KIM LEADBEATER: “CHANGING THE LAW IS THE RIGHT THING TO DO”
The Labour MP on the need for a balance between dignity and safety with the End Of Life Bill
“REGULATION IS PART OUR BLOODSTREAM”
In conversation with The London Clinic’s chief executive Al Russell
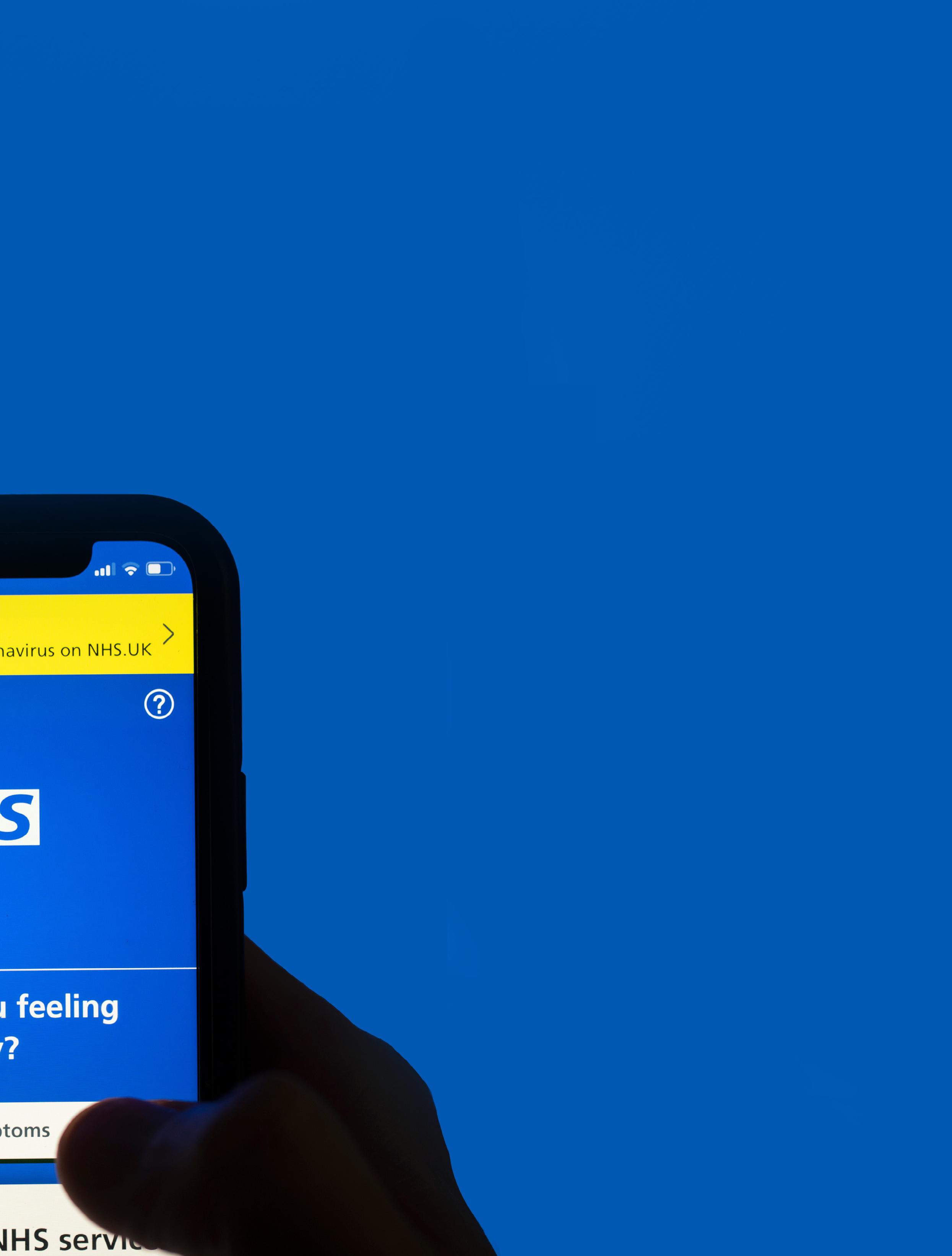
THE LEGACY OF THE NHS COVID APP
Looking at the app’s legacy in driving digital healthcare transformation
WELCOME
OCTOBER
“I strongly believe in personal choice and that people should be autonomous in the decisions that they make about their own lives.”
Kim Leadbeater, the Member of Parliament for Batley and Spen, has many times declared that she is “not a political person”. However, much to her own surprise, she is in the spotlight as one of the figureheads pushing the Terminally Ill Adults (End of Life) Bill into law.
Here, the Labour backbencher talks about safeguarding vulnerable people, the importance of making genuine choices and the need for a balance between dignity and safety.
Also in this issue, Australian GP Bhawani O’Brien explains why patient care remains at the heart of voluntary assisted dying; Rakeeb Chowdhury, the chief executive and founder of Hummingbirds Medical, explains why current recall systems are widely seen as fragmented, admin-led, and clinically unsafe; and much more...
We hope you enjoy!
Contact:
Contact: Glen Ferris, Editor In Chief
24-27 34-37
To
DISPARITIES REMAIN IN MATERNAL CARE
THE scandal of maternity care in the UK continues. The MBRRACEUK collaboration, co-led by Oxford Population Health’s National Perinatal Epidemiology Unit, has reported that 257 women died during or shortly after pregnancy in 2021-23, a rate of 12.8 per 100,000 women giving birth.
Although there was a slight improvement in the UK maternal death rate between 2021 and 2023, as Healthcare Today reported in February, the analysis finds that persistent disparities in maternal care remain.
Over the same period, black women were more than twice as likely to die during or up to six weeks after pregnancy when compared with white women. Asian women and women from mixed ethnic backgrounds also had a slightly, statistically non-significant increased risk of death when compared with White women. Women living in the most deprived areas of the UK were more than twice as likely to die when compared to women living in the least deprived areas.
The data also showed that 91% of the women who died during or up to a year after pregnancy faced multiple or interrelated challenges, including multiple and severe disadvantages, physical health problems, and mental health challenges.
“This latest national enquiry has identified several key actions which are needed to ensure women with medical, mental health and social challenges receive appropriate care,” said Marian Knight, director of the National Perinatal Epidemiology Unit and MBRRACE-UK programme lead.
The report presents a number of recommendations for maternal medicine networks in England, health boards and integrated care boards, NICE, and the NIHR to improve the care of women with complex medical, mental health and social needs.
Is suggests that urgent referral pathways must be set up to assess high-risk women for senior or specialist review in early pregnancy; that discharge summaries provided by hospitals for primary care (including local GP surgeries) should include a summary box of actions concerning conditions that require postnatal management; and that care guidelines for women with complex social needs should be updated to include clear steps for asking about and recording social risk factors early in pregnancy and again later.
It also recommends that codes for domestic abuse in women’s records are used and information is shared appropriately in the event of safeguarding concerns, and that specialist perinatal mental health teams undertake a leadership role for the care of pregnant or recently pregnant women with mental health conditions, even if women are not accepted for care under their services.
NHS COST NEGLIGENCE
THE annual cost of settling clinical negligence claims has more than tripled over the past two decades, from £1.1 billion in 2006-2007 to £3.6 billion in 2024-2025 due to increased claim numbers and the rising costs of settlements.
A new report from the National Audit Office (NAO) reports that between 2006 and 2007 and 2016 and 2017, the number of settled clinical negligence cases more than doubled, from 5,625 to 11,397.
The cost of clinical negligence in England appears much higher than in many other countries, as the UK offers universal healthcare, does not cap compensation, and has a more comprehensive understanding of the true cost compared to other nations.
NHS Resolution and the Government Actuary’s Department estimate that the cost of clinical negligence cases will continue to increase each year, with annual payments potentially reaching £4.1 billion by 2029-30.
“Despite progress in containing the number of clinical negligence claims in some specialities, the increasing cost of the small number of very high value claims is driving higher costs for taxpayers,” said Gareth Davies, head of the NAO.
“Reducing harm to patients is clearly the best way of containing this cost. Alongside this, DHSC [Department of Health and Social Care] should consider whether the existing approach to legal costs remains proportionate for all claims, including whether alternative methods to compensate for negligent treatment could provide better outcomes for patients, with less cost overall,” he continued.
The response unsurprisingly “The report an important negligence,” interim Services (HSSIB).
“Clinical the picture. data on reflection incidents suffering burden,” Organisation and Development this could potential England
The figures are on a par with those reported by NHS Resolution in August this year. It said that NHS negligence claims had risen almost billion.
COST OF SETTLING CLINICAL
NEGLIGENCE CLAIMS HITS £3.6BN
almost 11% over the past year to £3.1
response to the report was unsurprisingly bleak.
report from the NAO has shone important light on the cost of clinical negligence,” said Rosie Benneyworth, interim chief executive of the Health Services Safety Investigations Body (HSSIB).
“Clinical negligence costs are only part of picture. When combined with other on patient harms, it is a stark reflection on the true cost of safety incidents and failures – causing human suffering and carrying a huge financial burden,” she added, pointing out that the Organisation for Economic Co-operation Development (OECD) suggests that could be 13% of healthcare spend – a potential cost of £25 billion each year in England on safety failure.
To reduce the costs associated with unsafe care, the number of recurring safety incidents, and the resulting harm to people and their families, it was crucial to look “beyond the technical solutions to legal liability and focus on prioritising patient safety in a proactive way,” she said.
The Association of Personal Injury Lawyers (APIL) also focused on the human cost.
APIL executive committee member Suzanne Trask pointed out that one of the reasons for the increase in claims was that the cost of providing care has risen exponentially due to broader economic factors, including the provision of carers.
“Looking after the needs of people who have been harmed is inherently expensive,” she admitted.
But it cannot be overlooked that the rate of avoidable harm in the NHS has also increased. The bigger picture, she
emphasised, is the human cost. “Negligence and suffering are at the root of every penny spent on trying to put it right,” she said.
“Behind these figures are real people whose lives have been changed by avoidable harm - the focus must stay on prevention and accountability,” commented Matilda Blundell of specialist medical negligence law firm Tomlin & Partners.
The response from Steven Davies, head of legal services at Medical Protectio, said that it was right to question whether the sums paid out on NHS clinical negligence claims are sustainable and said it was welcome that this issue is starting to get attention.
“It is vital that quick steps can now be taken to introduce fixed recoverable costs in relation to legal fees combined with the development of a comprehensive strategy that balances fair compensation for patients and affordability for the NHS and society,” he said.
PUBLIC UNAWARENESS OF NHS CHOICE FRAMEWORK
HEALTHCARE review platform Doctify has found that many patients in England are unaware of their rights under the NHS Choice Framework, and only 20% in England have exercised these rights before.
Under the Choice Framework for NHS England, patients have the right to choose their provider and select their consultant, and in some cases to receive faster treatment.
The survey insights revealed that almost two-thirds (63%) of people in England were unaware of or unsure regarding their rights under the NHS Choice Framework.
“Under NHS law, you have the legal right to choose your healthcare provider at no extra cost. This right is guaranteed by the NHS Constitution in
England, giving you control over who manages your care,” said Stephanie Eltz, chief executive and co-founder of Doctify.
She went on to say that this right applies when a GP, dentist, or optometrist refers you for elective care (non-emergency treatment), and it’s not limited to NHS services. Patients can also choose from private providers that have an NHS commissioning contract.
Data split analysis revealed that men were more likely to be aware of their rights (40% for men versus 35% for women), and those aged 25-34 were the age group with the highest acknowledgement of this. Awareness dropped below 30% for those aged over 55.
There was also a disparity between regions. In South England awareness
stood at 40% and in Northern England at 37% while that slipped to 29% in South West England.
Overall, frequency of exercising these rights spanned between one and four occasions, with an average of 2.2 times.
Gender split data, however, showed that when women did exercise this right, they did so (marginally) more frequently than their male counterparts – 2.3 times for women versus 2.1 times for men.
“Despite these rights being clear in the NHS Constitution, the reality is that many patients are unaware of the freedom they have to choose beyond local hospitals or the first available specialist, which means they often miss the opportunity to take charge of their healthcare and make decisions that best suit their needs,” said Eltz.
EXCESS DEATHS ASSOCIATED TO LONG A&E WAITS IN SCOTLAND
THE Royal College of Emergency Medicine (RCEM) has highlighted more than 800 deaths associated with long A&E waits before admission in Scotland last year. This is an increase of a third – 202 people – from the figures in 2023.
Over the warmer months (1 June until 31 July 2025) one in 24 people (9,881) endured a stay of 12 hours or more from their time of arrival at an Emergency Department in Scotland. This is 7,003 more patients than the entire year of 2018.
When looking at July alone, 4,686 people experienced this extreme wait – over 2,400 more than in the winter month of January 2022 (2,266). Meanwhile, further analysis for last year reveals a record 76,510 patients waited 12 hours or more to be admitted, discharged or transferred from A&E. That’s 20,432 more people who endured an extreme wait compared to 2023.
Using the Standard Mortality Ratio – a method which calculates that
there will be one additional death for every 72 patients that experience an eight to 12-hour wait prior to their admission – RCEM estimates that there were 818 associated excess deaths related to stays of 12-hours or longer before being admitted in 2024.
Calling the deaths “a national tragedy”, RCEM Scotland’s vice president Fiona Hunter said: “It doesn’t have to be this way – the crisis is fixable and it comes down to patient flow in hospitals – getting people out of A&Eand into a ward bed and getting them out of hospital when they are well enough to go home.”
Responses for the census were received from 28 major emergency departments, along with three rural and remote hospitals.
It found that there is one whole time equivalent consultant for every 4,692 attendances. While it’s a significant improvement compared to RCEM’s census in 2021, it’s still
below RCEM’s recommended figure of 1:4,000.
There were 16 gaps in the consultant rota – the same when compared to RCEM’s last census in Scotland. Meanwhile, there were 32 in the specialist rota, up from 23, and 26 in the resident doctor rota, down from 28 compared to four years ago. Recruitment issues were highlighted among the main reasons for rota gaps.
The average weekday consultant presence was 14 hours a day, down from 15 hours in 2021. Given RCEM’s recommendation that consultants are present at least 16 hours a day in all medium and large systems, this decline is a worrying find.
“While there have been some slight improvements compared to our first census in 2021, it is still abundantly clear that A&E are not adequately staffed with senior decision makers to deliver high-quality patient care,” said Hunter.
MEDTRONIC CREATES AI AND ROBOTICS HUB
GLOBAL healthtech firm Medtronic has doubled both the size of its London office and grown its London workforce to over 200, to create a global hub for AI and robotics in surgery.
Located in London’s Old Street “Silicon Roundabout”, the Medtronic Centre of Digital Excellence wants to drive research and development in software for robotic-assisted surgery in the UK and globally.
The site is part of a multi-milliondollar investment in the Britain over five years and brings together some of the UK’s leading medical software engineers, including new software developer roles, to advance digital surgical capabilities and applications, across global healthcare systems.
“The future of surgery is increasingly digital. Our investment reflects the significant talent and innovation
here in the UK, including in AI, and is a statement of intent to transform healthcare outcomes for surgeons and patients worldwide, said George Murgatroyd, the company’s vice president of digital technologies.
The Medtronic London centre has already designed highly specialised computing and software for operating rooms – now installed in more than 30 countries worldwide. The team has developed and launched many AI algorithms to help surgeons automatically access data and analytics after performing surgery.
This digital technology supports surgical teams in their planning, learning, and collaboration with other experts around the world - including through secure live streaming.
The London centre is central to Medtronic’s surgical robotics innovation – with capabilities in development, including AI-powered
decision support capabilities for surgeons while they operate, in real-time.
The site also features a mock robotic operating theatre to test new technologies and allow healthcare professionals to engage directly in the future of digitised procedure rooms.
In March, Prokar Dasgupta, professor of surgery at King’s College, London, and chair of the Centre for Robotics at The London Clinic, highlighted how robotic surgery has become democratised.
He said that patients experience less blood loss, reduced pain, shorter hospital stays and faster recovery. More to the point: “Despite initial concerns over cost, studies have since demonstrated that the minimally invasive technology is cost-effective for most cancers when compared to open surgery,” he wrote.
X-ON HEALTH PARTNERS WITH DRINKAWARE
X-ON Health, a supplier of digital software for equal access to primary care, has partnered with Drinkaware to integrate the alcohol charity’s resources into X-on Health’s AI Surgery Assist chatbot.
Through the partnership, patients who engage with the chatbot and mention alcohol concerns, whether in the context of health, prescriptions, mental wellbeing or general enquiries, will automatically be signposted to Drinkaware’s information and self-help tools. These include access to the drinking check, advice on how to moderate your drinking, and links to mental health guidance.
The thinking behind the partnership is to take a community-first approach, empowering patients with accurate, non-judgmental advice at the very first point of contact, before they ever speak to a GP or nurse.
“It is exactly the type of collaboration the NHS Ten Year plan envisages, using AI and digital tools to help GP surgeries reduce demand,” said Drinkaware’s chief executive, Karen Tyrell.
X-on Health provides digital telephony services to over 60% of England’s GP practices.
MHRA ENFORCE NEW RULES FOR WEIGHT-LOSS MEDICINES
THE Medicines and Healthcare products Regulatory Agency (MHRA), in partnership with the Advertising Standards Authority (ASA) and General Pharmaceutical Council (GPhC), has jointly released an updated enforcement notice to reiterate the rules around the advertising of prescriptiononly medicines used for weight management.
The rules around prescription-only medicines for weight management continue to be broken.
Towards the end of April, the GPhC issued a joint enforcement notice making clear that adverts for named prescription-only medicines for weight management are prohibited.
“It is vital that people receive prescription-only medicines, such as those used for weight management, only after having an appropriate consultation, and when their prescriber has independently verified that the medicines are clinically appropriate for them,” said chief enforcement officer at the GPhC, Dionne Spence.
This was followed up in August with a letter to pharmacists. Roz Gittins, the chief pharmacy officer at the GPhC, raised concerns about a number of patient safety risks.
The letter was written to “raise awareness of some emerging issues which have led to concerns being raised with us”. She went on to emphasise that “pharmacy owners, pharmacists and pharmacy technicians have a responsibility to make sure there are appropriate arrangements for the management of medicines.”
The updated notice is directed at businesses, primarily pharmacies, that make these medicines available to the public and provides clarity on the kinds of claims and images in an ad that are likely to break the rules.
Advertisers should avoid language that refers to prescription-only medicines, such as “weight-loss injection”, “obesity treatment jab” or “GLP-1”, imagery likely to be understood by consumers as denoting a prescription medicine, and ads for general weight-loss products or services that direct consumers to other ads, such as website landing pages, promoting prescription-only medicines.
The MHRA re-emphasised that it takes the illegal advertising of prescription-only weight-loss medicines to the public seriously. The MHRA said that it had already taken action against more than 25 businesses that had promoted prescription-only medicines for weight loss to the public.
MENTAL HEALTH ACT DETENTIONS SHOW DISPARITIES BASED ON ETHNICITY
LATEST official figures from NHS England show that black people are more likely to be detained than other people under mental health laws. Detention rates under the Mental Health Act in 2024-25 were high for black people while detention rates among white people were negligible. The figures stood at 262.4 per 100,000 people versus 65.8 per 100,000 for white people. The gap between the use of Community Treatment Orders – requiring patients to comply with court-ordered treatment – for black and for other people has also widened.
Daniel Elkeles, chief executive of NHS Providers, called the figures “concerning”.
“NHS trusts and partners are working hard to understand why these inequalities exist and to better meet the mental health needs of people from ethnic minorities earlier. The figures, showing a disturbing discrepancy in detention rates, emphasise the value and significance of that work,” he said.
Rebecca Gray, mental health director at the NHS Confederation, said that “worrying disparities” in detention rates based on ethnicity which is causing significant concerns to those providing mental health services.
“There is also a clear connection between deprivation and acuity of mental illness visible in today’s figures. Living in areas with the most
deprivation can lead to increased social stressors for people with ongoing or emerging serious mental illnesses – such as poverty and a lack of secure housing or employment. These can drive detention levels and also impact how long people stay in inpatient wards,” she said.
She pointed out that the revised Mental Health Act would hopefully reduce the number of and length of detentions when fully implemented. “Increasing NHS and voluntary, community and social enterprise crisis services in the community designed with communities most impacted by severe mental illness will be an essential part of the evolution of mental health services,” she added.
ASKER HEALTHCARE CONTINUES ACQUISITION SPREE
SWEDEN’S provider of medical products and solutions Asker Healthcare Group continues its acquisition spree in the UK.
It has added endoscopic surgery specialists Novus Med to the group.
Financial terms have not been disclosed.
Kenilworth-based Novus Med has 12 employees and turned over £6.3 million in the year to June. Asker has said that the acquisition is a bolt-on and is expected to contribute positively to the group’s EBITA margin.
Asker’s chief executive Johan Falk called the acquisition an “excellent
complement” to the group. “With this acquisition, we are adding new and innovative technologies in minimally invasive surgery and becoming a more comprehensive partner to the hospitals in the country,” he added.
Earlier this month, Asker acquired British healthcare software firm Health Net Connections (HNC).
EARLY ALZHEIMER’S DETECTION TEST LAUNCHED BY NEUROCLIN
GLASGOW-BASED NeuroClin has partnered with diagnostic testing firm Advance Tests to bring to market Scotland’s first commercially available, blood biomarker test for the detection of early Alzheimer’s.
The test, developed by US Biotech innovators, Lucent Diagnostics, is already in widespread use across the US and is covered by the Medicare system.
Designed for people with symptoms of mild cognitive impairment, the test helps determine whether these symptoms are likely due to Alzheimer’s.
It marks the first time a clinically validated blood test for Alzheimer’s is available in Scotland, outside of a research trial setting, and comes after recent widespread national coverage of NHS clinical trials exploring single-marker biomarker tests.
“We know that changes in the brain linked to Alzheimer’s begin years before symptoms appear,” said Jennifer Lynch, medical director at NeuroClin.
“This new blood biomarker test helps us detect potential Alzheimer’s earlier, giving people access to
lifestyle advice and access to new disease-modifying treatments or research opportunities,” she added.
YouGov research commissioned by Advance Tests shows strong public interest in accessing early diagnosis, but only if patients are aware that it’s possible. The survey found that 76% of people were either unaware, unsure, or didn’t think that rapid blood tests are available in the UK that can help diagnose Alzheimer’s in a matter of days. In contrast, 85% of respondents said they would want to be tested if effective treatment were available, highlighting a clear desire for early diagnosis if patients are made aware of the benefits.
There has been a flurry of advances in research in Alzheimer’s so far this year. Earlier this year, the government backed four new research projects with £6.7 million funding to focus on developing technologies to help dementia patients manage memory loss, communication difficulties and cope better with everyday tasks.
Elsewhere, research has also focused on early identification. A simple brainwave test developed by researchers at the University of Bath and University of Bristol has been shown to detect signs of memory
impairment linked to Alzheimer’s disease years before clinical diagnosis is typically possible. At the same time, a study at UCL has been investigating whether a blood test that measures the protein p-tau217 can improve the early and accurate diagnosis of Alzheimer’s disease.
Earlier this year, the World Health Organization pointed out that dementia is currently the seventh leading cause of death and one of the major causes of disability and dependency among older people globally and costs economies globally £960 billion in 2019.
Although one in three of us is likely to develop dementia – a figure that is probably accurate and rising with age – Laurence Geller, Britain’s largest philanthropic supporter of dementia care research, pointed out that just 20-25% of the funding that goes into cancer research is allocated to dementia.
“With newly approved drugs now available, and growing evidence that lifestyle changes can delay progression, early diagnosis has never been more valuable. This is about giving people time - time to act, time to plan, and time to hope,” said Simon Worrell, chief medical officer at Advance Tests.
Trusted by Clinicians, Chosen by Patients
Located in the Harley Street Health District, Pharmacierge supports over 4,500 GPs and Consultants with seamless, secure e-Prescribing apps tailored for private practitioners.
With our state-of-the-art robotically enabled dispensary and nationwide delivery, we ensure your patients receive their medications promptly, while you prescribe with confidence - anytime, anywhere.
mPrescribe®
Revolutionises private prescribing by allowing you to prescribe flexibly without a laptop, for delivery to your patients nationwide.
Medication range
Due to the range of specialists we support, we stock and source medication not typically found outside of a hospital setting, including refrigerated, controlled, injectable and biologic medication.
Courier delivery
We include same weekday delivery to London postcodes, or next weekday nationally as standard. International deliveries are also available.
"Your mobile app changed my life!"
— Dr Dominic Paviour, Consultant Neurologist "Intuitive and secure."
— Dr Tim Wigmore, Consultant Intensivist & Anaesthetist
Join thousands of clinicians today. Download the app and register online www.pharmacierge.com/register
NHS CHANGES APPROACH TO MEDTECH
THE NHS has revamped its approach to buying the latest medical technology. Rather than buying techbased primarily on cost rather than effectiveness, the new approach could save what it considers “billions of pounds”.
The new approach will consider how well the equipment works for patients in the long term, supports patient and staff safety, and drives down future costs, including warranty.
Following early trials of the value-based procurement guidance and extensive engagement across the health system, including with industry and patient groups, 13 NHS trusts will pilot the new guidance, with rollout across the NHS expected early next year.
“This is about more than cost. It’s about working with suppliers to deliver technologies that bring real value –with better outcomes for patients, greater efficiency for the NHS and sustainable care for the future,” said Fiona Bride, interim chief commercial officer and director of medicines value and access at NHS England.
As well as supporting individual trusts to purchase medtech, the government is partnering with NHS Supply Chain and the NHS London Procurement Partnership to roll out value-based procurement across the country – including for purchasing technology and devices used in cardiology and vascular treatment and the use of AI in clinical settings. The NHS Supply Chain’s Cardiology and Vascular Framework alone is worth approximately £1 billion.
How NHS trusts purchase medical technology differs across the health service, with the absence of any standard guidance. This makes it difficult for medtech suppliers to do business with the NHS and drives suppliers away. It blocks innovation from getting to the front line of patient care.
“The value-based procurement initiative signals a watershed moment in commercial innovation in the NHS and DHSC,” said Lee Joseph, managing director of the NHS London Procurement Partnership.
“I am convinced that one of the best ways to improve the patient journey is to involve the supplier base in ownership and accountability of pathways and outcomes,” he continued.
MATERNITY SAFETY FOR BLACK WOMEN IN THE SPOTLIGHT
THE General Medical Council (GMC) and the Nursing and Midwifery Council (NMC) have published new maternity resources to support patient mental health, tackle discrimination and poor workplace behaviours, and remain compassionate under pressure.
Publication of the resources follows a stark warning from the GMC that harmful cultures are putting mothers and babies at risk.
Healthcare Today has consistently highlighted the issue of maternity safety, such as maternity services at Swansea Bay University Health Board and those at Leeds Teaching Hospitals NHS Trust.
At the beginning of September, a report from the Health Services Safety Investigations Body (HSSIB) reiterated that challenges in maternity and neonatal safety are the result of
systemic issues at a national level, rather than isolated issues within local areas.
What has been dubbed by the GMC as an “ethical hub” is an attempt to place a spotlight on the need to tackle inequalities in perinatal care and address disparities – particularly for patients from ethnic minority backgrounds.
The advice comes as the publication of The House of Commons Health and Social Care Committee Report on Black Maternal Health highlights the stark inequity in maternity outcomes and care experienced by black women in England.
It follows a 2016 report which found that “[B]abies that are black or black British Asian or Asian British have a more than 50% higher risk of perinatal mortality”. It was backed up by a study from Mothers and Babies: Reducing Risk through Audits and Confidential
Enquiries that found that between 2021 and 2023, black women were 2.3 times more likely to die in pregnancy, childbirth or the postnatal period than white women.
Publication of the report follows an inquiry in June last year to examine the reasons for slow progress in improving outcomes for black and brown women giving birth, despite government policies and taskforces. The committee heard from black mothers who had experienced poor maternity care, including concerns being dismissed, delayed clinical responses, and patchy postnatal care.
“The UK must tackle the unequal and unfair differences in maternal health outcomes and experiences of care for Black and minoritised women. We have known about these disparities for many years,” said Marian Knight, director of the National Perinatal Epidemiology Unit (NPEU).
SHEMED RAISES $50M SERIES A FUNDING
LONDON-BASED health tech company SheMed has raised $50 million (£37.3 million) in Series A funding. The firm has said that it is not disclosing its investors for this round.
The funding will be used to expand SheMed’s UK operations, scale its medical and technology teams, strengthen clinical infrastructure and enhance its data-driven capabilities. The investment will also support new research and patient-experience initiatives designed to improve access to care for women across the country.
Founded in April last year by sisters Olivia and Chloe Ferro [pictured above], SheMed has grown rapidly to address the gap in women’s healthcare: access to customised, trustworthy and sustainable solutions.
Its programme integrates medical oversight, wellness tracking and 24/7 support through an all-in-one digital platform, which ensures every woman receives tailored individual care while providing a platform that is redefining the healthcare space.
SheMed is best known for its GLP-1 and weight-management platform,
which blends medical expertise, data insights and support to help women achieve health results. The company claims more than 60,000 members and is one of the fastest-growing GLP-1 programmes in the country.
There is a clear market need for the platform. The Medicines and Healthcare products Regulatory Agency (MHRA) has had to take repeated action against rogue advertising of prescription-only weight loss medicines.
As Rachael Joy, the firm’s chief clinical officer, pointed out in Healthcare Today recently, GLP-1 treatment is a “welcome shortcut for overweight Brits, but it also increases the risk of health complications by allowing medications to be taken by the wrong cohort”.
Relying exclusively on body mass index (BMI) and a short questionnaire fails to identify pre-existing health issues that would contraindicate GLP-1 treatment, she wrote.
Joy cited a SheMed study of 16,000 women who took the company’s mandatory blood test before enrolling in their medically supervised weight-loss programme, nearly 500 had underlying conditions that would disqualify them from GLP-1 use or that needed to be addressed before beginning a GLP-1 regimen, and 99% showed some abnormality of which participants were not previously aware.
The SheMed programme includes a follow-up programme with suggested blood tests at six and twelve months to identify adverse reactions; weekly weigh-in calls, monthly questionnaires and check-ins to track participants’ progress and safety; and live check-ins and refill questionnaires to continue receiving GLP-1 medications.
Later this month, SheMed says that it will publish results from the first female-focused GLP-1 clinical study. The findings should provide insights into how GLP-1 medications affect women’s hormonal and metabolic responses.
BUPA ACQUIRES KING EDWARD VII’S HOSPITAL
INTERNATIONAL healthcare group
Bupa will acquire King Edward VII’s Hospital, an independent private hospital located within London’s Harley Street Health District.
Financial terms have not been disclosed, but this is the group’s second acquisition since it announced plans in July to acquire New Victoria
Hospital, an independent private hospital in Kingston upon Thames.
King Edward VII’s Hospital has 56 beds, three operating theatres and a specialist outpatient and diagnostic medical clinic that opened in 2022.
“The addition of King Edward VII’s Hospital creates a hub of specialist
services within the London region, enabling patients to get fast access to care,” said Sarah Melia, general manager of Bupa Health Services.
In August, Melia told Healthcare Today that acquisitions would occur: “Where it’s appropriate, and where we can provide more care directly to our customers and patients.”
GOVERNMENT PUSHES INTO AI
A NEW AI research screening platform dubbed AIR-SP and backed by nearly £6 million in government funding is being built by NHS England to enable trusts across the country to join trials of AI in screening to help speed up diagnosis.
At the same time, a new national commission will help accelerate safe access to AI in healthcare and across the NHS by advising on a new regulatory rulebook, which is set to be published next year.
The new NHS-wide cloud will hold multiple AI tools in a single environment that will have secure connections to all NHS trusts. It should cut down the time and costs associated with rolling out AI research studies.
The new platform, which will take two years to build, means that futuristic tools could be tested and trialled at the same time, in any trust across the health service, with a view to rolling them out to the NHS frontline if they are proven effective.
It will first be used to support 700,000 women across the country taking part in a National Institute for
Health and Care Research (NIHR)funded trial, identifying changes in breast tissue that show possible signs of cancer and referring them for further investigations if required.
Simon Vincent, chief scientific officer at Breast Cancer Now, welcomed the investment.
“We hope that the introduction of this single shared system will make it both quicker and easier for trusts across the UK to test AI tools that could hold the potential to improve early detection and make the breast screening programme even more effective,” he said.
The UK National Commission on the Regulation of AI in Healthcare will bring in experts from tech companies – like Google and Microsoft – as well as clinicians, researchers and patient advocates, to advise regulators on how to speed up access to the latest tech.
The commission will be chaired by Alastair Denniston, head of the UK’s Centre of Excellence in Regulatory Science in AI & Digital Health (CERSI-AI), and deputy chaired by patient safety commissioner Henrietta Hughes. It will guide the
Medicines and Healthcare products Regulatory Agency (MHRA) on how AI technologies can be safely and effectively integrated into everyday healthcare.
Supported by the Health Foundation, the commission will shape the new rulebook. This will help enable commitments in the government’s 10 Year Health Plan for England and Life Sciences Sector Plan to transform the NHS.
AI is already being used to analyse and interpret acute stroke brain scans to support doctors when diagnosing and making treatment decisions in all stroke units in England. Thanks to the AI Diagnostic Fund, half of hospital trusts are now deploying AI to help diagnose conditions like lung cancer. Separate research has indicated that hospitals using AI-supported diagnostics have seen a 42% reduction in diagnostic errors.
Representatives, including other regulatory bodies, from across the healthcare ecosystem in the UK and internationally, will have voices in the AI National Commission, ensuring advice balances innovation with patient safety.
CALLS TO CUT RED TAPE FOR CANCER TREATMENT
IN A briefing note, the Royal College of Radiologists (RCR) and the Society of Radiographers (SoR) have warned that current commissioning and funding structures are stifling innovation and causing unequal access to cancer treatments.
They say that problem with the current funding model is that Trusts are not incentivised to offer innovative cancer treatment. Cutting unnecessary red tape will give patients faster and fairer access to the best cancer treatments closer to home, they say.
“Our NHS pioneers and delivers some of the most cutting-edge cancer treatments in the world. However, red tape is preventing equal access to innovative types of radiotherapy and new drugs that can transform lives,” said Nicky Thorp, vice-president for clinical oncology at the RCR.
“The upcoming Cancer Plan presents a fantastic opportunity to
commit to reconsider how these are commissioned and funded. This would shift the dial by encouraging trusts to embrace innovation and helping more patients benefit from the latest treatments,” he continued.
The RCR and SoR propose that the Cancer Plan should include a commitment to reconsider how innovative cancer treatments are commissioned and funded. Any new approach should consider the elimination of treatment funding tariffs. This, the briefing note says, would eliminate “perverse financial incentives” and promote the use of “cost-effective, patient-focused innovative treatments”.
Funding should also include both workforce costs and the full cost of treatments of those like stereotactic ablative body radiotherapy (SABR), a method of accurately targeting radiotherapy to a tumour from many different directions. At the same time, an incentive payment would help trusts to facilitate new treatments that require additional expertise or training.
Finally, services should be designed to enable patients to access them no matter where they live, and medical royal colleges and other professional bodies should work with regulators to produce consensus and guidance.
“Our shared goal is to ensure every patient has timely access to the best cancer care. The Cancer Plan is a vital opportunity to ensure radiotherapy is properly supported, professionals are empowered, and patients can benefit wherever they live,” said Charlotte Beardmore, executive director of professional policy at the SoR.
AI PLATFORM ANTICIPATES VASO-OCCLUSIVE CRISES
AN artificial intelligence platform developed by London-based digital health company Sanius Health has been developed to anticipate painful vaso-occlusive crises – a significant breakthrough for rare haematology care and managing sickle cell disease.
The platform uses predictive analytics to forecast crises with up to 92% sensitivity, giving patients actionable lead time and enabling clinicians to intervene earlier.
“Imagine knowing a crisis is coming before it strikes,” said Orlando Agrippa, founder and chief executive of Sanius Health.
“This is about moving from reactive care to proactive care. Instead of waiting for pain to send someone to the emergency room, we can anticipate problems and step in early. For families and healthcare systems alike, the benefits are enormous,” he added.
Sanius Health’s technology is designed to integrate into patient lives and clinical workflows. Data captured from smartwatches (such as activity, sleep and heart rate), alongside mood, fatigue, and hydration reports, feeds into machine-learning models that identify changes in physiology and lifestyle.
When risks rise, the system provides them with clear advice on whether to rest or hydrate, or contact their healthcare provider.
Sanius Health has presented results from its predictive models at a number of global scientific haematology conferences.
In one study involving 399 patients and 1.2 million data points, the AI achieved 92% sensitivity in predicting crises.
Patients using the system reported fewer emergency admissions, shorter hospital stays, and improvements in quality of life.
Providing first class medical consulting and therapy rooms at prime locations in Central London and Liverpool
London
tenharleystreet.co.uk 020 7467 8300 Liverpool eightyeightrodneystreet.co.uk 0151 709 7066
Harley-quarter-ad-60x100.indd 1
CALL FOR URGENT ACTION ON WELSH MEDICAL WORKFORCE CRISIS
THE Royal College of Physicians (RCP) has launched a manifesto for the 2026 Senedd election, calling on all political parties to commit to urgent action to address the medical workforce crisis, tackle health inequalities and fix social care in Wales.
It comes as new figures show that there has been a rise in the longest waits for consultant-led hospital treatment in Wales.
The total number of patient pathways waiting longer than two years in July 2025 stands at 8,005, a slight increase from 7,447 in June 2025. The number of patient pathways waiting longer than a year has seen a small fall, standing at 156,143, compared to 157,027 in June 2025. Overall, 793,058 patient pathways were waiting for treatment, down slightly from 794,543 in June 2025. The latest figures demonstrate that progress on reducing waiting lists in Wales remains inconsistent. While some headway was made earlier this year on two-year waits, with four months of progress between November 2024 and March 2025, these long waits have seen a rise again this month.
13/10/2016 11:08
The RCP is calling on the next Welsh government to develop a long-term NHS workforce plan to recruit, retain and support doctors across Wales. More than four in five (81%) of doctors in Wales say that NHS staffing is inadequate (compared with 72% across the UK), and 66% work beyond their contracted hours at least once a week (compared with 62% across the UK), risking burnout and impacting patient safety.
A long-term health and care workforce plan should set out a new approach to recruitment and retention in Wales, consider the impact of changing working patterns, tackle rural recruitment issues and address wider issues with infrastructure, technology and working environments. It is also calling for a crossgovernment action plan on health inequalities. Nearly one-quarter of Welsh households and 31% of children are thought to live in poverty. Finally, the college is demanding a transformation of social care with a fully costed plan to increase capacity and reduce delayed discharge.
More than two-thirds (69%) of doctors in Wales say that poor patient flow and a lack of bed capacity are barriers to good care, compared with a UK average of 56%. This pressure on the Welsh NHS leads to unsafe and unacceptable corridor care and often stems from delays in transferring patients out of hospital, which takes several weeks on average.
NHS INPATIENT SURVEY SHOWS IMPROVEMENTS IN PATIENTS’ EXPERIENCES
WHILE the most notable improvements have been around people’s experiences with staff, large numbers of patients report long waits and poorly coordinated discharges from hospital.
This is the headline result of a survey coordinated by Picker for the Care Quality Commission (CQC), which looks at people’s experiences of hospital treatment, including at least one overnight stay, and asks about every element of their care from referral to after discharge.
Patients’ overall ratings of their care improved compared to 2023: The proportion of those who rated their care very highly rose from 50.8% to 52.1%. The most notable improvements were around the availability of healthcare staff and the care that they provided.
Almost six out of ten patients (58%) said that there were “always” enough nurses on duty to care for them in
hospital, which is up from 56% in 2023 and only 52% in 2022. At the same time, almost two-thirds (65%) of patients said that they could “always” get a member of staff to help when they needed attention, which is an improvement from 63% in 2023 and 62% in 2022.
“The latest large-scale survey data shows modest improvements in people’s experiences of NHS hospital care up to the Autumn of 2024,” said Chris Graham, chief executive of Picker.
The problem remains, however, patients’ journeys through care, with challenges at the front door and as people leave hospital. Two out of five people (42%) who had a planned admission said that they would have liked to have been admitted to hospital sooner, and 43% said that their health got “a bit” or “much worse” whilst they were on the waiting list.
As Healthcare Today reported in June, analysis by the Royal College of Emergency Medicine (RCEM) shows that there were more than 16,600
deaths associated with long A&E waits before admission in England last year. That’s an increase of 20% (2,725) compared to 2023.
At the end of their hospital stay, only half (49%) said that they were “definitely” given enough notice about when they would leave, and 40% said that hospital staff involved their family or carers in discussions about their discharge “not very much” or “not at all”.
“Although these improvements are welcome news for patients, far too many people are still reporting problems in their care,” said Graham.
“Being fully involved in one’s own care remains the exception rather than the rule, and the coordination of care across and between services – such as when people are discharged home – is too often lacking,” he continued.
This year, 131 Trusts took part in the survey, and more than 62,400 patients responded. Fieldwork for the survey took place between January and April this year.
NHS CHANGES APPROACH TO MEDTECH
THE NHS has revamped its approach to buying the latest medical technology. Rather than buying techbased primarily on cost rather than effectiveness, the new approach could save what it considers “billions of pounds”.
The new approach will consider how well the equipment works for patients in the long term, supports patient and staff safety, and drives down future costs, including warranty. Following early trials of the value-based procurement guidance and extensive engagement across the health system, including with industry and patient groups, 13 NHS trusts will pilot the new guidance, with rollout across the NHS expected early next year.
“This is about more than cost. It’s
about working with suppliers to deliver technologies that bring real value – with better outcomes for patients, greater efficiency for the NHS and sustainable care for the future,” said Fiona Bride, interim chief commercial officer and director of medicines value and access at NHS England.
As well as supporting individual trusts to purchase medtech, the government is partnering with NHS Supply Chain and the NHS London Procurement Partnership to roll out value-based procurement across the country –including for purchasing technology and devices used in cardiology and vascular treatment and the use of AI in clinical settings. The NHS Supply Chain’s Cardiology and Vascular Framework alone is worth approximately £1 billion.
How NHS trusts purchase medical technology differs across the health service, with the absence of any standard guidance. This makes it difficult for medtech suppliers to do business with the NHS and drives suppliers away. It blocks innovation from getting to the front line of patient care.
“The value-based procurement initiative signals a watershed moment in commercial innovation in the NHS and DHSC,” said Lee Joseph, managing director of the NHS London Procurement Partnership.
“I am convinced that one of the best ways to improve the patient journey is to involve the supplier base in ownership and accountability of pathways and outcomes,” he continued.
ALL CIRCLE HEALTH HOSPITALS ACCREDITED
THE Association for Perioperative Practice (AfPP) has accredited all 49 hospitals with operating theatres within Circle Health Group and more than 155 operating theatres under AfPP’s Theatre Accreditation and Audit programme.
This makes Circle the first provider in the independent sector to achieve AfPP accreditation across all its theatres.
“AfPP Theatre Accreditation is about far more than compliance. It provides reassurance for patients, confidence for staff, and a culture of continuous improvement. Circle Health Group’s achievement sets a powerful benchmark for others in the independent sector and beyond,”
said AfPP CEO Alex Duke. Circle Health started in 2020 and concluded this year with the accreditation of The Ridgeway Hospital in Wroughton.
AfPP Theatre Accreditation is a structured process that evaluates a hospital’s perioperative services against evidence-based standards. Built on the AfPP Standards & Recommendations for Safe Perioperative Practice (2022), Accreditation ensures services are aligned with recognised national frameworks. The process is not an inspection, but a supportive review that helps theatre teams reflect on practice, celebrate successes, and identify areas for improvement. Accreditation is valid
for two years, with reaccreditation visits ensuring standards are continuously upheld.
Beyond accreditation, AfPP also provides policy reviews, staffing reviews, perioperative peer reviews, and bespoke audit visits – all designed to help hospitals maintain safe, effective, and resilient perioperative services.
The AfPP is a membership organisation that promotes excellence in surgical practice by promoting education, networking and innovation within the sector. By working with healthcare professionals, AfPP’s aim is to provide patient care and safety during operative procedures.
KIM LEADBEATER: “CHANGING THE LAW THE RIGHT THING TO
HAVING been elected as the Member of Parliament for Batley and Spen in the wake of the tragic killing of her sister Jo Cox, Kim Leadbeater has many times declared that she is “not a political person”. Now, much to her own surprise, she is in the spotlight as one of the figureheads pushing the Terminally Ill Adults (End of Life) Bill into law.
Here, the Labour backbencher talks to Healthcare Today about safeguarding vulnerable people, the importance of making genuine choices and the need for a balance between choice, dignity, and safety.
You’ve spoken about the importance of compassion and dignity in end-of-life care. What shaped your own views on assisted dying?
A lot of Members of Parliament (MPs) come into Parliament with a vision: “If I ever got a chance to change an aspect of the law, this is what I would do”.
I didn’t have that. My journey into politics was unique, because of, obviously, Jo’s murder, and my being a reluctant politician. I still don’t think of myself as a politician at all, if I’m honest.
As I have a background in health and wellbeing –via prevention, early intervention, physical, mental and social health – I wrote a report in March 2023 called Healthy Britain, which was about how we could embed wellbeing if the Labour Party did get into government.
I have also always strongly believed in personal choice and that people should be autonomous in the decisions that they make about their own
As one of the figureheads pushing the Ill Adults (End of Life) Bill into law, the Labour talks about safeguarding vulnerable people, importance of making genuine choices need for a balance between dignity and
Written by Glen Ferris.
lives. If you put all those things together, it meant that my view on assisted dying and the choice at the end of life was very much about believing that people should have a choice if the inevitable was to happen.
Every year, you can put your name into a private members’ bills ballot, and if you get drawn out, you get a chance to put a piece of legislation forward. In September 2024, I was in the ladies’ loos in Parliament and my telephone started going bonkers with colleagues and journalists asking what I was going to do with my bill?
I was aware that it was a privileged position to be in and an opportunity to do something which would make a difference to many people.
Having spoken to people who had either lost loved ones through difficult, traumatic deaths or had had loved ones who were terminally ill take their own lives, I believed that I had a duty to do something about this situation.
The Assisted Dying Bill has passed the Lords. How realistic is it that MPs will now get the chance to debate and vote on it?
It has gone through Commons, and it has of scrutiny, debate had more scrutiny than other legislation, certainly Parliament.
Now, the House of Lords job to do. I’m respectful also clear that while and, if necessary, refine House’s job to block
I want to give them they need before the improve the bill, if that’s to happen.
I was, however, a bit from certain colleagues might be an opportunity legislation passing.
That is something I would be upset about, unelected chamber suggests the vast majority country want.
LEADBEATER: LAW IS TO DO”
Terminally Labour MP people, the choices and the and safety.
through all the stages in the has faced huge amounts and discussion. It has than probably any certainly since my time in
Lords has an important respectful of that job, but I’m while they need to scrutinise refine legislation, it isn’t the block legislation.
the time and the space the end of this Parliament to that’s what they think needs
bit disturbed by comments colleagues suggesting that there opportunity for them to stop this
personally, and the public too, about, given that you’ve got an chamber vetoing something that polling majority of people across the
As you say, polls show strong public support for assisted dying. Do you think Parliament is behind the curve on this issue?
Some people have presented this as a new debate and a new subject, but that’s simply not true. It is a debate that’s been going on for decades in this country and across the world.
Polling for a long period of time has suggested that between 70% and 80% of the public support a change in the law to give people the choice of an assisted death.
Some of the most powerful conversations I’ve had have been with people, often people of faith, who have said: “This isn’t something I would want, but who am I to deny other people this choice if it’s something they would want?”
The option of taking control provides such a huge amount of comfort and relief for people and enables them to live out the time that they’ve got left in a much less stressful way.
If the bill does pass, how do you envisage assisted dying fitting into the UK’s healthcare system?
It’s a big change, and it would be wrong to pretend otherwise. What the bill will do is to give a much more holistic approach to endof-life care.
Let’s be honest, health professionals across the country are having conversations about death and dying every single day.
While it is a big change, it’s not something which is totally new, certainly not to them or to many families who’ve experienced the loss of a loved one.
We have to acknowledge what an important change it is, and what a positive change it will make to the choices we give to terminally ill people.
There is a vocal trope, particularly in the British press, that legalisation could put vulnerable people at risk – one that was rubbished by the Australian doctors [see page 34] that we have talked to. What are your thoughts on this matter?
The option of taking control provides such a huge amount comfort and relief for people.
For me, there are two key points around protecting vulnerable people and making sure that only people who want to make this choice actually make this choice.
One is that the bill provides a level of safeguarding which, quite simply, does not exist at the moment. If somebody who has a terminal illness takes their own life, there is currently no legal framework.
The bill creates a robust legal framework that gives clarity to loved ones and stops them from being prosecuted, which can happen at the moment.
The other thing is, because of the many layers of safeguards set out in the bill, there are multiple opportunities for healthcare professionals and others involved in that patient’s care to make sure that this is absolutely the patient’s choice. Whether that’s around capacity or coercion, we have many types of pertinent healthcare professionals involved. What experts from other countries tell us is that if coercion does happen, it actually happens the other way.
Nobody wants to lose their loved one, and they will actually discourage someone from pursuing an assisted death because they don’t want to lose them.
What responses are you getting from the medical profession?
It has been really clear, and this has certainly
played out in the last year, range of views within the medical professions.
I’m respectful of those opinions, why strong protections for professionals who do not want in giving patients this choice included in the bill.
Some of the most powerful had have been with doctors have talked about the time people who are dying.
Sadly, far too many stories patients who have died under deeply traumatising circumstances.
When I compare those stories I’ve spoken to from other countries about the voluntary assisted and what that can look like families, there’s a stark contrast.
Doctors who have a lot of experience end-of-life care hold mixed there are many who really needs to change to give patients a legal perspective.
Everything is about achieving between the emotional side the technical and legal sides.
Whichever way you look at has got to be the right thing
control amount of people.
that there is a medical and legal opinions, and that’s healthcare want to participate choice have been
powerful conversations I’ve doctors and nurses who they’ve spent with have been of under difficult and circumstances.
stories to the doctors countries who talk assisted dying process like for patients and for contrast.
experience in mixed views, but certainly, do think the law patients a choice from
achieving that balance side of this debate and sides.
it, changing the law thing to do.
THE LEGACY OF THE
THIS time five years ago, the NHS faced an urgent need for rapid innovation as the Covid-19 pandemic strained every part of the system – from overwhelming waits for care, to staff buckling under the immense pressure and patients unable to receive treatment for serious illnesses that weren’t Covid.
Because of these unmitigated pressures, the NHS’s Covid App emerged as a swift, but vital response to the problem at hand, showing how quickly technology could be implemented and scaled even at a national level - even under relentless scrutiny.
Now, half a decade after the app’s rollout, its impact is still being felt across the health service, pioneering a more digital-first NHS. From streamlining vaccination appointments to giving patients greater control over their care, the pandemic marked a turning point for innovation. But things like waiting lists remain stubbornly high, posing the question: how can we rebuild this momentum to once again transform our everyday NHS services? How do we make sure we’re not distracted by the latest and greatest procurement projects, and instead focus on scaling the technology that already exists, and integrating it in the right places?
For years before 2020, digital transformation in the NHS had been a slow, often frustrating process – for patients and staff. Efforts to modernise the patient journey and administrative systems weren’t widely adopted (or even accepted). If they were adopted, they were usually limited by outdated processes and fragmented IT infrastructure.
The pandemic, put frankly, was the forcing hand for accelerated
transformation. It ensured the system’s digital maturity had no place to go but up. Solutions were scaled quickly, something that previously would have been a lengthy, slow and costly process. The impact of this transformation has echoed across the countryreshaping what healthcare looks like today, and in the future.
The government recently announced its plan for change, to shift the NHS from analogue to digital. But, according to the Health Foundation, this is going to cost £21 billion over the next five years, requiring additional funding.
Naturally, I support the plans to move from analogue to digital. However, I fear that simply investing in new technology is not enough – and in some places, it’ll be a distraction from where and how we can have the most impact. We need to champion a level of behavioural change within healthcare if we’re to build on the progress that we’ve already made. That means reinvesting in how we realise the benefits of the technology that already exists, on a much greater scale. To do this, we’re going to need to rely on greater collaboration between the public and private sectors. No single organisation can solve the challenges that we currently face. Instead, a multivendor approach would give us the ability to lean into existing technologies (many of which were born out of the pandemic), and integrate them effectively. So, how do we do this?
Focusing on interoperability, patient outcomes, and ensuring long-term sustainability of design will be critical to laying a foundation for further growth and digitisation
Tom Whicher, chief executive DrDoctor, looks at the legacy app in driving digital healthcare
at scale, just like we saw with the Covid app.
Tools that can connect hospitals, GP surgeries, mental health and community services reduce duplication, fractured communications, free up staff time, and improve outcomes for patients.
As the 10 Year Health Plan stated, care needs to move closer to home. By integrating community
THE NHS COVID APP
executive and co-founder of legacy of the NHS Covid healthcare transformation.
healthcare into mainstream digital platforms, patients can expect more accessible and impactful care. This may have seemed ambitious even ten years ago, but with a strong, connected digital backbone, the NHS can achieve such an ambition. Integrations such as community trusts connecting to the NHS App demonstrate how solutions that were born out of crisis can be translated into permanent stalwarts of our healthcare.
One great example of this is the Central London Community Healthcare NHS Trust (CLCH). It recently became the first community healthcare trust in the country to go live in the NHS App, via an integration using DrDoctor.
By connecting the trust’s community services to the wider NHS digital ecosystem, patients can now book and amend appointments, receive notifications, and access information through a single interface, just as they would for hospital care. Through this, they have already seen a 20-30% drop in Did Not Attends.
This shows that the right, interoperable technology can make community care a tangible part of the system rather than a separate bolt-on. Tools like these not only streamline administrative tasks for clinicians but also allow for proactive patient management, such as autorescheduling, follow-up reminders and digital triage, which in turn reduces pressures on clinics. Early adopters like CLCH have led the charge in this respect – when digital infrastructure is properly funded, designed for integration, and part of day-to-day workflows, the ambition of moving care closer to home becomes a reality.
Now, we can’t forget about the data. The pandemic showed that real-time, accurate data can shape proactive care, whether that’s spotting patterns in patientreported symptoms, identifying at-risk populations, or directing resources efficiently. Systems that combine appointment management, patient communications and predictive analytics can use the data to reduce missed appointments,
optimise capacity, and even prevent conditions from worsening. This is such a crucial element of modern healthcare management. Everything in our world is so intuitive, personalised and proactive – so why not our healthcare?
The success of the Covid app has created the conditions for these tools to be adopted more widely and confidently across trusts, proving that digital transformation isn’t just about convenience; it’s about building a resilient health service that works under pressure, instead of faltering.
The legacy of the Covid app extends beyond the technology itself. It has emboldened us to embrace the future. It’s proven the NHS can adapt quickly when the need is urgent and should continue adapting and innovating even when the need is not. It has provided a critical, systemwide mindset shift that the NHS desperately needed. The confidence to say, we can do this. Because we have now shown that radical change at speed and scale is absolutely possible.
So, reflecting on the anniversary of the NHS Covid app, it’s clear that its impact goes far beyond a single moment in time. The app was a catalyst for change, proving the strides we can make when technology meets urgency, and to this day, it continues to shape the way we interact with our care.
That legacy is like a roadmap. It highlights both the progress made and the opportunities still ahead to modernise the NHS. Reflecting on this milestone is not just about looking back, but about learning from the past as we drive the next wave of digital transformation across our health service.
“REGULATION IS PART OF OUR BLOODSTREAM”
AL RUSSELL has not come to The London Clinic by a familiar route.
Rather than medicine, he began his career in technology-related businesses and spent 14 years in business roles at telco Vodafone UK.
Since September 2017, he has been chief executive at The London Clinic, where he oversaw the international collaboration with US healthcare organisation Northwestern Medicine.
Here, he talks to Healthcare Today about how to handle a partnership without losing your own culture, the growth in private medical insurance, and why regulation is embedded in how The London Clinic operates.
You came into The London Clinic from a technology company. Has that influenced your approach to healthcare?
Having done a lot in technology and telecoms, certain things become second nature – both in management practice and in applying processes at scale.
What struck me was how useful that experience could be in healthcare.
Of course, healthcare is about clinical excellence, but it also depends on reliable processes and infrastructure. The common principles of leadership translate across any industry, and hopefully I’ve been able to apply that here as well.
Almost a year on, Al Russell, the chief executive of The London Clinic talks about how he has negotiated the international collaboration with the US’s Northwestern Medicine.
Written by Adrian Murdoch.
The London Clinic has been in partnership with Northwestern for almost a year. What has the experience been like?
The partnership and collaboration with Northwestern Medicine is, without question, an inflexion point for The London Clinic. We’re 93 years old, and this moment is as important in our history as when the foundation stone was first laid.
So, what does the collaboration mean for The London Clinic, and what do we bring to Northwestern Medicine in return? There are several dimensions.
First, resources – to support the growth that both the market and this hospital are seeking.
Second, expertise – particularly in pathways. By that, I mean digitisation of patient pathways and the application of artificial intelligence to support productivity.
Northwestern is already far along that journey in Chicago, and we’re now infusing that expertise into The London Clinic. It’s hugely valuable, and crucially, it works because we share the same values and culture.
What it allows us to do is adopt areas of expertise where we know we can improve, and where Northwestern is already excelling. We’ve deployed people across the organisation to accelerate progress – whether in workforce management, supply chains or translating revenue into cash. These may sound like process details, but they’re essential because without money, there is no mission.
And then, of course, there’s clinical excellence. We’re identifying a series of services that will be unique to The London Clinic, but which are already well established in Chicago. That includes areas such as motility and endoscopy, some cancer pathways, and others we’re exploring.
Were you worried about your culture being subsumed?
The first point to make is that this partnership would never have happened if we hadn’t recognised a shared culture. That alignment was essential, and our discussions over time confirmed it. I never had concerns on that front.
What I have really enjoyed, as chief executive, is infusing the best of Northwestern Medicine into The London
PART BLOODSTREAM”
Clinic, while staying true to who we are. Every organisation can improve, and there are elements of Northwestern’s approach that are outstanding. My aim has been to bring those into our hospital without trying to become something we’re not.
Importantly, it feels like a genuine partnership. They don’t overwhelm us or dictate. Instead, we choose the areas where we want support, and they sit alongside us to help us improve. For our staff, it has been a real development opportunity.
It’s been motivating not just for me and my immediate team, but for the leaders running services day-to-day.
The London Clinic is rare in that it has a Rapid Diagnostics Centre. How important is fast diagnosis versus treatment?
We are very much a cancer-leading hospital. Around 60% of what we do is cancer-related, and of course, the earlier you catch cancer, the better the outcomes.
Consultants increasingly want to work in teams, and that also creates opportunities for us to help ease
some of the indemnity pressures they
face.
The difference in survival between stage one and stage four breast cancer, for example, is dramatic. Yet far too many cancers are still detected at stage three or four. As a not-for-profit charity, our purpose is to advance healthcare for the wider community, and that means giving people rapid access. If I’m worried about something, I want an appointment tomorrow, an answer the next day, and – if it’s bad news – a team around me immediately to support me. That is the gap we’re trying to address.
We make deliberate choices to release capacity. Some of our GPs are not fully booked, and our scanners are not run at maximum every day. That flexibility allows us to deliver very fast turnaround times. We’ve also extended our rapid diagnostic services to neighbouring NHS hospitals, where waiting lists are under pressure.
We’ve written widely about growth in private medical insurance in the UK – how is that affecting demand at The London Clinic?
The commentary and the statistics are clear – private medical insurance is very much the driver of growth for us at the moment, and we’re seeing that borne out here at The London Clinic.
There are, of course, wider factors at play: cancer incidence is rising, PMI membership is increasing, and together those trends are fuelling demand. Our role is to meet that need – to serve that community, and to ensure we are ready to provide leading cancer treatment as that demand continues to grow.
Are you noticing a shift in the balance between insured, self-pay and international patients?
I don’t think the shifts are as dramatic for us as some of the commentary suggests. Yes, we’ve seen one or two percentage point changes, but nothing revolutionary. International patients still account for up to 15% of turnover, private medical insurance (PMI) is now around 60%, and self-pay sits fairly flat at about 15%.
The main difference is simply that PMI is growing a bit faster. At the macro level, health insurance is clearly the main growth area, while embassy work has probably plateaued – though London’s geopolitical advantages offset some of the decline.
Self-pay also feels steady; it certainly still has a role, but it’s no longer a booming part of the market.
Rising indemnity costs are a concern across healthcare. How is this
playing out for consultants working at The London Clinic?
Our consultants are independent of the hospital, and so far, we haven’t seen a major impact on them from these issues. Certain specialisms, in higher-risk areas, do carry traditionally higher indemnity costs, and we’re looking at models to help support and offset that for consultants in the future. But at this stage, it’s not a burning platform for us.
Do you see opportunities for private healthcare operators to develop new models of indemnity or claims resolution? In partnership with insurers or regulators?
The question for us is what role the hospital can play. We want to nurture more group work among consultants, because we believe that’s what the consultant of the
future will expect. It delivers a stronger patient experience, fosters cultures of quality and collaboration, and helps address the professional isolation that has historically characterised the independent sector.
Consultants increasingly want to work in teams, and that also creates opportunities for us to help ease some of the indemnity pressures they face. It is an important dimension we are actively exploring, and it underpins our wider move toward fostering more group work within specialisms.
How do you work with regulators? Does that help or hinder private sector growth?
Working with regulators is simply part of doing business. Even in a relatively small hospital like ours, with 1,400 staff, the cost of
supporting regulation has grown significantly over the past 10 to 15 years.
On a national scale, those costs must be vast. But I see it as business as usual – regulation is part of our bloodstream.
We’re inspected every three months, and while the process can be onerous at times, it is well understood and generally works well.
The Care Quality Commission’s current reassessment of its role is something we welcome and want to collaborate with, but of course, we’re also regulated by other bodies, from the United Kingdom Accreditation Service to the Joint Advisory Group on Gastrointestinal Endoscopy in pathology. The cost has increased, but regulation is embedded in how we operate.
BHAWANI O’BRIEN: “PATIENTS WANT CONTROL OVER HOW THEY
BHAWANI O’BRIEN is a Western Australian GP with decades of end-oflife experience. Following the Assisted Dying Bill’s Second Reading in the House of Lords, she talks to Healthcare Today about capacity assessments, safeguards and why voluntary assisted dying isn’t about rushing death, it’s about reassurance.
The UK is debating assisted dying again. What do you think lawmakers here most need to understand from the Australian experience?
For me, sharing this experience is about reassuring colleagues in Britain that it is safe, compassionate, and that it works. What we are achieving here are calm, peaceful deaths for people whose deaths are already imminent. These patients aren’t afraid of dying itself – what they fear is how they will die.
As doctors, we see deaths that the public often doesn’t. We witness people bleed to death from cancer, suffer intestinal blockages so severe they vomit their own faeces, or gasp for air with end-stage emphysema.
These are deeply traumatic experiences, and while pain is one element, it is far from the only one. Patients also endure intractable nausea, breathlessness, and other symptoms that cannot always be controlled. When you are told this is how your final days will be, and
The Western Australian GP explains why patient care remains at the heart of voluntary assisted dying.
Written by Adrian Murdoch.
it will only worsen, of course you want a choice. That’s what voluntary assisted dying (VAD) has given patients here: choice and control at the end of life, when they are already dying. And that has been transformative.
How has the introduction of VAD changed conversations about death and dying in Western Australia?
There’s sometimes a fear that voluntary assisted dying and palliative care are in conflict. In practice, the opposite is true. In Australia, they work hand in hand.
One of my responsibilities as a VAD assessor is to make sure every patient is receiving palliative care. If they aren’t, I refer them. And under the Act, I can only have conversations about VAD if I also discuss palliative care options, treatments and likely outcomes.
What that has created is a strong and respectful relationship with palliative care teams. They continue to support patients’ rights until the end, knowing the patient may have
VAD in their back pocket if they wish to use it.
Of course, there are still challenges, particularly in some Catholic institutions where conversations are harder. But overwhelmingly, people are reassured when they see their loved ones have calm, peaceful deaths.
Can you describe the impact it’s had on your patients and their families?
I’ve probably assessed more than 200 patients. Every time I ask why they want VAD, the same two words come up unprompted: choice and control. Patients tell me that they have lost control of everything else in their lives because of a disease, but they want control over how they die.
Once patients are found eligible, another word emerges again and again: relief. Families tell us the same – that their loved one seems to gain a new lease on life once the fear of a horrific death is lifted. They can focus on living whatever time remains, reassured that they won’t
O’BRIEN: CONTROL DIE
There’s sometimes a fear that voluntary assisted dying and palliative care are in conflict.
care – in fact, one of my responsibilities at the first assessment is to make sure they are receiving it. If they aren’t, I refer them, whether that means linking them to a consultant in the city via telehealth or community nurses who can visit regularly.
The reality is that many patients are exhausted by their illness, juggling oncology appointments, GP visits, and treatment schedules. They don’t always have the strength to advocate for themselves. Part of our role is to do that for them – to make sure their palliative care needs are being met, while also giving them the reassurance of choice and control through VAD.
Are there any misconceptions in the UK debate that you would like to challenge?
Capacity assessment seems to be a
big fear. But honestly, there’s nothing to fear. We assess capacity every single day. When a patient walks into my room, I assume they have capacity unless my conversation with them shows otherwise. It’s usually very clear when someone doesn’t. With VAD patients, it’s the same – it becomes obvious if capacity is lacking. This is no different to the consent we take for any other medical decision.
The other concern is coercion. In four years of practice in Western Australia, we haven’t seen it. In fact, it’s usually the opposite: families urging their loved one not to consider VAD too soon because they don’t want to lose them. Sometimes patients have to stand firm and say: “I love you, but I can’t go on like this”.
How do we assess coercion? The same way we would in everyday practice – by asking direct questions,
having conversations and observing dynamics. In general practice, I often coach patients to ask their oncologists difficult but direct questions, because clinicians can sometimes shy away from them. The same applies in VAD: it’s a process built on repeated, honest conversations.
What safeguards or practices do you consider most important to ensure VAD is ethical and patientcentred?
Talking is a big part of what we do, but ultimately, we are bound by the Act. Every patient must be assessed by two independent doctors. I explain to people that the second doctor isn’t there to check on them, but to check on me – to make sure I’ve done everything correctly under the law. Patients sometimes find the process long and tiring, so we talk about why: the safeguards,
the safety nets, the double-checks. Everything is carefully scrutinised. After each visit, I complete detailed paperwork that goes to the oversight board, covering everything from the patient’s medical history to whether they’ve been referred to palliative care. The system is designed to keep patients safe and to ensure their options are never limited.
One example stays with me. I saw a man with end-stage renal failure who was living alone in very poor conditions, with almost no support.
At the end of my assessment, I told him he was eligible for VAD, but I also urged him to consider a short stay in palliative care to get his symptoms under control and improve his quality of life. With the help of one of our excellent navigators – nurses, occupational therapists, social workers who guide patients through the system – he agreed. A few days
later, I heard back: he was in a hospice, feeling pampered, and his symptoms were 80% better.
That’s what people need to understand: this isn’t a system where someone applies for VAD, is deemed eligible, and then simply chooses a date. Our role is to look at the whole patient, ensure they are supported by palliative care, and help them live as well as possible until the end. VAD is part of that, but it’s never the only part.
You’ve described this work in the past as “deeply meaningful”. Has it changed how you view your role as a doctor?
I don’t think VAD has changed my view of what it means to be a doctor, but it has transformed my life. I’ve always been passionate about medicine. I chose general practice because I loved cradle-to-grave
care. But over the past decade, GP work has changed; it often feels like a rushed checklist, and I had lost some of the fulfilment I once had.
With VAD, I’ve found that connection again. This work has made my life more meaningful. I find joy in the everyday. It has taught me how precious time is.
What patients remind me, again and again, is that at the end of life, no one talks about career achievements, wealth, or possessions. They talk about love and connection. I’ve witnessed extraordinary moments: families reconciling, relationships healing.
These moments move you deeply. They strip life back to what really matters, and for me, the fulfilment comes from being able to walk alongside people in those final days.
“SAFEGUARDING ACCESS A CRISIS OF CONFIDENCE”
THIS September, GPs in England delivered a stark message: they have voted to re-enter dispute with the government over the changes due to take effect from 1 October, including a requirement to keep online consultation systems open throughout core hours.
Their reasoning? The proposed “unlimited” online consultation requirement threatens patient safety, staff wellbeing, and the very fabric of primary care.
This is not a straw-man protest. It is the frontline’s insistence that policy must meet operational reality. The BMA’s own statement describes “confusion and anger” among GPs, who warn that opening the floodgates of unrestricted online access offers no guarantee of improved care, only the risk of urgent cases drowning in a sea of unmet demand.
If policymakers truly want to strengthen access while preserving safety, it is time to recognise that technology partners are not optional extras; instead, they must be central collaborators in whatever online access model emerges.
The stakes are high
The stated driver of this policy is laudable: reduce the 8am scramble, relieve pressure on phone lines, and broaden digital access. But the BMA’s concern is that unfiltered open access risks becoming a “needle in the haystack” challenge, where urgent patient need is masked by volume.
The concern is not hypothetical. The Health Services Safety
Ric Thompson, senior vice-president of health and care at OneAdvanced, explains why technology partners must be in the room.
Investigations Body (HSSIB) has already documented instances in which online GP consultations contributed to misdiagnoses, delays in escalation, or harm, particularly when symptoms were under-triaged or misunderstood. (For example, see cases where online submissions of pain, infection or cardiac symptoms were underestimated.)
The BMA’s central ask is therefore understandable – that the changes only be introduced once agreed safeguards are in place: functionality to distinguish urgent from nonurgent requests, plus safe overflow routing to telephone or walk-in services when online volume becomes overwhelming.
In short, digital access is powerful and necessary, but dangerous when mis-designed or unmoderated.
Why the GP vote changes the framing
GPs who have rejected this component of the contract should not be treated as bureaucratic resistance. It is, in fact, a demand for a smarter, safer architecture. Their vote is a signal that the profession will not implement mandates without structural supports.
The October deadline should therefore be reframed: as a moment
of transition, not mere compliance. Policymakers should consider phasing implementation based on demonstrable capability. Practices that deploy validated triage tools could be required first; others could follow when ready.
Integrated Care Boards and NHS England should also openly fund and coordinate the deployment of digital infrastructure rather than penalise practices that cannot absorb the changes unaided.
Creating powerful technology partnerships
It’s clear that embedding AI into online consultation systems can have a powerful impact.
NHS-backed studies have shown AI triage tools can cut GP waiting times by as much as 73%, while national think tanks such as the Tony Blair Institute suggest that effective AI navigation could free up 29 million appointments annually and deliver productivity gains of around £340 million per year.
But not all digital triage is created equal. It’s therefore clear that technology providers should be treated not as retrofit vendors, but as core collaborators who deliver solutions to specific problems:
ACCESS IN CONFIDENCE”
1. Co-design from the start: Systems must be built with frontline clinicians, not for them. The triage engine should slot into practice workflows, whether in reception, clinical triage, or GP review.
2. Clinical validation and audit: Any AI or algorithmic system must be safety-tested, continuously monitored, and performance must be disaggregated by demographic groups to detect bias or error.
3. Explainability and transparency: Clinicians should see why an algorithm flagged or downgraded an input; the decision logic must be auditable and interpretable.
4. Safe fallback and overflow: When load surges occur,
tools must permit overflow to telephone or walk-in options. Practices must never be left stranded by a failed digital front door.
5. Incremental rollout and feedback loops: Begin with pilots, collect real-world data, refine, then scale. Don’t force full rollout before hidden issues are surfaced and resolved.
6. Ongoing support, adaptation and governance: These tools must evolve with feedback, changing clinical evidence, and user experience.
A vision for smarter digital access
The NHS Long Term Plan aims for better access, integrated care,
and sustainable workloads. But mandating open access without designing for scale, safety, and variability undermines those goals.
The GP vote is not about rejecting digital access. It is a demand for smart, safe, practical access.
The government’s October deadline should be a digital inflexion point, a chance to reset how access is delivered, not a race to compliance.
If we design access pathways that include robust triage, human oversight, safe fallback and strategic scaling, we can turn this tension into progress, rather than conflict. The tools exist. The evidence is emerging. The frontline is speaking. What remains is collective will.
HEALTHSPAN: THE STANDARD THAT
ANEW global analysis shows that while life expectancy is rising almost everywhere, the number of years lived in good health is not keeping pace. Researchers examined data from 183 countries and found that the healthspan/ lifespan gap is widening, with many societies projected to face decades where added years are lived in disability or decline by the end of the century.
The truth behind those numbers is stark: people are surviving longer but often without vitality. The gap between years lived and years lived well is where human dignity falters.
In the US, the statistics are especially sobering. A study found that Americans now spend an average of 12.4 years of their lives in poor health before death –the highest burden among high-income countries. Twelve birthdays marked not with joy but with pain, dependency, or confusion. Twelve years when life is extended, but living is diminished.
Survivors’ accounts echo this reality. Many describe a paradox: they lived through treatment, but they do not feel alive. Anxiety, fatigue, and withdrawal often replace the vitality they once had. Medicine counts them among its victories. They count themselves among the forgotten.
This is why our fixation on survival alone distorts priorities. The question is not only how long people live, but how they live.
Anastasia Bystritskaya, senior global life science market analyst at Thermo Fisher Scientific, explains why healthspan, not lifespan, should the true measure of progress.
Measuring healthspan
Science is beginning to catch up. In June, researchers introduced a new blood-based biomarker tool. Called the Healthspan Proteomic Score, it was derived from more than 50,000 participants in the UK Biobank. The score can predict disease risk and mortality independent of chronological age, offering a way to estimate how many of our years are likely to be lived in health rather than decline. For the first time, healthspan is not just a concept. It is quantifiable. Interventions are advancing as well. A randomised controlled trial in Switzerland followed older adults over three years. Those who combined daily omega-3 supplementation with vitamin D and exercise showed measurably slower biological ageing, as assessed by epigenetic clocks. The change was measured in months rather than years, but across populations, the potential is enormous. Small shifts in individual healthspan could mean vast improvements at scale.
Why systems resist change
So why do we continue to reward lifespan over healthspan? Because our systems are
built that way. Clinical trials prize survival endpoints and side effects. Regulators approve drugs that add months of even if those months are filled with Insurers reimburse treatments that survival while ignoring whether patients remain independent. Investors cheer pipelines that promise longevity but ask about quality of life. This is a distortion, and it carries real costs.
The same distortion has shaped philanthropy and funding priorities. For years, initiatives have emphasised projects that extend human lifespan. But when data showed that many of those added years were spent in disability, perspectives began to shift. Increasingly, research proposals emphasise independence, cognitive function, resilience – not just survival curves. mission grows sharper, not weaker.
What needs to change
That shift is possible across the entire ecosystem. Public health agencies integrate health-adjusted life years national reporting. Regulators could require healthspan endpoints in pivotal trials. Payers could reward therapies keep people strong and independent.
HEALTHSPAN: MATTERS
Universities could train scientists to ask how long people live well, not just how long they live.
survival Regulators life, with frailty. that extend patients cheer but rarely distortion, priorities. emphasised lifespan. in shift. emphasise and curves. The weaker. entire could years into could pivotal therapies that independent.
The economic case is undeniable. A report from Columbia University’s Mailman School of Public Health argued earlier this year that adding even a single healthy year of life for every older adult could deliver trillions of dollars in global economic value. The savings come from reduced medical costs, greater workforce participation, and more active engagement in communities. At a time of strained budgets, this return on investment is extraordinary.
Yet the moral case is even stronger. To define success by lifespan alone is to accept survival without dignity. It is to measure progress in numbers that ignore lived experience. Patients deserve more than endurance.
Families deserve more than prolonged caregiving. Societies deserve more than decades of decline dressed up as achievement.
A different future
Imagine a future where added years are marked not by dependency but by mornings free of pain, evenings filled with companionship, confidence in memory, and joy in work. That is healthspan. That is the standard that matters. Until we measure healthspan with the same seriousness as lifespan, our vision of longevity will remain incomplete. We can do better. We can aspire not just to help people survive, but to help them thrive.
TREATING A LACK
Rakeeb Chowdhury, the chief executive and founder of Hummingbirds Medical, explains why current recall systems are widely seen as fragmented, admin-led, and clinically unsafe.
Written by Adrian Murdoch.
RAKEEB CHOWDHURY
is the founder of Hummingbirds Medical, a practising GP and the developer of BookYourGP. A fully automated patient review and recall system, the digital platform is designed to improve patient safety across the UK and has already been recognised by Health Innovation Yorkshire & Humber, Propel Digital Accelerator, the RCGP IMP accelerator, and the NHS Clinical Entrepreneur Programme.
Here, he talks to Healthcare Today about patient review and recall systems and how he is addressing patient safety.
What problem are you trying to fix? What is the problem with most fully automated patient review and recall systems?
The simplest way of putting it is that there is a lack of oversight, and many of the systems we use are really unsafe.
Too often, we rely on proxies as evidence that care has been provided, rather than checking whether the right care has actually been delivered.
Take blood pressure as an example: we measure it in the arm as a
proxy for what is happening in the heart. No one really cares about the blood vessel in your arm – what matters is whether we can prevent heart attacks and strokes. Yet there are plenty of drugs that reduce blood pressure without meaningfully reducing those risks.
That same problem of using the wrong proxy runs right through healthcare. Pay-for-performance schemes like the Quality of Framework (QOF) reward ticking boxes.
The dashboard turns green, but a decade later, we discover that outcomes haven’t actually improved.
That’s where our approach is different. We tie everything to human physiology and actual clinical parameters – surfacing whether the work was truly done.
It’s embedded in the surgery’s workflow so patients understand why they are contacted, and the team has a clear view of what’s needed.
LACK OF ALIGNMENT
shocking NHS Resolution figures earlier this year and the 10% rise in litigation a year, why has patient safety been neglected?
I think several things have come together here. The core issue is that the systems we use today –electronic health records like EMIS or SystmOne – were built decades ago, in the 1980s and 1990s. That was even before QOF was introduced.
What we’re left with now is a kind of Frankenstein system. In practice, it’s a mishmash of tasks and workarounds: sending tasks, waiting for patients to contact us, seeing alerts when prescribing, maybe getting a flag to do a medication review, running searches in the background, and delegating jobs to different staff. You might have a diabetes champion, an antibiotics lead, a pharmacist doing reviews, and so on. It all seems fine when you walk into a surgery – everyone looks busy and purposeful – but the truth is there is no real clinical oversight.
Doesn’t this require a change in the mindset of staff, rather than just software?
That’s why we describe what we’ve built as clinical oversight infrastructure. The software allows you to embed care pathways directly into the system.
This goes far beyond the traditional idea of recalls. Anyone can create a static patient list and send out bulk text messages. What we’re doing
is embedding care: defining the physiological parameters that need to be checked, assigning responsibilities, surfacing what’s missing, and ensuring patients are contacted appropriately.
Everything flows into the clinical record, so admin teams aren’t jumping between systems. They can see why a patient has been recalled, who they need to see, and what needs to be done. Nurses know which checks are outstanding. If something is missed, the system shows what wasn’t done, by whom, and why – creating accountability.
How does the system help ensure that people don’t slip through the cracks?
We often show surgeries a demo of how the software works. Traditional systems rely on static filters, which are dangerous because they simply flag that a patient is on a list without showing what’s missing. By contrast, our system tracks everything down to the physiological level. In a patient record, anything overdue is shown clearly in red, with the date it was last done and what is now due.
It also keeps a full audit trail. You can see exactly who has been recalled, when, and by which method. Messages are sent automatically – email, text, WhatsApp or letter – according to the practice’s settings. If a text fails because a number is wrong or the network is down, the system automatically escalates to the next method. If a patient has been contacted multiple times without responding, they appear in a pending tab, so practices only need to follow up manually on a handful rather than hundreds or thousands.
Every action is recorded directly in the patient’s notes: when a recall was sent, why, what is due, and with whom the patient should be booked. That makes mistakes far less likely. Our platform removes guesswork and ensures the process is both transparent and accountable.
Do you have early evidence showing improvements in patient outcomes or safety from practices using the system?
We started in 2020 with our first site in a very deprived surgery where all the partners had left, and there were no GPs. They’ve now sent around 40,000 recalls using our system. Since then, we’ve grown organically and are now working with practices across York, Newcastle, Leeds, Manchester, London, Norwich and elsewhere.
In London, Strong Green Surgery recently started with us. It has already sent 1,000 recalls with only one query – which, when checked, turned out not to be an error but a clinical marker being misread. That shows how the system works silently in the background, surfacing the right needs without confusion.
It always comes down to money. How are you funded?
We’re self-funded and haven’t raised any external money, which makes us a bit unusual. The reason we started goes back to a case I saw as a trainee. A patient with back pain missed his blood tests, went through physio and other care, and eventually returned years later with prostate cancer that had spread. By then, three of the GP partners were facing legal action. I was astonished – in an age of computers, how could something so critical have been missed? It became clear there was simply no system of oversight.
That experience convinced me that something needed to change.
When I first floated the idea, people didn’t believe it would work, and we never fitted the mould for grants or funding. So we just built it ourselves. Within a year or two, it was selfsustaining.
Are you helped by the government’s focus on digital transformation?
We often end up working outside the usual remit of technology vendors. Behind the scenes, we think of ourselves a bit like Stripe in payments. Stripe doesn’t just move money; it detects fraud and keeps the system safe. In the same way, we can’t just automate healthcare recalls and walk away.
The NHS talks about but the infrastructure allow it.
The problem is the NHS often sees things differently. It commissions new tools – triage platforms, patches, connectors – and once they’re deployed, it sees it as a job done.
about prevention, infrastructure doesn’t
That makes the system look fine on paper, but in reality, it isn’t. We’d never accept that level of risk management in another safetycritical industry.
That’s why this issue has been overlooked. The technology to provide genuine oversight hasn’t existed until now. But once you see it, it’s obvious: you need a system that goes beyond static lists,
that can show what’s needed, when, why, and with whom – and that can be audited. That’s the only way to make this truly safe. What are the biggest barriers to adoption in primary care?
The big barrier here is business. In software, you usually have two models: low-cost, mass-market subscriptions like Netflix, where millions of customers cover the costs; or enterprise contracts like Palantir, where one deal is worth hundreds of thousands. General practice falls into a difficult no man’s land. Sales are complex, but GP surgeries have no tech budget, no r&d budget, and very little resource compared to other countries.
If you approach an integrated care board (ICB) as a small company, they’ll ask for evidence. But to generate evidence, you need adoption first – it’s a Catch-22.
The second problem is misalignment in care pathways. The theory is that if innovation reduces pathway costs, it should be adopted. But in practice, it doesn’t work. If you develop an app that helps women detect breast cancer recurrence earlier, the GP won’t pay for it – not their budget. The breast team won’t pay either – they’re funded for surgery, not prevention. So innovations fall through the cracks.
The NHS talks about prevention, but the infrastructure doesn’t allow it.
The bigger challenge is higher up. Many decision-makers are nonclinicians. They don’t understand what’s happening under the hood – the lack of oversight, the safety risks, the missed opportunities for prevention.
We’re left with a system where surgeries can’t afford innovation, structures above them can’t enforce it, and everything gets stuck in the middle.
DIABETES is one of the defining health challenges of our time. In the past three decades, the number of people living with the disease has quadrupled worldwide. By 2050, Africa alone is projected to see a 142% increase in prevalence, with 60 million adults affected. This trajectory is unsustainable. It places enormous strain on healthcare systems, threatens economic productivity, and affects the lives of millions of families.
What is needed is a shift towards earlier detection, personalised care, and scalable innovation. Artificial intelligence (AI) is uniquely positioned to deliver this shift, providing new tools to predict, prevent, and treat diabetes more effectively.
One of the most powerful applications of AI is the ability to detect early warning signs of diabetes. By analysing large and complex datasets, from electronic health records and lab results to imaging scans, AI systems can identify patterns invisible to the human eye.
For example, AI models trained on longitudinal health data can flag subtle changes in blood glucose trends, BMI, and metabolic markers. These predictive tools support proactive interventions, such as lifestyle coaching or targeted therapies, which can delay or prevent disease onset.
AI is also being used to forecast complications like cardiovascular disease, kidney damage, and diabetic retinopathy. By anticipating these risks earlier, clinicians can tailor preventive strategies and reduce long-term healthcare costs.
For those living with diabetes, management has relied on periodic clinical visits and selfreporting, approaches that provide only a partial picture of disease
HOW AI IS TRANSFORMING THE FUTURE OF MANAGEMENT
progression. AI is changing this by enabling continuous, personalised monitoring.
Wearable devices and continuous glucose monitors (CGMs) collect real-time data on blood sugar levels, physical activity, and dietary habits. AI algorithms analyse this data instantly, offering tailored recommendations and alerts. For example, some systems predict glucose spikes and suggest insulin adjustments or dietary changes before symptoms occur.
Importantly, this empowers patients. With timely feedback and personalised insights, individuals can take greater ownership of their health, while clinicians benefit from a richer and more accurate understanding of disease management outside the clinical setting.
Imane Motaib, professor diabetology and metabolic the University Mohammed examines the evolving reshaping diabetes
AI’s impact is not limited to frontline care. It is revolutionising the pace and scope of research. Drug discovery has been a slow and resource-intensive process, taking years to move from concept to trial. AI shortens timelines dramatically by analysing vast molecular datasets, identifying potential compounds, and predicting their effectiveness.
In the context of diabetes, this means accelerating the development of new therapies, from glucoselowering agents to treatments that address complications. Equally, AI
TRANSFORMING OF DIABETES MANAGEMENT
professor of endocrinology, metabolic
diseases
at Mohammed VI
Polytechnic,
evolving role of AI in diabetes care.
can support efficient clinical trials by identifying suitable participants and monitoring outcomes with greater precision. The result is a faster, more targeted pipeline of innovation, critical in the ongoing search for therapies that improve outcomes and, ultimately, work towards a cure.
A major advancement in diabetes technology is the development of AI-powered closed-loop insulin delivery systems, often referred to as artificial pancreas devices. These systems integrate CGMs with insulin pumps and AI algorithms
to automatically adjust insulin delivery in real time. By continuously analysing glucose levels and predicting future trends, closedloop pumps help maintain optimal glycaemic control with minimal manual input. This not only improves clinical outcomes but also enhances quality of life and significantly reduces anxiety for patients, who no longer need to make frequent dosing decisions.
AI is also playing a growing role in therapeutic education, particularly for patients with type 2 diabetes. AIpowered chatbots offer interactive, cost-effective, and accessible guidance on disease management, lifestyle changes, medication adherence, and more.
Virtual assistants answer questions, provide reminders, and deliver personalised educational content in
multiple languages and formats. For patients in remote or underserved areas, chatbots offer a scalable solution to bridge gaps in diabetes education and support.
Diabetes is a global challenge that requires a global response. AI creates opportunities for collaboration that transcend borders.
Shared data platforms and research networks can accelerate discovery and ensure that breakthroughs benefit diverse populations rather than being concentrated in a handful of regions.
Equitable access is, however, essential. The steepest increases in diabetes are expected in low- and middle-income countries, where healthcare resources are often limited. AI can help bridge these gaps if its deployment is guided by principles of fairness, accessibility, and cultural relevance.
The trajectory of diabetes prevalence is deeply concerning, but not inevitable. AI can fundamentally change the way we approach the disease: from predictive analytics that enable earlier intervention, to personalised care that adapts in real time, to accelerated discovery that expands treatment options.
These capabilities do not replace clinical expertise; they enhance it. By combining the power of AI with the knowledge of healthcare professionals, we can transform diabetes care from reactive crisis management to proactive, patientcentred prevention and treatment.
As healthcare systems continue to grapple with rising demand and constrained resources, the integration of AI is a necessity. The challenge is to ensure that its promise is realised equitably and sustainably, so that every individual living with or at risk of diabetes can benefit.
AI AND MEDICAL MALPRACTICE
WHY CLINICIANS MUST
ARTIFICIAL Intelligence
(AI) is rapidly becoming a familiar tool in healthcare, from clinical diagnostics to administrative efficiency. Increasingly, clinicians are also turning to AI-driven platforms to help with professional decisions outside the consulting room; including comparisons of medical malpractice indemnity policies.
While AI has its place, caution is essential. The complexities of indemnity cover mean that clinicians should not rely solely on AI outputs. Instead, professional advice from a broker or product specialist remains indispensable.
The risk of oversimplification
Medical malpractice indemnity policies are nuanced, and their terms can vary significantly depending on the insurer, the scope of cover,
George Maughan, THEMIS
Clinical Defence’s head of client relations, explains why the complexities of indemnity cover mean that clinicians should not rely solely on AI outputs.
the medical specialty, and even the jurisdiction in which a clinician practises. AI tools often work by scanning available policy data and generating comparisons based on surface-level features, such as premium price or headline coverage limits.
This creates the risk of oversimplification. An AI system might flag one policy as “cheaper” or “more comprehensive” without
recognising hidden limitations – for example, exclusions for certain procedures, restrictions on telemedicine, or differences between occurrence-based and claimsmade cover. These subtleties are critical, and misinterpreting them could leave clinicians dangerously exposed.
The problem of inaccuracy
AI tools depend on the data they are trained on. If the information available to them is incomplete, outdated, or inconsistent, their recommendations may be inaccurate. For example, policy wordings often change, and insurers regularly update underwriting appetite. A clinician relying on AI might receive advice based on last year’s terms rather than today’s.
Moreover, AI has a well-documented tendency to “hallucinate”, confidently presenting incorrect or invented information as fact. In the context of
PROCEED WITH CAUTION
indemnity policies, this could mean highlighting exclusions that do not exist, or worse, failing to mention crucial conditions that materially affect coverage.
In my own work with clinicians, I have already seen this first-hand. Some doctors have approached me after running AI-generated comparisons of indemnity policies, only to find that the results were not just misunderstood, but completely wrong. In several cases, the AI had either misrepresented key terms or failed to identify critical exclusions – creating a false sense of security that could have left those clinicians without the protection they thought they had.
Why expert advice still matters
Brokers and product specialists bring a depth of understanding that AI cannot replicate. They know how to navigate the small
print, interpret grey areas, and tailor advice to the unique profile of a clinician’s practice. They can also identify potential risks that AI would never pick up on, for instance, the reputational and legal considerations linked to a specific specialty or jurisdiction.
Crucially, human advisers are also accountable. If an error is made, a regulated broker can be held responsible for the guidance they provide. By contrast, AI tools bear no such responsibility; if they get it wrong, the consequences fall solely on the clinician.
The right way to use AI
This is not to say that AI has no role to play. It can be a useful starting point, a way of gathering broad market intelligence quickly or highlighting policies worth investigating further. But it should never replace professional advice. At best, clinicians can use AI as a
supplement, bringing their findings to a broker or product specialist who can then validate, challenge, or refine the information.
Conclusion
AI is a powerful tool, but when it comes to medical malpractice indemnity, it is not a substitute for expertise. The stakes are simply too high. Clinicians who rely solely on AI risk overlooking critical details and exposing themselves to gaps in cover that could jeopardise their careers.
My experience has shown that these risks are not theoretical, they are happening now. The safest approach is clear: use AI cautiously, but always seek professional guidance from a trusted broker or product specialist. In matters of indemnity, nothing can replace human judgment and accountability.
To discover more about THEMIS Clinical Defence, click here.
FUNDAMENTAL DISHONESTY:
Introduction
In clinical negligence and personal injury litigation, an allegation of “fundamental dishonesty” (FD) under the Criminal Justice and Courts Act 2015 (s.57) is a weapon for defendants - but a double-edged one. If successfully made, it allows a defendant to dismiss the claim and recover full costs; if unsuccessfully pursued, even a winning defendant can suffer cost sanctions. Two recent High Court judgments - Hakmi v East & North Hertfordshire NHS Trust & Anor (2025) and Zakia Din v Aviva Insurance Ltd (26 September 2025) - illustrate the stark contrast in potential cost outcomes from a defendant’s perspective.
Case
1: Hakmi v East & North Hertfordshire NHS Trust & Anor (2025)
Brief facts: The claimant, a consultant orthopaedic surgeon, alleged that after a second stroke the hospital defendants failed to offer thrombolysis, resulting in serious disability. Quantum was agreed at c.£1m subject to liability. The defence denied negligence and causation and also pleaded FD: it alleged the claimant deliberately underperformed neuro-psychological tests to bolster his claim. At trial, the defendant won: the court found the claim failed on causation; even if thrombolysis had been offered, the outcome may not have improved.
Evidence of exaggeration / dishonesty: what was advanced and the court’s analysis
The defendants contended that the claimant manipulated the neuro-psychological testing: e.g., intentionally performing poorly in cognitive assessments, leading to an inflated picture of impairment. The court noted the five requirements under s 57: pleading, burden on
Neil Rowe, Head of Practice at Maulin Law, looks at the high-stakes outcomes in two recent fundamental dishonesty judgments.
defendant, finding of dishonesty, that it be fundamental (not incidental) and that it substantially affect the presentation of the claim. However, the judge found that the poor performance could be explained by organic effects of the stroke, fatigue from family issues and psychological reaction – not deliberate malingering. In short, the evidence did not support the inference of dishonesty to the civil standard. Additionally, because the claimant was a medical professional, the court considered the reputational impact of an FD finding on him. The fact the evidence was “increasingly wanting” yet the allegation was pursued to the end was reported to contribute to the costs decision.
Judgment
& costs orders
While the claim failed on liability/ causation, the FD allegation itself also failed. On costs the court ordered:
• The claimant to pay the defendant’s costs of the action— but not to be enforced without leave of the court. Presumably the defendant will now need to pursue the enforcement and means assessment process - and recovery from the claimant in full or even part is not guaranteed depending on his financial situation having lost his claim.
• The defendants to pay 15% of the claimant’s costs from the date the FD allegation was formally raised to trial [around 6 months], on the standard basis.
In doing so, the court recognised that some defendant costs would have been incurred regardless, but the claimant’s extra burden of defending the FD allegation which failed justified the sanction against the defendant.
Defendant’s perspective
Despite winning the substantive claim, the defendants incurred a cost penalty due to a failed FD allegation. It reinforces the point: if you raise FD, you must have a robust evidential basis and be prepared to abandon it if it falters. Otherwise, you risk weakening your costs position.
Case 2: Zakia Din v Aviva Insurance Ltd (2025)
Brief facts
The claimant, a front-seat passenger in a vehicle accident, alleged neck/ right upper limb injury, chronic pain, PTSD and consequential losses. The defendant insurer admitted breach but denied causation/quantum and pleaded FD as to both the accident mechanism and alleged consequences. The court found the accident was a minor low impact event contrary to the claimant’s dramatic narrative. Surveillance showed the claimant actively shopping without the shoulder immobiliser she had claimed to need. Psychological and painmedicine expert testimony adduced by the claimant was rejected. The judge found the claimant had invented or grossly exaggerated both mechanism and effects, and that the dishonesty went to the heart of the claim.
Evidence of exaggeration / dishonesty
Key evidential pointers:
• Engineering/accident evidence: photographs and expert evidence contradicted the claimant’s version of a violent impact.
COSTLY CONSEQUENCES
• Surveillance: the claimant wore a shoulder immobiliser in examination, then left it in a taxi and carried on shopping unaided.
• Expert evidence: the defence psychiatrist discredited the claimant’s PTSD claim; the claimant’s psychologist’s evidence was disregarded due to telephone-only assessment, patchy record annotation and role-blurring as advocate.
Judgment & costs orders FD was found. Consequently:
• QOCS (qualified one-way costs shifting) was disapplied pursuant to CPR 44.16 because FD succeeded.
• The claimant was ordered to pay the defendant’s costs on an indemnity basis, fully enforceable.
• An interim payment on account of costs of £140,000 was ordered to be paid by the claimant to the defendant.
• The claimant was also ordered to repay an interim payment of damages plus interest – which presumably had already been spent in full or at least in part.
Defendant’s perspective
This case shows the full upside for the defence: a successful FD allegation converts what might be a cost-risk into a cost-reward, and claimant representatives will note a significant deterrent effect. The total costs payable by the claimant will presumably total much more than £140,000 and together with repayment of the interim on damages will have a catastrophic financial impact on the family.
Comparative costanalysis & key lessons
The contrast between the two cases is instructive for defendants:
• In Hakmi, the defence won the substantive claim but lost on FD; cost result: potential cost recovery, but liability to pay 15% of claimant’s costs from the FDissue date and restrictions on enforcement.
• In Din the defence succeeded on FD; cost result: QOCS disapplied, full cost recovery, indemnity basis, interim costs payment –strong financial win.
Thus, the strategic decision to raise FD must be made with eyes wide open: the risk of failing is real, and the cost sanctions meaningful. A well-founded FD allegation can however shift the balance by reversing the cost regime; one which the court deems to be poorly supported can reduce your cost recovery even if you succeed in defeating the claim on liability.
Considerations for defendant advisers: Raising fundamental dishonesty
From a defendant’s standpoint (hospitals/Trusts, insurers, legal teams) the decision to plead FD requires careful planning:
1. Evidential strength – Just as in Din, strong surveillance and expert evidence is crucial. In Hakmi, the court felt the evidence lacked a clear foundation.
2. Clarity in pleading and timing – The FD allegation should be clearly pleaded early and you must keep under review whether the evidence remains sufficiently strong to pursue. Hakmi shows the consequences where the allegation is maintained despite apparently weakening evidence.
3. Cost-risk analysis – You must weigh the cost-reward. If you lose the FD component you may face cost sanctions (e.g., percentage of claimant’s costs).
4. Interplay with QOCS/CPR 44.16 – Where FD is found, QOCS is disapplied and full costs shifting may apply; where it is not, you remain under the conventional regime and may face an adverse order.
5. Evidence-gathering –Surveillance, incident documentation, expert testing are vital. In claims involving diagnostic testing, evidence of deliberate under-performance may be difficult to establish.
6. Professional and reputational context – Courts may take into account the claimant’s standing when faced with an allegation of FD. In Hakmi, the claimant’s status as consultant surgeon influenced the court’s cost discretion.
7. Negotiation and settlement strategy – Raising FD may complicate settlement: claimants may refuse early offers, expecting a full hearing to avoid FD findings.
8. Isolation of the FD issue –Consider whether you can isolate the FD allegation (e.g., by issues-based cost order) or reserve the right to abandon it if new evidence undermines it.
Conclusion
From the defence perspective, FD allegations are high stake. The contrasting outcomes in Hakmi and Din show that FD can be either a cost-advantage or a cost-trap. The take aways are clear: only raise FD with a robust evidential foundation and a clear strategy.
Proper preparation, early investigation and dynamic casemanagement are essential. Successful FD outcomes can make spectacular headlines involving contempt of court and imprisonment, but if the court goes against you there can be a costs sting in the tail.
AGILIO STRENGTHENS LEADERSHIP TEAM TO POWER NEXT STAGE OF GROWTH
AGILIO SOFTWARE, the UK’s leading provider of healthcare operations software, has unveiled three senior appointments that will help propel its next phase of expansion across the Dental, Primary Care, Pharmacy and Veterinary sectors.
The new hires mark a major investment in Agilio’s growth strategy, focused on mergers and acquisitions (M&A), international expansion and continued organic growth. Together, they join a wellestablished leadership team, adding further depth and experience as the company continues to scale.
The new appointments are:
Tom Cornwell, Chief Financial Officer (CFO) – Tom brings more than a decade of financial leadership and growth expertise from The Access Group, where he helped scale the company from £60 million to £1.2 billion through strategic M&A and sustainable expansion
Bruce Fair, Chief Revenue Officer (CRO) – Following a successful consulting period, Bruce now joins
permanently. With a strong track record in scaling SaaS (Softwareas-a-Service) and digital platforms, and global experience across the UK, USA and Australia, he will accelerate Agilio’s revenue growth and international reach
Mike Osborn, Chief Customer Officer (CCO) – A seasoned leader in healthcare and technology, Mike is known for building highperforming teams and delivering exceptional customer experiences. At OneAdvanced, he drove significant organic growth through customer-centric innovation.
These appointments complement Agilio’s existing executive team, led by CEO Ben Betts and CMO Mike Beech, ensuring a blend of continuity and new perspective as the company moves into its next chapter.
Ben said: “Healthcare providers across the UK are under immense
pressure to deliver better care with fewer resources. At Agilio, we’re committed to giving them time back by simplifying compliance and operations, and by enabling practices to grow and improve patient care.
“Strengthening our leadership team ensures we have the expertise to deliver at scale across Dental, Primary Care, Pharmacy and Veterinary. This is a crucial moment for Agilio as we enter our next phase of growth — through M&A, international expansion and by growing our footprint of solutions with existing customers.”
Today, Agilio supports more than 8,000 dental practices and thousands of GP surgeries, pharmacies and veterinary practices across the UK. The company has grown rapidly through acquisitions, partnerships and product development, and its investment in leadership underscores its long-term commitment to redefining healthcare operations and empowering professionals to deliver better care.
For more information on Agilio’s leadership team, click here.
ARE YOU MISSING PRIVATE HEALTHCARE ENQUIRIES?
IF YOU rely on first- or last-click attribution, enquiries are slipping through the cracks. These may be straightforward metrics, but they hide the real touchpoints that influence appointments. Was it a PPC ad or a brochure they downloaded while researching, for example?
Without visibility of the patient journey, you’re missing vital insights that drive conversions.
Missing attribution data = ineffective decision-making
With tight budgets, NHS overflow pressures, and competition, attribution is essential.
Clinics lack insights into how different activities guide patients through the complex healthcare landscape. A call may have been triggered by PPC –but most analytics platforms can’t make that connection.
Without visibility into channel performance, there’s no way to know if you’re using the right messages or targeting the right touchpoints.
“If you’re not collecting the data needed to identify which touchpoints drive enquiries and appointments, you’re risking investment and efficiency,” explains Faye Thomassen, Head of Marketing, Mediahawk.
Call tracking is key for tracing the patient journey from initial contact to treatment, says Mediahawk
The middle phase: Where trust builds and insights hide
Patients researching health concerns, procedures, and providers can easily fall into a research rabbit hole. They need confidence that they’re making the right decision about when and where to seek care.
This makes healthcare marketing high-touch, with many opportunities to lose patients if you miss the moment to convert.
“Momentum builds between the first and last clicks,” says Faye. “Those middle touches - where prospects explore your services are where you establish trust. That’s when your marketing needs to work the hardest.”
This is why clinics increasingly use call tracking to connect effort to outcomes; enabling 100% attribution, and allowing marketers to trace the patient journey from initial contact to appointment.
Call tracking connects the journey
More than 75% of marketers surveyed by Mediahawk use call tracking. With it, you can:
• Report on how each channel, campaign, activity, and keyword performs
• Identify which strategies deliver the best ROI
• Make informed decisions about campaigns, messaging, and targeting
• Understand the research journey to ensure your website builds confidence
• Optimise every touchpoint so your clinic is top of mind when patients book.
Summary
First- or last-click attribution leaves critical gaps in the journey.
To maximise enquiries and make smarter decisions, clinics need complete visibility – capturing every touchpoint where trust is built.
Call tracking connects the journey, giving marketers the insights to optimise campaigns, prove ROI, and ensure their clinic is the first choice when patients are ready to act.
For more information about Mediahawk, click here.
AVOIDING BILLING HORROR SHOWS THIS HALLOWEEN
BEHIND the scenes of many private practices lurk frightening problems that can spook even the most experienced consultant:
• The phantom invoice: Sent but never seen again, drifting endlessly without payment.
• The vanishing excess: That small but important amount patients owe, which mysteriously disappears and is never collected.
• The zombie admin load: Billing tasks that keep rising from the dead, eating away at your time and energy.
• The ghostly cash flow: Income that should be there, but isn’t, leaving your practice finances looking pale.
For consultants, these billing terrors don’t just keep you up at night, they threaten the health of your practice. Unpaid invoices mean cash-flow uncertainty. Chasing patients or insurers takes precious time away from patient care. And confusing or outdated reporting leaves you in the dark.
Turning financial nightmares into peace of mind
The good news? You don’t need
October brings pumpkins, costumes, and the occasional scare. But for many private consultants, the real nightmare isn’t Halloween, it’s the billing horror show that comes with missed payments, insurance confusion and endless admin, says Medserv’s Derek Kelly.
With Medserv, you’re always in control, but never haunted by uncertainty.
Why consultants choose Medserv
Private consultants come to us because they want billing that feels professional, predictable, and transparent. With our systems in place, you can:
• See exactly where your money is - no more phantom invoices.
garlic, holy water, or a witch’s spell to banish these horrors. What you need is a billing partner who knows how to stop them before they begin.
That’s where Medserv comes in... We specialise in transforming billing nightmares into smooth, stress-free processes with:
• Simple, transparent pricing - no tricks, just clear fees.
• 24/7 live reporting dashboards - giving you real-time visibility into every invoice and payment.
• Professional collections of patient excesses - ensuring no money goes missing.
• Expert handling of insurers and claims - so you don’t have to fight financial monsters alone.
• Trust that patient excesses are collected efficiently - no more disappearing payments.
• Spend your time caring for patients - not wrestling with zombie admin.
• Sleep easy knowing your finances are in good health.
This Halloween, the only scares you should be dealing with are carved pumpkins and trick-or-treaters at the door. If your practice is still facing billing horror shows, it’s time to let Medserv take the fright out of finance.
Because in private practice, there’s nothing scarier than not getting paid!
Contact Medserv today to banish billing nightmares for good.
WHEN PATIENTS THE ETHICS AND RISKS OF
WHILE clinicians are well-versed in obtaining consent for interventions, fewer feel confident navigating situations where patients decline treatment. Yet from a medico-legal and investigative standpoint, informed refusal can be just as consequential.
The other side of consent
At its heart, informed refusal is about respecting patient autonomy in its fullest sense, not just the right to agree to care, but the right to decline it. Whether the decision involves refusing surgery, medication, or even diagnostic tests, the legal and ethical principles remain the same: patients must be provided with enough information to make an informed choice, including the risks of not proceeding.
However, in practice, this process is often informal or poorly documented. Clinicians might accept a patient’s refusal without fully exploring whether the decision is
Informed consent has long been a cornerstone of ethical medical practice, but its quieter twin, informed refusal, remains less clearly understood and inconsistently applied, says TMLEP’s lead healthcare investigator Nina Vegad.
based on misunderstanding, fear, or misinformation. In the eyes of the law, that can be as problematic as failing to obtain valid consent.
Why it matters in investigations
From an investigative perspective, cases involving informed refusal often reveal deeper systemic tensions. These are not simply about communication lapses, but about the culture surrounding shared decision-making.
When reviewing such cases, one of the first questions investigators must ask is: Was the refusal truly informed?
• Did the clinician clearly explain the risks of declining treatment?
• Was the patient’s capacity assessed and recorded?
• Were alternative options discussed?
• And crucially, was this all documented clearly and contemporaneously?
Too often, the record contains a brief note such as “patient declined” or “refused treatment,” which provides little insight into the quality of that conversation. In the event of an adverse outcome, that gap becomes the focal point of scrutiny.
Balancing autonomy and duty of care
There is also a subtle emotional and ethical tension at play. Clinicians have a professional duty to act in the patient’s best interests, and yet,
PATIENTS SAY NO: OF INFORMED REFUSAL
they must also respect a competent patient’s right to make what might appear to be an unwise decision.
This can be particularly challenging in high-stakes scenarios: a patient declining life-saving surgery, refusing blood products, or opting out of investigations that could reveal a serious diagnosis. The instinct to protect often clashes with the obligation to respect choice.
For investigators, recognising this tension is vital. It reframes the incident not as a failure of care, but as an ethical crossroads, one that requires careful documentation, communication, and compassion from all parties involved.
Documentation: The deciding factor
Informed refusal, like consent, lives or dies on the quality of its documentation. A well-written note should capture the essence of the discussion, not simply that a patient refused, but why, what
was explained, and how the clinician ensured understanding. This not only supports good clinical practice but also protects both the clinician and the organisation in the event of a complaint or claim. From an investigative lens, clear documentation demonstrates that autonomy was respected and the process was handled professionally, even if the outcome was poor.
Towards a culture of shared decision-making
The broader challenge is cultural. True shared decision-making goes beyond form-filling or compliance with policy. It involves meaningful dialogue, understanding what matters most to patients and ensuring they feel empowered to make decisions about their care, even when those decisions are difficult.
Healthcare systems are beginning to recognise this, but variability remains. Some organisations have robust processes for documenting
and reviewing refusals; others still treat them as administrative anomalies rather than clinical events worthy of reflection and learning.
Learning from refusal
When investigated well, cases involving informed refusal can offer powerful insights into communication, empathy, and trust. They remind us that safety is not only about preventing harm through action, but also about understanding harm that can occur through inaction.
As investigators, our role is to illuminate the nuances, to see beyond the decision itself and explore the context in which it was made. When a patient says no, it is not the end of the conversation; it is the beginning of a deeper one about understanding, respect, and the shared responsibility at the heart of healthcare.
For more information on TMLEP’s services, click here.
Published by Healthcare Today Media Ltd. Healthcare Today is editorially independent. Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment.