“Doug Ford has given the wrong kind of power to employers. He’s just breaking the healthcare system apart piece by piece and with that decimation comes the inability for us to communicate and stand up to what’s happening to our beloved health-care system.”
Home
care nurses are demanding better.
s Cover story: Little patients, big lessons: SickKids putting their own stamp on pediatric emergency medicine eductaion
16
s Compassion in aging: Celebrating a year of Southlake’s Acute Care of the Elderly Unit
10
s New RSV immunization catch-up clinic 24
Reshaping robotic rehabilitation
8
s Signs of progress. Transforming child health in Canada
14
Special focus: Pediatrics
s Pediatric surgical care helps young hockey players back on the ice
30
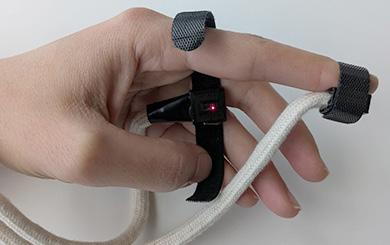
Smart wearables for faster cardiac arrest emergency response
26
Canada is falling behind on Alzheimer’s disease treatments
By Andrew Frank and Katherine C. Pearson
Alzheimer’s disease is an insidious and relentless loss of memory and thinking, accompanied by a gradual yet devastating deterioration in ability to function independently. It’s a terrifying diagnosis for patients and families alike.
Dementia is defined as a loss of memory or thinking, which takes away daily independence. Alzheimer’s disease is the buildup of amyloid and tau proteins in the brain -- proteins which begin as helpful yet become toxic as they accumulate. Alzheimer’s disease is therefore the cause, and dementia is the effect.
Unfortunately, medical treatments for Alzheimer’s disease and dementia have remained minimal for over 25 years, and with a growing aging population, Alzheimer’s disease has become one of the greatest unmet medical needs in the world.
THERE IS HOPE ON THE HORIZON.
Recently, two new intravenous medications, lecanemab and donanemab, have shown they can clear away toxic accumulations of the amyloid protein in Alzheimer’s disease. One or both of these medications have been approved in the United States, the European Union, United Kingdom, China, Japan, Mexico, Brazil and Australia. Yet, these medications have not been approved in Canada.
UPCOMING DEADLINES
SEPTEMBER 2025 ISSUE
EDITORIAL: August 8
ADVERTISING:
Display – August 22 | Material – August 26
Monthly Focus:
Emergency Services/Critical Care/Trauma/ Emergency/Online Education: Innovations in emergency and trauma delivery systems. Emergency preparedness issues facing hospitals and how they are addressing them. Advances in critical care medicine.
+ ONLINE EDUCATION SUPPLEMENT
Canada is falling behind, and families are suffering. It’s time we made new Alzheimer’s disease medications available to Canadians in a timely and accessible manner.
Clinical trials research into lecanemab and donanemab demonstrated a 27 per cent to 35 per cent slowing of cognitive decline in individuals with Alzheimer’s disease versus a placebo, with greater benefit experienced the earlier in the disease process the treatment was started. The treatments slow the rate at which Alzheimer’s disease worsens, though do not fully stop or reverse the damage.
Both lecanemab and donanemab remain under review by Health Canada and are not yet approved for use in Canada. The decision to approve these medications has been complex, as a slowing of cognitive deterioration by 27 per cent may not be viewed as enough of a benefit, especially when weighing against potential side effects.
Indeed, as these medications cross into the brain and trigger clearance of amyloid by the immune system, there can be development of swelling or bleeding in the brain. While most clinical trial participants who developed swelling or bleeding had no associated symptoms, three to six per cent experienced headache, dizziness, confusion or occasionally stroke-like symptoms.
Continued on page 6
OCTOBER 2025 ISSUE
EDITORIAL: September 12
ADVERTISING: Display – September 19 | Material – September 23
Monthly Focus:
Mental Health and Addiction /Patient Safety / Research /Infection control: New treatment approaches to mental health and addiction. Developments in patient-safety practices. Developments in the treatment of neurodegenerative disorders (Alzheimer’s, Parkinson’s etc.), traumatic brain injury and tumours. Developments in the prevention and treatment of drug-resistant bacteria and control of infectious (rare) diseases. Programs implemented to reduce hospital acquired infections (HAIs).
+ANNUAL INFECTION CONTROL SUPPLEMENT
200 North Service Road West, Suite 517 Oakville Ontario L6M 2Y1 TEL. 416.580.3450|EMAIL info@hospitalnews.com www.hospitalnews.com
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:
THANKS TO OUR ADVERTISERS
When you visit our advertisers, please mention you saw their ads in Hospital News.
Hospital News is published for hospital healthcare professionals, patients, visitors and students. It is available free of charge, accessed by our website (hospitalnews.com) and also available through our digital subscription. The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
For changes in email subscriptions please send requests to info@hospitalnews.com. Hospital News does not share email information and subscriptions can be cancelled at any time.
‘Nothing about us without us’: How Waypoint puts patient voices at the centre of
By Travis Mealing
By listening to the voices of those with lived experience, Waypoint Centre for Mental Health Care is setting a standard for client engagement in mental health services, policy development and research.
Through initiatives such as the Ontario Structured Psychotherapy (OSP) Client Advisory Committee (CAC), the Waypoint Research Institute (WRI) and the Patient/Client and Family Council (PCFC), patients are more than participants — they’re partners shaping care.
Launched in 2021, the CAC brings together five to seven current and former clients of the OSP program who volunteer to share their insights in virtual meetings every two months. Led by two clinicians and a member of the PCFC, committee members receive an honorarium for their time and play a direct role in guiding changes to services.
When big decisions or changes are being contemplated, it’s important to be able to engage people who actually went through the program, said OSP Manager Jessie Daniel.
“Any time we do a client-facing change — with our website, with our referral form, or how questions are asked — we run it by our CAC,” she said. “We had a demo for our web page, and we went through it with our CAC because they’re the ones that are going to be looking at it. So how does it visually look? What else should we include? What should we not include? How does this wording feel for you? If you were referring yourself, does this make sense?”
This isn’t just tokenistic consultation. The committee’s suggestions have led to tangible improvements. When the CAC flagged the welcome package as too lengthy and filled with clinical jargon, the OSP team made it more accessible. When members identified a gap in peer connection, the result was a client appreciation event. Even the implementation of a new scheduling system was adjusted based on CAC feedback — specifically, ensuring cli-
mental health care
ents leave their intake appointment with a treatment date in hand.
“We’ve attempted to implement every suggestion that has come out, even if it didn’t necessarily align with what we thought,” said fellow OSP Manager Melissa Moreau. “You have to come in with an open mind and not have preconceived notions of what you think will work best.”
That collaborative spirit not only improves services, but also boosts trust, engagement and the likelihood that clients will refer others to OSP.
This level of patient involvement extends beyond services into research.
Dr. Christopher Canning, Director of the WRI, views experiential expertise as equal in value to academic credentials. “For me, it’s not about an invitation in,” he said. “It is about recognizing the multiple forms of expertise that should inform what we do.”
For example, the WRI is working with an advisory group of patients from Waypoint’s high-secure forensic programs to co-design guidelines for patient involvement in research. These contributions do more than inform — they offer meaning and purpose to participants and reveal some of the realities of the forensic system to researchers.
“This isn’t a new conversation,” said Dr. Canning. “For years, patients have been calling for their voices to shape the mental health care system — from how they’re treated to the therapies they receive and the policies that shape their care.”
Dr. Canning credits Waypoint’s leadership for fostering an organiza-
tional culture where client and family input is not just welcomed, but essential: “It’s baked into who we are and what we need to do.”
As an academic and research hospital providing specialized mental health, addiction and geriatric care to some of the most complex and disadvantaged people in Ontario, Waypoint’s belief in patient involvement is bolstered by the work of the PCFC — a non-profit organization composed entirely of indi-
viduals with lived experience.
“Each patient and client we speak to brings bravery and expertise to the information they share,” said Jodie Erb, the PCFC’s Executive Director. “It’s so important that we as professionals continue to learn and grow based on their expertise.”
The PCFC plays a key role in supporting clients, navigating services, and representing patient voices across committees and working groups. Their guiding philosophy — “nothing about us without us” — echoes throughout Waypoint’s programs and research.
This model illustrates what’s possible when patient voices are treated not as optional, but foundational. Doing so not only delivers better care — it builds a system where clients are seen, heard and respected.
Travis Mealing is a Communications Officer at Waypoint Centre for Mental Health Care. n H
Travis Mealing is a Communications Officer at Waypoint Centre for Mental Health Care.
Growing crisis of communicable disease in Canada in tandem with US cuts
Canada must address the growing crisis of communicable diseases that has occurred in tandem with a rise in misinformation that threatens our health systems, argue authors in an editorial in CMAJ (Canadian Medical Association Journal).
“A crisis of communicable diseases is unfolding in North America, just as Canada’s health systems’ responses are being hampered by the dismantling of public health and research infrastructure in the United States,” writes family physician Dr. Shannon Charlebois,
Continued from page 4
medical editor, CMAJ, with coauthor Dr. Jasmine Pawa, Dalla Lana School of Public Health, University of Toronto, Ontario. “Coordinated attacks on US health institutions by the country’s executive office have drastically reduced their capacity to collect, interpret, and share data in the service of public health delivery. This coincides with a concerning spread of novel and existing communicable diseases across the continent, including in Canada.”
The spillover effect of changes in the US will likely affect Canada and other countries around the globe, as
Canada is falling behind on Alzheimer’s disease treatments
Often these symptoms resolved when treatment was stopped, though in rare cases, the symptoms were permanent.
In some ways, arrival of these medications ushers in a new era of Alzheimer’s disease treatment, reminiscent of the approach we now take towards cancer -- detection of disease at the earliest possible stage, and potential treatment with medications capable of serious side effects.
Canadians who have been diagnosed with Alzheimer’s disease deserve the chance to evaluate the potential benefits and side effects of these new medications, to determine, for themselves and their families, if they wish to proceed to treatment. The decision process must include fully informed consent, guided by real-world results from patients across the world.
Indeed, patient registries (collections of anonymous patient data) play a critical role in tracking benefits and side effects of new medications over time. Vaccinations for COVID-19 were subject to similar monitoring for
serious side effects, after the vaccines were approved for general use. A similar patient registry for those treated with new Alzheimer’s disease treatments in Canada will be essential.
At the end of July 2025, Canada will welcome the world’s Alzheimer’s disease clinical and research community to the Alzheimer’s Association International Conference (AAIC), held in Toronto this year. The message will be clear: Canada should provide the same treatment opportunities to its citizens as other jurisdictions around the world.
The memories and autonomy destroyed by Alzheimer’s disease continue to make it one of the greatest health challenges faced by Canadians. New anti-amyloid treatments are not a cure, though they represent desperately needed progress. They represent hope that we will one day live a long and full life without the ravages of dementia.
A long and full life, for ourselves and those we love.
Dr. Andrew Frank is a cognitive neurologist at Bruyère Health, and investigator at Bruyère Health Research Institute in Ottawa.
Katherine C. Pearson is a Professor of Law and Arthur L. and Sandra S. Piccone Faculty Scholar at Dickinson Law, Pennsylvania State University, and the 2024-25 Visiting Research Fellow in Health Law, Policy and Ethics at the University of Ottawa’s Centre for Health Law.
programs to track infectious diseases and address potential pandemic threats like avian flu have been cut or cancelled, and specialized staff with the capacity to rapidly develop reliable tests have been fired. Canada and other countries have relied on this work for disease surveillance and public health preparedness.
Now is the time for Canada to act on long-standing calls to strengthen health surveillance systems, improve interoperability and data exchange between electronic medical records and health systems, and better document and report rates of vaccine coverage.
The editorial outlines the threats from several infectious diseases to
Canadians — information the public should be made aware of. However, “[p]eople living in Canada are vulnerable to a cross-border bleed of not only microorganisms, but also of attitudes, health misinformation, and exposure to biased US media.” write Charlebois and Pawa.
“Canada does not have control over the situation south of the border, but strengthening national capacity to manage communicable diseases by optimizing data collection and interprovincial sharing of the information required to do this is possible.”
“Tackling communicable disease surveillance and misinformation in Canada” was published July 2, 2025. n H
Iron deficiency in females is common but treatable
Iron deficiency is common, especially in females of reproductive age and pregnant people, yet it is preventable and easily treated. A review article in CMAJ (Canadian Medical Association Journal) provides guidance to clinicians on diagnosing and managing iron deficiency in females.
The 2 types of iron deficiency are nonanemic iron deficiency (NAID) and iron-deficiency anemia (IDA). Both can have health consequences, such as fatigue, poor cognitive function, and reduced work performance with NAID and more serious effects with IDA, including an increased risk of death.
It is estimated that almost 50% of the entire population in some low- and middle-income countries is iron deficient, and higher-income countries are not immune. A 2022 Ontario study estimated from blood screening samples that 38% of nonpregnant females had NAID and 13% had IDA. Another Ontario study based on samples from 2013 to 2018 found that 53% of pregnant patients screened had NAID.
“Iron deficiency is the most common cause of anemia despite being preventable and easily treated,” writes Dr. Michelle Sholzberg, Unity Health Toronto, Toronto, Ontario, with coauthors. “Treatment of iron deficiency is usually straightforward and, given the burden of disease, its diagnosis and management should be prioritized.”
In people with symptoms of iron deficiency, clinicians should ask detailed questions about menstruation since heavy bleeding contributes to iron deficiency. The authors suggest testing complete blood count and ferritin for asymptomatic females every 3 years, especially in patients with heavy menstruation or who are planning to get pregnant.
“Testing of asymptomatic females and females at risk for iron deficiency is appropriate given the subtle nature of some symptoms, which will sometimes be accepted as normal by patients.”
“Diagnosis and management of iron deficiency in females” is published July 2, 2025. n H
Youth at risk of suicide show early warning signs that adults often miss
Drawing on a landmark 25-year study that followed Quebec children into adulthood, McGill University researchers have identified two distinct patterns in how suicidal thoughts emerge and the early signs that are often missed.
Suicidal thoughts are increasingly common among youth, but how they begin and what mental health symptoms often precede them are poorly understood, the researchers said.
The study, published in JAMA Psychiatry, analyzed data from the Quebec Longitudinal Study of Child Development, one of only two studies in the world to follow a large group of young people over time and repeatedly track suicidal thoughts.
While most of the 1,600 youth in the study never or rarely reported suicidal thoughts, there were two clear pathways among those who did: about seven per cent began experiencing suicidal ideation in early adolescence (ages 12 to 13), while another five per cent first reported such thoughts for the first time as young adults (ages 20 to 25).
In the early-onset group, many had shown signs of mental health struggles in childhood. These included symptoms like disruptive behaviour, which tend to be more noticeable (external symptoms), and depression and anxiety, which are often harder to detect (internal symptoms).
“A striking finding is that parents and teachers often noticed the be-
havioural problems but overlooked the internal emotional distress,” said lead author Marie-Claude Geoffroy, associate professor in McGill’s Department of Psychiatry, researcher at the Douglas Research Centre and Canada Research Chair in Youth Suicide Prevention.
In contrast, those whose suicidal thoughts began in young adulthood typically showed only internal symptoms, starting in their teen years.
“When taken seriously, these warning signs can lead to early interventions that could help safeguard children’s development,” said co-author Charles-Édouard Notredame, a child and youth psychiatrist at Lille University Hospital.
Age-appropriate support, including
mental health programs in schools, could be especially effective in reaching children and teens at the right time, before suicidal thoughts take hold, he added.
Suicide is the second leading cause of death among youth and young adults in Canada, according to national data.
“Suicidal ideation in youth is still too often dismissed as a ‘phase’ that will pass,” said Geoffroy. “Our findings highlight the need to start suicide prevention early.”
“Mental Health Antecedents and Correlates of 2 Distinct Developmental Pathways to Suicidal Ideation” by Marie-Claude Geoffroy, Sasha MacNeil and Vincent Paquin et al., was published in JAMA Psychiatry. n H
Nation-leading hospital efficiency freed up billions but further gains are unrealistic
The Ontario Hospital Association (OHA) today released the third edition of Ontario Hospitals – Leaders in Efficiency, a report detailing the nation-leading efficiency of Ontario’s hospitals. Unfortunately, further gains using traditional approaches are no longer realistic due to enormous demand for services from a growing and aging population and, like all other parts of the economy, rising pressures on costs.
“When it comes to efficiency, Ontario’s hospitals continue to lead the country. Ontario spends $1,935 per person on hospitals, the lowest in Canada, while ensuring access to high quality services for millions of patients every year,” said Anthony Dale, President and CEO of the OHA. “While the degree of efficiency achieved over the years has been remarkable, it’s clear that addressing the challenges of
the future will require further capacity planning and long-term investments in technological and clinical innovation, rather than relying on traditional ideas and approaches.”
As reflected in this year’s annual efficiency dividend, if Ontario spent the average rate per capita on hospitals as all other provinces, the additional cost to the province would be $4.4 billion. Ontario is unique in Canada – only here do independent boards, made of local volunteer community leaders, have accountability for hospital governance and oversight. This local governance and prudent stewardship enabled hospitals to remain resilient for many years by focusing on cost containment while serving their local communities and regions, despite capacity challenges within the hospital sector and across the health services continuum. For years, this freed up billions
of dollars each year for the provincial government to invest in other public services and programs that benefit Ontarians.
However, Ontario hospitals are facing very significant financial challenges today and the underlying financial position of the sector is under considerable pressure. Demand for health care is rising. Not only has Canada’s population rapidly grown in recent years, but as confirmed in last year’s release of the Patterns of Illness Report by the Dalla Lana School of Public Health, Ontarians will live longer with chronic disease. Many people will have multiple illnesses and there are rising rates of illness across all age groups.
“Hospitals today are doing everything they can to ensure that the taxpayers’ dollars are spent effectively. But we’re looking at rising demands, various cost pressures, aging infrastructure
and changing population demographics that are expected to intensify in the coming years,” Dale said. “Just as we’re adapting our economy in the face of trade conflicts and a changing world, we need to prioritize health care as one of our competitive advantages. Technical and clinical innovation within health care will also become increasingly important.
Continuous improvement efforts have resulted in Ontario achieving the second lowest hospitalization rate, the lowest average length of stay in acute care hospitals, and the lowest cost of an inpatient stay among all provinces. Building on this track record of operational excellence will require thoughtful planning to expand hospital capacity where needed, ongoing investment in broader system capacity and innovative approaches that shape the future of health care in Ontario. n H
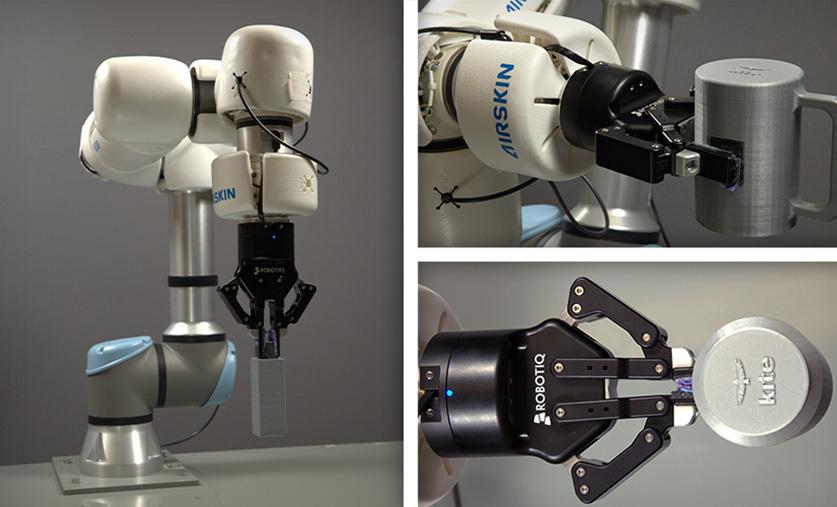
Reshaping robotic rehabilitation
For individuals recovering from a stroke or spinal cord injury, restoring hand and arm function is essential to regaining independence.
Robot-assisted therapy is an emerging rehabilitation tool that offers consistent and precise movement training. However, its real-world applicability remains limited due to variability in hand use during daily activities outside clinical settings.
Researchers from UHN’s KITE Research Institute are addressing this challenge by integrating real-world objects into robot-assisted therapy.
The research team, led by Dr. Milos Popovic, senior author of the study, Senior Scientist and Director of the KITE Research Institute, and a professor and Director of the Institute of Biomedical Engineering at the University of Toronto, adapted a common clinical assessment tool — the Toronto Rehabilitation Institute-Hand Function Test (TRI-HFT) — for use in robot-assisted therapy.
Traditionally, the TRI-HFT involves manipulating everyday objects that require different grips, including a mug, a sheet of paper, a book, a credit card and a pencil. By redesigning these objects for robotic compatibility, the team enabled the robotic arm to inter-
act with them, allowing the test to be used during therapy.
The team redesigned and 3D-printed 11 TRI-HFT objects. Testing demonstrated that the robotic arm successfully picked up and moved each object, achieving a 100 per cent success rate.
Additionally, five participants with normal arm and hand function evaluated the system’s safety and usability, reporting that it was comfortable, engaging and easy to use.
By combining advanced robotics with traditional rehabilitation tools, this approach enhances the functionality, personalization, and real-world application of robot-assisted therapy.
Modified, 3D-printed TRI-HFT objects and the robotic arm gripping them. (Phots: UHN’s KITE Studio)
The research, whose co-author is Dr. César Márquez Chin, scientist at the KITE Research Institute and a faculty affiliate at the Institute of Biomedical Engineering at the University of Toronto, explores a new approach to robotic rehabilitation and the findings lay the groundwork for more effective recovery strategies and improved longterm outcomes.
Future research will explore broader clinical applications and adaptability across different robotic systems. n H
Investigating leukemia cell lineages
B lymphocytes (B-2cells) are a type of white blood cell important for immune function. They develop from stem cells through several stages. Malignancies in this lymphoid lineage can lead to acute lymphoblastic leukemia. (Photo: Getty Images)
Pediatric patients with B-cell acute lymphoblastic leukemia (B-ALL) — a cancer of the blood and bone marrow — can sometimes relapse with features of both B-ALL and a different type of
blood cancer, acute myeloid leukemia (AML).
In a study published in Nature Cancer, Dr. John Dick at UHN’s Princess Margaret Cancer Centre (PM) and Dr. Charles Mullighan at St. Jude Children’s Research Hospital investigated the ability of cells to change from one type to another in B-ALL, and how it affects treatment response.
B-ALL is characterized by the abnormal proliferation of immature lym-
phoid cells — immune cells that develop into specific types of white blood cells, such as B lymphocytes (B-cells).
Categorizing patients into B-ALL subtypes and identifying associated risk levels can predict treatment response and likelihood of relapse. Although pediatric B-ALL cure rates have improved, high-risk children still face poor outcomes, and relapse remains a major cause of death. Evidence suggests that B-ALL can
switch from lymphoid to myeloid lineages after certain immunotherapies or chemotherapy. This phenomenon occurs when a cancerous cell originally classified as lymphoid (ie: a B-cell precursor) transforms into a myeloid-like cell, such as a granulocyte or macrophage precursor.
Malignancies in these lineages lead to different blood cancers, such as ALL from lymphoid cells and AML from myeloid cells.
Robot-assisted therapy combines technology and movement to support motor recovery, offering more precise, consistent and personalized care. Aisha Raji, the study’s first author, is pictured adjusting a robotic arm used in therapy. (Photo: UHN’s KITE Studio)
Modified, 3D-printed TRI-HFT objects and the robotic arm gripping them. (Photo’s: UHN’s KITE Studio)
ALL and AML have different molecular features and require different treatment targets.
These findings underscore the importance of understanding B-cell development and lineage switching to predict treatment response. To achieve this, the team analyzed the active and expressed genes (i.e., the transcriptome) of individual leukemia cells from 89 B-ALL patient samples and compared them to normal human B-cell development.
To do this, they developed the first comprehensive single-cell reference atlas of normal human B-cell development, spanning over 100,000 cells from various tissue sources.
In constructing this atlas, they discovered that a population of stem cells previously thought to only be capable of producing lymphoid cells (such as B cells) had the hidden ability to produce myeloid cells in the experimental setting.
The researchers found that some B-ALL patient samples contained leukemia cells that highly resemble this population of stem cells with myeloid
potential. B-ALL patients who had more of these specific leukemia cells were also more likely to have genomic alterations associated with lineage shifts from lymphoid leukemia to myeloid leukemia at disease relapse.
“Some of these immature lymphoid
cells can still develop into myeloid cells,” says Dr. Dick, a Senior Scientist at PM, professor in the Department of Molecular Genetics at the University of Toronto and the Helga and Antonio De Gasperis Chair in Blood Cancer Stem Cell Research.
“This ability, called multipotency, may explain the transition from ALL cases to AML in response to B-cell-specific immunotherapy,” adds Dr. Dick, co-senior officer of the study.
“We developed a Multipotency Score to describe the abundance of multipotent leukemic cells in patient samples. This score can help predict clinical outcomes,” says Dr. Andy Zeng, cofirst author of the study. When tested in independent B-ALL patient datasets, a higher Multipotency Score was associated with higher-risk disease and older age. A high score in pediatric patients was also found to be linked to chemo-resistance and worse overall survival.
“Our research advances our understanding of normal and cancerous B-cell development, which may ultimately enhance risk stratification and therapy development for B-ALL patients,” says Dr. Mullighan, co-corresponding author of the study. This article was submitted by UHN News.
Compassion in aging: Celebrating a year of Southlake’s Acute Care of the Elderly Unit
By Lindsey Furlanic
When Southlake Health first opened over a century ago, the population it served looked very different. It was smaller and younger. Since then, things have changed significantly. Seniors now make up more than half of all patients admitted through Southlake’s Emergency Department — a demographic shift that has forced the hospital to reimagine how it cares for older adults.
Enter Southlake’s Acute Care of the Elderly (ACE) Unit, a new kind of hospital unit created specifically to meet the complex needs of older adults. Since opening in June 2024 during Seniors Month, the ACE Unit has become a cornerstone of specialized senior care in northern York Region and southern Simcoe County. Now, just over a year later, more than 750 patients, with an average age of 85 years old, have come through the ACE Unit for leading edge care, close to home. Designed to promote mobility, independence, and recovery, the unit offers early rehabilitation, function-based assessments, and personalized care plans that help improve outcomes and support a safe return home or to the community. The results speak for themselves: 61 per cent of patients have been able to return home with additional supports, reducing the need for long-term care or extended hospital stays.
“The ACE Unit is more than just rooms and beds in a hospital,” says Jennie Popplow, Director of Senior Care at Southlake. “Our team has created a space where seniors feel seen, heard, and supported, and we’re just getting started.”
Traditional hospital units, while well-equipped for acute interventions,
aren’t typically tailored to the needs of older adults, who are more vulnerable to complications and functional decline. Southlake has collaborated with leading geriatricians from hospitals across Ontario to implement best practices in senior care in the ACE Unit, including staff training, the creation of a senior-friendly environment, and models of care tailored to the needs of elderly patients. Today, patients on Southlake’s ACE Unit are significantly less likely to experience functional decline or require long-term care when compared to other units. In fact, 95 per cent of patients have maintained or improved their level of function from admission to discharge. Beyond the walls of the unit itself, the ACE team is scaling its learnings to other parts of the hospital. Starting with the Senior Friendly 7 learn-
ing series that focused on topics like delirium, mobility, and continence, the ACE Unit is working with teams across Southlake to enhance care for older adults.
Dr. Youmna Ahmed, a geriatrician at Southlake, believes the team-based model is what sets the ACE Unit apart. “Caring for seniors requires a different approach that considers the whole person, not just their diagnosis,” she said. “We work together as a team to focus on what matters most to our patients: maintaining their independence, preventing decline, and supporting recovery. It’s truly rewarding work.”
Southlake’s approach focuses deeply on people, and for patients and their families that has made all the difference. One family member whose loved one, Emil, 89, received care on the
unit described it this way:
“We’ve been pleased with the quality of care and compassion from the medical team in the ACE Unit. In communicating with the staff, they made it clear they love ACE because it allows them the opportunity to connect with their patients in a meaningful way. It’s not easy to have a loved one in the hospital, but the unit felt peaceful and welcoming.”
That sense of connection and calm is exactly what the team set out to create – a unit that doesn’t just manage symptoms, but also restores autonomy and protects the dignity of seniors.
“The success of the ACE Unit is a direct result of the incredible passion and dedication of our team,” said Jennie Popplow, Director of Senior Care at Southlake Health. “They’ve created a space where older adults feel respected, safe, and empowered. This is just the beginning of how we’ll continue to transform senior care at Southlake.”
The ACE Unit is part of a broader network of programs at Southlake focused on the needs of older adults, including the Aging Well Clinic and Geriatric Outreach Team. These programs are designed to help older adults “age in place” by promoting independence, mobility, and safe transitions back to the community. Together, they help ensure seniors receive connected, compassionate care both inside Southlake and beyond.
With Canada’s population aging rapidly, the stakes couldn’t be higher. For hospitals like Southlake, the future is already here, and the first year of the ACE Unit offers a glimpse into what that future can look like: patient-centred, team-based, and grounded in compassion. n H
Lindsey Furlanic is a Communications Strategist at Southlake Health.
New podcast delivers cutting-edge geriatric care insights
By Lindsey Furlanic
The Geras Centre for Aging Research based at Hamilton Health Sciences’ (HHS) St. Peter’s Hospital is bringing the latest breakthroughs in healthy aging and geriatric care to listeners across Canada and around the world through its newly launched podcast series, GeriEvidence.
Geras is a centre at HHS that’s affiliated with McMaster University. It’s home to top Canadian researchers, including HHS health-care providers who also lead groundbreaking studies into healthy aging and geriatric care.
Sharing the latest research on digital airwaves
The podcast series features guest experts from Geras, HHS, McMaster and around the world, and is available on Spotify and the Geras website. It’s hosted by Dr. Alexandra Papaioannou, Geras’ executive director and an award-winning geriatrician, professor of medicine at McMaster, and Tier 1 Canadian Institutes of Health Research (CIHR) chair. GeriEvidence is supported by the CIHR Institute of Aging and the Betty Havens Prize for Knowledge Mobilization in Aging, which Papaioannou received in 2023.
“GeriEvidence is a great way for us to share the important work and research happening here in Hamilton and around the world,” says Papaioannou, adding that episodes are released monthly, with each lasting about 25 minutes. “We’re filling a niche market, because there are very few podcasts offering such information at this level of expertise.”
Each episode focuses on a different aspect of aging research and geriatric care, with topics so far including fall prevention, delirium, dementia, innovations in hospital care, and geroscience — the biological processes that drive aging and increase the risk of age-related disease.
Launched in December 2024, the
first few episodes were aimed at healthcare professionals, but in the spring of 2025 the focus shifted to the general public.
“What we do in geriatrics is so important to people’s quality of life, so we want to share the very best evidence-based information with as wide an audience as possible,” says Papaioannou, who produces GeriEvidence with a small team that includes Dr. Tricia Woo, an HHS geriatrician and professor in McMaster’s department of medicine; Dr. Patricia Hewston, an occupational therapist, Geras research associate and assistant clinical professor of rehabilitation science at McMaster; and Geras research assistant Caroline Marr.
Welcoming renowned guests
The most recent episode welcomed geriatrician Dr. Kenneth Rockwood, professor of medicine and clinical research professor of frailty and aging at Dalhousie University, and one of the world’s leading voices on frailty. A member of the Order of Canada, Rockwood has shaped the field through more than 600 peer-reviewed publications and nine books, transforming how clinicians and policymakers think about aging.
In conversation with Papaioannou, Rockwood unpacks Frailty: What It Is and What Can Be Done, explaining why frailty matters for every healthcare setting, how to recognize it early, and which practical, evidence-based steps can turn the frailty journey into an opportunity for healthier, more person-centred aging.
Renowned Hamilton geriatricians Dr. Irene Turpie and Dr. Christopher Patterson were interviewed for a segment on the history of geriatric care nationally and globally. Both worked at HHS St. Peter’s Hospital before retiring and are now professors emeriti at McMaster.
Guest experts from HHS have also included Dr. Anthony Levinson, a psychiatrist at HHS Juravinski Hospital and Cancer Centre, where many of his patients are older adults. Levinson is also a researcher and the director of McMaster’s division of e-learning innovation.
Levinson chatted with Papaioannou about online solutions for delivering high-quality health education on aging to the public and health-care professionals. The dementia risk reduction e-lesson developed by Levinson and his
team is an excellent example of how evidence-based research translates into practical, hands-on support for Canadians interested in improving their brain health and reducing their risk of dementia.
Future podcasts will revisit delirium, fall prevention and healthy aging as topics, because they’re pressing issues for many older adults and the people caring for them, says Papaioannou. “We want to be evidence-informed and helpful for the public in a very practical way.”
Other guests have included Dr. Gustavo Duque, a distinguished geriatrician and biomedical scientist in Montreal and geriatrician Dr. Roger Wong from British Columbia, who was appointed to the Order of Canada. Dr. Kelly Kay, executive director of Provincial Geriatrics Leadership Ontario (PGLO), joined Papaioannou to share her leadership journey in health-care transformation and highlight the importance of collaboration in improving geriatric care across Ontario and beyond.
Toronto physicians Dr. Amy Freedman and Dr. Morna McDougall, coleads of the Preventative Care for Older People (PCOP) tool, were also guests. The PCOP tool is a resource created to help doctors and health-care teams provide better care for adults aged 65 and older. It’s designed to streamline preventive care for older adults, particularly those with multiple complex conditions.
“Our podcast is an exciting new way for us to share pearls of wisdom and the incredible research happening in Hamilton, Canada and around the world,” says Papaioannou.
“With GeriEvidence, everyone has the opportunity to have the most leading-edge, up-to-date information from geriatric care experts, scientists and researchers at their fingertips.”
Have an idea for a future episode or feedback to share? Email the GeriEvidence team at gerievidence@gmail.com.
Dr. Alexandra Papaioannou is the host of GeriEvidence, a recently launched podcast by the Geras Centre for Aging Research that brings the latest research findings to listeners. Papaioannou is Geras’ executive director and an award-winning geriatrician. Recent guests included geriatrician Dr. Kenneth Rockwood, professor of medicine and clinical research professor of frailty and aging, who was visiting from Geras from Dalhousie University in Halifax. Photo by Josh Carey
Lise Diebel works in communications at HHS.
Empowering change through patient and community engagement at Humber River
At Humber River Health (Humber), community engagement and patient advocacy are more than just strategic priorities, they are commitments rooted in equity, listening, and action. One recent example of this is the series of Anti-Black Racism (ABR) Listening Sessions, held with both internal and external stakeholders, to understand and address how systemic racism affects access to care, patient experience, and workplace belonging.
These sessions were part of Humber’s broader strategic direction to embrace Equity, Diversity, and Inclusion (EDI), a key pillar within their 2023–2026 Strategic Plan. This direction includes a clear objective, to address racism, with a particular focus on anti-Black racism. Given that a significant portion of the community served by Humber identifies as African, Caribbean, and Black (ACB), this work is essential to ensuring safe, equitable, and inclusive healthcare.
The sessions
Between February 2024 and March 2025, Humber hosted 15 ABR listening sessions, nine internally with staff, physicians, and volunteers, and six externally in community settings across North West Toronto. These sessions were not designed to solve problems in the moment, but to deeply understand the lived experiences of those impacted by anti-Black racism. From patients hesitant to share sensitive information with providers due to fear or past harm, to staff and volunteers describing feelings of exclusion, the stories shared were a powerful reminder of how racism can manifest across all aspects of the healthcare journey.
Importantly, these sessions were led by trained internal facilitators, including members of the hospital’s leadership
“EVERY STORY IS A LIVED TRUTH,” SHARED ONE OF THE SESSION FACILITATORS. “OUR ROLE WAS TO LISTEN, NOT TO CORRECT OR EXPLAIN. THIS WAS ABOUT HEARING WHAT PEOPLE HAVE EXPERIENCED, WITHOUT DEFENSIVENESS, AND UNDERSTANDING WHAT NEEDS TO CHANGE.”
team. This choice highlighted the responsibility of leaders to actively listen, not just observe from a distance. Facilitators underwent training to ensure they could create safe spaces and practice active, nonjudgmental listening.
“Every story is a lived truth,” shared one of the session facilitators. “Our role was to listen, not to correct or explain. This was about hearing what people have experienced, without defensiveness, and understanding what needs to change.”
The results
The insights gathered through the listening sessions have since been thematically analyzed and validated by participants. This analysis formed the foundation of an internal Anti-Black Racism Action Plan, co-created with over 25 staff, physicians, and volunteers who stepped forward to help shape the hospital’s next steps.
Key areas of action include:
• Continue to foster workplace diversity and associated recognition opportunities
• Strengthen employee support and incident reporting mechanisms
• Education and training centered in compassionate, culturally inclusive care
• Better communication around wait times, process and care transitions
• Improvement for greater privacy when asking personal information and enhanced access to translational ser-
vices in treatment areas
• Continue to strengthen relationships with community service providers who support the African, Caribbean, and Black community to deepen understanding and enhance the overall patient experience
One example of progress already underway is the inclusion of equity and inclusion-based questions in Humber’s most recent engagement survey. Other efforts include the rollout of an anti-Black racism eLearning module for staff, and ongoing cultural celebrations and professional development focused on equity.
Empowerment and engagement
Patient education and empowerment is about making sure patients feel safe, respected, and heard. The ABR Listening Sessions revealed that when patients feel discriminated against or misunderstood, it directly affects their willingness to share important information, which can impact diagnoses, treatment adherence, and overall health outcomes.
By engaging directly with the community, both within the hospital and externally, Humber is helping to build trust and foster long-term relationships. These relationships, particularly with local organizations such as the Jamaican Canadian Association, have helped ensure that engagement is grounded in
real, lived experiences and that recommendations reflect the needs of those most affected.
Another key success of the initiative was the hospital’s commitment to communication and accountability. Humber shared the findings of the listening sessions first with those who participated, followed by a hospital-wide town hall, an all-staff memo, and opportunities for anonymous feedback through digital forms. In addition, Humber also followed up with all six participating community organizations, ensuring that the external voices who contributed were kept informed and engaged in the outcomes of the sessions. This transparent approach helped reinforce that the sessions were part of a genuine process of listening, learning, and change.
Moving forward
While the listening sessions have concluded, the work continues. The ABR Action Plan is just one part of Humber River Health’s long-term commitment to addressing racism and creating a more equitable system for patients and staff. Equity-focused leadership, culturally responsive care practices, and community-based partnerships are the building blocks for the inclusive, compassionate health system that Humber is striving to build.
“The act of listening itself can be healing, but listening must lead to action,” said one of the facilitators. “When we carry what we have learned into our policies, our practices, and our decision-making tables, that is when we begin to create true change.”
By elevating the voices of those historically marginalized, and embedding equity into its operations, Humber River Health is demonstrating how hospitals can be catalysts for trust, empowerment, and community-led transformation. n H
Signs of progress Transforming child health in Canada
By: Emily Gruenwoldt
veryone remembers March 2020, as the world was taken over by the COVID-19 virus, and the years of chaos and adaptation that ensued. It’s undeniable that COVID-related school closures, lockdowns and restrictions have had a major impact on Canada’s children.
COLLABORATION AND PARTNERSHIP ACROSS THE SECTOR
We wanted to know what else had changed in child health in that period. So, we asked our member organizations, a diverse network of health experts, families, and health system leaders dedicated to advancing the health and wellbeing of the 8 million children and youth in Canada. Here are four new trends that are worth celebrating.
MORE FOCUS ON DEVELOPMENTAL HEALTHCARE
Last year, the Ministry of Children, Community and Social Services of Ontario said that one third of all kids starting school need clinical care from developmental health providers. This means that demand for services is growing, along with the recognition that this type of care is foundational to lifelong health. Concurrently, the sector has also seen its first significant funding boost in over a decade—with $60 million in 2021 and an additional $45 million in 2023 as part of the $331 million interministerial Make Kids Count initiative. This cross-sectoral initiative was based on a recognition that different sectors in child health need to work together so that care is seamless for kids.
This type of collaboration is also developing in the research sector, as exemplified by the fun-named POPCORN (Pediatric Outcome ImProvement through Coordination of Research Networks) Network. POPCORN brings together the largest pediatric Canadian networks that currently exist to study child health. By harmonizing definitions, outcomes, and processes to create a uniform data structure, making logistics easier for starting a new study in children’s health, and enabling new collaborations, the platform will greatly advance pediatric research in Canada.
Similarly, the Canadian Institutes of Health Research’s investments in preterm birth research, particularly in the Canadian Neonatal Network, have led to healthier preterm infants. Over a 10-year period, Canada moved from last place (among 10 comparable countries) for preterm birth outcomes (death or severe complications) to being among the top globally.
INDIVIDUALIZED CARE AND PRECISION MEDICINE
At SickKids in Toronto, the Precision Child Health movement was launched in 2020, challenging a onesize-fits-all approach to medicine by using integrated data about each child’s unique genes, biology and environment to tailor care. One impressive milestone was the delivery of
the first individualized gene therapy in a single patient. SickKids is also building this network through partnerships with CHU Sainte-Justine in Montreal.
Also in Toronto, Holland Bloorview Rehabilitation Hospital is bringing together a first of its kind cohort of expert scientists, clinicians and people with lived experience, across several institutions through the Canadian Precision Health Initiative (CPHI). Together, they will create the largest genomics dataset, dedicated to understanding childhood onset neurodevelopmental, mental health and brain injury conditions. These efforts will democratize knowledge on genetic differences underlying neurodiversity, brain injury and mental health to support personalized health solutions for all.
WRAPAROUND SERVICES THAT FOCUS ON SUPPORTING THE WHOLE FAMILY
We now know that supporting caregivers enhances children’s health outcomes. At Kids Brain Health Network, they have expanded beyond discovery research to focus on implementation: scaling and spreading proven solutions that support families of children with disabilities. They are investing in project teams that are ready to implement evidence-based solutions in real-world settings.
Another example is the Extensive Needs Service (ENS) program at Holland Bloorview. ENS provides individualized and personalized care, ensuring each client receives the care they need, at the right time, in the
right place, and in a manner centred around their unique needs.
WE CAN’T DO THIS ALONE
Despite all these successes, we also know that children, youth and their families are experiencing long and costly delays for essential and time-sensitive healthcare services. In many jurisdictions, and for many services, children are now waiting longer for these services than adults. As a wealthy nation, Canada has all the resources necessary to meaningfully and measurably improve children’s health and wellbeing, but what will it take? It will take everyone – all levels of government, elected officials, corporate and philanthropic partners, community and healthcare leaders – working together to improve children’s health outcomes in Canada. The issues are complex but better is possible. n H
Emily Gruenwoldt is CEO and President, Children’s Healthcare Canada.
Emily Gruenwoldt
Child Health & Health
Child Health & Health
System Researchers System Researchers
SPARK: SPARK:
I M P A C T I M P A C T
Your go-to resource for knowledge mobilization products and services.
Free consultation on your grant
Free consultation on your grant development & knowledge development & knowledge mobilization plan. plan.
Costs covered through grant budget.
Access to a variety of knowledge
Access to a variety of knowledge tools and platforms. tools and platforms. Costs covered through grant budget.
Little patients, big lessons: SickKids putting their own stamp on pediatric emergency medicine education
SickKids
Emergency Department is a global leader in medical education, with physicians training the next generation while delivering world-class clinical care.
By: Sherina Harris
In the Emergency Department (ED) at The Hospital for Sick Children (SickKids), it’s not unusual to see a physician racing down the hallway while reviewing a differential diagnosis or doing “just-in-time training” with a trainee to offer a refresher before a procedure.
That balance takes a lot of practice, notes Dr. Jason Fischer, division head of Paediatric Emergency Medicine (PEM) at SickKids — but it’s something the team’s “incredible staff” of teachers excel at.
“The emergency department is not a very predictable environment, but then on top of that, what makes our place very special is that we have people that have found ways to deliver high quality education on the fly, at the bedside,” he says.
including medical students, physician assistant students, residents and fellows. The opportunity to teach the next generation is something that keeps staff working in the ED sometimes for decades, on top of the rewarding clinical work of taking care of the sickest kids.
“The clinical work can become routine after a while, so that academic outlet, that ability to put their own stamp on medical education, is so important to allow people to stay invigorated and enthused,” Fischer says.
Meet five ED physicians who excel at their unique approaches to medical education.
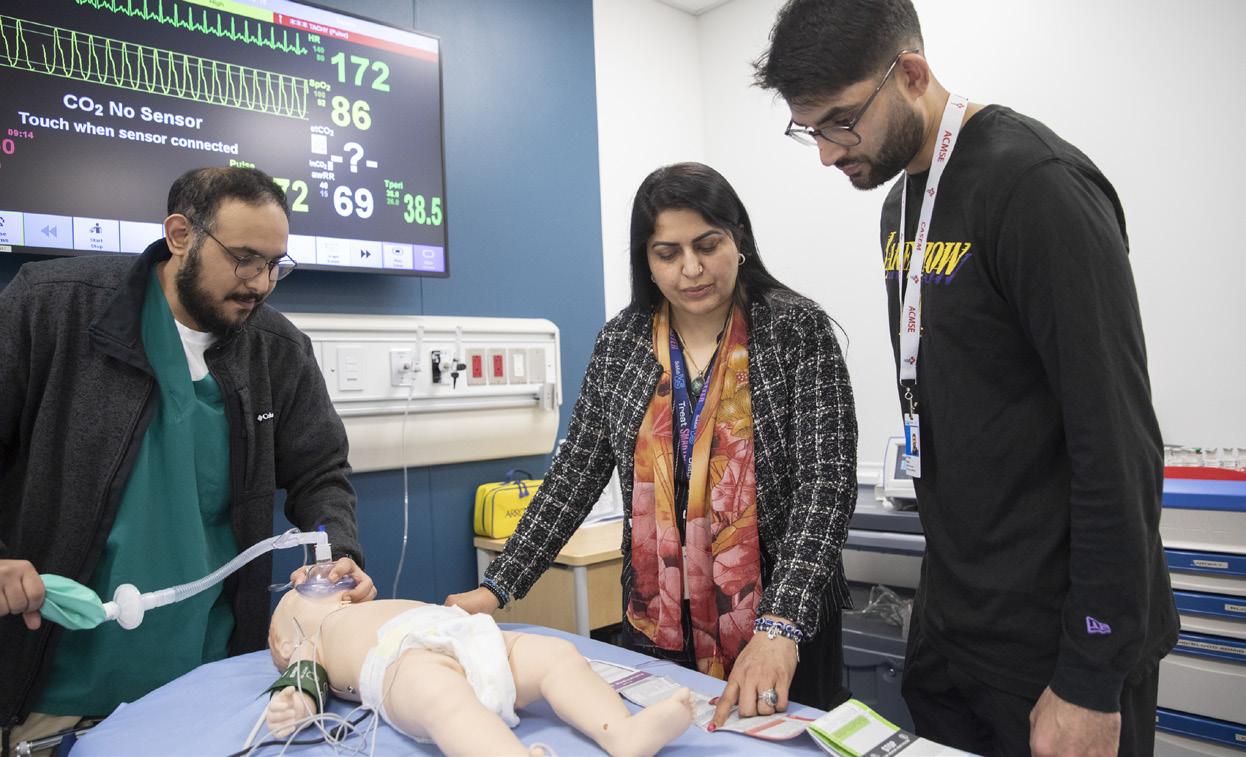
Dr. Jabeen Fayyaz
SickKids Emergency Room Physician
Dr. Jabeen Fayyaz is motivated by her desire to care for the sickest patients.
“Minutes matter,” she says, “and you
SickKids’ ED is a global leader in medical education and international training. As a teaching hospital affiliated with the University of Toronto, it welcomes between 350-400 medical learners a year from all over the world,
can make a huge difference in their lives by providing the best care, the safest care, in the first hour of them presenting with critical symptoms.”
Fayyaz started her medical career in Karachi, Pakistan. She came to Sick-
Kids as a fellow in 2016, and is now a staff physician in the division of paediatric emergency medicine and Medical Director of SimKIDS simulation program. Fayyaz was also recently voted President-Elect of the International Paediatric Simulation Society.
“It’s a humbling journey to come from a different setting, different perspective and to get to be a faculty member here,” she says.
“When I joined SickKids as a fellow, it was a very ‘aha’ moment for me when I realized simulation can play such an important role at different levels of teaching and learning.”
Fayyaz has a particular interest in exploring the impact of simulation on patient care and workflow and processes: looking at whether the ways of teaching using simulation are effective – and whether they are actually improving patient care.
“My passion is education, but as an acute care physician, I always want to see whether the simulation is actually making a difference, whether what I’m teaching is actually making the care better,” she says.
Dr. Savithiri Ratnapalan
Dr. Savithiri Ratnapalan starts each shift in the ED with “juice rounds.” She visits every patient, whether they’re admitted or not, to check on the child and see if parents or caregivers have eaten or need a bathroom break.
SickKids’ ED has a small supply of food like milk, juice, popsicles and crackers. The help she offers, whether a bite to eat, directions to the cafeteria or a person to stay with their child while they make a phone call, is sometimes exactly what caregivers need.
Ratnapalan, who has been at SickKids for 25 years, traces this practice back to an early experience at the hospital working with mentor Dr. Anna Jarvis. It has become a key learning she tries to impart on the trainees she now works with.
“You are a human being first, and so is the patient and their family — be human,” she tells trainees. “It’s a big privilege to take care of someone else’s child.”
One of her rewarding experiences was when one trainee told her recently “I learned how to be kind through watching you.” Ratnapalan says she
Dr. Fayyaz in a simulation with resident Dr. Faraz Damji and clinical fellow Dr. Rakan Alasqah.
Dr. Savithiri Ratnapalan
hopes the trainees she’s worked with will take their learnings throughout their career and that would have a ripple effect on the patients they care for and the people they train.
Dr. Suzan Schneeweiss
Working in emergency medicine means becoming accustomed to the fast-paced environment: as Dr. Suzan Schneeweiss says, “Things are always changing.”
That’s why Schneeweiss’s work on continuing professional development is so valuable. She has been on staff at SickKids for 32 years, and she is passionate about making education more effective.
“As physicians, we need to keep upto-date, find ways to keep education interesting and make it stick,” she says.
One way Schneeweiss does this is by organizing the SickKids’ Annual Paedi-
atric Emergency Medicine Conference, which ran for its 21st year in 2024. It’s open to learners from across the world. She also helped create SickKids’ Paediatric Emergency Procedural Sedation course, which combines lectures and simulation to allow participants to experience providing sedation and its challenges.
“We are training the next generation of physicians, including paediatric and adult emergency medicine specialists,” Schneeweiss says. “The education and experiences we provide our trainees is essential in shaping a healthier future for every child.”
Dr. Deborah Schonfeld
When teaching in SickKids’ Emergency Department, Dr. Deborah Schonfeld is motivated by the “lightbulb moments” where she can see a trainee get excited
and start to apply their learning.
Recognizing the unique, highly acute nature of the cases seen in the SickKids Emergency Department, Schonfeld created “acuity rounds” — a chance for trainees and staff to gather several times a year to review the most complex, rare or challenging cases they’ve seen.
“There are so many learning opportunities in those cases, the kind you don’t see unless you work at SickKids,” she says. “If there’s no forum to discuss them, the learning goes untouched.”
Schonfeld, who has been at SickKids since 2013, also got a chance to review the wide breadth of conditions she may come across in the ED as the co-editor, with paediatrician Dr. Shawna Silver, of the most recent 12th edition of The Hospital for Sick Children Handbook
Dr. Jonathan Pirie
Dr. Jonathan Pirie finds being an educator “balances the wear and tear” of the difficult specialty of emergency medicine.
“It’s an incredible experience to have an impact on someone’s journey or their discipline,” he says.
During his more than 30 years at SickKids, Pirie has helped to grow the hospital’s simulation program as the division of Paediatric Emergency Medicine’s first Simulation Director. He also created the Paediatric Emergency Medicine Simulation Fellowship, advanced training for trainees who have completed the PEM fellowship.
Pirie was drawn to simulation because it’s an uplifting learning experience. Occasionally cases can be emotional for
of Paediatrics — an internationally recognized reference guide for healthcare professionals caring for children. She felt uniquely suited to work on this project since “ED doctors are commonly described as ‘Jacks of all trades,’ because we need to be able to handle a wide range of medical issues that touch on every subspecialty.”
She and Silver, her co-editor, worked with more than 100 SickKids trainees, staff physicians, nurses, pharmacists and lab specialists to complete this resource designed to be used for bedside teaching, study and practice. Working on the book was a labour of love, she says. Schonfeld dedicated it to all the trainees whom she has taught and who have taught her.
participants, but he notes most simulations are a positive experience in a “psychologically safe” environment.
“We’re here to learn,” he says. “There’s no such thing as a perfect case. It’s a chance to practice and learn from each other.”
Trainees, he says, love simulation and always ask for more. SickKids PEM faculty are also expected to complete annual competency-based simulation education, a unique program that he developed in 2016.
“This is how we stay prepared. If everyone doesn’t have the opportunity to practice through simulation and develop their skills beforehand, they may not be prepared when it happens in real life.”
n H
Dr. Suzan Schneeweiss
Dr. Deborah Schonfeld
Dr. Jonathan Pirie
This article was submitted by the Hospital for Sick Children. Photo credit: Marta Iwanek.
Increasing access to autism assessments nationwide in partnership with families and autistic advocates
By Suelan Toye
Autism is a complex and diverse neurodevelopmental condition that is diagnosed in one in 50 children and youth in Canada. It affects how people communicate, learn and experience their world. No two individuals are alike.
The wait times, however, for a diagnostic assessment by an autism specialist are often over a year for families. These wait times are delaying access to essential services that have the potential to impact function and quality of life for children and their families.
To reduce these long wait times and ensure families can access assessments closer to home, Holland Bloorview Kids Rehabilitation Hospital is scaling up capacity nationwide.
A team of scientists and clinicians led by Dr. Melanie Penner, a developmental pediatrician and senior clinician scientist at the hospital’s Bloorview Research Institute, is engaging nearly 600 community-based clinicians across Canada each year to improve early diagnosis, support the development of integrated care models and build stronger connections –in close partnership with parents of neurodivergent children and autistic advocates.
“We know that long wait times for autism diagnoses can cause children to miss out on opportunities for therapy. We also know that after a diagnosis, it’s hard for kids to receive the ongoing care they need,” says Dr. Penner. “Through our ECHO Autism and ECHO AuDIO initiatives, we can democratize knowledge about autism diagnosis and ongoing care so that community-based physicians, nurse practitioners and other professionals across Canada can provide care that is tailored to the families living in their local communities.”
Using an inclusive teaching and learning approach, Dr. Penner co-developed the ECHO Ontario Autism hub with the vision of providing community practitioners the knowledge
and support they need to diagnose autism and provide ongoing care for autistic children and youth within their practice so that more families can receive timely care, closer to home.
Since 2018, the multidisciplinary team comprised of parents of neurodivergent children, autistic individuals and clinicians have supported the online education program funded by the province for over 500 community physicians, nurse practitioners, psychologists and physician assistants. Physicians and nurse practitioners, for example, can sign up for virtual sessions beginning each September. The sessions cover a range of topics, including understanding autism, the diagnostic process, promoting autism acceptance, school supports and strategies parents can use to support their child’s social communication skills while waiting for an assessment.
Maddy Dever, one of the ECHO Autism Hub team members and an autistic advocate and parent advisor, is passionate about their work with the hub. As a parent to four autistic children, they are a strong advocate for the inclusion and acceptance of autistic individuals.
“I’m grateful to work alongside health-care professionals who value my lived experience. Autism accep-
tance starts when providers truly listen to autistics and caregivers—and through ECHO’s ‘all teach, all learn’ model we all turn that listening into co-design, building pediatric care that centers every child.”
Building national capacity through ECHO AuDIO
To scale up capacity for autism assessments and ongoing care across Canada, Dr. Penner and her research team are conducting a national study called ECHO AuDIO (Extension for Community Healthcare Outcomes
Autism Diagnosis and Integrated Care Opportunities). This study is asking pediatricians coast-to-coast-tocoast about what they think providing good autism care in their communities looks like. The study is also reaching out to people who traditionally haven’t been asked what they think about autism care, including autistic people and people from equity-deserving groups.
Munira Khilji, a community advisor with ECHO AuDIO and parent of neurodivergent teenagers, believes that her family’s lived experiences can help to lift the voices of other culturally diverse families with autistic children.
“A big part of my role is to ensure this study meets the needs of equity-deserving groups. We want to ensure that we are advocating for culturally responsive care in communities.”
Dr. Penner and her team are now developing toolkits to support pediatricians provide the best possible care for even more families in their own communities.
“I’m excited to see how our initiatives can scale up to support more autistic children and youth with the right care, when and where they need it.” n H
Suelan Toye is a senior communications associate at Holland Bloorview Kids Rehabilitation Hospital.
ECHO Ontario Autism Hub team members
Munira Khilji, a community advisor with ECHO AuDIO and parent of neurodivergent teenagers and Dr. Melanie Penner, senior clinician scientist and developmental pediatrician.
By Lauren Ettin & Dr. Paul Gibson
A Childhood cancer care is closer to home thanks to POGO’s Satellite Clinic Network
childhood cancer diagnosis changes every aspect of life as families know it.
For Drago and Shanley Pavletic, their new reality also came with many 17-hour drives when their son, Luke, was diagnosed with acute lymphoblastic leukemia, a common childhood cancer with treatment that stretches over years. With limited care options close to home, it meant countless trips from Thunder Bay to London—1,500 kilometres each way—to access specialized care at Children’s Hospital at London Health Sciences Centre (CH, LHSC).
Every trip came at a cost—financially, emotionally, and logistically. While their daughter, Petra, stayed home with grandparents, the rest of the family navigated flight schedules, and when flights were cancelled, they made the hours-long drive—at times through bad weather and car trouble. The family relied on the kindness of friends and extended family, both in Thunder Bay and in London, to hold their life together.
For families like the Pavletics in Northwestern Ontario, that burden has now eased. In June, we at the Pediatric Oncology Group of Ontario (POGO) in partnership with Thunder Bay Regional Health Sciences Centre and Children’s Hospital at London Health Sciences Centre launched the ninth POGO Satellite Clinic. The Clinic provides local outpatient care for children and youth with cancer, closer to home and their support networks. The impact for families is significant. The ability to be at home more often allows families to maintain some semblance of normalcy and return to the daily rhythms of life—like work, school, socializing with friends and family, and participating in favourite activities.
POGO, as the official advisor to the Ontario government on childhood cancer, is the leader of Ontario’s world-class childhood cancer system. Our work is made possible thanks to
both provincial government funding, as well as donor support. Together with our partners, we have built a system of care that wraps around families supporting their physical and mental health needs from diagnosis to treatment, to survivorship and, when needed, to end-of-life care.
The existence and expansion of our Satellite Clinic Network isn’t just about convenience. It’s about improving access, ensuring equity, and opti-
mizing outcomes for the 500 children diagnosed with cancer every year in Ontario, and just as many who are seen annually in these Clinics. While children receive their primary cancer care at one of the five specialized pediatric cancer programs in Ontario—in London, Hamilton, Ottawa, Kingston or Toronto—at the appropriate time in their treatment, there is a smooth transition to a care team at a Satellite Clinic to receive aspects of their care
locally. The hospital care teams work in tandem, collaborating to deliver quality care in the setting that’s most appropriate to the child’s needs. Satellite Clinic care in community hospitals also frees up much-needed capacity in specialized pediatric cancer programs, while ensuring continuity and timeliness of care. This is a win-win for families and the system.
In 2024 alone, families made 6,500 visits to POGO Satellite Clinics for such services as chemotherapy, x-rays, ultrasounds and managing complications of cancer therapy. That’s 6,500 long-distance trips not taken. With less disruption to family life, it’s improved quality of life.
Care closer to home also lessens the overall financial burden on families. It is estimated that in the first three months after a child’s cancer diagnosis, families spend more than a third of their after-tax income on out-of-pocket costs—much of it on travel. That’s before accounting for lost income when a parent or caregiver leaves work to care for their child.
Outpatient care at POGO Satellite Clinics has also enabled patients to enroll in clinical trials, a core component to continued improved outcomes in pediatric cancer. This is thanks to a framework created by POGO with the Ontario Research Ethics Board (OCREB) to remove geographic barriers to clinical trials typically only accessed in major centres.
Through successive five-year provincial Childhood Cancer Care Plans, produced by POGO and our partners, our vision for care closer to home is clear: timely, equitable care in the right place. This requires strong, ongoing collaboration between POGO, care teams, hospitals, government and other partners. At its core, the POGO Satellite Clinic Network is a care delivery model that supports families like the Pavletics and others with the compassion they require at the most challenging time of their lives. n H
Lauren Ettin is CEO & Dr. Paul Gibson is Associate Medical Director, Pediatric Oncology Group of Ontario.
The Pavletic family
A The Transition Hub: Reimagining the transition to adult care through collaboration
‘transfer’ of care is defined as a single event where the responsibility for a patient’s medical care shifts from a pediatric to an adult provider. Up to 15% of youth in North America are living with a chronic condition and will progress to adult care1. Many patients experience disruptions in care during this transfer, often leading to negative health outcomes.
Those with complex medical conditions are particularly vulnerable and at risk of adverse health outcomes such as increased emergency room visits and hospitalizations, treatment nonadherence, and missed medical appointments2,3,4. These vulnerabilities are exacerbated by the addition of common psychosocial and developmental changes that youth undergo when entering young adulthood.
A ‘transition’ of care, on the other hand, is defined as the purposeful and planned process of moving from pediatric to adult care services beginning in adolescence and continuing into early adulthood5. One study done in the U.S. found that only about one in five adolescents with special health care needs successfully transitioned to adult health care services6. A successful transition was defined as a young adult having regular contact with an adult healthcare provider, adequate insurance, recent preventative care, satisfaction with services, and no recent delays in care.6
Established in 2019, the Health Hub in Transition to Adult Healthcare (Transition Hub) is a Canada-wide initiative that seeks to minimize barriers to a young adult’s transition to adult care. Pediatric care is often family-centered and offers centralized care, with parents and caregivers usually designated as primary advocates in a patient’s care. On the other hand, adult care can be turbulent, with emerging adults having to navigate multiple subspecialist appointments while managing their health conditions independently.
Dayle McCauley, the Transition Hub Manager, noted that while some
The Health Hub in Transition to Adult Healthcare (Transition Hub) is a Canada-wide initiative that seeks to minimize barriers to a young adult’s transition to adult care.
youth are prepared to transition independently, “for those that aren’t, they kind of fall through the cracks.” Without adequate preparation and development of self-efficacy, patients can become disengaged in their adult care.
Currently, the Transition Hub is advancing research and collaborations that further the landscape of transition care across Canada. An environmental scan was conducted to map the current state of transition resources and services. In response to inconsistent evaluation of transition, the health quality indicators project was established to identify a universal set of quality indicators for
youth with any chronic health condition transitioning to adult care. Furthering the Hub’s reach, the Comite Francophone was convened in 2021 with the aim of expanding the Canadian Francophone network, fostering collaborations amongst those working in transition care, and ensuring resources are available in both English and French.
“Everyone is working in silos,” says Dr. Anne Fournier, Chair of the Transition Hub, highlighting the need for collaboration amongst those looking to improve transition. The Hub aims to fill this gap through the mobilization of key stakeholders involved in the transition process. There are cur-
rently approximately 250 members situated across Canada. The Hub’s diverse membership – comprised of researchers, healthcare providers, youth with special healthcare needs, and caregivers – emphasizes the value in considering interdisciplinary viewpoints for facilitating a smooth transition for emerging adults.
The process of transition requires not only ongoing support from the patient’s pediatric team, but also collaboration and early engagement with adult healthcare providers. “We can’t stop at age 18 and call it done,” says Dr. Alene Toulany, Adolescent Medicine Specialist and Co-Lead of the Transition to Adult Care Program at SickKids (Toronto). “To truly improve outcomes, we need adult specialists and primary care providers engaged from the start. Transition is only halfway complete at transfer. We need ongoing support for both youth and their families on the adult side of care.” n H
Areputable ranking of the world’s top hospitals this year confirmed what many grateful parents and kids across Canada already know: this country’s children’s hospitals are among the best anywhere. That recognition reflects decades of investment, collaboration, and community trust.
Recently, we released our latest Impact Report, and the results are inspiring: there is remarkable, forward-looking work happening every day in children’s hospitals across Canada. We want to celebrate that work — the care teams innovating in real time, the researchers pushing boundaries, the families finding hope, and the communities that stand with them.
At Canada’s Children’s Hospital Foundations (CCHF), we are proud to support the 13 Canadian children’s hospitals that together see over three
million patient visits annually. These institutions are home to Canada’s most specialized pediatric care, and their impact reaches far beyond the bedside. What happens in children’s hospitals today fundamentally shapes the physical, emotional, and economic well-being of tomorrow’s communities.
No one knows when they’ll need a children’s hospital. But when a child needs treatment or care, nothing matters more. To illustrate this further, we invite you to explore our Impact Report at childrenshospitals. ca/impact-report. It shares real-world examples of how donor-supported initiatives are driving meaningful improvements — from innovations like wireless wearable sensors to monitor hospitals’ smallest patients, brain-computer interface technology for kids with disabilities, culturally appropriate indigenous-lead support, and advanced neonatal training —
that all transform children’s care.
In 2024, Canada’s Children’s Hospital Foundations (CCHF) raised over $60 million to help kids across the country access the specialized care, equipment, research, and family supports they rely on. This impact is made possible by the commitment of our corporate partners who continuously find meaningful ways to support their
Anew clinical research strategy at The Hospital for Sick Children (SickKids) seeks to transform how care is delivered for paediatric patients and families by accelerating discoveries and embedding research directly into the care experience.
It takes an average of 17 years for medical research to be translated into clinical practice. For children and families waiting for answers, that’s a lifetime. The new SickKids clinical research strategy, the first of its kind to encompass the entire enterprise, plans to close that gap by accelerating the translation of discoveries into care.
Aiming to foster cross-disciplinary collaboration, the strategy puts patients and families at the centre of research, driving more personalized and meaningful care. “This strategy reflects our shared commitment to advancing child health through world-class clinical research,” says Dr. Ronald Cohn, SickKids President and CEO. “As a key enabler of the
SickKids 2030 strategic plan and the Precision Child Health movement to individualize care for patients and families, it empowers us to ask bolder questions, uncover more meaningful answers and deliver care that is truly personalized for every child.”
The strategy focuses on collectively redefining how research is designed, conducted and integrated into care, anchored by six strategic directions:
• Commit to Patients & Families as Partners
• Advance Safety, Quality & Accountability
• Develop & Support a Skilled Clinical Research Workforce
• Enable a Seamless Clinical Research Ecosystem
• Adopt Innovative Digital Solutions
• Ensure Sustained Impact of Clinical Research
“While each direction plays a critical role, the commitment to partnering with patients and families is foundational to the strategy,” says Dr. Padmaja Sub-
barao, Associate Chief of Clinical Research. “By integrating clinical research across SickKids, investing in people and digital tools, advancing safety and quality, and partnering closer than ever before with patients and families, we will build up a learning health system that ensures every research question starts with patient needs and fuels innovation across our campus and beyond.”
More than 500 individuals, including clinicians, researchers, staff, and 30 patient families, contributed to the development of the strategy. Drawing on SickKids’ deep clinical research expertise, with over 3,000 active studies underway at any given point in time, their collective input helped define a shared vision for research, focusing on three core drivers: patient partnership, integration and impact.
Dr. Subbarao sees the development of the strategy as a significant milestone, setting the stage for a lasting culture shift that will benefit patients, families, and staff.
local children’s hospital foundations in the communities where their teams and customers live, work, and raise families.
CCHF is proud to stand alongside our member foundations, hospital partners, and Children’s Healthcare Canada — because when we invest in children’s health, we all benefit. n H
New Clinical Research Strategy for children puts patients and families at its centre Investing in children’s health: A fresh look at impact — and a reason to celebrate
“Rather than being passive participants, patients and families will be active co-creators, helping shape the questions researchers ask and the solutions sought,” she says. “Their lived experiences will inform the life cycle of research, from study design to how findings are translated in real-world care settings.” By embedding patient perspectives throughout the research journey, the hospital is working toward a more integrated, responsive, and patient-informed health system. The goal? Research that is not only scientifically rigorous but also equitable, inclusive, and reflective of the diverse communities it serves.
“Better clinical research means better care for patients,” says Dr. Subbarao. “By integrating research into the care experience, we can ensure that discoveries translate into meaningful improvements for children and families at SickKids and beyond.” Read the full strategy n H
Blaze, a patient of Jim Pattison Children’s Hospital. Photo courtesy of Jim Pattison Children’s Hospital Foundation
R Supporting families: Expanding in-hospital support amid rising demand
onald McDonald House was founded on the belief that when a child is sick, the whole family hurts, and both deserve to be surrounded by care.
For the 65 per cent of families that live in a city or town without a children’s hospital, travelling long distances to access their child’s medical treatment is essential. And as families leave their communities and support systems behind, often on short notice, they are met with unexpected challenges, including financial, emotional, and mental strain. This is the gap that Ronald McDonald House helps bridge by providing essential support and resources to ensure families can actively participate in their child’s medical journey.
As the only national organization enabling access to Canada’s paediatric healthcare system, Ronald McDonald House is proud to stand together with its hospital partners in service of the country’s most medically vulnerable children to complete the circle of care.
A GROWING NEED TO SUPPORT FAMILIES IN-HOSPITAL
Since opening doors in 1981, Ronald McDonald House has been a pillar in local communities, having served nearly 500,000 families across Canada through two core programs: Ronald McDonald House and Ronald McDonald Family Room.
While the 16 Ronald McDonald House programs across Canada provide out-of-town families with a place to rest, have a warm meal and be surrounded by a community of care close to their child in hospital, the 20 Ronald McDonald Family Room programs bring that same spirit of care directly into the hospital. These comforting spaces provide families with a place to rest, recharge and fuel without having to leave the hospital.
Remarkably, the demand for
in-hospital support has never been greater. Last year, Ronald McDonald House welcomed nearly 300,000 visits to Ronald McDonald Family Room programs across Canada, representing a 65% increase in families served in-hospital compared to 2023, and a new visitor every two minutes or less. This increase in visits led to 58% more meals being served to families inside the hospital.
THE JOURNEY TO SERVING MORE FAMILIES
As demand increases and family needs evolve, Ronald McDonald House remains steadfast in its commitment to surrounding families with the compassionate care and support they need to ensure they are at the heart of their child’s care, enabling the best possible health outcomes.
Following the opening of the new Ronald McDonald Family Room in
Niagara, O.N., last year, Ronald McDonald House has embarked on its largest growth year in Canada since 1985, with plans to add three new Ronald McDonald Family Room programs and expand three Ronald McDonald House programs in Calgary, Halifax and Ottawa.
In June, Ronald McDonald House opened the 20th Ronald McDonald Family Room in Canada in Kamloops, B.C., and later this year, Ronald McDonald House plans to open a new Ronald McDonald Family Room in
Prince George, B.C., and a second in Toronto, O.N.
The combined footprint expansion of Ronald McDonald House and Ronald McDonald Family Room programs across the country will increase national programming by nearly 20% and support an estimated 6,000 more families each year.
Despite this remarkable growth in 2025, more families across the country need Ronald McDonald House. In fact, it’s estimated that Ronald McDonald House is unable to serve up to four out of five families who need support. This is why Ronald McDonald House has bold plans in place to grow its footprint across Canada by 50 per cent by 2030 and expand core programs to better support the holistic needs of families navigating their child’s medical diagnosis.
Ronald McDonald House follows a diligent and data-informed approach to program growth, guided by global best practices and focused on areas of greatest need. Today, Ronald McDonald House is working closer than ever with the sector to ensure systems are accessible, equitable and connected to meet the needs of more children, youth, and their families.
Families like the Hart’s who stayed with Ronald McDonald House South Central Ontario.
For more information about how Ronald McDonald House and its hospital partners care for families inside the hospital, just steps from their child’s bedside, hear from the Hart family, here. n H
S Intervening early and effectively: Sunnybrook redefines neonatal developmental care
umaiya can’t believe how far her son has come. Born at 23 weeks of pregnancy and weighing only a pound, he was intubated in Sunnybrook’s neonatal intensive care unit (NICU) for four months. Today, her son is preparing to attend junior kindergarten, a milestone that once seemed out of reach.
“Sunnybrook’s Neonatal Follow-Up Clinic: his thriving is all down to them,” Sumaiya says, explaining that the team of occupational therapists, physical therapists, nurses, and neonatologist/developmental pediatricians have provided support since before his discharge from the hospital. “They got to know every aspect of his development, and truly walked alongside us, seeking to recognize my son’s potential.”
For over five decades, Sunnybrook’s Neonatal Follow-Up Clinic has been a leader in developmental care for infants born before 30 weeks’ gestation or those who experienced significant medical complications during their NICU stay. What makes the clinic especially unique is its leadership by a physician dually trained in neonatology and developmental pediatrics, an integrated subspecialty shared by only a handful of programs across the country.
This dual expertise bridges acute neonatal care with long-term developmental support, allowing for a model that is proactive, coordinated, and relationship-based. The clinic provides specialized consultation in physical, motor, and cognitive development and follows children through to nine years of age. This long-term support helps families navigate school transitions and engage early with educators to foster success in learning environments.
Sunnybrook’s team brings nationally recognized expertise in the early identification of cerebral palsy. It has helped establish provincial benchmarks for screening, referral, and early intervention through the Canadian
Neonatal Follow-Up Network. More recently, the clinic has incorporated the Rapid Interactive Screening Test for Autism in Toddlers (RITA-T) into its routine assessments, along with other standardized tools, offering a timely and reliable way to identify early social communication differences and autism spectrum disorders, and to tailor supports accordingly.
Sumaiya recalls that many of her son’s early visits to the clinic centred on play. “An occupational therapist would sit with him, some toys, and gently observe and interact with him,” she explains.
Dr. Rudaina Banihani, neonatologist and developmental pediatrician, and director of the clinic, explains that this approach is both intention-
al and evidence-based. “The clinic has shifted toward targeted, playbased interventions during the first year of life,” she says. “We know that the most effective supports happen early, before concerns fully emerge. Through play, we’re laying the neural groundwork for communication, self-regulation, and relationships. Our occupational therapists coach caregivers to engage with their children with intention.”
These early sessions are more than developmental observation; they are collaborative moments where the care team partners with families to embed strategies into everyday routines such as feeding, dressing, diapering, and shared play.
“They really followed his cues, and
went from there,” says Sumaiya, explaining that eventually he was diagnosed with autism spectrum disorder.
“They have been there every step of the way, from practical tips for simple things like putting on his socks, to support for classroom interventions and liaising with my workplace when I required additional time off.”
Dr. Banihani emphasizes that the clinic’s mission is not only to “follow up,” but to “follow through”—building long-term, strengths-based partnerships with families and systems, and holding steady to the belief that every child has the capacity to thrive.
“It takes a village to raise a kid, and I got my village through Sunnybrook,” says Sumaiya. n H
New RSV immunization catch-up clinic: An innovative model for community hospitals to prevent severe lung disease
As paediatric teams across Ontario prepare for the upcoming respiratory season, Halton Healthcare is proud to share an innovative and effective model of care that has already made a significant impact in Halton region. In collaboration with Halton Region Public Health, Halton Healthcare launched the region’s first and only seasonal Paediatric Respiratory Syncytial Virus (RSV) Immunization Clinic at Milton District Hospital. This clinic, operational for the first time last season, stands as a best practice in community-based paediatric care and infectious disease prevention. The clinic was established in alignment with the Ministry of Health’s expanded universal infant RSV prevention program, which broadened the eligibility for RSV immunization.
Previously targeted mainly at a limited subset of high-risk infants, the new program enabled access for all infants born in 2024, as well as high-risk children under two years of age. The new medication Nirsivemab has proven to reduce doctor visits and admissions by 80% and paediatric ICU admissions by 90 per cent in large studies across the world. RSV is the most common respiratory infection affecting infants and young children, but its impact can be severe.
At Halton Healthcare, RSV accounts for up to 30 per cent of all paediatric hospitalizations during the colder months. Recognizing the need for early intervention, the clinic aimed to protect the most vulnerable before they ever reached the Emergency Department. “From a health system perspective, prevention is always the best medicine,” said Dr. Jonathan Sam, Corporate Paediatric Strategy Lead at Halton Healthcare and Regional Paediatric Lead at Ontario Health Central. “By delivering timely immunizations, we not only protect infants and young children, but we also ease the seasonal burden on paediatric and emergency services.”
“RSV infection can be serious, especially for infants under six months of age
or those with underlying health conditions,” said Dr. Patrick Galange, Associate Medical Officer of Health, Halton Region Public Health. “That’s why we are happy to collaborate with Halton Healthcare on this innovative clinic model. Immunization with preventative antibodies is highly effective and can significantly reduce the risk of severe illness and hospitalization. By expanding access to this protection, we’re using every public health tool to keep children safe this RSV season.”
While Halton Healthcare began offering RSV immunization to newborns in-hospital, the need to reach infants in the community – especially those recently discharged or without easy access to primary care – prompted the launch of the dedicated clinic. Designed to be convenient and low-barrier, the seasonal clinic created an accessible entry point for families across the region seeking preventive care. The clinic was staffed by
paediatric nurses and supported through integrated communication with local healthcare providers and public health. The clinic ensured caregivers were informed and empowered to make preventative health decisions for their families.
During last winter season, and over just three months, the clinic immunized more than 500 babies – a significant milestone that reflected both the demand for this service and the effectiveness of the delivery model. The clinic also supported the provincial strategy of shifting care closer to home. By preventing illness in the community, it reduced the need for acute care and supports families proactively. This initiative offers a scalable model for other regions, demonstrating the success of hospital–public health collaboration, community-based infrastructure, and alignment with provincial programs.
As we prepare for the upcoming RSV season, the importance of ear-
ly and equitable access to immunization cannot be overstated. This model shows how cross-sector collaboration and patient-centered design can effectively meet public health goals. “The RSV immunization clinic has been a game-changer for families in our region,” said Cheryl Hoare, Clinical Program Director for the Women & Children Program at Halton Healthcare. “It’s about meeting people where they are, reducing preventable illness, and ultimately ensuring healthier beginnings for our youngest patients.”
By combining evidence-based prevention, health system collaboration, and communitycentered delivery, Halton Healthcare’s Paediatric RSV Immunization Clinic exemplifies the kind of forward-thinking innovation that strengthens Ontario’s paediatric healthcare landscape. n H
Bringing critical care closer to home:
Transforming pediatric and neonatal
outreach in Alberta
When a child or newborn becomes critically ill, every moment matters. For families living in rural, remote, and northern communities across Alberta, access to specialized pediatric and neonatal care can be limited by geography, resources, and distance. At the Stollery Children’s Hospital in Edmonton, our Pediatric and Neonatal Intensive Care Outreach Program is working to change that.
Our program is built on a simple belief: no matter where a child lives, they deserve access to high-quality, timely care. By bringing expert knowledge and practical skills directly to healthcare teams across the province, we help ensure that critically ill infants and children receive the best possible care, from the very first moments.
FROM THE ICU TO THE COMMUNITY: SUPPORTING TEAMS BEFORE CRISES OCCUR
Our outreach work focuses on proactive education and support. We don’t wait for emergencies to happen. Instead, our team of pediatric and neonatal intensive care specialists, including intensive care physicians, critical care transport nurses, respiratory therapists, and simulation educators, travels to hospitals and health centers throughout Alberta.
Our transport team members bring valuable frontline experience from caring for critically ill children and newborns in high-pressure, time-sensitive situations. By sharing their practical insights and lessons learned, they work alongside rural teams to build local capacity and strengthen confidence in managing critical situations. Together, we focus on preparing for rare but high-stakes events—such as neonatal resuscitation, pediatric respiratory failure, difficult vascular
access, and post-resuscitation care— while ensuring that education remains practical, relevant, and tailored to each team’s specific realities and resources.
Above all, our goal is to collaborate, not to replace or direct care. We recognize that rural teams bring deep knowledge of their patients, their communities, and the realities of delivering care in diverse settings. Our role is to offer additional specialized expertise and support when it’s needed most, working together to ensure that every child receives the best possible care, regardless of their location.
ENHANCING THE USE OF VIRTUAL HEALTH
Virtual health has long been part of our care model, allowing rural healthcare providers to connect in real-time with our PICU and NICU teams through video consultations. These virtual connections allow for immediate visual assessment, facilitate collaborative decision-making, and provide specialized guidance, thereby bridging the gap between distance
and timely critical care.
In recent years, we have dedicated new resources to expanding the number of sites actively utilizing virtual health and to enhancing the system to make it more accessible and user-friendly. Through outreach education and ongoing collaboration, we help teams understand when and how to activate virtual health support, and we work alongside them to identify barriers and co-create solutions that enhance the process. By integrating virtual care into both educational and clinical workflows, we aim to ensure that this valuable tool is familiar, efficient, and readily available when needed most.
PARTNERSHIPS THAT STRENGTHEN THE SYSTEM
At its heart, our outreach program is about relationships. We work alongside healthcare teams, not above them. By building trust and fostering ongoing communication, we create partnerships that extend beyond oneoff education sessions.
These relationships also allow us to better understand systemic challenges. We see firsthand the impact of staffing shortages, equipment limitations, and the need for ongoing skill development. Armed with this knowledge, we can advocate for change not only within individual sites but also across the broader healthcare system.
LOOKING FORWARD: INNOVATION FOR SUSTAINABLE IMPACT
As we continue to grow, we are exploring new ways to expand our reach and impact. This includes:
• Increasing the use of virtual health for more frequent support and consultation.
• Developing on-demand, digital education tools to supplement in-person learning.
• Collaborating with provincial networks to align efforts and share best practices in pediatric and neonatal resuscitation and emergency care. The true measure of our program’s success isn’t just the number of kilometres travelled, or sessions delivered. It’s found in the quiet moments: a nurse who confidently aids in the resuscitation of a newborn because she practiced it in simulation; a rural physician who feels supported during a complex case; a family who receives life-saving care without the delays of distance.
Through innovation, compassion, and collaboration, we are transforming how care is delivered, ensuring that geography never stands in the way of a child’s chance to thrive. Our outreach program is made possible thanks to the generous support of the Stollery Children’s Hospital Foundation, which provides the funding for this vital work. Their commitment ensures that we can continue to bring critical care closer to home for Alberta’s children and families, one community at a time. n H
Pediatric surgical care helps get young hockey players back on the ice
Scarborough Health Network’s (SHN) Kids Care and Surgery programs are always ready to make the game-winning play for young patients, with a team of paediatric surgical stars who consistently deliver the best outcomes for kids. For two young hockey players, getting referred to SHN for their procedures was a real game-changer—the Network’s paediatric and orthopaedic centres of excellence bring together the top doctors, teams, programs, and clinics to provide the best possible care.
Anna Mulhall, a 10-year-old from Stayner, Ontario, was born with an extremely rare birth defect called congenital femoral deficiency, which caused her left femur (thigh bone) to grow slower than her right. Without surgery, she could end up having a significant difference in the length of her legs, which could lead to a severely impaired gait, hip instability, knee deformities, and potential complications like scoliosis (a sideways curvature of the spine).
Despite this, Anna began playing hockey when she was seven years old. As the years passed, she faced challenges with maintaining
balance, and walking and skating for prolonged periods of time. If her condition was not corrected quickly, her chances of future complications, including arthritis and chronic pain, would increase.
Anna’s parents got her on the surgical waitlist at The Hospital for Sick Children (SickKids), where she had been a patient her entire life. But when it was final-
ly time for her corrective surgery last summer, the Mulhalls were informed that their surgeon was no longer available.
BETTER ACCESS AND OUTCOMES RESULTING FROM HOSPITAL TEAMWORK
To help alleviate its surgical waitlist and help kids like Anna more quickly, SickKids partnered with five community hospitals in April 2023, working together to transfer patients who were able receive their care at a community hospital. That is how Anna’s case was referred to SHN—SickKids’ largest partner within the Surgical and Endoscopy Community Part-
nerships Program—which has successfully completed over 300 surgical cases from SickKids. This has significantly benefitted paediatric patients who would otherwise face months or even years of waiting for much-needed procedures.
Through this collaboration, SickKids surgeons may also perform surgeries at SHN when their own operating rooms are at capacity. In addition to increasing SickKids’ surgical capacity, it provides valuable training opportunities for SHN staff, ensuring a smoother transition for patients between the hospitals and enhancing overall care coordination.
“Partners like SHN have been essential to the success of SickKids’ Surgical and Endoscopy Community Partnerships Program, helping to ensure that children receive more timely access to surgical care,” said Jessica Ivan, who manages the program at SickKids.
“We have received such positive feedback from patient families about their experience being referred to our community hospital partners, and are grateful for the care, compassion, and expertise that SHN has provided through this collaboration.”
With the assist from SickKids and a longstanding reputation for excellence in paediatric care, SHN was ready to make the winning shot with Anna’s procedure. Leading the line was Dr. Ryan Katchky, a paediatric orthopaedic surgeon.
“We had been with SickKids since Anna was eight months old, and at first it felt daunting to go to a hospital we’d never been with a doctor we didn’t know. But when we met Dr. Katchky, he put our minds at ease immediately,” said Kim, Anna’s mother.
To help reassure Anna’s parents, Dr. Katchky explained that he had trained at SickKids and had a close working relationship with them, particularly because of the strong partnership between the hospitals.
“He won Anna over in five seconds flat. She was so comforted
by Dr. Katchky and the kindness of the SHN team,” added Anna’s father, Mat.
Anna had her surgery at Centenary Hospital in July 2024 to positive results, and she was back gliding around the rink by October. Her story is an example of the positive impact SHN is making in the lives of patients and their families.
“By helping SickKids to free up resources for more complex cases, we are relieving children and their families of the emotional and physical distress that comes with waiting for a procedure, and helping get kids back to doing what they love faster,” said Lori-Lee James, Director of Surgery.
“We are providing a wide range of services—including orthopaedics, ophthalmology, otolaryngology (ear, nose and throat, or ENT), plastic surgery, urology, and dental surgery to the patients coming to us from SickKids.”
Plus, MyChart Central East Ontario—a free, secure, online portal to view personal health information—gives parents who have MyChart the option to establish proxy
causing pain and sometimes even falling due to a loss of control. Worse yet, he was going to have to deal with that for some time, because the kind of surgery he required could potentially damage the growth plates in someone so young.
Nolan’s family spent two years searching for a surgeon who was willing to undertake the procedure and were referred to Dr. Katchky. Nolan’s mother knew they had found their clutch surgeon.
“He said he could do it. He said he would do it. And he said he was confident that all would be well,” said Layal Scheirich, his mother. “He was calm and reassuring, and both pre- and post-surgery, he and the entire staff at the hospital were there for Nolan and for us. It was such a great experience.”
access with their child’s MyChart account and link their SHN and Sick Kids accounts. This allows parents to manage their child’s health records from both SHN and SickKids securely, including viewing test results, immunizations, and more.
RARE EXPERTISE, RIGHT HERE IN SCARBOROUGH
On Halloween day 2021, another young hockey player, 7-year-old Nolan Scheirich from Toronto was playing with friends on the school playground when he ran into a bench and dislocated his knee. Even though it hurt, he did not tell anyone until he got home, still planning to go to hockey practice.
“I was expecting it to be bruised, but when I saw the severity of his injury, I went pale as a ghost,” said Scott Sheirich, Nolan’s father.
They brought Nolan to SickKids, where they learned that he had obligatory patellar dislocation. This meant that every time Nolan flexed his knee, it would dislocate,
Dr. Katchky says clinching the victory was a case of having the right skills and focus, and he was glad to have been available.
“Fixing dislocated kneecaps is done very commonly in teenagers and adults. But the pathology, and therefore the surgery, is very different in a child. Nolan needed a paediatric surgeon with the confidence and experience in this procedure, and I was grateful that my team and I could offer that support.”
The surgery was in April 2024 at General Hospital, and today Nolan is recovered and playing hockey again, stronger than before.
“I’m proud of SHN’s growing reputation for paediatric surgical expertise, and credit everyone from the administrative staff, to unit teams, to clinic staff,” said Dr. Katchky.
As SHN continues to provide families with the care they need when they need it, the Network’s exceptional quality surgical and paediatric care can be summed up in two words: All Star. n H
Dr. Ryan Katchky, a paediatric orthopaedic surgeon.
Can the Hub Model solve Ontario’s healthcare woes?
By Helen Reilly
Ontario’s healthcare system faces growing pressure from ED backlogs, physician shortages and a rising demand for mental health and social services. In the meantime, Flemingdon Health Centre (FHC) has steadily built an integrated model of care over the last 50 years, addressing the complexity, resilience, and diversity of the community it serves.
In a city as culturally diverse and fast-growing as Toronto, access to wraparound support has never been more essential. The health centre’s approach has evolved to weave together healthcare with social support and a deep commitment to equity.
This past winter, as FHC marked its 50th anniversary, it launched The Thorncliffe Park Community Hub in partnership with The Neighbourhood Organization (TNO) and Michael Garron Hospital. The model is a collaborative and transformational response that offers individuals and families convenient access to co-located programs and services.
The Hub evolved around a longstanding collaboration and a shared vision between the three trusted community organizations, united under one roof. Here, residents access primary healthcare, mental health supports, food programs, health education, English-as-a-Second-Language classes, employment counselling, legal services, midwifery, home care, dental services and newcomer settlement support as part of a seamless, integrated experience.
The Hub model of care delivery is uniquely suited to this community because it does so much more than just respond to illness. It recognizes unique challenges, tackling the root causes of illness and disease addressing social determinants of health such as housing, food insecurity, income, language proficiency, racism, and social isolation.
LOUIS FLISS, CHIROPODIST AT FLEMINGDON HEALTH CENTRE, FOR MORE THAN 30 YEARS WAS PROUD TO SHARE NEWS OF THE HEALTH CENTRE’S 50TH ANNIVERSARY CELEBRATION WITH THE COMMUNITY.
“The cooperation and collaboration our organizations have harnessed to make the Thorncliffe Park Community Hub a reality is a transformational solution to the challenges facing so many urban neighbourhoods,” says Jennifer Quinlan, CEO of FHC. “Together with our community partners, we are building upon FHC’s tradition by eliminating barriers and building a system that truly reflects the community’s needs and strengths.”
Under Quinlan’s leadership, FHC nurtures a collaborative, equity-focused model that eliminates silos, making people the focus of care. Always with an eye to the future and upstream thinking, Quinlan sees the Hub model of care delivery as responsive, scalable, and replicable.
Quinlan’s upstream approach is grounded in building consensus
Written by Helen Reilly, Pages for Good, on behalf of Flemingdon Health Centre.
that recognizes and invests in local strengths. “FHC has a 50-year tradition as a natural gathering place, acting as a source of support for so many families. This tradition brings the Hub to life, along with our cherished community partners as a milestone on our journey,” she says.
According to the Institute for Clinical Evaluative Sciences (ICES), community-based primary healthcare organizations serve patients with more complex needs than other models, and overall, they achieve better outcomes. By coordinating and integrating care founded on trust, there is less fragmentation, which helps people stay healthier and out of hospital emergency rooms. In turn, this improves both patient experience and health system sustainability. (Alliance for Healthier Communities,
“Investing in Primary Health Care,” 2023)
The numbers can be compelling, but stories like Noel’s bring the value of this work to life. As a newcomer from the Philippines, he walked through FHC’s doors for the first time in 1975. He is still a client and has benefitted from consistent, compassionate care, with only three family doctors over 50 years.
Years ago, his physician noticed something unusual during a routine visit. Although Noel felt great, had no symptoms, and was doing 50 push-ups a day at the time, his doctor referred him to a cardiologist. The resulting bypass surgery saved his life. Throughout his recovery, he benefited from a full circle of care, relying on FHC’s dietitians, prevention programs, and follow-up care to regain his strength and return to wellness.
As a way of giving back, Noel became an FHC Board member nine years ago. In his role, he supported FHC’s strategy to embrace innovative solutions, including the Hub model that continues to serve newcomers in the same way he was supported when he first came to Canada.
The Thorncliffe Park Community Hub proves what’s possible when health and social systems work together to remove silos and focus on community-specific solutions that deliver care that’s connected, inclusive, and ready for the future.
As the demand for primary care continues to grow, the Hub isn’t just a milestone for this community; it’s a model for other healthcare systems. FHC’s 50-year legacy of community-led care and partnership is a blueprint for what the health system needs - disease prevention, strategic partnership, and equity in action. The time for integrated, upstream solutions is now. Noel reminds what the Hub model brings, saying, “You belong here. We’ve got you.” n H
Learning Health Systems strives to elevate patient-centred care
A framework that supports a systematic approach to meeting patient needs in care delivery is gaining traction among teams at Vancouver Coastal Health.
Learning Health Systems is an increasing priority at Vancouver Coastal Health (VCH) and Vancouver Coastal Health Research Institute (VCHRI) that champions continuous learning through knowledge, practice and data collection to improve patient outcomes and experiences. Driven by the VCH value “we are always learning,” the Centre for Clinical Epidemiology and Evaluation (C2E2) at VCHRI is working to expand the reach and adoption of Learning Health Systems at VCH.
“Learning Health Systems enhances quality improvement at VCH by explicitly integrating research and implementation science into care delivery,” says VCHRI researcher Dr. Donald Griesdale. “Importantly, the approach emphasizes the inclusion of patient-identified priorities and patient partners in decision-making.”
A recent example of Learning Health Systems in action at VCH was a review of antipsychotic reduction strategies at VCH long-term care facilities conducted in collaboration with patient partners. The project was led by UBC School of Social Work PhD student Karen Wong and supervised by VCHRI researcher Dr. Lillian Hung and senior Learning Health Systems lead Dr. Krisztina Vasarhelyi.
“We had on the team a patient partner living with dementia who provided in-depth and valuable feedback: from the formation of the research questions all the way through to the research process,” says Vasarhelyi. “Other patient partners with lived experience and their family members also regularly attended project team meetings, informing and co-creating our research.”
The antipsychotic reduction strategies project team also conducted interviews with VCH clinicians, pharmacists and staff involved in implementing a provincial antipsychotic reduction strategy to glean insights and best prac-
tices. Identified as a high-priority area of investigation at VCH, the project integrated knowledge translation, providing other VCH team members with information on project research findings and implementation to scale impacts and insights across the health authority.
Better alignment of care delivery and outcomes that are important to patients
A second example of Learning Health Systems at VCH — conducted in partnership with VCHRI researcher and liver transplant surgeon Dr. Maja Segedi and liver transplant surgeon Dr. Stephanie Chartier-Plante — aimed to identify outcomes important to patients and caregivers.
Importantly, patients and caregivers were integral members of the study team itself. C2E2 team members initially conducted a literature review of existing outcomes that have been reported in patients who have received a liver transplant. The next phase of the ongoing study involves interviewing
“THE PROCESS EMBEDS SCIENTISTS WITHIN CARE TEAMS TO OFFER ADVANCED RESEARCH METHODOLOGY AND PATIENT ENGAGEMENT FOR SUSTAINED CARE ENHANCEMENT.”
health professions, transplant recipients and caregivers to understand what outcomes are important to them.
“Engaging with our patient partners on the liver transplant project has been such a rewarding experience for me,” says Dr. Nitya Suryaprakash, a qualitative researcher with C2E2. “Besides directly impacting the project with their insights, the enthusiasm and commitment of our patient partners to the project has fostered a sense of shared purpose, encouraging me to do better at my job and making work fun again.”
“Through this project, we are trying to address a knowledge gap in identifying the outcomes that are important to patients and their caregivers,” states
Griesdale. “This is the outcome that we strive for in all Learning Health Systems initiatives at VCH.”
“At the end of the day, clinicians and allied health team members want to deliver the best possible care to patients; however, the patient voice has not necessarily been represented in health care delivery decision-making,” Griesdale adds. “Learning Health Systems gives us a path forward to better embed patient priorities into our care.”
For more information about Learning Health Systems, visit the Institute for Better Health or contact the Centre for Clinical Epidemiology and Evaluation n H
Corticosteroids: Safe medication use considerations in the pediatric population
By Samir Kanji, Laura Brady, and Certina Ho
LS is an 8-year-old girl who has been having a tough time with her asthma. After a recent flare-up that sent her to the emergency room, her doctor prescribed a short course of oral corticosteroids to help reduce the inflammation in her lungs. Her parents were nervous as they had heard about corticosteroids side effects and were not sure what to expect.
If you are a parent or caregiver facing similar questions, this article is the second of a three-part series that will cover some of the considerations for safe pediatric medication use. Corticosteroids are available in different dosage forms. We would like to invite you to read our July 2025 article on “Pediatric Dosage Forms: Safe Medication Use Considerations”. Here we highlight how corticosteroids work, how to use them safely, and what steps you can take to protect your child’s health.
How Corticosteroids work
Corticosteroids are medications similar to hormones made naturally by the adrenal glands in our body. There are two main types – glucocorticoids, which help reduce inflammation, control the immune system, and narrow blood vessels; and mineralocorticoids, which help mqanage electrolyte and water balance in the body.
Corticosteroids are used to treat many different health conditions in children, including, but not limited to:
• Breathing conditions, like asthma, croup
• Skin conditions, such as eczema, alopecia, vitiligo
• Digestive issues caused by inflammation, like ulcerative colitis, Crohn’s disease
• Other autoimmune and inflammatory conditions, including those that affect joints, blood, hormones, nerves, or kidneys
Common side effects of corticosteroids
Corticosteroids can be prescribed for
either short-term use (less than 14 days) or long-term use (more than 15 days). Depending on the duration of use, different side effects may occur.
For short-term courses of corticosteroids (e.g., for allergic reactions, asthma flare-ups, or sudden worsening of autoimmune conditions), some children may experience side effects like nausea, vomiting, behavioural changes (e.g., anxious, restless, or hyperactive), sleep disturbances, etc. For long-term courses of corticosteroids (e.g., for chronic conditions like asthma, chronic obstructive pulmonary disease (COPD), inflammatory bowel disease (IBD)), side effects may include weight gain, slower growth, fatigue, slower wound healing, bone pain, etc.
Safe medication use considerations
Prescribers generally aim to use corticosteroids in the safest way possible for your child. This means giving the lowest possible dose for the shortest duration needed. If long-term corticosteroid therapy is necessary, prescribers would monitor certain aspects of your child’s
health conditions (e.g., weight, height, bone health, nutrition, blood sugar level, stage of puberty, mood, behaviour, sleep, etc.).
It is important to note that certain side effects may occur as early as one week after starting corticosteroids therapy, and some are more likely to occur with higher doses. If corticosteroids need to be discontinued, it should always be done slowly and under a health care professional’s guidance and monitoring.
Resources for safe pediatric medication use
Helping your child use corticosteroids safely starts with good communication and staying organized. One helpful tool that can be recommended to LS and her parents is the Institute for Safe Medication Practices Canada (ISMP Canada) “5 Questions to Ask About My Medicine - For Kids” – a pediatric focused medication safety resource that was co-designed by children, caregivers, and health care providers to facilitate conversations with prescribers or pharmacists during a medical appointment or
patient consultation, respectively. An implementation guide is also available to accompany this resource.
In addition, it is also helpful to keep a list of all medications that your child is taking, including any over-the-counter drugs or supplements, as some of them may interact with corticosteroids. Using a calendar or a reminder system can keep doses on track, especially if corticosteroids need to be taken at certain times or if they need to be slowly tapered or reduced in doses. Be sure to store medications safely. If a dose is missed or if you are unsure what to do after a missed dose, reach out to your healthcare provider for guidance. With communication and support, you can help ensure your child’s corticosteroids use is safe and effective.
Samir Kanji and Laura Brady are PharmD Students at the Leslie Dan Faculty of Pharmacy, University of Toronto; and Certina Ho is an Assistant Professor, Teaching Stream, at the Leslie Dan Faculty of Pharmacy and Department of Psychiatry, University of Toronto. n H
Samir Kanji and Laura Brady are PharmD Students at the Leslie Dan Faculty of Pharmacy, University of Toronto; and Certina Ho is an Assistant Professor, Teaching Stream, at the Leslie Dan Faculty of Pharmacy and Department of Psychiatry, University of Toronto.
Socially conscious and digitally fluent, Gen Z’s strengths are proving helpful in health-care
By Alexa Battler
Gen Z is now well into its “internship era,” and a slew of research on the cohort’s first few years working in health-care signals a promising coincidence—it seems the TikTok generation’s life online may have inadvertently given it the tech-savviness, social consciousness and destigmatized view of mental health that the health-care system needs to modernize.
In a report this summer, the C.D. Howe Institute stated Canadian hospitals are “near the limit of the improvements that can be achieved” with their patchwork approach to adopting innovations in health-care. Meanwhile, a research review in Nurse Education Today looked at 14 studies on the perceptions of Gen Z’s health-care debut, and found they’ve been widely deemed the most tech-savvy the field has ever seen. They can pick up new tech easily and, crucially, they’re enthusiastic to continue using the latest versions of it (that tracks, after a childhood of bombastic smartphone and console launches).
Gen Z has also become known for a strong sense of social justice and high levels of empathy, compassion and self-confidence, which a study in RSIS International attributes to its formative years on social media. That study also points to social media as a driver of not just Gen Z’s openness in talking about mental health conditions, but its skyrocketing rates of experiencing them firsthand.
Gen Z’s strengths have been a boon for Dr. Jennifer Crosbie and her team at Toronto’s Hospital for Sick Children. The Crosbie Lab works to tease apart the complex biological and environmental factors that contribute to neurodevelopmental disorders in children, particularly ADHD, as well as the impacts on child and youth mental health. For over six years, the lab has hired two to three students from the University of
Toronto Scarborough’s Arts and Science Co-op Program, and Dr. Crosbie says her team is constantly surprised by how quickly these young students can adapt to the demands of a complex research environment, even with limited exposure and experience.
“Within a few weeks, they gain great confidence in navigating databases, contributing to discussions and managing their own deliverables,” says Dr. Crosbie, whose two current co-op students have been extracting data from clinical patient files and organizing them in the lab’s REDCap databases. “This level of professionalism is quite impressive, and it acts as a strong reminder of the potential young researchers bring when given the right environment and mentorship.”
Dr. Crosbie and her team have come to trust the co-op students from U of T
Scarborough so much that their current ones are directly gathering and contributing data for a major province-wide project on the drivers of neurodevelopmental disorders. The co-op students must keep their study participants, many of whom are children with ADHD, engaged while administering cognitive tasks and gathering high-quality data.
Student Cameron Gilbert says the kids enjoy some activities more than others (she and fellow co-op student Ayeza Ahmed use video games, virtual reality and other engaging mediums when able), but they’ve always found a way.
“We adapt to their moods, preferences and strengths to give them a better experience,” Gilbert says of their work with the kids. “Through the cognitive tasks we administer ... I have come to love learning about how different peo-
ple come to the same conclusion.”
Both Gilbert and Ahmed credit the lab for giving them a far more complex understanding of health-care and research. They’ve attended workshops, seminars and conferences with a gamut of researchers and professionals, expanding their networks and exposing them to the seeds of ideas they may eventually dedicate their careers to (Gilbert is expressly on the hunt to discover her “research niche”). They attend and participate in daily lab meetings, and while they both speak at length about the practical skills they’ve developed, Ahmed says what she’s working to gain from this experience is deeper than that.
“I wish to strengthen the way I operate in team environments, especially in a team where every individual wears multiple hats,” she says. “From acquiring new skills to adapting current ones, I want to continue expanding my skillset to continue being an asset in more ways than one.”
U of T Scarborough’s Arts and Science Co-op Program also supports the administrative side of recruitment and prepares its students with the tools, skills and goals to quickly start making an impact at their workplace.
“The structure of the co-op program at U of T ensures that students come in with clear goals, timelines, and academic support, which helps streamline onboarding and supervision,” Dr. Crosbie says. “We have also found it a great way to identify strong candidates for future roles, since co-op placements can often turn into longer-term opportunities.”
The co-op team at U of T helps health-care organizations get the support they need for short-term projects (of four, eight or 12 months), with students ready to help with research, communications, data analysis and much more. Connect with an expert and learn more about hiring a co-op student for your team. n H
Left to Right - Ayeza Ahmed (Mental Health Studies Co-op Student), Dr. Jennifer Crosbie (Senior Scientist at The Hospital for Sick Children), Cameron Gilbert (Population Health Co-op Student)
Prototypes of smartwatches and rings are driving forward advances in wearable technology that instantly alert emergency personnel
A Smart wearables for faster cardiac arrest emergency response
pioneering study led by Vancouver Coastal Health Research Institute (VCHRI) researcher Dr. Calvin Kuo and Dr. Mahsa Khalili has demonstrated that consumer wearable technology may hold the key to transforming how out-of-hospital cardiac arrests (OHCAs) are detected, potentially saving countless lives. With more than 4.4 million OHCAs occurring globally each year — and over 75 per cent of them unwitnessed — the study’s findings pave the way for Canadian-made technological advances to alert emergency response personnel as soon as a cardiac arrest occurs.
“This research shines a spotlight on a critical barrier to timely care in OHCA: the absence of a witness,” explains VCHRI researcher Dr. Brian Grunau, head of the Canadian Saving Cardiac Arrest Victims Everywhere (CanSAVE) research excellence cluster overseeing the award-winning broader project that encompasses the present study. “When unnoticed, the chance of surviving a cardiac arrest drops dramatically to almost zero.”
The study involved integrating the photoplethysmogram (PPG) sensors commonly used in smartwatches and fitness trackers into novel, wearable PPG heart rate monitoring devices.
Research in real-world settings is needed to further advance wearable technology.
The research team tested three different PPG sensor prototypes on 31 healthy adult participants who wore the devices on their wrists, fingertips and base of their fingers simultaneously. Researchers used an advanced machine learning computer algorithm — a type of artificial intelligence — to test prototype performance.
The PPG device prototypes were tested under three conditions: normal cardiac state, occlusion and off-body. Occlusion tests involved restricting blood flow through participants’ arms to mimic a pulseless cardiac arrest
While some smartwatches featuring an emergency services alert system have been approved in other parts of the world, including the United States, the technology is not yet approved in Canada. The present study underscores the importance of real-world testing to prevent false cardiac arrest alerts that could unnecessarily deploy emergency services personnel.
event. The off-body scenario tested the performance of devices when not worn by the participant, attempting to capture instances of false positives when the device may erroneously detect cardiac arrest when the wearer takes it off.
“This technology could be used by anyone, with particular clinical indications for people at risk of heart disease and cardiac arrest.”
Data collected from testing the PPG fingertip prototype under ideal conditions achieved almost a 94 per cent detection rate for occluded, pulseless states — approaching the level of sensitivity needed for clinical utility. Devices using finger-based PPG sensors consistently outperformed wrist-worn models, which only identified approximately 78 per cent of pulseless events under ideal conditions.
However, when used under conditions more similar to real-world settings, fingertip prototype performance in detecting pulseless events dropped to 90 per cent and wrist prototype performance dropped to 44 per cent.
“In this proof-of-principle study, we were able to show that the technology can detect cardiac arrest under ideal, controlled conditions.”
“Given the success of this study, our team has embarked on national clinical trials to test the efficacy of these wearables — including prototypes with enhanced technology and additional functionality — under real-world conditions in clinical and other settings,” notes Khalili.
On top of alerting emergency service personnel, subsequent iterations of the technology could also send vital medical information to first responders for a rapid response informed by the unique needs and health status of each patient.
The study also highlighted the limitations of current wrist-worn consumer devices. Nearly half of wrist PPG recordings were of low quality, undermining detection accuracy. This information is a wake-up call to improve the technology’s hardware and data processing algorithms further before moving to the next, highly anticipated step of commercialisation, Khalili says. The implications for health care systems are profound. Equipping everyday people with passive cardiac monitoring could significantly improve early recognition and emergency medical service activation in unwitnessed OHCA cases — dramatically increasing survival rates.
“Our study demonstrates the concept and the challenges that need to be addressed to make accurate cardiac arrest detection using smartwatches a reality in Canada,” says Kuo. “With continued innovation, wearable technology can evolve from fitness trackers into powerful medical tools, revolutionizing cardiac care and saving lives when every second counts.” n H i
Screening for malnutrition in community care
Malnutrition is high among seniors referred to home care service from hospital, but a rapid screening test could turn the tide.
Malnutrition puts older adults at greater risk of hospital readmission from consequential injuries such as falls, fractures and infections, as well as being a risk factor for death. Vancouver Coastal Health Research Institute (VCHRI) researcher Leila Goharian’s recently published research is the first in Canada to describe the prevalence of malnutrition among older adults newly referred to home care services from hospitals in British Columbia.
In Canada, hospital care costs for patients with malnutrition are between $1,500 and $2,000 more than for well-nourished patients.
Goharian’s study clearly underscores the importance of screening for malnutrition as an effective and proactive intervention to prevent its health impacts from spiraling out of control.
“A person may become malnourished as a result of barriers to adequate food intake related to dementia, depression, chronic diseases, medications, poverty and food insecurity, among other reasons,” Goharian explains. “Early interventions can save a life.”
Goharian’s research examined the chart records of patients referred from hospital to Vancouver Coastal Health (VCH) home care services in B.C. that offered care through an out-of-hospital ambulatory clinic or within a client’s home between January and December 2019. “The goal of home care services is to help restore, maintain or provide palliative care to ensure clients will achieve the most efficient use of resources while main-
“AROUND ONE IN THREE OLDER ADULTS OVER THE AGE OF 65 FACE OBSTACLES TO MEETING THEIR DIETARY NUTRITIONAL NEEDS.”
taining a safe, optimal level of care at home,” notes Goharian.
Of the 1,537 clients included in the study, the research team found that around 25 per cent (377 individuals) were malnourished, approximately 55 per cent were at risk of malnutrition (848 individuals) and just over 20 per cent (312 individuals) had normal nutrition status.
The research team also looked at a subset of 324 clients who received an
unplanned referral to hospital within 30 days of being discharged from hospital. Of these, 29 per cent (110 individuals) were identified as being malnourished, 21 percent (179 individuals) were at risk of malnutrition and 11 per cent (35 individuals) had normal nutrition.
“Malnutrition can be a gradual or rapid process that can be very time-sensitive and challenging to address,” explains Goharian. “Its effects
can lead to increased frailty and an over 50 per cent higher risk of falls due to deficiencies in nutrients causing muscle breakdown and brittle bones.”
Rapid identification of malnutrition with a short questionnaire
In 2018, VCH home and community care services began using the validated nutrition screening tool — the Mini Nutritional Assessment–Short Form (MNA‐SF) — which was also used by the home care services included in Goharian’s study to assess the nutritional status of clients. The six-question, shorter version of the Mini Nutritional Assessment questionnaire identifies whether an older adult over the age of 65 years is malnourished or at risk of malnutrition.
\MNA‐SF questions range from checking a person’s weight loss within the past three months to their food intake, mobility, mood and cognitive function. “The screening tool is designed to be completed by the client or their caregiver for a person-centred approach,” Goharian explains. “However, when needed, some questions can be informed by details from a client’s medical record.”
Across VCH, individuals identified as being malnourished are often referred to a registered dietitian for timely nutrition intervention. Dietitians can assist clients by tailoring a nutrition care plan to clients’ unique dietary needs — including cultural and personal needs — medical history, mobility and other considerations.
“By implementing the MNA‐SF across VCH, we can help to mitigate the negative implications associated with malnutrition,” says Goharian. “The benefits of screening include decreased hospital readmission rates, length of stay, mortality and morbidity, as well as increased overall satisfactory care experiences for clients and their families.”n H
Canadian Surgeons Volunteer Onboard the World’s Largest Civilian Hospital Ship
In April 2024, Quebec surgeons Dr. Jean-Martin Laberge and Dr. Louise Caouette-Laberge volunteered on the Global Mercy in Freetown, Sierra Leone, to offer free surgery to the population.
As President Julius Maada Bio of Sierra Leone stated just prior to Mercy Ships’ field service, “Mercy Ships, provides a continuous humanitarian and medical support towards providing treatment to people with various medical conditions worldwide”. At the time if the announcement, the partnership agreement included a 10-month deployment of the Global Mercy, offering free surgical care in and training healthcare professionals to build capacity within Sierra Leone’s national health system.
As she prepared to come aboard, Dr. Caouette-Laberge shared her excitement at being able to work aboard the Global Mercy. “The advantage of having a state-of-the-art hospital like this is that it has international standards. It allows us to perform complex surgeries that we wouldn’t be able to do in an African country because they don’t have the necessary infrastructure.”
The couple was recognized for their humanitarian work by the Collège des Médecins du Québec, which jointly awarded them the Prix d’humanisme in 2013. As for Dr. Laberge, in addition to participating in missions with his wife, he has contributed to the training of pediatric surgeons in Kigali, Rwanda. Through their respective work in pediatric surgery, they have between them changed countless lives of children both in Canada as well as Africa.
“We receive much more than we give! The people we operate on for free are so pleased, they thank us and are happy. We take for granted the training we receive and how lucky we are to be able to study. There are no teachers there. You don’t realize it until you leave home and see the reality of others,” says Dr. Louise Caouette-Laberge. After all
these years in the field, they are now part of an international team of medical specialists that serve onboard Mercy Ships.
The Global Mercy’s volunteer crew of nearly 600, both short- and longterm, works with dedication and excellence to welcome patients for life-changing surgeries. Darryl Anderson, Executive Director of Mercy Ships Canada, stated, “We are grateful for medical staff and all hospital volunteers who, like Dr. Laberge and Dr. Caouette-Laberge, share a passion for our mission of Hope and Healing.” Anderson also announced, “We are excited that the President of Sierra Leone has extended our partnership for another field service into 2024.”
Mercy Ships Canada is one of 16 National Offices dedicated to raising funds, building awareness, recruiting volunteers, and supporting impactful projects for Mercy Ships’ global programs. Mercy Ships operates the world’s two largest civilian hospital ships, delivering free, life-changing surgeries and healthcare, along with training and mentoring for local healthcare professionals, ensuring communities have sustainable healthcare long after the ships depart.
Mercy Ships believes that everyone deserves a life full of promise and potential. That every mother deserves to see her child grow healthy and thrive. We believe that healthcare is a human right, and we are committed to reaching children and families in need of safe surgical care with state-of-the-art hospital ships filled with compassionate volunteer healthcare providers.
Dr. Louise Caouette-Laberge, conducting a surgery with her husband Dr. Jean-Martin Laberge, onboard the Global Mercy
To learn more on volunteering visit mercyships.ca/en/get-involved/volunteer WITH VOLUNTEERS LIKE YOU OUR SHIPS BECOME HOSPITALS