“ We’re doing just as many things in people’s homes as in hospitals – relieving overburdened hospitals and helping people be more comfortable at home. And it’s not being respected.”
Home care nurses are demanding
s Cover story: Churro-inspired innovation that could transform bypass surgery
s St. Michael’s Hospital performs 10 TAVIs in a day, paving the way for more efficient care, faster healing
s Humber River Health’s journey toward onsite cardiac catheterization
Botox at 40: From medical curiosity to a wide range of uses
s Canada needs to move from patchwork to progress to unlock the full potential of our national framework for diabetes
s Canada’s first endovascular hemispherectomy
Canadian first: One-of-a-kind imaging platform for mental health
Doing more for Manitobans with heart failure would help our whole health system
By Dr. Shelley Zieroth
When Manitoba’s new government was elected 18 months ago, it promised to do things differently. In healthcare, it added a simple yet vital goal: take better care of people. In its first year and a half we have seen movement towards this, but significant opportunities for transformation in our healthcare system remain.
One opportunity for impactful change is for Manitobans with heart failure to be treated through a coordinated, province-wide diagnosis and care system. Implementing it would take better care, not just of those patients, but of our whole health system.
Heart failure is one of our most serious medical challenges and Manitoba has one of the highest rates of the life-changing and life-shortening condition in Canada. About 30,000 Manitobans are living with heart failure and nearly 5,000 are diagnosed each year – equivalent to the population of Flin Flon or Stonewall. This puts a significant burden on the province’s healthcare system, including hospitals and emergency departments.
Heart failure means exactly what the name says. The diseased heart is unable to pump sufficient blood throughout the body, and over time, it gets worse. This makes exertion difficult, so even small activities can be impossible or leave the patient short of breath. It is a
UPCOMING DEADLINES
AUGUST 2025 ISSUE
EDITORIAL: July 11
ADVERTISING:
Display – July 25 | Material – July 29
Monthly Focus:
Paediatrics/Community Engagement and Patient Advocacy/Social Work: Paediatric programs and developments in the treatment of paediatric disorders including autism. Specialized programs offered on an outpatient basis. Community engagement initiatives. Empowering patients –tools and strategies for improving patient education and self-management. The role of patient advocates and how healthcare professionals can support advocacy efforts. Social work programs helping patients and families address the impact of illness .
+ PAEDIATRICS SUPPLEMENT
THANKS TO OUR ADVERTISERS
progressive disease that can be effectively managed to improve symptoms, slow patient decline and prevent hospitalizations, but there is no cure.
By its very nature, heart failure causes many patients to require periodic hospitalization to stabilize symptoms and adjust medications. Overall, in Canada, heart failure is the third most common cause of hospitalization, behind only giving birth and lung diseases. It also results in the longest average hospital stay of the top eight causes of hospitalization – 9.6 days.
In fact, Manitoba’s healthcare system has the highest average hospital stay for heart failure in Canada at 13.4 days – 40 per cent longer than the Canadian average.
There is clearly room for improvement to provide better care. Early diagnosis, the right treatment plan that includes guideline-directed medical therapy and effective follow-up are the critical keys for keeping patients out of hospital, extending their life expectancy and improving their quality of life.
There are three things we can and must do in Manitoba to help achieve this for those with heart failure and, at the same time, lessen the burden on the health system for the benefit of all Manitobans.
First, we need to address the lack of equitable access to a blood test that is an important symptomatic screening tool doctors use for heart failure.
Continued on page 6
SEPTEMBER 2025 ISSUE
EDITORIAL: August 8
ADVERTISING: Display – August 22 | Material – August 26
Monthly Focus:
Emergency Services/Critical Care/Trauma/ Emergency/Online Education: Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine.
+ ONLINE EDUCATION SUPPLEMENT
When you visit our advertisers, please mention you saw their ads in Hospital News.
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:
Hospital News is published for hospital health-care professionals, patients, visitors and students. It is available free of charge, accessed by our website (hospitalnews.com) and also available through our digital subscription.
The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
For changes in email subscriptions please send requests to info@hospitalnews.com. Hospital News does not share email information and subscriptions can be cancelled at any time.
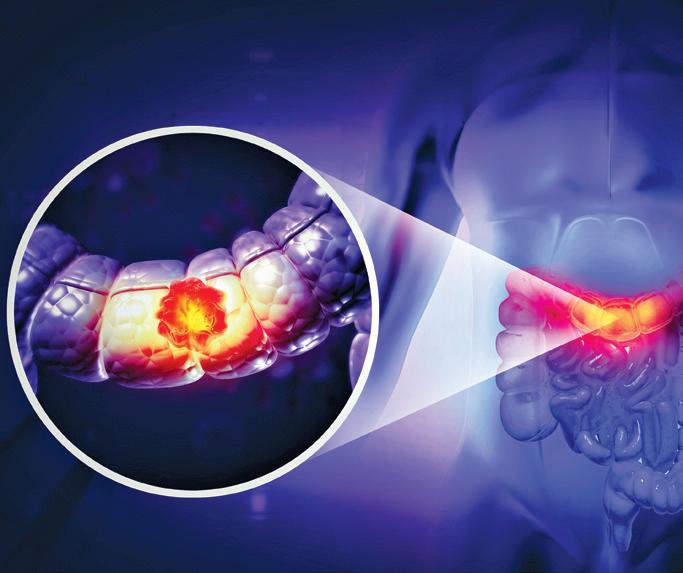
World-first clinical trial confirms exercise improves survival for colon cancer
Agroundbreaking clinical trial funded by the Canadian Cancer Society (CCS) shows that physical activity can significantly improve outcomes for people with colon cancer. Researchers say the study is the first in the world to use structured exercise to increase cancer survival.
The trial results, presented today at the American Society of Clinical Oncology annual conference and published in the New England Journal of Medicine, have the potential to change clinical practice. They show that, when incorporated into cancer care for people with colon cancer, a structured exercise program reduces the risk of cancer recurrence and of new primary cancers developing.
“Our findings show that exercise is no longer just a quality-of-life intervention for cancer patients that can be offered when and where possible,” says study co-chair Dr Kerry Courneya, a professor of kinesiology at the University of Alberta and Canada Research Chair in Physical Activity and Cancer. “It is a treatment for colon cancer that must be made available to all patients.”
Colorectal cancer is the second leading cause of cancer death in Canada. Last year, an estimated 25,200 Canadians were diagnosed with colorectal cancer and 9,400 people died from it. To improve outcomes, a team led by Dr Courneya and Dr Chris Booth – study co-chair, medical oncologist at Kingston Health Sciences Centre and professor of oncology at Queen’s University – has been working with the Canadian Cancer Trials Group (CCTG) on this first-of-its kind trial.
The 17-year international trial involved 889 people, all of whom had been diagnosed with and treated for colon cancer. After having surgery and chemotherapy, participants were given a 3-year structured exercise program or standard health education materials that are currently given to patients. Each participant in the ex-
ercise program chose their own forms of moderate-intensity exercise – from walking to pickleball – with the goal of adding 2.5 hours of exercise per week to their regular activity schedule. The outcome: those who received the exercise program had a 28 per cent lower risk of recurrence and new cancers and a 37 per cent lower risk of death.
“This is the first clinical trial in the world designed to answer whether exercise can improve cancer survival, and the results are clear,” says Dr Booth.
“The next step is to put this into practice. That means health systems will need to invest in behaviour support programs as part of standard care.”
The researchers are currently conducting a comprehensive health economic analysis. According to Dr Booth, they anticipate that the program will be “remarkably cost-effective compared to many new cancer drugs,” making it sustainable for health systems.
TERRI’S STORY
Terri Swain-Collins was diagnosed with stage 3 colon cancer in 2021 after a screening test led to further investigation. Following treatment including surgery and chemotherapy, she was invited to join Dr Booth and Dr Courneya’s clinical trial. During the trial, she worked closely with a physiotherapist to establish and maintain a fitness routine personalized to her needs.
“One of the biggest benefits was having a semi-structured routine that works for my lifestyle with someone to hold me accountable,” says Terri.
“Simply being told to exercise by a physician wouldn’t have been enough to get me to where I am today; having someone walk alongside me, guide me and check in regularly was what truly made it possible.”
Now, 3 years later, Terri continues to walk 3 times a week, feels fit and remains cancer-free. She says she is grateful for the impact of the program on her health and well-being.
“By bridging the gap between bold ideas and routine practice, clinical
trials are essential to driving research progress that can benefit patients,” says Dr Stuart Edmonds, Executive Vice President, Mission, Research and Advocacy at CCS. “The results of this trial have the potential to save and improve lives for the tens of thousands of people in Canada affected by colorectal cancer each year, and we are proud our donors enabled us to support it.”
The international study co-chair was Dr Janette Vardy, from The University of Sydney (Australia) with funding from National Health and Medical Research Council. The UK team was led by Dr Victoria Coyle at Queen’s University of Belfast, supported by Cancer Research UK.
The Canadian Cancer Society works tirelessly to save and improve lives. We raise funds to fuel the brightest minds in cancer research. We provide a compassionate support system for all those affected by cancer, across Canada and for all types of cancer. Together with patients, supporters,
donors and volunteers, we work to create a healthier future for everyone. Because to take on cancer, it takes all of us. It takes a society.
ABOUT THE CANADIAN CANCER TRIALS GROUP
The Canadian Cancer Trials Group (CCTG) is a cancer clinical trials research cooperative that runs phase I–III trials to test anti-cancer and supportive therapies at over 85 hospitals and cancer centres across Canada. From their operations centre at Queen’s University, CCTG has supported more than 600 trials enrolling 100,000 patients from 40 countries on 6 continents through a global network of 20,000 investigators and clinical trial staff. CCTG is the Canadian Coordinating Clinical Trial Network for the US NCTN and is a national program of the Canadian Cancer Society. CCTG’s aim is to improve survival and quality of life for all people with cancer. Learn more at cctg.ca. n H
Immunity’s impact on spine recovery
Arecent study from UHN’s Krembil Brain Institute has revealed the essential role of the immune system in response to treatments for spinal cord injury (SCI).
Comparing different laboratory models of SCI, a research team led by Dr. Michael G. Fehlings, Senior Scientist at the Krembil Brain Institute, discovered that cell therapy outcomes vary significantly between immunocompromised or immunodeficient models – which lack a fully functioning immune system – and immunocompetent models.
Cell therapies, such as human induced-pluripotent stem cell-derived neuron progenitor cell (hiPSC-NPC) transplants, are promising treatments for patients with SCI, many of whom have no other treatment options.
However, to ensure cell survival and minimize rejection, preclinical
Continued from page 4
PREVIOUS STUDIES HAVE SHOWN THAT THE INTERACTION BETWEEN IMMUNE CELLS AND TRANSPLANTED CELLS POST-SCI IS COMPLEX AND MULTI-DIRECTIONAL. IMPROVING SCI TREATMENTS REQUIRES MORE ACCURATE MODELS THAT INCLUDE A FUNCTIONAL IMMUNE SYSTEM.
models that scientists use to study the safety and feasibility of cell therapies, often exclude or downplay the immune system’s role. This trade-off affects how well these models replicate the real-world response to treatment.
Findings from this study suggest that this approach limits the relevance of these models to actual patients.
Researchers observed that some immunodeficient lab models favour the development of neurons and oli-
Doing more for Manitobans
While this test is available in 70 per cent of clinics across Canada, it’s available in less than 30 per cent of Manitoba facilities. As a result, for many patients, heart failure is being diagnosed only at later stages, negatively impacting both the patient prognosis and the need for health system resources.
Second, echocardiography is the cornerstone imaging test for diagnosis and follow-up of heart failure patients and must be linked to their clinical care. However, access to echocardiography in Manitoba is among the lowest in Canada. This limits the effective and timely follow-up of patients, increasing the likelihood they will eventually appear at a hospital emergency room requiring urgent care.
Third, we need a much better coordinated provincial cardiac care system to ensure better screening, diagnosis and follow-up throughout the province. This should be the responsibility of Cardiac Sciences Manitoba (CSM), but its current structure is fragmented, preventing the integration necessary to deliver consistent cardiac care province-wide.
We urgently need to achieve the CSM goal of establishing a province-wide cardiac hub with central referral and appointment services so heart failure patients get the care they need close to home that will keep them in better health and out of hospital.
CSM, together with Heart & Stroke and the HeartLife Foundation, have combined to alert the Manitoba government of the urgent need to improve services for Manitobans with heart failure and to urge action as quickly as possible. The government has acknowledged the importance of co-ordinated cardiac care and we look forward to working together to achieve that goal.
Better access to diagnosis and care for Manitobans with heart failure through a coordinated system would be a win for us all by reducing the time patients need to spend in hospital and keeping them away from our emergency departments, while allowing them to live easier and longer lives. What better goal could we have? n H
Dr. Shelley Zieroth is a cardiologist in Winnipeg, Director of the St. Boniface Hospital Heart Function Clinic and Past President of the Canadian Heart Failure Society. She is an internationally recognized clinical trialist who focuses on improving patient outcomes in heart failure.
godendrocytes from hiPSC-NPCs at the expense of the development of astrocytes, while astrocytes are the most common cell type that develop in immunocompetent models.
“Immunodeficient models seem to lack the intricate interplay between the transplant recipient’s immune system and the transplanted cells, resulting in an altered ratio of cells compared to what is expected in patients,” explains Dr. Fehlings, who is also the
Head of the Spinal Cord Program at UHN’s Toronto Western Hospital and a professor in the Department of Surgery at the University of Toronto.
Further investigation also found that immunodeficient lab models show lower levels of cell death and stress along with higher levels of nervous system development and cell growth signalling.
Although it is not possible to replicate every aspect of SCI in preclinical models, this work highlights the need for more comprehensive models that better reflect the immune system’s role with transplant survival. Successfully addressing this challenge will bring cell therapies for SCI closer to clinical application than ever before.
The lead author of this study is Dr. Zijian Lou, a graduate research student at the Krembil Brain Institute in the Fehlings Lab. n H
England’s diabetes prevention program as blueprint for Canada
Canada can learn from England’s successful diabetes prevention program to build its own programs to tackle diabetes prevention across the country, argue authors in an analysis in CMAJ (Canadian Medical Association Journal)
In 2022, Canada released a diabetes framework that calls on provincial and Indigenous governing bodies to build community-based programs to help address increases in new cases of diabetes.
Based on evidence showing positive preventive benefits of diet and exercise on type 2 diabetes, England’s National Health Service (NHS) created publicly funded prevention and remission programs that have been successful.
The initiative has reduced diabetes rates from 64.3 to 53.4 per 1000 person-years in people with prediabetes and is projected to save $121 million over 35 years.
A Quebec-based team of clinician–scientists, legal experts, and health economist researchers, with funding from the Canadian Institutes of Health Research, several of whom are Diabetes Quebec professional council
members, have partnered with leaders from the NHS to investigate whether a similar program could be rolled out in Quebec. The idea is to start in Quebec and trigger action in other parts of Canada. It would be akin to what happened with Quebec’s early child education and care program, which Canada’s federal government has adopted to deliver similar programs across the country.
“Our goal is to build successful programs in Quebec that will catalyze programs across Canada,” writes Dr. Kaberi Dasgupta, Research Institute of the McGill University Health Centre, Montréal, Quebec, with coauthors.
“In our view, if 1 province successfully builds a program, it will catalyze others and attract federal funding.”
As another example of change in one part of the country leading to change in other parts, medicare, which was originally a provincial initiative in Saskatchewan, was rolled out nationally and is the basis of Canada’s publicly funded health systems.
“Building diabetes prevention and remission programs across Canada: learning from England” was published June 16, 2025. n H
Air pollution may increase epilepsy risk, new study suggests
Anew study reveals air pollution may contribute to the development of epilepsy, a brain condition that causes seizures. Published in Epilepsia, researchers at London Health Sciences Centre Research Institute (LHSCRI) and Western University’s Schulich School of Medicine & Dentistry found an association between long-term exposure to air pollution with new cases of epilepsy in adults in Ontario.
The study utilized data from the Canadian Urban Environmental Health Research Consortium which was linked to Ontario’s health administrative databases and analyzed at ICES. It began with the population of Ontario residents with a health card as of January 1, 2010. After focusing on adults without other major health conditions like brain cancer, researchers found 24,761 new epilepsy cases over six years. The study found that higher exposure to fine particulate matter, a component of air pollution, increased the likelihood of developing epilepsy by 5.5 per cent, while ozone, another component of air pollution, increased it by 9.6 per cent.
The study is the first time databases were used to make a direct connection between new cases of epilepsy in adults in Ontario and long-term exposure to air pollution. “Our hope is that this research can help inform environmental policy and ensure there are adequate resources and health care for epilepsy in areas that have significant air pollution,” says Dr. Jorge Burneo, Scientist at LHSCRI, Neurologist at London Health Science Centre (LHSC) and Professor at Schulich School of Medicine & Dentistry.
According to the World Health Organization (WHO), 99 per cent of the world’s population breathes air that exceeds WHO air quality limits. Scientific studies have linked air pollution to a wide variety of health issues and now there is additional evidence on its association with new onset epilepsy.
“THIS RESEARCH IS IMPORTANT BECAUSE IT HAS THE POTENTIAL TO DRIVE CHANGES THAT COULD ULTIMATELY REDUCE THE NUMBER OF NEW EPILEPSY CASES.”
Epilepsy is one of the most common neurological disorders worldwide, affecting about six in every 1,000 people at any given time. People with epilepsy are three times more likely to die earlier in life and some do not respond to anti-seizure medications.
“This research is important because it has the potential to drive changes that could ultimately reduce the number of new epilepsy cases,” says Tresah Antaya, PhD, Postdoctoral Associate at Western University in the Department of Clinical Neurological Sciences. “We know seizures
can significantly affect quality of life – limiting a person’s ability to work in certain industries, drive, or live independently. Our hope is that this work will contribute to a future where fewer people are affected by epilepsy.”
As a next step in this work, the research team plans to explore the effects that forest fires may have on health, including epilepsy.
“Our environment plays a big role in our health,” adds Dr. Burneo. “Our research aims to better understand these connections with a goal of improving both planetary and human health.” n H
Clinical trial significantly improves detection of hidden blood clots in stroke patients
Agroundbreaking clinical trial led by London Health Sciences Centre Research Institute (LHSCRI) and Western University’s Schulich School of Medicine & Dentistry may enhance how medical professionals detect hidden blood clots responsible for strokes. The study, published in The Lancet Neurology, is the first to show that extending imaging to include the heart within minutes of a patient’s arrival to hospital with an acute stroke significantly improves the ability to determine the stroke’s underlying cause. This innovative diagnostic approach can be used to determine an effective and tailored treatment plan for preventing future strokes.
Strokes caused by blood clots or other mechanisms that obstruct blood flow in the brain account for about 85 per cent of all strokes. In this study, scientists from LHSCRI and Schulich Medicine & Dentistry
“IF THE CLOT ORIGINATED IN THE HEART, WE TYPICALLY USE BLOOD THINNERS TO PREVENT FUTURE STROKES.”
set out to determine whether strokes with undetermined causes could be identified using computed tomography (CT) scans that include images of the heart and aorta, a main blood vessel.
“Identifying where the clot came from is essential because it determines the safest and most effective treatment,” says Dr. Luciano Sposato, Scientist at LHSCRI, Head of the Southwestern Ontario Regional Stroke Centre at London Health Sciences Centre (LHSC), and Professor of Neurology at Schulich Medicine & Dentistry. “If the clot originated in the heart, we typically use blood thinners to prevent future strokes.”
The clinical trial included 465 patients admitted to LHSC’s Universi-
ty Hospital who were treated for an acute stroke or transient ischemic attack. The study found that using the extended CT scan increased the detection of blood clots in the heart by 500 per cent compared to standard imaging practice. They also found the extended CT scan did not delay completion of CT imaging in these emergency situations. The study found one clot for every 14 patients scanned with the new approach.
“If we did not extend the CT scan, some of these blood clots may not have been found and these strokes would have been classified as having an undetermined cause,” says Dr. Rodrigo Bagur, researcher at LHSCRI, Cardiologist at LHSC, and Professor at Schulich Medicine & Dentistry. n H
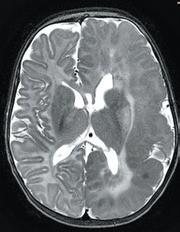
Dr. Prakash Muthusami runs through his typical preparation for a procedure. Inset: Brain MRI image showing Maryam’s enlarged left hemisphere.
2024
Canada’s first endovascular hemispherectomy
Maryam experienced unrelenting seizures from her very first moments of life.
Born in December of 2023 in Toronto, Maryam was admitted to the NICU after doctors noticed unusual twitching on the right side of her body.
Her seizures would occur about every two minutes – sometimes every few seconds – leaving her struggling to feed and even breathe.
An MRI revealed that Maryam had hemimegalencephaly, a rare neurological condition where one half of the brain is enlarged and can cause epilepsy, developmental delays and muscle weakness. In this case, it had affected the left hemisphere of Maryam’s brain. She was immediately rushed to The Hospital for Sick Children (SickKids).
Clinical tests suggested Maryam had tuberous sclerosis complex (TSC) – a rare genetic disorder that can cause atypical tissue growth in multiple organs, including the brain. In combination with the malformation in her brain and ongoing seizures that became uncontrollable, Maryam’s parents feared the worst.
“At that point, we thought she’d have debilitating seizures for the rest of her life, that she wouldn’t be able to live like other kids,” said Maryam’s mother, Muzna Nafees.
But that wasn’t how Maryam’s story turned out. Instead, her case would go
on to mark a turning point in paediatric epilepsy care in Canada. Facing numerous obstacles for treatment, her medical team at SickKids had to think differently, turning to a novel approach – the first of its kind in Canada for children – which changed the course of her life.
“In the early days, we were faced with a child who was seizing hundreds of times a day, and we needed to act fast,” says nurse practitioner Ivanna Yau, who coordinates the Epilepsy Surgery Program at SickKids and was a close contact for Maryam’s family throughout their journey.
As both an advocate and key point of connection for families, Yau spearheaded the coordination of several different specialties to figure out a new approach for Maryam.
“That level of collaboration and trust from Maryam’s family is what allowed us to move forward,” says Yau.
A clinical team including neurosurgery, neurology, and neurointerventional specialists assembled quickly to discuss possible next steps.
Despite repeated attempts at controlling Maryam’s seizures with medication, none of the available medications were effective in significantly decreasing them or their impact on her body.
Epilepsy that doesn’t respond to medication – also known as intracta-
ble epilepsy – can be treated with surgery, and the most common surgery to treat conditions like Maryam’s is a functional hemispherectomy. This type of surgery disconnects the part of the brain that is having seizures from the rest of the brain. While the approach has a long-established track record of success in children, it is highly invasive and carries significant risks – particularly for infants as young as Maryam.
Planning for SickKids’ first endovascular hemispherectomy involved using EEG-lead placements on a neonatal mannequin for continuous recording during the staged procedures (pictured left) and mapping out Maryam’s brain arteries using MR Angiography (right).
“With the open surgery approach, there is a major risk of blood loss requiring a transfusion. In a very young infant like Maryam, the risks are even greater. But there was no established alternative at the time,” says Maryam’s neurosurgeon, Dr. James Rutka.
Over the course of the next few months, the team did their best to keep Maryam’s seizures at bay while she could get stronger – the hope was that she could undergo surgery in the future. But Maryam would go on to continue to have significant daily seizures – at times spreading to the rest of her body – an alarming shift that
suggested this increase in epileptic activity might now be affecting her previously healthy right hemisphere.
The clusters were so frequent and resistant to medication that Maryam’s oxygen levels dropped. There was even a time when Maryam had to be placed on a ventilator temporarily to help her breathe. SickKids’ Paediatric Advanced Care Team (PACT) were engaged to provide additional palliative support in what were expected to be her final days with her family.
But then, Maryam did something unexpected.
“She started feeding from a bottle, even without any feeding tubes. It showed us she wasn’t ready to give up,” says Nafees.
Maryam’s team held an emergency meeting, and turned their attention to a novel, minimally invasive surgery that had only been attempted a handful of times globally before.
“Things developed quickly, and we changed our focus. The fact that we had a multidisciplinary team, and an outstanding neurointerventionist like Dr. Prakash Muthusami, enabled us to explore other, more creative possibilities for Maryam’s case,” says Rutka.
The novel procedure was an endovascular hemispherectomy, and while it was still an emerging approach, the published literature was promising.
Continued on page 19
Maryam at SickKids in February
Cardiac patients deserve more for heart surgery recovery.
Mepilex Border Post-Op Dressing has been clinically shown to optimize the patient healing journey. This highly absorbent pad with a shower proof backing can stay on for up to 14 days and helps support undisturbed wound healing.
Learn more at Molnlycke.ca
Clinical trial for teens shows improved health outcomes for type 1 diabetes
Anew study in teenagers with type one diabetes shows promise in reducing chronic kidney disease and informing future precision care.
A clinical trial involving adolescents with type 1 diabetes (T1D) has found a combination therapy may reduce chronic kidney disease and improve health outcomes. The findings could help guide more precision care for young people with T1D.
Led by Dr. Farid Mahmud, Associate Scientist in the Translational Medicine program and Staff Physician in the Division of Endocrinology at The Hospital for Sick Children (SickKids), and published in Nature Medicine, the study evaluated a therapy that combines standard insulin treatment with the investigational drug dapagliflozin. Results of this combination therapy showed improved blood sugar control and kidney function, and reduced weight gain in adolescents with T1D.
T1D is a chronic autoimmune
“OUR FINDINGS SHOWED THAT ADOLESCENTS WHO RECEIVED THIS COMBINATION THERAPY WERE ABLE TO IMPROVE MANY SYMPTOMS TYPICALLY ASSOCIATED WITH INSULINMANAGED TYPE ONE DIABETES.”
condition that causes the pancreas to stop producing insulin, a hormone that controls blood sugar levels. While most people with T1D are diagnosed as adults, the condition often starts in childhood and early adolescence.
T1D requires insulin therapy throughout a person’s life, which can lead to side effects such as weight gain and chronic kidney disease. In the trial, participants who received dapagliflozin alongside insulin had fewer of these side effects and better overall health outcomes.
“Our findings showed that adolescents who received this combination therapy were able to improve many
symptoms typically associated with insulin-managed type one diabetes,” says Mahmud. “This could inform a new early intervention strategy for the growing population of teenagers with type one diabetes.”
PATIENT PARTNER KEY TO TRIAL SUCCESS
While previous research has shown similar results in adults, Mahmud’s team focused on designing a clinical trial specifically for teenagers, a group often underrepresented in clinical trials. Hormonal changes, psychological development, and the shared responsibility between teens and their parents
for managing treatment protocols can make trial participation more complex for this age group.
To address these challenges, the research team worked closely with patient partner Lynne McArthur. Together, they enrolled 98 participants between 12 and 18 years old in the study, known as the ATTEMPT study, across three sites.
McArthur’s involvement in research began when one of her twin sons was diagnosed with T1D following a trip to the SickKids emergency department at just 18 months old. A few years later, his twin was also diagnosed. That experience led McArthur to become more involved in research efforts to improve diagnosis and treatment options for families like hers.
“Deciding to participate in a clinical trial is an important decision, but my goal has always been disease prevention. I knew that our participation could help build a future where children don’t get T1D,” says Lynne.
Now that her sons are older, McArthur continues to be involved as a patient advisor. She reviews recruitment materials and provides feedback on trial design, helping ensure the research stays connected to the lived experience of people managing T1D.
“Participating in research, whether in a trial or as an advisor, is hugely rewarding. With my experience as trial participant, I can see how the plans on paper would impact the real lives of people living with diabetes,” explains McArthur.
MOVING TOWARD TAILORED TREATMENTS FOR T1D
The trial provides a valuable foundation for future research into precision medicine for children and adolescents with T1D. One of those opportunities is the Empowering diVERse Youth with diabetes thrOugh precisioN mEdicine, or ‘EVERYONE’, study, which builds on this approach by focusing on how individual factors influence treatment response.
Aligned with Precision Child Health, a movement to individualize care for patients and families at SickKids, the EVERYONE study will explore how a youth’s unique characteristics such as their insulin sensitivity, immune response, metabolism, genetics and social health impact how they respond to insulin treatment. By understanding these differences between patients, the team hopes to one day inform tailored treatments to optimize outcomes for youth with T1D.
“This is opening exciting new treatment opportunities for youth with type one diabetes,” says Mahmud, who is also an Associate Professor in the Department of Paediatrics and Institute of Medical Science at the University of Toronto. “We’re giving them options that are grounded in science and designed to help them thrive throughout their lives.”
This study was funded by Breakthrough T1D (formerly known as Juvenile Diabetes Research Foundation, JDRF) and Canadian Institutes of Health Research (CIHR) Strategies for Patient Oriented Research (SPOR). n H
Jade Vyfhuis & Marlene Leung work in communications at Unity Health.
Heart Program.
Sunnybrook leads in novel approach to controlling treatmentresistant high blood pressure
With nearly 25 per cent of Canadians living with high blood pressure, Sunnybrook Health Sciences Centre is using a new minimally invasive procedure to help patients reduce their risk of heart attack and stroke.
About a third of those with high blood pressure have ‘uncontrolled hypertension’, a condition in which high blood pressure levels continue despite treatment. Renal denervation is a minimally invasive therapy to safely and effectively reduce blood pressure in patients with uncontrolled hypertension.
The Sunnybrook team uses radio-frequency heat energy, delivered by a catheter, to disrupt electrical signals travelling to and from the kidneys through the renal nerves. Renal nerves help to regulate blood pres-
sure by influencing kidney function; reducing their activity causes blood pressure to lower and become stable in most patients.
“Our first line of treatment if you have high blood pressure is always lifestyle changes, like weight reduction, more physical activity and decreasing alcohol and sodium, in addition to medications,” explains Dr. Mina Madan, interventional cardiologist and medical director of the cardiac catheterization laboratory for Sunnybrook’s Schulich Heart Program. “When this course of action doesn’t sufficiently lower your blood pressure, renal denervation is proving to be an excellent option and a new addition to the toolkit for lowering uncontrolled high blood pressure. In our experience, it has been a safe and effective approach for most patients.”
Since beginning the program in 2023, Dr. Madan and her multidisciplinary team have selected patients with resistant blood pressure who have been taking at least two or three medications to control their blood pressure without success. Following the one-to-two-hour procedure, patients remain in hospital overnight.
To date, 11 patients have been treated, with catheters obtained with support from generous donors to the New Device & Practice Fund at the Sunnybrook Foundation.
“Uncontrolled high blood pressure is one of the leading risk factors for heart disease and premature death. Renal denervation offers a great option for so many who have been taking prescribed medication and it’s just not working,” adds Dr. Madan. “This has the potential to impact thousands of lives in Canada.” n H
Dr. Mina Madan, interventional cardiologist and medical director of the cardiac catheterization laboratory for Sunnybrook’s Schulich
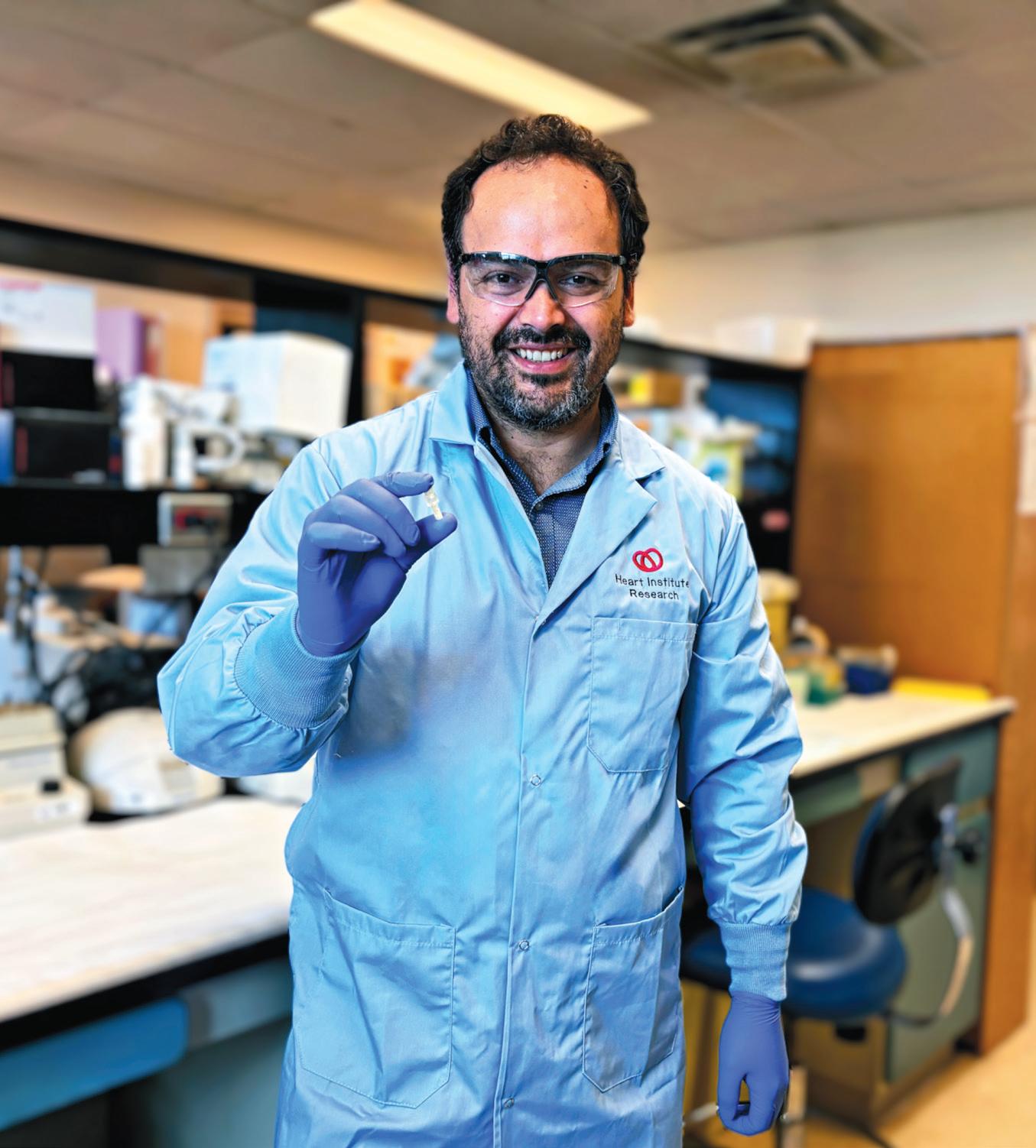
Churro-inspired innovation that could transform bypass surgery
arcelo Muñoz was waiting in line at a festival food truck, eyeing a batch of fried churros, when inspiration struck – an idea so sweet it could mark a seismic shift in the future of coronary artery disease treatment.
A pharmacist and chemist in the Bio-Engineering and Therapeutic Solutions (BEaTS) Laboratory at the Ottawa Heart Institute, Muñoz (PhD) and BEaTS director Emilio Alarcón, PhD, had spent weeks with their team exploring new ways to make
bypass surgery procedures safer and more efficient using bioengineered materials.
“We’d been trying to figure out how to create blood vessels for use inside the body quickly and reliably,” he recounted. “That churro machine was
the spark we needed that showed a possible path forward.”
As dough was extruded from a machine, Muñoz observed how it wrapped perfectly around a central rod to form a hollow cylinder before being dropped in bubbling oil, crisping
into a golden, cinnamon sugar-coated tube.
“I thought – why not do something similar for a blood vessel,” he said. That churro-stand moment became a turning point. In the years since, Muñoz, Alarcón, and the BEaTS team have worked to miniaturize the process and adapt it using biopolymers – naturally derived or engineered materials that are safe for use inside the body.Churros are deep-fried dough pastries, typically coated in sugar and often served with chocolate or caramel dipping sauce.
Affectionately dubbed The Churro Project among colleagues, Muñoz’s idea is now the basis for a bold new device designed to fabricate vascular grafts directly inside the human body – potentially eliminating the need for open-chest surgery.
Their concept was recently detailed in the peer-reviewed journal Advanced Materials Technologies.
THE NEED FOR INNOVATION
Each year, thousands of patients in Canada undergo coronary artery bypass graft (CABG) surgery.
The standard procedure involves removing a healthy blood vessel from elsewhere in the patient’s body and grafting it onto the heart to bypass blocked arteries. It’s like making a detour around a road that’s closed.
But CABG surgery isn’t perfect. Sometimes it’s hard for doctors to find the right kind of blood vessel to use, and the grafts (replacement blood vessels) can fail over time.
Marc Ruel, MD, head of minimally invasive cardiac surgery at the Ottawa Heart Institute, estimates about 80–90 per cent of his CABG patients have ideal vessels for grafting. But for the remaining 10–20 per cent – often older adults or individuals with diabetes – the available vessels are suboptimal, potentially affecting how long the surgical outcome remains effective or successful over time.
At the Heart Institute, Ruel and his team perform about 1,000 CABG procedures annually, meaning 100 to 200 patients may face increased risk due to less-than-ideal grafts.Nationwide, with about 25,000 CABG surgeries performed annually in Canada, this means that between 2,500 and 5,000 patients may undergo surgery using less-than-optimal conduits – highlighting a clear need for innovation in this field.
“These people try to manage their condition with medication or stents,” said Ruel. “But for many, especially those with diabetes, bypass surgery is still the most effective option.”
The risks of CABG extend beyond graft availability.
As Ruel explained, traditional CABG procedures often require “cracking open” the chest through a sternotomy – an incision that splits the breastbone. While newer, minimally invasive techniques aim to avoid this step, sternotomies remain common and are associated with longer recovery times and higher complication rates.
A MINIATURE BREAKTHROUGH WITH ENORMOUS POTENTIAL
Their innovation centres on a device no larger than a thumb.
As described in Miniaturized Devices for On-the-Spot Generation of Small-Diameter Vascular Grafts, the nozzle of the device can extrude a synthetic vascular graft from a liquid biopolymer in real time.
As the polymer passes through the nozzle – imagine gelatin squeezing through the tip of a glue gun – it forms a tube with fibres aligned in a circular pattern, closely mimicking the natural structure of blood vessels.
To cure the polymer into a solid tube, the team uses a small optical fibre to shine blue light on the material as it exits the nozzle. It’s like how dentists use a special light to harden a filling, but on a much smaller and more precise scale.
Under the leadership of international visiting student Manuel Calderon, the team also developed a “landing pad” that can attach to the inside of the aorta. This pad could further enable doctors to perform CABG surgery with just a small incision, a technique the Ottawa Heart institute has pioneered on the global scene.
FROM FOOD TRUCK TO THE OR
Though the research is still in its early stages, the implications are significant.
Muñoz and his team envision a future where the device is deployed via catheter, like how TAVI (transcatheter aortic valve implantation) transformed valve replacement. Once in place, surgeons in the OR could effectively “print” a new blood vessel directly onto the heart.
For now, the work remains preclinical. The team has tested the nozzle in lab settings, assessing how well the material holds up, how it interacts with blood, and whether it supports the growth of new blood vessels – all with promising results.
The current material – gelatin methacrylate – was chosen for its affordability and responsiveness to light, making it ideal for rapid prototyping. But it’s
not the final solution. The team plans to shift toward peptide-based biomaterials that encourage cell growth and long-term integration into the body.
Muñoz and his colleagues in the BEaTS Laboratory believe that with further testing, better materials, and the right support, their device could one day offer a minimally invasive lifeline to patients who currently have no surgical option. n H
Left: Piped into their signature ridged tube shape, churros are the inspiration behind a bold new breakthrough from the BEaTS Laboratory at the Ottawa Heart Institute. Right: First author Deyanira Hernandez Sanchez, a PhD student in biochemistry at the Ottawa Heart Institute, holds the churro-inspired innovation between her thumb and index finger. Primary care and Urologist level resource
to prostate cancer
Canada needs to move from patchwork to progress to unlock the full potential of our national framework for diabetes
By Glenn Thibeault
Over four million Canadians live with diabetes – with many more undiagnosed – and that number continues to climb. This chronic condition affects almost every family and stretches our healthcare system in ways that are both urgent and preventable.
While the federal government took a promising first step by implementing the Framework for Diabetes in Canada in October 2022, the work is far from over. What Canada needs now is political will, targeted investment and a commitment to three fundamental priorities: alignment, accessibility and affordability. Without strategic alignment between federal, provincial and territorial governments, the promise of the national framework remains aspirational. Accessibility to timely care, medications and life-saving devices remains uneven across jurisdictions. And with
inflation and international pharmaceutical tariffs looming, affordability is becoming an even more precarious reality for Canadians who rely on critical diabetes supports.
If we are serious about reducing emergency room visits, preventing amputations, improving quality of life and managing the financial burden of diabetes on our health system, we need a comprehensive approach rooted in these three priorities.
The federal government has a strong role to play.
ALIGNING SYSTEMS, STANDARDS AND SUPPORT
Healthcare may be a provincial jurisdiction, but chronic disease management requires consistency nationally. Diabetes doesn’t respect provincial borders, and neither should our response.
The Framework for Diabetes in Canada outlines a strong foundation,
but implementation has been uneven and under-resourced.
For example, access to medications and continuous glucose monitors (CGMs) differs vastly between Nova Scotia, British Columbia and Northern Ontario. Some provinces have signed bilateral agreements under the new pharmacare initiative that expands access and affordability while many other regions are still waiting for similar agreements.
This patchwork approach leaves too many Canadians behind.
What we need is federal leadership that goes beyond coordination toward action, including meaningful funding to incentivize provinces and territories to implement the framework fully and consistently. It also means building mechanisms to share best practices and evaluate outcomes so that a person in rural Newfoundland and Labrador receives the same standard of care as someone in downtown Toronto.
IMPROVING ACCESSIBILITY TO MEDICATIONS, DEVICES AND CARE
Accessibility to medications and life-saving technologies is another critical piece of the puzzle. CGMs, insulin pumps and personalized medications are more than conveniences – they are life-changing for people living with diabetes. They help prevent complications, reduce hospital visits and empower individuals to manage their conditions with dignity and control.
The recently announced national pharmacare program has the potential to dramatically improve access to medications, particularly for those without private insurance. However, the preliminary formulary does not yet reflect the reality of living with diabetes. A one-size-fits-all approach is insufficient. The federal list must include a broader range of medications and de-
By Marlene Yeung
A Stroke inspires hospital employee to go to medical school
rthur Tung was at the gym when he realized something was wrong. The night before that day in October 2023, he had had a terrible headache and struggled to use the apps on his phone. The 23-year-old chalked it up to not getting enough sleep, but when he went to meet his personal trainer, he couldn’t communicate.
“I couldn’t say ‘Hi’ and I couldn’t tell you what an object – like a water bottle – was. It was terrifying,” he said.
Tung was experiencing aphasia, a sign of stroke where a person’s ability to understand or formulate language becomes impaired due to damage to the brain.
Tung’s trainer called 911, and Tung was rushed to St. Michael’s Hospital where he was triaged as a stroke patient.
Tung had worked as a research assistant at St. Michael’s two years earlier.
“I was only mostly worried about my family’s reaction,” he said. “Otherwise I was calm because I had a lot of trust in St. Michael’s. I never had any doubt that I was receiving the best treatment.”
Neurologist Dr. Jose Danilo Diestro gave Tung a series of tests and determined he had an abnormal development of atherosclerosis, the buildup of plaque inside his artery walls. This plaque buildup likely caused an ischemic stroke or a transient ischemic attack, which in turn caused Tung’s aphasia. He was started on a standard treatment of dual antiplatelet therapy and statins.
While recovering, Tung had another bout of strong headaches. Additional tests revealed that he had antiphospholipid syndrome, an autoimmune disorder where the body mistakenly attacks phospholipids, which are essential for blood clotting. Antiphospholipid syndrome has no cure
and can cause serious complications, including stroke or heart attack. It can also lead to accelerated atherosclerosis.
After the diagnosis, Tung was put on blood thinners and educated on how to manage the syndrome. Within days, he started to regain his speech.
“I was unlucky to have this condition, but I feel like everything else was lucky,” Tung said. “My presentation was very mild, I was treated at St. Mike’s of all places. I met physicians and clinicians from different departments – neurologists, hematologists, interventional radiologists – a full spectrum, and I never had a bad interaction with any of them.”
STROKE IN YOUNG ADULTS
Neurologist Dr. Adam MacLellan, who also treated Tung, said that while young stroke survivors may have an earlier, more rapid physical
recovery than older patients, there can be a great deal of “invisible impairment,” such cognitive impairment, fatigue, executive dysfunction, post-stroke depression and anxiety. What’s more, stroke often impacts young patients during a time when they are developing their personal lives and careers.
“Stroke recovery can be isolating for a young adult. Patients may not show obvious physical impairment anymore, and many people do not realize that young individuals can even experience a stroke,” MacLellan said.
“We at Unity Health and the surrounding GTA hospitals are fortunate to have great colleagues in rehabilitation who can address how to best help young stroke survivors in their recovery, and help minimize the disruption to their life trajectory as much as possible, setting them up to lead long, fulfilling lives.”
Glenn Thibeault is the Executive Director of Government Affairs, Advocacy and Policy for Diabetes Canada.
vices to accommodate individualized care plans developed between patients and their healthcare providers.
Some provinces are moving in the right direction – Manitoba’s agreement added 18 additional medications to the federal background list, for instance – but this is not yet standard. Without inclusive formularies, patients are forced to ration medications or rely on less effective alternatives, jeopardizing their long-term health and adding stress to an already overwhelmed health system.
Another critical area to address is the structure of the federal diabetes device fund, which was announced alongside pharmacare agreements. While welcome, the funding is time-limited and unclear in scope. What happens after four years, when the money runs out?
Without sustained investment, we risk pulling the rug out from families who depend on these devices for dayto-day survival.
PRIORITIZING AFFORDABILITY IN AN UNCERTAIN GLOBAL MARKET
Affordability must be a guiding principle across all diabetes policies. Rising inflation, shifting pharmaceutical markets and international trade dynamics threaten access to affordable medications for millions of Canadians.
Consider the potential impact of pharmaceutical tariffs. Many essential diabetes medications and devices – such as Ozempic, insulin pumps and test strips – are either manufactured in or processed through the U.S. With growing uncertainty around American policies, including the possible roll-
back of insulin price caps under this U.S. administration, people living in Canada may face steep price increases and reduced availability.
Generic drugs may offer long-term relief – Canada could approve generic Ozempic alternatives by 2026 – but immediate protections are still necessary. The federal government must act now to shield Canadians from the fallout of global pharmaceutical disruptions.
When people can’t afford their medications, they don’t take them. They cut doses, delay refills or go without entirely. The results are predictable: hospitalizations, amputations, complications and premature death.
A CALL FOR LEADERSHIP
It is encouraging that the federal government has shown initiative by launching the diabetes framework and pharmacare program. But implementation without alignment, access without equity, and affordability without sustainability are not enough.
The costs of inaction, both financial and human, are far too high. Canada has the tools. It now needs the political will to finish the job. n H
National Caucus Chair, MPP and Minister of Energy in Ontario.
CHANGING LIVES
Before his stroke, Tung had been in the process of applying for medical school, an idea he had considered for a long time. The care he received at St. Michael’s re-confirmed his desire to become a doctor.
“I was impressed with both the clinicians’ medical knowledge, but also the communication and non-technical skills needed to interface with patients. Dr. Diestro always took the time to explain everything thoroughly to me in a kind but professional way,” he said.
Tung began interviewing with medical schools a few months after being discharged.
He was accepted into the University of Alberta, where he’s finishing up his first year and looking forward to becoming a clerk and interacting with patients. He’s even considering
pursuing a specialty in neurology, hematology or rheumatology – the three specialties most closely related to his own condition.
“I am one of thousands of Dr. Diestro’s patients, and he’s just in the beginning of his career. He’s going to go on to see thousands and thousands more patients. He will be changing lives, just like how he changed mine. I want to do the same.”
Diestro is equally inspired by Tung.
“I feel privileged to be part of Arthur’s care. He is an impressive young man! Not many people can take the Casper exam after having a stroke. He also decided to write his own case report. These are testaments to his strong will and dedication,” said Diestro. “I look forward to becoming his colleague once he finishes medical school. I hope he considers U of T Neurology for residency when the time comes.” n H
(L-R): Arthur Tung, a medical school student studying at the University of Alberta, is pictured with St. Michael’s Neurologist Dr. Danilo Diestro. Diestro was one of the physicians who cared for Tung when Tung was rushed to St. Michael’s for a stroke in 2023.
Glenn Thibeault is the Executive Director of Government Affairs, Advocacy and Policy for Diabetes Canada. He is also a former MP,
Marlene Yeung works in communications at Unity Health.
Photo: Katie Cooper
Improving the safety of ventilation
Scientists at UHN have tested a method to protect critically ill patients who need help breathing with a ventilator against complications such as damage to the diaphragm and lungs. When patients rely fully on machines to breathe, their diaphragm – the main muscle used in breathing –
When critically ill patients require a ventilator to breathe, their breathing muscles, especially the diaphragm, can become inactive. This inactivity can lead to complications such as lung collapse and diaphragm injury. Stimulating the diaphragm nerve may help prevent lung and muscle damage in these patients.
can become weak or even injured from lack of use. Maintaining diaphragm activity during ventilation may help prevent these complications, enhance circulation and preserve muscle mass and function.
Stimulation of the nerve that provides motor control of the diaphragm – called diaphragm neurostimulation –is a way to make the diaphragm muscle contract without the patient having to breathe on their own.
However, the feasibility, tolerability and safety of preventing diaphragm inactivity with temporary, continuous neurostimulation during ventilator use have not been investigated.
A Phase 1 clinical trial was conducted to assess the feasibility of this technique for up to seven days. The trial involved 19 participants recovering from lung surgery or experiencing severe lung failure. Neurostimulation was applied during periods when the patients were not breathing on their own.
Results showed that 95 per cent of participants maintained adequate diaphragm activity during the first 24
hours. Throughout the trial, all participants sustained sufficient diaphragm activity when stimulation was needed, demonstrating the feasibility of this procedure.
Importantly, the treatment was well-tolerated with no serious complications. Patients also showed an increase in diaphragm thickness and the likelihood of diaphragm atrophy appeared lower than in those who did not receive stimulation in past cases.
COULD PREVENT LONG-TERM DAMAGE, INCREASE THE CHANCE OF SURVIVAL
“These findings indicate that diaphragm neurostimulation is highly feasible in patients receiving mechanical ventilation,” says Dr Ewan Goligher, a Senior Scientist at UHN’s Toronto General Hospital Research Institute and senior author of the study.
First author of the study is Dr. Idunn Morris, a postdoctoral researcher at UHN and a faculty member at the University of Sydney.
“This method could help prevent long-term damage, increase the chances of survival and improve recovery for ventilated patients,” adds Dr. Goligher, who is also an associate professor of Medicine and Physiology at the University of Toronto.
Future clinical trials are required to confirm the long-term safety and effectiveness of this intervention in critically ill patients, with a Phase 2 clinical trial of this treatment strategy getting underway at UHN and other centres in the United States and Canada.
Results from a Phase 3 trial have been recently published and indicate that neurostimulation helps patients on prolonged ventilation wean off faster, strengthen breathing muscles and gain more days alive and free of mechanical ventilation, highlighting the potential benefits of this technique for patients in critical care who have difficulty weaning from mechanical ventilation.
This work was supported by the National Sanitarium Association, Interdepartmental Division of Critical Care Medicine and UHN Foundation. n H
Canadian first: One-of-a-kind imaging platform for mental health
The Royal has received a $1.9 million grant from Brain Canada to launch a one-of-a-kind brain imaging platform – the first of its kind in Canada.
This major support will help build a new research tool called the BIC Advanced Multi-modal neuroimaging Platform for Psychiatry (or BIC-AMPP) at The Royal’s Brain Imaging Centre. The platform will bring together specialized equipment, expert staff, and pioneering research to enable simultaneous MRI, PET, and EEG imaging. Using these three powerful techniques at the same time will give researchers a complete picture of the brain’s structure, function, chemistry, and electrical activity, and how these are disrupted in mental illness and addiction.
“This grant puts Canada at the forefront of brain research for mental health,” says Dr. Florence Dzierszinski, president and CEO of the University of Ottawa Institute of Mental Health
Research and vice-president of research at The Royal. “The extremely rich datasets generated through the BIC-AMPP are ideally suited for integration with AI tools, helping to transform our understanding of mental illness and improve care in the future.”
Recipients of the grant include a cross-disciplinary team of brain imaging experts led by Georg Northoff, and including Katie Dinelle, Florence Dzierszinski, Stuart Fogel, Natalia Jaworska, Tram Nguyen, Jennifer Phillips, Gayatri Saraf, Reggie Taylor, and Lauri Tuominen.
The Royal’s Brain Imaging Centre is a regional hub and leader in multi-modal brain imaging. Now, with the BIC-AMPP, it will become the first in Canada, and one of only three teams worldwide, with the advanced technology and expert staff needed to scan the brain in three different ways at the same time.
“This is an exciting step forward for brain imaging research in Canada,”
says Katie Dinelle, administrative director of The Royal’s Clinical Brain Research Centre. “This platform offers an extraordinary opportunity to build capacity and advance training in this challenging field, and unlock discoveries about our most complex organ.”
This project is funded through the Platform Support Grant program,
led by Brain Canada, supported by the Government of Canada and a handful of generous donors to The Royal.
The goal of the program is to strengthen the research infrastructure behind some of the country’s most promising mental health and neuroscience work. n H
From left: Dr. Florence Dzierszinski; Katie Dinelle, Dr. Viviane Poupon (Brain Canada); and Parlimentary Secretary for Health Maggie Chi.
As a former school principal, Jim has always looked at each day as an opportunity to learn something new. He still does. Now, as part of Christie Gardens, Jim is in a unique community that respects his passion for learning and invites him to share it with others.
New Cardiovascular Institute will improve heart health worldwide
The Vancouver Coastal Health Research Institute (VCHRI) is excited to expand its premier roster of research centres and programs with the addition of a new cardiovascular powerhouse. The Dilawri Cardiovascular Institute, a global centre of excellence, launched in June 2025. Its establishment was made possible by a record-setting $60 million philanthropic gift from the Dilawri Foundation.
Led by Dr. David Wood, a world-renowned cardiologist and head of the Division of Cardiology at Vancouver General Hospital, the Dilawri Cardiovascular Institute will provide exceptional cardiovascular care through advanced technology, evidence-based practice and a patient-centered approach. With dedicated infrastructure and a one-of-a-kind Innovation Fund, the Institute will have the capacity to accelerate clinical trials, develop new therapies and move breakthrough discoveries into patient care.
More than 200 clinicians, researchers, health care leaders and philanthropists gathered on June 5, 2025, to celebrate the historic launch of the Dilawri Cardiovascular Institute at Vancouver General Hospital.The Institute’s future home will be located on the 900 block of West 12th Avenue at Vancouver General Hospital. Learn more about the launch of the Dilawri Cardiovascular Institute.
“THE ESTABLISHMENT OF THIS NEW INSTITUTE SIGNALS THE BEGINNING OF A BOLD NEW ERA IN HOW WE TREAT HEART DISEASE, MENTOR THE NEXT GENERATION OF SPECIALISTS AND IMPROVE OUTCOMES FOR PATIENTS IN BRITISH COLUMBIA AND BEYOND.”
Bringing together internationally recognized leaders across multiple fields, the Institute will also build a collaborative network to connect with institutions and experts across Canada, North America and Europe. This highly collaborative environment will recruit top-tier talent, train early-career scientists and foster the next generation of cardiac innovators who will shape the global cardiac ecosystem for decades to come.
“The establishment of this new Institute signals the beginning of a bold new era in how we treat heart disease, mentor the next generation of specialists and improve outcomes for patients in British Columbia and beyond,” says Wood. “Our clinicians and researchers are focused on using new technology and discoveries to improve access to care, shorten wait times, improve outcomes, and decrease recovery times.”
“This milestone highlights our dedication to advancing cardiac research so that people with heart disease have a better chance to live longer and symptom-free, with hope and dignity.”
Core centres set new standards for research excellence across specialties
The new Dilawri Cardiovascular Institute is comprised of 16 specialized centres, including eight core research centres:
The Centre for AI, Data Science and Imaging, directed by Dr. Teresa Tsang, will build on years of expertise in data-driven analytics and advanced imaging, and integrate genomics to advance precision health and personalized medicine. The multidisciplinary team works together to harness largescale data and AI to improve cardiovascular disease diagnosis, treatment
and prevention. A cornerstone of the Centre is the AI Echo Core Lab, which enables large-scale, collaborative studies across local, provincial, national and international settings. Focused on real-world impact, the Centre aims to detect heart disease earlier, support clinical decisions, and tailor care using genetics, imaging and social factors, ultimately closing cardiac care gaps and improving outcomes for all British Columbians.
As an established Centre within VCH and UBC, the Centre for Cardiovascular Innovation (CCI) is dedicated to improving the health of patients with cardiovascular disease. Led by Brady Robinson, Jackie Chow and Elizabeth Grieve, CCI offers services to cardiovascular investigators to facilitate national and international clinical trials and provides physical and personnel infrastructure to enhance the research capacity of its member investigators.
The Centre for Cardiovascular Translational Science offers handson experiences that connect basic science, engineering and clinical applications. Under the guidance of Dr. Stephanie Sellers, trainees at the Centre are immersed in cutting-edge research projects, exposed to advanced technologies and mentored by leading multidisciplinary experts. Through tailored workshops and translational research training programs, the Centre cultivates a new generation of innovators equipped to transform cardiovascular health through scientific discovery, technological advancement and clinical impact.
The Centre for Pulmonary Vascular Disease is dedicated to furthering the
understanding of pulmonary hypertension: a severe and progressive disease that results in high blood pressure in pulmonary arteries, which carry oxygen-poor blood from the heart to the lungs. Directed by Dr. John Swiston and supported by Dr. Nathan Brunner, Centre researchers are actively involved in national and international clinical research trials, working on therapies that have shown the potential to dramatically change the disease course and improve patient quality of life.
The Centre for Structural Heart Interventions, overseen by Dr. David Wood and Dr. Scott Lim, employs cutting-edge minimally invasive techniques and exciting new treatments aimed at improving care and outcomes for patients, including early recovery following transcatheter aortic valve replacement and advanced interventions for tricuspid and mitral valve diseases. Guided by principles of equity and accessibility, the Centre ensures that life-saving procedures are available to diverse populations, striving to eliminate barriers to care and deliver outstanding outcomes.
The Centre for Thoracic Aortic Disease provides comprehensive, coordinated care for patients with thoracic aortic conditions under the guidance of Dr. Joel Price and supported by Dr. Ed Percy. Surgeon-scientists at the Centre specialize in complex aortic procedures, using advanced, innovative techniques to deliver timely and effective interventions. With a commitment to long-term monitoring, patients receive tailored follow-up and ongoing assessment. Program outcomes are continually evaluated, driving ongoing quality improvement and research.
The mandate of the Centre for Women’s Heart Health Research is to stop and prevent the progression of heart disease in women via a comprehensive outpatient risk reduction program. The Centre, directed by Dr. Tara Sedlak and Dr. Jackie Saw, comprises a team of experts on the identi-
fication and treatment of heart conditions, whose impressive catalogue of publications and ongoing research studies aim to increase the representation of women in clinical trials, with significant impacts on quality of care and patient outcomes.
SportsCardiologyBC strives to make exercise and athletics safer for everyone. Investigators lead studies that are exploring risk factors and warning signs for cardiovascular events, as well as optimal training processes. Dr. Saul Isserow leads the Centre, in collaboration with Dr. Nate Moulson and Dr. James McKinney. The Centre collaborates with local, national and international medical, health and athletic organizations to provide public education about the importance of cardiovascular health and safe participation in athletics.
The Dilawri Cardiovascular Institute will be a global centre of excellence – where care, research, innovation, and education converge in one fully integrated, world-class institute.]
In addition to these core centres, several emerging centres are under development, including the Centre for Cardiovascular Critical Care (Dr. Chris Fordyce and Dr. Gord Finlayson); the Centre for Cardiovascular Disease in the Young (Dr. Thomas Roston); the Centre for Cardiovascular Medical
Continued from page 8
Endovascular hemispherectomy
“Instead of traditional surgery, which would have required opening her skull and cutting connections in her brain, this approach allowed us to work through her blood vessels, minimizing risks and recovery time,” explains Dr. Prakash Muthusami, an interventional neuroradiologist at SickKids who led the eventual series of procedures and leads the hospital’s Neurointerventional Program.
As opposed to an open surgical procedure, the endovascular approach involves using catheters introduced inside blood vessels to selectively block blood flow to the abnormal areas of the brain, effectively “disconnecting” the problematic hemisphere while preserving healthy tissue.
The technique essentially targets dysfunctional areas of the brain, and by cutting the connection, protects the functioning half of the brain.
“At that point we had shifted drastically from comfort care to exploring potentially life-saving interventions,” says Yau. “Our role was to guide the family
through this innovative approach, and they put their trust in our team with something that was entirely new.”
Between February and April 2024, four carefully planned embolization procedures, spaced two to three weeks apart, successfully isolated Maryam’s left hemisphere.
“In the three cases in Washington, the endovascular approach bought them time while they waited for the more invasive surgery. Our hope was that this approach could do the same for Maryam time until she was strong enough for surgery,” says Muthusami.
“But we were amazed by how well she responded,” he says.
With each procedure, Maryam’s seizures became less frequent.
And at every step, the Interventional Neuroradiology team, Epilepsy and Neurosurgery teams worked together, using detailed electroencephalogram (EEG) and brain MRI scans to ensure precision and safety.
Now, months later, Maryam has not had a single seizure since July 2024.
Education (Dr. Parvathy Nair and Dr. Graham Wong); the Centre for Cardiovascular Health and Prevention (Dr. Nate Moulson); the Centre for Heart Rhythm Interventions (Dr. Jason Andrade); the Centre for Indigenous Cardiovascular Health (Dr. Miles Marchand); the Centre for Knowledge Translation and Implementation Science (Dr. Katherine Kulyk); and the Centre for Minimally Invasive Surgery (Dr. Richard Cook). n H
“She went from having seizures about every two minutes to having one or two per day, to then having zero, which is incredible,” says Muthusami.
In the months that followed, Maryam began meeting milestones her parents never thought possible. She learned to sit up, eat solids and engage with her environment.
“Because of the procedure, she’s making developmental gains that were not previously possible due to her unrelenting seizures. And she’ll now be able to develop at her own pace,” says neurologist, and Director of the SickKids Tuberous Sclerosis Complex Program, Dr. Lauren Sham, who will continue to follow Maryam until she’s 18 years old.
Maryam now understands two languages and loves to hum a tune with her mom at bedtime. During a threemonth family trip to India in the summer, she amazed relatives with her bright, playful personality and curiosity about the world around her.
In December 2024, Maryam celebrated her first birthday – a milestone
her parents once feared she would never see.
“She’s a miracle,” Muzna shared, beaming. “All the nurses would call her our little miracle baby. She now has her entire life ahead of her and it’s the greatest gift.”
Long-term monitoring will be crucial, say Muthusami, Sham and Rutka – but the outcomes of the procedures have opened new potential pathways for the future.
“This approach has shown us what’s possible with minimally invasive techniques for Precision Child Health,” Muthusami says. “It’s a major milestone in paediatric epilepsy care and Maryam’s journey could pave the way for other infants facing similar circumstances.”
While the future remains unknown, one thing is certain: Maryam is here and she’s thriving. Muzna says their family can now look forward to what’s next.
“She will be able to learn, she will play, she will do things other children can do,” says Muzna. “How simply beautiful is that?” n H
AI receptionist answers the call for busy medical clinics
A Hospital patients/family members test drive AI phone software co-created by HHS doctor
Hamilton Health Sciences (HHS) rheumatologist, a Niagara family doctor and a Toronto-area software engineer have teamed up to develop a high-tech remedy for busy medical clinics – an artificial intelligence (AI) receptionist that can answer unlimited phone calls at once so no caller is ever on hold or transferred to voicemail.
Their Strello Health AI-powered phone software sounds so realistic, it’s hard to tell that the virtual receptionist’s voice isn’t human. The fully integrated voice platform can book appointments, process prescription refills, answer questions, and more, freeing up about four hours a day for busy office staff to focus on their other duties.
“Office staff are incredibly busy, and don’t always have time to answer phones,” says Dr. Reza Mirza, an HHS rheumatologist, internist, innovator and Strello Health co-founder. “As a result, it has become increasingly common across Canada for patient calls at medical clinics to be placed on hold or sent directly to voicemail.”
Mirza co-founded Strello Health with Thorold family physician Dr. Ali Qamar and Toronto area software engineer Ali Sharif. Mirza and Qamar met as medical students at McMaster University, and looped in friend Sharif for the partnership.
As well as being a huge time-saver for clinic staff, the technology cuts down on patient frustration since calls are always answered by a friendly, helpful AI voice with infinite time and patience.
Their Strello Health system is currently being marketed to family doctors’ offices across Ontario, but it could also benefit other busy healthcare settings such as hospitals,” says Mirza, emphasizing the goal isn’t to replace staff.
Dr. Reza Mirza is an HHS rheumatologist and internist. He was inspired to co-found Strello Health to solve an increasingly common problem – medical clinics that have become so busy, office staff don’t have time to answer the phone. AS WELL AS FIELDING UNLIMITED CALLS EFFICIENTLY, AND POLITELY, THE AI RECEPTIONIST CAN BOOK APPOINTMENTS, ANSWER QUESTIONS, AND ORDER MEDICATION REFILLS. THIS SYSTEM CAN ALSO SEND APPOINTMENT REMINDERS OVER TEXT AND EMAIL TO MINIMIZE NO-SHOWS, AND ARRANGE OUTGOING FAXES FOR LABS AND IMAGING REQUESTS SUCH AS CT SCANS AND MRIS.
“The idea is that staff can spend more time checking in patients, managing the office, and doing things that require a human touch instead of spending their day on the phone.”
TEST DRIVING AI TECHNOLOGY
When Strello Health soft-launched in June 2024, members of the HHS Patient and Family Advisory Council were invited to test drive the system
and provide feedback to the co-founders, so any fine tuning could be done before the product went to market.
The Patient and Family Advisory Council is made up of HHS patients and family members who share their hospital experiences and give feedback to help make care better. They play an important role in improving how HHS delivers health care across the region, and council participation also includes opportunities to take part in focus
groups with hospital doctors, staff and industry partners designing innovative new health technology.
“It’s a great way for our physicians, staff and industry partners who develop products to receive feedback from potential end users,” says Andrea Lee, manager of research development, innovation and partnerships at HHS. Lee recruited several Patient and Family Advisory Council members to test drive Strello Health. The testers found it to be far superior to automated phone systems where callers are given a range of options such as, “Press 1 for customer service,” with menus that can be long and confusing.
FUTURE PLANS
INCLUDE
MAKING THE SYSTEM AVAILABLE IN MULTIPLE LANGUAGES.
“It felt like I was talking to a person,” says Emily Brown, an HHS patient advisor. “I was pleasantly surprised. I think it’s a really good solution for an issue that’s annoying for many patients.” The AI receptionist was able to handle tricky questions posed by Brown, and when she asked to speak with a real person, the AI receptionist promptly connected Brown to the front desk.
Jeff Brinson became a family member advisor because his daughter is an HHS patient. He tried out the system last year, and recently returned to demonstrate it for an HHS video. “I thought it was really good – easy to use and convenient,” says Brinson. He pushed the technology’s capabilities by changing his appointment availability multiple times, griping about parking, and asking whether his prescriptions would be covered by insurance. He interrupted the AI receptionist repeatedly, and at one point called ‘her’ rude to see how the technology would respond. But since the
“STRELLO HEALTH IS AN INNOVATIVE AND CREATIVE USE OF NOVEL TECHNOLOGY THAT MAY HAVE MUCH BROADER IMPLICATIONS WHEN IT COMES TO STREAMLINING WAYS THAT PATIENTS CONNECT WITH THEIR HEALTH CARE PROVIDERS.” – DR. MARC JESCHKE,
HHS VICE PRESIDENT, RESEARCH, AND CHIEF SCIENTIFIC OFFICER
receptionist is machine-generated, the voice remained calm and unflappable. Brinson even faked heart attack symptoms, prompting the technology to calmly instruct him to call 911.
A MASTER MULTITASKER
As well as fielding unlimited calls efficiently, and politely, the AI receptionist can book appointments, answer questions, and order medication refills. This system can also send appointment reminders over text and email to minimize no-shows, and arrange outgoing faxes for labs and imaging requests such as CT scans and MRIs. There’s seamless integration with clinics’ electronic medical records and phone systems, without a change to workflows. And if callers want to reach a real person, they can ask to be put through to the front desk. Future plans include making the system available in multiple languages.
“Strello Health is an innovative and creative use of novel technology that may have much broader implications when it comes to streamlining ways that patients connect with their health care providers,” says Dr. Marc Jeschke, vice president of research and chief scientific officer for HHS.
FROM THE FRONT LINES
After Strello Health launched last year, it went live with pilot trials in two family doctors’ offices including the Nobleton Medical Clinic, north of Vaughan. Results were so impressive, both clinics became customers.
More launches are currently underway in southwestern Ontario, with another 30 clinics on a wait list to have the technology installed.
“I’m quite impressed with its performance so far,” says Dr. Eric Da Silva, a family doctor with the Nobleton clinic.
Da Silva was the first of five doctors at his clinic to try out the system. Since then, two more Nobleton clinic doctors have started using it. “The system was well received by my patients, so we expanded it,” says Da Silva.
Prior to introducing this technology, 70 to 80 per cent of calls to the Nobleton clinic were going to voice mail, with office staff having dedicated time each workday to return messages. “The advantage with this system is that 100 per cent of calls are answered,” says Da Silva, adding that based on the latest metrics, 50 per cent of calls were handled by the AI receptionist without human involvement.
When patients’ requests were too complex for AI to manage, or when callers asked to speak to a human, they were forwarded to the front desk.
“The system is equipped to recognize what’s beyond its scope and it does a good job of transferring to the front desk when necessary,” says Da Silva. “And because it’s an AI system, it’s continuously learning, and getting better at recognizing what it can and can’t handle.”
While the system has provided welcome relief for Nobleton’s front desk staff, Da Silva says he’s especially glad that it helps even the playing field for patients when it comes to booking their own appointments using technology. Offering the service in multiple languages down the road is another exciting feature.
“The province has said it would like all family practices in Ontario to offer a way for patients to book their own appointments,” says Da Silva, who’s not in favour of directing patients to a website or app for self-booking because some patients may struggle with using computers.
Phones, though, have been part of our lives for decades so using
Thorold family physician Dr. Ali Qamar is a Strello Health co-founder. Drs. Qamar and Mirza have been friends since medical school, and have heard many of their peers share concerns about overwhelmed office staff.
them feels natural to most people, he says.
“With Strello Health, everyone has equal access. That was my primary motivation for bring the system to our
Nobleton clinic. It’s our way of meeting the province’s aspirational goal, and if autonomous patient booking becomes a requirement down the road, we’ll be ready.” n H
The best way to free patients from the burden of pressure injuries is to prevent them.
Pressure injuries have long been a challenge for patients and healthcare providers. When traditional methods fall short, it’s time to rethink your approach.
Clinical trial comparing methods of controlling bleeding in cardiac patients
Royal Columbian Hospital is one of 12 North American hospitals involved in a study that has been published in the Journal of the American Medical Association (JAMA).
Even though blood is red, the main ingredient–plasma–is a straw colour. Plasma is the liquid portion of blood and, for decades, has been the standard for treating excessive bleeding in trauma and surgical patients. According to Canadian Blood Services, some of this so-called “liquid gold” goes to hospitals for transfusions, but the majority is used to make life-saving medications, such as prothrombin complex concentrate (PCC), which is used to prevent bleeding and reverse the effects of blood thinners (anticoagulants).
Plasma arrives at hospitals in frozen form, and once thawed, has a limited shelf life. PCC comes in
powder form and is stored at room temperature, making it a good option for remote communities or hospitals that don’t have ready access to donated blood products. Both compounds are effective at controlling bleeding and have saved countless lives.
It’s estimated that 15 per cent of patients suffer excessive bleeding during cardiac surgery. The study Prothrombin Complex Concentrate vs Frozen Plasma for Coagulopathic Bleeding in Cardiac Surgery: The FARES-II Multicenter Randomized Clinical Trial, set out to compare the efficacy of PCC to frozen plasma when treating cardiac patients.
A total of 420 patients at 10 hospitals in Canada and two in the United States received either a PCC product with four blood clotting factors or frozen plasma. Royal Columbian Hospital recruited 63 patients for the
study, making it the second highest recruiting site in North America.
The study found that PCC was better than frozen plasma at controlling bleeding in cardiac patients who required blood products.
“The results show us that patients who receive PCC have less blood loss and massive bleeding, fewer adverse events, lower rates of transfusion and better clotting,” says Dr. Sukh Brar, one of the study’s principal investigators and an anesthesiologist at Royal Columbian Hospital. “This is a pivotal study because it gives us the clinical data to help optimize how we manage bleeding in patients who require a lot of blood products.”
According to Dr. Brar, this study will change clinical practice immediately.
“In Fraser Health, many of our sites already use PCC and I expect the ratio of PCC to frozen plasma to increase,
given the results of this study,” he says.
Dr. Brar is quick to credit the anesthesiology, cardiology, intensive care, perfusion, laboratory medicine, pharmacy, and nursing teams for their collaboration on the study. It is one of more than 90 active trials involving Fraser Health clinicians and staff in areas such as cardiology, gastroenterology, neurology, orthopedic surgery, and critical care.
“The FARES-II study is a great example of how Fraser Health clinicians and staff are working to integrate research with care,” says Kate Keetch, director, Evaluation and Research Services, Fraser Health. “Clinical trials provide our patients with advanced treatment options while at the same time supporting clinical sites to conduct research as important drivers of quality improvement and innovation in the system.”
n H
Researchers at UHN’s Toronto General Hospital Research Institute (TGHRI) have found that a class of diabetes medications, including dapagliflozin – used with diet and exercise to lower blood sugar in adults with Type 2 diabetes – is associated with reducing risk factors linked with cardiovascular disease and end-stage kidney disease (ESKD) in patients with Type 1 diabetes (T1D).
People with T1D have an increased risk of cardiovascular disease and kidney failure. They are 10 times to 30 times more likely to develop kidney failure compared to the general population.
Additionally, a diagnosis of T1D before the age of 10 can lead to a threefold increase in the risk of heart disease.
Thus, identifying therapies to help reduce these risks is essential.
Sodium-glucose cotransporter-2 (SGLT2) inhibitors, a class of drugs that includes dapagliflozin, have been shown to lower these risks in people with Type 2 diabetes and in people with kidney and cardiovascular disease associated with other conditions.
mately eight per cent compared to the placebo after 52 weeks of treatment.
The benefits on kidney health were especially pronounced in participants with chronic kidney disease (CKD).
These findings suggest that SGLT2 inhibitors like dapagliflozin could play an important role in protecting the heart and kidneys in people with T1D.
The authors have also been able to show similar potential benefits in separate models with another SGLT2 inhibitor called empagliflozin, which was used in the EASE clinical trials, and have published this work in the journal Diabetes Care. This study found that participants with T1D with the highest cardiovascular risk at the beginning of the trial may particularly benefit from these therapies.
Together, the study authors emphasize the need for dedicated clinical trials to confirm these benefits.
Even with intensive management of blood sugar and blood pressure, people with Type 1 diabetes face elevated risks of cardiovascular and kidney disease. There is a need for additional treatments to help mitigate these risks.
As part of this effort, the team has initiated a new trial called “SUGARNSALT,” funded by the Canadian Institutes of Health Research, the Kidney Foundation of Canada, and Breakthrough-T1D, which will determine if there are long-term kidney benefits in this unique patient population.
If proven effective, these medications could help individuals with T1D reduce their risk of life-threatening complications.
Evaluating diabetes risks Study offers new insights on how to limit brain tumour spread
However, no major studies have confirmed similar benefits for people with T1D.
To investigate this, the research team conducted a post hoc analysis of previous clinical trial data from the DEPICT-1 and DEPICT-2 studies. These trials were multicentre, phase 3, randomized studies that evaluated the safety and efficacy of dapagliflozin as an add-on therapy to insulin in lowering blood sugar levels.
The researchers used two risk prediction models to estimate changes in the 10-year cardiovascular disease risk and five-year ESKD risk in 1,473 participants with T1D who took dapagliflozin.
After 24 weeks of treatment, participants taking dapagliflozin had an approximately six per cent lower estimated risk of cardiovascular disease, as determined by one risk model, and a nine per cent lower risk, as determined by another, compared to those taking a placebo. Additionally, dapagliflozin lowered the risk of ESKD by approxi-
Approximately 90 per cent of cases of glioblastoma, a highly malignant and aggressive brain tumour, recur because of the tumour’s ability to spread into healthy brain tissue.
Therefore, specifically studying the cells that spread into the normal brain tissue is key to preventing recurrence in the disease.
A new study published in Developmental Cell found that glioblastoma cells hijack normal brain development processes to infiltrate brain tissue, suggesting new ways to control the spread of the cancer.
The study was led by Dr. Federico Gaiti, a scientist at UHN’s Princess Margaret Cancer Centre, in collaboration with the team in the lab of Dr. Gelareh Zadeh.
“We found that infiltrating glioblastoma cells – tumour cells that spread into healthy brain tissue – adopt features of early-stage brain cells called
oligodendrocyte precursor cells (OPCs),” says Dr. Gaiti, who is also an assistant professor in the Department of Medical Biophysics at the University of Toronto (U of T).
“These cells normally interact with neurons during brain development. Glioblastoma cells mimic them by switching on similar regulatory programs, helping them integrate into brain circuits and spread more effectively.”
The team used techniques called single-cell sequencing and spatial transcriptomics to study the regulation of infiltrating glioblastoma cells. By analyzing which genes were active, chemical modifications to the DNA, how open or closed different regions of DNA were, and how tumour cells physically and molecularly interacted with nearby neurons, they identified key developmental pathways that invasive glioblastoma cells hijack to spread through the brain.
The first author of the study published in CJASN is Dr. Massimo Nardone, postdoctoral researcher at TGHRI. The co-first authors of the study published in Diabetes Care are Luxcia Kugathasan, PhD candidate at the University of Toronto (U of T) and TGHRI, and Dr. Pritha Dutta, postdoctoral researcher at the University of Waterloo. The senior author of both studies is Dr. David Cherney, Senior Scientist at TGHRI and a professor in the Department of Medicine at U of T. n H
One such pathway is called NOTCH signaling – a cell communication system used by multicellular organisms to control cell fate decisions, such as differentiation, proliferation and apoptosis. The tumour cells hijack this pathway to activate oligodendrocyte lineage programs, effectively masquerading as normal OPCs.
The findings suggest that targeting this pathway and the regulatory programs involved may help limit tumour spread.
“We were able to confirm that these programs play a key role in driving the tumour’s ability to spread, by disrupting their control of tumour cells’ invasive behavior,” says Yiyan Wu, one of the first authors of the paper and a PhD student at U of T.
As a next step, the team is conducting experiments to pharmacologically target the pathway and related gene regulatory programs to assess their potential in reducing tumour invasion. n H
Photo:
A life’s mission: My story and the transformative role of The Royal
By Cara Vaccarino
believe mental health is the most important health – and I say that with the full weight of lived experience. This belief isn’t just professional or philosophical. It’s personal. It’s in my bones.
Today, I serve as President and CEO of The Royal, one of Canada’s leading mental health and addiction hospitals. But my mission didn’t begin in a boardroom. It began in grief.
I was 10 years old when my mother, Joan, died by suicide. She was a mother of four, including twin girls, who struggled silently with what we now recognize as treatment-resistant depression. At the time, she was prescribed multiple medications, but the exhaustion and despair never lifted. She lived with stigma, isolation, and a lack of understanding that still echoes too loudly in society today. We knew something was wrong, but no one talked about it. No one had the words – or the tools – to help.
And then, just like that, she was gone.
That kind of loss changes you forever. For me, it became a guiding force. I knew – even then – that I would spend my life working to ensure no other child had to lose a parent to an illness that could, and should, be treated with the same urgency and innovation as any physical health condition. I often ask myself, “How have we made so little progress in the last 40 years?” And I carry that question into every room I enter, determined to answer it through action.
My journey led me into social work, where I built a meaningful career helping others navigate their mental health challenges. But for me, it wasn’t enough to care. I wanted to change the system itself. That desire led me to The Royal.
What drew me to The Royal was more than its reputation. It was its purpose: reclaiming lives from mental illness and addiction through treat-
ment, research, and education. Here, I see not just a hospital, but a catalyst for transformation.
This is a place where some of the brightest minds in mental health are working on the frontlines of innovation – developing suicide biomarkers, launching pioneering clinical trials, and bringing new treatments to Canada for the very first time. At The Royal, research and care don’t live in silos. They’re integrated. Our patients benefit directly from discoveries happening in-house, and our researchers
are inspired every day by the people they serve.
That model, to me, is the key to closing the mental health gap – a gap that currently leaves 14 out of 15 people without the care they need. This isn’t because we lack compassion, but because of decades of stigma and underfunding. If we’re going to truly move forward, we need to invest in science, in systems, and in solutions that work.
And that’s exactly what we’re doing. The Royal is home to Canada’s
foremost mental health research institute, led by trailblazers like Dr. Florence Dzierszinski. Together, we are redefining what specialized care can be: more personalized, more accessible, and more grounded in evidence than ever before.
Still, I often say, what we know about the human brain is far outweighed by what we don’t. Compared to conditions like cancer or heart disease, we are decades behind in our understanding of mental illness. And yet, by 2030, depression is expected to be the leading global health crisis.
That sense of urgency is what drives me every day.
I can’t help but wonder – what if my mom had access to the kinds of treatments we’re developing now at The Royal? What if her suffering could have been eased, her story rewritten?
Those “what ifs” have become a rallying cry – not just for me, but for everyone at The Royal. They are at the heart of our bold and unapologetically hopeful vision: lives reclaimed from mental illness and addiction.
That vision is now embedded in our new mission: to advance specialized care and strengthen our region’s capacity to help people with mental illness and addiction through treatment, research, and education.
But I know this work can’t be done alone.
It’s not enough to be passionate. We need partners, advocates, and champions. We need you. To invest in research. To support education. To expand care. To help us save lives. Because in the end, my story isn’t just about loss. It’s about hope. It’s about leadership rooted in lived experience. It’s about a hospital that refuses to accept the status quo.
And it’s about building a future where fewer children grow up wondering what might have been – because the care their families need is finally within reach. n H
Cara Vaccarino is President and CEO, The Royal.
Cara Vaccarino
Reducing waitlists for patients with heart valve disease
The Montreal Heart recently opened the MHI’s Heart Valve Centre, a large-scale medical and scientific endeavour that aims to become a national hub of expertise. The new Centre will enable the MHI to double the number of patients with valve disease it can treat by 2028. The goal is to become a Canadian leader of heart valve disease and rank one of the world’s top ten most advanced centres in this quickly evolving field.
“This new centre for highly specialized care represents a major advance in how valve disease is treated. It also perfectly embodies our vision to make medical excellence accessible to patients both here and abroad. It’s a cutting-edge centre that will allow us to save more lives,” said Dr. Peter Guerra, Head of Specialized Medicine at the MHI.
“SIXTY FIVE PER CENT OF PATIENTS WHO ARE HOSPITALIZED AT THE MHI ARE DISCHARGED THE DAY AFTER THIS NEW PROCEDURE. AND MOST CAN RESUME THEIR DAILY ACTIVITIES A WEEK LATER.”
Heart valve disease affects 1 in 40 Canadians and is a significant cause of heart failure, morbidity, and mortality. Unfortunately, heart valve disease will become more prevalent as the population continues to age. It is estimated that by 2040, 1.5 million Canadians aged 65 and over will be living with heart valve disease.
Over the past few years, percutaneous valve therapies have transformed the way these pathologies are treated. These procedures do not require openheart surgery or general anaesthesia. Pa-
tients recover more quickly, experience less pain, need less medication, and require shorter hospital stays. These safe approaches are making treatments accessible to more patients while lessening the burden on the health care system.
“Sixty five per cent of patients who are hospitalized at the MHI are discharged the day after this new procedure. And most can resume their daily activities a week later,” said Dr. Walid Ben Ali, a heart surgeon at the MHI.
The MHI recently recruited Dr. Ralph Stephan von Bardeleben a
physician renowned for his in-depth expertise in the clinical, research, and educational aspects of minimally invasive valve therapies. Dr. von Bardeleben has performed a record number of percutaneous mitral and tricuspid procedures. The MHI hired Dr. von Bardeleben as part of a strategy to reaffirm its expertise in valve therapies and become a world-class centre.
In only one week, the MHI’s teams carried out mitral and tricuspid procedures in 23 patients in a single operating room. A record in North America. The MHI also aims to each year carry out 1,000 percutaneous aortic valve replacements (+100%) and 400 percutaneous mitral and tricuspid procedures (+300%), for a total of 1,400 valve procedures – a figure that would place it alongside the most advanced health institutions in Europe. n H
Humber River Health’s journey toward onsite cardiac catheterization
By Chiara Marcello
As the prevention and treatment of vascular disease continues to advance, Humber River Health (Humber) is taking steps to ensure patients in North West Toronto have equitable access to high-quality, life-saving cardiac care. As one of Ontario’s busiest cardiology programs, Humber sees more than 17,000 patients each year. To meet the rising complexity and urgency of cardiovascular needs, the Hospital is making significant upgrades to its Cardiology Program, including the expansion of its device clinic to include an Implantable Cardioverter Defibrillator (ICD) program and the development of a state-of-the-art Cardiac Catheterization (Cath) Lab. Currently, patients who experience certain cardiac emergencies, such as those requiring catheter-based diagnostics or interventions, must be transferred to another facility. These transfers not only delay critical care, but also contribute to longer hospitalizations and fragmented care experiences. As Humber continues to lead the charge in building a more integrated and responsive healthcare system, its vision is to perform essential procedures like angiograms and angioplasties on-site, improving the speed, continuity, and quality of care.
The proposed Cardiac Cath Lab will serve as the cornerstone of this transformation. As a critical tool in the diagnosis and treatment of cardiovascular disease, a Cath Lab enables clinicians to assess coronary blockages and perform interventional procedures in real time. For patients, this means fewer delays and safer outcomes, particularly in time-sensitive cardiac events. For the health system, it represents a more efficient and coordinated model of care delivery, especially in a high-demand region like North West Toronto.
Complementing the future Cath Lab is the recent and successful launch of Humber’s ICD program, which is
part of Humber’s Device Clinic, alongside pacemakers. Earlier this year, the Hospital implanted its first Implantable Cardioverter Defibrillator, a small device that monitors heart rhythms and delivers life-saving shocks to restore normal rhythm when needed.
The device was placed in a patient named Silvino, who was admitted to Humber’s Intensive Care Unit and became the first individual to receive this treatment entirely within the Hospital.
Before this advancement, patients like Silvino would have been transferred to a different institution for implantation and then returned to Humber for recovery and follow-up. With the implementation of the ICD program, this entire care pathway is now delivered on-site, increasing convenience, safety, and peace of mind for both patients and their families. The new ICD Clinic also represents a key step in Humber’s broader commitment to modernizing cardiac services and offering a full continuum of cardiovascular care under one roof.
Another major milestone in Humber’s cardiac care expansion is the relaunch of its Heart Failure (HF) Clinic. The Clinic serves patients who have been recently diagnosed with heart failure, are experiencing uncontrolled symptoms, or have been hospitalized for heart failure-related complications. By offering rapid access to specialized care, education, and monitoring, the HF Clinic plays a crucial role in preventing readmissions and improving patients’ quality of life.
The relaunch was made possible through the collaborative efforts of multidisciplinary teams, and by engaging patients and families in the redesign process. One notable contributor is Marjan Dehghani, a member of Humber’s Patient and Family Advisory Committee (PFAC), who joined after her mother, Rouhi, was diagnosed with heart failure and atrial fibrillation at age 90. Following a serious case of Digoxin toxicity that required emergency intervention, Rouhi received
exemplary care at Humber. This experience inspired Marjan to get involved and advocate for improved cardiac services from the patient’s perspective.
As part of the HF Clinic planning team, Marjan brought critical insights into what patients and caregivers need, whether it be improved educational resources, clearer care plans, or more compassionate communication. Thanks to regular visits to the HF Clinic, Marjan and her now 94-year-old mother have successfully avoided hospital readmissions and continue to manage Rouhi’s condition safely at home.
These initiatives, combined with Humber’s clinical expertise, underscore the Hospital’s commitment to continuous quality improvement and innovation
in cardiac care. They also reflect Humber’s larger vision: to build a comprehensive cardiac program that includes diagnosis, intervention, rehabilitation, and long-term management, all delivered locally, efficiently, and equitably.
With the growing prevalence of heart disease and an aging population, the need for advanced cardiovascular services has never been more urgent. “By investing in the infrastructure and programming required to meet these needs, Humber River Health is lighting new ways in cardiac care, and ensuring that patients and families can access the life-saving services they need, close to home,” says Jhanvi Solanki, Vice President of Clinical Programs. n H
Chiara Marcello works in communications at Humber River Health.
Dr. Irving Tiong implanting an ICD at Humber River Health.
Partnering to improve outcomes for high-risk breast cancer patients
The Hamilton Health Sciences (HHS)’ Centre for Data Science and Digital Health (CREATE) is partnering with cancer genetics expert Dr. Andrea Eisen to expand the hospital’s artificial intelligence (AI) Learning Health System for Breast Cancer to include genetics information from patients.
Eisen, who joined HHS last summer, is a leading expert in cancer genetics and high-risk breast cancer. She’s providing expertise from a medical perspective, while the CREATE team provides the technical knowhow. CREATE is staffed with experts in software engineering, AI and data sciences, all with a niche specialty in health care.
“We’re looking at using the Learning Health System to, for example, identify people diagnosed with breast cancer who might have benefitted from genetic testing but weren’t offered it,” says Eisen. “For instance, the criteria for qualifying for genetic testing may have been more restrictive when they were diagnosed. Or they may have felt that the timing wasn’t right because they were in the middle of treatment.”
Eisen is the Buffett Taylor Chair in Breast Cancer Research, a position previously held by retired HHS medical oncologist and renowned breast cancer researcher Dr. Mark Levine.
CREATE-ing and expanding the Learning Health System
Several years ago, before Levine retired, he reached out to CREATE with the idea to develop an AI-driven learning health system, using records from JHCC breast cancer patients, in order to better understand this population and drive improvements in care. The system uses AI to rapidly collect, sort and interpret patients’ medical information, providing HHS doctors, leaders and researchers with data they request in real time.
The AI database currently includes diagnoses, scans, tumor pathology, demographics, social determinants of health, medications, treatments, sur-
Hamilton Health Sciences is expanding the hospital’s AI Learning Health System for Breast Cancer to include genetics information from patients. This next step for the Learning Health System was made possible thanks to the work of Dr. Jeremy Petch, Dr. Andrea Eisen and Dr. Mark Levine.
geries and survivorship. Prior to this platform, it took months or even years, to search for and collect data to determine, for example, if certain patient groups faced barriers to care. Using AI, this information can be gathered and made available almost instantly.
The CREATE team is now building genetics into the system, with Eisen providing the clinical leadership as a medical oncologist and leader in cancer genetics and high-risk breast cancer. “Currently we can’t, for example, use this platform to look at the care for all HHS patients with the BRCA genes,” says Dr. Jeremy Petch, CREATE’s director.
BRCA1 and BRCA2 are the most common genes associated with hereditary breast and ovarian cancer. The risk of developing breast cancer is about 60 per cent for patients with these genes. The chances of being diagnosed with ovarian cancer is as much as 40 per cent for BRCA1 mutation carriers and up to 20 per cent for BRCA2.
By identifying people with BRCA genes early, they can take preventative measures such as surgery to avoid getting breast or ovarian cancer.
“By including genetics, we’re opening up an incredibly powerful resource to ask critical questions about how our system is doing at delivering care, and
the quality of the outcomes we’re getting,” says Petch. “This means we can take a much closer look at this patient
population, to help ensure they receive the care they need.”
Eisen, Levine and the CREATE team secured a grant from the Canadian Cancer Society to expand the system to include genetics information from HHS patients. It’s also expected to include data from St. Joseph’s Healthcare Hamilton, since some breast cancer patients receive care from both hospital systems. For example, a patient may receive cancer surgery at St. Joe’s and chemotherapy and radiation at HHS.
“By populating the platform with data from both hospital systems, we’ll have a more a complete, comprehensive picture of all of our patients’ breast cancer journeys,” says Petch, adding, “This will provide us a lot of very powerful insights, that will, in turn, drive improvements for breast cancer patients across our city’s health care system.” n H
New hope for people with stimulant use disorder
very day in British Columbia, five people lose their lives to unregulated drug toxicity. It is a crisis that demands new solutions.
April 14, 2025 marked the ninth anniversary of BC declaring the toxic drug crisis a public health emergency. Thousands have passed away from drug poisoning in the last nine years. Thousands more – including their family and friends – continue to suffer.
Communities across the province are working urgently to address the devastating impacts. In Vancouver, Dr. Paxton Bach is partnering with people with substance use disorders to improve treatment options and create new pathways to recovery.
As an addiction medicine specialist at St. Paul’s Hospital, Paxton has seen firsthand the complex health challenges linked to stimulant drugs like crystal methamphetamine (“crystal meth”). The rise in stimulant use has led to more chronic diseases, emergency room visits, hospitalizations, and overdose deaths.
Paxton says the use of both opioids and stimulants is a growing concern in the overdose crisis.
“While fentanyl and other opioids are the primary drivers of rising overdose deaths, up to 80% of overdose deaths in BC also involve stimulants,” he says. “Yet the role of stimulants gets little attention – and treatment options are limited.”
Paxton is leading research to explore new treatments for people living with methamphetamine use disorder – offering hope for better health and stronger support systems.
He is supported by Michael Smith Health Research BC through a Health Professional-Investigator (HP-I) award, in partnership with the BC Centre on Substance Use and St. Paul’s Foundation.
The HP-I award enabled Paxton to focus his research on how people use methamphetamines and the effects on their health, relationships, and daily lives. Understanding this will help determine the most effective treatments.
His findings are helping decision-makers better understand the issue to consider more effective solutions. He has shared his research insights with Health Canada’s expert advisory group on safer supply, which advises the federal government on preventing stimulant-related harms.
He also sits on the BC Coroners Service’s drug toxicity death review panel, which provides recommendations to the provincial government about interventions to prevent overdose deaths.
The HP-I award helped Paxton’s team lay the foundation for a national clinical trial on treating methamphetamine use disorder and secure $5 million from the Canadian Institutes of Health Research. The trial is looking at the impacts of using medication alone and in combination with a behavioral intervention.
Colin Johnson, co-chair of the Toronto Harm Reduction Alliance, sits on the national research committee guiding the clinical trial. He says there’s a significant lack of research in this area, making the study an essential part of finding solutions.
Colin is a strong advocate for research that meaningfully involves the communities it impacts – and returns value to them. He and other peers with lived and living experience helped design the trial, ensuring research questions reflect the needs of the people most affected.
“There’s a lot of research that investigates a topic without asking affected communities what they would like to have researched,” says Colin. “And then when you get to what was found, it benefits no one. Because the questions that researchers are asking do not answer the questions that people want answered.”
He adds that stigma can lead to silence.
“People who use drugs have been treated so negatively by society that after awhile, they don’t even bother trying to say anything because they’re dismissed,” says Colin. “It’s critical that they be heard. I want to ensure their voices count.”
The clinical trial is being carried out at five sites across Canada, including Vancouver, and is the largest study
on methamphetamine use disorder. Its findings will impact patients, clinicians, and policymakers – guiding responses to the ongoing overdose crisis and helping to shape future treatment guidelines across the country and beyond.
“It’s crucial to recognize the role of stimulants in the drug crisis – and to develop real solutions for this highly vulnerable and underserved community,” says Paxton.
Dr. Paxton Bach is Co-Medical Director at the BC Centre on Substance Use and Clinical Assistant Professor in the Department of Medicine in the Faculty of Medicine at the University of British Columbia.
The Vancouver site is currently enrolling participants into the clinical trial. People from the Lower Mainland aged 18-55 with moderate to severe methamphetamine use disorder may be eligible for the study. For more information, view the study poster.
This story was originally published on the Health Research BC website. n H
Dr. Paxton Bach with research team members Sahar Shahidi and Maddie Newby.
Pediatric dosage forms: Safe medication use considerations
By Laura Brady, Samir Kanji, and Certina Ho
As a parent, when your child is sick, it is not uncommon to have questions about the medications or the type of medications (including the dosage forms, such as tablets, capsules, liquids, suspensions, suppositories, etc.) that you are going to give them. This article is the first of a three-part series that we will cover some of the considerations for safe pediatric medication use. Here we highlight some frequently asked questions by parents regarding pediatric dosage forms and the safety of children medications.
WHICH DOSAGE FORM IS APPROPRIATE FOR MY CHILD?
Choosing the right medication dosage form for a child will depend on many factors – e.g., how the medication works in the body, how it tastes, and how easy it is to give, etc. These factors are also closely related to the age and the stage of development of the child. In both hospital and community settings, healthcare providers often select a dosage form based on the patient’s age group, since children at different stages will have varying physical and mental abilities. Some general age-based guidelines are as follows:
• Neonates (i.e., under 1-month old): Consider liquid formulations; or drops (limited volume)
• Toddlers: Consider liquids; or suspensions
• Pre-school (i.e., 2-5 years old): Consider liquids; crushable tablets (powder); or dispersible tablets
• Early school age (i.e., 6-8 years old): Consider liquids, crushable tablets (powder); dispersible tablets; chewable tablets; or tablets/capsules (smaller ones)
• Later school age (i.e., 9-12 years old): Consider all solid dosage forms
CHOOSING THE RIGHT MEDICATION
DOSAGE
FORM FOR A CHILD WILL DEPEND ON MANY FACTORS – E.G., HOW THE MEDICATION WORKS IN THE BODY, HOW IT TASTES, AND HOW EASY IT IS TO GIVE, ETC.
However, it is important to consider that every child is unique. Preferences and capabilities can vary widely, even within the same age group. The best type of medication may also depend on what medical condition is being treated. For these reasons, each pediatric case should be considered individually to ensure safety, efficacy, and accessibility of medication therapy options.
WHAT CAN I DO IF MY CHILD REFUSES TO TAKE THEIR MEDICATION BECAUSE OF THE TASTE?
Studies have shown that children often refuse to take their medication due to its bitter or unpleasant taste. Fortunately, there are several ways to address this. For instance:
• Offer a small amount of food or drink directly before and after giving the medication to reduce the degree or extent that they can taste the medication.
• Let them taste something cold first, like a popsicle, prior to giving the medication.
• Ask the prescriber if it is possible to minimize the dosing frequency of the medication; if a better-tasting option is available; or if a different route of administration is available (e.g., a rectal suppository instead of an oral liquid, etc.)
• Use a straw or an oral syringe to avoid the taste buds at the front of the tongue/mouth
• Ask your pharmacist if the medication can be flavoured at a compounding pharmacy
Note: Always check with your pharmacist or prescriber before trying any of the above options. Some medications cannot be mixed with food or flavouring, as it could affect the efficacy of the medication.
WHAT CAN I DO IF MY CHILD’S MEDICATION ISN’T AVAILABLE IN THE RIGHT DOSAGE FORM OR IF IT IS ON BACKORDER?
If the medication your child needs isn’t commercially available in the right dosage form or if there’s a drug shortage, discuss alternative options with your doctor and/or your pharmacist. They can help determine whether another medication can be used or if the original medication can be safely compounded into another dosage form without affecting how it works. These are usually prepared by specialty compounding pharmacies that are accredited and regulated by provincial pharmacy regulatory authorities (or Colleges). Additionally, it’s also important to note that some compounded medications may not be covered, depending on your insurance coverage. In some cases, certain medication tablets can be crushed into a powder and mixed with food (such as apple sauce) if the liquid formulation isn’t
available. However, not all medications can be safely crushed or split, so always ask your pharmacist before doing so.
HOW CAN I BE SURE MY CHILD IS GETTING THE RIGHT DOSE OF THEIR MEDICATION, AND WHAT TOOLS CAN HELP ME GIVE IT SAFELY?
Always follow your healthcare provider’s instructions and use proper measuring tools, such as medicine syringes, droppers, or cups that come with the medication, instead of household spoons, which can lead to inaccurate dosing. These tools help prevent giving too much or too little medicine to your child.
To stay organized, try keeping a written list or using a simple routine to remember when to give each dose. Always read the medication label and instructions carefully. Ask your pharmacist if you’re unsure about the medications. As your child grows or their health changes, regular checkins with your healthcare provider can help make sure the dose stays appropriate.
WHERE CAN I READ MORE ABOUT SAFE PEDIATRIC MEDICATION USE?
Examples of resources are as follows:
• From the Government of Canada
• From ISMP Canada
• From the Canadian Paediatric Society
• From SickKids
By utilizing these resources and maintaining open communication with healthcare professionals, you can play an active role in ensuring the safe use of medications for your child. n H
Laura Brady and Samir Kanji are PharmD Students at the Leslie Dan Faculty of Pharmacy, University of Toronto; and Certina Ho is an Assistant Professor, Teaching Stream, at the Leslie Dan Faculty of Pharmacy and Department of Psychiatry, University of Toronto.
Botox at 40: From medical curiosity to a wide range of uses
By Sara Yuan
Originating in a lab in San Francisco in the 1970s, botulinum toxin – best known by its trade names Botox, Xeomin and Dysport – is well known for its cosmetic uses, being the most common cosmetic procedure performed worldwide. What many people do not know is that Botox was originally developed to treat ophthalmological and neurological conditions.
In 1985, Dr. Stephen Kraft, a staff ophthalmologist at UHN’s Donald K. Johnson Eye Institute, treated the first patient in Ontario using Botox – then called Oculinum – at Toronto General Hospital. Dr. Kraft recently sat down with UHN News to discuss the history of Botox, its medical uses, how it has evolved over the past 40 years and future research.
WHAT IS BOTOX AND WHAT CONDITIONS DOES IT TREAT?
Botox is a purified form of a bacterial toxin called botulinum toxin, which disrupts communication between nerves and muscles. In the body, when a nerve signals a muscle to contract, it releases a chemical called acetylcholine. What Botox does is stop the release of the chemical, creating a nerve block, which will stop muscles from contracting.
Botox was originally developed only for one purpose: to straighten crossed eyes and lazy eyes. It was formulated to be injected into the eye muscles as an alternative to surgery. We used dosages in the billionths of a gram, which were still strong enough to change the muscle activity and straighten the eyes. Then it was found to be very helpful for various disorders involving overactive facial muscles, some confined to the eyes, some on the face and some involving the neck.
Today, there are at least 50 different medical uses of Botox and other botulinum toxin products, including treating chronic migraines, facial dystonia, excessive sweating and spastic disorders.
Dr. Stephen Kraft was the first physician in Ontario –and second in Canada – to use Botox to treat patients with ophthalmological and neurological conditions.
WHAT WAS YOUR EARLY EXPERIENCE USING BOTOX? HOW WAS IT RECEIVED BY
THE MEDICAL COMMUNITY?
It was really just curiosity. In medical school, we learned about all sorts of toxins, from snakes, spiders and other sources, and here we have one of the most dangerous toxins being developed to treat medical problems. It was very much like when Alexander Fleming discovered penicillin. Who would’ve thought that a fungal contaminant he chanced upon would transform the way we treat infections?
At the time, I was part of a small group of ophthalmologists who were exploring ways to use botulinum toxin. You can imagine the concern of our research ethics boards! We had to show them data from our early studies, including the precise dosage levels and safety margins. Once we proved that the drug was safe and showed great results, we started receiving interest from the broader medical community. Colleagues in other specialties, including orthopedics, neurology, rehab medicine and oral surgery, imagined additional uses of the toxin and started their own studies.
It was a really rewarding experience, not just being part of the initial break-
through, but also seeing the ripple effect of the knowledge we gained. The people I taught went on to teach others, and seeing the applications of Botox expand across so many disciplines has been incredible.
ARE
YOU SURPRISED
BY THE WIDE RANGE OF BOTOX USES?
DID YOU EXPECT THIS WHEN YOU STARTED USING IT?
No, I didn’t predict the expansive number of things it’s being used for now, but I suspected that it would have broader applications. Early on, my neurology colleagues and I knew that since Botox worked for muscles around the eyes, it could also treat muscles in spasm in other areas of the body. One of my closest collaborators in early studies of Botox for neurological applications was Dr. Anthony Lang – now neurologist and Senior Scientist at UHN’s Krembil Brain Institute – who was exploring the use of Botox to treat movement disorders. Some of my orthopedic surgeon friends also recognized that Botox had potential for muscular therapy. Thanks to these collaborations, I knew that it would probably be used for a range of neurological and muscular conditions affecting different parts of the body, but early on, nobody among my small
cohort of investigators had any notion of the cosmetic boom that it would cause.
TAKE US BACK TO THE CLINICAL TRIAL DAYS. WHAT WAS IT LIKE BEING THE FIRST PHYSICIAN IN ONTARIO TO TREAT PATIENTS
USING BOTOX – THEN OCULINUM?
It was kind of awesome because this was the first time that, as a medical practitioner, I had the opportunity to be involved in the early stages of developing a new therapy.
On January 12, 1985, I treated the first three patients using Oculinum at Toronto General Hospital. They were the only patients I booked that day because I wanted to talk to them, explain the treatment to their family members, and also tell them about possible side effects to look out for. The patients were quite excited, especially when they started seeing results within a few days after just one treatment session. They were really thankful.
Many of my patients had tried all the other therapies available at the time, so this treatment was really the last resort. Some of them had lived with the condition for decades – it had seriously disrupted their daily lives, and in many cases, their occupations. Knowing that I was able to help them to get their lives back was extremely satisfying.
HOW COMMON
IS THIS
TREATMENT NOW? HOW MANY PATIENTS DO YOU SEE IN THE CLINIC?
I see around 40 patients in my clinic at Toronto Western Hospital every month, and they are mostly patients with blepharospasm, hemifacial spasm and migraine. Because Botox wears off over time, most of my patients come in for another treatment session every three to four months. Even though strabismus was one of the original conditions treated with Botox, most
Photo: UHN
patients now choose to have surgery instead, to avoid potentially going through multiple treatments.
IN
YOUR OPINION, WHAT ARE THE MOST EXCITING NEW MEDICAL APPLICATIONS FOR BOTOX?
In the last 10 to 20 years, Botox and its sister products have been used to treat numerous conditions, including spastic bladders, stomach spasms, Achilles tendon spasticity (a serious problem for wheelchair users), excessive sweating, and various ophthalmological and neurological conditions.
I recently read an exciting study about a new form of botulinum toxin
that is said to last up to six months. If this new compound proves to be safe and effective, some patients will be able to come in for treatment
Yuan works in communications at University Health Network.
AUGUST 2025
Paediatrics Supplement Paediatrics Supplement
AUGUST FOCUS: Paediatrics, Community Engagement and Patient Advocacy and Social Work:
Paediatric programs and developments in the treatment of paediatric disorders including autism. Specialized programs offered on an outpatient basis. Community engagement initiatives. Empowering patients – tools and strategies for improving patient education and self-management. The role of patient advocates and how healthcare professionals can support advocacy efforts. Social work programs helping patients and families address the impact of illness.
Advertising Booking Deadline July 25th
Material Deadline July 29th
For more info email advertising@hospitalnews.com
Dr. Stephen Kraft, (L), a staff ophthalmologist at UHN’s Donald K. Johnson Eye Institute, in 1985 became the first physician in Ontario to use Botox to treat patients with ophthalmological and neurological conditions. Here, he uses it to treat a patient with blepharospasm, a neurological condition marked by uncontrollable blinking or spasm around the eyelids.
twice a year, instead of every 10 to 12 weeks. Another idea that was researched some years ago was to combine Botox with a drug that inhibits
nerve growth, to extend its effects. We don’t have such a product yet, but this is an interesting avenue for research. n H
UPCOMING EDITIONS
SEPTEMBER 2025
SEPTEMBER FOCUS: Emergency Services, Critical Care, Trauma, Emergency and Online Education:
Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine.
Advertising Booking Deadline August 22nd
Material Deadline August 26th
For more info email advertising@hospitalnews.com
OCTOBER 2025
OCTOBER FOCUS: Mental Health and Addiction, Patient Safety, Research and Infection control:
New treatment approaches to mental health and addiction. Developments in patient-safety practices. Developments in the treatment of neurodegenerative disorders (Alzheimer’s, Parkinson’s etc.), traumatic brain injury and tumours. Developments in the prevention and treatment of drug-resistant bacteria and control of infectious (rare) diseases. Programs implemented to reduce hospital acquired infections (HAIs). Annual National Infection Control Week (Oct.20-24) Supplement
Advertising Booking Deadline September 19th
Material Deadline September 23rd
For more info email advertising@hospitalnews.com
Sara
Photo:
Canadian Surgeons Volunteer Onboard the World’s Largest Civilian Hospital Ship
In April 2024, Quebec surgeons Dr. Jean-Martin Laberge and Dr. Louise Caouette-Laberge volunteered on the Global Mercy in Freetown, Sierra Leone, to offer free surgery to the population.
As President Julius Maada Bio of Sierra Leone stated just prior to Mercy Ships’ field service, “Mercy Ships, provides a continuous humanitarian and medical support towards providing treatment to people with various medical conditions worldwide”. At the time if the announcement, the partnership agreement included a 10-month deployment of the Global Mercy, offering free surgical care in and training healthcare professionals to build capacity within Sierra Leone’s national health system.
As she prepared to come aboard, Dr. Caouette-Laberge shared her excitement at being able to work aboard the Global Mercy. “The advantage of having a state-of-the-art hospital like this is that it has international standards. It allows us to perform complex surgeries that we wouldn’t be able to do in an African country because they don’t have the necessary infrastructure.”
The couple was recognized for their humanitarian work by the Collège des Médecins du Québec, which jointly awarded them the Prix d’humanisme in 2013. As for Dr. Laberge, in addition to participating in missions with his wife, he has contributed to the training of pediatric surgeons in Kigali, Rwanda. Through their respective work in pediatric surgery, they have between them changed countless lives of children both in Canada as well as Africa.
“We receive much more than we give! The people we operate on for free are so pleased, they thank us and are happy. We take for granted the training we receive and how lucky we are to be able to study. There are no teachers there. You don’t realize it until you leave home and see the reality of others,” says Dr. Louise Caouette-Laberge. After all
these years in the field, they are now part of an international team of medical specialists that serve onboard Mercy Ships.
The Global Mercy’s volunteer crew of nearly 600, both short- and longterm, works with dedication and excellence to welcome patients for life-changing surgeries. Darryl Anderson, Executive Director of Mercy Ships Canada, stated, “We are grateful for medical staff and all hospital volunteers who, like Dr. Laberge and Dr. Caouette-Laberge, share a passion for our mission of Hope and Healing.” Anderson also announced, “We are excited that the President of Sierra Leone has extended our partnership for another field service into 2024.”
Mercy Ships Canada is one of 16 National Offices dedicated to raising funds, building awareness, recruiting volunteers, and supporting impactful projects for Mercy Ships’ global programs. Mercy Ships operates the world’s two largest civilian hospital ships, delivering free, life-changing surgeries and healthcare, along with training and mentoring for local healthcare professionals, ensuring communities have sustainable healthcare long after the ships depart.
Mercy Ships believes that everyone deserves a life full of promise and potential. That every mother deserves to see her child grow healthy and thrive. We believe that healthcare is a human right, and we are committed to reaching children and families in need of safe surgical care with state-of-the-art hospital ships filled with compassionate volunteer healthcare providers.
Dr. Louise Caouette-Laberge, conducting a surgery with her husband Dr. Jean-Martin Laberge, onboard the Global Mercy
To learn more on volunteering visit mercyships.ca/en/get-involved/volunteer WITH VOLUNTEERS