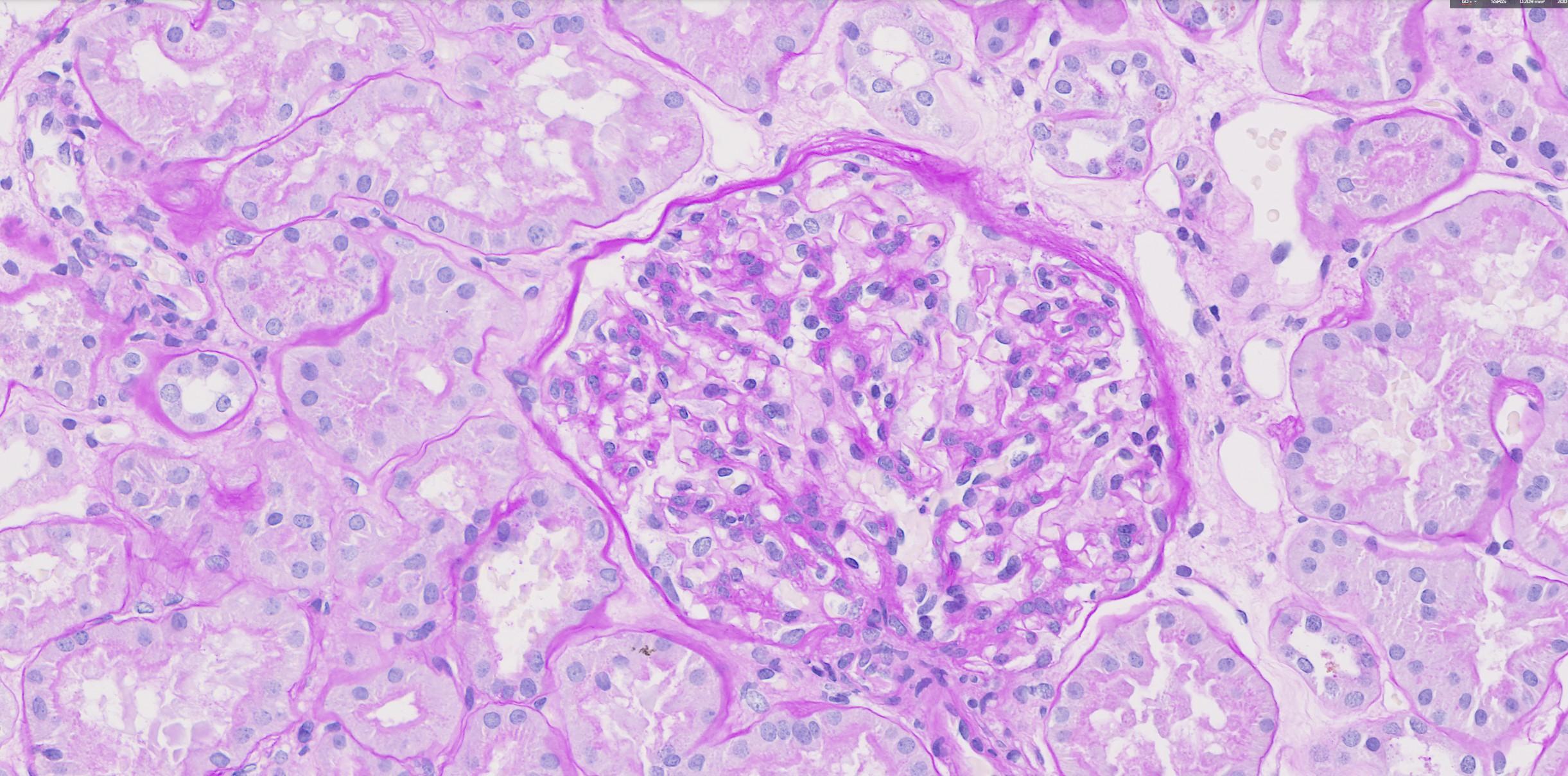
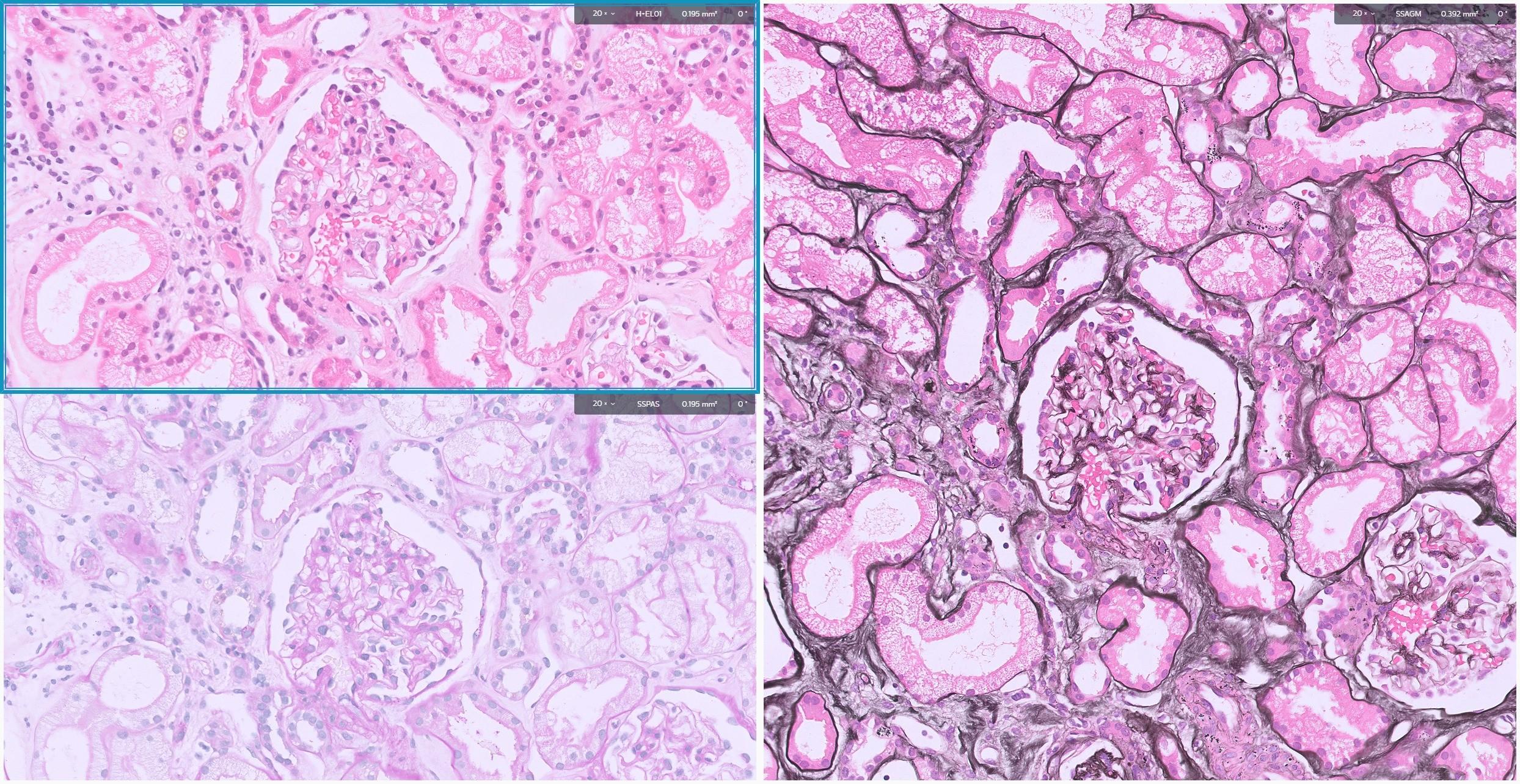
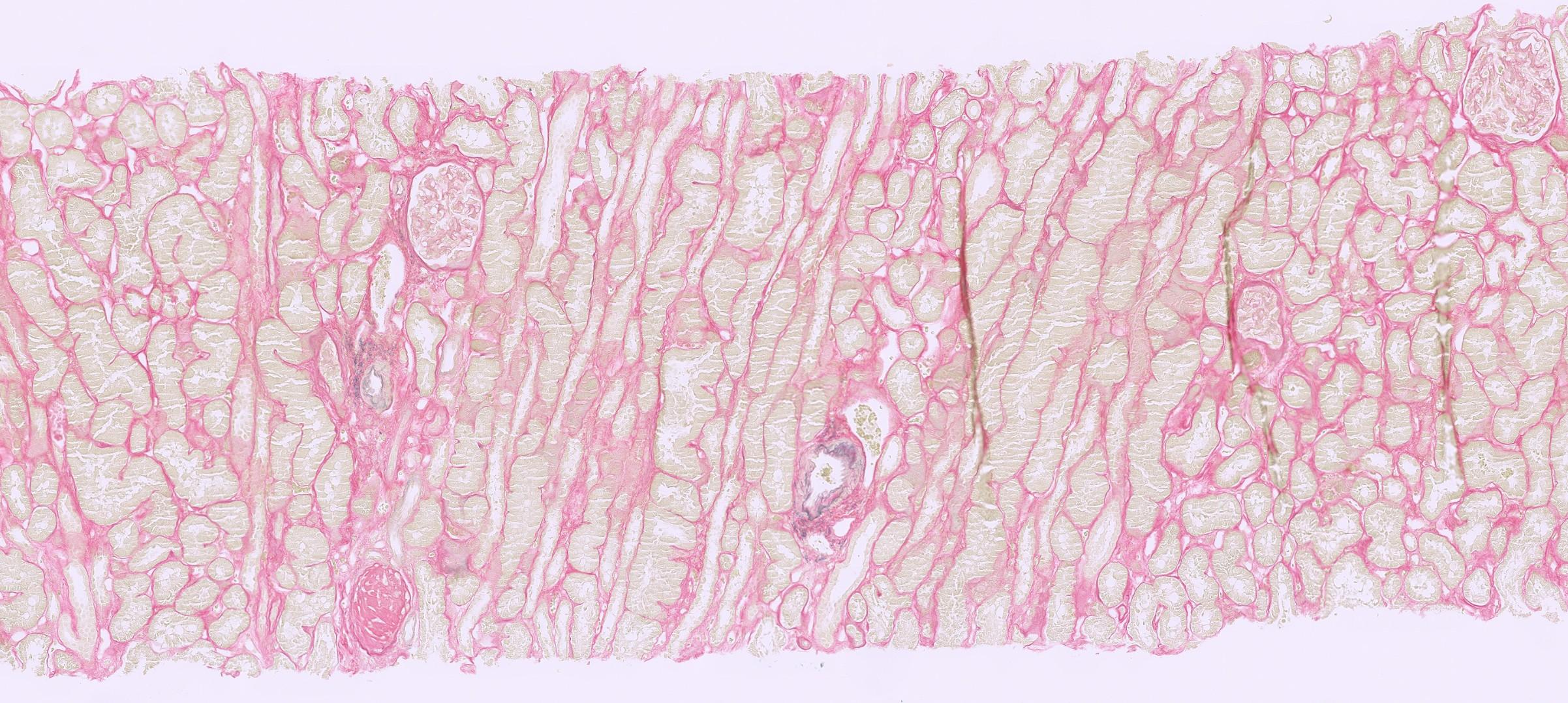
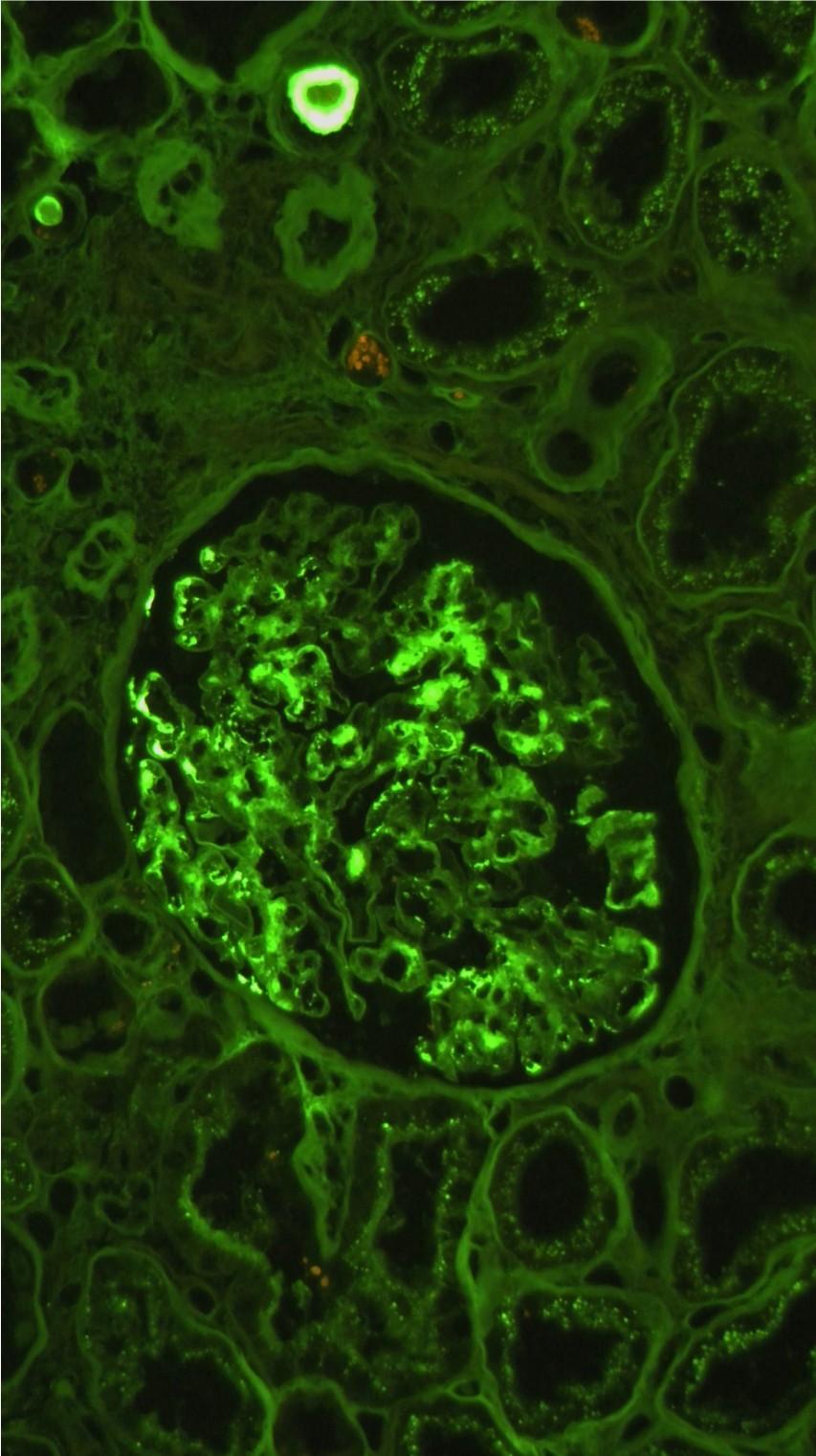
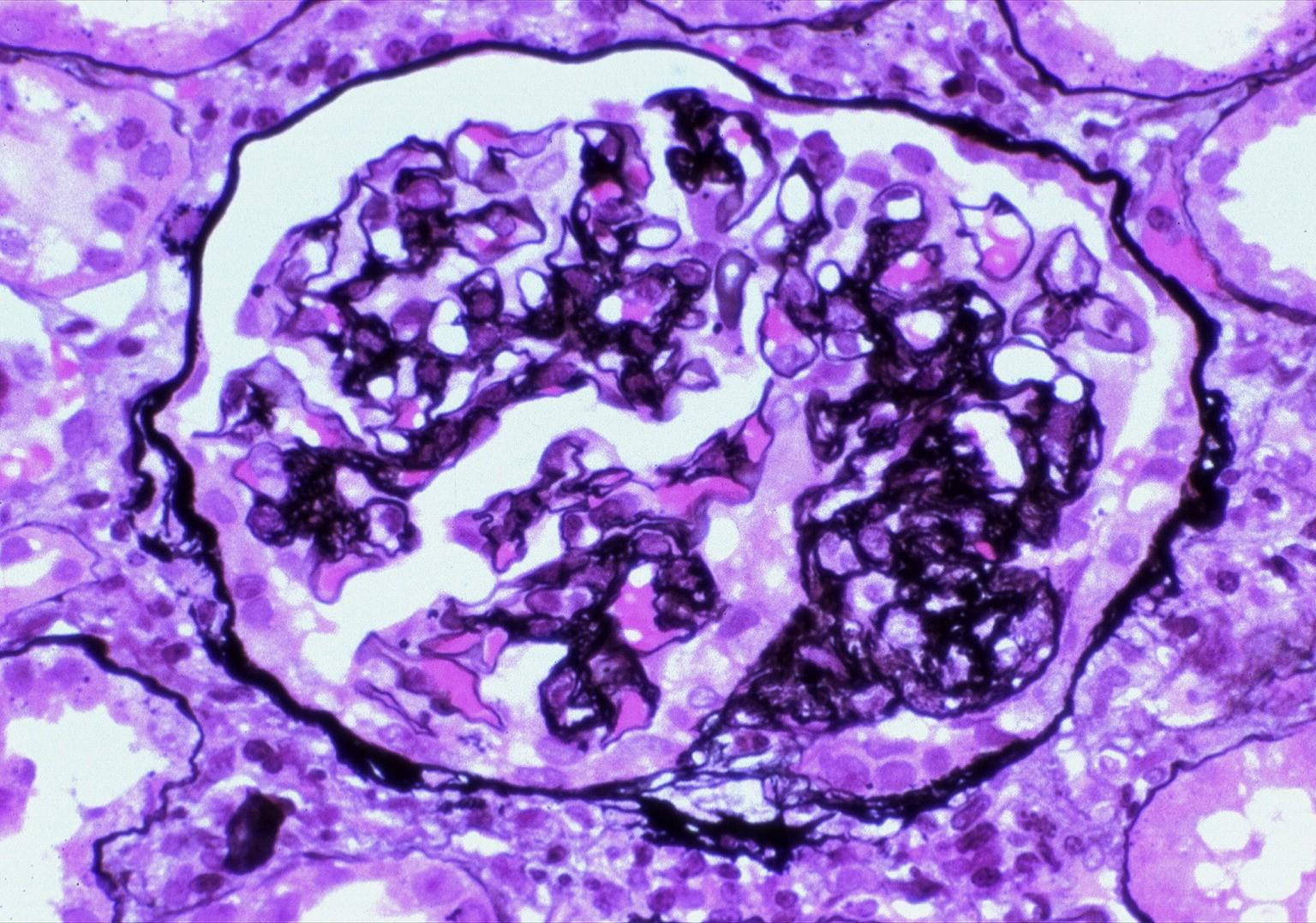
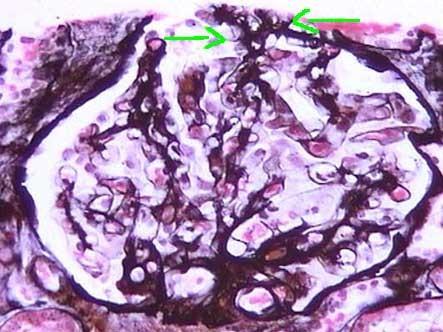
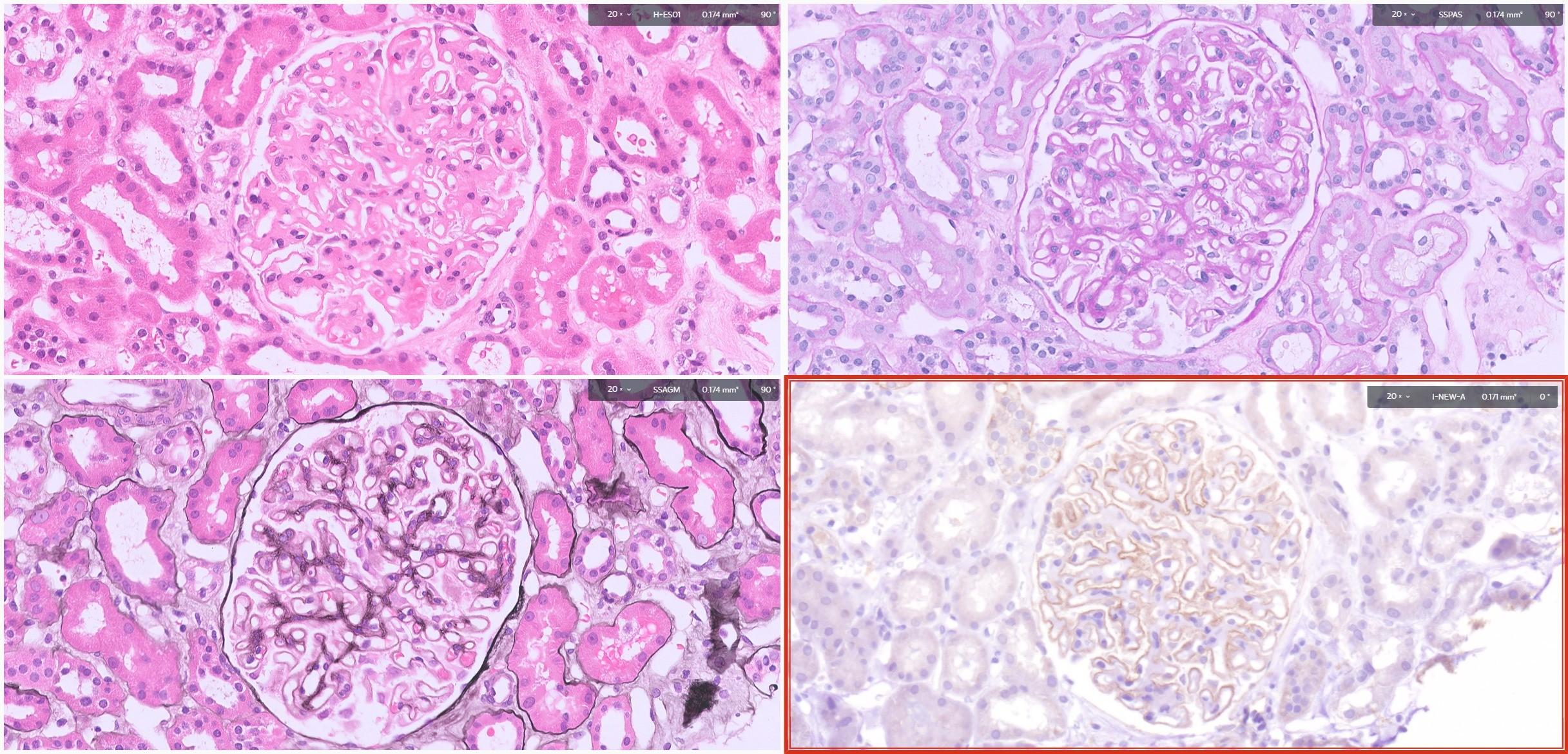
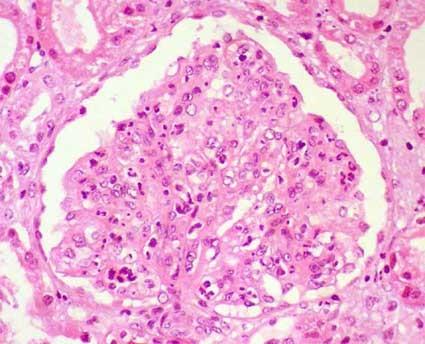
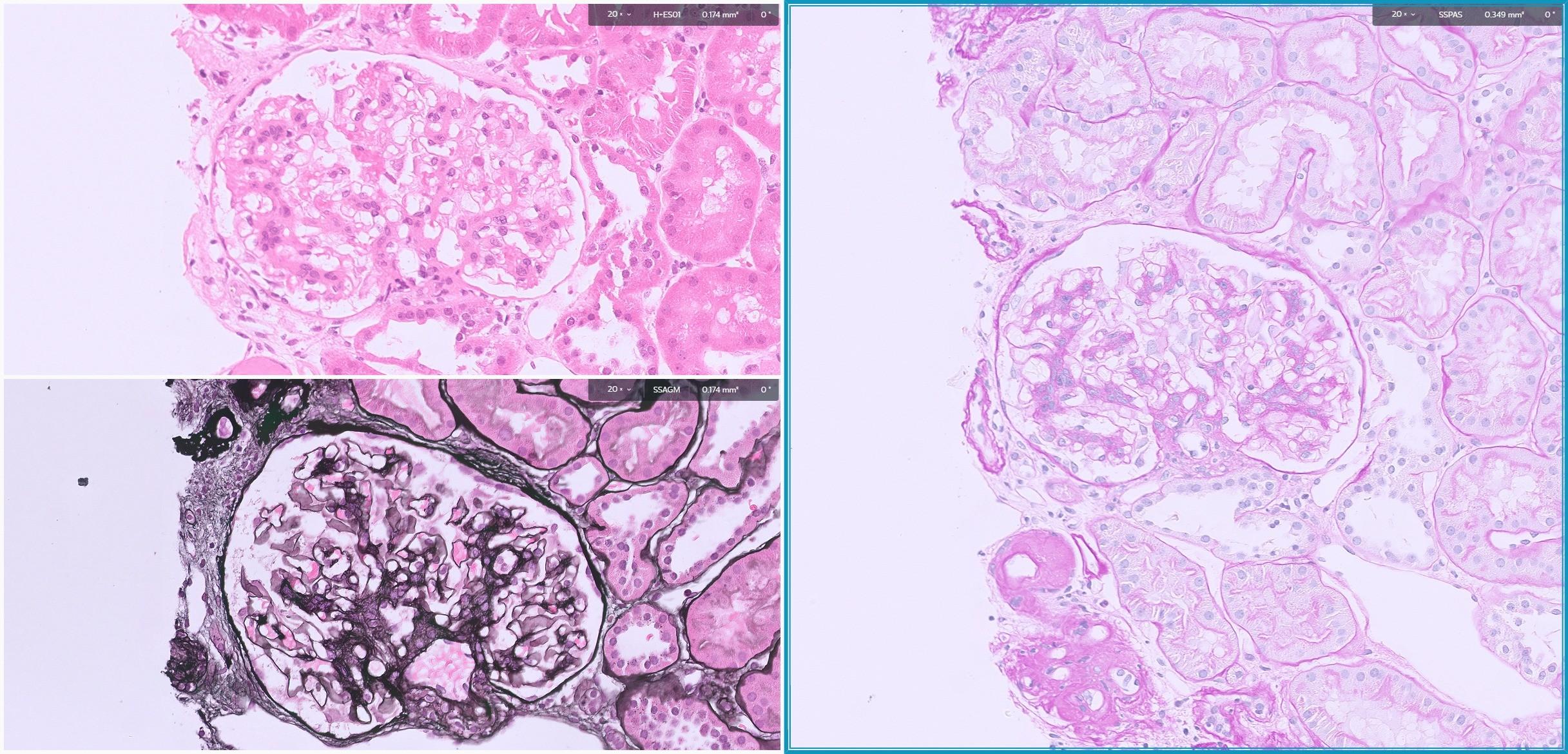
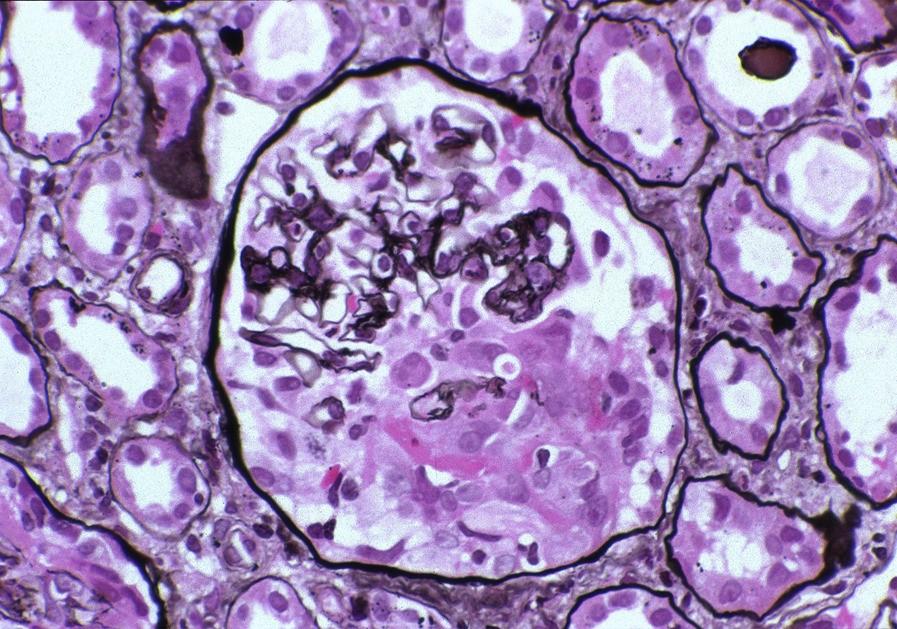
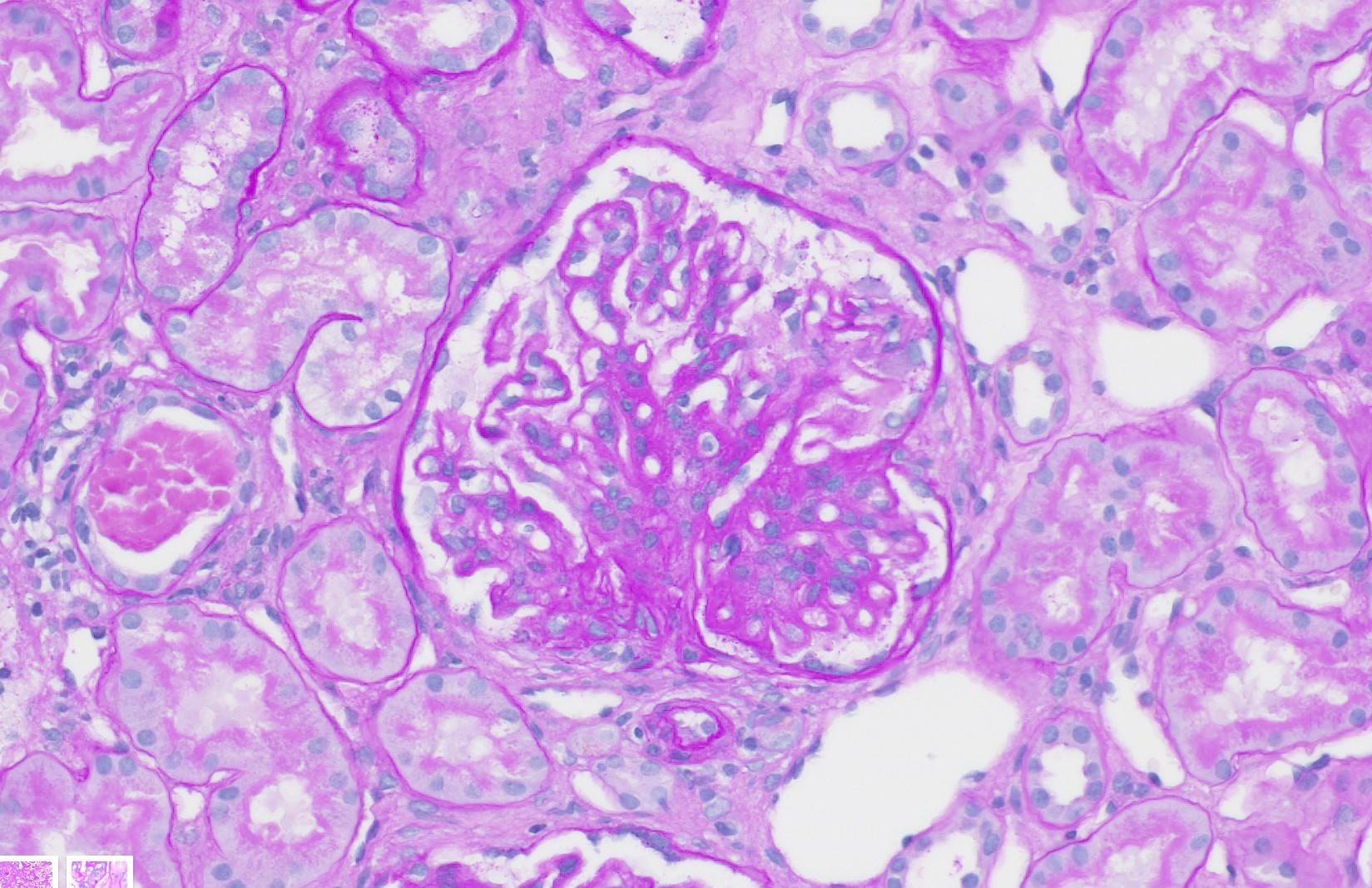
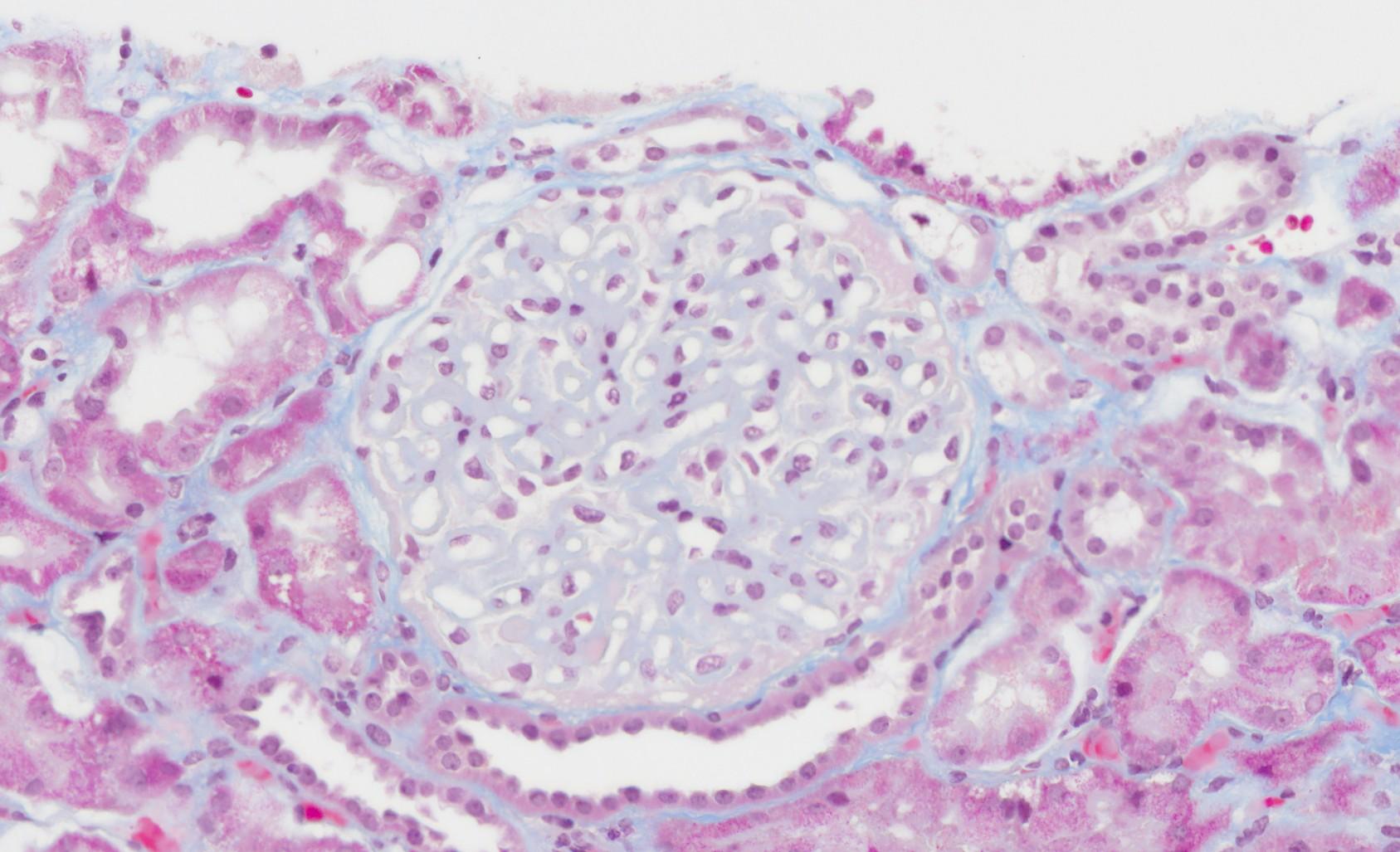
A 12-year-old boy presents with a 2-week history of periorbital and lower limb oedema. His urine dipstick shows 4+ proteinuria and his serum albumin level is low. A renal biopsy is performed. No immunoglobulin deposits were seen under immunofluorescence.
(Representative PAS-stained section)
Based on the light microscopic appearance of the renal biopsy and the clinical presentation, which of the following findings is MOST likely to be observed on electron microscopy (EM)?
A. Subepithelial "humps“
B. Extensive foot process effacement
C. Mesangial interposition
D. Subendothelial deposits with a "tram-track" appearance
E. Fibrillary material deposited in the mesangium and capillary walls
DON’T BE AFRAID!
■ Read the actual question first then the rest of the question stem
■ Use the clinical information to narrow down your differentials
■ Identify features in the picture provided
– The stain used in the picture can be a hint to what they want you to look at
■ Pick the correct answer
– If unsure, eliminate the answers you know are clearly wrong
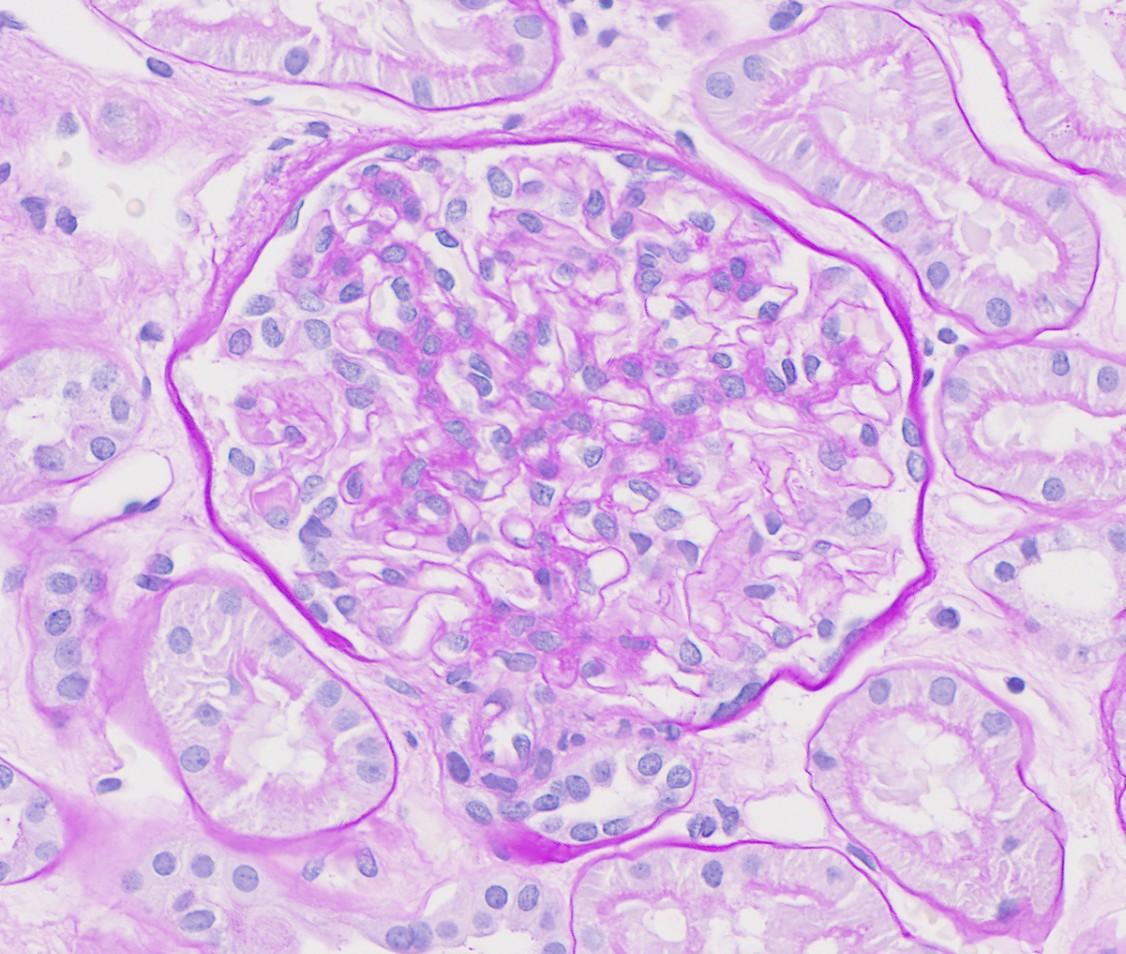
A 12-year-old boy presents with a 2-week history of periorbital and lower limb oedema. His urine dipstick shows 4+ proteinuria and his serum albumin level is low. A renal biopsy is performed. No immunoglobulin deposits were seen under immunofluorescence.
(Representative PAS-stained section)
Based on the light microscopic appearance of the renal biopsy and the clinical presentation, which of the following findings is MOST likely to be observed on electron microscopy (EM)?
A. Subepithelial "humps“
B. Extensive foot process effacement
C. Mesangial interposition
D. Subendothelial deposits with a "tram-track" appearance
E. Fibrillary material deposited in the mesangium and capillary walls
A 12-year-old boy presents with a 2-week history of periorbital and lower limb oedema. His urine dipstick shows 4+ proteinuria and his serum albumin level is low. A renal biopsy is performed. No immunoglobulin deposits were seen under immunofluorescence.
(Representative PAS-stained section)
Based on the light microscopic appearance of the renal biopsy and the clinical presentation, which of the following findings is MOST likely to be observed on electron microscopy (EM)?
A. Subepithelial "humps“
B. Extensive foot process effacement
C. Mesangial interposition
D. Subendothelial deposits with a "tram-track" appearance
E. Amorphous material deposited in the mesangium and capillary walls
Q1 - Explained
■ Correct Answer (B): Extensive foot process effacement is the characteristic EM finding in minimal change disease (MCD), which is the most common cause of nephrotic syndrome in children and has normal or near-normal glomeruli under light microscopy.
■ Incorrect Answer (A): Subepithelial "humps" are most characteristic of post-infectious glomerulonephritis (PIGN), which often presents as nephritic syndrome, not nephrotic, and has obvious glomerular changes on light microscopy (hypercellularity). Also seen in C3 glomerulopathy.
■ Incorrect Answer (C): Mesangial interposition is typical of membranoproliferative glomerulonephritis (MPGN), which usually presents with nephritic or mixed nephritic-nephrotic features and shows changes on LM
■ Incorrect Answer (D): Subendothelial deposits with a "tram-track" appearance are also associated with MPGN, and usually has associated light microscopy findings such as mesangial hypercellularity
■ Incorrect Answer (E): Amorphous material in mesangium/capillary walls is suggestive of amyloidosis or other proteinaceous deposits, not commonly associated with the specific presentation of primary childhood nephrotic syndrome. This is a light microscopy finding, not an EM finding.
BASIC PRINCIPLES REVIEW
Processing of the biopsy
■ Biopsy material should be sent ‘fresh’
– Not in any fixative
– Ideally in a saline wrapped gauze and refrigerated (4ºC)
■ Once received in lab, dissected microscopically
– Tissue for LM & IF/IP fixed in formalin or Bouin’s
– In some places IF (done with frozen) is fixed in Michel’s medium
– Tissue for EM fixed in glutaraldehyde
Renal Biopsy Basics
■ Assess the biopsy by dividing it into four compartments
■ The special stains help us with Light Microscopy
– H&E, PAS, Jones Methanamine Silver, Masson’s Trichrome, EVG, Congo Red
■ Immunofluorescence (IF) or Immunoperoxidase (IP) assessment tells us if there is immunecomplex activity and detect immune deposits
– IgG, IgA, IgM, C3, C1q, Kappa, Lambda
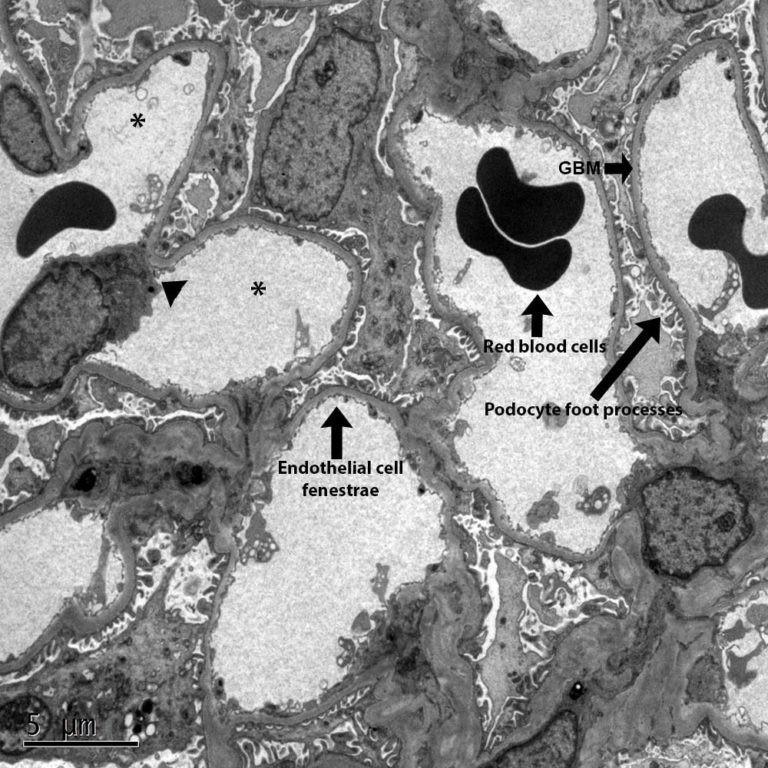
■ Electron microscopy (EM) is used to assess the ultrastructure of the glomerulus
■ Clinicopathologic correlation is extremely important to arrive at the correct diagnosis. Never give a renal biopsy diagnosis without clinical information.
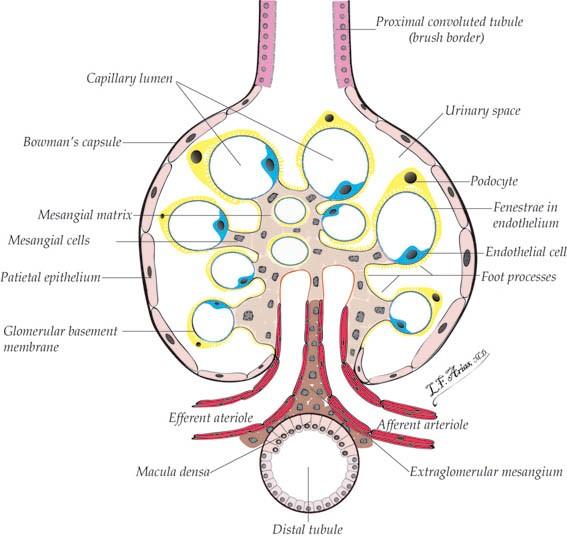
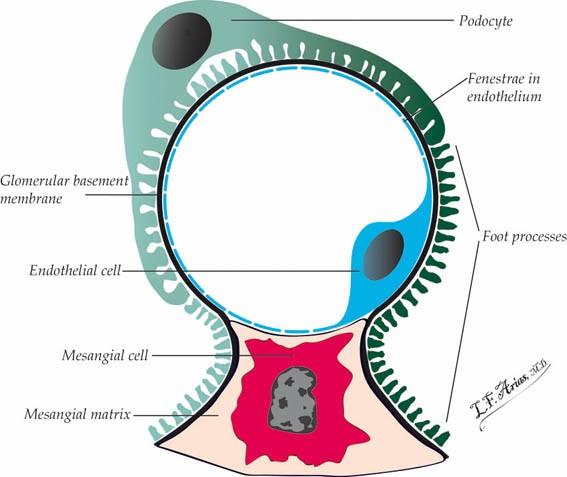
The Glomerulus
■ Imagine it as a 3D structure that we view in 2D
■ Multiple areas of interest
■ Mesangium made of mesangial matrix containing mesangial cells
■ Tufts composed of capillary walls made of endothelial cells
■ Outer lining of glomeruli covered by podocytes which have foot processes
■ Bowman’s capsule lined by visceral epithelial cells
The Glomerulus
The Glomerulus
■ The tuft is formed by lobules of capillaries
■ The mesangial matrix is composed of Collagen III, IV, V & VI
■ The glomerular filtrate from the afferent arteriole must cross into the urinary space (Bowman’s Space) through the capillary wall
■ The capillary wall (from in to out) is formed by the endothelial cell, glomerular basement membrane (GBM) and the podocyte foot processes
■ The GBM is contains type IV collagen and is between 240 and 360 nm in adults
The Glomerulus
■ The tuft is formed by lobules of capillaries
■ The mesangial matrix is composed of Collagen III, IV, V & VI
■ The glomerular filtrate from the afferent arteriole must cross into the urinary space (Bowman’s Space) through the capillary wall
■ The capillary wall (from in to out) is formed by the endothelial cell, glomerular basement membrane (GBM) and the podocyte foot processes
■ The GBM is contains type IV collagen and is between 240 and 360 nm in adults
Special Stains
■ H&E
– Used for general overview of the biopsy
■ PAS
– Used to assess the GBM
■ Jones Methanamine Silver (JMS / Jones / Jones Silver)
– Used to assess the GBM
■ Congo Red (CR)
– Used to detect amyloid
■ Masson’s Trichrome (MT)
– Used to assess fibrosis in the interstitium, in crescents etc.
■ Elastic Van Gieson (EVG)
– Used to assess intima of vessels
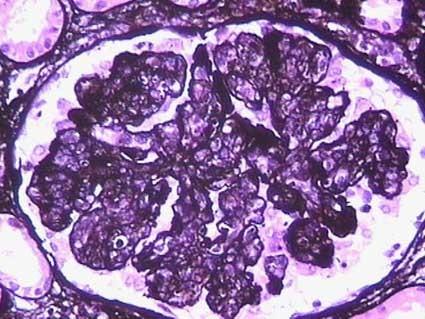
Normal Glomerulus
Congo Red Congo Red
Masson’s Trichrome
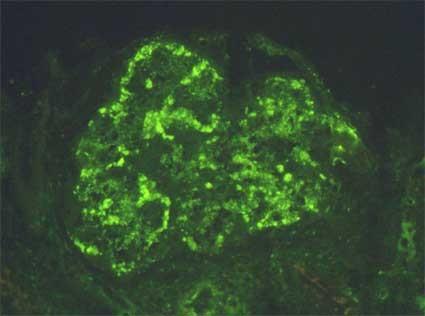
Immunofluorescence
(Positive Deposits in Disease)
Kappa
PATTERNS OF RENAL DISEASE
Patterns / Classification of Renal Diseases
■ Multiple ways to classify
– Clinical Manifestations
– Aetiology
– Immunopathology
– Morphological Patterns
■ There is a low amount of morphological patterns but caused by a large number or aetiological factors
■ There is a limited number of clinical manifestations for many conditions
■ The glomerular pathologic changes can produce any type of clinical syndrome, but, in general, some patterns of renal changes are associated to certain syndromes
■ Nephrotic Syndrome
– MCD, FSGS, Membranous GN
■ Haematuria & Proteinuria (Sub-Nephritic)
– IgA Nephropathy, Alport’s Syndrome, Thin Basement Membrane disease
■ Nephritic Syndrome
– Postinfectious & diffuse proliferative endocapillary forms of GN, membranoproliferative GN
Nephrotic Syndrome
■ Massive proteinuria (>3.5 g/24hrs for adults or >40 mg/m2/hour in children)
hypoalbuminemia, oedema and hyperlipidaemia
■ Caused by extensive or diffuse damage to podocytes
– Remember they are the main barrier to protein leakage
■ Could be caused by inherent damage/alteration to podocytes (podocytopathies) or external factors e.g immune complexes, damage to basement membrane, haemodynamic factors etc.
A 12-year-old boy presents with a 2-week history of periorbital and lower limb oedema. His urine dipstick shows 4+ proteinuria and his serum albumin level is low. A renal biopsy is performed. No immunoglobulin deposits were seen under immunofluorescence.
(Representative PAS-stained section)
Based on the light microscopic appearance of the renal biopsy and the clinical presentation, which of the following findings is MOST likely to be observed on electron microscopy (EM)?
A. Subepithelial "humps“
B. Extensive foot process effacement
C. Mesangial interposition
D. Subendothelial deposits with a "tram-track" appearance
E. Fibrillary material deposited in the mesangium and capillary walls
A 12-year-old boy presents with a 2-week history of periorbital and lower limb oedema. His urine dipstick shows 4+ proteinuria and his serum albumin level is low. A renal biopsy is performed. No immunoglobulin deposits were seen under immunofluorescence.
(Representative PAS-stained section)
Based on the light microscopic appearance of the renal biopsy and the clinical presentation, which of the following findings is MOST likely to be observed on electron microscopy (EM)?
A. Subepithelial "humps“
B. Extensive foot process effacement
C. Mesangial interposition
D. Subendothelial deposits with a "tram-track" appearance
E. Amorphous material deposited in the mesangium and capillary walls
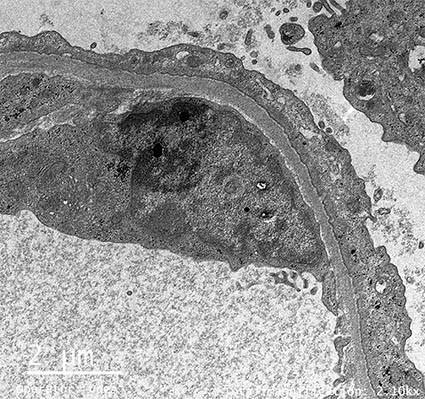
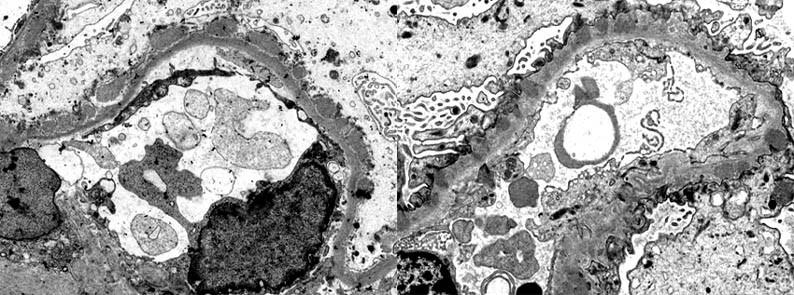
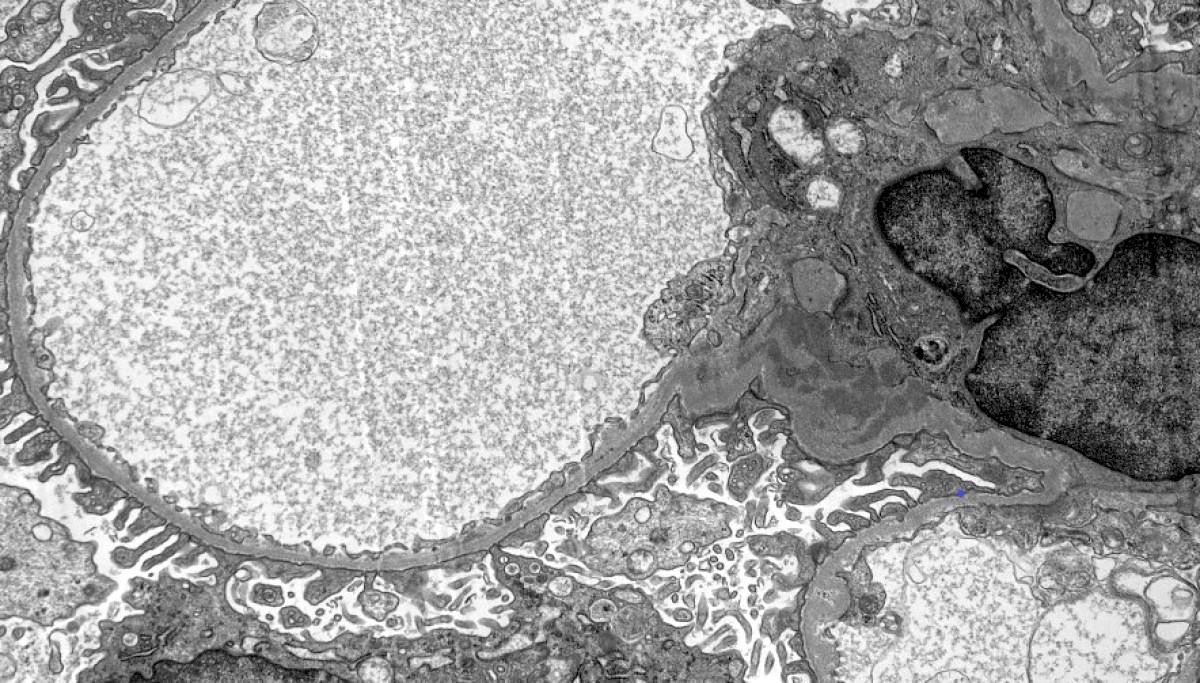
Minimal Change Disease
EM – Microvillous Transformation
– Effaced Foot Processes
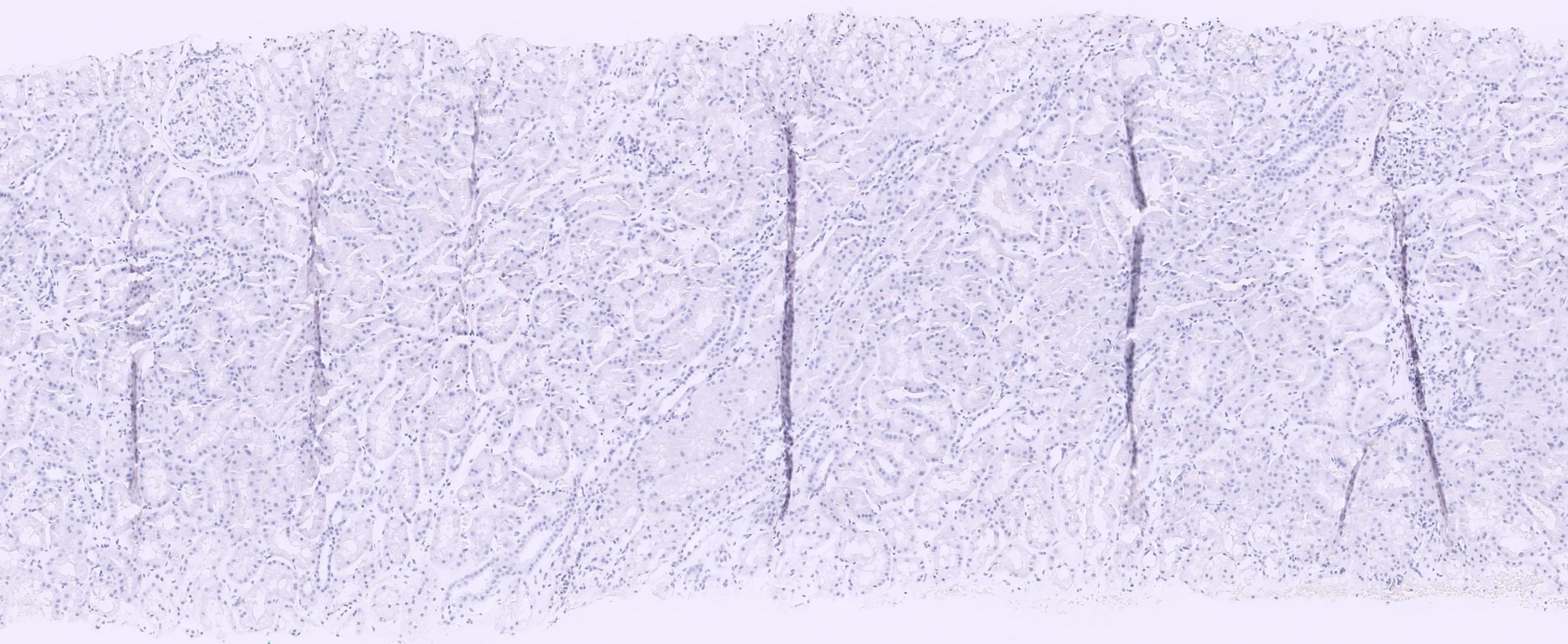
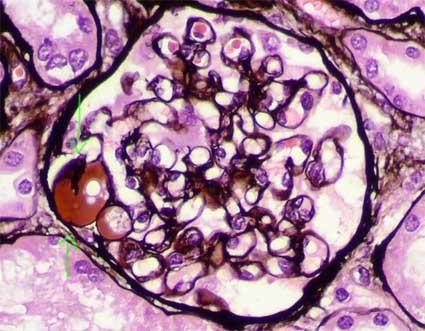
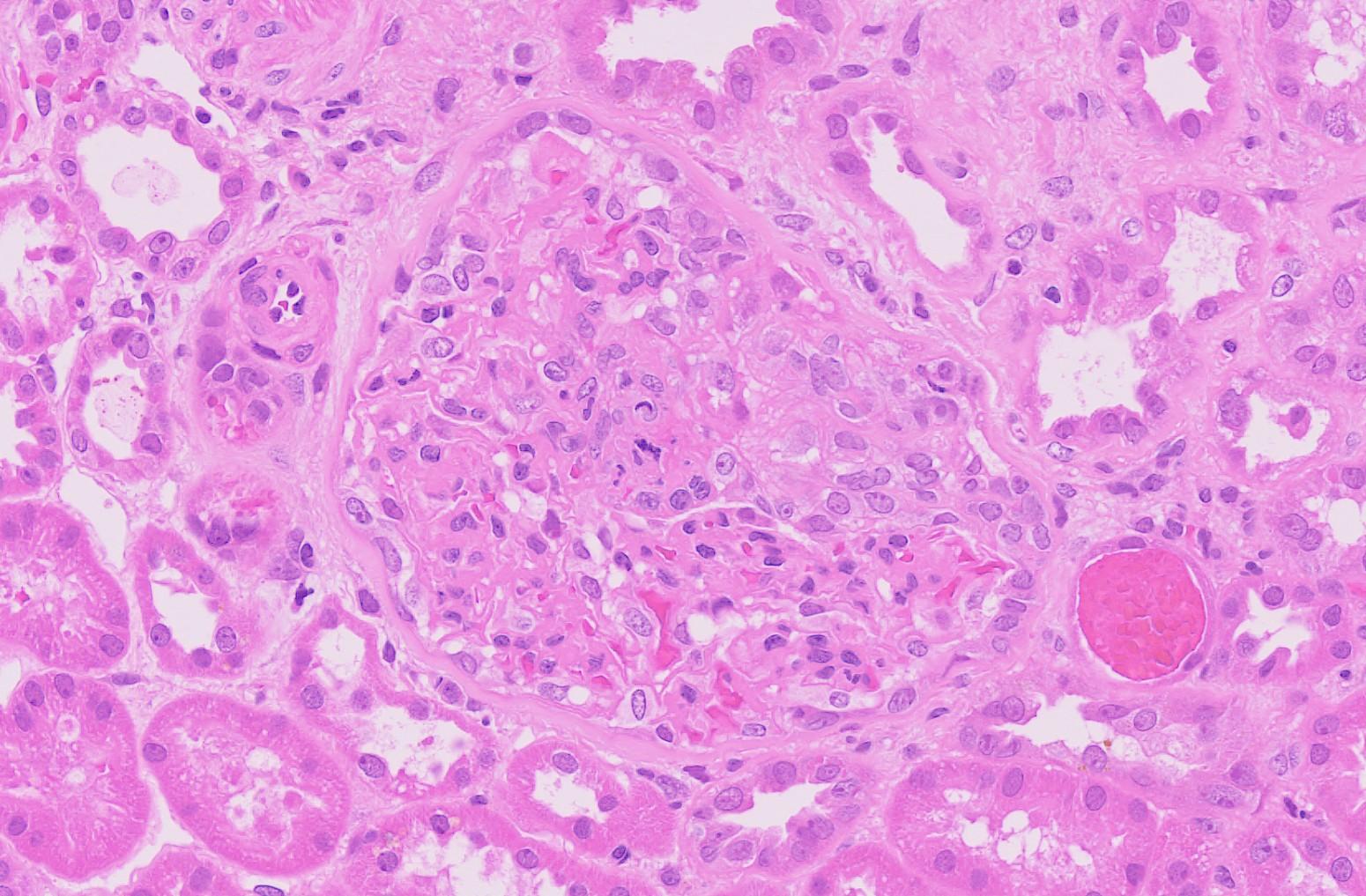
A 45-year-old male presents with significant lower limb oedema and foamy urine. His blood pressure is 150/90 mmHg. Laboratory studies reveal a 24-hour urine protein excretion of 4.5 grams. He denies any history of intravenous drug use or other medical conditions. A renal biopsy is performed. (Representative PAS Image)
Based on the light microscopy findings and clinical scenario, which of the following is the most important next step in further characterizing this patient's kidney disease?
A. Immunofluorescence for IgA
B. Electron microscopy to assess foot processes and rule out specific deposit patterns
C. Genetic testing for podocyte mutations
D. Staining for amyloid
E. Measurement of serum complement levels
A 45-year-old male presents with significant lower limb oedema and foamy urine. His blood pressure is 150/90 mmHg. Laboratory studies reveal a 24-hour urine protein excretion of 4.5 grams. He denies any history of intravenous drug use or other medical conditions. A renal biopsy is performed. (Representative PAS Image)
Based on the light microscopy findings and clinical scenario, which of the following is the most important next step in further characterizing this patient's kidney disease?
A. Immunofluorescence for IgA
B. Electron microscopy to assess foot processes and rule out specific deposit patterns
C. Genetic testing for podocyte mutations
D. Staining for amyloid E. Measurement of serum complement levels
Question 2 - Explained
■ Correct Answer (B): Electron microscopy to assess foot processes and rule out specific deposit patterns - Explanation: While light microscopy has revealed segmental sclerosis, which is diagnostic for FSGS, EM is crucial for further characterization and classification. Firstly, it will confirm the presence of foot process effacement, a hallmark of glomerular diseases presenting with nephrotic syndrome. Secondly, it can help differentiate subtle subtypes of FSGS based on the extent of effacement and other fine details. Thirdly, it will rule out conditions which can mimic FSGS, such as fibrillary/immunotactoid glomerulonephritis (which have characteristic EM features that may not be apparent on light microscopy). In this specific scenario where secondary causes are not obviously implicated on history, the key consideration at this stage is whether this is a primary or secondary form of FSGS, and EM is the most useful tool for that.
■ Incorrect Answer (A): Immunofluorescence for IgA - Explanation: IgA immunofluorescence is most relevant for the diagnosis of IgA nephropathy (Berger’s disease). This condition typically presents with macroscopic haematuria and, less commonly, nephrotic-range proteinuria. The light microscopy would typically show mesangial proliferation and deposition of IgA in the mesangium. It is not the first-line test in the setting of a FSGS pattern on LM and nephrotic syndrome.
■ Incorrect Answer (C): Genetic testing for podocyte mutations - Explanation: Genetic testing is important for identifying patients with inherited forms of FSGS, especially in children and young adults presenting with steroid-resistant disease. However, it is not the most important next step in this specific case and would be of lower priority initially. Genetic testing is usually done after initial investigations are completed or when other forms of FSGS have been excluded.
■ Incorrect Answer (D): Staining for amyloid - Explanation: Amyloidosis can present with nephrotic syndrome and may show glomerular changes, but the characteristic findings on light microscopy are markedly different from FSGS. Amyloid will appear as an eosinophilic, amorphous, acellular material, which will stain positive with Congo red stain and show apple-green birefringence under polarised light. Additionally, this clinical scenario is not suggestive of amyloidosis based on the patient history.
■ Incorrect Answer (E): Measurement of serum complement levels - Explanation: Serum complement levels are more relevant in the work-up of glomerulonephritis conditions like post-infectious GN and membranoproliferative glomerulonephritis (MPGN). These conditions typically present with a nephritic picture and have distinct light microscopy and immunofluorescence features. Complement levels are not relevant to the diagnosis or subclassification of FSGS, and therefore measuring these would be an inappropriate next step.
Focal Segmental Glomerular Sclerosis (FSGS)
■ Primary and secondary forms
– Secondary form very common – related to hypertension
■ Often presents with nephrotic syndrome
■ Multiple morphological variants
– Refer to Oxford classification of FSGS
■ Keep in mind collapsing variant of FSGS, which is associated with HIV (HIVAN) and Covid-19 (COVAN)
IF – Serum Staining
Hyalinosis – Negative for silver MT – Segmental Sclerosis
Tip Lesion
Foam Cells
Collapsing Variant
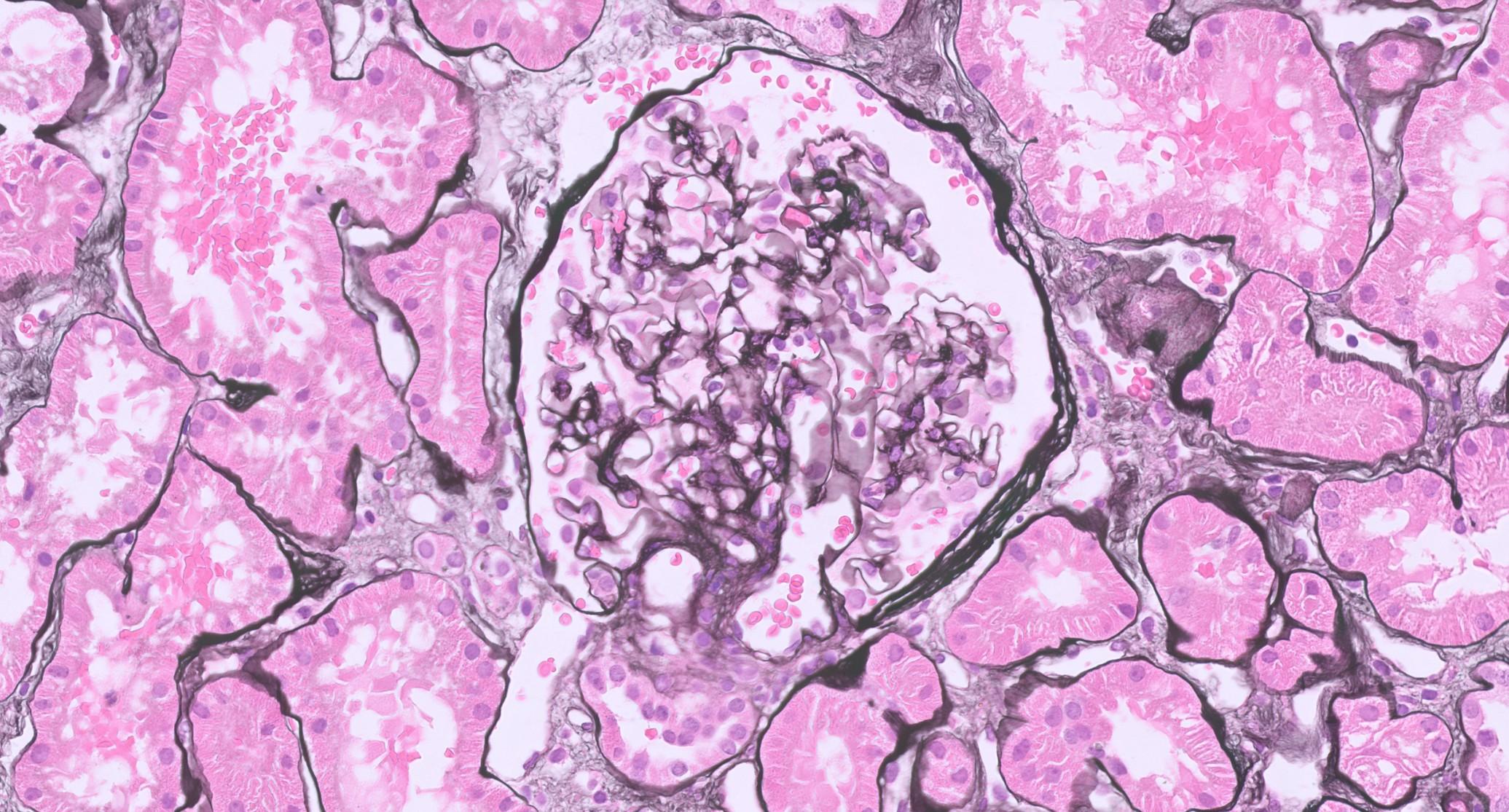
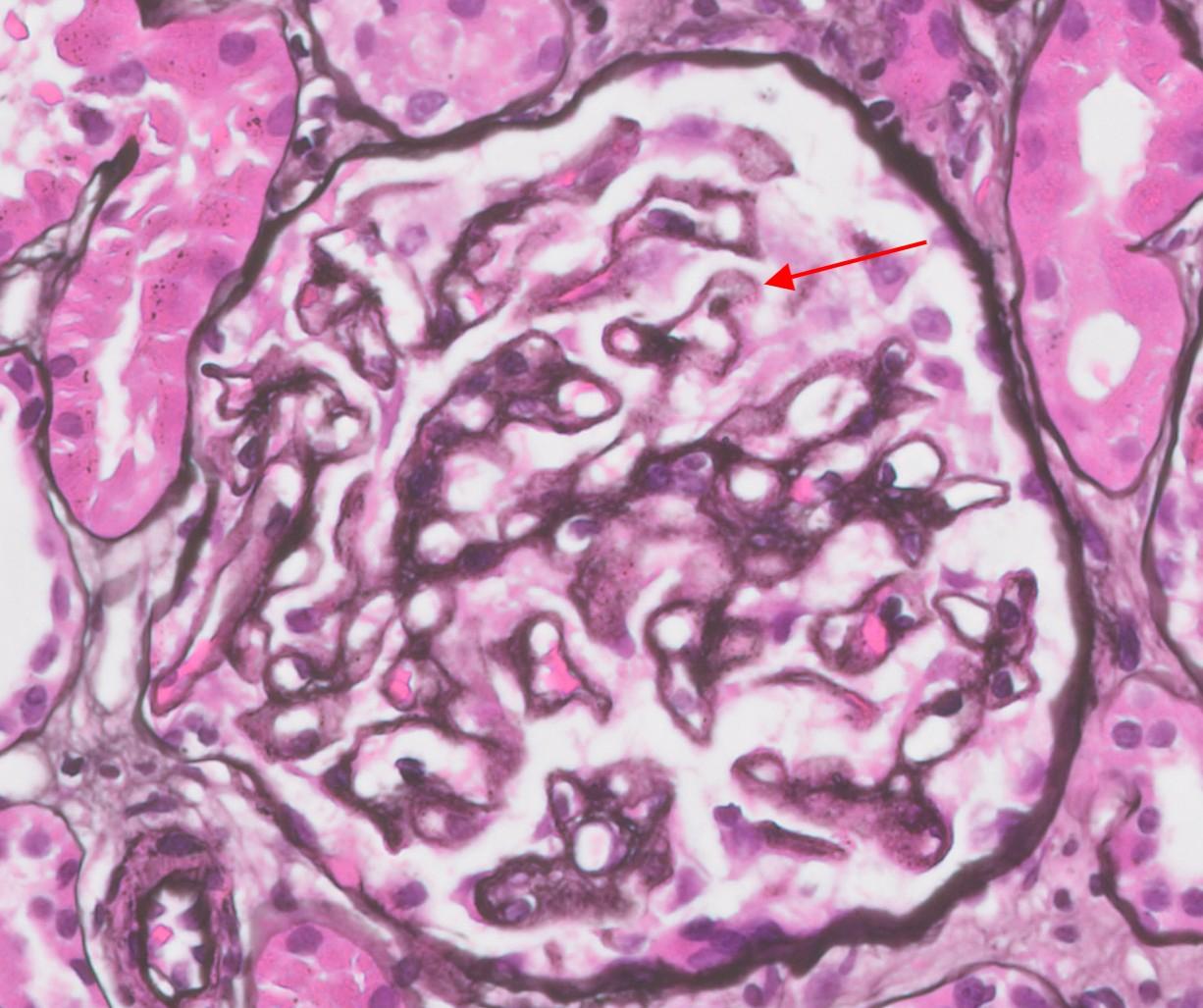
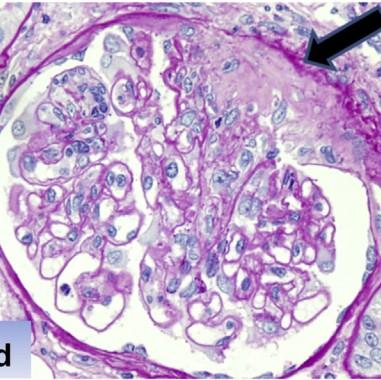
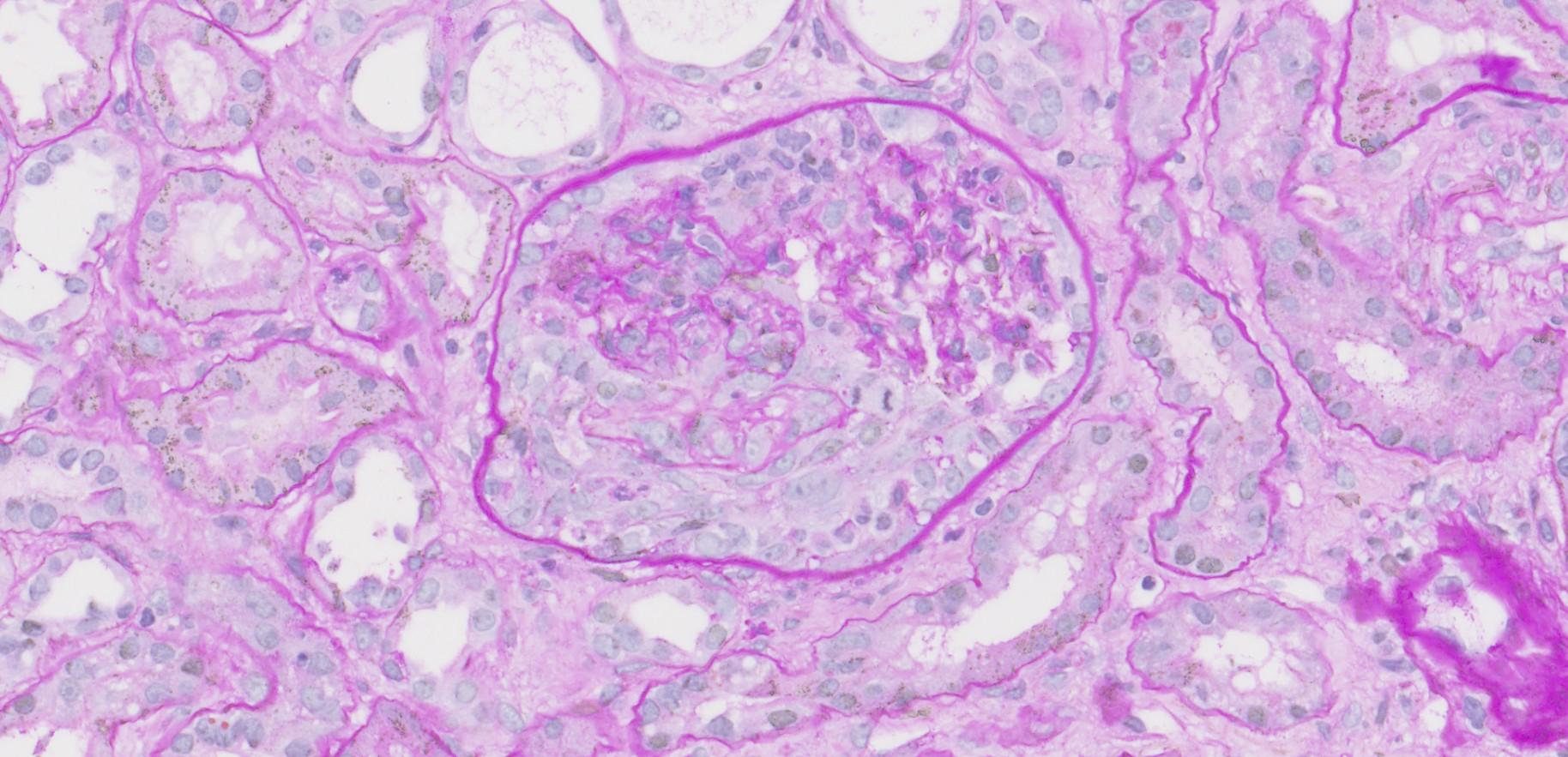
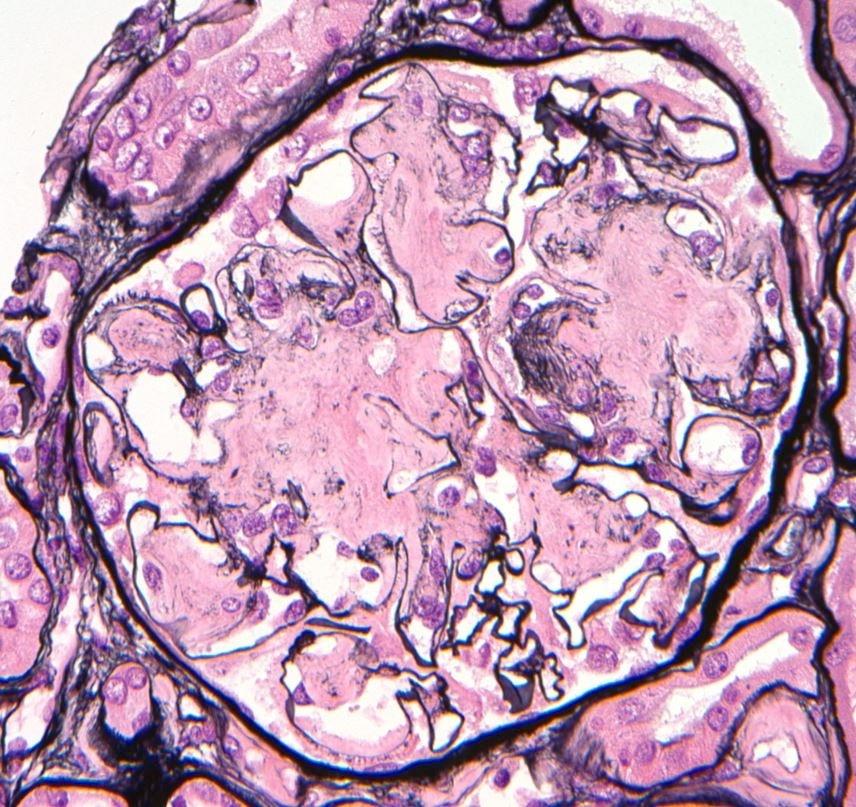
A 65-year-old male presents with insidious onset of lower limb oedema and fatigue. He has a history of smoking but no other significant medical problems. A 24-hour urine protein measurement shows 6.0 grams, and serum albumin is low. A renal biopsy is performed. There are basement membrane spikes and fenestrations visible on the Jones Silver stain (see image). Serum dsDNA and ANA titres are negative.
Based on the light microscopy findings and clinical scenario, which of the following findings on Immunofluorescence (IF) is MOST likely to be present in this patient?
A. Diffuse linear deposition of IgG along the glomerular basement membrane
B. Granular deposition of IgA in the mesangium
C. Granular deposition of IgG and C3 along the glomerular basement membrane
D. No significant immune deposits
E. Mesangial deposition of IgM
A 65-year-old male presents with insidious onset of lower limb oedema and fatigue. He has a history of smoking but no other significant medical problems. A 24-hour urine protein measurement shows 6.0 grams, and serum albumin is low. A renal biopsy is performed. There are basement membrane spikes and fenestrations visible on the Jones Silver stain (see image). Serum dsDNA and ANA titres are negative.
Based on the light microscopy findings and clinical scenario, which of the following findings on Immunofluorescence (IF) is MOST likely to be present in this patient?
A. Diffuse linear deposition of IgG along the glomerular basement membrane
B. Granular deposition of IgA in the mesangium
C. Granular deposition of IgG and C3 along the glomerular basement membrane
D. No significant immune deposits
E. Mesangial deposition of IgM
Question 3 Explained
■ Correct Answer (C): Granular deposition of IgG and C3 along the glomerular basement membrane is the classic IF pattern of primary membranous glomerulonephritis. This is due to the formation of subepithelial immune complexes.
■ Incorrect Answer (A): Diffuse linear deposition of IgG along the glomerular basement membrane is characteristic of Anti-GBM disease. This would typically have a more rapid onset, and present as a rapidly progressive glomerulonephritis and shows crescents on light microscopy, which are not present in MGN.
■ Incorrect Answer (B): Granular deposition of IgA in the mesangium is the hallmark of IgA nephropathy, which usually presents with haematuria, not nephrotic syndrome.
■ Incorrect Answer (D): No significant immune deposits is characteristic of minimal change disease (MCD), which has normal appearing glomeruli on LM and is not usually seen in a 65year-old.
■ Incorrect Answer (E): Mesangial deposition of IgM is not a typical finding in membranous GN and is not diagnostic. It can be seen in a number of conditions and often represents nonspecific trapped protein.
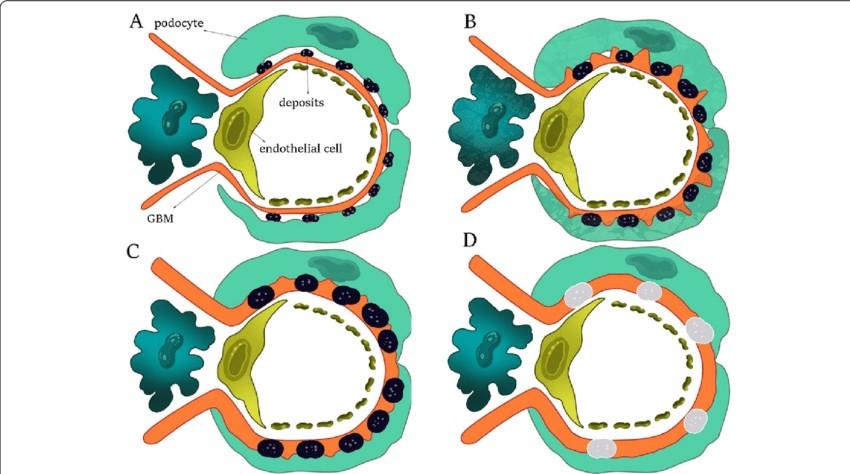
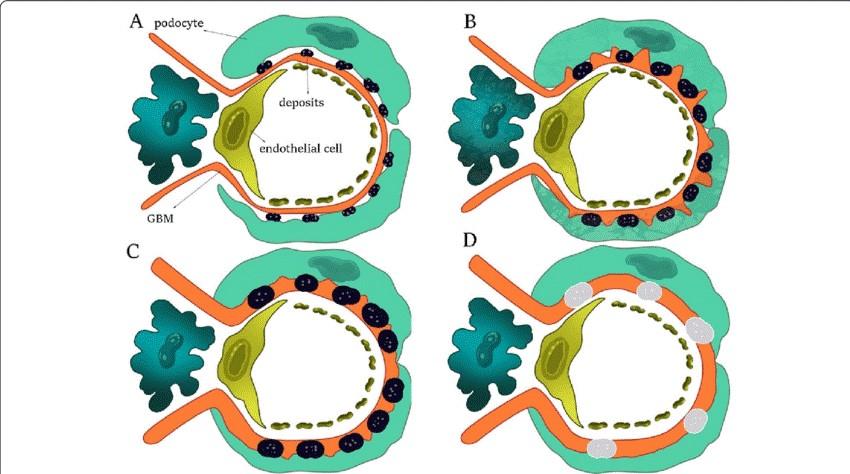
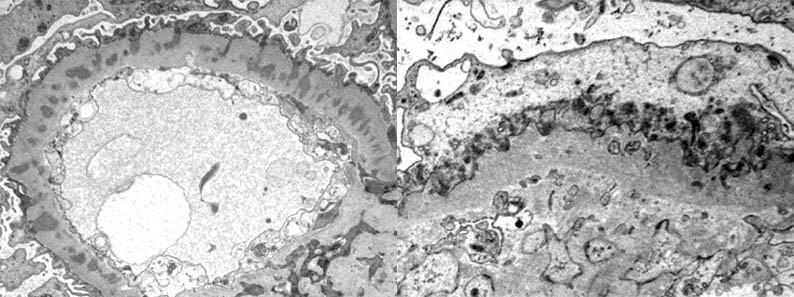
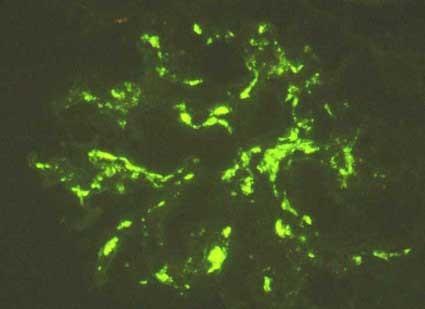
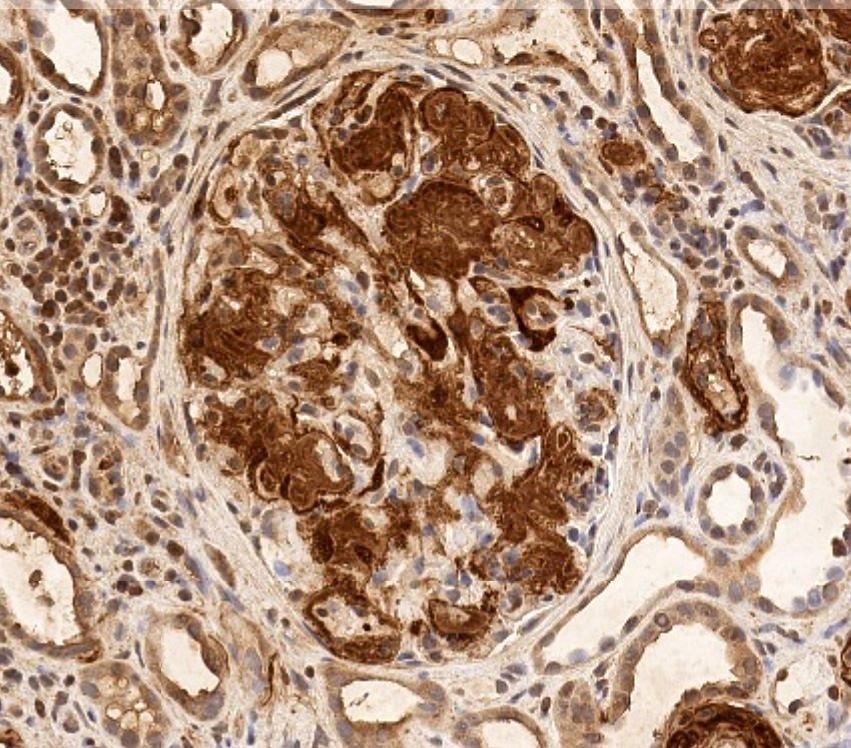
Membranous Glomerulonephritis (MGN)
■ Characterised by sub-epithelial deposits of immune complexes
– The GBM can then proliferate and engulf these deposits which corresponds to the spikes and in a later stage, fenestrations (‘chain-links’) seen on a basement membrane stain (typically Jones Silver but also PAS)
■ Primary or Secondary forms of which primary is most common
Membranous Glomerulonephritis
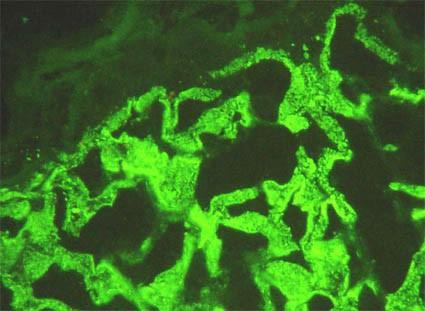
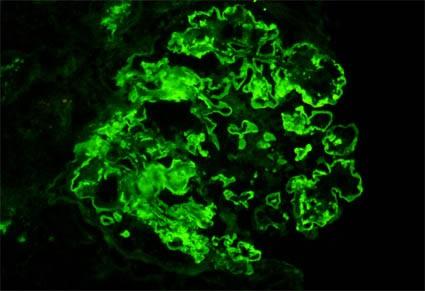
IF – Granular Capillary Deposits
Membranous Glomerulonephritis
IF – Granular Capillary Deposits
Subepithelial Deposits – Stage I
Glomerulonephritis
Membranous
Stage
Membranous Glomerulonephritis (MGN)
■ Most frequently present with nephrotic range proteinuria
■ Important to determine the cause – primary or secondary
– Malignancy – typically lung, breast, GI, renal carcinomas, lymphomas
– Drugs – Penicillamine, gold, mercury
■ Primary – considered idiopathic autoantibodies that localise at the podocyte membrane
– PLA2R
– THSD7A, NELL-1, EXT1/EXT2
– and many many more being found
Nephritic Syndrome
■ Decreased glomerular filtration rate (evidenced by elevated creatinine or BUN or decreased creatinine clearance), haematuria, oedema, mild proteinuria, and hypertension (in many cases there is oliguria)
■ Usually caused by alterations to the glomerular capillaries that prevent the elimination of water and metabolic end products
– Can be due to luminal obstruction by inflammatory cells, endothelial oedema or thrombosis
■ Manifests morphologically as endocapillary proliferative GN or membranoproliferative GN
■ Associated with hypocomplementaemia
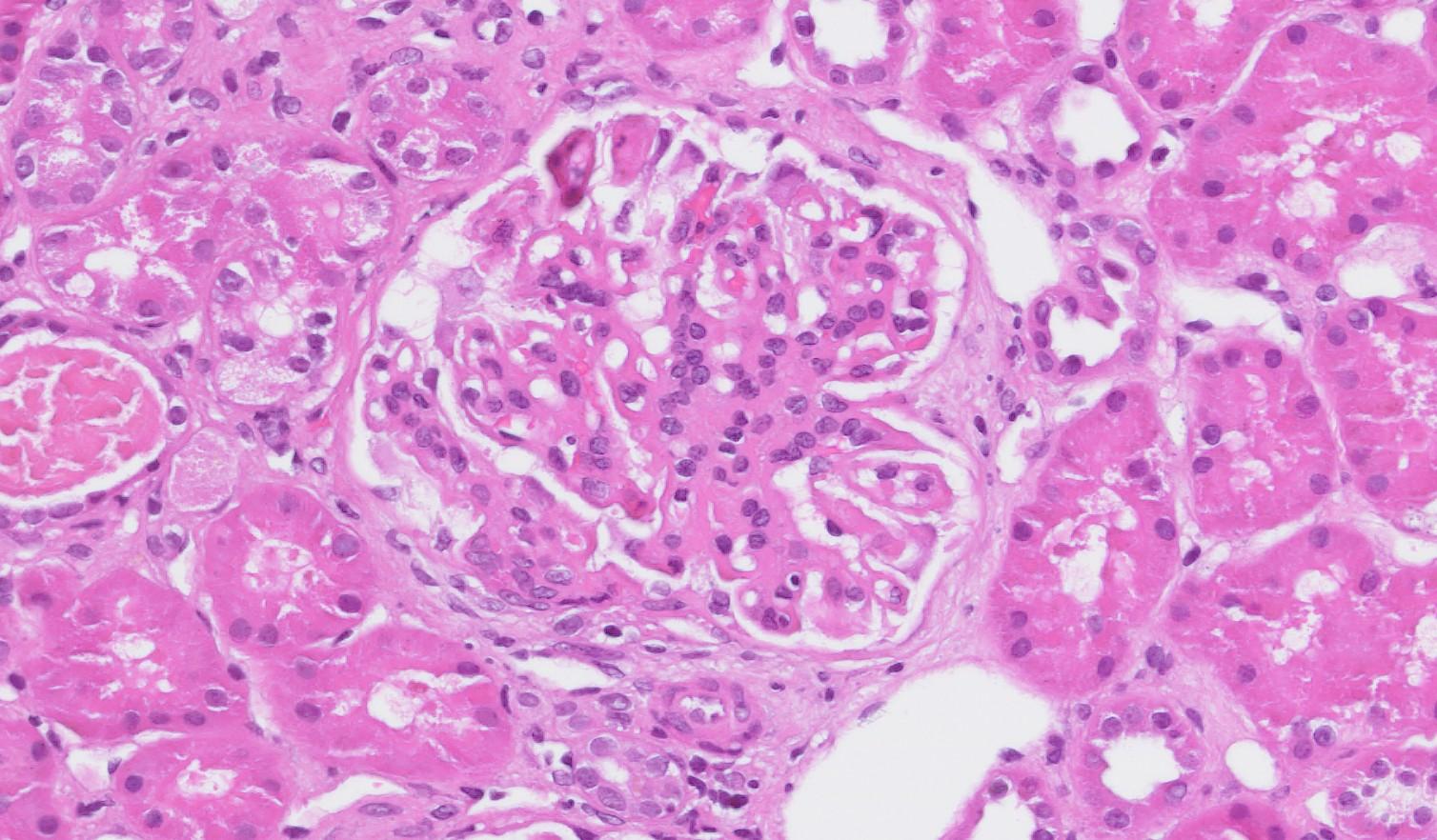
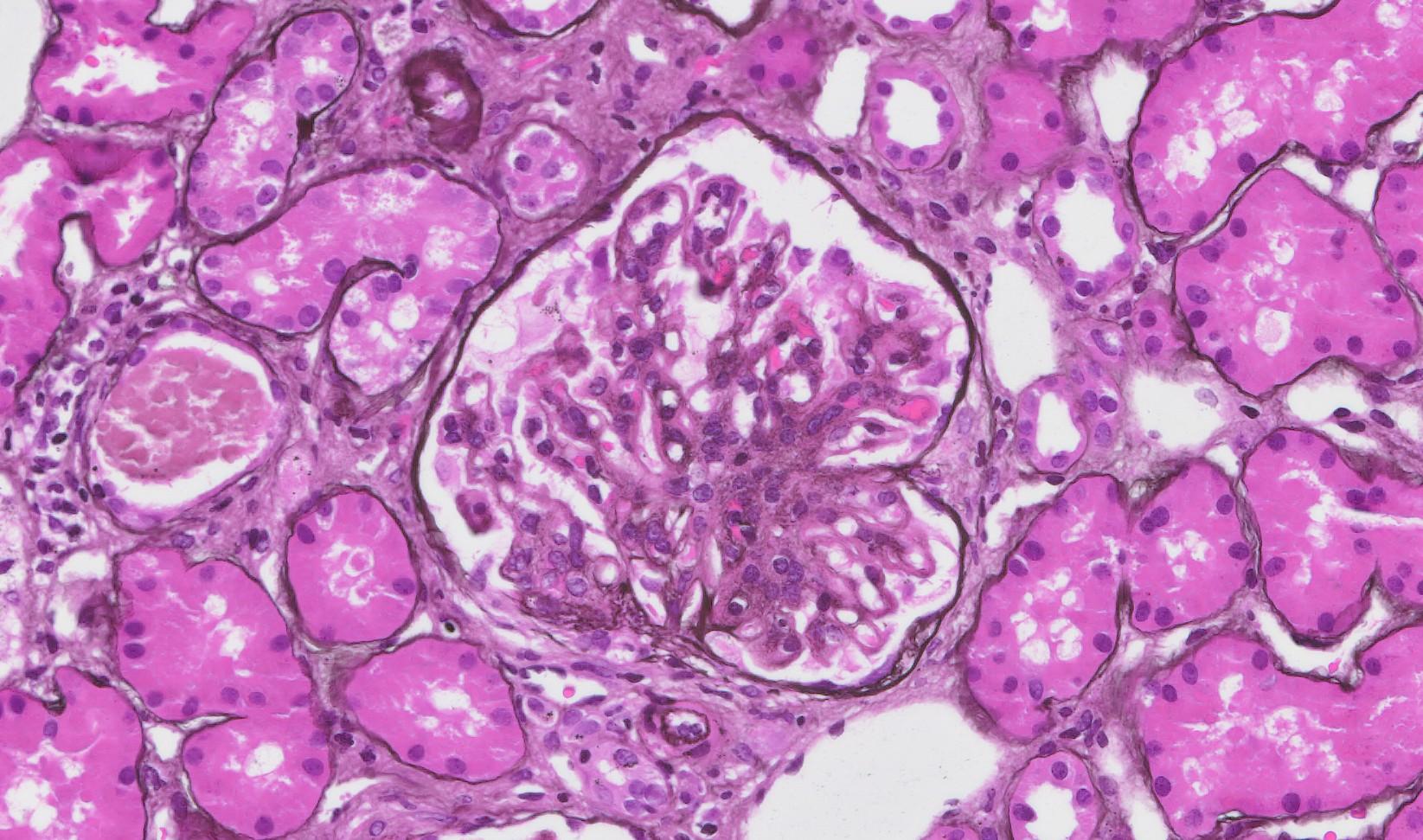
A 7-year-old boy presents with facial oedema, dark urine, and decreased urine output one week after recovering from a sore throat. His blood pressure is 140/90 mmHg. Laboratory investigations reveal elevated creatinine, haematuria, and low serum C3 complement level. A renal biopsy is performed.
Based on the clinical history, laboratory findings, and light microscopic appearance of the renal biopsy, which of the following is the most likely diagnosis?
A. IgA nephropathy
B. Anti-GBM disease
C. Post-infectious glomerulonephritis
D. Pauci-immune ANCA-associated glomerulonephritis
E. Minimal change disease
A 7-year-old boy presents with facial oedema, dark urine, and decreased urine output one week after recovering from a sore throat. His blood pressure is 140/90 mmHg. Laboratory investigations reveal elevated creatinine, haematuria, and low serum C3 complement level. A renal biopsy is performed.
Based on the clinical history, laboratory findings, and light microscopic appearance of the renal biopsy, which of the following is the most likely diagnosis?
B. Anti-GBM disease
D. Pauci-immune ANCA-associated glomerulonephritis
E. Minimal change disease
A. IgA nephropathy
C. Post-infectious glomerulonephritis
Q4 Explained
■ Correct Answer (C): Post-infectious glomerulonephritis (PIGN) is the MOST likely diagnosis. The clinical history of recent infection, acute nephritic syndrome, low C3 complement, and diffuse endocapillary proliferation are all consistent with this diagnosis.
■ Incorrect Answer (A): IgA nephropathy typically presents with recurrent macroscopic hematuria often coinciding with or following an upper respiratory tract infection, and usually has normal C3 levels. While it can occur in children, the history is less typical. The histology will also typically show mesangial proliferation.
■ Incorrect Answer (B): Anti-GBM disease typically presents with rapidly progressive glomerulonephritis (RPGN) with crescent formation on the renal biopsy, and linear IgG deposition on IF, neither of which are described in the scenario.
■ Incorrect Answer (D): Pauci-immune ANCA-associated GN typically presents as a rapidly progressive glomerulonephritis (RPGN), often with systemic features, including constitutional symptoms, arthralgia, weight loss and is less common in children. A preceding infection is unusual.
■ Incorrect Answer (E): Minimal change disease presents with nephrotic syndrome and normal appearing glomeruli on light microscopy. The renal function is also typically normal.
Post-Infectious Glomerulonephritis
■ Commonly affects children
■ Classically associated with Streptococcus infection
– But can also occur with Staphylococcus, Gram-ve Bacteria, Treponema, Mycobacteria, Plasmodium etc – But morphological changes can vary slightly in these
■ Morphological pattern is of a proliferative exudative endocapillary GN that is diffuse
– Exudative = neutrophils
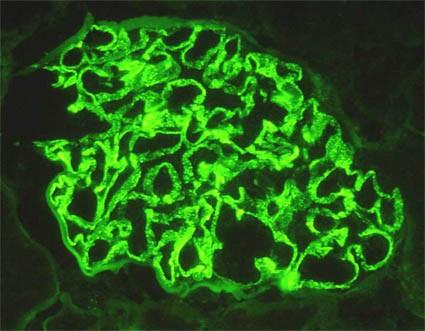
■ IF / IP will show chunky, granular IgG and C3 deposits in the capillary walls
– In later stages there can be paramesangial and mesangial deposits as well
– The IgA Dominant (or Co-Dominant) Variant will have strongly IgA +ve deposits
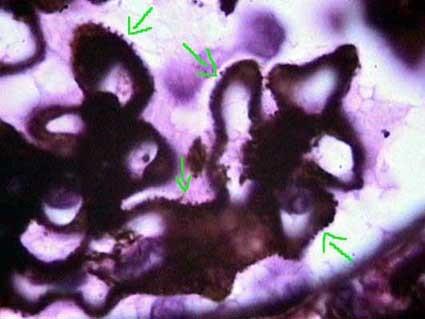
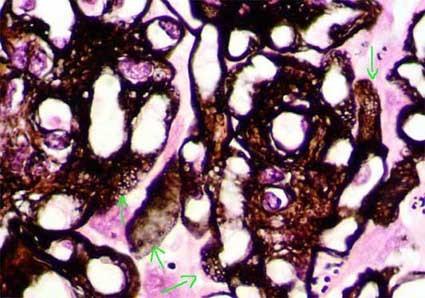
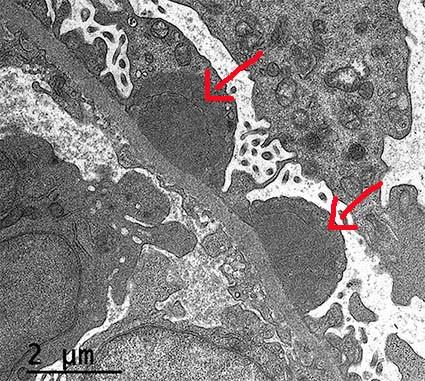
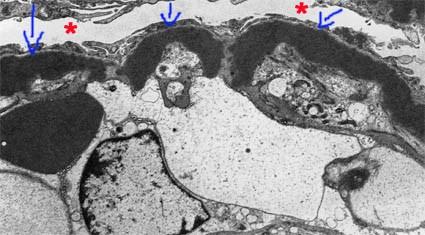
■ EM will show subepithelial hump-like electron dense deposits on the capillary walls
IF – Granular capillary deposits EM – Subepithelial Hump-like deposits
PIGN
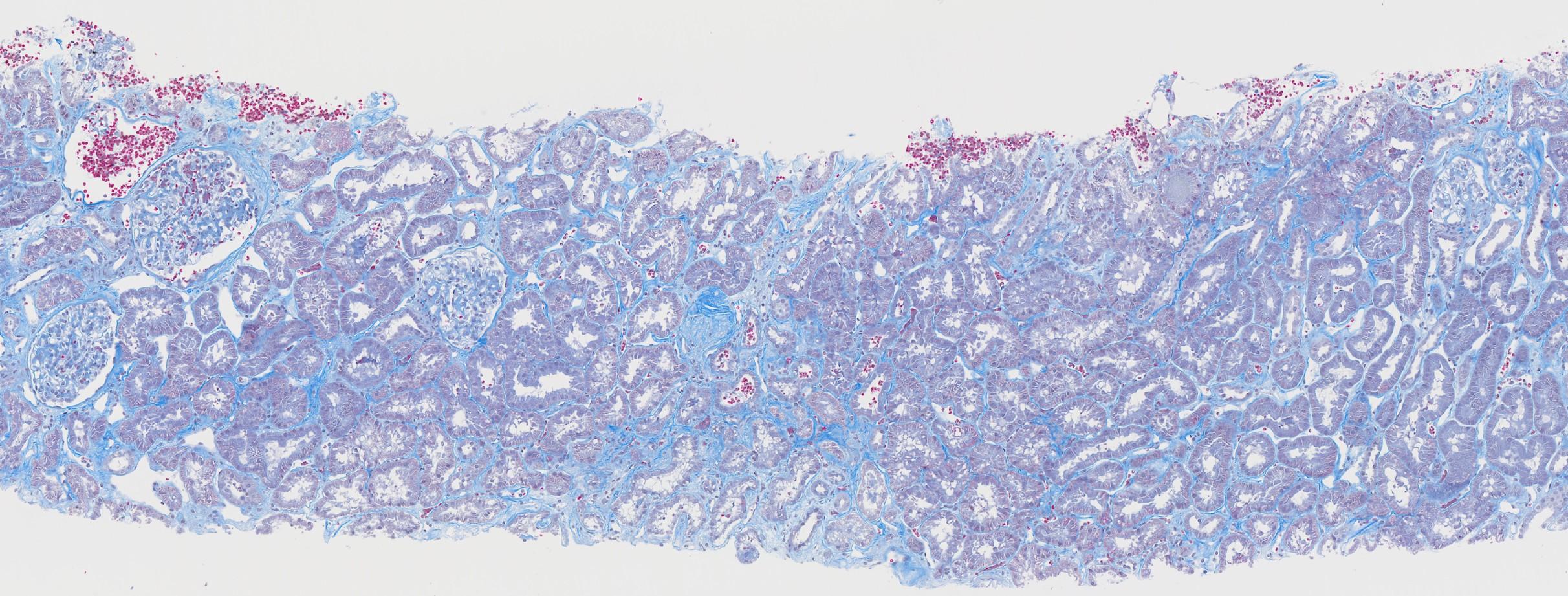
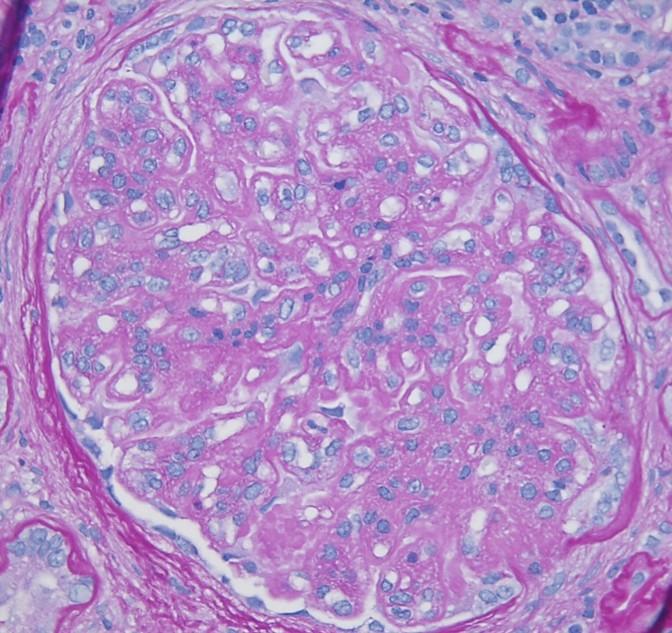
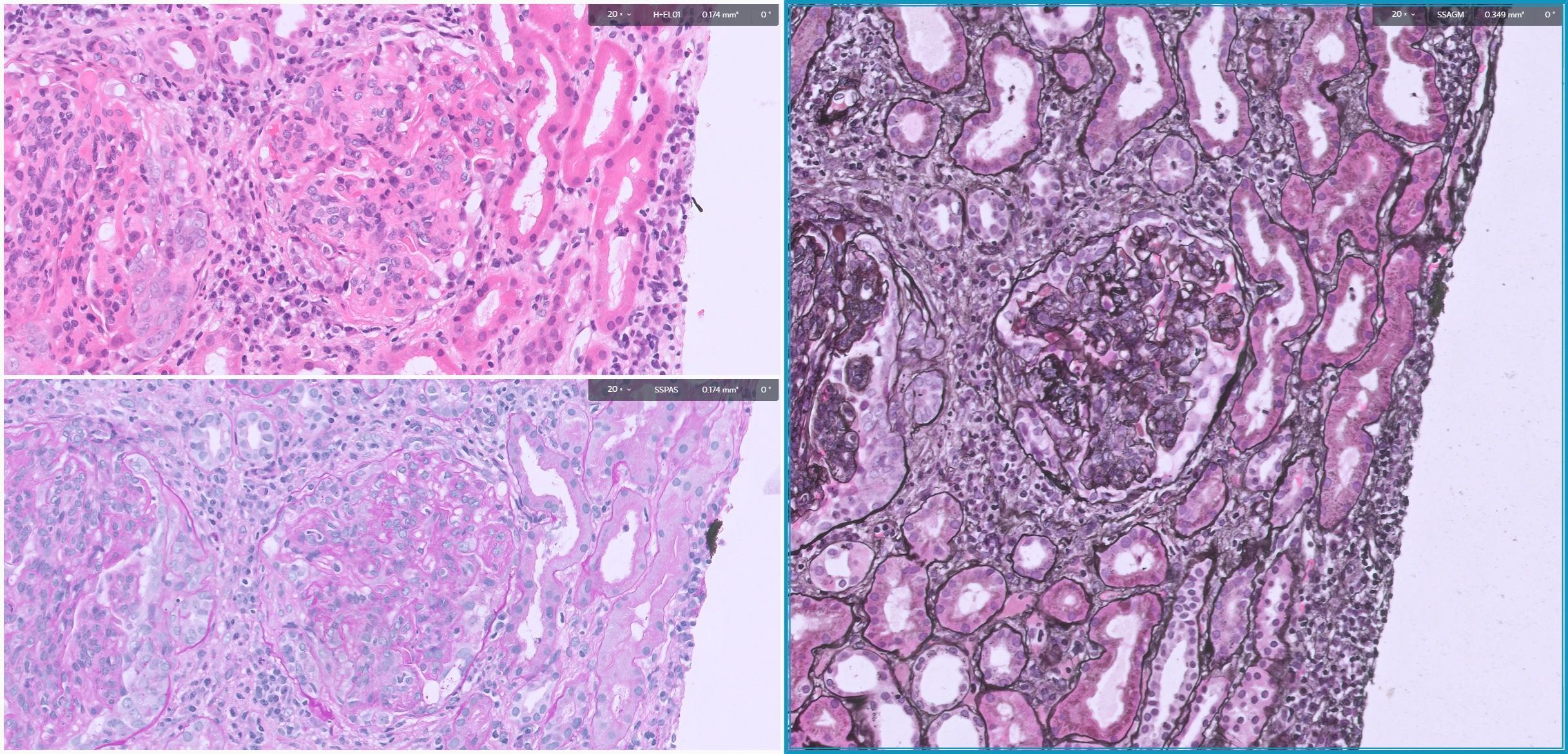
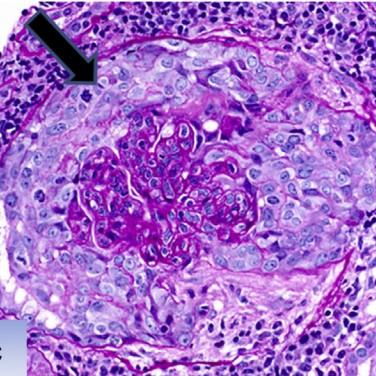
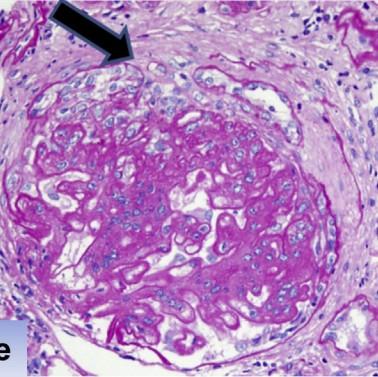
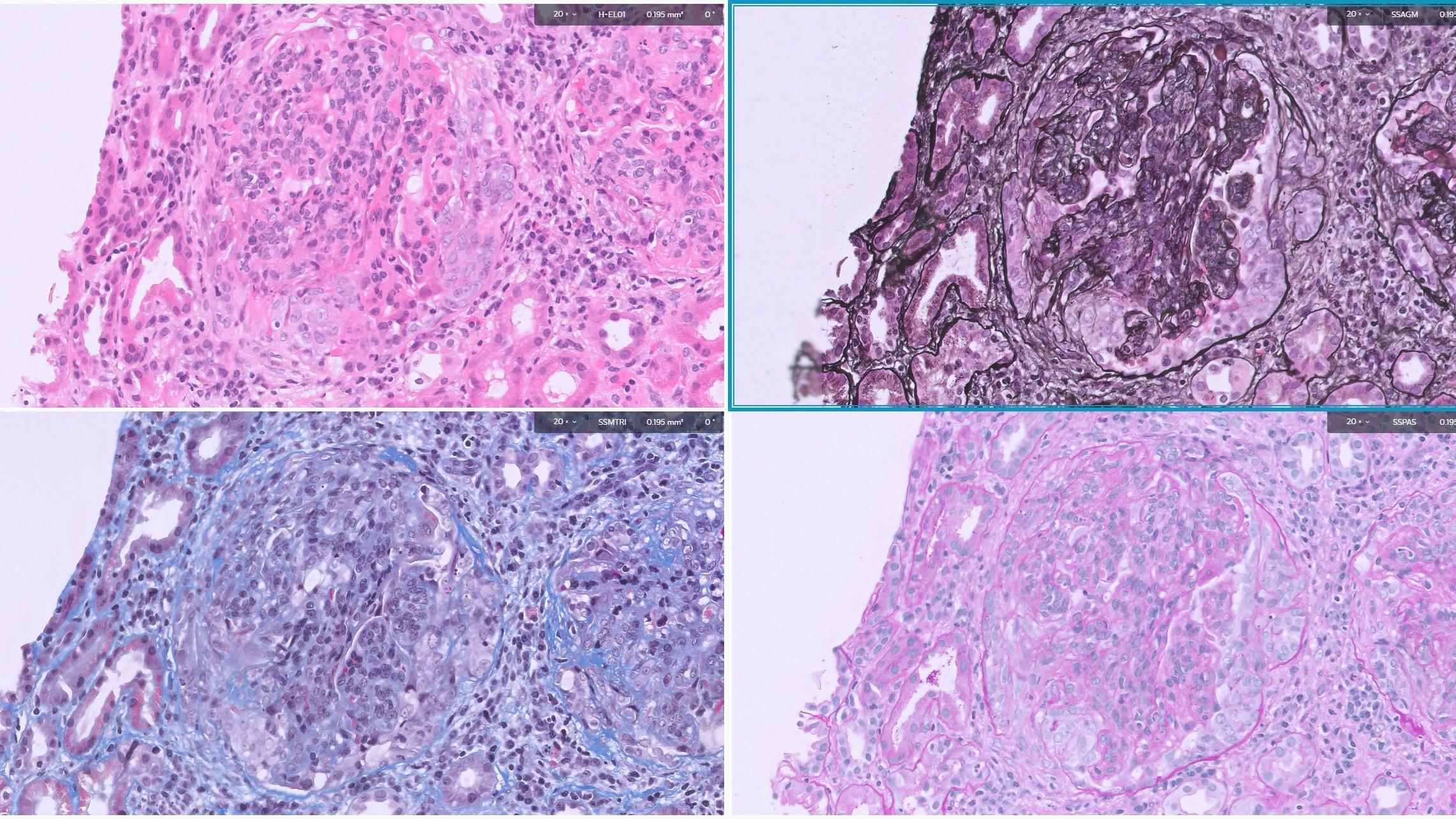
A 40year old male presents with lower limb oedema, mild hypertension and microscopic haematuria. His 24hour urine output is 4g. Serum C3 and C4 levels are low and he does not have dsDNA or ANA positive titres. A renal biopsy is performed (see provided PAS picture). On immunofluorescence there is granular IgG and C3 staining along the capillary walls and mesangium. Electron microscopy shows subendothelial and mesangial electron dense deposits.
Based on these findings, what is the most likely diagnosis:
A. Immune-complex-mediated
Membranoproliferative Glomerulonephritis
B. C3 Glomerulopathy
C. Membranous Glomerulonephritis
D. Anti-GBM disease
E. Lupus Nephritis
A 40year old male presents with lower limb oedema, mild hypertension and microscopic haematuria. His 24hour urine output is 4g. Serum C3 and C4 levels are low and he does not have dsDNA or ANA positive titres. A renal biopsy is performed (see provided PAS picture). On immunofluorescence there is granular IgG and C3 staining along the capillary walls and mesangium. Electron microscopy shows subendothelial and mesangial electron dense deposits.
Based on these findings, what is the most likely diagnosis:
A. Immune-complex-mediated
Membranoproliferative Glomerulonephritis
B. C3 Glomerulopathy
C. Membranous Glomerulonephritis
D. Anti-GBM disease
E. Lupus Nephritis
Q5 Explained
■ A - Immune-complex Mediated Membranoproliferative Glomerulonephritis [Correct Answer]: This is the correct answer because all findings point towards this diagnosis. The clinical picture, low C3/C4, specific IF and EM findings are all classic for Type I MPGN.
■ B - C3 Glomerulopathy: C3 glomerulopathy would also have low complement, however, on IF you would only see C3 deposition (with usually minimal to no IgG), and on EM you would only have intramembranous deposits with no subendothelial deposits. The light microscopy features may also differ.
■ C - Membranous Glomerulonephritis: Membranous GN presents with nephrotic range proteinuria but not microscopic haematuria. IF would show granular IgG and C3 staining along capillary walls (no mesangial deposition). EM would show subepithelial deposits with no mesangial changes. Complement levels are usually normal.
■ D - Anti-GBM disease: Anti-GBM disease typically presents with a rapidly progressive glomerulonephritis, with crescents on LM, linear IgG capillary wall positivity on IF and lacks the presence of electron dense deposits on EM.
■ E - Lupus Nephritis: Lupus nephritis is associated with dsDNA/ANA positivity (which is absent in this scenario), and is can also be associated with mesangial, subendothelial and subepithelial deposits, and does not usually cause low complement C3/C4 levels by themselves. IF classical shows full house positivity (IgG, IgA, IgM, C3, C1q).
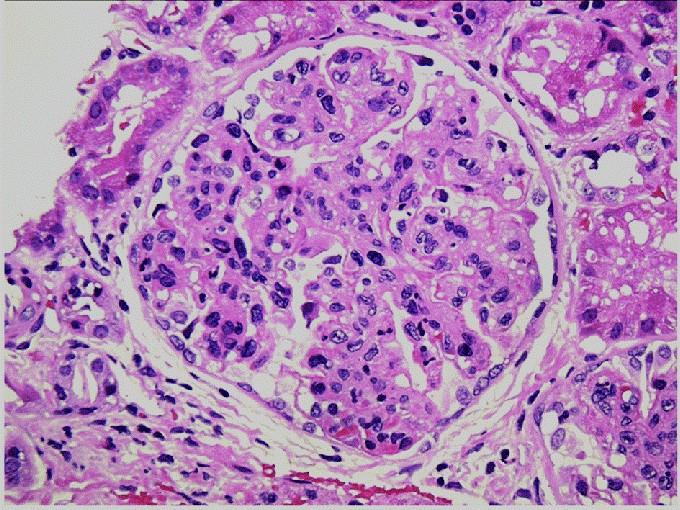
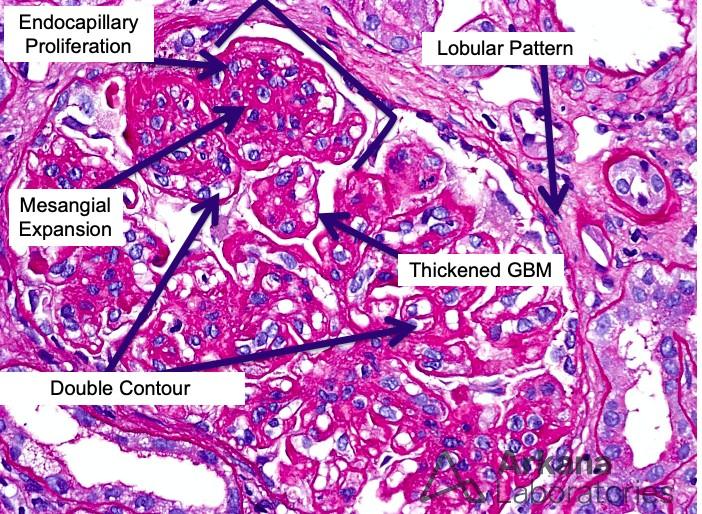
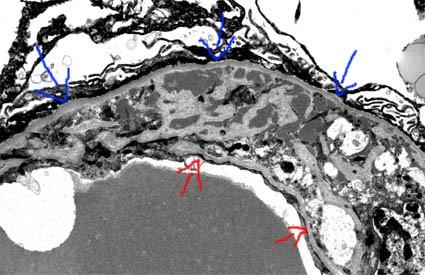
Membranoproliferative GN
■ Characterized by thickening of the capillary walls accompanied by cellular, predominantly mesangial, proliferation in all or almost all the glomeruli
– The increase in cellularity and mesangial matrix produces accentuation of the lobular aspect of the glomerular tuft (lobular GN)
– The thickening of the capillary walls is due to subendothelial deposits and mesangial interposition with formation of material similar to the glomerular basement membrane (GBM) in the internal aspect of the wall (subendothelial space)
■ Either immune complex deposits in the glomeruli or abnormal proteins affecting the alternative pathway.
Membranoproliferative
GN
■ Lobulated appearance of Glomerulus
■ Endocapillary Proliferation
■ Mesangial Expansion
■ Mesangial hypercellularity
■ Double contours (on Silver and PAS)
■ Thickened GBM
Membranoproliferative GN
Membranoproliferative GN – Pattern of
Injury
■ Primary forms previously classified into Type I, II & III but now thought of as a morphological pattern
■ Immune complex mediated MPGN
■ Complement Mediated Glomerulopathies
– C3 GN
– Dense Deposit Disease (DDD)
■ Secondary MPGN
– Lupus Nephritis Class III & IV
– Cryoglobulinaemia
– Monoclonal gammopathy
– Infections – Hep C, Hep B
– IgA Nephropathy with MPGN pattern
– Thrombotic Microangiopathy
MPGN Pattern Table
Diagnosis
Clinical Findings
Light Microscopy
Immunofluorescence
Nephrotic or mixed nephritic-nephrotic picture.
Low C3, C4. May have infection history (Hep B, Hep C) or other hx of secondary causes.
Child or Young adult.
Nephritic or mixed picture.
Low C3 / C4.
EM
Granular, strongly IgG and C3 positive deposits in capillary walls and occasionally in mesangium. May have some IgM and C1q.
Subendothelial electron dense deposits
Granular deposits in capillary walls which are C3 positive only.
Children and young adults.
Nephritic or mixed picture.
Low C3/C4.
Young adults skewed towards females.
Nephrotic or mixed nephritic-nephrotic picture. Other systemic findings of lupus. Anti-ANA/dsDNA and others.
pattern
Irregularly distributed ‘ribbon’-like C3 deposits on capillary walls. Sometimes mesangial as well.
Subendothelial electron dense deposits
‘Full House’ of IgG, IgM, IgA, C3 and C1q positive deposits in capillary walls and mesangium.
Electron dense ribbon-like deposits with the lamina dense of the capillary basement membranes
Subendothelial electron dense deposits. Also frequently paramesangial and mesangial deposits.
Membranoproliferative GN Pattern
Membranoproliferative GN Pattern
Duplication
IgA Nephropathy
IgA Nephropathy (Berger’s Disease)
■ Defined by the presence of diffuse dominant or codominant mesangial deposits of immunoglobulin A (IgA)
■ Globally the most frequently occurring primary glomerulonephritis
■ Clinical findings
– Second to third decade of life
– More common in males (2:1)
– Persistent or intermittent microscopic haematuria
– Episodic macrohaematuria
■ Can occur in association with hepatobiliary disease, autoimmune conditions, infections, malignancy
■ Henoch-Schönlein Pupura (HSP)
– Extrarenal manifestation of IgA
– Purpuric lesions skin lesions on the buttocks and lower extremities, migratory arthralgias, GI haemorrhage.
IgA Nephropathy – Findings
■ Light Microscopy (Classically)
– Mesangial expansion
– Mesangial hypercellularity
■ Immunofluorescence
– Mesangial deposits
– Dominant IgA staining. Variable IgG and IgM.
– C3 often equal or less to IgA intensity.
■ EM
– Mesangial electron dense deposits
– Increased mesangial matrix and density
Silver
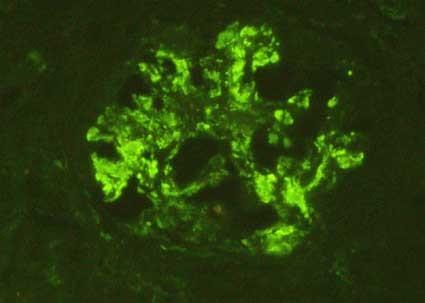
IgA Nephropathy
IF – Mesangial Deposits
– Mesangial
& Capillary Deposits
EM – Mesangial Deposits EM – Mesangial and Subendothelial Deposits
IgA Nephropathy
Oxford Classification of IgA Nephropathy
Mesangial hypercellularity M
Endocapillary hypercellularity E
Segmental glomerulosclerosis S
Tubular atrophy/interstitial fibrosis T Crescents
• <0.5 M0
• Absent E0
• Absent S0
• ≤25% T0
• >0.5 M1
• Present E1
• Present S1
• 26-50% T1
• 0: <4 Mesangial cells/mesangial area
• 1: 4–5 Mesangial cells/mesangial area
• 2: 6–7 Mesangial cells/mesangial area
• 3: >8 Mesangial cells/mesangial area
• Hypercellularity due to increased number of cells within glomerular capillary lumina causing narrowing of the lumina
• Any amount of the tuft involved in sclerosis, but not involving the whole tuft or the presence of an adhesion
• >50% T2
• Percentage of cortical area involved by the tubular atrophy or interstitial fibrosis, whichever is greater
• Predictive of ESRF No crescents Atleast 1 crescent Crescents in ≥25% glomeruli
CRESCENTIC GLOMERULONEPHRITI
Crescentic Glomerulonephritis
■ Proliferative extracapillary glomerulonephritis (GN) or crescentic GN is not a specific disease, but a histologic manifestation of severe glomerular damage
■ Extracapillary proliferation = cellular or fibrous proliferation arising from Bowman’s capsule that occupies the Bowman’s space (outside capillary tuft)
■ The mechanism is typically due to rupture of the capillary walls and presence of fibrin in the urinary space which together with other chemokines and mediators in blood stimulate proliferation of epithelial cells.
– Gradually over time evolve from cellular to fibrous and may eventually disappear
Crescents
• The term crescent is used for a lesion consisting of extracapillary hypercellularity, composed of a variable mixture of cells.
• Fibrin and fibrous matrix may be present.
• 10% or more of the circumference of Bowman’s capsule should be involved.
• Cellular Crescent
more than 75% cells and fibrin and less than 25% fibrous matrix
• Fibrocellular Crescent25%–75% cells and fibrin and the remainder fibrous matrix
• Fibrous Crescent
more than 75% fibrous matrix and less than 25% cells and fibrin
Crescents
Cellular Crescent
more than 75% cells and fibrin and less than 25% fibrous matrix
Fibrocellular
Crescent
25%–75% cells and fibrin and the remainder fibrous matrix
Fibrous Crescent
more than 75% fibrous matrix and less than 25% cells and fibrin
Cellular Crescent
A 60-year-old male presents with a 3-day history of rapidly worsening fatigue, oliguria, and hemoptysis. Laboratory studies show elevated creatinine, hematuria, and a 24-hour urine protein of 2.8 grams. A renal biopsy is performed (representative image provided). Immunofluorescence shows linear deposition of IgG along the glomerular basement membrane. Electron microscopy demonstrates no significant electron-dense deposits, but widespread effacement of podocyte foot processes.
Based on these findings, which of the following is the most likely diagnosis?
A. Post-infectious glomerulonephritis
B. Pauci-immune ANCA-associated glomerulonephritis
C. IgA nephropathy
D. Anti-GBM disease
E. Membranous glomerulonephritis
A 60-year-old male presents with a 3-day history of rapidly worsening fatigue, oliguria, and hemoptysis. Laboratory studies show elevated creatinine, hematuria, and a 24-hour urine protein of 2.8 grams. A renal biopsy is performed (representative image provided). Immunofluorescence shows linear deposition of IgG along the glomerular basement membrane. Electron microscopy demonstrates no significant electron-dense deposits, but widespread effacement of podocyte foot processes.
Based on these findings, which of the following is the most likely diagnosis?
A. Post-infectious glomerulonephritis
B. Pauci-immune ANCA-associated glomerulonephritis
C. IgA nephropathy
D. Anti-GBM disease
E. Membranous glomerulonephritis
Q6 Explained
■ Correct Answer (D): Anti-GBM disease is the MOST likely diagnosis. The rapidly progressive renal failure, haemoptysis (suggestive of Goodpasture's syndrome), linear IgG deposition along the GBM, lack of electron-dense deposits, presence of foot process effacement, and the cellular crescent on light microscopy all point to this diagnosis.
■ Incorrect Answer (A): Post-infectious glomerulonephritis is associated with a preceding infection, low C3 complement, and granular deposits on IF with subepithelial humps on EM. The presentation is usually more gradual, with a preceding infection, and without haemoptysis.
■ Incorrect Answer (B): Pauci-immune ANCA-associated glomerulonephritis is also an RPGN, but would not show linear IgG staining on IF. Instead, it would have minimal or no deposits on IF, and is often associated with a positive ANCA level.
■ Incorrect Answer (C): IgA nephropathy is less likely to present with RPGN, usually presenting with more recurrent haematuria and has mesangial deposits on IF. It also lacks the feature of haemoptysis.
■ Incorrect Answer (E): Membranous glomerulonephritis typically presents with nephrotic syndrome, shows subepithelial deposits on EM and granular IgG/C3 staining along the capillary wall on IF. It also does not cause crescentic GN.
Rapidly Progressive Glomerulonephritis
■ Clinical term used to describe subacute renal failure over weeks to months
– Active urine sediment
– Hypertension
– Oedema
– Proteinuria and Oliguria
■ Usually related to proliferation of cells in the urinary space (crescents)
■ Crescents form over weeks and therefore there is rapid progressive deterioration of glomerular filtration
A 65-year-old female presents with a two-week history of fatigue, weight loss, and rapidly worsening renal function. She also reports recent onset of arthralgias and a mild cough. Laboratory studies show elevated creatinine, haematuria, and a 24-hour urine protein of 1.5 grams and positive antiMPO antibodies. A renal biopsy is performed (see representative image). Immunofluorescence demonstrates minimal to no immunoglobulin or complement deposits in the glomeruli. Electron microscopy reveals no significant electron-dense deposits.
Based on these findings, which of the following is the most likely diagnosis?
A. Post-infectious glomerulonephritis
B. Anti-GBM disease
C. IgA nephropathy
D. Pauci-immune ANCA-associated glomerulonephritis
E. Immune complex-mediated membranoproliferative glomerulonephritis
A 65-year-old female presents with a two-week history of fatigue, weight loss, and rapidly worsening renal function. She also reports recent onset of arthralgias and a mild cough. Laboratory studies show elevated creatinine, haematuria, and a 24-hour urine protein of 1.5 grams and positive antiMPO antibodies. A renal biopsy is performed (see representative image). Immunofluorescence demonstrates minimal to no immunoglobulin or complement deposits in the glomeruli. Electron microscopy reveals no significant electron-dense deposits.
Based on these findings, which of the following is the most likely diagnosis?
A. Post-infectious glomerulonephritis
B. Anti-GBM disease
C. IgA nephropathy
D. Pauci-immune ANCA-associated glomerulonephritis
E. Immune complex-mediated membranoproliferative glomerulonephritis
Q7 Explained
■ Correct Answer (D): Pauci-immune ANCA-associated glomerulonephritis is the most likely diagnosis. The clinical picture of RPGN with systemic features (fatigue, weight loss, arthralgias, cough), the minimal immune deposits on IF, absence of electron-dense deposits, and a positive ANCA test (anti-MPO) are all classic findings for this condition.
■ Incorrect Answer (A): Post-infectious glomerulonephritis typically presents with a preceding infection, low C3 complement levels, and granular immune deposits on IF and EM. It does not usually present with systemic features as in this case.
■ Incorrect Answer (B): Anti-GBM disease typically shows linear IgG deposition on IF, and lacks systemic symptoms like arthralgia and cough. Furthermore, the ANCA test would be negative in Anti-GBM disease.
■ Incorrect Answer (C): IgA nephropathy presents with recurrent macroscopic hematuria, and has mesangial IgA deposits on IF, and also typically lacks the systemic features described in this case.
■ Incorrect Answer (E): Immune complex-mediated membranoproliferative glomerulonephritis typically shows granular deposition of IgG and C3 on IF, with deposits on EM, and would also lack the systemic features seen in ANCA-GN. It would also not cause segmental necrosis.
Anti-GBM Disease
■ Presents with RPGN
■ Also frequently associated with a pulmonary-renal syndrome – typically severe haemoptysis
– First described by Ernest Goodpasture (Goodpasture’s Syndrome)
■ Caused by circulating anti-GBM antibodies directed against the alpha-3 chain in the Cterminal non-collagenous domain of type IV collagen (alpha-3 [IV] chain of NC1 domain)
■ Typical age is 20-40 but can occur at any age.
■ Male>Female
■ Treatment is based on high doses of steroids, other immunosuppressors and plasma exchange
■ Anti-GBM disease has worse prognosis than immune complexes GN and pauci-immune GN
Anti-GBM Disease
■ Light Microscopy
– Breaks of GBM due to fibrinoid necrosis resulting in crescents
– Crescents are widespread affecting most gloms
– All crescents typically of similar age and chronicity
– Glomeruli that have disrupted capsules can be surrounded by granulomatous inflammation
– No proliferative glomerular lesions in uninvolved segments
■ IF / IP
– Strong linear IgG staining along GBM
– C3 positive in most cases but weaker than IgG
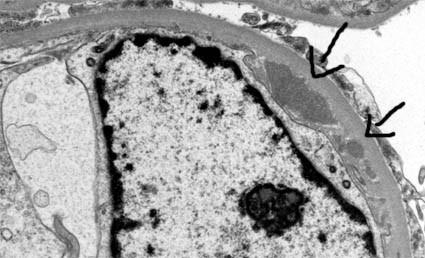
■ EM
– No electron dense deposits
– Breaks in GBM with necrosis and crescents may be seen
Pauci-Immune ANCA-Associated Glomerulonephritis
■ Presents with RPGN
■ Fever, arthralgias, myalgias, respiratory alterations, signs of vasculitis, pupura
■ Systemic features of ANCA vasculitis
– Granulomatous with polyangiitis (Wegener’s)
■ ANCA directed against myeloperoxidase (MPO) – P-ANCA
– Microscopic polyangiitis
– Eosinophilic granulomatosis with polyangiitis (Churg-Strauss)
■ ANCA directed against proteinase 3 (PR3) – C-ANCA
■ Treatment is with aggressive immunosuppression – cyclophosphamide and steroids
■ Approx 25% of patients with Anti-GBM have detectable ANCAs
– Clinical course dominated by anti-GBM disease – poor prognosis
Pauci-Immune ANCA-Associated Glomerulonephritis
■ Light Microscopy
– Focal and segmental glomerular inflammation with necrotising lesions (but can sometimes be global and diffuse)
– Necrotising lesions accompanied by crescents
– Glomeruli that have disrupted capsules can be surrounded by granulomatous inflammation
– Crescents at different ages and chronicity ranging from cellular to fibrocellular to fibrous
– No proliferative glomerular lesions in uninvolved segments
■ IF / IP
– No or very limited staining for immunoglobulins
■ EM
– No electron dense deposits
– Breaks in GBM with necrosis and crescents may be seen
■ This is a light microscopy pattern of glomerular disease whereby the mesangium is expanded by material producing a nodular appearance
■ Depending on the material being deposited / formed in the mesangium, this could be one of a (usually) limited number of things
– Diabetic Nephropathy (nodular sclerosis)
– Amyloidosis
– Light Chain Deposition Disease
– Fibrillary GN
– Immunotactoid GN
■ As expected, the clinical presentation and staining of the material under different special stains and some specific features will help determine the nature of the nodules and therefore the diagnosis
Key features of key conditions
Diabetic Nodular Sclerosis
Eosinophilic nodules
Amyloidosis
Amorphous pale staining nodules PAS –ve Silver –ve
Fibrillary GN Pale staining nodules
Congophilic, birefringence on polarisation
Serum (trapping) of IgG Thickened BM
Depending on type of Amyloid –Kappa or Lambda restricted. Heavy chain amyloid can be positive for immunoglobulins
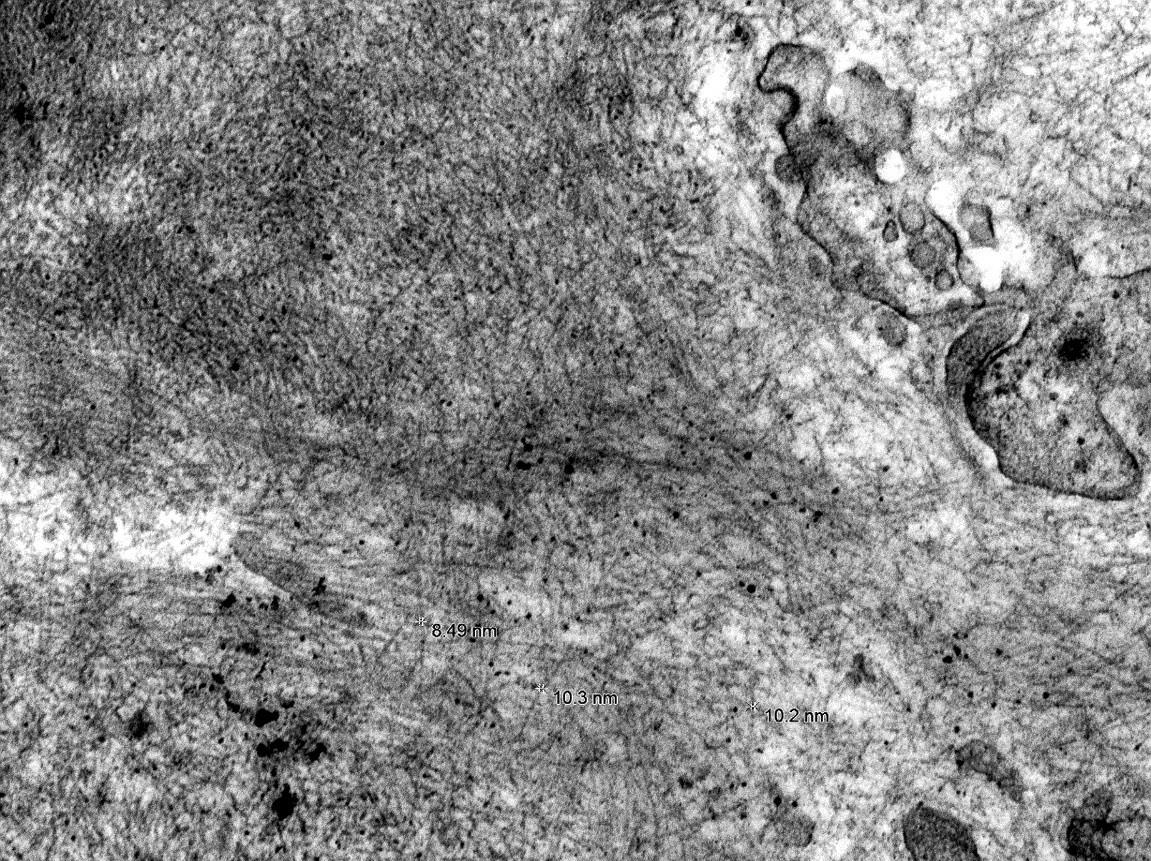
Amyloid fibrils that are 8-12nm diameter
Accompanied by capsular drops / hyaline caps and hyaline arteriolosclerosis
Depending on cause of amyloid. If inflammatory will be SAA+ve and Lambda restricted. If related to MM then variable
IgG and
Fibrils of 1222nm diameter
Membranoprolife rative pattern can be present with thickened GBM and crescents
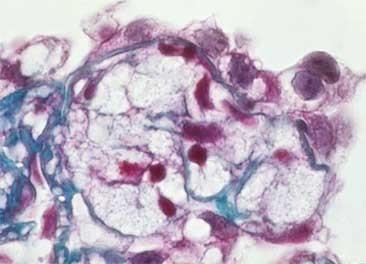
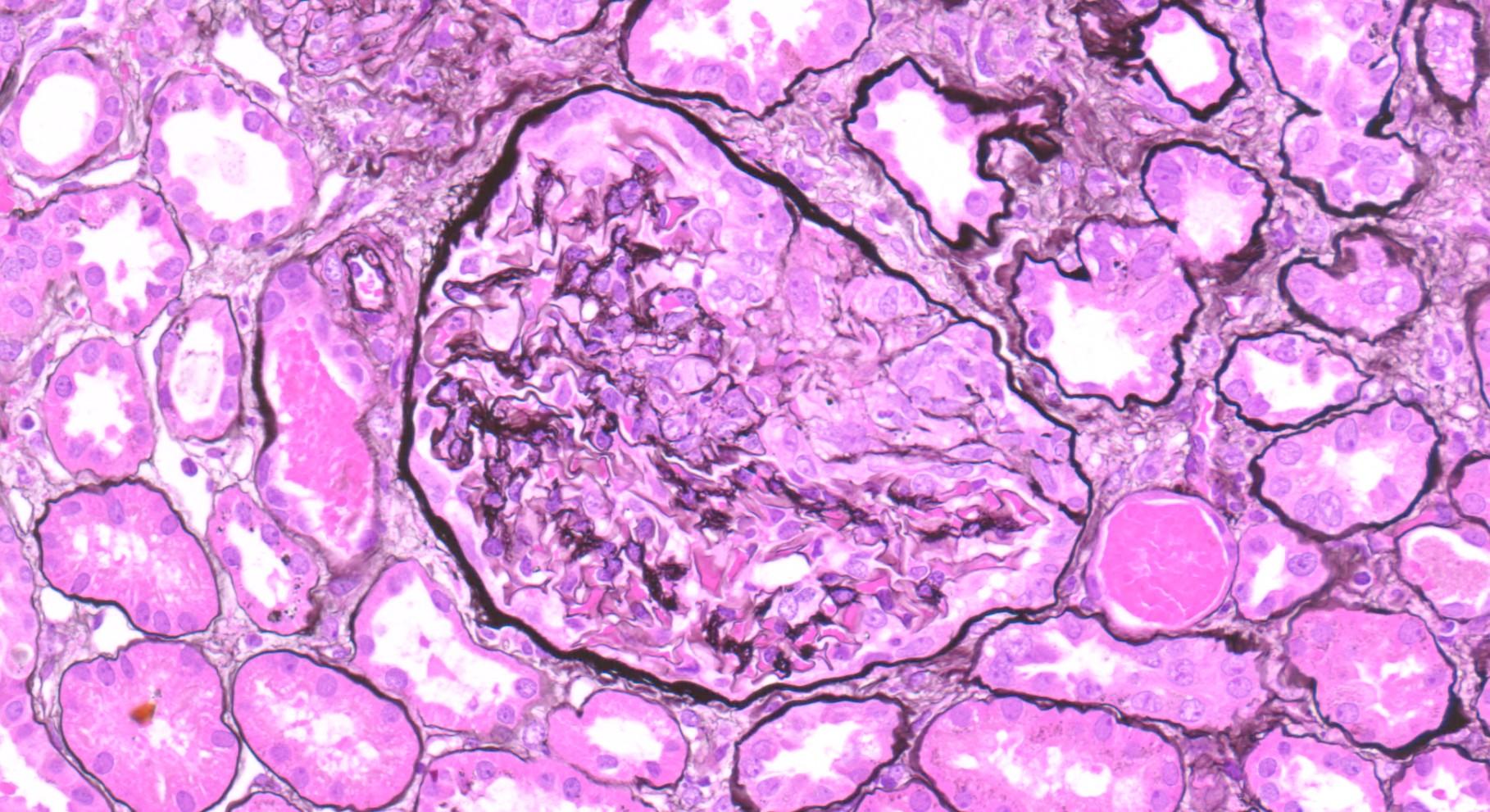
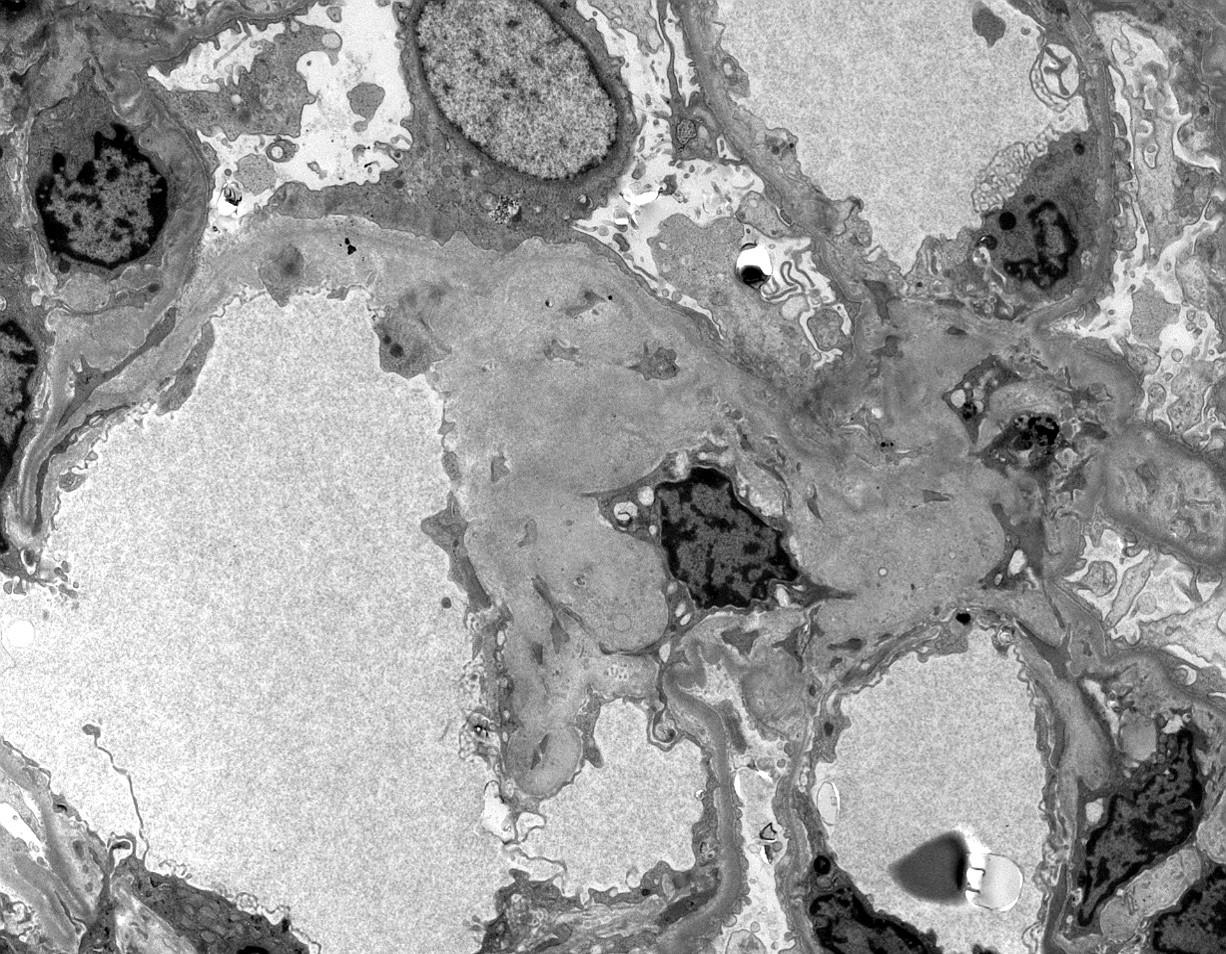
A 62-year-old male presents with increasing fatigue and frequent urination. Laboratory studies show a 24-hour urine protein of 2 grams, elevated serum creatinine, and HbA1c of 45. A renal biopsy is performed (See representative image provided). Immunofluorescence shows mild, non-specific staining for IgG in the mesangium. Electron microscopy shows a diffuse thickening of the glomerular basement membrane.
Based on these findings, which of the following is the MOST likely diagnosis?
A. Amyloidosis
B. Fibrillary glomerulonephritis
C. Diabetic nephropathy
D. Membranous glomerulonephritis
E. Minimal change disease
A 62-year-old male presents with increasing fatigue and frequent urination. Laboratory studies show a 24-hour urine protein of 2 grams, elevated serum creatinine, and HbA1c of 45. A renal biopsy is performed (See representative image provided).
Immunofluorescence shows mild, non-specific staining for IgG in the mesangium. Electron microscopy shows a diffuse thickening of the glomerular basement membrane.
Based on these findings, which of the following is the MOST likely diagnosis?
A. Amyloidosis
B. Fibrillary glomerulonephritis
C. Diabetic nephropathy
D. Membranous glomerulonephritis
E. Minimal change disease
Q8 Explained
■ Correct Answer (C): Diabetic nephropathy is the most likely diagnosis. The clinical history of proteinuria, elevated creatinine, elevated HbA1c and the characteristic PAS+ve mesangial nodules, GBM thickening on light microscopy and EM, and minimal IF staining for IgG, are all features of this condition.
■ Incorrect Answer (A): Amyloidosis presents with similar nodular mesangial changes, but amyloid will stain negative for PAS & Silver and positive with Congo red, displaying apple green birefringence. On EM you would see 8-12nm fibrils.
■ Incorrect Answer (B): Fibrillary glomerulonephritis typically presents with severe proteinuria, often with nephrotic range, and features mesangial deposits which are not PAS positive. Also, on EM there will be 12-22nm fibrils.
■ Incorrect Answer (D): Membranous glomerulonephritis typically presents with nephrotic syndrome but has subepithelial deposits on EM and granular IgG/C3 along capillary walls on IF. The LM will also show diffuse capillary loop thickening.
■ Incorrect Answer (E): Minimal change disease typically shows normal glomeruli on light microscopy, and has effacement of foot processes on EM. It also has no immune deposits on IF and occurs usually in younger people.
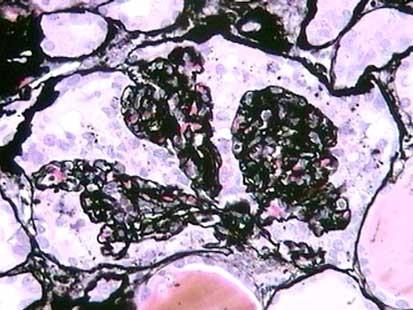
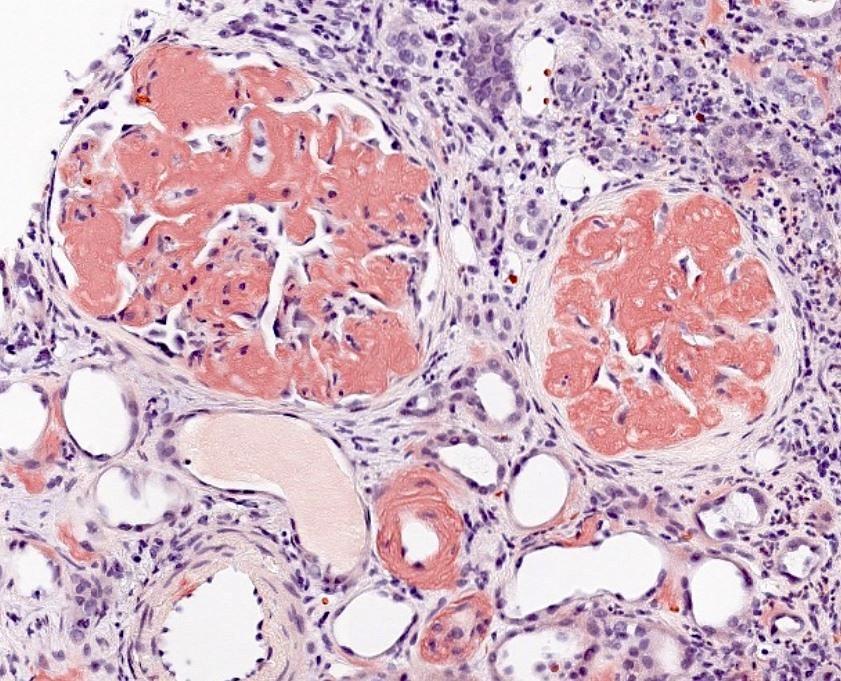
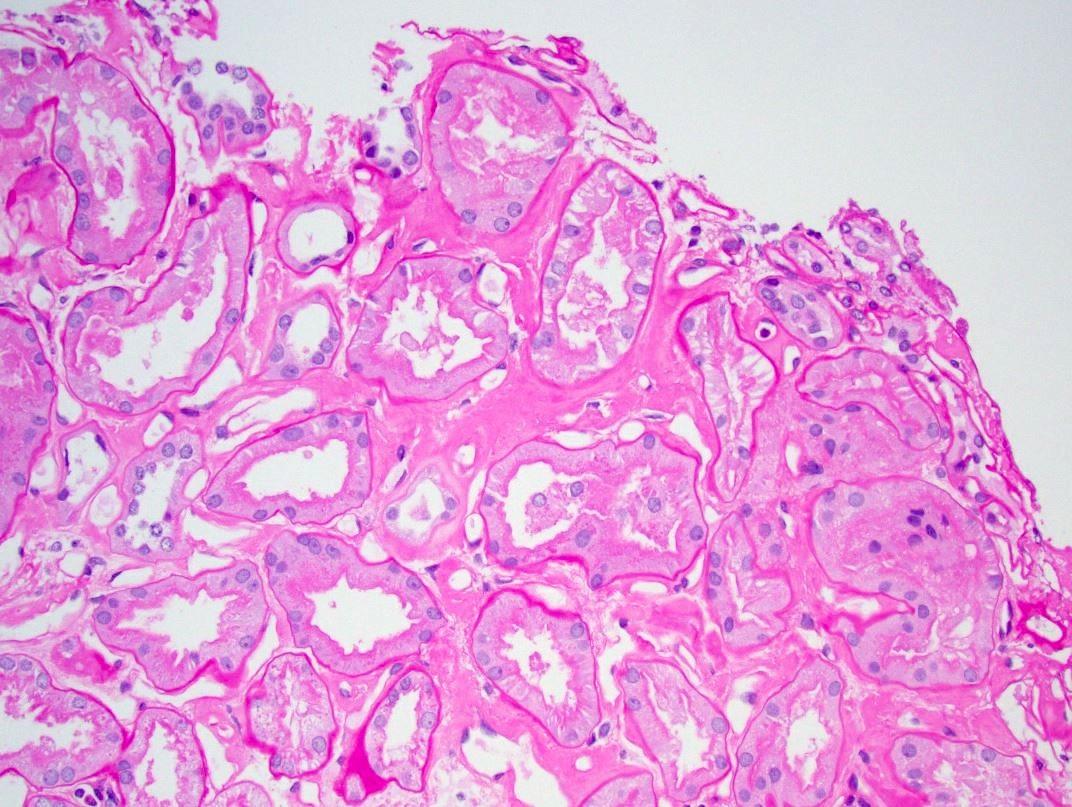
A 40 year old female with a history of rheumatoid arthritis presents with deteriorating renal function, elevated creatinine and proteinuria of 1g/24hrs. A renal biopsy is performed (see representative image).
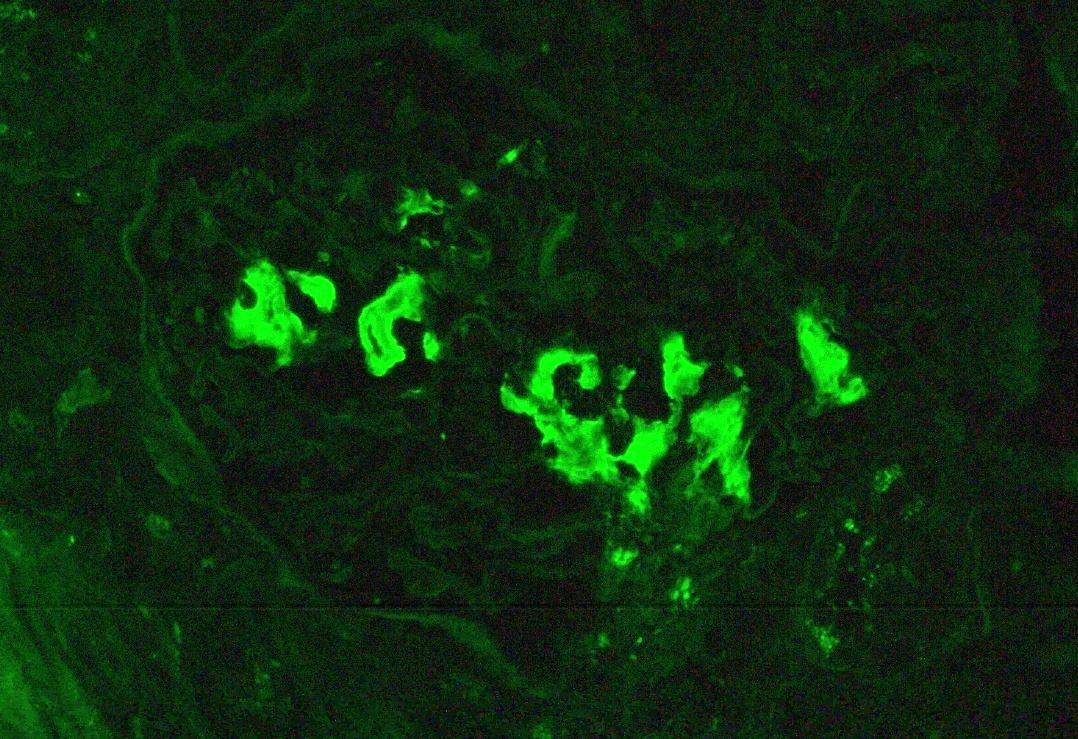
Immunofluorescence shows lambda restricted material in the mesangium. On electron microscopy, these deposits are composed of 8-12nm fibrils.
Based on these findings, which of the following is the most likely diagnosis?
D.
E.
A. Diabetic nephropathy
B. Fibrillary glomerulonephritis
C. Amyloidosis
Membranous glomerulonephritis
Minimal change disease
A 40 year old female with a history of rheumatoid arthritis presents with deteriorating renal function, elevated creatinine and proteinuria of 1g/24hrs. A renal biopsy is performed (see representative image).
Immunofluorescence shows lambda restricted material in the mesangium. On electron microscopy, these deposits are composed of 8-12nm fibrils.
Based on these findings, which of the following is the most likely diagnosis?
E.
A. Diabetic nephropathy
B. Fibrillary glomerulonephritis
C. Amyloidosis
D. Membranous glomerulonephritis
Minimal change disease
Congo Red
IF - Lambda
Renal Amyloidosis
Renal Amyloidosis
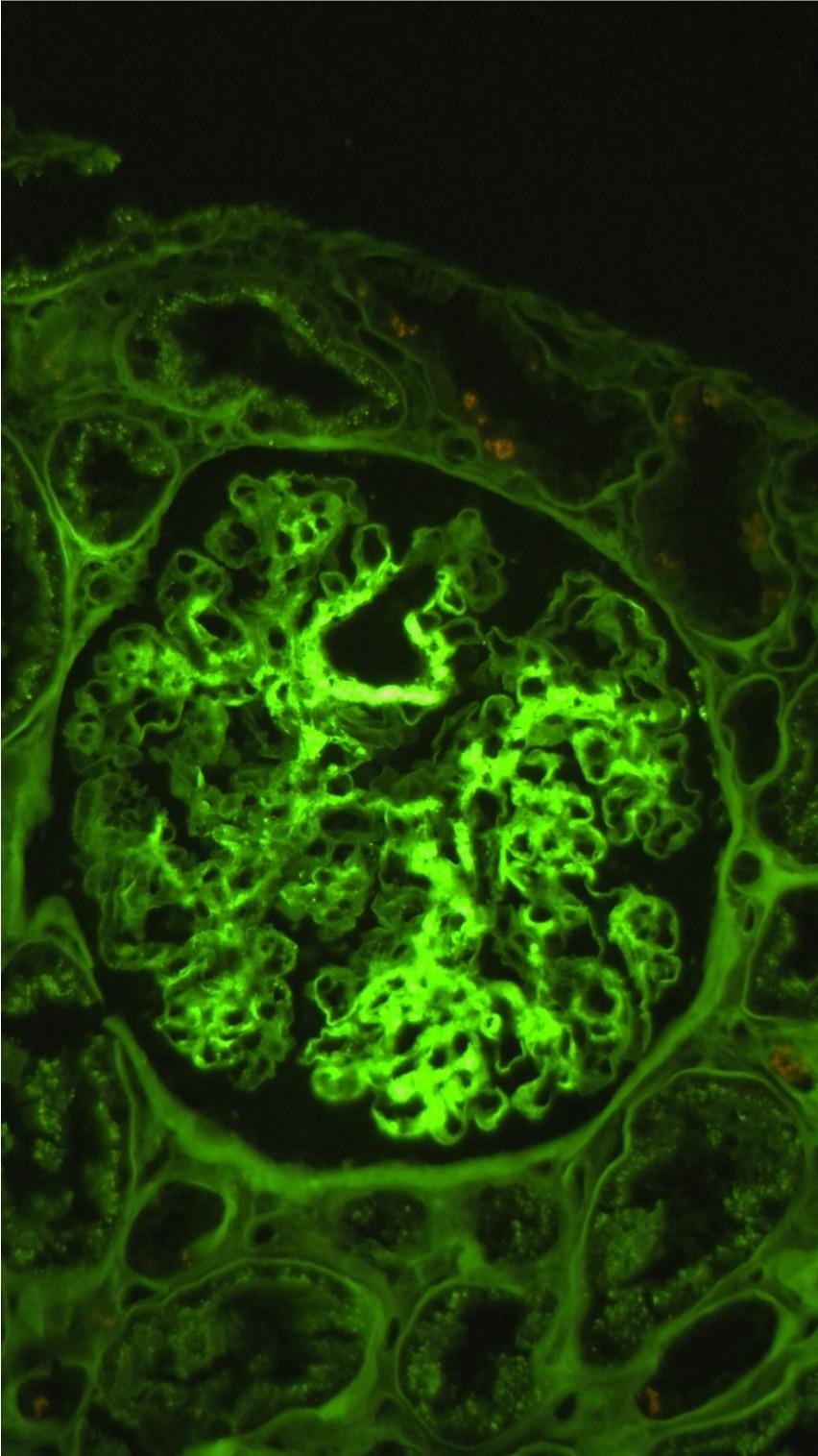
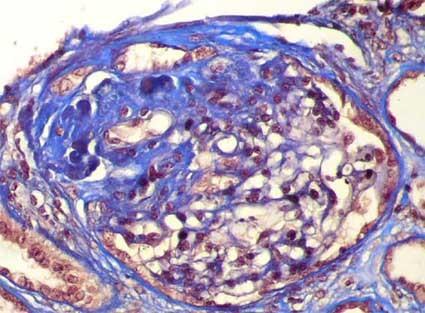
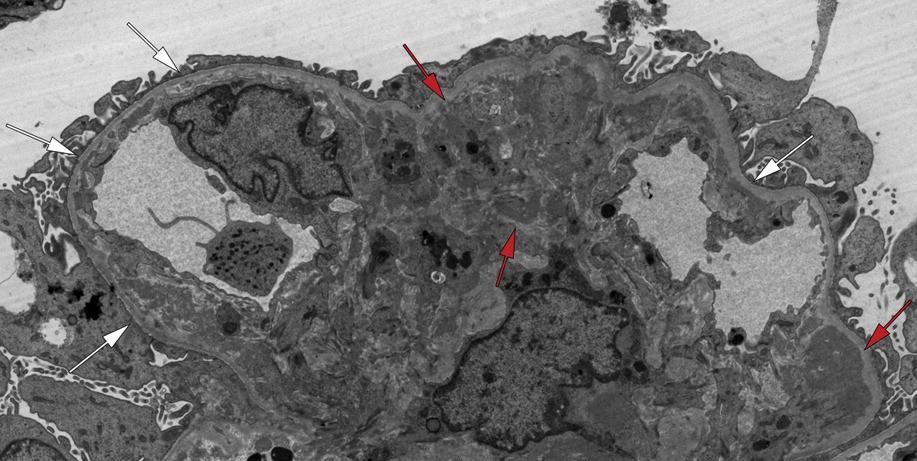
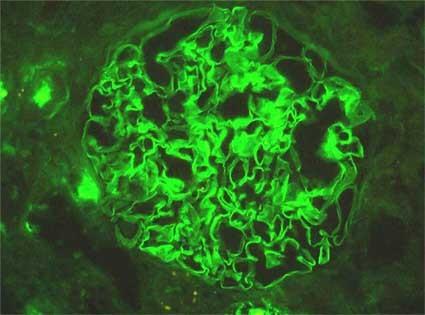
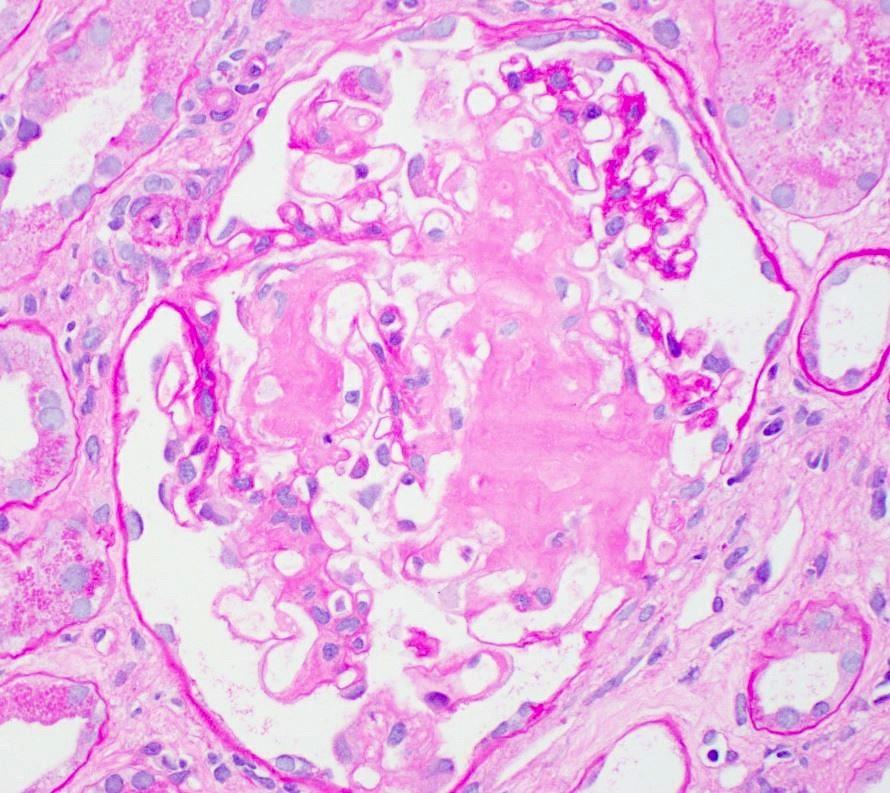
A 30-year-old female presents with a malar rash, lower limb oedema, fatigue, and increased blood pressure. Laboratory studies show a 24-hour urine protein of 5.8 grams, microscopic haematuria, and an elevated serum creatinine. She also has a positive ANA titre and high levels of anti-dsDNA antibodies. A renal biopsy is performed, revealing glomeruli with increased mesangial cellularity and matrix, as well as some thickening of the capillary walls (representative image provided). Immunofluorescence shows granular deposits of IgG, IgA, IgM, C3, and C1q along the glomerular basement membranes and in the mesangium. On Electron microscopy there are subendothelial and mesangial electron-dense deposits
Based on these findings, which of the following is the MOST likely diagnosis?
A. Membranous glomerulonephritis
B. Anti-GBM disease
C. Lupus nephritis
D. Post-infectious glomerulonephritis
E. Amyloidosis
A 30-year-old female presents with a malar rash, lower limb oedema, fatigue, and increased blood pressure. Laboratory studies show a 24-hour urine protein of 5.8 grams, microscopic haematuria, and an elevated serum creatinine. She also has a positive ANA titre and high levels of anti-dsDNA antibodies. A renal biopsy is performed, revealing glomeruli with increased mesangial cellularity and matrix, as well as some thickening of the capillary walls (representative image provided). Immunofluorescence shows granular deposits of IgG, IgA, IgM, C3, and C1q along the glomerular basement membranes and in the mesangium. On Electron microscopy there are subendothelial and mesangial electron-dense deposits
Based on these findings, which of the following is the MOST likely diagnosis?
B. Anti-GBM disease
C. Lupus nephritis
D. Post-infectious glomerulonephritis
E. Amyloidosis
A. Membranous glomerulonephritis
Q10 Explained
■ Correct Answer (C): Lupus nephritis is the MOST likely diagnosis. The clinical history of SLE symptoms, the combined nephritic-nephrotic presentation (proteinuria, hematuria, elevated creatinine), the positive ANA and anti-dsDNA antibodies, the granular deposition of IgG, C3 and C1q on IF, and the subendothelial deposits on EM are all consistent with lupus nephritis.
■ Incorrect Answer (A): Membranous glomerulonephritis usually presents with nephrotic syndrome and has subepithelial deposits on EM. While some forms of lupus nephritis have a membranous pattern, this diagnosis is much less likely given the mesangial and subendothelial pattern of the electron dense deposits. Also, the IF of membranous is usually granular IgG and C3 only.
■ Incorrect Answer (B): Anti-GBM disease presents with RPGN and has linear IgG staining on IF, and the clinical features of this scenario are against Anti-GBM disease.
■ Incorrect Answer (D): Post-infectious glomerulonephritis typically presents as an acute nephritic syndrome following an infection. Whilst it may have low C3, it is typically not associated with C1q and dsDNA positivity and would show subepithelial deposits on EM.
■ Incorrect Answer (E): Amyloidosis is associated with nodular mesangial deposits on LM, and amyloid fibrils on EM, and lacks granular complement staining on IF.
LUPUS NEPHRITIS
Lupus Nephritis
■ Renal manifestation of SLE
■ Presents with nephrotic or nephritic-nephrotic mixed picture. Can also present with RPGN in active lupus nephritis
■ Variety of patterns and associated lesions morphologically
– Near normal gloms – Class I
– Mesangial expansion and hypercellularity – Class II
– Membranoproliferative pattern – Class III & IV
– Membranous pattern – Class V
– Advanced sclerosis – Class VI
■ Can be mixed e.g Class III + V
■ Morphologically can mimic other glomerulopathies
Lupus Nephritis
■ More frequent in young adults – 1:9 male to female ratio
■ Renal manifestations are very variable, from asymptomatic hematuria or proteinuria until rapidly progressive renal failure and terminal renal damage.
■ Treatment is based on corticosteroids and other immunosuppressors
■ A variety of autoantibodies that can be detected in the serum: ANAs, anti-dsDNA, anti-Sm (very specific but few sensible), anti-RNP, anti-Ro, anti-La, anti-histone, and others; anti-DNA antibodies seem important in the pathogenesis of the active lupus nephritis
Silver Trichome
Lupus Nephritis
‘Full House’ Positivity
Lupus Nephritis
ISN/RPS Classification of Lupus Nephritis
ISN/RPS Classification of LN
■ Class I:
■ Class
II:
■ Class
III:
Kidney Int. 2004
Feb;65(2):521-30.
Minimal mesangial LN (normal LM, +deposits)
Mesangial proliferative LN
Focal LN (<50% of all glomeruli) (Global or Segmental)
III (A): Active lesions: focal proliferative LN
III (A/C): Active and chronic lesions
III (C): Chronic inactive lesions with scars
■ Class
IV:
IV-S (A): Diffuse LN (≥50% of all glomeruli) (Diffuse Global or Segmental)
IV-G (A):
Active lesions: diffuse segmental proliferative LN
Active lesions: diffuse global proliferative LN
IV-S (A/C): Active and chronic lesions
IV-G (A/C): Active and chronic lesions
IV-S (C): Chronic inactive lesions with scars
IV-G (C): Chronic inactive lesions with scars
■ Class
V: Membranous LN
■ Class VI: Advanced sclerotic LN (90% sclerosed, no activity)
Modified NIH Lupus Nephritis Activity and Chronicity Scoring System
Modified NIH activity index Definition Score
Endocapillary hypercellularity
Neutrophils/karyorrhexis
Endocapillary hypercellularity in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
Neutrophils and/or karyorrhexis in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
Fibrinoid necrosis
Fibrinoid necrosis in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
Hyaline deposits
Cellular/fibrocellular crescents
Wire loop lesions and/or hyaline thrombi in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
(0–3) × 2
Interstitial Inflammation
Cellular and/or fibrocellular crescents in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
(0–3) × 2
Interstitial leukocytes in <25% (1+), 25%–50% (2+), or >50% (3+) in the cortex 0–3
Modified NIH Lupus Nephritis Activity and Chronicity Scoring System
Total glomerulosclerosis score
Global and/or segmental sclerosis in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
0–3
Fibrous crescents
Tubular atrophy
Fibrous crescents in <25% (1+), 25%–50% (2+), or >50% (3+) of glomeruli
Tubular atrophy in <25% (1+), 25%–50% (2+), or >50% (3+) of the cortical tubules
0–3
0–3
Interstitial fibrosis
Interstitial fibrosis in <25% (1+), 25%–50% (2+), or >50% (3+) in the cortex