
LEGAL CATEGORY: POM (S1A). MARKETING AUTHORISATION NUMBERS/PRESENTATIONS: 10mg film-coated tablet, 14 tablets, EU/1/16/1138/002; 50mg film-coated tablet, 7 tablets, EU/1/16/1138/004; 100mg film-coated tablet, 7 tablets, EU/1/16/1138/005;100mg film-coated tablet, 14 tablets, EU/1/16/1138/006; 100mg film-coated tablet, 112 tablets, EU/1/16/1138/007. MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany. Further information is available from AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. † Indications are not reimbursed. * Indications are reimbursed. References: 1. VENCLYXTO ® Summary of Product Characteristics, available at www.medicines.ie. IE-VNCCLL-220013 Date of Preparation: February 2022 ▼
VENCLYTXO® REGIMENS ARE NOW AVAILABLE FOR THE TREATMENT OF ALL ADULT PATIENTS WITH CLL1
PROFESSIONALHOSPITALNEWS IRELAND Ireland’s Dedicated Hospital Professional Publication HPN September HOSPITALPROFESSIONALNEWS.IEIssue2022100 This Publication is for Healthcare Professionals Only IN THIS HealthONCOLOGYInternationalPrescriptionRiseNEWS:ISSUE:inGenericMedicinesinMarketPage7PHARMACY:RoleofPharmacistsinDosageFormsPage13REPORT:PharmacyPrescribing–LearningfromModelsPage20FEATURE:TypeAAorticDissectionPage20CPD:ManagementofTransthyretinAmyloidosisPage31FOCUS:EconomicsofColorectalCancerPage38SYMPOSIUM:InnovationsinPsoriasisandAtopicDermatitisPage49INDICATIONS1: VENCLYXTO ® in combination with obinutuzumab is indicated for the treatment of adult patients with previously untreated chronic lymphocytic leukaemia (CLL) (see section 5.1). VENCLYXTO ® in combination with rituximab is indicated for the treatment of adult patients with CLL who have received at least one prior therapy*. VENCLYXTO® monotherapy is indicated for the treatment of CLL in the presence of 17p deletion or TP53 mutation in adult patients who are unsuitable for or have failed a B cell receptor pathway inhibitor or in the absence of 17p deletion or TP53 mutation in adult patients who have failed both chemoimmunotherapy and a B cell receptor pathway inhibitor.* VENCLYXTO ® in combination with a hypomethylating agent is indicated for the treatment of adult patients with newly diagnosed acute myeloid leukaemia (AML) who are ineligible for intensive chemotherapy.† Full Summary of Product Characteristics is available at www.medicines.ie. ▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; Website: www. hpra.ie. Suspected adverse events should also be reported to AbbVie Limited on 01-4287900.


In ORAL Solo, XELJANZ delivered rapid reduction in the signs and symptoms of RA as early as week 2, with significant reductions at month 3 vs placebo (P<0.001).1
aFrom the start of treatment with XELJANZ in patients with moderate to severe RA who responded inadequately to, or who are intolerant to one or more DMARDs. 4
All rights reserved. April 2022
CAN
WITH RAPID
XELJANZ® (tofacitinib) Prescribing Information: Please refer to the Summary of Product Characteristics (SmPC) before prescribing XELJANZ 5 mg or 10 mg film-coated tablets, XELJANZ 11 mg prolonged release tablets or XELJANZ 1 mg/mL oral solution. Presentation: Film-coated tablet containing tofacitinib citrate, equivalent to 5 mg or 10 mg tofacitinib. Prolonged-release tablets containing tofacitinibcitrate, equivalent to 11 mg tofacitinib. Oral solution containing tofacitinib citrate, equivalent to 1 mg/mL tofacitinib. Indications: Please note not all presentations are licensed for all indications, please see dosage section for details: In combination with methotrexate (MTX) for the treatment of moderate to severe active rheumatoid arthritis (RA) in adult patients who have responded inadequately to, or who are intolerant to one or more disease-modifying antirheumatic drugs. Can be given as monotherapy incase of intolerance to MTX or when treatment with MTX is inappropriate. In combination with MTX for the treatment of active psoriatic arthritis (PsA) in adult patients who have hadan inadequate response or who have been intolerant to a prior disease modifying antirheumatic drug (DMARD) therapy. For the treatment of adult patients with active ankylosingspondylitis (AS) who have responded inadequately to conventional therapy. For the treatment of adult patients with moderately to severely active ulcerative colitis (UC) who have had an inadequate response, lost response, or were intolerant to either conventional therapy or a biologic agent. For the treatment of active polyarticular juvenile idiopathic arthritis(rheumatoid factor positive [RF+] or negative [RF-] polyarthritis, and extended oligoarthritis), and juvenile psoriatic arthritis in patients 2 years of age and older, who have responded inadequately to previous therapy with DMARDs. Can be given in combination with MTX or as monotherapy in case of intolerance to MTX or where continued treatment with MTX is inappropriate. Dosage: Treatment should be initiated and supervised by specialist physicians experienced in the diagnosis and treatment of the condition for which tofacitinib is indicated. Tofacitinib is given orally, with or without food. RA and PsA: The recommended dose is 5 mg twice daily or 11 mg once daily which should not be exceeded. Treatment with tofacitinib 5 mg film coated tablets twice daily and tofacitinib 11 mg prolonged release tablet once daily may be switched between each other on the day following the last dose of either tablet. AS: The recommended dose is 5 mg twice daily. Available data suggest that clinical improvement in AS is observed within 16 weeks of initiation of treatment. Continued therapy should be carefully reconsidered in AS patients exhibiting no clinical improvement within this timeframe. UC: The recommended dose is 10 mg twice daily for induction for 8weeks. For patients who do not achieve adequate therapeutic benefit by week 8, the induction dose of 10 mg twice daily can be extended for an additional 8 weeks (16 weeks total), followed by 5 mg twice daily for maintenance. Tofacitinib induction therapy should be discontinued in any patient who shows no evidence of therapeutic benefit by week 16. The recommended dose for maintenance treatment is tofacitinib 5 mg twice daily. Tofacitinib 10 mg twice daily for maintenance treatment is not recommended in patients with UC whohave known venous thromboembolism (VTE) risk factors, unless there is no suitable alternative treatment available. For patients with UC who are not at increased risk for VTE, tofacitinib 10 mg twice daily may be considered if the patient experiences a decrease in response on tofacitinib 5 mg twice daily and failed to respond to alternative treatment options for UC such as tumour necrosis factor inhibitor treatment. Tofacitinib 10 mg twice daily for maintenance treatment should be used for the shortest duration possible. The lowest effective dose needed to maintain response should be used. Polyarticular JIA and juvenile PsA: The recommended dose in patients 2 years of age and older: 10 kg - < 20 kg: 3.2mg (3.2 mL oral solution) twice daily, 20 kg - < 40 kg: 4 mg (4 mL oral solution) twice daily, and ≥ 40 kg 5 mg (5 mL oral solution or 5 mg tablet) twice daily. Patients ≥ 40 kg treated with tofacitinib 5 mL oral solution twice daily may be switched to tofacitinib 5 mg tablets twice daily. Available data suggest that clinical improvement is observed in paediatric patients within 18 weeks of initiation. Continued therapy should be carefully reconsidered in a paediatric patient exhibiting no clinical improvement within this timeframe. Dose interruption and adjustment: Tofacitinib treatment should be interrupted if a patient develops a serious infection until the infection is controlled. Interruption of dosing may be needed for management of dose-related laboratory abnormalities including lymphopenia, neutropenia, and anaemia. It is recommended not to initiatedosing in patients with an absolute lymphocyte count (ALC) less than 0.75 x 10 9/L, an absolute neutrophil count (ANC) less than 1x10 9 /L or with haemoglobin less than 9 g/dL. It is recommended not to initiate dosing in paediatric patients with an absolute neutrophil count (ANC) less than 1.2 x 10 9/L or with haemoglobin less than 10 g/dL. Renal impairment: No dose adjustment is required in patients with mild or moderate renal impairment. Patients with severe renal impairment the dose should be reduced to 5 mg once daily when the indicated dose in the presence of normal renal function is 5 mg twice daily or 11 mg prolonged-release tablet once daily. Dose should be reduced to 5 mg twice daily when the indicated dose in the presence of normal renal function is 10 mg twice daily. Patients with severe renal impairment should remain on a reduced dose even after haemodialysis. Hepatic impairment: No dose adjustment is required in patients with mild hepatic impairment. Patients with moderate hepatic impairment dose should be reduced to 5 mg once daily when the indicated dose in the presence of normal hepatic function is 5 mg twice daily or 11 mg prolonged-release tablet once daily. Dose should be reduced to 5 mg twice daily when the indicated dose in the presence of normal hepatic function is 10 mg twice daily. Tofacitinib should not be used in patients with severe hepatic impairment. Elderly: No dose adjustment is required in patients aged 65 years and older. Use with caution as increased risk and severity of adverse events. See also Warnings & Precautions for use in patients over 65 years of age. Paediatric population: The safety and efficacy of tofacitinib in children less than 2 years of age with polyarticular JIA and juvenile PsA has not been established. The safety and efficacy of tofacitinib inchildren less than 18 years of age with other indications (e.g. ulcerative colitis) has not been established. The safety and efficacy of tofacitinib prolongedrelease formulation in children aged less than 18 years have not been established. Interactions: TTofacitinib total daily dose should be reduced by half inpatients receiving potent inhibitors of cytochrome P450 (CYP) 3A4 (e.g. ketoconazole) and in patients receiving 1 or more products that result in bothmoderate inhibition of CYP3A4 and potent inhibition of CYP2C19 (e.g. fluconazole). Coadministration with potent CYP inducers (e.g. rifampicin) may result in a loss of or reduced clinical response. Coadministration with potent inducers of CYP3A4 is not recommended. Contraindications: Hypersensitivity to anyof the ingredients, active tuberculosis (TB), serious infections such as sepsis, or opportunistic infections, severe hepatic impairment, pregnancy and lactation. Warnings and Precautions: Patients treated with tofacitinib should be given a patient alert card. Use in patients over 65 years of age: Considering the increased risk of serious infections, myocardial infarction, and malignancies with tofacitinib in patients over 65 years of age, tofacitinib should only be used in patients over 65 years of age if no suitable treatment alternatives are available. Combination with other therapies: There was a higher incidence of adverse events for the combination of tofacitinib with MTX versus tofacitinib as monotherapy in RA clinical studies. Tofacitinib should be avoided in combination with biologics and potent immunosuppressants such as azathioprine, 6-mercaptopurine, ciclosporin and tacrolimus. Venous thromboembolism (VTE): Serious VTE events including pulmonary embolism (PE), some of which were fatal, and deep vein thrombosis (DVT), have been observed in patients taking tofacitinib. In a randomised post authorisation safety study in patients with rheumatoid arthritis who were 50 years of age or older with at least one additional cardiovascular risk factor, a dose dependent increased risk for VTE was observed with tofacitinib compared to TNF
Xeljanz in combination with MTX is indicated for the treatment of moderate to severe active rheumatoid arthritis in adult patients who have responded inadequately to, or who are intolerant to one or more DMARDs. Xeljanz given as monotherapy in case of intolerance to MTX or when treatment with MTX is inappropriate.
In patients over 65 years of age, patients who are current or past smokers, patients with other cardiovascular risk factors, and patients with other malignancy risk factors, XELJANZ should only be used if no suitable treatment alternatives are available. RESPONSE THE DIFFERENCE XELJANZ®
AND THE LARGEST SEE
PP-XEL-IRL-0722 © 2022 Pfizer Inc.
bPublished as of October 2020. Clinical trial program includes patients with RA who received ≥1 XELJANZ dose across the completed 2 phase 1, 10 phase 2, 6 phase 3, 1 phase 3b/4 index studies, and 2 open-label LTE studies. 2 RA=rheumatoid arthritis; JAKi=Janus kinase inhibitor; DMARDs=disease-modifying antirheumatic drugs; IR=inadequate responder; ACR=American College of Rheumatology; MTX=methotrexate.
At month 3, significantly more DMARD-IR patients with RA who received XELJANZ monotherapy achieved ACR20 response (primary endpoint) vs placebo (59.8% vs 26.7%; P<0.001) in a phase 3, randomised, double-blind, placebo-controlled study (N=610)1
Proven in 6 phase 3 trials, with >7000 patients evaluated across treatment arms in the clinical trial program2,b inhibitors. In a post hoc exploratory analysis within this study, in patients with known VTE risk factors, occurrences of subsequent VTEs were observedmore frequently in tofacitinib-treated patients that, at 12 months treatment, had D-dimer level greater than or equal to twice the upper limit of normal (2×ULN) versus those with D-dimer level <2×ULN. For patients with RA with known risk factors for VTE, consider testing D-dimer levels after approximately 12 months of treatment. If D-dimer test result is ≥ 2× ULN, confirm that clinical benefits outweigh risks prior to a decision on treatment continuation with tofacitinib. Tofacitinib should be used with caution in patients with known risk factors for VTE, regardless of indication and dose. Tofacitinib 10 mg twice daily for maintenance treatment is not recommended in patients with UC who have known VTE risk factors, unless there is no suitable alternative treatment available. Promptly evaluate patients with signs and symptoms of VTE and discontinue tofacitinib in patients with suspected VTE, regardless of dose or indication. Infections: Serious and sometimes fatal infections have been reported in patients administered tofacitinib. Rheumatoid arthritis patients taking corticosteroids may be predisposed to infection. Patients should be closely monitored for infections, with prompt diagnosis and treatment. Treatment should be interrupted if a serious infection develops. As there is a higher incidence of infections in the elderly and in the diabetic populations in general, caution should be used when treating the elderly and patients with diabetes. Tuberculosis: Patients should be evaluated for both active and latent TB prior to being treated with tofacitinib. Patients who test positive for latent TB should be treated with standard antimycobacterial therapy before administering tofacitinib. Viral Reactivation: In clinical studies viral reactivation and cases of herpes zoster have been observed. Screening for viral hepatitis should be performed in accordance with clinical guidelines prior to starting therapy with tofacitinib. The impact on chronic viral hepatitis is not known. Major adversecardiovascular events (MACE): MACE have been observed in patients taking tofacitinib. In a randomised post authorisation safety study in patients with RA who were 50 years of age or older with at least one additional cardiovascular risk factor, an increased incidence of myocardial infarctions was observed with tofacitinib compared to TNF inhibitors. In patients over 65 years of age, patients who are current or past smokers, and patients with other cardiovascular risk factors, tofacitinib should only be used if no suitable treatment alternatives are available. Vaccinations: Prior to initiating tofacitinib, it is recommended that all patients, particularly pJIA and jPsA patients, be brought up to date with all immunisations in agreement with current immunisation guidelines. Live vaccines should not be given concurrently with tofacitinib. Malignancy and lymphoproliferative disorder: Tofacitinib may affect host defences against malignancies. In a randomised post authorisation safety study in patients with RA who were 50 years of age or older with at least one additionalcardiovascular risk factor, an increased incidence of malignancies excluding non-melanoma skin cancer (NMSC), particularly lung cancer and lymphoma, was observed with tofacitinib compared to TNF inhibitors. Lung cancers and lymphoma in patients treated with tofacitinib have also been observed in other clinical studies and in the post marketing setting. Other malignancies in patients treated with tofacitinib were observed in clinical studies and the post marketing setting, including, but not limited to, breast cancer, melanoma, prostate cancer, and pancreatic cancer. In patients over 65 years of age, patients who are current or past smokers, and patients with other malignancy risk factors tofacitinib should only be used if no suitable treatment alternatives are available. NMSCs have been reported in patients treated with tofacitinib; the risk of NMSC may be higher in patients treated with tofacitinib 10 mg twice daily than in patients treated with 5 mg twice daily. Periodic skin examination is recommended in patients at increased risk for skin cancer. Interstitial lung disease: Caution is recommended in patients with a history of chronic lung disease as they may be more prone to infection. Asian patients are known to be at higher risk of ILD, caution should be exercised with these patients.
Legal Category: S1A. Marketing Authorisation Number: EU/1/17/1178/003 – 5 mg (56 film-coated tablets); EU/1/17/1178/007 – 10 mg (56 film-coated tablets); EU/1/17/1178/012 – 11 mg (28prolonged-release tablets); EU/1/17/1178/015 1mg/mL oral solution. Marketing Authorisation Holder: Pfizer Europe MA EEIG, Boulevard de la Plaine 17, 1050 Bruxelles, Belgium. For further information on this medicine please contact: Pfizer Medical Information on 1800 633 363 or at medical.information@pfizer.com For queries regarding product availability please contact: Pfizer Healthcare Ireland, 9 Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24, + 353 1 467 6500. Last revised: 03/2022. Ref: XJ 15_0.
LARGEST DATASET OF ANY JAKi IN RA, CAN MAKE FROM THE START 1-3,a,b
Starting as early as 2 weeks, DMARD-IR patients with RA who received XELJANZ monotherapy demonstrated a greater ACR20 response (secondary endpoint) vs placebo (30% vs 12%; P<0.001) in a phase 3, randomised, double-blind, placebo-controlled study (N=610)1,3
2. Cohen SB, Tanaka Y, Mariette X, et al. Long-term safety of tofacitinib up to 9.5 years: a comprehensive integrated analysis of the rheumatoid arthritis clinicaldevelopment programme. RMD Open. 2020;6(3):1-15.
Gastrointestinal perforations: Tofacitinib should be used with caution in patients who may be at increased risk, e.g. history of diverticulitis or concomitant use of corticosteroids or NSAIDs. Hypersensitivity: Cases of hypersensitivity associated with tofacitinib administration have been reported. Allergic reactions included angioedema and urticaria; serious reactions have occurred. If any serious allergic or anaphylactic reaction occurs, tofacitinib should be discontinued immediately. Laboratory Parameters: Increased incidence of lymphopenia and neutropenia have been reported, and decreases in haemoglobin, which should be monitored in accordance with the SmPC. Monitor ANC and haemoglobin at baseline, 4-8 weeks and 3 monthly, ALC at baseline and 3 monthly. Tofacitinib has been associated with increases in lipid parameters, maximal effects were observed within 6 weeks. Monitoring should be performed 8 weeks after initiation and managed according to hyperlipidaemia guidelines. Increases in liver enzymes greater than 3x ULN were uncommonly reported; use caution when initiating with potential hepatotoxic medicinal products. Gastrointestinal obstruction with a non-deformable prolonged-release formulation: Caution should be used when administering tofacitinib 11 mg prolonged release tablets to patients with pre-existing severe gastrointestinal narrowing(pathologic or iatrogenic). Pregnancy & Lactation: Use of tofacitinib during pregnancy and breast-feeding is contraindicated. Side Effects: RA: The most common serious adverse reactions were serious infections; pneumonia, cellulitis, herpes zoster, UTIs, diverticulitis, appendicitis and opportunistic infections. The most commonly reported adverse reactions during the first 3 months in controlled clinical studies were headache, upper respiratory tract infections, nasopharyngitis, diarrhoea, nausea and hypertension. UC: The most commonly reported adverse reactions in patients receiving tofacitinib 10 mg twice daily were headache, nasopharyngitis, nausea, and arthralgia. Commonly reported adversereactions (>1/100 to <1/10) across all indications were pneumonia, influenza, herpes zoster, urinary tract infection, sinusitis, bronchitis, viral upper respiratory tract infection, pharyngitis, anaemia, headache, hypertension, cough, abdominal pain, vomiting, diarrhoea, nausea, gastritis, dyspepsia, rash, arthralgia, pyrexia, peripheral oedema, fatigue, increased creatine phosphokinase. Refer to section 4.8 of the SmPC for further information on side effects, including description of selected adverse reactions.
1.References: Fleischmann R, Kremer J, Cush J, et al; for the ORAL Solo Investigators. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N EnglMed.2012;367(6):495-507.
3. Pfizer data on file. 4. XELJANZ Summary of Product Characteristics.
Pregnancy and Lactation: Women of childbearing potential should be advised to avoid becoming pregnant whilst receiving Calquence. Calquence should not be used during pregnancy unless the clinical condition of the woman requires treatment with acalabrutinib. A risk to the breast-fed child cannot be excluded therefore breast-feeding mothers are advised not to breast-feed during treatment with Calquence and for 2 days after receiving the last dose. Ability to Drive and Use Machines: Fatigue and dizziness have been reported and patients who experience these symptoms should be advised not to drive or use machines until symptoms abate. Undesirable Events: Consult SmPC for full list of side effects. For monotherapy: Very common (≥ 1/10): Upper respiratory tract infection, sinusitis, second primary malignancy (SPM); neutropenia, anaemia, headache, dizziness, bruising, contusion, petechiae, haemorrhage/haematoma, diarrhoea, nausea, constipation, vomiting, abdominal pain, rash, musculoskeletal pain, arthralgia, fatigue, haemoglobin decreased, absolute neutrophil count decreased, platelets decreased. Common (> 1/100 to < 1/10): Pneumonia, urinary tract infection, nasopharyngitis, bronchitis, herpes viral infections, non-melanoma skin malignancy, SPM excluding non-melanoma skin, thrombocytopenia, atrial fibrillation/flutter, ecchymoses, gastrointestinal haemorrhage, intracranial haemorrhage, epistaxis, asthenia. Uncommon (≥ 1/1,000 to < 1/100): Aspergillus infections, hepatitis B reactivation, lymphocytosis, tumour lysis syndrome. For combination therapy: Very common (≥ 1/10): Upper respiratory tract infection, sinusitis, nasopharyngitis, urinary tract infection, pneumonia, SPM, neutropenia, thrombocytopenia, anaemia, headache, dizziness, bruising, contusion, petechiae, haemorrhage/haematoma, diarrhoea, nausea, constipation, vomiting, abdominal pain, rash, musculoskeletal pain, arthralgia, fatigue, absolute neutrophil count decreased, platelets decreased, haemoglobin decreased. Common (> 1/100 to < 1/10): Bronchitis, herpes viral infections, non-melanoma skin malignancy, SPM excluding non-melanoma skin, atrial fibrillation/flutter, ecchymoses, gastrointestinal haemorrhage, epistaxis, asthenia. Uncommon (≥ 1/1,000 to < 1/100): Progressive multifocal leukoencephalopathy, hepatitis B reactivation, lymphocytosis, tumour lysis syndrome, intracranial haemorrhage.
Drug Interactions: Concomitant use with strong CYP3A/P-gp inhibitors should be avoided. If strong CYP3A/P-gp inhibitors (e.g. ketoconazole, conivaptan, clarithromycin, indinavir, itraconazole, ritinovair, telaprevir, posaconazole, voriconazole) are used short-term, treatment with Calquence should be interrupted. No dose adjustment is required in combination with moderate CYP3A inhibitors. Monitor patients closely for adverse reactions (see Section 4.2 of the SmPC). CYP3A inducers may decrease acalabrutinib plasma concentrations. Concomitant use of strong inducers (e.g. phenytoin, rifampicin, carbamazepine) should be avoided. Concomitant use of St. John’s wort should be avoided. If treatment with a gastric acid reducing agent is required, consider using an antacid (e.g. calcium carbonate) or H2-receptor antagonist (e.g. ranitidine or famotidine). Due to the long-lasting effect of proton pump inhibitors, separation of doses with proton pump inhibitors may not eliminate the interaction with Calquence and therefore concomitant use should be avoided. Exercise caution if co-administering acalabrutinib with CYP3A4 substrates with narrow therapeutic range administered orally (e.g. cyclosporine, ergotamine, pimozide). Co-administration with CYP1A2 substrates (e.g. theophylline, caffeine) may decrease their exposure. Acalabrutinib may increase exposure to co-administered BCRP substrates (e.g. methotrexate) by inhibition of intestinal BCRP. To minimise the potential of an interaction in the gastrointestinal tract, oral narrow therapeutic range BCRP substrates such as methotrexate should be taken at least 6 hours before or after acalabrutinib. ACP-5862 (active metabolite of acalabrutinib) may increase exposure to co-administered MATE1 substrates (e.g. metformin) by inhibition of MATE1. Patients should be monitored for signs of changed tolerability as a result of increased exposure of the concomitant medication whilst taking Calquence.
CALQUENCECONFIDENCE
Date of API Preparation: 05/2022 Veeva ID: IE-3859
A selective BTKi1 CALQUENCE Indications available in the high tech scheme: • Calquence as monotherapy for the treatment of previously untreated Chronic Lymphocytic Leukaemia (CLL) in the presence of 17p deletion or TP53 mutation in adult patients unsuitable for chemoimmunotherapy.* • Calquence as monotherapy for the treatment of adult patients with CLL who have received at least one prior therapy. *Please see the below prescribing information or SmPC for full detail on licensed indications.
Legal Category: Product subject to medical prescription which may not be renewed (A) Marketing Authorisation Number: EU/1/20/1479/001, EU/1/20/1479/002
1. CALQUENCE 100mg Hard Capsules Summary of Product Characteristics. November 2021. BTki = Bruton tyrosine kinase inhibitor Veeva ID: IE-3841 | Date of Preparation: May 2022
CALQUENCE® 100mg HARD CAPSULES (acalabrutinib) Consult Summary of Product Characteristics (SmPC) before prescribing. Indication: Calquence as monotherapy or in combination with obinutuzumab is indicated for the treatment of adult patients with previously untreated chronic lymphocytic leukaemia (CLL). Calquence as monotherapy is indicated for treatment of adult patients with CLL who have received at least one prior therapy. Presentation: Each hard capsule contains 100mg of acalabrutinib. Dosage and Administration: Treatment should be initiated and supervised by a physician experienced in the use of anticancer medicinal products. The capsules should be swallowed whole with water at approximately the same time each day, with or without food and should not be chewed, dissolved or opened. Recommended dose is 100mg acalabrutinib twice daily. Refer to obinutuzumab prescribing information for recommended obinutuzumab dosing information. The dose interval is 12 hours approximately and treatment should be continued until disease progression or unacceptable toxicity. Refer to SmPC for recommended dose modifications of Calquence for Grade ≥ 3 adverse reactions and interactions with CYP3A inhibitors or inducers and gastric acid reducing agents. Elderly: No dose adjustment required for patients (aged ≥ 65 years). Renal impairment: No dose adjustment needed in patients with mild to moderate renal impairment (greater than 30mL/min creatinine clearance). Maintain hydration and monitor serum creatinine levels periodically. Only use in patients with severe renal impairment (<30mL/min creatinine clearance) if benefit outweighs risk. Monitor closely for signs of toxicity. Hepatic impairment: No dose adjustment recommended in patients with mild or moderate hepatic impairment (Child-Pugh A, Child-Pugh B, or total bilirubin between 1.5-3 times the upper limit of normal [ULN] and any AST). Patients with moderate hepatic impairment should be closely monitored for signs of toxicity. Calquence is not recommended in patients with severe hepatic impairment (Child-Pugh C or total bilirubin >3 times ULN and any AST). Severe cardiac disease: Patients with severe cardiovascular disease were excluded from studies. Paediatric population: The safety and efficacy of Calquence in children and adolescents aged 0 to 18 years have not been established. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Warnings and Precautions: Haemorrhage: Major haemorrhagic events including central nervous system and gastrointestinal haemorrhage, some with fatal outcomes, have occurred in patients with haematological malignancies treated with Calquence monotherapy and in combination with obinutuzumab. Patients receiving antithrombotic agents may be at increased risk of haemorrhage. Exercise caution with antithrombotic agents and consider additional monitoring for signs of bleeding when concomitant use is medically necessary. Warfarin or other vitamin K antagonists should not be administered concomitantly with Calquence. Consider benefit-risk of withholding Calquence for at least 3 days pre- and post-surgery. Infections: Serious infections (bacterial, viral or fungal) including fatal events have occurred in patients with haematological malignancies treated with Calquence monotherapy and in combination with obinutuzumab. These infections predominantly occurred in the absence of Grade 3 or 4 neutropenia. Infections due to hepatitis B virus (HBV) and herpes zoster virus (HZV) reactivation, aspergillosis and progressive multifocal leukoencephalopathy (PML) have also occurred. Viral reactivation cases of hepatitis B have been reported and therefore HBV status should be established before initiating treatment with Calquence. A liver disease expert should be consulted before initiation of treatment if patients have a positive Hepatitis B serology and the patient should be monitored and managed to prevent hepatitis B reactivation. Progressive multifocal leukoencephalopathy (PML): Cases of PML including fatal ones have been reported following use of Calquence within the context of a prior or concomitant immunosuppressive therapy. Consider PML in differential diagnosis where there are new or worsening neurological, cognitive or behavioural signs or symptoms. If PML is suspected, appropriate diagnostic evaluations should be undertaken and treatment with Calquence should be stopped until PML is excluded. Prophylaxis should be considered in patients who are at increased risk for opportunistic infections. Monitor for signs and symptoms of infection. Cytopenias: Treatment-emergent Grade 3 or 4 cytopenias, including neutropenia, anaemia and thrombocytopenia, occurred in patients with haematological malignancies treated with Calquence monotherapy and in combination with obinutuzumab. Monitor complete blood counts as medically indicated (refer to section 4.8 of the SmPC). Second primary malignancies: Skin and non-skin cancers, occurred in patients with haematological malignancies treated with Calquence monotherapy and in combination with obinutuzumab. Monitor for appearance of skin cancers and advise protection from sun exposure. Atrial fibrillation/flutter: Atrial fibrillation/flutter occurred in patients with haematological malignancies treated with Calquence monotherapy and in combination with obinutuzumab. Monitor for symptoms (e.g. palpitations, dizziness, syncope, chest pain, dyspnoea) and obtain ECG as medically indicated (see section 4.5 and 4.2 of the SmPC). If atrial fibrillation is developed on therapy with Calquence, a thorough assessment of risk for thromboembolic disease should be undertaken. Patients at high risk for thromboembolic disease, tightly controlled treatment with anticoagulants and alternative treatment options should be considered.
Marketing Authorisation Holder: AstraZeneca AB, SE-151 85 Södertälje, Sweden. Further product information available on request from: AstraZeneca Pharmaceuticals (Ireland) DAC, College Business and Technology Park, Blanchardstown Road North, Dublin 15. Tel: +353 1 609 7100. CALQUENCE is a trade mark of the AstraZeneca group of companies.
ABRIDGED PRESCRIBING INFORMATION
This medicinal product is subject to additional monitoring Adverse events should be reported directly to: HPRA Pharmacovigilance, Website: www.hpra.ie Adverse events should also be reported to AstraZeneca Patient Safety on Freephone 1800 800 899

Chairperson for Medicines for Ireland, Padraic O’Brien said, “Every time a generic medicine is dispensed, it represents a cost saving to the State and an opportunity for additional funding to be channelled to other areas of the healthcare system. Now more than ever a focus on quality and value is crucial for the State and the patients who rely on timely access to affordable medicines.” Turn to page 7 to read more about this.
On page 13, Clinical Pharmacist Emer Cronin discusses the role of the pharmacist in dosage forms. Pharmacists are crucial decision makers in the manipulation of dosage forms for patients with swallowing difficulties. In order to appropriately assess the suitability of manipulating a medication, a number of questions need to be asked. “Firstly, back to pharmacy school basics, we need to know if modifying a dosage form will be safe, effective and efficient,” she says.
Biomarkers play an important and sometimes vital role in cancer detection and patient management (i.e., follow-up of patients following a diagnosis of cancer). Thus, in well or asymptomatic individuals, some biomarkers may be used in screening for early cancer. On page 58, Professor Joe Duffy examines the role played by biomarkers in cancer detection whilst on page 60, Professor William Gallagher and colleagues explain more about the vital work being carried out by the All Ireland Cancer Research Institute.
One of our lead news stories for this issue looks at a recent report on the value of generic medicines to the prescription market. According to findings commissioned by Medicines for Ireland (MFI) and compiled by IQVIA Ireland generic medicines now account for 57% of the volume of the total prescription market in Ireland.
EditorForeword
Independent and supplementary/ collaborative prescribing, also known as non-medical prescribing, has been introduced in many countries in recent decades. Mary-Claire Kennedy, Programme Lead for Independent and Supplementary Prescribing gives readers an overview as to learning potential for pharmacists from international models and presents some exciting opportunities. Turn to page 70 to read the full article. I hope you enjoy the issue.
Our Special Focus this month is in the field of oncology.
Cross border research on medical devices P6 Warnings issued on Ireland’s public hospitals P8 Huge funding boost for Crohn’s Disease P10 The role of pharmacists in dosage forms P13 Recognising Pain Awareness Month P14 The best shots this Autumn P63 Pharmacist Prescribing: Learning from International models P70 REGULARS CPD: Transthyretin Amyloidosis P31 Oncology Focus: Secondary Risk Reduction Strategies in Irish Breast Cancer Care P42 Oncology Focus: Sequencing treatment in Multiple Myeloma P52 Oncology Focus: Cancer Research across Ireland P56 Clinical R&D: P82 10 8 20 PROFESSIONALHOSPITALNEWS IRELAND Ireland’s Dedicated Hospital Professional Publication HOSPITALPROFESSIONALNEWS.IE HospitalProfessionalNews@HospitalProNews Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system of transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors. PUBLISHER IPN Communications Ireland Ltd Clifton House, Lower Fitzwilliam Street, Dublin 2 (01) 669 0562 GROUP DIRECTOR Natalie n-maginnis@btconnect.comMaginnis EDITOR Kelly Jo Eastwood DIGITAL MARKETING & EDITORIAL EXECUTIVE Danielle Norton danielle@hospitalprofessionalnews.ie EDITORIAL editorial@hospitalprofessionalnews.ie ACCOUNTS Rachel cs.ipn@btconnect.comWilson SALES EXECUTIVE Aoife aoife.t@hospitalprofessionalnews.ieTremere CONTRIBUTORS Emer Cronin | Professor Dominic Hegarty Saleem Jahangeer | Dr Katie Liston Dr Ciara O’Rafferty | Dr Zara Togher Mr Gerard Fitzmaurice | Ciara Steele Dr Jonathan Briody | Dr Stuart Macleod Professor Seamus O’Reilly | Brona Fullen Dr Barry Kevane | Caoimhe O’Leary Klaus Meier | Professor Siobhan Glavey Dr Roisin McAvera | Dr Claire Kilty Dr Rebecca Amet | Nikolett Warner Professor Joe Duffy | Ciaran Briscoe Rose Culhane | Professor William Gallagher Dr Rosemarie Gannon | Dr Tom Barrett Grainne Sheil | Dr Dermot O’Callaghan Dr Margaret Higgins | Mary-Claire Kennedy Ashley Costello | Theresa Lowry-Lehnen Gerard Clarke | Michelle Greenwood Professor Sinéad M Murphy
5 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 September Issue Issue 100 6 Contents






Both Ireland’s second One Health National Action Plan on
Researchers at NUI Galway and Queen’s University Belfast are investigating how attaching sugar molecules to plastics could give medical devices a new layer of protection from infection.
Aengus McMahon
A new network was launched last month, for pharmacists working across all settings in Ireland.
2025ActionandResistanceAntimicrobial(iNAP2)HSEAMRICplan2022-identify pharmacists as a key stakeholder and highlight the need to maximise engagement of pharmacists with Thestewardshipantimicrobial(AMS).functionsofthe network are:
CrossNewsBorder
The team is attempting to harness the science behind the interaction of sugar molecules with bacterial proteins to make fluorescent materials which glow at first, darkening when they become compromised by bacteria. The technology would be attached to plastics which coat medical devices - such as urinary catheters or endotracheal tubes - allowing clinicians to spot potential infection at an early opportunity and react faster.
• To share knowledge, information, learning and experience in AMS, both across and within sectors
Dr Joseph Byrne holding a polymer hydrogel, like those being developed in this research.
6 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE New Network for Pharmacists
The project is being supported with ¤193,000 from the Government’s Shared Island initiative.
• To share AMS work and foster creativity and innovation in AMS
Research on Medical Devices
Early-career researchers Dr Joseph Byrne, NUI Galway, and Dr Matthew Wylie, Queen’s University Belfast, are working together to tackle the issue of hospital acquired infections associated with devices by taking preventative science to a new level.
The research team is supported by senior colleagues Professor Abhay Pandit, Director of CÚRAM, the SFI Research Centre for Medical Devices at NUI Galway, and Professor Colin McCoy, Head of School of Pharmacy in Queen’s University Belfast. Medical device-associated infections account for up to half of healthcare-associated infections and people who are immunocompromised people and those with cystic fibrosis (CF) are particularly at risk, with the island of Ireland having one of the highest number of people with CF per capita. This project hopes to minimise the impact of this challenge by producing innovative coatings, which will prevent or detect bacterial build-up on widely-used medical devices before they lead to infection in a patient.
Dr Byrne, Honorary Research Lecturer in the School of Biological and Chemical Sciences, NUI Galway, explained the concept, “Prevention of bacterial infections is key to fighting the challenge of antimicrobial resistance and if this isn't possible, then early detection through innovative sensing materials could act as an alarm, allowing devices to be removed and replaced before infection becomes a more serious risk to patient health.”
The HSE Antimicrobial Resistance and Infection Control (AMRIC) team and Irish Institute of Pharmacy (IIOP) have collaborated to develop a AntimicrobialPharmacistStewardship Network (PAMS-net). The PAMS-net launched on the 15th August 2022. The network aims to support pharmacists across all sectors to work towards the common goal of promoting responsible use of antimicrobials in all patients and limiting the emergence of antimicrobial resistance. Antimicrobial stewardship (AMS) can encompass any action that promotes responsible use of antimicrobials. Some examples of antimicrobial stewardship (AMS) in pharmacy practice include: checking if antibiotic prescriptions align with antibiotic prescribing guidelines; recognising when an antibiotic agent, dose or duration is not in line with guidelines and highlighting this to the prescriber; providing advice when a patient presents with a self-limiting or viral infection. All pharmacists with an interest in responsible antimicrobial use are welcome to join this network. The network aims to bring together pharmacists from a diverse range of settings including community, hospital, education, researchers, Outpatient Parenteral Antimicrobial Therapy (OPAT) services, other HSE and national bodies. The network welcomes pharmacists from all professional backgrounds, those who are considered experienced antimicrobial pharmacists and those who wish to further their knowledge. Pharmacists working in all sectors play a pivotal role in antimicrobial stewardship (AMS) due to their expertise in medicines and accessibility to patients.
• To assist in the provision of CPD for pharmacists with an interest in AMS The PAMS-net webpage is hosted on the IIOP website. It provides a discussion forum and resources section. Members receive updates through the network and network events are organised regularly. To become a member of the network go to the “Courses and Events” page on the IIOP website and select the "Forum" tab. To learn more about antimicrobial stewardship and view national antibiotic prescribing guidelines and resources visit antibioticprescribing.ie
The SUGARCOAT project is among 62 research collaborations supported by the Government’s Shared Island fund.
• To provide a discussion forum for members


Report shows Hospital Pharmacy Contribution
The greater use of generic medicines in Ireland helps patients access high quality treatments at considerably lower costs, it also produces significant savings for the State. This data for IQVIA also indicates treatment costs in Ireland have decreased
Reflecting on the past two years during which hospital pharmacists supported efforts to combat the COVID-19 pandemic, EAHP President András Süle underlined that, "The roles of our profession have expanded tremendously. Hospital pharmacists engage more in multi-disciplinarily teams and have become more visible on wards through an increased provision of clinical services. This momentum needs to be used to ensure that our profession remains one of the key players in the delivery of care to patients across Europe. In particular, I hope that the recommendation contained in EAHP's COVID-19 Report will be a step toward ensuring a high degree of safety and quality during times of crisis due to the contributions of hospital pharmacists – as valued members of the interprofessional healthcare team – that can and should play an integral role, focusing on medication management, medication reconciliation, preventive care and patient education."
7 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 News
sizably since 2013, with a notable reduction in 2021.
“At MFI we look forward to engaging with Government and State bodies like the HSE on bringing forward new initiatives to boost use of generic medicines in Ireland, with the dual objective of helping to reduce State expenditure and delivering greater equality of access for patients,” concluded Mr O’Brien This data also shows that 8 out of 10 of companies supplying the prescription market are generic medicines companies, 75% of these companies are MFI members.
“Despite the considerable progressions presented in these findings we have still not reached the European average of 70% generic medicines usage, so there is still work to be done to improve Ireland’s position,” said Chairperson for the Medicines for Ireland Generics Committee, Melissa Fisher. Since its foundation in 2016, Medicines for Ireland has been promoting the benefits of the increased use of generic medicines in Ireland. The organisation’s core objective is to improve the way Ireland procures and supplies medicines, in order to expand patient access to affordable, lifesaving and lifeenhancing treatment.
Rise in Generic Medicines
Medicines now account for 60%
The COVID-19 Report of the European Association of Hospital Pharmacists (EAHP) outlines how both the Association and its members across Europe contributed to combatting the pandemic. As experts in medications, hospital pharmacists have been instrumental in ensuring that hospital patients were able to access their medicines. For instance, they participated in and supported vaccination campaigns across Europe, engaged in the development of clinical trials and carried out pharmacovigilance activities linked to medication interactions in COVID-19 patients. In addition, the hospital pharmacy profession adapted itself to the new normal by further integrating its expertise in multi-professional care teams. For example, hospital pharmacists supported nurses with the preparation of medicines for intensive care units and worked collaboratively with doctors on medication reviews to ensure the best possible therapeutic management for COVID-19 patients. Besides showcasing the contributions of the hospital pharmacy profession, EAHP's COVID-19 Report contains several recommendations that will not only help to respond to future health threats but also support the overall activities of the hospital pharmacy service to obtain better outcomes for patients.
“As an organisation MFI are proud that our membership will supply over 60 million packs of prescription medicines to Irish patients this year. This equates to an average of 2 packs of medicines every second.”
Chairperson for Medicines for Ireland, Padraic O’Brien
The recommendations focus on the need for a robust healthcare workforce, addressing medicine shortages, the importance of prospective risk assessment and communication, the value of multidisciplinary collaboration, the need for pharmacy specialisation programmes and the recognition of the role of hospital pharmacists in multi-professional care teams and vaccination campaigns.
Chairperson for Medicines for Ireland, Padraic O’Brien said, “Every time a generic medicine is dispensed, it represents a cost saving to the State and an opportunity for additional funding to be channelled to other areas of the healthcare system. Now more than ever a focus on quality and value is crucial for the State and the patients who rely on timely access to affordable medicines.
According to commissionedfindingsbyMedicines for Ireland (MFI) and compiled by IQVIA Ireland generic medicines now account for 57% of the volume of the total prescription market in Ireland.
Generic Prescription Market
Over the past ten years the volume of generic medicines across Ireland has risen by 24%, this is due to effective Government policies and legislative changes regarding procurement and supply, as well as consistent activity for MFI members to promote the advantages associated with increased usage of generic medicines.


Impact on Children
Conditions such as narrowing of bowels, vascular malformations or delivery of chemotherapy to tumours can be treated in this way. These techniques are used widely among adults but the necessary funding to adequately resource the theatre space, capacity and Consultant posts for interventional radiology in children have not been delivered.
CareNewsCan’t
A Disheartening Environment
Professor Stephanie Ryan, who recently retired as a Consultant Paediatric Radiologist, said that many of the problems that were present in the Irish health service 25 years ago are still present or worse today. During her career, Professor Ryan worked as a Paediatric Radiologist at Temple Street Hospital in Dublin (Children’s Health Ireland). Her work involved using medical imaging, for example X-rays, MRI scans and ultrasounds, to diagnose conditions such as tumours and congenital abnormalities, and to guide their treatment.
“While all these improvements have taken place, the system hasn’t been able to respond to the advances that are available, as quickly as it should or as completely as it should – so that we remain behind in our ability to provide the service that children need,” according to Professor Ryan.
“I really would like to see a system whereby when a need is identified, there would be a response that would approve extra staffing needs in a reasonable amount of time. It’s not terribly complex to calculate that to provide a given number of scans, you need a certain level of staff. It should not take years to get that staff.”
Professor Ryan also spoke about “interventional radiology”, and “minimally invasive treatment”.
Following her recent retirement, Professor Ryan has been considering her time spent working in the Irish health system.
According to Professor Ryan, the pressures of managing waiting lists, in addition to onerous on-call duties, shortages of resources and unfilled Consultant posts have made Ireland a less attractive place to work compared to other countries around the world.
8 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
“It really shouldn’t be a battle that’s taking up time and wearing people down and causing people to become disheartened.
For Consultant Radiologists, including those specialising in Paediatrics, the challenge of trying to prioritise access to care is especially complicated, “by the very nature of the fact that you need the scan to make a diagnosis, it is difficult to identify those with more serious problems before the scan.” explains Professor Ryan.
In addition, the pay discrimination imposed on Consultants contracted after 2012 has acted as a deterrent for applicants for Consultant posts. The IHCA has long campaigned for the Government and health service management to end this pay discrimination, which is a vital step to attract applicants for Consultant posts in Ireland.
“When I look back over the nearly 25 years as a paediatric radiologist, I can see vast improvements in the care that is available to children.
Wait – Warning Issued
The failure of staffing and capacity resourcing to keep pace with medical advances over the past quarter of a century has left Ireland’s public hospitals lagging behind in their ability to deliver timely care to children. That was a recent warning from the Irish Hospital Consultants Association.
Consultant Recruitment and Retention
More than 101,000 children were waiting for an appointment to be assessed or treated in public hospitals at the end of June.1 However, these figures from the National Treatment Purchase Fund (NTPF) fail to provide an accurate picture of the scale of the number of children waiting for care, as hospital diagnostics are not included in the NTPF data. When the additional 8,294 children awaiting CTs, MRIs or ultrasounds at the end of March 2022 are added, the total number is close to 110,000. With 30,500 children now waiting longer than a year for an appointment with a hospital Consultant or access to essential care and treatment1, Professor Ryan is concerned about the impact these long delays can have on children’s healthcare outcomes.
“Delays in diagnosis can delay treatment and there can be lifelong impacts as well. For example, with simple ear problems in young children, this can affect their language learning at a critical time. Sometimes the treatment of children with special needs or the formation of a plan for their care, can be delayed by waiting for an MRI scan. This could mean a long wait for access to treatment at a critical age in a child’s development. If a child needs a scan, I just wish we could provide the service and not have them waiting. No Consultant or parent wants this.”
Professor Ryan spoke of her disappointment that many of the same issues continue to negatively affect the provision of timely care to children in Ireland’s public hospitals. The Consultant recruitment and retention crisis, capacity shortages and long waiting lists for children have plagued the system for over a quarter of a century, despite the efforts of specialists like Professor Ryan advocating for adequate resources.
“These are techniques that use x-rays and scans to guide a procedure as an alternative to full surgery,” explained Professor Ryan, who trained in minimally invasive treatment in the United States. “When procedures are done by interventional radiology rather than traditional surgery, recovery and hospital stays are shorter and scars are avoided.”
Speaking on behalf of the IHCA as part of its Care Can't Wait campaign, Professor Ryan pointed out the potential negative consequences for children of facing delays in accessing care.


IMPORTANT NOTICE: Breastfeeding is best. Aptamil Pepti Syneo is a food for special medical purposes for the dietary management of Cow’s Milk Allergy. It should only be used under medical supervision, after full consideration of the feeding options available including breastfeeding. Suitable for use as the sole source of nutrition for infants under one year of age. Refer to label for details.
* Short chain galacto-oligosaccharides / long chain fructo-oligosaccharides; ^Single arm UK study in infants with non-IgE mediated CMA, baseline non-synbiotic formulas vs Aptamil Pepti Syneo, 4 week intervention; † Subgroup of n=48 infants with IgE associated AD, difference in SCORAD score Aptamil Pepti Syneo vs EHF without synbiotics, -4.6, 95%CI, p=0.04. ‡ Products can be provided to patients upon request of a healthcare professional. They are intended for the purpose of professional evaluation only. 1. MIMS Ireland, March 2022.
APTAMIL PEPTI SYNEO THIS INFORMATION IS INTENDED FOR HEALTHCARE PROFESSIONALS ONLY NEW OURP For more information or to avail of our sampling service ‡ scan the QR code, freephone 1800 923 404 or visit www.nutricia.ie Use your phone to scan the QR code GREATER REDUCTION constipation,3,4^ dry stools,3 abdominal discomfort 4^ and atopic dermatitis severity3†,4^ SUPERIOR PALATABILITY compared to other EHFs in Ireland5 The only 1 Extensively Hydrolysed Formula (EHF) to contain clinically proven to manage cow’s milk allergy symptoms in formula fed infants modulate the gut Bifidobacteriummicrobiome breve M-16V+scGOS / lcFOS* fibres
2. Giampietro PG et al. Pediatr Allergy Immunol 2001;12:83-86. 3. Van der Aa LB et al. Clin Exp Allergy. 2010;(40):795–804 4. Hubbard G et al. Immun Inflamm Dis. 2022;10:e636
5. Data on file, updated independent taste panel report, Campden BRI, October 2020. n=102 HCPs, Campden BRI home usage taste testing. N=102 Dietitians and GPs. Aptamil Pepti 1 & Aptamil Pepti Syneo vs all UK EHFs suitable from birth. Ireland, Block 1 Deansgrange Business Park, Deansgrange, Co. Dublin. Date of publication: 06/2022
Nutricia




Students undertake placements throughout the course and the 2nd-year placement is the first of these placements. These placements take place in two different ways: a two-week block for UCC and TCD students (16th - 27th January) and a longitudinal placement every Tuesday afternoon for RCSI students (10th January – 4th April).
CD drastically impacts the quality of life of affected patients - and that of their families, friends, and caregivers. Most significantly, however, there is no satisfactory treatment. Despite advances, there is a pressing need for novel, advanced therapies.
Could you help a future pharmacist?
Pharmacists who have previously facilitated APPEL placements have found the experience enjoyable and rewarding. In surveys, 90% of pharmacists said they would recommend facilitating a placement to other pharmacists. The advantages of facilitating an APPEL placement include:
Over the course of four years, GENEGUT’s aim to develop a non-invasive, safe, effective, and targeted treatment will be realised in the form of a first-in-class, orally administered RNA-based therapy. This breakthrough RNA therapy will be developed using complementary technologies that selectively target inflamed intestinal cells that reside in specific regions of the small intestine.
A University College Cork-led research project that seeks to revolutionise how Crohn’s disease is treated has just been awarded ¤5.4 million in funding by the European Union (EU).
Now GENEGUT, a four-year research project led by UCC's School of Pharmacy in partnership with APC Microbiome Ireland SFI Research Centre at UCC and funded by Horizon Europe, is to develop the first oral RNA-based therapy for ileal Crohn’s Disease.
“The multidisciplinary team in GENEGUT will pioneer the development of the next generation of therapeutics for the treatment of Crohn’s Disease by producing a patient friendly orally administered RNA medicine. The project will span the pre-clinical to clinical space thus accelerating the clinical translation of orally available RNA therapeutics and ensuring early access of lifealtering medicines for the patient. For these patients, this would be the first option to finally manage the chronic disease and lead a life of improved quality,” said Professor Caitriona O’Driscoll, GENEGUT Project Coordinator Through a patient-centred approach, the project, coordinated by the School of Pharmacy of University College Cork, brings together the European Federation of Crohn's & Ulcerative Colitis Associations with renowned researchers, expert clinical scientists, SMEs and large pharma companies with expertise and patented technologies in global proteomics, nanotechnologies, novel biomaterials, multicellular models, drug delivery systems and production as well as innovation management, stakeholder involvement and science communication.
Dr Joey O’Shea, Professor Caitriona O’Driscoll, Dr Piotr Kowalski and Dr Patrick O’Dwyer, School of Pharmacy, UCC
APPEL (Affiliation for Pharmacy Practice Experiential Learning) is now seeking expressions of interest from pharmacists in community and hospital pharmacy settings who would like to facilitate an experiential learning placement for a 2nd-year pharmacy student in 2023.
• Continuing experiencepharmacistsTrainingDevelopmentProfessional-APPELTrainercancontributetoCPD,ascantheoffacilitatinga placement.
• Development of your talent pipeline – many students will look to start their career in the organisations or practice settings where they undertook their placements
• Engagement – participating in the APPEL programme provides you with the opportunity to increase awareness of APPELpharmacy/organisation.yourtrainingandevents provide fantastic networking opportunities. The deadline to confirm your interest in offering placements is the 16th of September 2022. You can do this by clicking on the link below: furtherIfR9v2G2rXhrxpJnhJ6.https://forms.gle/youhaveanyquestionsorwantinformation,pleaseemail ops@appel.ie.
10 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE News
¤5.4m funding for Crohn’s Disease
Experiential learning placements are a key part of the integrated pharmacy masters (M.Pharm).


This information is intended for healthcare professionals only. The Fortini range are Foods for Special Medical Purposes for the dietary management of disease related malnutrition and growth failure in children from one year onwards and must be used under medical supervision. *Datacards reviewed form competitor websites June 2021 ** ONS: Oral Nutritional Supplement ^ Product can be provided to patients upon the request of a Healthcare Professional. They are intended for the purpose of professional evaluation only. Nutricia Ireland, Block 1, Deansgrange Business Park, Deansgrange, Co. Dublin. Date of publication, June 2021 PRODUCTS AVAILABLE FOR PROFESSIONAL EVALUATION^: SCAN THE QR CODE CONTACT NUTRICIA FOR A LOLLY MOULD AND RECIPE CARD FOR YOUR PATIENTS FREEPHONE 1800 923 404 ENJOY SUMMER FUN WITH FORTINI SMOOTHIE 3007.2 6.8 2.8 THE ONLY * PAEDIATRIC SMOOTHIE STYLE ONS** WITH 15% REAL FRUIT FORFREEZEICELOLLIES! NUTRITIONALLY COMPLETE FOR CHILDREN AGED 1+ APPROVEDGMSYEARS







































































































“The development of this lab-based model is a milestone in heart failure research as it enables devices to be tested that have the potential to treat a condition that affects millions of people around the world”
New heart model to help treat patients with heart failure
Researchers from RCSI University of Medicine and Health Sciences have developed a new lab-based model of a heart and circulatory system that will help test devices to treat patients with one of the most common forms of heart failure. The study, which used two different types of circulatory models including a silicone heart model, was carried out by RCSI in collaboration with the National College of Art and Design (NCAD).
Findings from a research study exploring the mental health of Dublin’s general hospital staff during the COVID-19 pandemic reveal significant impacts on doctors, nurses and radiographers, including high levels of symptoms of posttraumatic stress disorder (PTSD), depression and suicidal thinking.
This concept arose in military mental health research but has gained importance in research studying healthcare worker mental health due to COVID-19-related scenarios. For example, healthcare workers may have had no option but to ration care when resources were scarce, or they may have had to stop family from visiting their loved-ones due to restrictions.
12 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
The COWORKER Study, developed to investigate the mental health impact of the pandemic on Dublin general hospital staff and help inform appropriate responses, involved researchers from Trinity, St Patrick’s Mental Health Services and RCSI University of Medicine and Health Services. It was led by Declan McLoughlin, Research Professor of Psychiatry at Trinity and Consultant Psychiatrist at St Patrick’s Mental Health Services.
This model can test devices to examine the left atrium, the top chamber responsible for receiving oxygen-rich blood from the lungs, as well as the left ventricle, the lower chamber responsible for pumping the oxygen-rich blood around the body.
• 13% of respondents reported thinking of ending their life over the previous week and 5% reported planning to end their life Staff also reported high levels of moral injury, which is the psychological distress experienced when one is forced to witness or perform acts that go against one’s ethical beliefs.
In recent years, the number of patients presenting with heart failure with normal or preserved ejection fraction measurement is increasing, most likely due to the increase in prevalence of common risk factors, including old age, high blood pressure and obesity. Women are at greater risk than men.
Staff in three large Dublin general hospitals (St James’s Hospital, Tallaght University Hospital and Beaumont Hospital) were invited to participate, with the study also aiming to provide an opportunity for doctors, nurses and radiographers to recognise if they have been experiencing mental health difficulties during the pandemic and to seek support if required.
Staff report High Stress Levels
• 45% of respondents reported moderate or severe symptoms of post-traumatic stress disorder (PTSD)
Drs Hameed and Malone worked with RCSI colleagues, Jemil Saidi and Gina Rizq, and collaborators, Sean Gallagher, Enda O’Dowd and Derek Vallence, in NCAD.
Dr Aamir Hameed RCSI
Among the key findings, which came from a cross-sectional anonymous survey of 377 Dublin healthcare staff during the third wave of the COVID-19 pandemic in early 2021, are:
DublinNewsHospital
Senior author on the study, Dr Aamir Hameed, Lecturer in the Department of Anatomy and Regenerative Medicine and a Principal Investigator with the Tissue Engineering Research Group at RCSI said: “Half of the patients presenting with heart failure have heart failure with preserved ejection fraction and the numbers are increasing in the developed world in particular due to the increase in the prevalence of risk factors. The condition can be difficult to treat with medicines
The research is published in the current edition of ‘Frontiers in Cardiovascular Medicine’.
These pages were unfortunately published in the incorrect order. We have rectified this error and have the correct order running in this (September) issue of Hospital Professional News on pages 48-50. This was an error on the part of Hospital Professional News and we apologise for any confusion or disruption caused.
Researchers also examined whether there were any differences in the levels of mental health difficulties between staff based on their roles. The findings show that doctors were significantly less likely to report symptoms of PTSD, low mood and moral injury than nurse or radiographers, while radiographers were significantly more likely to report low mood. and is causing a considerable burden to health services throughout the world. “The development of this labbased model is a milestone in heart failure research as it enables devices to be tested that have the potential to treat a condition that affects millions of people around the world, improving their quality of life and reducing the burden on health services.”
• 52% of respondents reported low mood
In this research from RCSI, a model called a ‘mock circulatory loop’ was developed to mimic both a healthy heart and a heart in failure with preserved ejection fraction. The model enables potential heart failure treatment devices to be examined in terms of their effect on both chambers in the left side of the heart.
There are two common types of heart failure: Heart Failure with Preserved Ejection Fraction (HFpEF) and Heart Failure with Reduced Ejection Fraction (HFrEF). Ejection fraction is the measurement used to determine the heart’s ability to pump oxygenrich blood through the body.
Correction In the August issue of Hospital Professional News, we carried a three page advertisement special section which included 2 A4 Adverts for Rinvoq and Skyrizi alongside an editorial page on an educational symposium entitled, ‘A meeting entitled Abbvie Innovations in Psoriasis and Atopic Dermatitis.’

Having assessed these 3 important factors, a number of additional issues need to be addressed.
In order to appropriately assess the suitability of manipulating a medication, a number of questions need to be asked. Firstly, back to pharmacy school basics, we need to know if modifying a dosage form will be safe, effective and efficient.
Safe: Could administering this modified medicine adversely affect the patient and cause harm? For example, if a medication is inappropriately crushed, its absorption profile can become erratic and subsequently cause toxicity or a complete lack of effect.
13 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 Pharmacy
Calculations, Conversions and Corrections
The Role of Pharmacists in Dosage Forms
Effective: Will delivery of this drug ensure the intended therapeutic effect for the patient? For example, if a patient with a jejunal tube receives cephalexin, the site of absorption (the duodenum) will be bypassed and so the active ingredient will not achieve therapeutic levels or have any therapeutic effect.
Efficient: Are there more appropriate and easier to administer dosage forms at hand? It is important to consider the practicality of the user involvement which may include the patient, carer or nursing staff administering the medication. Crushing tablets or opening capsules can cause aerosolization of drug powder which can pose a health risk particularly if a medication is cytotoxic or a hormonal preparation deeming it unsafe practice.
It is important to be aware that crushing most medicines is an unlicensed activity and transfers liability from the manufacturer to the administrator and prescriber. Many film coated tablets are suitable for crushing which can make for a simple manipulation. Similarly, switching to a dispersible formulation when available makes for a straightforward modification. However, enteric coated or gastroresistant tablets are generally unsuitable for crushing as doing so could increase toxicity or reduce effectiveness as well as having the potential to cause a blockage in a feeding tube. Some coated tablets may also cause taste disturbances for a patient when crushed. E.g. amiodarone tablets have a very bitter Sometaste.capsules can be opened and dispersed in water provided the enclosed granules are not enteric coated or prolonged release.
Useful resources for information on manipulation of dosage forms include “The Handbook of Drug Administration via Enteral Feeding Tubes”, “The NEWT Guidelines” and the Summary of Product Characteristics. However, if faced with a query, it is always worthwhile contacting the pharmacist in your department who will serve as another medication expert to aid you in the minefield of the manipulation of medicines.
Manipulation of dosage forms for patients with trouble swallowing/feeding tubes
One alternative route to the oral route is the transdermal route which will require a dose conversion. Many dose conversion calculators and tables can be sourced online e.g. opioids, Parkinson’s disease medications. It takes time for medication delivered via the transdermal route to reach steady state and sufficient therapeutic cover in this interim period needs to be ensured. It is particularly important to monitor the patient for signs of toxicity or withdrawal at this stage and to make corrections to dosages based on Calculationsthis.may also need to be performed when manipulating drugs with narrow therapeutic indexes as bioavailability can vary across different formulations. For example, a dosage of 90 milligrams of phenytoin liquid is equivalent to a dosage of 100 milligrams of a phenytoin capsule.
Excipients: When considering switching to an alternative formulation such as a liquid, it is vital to assess the excipient content, which can include sucrose, sorbitol, sodium and ethanol that in high quantities can cause adverse effects in a patient. These adverse effects can include raised blood glucose levels, gastrointestinal disturbances, raised blood pressure, and profound drowsiness. It is also worth noting that excipients can vary across different liquid products of the same active ingredient. High osmolarity liquids will also require further dilution before administration via feeding tubes to reduce a patient’s risk of diarrhoea.
Duration: Manipulation of a medicine required for a short period of time versus a long term strategy may alter the course of action. For example, Carbamazepine suppositories are recommended for a maximum duration of 7 days due to an increased risk of rectal irritation.
To crush or not to crush?
Interactions: There are many additional interactions to consider when a medication is being modified for administration, particularly via a feeding tube. For example, the high protein content of some nutritional feeds can reduce the absorption of levodopa. Drugs including phenytoin, ciprofloxacin and warfarin have significantly reduced bioavailability unless administered following a recommended 2 hour feeding break and the feed must then be stopped for a further 2 hours following administration. It is also very important to ensure medicines are never mixed when administered via feeding tubes and that each medication is flushed well.
Pharmacists are crucial decision makers in the manipulation of dosage forms for patients with swallowing difficulties. There are a wide range of patients who will require pharmacist input to alter delivery of their medication. Patient profiles can vary considerably and range from a post- stroke patient, an older adult with reduced saliva production, a woman with metastatic oesophageal cancer, a young man with an oesophageal perforation and a paediatric patient with dysphagia. As pharmacists, we advise how medicines can be manipulated safely for each of these different types of patients. Medication comes in many different forms often allowing for different routes of administration. These routes include the oral route (tablets, capsules and liquids), rectal route (suppositories, rectal foams and enemas), nasal route (nasal sprays), transdermal route (patches), parenteral route (bolus injections, depots, infusions) inhalation (inhalers), nebulisation (nebules), buccal and sublingual route. However, deciding on the correct manipulation for a patient’s needs is not always straight forward.
Written by Emer Cronin, Clinical Pharmacist, University Hospital Waterford
A drug not suitable for crushing can be switched to a drug at an equivalent dosage in the same class or can be switched to a drug in a different class with a similar therapeutic effect. E.g. Olmesartan tablets could be switched to Losartan or Lisinopril.
Modified release medications are not suitable for crushing and may be recognised by a number of different names: XL (extended release), SL (slow release) LA (long acting), Retard, Slo or Slow, and PR (prolonged release). However, prolonged release medication can be converted to immediate release tablets when applicable.

Global Year of Pain 2022
Written by Professor Dominic A. Hegarty, BSc., BMedSc., MB., MSc. (Pain Management), PhD. FCARSCI, FFPMCAI, ConsultantFIPPinPain Management & Neuromodulation, Mater Private Hospital, AssociateCorkProfessor of Pain Medicine, UCC, Ireland
The value of multidisciplinary (MDT) approaches in pain management are well recognised.
14 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE At present the physical limits of an andoverburdenedalreadyunderfundedpainserviceareevident.Forthisreason,onemustconsiderallpossibleoptionstosupportindividuals.Butthereishope.
Treatments that help—and barriers to access
Recognising Pain Awareness Month
The same resources are not equally available nationally and in some regions the concept is no more than a long-term ambition. However, not everyone in pain needs access to all aspects of MDT. For example, the top strategies used in MDT including activity restriction or modification (73%), stress reduction techniques (42%), heat therapy (41%), and meditation and mindfulness (40%). In fact, activity restriction or modification is the most-used specific “therapy” of any kind across all categories, aside from prescription medications as an entire category.
The aim of the IASP 2022 Global Year in Pain is to increase awareness of pain knowledge and how it can benefit those living with pain. The key objective is to increase the awareness of clinicians, scientists, and the public of our accumulating pain knowledge and of how this may be used for the benefit of those living with pain.
When it comes to medications, a majority (77%) said prescription medications are the most helpful treatment in managing their pain. Access to interventional pain procedures continue to be the Holy Gail for many but with demand out stripping supply there is an obvious bottle-neck.
Change is needed
References To learn more about the results and download the full report, visit surveyreports/a-chronic-pain-uspainfoundation.org/ crisis. Web: pain-knowledge-to-practice/advocacy/global-year/translating-https://www.iasp-pain.org/www.chronicpain.ie
Honorary Consultant Guy's & St. Thomas' Hospital, London Clinical Lead Neuromodulation Research, Tyndall National Institute, PresidentUCCElect World Institute Of Pain (WIP) Clinical Director Pain Relief Ireland www.painreliefireland.ie
Pain
Every September since 2001, when the American Chronic Pain Association first led a coalition of groups to highlight the needs of those with living with chronic pain the spotlight is shone on one of the most common illnesses that effects so many individuals. Every year the same staggering number of 1 in every 4 individuals attend healthcare professionals with chronic pain does not seem to change. Every year we lament the cost chronic pain has on society. Under-recognised and under treated “Chronic pain is vastly underrecognized, funded, and treated when considering its significant impact on American lives,” so says U.S. Pain Foundation CEO Nicole Hemmenway. In fact, the recently published report from the US Foundation on Pain (2022) highlights that nearly three-quarters (74%) of the 2,378 respondents had lived with pain for more than 10 years. The most common pain conditions were primarily musculoskeletal in nature: back pain (67%), arthritis (56%), chronic low back pain (56%), nerve pain or neuropathy (53%), and neck pain (51%). Over half (52%) said their average pain level is 7 or more on a scale of 1-10. 95% of respondents had at least one comorbidity, and almost all report that pain restricted their ability to engage in routine activities, like exercise, household chores, sleeping, and socializing. The majority (60%) said they feel anxiety-like symptoms daily or a few times a week, and a similar portion (59%) feel depression-like symptoms
How timely it is especially when the majority of people with chronic pain feel stigmatized by their medical providers. This was a key finding of a comprehensive survey by the U.S. Pain Foundation. The report’s identified that people with pain often feel their health care providers are not equipped to manage their pain effectively. Over two-thirds (69%) either did not feel, or only “rarely” or “sometimes” felt, that their provider was on a team with them.
At present the physical limits of an already overburdened and underfunded pain service are evident. For this reason, one must consider all possible options to support individuals. But there is hope. For example, University College Cork, recognised that ensuring our graduate doctors appreciate the importance of pain management, and to reduce the risk to those with chronic pain of feeling stigmatized by their medical providers, appoint of the first Associate Professor in Pain Medicine. Also, Chronic Pain Ireland is once again supporting the Pain Awareness September campaign and their 2022 theme is “Inspiring pain freedom”. They inspire and empower people by ensuring they have knowledge, skills and self-awareness to take control and improve their quality of life. For certain individuals’ part of that healing journey starts with self-management strategies and tools. Chronic Pain Ireland are collaborating with the HSE for Pain Awareness Month and running the Living Well with Chronic Pain Programmes with several informative talks and webinars throughout the month. By directing some individuals to this pathway, they can be provided with timely and effective support. Future planning
In this context perhaps we should assess individuals on a case-bycase basis to identify the clinical need to maximise outcome and not simply take a one-size fits all approach referring individuals into an already overcrowded healthcare system.
The Pain Awareness month allows us to recognise the importance of what we can do for our individual patients. It highlights that not enough is being done for the management of chronic pain in Ireland. Clearly the are ample opportunities for all of us—patient groups, health care providers, insurers, and policymakers—to work together to better serve people with pain and improve pain care for everyone.
Author Professor Dominic A. Hegarty. BSc., BMedSc., MB., MSc. (Pain Management), PhD. FCARSCI, FFPMCAI, FIPP Consultant in Pain Management & Neuromodulation, Mater Private Hospital, AssociateCorkProfessor of Pain Medicine, UCC, Ireland
daily or a few times a week. Closer to home these statistics reflect a similar pattern in the Irish healthcare service.

19763_FK_Pemetrexed_A4_4pp_Brochure_v4_Option_A.indd 27/04/202114:42
Paediatric population – No relevant use in malignant pleural mesothelioma and non-small cell lung cancer. Renal impairment – (Standard Cockcroft and Gault formula or GFR measured Tc99m-DPTA serum clearance method). In clinical studies patients with creatinine clearance of ≥ 45ml/min required no dose adjustments other than those recommended for all patients. Not recommended in patients with creatinine clearance below 45ml/min. Hepatic impairment – Patients with hepatic impairment have not been specifically studied. Contraindications: Hypersensitivity to the active substance or to any of the excipients, breast-feeding, concomitant yellow fever vaccine. Special warnings and precautions for use: Monitor patients for myelosuppression. Pemetrexed should not be given until ANC returns to ≥ 1500 cells/mm3 and platelet count to ≥ 100,000 cells/mm3. Dose reductions for subsequent cycles based on nadir ANC, platelet count and maximum non-haematologic toxicity seen from previous cycle. All patients must be instructed to take folic acid and vitamin B12 as a prophylactic measure to reduce treatment-related toxicity. Pre-treatment with dexamethasone (or equivalent) can reduce the incidence and severity of skin reactions. Not recommended in patients with creatinine clearance of < 45ml/min. Patients with mild to moderate renal insufficiency (creatinine clearance 45-79ml/min) should avoid taking NSAIDs, or acetylsalicylic acid (> 1.3g daily) for 2 days before, on the day of, and 2 days following pemetrexed administration. In patients with mild to moderate renal insufficiency NSAIDs with long elimination half-lives should be interrupted for at least 5 days prior to, on the day of, and at least 2 days following pemetrexed administration. Patients should be regularly monitored for acute tubular necrosis, decreased renal function and signs and symptoms of nephrogenic diabetes insipidus. Drainage of third space fluid collection prior to pemetrexed treatment should be considered but may not be necessary. Patients should receive adequate antiemetic treatment and appropriate hydration prior to and/or after receiving treatment. Serious cardiovascular and cerebrovascular events have been uncommonly reported during clinical studies with pemetrexed, usually when given in combination with another cytotoxic agent. Concomitant use of live attenuated vaccines is not recommended. Sexually mature males are advised not to father a child during treatment and up to 6 months thereafter. Contraceptive measures or abstinence are recommended. Possibility of irreversible infertility; men advised to seek counselling on sperm storage before starting treatment. Women of childbearing potential must use effective contraception during treatment with pemetrexed. Cases of radiation pneumonitis reported in patients treated with radiation either prior, during or subsequent to pemetrexed therapy; particular attention should be paid to these patients and caution with other radiosensitising agents. Cases of radiation recall reported in patients who received radiotherapy weeks or years previously. Accumulation of cyclodextrins may occur in patients with moderate to severe renal dysfunction. May cause fatigue, patients should be cautioned against driving or operating machinery if this occurs. Undesirable effects: (Associated with pemetrexed monotherapy or in combination with cisplatin) Infection, pharyngitis, sepsis, dermo-hypodermitis, neutropenia, leukopenia, decreased haemoglobin, febrile neutropenia, decreased platelet count, pancytopenia, autoimmune haemolytic anaemia, hypersensitivity, anaphylactic shock, dehydration, taste disorder, peripheral motor neuropathy, peripheral sensory neuropathy, dizziness, cerebrovascular accident, ischemic stroke, intracranial haemorrhage, conjunctivitis, dry eye, increased lacrimation, keratoconjunctivitis sicca, eyelid oedema, ocular surface disease, cardiac failure, arrhythmia, angina, myocardial infarction, coronary artery disease, supraventricular arrhythmia, peripheral ischaemia, pulmonary embolism, interstitial pneumonitis, stomatitis, anorexia, vomiting, diarrhoea, nausea, dyspepsia, constipation, abdominal pain, rectal haemorrhage, gastrointestinal haemorrhage, intestinal perforation, oesophagitis, colitis, increased alanine aminotransferase, increased aspartate aminotransferase, hepatitis, rash, skin exfoliation, hyperpigmentation, pruritis, erythema multiforme, alopecia, urticaria, erythema, Stevens-Johnson syndrome, toxic epidermal necrolysis, pemphigoid, dermatitis bullous, acquired epidermolysis bullosa, erythematous oedema, pseudocellulitis, dermatitis, eczema, prurigo, decreased creatinine clearance, increased blood creatinine, renal failure, decreased GFR, nephrogenic diabetes insipidus, renal tubular necrosis, fatigue, pyrexia, pain, oedema, chest pain, mucosal inflammation, increased GGT, radiation oesophagitis, radiation pneumonitis, recall phenomenon. Legal Category: POM Marketing Authorisation Numbers: EU/1/16/1115/003, EU/1/16/1115/004, EU/1/16/1115/005. Marketing Authorisation Holder: Fresenius Kabi Deutschland GmbH, Else-Kroner-Straße 1, 61352 Bad Homburg v.d.Höhe, Germany. Further Information: See the SmPC for further details. Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2, Tel: +353 1 6764971, Fax: +353 1 6762517. Website: www.hpra.ie, E-mail: medsafety@hpra.ie. Adverse events should also be reported to Fresenius Kabi Limited via email Pharmacovigilance GB@Fresenius Kabi.com. Date of Preparation: May 2021 Job code: API/Pemetrexed/02 Fresenius Kabi Limited Fresenius Kabi Ireland Unit 3B Fingal Bay, Balbriggan, Co. Dublin, Ireland Website: www.fresenius-kabi.com/ie/ Email: Phone:FK-enquiries.ireland@fresenius-kabi.com+353(0)18413030 19763_FK_Pemetrexed_A4_4pp_Brochure_v4_Option_A.indd 27/04/202114:42
25 mg/mL A multi-targeted anti-cancer antifolate agent In three presentations Pemetrexed 25 mg/mL A room temperature stable ready-to-dilute concentrate
Neurotoxicity – Patients should discontinue therapy if Grade 3 or 4 neurotoxicity is observed. CTC Grade 0-1: 100% of previous pemetrexed and cisplatin dose (mg/m2). CTC Grade 2: 100% of previous pemetrexed dose (mg/m2) and 50% of previous cisplatin dose (mg/m2). Discontinue treatment with pemetrexed Fresenius Kabi if a patient experiences any haematologic or non-haematologic Grade 3 or 4 toxicity after 2 dose reductions or immediately if Grade 3 or 4 neurotoxicity is observed. Elderly – No dose reductions other than those recommended for all patients are necessary.
Fresenius Kabi Limited Fresenius Kabi Ireland Unit 3B Fingal Bay, Balbriggan, Co. Dublin, Ireland Website: www.fresenius-kabi.com/ie/ Email: Phone:FK-enquiries.ireland@fresenius-kabi.com+353(0)18413030
Date of Prep: May 2021 Ref: IV/ONCO/PEME/01/2021 Pemetrexed 25 mg/mL A multi-targeted anti-cancer antifolate agent In three presentations Pemetrexed 25 mg/mL A room temperature stable ready-to-dilute concentrate 19763_FK_Pemetrexed_A4_4pp_Brochure_v4_Option_A.indd 1 27/04/2021 14:42
PRESCRIBING INFORMATION: Consult the Summary of Product Characteristics for further information. Additional information is available upon request Pemetrexed Fresenius Kabi 25mg/ml concentrate for solution for infusion. Active ingredients: Pemetrexed diacid. One vial of 4ml concentrate contains 100mg pemetrexed. One vial of 20ml concentrate contains 500mg pemetrexed. One vial of 40ml concentrate contains 1,000mg pemetrexed. Excipients with known effect – 4ml vial - 964mg hydroxypropylbetadex, 20ml vial – 4820mg hydroxypropylbetadex, 40ml vial – 9640mg hydroxypropylbetadex. Indications: In combination with cisplatin - treatment of chemotherapy naïve patients with unresectable malignant pleural mesothelioma, first line treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology. Monotherapy – Maintenance treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology in patients whose disease has not progressed immediately following platinum-based chemotherapy, second line treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology. Posology and method of administration: Only administer under the supervision of a physician qualified in the use of anti-cancer chemotherapy. Administer as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. See SmPC for further information on handling, administering and dilution. In combination with cisplatin – Recommended dose is 500mg/m2 of body surface area (BSA) administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. Recommended dose of cisplatin is 75mg/m2 BSA infused over two hours approximately 30 minutes after completion of the pemetrexed infusion on the first day of each 21-day cycle. Patients must receive adequate anti-emetic treatment and appropriate hydration prior to and/or after receiving cisplatin (see also cisplatin SmPC). As single agent – In the treatment of non-small cell lung cancer after prior chemotherapy, recommended dose is 500mg/m2 BSA administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. Pre-medication regimen: To reduce the incidence and severity of skin reactions, a corticosteroid should be given the day prior to, on the day of, and the day after pemetrexed administration. Corticosteroid should be equivalent to 4mg of dexamethasone orally twice daily. Patients must also receive vitamin supplementation; oral folic acid or a multivitamin containing folic acid (350 to 1000 micrograms) on a daily basis. At least five doses of folic acid must be taken during the seven days preceding the first dose of pemetrexed and dosing must continue during the full course of therapy and for 21 days after the last dose of pemetrexed. Patients must also receive an intramuscular injection of vitamin B12 (1000 micrograms) in the week preceding the first dose of pemetrexed and once every three cycles thereafter. Subsequent vitamin B12 injections may be given on the same day as pemetrexed. Monitoring: Before each dose complete blood count including differential white cell count (WCC) and platelet count. Prior to each chemotherapy administration blood chemistry tests should be collected to evaluate renal and hepatic function. Before the start of any cycle of chemotherapy, patients are required to have absolute neutrophil count (ANC) ≥ 1500 cells/mm3 and platelets ≥ 100,000 cells/mm3 Creatinine clearance should be ≥ 45 ml/min. Total bilirubin should be ≤ 1.5 times upper limit of normal. Alkaline phosphatase (AP), aspartate aminotransferase (AST or SGOT) and alanine aminotransferase (ALT or SGPT) should be ≤ 3 times upper limit of normal. AP, AST and ALT ≤ 5 times upper limit of normal is acceptable if liver has tumour involvement. Dose adjustments: At the start of a subsequent cycle should be based on nadir haematologic counts or maximum non-haematologic toxicity from the preceding cycle of therapy. Treatment may be delayed to allow sufficient time for recovery. Upon recovery patients should be retreated using the guidelines as follows, which are applicable for pemetrexed Fresenius Kabi used as single agent or in combination with cisplatin. Haematologic toxicities (dose modify both pemetrexed and cisplatin) – Nadir ANC < 500/mm3 and nadir platelets ≥ 50,000/mm3 or nadir platelets < 50,000/mm3 regardless of nadir ANC: 75% of previous dose. Nadir platelets < 50,000/mm3 with bleeding regardless of nadir ANC: 50% of previous dose. Non-haematologic toxicities ≥ Grade 3 (excluding neurotoxicity) - pemetrexed Fresenius Kabi should be withheld until resolution to less than or equal to the patient’s pre-therapy value. Treatment should be resumed accordingly – Any grade 3 or 4 toxicities except mucositis, or any diarrhoea requiring hospitalisation or grade 3 or 4 diarrhoea: 75% of previous dose (mg/m2) of pemetrexed and cisplatin. Grade 3 or 4 mucositis: 50% of previous pemetrexed dose (mg/m2) and 100% of previous cisplatin dose (mg/m2).
PRESCRIBING INFORMATION: Consult the Summary of Product Characteristics for further information. Additional information is available upon request Pemetrexed Fresenius Kabi 25mg/ml concentrate for solution for infusion.
Paediatric population – No relevant use in malignant pleural mesothelioma and non-small cell lung cancer. Renal impairment – (Standard Cockcroft and Gault formula or GFR measured Tc99m-DPTA serum clearance method). In clinical studies patients with creatinine clearance of ≥ 45ml/min required no dose adjustments other than those recommended for all patients. Not recommended in patients with creatinine clearance below 45ml/min. Hepatic impairment – Patients with hepatic impairment have not been specifically studied. Contraindications: Hypersensitivity to the active substance or to any of the excipients, breast-feeding, concomitant yellow fever vaccine. Special warnings and precautions for use: Monitor patients for myelosuppression. Pemetrexed should not be given until ANC returns to ≥ 1500 cells/mm3 and platelet count to ≥ 100,000 cells/mm3. Dose reductions for subsequent cycles based on nadir ANC, platelet count and maximum non-haematologic toxicity seen from previous cycle. All patients must be instructed to take folic acid and vitamin B12 as a prophylactic measure to reduce treatment-related toxicity. Pre-treatment with dexamethasone (or equivalent) can reduce the incidence and severity of skin reactions. Not recommended in patients with creatinine clearance of < 45ml/min. Patients with mild to moderate renal insufficiency (creatinine clearance 45-79ml/min) should avoid taking NSAIDs, or acetylsalicylic acid (> 1.3g daily) for 2 days before, on the day of, and 2 days following pemetrexed administration. In patients with mild to moderate renal insufficiency NSAIDs with long elimination half-lives should be interrupted for at least 5 days prior to, on the day of, and at least 2 days following pemetrexed administration. Patients should be regularly monitored for acute tubular necrosis, decreased renal function and signs and symptoms of nephrogenic diabetes insipidus. Drainage of third space fluid collection prior to pemetrexed treatment should be considered but may not be necessary. Patients should receive adequate antiemetic treatment and appropriate hydration prior to and/or after receiving treatment. Serious cardiovascular and cerebrovascular events have been uncommonly reported during clinical studies with pemetrexed, usually when given in combination with another cytotoxic agent. Concomitant use of live attenuated vaccines is not recommended. Sexually mature males are advised not to father a child during treatment and up to 6 months thereafter. Contraceptive measures or abstinence are recommended. Possibility of irreversible infertility; men advised to seek counselling on sperm storage before starting treatment. Women of childbearing potential must use effective contraception during treatment with pemetrexed. Cases of radiation pneumonitis reported in patients treated with radiation either prior, during or subsequent to pemetrexed therapy; particular attention should be paid to these patients and caution with other radiosensitising agents. Cases of radiation recall reported in patients who received radiotherapy weeks or years previously. Accumulation of cyclodextrins may occur in patients with moderate to severe renal dysfunction. May cause fatigue, patients should be cautioned against driving or operating machinery if this occurs. Undesirable effects: (Associated with pemetrexed monotherapy or in combination with cisplatin) Infection, pharyngitis, sepsis, dermo-hypodermitis, neutropenia, leukopenia, decreased haemoglobin, febrile neutropenia, decreased platelet count, pancytopenia, autoimmune haemolytic anaemia, hypersensitivity, anaphylactic shock, dehydration, taste disorder, peripheral motor neuropathy, peripheral sensory neuropathy, dizziness, cerebrovascular accident, ischemic stroke, intracranial haemorrhage, conjunctivitis, dry eye, increased lacrimation, keratoconjunctivitis sicca, eyelid oedema, ocular surface disease, cardiac failure, arrhythmia, angina, myocardial infarction, coronary artery disease, supraventricular arrhythmia, peripheral ischaemia, pulmonary embolism, interstitial pneumonitis, stomatitis, anorexia, vomiting, diarrhoea, nausea, dyspepsia, constipation, abdominal pain, rectal haemorrhage, gastrointestinal haemorrhage, intestinal perforation, oesophagitis, colitis, increased alanine aminotransferase, increased aspartate aminotransferase, hepatitis, rash, skin exfoliation, hyperpigmentation, pruritis, erythema multiforme, alopecia, urticaria, erythema, Stevens-Johnson syndrome, toxic epidermal necrolysis, pemphigoid, dermatitis bullous, acquired epidermolysis bullosa, erythematous oedema, pseudocellulitis, dermatitis, eczema, prurigo, decreased creatinine clearance, increased blood creatinine, renal failure, decreased GFR, nephrogenic diabetes insipidus, renal tubular necrosis, fatigue, pyrexia, pain, oedema, chest pain, mucosal inflammation, increased GGT, radiation oesophagitis, radiation pneumonitis, recall phenomenon. Legal Category: POM Marketing Authorisation Numbers: EU/1/16/1115/003, EU/1/16/1115/004, EU/1/16/1115/005. Marketing Authorisation Holder: Fresenius Kabi Deutschland GmbH, Else-Kroner-Straße 1, 61352 Bad Homburg v.d.Höhe, Germany. Further Information: See the SmPC for further details. Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2, Tel: +353 1 6764971, Fax: +353 1 6762517. Website: www.hpra.ie, E-mail: medsafety@hpra.ie. Adverse events should also be reported to Fresenius Kabi Limited via email Pharmacovigilance GB@Fresenius Kabi.com. Date of Preparation: May 2021 Job code: API/Pemetrexed/02
Launching
Launching
19763_FK_Pemetrexed_A4_4pp_Brochure_v4_Option_A.indd 1 27/04/2021 14:42
Date of Prep: May 2021 Ref: IV/ONCO/PEME/01/2021
Neurotoxicity – Patients should discontinue therapy if Grade 3 or 4 neurotoxicity is observed. CTC Grade 0-1: 100% of previous pemetrexed and cisplatin dose (mg/m2). CTC Grade 2: 100% of previous pemetrexed dose (mg/m2) and 50% of previous cisplatin dose (mg/m2). Discontinue treatment with pemetrexed Fresenius Kabi if a patient experiences any haematologic or non-haematologic Grade 3 or 4 toxicity after 2 dose reductions or immediately if Grade 3 or 4 neurotoxicity is observed. Elderly – No dose reductions other than those recommended for all patients are necessary.
Active ingredients: Pemetrexed diacid. One vial of 4ml concentrate contains 100mg pemetrexed. One vial of 20ml concentrate contains 500mg pemetrexed. One vial of 40ml concentrate contains 1,000mg pemetrexed. Excipients with known effect – 4ml vial - 964mg hydroxypropylbetadex, 20ml vial – 4820mg hydroxypropylbetadex, 40ml vial – 9640mg hydroxypropylbetadex. Indications: In combination with cisplatin - treatment of chemotherapy naïve patients with unresectable malignant pleural mesothelioma, first line treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology. Monotherapy – Maintenance treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology in patients whose disease has not progressed immediately following platinum-based chemotherapy, second line treatment of locally advanced or metastatic non-small cell lung cancer other than predominantly squamous cell histology. Posology and method of administration: Only administer under the supervision of a physician qualified in the use of anti-cancer chemotherapy. Administer as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. See SmPC for further information on handling, administering and dilution. In combination with cisplatin – Recommended dose is 500mg/m2 of body surface area (BSA) administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. Recommended dose of cisplatin is 75mg/m2 BSA infused over two hours approximately 30 minutes after completion of the pemetrexed infusion on the first day of each 21-day cycle. Patients must receive adequate anti-emetic treatment and appropriate hydration prior to and/or after receiving cisplatin (see also cisplatin SmPC). As single agent – In the treatment of non-small cell lung cancer after prior chemotherapy, recommended dose is 500mg/m2 BSA administered as an intravenous infusion over 10 minutes on the first day of each 21-day cycle. Pre-medication regimen: To reduce the incidence and severity of skin reactions, a corticosteroid should be given the day prior to, on the day of, and the day after pemetrexed administration. Corticosteroid should be equivalent to 4mg of dexamethasone orally twice daily. Patients must also receive vitamin supplementation; oral folic acid or a multivitamin containing folic acid (350 to 1000 micrograms) on a daily basis. At least five doses of folic acid must be taken during the seven days preceding the first dose of pemetrexed and dosing must continue during the full course of therapy and for 21 days after the last dose of pemetrexed. Patients must also receive an intramuscular injection of vitamin B12 (1000 micrograms) in the week preceding the first dose of pemetrexed and once every three cycles thereafter. Subsequent vitamin B12 injections may be given on the same day as pemetrexed. Monitoring: Before each dose complete blood count including differential white cell count (WCC) and platelet count. Prior to each chemotherapy administration blood chemistry tests should be collected to evaluate renal and hepatic function. Before the start of any cycle of chemotherapy, patients are required to have absolute neutrophil count (ANC) ≥ 1500 cells/mm3 and platelets ≥ 100,000 cells/mm3 Creatinine clearance should be ≥ 45 ml/min. Total bilirubin should be ≤ 1.5 times upper limit of normal. Alkaline phosphatase (AP), aspartate aminotransferase (AST or SGOT) and alanine aminotransferase (ALT or SGPT) should be ≤ 3 times upper limit of normal. AP, AST and ALT ≤ 5 times upper limit of normal is acceptable if liver has tumour involvement. Dose adjustments: At the start of a subsequent cycle should be based on nadir haematologic counts or maximum non-haematologic toxicity from the preceding cycle of therapy. Treatment may be delayed to allow sufficient time for recovery. Upon recovery patients should be retreated using the guidelines as follows, which are applicable for pemetrexed Fresenius Kabi used as single agent or in combination with cisplatin. Haematologic toxicities (dose modify both pemetrexed and cisplatin) – Nadir ANC < 500/mm3 and nadir platelets ≥ 50,000/mm3 or nadir platelets < 50,000/mm3 regardless of nadir ANC: 75% of previous dose. Nadir platelets < 50,000/mm3 with bleeding regardless of nadir ANC: 50% of previous dose. Non-haematologic toxicities ≥ Grade 3 (excluding neurotoxicity) - pemetrexed Fresenius Kabi should be withheld until resolution to less than or equal to the patient’s pre-therapy value. Treatment should be resumed accordingly – Any grade 3 or 4 toxicities except mucositis, or any diarrhoea requiring hospitalisation or grade 3 or 4 diarrhoea: 75% of previous dose (mg/m2) of pemetrexed and cisplatin. Grade 3 or 4 mucositis: 50% of previous pemetrexed dose (mg/m2) and 100% of previous cisplatin dose (mg/m2).
Pemetrexed

ofandGastroenterologyUlsterSocietyGastroenterologyaredelightedtowelcomedelegatesfromacrossIrelandtohearaboutexcitingdevelopments
The Irish Society of Gastroenterology & Ulster Society of Gastroenterology recently held their annual All Ireland Summer Meeting at the Europa Hotel in Belfast. The meeting took place in a hybrid format, with a varied programme covering topics including Endoscopy ‘Tips and Tricks’, Managing refractory oesophageal strictures, Drug induced liver injury and Managing colorectal metastases in the liver. Dr Tony Tham, President of USG welcomed delegates to Belfast
“We are all very much working together towards the same goal, he said. Other speakers over the twoday event included Professor Séverine Vermeire, Consultant Gastroenterologist, University Hospitals Leuven, Belgium who spoke about ‘Small molecules in IBD, where will we position them?’ Dr Christine J. Buskens, Consultant Colorectal Surgeon Academic Medical Centre, Amsterdam, The Netherlands who discussed ‘Surgery for Perianal Corhn’s and Dr Jeremy Woodward Consultant Cambridge,Addenbrooke’sGastroenterologistHospital,UK.DrWoodward discussed Coeliac disease management when the gluten free diet fails. Sarah White from the DGBI team at Tallaght University Hospital won the prize for one of the best oral poster presentations at the All Ireland summer meeting. Her abstract was entitled, ‘Clinical outcomes following Dietetic- led in-person or virtual education for the management of irritable bowel syndrome. Her poster main finding concluded, “A greater proportion of pts (n=255) achieved satisfactory relief of their IBS symptoms following virtual rather than face to face consultation72.6% Vs 55.7%”
Professor Nuala Murphy, Chair of the National Paediatric Diabetes Audit Feasibility Steering Committee commented "As a country, we invest a lot of money in diabetes care over each patients journey but at the moment, most of this spend is in treating preventable diabetes related complications. We know that tight blood glucose control has been shown definitively to prevent diabetes related complications, so investing early and empowering patients to achieve good control makes sense. Audit allows us to see what we are doing well and what we need to improve and we are outliers in international terms as we do not currently have a national paediatric diabetes audit. This feasibility study supports the need for an audit and the next phase is audit development and implementation.”
16 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE News All Ireland ISG/USG Summer Meeting
Calls to Establish National Audit of Diabetes
Sarah White, DGBI team, Tallaght University Hospital and voiced their delight that this was the face-to-face meeting since the start of the Covid pandemic. We have a fantastic programme for this years’ meeting which we are extremely excited about,” he noted. Dr Tham also made reference to the ongoing working partnership between the Ulster Society Gastroenterology and the Irish Society of Gastroenterology.
“The Irish Society of within this field and emerging new developments”
The National Office of Clinical Audit (NOCA) has announced the publication of the National Paediatric Diabetes Audit Feasibility Study Report. The incidence of type 1 diabetes mellitus (T1DM) among children and young people in Ireland is one of the highest in Europe, with diabetes incidence rates in the top 25% worldwide. Over the last 25 years, the incidence rate has risen from 16.3 cases per 100,000 population <15yrs in 1997 to 27.3 per 100,000 in 2008 but more recent data shows a stabilisation of the rate to 27.1 cases per 100,000 population in 2018. Management of this chronic condition places huge demands on affected individuals, their families, and the health service. Paediatric T1DM care requires prioritisation because of its high incidence and the significant long-term consequences of suboptimal care. No national paediatric diabetes audit (NPDA) exists in Ireland, and available data originate from single-centre, stand-alone, or retrospective studies. The lack of reliable data precludes healthcare professionals from making informed decisions about how to improve services, and means that disparities in paediatric diabetes care may not be identified. A national audit of paediatric T1DM will highlight areas of good practice, identify areas for improvement and will support data-driven resource allocation. This study recommends the development of a National Audit of T1DM, with a phased approach. The first phase includes all paediatric T1DM patients aged under 16 years who attend the 19 paediatric centres nationally. Phase 2 involves extending the audit to include affected young adults aged 16-25 years and Phase 3 will incorporate all patients with T1DM nationally. An Individual Health Identifier (IHI) for all with T1DM would support successful implementation of this audit and would allow linkage to existing datasets. Electronic data capture is essential to allow complete, accurate and efficient data collection.



























Professor H. Paul Redmond, Chair, RCSI Short Life Working Group (SLWG), said, "These guidelines have been drafted to acknowledge the vital role that multi-disciplinary collaboration plays in kidney surgery in Ireland. There is now a wonderful opportunity for experts in the area to work together with colleagues to attain widespread best practices for optimum patient outcomes in kidney surgery in this country. We would like to thank all our colleagues on the SLWG for their support in preparing these important guidelines."
Professor H. Paul Redmond, Chair, RCSI Short Life Working Group (SLWG)
CollaborationNews
The guidelines recommend that centres undertaking kidney surgery should offer seamless, timely and expert care within a multidisciplinary team.
The guide outlines the best practices in adrenal surgery with a particular focus on endocrine adrenal surgery.
HPRA Invites Experts to Join Panel
The SLWG observed that within the republic of Ireland, adrenal surgery is undertaken in some high-volume centres and some low-volume centres across the health service.
Membership of the HPRA’s panel will provide clinical experts with an opportunity to develop a greater understanding of how health products are regulated nationally and in Europe, gain an insight into the development of innovative health products and contribute to ensuring that health products are safe and effective for patients. The HPRA both values the expertise of clinical specialists in Ireland and recognises the beneficial role their contribution adds to regulatory evaluation and assessment of health products.
Key amongst Clinicians
New guidelines published on adrenal surgery by the Royal College of Surgeons in Ireland (RCSI) emphasise the importance of collaboration amongst clinicians involved in kidney surgery in Ireland.
Novartis Ireland are delighted to announce the appointment of Caitriona Walsh as Novartis Ireland Country President.
The Health Products Regulatory Authority (HPRA) is inviting clinical experts to register their interest in contributing to the regulatory evaluation and assessment of medicines and medical devices through joining a new external expert panel. Collaborating with external clinical specialists, including doctors, pharmacists and other healthcare professionals, is an important part of how the HPRA continues to ensure public health is protected.
• Cardiovascular,
The guidelines were developed by a Short-Lived Working Group convened by immediate past RCSI President, Professor Ronan O’Connell.
• Oncology
18 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
The national regulator is seeking clinical expertise in the following areas: and Haematology Endocrinology,
Renal, Respiratory • DermatologyRheumatology,Gastroenterology,Immunology, • Neurology, Pain and Psychiatry • Infectious Diseases • Ophthalmology • Paediatrics and Geriatrics • Clinical Pharmacology • Diagnostic & Therapeutic • Radiopharmaceuticals
External experts may be requested to provide clinical input in relation to clinical studies and scientific advice for new products under development, applications to market innovative medicines that offer new treatment options for patients, and any emerging quality or safety concerns in relation to medicines and medical devices on the market.
They also advise that kidney surgeons should undertake a minimum of six adrenalectomies a year and 12 per year per centre where adrenocortical cancers are being performed.
The group reviewed international literature and guidelines from allied organisations on either side of the Atlantic, including the recently published 2021 UK GIRFT (Get It Right the First Time) report, the European Society of Endocrine Surgeons (ESES) consensus statement of 2019 and the Dutch Adrenal Network (DAN) guidelines.
A native of Galway and graduate of NUIG and Trinity College Dublin, Caitriona started her career in Novartis Ireland and has worked in senior leadership roles in Switzerland and the UK before returning to Ireland to take up this new position.
The agreed output is a short document outlining the current service, relevant issues and recommendations for the future.
New Appointment for Novartis


strains.+
SciencePrecision
Contains a unique combination of two clinically researched synergetic
The E volution of Precision Science
ScientificallyStudied
Pantothenic Acid, Vitamin B6: Contribute to the reduction of tiredness and fatigue.
TM Group ✝Calcium: Contributes to the normal function of digestive enzymes. Pantothenic Acid, Vitamin B6: Contribute to the reduction of tiredness and fatigue. 1714
Calcium: Contributes to the normal function of digestive enzymes.
NEW ScientificallyStudied
The Evolution of
Contains a unique combination of two clinically researched synergetic strains



Type A Aortic Dissection –The Facts Most lethal condition of the aorta Worldwide prevalence of 0.5 to 2.95 per 100,000 per year. Recent data : 10.4 cases per 100,000/year. 65% males. Up to 26% of aortic dissections die prior to hospital admission. 58% to 68% of acute dissection cases die prior to definitive operative intervention. Mortality is often quoted at 1% per hour. About 74% of patients die within the first two weeks. Less than 10% of untreated patients live for one year, and almost all patients die within 10 years. 33% of patients with a dissection are misdiagnosed. Over 2000 lives per year are lost to dissections in the UK and Ireland. 10 lives per week can be saved with the correct diagnosis and treatment.
Aortic Disease
The most common risk factors for acute dissection are hypertension, connective tissue disease and known aortic aneurysm. Other significant risk factors include:
20 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE Figure 1
Figure 2: Stanford and DeBakey aortic dissection classifications, taken from Gawinecka et al.8
• Vasculitis - Takayasu’s arteritis, Giant cell arteritis
Risk Factors
• Family history • Trauma • Pregnancy • Illicit drug use Clinical Presentation
This separation results in the creation of a false channel of blood. This false lumen may extend into branches of the aorta in the chest or abdomen, causing malperfusion, ischemia, or occlusion with resultant complications. The dissection can also progress proximally, to involve the aortic sinus, aortic valve, and coronary arteries. Dissection can lead to aneurysmal change and early rupture, which represents a life- threatening emergency.
Type A Aortic Dissection
• Atherosclerosis • Iatrogenic trauma Previous aortic manipulation (including cardiac surgery)
• Congenital abnormalities - Bicuspid Aortic valve, Coarctation of the aorta • Age (60-80 yrs. old)
Written by Saleem Jahangeer, Consultant Cardiothoracic and Aortic Surgeon, St James’s Hospital, Dublin
Aortic dissections are classified using the Stanford or DeBakey Classification (Figure 2). A Stanford A represents an intimal tear proximal to the left subclavian artery.
The vast majority of patients with dissection present with chest pain. This can be described as a ripping or tearing pain. The onset is very often abrupt and sudden in nature. Patients can also present with clinical features underlying malperfusion: acute organ ischaemia, neurological symptoms or acute heart failure. Unfortunately, in some patients the first sign can be sudden death, caused by free rupture or shearing of the coronary arteries. The physical signs and clinical features are summarised in Figure 3. Since the most common presentation is chest pain, acute dissections are very often misdiagnosed as acute coronary syndromes (ACS). Up to 33% of dissection patients are misdiagnosed. This can have very drastic consequences. Not only does this represent a delay in
The 19th of September is the global Aortic Dissection Awareness Day. To raise awareness, especially among healthcare professionals, about this silent killer, this article will focus mainly on Acute Type A Aortic Dissection (ATAD). ATAD is a life-threatening, time sensitive emergency with a high pre-hospital and peri-operative mortality.
•
Introduction An aortic dissection is a partial tear in the wall of the aorta between the intimal and the medial layer of the aortic wall (Figure 1).
• Infection – Syphilis, Tuberculosis



Imaging modalities in aortic PlaindissectionChest X-ray (CXR)
Most if not all patients presenting to ED will have a CXR as part of their investigations. Patients with an acute dissection may have some radiological signs on CXR such as a widened mediastinum or a pleural effusion. Comparison with old films can be very helpful but a normal CXR should not deter further investigations. CT scan CT scan remains the gold standard diagnostic imaging modality. It is 95% sensitive and shows both the true and false lumens with an intimal flap often visible (Figure 4). It is critical to emphasise that diagnosis of a dissection might not be visible on a Non-contrast CT or one with the wrong contrast phase (e.g. CTPA). In such cases, it is paramount that a proper arterial, ideally gated CT aorta is performed straight away.
21 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 diagnosis and ultimately treatment, but mis-managing a dissection as an ACS with antiplatelets or even an angiogram can lead to severe complications including rupture.
Blood Pressure Management
The European Society of Cardiology has published a risk-scoring method based on High Risk Condition, High Risk Pain features, High Risk Examination features (Figure 6Table 2 on page 22).
3: Clinical signs and presentation of Acute Type A Dissection Pulse deficit (30% Type A ) Variation in BP between the arms (>30mmHg) Hypertension or hypotension Acute Aortic Insufficiency - Diastolic murmur Acute MI - RCA most commonly involved Cardiac tamponade Haemothorax or pleural effusion Neurological deficit - 15-40%, CVA or reduced consciousness Malperfusion Mesenteric ischaemia <5% Renal insufficiency 20% in Type A Lower extremity ischemia Spinal cord ischemia 1% Figure 4: CT scan of aortic dissection. TL - True Lumen Figure 5: TTE and TOE images showing acute dissection with a distint flap
Figure
The diagnosis of an acute aortic dissections always requires a high level of suspicion.
Blood Pressure control is critical in the first line management and should be initiated immediately – Anti-impulse therapy. The aim is to decrease δP/ δT – the force of ejection of blood, while maintaining organ perfusion. Antiimpulse therapy aims to titrate systolic BP to less than 120mmHg and HR to less than 60bpm.
Surgical Management of Acute Type A Dissection
The definitive treatment for acute type A dissection is surgery. Once the diagnosis is confirmed, immediate referral needs to be made to the cardiothoracic on call team, with preparation for prompt patient transfer.
The definitive management remains surgical repair. The surgical strategy aims at resecting
Transthoracic echocardiogramTransoesophagealand(TTE and TOE)
TTE and TOE have a sensitivity of 80% and 89% respectively. There has been recent interest in the use Point of Care Ultrasound (POCUS) at the bedside upon presentation to diagnose an acute dissection (Figure 5). It is important to note that the use of TTE and TOE might be limited to the proximal aortic segment and a tear in the proximal arch may be missed. Any suspicious findings on echocardiogram should trigger an immediate CT scan to confirm the diagnosis.
The diagnosis of an acute aortic dissections always requires a high level of suspicion. Unless you think of an aortic dissection, it will be missed. And if you think of an aortic dissection, it needs to be immediately confirmed or ruled-out by a contrast CT scan without delay.
Management of Acute Type A Dissection
The first line agent is usually intravenous labetolol. GTN or nipride should generally be avoid as they can cause a reflex tachycardia which may increase δP/ δT.


The aortic arch should be inspected at the time of surgery to ensure there are no intimal tears. This is accomplished during Deep Circulatory Hypothermic Arrest (DHCA). Presence of any intimal tears in the arch would warrant a hemi-arch or a total arch replacement (Figure 8).
Table modified from Rogers AM et al Circulation 2011;123:2213-8. Risk score varies from 0-3 according the number of positive categories (I per column). the primary tear/tears and obliterating the false lumen. The aortic valve is usually resuspended to maintain competence. If the initial tear involves the root, a root replacement with a composite conduit and re-implantation of the coronary arteries is warranted (Figure 7).
Surgical repair of Acute Type A Dissections are high risk surgeries. The operative and in-patient mortality rates are around 18% and 33% respectively. In an effort to improve surgical outcomes, surgical management of Type A dissections has been centralised to specialist “Aortic” centres in many European countries and in the UK. This has seen an improvement in outcomes, mainly due to a volume-outcome relationship.
Risk
Table 2 score according to positive categories (I per column)
22 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE Figure 8: Hemi-arch and total arch Figurereplacement6:ESCrisk-scoring mehod Figure 7: (A) Dissected ascending aorta (B) Replacement of ascending aorta (C) Aortic root replacement Aortic Disease High-risk conditions Marfan syndrome (or other connective tissue diseases) Family history of aortic disease Known aortic valve disease Known thoracic aortic aneursym Previous aortic manipulation (including cardiac surgery) High-risk pain features Chest, back or abdominal pain described as any of the following: - abrupt onset# - severe intensity - ripping or tearing High-risk examination features Evidence of perfusion deficit: - pulse deficit - systolic blood pressure difference - focal neurological deficit (including with pain) Aortic diastolic murmur (new with pain) Hypotension or shock
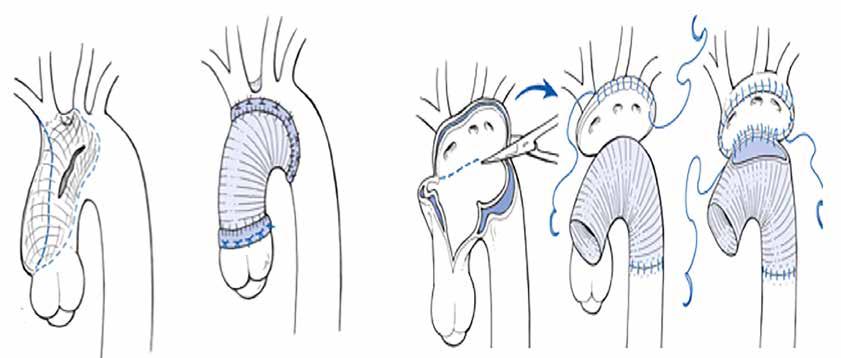
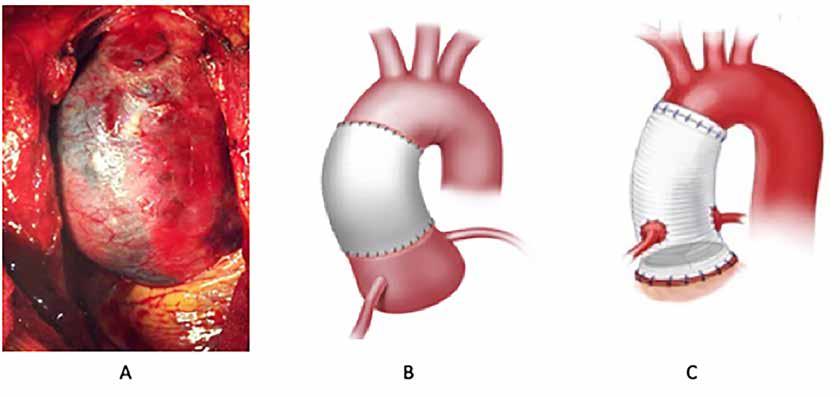
Our annual listing celebrating innovation and excellence in healthcare is coming soon. PROFESSIONAL 100 PROFESSIONAL 100 To request an entry or nomination form please sarah@hospitalprofessionalnews.iecontact: 2 0 2 2 NO M I N A T I O N S NO W O P E N PROFESSIONALHOSPITALNEWS IRELAND Ireland’s Dedicated Hospital Professional Publication To request an entry or nomination form please contact: kelly-jo@ipn.ie danielle@hospitalprofessionalnews.ieor

24 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Figure 10: Trifurcated FET prosthesis with extra-anatomical bypass of the left subclavian artery
The poor long-term prognosis related to a Type A dissection has led to a shift in the treatment paradigm of these patients. The focus currently has changed to performing a lifesaving, durable repair which will address the poor long-term prognosis of this condition.
The Frozen Elephant Trunk (FET) technique is invaluable in patients with distal aortic malperfusion with compression of the true lumen, complex primary and re-entry tears involving the distal arch or proximal descending thoracic aorta (DTA). FET prosthesis can fully open the compressed true lumen and also cover additional entry tears located in the proximal DTA. The presence of the stented graft of the FET prosthesis also provides a landing zone for future aortic endovascular stenting if required. This facilitates the long-term management of patients who might have an expanding false lumen after their index operation. Currently, both in the USA and the UK, FET procedures are performed by aortic surgeons trained in such procedures. Figure 10 shows a recent trifurcated FET prosthesis done by our Aortic team at St James’s Hospital, with excellent clinical and radiological outcome.
Follow-up following Acute Type A Dissection
Frozen Elephant Trunk procedure in acute dissection
Survivors of Type A dissection need long-term/life-long surveillance as the rate of post dissection complications and reintervention are quite high. Strict BP control along with enrolment in a surveillance programme are mandatory for these patients. Interval CT imaging is required to monitor the aorta. Echocardiograms are required to monitor the competence of the aortic valve if affected during the initial presentation.
Aortic Disease
The introduction of the Frozen Elephant Trunk (FET) graft
Even in patients who underwent successful surgery for a Type A dissection, the rates of reintervention or aortic-related complications can be as high as 70%.
Figure 9: Frozen elephant trunk procedure C Singh et al - AIMS bioengineering 2017
prosthesis has revolutionised the acute surgical management of acute Type A dissections. A FET prosthesis allows for a ‘2 in 1’ hybrid procedure which includes both a surgical repair and an endovascular stenting performed simultaneously (Figure 9).
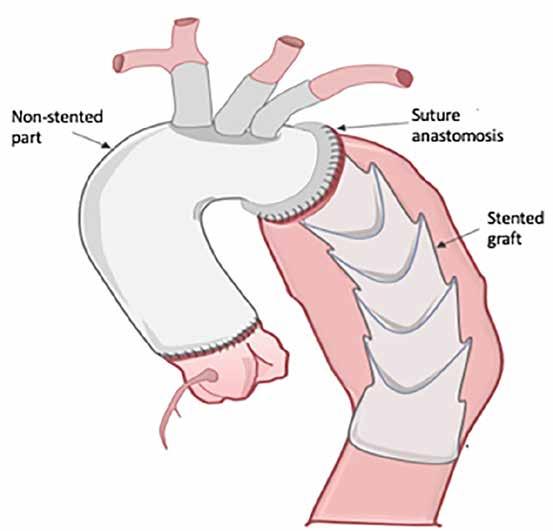

MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany. Further information is available from AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie. LEGAL CLASSIFICATION: POM (S1A). Full Summary of Product Characteristics is available at www.medicines.ie Reference 1. RINVOQ Summary of Product Characteristics, available on www.medicines.ie ©2022 AbbVie Inc. All rights reserved. IE-RNQ_AD-220036 | March 2022 INTRODUCINGFORTHETREATMENT OF MODERATE TO SEVERE atopic dermatitis in adults and adolescents 12 years and older who are candidates for systemic therapy 1



In 2012, in the UK, the National Institute for Clinical Excellence (NICE) published a guideline on VTE prevention and this was rolled out across all UK hospitals, with the help of financial incentives to encourage compliance. Such incentives allowed hospitals to develop an infrastructure for a VTE prevention protocol. Data from the implementation of this programme showed that hospitals that achieved risk-assessment targets had a reduced mortality from PE in both inpatients and also in the 90 days post discharge. This was demonstrable in both medical and surgical patients. NICE have also published data to show that VTE prophylaxis is cost effective.
The epidemiology and relevance of Hospital-Acquired Thrombosis Venous thromboembolism (VTE) is defined as the development of a blood clot within the venous system. These blood clots commonly arise within the deep veins of the leg, known as a deep vein thrombosis (DVT). Clots formed in this area have the potential to migrate to the vasculature of the lung, known as a pulmonary embolus (PE). In situ pulmonary thrombosis also occurs, particularly with Covid-19 infection. PE is associated with significant morbidity and mortality. Large PEs can lead to hypoxia, right heart strain, arrhythmia, systemic shock and death. The HSE estimated that VTE affected 6,772 patients in acute public hospitals in Ireland in 2021. VTE is a causative factor in 10% of deaths.
In 2018, the HSE carried out a quality improvement project and have subsequently published recommendations based on this project. Having an adequately resourced VTE prevention team, a VTE prevention committee and a clinically accessible VTE prevention protocol as well as individual risk assessment for every patient are the cornerstones of these recommendations, as is regular data collection and auditing. Patient advocacy now plays a large role in the driving of change and healthcare policy. The importance of educating the patient about the risk factors for VTE, the signs and symptoms of a clot and the role they can take themselves post discharge to reduce their personal risk of clot has become more widely recognised. The need to routinely deliver education to each patient and the need to audit this parameter are key areas highlighted in the HSE recommendations.
Hospital-Acquired-Thrombosis (HAT) Killshow we should we protect against it?
through the use of appropriate thromboprophylaxis methods.
How can HAT be prevented?
Hospital-acquired thrombosis (HAT) refers to VTE that occurs during hospitalisation or in the 90 days post-discharge. Hospitalisation is one of the leading risk factors for VTE. This is partly due to the close relationship that exists between inflammation and activation of the coagulation cascade. Hospitalised patients are more likely to have multiple acquired risk factors for VTE such as immobilisation, dehydration, malignancy, infection and surgery. Epidemiological studies have shown that before the use of thromboprophylaxis in hospital, up to 60% of all VTE events were hospital-acquired.
26 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE HAT
There are various methods of pharmacological and non-pharmacological VTE prophylaxis. General measures that should be considered in all patients include adequate hydration, maintaining mobility, especially post-operatively and the avoidance of the combined oral contraceptive pill or HRT, where appropriate. Antiembolic stockings are a method of mechanical prophylaxis in widespread use throughout Irish hospitals. They are fitted compression stockings that introduce a pressure gradient from ankle to calf working against venous stasis and clot formation, although evidence to support their use is limited. Intermittent pneumatic compression devices can also be used for mechanical prophylaxis. Pharmacological VTE prophylaxis is the most effective method of reducing VTE events in hospitalised patients. LMWH is the agent of choice in most international guidelines for most patient cohorts. The benefits of LMWH include its short duration of action, partial reversibility, a good safety profile and the extensive published and unpublished experience with its use. Direct oral anticoagulants may be used more extensively in the future for prophylaxis, but evidence to support their net benefit in the majority of patients is currently lacking. The patient’s weight and renal function must be taken into account when calculating the correct dose of LMWH prophylaxis. Evidence supports the use of higher dose LMWH as thromboprophylaxis in the setting of moderate Covid-19 infection.
However, patients vary in their risk of thrombosis and their risk of bleeding so the universal prescription of VTE prophylaxis may result in harm. Individual risk assessment for thrombosis and bleeding is considered to be the standard of care on admission to hospital. Prophylaxis should be administered according to a decision support tool. As hospital admissions are dynamic, the risk balance may change over time, so that patients may require further risk assessments when their clinical circumstances change.
In recent years, more recognition has been given to the need for a systematic and coordinated approach towards the prevention of HAT both across national healthcare systems and also across individual hospitals. Whilst healthcare staff may be aware of the prophylactic modalities available to their patients, they may not have the resources to implement risk assessment and prophylaxis. Care pathways may not facilitate VTE risk assessment. Variation in education and seniority also exists between clinicians. It is therefore important for a hospital/healthcare system to have a VTE prevention protocol. Such a protocol should combine international evidence and local knowledge of patient pathways and practice. Each hospital should have a VTE prevention committee to provide governance for protocol development. Some preventative strategies have proven more effective than others. For example, having a dedicated thromboprophylaxispre-printedprescription in the drug chart has been shown to increase compliance with VTE prevention protocols. Key performance indicator data should be collected and audited.
HAT is one of the leading causes of preventable hospital acquired death. In a major study sponsored by the World Health Organization, HAT accounted for more deaths and disability than nosocomial pneumonia, preventableincomedrugbloodstreamcatheter-relatedinfections,oradverseeventsinlowandmiddle-countries.HATispotentiallyin65%ofcases
The Challenges of rolling out a hospital-wide VTE prevention programme
Whilst HSE recommendations provide useful standards and advice for hospitals trying to implement their own VTE prevention programme, they are somewhat idealised, in that adequate resourcing of such a programme is assumed. Irish hospitals have struggled to get funding for VTE prevention nurses,
Authors: Dr Katie Liston and Dr Ciara O’Rafferty, Department of Haematology, Tallaght University Hospital, Dublin

News
Professor Afif EL-Khuffash, Clinical Professor of Paediatrics at RCSI and Consultant Neonatologist, at the Rotunda Hospital, said: "Until this point, there has been a dearth of evidence to explain why babies with Down Syndrome experience these issues. The results of this study show us that babies with Down Syndrome experience changes in the heart function that leads to increased blood pressure in the lungs."
In spite of the challenges in implementing such a programme, the clear need for a hospitalwide VTE prevention strategy is unquestionable. Routine risk assessment for VTE and thrombosis should be implemented as standard of care in all hospitals, but the required staff supports for this are crucial. There is an impetus on all clinical staff and hospital managers to support a VTE prevention programme in order to achieve best outcomes for patients.
Approximately half of babies born with Down Syndrome also have congenital heart disease. In this study, 48 babies with Down Syndrome had congenital heart disease and 22 did not. The results from the babies with Down Syndrome were compared to 60 babies without Down Syndrome (controls). All babies enrolled in the study underwent a heart scan (echocardiogram) to assess heart function at six months, one year and two years of age. The research was conducted by RCSI in collaboration with the Rotunda, Coombe and National Maternity Hospitals in Dublin; the Department of Paediatric Cardiology, Children's Health at Crumlin Hospital, Dublin; Department of Paediatrics and Child Health, Trinity College Dublin, Boston Children's Hospital and Harvard Medical School, Boston, Massachusetts, USA. The study was funded by the Health Research Board Ireland and the National Children's Research Centre.
Date for your Diary: Retina Conference
Published in the Journal of the American Society of Echocardiography, the study is the first of its kind to follow babies with Down Syndrome over the first two years of age to investigate heart function and increased blood pressure in the blood vessels in their lungs. Seventy babies with Down Syndrome were followed in this study through collaboration between three neonatal intensive care units in Dublin, Ireland. This research found that the babies with Down Syndrome have impaired changes in heart function and blood pressure in the lungs over the first two years of age Importantly, there were no differences in heart function between those babies with Down Syndrome who had congenital heart disease compared to those without over the study period. This is a significant finding and indicates that all babies with Down Syndrome should have their heart function and blood pressure in their lungs monitored during childhood.
Fighting Blindness is an Irish patient-led charity with a vision to cure blindness, support people living with sight loss and empower patients. It is the only Irish charity funding research into treatments for sight loss. Fighting Blindness is announcing the details about their awardwinning Retina conference: after two years of successfully hosting the conference virtually, they will be back to a fully hybrid event. This year Retina conference will be running on November 3, 4 and 5 at the Radisson Blu Royal Hotel Dublin City. Fighting Blindness will be bringing together top international and Irish researchers and clinicians in the global effort to find treatments and cures for conditions causing vision impairment and blindness. For more info visit: www.fightingblindness.ie or email at info@fightingblindness.ie
Furthermore, many different VTE risk assessment tools exist, none of which has been shown to be superior. Prescribing algorithms and recommendations differ between international guidelines mainly due to gaps in the evidence base and varying interpretations of evidence, making institutional consensus on the best approach difficult to achieve. As a VTE prevention programme has farreaching implications for nearly every clinical staff member and patient, multiple stakeholder involvement in the drafting of a VTE protocol is essential, but not always easy. Complex system change is always difficult to implement, with unforeseen setbacks occurring.
27 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 pharmacists and consultant posts. Staff shortages amongst non-consultant hospital doctors and nursing staff mean that priority has to be placed on dealing with emergent situations with preventative medicine often coming in second place.
New Study on Babies with Down Syndrome
Heart and lung conditions are common in babies born with Down Syndrome and can contribute to the requirement for intensive care and longer hospital admissions for babies with Down Syndrome compared to babies without Down Syndrome. The findings of this work will help clinicians to better asses one in 600 babies who are born with Down Syndrome in Ireland every year.
A study from RCSI University of Medicine and Health Sciences has gained new insights into changes in heart function and blood pressure in the lungs of babies born with Down Syndrome.

Please refer to the Summary of Product Characteristics for further information.
Now reimbursed in Republic of Ireland.
Name of the Medicinal Product: Onpattro (patisiran) 2 mg/mL concentrate for solution for infusion. Qualitative and quantitative composition: Each mL contains patisiran sodium equivalent to 2 mg patisiran. Each vial contains patisiran sodium equivalent to 10 mg patisiran formulated as lipid nanoparticles. Therapeutic Indication: Onpattro is indicated for the treatment of hereditary transthyretin-mediated amyloidosis (hATTR amyloidosis) in adult patients with stage 1 or stage 2 polyneuropathy. Posology and method of administration: The recommended dose of Onpattro is 300 micrograms per kg body weight administered via intravenous (IV) infusion once every 3 weeks. Dosing is based on actual body weight. For patients weighing ≥ 100 kg, the maximum recommended dose is 30 mg. Vitamin A supplementation at approximately 2500 IU vitamin A per day is advised for patients treated with Onpattro. All patients should receive premedication prior to Onpattro administration to reduce the risk of infusion- related reactions (IRRs). Each of the following medicinal products should be given on the day of Onpattro infusion at least 60 minutes prior to the start of infusion: • Intravenous corticosteroid (dexamethasone 10 mg, or equivalent) • Oral paracetamol (500 mg) • Intravenous H1 blocker (diphenhydramine 50 mg, or equivalent) • Intravenous H2 blocker (ranitidine 50 mg, or equivalent). If clinically indicated, the corticosteroid may be tapered in decrements no greater than 2.5 mg to a minimum dose of 5 mg of dexamethasone (intravenous, IV), or equivalent. The patient should receive at least 3 consecutive IV infusions of Onpattro without experiencing IRRs before each reduction in corticosteroid premedication. Therapy should be initiated under the supervision of a physician knowledgeable in the management of amyloidosis. Consult the summary of product characteristics for further details about the method of administration. Contraindications: Severe hypersensitivity (e.g., anaphylaxis) to the active substance or any of the excipients. Special warnings and precautions for use: IRRs have been observed in patients treated with Onpattro. In patients experiencing an IRR, Onpattro® (patisiran)
Abbreviated Prescribing Information - Republic of Ireland the majority experienced the first IRR within the first 2 infusions. Across clinical studies, the most common symptoms (reported in ≥ 2% of patients) of IRRs were flushing, back pain, nausea, abdominal pain, dyspnoea, and headache. IRRs may also include but are not limited to hypotension, syncope and pruritus. To reduce the risk of IRRs, patients should receive premedications on the day of Onpattro infusion, at least 60 minutes prior to the start of infusion. If an IRR occurs, slowing or interrupting the infusion and institution of medical management (e.g., corticosteroids or other symptomatic treatment) should be considered, as clinically indicated. If the infusion is interrupted, resumption of the infusion at a slower infusion rate may be considered after symptoms have resolved. The Onpattro infusion should be discontinued in the case of a serious or life-threatening IRR. Some patients who experience IRRs may benefit from a slower infusion rate or additional or higher doses of one or more of the premedications with subsequent infusions to reduce the risk of IRRs. By reducing serum TTR protein, Onpattro treatment leads to a decrease in serum vitamin A (retinol) levels. Serum vitamin A levels below the lower limit of normal should be corrected and any ocular symptoms or signs due to vitamin A deficiency should be evaluated prior to initiation of treatment with Onpattro. Patients receiving Onpattro should take oral supplementation of approximately 2500 IU vitamin A per day to reduce the potential risk of ocular toxicity due to vitamin A deficiency. Referral for ophthalmological assessment is recommended if patients develop ocular symptoms suggestive of vitamin A deficiency, including reduced night vision or night blindness, persistent dry eyes, eye inflammation, corneal inflammation or ulceration, corneal thickening or corneal perforation. Serum vitamin A levels should not be used to guide vitamin A supplementation during treatment with Onpattro. Fertility, pregnancy and lactation: There are no data on the effects of Onpattro on human fertility. No impact on male or female fertility was detected in animal studies.There are no data on the use of Onpattro in pregnant women. Animal studies are insufficient with respect to reproductive toxicity. Due to the potential teratogenic risk

Adverse events should be reported. Reporting forms and information can be found at HPRA Pharmacovigilance, Website: report-an-issue/human-adverse-reaction-formhttps://www.hpra.ie/homepage/about-us/
ONPATTRO® (patisiran) is indicated treatment of hATTR amyloidosis in adult patients with stage 1 or stage 2 polyneuropathy1
arising from unbalanced vitamin A levels, Onpattro should not be used during pregnancy, unless the clinical condition of the woman requires treatment. As a precautionary measure, vitamin A and thyroid stimulating hormone (TSH) levels should be obtained early in pregnancy. Close monitoring of the foetus should be carried out in the event of an unplanned pregnancy, especially during the first trimester. Women of childbearing potential have to use effective contraception during treatment with Onpattro. It is unknown whether Onpattro is excreted in human milk. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from Onpattro, taking into account the benefit of breast feeding for the child and the benefit of therapy for the woman. Undesirable effects: The most frequently occurring adverse reactions reported in Onpattro-treated patients were peripheral oedema (29.7%) and infusion-related reactions (18.9%). The only adverse reaction resulting in the discontinuation of Onpattro was an infusion-related reaction (0.7%).
Regardless of the mutation or predominant symptomatology, all patients with hereditary ATTR amyloidosis develop mixed symptoms2
ONPATTRO® has demonstrated benefits vs placebo across the multi-system manifestations typically seen in patients with hereditary ATTR amyloidosis with stage 1 or 2 polyneuropathy1,3,4
1.ReferencesONPATTRO®. Summary of Product Characteristics, November 2020. 2. Coelho T, et al. Curr Med Res Opin. 2013;29(1):63–76. 3. Adams D, et al. N Engl J Med. 2018;379(1):11–21. 4. Solomon SD, et al. Circulation. ATTR,2019;139(4):431–443.TTRamyloidosis; hATTR, hereditary ATTR amyloidosis; TTR, transthyretin. Developed and produced by Alnylam Pharmaceuticals
ONPATTRO®: Your opportunity to reset treatment expectations in hereditary ATTR amyloidosis with polyneuropathy
The adverse reactions are presented below as MedDRA preferred terms under the MedDRA System Organ Class (SOC) by frequency. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. The frequency of the adverse reactions is expressed according to the following categories: Very common ( ≥ 1/10): Infusion-related reaction, Peripheral oedema. Common ( ≥ 1/100 to < 1/10): Bronchitis, Sinusitis, Rhinitis, Vertigo, Dyspnoea, Dyspepsia, Erythema, Arthralgia, Muscle spasms. Uncommon ( ≥ 1/1,000 to < 1/100): Extravasation. Prescribers should consult the Summary of Product Characteristics for further details of the above and for details of other adverse reactions. Marketing Authorisation Number: EU/1/18/1320/001. Additional information is available from the Marketing Authorisation Holder: Alnylam Netherlands B.V. Antonio Vivaldistraat 150 1083 HP Amsterdam, Netherlands. Legal Classification: Medicinal product subject to restricted medical prescription. Pack size and Price: €8520.84 per vial (10mg/5ml) of Onpattro (patisiran) concentrate for solution for infusion. Date of last revision: 09/2021. Version Final: TTR02-IRL-00016.
for the
Adverse events should also be reported to Alnylam Netherlands B.V. at 1800 924260 (+353 7 667 05596) or medinfo@alnylam.com
For Healthcare Professionals only. ONPATTRO® is a trademark of Alnylam Pharmaceuticals, Inc. © 2021 Alnylam Pharmaceuticals, Inc. All rights reserved. October 2021 | TTR02-IRL-00028
7. González-López E, Gallego-Delgado M, Guzzo-Merello G, et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J. 2015;36(38):2585-2594. 8. Narotsky DL, Castano A, Weinsaft JW, Bokhari S, Maurer MS. Wild-type transthyretin cardiac amyloidosis: novel insights from advanced imaging. Can J Cardiol. 2016;32(9):1166.e1-1166.e10. 9. Brunjes DL, Castano A, Clemons A, Rubin J, Maurer MS. Transthyretin cardiac amyloidosis in older Americans. J Card Fail. 2016;22(12):996-1003. 10. Castaño A, Drach BM, Judge D, Maurer MS. Natural history and therapy of TTR-cardiac amyloidosis: emerging disease-modifying therapies from organ transplantation to stabilizer and silencer drugs. Heart Fail Rev. 2015;20(2):163-178. 11. Carroll JD, Gaasch WH, McAdam KP. Amyloid cardiomyopathy: characterization by a distinctive voltage/mass relation. Am J Cardiol. 1982;49:9-13. 12. Cyrille NB, Goldsmith J, Alvarez J, Maurer MS. Prevalence and prognostic significance of low QRS voltage among the three main types of cardiac amyloidosis. Am J Cardiol. 2014;114(7):1089-1093. 13. Quarta CC, Solomon D, Uraizee I, et al. Left ventricular structure and function in transthyretin-related versus light-chain cardiac amyloidosis. Circulation. 2014;129(18):1840-1849. 14. Connors LH, Prokaeva T, Lim A, et al. Cardiac amyloidosis in African Americans: Comparison of clinical and laboratory features of transthyretin V122I amyloidosis and immunoglobulin light chain amyloidosis. Am Heart J. 2009;158(4):607-614. 15. Nakagawa M, Sekijima Y, Yazaki M, et al. Carpal tunnel syndrome: a common initial symptom of systemic wild-type ATTR (ATTRwt) amyloidosis. Amyloid. 2016;23(1):58-63. 16. Rapezzi C, Merlini G, Quarta CC, et al. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation. 2009;120(13):1203-1212. 17. Sperry BW, Reyes BA, Ikram A, et al. Tenosynovial and cardiac amyloidosis in patients undergoing carpal tunnel release. J Am Coll Cardiol. 2018;72(17): 2040-2050. 18. Westermark P, Westermark GT, Suhr OB, Berg S. Transthyretin-derived amyloidosis: probably a common cause of lumbar spinal stenosis. Ups J Med Sci. 2014;119(3):223-228. 19. Yanagisawa A, Ueda M, Sueyoshi T, et al. Amyloid deposits derived from transthyretin in the ligamentum flavum as related to lumbar spinal canal stenosis. Mod Pathol. 2015;28(2):201-207. 20. Sueyoshi T, Ueda M, Jono H, et al. Wild-type transthyretin-derived amyloidosis in various ligaments and tendons. Hum Pathol. 2011;42(9):1259-1264. 21. Phelan D, Collier P, Thavendiranathan P, et al. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart. 2012;98(19):1442-1448. 22. Ternacle J, Bodez D, Guellich A, et al. Causes and consequences of longitudinal LV dysfunction assessed by 2D strain echocardiography in cardiac amyloidosis. JACC Cardiovasc Imaging 2016;9(2):126-138. 23. Coelho T, Maurer MS, Suhr OB. THAOS - The Transthyretin Amyloidosis Outcomes Survey: initial report on clinical manifestations in patients with hereditary and wild-type transthyretin amyloidosis. Curr Med Res Opin. 2013;29(1):63-76. 24. Swiecicki PL, Zhen DB, Mauermann ML, et al. Hereditary ATTR amyloidosis: a single-institution experience with 266 patients. Amyloid. 2015;22(2):123-131.
heart failure with preserved ejection fraction in patients typically over 60 years old5-7 Life-threatening, underrecognized, and underdiagnosed, ATTR-CM is a rare condition found in mostly older patients in which misfolded transthyretin proteins deposit in the heart.1-7 It is vital to recognize the diagnostic clues so you can identify this disease. to standard heart failure therapies (ACEi, ARBs, and beta blockers)8-10 between QRS voltage and left ventricular (LV) wall thickness11-13 of carpal tunnel syndrome or lumbar spinal stenosis3,8,14-20 showing increased LV wall thickness6,13,16,21,22 —autonomic nervous system gastrointestinaldysfunction-includingcomplaints or unexplained weight loss6,16,23,24 Sipe JD, Benson MD, Buxbaum JN, et al. Amyloid fibril proteins and amyloidosis: chemical identification and clinical classification International Society of Amyloidosis 2016 Nomenclature Guidelines. Amyloid. 2016;23(4):209-213. 2. Maurer MS, Elliott P, Comenzo R, Semigran M, Rapezzi C. Addressing common questions encountered in the diagnosis and management of cardiac amyloidosis. Circulation. 2017;135(14):1357-1377. 3. Connors LH, Sam F, Skinner M, et al. Heart failure due to age-related cardiac amyloid disease associated with wild-type transthyretin: a prospective, observational cohort study. Circulation. 2016;133(3):282-290. 4. Pinney JH, Whelan CJ, Petrie A, et al. Senile systemic amyloidosis: clinical features at presentation and outcome. J Am Heart Assoc. 2013;2(2):e000098. 5. Mohammed SF, Mirzoyev SA, Edwards WD, et al. Left ventricular amyloid deposition in patients with heart failure and preserved ejection fraction. JACC Heart Fail. 2014;2(2):113-122. 6. Maurer MS, Hanna M, Grogan M, et al. Genotype and phenotype of transthyretin cardiac amyloidosis: THAOS (Transthyretin Amyloid Outcome Survey). J Am Coll Cardiol. 2016;68(2):161-172.
1.References
The health information contained in this ad is provided for educational purposes only. Date of Preparation: February 2021 GCMA code: PP-RDP-IRL-0105
LEARN HOW TO RECOGNIZE THE CLUES OF ATTR-CM AT: S U S P E C T A N D D E T E C T . I E CONSIDER THE FOLLOWING CLINICAL CLUES, ESPECIALLY IN COMBINATION, TO RAISE SUSPICION FOR ATTR-CM AND THE NEED FOR FURTHER TESTING SUSPECT A(TRANSTHYRETINATTR-CMAMYLOIDCARDIOMYOPATHY)LIFE-THREATENING DISEASE THAT CAN GO UNDETECTED H FpEF I NEDDNTOLERANCEISCORDANCEIAGNOSISCHOERVOUSSYSTEM




1. REFLECT Before reading this module, consider the following: Will this clinical area be relevant to my practice?
Dr Zara Togher is a Specialist Registrar in Neurology currently working in University Hospital Limerick. She has an interest in neuropathies and neuromuscular disorders having spent time in dedicated Neuropathy and Neuromuscular clinics in Tallaght University Hospital (TUH).
Dr Zara SinéadProfessorMurphy
Prof. Sinead Murphy is a Consultant Neurologist at TUH and Clinical Associate Professor in Trinity College Dublin. She has particular subspecialty interest and expertise in inherited neuropathies and ataxias, runs Neuropathy and Neuromuscular clinics and co-leads the National Ataxia Clinic in TUH. She is lead of the Irish Consortium for Rare Neurological Disorders, with TUH recently being recognised as a site for the European Reference Network in Rare Neurological Diseases (ERN-RND). She chaired the Neurology sub-group of the HSE Amyloidosis Working Group which developed the Amyloidosis Model of Care and Guideline recently approved by the HSE.
AUTHORS: Dr Zara Togher, Professor Sinéad M Murphy
Transthyretin amyloidosis (ATTR) is a progressive and fatal disease caused by deposition of abnormal transthyretin-derived amyloid fibrils in the extracellular tissues of various organs.1 Transthyretin protein (TTR) is predominantly produced by the liver, although small amounts are also produced in the eye by the retinal and ciliary pigment epithelia, and in the brain by the choroid plexus.2,3 Normally TTR circulates in the form of a tetramer made up of four identical monomeric subunits in both the serum and cerebrospinal fluid (CSF). Its main function is as a transporter of both thyroxin and retinol-binding protein, hence the name.2 In ATTR, dissociation of the tetrameric TTR occurs followed by misfolding, aggregation and formation of insoluble amyloid fibrils which are then deposited systemically. Accumulation of amyloid fibrils in tissues progressively disrupts their structure and function, leading to loss of function in various organs, particularly heart and peripheral nerves. There are two sub-types of ATTR: wild-type ATTR (ATTRwt) and hereditary or variant ATTR (ATTRv).
ATTRv In ATTRv pathogenic genetic variants destabilise TTR, causing misfolding and aggregation.3 The TTR gene is located on chromosome 18, and over 120 TTR mutations have been identified to date3,4 Worldwide V30M (p.V50M) is the most frequent, accounting for approximately half of all cases.5 However, with regard to Irish patients, in 1995 Reilly et al. described a cluster of cases concentrated in North West Donegal. This cluster was associated with the T60A (p.T80A) variant. Further population-based studies showed a carrier rate for this mutation of approximately 1.1% in this region.6 This is the most common TTR mutation in the Irish population, although other variants also occur. It is important to note that there can be significant differences in presentation depending on the particular genetic variant. For example, while the typical presentation of ATTRv is with a combination of cardiomyopathy and neuropathy, patients with ATTRL12P usually present with oculoleptomeningeal disease.7 In addition, penetrance and age of onset varies between populations even with the same mutation. For example, patients with ATTRV30M of Portuguese origin have mean age of onset of 33 years with penetrance of 91% at 70 years, whereas patients of Swedish origin with the same variant have a later age of onset of 56 years and lower penetrance of 36% at 70 years.8
The clinical presentation of ATTR varies between patients depending on the subtype (ATTRwt vs ATTRv) and, in ATTRv, the specific mutation and the origin of the patient. However, the heart and peripheral nerves are the most common clinically involved organs in patients with ATTR. Cardiac symptoms classically consist of heart failure and arrhythmias, whereas neurological symptoms are due to involvement of peripheral
Transthyretin Amyloidosis
31
yes, I should identify any knowledge gaps in the clinical area. 3. PLAN If I have identified a knowledge gap - will this article satisfy those needs - or will more reading be required? 4. EVALUATE Did this article meet my learning needs - and how has my practise changed as a result?Have I identified further learning needs? 5. WHAT NEXT At this time you may like to record your learning for future use or assessment. Follow the 4 previous steps, log and record your Publishedfindings.by HPN. Copies can be downloaded copyright,Disclaimer:www.irishpharmacytraining.iefromAllmaterialpublishedisnopartofthiscanbeused in any other publication without permission of the publishers and author. Pfizer has no editorial oversight of the CPD programmes included in these modules CPD ContinuingDevelopmentProfessional
Introduction
ATTRwt ATTRwt (previously called senile systemic amyloidosis) is generally considered a disease of older adults in which amyloid fibril deposition occurs due to agerelated structural changes of the TTR protein which cause it to misfold. Studies which examined autopsy specimens revealed increasing amounts of wt TTR deposition in cardiac tissues with age.9,10 It is likely that ATTRwt is significantly underdiagnosed; it is estimated that up to 25% of patients with heart failure with preserved ejection fraction (HFpEF) have ATTRwt. In two autopsy studies specifically looking at supercentenarians (individuals who have reached the age of 110 years or more), the primary cause of death in 70% of patients was related to cardiac deposition of wt TTR.11
Clinical Features
If the answer
2. IDENTIFY If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). is CPD
60 Second Summary
Transthyretin amyloidosis (ATTR) is a multi-system fatal disease which occurs as a result of deposition of abnormal transthyretin-derived amyloid fibrils in a variety of body tissues. Both inherited (ATTRv) and acquired i.e. wild-type forms (ATTRwt) can occur. Due to the variety of systems affected there can be a wide variability in symptom manifestation, although cardiac and neurological symptoms generally Commonlypredominate.symptomsare nonspecific and may be mistaken for symptoms of other more frequently occurring causes (e.g. orthostatic hypotension being attributed to medication rather than to an underlying autonomic neuropathy). This, along with a lack of awareness among healthcare professionals, can lead to significant delays in diagnosis. With emergence of treatment,disease-modifyingpromptdiagnosis is of increasing importance. Licensed treatment options now include transthyretin stabilisers and small interfering RNA therapeutics, while gene editing with CRISPR-Cas9 based therapy is showing promise in clinical trial. This CPD piece will provide a general overview of ATTR including subtypes, clinical presentation, diagnosis and disease-modifying treatment strategies. Symptomatic management is outside the scope of this piece. The HSE Model of Care for Amyloidosis which aims to improve standards of care for patients with amyloidosis in Ireland is discussed; an important aspect of this is improved awareness and earlier diagnosis. We also discuss methods for earlier or potentially identificationpre-symptomaticofpatients.
CPD 91: ATTR
Togher



1: Diagnostic clues to ATTRCardiac Diagnostic Clues Neurological Diagnostic Clues Right sided heart failure UnexplainedHFpEF atrial arrhythmia or cardiac conduction disease/need for pacemaker Infiltrative phenotype on cardiac imaging Aortic stenosis with RV thickening (particularly if low flow/low Abnormalgradient)QRSvoltage to LV thickness ratio on ECG Cardiac imaging features: • Diffuse subendocardial/transmural late gadolinium enhancement/increased ECV fraction on MRI • Myocardial uptake on DPD • Apical sparing on longitudinal strain Particularlyimaginginthe presence of: • Bilateral carpal tunnel • Lumbar spinal stenosis • Biceps tendon rupture • Peripheral neuropathy • Autonomic complaints • Weight loss • Renal abnormalities • Vitreous abnormalities • Family history ATTRv/family story consistent with ATTRv Progressive sensory / sensorimotor axonal AutonomicORpolyneuropathycomplaints (e g chronic diarrhoea and/or constipation, erectile dysfunction, postural AtypicalORhypotension/syncope)CIDP/CIDPunresponsive to usual PLUStherapiesone or more of: • Family history ATTRv/family story consistent with ATTRv • Unexplained weight loss • Arrhythmias/cardiac failure • Renal abnormalities • Vitreous opacities • Bilateral carpal tunnel syndrome • Lumbar spinal stenosis Table 1: Diagnostic clues to ATTR CIDP = chronic inflammatory demyelinating polyradiculoneuropathy; DPD = diphosphono 1,2 propanodicarboxylic acid; ECG = electrocardiogram; ECV = extracellular volume; HFpEF = heart failure with preserved ejection fraction; LV = left ventricle; RV = right ventricle Cardiac Diagnostic Clues Neurological Diagnostic Clues Right sided heart failure UnexplainedHFpEF atrial arrhythmia or cardiac conduction disease/need for pacemaker Infiltrative phenotype on cardiac imaging Aortic stenosis with RV thickening (particularly if low flow/low Abnormalgradient)QRSvoltage to LV thickness ratio on ECG Cardiac imaging features: • Diffuse subendocardial/transmural late gadolinium enhancement/increased ECV fraction on MRI • Myocardial uptake on DPD • Apical sparing on longitudinal strain Particularlyimaginginthe presence of: • Bilateral carpal tunnel • Lumbar spinal stenosis • Biceps tendon rupture • Peripheral neuropathy • Autonomic complaints • Weight loss • Renal abnormalities • Vitreous abnormalities • Family history ATTRv/family story consistent with ATTRv Progressive sensory / sensorimotor axonal AutonomicORpolyneuropathycomplaints (e g chronic diarrhoea and/or constipation, erectile dysfunction, postural AtypicalORhypotension/syncope)CIDP/CIDPunresponsive to usual PLUStherapiesone or more of: • Family history ATTRv/family story consistent with ATTRv • Unexplained weight loss • Arrhythmias/cardiac failure • Renal abnormalities • Vitreous opacities • Bilateral carpal tunnel syndrome • Lumbar spinal stenosis Table 1: Diagnostic clues to ATTR CIDP = chronic inflammatory demyelinating polyradiculoneuropathy; DPD = diphosphono 1,2 propanodicarboxylic acid; ECG = electrocardiogram; ECV = extracellular volume; HFpEF = heart failure with preserved ejection fraction; LV = left ventricle; RV = right ventricle
32 CPD 91: ATTR nerves which can include large fibre, small fibre or autonomic involvement.12 In both subtypes, amyloid deposits in connective tissues may cause carpal tunnel syndrome, spinal stenosis, rotator cuff tears and joint pain which often predate the neurological or cardiac symptoms.13,14,15
Table
ATTRwt Historically ATTRwt has been regarded as a cardiomyopathy affecting elderly males.9 However; it is a disease of aging, with the amount of amyloid deposition increasing in proportion to age. A Finnish study demonstrated that 25% of the autopsied population over 85 years had evidence of wt TTR deposition in myocardium, with no difference in prevalence between males and females although the severity of deposition was more in males.25 ATTRwt is an important differential to consider when patients present with HFpEF, accounting for up to 25% of cases.26 It also manifests as carpal tunnel syndrome which often predates symptoms of cardiomyopathy.27 Neuropathy is usually a less prominent clinical feature in ATTRwt; however, some smaller studies28,29 suggest a higher prevalence than previously thought and occasionally it can be the presenting feature.30 Prognosis is poor as most patients have cardiac involvement at time of diagnosis, with mean survival 3.5 years. Diagnosis As previously discussed, there may be a wide variability in presenting symptoms many of which are non-specific. This can lead to misdiagnosis or often significant delays in diagnosis. Previous studies into ATTRv report rates of
Average survival depends on the mutation, overall 10-15 years following onset of symptoms, but only 2.5-5.5 years following diagnosis for ATTRT60A.17,18 With regard to ATTRT60A, the common Irish variant, a case series of 60 patients published by Stangou et al. in 2012 showed that cardiac involvement was present in nearly all cases by time of diagnosis, in contrast to Portuguese patients with ATTRV30M where cardiac involvement occurs much later.19 A review of 15 patients attending the Irish cardiac amyloidosis referral centre in 2020 demonstrated that patients presented with a mixed phenotype of neuropathy and heart failure, with cardiac scanning using 99m Tc-DPD tracer (Tc-DPD) showing an advanced stage of cardiac disease by the time of diagnosis.20 Mean age of symptom onset is 62 years. The first symptom in more than half of patients with ATTRT60A is of carpal tunnel syndrome (usually bilateral) which occurs approximately 7 years before other symptoms develop.21 Sensory symptoms typically predominate initially with numbness, burning, paraesthesiae and occasionally lancinating pains. Motor weakness is a later feature. Although typically the neuropathy is length-dependent, some patients have early upper limb involvement out of proportion to lower limb involvement.22 Autonomic dysfunction is common, with symptoms including alternating diarrhoea/constipation, orthostatic hypotension, nausea and vomiting, early satiety, urinary symptoms and erectile dysfunction.23 Weight loss results from a combination of autonomic and gastrointestinal involvement. Cardiac features include those of heart failure: shortness of breath, oedema, exercise intolerance, orthopnoea, syncope, as well as palpitations, arrhythmias and electrical conduction abnormalities.24 Table 1 lists diagnostic clues to ATTR.
ATTRv Clinical presentation in ATTRv can show a wide heterogeneity depending on the specific TTR mutation (Image 1). Diagnostic delay is frequent, typically 4 years from onset of symptoms.16
Disease-modifying treatment
Initially, disease-modifying therapy had relied predominantly on liver transplantation, the concept being that this would prevent further variant TTR being produced by the liver. This improved outcomes in some patients (especially those with early-onset ATTRV30M) but was not a viable option for patients with cardiac disease (and therefore was not usually considered in those with ATTRT60A who usually have cardiac disease at presentation).19,35 Thankfully, there have been significant advances in the last number of years in ATTR therapies. Tafamidis is a TTR stabiliser which was approved for use in the treatment of adults with ATTR cardiomyopathy in the European Union in 2016. However, it is not approved for, nor has shown a significant improvement in ATTRv associated neuropathy therefore use is currently limited in Ireland to patients with ATTR (either ATTRwt or ATTRv) with cardiomyopathy.36 Diflusinal is an oral non-steroidal antiinflammatory drug which has been repurposed for use in ATTR (off-license) as it stabilises the TTR tetramer in vitro. It has been shown to stabilise neuropathy progression and reduce cardiac dysfunction, however with potential side effects including gastrointestinal symptoms and renal impairment.36 Newer treatments including gene silencing therapies and gene editing have recently emerged as effective treatment strategies for ATTRv. Gene silencing therapies for ATTRv include antisense oligonucleotides (Inotersen) and small interfering RNAs (siRNAs), namely patisiran. The APOLLO trial37 demonstrated biochemical and clinical efficacy of intravenous patisiran in ATTRv, with significant reductions in circulating TTR and improvements in autonomic neuropathy, quality of life, peripheral neuropathy symptoms, nutritional status and cardiac function. An open label extension reported sustained benefits supporting the long-term effectiveness of this therapy.38 Similar benefits were reported with subcutaneous Inotersen therapy in the NEURO-TTR trial, although it has additional monitoring requirements due to the occurrence of thrombocytopaenia and glomerulonephritis39,40 At present only patisiran is reimbursed in Ireland for patients with ATTRv associated neuropathy and is given by three-weekly intravenous infusion; the initial three doses are given in hospital and subsequent doses can be given at home if tolerated. With regards to gene editing, the first ATTRv patient cohort treated with a single dose of CRISPRCas9 based therapy showed a significant dose-dependent and long-lasting reduction of serum TTR protein levels.41 Clinical outcomes are eagerly awaited. Given that gene silencing and gene editing therapies only affect TTR production by the liver, as they do not cross the blood brain barrier, there is concern that with prolonged survival will come the development of a new phenotype of ATTRv due to continued unchecked production of mutant 1: Varied systemic manifestations of
33 misdiagnosis of up to 32-74%.31,32 The Amyloidosis Research Consortium reported that 47% of patients received at least one misdiagnosis before being diagnosed with amyloidosis.33 In this survey, ATTR patients went undiagnosed for more than 4 years (27% ATTRwt and 15% ATTRv). 19% of patients also reported having to travel over 2 hours to get diagnosed. While this is data from the US, this would likely be mirrored in Irish patients, with the majority of patients until recently travelling to the UK for diagnosis. An amyloid Model of Care has been drafted by the HSE Amyloidosis Working Group to improve the standard of care for patients in Ireland 34. As part of this, a number of symptom ‘gates’ are highlighted where physicians are encouraged to think of a diagnosis of amyloidosis where it may not already be under consideration to aid in timely diagnosis. We will briefly mention here the symptoms of relevance to ATTRv and ATTRwt.
Image
The first of the symptom gates is carpal tunnel syndrome, with a rationale that patients (in particular with ATTRwt) may present with carpal tunnel syndrome up to 10 years before developing symptomatic cardiomyopathy. Therefore the recommendation is for patients who undergo surgical decompression to have a biopsy of the flexor retinaculum taken at the time of surgery to exclude ATTR. Another symptom gate is that of aortic stenosis with low flow-low gradient. It is advised that these patients be referred for DPD scan to exclude the presence of ATTR. Other presentations that should prompt consideration of ATTR are unexplained spinal stenosis, or an unexplained combination of autonomic and peripheral neuropathy. Several diagnostic algorithms have been proposed as part of the Model of Care, depending on the presenting symptom, a modified version of the neuropathy algorithm is shown below in Image 2. (page 34)
ATTRvOcular Pupil abnormalities Dry AbnormalVitreousGlaucomaeyesopacitiesconjunctival vessels Retinal neovascularisation Orthopaedic/Rheumatological Spinal stenosis Biceps tendon rupture Rotator cuff tear Neurological Peripheral MyopathyCarpalAutonomicneuropathyneuropathytunnelsyndrome Cardiac Heart AorticArrhythmiafailurestenosis Gastrointestinal Nausea/vomitingEarlyWeightConstipationDiarrhoealosssatiety Renal RenalProteinuriafailure
In this section we will focus primarily on disease-modifying treatment for ATTRv. Symptomatic management is equally important, especially for quality of life, but is outside the scope of this article.
References available
TTR in the eye and brain.42 Indeed, symptomatic cerebral amyloid angiopathy has been seen in ATTR patients surviving after liver transplantation.43 In contrast to the systemic circulation where other thyroxin carriers exist, TTR is required for thyroxin transport centrally as well as having some neuroprotective effects. Thus, novel approaches will be needed as prognosis improves with the recent advances in therapy.
Another consideration is of genetic testing of patients with family members with ATTRv. Although the dominant genotype in the Irish population (p.T80A) shows incomplete penetrance, screening allows mutation carriers to be followed in order to identify early symptomatic disease and offer early treatment. A recent consensus paper suggests that adult firstdegree relatives of ATTRv patients may be offered genetic counselling and screening and, if positive, should start having neurological and cardiac assessments within 10 years of anticipated onset of symptoms.47 The frequency of such assessments has yet to be clarified.
34 CPD 91: ATTR
One avenue for improvement is the potential for identification of pre-symptomatic disease in both ATTRwt and ATTRv. As mentioned, carpal tunnel disease may present up to 10 years before development of systemic symptoms. Sperry et al published an observational study of 98 patients where the flexor retinaculum in men ≥50 years and women ≥60 years undergoing carpal tunnel release surgery was routinely sent for analysis with Congo red staining to determine the prevalence of amyloid.44 This detected amyloid deposits in 10.2% of patients (in this study due to a combination of ATTRv, ATTRwt and light chain amyloidosis). In a similar Japanese study, 34% of patients had amyloid deposition in the tenosynovial tissue sample.45 Similar studies looking at ligamentous tissue in patients undergoing surgery for lumbar spinal stenosis showed amyloid deposition in 88.4%13 and 96%46 of patients respectively. We suggest that routine analysis of surgical tissue would be an easy way to diagnose presymptomatic patients and therefore enable earlier treatment, improving outcomes.
Future of ATTR in Ireland
As mentioned, a Model of Care has been drafted by the HSE Amyloidosis Working Group34 which aims to improve standard of care for Irish patients with amyloidosis. It aims to reduce burden of disease by improved awareness and earlier diagnosis in order to prevent less endorgan sequelae. It also aims to avoid patients having to travel abroad (usually to the UK National Amyloid Centre in London) as part of their diagnostic journey by creating a complex care centre or network in Ireland. With the advent of diseasemodifying treatment, the outlook for patients with this hitherto progressive terminal disease is certainly more hopeful although many challenges remain. An active patient group has been set up (the All Ireland Amyloidosis Support Group), and the first all Ireland ATTR Conference, Emerging from the Shadows, was recently held in Gweedore, Co. Donegal, bringing together patients and their families, amyloidosis experts and other health care professionals interested in learning more about the disease. on
request Symptoms, examination, NCS, MR Neurography suggestive of neuropathy due to amyloidosis Screen for presence of monoclonal protein Serum & urine protein electrophoresis Serum free light chains abnormal Refer to Haematology Biopsy of clinically involved organ +/ fat pad Amyloid staining confirmed Amyloid typing Yes No AL, TTR, other Amyloidosisunlikely Tc availableDPD Tc DPD ATTRvGeneticATTRabnormaltestingATTRwt ATTR neuropathy with cardiac phenotype unlikely Consider nerve & muscle biopsy if high suspicion Refer for Tc DPD / nerve & muscle biopsy / carpal tunnel biopsy Amyloid staining confirmed Amyloid typed normal Tc DPD negative or indeterminate yes ALATTR AGelsolin AApoA no Geneticabnormaltesting ATTRv abnormal normal AGelsolin AApoA Image 2 Neuropathy Algorithm















Unexplained bone pain / neurological symptoms
Lung cancer comprises two broad types namely small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) representing about 15% and 85% of lung cancer cases respectively. Small cell lung cancer is a particularly aggressive malignancy that is generally managed with systemic cytotoxic chemotherapy and radiotherapy; there is a limited role for surgery except in very select cases. Non-small cell lung cancer, being the more common, can be
PersistentHaemoptysisinclude:cough (> 3 weeks) or alteration of chronic cough
Figure 1: Projected incidence of lung cancer cases amongst females Cancer Registry Ireland]
There is also a greater awareness of the risk factors for lung cancer that include smoking (including a history of passive smoking, be that occupational or partner / family member), family history, radon exposure, prior radiation exposure, known or suspected exposure to asbestos, and / or a history of prior cancer. Patients referred via the RALC pathway will be assessed within 2 weeks of the receipt of a request by the referring clinician which has streamlined patients prompt access to appropriate secondary care, however patients do present via numerous other pathways.
Lung Cancer – a Brief Overview
Lung cancer is the leading cause of cancer related mortality amongst both men and women in Ireland. Based on median projections from the National Cancer Registry, annual cases of lung cancer are projected to increase to 2,633 (+94%) in men and to 3,124 (+176%) in women by 2045. That is an overall increase to 5,757 cases annually for men and women combined (+132%) highlighting the importance of optimising the prevention, early diagnosis, and treatment of lung cancer in Ireland (Figure 1).
Indications for urgent chest x-ray
Clinical signs such as finger clubbing, lymphadenopathy, focal chest signs, or hepatomegaly
ONCOLOGY FOCUS: LUNG CANCER
we have a variety of options to obtain tissue, including a CT-guided biopsy, ultrasoundguided biopsy, transbronchial biopsy under fluoroscopic guidance, ultrasoundEndobronchial(EBUS),andin certain cases surgical biopsy. When a diagnosis of lung cancer has been made, the patient will complete staging. For early-stage lung cancers, that can generally involve a PET-CT whereas more advanced cancers may need invasive staging modalities to accurately determine their clinical
Written by Mr Gerard J. Fitzmaurice MSc FRCSI (CTh), Consultant Cardiothoracic Surgeon s.i. Thoracic Surgical Oncology, St. James’s Hospital, Dublin
Written by Mr Gerard J. Fitzmaurice MSc FRCSI (CTh), Consultant Cardiothoracic Surgeon s.i. Thoracic Surgical Oncology, St. James’s Hospital, Dublin
Figure 1: Projected incidence of lung cancer cases amongst females and males [National Cancer Registry Ireland]
Lung cancer is the leading cause of cancer related mortality amongst both men and women in Ireland. Based on median projections from the National Cancer Registry, annual cases of lung cancer are projected to increase to 2,633 (+94%) in men and to 3,124 (+176%) in women by 2045. That is an overall increase to 5,757 cases annually for men and women combined (+132%) highlighting the importance of optimising the prevention, early diagnosis, and treatment of lung cancer in Ireland (Figure 1)
• An abnormal chest x-ray suspicious for lung cancer, or a patient with haemoptysis and / or other concerning symptom, even with a normal chest x-ray
Lung Cancer – a Brief Overview considered any type of epithelial lung cancer that is not smallcell. There are a variety of types with the most common being Squamous cell carcinoma and Adenocarcinoma; other tumour types include large cell carcinoma and pleomorphic carcinoma. Although they are heavily associated with cigarette smoking, Adenocarcinoma may be found in non-smokers, something that is becoming slightly more common. Our latest three-year cancer audit report 2018-2020 highlighted only 8% of patients who underwent treatment for lung cancer at St. James’s were never smokers. One of the major problems historically with lung cancer is delayed diagnosis with the majority of patients presenting with advanced disease that is not amenable to curative intent treatment. To counter this, the National Cancer Control Programme (NCCP) was established in Ireland in 2007 following the publication of the second National Cancer Strategy and led to the establishment of 8 cancer centres with rapid access lung cancer clinics (RALC) in each. General practitioners, as the gatekeepers to secondary care, were provided with a referral guideline to RALCs, which includes:
•
Figure 1: Projected incidence of lung cancer cases amongst females and males [National Cancer Registry Ireland]
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 35
Unexplained chest pain or Unexplaineddyspnoea weight loss
Written by Mr Gerard J. Fitzmaurice MSc FRCSI (CTh), Consultant Cardiothoracic Thoracic Surgical Oncology, St. James’s Hospital, Dublin
Lung Cancer – a Brief Overview
Lung cancer is the leading cause of cancer related mortality amongst in Ireland. Based on median projections from the National Cancer Registry, lung cancer are projected to increase to 2,633 (+94%) in men and to 3,124 by 2045. That is an overall increase to 5,757 cases annually for men (+132%) highlighting the importance of optimising the prevention, treatment of lung cancer in Ireland (Figure 1).




We are currently involved in a more detailed prehabilitation trial (PREHIIT) in conjunction with our upper gastrointestinal surgery colleagues, to evaluate the benefit of high intensity interval training in preparation for major thoracic surgery. These interventions improve patients fitness for surgery reducing post-operative complications and optimising their overall journey. All patients who continue to smoke are offered review by the smoking cessation clinical nurse specialist to optimise their chances of stopping smoking at what is an opportune time. We also provide a pre-assessment clinic for detailed evaluation of moderate and highrisk surgical candidates. At St. James’s, we offer a comprehensive minimally invasive thoracic surgical program – about 70% of all resections for lung cancer are undertaken via a minimally invasive approach. We offer both video-assisted and more recently robotic-assisted thoracic surgery using the latest da Vinci Xi model. We have an enhanced recovery after thoracic surgery (ERATS) program to optimise our patient’s peri-operative journey with an average length of stay of 4-days. For patients with advanced malignancies involving part of their airway or major vascular structures or chest wall, surgery is generally offered via a posterolateral thoracotomy to facilitate resection and reconstruction of the involved structure(s). That may involve a sleeve bronchoplastic repair, resection and reconstruction of the pulmonary artery, and / or resection and reconstruction of the chest wall with a variety of materials used to optimise the patients function and recovery.
Adjuvant treatment, which is additional treatment delivered following surgery in patients with stage IIA – III disease, comprises systemic cytotoxic chemotherapy. This, as with neoadjuvant treatment, is a platinum-based doublet that generally includes cisplatin or carboplatin and an additional agent. In general, patients are assessed by a medical oncologist with a special expertise in lung cancer care and appropriate treatment is delivered once they have fully recovered from surgery. This can provide a 5-year additional survival benefit of about 5.3% in appropriate patients. There is currently great debate about the role of adjuvant radiotherapy amongst this patient group and in general, it is only recommended in very select cases. As the largest centre for lung cancer surgery in Ireland, we are also involved in regular trials including neoadjuvant surgical trials using immunotherapy. We have a clear interest in research and have an active biobanking program to facilitate translational research. Patients will find that they are approached to be involved in research opportunities, should they wish, during their journey at St. James’s with an aim to improve overall lung cancer care. The future of lung cancer management is very dynamic at present. The landscape for neoadjuvant treatment strategies is evolving and in the next 6-12 months there should be definite changes to the treatment strategy to optimise patients access to optimal curative intent care in Ireland. The recent seminal paper by Forde et al (NEJM 2022) demonstrating the significantly longer event-free survival and pathological complete response rates with neoadjuvant Nivolumab and chemotherapy in resectable lung cancer is practice changing. Screening for lung cancer is also moving to centre stage following the Dutch-Belgian NELSON study that evaluated 50 – 74 year olds with a history of smoking who underwent a screening CT Thorax at 1, 3, and 5.5 years. At ten years follow-up, they demonstrated a 24% reduction in lung cancer mortality amongst the screened population. The clear benefit of screening is the detection of more patients with early-stage disease who could be offered curative intent treatment and consequently it is an important area of development in Ireland.
Save the date: The 10th All Ireland Lung Cancer Conference September 23rd / 24th Barberstown Castle, Straffan, Co Kildare
At St James’s we perform approximately 55% of all curativeintent lung cancer surgery in Ireland and consequently we have a special expertise in lung cancer care. We have a special interest and experience in the management of advanced malignancies, such as proximal airway tumours, tumours involving the major blood vessels, and chest wall tumours including Pancoasts (superior sulcus tumours). That experience can allow optimal preservation of lung parenchyma in “lung sparing” surgery. In certain cases, patients may undergo neoadjuvant treatment to include systemic chemotherapy and in some cases radiotherapy in preparation for surgical resection.
All patients who are considered potential candidates for surgery are seen by a cardiothoracic surgeon specialising in thoracic surgical oncology and a decision is made, in consultation and discussion with the patient, regarding the optimal management approach. Should they be fit for surgery, then they will be enrolled in our prehabilitation program to optimise their fitness for surgery under the guidance of a thoracic physiotherapist.
All patients diagnosed with lung cancer via the RALC at St James’s are discussed at the multi-disciplinary meeting where the clinical stage is determined following completion of all investigations and a treatment plan decided. The optimal treatment for lung cancer is surgical resection if that’s possible and appropriate. The more advanced the stage, the type of treatment offered will change. For patients with evidence of systemic disease, systemic treatment options are offered including systemic cytotoxic chemotherapy and / or immunotherapy. More recently there have been advances in the genetic evaluation of lung cancer with identification of mutations that may be amenable to targeted therapy such as third generation tyrosine kinase inhibitors (TKIs) for EGFR mutant NSCLC.
For patients with early-stage disease who are not fit or otherwise decline surgical resection, there is the option of stereotactic ablative radiotherapy which has clear benefits and a very acceptable risk profile. In some select cases, there may also be the option of radiofrequency ablation which is a local control treatment strategy.
Our lung cancer team at St. James’s includes respiratory physicians, thoracic radiologists, thoracic histopathologists, thoracic surgeons, thoracic medical oncologists, thoracic radiation oncologists, and a team of allied health professionals including advanced nurse practitioners, lung cancer co-ordinators, clinical nurse specialists, thoracic physiotherapists, speech and language therapists, dieticians, thoracic nurses, and social workers who provide a 360-degree patient centred model of care. We support our excellent respiratory and oncology colleagues in outside centres across Ireland and we are dedicated to providing the best possible treatment to our lung cancer patients while being actively involved in promoting and developing lung cancer care into the future.
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 36 ONCOLOGY FOCUS: LUNG CANCER stage and guide treatment. These include advanced bronchoscopic techniques (EBUS), and in certain cases surgical staging via mediastinoscopy or video-assisted thorascopic surgery (VATS).

KEYTRUDA as monotherapy is indicated for the first line treatment of metastatic microsatellite instability high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer in adults.
KEYTRUDA as monotherapy is indicated for the treatment of the following MSI H or dMMR tumours in adults with (a) unresectable or metastatic colorectal cancer after previous fluoropyrimidine based combination therapy, (b) advan ced or recurrent endometrial carcinoma, who have disease progression on or following prior treatment with a platinum containing therapy in any setting and who are not candidates for curative surgery or radiation, (c) unresectable or metastatic gastric, small intestine, or biliary cancer, who have disease progression on or following at least one prior therapy.
3.
PACKAGE QUANTITIES KEYTRUDA 25 mg/mL: 4 mL of concentrate in a 10 mL Type I clear glass vial. Legal Category: POM. Marketing Authorisation numbers EU/1/15/1024/002 Marketing Authorisation holder Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands. Date of revision: May 2022. © 2022 Merck & Co., Inc., Rahway, NJ, USA and its affiliates.. All rights reserved. Further information is available on request from: MSD, Red Oak North, South County Business Park, Leopardstown, Dublin, D18 X5K7 or from www.medicines.ie. II109_II117_II110 Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to MSD (Tel: 01-2998700)
2. Gandhi L, et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378:2078-2092. Paz-Ares L, et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N Engl J Med. 2018;379:2040–2051. Reck, M et al. Pembrolizumab versus chemotherapy for PDL1 positive-non-small cell lung cancer, N Eng J Med 2016, 375(19)1823-1833. lymphoma kinase; EGFR=epidermal
KEYTRUDA, in combination with platinum and fluoropyrimidine based chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic carcinoma of the oesophagus or HER-2 negative gastroesopha geal junction adenocarcinoma in adults whose tumours express PD-L1 with a CPS ≥ 10. KEYTRUDA, in combination with chemotherapy as neoad juvant treatment, and then continued as monotherapy as adjuvant treatment after surgery, is indicated for the treatment of adults with locally advan ced, or early stage triple negative breast cancer at high risk of recurrence. KEYTRUDA, in combination with chemotherapy, is indicated for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumours express PD L1 with a CPS ≥ 10 and who have not received prior chemotherapy for metastatic disease. KEYTRUDA, in combination with lenvatinib, is indicated for the treatment of ad vanced or recurrent endometrial carcinoma in adults who have disease progression on or following prior treatment with a platinum containing thera py in any setting and who are not candidates for curative surgery or radiation. KEYTRUDA, in combination with chemotherapy with or without beva cizumab, is indicated for the treatment of persistent, recurrent, or metastatic cervical cancer in adults whose tumours express PD L1 with a CPS ≥ 1. DOSAGE AND ADMINISTRATION See SmPC for full details. Therapy must be initiated and supervised by specialist physicians experienced in the treatment of cancer. The recommended dose of KEYTRUDA in adults is either 200 mg every 3 weeks or 400 mg every 6 weeks administered as an intravenous infusion over 30 minutes. The recommended dose of KEYTRUDA as monotherapy in paediatric patients aged 3 years and older with cHL is 2 mg/kg bodyweight (up to a maximum of 200 mg), every 3 weeks administered as an intravenous infusion over 30 minutes. For use in combination, see the Summary of Product Characteristics (SmPC) for the concomitant therapies. KEYTRUDA must not be administered as an intra venous push or bolus injection. When administering KEYTRUDA as part of a combination with intravenous chemotherapy, KEYTRUDA should be administered first. Treat patients until disease progression or unacceptable toxicity (and up to maximum duration of therapy if specified for an indica tion). For the adjuvant treatment of melanoma or RCC, KEYTRUDA should be administered until disease recurrence, unacceptable toxicity, or for a duration of up to one year. Refer to the SmPC for dosing in neoadjuvant and adjuvant treatment of locally advanced, or early stage triple-negative breast cancer at high risk of recurrence. KEYTRUDA, as monotherapy or as combination therapy, should be permanently discontinued (a) For Grade 4 toxicity except for: endocrinopathies that are controlled with replacement hormones; or haematological toxicity, only in patients with cHL in which KEYTRUDA should be withheld until adverse reactions recover to Grade 0-1; (b) If corticosteroid dosing cannot be reduced to ≤10 mg prednisone or equivalent per day within 12 weeks; (c) If a treatment-related toxicity does not resolve to Grade 0 1 within 12 weeks after last dose of KEYTRUDA; (d) If any event occurs a second time at Grade ≥ 3 severity. Patients must be given the Patient Alert Card and be informed about the risks of KEYTRUDA. Special populations Elderly: No dose adjustment necessary. Renal impairment: No dose adjustment needed for mild or moderate renal impairment. No studies in severe renal impairment. Hepatic impairment: No dose adjustment needed for mild hepatic impairment. No studies in moderate or severe hepatic impairment. Paediatric population: Safety and efficacy in children below 18 years of age not established except in pae diatric patients with cHL. CONTRAINDICATIONS Hypersensitivity to the active substance or to any excipients. PRECAUTIONS AND WARNINGS Assessment of PD-L1 status When assessing the PD-L1 status of the tumour, it is important that a well-validated and robust methodology is chosen to minimise false negative or false positive determinations. Immune-related adverse reactions Immune-related adverse reactions, including severe and fatal cases, have occurred in patients receiving pembrolizumab. Most immune related adverse reactions occurring during treatment with pem brolizumab were reversible and managed with interruptions of pembrolizumab, administration of corticosteroids and/or supportive care. Immune re lated adverse reactions have also occurred after the last dose of pembrolizumab. Immune-related adverse reactions affecting more than one body system can occur simultaneously. Immune-related adverse reactions are immune-related pneumonitis, immune-related colitis, immune-related he patitis, immune-related nephritis, immune-related endocrinopathies (including adrenal insufficiency, hypophysitis, type 1 diabetes mellitus, diabetic ketoacidosis, hypothyroidism, and hyperthyroidism), Immune-related skin adverse reactions (also including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN)), Refer to SmPC for more information and management of immune-related adverse reactions. Complications of allogeneic Haematopoietic Stem Cell Transplant (HSCT): Cases of graft-versus-host-disease (GVHD) and hepatic veno-occlusive disease (VOD) have been observed in patients with classical Hodgkin lymphoma undergoing allogeneic HSCT after previous exposure to pembrolizumab. Infu sion-related reactions: Grades 1, 2, 3 or 4 infusion reactions including hypersensitivity and anaphylaxis, could be seen with pembrolizumab treat ment. Refer to SmPC for more information and management of infusion-related reactions. Overdose: There is no information on overdose with pembrolizumab. In case of overdose, monitor closely for signs or symptoms of adverse reactions and treat appropriately. INTERACTIONS No formal pharmacokinetic drug interaction studies have been conducted with pembrolizumab. No metabolic drug drug interactions are expected. The use of systemic corticosteroids or immunosuppressants before starting pembrolizumab should be avoided because of their potential interference with the pharmacodynamic activity and efficacy of pembrolizumab. Corticosteroids can be used as premedication, when pembrolizumab is used in combina tion with chemotherapy, as antiemetic prophylaxis and/or to alleviate chemotherapy-related adverse reactions. FERTILITY, PREGNANCY AND LACTATION Women of childbearing potential Women of childbearing potential should use effective contraception during treatment with pembrolizu mab and for at least 4 months after the last dose of pembrolizumab. Pregnancy No data on use in pregnant women. Do not use during pregnancy unless the clinical condition of the woman requires treatment with pembrolizumab. Breast-feeding It is unknown whether pembrolizumab is secreted in human milk. A risk to newborns/ infants cannot be excluded. Fertility No clinical data available. SIDE EFFECTS Refer to SmPC for complete infor mation on side effects. Pembrolizumab is most commonly associated with immune-related adverse reactions. Most of these reactions resolved with appropriate medical treatment or withdrawal of pembrolizumab. The most serious adverse reactions were immune-and infusion-related adverse re actions. When pembrolizumab is administered in combination with axitinib or lenvatinib, refer to the SmPC for axitinib or lenvatinib prior to initiation of treatment. For additional lenvatinib safety information related to advanced RCC see the SmPC for Kisplyx and for advanced EC see the SmPC for Lenvima. Monotherapy: Very Common: anaemia, hypothyroidism, decreased appetite, headache, dyspnea, cough, abdominal pain, nausea, vomi ting, constipation, musculoskeletal pain, arthralgia, asthenia, oedema, pyrexia, diarrhoea, pruritus, rash, fatigue. Common: pneumonia, thrombocyto penia, neutropenia, lymphopenia, hyponatraemia, hypokalaemia, hypocalcaemia, insomnia, neuropathy peripheral, lethargy, dry eye, cardiac arr hythmia (including atrial fibrillation), hypertension, hyperthyroidism, insomnia, dizziness, dysgeusia, pneumonitis, colitis, dry mouth, severe skin reactions, vitiligo, dry skin, alopecia, eczema, dermatitis acneiform, erythema, dermatitis, myositis, pain in extremity, arthritis, influenza like illness, chills, AST and ALT increases, increase in blood alkaline phosphatase, hypercalcaemia, blood bilirubin increased, blood creatinine increased, infu sion related reaction. In combination with chemotherapy: Very Common: neutropenia, anaemia, thrombocytopenia, leukopenia, hypothyroidism, hypokalaemia, decreased appetite, insomnia, neuropathy peripheral, headache, dizziness, dysgeusia, dyspnoea, cough, nausea, diarrhoea, vomi ting, abdominal pain, constipation, alopecia, rash, pruritus, arthralgia, musculoskeletal pain, myositis, pyrexia, fatigue, asthenia, oedema, ALT increa se, AST increased. Common: pneumonia, febrile neutropenia, lymphopenia, infusion related reaction, adrenal insufficiency, thyroiditis, hyperthyroi dism, hyponatraemia, hypocalcaemia, lethargy, dry eye, cardiac arrhythmia (including atrial fibrillation), hypertension, pneumonitis, colitis, gastritis, dry mouth, hepatitis, severe skin reactions, erythema, dermatitis acneiform, dermatitis, dry skin, eczema, pain in extremity, arthritis, acute kidney injury, influenza-like illness, chills, blood creatinine increased, blood alkaline phosphatase increased, hypercalcaemia, blood bilirubin increased. In combination with axitinib or lenvatinib: Very Common: urinary tract infection, anaemia, hypothyroidism, decreased appetite, headache, dysgeu sia, hypertension, dyspnoea, cough, diarrhoea, abdominal pain, nausea, vomiting, constipation, rash, pruritus, arthralgia, musculoskeletal pain, myositis, pain in extremity, fatigue, asthenia, oedema, pyrexia, lipase increased, alanine aminotransferase increased, aspartate aminotransferase increased, blood creatinine increased. Common: pneumonia, neutropenia, thrombocytopenia, lymphopenia, leukopenia, infusion-related reaction, adrenal insufficiency, hyperthyroidism, thyroiditis, hyponatraemia, hypokalaemia, hypocalcaemia, insomnia, dizziness, neuropathy peripheral, lethar gy, dry eye, cardiac arrhythmia (including atrial fibrillation), pneumonitis, colitis, pancreatitis, gastritis, dry mouth, hepatitis, severe skin reactions, dermatitis, dry skin, erythema, dermatitis acneiform, alopecia, arthritis, nephritis, influenza like illness, chills, amylase increased, blood bilirubin in creased, blood alkaline phosphatase increased, hypercalcaemia.
4.
KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults with Stage III melanoma and lymph node involvement who have undergone complete resection.
KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic NSCLC in adults whose tumours express PD-L1 with a ≥1% TPS and who have received at least one prior chemotherapy regimen. Patients with EGFR or ALK positive tumour mutations should also have received targeted therapy before receiving KEYTRUDA.
KEYTRUDA as monotherapy is indicated for the treatment of adult and paediatric patients aged 3 years and older with relapsed or refractory classical Hodgkin lymphoma (cHL) who have failed autologous stem cell transplant (ASCT) or following at least two prior therapies when ASCT is not a treatment option. KEYTRUDA as monotherapy is indicated for the treatment of locally ad vanced or metastatic urothelial carcinoma in adults who have received prior platinum-containing chemotherapy. KEYTRUDA as monotherapy is in dicated for the treatment of locally advanced or metastatic urothelial carcinoma in adults who are not eligible for cisplatin-containing chemotherapy and whose tumours express PD L1 with a combined positive score (CPS) ≥ 10. KEYTRUDA as monotherapy or in combination with platinum and 5-fluorouracil (5-FU) chemotherapy, is indicated for the first-line treatment of metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC) in adults whose tumours express PD-L1 with a CPS ≥ 1. KEYTRUDA as monotherapy is indicated for the treatment of recurrent or metastatic HNSCC in adults whose tumours express PD-L1 with a ≥ 50% TPS and progressing on or after platinum-containing chemotherapy.
Reference 1. Keytruda Summary of Product Characteristics, June 2022, available at www.medicines.ie.
growth factor receptor; mNSCLC=metastatic non–small cell lung carcinoma; PDL1=programmed death ligand 1. Red Oak North, South County Business Park, Leopardstown, Dublin D18 X5K7, Ireland. 2022JunePreparation:ofDateIE-KEY-00596 Line Histology PD-L1 <1% or unknown 1-49%PD-L1 PD-L1>50% 1st line TherapyCombination*2 SQUAMOUSNON- √ √ √ 1st line TherapyCombination**3 SQUAMOUS √ √ √ 1st Monotherapyline***4 ANDNON-SQUAMOUSSQUAMOUS X X √ * KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of metastatic non-squamous NSCLC in adults whose tumours have no EGFR or ALK positive mutations. ** KEYTRUDA, in combination with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of metastatic squamous NSCLC in adults. *** KEYTRUDA, as monotherapy, is indicated for the first-line treatment of metastatic non-small cell lung carcinoma (NSCLC) in adults whose tumours express PD-L1 with a≥ 50% tumour proportion score (TPS) with no EGFR or ALK positive tumour mutations. KEYTRUDA: helping to redefine overall survival expectations for more patients with mNSCLC1-4 (pembrolizumab) Infusion 25mg/ml
KEYTRUDA, in combination with axitinib, is indicated for the first-line treatment of advanced renal cell carcinoma (RCC) in adults. KEYTRUDA, in combination with lenvatinib, is indicated for the first line treatment of advanced renal cell carcinoma in adults. KEYTRUDA as monotherapy is indica ted for the adjuvant treatment of adults with renal cell carcinoma at increased risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions.
ALK=anaplastic
KEYTRUDA® (pembrolizumab) ABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics before prescribing. PRESENTATION KEYTRUDA 25 mg/mL: One vial of 4 mL of concentrate contains 100 mg of pembrolizumab. INDICATIONS KEYTRUDA as monotherapy is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults.
KEYTRUDA as monotherapy is indicated for the first-line treatment of metastatic non-small cell lung carcinoma (NSCLC) in adults whose tumours express PD-L1 with a ≥50% tumour proportion score (TPS) with no EGFR or ALK positive tumour mutations.
KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of metastatic non-squamous NSCLC in adults whose tumours have no EGFR or ALK positive mutations. KEYTRUDA, in combi nation with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of metastatic squamous NSCLC in adults.



Colorectal cancer (CRC), sometimes referred to as bowel cancer, colon cancer, or rectal cancer, is the development of cells which grow out of control in the colon or rectum (parts of the the Health Economics of Colorectal Cancer: A COLOSSAL undertaking
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IEWrittenbyDrJonathan
Understanding
38 ONCOLOGY FOCUS: COLORECTAL CANCER
large intestine). As the third most commonly diagnosed, and second deadliest cancer, on average 10% of cancer diagnoses and 9.4% of deaths are attributed to CRC annually. A global burden of 1.93 million new diagnoses and 0.94 million deaths in 2020, coupled with projections of 3.2 million annual cases in 2040, suggests a growing global public health challenge. A key determinant of patient prognosis, metastatic colorectal cancer (mCRC) accounts for most recorded colorectal cancer-related deaths. CRC cells may break away from the original tumour and travel to other parts of the body via the blood or lymphatic system. Typical locations for this CRC metastasis include the liver, lungs, and brain.
mCRC is a heterogeneous disease, and subtyping captures the significance of this heterogeneity in predicting clinical outcomes, such as expected therapeutic response and patient survival. At least half of mCRC cases have disruptions in the RAS gene, a
Briody. Dr Briody is a health economist conducting an economic evaluation of the cost-effectiveness of precision medicine for metastatic colorectal cancer (mCRC) at RCSI University of Medicine and Health Sciences


gene which manages cell growth and division. Such disruptions lead to uncontrolled growth, making cells cancerous as they stop responding to the natural defences of the body. Microsatellite stable or MSS RAS mutant metastatic CRC cells additionally have a repair mechanism to address mutations in genes. While such mutational status currently does not significantly alter the initial treatment of mCRC from the frontline treatment traditionally provided in colorectal cancer, there is a growing consensus that targetted therapies may pose an important step in reducing mortality, and improving prognosis in mCRC.
COLOSSUS is an EU-funded Horizon 2020 project of 14 different partner organisations from 8 different countries that aims to provide more effective ways to index patients with mCRC and to develop subtypespecific treatment options for these patients. As part of this work, the consortium is analysing colorectal tissue and blood samples from MSS RAS mt mCRC patients in Spain, Germany and Ireland. Colossus has identified new methods for classifying mCRC via advanced multi-omic computational and mathematical modelling. These approaches have been applied to discover new MSS RAS mt specific subtypes, with contemporary clinically applicable diagnostic test prototypes in progress to stratify these patients. Now, specific novel combinatorial treatment options are under development based on these new targetedpredictiveAppropriatelyclassifications.establishingbiomarkerswiththerapyoptionsis not, however, the only step required for adoption in the clinic. With greater than 5 million people worldwide estimated to be living with CRC, efforts to expand treatment options for mCRC are expected to have a significant impact on healthcare costs. Against a background of increasing demands on limited resources, the financial consequences of novel therapies are quickly becoming an important consideration in clinical Healthdecision-making.economics exists to analyse whether interventions in health are both effective, and an efficient use of strained resources. However, health economics is about more than just money. Healthcare budgets are finite; investments in one area of the healthcare system will necessarily be at the expense of others. For example, given a national recommendation to increase cardiac screening, careful thought is needed on whether providing this additional service may require contracting other areas of care, and whether such shifts will lead to a net gain or loss in the total health produced in the current system. This discipline facilitates optimal decision making by providing a clear framework in which options that maximise the expected overall benefits from available resources in the health system are preferred. Particularly, economic evaluation relates the expected costs and benefits of alternative means of health care, such that it is possible to determine whether the gains from introducing an intervention outweigh those foregone when reallocating existing health budgets. This basic principle of health economics, the production of the maximum level of net health available in the health care system, is the cornerstone of the economic evaluation of any new screening strategy, model of care or medical therapy - such as the delivery of a personalised medicine approach for patients with MSS RAS mt mCRC. In COLOSSUS, clinically relevant outcomes, such as improved patient survival, are of significant interest. However, the health economics of the proposed treatment strategy, when compared to current best practice, is also considered meaningful and explicitly modelled to estimate whether increments in expected benefit justify proposed shifts in resource allocation.
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 39
In this project, the cost per qualityadjusted life-year (QALY) gained from testing and associated novel subtype-specific treatment options, compared with standard of care without testing, is estimated in a cost-effectiveness analysis. Cost-effectiveness analysis takes it's name from the manner in which the benefit of the proposed intervention is measured, typically valuing outcomes in terms of natural units, such as deaths prevented or life years gained from one treatment when compared to another. When making choices on allocating resources to a new method of care, it is necessary to understand how much this intervention may cost (per unit of health gained) when compared with possible alternatives and whether this choice may lead to a net loss or gain in the total level of health currently produced in the health care system.
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 40
FOCUS: COLORECTAL CANCER
The results of such an analysis can thus be useful to decision makers, such as a national health authority, who will be able to identify interventions which will be more effective and less costly. In such cases, the proposed intervention will result in improvements in health and savings in resources - which can be redirected back into the health care system. Even when interventions are more costly than the existing standard of care, the health economic analysis provides a transparent structure to determine when health improvements warrant increased demands on health care services.
The EU Commission takes no responsibility for any use made of the information set out.
While placing a financial value on patient health is contentious, decision makers must prioritise amongst competing demands for healthcare resources. Health economics provides a fair and explicit framework to maximise patient benefit from finite budgets and thus maximise efficiency in the healthcare system. Whilst the design of more targeted and personalised regimens is something which is welcomed in mCRC, in the provision of health care, difficult choices are inevitable. The discipline of health economics provides a framework to make such decisions equitable and explicit. To support realworld advancements in patient care at all stages, from the bench to the bedside, COLOSSUS is embracing a robust analysis of the expected clinical effectiveness and the cost-effectiveness of its proposed personalised medicine approach for patients with MSS RAS mt mCRC. For further information on the COLOSSUS project, please visit www.colossusproject.eu or follow COLOSSUSEU on Facebook and Twitter. Dr Briody can be found at: @JonathanBriody This project has received funding from the European Union's Horizon 2020 research and innovation programme under grant agreement No 754923. The material presented and views expressed here are the responsibility of the author(s) only.
ONCOLOGY
Particularly, the use of a common measure of outcome facilitates comparisons across every disparate healthcare sector. For example, as the most popular outcome studied in costeffectiveness analysis, the QALY simultaneously captures both elements of health, increased life expectancy and the healthrelated quality of this increased expectancy. By it's nature, a QALY gained in neonatal care has equal merit to one gained in rehabilitation interventions for the ageing. Consequently, it is possible in health economic evaluation for decision makers to establish allocative efficiency, that is, to make decisions to maximise the health of society as a whole.

decreased. Uncommon
increased, blood
WARNINGS *: Bone marrow suppres sion: Complete blood cell counts must be obtained prior to initiation of therapy, prior to each cycle and as needed. Treatment must not be start ed if absolute neutrophil count < 1.5 x 109/L, if platelet counts < 75 x 109/L, or if unresolved Grade 3 or 4 non-haematological clinically relevant toxicity. Patient should be monitored closely for infections, appropriate measures should be administered as clinically indicated. Gastrointestinal toxicity: anti-emetic, anti-diarrhoeal and other measures should be administered as clinically indicated, dose modifications should be applied as necessary. Renal impairment: not recommended if end-stage renal disease. Patients with renal impairment should be monitored closely; patients with moderate or severe renal impairment should be more frequently monitored for haematological toxicities. Hepatic impairment: not recommended if baseline moderate or severe hepatic impairment. Proteinuria: monitoring by dipstick urinalysis recommended prior to starting and during therapy. Excipients: contain lactose. INTERACTIONS*: Precautions: medicinal products that interact with nucleoside transporters CNT1, ENT1 and ENT2, inhibitors of OCT2 or MATE1, human thymidine kinase substrates (e.g. zidovudine), hormonal contraceptives. FERTILITY*. PREGNANCY AND BREASTFEEDING*: Not recommended. CONTRACEPTION*: For women and men, highly effective contraceptive measures must be used during treatment and for 6 months after stopping treatment. DRIVE & USE MACHINES*: Fatigue, dizziness or malaise may occur. UNDESIRABLE EFFECTS*: Very common: Neutropenia, leukopenia, anaemia, thrombocytopenia, decreased appetite, diarrhoea, nausea, vomiting, fatigue. Common: Lower respiratory tract infection, febrile neutropenia, disorder, hyperbilirubinaemia, Palmar-plantarerythrodysaesthesia syn inflammation, enzyme alkaline phosphatase weight : Septic shock, enteritis infectious, lung infection, biliary tract infection, influenza, urinary tract infection, gingivitis, herpes zoster, tinea pedis, candida infection, bacterial infection, infection, neutropenic sepsis, upper respiratory tract infection, conjunctivitis, cancer pain, pancytopenia, granulocytopenia, monocytopenia, erythropenia, leukocytosis, monocytosis, dehydration, hyperglycaemia, hyperkalaemia, hypokalaemia, hypophosphataemia, hypernatraemia, hyponatraemia, hypocalcaemia, gout, anxiety, insomnia, neurotoxicity, dysaesthesia, hyperaesthesia, hypoaesthesia, syncope, paraesthesia, burning sensation, lethargy, dizziness, headache, visual acuity reduced, vision blurred, diplopia, cataract, dry eye, vertigo, ear discomfort, angina pectoris, arrhythmia, palpitations, embolism, hyperten sion, hypotension, flushing, pulmonary embolism, pleural effusion, rhinorrhoea, dysphonia, oropharyngeal pain, epistaxis, cough, enterocolitis haemorrhagic, gastrointestinal haemorrhage, pancreatitis acute, ascites, ileus, subileus, colitis, gastritis, reflux gastritis, oesophagitis, impaired gastric emptying, abdominal distension, anal inflammation, mouth ulceration, dyspepsia, gastrooesophageal reflux disease, proctalgia, buccal polyp, gingival bleeding, glossitis, periodontal disease, tooth disorder, retching, flatulence, breath odour, hepatotoxicity, biliary dilatation, skin exfoliation, urticaria, photosensitivity reaction, erythema, acne, hyperhidrosis, blister, nail disorder, joint swelling, arthralgia, bone pain, myalgia, musculoskeletal pain, muscular weakness, muscle spasms, pain in extremity, renal failure, cystitis noninfective, micturition disorder, haema turia, leukocyturia, menstrual disorder, general physical health deterioration, pain, feeling of body temperature change, xerosis, discomfort, blood creatinine increased, electrocardiogram QT prolonged, international normalised ratio increased, activated partial thromboplastin time prolonged, blood urea increased, blood lactate dehydrogenase increased, protein total decreased, C-reactive protein increased, haematocrit decreased. Post-marketing experience: interstitial lung disease. OVERDOSE* PROPERTIES*: Trifluridine is an antineoplastic thymidine-based nucleoside analogue and tipiracil hydrochloride is a thymidine phosphorylase (TPase) inhibitor. Following uptake into cancer cells, trifluridine, is phosphorylated by thymidine kinase, further metabolised in cells to a deoxyribonucleic acid DNA substrate, and incorporated directly into DNA, preventing cell proliferation. However, trifluridine is rapidly degraded by TPase and readily metabolised by a first-pass effect following oral ad ministration, hence the inclusion of the TPase inhibitor, tipiracil hydrochloride.PRESENTATION* Pack of 20 or 60 film-coated tablets. Marketing Authorisation Holder LES LABORATOIRES SERVIER, 50 rue Carnot, 92284 Suresnes cedex France. www.servier.com. Marketing Authorisa tion: EU/1/16/1096/001-006. Legal Classification for Supply: POM. Further information available from: Servier Laboratories (Ireland) Ltd., Second Floor, 19 Lr. George’s Street, Dun Laoghaire, Co. Dublin A96 ER84, Ireland, Tel (01) 6638110, www.servier.ie. *For complete information, please refer to the Summary of Product Characteristics available on medicines.ie. Date of last revision of text: January 2021 (Date of last approved SmPC: December 2020)
malaise, hepatic
increased,
Reference: 1. Lonsurf SmPC December 2020 Date of preparation of item September 2021. 2122c1LNPressAd A4 Extend overall survival for patients in 3rd line mCRC1 matter
lymphopenia, hypoalbuminaemia, dysgeusia, neurop athy peripheral, dyspnoea, abdominal pain, constipation, stomatitis, oral
CONTRAINDICATIONS*: Hypersensitivity to the active substances or to any of the excipients.
MAKE TIME for more moments that
trifluridine/tipiracil Lonsurf® (Trifluridine/ tipiracil): Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics before prescribing COMPOSITION*: Lonsurf 15 mg/6.14 mg: film-coated tablet containing 15 mg trifluridine and 6.14 mg tipiracil (as hydrochloride). Lonsurf 20 mg/8.19 mg: film-coated tablet containing 20 mg trifluridine and 8.19 mg tipiracil (as hydrochloride). INDICATION*: As monotherapy for the treatment of adult patients with metastatic colorectal cancer who have been previously treated with, or are not considered candidates for, available therapies including fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapies, anti-VEGF agents, and anti-EGFR agents. As monotherapy for the treatment of adult patients with metastatic gastric cancer including adenocarcinoma of the gastroesophageal junction, who have been previously treated with at least two prior systemic treatment regimens for advanced disease. DOSAGE AND ADMINISTRATION*: Recommended starting dose: 35 mg/m2/dose taken orally twice daily on Days 1 to 5 and Days 8 to 12 of each 28-day cycle, within 1 hour after completion of the morning and evening meals (20mg/m2/dose for patients with severe renal impairment). Dosage calculated according to body surface area, not exceeding 80 mg/dose. Possible dosing adjustments based on individual safety and tolerability: permitted dose reductions to a minimum dose of 20 mg/m2 twice daily (15mg/m2/dose for patients with severe renal impairment), dose escalation not permitted after a dose reduction.
drome, rash, alopecia, pruritus, dry skin, proteinuria, pyrexia, oedema, mucosal

One UK based study in women attending breast screening showed that awareness of alcohol as a risk factor was associated with the knowledge necessary for behaviour change. Increased body mass, low physical activity, poor quality diet, alcohol and smoking are modifiable risk factors for primary and secondary cancer development.
References
on request 42
ONCOLOGY FOCUS: BREAST CANCER
Several studies have shown benefit of lifestyle interventions involving a combination of dietary education, behavioural change advice and physical activity resulting in improvement in anthropometric measures. The efficacy of these interventions is greater amongst patients who were aware of the risk associated with disease recurrence. Increased physical activity in breast cancer survivorship has been shown to be associated with lower cancer related and all-cause mortality.
Modifiable lifestyle risk factors including poor diet quality, low physical activity, high body mass index, smoking and alcohol intake, are associated with increased risk in many cancer diagnoses as well as contributing to increased morbidity and mortality. The Irish National Cancer Strategy Program 2017-2026 estimates that between 30% to 40% of cancer incidence in Ireland is attributable to modifiable lifestyle and environmental factors alone. The report lists several dietary and lifestyle goals including weight reduction and increasing physical activity as targets for primary and secondary disease prevention in Ireland.3 Considering the modifiability of these risk
Breast cancer survivors who are obese are at increased risk of both cancer related mortality and death from all-causes, reported as 33% and 41% respectively.
Clara Steele Over the past three decades in Ireland breast cancer survival rates have increased. Improvements in cancer diagnostics and treatments have resulted in age standardised survivorship of over 75% at ten years. Cancer survivorship is causing a shift to that of a chronic condition and is associated with an increased risk of recurrence, new cancer diagnosis and development of other noncommunicable diseases. Over the last fifteen years a substantial body of evidence has emerged on the impact of lifestyle modification on breast cancer related outcomes with studies showing targetable interventions. Secondary risk reduction services are an integral part of cardiovascular disease management and therefore similar strategies should be considered as part of an early breast cancer care treatment plan.
Furthermore, sufficient awareness and engagement of healthcare professionals in risk reduction strategies is imperative and is a fundamental principle of the HSEs ‘Making Every Contact Count’ Program. Research has been conducted at Cork University Hospital looking at breast cancer survivors and oncology clinicians awareness of modifiable risk factors and willingness to engage in or refer to secondary risk reduction services, if available. The study included over 300 patients and 30 clinicians and preliminary results will be presented at The European Society of Medical Oncology Conference this September.
Alcohol is a known carcinogen however awareness of alcohol as a risk factor for cancer development has been reported as low. Increased lifetime alcohol consumption and heavy episodic drinking amongst moderate lifetime drinkers has been associated with increased risk of breast cancer. Breast cancer screening and or diagnosis may be an important moment for behavioural change education and advice on alcohol reduction.
In addition, a 2018 metanalysis showed an association between increased physical activity and improved quality of life in breast cancer survivors. Furthermore, a randomised control trial involving at a four month supervised exercise program in breast cancer survivors showed improved bone health, physical fitness and improved quality of life.
Full results are expected to be published later this year. There is a need for diagnosis specific lifestyle based interventions however, to our knowledge, no large scale secondary risk reduction service is currently available in Ireland. A strategy such as, the Irish Heart Foundation’s Cardiac Rehabilitation program could be utilised as a blueprint for this urgent public health issue.
Written by Clara Steele, Final Year Medical Student, Department of Medicine, School of Medicine, University College Cork and Professor Seamus O’Reilly, Consultant Medical Oncologist, Department of Medical Oncology, Cork University Hospital and Cancer Research @UCC, University College Cork Professor Seamus O’Reilly
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Increasing awareness amongst breast cancer survivors and encouraging engagement to achieve beneficial lifestyle changes is of paramount importance. The evidence outlined above identifies that the time around breast cancer diagnosis is a pivotal moment for lifestyle modification advice and this should be a core focus of secondary risk reduction guidance and clinical practice.
Poor quality diet, high in saturated fat and sugar and low in fruit and vegetables is associated with increased cancer risk.2 A systematic review assessing dietary patterns, mortality and recurrence in cancer survivors concluded that reduction of dietary fat after breast cancer diagnosis was associated with increased relapse free time. Furthermore, the study identified that a highquality diet may be beneficial for reducing non breast cancer related mortality. This benefit was confirmed in a recent intervention trial where breast cancer survivors, provided with advice for a low-fat diet post diagnosis, had significantly reduced mortality from bybreastanalysisdevelopment.modifiableSmokingall-causes.isthesignificantriskfactorforcancerAlargescalemeta-showedanincreaseincancer-associatedmortalityalmostonethirdinthose who continued to smoke post diagnosis. The study also found that mortality in former smokers was the same as never smokers showing that smoking cessation post diagnosis can decrease breast cancer related deaths.
factors there should be greater emphasis placed on lifestyle interventions for cancer survivors with the aim to integrate these services into Irish breast cancer care treatment pathways.
In summary, the focus in breast cancer care is often pharmacological prescribing however the evidence supports lifestyle intervention as an important part of the treatment course in this cohort. Patients should be offered counselling on the importance of diet, weight management, increased physical activity, alcohol reduction and smoking cessation at an appropriate time point for them. These interventions have the potential to impact breast cancer related mortality and morbidity as well as decrease chronic disease related risk. available
A recent French review illustrated that one third of patients who were provided information on smoking post diagnosis quit with the main motivating factor reported as risk of recurrence. This review also identified that about one third of baseline assessments did not include a record of smoking status, an important finding for clinician education.
Secondary Risk Reduction Strategies in Irish Breast Cancer Care


ONCOLOGY FOCUS: THROMBOSIS
Tumour sub-type may also influence thrombosis risk due to the varying propensity of different tumours to activate coagulation, with particularly high-rates of Dr Stuart Macleod
Figure
‘high-risk’ patients. Similarly, it remains to be determined if novel drug targets may represent a means of addressing the high rates of VTE recurrence and bleeding which continue to arise in this patient population despite current best therapy.
Swelling or pain in one leg or calf Warmth or redness in the leg
WHAT IS A BLOOD CLOT?
CSN: 20154240
➢Short of breath or rapid breathing Chest pain (particularly when breathing deeply) Coughing or coughing up blood If you have one or more of these, you may have a clot and need urgent treatment
The precise molecular mechanisms underlying the increased thrombosis risk among patients with cancer remain to be fully elucidated. However, a number of investigators have demonstrated clear evidence of a complex relationship between tumour cells and the haemostatic system.8,9 In particular, the aberrant expression of tissue Factor (TF, a procoagulant glycoprotein) on the surface of tumour cells and on circulating tumour-derived microvesicles has been implicated in the pathogenesis of hypercoagulability in this population. Tumour cells have also been shown to directly activate coagulation through a number of other distinct mechanisms including through the expression/release of various other pro-coagulant substances which directly activate elements of the haemostatic system including coagulation factors and platelets.8
WHAT CAN I DO TO HELP MYSELF?
BLOOD CLOT ALERT CARD For more www.thrombosis.ieinformation:
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 43
Introduction Venous Thromboembolism (VTE) is a potentially devastating and yet frequently under-recognised complication of active cancer and cancer therapy. The risk of VTE is thought to be at least 5-fold higher among patients receiving cancer therapy than that which is observed in the general population and it is estimated that up to 20% of all patients with cancer will experience some form of venous thrombosis during the course of their disease.1-3 Acute VTE among patients with cancer is associated with a particularly high burden of morbidity and mortality risk. Cancer patients who develop VTE have a risk of recurrent thrombosis (despite optimal anticoagulant therapy) which may be as high as 20% at 12 months.4, 5 Patients
Advances in the Prevention and Treatment of Cancer-Associated Thrombosis with cancer also experience more anticoagulant-related bleeding events than that observed in the general population.5 The risk of death following VTE recurrence is also substantially higher among patients with cancer, estimated to be in the region of 15% in some subgroups.6 In fact it is widely recognised that VTE represents the second-leading cause of death among patients with cancer, second only to the progression of cancer itself.7 While significant advances have been made in recent years, several important clinical questions have yet to be addressed. The development of strategies for individualised prediction of VTE risk has proven to be challenging. Consequently, there is a degree of uncertainty among clinicians regarding the optimal approach to the use of primary thromboprophylaxispharmacologicalforpotentially
Mechanisms hypercoagulabilityof in cancer
Dr Barry Kevane
Ask for your risk of blood clots to be assessed, especially if you are in one of the higher risk groups listed opposite ➢Walk and move as much as ➢Drinkpossibleplenty of fluids ➢If directed to use stockings or medication to prevent or treat a clot follow instructions exactly Remember, a clot can form up to 90 days after being in hospital If you have any signs or symptoms of a clot, take immediate action to seek medical help YOU MAY BE AT HIGHER RISK IF YOU: are admitted to hospital and for 90 days after you go havehomeactive cancer or receiving cancer treatment are pregnant or have had a baby less than 6 weeks ago become immobile (more than 3 days in bed / travel non-stop more than 6 hours / in a leg cast)
RISK MAY INCREASE FURTHER IF: you or a close relative had a blood clot you had surgery in the last 90 days you have thrombophilia (tendency to clot) you are on the oral contraceptive pill or HRT you have heart, lung or inflammatory disease you are over 60 years of age or are overweight you have varicose veins that become red and sore BLOOD CLOT ALERT CARD Am I at risk?
You have a HIGHER CHANCE of getting a clot in HOSPITAL than on an AEROPLANE!
Written by Dr Stuart Macleod & Dr Barry Kevane, Department of Haematology, Mater Misericordiae University Hospital, Dublin 1
This is the formation of a clot inside a blood vessel, usually in the leg, which may break off and go to the lungs. This can be fatal. Blood clots can be very serious - but there are effective treatments to deal with them and help prevent them 60%of clots happen in HOSPITAL or in the 90 DAYS following admission.
SIGNS AND SYMPTOMS OF A BLOOD CLOT


SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 44 ONCOLOGY FOCUS: THROMBOSIS
Prevention of cancer-associated thrombosis
Personal risk factors including prior VTE and elevated body mass index have been reported to be associated with an increased risk of thrombosis following a cancer diagnosis.3 Numerous specific cancer treatments including traditional chemotherapies such as certain platinum-based agents (e.g. cisplatin, carboplatin) as well as some more novel treatments, including novel immunotherapies (such as the immune checkpoint inhibitors) have also been reported to increase risk.10 Cancer surgery, radiation therapy and the use of central venous catheters have also all been shown to contribute to the VTE risk profile of patients with cancer requiring therapy.3
education programs relating to cancer therapy may assist clinicians in ensuring that at-risk patients are sufficiently educated with regard to these risks. Given the magnitude of VTE risk associated with cancer and cancer therapy, many experts believe that primary thromboprophylaxis should be offered to selected patients with cancer during periods of cancer treatment or in other high-risk scenarios. Current national and international clinical practice guidelines recommend that all patients with cancer who are admitted to hospital should be risk assessed with regards to thrombosis and bleeding risk and that pharmacological thromboprophylaxis with low molecular weight heparin (LMWH) be considered for the period of hospitalisation unless contraindicated due to a competing risk of bleeding.13, 14 Similarly, the use of pharmacological thromboprophylaxis with LMWH, aspirin or a low-dose direct oral anticoagulant (DOAC) has become standard of care for out-patients receiving therapy for myeloma (a haematological cancer associated with a high risk of thrombosis).13, 14 The role of pharmacological thromboprophylaxis for other cancer out-patients is an area of significant debate. A key obstacle to determining whether prophylaxis is warranted is the difficulty in accurately identifying the patients who are most at risk of VTE (and for whom the potential risks of pharmacological thromboprophylaxis could be justified). Several VTE risk predication models have been proposed for use in the cancer population, with the Khorana score being the most widely validated (Table 1). This algorithm stratifies cancer patients who are about to commence cancer therapy based on specific clinical and laboratory parameters as being at low (score 0), intermediate (score 1-2) or high risk (score 3+) for VTE. In validation studies, these thresholds have corresponded to predicted 6-month cumulative VTE risks in the region of 5%, 6.6% and 11% respectively – although absolute risk appears to vary considerably across tumour types and a key limitation of the Khorana score is that it seems to perform less well in some populations (e.g. patients with lung cancer). Consequently the reported risk estimates in different validation studies have been variable. In addition, up to 50% of patients who eventually experience VTE would not have been identified as being at intermediate (or higher) risk, which suggests that efforts to enhance the sensitivity of the Khorana score may also be warranted.15, 16
thrombosis observed with tumours such as pancreatic carcinoma and multiple myeloma. The importance of this direct tumour effect in driving hypercoagulability is reflected in the observation that the risk of thrombosis appears to be greatest during periods of increased tumour activity, with the incidence of cancer-associated thrombosis being greatest in the first 6-months following diagnosis (as well as also being increased during periods of relapsing disease and at Patient-specificend-of-life).and treatmentspecific factors also appear to significantly modulate thrombosis risk in the cancer population.
The interaction of these tumourspecific, patient-specific and treatment-specific factors largely determine the risk of thrombosis in an individual patient. However, using this information to accurately risk-stratify an individual or to identify a patient who might derive benefit from controversyandthromboprophylaxisprimaryischallengingremainsanareaofsignificantanddebate.
The provision of education relating to thrombosis risk should represent an integral component of the supportive care programme provided to patients who are about to commence cancer therapy. In recent years we have seen numerous reports of patients’ experiences with cancerassociated thrombosis where the diagnosis and time to treatment initiation had been delayed as a consequence of patients being unaware of the symptoms of VTE (and the need to seek urgent medical attention).11 This lack of awareness may lead to adverse clinical outcomes as well as substantial psychological distress.11 The HSE have recently launched the VTE Alert Card initiative which provides patients with written information regarding VTE risk and the signs of symptoms which should prompt them to seek medical advice (Figure 1 on page 43).12 These cards have been issued to all hospitals in Ireland and current HSE recommendations state that all patients being discharged from hospital should be provided with this written information. Incorporating the VTE alert card initiative into current patient
Most recently, the Khorana score has been utilised in large randomised trials which have evaluated the safety and efficacy of low dose DOACs for patients with cancer commencing chemotherapy. The AVERT and CASSINI randomised trials (which sought to investigate the safety and efficacy of apixaban Table 1.
Khorana Score Table 1. Khorana Score PATIENT CHARACTERISTIC SCORE Tumour site 1. Very high risk (Stomach, pancreas) 2. High risk (lung, lymphoma, gynaecologic, bladder, testicular) 12 Pre chemotherapy Platelet count ≥350x109/L 1 Pre-chemotherapy Haemoglobin <10g/dL/or use of red cell growth factors 1 Prechemotherapy Leukocyte count >11 x109/L 1 BMI ≥35 kg/m2 1 TOTAL SCORE RISK CATEGORY 0 Low 1 2 Intermediate 3 + High References available on request
Prescribing information
IE2022/005/00Ref:2022Junepreparation:ofDate
Please refer to the Summary of Product Characteristics (SmPC) before prescribing.
Therapeutic Indications
Non-small cell lung cancer - Docetaxel is indicated for the treatment of patients with locally advanced or metastatic non-small cell lung cancer after failure of prior chemotherapy.
Docetaxel in combination with cisplatin is indicated for the treatment of patients with unresectable, locally advanced or metastatic non-small cell lung cancer, in patients who have not previously received chemotherapy for this condition. metastatic castration-resistant prostate cancer. Docetaxel in combination with androgen-deprivation therapy (ADT), with or without prednisone or prednisolone, is indicated for the treatment of patients with metastatic hormone-sensitive prostate cancer. Gastric adenocarcinoma - Docetaxel in combination with cisplatin and 5‑fluorouracil is indicated for the treatment of patients with metastatic gastric adenocarcinoma, including adenocarcinoma of the gastroesophageal junction, who have not received prior chemotherapy for metastatic disease. Head and neck cancer - Docetaxel in combination with cisplatin and 5‑fluorouracil is indicated for the induction treatment of patients with locally advanced squamous cell carcinoma of the head and neck.
Docetaxel concentrate20mg/ml for solution for infusion
Adverse reactions should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by email medsafety@hpra.ie . Adverse events should also be reported to Kent Athlone Pharma Group on (090) 666 1109 or medical@kent-athlone.com. Additional information available on request.
Breast cancerdoxorubicin and cyclophosphamide is indicated for the adjuvant treatment of patients with: operable node-positive breast cancer operable node-negative breast cancer
Docetaxel 20mg/ml concentrate for solution for infusion requires NO prior dilution with a solvent and is ready to add to the infusion solution.
Name and active ingredient: Docetaxel 20mg/ml concentrate for solution for infusion. Each ml of concentrate contains 20mg docetaxel anhydrous. Each vial of 8ml concentrate contains 4ml of ethanol anhydrous (3.16g). Indications: Treatment of breast cancer, non-small cell lung cancer, prostate cancer, gastric adenocarcinoma, head and neck cancer. Treatment can be in combination with other medications (see SmPC section 4.1). Docetaxel treatment should be confined to units specialised in the administration of cytotoxic chemotherapy and only under the supervision of a physician qualified in the use of anticancer chemotherapy (see SmPC section 6.6). Posology and method of administration: The daily dose is determined by the indication being treated. See SmPC section 4.2 for dosage, preparation and administration. Contraindications: Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 of the SmPC. Patients with baseline neutrophil count of < 1,500 cells/mm3. Patients with severe liver impairment since there are no data available (see SmPC section 4.2 and 4.4). Contraindications for other medicinal products also apply, when combined with docetaxel. Special warning and precautions for use: Precautions should be taken regarding haematology, gastrointestinal reactions, hypersensitivity reactions, cutaneous reactions, fluid retention, respiratory disorders, patients with liver impairment, patients with renal impairment, nervous system, cardiac toxicity, eye disorders, second primary malignancies, tumour lysis syndrome, congestive heart failure, patients with 4+ nodes and the elderly (see SmPC section 4.4). Interactions: The amount of alcohol in this product may alter the effects of other medicinal products. Caution should be exercised with concomitant use of Ciclosporine, Ketoconazole and Erythromycin. An increase in adverse reactions may be seen when used in combination with itraconazole, clarithromycin, indinavir, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin and voriconazole (see SmPC section 4.5). Adverse reactions: The most commonly reported adverse reactions of docetaxel alone are: neutropenia (which was reversible and not cumulative; the median day to nadir was 7 days and the median duration of severe neutropenia (< 500 cells/mm3) was 7 days), anaemia, alopecia, nausea, vomiting, stomatitis, diarrhoea and asthenia. The severity of adverse events of docetaxel may be increased when docetaxel is given in combination with other chemotherapeutic agents. For full information on adverse reactions, see SmPC section 4.8). Presentation: 15ml colourless type-I glass vial, closed with a 20mm grey chlorobutyl rubber stopper and a red flip-off seal consisting of an aluminium shell and a red plastic flip-off button. The rubber stopper is coated with a Teflon® barrier film. Pack Size: Each box contains one vial with 8ml fill volume. Legal Classification: POM. Marketing Authorisation Number: PA22766/001/001. Distributed by: Uniphar on behalf of Athlone Pharmaceuticals Ltd. For a copy of the SmPC or further medical information, please contact (00353) 86 8394447 or medical@kent-athlone.com Date of preparation: May 2021. Ref: IE21/005/SmPC Feb 2021.
For further information on this product, please contact Gavin Butler, Key Account Manager, Athlone Pharmaceuticals Ltd., Ballymurray, Co. Roscommon Tel: + 353 (0) 87 3354523 | Email: Gavin.Butler@kent-athlone.com



References available on request
Notwithstanding these recent recommendations, the widespread use of primary thromboprophylaxis in patients with cancer has yet to be adopted into routine clinical practice. It is clear that concerns remain among clinicians regarding the potential risks and challenges associated with implementing this approach in a ‘real-world setting’ as opposed to in the highlyselected clinical trial setting where certain patient groups, such as the elderly, are generally underrepresented. Moreover, some experts point to the fact that while primary thromboprophylaxis does appear to reduce thrombosis risk, this has not yet been shown to deliver a survival benefit, at least in the studies conducted to date.
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 46
When patients with cancer present with suspected VTE it is crucial that diagnostic testing and initiation of appropriate anticoagulant therapy is not delayed. Clinical decisions rules for exclusion of acute VTE, such as the Wells score for pulmonary embolism or deep vein thrombosis, have been widely validated in the general population and lead to reductions in unnecessary use of diagnostic imaging tests. The value of these pre-test probability predictive algorithms in the cancer population is less clear due to the higher prevalence of VTE and due to concerns regarding the predictive value of the d-dimer in this group.21 Consequently, clinicians must rely heavily on their clinical judgement when assessing cancer patients and will frequently need to resort to invasive diagnostic imaging tests. Efforts to determine the efficacy of pre-test probability algorithms in the cancer population are ongoing and most notably the HYDRA Study, a randomised trial comparing the use of the YEARS algorithm (which comprises of specific clinical signs in combination with a two-level d-dimer cut-off positivity threshold) versus diagnostic imaging with computed tomography for rapid exclusion of PE is currently recruiting worldwide.22 The results of this trial are eagerly awaited.
Treatment cancer-associatedof thrombosis anticoagulationTherapeutic-intensitywithLMWH was established as the standard of care for cancer-associated thrombosis following the publication of the CLOT randomised controlled trial in 2003 which confirmed the superiority of this agent over warfarin therapy in the cancer population.23 More recently the publication of the HOKUSAI cancer VTE trial, the SELECT-D trial and the CARAVAGGIO trial have confirmed the non-inferiority of the DOACs edoxaban, rivaroxaban and apixaban to LMWH for the treatment of cancer-associated thrombosis.24-26 All major international clinical practice guidelines now endorse the use of these agents as first-line alternatives for the management of cancer-associated thrombosis.13, 14 DOACs do appear to confer a higher risk of bleeding in some sub-groups of patients with cancer, specifically patients with luminal gastrointestinal tumours or genito-urinary tumours. Most clinicians continue to favour LMWH in these patient subgroups. LMWH may also be favoured for patients when there are potentially significant drugdrug interactions present between DOACs and cancer therapies, in the setting of treatment or disease-related thrombocytopenia and where there are concerns regarding the potential for impaired gastrointestinal DOAC absorption. Despite the advances in thrombosis therapy which have been achieved in recent years, outcomes for patients with cancer remain inferior to those which are observed in the general population. Even with the use of appropriate anticoagulant therapy, the risk of recurrent thrombosis remains unacceptably high in the cancer patient population with 6-month recurrence rates in the region of 6-10% being reported in the recent large DOAC clinical trials.24-26 Similarly, the risk of bleeding complications on anticoagulant therapy is higher in this population, with rates of major bleeding of approximately 4-6% at 6-months also reported. Given the clear danger associated with both recurrent thrombosis and major bleeding (which may have case-fatality rates in the region of 10-15% in the cancer population), more therapeutic options are urgently required to mitigate these competing risks. The contact pathway of coagulation activation (comprising of the clotting factors pre-kallikrein, high-molecularweight kininogen, factor XII and factor XI) has emerged as an attractive novel drug target for the prevention and treatment of thromboembolism.27 In preclinical models, the inhibition of the contact pathway does not appear to impair normal physiological haemostasis but does appear to inhibit pathological coagulation activation. Therefore, a drug which inhibits the contact pathway might be predicted to reduce the risk of thrombosis without significantly increasing the risk of bleeding.27 Coagulation factor XI appears to be the most promising drug-target for this novel class of anticoagulant and clinical trials evaluating factor XI inhibitors for the treatment of cancer-associated thrombosis are ongoing, including the ASTER & MAGNOLIA randomised trials which are comparing the FXI inhibitor abelacimab to apixaban or dalteparin in the management of cancer-associated thrombosis (ClinicalTrials.gov Identifier NCT05171049). Conclusion VTE remains a common complication of cancer therapy despite the advances in preventative and therapeutic strategies which have been made in recent decades. As our population ages and as more people with cancer survive longer with their disease as a result of advances in cancer therapy, it is likely that the number of patients at risk of strategiesasassociatedGiventhrombosiscancer-associatedwillcontinuetorise.theburdenofmorbiditywithVTEaswellthepotentialmortalityrisk,forimprovedprevention, diagnosis and treatment of cancer-associated thrombosis are clearly needed. The level of awareness of VTE risk among patients with cancer appears to be low. Patient organisations such as Thrombosis Ireland have recognised this deficit and have championed efforts to prioritise patient education in our hospitals. This can only succeed with the support of healthcare providers, healthcare administrators and all other stakeholders involved in cancer care in this country. As we look to the future it is clear that a number of other key issues need to be addressed. Firstly, while current evidence appears to support primary settinginterventionofMoreover,derive‘at-risk’meanshaveambulatorythromboprophylaxispharmacologicalforselectedcancerpatients,weyettodeterminetheoptimalofidentifyingthemostpatientswhowouldlikelybenefitfromthisstrategy.theabsolutebalancebenefitversusriskforthisinthe‘real-world’isuncertain.Secondly, while the recent clinical trials of DOAC therapy for cancerassociated thrombosis have increased the number of potential therapeutic options available to clinicians for managing VTE, rates of VTE recurrence and bleeding remain high. It remains to be seen if new strategies aimed at novel coagulation targets may help to bridge this gap. Addressing these important clinical questions will represent a major challenge for clinicians and researcher alike but will be crucial if we are to continue to improve outcomes for patients, their families and care-givers.
While the debate regarding the optimal use of thromboprophylaxisprimaryinthe cancer population is likely to continue over the coming years, all stakeholders appear to be united in agreement that improving awareness of thrombosis risk among patients and healthcare providers should be prioritised. Taking simple steps, such as providing patients with written information relating to their VTE risk and the associated symptoms may reduce the risk of delaying treatment of a potentially life-threatening event.
Diagnosis cancer-associatedof VTE
ONCOLOGY FOCUS: THROMBOSIS 2.5mg BD and rivaroxaban 10mg OD respectively in patients with Khorana scores of 2 or more) demonstrated that prophylaxis with these reduced the risk of thrombosis in patients commencing cancer therapy (although this did not achieve statistical significance in the CASSINI trial).17, 18 A systematic review and metaanalysis incorporating data from both these DOAC trials as well as several earlier LMWH trials (using a post-hoc application of the Khorana Score), suggested that the use of pharmacological thromboprophylaxis in patients with a Khorana score of 2 or more significantly reduces the risk of thrombosis in that population (relative risk 0.51; 95% CI 0.34-67) with a number needed to treat (NNT) of 25; without significantly increasing the risk of bleeding (but also without any significant difference in all-cause mortality).19 These and other data have subsequently shaped international clinical practice guidelines with recent guidance from bodies such as the American Society of Hematology, American Society of Clinical Oncology and the National Comprehensive Cancer Network suggesting that primary prophylaxis be considered for cancer outpatients who are about to commence chemotherapy and who are deemed to be at intermediate to high risk of thrombosis based on Khorana score.13, 14, 20










DATE OF REVISION: December 2021. PI-1404-005 Abbreviations: EASI – eczema activity and severity index; NRS – numerical rating scale; QD – once daily; EU European Union. * The recommended dose of RINVOQ is 15mg once daily for adolescents weighing at least 30kg. The safety and efficacy of RINVOQ in children with atopic dermatitis below the age of 12 years have not been established. No data are available. No clinical exposure data are available in adolescents <40kg. The posology in adolescent patients 30kg to <40kg was determined using population pharmacokinetic modelling and simulation.2 Reference: 1. Langan S. et al. Atopic dermatitis. The Lancet. 2020;396(10247):345-360. DOI: https://doi.org/10.1016/ S0140-6736(20)31286-1. 2. RINVOQ Summary of Product Characteristics, available on www.medicines.ie 3. Baricitinib Summary of Product Characteristics, available on www.medicines.ie 4. Abrocitinib Summary of Product Characteristics, available on www.medicines.ie ©2022
Venous thromboembolism: Deep vein thrombosis (DVT) and pulmonary embolism (PE) have been reported in patients receiving JAKi, including upadacitinib. Use therapy with caution in patients at high risk for DVT/PE. Risk factors should be determined by patients age, obesity and medical history of DVT/PE, patients undergoing major surgery and prolonged immobilisation. If clinical features of DVT/PE occur discontinue therapy, evaluate and treat promptly.
Hepatic transaminase elevations: Monitor liver enzymes at baseline and thereafter according to routine patient management. Prompt investigation of the cause of liver enzyme elevation is recommended to identify potential cases of drug-induced liver injury. In such cases therapy should be interrupted until this diagnosis is excluded.
AbbVie Inc. All rights reserved. IE-RNQ_AD-220017 | February 2022 THE ITCH & RASH OF MODERATE TO SEVERE ATOPIC DERMATITIS 1 HELP YOUR PATIENTS RINVOQ demonstrated in an integrated analysis of the MEASURE UP 1 & 2 monotherapy studies at Week 16: • EASI 75 skin clearance rates of 76% and 65% for patients treated with RINVOQ 30 mg QD and 15 mg QD, respectively, vs 15% with placebo (p<0.001 for both comparisons)2 • Itch reduction (mean percent change from baseline in Worst Pruritus NRS) of –70% and –58% for RINVOQ 30 mg QD and 15 mg QD, respectively, vs –24% with placebo (p<0.001 for both comparisons)2 RINVOQ, the first and only oral JAK inhibitor indicated for the treatment of both adults and adolescents ≥12 years* with moderate to severe Atopic Dermatitis in the EU2-4 page 1 of 3. This is a paid advertisement sponsored by AbbVie, it is part of a 3-page advertisement. Prescribing information for RINVOQ can be found on page 1 and for SKYRIZI on page 3
PRESCRIBING INFORMATION (PI) RINVOQ® (upadacitinib) 15 mg and 30mg prolonged-release tablets. Refer to Summary of Product Characteristics (SmPC) for full prescribing information. PRESENTATION: Each 15 mg prolonged-release tablet contains upadacitinib hemihydrate, equivalent to 15mg of upadacitinib. Each 30mg prolonged-release tablet contains upadacitinib hemihydrate, equivalent to 30 mg of upadacitinib. INDICATION: Treatment of moderate to severe active rheumatoid arthritis (RA) and active psoriatic arthritis (PsA) in adult patients who have responded inadequately to, or who are intolerant to one or more disease-modifying anti-rheumatic drugs (DMARDs). RINVOQ may be used as monotherapy or in combination with methotrexate. Treatment of active ankylosing spondylitis (AS) in adult patients who have responded inadequately to conventional therapy. Treatment of moderate to severe atopic dermatitis (AD) in adults and adolescents 12 years and older who are candidates for systemic therapy. DOSAGE AND ADMINISTRATION: Intended for use under guidance and supervision of a physician experienced in diagnosis and treatment of conditions for which upadacitinib is indicated. Dosage: RA, PsA and AS: The recommended oral dose is 15mg once daily. Consideration should be given to discontinuing treatment in patients with AS who have shown no clinical response after 16 weeks of treatment. Some patients with initial partial response may subsequently improve with continued treatment beyond 16 weeks. AD (adults): The recommended oral dose is 15 mg or 30 mg once daily based on individual patient presentation. 30 mg once daily dose may be appropriate for patients with high disease burden and for patients with an inadequate response to 15 mg once daily. The lowest effective dose for maintenance should be considered. For patients ≥ 65 years of age, the recommended dose is 15mg once daily. AD (adolescents from 12 to 17 years): The recommended oral dose is 15mg once daily for adolescents weighing at least 30 kg. Adults and adolescents 12 years and older: Upadacitinib can be used with or without topical corticosteroids. Topical calcineurin inhibitors may be used for sensitive areas such as the face, neck, and intertriginous and genital areas. Consideration should be given to discontinuing upadacitinib treatment in any patient who shows no evidence of therapeutic benefit after 12 weeks of treatment. Special Populations: Elderly: For AD, doses higher than 15mg once daily not recommended in patients aged 65 years and older. Limited data for patients aged 75 and older. Renal: No dose adjustment required in mild-moderate renal impairment. Upadacitinib 15mg once daily should be used with caution in patients with severe renal impairment. Upadacitinib 30 mg once daily is not recommended for patients with severe renal impairment. Upadacitinib has not been studied in subjects with end stage renal disease. Hepatic impairment: No dose adjustment is required in patients with mild (Child Pugh A) or moderate (Child Pugh B) hepatic impairment. Should not be used in patients with severe (Child Pugh C) hepatic impairment. Paediatric Population: No data available in the following paediatric patient populations: children with AD below the age of 12 years; children and adolescents with RA, PsA and AS aged 0 to less than 18 years. CONTRAINDICATIONS: Hypersensitivity to active substance or excipients. Active tuberculosis (TB) or active serious infections. Severe hepatic impairment. Pregnancy. SPECIAL WARNINGS AND
INTERACTIONS: Upadacitinib is metabolised mainly by CYP3A4 and plasma exposures may be affected by CYP3A4 inhibitors or inducers. Upadacitinib 15 mg once daily should be used with caution in patients receiving chronic treatment with strong CYP3A4 inhibitors. Upadacitinib 30 mg once daily dose is not recommended for patients receiving chronic treatment with strong CYP3A4 inhibitors. See SmPC for full details. FERTILITY, PREGNANCY AND LACTATION: Upadacitinib is contraindicated during pregnancy. Women of childbearing potential should be advised to use effective contraception during treatment and for 4 weeks following the final dose of upadacitinib. Female paediatric patients and/or their parents/caregivers should be informed about the need to contact the treating physician once the patient experiences menarche while taking upadacitinib. Upadacitinib should not be used during breast-feeding. The effect of upadacitinib on human fertility has not been evaluated. ADVERSE REACTIONS: Refer to SmPC for full details on adverse reactions. Very common adverse reactions (≥1/10): upper respiratory tract infections, acne. Common adverse reactions (≥1/100 to <1/10): bronchitis, herpes zoster, herpes simplex, folliculitis, influenza, anaemia, neutropaenia, hypercholesterolaemia, cough, abdominal pain, nausea, urticaria, fatigue, pyrexia, increased blood CPK/ALT/AST, increased weight and headache. This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie. LEGAL CLASSIFICATION: POM (S1A). MARKETING AUTHORISATION NUMBER/ PRESENTATION: EU/1/19/1404/001 and EU/1/19/1404/006 – Calendar blister packs containing 28 prolonged-release tablets. MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany. Further information is available from AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24, Ireland.
PRECAUTIONS: See SmPC for full details. Immunosuppression: Combination use, with immunosuppressants e.g. azathioprine, ciclosporin, tacrolimus, and biologic DMARDs or other JAK inhibitors has not been evaluated in clinical studies and is not recommended as the risk of additive immunosuppression cannot be excluded. Serious infections: Serious and fatal infections have been reported. Caution when treating patients ≥65 years. Frequently reported – pneumonia and cellulitis. Bacterial meningitis has been reported. Opportunistic infections reported –TB, multidermatomal herpes zoster, oral/oesophageal candidiasis, and cryptococcosis. Do not initiate treatment in patients with active, serious infection, including localised infections. Consider the risk/benefit of treatment in patients with: chronic or recurrent infection, history of serious or opportunistic infection, those exposed to TB, those who have resided or travelled in areas of endemic TB or endemic mycoses, those with underlying conditions that may pre-dispose patients to infection. Closely monitor patients and interrupt treatment if there are signs and symptoms of infection pre and post treatment. Tuberculosis: Pre-screen patients for active or latent TB. RINVOQ should not be given to patients with active TB. Consider anti-TB therapy in patients with previously untreated latent TB or in patients with risk factors for TB infection. Consult with a physician with experience in TB therapy to assess whether initiating anti-TB therapy is appropriate for an individual patient. Monitor patients for the development of signs and symptoms of TB, including patients who tested negative for latent TB infection prior to initiating therapy. Viral reactivation: Cases of herpes virus reactivation have been reported e.g. herpes zoster. If herpes zoster is reactivated, consider interruption of upadacitinib therapy until the episode resolves. Screen for viral hepatitis and monitor regularly for reactivation before starting and during therapy with upadacitinib. Patients, positive for hepatitis C antibody/hepatitis C virus RNA and hepatitis B surface antigen/hepatitis B virus DNA were excluded from clinical studies. If hepatitis B virus DNA is detected while receiving RINVOQ, a liver specialist should be consulted. Vaccination: Use of live, attenuated vaccines during or immediately prior to therapy is not recommended. It is recommended that patients be brought up to date with all immunisations, including prophylactic zoster vaccinations prior to starting therapy, in agreement with current immunisation guidelines. Malignancy: Immunomodulatory therapies may increase the risk of malignancies including lymphoma and nonmelanoma skin cancer in RA patients. Malignancies were observed in clinical studies. Periodic skin examination recommended for patients who are at increased risk for skin cancer. See SmPC for full details. Haematological abnormalities: Do not start therapy if Absolute Neutrophil Count <1 x 109 cells/L, Absolute Lymphocyte Count <0.5 x 109 cells/L and Hb <8 g/dL. Monitor patients and temporarily stop therapy if abnormal haematological parameters as specified are detected during routine patient management. Diverticulitis: Events of diverticulitis have been reported in clinical trials and post-marketing. Upadacitinib should be used with caution in patients with diverticular disease and especially in patients chronically treated with concomitant medications associated with an increased risk of diverticulitis. Patients presenting with new onset abdominal signs and symptoms should be evaluated promptly for early identification of diverticulitis to prevent gastrointestinal perforation. Cardiovascular Risk: RA patients have an increased risk for cardiovascular disorders. Manage patient’s risk factors for e.g. hypertension, hyperlipidaemia as per usual standard of care. Lipids: Monitor total cholesterol, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) at 12 weeks and thereafter according to international guidelines. Elevated LDL in clinical trials decreased to pre-treatment levels in response to statin therapy, although evidence is limited. The effect of these lipid parameter elevations on cardiovascular morbidity and mortality has not been determined.


Among the good news shared was the recent reimbursement of SKYRIZI for Psoriasis and RINVOQ for Atopic Dermatitis. Keynote speakers on the evening were Prof. Caitriona Ryan who presented on IL23 inhibition in Practice: Clinical Case Studies and Dr. Andrew Blauvelt who presented on Challenging AD Expectations: Challenging treatment goals for patients with moderate to severe Atopic Dermatitis. The interactive nature of both sessions was greatly received by all those in attendance. Dr. Andrew Blauvelt, President of Oregon Medical Research Center, a small business dedicated to performing high quality clinical research studies in dermatology. Professor Caitriona Ryan, Consultant Dermatologist and Co-Founder at the Institute of Dermatologists and an Associate Clinical Professor at University College Dublin. * SKYRIZI for Psoriasis and RINVOQ for Atopic Dermatitis ©2022 AbbVie Inc. All rights reserved. IE-RNQ_AD-220057 | June 2022 IN PSORIASIS ATOPIC DERMATITIS”*
AND
A MEETING ENTITLED “ABBVIE INNOVATIONS
Thursday May 5th, 2022 AbbVie were delighted to host the first face-to-face symposium since 2019 at the Irish Association of Dermatologists Spring Meeting 2022 which took place on May 5th in the Grand Hotel, Malahide, Dublin.
and
on page 3
L-R: Isobel Bird, Brand Manager, AbbVie; Dr. Andrew Blauvelt; Marie Kennedy, Senior Product Specialist, AbbVie; Deirdre Callaghan, Senior Product Specialist, AbbVie L-R: Dr. Andrew Blauvelt and Prof. Caitriona Ryan page 2 of 3. This is a paid advertisement sponsored by AbbVie, it is part of a 3-page advertisement. Prescribing information for RINVOQ can be found on page 1 for SKYRIZI










▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; Website: www.hpra.ie. Suspected adverse events should also be reported to AbbVie Limited on 01-4287900.
REFERENCES: 1. Gordon KB, et al. Lancet 2018; 392: 650-661. 2. Ryan C et al. Poster presented at the 27th European Academy of Dermatology & Venerology (EADV) Congress 2018; September 12–16; Paris, France.
PREGNANCY AND LACTATION: Women of Childbearing potential: An effective method of contraception during treatment and for at least 21 weeks after treatment should be used. Pregnancy: Limited data available. It is preferable to avoid the use of Skyrizi during pregnancy as a precautionary measure. Lactation: It is not known whether Skyrizi is excreted in breast milk. Human IgGs are known to be excreted in breast milk during the first few days after birth, which decreases to low concentrations soon afterwards; consequently, a risk to the breast-fed infant cannot be excluded during this short period. A decision should be made whether to discontinue/abstain from Skyrizi therapy, taking into account the benefit of breastfeeding to the child and the benefit of Skyrizi therapy to the woman. Fertility: The effect of Skyrizi on human fertility has not been evaluated.
WARNINGS AND PRECAUTIONS: See SmPC for full details. In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Skyrizi may increase the risk of infections. In patients with a chronic infection or history of recurrent infections, or known risk factors for infection, Skyrizi should be used with caution. Treatment with Skyrizi should not be initiated in patients with any clinically important active infection until the infection resolves or is adequately treated. Patients should be evaluated for tuberculosis infection prior to initiating treatment. Anti-TB therapy should be considered prior to initiating Skyrizi in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed. Completion of all appropriate immunisations should be considered prior to initiating therapy. If a patient has received live vaccination (viral or bacterial), it is recommended to wait at least 4 weeks prior to starting treatment with Skyrizi. Patients treated with Skyrizi should not receive live vaccines during treatment and for at least 21 weeks after treatment. If a serious hypersensivity reaction occurs, administration of Skyrizi should be discontinued immediately and appropriate therapy initiated. Excipients with known effect (75 mg solution for injection only): Skyrizi contains 68.0 mg sorbitol and less than 1 mmol sodium (23 mg) per 150 mg dose. INTERACTIONS: The safety and efficacy of Skyrizi in combination with immunosuppressants, including biologics or phototherapy have not been evaluated.
When it comes to your patient’s psoriasis treatment goals
* Nothing on the skin: Defined as 75% achievement of PASI90 at Week 16 and ≥50% achievement of PASI 100 at Week 52 in UltIMMa-1 and UltIMMa-2.1 High skin clearance matters to patients: Patients who achieve and maintain high levels of skin clearance (PASI 90-99 or PASI 100) have significantly better HRQoL than those with lower levels of skin clearance (PASI 75-89).2 Sustaining high skin clearance or complete skin clearance is associated with incremental and durable benefits in HRQoL and mental health of psoriasis patients.2
What means everything to the patient?
PRESCRIBING INFORMATION (PI). SKYRIZI®▼ (risankizumab) 75 mg solution for injection in prefilled syringe; Skyrizi 150 mg solution for injection in pre-filled pen and Skyrizi 150 mg solution for injection in prefilled syringe. Refer to Summary of Product Characteristics (SmPC) for full information before prescribing. PRESENTATION: Skyrizi 150 mg solution for injection in pre-filled pen/syringe: each prefilled pen/syringe contains 150 mg risankizumab in 1 mL solution. Skyrizi 75 mg solution for injection in pre-filled syringe: each pre-filled syringe contains 75 mg risankizumab in 0.83 ml mL solution. INDICATION: Plaque Psoriasis: For treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy. Psoriatic Arthritis: alone or in combination with methotrexate (MTX), is indicated for the treatment of active psoriatic arthritis in adults who have had an inadequate response or who have been intolerant to one or more disease-modifying antirheumatic drugs (DMARDs). DOSAGE AND ADMINISTRATION: Intended for use under guidance and supervision of a physician experienced in diagnosis and treatment of psoriasis. Dosage: The recommended dose of Skyrizi is 150 mg by subcutaneous injection at weeks 0, 4, and every 12 weeks thereafter (either as two 75 mg pre-filled syringe injections or one 150 mg pre-filled pen or pre-filled syringe injection). Two 75mg pre-filled syringes should be injected for the full 150 mg dose. Consider discontinuation of treatment in patients showing no response after 16 weeks of treatment. Some patients with initial partial response may subsequently improve with continued treatment beyond 16 weeks. Special Populations: Elderly: No dose adjustment required. Renal or hepatic impairment: No dose adjustment required. Paediatric Population: No data available. Overweight patients: No dose adjustment required. CONTRAINDICATIONS: Hypersensitivity to any of the active substances or excipients. Clinically important active infections (e.g. active tuberculosis). SPECIAL
Skyrizi® Summary of Product Characteristics, available on www.medicines.ie.
ADVERSE REACTIONS: See SmPC for full details on adverse reactions. Very common adverse reactions (≥1/10): Upper respiratory infections. Common adverse reactions (≥1/100 to <1/10): Tinea infections, headache, pruritus, fatigue and injection site reactions.
The potential for nothing left on their skin.1,2
Date of preparation: April 2022 | IE-RISN-220005 page 3 of 3. This is a paid advertisement sponsored by AbbVie, it is part of a 3-page advertisement. Prescribing information for RINVOQ can be found on page 1 and for SKYRIZI on page 3
LEGAL CLASSIFICATION: POM (S1A). MARKETING AUTHORISATION NUMBERS/PRESENTATIONS: Skyrizi 75 mg solution for injection in pre-filled syringe (Pack of 2 pre-filled syringes): EU/1/19/1361/001; Skyrizi 150 mg solution for injection in pre-filled pen: EU/1/19/1361/002; Skyrizi 150 mg solution for injection in prefilled syringe: EU/1/19/1361/003. Not all presentations may be marketed. Further information is available from: AbbVie Ltd., 14 Riverwalk, Citywest Business Campus, Dublin 24, D24XN32. DATE OF REVISION: November 2021 PI/1361/004 HRQoL, Health-Related Quality of Life; PASI, Psoriasis Area Severity Index.


ECOP 5 included two main exhibition areas - an exhibition space for pharmaceutical companies, and a second space for display of posters. The industry exhibition included demonstrations of automated and semi-automated devices for use in aseptic compounding units, including robotic systems for compounding of chemotherapy, and filling devices to reduce the risk of repetitive strain industry. Other booths had clean room equipment and consumables on display, and there was ample opportunity for conference attendees to liaise with industry colleagues.
The conference schedule, along with organised social events, allowed conference attendees to forge new friendships, share experiences and discuss differences and similarities in oncology pharmacy practice worldwide.
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 51
The programme for the conference was varied, with topics ranging from updates in cancer research and treatment to lectures on recent developments in robotics and automation in aseptic preparation to practicebased sessions on drug shortages, complementary and alternative medicine, and the role of pharmacy in CAR T-cell therapy. Some workshop sessions included interactive components, for example, during a workshop session on drug stabilities, the audience were invited to submit answers live on an app during the workshop, with the results of the interactive polls and multiplechoice questions displayed on screen. This allowed for
Over 150 abstracts were chosen by the ECOP 5 Scientific Committee for poster presentation at the conference. The posters covered a broad range of topics in relation to oncology pharmacy, ranging from research to practicebased studies. The posters were categorised into several key areas including cytotoxic drug preparation, clinical pharmacy and pharmaceutical care, drug stability and quality management. A section of the poster exhibition was dedicated to “One Day in Oncology Pharmacy” posters. ESOP members had previously been distributed a brief survey which included questions about typical oncology pharmacy work tasks, ranging from dispensing of oral anti-cancer medications, compounding versus outsourcing of parenteral anti-cancer medications, patient counselling etc. For each country that responded to the survey, a liaison for that country had an opportunity to compile results from the surveys received, and to present the findings in a poster. These posters showcased the work carried out in relation to oncology pharmacy in countries across the world.
The European Society of Oncology Pharmacy (ESOP), founded in 2000 in Prague, is the largest organisation of oncology pharmacists in the world, with a membership of over 4000 members from 66 countries. The overall aim of ESOP is to support optimal treatment for cancer patients.
Membership of ESOP offers many benefits, including access to standards and evidencebased materials, opportunity to participate in further education in oncology pharmacy, and the chance to be part of a global community. While most ESOP members work in oncology pharmacy, membership is open to all healthcare professionals with an interest in oncology pharmacy. The membership fee for Irish members in 2022 is ¤5 (per person, per year). If you would like to join ESOP, please contact the Irish liaison for ESOP, Caoimhe O’Leary, at co@esop.li or for general enquiries, membershipservice@esop.li.contact
Caoimhe O'Leary
ECOP 5 presented an opportunity to once again have an in-person conference after a hiatus due to the Covid-19 pandemic, allowing face-to-face exchange of knowledge and ideas, and the meeting of colleagues from all over the world with an interest in oncology pharmacy.
ONCOLOGY FOCUS: ONCOLOGY PHARMACY
European Conference of Oncology Pharmacy audience interaction, and sparked discussion among presenters and attendees.
ECOP 5 included over 30 hours of advanced education, held over 3 days, with keynote lectures, practical and clinical lecture sessions, workshops, scientific symposia, and poster sessions. The target audience for the conference included oncology pharmacists, hospital and community pharmacists, physicians and nurses working in oncology and those working in the pharmaceutical industry with an interest in oncology pharmacy. The aim of ECOP 5 was to equip oncology pharmacy practitioners with knowledge about recent developments in oncology, to advance the effectiveness of healthcare delivery and to increase the quality of patient care.
Written by Caoimhe O'Leary, Senior Pharmacist, National Cancer Control Programme & Klaus Meier, President of the European Society of Oncology Pharmacy Klaus Meier
ECOP 5 also presented an opportunity to develop a network of international colleagues with an interest in oncology pharmacy. The conference schedule, along with organised social events, allowed conference attendees to forge new friendships, share experiences and discuss differences and similarities in oncology pharmacy practice worldwide.
There were several joint symposia offered between ESOP and other organisations, including symposia with speakers from the European Cancer Patient Coalition, the European Society for Paediatric Oncology, and the International Society of Geriatric Oncology. Updates on ESOP research projects and activities were also presented. Most of the sessions were delivered in English, with a small minority delivered in German. For the German sessions, simultaneous translation via a headset was available, which worked smoothly.
The 5th European Conference of Oncology Pharmacy (ECOP 5) was recently held in Hamburg from June 30th to July 2nd, 2022.


SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Written by Dr Roisin McAvera (Postdoctoral researcher) and Professor Siobhan Glavey (consultant haematologist & clinician scientist), Royal College of Surgeons in Ireland & Beaumont Hospital Dublin
52 ONCOLOGY
Treatment of MM normally consists of a combination of two, three or even four drugs from different classes. With so many drugs available now, it can be difficult for clinicians to decide in which sequence therapies should be given. There is no one-size-fits-all approach to treatment as each patient is different. Treatment approaches vary, depending on patient fitness, co-morbidities, disease features and eligibility for an autologous stem cell transplant (ASCT). Additionally, practice is moving towards trying to personalise therapy options for high-risk patients, however clinically available biomarkers to direct this approach are lacking. High-risk patients are most commonly defined by their cytogenetic profile,
Alkylating agents are described as DNA intercalating agents causing DNA damage and later cell death.
Introduction Multiple myeloma (MM) is a haematological malignancy characterised by the clonal expansion of malignant plasma cells in the bone marrow. MM manifests clinically as hypercalcaemia, renal failure, anaemia and bone lesions (known as CRAB features), and is most common in people aged over 65 years. MM affects around 361 people in Ireland each year,1 and despite advancements in treatments remains incurable in 2022.
important than numerical age. Regimens like VMP and Rd are preferable for older, frailer patients who are not transplant eligible. Despite the discovery of effective monoclonal antibodies (daratumumab, isatuximab), immune modulators (lenalidomide) and other therapies, MM remains an incurable disease. Even with successful initial treatment, the disease follows a remitting and relapsing course with accumulation of toxicity and a decline in bone marrow function over time. Treatment at relapse is decided based on disease and patient factors, with resistance to prior therapies being a major issue. There is much debate on whether an aggressive multidrug approach that ensures a better response should be prioritised over a sequential disease control approach that considers quality of life as well as overall survival.2
Bone marrow microenvironment cells offer MM cells a protective niche – interrupting this relationship has been a major source of breakthroughs in MM therapy. The main target of IMiDs FOCUS: MULTIPLE MYELOMA
In this article, we briefly outline the available therapies for MM and their mechanisms of action. We discuss treatment options at diagnosis followed by treatment at each relapse and how they can be sequenced to aim for optimal outcome. Finally, we also discuss some novel agents in clinical trials for MM and how they are likely to influence the future disease landscape.
Dr Roisin McAvera
Prof. Siobhán Glavey Consultant Haematologist/Clinician Scientist, Beaumont Hospital and RCSI
Initial treatment in Ireland at present consists of one of the following National Cancer Control Programme (NCCP) approved regimens; RVD (bortezomib, lenalidomide, dexamethasone), VMP (bortezomib, melphalan, prednisone), factor,frailtybyTreatmentthalidomide,D-VTDdexamethasone)dexamethasone),(cyclophosphamide,CyBorDbortezomib,Rd(lenalidomide,ormostrecently(daratumumab,bortezomib,dexamethasone).choiceislargelyguidedpatient“fitness”intermsofandco-morbidities,ageisabutbiologicalageismore
with the presence of del(17p), t(4;14), t(14;16), t(14;20), or gain(1q) associated with high-risk disease. Generally, this indicates a predicted overall survival of approximately 3 years.2 Alternatively, standard-risk patients have an overall survival of 7-10 years and cytogenetic abnormalities associated with this outcome include t(11;14), t(6;14) and trisomies of odd numbered chromosomes 3, 5, 7, 9, 11, 15, 19 and Treatment21.2
Proteasome inhibitors have been approved for MM for the last two decades and are largely responsible for the unprecedented improvement in overall survival seen in Ireland in recent data. MM cells rely heavily on proteasome, and proteasome inhibition prevents the degradation of pro-apoptotic proteins, inhibition of NF-κB and ultimately cell death.4 Bortezomib was the first proteasome inhibitor approved in 2003 for both newly diagnosed and relapsed/refractory MM and since then has been followed by carfilzomib and ixazomib which are currently approved for relapsed/ refractory MM.3
Sequencing of Treatment in Multiple Myeloma
Thalidomide, lenalidomide and pomalidomide are IMiDs - they alter the immune system, namely the interaction between MM cells and the surrounding bone marrow.
at diagnosis is focused on getting the patient into a deep remission – measured by a reduction in serum paraprotein, normalisation of the light chain ratio and reduction in the percentage of bone marrow plasma cells.
Myeloma Therapies
Corticosteroids work by inhibiting cytokines and NF-κB signalling which is vital for myeloma growth.
Professor Siobhan Glavey
Sullivan Research Fellow, Therapeutics in Cancer RCSI Dr. Tríona Ní Chonghaile Group Leader, Targeted Therapeutics in Cancer Laboratory, RCSI
There are various therapies approved by the US Food and Drug Administration (FDA), the European medicines agency (EMA) and the NCCP for the treatment of MM. These can be divided into several main classes: corticosteroids, alkylating agents, anthracyclines, proteasome inhibitors, immunomodulatory agents (IMiDs), monoclonal antibodies (mAbs), and nuclear export inhibitors (outlined in Table 1). Additionally, at diagnosis, patients who are well enough will be considered for an ASCT.
Corticosteroids and alkylating agents have been available for many decades for MM treatment, with the alkylating agent melphalan and corticosteroid prednisone previously being the most common treatments used. Corticosteroids remain a backbone of MM treatment and are directly toxic to MM cells while also sensitising cells to newer therapies.3



Treatment of Newly Diagnosed Multiple Myeloma
Patients deemed eligible to receive an ASCT will typically receive 4-6 cycles of induction therapy followed by a stem cell harvest. A patient’s stem cells are harvested and stored until they are ready to receive them back as a stem cell transplant. Following treatment for MM, the aim is that malignant cells will have been reduced or completely removed, and are then replaced with the patient’s healthy stem cells which can become new healthy blood cells.
Transplant-Ineligible
10 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 53 Drug Class Approved agent Corticosteroids DexamethasonePrednisone Alkylating Agents CyclophosphamideMelphalan Anthracyclines Doxorubicin Immunomodulatory Drugs (IMiDs) PomalidomideLenalidomideThalidomide Proteasome Inhibitors (PIs) IxazomibCarfilzomibBortezomib Monoclonal Antibodies (mAb) Daratumumab (anti-CD38) Elotuzumab (anti-SLAMF7) Isatuximab (anti-CD38) Nuclear Export Inhibitors Selinexor (XPO1) Table 1. Current FDA-approved therapies for MM
At diagnosis, MM patients can be widely classified as either eligible for an ASCT, or ineligible for an ASCT. The factors considered for eligibility are based on a patient’s ‘fitness’ given the intensive nature of an ASCT, namely existing comorbidities (such as renal failure, cardiovascular disease etc.) and age. Patients over 75 years old are unlikely to be considered eligible due to the higher risk of toxicity and the availability of effective treatments for these patients. Initial treatment will vary depending on if a patient is to receive an ASCT or not.
As outlined above, various regimens are approved for the initial treatment of patients who are not transplant eligible. Results from recent clinical trials have shown that the addition of daratumumab can enhance the depth of response at diagnosis and improve outcomes.2 Generally, induction therapy is administered for 8-12 cycles followed in some cases by maintenance therapy. Maintenance therapy is most commonly lenalidomide, and in frail, elderly patients, a lower dose of lenalidomide may be better tolerated. Maintenance with bortezomib or lenalidomide is recommended for patients with high-risk myeloma, however in some frail patients, this may not be well tolerated and an important consideration is quality of life.
Treatment of Relapsed & Refractory Myeloma MM remains incurable as patients will eventually become relapsed or refractory to treatment following remission, with treatment being required once a patient is symptomatic. This can occur multiple times and thus adequate sequencing of therapies at this point is carefully considered to ensure the best outcome. The choice of treatment at relapse will depend on which regimen the patient received as their previous line(s) of therapy and their initial response, cytogenetics, aggressiveness of the relapse, and again the patient’s fitness and quality of life (Figure 1).8, 9 Many MM patients will receive five or more lines of therapy over many years, while other life circumstances and co-morbidities also develop. These patients are ideally treated on a clinical trial, which can provide access to the best standard of care and novel agents for MM.
is thought to be cereblon which targets two transcription factors IKZF1 and IKZF2 which are important for MM survival.2 For many years, there was a lack of effective mAb therapy for MM patients, in contrast to diseases like lymphoma. The discovery of CD38 as a target has changed the treatment landscape in MM and patients now have access to Daratumumab, and isatuximab in the relapsed and clinical trial setting, respectively.2 More recently the nuclear export inhibitor Selinexor has been FDA approved in the US (not available in Ireland currently) for treatment of relapsed MM. Selinexor inhibits exportin 1 (XPO1) which normally exports tumour suppressor and growth regulatory proteins out of the nucleus. When inhibited this ultimately results in suppression of NF-κB and upregulation of apoptosis.2
In Ireland, there are several NCCP approved regimens for treatment of relapsed and refractory myeloma; RVD (bortezomib, lenalidomide and dexamethasone), bortezomib and dexamethasone (VD), CyBorD/cyclophosphamide, VD (bortezomib Atanddexamethasone),(ixazomib,and(daratumumab,andKRd(carfilzomibandmonotherapy,dexamethasone),anddaratumumabpomalidomidedexamethasone,Kdanddexamethasone),(carfilzomib,lenalidomidedexamethasone),DVdbortezomibdexamethasone),IRDlenalidomideandandlenalidomidedexamethasone.firstrelapse,generallyatriplet
Transplant-Eligible Due to superior response rates and greater progression free (PFS) and overall survival (OS) standard of care induction regimens now include both a proteasome inhibitor and an immunomodulatory drug for transplant eligible patients
Induction regimens incorporating novel therapies have resulted in median PFS of more than 30 months and 5-year OS rates of more than 70%.5 Ideally, patients will be treated on a clinical trial which can help to provide the highest standard of care to cancer patients.
regimen is recommended with the incorporation of a therapy the patient has not been exposed to in the recent past.2, 8 Treatment is continued until progression unless the patient cannot tolerate the regimen. If a patient received first line bortezomib-based therapy, they can receive a lenalidomidebased regimen at relapse. Vice versa, if a patient becomes refractory during continuous lenalidomide maintenance, a patient may receive a bortezomibbased regimen.
There is much international debate regarding timing of ASCT, with some experts favouring to delay ASCT beyond the initial treatment phase due to the success of newer therapies. However, the IFM-2009 trial prospectively confirmed that, combined with novel agent triplet induction, upfront ASCT was associated with a superior PFS (50 vs. 36) months.6, 7 In Ireland, ASCT is offered as part of induction to patients who are transplant eligible. Studies have also investigated the role of a second, tandem ASCT with results being contradictory as to whether it is beneficial for overall survival. Generally, routine tandem ASCT is not recommended outside of clinical trials, but may be considered for high-risk patients or patients who did not show a complete response after their first ASCT.2
Future Treatment of Myeloma
Biomarkers which can be used to decide in advance, which patients might benefit from a more intensive or less intensive approach are now even more essential.
Treatment of MM is changing rapidly and there are now several clinical trials internationally, which are exploring the utility of entirely new mechanisms of killing MM cells. This includes chimeric antigen receptor-T (CAR-T) cell therapy which is likely to change the life expectancy and treatment approach for MM patients drastically in the near future. In brief, this immunologic approach uses T-cells harvested from the patient, which are then genetically engineered to make them target MM cells and kill those cells. These T-cells are then re-infused back to the patient where they specifically home to and kill MM cells. CARs are hybrid molecules that contain both an antigenrecognition domain and T-cell activation domains. T- (11). Most CAR-T therapies, in trial, target BCMA, but SLAMF7, CD19 and CD38 CAR-T approaches are also used in clinical trials for MM. Most of these therapies are being trialled in relapsed refractory patients, and research should aim to determine at what point receiving these therapies is most beneficial. It is possible in the future that CAR-T cells will replace ASCT in MM patients. Other targeted approaches in clinical development aim to focus on specific subgroups of MM patients who have individual genetic signatures, in a more personalised approach. Venetoclax is an inhibitor of anti-apoptotic protein BCL-2 which has shown promise specifically in patients with a t(11;14) translocation.12 There are several trials investigating this, focusing on this subgroup of patients at relapse, and venetoclax has potential to become one of the first genetically targeted drug for MM patients. Bispecific antibodies are another emerging immunologic approach, these can bind both plasma myeloma cells and T-cells simultaneously to target plasma cells for T-cell mediated death. Several trials are investigating bispecific antibodies that bind B-cell maturation antigen (BCMA) which is specifically expressed on plasma cells, and CD3 expressed on T-cells.2 Teclistamab and Elranatamab are both BCMAtargeting bispecific antibodies in trial, which may be accessed in Ireland through managed access programs. Both of these have shown clinical efficacy in relapsed refractory MM. Additionally, novel mAb Belantamab can also be accessed through such trials and also targets BCMA.
ASCT- autologous stem cell transplant; IMiD - immunomodulatory agent; PI – proteasome inhibitor
Magazine July
Future of pharmacIE Event
versa, if a patient becomes refractory during continuous lenalidomide maintenance, a patient receive a bortezomib based regimen (10).
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 54 ONCOLOGY FOCUS: MULTIPLE MYELOMA
1. Considerations for therapy options at relapse autologous stem cell transplant; IMiD immunomodulatory agent; PI proteasome inhibitor.
Future Treatment of Myeloma
Treatment of MM is changing rapidly and there are now several clinical trials internationally, which are exploring the utility of entirely new mechanisms of killing MM cells. This includes himeric antigen receptor T (CAR T) cell therapy which is likely to change the life expectancy treatment approach for MM patients drastically in the near future. In brief, this immunologic approach uses T cells harvested from the patient, which are then genetically engineered to make them target MM cells and kill those cells. These T-cells are then re infused back to the patient where they specifically home to and kill MM cells. CARs are hybrid molecules that contain both an antigen-recognition domain and T-cell activation domains. T Most CAR T therapies, in trial, target BCMA, but SLAMF7, CD19 and CD38 CAR approaches are also used in clinical trials for MM. of these therapies are being trialled in relapsed refractory patients, and research should to determine at what point receiving these therapies is most beneficial. It is possible in future that CAR T cells will replace ASCT in MM patients. Other targeted approaches in clinical development aim to focus on specific subgroups of MM patients who have individual genetic signatures, in a more personalised approach. Venetoclax is an inhibitor of anti Figure 1. Considerations for therapy options at relapse
The Future of pharmacIE, hosted by APPEL, will return on October 20th, 2022. This event is an online careers event for pharmacy students and professionals. Panel discussions will take place with pharmacy professionals which will showcase the varied and exciting career paths for pharmacists. Those who attend will get inspiration for their future in pharmacy and the chance to meet future colleagues. Exhibition booths will allow APPEL placement providers to promote their business or practice area to the pharmacists of the future and build their talent pipeline. This is a unique networking event with many opportunities for pharmacy students and professionals alike. Visit www.appel.ie to register your interest in attending.
References available on request 2022
Conclusion The number of therapies available for MM has rapidly increased in recent decades with 5-year survival rates now approaching 70%. Whilst this is undoubtedly a major success, it can be challenging for clinicians to decide on the most appropriate treatment sequence. Since MM is a complex disease and each patient responds differently, treatment at diagnosis is initially based on whether a patient is deemed eligible for an ASCT or not. At relapse, the sequence of treatment becomes more complex and largely depends on a patient’s previous response and which therapies they have already been exposed to. There is no doubt that within the next decade even more MM therapies will become available and therefore it is important that clinical trials answer questions about the timing of treatment. It is also important to emphasise that many MM patients have a lower risk and a more indolent disease course, and may benefit from less treatment or time off therapy.
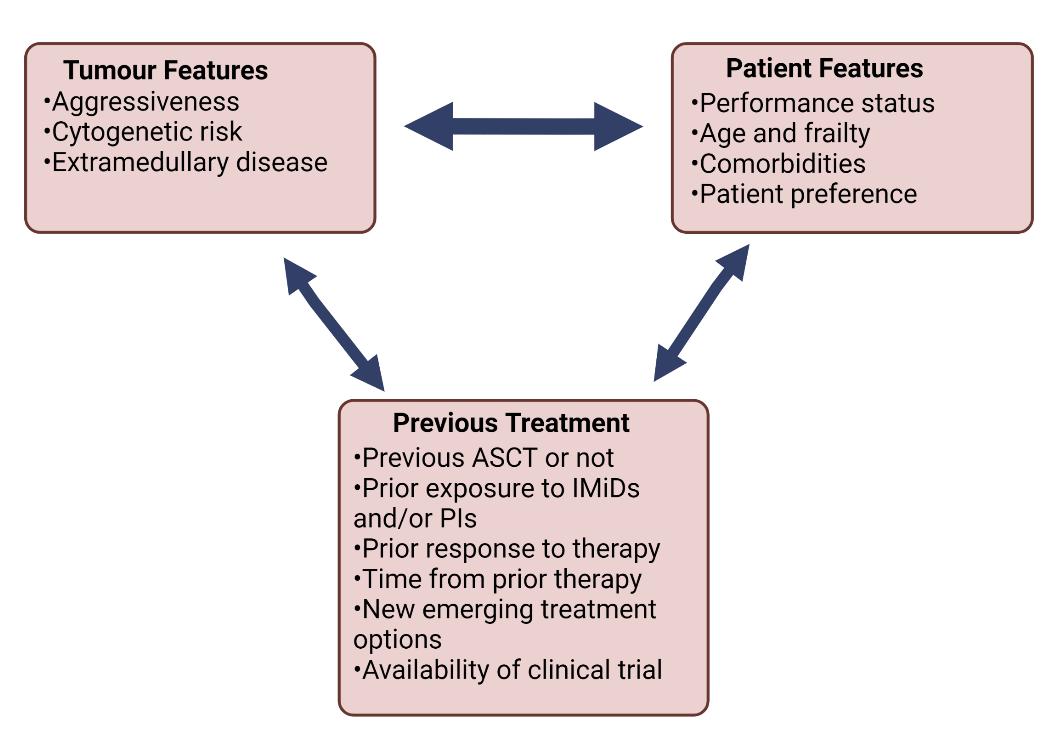
For a DEEP & DURABLE response when multiple myeloma relapses choose KYPROLIS ® DURABLEMedianRESPONSEPFS1 (Primary Endpoint n=792) months26.3vs Rd 17.6 months (HR 0.69,95% CI:0.57-0.83; 1-sided p<0.0001) Median follow-up 32 months DEEP ORRRESPONSE1,2 (Secondary Endpoint) 87.1%vsRd66.7% (OR 3.47, 95% CI: 2.41-5.00; 1 sided p<0.0001) Median follow-up 32 months ExtendedOSSurvival3 (Secondary endpoint) months48.3vs Rd 40.4 months (HR 0.79, 95% CI: 0.67-0.95; 1 sided p<0.0045) Median follow-up 67 months In the phase 3 ASPIRE trial, Kyprolis (carfilzomib), lenalidomide and dexamethasone (KRd) delivered: 32% of KRd patients achieved a CR or better vs 9% in the Rd arm 3,4 Kyprolis® (car lzomib) Brief Prescribing Information
Please refer to the Summary of Product Characteristics (SmPC) before prescribing Kyprolis. Pharmaceutical Form: Powder for solution for infusion presented as a single use vial. Indication: Kyprolis in combination with daratumumab and dexamethasone, with lenalidomide and dexamethasone or with dexamethasone alone is indicated for the treatment of adult patients with multiple myeloma who have received at least one prior therapy. Dosage and Administration: Intravenous (iv) infusion on two consecutive days each week for 3 weeks (days 1, 2, 8, 9, 15 and 16), followed by a 12 day rest period. Each 28-day period is considered one treatment cycle. Kyprolis in combination with lenalidomide and dexamethasone (KRd): Infuse over 10 minutes at a starting dose of 20mg/m2 (max dose 44mg) on days 1 & 2 of cycle 1. If tolerated, increase dose to 27mg/m2 (max dose 60mg) on day 8 of cycle 1. From cycle 13, omit doses on day 8 & 9 of each cycle. In combination with Kyprolis, lenalidomide is administered as 25 mg orally on days 1–21 and dexamethasone is administered as 40 mg orally or iv on days 1, 8, 15, and 22 of the 28 day cycles. Continue treatment until disease progression or until unacceptable toxicity occurs; treatment beyond 18 cycles should be based on an individual bene t:risk assessment as data are limited. Consider appropriate dose reduction for lenalidomide according to the current lenalidomide SmPC. Kyprolis in combination with dexamethasone (Kd): Infuse over 30 minutes at a starting dose of 20 mg/m2 (max dose 44 mg) on days 1 and 2 of cycle 1. If tolerated, increase dose to 56 mg/m2 (max dose 123 mg) on day 8 of cycle 1. Dexamethasone is administered as 20 mg orally or iv on days 1, 2, 8, 9, 15, 16, 22, and 23 of the 28 day cycles. Continue treatment until disease progression or until unacceptable toxicity occurs. Kyprolis in combination with daratumumab and dexamethasone (KdD): Infuse over 30 minutes at a starting dose of 20mg/m2 (max dose 44mg) on days 1 & 2 of cycle 1. If tolerated, increase dose to 56mg/m2 (max dose 123mg) on day 8 of cycle 1. If given intravenously, daratumumab is administered at 8mg/kg on days 1 & 2 of cycle 1, then 16mg/kg weekly from day 8 for cycles 1&2, then every 2 weeks for cycles 3-6, and every 4 weeks thereafter . If given subcutaneously, daratumumab is administered at 1800mg weekly from day 1 of cycles 1&2, then every 2 weeks for cycles 3-6, and every 4 weeks thereafter. Administer preinfusion medication to reduce risk of infusion-related reactions with daratumumab. Dexamethasone is administered as 20 mg orally or iv on days 1, 2, 8, 9, 15, & 16, then 40mg on day 22 of each cycle. For patients > 75 years of age, dexamethasone is administered as 20 mg orally or intravenously weekly after the rst week. Order of administration on days when more than one medicine is administered: dexamethasone, preinfusion medication for daratumumab, car lzomib, daratumumab, post infusion medication for daratumumab. Continue treatment until disease progression or until unacceptable toxicity occurs. Refer to the current daratumumab SmPC for additional detail regarding concomitant medication and appropriate dose reduction for daratumumab. All regimens: Modify dosing based on haematologic, renal and other non-haematologic toxicity as de ned in the SmPC. Consider antiviral prophylaxis in patients treated with Kyprolis to decrease the risk of herpes zoster reactivation. Monitor platelet counts frequently. Thromboprophylaxis is recommended based on an individual bene t:risk assessment. Adequate hydration is required before Kyprolis administration in cycle 1, especially in patients at high risk of tumour lysis syndrome or renal toxicity, give additional uids after Kyprolis administration in cycle 1 as needed. Monitor all patients for evidence of volume overload and tailor uid requirements to individual patient needs. Oral and/or intravenous hydration is not required on days when intravenous daratumumab is dosed in the KdD regimen. Monitor serum potassium monthly or more frequently as clinically indicated. Assess renal function at treatment initiation and monitor at least monthly, particularly in patients with lower baseline creatinine clearance (CrCL < 30 mL/min) for whom there are limited ef cacy and safety data. Assess liver enzymes and bilirubin at treatment initiation and monitor monthly during treatment, regardless of baseline values; pay special attention to patients with moderate and severe hepatic impairment for whom there are very limited ef cacy and safety data.
Adverse reactions/events should be reported directly to Health Products Regulatory Authority (HPRA) using the available methods via www.hpra.ie. Adverse reactions/events should also be reported to Amgen Limited on +44 (0)1223 436441 or Freephone 1800 535 160
Contraindications: Hypersensitivity to the active substance or to any of the excipients; women who are breast-feeding. Refer to relevant SmPC for contraindications, special warnings and precautions for products used in combination with Kyprolis. Special Warnings and Precautions: For patients who experience grade 3 or 4 cardiac events or dyspnoea, or pulmonary toxicities/hypertension or hypertensive crisis, stop Kyprolis until recovery and consider whether to restart Kyprolis at 1 dose level reduction based on a bene t/risk assessment. Cardiac disorders: New or worsening cardiac failure, myocardial ischaemia and infarction have occurred, including fatal outcomes. The risk of cardiac failure is increased in elderly (≥ 75 years) and Asian patients. A thorough assessment for cardiovascular risk factors prior to starting treatment is recommended. Patients with signs or symptoms of NYHA Class III or IV cardiac failure, recent history of myocardial infarction (in the last 4 months), and in patients with uncontrolled angina or arrhythmias should have a comprehensive cardiological assessment prior to starting treatment. Electrocardiographic changes: Cases of QT interval prolongation and of ventricular tachycardia have been reported. Pulmonary toxicity: Acute respiratory distress syndrome (ARDS), acute respiratory failure, and acute diffuse in ltrative pulmonary disease such as pneumonitis and interstitial lung disease have occurred, some events have been fatal.
4. KYPROLIS® SPC available at www.medicines.ie. © 2022 Amgen Inc. All rights reserved. IE-KYP-0322-00011. April 2022 Amgen Ireland Limited 21 Northwood Court, Santry, Dublin 9 Results are from ITT population (1-3 prior lines of treatment).
3. Siegal DS, et al. J Clin Oncol 2018;36:728-34.
1.References Stewart AK, et al. N Engl J Med 2015;372:142-52.
KRd was generally well tolerated. For full details of the Kyprolis safety pro le, please refer to the Summary of Product Characteristics (SPC) available online www.medicines.ie/medicines/kyprolis-32623/spc.at KRd KYPROLIS® in combination with lenalidomide and dexamethasone (KRd) is indicated for the treatment of adult patients with multiple myeloma who have received at least one prior therapy.4
Pulmonary hypertension: Pulmonary hypertension has been reported, some events have been fatal. Dyspnoea: Evaluate dyspnoea to exclude cardiopulmonary conditions including cardiac failure and pulmonary syndromes. Hypertension: Hypertension, including hypertensive crisis and hypertensive emergency, has been observed, some events have been fatal. Control hypertension prior to starting and during treatment. Evaluate all patients for hypertension during treatment. If hypertension cannot be controlled, reduce dose. Acute renal failure: Cases of acute renal failure have been reported, some of these events have been fatal. Tumour lysis syndrome (TLS): Cases of TLS, including with fatal outcome, have been reported. Consider patients with a high tumour burden at greater risk. Ensure patients are well hydrated before Kyprolis administration in cycle 1 and subsequent cycles as needed. Consider uric acid lowering medicinal products in patients at high risk for TLS. Monitor for evidence of TLS during treatment. Stop Kyprolis until TLS is resolved. Infusion reactions: Infusion reactions, including life-threatening reactions, have been reported in patients who received Kyprolis. Reactions can occur immediately following or up to 24 hours after administration of Kyprolis. Dexamethasone should be administered prior to Kyprolis to reduce the incidence and severity of reactions. Haemorrhage and thrombocytopenia: Haemorrhage, often associated with thrombocytopenia has been reported; some events have been fatal. Venous thromboembolic events: Events, including deep vein thrombosis and pulmonary embolism with fatal outcomes, have been reported. Closely monitor patients with known risk factors for thromboembolism, minimise all modi able risk factors (e.g. smoking, hypertension and hyperlipidaemia), and administer other agents that may increase the risk of thrombosis with caution (e.g. erythropoietic agents or hormone replacement therapy). Hepatic toxicity: Cases of hepatic failure, including fatal cases, have been reported. Thrombotic
2. Amgen data on le. CSR 20130395. 24 September 2017; Table 7-3.
microangiopathy: Cases of thrombotic microangiopathy, including thrombotic thrombocytopenic purpura and haemolytic uraemic syndrome (TTP/HUS) have been reported, some events have been fatal. Monitor for signs and symptoms of TTP/HUS and stop treatment if suspected. Once excluded, Kyprolis can be restarted. The safety of reinitiating Kyprolis in patients previously experiencing TTP/HUS is unknown. Posterior reversible encephalopathy syndrome (PRES): Cases of PRES have been reported. Kyprolis should be discontinued if PRES is suspected. The safety of reinitiating Kyprolis therapy in patients previously experiencing PRES is not known. Hepatitis B Virus (HBV) reactivation: Cases of HBV reactivation have been reported. Patients should be screened for HBV before initiation of treatment. For patients with positive HBV serology, consider prophylaxis with antivirals. Monitor for clinical and laboratory signs of HBV reactivation during and after the end of treatment. The safety of resuming car lzomib after HBV is adequately controlled is not known. Resumption of therapy should be discussed with experts in managing HBV. Progressive Multifocal Leukoencephalopathy (PML): Cases of PML have been reported in patients receiving car lzomib who have had prior or concurrent immunosuppressive therapy. Patients should be monitored for any new of worsening neurological, cognitive or behavioural signs and symptoms that may be suggestive of PML. If PML is suspected, further administration must be suspended until PML has been excluded by a specialist with appropriate diagnostic testing. If PML is con rmed, car lzomib must be discontinued. Contraception: Female patients of child bearing potential (and/or their partners) must use effective contraception measures during and for one month following treatment. Kyprolis may decrease the ef cacy or oral contraceptives. Patients using oral contraceptives or hormonal contraception associated with a risk of thrombosis should switch to an alternative method. Male patients must use effective contraception measures during and for 3 months following treatment if their partner is pregnant or of childbearing potential not using effective contraception. Sodium content: Each 10mg, 30mg and 60mg vial contains 37, 109 and 216 mg sodium, respectively. Cyclodextrin content: Each 10mg, 30mg and 60mg contains 500, 1500 and 3000 mg of cyclodextrin (betadex sulfobutyl ether sodium), respectively. Interactions: Caution should be observed when car lzomib is combined with medicinal products that are substrates of CYP1A2, 2C8, 2C9, 2C19 and 2B6 (e.g. oral contraceptives), or with substrates of P-gp (e.g. digoxin, colchicine). Fertility, pregnancy and lactation: No available data on use of Kyprolis in pregnant women; should not be used during pregnancy unless the potential bene t outweighs the potential risk to the foetus. Breast-feeding is contra-indicated during and for at least 2 days after treatment with Kyprolis. No fertility studies have been performed. Undesirable Effects: Adverse reactions in patients receiving Kyprolis: very common (≥ 1/10) pneumonia, respiratory tract infection, thrombocytopenia, neutropenia, anaemia, lymphopenia, leukopenia, hypokalaemia, decreased appetite, insomnia, dizziness, peripheral neuropathy, headache, hypertension, dyspnoea, cough, vomiting, diarrhoea, constipation, abdominal pain, nausea, back pain, arthralgia, pain in extremity, muscle spasms, increased blood creatinine, pyrexia, peripheral oedema, asthenia, fatigue, chills; common (≥ 1/100 to < 1/10) sepsis, lung infection, in uenza, herpes zoster, urinary tract infection, bronchitis, gastroenteritis, viral infection, nasopharyngitis, rhinitis, febrile neutropenia, dehydration, hyperkalaemia, hypomagnesaemia, hyponatraemia, hypercalcaemia, hypocalcaemia, hypophosphataemia, hyperuricaemia, hypoalbuminaemia, hyperglycaemia, anxiety, confusional state, paraesthesia, hypoaesthesia, cataract, blurred vision, tinnitus, cardiac failure, myocardial infarction, atrial brillation, tachycardia, ejection fraction decreased, palpitations, deep vein thrombosis, hypotension, ushing, pulmonary embolism, pulmonary oedema, epistaxis, oropharyngeal pain, dysphonia,wheezing, pulmonary hypertension, gastrointestinal haemorrhage, dyspepsia, toothache, increased alanine aminotransferase, increased aspartate aminotransferase, increased gammaglutamyltransferase, hyperbilirubinaemia, rash, pruritus, erythema, hyperhidrosis, musculoskeletal pain, musculoskeletal chest pain, bone pain, myalgia, muscular weakness, acute kidney injury, renal failure, renal impairment, decreased creatinine renal clearance, chest pain, pain, infusion site reactions, in uenza-like illness, malaise, increased c-reactive protein, increased blood uric acid, infusion related reaction; uncommon (≥ 1/1,000 to < 1/100) clostridium dif cile colitis, cytomegalovirus infection, hepatitis B virus reactivation, drug hypersensitivity, HUS, TTP, tumour lysis syndrome, intracranial haemorrhage, cerebrovascular accident, PRES, cardiac arrest, cardiomyopathy, myocardial ischaemia, pericarditis, pericardial effusion, ventricular tachycardia, hypertensive crisis, haemorrhage, ARDS, acute respiratory failure, pulmonary haemorrhage, interstitial lung disease, pneumonitis, gastrointestinal perforation, acute pancreatitis, hepatic failure, cholestasis, multi-organ dysfunction syndrome. In a phase III study comparing KdD with Kd, secondary primary malignancies were reported (1.9% in KdD; 1.3% in Kd arm). Please consult the Summary of Product Characteristics for a full description of adverse reactions. Pharmaceutical Precautions: Do not mix or administer as an infusion with other medicinal products. Store at 2°C to 8°C (in a refrigerator). Do not freeze. Store in original carton to protect from light. Reconstitute with sterile water for injections. Reconstituted solutions in the vial, syringe, or intravenous bag may be stored at 2°C – 8°C for up to 24 hours or at 25°C for up to 4 hours. Inspect visually before administration; do not administer if any discoloration or particulate matter is observed. Legal Category: POM. Presentation, Basic Costs and Marketing Authorisation Number: Kyprolis 60 mg, pack of 1: EU/1/15/1060/001. Kyprolis 30 mg, pack of 1: EU/1/15/1060/003. Kyprolis 10 mg, pack of 1: EU/1/15/1060/002. Price in Republic of Ireland is available on request. Marketing Authorisation Holder: Amgen Europe B.V., Minervum 7061, NL-4817 ZK Breda, The Netherlands. Further information is available from Amgen Ireland Limited, 21 Northwood Court, Santry, Dublin D09 TX31. Kyprolis is a registered trademark owned or licensed by Amgen Inc., its subsidiaries, or af liates. Date of PI preparation: April 2022 (Ref: IE-KYP-0322-00001)




Dr Rebecca Amet Nikolett Warner
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 56 ONCOLOGY FOCUS: CANCER RESEARCH
This partnership is important for many reasons: firstly, it ensures that the research we are carrying out is relevant and meaningful to those who are affected by cancer. Importantly, by promoting equity in the research decisions, it can increase the trust between people who are affected by cancer and the research community, as well as improving interactions
Researchers need to be flexible when it comes to their PPI methodology. Not all PPI contributors will feel comfortable or be able to contribute in a standard group setting, whether it be online or in person. Genuine involvement means making sure that we accommodate PPI contributors to share their voices in ways that works best for them. Researchers also need to have the ability to change and adapt when it comes to PPI, they need to be able to work with PPI contributors to reflect on things that haven't worked well, identify difficulties or challenges they had with including PPI, so that their PPI methodology can be refined and improved as required.
As the largest voluntary funder of cancer research in Ireland, the Irish Cancer Society is committed to putting patients, survivors, families, carers, supporters and the public at the very heart of what we do. To do this, we work directly with people affected by cancer to ensure that they are embedded as partners within the cancer research processes in Ireland through public and patient involvement in research (PPI).
Written by Dr Claire Kilty, Dr Rebecca Amet, Nikolett Warner - Irish Cancer Society
Cancer impacts the lives of everyone, unfortunately, no one is immune to the devastation it can cause. In order to achieve equitable access to world-class treatment, care and support; everyone must have a seat at the table. Historically, those from underserved and minority groups often have poorer outcomes from cancer than the general population. It is important that the benefits of cancer research reach everyone, especially people from these communities who might struggle with access to care and services. Including PPI contributors who are members of underserved communities ensures that the scientific research agenda is more equitable and impactful to their Inclusionneeds1.atthe planning stage guarantees that the research topic is relevant and will include individuals from all backgrounds; whilst including inclusive PPI at the dissemination stage will ensure that those who may benefit from the research findings will know about it. Some contributors may not have the same access to resources to participate in PPI. In these instances, researchers must be proactive in accommodating these individuals, for example, travelling to the contributors or creating bespoke methods of research communication. This may seem initially challenging, however, it is important to remember that that this can be a dynamic process whereby co-designed strategies for more inclusive research can be developed. This investment in inclusion will likely result is more just, equitable and impactful cancer research for all.
Dr Claire Kilty
Finally, the Society advises researchers to spend time developing their PPI network. A growing number of organisations are developing best practice in PPI in Ireland and are there to offer support to researchers. Health Research Charities Ireland have an excellent toolkit available guiding researchers on beginning a PPI relationship2. The National PPI Ignite network, and associated seven lead university sites offers supports to scientific, health, and social care researchers within academic institutions in Ireland, and are a vital resource for PPI within research. At the Irish Cancer Society, we are always willing to provide advice to cancer researchers during their PPI journey, and we advise researchers to get in touch with us on ppi@irishcancer.ie if you have any PPI related questions. available on request
between patients and health care professionals. Being involved in research can also create a sense of empowerment and value for all involved. In terms of the research community, it ensures that researchers are made aware of the true meaning of their research; it gives them a different perspective to consider, and helps them understand the real-world barriers and enablers of the research that they are Researchersproposing.canembed
References
PPI in cancer research involves carrying out research in partnership with people affected by cancer, ultimately whereby all contribute collaboratively in varying amounts towards the research. With true PPI, each voice is of equal importance in the research process.
Embedding Public and Patient Involvement in Cancer Research across Ireland
PPI at any stage of the research cycle, from the development and design stage of the project, to the grant application stage, to inputting directly into the methodology and direction of the research project, to helping interpret the results, and dissemination and communication of the results. Ideally, people affected by cancer should be involved as PPI contributors as early as possible in the research process, working together with researchers to identify and prioritise the initial research questions i.e. long before that grant application is due. Key to building this partnership is ensuring trust and respect. This includes having empathy and understanding for each other, communicating with respect and honesty, putting time in to developing the PPI relationship, as well as listening to the PPI contributor and making sure that their voice is heard. Managing and setting the expectations of both the researcher and the PPI contributor from the onset is a vital part of building this PPI relationship, as it ensures that everyone is clear what their role in the project will be. Completing a role description for the PPI contributor and the researcher is a good way of providing this clarity. In addition, following up with PPI contributors to communicate results and the impact of their involvement throughout the research project and afterwards is an important part of maintaining trust and respect. A piece of feedback that the Society continually receive from PPI contributors working with researchers is about the lack of follow-up and communication about how their contribution was utilised.
A major priority of the Society is making sure that cancer researchers around the country understand what PPI is and the value of PPI in research. The Society work with all researchers from traditional lab-based scientists to data scientists and doctors, and even nurses and allied health professionals; helping them incorporate PPI into their research projects.



BRIDION® 100 MG/ML SOLUTION FOR INJECTION Sugammadex ABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics (SmPC) before prescribing PRESENTATION Vials of 200mg (2 ml) or 500mg (5 ml). INDICATIONS Reversal of rocuronium (ROC) or vecuronium (VEC) induced neuromuscular (NM) block in adults. For routine reversal of ROC-induced block in children and adolescents aged 2 to 17 years. DOSAGE AND ADMINISTRATION I.V. as a single bolus injection administered rapidly (within 10 seconds), into an existing I.V. line, by/under the supervision of an anaesthetist. Use appropriate technique to monitor recovery of NM block. Dose depends on the level of block to be reversed, not the anaesthetic regimen. Adults: Routine reversal following ROC- or VEC-induced block: • 4 mg/kg if recovery has reached at least 1 2 post-tetanic counts (PTC). Median recovery time (T4/T1 = 0.9) ≅ 3 minutes. • 2 mg/kg if recovery has occurred up to at least T2 following ROC- or VEC-induced block. Median recovery time (T4/T1 = 0.9) ≅ 2 minutes. Median recovery time (T4/T1= 0.9) is slightly faster with ROC- than VEC-induced block. Immediate reversal of ROC-induced block: 16 mg/kg. Median recov ery time (T4/T1 = 0.9) ≅ 1.5 minutes when 16 mg/kg is given 3 minutes after a bolus dose of 1.2 mg/kg ROC. Not recommended for immediate re versal of VEC-induced block. Re administration of sugammadex: For post-operative recurrence of block after an initial dose of 2 mg/kg or 4 mg/kg, repeat dose of 4 mg/kg is recommended. Following a second dose of sugammadex, monitor the patient closely to ascertain sustained return of neuromuscular function. Re-administration of ROC or VEC after sugammadex: Up to 4 mg/kg Sugammadex a waiting time of 5 minutes for re-use of 1.2 mg/kg ROC; 4 hours waiting time for re-use of 0.6 mg/kg ROC or 0.1 mg/kg VEC. With ROC onset of NM block may be prolonged and dura tion of NM block may shortened. After immediate reversal, 16 mg/kg sugammadex, a waiting time of 24 hours is recommended. See SPC for patients with mild or moderate renal impairment. Special populations: Renal impairment: For mild and moderate renal impairment use adult dose. Not recommended in severe renal impairment (including patients requiring dialysis). Elderly: Use adult dose although recovery times are slower. Obese: In obese patients, including morbidly obese patients (body mass index ≥ 40 kg/m2), adult dose based on actual body weight. Hepatic impairment: Caution in patients with severe hepatic impairment, or impairment with coagulopathy. Children and adolescents (2-17 years): Bridion 100 mg/ml may be diluted to 10 mg/ml to increase the accuracy of dosing in the paediatric population. Routine reversal: A dose of 4 mg/kg sugammadex is recom mended for reversal of rocuronium induced blockade if recovery has reached at least 1-2 PTC. A dose of 2 mg/kg is recommended for reversal of rocuronium induced blockade at reappearance of T2 Immediate reversal: Immediate reversal in children and adolescents has not been investigated. Term newborn infants and infants: Not recommended. CONTRA-INDICATIONS Hypersensitivity to sugammadex or to any excipients.
PREGNANCY AND LACTATION Pregnancy and Lactation: Caution in pregnant women. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from sugammadex therapy, taking into account the benefit of breast feeding for the child and the benefit of therapy for the woman. The effects on human fertility have not been investigated. SIDE EFFECTS Refer to SmPC for complete in formation on side effects Common (≥ 1/100 to < 1/10): Anaesthetic complications including movement of limbs or body or coughing during anaes thesia, grimacing, or suckling on the endotracheal tube, airway complication of anaesthesia, procedural hypertension and procedural complication. Uncommon (≥ 1/1,000 to < 1/100): Hypersensitivity reactions, including anaphylaxis, have occurred in some patients and volunteers. Other less common and rarely reported side effects are listed in the SmPC. In clinical studies with subjects treated with rocuronium or vecuronium, where sugammadex was administered using a dose labelled for the depth of neuromuscular blockade, an incidence of 0.2% was observed for recurrence of neuromuscular blockade as based on neuromuscular monitoring or clinical evidence. The use of lower than recommended doses may lead to an increased risk of recurrence of neuromuscular blockade after initial reversal and is not recommended. HANDLING See SmPC for details of compa tability with infusion solutions. Physical incompatibility has been reported with verapamil, ondansetron and ranitidine. PACKAGE QUANTITIES 10 vials of 2 ml 10 vials of 5 ml LEGAL CATEGORY POM Marketing Authorisation Numbers EU/1/08/466/001-002 Marketing Authorisation Holder Merck Sharp & Dohme B.V., Waarderweg 39, 2031 BN Haarlem, The Netherlands Date of review of prescribing information: January 2022 © Merck Sharp and Dohme B.V., 2022. All rights reserved. Further information is available on request from: MSD, Red Oak North, South County Business Park, Leopardstown, Dublin 18 or from www.medicines.ie. EMEA/H/C/000885/II/0042
IE-XBR-000792022.Marchpreparation:ofDateRed Oak North, South County Business Park, Leopardstown, Dublin D18 X5K7 Ireland ➜ Scan the QR code to register an account with MSDConnect.ie ➜ Registering only takes two minutes ➜ Discover videos and product information in our portal that will help to support you and keep you informed ➜ Keep up-to-date with news, announcements and events If you would like to hear more from MSD and keep up-to-date with the most useful clinical content across all our therapy areas then register now for MSDConnect.ie MSDCONNECT
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to MSD (Tel: 01-299 8700)
OVERDOSE No dose related ad verse events nor serious adverse events were reported. Sugammadex can be removed using haemodialysis with a high flux filter. INTERACTIONS Toremifene and fusidic acid may displace rocuronium or vecuronium from sugammadex and delay recovery (no clinically relevant capturing interac tions are expected). Interaction of sugammadex with hormonal contraceptives may lead to a decrease in progesterone exposure equivalent to one missed daily dose of oral contraceptive (no displacement interactions are expected). In general sugammadex does not interfere with laboratory tests, with the possible exception of the serum progesterone assay where interference is observed at sugammadex plasma concentrations of 100 µg/ml plasma. In a study doses of 4 mg/kg and 16 mg/kg sugammadex resulted in maximum mean prolongations of the activated partial thrombo plastin time by 17 and 22% respectively and prothrombin time by 11% and 22% respectively. These were of short duration (≤ 30 minutes). In in vitro experiments pharmacodynamic interaction was noted with vitamin K antagonists, unfractionated heparin, low molecular weight heparinoids, rivarox aban and dabigatran.
PRECAU TIONS AND WARNINGS Ventilatory support is mandatory for patients until adequate spontaneous respiration is restored following reversal of block. Should block reoccur following extubation, adequate ventilation should be provided. The use of lower than recommended doses may lead to an in creased risk of neuromuscular blockade after an initial reversal and is not recommended. Caution should be exercised when considering the use of sugammadex in patients receiving anticoagulation for a pre-existing or co-morbid condition. An increased risk of bleeding cannot be excluded in patients with hereditary vitamin K dependent clotting factor deficiencies; with pre-existing coagulopathies; on coumarin derivatives and at an INR above 3.5; using coagulants who receive a dose of 16mg/kg sugammadex. If re administration of ROC or VEC is required in patients with mild or moderate renal impairment after routine sugammadex reversal a waiting time for re-use of 0.6 mg/kg ROC or 0.1 mg/kg VEC should be 24 hours. If a shorter waiting time is required, the ROC dose for a new NM blockade should be 1.2 mg/kg within 30 minutes after Sugammadex administration. For re-administration of ROC or VEC after immediate reversal a waiting time of 24 hours is recommended. If neuromuscular block is required before the recommended waiting time has passed, a nonsteroidal neuromuscular blocking agent should be used. The use in patients with severe renal impairment is not recommended including those requiring dialysis. If neuromuscular block is reversed, while anaesthesia is continued, additional doses of anaesthetic and/or opioid should be given as clinically indicated. Marked bradycardia with cardiac arrest have been observed within min utes after administration, closely monitor patients for haemodynamic changes during and after reversal. Treat with anti-cholinergic agents such as atropine if clinically significant bradycardia observed.Sugammadex has not been investigated in patients receiving ROC or VEC in the ICU setting.
Do not use sugammadex to reverse block induced by nonsteroidal blockers such as succinylcholine or benzylisoquinolinium compounds, or ste roidal blockers other than ROC or VEC. Conditions associated with prolonged circulation time such as cardiovascular disease, old age, or oedem atous state may cause longer recovery times. Be prepared for possible drug hypersensitivity reactions. This medicinal product contains up to 9.7 mg sodium per ml, equivalent to 0.5% of the WHO recommended maximum daily intake of 2 g sodium for an adult.

Another problem with the PSA test is that abnormal values are not confined to men with prostate cancer but may also occur when benign prostate hypertrophy (BPH) or prostatitis is present. Differentiation between BPH and prostate cancer necessitates a prostate biopsy with the possibility for complications such as infection, pain, bleeding, urinary retention or haematuria.
Monitoring Patients Following a Diagnosis of Cancer
Biomarkers Play Important Roles in Cancer Detection and Patient Follow-up
The aim of screening for cancer is to detect it at an early stage before it causes symptoms and when it may be easier to treat successfully. It is widely accepted that the earlier a cancer is detected, the better the outcome. An effective cancer screening test should therefore reduce mortality from the particular cancer being screened for.
One of the most widely used biomarkers in cancer screening is PSA which is used for detecting early prostate cancer. Although opportunistic screening with PSA is widely performed, this practice is highly controversial with arguments for and against
One of the cancers in which such biomarkers are widely used is breast cancer. Currently, when a woman is diagnosed with breast cancer, 3 important biomarkers are measured, estrogen receptors (ER), progesterone receptors (PR) and HER2. Depending on which of these biomarkers are positive, a particular therapy may be administered. For example, if ER or PR is present, the woman is likely to receive some type of endocrine therapy such as tamoxifen or an aromatase inhibitor. If however, the woman is HER2-positive, she is likely to receive the drug, Herceptin. If all 3 biomarkers are negative, i.e., the tumor is triple-negative, chemotherapy is the treatment of choice. However, it should be stated that there is currently intensive ongoing research into developing new non-chemotherapy treatments for patients with the triple-negative type of breast cancer. One of the most promising of these new treatments is immunotherapy which boosts ones’ immune system to fight the cancer.
Following initial diagnosis of a cancer, most patients are now followed up at regular intervals, a practice referred to as surveillance. The main aim of surveillance is to detect any emerging recurrent/ metastatic disease at a potentially curable stage, the assumption being that early detection followed by the initiation of treatment will result in better outcome than starting treatment when a recurrence is clinically evident. Indeed, in several different cancer types, regular measurement of biomarkers can predict the presence of early recurrent/ metastatic disease and provide a lead-time vis-à-vis clinical
58
Another biomarker that is used in screening for cancer is faecal occult blood testing (FOBT) for colorectal cancer (CRC). In contrast to PSA screening for prostate cancer, most countries have organized screening programmes for CRC using FOBT. Several years ago, an early version of the FOBT, known as the guaiac test, was shown to reduce mortality from colorectal cancer in several different large randomized trials. In Ireland, the National Screening Service (NSS) currently offers an improved version of the original FOBT, known as a faecal immunochemical test (FIT), to all individuals aged 60 to 69. Individuals in this age range are contacted by post and invited to participate in the programme. The small numbers of individuals with positive results are then offered a colonoscopy.
the practice. Although a large trial carried out across 8 European countries showed that screening men 55-69 years of age with PSA significantly reduced mortality from prostate cancer, the trial also showed that many men had a prostate malignancy detected that might not have caused any problems, i.e., screening led to many cases of overdiagnosis of non-life-threatening disease. The problem with overdiagnosis is the possibility of overtreatment with further potential for harm. Overdiagnosis of prostate cancer however, can be reduced by performing additional tests such as multiparametric magnetic resonance imaging (mpMRI).
Another cancer in which biomarkers are widely used in selecting the optimum treatment is a form of lung cancer known as non-small cell lung cancer (NSCLC). Lung cancer is the most common cancer world-wide and causes of most cancer-related deaths. Traditionally, this cancer was difficult to treat with the only form of drug-related therapy been chemotherapy. However, in the last few years, a large range of new treatments have become available, including immunotherapy and drugs which block genes involved in driving the growth of the cancer. To determine the most appropriate drug for an individual patient, a series of biomarkers may be measured and depending on which biomarker is present, a particular drug is recommended.
ONCOLOGY FOCUS: BIOMARKERS
Biomarkers in Screening for Early Cancer
Since PSA is less than an ideal screening test for prostate cancer, most guidelines published by international expert panels are opposed to mass population screening for the disease. Many guidelines however, recommend screening in men 55 to 69 years of age under specific conditions such as following the practice of shared decision making and informed consent. The shared decision making should include a discussion between the man and his doctor about the potential harms and benefits of the screening process and the likely ensuing impact on the man’s health and quality of life.
Use of Biomarkers in Guiding the Most Appropriate Therapy Few if any of the currently available drug-related treatments for disease are effective in all of those receiving it. This certainly applies in cancer treatment, especially with some of the newer molecularly therapies and immunotherapy where response are usually confined to a minority of patients. In addition, most cancer treatments can cause unpleasant side-effects. Clearly, in such a situation, biomarkers that predict response in advance of starting the treatment are important to identify those most likely to benefit.
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Written by Professor Joe Duffy UCD Clinical Research Centre, St. Vincent’s University Hospital, Dublin and UCD School of Medicine, Conway Institute of Biomolecular and Biomedical Research, University College Dublin, Dublin Biomarkers play an important and sometimes vital role in cancer detection and patient management (i.e., follow-up of patients following a diagnosis of cancer). Thus, in well or asymptomatic individuals, some biomarkers may be used in screening for early cancer. Following a diagnosis of cancer, biomarkers can help in planning the most appropriate therapy for a specific patient, in detecting the early emergence of cancer spread and in monitoring the effectiveness of an ongoing therapy. Below, I discuss the use of biomarkers in these different settings.
Early detection is key to improve the chances of cure but also to minimise the extent and amount of treatment needed for patients.
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 59
Advances in radiotherapy technology and high quality radiotherapy have been shown to improve patients’ chances of survival by up to 20% and also importantly reduce side effects and improve patient’s quality of life.
Clinical trials offer patients the opportunity to access novel treatments and new methods of treating cancer. Participating in clinical trials has been shown to have a survival benefit for patients.
Are treatments successful?
Head and neck cancers represent 6 % of all new cancer diagnoses worldwide. Historically oral cavity cancer and laryngeal cancer were the most common subsites, but these are now decreasing in frequency as a direct result of public health campaigns to reduce tobacco and alcohol consumption. However there has been a rise in the incidence of oropharyngeal cancer due to the increasing prevalence of HPV infection. Internationally in the western world almost 70% of all head and neck cancer is related to the Human papilloma virus.
To mark World Head and Neck Cancer Day (27th July 2022) Professor Sinead Brennan, Consultant Radiation Oncologist and Clinical Associate Professor in Clinical Medicine, at the School of Medicine talks about head and neck cancers, treatments available and what can be done to protect from this type of cancer.
What treatments are available?
Acknowledgement: MJD’s research is funded by the Cancer Clinical Research Trust
80% of all head and neck cancer patients require radiotherapy treatment at some stage of their illness and for many patients it can cure cancer without the need for potentially debilitating surgery which can sometimes involve removal of parts of the mouth, throat or the voice box which can have a significant impact on patient’s quality of life. Radiotherapy is a type of high energy ionising radiation that destroys cancer cells. Chemotherapy is used in advanced stage cancer in combination with radiotherapy treatment.
Unfortunately, some of the patients being following-up will develop recurrent or metastatic disease and will have to undergo further therapy. Although radiological imaging is the gold standard method for monitoring response to therapy, the use biomarkers is considerable more convenient for patients and is less expensive.
Generally, decreasing levels of biomarkers following the initiation of therapy correlate with tumor shrinkage while increasing levels tend to predict disease deterioration. The biomarkers used in monitoring therapy are the same as those mentioned above for postoperative surveillance Conclusion From above, it is clear that biomarkers are making a major contribution to cancer detection therapy selection and patient monitoring. Hopefully, the use of biomarkers in these different settings is helping with personalized treatment and improved outcome. Looking to the future, one of the most exciting research areas currently is in the development of a blood-based pan-cancer screening test. These tests involve analysing genetically altered DNA shed by tumor cells into the blood stream. Thus, with a sample of blood, it may in the future be possible to screen for up to 50 different cancer types, simultaneously. If so, the holy grail of a simple blood test for early cancer may finally be achieved.
What are the incidence rates internationally?
or radiological findings. Some examples of biomarkers that can identify the emergence of early recurrences include PSA in prostate cancer, CEA in colorectal cancer, AFP and HCG in patients with germ cell tumors of the testis (non-seminomatous type), CA 15-3 in breast cancer and CA 125 in ovarian cancer.
What can we do to prevent head and neck cancer?
smokers, where cure rates are over 90%. However, treatment for head and neck cancer is still associated with significant side effects such as dry mouth and swallowing problems. At St Luke's Radiation Oncology Network (SLRON) there is a large multidisciplinary team to support patients during their treatment and help manage any side effects that patients may have, including radiation oncologists, specialist nurses, radiation therapists, dieticians, speech and language therapists, physiotherapists, social workers and psycho-oncologists.
is the highest volume head and neck cancer centre in Ireland. All patients are discussed at a multidisciplinary meeting where recommendations are made for treatments for each individual patient. Patients often present at an advanced stage of disease and therefore may require both surgery and radiotherapy treatment.
The new HRB funded Irish Research Radiation Oncology Group (IRROG) is a national dedicated radiotherapy clinical trials group which is partnered with Trinity College Dublin and the Wellcome-HRB CRF at St James Hospital, and will be part of the Cancer Trials Ireland Network. As Clinical Lead for IRROG, Professor Brennan hopes to provide more patients the opportunity to become involved in clinical trials and expand our international collaborations to give Irish patients access to the latest treatment advances.
We know that the majority of head and neck cancers are caused by either smoking and alcohol or Human Papilloma Virus (HPV) infection. Therefore, the majority of head and neck cancers are actually preventable by avoiding smoking, reducing alcohol intake and ensuring all teenagers get their HPV vaccination.
Treatment includes combinations of surgery, immunotherapy.chemotherapyradiotherapyandsometimesStJamesHospital
Overall cure rates are improving especially for patients whose cancers are caused by HPV infection and who are non-
Do clinical trials have a role in the treatment of head and neck cancers?
Cancer News - World Head and Neck Cancer Day
Many clinical trials also look at ways of reducing side effects of treatment. St Luke's Radiation Oncology Network and St James Hospital have participated in many clinical trials in head and neck cancer with international collaborative groups such as CRUK in the UK, NRG in the USA and also with the Canadian Cancer Trials Group. These trials have focussed on reducing side effects and improving quality of life in patients with HPV positive oropharyngeal cancer who are often long-term cancer survivors, preventing dysphagia in patients with laryngeal cancer, individualising radiotherapy in patients who have undergone surgery in oral cavity cancer, combining immunotherapy with chemotherapy and radiotherapy, and currently the use of neoadjuvant immunotherapy for patients undergoing surgery for oral cavity cancer and post operative chemotherapy and radiotherapy, which is the first study to involve all four cancer treatment modalities in Ireland.

HOSPITALPROFESSIONALNEWS.IEProfessorofCancerBiology,UCDSchoolofBiomolecular
Significant Funding Successes
Significant Funding Successes
Four Cancer Research Workshops
Vision and Progress
Dr. Rosemarie Gannon Project Manager, All-Island Cancer Research Institute (AICRI) Member, AICRI Steering Committee and Core Working Group
About AICRI
The vision for All-Island Cancer Research Institute (AICRI) is to bring together the combined strengths of cancer researchers across the island of Ireland to create an overarching framework for cancer research.1 Over the last 18 months, AICRI has brought together ten academic institutions and multiple other stakeholders from the healthcare sector, cancer patients, cancer charities, industry partners and government agencies. It has a broad research programme from cancer prevention to cancer diagnosis and treatment to survivorship and quality of life. AICRI has taken a bottom-up approach in its activities and has achieved considerable success over the past year, particularly in relation to acquisition of initial funding. Moreover, it has organised a series of highly successful research and other stakeholder workshops which have been key in honing the AICRI vision.
On 24th March 2022, AICRI held an online workshop on ImmunoOncology and the Microbiome which was led by the Royal College of Surgeons in Ireland and University College Cork and attended by 72 people. Topics covered in this workshop included tumour immunology, immune cell therapy for cancer and other forms of immunotherapy, as well as the role of the microbiome as a modulator of cancer risk and cancer development. This workshop again highlighted the 60
AICRI receives its first funding success in December 2021 In December 2021, AICRI received a New Foundations Award from the Irish Research Council. This €20,000 award from the Shared Island Fund has allowed AICRI to hold a series
SEPTEMBER 2022 • HPN |
About AICRI
AICRI makes huge strides in developing an Overarching Framework for Cancer Research on the Island of Ireland
Ciaran Briscoe CEO, North East Cancer Research Trust (NECRET) Member, AICRI Steering Committee and Core Working Group
Ciaran Briscoe CEO, North East Cancer Research Trust Member,(NECRET)AICRI Steering Committee and Core Working Group
All-Island Cancer Research Institute (AICRI) Deputy Director, Precision Oncology Ireland
ONCOLOGY FOCUS: AICRI
Island Fund has allowed AICRI to hold a series of key stakeholder workshops in 2022 and to develop a dedicated website. These activities help raise the profile of the project, as well as make sure its objectives take on board relevant stakeholder input, including those with a lived experience of cancer. AICRI receives its foundation stone funding in March 2022 In March 2022, AICRI was awarded ¤4 million in funding from the Shared Island Fund as a Strand III (Partnerships of Scale) award under the HEA North-South Research Programme. This award allows for the creation of an All-Island Doctoral and Post-Doctoral Research Training Programme in Precision Cancer Medicine (AICRIstart), led by Prof. William Gallagher (University College Dublin) and Prof. Mark Lawler (Queen’s University Belfast). The AICRIstart programme will train ten doctoral students and ten postdoctoral fellows with significant expertise in precision cancer medicine and is due to begin in September 2022 and run for four years. By bringing together ten academic institutions on the island of Ireland (UCD, TCD, RCSI, TU Dublin, DCU, QUB, UU, NUIG, UL and UCC) in this foundational initiative, AICRIstart will catalyse a unique all-island network of excellence in cancer research.
Professor William Gallagher Professor of Cancer Biology, UCD School of Biomolecular and Biomedical Science Conway Fellow, UCD Conway Institute Co Lead, All Island Cancer Research Institute (AICRI) Deputy Director, Precision Oncology Ireland
AICRI receives its first funding success in December 2021
The All-Island Cancer Research Institute (AICRI):
Dr. Rosemarie Gannon Project Manager, All Island Cancer Research Institute (AICRI) Memb er, AICRI Steering Committee and Core Working Group
and Biomedical Science Conway Fellow, UCD Conway Co-Lead,Institute
In December 2021, AICRI received a New Foundations Award from the Irish Research Council. This ¤20,000 award from the Shared
On 26th November 2021, AICRI held an online workshop on Living With and Beyond Cancer which was led by Trinity College Dublin and attended by 100 people. Topics covered in this workshop included exercise and nutrition, communication and psychosocial needs and systems change and supporting optimum quality of life across the life span. The findings of the workshop highlighted the added value of research in this area of survivorship and living with and beyond cancer is to meet the needs of cancer patients to recover after a cancer diagnosis and to optimise their quality of life and that of their families.
The All-Island Cancer Research Institute (AICRI): Vision and Progress
Through its broader work, AICRI will contribute to policy development relevant to the Shared Island initiative, particularly in terms of building a healthier island. Under the same HEA NorthSouth Research programme, two additional large-scale AICRI-linked cancer research awards (circa. ¤4 million each) were announced in the areas of eHealth - An All-Island eHealth Hub for Cancer (led by Prof. Aedin Culhane, University of Limerick and Prof. Mark Lawler, Queen’s University Belfast) and liquid biopsies - All-Ireland Cancer Liquid Biopsies Consortium (CLuB) (led by Prof. Lorraine O’Driscoll, Trinity College Dublin and Prof. Paul Mullan, Queen’s University Belfast). Indeed, more than one third of the funding under the initial tranche of the scheme was allocated, as jointly announced by Taoiseach Micheál Martin and Minister Simon Harris on 2nd March 2022 to cross-border cancer research projects, largely linked to AICRI’s collaborative process.
AICRI makes huge strides in developing an Overarching Framework for Cancer Research on the Island of Ireland
The vision for All-Island Cancer Research Institute (AICRI) is to bring together the combined strengths of cancer researchers across the island of Ireland to create an overarching framework for cancer research (1) Over the last 18 months, AICRI has brought together ten academic institutions and multiple other stakeholders from the healthcare sector, cancer patients, cancer charities, industry partners and government agencies. It has a broad research programme from cancer prevention to cancer diagnosis and treatment to survivorship and quality of life. AICRI has taken a bottom up approach in its activities and has achieved considerable success over the past year, particularly in relation to acquisition of initial funding. Moreover, it has organised a series of highly successful research and other stakeholder workshops which have been key in honing the AICRI vision
Following a request for project ideas from the cancer research community across the island of Ireland, AICRI organised four very engaging and stimulating research workshops over the past year covering key thematic areas which were well attended.




AICRI Digital Health in Cancer Workshop, 27th April 2022, Limerick.
HOSPITALPROFESSIONALNEWS.IE
AICRI/PVCR Patient Stakeholder Workshop, 30th March 2022, Cork.
Engagement with Cancer Charities Active in Research
need for greater collaboration between academics and clinicians. The workshop also pointed out the need for greater patient involvement in research and that patient input should be an integral part of clinical research projects.
Finally, on 26th May 2022, AICRI held an online workshop on Functional Cancer Genomics and Precision Oncology, led by Trinity College Dublin and University College Dublin, which was attended by 180 people. Topics covered in this workshop included harnessing functional genomics to develop targeted therapies for cancers, genomics-driven RNA therapeutics in oncology, digital twins for precision oncology, and adaptive clinical trial designs to facilitate precision oncology. The workshop highlighted the importance of training in stateof-the-art technology and analysis, as well as the natural progression from functional cancer genomics to precision oncology. The workshop also pointed out the need for more collaboration between scientists and clinicians, as exemplified by ongoing discussions in relation to national policy on genomics and genetics which the HSE is currently developing together with a variety of stakeholders. Engagement with Patients Living with Cancer Patients are at the core of our work and indeed our ethos is “With the patient; around the patient; for the patient”. On 30th March 2022, we held a hybrid Patient Stakeholder Workshop, held in Cork and co-led by AICRI representatives and the Patient Voice in Cancer Research (PVCR) at UCD. This workshop was attended by 64 people (24 in-person and 40 online). This was a key event as one of AICRI’s main objectives is to engage with cancer patient advocacy groups across the island to ensure the voice of patients living with and beyond cancer is heard. This is central to AICRI’s vision.
61
Left to right: Prof. Amanda McCann (UCD and Lead, Patient Voice in Cancer Research), Prof. William Gallagher (UCD and Co-Lead, AICRI), Stephen Teap (Facilitator for Workshop and Co-Founder, 221+ Group), Ciara McNamara (Patient Advocate), Prof. Mark Lawler (QUB and Co-Lead, AICRI), Tom Hope (Patient Advocate), Kay McKeon (UCD and Patient Advocate) and John Wall (Patient Advocate)
On 30th June 2022, we held an online Cancer Charities workshop with seven key cancer researchsupporting charities on the island of Ireland as follows: Cancer Focus NI, Friends of the Cancer Centre Northern Ireland, Northern Ireland Pancreatic Cancer, the Irish Cancer Society, Breakthrough Cancer Research, the Oesophageal Cancer Fund and the National Children's Research Centre. This was a very engaging workshop as we explored how these cancer charities could collaborate with one another and learned more about their current research activities and priorities. Interestingly, several of these cancer charities have recently expanded their remit to include funding for all-island cancer research programmes in certain areas, such as survivorship (Irish Cancer Society) and oesophageal cancer (Breakthrough Cancer Research). | HPN • SEPTEMBER 2022
Left to right: George Maybury (Dell Technologies), Prof. William Gallagher (UCD and Co-Lead, AICRI), Prof. Aedin Culhane (UL and Co-Lead, All-Island eHealth Hub for Cancer) and Prof. Mark Lawler (QUB and Co-Lead, AICRI).
On 27th April 2022, AICRI held a hybrid Digital Health in Cancer Workshop at Dell Technologies, Limerick, led by the University of Limerick and Queen’s University Belfast with over 120 attendees. Topics covered in this workshop included digital health in the cancer landscape on the island of Ireland, data sharing, patient involvement and federated eHealth, mining ‘omic’ and image data in cancer research. Findings from this workshop highlighted the need for transparency and the importance of developing trust from the outset and clearly explaining what data is being used for. The workshop also pointed out that there is a need for more training in digital pathology and in the use of artificial intelligence (AI). We heard about the potential of AI-enabled digital twins in enabling the development of personalised diagnostics and treatments for cancer patients. We were reminded that clinicians need more support as technology at the point of care continues to evolve.


Political Engagement Over the past year, AICRI team have had a variety of productive meetings with key political stakeholders. Highlights included a meeting in Leinster House with the Joint Committee on the Implementation of the Good Friday Agreement (JCIGFA) on 21st October 2022. At this meeting, with public representatives from Ireland and Northern Ireland, the AICRI Core Working Group team presented its vision for AICRI and discussed its future plans.2 On 20th July 2022, we presented the AICRI vision at a panel discussion on 'The Future of Precision Medicine: FastTracking Innovation’, at the British Ambassador's Private Residence, Glencairn, Dublin. On 29th July 2022, there was also a very productive meeting on future US-facing engagement and collaboration with the US Ambassador to Ireland Claire Cronin, US Embassy, Ballsbridge, Dublin. Upcoming Event On 28th September 2022, we will hold the AICRI Showcase: Vision and Progress event in collaboration with 15th International Symposium on Translational Research in Oncology, Herbert Park Hotel, Dublin, organised by Prof. John Crown and colleagues. This inperson workshop will provide an opportunity for AICRI to showcase its achievements to date and roadmap future activities. All of our stakeholders are welcome and encouraged to attend this free event. The Future Considerable progress has been made over the last 12 months in terms of progressing the AICRI vision of creating an overarching framework for cancer research across the island of Ireland. Key next steps will be to attract significant core funding to place AICRI on a longer term footing, while also ensuring that the priority areas of focus highlighted in research workshops are supported. Contact Details Prof. William Gallagher, AICRI Co-Lead (william.gallagher@ucd.ie)
ONCOLOGY FOCUS: AICRI
Left to right: Senator Emer Currie, Deputy Fergus O’Dowd, TD (JCIGFA Chairperson), Prof. William Gallagher (UCD and Co Lead, AICRI), Prof. Maeve Lowery (TCD and Medical Oncologist St. James’s Hospital), Senator Erin McGreehan, Prof. Mark Lawler (QUB and Co Lead, AICRI), Eibhlin Mulroe (CEO, Cancer Trials Ireland), Brendan Smith, TD and Ciaran Briscoe (CEO, NECRET).
AICRI team meet with the Joint Committee for Implementation of the Good Friday Agreement (JCIGFA), 21st October 2021, Leinster House, Dublin.
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 62
Dr. Rosemarie Gannon, AICRI Project @AICRIprojectFollowWebsite:(rosemarie.gannon@ucd.ie)Managerwww.aicri.orgusonTwitter: References 1 Gallagher, W. (2021) “Progressing the Vision of an AllIsland Cancer Research Institute (AICRI)”, September Issue, Hospital Professional (Hospitalprofessionalnews.ie)News pp 24 and 26 2 Joint Committee on the Implementation of the Good Friday Agreement committees/4804/oireachtas-tv/video-archive/https://www.oireachtas.ie/en/Meeting
On 20th July 2022, we presented the AICRI vision at a panel discussion on 'The Future of Precision Medicine: Fast Tracking Innovation’, at the British Ambassador's Private Residence, Glencairn, Dublin. On 29th July 2022, there was also a very productive meeting
AICRI team meet with the Joint Committee for Implementation of the Good Friday Agreement (JCIGFA), 21st October 2021, Leinster House, Dublin.
Left to right: Senator Emer Currie, Committee Chair Fergus O’Dowd, TD, Prof. William Gallagher (UCD and Co-Lead, AICRI), Prof. Maeve Lowery (TCD and Medical Oncologist St. James’s Hospital), Senator Erin McGreehan, Prof. Mark Lawler (QUB and Co-Lead, AICRI), Eibhlin Mulroe (CEO, Cancer Trials Ireland), Brendan Smith, TD and Ciaran Briscoe (CEO, NECRET) meeting, with public representatives from Ireland and Northern Ireland, the AICRI Core Working Group team presented its vision for AICRI and discussed its future plans (2).

Most patients underwent primary surgical resection (80%, n = 289). Organ preserving surgery was performed in 71% of cases (n = 206), six of whom subsequently underwent total penectomy, while 28% of patients were treated with primary total penectomy (n = 81). The rate of organ preserving surgeries performed did change over time, with a gradual decrease between 1995 and 2002, and a gradual increase from 2003 to 2010 as shown in Fig. 1, however this change was not found to be statistically significant (p = 0.06). Details on specific type of organ preserving surgery were not available.
PatientResults demographics
PENILE CANCER Dr Anderson Written
cThe Department
Penile Cancer in Ireland – A National Review
Stage, grade and tumour location
The extent of direct tumour invasion was recorded in 66% of cases (n = 236), the majority of which were ≥T2 (54%, n = 127).
ONCOLOGY FOCUS: by S.Andersonac of Urology, Mercy University Hospital, Co. Cork, Ireland Ireland, Ireland of Surgical Affairs, RCSI University of Medicine Health Sciences,
,K.J.Breena1 ,N.F.Davisa1 ,S.Deadyb1 P.Sweeneya1 aDepartment
Survival outcomes Mean OS was 96 months (95% CI 102–124), and penile cancer
Although 70 patients were recorded as being lymph node positive, information on lymph node management was only available for 55 patients. Of those 55 patients, 51% underwent a biopsy or excision of a single inguinal node (n = 28), while 49% underwent nodal clearance surgery (n = 27). No information on the extent of lymph node clearance was available. Of the cases where stage and grade data was available, 183 cases were classified as either intermediate or high risk of lymph node involvement based on European Association of Urology (EAU) guidelines, though only 23% (n = 42) had some form of invasive lymph node staging recorded.10 There was however a steady increase in the percentage of intermediate or high risk patients who underwent invasive lymph node sampling over time (p = 0.026) (Fig. 2).
Clinical or pathological nodal status was recorded in 47% of cases (n = 171). Of these, 59% were N0 (n = 101), 17% were N1 (n = 29), 18% were N2 (n = 31) and 6% were N3 (n = 10).
A total of 65 (18%) patients received radiotherapy (RT), of whom 20 were treated with primary RT and 45 received adjuvant RT. Of those who received primary radiotherapy, the median time to treatment was 102 days, compared to 112 days for those receiving adjuvant RT. Only 27 patients received chemotherapy (8%), with a median of 76 days to start treatment.
Tumour grade was recorded in 80% of cases (n = 289). Of those, 30% were grade 1 (n = 87), 42% were grade 2 (n = 123), 27% were grade 3 (n = 1), and only one case was grade 4. No data on presence of lymphovascular invasion was available.
Information regarding sites of disease treated by RT, RT regimes or chemotherapy agents used were not available.
Treatment modality
The vast majority of cases were classified as SCC (91%, n = 328), 3% were melanoma (n = 9), and the remaining 6% were unspecified.
bNational Cancer Registry of
A total of 360 cases of penile cancer were identified through the NCRI, with an average of 24 new cases per year. The median age at diagnosis was 67 years. Limited data was available regarding risk factors for penile cancer. Smoking status was recorded in 77% of cases, of which 60% were either current or ex-smokers (n = 165). No information regarding history of phimosis, prior circumcision, or HPV status was available.
and
HOSPITALPROFESSIONALNEWS.IEIreland | HPN • SEPTEMBER 2022 63
Similarly, data on metastatic disease was available on 159 patients (44%), of which only 8% (n = 12) were M1 at diagnosis.
Materials and methods Overview of study design
Cases were identified through the National Cancer Registry Ireland (NCRI). The NCRI was established in 1991 by the Minister for Health in order to record information on all cancer cases in Ireland. This data is used to publish annual reports on incidence trend and to provide advice to the Minister for Health and to facilitate collaborative research. Following application to the NCRI in January 2017, we identified all cases of primary penile cancer in Ireland between 1995 and 2010. A database of patient demographics and clinicopathological characteristics was created and a retrospective review was undertaken. Primary outcome measurements were overall survival (OS) and disease specific survival (DSS). Secondary outcome measurements were prognostic factors. Staging is based on the 5th version of the penile cancer TNM classification.
Tumour location was recorded in 43% of cases (n = 156). Of those, the glans was affected in 52% of cases (n = 82), followed by the prepuce (32%, n = 53), the shaft (13%, n = 20), and overlapping lesions (<1%, n = 1).
Introduction Penile cancer is a rare malignancy, with an average incidence of around 1 per 100,000 in Europe, though significantly higher rates are seen in the developing world.1 The incidence increases with age and peaks during the sixth decade of life. Squamous cell carcinoma (SCC) accounts for >95% of cases of primary penile cancer.2 Well documented risk factors include a history of phimosis, chronic inflammation, smoking, poor hygiene, and Human papilloma virus (HPV) infection; in particular HPV types 16 and 18.3 The presence of HPV is associated with SCC of the penis in ≤50% of cases, which may explain the higher incidence of penile cancer in countries where HPV is more prevalent such as Brazil and Uganda.4 Lymph node status at diagnosis is the most important prognostic marker.5 The management of clinically node negative patients is challenging, as micro metastatic disease is not readily detectable and is present in 25% of patients with non-palpable inguinal nodes at presentation. While early lymphadenectomy in such patients offers a significant survival benefit, it carries a high risk of morbidity.6 There is a paucity of large, prospective randomised studies in the literature due to the rare nature of the disease, and as such, defining optimal management of penile cancer remains challenging. To address these challenges, there has been a recent move towards centralisation of treatment in many countries with improved patient outcomes demonstrated.7 While discussions regarding the centralisation of penile cancer services in Ireland have begun, it has yet to be implemented, despite a growing body of evidence to support it.8,9 The aim of this study was to perform the first review of national data on penile cancer in Ireland.

Opjordsmoen et al., in which patients treated with total penectomy reported that, if given the choice, they would choose reduced long-term survival if they were able to retain sexual function.16 The rate of total penectomy performed in this study remains relatively high when compared to previously reported data from our institution (28% vs 16% respectively), despite patients being closely matched for stage of disease.9 Such differences can also be seen when examining lymph node management.
Lymph node involvement is the most important prognostic factor influencing survival.5 Clinical examination and radiological assessment are insufficient for establishing nodal involvement, as 25% of patients without palpable inguinal adenopathy have radiologically occult nodal metastases.17,18 Therefore, international guidelines recommend lymph node staging for intermediate and high risk patients based on T stage and grade of disease (≥T1G2).10 There is currently no defined national standard for managing clinically node negative penile cancer patients in Ireland. This is reflected in this study, as only 15.3% of all patients, and 23% of intermediate or high risk patients were recorded as undergoing some form of invasive lymph node sampling, compared to 88% of high risk patients in data previously published from our institution.9 Also of note is the low rate of treatment with chemotherapy (7.5%). Although limited data was available, there was no measurable change in chemotherapy use over time in this study. Due to the limited data available from the NCRI it is not possible to definitively explain the high rates of total penectomies performed and low rates of inguinal node sampling seen in this study. However, given the lack of centralisation of care, and the low numbers of cases seen each year in Ireland, it is certainly possible that surgeon inexperience may account for these findings. This may also Figure 1
Figure SEPTEMBER2 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 64
Primary surgical resection remains the standard of care for local disease control. Organ preserving surgery has grown in popularity as it has been shown to offer patients equivalent oncological outcomes compared to total penectomy, while maintaining organ function.15 Furthermore, total penectomy imposes a significant psychological impact on patients, the extent of which was highlighted in a survey by
ONCOLOGY FOCUS: PENILE CANCER related mortality was 28% (n = 100). DSS was 74%, 70% and 67% at three, five and ten years respectively. DSS was significantly worse in node positive patients (Fig. 3). DSS for node negative patients was 79%, 75% and 70% at three, five and ten years respectively, compared to 44%, 41% and 38% in node positive patients (p < 0.001). On univariate analysis, age, marital status, T stage, N stage, M stage, grade and treatment modality (lymph node resection, RT and CT) were found to be statistically significant prognostic indicators. However, on multivariate analysis, only age, nodal status and presence of metastatic disease were independent prognostic indicators of DSS. Discussion The overall incidence and age profile of patients in this study are comparable to the figures reported across the globe.1,2,11,12 The majority of patients presented with pT1-pT2 disease. While this is comparable to rates in Europe, the rates of non-invasive disease are considerably lower in the Irish cohort. A total of 1.3% (of cases where T stage was recorded) were stage pTis or pTa nationally, compared to 7% and 20% of recently reported data from the Netherlands and the United Kingdom (UK) respectively.13 14 Previously published single-centre data from our institution has shown that Irish patients present late after symptom onset, which may explain the low rates of non-invasive disease seen nationally.9 However, to date no data has been published to explain this finding and perhaps greater public awareness is needed to prevent late presentations.


Figure
While this study is the first to report national data on the management of penile cancer in Ireland, there are several important limitations. As a retrospective study, there is the acknowledged risk of bias. In order to ensure a minimum of 5-year follow-up data was available, no cases after 2010 were included in this study.
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 65 explain the low rate of patients treated with chemotherapy. An interesting finding in this study is that age at diagnosis was found to be an independent prognostic marker for DSS (Fig. 3a). One potential explanation for this is that older patients may have been treated less aggressively than younger patients. When comparing treatment modalities, 28% (n = 28) of patients ≥75 years of age received no primary surgical treatment compared to only 16% (43) of those under the age of 75 (Chi-square 5.3, p = 0.021), despite there being no significant difference in stage or grade of disease. A similar finding was reported in a study by Ary et al., in which relative survival was much lower in men ≥80 years of age compared to those under 80.19 The potential presence of significant underlying comorbidities in this age group precluding them from radical treatment options, as well as patient preference for more conservative treatment may explain the reduced DSS in elderly patients, however insufficient data is available in this study to analyse these factors.
Importantly, the dataset from the NCRI is incomplete, with unknown data accounting for up to 50% of certain datapoints such as stage and grade of disease. While this significantly limits the comparison of this data to the Irish series reported to date, and to previously reported European figures, it is the authors’ opinion that the available data still provides valuable information on the management of penile cancer in Ireland.
In recent years, the centralisation of the management of penile cancer in the UK has led to significantly higher rates of organ preserving surgery and improved lymph node management.7 20 Centralisation has yet to be implemented in Ireland however the issue has been highlighted by the Irish Society of Urology and the Royal College of Surgeons Ireland with the National Cancer Control Programme (NCCP). Although survival rates from the NCRI database are equal to European figures (70% 5-year DSS), higher rates were seen in our data from the Mercy University Hospital which offers a rapid access penile cancer referral pathway and management by a fellowship trained uro-oncologist (92% 5-year DSS).1,9 The difference in DSS, as well as the higher rates of organ preserving surgery and invasive inguinal lymph node staging performed in the Mercy University Hospital data compared to the national figures reported here provides further evidence to support the centralisation of penile cancer management in Ireland. However, the authors acknowledge that there are significant challenges surrounding centralising the management of penile cancer in Ireland, the most notable being the number and location of designated centres. Guidelines from the UK advocate for supra-regional networks covering a population of 4 million people, with an expected 25 cases of penile cancer per year.21 This would suggest that only one centre is needed in the Republic of Ireland. However, the population density of the Republic of Ireland (around 70 persons per square kilometre) is significantly lower than that of the UK (around 275 persons per square kilometre), a factor that must be considered when structuring any potential centralisation proposal.22 23
Conclusion This study, the largest to report on penile cancer data in the Republic of Ireland, has shown that overall patient demographics and outcomes are similar in Ireland to European and American figures. However, superior DSS and adherence to European guidelines on nodal management has been reported from high volume centres in Ireland.9 This supports the growing body of evidence that in order to meet current international standards of care, penile cancer patients in Ireland should be managed in designated specialised multi-disciplinary centres, which can only be achieved through centralisation agreed and funded by the NCCP.3

• Provide best practice, evidencebased rehabilitation information to patients and carers of those living with, and beyond cancer.
Domains Intervention
to optimise function for those who experience disability aftertreatmentscancer Palliative Intervention to maintain functional and quality of life
Written by Grainne Sheill, Trinity St James’s Cancer Institute, Dublin
• Provide individual assessments, treatment programmes and group exercise programmes to approximately 500 patients experiencing cancer-related impairments in St James’s Hospital annually – both on-line and in-person.
Evidence Supporting the Role of Exercise in Cancer Rehabilitation
The main aims of the service are to:
ONCOLOGY REHABILITATION
The Cancer Rehabilitation Exercise Service in St James’s Hospital
FOCUS:
intervention. Anyone diagnosed with cancer is advised to engage in 150 minutes of aerobic activity and 2 strengthening sessions a week. Despite this, many cancer survivors do not engage in sufficient levels of exercise. Cancer survivors report a need for guidance, education and support when increasing physical activity levels following cancer treatment.
In October 2021 the Physiotherapy Department in St James’s Hospital started an exercise-based cancer rehabilitation service for patients during and after cancer treatment.
• Develop cancer rehabilitation pathways from acute cancer centers to primary care.
The Development of a Cancer Rehabilitation Exercise Service in a National Cancer Centre
Data on 250 patients referred to the service between October 2021 and May 2022 found that 56% of those were male. The mean age of clients was 64±11 years (Range 31-83 years). The main tumour groups presenting were thoracic cancer (n=78), prostate cancer (n=55), breast cancer (n=30), head and neck cancer (n=29), GI cancer (n=25), gynaecological (n=16) and colorectal (n=11). In total 73% of patients were in the first-year post treatment and 18% more than a year post treatment while 9% were on treatment at the time of physiotherapy review. Patient assessment identified physical impairments such as frailty, cancer related fatigue, and decreased strength. Patients attended on average 4 physiotherapy sessions, for input including exercise assessment and advice sessions (24%), 1:1 physiotherapy input (37%), group based supervised exercise programmes (22%) and onward referral (13%). The most common onward referral was to primary care physiotherapy (n=27) for patients to receive physiotherapy input close to their homes.
An online cancer rehabilitation exercise class
The Cancer Rehabilitation Exercise Physiotherapy service in St James’s Hospital provides one of the first dedicated exercise oncology services nationally. Patients presenting to the cancer rehabilitation service attend with a variety of cancer related impairments and cancer rehabilitation needs. Screening to identify rehabilitation needs combined with exercise prescription can effectively improve the quality of survivorship in cancer patients. Referral to cancer rehabilitation is indicated for patients during and after cancer treatment and there is a need to further develop and expand the cancer rehabilitation exercise services available to patients.
References: Campbell, K.L., Winters-Stone, K., Wiskemann, J., May, A.M., Schwartz, A.L., Courneya, K.S., Zucker, D., Matthews, C., Ligibel, J., Gerber, L. and Morris, S., 2019. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Medicine and science in sports and exercise, 51(11), p.2375. Wolin KY, Schwartz AL, Matthews CE, Courneya KS, Schmitz KH. Implementing the exercise guidelines for cancer survivors. J Support Oncol. 2012 SepOct;10(5):171-7. doi: 10.1016/j. suponc.2012.02.001. Epub 2012 May 10. PMID: 22579268; PMCID: PMC3543866.
Introduction Approximately 4,4860 patients are diagnosed and/or treated for cancer in St. James’s Hospital annually. As the number of cancer survivors and the length of their survival continue to increase, the long-term health issues related to cancer and its treatment are becoming more prevalent. Many adverse consequences of cancer treatment are amenable to physiotherapy led interventions; however, the integration of rehabilitation into standard cancer care continues to remain the exception rather than the norm in Ireland. Irish cancer survivors have identified a striking lack of care from healthcare professionals that would be influential in facilitating cancer recovery and rehabilitation.
of Cancer Rehabilitation Preventative Screen, monitor, educate and intervene to prevent or mitigate the effects of treatmentcanceronfunction Restorative interventionTargeted to alleviateimpairmentsfunctionalandrestorefunction Supportive
SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE 66
Systematic reviews demonstrate that exercise in cancer survivors improves quality of life, cardiorespiratory fitness, physical functioning, and fatigue. Exercise is an effective non-pharmacologic intervention to ameliorate the impact of cancer-related fatigue and improve patients’ quality of life. Increasing physical activity levels may also decrease the risk of additional late effects of cancer, for example, the cardiac, pulmonary, endocrine, or bone complications of cancer treatment and may even reduce the risk of secondary malignancies. Research on the cost-effectives of individualised cancer rehabilitation interventions also demonstrate positive effects of exercise oncology during cancer care, in terms of reductions in overall cost per patient pre- to post-exercise
• Act as an educational resource on the role of exercise in the management of the physical side-effects of cancer to healthcare professionals, patients and the public.

Reporting of Suspected Adverse Reactions
Further information can be found in the Summary of Product Characteristics or from: LEO Pharma, Cashel Road, Dublin 12, Ireland. E-mail: medical-info.ie@leo-pharma.com ® Registered trademark IL, interleukin. References: 1. Adtralza® SPC. 2. Bieber T. Allergy 2020;75:54–62. patient. purposes
For the treatment of moderate to severe atopic dermatitis in adult patients who are candidates for systemic therapy1NEW This is a promotional advertisement from LEO Pharma for IE healthcare professionals. Learn more at www.adtralza.ie Introducing Adtralza® The first licensed biologic that inhibits IL-13 alone,1 a key driver of atopic dermatitis signs and symptoms.2
Method of administration: Subcutaneous use. The pre-filled syringe should be not shaken. After removing the pre-filled syringes from the refrigerator, they should be allowed to reach room temperature by waiting for 30 minutes before injecting. Tralokinumab is administered by subcutaneous injection into the thigh or abdomen, except the 5 cm around the navel. If somebody else administers the injection, the upper arm can also be used. For the initial 600 mg dose, four 150 mg tralokinumab injections should be administered consecutively in different injection sites. It is recommended to rotate the injection site with each dose. Tralokinumab should not be injected into skin that is tender, damaged or has bruises or scars. A patient may self-inject tralokinumab or the patient’s caregiver may administer tralokinumab if their healthcare professional determines that this is appropriate. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: If a systemic hypersensitivity reaction (immediate or delayed) occurs, administration of tralokinumab should be discontinued and appropriate therapy initiated. Patients treated with tralokinumab who develop conjunctivitis that does not resolve following standard treatment should undergo ophthalmological examination. Patients with pre-existing helminth infections should be treated before initiating treatment with tralokinumab. If patients become infected while receiving tralokinumab and do not respond to antihelminth treatment, treatment with tralokinumab should be discontinued until infection resolves. Live and live attenuated vaccines should not be given concurrently with tralokinumab. Fertility, pregnancy and lactation: There is limited data from the use of tralokinumab in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. As a precautionary measure, it is preferable to avoid the use of tralokinumab during pregnancy. It is unknown whether tralokinumab is excreted in human milk or absorbed systemically after ingestion. Animal studies did not show any effects on male and female reproductive organs and on sperm count, motility and morphology. Side effects: Very common (≥1/10): Upper respiratory tract infections. Common (≥1/100 to <1/10): conjunctivitis, conjunctivitis allergic, eosinophilia, injection site reaction. Uncommon (≥1/1,000 to <1/100): keratitis. Precautions for storage: Store in a refrigerator (2°C-8°C). Do not freeze. Store in the original package in order to protect from light. Legal category: POM. Marketing authorisation number and holder: EU/1/21/1554/002. LEO Pharma A/S, Ballerup, Denmark. Last revised: June 2021 Reference number: REF-19238(1)
Adverse events should be reported. Reporting forms and information can be obtained from: HPRA Pharmacovigilance, Website: www.hpra.ie Adverse events should also be reported to Drug Safety at LEO Pharma by calling +353 1 4908924 or e-mail medical-info.ie@leo-pharma.com
Date of preparation: February IE/MAT-544632022V1
For illustrative
Not an actual
only.
Prescribing Information for Adtralza® (tralokinumab) 150 mg solution for injection in pre-filled syringe Please refer to the full Summary of Product Characteristics (SmPC) (www.medicines.ie) beforeThisprescribing.medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. Indications: Treatment of moderate-tosevere atopic dermatitis in adult patients who are candidates for systemic therapy. Active ingredients: Each pre-filled syringe contains 150 mg of tralokinumab in 1 mL solution (150 mg/mL). Dosage and administration: Posology: The recommended dose of tralokinumab is an initial dose of 600 mg (four 150 mg injections) followed by 300 mg (two 150 mg injections) administered every other week as subcutaneous injection. Every fourth week dosing may be considered for patients who achieve clear or almost clear skin after 16 weeks of treatment. Consideration should be given to discontinuing treatment in patients who have shown no response after 16 weeks of treatment. Some patients with initial partial response may subsequently improve further with continued treatment every other week beyond 16 weeks. Tralokinumab can be used with or without topical corticosteroids. The use of topical corticosteroids, when appropriate, may provide an additional effect to the overall efficacy of tralokinumab. Topical calcineurin inhibitors may be used, but should be reserved for problem areas only, such as the face, neck, intertriginous and genital areas. If a dose is missed, the dose should be administered as soon as possible and then dosing should be resumed at the regular scheduled time. No dose adjustment is recommended for elderly patients, patients with renal impairment or patients with hepatic impairment. For patients with high body weight (>100 kg), who achieve clear or almost clear skin after 16 weeks of treatment, reducing the dosage to every fourth week might not be appropriate. The safety and efficacy of tralokinumab in children below the age of 18 years have not yet been established.
TIME TO PRESS PLAY




SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Dr Margaret Higgins, Respiratory Registrar, Mater University Hospital and Dr Dermot O’Callaghan, Consultant Respiratory Physician, Mater University Hospital
For those patients who contracted COVID-19, the initial mandatory period of self-isolation in the context of infection (or as a result of being a close contact with another infected person) also resulted in delays in initial clinic reviews. Furthermore, patients who developed more severe disease frequently experienced a clinical deterioration in pulmonary status that negatively impacted these individuals’ suitability to undergo invasive testing and/or treatment.
Under the auspices of the National Cancer Control Programme (NCCP), specific referral pathways were established over a decade ago from primary care to urgent hospital outpatient clinic evaluation for patients with symptoms suggestive of lung cancer. These individuals can expect an appointment for evaluation at a specialized cancer centre within 10 working days. Since the program’s establishment up to and including 2019, there was a year-on-year increase in the numbers of new patients assessed across the 8 Rapid Access Clinics in Ireland overall through this pathway. A report published by the NCCP in Ireland however found that new clinic attendances dropped by 33% with the onset of the pandemic, though did recover thereafter (fig 1). In March and April 2020 there was a 29% and 49% reduction, respectively, in electronic-referrals to expert centres, the preferred method of referral. Cancer Research UK similarly found that referral rates were 40% lower than before the pandemic-enforced lockdown across Britain.
the development of hybrid models of care, with establishment of virtual clinics, modification of diagnostic pathways and scaling up of surgical and medical and radiation oncology activity at private hospitals in an effort to expedite patient treatments.
COVID-19 Effects on Diagnostic and Therapeutic Pathways Clinic Referrals and Patient Attendance
1. New attendances at the lung rapid access clinics in 2019 vs 2020, WrittenNCCPby
Access to Diagnostics
The Impact of COVID-19 on Lung Cancer Care
There are a number of factors which accounted for the decrease in patient clinic attendances during the initial phase of the pandemic. Patients with symptoms concerning for lung cancer frequently postponed outpatient appointments through concerns about acquiring the infection in the hospital setting. The overlap in symptomology between COVID-19 and lung cancer led to some patients self-isolating further due to concern about being infectious, particularly at periods when access to testing for the virus was delayed, such as was the case in early waves of the pandemic.
68 ONCOLOGY FOCUS: LUNG CANCER
A recent publication by Flores et al in the Journal of Thoracic Oncology reported on evidence of a stage migration among patients attending the Mount Sinai Cancer Centre in New York City. These investigators reported that the proportion of those with stage III/IV disease at presentation in the early phase of the pandemic was nearly double that of the pre-pandemic annual average, whereas there was a 50% decrease in the numbers presenting with stage 0, I and II disease. This is reflected in other centres in the U.S. including Cornell Health, also in New York City, and Washington State. In a centre in Turkey, Can Guven et al. reported that new referrals of localised non-small cell lung cancer (NSCLC) were greater in 2019 than in 2020, whereas there was an increase in the numbers presenting with advanced stage disease. In Australia, Degeling et al. developed an inverse stage-shift model to estimate the impact of COVID-19 on mortality and health economics. They estimated that the proportion of stage I lung cancers in 2020 that would progress during a 3- and 6-month delay were 2.1% and 8% respectively. This is of particular importance, given the strong inverse relationship between increasing stage and survival.
Figure
In 2020, lung cancer was the second most common cancer diagnosis across the globe, with 2.2 million new cases (equivalent to 12.2% of all cancers worldwide) and accounting for 1.8 million deaths. In Ireland, there are approximately 2,700 people diagnosed with lung cancer each year and the disease represents an enormous national health and socioeconomic burden. On the 11th of March 2020, COVID-19 was declared a global pandemic by the World Health Organisation. COVID-19 has enforced many changes to lung cancer care, affecting the numbers of patients attending for clinic appointments, resulting in delayed access to diagnostics and negatively impacting treatment timelines. Because of the pandemic and the resultant societal lockdowns, clinicians have been forced to adapt how rapid access clinics are run, leading to
Dr. Margaret Higgins Dr. Dermot O’Callaghan
Bronchoscopy is a critically important component and diagnostic tool in the assessment of lung cancer. However, access to this diagnostic tool early in the COVID-19 pandemic was significantly reduced, in order to protect both healthcare workers and patients, due to its aerosolgenerating nature and high risk of virus transmission. While it was later demonstrated that bronchoscopy can be safely undertaken with protective measures in place, it had a significant impact on access to diagnostics in Ireland initially. This was reflected in other reported international experiences also. For example, a study involving 37 units across Portugal published by Guedes et al noted a 31% decrease in the number of bronchoscopies performed, with the mean of 345 (±249) procedures carried out in each centre in 2020 compared to 500 (±346) the year prior. Indeed, in some jurisdictions, aerosol-generating bronchoscopic procedures (including endobronchial ultrasound (EBUS)) were completely suspended. A study across 58 cancer centres in the U.K. by Bartlett-Pestell and co-authors reported that bronchoscopy and EBUS services were completely suspended in 16 (27.6%) and 10 (17.2%) sites, respectively, in the early phase of the pandemic. Because of this significant risk of virus transmission, alterations in bronchoscopy unit operating procedure have become necessary. Protective measures, including routine pre-procedural swab/safety questionnaire and careful adherence to full personal protective equipment use (PPE),


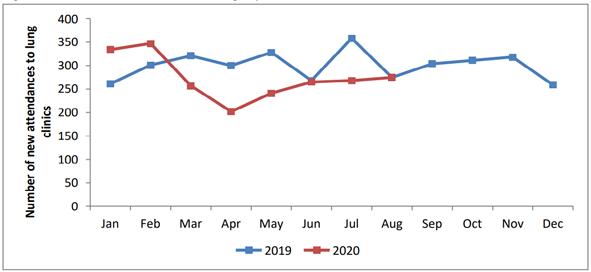
Over the subsequent course of the pandemic, further bespoke local arrangements between the HSE and various private hospitals have been established across the county in order to ensure timely access to predominantly curative-intent surgical intervention, but also to other cancer therapeutic modalities.
There have been arguments for and against pausing screening during the pandemic. Proponents in favour of temporarily suspending these programs point to the potential exposure of patients to the virus through hospital attendances leading to speculation that this risk competes with the mortality benefit conferred by early cancer detection, particularly given the pressures on acute health care systems in flux. Advocates for continuing LDCT screening in spite of the ongoing widespread virus spread highlight that risk of transmission can be minimised in an outpatient setting where mask wearing is mandatory, particularly with the widespread rollout of COVID-19 vaccination programs, in conjunction with readily available PCR and/or antigen virus testing, and highlight the potential of this program to detect early stage (i.e. curable) cancers. This benefit is particularly evident among marginalised populations that have particularly high risk of the disease. The National Cancer Institute (NCI) have acknowledged that the pandemic-associated
The implementation of new infection control and procedure room disinfection protocols however has led to an ubiquitous lengthening of interprocedural time delays, resulting in reduced capacity throughout the country, particularly for single procedure room units. The requirement for pre-procedural COVID-19 nasopharyngeal swab to help identify patients with potentially asymptomatic infection also posed logistic challenges to both patients and endoscopy units and procedure cancellations. Screening While there is as yet no screening program for early detection of lung cancer in Ireland, the COVID-19 pandemic saw a significant reduction, and, in certain regions, suspension of annual low-dose computed tomography (LDCT) screening in territories where it has been established. Pre-pandemic, the U.S. Centre for Disease Control and Prevention (CDC) reported that only approximately one in eight adults who met the eligibility criteria for LDCT screening attended for screening and most centres reported a significant reduction in patients undergoing this assessment as a result of COVID-enforced restrictions and patient preferences.
reduction in the numbers screened will inevitably lead to an increase of patients diagnosed with later stage disease. Cancer Management COVID-19 has caused significant disruption in the delivery of systemic treatment for oncology patients. A study from McGill University in Montreal noted that of 211 patients who were receiving active treatment at the onset of the pandemic, 121 (57%) experienced at least one change in the lung cancer treatment plan. In Ireland, although potentially overestimated due to movement of treatments off-site, day case attendance for chemotherapy reached its lowest point in April 2020, with an approximate 30% reduction from expected levels (across all cancer types) compared to previous years.
including use of FFP2/3 masks as standard, were rolled out. In Ireland, a protocol on guidance for safe bronchoscopy unit operations was published in 2020 by the Health Service Executive (HSE) in conjunction with the Irish Thoracic Society (ITS). Similar guidelines were published by the British Thoracic Society and other international respiratory groups.
During the COVID-19 pandemic, there was a marked increase in virtual consulting and telehealth. This has allowed the timely review and management planning for lung cancer patients in both the immediate and remote setting. There has been also greater emphasis placed on virtual multidisciplinary meetings which has also allowed specialist input outside of tertiary centres. A telehealth study published earlier this year by West et al in the AccessHope Cancer Centre in California reported on the benefit of a remote subspecialist second opinion availability to assist on management decisions of lung cancer cases. This study identified evidence-based management changes affecting initiallyrecommended treatments in 28% of study subjects and confirmed the potential role of integrated subspecialist care for patients, irrespective of location. This was of particular relevance during periods of travel restrictions and/ or for patients otherwise having to ordinarily travel long distances to attend expert centres in person.
Systemic anti-cancer therapy services were similarly routinely moved offsite from some NCCP specialised centres as the number of COVID-19 admissions began to rise in HSE hospitals. Protocols were regularly updated throughout the pandemic by cancer centres to limit risk of COVID-19 spread among day-case patients receiving systemic anticancer treatments, with arrangements similar to those for surgical caseload.
HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 69
Future considerations The COVID-19 pandemic brought previously unimaginable challenges to cancer care around the world, and healthcare teams and systems have had to adapt to a dynamic situation accordingly. Delays in patients being assessed and diagnosed with lung cancer will inevitably result in delays in initiation of their treatments. Moreover, the backlog of patients with delayed initial presentation as a result of lockdowns will have knock on effects on access to diagnostic services at hospitals dealing with a significantly increased burden of unscheduled care overall. As a result, their tumour management risks moving potentially from one of curative intent to disease control, with resultant reduced survival prospects. This is especially worrisome when one considers the comparatively poor outcomes for lung cancer patients overall. In contradistinction to those diseases that typically present with acute symptoms through emergency pathways (e.g. cardiovascular disease), the true excess mortality due to COVID-19 wrought disruption to cancer pathways will likely not be fully evident for several years. Indeed, the NCCP acknowledge that the full impact of the pandemic on survival rates for lung cancer patients in Ireland will not be known until long term outcome data are available through the National Cancer Registry. However, despite this, it is clear from our experience of the COVID-19 pandemic to date that we must continue to improve provision of cancer services as we hopefully move towards the post-COVID 19 era. While there were initial concerns regarding the potential for missed cancers during virtual reviews, overall, this modality of patient assessment has been a success and has now become embedded as a core element in the model of cancer care.
Changing approach to Lung Cancer Care Virtual consults and Telehealth
In the United States, the Presidents Cancer Panel (PCP) under the Biden Administration hopes to increase uptake in cancer screenings to counteract the poor uptake prior to the pandemic and the subsequent reduction since the emergence of COVID-19. In Ireland, the Department of Health (DoH) and the NCCP worked closely with key stakeholders, including the ITS and the clinical leads from the national expert centres throughout the pandemic in order to prioritize continued provision of cancer services, in spite of extraordinarily challenging circumstances. There was a restoration of services funding in 2019, followed by further funding for the implementation of the National Cancer Strategy in 2021 which will have lasting benefit though 2022 and beyond. The DoH and NCCP, like all healthcare staff, hope that the ‘spirit of innovation’ demonstrated throughout the pandemic will continue into the future, to better serve patients with lung cancer. References available on request
In Ireland, there was an early focus on migrating much of the complex, time-sensitive surgical workload (thoracic oncology activity included) to private hospitals with equivalent facilities and expertise, including post-operative critical care, in order to allow an outlet for public hospitals that were regularly operating at surge capacity. This move was supported by the Private Hospital Agreement and was in place until June 2020, with private hospital utilisation enabling urgent treatments to be undertaken in a timely fashion for public patients.
Changes in Treatment Paradigms
Among patients who progressed to cancer-directed therapy but contracted COVID-19 during their treatment, unscheduledinfection-enforcedbreaksintherapy posed a risk of worse outcomes. A study by authors based at Memorial Sloan Kettering Cancer Centre in the U.S. reported that 62% of those with lung cancer who contracted COVID-19 were hospitalised and 25% of patients died. The pandemic caused a similar major disruption to surgical services. An Annals of Oncology study found that a delay in surgery beyond 6 months is associated with a 5-35% decline in 5-year survival depending on age and tumour stage. In Ireland, between March to June 2020 inclusive, there were 740 less cancer resections performed (among all fields of surgical oncology), corresponding to a reduction of 14% overall.
Indeed, The HSE is establishing a framework through which public hospitals will be able to routinely access private hospitals’ services in order to expedite treatments for patients where this is deemed optimal with respect to adherence to nationally agreed key performance indicators.
Supplementary prescribing is defined as a partnership between an independent prescriber and supplementary prescriber to implement an agreed patient specific clinical management plan (CMP) with the patient’s agreement, particularly but not only in relation to prescribing for a specific non-acute medical condition or health need affecting the patient. For example, if managing a patient with hypertension, the supplementary prescriber might be able to implement dose adjustments or introduce new medications to the management plan, provided this has been set out in the CMP and has been agreed with an independent prescriber.
PharmacistPrescribingPrescribing: Learning from international models and opportunities for pharmacists in Ireland
70 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Written by Mary-Claire Kennedy PhD SFHEA MRPharmS, Programme Lead for Independent and Supplementary Prescribing, University of Leeds
Usually commissioned places can only be offered to healthcare professionals working within the geographical proximity of the HEI and providing care to patients through the NHS. Those who wish to attend an HEI outside of their geographical area or those caring for patients outside of the NHS, can opt to pay privately for a place on an accredited course.
Independent and supplementary/ collaborative prescribing, also known as non-medical prescribing, has been introduced in many countries in recent decades. Since 2007, nurses and midwives in the Republic of Ireland have been able to become registered prescribers with An Bord Altranais, upon completion of a programme of study1. The contribution of independent prescribers to the quality and safety of patient care has been studied and discussed within published literature. Pharmacist prescribers can make a meaningful impact on patient care, enhancing timely access to care which is delivered in a safe and effective manner. Focusing on a specialty or specific clinical area helps pharmacists to become established and integrated as prescribers in a multidisciplinary team. Within secondary care pharmacist prescribers have been demonstrated to make a positive contribution to the management of acute conditions in addition to the ongoing management of chronic conditions through outpatient clinics2,3. There are also studies currently being conducted to understand the contribution of pharmacist prescribers to care home or nursing home settings4 A Cochrane review examining prescribing by medical and nonmedical prescribers for chronic disease management in primary and secondary care concluded that specific outcomes such as the extent of diabetes control, adverse events and patient adherence were comparable when care was overseen by a medical practitioner or independent prescriber5. Furthermore, a study examining prescribing errors has demonstrated that independent pharmacist prescribers make fewer errors than their medical counterparts6. It is reasonable to say that pharmacist prescribers make a meaningful and highquality contribution to patient care.
I have been Programme Lead for Independent and Supplementary Prescribing at the University of Leeds since 2016 so I have first-hand experience of the education of trainee prescribers who are pharmacists, nurses, midwives, physiotherapists, paramedics and podiatrists. Since I joined the University, more than 500 healthcare professionals working in many different practice settings across Yorkshire and the Humber, including small and large hospitals, GP surgeries, community pharmacies, prison and custody settings, nursing homes and palliative care have completed the prescribing programme at Leeds. Having arrived as a novice Lecturer in Pharmacy Practice to the University in 2015, scarcely aware of the existence of prescribing pharmacists, it has been a source of pride (and sometimes bemusement) that I could play such an instrumental role in the progression of the profession in the UK, while longing to see similar advancements in Ireland.
Until now only pharmacists who were more than two years qualified could apply to complete a prescribing programme offered by one of the more than forty accredited HEIs within the UK. These courses focus primarily on developing pharmacists’ clinical evaluation, communication, diagnostic and decision-making skills. Courses usually combine a number of face-to-face study days as well as online learning materials. All teaching, learning and assessment materials are mapped to the thirty-two learning outcomes defined by the GPhC11
The Royal Pharmaceutical Society’s Core Competency Framework for All Prescribers, which details the skills, knowledge and behaviours that all prescribers should demonstrate, also informs teaching and assessment for many courses. The RPS Framework can also assist with planning learning and undertaking reflection when working as prescriber12
At present in the UK, becoming an independent or supplementary prescriber requires that the pharmacist undertakes an accredited training programme with a Higher Education Institution (HEI) and completes a specified period of training in practice. There is an established model of funding of prescribing programmes and accreditation of these programmes by professional regulators. Health Education England (HEE), an executive non-departmental public body of the Department of Health and Social Care, which commissions places on prescribing training programmes in HEIs.
During the period of learning with the HEI, pharmacists are also required to complete 90 hours in practice under the supervision of a Designated Prescribing Practitioner (DPP). DPPs can be a medic, pharmacist, nurse or allied health professional with more than 3 years’ prescribing experience and who have sufficient training or experience of clinical supervision in the workplace. During this period of supervised practice, pharmacists have an opportunity to develop the knowledge and skills specifically relevant to their specialist area so that they can become a competent prescriber. It is therefore essential that a trainee pharmacist prescriber has the full support of their employer and the clinical team they work with,
The UK could be considered to have the most advanced model of independent and supplementary prescribing, which has evolved over time, having existed in some form since 1992. It was introduced following the publication of the Cumberlege Report (1986) and the Crown Report (1989), these reports suggested that patient care would be enhanced by permitting nurses to prescribe medications, although limited these items to the Nurse Prescriber Formulary7
There are currently around 9000 pharmacists registered as prescribers in the UK, representing approximately 15% of the total number of registered pharmacists 9 However, this number will increase considerably in the coming years, as from this academic year onwards, prescribing training will be integrated into the MPharm curriculum, such that pharmacists will be automatically permitted to prescribe upon initial registration with the General Pharmaceutical Council (GPhC) or Pharmaceutical Society of Northern Ireland (PSNI)10
From 2003, pharmacists were permitted to become supplementary prescribers, and in 2006 could become independent prescribers. Independent prescribing powers enable pharmacists to prescribe licensed and unlicensed medications, and controlled drugs, although there are some exceptions (i.e. drugs prescribed to treat addiction)8
A large part of the success of the prescribing pharmacist role within the UK is the development of roles such as advanced clinical pharmacists in secondary care or GP based pharmacists where prescribing is a fundamental part of effective care, and also the allocation of specific funding for training of these pharmacists.

71 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 as they will need to work closely with these individuals to gain a sufficient depth and breadth of experience in practice.
The role of pharmacist prescribers differs considerably among countries, this is likely to be a product of many different factors such as health service systems and structure, the legislative context and the perceived need for pharmacist prescribers by key stakeholders. A common feature amongst many countries is the evolution of prescribing powers over time, initially restricted to a limited formulary or collaborative/ supplementary prescribing and moving to independent or autonomous prescribing over time, with fewer restrictions on what can be prescribed. Additionally, the introduction of independent and supplementary prescribing rights is rarely implemented in isolation, they are combined with advanced practice skills such as diagnostic and clinical decision-making skills, which further enable the pharmacist to work autonomously and effectively in a range of settings.
The Future of Pharmacy Practice report identified opportunities for pharmacist prescribing in Ireland17. Indeed, there are pockets of innovative practice within some of our hospitals, striving to upskill pharmacists as prospective prescribers, supported by medical staff. However, there are undoubtedly several major changes required before such an advancement can be widely introduced in Ireland. Firstly, there is the legislative change which would rely upon the support and leadership of key stakeholders. Training and education programmes would need to be established and models of funding for such programmes considered. Support of medical and nursing colleagues will be essential for training of pharmacist prescribers in practice. There is also the challenge of placing pharmacists within roles and practice settings where their contribution as a prescriber is routinely incorporated into the delivery of care to patients, such as outpatient clinics or GP-based consultations. Consideration also needs to be given to pay and reimbursement for an enhanced role and responsibility. Perhaps of greatest consequence is the acceptability of pharmacist prescribers to other groups of healthcare professionals, to patients and to the pharmacy profession itself. It must be acknowledged that gaining annotation as a prescriber without then utilising the skill will not benefit the healthcare system nor will introduction of the qualification with relatively few pharmacists seeking to become annotated as prescribers. In other words, there must be a determination and willingness for the profession to embed prescribing as part of our professional practice. Gaining acceptability and support is likely to be incremental. Perhaps starting with prescribingsupplementary/collaborativecouldprovideevidence of the value of pharmacist prescribers. Over time, as has been the case in many countries, this can evolve into a greater breadth of prescribing powers. References available on request.
Other International Models
Many other countries have a version of independent and prescribingsupplementary/collaborativeforpharmacists, although the latter is most common. I will mention a few different models here to give you a sense of the various approaches that are adopted by different countries. Prescribing rights for pharmacists in Canada differ between provinces. Pharmacist practising within the province of Alberta are permitted to prescribe all Schedule 1 drugs (those requiring a prescription) and blood products. There are no lists of drugs; instead, all pharmacists are expected to limit their prescribing to situations where they have an adequate understanding of the patient, the condition being treated, and the drug being prescribed. Pharmacists may not prescribe drugs regulated by the Controlled Drugs and Substances Act such as accesscansteroids.benzodiazepinesnarcotics,andanabolicPrescribingpharmacistsorderlaboratorytests,laboratorytestresultsand authorise the administration of medications and blood products. Pharmacists are reimbursed for their prescribing in a deal brokered between the advocacy body, Pharmacists Association of Alberta and Alberta Health13 One of the key drivers for independent prescribing in New Zealand was the number of GPs due to retire within the next decade, this mirrors issues with the number of GPs in Ireland that have been widely discussed within the media. Prescribing powers were therefore broadened to other groups of healthcare professionals in New Zealand to enable equitable access to healthcare and timely access to medications. Pharmacist prescribers must work collaboratively with a medical prescriber whereas nurse prescribers can work independently 14. Recently a further 200 medications were added to the list of medications that be prescribed by pharmacists. However, the number of registered pharmacist prescribers remains relatively low with only 37 currently registered as such in New Zealand. These pharmacists generally work as part of a multidisciplinary team15
There are four broad models of prescribing in place in the USA, patient specific collaboration of prescribing through collaborative prescribing agreements (CPAs), population specific prescribing, state-wide protocols and class specific prescribing16. CPAs create a formal practice relationship between pharmacists and other health care professionals, whereby the pharmacist assumes responsibility for specific patient care functions that are otherwise beyond their typical “scope of practice,” but aligned with their education and training. Services can include initiation and modification of drug therapy. The extent of the services authorised under the collaborative agreement depends on the state’s statutory and regulatory provisions, and the specific agreement between the pharmacist and other health care professionals. There are acknowledged to be a number of opportunities for further
development of pharmacist prescribing in the USA including standardisation of prescriptive authority and giving pharmacists greater access to electronic medical records16
Prescribing Pharmacists in Ireland: The opportunities and challenges

Gerard Clarke MD FRCPI Graduate entry medical school, University of Limerick
Age: The most common age of onset for UC is between 15 and 30 years of age. However, a second peak occurs between 50-80 years of age representing a bimodal age distribution.11, 15
Written by Ashley Costello Bpharm, Mpharm, Graduate entry medical school, University of Limerick - Rosie Culhane B.Sc. Graduate entry medical school, University of Limerick and Gerard Clarke MD FRCPI, Graduate entry medical school, University of Limerick
Epidemiology UC was the first subcategory of IBD to be characterised as a separate entity and was first described by Samuel Wilks in 1859.6, 7 The prevalence of IBD has been trending upwards on a global scale; from 3.7 million affected individuals in 1990 to 6.8 million in 2017.8 UC is more common than Crohn’s disease with an incidence of 9 to 20 cases per 100,00 persons per year and a prevalence of 156 to 291 cases per 100,000 per year.9, 10 Highest incidences of UC have been reported in northern Europe, Canada and Australia with incidences of 24.3 per 100,000, 19.2 per 100,000 and 17.4 per 100,000 respectively.11-13
While the exact cause of UC remains unknown, the pathogenesis appears to be multifactorial; related to a combination of genetic predisposition, altered immune responses, defects in epithelial barriers along with environmental factors. Studies have reported a number of risk factors for UC:
However, nicotine replacement therapy in individuals with UC has not been shown to reduce disease severity which suggesting a tobacco effect on UC rather than nicotine alone.
Etiology and Risk Factors
Gut microbiota: A twin study described a loss of interaction between the transcriptional profile of the mucosa with the colonic microbiota in patients with UC.34
Ingestion of a diet high in total fat, animal fat and polyunsaturated fatty acids has been correlated with an increased incidence of UC as well as Crohn’s disease while a diet high in vegetables was associated with a reduced risk of UC.31-33
Pathophysiology Epithelial cells of the colon (colonocytes), mucous and epithelial barrier defects are implicated in the pathogenesis of UC. There is reduced expression of peroxisome proliferator-activated receptor gamma (PPAR-y) in the colonocytes of patients with UC, which normally functions as a negative regulator of NF-kB dependent inflammation.38, 39
Infection and Immune system: Studies have suggested that episodes of infectious gastroenteritis such as Salmonella or Campylobacter gastroenteritis may play a role in the initiation and/or exacerbation of IBD.35, 36
Dietary factors: Findings from epidemiology studies have suggested that dietary factors may play a role as factors for developing IBD. Consumption of a Westernstyle diet has been postulated to increase the risk of UC.
Sex: Whilst several studies suggest there is no sex predominance in UC,11, 16, 17 other studies have shown higher incidence rates of UC amongst males versus their female counterparts.18, 19
Other: Breast feeding has been shown to decrease the risk of developing UC.37
Ulcerative Colitis
Smoking: While previous cigarette smoking is an important risk factor associated with UC, active cigarette smoking confers a protective effect against development of UC compared to non-smokers and tend to have a milder course of disease.14, 25-28
Family history: Individuals with UC have a family history of UC from 7 to 11% and a family history of any type of IBD ranging from 8-14%.24
Genetics: Previous studies have identified 200 risk loci for IBD, with most genes contributing to both UC and Crohn’s disease phenotypes.21, 22 Of note, many of these IBD loci are implicated in other immune disorders such as ankylosing spondylitis and psoriasis.22 Human leukocyte antigen (HLA) and genes associated with barrier functionality such as HNF4A and CHH1 have been associated with an increased risk of UC.22, 23 Despite this, genetics have very little predictive capacity for phenotype and are of limited clinical use.
Furthermore, geographical locations previously considered as “low-risk” such as India and Japan have been experiencing a rise in the incidence of UC.14
Appendectomy: Appendectomy, in particular when performed for acute appendicitis in young patients appears to confer a protective effect against development of UC, suggesting that the appendix may have a role in the development of IBD.29 Findings from a large cohort study suggested that the inverse relationship between appendectomy and the risk of UC was found only for those who underwent surgery before the age of 20 (p<0.001) (N=212,963).30 Despite this association, this is not proof of causality nor is there any evidence of a therapeutic utility for it in established UC.
72 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Ashley Costello Bpharm, Mpharm, Graduate entry medical school, University of Limerick
Rosie Culhane B.Sc. Graduate entry medical school, University of Limerick
Current Overview and Management of Ulcerative Colitis
Introduction
Ulcerative colitis (UC), a subcategory of inflammatory bowel disease (IBD) is a chronic idiopathic inflammatory disorder of the bowel and the most common form of IBD worldwide. It is characterised by continuous inflammation of colonic mucosa and follows a relapsing-remitting course. Typically, inflammation in UC starts in the rectum and may extend proximally resulting in inflammation affecting a variable length of colon.1-3 Depending on the site and extent of anatomical involvement UC can be classified as proctitis, left-sided colitis or pancolitis.2, 4 The Montreal classification categorises UC patients based on maximal disease extent; with E1 or proctitis representing disease limited to the rectum, E2 representing a leftsided colitis and E3 representing extensive colitis which extends proximally to the splenic flexure.5
Ethnicity and race: UC is more common in Jewish populations than other ethnicities.14, 20 Earlier studies reported a lower prevalence of IBD in African-
American and Hispanic ethnicities compared to white population, however, more recent studies have shown that the difference in incidence between white and nonwhite populations is much smaller than previously thought.3



2. ASACOLON® 1600 mg modified-release tablets, Summary of Product Characteristics available at www.medicines.ie
DOSAGE AND ADMINISTRATION: Oral use. To be swallowed whole (not chewed, crushed, or broken) with water, with or without food. Acute ulcerative colitis: Adults and elderly: Adjust the dosage to the severity of the disease and tolerance. During exacerbation, the dose may be increased to 4800 mg daily, once daily or in 2-3 divided doses. Once remission is achieved, reduce the dose gradually to the maintenance dose. Monitor by week 8. Maintenance of remission: 1600 mg once daily. Elderly: As for adults, provided renal or hepatic function is not severely impaired. No study data. Children: Not for use in children or adolescents.
INDICATIONS: Ulcerative colitis. For the treatment of mild-to-moderate acute disease. For the maintenance of remission.
SPECIAL WARNINGS AND PRECAUTIONS: Conduct blood count, liver function tests, serum creatinine and urinary status (dip stick) prior to and during treatment. Follow up after 14 days, then every 4 weeks for 12 weeks, 3 monthly thereafter or immediately if signs appear. Not for use in patients with renal impairment. Stop treatment immediately if signs of renal impairment develop, or if there is suspicion or evidence of blood dyscrasia. Nephrolithiasis has been reported: ensure adequate fluid intake. Caution in patients with hepatic impairment, gastric or duodenal ulcer. Not for use in patients with a history of mesalazine-induced cardiac hypersensitivity. Caution in patients with any previous myo- and pericarditis of allergic background. Monitor closely: Patients with pulmonary disease, particularly asthma; patients sensitive to sulfasalazine. Stop treatment immediately if acute symptoms of intolerance (e.g. abdominal cramps, acute abdominal pain, fever, severe headache and rash). Caution in elderly; use subject to renal and hepatic function. Limited data in children.
UNDESIRABLE EFFECTS: Common: Headache, abdominal pain, ulcerative colitis, dyspepsia, rash, haematuria, proteinuria. Uncommon: Eosinophilia (as part of an allergic reaction), paresthesia, urticaria, pruritus, pyrexia and chest pain. Rare: Dizziness, myocarditis, pericarditis, diarrhoea, flatulence, nausea and vomiting, photosensitivity.
Very rare: Altered blood counts (aplastic anemia, agranulocytosis, pancytopenia, neutropenia, leukopenia, thrombocytopenia), blood dyscrasia, hypersensitivity reactions such as allergic exanthema, drug fever, lupus erythematosus syndrome, pancolitis, peripheral neuropathy, allergic and fibrotic lung reactions (including dyspnoea, cough, bronchospasm, alveolitis, pulmonary eosinophilia, lung infiltration, pneumonitis), interstitial pneumonia, eosinophilic pneumonia, lung disorder, acute pancreatitis, changes in liver function parameters (increase in transaminases and cholestasis parameters), hepatitis, cholestatic hepatitis, alopecia, myalgia, arthralgia, impairment of renal function including acute and chronic interstitial nephritis and renal insufficiency, nephrotic syndrome, renal failure which may be reversible on early withdrawal, oligospermia (reversible). Frequency not known: nephrolithiasis, lupus-like syndrome, changes in weight and blood parameters. Refer to Summary of Product Characteristics for details.
LEGAL CATEGORY: POM. MARKETING AUTHORISATION NUMBER: ASACOLON® 1600 mg MR Tablets PA MA2018/4/1.HOLDER: TILLOTTS PHARMA GMBH, Warmbacher Strasse 80, DE- 79618 Rheinfelden, Germany.
modified-release mesalazine
Abbreviated Prescribing Information ASACOLON®1600 mg modified-release tablets: Red-brown, oblong, film-coated tablets each containing 1600 mg mesalazine.
DATE OF PREPARATION: August 2021 CODE: 2021/20 FULL PRESCRIBING INFORMATION AVAILABLE ON REQUEST FROM THE MARKETING AUTHORISATION HOLDER OR FROM TILLOTTS PHARMA LIMITED, 25 SANDYFORD OFFICE PARK, DUBLIN 18, IRELAND, TEL: (00 353 1) 294 2015. ASACOLON® is a trademark.
INTERACTIONS: Caution recommended for the concomitant use of mesalazine with known nephrotoxic agents, including NSAIDs and azathioprine, or methothrexate as these may increase the risk of renal adverse reactions. Mesalazine can increase the myelosuppressive effects of azathioprine, 6 mercaptopurine, or thioguanine. Life threatening infection can occur. Monitor closely for signs of infection and myelosuppression. Haematological parameters, especially the leukocyte, thrombocyte and lymphocyte cell counts should be monitored weekly, especially at initiation of combination therapy. May decrease the anticoagulant effect of warfarin.
USE DURING PREGNANCY AND LACTATION: Limited data on use in pregnancy. One case of neonatal renal failure was reported. Mesalazine crosses the placental barrier; use only if benefit outweighs risk. Limited data on lactation are available.
References: 1. downloadeda-medicine/results?query=MESALAZINE&field=ACTIVESUBSTANCEShttps://www.hpra.ie/homepage/medicines/medicines-information/find-on29thApril2021
CONTRAINDICATIONS: Hypersensitivity to salicylates, mesalazine or any excipient. Severe hepatic or renal (GFR < 30 mL/min/1.73 m²) impairment.
N-acetyl-5-aminosalicylic acid and mesalazine are excreted in breast milk. The clinical significance has not been determined. Hypersensitivity reactions such as diarrhoea in the infant cannot be excluded. Use only if the benefit outweighs the risk. If the infant develops diarrhoea, discontinue breast-feeding.

Treatment – pharmacological versus surgical interventions
There are a growing number of effective biologic agents for moderate to severe UC, including anti-tumor necrosis factor (TNF) therapy (infliximab, adalimumab), anti-integrin therapy (vedolizumab), and anti-interleukin 12/23 therapy (ustekinumab).54-56 Small molecules including tofacitinib (an oral Janus kinase [JAK] inhibitor), upadacitinib (an oral JAK inhibitor), and ozanimod (an oral sphingosine-1-phosphate [S1P] receptor modulator), have also shown effectiveness as induction therapies in UC.57-60 However, due to possible risks associated with these medications (thromboembolic, cardiovascular, and malignancy risks with JAK inhibitors, and cardiovascular risks with ozanimod), they are reserved as second-line options in patients who do not achieve remission with anti-TNF-based therapy.61
Alterations in goblet-cell derived proteins which contribute to the integrity of the mucosal barrier have also been described in UC.40, 41 Gut dysbiosis has also been reported in individuals with UC.42 Reduced biodiversity, in particular lower proportions of Firmicutes and increased proportions of Gamma-proteobacteria and Enterobacteriaceae.43 Although, it remains unclear whether dysbiosis is the cause or effect of mucosal inflammation.
Although the likes of biologics and novel small molecule drugs targeting different immune pathways have revolutionised the treatment of autoimmune disorders including IBD in recent decades, unmet needs remain. Novel treatment concepts such as bispecific biologics and biologic/ small molecule drug combination therapies are also being developed (70, 71). Numerous head-to-head trials are underway to investigate what combinations of biologics can induce clinical response and remission.72 A new generation of drugs for IBD are in clinical development, including S1P modulators, IL-23 inhibitors, leukocyte adhesion inhibitors, and preferential JAK1 inhibitors.57, 71, 73 In parallel, the clinical management of IBD is being improved through introducing personalised treat-totarget strategies, biomarker-based disease activity monitoring, along with empowerment of patients through better education.74, 75
The goals of therapy encompass induction and maintenance of remission, risk reduction of complications and improvement of quality of life. The choice of therapy can be decided based on the extent and severity of disease. The modified Truelove and Witts criteria incorporates both clinical and laboratory parameters as a measurement of disease severity.5 Induction treatment for mildmoderate distal ulcerative colitis e.g. mild to moderate proctitis or proctosigmoiditis, includes mesalazine that can be administered as a foam enema usually at a dose of 2g once daily at bedtime.49 Emerging data suggests that a Multimatrix® (MMX®) mesalazine formulation may be just as effective at inducing remission in these UC patients. This drug formulation facilitates homogenous delivery of high concentrations of drug into the colon, particularly to distal segments which is often difficult to achieve using normal oral delivery.50 Maintenance can be achieved by 1g mesalazine suppositories each night.51 While the mechanism of action of mesalazine is unknown, it is closely related to salicylic acid which has anti-inflammatory properties mediated by inhibition of prostaglandin synthesis. More extensive or proximal disease, including left-sided colitis and colitis extending proximal to the splenic flexure, can be treated with oral 5-aminosalycylic acid (5-ASA) at maintenance doses of 3.0 to 3.2 g daily and induction doses of 4.8 to 5 g daily.52 In terms of treating moderate to severe ulcerative colitis systemic glucocorticoids were once the mainstay of therapy, but are avoided now due to significant toxicity; major adverse effects arise from the suppression of the skin,bone,axishypothalamic–pituitary–adrenalandinvolvemetabolism,centralnervoussystem,arterialpressureandthe gastrointestinal tract.50 There is positive data to suggest advance MMX® technology could encourage glucocorticoid use as it becomes more targeted to the distal colon, trials have shown that MMX® budesonide has been particularly useful in treating mild to moderate left sided UC.53
Surgery remains a valuable option in UC. Surgical management of ulcerative colitis is required when patients fail medical therapy or when serious complications arise.
Emergency surgery is indicated in patients with colonic perforation, life-threatening gastrointestinal hemorrhage, or toxic megacolon.62
Urgent surgery during the same hospital admission is indicated in patients with acute fulminant colitis that is refractory to medical therapy.63 A total abdominal colectomy with end ileostomy is the procedure of choice in both situations. Elective surgery is indicated in patients with persistent symptoms despite best medical management and in those with increased cancer risk.64 Most patients undergo a restorative proctocolectomy with ileal pouchanal anastomosis (RPC-IPAA). The overall mortality rate associated with surgical treatment of ulcerative colitis is less than 1 percent; the overall morbidity is about 30 percent.65 Major complications include stricture, pelvic sepsis, pouch failure, fecal incontinence, pouch anddevelopment,dysplasia/cancersexualdysfunction,femaleinfertility.66-69
References available on request
Bilsborough J, Targan S, Snapper S. Therapeutic Targets in Inflammatory Bowel Disease: Current and Future. The American Journal of Gastroenterology Supplements. 2016 Dec 1;3:27–37.
Ulcerative Colitis
Future developments
Clinical presentation Abdominal pain, bloody diarrhoea, urgency and tenesmus are typical presenting features.1, 3 Diagnostics Diagnosis of UC is based on clinical presentation, endoscopic findings and histological evaluation.44 Stool assessments should include stool culture and a Clostridium difficile assay to rule out superimposed infectious agents. Fecal calprotectin, a biomarker more specific for intestinal inflammation can be useful for ruling out IBD as individuals with low levels have a <1% chance of having IBD.45, 46 Endoscopy with biopsies is the only definitive method to establish the diagnosis of UC. Classical endoscopic findings consistent with UC include erythema, oedematous mucosa, friability, bleeding and ulcerations.47, 48
74 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE

IMFINZI® (durvalumab) 50mg/ml Concentrate for Solution for Infusion Consult Summary of Product Characteristics (SmPC) before prescribing.
Marketing Authorisation Holder: AstraZeneca AB, SE-151 85, Södertälje, Sweden. Further information available on request from: AstraZeneca Pharmaceuticals (Ireland) DAC, College Business and Technology Park, Blanchardstown Road North, Dublin 15 Tel: +353 1 6097100.
In a post-hoc subgroup analysis of the PACIFIC study, WITH IMFINZI, the median overall survival (OS) at 5 years, was 63.1 months versus 29.6 months for the placebo arm (HR: 0. 61; 95% CI, 0.44-0.85)1*
Marketing Authorisation Number: EU/1/18/1322/001; EU/1/18/1322/002.
Pregnancy and Lactation: Durvalumab may cause foetal harm when administered to a pregnant woman and is not recommended during pregnancy and in women of childbearing potential not using effective contraception during treatment and for at least 3 months after the last dose. A decision must be made whether to discontinue breast feeding or to discontinue or abstain from durvalumab therapy taking into account the benefit of breast feeding for the child and the benefit of therapy for the woman.
IMFINZI is a trademark of the AstraZeneca group of companies. ©2022 AstraZeneca. All rights reserved. Veeva ID: IE-4108 | DOP: August 2022
The most frequent any grade (>10%) adverse reactions were cough/productive cough (21.5%), diarrhoea (16.3%), rash (16.0%), pyrexia (13.8%), upper respiratory tract infections (13.5%), abdominal pain (12.7%), pruritus (10.8%), and hypothyroidism (10.1%)1 See SmPC for recommended treatment modifications for IMFINZI and management considerations.
*Patients were retrospectively tested for PD-L1 expression on tumour cell using the Ventana PD-L1 (SP263) IHC assay, where available. 63% of patients provided a tissue sample of sufficient quality and quantity to determine PD-L1 expression and 37% were unknown. This exploratory post-hoc 5-year OS analysis was conducted at ~5 years after last patient was randomised and was not powered to show statistical significance.
All immune-mediated adverse events should be managed as recommended in Table 2 Section 4.2 of the SmPC. Patients excluded from clinical trials: Patients with: a baseline ECOG performance score ≥ 2; active or prior documented autoimmune disease within 2 years of initiation of the study; a history of immunodeficiency; a history of severe immune-mediated adverse reactions; medical conditions that required systemic immunosuppression, except physiological dose of systemic corticosteroids (≤ 10 mg/day prednisone or equivalent); uncontrolled intercurrent illnesses; active tuberculosis or hepatitis B or C or HIV infection or patients receiving live attenuated vaccine within 30 days before or after the start of IMFINZI. Durvalumab should be used with caution in these populations after careful consideration of the potential benefit/risk on an individual basis. The safety of concurrent prophylactic cranial irradiation (PCI) with IMFINZI in patients with ES-SCLC is unknown.
50 mg/mL concentrate for solution for infusion
Drug Interactions: The use of systemic corticosteroids or immunosuppressants before starting durvalumab, except physiological dose of systemic corticosteroids (≤ 10 mg/day prednisone or equivalent), is not recommended because of their potential interference with the pharmacodynamic activity and efficacy of durvalumab. However, systemic corticosteroids or other immunosuppressants can be used after starting durvalumab to treat immune-related adverse reactions. PK drug-drug interaction between durvalumab and chemotherapy was assessed and showed concomitant treatment did not impact the PK of any of the drugs involved. Additionally, based on population PK analysis, concomitant chemotherapy treatment did not meaningfully impact the PK of durvalumab.
Non-immune-mediated adverse reactions: Withhold IMFINZI for Grade 2 and 3 adverse reactions until ≤ Grade 1 or baseline. IMFINZI should be discontinued for Grade 4 adverse reactions. Special populations: Elderly: No dose adjustment is required for elderly patients (≥ 65 years of age). Renal impairment: No dose adjustment is recommended in patients with mild or moderate renal impairment. Data from patients with severe renal impairment are too limited to draw conclusions on this population. Hepatic impairment: Data from patients with moderate and severe hepatic impairment are limited. Due to minor involvement of hepatic processes in the clearance of durvalumab no dose adjustment of IMFINZI is recommended for patients with hepatic impairment as no difference in exposure is expected. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Warnings and precautions: Traceability: In order to improve the traceability of biological medicinal products, the tradename and the batch number of the administered product should be clearly recorded. Immune-mediated pneumonitis: Monitor for signs and symptoms of pneumonitis or radiation pneumonitis. Suspected pneumonitis should be confirmed with radiographic imaging and other infectious and disease-related aetiologies excluded. Immune-mediated hepatitis: Monitor for abnormal liver tests prior to and periodically during treatment with IMFINZI, and as indicated based on clinical evaluation. Immune-mediated colitis: Monitor for signs and symptoms of colitis or diarrhoea. Immune-mediated hypothyroidism, hyperthyroidism and thyroiditis: Monitor for abnormal thyroid function tests prior to and periodically during treatment and as indicated based on clinical evaluation. Immune-mediated adrenal insufficiency: Monitor for clinical signs and symptoms of adrenal insufficiency. Immune-mediated type 1 diabetes mellitus: Monitor for clinical signs and symptoms of type 1 diabetes mellitus including diabetic ketoacidosis. Immune-mediated hypophysitis/hypopituitarism: Monitor for clinical signs and symptoms of hypophysitis or hypopituitarism. Immune-mediated nephritis: Monitor for abnormal renal function tests prior to and periodically during treatment with IMFINZI. Immune-mediated rash: Events of Stevens-Johnson Syndrome or toxic epidermal necrolysis have been reported in patients treated with PD-1 inhibitors. Patients should be monitored for signs and symptoms of rash or dermatitis (including pemphigoid). Immune-mediated myocarditis: Patients should be monitored for signs and symptoms of immunemediated myocarditis. Other immune-mediated adverse reactions: Myasthenia gravis, myositis, polymyositis, meningitis, encephalitis Guillain-Barre syndrome, immune thrombocytopenia, cystitis noninfective and pancreatitis have been observed. Monitor for signs and symptoms. Infusion related reactions: Monitor for signs and symptoms of infusion related reactions.
Presentation: Each ml of concentrate for solution for infusion contains 50mg durvalumab.
Primary analysis in the ITT population
References: 1. Imfinzi-Ireland Summary of Product Characteristics. July 2022. 2. Antonia SJ, et al. N Engl J Med 2018;379:2342−2350.
ABRIDGED PRESCRIBING INFORMATION
3. Antonia SJ, et al. N Engl J Med 2017;377:1919-1929.
IMFINZI is reimbursed for the treatment of locally advanced, unresectable non-small cell lung cancer (NSCLC) in adults whose tumours express PD-L1 on ≥1% of tumour cells and whose disease has not progressed following platinum-based chemoradiation therapy.
Median OS†: Not reached vs 28.7 months with placebo (HR=0.68; 99.73% CI, 0.47-0.997); P=0.00252
This medicinal product is subject to additional monitoring. Adverse events should be reported directly to: HPRA Pharmacovigilance. Website: www.hpra.ie. Adverse events should also be reported to AstraZeneca Patient Safety on Freephone 1800 800 899
Undesirable events: Consult SmPC for full list of adverse events. IMFINZI Monotherapy: Very common (≥ 1/10; any grades): Upper respiratory tract infections, hypothyroidism, cough/productive cough, diarrhoea, abdominal pain, rash, pruritus, pyrexia, arthralgia. Common (≥ 1/100 to < 1/10; any grades ): Pneumonia, dental and oral soft tissue infections, oral candidiasis, influenza, hyperthyroidism, pneumonitis, dysphonia, aspartate aminotransferase increased or alanine aminotransferase increased, night sweats, myalgia, blood creatinine increased, dysuria, peripheral oedema, infusion related reaction. Uncommon (≥ 1/1,000 to < 1/100; any grades): Thyroiditis, adrenal insufficiency, interstitial lung disease, colitis, pancreatitis, hepatitis, dermatitis, myositis, nephritis. Rare (≥ 1/10,000 to < 1/1000; any grades): Type 1 diabetes mellitius, hypophysitis/hypopituitarism, diabetes insipidus, myocarditis, polymyositis, myasthenia gravis, meningitis, pemphigoid, immune thrombocytopenia, cystitis noninfective. Not known: Noninfective encephalitis, Guillain-Barre syndrome. IMFINZI Combined with Chemotherapy: Very common (≥ 1/10; any grades): Neutropenia, anaemia, thrombocytopenia, leukopenia, decreased appetite, cough/productive cough, nausea, constipation, vomiting, alopecia, fatigue. Common (≥ 1/100 to < 1/10; any grades): Upper respiratory tract infections, pneumonia, dental and oral soft tissue infections, febrile neutropenia, pancytopenia, hypothyroidism, hyperthyroidism, thyroiditis, adrenal insufficiency, pneumonitis, diarrhoea, abdominal pain, stomatitis, aspartate aminotransferase increased or alanine aminotransferase increased, hepatitis, rash, pruritus, dermatitis, myalgia, arthralgia, blood creatinine increased, dysuria, pyrexia, peripheral oedema, infusion-related reaction. Uncommon (≥ 1/1,000 to < 1/100; any grades): Oral candidiasis, influenza, Type 1 diabetes mellitus, dysphonia, interstitial lung disease, colitis, night sweats. Legal Category: Product subject to prescription which may not be renewed (A).
Median PFS ‡: 16.8 vs 5.6 months with placebo (HR=0.52; 95% CI, 0.42-0.65; P<0.0001)1
†The primary 2-year OS analysis was conducted after 299 deaths for 42% maturity (61% of targeted events) with a median follow-up of 25.2 months. Reduction in the risk of death vs placebo was 32% (95% CI, 0.53-0.87). Median OS was NR with IMFINZI (95% CI, 34.7-NR) vs 28.7 months with placebo (95% CI, 22.9-NR).1,2 ‡Measured based on RECIST v1.1 criteria by BICR. The primary PFS analysis was conducted after 371 events (81% of targeted 458 events) with a median follow-up of 14.5 months. Reduction in the risk of progression or death vs placebo was 48% (HR=0.52; 95% CI, 0.42-0.65). Median PFS was 16.8 months with IMFINZI (95% CI, 13.0-18.1) vs 5.6 months with placebo (95% CI, 4.6-7.8).3
IMFINZI® is a registered trade mark of the AstraZeneca group of companies. Date of API Preparation: 07/2022 Veeva ID: IE-4002
Dosage and administration: Treatment must be initiated and supervised by a physician experienced in the treatment of cancer. Patients with locally advanced NSCLC should be evaluated for treatment based on the tumour expression of PD-L1 confirmed by a validated test. For locally advanced NSCLC, the recommended dose of IMFINZI is 10 mg/kg administered as an intravenous infusion over 1 hour every 2 weeks or 1500 mg every 4 weeks, until disease progression, unacceptable toxicity, or a maximum of 12 months. For ES-SCLC, the recommended dose for IMFINZI in combination with chemotherapy (etoposide and either carboplatin or cisplatin) is 1500 mg, administered as an intravenous infusion over 1 hour, every 3 weeks (21 days) for 4 cycles, followed by 1500 mg every 4 weeks as monotherapy, until disease progression or unacceptable toxicity. Patients with a body weight of 30kg or less must receive weight-based dosing, please consult Section 4.2 in the SmPC for more information. Dose escalation or reduction is not recommended. Dose withholding or discontinuation may be required based on individual safety and tolerability. Suspected immune-mediated adverse reactions: Adequate evaluation should be performed to confirm aetiology or exclude alternate aetiologies. Based on the severity of the adverse reaction, IMFINZI should be withheld and corticosteroids administered. Guidelines for the management of immune mediated adverse reactions are described in Table 2, Section 4.2 in the SmPC. Consider increasing dose of corticosteroids and/or using additional systemic immunosuppressants if there is worsening or no improvement. Upon improvement to ≤ Grade 1, corticosteroid taper should be initiated and continued over at least 1 month. After withhold, IMFINZI can be resumed within 12 weeks if the adverse reactions improved to ≤ Grade 1 and the corticosteroid dose has been reduced to ≤ 10 mg prednisone or equivalent per day. IMFINZI should be permanently discontinued for recurrent Grade 3 (severe) immune-mediated adverse reactions and for any Grade 4 (life-threatening) immune-mediated adverse reactions, except for endocrinopathies that are controlled with replacement hormones. For myasthenia gravis, if there are signs of respiratory or autonomic insufficiency, IMFINZI should be permanently discontinued.
Indication: IMFINZI as monotherapy is indicated for the treatment of locally advanced, unresectable non-small cell lung cancer (NSCLC) in adults whose tumours express PD-L1 on ≥ 1% of tumour cells and whose disease has not progressed following platinum-based chemoradiation therapy. IMFINZI in combination with etoposide and either carboplatin or cisplatin is indicated for the first-line treatment of adults with extensive-stage small cell lung cancer (ES-SCLC).
SAFETY INFORMATION


Onset of signs and symptoms in the first two years of life
The causes of this common inflammatory skin disease are complex, and comprises an interplay of genetics, immunologic and environmental triggers, that contribute to a skin barrier disruption and abnormal immune system response.
Taking a careful history to help identify any relationship between suspected triggers and AE skin symptoms is important. Identification, elimination and/or control of exacerbating triggers maybe helpful in preventing recurrent symptoms and disease deterioration. Irritants in the environment, such as physical (fabrics such as wool) household chemicals (bleaches or solvents) can aggravate affected skin in people living with AE. Consideration for nonallergic triggers, may include, psychological stress, temperature extremes, and dry wintery or conditioned air.
Emollients: Ongoing, practical application of over-the-counter emollients is the cornerstone of treatment for the condition, as dry skin is one of the predominant manifestations of AE. The purpose of emollients is to improve the skin barrier by restoring and maintaining skin hydration, therefore soothing the skin and reducing pruritus. Emollients are also a crucial element of maintenance treatment and also in the prevention of flares. Adults
The epidermis acts as a barrier, preventing water loss, as well as entry of foreign substances such as irritants, microbes and allergens. The epidermal barrier is made up of structural proteins including filaggrin (FLG). FLG deficiencies or mutations in the epidermis result in a weakened skin barrier, as it is less able to retain water, and the lipids that surround and support the cells break down more quickly. The impaired skin barrier allows loss of moisture and irritants or allergens to pass through the skin more easily. This can ultimately prompt an inflammatory cascade.
Presentation
Cause and risk factors
FocusingEczemaon
Eczema in Pharmacy
Assessment and management of atopic eczema
Itch is a major symptom of AE, and scratching only provides temporary relief, and leads to more itching and scratching, which is often referred to as the ‘itch-scratch-cycle’. The clinical appearance of AE may be modified by scratching, which in time may produce lichenification, broken skin surface resulting in excoriations, exudate and secondary infection. Appearance and location of eczematous lesions of AE may vary with age, and three stages have been recognised, infancy, childhood and adolescent/adult.
A really useful health-related quality of life measurement tool used in clinical practice is the Dermatology Life Quality Index (DLQI). This tool is not AE specific, however it helps clinicians to assess the impact of AE on the person’s life and assists the clinician to measure effectiveness of treatments. DLQI scores range from 0 (no impairment of quality of life) to 30 (maximum impairment). For children, there is the Children’s Dermatology Life Quality Index (CDLQI) which is also available with added cartoons. The aim of the questionnaire is to measure how much did the child’s skin condition affect them in the last Onceweek.adiagnosis of AE is established, treatment decisions are based on disease activity and impact of the disease on the patient’s quality of life. Management AE is a life-long skin condition, so the main aim of treatment is to improve symptoms and achieve long-term control. Typically a multistep treatment approach may be considered, according to severity of the disease, patients age, its extent and distribution. Key principals in AE management are: restoring the skin barrier with emollient therapy, baseline trigger avoidance, anti-inflammatory treatment with topical steroids or topical calcineurin inhibitors. In moderate to severe AE, phototherapy or systemic agents may be considered Trigger avoidance and Topical Triggertreatmentsavoidance:
The
A strong risk factor for AE is a positive family history. The strongest known genetic risk factor in AE is associated with null mutations in filaggrin gene (FLG), which encodes a key epidermal structural protein filaggrin, which is necessary for skin barrier function.
Validated measures of severity in AE, include SCORing Atopic Dermatitis (SCORAD), Eczema Area and Severity Index (EASI) and Patient Orientated Eczema Measure (POEM). Measurement techniques can be helpful in assessment, monitoring and guidance on effective management.
Clinical presentation varies from mild to severe and depending on severity, symptoms can include severe dryness caused by a dysfunctional epidermal barrier, intense itching, cutaneous inflammation and vesicle formation. AE symptoms have a chronic, or relapsing disease course.
Triggers of AE may include, allergen exposure such as house dust mite, whereas, non-allergic factors such as Staphylococcus aureus infection, abrasive garments, temperature changes, stress, and exposure to irritants such as detergents, harsh soaps and fragrances and habitual scratching can disrupt the skin barrier function.
highlights World Eczema Day: 14 September
Written by Michelle Greenwood, Health Promotion Manager, Irish Skin Foundation Irish Skin Foundation 2022
According to the UK Working Party diagnostic criteria, a diagnosis for AE requires: patients must have a history of itchy skin plus a minimum of 3 of the following; Flexural involvement, involving skin creases such as behind the knees, bends of elbows, wrists, front of ankles, or neck History of generally dry skin in the last 12 months Visible flexural eczema Personal history of asthma or hay fever (or history of atopic disease in a first degree relative, if patient is under 4 years)
76 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
Atopic eczema (AE), also known as atopic dermatitis, is a chronic, inflammatory skin condition characterised by intense itch and recurring eczematous lesions. This common inflammatory skin disorder affects people of all ages and ethnicities, approximately affecting up to 20% of children and 10% of adults.


The British Association of Dermatologists (BAD) released a statement on their website in July 2020 on fire risk associated with emollient use. According to the BAD “emollients represent a safe treatment option, for most patients. That said, it is important that patients, carers, and healthcare professionals are aware of the potential fire risks associated with these products, and how to minimise them. It is important to stress that emollients are not flammable in themselves, nor when they are on the skin. The risk comes when emollient residue dries onto fabrics such as clothing or bedding and then comes into contact with a naked flame or lit cigarette causing them to catch fire. To reduce the fire risk, patients using these products are advised to avoid naked flames completely, including smoking cigarettes and being near people who are smoking or using naked flames. It is also advisable to wash clothing and bed linen regularly.”
In July 2020 the Medicines and Healthcare products Regulatory Agency (MHRA) in the UK, in partnership with the National Fire Chiefs Council, launched a campaign to raise awareness around the potential fire risks of emollients (moisturisers) often used in the management of skin disease.
Topical corticosteroids: Recognised as first-line antiinflammatory prescribed treatments in acute exacerbations. Selection of agent varies depending on potency, the location and severity of skin affected by AE, patient age and formulation. Topical corticosteroids are grouped into classes depending on their potency, ranging from mild, moderate, potent and very potent. A fingertip unit (FTU) is a useful method for individuals to apply topical corticosteroid in safe quantities. A FTU refers to the amount of ointment or cream applied from the end of an adult index fingertip, to the distal crease (first joint) in the finger, and is equivalent to approximately 0.5grams. The recommended FTU of topical corticosteroid will depend on the part of the body being treated and whether the patient is an adult or child. The Irish Skin Foundation has a useful guide describing the number of FTU’s required for different parts of the body in adults and children in the eczema booklet on https://irishskin.ie/eczema/ Topical calcineurin inhibitors (TCI): Considered as a secondline option for short-term and intermittent treatment of AE. These prescribed non steroidal, anti-inflammatory agents do not cause skin atrophy, and are beneficial in treating sensitive skin areas such as the face and groin. Stinging on application is the most common side-effect, but this usually settles within a few days, also sun protection is advised, in patients treated with TCI.
Newer systemic agents which can be prescribed in secondary care for patients with moderate to severe AE, through the HSE managed access programme include; abrocitinib (Cibinqo®), dupilumab (Dupixent®), tralokinumab (Adtralza®) and upadacitinib (RINVOQ®). These agents are available to patients that meet a certain criteria set out by the Managed Access Protocol and prescribing is confined to consultant dermatologists.
Itch AE is often referred to as the “itch that rashes” due to the pruritus that patients with AE often experience. The urge to scratch can be overwhelming but only provides temporary relief, leading to more itching and scratching (the itch-scratch cycle) which may lead to excoriation and skin barrier damage. Itch interferes with sleep and negatively impacts on an individual’s quality of life, as well as that of the wider family, with sleep deprivation contributing to difficulties concentrating at school, and/or work. Sufficient sleep is crucial for health and well-being. In children, both acute and chronic sleep disruption has been associated with a range of ‘cognitive, mood and behavioural impairments’, as well as poor performance in school. In a ISF ‘Living with Atopic Eczema Survey’ in 2019, respondents reported interrupted/loss of sleep in 86% of children and 84% of adults. Additionally, 26% of carers of children with AE, reported that their child missed 1-2 days of school per month due to their skin condition. Quality of life For some, the burden of AE often extends beyond the immediate dermatological effects of this disease. AE can place a serious mental health burden on patients, particularly those living with moderate-to-severe disease, with research indicating that the more severe the AE, the more quality of life is impacted. It has been associated with anxiety, depression and attention deficit hyper-activity disorder. Research has indicated that the health related quality of life in children with AE is comparable to that of other chronic childhood diseases such as diabetes or asthma.
Wet-wrap therapy: This is a technique used in people with moderate to severe eczema by using two layers of open-weave tubular bandage applied over emollients. The bottom layer is soaked in warm water, squeezed out and then put onto the skin over the emollient wet and then followed by the top layer which is dry. This treatment is reported to introduce moisture, soothe and protect irritated skin from damage caused by scratching and is applied for short periods of time.
Conclusion AE is often associated as a disease of childhood, but it is important not to forget that AE can be a very distressing condition for adults as well. While severity of AE varies greatly, most are affected by mild disease. Due to a variety of treatments for AE and different individual symptoms, it is important to educate patients and their families about the disease, and selfcare to ensure compliance and effective management. These include, basic skin care routines that fits in with the individual’s lifestyle, management of future flares and trigger avoidance. Also consideration around any potential fears with regards to side-effects of medications such as topical steroids should be addressed, as this may impede sufficient treatment. Education for self-managing AE, are reported to improve the severity of the disease and also improve the quality of life for these individuals and their carers. The Irish Skin Foundation operates a Ask-a-Nurse Helpline that provides free, direct, accessible and specialist guidance about skin conditions, delivered by dermatology clinical nurse specialists on an appointment model. For information on eczema or other skin conditions log onto www.irishskin.ie
Caution should be taken when wet wrapping using topical steroids, as absorption is increased. Occlusive medicated dressings or dry bandages should not be used in infected AE.
77 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 require at least 500g/per week and children at least 250g/per week. Pump dispensers are preferable, in order to prevent contamination. The use of emollient wash products instead of ordinary soaps and bubble baths are also recommended. Bathing should be limited to short periods of time (e.g. 5-10 minutes) with warm water, and when finished, followed by application of emollients. When choosing an emollient, individual preference, skin type, skin dryness, inflammation and body area may be considered to help promote adherence.
AE associated infections AE is often complicated by bacterial, viral and fungal infections, due to a weakened skin barrier, trauma from scratching and impaired cellular immunity. Staphylococcus aureus, is the most common organism, to cause bacterial infection in AE. Distinctive signs may include honey-coloured crusts, weeping and pustules, and folliculitis in hair-bearing areas. Topical or oral antimicrobials may be prescribed. Common viral Infections seen in individuals with AE include molluscum contagiosum, cutaneous warts and herpes simplex virus.
Phototherapy Phototherapy is a form of artificial ultraviolet light treatment, comprised of either ultraviolet A (UVA) or ultraviolet B (UVB) wavelengths of light, delivered in hospital dermatology day care centres. Phototherapy may be given in combination with topical steroids and emollients to prevent flare-up.
Systemic agents
In circumstances where AE is moderate to severe or widespread, and has not responded to topical or phototherapy treatments or when quality of life is significantly impacted, systemic immunosuppressive treatments may be prescribed. Current options include, methotrexate, ciclosporin, mycophenolate mofetil, and azathioprine. The individual patient profile, lifestyle factors, associated comorbidities, side effect profile along with patient preference all influence choice of drug. These medications have different toxicity profiles, therefore patients are reviewed and monitored regularly to avoid any potential side effects.

As we head into autumn the 2022/2023 influenza season presents a significant challenge to the delivery of healthcare services both in primary care and in hospitals, especially as there may also be a resurgence of cases of COVID-19. During the 2020-2021 flu season, the first flu season of the pandemic, influenza cases were not reported in Ireland because the public health measures recommended to prevent COVID-19 infection were very successful in preventing influenza virus transmission. In the 2021-2022 flu season, though influenza cases numbers increased, they remained far below pre-pandemic levels because of ongoing COVID-19 preventative measures. However, throughout the 2022/2023 influenza season there is likely to be a limited recent community natural immunity to influenza, especially for children born since 2020. In this year’s southern hemisphere flu season, Australia reported
For the 2022/2023 influenza season the Department of Health, will continue to provide funding to the HSE to offer Quadrivalent Live Attenuated Influenza (LAIV) vaccine free to all children aged 2 to 17 years inclusive. This vaccine was introduced during the 2020/2021 influenza season, however uptake of the LAIV vaccine remains very low. For 2021/2022 Flu season vaccine uptake in children aged 2 to 17 was 16.6%. Therefore it is important to encourage up take of the LAIV vaccine.
Written by Dr Tom Barrett, Senior Medical Officer, National Immunisation Office
Quadrivalent Live Attenuated Influenza vaccine (LAIV) Fluenz Tetra is manufactured by Astra Zeneca. It is administered intra-nasally. The vaccine contains the following four vaccine virus strains as recommended by the World Health Organization (WHO): Egg-based influenza vaccines • an A/Victoria/2570/2019 (H1N1) pdm09-like virus; • an A/Darwin/9/2021 (H3N2)-like virus; • a B/Austria/1359417/2021 (B/ Victoria lineage)-like virus; and • a B/Phuket/3073/2013 (B/ Yamagata lineage)-like virus.
Between the 2009/2010 and 2018/2019 influenza seasons: 4750 children aged 0-14 years have required hospitalisation as a result of influenza.
The Best Shots this Autumn: Influenza and COVID-19 vaccination
Influenza vaccination of young children can not only protect against severe illness in children but may also assist in reducing influenza transmission to other vulnerable populations, such as those aged 65 years or older who due to immunosenescence develop less immunity after vaccination. Approximately 10% of children under 15 attend their GP with influenza in an average influenza season. Influenza is an important cause of pneumonia, bronchitis, otitis media, croup and bronchiolitis in children. Incidence rates are highest in the younger age groups leading to high rates of excess GP and outpatient visits, hospital admissions and medicines prescriptions, increasing pressure on the healthcare system.
LAIV effectiveness Since LAIV contains live attenuated viruses, it mimics natural infection with wild-type viruses, with the development of both mucosal and systemic immunity. Local mucosal antibodies protect the upper respiratory tract and may be more important for protection than serum antibodies, inducing more durable immune memory and so providing better longterm protection to children than inactivated influenza vaccines such as QIV. In some studies, LAIV has been shown to be more effective in children compared with
In Finland, annual inactivated influenza vaccine was recommended for children aged 6–35 months in 2007. LAIV was introduced in 2015 to enhance vaccine uptake. Since then, all 2 and 3 year old children have been eligible for vaccination with either LAIV or inactivated influenza vaccine. The programme is now extended to include all children to 6 years of age. Live Attenuated Influenza vaccine (LAIV) for 2022/2023 influenza season
influenza–like-illness notifications that peaked at the beginning of the influenza season and the weekly number of notifications has exceeded the 5 year average. During this influenza season in Australia, the groups with the highest rates of disease are among children aged 5-9 years, followed by children aged under 5 years, and adolescents. Influenza in children
Nine European countries, US, Canada and Australia recommend influenza vaccine for children. The UK offer LAIV to children. Finland, US and Canada offer LAIV or QIV to children. In the US, LAIV has been recommended since 2004. LAIV has been authorised for use in Canada since 2011. In 2013, the UK introduced trivalent LAIV for 2 and 3 year olds with pilot programmes for primary school children. Quadrivalent LAIV was introduced during the 2014/2015 influenza season. The programme has extended year on year to include all children from 2 up to 11 years.
In Ireland during the 2018/2019 influenza season, 1245 children were hospitalised with influenza. Children aged less than 5 years had the second highest hospitalisation rates for influenza after those aged 65 years and older.
Children are among the most susceptible to influenza infection.
LAIV does not contain any adjuvants, or preservatives.
Immunisations
LAIV may contain residues of egg proteins (ovalbumin), with a maximum amount of less than 0.024 micrograms and gentamicin.
transmission to health care workers in families with children absenteeism of children from school and their parents from work Influenza vaccination for children in other countries
Influenza Influenza is a very common acute viral respiratory illness which affects all age groups. The virus is seen all year round but peaks every winter. The degree of influenza infection is unpredictable, however, each year in Ireland influenza is responsible for between 200 and 500 deaths and as many as 1,000 during a particularly severe season (2008/2009).
It is estimated that 20-30% of children develop influenza during each influenza season compared to 5 to 10% of adults. Children, because they have limited preexisting immunity, are primary vectors of influenza transmission in the community and shed the virus at higher viral titres. Children transmit the influenza virus for a longer period than adults; they can transmit the influenza virus for 10 or more days, compared to 6 days in adults, therefore increasing spread of the disease and contributing significantly to influenza outbreaks.
transmission of influenza to the elderly and persons in risk groups the number of hospital admissions
Influenza vaccination for children in Ireland
The aim of the childhood influenza programme is to reduce: morbidity and mortality from influenza in children
78 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE

Each LAIV vaccine comes as a prefilled nasal applicator and each applicator contains 0.2ml nasal suspension. The vaccine is administered by the nasal route. One dose of LAIV is 0.2ml administered in divided doses into each nostril i.e. 0.1ml in each nostril.
• Children receiving topical or corticosteroidsinhaled low dose systemic corticosteroids replacement therapy corticosteroids (e.g. adrenal insufficiency). Contraindications to LAIV:
Increasing uptake of influenza vaccine Influenza remains a major public health issue and never more than after more than two years of the COVID-19 pandemic.
• Concomitant use of aspirin/ salicylates
Influenza vaccination is the best intervention available to prevent
Avoid influenza antiviral medication for 2 weeks post vaccination. Children aged 2 to 17 years for whom LAIV is contraindicated should be offered QIV vaccine (provided there are no contraindications to QIV).
The vaccine is immediately absorbed after administration. For the same reason, the vaccine does not need to be repeated if the child sneezes or blows their nose after vaccination.
• Asymptomatic HIV infection
LAIV dose and administration
Vaccinated children can shed the attenuated virus for a few days after vaccination but the virus that is shed cannot cause infection. Peak incidence of shedding occurred 2-3 days post-vaccination in Fluenz clinical studies. Therefore the weakened viruses do not cause flu infection in others, or in the person vaccinated.
If the child’s nose drips after vaccination, the vaccine dose does not need to be repeated.
59% reduction in adults GP influenza-like illness consultations.
The UK pilot primary school programme introducing LAIV was evaluated in 2014/2015 and showed:
LAIV can be given together with or at any time before or after the administration of any other live attenuated (e.g. MMR) or inactivated vaccines including COVID-19 vaccines. In Ireland the National Immunisation Advisory Committee (NIAC) has recommended healthy children require one dose of LAIV. However children in a medically at risk group aged 2 to 8 years inclusive are recommended 2 doses of LAIV if they have never had any influenza vaccine before. (Table 1). The two doses should given 4 weeks apart.
The following are NOT contraindications
vaccine before. (Table 1). The two doses should be given 4 weeks apart. Table 1. Doses of LAIV required for children aged 2-17 years Group Age Previous vaccination Dose Medically at risk 2 to 8 years Have never had any influenza vaccine Two doses 4 weeks apart Have had any influenza vaccine before One dose 9 to 17 years Not relevant One dose Healthy 2 to 17 years Not relevant One dose The following are NOT contraindications • Asymptomatic HIV infection • Children receiving o topical or inhaled corticosteroids o low dose systemic corticosteroids o replacement therapy corticosteroids (e.g. adrenal insufficiency). Contraindications to LAIV: • Anaphylaxis following a previous dose of influenza vaccine or any of its constituents 1 (other than ovalbumin see Precautions) • Asthma • Acute exacerbation of symptoms increased wheezing and/or additional bronchodilator treatment in the last 72 hours • Seek specialist advice if on regular oral steroids or previous ICU admission • Significant immunosuppression due to disease or treatment • Children who live with severely immunosuppressed persons (i.e. post haematopoietic stem cell transplant) • Concomitant use of aspirin/salicylates • Children who live
Table 1. Doses of LAIV required for children aged 2-17 years inactivated influenza vaccines. In addition, LAIV may offer some protection against strains not contained in the vaccine, as well as virus strains that have undergone antigenic drift.
A recent meta-analysis of LAIV suggested an efficacy against confirmed disease of 83% (95% confidence interval 69-91%).
association with immune related adverse reactions. Precautions Defer until recovered from an acute severe febrile illness.
• Anaphylaxis following a previous dose of influenza vaccine or any of its constituents1 (other than ovalbumin – see Precautions)
Very rare (less than 1 in 10,000): Immediate allergic reactions.
• Those with severe neutropoenia (absolute neutrophil count <0.5 × 109/L) to avoid an acute vaccine related febrile episode
• Those on becauseipilumumabcheckpointcombinationinhibitors(e.g.plusnivolumab)ofapotential
• Children who live with severely immunosuppressed persons (i.e. post haematopoietic stem cell transplant)
• Influenza antiviral medication within the previous 48 hours
• Seek specialist advice if on regular oral steroids or previous ICU admission • Significant immunosuppression due to disease or treatment
As LAIV has an ovalbumin content <0.1 micrograms per dose, it can be given to children with confirmed egg anaphylaxis or egg allergy in a primary care setting except children who have required ICU admission to hospital for a previous severe anaphylaxis to egg who should be given LAIV in Aspirin/salicylateshospital.should not be be used for 4 weeks after vaccination unless medically indicated, as Reye’s syndrome has been reported following the use of salicylates during wild-type influenza infection.
• Asthma • Acute exacerbation of symptoms increased wheezing and/or additional bronchodilator treatment in the last 72 hours
The attenuated vaccine viruses in LAIV are cold adapted. They can replicate at the lower temperatures found in the nose but cannot replicate efficiently at body temperature elsewhere in the body.
Very rare cases of Guillain-Barré syndrome (GBS) have been observed in the post-marketing setting following influenza vaccination. The risk of GBS following influenza infection is significantly greater than that following influenza vaccination. Can LAIV vaccine cause virus shedding?
94% reduction in primary school age children GP influenza-like consultations 74% reduction primary school age Emergency Department attendances with respiratory complaints 93% reduction in primary school age confirmed influenza hospitalisations
79 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022
LAIV side effects Very common or common (More than 1 in 10 to 1 in 100): Nasal marketingheadache,decreasedcongestion/rhinorrhoea,appetite,malaise,fever,andmyalgia.Inpostsurveillance,overall rates of fever were similar to the rates following other childhood vaccines and were generally mild and of short duration.
• Those with morbid obesity (Body mass index >40)
• Those immunosuppressionwith due to disease or treatment, including asplenia or hyposplenism, and all cancer patients
3. A second mRNA COVID-19 booster vaccine is recommended for • healthcare workers, and when practicable, should be given at the same time as seasonal influenza vaccine (4th COVID-19 vaccine).
NIAC strongly recommends those who to date are unvaccinated or are incompletely vaccinated should complete a primary COVID-19 vaccination course and booster vaccination to protect themselves against COVID-19 infection.
• aged 12-29 years: Comirnaty® (0.3ml/30 mcg) • aged 5-11 years: Comirnaty® (0.2ml/10mcg) Nuvaxovid® Novavax vaccine is recommended if there is a contraindication to an mRNA vaccine. Jcovden® Jansen vaccine is recommended only if there is a contraindication to both Novavax and the mRNA vaccines. Implementation of these new NIAC COVID-19 vaccine recommendations has now commenced. References available from National Immunisation age Chapter 5a COVID-19 COVID-192022July29
• those aged 12–64 years with immunocompromise associated with a sub optimal response to vaccines at the time of their primary or booster vaccination (6th COVID-19 vaccine). When practicable, these booster doses of COVID-19 vaccine and influenza vaccine can be given at one visit.
Office Table 5a.1 Recommendations for COVID-19 vaccines by
and immune - status July 2022
influenza. Extending the influenza vaccination programme to all children aged 2-17 years aims to protect children and reduce transmission to others, thereby reducing the burden on our health services at this crucial time. Research, both in Ireland and elsewhere, has consistently shown that doctors and other healthcare professionals are the most trusted sources of information on vaccination. A recommendation by a trusted healthcare professional for their patients who are at an increased risk of influenza-related complications to attend their GP or pharmacist for vaccination has been shown to increase vaccine uptake.
Using currently available mRNA COVID-19 vaccines, NIAC advise the following groups are recommended COVID-19 booster vaccination 4 months after their last COVID-19 vaccination (a 3 months interval may be used in exceptional circumstances):
80 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
• Those with chronic illness, e.g. chronic heart disease (including acute coronary syndrome), chronic liver disease, chronic neurological disease (where the neurological condition compromises clearance of respiratory secretions), chronic renal failure, chronic respiratory disease (including chronic obstructive pulmonary disease, cystic fibrosis, moderate or severe asthma, and dysplasia),bronchopulmonarydiabetesmellitus, or haemoglobinopathies
Medical conditions that are associated with an increased risk of influenza-related complications:
4. To enhance maternal protection and provide optimal benefit to the infant, an additional mRNA COVID-19 booster vaccine is recommended in pregnancy at 16 weeks gestation or later for those who have not received a booster vaccine in the current pregnancy (4th COVID-19 vaccine). This timing is to enhance protection to the mother and the infant. New recommendations for children aged 5 to 11 years with immunocompromise 5. A first mRNA COVID-19 booster vaccine is now recommended for those aged 5–11 years with immunocompromise associated with a sub optimal response to vaccines at the time of their primary or additional vaccination (3rd COVID-19 vaccine). See Table
2. A second mRNA COVID-19 booster vaccine is now recommended for • those aged 50-64 years (4th COVID-19 vaccine).
• those aged 12–49 years who have underlying medical conditions who are residents of long term care facilities (4th COVID-19 vaccine).
Click here to return to contents Table 5a.1 Recommendations for COVID-19 vaccines by age and immune status July 2022 Group Primary course* Additional dose 1st booster 2nd booster 3rd booster 65 years and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years tions medicalUnderlyingcondi √√ √ √ Residents of long term care facilities √√ √ √ workers Healthcare √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11 years √√ 12 years and older vaccines responseaassociatedcompromiseImmunowithsuboptimalto √√ √ √ √ √ 5-11 years √√ √ √ *two dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen) **at 16 weeks gestation or later if not already boosted in this pregnancy Chapter 5a COVID-19 COVID-192022July29 Click here to return to contents Table 5a.1 Recommendations for COVID-19 vaccines by age and immune status July 2022 Group Primary course* Additional dose 1st booster 2nd booster 3rd booster 65 years and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years tions medicalUnderlyingcondi √√ √ √ Residents of long term care facilities √√ √ √ workers Healthcare √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11 years √√ 12 years and older vaccines responseaassociatedcompromiseImmunowithsuboptimalto √√ √ √ √ √ 5-11 years √√ √ √ *two dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen) **at 16 weeks gestation or later if not already boosted in this pregnancy Chapter 5a COVID-19 COVID-192022July29 Click here to return to contents Table 5a.1 Recommendations for COVID-19 vaccines by age and immune status July 2022 Group Primary course* Additional dose 1st booster 2nd booster 3rd booster 65 years and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years tions medicalUnderlyingcondi √√ √ √ Residents of long term care facilities √√ √ √ workers Healthcare √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11 years √√ 12 years and older vaccines responseaassociatedcompromiseImmunowithsuboptimalto √√ √ √ √ √ 5-11 years √√ √ √ *two dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen) **at 16 weeks gestation or later if not already boosted in this pregnancy Immunisations
• Children on long-term aspirin therapy (because of the risk of Reye syndrome)
• Residents of nursing homes, old people’s homes, and other long stay facilities where rapid spread is likely to follow introduction of infection
new COVID-19 recommendationsvaccines(July2022)
• Children and adults with Down syndrome • Children with moderate to severe disordersneurodevelopmental such as cerebral palsy and intellectual disability
1. A third mRNA COVID-19 booster vaccine is recommended for • those aged 65 years and older (5th COVID-19 vaccine)
•givenmRNAcovid19.pdfimmunisation/hcpinfo/guidelines/https://www.hse.ie/eng/health/leftboostervaccinesshouldbeasfollows:aged30yearsandolder:Comirnaty ® (0.3ml/30 mcg) or Spikevax® (0.25ml/50 mcg)
COVID-19 vaccinations: National Immunisation Advisory Committee (NIAC)
• those aged 12–49 years who have underlying medical conditions associated with a higher risk of severe COVID-19 e.g. DM (4th COVID-19 vaccine)
• Those with any condition that can compromise respiratory function (e.g. spinal cord injury, seizure disorder, or other neuromuscular disorder,) especially those attending special schools/ day centres
Written by Brona Fullen, PhD, MSc, BSc, Associate Professor, UCD School of Public Health, Physiotherapy and Sports Science, Director, MSc Advanced Physiotherapy Studies programme, Belfield Campus, Dublin
EFIC’S Health Literacy Campaign
The World Health Organisation has declared HL a global health concern and state that efforts to raise HL will be vital in realising the social and economic ambitions described in their 2030 Agenda for Sustainable Development2
Readable.com is a useful online website to gauge reading level difficulty18 Teach Back Method19 Ask your patients to repeat back what you have said to them in their own words.
81 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022 EFIC
If necessary rephrase the information until the patient understands. Ask Me 3®20 Empower your patients by encouraging them to ask these three questions during all healthcare consultations: What is my main problem? What do I need to do?
Why is important for me to do this?
Active self-management is key to the long term management plans of pain conditions1. For this to be effective patient education is key7. However, limited HL can be a barrier as it impacts on disease related knowledge8 – a vital component for developing effective self management skills9 Limited HL results in poorer health outcomes for those with chronic diseases; worse symptom control, an increase in healthcare utilisation, lower adherence to treatment and inadequate communication between the patient and clinician10. The economic cost has been estimated to account for 3–5% of total healthcare costs at health system levels11 due to medical errors, increased illness and disability, loss of wages and compromised public health12
Identifying People with limited Health Literacy Patients with lower levels of HL tend not to ask questions and engage less with their clinicians, frequently miss appointments, and show poor adherence to treatment. Whilst questionnaires13,14, 15 and scales offer a method to potentially identify those with limited HL, healthcare professionals should assume that all patients, regardless of their educational or socioeconomic background may struggle to understand and absorb health-related information.
Health Literacy Interventions To support patient selfmanagement education HLsensitive approaches should be implemented by all healthcare professionals to enable patients develop and improve their levels of HL16. The following tools can be successfully integrated into everyday clinical practice: Plain Language Use lay language and explain complex medical terminology when it is used.
The European Pain Federation EFIC is a psychologistsdoctors,scienceorganisationmultiprofessionalinthefieldofpainrepresenting20,000physiotherapists,nurses,andresearchers
across Europe who are involved in pain management and pain research. Its overarching vision and mission are to advance education, research, and the clinical management of pain, serving as an authorative sciencebased resource on issues related to pain.
This allows you to gauge your patient’s understanding of the information you have given them.
Limit information given in a consultation to 3 to 5 messages per session Implementing the Teach Back Method and Plain English strategies lead to greater improvements in treatment adherence21, and increased engagement in self-management practices and disease-related knowledge22, regardless of prior HL levels. Similarly, Ask Me 3® encourages patients to be more engaged while attending physiotherapy sessions23 Health services also have a role in supporting patients to separate evidence-based information from false or misleading information, to provide new information that is accessible, and to deliver it at a pace that suits the patient.24 This will ultimately allow patients to make informed decisions and become actively engaged in their own healthcare. Limited HL is a global health issue with social and economic implications. Increasing HLsensitive interventions in existing health services have the potential to improve health outcome for those living with pain. Health services need to consider their role in, and develop strategies for improving the public’s levels of HL and accessibility to evidencebased health information.
For further information on EFIC and the health literacy campaign please see www.efic.org
EFIC President Brona Fullen (Associate Professor, UCD School of Public Health, Physiotherapy and Sports Science) chose the theme of health literacy (HL) for her term in office with the ‘Plain Talking’ campaign Health literacy is an individual’s capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions1.
A pan European study found that 47% of respondents had limited HL3, with certain populations (e.g., older people, those with lower social status and education) more likely to be affected. Similar levels of limited HL have been reported in people living with chronic pain4,5,6
Plain Talking: The European Pain Federation
Provide written information in a style that is accessible to all, by considering the average reading level, the language used, and the design of the leaflet 17 Include diagrams to help explain.
Authors: The EFIC Health literacy Working Group Dr Laura Mackey (Chair, Working Group on Health literacy), Professor Harriet Wittink, Dr Magdalena Kocot-Kępska, Dr Brona Fullen, Dr Nadja Nestler References available on request


540 people have completed treatment under the scheme as of the end of February 2022, with over £3 million spent in reimbursing patients for the cost of treatment, according to data released by the Health and Social Care Board.
BOOTS IRELAND LAUNCHES
Managing Director at Boots Ireland, Stephen Watkins, said, “This year the Boots Night Walk is back in person and hopes to be the biggest one yet The Boots Night Walk helps to raise funds and awareness of the incredible work these Night Nurses undertake. Over the past 10 years an incredible ¤2.5 million has been raised for this service so we want to say a big thank you from Boots Ireland to the public as this cannot be done without your fundraising and support.”
EDWARDS LIFESCIENCES
The Department of Health has announced that it has allocated a further £5m to continue to operate The Health Services Republic of Ireland Reimbursement Scheme beyond the original 30 June 2022 deadline for another year. Introduced under the Elective Care Framework for an initial period of 12 months on 1 July 2021, the scheme provides an option for patients who are ordinary residents of Northern Ireland to access private treatment in the Republic of Ireland. The scheme is based on the EU Cross Border Healthcare Directive. Patients who are on a waiting list for surgery or medical treatment through the National Health Service (NHS) or Health & Social Care (HSCNI) Board may wish to avail of the scheme. Once approved by the HSCNI Board, patients usually pay for treatment themselves and can be reimbursed afterwards for approximately 5080% of these costs.
Mater Private Network are one of the leading hospital networks in the Republic of Ireland providing treatment under the scheme.
Boots Night Walks Campaign ambassador TV Presenter and Broadcaster Darren Kennedy, launches the Boots Night Walks in aid of the Irish Cancer Society Night Nursing service
Speaking on the scheme renewal Mater Private Network CEO, David Slevin said, “I am very pleased that the scheme has been granted additional funding. The popularity of the scheme speaks for itself of the need for a programme like this and it only made sense to extend it further. Applications have grown and continue to grow with the long waiting lists in Northern Ireland. People should not have to wait unnecessarily with chronic pain.
Common treatments include orthopaedic surgery, such as hip and knee replacements, cataract surgery and hernia repairs, according to the HSCB.
Anyone who might be waiting for a procedure in Northern Ireland should contact their local HSCNI services to see if they qualify for the scheme. Mater Private Network is standing by, ready with our team of specialists and patient coordinators in Dublin and Cork, to help patients on their journey back to good health”
New applications of the scheme are now being accepted. They will be processed in chronological order, and the scheme will continue under further funding has been committed.
THIS YEAR’S BOOTS NIGHT WALK IN AID OF THE IRISH CANCER SOCIETY
82 SEPTEMBER 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE Clinical R&D
HEALTH SERVICES EXECUTIVE NI EXTENDS THE REIMBURSEMENTROISCHEME
Boots Ireland has partnered with TV presenter and broadcaster Darren Kennedy, to launch this year’s Boots Night Walk in aid of the Irish Cancer Society Night Nursing service which provides end-of-life care for people living with cancer in Ireland. The Irish Cancer Society Night Nursing service provides up to 10 nights of care, free to people who avail of it, and it is funded almost entirely by donations. Boots Ireland has partnered with the Irish Cancer Society since 2012 and through the su pport of their Team Members, patients and customers have raised ¤2.5 million for the service so far, helping to provide 7,200 nights of care. This year, the Boots Night Walk is back in person and hopes to be the biggest one yet, with Boots Ireland calling upon the public to sign up and walk 5km together this autumn in support of the Irish Cancer Society Night Nurses. Alongside the walk, Honour Tags are now on sale in Boots stores nationwide for ¤2. Customers can purchase a tag in honour of someone who has survived or passed away from cancer. The front of the tag allows for the name of the individual with space on the back for a personal message. One metre will be walked in honour of that person by members of the Boots Ireland team. All funds raised from the Boots Night Walk will go towards the Irish Cancer Society Night Nursing service which provides end-of-life care for cancer patients, allowing them to spend their final days at home surrounded by family and loved ones, as well as giving much needed respite for the family caring for them.
BEGINS RENOVATIONS Edwards Lifesciences has announced it has begun renovations to convert its existing Shannon facility into a manufacturing centre to produce components that are an integral part of Edwards’ life-saving transcatheter heart valves. “The expanded capability at our Shannon facility demonstrates that our operations in Ireland are a key enabler for Edwards to continue helping patients across the globe,” says Andrew Walls, Edwards’ general manager for its manufacturing facilities in Ireland. Edwards established its operations in Shannon in 2018, and officially opened its plant in Limerick in October. At that time, Edwards announced that it will employ up to 850 people in the region by 2025. The Limerick plant manufactures transcatheter therapies to repair or replace damaged heart valves, enabling patients to live longer, healthier lives. Edwards Lifesciences is the global leader of patient-focused innovations for structural heart disease and critical care monitoring. We are driven by a passion for patients, dedicated to improving and enhancing lives through partnerships with clinicians and stakeholders across the global healthcare landscape. For more information, visit Edwards.com and follow us on Facebook, Instagram, LinkedIn, Twitter and YouTube. Edwards, Edwards Lifesciences, the stylized E logo, are trademarks of Edwards Lifesciences Corporation and its affiliates.
Pfizer Healthcare Ireland has today announced the availability of the 50 mg, 100 mg and 200 mg doses of CIBINQO® (abrocitinib), an oral, once-daily, Janus kinase 1 (JAK1) inhibitor, for the treatment of moderate-to-severe atopic dermatitis (AD) in adults who are candidates for systemic therapy, in Ireland.
Innovent and Sanofi will jointly explore the development of SAR444245 in China in various cancer types, where Innovent will lead the clinical development.
Subject to mutual agreement of both parties in the future, Sanofi will have the right to acquire additional Innovent new common shares for ¤300 million, at a subscription price that represents 20% premium to Innovent 30-trading-day average share price as the date of the separate agreement that may be entered into by both parties.
Clinical development and commercialization of tusamitamab ravtansine SAR408701 (tusamitamab ravtansine) is a potential first-inclass antibody-drug conjugate (ADC) targeting NSCLCcurrentlyandcancerexpressedsurfacecell(carcinoembryonicCEACAM5antigen-relatedadhesionmolecule5),acell-glycoproteinthatishighlyinnon-smallcelllung(NSCLC),gastriccancerothercancers.SAR408701isinaPhase3studyfor2LgloballyincludingChina, and global Phase 2 studies in additional indications including 1L NSCLC, gastric cancers and other solid tumors. According to the agreement, Innovent will be responsible for developing and exclusively commercializing tusamitamab in multiple indicationsoncology-basedinChina.Sanofi will be entitled to receive up to ¤80 million development milestone payment and royalties on the net sales of the product in China upon approval.
The panel recommended 16 changes to be continued beyond COVID-19 in Ireland, rather than reverting to pre-pandemic practices. The agreed statements related to facilitating safe access to OAT with minimal waiting time, supporting patient-centred care to promote health and well-being, and preventing drug overdose. Consensus was not achieved for OAT drug dosing and frequency of urine testing.
In one trial including an active control arm with dupilumab, which evaluated patients on background topical medicated therapy, abrocitinib 200 mg was associated with a greater improvement in itch relief after two weeks than dupilumab.1 Abrocitinib also demonstrated a consistent safety profile across trials, including in a long-term extension study, showing a favorable benefit-risk profile.
Clinical development and commercialization of SAR444245 SAR444245 is a potential first-in-class bindingaffinityspecificallyvariantrecombinantsite-directed,reprogrammed,singlePEGylated,humanIL-2(rIL-2)withextendedhalf-lifethatbindstothelow-IL-2receptorbutlacksaffinityforthe αlpha chain of the high-affinity IL-2 receptor.
The availability of abrocitinib in Ireland is based on the results of five clinical studies of more than 2,800 patients including four Phase 3 studies and an ongoing long-term open label extension study. Abrocitinib demonstrated meaningful improvements across measures of symptom relief and disease control versus placebo.
CIBINQO is indicated for the treatment of moderate-to-severe atopic dermatitis in adults who are candidates for systemic therapy.2 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See section 4.8 of the SmPC for how to report adverse reactions.
Commenting on the announcement, Caitriona McCarthy, Medical Lead I&I, Pfizer Healthcare Ireland said; “Abrocitinib has shown significant efficacy, including relief from the trademark itch symptom, rapid improvements in skin clearance, extent and severity of disease versus placebo, and a favourable risk-benefit profile.”
Emergency contingency guidelines for opioid agonist treatment (OAT) were introduced in Ireland in March 2020, to ensure rapid and uninterrupted access to treatment while mitigating COVID-19 risk.
New research from RCSI University of Medicine and Health Sciences recommends that several measures implemented during COVID-19 to maintain access to opioid agonist treatment (OAT) led to improvements in the service and should be continued
SAR444245(IL-2) is currently under global Phase 2 studies for skin cancers, gastrointestinal cancer, NSCLC / mesothelioma, head and neck tumors, and lymphoma.
OAT is type of a treatment in which ‘opioid agonists’ – most commonly methadone – are prescribed for people who are dependent on opioids such as heroin. OAT helps to suppress heroin use, improves mental and physical well-being, and reduces risk of death including drug overdose deaths. A 2019 study showed there were over 10,000 people receiving OAT in Ireland.
CHANGES TO METHADONE TREATMENT GUIDELINES IN RESPONSE TO COVID-19 LED TO IMPROVEMENTS IN OVERALL SERVICE, STUDY FINDS
This study, consulted a panel of experts and stakeholders including psychiatrists, GPs and pharmacists, as well as people who were accessing OAT for opioid dependency, to identify which of the OAT contingency measures implemented as a result of COVID-19 should be continued.
Thepost-pandemic.study,ledby
Sanofi remains the sole Marketing Authorization holder for both assets and will be fully responsible for SAR245 commercialization.
Certain measures, such as rapid assessments and telehealth, enabled services to overcome many of the usual barriers to providing treatment. As a result, waiting lists for OAT were drastically reduced, with over 11,000 people accessing treatment in 2021.
83 HOSPITALPROFESSIONALNEWS.IE | HPN • SEPTEMBER 2022
Dr Gráinne Cousins, Senior Lecturer in the RCSI School of Pharmacy and Biomolecular Sciences and the study’s principal investigator, commented on the findings: “The emergence of the COVID-19 pandemic transformed how OAT was delivered, in Ireland and internationally. While many authors have suggested that recent innovations should be continued beyond the pandemic, this is the first study to seek consensus, among a wide range of stakeholders, on whether recommendations introduced in emergency clinical guidelines should be retained beyond the pandemic.
This research was funded by the Health Research Board, Research Collaborative in Quality and Patient Safety [RCQPS-2020-016].
Innovent will be entitled to receive up to ¤60 million development milestone payments and royalties on the net sales of the product in China upon approval.
Sanofi and Innovent Biologics (HKEX: 1801.HK, “Innovent”) announced a collaboration to bring innovative medicines to patients in China with difficult-to-treat cancers. Innovent is a leading biopharmaceutical company with strong clinical development capabilities and a broad commercial footprint in China. Both companies are committed to accelerating the development and commercialization of two Sanofi key clinical stage oncology assets: Phase III SAR408701 (tusamitamab ravtansine; theIL-2),Phaseantibody-druganti-CEACAM5conjugate)andIISAR444245(non-alphacombiningwithsintilimab,leadingcheckpointinhibitor in China. In addition to the collaboration and license agreement, Sanofi will invest ¤300 million in Innovent through subscription of new common shares.
PFIZER AVAILABILITYANNOUNCESOFCIBINQO® (ABROCITINIB) FOR THE TREATMENT OF ADULTS WITH MODERATE-TO-SEVERE ATOPIC DERMATITIS IN IRELAND
SANOFI AND INNOVENT BIOLOGICS ENTER STRATEGIC COLLABORATION TO ACCELERATE DEVELOPMENT OF ONCOLOGY MEDICINES AND EXPAND PRESENCE IN CHINA
researchers in the RCSI School of Pharmacy and Biomolecular Sciences, has been published in the International Journal of Drug Policy.
“These recommendationsconsensus are intended to inform future policy decisions and discussions regarding the delivery of OAT, identifying which changes should be considered for integration into care models beyond COVID-19. For example, all people on OAT should be prescribed and encouraged to take a supply of Naloxone (a medicine that rapidly reverses an opioid or heroin overdose), particularly during high-risk periods. They should also be trained on how to use Naloxone.”
Sanofi’s initial strategic equity investment in Innovent for ¤300 million In addition to the strategic multiproduct collaboration and license agreement, Sanofi, subject to conditions precedent including regulatory approval and customary closing conditions, will invest in new common shares issued by Innovent for ¤300 million, at a price of HK $42.42 per share, representing a 20% premium to the Innovent 30-trading-day average share price as of August 3, 2022, one day prior to the signing of the agreements.
CIBINQO® is a once-daily oral treatment with proven efficacy demonstrated in a large-scale clinical trial program
PRESCRIBING INFORMATION CIBINQO® ▼ (ABROCITINIB)
A once-daily
Significant skin clearance at week 12, with sustained control at week 481,5 Rapid itch relief, superior to dupilumab + TCS at week 2 for CIBINQO 200 mg + TCS, with significant results as early as day 41,6 pill available doses with therapies
Renal impairment: No dose adjustment is required in patients with mild renal impairment, i.e., estimated glomerular filtration rate (eGFR) of 60 to < 90 mL/min. In patients with moderate (eGFR 30 to < 60 mL/min) renal impairment, the recommended dose of Cibinqo should be reduced by half to 100 mg or 50 mg once daily. In patients with severe (eGFR < 30 mL/min) renal impairment, 50 mg once daily is the recommended starting dose. The maximum daily dose is 100 mg. Cibinqo has not been studied in patients with end-stage renal disease (ESRD) on renal replacement therapy.
that can be used
Elderly: The safety profile observed in elderly patients was similar to that of the adult population with the following exceptions: a higher proportion of patients 65 years of age and older discontinued from clinical studies and were more likely to have serious adverse reactions compared to younger patients; patients 65 years and older were more likely to develop low platelet and ALC values; the incidence rate of herpes zoster in patients 65 years of age and older was higher than that of younger patients. There are limited data in patients above 75 years of age. Immunosuppressive conditions or medicinal products: Patients with immunodeficiency disorders or a first-degree relative with a hereditary immunodeficiency were excluded from clinical studies and no information on these patients is available. Combination with biologic immunomodulators, potent immunosuppressants such as ciclosporin or other Janus kinase (JAK) inhibitors has not been studied. Their concomitant use with abrocitinib is not recommended as a risk of additive immunosuppression cannot be excluded.
Breast-feeding: There are no data on the presence of abrocitinib in human milk, the e ects on the breast fed infant, or the e ects on milk production. Abrocitinib was secreted in milk of lactating rats. A risk to newborns/infants cannot be excluded and Cibinqo is contraindicated during breast feeding. Fertility: Based on the findings in rats, oral administration of Cibinqo may result in temporary reduced fertility in females of reproductive potential. The e ects on female rat fertility were reversible 1 month after cessation of abrocitinib oral administration. Driving and operating machinery: Cibinqo has no e ect on the ability to drive or use machines. Side E ects: The most commonly reported adverse reactions are nausea (15.1%), headache (7.9%), acne (4.8%), herpes simplex (4.2%), blood creatine phosphokinase increased (3.8%), vomiting (3.5%), dizziness (3.4%) and abdominal pain upper (2.2%). The most frequent serious adverse reactions are infections (0.3%) including herpes simplex, herpes zoster, and pneumonia. Refer to SmPC for further information on side e ects. Legal Category: S1A. Marketing Authorisation Numbers: EU/1/21/1593/002 - Cibinqo 50 mg (28 film-coated tablets), EU/1/21/1593/007 - Cibinqo 100 mg (28 film-coated tablets); EU/1/21/1593/012 - Cibinqo 200 mg (28 film-coated tablets). Marketing Authorisation Holder: Pfizer Europe MA EEIG, Boulevard de la Plaine 17, 1050 Bruxelles, Belgium.
so you can tailor treatment to meet the individual needs of your patients1-3,7,8
in multiple
Lactose: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product. Drug Interactions: Potential for other medicines to a ect pharmacokinetics of abrocitinib: Abrocitinib is metabolised predominantly by CYP2C19 and CYP2C9 enzymes, and to a lesser extent by CYP3A4 and CYP2B6 enzymes, and its active metabolites are renally excreted and are substrates of the organic anion transporter 3 (OAT3). Therefore, exposures of abrocitinib and/or its active metabolites may be a ected by medicinal products that strongly inhibit or induce theses enzymes and transporter. Dose adjustments, as appropriate, may be required. Co-administration with products which increase gastric pH: The e ect of elevating gastric pH with antacids, H2-receptor antagonists (famotidine), or proton pump inhibitors (omeprazole) on the pharmacokinetics of abrocitinib has not been studied and may reduce the absorption of abrocitinib due to the low solubility of abrocitinib at pH above 4. Potential for Cibinqo to a ect pharmacokinetics of other medicinal products: No clinically significant e ects of Cibinqo were observed in drug interaction studies with oral contraceptives. Caution should be exercised for concomitant use of abrocitinib with dabigatran. Caution should be exercised as the levels of P-gp substrates with a narrow therapeutic index, such as digoxin, may increase. The exposures of medicinal products metabolised by CYP2B6 (e.g., bupropion, efavirenz) and CYP1A2 (e.g., alosetron, duloxetine, ramelteon, tizanidine) may be decreased and of those metabolised by CYP2C19 (e.g., S mephenytoin) may be increased initially and then decreased, when used concomitantly with abrocitinib. Fertility, pregnancy, and lactation: Women of childbearing potential: Women of reproductive potential should be advised to use e ective contraception during treatment and for 1 month following the final dose of Cibinqo. Pregnancy planning and prevention for females of reproductive potential should be encouraged. Pregnancy: There are no or limited amount of data on the use of abrocitinib in pregnant women. Studies in animals have shown reproductive toxicity. Abrocitinib has been shown to cause embryo-foetal lethality in pregnant rats and rabbits, skeletal variations in the foetuses of pregnant rats and rabbits and to a ect parturition and peri/postnatal development in rats. Cibinqo is contraindicated during pregnancy.
References: 1. Bieber T, Simpson EL, Silverberg JI, et al. N Engl J Med. 2021;384(12):1101-1112. 2. Simpson EL, Sinclair R, Forman S, et al. Lancet. 2020;396(10246):255-266. 3. Silverberg JI, Simpson EL, Thyssen JP, et al. JAMA Dermatol 2020;156(8):863-873. 4. Boeri M, Sutphin J, Hauber B, et al. J Dermatolog Treat. 2020 Nov 2:1-10. doi:10.1080/09546634.1832185. 5. Reich K, Silverberg JI, Papp K, et al. Presented at the Revolutionizing Atopic Dermatitis Virtual Conference; 13 June 2021. 6. Ständer S, Yosipovitch G, Simpson EL, et al. Presented at the American Academy of Dermatology Virtual Meeting Experience 2021; 23-25 April 2021. 7. Cibinqo Summary of Product Characteristics. 8. Blauvelt A, Silverberg JI, Lynde CW, et al. J Am Acad Dermatol. Published online 17 August 2021. doi: 10.1016/j.jaad.2021.05.075.
9. Cork MJ, Deleuran MS, Geng B, et al. Presented at the European Academy of Dermatology and Venereology Virtual Congress 2021; 29 September-2 October 2021. Although some clinical trials included adolescents, please note that CIBINQO is indicated for the treatment of moderate-to-severe atopic dermatitis in adults who are candidates for systemic therapy.
TCS includes low- to medium-potency topical corticosteroids, topical calcineurin inhibitors, or topical phosphodiesterase 4 inhibitors, per protocol guidance in JADE COMPARE. Nonmedicated topicals were also required.1 AD=atopic dermatitis; JAK=Janus kinase; LTE=long-term extension. © 2022 Pfizer Inc. All rights reserved. July 2022. PP-CIB-IRL-0035
FIERCE or TAMER,
SAFETY PROFILE: Rigorously studied in >3100 patients across 7 clinical trials, including one ongoing LTE 9 moderate-to-severepatients’AD is
Presentation: Film-coated tablets containing 50 mg, 100 mg, or 200 mg abrocitinib. Each tablet contains 1.37 mg, 2.73 mg, and 5.46 mg of lactose monohydrate, respectively. Indications: For the treatment of moderate-to-severe atopic dermatitis in adults who are candidates for systemic therapy. Dosage: Treatment should be initiated and supervised by a healthcare professional experienced in the diagnosis and treatment of atopic dermatitis. Posology: The recommended starting dose is 200 mg once daily. A starting dose of 100 mg once daily is recommended for patients ≥ 65 years of age. For other patients who may benefit from a starting dose of 100 mg, see sections 4.4 and 4.8 of the SmPC. During treatment, the dose may be decreased or increased based on tolerability and e cacy. The lowest e ective dose for maintenance should be considered. The maximum daily dose is 200 mg. Can be used with or without medicated topical therapies for atopic dermatitis. Discontinuation of treatment should be considered in patients who show no evidence of therapeutic benefit after 24 weeks. Treatment initiation: Treatment should not be initiated in patients with a platelet count < 150 × 103/mm3, an absolute lymphocyte count (ALC) < 0.5 × 103/mm3, an absolute neutrophil count (ANC) < 1.2 × 103/mm3 or who have a haemoglobin value < 10 g/dL. Dose interruption: If a patient develops a serious infection, sepsis or opportunistic infection, dose interruption should be considered until the infection is controlled. Interruption of dosing may be needed for management of laboratory abnormalities. Missed doses: If a dose is missed, patients should be advised to take the dose as soon as possible unless it is less than 12 hours before the next dose, in which case the patient should not take the missed dose. Thereafter, dosing should be resumed at the regular scheduled time. Interactions: In patients receiving dual strong inhibitors of cytochrome CYP2C19 and moderate inhibitors of CYP2C9, or strong inhibitors of CYP2C19 alone (e.g., fluvoxamine, fluconazole, fluoxetine and ticlopidine), the recommended starting dose of Cibinqo should be reduced by half to 100 mg or 50 mg once daily. Treatment is not recommended concomitantly with moderate or strong inducers of CYP2C19/CYP2C9 enzymes (e.g., rifampicin, apalutamide, efavirenz, enzalutamide, phenytoin).
or without medicated topical
Last revised: December 2021. Ref: CQ 1_0 IE.
CIBINQO is a convenient once-daily oral JAK1 inhibitor for moderate-to-severe atopic dermatitis (AD) that o ers1-4 CONSISTENT
For further information on this medicine please contact Pfizer Medical Information on 1800 633 363 or at medical.information@pfizer.com. For queries regarding product availability please contact: Pfizer Healthcare Ireland, Pfizer Building 9, Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 + 353 1 467 6500.
Hepatic impairment: No dose adjustment is required in patients with mild (Child Pugh A) or moderate (Child Pugh B) hepatic impairment. Cibinqo must not be used in patients with severe (Child Pugh C) hepatic impairment. Elderly: The recommended starting dose for patients aged 65 years or more 100 mg once daily. Paediatric population: The safety and e cacy of Cibinqo in children under 12 years of age have not yet been established. No data are available. Cibinqo has been studied in adolescents 12 to < 18 years of age. However, because of bone findings in juvenile rats (comparable to a 3 month old human), additional long-term data in growing adolescents is needed to conclude that the benefits outweigh the risks. Method of administration: This medicinal product is to be taken orally once daily with or without food at approximately the same time each day. In patients who experience nausea, taking Cibinqo with food may improve nausea. Tablets should be swallowed whole with water and should not be split, crushed, or chewed because these methods have not been studied in clinical trials. Contra-indications: Hypersensitivity to the active substance or to any of the excipients. Active serious systemic infections, including tuberculosis (TB), severe hepatic impairment, pregnancy, and breast-feeding. Warnings and Precautions: Serious infections: Serious infections have been reported in patients receiving Cibinqo. The most frequent serious infections in clinical studies were herpes simplex, herpes zoster and pneumonia. Treatment must not be initiated in patients with an active, serious systemic infection. Risks and benefits of treatment prior to initiating Cibinqo should be considered. Patients should be closely monitored for the development of signs and symptoms of infection during and after treatment with abrocitinib. A patient who develops a new infection during treatment should undergo prompt and complete diagnostic testing and appropriate antimicrobial therapy should be initiated. The patient should be closely monitored, and therapy should be temporarily interrupted if the patient is not responding to standard therapy. Tuberculosis: Patients should be screened for TB before starting treatment and yearly screening for patients in highly endemic areas for TB should be considered. Abrocitinib must not be given to patients with active TB. For patients with a new diagnosis of latent TB or prior untreated latent TB, preventive therapy for latent TB should be started prior to initiation of treatment. Viral reactivation: Viral reactivation, including herpes virus reactivation (e.g., herpes zoster, herpes simplex), was reported in clinical studies. The rate of herpes zoster infections was higher in patients 65 years of age and older and patients with severe atopic dermatitis at baseline. If a patient develops herpes zoster, temporary interruption of treatment should be considered until the episode resolves. Screening for viral hepatitis should be performed in accordance with clinical guidelines before starting therapy and during therapy. Patients with evidence of active hepatitis B or hepatitis C (positive hepatitis C PCR) infection were excluded from clinical studies. Patients who were hepatitis B surface antigen negative, hepatitis B core antibody positive, and hepatitis B surface antibody positive had testing for hepatitis B virus (HBV) DNA. Patients who had HBV DNA above the lower limit of quantification (LLQ) were excluded. Patients who had HBV DNA negative or below LLQ could initiate treatment; such patients had HBV DNA monitored. If HBV DNA is detected, a liver specialist should be consulted. Vaccination: No data are available on the response to vaccination in patients receiving Cibinqo. Use of live, attenuated vaccines should be avoided during or immediately prior to treatment. Prior to initiating treatment with this medicinal product, it is recommended that patients be brought up to date with all immunisations, including prophylactic herpes zoster vaccinations, in agreement with current immunisation guidelines. Thrombotic events including pulmonary embolism: Events of deep venous thrombosis (DVT) and pulmonary embolism (PE) have been reported in patients receiving abrocitinib. Cibinqo should be used with caution in patients at high risk for DVT/PE. Risk factors that should be considered in determining the patient’s risk for DVT/PE include older age, obesity, a medical history of DVT/PE, prothrombotic disorder, use of combined hormonal contraceptives or hormone replacement therapy, patients undergoing major surgery or prolonged immobilisation. If clinical features of DVT/PE occur, treatment should be discontinued and patients should be evaluated promptly, followed by appropriate treatment. Malignancy (including non-melanoma skin cancers): Malignancies, including non-melanoma skin cancer (NMSC), were observed in clinical studies with abrocitinib. Clinical data are insu cient to assess the potential relationship of exposure to abrocitinib and the development of malignancies. Long-term safety evaluations are ongoing. The risks and benefits of Cibinqo treatment should be considered prior to initiating in patients with a known malignancy other than a successfully treated NMSC or cervical cancer in situ or when considering continuing Cibinqo therapy in patients who develop a malignancy. Periodic skin examination is recommended for patients who are at increased risk for skin cancer. Haematologic abnormalities: Confirmed ALC < 0.5 × 103/mm3 and platelet count < 50 × 103/mm3 were observed in less than 0.5% of patients in clinical studies. Treatment with abrocitinib should not be initiated in patients with a platelet count < 150 × 103/mm3, an ALC < 0.5 × 103/mm3, an ANC < 1.2 × 103/mm3 or who have a haemoglobin value < 10 g/dL. Complete blood count should be monitored 4 weeks after initiation of therapy and thereafter according to routine patient management. Lipids: Dose dependent increases in blood lipid parameters were reported in patients treated with abrocitinib compared to placebo. Lipid parameters should be assessed approximately 4 weeks following initiation of therapy and thereafter according to the patient’s risk for cardiovascular disease. The e ect of these lipid parameter elevations on cardiovascular morbidity and mortality has not been determined. Patients with abnormal lipid parameters should be further monitored and managed according to clinical guidelines, due to the known cardiovascular risks associated with hyperlipidaemia. In patients with a high burden of cardiovascular risk factors, the risks, and benefits of abrocitinib compared to that of other available therapies for atopic dermatitis should be considered. If abrocitinib is chosen, interventions to manage lipid concentrations should be implemented according to clinical guidelines.
▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See section 4.8 of the SmPC for how to report adverse reactions.
Please refer to full Summary of Product Characteristics (SmPC) before prescribing Cibinqo®.
Whether your










































