



The Spokane County Firearm Violence Prevention Community Needs Assessment is a crucial and timely contribution to the health and well-being of our region. At Excelsior Wellness, we believe that every person deserves the opportunity to grow, heal, and thrive in a safe and supportive community. This assessment highlights that firearm violence remains an urgent public health issue, fundamentally connected to our mission of providing whole-person, integrated care for individuals and families.
Firearm-related injuries and deaths do not occur in isolation; they reflect broader systemic challenges, including limited access to mental health care, cycles of trauma, and a pressing need for more effective prevention strategies. The findings of this report reaffirm what we witness every day: communities are demanding deeper investment in behavioral health, early intervention, and culturally responsive care. These services are not just what we offer; they are the foundation of our mission.
I extend my gratitude to Excelsior Wellness’s Office of Research and Evaluation for their thoughtful and rigorous approach. This work not only amplifies the community’s voice but also establishes a clear path forward—one rooted in equity, healing, and actionable steps.
At Excelsior Wellness, we are committed to being part of the solution. As we continue to build integrated systems of care and expand access for underserved populations, we carry the insights from this report with us. To effectively prevent firearm violence, we must address its root causes with compassion, data-informed strategies, and a collective belief that a better future is possible for everyone.
With appreciation,
Andrew Hill President & CEO Excelsior Wellness

The Spokane County Firearm Violence Prevention Community Needs Assessment (CNA) is a groundbreaking effort. This comprehensive report focuses on Eastern Washington, particularly Spokane County, providing a deep dive into firearm-related incidents, deaths, injuries, and community perspectives to help shape evidence-based prevention strategies. Nothing like this has been done before at this scale, making it an invaluable resource for community-based organizations across our region. Between 2018 and 2022, Spokane County saw 348 firearm-related deaths. Firearms remain the leading cause of death in the county. There are significant racial disparities, with Black and Hispanic residents facing disproportionately high rates of firearm-related deaths. Youth firearm violence is a growing concern, with death rates for ages 0-24 in Spokane County consistently exceeding state averages. This assessment goes far beyond statistics. The team employed a mixedmethods approach to support not only salient statistics but also stories from our partners with lived experiences. Community members pointed to mental health access, suicide prevention, and domestic violence interventions as top priorities, and this report dives deep into each topic for Spokane County.
I would like to extend special thanks to Andrew Ogwang and Lauren Dodier, members of our Research and Evaluation team, for their leadership in productive community meetings, their tireless pursuit of data wrangling, and the time they devoted to assembling this complex document. I would like to thank Anastacia Lee and Malecka Nachtsheim for their support throughout this project. Finally, I would like to extend my sincere appreciation to Dr. Yunhee Bae, who created many of the data figures in this document and served as our data engineer. I sincerely thank all our community partners for their engagement and participation. Their voices and lived experiences are critical in developing practical and lasting solutions to improve the quality of life for residents of Spokane County.
Best Regards
Anna Tresidder, Ph.D.
Vice President, Office of Research and Evaluation
Excelsior Wellness, Office of Research and Evaluation
This project was funded by the generous support of the Office of Firearm Safety and Violence Prevention—Community Safety Unit within the Washington State Department of Commerce.
The Office of Research and Evaluation and Excelsior Wellness extend their sincere gratitude to all community partners who generously contributed their time, expertise, and valuable insights to the development of this community needs assessment report. We value your collaboration and eagerly look forward to our continued joint efforts in addressing the identified areas of concern and creating sustainable solutions that uplift and empower our community.
We strive to ensure that this report reflects the voices and concerns of our esteemed community partners, whose contributions have been instrumental in its development.
This report was authored by:
• Andrew Ogwang, MPH, FRSPH — Public Health Systems Administrator
• Lauren Dodier, BA — Research Assistant
With support from:
• Anna Tresidder, MPH, PhD — Vice President, Research and Evaluation
• Yunhee Bae, PhD –Senior Data Scientist
• Malecka Nachtsheim, M.Ed—Research Assistant
County Data Resource Partnerships:
• Spokane Regional Health District
• Spokane County Sheriff’s Office
• Washington State Department of Health, Office of Healthy and Safe Communities
• Washington Emergency Medical Services Information System

Excelsior Wellness is an integrated health and wellness organization dedicated to empowering individuals and families in the Spokane community. We offer a wide range of services that provide physical, mental, and behavioral health, ensuring holistic care for all those seeking care. Our team of compassionate professionals works collaboratively to provide personalized care, fostering wellness and resilience in every stage of life.
We believe that every person has the potential to be safer, stronger, and more satisfied in thelivesthey lead. Tothatend, weprovideequitableaccess to care, respect, and hope as we empower them to live and stay well.
Our vision is to serve a broad base of individuals and families with the primary aim of identifying goals and making positive steps towards accomplishing them. In ourcommunity, weare advocatesand hold fastto the belief that children and families have the potential to be safer, stronger, and more satisfied in the lives they lead.






This Spokane County Firearm Violence Prevention Community Needs Assessment (CNA) presents a comprehensive analysis of firearm-relatedincidents, deaths, injuries, andcommunity perspectives to inform evidence-based prevention strategies. Thisassessment utilizes extensive mixed-methods research, including quantitative and qualitative analyses from multiple sources. It highlights critical areas that need active intervention for Spokane County’s 553,170 residents.
From 2018-2022, Spokane County experienced 348 firearm-related deaths, representing a rate of 13.1 deaths per 100,000 residents. Firearms consistently caused the highest number of deaths in the county, with approximately 31-34 annual deaths from 2017 to June 2024. The analysis illustrates that suicides significantly outnumber homicides, with suicide rates peaking at around 54 deaths per 100,000 people in 2017. This assessment revealed significant racial disparities in firearm violence, with Black residents experiencing the highest rates of both homicides (15.1 per 100,000) and suicides (12.37 per 100,000), followed by Hispanic residents with homicide rates of 3.9 per 100,000. Males consistently exhibited substantially higher rates of firearm-related deaths compared to females, with male suicide rates reaching 16.54 per 100,000 from 2018-2022, while female rates remained around 3.5 per 100,000.
Youth firearm violence data shows trends with death rates for ages 0-24 in Spokane County generally trending higher than statewide rates, ranging from 5.8 to 10.9 per 100,000 people compared to Washington State’s 4.9 to 7.2 per 100,000 people. People aged 18-24 experienced the highest death rates, with 589 deaths at a rate of 17.3 per 100,000 people statewide and 43 deaths at a rate of 14.6 per 100,000 people in Spokane County from 2018 through 2022. The highest death counts for youth occurred in home settings, with 458 deaths statewide (50.2%) and 52 deaths in Spokane County (76.5%).
Emergency Medical Services data from 2018-2024 provides additional context, showing that 69% of firearm-related incidents were classified as lower acuity cases, while 2% required emergency response and 1% were critical cases. Approximately 81% of incidents resulted in hospital transport. The hospitalization data demonstrates notable racial disparities, with White Non-Hispanic patients showing the highest overall numbers but disproportionate rates affecting minority communities.
Through extensive community engagement, community partners identified mental health as the primary concern, with 82% of community partners ranking it as the top priority. They highlighted limited access to services and long waitlists, particularly for Medicare and Medicaid recipients. Suicide prevention emerged as the second highest priority at 71%, with community members emphasizing the need for improved
prevention strategies, including safe storage protocols and mental health support. Domestic violence ranked third at 53%, with community partners calling for enhanced support services and firearm relinquishment enforcement. Community members also expressed significant concern about school shootings and their impact on youth mental health.
Based on these findings, the CNA highlights four primary areas for intervention:
• Expanding access to behavioral health services including mental health, suicide prevention, and substance use treatment
• Implementing comprehensive safe storage protocols with education and access to safety devices
• Strengthening domestic violence prevention through enhanced firearm relinquishment processes and extreme risk protection orders
• Developing targeted educational initiatives and community-based violence prevention programs
These evidence-based recommendations will inform the development of a comprehensive Community Firearm Violence Strategic Action Plan in 2025, focusing on implementing strategies to reduce firearm violence and enhance community safety in Spokane County.
This assessment represents a crucial first step in understanding and addressing firearm violence through a data-driven, community-informed approach. The findings highlight the complex intersection of mental health, social factors, and access to firearms, emphasizing the need for collaborative, multi-faceted solutions to create lasting positive changes in community safety and well-being.

irearm violence is a serious public health crisis in the United States with devastating impacts on individuals, families, and communities. In June 2024, the U.S. Surgeon General declared an advisory on firearm violence.1 This advisory aimed to raise national awareness and mobilize a whole-of-society response to address this public health crisis. In 2022, over 48,000 people died from firearm-related injuries in the United States, with firearm suicides reaching the highest rate since 1968 2.3 . According to the American Public Health Association, the United States has a firearm homicide rate of 4.5 to 11 times higher than comparable high-income countries 4 . Firearm-related injuries are now the leading cause of death for children and adolescents. 5 Beyond fatalities, firearm violence causes lasting trauma, with 58% of American adults or their family members having experienced gun violence in their lifetime. 6 The economic cost is also substantial, estimated at $557 billion annually. 7 The Centers for Disease Control and Prevention (CDC) recommends that public health approaches to prevention should focus on addressing the risk factors (needs of people at greatest risk), promoting safe storage practices, and implementing evidence-based policies and programs to reduce firearm violence.8
Firearm violence the use of firearms to cause harm, often used interchangeably with “gun violence” describes both injuries and deaths from the use of firearms. A firearm is defined as any weapon that uses explosive force to discharge a projectile, including handguns, rifles, and shotguns. See Figure 1 below.

Source: History. (2023). Firearms. https://www.History.Com/Topics/Inventions/Firearms.
1 U.S. Surgeon General. (2024). Firearm Violence: A Public Health Crisis in America. https://www.hhs.gov/sites/default/files/firearm-violence-advisory.pdf
2 Centers for Disease Control and Prevention (CDC). (2024). Fast Facts: Firearm Injury and Death. Firearm Injury and Death Prevention. https://www.cdc.gov/firearm-violence/data-research/facts-stats/index.html
3 Friar, N. W., MPH, Merrill-Francis, M., PhD, Parker, E. M., PhD, Siordia, C., PhD, & Simon, T. R., PhD. (2024) Firearm Storage Behaviors Behavioral Risk Factor Surveillance System, Eight States, 2021–2022. Morbidity and Mortality Weekly Report, 524–529.
4 American Public Health Association (APHA). (n.d.). Gun Violence Prevention Fact Sheet. In https://www.apha.org/topics-and-issues/gun-violence. American Public Health Association.
5 Goldstick, J. E., Cunningham, R. M., & Carter, P. M. (2022). Current Causes of Death in Children and Adolescents in the United States. New England Journal of Medicine, 386(20), 1955–1956. https://doi.org/10.1056/nejmc2201761
6 Everytown for Gun Safety Support Fund. (2024). When the Shooting Stops: The Impact of Gun Violence on Survivors in America. Everytown Research & Policy. https://everytownresearch.org/report/the-impact-of-gun-violence-on-survivors-in-america/
7 Everytown for Gun Safety Support Fund. (2024). The Economic Cost of Gun Violence. Everytown Research & Policy. https://everytownresearch.org/report/the-economic-cost-of-gun-violence/
8 Centers for Disease Control and Prevention (CDC). (2024). Preventing Firearm Injury and Death. CDC Firearm Injury and Death Prevention. https://www.cdc.gov/firearm-violence/prevention/index.html
9 Kena, G., Ph. D., & Truman, J. L., Ph. D. (2022). Trends and Patterns in Firearm Violence, 1993–2018. In Special Report (NCJ 251663). https://bjs.ojp.gov/content/pub/pdf/tpfv9318.pdf
In addressing firearm violence in Spokane County, we used a public health approach to violence prevention. A public health approach is a comprehensive strategy that focuses on improving the entire population’s health, safety, and well-being. It aims to provide maximum benefits for the largest number of people by applying scientific methods to prevent violence. This approach utilizes a four-step process rooted in public health to address and mitigate violence.10
The CDC’s public health approach has been adopted and used to provide guidance to Spokane County’s firearm violence prevention through four systematic steps:
Figure 2: A Public Health Approach to Firearm Violence Prevention

DefineandMonitor theProblem By collecting local data on firearm incidents, demographics, and trends.
1
4 Assure Widespread Adoption
IdentifyRiskand Protective Factors Specific to Spokane communities through data analysis and community engagement.
2
3 Through policy advocacy, community partnerships, and program evaluation.
DevelopandTest Prevention Strategies By implementing evidence-basedinterventions tailored to local needs.
The Spokane County assessment systematically collected data, identified risk factors, gathered community perspectives, anddeveloped evidence-basedstrategies following a comprehensive public health framework. 10 Centers for Disease Control and Prevention (CDC). (2024). About The Public Health Approach to Violence Prevention. Violence Prevention https://www.cdc.gov/violence-prevention/about/about-the-public-health-approach-to-violence-prevention.html
The social-ecological model (SEM) provides a comprehensive framework for addressing firearm violence prevention at multiple levels of society. According to the CDC, interacting factors are considered at the individual, relationship, community, and societal levels.11 The SEM recognizes that violence prevention requires addressing factors at all levels, not just individual behavior.
Source: CDC. (2024). About Violence Prevention. https://www.cdc.gov/violence-prevention/about/?CDC_AAref_Val=https://www.cdc.gov/ violenceprevention/about/social-ecologicalmodel.html
The needs assessment addressedfirearms violence prevention through individual mental health, relationship dynamics, community collaboration, and societal factors-examining risk at every ecological level:
AttheIndividuallevel: By examining personal factors like mental health access barriers, substance use treatment needs, suicide risk factors, firearm safety education, and access to firearms.
AttheRelationshiplevel: Familysupportprograms andpeermentorshipinitiatives shouldbeestablishedat the relationship level through different organizations.
AttheCommunitylevel: Neighborhood watch programs (bystander awareness), school safety measures, local firearm storage programs, healthcare-community partnerships, and collaboration between law enforcement and community organizations should be strengthened through town hall meetings and coalitions.
At the Societal level: Supporting state and local policy initiatives like the WA state law initiative I-1639, city ordinance Gun Violence Prevention for Safer Spokane, conducting public education campaigns, and working with media outlets for responsible reporting of firearm incidents.
This approach aligns with including a broadarray of community partners who emphasize addressing upstream factors and immediate interventions.
11 Centers for Disease Control and Prevention (CDC). (2024). About Violence Prevention. Violence Prevention. https://www.cdc.gov/violence-prevention/about/index.html
Excelsior Wellness was awarded a grant by the Washington State Department of Commerce’s Office of Firearm Safety and Violence Prevention Community Safety Unit in December 2023 to facilitate community participation in addressing firearm violence in Spokane County. The project’s ultimate goal is to convene and facilitate Spokane County organizations interested in reducing violence to implement evidence-based strategies for firearm violence reduction, thereby developing a Community Violence Strategic Action Plan.
Excelsior Wellness utilized the public health expertise within their Office of Research and Evaluation (ORE) to collect and analyze data to define Spokane County communities’ most prominent areas of need related to firearm violence through data-driven initiatives. The ORE convened a Firearm Violence Prevention Planning Team (hereafter referred to as “community partners”) of representatives from diverse community organizations and concerned community members throughout Spokane County. The goal was to collaborate on producing project deliverables, including a Community Needs Assessment (CNA) in 2024 and a Community Violence Strategic Action Plan (SAP) in 2025. This CNA will inform the SAP by using evidence to demonstrate the root causes and impacts of firearm violence in the community and identify service gaps and barriers, which, if addressed using the SAP, will organize community resources to lower overall rates of firearm violence in Spokane County.

This list includes diverse community partners from law enforcement, healthcare, public health, mental health, domestic violence prevention, education, and community advocacy organizations. These multidisciplinary partners were essential contributors to the Firearm Violence Prevention Community Needs Assessment, providing critical expertise, community perspectives, and collaborative input to develop comprehensive understanding and solutions for firearm violence in Spokane County.
AnastaciaLee,MPH, Board Member, Asians for Collective Liberation in Spokane (ACLS)
Salliejo Evers, Regional Prevention Coordinator, Department of Homeland Security – CP3
Taffy Hunter, MSHS, HS-BCP, Interim Executive Director, Spokane Regional Domestic Violence Coalition
Melody Youker, Community Outreach, Prevent Suicide Spokane Coalition
BobLutz,MD,MPH,PublicHealth Physician
Sabrina Votava, Founder and Executive Director, Fail Safe For Life
Michael Van Dyke, DO, Pediatric Intensivist, Sacred Heart Children’s Hospital / Washington Chapter of the American Academy of Pediatrics
PaulDillon, CityCouncil Member, District 2, Spokane City Council
RobinBall,Retired, Sharp Shooting Indoor Range & Gun Shop
Rick Scott, Community Safety Partnerships Coordinator, GSSAC’s Prevention Center
Khris Thompson, Undersheriff, Spokane County Sheriff’s Office
DeniseMcCurdy,MBA,RN, Regional Nurse Manager Trauma Services INWA, Providence Hospital
AngelaSvastisalee, GrantCoordinator, Spokane Regional Domestic Violence Coalition
MiaParker,MPH,Fatality Review and Prevention Coordinator, Spokane Regional Health District
VirginiaRamos,LegislativeAssistant, Spokane City Council
JerrieNewport,LevelIIThreatAssessment Coordinator, North East Washington Educational Service District 101
VeenaSingh,MD,MPH,ChiefMedical Examiner, Spokane County Medical Examiner’s Office
Shayla Maxey, Assistant Program Manager, Carl Maxey Center/ Sandy Williams Justice Center
JohnathanWaldrop,Medical Examiner Operations Manager, Spokane County Medical Examiner’s Office
RumyanaKudeva,DSW,MPH, LICSW, Early Childhood Specialist, Spokane Regional Health District
HeatherWallace, SeniorProgramManager of Equity and Engagement, Better Health Together
Kami LaMoreaux, Violence Prevention Coordinator, Spokane Regional Domestic Violence Coalition
Dr. Deborah Svoboda, MSW, Associate Professor of Social Work, Eastern Washington University
JaredKiehn,Lieutenant, Investigative Division, Spokane County Sheriff
ChiefDavidEllis,SpokaneValleyPolice Department
During the CNA period, the community partners provided valuable feedback regarding where and how to collect data from their respective populations. They helped suggest additional community leaders and members for the focus groups. The community partners served as the ultimate source of feedback for editing this report, ensuring that the presented data represented diverse voices. Once the community partners approved the CNA in its final form it was shared with the community via paper and virtual options. Notably, the digital version of this document is more comprehensive and includes all supplementary information.
The work of the community partners and ORE will be shared with the Spokane County community at the 2025 Firearm Violence Prevention Conference to engage organizations with a shared goal and values from across the region in this work.
The methodology employed in this project reflects a systematic approach to community engagement, data collection, and collaborative planning across clearly defined phases. Beginning in January 2024, the project initiated quantitative data collection and established relationships with community partners to form a planning team. Over subsequent months, the team facilitated meetings, recruited additional partners, and conducted focus groups, culminating in the drafting and refining of the CNA with input from community partners.
JANUARY-MARCH2024
• Research: quantitative data collection
• Identified community partnersfor planning team and focus groups


• Second planning team meeting occurred in June with 13 participants
• Recruited 3 new community partners
•Created SharePoint for participants' ease of accesstoproject filesandresearch/resource submissions
• Identified focus group population
• First focusgroup meeting occurred in July with 13 participants
• Recruited 2 new community partners
OCTOBER 2024
• Complete initial draft of CNA

















DECEMBER2024
• Produce final CNA
• Group assessment survev








APRIL-MAY2024
• Recruited organizations for planning team
• Scheduled first planning team meeting
• First planning team meeting occurred in May with 12 participants
• 8 Additional community partners identified through attendee referrals
• Second focusgroup meeting occurred in August with 9 participants
• Recruited 5 new community partners
• Began drafting CNA in September
NOVEMBER2024
• Community partners provide feedback on initial CNA draft
Mixed-methods research combines and integrates both qualitative and quantitative data in a single study.12 Qualitatively, this report includes listening sessions and focus group data to identify common themes and highlight areas of need for firearm violence prevention. Facilitators and scribes captured detailed notes, recordings, and transcripts of the listening sessions and focus groups, which were later analyzed using the qualitative analysis software tool NVivo. Quantitatively, this report incorporates survey data, peer reviewed research, and statistical analyses of relevant data metrics to provide measurable evidence and a broader context to the community partners’ experiences. The findings from both data types are presented individually and in tandem to highlight the large scope of this work.
The diagram in Figure 4 illustrates how we organized and categorized our qualitative findings:
This section describes how the project gathered information on firearm violence in Spokane County through surveys, focus groups, and data-sharing agreements with various organizations in addition to the limitations we faced. The purpose of this data is to gain insight into the impact of firearm violence and investigate viable harm-reduction strategies by collecting both professional insights and personal experiences from community partners and members.

Kajamaa, A., & Mattick, K. (2020). How
A series of surveys (see Appendix C: Community Survey and Appendix D: Professional Survey) were conducted by gaining insight into the more significant Spokane population’s attitudes and beliefs and those of our focus group respondents. The professional and community surveys were distributed via “snowballing” through community partners, posts on LinkedIn and Reddit (r/Spokane), and flyers containing QR codes posted around Excelsior’s main campus and the SRHD Community Health Department. Both surveys aimed to gain insight into the impact of firearm violence in Spokane County to investigate viable harmreduction strategies later.
The professional survey was designed for professionals who are concerned for or work with people impacted by firearm violence. It asks questions such as “What types of firearm violence does your work engage with?” and “What are some of the main challenges or barriers faced by you…or your organization to reducing firearm violence?” to learn how communities have been affected by violence and investigate potential solutions. The community survey was open to all Spokane County residents to report personal experiences with firearm violence, including how it has impacted friends or family. Professionals were allowed to respond to one or both of the surveys. Participants in the community violence survey (whether or not they reported experiencing violence) were provided with resources such as the national domestic violence hotline number, regional 24-hour crisis line, and the SRDVC community advocate’s contact information.
The activation period for both surveys began on June 24, 2024, and ended on September 25, 2024, allowing participants three months to submit their responses.

The project’s work group was formed through networking and outreach communications and was nearly identical to the Planning Team. The Program Director initially contacted 61 community organizations in fields related to the project’s target issues and formed a contact list of 15 community partners interested in joining the project’s planning team. Outreach began with organizations such as Spokane Regional Health District (SRHD) and law enforcement. Interested parties were encouraged to invite colleagues and professionals in related fields to join the work group. This group evolved as members navigated factors impacting their ability to participate; however, the work group had consistently strong participation as word spread of the project and additional community partners joined. The work group met four times between May and August.
The focus groups mainly consisted of the project’s pre-existing work group members and a few additional interested community partners. The first of two focus group meetings explored the topics of suicide, mental health, domestic violence, determinants of health, and substance use. In the second meeting, members returned to discuss mass and school shootings, community safety, news/media, public discourse, and safe storage options. Focus group participants were allowed to complete a follow-up survey after the meetings to provide further comments on each topic.
From July to August 2024, two focus group meetings were conducted at the Spokane Public Library— Hillyard to better understand the concerns and key findings of firearm violence in Spokane County. The July focus group meeting had 13 community partners in attendance, both in person and virtually. The group was subdivided into two, with different facilitators guiding the discussions using a formal interview guide (Appendix B: Community Partner Listening Session and Focus Group Questions). The August focus group met to finalize the remaining topics that were not completed in the first meeting, and the group used a formal interview guide (Appendix B: Community Partner Listening Session and Focus Group Questions).
The focus groups provided an opportunity for in-depth discussions on the topics from the listening sessions about their communities.
The facilitators used techniques to ensure that all community partners could participate in the discussion, which lasted about 120 minutes (about 2 hours).
In addition to data collected from public online sources, Excelsior entered into data-sharing agreements with the Washington Department of Health (DOH), the Spokane Regional Health District (SRHD), Spokane County Sheriff’s Office (SCSO), and the Washington Emergency Medical Services Information System (WEMSIS).
The Community Needs Assessment utilized current secondary datasets while engaging community partners to identify relevant topics and data sources for understanding firearm violence in Spokane County. Access to the WEMSIS data was delayed, and the medical examiner’s office data was unavailable for this report. The available data spans from 2002 to June 2024 and represents the region’s first comprehensive analysis of firearm violence. The assessment relied on non-partisan, routinely collected data, such as crime statistics, mortality rates, injuries, and hospitalizations. The demographic data collected from these sources categorized gender in binary terms (male and female), which limits our understanding of how firearm violence affects individuals across the full spectrum of gender identities. National data shows that 2020 had the highest firearm violence rates in two decades13 , with many cities experiencing increased violent crime14 , though analyzing 2020’s specific patterns was beyond this study’s scope. These limitations should be carefully considered when concluding the available data.
13Johns Hopkins Center for Gun Violence Solutions. (2022). A Year in Review: 2020 Gun Deaths in the U.S. In https://publichealth.jhu.edu/gun-violence-solutions
14Braga, Anthony A., and Philip J. Cook, Policing Gun Violence: Strategic Reforms for Controlling Our Most Pressing Crime Problem (New York, 2023; online edn, Oxford Academic, 19 Jan. 2023), https://doi.org/10.1093/oso/9780199929283.001.0001
This needs assessment explores firearm violence in Spokane County using various data sources, including mortality records, hospital data, emergency services data, and crime statistics. The analysis presents findings using standardized rates per 100,000 to facilitate meaningful comparisons across geographic areas, demographic groups, and time periods within Spokane County. Additionally, for each topic area (deaths, injuries, crimes, and EMS events), the assessment provides overall counts followed by detailed breakdowns of geographic distributions, demographics, and circumstances specific to Spokane County. Finally, the standardized rates are calculated and presented at various levels, including state and county-wide annual rates, multi-year average rates, geographic area-specific rates, and demographic-specific rates, which analyze disparities by race, gender, and age.
Population Density
Spokane County, Washington’s estimated 2024 population is 553,170 with a growth rate of 0.31% in the past year according to the most recent United States census data15 . Spokane County is the 4th largest county in Washington State.16
Race, Ethnicity, and Firearm Violence
Spokane County racial demographics17
• White: 80.96%
• Black orAfrican American:2.69%
• American Indian and Alaska Native: 1.31%
• Asian: 2.63%
Racial demographics and firearm violence:18
Washington
• NativeHawaiianandotherPacific Islander: 0.81%
• Some other race: 2.06%
• Multiracial: 9.29%
• Black people are2x morelikelythanwhitepeopleto die byfirearms
• White people are2x more likely than Black peopleto die by firearm suicide
• Black people are 9x more likely than white people to die by firearm homicide
National
• Black people are 2.7x more likely than white people to die by firearms
• White people are2x more likely than Black peopleto die by firearm suicide
• Black people are 12x more likely than white people to die by firearm homicide
Spokane County
• Total deaths 2018-2022= 348
• Rate per 100,000= 13.1
• Population= 541,125
15 United States Census Bureau. (2025). County Population Totals and Components of Change: 2020-2024. https://www.census.gov/data/datasets/time-series/demo/popest/2020s-counties-total.html
16 Spokane County, Washington Population 2024. (n.d.). https://worldpopulationreview.com/uscounties/washington/spokane-county
17 Research, N. (2025). Spokane, WA Population by race & ethnicity. https://www.neilsbera.com/insiahts/spokane-wa-population-bv-race/
18 EveryStat - EveryStat.org. (n.d.). EveryStat.Org. https://everystat.org/#Washington|
As illustrated in Figure 5, from 2017 to June 2024, firearms caused the highest number of deaths in Spokane County, with approximately 31-34 death counts annually, with similar numbers across homicides, deceased, and categories of suspects/arrests. Motor vehicles were the second leading cause with about 12-13 death counts, followed by knife-related deaths at roughly 9-10 death counts. Approximately eight deaths occurred at various physical locations, including residences, unknown sites, jails, drug stores, doctor’s offices, hospitals, bars, nightclubs, and motels or hotels. Other causes showed lower frequencies, with “Other” atabout three deaths, drugs atapproximately threedeaths, andblunt objects causing about two deaths per year.







Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than do does not show but rate shows calculated
*n=69
*Source: Spokane County Sheriff's Office

Figure 6 shows the average annual suicide deaths in Spokane County from 2004 to 2022. The data includes various categories, such as firearms, suffocation, poisoning, and other rates per 100,000 people. The data indicates fluctuating trends over the years, with firearms consistently accounting for a significant portion of death count cases in Spokane County.
100
0 0
-SumofCount
- Sum of Count
- Sum of Count Other-Sum ofCount Other - Average of Rate


- Average of Rate Suffocation-Average of Rate Firearm-Average of Rate
Note: *Population Multiplier: per100.000: Average across categories. *Count Sum across categories; Less than 10 shows neithercount nor rate. *n=1,570 * Data source: Spokane Regional Health District
Geography of Firearm-Related Deaths per 100,000 People
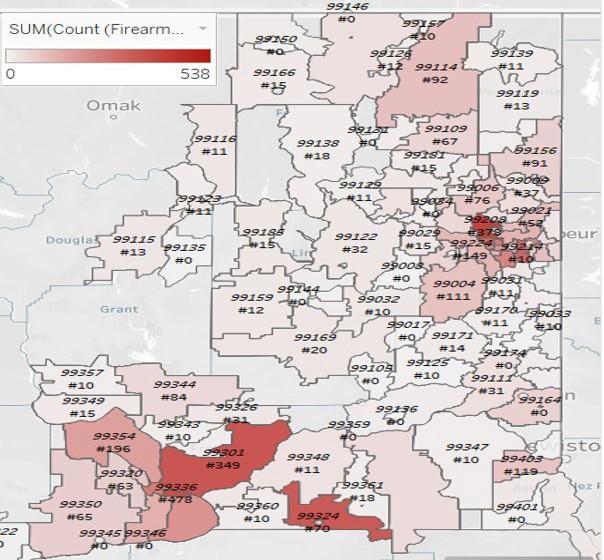
The heat map depicted in Figure 4 displays all firearm injuries by ZIP code in Spokane County and surrounding counties from 2016 to 2023. The map uses varying shades of red to represent the concentration of incidents, with darker areas indicating a higher number of firearm injuries in specific ZIP codes. The numbers (#) displayed within each ZIP code region indicate the total count of firearm injuries reported in that specific area.
The map in Figure 8 shows firearm-related homicide and suicide counts by ZIP code in Spokane County (2013-2022), with darker red areas indicating higher concentrations of up to 111 incidents. Yellow dots represent assaults, while blue dots indicate self-inflicted injuries, showing clustering patterns across different ZIP codes.
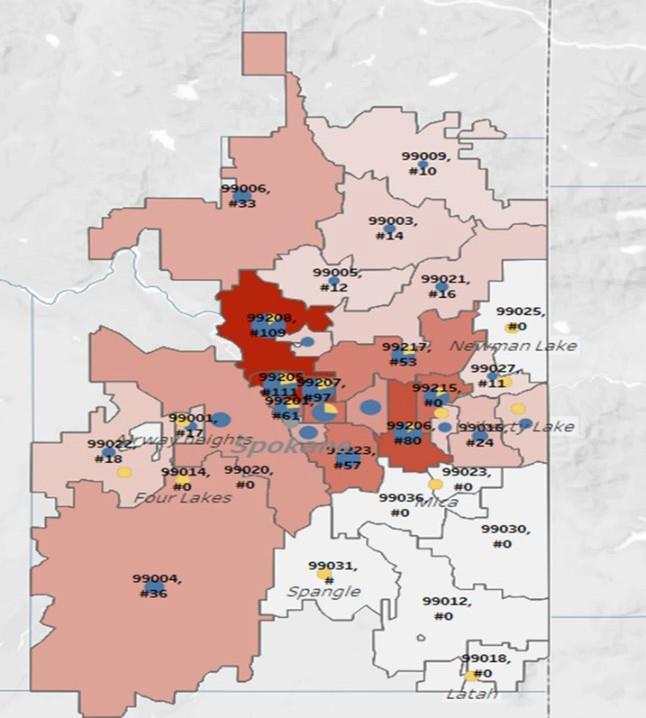
n=1,063 Data source: Spokane Regional Health District
The data below highlights firearm-related deaths in Spokane County by race and ethnicity. Figure 9 reveals significant racial disparities from 2018 to 2022. The “Black Only Non-Hispanic” population experiences the highest rates of both homicides (15.1 per 100,000) and suicides (12.37 per 100,000). Followed by the “Hispanic” population, which has a homicide rate of 3.9 per 100,000. Additionally, “Native Americans and Pacific Islanders” report the highest suicide rates at 8.62 per 100,000. Meanwhile, “White Only NonHispanic” populations have the highest total number of firearm-related death counts (228) and elevated suicide rates.
Figure 9: Average Annual Firearm-Related Deaths by Race/Ethnicity in Spokane County from 2018-2022










Suicide - Sum of Count
Homicide - Sum of Count
Suicide-AverageofAge-AdjustedRate(per100,000)
Homicide - Average of Age-Adjusted Rate (per 100,000)
Note: *2023 & 2024 death date is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=287
*Source: Washington State Violent Death Reporting System (WA-VDRS)
Figure 10 presents trends from 2004 to 2024 in five-year intervals, demonstrating a general increase in overall firearm deaths while suicides have consistently outnumbered homicides over the last five years (2018-2022).
10: Average Annual Firearm-Related Death by All Races/Ethnicities in Spokane County







Suicide - Sum of Count Homicide-SumofCount
Suicide - Average of Age - Adjusted Rate (per 100,000)
Homicide -Average of Age -AdjustedRate (per 100,000)
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count Sum across categories; Less than 10 does not show but rate shows calculated. *n=1,052
"Source: Washington State Violent Death Reporting System (WA-VDRS)
The following graphs show firearm-related deaths in Spokane County, comparing age groups and types of death (suicide vs. homicide). Figure 11 provides an age-group overview from 2018-2022, with Figure 12 and Figure 13 focusing on the 25-44 and 65+ age groups from 2004-2024. These differences might be attributed to increased exposure to high-risk situations, social dynamics, and lifestyle differences between working-age adults and seniors.








Suicide-SumofCount
Homicide -Sum of Count
Suicide-AverageofAge-AdjustedRate(per100,000)
Homicide -Average of Age-Adjusted Rate (per 100,000)
Note: *Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
* n=315
*Source: Washington State Violent Death Reporting System (WA-VDRS)
Figure 12 shows the 25-44 age group experiencing consistently higher rates of both suicide and homicide, with suicide rates peaking at 78 death count in 2018-2022.
Figure 12: Average

Figure 13 reveals that the 65+ age group has primarily suicide-relateddeaths (peaking at 73 death counts in 2018-2022) with nearly negligible homicide rates.
Figure



Figure 14 illustrates the average number of firearm-related deaths by suicide and homicide in Spokane County from 2004 to 2024. Figure 15 and Figure 16 show a breakdown by gender. Males exhibit significantly higher rates of both firearm-related suicides and homicides compared to females. From 2018 through 2022, there have been 233 male suicide death counts by firearms at a rate of 16.54 per 100,000 people, whereas female suicides reached a high of approximately 45 death counts at a rate of 3.5 per 100,000 people from 2014 through 2018. This substantial gender disparity may be attributed to factors such as higher firearm ownership rates among males19 , different chosen methods for suicide attempts, and varying rates of seeking mental health support between genders.20
Figure 14: Average Annual Firearm-Related Deaths by Gender in Spokane County from 2004-2024, Categorized by 5-Year Groups


Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated. *n=1,130
*Source: Washington State Violent Death Reporting System (WA-VORS)

19 Mitchell, T., & Mitchell, T. (2024). The demographics of gun ownership. Pew Research Center. https://www.pewresearch.org/social-trends/2017/06/22/the-demographics-of-gun-ownership/ 20 Griffith, D. (2024). Men and mental health: What are we missing? AAMC. https://www.aamc.org/news/men-and-mental-health-what-are-we-missing

*n=124
*Source:
Figure 17 and Figure 18 show firearm-related deaths by homicides and suicides in Spokane County from 2004 through 2024 by gender. Figure 17 shows homicides increasing over time, with rates rising from 2.0 4.2 per 100,000 (22–52 death counts annually) for males from 2004 through 2022 and remaining relatively stable at around 0.6 per 100,000 for females.
Figure 17: Average Annual Firearm-Related Homicides by Gender in Spokane County from 2004-2024, Categorized by 5-Year Groups
-Sum of Count

- Sum of Count Female - Average ofAge-Adjusted Rate (per 100,000) Male-AverageofAge-AdjustedRate(per100,000)
Note:
Washington State Violent Death Reporting System (WA-DRS)
Figure 18 depicts suicides, showing significantly higher rates among males (ranging from 15.3 16.5 per 100,000)compared to females (around1.7–3.5 per 100,000 people), withmalesuicides reachinga peakof 235 death counts from 2018 through 2022. Figure 18: Average Annual Firearm-Related Suicides by Gender
Figure 19 illustrates the average number of firearm-related death rates per 100,000 people over a ten-year period (2004-2024) for youth 0-24 in Spokane County compared to the statewide rates for Washington State. The rates for Spokane County, which range from 5.8 to 10.9 per 100,000 people, generally trend higher than those for Washington State, which range from 4.9 to 7.2 per 100,000. The most significant difference occurred around the years 2016-2017, when Spokane County reached approximately 9.9 per 100,000, while the statewide rate was closer to 5.9 per 100,000. This represents a difference of about four deaths per 100,000 people during that peak period.






















Spokane County - Sum of Court Statewide-SumofCount
SpokaneCounty-AverageofAge-SpecificRate(per100,000)
Statewide - Average of Age-Specific Rate (per 100,000)
Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=2,606
*Source: Washington State Violent Death Reporting System (WA-VDRS)
Figures 20 – 21 illustrate the average number of firearm-related deaths and average rates per 100,000 people for specific age groups in Spokane County and Washington State over a ten-year period from 20042024. Figure 20 indicates that people aged 18-24 experienced the highest death rates, with 589 deaths at a rate of 17.3 statewide and 43 deaths at a rate of 14.6 in Spokane County from 2018 through 2022.
Figure 20: Average Annual Firearm-Related Deaths by Age Group for Ages 0-24 in

Spokane County - Sumof Court Statewide - Sum of Count
Spokane County - Average of Age-Specific Rate (per 100,000)
Statewide-AverageofAge-SpecificRate(per100,000)
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count:
Figure 21 presents trends from 2004 - 2024 for the 18-24 age group, showing that statewide rates consistently exceed those of Spokane County, peaking at 17.3 per 100,000 (589 death counts from 2018 - 2022).
Figure 21: Average Annual Firearm-Related Deaths by Age Group (18-24) in Spokane County Compared to Washington State from 2004-2024, Categorized by 5-Year Groups

Spokane County - Sum of Court Statewide - Sum of Count
County - Averageof Age-Specific Rate (per100,000) Statewide-AverageofAge-SpecificRate(per100,000)
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated. *n=2,211 *Source: Washington State Violent Death Reporting System (WA-DRS)
Figure 22 shows that from 2018 - 2022, the average male firearm-related death rates experienced a significant increase, rising from 6.9 to 12.1 per 100,000 people. During this five-year period, the number of deaths peaked at 54. In contrast, female firearm-relateddeath rates remained relatively low, at 1.2 per 100,000 people.
Figure 22: Average Annual Firearm-Related Deaths by Gender for Age Group 0-24 years in Spokane County from 2004-2024, Categorized by 5-Year Groups






Female -Sum of Count Male - Sum of Count
Female - Average of Age-Specific Rate (per 100,000)
Male-AverageofAge-SpecificRate(per100,000)
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=165
*Source: Washington State Violent Death Reporting System (WA-DRS)
Figure 23 compares the average firearm-related deaths and percentages among people aged 0-24 in Spokane County and Washington State from 2018 through 2023, categorized by the location of the incidents.Thehighestdeathcountsoccurredinthe “Home” category,with 458 deaths statewide (50.2%)and 52 deaths in Spokane County (76.5%). Additionally, there were 181 deaths in the “Other specified places” category, accounting for 19.8% statewide. Both areas show a declining trend in deaths when considering other locations, such as streets/highways and schools/institutions.
23: Average Annual Firearm-Related Deaths by Location for Ages 0-24 years in Spokane County Compared to Washington State from 2018-2023





AverageofAge-SpecificRate(per100,000)
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=955 *Source: Washington State Violent Death
System (WA-DRS)
Figure 24 presents a comparison of average annual firearm-related deaths by race and ethnicity for people aged 0-24 in Spokane County versus Washington State from 2018 to 2022. The highest death rate is observed among Black and Non-Hispanic people, with rates of 26.9 per 100,000 in Spokane County and 21.9 per 100,000 statewide. Additionally, American Indian/Alaskan Native and Hispanics exhibit higher death rates compared to White and Asian Only (Non-Hispanic). However, White Only (Non-Hispanic) had a higher total death count of 354; their rates were lower compared to the other racial and ethnic groups.
Figure 24: Average Annual Firearm-Related Deaths by Race/Ethnicity for Ages 0-24 years in Spokane County Compared to Washington State from 2018-2022











Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=788 *Source: Washington State Violent Death Reporting System (WA-DRS)
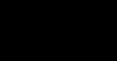
From 2018-2022, the average annual firearm-related deaths in Washington State shows suicide (96%) significantly outweighing homicide (94%) as the primary cause with known circumstances. Mental health problems (42%) anda history ofsuicidal thoughts, plans, or attempts (40%) are the most common circumstances for suicides, while injury that occurred during an argument (35%) is the leading factor for homicides, as shown in Figure 25.
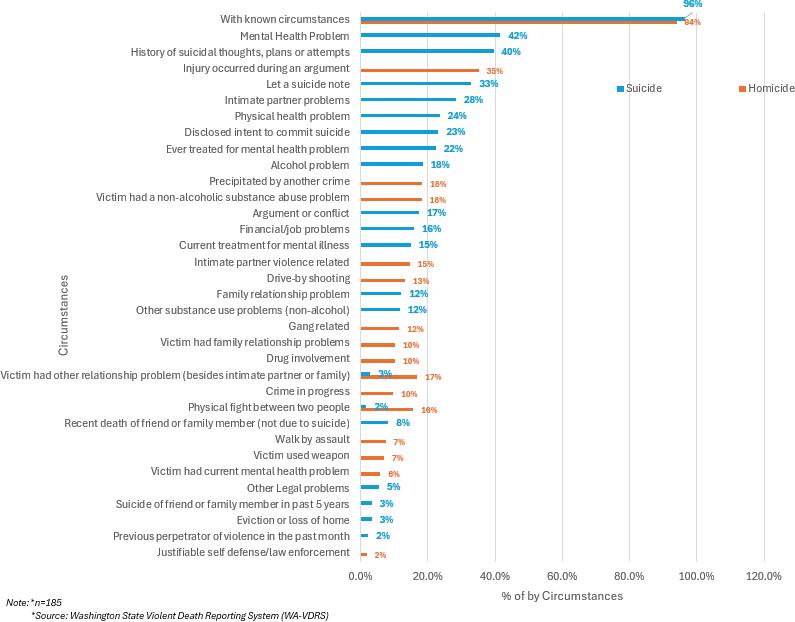
Figure 26 shows the average annual firearm-related death circumstances by gun ownership from 20182022. The “Unknown” category shows the highest percentage, increasing from 67.9% in 2020 to 79.2% in 2021 and then declining. “Shooter” declined from 21% in 2018 to 9.3% in 2022. Other categories like “Friend/Acquaintance” and “Parent” remained relatively stable at lower percentages.
Figure 26: Average Annual Firearm-Related Death Circumstances by Firearm Ownership in Washington State from 2018 to 2022 per 100,000 People


Spouse / Intimate Partner Friend/Acquaintance
Note: *n=1,130
*Source: WashingtonState Violent Death Reporting System (WA-VORS)
From 2018-2022, data from Washington State in Figure 27 shows the average annual firearm-related deaths by three circumstances: hunting, weapon cleaning, and victims playing with a firearm when discharged. Deaths from victims playing with a gun when discharged dropped significantly from 0.5% to 0.0% from2018 to 2020 and peaked in 2021, while hunting and weapon cleaning deaths remained consistently low, never exceeding 0.1%.
27: Average Annual Firearm-Related Death Circumstances by Firearms from 2018 to 2022 per 100,000 People in Washington State
Victimplaying withgun when discharge WeaponCleaning
Note: *Age-Specific Rate (per 100.000): Average across categories
Sum across categories; Less than 10does not show butrate shows calculated. *n=15
In Figure 28, between 2018-2022 Washington State’s average annual firearm-related death data reveals that handguns were consistently the predominant type of weapon used, accounting for 75-80% of deaths by circumstances, with a peak of 84.3% in 2020.
28: Average Annual Firearm-Related Death Circumstances by Firearm Type from 2018 to 2022 per 100,000 People in Washington State
Note: *Age-Specific Rate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated *n=30 *Source: Washington State Violent Death Reporting System (WA-VDRS)
Figure 29 highlights youth and school-related death circumstances in Washington State. “Firearm victims with known circumstances” rates were consistently highest (96.2-99.1%) from 2018 to 2021 and dropped in 2022, while other youth and school-related death circumstances remained low. Gang-related deaths showed moderate rates between 21.2-30.8%, peaking in 2020.
Figure 29: Average Annual Firearm-Related Death Rates among Youth and School-Related Incidents from 2018 to 2022 per 100,000 People in Washington State
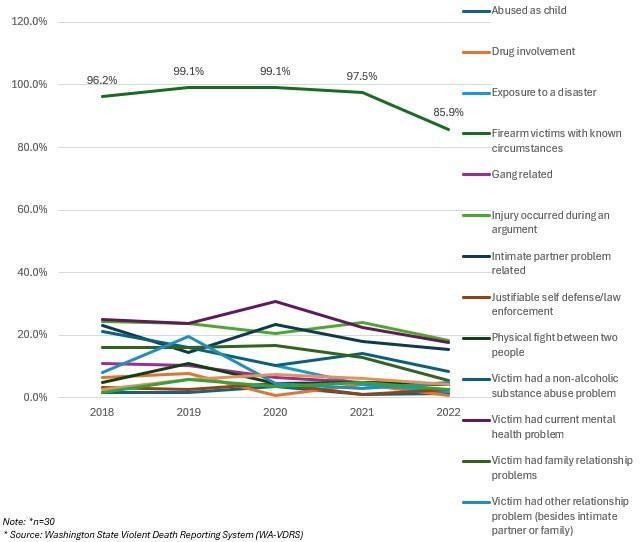
From 2016-2023, the average annual firearm-related hospitalizations in Washington State demonstrated notable racial disparities. White Only Non-Hispanic death counts remained the highest overall, climbing from 154 in 2018 to 268 in 2022. Hispanic death counts saw the most dramatic increase, rising from 49 in 2016 to reaching 118 in 2022 before declining. Black Only Non-Hispanic death counts increased steadily from 67 in 2018 to 146 in 2023, while Asian and Pacific Islander Only Non-Hispanic death counts stayed consistently below 50 per 100,000 people. Refer to Figure 30 for further details.
Figure 30: Average Annual Firearm-Related Hospitalization Cases by Race/Ethnicity from 2016 to 2023 per 100,000 People in Washington State
Suicide
Data from the Spokane County Sheriff’s Office shows a trend in the average annual firearm-related deaths by suicide from 2017 to June 2024. Of note, data from 2024 is still preliminary.
Figure 31 displays cases by age group (15-24, 25-44, 45-64, 64+); the 64+ age group experienced the highest death counts, with 7-19 deaths yearly, peaking at 19 in 2021. The middle-aged adults (25-64) showed fluctuating numbers between 7-19 cases, while the younger age group (15-24) maintained lower but persistent death counts.
Figure 31: Average Annual Firearm-Related Suicide Death Cases by Age Group in Spokane County from 2017 to (June) 2024



Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=293
*Source: Spokane County Sheriff's Office
Group=15-24

Group=64+

Group=25-44 NA
Group=45-64
Figure 32 shows that nearly all cases involve adults rather than juveniles, with annual adult cases ranging from 24-45 and minimal juvenile cases (0-3).
Figure 32: Average Annual Firearm-Related Suicide Death Cases by Adult/Juvenile in Spokane County from 2017 to (June) 2024
Note: *2023 & 2024 death data is still preliminary and will change *Age-Specific Rate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated.
From 2017-2024, data in Figure 33 shows varying patterns of firearm-related homicides across age groups in Spokane County for both victims and suspects. The highest victim counts appear in the age groups 25-44 and 45-64, with peaks in 2020-2023. For suspects/arrestees, there is a consistent trend in the 18-24 and 25-34 age brackets. The data suggests that while various age groups are affected, the 25-44 demographic is most heavily impacted by firearm-related deaths for both victims and suspects.
AgeGroup-25-44
#Suspect/Arrestee (blank) -#Suspect/Arrestee
Age Group=15-24#Suspect/Arrestee
AgeGroup=64´+ #Suspect/Arrestee
AgeGroup=45-64
#Suspect/Arrestee
AgeGroup=<15 #Suspect/Arrestee
Age Group-25-44- #Victim (blank) - #Victim Age Group=45-64 - #Victim
Age Group=15-24 -#Victim Age Group=64 + #Victim Age Group <15 + #Victim
Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100,000): Average across categories
*Count Sum across categories; Less than 10 does not show but rate shows calculated. *n=107
*Source: Spokane County Sheriff's Office
Figure 34 shows the average annual firearm-related suicide death cases in Spokane County by gender from 2017 to June 2024. Males consistently account for the majority of cases, with annual numbers ranging from 20-37 death counts, while female death count cases range from 3-9 per year.


Note: *2023 & 2024 death data is still preliminary and will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=293
*Source: Spokane County Sheriff's Office
In Figure 35, from 2017 to 2024 homicide cases in Spokane County showed higher rates for male suspects and victims compared to females. The number of cases peaked between 2019 and 2022, with 10 incidents involving males, followed by a sharp decline through 2024.
The data from the Spokane County Sheriff’s Office shows the average annual firearm-related suicide and homicide death count cases by race from 2017 to June 2024. Figure 36 shows that suicide death counts were predominantly among the White population, ranging from 22-42 cases annually, followed by the Black population.


Figure 37 shows that homicide death count cases had more variation across racial groups, with a peak of 13 White victims in 2022.


Data from the Spokane County Sheriff’s Office shows the average annual circumstances of suspect firearmrelated death cases from 2018 to 2022. Figure 38 illustrates the manner of death, showing that homicide by firearms consistently represents the highest percentage (peaking at 94% in 2021) followed by cases involving legal intervention.
Figure 38: Average Annual Circumstances of Suspects in Firearm-Related Cases by Manner of Death from 2018 to 2022 in Spokane County
Homicide
Legal intervention (by police orotherauthority)
Undetermined intent
Unintentional Firearm-inflicted byotherperson
Unintentional Firearm-unknown whoinflicted
Note: *Age-Specific Rate (per100.000): Average across categories *Count:Sum across categories; Less than 10 does not show but rate shows calculated. *n=107
*Source: Spokane County Sheriff's Office
Figure 39 shows other circumstances, depicting a general declining trend across multiple categories, with “Contact with law enforcement in the last 12 months” by suspect peaking at around24.1% in 2019, followed by “Attempted suicide by the suspect.”
Figure 39: Average Annual Firearm-Related Cases by Other Circumstances of Suspects from 2018 to 2022 in Spokane County
Alcohol use suspectedby suspect
Attempted
Suicideby Suspect
Had contact with law enforcement inlast12 months

Had contact with law enforcement inlast12 months
Note: *Age-SpecificRate (per 100.000): Average across categories *Count: Sum across categories; Less than 10 does not show but rate shows calculated. *n=107 *Source: Spokane County Sheriff’s Office
From 2018-2022, Spokane County’s firearm-related cases show the category “Relationship Unknown” representing the highest percentage, reaching 60.8% in 2022, followed by “Injured by law enforcement officers.” Other relationships between suspects and victims, including “Acquaintances andcurrent/former partners,” remained relatively stable below 10% throughout the 5 years as shown in Figure 40.
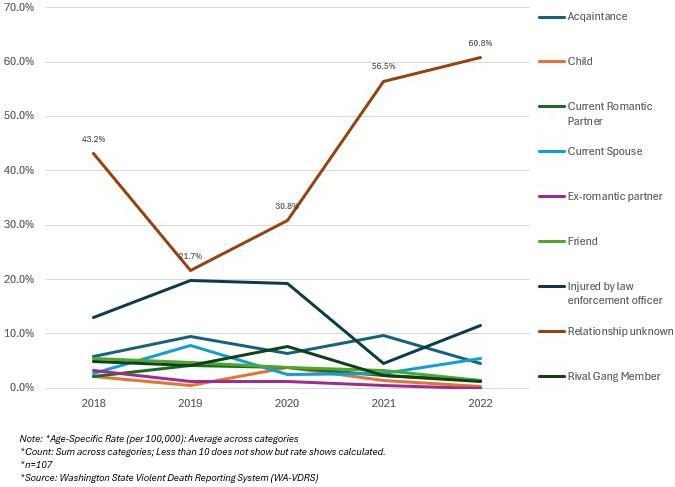
Figure 41 shows that Spokane County’s firearm-related homicides were predominantly concentrated in residential areas, with 35 cases of suspects and 32 cases of victims atresidence/apartment and 20 cases of victims and 21 suspects on highways/roads/alleys between 2017 and June 2024. Public spaces like fields/ woods, hotels/motels, and other places collectively accounted for fewer than 5 cases.

Homicides Deceased

Suspect/Arrestee
Victim
Note: *2023 &2024 death data is still preliminaryand will change
*Age-Specific Rate (per 100.000): Average across categories
*Count: Sum across categories; Less than 10 does not show but rate shows calculated.
*n=70 *Source:Spokane County Sheriff’s Office
From May to June 2024, the Office of Research and Evaluation conducted two listening sessions with diverse community partners at two locations of the Spokane Public Library (Indian Trail and Hillyard). The sessions were organized with an introduction, remarks on the project’s background, and prepared questions (see Appendix B: Community Partner Listening Session and Focus Group Questions). An overview of the current firearm violence data in Spokane County was presented to the community partners by the ORE facilitators.
These meetings were intended to establish an understanding of the community partners’ perspectives on the root causes of firearm violence in the community and identify service gaps and barriers. Topics of interest identified in the first listening session are represented in the “word cloud” in Figure 42. The size of each word correlates with the frequency with which it was mentioned by the community partners.
42: Listening Session Word Cloud

The listening sessions revealed several areas of concern related to firearm violence, including domestic violence, mental health, mass shootings, survivor’s aid, safe storage, social and political determinants of health,gang violence,suicide,andschoolormassshootings.Afteridentifyingthesekey concerns,community partners were invited to complete a survey ranking the topics by level of importance to discuss in the focus groups. A hierarchy pyramid was created to show the percentage of community partners who ranked each topic as highly important to be discussed in the upcoming focus group (Figure 43).


Many community partners (82%) cited Mental Health as the top priority for the focus group discussion, followed by Suicide (71%) and Domestic Violence (53%). School shootings and Substance use were split evenly (41%), while Mass shootings (35%) and Gangviolence (12%) followed.
Six main topics emerged from the work group’s ranking, which informed the types of questions that were posed to the focus group. Between the two focus group meetings, participants discussed suicide, mental health, domestic violence, determinants of health, substance use, andschool/mass shootings. Additional topics of news and social media and public discourse were posed after participants requested a second meeting. The six key concerns and two additional topics are mapped in Figure 44 below. Focus group members’ comments were categorized by these key concerns and are accompanied by supplemental research in the following data presentation.
Figure 44: Qualitative Themes










Mental health was the primary topic that community partners desired to be addressed in the focus group discussion (ranked highly by 82% of participants). The community partners’ discussion on mental health in Spokane County revealed a complex intersection between firearm ownership, healthcare access, and treatment quality.
Community partners expressed concern for rising mental health disorders, especially among youth, with one observation that “there’s so many undiagnosed mental illnesses among youth aged 18-24 and on college campuses.” Abrams (2022) supports this, stating that “By nearly every metric, student mental health is worsening. During the 2020–2021 school year, more than 60% of college students met the criteria for at least one mental health problem, according to the Healthy Minds Study, which collects data from 373 campuses nationwide.”21 This highlights the need for mental health services on college campuses as well as accessible mental health care for non-students of the same age category.
Community partners also mentioned the need for better approaches to firearm control, with one stating, “We shouldn’t ban gun ownership for everyone with a mental illness, but certain conditions should prevent ownership. Total gun bans may further stigmatize mental health, and people may evade help, treatment, or diagnosis because they want to own a gun. Those who own guns don’t want a punitive response for reaching out to get help.” Under federal law, any person attempting to purchase a firearm from a licensed dealer must undergo a background check. The National Instant Criminal Background Check System (NICS) is used to determine if an individual is prohibited from ownership due to certain criminal convictions or subjection to a protective/ restraining order. Current Washington laws and regulations prohibit gun ownership for individuals with a history of mental illness if they have been involuntarily committed for mental health treatment or were found not guilty of a crime by reason of insanity. State law also requires healthcare facilities to report involuntary commitments for mental health treatment to the NICS and local law enforcement agencies; however, under federal law, healthcare providers cannot disclose information regarding mental health status unless the patient poses an imminent threat of harm to themselves or others. Additionally, Washington’s Firearm Protection Order (FPO) law allows family members and law enforcement to petition for an individual’s firearms to be temporarily removed if they pose a significant danger to themselves or others due to mental illness. In most cases, individuals in Washington may petition in court to have their firearm rights restored, but they may remain disqualified under federal law.22, 23, 24, 25 There is a need for the effectiveness of these laws and regulations to be studied. If proven to be ineffective in preventing gun violence perpetrated by individuals with mental health disorders, further restrictions to gun purchase and ownership may be necessary.
21 Abrams, Z. (2022). Student mental health is in crisis. Campuses are rethinking their approach. https://Www.Apa.Org. https://www.apa.org/monitor/2022/10/mental-health-campus-care
22 Chow, C. (2024). Mental Health and Firearm Ownership in Washington – State Regs Today. https://www.stateregstoday.com/politics/gun-control/mental-health-and-firearm-ownership-in-washington

23 Petition to restore firearm rights. (2024). In Superior Court of Washington (pp. 1-3). https://www.courts.wa.gov/forms/documents/WS%20900_Pt%20to%20Restore%20Firearms%20Rights%202024%2001.pdf
24 Alexander Stoker. (n.d.). Firearms background checks Overview. https://www.hca.wa.gov/assets/program/fact-sheet-firearm-background-check.pdf
25 RCW 9.41.040: Unlawful possession of firearms—Penalties. (n.d.). https://app.leg.wa.gov/rcw/default.aspx?cite=9.41.040
The community partners also highlighted disparities in care quality and availability, with one participant pointing out a “...huge gap between the level of care the rich and poor can afford. Resources are often not available for the population that needs it most.” This gap emerged as a critical issue, particularly for Medicare and Medicaid recipients. As one community partner noted, “Medicaid patients trying to get mental health treatment face a long waitlist with unreasonable expectations to get off. They must call every day until a bed is available.” On a related note, insurance barriers were discussed extensively, with one insight being that “organizations may have their heart in the right place, but reimbursement rates aren’t sustainable to maintain staffing models and give adequate care.” This highlights a multidimensional deficit in healthcare, where the community’s need for mental health programs is in high demand, but the support necessary for organizations to provide care is lacking. Community partners noted that virtual programming can be effective for those with physical barriers to accessing care (such as transportation), but enrollment capacity of in-person counseling and inpatient treatment programs remains insufficient for the community’s needs.
Finally, community partners stressed the importance of collaborative, family-centered approaches to mental health care, especially for children. One community partner noted, “It takes adjustments to every factor of a person’s life to make a full change. People need support from services before, during, and after an episode of care.” This highlights the need for mental health services to target the family unit rather than just the individual. For children, collaboration between care teams working in and outside of schools could create more effective, well-rounded mental health treatment. As such, it is necessary for educators, school counselors, therapists, and other healthcare service providers to work together and communicate the child’s progress and continuing needs.
Overall, the community partners considered the need for a comprehensive, integrated approach to mental health care that addresses systemic barriers while promoting positive attitudes toward treatment and recovery.

Suicide was the second most important topic that community partners identified for the focus group discussion(rankedhighlyby71% of participants).Thecommunitypartners’discussiononsuicideinSpokane County revealed a complex intersection between lawful gun ownership, safe storage, and education for adults and children.
Community partners expressed concerns for the risk of suicide when firearms are present in the household: “Storing guns loaded with ammunition may increase suicide if impulsivity is involved.” Kellermann et al. (1992) support this claim, stating that, “Ready availability of firearms is associated with an increased risk of suicide in the home. Owners of firearms should weigh their reasons for keeping a gun in the home against the possibility that it might someday be used in a suicide.”26 One community partner highlighted fluctuation in risklevels, with an emphasis on the negative impact the presence of firearms contributes: “Suicide doesn’t occur in isolation; it builds up over time, reaching a peak that eventually deescalates. The risk increases when individuals have access to firearms during emergency situations.” This demonstrates that itis important for suicide risk levels to be assessed, both formally by mental health professionals and informally by friends or family members who may be able to provide timely intervention. The American Public Health Association (APHA) states that, “The most promising evidence-based strategies to reduce access to firearms during a period of high risk are (1) temporary relocation of household firearms away from home when [someone] is at risk for suicide, (2) safe storage at home if relocation is not possible, (3) working with leaders in the gun community to develop and implement messaging about [relocation and safe storage]...27

Several perspectives emerged on how to prevent firearm-related incidents involving children in the household.One partner calledfor a change in legal ownership laws, stating that, “If they can’t buy it, they shouldn’t have access to it even though legally [youth] can be gifted a gun at the age of 18. They can’t carry it, but they can have possession of it in their abode.” Stricterparametersongunownership,suchaseliminatingthe possibility of youth receiving weapons as gifts, may decrease the rate of gun violence perpetrated byyouth.
26 Kellermann, A. L., Rivara, F. P., Somes, G., Reay, D. T., Francisco, J., Banton, J. G., Prodzinski, J., Fligner, C., & Hackman, B. B. (1992). Suicide in the Home in Relation to Gun Ownership. New England Journal of Medicine, 327(7), 467–472. https://doi.org/10.1056/nejm199208133270705
27 American Public Health Association (APHA). (2018). Reducing Suicides by Firearms. https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2019/01/28/reducing-suicides-by-firearms
Another community partner emphasized using a multi-layered approach, combining primary prevention through mental health support and family counseling with secondary and tertiary measures like trigger locks: “Often people who have guns in safes don’t realize that kids and others in the household know how to access it. Guns aren’t always safe being locked up. Have you ever tried to hide Christmas presents from your kids? They’ll find them.”
Two community partners strongly advocated safe storage as the most critical element, stressing the importance of parents recognizing its significance: “Too many parents think their kids can’t get to their gunsordon’tknow how touse them, but accessleadsto accidentsorunsuperviseduse.” Thisissupported by Monuteaux et al. (2019), who estimate that up to 32% of youth (ages 0-19) firearm-related deaths by suicide and unintentional firearm injury could be prevented if adults with youth in the home engaged in safe household firearm storage practices: “…storing all firearms locked as opposed to unlocked, unloaded as opposed to loaded, and storing all ammunition locked andseparate from firearms have each been associated with a reduced risk of intentional self-inflicted and unintentional firearm injuries.”28 Other community partners stressed the importance of parental involvement, with one partner asking, “What is [the] general practice like for talking with students who might be experiencing suicidal ideation?” A suicide prevention specialist replied that, “When we’re talking about suicide prevention at those ages, we really have to be talking to the parents.” Suicide can be a difficult topic to approach, especially for parents who want to provide their children with age-appropriate information. While mental health disorders commonly begin in teenage years, psychiatrists have observed children as young as six years old reporting suicidal thoughts. Thus, for children who are asking questions or are known to have heard of or witnessed a tragic event, it is important for parents to discuss suicide to dispel misinformation and provide early intervention. Resources such as the University of Utah’s age-by-age guide are available for those unsure of how to broach the subject of suicide with children. 29
The overall qualitative data suggests that safe storage, education, and limiting access to firearms could be effective suicide prevention strategies, as they seek to remove a highly lethal means during critical moments when an individual might act on suicidal impulses.
Domestic violence (DV) emerged as a critical third topic for the focus group discussion (rankedhighly by 53% of participants). The gravity of the situation was marked by a recent tragedy as mentioned by a community partner: “I know of a young woman in Spokane who was recently shot and killed in a domestic violence case.” The incident served as a reminder of the lethal potential of domestic abuse, particularly when firearms are involved: “Firearms are a huge component of DV threats,” one community partner noted, explaining thatwith “firearms presentduring DV, lethality increases by five-fold.” ResearchconductedbytheEducationalFundto Stop Gun Violence (EFSGV) supports this claim: “Over half of all intimate partner homicides are committed with guns… a woman is five times more likely to be murdered when her abuser has access to a gun.”30 There is a need to reliably identify perpetrators of domestic violence and remove firearms from the household to prevent fatalities.
28 Monuteaux, M. C., Azrael, D., & Miller, M. (2019). Association of Increased Safe Household Firearm Storage with Firearm Suicide and Unintentional Death Among US Youths. JAMA Pediatrics, 173(7), 657.
https://doi.org/10.1001/jamapediatrics.2019.1078
29 University of Utah Health. (2022). How to Talk to Your Child About Suicide: An Age-By-Age Guide. University of Utah Health | University of Utah Health. https://healthcare.utah.edu/healthfeed/2022/09/how-talk-your-child-about-suicide-age-age-guide
30 Educational Fund to Stop Gun Violence. (2020). Domestic Violence and Firearms. Educational Fund to Stop Gun Violence. Domestic Violence and Firearms - The Educational Fund to Stop Gun Violence (efsgv.org)

One community partner who operates a free legal clinic noted, “I see a lot of domestic violence issues come in, and I see a lot of intimidation by firearms come up.” Another community partner mentioned that “Little data is collected on the non-lethal effects of gun violence, but particularly in cases of domestic violence, intimidation is a major factor. Many youths are unaware of what domestic violence and intimate partner violence looks like and have trouble identifying various forms of abuse.” Research corroborates these claims, as “Around 4.5 million women in the United States have been threatened with a gun, and nearly 1 million women have been shot or shot at by an intimate partner.” 31 Furthermore, “…because guns can be lethal quickly and with relatively little effort, displaying or threatening with a gun can create a context known as coercive control, which facilitates chronic and escalating abuse.”32 This indicates the need for further data collection on the mechanisms of coercive control (such as firearm intimidation) that are frequently used in DV cases to prolong abuse.
Community partners mentioned the complications of identifying and intervening in DV situations, as “DV and child abuse symptoms aren’t always visible.” One community partner pointed to signs in children, such as unexplained stomachaches, inappropriate age tantrums, and declining school performance as covert markers of trouble at home. This invisibility often leads to a “lack of resources provided through CPS,” with community partners agreeing on the “need [for] someone to intervene at the gray area stage, identify problems, and refer to services that exist.”
One community partner who is a Domestic Violence Prevention Executive shared insights on their evolving approach, including “Law Enforcement Officers (LEOs) doing a lethality assessment protocol (LAP) with victim survivors to get a better DV picture and connect them with an advocate over the phone.” This initiative, part of a study with Washington State University (WSU), aims to enhance victim safety and support. The group also discussed the implementation of Domestic Violence Protection Orders (DVPOs) and the challenges of firearms relinquishment, noting that, “in WA state it has to be relinquished to specific locations, not just another family member.” In addition to relinquishment challenges, there is a need to study the effectiveness of DVPOs in Spokane County.
31 Sorenson, S. B., & Schut, R. A. (2018). Nonfatal Gun Use in Intimate Partner Violence: A Systematic Review of the Literature. Trauma Violence & Abuse, 19(4), 431–442 https://doi.org/10.1177/1524838016668589
32 Ibid
Prevention emergedas a key focus, with community partners emphasizing the need to “create an intentional message when spreading awareness.” This included maintaining “regular dialogue about the issue and spread[ing] messages that counter violent behavior and make it clear that it isn’t right or acceptable.” The group recognized that “not discussing the issue hides its prevalence.” In addition to spreading messages through awareness campaigns, conducting an open dialogue with someone experiencing active DV may serve as the most effective intervention for concerned friends and loved ones. It is important to note that providing support for victims of DV does not always require expertise. The Washington State Coalition Against Domestic Violence (WSCADV) states that three strategies anyone can employ to help a victim of DV are asking questions, actively listening, and staying connected. 33
Asthe meeting concluded, community partnersagreedon the criticalneedto “bring all the coalitions together a couple times a year to share how they’re all working on prevention efforts.” This collaborative approach is essential to addressing the various challenges of domestic violence and creating safer, more resilient communities.
Schoolandmassshootings sharedthefourthhighestranking(alongside substance use) in importance for focus group discussion (ranked highly by 41% of participants). The community partners’ discussion on school and mass shootings in Spokane County revealed a complex intersection between children’s physical and mental health, school responses, and negative perceptions of public safety.
The impact of mass and school shootings on community mental wellbeing was discussed, raising questions like, “Is reporting mass violence events in the news responsible? How do these reports affect the community? Survivors may be unable to watch certain news or television programs due to PTSD triggers. Can reporting on these events inspire ‘copycat’ offenders?” and noting that, “Threats of gun violence and school lockdowns have risen in recent years. Not only has fear increased on school campuses, but compassion fatigue from the public has increased dueto thefrequency ofshootings.” Recentdata suggest continuedupward trends in school shootings and related deaths over the past 5 years.34 Imitation is a serious concern when mass violent events occur, and media coveragemust be made responsiblytoavoidsimilar crimes.Tocombat this issue, the Advanced Law Enforcement Rapid Response Training team and the Federal Bureau of Investigation developed the “Don’t Name Them” campaign. The campaign aims to “…curb media-induced imitational mass shootings and suggests minimizing naming and describing the individuals involved in mass shootings, limiting sensationalism, and refusing to broadcast shooter statements or videos” among other strategies.35

33 Washington State Coalition Against Domestic Violence (WSCADV). (2024). About Domestic Violence – Washington State Coalition Against Domestic Violence (WSCADV). https://wscadv.org/about-domestic-violence/
34 Katsiyannis, A., Rapa, L. J., Whitford, D. K., & Scott, S. N. (2022). An Examination of US School Mass Shootings, 2017–2022: Findings and Implications. Advances in Neurodevelopmental Disorders, 7(1), 66–76.
https://doi.org/10.1007/s41252-022-00277-3
35 Meindl, J. N., & Ivy, J. W. (2017). Mass Shootings: The Role of the Media in Promoting Generalized Imitation. American Journal of Public Health, 107(3), 368–370. https://doi.org/10.2105/ajph.2016.303611
While not a common occurrence in the Spokane County area, the effects of school shootings were of particular concern. Community partners noted that frequent drills and lockdowns can normalize the idea of violence for students. One community partner mentioned that “some kids are not allowed to use backpacks anymore, leading to physical problems carrying books and the emotional toll of knowing why you aren’t allowed to have a backpack.” Additional concerns include schools’ overall reactions to firearm violence, the presence of metal detectors, and reports that kids are more worried about threats originating within the school from other students than external threats to perpetrate harm.
Community partners also expressed concern for the ways that mass shootings have increased vigilance and changedperceptions ofsafety in publicspaces: “We have resigned ourselves to the fact that there’s always going to be gun violence. I’m always aware of exits and potential threats when in public, but it doesn’t have to be this way.” Even when a violent event is not local, national incidents have changed how people perceive risk in places like malls, theaters, and large events, indicating a shift toward general feelings of insecurity. Community partners revealed conflicting perspectives on how to address this issue. While some endorsed the “See something, Say something” campaigns,therewasalsocautionregardingpotentialunintendedconsequences, such as racial profiling and false reports.
As potential solutions to school and mass shootings, community partners recommended “focusing on upstream prevention and interventions to fill the gap before the crime has been committed.”
Substance use sharedthe fourth highest ranking (alongside school andmass shootings) of importance for thefocusgroup discussion(rankedhighlyby41% ofparticipants).Thecommunitypartners’discussionon substance use in Spokane County revealed an intersection between barriers to Substance Use Disorder (SUD) treatment and community dysregulation resulting from gun violence.
The intersection of substance use with firearm violence was highlighted when one community partner sharedapersonalstory:“There was a house on the corner that was known fordistributing opioids and other narcotics, drugs, and there has been a pretty significant threat of firearm violence in just my neighborhood because, in their process, these family members have come in to try to clean it up. Some people still want to frequent the house, and the family members who are trying to protect that property have said that they will shoot anyone who comes onto their property. So, every time there’s a bang in the neighborhood, we wonder if that’s what’s happening.” Research indicates that thisis not a unique phenomenon, as“Substance-relatedfirearm violence often starts with drug dealers, who get firearms to protect their drugs. This leads to more people in the neighborhood getting firearms because the drug dealers have them. Experts think this cycle leads to more violence in the community….
Bystanders are often victims of violence as well.”36 This highlights that the threat of firearm violence and accompanying fear destabilizes the community by causing residents to feel unsafe and distrustful of others’ motivations and actions.
Anothercommunity partnersharedthat a “neighbor was shot and killed over drugs” and highlighted the“ripple effects in the community” that such violence creates. Many community partners discussed the need for more behavioral health care services, seeing that “there is a shortage of inpatient beds for substance use treatment.” Community partners also recommended that “Approaches should be trauma-informed to address the complex needs of individuals struggling with substance use.”
36 The Recovery Village Drug and Alcohol Rehab. (2021). How Guns and Drugs Contributes to The Violence Across America. The Recovery Village Drug and Alcohol Rehab. https://www.therecoveryvillage.com/drug-addiction/how-guns-drugs-contribute-to-violence/
Determinants of health were a trending concern amongst community partners. The significance of addressing health determinants was emphasized when a community partner shared a personal experience fromtheirpreviousneighborhood: “I had the opportunity to move out of my old neighborhood because I didn’t feel safe. There was domestic violence occurring across the street from me. There was also a murder that happened four doors down from me. There was a shooting…a block away from me, and I was like, ‘I can’t raise kids in this.’ I was so scared even to leave my house. It’s very different from where I live now.” This reflects the disruption that firearm violence causes to the community. While relocation is an option for some, firearm violence largely affects low-income areas (see Figure 7, Figure 8 and Figure 73) where many residents feel “stuck” living and/or raising families amid turmoil. Furthermore, “outrunning” firearm violence through relocation is not a pragmatic solution. This indicates a robust need for the implementation of firearm violence prevention efforts which aim to make the community safer rather than the individual.
Regarding theneedforsurvivors’ aid, one community partnernoted, “A friend of mine in high school was a victim of a drive-by shooting, which impacted her life; she cannot necessarily watch many television shows because there is some firearm violence in it, and she cannot watch the news because there is firearm violence. Although she is healthy and happy, she still has some physical aftermath. How do we help those who have been impacted by firearm violence, because it doesn’t stop after the incident?” Theaftermathoffirearmviolencenotonlyaffects the individuals directly involved, but the surrounding community. Individuals may also experience vicarious trauma from witnessing violent events, hearing stories, or seeing reports of tragedies in the media. This is especially pertinent to children. It is important for survivors and affected individuals to know that there are resources available. Existing survivors’ aidservices in Spokane County include financial aid, victim advocacy, counseling and legal assistance, and 24/7 helplines provided by organizations such as the MacArthur Foundation’s Safety & Justice Challenge, YWCA Spokane, Kalispel Tribe Victim Assistance Services, and The Living Room for LGBTQ Youth. There is a need to evaluate these survivors’ aid programs to measure their accessibility and effectiveness in addressing the community’s needs.
Additionally, firearm access and its societal impacts surround many interconnected factors, from legal and illegal acquisition to the challenges of identifying potential perpetrators. One community partner highlightedtheneedforinnovative approachestoprevention,notingthat, “Perpetrators of firearm violence are hard to profile as there is not one ‘look.’” Warningsignssuch as direct threats, fascination with weapons or violent events, and a personal history of violence are among the primary means of identifying potential perpetration. Gang involvement also plays a role, although there are no dependable means of visually identifyingmembers.37 Gangviolence wasnoted as aconcern,with onecommunitypartnerstating, “Gang gun violence is on the rise and access to guns is high. Gang wars are on the rise in certain areas and are running longer than before, and that’s not just here in Spokane, but throughout all the other counties as well.”
While the Spokane Police Department admittedly “…does not track the specific number of people affiliated with gangs within city limits,”38 they reported “…almost four times as many shootings and drive-bys recorded by the Spokane Police Department…” in April of 2021 compared to the same time the previous year. 39 The motivating factors for gang violence can be linked to multiple determinants of health, such as poverty, lack of education andcommunity-belonging, andlimited access to healthcare. To address the widespread riseof this form of violence, access to mitigating resources must be made available to the community.
37 American Psychological Association. (2013). APA report on gun violence identifies precursors and promising solutions. [Press release]. https://www.apa.org/news/press/releases/2013/12/gun-violence
38 Epperly, E. (2022). Spokane leaders blame recent violence on county’s “850-1,500” gang members and soft-on-crime laws. Spokesman.Com https://www.spokesman.com/stories/2022/jun/30/gang-presser/
39 Mason, G. (2021). With gang violence on the rise, Spokane-area law enforcement leaders call for community action. Spokesman.Com. https://www.spokesman.com/stories/2021/mar/08/with-gang-violence-on-the-rise-spokane-area-law-en/
Finally, the motivations behind firearm ownership were diverse, driven by factors such as fear, family culture, and personal passions. One community partner notedthat, “when ‘everyone’ in the community owns and has access to guns, you are likely to own one or more too.” The discussions also touched on the evolving interpretation of theSecondAmendment, with one community partnerstating that, “the second amendment was initially the right to stand up to the government if things go awry; that’s not a relevant use nowadays.” With many firearm violence prevention advocates calling for stricter requirements for firearm ownership, it is imperative that current and prospective firearm owners evaluate their reasons for wanting to possess a firearm and weigh the perceived benefits against the potential costs.

News and social media were additional trending themes identified in the second focus group discussion. The community partners expressed deep concerns about the media portrayal of firearm violence, particularly with mass shootings: “Sensationalist coverage contributes to copycat incidents or increases fear.” One community partner emphasized the need for “more responsible reporting practices, including focusing on victims rather than perpetrators and providing more context and solution-oriented coverage.”
Community partners identified an interaction between media reporting and suicide, with concerns of the former influencing the latter: “I know that a lot of times, suicide is not reported in the media for safety reasons, but then we have an experience like we will see a mass violence event and that is reported on. I don’t know if that’s responsible reporting, and there are no guidelines for safe reporting on suicide and safe reporting on mass violence events.” While reporting guidelines should be well known and adhered to by journalists, the public may still have concerns over how tragic events are portrayed in the news. These concerns are founded, as research shows that the manner in which suicides are reported in the media can influence at-risk individuals. Guidelines for reporting on suicide have been well researched, and have helped inform reporting methods on other issues, such as mass shootings. 40 The American Foundation for Suicide Prevention’s top ten recommendations for reporting on suicide include modifying language in addition to avoiding the following: sensationalism, speculation, assigning one cause, featuring stories in a prominent place, immediately interviewing loss survivors, or sharing images.41
40 Meindl, J. N., & Ivy, J. W. (2017). Mass Shootings: The Role of the Media in Promoting Generalized Imitation. American Journal of Public Health, 107(3), 368–370. https://doi.org/10.2105/ajph.2016.303611
41 American Foundation for Suicide Prevention (AFSP). (2024). Safe Reporting Guidelines for Media. American Foundation for Suicide Prevention. https://afsp.org/safereporting/
Social media regulation and phone usage emerged as critical issues, with a focus on parental education: “Parents/guardians need to be the target of education on the negative impact of social media and phones in schools.” Parents are often at the center of the phone ban debate, with some arguing that phones merely serve as a distraction while others fear losing contact with their children during emergency situations. One community partner shared that, “in Victoria, AUS, kids were not allowed to have cell phones. High school kids could have phones, but they had to be locked away in their locker during the day. It started when kids were videotaping and recording school fights and then streaming it, so the schools banned phones – community norming helped there.”
Overall, the impact that banning phones has on gun violence is complex and context dependent. Proponents argue that cell phone bans are necessary to avoid everyday negative impacts, such as distractions, cheating, and cyberbullying, which outweigh their potential benefits in the relatively low risk of a school shooting. However, opponents contend that phones can be crucial for students to communicate with parents and authorities during a crisis, and that the educational and social harms of phones at school do not affect all kids equally. Banning phones might hinder communication, causing unnecessary anxiety among both parents and children. Proponents dispute this, stating that phones mostly operate as an “emotional safety blanket” for parents and do not decrease the limits in one’s ability to protect their child from an emergency remotely. Moreover, they argue that without phones students are less likely to be distracted during emergency drills and actual emergencies, allowing them to follow safety protocols more effectively. Still, parents opposing bans would argue that schools, with their bulletproof doors and active shooter drills, are guilty of the same wishful thinking. 42

Public discourse on firearms was another prominent theme discussed in the second focus group. Community partners expressed a desire for more productive conversations that incorporate diverse perspectives. One community partner pointed out the stigma that responsible firearm owners experience, saying, “As a firearm owner, I am demonized for others’ abuse of their weapons. Firearms do not kill people; people kill people, and that is the message that we really need to getoutthere to find the root cause!” Thishighlightsoneof the ways in which firearm violence can become a sensitive topic that leads to people feeling attacked. When messaging is not centered around violence prevention, conversations can become escalated as responsible owners may feel that advocates of firearm safety are calling for a total firearm ban and attacking their rights. Through the shared goals of improving community safety and saving lives lost to firearm violence, the community partners were able to identify several strategies to conduct productive conversations about firearm violence prevention. These included sharing statistics on firearm violence, promoting safe firearm ownership, sharing personal stories, and adopting a public health approach. This is captured in one community
partner’s key insight: “We should be educating others that it’s not about taking rights away. It’s about violence prevention and awareness. We need to focus on shared goals of community safety rather than divisive political ideologies.” Another community partner argued that “people want to blame mental health conditions to take focus away from the guns; people need to know that [perpetrators of gun violence] do not all have a mental health condition. Lots of folks blame mental health for taking the attention away from the firearm topic.”
As explored earlier in this report, while mental health disorders can be a contributing factor to firearm violence, they are not the sole cause, andconversations about prevention must be more nuanced andextend past this point. These diverse perspectives illustrate the complexity of firearm violence and emphasize the need for comprehensive, community-based strategies for firearm violence prevention and intervention in Spokane County. Overall, the community partners calledfor a more inclusive, informed, andsolutionoriented public discourse on firearms with a focus on prevention, education, and community safety.

Six main topics emerged from the work group’s ranking, which informed the types of questions that were posed to the focus group. Between the two focus group meetings, participants discussed suicide, mental health, domestic violence, determinants of health, substance use, andschool/mass shootings. Additional topics of news and social media and public discourse were posed after participants requested a second meeting. The six key concerns and two additional topics are mapped in Figure 44 below. Focus group members’ comments were categorized by these key concerns and are accompanied by supplemental research in the following data presentation.
Almost all participants in Spokane County, both community members (100%) and professionals (98%), reported working and living in the area.
Figure 45 illustrates the average age groups of participants. Community members had an average age of 45 to 54 years, while a significant number of professionals chose not to disclose their age, resulting in 42% falling into the “Not Applicable (N/A)” category. The data shows representation across various age ranges, from 18 to 84 years, although there was lower participation among the “18-24” and 65+ age groups for both categories.



Professionals and community members were asked the question, “Are you Hispanic, Latino, or Latina?” The majority of both groups identified as not Hispanic, with only 2% of community members and 4% of professionals identifying as Hispanic. Additionally, 17% of community members and 38% of professionals chose not to answer the question, which is categorized under “N/A.”
Community members and professionals were also asked, “Which of these groups do you say best represents your race?” The majority of respondents identified as White, with 60% from the community and 44% from the professional group. Additionally, 34% of community members and 42% of professionals preferred not to answer “N/A.” Smaller percentages identified as “Black/African American, Asian, American Indian/Native American,” or other races.
Among community members, the gender distribution was nearly equal, with “Females” at 34% and “Males” at 30%. Two percent identified as “Transgender,” while 34% chose not to disclose their gender identity “N/A.” Amongprofessionals,thegender distributionwas different:“Females” comprised50%, while“Males” accounted for 12%, and 38% did not disclose their gender identity “N/A.”
When survey respondents were asked, “What is the highest grade or year of school you completed?” Professionals reported higher rates of “Postgraduate or professional degree” education (37%), while community members had higher rates of “College graduates” (34%). 40% of professionals and 19% of community members preferred not to answer “N/A.”
This section presents community survey findings on firearm violence experiences, ownership patterns, and perceptions in Spokane County. Documenting both quantitative data (ownership rates and safety concerns) and qualitative insights (perceived causes, solutions, and needs) establishes an evidence base from the community’s perspective to inform targeted prevention strategies.
Of the community participants surveyed about firearm violence experiences in the last five years, 65% reportedno experience “No, no one,” while 14% of the participants indicated encounters through either family members, close friends 12%, or direct experiences 8% as shown in Figure 46.

No, no one Yes,someone inmyfamily Yes,a closefriend Yes, I have personally experienced this
Follow-up questions were given to those who had personally experienced firearm violence in the past five years.
Figure 47 illustrates that among the community participants, 33% of participants reported being “shot at but not hit” and “threatened by someone showing a gun,” 17% were “threatened to be shot at (though no gun was shown)” and “threatened by pointing a gun.”

Figure 48 shows that community participants were asked if they knew anyone at all who has been impacted by firearm violence, aside from themselves. The responses showed a range of relationships, with “My friend” being the most frequently mentioned, totaling 31% of cases. Other categories, such as “My neighbor,” “My parent,” “Another familymember,” and“My colleagueorco-worker,” had 13% each.
48: Participant’s Relationship to Person Who Was Injured or Killed



Community participants who had known someone injured or killed by a firearm in the last five years were asked, “What type of firearm violence was this?” According to Figure 49, the most common response was “Intentional assault by someone else,” which accounted for 33% of the responses. This was followed by “Suicide or attempted suicide” with 25% of the responses. Other categories included “Intentional assault relatedto domestic violence” and“Other” which received17% of the responses, and“Accidental” with8% of the responses.
Figure 50 shows that community participants were asked about firearm ownership. When asked “Is there a firearm in your home (such as a handgun, shotgun, rifle, etc.)?” 58% answered “Yes” and 43% with “No.”
50: Presence of Firearm(s) in the Home


When firearm owners were asked about their reasons for possession, the highest responses were for personal protection and household protection (43%), with sports/recreational shooting (37%), given or inherited from a family member or friend (15%) and for work being the least common reason (2%). Participants were also asked, “Is the firearmin yourhome safely stored(such asin a safe or locked container)?” 73% said “Yes” while 27% said“No.”
Community participants were asked about their experiences with firearm use in self-defense. When asked, “Have you ever used a firearm in self-defense (to protect yourself or someone else)?” 27% reported using a firearm in self-defense while 67% reported “No.”
Figure 51: Have You Ever Used a Firearm in Self-Defense (to protect yourself or someone else)? n=22
Whenparticipants were asked,“Whowere youdefending/protecting?” most(6)indicated “myself,” followed by a family member (2) and a colleague/co-worker (1) as shown in Figure 52.
Figure 52: Who Were You Defending/Protecting?
Regardingfirearmdischarge,whenasked, “Was theFirearmDischargedor Presented?” 83% ofthe participants only presented the firearm while one participant mentioned that the firearm was discharged (17%).
Amongthose who used a firearm in self-defense, 67% did not report the incident to law enforcement while 33% reported the incident.
Community participants expressed varying levels of concern about firearm violence in their community. When asked, “How concerned are you about firearm violence in your community (where you live, work, worship, go to school, etc.)?” 35% of members indicated that they were “Very concerned,” while another 20% reported being “Somewhat concerned” seen in Figure 53.
Figure 53: Participants’ Level of Concern for Firearm Violence in Their Community
Participants were also asked about their safety (Figure 54): “When thinking about community firearm violence(suchasstreetviolenceor gangviolence),howsafedo youfeel inyourcommunity?” 30%reported feeling “Very safe” and 8% reported feeling “Very unsafe.”
When participants were asked about their likelihood of becoming a victim of firearm violence in the future, responses were evenly distributed with 8% indicating it was “Very likely” and 28% saying it was “Somewhat likely,” though some participants also expressed lower levels of concern.
• Somewhat likely 28%
• Very unlikely 25%
• Somewhat unlikely 25% • Neither likely nor unlikely 15% • Verylikely8%
Community participants who indicated “Very likely” or “Somewhat likely” on the survey were asked, “You said that you think you or someone you know could possibly be the victim of firearm violence in the future. What type of firearm violence?” 77% indicated they were concerned about “Community violence (like street violenceandschoolshootings),” while15%mentioned“Accidental harm,” and8% cited “Suicide.”
Community participants identified “Mental health issues” (20%) and“Substance use” (18%) as the leading causes of firearm violence. “Gang violence” and “Access to firearms” followed, with “Domestic violence,” other causes, and lack of firearm safety training rated as the lowest.
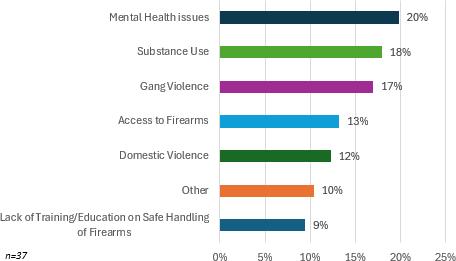
Community participants provided diverse responses when asked about solutions for reducing firearm violence. “Firearm Control and Regulation” led with the highest rate of responses (26%), followed by “Law Enforcement and Criminal Justice” (21%) and “Mental Health and Social Services” (18%). “Education and Training”(13%),“CulturalChange”(8%),“NoSolution” (8%),and“SocioeconomicApproaches”(5%)followed.
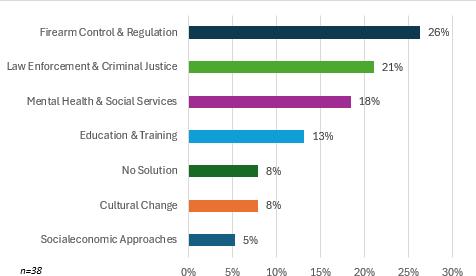
Domestic violence support center/services and substance use counseling/treatment emerged as the highestpriority needs, with 64% and 62% of community members rating these as vital and greatly needed. Mental health counseling, afterschool/youth programs, and general firearm safety training are followed closely aspriorities.
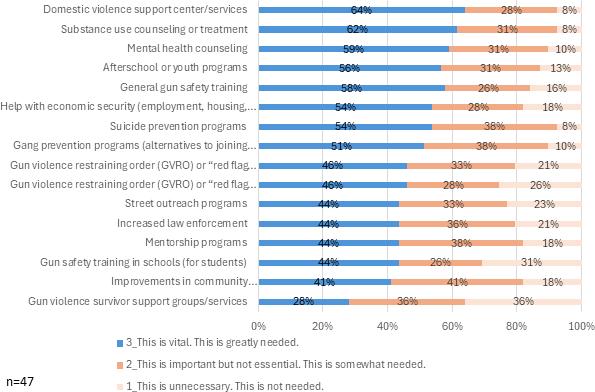
Participants were also asked the open-ended question, “What other resources, services, or programs are needed to help local communities impacted by firearm violence?” Many resources were mentioned including:
• Suicide prevention
• Universal health care, housing, basic income
• Weapons library
• Supportforindividualfirearm ownersto allowforrecurrenttraining
• Nonviolent solutions andhelpbefore shootingshappen.
• Committingacrimewithastolenfirearm should have serious consequences
• Outreach presence
• Education and awareness
• Resourceofficers
• Expanded jail
• Specific support groups
• More training andsupport forthose impacted
• Stopping criminals from getting firearms
• Address social isolation among males
• Suicidepreventionforyoungmenandmental healthresources
• Enforce current lawstohold offendersaccountable
• Mental health helpandsupportto thoseimpacted.
• Neighborhood watch.
• Educating people on the side effects SSRI drugs.
This section presents professional survey findings on firearm violence experiences, ownership patterns, and perceptions in Spokane County. Documenting both quantitative data (ownership rates and safety concerns) and qualitative insights (perceived causes, solutions, and community and needs) establishes an evidence base from the professional’s perspective to inform targeted prevention strategies.
Background
Professionals were asked about their primary profession/vocation, as shown in Figure 59. “Non-profit/ community-based organization employees” emerged as the most common (27%) response. “Victim advocate” (17%) and “Government administrators/employee/service providers” (15%) followed while professionals like “Researchers” (10%), “Social workers” (7%), “Security guards” (5%), “Mental health therapists” (5%), and“K-12 teachers” (2%) had fewer responses.
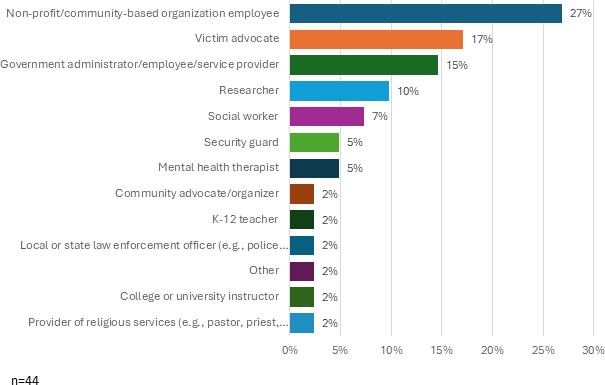
Professionals reported varying years of experience serving populations impacted by firearm violence, ranging from 0-5 years (n=11) to 26+ years (n=3). Most professionals were in the early stages of their careers,as21 had10 yearsorlessofexperience.Theaverageyearsofexperienceamong these professionals is 7.8 years.
When professionals were asked if they provided direct services to people impacted by firearm violence, 56% reported offering direct services against firearm violence, while 44% did not.
Figure 60: Professionals Offering Direct Services Related to Firearm Violence


Professionals providing direct services related to firearm violence were asked about the types of violence their work involves; “Community violence” was the most common (32%) followed by “Domestic violence” (28%).“Suicide” and“Accidental harm” had(21%)and(15%)respectively.

On average, professionals who serve those impacted by firearm violence report assisting between one and twenty-five people per month. Most professionals (8 out of 53) serve five or fewer people monthly, while seven manage moderate caseloads of six to twenty. Only two professionals serve more than twenty people monthly.
Figure 62 shows that when professionals were asked about barriers to serving their desired number of clients, they identified “Funding” (28%), “Staffing” (26%), and “Resources” (24%) as key limitations.
Professionals identified several critical needs to better serve those impacted by firearm violence. Top priorities included long-term funding (88%), guidance on how to identify those at risk of committing violence,andconflictde-escalation training(79%).Additionally,trainingongunsafety,victimidentification, and mental health referrals are also considered greatly needed by most professionals.
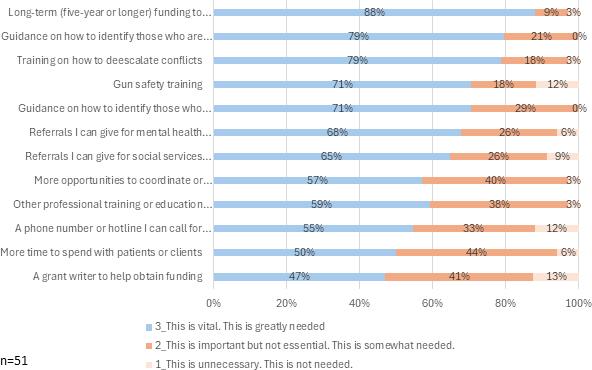
Professionals who participated were also asked, “You said that more opportunities to coordinate or network with other professionals is needed. What might that look like?”
Participants mentioned the following:
• Acoalition withfundingto supportfacilitation
• Collaboration between organizations such as updated contact lists for key staff within organizations, events coordinated to serve communitymemberstogether.
• Safer community meetings
• Quarterly meetings withother professionals who work with firearm violence prevention
• Partneringwithlaw enforcement,attorneys andjudges
• More multidisciplinary workgroups to stoppeoplefrom workinginsilos.More informationsharing.
• Monthly network meetings
• Start acoalitionandworkwithlocal lawenforcement
• Regular statistics on firearm incidents, shared anddiscussedwithaninterdisciplinary group
• More work with mental health agencies in Spokane around waitlists and services that are beingprovidedforyouth
Participants were then asked, “You said that professional training or education on firearm violence reduction is needed. What kind of training or education would be helpful?”
The professional training or education needs are as follows:
• Hands-on supervised training
• Gunsafety
• Trauma-informed training
• Firearm safety education
• Scenario-based training
• Evidence-based practices to prevent firearmviolence
• Pro-Gun community education
• De-escalation training
• Storage training
• Crisis intervention
• Regular safety training
When participants were asked, “What other resources, services, or programs are needed to help you or your organization better serve people impacted by firearm violence?” Many responses included:
• Expanded mentalhealthservices andcounseling
• Better connections with law enforcement
• Engagement with firearm sellers
• Trainingforserviceproviders and lawenforcement
• Dedicatedfundingforviolent crimeprevention
• Subsidized gun safety equipment (safes,locks)
• Crisis hotlines
• Public awareness campaigns
• Community responder programs
• Increased staffing for victim services
• Collaboration with advocacy organizations
• Victim advocacy services
• Clinical and professional training
• School-based education (elementary through highschool)
• Better marketing of available services
• Financial support for victim recovery
• Partnership with gang prevention programs
• Support groups for victims and professionals
All participants were asked, “How comfortable do you feel asking patients/clients about firearms (for example, if there is a firearm in the home or if they safely store their firearm)?”
Figure 64 shows that 55% of the participants felt “Very comfortable” asking their patients/clients about firearms while 12% of the participants felt “Somewhat uncomfortable” asking about firearms.
Figure 64: Professionals’ Needs for Serving People Impacted by Firearm Violence
When participants were asked, “Have you ever used a firearm in self-defense (to protect yourself or someoneelse)inaprofessional capacity orwhileon the job?”9% responded to“Yes” tohave had touse a firearm in self-defense in a professional capacity or while on the job whereas 91% of the participants responded “No.”
Perceptions of Firearm Violence
Figure 65 shows that professionals were asked about their perceptions of firearm violence in their workplaces.About9% reported feeling“Somewhatunsafe” atwork,whilethe majority(53%)reported feeling “Somewhat safe.”
65: Professionals’ Feelings of Safety at Workplace

n=32
The topreason for feeling unsafe (33%) was the neighborhood where they work and concerns about the patients/clients they serve, followed by mass shootings atthe workplace (17%) and retaliation (17%) as illustrated in Figure 66.
Figure 66: Reasons for Feeling Unsafe in the Workplace


When professionals were asked about future victimization, about 31% believed they were “Somewhat likely” to become victims, with 25% saying “Somewhat unlikely” while no responses indicated being “Very likely.”
Among professionals who expressed concern about future firearm violence, the majority cited community violence (100%) when asked about the type of firearm violence.
When professionals were asked, “What do you think are the main causes of firearm violence?” “Mental health issues” (22%) emerged as theleadingconcern,followed by “Access tofirearms” (20%) and“Domestic violence”(19%).Other identifiedcausesincluded“Substanceuse,”“Gangviolence,” “Lackofsafetytraining,” and “Other” reasons as shown in Figure 67.
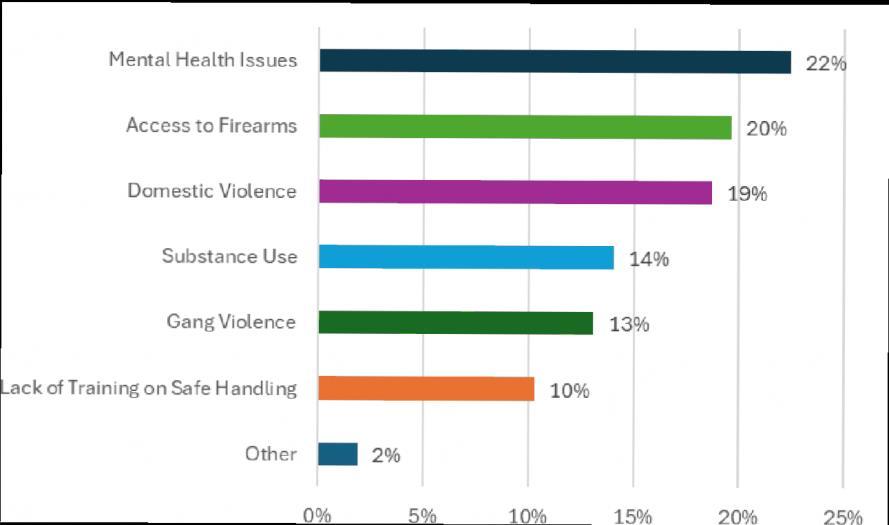
To reduce firearm violence, participants suggested implementing “Policy and legal restrictions” (40%), followed by “Education and training” (21%). Recommendations included “Mental health services” (17%), promoting“Safestorage” (13%)practices,anddeveloping“Socialandcommunitysupport” (10%)programs as shown in Figure 68.
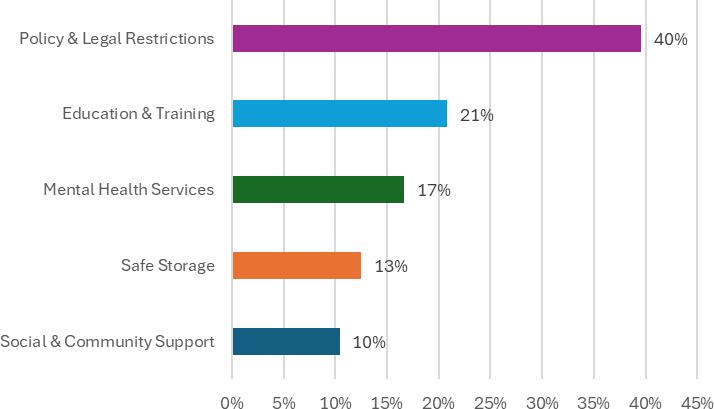
When professionals were asked about the key barriers to reducing firearm violence, six main challenges were identified. The most significant barriers include “Cultural and political” (22%) factors and issues related to “Access and availability” (22%). Following these, “Resource constraints and Enforcement/legal issues” (17%) were noted, while “Education and awareness” (17%), and “Social and safety implementation gaps” (9%) were considered lower priorities.
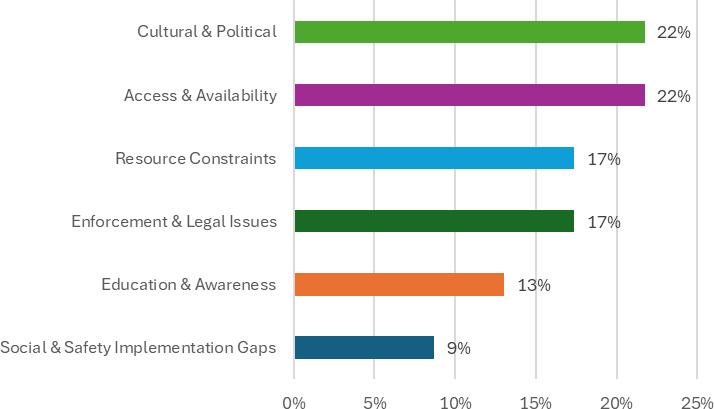
“Domestic violence support centers/services” (91%), mental health counseling (84%), “Gun violence restraining orders (GVRO)” (84%), and “Suicide prevention programs” (84%) were the professionals’ top priorities for reducing firearm violence when asked, “What services, programs, or resources do you think are most needed to help local communities impacted by firearm violence?” Other highly ranked needs include gun violence survivor support groups/services, substance abuse counseling or treatment, general gun safety training, and gang prevention programs.
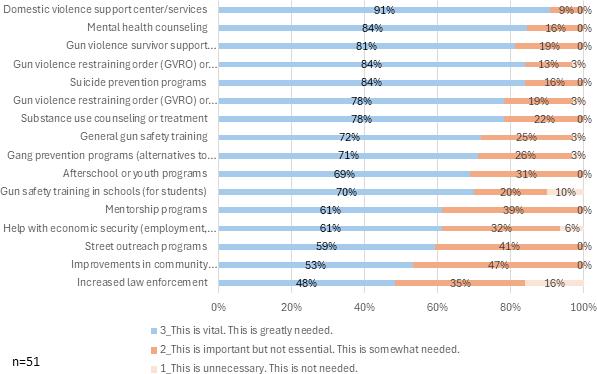

It is evident that firearm violence in Spokane County is a multifaceted issue requiring a collaborative, datadriven approach. This comprehensive analysis highlights several key areas of need and potential strategies for reducing firearm violence. A number of these strategies (listed below) show a broad applicability across multiple areas of firearm violence prevention, highlighting their potential for comprehensive community safety strategies. As such, it may prove to be most effective to invest in these prevention strategies early when implementing measures to address firearm violence.
1.Behavioral Threat Assessment:
• Mental Health: Helps identify individuals at risk of violence due to mental illness.
• SchoolShootings: Usedin schools to identify individuals atrisk and connectthem withservices to prevent potential threats of violence.
• Domestic Violence: Can identify potential DV perpetrators and address underlying issues to prevent the individual from carrying out violent acts.
2.Safe Storage and Education:
• Suicide: Prevents access to firearms during crises.
• School andMass Shootings: Promotes secure storage to preventunauthorized access (e.g., bringing parents’ weapons to school).
• SubstanceUse: Reduces the risk of individuals under the influence accessingfirearms.
3.Firearm Relinquishment and Extreme Risk Protection Orders (ERPOs):
• Suicide: Removes access to firearms during mental health crises.
• DomesticViolence: Ensures perpetrators do not have access to firearms while they have active court orders or are under investigation.
• Substance Use: Prevents individuals with substance abuse disorders from accessing firearms.
4.Increased Access to Mental Health Services:
• MentalHealth: Directly addresses mental health issues.
• Suicide: Provides support and intervention for at-risk individuals.
• SchoolShootings: Addressestheriseofyouthmentalhealthcrises.
• SubstanceUse: Integratesmentalhealthandsubstanceusetreatment,asSUDsareconsideredamental health disorder.
5.Education and Community Programs:
• DomesticViolence: RaisesawarenessforDVpreventionandsupports theneeds of abusevictims through topics such as “Domestic Violence 101, Teen Dating Violence, and the Effects of Domestic Violence on Children.” 43
• SchoolandMass Shootings: Fosters safe environments andaddresses the root causes of violence throughthreatidentification andassessmentprograms,securegunstorage education,andpromoting mental health resources.
• DeterminantsofHealth: Provides community-focusededucationon responsible gunownership.

Lack of accessibility, increased behavioral health workers, and limited program capacity emerged as the most prominent areas of need for reducing gun violence related to mental health disorders. The American Psychological Association (APA) states that, “For people at risk for violence due to mental illness, suicidal thoughts, or feelings of desperation, mental health treatment can often prevent gun violence.”44 Mental health treatment may be a viable avenue for reducing gun violence in Spokane County; however, when assessing the community’s current level of access to mental health services, the Firearm Violence Prevention Team discovered that there is a severe disparity in access to services based on individuals’ socioeconomic status. Particularly, recipients of Medicare and Medicaid reported facing various barriers to care, including long waitlists and lack of coverage for intermediate mental healthcare options such as intensive outpatient programs. While low reimbursement rates from insurance companies pose limitations, Spokane County residents would benefit greatly from an investment in increased access to mental health services; however, the Firearm Violence Prevention Team recognizes that increasing mental health care access and program capacity requires ample time and funding.
One avenue for early investment in effective gun violence reduction strategies may be behavioral threat assessment, which is gaining traction as “…a standard of care for preventing violence in schools, colleges, the workplace and against government and other public officials. Threat assessment teams gather and analyze information to assess if a person poses a threat of violence or self-harm, and if so, take steps to intervene.”45 Due to its wide range of applicability, investing in behavioral threat assessment for various organizations may lead to a reduction in the overall rates of gun violence in Spokane County. As community partners described a shortage of mental health professionals in the area, they called for an increase in the local behavioral health workforce. Implementing multidisciplinary behavioral threat assessment teams including trained mental health professionals who are incentivized to work in non-private practices may help to address this shortage and aid patients in navigating care and entering programs. Community partners also recounted extremely limited capacity in mental health programs with the highest level of need in the community, namely inpatient and local residential care. Particularly, inpatient care for youth ages 12 and under was described as severely limited.
43 Education and Outreach - The Women’s Safe House. (2018). The Women’s Safe House. https://twsh.org/community-education/education-and-outreach/
44 American Psychological Association (APA). (2013). Gun violence: Prediction, prevention, and policy. https://Www.Apa.Org. https://www.apa.org/pubs/reports/gun-violence-prevention
45 Ibid
Safe storage education and limiting firearm access during crises emerged as the most prominent violence reduction strategies for firearm-related suicide deaths. Research corroborates the need to store weapons safely and evaluate the pros and cons of firearm ownership as, “Most guns involved in self-inflicted and unintentional firearm injuries originate either from the victim’s home or the home of a friend or relative.”46 When assessing the community’s current level of knowledge towards safe storage practices, the majority of participants showed an awareness of popular methods such as lock boxes and trigger locks. However, of 23 community survey respondents who reported having any type of firearm in their home, 27% stated that their weapon was not stored using precautions such as a safe or locked container. This highlights the need for education on the importance of safe storage as well as access to safety devices. Currently, King County, WA is funded by the Department of Commerce’s Office of Firearm Safety and Violence Prevention to introduce the Lock It Up program throughout Washington State. SRHD has joined this effort to provide safe storage education and connect owners to safety device options. While this initiative shows promise, it is limited to the department’s scope of reach and firearm owner “buy-in.” Suggested interventions to expand this effort include requiring prospective owners to undergo safety training programs in order to purchase a firearm and stocking safety devices for need-based distribution at healthcare systems, firearm retailers, shooting ranges, fire departments, and police departments. In addition to safe storage education, recommendations to limit an individual’s access to firearms during crisis include firearm relinquishment through Extreme Risk Protection Orders (ERPOs) and temporary transfer laws. Both of these interventions currently exist in Spokane County, but there remains a need to assess their effectiveness in preventing suicides. In addition to safe storage, community partners identified a needfor increased access to suicide prevention andmeans safety education. Improving the continuity of care for at-risk individuals is also needed, with consistent safety planning and provider communication upon discharge from mental health programs identified as possible avenues for reducing the number of suicides and program re-admissions.
Early education, perpetrator resources, firearm relinquishment follow through, and police staffing emerged as the most prominent areas of need for domestic gun violence reduction strategies. Research has shown that abuse in childhood may make an individual susceptible to further victimization in the future. Through their meta-analysis, Li et al. (2018) discovered a significant association between childhood maltreatment and intimate partner violence (IPV) victimization later in life.47 It is important that as youth grow older, they receive education about warning signs, how to identify abuse, and what healthy relationships look like. Spokane County may address this need through avenues such as mandatory health courses or school assemblies with qualified guest speakers. Additionally, the community expressed a need to define the “gray area” between when CPS is restricted from or qualified to intervene as well as evaluate the effectiveness of the resources they refer out to. While victim survivor resources are essential, community partners also expressed a great need to establish services for perpetrators of DV in order to fully address the issue. They noted that perpetrators are largely neglected by mental health services (only 2 treatment programs are currently offered) and in cases where perpetrators are court ordered to complete treatment, even willing participants face financial barriers that prevent them from adhering to the orders. As such, there is a need to increase insurance coverage and/or establish funding streams from local or state organizations and grants to provide perpetrator rehabilitation services. Furthermore, community partners expressed that multiple processes are stunted by the Spokane Police Department’s lack of staffing, including the enforcement of DVPOs and timely firearm relinquishment. To reduce the number of domestic violence homicides, it is imperative that perpetrators of DV or IPV do not have access to firearms.
46 Grossman, D. C., Reay, D. T., & Baker, S. A. (1999). Self-inflicted and Unintentional Firearm Injuries Among Children and Adolescents. Archives of Pediatrics and Adolescent Medicine, 153(8), 875. https://doi.org/10.1001/archpedi.153.8.875
The primary means of identifying firearms as a factor in DV cases is through protective orders, such as DVPOs and ERPOs. While these orders place a temporary restriction on the respondent’s (i.e., DV perpetrator’s) right to possess firearms, it is known that follow-through with firearm relinquishment is not always enforced. Community partners indicated a need to evaluate how often Lethality Assessment Protocols (LAPs) are conducted with DV victims as well as their effectiveness in connecting survivors with resources. Additionally, there is a need to expand the range of accepted locations for firearms relinquishment to decrease barriers and encourage follow-through. To combat this issue, in 2018 King County, WA implemented the Regional Domestic Violence Firearms Enforcement Unit (RDVFEU), which was proven to have “…benefits at each stage of the protection order process with improvements in both judicial enforcement and respondent compliance. Overall, RDVFEU implementation was associated with improvements in granted orders to surrender weapons, respondent compliance, and relinquishment.”48 Therefore, Spokane County may see an increase in successful firearm relinquishment if a unit similar to the RDVFEU is implemented to enforce the terms of legal protective orders. Furthermore, establishing a separate DV court to handle these cases would improve processing times of court orders and ensure that essential parties such as LEOs and firearm retailers are appropriately notified of purchase prevention and firearm relinquishment orders.
Children’s mental health, threat assessment, and weakened perceptions of public safety emerged as the most prominent concerns related to school and mass shootings. Research has shown a connection between the rising youth mental health crisis and gun violence, particularly with depression, anxiety, suicidality, and PTSD.Ina longitudinal studyofhighschoolstudents,Riehmetal.(2021) discovered that “…kids whowere… more concerned [about experiencing a school shooting at baseline] were more likely to meet the criteria for generalized anxiety disorder and panic disorder six months later—suggesting that kids internalize these fears, which can then manifest as diagnosable mental-health issues.” 49 Further, young children (ages 2-9) are at heightened risk as they were found to develop psychological symptoms after both direct and indirect exposure to violence at higher rates than older kids (ages 10-19)50. This highlights the need for mental health intervention in schools, particularly surrounding anxiety disorders resulting from the perceived threat of gun violence. These adverse mental health effects sparked concern over current methods of intervention, with some questioning whether schools are reacting appropriately. Community partners agreed on the need for safety precautions, but some wondered whether banning backpacks and phones, installing metal detectors, and increasing active shooter drills were helping or hiking students’ anxiety. Research shows that common practices aimed to prepare students for emergencies, such as drills and simulations, actually cause more harm than good: “…schools that have active shooter drills were associated with a 42% increase in stress and anxiety and a 39% increase in depression.” 51 Alternatively, Everytown for Gun Safety found that “…threat assessment programs, access to mental health professionals and social support…coupled with commonsense gun laws and practices like secure storage” proved to be effective proactive school safety measures. 52
Community partners also suggested implementing social emotional learning (SEL) in early and mid- elementary schools to help kids cope with feelings, develop interpersonal skills, work in teams, and resolve conflicts.
47 Li, S., Zhao, F., & Yu, G. (2018). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. Child Abuse & Neglect, 88, 212–224 https://doi.org/10.1016/j.chiabu.2018.11.012
48 Ellyson, A. M., Adhia, A., Shanahan, S., Alsinai, A., DiMascolo, L., Reygers, M., Bowen, D., & Rowhani‐Rahbar, A. (2023). Firearm restrictions in domestic violence protection orders: Implementation, vetting, compliance, and enforcement. Criminology & Public Policy. https://doi.org/10.1111/1745-9133.12639
49 Chung, M. (2022). School shootings are raising anxiety and panic in U.S. children. TIME. https://time.com/6182235/mass-shootings-children-mental-health-anxiety-depression/
50 Cimolai, V., Schmitz, J., & Sood, A. B. (2021). Effects of Mass Shootings on the Mental Health of Children and Adolescents. Current Psychiatry Reports, 23(3) https://doi.org/10.1007/s11920-021-01222-2
51 Everytown for Gun Safety Support Fund. (2024). The Impact of Active Shooter Drills in Schools. Everytown Research & Policy. https://everytownresearch.org/report/the-impact-of-active-shooter-drills-in-schools/#key-findings
52 Ibid.
Additionally, community partners endorsed the establishment of Hope Squads in every school, noting the benefits of peer support, mental health education and awareness, suicide support training, positive relationship building, and student collaboration with school advisors. If implemented in Spokane County, these alternative interventions to preventing school shootings may decrease gun violence related to other factors, such as mental health and suicide. Finally, community partners reported a general decline in perceptions of public safety following national mass violent events. They expressed the need for better systems to report concerns about potential violence, which indicates the need for further study around current reporting methods in Spokane County as well as practical solutions.
Increased capacity for SUD treatment programs, trauma informed care, and multidisciplinary teams emerged as the community’s greatest needs for gun violence reduction strategies related to substance abuse. Research has shown an indivisible link between mental health, drug use, and the resulting effects on gun violence: “More than 25% of adults with a mental health problem also struggle with substance use. For this reason, it is hard to separate mental health from drug use when it comes to gun violence — consider that substance use itself is considered to be a mental health problem.”53 Comprehensive background checks, ERPOs, safe storage, and educational campaigns are all strategies that have proven to be effective in reducing overall rates of gun violence, including those related to substance use. In addition, investments in accessible, high-quality treatment programs that recognize SUD as a mental health condition may prove to be the most effective targeted intervention to address substance use related gun violence. To achieve this in Spokane County, community partners indicated a need to increase the capacity of inpatient SUD programs to meet the community’s demand for such services as well as incorporate trauma-informed care to address the complex needs of the individual. Additionally, re-establishing the Drug Endangered Children (DEC) Alliance emerged as an avenue to provide support to children and families affected by substance misuse through a multidisciplinary approach. The DEC Alliance works to raise awareness, create a supportive environment, and collaborate with local organizations to provide immediate support and long-term solutions for drug-endangered children. This includes connecting affected individuals with local resources and access to healthcare, counseling, and safe housing.
Community-focused intervention, education, and additional services emerged as the most prominent violence reduction strategies for addressing the social and political determinants of health alongside gun violence. Violent incidents causing relocation away from certain neighborhoods highlighted an express need for violence reduction strategies aiming to make the community a safe place to live. While many interventions focus on individual needs, context-specific resources may be more effective in addressing the community’s overall needs for violence reduction. For example, vulnerable populations in Spokane County, such as refugees, may have unique needs. As one community partner noted, “housing, language barriers, and job security are interconnected with secondary trauma and survival for refugee populations.” One of the main recommendations for addressing issues at a community level is education.
As community partners noted, the need for education persists well into adulthood; however, the means for delivering it (i.e., schools) is eliminated. Thus, spreading educational messages to adults emerged as a possible intervention with a heightened need for creativity. While adults could be required to complete educational programs in order to purchase firearms, “at-will” education is also necessary to ensure that individuals maintain responsible gun ownership. However, education on its own is an insufficient means of altering an individual’s behavior. Community partners observed a need for additional services related to social determinants of health, such as identifying food, healthcare, and social service deserts, increasing affordable housing and childcare, and raising the capacity and accessibility of respite care for youth and adults. Further, community partners expressed a desire for Sexual Assault Nurse Examiners (SANE) andnonfatal DV forensic exams to provide medical, psychological, and forensic services to victims of assault.
Based on the mixed methods analysis conducted for this CNA, the Office of Research and Evaluation identified the following needs as a priority for Spokane County:
1. Behavioral Health Services (Mental Health, Suicide, and Substance Use)
2. Safe Storage Protocols
3. Domestic Violence (Firearm Relinquishment and Extreme Risk Protection Orders)
4. Education and Community Programs
The criteria for prioritization were based on community partner feedback through qualitative and quantitative data collection (focus groups and surveys) as well as evidence-based strategies discovered through supplemental research from academic sources and reliable community organizations. The criteria included the magnitude of the problem, the severity of the problem, and the ability to impact the problem (through clear, realistic goals).
The priorities identified will be used to inform a comprehensive Spokane County Community Violence Strategic Action Plan in 2025.
Community partners, along with the ORE team, will develop and implement firearm violence reduction strategies to address these prioritized needs, resulting in the Community Violence Strategic Action Plan (CVSAP).
Community partners led by the ORE team will meet to create planning team committees. The planning team committee will utilize the CNA to create the CVSAP.
The Community Needs Assessment conducted by Excelsior Wellness and its community partners has delivered a comprehensive understanding of the multifaceted issue of firearm violence in Spokane County. The goal of the Community Needs Assessment was to collaborate with community partners to assess the needs of the community using qualitative and quantitative evidence. The findings from the Firearm Violence Prevention Team's assessment highlight critical areas of need for reducing firearm violence related to mental health disorders, suicide, domestic violence, school and mass shootings, substance abuse, and social determinants of health. By addressing these areas through evidence-based strategies highlighted in this report and continuing to foster collaboration among community partners, Spokane County can make significant strides in reducing firearm violence and enhancing community safety. It is the goal of this deliverable to inform a Community Violence Strategic Action Plan that will be carried out in 2025. This Strategic Action Plan should inspire more local organizations to take part in the effort to reduce firearm violence by providing realistic and meaningful action items that can be incorporated into existing workflows. Continued engagement, data sharing, and evaluation of implemented strategies will be essential to sustain progress and adapt to emerging challenges. Through these collective efforts, Spokane County can create a safer and more resilient community for all its residents.

Below is a list of community resources across all the main themes/topics. It's not a comprehensive list of resources in Spokane County:
If you need immediate help from the police, medics or fire department call 9-1-1.
If you or a loved one is actively experiencing a behavioral health crisis, call the 24-Hour Regional Crisis Line (Frontier Behavioral Health) at 1-877-266-1818 www.fbhwa.org or Suicide and Crisis Lifeline 988 www.988lifeline.org (text and online chatting available)
Safe Firearm Storage Brochures. They are available in English, Marshallese, Russian, Spanish, and Ukrainian near the bottom of this page on the Spokane Regional Health District website, srhd.org/injuryviolence-safety
YWCA Spokane
Provides 24-hour domestic violence helpline and answers your questions about options for safety, access to their safe shelter and other programs, and community resources
24/7 Domestic Violence Hotline (509)326-2255, Text Line (509) 220-3725 Website: www.ywcaspokane.org
SRDVC Community Advocate (509) 481-0798 Email; advocacy@srdvc.org
Lutheran Community Services Spokane
Provides free and confidential advocacy services to victims, survivors, loved ones, and witnesses of traumatic events.
Sexual Assault 24-hour Support Line (509) 624-7273 / Crime Victim Support Line (509) 747-8224. Website: www.lcsnw.org
Kalispel Tribe Victim Assistance Services
24/7 Hotline 1-877-700-7175
Mujeres in Action (MIA)
Provides free, confidential support to survivors of domestic violence and/or sexual assault, and their families. (509) 795-2028. Website: www.miaspokane.org
Lock to Live website
Prevention Resource Finder, U.S. Department of Homeland Security, provides information on the resources needed to help prepare for and prevent targeted violence and terrorism.
Reducing Gun Violence, U.S. Department of Justice, includes fact sheets on safe firearm storage, information on efforts to reduce violent crime, and other resources.
Resource for School Administrators on Importance of Safe Firearm Storage, U.S. Department of Education, provides tools that schools can use to communicate with parents and families about the importance of safe firearm storage.
Suicide Prevention is Everyone’s Business: A Toolkit for Safe Firearm Storage, U.S. Department of Veterans Affairs, guides communities through building coalitions to raise awareness about safe firearm storage.
Violence Prevention Resources for Action, CDC, provides information to help communities make decisions based on the best available evidence to prevent different forms of violence.
Crisis Text Line
Text NAMI to 741-741
Excelsior Wellness Center
Provides individual and group counseling, support, and advocacy services for young people with complex behavioral health needs and their families.
3754 W Indian Trail R., Spokane, WA 99208
509-559-3100.
Excelsior Teen Text Line: Call: 844-814-8336
Website: www.excelsiorwellnesscenter.org
YWCA of Spokane
Provides mental health therapy for survivors of intimate partner violence who are focusing on processing and healing trauma.
Call 509-326-1190 (CALL) or Text 509-220-3725
Lutheran Community Services Spokane
Provides behavioral healthcare and related services to individuals of all ages (509) 624-7273. Website: www.lcsnw.org
FailSafe for Life
Provides education and community events for Suicide Prevention
Email; info@failsafeforlife.org
509-475-7334
Suicide Prevention Resource for Action, CDC, describes the best available evidence for suicide prevention. Trauma and Violence, SAMHSA, provides additional information and resources for understanding and addressing trauma and its impacts.
Spokane Regional Health District Treatment Services
West 1101 College Avenue, Room 106, Spokane, WA 99201 in Spokane County
509-324-1420
Partners with Families and Children
106 West Mission Avenue, Spokane, WA 99201
509-473-4810
Thrive Treatment Center
300 North Argonne Road, Suite 201, Spokane, WA 99212 in Spokane County 509-868-0875
Detox Local
1-866-640-2212
Live Another Day
1-877-720-1044
Spokane Resource Center (509)867-8188
130 S Arthur St (2nd Floor), Spokane, WA 99202
Volunteers of America Eastern Washington (509)624-2378
525 W 2nd Ave, Spokane, WA 99201
Family Promise Open Doors
2002 E Mission Ave Spokane, WA 99202
Email : shelter@familypromiseofspokane.org
Phone : (509) 723-4663
Crosswalk Youth Shelter
525 W 2nd Ave Spokane, WA 99201
Email : crosswalk@voaspokane.org
Phone : (509) 688-1112
1. How familiar are you with firearm violence trends?
2. To what degree does your community experience firearm violence?
3. How have you or your community been affected by firearm violence?
4. What are your perceived needs to reduce firearm violence in your community?
Meeting 2
1. Rank topics/areas of interest from the key findings.
2. Further exploration of community concerns not fully developed or mentioned previously.
FOCUS GROUP MEETING 1 (7.16.2024)
BreakoutGroupQuestions
1. How do you think the presence of firearms in households impacts the risk of suicide?
2. What role, if any, can mental health resources play in reducing firearm-related suicides?
3. How informed do you feel you are about the signs that someone might be at risk of suicide, particularly with access to firearms?
4. What barriers exist for people seeking help for suicidal ideation?
5. How effective do you think suicide prevention resources are? Are people aware of these resources?
1. Are there specific risk factors related to both mental health and firearm violence?
2. How accessible are mental health services in the community?
a. Arethereculturalorcommunityspecificbarriers?
b. Howdostigma,cost,oravailabilityofservicesfactorin?
c. Howcanwereducestigmaandencourageopenconversations?
3. What role do you think schools/workplaces should play in mental health advocacy?
4. How can we encourage more community involvement in prevention and intervention efforts?
5. What community-based solutions have you seen or heard about that address both mental health and firearm violence?
6. How has the pandemic affected mental health generally and in relation to firearm violence?
1. What links, if any, do you think exist between domestic violence and firearm violence?
2. In what ways do you think easy access to guns exacerbates various factors of domestic violence?
3. What immediate and long-term impact does the presence of guns have on victims’ safety and well-being?
a. Howmightwitnessingorexperiencingviolenceaschildrenmakeindividualsvulnerable toactingviolentlyorexperiencingviolenceasadults?
4. What community-led efforts to disarm domestic abusers have you heard or been a part of?
5. How effective do you think restraining orders are in protecting victims? Are there more effective strategies?
6. Are you aware of any programs or organizations addressing both domestic violence and firearm safety in our community?
Topic 4: Determinants of Health (15 minutes)
1. How do economic conditions contribute to the determinants of health in our community?
a. Bydeterminantsofhealth,Imean,“Thesocialandeconomicenvironment,thephysical environment,andtheperson’sindividualcharacteristicsandbehaviors.Thecontextof people’slivesdeterminestheirhealth,soitisinappropriatetoblameindividualsforpoor healthorcreditthemforgoodhealth”(WHO,2024).
2. How do factors like income inequality, education level, and social mobility impact the prevalence of gun violence in our community?
3. Are there specific neighborhoods or demographics disproportionately affected by gun violence? If so, how can we address this in our violence prevention strategies?
4. How do job opportunities (or lack thereof) impact community well-being?
5. What role should businesses play in community mental health and firearm violence prevention?
Topic 5: Substance Use (15 minutes)
1. What links, if any, do you think exist between substance use and firearm violence?
2. How could substance use treatment programs incorporate firearm violence prevention strategies?
3. Are there any successful violence reduction models from other communities we could learn from?
4. Are there particular substances that you believe are more closely associated with firearm violence?
5. Are survivors of substance-related gun violence aware of available resources, such as counseling, legal assistance, and community support groups?
a. Whatbarriersexistinaccessingtheseservices,andhowcanweaddressthemtobettersupport survivors?
FOCUS GROUP MEETING 2 (8.20.2024)
BreakoutGroupQuestions
(Brief Intro to set ground rules for focus group)
Topic 1: Mass/School shootings (15 minutes)
1. Do you feel that the increase in mass/school shootings has changed your perception of safety at school or in public spaces compared to when you were younger? If so, how?
a. Do the children in your life feel safe at school? Why or why not?
b. How safe do you feel in public spaces?
c. If at all, how has your perception of crowded events changed?
d. How prepared do you think our community and local schools are for such incidents?
e. What measures do you believe could help prevent mass shootings in public spaces and
in schools? [Probe for specifics about Actions/inactions, Policies]
f. If there were stricter laws around firearm ownership and safety, do you think that school or mass shootings would still occur at the same frequency? [Probe: Why or why not?]
g. What other resources have you observed in other counties or states that could be adapted, or what do you believe is required to improve public and school safety in our community?
1. What affects your perception of safety in your community?
a. How do you think the presence of firearms/firearm ownership affects your community’s safety?
b. Whose job do you think it is to keep your community safe? How should they go about it?
c. What role should community members have in ensuring safety? How can they contribute to maintaining a safe environment?
d. What changes would make you feel safer in your community? Can you provide some specific examples or suggestions?
e. What other community educational programs or initiatives could be adapted from successful programs in different communities?
1. How do you feel about how firearm violence is discussed in the media?
a. By media, I mean both journalistic news sources and content by various creators on social media.
b. What are your thoughts on the way this issue is portrayed?
c. How do you decide which news outlets or creators to follow? How did you find these sources? Which platforms do you use to access their content?
d. How do you think their content shapes, aligns with or differs from your views on firearms, firearm ownership, and firearm violence?
a. What specific aspects of their content do you find most align with or differ from your own views?
b. Can you provide some specific examples?
e. How do you feel about the way they discuss other political issues? For example, voting, Supreme Court decisions, immigration, race relations, etc.?
f. How do you feel about the way that news outlets/ creators you do not follow talk about other political issues? For example, voting, Supreme Court decisions, immigration, race relations, etc.?
g. How did you initially come across the media sources you follow?
1. What do you wish the public knew about firearms, firearm ownership, and firearm violence?
a. What are some important facts you believe need to be addressed?
b. What, if anything, is absent from public discussions (in the news, on social media, etc.) concerning firearms and their connection to violence?
c. Why should we include these topics in public discussions about firearms?
(Adapted from Health Assessment and Research for Communities (HARC), 2023)
to this Community
The Office of Research and Evaluation (ORE) is conducting a Community Needs Assessment2024 about Firearm Violence Prevention in Spokane County. By “Firearm violence,” we mean any violence (or threat of violence) involving a firearm (A weapon that fires a projectile by force of an explosion, e.g., handguns, rifles, and shotguns). This includes community violence (for example, street violence, gang violence, etc.), domestic violence, suicide, or accidental harm.
This survey is for Spokane County residents only.
This survey takes about 10 minutes and can be completed later. Feel free to skip any question that does not apply to you.
You will have a chance to win a $100 Visa gift card. At the end of the survey, please provide your name and contact for a chance to win.
This survey contains questions about personal experience with firearm violence, including how it has impacted friends or family. Please proceed if you are ready to discuss this topic.
This survey is entirely anonymous. Responses will not contain identifying information; all survey responses will be combined at the group level and will not be reported individually.
If you have been a victim of firearm violence and need help, please reach out to these services or organizations:
• National Domestic Violence Hotline: 1.800.799.SAFE (7233)
• Regional Behavioral Health 24/7 Crisis Line: (877) 266-1818
• YWCA Spokane 24/7 Domestic Violence Hotline: (509)326-2255, Text Line (509) 220-3725, (https://www.ywcaspokane.org)
• SRDVC Community Advocate: (509) 481-0798, email; advocacy@srdvc.org
If you have any questions or concerns, contact the Program Director at andrew.ogwang@excelsiorwellness.org
Thank you for your time and participation.
Sincerely,
The Office of Research and Evaluation Team
[i.] Do you live in Spokane County?
oYes [continuestothesurvey]
oNo [exitssurvey]
[1.] Have you, a family member, or a close friend experienced firearm violence in the last five years? (This can include being threatened with a gun, being shot at, or being shot.) Please select all that apply.
o[a] Yes, I have personally experienced this.
o[b] Yes, someone in my family.
o[c] Yes, a close friend.
o[d] No, no one.
[If“Yes,Ihavepersonallyexperiencedthis”aboveforQuestion1…]
[2.] What type of firearm violence have you experienced in the last five years? Select all that apply.
o[a] Someone threatened to shoot me (but did not show a gun)
o[b] Someone threatened me by showing me a gun
o[c] Someone threatened me by pointing a gun at me
o[d] I was shot at (but I wasn’t hit)
o[e] I was shot
[Ifanswered“Yes,Ihavepersonallyexperiencedthis”aboveinQuestion1…]
[3.] What relationship do you/did you have to the person who committed the firearm violence against you? The person who committed the violence was…
o[a] My spouse or partner
o[b] A family member
o[c] My girlfriend/boyfriend
o[d] My neighbor
o[e] My classmate
o[f] My co-worker or colleague
o[g] A customer, client, or patient
o[h] My friend
o[i] A stranger (no relationship)
o[j] Myself
o[k] Other (Please specify): ________
[Ifanswered“Yes,Ihavepersonallyexperiencedthis”aboveinQuestion1…]
[4.] Are there any comments that you would like to share about your experience with firearm violence?
o[a] Yes: [Openresponse]
o[b] No
[5.] Have you known anyone, such as family, friend, co-worker, or neighbor, who has been injured or killed by a firearm in the last five years? This can include community violence, domestic violence, suicide, or accidental harm.
o[a] Yes
o[b] No
[If“Yes”aboveforQuestion5…]
[6.] What was your relationship to the person or persons who was injured or killed? Please select all that apply. The person (or persons) was…
o[a] My child
o[b] My parent
o[c] My sibling
o[d] My spouse or partner
o[e] Another family member
o[f] My girlfriend/boyfriend
o[g] My friend
o[h] My colleague or co-worker
o[i] My classmate
o[j] My neighbor
o[k] Myself
o[l] Other (Please specify):
[7.] What type of firearm violence was this?
o[a] Accidental (for example, unintended or a mistake)
o[b] Suicide or attempted suicide
o[c] Intentional assault by a domestic partner (for example, a spouse, boyfriend/girlfriend, etc.)
o[d] Intentional assault by someone else (for example, a friend, a stranger, etc.)
o[e] I don’t know
o[f] Other (Please specify): _____
Thenextfewquestionsareaboutfirearm(gun)ownership.Thissurveyisanonymous,andtheresponses willnotcontainidentifyinginformation.ThisinformationwillbeconfidentialwithOREresearchers(it won’tbeshared).Also,theresponsesfromallsurveyswillbecombinedatthegrouplevelandwillnotbe reportedindividually.
[8.] Is there a firearm in your home (such a handgun, shotgun, rifle, etc.)?
o[a] Yes
o[b] No
[If“Yes”aboveforQuestion7…]
[9.] Why do you have a firearm in your home? Please select all that apply.
o[a] It is for recreation/sport (for example, target shooting or hunting)
o[b] It is for self-defense/security (for example, defending yourself or your property)
o[c] It is for work (for example, for law enforcement)
o[d] It was given or inherited from a family or friend
o[e] Other (Please specify):
[If“Yes”aboveforQuestion7…]
[10.] Is the firearm in your home safely stored (such as in a safe or locked container)?
o[a] Yes
o[b] No
[11.] Have you ever used a firearm in self-defense (to protect yourself or someone else)?
o[a] Yes
o[b] No
[12.] Who were you defending or protecting? Please select all that apply.
o[a] Myself
o[b] A family member
o[c] A friend
o[d] A colleague or co-worker
o[e] A stranger
o[f] Other (please specify): ____
[13.] Did you discharge the firearm or was it just presented?
o[a] I discharged the firearm
o[b] I only presented the firearm
[14.] What was the reason for self-defense with a firearm?
[Open response]
[15.] Did you report this incident to law enforcement?
o[a] Yes
o[b] No
Perceptions
Thesenextquestionswillaskaboutyourthoughtsandperceptionsaboutfirearmviolence.Firearm violenceincludesanyviolencecausedbyguns,includingcommunityviolence,domesticviolence,suicide, andaccidentalharm.
[16.] How concerned are you about firearm violence in your community (where you live, work, worship, go to school, etc.)?
o[a] Very concerned
o[b] Somewhat concerned
o[c] Not too concerned
o[d] Not concerned at all
[17.] When thinking about community firearm violence (such as street violence or gang violence), how safe do you feel in your community?
o[a] Very safe
o[b] Somewhat safe
o[c] Neither safe nor unsafe
o[d] Somewhat unsafe
o[e] Very unsafe
[18.] How likely do you think that you or someone you know would be a victim of firearm violence in the future?
o[a] Very likely
o[b] Somewhat likely
o[c] Neither likely nor unlikely
o[d] Somewhat unlikely
o[e] Very unlikely
[Ifselected“Verylikely”or“Somewhatlikely”aboveforQuestion16…]
[19.] You said that you think you or someone you know could possibly be the victim of firearm violence in the future. What type of firearm violence?
o[a] Community violence (for example, street violence, school shootings, etc.)
o[b] Domestic violence
o[c] Suicide
o[d] Accidental harm
o[e] Other (Please specify): ________
[20.] What do you think are the main causes of firearm violence? This can include structural, root causes or immediate, everyday causes.
[Open response]
[21.] What do you think are the best solutions for firearm violence prevention? This could include shortterm solutions, long-term solutions, policy solutions, changes in your community, or anything else.
[Open response]
[22.] Below is a list of different services that are intended to prevent firearm violence. What services, programs, or resources do you think are most needed to help local communities impacted by firearm violence?
This is vital. This is Greatly needed. This is important but not essential. This is somewhat needed.
This is necessary. This is not needed.
Mental health counseling
Suicide prevention programs
Domestic violence support center/services
Substance use counseling or treatment
Gun violence survivor support groups/services
General gun safety training
Gun safety training in schools (for students)
Help with economic security
(employment, housing, childcare, etc.)
Improvements in community conditions/infrastructure (such as better street lighting, more parks, etc.)
Gang prevention programs (alternatives to joining gangs)
Afterschool or youth programs
Mentorship programs
Street outreach programs
Increased law enforcement
Gun violence restraining order (GVRO) or “red flag law” for those with mental health crises
Gun violence restraining order (GVRO) or “red flag law” for those at risk of committing violence
[23.] What other resources, services, or programs are needed to help local communities impacted by firearm violence?
[Open response]
[24.] Do you know of any local organizations, groups, or networks that are working on firearm violence prevention in your community? If so, please mention the exact organization names. [Open response]
Demographics
[25.] Are you Hispanic, Latino, or Latina?
o[a] Yes
o[b] No
[26.] Which one of these groups would you say best represents your race? For the purposes of this survey, Hispanic is not a race.
o[a] White
o[b] Black/African American
o[c] Asian/Asian American
o[d] American Indian/Alaska Native
o[e] Native Hawaiian or Other Pacific Islander
o[f] Multiracial/two or more races
o[g] Choose not to answer
o[h] Other (please specify): __________
[27.] How do you describe yourself?
o[a] Male
o[b] Female
o[c] Transgender
o[d] Do not identify as female, male, or transgender
[28.] Have you ever served in the U.S. military?
o[a] Yes
o[b] No
[29.] What zip code do you live in?
[Open response]
[30.] What is the highest grade or year of school you completed?
o[a] 8th grade or less
o[b] Some high school (grades 9-11)
o[c] Grade 12 or GED certificate (high school graduate)
o[d] Technical school graduate
o[e] Some college
o[f] College graduate
o[g] Postgraduate or professional degree
[31.] What is your age in years?
[Drop-down menu of number of years]
[32.] How many people, including yourself, live in your household?
[Drop-down menu of number of adults]
[Drop-down menu of number of children]
[33.] Do you have any other comments you would like to share?
[Open response]
If you have been a victim of firearm violence and need help, please reach out to these services or organizations:
• National Domestic Violence Hotline: 1.800.799.SAFE (7233)
• Regional Behavioral Health 24/7 Crisis Line: (877) 266-1818
• YWCA Spokane 24/7 Domestic Violence Hotline: (509)326-2255, Text Line (509) 220-3725, (https://www.ywcaspokane.org)
• SRDVC Community Advocate: (509) 481-0798, advocacy@srdvc.org
That concludes the survey! Thank you so much for your time and responses. We truly appreciate it. Go to the next page to enter your information for a chance to win a gift card!
If you have any questions or concerns regarding the survey and/or needs assessment, contact the Program Director at andrew.ogwang@excelsiorwellness.org
For a chance to win $100 Visa gift card. Complete the survey and leave your name and contact information to be entered into the drawing. Your name and contact information will not be linked to your survey responses. Winners will be selected at random. We will contact you if you are selected by the end of August 2024.
(Adapted from Health Assessment and Research for Communities (HARC), 2023)
Welcome to this Professional Survey!
The Office of Research and Evaluation (ORE) is conducting a Community Needs Assessment2024 about Firearm Violence Prevention in Spokane County. By “Firearm violence,” we mean any violence (or threat of violence) involving a firearm (A weapon that fires a projectile by force of an explosion, e.g., handguns, rifles, and shotguns). This includes community violence (for example, street violence, gang violence, etc.), domestic violence, suicide, or accidental harm.
The survey is designed for professionals who are concerned or work with or for people impacted by firearm violence. We are interested in learning how communities have been affected by firearm violence and potential solutions to overcoming firearm violence.
The data from this survey will be included in the Strategic Action Plan - 2025 report and will advise future actions in firearm violence prevention efforts.
This anonymous survey takes about 10 minutes and can be completed later. Feel free to skip any question that does not apply to you.
You will have a chance to win a $100 Visa gift card. At the end of the survey, please provide your name and contact for a chance to win.
If you have any questions or concerns, contact the Program Director at andrew.ogwang@excelsiorwellness.org
Thank you in advance for your time and participation.
Sincerely,
Office of Research and Evaluation Team
[i.] Do you work in Spokane County?
oYes [continuestothesurvey]
oNo [exitssurvey]
109
[ii]Are you 18 or older?
oYes [continuestothesurvey]
oNo [exitssurvey]
[iii] Do you provide professional services to people who are impacted by gun violence, or do you professionally support gun violence prevention efforts? (This can include a variety of professions, such as law enforcement, medical care, counseling, social work, research, education, etc.)?
o Yes [continuestothesurvey]
o No [exitssurvey]
[1.] What is your primary profession/vocation?
o Local or state law enforcement officer (e.g., municipal police department, County Sheriff, WA State Patrol, etc.)
o Federal law enforcement officer (e.g., Border Patrol, FBI, etc.)
o Security guard
o U.S. military service member
o K-12 teacher
o College or university instructor
o Researcher
o Social worker
o Mental health therapist
o Physician
o Nurse (RN or LVN)
o Paramedic/EMT
o Non-profit/community-based organization employee
o Community advocate/organizer
o Government administrator/employee/service provider
o Legal professional (e.g., judge, attorney)
o Victim advocate
o Firearm safety instructor
o Firearm dealer
o Provider of religious services (e.g., pastor, priest, rabbi, imam)
o Other (Please specify): ____
[2.] For how many years have you been serving people or populations impacted by firearm violence?
(Drop-down menu)
[3.] Do you provide direct services to people impacted by firearm violence?
o [a] Yes
o [b] No
[If“Yes”aboveforQuestion3…]
[4.] What type of firearm violence does your work engage with? Select all that apply.
o Community violence (e.g., gang violence, street violence, etc.)
o Domestic violence
o Suicide
o Accidental harm
o Other (Please specific):
o N/A (Not applicable)
[If“Yes”aboveforQuestion4…]
[5.] On average, how many people (who are impacted by firearm violence) do you as an individual serve each month?
(Drop-down menu)
[If“Yes”aboveforQuestion5…]
[6.] Some professions seek to serve as many clients as possible. If you are serving fewer people than you’d like to, what is the reason? [a] Accidental (for example, unintended or a mistake) (Open response)
[7.] Which of the following do you as a professional need to better serve people impacted by firearm violence?
This is vital. This is Greatly needed. This is important but not essential. This is somewhat needed. This is necessary. This is not needed.
Training on how to deescalate conflicts
Firearm safety training
Other professional training or education on firearm violence reduction
Long-term (five-year or longer) funding to support programs and services
A grant writer to help obtain funding
More time to spend with patients or clients
More opportunities to coordinate or network with other professionals on this issue
Guidance on how to identify those who are at risk of committing violence
Guidance on how to identify those who might be victims of violence
A phone number or hotline I can call for advice if I’m concerned about a patient or client
Referrals I can give for social services
(employment, housing, childcare, etc.)
Referrals I can give for mental health treatment
[Ifmarked“greatlyneeded”or“somewhatneeded”forcoordinationwithprofessionals…]
[8.] You said that more opportunities to coordinate or network with other professionals is needed. What might that look like?
(Open response)
[Ifmarked“greatlyneeded”or“somewhatneeded”forothertraining/education…]
[9.] You said that professional training or education on firearm violence prevention is needed. What kind of training or education would be helpful?
(Open response)
[10.] What other resources, services, or programs are needed to help you or your organization better serve people impacted by firearm violence?
(Open response)
[11.] How comfortable do you feel asking patients/clients about guns (for example, if there is a firearm in the home or if they safely store their firearm)?
oVery comfortable
oSomewhat comfortable
oNeither comfortable nor uncomfortable
oSomewhat uncomfortable
oVery uncomfortable
oN/A (I don’t provide direct services to clients/patients)
[12.] Have you ever used a firearm in self-defense (to protect yourself or someone else) in a professional capacity or while on the job?
oYes
oNo
Thesenextquestionswillaskaboutyourthoughtsandperceptionsaboutfirearmviolence.Firearm violenceincludesanyviolencecausedbyfirearms(guns),includingcommunityviolence,domestic violence,suicide,andaccidentalharm.
[13.] When thinking about firearm violence, how safe do you feel where you work (for example, in a hospital, at a school, in a community which you serve, etc.)?
oVery safe
oSomewhat safe
oNeither safe nor unsafe
oSomewhat unsafe
oVery unsafe
[Ifselected“Veryunsafe”or“Somewhatunsafe”aboveforQuestion13…]
[14.] You said you feel very or somewhat unsafe where you work. What is the reason for this?
Select all that apply.
oI’m afraid of mass shootings at my workplace
oI’m afraid of retaliatory shootings at my workplace
oI’m afraid that someone I serve (a client, patient, etc.) might have a gun
oThe neighborhood where I work feels unsafe
oOther (please specify): _
[15.] How likely do you think that you will be a victim of firearm violence in the future?
oVery likely
oSomewhat likely
oNeither likely nor unlikely
oSomewhat unlikely
oVery unlikely
[Ifselected“Verylikely”or“Somewhatlikely”aboveforQuestion15…]
[16.] You said that you think you could possibly be the victim of firearm violence in the future. What type of firearm violence?
oCommunity violence (for example, street violence, school shootings, etc.)
oDomestic violence
oSuicide
oAccidental harm
oOther (Please specify): _
[17.] What do you think are the main causes of firearm violence?
(Open response)
[18.] What do you think are the best solutions for firearm violence prevention? This could include shortterm solutions, long-term solutions, policy solutions, or anything else. (Open response)
[19.] What are some of the main challenges or barriers faced by you as a professional or your organization to reducing firearm violence?
[Open response]
[20.] Below is a list of different services that are intended to reduce firearm violence. What services, programs, or resources do you think are most needed to help local communities impacted by firearm violence?
This is vital. This is Greatly needed. This is important but not essential. This is somewhat needed.
This is necessary. This is not needed.
Mental health counseling
Suicide prevention programs
Domestic violence support center/services
Substance use counseling or treatment
Gun violence survivor support groups/services
General gun safety training
Gun safety training in schools (for students)
Help with economic security (employment, housing, childcare, etc.)
Improvements in community conditions/infrastructure (such as better street lighting, more parks, etc.)
Gang prevention programs (alternatives to joining gangs)
Afterschool or youth programs
Mentorship programs
Street outreach programs
Increased law enforcement
Gun violence restraining order (GVRO) or “red flag law” for those with mental health crises
Gun violence restraining order (GVRO) or “red flag law” for those at risk of committing violence
[21.] What other resources, services, or programs are needed to help local communities impacted by firearm violence? (Open response)
[22.] Do you know of any local organizations, groups, or networks that are working on firearm violence prevention in the County? If so, please mention the exact organization names. [Open response]
[23.] Have you experienced firearm violence in the last five years in the course of carrying out your
professional duties? (This can include being threatened with a gun, being shot at, or being shot while on the job.)
oYes
oNo
[If“Yes,Ihavepersonallyexperiencedthis”aboveforQuestion23…]
[24]. What type of firearm violence have you experienced in the last five years while on the job?
Select all that apply.
oSomeone threatened to shoot me (but did not show a gun)
oSomeone threatened me by showing me a gun
oSomeone threatened me by pointing a gun at me
oI was shot at (but I wasn’t hit)
oI was shot
[Ifanswered“Yes”aboveinQuestion23…]
[25.] What relationship do you/did you have to the person who committed the firearm violence against you? The person who committed the violence was…
oSomeone I know personally
oA co-worker or colleague
oA customer, client, patient, or someone else I professionally serve
oOther (Please specify):
[26.] Are you Hispanic, Latino, or Latin?
oYes
o No
[27.] Which one of these groups would you say best represents your race? For the purposes of this survey, Hispanic is not a race.
o[a] White
o[b] Black/African American
o[c] Asian/Asian American
o[d] American Indian/Alaska Native
o[e] Native Hawaiian or Other Pacific Islander
o[f] Multiracial/two or more races
o[g] Choose not to answer
o[h] Other (please specify): __________
[28.] How do you describe yourself?
o[a] Male
o[b] Female
o[c] Transgender
o[d] Do not identify as female, male, or transgender
[29.] What zip code do you live in?
[Open response]
[30.] What is the highest grade or year of school you completed?
o[a] 8th grade or less
o[b] Some high school (grades 9-11)
o[c] Grade 12 or GED certificate (high school graduate)
o[d] Technical school graduate
o[e] Some college
o[f] College graduate
o[g] Postgraduate or professional degree
[31.] What is your age in years?
[Drop-down menu of number of years]
[32.] Do you have any other comments you would like to share?
[Open response]
That concludes the survey! Thank you so much for your time and responses. We truly appreciate it.
If you have any questions or concerns regarding the survey and/or needs assessment, you may contact the Program Director at andrew.ogwang@excelsiorwellness.org

Washington Emergency Medical Services provided supplemental information on firearm-related incident rates, which provides more context for firearm-related incidents in the county.
Among 33,541 firearm-related incidents from 2018 to 2024, over 69% were classified as lower acuity cases, while 2% required emergency response. Critical cases comprised 1% of the incidents. Refer to Figure 71 for the severity levels of firearm-related incidents.
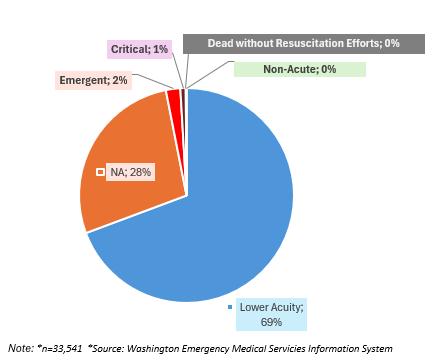
Washington emergency medical data reveals that 81% of firearm-related incidents were directed to hospitals, with law enforcement and other healthcare facilities, including mental health, nursing homes, and assisted living centers managing the remaining cases. Refer to Figure 72 for more details.
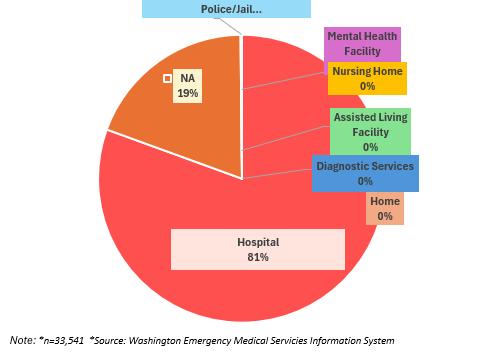
The map in Figure 73 provides a geographic context for emergency medical service (EMS) incidents related to firearms across the ZIP codes in Spokane County. The data is displayed in a color-coded format, where darker shades represent a higher number of firearm-related incidents. Each ZIP code is labeled with the corresponding count of EMS cases.
73: Firearm-Related Emergency Medical Services Events by Zip Code in Spokane County (2018-2024)
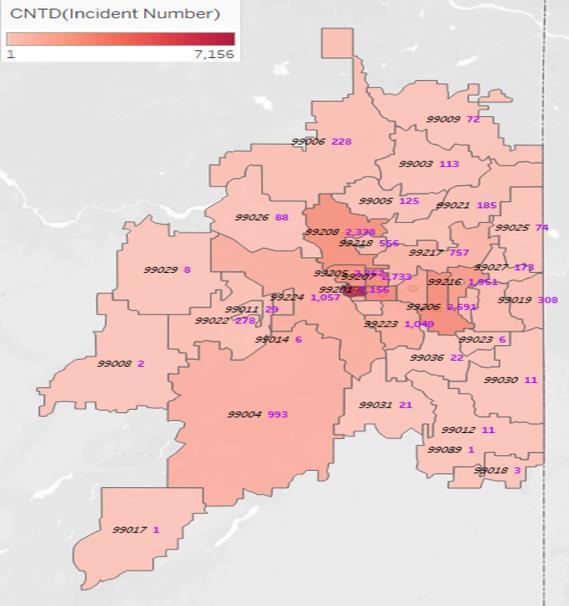
n=33,284 Source: Washington Emergency Medical Services Information System
Figure 74 shows the average rates of emergency medical services events over six years, from 2018 to 2024, categorized by race and ethnicity. The average event rates are highest among individuals who identify as white (57%) and Black or African American (4%). Additionally, 36% of patients did not identify their race or ethnicity, indicating “N/A.”
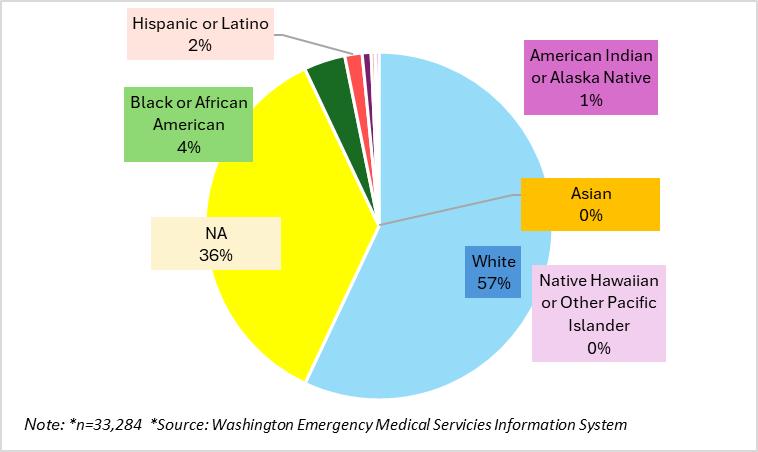
Figure 75 includes the average number of emergency medical services event rates by gender over six years (2018 through 2024). The average rate is higher among males (52%) than among females (41%).
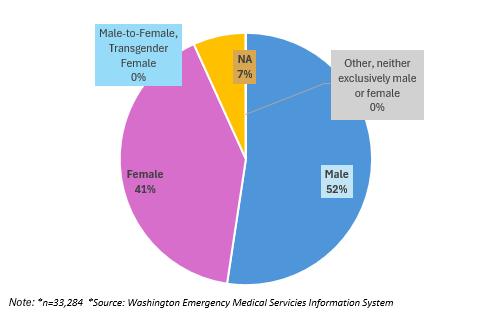
Firearm-related emergency medical services data in Spokane County from 2018-2024 (Figure 76) shows significant racial disparities, with the White population comprising the largest identified demographic at 57%. A substantial portion of cases (36%) lack racial/ethnic identification, while Black or African American (4%), Hispanic or Latino (2%), and American Indian or Alaska Native (1%) populations.
76: Average Firearm-Related Emergency Medical Services by Race/Ethnicity for the Years 2018-2024
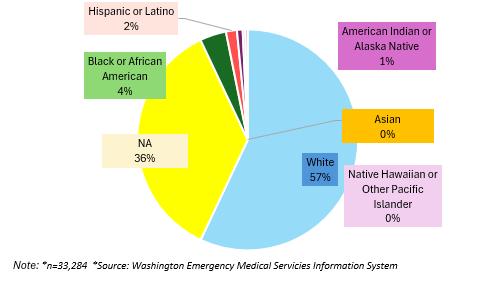

1. Abrams, Z. (2022). Studentmentalhealthisincrisis:Campusesarerethinkingtheirapproach. Https://Www.Apa.Org. https://www.apa.org/monitor/2022/10/mental-health-campus-care
2. American Foundation for Suicide Prevention (AFSP). (2024). SafeReportingGuidelinesforMedia. American Foundation for Suicide Prevention. https://afsp.org/safereporting/
3. American Psychological Association (APA). (2013). Gunviolence:Prediction,prevention,andpolicy. Https://Www.Apa.Org. https://www.apa.org/pubs/reports/gun-violence-prevention
4. American Psychological Association. (2013). APAreportongunviolenceidentifiesprecursorsand promisingsolutions.[Press release]. https://www.apa.org/news/press/releases/2013/12/gun-violence
5. American Public Health Association (APHA). (2018). ReducingSuicidesbyFirearms. https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policydatabase/2019/01/28/reducing-suicides-by-firearms
6. American Public Health Association (APHA). (n.d.). Gun Violence Prevention Fact Sheet. In https://www.apha.org/topics-and-issues/gun-violence. American Public Health Association. https://www.apha.org//media/files/pdf/advocacy/speak/220617_gun_violence_prevention_fact_sheet.pdf
7. Braga, A. A., & Cook, P. J. (2023). PolicingGunViolence:StrategicReformsforControllingOurMost PressingCrimeProblem. Oxford University Press. https://doi.org/10.1093/oso/9780199929283.001.0001 (2023)
8. Centers for Disease Control and Prevention (CDC). (2024). AboutViolencePrevention. Violence Prevention. https://www.cdc.gov/violence-prevention/about/index.html
9. Centers for Disease Control and Prevention (CDC). (2024). FastFacts:FirearmInjuryandDeath. Firearm Injury and Death Prevention. https://www.cdc.gov/firearm-violence/data-research/factsstats/index.html
10.Centers for Disease Control and Prevention (CDC). (2024). PreventingFirearmInjuryandDeath. CDC Firearm Injury and Death Prevention. https://www.cdc.gov/firearm-violence/prevention/index.html
11.Centers for Disease Control and Prevention (CDC). (n.d.). VetoViolence:Resourcesforviolence prevention. VetoViolence. https://vetoviolence.cdc.gov/apps/main/prevention-information/violenceprevention-fundamentals/
12.Chow, C. (2024). MentalHealthandFirearmOwnershipinWashington–StateRegsToday. https://www.stateregstoday.com/politics/gun-control/mental-health-and-firearm-ownership-inwashington
13.Chow, C. (2024, January). MentalHealthandFirearmOwnershipinWashington. State Regs Today: Home and State Regulations and Laws. https://www.stateregstoday.com/politics/gun-control/mentalhealth-and-firearm-ownership-in-washington
14.Chung, M. (2022, May 27). SchoolshootingsareraisinganxietyandpanicinU.S.children. Time. https://time.com/6182235/mass-shootings-children-mental-health-anxiety-depression/
15.Cimolai, V., Schmitz, J., & Sood, A. B. (2021). Effects of Mass Shootings on the Mental Health of Children and Adolescents. CurrentPsychiatryReports, 23(3). https://doi.org/10.1007/s11920-02101222-2
16.Educational Fund to Stop Gun Violence. (2020). Domestic Violence and Firearms. EFSGV. https://efsgv.org/learn/type-of-gun-violence/domestic-violence-and-firearms/
17.Ellyson, A. M., Adhia, A., Shanahan, S., Alsinai, A., DiMascolo, L., Reygers, M., Bowen, D., & RowhaniRahbar, A. (2023). Firearm restrictions in domestic violence protection orders: Implementation, vetting, compliance, and enforcement. Criminology&PublicPolicy. https://doi.org/10.1111/17459133.12639
18.Epperly, E. (2022). Spokane leaders blame recent violence on county’s “850-1,500” gang members and soft-on-crime laws. Spokesman.Com. https://www.spokesman.com/stories/2022/jun/30/gangpresser/
19.Everystat. (2023). Howdoesgunviolenceimpactthecommunitiesyoucareabout?EveryStat.Org; Everytown for Gun Safety Support Fund. https://everystat.org/#Washington
20.Everytown for Gun Safety Support Fund. (2024). BeyondMeasure:GunViolenceTrauma. Everytown Research & Policy. https://everytownresearch.org/report/gun-violence-trauma/
21.Everytown for Gun Safety Support Fund. (2024). TheEconomicCostofGunViolence. Everytown Research & Policy. https://everytownresearch.org/report/the-economic-cost-of-gun-violence/
22.Everytown for Gun Safety Support Fund. (2024). TheImpactofActiveShooterDrillsinSchools. Everytown Research & Policy. https://everytownresearch.org/report/the-impact-of-active-shooterdrills-in-schools/#key-findings
23.Everytown for Gun Safety Support Fund. (2024). TheImpactofGunViolenceonChildrenandTeens. Everytown Research & Policy. https://everytownresearch.org/report/the-impact-of-gun-violence-onchildren-and-teens/
24.Everytown for Gun Safety Support Fund. (2024c). WhentheShootingStops:TheImpactofGun ViolenceonSurvivorsinAmerica. Everytown Research & Policy. https://everytownresearch.org/report/the-impact-of-gun-violence-on-survivors-in-america/
25.Friar, N. W., MPH, Merrill-Francis, M., PhD, Parker, E. M., PhD, Siordia, C., PhD, & Simon, T. R., PhD. (2024). Firearm Storage Behaviors Behavioral Risk Factor Surveillance System, Eight States, 2021–2022. MorbidityandMortalityWeeklyReport, 524–529.
26.Goldstick, J. E., Cunningham, R. M., & Carter, P. M. (2022). Current Causes of Death in Children and Adolescents in the United States. NewEnglandJournalofMedicine, 386(20), 1955–1956. https://doi.org/10.1056/nejmc2201761
27.Griffith, D., Ogunbiyi, A., & Jaeger, E. (2024, April 2). Menandmentalhealth:Whatarewemissing? AAMC; Association of American Medical Colleges. https://www.aamc.org/news/men-and-mentalhealth-what-are-we-missing
28.Grossman, D. C., Reay, D. T., & Baker, S. A. (1999). Self-inflicted and Unintentional Firearm Injuries Among Children and Adolescents. ArchivesofPediatricsandAdolescentMedicine, 153(8), 875. https://doi.org/10.1001/archpedi.153.8.875
29.Health Assessment and Research for Communities (HARC). (2023). SanDiegoCountyGunViolence ReductionCommunityNeedsAssessmentComprehensiveReport. https://harcdata.org/wpcontent/uploads/2024/03/SD-Report.pdf
30.Johns Hopkins Bloomberg School of Public Health. (2023). CenterforGunViolenceSolutions. Center for Gun Violence Solutions | Johns Hopkins Bloomberg School of Public Health. https://publichealth.jhu.edu/gun-violence-solutions
31.Kajamaa, A., Mattick, K., & de la Croix, A. (2020). How to … do mixed-methods research. TheClinical Teacher, 17(3), 267–271. https://doi.org/10.1111/tct.13145
32.Katsiyannis, A., Rapa, L. J., Whitford, D. K., & Scott, S. N. (2022). An Examination of US School Mass Shootings, 2017–2022: Findings and Implications. AdvancesinNeurodevelopmentalDisorders, 7(1),
33.Kellermann, A. L., Rivara, F. P., Somes, G., Reay, D. T., Francisco, J., Banton, J. G., Prodzinski, J., Fligner, C., & Hackman, B. B. (1992). Suicide in the Home in Relation to Gun Ownership. New EnglandJournalofMedicine, 327(7), 467–472. https://doi.org/10.1056/nejm199208133270705
34.Kena, G., Ph. D., & Truman, J. L., Ph. D. (2022). Trends and Patterns in Firearm Violence, 1993–2018. In SpecialReport(NCJ 251663). https://bjs.ojp.gov/content/pub/pdf/tpfv9318.pdf
35.Legal Information Institute. (2022, May). Suspect(Wex Definitions Team, Ed.). Cornell Law School; Legal Information Institute. https://www.law.cornell.edu/wex/suspect
36.LegalClarity Team. (2025, January 21). What’saperpetratorincriminallaw?LegalClarity. https://legalclarity.org/whats-a-perpetrator-in-criminal-law/#google_vignette
37.LegalRampart. (2025). WhatisanArrestee?LegalRampart; LegalRampart.com. https://www.legalrampart.com/definitions/your-rights/arrestee/2725
38.Li, S., Zhao, F., & Yu, G. (2018). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. ChildAbuse&Neglect, 88, 212–224. https://doi.org/10.1016/j.chiabu.2018.11.012
39.Mason, G. (2021). With gang violence on the rise, Spokane-area law enforcement leaders call for community action. Spokesman.Com. https://www.spokesman.com/stories/2021/mar/08/with-gangviolence-on-the-rise-spokane-area-law-en/
40.Meindl, J. N., & Ivy, J. W. (2017). Mass Shootings: The Role of the Media in Promoting Generalized Imitation. AmericanJournalofPublicHealth, 107(3), 368–370. https://doi.org/10.2105/ajph.2016.303611
41.Monuteaux, M. C., Azrael, D., & Miller, M. (2019). Association of Increased Safe Household Firearm Storage With Firearm Suicide and Unintentional Death Among US Youths. JAMAPediatrics, 173(7), 657. https://doi.org/10.1001/jamapediatrics.2019.1078
42.Murray, S. H. (2024, June 9). What if the fearful families resisting stronger school phone bans have a point? Slate. https://slate.com/life/2024/06/phone-bans-schools-activism-shootings-parentsresistance.html
43.National Institute of Mental Health. (2023). Frequentlyaskedquestionsaboutsuicide. National Institute of Mental Health; U.S. Department of Health and Human Services, National Institutes of Health. https://www.nimh.nih.gov/health/publications/suicide-faq
44.Neilsberg Research. (2025, February 21). Spokane,WAPopulationbyRace&Ethnicity. Neilsberg. https://www.neilsberg.com/insights/spokane-wa-population-by-race/
45.Office for Victims of Crime. (n.d.). AchievingExcellence:ModelStandardsforServingVictimsand SurvivorsofCrime. Office for Victims of Crime; Office for Victims of Crime, U.S. Department of Justice. Retrieved March 17, 2025, from https://ovc.ojp.gov/sites/g/files/xyckuh226/files/modelstandards/6/glossary.html#top
46.Parker, K., Horowitz, J. M., Igielnik, R., Oliphant, J. B., & Brown, A. (2017, June 22). America’s ComplexRelationshipWithGuns. Pew Research Center. https://www.pewresearch.org/socialtrends/2017/06/22/the-demographics-of-gun-ownership/
47.Sorenson, S. B., & Schut, R. A. (2018). Nonfatal Gun Use in Intimate Partner Violence: A Systematic Review of the Literature. TraumaViolence&Abuse, 19(4), 431–442. https://doi.org/10.1177/1524838016668589
48.Stoker, A. (2024, October). Firearmsbackgroundchecks. Washington State Health Care Authority. https://www.hca.wa.gov/assets/program/fact-sheet-firearm-background-check.pdf
49.The Educational Fund to Stop Gun Violence (EFSGV). (2020). DomesticViolenceandFirearms:The EducationalFundtoStopGunViolence. The Educational Fund to Stop Gun Violence. https://efsgv.org/learn/type-of-gun-violence/domestic-violence-and-firearms/
50.The Recovery Village Drug and Alcohol Rehab. (2021). HowGunsandDrugsContributestoThe ViolenceAcrossAmerica. The Recovery Village Drug and Alcohol Rehab. https://www.therecoveryvillage.com/drug-addiction/how-guns-drugs-contribute-to-violence/
51.The Women’s Safe House. (2015, November 4). EducationandOutreach. The Women’s Safe House. https://twsh.org/community-education/education-and-outreach/
52.U.S. Surgeon General. (2024). FirearmViolence:APublicHealthCrisisinAmerica. https://www.hhs.gov/sites/default/files/firearm-violence-advisory.pdf
53.United States Census Bureau. (2025, March 13). CountyPopulationTotalsandComponentsof Change:2020-2024. Census.Gov. https://www.census.gov/data/datasets/timeseries/demo/popest/2020s-counties-total.html
54.University of Utah Health. (2022). How to Talk to Your Child About Suicide: An Age-By-Age Guide. UniversityofUtahHealth. https://healthcare.utah.edu/healthfeed/2022/09/how-talk-your-child-aboutsuicide-age-age-guide
55.Washington Courts. (2024, January). PetitiontoRestoreFirearmRights(pp. 1–3). Washington State Administrative Office of the Courts. https://www.courts.wa.gov/forms/documents/WS%20900_Pt%20to%20Restore%20Firearms%20Rig hts%202024%2001.pdf
56.Washington State Coalition Against Domestic Violence (WSCADV). (2024). AboutDomesticViolence. https://wscadv.org/about-domestic-violence/
57.Washington State Department of Social and Health Services (WA State DSHS). (n.d.). Typesand SignsofAbuse|DSHS. https://www.dshs.wa.gov/altsa/home-and-community-services/types-andsigns-abuse
58.Washington State Legislature. (2024). RCW9.41.040:Unlawfulpossessionoffirearmspenalties. Washington State Legislature. https://app.leg.wa.gov/rcw/default.aspx?cite=9.41.040
59.World Health Organization. (2022). Homicide:WHOGlobalHealthEstimates(2019update). WHO Violence Info; WHO. https://apps.who.int/violence-info/homicide/
60.World Health Organization. (2024). Determinantsofhealth. https://www.who.int/newsroom/questions-and-answers/item/determinants-of-health#
61.World Population Review. (2025). SpokaneCounty,WashingtonPopulation. World Population Review. https://worldpopulationreview.com/us-counties/washington/spokane-county
Arrestee: A person who has been apprehended by law enforcement due to suspected criminal activity.54
Firearm violence: The use of firearms to cause harm, encapsulating both injuries and deaths from the use of firearms. Often used interchangeably with “gun violence.”
Firearm: Any weapon that uses explosive force to discharge a projectile, including handguns, rifles, and shotguns.55
Homicide: The killing of a person by another with intent to cause death or serious injury, by any means. It excludes death due to legal intervention and operations of war.56
Needs assessment: A systematic effort to gather information from various sources that will help identify the needs of victims in the community and the resources that are available to them.57
Perpetrator: An individual who has committed a criminal act, directly engaging in conduct that violates statutory provisions.58
Suicide: When people harm themselves with the goal of ending their life, and they die as a result.57
Survivor: A person who has survived an ordeal or trauma; includes both direct and indirect victims of crime. The term survivoremphasizes the strength and courage needed to survive a traumatic event.57
Suspect: A person who is believed to have committed a crime but has not yet been found guilty.59
Victim: A person who experiences mental, physical, financial, social, emotional, or spiritual harm as the direct result of a specified crime committed on his or her person or property.57
Violence: The intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation.60
54 What is an Arrestee? - Definition from LegalRampart (n.d.). https://www.legalrampart.com/definitions/your-rights/arrestee/2725
55 Kena, G., Ph. D., & Truman, J L., Ph. D. (2022). Trends and Patterns in Firearm Violence, 1993–2018. In Special Report (NCJ 251663). https://bjs.ojp.gov/content/pub/pdf/tpfv9318.pdf
56 World Health Organization. (2019). Violence Info – Homicide. https://apps.who.int/violence-info/homicide/
57 Office for Victims of Crime (n.d.) OVC Model Standards. https://ovc.ojp.gov/sites/g/files/xyckuh226/files/model-standards/6/glossary.html#victims
58 Legal Clarity Team (2025). What’s a Perpetrator in Criminal Law? https://legalclarity.org/whats-a-perpetrator-in-criminal-law/#google_vignette
59 suspect. (n.d.). LII / Legal Information Institute. https://www.law.cornell.edu/wex/suspect
60 Krug E, Dahlberg L, Mercy J.et al World report on violence and health. Geneva: World Health Organization, 2002 Excelsior Wellness | 2025 Community Needs Assessment | Page 112
CDC Centers for Disease Control and Prevention
CNA Community Needs Assessment
CPS—Child Protective Services
CVSAP Community Violence Strategic Action Plan
DOH Department of Health
DV Domestic violence
DVPOs Domestic Violence Protection Orders
EMS Emergency Medical Service
EMS Emergency Medical Services
ERPOs—Extreme Risk Protection Orders
IPV Intimate partner violence
LAPs Lethality assessment protocols
MH—Mental health
NICS National Instant Criminal Background Check System
ORE Office of Research and Evaluation (Excelsior)
SCSO—Spokane County Sheriff’s Office
SEM—Social Ecological Model
SRDVC Spokane Regional Domestic Violence Coalition
LEOs Law Enforcement Officers
SRHD—Spokane Regional Health District
SUD Substance Use Disorder
WEMSIS Washington Emergency Medical Services Information System
EMS Emergency medical services
WSCADV—Washington State Coalition Against Domestic Violence