• New role now being introduced – to try to increase scrutiny in to non-coronial deaths
• Starting in acute trusts, but now being rolled our to examine all non-coronial deaths
• Functions of The Medical Examiner:
• to ensure that cases which should be reported to the Coroner are in fact reported
• to ensure that medical certificates of the cause of death are as accurate as possible.
• to provide opportunities for the bereaved to raise concerns
• to provide advice to the Coroner and doctors
• to have a local overview of patterns in reported deaths
Medical Examiner Role
• Medical Examiners
• Senior doctors contracted for a number of sessions per week alongside their other work
• Oversee ME process
• Medical Examiner Officers
• Staff the medical examiner office full time
• Come from a variety of backgrounds
• Provide continuity to the service
• Can perform roles such as scrutinise notes, discuss with clinicians and relatives etc
Who is going to fund Medical Examiners?
A. Home Office
B. NHS England
C. Primary care trusts
D. Charitable groups
E. LocalAuthorities
3. The Coroner
The Coroner’s rules relevant to the PM (in the Coroner’s and Justice Act)
– WHEN – rule 5: “as soon after the death of the deceased as is reasonably practicable”
– WHO – rule 6: “fully registered medical practitioner” whenever practicable, by a pathologist with suitable qualifications and experience
– WHO ELSE – rule 7: “Coroner to notify persons of post-mortem to be made” - a list of properly interested persons to be informed of the PM and who may be present, or represented, at the PM
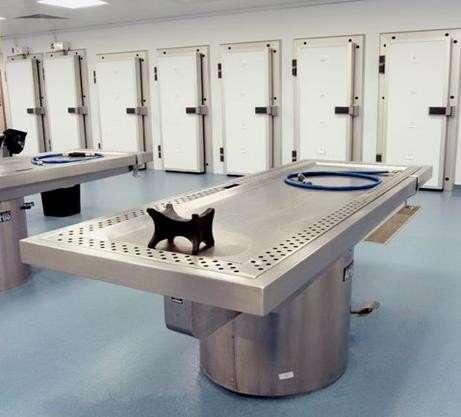
– WHERE - rule 11: “(1) No post-mortem examination shall be made in a dwelling house or in licensed premises. (2) Every post-mortem examination shall be made in premises which are adequately equipped for the purpose of the examination.”
Deaths reportable to the Coroner/PF:
• Need to establish cause of death
• Unknown cause of death
• Sudden unexpected death (SIDS, SADS, SUDEP)
• Deceased was not seen by the doctor within the 28 days before death
• Death may be unnatural
• Violent or suspicious
• Possible manslaughter/murder
• Due to an accident
• May be due to self-neglect or neglect by others
• Possible suicide
• Death may be related to poisoning/drugs/acute alcohol poisoning (though not other forms of alcohol-related death)
• Death may be a result of medical treatment
• Death occurred during an operation or before recovery from the effects of an anaesthetic
• Deaths secondary to medical treatment
• Deaths where the conduct of a member of staff is questioned
• May be due to abortion
• Other
• Deaths during or shortly after detention in police or prison custody
• Industrial disease or related to employment
The Coroner
• Independent judicial officer
• Must be legally qualified for 5 years
• Role of the coroner…
• Identify the deceased
• Determine how, when and where they came about their death
• Issue death certificate
• Maintain records
• Can order a post-mortem examination of the body, if needed to determine the cause of death.
• Each Coroner has a defined area of jurisdiction (and responsible for all bodies lying within their jurisdiction)
• A body can only be moved from one jurisdiction to a neighbouring one, by formal arrangement between the Coroners.
• Procurator Fiscal has a similar role in Scotland
Coroners Inquests
• Public legal inquiry held by the Coroner if:
– Death is violent or unnatural
– Death took place in prison or police custody
– Cause is still uncertain after a post-mortem
• Held in a court and may have a jury
• Consists of coroner and next of kin (as a minimum)
• May also have witnesses, GP, pathologist, hospital doctors, police etc
• Inquisitorial not adversarial, must not assign blame
Coroners Inquests
• The Coroner reaches a conclusion (verdict), which can be one of
o Death by natural causes
o Death by misadventure
o Accidental death
o Unlawful killing
o Suicide
o Occupational disease
o Drug abuse
o Self-neglect
o An open verdict
o A narrative verdict
Fatal Accident Inquiry (Scotland)
• Equivalent of an inquest
• FAI held by the Procurator Fiscal (Scotland) if:
– Death is caused by employment
– Death took place in legal custody
– Issue of public safety or general public concern
• Held much less often than Coroners inquests
• Held in private usually
Which of the following IS correct?
A. Any qualified doctor may issue a death certificate so long as they see the deceased after death.
B. The consultant may request a hospital post mortem before issuing a certificate of cause of death.
C. The Registrar may report deaths to the Coroner if the certified cause of death appears incorrect.
D. The Coroner must order a post-mortem examination on any death due to accident.
E. In UK, approximately 15% of deaths are reported to the Coroner.
Which one of these deaths would NOT need to be reported to a Manchester area Coroner?
A. Woman from Scotland who dies in a motor vehicle collision in Manchester
B. Manchester resident who dies in a climbing accident on holiday in Wales
C. Man from Liverpool who dies from drowning in France and body is returned via Manchester airport
D. Child from Leeds who dies suddenly whilst staying with relatives in Manchester.
E. Chinese visitor who unexpectedly collapses and dies on arrival in Manchester airport.
Which of these deaths would NOT need to be reported to the Coroner?
A. An ex-dockyard worker who dies due to known fibrotic interstitial lung disease.
B. Woman dies due to metastatic breast cancer. Seen regularly by her GP until last week but GP now away on holiday for 2 weeks.
C. A 45 year old who is taken to hospital after binge drinking, dying shortly after admission with a very high blood ethanol level.
D. A45 year old with hepatic cirrhosis due to excessive alcohol use who dies of liver failure in hospital.
E.Young woman who has taken 30g of paracetamol & dies of liver failure in hospital.
Which of these deaths would NOT need to be reported to the Coroner?
A. An ex-dockyard worker who dies due to known fibrotic interstitial lung disease.
B. Woman dies due to metastatic breast cancer. Seen regularly by her GP until last week but GP now away on holiday for 2 weeks.
C. A 45 year old who is taken to hospital after binge drinking, dying shortly after admission with a very high blood ethanol level.
D. A45 year old with hepatic cirrhosis due to excessive alcohol use who dies of liver failure in hospital.
E.Young woman who has taken 30g of paracetamol & dies of liver failure in hospital.
You have performed a Coroner’s autopsy on a case of death due to an industrial injury. To which ONE of the following legitimately interested parties must you give a copy of your PM report at their request?
A. The next of kin of the deceased
B. The Solicitor of the next of kin of deceased
C. Health & Safety Executive officers investigating the case
D. The senior police officer investigating the case
E. The Coroner responsible for the case
4. The Human Tissue Act
The Human TissueAct
• Set up in 2005 after a culture of retaining tissue and organs without consent was revealed
• Regulates “relevant material” for the following reasons:
• Autopsy
• Anatomical examination
• Public display of tissue
• Tissue used in education and research
• It covers England, Wales & N.Ireland; Scotland has a separate law - HT (Scotland) Act 2006.
• The Human Tissue Authority implements theAct
The Human TissueAct
• Exceptions:
• Does not apply to tissue removed before September 2006
• Does not apply to tissue removed from the living for diagnosis or treatment
• Does not apply to images - GMC standards for this
• Does not apply to Coronial or Home Office PMs (but does apply to the material once the coroner’s/home office purposes are complete)
“Relevant Material”
• Any material which consists of or includes human cells
• Therefore includes….
• Human bodies, organs, tissues, skin, bone, body fluids (bile, breast milk)
• processed tissues that contain cells,
• cell deposits or tissue sections on microscope slides
• aspirated serous fluids and cyst fluids
• pus, sputum, urine, stomach contents and bodily waste
• umbilical cord stem cells
• It does include hair and nails from the deceased
• Does not include….
• Gametes and embryos created outside the body (regulated separately by human fertilization and embryology act)
• Hair and nails from a living person (but does cover hair and nails from deceased person!)
• Any tissue collected from a living person for diagnosis or treatment
• Tissue collected before 2006
• Serum and sweat are thought to be acellular
• NB fetal tissue <24 weeks is counted as tissue belonging to the mother
“Scheduled Purposes”
ieActivities for which consent and licensing are required:
•Anatomical examination
•Determining cause of death
•Establishing effectiveness of treatment
•Public display
•Research
•Transplantation
•Audit, Teaching, QC, Public health monitoring
The HT Authority
• Established 2005, to implement the HTAct
• The Human Tissue Authority is an independent watchdog that protects public confidence by licensing and inspecting organisations that store and use tissue (for scheduled purposes under the Act)
• Provides advice and guidance about: the Human Tissue Act (2004) and the Quality and Safety Regulations (2007).
The HT Authority
• Codes of Practice – covering post-mortem practice, consent for use of human tissue, and disposal of human tissue.
• Regulation of people, premises and practices involved in post-mortems.Assessed by site inspections and audits.
• Sets rigorous standards for taking consent
• Disposal options must be offered to relatives for any tissue retained from PM
Consent under the HTA
• Consent required for all scheduled purposes involving any relevant material
• Except for Coroners’ or Home office PMs or samples retained for their investigations
• After the Coroner’s function has ceased, then consent is required for further use or storage of material under the HTArules.
Consent
• Can be given by the Deceased, or their Nominated Representative, otherwise:
• varies with region and lab method, correlate result with local lab ranges
• > 100,000 fibres/g dried lung for asbestosis
• Sample destroyed in processing
• Genetic studies - only with specific permission
• use fresh or paraffin embedded spleen
• Eg for inherited cardiomyopathy
Which of the following tests is most likely to be useful in investigating the death of a poorlycontrolled insulin-dependant diabetic man who was discovered dead at home, with no cause found grossly at autopsy?
A. Blood for glucose level
B. Blood for insulin level
C. Vitreous for ketones and glucose level
D. Blood cultures
E. Vitreous for insulin levels
A 22 year old female student collapses outside a bar late at night and cannot be resuscitated. Which ONE of the following PM toxicology results most likely indicates her cause of death?
A.Blood ethanol level 450 mg/dL (NB legal limit for driving is 80 mg/dL)
B.Cannabinoids present at high levels in blood and urine
C.Hair samples show chronic use of ecstasy, amphetamines, cannabis and sertraline
D.Codeine, morphine and morphine metabolites all present (at low levels) in blood and urine
E.Lack of anti-convulsant medication in blood or urine.
6. Important Autopsy Scenarios
RCPath Autopsy
Best Practice Scenarios
Sudden death with likely cardiac pathology
Epilepsy
Sudden Cardiac Death
These are likely to be one of the following, depending on age and circumstances of death:
• Ischaemic heart disease
• ?Familial hypercholesterolaemia if young age
• Hypertensive heart disease – dilated and hypertrophied
• or can be Familial (30%) – usually mutations in mitochondrial or cytoskeletal genes
• Causes congestive heart failure
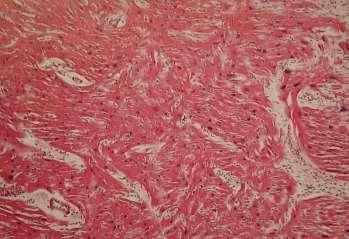
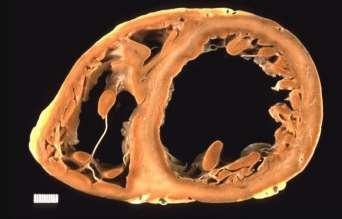
Cardiomyopathy - ARVC
Arrhythmogenic right ventricular cardiomyopathy
• Autosomal dominant inheritance
• Gross: Right ventricular thinning +/- fatty infiltration
•Micro: fibro-fatty replacement of myocytes, +/inflammation
Which of the following features is NOT associated with sudden arrhythmogenic death syndrome (SADS)?
A.Young age and previously fit and well
B.Heart appears structurally normal at autopsy
C.Death occuring during physical exertion
D.Inherited genetic mutation found on family screening
E.Histology of the myocardium shows myocyte disarray
Deaths Associated with Epilepsy
Types of epilepsy deaths:
• status epilepticus
• accident due to seizure - trauma or drowning
• aspiration or asphyxia due to seizure
• complication of treatment
• SUDEP
Epilepsy Deaths - Sampling
Ideally specialist referral and whole brain
fixation for 2-3 weeks before sampling
2 coronal slices of brain 1.5cm thick (pre and post midbrain): photograph and sample specific areas (x8, bilaterally)
Myocardium, Lung, other organs
Blood and Urine for drugs, alcohol and anticonvulsants
SUDEP
must have ante-mortem epilepsy diagnosis or strong history of seizures
no other cause of death found mechanism of death not known - thought to be neurogenic cardiac arrhythmia or respiratory arrest
A 18 year old man with a past history of epilepsy is found dead at home with evidence of urinary incontinence. No macroscopic abnormalities are seen at PM examination. You retain the brain. What are the most likely histological findings?
A. Amyloid plaques
B. Intranuclear inclusions within neurons
C. Ahistologically normal brain
D. Patchy demyelination
E. Diffuse spongiosis of the grey and white matter
Anaphylaxis
Modes of death from anaphylaxis:
• Airway: Asphyxia due to Laryngeal oedema - eg insect sting, food
• Lungs: Asthmatic attack - eg aspirin and food allergies
• Circulation: Shock - eg drug allergy
Misdiagnosed commonly as an MI orAsthma attack
• NB myocardial ischaemia inevitable in shock
• pulmonary oedema may be due to epinephrine use
• can differentiate acute from chronic asthma histologically
Anaphylaxis
Look for serological evidence of allergen:
• serum drug levels
• specific IgE levels for foods, beesting, drugs
Look for biochemical evidence of anaphylaxis
• Mast cell tryptase - samples useful up to 3 days post death
•Total IgE levels - stable at room temperature for 11 weeks
Mention the allergen on the death certificate where known.
A14 year old girl collapses and dies at a party after eating birthday cake. At post-mortem there is laryngeal oedema. What is the most useful sample to retain to confirm the cause of death?
A. Peripheral blood for mast cell tryptase
B. Histology of the larynx
C. Urine for drug screen
D. Peripheral blood for ketones
E. Stool sample for culture
Maternal Deaths
• International definition: death during pregnancy or within 6 weeks of delivery/miscarriage.
• UK definition includes deaths up to 12 months
‘early’(<6 weeks/ 42 days)
‘late’(>6 weeks)
• NB: all maternal deaths are scrutinised for the UK Confidential Enquiry into Maternal Death.
• eg road accident, illicit drug overdose, unrelated malignancy.
A 40 year old woman develops shortness of breath, collapses and dies following a complicated full-term delivery. Histology of the pulmonary vessels demonstrates intravascular squames and mucin. What is the most likely cause of death?
A. Pulmonary thromboembolism
B. Squamous cell carcinoma
C. Amniotic fluid embolism
D. Eclampsia
E. DIC
Occupational Lung Disease
• Dept for Work & Pensions classifies prescribed Occupational Diseases on advice of Industrial InjuriesAdvisory Council
• Once diagnosed, can apply for government compensation
• Deaths reportable to Coroner
Occupational lung disease
• Role of the autopsy?
• confirm lung disease
• evidence of occupational exposure
• relevance to cause of death
Commonest cases now are asbestos-related (coal, cotton, silica etc very rare)
• pleural plaques •mesothelioma
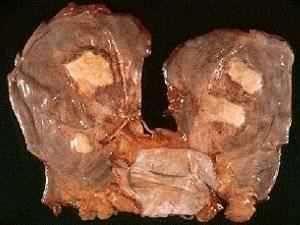
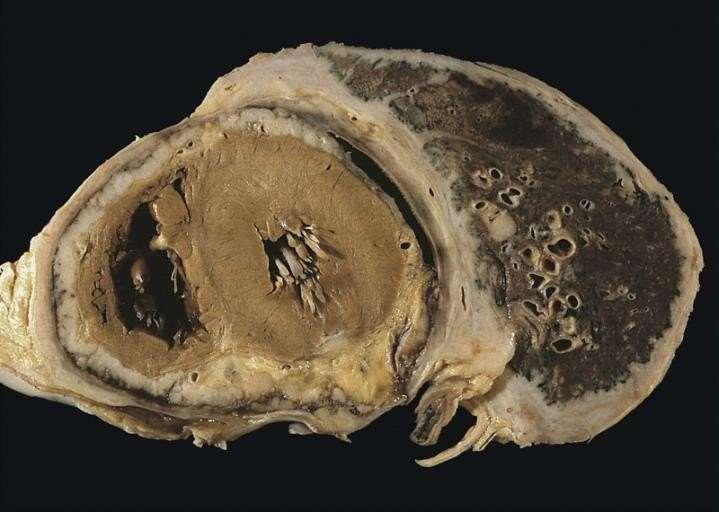
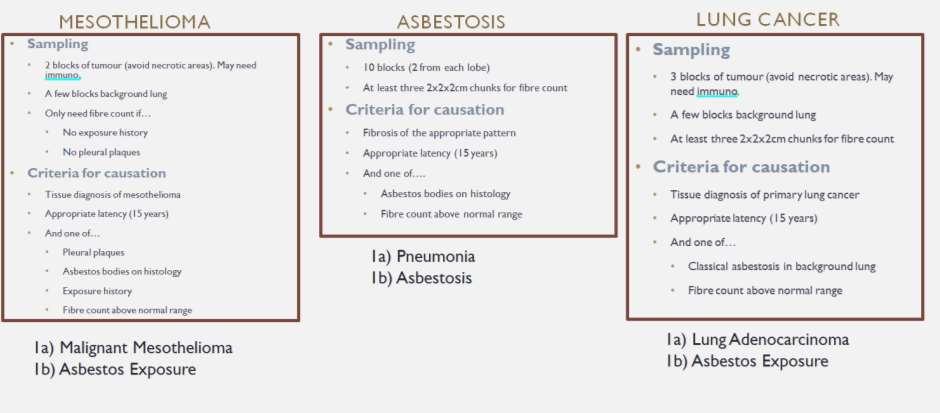
Asbestos
Asbestos-related deaths include any direct or indirect death resulting from:
• asbestosis (fibrosis)
• mesothelioma
• carcinoma of lung – any type
• diffuse pleural thickening or benign pleural effusions
Must demonstrate adequate asbestos exposure...
Asbestos
A 68 yr non-smoking dock worker dies following 6/12 history of increasing SOB and chest pain. PM examination finds an extensive tumour encasing the right lung. What is the most likely cause of death?
A. Squamous cell carcinoma of the lung
B. Metastatic colorectal carcinoma
C. Mesothelioma
D. Pulmonary fibrosis
E. Small cell lung carcinoma
7. Virtual Autopsies
Virtual Autopsies - MR scan
• Non Invasive technique
• Used for religious /cultural reasons, forensics or mass disasters
• Can yield high quality, 3D, high res images
• Disadvantages:
– Cannot sample body for microorganisms or toxins
– Cannot type tumours etc
– Limited availability and expense, of scanners and radiologists
– Not suitable for all cases
Suggested Reading
• Robbins Pathologic Basis of Disease
• Knight’s Forensic Pathology
• Simpson’s Forensic Pathology
• The HospitalAutopsy – GN Rutty, J Burton
• Gross pathology atlases
Resources
on College Website
• Guidelines onAutopsy Practice (RCPath, 2002)
• RCPath Best Practice Scenarios, 2005
• Autopsy andAudit
• Code of Practice and Performance Standards for Forensic Pathologists
• ABrief Guide on Consent for Pathologists
• NCEPOD CoronialAutopsy Study
For Further information
• www.e-lfh.org.uk/projects/medical-examiner : about medical examiner role and online training