPN Excellence in Patient Safety Honour for their work on penicillin allergy de-labelling. In 2019, she was honoured at the HPN Awards with the GSK Infectious Disease Project of the Year for her work on CPE and was a key member of the Consultant-Led Hospital Team of the Year.
A frequent presenter at conferences, Marie has won numerous awards for her research posters. A dedicated advocate for innovation and continuous improvement, she has earned two master’s degrees: an MSc in Clinical Pharmacy (self-funded) and an MSc in Digital Health Transformation (fully funded by the HSE during COVID), graduating with First-Class Honours from the University of Limerick.
Shane Ryan, General Manager, Takeda Ireland/ President, IPHA
With over 25 years in the pharmaceutical industry, Shane Ryan serves as General Manager of Takeda in Ireland. His commitment to excellence and ability to inspire his team have established Takeda Ireland as a leader in the pharmaceutical industry. Under his leadership, Takeda Ireland was recognized as Life Science Company of the Year in 2024.
Shane also plays a pivotal role in the life science industry. Newly appointed President of the Irish Pharmaceutical Healthcare Association (IPHA), Shane is motivated by IPHA’s mission to enhance health outcomes through innovative treatments and advancing the Ireland as a hub for life science innovation. A champion for diversity, Shane is committed to ensuring the sector represents individuals, carers and clinicians that it serves and volunteers his time to lead initiatives which drive this goal.
Professor Laura Sahm, University College Cork
Professor Sahm was at the forefront of a newly announced strategic partnership between the School of Pharmacy at University College Cork (UCC) and the Pharmacy Department at St Patrick’s Mental Health Services (SPMHS) based in Dublin will see the two organisations come together over the coming five years to advance research and clinical training in mental health pharmacy. Through a wide range of collaborative activities, the partnership aims to foster innovation and enhance collegiality, or cooperation. Facilitating clinical teaching for pharmacy students at UCC and advancing evidence-based research into mental health difficulties are central to the partnership, with the goal of improving service user outcomes and informing best practices in mental healthcare.
In August 2023, Professor Sahm was appointed as Professor of Clinical Pharmacy and Head of Clinical Pharmacy Practice.
Mr Sadiq Siddiqui, University Hospital Galway
Mr Siddiqui is the first in the country to start minimally invasive vessel harvesting program in a public sector hospital. Starting this program with endoscopic vein harvesting for coronary artery bypass surgeries in 2017, Mr Siddiqui started endoscopic radial artery harvesting in 2022. To date, Mr. Siddiqui has successfully completed 700 such cases (both veins and radial arteries) making it one of the biggest numbers in Europe and making University Hospital Galway the only public sector hospital in the country to do so.
Mr Siddiqui has published his work in renowned Cardiothoracic journals and is a frequent international faculty in European countries for endoscopic vessel harvesting. This year, he received HSE excellence award in Innovation in Service Delivery.
Dr Virginia Silvari, Cork University Hospital
Dr Silvari led her team to being shortlisted for the Haematology Project of the Year at the 2024 Hospital Professional Honours.
The aim of this project was to determine patients discharged with extended VTE prophylaxis post major abdominal surgery for a gynaecological malignancy in CUMH: (1) Are eligible for a DOAC post-discharge for VTE prophylaxis and receive counselling from a clinical pharmacist (2) Apixaban efficacy (postoperative VTE events) and safety (postoperative major bleeding) compared to tinzaparin. (3) Patient adherence and satisfaction to apixaban. A recent guideline was developed for Postoperative VTE Prophylaxis for Gynaecologic Oncology Patients post Major Abdominal Surgery at Cork University Maternity Hospital. This was an important tool in managing this risk safely and appropriately for these patients.
Dr Silvari is Hospital Pharmacist working in Cork University Hospital, where she delivers specialised advanced pharmaceutical care to patients with cardiovascular diseases. She is an adjunct lecturer at University College Cork and clinical lecturer in Trinity College Dublin. She sits on the Scientific Committee of the European Association of Hospital Pharmacists (EAHP).
Professional 100
Professor Alan Soo, University Hospital Galway
Professor Alan Soo is a senior Cardiothoracic Surgeon in University Hospital Galway. Professor Soo introduced a revolutionary non opioid solution for post-operative pain, making University Hospital Galway, the first centre in Ireland to do so. This procedure involves a unique freezing method to temporarily block pain signals from nerves in the affected area, providing an effect that is similar to a local anesthetic, but lasts for several months during the patients recovery period. Prof. Soo has been using this “Cryo Nerve Block Therapy’’ successfully in both his cardiac and thoracic surgery patients with excellent outcomes.
Professor Judith Strawbridge, School of Pharmacy and Biomolecular Sciences at RCSI University of Medicine and Health Sciences, has been appointed to the Expert Taskforce to Support Expansion of the Role of Pharmacy.
Established by Minister for Health Stephen Donnelly, the taskforce will examine how pharmacists in Ireland can be enabled to operate at the top of their licence for the benefit of patients and the wider health service.
Professor Strawbridge was a founding lecturer on the pharmacy degree programme at RCSI and is currently Deputy Head (Education) of the School of Pharmacy and Biomolecular Sciences and Director of the Masters of Pharmacy (MPharm) Programme. She is widely recognised nationally for her scholarly expertise and passion for standards in pharmacy education and practice.
Judith Strawbridge was a founding Lecturer in the School of Pharmacy, and has over 20 years of experience in designing, delivering and evaluating teaching and learning across the healthcare professions. She has experience in clinical pharmacy and a PhD in Pharmacy Education. Previous leadership positions include Programme Director of the BSc in Pharmacy 2011-2014, Associate Vice Dean for Student Affairs from 2008 - 2012, Year Lead for Year 3 of the integrated MPharm Programme 2017-2019. She was the inagural RCSI Lead for Patient and Public Engagement from 2018 - 2023. She is Programme Director of the MPharm Programme and Deputy Head (Education) of the School of Pharmacy and Biomolecular Sciences.
Professor Imran Sulaiman, RCSI Department of Medicine
Professor Imran Sulaiman, Honorary Clinical Associate Professor at RCSI's Department of Medicine, has received a ¤1.87 million Starting Grant from the European Research Council (ERC) for a research project focused on improving the early detection and treatment of lung cancer. This significant funding will enable Professor Sulaiman to explore innovative methods for identifying and diagnosing lung cancer.
Professor Sulaiman’s research aims to address these challenges by taking a multi-omic approach to discover new biomarkers specific to lung cancer.
Professor Judith Strawbridge, School of Pharmacy, RCSI
Professor Desmond Tobin, Charles Institute of Dermatology, University College Dublin
In May of this year Professor Tobin was announced as the new Chair of the Alopecia Society Research Committee.
Professor Tobin was a co-Chair of the Irish Melanoma Forum 12th Annual Scientific Meeting which took place earlier this year. Over the past 25+ years he has researched in basic and applied skin/hair sciences, with a particular focus on the regulation of hair growth in health and disease especially those conditions with an immune-medicated basis, and on the biology of human melanocytes/pigmentation in health and disease.
His lab was the first to identify antibodies to hair follicle-specific antigens in patients with acute alopecia areata and is working to identify targeted (auto)antigens in this common condition.
His lab was the first to establish melanocytes from the human hair follicles in long-term culture.
His lab also identified a ‘self-similarity’ between the POMC peptide system in the human hair follicle pigmentary unit and that of the central stress axis. Specifically, he examined how pigmentation can be regulated by CRF and POMC peptides (incl. beta endorphin), and more recently by bone morphogenetic proteins.
Dr Liam Townsend, St James’s Hospital
Dr Townsend and the PRECISE Study Team at St James’s Hospital were shortlisted in the Hospital Professional Honours 2024 for the GSK ViiV Infectious Diseases Project of the Year.
Healthcare workers (HCWs) are at increased risk of SARS-CoV-2 infection compared to the general population. Accurate estimates of COVID-19 seroprevalence in HCWs and the factors associated with HCW infection were necessary to understand infection transmission and dynamics of immunity within healthcare settings.
As the pandemic progressed, there was an increasing need to understand the durability of immunity within HCWs, especially with the introduction of COVID-19 vaccination and emerging variants of concern. COVID-19 continues to cause ill-health amongst HCWs, and the team here aimed to further explore the ongoing impact this has on HCW workplace attendance, the associated costs of HCW illness, and the mitigating role that vaccination may play. The principles employed in the PRECISE study can also be applied to other infections associated with HCW ill-health, most notably Influenza and Respiratory Syncytial Virus.
Jayne Tuthill, Mater Misericordiae University Hospital
Jayne was the winner of the ‘Young Hospital Pharmacist of the Year’ Honour at the 2024 Hospital Professional Honours. Jayne has worked in the MMUH since 2018 and has gained extensive experience across pharmacy services, with a strong clinical background and patient-centered focus. Jayne worked in a Chief II pharmacist post leading on multiple information technology projects for the organisation including a CATO upgrade, NCIS implementation and the introduction of a Drug Information App from January – September 2024. Currently, Jayne is the Acting MMUH Drug Safety Facilitator.
Professional 100
Dr Damir Vareslija
Dr Vareslija is the Co-Director of a new programme announced this year which will aim to improve survival rates and quality of life for patients with this challenging form of breast cancer. In Ireland, more than 3,000 new cases of breast cancer are diagnosed each year, many of which progress to metastatic disease, a form that is difficult to treat. PRISM brings together a team of researchers and experts to introduce the first national longitudinal multi-omic study for advanced breast cancer patients, using comprehensive genomic profiling to better understand and target the mechanisms of breast cancer spread (metastasis) and consequently, develop new, effective treatments.
Dr Vareslija is a Principal Investigator and Senior Lecturer in the School of Pharmacy and Biomolecular Sciences. The main themes central to his research are (i) understanding aberrant transcriptional regulation as a mechanism of breast cancer metastases; (ii) defining epigenetic reprogramming as a key regulator of drug resistance leading to disease progression and (iii) developing new models and tools to better study the physiology of metastatic disease.
Darren Walsh, University Hospital Waterford
Darren’s innovative role in the Geriatric Oncology Assessment and Liaison (GOAL) clinic in University Hospital Waterford, led by Dr Anne Horgan, has been recognised nationally when he was named the Pharmasource Hospital Pharmacist of the Year at the Hospital Professional Honours this year. His research activity on his role as a member of the GOAL MDT, being conducted as part of his PhD with the School of Pharmacy in University College Cork under the supervision of Professor Laura Sahm, Dr Michelle O’Driscoll and Dr Anne Horgan has been recognised internationally. He was named the International Society of Geriatric Oncology (SIOG) Nursing and Allied Healthcare investigator of the year in November 2023, and his research on medication management in older adults with cancer has been highlighted at several international conferences, including the French Society of Geriatric Oncology’s annual conference in Poitiers last September and the SIOG Annual Conference in Montreal last November.
Dr Sinead Walsh, Galway University Hospital/University of Galway
Dr Walsh is the Respiratory Lead in the Galway City Integrated Care hub, working on delivering specialist care in the community for patients with two respiratory conditions, asthma and COPD.
Dr Walsh was instrumental in setting up the COPD Virtual Ward in Galway University Hospital. Using remote patient virtual monitoring, COPD patients who are experiencing an exacerbation of their condition can be safely cared for in their home setting, keeping them out of hospital and the busy emergency department.
Dr Walsh and her team had the privilege of winning the ‘Excellence in Respiratory’ honour at the Hospital Professional News Honour in September 2024.
Dr Walsh was voted ‘Consultant Teacher of the Year’ by the final year medical students in June 2024.
Professor Leonie Young, Beaumont RCSI Cancer Centre
Professor Young is leading the PRISM (Precision Oncology Research Initiative for Metastatic Breast Cancer) programme with Beaumont RCSI Cancer Centre, a new ¤5 million research programme focused on advanced breast cancer has been announced this year.
This pioneering four-year initiative, funded by Breast Cancer Ireland, Carrick Therapeutics, and the Research Ireland Strategic Partnership Programme, represents a significant advancement in the fight against advanced breast cancer. Key collaborators include University College Dublin, University College Cork, the University of Galway and Cancer Trials Ireland.
Professor Leonie Young leads the Endocrine Oncology Research Group based at York House in the Royal College of Surgeons in Ireland. Prof. Young graduated from Trinity College Dublin and completed her PhD training at University College Dublin in 1997 and her research is focused on uncovering networks involved in SRC-mediated resistance in breast cancer to both tamoxifen and aromatase inhibitors.
ICO host Winter Meeting 2024
The Irish College of Ophthalmology held their annual Winter Conference recently. Discussions focused on the evolving landscape of public and private practice in Ireland with presenters and panelists sharing their impressions of the changing ownership and funding models, and how the development of medicine as a business with the entrance of investment capital, impacts the delivery of care.
The meeting took place on Friday, 15 November at the Albert Lecture Theatre, Royal College of Surgeons in Ireland, Dublin.
Annual Montgomery Lecture 2024
Professor Scott is a former Royal Air Force Lead Military Consultant Ophthalmologist at the Birmingham and Midland Eye Centre (BMEC) and Royal Centre for Defence Medicine (RCDM) at Queen Elizabeth Hospital in Birmingham,
sub-specialising in eye trauma, advanced cataract and vitreoretinal surgery. His lecture, titled "Traumateyesed: Coping with Major Ocular Injuries", offered a unique and invaluable clinical learning perspective on the management of severe ocular trauma, as well as practical guidance for ophthalmologists dealing with similar eye trauma cases in civilian healthcare settings.
During his lecture, he told the audience of ICO members and trainees, "All ophthalmologists, like myself, will be expected to deal with severe eye trauma. If you are not managing such patients day to day, it can be difficult to find a framework to work from. Eye injury is a disaster with life-changing functional, social and cosmetic effects. The role of the eye surgeon is to manage the patient, their family and the injury. Management should be staged with the aim of doing as little as is effective at any stage, initially aiming to stabilise the eye and then offering secondary management of longer-term complications. Eye protection prevents the worst effects of ocular injury and should be encouraged at a personal and
Keynote speakers and panelists Dr Shane McKeogh, ICGP/HSE GP Integrated Care Lead for Adult Respiratory Disease and Principle GP, Solas Medical Centre, Dublin, Mr Sean Gallagher, Entrepreneur and ICO Board Member, Mr James O'Reilly, Consultant Ophthalmic Surgeon, UPMC Aut Even Hospital, Kilkenny and Whitfield Hospital, Waterford, Mr John Doris, President, ICO and Consultant Ophthalmic Surgeon, University Hospital Waterford, Mr Richard Comer, Consultant Ophthalmic Surgeon, Bon Secours Hospital, Galway, Mr Aidan O'Reilly, Interim Secretary General, Irish Hospital Consultant Association and Professor Robert Scott, Consultant Ophthalmologist, St John and St Elizabeth Hospital, London
legislative level. Eye injury patients require life-long monitoring and patients must know this.
“For ease of memory, I organised the initial management of eye trauma cases into the acronym CLASSIC as follows. Perform a lateral Canthotomy and cantholysis for retrobulbar haemorrhage immediately if required. Take a detailed Log of history and examination with timings for any insurance or legal reports that will be required in the future. Make sure that systemic Antibiotics are prescribed if there is an open globe injury. Ensure that an appropriate Scan is performed, s-ray, CT scan or ultrasound ‘B’ scan. Perform a primary closure of the globe often with a Suture. Do not neglect
communication with the patient’s family, and sort any general Issues that they might have, that is what the hospital welfare department is for. Ensure your patient is in a Comfortable and quiet environment to minimise stress and reduce potential Charles Bonnet syndrome. Follow these guidelines and you can handle the worst eye trauma that presents to you."
Professor Scott also participated in the ICO Winter Meeting session earlier that day on the topic, “What Might the Future of Practice Look Like?" where he shared further expertise on ophthalmology healthcare delivery and discussed evolving management models for the specialty in light of his experience of the evolution of the UK healthcare system.
L-R Mr Richard Comer, Consultant Ophthalmic Surgeon, Bon Secours Hospital, Galway (ICO Winter Meeting Chair and Moderator) photographed with Mr Sean Gallagher, Entrepreneur and ICO Board Director
Professor Robert Scott (right), Consultant Ophthalmologist at St John and St Elizabeth Hospital, London, who delivered the Annual Montgomery Lecture 2024 at the Irish College of Ophthalmologists Winter Meeting on Friday, November 15th, is pictured with Mr John Doris, ICO President and Consultant Ophthalmic Surgeon, University Hospital Waterford
Chair and Moderator) photographed with Mr Sean Gallagher, Entrepreneur and ICO Board Director, Professor Robert Scott, Consultant Ophthalmologist, St John and St Elizabeth Hospital, London and Mr Aidan O'Reilly, Interim Secretary General, Irish Hospital Consultant Association
Ahead of World Diabetes Day (14 November), the HSE has highlighted the range of supports and services for people at risk of type 2 diabetes, as well as for people living with type 2 diabetes so they can manage their condition and live a healthy life. There are approximately 270,000 people living with type 2 diabetes in Ireland today.
Professor Derek O’Keeffe, Clinical Lead for the HSE National Clinical Programme for Diabetes, said, “A person living with pre-diabetes or diabetes requires time and support to understand what the condition is, how to treat and manage it, and the serious nature of the condition if not treated. The HSE diabetes programmes aim to empower people, providing them with the knowledge, skills and confidence required to engage in changes that will benefit their health for the long term. Participants learn how to self-care and manage the condition in partnership with their GP and healthcare teams, which helps avoid serious health complications.”
Data from pilot phases of the programmes show very positive results:
• 75% of people with pre-diabetes on the HSE National Diabetes Prevention Programme lost weight and 50% managed to bring their blood glucose levels back to within the normal range.
Dr Sarah O’Brien, HSE National Clinical Adviser and Group Lead for Chronic Disease
• There were significant improvements in outcomes for people with a new or existing diagnosis of type 2 diabetes on the HSE DISCOVER DIABETES programme, a free course, including management of blood glucose, body weight, body mass index and levels of diabetes distress associated with living with diabetes.
GP programme identifies 16,000 patients with pre-diabetes
The HSE delivers person-centred, integrated, accessible care to patients living with diabetes and other chronic diseases as close to home as possible. The Structured Chronic Disease Management (CDM) Programme, has had a positive impact for people with chronic diseases, including diabetes.
Dr Sarah O’Brien, HSE National Clinical Adviser and Group Lead for Chronic Disease, said, “In the first two years of the Opportunistic Case Finding Programme, over 16,000 patients were identified as having pre-diabetes and over 2,800 patients were newly diagnosed with type 2 diabetes and enrolled onto the Chronic
Disease Management Treatment and Preventive Programmes, as appropriate. Eligible patients have scheduled reviews with their GP and Practice Nurse, with a focus on lifestyle health behaviour improvements and/ or medical management of diabetes and associated risk factors.”
Earlier this year, a new Diabetes in Pregnancy model of care was launched, to support the estimated 7,000 women in Ireland
a year who develop gestational diabetes and/ or pre-eclampsia. Women diagnosed with gestational diabetes from 1 January 2023 are eligible for the Chronic Disease Management Programme and are being supported through an annual review with their GP and a care plan aimed at reducing their risks. More information on pre-diabetes and type 2 diabetes is available at the HSE website: www.hse.ie/diabetes.
Encouragment to Join in ‘Flunion’ this Winter
In a recent survey, commissioned by the Irish Patients Association, it has been revealed that 56% of Irish parents stated that their children have missed school days in the past year due to flu or flu-like conditions, which has an negative impact on their children’s learning opportunities and has forced 1 in 5 parents to rely more on grandparents for childcare when their children are ill.
Almost half of parents (49%) stated that the biggest impact of missed school days was their children missing learning opportunities and 24% cited that missing school activities was an issue too.
However, it seems that many parents are hesitant to get the winter flu vaccine for their children, with 53% of those surveyed revealing they hesitated to get their
children the winter flu vaccine in the last year. This has increased from survey results in 2023, which found that 44% hesitated to get the vaccine. While the research indicates that hesitation has increased this year this seems to be driven by time constraints on parents with 17% of those surveyed admitting that a lack the time was one of the reasons why they hesitated in getting their child vaccinated last year.
The Irish Patients Association is urging parents & guardians to avail of the free nasal flu vaccine for their children and is asking them to join in ‘Flunion’ in the battle against the flu this winter. In getting the free vaccine parents & guardians are not only protecting their children but they are also protecting the wider community too. It can also help to alleviate missed school days too!
The survey also found that half of respondents saw their GP up to 3 times as a result of flu-like symptoms in the past year and 1 in 10 admitted they had to visit their GP 4+ times over this period. Also, noted was the delay with being able to access a GP appointment with 49% of respondents experiencing delays of at least a day or more.
Speaking about the research, Consultant in Emergency Medicine & Prehospital Doctor, Dr. Lisa Cunningham, commented, “It’s encouraging to see that there is an increase awareness among parents as to the seriousness of the influenza virus, including the complications it can cause. What we would encourage is for parents to avail of the many opportunities to get the influenza nasal spray protection. Pharmacists are the corner stone for community
influenza vaccination for children, with appointments in many community pharmacies easier to access for parents. The schools are rolling out the influenza programme also which is currently underway. Of course, GPs are also providing this free service.”
Stephen McMahon of the Irish Patients Association, said, “The research shows that families are greatly impacted by flu and flu like condition and that an issue for parents when it comes to vaccination is time constraints. Therefore, we want to make it as easy as possible for parents and guardians to access the vaccination. It is very quick and easy to receive and free from local GPs or pharmacies, so parents / guardians can arrange an appointment at a time that works for them.”
The IRELAnD study—investigating the role of early lowdose aspirin in diabetes mellitus: a double-blinded, placebo-controlled, randomized trial
Written by Catherine Finnegan PhD 1 , Patrick Dicker MSc 1 , Denisa Asandei MPhil 1 , Mary Higgins MD 2 , Neil O’Gorman MD 3 , Mairead O’Riordan MRCOG 4 , Fidelma Dunne PhD 5 , Geraldine Gaffney MD 5 , Christine Newman MD 5 , Fionnuala McAuliffe FRCOG 2 , Vineta Ciprike MD 6 , Elena Fernandez MS 7 , Fergal D. Malone MD 1 , Fionnuala M. Breathnach MD 1
1RCSI Fetal Centre, Rotunda Hospital, Dublin, Ireland (PhD Finnegan, MSc Dicker, MPhil Asandei, MD Breathnach and MD Malone)
2UCD Perinatal Research Centre, University College Dublin, National Maternity Hospital, Dublin, Ireland (MD Higgins and FRCOG McAuliffe)
3Coombe Women and Infants University Hospital, Dublin, Ireland (MD O’Gorman)
4Infant Research Centre, Department of Obstetrics and Gynaecology, University College Cork, Cork, Ireland (MRCOG O’ Riordan)
5University College Hospital Galway, Galway, Ireland (PhD Dunne, MD Gaffney, and MD Newman)
6Our Lady of Lourdes Hospital, Drogheda, Ireland (MD Ciprike)
7Rotunda Hospital, Dublin, Ireland (MS Fernandez)
A global increase in the prevalence of type 1 (T1DM) and type 2 diabetes mellitus (T2DM) has been observed over the last 3 decades, with 1% of all pregnancies being complicated by pregestational diabetes mellitus (PGDM).1,2 When compared with women with normal glycemic control, women with PGDM have consistently higher rates of serious obstetrical and perinatal complications, which renders PGDM one of the highest-risk medical disorders of pregnancy.3 4 Placental dysfunction, manifesting as preeclampsia, preterm delivery, and growth restriction, is one example of the increased obstetrical risk in this population. Preeclampsia, a multisystem disorder characterized by elevated blood pressure and proteinuria during pregnancy, occurs more commonly in pregnancies complicated by PGDM. The repercussions of this intricate disorder manifest with greater intensity in this population, which accounts for much of the heightened risk of adverse perinatal outcome associated with PGDM. Rates of preeclampsia in women with PGDM range from 20% to 54% in those with microvascular disease and resultant nephropathy 5 6 A UK–based population study of pregnancies complicated by PGDM reported preterm delivery rates of 43% and 23% for T1DM and T2DM, respectively.7 Placenta-mediated growth restriction is observed in 9% to 24% of PGDM pregnancies 8 9 Aspirin has been investigated for the prevention of preeclampsia, yielding inconsistent results.10, 11, 12 The conflicting reports on aspirin
effectiveness in the prevention of preeclampsia may reflect heterogeneity in the selection of trial participants, including inconsistency in the definition of “high-risk pregnancy,” disparate study design, inconsistent dosing regimens, gestational age at initiation of aspirin, and nonuniformity in the definition of preeclampsia. Where aspirin has been shown to reduce the incidence of preeclampsia in certain at-risk groups, its benefits are most pronounced when started before 16 weeks of gestation.13 Aspirin is acceptable and has been shown to be cost-effective in the prevention of preeclampsia in low-risk women.14,15
Importantly, women with PGDM have typically been underrepresented in studies evaluating the impact of aspirin. Two notable studies that included women with PGDM failed to demonstrate a beneficial effect of aspirin in risk modification for this population.11,12 The ASPRE trial reported a 62% reduction in preterm preeclampsia among women deemed high-risk by firsttrimester ultrasound and biomarker evaluation.10 However, <7% of those recruited had PGDM.
Professional guidelines increasingly recommend considering low-dose aspirin for individuals with PGDM because of its reported positive impact on perinatal outcomes in similar high-risk groups.16, 17, 18 However, the consensus-based guidance (Grade E recommendation by the American Diabetes Association16) raises uncertainty about the shared pathophysiological mechanisms
for placental dysfunction or preeclampsia among diverse at-risk groups. It remains unclear whether the clinical benefits observed in one group will be replicated in others given that manifestations of preeclampsia may represent a final common pathway influenced by various pathophysiological determinants. We therefore designed a doubleblinded, randomized, placebocontrolled trial of 150-mg aspirin, initiated in the first trimester, to determine its effect on perinatal outcome in pregnancies complicated by PGDM.
Materials and Methods
A phase 3 multicenter randomized double-blinded placebo-controlled trial of daily low-dose 150mg aspirin initiated between 11+0 and 13+6 weeks’ gestation and continued until 36 weeks’ gestation was designed. Participants had a background history of prepregnancy T1DM or T2DM of at least 6-month duration, and a singleton viable intrauterine pregnancy. Women with a background of cardiovascular disease, diabetic nephropathy, or hypertension were excluded, as were those for whom aspirin was already recommended on the basis of other risk factors such as early-onset preeclampsia in a previous pregnancy or multifetal gestation. The study was conducted at 6 universityaffiliated perinatology centers across Ireland.
After screening and consent procedures, a computer-generated randomization system assigned study participants to aspirin or placebo groups. Participants were
prescribed low-dose 150-mg aspirin or matched placebo to be taken once daily (night-time dosing), initiated between 11+0 and 13+6 weeks of gestation. Treatment commenced after a satisfactory first-trimester assessment, which included sonographic confirmation of fetal cardiac activity, followed by 4-weekly clinical review visits including blood draws for renal profile, with quantification of microalbuminuria. Once a gestational age of 36 weeks was reached, medication was discontinued and weekly study visits took place until birth.
Participants took the medication once daily at night with water. Trial staff checked returned medication for discrepancies at dispensing, and discussed noncompliance during study visits. Noncompliance, defined as taking <80% of prescribed medication, resulted in trial withdrawal.
The primary outcome was a composite clinical measure of placental dysfunction that included preeclampsia (newonset hypertension after 20 weeks’ gestation and newonset proteinuria or maternal organ dysfunction19), preterm birth at <34 weeks, birthweight <10th centile,20 or perinatal mortality. Secondary outcome measures included mode of delivery, neonatal unit admission, and determination of glycemic control including insulin requirements and glycosylated hemoglobin (HbA1c) across gestation.
Owing to the variation in insulin regimens among study participants (basal bolus regimens and insulin pumps), insulin dosing in units
Figure 1. Study population: screening, randomisation, and follow-up PGDM, pregestational diabetes mellitus.
Finnegan. The IRELAnD study. Am J Obstet Gynecol MFM 2024.
per kilogram of body weight was calculated at each visit to facilitate comparison. HbA1c was measured at screening, once per trimester, and at any other time point in accordance with clinical need.
The planned study sample size was determined on the basis of a composite outcome of placental dysfunction consisting of preeclampsia, preterm delivery at <34 weeks’ gestation, low birthweight <10th centile, and perinatal mortality. The expected rate of the baseline composite outcome of placental dysfunction was assumed to be 30% (20% preeclampsia plus 50% of other outcomes, due to coincidental outcomes). A total sample size of 566 was required to achieve a 35% reduction in the composite outcome, assuming a 5% type I error and 80% statistical power.21 However, because of a lower than anticipated recruitment
rate during the COVID-19 pandemic, 134 patients were recruited and the primary outcome was therefore underpowered, with a retrospective power calculation of 64%.
The database was anonymized, encrypted, and stored in accordance with data protection law.
Treatment groups were analyzed by intention-to-treat analysis, with all randomized patients included in the composite outcome measure. Data were centrally managed using ClinInfo (ClinInfo, Lyon, France) and analyzed using SAS 9.4 (SAS Institute, Cary, NC). The 2 treatment groups were compared using t tests or chi-square tests, as required, and longitudinal data were compared using a repeated-measures analysis. A P value <.05 was considered statistically significant.
The trial protocol21 was reviewed and approved by the National Ethics Committee (EudraCT number 2018-000770-29), and the trial was registered prospectively on ClinicalTrials.gov (identifier: NCT03574909).
An independent monitor was assigned to visit the recruiting sites periodically to validate compliance with the protocol according to good clinical practice principles, the maintenance of the trial-related records, and the extensiveness and accuracy of a proportion of case report form entries relative to source data. The
study’s clinical trial governance was meticulously managed by the Trial Steering Committee (TSC), Trial Management Group (TMG), and Data and Safety Monitoring Board (DSMB). The TSC, consisting of key stakeholders and experts, provided strategic oversight and guidance, ensuring adherence to protocol and ethical considerations. The TMG handled day-to-day management, fostering communication and coordination among study sites. The independent DSMB monitored safety data, enhancing the overall integrity and reliability of trial results. This collaborative governance structure established a robust and ethical framework for the trial’s successful execution.
Results
In total, 437 women were screened for recruitment across 6 centers between February 2020 and September 2022. A total of 191 patients met the eligibility criteria for study inclusion, and 134 women were recruited. Figure 1 displays the screening, randomization, and follow-up study population. Reaching the target sample size was limited by the impact of the COVID-19 pandemic. Baseline characteristics were similar between treatment groups.
The composite primary outcome was observed in 25% of the aspirin group and in 21% of the placebo group. No statistically significant distinctions were observed between the treatment
groups in the composite primary outcome nor in any of its individual components. The mean gestational age at delivery was 37.3 weeks (range 23-40 weeks of gestation), and there was an overall cesarean birth rate of 70% in the study population. There was no significant difference between study groups for any listed secondary outcome (Table 1) nor for any pre-specified indicator of perinatal or neonatal morbidity. The median birthweight centile according to the Fetal Medicine Foundation growth centile standards was 94th (range, 73rd–98th) in the aspirin-treated group and 82nd (range, 60th–98th) in the placebo group (P=.126).
Glycemic control
To adjust premeal insulin levels, 55% of participants used a fixed-dosing regimen and 27% used carbohydrate counting. In total, 18% of participants used continuous subcutaneous insulin infusion therapy Participants in the aspirin group had a mean dose of insulin of 0.7 units/kg at screening (SD, 0.3), increasing throughout pregnancy to a mean of 1.1 units/kg (SD, 0.6) at 38 weeks, and decreasing to a mean of 0.5 units/kg (SD, 0.3) at 6 weeks postpartum. The placebo group had a mean dose of 0.7 units/kg at baseline (SD, 0.4), increasing throughout pregnancy to 1.3 units/kg at 38 weeks (SD, 0.4). The postnatal dose in the placebo group decreased to a mean of 0.6 units/kg (SD, 0.4).
Diabetes
Table 2. Primary and secondary outcomes per study group
CD, cesarean delivery; IV, intravenous; NICU, neonatal intensive care unit; OVD, operative vaginal delivery; SVD, spontaneous vaginal delivery.
Fetal Medicine Foundation weight standards: Nicolaides et al.22 Finnegan. The IRELAnD study. Am J Obstet Gynecol MFM 2024.
Table 2. Primary and secondary outcomes per study group
The mean change in insulin dose throughout pregnancy from baseline was calculated for each participant. The temporal change in insulin requirements between groups was statistically significant (P=.002). Insulin dosing in the aspirin group was notable for a mean increase in dose of 83% by 37 weeks (SD, 135), whereas those in the placebo group had escalating doses from an earlier gestation, reaching a mean increase in dose by 181% in the same period (SD, 353) (Figure 2, A). Improved HbA1c levels throughout pregnancy were observed in the study cohort (Figure 2, B), with a more marked mean decrease in HbA1c in the aspirin group of 5 mmol/mol (SD, 7.4 mmol/mol) and mean decrease in the placebo group of 3.2 mmol/mol (SD, 7.4 mmol/mol). This observed trend toward more favorable HbA1c levels in the aspirin group did not reach statistical significance (P=.222). Women with T1DM had a more marked mean decrease in HbA1c of 4.4 mmol/mol (SD, 7.0 mmol/mol), and those with T2DM a mean decrease of 3.3 mmol/mol (SD, 9.8 mmol/mol) (P=.021).
In a repeated-measures analysis of insulin use, we sought to determine if adverse perinatal outcome (fetal growth restriction, stillbirth, preeclampsia, or preterm delivery, or a composite of these) was associated with greater insulin requirements, in both an unadjusted and adjusted analysis for baseline insulin use (Figure 3). The analysis was performed for all participants and for T1DM patients alone. Stillbirth and fetal growth restriction were not modeled because of the small numbers of events. Adverse perinatal outcome was associated with higher insulin requirements, most notably among women with T1DM (+0.13 insulin/kg [P=.0002] for placental dysfunction, +0.08 insulin/kg [P=.0075] for preeclampsia, and +0.23 insulin/ kg [P=.011] for preterm delivery, over the course of pregnancy). The analysis of all participants (ie, including T2DM) also showed similar elevated levels in insulin requirements among those with adverse outcomes, but with less statistical significance.
Figure 2. Glycemic control data
A, Trends in insulin use in units/kg by treatment group. B, Trends in HbA1c levels across gestation by treatment group.
HbA1c, hemoglobin A1c.
Finnegan. The IRELAnD study. Am J Obstet Gynecol MFM 2024.
Principal findings
Although the trial was ultimately insufficiently powered to examine the composite primary outcome, the secondary observation of highly significant differences in glycemic control deserves close scrutiny. The aspirin group had an increase of 28% in insulin dosing from screening to 20 weeks, whereas the placebo group required more than double that increase in the same time period. By 37 weeks’ gestation, the statistically significant difference in insulin requirements between study groups was more marked, with an 83% increase in the aspirin group and a 181% increase in insulin dosing in the placebo group.
Results in the context of what is known
The magnitude of perinatal risk associated with PGDM pregnancies exceeds that of any other commonly observed medical complication in pregnancy. In recognition of the stark disparity in perinatal outcomes reported in this population, the St. Vincent Declaration of 1989 established a goal of achieving pregnancy outcomes in women with PGDM similar to those of the nondiabetic population.23 More than 30 years later, the aspirations of the St. Vincent Declaration have not been realized,24 with the prevalence of congenital abnormality, preeclampsia, preterm birth, and perinatal mortality being far in excess of that observed in women with normal glucose tolerance 25, 26, 27 Despite advances in glucose sensing and insulin delivery technology in recent years,28 rates of fetal macrosomia, birth trauma, and cesarean delivery remain much higher in women with PGDM compared with the background population.29 30 Furthermore, although advances in diabetes technology offer many advantages, the associated costs preclude
widespread use, particularly in resource-limited settings, where T2DM prevalence is rising.
Low-dose aspirin has been investigated for the prevention of preeclampsia and placental dysfunction for many years, with over 40,000 women recruited to randomized trials to date.31 The rationale for using aspirin to optimize placental function is based on its inhibitory effect on thromboxane production. However, evidence that aspirin influences biochemical, biophysical, and ultrasound markers of placental disease in low-risk women is sparse.32 33 Paradoxically, however, the high-risk nature of PGDM has led to exclusion of women with diabetes mellitus from many clinical trials,34 35 and thus there is a paucity of evidence to support the use of aspirin in this cohort.
Nonetheless, current guidance advocating for the consideration of aspirin treatment in PGDM pregnancies may have diminished the clinical equipoise required to recruit a sufficient number of participants for this study. Among screened patients deemed
ineligible for study participation, 40 of 206 (19%) were already on aspirin therapy. It is further plausible that the group that declined participation did so in favor of opting for aspirin. Recruitment was further impacted by the COVID-19 pandemic, which had the effect of limiting in-person hospital attendance, resulting in diminished opportunities for trial recruitment.
Clinical implications
Our data suggest that women using aspirin therapy during pregnancy require lower insulin dosing to attain normoglycemia. This observation suggests enhanced glycemic regulation linked to aspirin use. Nevertheless, the degree to which this reduction in insulin requirements signifies an ameliorated metabolic or vascular environment for the fetus remains uncertain. More specifically, the extent to which these findings should be considered to indicate a beneficial effect must be closely examined. Although decreasing insulin doses in pregnancy have previously been associated with worse neonatal outcome, and are considered to potentially reflect placental dysfunction,36 37 the
Diabetes
Figure 3. Adverse perinatal outcome and changes in insulin requirements across gestation
(*) Adjusted analysis: adjusted for baseline insulin use. (**) Placental dysfunction: composite outcome of any of the following: preeclampsia, preterm birth <34 weeks of gestation, fetal growth restriction <10th percentile, or stillbirth.
Finnegan. The IRELAnD study. Am J Obstet Gynecol MFM 2024.
most important determinant of optimal pregnancy outcome in the setting of PGDM is tight glycemic control.38 Our study supports the well-recognized association between higher insulin requirements and adverse perinatal outcome, such that the clearly demonstrated lesser escalation of insulin requirements among aspirin-treated women could be considered to indicate a beneficial effect of aspirin on perinatal outcome. Importantly, the benefit of aspirin among PGDM patients may be independent of any effect on platelet aggregation or endothelial dysfunction, but rather may depend on an effect on glycemic regulation.
The observation that aspirin reduces the incidence of glycosuria in patients with diabetes mellitus was first reported in 1957.39 Subsequently, Hundal et al40 also showed that hepatic glucose production was
reduced, and an improvement in insulin-stimulated peripheral glucose uptake was observed in nonpregnant individuals with diabetes mellitus taking aspirin.40 Those with poor glycemic control have been shown to have higher baseline platelet activity and incomplete suppression of platelet activity.41 42 43 Furthermore, patients taking aspirin with higher levels of HbA1c demonstrate higher rates of aspirin resistance compared with those with lower HbA1c levels.44 However, no genetic signatures associated with reduced platelet response to aspirin in pregnancy have been described to date.45 Therefore, better glycemic control is known to result in improved platelet suppression and improved responsiveness to aspirin, whereas aspirin itself appears to result in improved metrics of glycemic control (reduced insulin requirements and lower levels of HbA1c), thereby indicating a potentially beneficial effect of aspirin on diabetes mellitus–related morbidity.
In a secondary analysis of the Maternal-Fetal Medicine Units Network trial on aspirin for preeclampsia prevention, the association between HbA1c and thromboxane B2 levels was examined.44 Higher HbA1c levels correlated with increased thromboxane B2 before randomization (r=0.67; P<.05). Pregnancies with rising HbA1c had higher incomplete thromboxane B2
compared with those with decreasing levels (69.2% vs 18.1%; P=.02). The authors concluded that low-dose aspirin positively affects glycemic control, which is corroborated by findings from our study.
Although the exclusion of women with established diabetes mellitus–related microvascular disease may explain the lower than anticipated preeclampsia incidence in this study (overall incidence of 14%), preterm birth before 34 weeks was observed in 5% of the study cohort, and the stillbirth rate was 2.4%. The observed persistence of these perinatal complications in a selected population of women with “nonvascular” PGDM indicates a degree of perinatal risk that may be independent of the prothrombotic state of pregnancy and merits continued attention to alternative mechanisms underpinning adverse perinatal outcomes in this group. Importantly, improved glycemic control in the aspirin-treated group was not accompanied by lesser degrees of macrosomia.
Strengths and limitations
This study is notable for several strengths. The trial demonstrated high overall acceptability among participants, as indicated by the minimal number of withdrawals. Five of 6 withdrawals were at the request of the trial monitor during site visits, citing low compliance with the study medication. Among the remaining participants, compliance with study medication
and adherence to the study schedule were high, and complete outcome data were ascertained for 99%. However, because of a lower than anticipated recruitment rate during the COVID-19 pandemic, 134 patients were recruited and the primary outcome was therefore underpowered.
Research implications
Cord C-peptide levels may have yielded supporting evidence of improved glycemic control among aspirin-treated participants. However, procurement of cord samples was not included in the study schedule. A subset of participants provided serial serum samples at prespecified time periods throughout gestation, and interrogation of these samples for additional markers of glycemic control and for evaluation of thromboxane B2 levels is planned.
Conclusions
Despite showing no difference in the primary outcome (a composite measure of placental dysfunction), aspirin use in pregnancy among women with PGDM was associated with a significant reduction in insulin requirements and improvement in glycemic control when compared with placebo. A beneficial effect of aspirin therapy for PGDM pregnancies may be independent of its antiplatelet effect. Given the importance of optimal glycemic control for successful PGDM pregnancy outcomes, it is important to consider initiation
of aspirin therapy at the earliest opportunity, potentially in advance of conception. Future studies should investigate the potential benefits of preconception initiation of aspirin therapy and continuing it until term, including the possibility of reducing the risk of hyperglycemiarelated teratogenesis
Credit authorship contribution statement
Catherine Finnegan: Data curation, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. Patrick Dicker: Formal analysis. Denisa Asandei: Investigation, Project administration. Mary Higgins: Investigation. Neil O'Gorman: Investigation. Mairead O’ Riordan: Investigation. Fidelma Dunne: Investigation, Methodology, Writing – review & editing. Geraldine Gaffney: Investigation. Christine Newman: Investigation. Fionnuala McAuliffe: Investigation, Writing – review & editing. Vineta Ciprike: Investigation. Elena Fernandez: Conceptualization, Methodology. Fergal D. Malone: . Fionnuala M. Breathnach: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Supervision, Writing – review & editing.
Dana Kendall Appointed General Manager of AbbVie Ireland
Dana Kendall has been appointed General Manager of AbbVie Ireland, a leading global biopharmaceutical company.
Based at AbbVie’s commercial headquarters in Citywest, Kendall will lead AbbVie’s commercial business in Ireland, focusing on delivering innovative medicines that address complex health challenges and make a meaningful difference in patients’ lives.
Speaking about her appointment, Dana Kendall said: “I am honoured to step into the role of General Manager for AbbVie Ireland, a country where our commitment to innovation and patient care is strongly rooted. With a talented team and a robust presence across Ireland, we are well-positioned to continue delivering transformative medicines that address complex health challenges. I look forward to working closely with our partners and stakeholders to make a
meaningful impact on patients’ lives and contribute to the healthcare landscape in Ireland.”
Kendall joined AbbVie in 2020, where she successfully led the international launches of treatments for active psoriatic arthritis and ankylosing spondylitis. In 2022, she advanced to the role of International Marketing Director for a key dermatology therapy.
A Texas native, Kendall has over 18 years of extensive pharmaceutical industry experience across sales, marketing, and leadership roles in therapeutic areas such as urology, oncology, endocrinology, and
immunology. Her career began at Galderma Laboratories, followed by roles at inVentiv Health, Endo Pharmaceuticals, and UCB, where she gained expertise in commercial strategy with an international focus.
European Accreditation for Cancer Network
The HSE West North West –University of Galway Cancer Network has announced that it has been accredited by the Organisation of European Cancer Institutes (OECI).
OECI is an organisation of European cancer centres founded in 1979 to provide patients equal access to high quality cancer care through cooperation and knowledge exchange. HSE West North West – University of Galway Cancer Network is only the 20th such network to achieve cancer centre accreditation across Europe.
The highly sought after accreditation follows several years of rigorous review and engagement with the European team including a peer review visit which took place last May.
This saw a panel of European experts visit a number of hospitals across our region to assess all elements of the cancer programme.
The OECI team evaluated 345 standards across our Regional Cancer Programme. This process has helped to strengthen our clinical pathway, improve patient’s outcomes through enhanced processes and will ultimately help to increase the numbers of patients participating in clinical trials.
The European body has now confirmed that the HSE West North West –University of Galway Cancer Network met the quality standards for cancer care and research and has been designated as an OECI Cancer Centre.
The OECI Accreditation and Designation programme is considered internationally as the gold standard for cancer care. It focuses on enabling a complete quality system for cancer diagnosis, care, education and research.
In gaining this prestigious accreditation the HSE West North West – University of Galway Cancer Network has committed to ongoing quality improvement in cancer care through research, innovation, partnership and patient empowerment.
Professor Michael Kerin, Director of the HSE West North West – University of Galway Cancer Network welcomed the announcement adding: “This acknowledgement is a testament to the hard work of our incredible staff. This took an enormous amount of
With a significant manufacturing presence across five sites in Sligo, Mayo, Cork, and Dublin, AbbVie currently employs 2,900 people in Ireland. The company also markets medicines in over 175 countries globally.
work across our hospitals and a huge amount of support from the voluntary organisations working in our region.
“We were evaluated on 345 standards and we will now focus on the 33 point quality improvement plan which will deliver a fit for purpose cancer centre for the West and North West region. This was a commitment of the National Development Plan and we now need to ensure we have the resources, national support and infrastructure to deliver a fully accredited cancer network. The fact that we have been given cancer centre status is hugely valuable and our ability to recruit, retain and develop our staff and deliver really good care has been enhanced by this process,” he added.
Dana Kendall, General Manager, AbbVie Ireland
The Experience of Anaemia and Ingesting Oral Iron Supplementation in Pregnancy: A Qualitative Study
Written by F.E O'Toolea,b, E. Hokeya, F.M McAuliffea,b, J.M Walsha,b
aUCD Perinatal Research Centre, University College Dublin, National Maternity Hospital, Dublin,
bNational Maternity Hospital, Dublin, Ireland
Introduction
Iron deficiency anaemia is the most common haematological problem in pregnancy. It affects approximately 38 % of women in pregnancy globally.1 Crosssectional data from fifteen European countries gives a prevalence of iron deficiency anaemia in pregnancy of 35 %.2
Prevalence of iron deficiency anaemia in pregnancy from an audit encompassing 86 maternity units across the United Kingdom and Ireland was 30.4 %.3 It remains a common problem in Western well-nourished nations despite these countries being much less afflicted by helminths, malaria or haemolytic conditions.
Significant adverse pregnancy, maternal, foetal, neonatal and childhood outcomes are associated with iron deficiency anaemia.4, 5 Maternal complications include fatigue, post-partum haemorrhage, increased risk of caesarean section, postpartum anaemia, blood transfusion, and labour induction.4 Infant complications include preterm birth, low birth weight infant, increased risk of stillbirth, lower Apgar scores at delivery and increases in perinatal and neonatal mortality.4, 6 Symptoms of anaemia include fatigue, breathlessness, and dizziness. Postpartum anaemia has been linked to depression, fatigue, lactation failure and early cessation of breastfeeding.7, 8, 9, 10 Maternal anaemia has also been associated with behavioural and neurodevelopmental abnormalities in offspring.11, 12
Iron deficiency anaemia in pregnancy has a multitude of contributing causes including physiological changes and inadequate nutrient intake, rates will depend on baseline iron stores pre-conception. Women of reproductive age are at increased risk of anaemia due to menstruation. Acute blood loss can also occur from miscarriage, placental events such as abruption or praevia or recent childbirth resulting in postpartum haemorrhage. Both breastfeeding and pregnancy deplete maternal
iron stores. The iron demands of pregnancy can cause an iron deficit even in iron-replete women. Insufficient dietary iron intake may compound the problem.13
Iron deficiency anaemia in pregnancy can be challenging to treat. The hormonal and physiological effects of pregnancy predispose women to slowed gut transit, hemorrhoidal disease, heartburn, nausea, vomiting. Oral iron supplementation is the recommended first-line treatment and is often commenced as both a diagnostic and therapeutic trial without further investigations, as iron deficiency is commonly the underlying cause of anaemia. The commencement of oral iron in pregnancy may exacerbate pre-existing pregnancy-induced gastro-intestinal disturbances or may cause new unpleasant gastrointestinal side-effects to include nausea, vomiting, constipation, abdominal discomfort, and black stools. Advice on optimal absorption of oral iron will typically be to take in the morning, on an empty stomach and with a source of vitamin C. Women are generally advised to increase their dietary iron and often given advice on foodstuff that may hinder absorption. Compliance
with treatment can be limited secondary to side-effects, among other factors.14, 15 Rates of iron deficiency anaemia in pregnancy appear to be relatively unchanged over the past two decades, despite treatment being affordable, accessible and in theory straight-forward. The World Health Organization Global Health repository data only demonstrated a 4 % reduction over a twenty-year period to a prevalence of 37 %. The 2017 World Health Organization Global Nutrition Targets include a 50 % reduction of anaemia in women of reproductive age by 2025.16
There a paucity of published qualitative data from higher income countries on women’s experience of taking oral iron in pregnancy. This study was performed to examine the lived experience of ingesting supplemental oral iron to treat anaemia in pregnancy. We specifically wished to explore women’s awareness and experience of this problem both before and during pregnancy, their awareness of any potential negative sequelae of untreated anaemia, how they felt about the role of diet in its management, and what factors contributed negatively or positively to their compliance
Ireland
with oral iron supplementation in pregnancy. Feedback was also sought on acceptability of a proposed randomised controlled trial of daily versus alternate day oral iron for the treatment of confirmed iron deficiency anaemia in pregnancy. This project successfully answered these research questions.
Materials and methods
Recruitment for this qualitative study performed between 4th November 2021 and 17th December 2021. Ethical approval was obtained in advance of recruitment by the National Maternity Hospital Research Ethics Committee (EC23.2021). Informed written consent from each participant was obtained in advance of an interview. Pregnant or recently pregnant women who required iron supplementation in pregnancy were invited to take part in interviews. Women were invited to participate in the study via social media channels such as on the UCD Perinatal Research Centre Twitter account (supplementary material S1) and women were also approached for study participation during antenatal hospital visits. Ethically approved patient information
leaflets on the study and study-specific consent forms were provided in advance of participation and an opportunity to ask questions was provided.
Interviews were audio-recorded virtually or in person using the audio function in Zoom (Zoom Video Communications Inc. 2016). Interviews were then transcribed using Sonix (Sonix, Inc. San Francisco, 2021). To ensure patient confidentiality all transcripts were anonymised and allocated a unique study identifier (P1–P14) and the audio files were destroyed. Interviews were carried out by one member of the research team (FOT). This researcher was a female obstetric trainee performing research as part of an MD thesis. There was no prior relationship with any of the interviewees.
Participants were provided with clear typed information regarding the study and the researcher’s background and role as part of the consent process in advance of participation. Consent forms were stored on a secure server and could not be linked to the transcripts to ensure participant confidentiality. No medical records were accessed as part of this study and participants contact details were deleted following a two-week period after the interview. Participants were offered an opportunity to review their anonymized typed transcript for a two-week period after the interview. After this period, their contact details were destroyed as per the consent form and planned management of their data.
The interview took the following format: an interview tool comprising of 5 open-ended questions for semi-structured interviews was developed by the research team (supplementary material S2). Interview length varied between 14 and 17 min duration. There was scope for exploratory questions on new themes. Open-ended questions were asked of each participant surrounding their awareness of iron deficiency anaemia both before and during pregnancy, their knowledge of its symptoms and of potential sequelae, how big a role they felt diet played as part of management, and their experience of taking iron tablets in pregnancy. Factors affecting compliance with oral iron supplementation were explored. Finally, each participant was asked about how acceptable they felt participation in a randomized controlled trial of daily versus alternate day iron would be to other women. Details of what participation in the trial would involve was outlined and feedback was sought on how acceptable they felt this would be.
The anonymised transcripts were then analysed separately by two members of the research team (EH, FOT). Data saturation was felt to be reached with clear recurring themes. Individual analyses were compared, and agreement of themes and subthemes was reached through discussion. Rigour in the analytic process was ensured through review and confirmation of themes by other members of the team (FMcA, JW).
Results
Demographics
The participant demographics can be seen in Table 1. Fourteen women were interviewed. The mean age was 36 (range 32–40 years of age). Half of the participants (50 %) were currently pregnant at the time of interview, with a mean gestation of 27 weeks' gestation and a range of 11 to 36 weeks' gestation. Regarding the antenatal participants, 2/7 were primiparous and 5/7 were multiparous. In terms of parity of the postnatal participants, 4/7 had ≥2 children and 3/7 had delivered their first baby within the previous year. The majority (9/14) of participants were White Irish. Two participants were of Eastern European ethnicity, one was of Pakistani ethnicity, and one was of Indian ethnicity.
Main findings
Overall, there appeared to be a varied awareness that iron deficiency could become a problem in pregnancy. Prior awareness was sometimes from previous personal experience, and often from anecdotal reports from friends or family who had previously been pregnant. Personal experience ranged from experience of anaemia as a teenager, vegetarianism, and during work-up for a history of subfertility. Often, however, it was their first pregnancy that initially highlighted the problem to them. Women described being warned of it as a potential problem more in their initial pregnancies:
P8- “I did have people telling me in the first pregnancy that I looked pale, and they were like you’re anaemic. You need to take iron. Other Mums were telling me.”
P13- “I was aware, because of all my sisters who’ve gone through pregnancy. I know it’s quite common now.”
With regards to participants’ experience of symptoms of iron deficiency anaemia in pregnancy, significant and depleting fatigue was a recurring theme. Women described it as a more severe fatigue than previously experienced:
P2- “I was absolutely exhausted and the tiredness, it’s just inexplicable if you’ve never been pregnant. It’s a completely flattening experience.”
Knowledge and awareness on the potential effects of untreated anaemia on the pregnancy and baby were limited. Participants did not demonstrate good knowledge on the potential negative consequences/sequelae for themselves in their pregnancy or afterwards in the postpartum period. Awareness and knowledge of potential foetal sequelae such as childhood iron deficiency was poor:
P8- “No actually, I don’t. I’m not aware of any of the effects in pregnancy of untreated anaemia for me in pregnancy or for the baby in the long-term.”
With regards to the lived experience of ingesting oral iron in pregnancy, the unpleasant side-effects of ingesting oral
Anaemia
(11/12)
(31/40)
(11/40)
9/14 of our interviewees were recruited from Twitter and 5/14 from a public antenatal setting and majority were linked with the National Maternity Hospital, a tertiary referral centre in Dublin, Ireland.
9/14 of our interviewees were recruited from Twitter and 5/14 from a public antenatal setting and majority were linked with the National Maternity Hospital, a tertiary referral centre in Dublin, Ireland.
iron were a commonly recurring theme. Constipation and nausea appeared to be the most frequently described and troublesome:
P2- “It did not agree with me at all, it was absolutely horrendous to take. I got constipation, I got heartburn. It just really played havoc with my digestive system. Made me nauseous if I took it without food, it was really hard. It was really unpleasant to take.”
P12- “It helped me, but the sideeffects were horrible. It’s not nice to be constantly sick for 50 days.”
Barriers and enablers to oral iron supplementation in pregnancy were explored in this study.
Gastro-intestinal side-effects featured heavily in the interview transcripts and appeared to contribute to poor compliance with oral iron supplementation in pregnancy. Forgetfulness also
negatively impacted compliance. One participant commented that the cost of a more expensive brand of iron supplementation influenced compliance. A prior experience of poorly tolerating oral iron in the past also caused hesitation with compliance.
Factors that positively affected compliance included a noticeable or anticipated improvement in fatigue with oral iron supplementation. The benefit of a routine with ingestion of oral iron was also cited as an aid in terms of assisting compliance. A fear of worsening symptoms of anaemia and a desire to avoid the risks of a blood transfusion were other factors which appeared to motivate compliance with oral iron therapy. There was also evidence that reduced dose frequency positively impacted compliance with oral iron supplementation.
Table 1. Participant demographics
Pregnancy as motivating factor recurred as a theme in analysis of the interviews. Participants felt that most women were highly motivated to do everything in their power for the best possible outcome for themselves and their baby. This effect was described as greater than any motivation for compliance with treatment outside of pregnancy.
P6- “I presume, like most women, when they’re pregnant, you just want to do the best thing for your health and the baby’s health. In more normal times… I probably wouldn’t have been as compliant, but I think being pregnant, you just want to look after yourself and the baby. So that was definitely a motivating factor.”
P2- “I didn’t object to taking them because you do take whatever you need to take. You know, whatever they tell you. They tell you; you need coal. You’re going to take the coal. Your motivation is high in pregnancy.”
In terms of the role of diet in the management of iron deficiency anaemia in pregnancy, participants’ knowledge and awareness of iron-rich foods was generally good. There also was evidence that women believed and understood that diet alone would not rectify their anaemia:
P4- “For me, dietary stuff was ineffective. I’d go for all the iron-rich foods, and it was just neglible. It was just the impact was too tiny for the mountain I was trying to climb.”
Pregnancy symptoms and nausea negatively impacted appetite for some women. For some, they felt a reliance on supplementation due to this. Knowledge of facilitators and inhibitors of iron absorption was also widely good.
Themes that emerged in relation to trial acceptability included the benefit and attraction of extra supportive care in pregnancy and the time constraints women can be under. Participants highlighted the demands on women’s time and to try to work around this for convenience for any trial participants. Pregnancy alone requires planning for regular and frequent appointments in women who have busy lives and would not otherwise require planning for regular medical appointments outside of pregnancy.
The proposed trial generally received very positive feedback with participants feeling that this was an important area of research:
P1- “I think this trial is very important and it sounds like it’s going to be very educational for women in the longer term.”
P5- “I think it’s a very interesting study. So very, very much needed… I’m happy you are working on it”
P6- “There doesn’t seem to be a particularly large burden on the participants, and I think that it would be largely acceptable.”
There were mixed responses to the acceptability of taking alternate day versus daily iron. Some women felt alternate day iron would be acceptable and potentially beneficial for that arm of the trial. However, there was doubt among some participants about the willingness of patients to accept alternate day iron over daily iron.
Discussion
Main findings
Themes of awareness, compliance, the role of diet and pregnancy as a motivating factor recurred throughout our analysis. Fatigue emerged as the predominant and most troubling symptom. Knowledge and awareness of possible adverse consequences of iron deficiency anaemia in pregnancy were poor. Significant unpleasant gastrointestinal side-effects appeared to be experienced widely among interviewees and affected compliance. Factors that positively impacted compliance with oral iron supplementation included routine, a perceived or historical improvement in symptoms with supplementation, reduced dose frequency and a desire to avoid both worsening symptoms of anaemia and a blood transfusion.
Clinical significance
Awareness pre-pregnancy of iron deficiency anaemia varied in our cohort. When present, it stemmed from personal experience of friends and family and anecdotal advice. However, knowledge on symptoms and the potential need for iron supplementation in pregnancy was generally good. First pregnancy also appeared to be a time when women noticed an emphasis from health professionals on the problem. This may possibly be explained by health providers assuming prior knowledge from previous pregnancies in multiparous women. Participants knowledge on both iron-rich diets and foodstuff that could impact iron absorption was also good. This may be due to the population in our catchment area being generally well-educated, from a higher
socio-economic background and the mean age of our participants being 36. The appreciation that an iron-rich diet alone was not sufficient to rectify anaemia in pregnancy appeared to stem from personal experience of increasing dietary iron with no noticeable improvement in symptoms:
P4- “For me, dietary stuff was ineffective. I’d go for all the iron-rich foods, and it was just neglible. It was just the impact was too tiny for the mountain I was trying to climb.”
Knowledge on the possible negative sequelae of untreated iron deficiency anaemia in pregnancy however was poor. None of our participants commented on the potential for maternal complications or the negative associations including preterm birth, low-birth weight, Caesarean delivery, post-partum haemorrhage.4 Knowledge surrounding possible adverse outcomes for the foetus in the short and long-term were also poor. Only one participant commented on the effect maternal iron deficiency anaemia might have on the baby’s iron stores in the 6 months post-delivery.
Fatigue emerged as a pervasive and debilitating symptom women experienced with iron deficiency anaemia in pregnancy. The effects were dramatic and appeared worse than previously experienced tiredness. Significant fatigue is known to affect quality of life and increase the likelihood of depressive symptoms in pregnancy.17 Undetected and untreated antenatal depression is one of the strongest risk factors for postnatal depression.18
The feedback on trial acceptability from our study was used to inform our design for a planned randomized controlled trial of daily versus alternate day oral iron in pregnancy. Acceptability refers to determining how well an intervention will be received by the target population and the extent to which the new intervention or its components might meet the needs of the target population and organizational setting.19 It has become a key consideration in the design, evaluation and implementation of clinical trials.
Positive feedback noted from this qualitative study included the benefit of extra supportive care in pregnancy and the potential to improve side-effects of oral iron for women in pregnancy. Perceived research relevance has been shown to be an important factor for clinical trial recruitment in pregnancy.20 Advice on incorporating research visits
with routine antenatal care and limiting extra hospital visits was used to finalise our trial protocol. Time constraints on women has been shown to be a factor affecting both recruitment and retention in clinical research trials in pregnancy.20 It is useful to be aware that some participants may resist or refuse their randomized dosing regimen. Participants’ understanding that a scientific question is being answered and the nature of participation will need to be ensured prior to recruitment. Randomised trials in pregnancy face specific enrolment challenges and research in pregnancy can be limited due to an individual’s risk perception.21 Altruism and a wish to contribute to scientific research has been shown to be a previous motivating factor in trial participation in pregnancy. However, key motives which have previously been identified for non-participation in clinical trials in pregnancy include a dislike for the intervention, either because of a risk of harm or due to practical considerations.22
Comparison with other qualitative studies in this area
While there is a paucity of qualitative data from higher income countries on this subject, multiple qualitative studies have been carried out in lower- and middleincome countries.15, 23, 24, 25, 26, 27, 28 Rates and severity of anaemia and iron deficiency remain even higher in poorer nations, with a more pressing need for development of strategies and research to improve compliance with supplementation.1
While populations from lower income and developing countries will be hugely different from an economic and education perspective, forgetfulness has previously been highlighted as a barrier to compliance with iron supplementation in pregnancy from both higher income and lower income countries in studies from Zambia, Sweden, the United States of America, Senegal and India.15, 28, 29, 30, 31
In a less educated population in Mumbai where only 3 out of 31 interviewees had completed education to secondary level, the cause of anaemia was attributed to a poor diet but the link was frequently not made to iron deficiency.27 The respondents described weakness and dizziness as symptoms of anaemia. Similar our study, recognition of maternal complications associated with anaemia was low. The authors describe an urgency in maternal and child health programmes to emphasise the importance of the mother’s own health. They
Anaemia
describe anaemia interventions to have the potential to become proxies for women’s health and empowerment programmes. This concept also resonates in our study; there is huge potential in empowering women with knowledge on the potential adverse short and long-term maternal and foetal outcomes which may arise from sub optimally treated iron deficiency anaemia in pregnancy. This is particularly relevant given the recurring theme of pregnancy as a motivating factor that emerged from our data.
Gastrointestinal side-effects were found to be a major reason why pregnant women in Sweden stop taking iron supplements- they were cited as a reason for stopping oral iron
supplementation in 46 % of cases in data from over 900 patients.29 In this Swedish study approximately half of the women had experience of taking iron previously and 32 % reported noticing adverse effects. Of the women that ceased taking oral iron in pregnancy, 31 % was due to a perception of no longer needing it and 8 % reported that they forgot. Absence of side-effects with supplemental oral iron in pregnancy has also been shown in an Indian population to be positively associated with compliance.15
There was evidence that alternate day dosing positively affected compliance in our cohort. This compares well with published data from a randomized trial of weekly versus daily oral iron supplementation in pregnancy in
Bangladeshi women.32 This study noted a difference in compliance of 93 % in the weekly group versus 61 % in the daily group, although they found no significant association between side-effects and compliance.
Pregnancy as a motivating factor is well-described in the literature on health interventions in pregnancy.33 In a qualitative study from India, the most common reasons for adherence with oral iron supplementation were to improve mother’s health (40 %) and their baby’s health (46.5 %).15
Future research
Further qualitative research in this area could focus on a younger cohort and populations from lower socio-economic groups but who
Important New Alzheimer’s Research
Important new research is to be undertaken by a Consultant Neurologist at Tallaght University Hospital (TUH) to find out if blood tests can be used to diagnose Alzheimer’s disease in people with Down syndrome. Dr Antoinette O’Connor hopes this new study will also support future investigation of whether new medications to slow the progress of Alzheimer's could be effective for those with Down syndrome. This new study is necessary as people with Down syndrome have a significant risk of developing Alzheimer’s disease (AD). Recently new drugs have come on stream
Antoinette O'Connor, Consultant Neurologist
which have been shown to slow the progression of Alzheimer's for those in the early stages of the disease. The challenge for doctors is to determine if individuals with Down syndrome can also benefit from these treatments.
In order to properly test these treatments, there will need to be carefully designed studies. Traditional tests, cerebrospinal fluid sampling, and brain scans are invasive and expensive, therefore it would be easier for participants if blood tests could be used to detect and track potential treatment effects.
are still residing and receiving antenatal care in a higher income country. Purposive sampling from ethnicities more strongly affected by iron deficiency anaemia would also be of interest to ascertain if the same themes recur and if there are any cultural differences in the analyses.
Conclusion
In conclusion, women view sideeffects as a significant barrier to taking oral iron. Informing women on the important maternal and infant complications associated with iron deficiency may prove to improve compliance with oral iron treatment. Women clearly view this topic as an important research area.
References available on request
Dr O’Connor says, “We are entering a new era in AD treatment– for the first time there are therapies that can slow disease progression. Frustratingly, people with Down syndrome have been routinely excluded from AD drug trials, despite urgent clinical need in this population. Therefore, we do not know if these potentially life-altering treatments work in Down syndrome.”
The TUH Consultant Neurologist says, “Robust clinical trials involving those with Down syndrome will need to be undertaken to track the changes in them caused by Alzheimer's disease. These measures of change are called biomarkers. Blood tests represent an ideal AD biomarker as they are cheap, accessible and repeatable.”
Several important questions must be answered before blood tests for AD can enter routine use for those with Down syndrome. Dr O’Connor's new research study will address some of these, specifically:
• What blood tests are the most promising for the detection of AD in Down syndrome?
• Do blood test levels vary from day to day and does this variability impact their ability to diagnose AD and/or track change?
• What role does inflammation play in driving AD onset?
• How long, and how many people, are required to participate in AD clinical trials to show a treatment effect in Down syndrome?”
This new study will answer these questions by reviewing previous blood biomarker studies in people with Down syndrome and by collecting repeated blood samples from study participants. These blood samples will also enable Dr O’Connor and her team to investigate the role of inflammation in AD which could potentially open up new treatment avenues.
The Deputy CEO of TUH John Kelly who is also the executive lead for Research & Innovation at the Hospital says, “This kind of research is important as it can result in medical breakthroughs which can lead to the discovery of life-changing treatment. We at TUH are delighted to host this cutting-edge study as Dr O’Connor and her team strive to improve care for Down syndrome patients with Alzheimer's. This study reflects our commitment to the discovery of new treatments for wider health improvements.”
The research which will be undertaken at TUH, has been funded by the Health Research Board under their Emerging Clinician Scientist Award.
Dr
New HSE E-Learning Module
The National Clinical Programme in Surgery (NCPS) has launched a new HSE eLearning Module which provides education on the management of neck haematomas when they occur on the ward after thyroid surgery.
Neck haematomas are rare but life-threatening and can occur in approximately 1-3% of patients who have thyroid surgery. The haematomas can enlarge rapidly and compromise the patient’s airway requiring urgent intervention. There are a number of factors that can increase the risk including age, hypertension, Grave’s disease or history of previous thyroid surgery.
The eLearning module aims to provide education on recognition, escalation, and the management of this condition and is recommended for all doctors and nurses involved in the post-operative care of all patients who have undergone thyroid surgery.
The module was funded by the HSE and its development was led by the National Clinical Advisor for Otorhinolaryngology-Head and Neck Surgery, Professor Michael Walsh. It was developed by Aurion Learning and was supported by an expert working group that included a range of ENT consultants, nurses and anaesthesiologists.
Pictured (l-r): Ciara Hughes, Programme Manager, NCPS; Prof. Michael Walsh, National Clinical Advisor for OtorhinolaryngologyHead and Neck Surgery; Prof. Deborah Mc Namara, President RCSI; and Sharon Casey, Administration Officer, NCPS
Professor Walsh, National Clinical Advisor for Otorhinolaryngology
– Head and Neck Surgery, NCPS, said, “The development of this eModule was a collaborative effort involving multiple stakeholders and the NCPS is grateful to all those who contributed to this work, particularly to Mr Greg Sadler Consultant Endocrine Surgeon, John Radcliffe Hospital, Oxford, UK and Mr Shad Khan Consultant Endocrine and General Surgeon, Oxford University Hospitals for the use of their video.
“This module is easily accessible through HSELanD for all relevant healthcare staff and should give staff the knowledge and confidence to act quickly and safely in this emergency scenario which will ultimately save lives.”
The National Clinical Programme in Surgery is a strategic initiative between the HSE and RCSI. The programme aims to design and
implement change initiatives to improve and standardise the quality of care and access for all patients in a cost-effective manner.
The programme works closely with other National Clinical and Care Programmes under the governance of the HSE CCO to ensure integration across multiple areas of care.
Dr Siobhán Ni Bhriain, HSE National Clinical Director Integrated
Care, welcomed the launch, noting “the integrated approach taken in the development of the protocol, ensuring that it meets the highest standards internationally. It demonstrates the importance of continued collaboration between the HSE and RCSI in the development of these guidelines to support the delivery of high quality, standardised clinical care. Congratulations to Prof. Walsh and team and the NCPS for bringing this to completion.”
A Decade of Impact: Celebrating Our Journey
The Health Research Board recently hosted an event – A Decade of Impact: Celebrating our Journey which acknowledged ten years of HRB investment in trials methodology research and capacity building in Ireland, through the HRB-TMRN.
One of the speakers at this event was Dr Conor Judge, Consultant Nephrologist and Senior Lecturer in Applied Clinical Data Analytics who spoke on - Testing Artificial Intelligence Interventions in Pragmatic Trials. Here, he gives Hospital Professional News an overview.
“Artificial intelligence (AI) holds immense promise in transforming healthcare, particularly in areas like clinical decision support systems (CDSS). My talk at the HRB Trials Methodology Research Network event - ‘A Decade of Impact: Celebrating Our Journey’ explores the intersection of AI and pragmatic randomised controlled trials (RCTs), focusing on ensuring
these technologies are safe, effective, and scalable.
“The core of my research is developing an AI-CDSS for hypertension management. This project is funbded by the Health Research Board. The system integrates data from electronic health records (EHRs) and employs advanced machine learning techniques to provide clinicians with evidencebased recommendations for antihypertensive therapy. However, introducing AI into clinical care raises questions about trust, acceptability, and effectiveness, which can only be answered through robust testing frameworks like RCTs.
“Pragmatic trials are critical for evaluating AI interventions because they reflect real-world conditions. Unlike traditional RCTs, which often operate under idealised scenarios, pragmatic trials account for the variability and complexity of everyday
Dr Conor Judge, Consultant Nephrologist and Senior Lecturer in Applied Clinical Data Analytics
clinical settings. For example, a recent multicenter trial tested an AI-driven decision-making tool in stress echocardiograms. While the AI showed potential, it also highlighted the challenges of achieving non-inferiority compared to standard care, emphasising the need for careful evaluation.
“Building infrastructure for pragmatic trials is another focus of my work. In Ireland, we face gaps like the lack of fully integrated EHR systems, though we do have strong data linkage capabilities, such as connecting clinical data to mortality and audit registries. Collaborations with entities like the Health Service Executive (HSE)
are vital for leveraging existing datasets to support such trials.
“In conclusion, testing AI interventions requires blending technical innovation with rigorous research methodology. Through pragmatic trials, we can address unmet clinical needs while ensuring AI's safe integration into healthcare systems.”
Bladder Cancer
Bladder Cancer: Current Management and Future Direction
Written
by Dr Ishapreet Kaur1 and Mr David Galvin1
1Department of Urology, Mater Misericordiae University Hospital, Dublin Ireland
Bladder cancer affects around 540 people in Ireland every year. It accounts for 15 percent of cancer cases worldwide.1 Most cases (90%) are transitional cell carcinomas (TCC), arising from bladder lining cells, while squamous cell carcinoma (SCC), often linked to chronic infection, accounts for most of the rest.1
Major risk factors include smoking, occupational exposure to harmful chemicals, obesity, and the male sex. Inflammation of bladder tissue is the primary SCC risk, especially in regions with schistosomiasis.2-3
Bladder cancer commonly presents with painless haematuria (85%), up to 20% of patients present with urinary urgency or suprapubic pain. A small cohort of patients (3%) will present with non-visible haematuria.4
Diagnosis involves cystoscopy and upper tract imaging which includes either CT Urogram or a renal ultrasound. Some hospitals within the HSE have developed protocols with the triage of patients with Visible Haematuria including the introduction of Haematuria Clinics which echo principles of the triple-assessment breast clinics. Patients triaged into these clinics will have their urine cytology taken, flexible cystoscopy completed and upper tract imaging filmed on the day of their visit.
With their diagnosis, patients with frank haematuria will undergo CT Thorax Abdomen and pelvis with a Urographic phase to assess local spread and metastasis. The TNM staging system assesses tumour invasion, nodal involvement, and metastasis, while grading determines tumour cell differentiation.5
Treatment and management of bladder cancer depends on the invasive nature of the cancer. The bladder wall consists of three layers, the innermost mucosa, muscularis propria (or detrusor muscle), and the outermost serosa and peri-vesical fat. Patients are then classified to have non-muscle invasive bladder cancer (NMIBC), muscle invasive bladder cancer (MIBC), and metastatic disease.
Non Muscle Invasive Bladder Cancer
80% of patients have NMIBC.1 They will undergo a transurethral resection of bladder tumour (TURBT) with the intention of making a correct histological diagnosis and to remove all macroscopic lesions. This is sometimes followed by intravesical chemotherapy (Mitomycin C or Epirubicin) which has an ablative effect on residual tumour cells. It has shown to reduce recurrence soon after the TURBT, and is generally offered to high grade lesions.6
Over the past decade the use of immunotherapy can be considered in patients that are unfit for cisplatin/ carboplatin treatment.8 Additionally, the use of immune check-point inhibitors led to longer survival in patients with metastatic bladder cancer
Intravesical BCG (bacillus Calmette-Guérin) decreases the risk of recurrence in intermediate and high risk tumours. It is given at least two weeks after TURBT and the initial induction course involves six, weekly treatments. Following this, maintenance therapy as per the Lamm regime can be commenced.7 These involve once-weekly instillations for three weeks at three months, six months, and 12 months posttumour resection. Three onceweekly courses every six months are recommended thereafter up to three years post-resection.
Common side-effects include dysuria, frequency, and malaise with a mild fever for up to 24 hours post-instillation. If patients develop a symptomatic urinary-tract infection, BCG should not be administered until they have recovered.
Diagram 1: TNM Staging of Bladder Cancer16
Dr Ishapreet Kaur
Mr David Galvin
There is a small risk (0.4-2%) of developing BCG sepsis, which may present as persistent fever, arthralgia, headaches, rash, and increased malaise. This requires hospitalisation, blood cultures, resuscitation, and commencement of anti-tuberculous treatment.7
Follow up for patients with NMIBC according to current European Association of Urology (EAU) guidelines recommend regular follow-up with flexible cystoscopy accompanied by annual imaging for high-risk tumours.6
Muscle Invasive Bladder Cancer
Approximately 20% of patients are diagnosed with MIBC.1 It is treated with radical cystectomy, radiotherapy, chemotherapy, or immunotherapy, depending on the patient’s health status and tumour stage.
Radical cystectomy and radiotherapy are the standard for localised cancers, often combined with chemotherapy. Evidence shows that neo-adjuvant cisplatin containing chemotherapy has been shown to improve overall five-year survival rates by 8% compared to cystectomy alone.8
There is no difference shown between open and robotic cystectomies with regards to oncologic outcomes or major complications. Robot-assisted cystectomy has been shown to decrease length of stay and blood loss and is now the standard of care in our hospital.
Radiotherapy is delivered as part of a tri-modal treatment (TMT) option. It combines TURBT, chemotherapy and radiotherapy with the aim to achieve local tumour control in the bladder to preserve quality of life. Both cystectomy and radiotherapy have similar oncological outcomes over 5 years.
Metastatic Disease
Patients with metastatic disease can be categorised based on their fitness to undergo cisplatin-based chemotherapy, carboplatin-based chemotherapy, and finally platinum based therapy which has been the standard of care for decades.
Over the past decade the use of immunotherapy can be considered in patients that are unfit for cisplatin/carboplatin treatment.8 Additionally, the use of immune check-point inhibitors led to longer survival in patients with metastatic bladder cancer.9
Immunotherapy is also being considered in neoadjuvant
settings. Agents currently showing significant pathologic response includes Pembrolizumab and atezolizumab. These have yet to be included in routine practice.10
Looking forward
Emerging trials include CheckMate-901 that provided compelling results supporting the use of upfront chemotherapy and immunotherapy (Nivolumab + gemcitabine-cisplatin) in patients with previously untreated unresectable metastatic bladder cancer, or recurrence post-chemotherapy.11
An exciting second trial, called EV-302 (Ertofumab-Vedotin), compared the effectiveness of enfortumab plus pembrolizumab versus platinum-based chemotherapy as initial treatments for advanced bladder cancer. Tumours shrank or stopped growing in 67% of the enfortumabplus-pembrolizumab group versus 44% in the chemotherapy group. Pathological complete response was seen in 30% of the enfortumab-plus-pembrolizumab group, compared to 12% in the chemotherapy group. Most importantly, a median follow-up period of 18 months showed patients in the ertofumab-pluspembrolizumab group lived nearly twice as long as those in the chemotherapy group: a median of 31 months versus 16 months.12 It has recently been approved (September 2024) by the European Medicines Agency for its use for upfront chemotherapy for inoperable or metastatic bladder cancers that have not been treated before.13
The phase 3 NIAGARA is the first to challenge the standard neo-adjuvant approach for MIBC. Here, durvalumab was added to neoadjuvant chemotherapy before radical cystectomy and durvalumab monotherapy after surgery produced significant and clinically meaningful improvements in event-free survival and overall survival compared with NAC alone. Importantly, the addition of neoadjuvant durvalumab did not compromise the ability to complete radical cystectomy.14
Currently, HSE approved immunotherapies include:
1. Avelumab: First line maintenance for patients’ progression free after platinumbased therapy
2. Atezolizumab: Approved for patients post platinum or cisplatin- ineligible
3. Pembrolizumab: for prior platinum-treated or cisplatinineligible patients
4. Ertofumab-Vedotin: Approved for inoperable or metastatic bladder cancer in patients that have not been treated previously
Bladder cancer is increasing in incidence with an ageing population, and it varies in severity. With the progress currently made in bladder cancer treatment, there will be increased emphasis on tailored therapies. Ongoing studies looking at circulating tumour DNA is increasingly being investigated to assess which patients need perioperative systemic therapy after radical surgery.15 Bladder sparring treatment approaches are also being considered and evaluated to improve the quality of life of patients with MIBC.
References
1. Irish Cancer Society Bladder cancer. [Online]. Irish Cancer Society. Available at: www. cancer.ie/cancer-information-andsupport/cancer-types/bladdercancer [Accessed July 11, 2024]
2. Brennan P, Bogillot O, Cordier S et al. Cigarette smoking and bladder cancer in men: a pooled analysis of 11 case-control studies. International Journal of Cancer 2000; 86(2):28994
3. Rezaei F, Tabatabaee H, Rahmanian V, Mirahmadizadeh A, Hassanipour S. The correlation between bladder cancer and obesity, overweight, physical inactivity, and tobacco use: an ecological study in Asian Countries. Annal Global Health 2019; 85(1):102
4. National Cancer Registry Ireland. (2021). Incidence Statistics. NCRI. Available at: www.ncri.ie/data/incidencestatistic [Accessed 12 July 2024
5. Lin W, Pan X, Zhang C, Ye B, Song J. Impact of age at diagnosis of bladder cancer on survival: a surveillance, epidemiology, and end results-based study 2004. Cancer Control 2023. 30:1-14. doi: 10.1177/10732748231152322
6. EAU Guidelines. Edn. presented at the EAU Annual Congress Paris 2024. ISBN 978-94-92671-23-3.
7. Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression in Superficial Bladder Cancer, Lamm, Donald, European Urology Supplements, Volume 5, Issue 10, 654 – 659
8. Gunlusoy B, Arslan M, Vardar E et al. The efficacy and toxicity of gemcitabine and cisplatin
9. Maiorano B, Giorgi U, Ciardiello D et al. Immunecheckpoint inhibitors in advanced bladder cancer: seize the day. Biomedicines 2019; 10(2):411
10. Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY, Fradet Y, Oudard S, Vulsteke C, Morales Barrera R, Fléchon A, Gunduz S, Loriot Y, RodriguezVida A, Mamtani R, Yu EY, Nam K, Imai K, Homet Moreno B, Alva A; KEYNOTE-361 Investigators. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021 Jul;22(7):931-945. doi: 10.1016/S1470-2045(21)001522. Epub 2021 May 26. PMID: 34051178.
11. LBA7 Nivolumab plus gemcitabine-cisplatin versus gemcitabine-cisplatin alone for previously untreated unresectable or metastatic urothelial carcinoma: Results from the phase III CheckMate 901 trial van der Heijden, M.S. et al. Annals of Oncology, Volume 34, S1341
12. Powles, T. et al. (2024) ‘Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer’, New England Journal of Medicine, 390(10), pp. 875–888. doi:10.1056/ nejmoa2312117.
13. Authorisation details: EMA product number EMEA/ H/C/005392 Additional monitoring Padcev, European Medicines Agency (EMA). Available at: https://www.ema.europa.eu/en/ medicines/human/EPAR/padcev s
14. Powles TB, et al. A randomized phase 3 trial of neoadjuvant durvalumab plus chemotherapy followed by radical cystectomy and adjuvant durvalumab in muscle-invasive bladder cancer (NIAGARA). ESMO Congress 2024, LBA5
15. Ascione C, Napolitano F, Esposito D et al. Role of FGFR3 in bladder cancer: Treatment landscape and future challenges. Cancer Treat Rev 2023; 115(1):1
16. Staging and grading of bladder cancer, Macmillan Cancer Support. Available at: https:// www.macmillan.org.uk/cancerinformation-and-support/bladdercancer/staging-and-grading-ofbladder-cancer.
Clinical R&D
NEW
TREATMENT FOR PROSTATE CANCER PERFORMED FOR THE FIRST TIME IN IRELAND AT BEACON
HOSPITAL
A new and non-invasive treatment for prostate cancer has been successfully used in Ireland for the first time by Mr Mohammud Shakeel Inder in Beacon Hospital.
Focal Therapy (Sonablate HIFU System), involves the delivery of high intensity focused ultrasound energy (HIFU) to the affected area, which leads to a rapid rise in intracellular temperature, leading to instant cell death, while preserving surrounding tissue.
Unlike invasive surgery and radiotherapy, focal therapy does not impact on or damage surrounding cells, tissues or organs, significantly reducing the risks of erectile dysfunction, urinary incontinence and rectal toxicity. Compared to other treatments, focal therapy also provides patients with the highest chance to preserve ejaculation post-treatment.
The treatment is minimally invasive and performed under general anaesthesia. HIFU energy is delivered to an affected area of the prostate, externally via an ultrasound probe placed in the rectum. Treatment usually involves one session, which last an average of 1.5 - 2 hours. Most patients stay overnight in hospital and are discharged one day after surgery. Recovery is subjective but most patients are expected to be back to work within two weeks post treatment.
In studies on treatment outcomes for focal therapy for prostate cancer, survival rates are at 99 percent and treatment is best suited to those with localised prostate cancer that has not spread to other tissues or areas of the body.
Mr Mohammud Shakeel Inder, Consultant Urological Surgeon at Beacon Hospital said: “Prostate cancer is the most prevalent cancer in men in Ireland. One in seven men in Ireland will be diagnosed with the disease in their lifetime. With around 4,000 men affected yearly, it is important to adapt new technologies that provide better functional outcomes. By providing focal therapy in Ireland for the first time, patients suitable for the treatment can expect less downtime and a better quality of life without debilitating long-term side effects, often associated with prostate cancer treatment. Our first patient is on the road to recovery and a good prognosis is expected.”
Michael Cullen, CEO of Beacon Hospital said: “We are proud to announce yet another first-inIreland treatment being carried out here at Beacon Hospital. This innovative focal therapy is not only less invasive than traditional methods, but also significantly reduces common side effects and will have a dramatic impact on the lives of our patients. As one of the most technologically advanced private hospitals in Europe, we continue to invest heavily in the latest innovations to provide pioneering world-class medical and surgical care to our patients.”
DARZALEX® (DARATUMUMAB)SC BASED QUADRUPLET REGIMEN APPROVED BY THE EUROPEAN COMMISSION FOR PATIENTS WITH NEWLY DIAGNOSED MULTIPLE MYELOMA WHO ARE TRANSPLANT-ELIGIBLE
Janssen-Cilag International NV, a Johnson & Johnson company, has announced that the European Commission (EC) approved the indication extension for DARZALEX® (daratumumab) subcutaneous (SC) formulation in combination with bortezomib, lenalidomide and dexamethasone (daratumumab-VRd) in patients with newly diagnosed multiple myeloma (NDMM) who are eligible for an autologous stem cell transplant (ASCT). Patients will have the opportunity to receive this daratumumab SCbased quadruplet therapy at initial diagnosis, providing them with a new treatment shown to significantly improve outcomes.
This approval is supported by data from the Phase 3 PERSEUS study, which evaluated daratumumab SC-based quadruplet regimen for induction and consolidation therapy, followed by daratumumab SC and lenalidomide (D-R) maintenance therapy, compared to bortezomib, lenalidomide and dexamethasone (VRd) during induction and consolidation, followed by lenalidomide (R) maintenance in 709 patients with NDMM eligible for ASCT.
Michaela Hagenhofer, General Manager, Commercial Operations at Johnson & Johnson Innovative Medicine said: “Since daratumumab was first made available to Irish patients in 2018, it has become a foundational therapy for the treatment of multiple myeloma and has been used to treat more than 548,000 patients worldwide. At Johnson & Johnson, our ambition is to get in front of this incurable disease. The EC approval of this daratumumab SC based quadruplet regimen in frontline therapy marks a step towards a new standard of care. With a twenty-year heritage in
research and development in treating multiple myeloma, we are committed to continuing to deliver innovations to treat all patients across all stages of this disease.” Multiple myeloma is the second most common blood cancer.6 Approximately 352 people are diagnosed with multiple myeloma each year in Ireland, with an estimated 2,200 people living with the condition. Data shows that the five-year net survival for someone diagnosed with MM in Ireland has increased by 37% from 27% to 64% in the period from 1994-2018. However, global data shows that almost 29% of patients diagnosed with MM will die within the first year.
Findings from the PERSEUS study, after a median follow-up of 47.5 months, demonstrated a significant improvement in the primary endpoint of progressionfree survival (PFS), with the daratumumab-VRd regimen reducing the risk of disease progression or death by 58 percent compared to VRd (hazard ratio [HR], 0.42; 95 percent confidence interval [CI], 0.30-0.59; p<0.0001).1
Treatment with daratumumabVRd resulted in deeper responses compared to VRd with overall minimal residual disease (MRD)negativity rate assessed at 10-5 of 75.2 percent vs. 47.5 percent (p<0.001), complete response or better of 87.9 percent vs 70.1 percent (p<0.001) and importantly, sustained MRD negativity for ≥12 months of 64.8 percent vs 29.7 percent, respectively.
The overall safety profile of daratumumab-VRd was consistent with the known safety profiles for daratumumab SC and VRd. The most common haematologic adverse reactions (≥20 percent) in patients with multiple myeloma who received daratumumabVRd vs VRd were neutropenia (69.2 percent vs 58.8 percent), thrombocytopenia (48.4 percent vs 34.3 percent) and anaemia (22.2 percent vs 20.7 percent). The most common non-hematologic adverse reactions (≥20 percent) in patients with multiple myeloma who received daratumumabVRd vs VRd were peripheral neuropathy (53.6 percent vs 51.6 percent), fatigue (23.9 percent vs 26.5 percent), peripheral oedema (20.5 percent vs 21.3 percent), pyrexia (31.6 percent vs 31.4 percent), upper respiratory infection (31.6 percent vs 25.1 percent), COVID-19 (35 percent vs 23.9 percent), constipation (33.9 percent vs 34.0 percent), diarrhoea (61.0 percent vs 54.2 percent), back pain (22.8 percent vs 19.0 percent), insomnia (27.1 percent vs 17.6 percent), asthenia (26.8 percent vs 25.6 percent) and rash (23.4 percent vs 27.1 percent).
Daratumumab is currently approved in eight indications for multiple myeloma, four of which are in the frontline setting, including as part of treatment regimens for newly diagnosed patients who are transplant-eligible or ineligible for ASCT. Since 2015, DARZALEX® (daratumumab) has been manufactured at Johnson & Johnson’s biopharmaceutical manufacturing site in Ringaskiddy, Co Cork
EARLY PHASE TRIAL A FIRST FOR CHILDREN IN IRELAND
Children’s Health Ireland (CHI), in partnership with St. James’s Hospital have successfully opened Ireland’s first early phase clinical trial, enrolling eligible children with Duchenne muscular dystrophy (DMD). The global trial, called DELIVER, which started in August 2022 as the first-in-human (phase 1/2) trial of a therapeutic called DYNE-251 at sites around the world targets male children with a specific type of DMD (children amenable to exon 51 skipping). The trial is being delivered by the HRB CHI Clinical Research Centre and the Wellcome HRB Clinical Research Facility at St James’s Hospital and involves delivery of a next generation molecular therapy developed by Dyne Therapeutics, a Massachusetts based biotechnology company, specialising in the development of therapies for rare muscle diseases. The study is progressing through at sites around the world but is the first time such an early phase trial has been conducted in children in Ireland.
Duchene muscular dystrophy (DMD) is a rare neuromuscular disease that results in progressive deterioration in muscle strength and premature death. Symptoms are often first detected as early as age two, but diagnosis often occurs between four and five years of age. The disease is almost exclusively seen in boys. It is caused by gene mutations that affect a protein called dystrophin, which plays a critical role in muscle cell structure and function. As they grow, children with DMD become gradually weaker, losing the ability to walk and ultimately being confined to a wheelchair. Weakness of the muscles involved in swallowing, breathing and heart function are particularly serious and ultimately life threatening. Currently, very few treatments are available for this devastating disease, and children and their families are anxiously awaiting treatments that can target the basic defect in DMD, aimed at slowing or stopping the inevitable decline in muscle function.
Clinical trials can be extremely complex to undertake and are
governed by very strict and detailed safety codes. They involve years of careful planning by a large team of experts within the hospitals, regulators and industry. Global healthcare regulatory agencies comprehensively review data on investigational medicines before the clinical trial can start in humans.
Dr Declan O’Rourke, Consultant Paediatric Neurologist and principal investigator for the study at CHI, said, “This is a watershed moment for CHI. We have been working for many years to increase the number of trials we offer to our patients with progressive muscle diseases and have had some great successes already. DMD is a condition with very few treatment options currently, and with this trial, it is great to be at the very forefront of potentially bringing new, transformative therapies to children.”
The development of clinical trials in Neurology in CHI has been supported by a research grant from Children’s Health Foundation, CHI’s fundraising partner.
CHI’s Director of Research & Innovation, Paul McNally welcomed CHI’s participation in the ongoing study saying:
“This is an exciting day for everyone involved in clinical trials in CHI. These early phase trials are an enormous undertaking but a vitally important thing for us to be able to do if we really want to become a leading children’s hospital and offer our patients the very latest in cutting edge treatments in the world. Our partnership with St James’s Hospital has been critical here and is an example of the type of benefits that we can expect when working together on the same campus when we move to the new children’s Hospital.”
Having previously supported the CHI team to deliver gene therapy to many infants with a rare neurological disorder, the Wellcome HRB Clinical Research Facility at St James’s Hospital is no stranger to advanced paediatric trials. Director of the centre Prof. Martina Hennessy said:
“We are delighted to see this important ongoing trial finally becoming available in Ireland, resulting from the hard work and collaboration between the teams at CHI and St James’s. With the support of our funders and amazing colleagues, our centre has developed the facilities and expertise to be able to deliver the most advanced trials to both adults and children. This very productive partnership with CHI will allow us to explore new and potentially better types of medicines that may
offer a meaningful impact on this and other disease.”
DANDELION CLOCK SCULPTURES
This month, Children’s Health Ireland (CHI) proudly completed the installation of two Dandelion Clock sculptures at the west entrance of the New Children’s Hospital. These striking sculptures, designed by renowned artist, Remco deFouw, and fabricated by Hickeys Engineering, mark the final piece in a series that now visually connects all Children's Health Ireland sites, including CHI at Connolly and CHI at Tallaght.
The Dandelion Clocks, first installed at CHI at Connolly and CHI at Tallaght in July, feature prisms that refract sunlight to project rainbows into the hospital buildings at certain times of the year. This unique design brings light and colour into the hospitals, creating a calming and uplifting atmosphere for children, young people, families and staff.
The sculptures are part of CHI’s Arts in Health Programme, which commissions original artworks from leading artists to ensure that the new hospital and its satellite centres offer an engaging, healing and creative environment for children and young people. The Dandelion Clocks directly respond to the hopes expressed by patients
Remco deFouw, Christian Brodie, Sinead White and CHI staff at the launch of the Dandelion Clock sculptures
and staff that art within the hospital would bring brightness and joy to these spaces.
“We are thrilled to see these beautiful sculptures now installed across all CHI sites,” said Mary Grehan, Arts in Health Curator.
“The Dandelion Clocks not only enhance the environment, but they also reflect our commitment to supporting the emotional and psychological well-being of the children and families we care for.”
The Dandelion Clock sculptures and the broader Arts in Health Programme are generously supported by the Children’s Health Foundation, whose ongoing contributions ensure the hospitals remain places of inspiration, creativity and healing.
GSK PRESENTS POSITIVE DATA FOR AREXVY, ITS RESPIRATORY SYNCYTIAL VIRUS (RSV) VACCINE, INDICATING PROTECTION OVER THREE RSV SEASONS
GSK Ireland has announced new data from the AReSVi-006 (Adult Respiratory Syncytial Virus) phase III trial evaluating the efficacy of a single dose of Arexvy (respiratory syncytial virus vaccine, recombinant adjuvanted) against lower respiratory tract disease (LRTD) caused by respiratory syncytial virus (RSV) in adults aged 60 years and older, including those at increased risk over three RSV seasons (NCT04886596).
[i] This data was presented at the CHEST 2024 Annual Meeting, organised by the American College of Chest Physicians.
Arexvy was the first RSV vaccine approved in the EU based on efficacy results for the prevention of lower respiratory tract disease (LRTD) caused by respiratory syncytial virus (RSV) in individuals 60 years of age and older and it is now also approved for use in individuals aged 50-59 who are at increased risk due to certain underlying medical conditions. These results indicate that after a single dose of GSK’s RSV vaccine, cumulative efficacy over three RSV seasons was clinically meaningful at 62.9% against RSV-LRTD (97.5% CI, 46.7-74.8, 48 of 12,468 vs 215 of 12,498) and 67.4% against severe RSV-LRTD (95% CI, 42.4-82.7,15 of 12,468 vs 75 of 12,498) compared to placebo. In the third season, the vaccine’s efficacy was 48.0% against RSVLRTD (95% CI, 8.7-72.0, 16 of 4,988 vs 61 of 10,031).
These results include efficacy against different RSV subtypes, in adults with advancing age (70-79 years of age), and those with certain underlying medical conditions. Since RSV can exacerbate medical conditions and potentially lead to hospitalisations, cumulative efficacy over three RSV seasons has the potential for significant health impact. It has the potential to offer health care professionals flexibility to administer the vaccine year-round. Over time, revaccination is expected to be required to maintain an optimal level of protection.
Eavan Daly, Director of Medical Affairs, GSK Ireland, said: “We are excited by this new data which
Clinical R&D
shows that a single dose of Arexvy could protect older adults in Ireland at risk of RSV disease over three seasons to benefit public health. Arexvy has 94.6% efficacy in adults aged 60 years and older with at least one comorbidity of interest during the first season and is the only RSV vaccine with efficacy and safety data available through three seasons. We look forward to ongoing dialogue with the HSE and healthcare professionals to ensure equity of access to RSV vaccination, including those who are at high risk for severe outcomes and hospitalisation from RSV and account for the biggest burden on our healthcare system.”
RSV is a common contagious virus affecting the lungs and breathing passages and impacts an estimated 64 million people of all ages globally every year.[ii] Adults can be at increased risk for RSV disease due to comorbidities, immune compromised status, or advanced age. RSV can exacerbate multiple conditions, including COPD, asthma, and chronic heart failure, and can lead to severe outcomes, such as pneumonia, hospitalisation, and death.[iii] Each year RSV causes over 465,000 hospitalisations and 33,000 deaths in adults aged 60 and older in high-income countries.[iv]
Professor Patrick Mitchell, Consultant Respiratory Physician at Trinity College Dublin and Tallaght University Hospital, said: “In Ireland I continue to see a significant increase in hospital admissions caused by RSV. Reducing the burden of this virus is a key priority for healthcare professionals as unfortunately some patients do end up being admitted to hospital and even the intensive care units as a result. Ireland is among 16 countries globally that have national RSV vaccination recommendations for older adults and I hope we join other countries that already have national immunisation programmes in place.”
References
[i] Clinicaltrials.gov, “Efficacy Study of GSK's Investigational Respiratory Syncytial Virus (RSV) Vaccine in Adults Aged 60 Years and Above”. Available at: https://clinicaltrials.gov/study/ NCT04886596 - last accessed: September 2024
[ii] National Institute of Allergy and Infectious Diseases, Respiratory Syncytial Virus (RSV). Available at: https://www.niaid.nih.gov/ diseases-conditions/respiratorysyncytial-virus-rsv – last accessed: September 2024
[iii] Centers for Disease Control and Prevention (CDC), RSV in Older Adults, 2024. Available at: https://www.cdc.gov/rsv/olderadults/index.html - Last accessed: September 2024
[iv] Savic M, et al., “Respiratory syncytial virus disease burden in adults aged 60 years and older in high-income countries: a systematic literature review and meta-analysis”, in Influenza Other Respir Viruses, 2023, 17(1):e13031, DOI: 10.1111/irv.13031
APPOINTMENT OF NEW CHAIRPERSON OF THE NATIONAL CANCER REGISTRY BOARD (NCRB)
Following a States Board campaign, the Minister for Health Stephen Donnelly T.D. has appointed Dr Robert O'Connor as the new Chair of the National Cancer Registry. The appointment comes in the year the National Cancer Registry marks its 30th anniversary of collecting comprehensive cancer information for the population of the Republic of Ireland.
Robert O'Connor Ph.D. has been a member of the National Cancer Registry Board since 2019. Robert has served on multiple national charity, health and research boards and is Director of the HRB-funded National Clinical Trials Office. With over 25 years of experience in clinical trials, oncology, and translational health research, he brings a fount of knowledge and a deep commitment to advancing cancer research and improving patient outcomes, making him an ideal fit for this critical role.
Robert’s Postdoctoral research transitioned laboratory findings into early-stage clinical trials for cancer. He served as Executive Chair at ICORG (now Cancer Trials Ireland), fostering connections between laboratory and clinical researchers. A former lecturer at Dublin City University, Robert later became Director of Research for the Irish Cancer Society, where he delivered the research strategy of the organisation, helped support the inclusion of research into national cancer treatment policy and developed patient partnership initiatives.
Welcoming the appointment of Dr Robert O’Connor, Prof. Deirdre Murray, Director of the NCRI, said: “Robert brings a wealth of experience to the National Cancer Registry with a strong research background and governance experience. I look forward to working with Robert and the other Board members in implementing our ambitious strategy.”
As Chair, Robert will lead the seven member NCRB, overseeing governance, strategic direction, and management of the Registry to ensure transparency, ethics, and effectiveness in serving the cancer community.
“I am immensely honoured to have been nominated as Chair of the Board of the National Cancer Registry,” said Robert following his appointment. “Our community faces a growing tide of cancer challenges and accurate, timely and trusted insight on cancer will be of ever-greater importance if we are to keep driving
improvements in outcome for people affected by cancer.
“I look forward to our ongoing strategy and governance work with my excellent fellow members of the Board, the world class team within our National Cancer Registry, our ever-supportive colleagues in the Cancer Policy Unit of the Department of Health and our many other stakeholders. Together, we will ensure the Registry remains a vital, trusted resource for those affected by cancer, policymakers, researchers, and the public.”
THE NMH FOUNDATION ANNOUNCES SPONSORSHIP WITH BEPANTHEN NAPPY CARE OINTMENT ON WORLD PREMATURITY DAY
The National Maternity Hospital Foundation, in partnership with Bepanthen Nappy Care Ointment, marked World Prematurity Day with a special event welcoming families of children who were born prematurely at the hospital. Each year, over 4,500 babies are born prematurely in Ireland, with 1,202 babies born prematurely at the National Maternity Hospital last year.
As part of the sponsorship, Bepanthen will provide vital support to the NMH Foundation for the pioneering work taking place in The NMH’s Neonatal Intensive Care Unit (NICU), a world-class facility renowned for its dedication to saving and nurturing the lives of babies born too soon. The collaboration will focus on supporting cutting-edge research, fostering innovation, and developing new treatments and solutions to help premature infants to survive and thrive.
Bepanthen Nappy Care Ointment, which celebrates its 80th anniversary in 2024, is a breathable barrier cream designed to protect vulnerable skin from irritants and other causes of nappy rash.
Mary O’Donovan, Executive Director of The NMH Foundation, commented, “We are delighted to partner with Bepanthen in this meaningful initiative, particularly as we celebrate World Prematurity Day. The sponsorship funds will help us to accelerate vital research and innovation at The NMH, giving premature babies a better chance at survival and a healthier future. Together, we are committed to advancing neonatal care and ensuring every baby born too soon gets the best possible care.”
Lyndsey Ashe Byrne, Mother of Baby Stephen said, “If it wasn’t for the amazing staff at The National Maternity Hospital, we might not have our gorgeous baby Stephen with us this Christmas. Last year while I was pregnant with him,
accelerate the painstaking work of drug discovery and development. Ultimately, this collaboration has the potential to positively impact patient pathways.
Against this backdrop, partnerships between indigenous firms and multinationals such as the Novartis and Deciphex collaboration, can deliver positive economic, clinical and societal outcomes in the coming years.
The roundtable also heard that with AI set to transform sectors such as healthcare over the coming years, the public and patients are being engaged to ascertain the degree in which safeguards and regulation can provide comfort that with AI advances, a human will still be in the loop. The Irish public are being invited to share their insights for policymakers through important initiatives such as the IPPOSI ‘Citizens’ Jury on AI in Healthcare’.
Dr. Donal O’Shea, CEO of Deciphex said: “We are thrilled to collaborate with Novartis in leveraging AI technology to drive innovation in preclinical research. This partnership underscores our commitment to advancing healthcare through the development of cutting-edge solutions that address critical challenges in drug development lifecycles. Novartis is committed to innovating AI-based approaches with potential to accelerate drug discovery and development and bring life-changing medicines to patients faster.” Statement approved by stakeholder
he stopped moving at around 30 weeks. When he was born, he was so tiny, just 2lbs. The NMH NICU team saved him. They knew what to do, they gave him a fighting chance, and he is thriving now. We are so grateful”.
Holly Elliott-Gurr, Brand Manager, Bepanthen said, “We are honoured to partner with the NMH Foundation and contribute to their mission of funding lifechanging research happening at The National Maternity Hospital. Our commitment to baby health and wellbeing aligns perfectly with the Foundation's mission, and we are excited to see the impact this collaboration will have on premature infants and their families. That is why we will be donating to the NMH Foundation for every Bepanthen Nappy Care Ointment sold.”
NOVARTIS AND DECIPHEX HOST ROUNDTABLE ABOUT IRELAND’S AI SECTOR TO MARK COLLABORATION
Novartis Ireland has marked its Collaboration Agreement with Deciphex, a Dublin-based digital pathology company, at a specially convened roundtable on Artificial Intelligence (AI).
The collaboration is a global agreement between Novartis and Deciphex. Harnessing cuttingedge technology, it seeks to develop a suite of AI tools that will improve the efficiency and accuracy of preclinical studies and
In Ireland, Novartis and Deciphex marked the agreement at a panel discussion titled ‘How Ireland can be the Centre of Artificial Intelligence (AI) for Europe’. Taking place at Novartis Ireland and officiated by Minister of State for Digital Dara Calleary TD, the event featured contributions from Novartis and Deciphex leadership and representatives from IDA Ireland and patient-led platform, IPPOSI.
The event heard from panelists that government policies and State support, ongoing investment and a strong pipeline of tech talent from universities are key factors in creating a fertile ecosystem where the AI sector in Ireland is flourishing.
Minister of State for Digital Dara Calleary TD said: “I am delighted to officiate at today’s panel discussion. Ireland’s AI sector is flourishing, with a partnership approach between State bodies, enterprise and the public key to delivering transformative societal benefits in the coming years. The Novartis-Deciphex collaboration is a great example of how this approach works in practice, with an indigenous medtech collaborating with a global leader in pharma to harness cutting-edge technology and deliver better outcomes for patients.”
Michael Lohan, CEO, IDA Ireland said, “Artificial Intelligence is a cornerstone of Ireland’s strategy to drive innovation and fuel economic growth. By fostering a robust AI ecosystem, we are not only attracting leading global tech companies but also empowering local enterprises to compete on the world stage. The integration of AI across various sectors is pivotal in enhancing productivity, creating high-value jobs, and ensuring Ireland remains at the forefront of technological advancements”
Caitriona Walsh, Country President, Novartis Ireland said: “I’m excited that Novartis has entered into a collaboration agreement with Deciphex to develop Artificial Intelligencebased approaches aimed at improving the efficiency and accuracy of preclinical studies. We believe AI has transformative potential to accelerate the painstaking work of drug discovery and development. I look forward to seeing how our collaborative efforts can help us improve and streamline existing processes to deliver impactful medicines to patients more quickly.”
Pictured at the Novartis and Deciphex AI event are (from left): Caitriona Walsh, Country President, Novartis Ireland, Dr. Donal O’Shea, CEO of Deciphex and Laura Kavanagh, Research & Advocacy Manager, the Irish Platform for Patients’ Organisations (IPPOSI). Pictured taking part in the panel discussion are (from left); Moderator Elaine Burke; Minister of State for Digital Dara Calleary TD; Laura Kavanagh and Neasa McNabola, Senior Scientific Adviser, IDA BioPharma Team
Baby Stephen pictured here with Mum Lyndsey, Dad Stephen and Sister Layla