












Findings
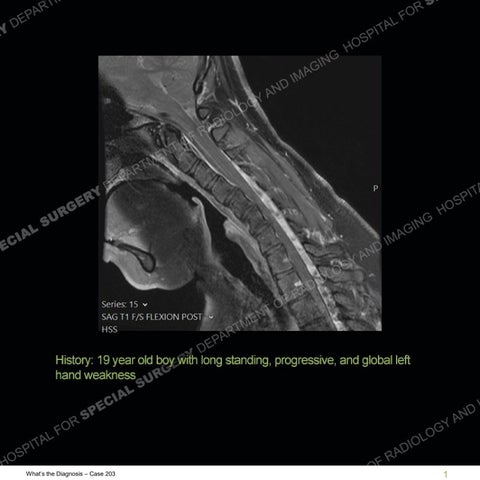
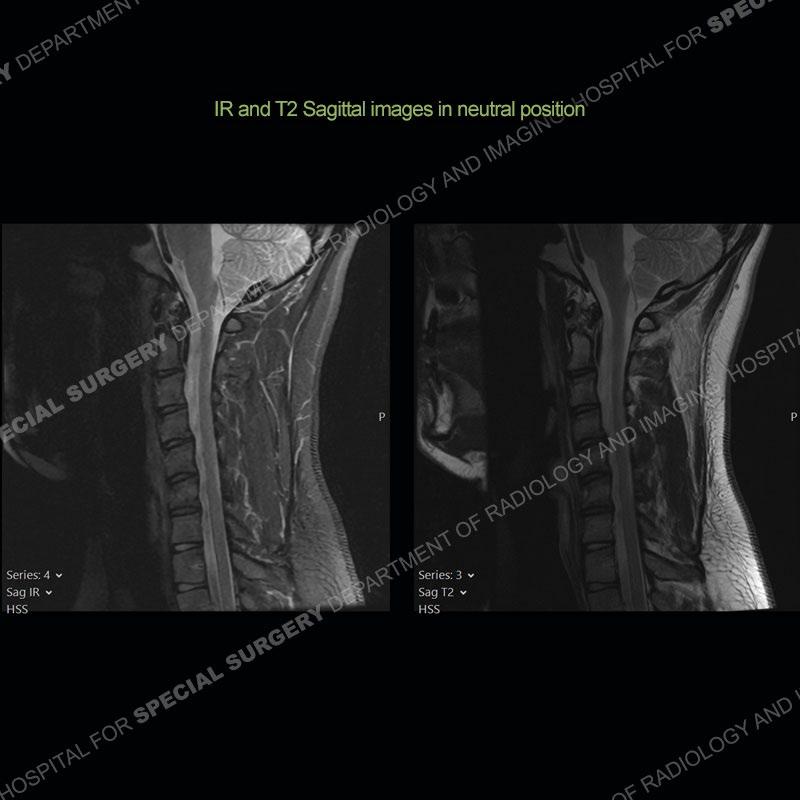
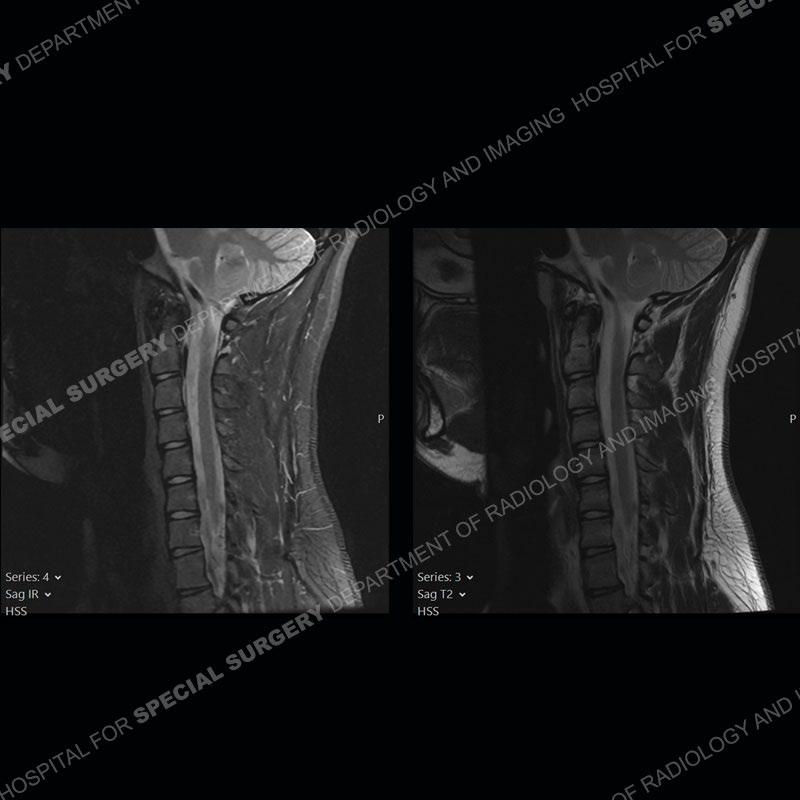
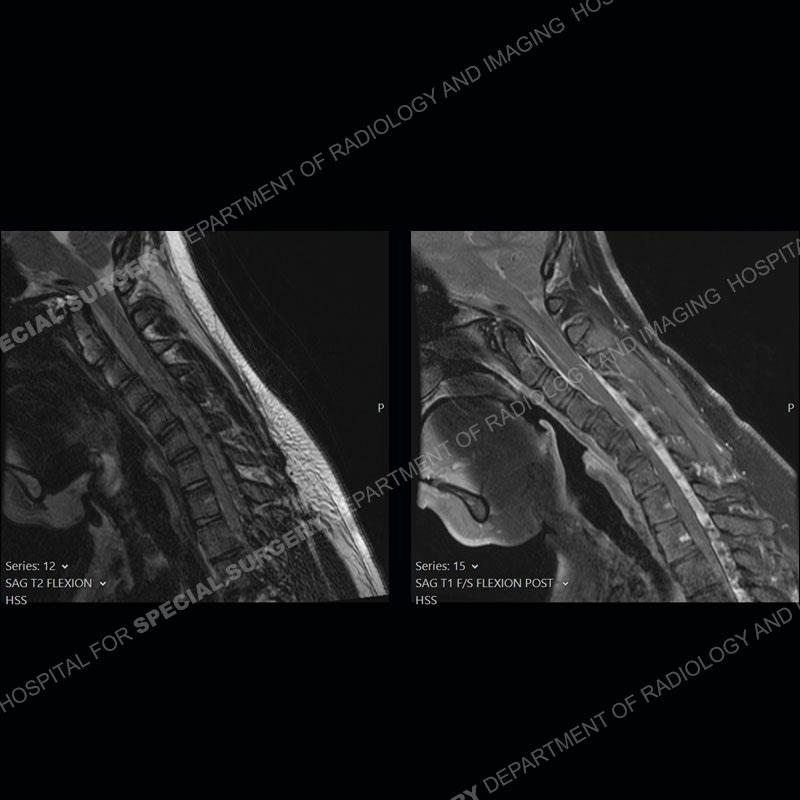
The images on the neutral sagittal images do not demonstrate any appreciable abnormality. On the flexion images, there is a forward displacement of the spinal cord centered on C6-C7. There is an expansion of the posterior dural sac which shows marked enhancement. Prominent flow voids are present of the expanded posterior dural sac on the T2 and T1 post contrast images.





Diagnosis: Hirayama Disease
Hirayama disease or non-progressive juvenile spinal muscular atrophy is an incompletely understood process related to infarct of the anterior horns of the lower cervical cord. It is most frequently found in young men and presents with an insidious onset of typically unilateral upper extremity weakness and muscle wasting involving the C7 through T1 myotomes. One current hypotheses of etiology relates to disproportionate growth of the vertebrae and thecal sac leading to the forward cord displacement on flexion. Other thoughts relate to imbalance of posterior epidural ligament resistance and strenuous exercise with neck flexion in the rapidly growing, younger male patients.
Not present in this case, but frequently found is abnormal T2 signal intensity of the lower cervical cord about the area of maximum forward displacement. This can be seen on the neutral and flexed position imaging. Shown well in this case is the marked, crescentic expansion of the posterior dural sac. The sac shows marked enhancement with prominent flow voids and is often hyperintense on T1 and T2 images. The spinal cord as shown in this case is typically anteriorly displaced about the lower cervical cord.
Progressive, unilateral involvement is typical. Although the process is self limiting early diagnosis is crucial as early treatment has been found to stop disease progression.
References
Yen-Lin Huang, Chi-Jen Chen, Hirayama Disease, Neuroimaging Clinics of North America, Volume 21, Issue 4, 2011, Pages 939-950, ISSN 1052-5149, https://doi.org/10.1016/j.nic.2011.07.009.