“Home care nurses are not recognized on the same level as hospital and long-term care nurses. The government needs to see that we’re valuable. We provide a service that keeps people out of hospitals, where it’s very expensive to care for a patient.”
Home care nurses are demanding better.
Expanding the Canada Health Act must include mental health and substance use health
By Dr.Mary Bartram and Dr. Kathleen Leslie
Patients should not “face charges for medically necessary care when a service would otherwise be covered if provided by a physician,” federal Minister of Health Mark Holland recently stated in his letter to provincial and territorial Ministers of Health on the importance of upholding the Canada Health Act. Starting in April 2026, the federal government says it will deduct any dollar paid “wrongfully” by Canadians for “physician-equivalent services provided by regulated health professionals, such as nurse practitioners” from federal health transfers.
This is an important move to safeguard medicare in Canada. Unfortunately, mental health and substance use health professionals seem to have been completely overlooked in the warning. By omitting them, the federal Minister has missed a golden opportunity to require provinces and territories to address long-standing gaps and inequities in access to much needed healthcare.
Mental health and substance use health professionals are a critical component of our health system. Physicians started to be able to bill provincial medicare plans for psychotherapy, an important treatment method for mental health and substance use health, soon after the Medical Care Act was passed in 1966.
The same services should be covered so long as the healthcare providers are regulated by statute, as physicians are, which would include psychotherapy provided by psychologists, social workers, psychotherapists, counselling therapists and occupational therapists. Provincial regulation of these providers started in earnest in the 1960s, and is almost complete today as the remaining five provinces work to regulate psychotherapy and counselling therapy.
UPCOMING DEADLINES
MAY 2025 ISSUE
EDITORIAL: April 11
ADVERTISING:
Display – April 25 | Material – April 29
Monthly Focus:
Surgical Procedures/Pain Management/ Palliative Care/Oncology: Non-invasive surgery, plastic surgery, orthopedic surgery and new surgical techniques including organ donation and transplantation procedures. New approaches to pain management and palliative care delivery. Approaches to cancer diagnosis and treatment.
+ NATIONAL NURSING WEEK SUPPLEMENT
THANKS TO OUR ADVERTISERS
So why not include them in the letter?
While we are at it, why not consider expanding medicare coverage to include certified peer support workers, as has been done across the United States – as well as certified addiction counsellors?
Expanded medicare coverage would go a long way to address longstanding gaps and inequities in access to mental health and substance use health services, which date back to the original exclusion of mental hospitals from hospital insurance in 1957 that was further entrenched in the Canada Health Act in 1984.
Today, many people in Canada still do not have access to needed mental health and substance use health services, with the ongoing impacts of the pandemic, the overdose crisis and the toxic illegal drug supply amplifying the gap between the needs of the population and the capacity of health workers to respond. Targeted federal health transfers are helping but are still falling short.
For mental health and substance use health to reach full parity with physical health, it’s time for it to be included in medicare through explicit inclusion in the Canada Health Act.
We understand that such a policy change requires a significant transfer from the private to the public purse, just as with recent steps towards medicare coverage for dental services and pharmacare. However, the case for public investment is rock solid.
Mental health and substance use health are the foundation of economic productivity as well the cornerstone of our health and wellbeing, and mental health and substance use concerns are each estimated to cost the economy close to $50 billion dollars a year.
Continued on page 6
JUNE 2025 ISSUE
EDITORIAL: May 9
ADVERTISING: Display – May 23| Material – May 27
Monthly Focus:
Precision Medicine and Genomics/Pharmacy and Medication Management/Research: Developments in the field of personalized medicine. Innovative approaches to fundraising and the role of volunteers in healthcare. An examination of safe and effective use of medications in hospitals including medication management.
+ ANNUAL HOSPITAL PHARMACISTS’ ASSOCIATION SUPPLEMENT
When you visit our advertisers, please mention you saw their ads in Hospital News.
610
www.hospitalnews.com
Editor Kristie Jones editor@hospitalnews.com
Advertising Representatives
Denise Hodgson denise@hospitalnews.com
Publisher Stefan Dreesen stefan@hospitalnews.com
Accounting Inquiries
accountingteam@mediaclassified.ca
Circulation Inquiries info@hospitalnews.com
Director of Print Media
Lauren Reid-Sachs
ADVISORY BOARD
Helen Reilly, Publicist Health-Care Communications
Bobbi Greenberg, Health care communications
Sarah Quadri Magnotta, Health care communications
Dr. Cory Ross, B.A., MS.C., DC, CSM (OXON), MBA, CHE Vice President, Academic George Brown College, Toronto, ON
ASSOCIATE PARTNERS:
Hospital News is published for hospital health-care professionals, patients, visitors and students. It is available free of charge, accessed by our website (hospitalnews.com) and also available through our digital subscription.
The statements, opinions and viewpoints made or expressed by the writers do not necessarily represent the opinions and views of Hospital News, or the publishers.
Hospital News and Members of the Advisory Board assume no responsibility or liability for claims, statements, opinions or views, written or reported by its contributing writers, including product or service information that is advertised.
For changes in email subscriptions please send requests to info@hospitalnews.com. Hospital News does not share email information and subscriptions can be cancelled at any time.
College of Physicians and Surgeons of Ontario welcomes Physician Assistants as registrants
hysician Assistants (PAs) are highly skilled professionals who provide a range of medical services within health-care teams under the supervision of a physician, acting as physician-extenders to improve access to care. They are broadly trained to complement existing services and improve access to health care.
Starting April 1, 2025, the College of Physicians and Surgeons of Ontario (CPSO) began regulating all PAs in Ontario under the Regulated Health Professions Act, 1991 (RHPA) and the Medicine Act, 1991. PAs must be registered with CPSO to continue using the title “physician assistant” or “PA” in the province. Hospitals and physicians working with PAs are encouraged to remind them to register with CPSO as soon as possible, if they have not already done so.
Ontario is now the eighth province to regulate PAs by a provincial medical regulator, joining Alberta, British Columbia, Saskatchewan, Manitoba, New Brunswick, Nova Scotia and PEI. Newfoundland has also passed legislation to regulate PAs, although it has not yet taken effect.
CPSO’s oversight of PAs will help ensure safe and high-quality health care for patients through clearly defined training, certification, and continuing education requirements. However, regulation is not intended to affect the core way physicians and PAs work together.
ELIGIBILITY FOR REGISTRATION
PAs may register with CPSO if they have:
1. graduated from an accredited PA education program offered in Canada or the US and
2. successfully completed a certifying examination in Canada (Physician Assistant Certification Council of Canada - PACCC) or the US (National Commission on Certification of Physician Assistants - NCCPA). The regulations also include a transitional grandparenting provision to enable two cohorts of trained and currently practising PAs who do not meet
the standards and qualifications set out in the regulation to register as members. The provision captures individuals who have successfully completed the Canadian Armed Forces Physician Assistant Program and the Physician Assistant Integration Program, a historical assessment-based program.
To register, PAs are required to create an account to submit an online application form, upload documents, and pay the required fees to CPSO directly through CPSO’s Member Portal.
PAS WILL CONTINUE TO PRACTISE VIA DELEGATION FROM A PHYSICIAN
Physicians and PAs in Ontario have long practised together through the delegation model, which is effective and well-established. The relationship between physicians and PAs, anchored in the delegation framework, will not change as a result of PA regulation. Delegation allows a regulated health professional (e.g., a physician) who is authorized to perform a controlled act to grant that authority to another person (whether regulated or unregulated) who is not legally authorized to perform the act independently. Delegation is not required for tasks that are not controlled acts (e.g., taking a patient’s history).
PAs can only perform controlled acts through delegation and with appropriate supervision by a physician, as set out in CPSO’s Delegation of Controlled Acts policy. Further guidance can be found in the accompanying Advice to the Profession document.
PAS’ SCOPE OF PRACTICE WILL NOT CHANGE
A PA’s scope of practice will reflect their supervising physician’s scope of practice and is determined by the PA’s own knowledge, skill, and judgment. This means that each PA’s scope of practice will vary according to a number of factors, including the individual’s education, training and experience.
PAs Will be Required to Participate in a Continuing Professional Development (CPD) Program
Quality Assurance Regulations (O. Reg. 114/94, General, Part VII) require PAs to participate in a program of CPD and to, each year, provide to CPSO proof of their participation that is satisfactory to CPSO.
PAs are required to complete the CPD requirements set by their certifying body, which is either the:
• Physician Assistant Certification Council of Canada (PACCC); or
• National Commission on Certification of Physician Assistants (NCCPA).
PAS MUST OBTAIN APPROPRIATE PROFESSIONAL LIABILITY INSURANCE
All regulated health-care professionals, including PAs, must have professional liability protection. PAs are required to hold at least $10 million in professional liability insurance issued by a company licensed to carry on business in the province.
PHYSICIANS, INSTITUTIONS, AND PAS WILL HAVE REPORTING REQUIREMENTS
Effective April 1, PAs will become regulated members under the Regulated Health Professions Act, 1991 (RHPA). As such, any requirement under the RHPA to report a member of a College, or for a member of a College to make a report, will include PAs. More information about reporting requirements can be found in the Guide to Legal Reporting Requirements. More details on PA registration, delegation, and other topics are available on CPSO’s website. If you have further questions, please get in touch with CPSO at inquiries@cpso.on.ca or contact an Advisor at 416-967-2617. n H
AI can predict premature deaths in people with inflammatory bowel disease
Almost half of people who died with inflammatory bowel disease (IBD) died prematurely, according to a study published in CMAJ (Canadian Medical Association Journal) that used machine learning models to predict death.
Canada has some of the highest rates of IBD worldwide, which includes Crohn disease and ulcerative colitis. People with IBD have shorter life expectancy than people without such diseases, and they can develop other chronic health conditions related to their IBD. The study found that people with IBD are at risk for premature death (defined as death before age 75) when they develop other chronic health conditions earlier in life.
As machine learning models can predict premature death in the general population, researchers applied the technology to determine whether it could predict premature deaths among people in Ontario with IBD and other
Continued from page 4
chronic conditions using health care data held at ICES.
“The clinical implication is that chronic conditions developed early in life may be more important in determining a patient’s health trajectory, although further causal research is needed to elucidate this relationship,” writes Dr. Eric Benchimol, a pediatric gastroenterologist and senior scientist at The Hospital for Sick Children (SickKids), professor of pediatrics and epidemiology at the Temerty Faculty of Medicine, University of Toronto, and a senior core scientist at ICES.
“Although our insights are not causal insights, they identify patients potentially at higher risk of premature death, and therefore who might benefit from more coordinated care of their IBD and other chronic conditions,” he says.
Of the total 9278 deaths in people with IBD between 2010 and 2020, almost half (47 per cent) were premature, with higher rates in males than in females (50 per cent v. 44 per cent).
Expanding the Canada Health Act
Our research team has just released Toward a Mental Health and Substance Use Health Workforce Strategy for Canada that draws on international best practices, the latest evidence, and advice from a diverse cross-section of experts from provider associations, the public and private sectors, and individuals with lived experience. It’s time Canada explicitly include mental health and substance use health in our public health insurance plans.
A first step is within reach. We urge the federal Minister of Health to clarify that psychotherapy provided by regulated mental health and substance use health professionals be added to an expanded interpretation of the
Canada Health Act. In so doing, the federal government would recognize that mental health and substance use health professionals have been providing psychotherapy that is at least equivalent to – and in many cases better than – what is provided by less specialized primary care physicians.
The United States, the UK, Australia and New Zealand all have national strategies for the mental health and substance use health workforce. Expanded public insurance coverage for psychotherapy should be the first step in the implementation of a ground-breaking mental health and substance use health workforce strategy for Canada. n H
Dr. Mary Bartram is the Chief Executive Officer of Rideauwood Addiction and Family Services, an Adjunct Research Professor at Carleton University, and co-lead of the Mental Health and Substance Use Health sector of the Canadian Health Workforce Network. Dr. Kathleen Leslie is an Associate Professor in the Faculty of Health Disciplines at Athabasca University and co-lead of the Regulation and Governance theme of the Canadian Health Workforce Network.
The most common chronic conditions at death were various types of arthritis (77 per cent), hypertension (73 per cent), mood disorders (69 per cent), kidney failure (50 per cent) and cancer (46 per cent). The researchers found that including chronic conditions diagnosed before age 60 and the age of diagnosis improved the models’ predictions.
“The use of premature death as the outcome more directly identifies opportunities for health system improvements, as premature deaths are considered avoidable through appropriate prevention or early and effective treatment,” write the authors.
The study was co-led by medical student Gemma Postill of the Temerty Faculty of Medicine, and Dr. Laura Rosella, professor and Canada
Research Chair in Population Health Analytics at the Dalla Lana School of Public Health.
The authors hope that their research will help pinpoint areas for more targeted follow up from a range of health care professionals, from dietitians to mental health professionals and specialists when required.
“These findings provide scientific support for providing multidisciplinary and integrated health care across the lifespan (particularly during young and middle adulthood),” the authors conclude.
“Machine learning prediction of premature death from multimorbidity among people with inflammatory bowel disease: a population-based retrospective cohort study” is published March 24, 2025. n H
Blood test shows promise for
early detection of dementia
For people with a certain sleep disorder, a simple blood test could help predict the development of dementia years before symptoms appear, a new study indicates.
Idiopathic REM sleep behaviour disorder (iRBD) causes people to physically act out their dreams while sleeping. The disorder is also associated with a very high risk of Parkinson’s disease and a related condition called Dementia with Lewy Bodies. This is a form of dementia that often causes memory and cognitive loss, as well as vivid visual hallucinations and movement difficulties similar to Parkinson’s.
McGill University researchers have discovered that a blood test, originally developed to detect Alzheimer’s disease, could also identify which patients with the iRBD sleep disorder are most likely to develop Dementia with Lewy Bodies. The blood test analyzes two proteins in the blood that serve as biomarkers for Alzheimer’s.
“Detecting dementia risk early could have significant implications for how doctors guide patients, helping them plan for the future and potentially allowing for more personalized, effective
treatments,” said Dr. Ronald Postuma, a Professor in McGill’s Department of Neurology and a clinical researcher at The Neuro (Montreal Neurological Institute-Hospital).
Researchers followed 150 iRBD patients, testing their blood for the biomarkers and tracking their health annually. Remarkably, the blood test, taken four years before, predicted dementia in almost 90 per cent of the patients who later developed the disease.
This study, published in the journal Brain, also suggests the early stages of Parkinson’s and Alzheimer’s have more in common than previously thought.
“Our findings suggest that Alzheimer’s treatments could also be tested in patients with this sleep disorder. Perhaps, if treatments start early enough, Dementia with Lewy Bodies can be prevented,” said first author Dr. Aline Delva, who was a research fellow at The Neuro during the study.
The research team plans to expand the study to confirm how well the test can predict dementia risk in patients with diagnosed Parkinson’s disease as well as other populations at risk for Dementia with Lewy Bodies. n H
CMA fighting to ensure access to health care is an all-party priority on the campaign trail
As political parties and their leaders hit the campaign trail today, the Canadian Medical Association (CMA) is here to stand up for Canadians’ access to health care. With uncertainty rising due to Donald Trump’s attack on our economy, Canadians shouldn’t also have to worry about whether they can access health care when they need it. Now more than ever, they need a strong health system to protect them from the harms of this economic uncertainty.
“Health care is political, but it is not partisan. It will always be a pressing issue for Canadians and those who care for them,” says Dr. Joss Reimer, CMA president. “We will all need the health system at some point in our lives. Political leaders must make sure that when that day comes, Canadians not only get timely access to care, but that they get the quality of care they deserve.”
As Canadians rally around our flag, nothing unites us more than our universal health system. While it may be hurting, it is worth fighting for – now more than at any other time. The CMA has outlined priorities that should be at the forefront of each party’s election platform:
• Make sure Canadians can get ongoing care from a family doctor and a primary health care team.
• Make it easier for clinicians to share digital health information with each other and their patients.
• Make it possible for doctors trained in other countries to safely see patients here.
• Fight against false information that is increasing preventable infections, childhood mental illness and other diseases.
• Improve the health and well-being of Indigenous Peoples through
supporting First Nations, Inuit and Métis-led led health care services.
In this election, the CMA will be working hard on behalf of physicians, their patients and communities to make sure that health care remains at the forefront of the conversation.
We can’t ask doctors and other health professionals to bear the weight of the health care system on their own. We must keep working together to offer a publicly funded health care system that will make Canadians proud. See our complete list of solutions here. n H
One-third of older Canadians at nutritional risk
One-third of Canadian adults aged 55 or older are nutritionally at risk, potentially leading to increased hospital stays, more emergency visits and physician consultations for possible infections, a new study found.
The University of Waterloo researchers assessed data from more than 22,000 community-dwelling adults aged 55 and over from the Canadian Longitudinal Study on Aging. After an initial evaluation, they followed up with participants up to three years later to track their health-service use over the previous year.
Researchers used the SCREEN-8 tool (Seniors in the Community Risk Evaluation for Eating and Nutrition) to measure an individual’s nutrition risk. They found that those with higher SCREEN-8 scores at the initial screening – indicating better nutrition – had significantly lower odds of reporting an overnight hospital stay, visiting a hospital emergency room, or seeing a
doctor for an infection when followed up three years later.
“While these results make sense intuitively, they highlight how a straightforward and inexpensive tool can easily be used to potentially make a vast difference in improving health-care outcomes and costs,” said Dr. Heather Keller, a professor in the Department of Kinesiology and Health Sciences and Schlegel Research Chair in Nutrition and Aging.
“SCREEN-8 should be a routine part of primary care practice, although it can be self-administered at home.”
Nutrition risk among older adults is a significant concern, especially among community-dwelling individuals, as it precedes malnutrition. The eight questions on SCREEN-8 gather information about weight change, appetite, eating challenges – such as choking or difficulty swallowing – meal preparation behaviours and fruit, vegetable and fluid intake.
The study sample included an equal number of males and females, with a
mean age of about 66 years. Most participants were living with a partner and two-thirds of people surveyed had post-secondary degrees. One of the study’s limitations was that the people sampled were predominately highly educated and white, meaning that it is not fully representative of Canadians.
“Knowing who’s at risk nutritionally allows individuals the possibility of modifying behaviours to avert negative health outcomes,” Keller said. “Further research can help determine how health-care practitioners can best triage and provide education, programming and services to offset high risk.”
The study, Baseline nutrition risk as measured by SCREEN-8 predicts self-reported 12-month healthcare service use of older adults 3 years later, was published in Applied Physiology, Nutrition, and Metabolism and is co-authored by Vanessa Trinca, a research associate in Kinesiology and Health Sciences at Waterloo. n H
Optimizing public placement of naloxone kits to save lives
Making it easy to access naloxone kits to reverse the effects of opioid poisoning will help save lives, according to research published in CMAJ (Canadian Medical Association Journal) that looks at the best placements for these kits.
Researchers wanted to understand the best placement for public-access naloxone kits in Vancouver, British Columbia, to help prevent deaths from opioid poisoning. They compared public access strategies for more than 14 000 opioid poisonings over 6 years. They looked at placement at existing locations of take-
home naloxone, at public locations like chain businesses, and at public transit locations. They found that kits placed at public transit locations, using criteria similar to those in an optimization strategy for placing automated external defibrillators, had the best coverage for reversing opioid poisonings, with fewer kits needing to be placed.
Placing publicly accessible naloxone kits at transit stations using the optimization-driven strategy and ensuring blanket placement at take-home naloxone program locations, which distribute free naloxone kits to community members, helped cover a ma-
jor proportion of opioid poisonings in Vancouver.
“Optimization-driven placement can identify locations where opioid poisonings are most concentrated and therefore where naloxone kits are most valuable, leading to coverage especially in areas not covered by other strategies,” writes Dr. K.H. Benjamin Leung, a research fellow in health systems engineering, Duke University, Durham, North Carolina, with coauthors. “Overall, a combination of blanket naloxone kit placement at take-home naloxone locations and optimization-driven placement in areas underserved by the take-home
naloxone program may be the best approach.”
The authors hope these findings will help decision-makers optimize accessibility of naloxone kits to prevent deaths from opioid poisoning.
“For public-access naloxone programs to be successful, naloxone kits must be easily accessible at all times, which may be achieved by placement on the exterior of buildings along with clear indicative signage,” the authors conclude.
“Optimizing placement of public-access naloxone kits using geospatial analytics: a modelling study” was published March 17, 2025. n H
UHN addressing care gap in women’s heart health
By Shauna Mazenes
lana Trainoff didn’t think it was possible to have a heart attack at age 40.
That is, until she was rushed to the hospital with shortness of breath and chest pain. Doctors discovered she had a STEMI – one of the most fatal types of heart attacks. She had total blockage in one artery; two others were 65 per cent blocked. She was taken into emergency surgery.
“I had this instinctive feeling that something was seriously wrong,” says Elana, now 50, who was saved at UHN’s Peter Munk Cardiac Centre (PMCC). “It was a very traumatic and scary experience.”
February is Heart Month and the 10th anniversary of Elana’s life-saving procedure. She wants women to know their risks, prevention strategies – and most importantly – that they’re not alone.
According to Professor Sherry Grace, Director of Research in the Cardiovascular Rehabilitation & Prevention Program at PMCC, what happened to Elana is becoming increasingly common. While heart disease has traditionally been viewed as an older man’s condition, they’re seeing more young women diagnosed.
“It’s being recognized in the research literature that something’s going on, because a lot more 40-year-old women are getting acute coronary syndrome than in previous years,” says Professor Grace, who is also a Senior Scientist at UHN’s KITE Research Institute and a professor in the Department of Medicine at the University of Toronto.
She says increased rates of heart risk factors in young women, such as stress and mental illness, as well as delayed diagnosis and sex-related biological differences, can all impact the disease pathway and health outcomes.
There’s been an effort to increase the number of women being recruited into heart research, including at UHN – to better understand how symptoms and treatment outcomes may differ compared to men.
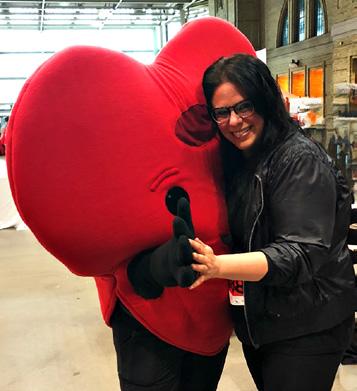
“I didn’t know if I was going to live 10 years, but I did. And now, I’m stable and thriving,” says Elana Trainoff, posing with a heart mascot. “I’ve made a lot of changes in my life since then, and I want other women to know that they can, too.”
For Elana, the first indication of a problem was shortness of breath and heartburn. Despite what may have seemed like minor discomfort, she knew something was wrong.
But her vitals were normal when she arrived at the hospital. Doctors initially thought it might be indi-
gestion – a common symptom of a heart attack in women. It wasn’t until she experienced crushing chest pain that she got an electrocardiogram and it was determined what was happening.
“I want to remind women if you feel these concerning symptoms, go
to the hospital,” she says. “Advocate for yourself if you know something is wrong.”
Professor Grace echoes this sentiment. The lack of research historically has resulted in a care gap in women’s heart health – women are more likely to have their symptoms misattributed, to not be tested or to receive inadequate care.
“It’s very typical for women to also present with symptoms other than chest pain,” says Professor Grace. “That’s why we want to encourage women to speak up for themselves, and to be aware of the unconscious bias that they’re more likely to have their symptoms dismissed.”
This is, in part, why heart and stroke are the leading causes of death amongst women worldwide.
“Physicians report feeling less confident treating heart issues in women,” she says.
Elana struggled with her mental health after the procedure. Not only did she feel lost and alone, but overwhelmed by all the lifestyle adjustments she had to make.
One of the most important parts of her recovery was seeing a cardiac psychiatrist at UHN. She says she needed to learn how to care about herself enough to make positive changes in her life.
“I had to wake up every morning and think: I’m going to make good choices for myself today,” she says.
Professor Grace says Elana is not alone. One in five people suffer with depression after a heart attack, a number that’s higher in women than it is in men.
It’s also more common, she says, to see people suffering with feelings of shame after being diagnosed with heart disease as opposed to a condition such as cancer, even though the risk factors are the same.
Professor Grace says for these reasons and more, women’s awareness of cardiac rehab programs is low, even
Photo: Courtesy Elana Trainoff)
though they have much to gain from participating.
Cardiac rehab aims to help patients recover from a heart issue by leading a healthier lifestyle. It promotes things such as stress management, exercise and awareness.
“Women need to be better informed about their risks and given psychosocial support,” Professor Grace says. “That’s why UHN is trying to promote women’s heart health clinics and increase access to heart doctors who understand and know how to treat women’s heart issues.”
Professor Grace’s research has guided the refinement of a woman-focused cardiac rehab program at UHN, which opened in 2005. The program addresses women-specific issues that can influence heart disease and consider socio-economic barriers that can impact access to care. This includes mental health challenges, care-giving demands, transportation difficulties and work-related priorities.
Since joining cardiac rehab, Elana has adopted a lifestyle that supports her needs. She quit smoking, limits her alcohol intake and exercises as best as she can. She also follows a heart, diabetes and anemia-friendly diet that isn’t too restrictive.
“IT’S BEING RECOGNIZED IN THE RESEARCH LITERATURE THAT SOMETHING’S GOING ON, BECAUSE A LOT MORE 40-YEAR-OLD WOMEN ARE GETTING ACUTE CORONARY SYNDROME THAN IN PREVIOUS YEARS.”
“Don’t ignore these metabolic, chronic conditions that can lead to heart problems,” says Elana, who started showing signs of blood sugar and cholesterol issues in her 20s but chose to look the other way.
“And, don’t discount your family history, even if you’re young.”
Both of her parents had heart issues as well.
But Elana says it doesn’t stop there. There’s a dire need for
“If there’s anything I want women to know, it that there’s a light at the end of the tunnel,” says Elana Trainoff, who 10 years ago had a heart attack at the age of 40.
more women in research and more funding towards women’s heart health. She’s committed much of her time towards raising awareness, advocating and reminding women that they’re not alone if they find themselves in the same position she was.
“If there’s anything I want women to know, it that there’s a light at the end of the tunnel,” she says. “I was in a dark, lonely place.
“But 10 years later, I’m healthy and I’m happy, and you can be, too.” n H
Shauna Mazenes works in communications at UHN.
Photo: Courtesy Elana Trainoff)
Timely wrap-around support for people with type 1 diabetes
A pilot project of the new REACHOUT app offered accessible and flexible support for people with type 1 diabetes
Around 30 to 50 per cent of Canadians living with type 1 diabetes (T1D) experience diabetes distress, a psychological state characterized by ongoing frustrations, worries and fears related to managing this complex condition. A pilot study headed by Vancouver Coastal Health Research Institute researcher Dr. Tricia Tang tested Tang’s novel REACHOUT peer-driven mobile application, which shows promise as a just-in-time, wrap-around and customizable mental health care support system for individuals with T1D.
T1D affects approximately five to 10 per cent of the over 560,000 British Columbians diagnosed with diabetes. More than half of new T1D cases are diagnosed in adulthood.
T1D is caused by the pancreas not producing insulin – an essential hormone for the control of blood sugar levels. People with the condition must take insulin and follow nutritional and lifestyle habits to protect against harmful or life-threatening complications, such as mental health issues, nerve damage, high blood pressure, eye damage, kidney disease, heart disease and stroke.
diabetes distress before and six months after using the REACHOUT app.
AN ACCESSIBLE MENTAL HEALTH SUPPORT INTERVENTION
Tang’s study included 38 adult participants living with T1D in rural and remote communities in the B.C. Interior, 76 per cent of whom were female. The study also included 36 peer supporters from the B.C. Interior and other parts of the province – all of whom received six hours of training after recruitment. Study participants filled out questionnaires surrounding their
The one-of-a-kind REACHOUT mobile app offered participants flexible approaches to connect with peer supporters as well as other participants with T1D. The three REACHOUT delivery modalities offered to participants were: 1) one-on-one support with a peer supporter of their own choosing; (2) access to group-based support from other participants and peer supporters through a 24/7 online chat room; and (3) community support through monthly virtual huddles.
Virtual huddles were pre-scheduled, 60-minute interactive seminars delivered by one or more peer supporters who were accompanied or monitored by a health care professional. Seminars touched on diabetes-related tips and topics such as managing T1D while downhill skiing, travelling with
“THE REACHOUT APP GAVE PARTICIPANTS THE SUPPORT THEY NEEDED IN THE MOMENT IT MATTERED MOST. THEY DECIDED THE FREQUENCY AND INTENSITY OF SUPPORT.”
T1D, addressing burnout and working towards greater resilience. Peer supporter facilitators presented in the first 10 to 15 minutes followed by a question-and-answer period. Attendees were invited to submit questions one to two weeks prior as well as during the session itself.
PARTICIPANTS REPORTED FEELING MORE SUPPORTED AFTER USING REACHOUT
Similar to dating apps, the REACHOUT platform invites partici-
pants to browse peer supporter profiles housed in the app’s peer supporter e-Library. Profiles included sociodemographic characteristics such as age, sex and city of residence, along with an overview of peer supporters’ diabetes history, hobbies, professional life, whether they had children and more.
Each participant was encouraged to review profiles and select a peer supporter to connect with based on their personal preferences.
“Participants had the option to switch to a different peer supporter mid-way through the study,” Tang
An example of a peer supporter profile on the REACHOUT app.
O Advancing health through innovation
n March 11, 2020, the world changed.
The World Health Organization declared COVID-19 a pandemic, launching an unprecedented global health crisis. At UHN, researchers, clinicians, and scientists rapidly mobilized, applying expertise and innovation to understand, combat, and ultimately shape the future of pandemic preparedness.
“COVID-19 reinforced what we have always known – scientific discovery, collaboration, and innovation are our best defences against global health crises,” says Dr. Brad Wouters, Executive Vice President of Science and Research at UHN.
“This is true for both the challenges we are aware of today and those that will continue to develop. At UHN, we are not just responding to pandemics; we are building the future of health care.”
As we mark the fifth anniversary of this defining moment, we reflect on the extraordinary contributions of UHN’s research teams and the lasting impact of this work on global health.
RESPONDING TO A GLOBAL CRISIS
The urgency of the pandemic demanded swift, coordinated action. UHN experts stepped up as leaders in public health strategy, ensuring data-driven decisions that would save lives.
Dr. Beate Sander’s data modelling provided critical insights to policymakers, shaping Ontario’s response and resource allocation. Meanwhile, UHN researchers played a key role in Canada’s $53-million Variants of Concern Strategy, identifying and tracking emerging threats such as the Delta variant.
notes. “This flexibility was designed to offer participants the freedom to connect with peers with whom they could best relate.”
“We often seek out people who share similar interests, are at a similar stage of life or have a related professional or family background,” adds Tang. “In the study, a young man in his 20s matched with a man in his 50s because both had a background in
These contributions ensured that UHN was not just responding to the crisis but actively shaping the scientific and public health response at both the national and international levels.
TRANSFORMING RESEARCH INTO ACTION
Clinical trials at UHN adapted in real time, ensuring research could continue without compromising patient safety.
The launch of STOP-CoV, UHN’s first fully virtual clinical trial demonstrated the power of remote participation in medical research. Innovations such as electronic consent and virtual monitoring redefined how trials were conducted, setting a new standard for accessibility in clinical research. A first-in-the-world trial led by Atul Humar and Deepali Kumar, has provided critical evidence on the effectiveness of third-dose COVID-19 vaccines for transplant recipients.
Additionally, a recent study, co-authored by Peter Wu and Moira Kapral, provides further information about nirmatrelvir-ritonavir’s role in reducing the risk of hospitalization for COVID-19 while highlighting key limitations for patients and health care providers.
These findings are reshaping global vaccination strategies, ensuring that immunocompromised individuals receive optimal protection against emerging variants.
DRIVING SCIENTIFIC DISCOVERY
The pandemic also catalyzed game-changing discoveries at UHN.
Dr. Eleanor Fish’s research on interferon-a2b showed its potential to
information technology. This pairing was intuitive from the standpoint of the participant but would have been difficult for us to make for him.”
Results from the study showed that participants experienced higher levels of support from friends, family and peers following the REACHOUT intervention. For women, the survey results showed significant reductions in their depressive symptoms and overall
On the five-year anniversary of the COVID-19 pandemic, UHN reflects on the extraordinary contributions of research teams and the lasting impact of this work on global health.
reduce COVID-19 viral load, offering a new avenue for treatment. Meanwhile, computational modeling by Dr. Donald Weaver identified furosemide as a promising candidate for mitigating severe infections, reinforcing the power of fundamental science in pandemic response.
These discoveries highlight how UHN’s scientific infrastructure is positioned to pivot quickly when new global health threats emerge, ensuring that research remains one step ahead of the next pandemic.
PROTECTING MENTAL HEALTH AND FRONTLINE WORKERS
Beyond virology and clinical breakthroughs, UHN recognized the deep mental health impact of the pandemic.
The development of UHN CARES initiative provided tailored mental health support, reinforcing UHN’s commitment to holistic well-being in health crises. The pandemic reinforced the need to integrate mental health support into frontline care environments, ensuring that those who dedicate their lives to protecting others receive the care they need to sustain their own well-being.
To further this commitment, UHN continues to develop innovative mental health programs and digital solutions that support resilience, en-
distress, including in three of the distress subscales of powerlessness, management distress and eating distress.
“Encouragingly, 20 of the 36 peer supporters involved in the pilot study are continuing on as peer supporters in our subsequent, large-scale REACHOUT randomized controlled trial (RTC),” Tang relays. “Likewise, of the 38 participants in our pilot study, nine completed training to become
suring that health care workers have access to the resources they need, both during crises and in everyday practice.
BUILDING A FUTURE ON INNOVATION AND COLLABORATION
The pandemic underscored the necessity of an integrated approach to health care, research, and public policy. UHN’s response exemplified a One Team mindset, uniting experts across disciplines to address urgent challenges.
As we move forward, the lessons learned will shape the next generation of pandemic preparedness – enhancing surveillance, refining rapid response frameworks, and advancing digital health solutions. Strengthening global collaborations and investing in pandemic prevention measures will be critical to mitigating the impact of future outbreaks before they escalate into crises.
UHN’s vision of A Healthier World is more than an aspiration; it is a commitment. The advanced research and innovations developed in response to COVID-19 will continue to drive progress, ensuring that global health systems are more resilient, responsive, and prepared for the challenges ahead. The fight against infectious diseases is ongoing, but with science, collaboration, and a relentless pursuit of excellence, TeamUHN is leading the way forward. n H
peer supporters for the REACHOUT RCT.”
“This development shows us that the low-barrier REACHOUT program could well have longevity should it be rolled out across the province, with a continuous influx of participants paying it forward by becoming peer supporters, along with volunteers from the broader community of people living with T1D.” n H
Photo: Getty Images)
Canadian first surgery to restore vision
By Ann Gibbon
Adecade ago, Gail Lane suffered a seizure so bad she needed to be hospitalized. But during that stay, things took a devastating turn for the Victoria resident, now 74. The anti-seizure medications she took triggered a reaction that led to a rare auto-immune disorder, Stevens Johnson Syndrome.
At age 64, she became completely blind.
“It was hard adjusting to blindness later in life,” she acknowledges, having to relearn everything sighted persons take for granted – walking, dressing so things matched, eating, using a cell phone.
But in late February this year, Lane, two other blind patients, one from the Vancouver area and one from Ontario, plus a team of surgeons and healthcare providers made Canadian medical history at Mount Saint Joseph Hospital in Vancouver: the patients underwent the first part of a two-phase surgery in which ultimately, one of their own teeth, outfitted with a plastic lens, will be sewn over their eyeball to restore their sight – often to 20/20 vision.
They were the first patients in Canada to receive the surgery.
When people hear about it, their jaws usually drop. Lane, too, thought it sounded like science fiction. But her fierce desire to see again overcame those thoughts and she is grateful to receive this potentially life-saving operation.
SURGERY IS FOR PATIENTS WITH SEVERE CORNEAL BLINDNESS
She was the first of the three Canadian patients. Her surgery took place February 25 and went well, her doctors say. She is back in Victoria, recuperating.
Colloquially known as “tooth-ineye” surgery, the medical name is Osteo-Odonto Keratoprostheseis (OOKP). This highly specialized and
rare surgery was not, until this week, available in North America.
The procedure is suited to certain patients whose severe corneal blindness is caused by scarring, conditions like autoimmune diseases (as in Lane’s case) or chemical burns and other traumas. In these situations, traditional corneal transplants don’t work. However, for patients whose retina and optic nerves are still healthy, OOKP surgery can restore full sight by implanting an optical lens or “telescope” within a tooth to replace the scarred eye surface. (The cornea is the clear tissue part covering the eyeball.)
Another of the other three patients to receive the surgery in Vancouver was Brent Chapman, a 33-year-old Vancouver-area resident. At just age 13, he took ibuprofen during a basketball game and had a horrific reaction that blinded him fully and left him in a coma for a period.
PATIENTS AND FAMILIES EXPEND TIME AND MONEY TO GET SIGHT BACK
Chapman and his family spent countless hours and dollars over the years trying everything to get him to see again. Brent’s ordeal has included
nine surgeries for in the US, a surgery using stem-cell tissue from his parents’ eyes, and 12 corneal transplants.
Nothing has worked. “That’s why this tooth-n-eye surgery is the last resort,” he says.
TWO STAGES TO TOOTH-IN-EYE SURGERY
The first surgery, about six hours long, begins with the extraction of a tooth from the patient (typically the canine, or ironically, “eye” tooth). It is then drilled down, shaped, and the lens, or telescope, is glued inside.
The tooth is sewn into the patient’s cheek for up to three months, allowing tissue to grow around it before it is used as the carrier for the new lens. Surgeons also remove a flap of skin from inside the cheek and sew it over the patient’s eye until the second surgery.
During the second surgery, about three months later (also lasting some six hours), the tooth is removed from the cheek.
Mount Saint Joseph Hospital ophthalmologist and surgeon Dr. Greg Moloney will pull back the flap of skin covering the eye and take out the patient’s damaged iris and lens. He and
The tooth before the insertion.
the team will then sew the tooth holding the plastic lens onto the eyeball. The tissue that formed around the tooth while implanted in the cheek allows the tooth to be sewn onto the eye. The flap, which helps the tooth stay in place on the eye, is then resewn over the eyeball. Dr. Moloney will create a small hole in the flap of skin so the patient can see.
WHY USE A TOOTH?
“A tooth contains dentin, which is the ideal tissue to house a plastic lens without the body rejecting it,” explains Dr. Moloney, who was recruited from his native Australia in 2021 to Vancouver to perform these surgeries. He and a medical team have done about seven in his home country. He adds, “The skin flap from the mouth recognizes the tooth that has been inside the cheek.”
He was joined at Mount Saint Joseph in February by fellow Aussie Dr. Shannon Webber (the two went to medical school together) who flew in from Australia specifically for the trio of Vancouver surgeries.
Dr. Webber is an oral-maxillofacial surgeon – a specialist in surgeries involving the face, jaw and mouth. For the three surgeries, he trained local
oral-maxillofacial surgeon Dr. Ben Kang, from Vancouver General Hospital, so that this expertise becomes local to Vancouver and other Canadian patients can be accommodated. Dr. Webber removed Lane’s, Chapman’s and the other patient’s tooth in the separate surgeries and insert it inside their cheek.
OOKP surgery has documented positive results dating back to 1973. However, it is an intricate procedure requiring multiple surgeons, which has discouraged many centres from offering the procedure.
To date, about 500 to 1000 patients have received the surgery in clinics in about 10 countries including the United Kingdom, Singapore, India, Australia – and now, Canada.
Dr. Moloney wants Mount Saint Joseph to be the Canadian OOKP clinic.
Prior to the Mount Saint Joseph clinic, patients like Brent Chapman shouldered a heavy financial burden in their quest to see again.
St. Paul’s Foundation and the Department of Ophthalmology at
Providence Health Care partnered to establish an OOKP clinic. The Foundation raised $430,000 to fund it for three years to support start-up costs, including training for the OR team and equipment, and yearly operating expenses. After that, Providence Health Care
will build the costs into its budget planning.
To Dr. Moloney and Dr. Webber, these are more than just surgeries. “We get emotional about them,” says Dr. Moloney.
“It is so rewarding when a patient regains their sight.” n H
Ann Gibbon works in communications at Providence Health.
Right: Tooth in eye. Middle: Gail Lane before her surgery Far Right : Dr. Greg Moloney.
Centralized booking and registration making hospital appointments easier
By Emily Santos
Scarborough Health Network (SHN) is delivering a superior experience for patients accessing healthcare services, right from the start of their hospital journey. Thanks to a new centralized patient scheduling model implemented last spring, which works in tandem with an easy and efficient registration process, SHN now operates the largest volume of centralized patient access interactions in Ontario – daily booking over 1,400 appointments and registering more than 3,000 patients across three hospitals and several community-based locations.
The organization-wide move to improve patient access (how patients obtain and use healthcare services, information, and resources, such as appointment booking and hospital registration) began with SHN’s adoption of the Epic clinical information system in December 2021. Now equipped with fully electronic health records, SHN was able to centralize Patient Registration at its Birchmount, Centenary, and General hospitals, each supported by self-serve registration kiosks.
The next step was to centralize a complex labyrinth of clinic schedules spread across more than 150 outpatient areas. SHN’s patient contact centre is a one-stop shop for booking, rescheduling, canceling, or inquiring about appointments through a single point of contact. It consistently scores 85 per cent or higher for patient satisfaction, due to exceptional customer service and accessibility, including extended operating hours on evenings and weekends. Patients are offered the earliest available appointment(s) with coordination across multiple clinics (if applicable), so they can spend less time waiting on the phone and select the clinic location that is closest to their home.
On arrival at the hospital, up to 90 per cent of patients are completing their check-in at kiosks in under a minute, a significant improvement from the previous average of over eight minutes.
For patients with multiple appointments on the same day, registration kiosks allow patients to register just once at a central location, instead of repeating the process at each clinic. The kiosks are supported by staff who provide assistance, answer questions, and help direct people to their appointment(s).
“When patients can easily book appointments, they are more likely to seek timely medical care, leading to earlier diagnosis and treatment of conditions,” explained Tobi Odueke, Director of Patient Access at SHN.
“Our booking and registration systems are strategically designed to break down barriers, making it easier for patients of all demographics and abilities to schedule and attend their appointments with ease and convenience.”
For instance, Patient Access Scheduling representatives are able to communicate with patients in their preferred language using interpretation services, as well as schedule an interpreter for their hospital visit. They can even help to reserve a volunteer if a patient needs on-site assistance when visiting the hospital, through the Call Ahead for Volunteer Assistance program.
“I treat every patient as if they were one of my family members; I love to
go above and beyond to make patients feel important and comfortable, and build trust,” added Sarah Cowal, Patient Access Scheduling representative.
“I work to find solutions by coordinating multiple appointments on a sin-
gle day to save them time, money, and stress. I also work closely with doctors and technologists to accommodate patients’ cultural and personal preferences, such as offering the option of a female-only staff.”
Grounded in SHN’s commitment to provide the best possible patient experience, the Network’s strategic centralization of Patient Access functions enabled by Epic also resulted in millions of dollars in annualized savings – funds that are being reinvested into clinical areas in support of exceptional quality care.
Looking ahead, the Patient Access team will focus on making additional improvements to the appointment booking and registration processes, seeking input from patients and conducting health equity analyses. With upcoming technology enhancements, patients will soon be able to schedule their hospital appointments online or through Epic’s patient portal, MyChart, a free, secure tool to view and share personal health information at any hospital across the Central East region of Ontario. n H
BUTTON: SIGN UP FOR MYCHART
MyChart.OurEpic.Ca
MyChart is an online tool where you can access all your health information in one place. Sign up today to:
• View upcoming appointments
• Use eCheckIn to save time during hospital registration
• View educational materials and discharge information from past visits
• Access medical information and test results
• Review healthcare history and prescribed medications
• Sign up for paperless billing to pay hospital bills with ease
MyChart offers secure online access to your health record for care you received at any of these hospitals in Central East Ontario:
• Campbellford Memorial Hospital
• Haliburton Highlands Health Services
• Lakeridge Health
• Northumberland Hills Hospital
• Peterborough Regional Health Centre
• Ross Memorial Hospital
• Scarborough Health Network
Learn more at SHN.ca/mychart.
Emily Santos is a Communications Officer at Scarborough Health Network.
To boldly go where no electronic medical records system has gone before
Fans of the original Star Trek TV series will remember Captain James T. Kirk and his crew of space explorers using a universal translator to communicate with extraterrestrial beings from other worlds.
Hamilton Health Sciences (HHS) CREATE (Centre for Data Science and Digital Health) is playing a key role in developing a universal translator of sorts for Canada’s health-care system. This innovative technology will instantly connect the different electronic medical records systems used, for example, by thousands of Canada’s family doctors, hospitals and long-term care facilities, allowing providers to quickly and confidentially access patient medical records for faster, better and safer care.
Currently, Canada’s primary care providers, hospitals and other providers such as long-term care facilities use a variety of different electronic medical record systems for storing confidential patient information. These systems are rarely compatible so information can’t be quickly or easily shared. This lack of connection translates into longer waits for patient care, because of the time it takes to transfer health information between providers using outdated technology like fax machines. If, for example, a Hamilton resident needs emergency care while in British Columbia, or even much closer to home in Niagara, there’s currently no way for emergency department doctors to instantly check the person’s entire medical history for vital information like chronic diseases, current medications, allergies and immunizations because the different systems aren’t linked.
A ROADMAP FOR INSTANT CONNECTION
Efforts to connect these systems are at the heart of an ambitious plan, called the Shared Pan-Canadian Interoperability Roadmap, that could allow health-care providers across Canada to be able to instantly access each other’s electronic patient medical records. This massive project is being led
by federally and provincially-funded Canada Health Infoway, which works with governments and health-care organizations to make health care more digital and connected, with a focus on accelerating digital health adoption across Canada.
“CREATE is providing expertise in interoperability – which is the ability of different systems to communicate and share data with each other, to support this,” says Dr. Jeremy Petch, CREATE’s director. Staffed with experts in software engineering, AI and data sciences, CREATE works to develop new ideas and digital solutions that fundamentally reimagine how health care is delivered. This includes working with HHS teams as well as organizations in both the public and private sector.
Infoway, in partnership with Ontario Health and British Columbia’s Provincial Health Services Authority, launched a joint design and development of a health application lightweight protocol framework, called HALO.
CREATE’s role for this project includes developing the pan Canadian specifications for the framework that will allow web applications from providers to plug into various electronic medical records and point-of-care solutions so they can be shared.
“Through our team’s contract with Infoway, we’re helping to establish an environment where information can confidentially flow between existing, differing electronic medical records across Canada,” says Dr. Ted Scott, vice president of innovation and partnerships for HHS.
CREATE-ING INSTANT COMMUNICATION
CREATE has significant expertise in FHIR (Fast Healthcare Interoperability Resources), the new and cutting-edge way to access health-care information instantly between different computer systems, regardless of how information is stored.
“We’re working with Infoway, Ontario and B.C. to build out one of the first components of this roadmap to demonstrate how it would work,” says
The HHS CREATE team is playing a pivitol role in an ambitious plan, called the Shared Pan-Canadian Interoperability Roadmap, that would allow providers, hospitals and institutions across Canada to instantly access each other’s electronic patient medical records. Dr. Jeremy Petch and Dr. Ted Scott are leaders in this work.
“THROUGH OUR TEAM’S CONTRACT WITH INFOWAY, WE’RE HELPING TO ESTABLISH AN ENVIRONMENT WHERE INFORMATION CAN CONFIDENTIALLY FLOW BETWEEN EXISTING, DIFFERING ELECTRONIC MEDICAL RECORDS ACROSS CANADA.” — DR. TED SCOTT, HHS VICE PRESIDENT OF INNOVATION AND PARTNERSHIPS
Petch. “The longer-term vision is an enormous undertaking because of the scope, but the work happening now is providing valuable first steps towards what the future could look like.”
CONNECTATHON CONFERENCE
Petch and CREATE senior software architects Mo Ibrahim and Nityan Khanna, and software architect Colin Kent-Sheppherd, are attending Healthcare Enterprise (IHE) North America Connectathon Week in Toronto, Feb. 3 to 7. It’s considered one of the world’s most significant digital health interoperability testing events, and this is its first time in Canada. The conference brings together hundreds
of health IT professionals from around the world to collaborate, innovate and advance the future of health care.
Hosted by Infoway, Connectathon is well-known for its rigorous testing protocols and ability to drive meaningful advancements in health care-interoperability. HALO is being presented by Infoway, with Ontario and B.C., and CREATE representatives will be there to help answer questions. CREATE is also giving a presentation on AI, as it relates to interoperability.
“CREATE has attended past Connectathons, and the team’s involvement in this highly regarded international event speaks to their reputation as globally recognized experts in interoperability and AI,” says Scott. n H
Advancing women’s health research and care
By Anna McClellan
Historically, women have faced barriers in the diagnosis, treatment and care of many health conditions. This year for International Women’s Day, we’re highlighting the extraordinary contributions female-identifying researchers and physicians at Sunnybrook are making to bridge gaps and advance women’s health research and care.
EXPANDING THE TREATMENT OPTIONS FOR UTERINE FIBROIDS
Uterine fibroids are a common but potentially debilitating gynecological condition. Approximately 70 per cent of women develop them before the age of 50. They are typically benign tumors that develop inside the wall of the uterus and can cause heavy menstrual bleeding, infertility and severe pain. Traditional treatment options include surgical treatments such as hysterectomy and myomectomy but these often require longer recovery times and can be quite invasive.
Dr. Elizabeth David, an interventional radiologist and affiliate scientist in the Odette Cancer Program, recently led a successful clinical trial, exploring the use of non-invasive MRI-guided focused ultrasound (FUS) for the ablation of uterine fibroids. Following the success of the trial, the device developed by Arrayus Technologies Inc., a Sunnybrook Research Institute spinoff company, received Health Canada Approval.
The Arrayus FUS system uses high-precision acoustic energy to precisely target and treat tissue deep within the body while protecting nearby tissue, without the need for incisions or general anesthesia. This research and technology are paving the way for Canadian health-care providers to offer a safe, non-invasive alternative to traditional surgical options thereby
giving women with fibroids more treatment options and hopefully improving their quality of life.
BRIDGING GAPS IN STROKE RESEARCH AND CARE
In the fall of 2024, a research team led by Dr. Amy Yu, neurologist and senior scientist in the Hurvitz Brain Sciences Program, was awarded $5M from the Heart & Stroke Foundation, Canadian Institutes of Health Research (CIHR) and Brain Canada Foundation for its work improving stroke care, treatment and recovery for women.
Every year, more than 30,000 women in Canada experience a stroke, and despite this prevalence, gaps in awareness, research, diagnosis, and care threaten women’s heart and brain health.
The pan-Canadian initiative, Stroke in Women: Growing Opportunities to Realize optimal Evaluation, Diagnosis, and outcomes, or StrokeGoRed, is the first formal research network in Canada dedicated to studying stroke in women. The interprofessional group aims to advance knowledge on how and why stroke affects women differently and provide mentorship to the next generation of stroke researchers and clinicians.
PERSONALIZED SUPPORT FOR YOUNG PATIENTS WITH BREAST CANCER
Sunnybrook is home to PYNK, the first program of its kind in Canada, designed to support Sunnybrook patients who are newly diagnosed with breast cancer at age 40 or younger.
Doctors are seeing a rise in breast cancer rates among young women in their 20s, 30s and 40s, and while women under 40 make up a small amount of all breast cancer patients, they have unique physical, psychological and social care needs. Young patients with breast cancer are more likely to expe-
rience fertility concerns, social isolation, financial and career-related distress, and difficulties caring for young children, among other hardships as a result from their cancer diagnosis and treatment.
The PYNK program provides patients and their families with a continuum of support from the time of referral through treatment and follow-up. PYNK educates patients about their breast cancer diagnosis and the impact of treatment, empowering them to make informed decisions about their care. PYNK also helps patients navigate a complex medical system involving multiple specialists, such as plastic surgeons and oncofertility experts.
PYNK offers professional and peer psychosocial support, as well as resources on nutrition, exercise, and hair preservation options like cold capping and wigs. Patients also have access to specialized support for their children, including age-appropriate books about a parent’s cancer experience, childcare resources, and a child life specialist who can provide in-home therapy sessions.
The PYNK program bridges gaps that young women may face during their cancer journey, and can help those recovering get back to a “new normal” life, including returning to
work or dealing with long-term effects of treatment.
CHAMPIONING ENDOMETRIOSIS DIAGNOSIS AND CARE
Endometriosis, affecting approximately 10 percent of patients with a uterus, occurs when tissue similar to the lining of the uterus grows outside of the uterus, which often results in pain or infertility. On average, patients wait 9-10 years to be diagnosed with the condition, delaying appropriate care and impacting their quality of life.
Dr. Jamie Kroft, an obstetrician gynaecologist in the DAN Women & Babies Program specializes in minimally invasive surgery, and cares for patients who have lived with endometriosis for years without a proper diagnosis, which can end up impacting other major organs, like the kidneys, GI tract or lungs.
Dr. Kroft is working closely with other specialists in the GTA to form a central intake clinic for patients with endometriosis. Her advocacy is helping women in the GTA gain access to first consult sooner, advancing earlier diagnosis, treatment and pain management of their endometriosis and ultimately improving quality of life. n H
Anna McClellan is a Communications Specialist at Sunnybrook Health Sciences Centre.
From the time she learned piano at 7 years old, Roberta has been in love with music.
A former teacher and music consultant, and now a member of our Christie Gardens community, she keeps that love and incredible talent alive by sharing her gift with those around her, who share her appreciation for beautiful things in life.
A health management solution for older adults and their family caregivers
By Melissa McDermott
When Rob Parker’s father got sick in his mid-70s, it took two years and 12 falls before he was accurately diagnosed with hydrocephalus, which can be tricky to detect because it often presents like dementia.
“My Dad couldn’t remember what he talked to the doctor about, he couldn’t remember the doctor’s in-
structions, and he couldn’t answer the questions,” explains Parker.
“Partly, this was due to his cognitive situation, but it’s also common for most of us to forget details from a medical appointment.”
A seasoned software designer and product leader, Parker says: “I saw small problems with massive ramifications that if we solved them, we could get people to earlier, more accurate diagnoses.”
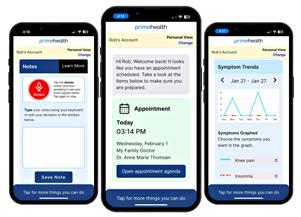
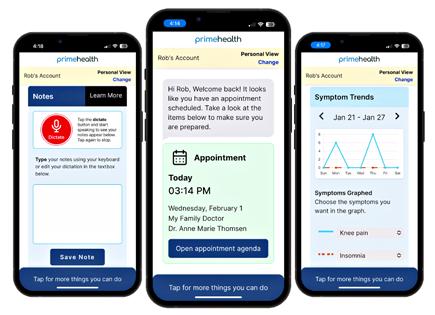
This experience led Parker to channel his 30-plus years of professional experience with his family caregiving experience to create PrimeHealth and develop its flagship product, also called PrimeHealth, with co-founder Carey-Jo Hoffman.
This app acts as the electronic medical record for older adults and their families, helping to accurately track and communicate health needs and information. It also records, retains
and securely shares doctors’ instructions. The goal is to reduce diagnostic and medication errors, improve health outcomes and extend seniors’ independence.
“In an older adult’s life, things get complicated, especially on the health care side,” notes Parker, whose company PrimeHealth is based out of Vancouver, B.C. and is an AGE-WELL startup affiliate. “We’re helping people make the most of their time with the
Virtual Urgent Care program tackling the digital divide with on-site kiosk
When a child is sick, it can be tough to know where to seek care, especially if you don’t have access to resources or technology to help make those decisions. While virtual care services are becoming more common across the health system, access to technology and internet services is not equal across communities – a health equity issue that The Hospital for Sick Children (SickKids) is looking to address through a pilot project at the Lawrence Allen Centre.
Situated on the ground floor of the Lawrence Allen Centre, SickKids has launched an in-person, greeter-assisted kiosk that provides access to the hospital’s Virtual Urgent Care (VUC) program where patients and families can use a symptom checker, obtain digital and printed health information and even engage in virtual care visits with SickKids Emergency Department (ED) physicians, if eligible. The pilot project – created through an innovative public-private partnership between SickKids and RioCan – aims to provide an additional way for one of Toronto’s most digitally underserved communities to access SickKids’ VUC program.
“Through detailed analysis, we know that our VUC is not being used equally across population groups. We wanted to be able to offer this service to all groups and equity-deserving populations. We will be robustly evaluating who is and isn’t using the service, in order to optimize it for all of our patients,” says Dr. Daniel Rosenfield, Staff Physician and Lead, Virtual Care in the Division of Paediatric Emergency Medicine at SickKids.
Launched in 2021, the SickKids VUC program offers patients and families a convenient way to help determine the most appropriate care setting for a medical concern, whether it is a virtual appointment with SickKids ED, a recommendation to visit a primary care provider or your local ED. To date, the VUC’s symptom checker has been accessed by patients and families close to 57,000 times, with more than 14,000 virtual visits completed with SickKids ED physicians.
Although successful, data on SickKids VUC program revealed that highneeds communities in Toronto did not use the program at the same rate as other neighbourhoods with higher socioeconomic status, a common occurrence known as the ‘digital divide’. To address these digital barriers, a greeter at the kiosk can help families use SickKids’ VUC program by providing access to technology and internet services at the on-site location. Interpretation services are also available in more than 230 languages.
“RioCan is excited to leverage this collaboration with SickKids to reinforce our commitment to vibrant community spaces,” said Jennifer Suess, Senior Vice President, General Counsel, ESG and Corporate Secretary at RioCan and Board Member for SickKids Foundation. “Lawrence Allen Centre is a cornerstone for local residents and is an ideal location for this strategic initiative that we hope will contribute to the health and well-being of children in our community.”
Through this novel, health-equity project, SickKids hopes to benefit the community by improving access to trusted, high-quality virtual care. n H
doctor by facilitating smooth communication within the circle of care.”
The PrimeHealth app is a one-stop digital hub for appointment information, medication lists, symptom tracking and questions for the health care team. The app synthesizes this information and produces an agenda format for patients and caregivers to follow at doctor appointments. PrimeHealth also has voice transcription so older adults can keep track of (with consent) their doctor’s consolidated points at the end of each appointment, which are captured in their PrimeHealth profile. Additionally, family members (with permissions) can con-
tribute to the health information and easily access a fuller picture of their loved one’s health. This is particularly helpful for family members who cannot be as involved in day-to-day care.
Parker, who is CEO of PrimeHealth, and his team engaged early on with older adults, families and health care professionals. “Some things really changed through the co-design process. A big shift was we needed to break many fundamental user experience rules to help older adults use PrimeHealth successfully.” For example, the team determined features in the app must remain constant and there needed to be a lot of inapp explanatory text as a useful guide.
Parker was introduced to AGEWELL, Canada’s technology and aging network, in the early days of PrimeHealth while attending the AGE-WELL Annual Conference in 2022. He credits that event for kickstarting important relationships and connections for the company.
Parker went on to enter PrimeHealth (then called ElderPRIME) in the National Impact Challenge 2023 –Bold Innovations for Living, powered by AGE-WELL and SE Health. His company was runner-up (and winner of the People’s Choice Award) in the Startup category. PrimeHealth has
since joined AGE-WELL’s Startup Affiliate Program to continue the supportive relationship.
“Those two AGE-WELL events have been big jumping-off points that have really helped propel our company forward,” Parker shares.
The company is working through its beta to refine the experience. The company’s first pilot program began with a home health care partner, and numerous other pilots are in development, including a large health authority in B.C. Parker and his team continue to work with potential partners across Canada to roll out PrimeHealth to older adults and families who need it. n H
Melissa McDermott is an Ottawa-based communications consultant. AGE-WELL is Canada’s technology and aging network. The pan-Canadian network has mobilized a vast community of researchers, older adults, caregivers, partner organizations and future leaders to accelerate the delivery of technology-based solutions for healthy aging. www.agewell-nce.ca
Transgender and gender diverse people less likely to receive follow-up after a mental health hospitalization
Transgender and gender diverse individuals who were hospitalized for psychiatric care were less likely to have a follow-up visit compared to the general population, suggesting they face transphobia in the hospital system.
In a new study from ICES and the Centre for Addiction and Mental Health (CAMH), findings demonstrate that transgender and gender diverse (TGD) people face an interesting paradox: they have lower access to appropriate mental health care and support following a psychiatric hospitalization, yet have better follow-up after an emergency department (ED) visit. According to Statistics Canada, TGD people account for 0.33 per cent of the Canadian population, with many living in large urban centres.
“Follow-up after an emergency department visit or hospitalization for mental health concerns is vital for people’s long-term well-being,” says lead author Dr. June Lam, associate scientist at CAMH and ICES Fellow. “It’s a risky time for folks, and we wanted to better understand if this population is being well supported after a mental health crisis.”
The researchers analyzed health data at ICES for all adults discharged
from the emergency department (ED) or hospital for psychiatric care between 2012 and 2018 in Ontario, Canada. The study included 728 TGD and over 581,708 individuals in the general population.
TGD individuals were identified through electronic health records from four primary care and hospital-based clinics specialized in working with this population. The data were then linked (anonymously) to hospital-based databases.
KEY FINDINGS
• Compared to the general population, TGD individuals were younger, and more likely to live in underserved urban areas and low-income neighbourhoods. They also had much greater prior psychiatric care service use.
• 55 per cent of TGD individuals had outpatient mental health-related physician follow-up in the 30 days after discharge from the ED, compared to 38 per cent for the general population.
• One-third of TGD individuals had a follow-up with a psychiatrist within one month of an ED visit, about double the rate of the general population.
• In contrast, TGD people were less likely to receive follow-up after a hospitalization.
• Even after accounting for other factors, TGD individuals were still 21 per cent more likely to have a follow-up after discharge from the ED than the general population, but they were 20 per cent less likely to have follow-up after a hospitalization.
“Lower follow-up after hospitalization is concerning because it suggests that there is something about the hospital experience that may be leading to avoidance of care after discharge,” says Lam, who is also a psychiatrist in the CAMH Gender Identity Clinic. “Patients may be experience misgendering and transphobia in the hospital setting, which could influence whether they’ll seek follow-up care.”
IMPROVING THE HOSPITAL EXPERIENCE
The authors suggest that one way to improve hospital care for TGD patients is to ask for their chosen name, gender identity and pronouns on the initial intake form, and make sure that all care providers are using the correct name and pronouns throughout the care experience.
Another approach is to tailor follow-up resources for TGD patients that address social determinants of health. Resources have been developed in the CAMH ED to provide
TGD-specific crisis lines, housing resources, and community organizations.
“Lack of social supports is often a perpetuating factor for mental health challenges for TGD people, so connecting them with community organizations that offer healthcare provider and peer connections is so crucial for TGD people’s wellness and recovery long-term,” says co-author Dr. Juveria Zaheer, a scientist with the Institute for Mental Health Policy Research and General Adult Psychiatry and Health Systems Division at CAMH.
One limitation of the study is that it didn’t capture nonphysician mental health care and there was no measure of need for follow-up. However, a higher rate of post-ED follow-up suggests that there is a greater need among TGD individuals, and standards of care recommend that follow-up should occur regardless.
“These findings underscore the urgent need to improve hospital experiences and make sure that all patients feel safe and supported in seeking care. By addressing barriers such as a lack of social support, misgendering and transphobia in hospital settings, we can help close this gap and create a more equitable mental health system,” says senior author Dr. Paul Kurdyak, a senior scientist with ICES and CAMH. n H
A new app can greatly improve ventriculostomy safety and accuracy
Access to potentially life-saving neurosurgical care remains very uneven worldwide, with potentially life-threatening consequences. This is especially true for a process called ventriculostomy, the most common neurosurgical procedure. Ventriculostomy involves the insertion of a catheter into the brain cavities called ventricles to drain cerebrospinal fluid and relieve intracranial pressure.
It’s a delicate, difficult process that requires extreme precision: misplacing the catheter, which happens in up to 30 per cent of freehand procedures, can result in hemorrhage, infection, prolonged hospital stays, morbidity and even death.
That’s why a group of Gina Cody School of Engineering and Computer Science researchers sought to improve access to low-cost technologies that can aid in improving ventriculostomy accuracy. Marta Kersten-Oertel, an associate professor in the Department of Computer Science and Software Engineering, and her team have developed an augmented-reality (AR)based platform. They say it may make the procedure far safer and more accurate, especially in low- and middle-income countries and resource-limited settings.
The iSurgARy system uses LIDAR, a light detection and ranging technology, to help surgeons identify specific landmarks on the skull and accurately map them to the patient’s preoperative images (CT/MRI). Augmented reality is then used to project the ventricles onto the patient. The creators describe the technology in the Healthcare Technology Letters journal.
“The technology offers better spatial awareness of patient anatomy, which provides surgeons better aim at their target points,” says co-author Joshua Pardillo Castillo, MSc 24. “The augmented reality overlays the patient’s medical images to better see how they can best position the catheter.”
PRECISION BRAIN MAPPING
LIDAR, available on Apple’s iOS devices, helps determine distances from the sensor to seven anatomical landmarks on the patient’s head: the tragus (the pointed eminence jutting out from the scalp at the front of the ear) on both sides of the head, the outer eyes, the inner eyes and the bridge of the nose. These landmarks are used to align the virtual models of the patient’s anatomy to the actual patient, providing the medical personnel with an augmented reality view that shows them where the ventricles are.
This visualization guides the clinician to the optimal location for catheter placement, while the catheter’s tracking tool can provide spatial understanding of the distance between the tip of the catheter and the ventricles.
“The AR view shows where the ventricles are so clinicians can decide on the best approach,” Kersten-Oertel explains. “The freehand technique relies on bony landmarks of the skull, and clinicians make their decision based on them. But if there is a brain tumour that is causing pressure or a traumatic brain injury, the brain may have shifted so the ventricles are not where they are expected to be. This system allows users to see the ventricles projected on the patient and accurately target them.”
The researchers point out that the platform emerged out of a practical need identified by an experienced clinician – David Sinclair, a clinical pro-
fessor in cerebrovascular and skull base neurosurgery in the Division of Neurosurgery of McGill University’s Department of Neurology and Neurosurgery and a co-author on the paper. Sinclair asked Kersten-Oertel if it was possible to develop a tool that improves visualization to target ventricles in emergent scenarios where time, cost and accuracy are of utmost importance.
“This kind of collaboration with a neurosurgeon in the design and discovery phase makes this whole project unique,” says Zahra Asadi, a PhD student and co-first author on the paper.
“Working with him and getting to know the needs of the people who will be using this application is critical.”
Read the cited paper: “iSurgARy: A mobile augmented reality solution for ventriculostomy in resource-limited settings.”
Watch a video of the researchers discussing how the iSurgaARy app works: https://youtu.be/b8Xg9Mlq8hc n H
Electronic health record enabling new solutions in delirium care
By Gaithre Kalainathan
In June 2024, Fraser Health launched the first iteration of the Advanced Analytics Platform for delirium care. Since then, this new solution – enabled by the electronic health record, MEDITECH Expanse – is showing great potential in changing the trajectory of outcomes in patients at risk for delirium, a critical patient care concern.
The Advanced Analytics Platform uses real-time patient data that has been entered by staff and medical staff into
the electronic health record. The electronic health record is the foundational element that eliminates the lag time we used to see when patient information was written on paper and then coded into computer systems at a later date.
Fraser Health’s Centre for Advanced Analytics, Data Science and Innovation, in collaboration with several clinical and non-clinical teams across Fraser Health, developed the delirium page in the Advanced Analytics platform along with a deliri-
um predictor solution, which scans relevant data to flag risk indicators, supporting proactive intervention and faster, more informed decisions regarding patient care.
The platform flags patients who are at risk for delirium. Once flagged, care providers can take action by incorporating treatments.
Delirium, characterized by sudden changes in thinking or behaviour, can result from various causes – including injury, infection, medication, surgery,
environmental changes or dehydration. While many patients recover, some may lose their independence and require long-term care.
Delirium remains a critical patient safety priority, and with the aid of advanced analytics and real-time data integration, we can make significant strides in its prevention and management. The platform’s ability to predict risk, guide interventions and monitor outcomes exemplifies its potential to enhance patient care and safety. n H
Marta Kersten-Oertel, right, with Zahra Asadi and Joshua Pardillo Castillo: “This system allows users to see the ventricles projected on the patient and accurately target them.”
Gaithre Kalainathan is the Director, Centre for Advanced Analytics Data Science and Innovation, (CAADSI), Fraser Health.
Genome Canada awards SickKids $11.7 million to advance Precision Child Health
The projects will support a national genomic dataset of 100,000 genomes that reflects Canada’s diverse population
Genome Canada awarded almost $12 million in funding to research projects led by The Hospital for Sick Children (SickKids), to build the largest-ever collection of human genomic data in Canada.
The funding is part of the Canadian Precision Health Initiative, which provided a total of $81 million in Government of Canada funding through Genome Canada, to create a coordinated, large-scale, diverse genomic data asset of 100,000 genomes that reflects Canada’s population. The initiative aims to drive genomics-enabled precision health for Canadians.
Of the $81 million awarded, $11,716,046 was given to two transformative projects led by SickKids, in
addition to several other projects involving SickKids scientists.
“We will leverage SickKids’ strengths as the most research-intensive paediatric centre in Canada to advance the utility of genomic health data to realize the vision of Precision Child Health, allowing all patients and families to have the opportunity to learn and benefit from research,” says Dr. Stephen Scherer, Chief of Research and Senior Scientist in the Genetics & Genome Biology program.
ysis. Matching of Genome Canada funding for the two projects will be facilitated by partnerships between the institutions and several co-funding partners.
Precision Child Health – comprehensive sequencing for childhood lifelong disorders (PCHSeq)
The genome sequencing for each of these projects will be conducted at The Centre for Applied Genomics (TCAG) at SickKids, part of CGEn, Canada’s National Platform for Genome Sequencing and Anal-
At SickKids, many children are diagnosed with genetic conditions that have a lifelong impact. Whole genome sequencing offers the potential to enable earlier and more accurate diagnosis, prediction of health trajectory, and identification of novel therapeutic targets.
Led by Dr. Stephen Scherer, this project will sequence the genomes of participants (and their parents) with a diverse range of childhood-onset
conditions. The project will recruit patients and families from a wide range of clinical areas at SickKids, as well as collaborate with scientific leaders to engage participants from existing research cohorts. The team will use cutting-edge technology to ensure data quality as well as build condition-specific artificial intelligence models to analyse the data.
The project will sequence a total of 10,000 genomes over a period of four years, with data made available through the Pan Canadian Genome Library.
Project value: $15,430,370, of which Genome Canada has provided $7,518,328 to SickKids.
Read more about the project on the Genome Canada website. n H
Celebrating 25 years of e-Health!
Join us in Toronto from June 1 – 3 for e-Health 2025! e-Health is the premier event for Canadian digital health professionals working to make a difference in health and healthcare delivery.
Since its inception in 2000, the e-Health Conference and Tradeshow has served as a vital epicentre of Canadian digital health discussion and debate. e-Health is the optimal spot for networking and knowledge sharing with peers nationally and around the globe.
e-Health 2025 will be at The Westin Harbour Castle, One Harbour Square, Toronto
PROGRAM
DETAILS
SUNDAY, JUNE 1
12:00 p.m.-8:00 p.m.
Registration
3:00 p.m.-4:00 p.m.
Newcomer Session
4:00 p.m.-5:00 p.m.
President’s Reception (by invitation only) Sponsored by Amazon Web Services
5:00 p.m.-7:00 p.m.
Welcome Reception Sponsored by Teladoc Health
7:00 p.m.-9:30 p.m.
Sponsor Receptions
MONDAY, JUNE 2
6:30 a.m.-7:00 p.m.
Registration
7:00 a.m.-8:00 a.m.
Networking Breakfast Sponsored by CANImmunize
7:00 a.m.-7:30 p.m.
Tradeshow Open
e-Health is hosted by Canada Health Infoway, Digital Health Canada, and Canadian Institute for Health Information.
MONDAY, JUNE 2
8:00 a.m.-9:45 a.m.
OPENING CEREMONIES + KEYNOTE PANEL: HEALTH
DATA GOVERNANCE, SECURITY AND PRIVACY, AND ARTIFICIAL INTELLIGENCE IN HEALTHCARE/MEDICINE
Sponsored by Oracle Health
This expert panel of thought leaders will discuss health data governance and the transformative role of artificial intelligence in advancing healthcare and public health outcomes. They will share valuable insights into the possibilities, challenges, and responsibilities surrounding patient health data governance and artificial intelligence in the health sector.
With Knowledge Keeper Gimaa R. Stacey Laforme, Retired Chief Of The Mississaugas of The New Credit First Nation; Emcees Cassie Frazer, Reliance Healthcare Consulting | Digital Health Canada and Alifa Khan, Holland Bloorview Kids Rehabilitation Hospital; Moderator Zayna Khayat, University of Toronto; and Panellists Dr. Ewan Affleck, College of Physicians & Surgeons of Alberta; Maureen Kelly, Canadian Institute of Health Information; Dr. Muhammad Mamdani, Unity Health Toronto; and Alies Maybee, Patient Advisors Network (PAN).
Program highlights
MONDAY, JUNE 2
9:45 a.m.-10:00 a.m.
Networking Break
Sponsored by Novartis
Ask the Patient
Connect with the e-Health 2025 Patient Partners at breaks near the e-Health Host booths (5/6). Look for “THE PATIENT IS IN” sign.
10:00 a.m.-11:00 a.m.
Concurrent Sessions
• AI-Powered Postoperative Monitoring Solution for Early Detection of Anatomic Leaks
• AI-Driven Phenotyping to Stratify Patient Populations for Personalized Healthcare
• Harnessing Epic Data to Cut Pediatric Anesthesia Emissions by 30 per cent
• One Patient, One Record, One System for multiple hospitals
• Key Drivers of Privacy: Enabling the flow of PHI for better health for all
• Integrating Pulmonary Function Testing into Medical Records: Enhancing Efficiency and Improving Healthcare Delivery
• Leveraging AI Video Generation for Digital Health Training
• Testing an Assessment Tool and Standardized Process for Virtual Care Development: A Design Thinking Approach
• How AI-enabled self-management care models divert ALC traffic, reduce ED
• visits, and 911 calls
• Empowering client engagement and enhancing experience through the development of a codesigned, AI-enabled Client Portal
Alies Maybee
Maureen Kelly
Zayna Khayat
Ewan Affleck
Muhammad Mamdani
Cassie Frazer
Alifa Khan
Gimaa R. Stacey Laforme
Program highlights
MONDAY, JUNE 2
• Simplifying Parental Consent for School Immunization Programs with a Digital Consent Collection and Tracking Platform
• Leading a Cultural Shift by Empowering Patients Through Access to a Unified, RegionalScale Patient Portal
• Technology Solutions for Mental Health; Virtual Care, Telemonitoring, and Remote Patient Care
• Co-designing implementation strategies for a suicide prevention app with clinicians, patient and care partners
• Enhancing Forensic Patient Safety
• Incorporating Patient’s Digital Preferences in the EHR: Impact and Lessons Learned
11:10 a.m.-11:40 a.m. P3 Showcases
Fireside Chat: The AI Threat to Patient Data
Hosted by Google Cloud Enhancing Security in Digital Health Hosted by CDW
Computer Assisted Coding: How this tool transforms clinical coding workflows
Hosted by Solventum
11:40 a.m.-12:30 p.m. Lunch Break
Sponsored by DCM Healthcare Solutions
12:30 p.m.-1:30 p.m.
Sponsor Symposia
Healthcare Leaders Driving Innovation: How TSSO, NYGH, and CA.M.H are Powering the Future with Oracle Health
Hosted by Oracle Health
Exploring Real-life Examples of How Generative AI is Making a Difference in Canadian Healthcare
Hosted by Deloitte: Collaborative Partnerships: An Essential Component in Digital Hosted by LGI Healthcare Solutions
AI Applications in Healthcare: Enhancing Efficiency, Improving Care, and Empowering Clinicians
Hosted by Meditech
1:40 p.m.-2:40 p.m.
Concurrent Sessions
• Much Ado aBOT SomethingStandardizing EMR Data for Transmission Between Clinicians
• Evaluating EMR interoperability across Canadian jurisdictions: A maturity model and roadmaps toward integration
• Optimizing health data design and use in British Columbia through a patient-led interprofessional collective approach
• A community-centred program using digital tools to advance health equity for multicultural and Indigenous communities
• Expanding Canada’s first Regional Digital Twin-Driving Clinical & Digital Change for Improved Access
• Digitizing Sickle Cell Disease Care-Reducing Inequities Across Emergency Departments
• Digital Technology and Healthcare Human Resources; Patient Engagement and Empowerment
• Enabling Clinical Best Practices Through Digital Referrals with Embedded CDS
• Digital Referral Form standardization – a transformative and clinically informed co-design approach
• Addressing Communication Challenges in Disconnected Indigenous Populations
• Policy recommendations for enhancing health data interoperability in Alberta with broad application for Canada
• Interoperability and Data Ownership: Lessons Learned from the Implementation of a ProvinceWide Interoperability Solution
• The impact of policy changes on virtual care use in Ontario: a population-based study.
• Virtual Care: Australian Learnings and Perspectives
• Addressing the Urgent Gap in Emergency Rooms Through
Virtual Care Collaboration
• Technology Solutions for Mental Health; Virtual Care, Telemonitoring, and Remote Patient Care
• Machine Learning Classification of Mental Health and Addiction Calls in Paramedic Services
• First Nations Community Paramedicine Service
2:40 p.m.-3:00 p.m. Networking Break Sponsored by PWC Ask the Patient Connect with the e-Health 2025 Patient Partners at breaks near the e-Health Host booths (5/6). Look for “THE PATIENT IS IN” sign.
3:00 p.m.-4:00 p.m. Concurrent Sessions
• Using AI/ML to translate youth language into a clinical context to support frontline staff.
• Using Artificial Intelligence and Machine Learning to Automate Injury Prevention Surveillance Data
• Delivering Health AI Literacy: A Principle-Based Framework for Enhancing Practical AI Competencies Among Healthcare Professionals
• The Current State of Interoperability in Canada
• Key Factors for True Interoperability: Lessons Learned during a Provincial Interoperability Journey
• Digital Technology and Healthcare Human Resources
• Transforming Clinical Documentation-Evaluating EHRIntegrated AI Scribe Technology in an Acute Care Setting
• The Introduction of a HHR Dashboard to Improve Operational Excellence
• Bridging Access Gaps in Chronic Pain Management with Patient-Centric Virtual Care and Telemonitoring
• Streamlining Healthcare Access and Navigation with ProvinceWide Digital Front Door Solutions
• Provincial Framework and Committee for Addressing Physician Shortages in Mid-Sized Rural and Remote Hospitals
• Virtual Nursing and Sitting to Elevate Safety and Add MuchNeeded Capacity
• Co-Designing Digital Health Tools to Minimize Burden and Improve Efficiency in Mental Health Care Delivery
Shelagh Maloney
Chris Carvalho
Dr Fahad Razak
Michael Green
Rachel Bartholomew
Chuck Anderson
Michael Anderson
As the largest digital health event in Canada, e-Health is the best place to grow your business, and forge important connections with industry peers, vendors, and thought leaders connect innovation, and real change. Join us at the Westin Harbour Castle Toronto from June 1 to 3 as and learning with the people and organizations driving change in Canadian health through inf
As the largest digital health event in Canada, e-Health is the best place to grow your business, expand your digital health knowledge, and forge important connections with industry peers, vendors, and thought leaders connections that spark collaboration, innovation, and real change Join us at the Westin Harbour Castle Toronto from June 1 to 3 as we celebrate 25 years of networking and learning with the people and organizations driving change in Canadian health through information and technology
Learn more and register at e-healthconference.com
Learn more and register at e-healthconference.com
MONDAY, JUNE 2
4:15 p.m.-6:00 p.m.
Awards + Host Plenary Session: Health Equity –
The Role of Digital and Data
Digital Health Canada Awards
Join us as we celebrate Canadian digital health leaders, innovators, and emerging professionals with the annual Digital Health Canada Awards: Digital Health Executive of the Year, Digital Health Leader of the Year, Clinical Innovator of the Year, Community Care Leader of the Year, Emerging Leader of the Year, StartUp Innovator of the Yea, and the Steven Huesing Scholarship recipients.
Host Plenary Session:
Health Equity – The Role of Digital and Data
Digital health has the power to transform healthcare, but how can we ensure these innovations advance equity rather than widen disparities? This panel brings together experts working at the forefront of health equity and digital innovation with representatives from the three e-Health host organizations (Canada Health Infoway, Canadian Institute for Health Information, and Digital Health Canada) to discuss how health data and digital solutions can drive equitable outcomes so we can create a more inclusive and accessible healthcare system for all Canadians.
With Awards Presenter Chris Carvalho, Digital Health Canada; Emcees Krista Balenko, Canada Health Infoway and Cyndi Peal, Indigenous Health | Vancouver Coastal Health; Moderator and Panellist Shelagh Maloney, Digital Health Canada; and Panellists Dr. Michael Anderson, University Health Network; Rachel Bartholomew, Hyivy Health Inc./Femtech Canada; Dr. Anderson Chuck, Canadian Institute of Health Information; Michael Green, Canada Health Infoway; and Dr. Fahad Razak, Unity Health Toronto | GEMINI
6:00 p.m.-7:30 p.m. 25th Anniversary Reception Sponsored by Oracle Health
Program highlights
TUESDAY, JUNE 3
7:00 a.m.-8:00 a.m.
Networking Breakfast
Sponsored by PWC
9:15 a.m.-9:30 a.m.
Networking Break
Sponsored by CANImmunize Ask the Patient Connect with the e-Health 2025 Patient Partners at breaks near the e-Health Host booths (5/6). Look for “THE PATIENT IS IN” sign.
8:00 a.m. to 9:15 a.m.
Opening Ceremonies + Opening Plenary Panel: Health Data Approach for Enabling Integrated Care Sponsored by Deloitte
This plenary panel features three Canadian healthtech leaders with deep experience in deploying technology innovation to improve patient and provider outcomes at hospitals across Canada. With Emcees Nasir Kenea, Canadian Institute of Health Information and Pam Dawson, Patient Voices Network and Panellists Dr. Peter Bak, Humber River Hospital; Noralyn (Lyn) Baluyot, TransForm Shared Service Organization; and Dr. Jeremy Theal, Alberta Health Services.
9:30 a.m.-10:30 a.m.
Concurrent Sessions
• Optimizing AI in Ontario Healthcare: From Point Solutions to Scale
• Addressing Clinician Cognitive Load: the role of an AI-based “Easy Button” that NEVER hallucinates.
• AI Powered Pan-Canadian Conformance Program
• Common Data Architecture is the foundation for data exchange standards – why FHIR isn’t enough
• The Canadian Core Data for Interoperability: Drawing from International Examples to Advance Connected Care
Noralyn (Lyn) Baluyot
Peter Bak
Jeremy Theal
• Enhancing Interoperability in Health Care Facilities through a New Digital Infrastructure Standard
• Digital Health, Equity, and Access in the Provincial Digital Pathology Initiative
• Triaging Referrals to eConsult (TReC): Increasing Access to Endocrinology and Osteoporosis Care in Ontario
• Evaluation of a secure messaging proof of concept pilot
• Health Data Governance, Security, and Privacy
• Leveraging AI to Improve Accuracy in Medical Audio Transcription
• Unlocking the Untapped Potential: The Power of Digital Twins in Healthcare
• National Eye Data Repository for Primary Care Optometry Optimization and AI Innovation
• Co-Created Principles for Organizational Digital Compassion in Health Care
• An APP keeps the doctor awayleveraging digital tools for surgical patients
• Optimizing virtual care: Lessons learned from a nurse practitionerled virtual episodic care program in Ontario
10:40 a.m.-11:10 a.m.
P3 Showcases
Revolutionizing Healthcare in Ontario: Oracle Health’s Impact on Patient Care and Efficiency
Hosted by Oracle Health
Scalable, Sustainable, Essential: The Case for Virtual Primary Care in Canada
Hosted by Teladoc Health Canada How Hybrid Care Models Drive the Quintuple Aim
Hosted by Teladoc Health Canada Moving healthcare forward through modernization and collaboration: Practical insights from an OHT
Hosted by Calian
11:10 a.m.-12:00 p.m.
Lunch Break
Sponsored by DCM Healthcare Solutions
12:00 p.m.-1:00 p.m.
Sponsor Symposia
Lessons Learned: A View from the Inside
Hosted by Baxter Re-imagining Central Intake at Horizon Health: A Candid Conversation on the Digitization Journey
Hosted by Process Fusion
Digital Solutions for Homecare
Hosted by EY AI Agents for Healthcare Technology-From Basics to Breakthrough Hosted by Google Cloud
Transforming Primary Care: Unlocking the Potential of AI in Ontario
Hosted by OntarioMD
1:10–2:10 p.m.
Concurrent Sessions
• Revolutionizing Patient & Staff Safety: The Impact of Breakthrough Ambient Perceptual AI Technology
• Topological Clustering of Complex Healthcare Data: Insights into Unmet Healthcare Needs Among Injured Patients
• Use of Artificial Intelligence in Post 48 hour Discharge Calls
• Passing Notes in Class
• A New Program to Drive National Interoperability in Canada
• From Notes to Insights: Enhancing Patient Care and Interactions through AI Documentation in Clinical Settings
• Rapid Response: Fast-Tracking Early Warning System Success
• Enabling Patient Access to Personal Health Information and Services Through a Digital Front Door
• Supporting primary care clinicians in diagnosing and managing patients with anxiety disorders and major depression
• Advancing Precision medicine: Pharmacogenomics testing with advanced Clinical Decision Support
• Promoting equitable access to digital population-level mental health portals: Lessons learned from this collaborative initiative
• Digital facilitators of the early implementation of a national crisis line
• A Novel Virtual Walk-In Counselling Service for Mental Health Support for Children, Youth, and Caregivers
• Supporting Complex Care Needs in Primary Care Through Virtual Care
• Building Canada’s Psychiatric Mental Health Care Workforce: Competency, Capacity, and Resiliency
2:10 p.m.-2:30 p.m.
Networking Break
Sponsored by AEGIS
2:30 p.m.-3:30 p.m.
Concurrent Sessions
• Creating a More Interconnected Future of Health in Canada
• AI for Better Health – AI Strategy & Governance Learnings
• Provincial Clinical Registries: Bridging Fragmented Clinical Information Systems and Improving Health Information Interoperability
3:45 p.m.-5:00 p.m.
• Lessons Learned from Building a Successful Data Exchange Network Strategy
• Enhancing Emergency Access: Lessons Learned from the Virtual Urgent Nova Scotia (VUNS) Program
• What is holding them back? Exploring barriers to patient portal activation
• Evaluating the usefulness of a mental health chatbot for people with arthritis and diabetes
• Streamline primary care and reduce administrative burden through provincial LOINC document standards: a grassroots success.
• Pan Canadian Health Workforce Data Dashboards to Support Planning
• Empowering and engaging patients to support their kidney health and wellbeing through customized virtual resources
• Digital Bridge: Supporting older adults with complex needs transition from hospital to home
• From Hospital to Home: Enhancing Post-Surgical Recovery with Remote Patient Monitoring
3:30 p.m.-3:45 p.m. Networking Break
Closing Ceremonies + Closing Keynote: From Mount Everest to the Sahara-A Tale of Resilience and Adaptation
Sponsored by Workday
Wrap up the conference with key takeaways and an inspiring talk from endurance athlete Sébastien Sasseville. With Knowledge Keeper Gimaa R. Stacey Laforme and Emcees Dana Greenberg, Diabetes Action Canada | CIHR SPOR Network and Shelagh Maloney, Digital Health Canada.
Sébastien Sasseville helps organizations to surpass themselves and to win the long ga.m.e. Supported by breathtaking visuals and world class storytelling, this session is an astonishing tale of resilience loaded with actionable insights to leverage change to win and adopt a collaborative posture. An endurance athlete, Sasseville’s extraordinary accomplishments – which include summiting Mount Everest, completing the mythical Sahara race, and running across Canada – are made all the more impressive by the fact that he lives with Type 1 Diabetes.
Sébastien Sasseville
The buzz around kidney stone research
Fruit-fly-fueled research could help solve kidney-stone mystery linked to antibiotic use
Tucked in the back of the Microbiome and Probiotic Research Lab at St. Joseph’s hospital sits the Fly Room – a small space that houses even smaller insects whose microscopic innards could hold clues into the link between antibiotic use and the formation of kidney stones. Kidney stones are a growing problem, especially among women and young children.
Researchers at Lawson Research Institute (Lawson) of St. Joseph’s Health Care London have turned to an unlikely source – the humble fruit fly as helper, not house pest - to see whether oral antibiotic use is partly to blame.
Previous research has shown that people with kidney stones have an imbalance in the gut microbiome and a genetic footprint that could suggest resistance to antibiotics. The question Lawson researcher Riley Fidler is trying to solve: Is antibiotic use shifting microbiome balance and making otherwise-healthy individuals more susceptible to kidney stones? At the centre of her research is an unlikely research ally.
No bigger than a sesame seed, fruit flies share about 70 per cent of their genes with humans - making the insects ideal stand-ins for genetic research into human diseases. This similarity is especially relevant in fruit flies’ Malpighian tubules, or excretory organs, and in human nephrons, the functional unit of the kidneys. If a fruit fly is the size of a sesame seed, their tubules are smaller than the hairs on a raspberry. And “kidney stones” within their tubules are even tinier.
“It is exacting and exciting research”, says Fidler, a Master of Science Student in Western University’s Department of Microbiology and Immunology and a researcher alongside Principal Investigator, Jeremy Burton, PhD, Chair in Human Microbiome and Probiotics and Co-Supervisor Dr. Kait F Al, PhD, post-doc researcher.
Fidler is fascinated by the human microbiome and its impact on health –from metabolism and stress to mental health, the ability to fight infection, and even to prevent and overcome cancer.
“A lot of people view bacteria as dangerous agents, but I would suggest that we view the microbiome almost as our ‘sidekick’,” says Fidler. “By maintaining good gut health, in turn, your gut microbiota will keep you healthier.”
If the team can identify whether antibiotic use could be an underlying
cause of kidney stones, prevention strategies that strengthen gut health could be used in tandem with an antibiotic to repair gut barrier integrity.
“Kidney stone disease has a high prevalence, high rate of recurrence and high pain. Finding the cause of the increased cases of kidney disease and knowing how to prevent stone-formation is critical for quality of life,” says Fidler.
Fidler’s research looks at four antibiotics commonly prescribed to fight infections (both related and unrelated to kidney function) in people: cefazolin, ciprofloxacin, penicillin and sulfamethoxazoletrimethoprim. Fidler places different fruit fly populations into containers with different antibiotics. Then she removes the insects’ two pairs of tubules and examines them with birefringence microsco-
py, a technique that uses light and special filters to see things otherwise invisible to the naked eye, to see the microscopic kidney stones that grew within the tubules after the flies were supplemented with antibiotics. Computer software then quantifies the stone load.
The hope is, once researchers understand the correlation between antibiotics and the formation of kidney stones, this could promote antibiotic stewardship – fewer unnecessary antibiotic prescriptions – and lead to more targeted treatment strategies. For children specifically, this research could help practitioners know which antibiotic is best for children to avoid kidney stones.
For Fidler, doing this research in a hospital-based research institute is critical. As she seeks guidance from urologists at St. Joseph’s and others affiliated with Western University, Burton works closely with other researchers and clinicians at St. Joseph’s in infectious diseases, urology and surgery to understand issues facing patients in clinical practice.
This knowledge directly improves the work being done in the Microbiome and Probiotic Lab, and other labs across Lawson. “I love research because I use each result to determine what experiments I should perform next. And in the end, I am able to communicate a story using all my results that can be tied together,” says Fidler. “To produce good work and overcome the many challenges in research, you must be very passionate about what you do.” n H
Using AI to improve hand hygiene and patient safety
The Ottawa Hospital (TOH) is the first in Canada to implement the Artificially Intelligent Monitoring System (AIMS) to understand and improve hand hygiene. AIMS is a Perception-Action AI platform technology that unites AI and 3D sensors, providing real-time feedback and generating predictive insights – helping improve hand hygiene compliance and enhance patient safety without using cameras or collecting personal data.
light. If someone approaches a patient without cleaning their hands, AIMS provides a proactive ‘nudge’ – a yellow light and soft chime – as a reminder. AIMS captures this data in real time and makes it available to unit managers and staff through a dashboard to track their hand hygiene practices. AIMS provides the equivalent of seven years of hand hygiene data daily compared to traditional human auditors.
The results have been significant. The E5 Unit at TOH saw a 27 per
EARLY RESULTS HAVE BEEN SIGNIFICANT
TOH installed AIMS in 2023 in a Transitional Care Unit (E5) at the Civic Campus. AIMS nodes were installed in patient rooms and hallways, first collecting baseline data before activating real-time reminders.
When someone cleans their hands, AIMS assesses the duration and quality, which is signalled by a pulsing blue
cent sustained, relative increase in daily hand hygiene events. There were no outbreaks in the 12 months after AIMS was implemented, which is particularly notable given that staff in E5 care for vulnerable populations who may be at higher risk for outbreaks and serious illness.
The technology has been embraced by patients, visitors and clinical staff with zero complaints.
ACCORDING TO THE WORLD HEALTH ORGANIZATION, 70 PER CENT OF THESE INFECTIONS ARE PREVENTABLE WITH PROPER HAND HYGIENE.
“We have positive feedback from our staff, our patients and our family members,” said Sybile Delice-Charlemagne, Clinical Manager at TOH. “When they understand what it does, they’re like, ‘Wow, that’s great that the hospital is taking a step to keep my loved one safe.”
Frontline health-care workers have shared positive feedback regarding the integration of AIMS into their daily routines. Nurses say AIMS has become an essential tool in promoting patient safety and reducing the risk of infections.
“It’s really been helpful in ensuring staff compliance with hand hygiene protocols,” said Colleen Menary, a Clinical Care Leader with TOH. “It’s like having a colleague that’s there to just give you a gentle nudge when you need a reminder on some things.”
HAND HYGIENE IS A KEY FACTOR IN REDUCING HOSPITAL-ACQUIRED INFECTIONS
Hospital-acquired infections (HAIs) are a serious issue in health care. According to the World Health Organization, 70 per cent of these infections are preventable with proper hand hygiene, but ensuring consistent compliance can be challenging.
The Public Health Agency of Canada estimates that HAIs affect more
than 200,000 patients annually and result in approximately 8,000 deaths annually.
“The Ottawa Hospital is committed to finding innovative solutions to health-care challenges and has actively integrated AI to improve patient care and operational efficiency,” said Suzanne Madore, Chief Operating Officer and Chief Nursing Executive at The Ottawa Hospital. “We recognized AIMS’ potential for hand hygiene during the COVID-19 pandemic and are impressed by the continued improvements since our collaboration began.”
THE OTTAWA HOSPITAL IS EXPANDING AIMS USE TO OTHER AREAS
AIMS is more than just a solution for hand hygiene, it also has the potential to address other patient safety challenges. Building on the successful implementation of AIMS for hand hygiene, TOH is currently planning to leverage AIMS for detection and prevention of falls.
Through strong collaboration with Canadian technology firm Lumenix, Lumenix, TOH will continue to explore innovative uses of the AIMS technology, ensuring ongoing improvements in patient care and operational efficiency and enhancing the overall patient experience. n H
Ground-breaking HIV, syphilis testing initiative
Amid soaring rates of HIV and syphilis in Canada –with Indigenous communities in the Prairies being hardest hit – a team of Indigenous leaders and HIV advocates, researchers, health care workers and people with lived experiences, including HIV, have created The Ayaangwaamiziwin Centre.
This Centre is a ground-breaking initiative to “test, treat and link to culturally safe care” 10,000+ people at risk for HIV and/or syphilis in the Prairies and an additional 2,500+ people in Yukon, Nunavut and Northwest Territories.
Launched on March 5, the Ayaangwaamiziwin Centre – an Ojibwe word for “carefulness and preparedness” –will consist of a constellation of organizations working together to provide access to testing, preventative care, harm reduction and treatment for HIV and syphilis in underserved and remote communities across the regions.
Co-led by Dr. Sean B. Rourke, director of REACH Nexus at the MAP Centre for Urban Health Solutions at St. Michael’s Hospital, the Ayaangwaamiziwin Centre is a collaborative effort involving leaders from community, the health system, public health, and regional governments in the Prairies and northern Territories. Following an initial $4 million in funding secured in 2024 from CIHR, Indigenous Services Canada (ISC), Staples Canada through the Even the Odds partnership, Jackman Foundation, and other foundations, the Ayaangwaamiziwin Centre recently received an additional $3.75 million from CIHR to expand its intervention work to support northern communities.
“HIV and infectious syphilis are public health emergencies in Canada, sweeping across communities, particularly in Alberta, Saskatchewan and Manitoba. The more people we can reach to test, diagnose and treat with HIV and syphilis, the faster we can help end these health crises,”
said Dr. Rourke, director of REACH and a MAP scientist at St. Michael’s Hospital.
“This is a historic Canadian health partnership – involving the community, health care system and public health sectors.”
But none of this will make an impact on the people and communities most affected, without the leadership, expertise and commitment from Communities, Alliances & Network (CAAN) and Indigenous Services Canada (ISC) and the following agencies and organizations: StreetWorks, Radius Community Health and Healing, Northreach Society, and Alberta Health Services in Alberta; The Wellness Wheel Medical Clinic, the Northern Inter-Tribal Health Authority, and All Nations Hope Network in Saskatchewan; Nine Circles Community Health Centre, Ka Ni Kanichihk, Siloam Mission, and the Manitoba
Harm Reduction Network in Manitoba; and One Yukon Coalition, the Chief Public Health Officers in Northwest Territories and Nunavut.
“Indigenous-led, culturally-grounded, trauma-informed, and community-oriented health services are an essential part of reducing the spread of sexually transmitted and blood borne infections in First Nations, Inuit and Métis communities,” said Dr. Tom Wong, Chief Medical Officer of Public Health, Indigenous Services Canada.
“We will continue to work alongside partners and leaders to support safe spaces for Indigenous Peoples to seek holistic care in their healing journey.”
Everyone in Canada has the right to access health services and to thrive, but for many this isn’t happening. Underserved and marginalized communities – especially First Nations, Inuit and Métis – have faced a history of colonization, residential schools, racism,
stigma, discrimination, overcrowding, food insecurity and other social determinants of health that have created significant systemic barriers (over decades) leading to progressive, profound and persistent health disparities.
The latest data from the Public Health Agency of Canada shows in 2023:
• New HIV diagnoses climbed more than 35 percent since 2022.
• In Saskatchewan, the rate of HIV was 19.4 per 100,000 people and in Manitoba it was 19.3 – more than three times the national rate.
• In 2022, there were nearly 14,000 reported syphilis cases, with rates increasing by 109 per cent overall compared to 2018.
• In Alberta, Manitoba, Saskatchewan rates have risen 105 percent, 123 per cent and over 1,400 percent respectively. In the Yukon, infectious syphilis rates jumped by an as-
tounding 2,344 per cent during that time period, while N.W.T. saw an 844 percent increase.
• Congenital syphilis cases have seen a seven percent increase from 2021 and a nearly 600 per cent increase from 2018. Consequences of congenital syphilis for mother and unborn infant can be severe, resulting in miscarriage, stillbirth, and death shortly after birth, in 20-30 per cent of cases.
SEARCHING FOR A SOLUTION
In March 2024, over 100 collaborators – who had been meeting for more than a year virtually – came together for a landmark two-day meeting in Winnipeg to address this dire health crisis.
Their goal: to develop innovative and pragmatic actions to address the health crises of HIV, syphilis and other sexually transmitted and blood-borne infections (STBBIs) in the Prairies and in the Yukon, Northwest Territories and Nunavut. The late Roger Roulette, an Ojibwe Language Specialist from Manitoba, shared the Ojibwe
MAY 2025
“THIS IS A HISTORIC CANADIAN HEALTH PARTNERSHIP – INVOLVING THE COMMUNITY, HEALTH CARE SYSTEM AND PUBLIC HEALTH SECTORS.”
philosophy, ayaangwaamiziwin –carefulness:preparedness, with team member Elder Albert McLeod. In addressing HIV-STBBI’s, this ancient tradition, ethic and value is highlighted in all aspects of the work that this project is undertaking in Canada.
At the heart of this initiative is the holistic and community-centred approach of our interventions and knowledge mobilization efforts involving people with lived and living experiences. Through a “Two-Eyed Seeing” approach, our teams in Alberta, Manitoba and Saskatchewan are working closely with Indigenous leaders, with Indigenous-led and non-Indigenous-led community-based HIV, harm reduction and health agencies, and with affected communities.
Together, along with Indigenous Ways of Knowing and Doing, the
MAY FOCUS: Surgical Procedures, Pain Management, Palliative Care and Oncology: Non-invasive surgery, plastic surgery, orthopedic surgery and new surgical techniques including organ donation and transplantation procedures. New approaches to pain management and palliative care delivery. Approaches to cancer diagnosis and treatment.
NATIONAL NURSING WEEK SUPPLEMENT
Advertising Booking Deadline April 25th
Material Deadline April 29th
For more info email advertising@hospitalnews.com
initiative is building a shared vision of a culturally responsive, community-driven healthcare model to reach people who might be at risk for HIV and/or syphilis. The initiative will provide options for treatment and care with community-based health care practitioners who can help to engage those affected in spaces of trust, empathy and safety.
“This community-centered initiative is a transformative approach to addressing health disparities among Indigenous populations,” said Nikki Williamson, a Registered Nurse with the Wellness Wheel Medical Clinic in Sask. “By integrating testing and treatment for multiple diseases, including HIV and syphilis, into a single, accessible framework, this initiative demonstrates the power of community-driven healthcare. Grounded in trusted partnerships and culturally safe care
spaces, this initiative offers a scalable, syndemic-focused solution that can be adapted to improve healthcare access and outcomes in underserved communities nationwide.”
Over the next five years, Ayaangwaamiziwin Centre will continue expanding our engagement bringing on more frontline agencies, people with lived experiences, and building community-driven partnerships in the Prairies and the northern Territories to reach those who have been failed by our traditional health care systems. This new testing, care and prevention initiative is critical towards ending the HIV and syphilis epidemics in Canada.
“The Ayaangwaamiziwin Centre changes the conversation and ways of reaching Indigenous peoples and other communities and key populations affected, and provides a new pathway for people who might have gone through trauma or faced discrimination when accessing the traditional health care system,” said Albert McLeod. “This new way forward is about giving people more choices and options to reclaim their health and wellbeing.” n H
UPCOMING EDITIONS
JUNE 2025
Pharmacists Supplement Pharmacists Supplement
JUNE FOCUS: Precision Medicine and Genomics, Pharmacy and Medication, Research: Developments in the field of personalized medicine. Innovative approaches to fund-raising and the role of volunteers in healthcare. An examination of safe and effective use of medications in hospitals including medication management. ANNUAL PHARMACY SUPPLEMENT
Advertising Booking Deadline May 23rd
Material Deadline May 27th For more info email advertising@hospitalnews.com
JULY 2025
JULY FOCUS: Cardiovascular Care, Respirology, Diabetes, Complimentary Health: Developments in the prevention and treatment of vascular disease, including cardiac surgery, diagnostic and interventional procedures. Advances in treatment for various respiratory disorders, including asthma and allergies. Prevention, treatment and long-term management of diabetes and other endocrine disorders. Examination of complementary treatment approaches to various illnesses.
Advertising Booking Deadline June 20th
Material Deadline June 24th For more info email advertising@hospitalnews.com
It is time the feds make the long-awaited diabetes device fund a reality
by Glenn Thibeault
It has been almost a year since the federal government announced that it would establish a Diabetes Device Fund to make devices and supplies for managing diabetes more accessible.
Canadians with diabetes are still waiting.
It is time to end the wait. The fund has the potential to transform diabetes care in Canada, making it crucial that the federal government act now to set up the fund.
Over four-million Canadians have been diagnosed with diabetes. Living with the chronic condition comes with significant health and financial challenges.
To prevent or delay serious health complications, people with diabetes need timely access to proper medications, supplies and devices – including continuous glucose monitors (CGMs) and insulin pumps – to help them manage the condition.
Yet, the costs to access diabetes management tools are substantial. The out-of-pocket costs for people with type 1 diabetes can be as high as $18,306 per year in certain parts of Canada. For those with type 2 diabetes, the annual costs can be as high as $10,014.
While provincial and territorial public health plans might fully or partially cover some devices and supplies, there are often eligibility restrictions and dollar caps.
Coverage also varies significantly from province to province, resulting in inequitable access across the country.
Those who live in jurisdictions without coverage or with limited coverage have to shoulder the costs themselves. While private health insurance can defray costs, for those without private coverage, devices can be unaffordable.
That is why the federal fund is vital. By providing funding to cover the costs of tools such as CGMs, insulin
FOR THOSE DIAGNOSED WITH DIABETES, ACCESS TO RELIABLE MONITORING SYSTEMS MEANS FEWER DAYS LOST TO ILLNESS, IMPROVED MENTAL HEALTH AND AN OVERALL BETTER QUALITY OF LIFE. IT MARKS A SHIFT TOWARDS PROACTIVE CARE RATHER THAN COSTLY, REACTIVE TREATMENT.
pumps, lancets, test strips and blood glucose meters, the fund can help alleviate the financial burden weighing on those living with diabetes and eliminate regional inequities in access.
Make no mistake. Diabetes management tools are not frivolous accessories. CGMs and insulin pumps have long been recognized as game-changing diabetes management tools.
By providing real-time glucose data and seamless insulin delivery, these devices empower people to manage their condition and help prevent complications like diabetic ketoaci-
dosis, heart disease and other chronic conditions.
Research has shown that people who regularly monitor their glucose levels and use insulin pumps or CGMs experience fewer hospitalizations and emergency room visits – making them important tools for helping to ease financial pressure on Canada’s healthcare system. Stable glucose levels also translate to better sleep, increased energy and a greater sense of personal agency – a stark contrast to the constant highs and lows people too often experience without these tools.
For people managing diabetes, these outcomes are not just health statistics, but life-changing realities.
The device fund symbolizes more than just financial support, though – it is an investment in the future of Canada’s collective health and prosperity.
For those diagnosed with diabetes, access to reliable monitoring systems means fewer days lost to illness, improved mental health and an overall better quality of life. It marks a shift towards proactive care rather than costly, reactive treatment.
The fund can promote patient-centred care by offering access to devices suited to individual needs – finding the right device often depends on a person’s lifestyle and budget.
When the federal government announced the fund last February – at the same time it tabled legislation to establish a national pharmacare plan covering diabetes and contraceptive medications – people living in Canada with diabetes cheered it as a way to address the significant financial and health challenges they face.
They are now getting discouraged. The federal government has not indicated when it will set up the fund, how much it will contribute to it or what it will cover – will it include only the basics or will it also cover maintenance costs like replacement sensors, batteries and other associated expenses?
The federal delay has also stalled efforts to get provinces and territories to reduce or eliminate coverage restrictions or caps or to standardize their coverage as they wait to hear what Ottawa is doing.
We need to move towards a future where no one in Canada struggles to afford the tools they need to manage their chronic condition. The Diabetes Device Fund is an important step in this direction.
It is time for the federal government to allocate money for the fund and get it up and running.
Canadians with diabetes have already waited too long. n H
a former
Glenn Thibeault is the Executive Director of Government Affairs, Advocacy and Policy for Diabetes Canada. He is also
MP, National Caucus Chair, MPP and Minister of Energy in Ontario.
Glenn Thibeault.
Heart failure patient recovers at home thanks to a Canadian first at HHS
By Lise Diebel
t felt like an elephant was sitting on my chest.”
That’s how Hamilton resident Peg Kelly describes chest pressure she experienced one night in December, during the holidays. Kelly has been living with heart failure (HF) for 10 years and recognized the seriousness of her symptoms.
“I couldn’t breathe when I tried lying down in bed. I was sitting up all night long, trying to breathe better, and I felt dizzy and faint. I knew something was very wrong, because these were the same symptoms I had 10 years ago when my heart problems started,” she said.
Kelly visited the emergency department at Hamilton Health Sciences (HHS) Hamilton General Hospital and was admitted for three days, until she was well enough to return home. While in the hospital, she was invited to take part in a new remote home monitoring program launched by HHS for patients living with HF and chronic obstructive pulmonary disease (COPD).
INNOVATIVE HHS SYMPTOM MONITORING PROGRAM
Thousands of HHS surgical patients recovering at home from their operations have benefited from remote home monitoring since this form of virtual care was introduced several years ago and expanded during the pandemic.
Recently, HHS launched a remote symptom monitoring program specifically for patients living with HF and COPD. This new program includes nurse practitioners, and is supported by MyChart Care Companion, a feature in Epic, the stateof-the-art, fully digital hospital information system launched at HHS in 2022.
If this program proves successful, it could be expanded to include patients with other health conditions. The clinical pathways developed through this model could also be shared with other Epic hospitals in Canada resulting in improved patient and health system outcomes. An area of efficiency could be the elimination of some costs associated with home monitoring equipment while also streamlining the data collection process.
DEVELOPING CUSTOM REMOVE MONITORING PROTOCOLS
“MyChart provides integrated clinical pathways for patients with HF and COPD who are discharged
Epic is considered among the best hospital information systems in the world and is used internationally by many top-ranked hospitals. MyChart is Epic’s patient portal that allows patients with a computer, tablet or mobile phone to connect with HHS and access their lab and test results, appointment information, doctors’ consult notes and more.
from HHS,” says Jennifer Lounsbury, chief nursing information officer for HHS. “This created an opportunity for HHS teams to develop MyChart Care Companion custom remote monitoring protocols and to test drive this approach to care starting in November 2024 with HF and COPD patient populations.”
Patients are remotely monitored from the comfort of their homes by a team of HHS virtual care nurses and nurse practitioners through a custom program created by HHS and made possible through the Care Companion platform.
HHS is the first Epic hospital system in Canada to develop a streamlined remote monitoring system integrated Care Companion model. Potential benefits include:
• Health equity and cost savings. By providing patients with hospital-owned kits containing home monitoring equipment, all patients have access to technology and there’s no need to rent this equipment from outside providers.
• A better provider experience for HHS virtual nursing staff and other team members. Since HHSowned monitoring equipment is integrated with Epic, nurses will not have to manually input data from another source into the Epic system.
• Improved patient care. For example, patients with HF and COPD rely on their primary care physicians, specialists, home care and other community providers when they return home after being in hospital. Remote symptom monitoring can enhance their care from their home with Care Companion, since with early intervention it’s possible to avoid the worsening of HF and COPD conditions. This can improve patients’ health outcomes, well-being, as well as system outcomes such as reducing emergency department visits and readmissions.
The Remote Monitoring team. Photo credit: Josh Carey
SEAMLESS INTEGRATION BETWEEN HOSPITAL AND HOME
Eligible patients with HF and COPD are identified by HHS teams and receive a home monitoring kit consisting of an HHS-owned iPad so they can log into MyChart’s health tracking application, says Prathiba Harsha, HHS interim director of clinical informatics and solutions delivery.
Kits also include an HHS-owned blood pressure cuff, a weight scale, a pulse oximeter for measuring blood oxygen levels and pulse, and a thermometer, with results for all the devices automatically entered into the patient’s electronic health record in the Epic system via MyChart.
“I had never used an iPad before,” says Kelly, who received support from the HHS team in learning how to use the equipment. Each morning, Kelly logs into Epic’s MyChart to input her vital signs. “It’s great because I’m constantly being monitored and if something doesn’t look right a nurse con-
tacts me right away,” says Kelly. “They really keep an eye on me, and it’s easy.”
Kelly also enjoys weekly video conferences with a member of the program’s nursing team. “The nurses are very agreeable, supportive and kind.”
Care Companion also provides medication reminders, education, questionnaires, links to community resources and on-demand video visits with a member of the HHS virtual care nursing team and nurse practitioners.
Patients’ vital signs seamlessly integrate into Epic, where HHS clinical informatics teams, clinical experts and operational leaders have worked together to create specific care pathways that empower patients to monitor their vital signs at home, respond to questions related to HF and COPD, and connect with virtual nursing and nurse practitioners to obtain required support.
IMPROVING PATIENT CARE
Kelly O’Halloran, director of community and population health
services for HHS, came up with the idea to offer remote home monitoring to HF and COPD patients, and partnered with the HHS informatics team on the development of custom MyChart Care Companion protocols.
“I believe patients discharged from hospital can really benefit from remote symptom monitoring overseen by registered nurses and nurse practitioners,” says O’Halloran, who elicited funding support from Ontario Health West/Ontario Health to develop and implement the custom Care Companion protocols.
“We have been fortunate to have the expertise of Dr. Catherine Demers, HHS director of heart function services, Dr. Natya Raghavan, HHS head of the service for respirology, and other clinicians to develop the clinical pathways,” says O’Halloran.
INSPIRED BY HHS PROTECT LAB
O’Halloran says she was inspired by the HHS PROTECT Lab and its
Continuus Health program, based at HHS Juravinski Hospital and Cancer Centre (JHCC).
The PROTECT Lab is a leading-edge HHS and McMaster University research lab that studies virtual care and remote home monitoring of hospital patients through its Continuus Health program. Care Companion is a satellite model build around the hub PROTECT Lab virtual care model, which has traditionally focused on post-surgery care, with plans to include JHCC cancer patients receiving treatments such as chemotherapy, radiation, and immunotherapy as outpatients.
The virtual nursing team supports pediatric and adult surgical patient populations. This further expansion to support patients with chronic medical conditions like COPD and HF continues to build on a virtual care model supporting person-centred integrated care for the people of Hamilton and surrounding regions. n H
Lise Diebel works in communications at Hamilton Health Sciences.
Canadian Surgeons Volunteer Onboard the World’s Largest Civilian Hospital Ship
In April 2024, Quebec surgeons Dr. Jean-Martin Laberge and Dr. Louise Caouette-Laberge volunteered on the Global Mercy in Freetown, Sierra Leone, to offer free surgery to the population.
As President Julius Maada Bio of Sierra Leone stated just prior to Mercy Ships’ field service, “Mercy Ships, provides a continuous humanitarian and medical support towards providing treatment to people with various medical conditions worldwide”. At the time if the announcement, the partnership agreement included a 10-month deployment of the Global Mercy, offering free surgical care in and training healthcare professionals to build capacity within Sierra Leone’s national health system.
As she prepared to come aboard, Dr. Caouette-Laberge shared her excitement at being able to work aboard the Global Mercy. “The advantage of having a state-of-the-art hospital like this is that it has international standards. It allows us to perform complex surgeries that we wouldn’t be able to do in an African country because they don’t have the necessary infrastructure.”
The couple was recognized for their humanitarian work by the Collège des Médecins du Québec, which jointly awarded them the Prix d’humanisme in 2013. As for Dr. Laberge, in addition to participating in missions with his wife, he has contributed to the training of pediatric surgeons in Kigali, Rwanda. Through their respective work in pediatric surgery, they have between them changed countless lives of children both in Canada as well as Africa.
“We receive much more than we give! The people we operate on for free are so pleased, they thank us and are happy. We take for granted the training we receive and how lucky we are to be able to study. There are no teachers there. You don’t realize it until you leave home and see the reality of others,” says Dr. Louise Caouette-Laberge. After all
these years in the field, they are now part of an international team of medical specialists that serve onboard Mercy Ships.
The Global Mercy’s volunteer crew of nearly 600, both short- and longterm, works with dedication and excellence to welcome patients for life-changing surgeries. Darryl Anderson, Executive Director of Mercy Ships Canada, stated, “We are grateful for medical staff and all hospital volunteers who, like Dr. Laberge and Dr. Caouette-Laberge, share a passion for our mission of Hope and Healing.” Anderson also announced, “We are excited that the President of Sierra Leone has extended our partnership for another field service into 2024.”
Mercy Ships Canada is one of 16 National Offices dedicated to raising funds, building awareness, recruiting volunteers, and supporting impactful projects for Mercy Ships’ global programs. Mercy Ships operates the world’s two largest civilian hospital ships, delivering free, life-changing surgeries and healthcare, along with training and mentoring for local healthcare professionals, ensuring communities have sustainable healthcare long after the ships depart.
Mercy Ships believes that everyone deserves a life full of promise and potential. That every mother deserves to see her child grow healthy and thrive. We believe that healthcare is a human right, and we are committed to reaching children and families in need of safe surgical care with state-of-the-art hospital ships filled with compassionate volunteer healthcare providers.
Dr. Louise Caouette-Laberge, conducting a surgery with her husband Dr. Jean-Martin Laberge, onboard the Global Mercy
To learn more on volunteering visit mercyships.ca/en/get-involved/volunteer WITH VOLUNTEERS