The Advertising Standards Authority spells out the law for doctors P18
The business journal for doctors in private practice
Defending medico-legal claims is eye-watering
What can be learned from the claims the MDU receives from ophthalmology members P20
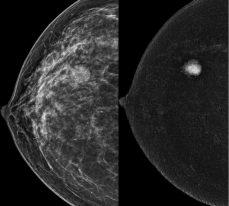
Self-pay still surging
By Robin Stride
The surge in the number of self-paying patients is continuing and is now being experienced nationwide, according to a leading analyst.
Self-pay expert Liz Heath says growth in demand for self-pay is being seen across all areas of the UK, including areas that have not traditionally been private healthcare ‘hot spots’, such as Wales and Scotland.
The author of the newly published fifth edition of LaingBuisson’s Private Healthcare Self-Pay UK Market Report states that research from multiple sources shows many patients are viewing a private doctor option for the first time.
But she warns they may have little knowledge of how to navigate the system and need support along the way.
In this issue of Independent Practitioner Today (page 12), she gives consultants who are aiming to boost their self-pay income some useful tips.
And she stresses it is crucial to ensure prospective patients receive prompt responses to their inquiries and are signposted to the right choice for them.
‘Inaccurate contact information or a lack of response gives a poor impression to a potential patient in a climate where we are all used to immediacy and “on demand” services,’ Mrs Heath says.
‘Affordability is frequently cited as a key decision-making factor by patients and visibility of consultant fees is a positive step.
‘LaingBuisson’s pricing analysis found that most procedure prices reviewed had increased broadly in line with general and medical inflation, but there is still a vast range in some cases between highest and lowest prices.’
She went on to explain that the guide price for a primary knee replacement varies across the UK between around £9,000 and £17,000, which is unhelpful and confusing for the consumer. The average guide price in 2023 is £13,781, a rise of 5.17% on 2021-22.
Despite inflation concerns, market analysts LaingBuisson observe a growing interest in self-payfunded procedures, ‘most likely fuelled by long NHS waiting lists’.
It reports that some providers
Our sponsors
SELFPAY KEY POINTS
➤ Confidence in the market remains high. Just over 53% of respondents to a LaingBuisson survey believe the selfpay market will grow by 1015% in the next three years.
➤ The NHS faces challenges in meeting elective treatment demands and experiences increased waiting times for diagnostic tests.
➤ Providers have diverse pricing strategies for selfpay and cosmetic procedures, with some adopting regionalised or harmonised pricing structures while others rely on local pricing.
➤ NHS private patient units (PPUs) have the potential to compete with the independent sector locally by improving their access to highquality NHS care. Some NHS trusts are making better efforts to attract selfpay customers.
➤ Future growth projects are challenging due to constraints on private sector capacity expansion, primarily related to staff and resourcing, However, all indicators are that selfpay growth will continue.
➤ The key legacy of Covid19 is greater use of technology across healthcare providers. Their challenge now is to embrace the opportunity to extend the patient relationship with the help of technology.
Source: 5th edition of LaingBuission’s Private Healthcare Self-Pay UK Market Report
have regionalised or harmonised their price structures across the UK while others stick to local pricing ‘with localism a large factor for consumers’.
There is little evidence of a ‘race to the bottom’ in price competitiveness. Prices for the highest volume self-pay and cosmetic surgery procedures have risen but are below overall inflation.
Some NHS private patient units (PPUs) are making efforts to attract self-pay customers, but Laing -
Buisson says consultants working in others are potentially missing out on an opportunity to compete locally with the independent sector. This is due to PPUs’ failure to capitalise on their access to highquality NHS care.
It warns that the scale of future growth is difficult to estimate due to constraints on the private sector’s ability to expand capacity –primarily related to staffing and resourcing shortages.
➱ continued on page 5
Liz Heath, author of the LaingBuisson selfpay report
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
This must be one of the most overused phrases we come across. We regularly hear it in speeches and conversations, and read it in reports and press releases from eager start-ups keen to impress potential clients.
The aspiration pops up regularly both in private healthcare and the NHS and may sound a bit obvious to many. ‘It’s all about patients, is it? Oh really? Well, what a surprise!’
With so much publicity, it is odd the ‘at the heart’ message so often gets lost in translation. We’ve all got stories about that.
One of our team went for a consultation with a private surgeon and was stunned to find out halfway through – after close questioning – that the guy was unavailable and was using one of his juniors instead.
But patients are very much at the centre of this issue of
Independent Practitioner Today
with a variety of articles following the current widespread agenda to ever improve services to them.
These include a feature on what is being called value-based healthcare – a patient-centred approach focusing on improving patient outcomes, cost-effectiveness and overall value in healthcare delivery (page 26).
There is some valuable feedback on private consultants from their patients (page 24) in Bupa’s report showing that, in both the positive and less positive circumstances, communication issues are a key theme affecting patients’ impressions.
When it comes to complaints, we thought it would also be useful to show you what advice patients nationwide are being given via the Patients Association (page 44 ) if they consider they have not, perhaps, been at the heart of everything you did.
Will self-pay keep on rising?
The 5th edition edition of LaingBuisson’s report into self-pay has just been published. Its author Liz Heath reflects on what the data tells us P12
Free yourself from drudgery
Outsourcing your administrative tasks in private practice has some big advantages, as Medserv’s marketing manager Derek Kelly explains P16
Patient safety is at a pivotal point
Quality and safety have been leading the Independent Healthcare Providers Network’s agenda. Now its clinical director asks for doctors’ help P22
Communication key to happy clients
People buying health insurance have high expectations of care, so their feedback is key to help improve service, explains Bupa’s Tricia Carley-White P24
How consent has become stricter
Medico-legal expert Dr Emma Green highlights some defining cases that have led to the principles of consent and how they apply in practice P33
The perils of social media
Rachel Levine explains who the law protects in social media and how you can shield yourself as an employer and/ or employee against its dangers P38
PLUS OUR REGULAR COLUMNS
Business Dilemmas: When asked to attend an adverse incident meeting
Dr Kathryn Leask gives her advice on two requests for help in our long-standing medico-legal series P42
Accountant’s tips: Tax changes you need to grasp
Richard Norbury of accountants Sandison Easson gives a round-up of changes to tax in the near future P45
Doctor on the Road: Is Tesla running out of sparks?
Our motoring correspondent Dr Tony Rimmer reckons Tesla has a job to do if is wants to stay in front P48
IT system promises to revolutionise booking
By Robin Stride
A new national initiative from online IT solutions experts promises to transform private healthcare access by easing the hassle of booking appointments with private doctors and hospitals.
With final testing of Healthcode’s integrated channel exchange (ICE) underway, the company’s managing director Peter Connor hailed the development as ‘a game-changer for our sector and for patients’.
He said: ‘At a time when demand for private healthcare is growing, it makes sense to have a booking process that’s efficient, convenient, secure and accurate, rather than something that demands perseverance and patience from users.’
Providers will be able to share real-time services and availability information so people can find what they need and make an online appointment.
The first sector-wide booking system, being tested with hospitals and insurers, is due to go live on 1 September.
A launch event in London
Healthcode’s integrated channel exchange (ICE) system is due to go live in September
attracted a strong turnout from stakeholders and answered many of their questions.
ICE was developed to replace ‘multiple and disparate booking processes’ used across the sector, from paper-based admin to oneoff IT solutions built for individual providers or software systems.
The developer says this fragmented approach does not meet today’s patients’ needs or expectations and often proves labour-
intensive and prone to inaccuracy like double-booking.
It labels most booking processes as inefficient, resulting in poor patient experience, empty appointment slots, wasted admin time and missed revenue.
Healthcode, inspired by online booking technology evolution in the travel sector, has responded with a bespoke Global Distribution System (GDS) – seen as the hidden engine room powering the booking process for private healthcare.
ICE allows providers, insurers and booking sites to link to a central hub to securely exchange and sync live information about services and availability. Private doctors will not have to change their front face booking system.
Third-party users – patients, GPs, insurers and call centres – can use their choice of booking site to search the network to find free slots and then book their appointment.
The provider’s diary system then automatically updates so the slot is no longer available.
Healthcode predicts it will process a record 10m invoices this
year after reaching 4.9m before the end of June.
Mr Connor told the launch event that business was ‘almost off the scale for us: 25% up on last year and 15% up on 2021’.
Most of the bookings for these treatments were likely to have been by phone rather than the greater choice offered by online.
He said ICE would make a ‘massive impact on our sector’ with its benefits transferring directly to patients.
Two major hospital groups, two major insurers and ‘a lot of independent hospitals’ were already committed to use ICE. Its fee structure has not yet been disclosed.
Mr Connor said the development was true to the firm’s principles: Using interoperable technology so that different organisations can connect seamlessly;
Meeting recognised data standards;
Encouraging industry collaboration in the interests of patients;
Finding innovative ways to work more efficiently within the private healthcare sector.
More ‘what’s new’ from Healthcode, see page 6
Have you got rise due on your NHS pension?
Doctors caught up
Doctors due to receive inflationary increases on their NHS pensions may have been missing out, according to specialist financial planners Cavendish Medical.
Members in receipt of their NHS pension should see their pension increase every year in line with inflation.
But some doctors have not received the standard annual increase, which should be at the Consumer Price Index inflation rate – from the preceding September – because of administration
in payment delays to statutory pension increases
issues with the NHS Business Services Authority that manages the pension scheme.
Patrick Convey, technical director at Cavendish Medical, exp lained: ‘We have seen more and more cases where the statutory inflationary increase has not been applied. We understand that there are even occurrences of payments being several years behind.
to have your own figures thoroughly checked by experts well versed in seeing these numbers.’
‘As we always advise, it can pay
Individuals who have recently retired may also be missing an additional pension payment –referred to as ‘second bite’.
This is based on the inflationary increase due on your pension since your retirement and is paid in the April following your retirement date.
Mr Convey told Independent Practitioner Today: ‘With more pension flexibilities coming into force in October, and the McCloud remedy due to be implemented from the same month, it is extremely important that doctors are checking their positions carefully now to ensure all figures are current and correct.
‘Small errors can have substantial impacts, particularly where the figures might be used as the foundation of significant life decisions.’
Patrick Convey of Cavendish Medical
Docs cancel their holidays to cope
By Olive Carterton
Pressures faced by consultants and their reported impacts on patient care are highlighted in the latest census from the Federation of the Royal Colleges of Physicians in the UK.
Around one-in-five doctors (18%) almost never feel in control of their workload and 42% of consultant physicians did not take all their annual leave last year – usually because they could not find cover or were too busy to arrange it.
The findings came as The Medical Defence Union (MDU) backed calls for immediate action to be taken to support dissatisfied and burnedout doctors, following the publication of a GMC report.
The ‘State of medical education and practice’ report found more doctors than ever were thinking of leaving the workforce and had taken hard steps to do so.
Three-quarters of doctors (70%)
reported working beyond their rostered hours on a weekly basis in their NHS jobs and just half said they were satisfied in their work, down from 70% in 2021.
How many will completely retire, take up private practice or try to do more of it remains to be seen.
Most say widespread NHS vacancies are significantly impacting patient care, the study from the three medical royal colleges representing UK physicians revealed.
The Royal College of Physicians, Royal College of Physicians of Edinburgh and Royal College of Physicians and Surgeons of Glasgow’s annual census found 58% of physicians reported consultant vacancies in their departments.
Forty-four per cent reported having an excessive workload almost always or most of the time.
Dr Sarah Clarke, president of the Royal College of Physicians in London, said: ‘It is alarming that
so many of our dedicated doctors feel that their workload is out of control.’
The census found 28% of consultant physicians were working less than full time. It projects that by 2027, this will rise to one third.
The proportion of men and women working less than full time is similar until age 35, where they diverge.
Over 49% of female consultants aged 35-44 are working less than full time compared to 10% of male consultants in that age bracket.
This year’s census survey was sent electronically to 19,187 consultant physicians and 5,244 (27%) responded
Dr Caroline Fryar, MDU director of medical services, said the GMC report should be a wake-up call to employers, the Government and regulators. ‘We know from our own survey that well-being among doctors is very low and that our members are really struggling.’
Surgical robot lands in Woking
Consultant surgeons at Nuffield Health Woking Hospital are pleased to be using a Mako robot to carry out more precise knee and hip replacements. Mr Dean Michael, consultant hip and knee surgeon at the Surrey Orthopaedic Clinic – who practices at Nuffield – said it improved the accuracy of hip and knee replacement component positioning and potentially reduce surgical soft tissue trauma.
Pictured at the installation of the Mako robot at Nuffield’s Woking Hospital are (L-R) deputy theatre manager Kat Truswell; scrub nurses Hazel Sigua and Janine Gibbs; Jason Eddy of manufacturer Stryker; and Keith Mawer, theatre manager
‘It’s hoped that this may lead to optimised recovery and shorter length of stay for patients, as well as improving the long-term survival of these joint replacements.’
Consultant orthopaedic surgeon Mr Constant Busch added: ‘Any experienced surgeon will be able to make accurate bony cuts, but evidence shows that the Mako® robot will increase the accuracy even further.’
BMA attacks former Health Secretary’s Covid claims
A doctors’ leader says former Health Secretary Matt Hancock’s apologies at the Covid Inquiry ‘will ring hollow for thousands of doctors and patients’.
The BMA council chairman said, as a doctor working on the front line during the pandemic, he took issue with Mr Hancock saying that if all the recommendations from pandemic planning exercises had been implemented, it ‘would not have been much help’.
Prof Philip Banfield added that if there had been adequate availability and provision of appropriate personal protective equipment (PPE), it would have made a huge difference to staff on the ground who had to fight a deadly disease, often without the right protection.
‘By saying the stockpile of PPE was “very significant” in early 2020 and that the problem was just one of distribution, he is glossing over the issues of quality and type of PPE.
‘Staff had to use items that were out of date, with multiple expiry stickers visibly layered on top of each other, leading to some PPE that was no longer fit for purpose snapping unpredictably while in use.’
In a BMA survey, 81% of doctors reported not feeling fully protected during the first wave of the pandemic.
The BMA’s Prof Philip Banfield
Self-pay predicted to continue on up
The author of the latest market report on self-pay says that the future looks quite rosy.
Liz Heath says: ‘Forward projections are always difficult to make, but based on the recent growth trajectory, all indicators are that selfpay growth will continue.
‘There are signs of some “recovery” in NHS private patient revenues, but these are very variable and may depend on geography, the existence of dedicated private patient beds and local pressures.
She adds: ‘We have noted that a
number of NHS trusts have taken the opportunity to re-evaluate their private patient offer, particularly for self-pay patients, and this is reflected in much wider availability of information and prices for procedures, including cosmetic surgery, within NHS private patient services.
‘Therefore, it is clear that some trusts are very well-placed to optimise the opportunity to recover private patient income in the future.
‘Many trusts report optimism about the future prospects for
their private activity growth overall.
‘Long term, there are favourable signals for growth in private spending on acute medical care in the UK, as individuals, companies and overseas customers have strong interest in the private healthcare product and its capabilities across the healthcare spectrum.
‘However, the strength of growth is likely to depend on the ability of providers to convert interest into realised demand, and effectively target varied customer needs.’
The Cleveland Clinic signs up some big-name specialists
Cleveland Clinic London has promoted Prof Richard Cohen to medical director and Prof Charles Knowles to chief academic officer.
Prof Cohen continues as consultant colorectal surgeon, chief of surgery and chairman of the Digestive Disease and Integrated Surgery Institutes.
A pioneer of new surgical techniques, he is professor of surgery at University College London.
Prof Knowles, the hospital’s lead for colorectal surgery and clinical director of research, is a champion for academics, education and research.
He is professor of surgery at Queen Mary University of London
and an honorary consultant colorectal surgeon at Barts Health NHS Trust and St Mark’s Hospital.
➤ Consultant gastroenterologist
Dr Sara McCartney and hip and knee surgeon Prof Justin Cobb have joined the Cleveland Clinic.
Dr McCartney is currently divisional clinical director in gastrointestinal services at University College Hospital London (UCLH) and has a subspecialty interest in managing complex ulcerative colitis and Crohn’s disease.
She has established and runs a large adolescent and young adult multidisciplinary inflammatory bowel disease (IBD) clinic at UCLH promoting optimal care for young
Clinic offers pledge to see the same GP every time
A new private concierge GP clinic is offering patients the convenience of seeing the same doctor every time and pledging to offer an appointment within three hours of their initial query.
HarleyDoc, in Harley Street, London, says it is dedicated to delivering exceptional patient care through a team of doctors from diverse healthcare backgrounds, each with at least ten years of post-qualification experience.
patients and a joint IBD and pregnancy clinic with the obstetric team.
Prof Cobb, awarded a CVO for services to the royal family, has moved his practice after 25 years at the King Edward’s VII Hospital.
He has been an orthopaedic surgeon at Imperial College NHS Trust and chairman of orthopaedics at Imperial College since 2005, having previously worked at UCLH.
His research and clinical team in the MSk Lab at Imperial focus on the development of less invasive alternatives to joint replacement such as H1, a novel all-ceramic hip resurfacing.
Chief executive and founder Dr Tony Banerjee, who has worked for over 20 years in the NHS, private and managerial sectors, aims to cater for clients wanting more individualised approaches to their healthcare.
The clinic’s range of services include travel medicine, mental health, chronic disease management, skin surgery and aesthetics.
Dr Banerjee said: ‘We are so excited to launch HarleyDoc and bring this elite healthcare model to market, offering patients the convenience of seeing the same doctor every time within three hours of their first contact, wherever they or their loved ones find themselves in the world.
‘We have clinic presence already between London, Dubai and Monaco, and look forward to further expanding in the near future as our client base grows yet further. We believe that this is the best way to provide patients with the care they need and deserve.’
New patients are currently being offered a special introductory membership.
Prof Richard Cohen
➱ continued from front page
Prof Charles Knowles
Dr Sara McCartney
Dr Tony Banerjee of HarleyDoc
e-bill service taps into self-pay surge
By Olive Carterton
Independent practitioners, hospitals, practices and clinics are being been offered ‘an efficient, secure and convenient’ way to send invoices directly to self-pay patients.
Online technology specialist Healthcode has expanded its customers’ popular online payment service with patientzone to take on board self-pay patient invoices for providers who use third-party software.
It said this would make it easy for the thousands of providers who use its clearing service to access the patientzone platform so they can send electronic invoices to patients.
As well as being more time-efficient than printing and posting paper invoices and more secure
NEW CHIEF NURSE FOR SPIRE HEALTHCARE
Spire Healthcare has appointed Prof Lisa Grant as group clinical director and chief nurse.
She said a key priority was to expand the hospital group’s professional development and clinical learning programmes, including opportunities for the 5% of colleagues who were apprentices.
Prof Grant added: ‘I’m also looking forward to developing a professional recognition award for our colleagues that recognises outstanding care delivery.’
than sending unencrypted emails, the solution is being promoted as cost-effective when compared with arranging a merchant account or paying with credit card processing fees.
Product marketing manager
Desné Marston said it would be more convenient for doctors, their secretaries and patients.
She told Independent Practitioner
Today secretaries would save time sending invoices and chasing payments, taking payments over the phone or having to take cheques to the bank.
‘This has worked really well for our ePractice customers and we are opening it to all our customers. It is also a great debt collection tool, because once the invoice is sent to patientzone, you can write your own debt collection letters and patientzone will send them out
automatically on your behalf at your timing.’
Patients settling their invoice online receive an electronic receipt to show their payment has been processed.
Healthcode launched online patient invoicing via patientzone to users of its ePractice software four years ago. In 2021, it began a shortfall collection service for hospitals, which automatically identified shortfalls and it used patientzone to send invoices and collect online payments.
Both have proved popular: more than 76,000 electronic patientzone invoices have been processed since launch and volumes have increased year on year.
Providers pay patientzone a fee of 2.5% per paid bill (+ VAT) and a charge of 10p (+VAT) for each reminder letter sent.
Beauty op clinic rated as inadequate again
Care Quality Commission (CQC) inspectors have given Alexandra Private Hospital in Chesterfield, Derbyshire, an ‘inadequate’ rating again following an unannounced inspection in February and March to follow up on previous concerns.
The independent hospital, run by Alexandra Health Care Limited, provides cosmetic surgery to selffunding patients.
Bosses have been told to display the current CQC rating at the hospital location and on their website; ensure they support patients to
TELL US YOUR NEWS
give informed consent for revision or return surgery following the original procedures; and ensure electrical items are safety tested and safe to use.
They must also implement effective governance processes to enable sufficient oversight of performance, quality and risk; see that all patient and staff information is stored as per General Data Protection Regul ations; and ensure patients are able to access appropriate and timely clinical advice after surgical procedures.
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@ip-today.co.uk
Healthcode managing director Peter Connor said: ‘Our clearing service paved the way for the private healthcare sector to adopt electronic billing for insurers and I’m proud to say we’re continuing to break new ground with a service that’s both necessary and timely.
‘As the self-funded market grows, it’s essential that providers can manage the patient journey as efficiently as possible rather than get bogged down with labour intensive and costly admin.
‘Online invoicing via patientzone is painless and more costeffective than alternatives, as well as being a secure and convenient option for patients.’
NHS GPs want to be allowed to charge for more private services
The BMA’s GP committee in England is considering NHS GPs’ calls to allow them to charge patients for more private services. Strong support for the move came from GPs around the country at their annual policy-making conference in London.
The GP committee’s deputy chair Dr Clare Bannon said: ‘The possibility of offering patients services privately that are not available on the NHS is something that is being explored. However, it’s worth noting that there is limited evidence to suggest that offering paid-for services for routine NHS care can help to improve access.’
Healthcode’s Desné Marston
Cromwell starts urgent care centre
By Douglas Shepherd
A new urgent care centre for patients with non-life-threatening injuries and illnesses which need immediate treatment has been opened by Cromwell Hospital. It is open from 8am to 8pm, 365 days of the year and operates a walk-in service. The service is led by emergency medicine consultants, who can refer patients to specialists within the hospital for ongoing care and treatment.
After seeing a nurse on arrival, one of the consultants is on hand to do a full assessment including X-rays, ultrasounds and blood tests, if needed.
Outpatient appointments with a specialist consultant or a GP are available and treatments and investigations may continue in the hospital’s recently opened new acute admissions unit.
Dr Sarah Frankton, hospital chief medical officer, said: ‘We’re really proud to open both our urgent care
centre and acute admissions unit to patients in need of immediate access to secondary care.
‘We know that medical emergencies can be incredibly stressful and having rapid access to consultants, diagnostics and the latest technology and equipment will provide high-quality care and peace of mind for our patients and their families.’
Eye group launches an academy
Independent eye surgery provider
OCL Vision has opened a free education and events platform for optical professionals: the OCL Vision Academy.
The surgeon-owned company, with locations in London and Hertfordshire, offers online webinars, in-person courses and events to give optometrists useful insights and expert knowledge from a team of consultant ophthalmologists.
Participants also have the opportunity to earn CPD points.
The platform runs alongside its shared-care partnership programme, which aims to improve patient choice in the community and connect optometrists and ophthalmologists.
Consultant ophthalmic surgeon Mr Allon Barsam, co-founder of the eye care brand, said the academy would strengthen its relationship with optometrists.
He believes the partnership programme is a powerful way to help surgeons and referrers work seamlessly together.
‘Community care is more important than ever as NHS hospital waiting lists are under significant pressure, meaning that many eye
patients are now relying on optometrists to avoid the difficulties with the NHS.
‘We hope the OCL Vision Academy educational platform will be a useful education and development tool for optical professionals at every stage of their career.’
The academy aims to cover all aspects of cataract, corneal and retinal eye health. It also features an online knowledge base, available to shared care partners, allowing them to search for topics they want to learn more about.
A thumbs-up for the shared care partnership programme and the
academy came from Justin Hardy, lead optometrist and owner of St Albans Eye Care Centre. ‘The scheme gives me confidence that the patients I refer will be looked after with professionalism and receive the highest quality of care available.
‘Once the patient has completed their surgery at OCL, it is reassuring to know that I will be able to provide the correct aftercare and the patient will be coming back to my practice with a personalised plan in place.’
Find out more about the OCL courses by emailing Sofia Carbognon at sofia@oclvision.com.
Chief executive Philip Luce said: ‘I’m delighted to open our new urgent care centre to help people access emergency treatment as and when they need it.
‘The centre is open seven days a week, taking walk-in patients as well as bookings and will be able to refer patients into further services for treatment at the hospital if needed.’
Welcome for private care option on NHS app
The Association of Medical Insurers and Intermediaries (amii) has welcomed a change meaning patients will be able to use the NHS app to opt for private hospital treatment.
It said the push to reduce waiting times relied on more patients opting to use private healthcare and the app would make life easier for those considering a private alternative.
Executive chairman Dave Middleton said: ‘It is pleasing to see steps being taken to support further collaboration between the NHS and the private sector.
‘At a time when the NHS is under unrelenting pressure, the Government has recognised that making the process easier for patients who are open to private healthcare is a key factor in reducing waiting times for routine treatment.
‘I’m looking forward to seeing further details of how it will work in practice for our members.’
Cromwell Hospital in Cromwell Road, south-west London
Optometrist Purvi Thomson, theatre lead nurse Marta Ramos and OCL ophthalmologist Mr Ali Mearza
Tie-up creates orthopaedic ‘super-centre’
Private orthopaedic group Fortius Clinic, a leading treater of professional sportspeople, has acquired Schoen Clinic’s orthopaedic and spinal hospital in London.
It said this would create the UK’s largest single specialty centre of excellence in orthopaedics and sports medicine.
The Affidea Group outfit aims to bring together a super-specialist group of clinical teams to provide ‘world-class orthopaedic care and elite sports medicine across the whole patient pathway – from consultation and imaging through to complex surgery and recovery’.
Fortius Clinic’s chief executive Jim McAvoy said: ‘Fortius has shown the value of super-specialism, with a strong clinical leadership underpinned by a focused governance framework guiding the highest-quality care and a culture of learning and innovation.
‘This acquisition enables us to
build on our vision to deliver outstanding patient care and improve outcomes through the latest techniques and research in orthopaedic medicine.’
Guy Blomfield, chief executive and chairman at Affidea Group, called the acquisition an important milestone for the company.
He said: ‘This strategic move propels our business to new heights, positioning us as a frontrunner in providing top-tier healthcare solutions in a specialised field and it signals our intent to selectively add more centres of excellence to our already extensive offer across the continent.
‘This is an exciting period of growth. I would like to express my gratitude to our Fortius clinical leaders for their contributions and to warmly welcome the Schoen Clinic clinicians to our network.
‘Equally, this presents a remarkable opportunity for our patients,
who will now have access to worldclass orthopaedics services tailored to their specific medical needs all along their medical pathway.’
Fortius Clinic offers a range of surgical treatments, including advanced joint replacements using the latest in robotic technology. It has a collaborative approach through subspecialty teams, sharing knowledge and combining experience.
The company said with its existing facilities, Fortius Clinic now had the extra capacity, options and flexibility to support its consultants and patients at a dedicated centre of excellence.
Schoen Clinic London becomes an integral part of Fortius Clinic and Affidea Group and is being
rebranded as Fortius Clinic London.
Affidea Group is the largest European provider of advanced diagnostics, out-of-hospital and cancer care services, operating over 330 clinics, plus centres of excellence in a variety of specialties where over 12,000 professionals are seeing more than 12m patients every year across 15 countries.
Fortius Clinic was founded in 2009 by a group of consultants and specialists. It is the largest single group of orthopaedic and MSK consultants in Europe, with more than 200 specialists, from surgeons to sports physicians, rheumatologists, pain management specialists, radiologists, and anaesthetists.
Vein specialists raise £1.5m to expand clinic chain
A chain of medical clinics specialising in treating varicose veins and thread veins has raised £1.5m in debt funding from Frontier Development Capital (FDC) to help it expand into new locations nationwide.
The UK Vein Clinic group, operating under the brands of Dr Newmans Clinic and UK Vein Clinic, is believed to be the largest independentlyowned chain of its type in the UK.
Based in London’s Harley Street, it has a presence in 16 cities including Brighton, Bristol, Exeter, Cardiff, Cambridge, Leeds, Sheffield, Liverpool, Manchester, Newcastle, Edinburgh and Glasgow.
It aims to use the funding to support its plans to open clinics in ten new locations over the next two years.
The group is run by Jason Powell, who was chief executive of Premier Medical Group before it was sold to Capita for £62m in 2010, and Dr Peter Finigan, a medical entrepreneur
with over 30 years’ experience in general practice and vascular medicine.
They joined forces in 2010 to acquire Dr Newmans Clinic, which specialises in the noninvasive treatment of thread veins and is the only service of its type where all procedures are done by GPs.
In 2020, it started UK Vein Clinic and has a
team of 65 clinicians and admin staff. It plans to create about 50 new jobs as part of the roll-out.
Director Jason Powell said the NHS and private medical insurers had restricted treatment for varicose veins to the most severe cases, so people were increasingly willing to fund the treatment themselves.
Justin Sorby of FDC added: ‘Jason and Peter lead an impressive team who have differentiated their service through the use of experienced vascular consultants and a care pathway that puts patient outcomes at the centre of the business.
‘The group is already the UK largest independent chain of its type. With the increased focus on health and well-being, an ageing population and restrictions on NHS treatments, their services will be in growing demand in the future. We are pleased to be able to provide the funding they need to support their expansion plans.’
The Fortius Clinic – formerly the Schoen Clinic – in Wigmore Street, London
Jason Powell of UK Vein and Justin Sorby of FDC, with Prof Stephen Black, Dr Peter Finigan and Mr Ed Sideso of UK Vein.
An NHS trust hikes its private service
Philip
Housden reports on private progress at one of London’s biggest NHS trusts, University College London Hospitals NHS Foundation Trust
The UCLH hospital boasts some of the country’s most respected teaching hospitals.
They include the University College Hospital flagship site and the highly specialist National Hospital for Neurology and Neurosurgery, among Newsweek magazine’s top three neurosurgical hospitals in the world in 2022.
UCLH has one of London’s most modern estates and the trust has invested many billions of pounds in it over the 20 last years.
Most recently, this included the opening of two new facilities: the Royal National ENT and Eastman Dental Hospitals (2020) and The Grafton Way Building, housing cancer services (2022).
UCLH directly offers private healthcare services in some specialties under the umbrella brand of UCLH Private Healthcare as well as a long-standing partnership with HCA to deliver a private adult blood cancers service on site.
Private patients have been seen for a range of conditions at UCLH for many years, but the service has only been consolidated under the UCLH Private Healthcare brand since 2019.
UCLH Private Healthcare currently offers private neurology, neurosurgery and maternity services in dedicated private facilities and a paediatric oncology and teenage haematology service integrated with the NHS service.
Patients present with conditions ranging from the most common, such as recurrent migraines or balance disorders, to very complex neurosurgery and teenager cancer cases.
Private patients have access to
the same world-class team of consultants and other health professionals, but with the customer service you would expect from a private setting; from consultantled care to private en suite bedrooms and enhanced menus.
As the service is part of a major NHS hospital group, patients additionally benefit from the high level of specialist infrastructure and back-up emergency support around the clock, including onsite intensive care and high dependency facilities, if required.
Many consultants hold dual clinical and academic contracts with UCLH and University College London, which supports the rapid translation of evidence-based research into clinical practice.
The high degree of specialism and complex work also attracts world-class specialist consultants, nurses and allied health professionals to the workforce, which then supports the development of highly expert teams.
Within complex specialties such as neurosciences, these subspecial-
underwent a £3m refurbishment of its 17-bedded ward and hotel finishes in all private rooms and shared spaces.
The ward also incorporates specialist diagnostic facilities for neurosciences: a video-telemetry suite supporting diagnosis of conditions such as epilepsy and a purpose-built diagnostic suite for autonomic system disorders, covering conditions such as excess sweating or fainting episodes. Both services are provided by UCLH’s expert diagnostic teams.
The University College Hospital Trust includes the highly specialist National Hospital for Neurology and Neurosurgery
In 2021, the private healthcare team took over the management of The Private Consulting Rooms in Queen Square, which provides outpatient facilities for neurological conditions. This helps support a seamless integration between outpatient and inpatient care.
In the last year, The Fitzrovia Private Maternity Ward at UCH has also had its five postnatal rooms refurbished to high specifications. The private maternity market has very high expectations of the physical environment and customer service, and feedback from patients about the new ward has been extremely positive.
ists work together as part of a multidisciplinary approach to care, with each team member providing a different perspective on the patient’s condition and treatment options.
As with all NHS private patient units, all the profits are reinvested back into services at the trust, ultimately benefiting NHS patients.
‘UCLH Private Healthcare as a brand is very much in its infancy, albeit with a long-established and respected clinical offer at its core,’ says director of private healthcare Kerensa Heffron.
‘Since our inception, we have been busy developing our infrastructure and have made significant investment in our private estate, which we are really proud of.’
The past three years have mostly been focused on developing the private healthcare facilities and services at UCLH alongside supporting the NHS team through the pandemic and into recovery.
In 2022, The Bloomsbury Private Ward at The National Hospital for Neurology and Neurosurgery
The refurbishment also included two new labour rooms, allowing the team to offer vaginal as well as C-section deliveries.
There are ambitions to expand UCLH Private Healthcare’s offer to accommodate even more specialist services.
Kerensa says: ‘We have some really exciting service developments in the pipeline which will open our private healthcare services up to a much wider cohort of patients in the future.’
Private patient income at the trust grew from £5.9m to £7.3m in 2021-22, the last published trust accounts. This is a 25% rise, but still well below the trust record of £21.7m achieved pre-pandemic in 2019-20.
The trust is ranked 14th in private patient earnings in the NHS and eighth in London. UCLH’s private patient income represents 0.59% of total trust revenues, again well down on the 2-3% achieved in the previous decade and demonstrating a likely significant headroom for future growth.
Philip Housden is director of Housden Group
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Pension tax trap for the unwary
High-earning independent practitioners who opted out of the NHS pension were shocked to find themselves unwittingly re-enrolled thanks to a new Government push to encourage retirement saving. Financial planning experts warned the move could invalidate precious ‘fixed protection’ on their pension savings and leave some vulnerable to huge tax penalties.
A senior London consultant on pensionable pay of £156,520 a year and with ‘added years’, for instance, could be hit by a £165,000 tax bill on retirement at 60 if protection on a £1.8m pension pot was chopped to £1.5m.
After taking advice from Cavendish Medical specialist financial planners, doctors were
able to restore their personal taxfree lifetime allowance to £1.8m –provided they began no new pension arrangement.
But it was feared other busy consultants could have missed the boat because many of them admitted they did not read their NHS payslips.
Part-timers lag behind in pay stakes
A consultants’ leader revealed why so many part-time independent practitioners were feeling the pay pinch – they were a decade behind.
BMA Consultants Committee
chairman Dr Paul Flynn said NHS remuneration in real terms was back where it was before contract changes in 2003.
An ongoing NHS pay freeze and ‘numerous below-inflation pay awards’ had all taken their toll.
And, with pension changes, it meant most consultants had seen their take-home pay fall in 2013, he said.
Clinical photo danger
The launch of an app for doctors wanting to share clinical photos sparked a defence body warning about the risks of doing so either through that medium or website.
Dr Mike Devlin, the Medical
Defence Union’s (MDU’s) head of advisory services, said: ‘There are many circumstances where doctors feel it may be beneficial to take a photograph of a patient’s clinical signs or record a consultation.
‘However, it is important that they have the patient’s informed consent before doing so and they must follow GMC guidance on making and using visual and audio recordings of patients.’
The MDU had received more than 100 calls in five years about taking and sharing photographs, audio and video recordings of patients. In some cases, doctors received complaints from patients after taking pictures of the recordings.
Welcome for doctors’ input into inspections
The Care Quality Commission (CQC) plans to beef up its inspections in the wake of severe criticism over well-publicised previous failings were given a cautious welcome in the independent hospital sector.
The Independent Healthcare Advisory Service backed many of the proposals, which included giving a quality rating to independent acute hospitals for the first time.
But the private body warned that, as all NHS trusts would be rated first, this would leave independent hospitals without a
rating, posing potential issues for the sector when tendering for NHS-commissioned services.
Patient trials can help boost profits
Independent practitioners should consider the possibility of doing clinical trials because it was a chance to grow their business, according to a consultants’ group director.
Chris Adams, director of development at Re:Cognition Health, said clinical trials also gave consultants something to ‘sell’ when talking about their services to NHS GPs.
The overall revenue per patient was significant, at over £14,000 per patient, so was a business opportunity in its own right.
Dating-style firm is a promotion tool
Private consultants found a new way of getting in front of potential GP referrers.
They were offering themselves as unpaid speakers for medical education programmes held at surgeries for doctors and nurses. Practices chose the specialties and a firm arranged for the relevant experts to go to them.
Are you offering your patients the full range of payment functionality they need?
Introduce smart payment solutions into your practice to meet the increasing patient demand
Civica Medical Billing and Collection service enables:
Will self-pay keep on
LaingBuisson’s Self-pay Report, 5th Edition, has now been published. Its author Liz Heath (right) reflects on what it tells us about the market – a market that has underpinned growth for many providers over the last two years and has led to a surge in demand for consultations and diagnostics
on rising?
PATIENTS ARE seeking out selfpay options for surgery in greater numbers, as well as the vast range of other self-pay services from virtual and online GP and medical services right through to complex cancer care.
Data from various sources backs this up, though it suggests demand has steadied a little over recent months. However, this is set in the context of higher self-pay activity than pre-2020.
Consumer confidence is key to discretionary healthcare spending, whether this is for an MRI scan, a knee replacement or a face lift. Perhaps surprising, then, that cosmetic surgery demand rose in the last 18 months, not just, it appears, as a result of post-pandemic catch-up.
For self-pay elective procedures, providers all view the over-60s market as their core self-pay market – the profiles are slightly different for cosmetic surgery.
The growth in this demographic and, to some degree, their insulation from some of the impacts of the current financial crisis, suggests a sustainable market in some of the core specialties such as orthopaedics, general surgery and ophthalmology.
For others, private healthcare is only affordable with the help of payment plans and other options to spread the cost. This segment of the self-pay market does appear to be most at risk from continuing economic uncertainty and high costs of living.
Covid’s effect
The cycle of growth and decline in self-pay treatment has historically tended to follow the UK economic cycle. However, Covid-19 has had a much more pronounced impact on self-pay activity since early 2020, leading into the current situation where NHS access appears to be overriding concerns around economic impact.
Nevertheless, we cannot ignore the influence of economic factors, whether macro-economic or those related to individual circumstances and personal consumer confidence.
Our research indicates the UK self-pay market continues to grow and that this trend will continue over the next three to five years.
The rate of growth may slow a
Our research indicates the UK self-pay market continues to grow and that this trend will continue over the next three to five years
little, but there is a genuine sense of optimism among almost everyone we engaged with, although a note of caution was raised by some around the constraints such as staffing and capacity on realising the growth potential.
Of note is that we are seeing growth in demand for self-pay across all areas of the UK, including areas that have traditionally not been private healthcare ‘hot spots’ such as Wales and Scotland.
What’s driving demand?
The highest demand for self-pay procedures remains in orthopaedics – for example, hip and knee replacements – and ophthalmology –cataract surgery.
These procedures and specialties very much reflect an ageing demographic with those over 60 being the largest self-pay group. But other specialties such as general surgery and gynaecology have also seen growth in younger age groups, who are more likely to seek out ways of spreading the cost of their treatment.
While frustration with long NHS waits and difficulty accessing NHS services is the primary driver, rapid access, affordability and the certainty in being able to plan treatment are also key decisionmaking factors.
We are also seeing the emergence of different types of self-pay consumers. There are those who weight up the pros and cons of waiting for NHS diagnosis or treatment and, having undertaken their research and perhaps had discussions with friends and family, make a specific choice to seek out a particular provider or treatment option.
For others, an element of desperation fuels their desire to seek out private treatment – maybe for the first time – when faced with
➱ continued on page 14
GoPrivate.com has seen its web traffic increase from two million to four million visits in just over two years
WHAT DOES ALL OF THIS MEAN FOR CONSULTANTS AND SPECIALISTS?
Research from multiple sources has indicated that many consumers are being drawn towards private healthcare options for the first time.
They may have little knowledge of how to navigate the system and need support along the way. Crucially, it is vital that they have prompt responses to their inquiries and are signposted to the right choice for them.
Inaccurate contact information or a lack of response gives a poor impression to a potential patient in a climate where we are all used to immediacy and ‘on-demand’ services.
the reality of long waits, the experience of demand management by commissioners or just their own deteriorating clinical situation.
Inquiries about private healthcare in general or how to navigate the system have grown significantly. GoPrivate.com has seen its web traffic increase from two million to four million visits in just over two years.
While younger consumers are often thought of as being much more digitally ‘savvy’, older generations are now much more engaged in the digital world and are actively seeking out information and options.
Talk about quality and safety
For those new to private healthcare, there may still be concerns around quality and safety. It is clear that many consumers undertake research to inform their decision-making, and prominent information about quality, safety and outcomes is becoming more important, as are reviews from trusted sources.
Openness, publication of quality data and outcomes by individuals and groups is becoming increasingly common and contributes to informed decision making.
Future prospects?
In 2019, only 11.1% of respondents to LaingBuisson’s survey intended to allocate more than 30% of their marketing budget to self-pay.
At the end of 2022, this had risen significantly to 41.7%. Investment in online, digital and patient acquisition are likely to feature strongly and were viewed as the most successful channels.
This is something that consultants and specialists can also take on board when considering how best to connect with potential patients.
Affordability is frequently cited as a key decision-making factor by patients and visibility of consultant fees is a positive step. LaingBuisson’s pricing analysis found that most procedure prices reviewed had increased broadly in line with general and medical inflation, but there is still a vast range in some cases between highest and lowest prices.
The guide price for a primary knee replacement varies across the UK between around £9,000 and £17,000, which, from a consumer perspective is unhelpful and confusing. The average guide price in 2023 is £13,781; a rise of 5.17% on 2021-22.
‘Value’ options offer a more affordable access route to diagnosis or treatment and we are seeing this with some NHS private patient units as well as providers such as Practice Plus Group.
The expansion of single specialty clinics, imaging and day surgery centres presents the opportunity to offer competitive pricing alongside rapid access and efficient clinical pathways.
From a consumer perspective, the important thing is that there is now a much bigger choice of provider, access and pricing options than just a few years ago.
In general, there is also improved pricing transparency, although some providers are still not publishing guide pricing on their websites.
Certainty is one of the factors cited by consumer research – whether this is related to date and time of consultation, diagnostics or surgery or around reassurance of a positive outcome.
The ability to have certainty around planned treatment is definitely one of the factors driving interest in selfpay. From a consultant perspective, clarity and discussion around the planning of treatment is therefore vital.
We found the view on growth prospects reasonably consistent, with high single-digit growth being viewed as achievable year on year.
However, while this projection is based on what appears to be a reasonably solid market at present, there is always concern that at
some point, economic concerns will provoke caution from consumers – whether or not NHS access improves.
Taking a different perspective, the recent rise in self-pay demand may be signalling a permanent shift in our expectations around NHS-funded care and may under-
pin a very different landscape in which a ‘mix and match’ approach to private and NHS funded care is the reality for many people.
LaingBuisson’s Self-pay Report 5th Edition is now available in digital and hard copy at www. laingbuisson.com/healthcarereport-store/
Choose protection that wants to help
Access to the advice line is unlimited, and the number of times you call has no impact on your subscription. Whatever the issue, you can be confident of 24/7 support, 365 days a year. Our experts are always there, ready to provide you with support when you need us.
For just £549, consultants working in the NHS can feel safe in the support membership brings. We also offer competitive, tailored prices for consultants working in Private Practice.
OUTSOURCING YOUR ADMINISTRATION
Free yourself from
Outsourcing your administrative tasks in private practice has some big advantages, says Derek Kelly
TIME IS a valuable asset and, in the fast-paced world of business, it holds true that time is money. This same principle applies to the field of medicine.
Doctors can attest that time plays a critical role in the difference between saving a life and losing a patient. When patients seek medical assistance, they expect immediate solutions to their problems, but ,unfortunately, the waiting time can often be excessively long.
The issue at hand extends beyond doctors being overwhelmed with patients; it is primarily due to their limited time to handle all tasks efficiently.
Many doctors face the burden of excessive clinical documentation, leaving them with insufficient time to nurture the doctor-patient relationship.
To address this challenge, outsourcing administrative tasks has emerged as a practical solution for doctors in private practice.
The growing trend of healthcare outsourcing stems from its proven benefits in the industry. Let’s explore some advantages of outsourcing medical tasks in private practice.
Enhanced focus on patient care
Private doctors constantly face the increasing demand for high-quality, patient-oriented and timely documentation.
However, this demand has led to time pressure and reduced job satisfaction among doctors, as they find themselves spending more time on clinical documentation rather than interacting with patients.
Doctors spend about three hours each day, on average, on documentation tasks. That’s equivalent to the time it takes to see an additional eight or nine patients. By outsourcing administrative documentation tasks and prioritising the value of face-to-face interactions, doctors can improve the most crucial aspect of healthcare: the doctor-patient relationship.
Outsourcing private practice administrative tasks proves to be an effective strategy. It allows doctors to focus on patient care, spend more time with their patients and minimise their computer-related tasks.
This not only eases the workload but also enhances overall efficiency in attending to patients’ needs. Outsourcing enables doctors to maximise their time, see
more patients and provide focused attention to each individual’s medical concerns.
Expert handling of jobs
Another significant advantage of outsourcing administrative tasks is the opportunity to delegate the job to an expert.
By doing so, doctors gain more time for quality patient interactions, enabling them to fulfil their primary function of diagnosing and treating patients.
Outsourcing offers access to a diverse pool of skilled professionals who excel in various administrative tasks.
While retaining control over core practice areas, doctors can delegate various tasks, including referrals, diary management, inbound and outbound phone calls, insurance verification and
drudgery
pre-authorisations, billing and other back-office responsibilities.
Time and cost savings
Saving time and money remains one of the primary motivations for businesses to embrace outsourcing. By outsourcing, private practices can significantly reduce the expenses associated with hiring additional office employees.
It eliminates the need to invest valuable time and money in training new employees, as the outsourcing partner takes charge of such training and management tasks.
Outsourcing also leads to substantial cost reductions in office supplies, furniture and computer hardware, enabling practices to reinvest in patient services and amenities that enhance overall patient care.
Improved patient experience
One of the most common patient complaints revolves around waiting time. Long waits lead to dissatisfaction, causing patients to seek alternatives and negatively impacting their perception of the clinic’s customer service.
Outsourcing billing and incoming calls can help reduce queues, thereby improving the overall patient experience.
By thoroughly examining eligibility requirements and completing pre-authorisations, practices can ensure insurance coverage and provide accurate information to patients.
Typically, patients spend an average of five to seven minutes on hold when calling a medical practice, while those waiting at the front desk may also experience delays. At Medserv, we can efficiently manage incoming calls, handle billing-related inquiries, schedule appointments, process prescriptions and address other patient needs.
Outsourcing these services sig-
Doctors spend about three hours each day, on average, on documentation tasks. That’s equivalent to the time it takes to see an additional eight or nine patients
nificantly contributes to enhancing the overall patient experience. It represents one of the most promising applications of technology in the medical field. By eliminating inefficiencies and delegating tasks that can be handled externally, doctors can achieve optimal practice efficiency.
Embracing technology presents an opportunity to spend more time cultivating the doctorpatient relationship rather than being consumed by excessive documentation. By outsourcing administrative tasks, doctors can eliminate the factors hindering their ability to perform their medical duties efficiently.
The benefits are not limited to doctors alone. Patients also stand to gain. Ultimately, the care provided to patients serves as the core product and ensuring their satisfaction relies on delivering value during their visits.
Allocating more time for each patient visit enables doctors to understand patients’ needs and deliver the quality they deserve. If you embrace the advantages of outsourcing, you will witness the positive impact on both your practice and patients.
Derek Kelly (pictured right) is marketing manager at Medserv
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
Don’t fall foul of drug
Make sure you get your adverts right when it comes to prescriptiononly medicines. Victoria Avery, of the Advertising Standards Authority, spells out the rules and offers help to doctors and clinics who want to ensure they comply
AS THE regulator for the advertising of prescription-only medicines, the Advertising Standards Authority takes its responsibility seriously and we expect any practitioners advertising their services to do the same.
And when it comes to prescription-only medicines, the rules are simple: they can’t be advertised to the public.
In practice, this strictly limits where and how ads can talk about products like Botox, Kenalog or Viagra, among others. It’s important that consumers are protected, and so advertisers need to understand and follow our rules or risk their ads being banned.
Following legislation, the UK Code of Non-broadcast Advertising and Direct and Promotional Marketing (the CAP Code) expressly states that prescription-only medicines or prescription-only medical treatments may not be advertised to the public.
This covers all forms of advertis-
ing, from websites to social media to leaflets.
Ads can mention the consultation for a treatment that would use a prescription-only medicine; for example, ‘a consultation for lines and wrinkles’ or ‘a consultation for erectile dysfunction’ is likely to be acceptable.
But we view virtually any reference to a prescription-only medicine as promoting that medicine, and therefore a breach of rules. Stick to talking about the consultation and don’t mention the medicine.
No celebrities
Ads must not use any celebrities or health professionals to market their products.
They mustn’t mislead consumers, exaggerate the efficacy of any treatments or omit any relevant terms and conditions for treatment.
They can’t use ‘before’ and ‘after’ pictures and they should be
An ad mentioning ‘Back-to-school Botox’ was banned by the ASA
responsible, avoiding playing on people’s insecurities or offering inappropriate pricing deals.
For example, this year we banned an ad that mentioned ‘Back-to-school Botox’, for both advertising a prescription-only medicine and also exploiting women’s securities about their bodies and the ageing process. When it comes to websites, very limited references to prescriptiononly medicines may be acceptable as long as they don’t appear on the home page and claims don’t go
drug advertising rules
beyond balanced and factual information typically found in the patient information leaflet, ‘summary of product characteristics’ or similar non-promotional information that comes with the product. It should also be presented as a potential outcome of a consultation. Casually browsing consumers must not be able to come across information relating to prescription-only medicines with ease.
Factual information only
You may include a price list – but not on the homepage – with a range of treatments available. But the price list should not include claims about the prescriptiononly products or actively encourage viewers to choose a product based on the price, such as a discount price offer.
There are a few exceptions. Prescription-only medicines can be advertised to the medical, dental, veterinary and allied professions but, again, the ads should
Working with Meta, we’ve seen 50,000 Botox ads removed from social media since 2020 and we’re consistently taking action against ads that break our rules in this space
only focus on balanced and factual information about the products and not make any claims outside of that.
The advertising of prescriptiononly medicines, particularly online, remains a high priority concern for us. That’s why we’re taking action to ensure that advertisers understand our rules and are following them.
Thanks to our data science team, we’re moving to a more pro-active method of regulation, processing more ads than ever before to quickly get those that are a problem banned.
Our rolling programme of monitoring and enforcement ensures that advertisers know what the rules are and follow them carefully. Working with Meta, we’ve seen 50,000 Botox ads removed from social media since 2020 and we’re consistently taking action against ads that break our rules in this space.
If you’re offering treatments
that use prescription-only medicines and you’re not sure if your ads follow the rules, the ASA can help.
We offer a copy advice service that offers free advice about any ad campaign you’re thinking of running. We provide a 24-hour turnaround service or, if your query is urgent, for a fee we can provide advice with a four-hour turnaround. Head over to our website www.asa.org.uk for more information.
We know the vast majority of advertisers want to get it right. Our rules are designed to protect consumers, so it’s vital that you understand how they work. And if you’re ever unsure, get in touch.
Victoria Avery (right) is an investigations executive at the Advert ising Standards Authority (ASA)
OPHTHALMOLOGY CLAIMS
Defending claims is eye-watering
Claims experts Claire Wratten and Pete Renwick (right) discuss what is to be learned from the claims they have received from ophthalmology members of the Medical Defence Union (MDU)
THE MDU regularly assists ophthalmologists with a variety of issues ranging from regulatory matters and inquests to complaints and medico-legal or ethical scenarios.
Many ophthalmologists work in private practice and this review focuses on the last ten years of experience in handling clinical negligence claims against ophthalmology members (see box on top of opposite page).
The most common reason for a claim was following cataract surgery.
Claims were often brought when the wrong lens had been used. Another common allegation was that the consent process had been inadequate and that the claimant had not anticipated they might continue to need glasses following surgery.
Claims were also brought follow-
ing postoperative complications such as glaucoma, retinal detachment, retained lens fragments and endophthalmitis.
There were a significant number of claims in relation to refractive surgery. Slightly more of these related to lens surgery than laser surgery, although both primarily occurred due to an alleged failure of the treatment or postoperative complications.
These issues often arose due to alleged failures to correctly assess suitability for treatment, alleged failure to obtain accurate optical values prior to surgery and alleged inappropriate choice of treatment.
Postoperative concerns and complications included an on-going need to wear glasses, corneal damage and dry eye syndrome.
There were also several claims related to lens surgery performed
for age-related macular degeneration, which concerned allegations about consent and, in particular, failing to advise the patient that they were not a suitable candidate for the surgery and an unsatisfactory outcome in terms of improvement in vision.
The primary cause of claims following blepharoplasty was postoperative scarring. Other issues raised were postoperative pain, blurred vision and a failure to pick up on other conditions.
Additional cosmetic procedures that were subject to claims included corneal tattooing, surgery to remove molluscum contagiosum and fat transfer procedures.
The majority of claims relating to an alleged delay in diagnosis were due to an alleged delay in diagnosis of an intracerebral
tumour, including prolactinomas, meningiomas or glioblastomas, or an alleged delay in diagnosis of glaucoma.
The potential for claims against ophthalmologists following diagnosis of an extra-ocular condition highlights the importance of examining the eyes holistically and considering pathology outside of the eye as a cause for visual impairment.
Outcome of the cases
A clinical negligence claim can either be settled by the defendant, with a payment of compensation being made to the claimant; or it can be discontinued, become statute-barred – out of time – or a case can be won at trial by either party to the claim.
There is a time limit for bringing a claim of three years from the date
MANAGING THE RISK
Claims involving ophthalmologists are made for a wide variety of reasons. However, there are some common risk factors, which, if managed appropriately, can help to reduce risks. These include:
Ensure patients understand the potential risks and benefits of the procedure in order to give their consent
Provide written information leaflets, if possible, as this may help the patient to remember what was said in a consultation so they can reflect on it later in their own time
Document discussions with patients and the consent process clearly
Be aware of relevant guidance such as from the GMC on consent, royal college guidance and NICE guidelines.
Ensure you have the appropriate training and experience to carry out a procedure. Consider referral to a specialist in those cases which fall outside your skill set or knowledge
If things go wrong, be open and honest with the patient by providing an explanation of what has happened and the possible short- and long-term effects of this. Say sorry and get advice from your defence body if you believe the incident triggers your organisation’s duty of candour requirements
of incident or three years from when the patient became aware that they may have received negligent care.
The date of knowledge may be some considerable time after the actual incident – for example, if the claim relates to a delayed diagnosis of malignancy – and these time limits do not apply to patients who lack mental capacity and for children, for whom the three-year period does not begin until they reach their 18th birthday – or in Scotland, their 16th birthday.
This means that a claim may be brought many years after the treatment in question, which underlines the importance of keeping clear and accurate records, but also it can be helpful to retain copies of any patient information leaflets that were available at the time.
The vast majority of claims brought against ophthalmologists were either discontinued or became statute-barred, with only 22% being settled, and one case was won at trial.
In general, very few clinical negligence claims end up at trial, because the whole claims process is designed to encourage exchange of information between the parties and resolution of the case without resorting to a trial.
The MDU will always involve the member in the management of their claim and, depending on the stage at which the case is resolved, this can include an
REASONS FOR A CLAIM
In the majority of cases, where the sum of damages paid was below £40,000, the costs were greater than the damages paid, sometimes by as much as four times the sum.
opportunity to discuss their case with the instructed solicitor, barrister and medico-legal experts. Views of the member are very important in decisions on how to manage the claim, including whether to make an offer of compensation to the claimant.
Compensation costs
For damages paid by the MDU on the claims that were settled, the sums ranged from £100 to almost £400,000 for a claim following complications arising from laser refractive surgery.
The purpose of compensation is to put the patient back in the position they would have been in had it not been for the problems caused by negligence.
In addition, when a claim is settled by a defendant, they are also responsible for payment of the legal and expert fees incurred by the claimant’s solicitor in bringing the claim. These fees can often outstrip the damages paid to the claimant.
For example, in a claim for which damages were agreed at only £85,000, the legal costs incurred by the claimant – and paid for by the MDU – amounted to £230,000.
Solicitors’ costs
The disproportionate impact of costs incurred by solicitors for the claimant is even more marked in cases where damages are lower.
Even if no payment of damages or claimant costs is made by the MDU, it can incur significant defence costs. These costs go to pay the solicitor, barrister and medico-legal experts instructed on behalf of the defendant ophthalmologist.
For example, in this ten-year period, we successfully defended a
claim leading to its discontinuation by the claimant, but incurred almost £60,000 in defence costs in doing so.
Due to legal reform called ‘qualified one-way costs shifting’, introduced in 2013 in relation to funding clinical negligence claims, it is very hard for the MDU even when we successfully defend a claim to recover any of the costs incurred.
Claire Wratten is claims team manager and Pete Renwick is lead claims handler at the MDU
CASE STUDY: INFECTION FOLLOWING CATARACT SURGERY
The following anonymised case example illustrates the type of scenario that can evolve into a clinical negligence claim.
An MDU member was notified of a claim from a former patient alleging that he had performed inappropriate cataract surgery, which resulted in postoperative complications causing considerable loss of vision in one eye.
The claimant had a history of chronic obstructive pulmonary disease (COPD) which had worsened around the time of the procedure. While still in hospital, the patient had started to suffer pain in his eye and was discharged and advised to take analgesia and use topical steroid drops.
A few days later, the claimant returned to hospital because of worsening vision, where a vitreous aspiration was performed and a provisional diagnosis of infective endophthalmitis was made.
The claimant was treated with intravitreal antibiotics and was monitored in hospital, and it was later decided he required a vitrectomy. He never fully recovered his vision in the affected eye.
It was alleged the member should not have performed the surgery while the patient was unwell with COPD, that he failed to diagnose the postoperative infection fast enough and should not have allowed the claimant to be discharged home. The claimant was seeking around £500,000 in compensation.
Experts instructed by the MDU were not critical of the member for operating at that time, although acknowledged that consent and the records could have been more detailed.
In the experts’ view, the claimant may not have suffered from infective endophthalmitis, but a sterile inflammation. The MDU was also able to show that the member’s postoperative management was appropriate and lodged a defence to the claim denying negligence on this basis. In light of this, the claim was discontinued by the claimant’s solicitors.
Patient safety is at a pivotal point
Quality and safety issues have been dominating the Independent Healthcare Providers Network (IHPN) agenda. Its clinical director Dr Howard Freeman (right) reports – and asks for consultants’ help
THE IHPN IS looking to welcome volunteer consultants to join our recently formed ‘share and learn’ sessions.
This is a small community of senior clinical leads from independent providers who meet in person – safely and maintaining strict confidences – to discuss reallife case studies and the associated patient safety issues.
Meetings are usually held in London and again, at our most recent session, we found it a very powerful process which throws up real challenges, opportunities to learn and to reflect and change clinical practice.
One of the things our year-old group would greatly value is for greater insight and perspective from senior consultants – surgeons or anaesthetists particularly. I suspect the value would be very much reciprocal.
So I would like to welcome and strongly encourage any consultants of any specialty reading this in Independent Practitioner Today to consider if you might be interested and able to spare an hour.
You could either bring forward a case of your own or just be willing to bring your own expertise and perspective to this group. Do please contact linda.jones@ihpn. org.uk if you are interested.
I was very pleased to chair the IHPN’s annual quality and safety conference recently at the Law Society, in central London.
Now in its fifth year, the meeting
had a particular focus around the theme of patient involvement in safety and quality.
Run by the IHPN in partnership with the Care Quality Commission (CQC), it is one of the highlights of our calendar. It brings together colleagues from member organisations, many of whom are clinicians, from across the network.
Participants learn from each other about what makes ‘great’ in quality and safety and they get tips from expert speakers to help deliver the safest possible services in the sector.
Changes afoot
The backdrop for this year’s event is that, over the course of the next 12 months, we are seeing significant changes in the patient safety world. These are both an opportunity to do things better but also may represent challenges we must rise to meet.
This conference provided a fantastic
and timely moment to hear from key leaders at the heart of the patient safety world, to understand the impact of upcoming developments on the independent healthcare sector and to share experiences and ideas.
The quality and calibre of speak-
ers this year was the highest I have ever seen.
Opening the conference, the CQC’s chief inspector of healthcare, Dr Sean O’Kelly, spoke about the importance of patient safety and how the watchdog is working to improve it across the healthcare system.
Other high-profile speakers included Dr Henrietta Hughes, patient safety commissioner for England; Nick Day, policy and programme lead at the National Medical Examiner System, and Dr Rosie Benneyworth, chief investigator at the Healthcare Safety Investigation Branch (HSIB).
They and others from the CQC shed light on the ways the patient safety system is changing and what the impacts might be –whether it be the CQC’s changing regulatory approach or the merger and restructure as HSIB becomes the Health Services Safety Investigation Body (HSSIB).
All these seismic moves, along with
the introduction of new policies, frameworks, and ways of working, such as the Patient Safety Incident Response Framework (PSIRF) could have a significant impact.
I believe this is an opportunity we must collectively grasp to make sure the safety issue is raised to the level of prominence, focus and attention it should always be. And that it remains there.
James Titcombe, of the Harmed Patient Alliance, was perhaps the most powerful speaker of all. He is an engineer by profession, but is also now an expert in patient safety, having sadly suffered the loss of his son Joshua after negligent care in the days immediately after his birth.
It was and is a difficult story to hear – I urge any reader unfamiliar to read James’ book, Joshua’s Story Despite the terrible circumstances he and his family have endured, James spoke on the day – and again in a short video featur-
ing the main speakers, which gives a flavour of their sessions and the day overall, available to watch on our website – of cause for optimism and positivity.
He spoke of the vital importance of creating a ‘just culture’ for both patients and staff, and what that entails: a recognition that errors in healthcare do happen, but most of the time when things go wrong, it is not the the fault of any individual but the wider system and the processes.
James was clear that we can only make progress if staff feel supported, confident and safe in engaging in those processes, so that we can be open and honest.
A positive reaction
Many people gave much positive feedback and found the networking opportunities invaluable. It is worth remembering in these days where Zoom and virtual events have become so widely used, that
Most of the time when things go wrong, it is not the the fault of any individual but the wider system and the processes
there is nothing which quite beats being there in person.
I believe this was particularly the case given the content and the stories several presenters told, with examples of patients, which were both emotive and powerful.
The patient stories which were told by Sean O’Kelly, by Henrietta Hughes and by James Titcombe especially did a quite remarkable job of making the need for patient safety ‘real’.
We all learn by taking the oppor-
tunity every now and again to reflect, to think about where things have gone right or wrong.
Let me return to some words of James Titcombe to sum up the very essence of what all this is all about and why it matters.
He said: ‘It’s been a huge journey. It’s coming up to 15 years since Joshua died and there have been changes. I think that they’ve been much slower than I would have liked to see, but right at the moment is a really interesting time for patient safety.
‘We’re at a really pivotal point, and what keeps me going really is, if I can use Joshua’s story to kind of reinforce – actually – what could the future look like if we got this right? What would that look like?
‘And I think “Keep that vision in our minds”. There is a better place and we can get there if we all carry on working together. So, yeah, that’s very much the message that I’d like to give people.’
IMPORTANCE OF PATIENT FEEDBACK
Communication is key
People buying health insurance have high expectations of the care they should receive, so their feedback is valuable in helping improve our service, writes Bupa’s Tricia Carley-White (right)
key to happy patients
While positive feedback is always great to hear, the learnings from when things don’t go so well are valuable in helping us to deliver for patients
OUR AMBITION at Bupa is to be the world’s most customer-centric healthcare company. This means having a commitment to excellent customer experience, through great service and value, frictionless access and quality healthcare.
We’ve set ourselves a performance indicator of achieving a net promoter score (NPS) of 80, in line with the most customer-centric organisations in the world. NPS is the likelihood of our customers recommending Bupa from -100 to +100.
We have a team focused on clinical quality and part of their job is to examine all the feedback we receive, both good and bad, to look at ways we can improve the patient journey.
To help us make sure we are on target, we gather feedback from Bupa patients in a number of ways. Depending on the care that they have had, people are sent our hospital inpatient survey, outpatient survey or GP appointment feedback survey to complete afterwards.
Information from the sixmonth period from November 2022 to April 2023 shows that those participating in our hospital inpatient survey gave their hospital an NPS of 80 and those completing our outpatient survey scored Bupa 81.
These high scores tell us that patients would recommend their hospital and Bupa to a friend or colleague.
Where the outpatient survey respondents referred to ‘staff’ in their feedback, 93% of these comments were positive.
If we look at the outpatient survey in more detail, we can see what patients were most satisfied with in their experiences with their consultant or other healthcare professional.
93% said they were extremely satisfied with the knowledge and expertise of their consultant.
92% said they were extremely satisfied with the friendliness and empathy of their consultant;
89% said they were extremely satisfied with how much their consultant involved them in decisions about their care.
Further insights from our outpatient survey show that Bupa patients who scored their consultants ten out of ten placed great importance on:
Their consultants being approachable and caring;
Feeling listened to;
Ease of booking of appointments;
Quick access to care.
Patients’ comments
This was evidenced through comments including:
‘My consultant was very helpful and reassuring and provided a clear path forward for treatment of my condition. He explained the procedure, the risks and the likely outcomes.’
‘Friendly, experienced, knowledgeable staff. Comfortable waiting room. My consultant is always very polite and gentle. He explains everything very clearly so I have confidence in him.’
‘My consultant is very approachable and answered all my questions.’
‘Very easy to book, quick to see a doctor, every person was helpful and friendly.’
Expressing dissatisfaction
Bupa patients also get in touch when things haven’t gone quite as they expected, although this is much rarer. The number of Bupa patients expressing dissatisfaction or making formal complaints about their care has remained low, at just over 1% for the last few years.
The three main reasons Bupa patients cited for their dissatisfaction or complaints were:
❶ Clinical care and treatment (34%);
❷ Appointment services (22%); ❸ The healthcare professional, hospital or clinic’s billing (22%).
When we took a closer look at this, the reasons why patients complained about clinical care and treatment related to the standard of clinical care, the length of time it took for them to receive their results and lack of confidence in their treatment or consultant.
Complaints about appointment services focused on the length of time to get an appointment and appointments being cancelled.
To avoid this happening, it’s important that patients are aware of any potential challenges with securing an appointment to help manage expectations. We also ask consultants to let us know if they are not taking new patients, so that we can let patients know.
The billing complaints focused on the healthcare professional, hospital or clinic’s invoicing process and what they believed were excessive charges.
Conclusion
While positive feedback is always great to hear, the learnings from when things don’t go so well are valuable in helping us to deliver for patients.
What our surveys show is that in both the positive and less positive circumstances, communication is a key theme in the patients’ feedback.
The reasons the patients gave are often rooted in how they are communicated with and not feeling sufficiently involved in decisions about their care. It’s encouraging that these patients’ expectations aren’t unrealistic, so this is something that we can easily remedy; they just want to be heard and involved.
Tricia Carley-White is head of clinical quality and governance at Bupa UK Insurance
Quality not quantity leads to happiness
With healthcare resources stretched worldwide and a situation where even those countries spending more are not achieving the best patient outcomes, the concept of valuebased healthcare offers a potentially transformative approach to improving patient outcomes and enhancing healthcare efficiency. Robert McGough reports
THE NHS has been slowly adopting principles of value-based healthcare (VBH), particularly in Wales, and it is equally crucial for doctors working privately to recognise the importance of embracing these.
This article explores why an understanding of VBH is important for independent practitioners, highlights its potential to optimise patient care and achieve better outcomes, and to do so through efficient use of scarce healthcare resources.
What is value-based health care?
VBH is a patient-centred approach that focusses on improving patient outcomes, cost-effectiveness and overall value in healthcare delivery.
Unlike the traditional fee-forservice model that focuses on the volume of medical services provided, VBH rewards the quality and effectiveness of care across the cycle of care delivery.
It emphasises outcomes which patients most want to see, aiming to provide broader elements of care that considers the patient’s well-being, preferences and goals.
And it encourages healthcare systems to measure and monitor patient outcomes, enabling datadriven decision-making and continuous quality improvement.
By adopting evidence-based practices and promoting preventative care, VBH seeks to optimise resource allocation, reduce unnecessary procedures and improve healthcare efficiency.
It recognises the importance of interdisciplinary collaboration, fostering partnerships between doctors, nurses, pharmacists and other healthcare professionals to enhance care co-ordination and the patient experience.
From a financial perspective, VBH promotes cost-effective care delivery, focusing on interventions that yield the greatest value for patients according to patient definitions of what that is.
The VBH approach has several potential benefits for private practitioners and their patients:
Enhancing patient care
➤ Holistic and patient-centred care: VBH emphasises provision of patient-centred care, focusing on
By adopting evidence-based practices and promoting preventative care, value-based healthcare seeks to optimise resource allocation, reduce unnecessary procedures and improve healthcare efficiency
This approach fosters a culture of learning, innovation and excellence, ultimately benefiting patients through better healthcare delivery.
Achieving financial benefit
➤ Economic sustainability: By adopting VBH principles, private practitioners can improve the financial sustainability of their practices.
By delivering high-value care and avoiding unnecessary procedures, doctors can optimise resource utilisation, reduce healthcare costs and ensure the longterm viability of their private practices.
➤ Enhanced reputation and patient referrals: Providing valuebased care allows doctors to build a reputation as high-quality and patient-focused practitioners.
and collaborate with peers to enhance their professional expertise and standing.
➤ Interdisciplinary collaboration: By focusing on full cycles of care, VBH promotes interdisciplinary collaboration, encouraging private practitioners to work closely with other healthcare professionals, such as nurses, pharmacists and therapists.
Collaborative care improves care co-ordination, reduces medical errors and enhances the overall patient experience.
➤ Professional and work-life balance: The focus on patientcentred care in VBH aligns with the intrinsic motivations of many doctors.
the overall well-being of patients rather than solely treating their diseases.
Together with the clear benefits for the patient, by adopting this approach, private practitioners can improve patient satisfaction and engagement, which should lead to better health outcomes.
➤ Outcome measurement and transparency: VBH encourages the measurement and monitoring of patient outcomes, enabling doctors to assess the effectiveness of different treatment approaches.
This data-driven approach empowers practitioners to make informed decisions, improve treatment plans and achieve better patient outcomes.
➤ Cost-effective care delivery: By emphasising value rather than volume, VBH encourages the delivery of cost-effective care.
Private practitioners can identify and reduce unnecessary medical procedures, promote preventive care and optimise resource allocation, resulting in improved efficiency and reduced healthcare costs for payers/patients.
➤ Continuous quality Improvement: VBH promotes continuous quality improvement by encouraging private practitioners to analyse outcomes, benchmark performance against peers and adopt evidence-based practices.
Satisfied patients are more likely to recommend doctors who prioritise their well-being, resulting in increased patient referrals and a broader patient base for private practitioners.
➤ Competitive advantage in the market: In an increasingly competitive private healthcare market, VBH can serve as a unique selling proposition for private practitioners.
Demonstrating a commitment to value-based care sets doctors apart, attracting patients who prioritise quality, outcomes and overall value in their healthcare choices.
➤ Insurance company collaboration: Value-based care aligns with the goals of insurance companies and payers, as it aims to optimise patient outcomes while minimising overall costs.
By embracing VBH, private practitioners can foster stronger relationships with insurance providers, negotiate favourable re-imbursement rates and potentially expand their patient coverage.
Professional development and collaboration
➤ Clinical innovation and research opportunities: VBH encourages doctors to actively participate in clinical innovation, research and quality improvement initiatives.
Private practitioners can contribute to medical advancements, explore new treatment modalities
By embracing this approach, private practitioners could experience greater professional satisfaction and purpose, ultimately contributing to improved worklife balance.
Likewise, pressures on healthcare resources are not purely financial, but stem from workforce availability as skilled professionals increasingly burn out and leave the profession.
Enabling professionals to provide more effective care through working within VBH approaches may encourage some who may otherwise have left to stay within the workforce.
Conclusion
As the healthcare landscape continues to evolve, private practitioners working outside of the NHS should recognise the opportunities available through adopting VBH principles.
Emphasising patient-centred care, achieving financial sustainability and enhancing professional development, VBH offers a comprehensive framework for doctors to optimise their practice’s efficiency, effectiveness and reputation.
By embracing value-based healthcare, private practitioners can contribute to a transformative shift in healthcare delivery, benefiting both patients and their practices in the process.
Robert McGough (right) is a partner at legal firm Hill Dickinson LLP
Take the pressure off your secretary
Is your medical secretary overwhelmed?
Simon Brignall pinpoints the key warning signs to watch for and offers a check list for you to assess why your practice might need help
THERE IS little doubt that, from all the reports we have been receiving, it is a good time to be in private practice.
At Civica Medical Billing and Collection, we partner with more than1,800 consultants, groups clinics and hospitals, and many are seeing record activity levels, all underpinned by a 50% increase in self-pay activity.
The knock-on effect of increasing NHS waiting times has driven demand in the private sector and this can create a virtuous circle as patients relate their positive experiences to friends and family.
A recent YouGov survey suggested one-in-eight Britons used private healthcare in the past year, with a third having used it for the first time. The survey also noted they had an average spend of £500 which, while not an amount affordable to all, is less than many would imagine.
This surge in activity, while a boon to consultants recovering from the pandemic, is putting considerable stress on administration teams across the private sector. Hospital administration staff along with medical secretaries are all feeling the strain.
I have had many conversations with consultants whose complaint is that they do not think their cash flow reflects their increased activity.
Judging by the frequency this issue is raised, it appears to be a more common problem than you might think. Demand-related issues are good problems to have, but they still need to be addressed.
Here are some early warning signs to look out for and some suggestions of what you can do.
Rising debt
When a practice is struggling to manage increased patient activity, the first task to be set aside is the reconciliation and chasing of outstanding debts.
A medical secretary is tasked with acting as a receptionist, medical PA, billing clerk, theatre manager, insurance guru and credit controller alongside managing their consultant. The increase in self-pay patients means more and more time must be spent chasing patients and taking payments.
Insurance companies are also harder to reach to resolve problems, which means many secretaries feel they are struggling just to keep up.
Added to this, many secretaries work for more than one consultant and are likely to be seeing similar increases in activity across all their practices. What was manageable before can now prove to be challenging and even impossible.
As a rising tide lifts all boats, it is more important to focus on aged debt rather than payments received. Increased demand will lead to more being invoiced each month, which is why tracking aged debt as a percentage of income is a more reliable guide.
Invoice delays
Another good indicator that a practice is getting into difficulties is if it starts to fall behind on invoicing.
This will not only impact the business’s cash flow but also be a sign that the practice’s administration is unprofessional. That can result in bad reviews. As this does not show up as part of your aged debt, it is a good idea to check how
This surge in activity, while a boon to consultants recovering from the pandemic, is putting considerable stress on administration teams across the private sector
up to date your practice is with this task.
It is vital to raise invoices in a timely manner because this is the first step in the payment pathway for all patient types. For insured patients, remember to consider the nuances of each private medical insurer and the correct Clinical Coding and Schedule Development group (CCSD) codes combined with the relevant fee schedule.
Delays not only will impact all subsequent steps in the payment cycle but can often increase the likelihood of losses or bad debts.
At Civica Medical Billing and Collection, we have a bad debt rate of less than 0.5% and often this can be as low as 0.3%
Lack of visibility
Where a practice has inadequate infrastructure and relies on the medical secretary to provide
DO YOU NEED HELP?
HERE’S A QUICK CHECK LIST TO HELP YOU REVIEW YOUR PRACTICE:
Do you have access to accurate up-to-date financial data?
How much debt is currently outstanding and what is this as a percentage of your income?
How old is your aged debt?
Have all your payments been reconciled?
When were your outstanding debts last chased?
What is your bad debt rate?
Are you up to date on invoicing patient activity and shortfalls?
Are your patients saying they have not received an invoice or have had difficulty making payment?
When was the last time the codes you use were reviewed?
When was the last time your practice carried out a fee review?
Are you using the latest fee schedules?
Do you have adequate infrastructure to support your increased activity?
reports, delays in the provision of accurate information can also be a warning sign.
It is self-evident that if a practice has no access to this information, then it is impossible to have a robust and effective chase procedure.
Our clients have access to a dashboard displaying key performance indicators as well as reports showing the following data at both a summary and granular level: invoices raised, payments received and aged debt.
Staffing
While not a warning sign per se, every business sector is finding recruitment challenging. We know the healthcare sector is no exception and finding a person with the skill set required to complete all these tasks as well as fit them all into a working week is not easy.
It can be an impossible task for one person to cope with once a practice starts to see exponential growth. The secretary is so busy dealing with the medical side of
things in many practices now that the billing and collection function gets neglected.
Administration staff can be reluctant to put their hand up and ask for assistance until it is too late. Often this results in previously unknown problems being discovered, including lost income.
When a secretary has been with the practice for some time, they can appear to have everything under control. But when they leave or retire, the impact on the practice can be devastating, particularly financially.
Many consultants make the common mistake of assuming their secretary would not welcome support provided from outsourcing work to a medical billing and collection company.
This is rarely the case, and when private practices take the plunge, it often leaves the medical secretary free to focus on the highvalue tasks aligned to the patient’s clinical journey.
This not only brings financial improvements to the practice but also to the patients’ experience.
Secretaries who support multiple practices find they are freed up to take on more activities they enjoy.
Our account managers ensure they form a strong partnership with medical secretaries so they can work as team and deliver care in line with your objectives.
So streamline your day-to-day operations, maximise revenues, and grow the practice – leaving your secretary free to focus on the patients without finance issues clouding the relationship.
Give your practice a review using the check list in the box to the left.
If any of your answers to these questions are a cause for concern, then I suggest you take steps to address them. Quite often the best solution is to reach out to a medical billing and collection company who can offer both expertise and functionality.
Simon Brignall (right) is director of business development at Civica Medical Billing and Collection
How to challenge the CQC inspector
Some doctors have been left badly shocked at the contents of inspection reports from the Care Quality Commission. If that happens to you, then be aware you have the right to reply about factual accuracy comments and warning notices. Samantha Guest (below) reports
AFTER REGISTERING a service with the Care Quality Commission (CQC), the next interaction a provider is likely to have with the regulator is via an inspection.
The result of this is a published inspection report that may be accompanied by a warning notice. Publication of these documents makes them readable to a wide audience and any independent practitioner affected should be well aware of their right to respond.
A thorough response by a provider aids the CQC in fulfilling its obligation to make sure information sitting in the public domain is an accurate and well rounded reflection of a service.
Draft inspection report
An onsite inspection can be a stressful and high-pressured situation, but coping with the resultant draft report can be equally challenging.
108 Harley Street introduces London's first private HOLOGIC Contrast Enhanced Mammography System, revolutionising breast cancer screening Mammography has long been the primary method for detecting breast cancer at an early, treatable stage However, with the advent of Contrast Enhanced Mammography (CEM), a specialised and advanced mammography test, breast imaging has reached new levels of precision and detail Our facility now offers this state-of-the-art technology, ensuring patients receive the highest quality breast cancer screening available
CEM goes beyond the capabilities of standard mammography by utilising a special dye (contrast) injected into the patient's arm, enhancing the visibility of breast tissue changes
CEM is recommended for several patient groups, including those who require assistance in resolving findings detected through conventional breast imaging, individuals needing pre-operative staging of breast cancer, patients with contraindications or intolerance to MRI (e g , pacemakers or claustrophobia), and patients over 40 who have suspected cancer based on ultrasound but normal mammography results Additionally, CEM can be employed as an alternative to MRI for women at an increased risk of developing breast cancer, such as those with dense breasts or a strong family history
Inspection reports are essentially the most compelling piece of marketing for any health or social care service, therefore the contents of an inspection report ought to accurately reflect what the regulator witnessed while inspecting.
In our experience, providers are often left shocked and disappointed when the draft inspection report is received. They are often unsure of how such a negative draft inspection report could have arisen from what appeared to be a positive period of inspection.
An overly negative, and inaccurate report, is likely to impact a provider’s business and result in reputational damage.
We always encourage providers to reflect carefully on a draft inspection report and to feel empowered to challenge them where there are clear errors or something simply does not feel fair or reasonable.
To learn more about CEM or refer a CEM patient please
This is particularly relevant for those with a highly technical, complex and/or specialised service. In these instances, it is often the case that the CQC has not fully understood the nature of the service provided and therefore fails to accurately report and analyse internal policies or procedures.
A draft inspection report is challenged by way of factual accuracy comments. At my legal firm, Ridouts, we have vast experience in challenging draft inspection reports. Some contained minor errors and others presented highly damaging and misleading portrayals of a service.
Critical eye
While a provider may have the time to prepare their own response to a draft inspection report, it may find its inability to be objective impacts its ability to address the right points from the right angle. We operate forensically and go through every comment, nuance and asserted ‘fact’ with a critical eye.
In a recent matter, a reading of the draft inspection report highlighted a clear misunderstanding of the CQC of how the provider operated.
This was not only evident in the explanation of the service but in how the CQC reviewed the provider’s internal processes, policies and procedures. We worked with the provider to accurately break down the information into an understandable format, which clearly outlined its safe practices.
The CQC is legally required to prepare a draft inspection report on the matters inspected. A copy of the report must be sent to the provider and manager ‘without delay’.
Providers should be clear that not only will an inspection be made up of findings unearthed during a physical onsite visit but also from information gathered remotely from other stakeholders – patients, family members, commissioners and whistleblowers.
The CQC often relies on subjective third-party opinion to demonstrate how a service is operating in practice. While this is a credible form of information-gathering, its reliability is often unchecked by the watchdog.
This can result in a disproportionate reliance on third-party
The CQC often relies on subjective third-party opinion to demonstrate how a service is operating in practice. While this is a credible form of informationgathering, its reliability is often unchecked by the watchdog
REPLYING TO WARNING NOTICES FROM THE CQC
Warning notices are issued by the CQC where a service is deemed to have failed, or is continuing to fail, to comply with a legal requirement.
The CQC can issue a warning notice for a current breach of regulation or for a past breach, which may have been rectified, if it considers that the past breach is serious enough.
The issuing of a warning notice can be classed as ‘low-level enforcement’ action and, if not actioned by a provider, may escalate to a greater form of enforcement action – for example, a ‘notice of proposal’.
opinion. In preparing factual accuracy comments on behalf of clients, we seek to remind the CQC of its obligation to triangulate, and fact-check, all information before passing comment within the inspection report.
In practice, a provider has ten working days to challenge any factual inaccuracies in the draft inspection report. This is a fairly tight time-frame and we strongly encourage a provider to obtain legal advice as soon as the draft inspection report is received.
Conclusion
It is natural for providers to get overwhelmed during periods of high CQC interest and involvement in their services. Onsite inspections are often targeted and fail to accurately review a service as a whole.
This is indicative of the CQC’s ‘risk-based approach’, meaning that a provider is likely to only be inspected where the watchdog believes there are issues to be found.
Also, the accuracy of information obtained at an inspection is only reflected to the extent of an inspector’s understanding of the services offered by a provider.
This is evidenced through the limited or inaccurate information provided in a draft inspection report and/or warning notice.
A provider is the only reliable expert on the nature of its service. If the CQC fails to accurately capture a provider’s service, then we strongly encourage a provider to exercise its right of reply through factual accuracy comments and/or warning notice representations.
Samantha Guest is a ‘registered foreign lawyer – New Zealand’ working for Ridouts Professional Services Ltd, London
Further, the CQC may, and frequently does, decide to publish a warning notice more widely than a final inspection report. This publication, or sharing of information, can lead to unwanted attention from relevant stakeholders, such as the local authority, professional regulators and clients.
In turn, this can have a detrimental impact on a provider’s business, reputation and will continuously appear as part of their CQC regulatory history.
It does not automatically follow that an onsite inspection will trigger the issuing of a warning notice. However, we have noticed an increase in the issuing of warning notices following the completion of an onsite inspection.
On these occasions, the CQC uses the information obtained during the inspection period to support its issuing of the warning notice. This often means providers are required to react quickly and begin to enact change from the point of receiving formal inspection feedback.
A warning notice must be issued in writing,and must state:
The relevant legal requirement that the registered provider is not complying with;
How the registered provider did not comply;
The time-scale within which the CQC expects the registered person to become compliant.
There is no legally set time-scale for complying with a warning notice and the CQC can set any period which it considers reasonable.
In accordance with its guidance, that period must reflect the degree of risk to the safety and welfare of people who use the service and must be a realistic and achievable time-frame.
It is important for providers to note that the time-frame to comply with the warning notice and the deadline to submit representations to the warning notice are two separate things and often fall on different dates.
A failure to produce a robust response to a warning notice is likely to result in the CQC concluding that the issuing of the warning notice was proportionate; in the public interest and accurately representative of the state of the service.
Lack of response by the provider is also indicative of an acceptance that it is failing to comply with its legal obligations.
How consent has become stricter
Dr Emma Green (right) highlights some defining cases that have led to the principles of consent and how they apply to current practice
CONSENT IS not a new topic; many articles have been written on it and usually raise further questions from practitioners about their own consent processes.
It is a common topic that doctors seek advice about and clinicians sometimes need to understand how the pragmatic application of the principles apply to their practice.
Doctors will find it useful to be aware of some of the key defining cases which have led to the current principles of consent.
CASE 1. Bolam v Friern Hospital Management Committee [1967]
A patient required electroconvulsive therapy (ECT) for treatment of a mental illness. No muscle relaxant was given and Mr Bolam sustained multiple fractures.
It was alleged that the doctor was in breach of duty for not giving muscle relaxant when, in fact, this omission accorded with usual practice of others giving ECT and the court did not consider there had been breach of duty. This resulted in the following judgment, which most clinicians are familiar with:
‘He is not guilty of negligence if he has acted in accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art.’
Bolitho [1997] later refined the Bolam test by clarifying that the experts opining as the responsible body for the basis on which Bolitho would be supported must have logical reasoning.
➱ continued on page 34
CASE 2. Sidaway vs Bethlem Royal Hospital Governors [1985]
The patient, Mrs Sidaway, underwent cervical decompression, which carried a risk of 1-2% of spinal injury even if performed perfectly, along with risk of peripheral nerve damage.
The case found that she was not advised of the risk of serious spinal injury and had she been warned, she would not have undergone the surgery.
It was also found that the patient was not advised that the operation was unnecessary and there was an option of doing nothing.
This case set the common law that a doctor must provide all material risk.
That means telling the patient about all those risks required for them to make a balanced judgement, unless there is considered to be exceptional reason not to – the so called ‘therapeutic exception’.
SO HOW DO THESE CASES APPLY TO CONSENT IN CURRENT PRACTICE?
Consent must not be considered in isolation as a static process, but a journey which considers patient factors and those which are of importance to the patient.
The assumed worst-case scenario from the doctor’s perspective can no longer be considered as blanket consent for all ‘less severe’ outcomes.
An example may be a patient undergoing ophthalmic surgery where there is a risk of blindness. The assumed position that this is the worst outcome may not be the case for a patient where diplopia renders them incapacitated.
Even where the doctor may not normally consider diplopia as a frequent risk, it may be of such importance to the patient that not discussing it would be indefensible in court, based on Montgomery and the clear message that consent has no place for medical paternalism.
When consent is delegated to other healthcare professionals, the same principles apply. The person taking consent must be able to sufficiently understand the risks which may be material to the individual patient, even where the risks may be small.
Consent also relies upon the person taking the consent having adequate insight into whether they have sufficient experience to undertake the task.
JUST A PAPER EXERCISE?
Many doctors ask about the use of consent forms. Are they worth the paper they are written on? Are they needed for every procedure?
The key to this question is not the patient’s signature on a written consent, but the quality of the consenting discussion – what the procedure entails, risks, benefits, alternatives, no action, if an option – which the clinician records themselves, for example, in bullet points.
When considering the Montgomery case, doctors should ensure they ask patients questions which focus on the specific concerns of the individual. This should be recorded and although prudent to use a consent form, space limitations may preclude a consent form being the most appropriate format.
The importance of genuine dialogue rather than form-filling was underlined in the case of Thefaut v Johnston [2017]. There, the doctor sought to rely on the fact that they had obtained consent from the patient shortly before the surgery.
The court held: ‘It is routine for a surgeon immediately prior to surgery to see the patient and to ensure that they remain wedded to the procedure. But this is neither the place nor the occasion for a surgeon for the first time to explain to a patient undergoing elective
surgery the relevant risks and benefits. …. There is no “adequate time and space” for a sensible dialogue to occur and for free choice to be exercised…’
Now this leads to a final consideration of whether a complication such as death from local anaesthetic should be disclosed to patients and whether written consent is required.
This complication is astonishingly rare and there is debate as to whether local anaesthetic administration is a drug delivery or a procedure, but regardless, the principles of consent should still be considered on the basis that a patient is choosing whether or not to receive this drug.
It may be defensible to not discuss the risk of death, but this would depend on whether the patient would consider this to be of significance to them, taking us back to the material risk to that individual.
An argument could be made that a patient with thanatophobia would want to know this risk, but unless the question of importance and beliefs is explored, any practitioner should be mindful that importance cannot be presumed.
But the risk of allergic reaction may be of importance to many patients and it could be argued where this is adequately explained, it would encompass the extreme end of allergic reactions and therefore the risk of death.
KEY POINTS
Consent is now judged by the principles of Montgomery and can be difficult to defend in clinical negligence cases
Clinicians should be mindful of the consent journey and record discussions with the patient in the records
Inadequate space on a consent form is not a reason to not document discussions
Risks cannot be considered purely as a percentage
A risk is ‘material’ if a reasonable person in the patient’s position would be likely to attach significance to it
CASE 3. Chester v Afshar [2004]
The claimant in this case had a sixyear history of back pain, mobility issues and bladder incontinence secondary to disc protrusion. She therefore opted to undergo surgery.
The consent process did not include the information that the operation carried a 1-2% risk of paralysis and the patient underwent the operation which caused her condition to worsen.
While it was found that the procedure itself was not negligent, the claimant argued that had she been aware of the risk, she would have delayed when she underwent the operation and it was found that the same operation, carried out on a different day, may have had a different outcome.
This outlined that a patient no longer had to prove they would not have undergone the procedure.
CASE 4. Montgomery v Lanarkshire Health Board [2015]
Nadine Montgomery was pregnant with her first child. She was concerned about the risk associated with being a diabetic patient and explicitly expressed concern about the risk of the size of her baby and vaginal delivery.
However, the risks of shoulder dystocia were not discussed and she was never offered the option of a Caesarean section.
When Mrs Montgomery went into labour, a shoulder dystocia occurred and her son was born with significant cerebral palsy. Mrs Montgomery claimed for negligence and the case was ultimately heard in the supreme court after the treating clinician advised they had not discussed a caesarean section, as they did not think it to be in her best interests.
The key finding in the judgment made at the supreme court was:
‘The doctor is under a duty to take reasonable care to ensure that the patient is aware of material risks involved in proposed treatment and of reasonable alternatives.
‘A risk is “material” if a reasonable person in the patient’s position would be likely to attach significance to it.
‘Or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.’
Three further points were raised which highlighted:
The significance of risk is factsensitive and cannot be reduced to percentages;
In order to advise, the doctor must engage in dialogue with their patient;
Therapeutic exception is limited and should not be abused.
Dr Emma Green is a medico-legal consultant at Medical Protection
BOOK YOUR DEMO Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
PRINCIPLES OF INVESTING
Don’t just take our word for it! Dr Benjamin Holdsworth sets out the key tenets of successful investing
Shield yourself against inferior investments
against investments
A SYSTEMATIC APPROACH to investing provides the best chance of experiencing a successful investing journey.
Sticking to some key guiding principles – which are grounded in evidence and logic – gives investors a solid foundation on which to build a sensible investment solution.
Although we repeat this doctrine often, there is no need to simply take our word for it.
Here below we provide an insight into five of our favourite quotes from experienced and accomplished academics and practitioners and explain how these link to our own investment philosophy.
1
A focus on risk management, rather than chasing performance
‘You don’t find out who’s been swimming naked until the tide goes out.’
The financial media enjoys reporting on top-performing fund managers. Humans like exciting stories. Good investing, however, should – to most – seem relatively boring through taking a ‘risk-first’ approach.
Ultimately, sensibly considered risks should be rewarded appropriately over time. The risk management process involves deciding which risks one wants to be exposed to in portfolios – such as broad global equity market risk –and which we do not,such as the use of leverage.
Managing these risks tightly over time and monitoring them on a regular basis is key.
2 Be diligent and act rationally, with due patience
‘Activity in investing is almost always in surplus.’
Charles D. Ellis, Winning the Losers Game, 1993
Ensuring any decision made is free from an emotional reaction is a must.
Many investors are prone to making knee-jerk – and sometimes permanently damaging – investment decisions. Taking steps to avoid this is well-advised.
Many investors are prone to making knee-jerk – and sometimes permanently damaging – investment decisions. Taking steps to avoid this is well-advised
being overly concentrated in a single stock.
4
Keep costs low
‘In investing, you get what you don’t pay for.’
John C. Bogle, Founder of The Vanguard Group, February 2005
Cost is by no means the only factor separating better and worse investment solutions, but it is a significant one.
Costs can be implicit – for example, trading costs – or explicit – for example, fund manager fees. Clearly, any saving made by an investor is retained in the portfolio, rather than being passed off to another party in the process.
5 Stick to the plan
‘Real-world application of fundamental investment principles produces superior outcomes.’
David F. Swensen, author and former chief information officer of Yale University Endowment, 2005
An investor who can recall their key investment principles stands in good stead to avoid making mistakes.
Abiding by some simple guidelines – such as those outlined by the investment experts in this note – enables investors to employ a robust and repeatable process for managing their wealth.
3
Take part and believe in capital markets
‘You’ve got to talk yourself out of the market portfolio.’
Eugene Fama, Nobel Laureate, speaking with The Rational Reminder Podcast, May 2020
Owning a share of companies through investing in capital markets is an effective way for investors to grow their wealth over time.
Owning a little bit of everything is not a bad place to start. Luckily for investors these days, one can do so with relative ease through investing in mutual funds. Doing so enables investors to participate in the growth of listed companies from around the world in a diversified manner, avoiding
Dr Benjamin Holdsworth (right) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
KEEP IT LEGAL
The perils of social
Rachel Levine (right) explains who the law protects in social media and how you can shield yourself as an employer and/or employee against its dangers
social media
POINTS FOR INDEPENDENT PRACTITIONERS TO WATCH
The examples in this article are the extreme cases, but they go some way in illustrating the current legal position in this ever-changing area. As you grow your medical business, social media should form a core part of your people-management planning.
There are actions that can be taken should our nightmare scenario at the start of the article happen to you. But it is easier to act if you have appropriate documentation in place.
The tribunals remain keen to maintain an employee’s right to privacy and right to freedom of expression except in the most extreme of circumstances.
But as seen in these cases, caution should certainly be taken when posting online, particularly in a profession necessitating high standards such as healthcare. See the list of advisory points on page 41 ➱
PICTURE THE scene: you have secured a lucrative new contract providing a range of health services to a large local business. Delivering this will require administrative support and additional medical team members.
You happily employ a new administrator and enter into contracts of service with a couple of local doctors you have known for years.
As the contract commences, your administrator launches a scathing attack on your client on their personal social media page due to a local contentious issue.
One of the new GP team members makes some unsavoury comments about the latest hot topic in the media and another sees these problems and raises concerns about your business on social media under the grounds of ‘whistle-blowing’.
What does the law say about these arrangements and what can you do to protect both your business and your reputation?
The rise of social media
Social media is a core part of everyday life for the vast majority of people, and the lines between personal and professional use of these apps are often blurred.
It can be used to transform patient experience. The #HelloMyNameIs campaign, started by late hospital doctor Kate Granger MBE, encourages medical professionals to introduce themselves by name to patients in their care and her recognisable name badges are now commonplace across healthcare settings.
The GMC notes that benefits of social media use can include ‘engaging the wider public in discussions about health policy, widening your professional network and facilitating patients’ access to information about health and the services available to them’.
On the other side of the same coin, however, disagreements and conflict can become more toxic and ferocious online than might ever occur face to face.
Contentious issues such as the doctors’ and nurses’ strikes, increasing perceptions of privatisation of the NHS and a hornets’ nest of other social and political issues may be hot topics for commentary but also represent legal and commercial risks.
To add to the complexity, as demonstrated in our example above, as an entrepreneurial independent practitioner, you may find you have problems relating to your own comments, the comments of your employees and of third-party contractors.
Being aware of this and the risks it represents should be a part of your risk management while growing your business.
So where is the line on appropriate social media use, and how can you ensure you are protected from any potential adverse repercussions? This is a developing area of law, as courts and tribunals try to keep pace with a rapidly changing world.
The law
When considering law in relation to independent healthcare, it is
➱ continued on page 40
important to ascertain the nature of the relationship between the parties.
Social media-related terms and conditions may be found in an employment contract, company policies, contracts for service and agreements with partner organisations. Each of these documents can be drafted in a multitude of ways and you will need to ensure they suit the needs of your business.
It is recommended you have a social media policy in place, either stand-alone or incorporated into an employee handbook.
This should specify company expectations for employee and worker use of social media, including the possibility of disciplinary action for conduct online that might breach employee policies.
When you start growing your team, it is necessary to confirm these policies exist and that they are applicable to all individuals working for you or on your behalf with your clients, regardless of the legal relationship between you.
It is also important to ascertain whether your clients have their own social media policies they expect your team to comply with.
A classic example is the provision of insourcing services where the client may have a general clause in the contract expecting compliance with their policies and procedures. Failing to identify and enforce this could result in your contract being terminated should your team be deemed in breach.
Another way that parameters are set is the rulings of courts and tribunals, which are vital for establishing the parameters of the law and how it relates to real-world situations.
Shooting yourself in the foot?
Social media can seem to offer a ‘safe space’ for the airing of complaints, with a community of likeminded people who might support your concerns.
In our example, this may be how your administrator felt when responding to a local issue perceived by her community to be caused by your client.
In recent rulings, the tribunals have confirmed the right of employers in certain circumstances to discipline – or in some
PERSONAL OPINIONS –WHAT’S APPROPRIATE?
lf almost all of the situations explored so far have connections to work, what happens in relation to private conversations had in a personal capacity?
This, predictably, is a particularly thorny subject due to the legitimate expectation of privacy and data protection laws.
However, certain professions have high standards expected as part of the job. This is particularly relevant for healthcare professionals, where patient and public trust in the profession and perception of doctors is crucial.
Clemmie Hooper, ‘mummy blogger’ and midwife, has just been handed a one-year caution order after being found to have posted inappropriate comments on social media intended to ‘undermine and humiliate’ the recipients, including one comment that was racially offensive and/or discriminatory – though Hooper denied being aware of that at the time.
Many people engage in negative comments online, but the discovery of Hooper’s comments led to a number of complaints to her NHS trust that her behaviour was incompatible with being a midwife.
While there is a general acceptance that WhatsApp conversations are private, there have also been examples where private messages have been disclosed to an employer, who has then acted on them.
Again, the status of the sender is likely to play an important factor here in deciding whether the employer was entitled to rely on those private messages. In a case involving a WhatsApp group operating between police officers – BC v Scottish Police – the offensive nature of the communications, coupled with the standards of conduct expected of a serving officer, meant that the officers had no reasonable expectation of privacy.
This expectation of high standards also includes those working within a healthcare setting.
In Nakash v MPC, an unlawful search by police found WhatsApp messages which were passed to the GMC. The GMC was then permitted to use those messages, despite them being unlawfully obtained, on the basis that they shed light on an allegation of sexual assault that had been made against a doctor.
cases dismiss – employees who have bad-mouthed them online.
In one case (Crisp v Apple Retail), the employer was found to have acted fairly in dismissing an employee who had posted negative comments about the business on his Facebook page.
The employer had a clear policy outlining that comments made outside of work which affected the company’s reputation would be covered by company policy, bringing him within its scope even when posting on his personal social media platform.
That is not to say that employers have unfettered access to your team’s social media pages: underpinning this area as a whole is an individual’s fundamental right to privacy.
The excessive monitoring of employees can cause significant
issues for employers under data protection laws, and companies must be able to show that data is processed fairly, there is a legitimate interest and any monitoring is proportionate and necessary in the circumstances.
Aside from airing general grievances, it may even be tempting for some people to use social media to blow the whistle on practices they identify and disagree with, as suggested in our example.
Particularly in a healthcare setting, patient safety comes first and foremost, regardless of it being a private setting, and they may feel there are strong public interest arguments for whistle-blowing via social media rather than by direct means.
However, while some protection is afforded to a whistle-blower who uses social media to raise their con-
While some protection is afforded to a whistle-blower who uses social media to raise their concerns, it is far less protective than if concerns are raised through the proper channels
cerns, it is far less protective and far more difficult to satisfy the requirements than if concerns are raised through the proper channels.
The ‘social media whistleblower’ would also be required to persuade a tribunal that their disclosure via social media was ‘reasonable’, which could be very difficult when they have bypassed their employer’s policies and posted straight to social media.
In balancing the employee’s right to privacy and the employer’s right to protect its reputation, the issue will often fall to whether the conduct in question relates to the employment relationship and the impact on the employer’s reputation, such as whether the employer was named or identifiable in the posts, as well as the potential reach of the posts.
While this is generally satisfied when employees are posting opinions or complaints specifically about the workplace, the line can be far less clear when considering personal opinions that may be fundamentally disagreeable and potentially incompatible with the person’s job.
Blurred personal and professional boundaries
One of the issues currently surrounding social media use is the increasing polarisation of views and opinions, which can be seen across the board.
As touched on above, freedom of expression is an overriding human right, protected internationally, including those views that might provoke negative reactions or cause some level of offence.
The question always being tested in this area is the extent to which employers are or should be required to respect and take account of employees’ freedom of expression and right to privacy when those opinions could be
substantially offensive to certain groups of people.
There can be a fine line between sharing controversial views and breaching legal protections against discrimination. In a recent high-profile case (Forstater v CGD Europe), the tribunal erred on the side of freedom of expression.
It held that although the employee had posted ‘gender critical’ views on social media which were intentionally provocative and mocking and which people found offensive, a decision to dismiss her based on those posts was discriminatory.
Yet where those views cross over into the workplace, causing harm or affecting an employer’s business, the tribunals are less protective of the employee. In Mackereth v DWP, the claimant was a doctor who refused to refer to transgender service users by their chosen pronouns. His dismissal by his employer was found to be fair.
These examples show the difficult balance between an individual’s right to express their views on social media and how this can seep into the working relationship, at which point the risk of disciplinary action or dismissal is far greater.
When the individual is not an employee, it would be reasonable to apply a similar test to ascertain whether they have breached the terms of engagement.
Ensuring your contracts for services have clauses which allow you to terminate in cases of potential damage to your reputation is reasonable, but it may be difficult to evidence.
These contracts are less restricted than employment terms, so you may be able to resolve the issue with short notice periods or other grounds of termination.
Rachel Levine is a solicitor in the employment team at Hempsons
IF YOU ARE AN EMPLOYER
1
As an employer, having social media policy (either a stand-alone document or as part of your employee handbook) will be the framework through which you can manage your team and set expectations.
2
Ensure you and your team understand your client’s social media polices and identify any topics which should be avoided.
3 Consider arranging training on the best uses of social media.
4
Review your whistle-blowing procedures to avoid any team members claiming they do not how to access it or that it is ineffectual.
IF YOU ARE AN EMPLOYEE
1
2
If you are a doctor with an employer, then familiarise yourself with your employer’s social media policy, if they have one.
Think before you post! The standards expected of a doctor does not change because they are communicating through social media rather than face to face.
3
Consider your position before posting directly about any employer online, particularly if your comments will paint them in a negative light.
4
Ensure you are posting in a personal capacity unless you have been instructed or are authorised to post on behalf of any employer.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
How should this consultant prepare for a meeting following an adverse incident?
Dr Kathryn Leask gives her response
Dilemma 1 Can you help with this meeting?
QI have been asked to attend a meeting following an adverse incident involving a medication error (I work as a consultant cardiologist).
I have put my account of the event in writing based upon my recollections and the appropriate records, but I was wondering if you could offer further advice in this area?
AFirstly, it is important not to jump to conclusions about the purpose of the meeting.
And remember that you have a professional duty to be open and honest when things go wrong and to learn lessons from any incident. It’s also advisable to contact your medical defence body for advice. The check list below will help you to prepare in advance. It is important to do this, even if there are no obvious concerns about your role in the incident.
1. Establish what process or policy
When asked to attend adverse event meeting
is being followed, who will be present at the meeting and if you can bring a trusted colleague for support.
2. If you do feel that your care could have been better, then be prepared to demonstrate that you recognise this and what remediation you have undertaken – or plan to – to address this.
Including mention of reflection and remediation in adverse incident statements or at meetings is not always necessary, but it can help you pre-empt any recommendation about steps you should take to improve your practice.
3. Ensure you have seen the relevant medical records, where applicable, so you are familiar with the original documentation about the event in question.
4. Consider drafting a statement, even if one has not been formally requested. Aim to create an aide memoire for the meeting that includes a full chronology and everything you would want to say about your role in events.
This way, you are less likely to leave the meeting feeling that key points were omitted from your evidence or that you didn’t make yourself clear. You can find our guide on writing reports at www. themdu.com/guidance-andadvice/guides/writing-a-report-orstatement.
5. Listen carefully to each question and only answer if you fully understand. You can ask for clarification if the question is unclear.
6. Take your time and consider your answer before speaking.
7. When you have answered a question, it is appropriate to stop talking and wait for the next question. Don’t be tempted to fill any silences.
8. If you don’t know something, it is fine to say so.
9. Do not speculate about what might have, should have, or could have happened, or not happened.
10. Do not comment on the actions or omissions of other people or go outside of your own area of expertise.
11. While the purpose of adverse
incident investigations is to factfind and not to apportion blame, if you do feel uncomfortable with the questions you are being asked, you can ask for a copy of the questions to take away.
This will allow you to seek support and get advice before you answer them. You can offer to reply to these in writing later.
12. Be mindful of the relevant GMC guidance when answering questions. It is important to be honest, take reasonable steps to check any information is accurate and that no relevant information is omitted.
13. Ask to see a copy of any report or statement that is prepared based on your answers so that you can check this is factually correct and your responses have not been misunderstood.
Your account will be relied on, so try to give an accurate report of your involvement in the incident, as the information could be used in processes such as a coroner’s inquiry or GMC investigation.
Insurer wants details of my care for a dead patient
A consultant requests help to respond to a request for information from an insurance provider. Dr Kathryn Leask (right) gives her advice
Dilemma 2
Why has insurer asked for data?
QI am an interventional radiologist and have been contacted by a patient’s private medical insurance company asking for details of their care and the reasons why specific decisions about their treatment was made.
Unfortunately, the patient died three weeks after treatment following a deterioration in their condition. The insurer has asked about the decision-making process including timings. It has also asked for some audit information about my practice. While I have no concerns about the care I provided and the family of the patient have not raised any issues, I am concerned about the reason for this request. Please could you advise?
AIt is likely that this request is based on the fact that the insurer is regulated by the Financial Conduct Authority and has a responsibility towards its customers to ensure they are receiving appropriate treatment.
From time to time, private medi-
cal insurers undertake quality assurance investigations which doctors generally have an ethical obligation to co-operate with, after taking into account their duty of confidentiality to the patient/deceased.
You may find that you have a contractual obligation to provide this type of information as part of your recognition agreement with the private insurer and it would, therefore, be worth reviewing the wording of your agreement.
If you have any specific concerns about the request for information or the reasons behind it, you are advised to contact your medical defence organisation for support.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union (MDU)
PATIENTS’ GRIPES
How patients are told to make a complaint
Doctors get advice on responding to complaints, but what are patients advised about making them? Solicitor Chris James (right) offers these tips on the Patients Association website – which both parties have agreed to share with Independent Practitioner Today readers
1
Consider who the best person is to deal with your complaint. There are a number of options, so look at available resources – for example, the Patients Association’s ‘making a complaint’ leaflet or the guidance offered by the NHS in relation to complaints.
You may want to raise the complaint informally first, without labelling it as a ‘letter of complaint’; for example, writing to say you have ‘concerns’.
You will also generally have the option to complain to the healthcare provider themselves – for example, the GP practice or your treating hospital – or, if you are uncomfortable doing that, to the body overseeing the care; for example, NHS England.
2
Think carefully about the important questions that you or the family want answered. The complaint process is probably the best opportunity for you to get answers or an explanation, so take your time.
If another person has an interest in the complaint, such as the rest of the family, it might be a good idea to have a discussion and ensure everyone’s concerns are included.
3 It is hard to do, but try to take the emotion out of what you write. You may well be very entitled to be angry and upset about what has happened, but it is unlikely to help your cause to write in that way.
Try to stick to the facts, ask the questions and raise the concerns you have. You want to get empathy from whoever is reading it and directing anger at them, however justified it may be, is unlikely to achieve that.
4
If you are considering bringing a clinical negligence claim, do not worry too much about ‘saying the wrong thing’ in a complaint letter or meeting.
The two processes are entirely separate. It would be quite unusual for something said by a patient or family member to damage any later claim. If you are honest, there shouldn’t be a problem.
5 Set out below are some tips on setting out the letter clearly.
The aim of any piece of writing is to make it as easy as possible for the reader to understand. If you are trying to persuade someone of something, make it as easy as possible for the person to come around to your point of view.
Practical tips include:
State the date that the incident/ issues that have occurred;
Use headings to break up the detail;
Use bullet points or numbers to separate your points or questions.
Try to keep only the most important bits in and ask the most
It is hard to do, but try to take the emotion out of what you write. You may well be very entitled to be angry and upset about what has happened, but it is unlikely to help your cause to write in that way
important questions. Of course, include all important details, but perhaps think to yourself ‘does the reader need to know this to understand my complaint or answer my concerns?’
Make your best point(s) first and ask your most important question(s) first. Don’t leave it to the end when people are less engaged. Be clear about the outcome(s) that you want. This could be an explanation of why something did or didn’t happen, an apology or proposals to ensure the same issue doesn’t happen again.
Leave the letter to go cold for a few days and then come back to it. It is amazing what a fresh mind can see: things you had forgotten or parts you realised you didn’t need or should reword.
Chris James is a solicitor with Bolt Burdon Kemp and his wording is taken from the Patients Association website and used with permission
Tax changes you need to grasp
Doctors are facing many changes around the tax system and rates – and these may have a significant impact on your private practice business. Some of these measures have already been introduced and others are planned for the near future.
Richard Norbury gives a round-up of some of the more important changes to consider
BASIS PERIOD REFORM
Basis period reform applies to sole traders and partnerships where their financial accounts are drawn up to a date that is not coterminous with the fiscal year-end, which is 5 April – or 31 March for many in practice.
These year-end dates have often arisen from the commencement of the business or, for older businesses, when the self-assessment tax system was introduced.
Legislation has now been introduced so that you have to report your profits to 31 March/5 April 2024, which may be a change to your usual year-end.
You do not officially have to change the date of your accounts, but it is expected that most busi-
nesses will, unless you are expecting significant differences between accounting years, in which case some planning may be required.
The impact of the change is that it can accelerate income tax due on the profits, as it unwinds the timing difference for the disclosure of earnings.
For example, if you started in private practice on 1 July 2010 and decided to draw up your first accounts to 30 June 2011, you will have been taxed in the tax year 2010-2011 for the period 1 July 2010 to 5 April 2011.
The following tax year, you are on the ‘current year’ basis, which means you will have paid tax on the year ended 30 June 2011 profits. ➱ continued on page 46
This creates overlap profit, or in other words, you have used the same profits twice on the first period of 1 July 2010 to 5 April 2011.
This can be a benefit if profits are rising, as it builds in a timing difference that you are effectively paying the tax on profits later.
Over the life of your practice, this would naturally unwind with usually a higher tax liability in the final year, often well after the business has, in fact, ceased.
The basis period reforms basically unwind the timing difference to align the disclosure for tax to the tax year-end. In doing so, the first period that was included twice is deducted from the longer period.
As the overlap profits are usually set at a time when the business is in its infancy, they do not normally extinguish the extra profit that is being included.
This gives rise to an acceleration of the tax point on these profits, resulting in the tax being payable sooner, which is ultimately why HM Revenue and Customs (HMRC) is making the change.
Calculations for this are complicated and if you do not have a financial year-end aligned with the tax year end, then you should discuss this with your accountant
who should be able to quantify the effect.
The good news is that any acceleration of tax from the forced change can be ring-fenced and paid to HMRC over a period of five years in equal instalments.
However, if you cease private practice during that period, then this would crystallise the remaining tax due in that particular tax year.
CORPORATION TAX
The main rate of corporation tax has increased to 25% from 1 April 2023. This means any company that earns over £50,000 in profits each year is likely to pay more tax.
A review is needed because this may make certain expenditure items – salary, pension or electric car, for example – more viable because the tax saving is greater.
The revised tax rate of 25% applies to profits in excess of £250,000, with the first £50,000 retaining the 19% tax rate. Profits between £50,000 and £250,000 are taxed at 26.5% and therefore costs incurred within this range attract higher tax relief.
Many consultants have interests in more than one company. From 1 April 2023, rules known as ‘associated companies’ become more important.
The main rate of corporation tax has increased to 25% from 1 April 2023. This means any company that earns over £50,000 in profits each year is likely to pay more tax
tax relief of 130% on the cost of the asset.
This was introduced so as not to encourage companies to delay capital expenditure and wait for the higher rate of corporation tax. This super-deduction no longer applies for companies because the higher tax rate provides additional tax relief for those with sufficient earnings.
Previously, the main rate and small rate of tax was mirrored at 19%, so, effectively, the associated company rules did not make any difference to the overall tax paid. But now you could find yourself having to spread the limit when the higher rate of tax kicks in.
For example, if you controlled two companies and they were considered to be associated, the £50,000 limit would be halved and the higher tax rate would apply from £25,000 for each company.
Some consultants may have arranged their affairs in a certain way to trade using multiple companies, meaning a review is now necessary to ensure this is still the best trading structure.
In recent times, companies have been able to claim a capital allowances super-deduction for any assets purchased. They enjoyed
PENSION ANNUAL ALLOWANCE
The pension annual allowance limit has now increased from £40,000 to £60,000 from 6 April 2023. Tapering – only to be considered if taxable income exceeds £200,000 – can still reduce the £60,000 annual allowance. The lowest tapered value has now increased from £4,000 to £10,000. Another change implemented from 6 April 2023 is how inflation is applied to your pension benefits.
This change will remove the problem of inflation-driven pension growth, which was becoming a significant risk in the current inflationary times.
Other changes have been made to more fairly calculate the overall pension growth where your benefits in the 1995 scheme may have fallen.
The reduction can now be offset against growth in the 2015 scheme.
Meanwhile, the impact of what’s known as the ‘McCloud remedy’ on doctors remains uncertain. NHS Pensions is currently working on restating members’ records. This is being carried out in stages, which will delay the issuing of annual allowance statements for 2022-23 because NHS Pensions needs to know the opening value of the pension after reinstatement for McCloud.
LIFETIME ALLOWANCE
From the 6 April 2023, the lifetime allowance (LTA) charge has been removed and, in a future fiscal event, the Government will make the necessary changes to entirely remove the LTA from pensions tax legislation.
Many independent practitioners will have different forms of lifetime allowance tax protection and
although the LTA tax no longer applies, there is a limit on the maximum tax-free lump sum that can be taken.
From 6 April 2023 it is £268,275 – 25% of the previous LTA limit. If your protection allows a larger lump sum, then this can be taken instead if you so wish, shielding more money from tax. If the tax-free lump sum is exceeded, then the excess is now taxed at an individual marginal rate of tax.
INCOME TAX
The additional rate threshold has now decreased from £150,000 to £125,140. This means that as soon as an individual reaches the income level where their personal allowance is lost, the 45% tax rate applies.
Total exposure for doctors in this situation is an additional 5% on income between these bands, boiling down to a total additional tax
liability of £1,243. In Scotland, the rate of 47% applies at the same interval.
Higher-rate taxpayers currently have the benefit of up to £500 as a tax-free allowance on interest, while additional rate taxpayers lose this allowance and pay tax on all interest.
The tax-free dividend allowance has now been reduced to £1,000 from 6 April 2023 and it goes down further to £500 from 6 April 2024.
The capital gains tax annual exemption has now reduced to £6,000 and then drops to £3,000 from 6 April 2024. Again, this offers planning opportunities.
MAKING TAX DIGITAL
The legislation for businesses to comply with making tax digital (MTD) rules has been delayed numerous times. Currently, VATregistered businesses, mainly medico-legal private practices, are required to keep digital records and
file returns using compatible software.
If you are self-employed or a landlord, then you will need to comply with the legislation from 6 April 2026 (income of more than £50,000) or 6 April 2027 (income of more than £30,000).
HMRC has stated that MTD will not be mandated for companies until April 2026.
Taking specialist professional advice will help you ensure that you have robust systems in place to deal with this legislation and help avoid unnecessary stress and risk.
Coming in September: Alec James gives a pensions update on the ‘McCloud remedy’
Richard Norbury (right) is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: TESLA MODEL Y
Is Tesla running out of sparks?
It’s a great package, but our motoring correspondent Dr Tony Rimmer (right) reckons Tesla has a job to do if it wants to stay in front
MEDICAL
INVESTIGATIONS , diagnoses and treatments change over time as new knowledge, techniques and medications advance.
Hopefully, each change also improves outcomes for our patients. Car makers must evolve too; there is too much competition around to remain complacent, even when you lead the pack.
In the world of electric vehicles (EVs), Tesla has been the go-to brand for most buyers for the last few years. However, it now faces increasing competition from the big brands as a steady stream of new electric rivals hit the showrooms.
The original Tesla Model S and Model X had the EV field to themselves, but remain niche products and are expensive to buy. In fact, Tesla has just withdrawn them from sale in the UK in RHD form.
Instant success
When the more affordable and smaller Model 3 went on sale here in 2019, it was an instant success. Many more buyers now had access to Tesla design and technology and could enjoy the benefits of access to the brand’s Supercharger network.
But it is a saloon and many families demand greater space and the
practicalities of a hatchback. So Tesla responded with the Model Y, a slightly larger hatchback evolution of the Model 3 that uses the same electric platform.
Like its smaller sibling, there are three versions available. The entry-level £44,990 Standard Range has one 275bhp electric motor powering the rear wheels and WLTP range of 283 miles.
The £52,990 Long Range has dual electric motors producing a combined 412bhp, four-wheel drive and a range of 331 miles.
If you go for the £59,990 flagship Performance model, it has bigger dual motors producing
473bhp, four-wheel drive and a range of 319 miles.
All Model Ys share a full and impressive set of standard features, the dominant one being Tesla’s unique in-car technology controlled via a huge and dominant 15” touchscreen.
Autopilot functions
Almost every feature of the car’s controls is operated via this screen.
As in the Model 3, there are no instruments, digital or otherwise, directly in front of the driver. Autopilot and autosteer functions also feature on all models, with
Almost every feature of the car’s controls is operated via the 15” touchscreen
TESLA MODEL Y long range
Body: Five-seat SUV hatchback
Engine: Dual electric motor. All-wheel drive
Power: 434bhp
Torque: 493Nm
Top speed: 135mph
Acceleration: 0-60mph in 4.8 seconds
WLTP claimed range: 331 miles
CO2 emissions: 0g/km
On-the-road price: £52,990
full autonomous driving elements available at significant extra cost.
You enter the Model Y with a credit-card sized key or use the phone App that is downloadable. The driving seat is comfortable and the interior feels light and airy, but some of the interior trim feels cheap and of poor quality for a car of this price.
Tesla has made the most of the packaging benefits afforded by the electric drive so there is plenty of space for all passengers. The hatchback boot is large and there is extra storage space below the boot floor.
So does the Model Y drive differ-
ently from the Model 3? Well, as with all EVs, the instantaneous torque and minimal noise is impressive and the car feels just as sprightly.
Stream of acceleration
You get up to speed really quickly with one long uninterrupted stream of acceleration. The suspension feels firm and a little unsettled when dealing with urban potholes at low speeds. In fact, the ride quality is really too firm for most people for most of the time, probably the Model Y’s biggest fault. The steering is very direct and contributes to an
almost go-cart feel in town; welcome when threading through busy traffic but a bit oversensitive for the open road.
The handling on A and B roads is pretty good and helped by the low centre of gravity from those big batteries, but this is not a sports car.
Strangely, the fast Performance model, which has had some suspension changes to suit higher speeds, actually rides better than the cheaper and slower variants. Perhaps Tesla should make these changes across the whole range.
The model Y is better suited to motorways where the low aerodynamic drag helps economy and the driver aids are at their most helpful.
Being a Tesla, it has access to the impressive Supercharger network with 1,000 UK stalls and 10,000 in mainland Europe.
Beware though, because Tesla has opened up many of its sites to third-party use, so you may find yourself competing with a Mercedes or Audi.
I suspect that most medic families will charge at home for most of the time and with a real-world range of 200-250 miles, this may only be necessary once a week.
So, the Model Y is a great package and I am not surprised that it is selling in big numbers. However, it is let down by a poor ride quality and does not feel as solidly put together as its rivals.
Tesla needs to tackle these issues soon or it will lose out more and more to competitors from Europe, South Korea and China.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The Model Y gets up to speed really quickly with one long uninterrupted stream of acceleration
WHAT’S COMING IN OUR SEPTEMBER ISSUE
Coming in our September issue, published on 5 September:
Breaking up is not so hard to do. Partnership dispute specialist Ross Clark of Hempsons looks at the major causes of disputes in consultants’ groups and partnerships and shows how much of the pain can be avoided
More big pension changes for thousands of doctors are on the way. Specialist medical accountant Alec James of Sandison Easson provides an important update on the forthcoming ‘McCloud Remedy’
Closing down your private practice. Dr Kathryn Leask gives a detailed and useful response to answer a private consultant who wants to start the process of retiring and closing her private practice
Digital solutions, such as electronic health records and virtual consultations, offer promising avenues for creating sustainable healthcare systems while ensuring efficient and accessible patient care. Robin Clarke, medical director, Bupa UK Insurance and Bupa Global, reports
The law gives the Care Quality Commission an important role in public health care protection. A solicitor gives some words of warning about dealing with the watchdog and concludes: ‘Be careful; recognise the role and work with the CQC not against it’
A Harley Street GP relates a heart-moving story about the setting up of his new private practice
INDEPENDENT PRACTITIONER
TODAY The business journal for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Psychiatrists under the cosh. We share an analysis of claims made against private psychiatrist MDU members, authored by claims team manager Dr Claire Wratten and Lee Lewis, high value claims handler
Sticking with a sensible portfolio strategy. In the past few years, obituaries for a traditional ‘balanced’ portfolio of, say, 60% equity and 40% bonds have been written by many journalists and fund managers. But our Cavendish Medical expert considers such a portfolio continues to be alive and kicking
True Alfa Romeo style? Our ‘Doctor On The Road’ columnist Dr Tony Rimmer tests the marque’s new Tonale
Withdrawal of consent – what are the doctor’s obligations?
Thousands of private doctors’ patients sign up for their private medical insurance through members of the Association of Medical Insurers and Intermediaries. We hear more about what it does and how it’s changing
Hound it out? A patient brings their large and boisterous assistance dog to a medical appointment – and frightens a nurse when it jumps up at her. Now the consultant owner writes: ‘Obviously, I do not want my staff to be frightened at work and am wondering whether we can refuse entry to the animal because of hygiene or patient safety?’ Dr Sally Old of the Medical Defence Union gives her view
Plus advice from Civica Medical Billing and Collection, the latest from the Independent Healthcare Providers Network and all the news and views
ADVERTISERS: The deadline for booking adverts in our September issue is 18 August
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140