

Update on Intraocular lenses


Eye Anatomy Overview


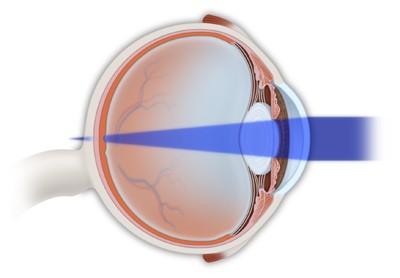
How the eye works
Light enters the eye through the cornea, pupil and lens
Light rays are focused directly onto the retina where they are converted into impulses
These impulses are sent to the brain through the optic nerve
Lens Anatomy
• Lens is suspended in the eye by zonules
• “Support capables”
• Zonules are attached to the ciliary body
• These attachments allow accommodation while young
• Presbyopia- decreased lens flexibility means less accommodation
• Reading glasses if >40

Lens anatomy
• The lens provides the remaining 25% of focusing power for the eye
• 9mm equatorially
• 5mm anteroposteriorly
• Involves a capsule, cortex and nucleus
• All of these structures have important surgical implications

Lens
Anatomy and Cataract
• With age, the lens losses its clarity
• This is called a cataract
• Cataracta= latin for waterfall
• Explains the symptoms patients develop

Cataract
• In developed world, cataracts are a source of impaired activities of daily living
• In the developing world, these are blinding and debilitating diseases
• Major socioeconomic impact as blindness impacts patient but also their family

Cataract Surgery
• Removing the cataract clears the visual axis

Intraocular Lenses

Cataract surgery

Cataract Considerations
• New era in cataract surgery
• Now can decrease need for glasses by determining the power of the lens to insert in the eye
Spectacle independence



Cataract surgery steps
• Use ultrasound probe to emulsify the cataract
• Most dangerous part of surgery
• Posterior capsule is 4um thick
• Separates anterior and posterior chamber
• Mistakes here can result in the cataract falling into the back of the eye

Cataract surgery steps
• The capsular complex is left intact
• The intraocular lens (IOL) is then inserted into the capsular complex to restore sight


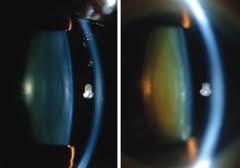
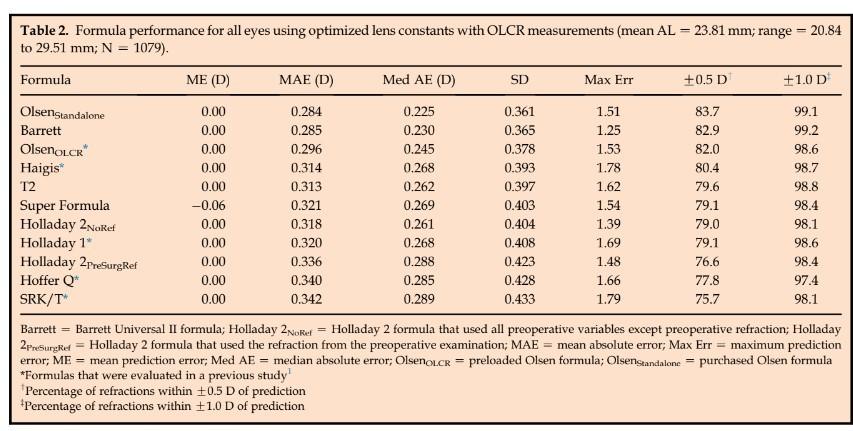
IOL calculations

IOL calculations- Lenstar

Refractive errors: myopia (nearsightedness)
There is too much optical power in the eye.
The distance between the cornea and the retina is too long
Light rays focus in front of the retina instead of on it.

Close objects will look clear, but distant objects will appear blurred.
Refractive errors: hyperopia (farsightedness)
There is too little optical power.
The distance between the cornea and the retina is too short.
Light rays are focused behind the retina instead of on it.
Distant and near objects are blurred
Hyperopia and Myopia
•
Hyperopia and myopia can be addressed with a monofocal IOL

IOL calculation- Normal Eyes
IOL calculation- Long Eyes

IOL calculation- Short Eyes

Refractive errors: astigmatism
Occurs when corneal is not spherical
Shaped more like a football than a basketball.
Light passing through the astigmatic cornea is focused in two or more locations.
Distant and close objects appear blurry.

Astigmatism and Toric IOL


Presbyopia


Multifocal IOL


Multifocal IOL

Multifocal IOL



LASIK
• Corneal based surgery to fix refractive errors
• Alters the anterior cornea without changing the posterior cornea
IOL calc prior refractive surgery

• 74 yo lady c/o glare and halos and difficulty driving
• h/o monovision lasik 20years ago in Chicago
• Desires spectacle independence with cataract surgery





• Proceeded with ce/iol OS Nov 2023
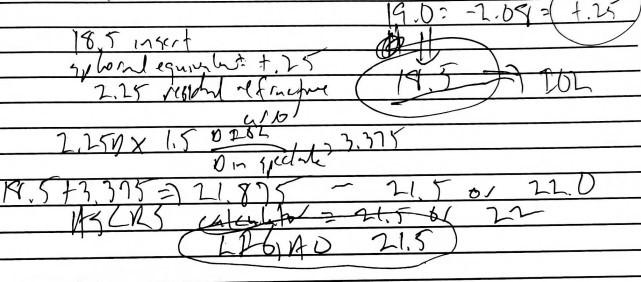
• Implanted LI61AO 18.5 with aim of2.0(nearsighted)
• Returned POW 6- spherical equivalent of +.25
• Perfect distance vision, but she wanted to be nearsighted


IOL exchange
Current Options for Residual Refractive Error
• Refractive surgery
• Many are post lasik
• PRK after lasik is less accurate
• Many have contraindications
• IOL exchange
• Intraocular surgery- more risk and more expense
• Return to the OR
Adjustability is Here



Optimize Visual Outcomes After Cataract & Lens Replacement Surgery


Why did we pursue this technology?


Delivers LASIK Level-Level
Refractive Outcomes
The World’s First Adjustable Intraocular Lens
High quality vision with no reduction in contrast or increased glare and halo (relative to a monofocal IOL)

Patient driven binocular outcomes with 90% achieving 20/20 & J21
Higher practice revenue and profits
Empowers a wide group of patients and doctors


Redefining the Patient Journey
All Fixed, Non-Adjustable Competitive IOLs Share a Common Limitation
High-stakes decisions that must be made before surgery
Patient is asked to describe priorities for post-operative vision
Doctor recommends specific IOL type

Patient’s eyes undergo pre-operative measurements
Doctor selects IOL sphere and astigmatism power
Perform Surgery
Deal with Consequences
Fixed IOLs limit options for those with sub-optimal outcome IOL power predictions are never perfect due to several factors.



Only RxSight IOLs Are Adjustable After Surgery Patient drives optimization
of their own vision
Streamlined patient discussions
pre-operative measurements
Choose LAL and approximate power

Office-based light treatments designed to customize LAL to patient’s optimal refraction using the RxSight Light Delivery Device (LDD)
Real life trial drives LALs adjustments Perform Surgery
Patients experience their vision at home after light treatment, return to clinic for additional adjustments, or to make the prescription permanent



First Ever “Patient Trial” of Final Outcome
Patient preferred prescription is determined after healing is complete and ocular media clear ~80% of LAL patients select customized blended vision1
Patients benefit from “test-driving” their vision
Digital correction of vision
Light Treatment After LAL Implantation


ActivShield
Blocks UV light except during LDD treatment

Adjustment Beam
Light from the RxSight LDD is directed by the surgeon to the Light
Adjustable Lens
Photopolymerizatio
Macromers in the path of the light are photopolymerized



Diffusion and Power Change
Unpolymerized macromers move into the polymerized area, causing precise shape and power change
Lock-In Beam
The entire lens is exposed to light to polymerize all the remaining macromers
Final Result
The outcome is a precise change in the LAL power to match the patient’s individual prescription
Light treatments are painless, non-invasive, and take approximately 90 seconds


Initial Light Treatment
At least 17 days after surgery
Secondary Light Treatment
At least 3 days after initial light treatment
Additional Light Treatments
If required. At least 3 days after each prior light treatment

Why Adjustability Matters
High Quality Customized Vision for Cataract Patients
Accuracy: measure refraction post-op rather than predict pre-op
Using both eyes, ~90% able to see:
• 20/20 at distance
• read 5-point font using both eyes2, 3
Quality: no loss of contrast or increased visual symptoms versus monofocal IOL1

Customization:
including optimization of blended vision between two eyes in ~80% of cases
Refractive Results
Absolute MRSE and astigmatism were within 0.50 D of emmetropia in targeted for emmetropia


No Difference Between Eyes With and Without
History of Prior Refractive Surgery
Refractive Accuracy Leads to Visual Excellence
Monocular uncorrected visual acuity of “distance” eyes was 20/20 or better in nearly 80% of subjects.

Binocular Outcomes
Uncorrected
Summary: The LAL Delivers Customized Vision for Every Patient
Adjustability offers better refractive outcomes for every patient
Outstanding binocular range and quality of vision
Dysphotopsias
• No increase in glare or halo versus monofocal
Low Light Conditions
• No reduction in contrast versus a monofocal lens