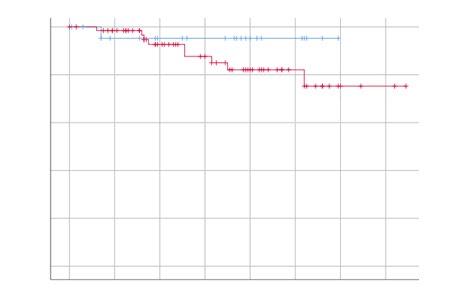
55 Long-Term Outcomes of Endoscopic Therapy in High-Risk Urinary Tract Carcinoma
Quereda-Flores et al.
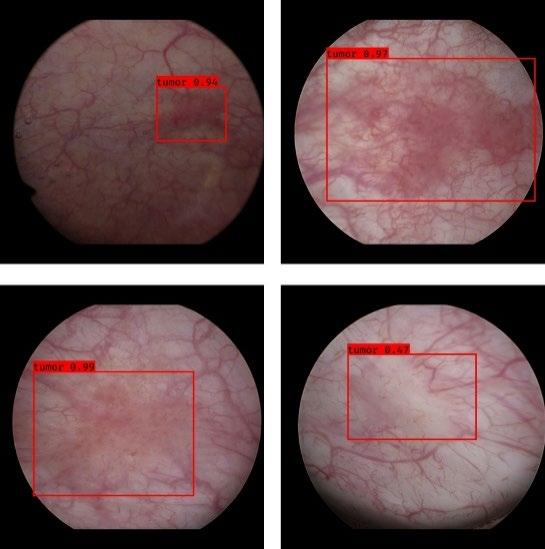
57 AI System for Detecting Flat Bladder Tumours in Cystoscopic Images
Mutaguchi et al.
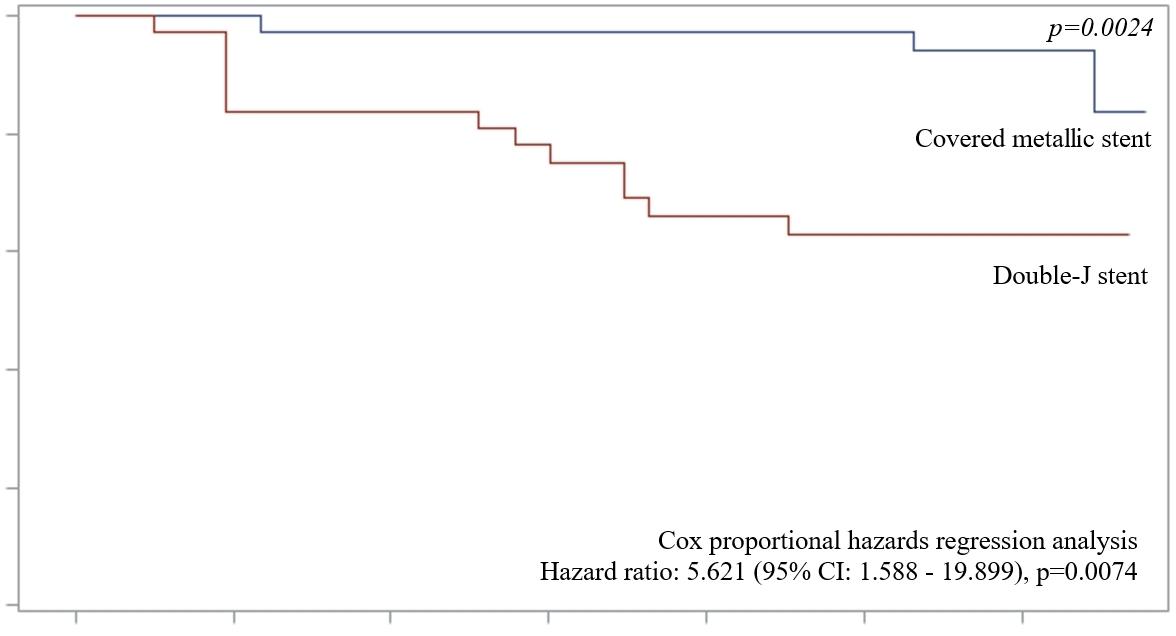
59 Silicon-Covered Metallic Mesh Stents for Malignant Ureteral Obstruction
Han et al. Congress Interviews
63 Maarten Albersen
66 Evangelos Liatsikos Interviews
69 Axel Heidenreich
77 Post-partum Urinary Retention: Under-recognised, Under-treated Tablazon and Hickman
82 Editor's Pick: Treatment of Urolithiasis: A Comprehensive Review
Dika et al.
98 Delayed Presentation of Transurethral Resection of Prostate Syndrome: A Case Presentation from a Rural Referral Hospital
103 Leiomyosarcoma Arising in Angiomyolipoma 5 Years Post-Embolisation:
"Over
4 days, attendees immersed themselves in cutting-edge research, live surgical demonstrations, and thought-provoking debates"
Editorial Board
Editor-in-Chief
Prof Abdullah Erdem Canda Koç University, Türkiye
Abdullah Erdem Canda is an esteemed expert in robotic urology, serving on the Board of the European Robotic Urology Society and as a trainer for leading institutions, including the Orsi Academy, Merelbeke-Melle, Belgium. With a focus on advancing robotic surgery through education, research, and international collaboration, he has played a pivotal role in shaping the field and mentoring future specialists.
Prof Riccardo Autorino
Rush University, USA
Dr Jean de la Rosette
Academic Medical Center, the Netherlands
Dr Selçuk Güven
Necmettin Erbakan University, Türkiye
Prof Jørgen
Bjerggaard Jensen
Aarhus University Hospital, Denmark
Dr Roberto Sanseverino
Azienda Sanitaria Locale Salerno, Italy
Prof Alan J Wein University of Pennsylvania, USA
Prof Henry Woo
Blacktown and Mount Druitt Hospitals, Sydney, Australia
Mr Marius Rebek
The Princess Alexandra Hospital NHS Trust, UK
Aims and Scope
EMJ Urology is an open access, peer-reviewed eJournal committed to helping elevate the quality of healthcare in urology by publishing content on all aspects of urological function and disease.
The journal is published annually, six weeks after the European Association of Urology (EAU) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. Additionally, this journal covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Urology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests.
EMJ Urology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
Our focus is on research that is relevant to all healthcare professionals. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance research and inform of coming trends affecting clinical practice in Urology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
Launch Date: 2013
Frequency: yearly ISSN: 2053-4213
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (EAU 2025) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Katie Wright, Katrina Thornber, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Creative Artworker
Dillon Benn Grove
Designers
Owen Silcox, Fabio van Paris, Shanjok Gurung
Senior Project Manager
George Roe
Senior Performance & Insight Lead
Darren Brace
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief Executive Officer
Spencer Gore
Welcome
Dear Readers,
I am delighted to welcome you to the latest edition of EMJ Urology. In this issue, our team shines a spotlight on the 40ᵗʰ Annual Congress of the European Association of Urology (EAU), which welcomed a record number of delegates in the organisation’s history.
This issue features a detailed review of the EAU Congress 2025, including summaries of key abstracts on topics such as MRI-based active surveillance in prostate cancer and advancements in imageguided navigation for enhanced precision in robotic surgery. Alongside these, we present in-depth features revisiting early detection strategies for prostate cancer and examining clinical decision making in patients with both overactive bladder and benign prostatic obstruction.
In keeping with EMJ’s commitment to showcasing the latest advancements in urology, this issue includes peer-reviewed articles on diverse clinical topics, including a review of current approaches to the treatment of urolithiasis and a feature exploring post-partum urinary retention, as well as two compelling case reports.
This issue also features exclusive interviews with distinguished experts in the field, offering insights into the latest developments in neurological urology and the current status of prostate cancer research.
I hope you find this issue informative and thought-provoking, and I would like to express my gratitude to the Editorial Board, contributors, and interviewees for their invaluable insights and support.
The EMJ team look forward to seeing everyone in 2026 at the next EAU Congress in London, UK.
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Foreword
Dear Colleagues,
It is a great pleasure for me to introduce you to the new issue of EMJ Urology.
The European Association of Urology (EAU) Congress, held annually, draws global attention. The latest advancements and cutting-edge research are showcased and discussed through its extensive programme featuring sessions, debates, presentations, and courses across all urology subspecialties.
This issue includes a comprehensive review of the 40ᵗʰ Annual EAU Congress, which took place in Madrid, Spain. The congress highlighted numerous technological developments, and I had the privilege of delivering a talk on 'Telesurgery Training in Robotic Urology'.
In this issue we also have a variety of very interesting papers, with peer-reviewed articles providing valuable insights into critical urologic conditions, including delayed transurethral resection of prostate
The congress highlighted numerous technological developments, and I had the privilege of delivering a talk on ‘Telesurgery Training in Robotic Urology’
syndrome in resource-limited settings, the malignant transformation of renal angiomyolipoma, and the management of urolithiasis. Additionally, we feature interviews with leading experts in the evolving field of neurological urology, and prostate cancer treatment.
I would like to take this opportunity to invite you all to submit your work to EMJ Urology
I hope you enjoy reading this new issue!
Abdullah Erdem Canda Professor of Urology, Koç University School of Medicine, İstanbul, Türkiye
EAU 2025
Over 4 days, attendees immersed themselves in cutting-edge research, live surgical demonstrations, and thought-provoking debates
Congress Review
Review of the European Association of Urology (EAU) Congress 2025
THIS YEAR the Spanish capital, Madrid, provided the backdrop for Europe’s biggest urological event, the 40th Annual European Association of Urology (EAU) Congress. Taking place from 21st–24th March 2025, this year’s congress hosted a record number of delegates in the organisation's history. Over 4 days, attendees immersed themselves in cutting-edge research, live surgical demonstrations, and thought-provoking debates that showcased the rapid advancements shaping the future of urology.
The Opening Ceremony set the stage for an exhilarating congress, beginning with a flamenco performance that captivated the audience. As the dancing concluded, the EAU Secretary General Arnulf Stenzl, University of Tübingen Medical School, Germany, took to the stage to extend a warm welcome to all participants. Stenzl highlighted the unprecedented number of abstract submissions this year, an impressive 5,745, which is a testament to the growing influence of the EAU as a global platform for innovation and scientific exchange. He also emphasised the importance of collaboration within the urological community, recognising the dedication of professionals working together to advance patient care.
A major highlight of the Opening Ceremony was the presentation of the EAU awards, where outstanding contributions to the field were recognised. Honorary membership was awarded to several distinguished urologists who have left a lasting impact on European urology. Truls-Erik Bjerklund Johansen, University of Oslo, Norway, was honoured for his instrumental role in shaping
guidelines on infectious diseases in urology. Ivan Minčík, University of Prešov, Slovakia, expressed heartfelt gratitude, noting that despite the rain outside, receiving this recognition was a sunny moment in his career. Meanwhile, David Winkle, UroMed South Brisbane, Australia, was acknowledged for his extensive leadership roles within urological societies, including his tenure as President of The Urological Association of Asia, Singapore.
The EAU Willy Gregoir Medal, named after the esteemed Brussels-based urologist and first Secretary General of the EAU, was awarded to Francesco Montorsi, University Vita-Salute San Raffaele, Milan, Italy. In his acceptance speech, Montorsi dedicated the award to his patients and their families, emphasising that “all we do is for them”. Another significant honour, the EAU Frans Debruyne Lifetime Achievement Award, was bestowed upon Anders Bjartell, Lund University, Sweden, acknowledging his decades of dedication and profound contributions to the EAU and the broader urological community.
Young talent in the field was also celebrated, with Isabel Heidegger, Innsbruck Medical University, Austria, receiving the EAU Crystal Matula Award for 2025, a prestigious distinction awarded to a promising young European urologist with the potential to shape the future of the specialty. The EAU Prostate Cancer Research Award, recognising the best published paper on clinical or experimental studies in prostate cancer, was presented to Jonas Hugosson, University of Gothenburg, Sweden.
The ceremony concluded just as it began, with live music and another dazzling flamenco performance, setting an energetic tone for the days ahead. Of the comprehensive scientific programme, some of the standout sessions were the muchanticipated 'Game Changer' sessions, which focussed on groundbreaking techniques in prostate cancer diagnosis. One of these sessions, chaired by Eamonn Rogers, National University of Ireland, Galway, and Jochen Walz, Institut Paoli-Calmettes Cancer Centre, Marseille, France, delved
into innovative methodologies that have the potential to revolutionise existing diagnostic protocols. Meanwhile, the European School of Urology offered hands-on training sessions, equipping young urologists with essential skills that will shape their future careers.
Beyond the scientific sessions, the exhibition floor buzzed with excitement as industry leaders unveiled cutting-edge technologies and innovations set to redefine the standard of urological care. EAU25 reaffirmed its commitment to pushing the boundaries of the field, providing a dynamic platform for knowledge exchange and professional development.
EAU25 proved to be a resounding success, and, as the event came to a close, anticipation was already building for EAU26, set to take place in London, UK. Stay tuned for further updates on what promises to be another exceptional gathering of the global urological community, but, for now, enjoy our review of EAU25.
A major highlight of the Opening Ceremony was the presentation of the EAU awards
Long-Term Outcomes of Open Urorectal Fistula Repair
URORECTAL fistulas (URF) following prostate cancer treatment are rare but significantly impact patients' quality of life. Despite various surgical approaches, long-term outcome data, particularly those incorporating patient-reported outcome measures (PROMs), remain limited. This study, presented at EAU25, details a decade-long retrospective analysis of URF repairs at a specialist centre, providing insights into survival rates and patient experiences.1
From 2014–2024, 29 men underwent open URF repair, with a median age of 68 years and a median BMI of 26. The interval between radical prostatectomy and URF repair was a median of 10 months. Notably, 17% of patients had undergone pelvic radiotherapy, and 41% required redo repairs. Common symptoms included rectal urine leakage (48%), pneumaturia (24%), recurrent infections (21%), alguria (21%), and faecaluria (10%). Surgical repair was predominantly transperineal (90%), with a smaller proportion requiring transabdominal intervention (10%). The median operative time was 90 mins, and long-term follow-up data were available for fistula recurrence (median 50 months) and reintervention (median 58 months).
The study reports excellent long-term outcomes, with estimated 5-year recurrencefree and reintervention-free survival rates of 96% and 75%, respectively. PROMs were evaluated at a median of 71 months post-repair, with complete data from 16 patients. The median six-item Lower Urinary Tract Symptoms score was four, the ICIQ-UI SF quality of life
questionnaire score was 11, and the Wexner faecal incontinence score was three, indicating that while voiding function and faecal continence were largely preserved, moderate urinary incontinence persisted in some patients. Patient satisfaction remained high, with a median ICIQ-Satisfaction score of 21 and an overall satisfaction score of nine.
This study highlights the durability of open URF repair, even in complex cases. While recurrence rates are low and patient satisfaction is generally high, persistent urinary incontinence remains a challenge, likely due to underlying disease-related factors.
The study reports excellent longterm outcomes, with estimated 5-year recurrence-free and reintervention-free survival rates of 96% and 75%, respectively
MRI-Based Active Surveillance for Gleason Grade 2 Prostate Cancer
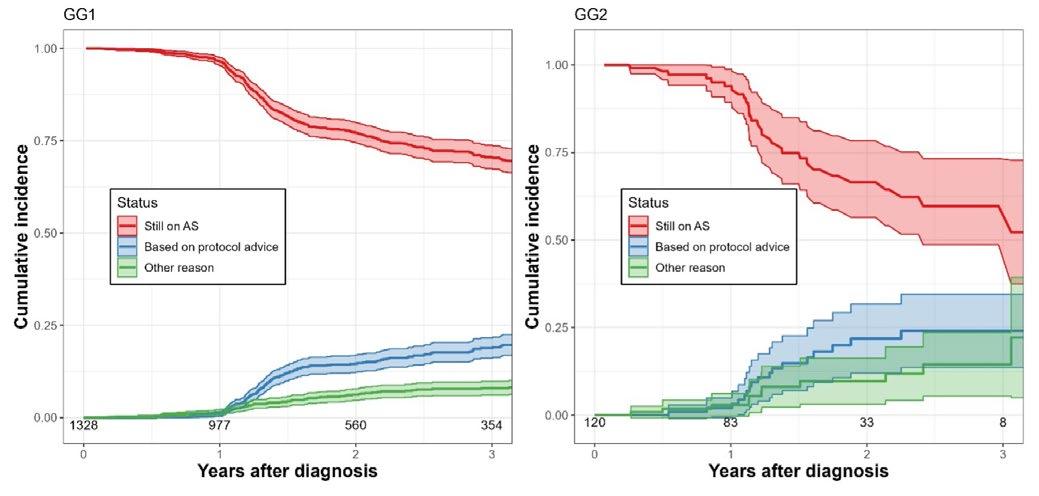
ACTIVE surveillance has shown to be a safe management option for patients with Gleason Grade (GG) 2 prostate cancer (PCa), according to data presented at EAU25.2
Researchers presented the first reported European series of patients with GG 2 PCa who were selected for active surveillance based on MRI imaging prior to biopsy. Whilst uptake of active surveillance in patients with GG 2 PCa has been historically low, it has been hypothesised that fine-tuning patient selection based on MRI may be a safe option. Hence, this multicentre study enrolled 139 patients with GG 2 PCa between 2016–2024 in 10 reference centres in France, Spain, Italy, Switzerland, and Germany, who had been selected for active surveillance based on MRI imaging prior to biopsy.
The first reported European series of patients with GG 2 PCa who were selected for active surveillance based on MRI imaging prior to biopsy
Baseline MRI showed a Prostate Imaging Reporting and Data System 4–5 lesion in 59% of patients. The median event-free follow-up was 38 months, and whilst there were two cases of metastasis, there were no deaths due to PCa. The estimated 5-year metastasis-free survival rate was 98%, the estimated 5-year treatment-free survival was 45%, and the estimated GG 3 reclassification-free survival was 77%.
During the follow-up, 56 patients underwent definitive treatment, and 26 patients underwent GG 3 reclassification.
The final analysis revealed an estimated 5-year GG 3 reclassification-free survival rate of 81% (95% CI: 69–94) for patients within the EU criteria, and 73% (95% CI: 62–86) for patients outside the criteria. Additionally, the estimated 5-year treatment-free survival rate was 43% (95% CI: 30–61) for patients within the EU criteria, and 49% (95% CI: 36–66) for patients outside. Importantly, the estimated 5-year metastasis-free survival rate was 100% (95% CI: 100–100) for patients within the EU criteria, and 96% (95% CI: 91–100) for those outside, and the estimated 5-year overall survival rate in patients within and outside the EAU criteria was 95% (95% CI: 90–100), and 91%, respectively.
These results demonstrate that active surveillance with an MRI-based selection process is a safe management option in patients with GG 2 PCa. The authors emphasise that future studies should prioritise redefining current active surveillence inclusion criteria to identify low-risk GG 2 subgroups, particularly those at low absolute risk of distant progression.
%
The estimated 5-year metastasis-free survival rate was 100% (95% CI: 100–100) for patients within the EU criteria, and 96% (95% CI: 91–100) for those outside
Barriers to Acceptance of Inclusive Prostate Cancer Measures
ACCEPTANCE of sexual and gender minorities has shown to vary across different parts of the UK, according to new research presented at EAU25.3 This, along with geographic inequities in disclosing sexual orientation or gender identity (SOGI), poses significant barriers to national implementation of SGM-inclusive prostate patient-reported outcome measures (PROM).
A nationwide search was conducted to determine the attitudes towards LGBTQ+ rights, hate crimes statistics, and individuals’ comfort levels in expressing their SOGI in healthcare settings. Examples of these metrics included ‘not open about sexuality in healthcare’, ‘not open about gender identity in healthcare’, ‘experienced a hate crime’, ‘think LGBTQ+ rights have “gone too far”’, and finally, ‘opposed to LGBTQ+ teaching’.
A nationwide search was conducted to determine the attitudes towards LGBTQ+ rights, hate crimes statistics, and individuals’ comfort levels in expressing their SOGI in healthcare settings
The results found that, compared to people in urban areas, those in rural areas were less likely to feel comfortable expressing their SOGI in healthcare settings. Additionally, the Northeast of England and London had the highest rates of reported LGBTQ+ hate crimes, at 35% and 25%, respectively. Moreover, the highest percentage of people (29%) that thought LGBTQ+ rights have 'gone too far' was seen in Wales, whilst the lowest (12%) was recorded in the Midlands.
These geographic disparities highlight the need for tailored local campaigns to help reduce stigma and encourage people to feel more comfortable disclosing their sexual orientation and gender identity in the healthcare setting. As a result, the implementation of national initiatives such as the Sexual Minorities and Prostate Cancer Scale (SMACS) should be better.
Northeast of England and London had the highest rates of reported LGBTQ+ hate crimes, at 35% and 25%, respectively
Day-Care Percutaneous Nephrolithotomy Proves Safe and Effective
PERCUTANEOUS nephrolithotomy (PCNL) can be safely performed as a day-care procedure in carefully selected patients, reducing hospital stay without increasing complications or readmissions, according to an abstract presented at EAU25.4
A structured Day-Care PCNL Checklist was formulated to identify the optimal patient cohort based on preoperative, intraoperative, and postoperative factors
This prospective observational study included patients with renal stones who underwent PCNL, with day-care defined as discharge within 24 hours post-surgery. The primary outcomes included readmission rates, unplanned emergency department visits, and complications classified using the ClavienDindo system. Statistical analyses were conducted using Student’s t-test, MannWhitney U test, and Chi-squared test. A structured Day-Care PCNL Checklist was formulated to identify the optimal patient cohort based on preoperative, intraoperative, and postoperative factors.
A total of 300 patients underwent day-care PCNL, with a mean age of 47 (±13.00) years and mean BMI of 27 (±13.52). The mean stone volume was 1,625 (±1,376.24) mm³, and the mean S.T.O.N.E. nephrolithometry score was 6.06 (±0.75). Tract size averaged 20.79 Fr (±5.34), with 169 patients undergoing miniPCNL (≤20 Fr) and 131 undergoing standard PCNL (>20 Fr). The overall stone-free rate was 93%. The unplanned revisit rate was 6.0%, with a 4.3% readmission rate, occurring on average 9 (±5.34) days post-surgery. Significant risk factors for readmission included a Charlson Comorbidity Index Score ≥2 (p=0.024) and stone volume >5,000 mm³ (P=0.021), while diabetes was associated with Clavien-Dindo ≥2 complications (P=0.039). Complications included five cases of Clavien-Dindo Grade 1, 12 of Grade 2, and one of Grade 3b.
These findings confirm that PCNL can be performed safely as a day-care procedure in selected patients, maintaining high stone-free rates and acceptable readmission risks. The proposed Day-Care PCNL Checklist may help clinicians optimise patient selection and ensure favourable outcomes.
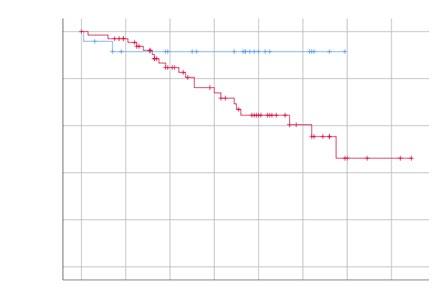
Predicting Long-Term Failure After Urethroplasty Surgery
URETHRAL stricture disease is a significant contributor to male lower urinary tract symptoms, often necessitating surgical intervention. According to an abstract presented at EAU25, urethroplasty is now considered the gold standard treatment for strictures that do not respond to endoscopic management; however, long-term recurrence-free survival rates, and the key predictors of treatment failure remain insufficiently explored.5
A total of 291 patients were included in the study, with 91 (31.27%) experiencing stricture recurrence
In this retrospective single-centre study, the authors analysed medical records of male patients who underwent urethroplasty from January 2003–December 2014. Failure was defined as the necessity for additional instrumentation for stricture release or confirmed anatomical failure with clinical implications, identified through cystoscopy or cystourethrogram. Various patient- and surgery-related factors that could predict long-term failure were assessed, including age, American Society of Anaesthesiologists (ASA) score, smoking habits, cardiovascular risk factors, stricture aetiology, location, length, preoperative urine cultures, and surgical technique. Statistical analyses, including Kaplan-Meier survival estimates and Cox-proportional hazards regression models, were utilised to determine significant predictors.
A total of 291 patients were included in the study, with 91 (31.27%) experiencing stricture recurrence. Among those who remained recurrence-free, the median follow-up period was 114.5 months. Notably, half of all recurrences occurred within 33 months post-surgery, while the
remaining failures were observed over the subsequent decade. Survival analyses identified age (p=0.003), ASA score (p=0.007), and smoking habits (p=0.035) as statistically significant predictors of recurrence. Stricture localisation (p=0.010), length (p=0.008), preoperative urine culture results (p=0.022), and surgical technique (p=0.042) also influenced recurrence risk. Multivariable Cox regression analysis further highlighted ASA score (p=0.007, HR=1.98, 95% CI: 1.20; 3.24), smoking (p=0.015; HR=1.76; 95% CI: 1.12; 2.78), and stricture localisation (p=0.005; HR=2.18; 95% CI:1.26; 3.77) as the most significant predictive factors.
The study findings confirm that urethroplasty failure can occur even years after surgery, emphasising the need for long-term patient monitoring. ASA score, smoking status, and stricture localisation are the strongest predictors of recurrence. Using these variables, the authors developed an accessible prediction model for recurrencefree survival, offering clinicians a valuable tool for patient counselling and aiding in future clinical decision-making.
Augmented Reality-3D Guidance System Enhances Lymph Node Detection in High-Risk Prostate Cancer
A NOVEL augmented reality (AR)-3D guidance system for extended pelvic lymph node dissection (ePLND) during robot-assisted radicalprostatectomy (RARP) is feasible, safe, and enhances identification of nodal metastases, according to research presented at EAU25.6
Prostate-Specific Membrane Antigen-PET (PSMA-PET) has redefined staging accuracy in high-risk prostate cancer (PCa), leading to increased identification of cN1 disease. Despite this advancement, the role of local therapies like RARP in cN1 disease remains underexplored, particularly due to challenges arising from the localisation of suspicious lymph nodes outside of standard templates. Therefore, researchers have developed an AR-3D-PSMA guided PLND based on preoperative PSMA-PET for real-time intraoperative identification of nodal metastases during RARP in high-risk patients.
In this study, 13 patients with PSMA-PETconfirmed cN1 PCa underwent RARP with AR-3D-guided ePLND between April 2023–June 2024. Preoperative 3D virtual models of pelvic anatomy and PSMA-avid nodal regions were integrated into the robotic console’s AR interface for real-time intraoperative navigation. The median operative time was 280 minutes, with 150 mL blood loss and 4-day hospitalisation. No intraoperative complications occurred, but one patient experienced a Clavien-Dindo Grade 3 complication.
Pathological nodal involvement was confirmed in in 69% of cases, with 15% showing metastases outside standard templates (pararectal/presacral). Among the 117 nodal regions analysed, AR-3D-PSMA guidance demonstrated 67% sensitivity, 89% specificity, 48% positive predictive value, 95% negative predictive value, and an area under the curve value of 0.77. Postoperatively, 46% of patients achieved PSA <0.1 ng/mL at 40 days.
Preoperative 3D virtual models of pelvic anatomy and PSMA-avid nodal regions were integrated into the robotic console’s AR interface
The results show that AR-3D-PSMA-guided ePLND during RARP is feasible and safe, and enhances intraoperative identification of nodal metastases both within and beyond traditional dissection templates. While the technique’s high negative predictive value (95%) supports its utility in excluding regions without disease, its moderate positive predictive value (48%) highlights the need for refined imagingpathology correlation. These findings advocate for integrating PSMA-PET-driven AR navigation into surgical planning for high-risk cN1 PCa, potentially optimising oncologic outcomes through precision dissection.
AR-3D-PSMA guidance demonstrated 67% sensitivity, 89% specificity, 48% positive predictive value, 95% negative predictive value, and an area under the curve value of 0.77
Objective Assessment of Intraoperative Skills for Bladder Tumour Resection
A STUDY, presented at EAU25, has highlighted the importance of objective performance metrics in evaluating the skills of urology residents performing Transurethral Resection of Bladder Tumour (TURBT), a common procedure for young urologists.7
Researchers sought to assess the reliability and validity of performance metrics defined through ProficiencyBased Progression (PBP), a training methodology aimed at ensuring optimal skill development. To do so, they compared the performances of 15 novice urologists (≤25 TURBT procedures) and 15 experts (≥100 TURBT procedures) by having two blinded experienced urologists score anonymised videos of the surgeries.
To do so, they compared the performances of 15 novice urologists (≤25 TURBT procedures) and 15 experts (≥100 TURBT procedures)
Compared to novices, experts made 77%, 71%, and 89% fewer total (tE), normal (nE), and critical (CE) errors. The median errors for expert surgeons were one (tE), zero (nE), and one (CE), while for novices, they were three (tE), five (nE), and two (CE). Statistical differences (p<0.05) were found between the two groups for all error categories, with p<0.005 for median tE, nE, and CE.
These results emphasise the reliability of performance metrics in distinguishing skill levels in TURBT procedures. Furthermore, they suggest that the PBP approach offers a valuable tool for establishing clear proficiency benchmarks. By using these objective metrics, residency programs can more accurately track progress and target areas for improvement, leading to higherquality training and, ultimately, better patient outcomes.
Compared to novices, experts made 77%, 71%, and 89% fewer total, normal, and critical errors.
Image-Guided Navigation Enhances Precision in Robotic Surgery
NEW research presented at EAU25 has demonstrated the feasibility of integrating image-guided navigation (IGN) into robotic sentinel lymph node biopsy (SLNB) for prostate cancer, offering improved anatomical orientation and surgical precision.8
Among 12 patients with 31 SNs, IGN successfully localised 25 SNs (81%)
This single-centre prospective feasibility study included patients with prostate cancer scheduled for robotic SLNB, with IGN integration assessed using electromagnetic (EM) tracking and ultrasound (US). Sentinel node (SN) locations were identified preoperatively via Single-photon emission computed tomography (SPECT)/CT scans and reconstructed into a 3D model. Intraoperatively, patient alignment with this model was achieved through US acquisition using an EM-tracked drop-in probe.
Surgical instruments were equipped with EM sensors for live tracking, with real-time stereoscopic visualisation displayed in the da Vinci Xi system. Surgeons navigated towards SNs using tracked instruments, with SN localisation confirmed intraoperatively via fluorescence, ex vivo radioactivity verification, or both. Feasibility was defined as a successful SN removal rate of over 75% using IGN.
Among 12 patients with 31 SNs, IGN successfully localised 25 SNs (81%). Intraoperative US acquisition and image registration were rapid (median: 10 min; interquartile range: 8–14 min), intuitive, and seamlessly integrated into the surgical workflow. The combination of 3D stereoscopic visualisation and instrument tracking enabled improved anatomical identification. IGN was not used in one patient (five SNs, 16%) due to technical failure, and in another, one SN (3%) was not identified by any method. No patient complications were reported.
These findings confirm that IGN is a safe and effective tool in robotic surgery, providing an intuitive and well-integrated approach for enhanced surgical precision.
Sentinel node locations were identified preoperatively via SPECT/CT scans and reconstructed into a 3D model
Anticholinergic Burden Increases Risk in Patients with Overactive Bladder Syndrome
RESEARCH presented at EAU25 assessed whether baseline anticholinergic burden, measured by the Anticholinergic Cognitive Burden (ACB) score, is associated with increased cardiovascular and urological complications after initiating anti-muscarinic therapy.9
The retrospective study analysed electronic health records from 43 hospitals and affiliated clinics between 2017–2021, and identified 13,947 adult patients who have recently begun antimuscarinic monotherapy. The ACB score was calculated for all patients based on prescription records. Patients with ACB≥1 were compared with the control group ACB=0. After propensity score matching, a total of 9,854 patients were analysed, and cardiovascular and urological complications were compared between groups.
Results showed that patient with ACB ≥1 experienced significantly higher rates of complications. For urological outcomes, the incidence of acute retention of urine was significantly higher in the group with baseline ACB ≥1 at 4.5% compared to 3.5% in the control group (relative risk [RR]: 1.25; p=0.028). ACB ≥1 was also associated with statistically higher incidence of urinary tract infections which occurred in 9.4% of patients versus 6.3% (RR: 1.50; p<0.001). Cardiovascular complications were also higher in patients with baseline ACB ≥1, including ischaemic heart disease (6.3% versus 3.8%; RR: 1.65; p<0.001), acute coronary syndrome (2.0% versus 1.2%; RR: 1.66; p=0.002), congestive heart failure (2.9% versus 1.7%; RR: 1.66; p<0.001), atrial fibrillation (3.5% versus 2.2%; RR: 1.59; p<0.001), and stroke (4.5% versus 3.4%; RR: 1.32; p=0.006).
This is the first study to report on the clinical importance of baseline anti-cholinergic burden in the treatment of patients with overactive bladder syndrome
The study authors emphasised that this is the first study to report on the clinical importance of baseline anti-cholinergic burden in the treatment of patients with overactive bladder syndrome. The results showed that the ACB score was associated with a higher incidence of urological and cardiovascular complications after initiation of anti-muscarinic drugs. Clinicians should assess the ACB score before starting therapy, especially in older adults or those on multiple medications, to minimise adverse outcomes.
Long-Term Study of Complications of Catheterisable Conduits in Patients with Bladder Exstrophy
NEW research presented at EAU25 evaluated continent catheterisable conduits (CCC) for effective bladder management in patients with bladder exstrophy-epispadias complex (EEC) who often rely on CCCs for effective bladder management.10 The aim was to to evaluate the incidence, timing, and clinical management of complications over an extended follow-up period.
The study was conducted at a specialist urology centre, where the researchers analysed 40 patients with EEC who underwent CCC, with a mean follow-up of 21 years. Most patients (92.5%) also had augmentation cystoplasty. Data on complication types, timing, and outcomes were reviewed using descriptive and Cox regression analyses.
Results showed that complications were common, occurring in 67.5% of patients. Catheterisation difficulties were the most frequent (66.6%), primarily due to distal conduit stenosis often linked with skin issues. Urinary incontinence occurred in one-third of cases, mainly due to bladder overactivity or conduit mechanism failure. Other complications included granulomas (30%) and polyps (22.2%). The median time to onset varied by complication, about 7 years for incontinence, nearly 10 years for stenosis, and over 22 years for polyps. While minimally invasive interventions were effective in 56% of cases, recurrences were common, particularly in stenosis and polyp-related issues.
Catheterisation difficulties were the most frequent (66.6%), primarily due to distal conduit stenosis often linked with skin issues
The results showed that CCCs present a substantial rate of long-term complications in patients with EEC, often emerging a decade or more after the initial procedure. The findings reinforce the necessity of life-long followup and proactive management to address functional decline, prevent recurrence, and preserve patient quality of life.
Results showed that complications were common, occurring in 67.5% of patients
References
1. Wagner MC et al. Long-term patientreported outcomes following urorectal fistula repair post-prostate cancer treatment. Abstract A0001. EAU25, 21-24 March, 2025.
2. Uleri A et al. Active surveillance of grade group 2 prostate cancer: oncological outcomes from a contemporary European cohort. Abstract A0032. EAU25, 21-24 March, 2025.
3. Wheeler LT et al. Barriers to acceptance of an inclusive prostate cancer PROM for sexual and gender minority patients: a narrative synthesis of national datasets. Abstract A0149. EAU25, 21-24 Madrid, 2025.
4. Viswanath K et al. Day care PCNL: who qualifies? Introducing the daycare PCNL checklist. Abstract A0100. EAU25, 21-24 March, 2025.
5. Adriaensen E et al. Long-term recurrence-free survival of urethroplasty and its possible predictors of failure: a retrospective single center analysis. Abstract A0324. EAU25, 21-24 March, 2025.
6. Bianchi L et al. Augmented reality PSMA-PET 3D guided lymph node dissection during robot-assisted radical prostatectomy. Abstract A0533. EAU25, 21-24 March, 2025.
7. Diana P et al. Objective assessment of intraoperative skills for Transurethral Resection of Bladder Tumor (TURBT):
construct validity of Proficiency Based Progression (PBP) training curriculum. A0782. EAU25, 21-24 March, 2025.
8. Aguilera Saiz L et al. Imageguided navigation during robotic surgery using electromagnetic tracking and ultrasound. A0835. EAU25, 21-24 March, 2025.
9. Liu AQ et al. Prediction of OAB treatments' outcomes: on the way to tailored treatment. Abstract A0857. EAU25, 21-24 March, 2025.
10. Osorio Iriarte JC et al. Complications of catheterizable conduits in patients with bladder exstrophy: a long-term study. Abstract A0136. EAU25, 21-24 March, 2025.
LEADING experts gathered at the European Association of Urology (EAU) Congress 2025 to explore the rapidly evolving landscape of prostate cancer screening, calling for risk-adapted, evidence-based strategies amid rising global mortality. From updated EU recommendations to genetic profiling and MRI diagnostics, this important session showcased how ‘smart’ screening can improve early detection, reduce overtreatment, and address healthcare disparities.
NEW HORIZONS IN CANCER SCREENING
Opening the session, Harry de Koning, Erasmus University Medical Centre, Rotterdam, the Netherlands, cited the latest EU cancer screening recommendations from 2022,1 which provide a key step towards improving early cancer detection throughout Europe. The goal was to increase participation in breast, cervical, and colorectal cancer screening programmes in those who qualify, and extend populationbased screening programmes to lung and prostate cancer (PCa). He stressed that cancer screening is necessary to reduce socioeconomic health disparities.
In light of the surge in PCa mortality worldwide, Peter Albers, Heinrich-HeineUniversity, Düsseldorf, Germany, continued that “smart screening is the only way”. Risk-adapted, organised screening for PCa, if started early, will likely detect all relevant cancers, and with personalised riskstratified active surveillance, overtreatment can be avoided. Importantly, he added that baseline prostate-specific antigen (PSA) also works in low-income countries.
Cancer screening is necessary to reduce socioeconomic health disparities
GENETIC MARKERS FOR INITIAL RISK STRATIFICATION
Rosalind Eeles, Royal Marsden NHS Foundation Trust, London, UK, leader in the field of genetic susceptibility to PCa, reminded that audience that 20% of individuals in the general population will have a relative risk >2 for PCa. Genome-wide association studies have now identified a total of 451 single nucleotide polymorphisms (SNP) as genetic risk variants for PCa.2 These common variants contribute to a large proportion of the genetic predisposition to prostate cancer (~44%), while rare germline variants, mostly found in DNA-repair genes, only account for 7%. The remaining 49% of genetic variation is still unknown: this is a significant pitfall for risk stratification.
On one hand, the National Comprehensive Cancer Network (NCCN) Guidelines recommend offering germline testing to men with high-risk localised PCa, metastatic PCa, or who met family history criteria. On the other hand, the European Society for Medical Oncology (ESMO) Guidelines recommend molecular testing for DNA-damage repair gene mutations in all patients with metastatic castrationresistant PCa, regardless of family history or disease burden. However, a negative result for somatic testing does not rule out germline variants, added Eeles. The European Guidelines for germline testing
in PCa recommend germline testing in men with multiple family members diagnosed with PCa <60 years of age or a family member who died from PCa. However, the UK National Testing Directory is slightly different, recommending germline testing for Ashkenazi Jewish ancestry or individuals with ≥1 grandparent from Whalsay, Shetland, as one in 43 have a BRCA2 c.5172A>G mutation.
The difference in founder mutations across the world inevitably leads us to a second pitfall for risk stratification: guidelines may differ significantly depending on populations.
“So, which genes should we test for in a germline test?” asked Eeles. She recommended testing for 10 genes, with a blood test preferred over saliva test: DNArepair genes BRCA1, BRCA2, ATM, CHEK2, and PALB2; mismatch repair genes MSH2, MSH6, MLH1, and PMS2; and the PCaspecific gene HOXB13, found at higher rates in Scandinavian populations. She added that not all mutations in the same gene are the same, and this is the next challenge. For instance, a truncation mutation in ATM has a higher odds ratio for PCa than a missense mutation, which also increases prostate cancer risk but to a lesser extent. Eeles added that another significant pitfall lies in variants of uncertain significance, which may be unrelated to the disease.
The IMPACT study,3 spanning 65 centres and 20 countries, recently provided data
on genetic markers for prostate cancer risk stratification. The study conducted annual targeted PSA screening for BRCA 1/2 and Lynch syndrome mutation carriers, and findings led to the development of EAU guidelines for BRCA2, stating that annual PSA screening should be undertaken from age 40 years. Results also showed that certain gene mutations are associated with more aggressive disease, such as a 77% elevated risk in BRCA2 carriers. Baseline data are currently being collected for Lynch syndrome mismatch repair genes MSH2/6. Eeles emphasised that targeted screening for individuals with monogenic higher-risk mutations is crucial to identify more PCa cases and target those with more aggressive disease.
With regards to common variants, the Prostate Cancer Association Group to Investigate Cancer Associated Alterations in the Genome (PRACTICAL), a large global consortium, has looked at case-control studies of common PCa variations in over 200,000 individuals. Recent data shows that men of African ancestry have a twofold greater lifetime risk for Pca compared to men of European ancestry, and reach this higher risk at an earlier age.2 Eeles highlighted that more diversity is needed in PCa research to tailor risk profiles and screening strategies to different populations.
Moving on to implications for real-world screening, Eeles explained findings from the pivotal BARCODE 1 study,4 which
assessed the feasibility of a communitybased PCa screening programme based on polygenic risk scores (PRS). Saliva samples were collected from healthy males aged ≥55 years across 69 general practices in London, UK. PRS for PCa was calculated by genotyping 130 PCa risk SNPs, and men with PRS above the 90th percentile were invited for prostate MRI and biopsy. A total of 187 PCa cases were identified in this group, with a median age at diagnosis of 64 years, and median PSA at diagnosis of 2.1 ng/mL. A total of 55% of identified cancers had a Gleason score ≥3+4, and 21% needed radical treatment.4 Eeles reinforced that genetic profiling is a valuable tool to risk-stratify populations, and BARCODE 1 suggests that PRS may be useful in population PCa screening programmes.
“We do have the technology, but the implementation needs cheaper tests and education about the promises and pitfalls of genetic markers,” concluded Eeles. Trials incorporating genetic results will also be crucial for individualised care in PCa.
MRI: BEST PRACTICE FOR RISK STRATIFICATION
Veeru Kasivisvanathan, University College London, UK, reinforced the importance of MRI in the initial assessment of PCa. MRI can determine PCa risk and prognosis, guide biopsy decisions, direct targeted prostate biopsies, and determine treatment plans. The 2024 VISION study recently provided Level 1A evidence that a PCa diagnostic pathway with MRI is more favourable than one without.5 “MRI signal through the PI-RADS score is one of the strongest predictors of significant cancer that we have today,” said Kasivisvanathan.
He asked: “What do we do with a negative MRI: does this mean we can avoid a biopsy?” Data have shown that the negative predictive value of MRI in detecting clinically significant PCa is as high as 91%, meaning that it misses, on average, 9% of men with Gleason ≥3+4 PCa.6 Furthermore, prostate volume obtained through MRI allows clinicians to calculate PSA density,
and combining PI-RADS with PSA density can improve MRI performance, allowing men with negative MRI and low clinical risk to safely avoid biopsy. One of the most underappreciated aspects of MRI, continued Kasivisvanathan, is that it is a good predictor of the absence of significant cancer in the medium term, with 98–99% of patients free of Gleason ≥3+4 PCa within 3–5 years. He added that PSA surveillance in these patients is also recommended.
“What about a positive MRI: should we do a systematic biopsy?” continued Kasivisvanathan. He explained key findings from the multicentre MRIFIRST study,7 where men with clinical suspicion of PCa underwent an MRI. If the MRI was suspicious, they underwent targeted systematic biopsy; if it was not suspicious, they underwent a transrectal ultrasound biopsy. In this study, the addition of systematic biopsy increased the detection of Gleason ≥3+4 PCa by 5%, but showed no added benefit for the detection of higher-grade PCa (Gleason ≥4+3).7 With perilesional biopsy gaining increased attention in the last 2 years, Kasivisvanathan cautioned that, while perilesional biopsy slightly increases detection of Gleason ≥3+4 PCa compared to targeted biopsy alone, taking more non-targeted biopsies also raises the risk of detecting more clinically insignificant cancer. He added that, for large PI-RADS 5 lesions, there is often limited value for additional biopsies.
EAU GUIDELINES ON PROSTATE CANCER: WHERE ARE WE GOING?
“We are aiming for timely detection of significant prostate cancer, while leaving insignificant prostate cancer undetected, and balancing diagnostic accuracy with the burden on an individual and healthcare provider,” said Philip Cornford, Chair of EAU Prostate Cancer Guidelines Panel. However, is this achievable?
Current EAU guidelines on prostate cancer screening focus on stratified PSA testing, recommending the use of risk stratification
nomograms before considering MRI. For patients who benefit from MRI, MRI should then drive targeted, perilesional biopsies only, rather than systematic biopsies. PSA testing should always follow thorough counselling on its potential risk and benefits, and should be offered to all men at elevated risk of PCa: men >50 years, men >45 years with a family history of PCa and/ or of African descent, and men >40 years carrying BRCA2 mutations.
“We need to avoid the temptation to find all the cancer that is present,” Cronford continued. Clinicians also need to be aware
References
1. European Commission. European Health Union: Commission welcomes adoption of new EU cancer screening recommendations. 2022. Available at: https://ec.europa.eu/commission/ presscorner/detail/en/ip_22_7548. Last accessed: 1 April 2025.
2. Wang A et al. Characterizing prostate cancer risk through multi-ancestry genome-wide discovery of 187 novel risk variants. Nat Genet. 2023;55(12):2065-74.
3. Page EC et al; IMPACT Study Collaborators. Interim Results from the IMPACT Study: Evidence for Prostate-specific Antigen Screening in BRCA2 Mutation Carriers. Eur Urol. 2019;76(6):831-42.
that MRI-targeted biopsies are associated with grade inflation. Citing recent data, he explained that post-screening radical prostatectomy was only associated with 0.2% mortality reduction at 15 years for patients with Grade Group 1 disease, and ≤5% mortality reduction for patients with Grade Group 2 with lower PSA and stage.8 He reminded the audience that screening is important, but weighing patient benefits and risks should remain a priority to avoid overdiagnosis and overtreatment.
4. Eeles RA et al. Effect of polygenic risk score for clinically significant prostate cancer in a screening program: the BARCODE 1 study results. JCO. 2024;42(16):10500.
5. Kasivisvanathan V et al; VISION Study Collaborators. VISION: An individual patient data meta-analysis of randomised trials comparing magnetic resonance imaging targeted biopsy with standard transrectal ultrasound guided biopsy in the detection of prostate cancer. Eur Urol. 2024;DOI:10.1016/j. eururo.2024.08.022.
6. Sathianathen NJ et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant
prostate cancer in the prostate imaging reporting and data system era: a systematic review and metaanalysis. Eur Urol. 2020;78(3):402-14.
7. Rouvière O et al; MRI-FIRST Investigators. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): a prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019;20(1):100-9.
8. Vickers A et al. Estimating the effect of radical prostatectomy: combining data from the SPCG4 and PIVOT randomized trials with contemporary cohorts. J Urol. 2024;212(2):310-9.
Clinical Decision-Making in Overactive Bladder and Benign Prostatic Obstruction
An expert-led session at the European Association of Urology (EAU) Congress 2025 examined how non-invasive assessment, evidence-based surgical approaches, and predictive strategies can support personalised care and improve outcomes for men with lower urinary tract symptoms (LUTS), benign prostatic obstruction (BPO), and overactive bladder (OAB).
NON-INVASIVE WORKUP OF MALE OVERACTIVE BLADDER
Marcio Augusto Averbeck, Moinhos de Vento Hospital, Porto Alegre, Brazil, began his session by providing a brief background on LUTS, a common complaint in an increasingly ageing male population. The objectives in assessing men with LUTS are to establish a differential diagnosis and define their clinical profile in order to assess patients’ values and preferences, set their expectations, identify those at risk of progression, and provide the best evidence-based care.
To provide a real-life example, Averbeck described a clinical case of a 64-yearold man with a history of benign prostatic enlargement diagnosed 10 years earlier, whose main complaint was mixed LUTS. The patient presented with bothersome urinary urgency, with a urinary frequency of 15 times a day and 2–3 times a night. The patient also had co-morbid systemic arterial hypertension, managed with losartan 50 mg/day.
What Should the Diagnostic Workup for This Patient Be?
Averbeck detailed the EAU guidelines on non-neurogenic LUTS, according to which non-invasive assessments are recommended first. These initial noninvasive assessments include a medical
history, symptom score questionnaire, urinalysis, physical examination, prostatespecific antigen, if the diagnosis of prostate cancer would impact management, and post-void residual (PVR) measurement.
Averbeck recommended using the symptom score questionnaire to assess quality of life, in line with EAU guidelines. He also noted that the bladder diary is strongly recommended, particularly for patients presenting with nocturnal symptoms, and that physical examination and urinalysis are key in the assessment of male LUTS.
Prostate-specific antigen should always be considered in two circumstances: 1) if the diagnosis of prostate cancer will change management, and 2) when it would assist in the treatment and/or decision-making process. Measurement of PVR urine is strongly recommended in the guidelines and should be performed using a noninvasive method. While the EAU guidelines indicate that uroflowmetry has a weak strength rating at initial assessment, it has a high strength rating for patients prior to medical or invasive treatment. Averbeck believes uroflowmetry is key and uses it in his clinical practice routinely. Urethrocystoscopy has a weak strength rating for patients with LUTS; however, should always be considered when a minimally invasive surgical procedure is a treatment option.
Urodynamics
Moving on to urodynamics (UDS) and the publication of the UPSTREAM trial,1 in which the UDS randomised group was noninferior to routine care for the International Prostate Symptom Score (IPSS), but did not reduce the surgical rates. The study showed that the routine use of UDS in the evaluation of uncomplicated LUTS has a limited role and should be used selectively. However, the EAU guidelines highlight factors that should be taken into account when considering urodynamics, which could be useful for patients under 50 and over 80 years old, such as performing UDS when considering invasive treatment in men with bothersome, predominantly voiding LUTS. UDS is also recommended if the voided volume is <150 mL or Qmax<10 mL/s before surgery. Averbeck believes that these are reasonable options and that it is important to map the need for UDS in these situations.
Other non-invasive assessments include ‘surrogates’, where clinicians sometimes use ultrasound or biomarkers to assess the risk of progression and their correlation with the Bladder Outlet Obstruction Index (BOOI). However, the heterogeneity is often
what limits the use of these assessments as routine in clinical practice. Additionally, Averbeck expressed that use of the novel Visual Prostate Symptom Score (VPSS) could be beneficial when uroflowmetry is unavailable, and when the patient has limited literacy.
To conclude, Averbeck circled back to the clinical case, where the patient had an IPSS of 22 points, a digital rectal examination of 35 g with normal consistency and no palpable nodules, Qmax at 11 ml/seg, PVR of 40 ml, and a bladder diary that excluded nocturnal polyuria. According to the EAU guidelines, this patient would fit into medical treatment initially with alpha blocker or PDE5 inhibitor monotherapy, and if after 4–6 weeks, the patient still experienced residual storage symptoms, treatment could involve the addition of anti-muscarinic receptor antagonist/beta3 agonist. In this case, the absence of elevated post-void residual volume and the presence of an adequate Qmax suggest that the patient may be appropriately managed with an anti-muscarinic agent, in line with guideline recommendations for persistent storage symptoms.
WHICH SURGERY IS BEST FOR PATIENTS WITH BENIGN PROSTATIC OBSTRUCTION/ OVERACTIVE BLADDER?
Malet Rieken, University of Basel, Switzerland, began his talk by introducing the current surgical options available for BPO based on the current EAU guidelines, which include resection, vaporisation, enucleation, and various types of alternative ablative techniques, as well as non-ablative techniques. The aim of Rieken’s talk was to determine which surgical option is the best for patients with BPO/OAB.
A closer look at how different techniques affect both symptom relief and obstruction is needed
Surgical techniques vary in how effectively they relieve obstruction, meaning that not all procedures achieve the same degree of de-obstruction in every patient. Rieken then described a systematic review by Creta et al.,2 which grouped patients based on improvements in outlet obstruction and the IPSS, which revealed that the holmium laser enucleation of the prostate (HoLEP) performs very well for both obstruction relief and IPSS improvement. In contrast, transurethral resection of the prostate (TURP) showed solid improvement in IPSS but less impact on obstruction. Laser vapourisation ranked even lower on both metrics, and techniques such as aquablation and UroLift were even further behind.
Therefore, the greater the obstruction relief, the higher the expected IPSS improvement. However, it is important to remember that IPSS doesn’t always equal obstruction, so a closer look at how different techniques affect both symptom relief and obstruction is needed.
Specific Technologies
Considering some specific technologies, Rieken described HoLEP as a therapy that has been associated with a significant reduction in OAB symptoms at 12-month follow-up, with improvements observed
across all age groups. Similar improvements in OAB-related symptoms such as urgency, frequency, nocturia, and IPSS have also been observed in patients undergoing other surgical procedures like TURP, GreenLight laser, or diode laser vaporisation.
Novel Techniques
Rieken continued by describing novel techniques, including aquablation. While there is a lack of specific data on its effect in OAB-dominant patients, IPSS analyses for frequency, urgency, and nocturia show a clear decline over 12 months.
Another notable technique was Rezum, which was featured in an interesting analysis by Wolters et al.3 According to Rieken, the analysis looked at a subgroup of 250 patients, including 19 with urodynamic assessments pre- and post-Rezum due to persistent OAB symptoms. Before surgery, most were clearly obstructed. Postsurgery, 26% still had obstruction, 31% were equivocal, and 42% were unobstructed. Rieken stated that this might explain why there was no significant change in the prevalence of detrusor overactivity in this selected group.
Combined Treatments
Moving onto combined treatments like TURP with botulinum toxin injection, Rieken described an RCT by Huang et al.,4 that compared TURP with an addition of 300 units of Dysport to TURP plus saline in patients with detrusor overactivity, but without urgent urinary incontinence. All patients had a BOOI of over 40. Results showed that the IPSS didn’t significantly differ between groups at 6 months; however urgency incontinence was significantly lower in the TURP + Botox group.
In conclusion, Rieken stressed that while many surgical options improve OAB symptoms, factors like anaesthesia risk, anticoagulation, prostate size, and patient preferences must guide treatment. HoLEP remains the only size-independent technique offering consistent relief, but no single approach suits all, and high-level evidence for OAB- or detrusor overactivitydominant cases remains limited.
HOW TO PREDICT PERSISTENT
OVERACTIVE BLADDER AFTER BENIGN PROSTATIC OBSTRUCTION SURGERY
Sanjay Sinha, Apollo Hospital, Hyderabad, India, began by explaining that most patients undergoing surgery for BPO present with a combination of voiding and storage symptoms. Importantly, it is often the storage symptoms, such as urgency and frequency, that prompt patients to seek medical consultation, and many ultimately undergo surgery because these symptoms significantly affect their quality of life. Fortunately, most patients who undergo BPO surgery experience an improvement in storage symptoms, and this improvement contributes significantly to their postoperative quality of life. Therefore, predicting whether a patient will benefit in this way is important for preoperative counselling.
Holmium laser enucleation of the prostate remains the only size-independent technique offering consistent relief
How Common is Persistent Overactive Bladder After Surgery?
Many patients undergoing surgery for BPO present with storage symptoms, and, while a significant proportion experience improvement postoperatively, a notable number may continue to have persistent or new symptoms over time. Long-term follow-up studies have also suggested that some patients may eventually require OAB medication after surgery.
What Are the Mechanisms Behind Persistent Symptoms?
Sinha emphasised that in order to better predict persistent OAB, it is important to understand why these symptoms might persist. Although the current evidence is not entirely robust, some conceptual mechanisms exist; for example, a common underlying factor, such as bladder ischaemia, could be driving both storage and voiding symptoms. Other potential mechanisms could include inadequate obstruction relief due to an incomplete procedure or a suboptimal surgical technique; postoperative underactive detrusor may also cause inefficient voiding that manifests as storage symptoms; and bladder wall changes due to longstanding obstruction may persist after surgery. Notably, patients with a known neurological condition are more likely to experience persistent symptoms.
Sinha highlighted that higher preoperative urgency scores and normal detrusor contractility are linked to better OAB symptom resolution after BPO surgery. In contrast, longer symptom duration, psychological comorbidities, and absence of obstruction may increase the risk of persistence. Although certain patterns of detrusor overactivity (DO) may play a role, evidence remains inconclusive, and the UPSTREAM trial1 showed that in men with DO, urodynamic indices like the BOOI and Detrusor Contractility Index (DCI) lose predictive value.
What Predicts the Resolution of Overactive Bladder?
Two strong predictors are unequivocal obstruction and normal detrusor contractility. Patients with both of these are more likely to see improvement in their OAB symptoms after surgery. However, the UPSTREAM study1 suggested that in the presence of DO, these predictors lose their value. Although, it is still unclear whether this applied to total IPSS or specifically to storage symptoms.
What Predicts Persistent Overactive Bladder?
Some predictors include: older age, possibly longer symptom duration, psychological comorbidities, severe preoperative storage symptoms, and early-onset DO, high-
References
1. Young et al. Prostate surgery for men with lower urinary tract symptoms: do we need urodynamics to find the right candidates? Exploratory findings from the UPSTREAM Trial. 2022;8(5):1331-5.
2. Creta M et al. Bladder outlet obstruction relief and symptom
pressure DO, or terminal DO. However, Sinha stressed that the mere presence of DO may not be a predictor of poor outcomes in itself.
CONCLUSION
To close the session, Sinha reminded the audience that persistent OAB following BPO is relatively common, but predictive tools, especially invasive urodynamics, are not routinely used.
These insightful presentations highlighted the importance of tailoring treatment strategies for male OAB and BPO, emphasising the role of patient-specific assessment, guideline-driven decisionmaking, and the need for stronger predictive tools to guide long-term management.
improvement following medical and surgical therapies for lower urinary tract symptoms suggestive of benign prostatic hyper-plasia: a systematic review. Eur Urol. 2024;86:315-26.
3. Wolters M et al. Real-world experience of water vapour therapy (Rezum) in patients with be-nign prostatic enlargement: a retrospective single-
center study. Prostate Cancer Prostatic Dis. 2025;28(1):160-6.
4. Huang MM et al. Intradetrusor OnabotulinumtoxinA injections at the time of holmium laser enucleation of the prostate for men with severe storage symptoms. J Endourol. 2023 Jul;37(7):801-6.
EAU 2025
Abstract Reviews
Drawing on insights from the European Association of Urology (EAU) Congress 2025, these abstract reviews spotlight notable new advancements and key focuses in the field of urology.
Prostate Assessment using Comparative Interventions – Fast MRI and Image-fusion for Cancer (IP7-PACIFIC): A Prospective,
Francesca Rawlins,1 Emma Cullen,1 Natalia Klimowska-Nassar,1,3 Thiagarajah Sasikaran,1,3 Puja Jadav,3 Heminder Sokhi,4,5 Andrew Smith,6 Darren Walls,7 Robert Oldroyd,8 Derek Price,8 Clare Robinson,9 Emily Lane,9 Andrea Rockall,10 Rakesh Heer,1,2 Luke Vale,11 Anwar R. Padhani,4,5 Mathias Winkler,1,2 Taimur T. Shah,1,2 Rhian Gabe,9 Hashim U. Ahmed1,2
1. Division of Surgery, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, UK
2. Department of Urology, Imperial College Healthcare National Health Service (NHS) Trust, London, UK
3. Imperial Clinical Trials Unit, School of Public Health, Imperial College London, UK
4. The Hillingdon Hospitals NHS Foundation Trust, London, UK
5. Paul Strickland Scanner Centre, Mount Vernon Hospital, Northwood, UK
6. Department of Pathology, Imperial College Healthcare NHS Trust, London, UK
7. Institute of Nuclear Medicine, University College London, UK
8. Patient and Public Involvement Co-Lead, Prostate Cancer UK, London, UK
9. Centre for Evaluation and Methods, Wolfson Institute of Population Health, Queen Mary University of London, UK
10. Division of Cancer, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, UK
11. Global Centre for Health Economics, London School of Hygiene and Tropical Medicine, UK
*Correspondence to n.mayor@imperial.ac.uk
Disclosure: Gabe and Ahmed share joint-senior authorship. The authors have declared no conflicts of interest.
Acknowledgements: The study was funded by Cancer Research UK (Early Detection and Diagnosis Committee, ref A30065) and was prospectively registered on ISRCTN (11171089).
The authors would like to thank all patients who have consented to take part in IP7-PACIFIC.
Multiparametric MRI (mpMRI) with contrast medium is recommended in the prostate cancer diagnostic pathway.1,2 It is unclear if MRI without contrast medium (biparametric [bp]) can be used instead whilst remaining sensitive to the detection of clinically significant cancers.3 Additionally, for those with a positive MRI, is image-fusion targeting better than visual-registration (cognitive) targeting in detecting clinically significant prostate cancer?4 And does bpMRI represent better value for money than mpMRI? A randomised controlled trial testing the clinical utility and costeffectiveness of these approaches is vital before changes in practice.
METHODS
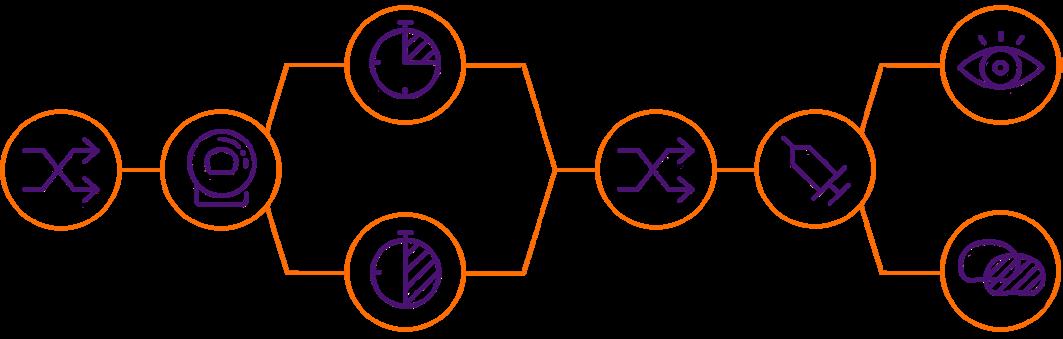
IP7-PACIFIC is a prospective, multicentre, co-enrolment trial with two randomisations and embedded economic evaluation (Figure 1). The first randomisation will evaluate non-inferiority of bpMRI compared to mpMRI in those with clinical suspicion of prostate cancer. Men with a suspicious MRI will undergo a second randomisation to evaluate if image-fusion targeting is superior to standard visual-registration targeted biopsy. Ethics committee approval has been granted by the London Bromley Research Ethics Committee.
1: Study schema.
15–20
MINUTES
RANDOMISE MRI BIOPSY
30–40
MINUTES
RANDOMISE
3,600 patients referred by their GP with a high PSA
Patients undergo a short duration MRI or long duration MRI
GP: general practitioner; PSA: prostate-specific antigen.
RESULTS
The primary objective for Randomisation 1 is to determine the non-inferiority of bpMRI to detect Gleason score ≥7 cancer (International Society of Urological Pathology Grade Group [GG] ≥2) compared to mpMRI. The objective for Randomisation 2 is to determine if image-fusion targeted biopsy is superior to visual-registration targeted biopsy for GG ≥2 cancer detection. An internal pilot phase will enrol 700 patients; the overall recruitment target is 2,600–3,600 pending interim analysis.
DISCUSSION
IP7-PACIFIC aims to provide randomised comparative evidence for the clinical utility and cost-effectiveness of using bpMRI and image-fusion biopsy. The findings will inform guidelines. The sequential randomised co-enrolment design allows simultaneous evaluation of two research
Patients with a suspicious MRI continue to biopsy
VISUAL REGISTRATION
IMAGE FUSION
Patients undergo a visual registration biopsy or image fusion biopsy
questions and avoids heterogeneity of trial populations. By contrast to previous pairedcohort studies, the randomised design will reduce reporter bias, providing the highest level of diagnostic evidence.
References
1. Mayor N et al. Prostate Assessment using Comparative Interventions – Fast MRI and Imagefusion for Cancer (IP7-PACIFIC): A prospective, multi-centre, dual sequential randomised controlled trial. Abstract A0074. EAU25, 21-24 March, 2025.
2. EAU. Prostate cancer- diagnostic evaluationuroweb. Available at: https://uroweb.org/guidelines/ prostate-cancer/chapter/diagnostic-evaluation. Last accessed: 1 March 2025.
3. Woo S et al. Head-to-head comparison between biparametric and multiparametric MRI for the diagnosis of prostate cancer: a systematic review and meta-analysis. AJR Am J Roentgenol. 2018;211(5):W226-41.
4. Hamid S et al. The SmartTarget Biopsy trial: a prospective, within-person randomised, blinded trial comparing the accuracy of visual-registration and magnetic resonance imaging/ultrasound image-fusion targeted biopsies for prostate cancer risk stratification. Eur Urol. 2019;75(5):733-40.
Figure
A Phase I/II Study of Detalimogene Voraplasmid Intravesical Monotherapy for Patients with High-Risk Non-Muscle Invasive Bladder Cancer
Authors: *Félix Guerrero-Ramos,1 Sam S. Chang,2 Rian J. Dickstein,3 Gautam Jayram,4 Scott Johnson,5 Shreyas Joshi,6 Jen-Jane Liu,7 Yair
Lotan,8 Gautier Marcq,9 Raj Satkunasivam,10 Anne Schuckman,11 Gary Steinberg,12 John Taylor,13 Tammy Linback,14 Raj Pruthi,14 Anthony Cheung,14 Christine Tosone,14 Ashish M. Kamat,15 Juan Palou16
1. Hospital Universitario 12 de Octubre, Madrid, Spain
2. Vanderbilt University, Nashville, Tennessee, USA
3. Chesapeake Urology, Hanover, Maryland, USA
4. Urological Associates P.C., Nashville, Tennessee, USA
5. Medical College of Wisconsin, Milwaukee, Wisconsin, USA
6. Emory University School of Medicine, Atlanta, Georgia, USA
7. Oregon Health & Science University, Portland, USA
8. University of Texas Southwestern Medical Center, Dallas, USA
9. Hospital Center University De Lille, France
10. Weill Cornell Medical College, Houston, Texas, USA
11. University of Southern California, Los Angeles, USA
12. RUSH University Medical College, Chicago, Illinois, USA
13. University of Kansas Cancer Center, Kansas City, USA
14. enGene Inc., Waltham, Massachusetts, USA
15. University of Texas MD Anderson Cancer Center, Houston, USA
16. Fundación Puigvert, Barcelona, Spain
*Correspondence to felixguerrero@gmail.com
Disclosure: This study was funded by enGene. Please click here for a full list of author disclosures.
High-risk, non-muscle-invasive bladder cancer (NMIBC) is generally treated with intravesical Bacille Calmette-Guérin (BCG); however, ~50% of patients experience recurrence and/or progression after BCG and are considered unresponsive.1 Detalimogene voraplasmid (EG-70) is an investigational, intravesically administered, non-viral gene therapy designed to elicit local stimulation of anti-tumour immune responses in the bladder and drive durable efficacy in BCG-unresponsive NMIBC, while mitigating the risk of systemic toxicities from immune stimulation. The Phase I portion of the open-label, multicentre LEGEND trial identified the selected dose for Phase II, which was generally well tolerated with an overall complete response (CR) rate of 73%.2 Here, the authors describe the ongoing Phase II portion of the trial, which is open to enrolment; where a new cohort of papillary-only (no carcinoma in situ [CIS]) disease is being included.
MATERIALS AND METHODS
The aim of the single-arm, open-label, Phase II portion of LEGEND (NCT04752722)3 is to evaluate the efficacy and safety of the identified Phase II dose in patients with high-risk NMIBC. Selected eligibility criteria: age ≥18 years; Eastern Cooperative Oncology Group (ECOG) performance status 0−2; with/without resected coexisting papillary tumours, ineligible for, or elected not to undergo, cystectomy; and satisfactory bladder function. Patients receive detalimogene 0.8 mg/mL in 50 mL by intravesical administration at Weeks 1, 2, 5, and 6 of a 12-week cycle for 4 cycles; patients with CR at the end of the 4th cycle enter maintenance treatment (2 instillations per cycle, at Weeks 1 and 2 for up to 8 cycles)in three cohorts: BCG-unresponsive with CIS ± papillary disease (Cohort 1); BCG-naïve (Cohort 2a) and BCG-exposed
(Cohort 2b) with CIS ± papillary disease; and BCG-unresponsive with high-grade papillary bladder cancer without CIS (Cohort 3).
The Phase II primary endpoints are efficacy (CR rate at Week 48) and safety. Secondary endpoints include: progression free survival; CR rate at Weeks 12, 24, 36, and 96; duration of response; and quality of life. The trial is being conducted in accordance with the ethical principles of the Declaration of Helsinki and is consistent with International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) good clinical practice(GCP). All patients provide written informed consent. The ongoing Phase II portion of the trial will recruit up to
300 patients, with sites planned in the USA, Canada, Europe, and the Asia-Pacific region.
References
1. Guerrero-Ramos F et al. A Phase 1/2 study of detalimogene voraplasmid (EG-70) intravesical monotherapy for patients with high-risk nonmuscle invasive bladder cancer – Trial in progress. Abstract A0081. EAU25, 21-24 March, 2025.
2. Kalota S et al. P2-08 LEGEND: A phase 1/2 study of EG-70 (Detalimogene Voraplasmid), a novel, non-viral intravesical gene therapy for patients with BCG-unresponsive non-muscle invasive bladder cancer with carcinoma in situ (CIS). J Urol. 2024;211(5S2):e5.
3. enGene, Inc. LEGEND study: EG-70 in NMIBC patients BCG-unresponsive and high-risk NMIBC incompletely treated with BCG or BCG-naïve. NCT04752722. https://clinicaltrials.gov/study/ NCT04752722?term=NCT04752722&rank=1.
Patient Satisfaction and Quality of Life in Long-Term Urinary Catheter Users in the Netherlands: A Nationwide Survey Study
Authors: *Coen Christiaans,1 Felice van Veen,1 Bertil Blok1
1. Erasmus MC, Rotterdam, the Netherlands *Correspondence to c.christiaans@erasmusmc.nl
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank JR Scheepe.
In recent decades, the use of urinary catheters in the Netherlands has substantially increased.1,2 Because of the ageing population, the prognosis is that this number will only rise.3 To improve the standard of care, it is important to know more about the catheter users in the Netherlands and their perspective on urinary catheters.
OBJECTIVE
To identify patient satisfaction and quality of life (QoL) in long-term (>6 months) urinary catheter users in the Netherlands.
METHODS
A cross-sectional study was conducted from August–September 2024 at the urology department of Erasmus MC Rotterdam. Patients who perform clean
intermittent catheterisation (CIC), or have an indwelling catheter (IDC), or a suprapubic catheter (SPC), were identified through the MediReva database, a Dutch medical specialty supplier. The survey consisted of a validated questionnaire (ICIq-LTCqol) and the EuroQol-5 Dimensions-5 Levels (EQ-5D-5L).
RESULTS
The survey was sent to 10,109 patients. Patients who completed at least 50% of the questionnaire were included in the study, resulting in a total of 3,320 participants (response rate 33%). Among them, 2,634 (79.3%) patients performed CIC, 383 (11.5%) had an IDC, and 303 (9.1%) had an SPC. In this study, 75.9% were male, the mean age was 72 years, and 19.2% had a urinary catheter because of a neurogenic problem.
There was no difference in urinary tract infection (UTI) incidence between the different groups. However, haematuria and bladder stone incidence were lower in the CIC group. Catheter function and concern scores were significantly lower in CIC patients compared to IDC and SPC patients. The lifestyle impact score was significantly lower in CIC patients compared to IDC and SPC patients, and in SPC compared to IDC patients. The EQ-5D-5L health value was significantly higher in CIC patients compared to IDC and SPC patients, and in SPC compared to IDC patients.
When corrected for multiple confounders, IDC and SPC were independently associated with lower patient satisfaction and QoL scores. The multivariate regression is shown in Table 1.
Table 1: Multivariate regression of the different patient satisfaction and EQ-5D-5L scores.
This is the largest study to date to compare patient satisfaction and QoL in different long-term urinary catheter users. IDC and SPC are related to lower patient satisfaction and (perceived) QoL and higher catheter-related complications. Therefore, CIC is strongly preferred over IDC and SPC for assisted bladder drainage if the patient is able to perform CIC. Healthcare providers should be aware of the impact of assisted bladder drainage. When selecting a type of catheterisation, the differences should be discussed using shared decision-making.
References
1. Christiaans C et al. Patient satisfaction and quality of life in long-term urinary catheter users in the Netherlands: a nationwide survey study. Abstract A0178. EAU25, 21-24 March, 2025.
2. Berendsen SA et al. Trends in the use and costs of intermittent urinarycatheters in the Netherlands from 1997 to 2018: a populationbased observational study. Neurourol Urodyn. 2021;40(3):876-82.
3. Fortune Business Insights. Europe urinary catheters market size, share & COVID-19 impact analysis, by product (indwelling catheters, intermittent catheters, and external catheters), by application (urinary incontinence, benign prostatic hyperplasia, surgery, and others), by gender (male and female), by end-user (hospitals, age care centers, and others), and regional forecast, 2023-2030. Available at: https://www.fortunebusinessinsights. com/enquiry/request-sample-pdf/europe-urinarycatheters-market-101442. Last accessed: 21 February 2025.
Active Surveillance in a Prostate Cancer Screening Trial in Young Men: Interim Results from the PROBASE Trial
Authors: Maxime De Vrieze,1 Rouvier Al-Monajjed,2 Jale Lakes,2 Kathleen Herkommer,3 Jürgen E. Gschwend,3 Lilly J. Schmalbrock,3 Markus Kuczyk,4 Nina N. Harke,4 Jürgen Debus,5
Christoph A. Grott,5 Lisa-Marie Stertz,5 Glen Kristiansen,6 Lars Schimmöller,7 Gerald Antoch,8 Frederik Giesel,9 Christian Arsov,10 Boris Hadaschik,11 Axel Benner,12 Agne Krilaviciute,1
Petra Seibold,1 Rudolf Kaaks,13 Nikolaus Becker,1 *Peter Albers1,2
1. Division of Personalized Early Detection of Prostate Cancer, German Cancer Research Center (DKFZ), Heidelberg, Germany
2. Department of Urology, University Hospital Düsseldorf, Medical Faculty, Heinrich-Heine University, Germany
3. Department of Urology, Klinikum rechts der Isar, School of Medicine and Health, Technical University of Munich, Germany
4. Department of Urology, Hannover Medical School, Germany
5. Department of Radiation Oncology, Heidelberg University Hospital, Ruprecht Karls University Heidelberg, Germany
6. Institute of Pathology, University of Bonn, University Hospital Bonn, Germany
7. Department of Diagnostic, Interventional Radiology and Nuclear Medicine, Marien Hospital Herne, University Hospital of the Ruhr-University Bochum, Germany
8. Department of Diagnostic and Interventional Radiology, University Hospital Düsseldorf, Medical Faculty, Heinrich-Heine University, Germany
9. Department of Nuclear Medicine, University Hospital Düsseldorf, Medical Faculty, Heinrich-Heine University, Germany
10. Department of Urology and Paediatric Urology, ElisabethKrankenhaus Rheydt, Städtische Kliniken Mönchengladbach, Germany
11. Department of Urology, University Hospital Essen, University of Duisburg-Essen, Germany
12. Division of Biostatistics, German Cancer Research Center (DKFZ), Heidelberg, Germany
13. Division of Cancer Epidemiology, German Cancer Research Center (DKFZ), Heidelberg, Germany
*Correspondence to p.albers@dkfz-heidelberg.de
Disclosure: Hadaschik has grants from DFG, Novartis, BMS, Janssen, and Amgen; royalties or licenses from Uromed; consulting fees from Janssen, Bayer, Novartis, BMS, ABX, Merck,
Onkowissen, Accord Healthcare, AstraZeneca, MSD/Pfizer, Amgen, Astellas, Lightpoint Medical, Point Biopharma, Ipsen, and Telix; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen, Amgen, Astellas, Monrol, and Novartis; support for attending meetings and/or travel from Janssen, AstraZeneca, Bayer, BMS, Ipsen, and Amgen; participation on a Data Safety Monitoring Board or Advisory Board with Janssen, ABX, Telix, and Novartis; leadership or fiduciary role in other board, society, committee, or advocacy group, paid or unpaid from DGU. The other authors have declared no conflicts of interest.
Acknowledgements: Published on behalf of the PROBASE study group and investigators.
Keywords: Active surveillance (AS), prostate cancer (PCa), risk-adapted screening.
The German PROBASE trial is an ongoing, randomised, risk-adapted prostate cancer (PCa) screening trial that primarily evaluates the start of prostate-specific antigen (PSA)based screening at 45 versus 50 years.1-3 Active surveillance (AS) is a treatment option that may reduce treatment-related harms in clinically insignificant screendetected PCa, especially in younger men.4 In this analysis, the authors present the first interim results of AS as a treatment modality within PROBASE.
MATERIALS AND METHODS
Basic descriptive statistics were used to report treatment choices and outcomes. A Kaplan–Meier time-to-event analysis was performed to analyse the rate of AS discontinuation. Since the start of the study in 2014, 364 PCa cases out of 46,495 PROBASE participants were registered at the time of data extraction (October 1, 2024). This analysis was limited to International Society of Urological Pathology (ISUP)
Grade Group (GG) 1 (n=83) and 2 (n=158) PCa cases with available first-line treatment data. For the Kaplan–Meier analysis, participants who either withdrew from the study (n=2) or were lost to follow-up (n=14) after the start of AS were excluded.
RESULTS
The median age at PCa diagnosis was 50 years (interquartile range [IQR]: 47–51).
A total of 91 patients started AS, including 72% of men diagnosed with ISUP GG 1 PCa (n=60). The remainder of ISUP GG 1 and 2 patients (n=150) underwent up-front radical prostatectomy (RP) or radiotherapy. Figure 1 shows the course of AS over time since the start of the AS protocol. The median time on AS was 41.2 months. In 85% (95% CI: 74.9–96.1%), 60% (95% CI: 45.3–78.8%), and 40% (95% CI: 24.2–65.1%) of men, AS delayed definitive treatment for at least 2, 3, and 4 years, respectively. So far, 19 patients have discontinued AS, with a median time to radical treatment of 24 months (IQR: 15–33; range 7–46). Importantly, of 13 patients with documented repeat biopsy prior to AS discontinuation, only seven had histological tumour upgrading (≥ISUP GG2 with >10% Gleason pattern 4) as a hard criterion for AS discontinuation.
Few of the 13 cases with available RP pathology reports had adverse pathological outcomes (R1: 3/13, pT3-4: 1/13, pN1: 0/13, ISUP GG 3–5: 0/13) at RP after AS discontinuation. After RP, 12 of 14 patients had a complete PSA response and remained free of biochemical recurrence with a median follow-up of 25.5 months (IQR: 13.5–35.4; range 5.3–66.5).
CONCLUSION
In PROBASE, AS deferred definitive treatment in half of the young men with low-risk and favourable intermediate-risk screen-detected PCa by nearly 3.5 years or longer, with acceptable short-term oncological outcomes after RP following AS discontinuation.
Figure 1: Course of active surveillance for International Society of Urological Pathology Grade Group 1 and 2 prostate cancer in PROBASE.
AS: active surveillance.
References
1. De Vrieze M et al. Active surveillance in a prostate cancer screening trial in young men: interim results from the PROBASE trial. A0023. EAU25, 21-24 March, 2025.
2. Arsov C et al. Prospective randomized evaluation of risk-adapted prostate-specific antigen screening in young men: the PROBASE trial. Eur Urol. 2013;64(6):873-5.
3. Arsov C et al. A randomized trial of risk-adapted screening for prostate cancer in young men—results of the first screening round of the PROBASE trial. Int J Cancer. 2022;150(11):1861-9.
4. Hamdy FC et al. Fifteen-year outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2023;388(17):1547-58.
Ureteral Stenting with Flexible Cystoscope Under Local Anaesthesia in an Outpatient Setting: Feasibility, Safety, Patient Satisfaction, and Lessons Learnt from European Prospective Study
Authors: Michele Rizzo,1 *Federico Zorzi,1 Fabio Traunero,2 Victoria Jahrreiss,3 Andrea Piasentin,1 Paolo Umari,1 Bhaskar Somani,4 Giovanni Liguori,1 Amelia Pietropaolo4
1. University of Trieste, Department of Urology, Italy
2. University of Udine, Department of Urology, Italy
3. Comprehensive Cancer Center, Medical University of Vienna, Austria
4. University Hospital Southampton NHS Trust, UK
*Correspondence to federicozorzi94@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Ureteral double J (DJ) stent placement and replacement are common urological procedures,1 typically performed in the operating room under general or locoregional anaesthesia.2 The advent of single-use cystoscopes has enhanced the manoeuvrability and efficiency of endourological procedures.3,4 Therefore, elective DJ stenting could benefit from a modified approach to reduce patient medicalisation and the number of surgical interventions.5 This study aimed to evaluate the feasibility, safety, and patient satisfaction of DJ ureteral stenting using a flexible, disposable cystoscope under local anaesthesia (LA).
MATERIALS AND METHODS
The authors analysed prospectively collected data from all patients who
underwent DJ stent insertion or replacement using a flexible, single-use cystoscope under LA between February 2022–April 2024 at two tertiary referral centres in Italy and England. Technical failure was defined as the inability to complete the scheduled procedure for positioning or replacing the ureteral stent. A visual analogue scale (VAS) was used for pain scores (range: 0–10, where 10 represented worst pain experienced). Patient satisfaction with the procedure and willingness to undergo future LA ureteral stenting were also inquired.
RESULTS
A total of 177 consecutive procedures were performed, comprising: unilateral stent changes (n=122; 68.9%), unilateral stent insertion (n=22; 12.4%), bilateral stent changes (n=28; 15.8%), and bilateral stent placements (n=5; 2.8%). The median age, Charlson Comorbidity Index, and hospital stay were 76 years (interquartile range [IQR]: 66–80), 8 (IQR: 6–12), and 0 days (IQR: 0–1), respectively (Table 1). Technical failure occurred in 13 (7.3%) cases (11 stent changes and two stent insertions). These failures were due to stent encrustation, unpassable ureteral strictures, or abnormal ureteral orifice anatomy due to malignancy, and were successfully managed by percutaneous nephrostomy or stent insertion under sedation. Complications included one Clavien-Dindo Grade III (0.56%) case of stent migration, which required ureteroscopy for repositioning, and 10 Clavien-Dindo Grade II (5.6%) cases of urinary infection. Overall, 88.1% (n=156) of patients were satisfied with LA ureteral stenting, and 89.8% (n=159) indicated they would be willing to undergo further LA ureteral stenting.
Table 1: Demographic features of the study population and their satisfaction with the procedure.
CONCLUSION
Results demonstrate that DJ stenting with a flexible dispensable cystoscope under LA in an outpatient setting is a feasible, safe, and well-tolerated procedure, even among elderly patients with multiple comorbidities. The procedure has a high success rate with low risk of minor complications. The risk of failure is associated with complex anatomy due to underlying pathologies or device encrustation. This approach enhances clinical efficiency, reduces anaesthesiarelated risks, and may offer significant cost savings for healthcare systems.
References
1. Finney RP. Experience with new double J ureteral catheter stent. J Urol. 1978;120(6):678-81.
2. Cousins J et al. Principles of anaesthesia in urological surgery. BJU Int. 2005;96(2):223-9.
3. Scotland K et al. Evaluation of a singleuse flexible cystoscope: a multiinstitutional international study. J Endourol. 2020;34(9):981-6.
4. Chen R et al. Time efficiency and performance of single-use vs reusable cystoscopes: a randomized benchtop and simulated clinical assessment. J Endourol. 2024;38(1):53-9.
5. Rizzo M et al. Ureteral stenting with flexible cystoscope under local anaesthesia in outpatient setting: feasibility, safety, patient satisfaction and lessons learnt from European prospective study. Abstract A0649. EAU25, 21-24 March, 2025.
Lower urinary tract symptoms (LUTS) in men are a growing problem as more men age. For a urological evaluation of LUTS in men, the International Prostate Symptom Score (IPSS) is the most frequently used questionnaire worldwide.1 The IPSS is intended to convert subjective symptoms into quantitative values, with questions on storage symptoms, irritative symptoms, and quality of life. The IPSS-scores are used for diagnosis, treatment choices, and evaluation of results.
However, several studies have shown problems regarding the completion of the IPSS.2,3 Self-completion resulted in an incomplete questionnaire in 53–73% of men.4,5 This, as well as poorer accuracy of symptom representation when completing the IPSS, was especially true for lower levels of education.6-8
A partner or another family member can provide an inexpensive and uncomplicated solution for assisting questionnaire completion. However, the question is: what if the patient himself cannot provide input? This study investigates the reliability of IPSS for men with LUTS when filled out by the ones closest to them: their partners.
MATERIALS AND METHODS
The study received approval from the local ethics committee. A power of 34 was calculated, and 43 couples were included. Men over 50 years of age attending the urology outpatient clinic were asked to participate. After approval, the individual and their partner were asked to separately fill out the IPSS for the man's complaints. If the man came to his appointment alone, after approval, the partner (relationship >1 year, at least 3 nights a week together) was called to answer the questions by phone. Individual questions, total scores, and subscores (obstructive and irritative) were compared. For statistics, Pearson and Spearman correlation, Bland-Altman plotting, and Kappa were calculated in SPSS version 25.0.
RESULTS
A Pearson and Spearman correlation between patients' and partners' total scores proved 0.62 and 0.61, respectively. Bland-Altman plotting showed substantial spread, and Kappa was 0.162 (slight). As men had higher scores, partners tended to score higher as well. As shown in Table 1, 20 couples (46.5%) scored the patient’s symptoms in the same severity category (mild [n=5], moderate [n=23], and severe [n=15]); 22 (51.2%) differed in one category; and one couple (2.3%) differed in two categories. Partners tended to slightly overscore, and therefore, seemed only moderately able to assess true symptom severity. Even for quality of life, partners proved only modestly reliable (Kappa 0.192). The irritative subscore proved slightly better assessed than the storage subscore, mainly because of the question on nocturia, which showed a fair correlation with a Kappa of 0.367.
CONCLUSION
For the first time, a study was performed in which the IPSS scores of male LUTS was completed by their partners. Partners were found to be only modestly able to reliably replace their husbands. Considering that the sudden request for partners to fill out the form does not conform to the reality where the questionnaire is sent in advance, the partner’s result in that situation may be better than the result tested in the authors’ study. If the IPSS is not sufficiently understood, another instrument could possibly be used, as shown in previous research.3,9 With an increase in men dependent on caregivers, especially those who are not as close as the spouses tested in this study, a reliable alternative assessment of symptoms by others is desirable.
Table 1: Correlation between International Prostate Symptom Scores completed by the patient himself and the scores completed by the partner on the male lower urinary tract symptoms.
References
1. Schlatmann FWM et al. How well can women assess their partner’s urinary symptoms? An IPSS-based study. Abstract A0892. EAU25, 21-24 March, 2025.
2. Olcücu MT et al. Comparison of a visual prostate symptom score and international prostate symptom score: a prospective multicenter study and literature review. Urology. 2020;146:230-5.
3. Schlatmann FWM et al. How do patients understand questions about lower urinary tract symptoms? A qualitative study of problems in completing urological questionnaires. Int J Environ Res Public Health. 2022;19(15):9650.
4. Cam K et al. The efficacy of an abbreviated model of the International Prostate Symptom Score in evaluating benign prostatic hyperplasia. BJU Int. 2003;91(3):186-9.
5. Van der Walt CL et al. Prospective comparison of a new visual prostate symptom score versus the International Prostate Symptom Score in men with lower urinary tract symptoms. Urology. 2011;78(1):17-20.
6. Ceylan Y et al. Is new visual prostate symptom score useful as International Prostate Symptom Score in the evaluation of men with lower urinary tract symptoms? A prospective comparison of 2 symptom scores in Turkish society. Urology. 2015;85(3):653-7.
7. Taneja Y et al. Comparison of Visual Prostate Symptom Score and International Prostate Symptom Score in the evaluation of men with benign prostatic hyperplasia: a prospective study from an Indian population. Prostate Int. 2017;5(4):158-61.
8. Johnson TV et al. Patient misunderstanding of the individual questions of the American Urological Association symptom score. J Urol. 2008;179(6):2291-4.
9. Schlatmann FWM et al. Developing a new urology questionnaire from the patient’s perspective. Inf Des J. 2025;29(2):92-107.
Reasons for Discontinuation of Active Surveillance in Men with Grade Group 1 and Grade Group 2 Prostate Cancer in the PRIAS Study
Authors: *Jeroen Lodder,1 Sebastiaan Remmers,1
Cristina Marenghi,2 Roderick van den Bergh,3 Francisco Lozano-Urunuela,4 Markus Graefen,5 Antti Rannikko,6 Frederic Staerman,7 Mikio Sugimoto,8 Rik Somford,9 Ivo de Vos,1 Pim van Leeuwen,10 Monique Roobol,1 the PRIAS consortium
1. Erasmus Medical Center, Rotterdam, the Netherlands
2. Fondazione IRCCS Instituto Nazionale dei Tumori, Milan, Italy
3. Sint Franciscus Hospital, Rotterdam, the Netherlands
4. Hospital Universitario de Navarra, Pamplona, Spain
5. Martini Klinik, Hamburg, Germany
6. Helsinki University Hospital, Finland
7. Polyclinique Reims-Bezannes, France
8. Kagawa University, Takamatsu, Japan
9. Canisius Wilhelmina Hospital, Nijmegen, the Netherlands
10. Antoni van Leeuwenhoek Hospital, Amsterdam, the Netherlands
*Correspondence to j.lodder@erasmusmc.nl
Disclosure: Marenghi has held a leadership or fiduciary role for Europa Uomo Italia. Rannikko has received academic research grants from State Research Funding (VTR) of HUS Helsinki University Hospital, Cancer Foundation Finland, Academy of Finland, and the Jane and Aatos Erkko Foundation, Finland; consulting fees from Janssen, Orion, Accord Healthcare, and Nanoform; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen, Orion, and Accord Healthcare; and held board membership for the Ida Montin Foundation and the Orion Research Foundation. Remmers has received support for the present manuscript for analysis and interpretation of data, critical revision for important intellectual content, and statistical analysis. Somford has received grants or contracts from any entity from the Dutch Cancer Society, Besins, Janssen, and AstraZeneca; consulting fees from Bayer, Janssen, and Blue Earth Diagnostics; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Mayumana; support for attending meetings and/or travel from Bayer and Pfizer; and has held leadership or fiduciary role for the Dutch Uro-Oncology Study Group and the Dutch Urological Association. Suigimoto has received payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from AstraZeneca, Novartis, Astellas, Janssen, and Takeda. The other authors have declared no conflicts of interest.
Keywords: Active surveillance (AS), disease progression, prognosis, prostate cancer (PCa).
Active surveillance (AS) is the preferred management strategy for low-risk prostate cancer (PCa), with evidence supporting its safety for both Grade Group (GG) 11 and favourable-risk GG2 disease.2,3 However, almost half of men discontinue AS within 5 years, often without clear evidence of disease progression but for reasons such as patient anxiety.4 Here, the authors compare the reasons for discontinuation between GG1 and GG2 PCa, questioning whether AS is equally tolerated from a psychosocial perspective in these groups.
MATERIALS AND METHODS
The authors evaluated men with GG1 (n=1328) and GG2 (n=120) PCa from the global Prostate Cancer Research International Active Surveillance (PRIAS) database who had an MRI at the time of diagnosis and attended at least one follow-up visit. Cumulative incidences (CIN) of remaining on AS, discontinuation based on protocol advice, and discontinuation for other reasons (e.g., patient anxiety) were calculated using competing risk analyses. Additionally, protocol-based reasons of discontinuation between GG1 and GG2 were compared.
RESULTS
Median follow-up for men still on AS was 1.68 years (interquartile range: 0.80–3.34) in GG1 and 1.44 years (interquartile range: 0.76–2.34) in GG2. The CIN of still being on AS at 3 years post-diagnosis was similar in both groups: 0.71 (95% CI: 0.67–0.74) in GG1 versus 0.60 (95% CI: 0.49–0.73) in GG2 (Figure 1).
Figure 1: Cumulative incidences of active surveillance discontinuation for Grade Group 1 and Grade Group 2 prostate cancer.
AS: active surveillance; GG1: Grade Group 1; GG2: Grade Group 2.
The CIN of discontinuation based on protocol advice was also similar: 0.19 (95% CI: 0.16–0.22) in GG1 versus 0.24 (95% CI: 0.14–0.35) in GG2. A CIN of 0.08 (95% CI: 0.06–0.10) in GG1 and 0.15 (95% CI: 0.05–0.24) in GG2 reflects discontinuation for other reasons. Among men who discontinued based on protocol advice within 3 years, biopsy upgrading was the main reason in both groups, with 85% in GG1 and 59% in GG2.
CONCLUSION
Both the overall probability of remaining on AS at 3 years post-diagnosis and discontinuing based on protocol advice are similar for men with GG1 and GG2 PCa, with biopsy upgrading being the most common reason for discontinuation in both groups.
Importantly, there seems to be no difference in the probability of discontinuation due to other reasons, such as patient anxiety, suggesting that patients and physicians tolerate AS as a management strategy for favourable GG2 PCa.
References
1. Newcomb LF et al. Long-term outcomes in patients using protocol-directed active surveillance for prostate cancer. JAMA. 2024;331(24):2084-93.
2. Lodder J et al. Reasons for discontinuation of active surveillance in men with Grade Group 1 and Grade Group 2 prostate cancer in the PRIAS study. Abstract A0028. EAU25, 21-24 March, 2025.
3. Baboudjian M et al. Active surveillance of grade group 2 prostate cancer: oncological outcomes from a contemporary European cohort. Eur Urol Oncol. 2025;DOI:10.1016/j.euo.2025.01.009.
4. Timilshina N et al. Factors associated with discontinuation of active surveillance among men with low-risk prostate cancer: a population-based study. J Urol. 2021;206(4):903-13.
Accuracy of a Large Language Model (ChatGPT) in Responding to Patient-Generated Queries Following Benign Prostatic Hyperplasia Surgeries
Authors: Jad Najdi,1 Bilal Alameddine,1
Alexandre Armache,1 Marwan Zein,1
William S Azar,2 Towfik Sebai,1 Yara Ghandour,1
*Albert El-Hajj1
1. American University of Beirut Medical Center, Lebanon
2. Georgetown University School of Medicine, Washington, District of Columbia, USA
*Correspondence to ae67@aub.edu.lb
Disclosure: The authors have declared no conflicts of interest.
Keywords: AI, minimally invasive surgical procedures, natural language processing, postoperative care, prostatic hyperplasia.
The rapid advancements in AI, especially in large language models like ChatGPT (OpenAI, San Francisco, California, USA), hold potential for various applications in healthcare.1-6 This study aims to assess the accuracy of ChatGPT in responding to postoperative patient enquiries after surgery for benign prostatic hyperplasia.
METHODS
Common post-operative questions were collected from discharge instruction booklets, online forums, and social media platforms. Surgeries of interest included transurethral resection of the prostate (TURP), simple prostatectomy, laser enucleation of the prostate, Aquablation, Rezum, greenlight photovaporisation of the prostate, Urolift, and iTIND. ChatGPT 3.5
outputs were graded by two independent senior urology residents using pre-defined evaluation criteria. A third senior reviewer resolved grading discrepancies. Response errors were categorised into different types. Categorical variables were analysed using the Chi-square test. Inter-rater agreement was measured using Cohen’s Kappa coefficient.
RESULTS
A total of 496 questions were evaluated by two reviewers, of which 280 were excluded. Of the 216 graded responses, 78.2% were comprehensive and correct, 9.3% were incomplete or partially correct, 10.2% were misleading or contained a mix of accurate and inaccurate information, and 2.3% were completely inaccurate (Figure 1). The highest percentage of correct answers was observed with newer procedures (Aquablation, Rezum, iTIND) as compared to older procedures (TURP, simple prostatectomy). Lack of context or incorrect information (36.6%) were the most common errors encountered.
CONCLUSION
ChatGPT demonstrates promise in providing accurate post-operative guidance for patients undergoing benign prostatic hyperplasia surgeries. However, incomplete or misleading responses raise concerns about its current clinical applicability, emphasising the need for further research to enhance its accuracy and ensure patient safety.
Figure 1: Percentage of answers in the four different grading categories divided by procedure type.
■ Incomplete/
■ Mixed with accurate and inaccurate data/ misleading
■ Completely inaccurate/ irrelevant
AQUA: aquablation; G-PVP: greenlight photovaporisation of the prostate; LEP: laser enucleation of the prostate; Simple P: simple prostatectomy; TURP: transurethral resection of the prostate.
References
1. Najdi et al. Accuracy of a large language model (ChatGPT) in responding to patient-generated queries following BPH surgery. Abstract A0901. EAU25, 21-24 March, 2025.
2. Wu J et al. The application of ChatGPT in medicine: a scoping review and bibliometric analysis. J Multidiscip Healthc. 2024;17:1681-92.
3. Wright BM et al. Is ChatGPT a trusted source of information for total hip and knee arthroplasty patients?. Bone Jt Open. 2024;5(2):139-46.
4. Kuşcu O et al. Is ChatGPT accurate and reliable in answering questions regarding head and neck cancer?. Front Oncol. 2023;13.
5. Harada Y et al. Performance evaluation of ChatGPT in detecting diagnostic errors and their contributing factors: an analysis of 545 case reports of diagnostic errors. BMJ Open Qual. 2024;13(2):e002654.
6. Briganti G. How ChatGPT works: a mini review. Eur Arch Otorhinolaryngol. 2024;281(3):1565-9.
The Practice of Perioperative Stone Cultures in Percutaneous Surgery: Results, Correlation with Urine Testing,
and Postoperative Systemic Inflammatory Response Syndrome
Authors: *Hugo W. Schuil,1,2 Justin van de Kamp,1 Tessa R. de Weijer,2 Joyce Baard,1 Michaël M.E.L. Henderickx,1 A. Carolien Bouma-Houwert,1 Katja (C.A.) Goossens-Laan,2 Joost A. van der Spruit,2 Harrie P. Beerlage,1 R. Jeroen A. van Moorselaar,1 Barbara M.A. Schout,2 Guido M. Kamphuis1
1. Amsterdam University Medical Center, the Netherlands
2. Alrijne Ziekenhuis, Leiderdorp, the Netherlands
*Correspondence to h.w.schuil@amsterdamumc.nl
Disclosure: The authors have declared no conflicts of interest.
Urolithiasis may cause urinary tract infections, infections can cause urolith formation, and surgery for urolithiasis carries risk of infectious complications.1,2 The European Association of Urology (EAU) guidelines recommend peri-operative antibiotic prophylaxis for stone removal, but do not specify the type or duration.3 The authors studied the results of stone cultures in percutaneous nephrolithotomy (PCNL), and its relationship to preoperative urine testing and postoperative systemic inflammatory response syndrome (SIRS).
MATERIALS AND METHODS
A total of 424 consecutive PCNL procedures performed in two medical centres during the period of January 2018–September 2023 were included. Urine was directly sent for culture in at-risk patients or if a urine test strip showed the presence
of leucocytes or nitrite. During PCNL, stone fragments were collected on sterile gauze and placed in a container that was sent to the microbiology laboratory. Following this, the entire specimen was inoculated in a brain heart infusion agar of thioglycolate broth, and then assessed after 5–7 days for signs of growth. If present, subculture was performed onto blood agar plates. These plates were incubated aerobically and anaerobically to identify the microorganism.
RESULTS
Stone cultures were obtained in 338 (80%) surgeries, with 145 (46%) being positive. Preoperative urine testing was performed before 391 (92%) procedures, of which 143 (41%) were positive. Enterococcus faecalis was the most commonly cultured microorganism on stones (n=28, 19%) and Escherichia coli was the most commonly cultured microorganism in urine (n=49, 34%; Figure 1). Of all patients with clean preoperative urine, 26% had a positive stone culture. Of patients with a positive preoperative urine culture, 47% had the same microorganism in the stone culture, 21% had a different microorganism, and 32% had a negative stone culture. Positive stone cultures were significantly associated with an increased risk of postoperative SIRS (odds ratio: 3.3; 95% CI: 1.3–8.2), while urine cultures were not (odds ratio: 1.7; 95% CI: 0.76–3.6).
CONCLUSION
Stone cultures are often positive, are poorly predicted by preoperative urine cultures, and are associated with an increased risk of postoperative SIRS. Intraoperative stone cultures provide additional information regarding the colonised status of the urinary tract.
Figure 1: Results of the preoperative urine cultures and perioperative stone cultures.
Figure 1: Continued.
References
1. Schuil HW et al. The practice of perioperative stone cultures in percutaneous surgery: results, correlation with urine testing and postoperative SIRS. Abstract A0091. EAU25, 21-24 March, 2025.
2. Razi A et al. Unraveling the association of bacteria and urinary stones in patients with urolithiasis: an update review article. Front Med (Lausanne). 2024;11:1401808.
3. European Association of Urology (EAU). Guidelines on Urolithiasis. 2024. Available at: http://uroweb. org/guideline/urolithiasis/. Last accessed: 11 January 2024.
Implementation of an Outpatient Major Surgery Programme in Mini-Percutaneous Nephrolithotomy
Authors: *Ermengol Moretó,1 Sergi Colom,1 José María Cuadrado,1 Núria De Fuentes,1 Manel Castells,1 Francesc Vigués1 1. Bellvitge University Hospital, Hospitalet de Llobregat, Barcelona, Spain
*Correspondence to emoreto@bellvitgehospital.cat
Disclosure: The authors have declared no conflicts of interest.
Percutaneous nephrolithotomy (PCNL) has traditionally been associated with a hospital stay of several days. In recent years, some international centres have reported successful outcomes with outpatient PCNL in selected cases, demonstrating its safety.1-6 This study presents the authors’ experience and results with mini-PCNL in an outpatient surgery setting in a total of 74 cases.
MATERIALS AND METHODS
A specific protocol was developed in collaboration with anaesthesiology and nursing teams, adapted to the characteristics of the procedure, hospital infrastructure, and target population. From April 2021–December 2024, a total of 74 patients eligible for miniPCNL or anterograde ureteroscopy meeting inclusion criteria were recruited. Exclusion criteria included age >75 years, unstable American Society of Anesthesiologists (ASA) Physical Status (PS) III or IV, non-steroidal anti-inflammatory drugs allergy, coagulation disorders, untreated positive urine cultures, and the presence of encrusted or calcified ureteral stents. A retrospective analysis was performed on demographic data, perioperative variables, complications, need for re-evaluation or re-intervention, and stone-free rate.
RESULTS
A total of 74 patients underwent surgery, with a median age of 59 years: 42 males (56.7%) and 32 females (43.2%). The median stone size was 15 mm (range: 10–30 mm), predominantly located in the renal pelvis (39.2%), followed by the lower calyx (29.7%), middle calyx (12.2%), upper ureter (6.8%), and upper calyx (5.4%). Single stones were treated in 54.0% of cases, two stones in 37.8% of cases, and three stones in 8.1% of cases. A single percutaneous access was used in 98% of cases (one case required dual access). The access tract sizes were 14 Ch (56%), 16 Ch (34%), and 21 Ch (10%). All patients were positioned in the Galdakaomodified supine position. Tract dilation was performed using Alken telescopic dilators for 14 Ch access or one-shot dilators for 17 and 21 Ch access. Lithotripsy was performed using a Holmium laser in 97% of cases, with a Thulium laser used in two patients.
The median operative time was 80 minutes (interquartile range: 61–100), with no intraoperative complications. A ureteral JJ stent was placed in 98% of cases, while one patient required a nephrostomy tube due to ureteral stricture pending reconstructive surgery. Out of a total of 74 patients, 68 patients (92%) were discharged home on the same day as an outpatient surgery, after a 6–8 hour observation period. The remaining six patients were hospitalised: four for inadequate pain control, one for dizziness, and one for haematuria, all classified as Clavien-Dindo I and discharged within 24 hours postoperatively. One patient presented with haematuria 10 days postoperatively without requiring transfusion or angioembolisation. Two patients consulted due to JJ stent-related discomfort, while another two required hospitalisations due to fever. The median time to JJ stent removal was 15 days. The overall stone-free rate was 79%, with four cases (6%) requiring reintervention via retrograde intrarenal surgery or extracorporeal shock wave lithotripsy for residual stone fragments.
CONCLUSION
The authors’ experience with mini-PCNL in an outpatient setting demonstrates favourable safety and patient satisfaction outcomes in selected cases, with satisfactory surgical results. These findings encourage further implementation of the outpatient surgery programme in the authors’ centre.
References
1. Moretó E et al. Implementation of an outpatient major surgery program in mini-percutaneous nephrolithotomy. Abstract A0099. EAU25, 21-24 March, 2025.
2. Beiko D et al. Ambulatory percutaneous nephrolithotomy: what is the rate of readmission?. J Endourol. 2015;29(4):410-4.
3. Fahmy A et al. Can percutaneous nephrolithotomy be performed as outpatient procedure?. Arab J Urol. 2017:15(1):1-6.
4. Bechis SK et al. Outpatient percutaneous nephrolithotomy: the UC San Diego Health experience. J Endourol. 2018;32(5):394-401.
5. Schoenfeld D et al. Outcomes for patients undergoing ambulatory percutaneous nephrolithotomy. J Endourol. 2019;33(3):189-93.
6. Wu X et al. Day-surgery percutaneous nephrolithotomy: a high-volume center retrospective experience. World J Urol. 2020;38(5):1323-8.
Long-Term Outcomes of Conservative Endoscopic Treatment in High-Risk Upper Urinary Tract Urothelial Carcinoma
Authors: *Francisco Quereda-Flores,1 Marta Trassierra,1 Juan Ortiz-Salvador,1 Domingo de Guzmán Ordaz,1 Álvaro José Beviá-Romero,1 Daniel López-Acón,1 Pilar Bahílo,1 Alberto Budía1 1. University and Polytechnical Hospital La Fe, Valencia, Spain
*Correspondence to francisco.quereda@goumh.umh.es
Disclosure: The authors have declared no conflicts of interest.
Upper urinary tract urothelial carcinoma (UTUC) is categorised into low-risk (LR) and high-risk (HR) groups based on patient and tumour-specific prognostic factors, according to European Association of Urology (EAU) guidelines.1,2 Traditionally, elective conservative endoscopic treatment (ET) has been reserved for low-risk tumours with a fairly restrictive definition. However, some high-risk patients may benefit from this approach,3,4 as shown by recent changes in the risk-stratification criteria in the 2024 EAU guidelines, where size, multifocality, and hydroureteronephrosis are considered as only weak high-risk factors.2
AIM
The aim of this study was to evaluate the long-term oncological outcomes and renal preservation (RP) rates in patients with HR UTUC undergoing conservative ET, either as an imperative or elective procedure.
MATERIALS AND METHODS
A prospective cohort analysis was conducted on patients with UTUC treated with conservative ET in a single centre from January 2011–January 2024. Exclusion criteria were nodal involvement or metastasis at diagnosis, invasive features on CT urography (uro-CT), tumour stage ≥T1, and histologic variants on initial endoscopic biopsy. Variables analysed included elective versus imperative indication, age, sex, urinary cytology, tumour grade, hydroureteronephrosis, tumour size, location, number, and multifocality, and their association with radical nephroureterectomy (NFU)-free survival, cancer-specific survival (CSS), and overall survival (OS) (Kaplan-Meier curves and Cox regression model).
RESULTS
Out of the 98 patients with UTUC undergoing ET, 71 (72%) met the HR criteria. Among them, treatment was elective in 45 (64%) and imperative in 26 (36%) patients. Eighteen patients (25%) had tumour size ≥2 cm, nine (13%) multifocality (renal and ureteral), 33 (46%) multiple tumours, 36 (51%) hydroureteronephrosis, 12 (17%) high-grade tumours, and 12 (17%) positive cytology.
Over a mean follow-up of 59 months (range: 12–145 months), RP was achieved in 46 patients (65%): 31 (69%) in elective and 15 (58%) in imperative patients. The estimated NFU-free survival was 89% (95% CI: 85–93), 75% (95% CI: 69–81), and 37% (95% CI: 28–46) at 3, 5, and 10 years, respectively, with no statistically significant differences between LR and HR UTUC (Figure 1).
No single criteria showed a significant association with RP in bivariate analysis. Multivariate analysis identified multiplicity as the only independent risk factor for NFU (hazard ratio [HR]: 2.1; 95% CI: 1.1–4.3; p=0.03). The CSS at 3, 5, and 10 years was 91% (95% CI: 88–94), 84% (95% CI: 79–89), and 80% (95% CI: 74–86), respectively. No statistically significant differences were found in terms of CSS with the LR group (Figure 1). An OS of 82% (95% CI: 77–87), 69% (95% CI: 63–75), and 49% (95% CI: 39–59) was observed at 3, 5, and 10 years, respectively, with significant differences between LR and HR groups (p=0.04) (Figure 1). Imperative indication was the only independent factor associated with worse OS in HR patients (HR: 4.6; 95% CI: 1.8–11.4). The estimated OS was 52% (95% CI: 42–62) versus 86% (95% CI: 80–92) at 5 years and 35% (95% CI: 25–45) versus 68% (95% CI: 58–78) at 10 years for imperative and elective cases, respectively.
CONCLUSION
The authors' results suggest that conservative ET may be extended to selected HR UTUC cases, including many with factors such as multifocal disease, tumour size ≥2 cm, or hydroureteronephrosis, that, until recently, would have been excluded from this approach according to previous EAU guidelines.
References
1. Quereda-Flores F et al. Long-term outcomes of conservative endoscopic treatment in highrisk upper urinary tract urothelial carcinoma. Abstract A0063. EAU25, 21-24 March, 2025.
2. Masson-Lecomte A et al. Upper Urinary Tract Urothelial Carcinoma. European Association of Urology Guidelines. Edn. ISBN 978-94-92671-23-3.
3. Kawada T et al. Oncologic and safety outcomes for endoscopic surgery versus radical nephroureterectomy for upper tract urothelial carcinoma: an updated systematic review and meta-analysis. Eur Urol Focus. 2023;9(2):236-40.
4. Grasso M et al. Ureteroscopic and extirpative treatment of upper urinary tract urothelial carcinoma: a 15-year comprehensive review of 160 consecutive patients. BJU Int. 2012;110(11):1618-26.
AI System for Detecting Flat Bladder Tumours in Cystoscopic Images
1. Department of Urology, Kyushu University Hospital, Fukuoka, Japan
2. Information Technology Center, Nagoya University, Japan
3. Graduate School of Informatics, Nagoya University, Japan
4. Research Center for Medical Bigdata, National Institute of Informatics, Tokyo, Japan
*Correspondence to mutaguchi.jun.674@m.kyushu-u.ac.jp
Disclosure: Olympus Corporation supported the following instruments to conduct this research (CLV-S400, OTV-S400, WM-NP2, LMD-X310S, HVO-4000ST, WA2TA430A, WA03200A, CH-S400-XZ-EB, WA05990A).
Bladder tumours have a high intravesical recurrence rate after transurethral resection of the bladder tumour (TURBT).1,2 Overlooking tumours during TURBT occasionally causes early intravesical recurrences. In particular, flat tumours are sometimes overlooked because those tumours are more difficult to detect than elevated papillary tumours.3 Detecting flat tumours is clinically beneficial because those tumours represent carcinoma in situ and are high-risk tumours amongst bladder tumours. Recently, AI has been developed as a new diagnosis system. You Only Look Once (YOLO) is a fast object detection AI system,4 and this is a deep neural network that detects objects in an image. This technique has the potential to improve flat tumour detection rate in cystoscopy; however, only a few studies reported the utility of AI for detecting flat tumours
in cystoscopy. In this study, the authors aimed to develop an AI system to detect flat tumours in cystoscopic images.
MATERIALS AND METHODS
The authors constructed an object detection system based on YOLO. They obtained cystoscopic images of bladder tumours during TURBT procedures at their institutions between December 2019–September 2021. Those cystoscopic images obtained were divided into training and testing data in an 8:2 ratio. YOLO was trained to detect bladder tumours in an image by learning the tumour features from training data. AI testing was conducted using YOLO, and its sensitivity, specificity, and area under the receiver operating characteristic curve were evaluated for flat tumour images.
RESULTS
The authors obtained 2,371 tumour images and 254 non-tumour images. In tumour images, 436 flat tumour images were included. They used 1,896 images for the AI training and assessed the accuracies of the AI system. The sensitivity and specificity were 90.0% and 90.6%, respectively. With a likelihood score of 0.163, the area under the receiver operating characteristic curve in detecting flat tumours was 93.4%. An example of the detection is shown in Figure 1
CONCLUSION
The system proposed by the authors can detect flat bladder tumours in cystoscopic images. This system has the possibility to improve detection accuracy during TURBT and might be beneficial to reduce the recurrence rate of bladder tumours after TURBT in the future.
The authors' proposed AI system could detect small and large flat bladder tumours. The lower right of images represents the whiteness lesion that was a carcinoma in situ, and their proposed AI could detect this flat lesion.
References
1. Mutaguchi J et al. Artificial Intelligence system for detecting flat bladder tumors in cystoscopic images. Abstract A0681. EAU25, 21-24 March, 2025.
2. Kausch I et al. Photodynamic diagnosis in non-muscle-invasive bladder cancer: a systematic review and cumulative analysis of prospective studies. Eur Urol. 2010;57:595-606.
3. Ye Z et al. A comparison of NBI and WLI cystoscopy in detecting non-muscle-invasive bladder cancer: a prospective, randomized and multi-center study. Sci Rep. 2015;5:10905.
4. Redmon J, Ali F. YOLOv3: an incremental improvement. arXiv. 2018;DOI:1804.02767.
Figure 1: Representative flat tumour detection by You Only Look Once.
Randomised Controlled Trials on Silicon-Covered Metallic Mesh Stents for Malignant Ureteral Obstruction
Authors: Deok Hyun Han,1
Chung Un Lee,2 *Jae Hoon Chung3
1. Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2. Department of Urology, Chungang University College of Medicine, Chungang University Gwangmyeong Hospital, Korea
3. Department of Urology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea
*Correspondence to dr.jhchung@gmail.com
Disclosure: This study was funded by a grant from the Ministry of Health & Welfare, Republic of Korea.
Keywords: Hydronephrosis, malignancy, quality of life, stents, ureter.
To evaluate the efficacy and safety of silicone-covered metallic ureteral stents (MUS) compared with double-J (D-J) stents in patients with malignant ureteral obstruction.1
MATERIALS AND METHODS
This was a prospective, randomised controlled trial. Patients diagnosed with ureteral stricture caused by a malignant tumour with a life expectancy of >3 months and those who had not previously undergone metal ureteral stent (MUS) placement were selected.2-9 Seventysix ureters (65 patients) were enrolled in this study between January 2020–November 2023. The 76 ureters were randomised 1:1 into the experimental and control groups.10 The experimental group received a covered MUS and the control group received D-J stenting. One ureter in the control group did not undergo stenting because patency was confirmed during retrograde ureterography. Analysis was conducted at 1, 3, and 6 months after the procedure, and the primary endpoint
was the primary patency rate determined using CT and diuretic renal scan during the study period. Secondary endpoints included technical success rate, adverse reaction rate, and degree of discomfort caused by the stent.
RESULTS
A total of 76 ureters from 65 patients were enrolled and randomised into two groups: 38 ureters in the experimental group (silicone-covered MUS) and 38 ureters in the control group (D-J stent). There were no statistically significant differences in age, BMI, underlying diseases, and previous treatment histories. However, right-sided ureteral involvement was more common in the experimental group (56.25% versus 27.27%; p=0.023). The experimental group had a higher proportion of right-sided ureteral strictures than the control group (63.16% versus 36.84%; p=0.038; Table 1).
The risk of occlusion within 6 months in the control group was 5.621 times greater than that in the experimental group (95% CI: 1.588–19.899; p=0.0074). Additionally, the log-rank test demonstrated a significant difference in patency survival rates between the two groups (p=0.0024; Figure 1). Stent removal occurred in 7/38 cases (18.42%) in the experimental group and 13/37 cases (35.14%) in the control group (Figure 1). In the experimental group, four stents were removed due to stent-related adverse events (stent migration in two cases, general weakness in one case, and gross haematuria in one case). Three other stents were removed due to worsening hydronephrosis and stent failure. In the control group, all 13 stent removals were attributed to worsening hydronephrosis and stent failure, with no stent-related adverse events reported.
Two patients (three ureters) in the control group were excluded from the study because of death from cancer progression during the follow-up period.
Table 1: Characteristics of ureteral stricture, intent-to-treat analysis.
*Student t test.
†Fisher's exact test.
SD: standard deviation.
Cox proportional hazards regression analysis
Figure 1: Patency survival rate and risk of occlusion within 6 months.
Multivariate analysis revealed that D-J stenting was an independent predictor of patency failure (hazard ratio: 6.358; 95% CI: 1.482–27.287; p=0.013; Table 2).
Patient-reported discomfort and quality of life, as measured by the Ureteral Stent Symptom Questionnaire, were compared between the two groups. There were no statistically significant differences between the groups in terms of urinary symptoms, body pain, general health, or work performance at 1, 3, or 6 months
after stenting. However, the global quality of life scores were significantly lower in the control group at 3 months (p=0.007) and 6 months (p<0.001).
CONCLUSION
The covered metallic stent for patients with malignant ureteral obstruction showed a higher patency maintenance rate than the D-J stent, with no differences in satisfaction and safety.
Table 2: Logistic regression analysis for patency failure.
1. Han DH et al. Randomized controlled trial to evaluate the efficacy and safety of silicon-covered metallic mesh stent compared to conventional polymeric stent in malignant ureteral obstruction patients. Abstract A0640. EAU25, 21-24 March, 2025.
2. Hyams ES, Shah O. Malignant extrinsic ureteral obstruction: a survey of urologists and medical oncologists regarding treatment patterns and preferences. Urology 2008;72(1):51-6.
3. Monsky WL et al. Quality-of-life assessment after palliative interventions to manage malignant ureteral obstruction. Cardiovasc Int Radiol. 2013;36(5):1355-63.
4. Cordeiro MD et al. A prognostic model for survival after palliative urinary diversion for malignant ureteric obstruction: a prospective study of 208 patients. BJU Int. 2016;117(2):266-71.
5. Hao P et al. Clinical evaluation of double-pigtail stent in patients with upper urinary tract diseases: report of 2685 cases. J Endourol. 2008;22(1):65-70.
6. Liatsikos EN et al. Ureteral metal stents: 10-year experience with malignant ureteral obstruction treatment. J Urol. 2009;182(6):2613-7.
7. Flueckiger F et al. Malignant ureteral obstruction: preliminary results of treatment with metallic selfexpandable stents. Radiology. 1993;186(1):169-73.
8. Ahmed M et al. Metal mesh stents for ureteral obstruction caused by hormone-resistant carcinoma of prostate. J Endourol. 1999;13(3):221-4.
9. Schoder M et al. Malignant biliary obstruction: treatment with ePTFE-FEP- covered endoprostheses initial technical and clinical experiences in a multicenter trial. Radiology. 2002;225(1):35-42.
10. Kim JW et al. A prospective randomized comparison of a covered metallic ureteral stent and a double-J stent for malignant ureteral obstruction. Korean J Radiol. 2018;19(4):606-12.
Congress Interviews
EMJ is delighted to introduce two Chairs of the European Association of Urology (EAU) Congress 2025, Maarten Albersen and Evangelos Liatsikos, as they discuss cutting-edge research in urology and the future of the EAU.
Featuring: Maarten Albersen and Evangelos Liatsikos
Maarten Albersen Chair of EAU Scientific Congress Committee, European Association of Urology (EAU); Professor of Urology, KU Leuven, Belgium.
As the incoming Chair of the European Association of Urology (EAU) Scientific Congress Committee, what are your main responsibilities, and what do you hope to bring to the role?
attractive and user-friendly remains a focus, with features designed to enhance the overall experience.
Q2
AI is rapidly transforming all aspects of medicine, and its impact on urology is becoming increasingly evident
As Chair, my main responsibilities include shaping the thematic structure and plenary sessions of the EAU Congress 2025, ensuring the quality and selection of submitted research, and overseeing the scientific office that drives the EAU Congress organisation. A key focus is to attract primary endpoint trial presentations, making EAU a key platform for major research breakthroughs. Additionally, I aim to enhance the delegate experience through structured navigation and innovative session formats that foster engagement. Accessibility is another priority as we strive to ensure better representation from underrepresented regions while strategically targeting high-growth areas. To support these efforts, we are expanding market research and membership insights for evidence-based decision-making. Lastly, making the congress more
The landscape of urological research is constantly evolving with emerging technologies such as AI and precision medicine. How do you see these shaping future EAU Congresses and discussions?
AI is rapidly transforming all aspects of medicine, and its impact on urology is becoming increasingly evident. Within the EAU Congress, AI will enhance planning and organisation while also assisting delegates with navigation, personalising their experience. Clinically, AI is revolutionising diagnostics in imaging and pathology, improving response prediction, and refining treatment selection, critical elements of precision and personalised medicine. These advances are particularly relevant in uro-oncology, where molecular profiling and AI-driven models are guiding tailored treatment strategies. However, challenges remain in validating AI applications and integrating them into routine practice. The EAU Congress is
committed to providing a platform for cutting-edge discussions on these developments, ensuring that urologists stay ahead of technological and scientific advancements. By fostering dialogue between researchers, clinicians, and industry leaders, we aim to drive innovation and ensure that these technologies translate into meaningful improvements in patient care.
Q3 Were there any particular sessions, presentations, or studies that stood out to you as especially groundbreaking or influential, particularly in your areas of expertise?
High-impact studies are featured at the EAU Congress under our Game-Changer platform, where new data are presented by authors and critically analysed by internationally renowned experts. This year, several pivotal studies stood out, particularly in prostate cancer, including research on surgery for metastatic disease, biopsy and imaging advancements, and the balance between oncological control and nerve-sparing using a neuroSAFE approach. Other highlights included urodynamics
in therapy-refractory overactive bladder, antibiotic prophylaxis in extracorporeal shock wave therapy, and perioperative outcomes in novel bladder cancer treatment paradigms. Many of these studies were simultaneously published in high-impact journals, a process coordinated by our Scientific Office in collaboration with editorial teams. This strategic approach maximises visibility for practicechanging trials and reinforces the EAU Congress as a premier platform for groundbreaking research in urology.
Q4 Can you tell us more about your background in urology and what initially drew you to the field, particularly uro-oncology and andrology?
My early research focused on stem cell therapy for erectile dysfunction following prostate cancer treatment, which formed the foundation of my PhD. This led to an active role in andrology during the early years of my clinical career. However, I have always been drawn to complex surgical cases, and oncology provided the greatest challenge and reward as a surgeon. Over
time, this dual background naturally guided my research focus toward uro-oncology of the genital region, particularly penile cancer. In this space, both the functional expertise from andrology and the oncological surgical principles are equally essential. Given the rarity of penile cancer, there is a unique opportunity to make significant advancements in understanding the disease and developing novel therapies. My work in this field is driven by the goal of improving treatment options and outcomes for these often-vulnerable patients, ensuring they receive both optimal cancer control and quality-of-life considerations.
Q5 As Chair of the Scientific Congress Committee, what was your most memorable or rewarding moment from this year’s congress?
While we’re still awaiting the full analysis of the delegate feedback, the initial responses have been overwhelmingly positive. Personally, one of the most rewarding moments was seeing several plenary rooms fill to capacity, proof of the strong interest and engagement our
sessions generated. We put considerable effort into enhancing the content and structure of the sessions this year, and that seems to have resonated with attendees. For next year, we’re planning even bolder changes to further elevate the experience. On a personal level, I find the informal, spontaneous conversations in the hallways truly enriching, those moments of connection where delegates share honest feedback and ideas for improvement. These interactions are not only memorable but also essential for shaping a better congress in the years ahead.
Q6 With the push to better integrate congress research with EAU journals, do you think this year's event made progress in that area and what would you say are the next steps?
This year marked real progress in aligning congress content with academic publishing, particularly through our Game-Changer sessions. Several of these presentations were accompanied by simultaneous high-impact journal publications, an effort made possible through close collaboration with editorial teams. Looking ahead, we aim to deepen these partnerships, especially with the EAU’s own journal family. A highlight this year was celebrating the 50th anniversary of European Urology, recognising the outstanding leadership of editors Claude Schulman, Francesco
Montorsi, Jim Catto, and Alberto Briganti, alongside Cathy Pierce’s pivotal editorial guidance. Their work has firmly positioned the journal family at the forefront of the field. Strengthening ties not only between the Scientific Congress Office and the journals but also across the EAU’s broader ecosystem, including guidelines, policy, sections, and the Young Urologists Office, is a key next step in creating a more integrated and impactful scientific network.
Q7
Looking ahead, what are your aspirations for the future of the EAU Congress, both in terms of scientific impact and global collaboration?
This year marked real progress in aligning congress content with academic publishing, particularly through our Game-Changer sessions
Our ambition is for the EAU Congress to be the leading global meeting in urology, not only in size but above all in scientific quality. We aim to attract the most cutting-edge research and deliver it through an enhanced, modern congress experience with dynamic, interactive session formats and reimagined session environments. Expanding our global reach, particularly by engaging underserved urology communities and embracing multidisciplinary care in urooncology, is a core part of our vision. Strengthening collaboration across the entire EAU ecosystem, guidelines, journals, sections, and education, will be key. Most importantly, we stand ready and highly motivated, together with the full Scientific Office and our congress consultants, to make these goals a reality. Our shared mission is to deliver the best possible educational experience for our delegates, ultimately advancing the quality of care we provide to patients worldwide.
Evangelos Liatsikos
Chair of EAU Education Office, European Association of Urology (EAU); Professor of Urology, Director of Urology Department, University Hospital of Patras, Greece
Since our last interview in 2020, you have continued to shape the future of urology education and research. What have been your most fulfilling achievements in these past 5 years, and what future goals still drive your passion for the field?
First of all, I would like to highlight that this is actually teamwork! One of the key achievements we have made is the standardisation of education. This is not just my personal achievement but a collective effort by the team. We have standardised education at all levels, beginning with first-year residents and continuing through to senior urologists. Every single approach and procedure has been standardised in a highly proficient, competency-based way. This ensures that all individuals, from the younger residents to the most experienced professionals, have unlimited access to comprehensive training activities. It is important to highlight that our primary focus is on younger urologists, who stand to gain the most from access to these resources. It is our responsibility to train them, creating the future experts in the field.
Q2
We now have scopes that are increasingly smaller, while at the same time offering exceptional image quality
As you chaired the joint European Association of Urology and Urological Society of Australia and New Zealand (EAUUSANZ) session on ‘Precision Medicine in Urologic Cancers’, how do you see AI and advanced imaging transforming the future of personalised treatments in urology?
I strongly believe that AI will transform medicine as a whole, totally revolutionising existing patterns. Significant
advancements are made each year, not only in imaging but also in other aspects of our medical practice. The next few years will bring even more progress, whilst what we are currently witnessing is just the beginning. The integration of AI into existing surgical approaches, diagnostics, and treatment will significantly improve these fields. I am convinced that AI is crucial, and we must embrace it. Otherwise, we take the risk of losing the game and falling behind. For example, look how pilots now rely on autopilot systems even for landing. AI will act as the 'autopilot' in our medical practice, particularly in diagnostics and therapeutics. Moreover, AI is supposed to play a crucial role in automated surgeries like robotic procedures, where the machine is a significant intermediary between the surgeon’s hands and the operating field.
Q3
The thematic session you co-chaired on ‘Seminal Developments in Upper Tract Endoscopy’ spotlighted key advancements. What were the most exciting innovations in this field that urologists should be aware of?
Upper urinary tract endoscopy has seen remarkable developments and progress over the past years. For example, we now have scopes that are increasingly smaller, while at the same time offering exceptional image quality. Furthermore, recent advancements in laser technology have revolutionised the current management of stones and tumours. Moreover, improvements in inflow and outflow systems have allowed us to maintain constant
pressure within the kidney. These developments are continuous, focusing on downsizing, image quality optimisation, development of more efficient lasers, and development of better monitoring systems to improve patient safety.
Q4
As Chair of the EAU Education Office, how do you ensure that the European School of Urology (ESU) continues to meet the evolving educational needs of urologists across Europe and beyond?
Let’s make something clear: our approach to education is driven by the needs of our stakeholders. We actively engage with them in order to understand their requirements. As you are already aware, our organisation is extensive, and various stakeholders, including national societies and all our members, communicate their needs to us. Following this communication, we assess their needs, and we adapt accordingly, striving to offer standardised treatments that can be implemented even in peripheral locations. This allows for a decentralised approach, with education being delivered
at national societies and national meetings, ensuring global dissemination of knowledge.
The EAU is a highly influential organisation and one of the strongest and leading organisations in the field of urology worldwide. The EAU’s mission extends beyond the provision of scientific knowledge; it aims to foster a global network of professionals who can exchange both scientific insights and engage in social networking. I am proud to be a part of such a distinguished organisation.
Q5 With ESU activities spanning specialised e-courses, URO webinars, podcasts, and hands-on training, which recent initiatives do you believe have had the most impact on postgraduate education in urology?
The COVID-19 pandemic significantly accelerated the adoption of online education, as it was our only viable option during that period. This shift to online learning has proven to be highly effective and has become an integral part of our educational
framework. Even surgical proctoring can now be conducted online. We offer a variety of educational formats, including webinars, e-courses, podcasts, and hands-on training, both remotely and at various sites. Whilst I don't dwell on this, I recognise that the impact of the COVID-19 pandemic on the education system has been transformative, totally altering the current algorithm of education.
Q6
From your perspective, what have been the biggest highlights or standout sessions of this year’s Congress?
One of the major highlights of this year’s Congress was undoubtedly the live surgery session held on Saturday, where attendees had the opportunity to witness the latest urological developments in real-time. This is why the room was constantly filled with over 2,000 attendees throughout the day, demonstrating the value placed on these sessions. In addition, breakthrough research was presented at the EAU25 Congress, which was really intriguing. Overall, this year’s meeting has been a resounding success, with participants from
all around the world. I think that at the end of the day, attendance reflects on how good or not a meeting is.
Q7With your extensive experience in endourology and laparoscopy, looking ahead, what do you see as the next major breakthroughs in minimally-invasive urologic surgery, and how do you envision these advancements shaping patient care in the coming years?
The introduction of minimallyinvasive surgery was a major revolution in the field of urology. Back in the days when we were residents, we were trained mainly in open surgery. However, open surgery is now becoming increasingly rare, especially in urology. We first transitioned to laparoscopy, followed by the use of scopes. Whilst these are distinct areas, significant progress has been made in both fields. One the one hand there’s the ‘endo’ part, which involves going through the lumen of the ureter and other organs. Scopes are becoming smaller and equipped with high-definition chips in their tips, improving image quality. Technology is doing very well! On the other hand is the laparoscopy and robotic surgery part, which is rapidly advancing. In the beginning, we had only one robotic company a couple of years ago. Now, we have another three that are Conformité Européenne marked, while multiple companies
are expected to offer additional certified robotic systems in the near future. This technological evolution is optimising surgical practice.
I think that these advancements ultimately improve patient care in a significant way. For example, the use of machines in surgery enables us to standardise and objectively assess performance, as everything is recorded. Now, there are curricula that can evaluate the performance of the surgeon, while accreditation is based on a standardised, stepwise teaching methodology. And I believe that everything is, at the end of the day, for the benefit of our patients. For example, our instructors in the past used to say, “Big surgeon, big incision,” but that has now completely changed to, “The smaller incision, the better the surgeon.” The shift from the traditional notion of the ‘god-like’ surgeon performing large incisions to the modern approach, where smaller incisions are seen as a sign of greater skill, demonstrates the significant changes in the field. The focus is now on precision, minimising invasiveness, and improving patient outcomes.
I believe that everything is, at the end of the day, for the benefit of our patients
Interviews
EMJ is delighted to introduce two key opinion leaders, Axel Heidenreich from the University of Cologne, Germany, and Marcus Drake, Imperial College London, UK, who discuss two dynamic areas of urology. Axel Heidenreich unpacks the role of precision medicine in prostate cancer treatment, whilst Marcus Drake explores the complexities of neurological urology and the future of neuromodulation therapies.
Axel Heidenreich Professor and Director, Department of Urology, University of Cologne, Germany
After your medical studies at the Johannes Gutenberg University of Mainz, Germany, and the University of Texas Health Science Center, USA, was there a specific moment, or aspect of urology, that drew you to this field?
AI probably makes it easier for the general pathologist to identify patients who have a high risk of progression and need active treatment
Yes, definitely. It was before I did my last year of medical school in San Antonio, when I had already started a doctoral thesis in urology. At that time, it was an experimental thesis, so I had to do a lot of micro-surgical surgeries in rats to perform what we call a portocaval anastomosis. Due to this portocaval anastomosis, the animals developed renal stones, so my task was to develop a stone model, to create a model to treat patients with urolithiasis, and how to prevent urolithiasis.
I thought that if you’re doing this type of doctoral thesis in urology, you have to go into this field to do some practical work in urology. I started at the Department of Urology in Mainz, Germany, which was at that time the largest urology department in Europe. You get exposed to numerous, very
large, and complicated surgeries in oncology, reconstructive urology, and also paediatric urology. So, I thought, this is my field, this is what I want to go into. Then I started my last year in medical school in San Antonio, where I also rotated into Urology, and once I had finished medical school, I went into Urology.
Q2
Given the impressive sensitivity and specificity results of the AI tool in detecting prostate cancer in biopsy samples in the recent paper you coauthored entitled ‘An international multi-institutional validation study of the algorithm for prostate cancer detection and Gleason grading’, what do you think are the main challenges and potential implications on patient experience of integrating this AI classifier into routine clinical workflows?
The challenge would be to validate this type of AI usage throughout all pathology departments, worldwide. Right now, it is essentially a single centre, single pathology study. The challenge is also to transfer this type of technology to other departments
of urology and pathology, and to still obtain the same results with the same high specificity and sensitivity. I estimate that it will take maybe 1, 2, or 3 years to validate this type of process.
But then, if I have a look at some other types of AI we use, like radiomics in patients with testicular cancer, we have already validated this type of AI by external institutions, and we know that we can achieve this high sensitivity and specificity to predict significant cancer in those patient cohorts.
I think the same is true with prostate cancer, we will have or will achieve this widespread use within the next 2 or 3 years. For the patients, it will have significant implications because what we see is that whenever you have pathologists evaluating prostate biopsy samples, there is still a high number of variations in the correct diagnosis, meaning the correct Gleason score.
So, it's not only that you have to identify prostate cancer, but you also have to identify the biological aggressiveness of prostate cancer.
If a patient has low biological aggressiveness, they don't need any type of treatment, and they are followed by what we call active surveillance. If they have high-grade cancer, they need to undergo radical prostatectomy or radiation treatment with longterm hormonal therapy, and we see that there is a discordance between central pathology review and peripheral pathology diagnosis in about 30% of the patients. So, this type of AI probably makes it easier for the general pathologist to identify patients who have a high risk of progression and need active treatment, differentiating these patients from those who can just be followed by active surveillance.
Q3
In the Phase II TRITON study, patients with BRCA and PALB2 mutations showed strong responses to rucaparib, but responses were limited in those with particular mutations. Could you elaborate on why PARP inhibition is more effective for certain DNA damage repair gene alterations than others, and what the results of this trial suggest about the future of precision medicine in treating metastatic castrationresistant prostate cancer?
That’s very difficult because right now we don't have good evidence to explain why different mutations result in different responses to these types of PARP inhibitors. However, we know that, for example, we have several PARP inhibitors like rucaparib, olaparib, and niraparib, and they act differently depending on the type of mutations we see in these HRD genes.
It is not clear why there is a difference, but the TRITON study, as well as some of the other prospective randomised clinical studies, give us the evidence that we have to perform a whole mutational analysis of all HRD genes which are available on a molecular basis. Then, depending on the specific type of this mutation in DNA damage repair genes, you select the specific drug which will then give the most optimal treatment response to your patient. The drawback of the TRITON study is that rucaparib will only work in BRCA1 and 2 mutations and the PALB mutations.
We have other studies on talazoparib, which also work in ATM mutations, for example. The bottom line is that we have to do a whole genomic sequence of all DNA damage repair genes. The other option is to include an analysis called an HRD score, which is the relative frequency of HRD mutations on the number of HRD genes that have been evaluated. If this score is above 50%, these patients will respond to PARP inhibitors.
This is a type of analysis already used for ovarian cancer. PARP inhibitors have been approved by the FDA and by the European authorities to be used in patients without a specific DNA-damage repair mutation but who have a high HRD score, and this is what we also use in clinical practice right now.
Q4In light of the findings from your real-world data study on 177Lu PSMA therapy, which identified prostatespecific antigen decrease after the first two cycles and ALP levels as potential predictive biomarkers, what do you see as the next steps for validating these markers in clinical practice to aid in treatment decision-making for patients with metastatic castration-resistant prostate cancer?
What we already know, which has already been integrated into daily clinical routine, is that patients typically receive just two cycles, or if a patient is started on radioligand therapy, then it is six cycles, which is according to the VISION trial as well as other prospective randomised trials. However, it's important to note that not every single patient needs six cycles in a row, because some of them respond after two or three cycles, and some of them don't respond at all.
Evaluating patients after two cycles of treatment will give you the direction of further treatment. If a patient shows minimal PSA reduction after two cycles, it indicates that they are unlikely to respond to subsequent cycles, whether it's the third, fourth, or even the sixth. In such cases, you can stop radioligand treatment, and start thinking about other treatment options, like PARP inhibitors, second-line
chemotherapy, and personalised treatment based on specific mutations. If a patient, however, responds very well after two cycles, for example, by PSA level decreasing by at least 80% or by demonstrating a significant objective response based on a PSMA PET CT scan, you could stop treatment after two cycles. You follow the patient and reintroduce another course of radioligand treatment in case of PSA or metastatic disease progression.
Having these two cycles as a threshold number of cycles to be delivered will give you the optimal strategy on who should continue, who could be interrupted, and in whom radioligand treatment should be stopped.
Q5 In the COTRIMS trial, nerve-sparing retroperitoneal lymph node dissection (nsRPLND) showed high oncological efficacy with minimal morbidity for low-volume metastatic seminoma. Given these promising results, how do you see nsRPLND fitting into the standard treatment landscape for clinical Stage IIA/B seminoma?
I think it will change the treatment landscape. Currently, most of the guidelines still recommend either chemotherapy or a combination of radiation therapy plus chemotherapy in patients who have clinical Stage IIA/B disease.
The problem is that chemotherapy and radiation treatment are highly effective, the cure rate in Stage 2A is in the range of about 95% and the cure rate in Stage 2B is in the range of 82–90%; however, the problem is that both of these established treatment options result in significant long-term toxicity.
Long-term toxicity means side effects that develop 30–40 years after treatment, and these could be cardiovascular disease, heart attacks, an apoplectic insult, metabolic disease, or secondary malignancies. We see that about 80% of patients who die after the treatment of testicular cancer, about 30–40 years after discontinuation of chemotherapy, have died not due to cancer but due to these long-term side effects.
Surgical therapy like RPLND, in our case, has a relapse rate of only about 10–15%, so 85–90% of patients are cured by surgery alone. This means that they will not develop long-term toxicity and that only about 10–15% of patients will need chemotherapy. So far, the American Urological Association and the National Comprehensive
Cancer Network (NCCN) guidelines have integrated RPLND for Stage 2A and B disease with a maximum lymph node diameter of 3 cm as the current treatment approach of choice within the European guidelines. We are still discussing this approach, but most probably it will be integrated in 2025 as one of the standard options for the treatment of those patients.
Q6
Do you think there is a possibility that nsRPLND could potentially replace or complement traditional chemotherapy or radiotherapy approaches, especially considering the goal of reducing long-term toxicities?
My idea would be that nsRPLND could replace chemotherapy or radiation therapy in specific patients who have to be markernegative, meaning that tumour markers in the serum have to be negative or only very, very slightly elevated. Patients should only undergo this type of surgery by an experienced surgeon, as relapse rates are likely to increase if the procedure is conducted by someone who performs only a few RPLNDs annually.
These types of surgeries need to be centralised. In Germany, for example, we perform about 100 procedures annually, which is half of all RPLNDs nationwide. Similarly, we also see that in some centres in the USA, such as those in Los Angeles, Indianapolis, and New York, about one-third of all RPLNDs are done in highly specialised centres. Relapse rates after RPLNDs in those specialised centres are around 10%, as we have published, compared to about 30–40% in not-soexperienced centres. So, this is a prerequisite, a good surgeon, good indication, marker negative, and then RPLND could replace chemotherapy or radiation therapy.
Relapse
rates after RPLNDs in those specialised centres are around 10% compared to about 30–40% in not-soexperienced centres
Looking to the future, what would you say are the most crucial areas for further research and clinical development to improve outcomes for patients with metastatic prostate and testicular cancers?
When it comes to testicular cancer, we have two goals. What we do currently is de-intensify the treatment by the use of active surveillance in clinical Stage I disease, primary RPLND in marker negative clinical Stage IIA/B disease. We also have patients who already have widespread metastatic disease at the time of diagnosis, and we separate those patients, depending on the localisation of their metastatic disease and the concentration of the tumour markers in the serum, into those who have a good, intermediate, or poor prognosis. Right now, the treatment of choice in patients with good prognosis is with three cycles of the cytotoxic PEB-regime (cisplatin, etoposide, and bleomycin).
Most recent studies show that there is a proportion of patients with a good prognosis who will have a very high cure rate with three cycles of PEB. However, we also know that there are some patients who have highly elevated lactate dehydrogenase (LDH) levels in their blood and will need four cycles of treatment. We are just in the process of setting up a prospective randomised trial in those patients based on clinical and molecular markers. So, personalised treatment with very easily available markers like LDH or the biomarker miR371 in the serum would be the next goal. This approach aims to identify the high-risk population of patients with testicular cancer, those who will have a poor prognosis, and to intensify treatment, and deintensify treatment in the rest of
the patients whose prognosis and long-term outcome will be good.
We also have a cohort of patients who have chemorefractory testicular cancer, who have undergone one or two rounds of chemotherapy but continue to experience disease progression and develop new metastatic sites. We don't have very good treatment options for such cases. Currently what we do is perform complete next-generation sequencing, a very intensive molecular analysis of progressing metastatic sites to identify druggable mutations, similar to the approach used with PARP inhibitors in prostate cancer. These are the three areas in testicular cancer where I would expect most of the development within the next years.
With regard to prostate cancer, it is still very important to focus on early detection. It is necessary to develop a type of individualised screening strategy and to omit the unnecessary annual screening visits, and one approach involves assessing baseline PSA levels. Ideally, men should have their first PSA test around the age of 50 years, and if this PSA level is below 1.0 ng/mL, the probability of this specific person developing clinically significant prostate cancer within the next 20 years is minimal. So, in such cases, men should only need to visit a urologist every 4–8 years. However, we know if the PSA level is above 1.0 ng/mL, even if it's only 1.2 ng/mL, the risk of developing locally advanced disease, or metastatic disease, is increased 25-fold compared to those men with a PSA level less than 1.0 ng/ mL. These patients need to undergo regular follow-ups every 1–2 years.
The next step would be to use a very sensitive method of detecting early prostate cancer, which would be multiparametric MRI, and
The next step would be to use a very sensitive method of detecting early prostate cancer, which would be multiparametric MRI
depending on the multiparametric MRI to identify those patients who will need a so-called MRI fusion biopsy and those who can be followed independently of the PSA level. When it comes to treatment, we still treat too many patients who have been diagnosed with organconfined disease. In Germany, we have a very high percentage of patients who have organ-confined disease, with prostate cancer of a very low biological aggressiveness. Most of these patients could be followed by active surveillance, as their 15-year overall and cancerspecific survival rates are 98%, even without treatment. This survival rate remains 98% with radical prostatectomy or radiation therapy, meaning most of these men will just be exposed to side effects, but not to an oncological benefit. Therefore, it’s crucial to educate urologists on the importance of adopting active surveillance for these patients.
On the other hand, you have patients with locally advanced disease, and we need to develop multi-modality treatments to increase the cure rate. This may involve not just radical prostatectomy or radiation therapy but a combination of specific treatment options to enhance the outcome of patients. When it comes to metastatic disease, it is more focused on the development of personalised, individual treatment decisions or treatment strategies depending on the molecular profile of patients with prostate cancer.
Marcus Drake
Professor of Neurological Urology, Imperial College London, UK
What inspired your decision to specialise in neurological urology, and how has this focus changed throughout your career so far?
There are two things that led me to pursue this really stimulating field. Firstly, there is so much unknown about the control of these functions, with important contributions from the brain and the spinal cord, and all the major divisions of the nervous system. Putting these together is a tremendous intellectual challenge. But the key motivation is the privilege of helping the patients themselves. Their need is great, and the support they receive is vital to them. This is truly a rewarding clinical area to work in.
Q2
Given the potential limitations of relying solely on symptom scores and flowmetry for assessing lower urinary tract symptoms, how can we ensure that healthcare providers are equipped to accurately interpret these tests and make informed decisions about the need for further investigations, such as urodynamic studies?
to bladder problems alongside prostate changes. Practitioners are now more pragmatic about the necessary tests and are better able to make use of sometimes suboptimal evaluations. Challenges still remain, nonetheless. Particularly, it is important to encourage practitioners to keep up to date with the latest findings; the algorithm produced by the UPSTREAM study is a prime example.2 It is practical, evidencebased, and clinically driven. We need to encourage all practitioners working in this area to engage with it, to the benefit of patients.
Q3
Could you discuss the potential impact of your research on point-ofcare testing for urinary tract infections (UTI) in GP practices? How could this innovation improve patient outcomes and reduce healthcare costs?
The key motivation is the privilege of helping the patients themselves. Their need is great, and the support they receive is vital
There has been a slow but steady improvement over the years, as practitioners come to realise the importance of properly understanding all aspects of a patient’s presentation. We are now much better at recognising the distinction of storage from voiding symptoms,1 and the potential for symptoms to arise from aspects of ageing and other comorbidities contributing
This technology is still early in the innovation pathway. The aim is to provide a more reliable approach to diagnosing infection than currently offered by dipsticks, but without the significant delay needed to culture and identify the infection organism. Immediate diagnosis and knowledge of the organism, combined with the detection of inflammation, will enable GPs to ensure antibiotics are given promptly to the right people. The technology is based on rapid detection of interaction between antibody and antigen, and this could be developed further to look at other indications, opening a rapid method of delivering more accurate diagnoses.
Q4
Given the challenges posed by indwelling urinary catheters and the limitations of current designs, what are the most promising avenues for future research and development to minimise the risk of UTIs and improve patient outcomes?
We do need to be realistic that the ability of microorganisms to thrive in challenging environments is remarkable, and the toxic and caustic nature of urine is remarkably challenging for physical structures like catheters. My personal feeling is that catheter design needs to focus on coping with inevitable microbiological challenges, rather than attempting to prevent UTIs. Designs that drain effectively and reduce the risk of blockage should be prioritised, and additional benefits to patients, such as reduced discomfort, should be encouraged.3 Prioritising solely UTI prevention is potentially unrealistic and may miss the possibility of other benefits.
Q5
What are the latest advancements in neuromodulation therapies, such as sacral neuromodulation and tibial nerve stimulation, for treating urinary incontinence?
Increasingly we are seeing incremental valuable benefits, with improvements in battery performance and the ability to recharge the battery efficiently being particularly helpful. We are also beginning to see convincing performance of non-invasive (transcutaneous) therapy, with clear potential to improve access to treatment and tolerability. We still need to see reduction in prices, and it is to be hoped that the economy of scale could make these treatments more affordable.
Q6
Given the complex bidirectional relationship between depression, anxiety, and urinary symptoms, how do you think healthcare providers effectively screen for and manage these conditions to improve patient outcomes?
Healthcare professionals can be quite protocol driven, and focused on direct measures, such as symptom scores. Of course, patients prioritise their lived experience, which is much harder to measure. Two areas where healthcare professions could really improve relate to the mental health impact of the condition and being up-front about potentially embarrassing topics. The mental health side ought to be considered alongside the physical aspects, as it is self-evident that incontinence could easily lead to depression or anxiety. It is interesting that our recent publication identified the reverse association,4 but more research will be needed to ascertain the implications of that and whether there could conceivably be benefit of screening for incontinence in people with depression or anxiety. More immediately, the profession must do a better job of leading discussions about supposedly embarrassing topics, such as sexual function and bladder or bowel symptoms. That is expected by the patients and would truly be valued by them, yet too often the profession ignores the issues.
Q7 Looking ahead, what do you see as the most promising areas for future research in your areas of research in urology, and how do you envision these advancements shaping the management of the most common conditions, including UTIs and urinary incontinence in the coming years?
It is so interesting to see how many opportunities for amazing research continue to emerge. My particular interest is to consider the implications of UTIs in major patient groups, such as those with neurological disease. In particular, people with conditions like dementia or multiple sclerosis, where the inflammation caused by infection can lead to deterioration in the neurological condition. In urinary incontinence, a key need is to consider it in conjunction with closely related issues such as bowel or sexual dysfunction. These three issues almost inevitably coexist in people with spinal cord or peripheral nerve disease, yet their treatment is siloed, each one being managed separately rather than in a coordinated fashion. Developing multidisciplinary approaches will be a huge step forward, and from there a rich stream of research would result.
The mental health side ought to be considered alongside the physical aspects, as it is selfevident that incontinence could easily lead to depression or anxiety
References
1. Ito H et al. Grading severity and bother using the international prostate symptom score and international consultation on incontinence questionnaire male lower urinary tract symptoms score in men seeking lower urinary tract symptoms therapy. J Urol. 2020;204(5):1003-11.
2. Ito H et al. Predicting prostate surgery outcomes from standard clinical assessments of lower urinary tract symptoms to derive prognostic symptom and flowmetry criteria. Eur Urol Focus. 2024;10(1):197-204.
3. Drake MJ et al. Development and first-in-human testing of FLUME urinary catheter with protected
tip and relocated drainage holes. Continence (Amst). 2023; DOI:10.1016/j.cont.2023.101054.
4. Joinson C et al. Bidirectional relationships between depression, anxiety and urinary symptoms in women: a prospective cohort study. J Affect Disord. 2025;369:516-22.
Pain, increased bleeding, nerve damage, and, at worst, bladder rupture are a few of the potential consequences of undertreated post-partum urinary retention (PUR). Despite these possible sequelae, PUR is often underreported, with a wideranging incidence in the literature ranging from 0.18–17.9%.1,2 Although its incidence is not entirely clear, PUR remains a common indication for post-partum urogynaecology referral. One prospective, cross-sectional survey study of obstetric providers at a tertiary care health system found that 53.8% of survey respondents identified PUR as an indication for a post-partum urogynaecology referral.3 However, despite these findings, provider knowledge and standardised protocols for identifying and addressing PUR are often lacking. In one study, only 17.1% of obstetrician/gynaecologist (OB/ GYN) resident respondents received formal didactics on the condition.1 In essence, PUR is under-recognised and under-reported, resulting in an unstandardised post-partum experience with noteworthy potential patient consequences. As such, it is important to consider the risk factors and clinical findings of this condition to appropriately develop management algorithms and direct potential future studies.
There are three types of PUR. Overt PUR is the complete inability to void at least 6 hours after a spontaneous vaginal
delivery or after Foley removal from a caesarean section (CS). Covert PUR is incomplete bladder emptying, which is often defined as a post-void residual amount of at least 150 mL measured by bedside ultrasound or straight catheterisation. Lastly, persistent PUR is urinary retention that continues after 3 days post-partum and, sometimes, lasts several weeks. If left untreated, this type of long-term bladder retention can lead to parasympathetic nerve and detrusor muscle damage, which can transform into non-contractile fibrosis.2 Of these types, covert PUR is, not surprisingly, the most often underdiagnosed. Risk factors for these conditions vary widely and include prolonged labour, episiotomy, nulliparity, epidural analgesia, and perineal injury.4,5 The risk factor with the strongest association, however, is operative delivery.5,6 Studies have suggested that instrument use during delivery can lead to pelvic floor, bladder, and direct nerve injury with resulting dysfunction and oedema. This oedema can result in mechanical outlet obstruction and, subsequently, impaired reflex and relaxation of the urethral sphincter, periurethral muscles, and pelvic floor. Delayed voiding can lead to overdistention, which can further cause stretch injury, nerve ischemia and injury, and impaired detrusor sensitivity and contractility. It has also been suggested that discomfort from delivery and hesitancy with voiding in unfamiliar places may further contribute to emptying issues.
MANAGEMENT OF POSTPARTUM
URINARY RETENTION
PUR management varies by institutional policy and PUR type. One algorithm, developed by Nutaitis et al.,1 recommends evaluating all patients for spontaneous voiding within 6 hours of delivery or catheter removal (Figure 1). For patients unable to void, overt PUR is identified using a bladder scan. For patients able to void, covert PUR can be evaluated based on urinary output, post-void residual volume, and/or symptomatology (e.g., suprapubic or lower abdominal discomfort). Depending upon the evaluation, patients are either observed or provided an indwelling urethral catheter. The timing of subsequent urethral catheter removal depends on the volume of retention and/or persistence of patient symptoms. Generally, catheter removal prior to discharge is appropriate for lower retention volumes, whereas arrangements for outpatient removal are made for larger retention volumes as delineated in Figure 1.1 It is important when evaluating the post-void residual to interpret the volume obtained by catheterisation in the context of the preceding voided volume to understand the patient’s voiding efficiency. These data can help inform management decisions. Without algorithms such as these, appropriate identification of covert PUR is significantly more challenging, as patients who spontaneously void do not automatically undergo a bedside bladder scan unless there are other concerning symptoms. In these circumstances, diagnosis is greatly dependent on a strong provider–patient relationship and the communication therein. Moreover, timely diagnosis is highly impacted by the providers’ abilities to identify suggestive symptoms, including suprapubic fullness, displaced uterine fundal height, urinary frequency, feeling of incomplete bladder emptying, changes in urinary stream, and increased vaginal bleeding.
Intermittent Self-Catheterisation
In addition to the algorithm by Nutaitis et al.,1 another potential intervention is to simply follow patient urinary output
(UOP). If UOP is less than 30 mL/kg/ hour, a bladder scan can be considered at that time to evaluate the PUR1. However, although following UOP is standardised care after a CS, it is less common after a vaginal delivery. For patients diagnosed with covert PUR, another management option is intermittent catheterisation. A randomised control trial by Bachar et al.7 evaluated the utility of intermittent versus continuous catheterisation for individuals with retained bladder volumes of at least 150 mL up to 6 hours after a vaginal delivery or Foley removal after CS. A total of 147 patients were enrolled, with 73 randomised to intermittent catheterisation and 74 to continuous drainage with an indwelling Foley. They found that the mean time to resolution was significantly shortened for the intermittent catheterisation group, with 99% of individuals in the intermittent catheterisation group experiencing PUR resolution by 24 hours, compared with 91% of patients undergoing continuous drainage. There were no significant differences between the groups for urinary tract infection or duration of hospitalisation.7 However, there were significant limitations to this study, including the impact of patient preference on intermittent versus indwelling catheter placement, variations in length of hospitalisation, and distorted anatomy. Still, this may suggest that intermittent catheterisation may have a role in the management of PUR.
Facilitating intermittent self-catheterisation is typically more labour-intensive, requiring additional time for patient education regarding the process of self-catheterisation, utilising clean techniques, and following up voided and residual volumes to direct patient care after discharge. It would also require the provision of additional resources, such as single-use lubricant, disposable catheters, and urine collection basins to measure residuals, bladder diaries, and other educational materials for those with PUR that does not resolve during their hospitalisation. These resources, in addition to patient preference and ability, may make self-catheterisation feasible for only a subset of patients.
Within 6 hours after prior bladder drainage or removal of catheter: Did patient spontaneously void?
Check for signs of Covert PUR:
Urinary discomfort, fullness
Voiding <30 mL/hour
Voided volume <150 mL
Immediate bladder scan: PVR ≥150 mL?
Place indwelling urethral catheter to confirm PVR: PVR ≥150 mL?
Observe
Overt PUR
Immediate bladder scan: Volume ≥300 mL?
Void within 2 hours and undergo bladder scan for PVR if voided volume <150 mL.
If <300 mL
Remove foley and restart algorithm.
Leave indwelling urethral catheter in place for 24 hours.
Perform AVT. If unsuccessful AVT
Postpartum urinary retention, Intermittent straight catheterization, Active Void Trial
Place indwelling urethral catheter and measure amount drained.
If 300–1,000 mL
Leave catheter in place for 24 hours. Perform AVT. If unsuccessful, restart algorithm when catheter removed.
If >1,000 mL
Place indwelling urethral catheter to gravity for remainder of hospital course
Shared decision making for discharge planning:
- ISC or indwelling urethral catheter
- Follow up in office in 5–7 days for AVT if indwelling catheter is selected
▪ If AVT is unsuccessful > Initiate ISC or replace indwelling catheter with return to clinic after 1 week to repeat evaluation
This figure was previously published in Nutaitis AC et al. Postpartum urinary retention: an expert review. Am J Obstet Gynecol. 2023;228(1):14-21. Copyright Elsevier (January 2023).
Persistent, or protracted, PUR is much less common, with an incidence as low as 0.05–0.18%.6,8. A study by Groutz et al.6 reviewed 37,757 women who delivered over a 3-year period. Among them, 55 individuals had persistent PUR beyond the third post-partum day. Of these patients, 65% achieved normal voiding within 2 weeks post-partum, while 35% achieved it within 28 days. Ultimately, only five developed long-term stress urinary incontinence, whereas four had overactive bladder symptoms. Findings were most suggestive of complete resolution of symptoms within 28 days without extraordinary long-term consequences. However, another study by Hickman et al.8 was significant for one patient with urinary retention up to 47 days after delivery. Generally, patients diagnosed further out from delivery were more likely to have protracted PUR. Management of protracted PUR may include pharmacologic therapy. Alpha-blockers, including prazosin or phentolamine, have been used in functional outlet obstruction.9 Cholinergic agonists, such as bethanechol, have been used for post-operative urinary retention. Both medications may be considered in the post-partum state; however, such use is complicated in the setting of breastfeeding patients due to the paucity of data on potential risks to the infant.9 Given the limited data on the efficacy of these agents, dosing considerations, maternal side effects, and neonatal considerations, non-pharmacologic management strategies should be prioritised, especially in breastfeeding mothers.
OTHER TREATMENT OPTIONS
Furthermore, an interesting potential area of study is the utility of acupuncture. A randomised control trial by Zhu et al.10 evaluated 1,200 patients across 12 hospitals in China over an 8-month period. Just more than 1,000 patients were enrolled in the study with approximately half undergoing routine care plus three sessions of a 4-hour acupoint hot compress involving the abdominal, lumbosacral, and plantar regions within 30 min, 24 hours, and 48 hours after vaginal delivery. They found that the intervention group had a significantly decreased incidence of PUR.10 The utility of acupuncture as a treatment for PUR in the USA is less clear but is likely to be low risk for patients who are interested.
CONCLUSION
The key components for facilitating early recognition and intervention for PUR include standardised post-partum care and patient education. It is imperative for institutions to develop a streamlined process for PUR identification and outpatient follow-up. Most importantly, post-partum patients should receive anticipatory guidance regarding expectations for spontaneous voiding and concerning signs/symptoms early in the post-partum period so that they may advocate for themselves. For those experiencing persistent or protracted PUR, it is important to have protocols in place for patient education regarding intermittent self-catheterisation and retrograde voiding trials in both inpatient and outpatient settings. Through anticipatory patient guidance, standardised protocols, and openness to potential interventions, PUR can be appropriately and expeditiously recognised and managed.
References
1. Nutaitis AC et al. Postpartum urinary retention: an expert review. Am J Obstet Gynecol. 2023;228(1):14-21.
2. Mohr S et al. Postpartum urinary retention: what are the sequelae? A long-term study and review of the literature. Int Urogynecol J. 2022;33(6):1601-8.
3. Propst K, Hickman LC. Peripartum pelvic floor disorder clinics inform obstetric provider practices. Int Urogynecol J. 2021;32(7):1793-9.
4. Li L et al. Risk factors for postpartum urinary retention:
an updated systematic review and meta-analysis. Int J Gynaecol Obstet. 2025;168(1):10-24.
5. Mulder FE et al. Postpartum urinary retention: a systematic review of adverse effects and management. Int Urogynecol J. 2014;25(12):1605-12.
6. Groutz A et al. Third- and fourthdegree perineal tears: prevalence and risk factors in the third millennium. Am J Obstet Gynecol.2011;204(4): 347.e1-4.
7. Bachar G et al. Intermittent vs continuous catheterization for postpartum urinary retention: a multicenter randomized controlled
trial. Am J Obstet Gynecol MFM. 2023;5(10):101084.
8. Hickman LC et al. Protracted postpartum urinary retention: incidence, risk factors, and natural history of a rare postpartum urinary retention subtype. Urogynecology (Phila). 2022;28(12):887-93.
9. Yip SK et al. Postpartum urinary retention. Acta Obstet Gynecol Scand. 2004;83(10):881-91.
10. Zhu Y et al. Effect of acupoint hot compress on postpartum urinary retention after vaginal delivery: a randomized clinical trial. JAMA Netw Open. 2022;5(5):e2213261.
Treatment of Urolithiasis: A Comprehensive Review
Editor's Pick
This paper provides an excellent summary of urolithiasis management, which significantly impacts both adults and children. Key takeaways include the observation that global warming appears to be contributing to an increase in urolithiasis diagnoses, as well as the role of recent advancements in endoscopic instruments, which have greatly enhanced minimally invasive treatment options.
Abdullah Erdem Canda
Professor of Urology, Koç University School of Medicine, Department of Urology, İstanbul, Türkiye
Authors:
*Živka
Dika,1,2 Marjan Marić,1 Marijana Živko1
1. University Hospital Centre Zagreb, Croatia
2. School of Medicine, University of Zagreb, Croatia *Correspondence to zivkadika1@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Urolithiasis is a highly prevalent and multifactorial disease, representing the most common urological condition globally. Its incidence continues to rise, posing a significant public health challenge. Management strategies are tailored to individual patients, considering factors such as stone size, composition, location, and underlying metabolic conditions. This review provides a comprehensive overview of both pharmacological and surgical approaches to urolithiasis, emphasising recent advancements and emerging technologies. Surgical treatments, particularly minimally invasive procedures, have shown considerable improvement, offering highly effective solutions with reduced morbidity. While surgical interventions are essential, pharmacological therapies play a key role in preventing recurrence and addressing metabolic abnormalities that contribute to stone formation. Advances in understanding the molecular mechanisms and pathophysiology of urolithiasis are crucial for developing targeted therapies. A holistic approach that integrates advanced surgical techniques with pharmacological interventions, tailored to individual metabolic profiles, is essential for optimising patient outcomes. Personalised management, supported by regular monitoring of urinary pH, metabolic profiles, and adherence to treatment regimens, is vital to reducing recurrence and improving the quality of life for patients with urolithiasis.
Key Points
1. Urolithiasis is a prevalent systemic disease with a rising incidence. Advances in treatment, including novel therapies, are essential to optimising outcomes and reducing the burden of this condition.
2. This review examines comprehensive management strategies for urolithiasis, including surgical innovations, pharmacological therapies, and non-pharmacological interventions. It highlights the importance of personalised treatment plans and emerging novel therapies.
3. Successful urolithiasis management requires a multifaceted approach, combining tailored surgical, pharmacological, and lifestyle interventions. Emphasising personalised care, novel therapies, and proactive patient management improves outcomes and reduces recurrence rates.
INTRODUCTION
Urolithiasis refers to the formation of stones in the urinary tract and is the most common urological condition globally. It is a multifactorial disease, with both prevalence and incidence increasing worldwide over recent decades. Urolithiasis poses a growing public health challenge, affecting populations across diverse demographics.1 Management strategies are tailored based on stone size, composition, location, and patient-specific factors. This review explores medical and surgical treatments, recent advancements, and innovative technologies, providing a comprehensive overview of urolithiasis management.
OVERVIEW OF MEDICAL (PHARMACOLOGICAL) TREATMENT OF UROLITHIASIS
The management of urolithiasis typically begins with non-invasive approaches that emphasise observation, conservative measures, and medical expulsive therapy (MET). For patients with small stones likely to pass spontaneously, observation is a practical option, particularly when the stones are asymptomatic or cause minimal symptoms. Conservative management strategies aim to alleviate symptoms, facilitate stone expulsion, and prevent recurrence, forming the cornerstone of initial treatment. These strategies are universally applicable, regardless of stone composition, and prioritise non-pharmacological measures such as adequate hydration, dietary adjustments,
and lifestyle modifications to promote natural stone passage and reduce recurrence risk.2,3
Adequate hydration is the cornerstone of conservative management, with a recommended daily fluid intake sufficient to achieve a urine output of 2 L or more. This reduces the concentration of stoneforming salts in the urine, supporting the expulsion of smaller stones while preventing new stone formation. Dietary modifications, including sodium restriction to lower urinary calcium excretion, are universally advised, as are adjustments to reduce intake of oxalate-rich foods and animal protein to limit recurrence. Additionally, urinary pH regulation is an important factor in the management of various stone types, as the solubility of certain stone components depends on the acidity or alkalinity of the urine. These general measures provide a strong foundation for managing urolithiasis and are often sufficient in cases without complex underlying conditions.3-6
Pharmacological treatment complements these general strategies and is essential in both acute and chronic urolithiasis management. During acute episodes, the primary goals are to alleviate pain and facilitate stone passage. Pain management is central, with non-steroidal antiinflammatory drugs (NSAID) being the firstline agents due to their combined analgesic and anti-inflammatory effects. For patients with severe pain or contraindications to NSAIDs, opioids may be used cautiously, while intravenous lidocaine has shown promise as an alternative in select cases.7
Antiemetics such as ondansetron or metoclopramide are frequently used to manage nausea and vomiting associated with acute renal colic.
MET is a pharmacological strategy primarily used for managing ureteral stones measuring 5–10 mm. Alpha-blockers, such as tamsulosin and doxazosin, relax ureteral smooth muscle, facilitating stone passage and reducing the time to expulsion. When combined with anti-inflammatory agents, MET has demonstrated significant efficacy in reducing the need for surgical intervention and improving patient outcomes.3,8 For stones ≤5 mm, the spontaneous passage rate is high, often making conservative management (observation without medication) sufficient. In contrast, MET is particularly effective for distal ureteral stones >5 mm, where spontaneous passage is less likely. However, its benefits are less pronounced for proximal stones due to their lower spontaneous passage rates and higher risk of obstruction. Clinical guidelines recommend considering alpha-blockers as MET for distal ureteral stones >5 mm as part of the treatment options for patients who are amenable to conservative management.3,8
Management of unilateral urological obstruction caused by a ureteral calculus requires a tailored approach based on stone characteristics, urinary tract anatomy, and clinical presentation. Small stones (<5 mm) typically pass spontaneously with conservative management (analgesia, hydration, and MET) for 4–6 weeks. Larger stones or those causing persistent obstruction, severe pain, or renal impairment require surgical intervention.
In cases complicated by infection, such as obstructive pyelonephritis or urosepsis, urgent renal pelvis drainage is necessary to relieve obstruction. Antibiotic therapy should be initiated promptly to control the infection. Definitive stone removal follows once the infection is resolved, and the patient’s condition stabilises.
Surgical intervention is also indicated for complications directly related to the stone or its treatment, such as perforation, avulsions, or infections.
Prompt intervention is essential to prevent further renal damage and manage sepsisrelated conditions. Hospitalisation and a combined medical and surgical approach are often required, especially when urosepsis, renal abscess, infected stones, and/or acute renal impairment are present.2,3,8
This approach effectively addresses both the stone and related complications, optimising patient outcomes and minimising long-term renal damage.
Specific Stone Composition Treatments
The treatment of urolithiasis becomes increasingly targeted once the stone composition is identified, as different stone types require distinct therapeutic strategies.
Calcium oxalate stones
Calcium oxalate stones, the most prevalent type, are managed through a combination of pharmacological and dietary measures. Thiazide diuretics are commonly prescribed to lower urinary calcium excretion, thereby reducing the likelihood of stone formation.9-11 Potassium citrate is also used to increase urinary citrate levels, which inhibit stone formation by preventing crystal aggregation. Dietary interventions play a crucial role, focusing on reducing the intake of oxalate-rich foods such as spinach, beets, and nuts while ensuring adequate consumption of calciumrich foods to minimise oxalate absorption in the gastrointestinal tract.12,13 Additionally, maintaining sufficient hydration is crucial to dilute urinary constituents and reduce the risk of stone formation.
In primary hyperoxaluria (PH), a rare genetic disorder causing excessive oxalate production, standard treatments may not suffice. PH leads to oxalate accumulation in the kidneys, causing recurrent kidney stones, nephrocalcinosis, and progressive renal impairment. As renal function declines and glomerular filtration rate (GFR) falls below 30–40 mL/min/1.73 m², liver oxalate production surpasses renal clearance, leading to systemic oxalate deposition and multi-organ failure.14
In PH1, the most common and severe form of the disorder, pyridoxine (vitamin B6) therapy plays a key role. Pyridoxine can significantly lower urinary oxalate excretion in about one-third of the patients with PH1, and its effectiveness should be assessed through monitoring urinary oxalate levels.14 If pyridoxine proves ineffective, newer therapies such as RNA interference (RNAi) treatments offer promising alternatives. Lumasiran, an RNAi agent targeting glycolate oxidase, has demonstrated a significant reduction in urinary oxalate excretion (65% versus 11%; p<0.001), with 84% of treated patients reaching urinary oxalate levels below 1.5 times the upper reference limit within 6 months.15 Another agent, nedosiran, which inhibits lactate dehydrogenase A (LDHA), a key enzyme in oxalate production, has demonstrated the potential to reduce urinary oxalate levels by approximately 55% in patients with PH1 or PH2, though its efficacy in PH2 remains uncertain.16
Despite these advances, no specific pharmacological treatments are available for PH2 or PH3.
These newer therapies bring hope, particularly for patients in the advanced stages of PH, where renal impairment and systemic oxalosis complicate treatment. In these cases, kidney replacement therapy should be considered before kidney failure develops. Intensified haemodialysis is recommended for patients who lack access to or do not respond to oxalatelowering therapies.
For patients with PH1 with advanced renal disease (estimated glomerular filtration rate [eGFR] <30 mL/min/1.73 m²) who fail to respond to pyridoxine therapy, combined liver and kidney transplantation is recommended, regardless of access to RNAi treatments. The decision to perform sequential or simultaneous liver and kidney transplantation should be based on the clinical situation and the surgeon’s preference. However, this may be challenging in low-resource countries due to the limited availability of diagnostic tools, renal replacement therapies, and novel therapies.14 Ongoing research is essential to assess the long-term impact of RNAi
therapies and their potential to reduce the need for liver transplantation in patients with multi-organ involvement.
Calcium phosphate stones
Calcium phosphate stones form in alkaline urine and are often associated with underlying metabolic conditions such as renal tubular acidosis. Treatment focuses on correcting hypercalciuria and managing urinary pH. Thiazide diuretics are prescribed to reduce urinary calcium excretion, while potassium citrate or sodium citrate may be cautiously used to balance urinary citrate levels. Monitoring and adjusting urinary pH are essential to prevent excessive alkalinity, which fosters calcium phosphate precipitation.3,6,12
Uric acid stones
Uric acid stones form in acidic urinary conditions and are primarily treated by alkalinising the urine. Potassium citrate or sodium bicarbonate is used to raise urinary pH, enhancing the solubility of uric acid and facilitating its excretion. In cases of hyperuricemia, xanthine oxidase inhibitors, such as allopurinol or febuxostat, are prescribed to reduce uric acid production. It is important to note that uric acid stones can also form in individuals with normal serum and urine uric acid levels but with low urine pH. In such cases, allopurinol and febuxostat have no role in treatment. Regular monitoring of urinary pH is critical, aiming to maintain it within the optimal range of 6.0–6.5 to prevent precipitation of uric acid and other salts.3,6,17
Struvite stones
Struvite stones, commonly associated with urinary tract infection (UTI) caused by urease-producing bacteria, require a multi-faceted treatment approach. The cornerstone of therapy includes antibiotics to eradicate the infection and prevent stone recurrence. Urease inhibitors, such as acetohydroxamic acid (AHA), may also be used to reduce the production of ammonia, which lowers urinary pH and inhibits struvite stone growth. AHA has demonstrated effectiveness in preventing stone growth and delaying recurrence. However, its side effects, including tremulousness and haemolytic anaemia, often limit its use.3,6,17
In some cases, surgical intervention is necessary to remove large or obstructive stones and restore normal urinary function.
Cystine stones
Cystine stones are rare and associated with the hereditary condition cystinuria, which leads to high urinary cystine levels. Treatment strategies emphasise management, primarily involving aggressive hydration to dilute the urine and reduce cystine concentration, often targeting a urine output of at least 3 L/day. Urinary alkalinisation with potassium citrate, targeting a pH of 7.0–7.5, is used to further enhance cystine solubility, and cystinebinding agents such as tiopronin or penicillamine are used for refractory cases. In refractory cases, cystine-binding agents such as tiopronin and D-penicillamine are used, as they form soluble cysteine complexes that facilitate excretion. Measuring free and bound cystine is clinically valuable for adjusting treatment doses, with a target-free cystine level of <100 mmol/ mmol creatinine. However, this test is not widely available, and further studies are needed to validate its clinical utility.18 Among cystine-binding drugs, tiopronin is preferred due to its superior efficacy, reducing urinary-free cystine levels approximately 1.5 times more than D-penicillamine, while also increasing soluble mixed disulfide formation.18,19 Unlike D-penicillamine, tiopronin is not excreted in the urine, making the cyanide–nitroprusside test an effective monitoring tool. It is also associated with a lower toxicity profile, leading to fewer treatment discontinuations (31% versus 69% for D-penicillamine in a multi-centre trial).20 In contrast, D-penicillamine, though effective, carries a higher risk of adverse effects, including rash, gastrointestinal symptoms, joint pain, and haematologic complications such as thrombocytopenia and neutropenia. Long-term use may also cause vitamin B6 deficiency, necessitating supplementation. Given its lower toxicity, tiopronin is generally the first choice for patients requiring pharmacological intervention. The dosing and adverse effect profiles of both agents are detailed in Table 1.
Regular monitoring of cystine levels in the urine and adherence to these interventions are critical for long-term management. Long-term management of cystinuria requires regular monitoring of urinary cystine levels, blood counts, and urinary protein excretion to optimise treatment and minimise complications.3,6,17,18
Captopril, an angiotensin-converting enzyme (ACE) inhibitor, has been explored for cystine stone treatment due to its sulfhydryl groups, which bind cystine and form a more soluble cystinecaptopril complex. While this mechanism theoretically enhances cystine solubility, its clinical efficacy remains controversial. Due to insufficient high-quality evidence, captopril is not recommended as monotherapy but may be considered as an adjunct to tiopronin in patients with high cystine excretion. It is also a potential alternative for those intolerant to tiopronin and D-penicillamine.6,12 Given these considerations, the authors hypothesise that zofenopril, another sulfhydryl-containing ACE inhibitor used for hypertension, could be a potential option for patients with both cystine stones and hypertension. Due to its structural similarity to captopril, it may also enhance cystine solubility while providing anti-hypertensive benefits. However, this hypothesis remains untested, and further research is needed to evaluate its potential role in cystinuria management.
Mixed stones
Mixed stones, such as those comprising calcium oxalate and uric acid or calcium oxalate and phosphate, present unique challenges due to their varied composition. Treatment strategies must address all components of the stone effectively:
• Calcium oxalate and uric acid stones: a combination of urinary alkalinisation with potassium citrate to enhance uric acid solubility and the use of thiazides to lower urinary calcium levels is effective. Xanthine oxidase inhibitors such as allopurinol and febuxostat may be added if hyperuricemia is present.
• Calcium oxalate and phosphate stones: addressing hypercalciuria with thiazides or thiazide-like diuretics and carefully managing urinary pH to avoid excessive alkalinity are critical.
• Urate and phosphate stones: these require precise management of urinary pH to prevent simultaneous precipitation of both components. Regular monitoring of pH ensures the balance needed to prevent further stone formation.8,12,17
In chronic management, pharmacological therapies are tailored to the stone’s composition and the patient’s metabolic profile to prevent recurrence. By addressing the unique metabolic abnormalities associated with mixed stones, clinicians can improve treatment outcomes and reduce recurrence risk.
To support clinical decision-making in pharmacological management, Table 1 provides a comprehensive summary of the available medical therapies for urolithiasis. It highlights the mechanisms of action, recommended dosages, specific indications, and potential side effects for each medication, aiding clinicians in tailoring treatment plans based on stone composition and patient-specific factors.
Innovative Treatments
Emerging therapies in the treatment of urolithiasis are focused on improving patient outcomes through advanced techniques and novel pharmacological interventions. One area of innovation involves the use of nanotechnology to deliver targeted treatments directly to the site of stone formation. These nanoparticles can carry drugs that inhibit crystal growth or dissolve existing stones, offering a minimally invasive alternative to traditional surgical approaches.2,21 Advances in genetic research have also paved the way for personalised medicine, with treatments tailored to an individual’s genetic predisposition to stone formation.2,22 Table 2 provides an overview of the genetic diseases associated with an increased risk of urinary stone formation, emphasising the role of specific genetic factors in stone development. Another
promising development is the use of probiotics, such as Oxalobacter formigenes, which degrade oxalates in the gut and reduce urinary oxalate levels. This approach is particularly beneficial for patients with recurrent calcium oxalate stones.13
Additionally, novel medications targeting specific metabolic pathways involved in stone formation are under investigation, offering the potential to prevent stones at their source.13,26,27 These innovations, while still in varying stages of research and clinical trials, represent the future of urolithiasis management, promising more effective and less-invasive treatment options for patients worldwide.
Dietary and Nutritional Strategies in the Prevention and Management of Urolithiasis
Dietary modifications play a crucial role in both the prevention and management of urolithiasis. Various dietary components, including calcium, oxalate, uric acid, hydration, and micronutrient intake, influence stone formation. Understanding these factors is essential for designing effective dietary interventions.
Hydration and fluid intake
Adequate fluid intake is the cornerstone of urolithiasis prevention. Increasing urine output dilutes stone-forming solutes, reducing their supersaturation. Water is the preferred choice, but certain beverages, such as citrus juices like lemonade and orange juice, may offer additional benefits due to their citrate content, which inhibits stone formation. Evidence suggests that orange juice has a protective effect, while apple and grapefruit juice have not been confirmed as risk factors. However, sugar-sweetened sodas and punch are linked to an increased risk of stone formation. Additionally, increased caffeine intake, particularly above 500 mg/day, has been associated with a lower risk of urolithiasis.28-30
Calcium intake and its role
Dietary calcium plays a paradoxical role in stone formation. While excessive calcium supplementation can contribute to stone formation, an adequate intake of dietary
Table 1: Pharmacotherapy for urolithiasis.6,12,13
Medication/ drug (class)
Hydrochlorothiazide (thiazide) Increases calcium reabsorption in tubules
12.5–50 mg/day
Chlortalidone (thiazide-like diuretic) Increases calcium reabsorption in tubules 25–50 mg/day
Indapamide (thiazide-like diuretic)
Reduces urinary calcium excretion and promotes calcium reabsorption
Potassium citrate Alkalinises urine and dissolves stones
Allopurinol (xanthine oxidase inhibitor)
Febuxostat (xanthine oxidase inhibitor)
Reduces uric acid levels and prevents hyperuricosuria; effective only in uric acid stones associated with hyperuricosuria
Reduces uric acid levels and prevents hyperuricosuria; effective only in uric acid stones associated with hyperuricosuria
Calcium supplements Binds to oxalate in the gut to reduce absorption
Tiopronin Binds to cystine to enhance its solubility in urine
Abnormal purine metabolism causing the formation of 2,8dihydroxyadenine stones.
Tubular dysfunction results in electrolyte imbalances, particularly hypercalciuria, promoting stone formation.
Impaired cystine transport in renal tubules leads to cystine crystal formation, causing stones.
Renal tubular dysfunction causes hypercalciuria and impaired oxalate handling, leading to stone formation.
Impaired hydrogen ion secretion in the distal tubule leads to severe metabolic acidosis, which causes calcium mobilisation from bones, increasing urinary calcium. This process favours calcium phosphate stone formation.
Partial impairment in acidification leads to mild metabolic acidosis, causing an imbalance of calcium and phosphate in urine, promoting calcium phosphate stone formation.
Defective phosphate handling increases calcium phosphate stone risk.
Hyperuricemia due to defective purine metabolism results in uric acid stones.
Tubular ectasia leads to urine stasis, which increases the risk of stone formation.
Hyperparathyroidism leads to hypercalcaemia, hypercalciuria, and increased risk of calcium-based stones.
Hyperparathyroidism (in MEN2A) results in hypercalcaemia and hypercalciuria, promoting calcium stone formation.
Impaired renal function leads to hyperuricemia and metabolic changes favouring stone formation. Tubular ectasia leads to urine stasis, which increases the risk of stone formation.
Increased oxalate production, leading to calcium oxalate stone formation.
Defective xanthine oxidase enzyme leads to xanthine accumulation and stone formation.
calcium is protective. It binds to oxalate in the intestines, reducing its absorption and urinary excretion. A normal calcium intake of about 1,200 mg/day, combined with a low-salt, low-animal-protein diet, has been shown to reduce the risk of stone recurrence by approximately 50% over 5 years compared to a low-calcium diet of 400 mg/ day.31 Dairy products such as milk, yogurt, and cheese are the recommended sources of calcium, while calcium supplements should be used cautiously.28,29
Oxalate consumption and reduction strategies
Oxalate is a major component of calcium oxalate stones, which are the most common type of kidney stone. Foods high in oxalate include spinach, rhubarb, nuts, tea, and chocolate. Reducing dietary oxalate intake, especially in individuals with hyperoxaluria, can help minimise stone risk. Pairing oxalate-rich foods with calcium sources may help reduce oxalate absorption. Oxalate absorption is variable, and in cases of low-calcium diets, increased intestinal absorption of oxalate can contribute to stone formation.28,29
Uric acid and protein intake
Excessive consumption of animal proteins, particularly red meat, poultry, and seafood, increases uric acid production, lowers urinary pH, and promotes uric acid stone formation. High-protein diets have been confirmed as risk factors for urolithiasis. Reducing the intake of beef, pork, shellfish, and chicken can help mitigate this risk. Alkalinising agents, such as potassium citrate, may also be beneficial for patients with recurrent uric acid stones.28,29
Sodium and potassium balance
High sodium intake enhances calcium excretion in urine, increasing the risk of stone formation. Reducing dietary sodium, primarily by limiting processed and fast foods, can help maintain a balanced calcium excretion rate. Conversely, potassiumrich foods such as bananas, oranges, and potatoes contribute to stone prevention by enhancing urinary citrate levels. Notably, only potassium citrate, not potassium chloride, has been found to have a protective effect against urolithiasis.28,29
Role of vitamin and mineral supplements
Certain vitamins and minerals influence kidney stone formation. Vitamin C, when consumed in excessive amounts (more than 1 g/day), increases oxalate production, which elevates the risk of calcium oxalate stones, particularly in men. However, vitamin B6 intake has not been associated with an increased risk of stone formation. Vitamin D supplementation has not been conclusively linked to an increased stone risk in men and younger women, although older women may experience a slight increase in risk.28,29
Among metal cations, dietary copper intake has been associated with an increased risk of kidney stones, while manganese intake appears to have a protective effect. Magnesium plays a critical role in reducing stone formation by binding to oxalate in the gastrointestinal tract, decreasing its absorption and subsequent urinary excretion. Additionally, magnesium enhances urinary citrate levels, further preventing calciumbased stone formation. Research suggests that individuals with low magnesium intake may be at a higher risk of developing kidney stones. Magnesium-rich foods include leafy greens such as spinach and kale, nuts such as almonds and cashews, seeds such as pumpkin and flaxseeds, legumes, whole grains, and bananas. Magnesium supplements, such as magnesium citrate and magnesium oxide, may provide additional benefits for patients with recurrent kidney stones, particularly those with low urinary magnesium levels.28,29 However, excessive supplementation should be avoided due to potential gastrointestinal side effects.
Probiotics and herbal products
Probiotics, particularly gut colonisation with O. formigenes, have been linked to lower urinary oxalate levels, potentially reducing stone formation. However, the effectiveness of oxalate-degrading probiotics remains inconclusive.28
Several herbal products have shown potential benefits in reducing stone formation and recurrence. While clinical evidence is still evolving, traditional medicine has used for long certain plants for their diuretic, anti-inflammatory, and crystallisation-inhibiting properties. Phyllanthus niruri (chanca piedra)
demonstrates anti-lithogenic properties by inhibiting calcium oxalate crystallisation, promoting stone dissolution, and reducing oxidative stress. Hibiscus sabdariffa contains natural citrate-enhancing compounds that may help prevent stone formation. Additionally, it has mild diuretic effects, increasing urinary volume and reducing stone supersaturation. Orthosiphon stamineus (Java tea), traditionally used in Southeast Asia for urinary tract health, has been found to exhibit diuretic and antioxidant properties that may help reduce stone formation. Urtica dioica (stinging nettle), known for its diuretic and anti-inflammatory effects, may support increased urine flow and decrease urinary crystallisation potential.28 While these herbal products show promise, more randomised clinical trials are needed to confirm their long-term efficacy and safety.
Dietary patterns and lifestyle modifications
Adopting a balanced diet, such as the Dietary Approaches to Stop Hypertension (DASH) diet, which is rich in fruits, vegetables, whole grains, and low-fat dairy, has been associated with a lower risk of kidney stones.32 A vegetarian diet that includes dairy products appears to be the most protective dietary pattern for urolithiasis prevention. High intake of fruits and vegetables contributes to increased urinary citrate excretion and a reduced stone formation risk. Maintaining a healthy weight and engaging in regular physical activity further support stone prevention.
In conclusion, dietary interventions are integral to urolithiasis management. A well-balanced diet that ensures proper hydration, adequate calcium intake, controlled oxalate and uric acid consumption, reduced sodium intake, and increased fruit and vegetable consumption can significantly reduce the risk of stone formation. The available scientific evidence supports a dietary approach that prioritises fluid intake, balanced calcium consumption, moderate protein intake, and increased consumption of plant-based foods.28,29,31,32 Further research into personalised nutrition strategies may enhance the effectiveness of dietary interventions in kidney stone prevention and management.
Overview of Surgical Treatment Options of Urolithiasis
Surgical interventions are a cornerstone in the management of urolithiasis, especially in patients where medical management proves insufficient, stones are particularly large, or complications arise. These procedures vary based on the stone characteristics and patient-specific factors, encompassing several modalities that differ in their indications, success rates, and potential complications.
Extracorporeal shock wave lithotripsy
Extracorporeal shock wave lithotripsy (ESWL) uses high-energy shock waves to fragment stones into smaller pieces, which are then passed naturally through the urinary tract. This method is particularly effective for kidney and proximal ureteral stones less than 2 cm in size.33,34 ESWL is favoured for its non-invasive nature and minimal recovery time. However, it is less effective for dense stones and stones located in the lower pole due to gravity-dependent fragment clearance.35,36 Temporary haematuria and incomplete fragmentation are common complications.37
Clinical outcomes of ESWL vary based on factors such as stone size, location, and patient-specific characteristics. The stone-free rate (SFR) after the first ESWL session ranges from 46.7% to 69%.38,39 Repeated treatments improve success rates significantly, reaching 70.5% to as high as 93%,39,40 highlighting the importance of repeat procedures in achieving optimal outcomes.
Potential contraindications for ESWL include pregnancy, uncorrected bleeding disorders, aortic aneurysms, severe skeletal deformities, and morbid obesity. The effectiveness of shock wave penetration and stone localisation may be compromised due to technical limitations, making alternative modalities such as ureteroscopy (URS) or percutaneous nephrolithotomy more suitable.33
These variations underscore the importance of individualised patient assessment when considering ESWL for stones less than 2 cm. Factors such as stone composition,
density, and anatomical considerations can significantly influence treatment outcomes. A thorough evaluation is essential to optimise the efficacy of ESWL and determine the necessity for additional treatment sessions.
Ureteroscopy
URS is a minimally invasive procedure that involves the insertion of a flexible or rigid ureteroscope through the urethra, enabling direct visualisation and fragmentation of stones using laser lithotripsy. This method is highly effective for treating ureteral and renal stones, particularly stones smaller than 1 cm, with SFR exceeding 90%.41,42 Flexible ureteroscopy (FURS) extends the capabilities of URS by allowing access to challenging locations such as the renal calyces and renal pelvis, which are difficult to reach with rigid scopes.
Despite its minimally invasive nature, URS is associated with potential complications, including ureteral injury, perforation, and post-operative strictures. Ureteral avulsion, though rare (0.06–0.45%), is one of the most severe complications of URS, often related to the use of an overly large ureteroscope or attempts to extract an inadequately fragmented or impacted stone from the proximal or midureter. It typically results from excessive stretching at the ureter’s weakest point, which may be further aggravated by factors such as impaired fluid irrigation during laser lithotripsy, weakening the ureter.43,44 Potential contraindications include untreated UTIs and severe ureteral strictures that may prevent safe scope passage. Advances in laser technologies, such as the holmium:yttrium–aluminium–garnet (holmium:YAG) and thulium fiber laser (TFL), have significantly improved the efficacy and safety of URS.29 The holmium:YAG laser, considered the gold standard, effectively fragments stones of all compositions, though it may lead to stone retropulsion. The TFL offers faster ablation rates and reduced retropulsion, making it particularly advantageous in complex cases.45
Percutaneous nephrolithotomy
Percutaneous nephrolithotomy (PCNL) is the gold standard for managing large stones (>2 cm) and complex staghorn
calculi. The procedure involves accessing the kidney through a small incision in the back, allowing for direct removal or fragmentation of stones. PCNL achieves high success rates, with SFRs reaching 92% for staghorn calculi.2,46
However, PCNL is not without risks. Common complications include bleeding, infection, and, in rare cases, injury to adjacent organs. Contraindications include active UTIs, severe cardiopulmonary comorbidities, or uncorrected coagulopathies. Recent innovations such as suction-assisted systems and laser integration have enhanced the procedure’s outcomes while minimising complications.2,3 These advancements have made PCNL a reliable option for patients with complex or large stone burdens.
Open and laparoscopic surgery
Open and laparoscopic surgeries are reserved for patients with complex anatomical abnormalities or other cases where minimally invasive methods are not feasible. These approaches allow for precise stone removal but are associated with longer recovery periods and higher morbidity compared to minimally invasive options.2,47
While their use has declined due to advancements in less invasive techniques, open and laparoscopic surgeries remain valuable in specific scenarios. Potential contraindications include severe medical comorbidities that preclude surgical interventions. The success rates for these procedures are high in appropriately selected cases but their risks include post-operative pain, infection, and extended hospital stays.
Advancements and Combination Modalities
Advancements
in technology
Disposable ureteroscopes have reduced the risk of cross-contamination and eliminated the need for sterilisation, enhancing procedural consistency. Studies demonstrate that disposable and reusable ureteroscopes have comparable SFRs, complication rates, and clinical outcomes. While disposables minimise infection risks and sterilisation needs, they generate significant waste, raising concerns about
long-term environmental sustainability. Reusable ureteroscopes, although generating less immediate waste, require extensive cleaning and maintenance, contributing to resource consumption. Despite these compromises, disposables are particularly beneficial in high-volume or resource-limited settings, where infection control and efficient turnover are prioritised.31,35–37
However, in regions such as sub-Saharan Africa, where the majority of patients pay for healthcare services out of their pocket, both the financial burden of procedures and the limited availability of disposable ureteroscopes can hinder their widespread adoption. Despite their advantages in infection control and procedural efficiency, these economic and logistical challenges faced by patients and healthcare providers may limit their feasibility in these settings.42,48–50
Robot-assisted FURS is another notable innovation, offering enhanced surgeon dexterity and precision in complex cases. These robotic systems help reduce surgeon fatigue and improve surgical outcomes.2,51 AI integration into FURS has further revolutionised the field by assisting in real-time stone detection and procedural guidance, which is particularly beneficial for less-experienced surgeons, ultimately improving patient outcomes.2
High-intensity focused ultrasound (HIFU) is an emerging non-invasive technology that is being explored as a potential alternative to conventional ESWL. HIFU uses focused ultrasound waves to fragment stones, offering the advantage of avoiding radiation exposure and eliminating the need for external shock waves. Although still in the experimental phase, HIFU presents a promising treatment modality for certain types of kidney stones, especially in patients who are contraindicated for more invasive procedures.52-54
Recent advances in laser technology, such as the TFL and holmium:YAG laser, have significantly improved the efficiency and safety of URS procedures. The TFL offers faster ablation rates, reduced stone
retropulsion, and more precise targeting, which is particularly beneficial in complex stone locations.45 The integration of these advanced lasers has enhanced the success rates of ureteroscopic treatments for both renal and ureteral stones.
Miniaturised percutaneous nephrolithotomy (mini-PCNL) is a less-invasive version of traditional PCNL, utilising smaller instruments and smaller incisions, which result in reduced blood loss, faster recovery, and fewer complications. This technique is particularly effective for large stones while still maintaining high SFRs. Mini-PCNL represents a key step forward in reducing the morbidity of patients undergoing complex stone removal procedures.46
Combination modalities
For complex cases, combining multiple surgical modalities can yield synergistic effects, improving stone clearance and minimising the need for repeated procedures.45 This approach is particularly beneficial for patients with staghorn calculi or other complex stone formations.
Endoscopic combined intrarenal surgery (ECIRS) is a modern, minimally invasive technique for treating large and complex renal stones. This method primarily integrates URS/FURS and PCNL to optimise SFRs. By enabling simultaneous visualisation and manipulation through both transureteral and percutaneous access, ECIRS enhances stone clearance compared to traditional approaches. Additionally, ECIRS may incorporate adjunctive techniques such as ESWL or mini-PCNL to further improve efficacy and patient outcomes.2
By leveraging the strengths of both PCNL and URS/FURS, surgeons can optimise SFRs while minimising patient morbidity.2,42,52 The flexibility of URS allows for precise stone localisation and fragmentation, while percutaneous access provides direct entry into the renal collecting system, facilitating removal of larger stone fragments and reducing intrarenal pressure. This approach lowers the incidence of post-operative sepsis and is particularly advantageous for patients with anatomical anomalies or complex
stone burdens. The integration of advanced technologies, such as holmium:YAG laser lithotripsy and digital endoscopes, further enhances procedural success.45
ECIRS is performed under general anaesthesia and requires a multidisciplinary team, including urologists and anaesthesiologists. Intraoperative ultrasound and fluoroscopy guide precise instrument placement. The supine position minimises anaesthetic risks and shortens operative time by eliminating the need for patient repositioning. Although risks such as bleeding, infection, or injury to adjacent structures exist, they are significantly lower than with traditional methods due to the controlled percutaneous renal access under ultrasound guidance. Additionally, the use of suction-assisted systems enhances stone fragment clearance, further improving procedural outcomes.2,42,45,47
Another innovative combination under research involves pairing HIFU with other modalities such as URS. While still being explored for its clinical efficacy, HIFU has the potential to fragment stones in challenging locations or those less amenable to traditional methods. URS or FURS can then be used to remove the resulting fragments. This multi-modal approach may improve patient outcomes by utilising the strengths of each technique, particularly for patients with stones in hardto-reach locations or those with multiple, fragmented stones.52-54 Further studies are required to establish its effectiveness and safety in routine clinical practice.
To assist in clinical decision-making, Table 3 provides a clear comparison of the various surgical approaches for urolithiasis treatment, outlining the advantages, complications, outcomes, limitations, and contraindications associated with each modality.
CONCLUSION
The management of urolithiasis has undergone substantial advancements in surgical (urologic) treatments, offering minimally invasive and highly effective solutions. However, pharmacological management, crucial for preventing recurrence and addressing metabolic abnormalities, requires further development. A holistic approach integrating surgical innovation with tailored medical interventions is essential to optimising outcomes and mitigating the burden of this disease.
Personalised management guided by regular monitoring of urinary pH, metabolic profiles, and adherence to dietary and pharmacological regimens forms the cornerstone of effective long-term care. Tailoring treatment to specific composition of kidney stones not only improves outcomes but also reduces recurrence, emphasising the importance of sustained patient education and support.
Advances in understanding the pathophysiology of urolithiasis, including molecular pathways such as crystal nucleation and aggregation, as well as genetic predispositions affecting metabolism and stone composition, are opening new avenues for more precise therapies. By integrating surgical expertise, personalised pharmacological care, and proactive monitoring within a comprehensive framework, clinicians can significantly enhance patient outcomes, reduce recurrence rates, and improve the quality of life for individuals affected by urolithiasis.
Table 3: Comparison of surgical modalities in urolithiasis treatment: advantages, complications, outcomes, and limitations.
1. Stamatelou K, Goldfarb DS. Epidemiology of kidney stones. Healthcare (Basel). 2023;11(3):424.
2. Papatsoris A et al. Management of urinary stones: state of the art and future perspectives by experts in stone disease. Arch Ital Urol Androl. 2024;96(2):12703.
3. Skolarikos A et al. EAU Guidelines for Urolithiasis. Available at: https:// d56bochluxqnz.cloudfront.net/ documents/full-guideline/EAUGuidelines-on-Urolithiasis-2024.pdf. Last accessed: 27 January 2025.
4. Bao Y et al. Water for preventing urinary stones. Cochrane Database Syst Rev. 2020;2(2):CD004292.
5. Fink HA et al. Diet, fluid, or supplements for secondary prevention of nephrolithiasis: a systematic review and meta-analysis of randomized trials. Eur Urol. 2009;56(1):72-80.
6. Jahrreiss V et al. Medical management of urolithiasis: great efforts and limited progress. Asian J Urol. 2024;11(2):149-55.
7. Motov S et al. Pain management of renal colic in the emergency department with intravenous lidocaine. Am J Emerg Med. 2018;36(10):1862-4.
8. Pearle MS et al.; American Urological Association. Medical management of kidney stones: AUA guideline. J Urol. 2014;192(2):316-24.
9. Hsi RS et al. Thiazide dose, urine calcium, and symptomatic kidney stone events. JAMA Netw Open. 2024;7(8):e2428953.
10. Dhayat NA et al. Hydrochlorothiazide and prevention of kidneystone recurrence. N Engl J Med. 2023;388(9):781-91.
11. Bargagli M et al. Thiazides for kidney stone recurrence prevention. Curr Opin Nephrol Hypertens. 2024;33(4):42732.
12. Segall M et al. Pharmacologic treatment of kidney stones: current medication and pH monitoring. Actas Urol Esp (Engl Ed). 2024;48(1):11-8.
13. Khanam A et al. Treatment and prevention of recurrent urolithiasis: insights on molecular mechanism of occurrence and medical care. Food Chem Adv. 2024;5:100751.
14. Groothoff JW et al. Clinical practice recommendations for primary hyperoxaluria: an expert consensus statement from ERKNet and OxalEurope. Nat Rev Nephrol. 2023;19(3):194-211.
15. Garrelfs SF et al. Lumasiran, an RNAi therapeutic for primary
hyperoxaluria type 1. N Engl J Med. 2021;384(13):1216-26.
16. Hoppe B et al. Safety, pharmacodynamics, and exposureresponse modeling results from a firstin-human phase 1 study of nedosiran (PHYOX1) in primary hyperoxaluria. Kidney Int. 2022;101(3):626-34.
17. Shastri S et al. Kidney stone pathophysiology, evaluation and management: core curriculum 2023. Am J Kidney Dis. 2023;82(5):617-34.
18. Servais A et al. Cystinuria: clinical practice recommendation. Kidney Int. 2021;99(1):48-58.
19. Harbar JA et al. Comparison of 2-mercaptopropionylglycine and D-penicillamine in the treatment of cystinuria. J Urol. 1986;136(1):146-9.
20. Chillarón J et al. Pathophysiology and treatment of cystinuria. Nat Rev Nephrol. 2010;6(7):424-34.
21. Houlihan I et al. Proof-of-concept for a novel nanotechnology-based treatment for urolithiasis. Urolithiasis. 2024;52(1):60.
22. Friedrich M, Aigner A. Therapeutic siRNA: state-of-the-art and future perspectives. BioDrugs. 2022;36(5):549-71.
23. Edvardsson VO et al. Hereditary causes of kidney stones and chronic kidney disease. Pediatr Nephrol. 2013;28(10):1923-42.
24. Gómez-Conde S et al. Hereditary distal renal tubular acidosis: genotypic correlation, evolution to long term, and new therapeutic perspectives. Nefrologia (Engl Ed). 2021;41(4):38390.
25. Alexander RT et al., Hereditary distal renal tubular acidosis - GeneReviews® [Internet] (2019) Seattle: University of Washington. Available at: https://www. ncbi.nlm.nih.gov/books/NBK547595/. Last accessed: 14 March 2025.
26. Allam EAH. Urolithiasis unveiled: pathophysiology, stone dynamics, types, and inhibitory mechanisms: a review. Afr J Urol. 2024;30:34.
27. Dika Ž et al. SGLT2 inhibitors and their effect on urolithiasis: current evidence and future directions. J Clin Med. 2024;13(19):6017.
28. Pedro RN et al. Nutrients, vitamins, probiotics and herbal products: an update of their role in urolithogenesis. Urolithiasis. 2020;48(4):285301. Erratum in: Urolithiasis. 2020;48(4):303.
29. Ferraro PM et al. Risk of kidney stones: influence of dietary factors, dietary patterns, and vegetarian-vegan diets. Nutrients. 2020;12(3):779.
30. Ferraro PM et al. Caffeine intake and the risk of kidney stones. Am J Clin Nutr. 2014;100(6):1596-603.
31. Borghi L et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. N Engl J Med. 2002;346(2):77-84.
32. Taylor EN et al. DASH-style diet associates with reduced risk for kidney stones. J Am Soc Nephrol. 2009;20(10):2253-9.
33. Turk C et al. EAU Guidelines on Urolithiasis 2021. Available from: https://uroweb.org/guideline/ urolithiasis. Last accessed: 28 January 2025.
34. Zumstein V et al. Surgical management of urolithiasis – a systematic analysis of available guidelines. BMC Urol. 2018;18(1):25.
35. Lingeman JE et al. Management of lower pole nephrolithiasis: a critical analysis. J Urol. 1994;151(3):663-7.
36. Sani A et al. Urolithiasis management: an umbrella review on the efficacy and safety of extracorporeal shock wave lithotripsy (ESWL) versus the ureteroscopic approach. Urologia. 2025;22:3915603241313162.
37. Tzelves L et al. Shockwave lithotripsy complications according to modified Clavien-Dindo grading system. A systematic review and meta-regression analysis in a sample of 115 randomized controlled trials. Eur Urol Focus. 2022;8(5):1452-60.
38. Wagenius M et al. Factors influencing stone-free rate of extracorporeal shock wave lithotripsy (ESWL); a cohort study. Scand J Urol. 2022;56(3):23743.
39. Nielsen TK, Jensen JB. Efficacy of commercialised extracorporeal shock wave lithotripsy service: a review of 589 renal stones. BMC Urol. 2017 27;17(1):59.
40. Snicorius M et al. A prospective study on the impact of clinical factors and adjusted Triple D system for success rate of ESWL. Medicina (Kaunas). 2023;59(10):1827.
41. Aboumarzouk OM et al. Flexible ureteroscopy and laser lithotripsy for stones >2 cm: a systematic review and meta-analysis. J Endourol. 2012;26(10):1257-63.
42. Juliebø-Jones P et al. Advances in ureteroscopy: new technologies and current innovations in the era of tailored endourological stone treatment (TEST). J Clin Urol. 2023;16(3):190-8.
43. Ge C et al. Management of complete ureteral avulsion and literature review: a report on four cases. J Endourol. 2011;25(2):323-6.
44. Kuddah Y et al. Inverted mucosa and avulsion ureteral injury in ureteroscopic procedure: a very rare complication of a common procedure in urology. Urol Case Rep. 2021;37:101605.
45. He M et al. Recent advances in the treatment of renal stones using flexible ureteroscopys. Int J Surg. 2024;110(7):4320-8.
46. Jones P et al. Safety and efficacy of day-case percutaneous nephrolithotomy: a systematic review from European Society of Uro-Technology. Eur Urol Focus. 2019;5(6):1127-34.
47. Meria P et al. 2022 recommendations of the AFU lithiasis committee:
open surgery and laparoscopy. Prog Urol. 2023;33(14):864-70.
48. Marchini GS et al. A comprehensive literature-based equation to compare cost-effectiveness of a flexible ureteroscopy program with single-use versus reusable devices. Int Braz J Urol. 2019;45(4):658-70.
49. Bragaru M et al. Single-use versus conventional reusable flexible ureteroscopes – an evaluation of the functional parameters. J Med Life. 2023;16(1):10-5.
50. Göger YE et al. Efficiency of retrograde intrarenal surgery in lower pole stones: disposable flexible ureterorenoscope or reusable flexible ureterorenoscope? World J Urol. 2021;39(9):3643-50.
51. Türk C et al. EAU guidelines on interventional treatment for urolithiasis. Eur Urol. 2016;69(3):475-82.
52. Ikeda T et al. Focused ultrasound and lithotripsy. Adv Exp Med Biol. 2016;880:113-29.
53. Do MT et al. Clinical application of the therapeutic ultrasound in urologic disease: part II of therapeutic ultrasound in urology. Investig Clin Urol. 2022;63(4):394-406.
54. Mosquera Seoane L et al. Technological innovations in shock wave lithotripsy. Actas Urol Esp (Engl Ed). 2024;48(1):105-10.
Delayed Presentation of Transurethral Resection of Prostate Syndrome: A Case Presentation from a Rural Referral Hospital
1. Department of Urology, St. Francis Referral Hospital, Ifakara, Tanzania
2. Department of Surgery, St. Francis University College of Health and Allied Health Sciences, Ifakara, Tanzania *Correspondence to magodaam@yahoo.co.uk
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements The author would like to thank the patient for consenting for publication of this work. The author expresses sincere gratitude to the urology team at St. Francis Regional Referral Hospital and the Intermediate Care Unit staff at St. Francis Hospital for their co-operation in managing this patient.
Received: 23.05.24
Accepted: 12.08.24
Keywords: Acute kidney injury, case report, delayed transurethral resection of prostate (TURP) syndrome, limited health resource, rural setting.
The authors report a case of delayed transurethral resection of prostate (TURP) syndrome. A 60-year-old man was diagnosed with obstructive prostatic enlargement where conservative medical treatment failed, and therefore he was scheduled for standard TURP under spinal anaesthesia. Six days post-discharge, the patient presented at the emergency department with signs of clot retention and transient hypertension with difficulty in passing urine, suprapubic pain, and abdominal distention; clot evacuation was endoscopically done. However, 5 days post-clot evacuation (11 days post-TURP), the patient presented signs of TURP syndrome with hypertension, difficulty breathing, and reduced oxygen saturation. Electrolyte analysis revealed hyponatraemia (sodium concentration of 105 mmol/L), hypokalaemia (potassium concentration of 2.7 mmol/L), and kidney injury with a serum creatinine level of 157.3 mmol/L. Medical treatment consisted of hypertonic saline 3%, intravenous potassium chloride, volume expansion, oxygen therapy, and renal haemodialysis. The case presented here describes a typical delayed TURP syndrome, a rare occurrence which was diagnosed and treated. The patient was discharged from the hospital for the second time without complications.
Key Points
1. Transurethral resection of the prostate (TURP) is one of the most common procedures worldwide. It has gained popularity over the years despite well-documented cases of intraoperative TURP syndrome. Many urologic surgeons are comfortable discharging patients 72 hours post-operation; however, this case report points out the persistent risk of TURP syndrome even after 72 hours, particularly in resource-limited settings.
2. This is a case report exploring unusually delayed TURP syndrome in a rural hospital setting.
3. The authors hope that clinicians and surgeons who are involved in endoscopic surgery will take note of this case and be vigilant in the management of post-TURP patients as life-threatening TURP syndrome may have a delayed onset.
INTRODUCTION
Transurethral resection of prostate (TURP) complications may be defined as postoperative complications that occur in patients who have undergone endoscopic prostatectomy.1,2 These include haemorrhage, clot retention, catheter blockage, and volumetric overload hypotension leading to volumetric overload shock as a result of massive fluid gain from either fluid absorption after prostatic surgery or massive fluid infusion.3
Haemorrhage and clot retention may be immediate or delayed, while vascular hypotension is the result of fluid absorption or excessive intravenous (IV) infusion that leads to reduced serum sodium, a condition known as dilution hyponatraemia (<120 mmol/L).4 They are all life-threatening and remain significant challenges in surgeries, especially in endoscopic urology surgery. Each complication is managed based on the underlying cause.5 The effective management of clot retention is clot evacuation, while management of volumetric overload is hypertonic sodium therapy (HST), including HST 3.0% NaCl, HST 5.0% NaCl, and 8.4% NaHCO₃. Haemorrhage is treated by endoscopic ligation of the bleeders in addition to blood transfusion, which may be in combination with fresh frozen plasma when available (or a whole package of blood).4 The management of concurrent haemorrhage, clot-induced urine retention, and volumetric hyponatraemia with limited resources requires a high suspicion index and this can mostly be possible by experienced surgeons.4,5 The authors present a case of a 60-year-old male patient who developed delayed post-TURP clot retention and volumetric hyponatremia. He was managed by endoscopic clot evacuation and bleeders’
electrocoagulation with continuous irrigation, but the patient developed volumetric hyponatraemia on Day 5 post-clot evacuation. The patient finally recovered completely and was discharged on the eleventh day after evacuation.
CASE PRESENTATION
A 60-year-old man presented at St. Francis Referral Hospital’s emergency department with difficulty passing urine for 3 days and lower abdominal distention for 24 hours, 7 days post-TURP. For 6 months before TURP, the patient has been visiting a urology clinic due to bothersome lower urinary tract symptoms. Conservative medical management was given but had no significant clinical improvements, so the best option for the patient then was to undergo standard TURP surgical intervention. Pre-operative clinical assessment and evaluations were done, which revealed stable vital signs with a temperature of 37.0 °C, blood pressure of 130/80 mmHg, pulse rate of 82 beats/ min, and respiratory rate of 19 breaths/min. Abdominal pelvic ultrasound was done and was normal with a residual urine volume of 200 mL and an estimated prostate size of 62 g. On digital rectal examination, the patient had normal anal verge, normal anal tone, smooth rectal mucosa, and a firm enlarged prostate.
Pre-operative preparations were done effectively, and the patient had no other comorbidities. Among the investigations done, full blood count was also analysed, and all parameters were normal, haemoglobin was 12.1 g/ dL, platelet count was 298x10³, and prostate-specific antigen was 4.9 ng/ mL. Other relevant investigations done were within normal ranges. TURP was
the best option, and it was done under spinal anaesthesia. Urethrocystoscopy intraoperative findings showed an enlarged median lobe and normal bladder mucosa. TURP was successfully done by using Storz sheath 27fr (KARL STORZ SE & Co. KG, Tuttlingen, Germany) and cutting loop number 27. Lastly, the urinary bladder was evacuated of prostatic chips and cleaned. Haemostasis was achieved through electrical coagulation.
A three-way indwelling urethral catheter was left in situ for 72 hours for postoperative continuous irrigation. The patient was admitted to the intermediate care unit (IMC). Following an uneventful postoperative period in IMC, the urethral catheter was removed after 72 hours, and the patient was discharged home in stable condition.
On the sixth day post-discharge, the patient reported at the emergency department presenting with difficulty in passing urine, suprapubic pain, and abdominal distention. On examination the patient looked like he was in pain, pale (conjunctiva), afebrile, blood pressure was 167/104 mmHg, pulse rate was 86 beats/min, respiration rate was 24 breaths/min, the temperature was 36.9 °C, and oxygen saturation was 98% on room air. An emergency abdominal pelvic ultrasound showed significant clot retention (21x17 cm). He was diagnosed with anaemia, clot retention, and transient hypertension. An emergency haemoglobin level investigation was ordered, which was 6.7 g/dL. Blood transfusion was performed, and the patient was taken to the theatre for an emergency clot evacuation and to arrest the bleeding. Clot evacuation was successfully done using Storz sheath 27Fr and a few bleeders found were electrofulgurated. The bladder was irrigated by using normal saline and the three-way indwelling urethral catheter was reinserted for continuous irrigation as indicated in the literature for TURP prevention of clot retention formation.
The patient was admitted and given empirical antibiotics and one unit of fresh frozen plasma, and he was monitored closely in the IMC. The patient was visited by doctors regularly every day, and he was
making good progress, but 5 days postreoperation the patient developed difficulty breathing, and restlessness, BP was 167/105 mmHg, pulse rate was 96 pulse/min regular, oxygen saturation was 86% on room air. On physical examination the chest was clear. The authors had a provisional diagnosis of TUR syndrome based on high BP of unknown cause. Emergency serum electrolyte was ordered that revealed sodium level was at 105 mmo/L, potassium level was at 2.7 mmo/L, and creatinine level raised to 157.3 mmo/L. Chest X-ray and CT scan were all normal. Hence post-TURP hyponatraemia, hypokalaemia, and acute kidney injury were confirmed (TURP with multiple organ failure). The patient was ordered 500 mL 3% hypertonic saline running slowly for 4 hours, IV KCl 40 mEq (milliequivalent) in 500 mL NS stat (normal saline single dose), then slow K4 tablets 8 hours, serial monitoring of serum sodium and potassium for 24 hours, three units of blood transfusion, IV tranexamic acid injection, furosemide 40 mg every 8 hours for 24 hours, oxygen therapy 3 L/min via nasal prong, and regular monitoring of vital signs, particularly blood pressure, pulse rate, and respiration rate.
DISCUSSION
TURP remains the gold standard and safe surgical procedure in prostate surgeries. However, like any other surgery, the procedure is rarely associated with complications, but some of them are lifethreatening, including TURP syndrome resulting from absorption of irrigant fluid during resection of the prostate.3 The common clinical presentations include nausea, vomiting, convulsions, coma, altered vision, and respiratory distress, which results from pulmonary oedema.1,6 Most of these clinical features were present in the case presented here (acute respiratory distress, restlessness, confusion, and convulsion). In the authors’ case, 5% glucose was the fluid used as an irrigant during TURP, as the authors have a monopolar resectoscope, and 0.9% normal saline was used as continuous irrigation fluid after prostatectomy.
In this case, the patient had multiple
complications involving clot retention, haemorrhagic anaemia, and hyponatraemic shock with multiple organ failures, which are reflected by clinical presentations (low blood pressure, raised pulse rate, acute respiratory distress, restlessness, and convulsions) and supported by laboratory investigation (low serum sodium and potassium and raised serum creatinine).7 Hyponatraemia and hypokalaemia may be the result of volumetric fluid overload caused by both fluid absorption following bladder clot irrigation and IV fluid administration, as reported in other literature.8 It should be noted that this patient had significant blood loss after TURP, which led to anaemia, and hence he had a significantly low haemoglobin level (6.7 g/dL) during his second admission, for which a blood transfusion of three units was administered.3,7
It has been reported that during transurethral resection of the prostate, TURP syndrome is one of the complications and results from excessive absorption of electrolyte-free irrigation fluids, causing acute hypervolaemia and hyponatraemia.9 The clinical parameters of hyponatraemia may be asymptomatic, or the patient may have electrocardiographic symptoms including hypertension, nausea, vomiting, pulmonary oedema symptoms (acute cardio-respiratory disease), convulsions, and coma.1,5 There are two roles of irrigation solution first is to distend the bladder and hence to clear the surgical site, and the second is to wash out the resected tissues and blood. The common fluids used include glycine, 5% glucose, sorbitol, mannitol, and normal saline in a bipolar or monopolar resectoscope.4
The authors’ patient presented clinical features of hyponatraemia 5 days postendoscopic clot retention evacuation. The case becomes contrary to other reported cases in literature, of which most of the reported cases occur intraoperatively or immediately after the operation.10 In this patient, hyponatraemia may have been attributed to several factors including multiple IV fluid administration during TURP, irrigant fluid (dextrose 5%) absorption in the monopolar resectoscope the authors used, and repeated urethrocystoscopy and clot evacuation. In published cases, signs
and symptoms are observed during surgery where, in patients under general anaesthesia, cardiovascular signs (marked by unexplained raised hypertension) and refractory bradycardia are predominant features followed by neurologic manifestations (convulsions and coma).11 This is a unique case as it happened several days after TURP.
The administration of hypertonic saline remains the gold standard in the management of TURP hyponatraemia. This case becomes similar to other reported cases where hypertonic saline administration was successful in rescuing a patient’s life.12 However, this case teaches a lesson that TURP syndrome may occur as a late complication and may result in multi-organ failure involving kidney injury, encephalopathy, and shock. At this moment, it requires a suspicion index based on clinical manifestation supported by diagnostic investigations, particularly serum electrolytes and renal function profile.
CONCLUSION
Syndromic delayed post-TURP hyponatraemia is rare, and limited healthresourced areas require a high suspicion index, which needs an experienced urology surgeon for early diagnosis and to avoid mismanagement. The authors therefore advise urologists to be careful for a few days following endoscopic procedures, to bear in mind and take into consideration everything, even in cases of patient-reported symptoms. Hence, the 72-hour discharge protocols adopted by many may be revisited, especially in limited health-resourced areas. Luckily, the authors’ patient was treated promptly due to the hospital’s proximity. Hypertonic saline remains a gold standard in TURP syndrome management, and hence it should be readily available in operating rooms and wards
Ethical Consideration
The patient signed informed consent prior to writing this case. Also, ethical clearance was obtained from the internal reviewer board at Saint Francis University College of Health and Allied Sciences, Ifakara, Tanzania.
References
1. Ghanem ANM. What exactly is the TUR syndrome and how should it be treated? Open Access J Urol Nephrol. 2022;7(4):1-7.
2. Boukatta B et al. Transurethral resection of prostate syndrome: report of a case. Pan Afr Med J. 2013;14:14.
3. Demirel I et al. TURP syndrome and severe hyponatremia under general anaesthesia. BMJ Case Rep. 2012;2012:bcr-2012-006899.
4. Pindoria N et al. Volumetric overload shocks in the patho-etiology of the transurethral resection prostatectomy syndrome and acute dilution hyponatraemia. Integr Mol Med 4. 2017;DOI:10.15761/IMM.1000279.
5. Tong Xuan H et al. Successful treatment of pulmonary edema caused by transurethral resection of the prostate syndrome. Res Rep Urol. 2021;13:297-301.
6. Hawary A et al. Transurethral resection of the prostate syndrome: almost gone but not forgotten. J Endourol. 2009;23(12):2013-20.
7. Olapade-Olaopa EO et al. Haematuria and clot retention after transurethral resection of the prostate: a pilot study. Br J Urol. 1998;82(5):624-7.
8. Rassweiler J et al. Complications of transurethral resection of the prostate (TURP)—incidence, management, and prevention. Eur Urol. 2006;50(5): 969-80.
9. Trépanier CA et al. Another feature of TURP syndrome: hyperglycaemia and lactic acidosis caused by massive absorption of sorbitol. Br J Anaesth. 2001;87(2):316-9.
10. Kumar V et al. TUR syndrome - a report. Urol Case Rep. 2019;26:100982.
11. Al-Hajjaj M et al. TURP syndrome: a rare case report from Syria. Int J Surg Case Rep. 2022;93:107021.
12. Vijayan S. TURP syndrome. Trends Anaesth Crit Care. 2011;1(1):46-50.
Leiomyosarcoma Arising in Angiomyolipoma 5 Years PostEmbolisation: A Case Report and Literature Review
Renal angiomyolipoma is a benign tumour characteristically composed of fat, smooth muscles, and thick-walled blood vessels. In extremely rare instances, transformation into the more sinister leiomyosarcoma causes potentially drastic differences in both management strategies and prognosis. In most cases, radical nephrectomy remains the standard modality of choice for these tumours as they exhibit aggressive biological behaviour with unfavourable prognosis. Herein, the authors describe a rare case of renal angiomyolipoma in a 33-year-old male, which showed malignant transformation into leiomyosarcoma 5 years post angioembolisation and was managed with radical nephrectomy.
Key Points
1. Renal angiomyolipoma (AML), although a benign entity, can transform into leiomyosarcomas, significantly altering prognosis and creating a need for more aggressive treatment, including surgical resection alongside additional adjuvant therapies.
2. This case report describes an unusual clinical scenario in which renal AML underwent a malignant transformation in a 33-year-old male 5 years post-angioembolisation and was managed with radical nephrectomy.
3. Sarcomatoid transformation of renal AML, although rare, can occur after angioembolisation. Due to its malignant potential, patients should undergo regular follow-up for early detection and timely intervention to improve outcomes.
BACKGROUND
Sarcomatous transformation of the angiomyolipoma (AML) is a rare event with a handful of cases reported in the literature.¹ It is marked by rapid growth, early metastasis, and cachexic symptoms.1 The exact cause and duration after which such a malignant change occurs is unknown. On the other hand, angioembolisation has recently become the mainstay of managing patients with AML, especially after rupture with stable haemodynamics, or in patients with syndromic associations, such as tuberous sclerosis (TS), where these tend to be bilateral and multiple. It is a common practice not to intervene surgically, with patients kept on radiological follow-up in the absence of well-defined advantages of the surgical intervention. Herein, the authors discuss a patient with TS and bilateral AMLs who underwent angioembolisation of a ruptured AML in the right kidney and presented to them 5 years later with a rapidly growing mass at the same site. They were found to have leiomyosarcoma of the embolised AML. The authors also conducted a review of the literature of all reported articles on sarcomatous change of the AML, and to the best of the author’s knowledge, such delayed transformation of a postembolisation AML into a leiomyosarcoma has never been reported. This report underscores the need and importance of regular, time-bound radiological follow-up in patients who undergo angioembolisation to ensure optimal outcomes.
CASE PRESENTATION
A 33-year-old male with a known case of TS (history of epilepsy and facial angiofibroma) presented to the emergency department in 2019 with signs of shock, right flank pain, and anaemia. After resuscitation, a contrastenhanced computed tomogram (CECT) abdomen was obtained, revealing multiple fat-dense lesions (-10HU) suggestive of angiomyolipoma in both kidneys with intralesional pseudoaneurysm in the segmental branch of the right renal artery and 19x15 cm perirenal haematoma with mass effect over the parenchyma
(Figure 1A–1B). Given the presence of multiple AMLs and the goal of preserving kidney parenchyma, surgery was deemed unnecessary. Instead, the patient underwent a successful glue embolisation and was discharged the following day in stable condition. Afterward, the patient was lost to follow-up and remained symptom-free for the next 5 years, without receiving any adjuvant treatment of any sort for those 5 years. However, after 5 years, the patient presented with malaise and loss of appetite and weight. A CECT of the abdomen revealed a 12x11 cm heterogeneous, avidly enhancing lesion, with prompt washout in the venous phase in the upper pole of the right kidney with blurred margins along the adjacent liver, as well as a 24 mm radiodensity at the midpole depicting postembolisation glue with a reported final impression of renal cell carcinoma (Figure 1C–1D). Given the significant increase in lesion size and cachexic symptoms, indicating sarcomatous change or new malignancy, an 18-fluorodeoxyglucose positron emission tomography (18F-FDG PET-CT) scan was performed. This showed an FDG-avid, ill-defined lesion in the upper pole of the right kidney having maximum standardised uptake value (SUVmax) of 5.3, with another mildly FDG-avid lesion in the right thigh muscle. A core needle biopsy was performed, which suggested a low-grade spindle cell lesion, likely benign. A preliminary diagnosis of RCC was made, and the patient underwent a right open radical nephrectomy with an uneventful postoperative course and discharge on the Day 7. Histopathological evaluation of the mass revealed all three hallmark diagnostic criteria of leiomyosarcoma; that is, the presence of spindle-shaped cells arranged in interlacing fascicles, bundles showing moderate to marked pleomorphism including the presence of multinucleated giant cells with brisk mitosis (>10/10 high power field), and necrosis involving <50% of the tumour mass (Figure 2A–2C). The tumour was breaching the renal capsule and extended into the hilar fat; however, resection margins of the renal vessels and the ureter were free. Hilar lymph node resected en bloc was also positive for similar histology. On immunohistochemistry (IHC), tumour cells were diffusely positive for the smooth muscle markers vimentin
A and B) CT images descriptive of ruptured right AML with large perinephric haematoma compressing the renal parenchyma.
C and D) CT images depicting heterogeneously enhancing, infiltrating mass from the right kidney with indistinct margins with liver and IVC.
AML: angiomyolipoma; IVC: inferior vena cava.
and smooth muscle actin (SMA), suggesting leiomyosarcoma. Interestingly, the histology also revealed focal presence of HMB45 in the background, a marker that is usually absent in primary leiomyosarcoma, suggesting a malignant transformation of the earlier angiomyolipoma into its more sinister malignant counterpart (Figure 2D–2F). After a multidisciplinary discussion, the decision was made not to initiate any adjuvant therapy, considering the patient’s intermediate Federation Nationale des Centers de Lutte Contre le Cancer (FNCLCC) grade. Instead, it was agreed to proceed with a 6-monthly follow-up for ongoing surveillance. During the follow-up in the 5th month, 18F-FDG PET CT showed no evidence of residual or recurrent tumour. The patient was doing well at the 6-month follow-up.
DISCUSSION
Renal angiomyolipoma usually has a benign course, and treatment is based on the lesion size, symptoms, and presentation. TS-associated AML tends to be multicentric and bilateral and has a higher likelihood of progression, whereas sporadic AML more commonly presents as a solitary lesion.2 Observation and selective embolisation are the mainstays of management options, while surgical excision is reserved for selective cases. Patients who undergo selective embolisation seldom undergo consolidation surgery, even when the embolisation is for a large or ruptured AML. The literature indicates that 85% experienced post-embolisation syndrome, with re-embolisation or surgical
Figure 1: CT images depicting renal lesions over respective timelines.
A) Interlacing fascicles of neoplastic cells along with branching slit-like blood vessels at low power. B) Brisk mitosis and necrosis were observed. C) Pockets of tumour deposits were seen invading the renal parenchyma, tumour nodules (thick arrows), and normal parenchyma (long arrow). D) Tumour cells were diffusely positive for vimentin. E) Tumour cells exhibited focal positivity for SMA. F) HMB showed focal positivity in nests and islands of tumour deposits infiltrating the renal parenchyma, brown-coloured tumour nodule suggesting HMB45 positivity (thick arrow). HMB: human melanoma black; SMA: smooth muscle actin.
intervention needed in 14% and 16% of patients, respectively.2
Sarcomatous change in AML is a rarity, with a handful of cases reported in the literature. The authors conducted a literature review with 13 case reports, including three diagnosed post-mortems (Table 1A–1B).1,3-14 The most common presenting complaint was flank pain (54%), followed by haematuria (23%) and incidental diagnosis (23%). All the patients were primarily managed surgically, with 54% receiving some sort of adjuvant treatment during the postoperative period. However, the prognosis remained dismal in most of the reports. To date, no genetic mutations have been identified that link the sarcomatous transformation of AML, which has precluded the development of targeted
therapies. Furthermore, the epithelioid variant of AML has aggressive characteristics with a high potential to become malignant, and it has been suggested to be treated in line with renal cell carcinoma.15
In the author’s case, either there was a transformation of the embolised AML into leiomyosarcoma or de novo development of leiomyosarcoma synchronously with the AML, with possible likelihood of the former, as supported by IHC expression of vimentin and SMA in the background of human melanoma black-45 (HMB45), suggesting that the sarcoma originated from the same site as the original AML. To the author’s knowledge, there have been no reports till now, that an AML can undergo sarcomatous change despite embolisation and is of
Figure 2: Histology of tumour mass.
Table 1A: Comparison between data obtained from the authors’ review and other case reports with respective follow-up and adjuvant therapy.
Current case report Right flank pain, anaemia Yes Vimentin, SMA, HMB45
Fish et al. 19462 Anaemia, fever, abdominal pain, Yes
Kargel et al. 19853 Fever, abdominal pain, nausea No Desmin
Byrne et al. 19884 Incidental No
De Sevilla et al.19885 Fever, abdominal pain Yes
Ferry et al. 19911 Flank pain No Vimentin, SMA, desmin
Lowe et al. 19926 Flank pain, haematuria, hypotension No Cytokeratin, SMA
Martignoni et al. 20007 Flank pain, haematuria No Actin, vimentin, desmin, HMB45, S-100, A103 CD68
Chandrasoma et al. 20048 Abdominal pain No Vimentin Chemotherapy Yes 3 months (death)
Inci et al. 20069 Abdominal lump, weight loss No
Pingali et al. 201210 Anaemia, chest discomfort, dyspnoea No
Vimentin, SMA, S-100 Chemotherapy Yes 7 months
HMB45, SMA, desmin
CD 68: cluster of differentiation 68; HMB45: human melanoma black–45; IHC: immunohistochemistry; A103: melan A monoclonal antibody; SMA: smooth muscle actin; S-100: soluble in 100% ammonium sulphate; TS: tuberous sclerosis.
Table 1B: Case reports with diagnosis on autopsy findings.
Author (year)
Burkitt 194911 No Lipoangioleiomyosarcoma arising from AML
John W. Berg 195512 No Lipoblasts with thick vessels with anaplastic sarcoma cells in periphery
et al. 196013 No
AML: angiomyolipoma; TS: tuberous sclerosis.
along with nodule showing angiolipomyosarcomatous changes
Robin
Hartveit
clinical significance as embolisation is being offered more commonly and surgical consolidation is seldom performed. AMLs with sarcomatous change have metastatic potential and tend to perform poorly.
There is no data on whether the outcomes of post-embolisation sarcomatous transformation are similar to those of de novo sarcomatous transformation, but it is safe to assume, that the possibility of a sarcomatous change in the long term, no matter how small, merits regular followup scans to assess for the development of the same at the very least and curative surgical options should be offered at the earliest. Follow-up protocols tend to vary but typically involve cross-sectional imaging, such as CT or MRI, conducted every 1–2 years to detect any potential transformation.
References
1. Ferry JA et al. Renal angiomyolipoma with sarcomatous transformation and pulmonary metastasis. Am J Surg Path 1991;15:1083-8.
2. Nelson CP, Sanda MG. Contemporary diagnosis and management of renal angiomyolipoma. The Journal of Urology. 2002;168(4 Pt 1):1315-25.
3. George W. Fish, William L. McLaughlin. Liposarcoma of kidney: report of a case presenting an unusual syndrome. J Urol. 1946;55(1):28-35
4. Kragel PJ, Toker C. Infiltrating recurrent renal angiomyolipoma with fatal outcome. J Urol 1985;133(1):90–1.
5. Byrne DJ et al. Malignant angiomyolipoma of the kidney associated with hypercalcemia. Br J Urol. 1988;62(1):89–90.
6. De Sevilla TF et al. Renal leiomyosarcoma in a patient with
CONCLUSION
Sarcomatoid transformation of renal AML is an extremely rare encounter and can possibly occur despite angioembolisation. Given its malignant potential and dismal prognosis, patients who undergo embolisation should be kept on regular follow-up to facilitate early detection and optimal management of sarcomatous transformation.
Consent for Publication
Informed consent for publication was obtained from the patient, ensuring their identity remains confidential. While we have the patient’s permission to share their case, all identifying information has been omitted to protect their anonymity and privacy throughout this article. This approach upholds ethical standards while contributing valuable insights to the field.
tuberous sclerosis. Urol Int. 1988;43(1):62-4
7. Lowe BA et al. Malignant transformation of angiomyolipoma. J Urol. 1992;147:1356–8
8. Martignoni G et al. Renal angiomyolipoma with epithelioid sarcomatous transformation and metastases: demonstration of the same genetic defects in the primary and metastatic lesions. Am J Surg Pathol. 2000;24(6):889-94.
9. Chandrasoma S et al. Angiomyolipoma of the kidney: expanding disease spectrum demonstrated by 3 cases. Appl Immunohistochem Mol Morphol. 2004;12(3):277-83.
10. Inci O et al. Renal angiomyolipoma with malignant transformation, simultaneous occurrence with malignity and other complex clinical situations. Int Urol Nephrol. 2006;38(3-4):417-26.
11. Pingali S et al. Renal angiomyolipoma - sarcomatous transformation and cavoatrial extension. Indian J Surg Oncol. 2013; 4(1):27-9.
12. Burkitt R. Fatal haemorrhage into a perirenal liposarcoma. Br J Surg. 1949;36(144):439.
13. Berg JW. Angiolipomyosarcoma of kidney (malignant hamartomatous angiomyolipoma) in a case with solitary metastasis from bronchogenic carcinoma. Cancer. 1955;8(4):759-63.
14. Hartweit F, Halleraker B. A report of three angiolipomyomata and one angiomyolipomyosarcoma. Acta Pathol Microbiol Scand. 1960;49:329-36.
15. Tsai HY et al. Clinicopathologic analysis of renal epithelioid angiomyolipoma: Consecutively excised 23 cases. Kaohsiung J Med Sci. 2019;35(1):33-8.