

2025 Neurology


Sports Neurology Highlights, the 2024 Revised McDonald Criteria, and Myasthenia Gravis Insights Congress Features: Novel Therapies and Targets for Parkinson’s Disease Editor’s Pick: An

10 Review of the American Academy of Neurology (AAN)
2025 Annual Meeting
Congress Features
21 Sports Neurology Highlights from the 2025 AAN Annual Meeting
Jonathan E. Attwood
26 The 2024 Revised McDonald Criteria: AAN 2025 Highlights
Andrew Dugue
30 What Is Next in Myasthenia Gravis? Insights on Ocular and MuSK Forms from AAN 2025
Bertie Pearcey
Abstract Reviews
34 Personalized Locomotor Training with Non-Invasive Spinal Cord Stimulation for Functional Recovery After Spinal Cord Injury
Rafay et al.
35 Outcomes of a 3-Week Interdisciplinary Intensive Outpatient Treatment Program for Mild-Moderate Traumatic Brain Injury in Veterans and First Responders
Bryant et al.
37 Comprehensive Efficacy and Safety Analysis of Levetiracetam versus Phenytoin in Brain Injury: An Umbrella Review
Maryam et al.
39 Characterizing Cerebrospinal Fluid Profiles of Immunocompromised Patients with Infectious Meningitis/Encephalitis
Thomas et al.
40 Neurological Complications in Dengue: The Neuroinfections Emerging in the Americas Study (NEAS) in Colombia
Villegas et al.
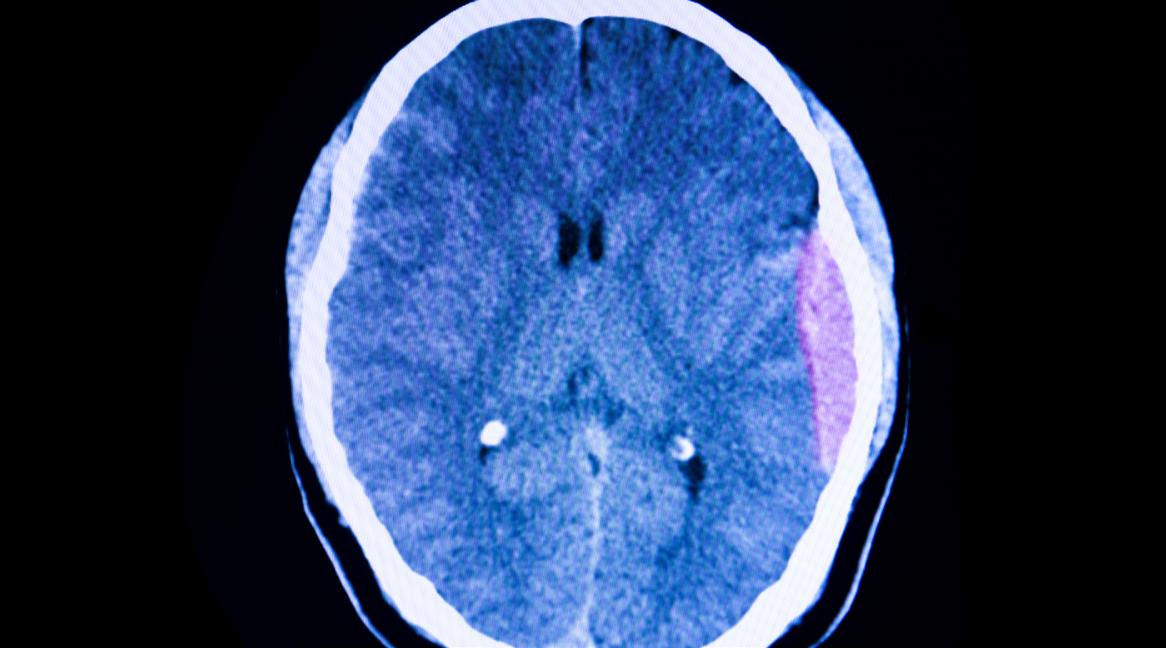
42 Relationship of Rehabilitation Insurance Payor to Functional Status at One-Year Post-Traumatic Brain Injury
Shah et al.
44 Risk Factors Associated with Neurocognitive Disorder and Depression Among Adults from an Urban-Marginalized Area of Lima, Peru
Diaz et al.
46 Grapheme-Color Synesthesia in Patients with Epilepsy: A Pilot Study on Prevalence and Seizure Characteristics
Chu et al.
50 Atypical Presentation of Neurosyphilis: A Case Report
Vyas et al.
Congress Interviews
52 Joseph Sirven
55 Larry B. Goldstein Interviews
57 Courtney Wusthoff
61 Ryan Hakimi Feature
64 Non-rapid Eye Movement Sleep Homeostatic Plasticity Carries the Risk of Epileptic Transformation
Halász, Szűcs
Articles
71 Editor's Pick: Novel Therapies and Targets for Parkinson’s Disease
Ledingham, Pavese
83 MRI and Vascular Cognitive Impairment: A Systematic Review of Randomized Controlled Trials from the Last 10 Years and Implications for Future Interventions
da Silva et al.
96 Seizure Disorders: Clinical Insights and Review of the Major Clinical Topics Impacting the Reproductive Lifespan
Oster
112 Reversible Cerebral Vasoconstriction Syndrome Presenting with Multifocal Infarcts: A Case Report
Kaleel et al.
117 Cocaine-Induced Leukoencephalopathy: A Case Report
Montion et al.
Editorial Board








Prof Nils Erik Gilhus
University of Bergen, Norway
Prof Amos Korczyn
University of Bergen, Norway
Dr Natan Bornstein
Shaare-Zedek Medical Center, Israel
Dr Giuseppe Lanza
University of Catania, Italy
Dr Simy Parikh
Thomas Jefferson University, Pennsylvania, USA
Dr Rajiv R. Ratan
Weill Cornell Medicine, New York, USA
Aims and Scope
AMJ Neurology is an open access, peer-reviewed eJournal committed to committed to publishing the highest quality medical research concerning all aspects of the function and disease of the nervous system to help advance the development of this field.
The journal is published annually, 6 weeks after the American Academy of Neurology (AAN) Annual Meeting, and features highlights from this event, alongside interviews with experts in the field, reviews of abstracts presented at the event, and indepth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house Editorial team.
AMJ Neurology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field, and broaden readers’ professional interests. The journal is managed by a dedicated Editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copyediting, and ensures timely publication.
AMJ endeavours to increase knowledge, stimulate discussion, and contribute to the delivery of world-class updates in the clinical realm. We do not publish veterinary science papers or laboratory studies that are not linked to patient outcomes. Further details on coverage can be found here: www.emjreviews.com/en-us/amj/.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial Team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
Every review article, case report, feature, and research article published in AMJ Neurology undergoes peer review by at least two independent experts.
On submission, all manuscripts are assessed and undergo a technical check by the AMJ Editorial staff to determine their suitability for the journal and appropriateness for peer review. Editorial staff identify appropriate reviewers who are selected based on their specialist knowledge in the relevant area. All peer review is double-blind.
Following review, manuscripts are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff are responsible for ensuring that necessary amendments to the manuscript have been made, with input from our Editorial Board or the original reviewers where necessary. The Editor of AMJ has final discretion over any proposed amendments. Manuscripts authored by members of the Editorial Board are subjected to the same double-blind process. Short opinion pieces are published following internal review and publication is at
the discretion of the Editor. Congress-related content sponsored or funded by our industry partners undergoes quality control checks independently. Industry-supported content that falls into any of the categories that are eligible for peer review, undergoes the same peer review process.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in neurology and accept original research, review articles, case reports, and features.
To discuss potential submissions, please email: editorial@americanmedicaljournal.com.
To submit a paper, use our online submission site: emj.kriyadocs.com/submissions/submit/emj/emj/login.
Submission details can be found through our website: www.emjreviews.com/en-us/amj/contributors/authors/.
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
AMJ is available through the websites of our leading partners and collaborating societies. AMJ publications are all available via our website: www.emjreviews.com/en-us/amj/.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2024 Frequency: Yearly Online ISSN: 3033-375X
All information obtained by AMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, AMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. This content was developed independently and is not endorsed by the the American Academy of Neurology. The content does not constitute a media partnership in any form whatsoever. The cover photo is of San Diego, California, USA, the location of AAN 2025. Front cover and contents photograph: San Diego, California © jonbilous / stock.adobe.com
Editor
Evgenia Koutsouki
Vice President of Content
Anaya Malik
Managing Editor
Darcy Richards
Copy Editors
Sarah Jahncke, Aranii Nagarajah
Editorial Co-ordinators
Jenna Lorge, Bertie Pearcey
Editorial Leads
Helena Bradbury, Ada Enesco
Editorial Assistants
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Designers
Shanjok Gurung, Owen Silcox, Fabio van Paris
Creative Artworker
Dillon Benn Grove
Head of Marketing
Stephanie Corbett
Vice President of Customer Success
Alexander Skedd
Senior Vice President of Business Development
Rober t Hancox
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and CEO
Spencer Gore
Contact us
Welcome
Dear Readers,
We are proud to share our latest issue of AMJ Neurology, starting with our comprehensive review of the American Academy of Neurology (AAN) 2025 Annual Meeting. Whether you were one of the 14,500 attendees navigating the conference or are catching up on the latest in your discipline, consider this your comprehensive recap. This issue boasts broad coverage of the meeting curated in one place.
As an advocate of lifestyle medicine, I was most eager to delve into the latest data on the intersection between sleep and neurological health. The critical role of sleep in cognitive function, immune health, and many other factors were featured heavily in seminars, abstracts, and in the Wellness and Innovation Hubs. It is well-established that sleep is indispensable for cognitive function, yet the precise mechanisms are not fully known. As our understanding of this relationship deepens, we now know that prioritizing sleep, with or without neurodegenerative diseases, is not only beneficial, but essential for maintaining optimal brain function.1
The journal also features original peer-reviewed content spanning the breadth of neurological science and clinical care. I’d like to thank the Editorial Board, authors, peer reviewers, interviewees, and editorial team for bringing this journal together. We strive to deliver timely and innovative content to impact patient outcomes for the better. I hope that this issue exemplifies that commitment.

Editorial enquiries: editorial@americanmedicaljournal.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
1. Nature. Sleep is essential — researchers are trying to work out why. Nature. Available at: https://www. nature.com/articles/d41586-025-00964-w. Last accessed: May 5 2025.
Anaya Malik Vice President of Content
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com


We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Foreword
Dear Colleagues,
I am pleased to introduce the latest issue of AMJ Neurology, which celebrates the success of the 2025 American Academy of Neurology (AAN) Annual Meeting in Chicago, Illinois, with a curated review of conference highlights.
The meeting shared cutting-edge contributions to science and enriched the knowledge of over 14,500 healthcare professionals in neurology care from 110 countries and all 50 U.S. states in attendance. The comprehensive review in this publication is a distilled selection of learnings from the meeting, including a recap of the 2025 Abstracts of Distinction, expert-led commentaries on the revised McDonald criteria and myasthenia gravis, abstract reviews authored by the presenters, and exclusive interviews with leaders from the AAN.
This publication also features a diverse range of peer-reviewed articles addressing emerging areas of neurological care. The role of non-rapid eye movement sleep plasticity in increasing vulnerability to epileptic transformation is explored. A focused review on seizure disorders across the reproductive lifespan highlights the importance of tailored care in hormonal transitions, while


updates in Parkinson’s disease uncover novel therapeutic targets and strategies in development. Finally, two striking case reports expand our clinical understanding of rare, but important considerations in neurological conditions.
We hope these insights will encourage continued learning and efforts toward better outcomes for patients in daily clinical practice.
We hope these insights will encourage continued learning and efforts toward better outcomes for patients in daily clinical practice.
Rajiv R. Ratan Weill Cornell Medicine, New York, USA
AAN 2025

Keynote speakers reflected on the evolving role of neurologists in a changing world; from harnessing cutting-edge neurotechnologies to addressing health disparities across populations
Congress Review
Review of the American Academy of Neurology (AAN) 2025 Annual Meeting
Location: San Diego, California, USA
Date: April 5th–9th, 2025
Citation: Neurol AMJ. 2025;2[1]:10-20. https://doi.org/10.33590/neurolamj/SZNT3118
THE VIBRANT city of San Diego, California, USA, welcomed the global neurology community at the American Academy of Neurology (AAN) 2025 Annual Meeting and proved to be an optimal meeting place for collaboration and innovation. With over 14,500 experts in neurological health from 110 countries and all 50 U.S. states, the AAN 2025 Annual Meeting boasted the best of this expertise. The gathering transcended borders to expand, build on, and strengthen knowledge in research and clinical practice.
The Presidential Plenary set the tone for an inspiring week, spotlighting not only scientific innovation, but also the profound human impact of neurology. Keynote speakers reflected on the evolving role of neurologists in a changing world; from harnessing cuttingedge neurotechnologies to addressing health disparities across populations. The plenary also honored pioneers whose contributions continue to shape the field, reminding us that behind every breakthrough lies a commitment to improving lives.
Over the course of the meeting, sessions continued to provide breadth on the major topics dominating the field. Breakthrough findings included neurodegenerative disease research, advances in neuroimaging and biomarkers, the expanding role of AI, and a renewed
focus on neuroinflammatory conditions. In particular, health equity took center stage, as the community works to ensure neurology care reaches every patient in need.
This community demonstrated what it means to work as a multifaceted team. From mentorship programs and networking events to wellness activities and social gatherings, the attendees connected at every opportunity out of necessity to drive the field forward.
In our reflection of this year’s meeting, we have curated the 2025 Abstracts of Distinction, expert-led session summaries, and abstract reviews authored by the presenters themselves. These works represent the cutting edge of scientific discovery and the heart of the AAN mission to advance brain health for all.

Mouse Model Gives Hope for Anti-N-Methyl-D-Aspartate Receptor Encephalitis Treatment Development
ALTHOUGH many patients with anti-N-methyl-D-aspartate receptor encephalitis (NMDARe) improve with immunotherapy, current animal models have failed to replicate the full complexity and duration of the disease, limiting progress in the development of new therapies. Researchers at the AAN 2025 Annual Meeting presented an abstract describing the development of a novel mouse model that more accurately captures the pathophysiological and clinical trajectory of NMDARe, creating an opportunity for comprehensive therapeutic assessment and further research.1
In the model, 8-week old female C57BL/6J mice were immunized with a GluN1356-385 peptide combined with AddaVax (adjuvant that favors B cell autoimmunity) and pertussis toxin, while control mice received saline. Mice were then monitored for a range of behavioral, immunological, and neurological changes. Treatment arms included anti-CD20 therapy, a positive allosteric modulator of NMDAR (NMDAR-PAM, SGE-301), or a combination of both. The researchers used a range of techniques to assess factors including GluN1-antibody synthesis and microglial activation. A panel of behavioral tests and brain-implanted electrodes were used to asses changes in memory and clinical/ subclinical seizures, respectively.
Results showed that mice receiving the GluN1356-385 peptide developed both serum and cerebrospinal fluid NMDAR antibodies, with epitope spreading and a reduction in synaptic NMDAR clusters and hippocampal plasticity seen. The researchers also observed brain-bound antibodies, B cell and plasma cell
infiltration, microglial activation, and NMDAR/ IgG complexes within microglial endosomes. Cultured deep cervical lymph nodes showed NMDAR-antibody synthesis. Clinically, these mice displayed psychosis-like behavior, memory deficits, abnormal movements, and heightened seizure susceptibility. Notably, treatment with anti-CD20, NMDAR-PAM, or both, reversed most behavioral and neurobiological abnormalities. Furthermore, B cell repopulation led to a resurgence of clinical-neurobiological alterations, which were mitigated by NMDAR-PAM.
The study presents a comprehensive and clinically relevant model of NMDARe that not only elucidates the immunopathogenesis of the disease but also facilitates the testing of novel treatments. Of particular clinical interest is the demonstrated efficacy of NMDARPAM in both symptom reversal and disease suppression following B cell repopulation. This model may inform future therapeutic strategies, and supports more refined immunological approaches in managing NMDARe in clinical practice.
New Insights into the Role of APOE e4 in Dementia with Lewy Bodies
NEW research presented at the AAN 2025 Annual Meeting has revealed that the APOE e4 allele exacerbates Lewy body pathology independently of Alzheimer’s disease (AD) co-pathology, and differentially influences core clinical features in dementia with Lewy bodies (DLB).2
The APOE e4 allele is a well-established genetic risk factor for AD, but its role in DLB remains debated. While AD neuropathology in DLB correlates with accelerated cognitive decline, the independent contribution of APOE e4 to Lewy body pathology and its impact on hallmark symptoms such as fluctuating cognition, visual hallucinations, rapid eye movement sleep behaviour disorder (RBD), and parkinsonism have been unclear. This study aimed to resolve these uncertainties using a large, multi-group cohort to dissect genetic
The analysis included 38,414 participants: 1,170 with DLB, 1,032 with Parkinson’s disease (PD), 17,416 with AD, and 18,796 controls. Logistic regression models assessed associations between APOE genotypes, Lewy body pathology severity, and clinical features. Results demonstrated that APOE e4 correlated with more severe Lewy body pathology even in cases with minimal AD co-pathology (odds ratio [OR]: 1.39; 95% CI: 1.01–1.94; p=0.049), suggesting an independent role in α-synucleinopathy progression. Clinically, two-thirds of participants with DLB exhibited fluctuating cognition, visual hallucinations, or RBD, while 86.9% developed parkinsonism. Intriguingly, higher APOE genetic risk scores reduced the likelihood of fluctuating cognition (OR: 0.72; 95% CI: 0.53–0.97; p=0.031), RBD, and parkinsonism but increased visual hallucinations (OR: 1.16; 95% CI: 1.12–1.20; p<0.001), indicating allele-specific modulation of symptom profiles.
Results demonstrated that APOE e4 correlated with more severe Lewy body pathology even in cases with minimal AD co-pathology
These findings demonstrate that the link between APOE e4 and Lewy body pathology is independent of the severity of AD pathology, and exerts divergent effects on clinical phenotypes. For clinical practice, this highlights the need for APOE genotyping in patients with DLB to predict pathological burden and symptom trajectories, particularly visual hallucinations, which may require tailored interventions.

National Survey Shows Missed Opportunities in Amyotrophic Lateral Sclerosis Care
AN ABSTRACT presented at the AAN 2025 Annual Meeting has highlighted both the strengths and limitations in the provision of palliative care (PC) for individuals diagnosed with amyotrophic lateral sclerosis (ALS), based on a nationwide survey of interdisciplinary ALS and PC clinicians.3
The study, designed to inform future educational initiatives, program development, and quality improvement strategies, revealed a consistent recognition of the benefits of PC in enhancing symptom management and overall well-being for patients and their care partners. However, its implementation remains suboptimal.
Survey responses were collected from 118 ALS clinicians and 145 PC clinicians representing 28 and 26 states, respectively. Among ALS clinicians, including physicians, rehabilitation therapists, and nurses, only approximately half reported high confidence in effectively managing pain (56.6%) and mood symptoms (53.1%). Notably fewer clinicians reported proficiency in addressing spiritual or existential distress (31.0%) and family or care partner needs (43.4%).
While ALS clinicians generally expressed satisfaction with the quality of care delivered by PC teams (with satisfaction rates ranging from 77.0–97.6% across different care aspects), many PC clinicians reported lower confidence in managing ALS-specific
concerns. For example, 78.3% expressed discomfort with managing assistive equipment, and 56.6% were uncertain about counseling patients on the discontinuation of ALS-specific pharmacologic therapies.
Despite these identified challenges, there was strong consensus regarding the value of integrated PC: 76.1% of patients with ALS and 79.2% of PC clinicians supported the inclusion of PC for all individuals with ALS as part of standard, comprehensive care. Additionally, most ALS clinicians rated the quality of outpatient PC as excellent (53.7%) or good (38.8%).
Many PC clinicians reported lower confidence in managing ALSspecific concerns
These findings highlight critical areas for targeted training and interprofessional collaboration to optimize the delivery of PC in ALS, and support future efforts in system-level improvement and advocacy.
Is Ang2 a Biomarker for Microvascular Injury Following Traumatic Brain Injury?
AS AN antagonist of the TIE2 receptor, Ang2 is involved in vascular injury and repair processes, which are often disrupted following traumatic brain injury (TBI). Given the potential for Ang2 to serve as a biomarker of microvascular injury, an abstract presented at the AAN 2025 Annual Meeting aimed to assess the relationship between Ang2 plasma levels, TBI severity, CT findings, and the temporal evolution of Ang2 levels in the weeks following TBI.4
The key finding was that Ang2 levels were elevated in TBI cases and correlated with injury severity, with higher levels persisting in more severely injured patients for up to 2 weeks.
The study was part of the TRACK-TBI cohort and included 362 adults with TBI, 89 individuals with orthopedic injuries (OI) as controls, and 64 healthy controls (HC). Plasma samples were collected at three time points: 1 day (D1), 2 weeks (W2), and 6 months (M6) post-injury. Ang2 levels were measured using the Meso Scale Discovery (MSD) R-PLEX assay, and additional biomarkers were assessed on the MSD Neurology Panel S-Plex. This allowed for a comprehensive analysis of the biomarkers associated with TBI.
The mean age of the participants with TBI was 39.8 years. Among them, 174 participants (48%) had a Glasgow Coma Scale (GCS) score of 13–15, while 188 participants (52%) had a GCS score of 3–12. On D1, participants in the TBI group had significantly higher Ang2 levels (2.4 ng/mL [1.8–3.9]) compared to healthy controls (1.7 ng/mL [1.3–2.1]; p<0.001) and OI participants (2.2 ng/mL [1.6–2.7]; p=0.008). Ang2 levels remained elevated at W2 in patients with GCS 3–12 (3.3 ng/mL [2.3–5.1]), but returned to normal by M6. In contrast, Ang2 levels
in patients with GCS 13–15 had returned to baseline by W2. Furthermore, higher Ang2 levels on D1 were associated with abnormal CT findings, with a median of 2.9 ng/mL (2.0–4.5) in cases with abnormal CT compared to 2.0 ng/mL (1.5–2.5) in CT-negative cases (p<0.0001).
Ang2 is an important biomarker for TBI, particularly for identifying microvascular injury
In conclusion, the study demonstrated that Ang2 is an important biomarker for TBI, particularly for identifying microvascular injury. Elevated Ang2 levels in the first 2 weeks post-injury, especially in severe cases, suggest its potential role in monitoring TBI severity and progression. However, the study is limited by its observational design and the absence of long-term follow-up beyond 6 months, and further research is needed to validate Ang2 as a clinical tool for TBI management. Nonetheless, these findings could inform future clinical practice by offering a promising biomarker for assessing the severity and recovery of patients with TBI.
Participants in the TBI group had significantly higher Ang2 levels (2.4 ng/mL [1.8–3.9]) compared to healthy controls (1.7 ng/mL [1.3–2.1]; p<0.001) and OI participants (2.2 ng/mL [1.6–2.7]; p=0.008)
Mapping the Genetics of the Hypothalamus: Implications for Neuropsychiatric Disease
THE
FIRST comprehensive genetic map of the human hypothalamus, with data on how subregions link to various neuropsychiatric traits and disorders, was presented at the AAN 2025 Annual Meeting.5 This study identifies key genetic loci influencing hypothalamic anatomy and links them to neuropsychiatric traits, offering new avenues for understanding brain-behaviour relationships.
The hypothalamus is a critical brain region governing neurological and metabolic functions, yet its genetic underpinnings remain poorly characterized. Previous studies have been limited by small sample sizes and manual segmentation methods, constraining insights into its genetic associations with neuropsychiatric conditions. This study aimed to address this gap by systematically investigating the genetic architecture of the hypothalamus and its association with neuropsychiatric conditions.

Using advanced imaging and genomic techniques, multivariate genome-wide association studies were conducted on hypothalamic structural data. Automated segmentation of the hypothalamus and its subregions enabled large-scale analysis. Functional annotation, gene mapping, and causal inference methods were applied to prioritize relevant pathways.
Twenty-three genomic loci were significantly associated with hypothalamic structure, with enrichment for genes involved in intracellular trafficking and steroid-related metabolism. Genetic correlations linked hypothalamic anatomy to neuropsychiatric traits such as chronotype, risk-taking behaviour, cognition, and autonomic regulation. Shared genetic architecture was observed between the hypothalamus and schizophrenia, Parkinson’s disease, and stroke. The strongest genetic signal, located near the ADAMTS8 gene, was replicated in three independent datasets (N=1,685–4,321), and demonstrated a causal relationship with hypothalamic volume, suggesting a role in neurodevelopmental processes.
Shared genetic architecture was observed between the hypothalamus and schizophrenia, Parkinson’s disease, and stroke
These findings advance understanding of the hypothalamus’s genetic complexity and its influence on neuropsychiatric health. Integrating hypothalamic genetic profiles into clinical frameworks may enhance precision medicine approaches in psychiatry and neurology.

How Four Women Shaped EEG History
THE HISTORY of EEG is often told through the achievements of prominent male scientists including W. Grey Walter, Hallowell Davis, and Alexander Forbes; however, behind the evolution of EEG as a clinical tool lies a cohort of pioneering women whose vital contributions remain largely under-recognized. A recent study presented at the AAN 2025 Annual Meeting aimed to spotlight four of these trailblazers: Erna L. Gibbs, Pauline A. Davis, Ellen Grass, and Mary A.B. Brazier.6
Despite their foundational work, few historical records or dedicated articles acknowledge their influence. For instance, only one article focusing solely on Grass’s contributions was found, while none were retrieved for Gibbs, Davis, or Brazier. Nevertheless, their work shaped the field in critical ways.
Gibbs and Davis were instrumental in the first recordings of the characteristic 3 Hz spikeand-wave patterns associated with absence epilepsy. Gibbs also authored the first EEG manual, cataloguing over 10,000 traces, and conducted pioneering work on seizure localization to support epilepsy surgery. Davis made a breakthrough by reporting the first evoked potentials in response to auditory stimuli, an innovation that would prove essential in clinical and research contexts.
Gibbs also authored the first EEG manual, cataloguing over 10,000 traces
Brazier was a pioneer of computational approaches in EEG, introducing correlation and auto-correlation analyses to interpret brain signals. Her leadership roles, including presidency of the International Federation of Clinical Neurophysiology, further highlight her impact. Grass contributed significantly to the technical advancement of EEG through her role in founding The Grass Instruments Company.
These women not only propelled EEG research forward but also laid foundational stones for modern neurophysiology. Their legacy, though monumental, remains undervalued. This study underscores the need to reframe historical narratives to rightly honor the women whose work helped define an entire scientific field.
These women not only propelled EEG research forward but also laid foundational stones for modern neurophysiology
Early-Onset Parkinson Disease Autonomic Impairment Linked to Increased Risk of Mortality
EXPERIENCING
autonomic dysfunction is common in patients with Parkinson's disease (PD) and has also been associated with increased cardiovascular mortality. Authors from Mayo Clinic, Rochester, Minnesota, USA, presented new findings on the frequency and time of onset of autonomic dysfunction relative to PD onset in early-onset parkinson disease (EOPD), and explored its association with mortality.7 The study was presented at the AAN 2025 Annual Meeting as part of the 2025 Abstracts of Distinction.
The team collated information on 829 incident PD cases with EOPD (motor symptom onset before 50 years of age), and 829 controls evaluated at Mayo Clinic between 1990–2022. The median age at PD onset was 42 years (interquartile range: 37–46). Medical records confirmed clinical diagnosis, and assessment of presence and time of onset of autonomic symptoms, including constipation, bladder urgency, sweat dysfunction, orthostatic hypotension, and erectile dysfunction, relative to PD motor onset. Sex- and age-matched controls were also included for each patient.
Of the patients with EOPD, 63.4% had autonomic symptoms, compared to 27.0% of unaffected controls, and these preceded motor symptoms in 91.4% of EOPD cases. The patients with EOPD experienced constipation (47%), bladder urgency (27.4%), orthostatic hypotension (19.3%), and sweat dysfunction (15.4%). Among male patients with EOPD, 36.8% had erectile dysfunction. In EOPD, the presence of any symptoms of autonomic impairment was associated with a 3.06 increased mortality risk. For each additional such reported symptom, the relative mortality
Autonomic impairment affects 63.4% of patients with EOPD and is associated with a threefold higher mortality risk.
risk increased by 63% (p<0.001). Patients with constipation or orthostatic hypotension had a 2.84 and 2.16 fold higher mortality risk, respectively, compared to patients without these symptoms.
In EOPD, the presence of any symptoms of autonomic impairment was associated with a 3.06 increased mortality risk
Autonomic impairment affects 63.4% of patients with EOPD and is associated with a three-fold higher mortality risk. The mortality risk increases with each additional autonomic failure symptom reported. In this disease cohort, autonomic symptoms were most commonly postdromal features, contrasting with prodromal autonomic impairment seen in late-onset PD.


RAG-17 siRNA Therapy Shows Promise in Amyotrophic Lateral Sclerosis Trial
A NEW investigational therapy may offer hope for patients with SOD1associated amyotrophic lateral sclerosis (ALS). RAG-17, an siRNA therapy designed to silence the SOD1 gene, was evaluated in a first-in-human trial conducted in China. The treatment uses a smart chemistry aided delivery (SCAD) system to enhance delivery to the central nervous system via intrathecal injection, and the study was presented at the AAN 2025 Annual Meeting as part of the 2025 Abstracts of Distinction.8
In the small open-label dose-escalation study, six participants with SOD1-ALS received between 6 and 7 doses of RAG-17 over 240 days, with doses escalating up to 180 mg. The therapy was well tolerated, with no serious adverse events or doselimiting toxicities. Side effects such as muscle tremors and headaches were reported in a few participants.
Biological markers showed promising changes: cerebrospinal fluid levels of the SOD1 protein dropped by more than 50% in five patients, and plasma neurofilament light chain, a marker of neuronal injury, also declined. Importantly, the average rate of ALS progression, measured by the ALS Functional Rating Scale-Revised (ALSFRS-R), was slower than expected, with participants losing only 0.29 points per month. Respiratory function (forced vital capacity) remained stable or improved in most individuals.
Although the study’s size limits broad conclusions, these preliminary results suggest that RAG-17 is safe and biologically active, meriting further clinical investigation as a disease-modifying treatment for ALS.
Cerebrospinal fluid levels of SOD1 protein dropped by more than 50% in five patients 50 % >
References
1. Maudes E et al. Animal model of anti-NMDAR encephalitis by active immunization: insights into the neuroimmunobiology and therapeutic interventions. Abstract 1869. AAN 2025, April 5-9, 2025.
2. Ye R et al. APOE e4 linked effects on neuropathology and clinical features in dementia with lewy bodies. Abstract 4641. AAN 2025, April 5-9, 2025.
3. Maiser S et al. Clinicians’ perceptions of palliative care for amyotrophic lateral
sclerosis (ALS): national survey results. Abstract 186. AAN 2025, April 5-9, 2025.
4. Nunez A et al. Angiopoietin2 (Ang2) Levels are Associated with Increased Severity and Unfavorable Outcomes in Traumatic Brain Injury (TBI): A TRACKTBI Study. Abstract 3980. AAN 2025, April 5-9, 2025.
5. Chen SD et al. The genetic architecture of the human hypothalamus and its involvement in neuropsychiatric behaviours and disorders. Abstract 4473. AAN 2025, April 5-9, 2025.
6. Ahmad B et al. The pioneering women of EEG. Abstract 2028. AAN 2025, April 5-9, 2025.
7. Piat C et al. Autonomic impairment and risk of mortality in early-onset parkinson disease. Abstract 3019. AAN 2025, April 5-9, 2025.
8. Ye J et al. RAG-17, a novel siRNA therapy for SOD1-ALS: safety and preliminary efficacy from a firstinhuman trial. Abstract 5451. AAN 2025, April 5-9, 2025.
Sports Neurology Highlights from the 2025 AAN Annual Meeting
Author: *Jonathan E. Attwood1
1. Nuffield Department of Clinical Neurosciences, University of Oxford, UK
*Correspondence to jonathan.attwood@ndcn.ox.ac.uk
Disclosure: The author has declared no conflicts of interest.
Keywords:
Autonomic dysfunction, biomarkers in concussion, endocrine dysfunction, glymphatic system, mild traumatic brain injury (mTBI), neurodegeneration, post-traumatic headache, sports neurology, traumatic brain injury (TBI), traumatic brain injury biomarkers.
Citation: Neurol AMJ. 2025;2[1]:21-25. https://doi.org/10.33590/neurolamj/PGND2630
The Annual Meeting of the American Academy of Neurology (AAN) continues to attract neurologists from around the world due to its highquality clinical education sessions and groundbreaking research updates. Sports neurology has featured at the conference since 2010, reflecting sustained attention on mild traumatic brain injury and increasing interest in the care of athletes with other neurological conditions. This year in San Diego, California, sessions dedicated to sports neurology and mild traumatic brain injury ran throughout the meeting, beginning with a comprehensive day of talks directed by Meeryo Choe, University of California Los Angeles, and Nicole Reams, NorthShore University HealthSystem, Evanston, Illinois. This report summarises key themes and take-home messages from these presentations.
ENDOCRINE DYSFUNCTION AFTER MILD TRAUMATIC BRAIN INJURY
Jeffrey Bazarian, University of Rochester School of Public Health-Bloomington, Indiana, gave an illuminating presentation on endocrine dysfunction following concussion, highlighting a relatively underexplored aspect of traumatic brain injury (TBI) pathophysiology. After detailing the vulnerability of the pituitary stalk to traction, ischemia, and potential autoimmune damage, Bazarian addressed how little is known about the acute endocrine response to mild TBI (mTBI). He summarized compelling evidence indicating pituitary dysfunction in the subacute phase post-
injury. For example, although concussion does not appear to affect hormone levels at the group level, lower hormone levels are associated with prolonged recovery, and a diminished cortisol awakening response correlates with more severe symptoms after mTBI.1,2
Bazarian also presented work from his group on gene expression changes following concussion, particular involving the folliclestimulating hormone/luteinizing hormone pathway, which may go some way to explaining the link between concussion and menstrual irregularities.3 Chronic endocrine dysfunction was also discussed, illustrated by a study of female ice hockey players
with mTBI, revealing that more than 60% had persistently abnormal hormone levels, necessitating medical treatment in 10%.4 This session strongly highlighted the need for further research in this area.
BRAIN INJURIES FROM INTIMATE PARTNER VIOLENCE
Carrie Esopenko, Icahn School of Medicine at Mount Sinai, New York, delivered a powerful talk on brain injuries resulting from intimate partner violence (IPV). Although IPV differs from sports-related concussion, Esopenko clarified its relevance to healthcare providers who care for athletes. IPV affects one in three women, disproportionately impacting young women, women of color, individuals with disabilities, and military service members. At least 50% of women affected by IPV report head trauma, though the actual prevalence may be even higher.
Esopenko described IPV-related brain injury, involving impact, shaking, and strangulation mechanisms, resulting in a distinctive combination of focal, diffuse,
and hypoxic insults.5 The overlap with psychological trauma, post-traumatic stress disorder, and other mental health conditions presents significant diagnostic, prognostic, and management challenges, spotlighting IPV-related brain injury as an urgent, underserved research area.
BIOMARKERS OF MILD TRAUMATIC BRAIN INJURY
Ramon Diaz-Arrastia, University of Pennsylvania Perelman School of Medicine, Philadelphia, provided a reflective update on mTBI biomarkers. While acknowledging the slow clinical adoption of blood-based biomarkers, and noting their narrow FDA approval criteria, he emphasized their potential utility in pitch-side, military, and low-resource environments. Although these biomarkers may have limited applications in the diagnosis of concussion, they hold promise for identifying which patients require urgent evaluation in the emergency department, counselling on symptom duration, guiding return-to-play decisions, and informing discussions about when

In a more clinically-focused session, Erik Beltran, NorthShore University HealthSystem, Evanston, Illinois, discussed concussion mimics, noting that up to 20% of athletes and military personnel without a history of brain injury report symptoms meeting International Classification of Diseases, 10th Revision (ICD10) criteria for post-concussion syndrome.7 Beltran explored differential diagnoses for the unwell athlete such as dehydration, electrolyte disturbances, vestibular disorders, ocular and cervical injuries, and autonomic disorders like postural orthostatic tachycardia syndrome.
John Leddy, University of Buffalo, New York, summarized his influential research on posttraumatic autonomic dysfunction, including the effects of concussion on sympathetic and parasympathetic function and baroceptor sensitivity.8-10 Leddy stressed the clinical significance of both orthostatic and exercise intolerance, and detailed his approach to the diagnosis and management of postural orthostatic tachycardia syndrome, a theme expanded on by Rachel Pearson, University of California Irvine, later in the week.
after mTBI.
THE GLYMPHATIC SYSTEM, SLEEP DISRUPTION, AND NEURODEGENERATION IN TRAUMATIC BRAIN INJURY
Michael Jaffee, University of Florida, Gainesville, delivered a keynote highlighting the potential role of the glymphatic system in TBI-related neurodegeneration. Extending arguments from his 2018 review, he proposed connections between reduced glymphatic flow, impaired waste clearance, and chronic traumatic encephalopathy pathology.12 He also discussed advanced neuroimaging techniques for assessing the glymphatic system, including magnetic resonance imaging-visible perivascular spaces and diffusion tensor imaging along perivascular spaces.
In a later talk, Juan Piantino, Oregon Health and Science University, Portland, Oregon, focused on the impact of sleep dysfunction on glymphatic flow after mTBI.13 Piantino shared his group’s recent work confirming that intrathecal gadolinium moves through
the perivascular space into the brain parenchyma in humans.14 He also examined evidence that interstitial flow through the brain is driven by vasomotor oscillations and hypothesized that cerebral edema after TBI may interfere with this pump-like action.

References
1. Di Battista AP et al. Peripheral blood neuroendocrine hormones are associated with clinical indices of sport-related concussion. Sci Rep. 2019;9(1):18605.
2. Villegas E et al. Association between altered cortisol profiles and neurobehavioral impairment after mild traumatic brain injury in college students. J Neurotrauma. 2022;39(1112):809-20.
MILD TRAUMATIC BRAIN INJURY RESEARCH: YEAR IN REVIEW
To round off the day, Chris Giza, University of California Los Angeles, updated the ‘neurometabolic cascade’ model of concussion, emphasizing that: “mTBI pathophysiology is more than neuronal
and more than metabolic”. Specifically, Giza discussed the effects of mTBI on astrocytes, with implications for blood–brain barrier integrity and glymphatic function, microglial-mediated neuroinflammation, and synaptic reconfiguration. Looking to the future, Giza highlighted the application of biomarkers in characterizing the endophenotypes of individuals with persistent symptoms.15 Finally, Christina Master, University of Pennsylvania Perelman School of Medicine, Philadelphia, concluded with a succinct review of clinical mTBI studies, covering the effectiveness of helmets, the effect of sport-related etiology on outcomes, and social determinants of health impacting recovery.16-20
CONCLUSION
The AAN 2025 Annual Meeting reaffirmed the importance and increasing complexity of sports neurology, highlighting key knowledge gaps and new research directions in mTBI care. These highlights offer a snapshot of how the field continues to evolve, emphasizing opportunities for collaboration and innovation in the search for diagnostic and therapeutic strategies to ultimately enhance patient outcomes and performance.
3. Snook ML et al. Association of concussion with abnormal menstrual patterns in adolescent and young women. JAMA Pediatr. 2017;171(9): 879-86.
4. Claessen LÓE, et al. Pituitary dysfunction following mild traumatic brain injury in female athletes. Endocr Connect. 2024;13(2):e230363.
5. Esopenko C et al. Intimate partner violence-related brain injury: unmasking and addressing the gaps. J Neurotrauma. 2024;41(19-20):2219-37.
6. Cooper JG et al. Age specific reference intervals for plasma biomarkers of neurodegeneration and neurotrauma in a Canadian population. Clin Biochem. 2023;121-122:110680.
7. Caccese JB et al. Factors associated with symptom reporting in U.S. service academy cadets and NCAA student athletes without concussion: findings from the CARE Consortium. Sports Med. 2021;51(5):1087-105.
8. Johnson BD et al. Face cooling exposes cardiac parasympathetic and
sympathetic dysfunction in recently concussed college athletes. Physiol Rep. 2018;6(9):e13694.
9. La Fountaine MF et al. Attenuation of spontaneous baroreceptor sensitivity after concussion. Med Sci Sports Exerc. 2019;51(4):792-7.
10. Haider MN et al. Symptoms upon postural change and orthostatic hypotension in adolescents with concussion. Brain Inj. 2021;35(2):22632.
11. McAllister TW et al. Randomized placebo-controlled trial of methylphenidate or galantamine for persistent emotional and cognitive symptoms associated with PTSD and/or traumatic brain injury. Neuropsychopharmacology. 2016;41(5):1191-8.
13. Piantino JA et al. The bidirectional link between sleep disturbances and traumatic brain injury symptoms: a role for glymphatic dysfunction? Biol Psychiatry. 2022;91(5):478-87.
14. Yamamoto EA et al. The perivascular space is a conduit for cerebrospinal fluid flow in humans: a proof-of-principle report. Proc Natl Acad Sci USA. 2024;121(42):e2407246121.
15. Kamins JL et al. Biomarkers and endophenotypes of post-traumatic headaches. Curr Pain Headache Rep. 2024;DOI:10.1007/s11916-024-01255-1.
12. Sullan MJ et al. Glymphatic system disruption as a mediator of brain trauma and chronic traumatic encephalopathy. Neurosci Biobehav Rev. 2018;84:316-24.
16. Hammer E et al. The association between Guardian Cap use during practices and sport-related concussion risk in high school American football players. Br J Sports Med. 2025;59(4):257-62.
17. Corwin DJ et al. Community and patient features and health care point of entry for pediatric concussion. JAMA Netw Open. 2024;7(10):e2442332.
18. MacEachern T et al. The prevalence of Black/African American individuals in concussion literature: a systematic review and meta-analysis. Front Public Health. 2024;12:1430428.
19. Kinney AR et al. Relationships between neighborhood disadvantage, race/ethnicity, and neurobehavioral symptoms among veterans with mild traumatic brain injury. J Head Trauma Rehabil. 2025;40(2):65-75.
20. Ntikas M et al.; CENTER-TBI participants and investigators. Contrasting characteristics and outcomes of sports-related and non–sports-related traumatic brain injury. JAMA Netw Open. 2024;7(1):e2353318.
The 2024 Revised McDonald Criteria: AAN 2025 Highlights
Author: *Andrew Dugue1
1. Department of Neurology, NYU Grossman School of Medicine, New York City, USA
*Correspondence to Andrew.Dugue@nyulangone.org
Disclosure: The author has declared no conflicts of interest.
Keywords:
Biomarkers, central vein sign, cerebrospinal fluid, diagnosis, McDonald criteria 2024, MRI, multiple sclerosis (MS), optic nerve, optical coherence tomography.
Citation: Neurol AMJ. 2025;2[1]:26-29.
https://doi.org/10.33590/neurolamj/ZSFM1010
The 2025 American Academy of Neurology (AAN) Annual Meeting was held in San Diego, California, USA, April 5th–9th, and provided the most recent updates in the field of neurology. The upcoming publication of the 2024 Revised McDonald criteria for the diagnosis of multiple sclerosis (MS) was particularly highlighted in multiple sessions at the conference as described below.
UPDATING THE FRAMEWORK FOR MULTIPLE SCLEROSIS DIAGNOSIS
In the Fall of 2023, a group of international experts convened to examine the McDonald criteria for the diagnosis of MS. There was an imperative for revision of the 2017 criteria, given the substantive MS research, particularly involving paraclinical testing and biomarkers, that had since emerged. They utilized a modified nominal group technique, requiring agreement of 80%, on statements and recommendations deemed important in the diagnosis of MS.1 According to Aaron Miller, Icahn School of Medicine at Mount Sinai, New York, USA, these statements and recommendations were derived from the past year of presentations and evidence from the National Multiple Sclerosis Society and European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).1 Over 70 questions were discussed and voted upon, culminating in the inclusion of new parameters to increase the sensitivity of the
McDonald criteria. These parameters added to the definitions of dissemination in time and dissemination in space. A diagnostic algorithm based on the proposed criteria is provided in Figure 1 1
WHAT’S NEW IN THE 2024 CRITERIA
Miller stated that the goal of the McDonald criteria is to facilitate the early diagnosis of MS, and that they were designed to be applied to only typical cases of MS.1 For example, unilateral optic neuritis, focal supratentorial syndrome, focal brainstem or cerebellar syndrome, or a partial myelopathy. He cautioned that they were not designed to be applied to atypical presentations, such as bilateral optic neuritis, complete ophthalmoplegia, complete transverse myelopathy, encephalopathy, headache, isolated fatigue, dizziness, or isolated vertigo.1
Typical MS Presentation
Objective Progression
History and examination, imaging, laboratory testing, and differential diagnosis supporting MS without a better diagnosis.
Lesions in at least two CNS locations or
Progressive symptoms for at least 12 months with at least two spinal cord lesions
MS diagnosis is met with the addition of at least one of the below:
• CVS
• Positive CSF (presence of oligoclonal bands or kappa free light chains)
• Presence of lesions in 4 of 5 CNS locations
• Dissemination in Time
*Diagnostic algorithm is adapted from Miller et al., 20251
Lesion in one CNS location
MS diagnosis is met with the addition of at least one of the below:
• Dissemination in Time and CVS
• Dissemination in Time and PRL
• Positive CSF and PRL
• Positive CSF and CVS
CNS: central nervous system; CVS: central vein sign; CSF: cerebrospinal fluid; MS: multiple sclerosis; PRL: paramagnetic rim lesion.
THE ROLE OF IMAGING AND BIOMARKERS
Laura Balcer, NYU Grossman School of Medicine, New York, USA, introduced the optic nerve as the fifth topographic site for MS lesions in the 2024 Revised McDonald criteria (Table 1). Evidence of a symptomatic or asymptomatic optic nerve lesion can be determined through paraclinical testing with orbital MRI, optical coherence tomography (OCT), and/or visual evoked potentials (VEP) (Table 2). 1 Orbital MRI findings of optic nerve injury, through gadolinium enhancement and/ or T2 hyperintensity, will be included in the same manner as other topographic sites. It
was stressed that in order to make an accurate diagnosis, these findings must be interpreted in the correct clinical context, such as during an acute episode of optic neuritis with classic findings (eye pain, relative afferent pupillary defect, and dyschromatopsia).1 Work by Rachel Kenney, NYU Grossman School of Medicine, on OCT showed that an inter-eye asymmetry in retinal nerve fiber layer (RNFL) thickness and/or ganglion cell layer (GCL) thickness could distinguish eyes with prior optic neuritis amongst patients with MS.2 VEP demonstration of delayed latency could also indicate an optic nerve lesion. Steven Galetta, NYU Grossman School of Medicine, noted that studies by Brownlee, Bsteh, and Vidal-Jordana using the
Figure 1: Diagnostic algorithm for multiple sclerosis diagnosis.*
Table 1: Topographic locations for multiple sclerosis diagnosis.
CNS locations fulfilling Dissemination in Space
Optic nerve
Periventricular
Juxtacortical/cortical
Infratentorial
Spinal cord
CNS: central nervous system.
Table 2: Paraclinical test criteria for optic nerve lesions.*
Significant intereye difference in OCT RNFL and/or ganglion cell layer (5 microns RNFL, 4 microns GCL)
Delayed P100 latency on visual evoked potentials
Presence of optic nerve T2 hyperintensity and/or gadolinium enhancement on MRI orbits
*Official retinal nerve fiber layer and ganglion cell layer intereye difference measurement to be announced in the upcoming McDonald Criteria 2024 publication. The numbers provided in the Figure are based on research by Kenney et al.2
GCL: ganglion cell layer; OCT: optical coherence tomography; RNFL: retinal nerve fiber layer.
optic nerve as a fifth site with these paraclinical tests maintained McDonald criteria accuracy, while increasing their sensitivity.3-6 He stated that one cannot make the diagnosis of MS using the optic nerve as a fifth site without the correct clinical context. He noted that there are other causes of optic nerve abnormalities, such as glaucoma, a highly myopic eye, and maculopathies that can confound paraclinical testing.3 He also remarked that these tests (VEP, OCT, MRI) had been verified in wellcharacterized cohorts of patients, underscoring the importance of applying the criteria to those with a typical MS presentation.3
Balcer discussed cerebrospinal fluid (CSF) biomarkers in the 2024 McDonald criteria. She stated that the kappa-free light chain index is reflective of intrathecal B cell activity and is increased in MS1 It was added to the new McDonald criteria as a marker fulfilling dissemination in time. This marks the addition of a second CSF biomarker, aside from oligoclonal bands, fulfilling dissemination in time criteria. It was noted that there is approximately 87% concordance between the kappa-free light chain index and oligoclonal bands.1
APPLYING THE CRITERIA IN CLINICAL PRACTICE
Jiwon Oh, University of Toronto, Canada, reviewed the MRI findings in the 2024 criteria and remarked that this is the first time in McDonald criteria history that MRI has been incorporated beyond simply detecting new lesions. Two MRI findings were added: the central vein sign (CVS) and paramagnetic rim lesions (PRL). The CVS, a line or dot centrally located within a lesion on susceptibility sequences, reflects the pathologic mechanism of MS (perivenular inflammation and demyelination). The CVS’ sensitivity and specificity for MS is greater than 90%. It can be applied through the Select 6 and Rule of 6 rating methods. The Select 6 method supports MS if at least 6 lesions have central veins, while the Rule of 6 is used if there are fewer than 6 lesions and supports a diagnosis of MS if the majority of lesions have a central vein. PRLs, lesions from inflammation and demyelination related to paramagnetic effects
References
1. Miller A et al. Revised McDonald Criteria (2024): Diagnosis and Misdiagnosis of MS in 2024 and Beyond. AAN 2025, April 5-9, 2025.
2. Nolan-Kenney RC et al. Optimal intereye difference thresholds by optical coherence tomography in multiple sclerosis: An international study. Ann Neurol. 2019;85(5):618-29.
of iron-laden microglia and macrophages at the lesion edge, are regarded as a marker of MS disease progression and confer over 90% specificity for MS.1 Shamik Bhattacharyya, Brigham and Women's Hospital, Boston, Massachusetts, USA, cautioned that in periventricular lesions, there is a high rate of positive CVS even in people with non-MS pathologies. He noted that a combination of susceptibility and T2 weighted images allows for the best visualization of the CVS, particularly T2* or FLAIR* imaging.7 Critically, these imaging signs facilitate earlier diagnosis in patients across the spectrum of MS, particularly in those with radiologically isolated syndrome. The high specificity of these signs was noted to act as guard rails against MS misdiagnosis. Oh again emphasized that the new criteria should be used in those presenting with typical clinical syndromes, and that adherence to strict definitions of characteristic lesion topographies is important to minimize misdiagnosis.1
3. Biousse et al. Neuro-ophthalmology 2: Optic Neuritis, Visual Fields, and Anisocoria, AAN 2025. AAN 2025, April 5-9, 2025.
4. Brownlee WJ et al. Inclusion of optic nerve involvement in dissemination in space criteria for multiple sclerosis. Neurology. 2018;91(12):e1130-e1134.
5. Bsteh G et al. Diagnostic performance of adding the optic nerve region assessed by optical coherence
tomography to the diagnostic criteria for multiple sclerosis. Neurology. 2023;101(8):e784-e793.
6. Vidal-Jordana A et al. Adding the optic nerve in multiple sclerosis diagnostic criteria: a longitudinal, prospective, multicenter study. Neurology. 2024;102(8):e209214.
7. Bhattacharyya S et al. Neuroimaging for the Neurologist: Brain. AAN 2025, April 5-9, 2025.
What Is Next in Myasthenia Gravis? Insights on Ocular and MuSK Forms from AAN 2025
Author: Bertie Pearcey, EMJ, London, UK
Citation: Neurol AMJ. 2025;2[1]:30-33 https://doi.org/10.33590/neurolamj/SDSW2308
THE 2025 American Academy of Neurology (AAN) Annual Meeting saw experts in the field travel to San Diego, California, for the field’s latest insights. Attendees were presented with these updates in the form of fascinating abstracts, captivating presentation sessions, and exciting discussions around the future of neurology. One of these talks, entitled "Neuromuscular junction disorders: myasthenia gravis, ocular, and MuSK myasthenia", and expertly chaired by Neelam Goyal, Stanford University, California, detailed many aspects of myasthenia gravis (MG), ranging from the current standard-of-care to treatments of the future.
RETHINKING THE FOUNDATIONS OF MYASTHENIA GRAVIS: WHEN TO TREAT, HOW TO TREAT, AND WHY IT MATTERS
Stephen Reddel, University of Sydney, Australia, opened the session by reframing the treatment landscape of MG, emphasizing that: “It’s a bad disease, but also a treatable disease,” and often dramatically so. He argued strongly for early intervention to avoid unnecessary disability. “Why make people live with disability rather than treat it as early as possible?” he asked, reflecting a key message from his talk: timely therapy can transform lives.
Reddel alluded to the privilege of travelling from Australia to present his talk; a reflection on the privilege afforded by the Australian healthcare system. In Australia, where there is broad access to immunotherapies under a single-payer system, Reddel described a flexible treatment paradigm, where there is no mandated drug sequence, allowing clinicians to tailor treatment to disease severity and patient preference
across different stages. This pragmatic flexibility allows for the use of both traditional therapies, such as corticosteroids and azathioprine, as well as newer immunomodulators and biologics.
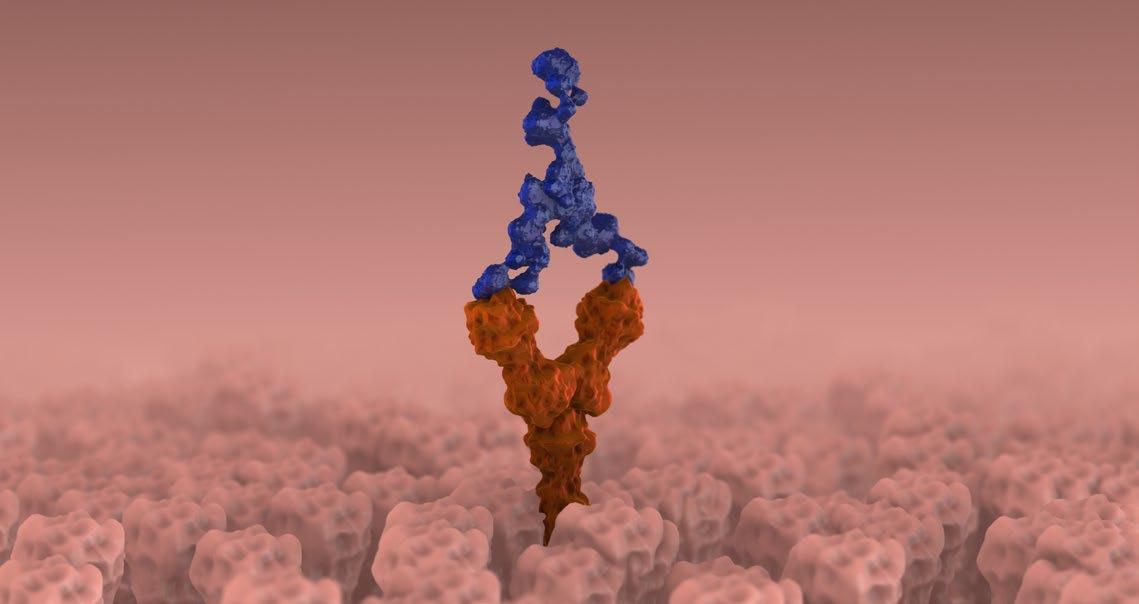
PATHOPHYSIOLOGY OF MYASTHENIA GRAVIS
One of the central themes of Reddel’s talk was the pathophysiological underpinnings of MG, particularly acetylcholine receptor (AChR)-positive disease. He began his discussion with a figure of normal mouse neuromuscular junctions (NMJ) in the background, remarking that: “They’re really pretty things,” which is testament to his passion for the field. He continued with a brief explanation of the classic synapse and the tests that are currently available for MG. Importantly, Reddel challenged the conventional dogma that AChR antibody levels do not correlate with disease severity. Citing a 23-year longitudinal case study, he showed that antibody titres, when carefully tracked over time, can correlate with clinical
fluctuation; a valuable point for those managing complex cases in the long term.
After detailing the strategy for the clinical management of MG, he continued by explaining the four pathogenic antibody mechanisms in MG: receptor blockade, complement activation, receptor internalization, and antibody-dependent cellular cytotoxicity. He noted that treatments, must be matched to mechanism accordingly. Reddel presented a structured approach to MG therapy, ranging from the perhaps underutilised thymectomy, to targeted B cell depletion (e.g., rituximab in muscle-specific kinase [MuSK] MG) and upstream agents targeting BAFF/APRIL and CD19. He stressed that: “The critical issue that people get wrong is the timeto-treatment onset of the therapies,” while explaining the time-to-treatment onset of the available therapeutic options.
He stressed that while some treatments like corticosteroids are widely available and effective, they come with well-established longterm toxicities. “The toxicity is horrendous,”
he expained, which he underscored with sobering epidemiological data. For upstream therapies like azathioprine or mycophenolate, he emphasized realistic timelines: no clinical benefit before 12–15 months. Hence, bridging agents or more rapid-acting therapies (e.g., intravenous immunoglobulin [IVIG], plasma exchange [PLEX], and calcineurin inhibitors) may be needed in patients with significant disease burden.
OCULAR AND MuSK MYASTHENIA GRAVIS DIAGNOSIS AND TREATMENT
On ocular MG, he advocated for careful diagnostic scrutiny, especially in seronegative cases. Treating early with corticosteroids may reduce generalization, but overtreatment carries its own risks. As for MuSK MG, he emphasized its distinct phenotype; bulbar features, poor steroid response, and excellent response to PLEX or rituximab; and highlighted emerging challenges in combining therapies like anti-neonatal Fc receptors (FcRn) with B cell depleting agents.
The critical issue that people get wrong is the time-totreatment onset of the therapies
He closed with a poignant case of a patient who recovered from a ventilator-dependent state that began in their 20s, including being on a ventilator at home for an extended period. He mentioned that this must have been traumatic, and described the patient’s slow journey into remission, leaving the audience to ponder his take home message: MG is a plastic but manageable disease.
TARGETING THE IMMUNE CASCADE: COMPLEMENT BLOCKADE AND NEONATAL
Fc RECEPTOR INHIBITION
Francesco Saccà, Federico II University of Naples, Italy, followed with an in-depth look at the immunological mechanisms that are now shaping the next generation of MG therapies. He reflected on how far the field has come since his medical training, when AChR blockade was the only described mechanism. Today, complement activation and FcRn pathways are known to be central drivers of pathology, and thus prime therapeutic targets.
Saccà structured his talk around two major downstream strategies: complement inhibition and IgG reduction via FcRn inhibition. He began with a clear primer on the complement cascade, outlining how antibody–antigen complexes (such as those in AChR-positive MG) activate the classical pathway, ultimately damaging the NMJ. Blocking C5 with agents like eculizumab and ravulizumab halts this cascade. Ravulizumab, a long-acting C5 inhibitor requiring only bimonthly infusion, has demonstrated durable benefits in clinical trials such as CHAMPIONMG,1 including rapid Quantitative Myasthenia Gravis (QMG) score improvement and long-term reduction in corticosteroid use.
Further innovations, including zilucoplan, a subcutaneous macrocyclic peptide, offer promising dual-action complement inhibition with the potential for homebased administration and compatibility with other therapies like IVIG and anti-FcRn.
ANTI-NEONATAL Fc RECEPTORS
Following his discussion of complement inhibition, Saccà shifted focus to another promising strategy: FcRn inhibition, describing it as: “An entire new chapter in therapy.” FcRn normally rescues IgG from lysosomal degradation, giving them a long half-life. Drugs like efgartigimod, rozanolixizumab, nipocalimab, and batoclimab disrupt this process, lowering circulating IgG (including pathogenic autoantibodies) by up to around 80%. Unlike complement inhibitors, some anti-FcRn (efgartigimod and rozanolixizumab) are given cyclically, and show a pattern of clinical improvement followed by deterioration between treatment cycles, a feature absent in continuously administered agents.
Real-world data comparing complement inhibitors to anti-FcRn was another highlight of Saccà’s presentation. A retrospective Italian study showed both were effective in improving MG-Activities of Daily Living, but complement inhibitors achieved deeper QMG improvements and greater steroid reduction.2 Similarly, U.S. data from electronic medical records showed faster and more substantial corticosteroid tapering with C5 inhibitors compared to efgartigimod.3 However, Saccà also presented a German cohort where outcomes between the two strategies were more closely matched, emphasizing that clinical context and patient-specific factors remain key.4
In summarizing, Saccà evaluated the differences between the two approaches. The effect of complement inhibitors results in complete complement blockade, whereas anti-FcRn can only reduce IgG by 60–70%. The administration of C5 inhibitors is continuous, whereas anti-FcRn are administered both cyclically (in the
case of efgartigimod and rozanolixizumab) or continuously (with nipocatimab and satoclimab). He briefly mentioned how intercycle fluctuations are not seen for complement inhibitors but are seen with cyclically administered anti-FcRNs. When describing the steroid-sparing effect, he noted that the effects are reported in open-label extension trials for complement inhibitors, and observed to be greater for complement inhibitors in many real-world evidence studies. For anti-FcRns, effect is not reported in open-label extension trials, yet is seen to be lower in many real-world evidence studies, but not all of them.4 He concluded with the safety considerations for complement inhibitors, including meningococcal infections and the need for vaccinations, and anti-FcRNs, including bacterial infections of the respiratory or urinary tract.
References
1. Vu T et al. Terminal complement inhibitor ravulizumab in generalized myasthenia gravis. NEJM Evid. 2022;1(5):EVIDoa2100066.
2. Pane C et al. A real-life experience with eculizumab and efgartigimod in generalised myasthenia gravis patients. J Neurol. 2024;271(9):6209-19.
Looking to the future, Saccà hinted at even more upstream immunomodulation, including agents targeting C1 and early components of the immune cascade. These therapies may balance efficacy with safety by preserving alternative immune pathways.
CONCLUDING THOUGHTS
This two-part session offered both a grounded clinical approach and a visionary outlook on MG management. Reddel’s practical treatment strategies and pathophysiological insights were the ideal prelude to Saccà’s discussion of precision immunotherapies. Together, they made one point abundantly clear: MG is no longer a disease of therapeutic despair. With smart strategy and evolving tools, clinicians can now aim not just for symptom control, but for remission, and perhaps one day, a cure.
3. Blackowicz M et al. Long-term corticosteroid treatment patterns and steroid-sparing effects of approved treatments for generalized myasthenia gravis in the United States. Abstract 145. AANEM Annual Meeting. 15-18 October, 2024.
4. Scheiner CA et al. Outcomes for patients with generalized myasthenia gravis prescribed ravulizumab, eculizumab, or efgartigimod treatment: interim analysis of a retrospective medical record analysis (ELEVATE). AANEM Annual Meeting. 15-18 October, 2024.
Personalized Locomotor Training with Non-Invasive Spinal Cord Stimulation for Functional Recovery After Spinal Cord Injury
Authors: Umema Rafay,1 Muhammet B. Kocer,1
Attiyeh Vasaghi,1 Katrina Armstrong,1 Sydney
Sass,2 Kristine C. Cowley,1,3 *Katinka Stecina1,3
1. University of Manitoba, Winnipeg, Canada
2. University of Winnipeg, Canada
3. Spinal Cord Research Centre, University of Manitoba, Winnipeg, Canada *Correspondence to katinka.stecina@umanitoba.ca
Disclosure: Cowley has served on a scientific review advisory board for research grants with Craig Neilsen Research Foundation. The remaining authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank all study participants and Peisan Lew and Matt Ellis for technical support.
Keywords: Electromyography (EMG), functional electrical stimulation, locomotor training, metabolic outcomes, neurorehabilitation, spinal cord injury (SCI), trans-spinal electrical stimulation (ts-ES).
Citation: Neurol AMJ. 2025;2[1]:34-35. https://doi.org/10.33590/neurolamj/QHXD8365
BACKGROUND
Spinal cord injury (SCI) is a central nervous system injury that often leads to motor, sensory, and autonomic dysfunction. Noninvasive trans-spinal electrical stimulation (ts-ES) has been shown to activate neural networks below the injury and improve motor,1,2 as well as autonomic function recovery after SCI.3 The objective of this study4 was to compare changes in motor and autonomic function attributable to ts-ES in individuals with incomplete SCI after 4 weeks of personalized locomotor (treadmill-walking-based) training.
METHODS
Participants (n=6, 1 female) received 4 weeks of treadmill training with personalized step-
cycle based peripheral functional electrical stimulation (FES) with or without additional, non-invasive lumbar ts-ES. Spinal stimulation was done by rectangular, monophasic current pulses (1 ms) at 40 Hz frequency for max 1–3-minute bouts, with intensity adjusted for each participant (17–35 mA). Clinical outcome measures of motor function (2-minute walk test, Berg Balance, and modified SCIMMobility) and metabolic analysis were assessed before and after training. Metabolic analysis of oxygen consumption was performed at the start and at the end of the training, which consisted of automatic, breathby-breath analysis of oxygen consumption (VO2 sub-max), and heart rate measurements during graded treadmill tasks (from seated rest, standing, to walking at increasing speeds). Ground forces and electromyography (EMG) recordings while walking on a treadmill allowed quantification of muscle activity, and a combination of locomotor assessment tools were used to create cycle-based analysis of each person’s locomotor EMG profile from randomly selected steps (n=18–28). Averaged EMGs obtained with and without ts-ES were compared by using a 500 ms window aligned to maximum vertical force loading on the left leg. Changes induced by ts-ES in each muscle’s root-mean square (RMS) in the raw EMG, and mean amplitude of the filtered and rectified EMG were measured in this window and calculated as percent of the EMG activity during no ts-ES condition.
RESULTS
Quantitative analysis of EMG activity showed facilitation of muscle activity in ankle and knee extensors with about 10–25% increases during forward walking. Qualitatively, based on participant feedback, ts-ES in addition to FES during locomotor training was tolerable, and improved leg movement EMG output, even during backward walking and step-
arm-reach tasks. Moreover, ts-ES tended to increase heart rate and VO2 sub-max when applied acutely, i.e., within one session for 1–2 minutes.
CONCLUSIONS
Personalized rehabilitation strategies combining ts-ES with locomotor training with not only forward walking, but also backward walking or step-and-reach tasks, in addition to FES, have a realistic potential to improve metabolic output during recovery in people living with SCI.
References
1. Flett S et al. Spinal electrical stimulation to improve sympathetic autonomic functions needed for movement and exercise after spinal cord injury: a scoping clinical review. J Neurophysiol. 2022;128(3):649-70.
2. Nardone R et al. Noninvasive spinal cord stimulation: technical aspects and therapeutic applications. Neuromodulation. 2015;18(7):580-91.
3. Zaaya M et al. Transspinal stimulation and step training alter function of spinal networks in complete spinal cord injury. Spinal Cord Ser Cases. 2021;7(1):55.
4. Rafay U et al. Personalized locomotor training with non-invasive spinal cord stimulation for functional recovery after spinal cord injury. Poster 6. AAN Annual Meeting, April 5-9, 2025.
Outcomes of a 3-Week Interdisciplinary Intensive Outpatient Treatment Program for Mild-Moderate Traumatic Brain Injury in Veterans and First Responders
Authors: *Vaughn E. Bryant,1 Jade Hannan,1 Ramon Bautista,1 Scott Silliman1
1. University of Florida College of Medicine –Jacksonville, USA
*Correspondence to vaughn.bryant@jax.ufl.edu
Disclosure: Bryant has received support for attending meetings and/or travel from a grant provided by the Avalon Action Alliance. The other authors have declared no conflicts of interest.
Acknowledgements: The authors would like to give special thanks to the Avalon Action Alliance, the Marcus Institute for Brain Health, their collaborators, and all Veterans and First Responders.
Keywords: Concussion, first responders, neurorehabilitation, post-concussion syndrome, rehabilitation, traumatic brain injury (TBI), veterans.
Citation: Neurol AMJ. 2025;2[1]:35-37. https://doi.org/10.33590/neurolamj/UYVS2448
OBJECTIVE
To evaluate the outcomes of a threeweek interdisciplinary intensive outpatient
treatment program for mild-moderate traumatic brain injury (TBI) in veterans and first responders.1
BACKGROUND
Military service members and first responders are at elevated risk for TBI. While most individuals with mild TBI report no persisting symptoms >6 months postinjury, approximately 15% experience persisting cognitive, mood, and/or somatic consequences. Currently, there is no standard of care for treating persistent symptoms associated with mild-to-moderate TBI.
METHODS
The Haley Brain Wellness Program (HBWP) is a 3-week, interdisciplinary outpatient treatment program for veterans and first responders with persisting symptoms from TBI. Descriptive statistics and paired samples t-tests were conducted to examine intensive
outpatient program (IOP)-associated changes in self-reported neurobehavioral symptoms, as well as measures of cognitive, vestibular, and sensory-integration functioning, for 128 participants (Table 1).
Table 1: Selected results from patient-reported and objective clinical outcomes at the start and end of the 3-week intensive outpatient program.
ACE-III: Addenbrooke’s Cognitive Examination-III; IOP: intensive outpatient program; LiSat-11: Life Satisfaction Questionnaire-11; mCTSIB: Modified Clinical Test for Sensory Interaction on Balance; NSI: Neurobehavioral Symptom Inventory; PCL-5: Posttraumatic Stress Disorder Checklist for DSM-5; SD: standard deviation; SOT: sensory organization test.
RESULTS
The majority of attendees were male (81%, n=104). The average age was 49 years (standard deviation [SD]:11.7, range: 23–78). The average time since the last TBI with loss of consciousness was 18.4 years (SD:13.9), with 76% of individuals reporting any TBI with loss of consciousness. Upon discharge, HBWP participants reported a mean decrease of 15.570 points (41%) on the Neurobehavioral Symptom Inventory (NSI;
Cohen’s d=1.111). Scores on Addenbrooke’s Cognitive Examination-III (ACE-III) improved by an average of 6.837 points (Cohen’s d=1.408). Furthermore, participants increased their forward (Cohen’s d=0.679) and reverse gait speed (Cohen’s d=0.758), and demonstrated large improvements on tests of sensory integration (Bertec sensory organization test [SOT] composite; Cohen’s d=0.874) and vestibular function (PropriomCTSIB#4; Cohen’s d=0.850).
CONCLUSION
The HBWP model demonstrates strong preliminary efficacy in reducing symptoms associated with mild-moderate TBI and improving performance on clinical measures of cognition, vestibular function, and sensory integration. These results have implications for the development of a standard of care for persistent post-TBI symptoms in this patient population.
Further studies are necessary to determine whether these short-term results are sustained over time.
Reference
1. Bryant VE et al. Outcomes of a three-week interdisciplinary intensive outpatient treatment program for mild-moderate traumatic brain injury in veterans and first responders. Abstract 2899. AAN Annual Meeting, 5-9 April, 2025.
Comprehensive Efficacy and Safety Analysis of Levetiracetam versus Phenytoin in Brain Injury: An Umbrella Review
Authors: Areeba Maryam1, Muhammad Hassan Waseem,2 Muhammad Ahmad Sohail,3 *Zain ul Abideen,4 Brandon Lucke-Wold,5 Syeda Nimra Qadri,6 Esha Chaudhary,7 Azka Shahab,8 Sassi Abbasi,9 FNU Deepak,10 Aimen Zulfikar,6 Zunaira Saeed,6 Sania Aimen11
1. Rawalpindi Medical University, Pakistan
2. Allama Iqbal Medical College, Lahore, Pakistan
3. Shifa College of Medicine, Islamabad, Pakistan
4. King Edward Medical University, Lahore, Pakistan
5. University of Florida, USA
6. Dow University of Health Sciences, Karachi, Pakistan
7. Islamic International Medical College, Rawalpindi, Pakistan
8. Bahria University Medical and Dental College, Karachi, Pakistan
9. Sindh Institute of Urology and Transplantation, Pakistan
10. Shaheed Mohtarma Benazir Bhutto Medical College, Karachi, Pakistan
11. Quetta Institute of Medical Sciences, Pakistan
*Correspondence to mzainulabideen@kemu.edu.pk
Disclosure: The authors have declared no conflicts of interest.
Keywords: Brain injury, levetiracetam, phenytoin, seizure prophylaxis, traumatic brain injury.
Citation: Neurol AMJ. 2025;2[1]:37-38. https://doi.org/10.33590/neurolamj/VFNB9163
AIMS AND OBJECTIVES
New research presented at the American Academy of Neurology (AAN) Annual Meeting 20251 reveals critical insights into the comparative efficacy and safety of levetiracetam and phenytoin for seizure prophylaxis in patients with brain injury. Traumatic brain injury is a major cause of disability worldwide, with seizures affecting a significant number of individuals. This umbrella review, synthesizing data from six systematic reviews and meta-analyses, aims to address ongoing uncertainties regarding the effectiveness of these two common anti-epileptic drugs.
METHODS AND RESULTS
A total of 14 randomized controlled trials (RCT) and 43 observational studies were included, with a focus on key outcomes, including seizure prevention, early and late seizure response, mortality, and adverse effects. The findings suggest that
while levetiracetam showed a favorable safety profile, with fewer adverse effects (p=0.0003) such as nausea and hypotension, it did not significantly reduce the incidence of seizures (Figure 1) compared to phenytoin. Notably, levetiracetam was associated with a significantly higher mortality rate (p=0.04), which warrants attention in clinical practice.
Interestingly, both drugs showed similar outcomes in terms of seizure control, length of ICU and hospital stays, and early or late seizure responses. These findings highlight the need for further research to assess the precise role of levetiracetam in managing patients with brain injury, especially given the higher mortality rate observed with its use.
1: Forest plot demonstrating the response rate of overall seizures.
Chaari et al., 2017
Zhao et al., 20185
Test for overall effect: Z=1.39 (p=0.16)
Heterogeneity: Tauz= 0.14; Chiz= 8.41, df=3 (p=0.04); Iz=64%
CONCLUSION
The study highlights the importance of ongoing monitoring and research in refining treatment protocols and enhancing patient outcomes. It also points to the critical need for clinicians to carefully evaluate the riskbenefit profile of anti-epileptic drugs in brain injury care, considering both efficacy
References
1. Maryam A et al. Comparing efficacy and safety of levetiracetam versus phenytoin in brain injury: an umbrella review. Abstract 4956. AAN Annual Meeting, 5–9 April, 2025.
2. Xu JC et al. The safety and efficacy of levetiracetam versus phenytoin for seizure prophylaxis after traumatic brain injury: a systematic review and metaanalysis. Brain Inj. 2016;30(9):1054-61.
3. Yang Y et al. Levetiracetam versus phenytoin for seizure prophylaxis following traumatic brain injury: a systematic review and meta-analysis. CNS Drugs. 2016;30(8):677-88.
4. Chaari A et al. Levetiracetam versus phenytoin for seizure prophylaxis in brain injured patients: a systematic review and meta-analysis. Int J Clin Pharm. 2017;39(5):998-1003.
5. Zhao L et al. Efficacy of levetiracetam compared with phenytoin in prevention of seizures in brain injured patients: a meta-analysis. Medicine (Baltimore). 2018;97(48):e13247.
Figure
Characterizing Cerebrospinal Fluid Profiles of Immunocompromised Patients with Infectious
Meningitis/Encephalitis
Authors: Sarah Thomas,1 Kailyn Hayes,2 Hai Ethan Hoang,3 Kiran Thakur,4 *Rachelle Dugue5
1. Morehouse School of Medicine, Atlanta, Georgia, USA
2. Meharry Medical College, Nashville, Tennessee, USA
3. Weill Cornell Medical College/New York Presbyterian Hospital, USA
4. Columbia University Irving Medical Center, New York, USA
5. Stanford University School Medicine, California, USA
*Correspondence to rdugue@stanford.edu
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank the REACH-HBMC program.
Keywords: Bacterial meningitis, cerebrospinal fluid (CSF), encephalitis, immunocompromised, meningitis, viral meningitis, white blood cell (WBC).
Citation: Neurol AMJ. 2025;2[1]:39-40. https://doi.org/10.33590/neurolamj/XIMM6666
BACKGROUND
There are widely accepted ranges of typical cerebrospinal fluid (CSF) values used to guide diagnosis and treatment of suspected infectious meningitis/encephalitis in healthy individuals.1,2,3 However, it is unclear whether these values should routinely be applied to immunocompromised patients. Atypical CSF profiles may impact timely diagnostics and treatment, affecting clinical outcomes.4 In this study,5 the authors aimed to characterize CSF of immunocompetent versus immunocompromised patients with confirmed infectious meningitis/encephalitis.
METHODS
A retrospective database of patients with confirmed infectious bacterial or viral meningitis/encephalitis, admitted between 2010–2021, was constructed. Patients ≥18 years old, identified via International Classification of Diseases (ICD)-9/10 codes for infectious meningitis/encephalitis, were included. Demographic data, serum, CSF, imaging, and clinical data including immune status were collected.
RESULTS
Of 71 definitive bacterial meningitis/ encephalitis cases, 46 patients were immunocompromised. Immunocompromised patients had a mean adjusted CSF white blood cell (WBC) count of 3,035±558 cells/ μLwith 76.77±3.66% neutrophils, CSF protein of 245±31.4 mg/dL, and glucose ratio of 0.35±0.05. Immunocompetent patients had a mean CSF WBC count of 3192±1147 cells/μL with 77.52±5.58% neutrophils, CSF protein of 245±31.4 mg/dL, and glucose ratio of 0.32±0.05. There were 110 definitive viral meningitis/encephalitis cases. Fiftyeight patients were immunocompromised, with a mean CSF WBC count of 120.18 cells/ μL±36.8 with 63.5±3.9% lymphocytes, CSF protein of 116±23.2 mg/dL, and glucose ratio of 0.49±0.02. Immunocompetent patients had a mean CSF WBC count of 422.1 cells/ μL±71.5 with 72.4±3.5% lymphocytes, CSF protein of 103.3±6.1 mg/dL, and glucose ratio of 0.52±0.01.
DISCUSSION AND CONCLUSION
There were no differences in bacterial meningitis/encephalitis CSF profiles between immunocompetent and immunocompromised
patients. However, atypical CSF WBC counts were noted in immunocompromised patients with viral meningitis/encephalitis. Immunocompromised patients with viral meningitis/encephalitis had lower CSF WBC counts compared to immunocompetent patients, with a trend towards lower lymphocyte counts and greater monocyte counts in immunocompromised patients.
Immunocompromised patients have a less robust immune response to pathogens, which may make detecting a CSF signature of disease activity to particular pathogens more difficult.5 Notably, 14 cases of the viral meningitis cases had a CSF WBC count of less than five cells, a result consistent with a normal CSF profile. This was most commonly seen in immunocompromised patients infected with HHV-6 (n=10). Such atypical infectious profiles may delay appropriate workup, diagnosis, and management, suggesting the need for more tailored guidelines for immunocompromised
patients. Multi-site collaboration with pooling of retrospective databases to increase generalizability of findings and validate this hypothesis is pending.
References
1. Spanos A et al. Differential diagnosis of acute meningitis. JAMA. 1989;262(19):2700-7.
2. Tunkel AR et al. Infectious Diseases Society of America. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2008;47(3):303-27.
3. Fouad R et al. Role of clinical presentations and routine CSF analysis in the rapid diagnosis of acute bacterial meningitis in cases of negative gram stained smears. J Trop Med. 2014;2014:213762.
4. Habis R et al. Absence of cerebrospinal fluid pleocytosis in encephalitis. Clin Infect Dis. 2024;ciae391.
5. Thomas S et al. CSF Profiles of Immunocompromised Patients with Bacterial and Viral Meningitis. Poster 003. AAN Annual Meeting, April 5-9, 2025.
6. Fodor PA et al. Atypical herpes simplex virus encephalitis diagnosed by PCR amplification of viral DNA from CSF. Neurology. 1998;51(2):554-9.
Neurological Complications in Dengue: The Neuroinfections Emerging in the Americas Study (NEAS) in Colombia
Authors: Ana C. Villegas,1 Mariana Medina,1 David Acero-Garcés,2 Federico Silva,3 Melissa Medina,3 Catalina Vallejo C,4 Thanya Lagos,4 Katherine Claros,5 Susana C Dominguez-Peñuela,2 Martha Moyano,6 Lyda Osorio,6 Beatriz Parra,2 Carlos A Pardo-Villamizar,2 Guillermo González,6 *María I Reyes-Mantilla1,2
1. Department of Neurology, Hospital Simón Bolívar, E.S.E. Subred Integrada de Servicios de Salud Norte, Bogotá, Colombia
2. Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
3. Fundacion Cardiovascular de Colombia, Floridablanca, Colombia
4. Hospital Universitario Departamental de Nariño, Pasto, Colombia
5. Universidad Surcolombiana, Neiva, Colombia
6. Universidad del Valle, Santiago de Cali, Colombia
*Correspondence to mreyesm2@jhmi.edu
Disclosure: Pardo-Villamizar has received funding and support provided by the Bart McLean Fund for Neuroimmunology Research for GBS research in Colombia, NIH R01 NS110122, European Union’s Horizon 2020 ZikaPLAN Grant Agreement 734584, and Wellcome Trust Grants 092805 and 202789. The remaining authors have declared no conflicts of interest.
Acknowledgements: This work was carried out on behalf of The Neuroinfections Emerging in the Americas Study (NEAS) network.
Keywords: Dengue, dengue virus (DENV) serotype, Guillain-Barré syndrome, NEAS study, neurological complications of dengue.
Citation: Neurol AMJ. 2025;2[1]:40-41. https://doi.org/10.33590/neurolamj/UNCW5913
OBJECTIVE
To characterize the demographic, clinical, and laboratory features of neurological complications of dengue virus (DENV) enrolled in the NEAS cohort.1
BACKGROUND
The global incidence of neurological complications of DENV varies between 5% and 21%. In Colombia, epidemic outbreaks of DENV occur every 2–3 years, with all four serotypes circulating. Neurological manifestations could be classified as direct (e.g., encephalitis), indirect (e.g., encephalopathy), or postinfectious complications (e.g., myelitis, Guillain-Barré syndrome [GBS]).
DESIGN/METHODS
All newly diagnosed patients who fulfilled established criteria for encephalitis or encephalopathy, myelitis, meningoencephalitis, or GBS were recruited as part of an observational cohort. The authors examined the demographic, clinical, and epidemiological features of all cases accrued between January 2017 and December 2024.
RESULTS
In the period 2017–2024, a total of 25 patients were diagnosed with neurological complications of dengue, most presenting with encephalopathy or encephalitis (56%, n=14). Eight patients (32%) were diagnosed with GBS. The median age was 36 years (interquartile range: 20-52) and 56% (n=14) were male. Laboratory blood testing showed
positive serum DENV IgM in 24 (96%), serum DENV IgG in 16 (64%), and DENV serotype 1 by RT-PCR in the blood of two patients (8%). Cerebrospinal fluid (CSF) findings included a median cell count of 0 (range 0–9), glucose of 65 mg/dL (range: 53–77), and proteins of 42 mg/dL (range: 23–64). Neuroimaging was abnormal in only one case. In two patients with GBS, neurophysiological studies showed a case of axonal motor neuropathy and one case of demyelinating polyneuropathy. In the cases evaluated in 2024, ICU admission was required in 80% (n=8) of the cases, with three of them (30%) needing ventilatory support. Mortality was reported in one case (10%).
CONCLUSIONS
Dengue brain involvement can be classified as encephalopathy, encephalitis, or autoimmune/postinfectious processes. Although neurological problems in dengue are rare and emerging in the setting of severe dengue, the majority of cases require ICU admission. In the author's cohort, neurological complications of DENV infection were primarily associated with encephalopathy, which presented with normal CSF and neuroimaging findings. To clarify the diagnosis of dengue encephalitis, neuroinvasion must be demonstrated through serological or molecular tests (NS1, IgM, or RNA) in CSF and pleocytosis. However, these tests are often difficult to access in endemic countries. Standardizing these criteria is essential, but clinical application faces biases due to limited access and varying diagnostic performance based on the timing of sample collection.
Reference
1. Villegas AC et al. The spectrum of neurological complications in dengue: the Neuroinfections Emerging in the Americas Study (NEAS) in Colombia. Poster 008. AAN Annual Meeting, April 5-9, 2025.
Relationship of Rehabilitation Insurance Payor to Functional Status at One-Year Post-Traumatic Brain Injury
Authors: Rajit J. Shah,1 *Angelle M. Sander,2,3
Shannon B. Juengst,3,4 Abdulaziz Bako,5 Librada
Callender,6 Jeanne Hoffman,7 Raj Kumar,8 Anthony Lequerica, 9,10 Amanda Rabinowitz11,12
1. Tilman J. Fertitta Family College of Medicine, University of Houston, Texas, USA
2. H. Ben Taub Department of Physical Medicine and Rehabilitation, Baylor College of Medicine, Houston, Texas, USA
3. Brain Injury Research Center, TIRR Memorial Hermann, Houston, Texas, USA
4. Department of Physical Medicine and Rehabilitation, University of Texas Health Sciences Center at Houston, USA
5. Center for Health Outcomes and Informatics Research, TIRR Memorial Hermann, Houston, Texas, USA
6. Baylor Scott and White Institute for Rehabilitation, Dallas, Texas, USA
7. Department of Rehabilitation Medicine, University of Washington School of Medicine, Seattle, USA
8. Department of Rehabilitation and Human Performance, Icahn School of Medicine at Mount Sinai, New York, USA
9. Center for Traumatic Brain Injury Research, Kessler Foundation, East Hanover, New Jersey, USA
10. Department of Physical Medicine and Rehabilitation, Rutgers Health New Jersey Medical School, Newark, USA
11. Department of Rehabilitation Medicine, Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, Pennsylvania, USA
12. Jefferson Moss Rehabilitation Research Institute, Philadelphia, Pennsylvania, USA
*Correspondence to angelle.sander@memorialhermann.org
Disclosure: The contents of this publication were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) grant numbers 90DPTB0025 [PIs: Sander, Juengst], 90DPTB0024 [PI: Hoffman], 90DPTB0032 [PI: Chiaravalloti], 90DPTB0023 [PI: Driver], 90DPTB0028 [PI: Dams-O’Connor], and 90DPTB0019 [PI: Rabinowitz]. NIDILRR is a center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this publication are solely the responsibility of the
authors and do not necessarily represent the policy or official views of NIDILRR, ACL, NIH/NIA, NIH/ NIMHD, or HHS, and should not be assumed to be endorsement by the Federal Government. Sander, Juengst, Bako, and Rabinowitz are Executive Committee members for the American Congress of Rehabilitation Medicine’s Brain Injury Interdisciplinary Special Interest Group. Hoffman has received grants to their institution from PCORI, NIH, and CDMRP. Kumar has received consultancy fees from the University of Colorado.
Keywords: Assessments, insurance, patient outcomes, traumatic brain injury (TBI).
Citation: Neurol AMJ. 2025;2[1]:42-44. https://doi.org/10.33590/neurolamj/JRIL2272
BACKGROUND AIMS
Insurance is an important social determinant of health that can contribute to health inequities. Many patients with traumatic brain injury (TBI) lack health insurance. Between 2017 and 2020, 15.7% of patients with severe TBI in the United States lacked insurance coverage.1 Previous research has shown a relationship between insurance and outcomes following acute trauma care for TBI, such that uninsured patients had shorter hospital lengths of stay, decreased likelihood of discharge to rehabilitation, higher likelihood of mortality, and increased recurrence of TBI compared to those with health insurance.2-5 Few studies have investigated the contribution of insurance to outcomes in patients with TBI who have undergone inpatient rehabilitation.
METHODS
The authors conducted an analysis of the Traumatic Brain Injury Model Systems (TBIMS) national database to investigate the relationship between insurance payor and functional status 1-year post-injury
in individuals with TBI who had received acute level-one trauma care and completed comprehensive inpatient brain injury rehabilitation.6 The TBIMS national database enrolls individuals who meet the following criteria: at least 16 years old at the time of injury; admitted to a TBIMS level-one trauma center within 72 hours of injury; admitted to TBIMS comprehensive inpatient rehabilitation; and a complicated mild, moderate, or severe injury.7 Rehabilitation insurance payor status was classified as charity, private, public (Medicare/Medicaid), worker’s compensation/ auto, or self-pay (Figure 1). Functional status was assessed by the 1-year post-injury Functional Independence Measure (FIM)8 motor and cognitive domain scores. The contribution of insurance group to 1-year FIM scores was investigated by linear regression, covarying for age and FIM scores at rehabilitation discharge.
FIM motor and cognitive scores at 1 year were analyzed for 5,925 and 7,403 patients, respectively. Self-pay or private pay patients had the highest mean motor scores, while publicly insured patients had the lowest. Privately insured patients had the highest mean cognitive scores, while publicly insured patients had the lowest. After controlling
for age and FIM scores at rehabilitation discharge, insurance payor contributed significantly to 1-year FIM motor and cognitive scores. Publicly insured and worker’s compensation and auto insurance patients had lower scores compared to self-pay.
CONCLUSION
The results indicate that publicly insured patients achieved less independent functioning at 1 year, even after controlling for age and functioning at discharge. While the exact mechanism for this disparity cannot be determined from the current data, less access to outpatient therapy and other services to improve functioning should be investigated in future research. The results suggest that publicly insured patients and those with worker’s compensation/auto insurance should be targeted for monitoring to reduce risk factors for poor functional outcomes after inpatient rehabilitation. Future studies should also include other factors that may underlie the relationship of insurance to functional outcomes, including length of stay, geographic characteristics (e.g., urban versus rural areas), and health literacy.
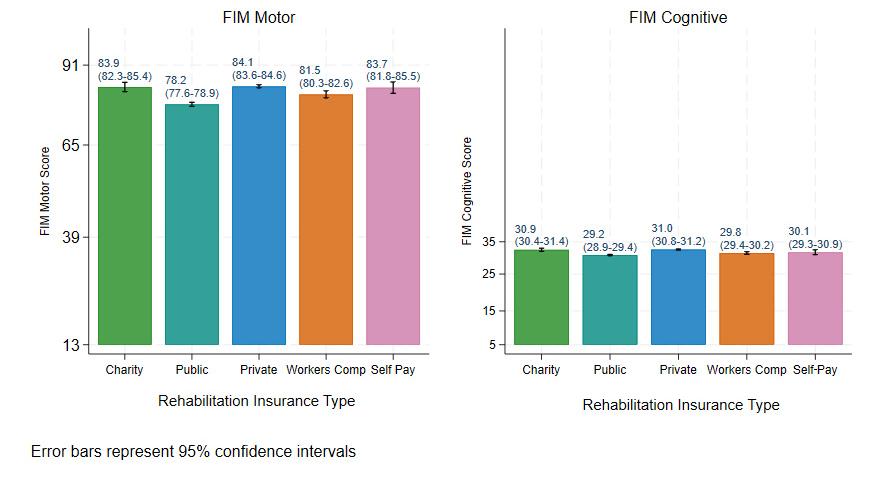
Figure 1: FIM scores at 1 year by rehabilitation insurance type.
References
1. Malhotra AK et al. Influence of health insurance on withdrawal of life sustaining treatment for patients with isolated traumatic brain injury: a retrospective multi-center observational cohort study. Crit Care. 2024;28(1):251.
2. Galicia KE et al. Association between health insurance and outcomes after traumatic brain injury: a national ACSTQP-PUF database study. J Surg Res. 2023;290:16-27.
3. Kane WG et al. Racial/ethnic and insurance status disparities in discharge to posthospitalization care for patients
Risk
with traumatic brain injury. J Head Trauma Rehabil. 2014;29(6):E10-7.
4. Moffet EW et al. Race, insurance status, and traumatic brain injury outcomes before and after enactment of the Affordable Care Act. Surgery. 2018;163(2):251-8.
5. Saunders LL et al. Pre-existing health conditions and repeat traumatic brain injury. Arch Phys Med Rehabil. 2009;90(11):1853-9.
6. Shah RJ et al. Relationship of rehabilitation insurance payor to functional status at one year post
traumatic brain injury. Poster presented at the annual meeting of the American Academy of Neurology, San Diego, CA, USA, April 5–9, 2025.
7. Dijkers MP et al. Thirty years of National Institute on Disability, Independent Living, and Rehabilitation Research Traumatic Brain Injury Model Systems Centers research—an update. J Head Trauma Rehabil. 2018;33(6):363-74.
8. Granger CV et al. Advances in functional assessment for medical rehabilitation. Top Geriatr Rehabil. 1986;1(3):59-74.
Factors Associated with Neurocognitive Disorder and Depression Among Adults from an Urban-Marginalized Area of Lima, Peru
Authors: *Monica M. Diaz,1 Eder Herrera-Perez,2,3 Nilton Custodio,4,5 Rosa Montesinos,4 Chhitij Tiwari,1 Serggio C. Lanata6
1. University of North Carolina at Chapel Hill, USA
2. University of California, San Francisco, USA
3. Vicerrectorado de Investigación, Universidad
San Ignacio de Loyola, Lima, Peru
4. Centro de Excelencia en Biotecnología e Investigación Traslacional (CEBIT LATAM), Lima, Peru
5. Unidad de Investigación, Instituto Peruano de Neurociencias, Lima, Peru
6. Escuela Profesional de Medicina Humana, Universidad Privada San Juan Bautista, Lima, Peru
*Correspondence to monica.diaz@neurology.unc.edu
Disclosure: The authors have declared no conflicts of interest.
Keywords: Depression, neurocognitive disorders, socioeconomic, urban-marginalized.
Citation: Neurol AMJ. 2025;2[1]:44-45. https://doi.org/10.33590/neurolamj/BHYM3864
BACKGROUND AND AIMS
This study investigates the prevalence and risk factors of neurocognitive disorders (NCD) and depression among community-dwelling younger and older adults in Puente Piedra, an urban-marginalized district of Lima, Peru.1
NCDs and depression pose substantial public health challenges, particularly in urbanmarginalized areas of low-to-middle-income countries, where socioeconomic disparities amplify mental health concerns. The risk factors for NCDs among both younger and older adults in urban-marginalized areas of Latin America have been inadequately studied.
METHODS
A population-based study was conducted from July–September 2022, incorporating door-to-door visits and structured questionnaires to collect demographic, health, and socioeconomic data from 900 community-dwelling adults aged 30 years and older. Neurocognitive assessments included the Addenbrooke's Cognitive Examination for younger adults,
Rowland Universal Dementia Assessment Scale for older adults, and Patient Health Questionnaire for depression screening.
RESULTS
The authors found that 75.6% of participants were cognitively normal, 20.1% had possible NCDs without functional impairment, and 4.2% had possible NCDs with functional impairment. Additionally, 40% had depression. After controlling for covariates, lower educational levels and lower socioeconomic levels were risk factors for NCDs among older adults. Among younger adults, lower educational levels, a native language other than Spanish, hypertension, and depression were risk factors for NCDs. Risk factors for depression included female sex, lower educational level, a native language
other than Spanish, overcrowding in the home, and a history of chronic diseases.
CONCLUSION
The results highlight that potentially modifiable risk factors, such as hypertension, educational level, and depression, may play a role in NCDs among residents of an urban-marginalized area of Peru. These findings underscore the critical need for targeted interventions and policies to address mental health and healthcare disparities in urban-marginalized areas of low-to-middle-income countries.
Reference
1. Diaz M et al. Risk factors associated with neurocognitive disorder and depression among adults from an urban-marginalized area of Lima, Peru. Abstract S24.007. AAN Annual Meeting, April 5-9, 2025
Grapheme-Color Synesthesia in Patients with Epilepsy: A Pilot Study on Prevalence and Seizure Characteristics
Authors: Irene Chu,1 Atef Kokash,1 Snow P. Li,1
*Martina Vendrame1
1. Lehigh Valley Fleming Neuroscience Institute, Lehigh Valley Health Network, Allentown, Pennsylvania, USA
*Correspondence to martina.vendrame@lvhn.org
Disclosure: The authors have declared no conflicts of interest.
Keywords: Epilepsy, focal onset, generalized onset, grapheme-color, motor seizures, non-motor seizures, synesthesia.
Citation: Neurol AMJ. 2025;2[1]:46-49. https://doi/org/10.33590/neurolamj/IFLE7494
BACKGROUND
Synesthesia, a condition where stimulation of one sensory pathway involuntarily triggers another (e.g., seeing colors when reading letters), has been a longstanding topic of neurological curiosity. Graphemecolor synesthesia (GCS), where individuals associate letters and numbers with specific colors, is one of the most common forms. This phenomenon, while benign, is believed to provide insight into cortical connectivity and cross-modal sensory processing. Prior studies have suggested associations between synesthesia and specific neurological profiles, including autism spectrum disorder and migraine.1,2 However, little is known about the prevalence and characteristics of synesthesia among patients with epilepsy.
METHODS
This pilot study3 aimed to investigate the occurrence of GCS in individuals with epilepsy and to explore the relationship between synesthetic experience and seizure type. The methodology was straightforward: 40 participants with epilepsy were surveyed regarding subjective GCS experiences.
Those affirming these experiences underwent further assessment using a standardized synesthesia battery hosted on The Synesthesia Battery website, which evaluates both consistency (stability of color associations over time) and congruency (accuracy and speed of matching graphemes with colors).4
RESULTS AND DISCUSSION
Out of 40 participants, 21 reported subjective GCS experiences, and three (7.5%) met objective criteria for synesthesia based on the battery (Table 1). This prevalence is notably higher than that reported in the general population, estimated between 0.05–4.4%.5,6 A key finding was that individuals with focal seizures exhibited significantly lower consistency scores (median 1.2) and higher congruency scores (76.4), indicating more accurate and quicker color-grapheme responses but less consistency in repeated associations. In contrast, those with generalized-onset seizures had higher consistency scores (2.9) and lower congruency scores (51.4), suggesting more stable associations but slower processing. These differences were statistically significant (p=0.006 for consistency and p=0.001 for congruency).
Moreover, participants with non-motor seizures had similar trends: lower consistency (1.1) and higher congruency (79.2) compared to patients with motor seizures (2.8 and 52.8, respectively), again with statistical significance (p=0.011 and p=0.036). These patterns suggest that certain seizure types may influence cross-modal sensory integration and perceptual processing.
The authors hypothesize that the heightened prevalence of GCS in this sample could reflect underlying neural hyperconnectivity or
Table 1: Demographic and clinical characteristics, synesthesia battery results of all tested participants.
MRI findings: side of lesion type of lesion
Table 1: Continued.
disinhibition in sensory regions, particularly within the temporo-parietal junction, known to be implicated in synesthesia.7,8 Focal seizures, especially those arising from temporal lobe structures, may amplify or uncover latent synesthetic networks by disrupting inhibitory gating mechanisms.8 Similarly, non-motor seizures might affect perception and sensory integration more subtly than motor seizures, thus predisposing to synesthetic traits.
This study adds to a growing body of literature that views synesthesia not merely as a curiosity, but as a window into atypical brain organization. Though limited by sample size and reliance on self-report for initial screening, the findings warrant largerscale investigations. Future studies should incorporate neuroimaging to explore functional connectivity patterns in synesthetes with epilepsy and investigate whether antiepileptic medications modulate synesthetic experiences.
CONCLUSION
In conclusion, GCS may occur more frequently in individuals with epilepsy, particularly those with focal or non-motor seizure types.
The observed differences in synesthetic test performance point to potential neural correlates of sensory cross-activation in epilepsy, meriting further investigation.
References
1. Cytowic RE. Synesthesia: a union of the senses. 2002. Available at: https://direct.mit.edu/books/ monograph/1882/SynesthesiaA-Union-of-theSenses. Last accessed: April 15, 2025.
2. Baron-Cohen S et al. Synesthesia: prevalence and familiality. Perception. 1996;25(9):1073-9.
3. Chu I et al. Grapheme-color Synesthesia in Patients with Epilepsy: a Pilot Study. Poster 011. AAN Annual Meeting, April 5-9, 2025.
4. Eagleman DM et al. A standardized test battery for the study of synesthesia. J Neurosci Methods. 2007;159(1):139-45.
5. Simner J et al. Synaesthesia: the prevalence of atypical cross-modal experiences. Perception. 2006;35(8):1024-33.
6. Chun CA, Hupé JM. Are synesthetes exceptional beyond their synesthetic associations? A systematic comparison of creativity, personality, cognition, and mental imagery in synesthetes and controls. Br J Psychol. 2016;107(3):397-418.
7. Hubbard EM, Ramachandran VS. Neurocognitive mechanisms of synesthesia. Neuron. 2005;48(3):509-20.
8. Neufeld J et al. Are synesthetes exceptional? Cognition. 2012;122(1):25-30.
Atypical Presentation of Neurosyphilis: A Case Report
Authors: *Abhishek Vyas,1 Samir Cayenne,1 Suraj Vodnala,1 Camila Narvaez Caicedo,2 Hashem Shaltoni2
1. The University of Texas Medical Branch, Galveston School of Medicine, USA
2. The University of Texas Medical Branch, Galveston Department of Neurology, USA *Correspondence to abvyas@utmb.edu
Disclosure: The authors have declared no conflicts of interest.
Keywords: Atypical stroke, incarcerated populations, neurosyphilis.
Citation: Neurol AMJ. 2025;2[1]50-51. https://doi.org/10.33590/neurolamj/KAAO3210
BACKGROUND
Neurosyphilis can manifest in various ways, often complicating the clinical picture.1 This condition is frequently overlooked, particularly when presenting alongside stroke symptoms.2 While cerebrospinal fluid (CSF) venereal disease research laboratory (VDRL) is the gold standard for diagnosis, it is known to have low sensitivity and can yield false negatives in patients with compatible symptoms.3
CASE PRESENTATION
A 45-year-old incarcerated male with a medical history of hypertension, Type 2 diabetes, and hyperlipidemia presented with acute onset altered mental status and expressive aphasia.4 Imaging studies, shown in Figure 1, revealed an acute/subacute left middle cerebral artery infarct with proximal inferior trunk occlusion and a chronic right cerebellar infarct, prompting an extensive workup for stroke in younger patients.
Further evaluation through a cerebral angiogram revealed subtle irregularities of the intracranial arteries. As a result, a lumbar puncture was performed, which indicated slightly elevated protein and leukocyte counts. Serological testing confirmed latent syphilis. Despite a negative CSF VDRL test, the diagnosis of neurosyphilis was established based on the clinical presentation and positive treponemal blood test. 5 The patient was treated successfully with a 14-day course of intravenous penicillin.
CONCLUSION
This case emphasizes the necessity of considering neurosyphilis in patients presenting with atypical stroke symptoms, particularly young patients with stroke and those with risk factors, such as incarcerated populations, unprotected sex, and multiple sexual partners.6 As neurological complications are often disabling, early recognition along with a multidisciplinary approach is crucial for preventing long-term neurological complications and preserving quality of life, while reinforcing the evolving understanding of neurosyphilis in clinical practice.
References
1. Feitoza LM et al. Neurosyphilis vasculitis manifesting as ischemic stroke. Rev Soc Bras Med Trop. 2020;53:e20190546.
2. Gonzalez H et al. Neurosyphilis. Semin Neurol. 2019;39(4):448-55.
3. Zhou J et al. An updated review of recent advances in neurosyphilis. Front Med (Lausanne). 2022;9:800383.
4. Vyas A et al. Atypical Presentation of Neurosyphilis: A Case Report. Poster 009. AAN Annual Meeting, April 5-9, 2025.
5. Jum'ah A et al. Neurosyphilis in disguise. Neuroradiology. 2022;64(3):433-41.
6. Hobbs E et al. Neurosyphilis in patients with HIV. Pract Neurol. 2018;18(3):211-8.
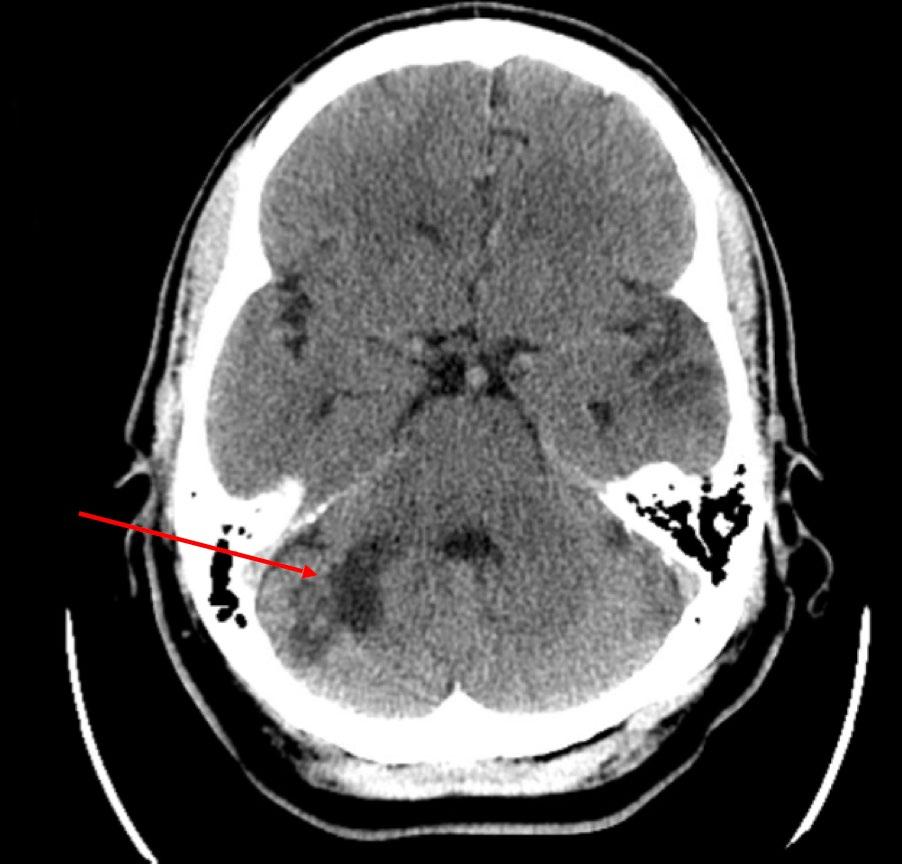
Figure 1: CT demonstrating a region of encephalomalacia within the right cerebellar hemisphere, suggesting chronic infarction.
Congress Interviews
These interviews feature leading voices in neurology who share their experiences and roles in the American Academy of Neurology (AAN), as well as highlights from their celebrated careers in neurology care. Joseph Sirven shares insights on epilepsy care inequities, workforce challenges, and age-specific treatment gaps; and Larry B. Goldstein delivers a global perspective on stroke innovation, health policy, and the future of recovery and prevention.


Joseph Sirven
Professor of Neurology and Chairman Emeritus, Department of Neurology, Mayo Clinic, Arizona; Professor of Practice, College of Health Solutions, Arizona State University; and Chair, Education Committee, American Academy of Neurology (AAN), USA.
Citation:
Q1Access to epilepsy surgery and advanced treatments continues to be uneven, particularly for patients in under-resourced or safety-net settings
Neurol AMJ. 2025;2[1]:52-54. https://doi.org/10.33590/neurolamj/XRFW4394
Much of your work highlights the influence of psychosocial factors on epilepsy care, particularly within Hispanic communities. Can you elaborate on how these factors contribute to delays in diagnosis and treatment? What communitydriven interventions have proven most effective in bridging these care gaps?
As a Cuban American, this issue is personal for me. Psychosocial factors such as stigma, language barriers, and cultural dynamics play a significant role in delaying epilepsy diagnosis and treatment in Hispanic communities. Stigma surrounding epilepsy often leads to secrecy about seizures, preventing individuals from seeking medical care promptly. Language discordance further complicates access to care, as many Hispanic patients primarily speak Spanish, which can hinder effective communication with healthcare providers and limit understanding of treatment options. Additionally,
the cultural emphasis on familycentered decision-making can sometimes conflict with traditional medical protocols, leading to delays in pursuing specialized care. These barriers contribute to significant disparities, with Hispanic individuals being less likely to access epilepsy specialists and more likely to rely on emergency departments for seizure management.
Community-driven interventions have proven effective in addressing these gaps. For example, bilingual epilepsy clinics like the Spanish Clinic for Epilepsy at Lurie Children’s Hospital of Chicago, Illinois, USA, have successfully reduced care delays by employing culturally sensitive practices and improving communication between providers and patients. Programs like Project UPLIFT, which offer telephonebased depression self-management tailored to Hispanic populations, have also demonstrated success in reducing comorbid conditions that exacerbate epilepsy outcomes. Additionally, partnerships with
community organizations to distribute translated educational resources and expand telemedicine access have helped overcome logistical challenges such as transportation barriers. By combining linguistic accessibility with cultural competency, these interventions provide a roadmap for addressing systemic disparities and ensuring timely, equitable care for Hispanic patients with epilepsy.
Q2Your 2021 American Academy of Neurology (AAN) study highlighted that disparities in epilepsy treatment are tied to race and homelessness. How has this work influenced AAN’s health policy initiatives to address systemic inequities in neurology, and what gaps remain?
Thank you for the thoughtful question. Our 2021 AAN study on disparities in epilepsy care, specifically the role of race and housing instability, joined a growing body of research that underscores how systemic inequities continue to shape access to neurologic treatment. While the findings were
sobering, they were not entirely surprising to those of us working with vulnerable populations.
This study, alongside others, helped reinforce the need for policy solutions that address social determinants of health in neurology. The AAN has increasingly recognized these challenges, and its health policy initiatives now reflect a broader commitment to promoting neurologic equity. These efforts include support for Medicaid expansion, greater investment in tele-neurology to reach underserved areas, and the inclusion of health equity principles in quality improvement and reimbursement models.
Still, significant work remains. Access to epilepsy surgery and advanced treatments continues to be uneven, particularly for patients in under-resourced or safetynet settings. Minoritized groups are underrepresented in clinical research, and implicit bias and structural barriers still influence referral patterns and care delivery.
Going forward, we must prioritize policies that close these gaps by expanding access, diversifying our workforce, and embedding equity into the way we train, practice, and advocate. Studies like ours serve as reminders: the disparities are real, the data is there, and the time to act is now.
Q3
As Chair of the AAN Education Committee, how do initiatives like the Neurology Education Room or Pipeline Subcommittee address workforce gaps in epilepsy care, especially in rural areas or low- and middleincome countries?
As Chair of the AAN Education Committee, I’ve seen how intentional educational initiatives can help address workforce gaps in neurology, particularly in rural areas and low- and middle-income countries, by building both teaching capacity and a more diverse, prepared pipeline of neurologists.
The Neurology Education Room was created as a dedicated, inperson space for those passionate
about medical education to come together, learn how to teach more effectively, and exchange ideas in a personalized, interactive setting. It serves as a haven for anyone seeking to deepen their skills as an educator and contribute meaningfully to the learning environment within our field.
Meanwhile, the Pipeline Subcommittee focuses on longerterm strategies by identifying and mentoring future neurologists, often reaching learners in communities historically underrepresented in medicine or located far from academic medical centers. The goal is to cultivate interest early and support individuals throughout their journey into neurology.
While these initiatives don’t solve every challenge, they are important building blocks. Expanding educational excellence and nurturing future talent are essential to ensuring that all communities, regardless of geography or income level, have access to skilled neurologic care. Education remains one of our most powerful tools in narrowing workforce disparities and strengthening the future of the field.
Q4At the recent AAN Annual Meeting, you led a session on aviation and driving safety in neurological disorders, featuring experts from the Federal Aviation Authority (FAA) and the Department of Transportation (DOT). What were the key insights from this session?
The session on aviation and driving safety in neurological disorders at the recent AAN Annual Meeting brought together experts from the FAA, the DOT, and neurology, to examine how neurologic conditions intersect with public safety, personal mobility, and regulatory frameworks.
One of the key insights was the vital role neurologists play in navigating the balance between patient autonomy and safety, both for individuals and the public. We discussed how conditions like epilepsy, stroke, cognitive impairment, and sleep disorders can impact a person’s ability to safely operate vehicles or aircraft, and how guidance varies significantly between aviation and road travel.
Our FAA colleagues emphasized the importance of clear, thorough documentation in medical evaluations for pilots, along with the rigorous protocols they follow when reviewing neurologic cases. The DOT representatives highlighted the patchwork nature of state driving laws and the need for more standardized communication between neurologists and licensing authorities.
Another important takeaway: clinicians often feel caught between advocating for their patients and adhering to complex legal or ethical responsibilities. We explored how to counsel patients more effectively about these issues and the need for education and support for neurologists making these difficult determinations.
Ultimately, the session underscored that mobility is not just a medical issue, it’s a deeply human one. Our job as neurologists is to support both safety and dignity, working within evolving regulatory frameworks while ensuring our patients remain informed, empowered, and treated with empathy.


Larry B. Goldstein
Judy and Byron Young Neuroscience Institute Endowed Professor, Chair of the Department of Neurology, Associate Dean for Clinical Research at the College of Medicine, Co-Director, Kentucky Neuroscience Institute, Co-Director of UK Neuroscience Research Priority Area, Medical Director of UK-Norton Stroke Care Network KY Clinic, University of Kentucky, Lexington, USA; Board Director, American Academy of Neurology (AAN), USA.
Citation: Neurol AMJ. 2025;2[1]:55-56. https://doi.org/10.33590/neurolamj/ESRA5449
Disclaimer:
The single most important change was the advent of thrombolytic therapy based in large part on the results of the National Institute of Neurological Disorders and Stroke tissue plasminogen activator (NINDS-tPA) trial
Goldstein’s responses represent his own opinions and are not necessarily the positions of the AAN.
Q1 As an expert in cerebrovascular disease and stroke, your career spans laboratory research, clinical trials, and policy work. Over the past 30 years, which area has undergone the most transformative evolution, and how has this shaped the current stroke prevention strategies?
The single most important change was the advent of thrombolytic therapy based in large part on the results of the National Institute of Neurological Disorders and Stroke tissue plasminogen activator (NINDS-tPA) trial. This provided evidence that timely treatment of selected patients with an acute ischemic stroke (caused by a blood clot blocking a brain artery) can meaningfully improve outcomes. This led to the development of stroke systems of care, including public education that stroke is treatable with timely care, integration of emergency medical services, and the designation of different levels of stroke centers.
Q2
Despite advances, many neuroprotective agents fail in clinical trials. What systemic barriers hinder the translation of preclinical discoveries into viable therapies?
There are a wide variety of reasons for the lack of translation of animal model data related to neuroprotective agents into clinical care. For example, laboratory studies are most often conducted
in rodents that have brains that are structurally different from those of humans. Animal models are typically homogeneous and do not reflect the underlying variability in age, comorbid conditions, medication exposures, and other characteristics inherent in humans. Drug dosages, timing, and metabolic factors differ as well. Additionally, behavioral outcome measures used in animal models may not directly correlate with the functional effects of stroke in humans.
Q3 In your opinion, what novel targets hold the most promise for improving poststroke recovery?
One set of observations that has emerged is that structured practice can improve functional outcomes after stroke, even when done months after the acute event. Pharmacological approaches to improve functional outcomes, stem cell therapies, and physiologic modulation with transcranial magnetic stimulation and related technologies are all being explored.
Q4
Reflecting on this year’s American Academy of Neurology (AAN) Annual Meeting, what do you consider to be the most significant piece of research or the most impactful discussion?
There were hundreds of presentations at the meeting. An analysis of data from two Phase IV studies (MINORE and SOPRANINO)
found minimal placental and breast milk transfer, and no B cell reduction in infants of mothers being treated with ocrelizumab for multiple sclerosis. Treatment with tolebrutinib slowed progression to disability in trial participants with non-relapsing secondary progressive multiple sclerosis (HERCULES). A retrospective observational study in military veterans suggests an association between obstructive sleep apnea and Parkinson’s disease, which might be moderated with continuous positive airway pressure. A Phase III trial found that fremanezumab may have benefit as a preventive therapy in children and adolescents with episodic migraine (SPACE).
Q5 Can you tell us how AAN health policy initiatives address racial or rural disparities in US stroke care access?
The AAN mission includes optimizing brain health for all. Support of measures that improve preventive approaches, including lifestyle interventions, access to care, and fostering emergent treatment, when necessary, are all components of optimizing brain health.
Q6 What impact have collaborations between the AAN and international bodies like the UEMS-SN and African Task Force achieved in addressing global disparities in post-stroke rehabilitation?
Improving global health is critical, as one in three persons worldwide will have a neurological condition that can lead to early mortality, disability, and socioeconomic loss. What we have learned in providing neurological care can be used in other parts of the world, and lessons learned in underserved regions may also be applicable to areas of our country with limited access to care.
Q7
As an AAN Media Expert, what strategies does the AAN employ to counteract misinformation about stroke recovery timelines or novel interventions in public health campaigns?
Consistently conveying evidence-based information, educating both the public and healthcare providers, and being a relied-on source of scientifically reliable recommendations are the cornerstones of combating misinformation.
Q8 What new projects or initiatives are you most excited about in the coming years, and how do you envision them contributing to the broader landscape of stroke prevention, treatment, and recovery?
The organization of the country’s health care and research infrastructural support is changing rapidly ,and it is unclear what resources will be available moving forward. Because approximately 90% of strokes are potentially preventable, given our emphasis on brain health, I would hope that we would be able to develop better, more effective strategies to empower people to take whatever steps they can to live a healthy life.

Interviews
This expert interview section begins with Courtney Wusthoff, who shares her expertise on neonatal seizure monitoring, electroencephalogram innovations, and long-term neurodevelopment in pediatric neurology. Ryan Hakimi then explains the latest advances in neurocritical care, transcranial Doppler ultrasound, and the evolving role of therapeutic hypothermia in acute neurologic management.

Courtney Wusthoff
Professor, Department
Neurology,
Section
of
and Child Neurology
Chief, University of California, Davis (UC Davis) School of Medicine, USA
Citation: Neurol AMJ. 2025;2[1]:57-60. https://doi.org/10.33590/neurolamj/OCAP7324
Q1
As a specialist in pediatric epilepsy and neonatal neurology, a large part of your work involves electroencephalogram (EEG) monitoring of infants and children in the intensive care unit (ICU). This often involves guiding families through difficult situations. How do you approach these interactions, and how does this influence your clinical decision-making?
Technological advances in cEEG allow us to safely refine our care for newborns with suspected seizures
In pediatric neurology, we often face the challenge of needing to make important decisions, knowing that there may be unavoidable uncertainty in the evidence available to guide those decisions. When first meeting a family, I ask what they already know, and what questions or goals they have for the situation at hand. This is helpful for framing a discussion and decisions. For example, if the team assumes the goal is perfect seizure control, but the family really prioritizes decreased sedation, we need to understand that before making choices. Letting the family show me the starting point sets us up to work together more effectively.
In turn, I strive to be direct and transparent with families about what we do and don’t know, and why we might suggest a particular course of action. Admitting there is some uncertainty is important for building trust with families; we need to admit there are things that medicine doesn’t know. I believe it also lays the foundation for when or why we might need to reconsider a decision if things aren’t going as we’d hoped. We are all doing our best with the information we have, but if we see we are not heading down the right path, we may need to take a step back and reassess.
Q2 Can you elaborate on how advancements in EEG technology, such as continuous EEG (cEEG) or machine learning tools, have improved the detection and management of seizures in neonates?
Not too long ago, EEG was recorded on bulky machines that provided recordings on paper printouts at the bedside. Now, we have digital equipment with a
smaller footprint at the bedside, synchronized video recording, and the ability to remotely access and review EEGs in real time. This has prompted a paradigm shift in how we approach neonatal seizures. It turns out that many of the unusual movements or sudden vital sign changes that would have been diagnosed as seizures in the past, we find are not seizures when we use EEG for confirmation. The International League Against Epilepsy (ILAE) has changed their entire system for neonatal seizure classification to reflect this. Whereas 5 years ago it was entirely based on semiology, it is now based on whether there is EEG confirmation that a suspicious clinical event correlates with ictal activity in the brain. In fact, the only way to diagnose a “definite seizure” is when an EEG shows that a seizure occurs. The good news is that using EEG has allowed us to be far more accurate in diagnosing seizures. Multiple studies have shown that the implementation of cEEG in neonatal ICUs (NICU) leads to an
overall decrease in the number of babies who receive antiseizure medications (ASM), and a decrease in the total doses used for those babies who do receive ASMs. Technological advances in cEEG allow us to safely refine our care for newborns with suspected seizures.
The clear next step will be to develop seizure detection programs that can alert the bedside team to a likely seizure in real time, without a highly trained neurophysiologist constantly monitoring the recording. I have no doubt that these will be ready for clinical use in the next few years. Initially, these will screen the EEG and alert a neurophysiologist when suspected seizures occur, so that they may confirm the diagnosis. At the same time, we’ve seen with AI in other areas that we can’t just jump to assuming the output is always correct. It will be important to train systems up with quality information.
Q3You recently spearheaded the American Clinical Neurophysiology Society (ACNS) project, “The American Clinical Neurophysiology Society Guideline on Indications for Continuous EEG Monitoring in Neonates.” As the first update on this topic in 12 years, why was this project so critical, and what are the key changes introduced?
It was such a privilege to work with the exceptional group of co-authors who put this guideline together. ACNS is the professional society for clinical neurophysiologists. A particular strength of the group is that they have a clear focus on neurophysiology and there are amazing experts in the membership. ACNS had developed guidance on topics like technical standards for how to record an EEG or a standardized nomenclature for interpreting EEG in critically ill adults and children. It has been a way to promote best practices and to bring together different ways of doing things to make sure the most important aspects are consistent.

In the first version of the ACNS guideline on neonatal EEG, a group of pediatric neurophysiologists came together and issued what was essentially an expert consensus on when cEEG monitoring should be used in neonates. Renée Shellhaas, WashU Medicine, St. Louis, Missouri, USA, was the lead author, and Robert R. Clancy, The University of Pennsylvania Health System, Philadelphia, USA, was the senior author on the final publication. I was extremely fortunate to be included in the writing group. We shared what we considered key papers to inform our opinions, and the group discussed back and forth to come to the final guideline. When it was published in 2011, cEEG was just beginning to enter use in the NICU outside of tertiary pediatric hospitals. It was the first guidance available to suggest how this new tool might be most useful. That was a huge first step.
In the more than decade since, so much has evolved. Many more centers have access to cEEG for neonates. Rather than facing the question of: “Why should we use this technology?”, at some centers, people are even asking: “Why wouldn’t we use this technology for every baby in the NICU?” Fortunately, we now have far more evidence to show what the yield is of cEEG for various indications. Over the past 10–15 years, there also has been a muchneeded raising of the bar for what methodology is accepted when creating a clinical guideline. For all these reasons, we knew it was time to update the original.
The result is an evidencebased clinical guideline on indications for neonatal cEEG. We
performed a systematic review and summarized the available evidence regarding the use of cEEG for various purposes. We couldn’t apply the typical Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology for diagnostic tests, because cEEG is, in fact, the gold standard for diagnosing neonatal seizures. At the same time, we were able to adapt the GRADE approach for our guideline to include many of the key features to ensure transparency and reproducibility. Many of our recommendations have not changed since the first version. As an example, we still recommend that cEEG be used for the diagnosis of seizures in neonates. There were some specifics that were new, based on evidence we did not have 15 years ago. For example, we recommend cEEG to screen for seizures in neonates on extracorporeal membrane oxygenation (ECMO), for those with hyperammonemia, and immediately post-operatively following repair of congenital heart disease. This was based on moderate quality evidence that cEEG has particularly high yield for seizures in patients with those conditions.
Probably the biggest surprise to clinicians was that all of our recommendations were conditional, meaning that whilst cEEG would be recommended for these indications, we recognize that there are feasibility considerations that might limit using cEEG in some situations. I think some expected us to issue strong recommendations that cEEG must be used without exception, but we absolutely needed to take into account that it may not be possible in every circumstance. The hope is that having the
indications recommended, even if as a conditional recommendation, helps move the field toward having cEEG more consistently available for these patients.
Q4
What are the current barriers to implementing cEEG monitoring for neonates, and how do you envision these guidelines influencing monitoring practices in NICUs?
Without a doubt, cEEG is a highresource tool. This includes not just the EEG recording device, but also the skilled neurodiagnostic technologists who initiate and troubleshoot recordings at the bedside, and clinical neurophysiologists who are available to interpret the recordings. Having that equipment and those experts available 24/7 requires a big investment, and that is a very real barrier. Our hope is that these guidelines show which patients might benefit the most from cEEG; it is certainly not a tool that can or should be used on every newborn in the NICU. Additionally, if a center makes the investment to have cEEG monitoring available, these guidelines will help establish how best to apply that investment to maximize clinical benefit.
Q5 What do you consider the most significant challenges in managing neonatal seizures today? Are there gaps in research or clinical practice that require urgent attention?
We desperately need better medications to treat neonatal seizures. It is mind-boggling that the first-line treatment for neonatal seizures is still phenobarbital. Phenobarbital can have nasty side effects and doesn’t always
stop seizures; we need something more effective that is also safer to use. There have not been enough drugs developed to treat neonatal seizures. Most ASMs are only available in oral formulations, and most of those that can be given intravenously haven’t been properly studied in newborns. There is an urgent need for attention, funding, and collaboration to perform the studies needed to learn which medications might be better for neonates with seizures than the handful we have now.
On a brighter note, a significant gap that currently exists in clinical practice is one that we can change now. It had been common practice that once a baby was started on phenobarbital for seizures, they were sent home on that medication, and would continue it for months or even years. The Neonatal Seizure Registry (NSR) group, led by Hannah Glass and Renée Shellhaas, conducted a comparative effectiveness study that demonstrated for neonates with acute symptomatic seizures (seizures that are known to be due to an acute injury like hypoxic ischemic encephalopathy or stroke), it is safe to stop ASMs before babies are discharged home. While approximately 13% will go on to have epilepsy, the large majority don’t need medication beyond the immediate neonatal period. Furthermore, continuing medication doesn’t prevent the development of epilepsy. This work was so important, and I hope that message continues to get out so we can change practice to stop sending babies home on medicine that doesn’t help them.
Q6
While seizures are a focus, EEG also assesses brain injury severity. How do EEG background patterns or sleepwake cycling inform prognosis and guide therapies like hypothermia?
This is where EEG for neonates is really starting to take off. We so often think of EEG as just a seizure detection tool for newborns, but there is such a wealth of information it can provide about brain function. EEG can show whether a newborn’s brain is developing as expected, or if it is dysmature. Certain features, like normal sleep-wake cycling after brain injury are very reassuring for prognosis, which is incredibly valuable for families. Specific patterns can indicate a brain is at risk, or that function is worsening, which may help us target prompt intervention for a newborn. As technology improves, we will increasingly see EEG analyzed not by human experts recognizing patterns, but rather by quantitative analysis to uncover features that go beyond simple visual patterns. There is very exciting early work showing that the features revealed by these approaches outperform conventional interpretation in identifying newborns with injury and in informing prognosis.
Q7 Looking ahead, what areas of pediatric neurology research do you believe will see the most progress over the next decade? Are there specific innovations or collaborations you're excited about pursuing?
The best part of child neurology is the constant discovery
The best part of child neurology is the constant discovery. I love taking care of my patients, and I need that other side to my work to know that I am helping bring about cures for tomorrow’s patients as well. There is so much potential. I’m working with the NSR on methods to identify which babies are at highest risk to develop later epilepsy, in the hope that we might be able to give treatments to prevent epilepsy, not just treat it once it occurs. At UC Davis, we have a group of outstanding scientists, like Kyle Fink and Caren Armstrong, working to bring precision therapies for genetic conditions into clinical use for children. I’m awestruck by the potential this could unlock. As these discoveries become available, we will need to ensure that as many children as possible can benefit from them. We need talented scientists to advance discovery, and we need educators, to train more child neurologists who will practice in communities where access is a barrier. We also need advocates to ensure we never give up on our search for cures, and that we bring them to every child who needs them, not just a select few. Child neurology is exciting because we can all use our individual skills toward that common goal of protecting infants and children from nervous system injury, and treating disease when it occurs.

Ryan Hakimi
President, American Society of Neuroimaging (ASN); Executive Committee Member, Neurocritical Care Society Board of Directors, Neuroimaging Section Chair, American Academy of Neurology (AAN); Professor, Department of Medicine (Neurology Division), School of Medicine Greenville, University of South Carolina; Founding Medical Director, Transcranial Doppler Ultrasound Laboratory, Prisma HealthGreenville Memorial Hospital, South Carolina, USA
Citation: Neurol AMJ. 2025;2[1]:61-63. https://doi.org/10.33590/neurolamj/SEIU6239
Q1
You began your academic journey as a United States Department of Energy (USDOE) Applied Health Physics Fellow. Could you share how this unique foundation led to your transition into neurology, and specifically into the specialized fields of neurocritical care and neurosonology?
Q2
You played a key role in developing the neurology curriculum for medical students at Oklahoma State University College of Osteopathic Medicine (OSUCOM) in Tulsa, Oklahoma. What core areas of neurology did you prioritize, and how do these align with the evolving needs of future physicians?
The number one cause of death for cardiac arrest survivors who make it to hospital admission is neurological death
Initially, my career goal was to become a radiologist. I had the unique opportunity to be one of 24 individuals in the US to be accepted to the USDOE Applied Health Physics Fellowship, a 2-year fully funded fellowship that would prepare me for the technical aspects of radiological care and strengthen my scientific basis for the field. As a medical student, I rotated on two radiology rotations and quickly found that I desired to be part of a clinical care team, and hence selected neurology for my residency, as it integrated neuroimaging into daily care. Neurocritical care was a new field in the mid-2000’s and I enjoyed the challenge of integrating neurology with acute care medicine, as well as being the first Doctor of Osteopathic Medicine (DO) to enter the field. During my time as a fellow, I fell in love with neurosonology and elected to make it my life’s passion, ultimately ascending to the President of the American Society of Neuroimaging (ASN).
Owing to the fact that ≤1% of medical students select neurology for their residency, it is important to prioritize what every physician (regardless of specialty) should know about neurology. This includes how to do a neurological examination, as well as the basics of diagnosis and treatment for common neurological conditions including stroke, epilepsy, multiple sclerosis, and dementia; all of which are becoming more common as the population ages.
Q3 You authored postcardiac arrest hypothermia protocols for Durham County Emergency Medical Services (EMS) in North Carolina, and later co-developed Oklahoma’s statewide protocol for post-cardiac arrest treatment. How have these protocols impacted patient care at both local and state levels?
The number one cause of death for cardiac arrest survivors who make it to hospital admission is neurological death from brain swelling. At the time, data suggested that pre-hospital cooling of cardiac arrest survivors
by EMS would improve outcomes. I chose to partner with the EMS leadership teams, first in Durham County, North Carolina, where EMS were governed on a county level, and later in Oklahoma, where it was centralized at a state level, to determine the best way to implement this process for the communities that they served, including purchase of special refrigerators to carry cold IV fluids in EMS trucks. This allowed me to develop my expertise in the field and ultimately establish neurocritical care as the admitting service for all patients with cardiac arrest at the University of Oklahoma Medical Center. We set up our own resuscitation bay in the emergency room to facilitate this time-sensitive care, leading to improved outcomes in our patients.
Q4
As a collaborator in the Curing Coma Campaign, what are some of the most groundbreaking research projects you’ve been involved in? How do these findings translate into improvements in clinical practice for neurologists and intensivists?
We are just now learning about disorders of consciousness, which were not well differentiated in the past. The description of a minimally-conscious state and the concept of covert consciousness has led to a greater amount of patience with brain injury survivors, affording them more time to demonstrate clinical improvement.
Q5 As Director of Transcranial Doppler
Ultrasound Services at Prisma Health-Upstate, what initiatives have you spearheaded to enhance patient care? Additionally, could you explain the clinical applications and benefits of transcranial Doppler (TCD) ultrasound in neurology?
TCD ultrasound is a safe, bedside, portable, non-invasive tool which allows one to evaluate cerebral blood flow in the major blood vessels in the brain. It is part of standard of care during the daily evaluation of patients with subarachnoid hemorrhage from ruptured brain aneurysms, allowing the identification of patients at risk for strokes, thereby guiding medical decision making. TCD

is also used for diagnosis and guidance of treatment decisions in patients with acute ischemic stroke, patent foramen ovale (the persistent presence of a hole between the right and left side of the heart), and for guiding blood thinner management. Less than 10% of the 350+ Comprehensive Stroke Centers in the US are accredited to perform and interpret TCD, although they all require the availability of TCD. We were able to establish our program in 2019, achieve site accreditation in 2021, and have the largest number of TCD certified technologists in the nation.
Q6
You were the first fellowship-trained DO neurointensivist and the first DO to be designated as a Fellow of the Neurocritical Care Society (NCS). What advancements have you witnessed in neurocritical care since your training?
In the US there are two kinds of physicians that practice medicine. Medical Doctors (MD) and DOs. Both have equal scope to practice in all disciplines of medicine
in all 50 states. However, prior to 2015, when the two entities merged the accreditation body of their residencies, DO physicians were not afforded all of the same opportunities as MD physicians for training and hospital practice. At the time of my training, neurocritical care was a new field whose legitimacy was not uniformly accepted, and thus, there were very few residents who were entering the handful of fellowship programs available. I was the first DO to complete a 2-year neurocritical care fellowship program. I have been the founding Medical Director of two academic neurocritical care units; first at the University of Oklahoma and now at the University of South Carolina-Greenville (Prisma HealthUpstate). For this accomplishment, and my contributions as one of the world leaders in neurovascular ultrasound, as well as education and advocacy for the NCS, I was fortunate to achieve the designation of Fellow of NCS, a designation held by about 50 individuals worldwide at the time. In the past 15+ years of practice, I have seen the establishment
of mechanical thrombectomy (removal of a blood clot from a brain artery) become the standard of care for acute ischemic stroke, allowing neurointensivists and neurointerventionalists to help minimize brain injury in patients with stroke, thereby reducing their level of disability and improving survival.
Q7 Therapeutic
hypothermia is one of your key research interests. Could you elaborate on its mechanisms and how it improves patient outcomes, particularly in neurocritical care settings?
It is uniformly known now that fever worsens neurological outcome in patients with a brain injury by increasing the brain’s metabolic demand. The increased metabolic demand ultimately leads to greater brain swelling, which can lead to death. Targeted temperature management reduces the brain’s metabolic demand by cooling the patient, and therefore minimizes the brain injury and reduces the probability of death.

Non-rapid Eye Movement Sleep Homeostatic Plasticity Carries the Risk of
Epileptic Transformation
Authors: *Péter Halász,1 Anna Szűcs1
1. Semmelweis University, Budapest, Hungary
*Correspondence to halasz35@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Received: 01.14.2025
Accepted: 05.01.2025
Keywords: Derailment of sleep-homeostatic plasticity, epileptic networks, strong link between sleep and epilepsy, system epilepsies.
Citation: Neurol AMJ. 2025;2[1]:64-70. https://doi.org/10.33590/neurolamj/DUUT3368
INTRODUCTION
This paper aims to review and redefine certain concepts of epilepsy in the light of contemporary brain research, and highlight the involvement of non-rapid eye movement (NREM) sleep homeostasis. This robust biological healing force carries a risk of epileptic upregulation; therefore, epileptogenesis is interconnected with homeostatic plasticity. The diversity of epileptic syndromes originates from the differences in brain networks and epilepsyhosting functions; that undergo latent, longlasting histological reorganization during periods of clinical silence. The system-epilepsy approach may provide a “royal” conceptual framework of understanding epilepsies.
The link between NREM sleep and epilepsy has attracted the attention of clinicians and neuroscientists in recent decades. In most clinical papers, authors have recognized the high prevalence of sleep disorders in the epileptic population; also calling attention to the interconnection between sleep and epilepsy: epilepsy impairs sleep-quality, and changes in sleep-physiology may activate
epilepsy.1,2 The acquisition of knowledge on NREM sleep microstructure provides several examples for both effects.3 The idea that sleep physiology may be connected to epilepsy is becoming a subject of interest.4,5The recognition of homeostatic use-dependent slow-wave regulation (Figure 1)6 was an important step. Sleep researchers have recognized why NREM sleep is so important and why it is preserved throughout phylogeny, constituting about two-thirds of human life. An increased sleep-propensity after sleep deprivation shows that slow wave-power needs to be compensated. The compensatory elevation of sleep pressure resulting in slow waves, recovers synapses loaded by daytime information.7,8 However, the physiological mechanisms of this process need further clarification.
The significance of NREM sleep and its use-dependent homeostatic regulation is now better understood. NREM sleep as the main cradle of our cognitive and plastic operations has been recognised. Sleep might have been one of the powerful vehicles helping humans to stand out from the animal world.
Slow wave increase
Slow wave decrease
Epileptic interictal manifestations
Increasing homestatic pressure and sleep propensity
Synaptic load increasing
Decreasing homeostatic pressure and sleep propensity
Synaptic refreshing
Homeostatic pressure, sleep propensity, slow sleep waves, and synaptic economy; changes in waking and NREM sleep. The homeostatic pressure, slow wave power and synaptic load increase exponentially in waking; reaching their highest levels during the first cycles of sleep. Later, each of them decreases exponentially with the synaptic recovery. The red/yellow insert indicates the degree and timing of interictal epileptic manifestations at the end of the day and the first sleep cycles. Yellow quadrate: waking state, blue quadrate: sleeping.
The co-elevation of homeostatic sleep plasticity with slow wave pressure is another important point.9 The idea that epilepsy would be resulted from the exaggeration and derailment of plasticity,10,11 brings sleep and epilepsy into a close relationship.
In a cat model of postinjury epilepsy, the Timofejev school (CERVO Brain Research Centre, Université LAVAL Québec, Canada) observed a strong increase of slow wave down-states during NREM sleep; it penetrated into REM sleep and even into wakefulness.12,13 The increase of slow wave down-states paralleled an accumulation of seizures. Recently, Massimini et al.14 have observed the increase of similar sleep-like down-states in a stroke patient, during their recovery period.
THE PRESENT VIEW ABOUT THE PLAYERS OF EPILEPTIC MECHANISMS
Clinical epileptologists and researchers have an implicit agreement that epileptogenesis is the result of exaggerated synaptic excitation in certain parts of the brain, affected by a
lesion or a genetic abnormality.15,16 Brainfunctions are not organised in centers; rather in networks. The networks of simple brain functions are easy to locate, but tracing them in case of more complex ones is more difficult. For example, the executive memory system works in the hippocampus and is connected to cortico-frontal areas; in addition it may execute different tasks in the daytime versus during NREM sleep.
THE UPGRADING (EXAGGERATION) OF BRAIN NETWORKS IS REPRESENTED BY ELECTROPHYSIOLOGICAL MANIFESTATIONS
Since EEG has become an essential tool of epilepsy-diagnostics, the enhancement of sleep-related interictal epileptiform discharges (IED)- spikes and ripples -has been noticed, and recent ultra-long EEG observations have alighted the features of IEDs even better. Their continuous presence in epilepsies has suggested important roles, and neuroimaging studies have identified their morphological substrates.16,17
Figure 1: Dynamics of sleep pressure, synaptic load, and epileptic activity.
Awake state
NREM sleep
The links between IEDs and ictal events remain unclear. It is difficult to explore the direct relation between ictogenesis and the clinically silent IEDs; their participation in epileptogenesis can be considered just retrospectively in most cases. The idea about IEDs’ important role in the epileptic mechanism comes primarily from their presence in almost all types of epilepsy. In even severe epilepsies (see Electrical Status Epilepticus in Sleep [ESES]), seizures may be lacking or scarce, and IEDs be the effective players. In the major epileptic syndromes, IEDs are found close to the seizure-onset zones; typically in NREM sleep. It seems that IEDs act latently in epileptogenesis. The seizure-onset zones can be identified, but the ictogenic factors may be hidden.
Ictal triggers have been discussed recently. They can be categorized as sensory stimuli, cognitive or emotional cues,18 and sleep-related processes such as falling asleep, or arousing from sleep,19 which are special, newly considered mechanisms.
The group of IEDs has been extended to fast, pathological ripples (>200 Hz; high-frequency oscillations [HFO]) that have qualified as the most accepted biological markers of epilepsy.20 HFO cannot be detected with scalp electrodes in most EEG-labs; therefore their routine clinical use is delaying.
While the details of electrophysiological features exceed the frames of this paper, some essential phenomena deserve to be mentioned; such as the ubiquity of interictal, and (less so) the ictal spiking and the recognition of IEDs’ significance. HFO, identified recently, have been associated with cognitive processes. The extension of detected EEG oscillations to the 200–500 Hz range has revealed that HFO are valid biological markers of epilepsy20 and good tools to define the epileptogenic zone for epilepsy surgery.
The registration of HFO activity might also indicate the progress or regress of the epileptic process.
The close correlation between sleep slow waves and IEDs was described early, and has been confirmed in several papers.3,21 Later, seminal publications pointed out the transformation of sleep EEG-patterns to epileptic spikes and pathological (>500 Hz) ripples.11,22 The evident correlation of sleep slow waves with IEDs is another argument for the connection of NREM sleep with epilepsy.1 Clinically, the significance of NREM sleep as an enhancing factor is confirmed; boosting IEDs’ networks and IEDs themselves; both spikes and pathological ripples (≤500 Hz).23
NETWORK-BASED VIEW OF EPILEPSIES AND THE ROLE OF NREM SLEEP
The network-view of brain functions has appeared in the network-approach of epilepsy as well Beenhakker and Huguenard stated in their emblematic paper that “normal brain circuits provide a template that epileptic circuits use to generate seizures.”24 In other words, normal and epileptic brain circuits share common features. They demonstrated the epileptic transformations in two syndromes: medial temporal lobe epilepsy and absence epilepsy. This view automatically brought back the idea of approaching different epileptic syndromes as system (-function) epilepsies.25-28
INTERRELATIONS OF BRAIN SYSTEMS AND MAJOR EPILEPSY SYNDROMES
In the last 7 years, the authors have tried to discuss the association of well-known, frequent epileptic syndromes with established functional brain networks. Here, they provide a summary (Table 1) of this work. Out of the 10 discussed epilepsy syndromes, sleep studies are missing for reading epilepsy and human post-traumatic epilepsy, but in the rest of syndromes, a close connection with NREM sleep could be established.
Table 1: A system-based classification of known epilepsies.
Epilepsy type
Medial temporal lobe epilepsy as an epilepsy of the declarative memory-system.
Absence epilepsy as a disorder linked to sleep promotion.
Function of the affected brain system
Short-term memory-store in the hippocampus; replaying engrams during NREM sleep; frontal transmission and consolidation.
Players: Hippocampal sharp wave-ripple, fronto-thalamic slow waves and spindles.
Thalamocortical integration, slow-wave sleep and spindleproduction; participation in consciousness.
Burst-firing mode during NREM sleep.
Juvenile myoclonic epilepsy as a system epilepsy of the thalamocortical network with extended cortical involvement.
Extended thalamocortical system, with increased visual, cortico-motor sensitivity, and special frontal personality type.
Structural or genetic background
Early temporal lobe pathology; hippocampal involvement; histological reorganization (6–7 years latency).
Mutations in the GABAergic intrareticular neurons.
Epileptic consequences built on brain networks
Epileptic transformation from sharp-wave ripple to mesio-temporal spiking and ≤500 Hz ripples.
Memory disturbances in seizures; chronic side-specific memory-loss in the long term.
Transformation of nRE spindle-production to bilateral spike-wave pattern (absences) in the process of falling asleep.
A long-term cognitive effect may evolve.
Epileptic facilitation in the visuo-motor system.
Spontaneous myocloni and generalised tonic-clonic seizures are activated by sleep deprivation.
Self-limiting childhood epilepsy as a system epilepsy of the perisylvian human communication system.
Perisylvian human communication network (speech, reading, writing, singing, instrumental music).
Family accumulation supporting genetic origin.
Reflex epilepsies of the human communication network (assumed to be system epilepsies).
Cognitive fields; parts are linked to the perisylvian network with reading*, writing, auditory, or other appropriate communication functions.
Neuroimaging alterations behind the centrotemporal spikes (presumably mild developmental abnormalities).
Early intrathalamic hemorrhage, in those cases where ESES encephalopathy develops.29
EEG: fast type of bilateral spikewave paroxysms are elicitable by photic and cognitive triggers.
Absence of epilepsy may progress to juvenile myoclonic epilepsy after puberty and remain throughout the lifespan.
Neuropsychological impairments of human communication; bilateral independent self-limiting (3 to 13–15 years) centrotemporal spikes as endophenotypes; focal and sec. generalised sensorimotor seizures in typical and atypical rolandic epilepsy.
In approx. 6–30 % of patients with atypical and typical Rolandic epilepsy, ESES develops by the transformation of centrotemporal spikes to the ESES pattern, from focal to regional or bilateral augmented discharges.30 If this is maintained for more than 1–1.5 years, there can be long-term mental regression.
Genetic or structural.
Example: reading epilepsy, musicogenic epilepsy.
Table 1: Continued.
Epilepsy type
Sleep-related hypermotor epilepsy as a system epilepsy of arousal from sleep.
Somatosensory epilepsy as a system epilepsy of the somatosensory network.
Visual epilepsy as a system epilepsy of the visual network.
Post-traumatic epilepsy* as a system epilepsy of any brain network.
Function of the affected brain system
Ascending brainstem cholinergic arousal system
Different degrees of arousal from slow-wave sleep.
Sensory-motor gyrus (Brodmann 1,2) with involvement of the supplementary motor area, particularly the supplementary eye field.
Visual afferentation pathways affecting the pulvinar thalami and the visual cortex.
Photosensitivity increases.
Any cortical area with frontal and temporal emphasis.
Structural or genetic background
Autosomal dominant mutation in the second transmembrane domain of the neuronal nicotinic acetylcholine receptor alpha-4 subunit gene, located on chromosome 20q13.2-13.3.31
In ascending cholinergic brainstem arousal system.
Structural or genetic changes in the ascending arousal system.
Structural abnormalities around the visual system.
Genetic origin of increased photosensitivity.
Post-traumatic and post-stroke with ≥2 years latency.
Epileptic consequences built on brain networks
Epileptic level facilitation in the brainstemarousal-system.
Pathological arousals ignite differentdegree hypermotor frontal lobe seizures.
Cortical epileptic reorganization, with epileptic upregulation, resulting in increased excitation.
Epileptic seizures and spiking in the affected cortical fields.
Photoparoxysmal response as an endophenotype; increased propensity to spiking in response to photic stimuli
Cortical reorganization with increased excitability. Sleeplike bistability penetrates to REM sleep and wakefulness.
The first column shows the epilepsy type, the second describes the function of the brain system hosting epilepsy; the third one highlights etiologies; and the fourth column indicates the transformation (upgrading) to an epileptic mechanism with some consequences. However different the etiologies may be, the underlying mechanisms and the clinical and electrophysiological features seem to be common.
CHRNA4 gene: neuronal nicotinic acetylcholine receptor alpha-4 subunit gene; CTS: centro-temporal spike; EEG: electroencephalogram; ESES: Electrical Status Epilepticus in Sleep; GABA: gamma-aminobutyric acid; GTC seizure: generalised tonic–clonic seizure; HFO: high frequency oscillations; LKS: Landau-Kleffner Syndrome; nRE: reticular nucleus of the thalamus.
*For reading and post-traumatic epilepsies, sleep studies are missing.
The work of Wolf has offered much insight into the nature of ictogenesis.18 The key syndrome is juvenile myoclonic epilepsy with reflex-traits (photosensitivity, eye closure sensitivity, praxis- and language-induction). Multimodal investigations of cerebral functions indicate that ictogenesis (ab-) uses pre-existing functional brain-networks (central nervous system subsystems) normally serving physiological functions; supporting the concept of system-epilepsy.
Thus, the actual epileptic trigger is the activation of an epileptically upgraded functional network. Accordingly, absence epilepsy is perceivable as the epilepsy of NREM sleep-promotion; sleep-related hypermotor epilepsy as the epilepsy of the arousal from NREM sleep19; and self-limiting childhood epilepsies as those of the human communication network (Table 1).
Shared Features of Epileptogenesis:
• Epileptogenesis prefers those networks involved in plasticity; it favours developmental periods, and may resolve.
• The long process of epileptogenesis is ignited by a ‘‘first hit”, which is a genetic mutation or a lesion (sometimes shown by neuroimaging, e.g. in medial temporal lobe epilepsy and lesional epilepsies upon developmental anomalies).
• It carries a risk of escalation in both localization and severity, e.g. to epileptic encephalopathies (Table 1).28
• Epileptogenesis and epileptic progression are both underlain by an increase and spreading of excitation, shown by the shared presence of pathological HFO.32–34
• NREM sleep enhances IEDs, promoting epileptogenesis. Sleep oscillations become templates for IEDs, the clearest example being the transformation of hippocampal sharp wave-ripple to epileptic spike-pathological ripple.11,22
• IEDs have crucial role in epileptogenesis. They have specific distributions in relation with the up- and down-states of sleep slow waves.1 Sleep spindles link to the “up” states, and HFO predominantly occur in the transition-zones from the “up” to the “down” state. These data highlight the socalled ‘‘bistability” (or alternating polarity) of sleep slow waves as a potential factor driving epileptogenesis in sleep.
INTERRELATIONS OF BRAIN SYSTEMS AND MAJOR EPILEPSIES
Epilepsy is a colourful ensemble of syndromes; a few of them are frequent, while the large majority appear rarely.
The authors are focusing here on those epilepsies frequently encountered by neurologists (Table 1).
For dealing with system epilepsies, one needs to be familiar with the affected brain systems’ neuroanatomy. The criteria of system epilepsies are simple: seizure symptoms reflect, by an excitatory or inhibitory way, the function of the system; the localization of epileptic EEG-changes covers the anatomy of the system; if there is a lesion, it is in anatomical relation with the epilepsy-network; a long-term dysfunction may evolve in the affected system(s); and if a reflex seizuretrigger can be identified, it is congruent with the afferentation of the system.
The diversity of epilepsy-presentations does not contradict the existence of a common way of epileptogenesis. The multifariousness of epilepsies is related to the diversity of involved brain-networks.
SYSTEM EPILEPSY AND EPILEPSY TAXONOMY
The classification of epilepsies needs to reflect contemporary perception. The International League Against Epilepsy (ILAE) taxonomy is struggling to maintain the focal/ generalized dichotomy, despite convincing evidence that “focal” epilepsies are not circumscribed enough and “generalized” epilepsies are insufficiently generalized.35 The network concept now prevailing in brain research may resolve this contradiction and the untenable separation of epilepsyresearch from the mainstream of networkbased approaches in neuroscience.
The system-view of epilepsy raises several questions; nonetheless it seems to provide a uniform comprehensive approach with flexible frames.
References
1. Frauscher B et al. Facilitation of epileptic activity during sleep is mediated by high amplitude slow waves. Brain. 2015;138(Pt 6): 1629-41.
2. Halász P et al. Strong relationship between NREM sleep, epilepsy and plastic functions - A conceptual review on the neurophysiology background. Epilepsy Res. 2019;150: 95-105.
3. Nobili L et al. Sleep and epilepsy: A snapshot of knowledge and future research lines. Journal of Sleep Research. 2022;31(4): e13622.
4. Halász P, Szűcs A. Sleep and epilepsy link by plasticity. Front Neurol. 2020;11: 911.
5. Sheybani L et al. Mechanistic insights into the interaction between epilepsy and sleep. Nat Rev Neurol. 2025;21: 177-92.
6. Borbély AA, Achermann P. Sleep homeostasis and models of sleep regulation. J Biol Rhythms. 1999;14(6): 557-68.
7. Tononi G and Cirelli C. Sleep and synaptic homeostasis: a hypothesis. Brain Research Bulletin. 2003;62: 143-50.
8. Tononi G and Cirelli C. Sleep function and synaptic homeostasis. Sleep Med Rev. 2006;10(1): 49-62.
9. Halász P et al. Derailment of Sleep Homeostatic Plasticity Affects the Most Plastic Brain Systems and Carries the Risk of Epilepsy. J Integr Neurosci. 2023;22(5): 111.
10. Tononi G, and Cirelli C. Sleep and the price of plasticity: from synaptic and cellular homeostasis to memory consolidation and integration. Neuron. 2014;81: 12–34.
11. Buzsáki G. Hippocampal sharp wave-ripple: a cognitive biomarker for episodic memory and planning. Hippocampus. 2015;25(10): 1073-88.
12. Houweling AR et al. Homeostatic synaptic plasticity can explain posttraumatic epileptogenesis in chronically isolated neocortex. Cereb Cortex. 2005;15(6): 834-45.
13. Avramescu S, Timofeev i. synaptic strength modulation after cortical trauma: a role in epileptogenesis. J Neurosci. 2008;28(27): 6760-72.
14. Massimini M et al. Sleep-like cortical dynamics during wakefulness and their network effects following brain injury. Nat Commun. 2024;15: 7207.
15. Pitkänen A, Lukasiuk K. Molecular and cellular basis of epileptogenesis in symptomatic epilepsy. Epilepsy Behav. 2009;14(Suppl 1): 16-25.
16. Ciumas C et al. Neural correlates of verbal working memory in children with epilepsy with centro-temporal spikes. Neuroimage Clin. 2020;28: 102392.
17. Bourel-Ponchel E et al. Functional and structural network disorganizations in typical epilepsy with centro-temporal spikes and impact on cognitive neurodevelopment. Front Neurol. 2019;10: 809.
18. Wolf P. Reflex epileptic mechanisms in humans: Lessons about natural ictogenesis. EBR. 2017;71(Pt B): 118-23.
19. Halász P. Are absence epilepsy and nocturnal frontal lobe epilepsy system epilepsies of the sleep/wake system? Behav Neurol. 2015: 231676.
20. Frauscher B, et al. High-frequency oscillations: the state of clinical research. Epilepsia 2017;58(8): 1316–1329.
21. Gibbs FA, Gibbs EL. (1941). Atlas of electroencephalography. F. A. Gibbs, Boston City Hospital.
22. Gulyás AI, and Freund TT. Generation of physiological and pathological high frequency oscillations: the role of perisomatic inhibition in sharp-wave ripple and interictal spike generation. Curr Opin Neurobiol. 2015;31: 26–32.
23. von Ellenrieder N, et al. Physiological and pathological high-frequency oscillations have distinct sleephomeostatic properties. NeuroImage: Clinical. 2017;14: 566–73.
24. Beenhakker MP, Huguenard JR. Neurons that fire together also conspire together: is normal sleep circuitry hijacked to generate epilepsy? Neuron. 2009;62(5): 612–32.
25. Avanzini G et al. The system epilepsies: a pathophysiological hypothesis. Epilepsia. 2012;53: 771–8.
26. Wolf P et al. Juvenile myoclonic epilepsy: A system disorder of the brain. Epilepsy Research. 2015;114: 2–12.
27. Capovilla G et al. Epileptic encephalopathy as models of system epilepsy. Epilepsia. 2013;54: 34–7.
28. Halász P et al. Perisylvian epileptic network revisited. Seizure. 2019;65:31–41.
29. Tassinari CA et al. Encephalopathy with electrical status epilepticus during slow sleep or ESES syndrome including the acquired aphasia. Clin Neurophysiol. 2000;111(Suppl 2): S94-S102.
30. Lu G et al. The prevalence and risk factors of electrical status epilepticus during slow-wave sleep in self-limited epilepsy with centrotemporal spikes. Clin EEG Neurosci. 2023;55(2):265-71.
31. Yang Y et al. Pathogenic genes implicated in sleep-related hypermotor epilepsy: a research progress update. Front Neurol. 2024;15:1416648.
32. van Klink NE, et al. Ripples on rolandic spikes: a marker of epilepsy severity. Epilepsia. 2016;57(7): 1179-89.
33. Kilic H et al. Electrical status epilepticus in sleep: The role of thalamus in etiopathogenesis. Seizure. 2021;93:4450.
34. Gong P et al. Scalp-recorded highfrequency oscillations in childhood epileptic encephalopathy with continuous spike-and-wave during sleep with different etiologies. Brain Dev. 2018;40(4): 299-310.
35. Halász P, Kelemen A. New vistas and views in the concept of generalized epilepsies. Ideggyogy Sz. 2009;62(1112): 366-80.
Novel Therapies and Targets for Parkinson’s Disease
Editor's Pick
This article explores the evolving landscape of Parkinson’s disease treatment, from newly licensed symptomatic therapies to emerging disease-modifying approaches targeting α-synuclein. With a focus on non-motor symptoms and innovations in trial design, the article offers timely insights into how the future of Parkinson’s disease care is being reshaped at both the clinical and research levels.
Rajiv R. Ratan
Weill Cornell Medicine, New York, USA
Authors: *David Ledingham,1 Nicola Pavese1,2
1. Clinical Ageing Research Unit, Newcastle University, Campus for Ageing and Vitality, Newcastle upon Tyne, UK
2. Department of Nuclear Medicine and PET Centre, Aarhus University Hospital, Denmark *Correspondence to david.ledingham1@nhs.net
Disclosure: The authors have declared no conflicts of interest.
Received: 11.19.24
Accepted: 04.14.25


Keywords: Alpha-synuclein, clinical trials, deep brain stimulation (DBS), device-aided therapies (DAT), disease-modifying therapies, motor complications, non-motor symptoms (NMS), Parkinson's disease (PD).
Citation: Neurol AMJ. 2025;2[1]:71-82. https://doi.org/10.33590/neurolamj/XNGP3532
Abstract
In this editorial, the authors highlight newly licensed medications for the symptomatic treatment of Parkinson’s disease (PD) and their role in the current management of PD. Non-motor symptoms (NMS), which cause significant disability in this patient group, are highlighted to emphasize their importance as targets for treatment, both in current and in future research. The clinical trial pipeline for disease-modifying treatments for PD is discussed with an emphasis on therapies targeting α-synuclein propagation and aggregation within the central nervous system. Newly licensed treatments and advances in the management of motor complications are discussed. Finally, the current state of clinical trial design is highlighted, with a focus on how study design is evolving and the potential implications for both the treatment and prevention of PD.
Key Points
1. Parkinson’s disease (PD) is the fastest rising cause of neurological disability and death worldwide. Over the last decade, significant advancements in understanding the clinical spectrum and biological underpinnings of PD have led to the introduction of new medications and therapies.
2. This article provides a comprehensive overview of new infusion therapies, sublingual and inhaled formulations of established compounds, and the evolution of deep brain stimulation (DBS) capabilities.
3. Health care professionals should understand the significant impact of non-motor symptoms (NMS) on patients' clinical course. They should also be aware of the marked expansion of clinical drug and device trials for PD, highlighting the ongoing efforts to develop disease-modifying therapies.
INTRODUCTION
Parkinson’s disease (PD) is a progressive neurodegenerative disorder. Current diagnostic criteria rely predominantly on clinical features, specifically the presence of motor symptoms, including bradykinesia, in combination with extrapyramidal rigidity and/or resting tremor.1 Of all the neurological disorders, PD is now recognized to be the fastest rising cause of disability and death worldwide.2 Over the last decade, there have been dramatic steps in our understanding of both the clinical spectrum and biological underpinnings of the disease. These developments have led to the introduction of new medications into clinical practice, including novel infusion therapies and both sublingual and inhaled formulations of established compounds. There has also been an ongoing evolution of the capabilities of established therapies, including deep brain stimulation (DBS), which is generally used for individuals with advanced PD, but is potentially beneficial also in early-stage PD.3 This has paralleled a significant expansion in the number of clinical drug and device trials for PD. As of January 31, 2024, there were 136 active trials investigating medications for PD. A total of 44% was considered as diseasemodifying therapies and the remaining 56% was symptomatic therapies. McFarthing et al.4 have described these trials in detail.
THE CLINICAL SPECTRUM OF PARKINSON’S DISEASE
“Early” Parkinson’s Disease
The motor symptoms of early PD are often the clinician’s focus over the first few years following diagnosis, which in most cases remains based on the detection of clinical symptoms. In this regard, the Movement Disorder Society (MDS) has provided clinical diagnostic criteria for PD that are intended for use in clinical research and for guiding clinical diagnosis.1 First-line symptomatic therapies for motor symptoms remain unchanged over the last decade and include levodopa preparations, dopamine agonists, and monoamine oxidase inhibitors (MAOi). The evidence base and rationale for selecting between medications is summarized in the evidence-based medicine review commissioned by the MDS.5 Non-motor symptoms (NMS), including neuropsychiatric, neurocognitive, sleep, and autonomic impairment, are now also recognized to have a significant impact on a patient’s clinical course.6,7 It has recently been observed that, in patients with early PD, the presence of depression may be as significant a predictor of impairment in activities of daily living as motor function (Stewart et al., unpublished data). Depression is significantly associated with the development of cognitive decline in PD,8 and there is observational evidence that early treatment of depression and
anxiety may improve both non-motor and motor outcomes.7 Hence, for clinicians, it is important to remember that NMSs should be actively explored, rather than focusing solely on easily visible motor symptoms.
“Advanced” Parkinson’s Disease
As the disease progresses, many of the early motor and NMSs worsen. A diverse range of symptoms, including gait impairment, postural instability, freezing, and neuropsychiatric and neurocognitive impairment, are more likely to occur and progressively worsen in the later stages of the disease.6 Where patients initially have a good clinical response to dopaminergic therapy, typically, the severity of motor symptoms and the probability of developing motor complications increase as time passes.9
Motor complications encompass OFF periods, which are specific times during the day when dopaminergic medications exhibit reduced efficacy; OFF dystonia, which typically presents painful posturing of a limb during an OFF period; and dyskinesias, characterized by involuntary hyperkinetic movements affecting any part of the body. These can all greatly affect a person’s quality of life. In clinic, first-line management strategies for motor complications include increasingly complex medication regimens. Clinicians and their patients can select one or a combination of different strategies, including increasing the dosing intervals of standard-release dopaminergic medications, the addition of dopamine agonists, prolonged-release levodopa formulations, or enzyme inhibitors, including MAOis and catechol-O-methyl transferase inhibitors (COMTi). Although it is not available in Europe, in 2019, the FDA approved a drug with a new mechanism of action, istradefylline (a selective A2A receptor antagonist), for the treatment of motor complications. A pooled analysis of all studies showed a reduction in OFF time of 0.45 hours compared to placebo (p<0.0001).10
Whereas enzyme inhibitors prolong the ON time and minimize the OFF time over a 24-
hour period, over the last few years, several drugs have been released, which provide ‘ondemand’ relief for the same symptoms. In 2018, the FDA approved Inbrija® (Merz, Frankfurt, Germany), an inhaled levodopa formulation. When taken at a single dose, an individual’s PD motor symptoms begin to show a significant improvement compared to placebo at 10 minutes post-dose.11 The FDA approved a further ‘on-demand’ therapy, sublingual apomorphine, in 2020. Again, significantly more patients demonstrated improvement in their PD motor scores compared to placebo at 15 minutes.12 Both therapies, which are modified formulations of established drugs, enhance outcomes notably in patients with unreliable gastrointestinal absorption of oral medications, a frequent symptom in individuals with PD.
If first-line oral and ‘on-demand’ medications fail to sufficiently improve an individual’s quality of life, then device-aided therapies (DAT) are often considered. These therapies aim to minimize the fluctuation index of dopaminergic preparations by either instilling them as a continuous infusion or bypassing peripheral dopaminergic pathways and applying highfrequency stimulation directly to targets within the basal ganglia network, which have been identified as playing a key role in mediating the motor symptoms of PD, i.e., DBS.
Prodromal Disease
It is well established that the neurodegenerative process in PD begins decades before the onset of clinical symptoms (preclinical phase), and later, symptoms and signs may be present but be insufficient to define the disease (prodromal phase). In fact, patients with PD have frequently experienced one or multiple NMSs for years prior to their diagnosis. Autonomic dysfunction, including constipation and urinary urgency, as well as rapid eye movement sleep behavioural disorder (RBD), depression, anxiety, and hyposmia are among the most recognized prodromal disorders. The annual risk of developing a synucleinopathy,
such as PD, dementia with Lewy bodies, or multiple system atrophy, for someone with RBD is 6–7%. After 12 years of follow-up, 73.5% of patients will have converted.13
There is an increasing emphasis on developing tests to aid researchers and clinicians in predicting which patients may be at increased risk of phenoconverting soon, potentially providing a further avenue for intervention before the onset of motor symptoms. The MDS has released the research criteria for prodromal PD, which provide an evidence-based methodological framework to statistically estimate the likelihood that an individual has prodromal PD.14 The utility of these criteria in clinical settings, however, remains to be established.
The Parkinson Associated Risk Syndrome (PARS) study found that a positive cerebrospinal fluid (CSF) α-synuclein seed amplification assay (SAA) was detected in 48% of individuals with hyposmia, compared to 4% of normosmics. Individuals with hyposmia who tested positive for SAA had an increased relative risk (RR) of reduced dopamine transporter activity, as identified by a dopamine transporter scan (RR: 3.26; 95% CI: 1.16–9.16). Additionally, seven out of 12 SAA-positive individuals with hyposmia and a dopamine transporter deficit subsequently developed symptoms consistent with synucleinopathy.15 This and other supporting data suggest that biomarkers such as SAA positivity and dopamine transporter deficit may precede the onset of clinical synucleinopathy.15 Stratifying individuals with symptoms more common in the years prior to PD, depending on these biomarkers, provides a potential mechanism wherein their chance of developing diagnostic motor or cognitive symptoms may be predicted in the future. The Parkinson’s Progression Marker Initiative (PPMI), a large multicenter observational study, has recently embarked on a large effort to recruit individuals with hyposmia and RBD to advance research in this area.16
THE BIOLOGICAL UNDERSTANDING OF PARKINSON’S DISEASE
The Role of α-Synuclein
PD is a heterogeneous condition, both in terms of its clinical picture and of its underlying biological mechanisms. Histopathological examinations reveal that most patients exhibit the characteristic findings of neuronal Lewy bodies. These are abnormal protein deposits composed of multiple different proteins, including abnormally folded α-synuclein. A leading hypothesis in the field is that misfolded α-synuclein monomers exhibit prion-like activity. They propagate throughout the nervous system, leading to subsequent characteristic but variable patterns of neuronal damage and subsequent clinical symptoms that reflect the topographical burden of Lewy body deposition. For a recent update on the scientific background of this hypothesis, refer to Jan et al.17
Many clinical trials are either ongoing or have recently been completed, wherein interrupting the spread of α-synuclein or enhancing its clearance is the main goal of treatment. However, no trial has yet met its primary outcome. Post-hoc analyses have provided some hope that a potential diseasemodifying therapy may be anticipated. The PASADENA study investigated whether prasinezumab, a monoclonal antibody that binds to aggregated α-synuclein, thereby potentially enhancing its clearance, slowed disease progression in early PD.18 While there was no significant difference compared to placebo over 1 year in the primary outcome, minimal progression was observed in motor outcomes in both the treated and untreated groups. Overall, there was a lower level of motor progression in the treatment group. In the open label extension study, patients on active treatment had better motor outcomes over 4 years when compared to controls from an external comparator natural history study, the PPMI study.19 Post-hoc analyses of the PASADENA study also suggested that patients in a prespecified subgroup with
faster motor progression had better motor outcomes on treatment.20 Consequently, a larger and longer Phase III study has recently completed and is due to read out shortly. As of January 2024, there are nine clinical trials underway using different molecules that directly target α-synuclein.4
In 2019 and 2021, two studies were published that validated a highly sensitive and specific diagnostic test for PD: the CSF α-synuclein SAA.21,22 The test is positive in 95% of post-mortem confirmed PD.23 The pooled sensitivity and specificity of the test to differentiate synucleinopathies from controls were 0.88 and 0.95, respectively.24 In addition to providing an extra diagnostic tool, a reliable biomarker also means that clinical trials can be enriched, i.e., patients who are α-synuclein-negative need not be enrolled in studies of compounds targeting the α-synuclein pathway. It has also led to two proposals for a biological definition of PD, and one of these groups has proposed a subsequent staging system, akin to that observed in Alzheimer’s disease.25-27 The staging system proposes the use of the term “neuronal α-synuclein disease,” taking into account that patients with prodromal disorders may have positive SAA assays and are at increased risk of developing PD, compared to SAA-negative individuals.28,29 These proposals are currently intended as research criteria, as SAA testing and, to a lesser extent, genetic evaluation are not widely available in clinical practice. The concept, however, is particularly exciting as it has led academic and industry partners to consider disease-modifying treatment trials in patients with prodromal disease, with the aim of preventing the development of PD in these patients (see section Approaches to Clinical Trials in Parkinson's Disease).
Other Molecular Mechanisms
Underlying Parkinson’s Disease
There remain, however, several unanswered questions. The most intriguing question for the authors is what are the upstream mechanisms that have triggered the initial
seeding of abnormal α-synuclein monomers and what is the mechanism behind the development of PD in patients who are both SAA-negative and have no evidence of Lewy body disease at post-mortem. Indeed, while α-synuclein is widely considered an important pathology and therapeutic target, several researchers have proposed that the field may be overly focused on the pathogenic role of α-synuclein in PD, with important implications for a large number of anti-synuclein therapies in development.30,31 Genetic differences in patients with PD may provide important clues. Variants in the GBA and LRRK2 genes are the most common cause of autosomal dominant PD, while mutations in the PRKN gene are the most common cause of autosomal recessive PD.32 In one large analysis, only 67.5% of patients with LRRK2 PD were SAA-positive29 compared to 93.3% of patients with sporadic PD and 95.9% of patients with GBA PD. The CSF SAA has not been used in a large population of individuals with PRKN PD, but previous post-mortem studies have suggested that more than 50% of PRKN PD do not have Lewy body pathology.33
Anti-synuclein therapies are unlikely to have a significant impact on SAA-negative PD. It remains unclear whether these individuals require an entirely different approach to disease-modifying therapies. Initiatives such as the LRRK2 Initiative Therapeutics Exchange (LITE)34 seek to explore new biomarkers for individuals who carry the LRRK2 variant and are more likely to be SAA-negative. In the interim, there are also a number of drugs in therapeutic trials that do not directly target the removal of α-synuclein. Currently, there are nine compounds targeting LRRK2 and GBA, which are encoded by the LRRK2 and GBA genes, respectively, undergoing clinical trials. The studies are divided between those targeting discrete subpopulations of individuals with confirmed genetic variants and those that have incorporated individuals with PD, unaware of their underlying genetic background on the basis that the activity of these enzymes is also abnormal in sporadic PD.
Trial Design Intervention Arms
Traditional Trials
Platform (Multi-arm) Trials
Open-Label
Extension Trials
Leveraging Data from Natural History Studies
Trials in Prodromal Disease
Trials in Prodromal Disease
Phase I-IV trials in PWP
EEG: electroencephalogram; GCS: grapheme-color synesthesia; F: female; M: male.
Open-label extension
Legend
Placebo arm
Placebo arm based on matched natural history group
Intervention arm
In addition to the aforementioned drug classes, current disease-modifying trials target other mechanisms, such as neuroinflammation suppression, antioxidant activity, gut microbiome manipulation, neuronal survival, and lysosomal and mitochondrial function. A full review is beyond the scope of this editorial but readers are recommended to read the recent summary by Vijiaratnam et al.35
DEVICE-AIDED THERAPIES
Infusion Therapies
Data from large cohorts of individuals with PD show that motor fluctuations (characterized by the development of OFF periods) occur in 54.3% and 100% of patients at 5 and 10 years,
respectively. Levodopa-induced dyskinesias occur in 14.5% and 55.7% over the same period (Figure 1).36 While a significant number of patients can be managed with adjustments to oral medications, many will develop motor complications that are unresponsive to these treatments. At this stage, provided there are no clear contraindications, there is an expanding array of DAT available, which can effectively address dopamineresponsive symptoms. It is important to note that symptoms which do not respond to oral dopaminergic therapies, such as cognition issues, balance problems, and ON freezing, will also not respond to continuous dopamine delivery via DAT. This underscores the necessity of conducting a clinician-observed levodopa challenge test as part of the evaluation process for all DAT candidates.
Figure 1: An outline of novel trial designs for testing disease modifying treatments in Parkinson’s disease.
DAT can be divided into continuous infusions and DBS. Apomorphine is a D2, D3, and D5 receptor dopamine agonist. It is currently available as cartridge for subcutaneous injection and as a sublingual film in the USA, but in Europe it is also widely available as a continuous subcutaneous infusion. As an infusion, it has been shown to reduce OFF time by a mean of 1.89 hours when compared to placebo (p=0.0025).37
Continuous subcutaneous infusions for PD have gained significant physician and public interest over the last year with the introduction of foslevodopa–foscarbidopa, a prodrug of levodopa. Similar to apomorphine, trial data have demonstrated that it can reduce OFF time by a mean of 1.79 hours (p=0.0054) compared to placebo.38
Levodopa can also be administered through infusion directly into the small intestine via a percutaneous endoscopic gastrostomy with jejunal extension (PEG-J). Carbidopa/ levodopa (Duopa/Duodopa®, AbbVie Inc., Chicago, Illinois, USA) was first licensed in 2015 and it is effective at improving motor complications (OFF time was reduced by a mean of 1.91 hours compared to placebo; p=0.0015 in the pivotal Phase III study).39
In 2019, Sweden approved an alternative intestinal infusion that combines levodopa, carbidopa, and entacapone, which has gained wider use in Europe but, is yet to pass FDA regulatory approval. The addition of entacapone, a COMTi, allows for lower doses of levodopa, meaning the pumps are smaller and potentially reducing levodoparelated side effects, such as peripheral neuropathy, although there have been no head-to-head studies.40
Deep Brain Stimulation
DBS of either the subthalamic nucleus (STN) or globus pallidus interna is the primary neurosurgical alternative to infusion therapies for refractory motor complications. The original studies and a subsequent metaanalysis highlighted that STN DBS reduces OFF symptoms by an average of 60%. Dyskinesias are reduced by 60–80%, in part, due to an average of 30–50% reduction in the
dose of oral dopaminergic medications.41–43
DBS has the added advantage over other forms of DAT in providing a significant degree of tremor control beyond what dopamine-based treatments can provide, through the stimulation of non-dopaminergic tremor networks. This makes it first-line when considering DAT for individuals with significant tremor.
DBS has experienced numerous substantial advancements in recent years. Improvements in battery life and electrode design have meant that patients need to recharge less frequently and clinicians can compensate for electrode misplacement using multisegmented electrodes. These allow steering of current toward target structures, thereby improving clinical outcomes, minimizing side effects, and reducing the need for repeat operations to move mildly misplaced electrodes. While not available across all devices, one company has developed the ability to perform remote (out of clinic) programming, reducing the number of inpatient clinic visits for patients.44 Other manufacturers have focused on the ability to incorporate anatomical imaging into programmers, allowing clinicians to target the “sweet spot” areas of stimulation using multicontact electrodes. This reduces the time needed for traditional trial–and-error programming, wherein each contact along electrodes containing 4–16 different points of stimulation needs to be tested for both efficacy and side effect thresholds, before selecting the optimal contact.
In 2021, the FDA approved a novel device the Percept™ PC (Medtronic, Minneapolis, Minnestoa, USA), which has the unique ability among currently available commercial DBS models of being able to detect electrical activity as well as deliver stimulation. The electrodes record local field potentials (LFP). LFPs are created by synchronous activity in interconnected populations of neurons, occurring due to the synchronizing effects of emergent network oscillations.45 A specific signal in the low beta frequency is a reliable
and reproducible correlate of clinically detectable bradykinesia and rigidity.46 It is supressed by both dopaminergic medications and stimulation.47,48 The band can be tracked, allowing clinicians to focus stimulation on contacts recording the highest beta peak and target the degree of stimulation to the peak in real-time. As the stimulation increases, the spectral power of the peak reduces, with concomitant improvement in motor symptoms. This has resulted in a new way of programming that does not rely on trial-and-error approaches or anatomical review. The ability to track LFPs in real-time means that patients can also log when they experience specific symptoms. The LFP data can be interrogated in clinic, and stimulation parameters or medications can be subsequently adjusted to improve clinical outcomes.
The Adapt-PD trial has taken this a step further and used LFP data to vary stimulation parameters in real time, increasing and decreasing stimulation amplitude in response to variation in beta peak power.50 The study has not been published yet, but early presentations at international conferences have suggested that using “adaptiveDBS” improved patient “ON” time by up to 1.4±3 hours compared to continuous DBS (p<0.0125).49,50 This may lead to a system that can vary treatment in a much more physiological manner than any other symptomatic treatment so far. Although oral therapies lead to pulsatile pharmacokinetics of levodopa and infusion therapies result in continuous levodopa pharmacokinetics, it has become increasingly recognized from LFP data that the network oscillations that reflect the akinetic-rigid symptoms of PD are neither fixed-interval pulsatile nor continuous and constant. They vary depending on diurnal rhythms, physical activity, and emotional state.51 This should be evident from the fact individuals with PD still experience OFF time and dyskinesias, albeit to a lesser degree, even on continuous infusion therapies. One small study effectively demonstrated that LFP activity can be influenced by emotional state. They documented that the beta frequency
band was suppressed over Christmas in four patients in the absence of any medication changes, demonstrating how LFP activity, and by inference bradykinesia and rigidity, can improve over festive periods.51,52 A system that can vary treatment of network oscillations in a more physiological manner has the potential to provide better control of motor complications (Figure 2).
NOVEL TREATMENTS FOR PARKINSONIAN TREMOR
There is increasing recognition that, as well as being a key diagnostic marker for PD, parkinsonian tremor is one of the most troublesome symptoms for many. Pasquini et al.53 highlighted that 96% of individuals with PD will experience tremor in the first 7 years of their condition. While classically this tremor may be considered predominantly a rest tremor, 85% of individuals will have a postural tremor and 79% will have a kinetic tremor.53 Recent patient survey data have revealed that 49% of individuals with PD feel that there is either no or minimal improvement in their tremor from current medications.54 Postural and kinetic tremors lead to higher functional impairment and are less likely to respond to medications.53 As discussed, DBS is an effective treatment for tremor; however, there is a group of individuals who may be unsuitable for invasive surgery, develop significant tremor at an advanced age, or be concerned about the risks inherent to a neurosurgical procedure. There are various pharmacological and non-pharmacological strategies currently in development. The authors would like to highlight two potential strategies that have gained recent interest: targeted botulinum toxin injections and MRIguided focused ultrasound.
Targeted Botulinum Toxin Injections
A double-blind, placebo-controlled crossover trial demonstrated that injections of botulinum toxin into arm muscles can improve clinical rating scores for rest, action, and postural tremor, alongside
Figure 2: A pictograph demonstrating the development of motor complications in Parkinson’s disease and the current and potential future management strategies.
Response to levodopa therapy in Parkinson's disease
Early PD Development of motor complications
Dyskinesia:
15% at 5 years
Clinical State
DBS Beta peak power
Beta peak power
Clinical State
Levodopa doses
56% at 10 years OFF:
54% at 6 years
100% at 10 years ON with Dyskinesia ON with Dyskinesia ON with Dyskinesia ON with Dyskinesia Non-continuous therapies
Management strategies for motor complications
therapies
Levodopa doses ON ON ON ON ON OFF OFF OFF OFF
Levodopa doses/ Adjuncts
Infusions with bolus/ Continuous DBS
Adaptive stimulation/ Levodopa doses
A) In early PD clinical symptoms and local field potential activity (beta peak power) are controlled with doses of oral levodopa (grey vertical arrows). B) When motor complications develop, the therapeutic window narrows, individuals with PD experience OFF periods and dyskinesia. Clinical symptoms correlate with a fluctuation in beta peak power. C) The doses of levodopa can be fractionated, and adjuncts such as monoamine oxidase inhibitors (MAOi) and catecholO-methyl transferase inhibitors (COMTi) added (blue vertical arrows), to improve time within the therapeutic window. D) Continuous infusions increase time within the therapeutic window. Fluctuations in clinical symptoms and concomitant beta peak power still occur but are managed by bolus doses of the same infusion. E) Potential role of adaptive DBS, stimulation is varied in response to beta peak power in real-time allowing adjustment of stimulation amplitude over seconds, thereby minimizing motor complications. Oral dopaminergic medications are still required but at lower doses (grey vertical arrows). Adaptive DBS will vary over the course of seconds to minutes, rather than hours as shown in the figure. The slower time course was used because it is more suitable for the visual representation.
DBS: deep brain stimulation; PD: Parkinson’s disease.
patient perception of improvement. In experienced hands, there were minimal side effects.55,56 Patient outcomes may be improved by using electromyography guidance, i.e., the “Yale technique” or sensor-based kinematics to aid selection of the appropriate muscles at effective doses.
MRI-Guided Focused Ultrasound
MRI-guided focused ultrasound (MRgFUS) is now increasingly available for the treatment of essential tremor (ET), and there is renewed interest in its potential role in PD. A randomized trial of unilateral MRgFUS thalamotomy (targeting the ventralis intermediate nucleus [Vim], a target typically considered in the management of ET) for individuals with tremor-dominant PD demonstrated that patients’ tremor scores improved by a median of 62%.57 Ablation of the Vim is expected to affect tremor significantly but it may not substantially improve bradykinesia or rigidity. Unilateral ablation of the subthalamic nucleus (STN; the same target as that often used in DBS for PD) has also been explored in open label studies and appears to have potential for providing a meaningful and sustained improvement in contralateral motor function.58 While early data suggest that the clinical improvement from MRgFUS thalamotomy (Vim) may not be sustained to the same degree as in ET, and the therapy is currently limited to unilateral or staged bilateral use, the therapy remains a potential option for surgically unsuitable patients with disabling tremor. Further research is needed before this can be considered an established therapy.
APPROACH TO CLINICAL TRIALS IN PARKINSON’S DISEASE
Alongside the increase in drug trials for PD, there is a growing recognition that current research trial design is cumbersome and expensive. An individual study drug takes, on average, 7.3 years to progress from Phase I studies to subsequent market authorization.59 Several initiatives have
been proposed to make the process more economical in terms of both time and cost. The PD multi-arm platform study60 is in late stage setup, with the goal of mimicking the success of the prostate cancer platform study “STAMPEDE”61 in creating a “‘platform” for a continuous study design with multiple trial arms so that multiple agents can be explored in parallel. There are also initiatives by longitudinal natural history studies, such as PPMI, to incorporate treatment trials into their study protocol, thereby providing the advantage of already having a substantial number of healthy controls and patients at different stages of PD enrolled, cutting down recruitment and investigation costs. The natural history of the disease from well-phenotyped cohorts can also be used as a surrogate (with caveats) for a placebo treatment arm in open-label extension studies, providing the pharmaceutical industry and the scientific community added confidence that longer studies for a specific agent may be worthwhile.19 The availability of SAA assays to identify CSF α-synuclein in prodromal PD has led to the recruitment of individuals with prodromal disorders, such as hyposmia and RBD, into large natural history studies such as PPMI. This offers a potential mechanism whereby trials of PD prevention can also be considered (Figure 1).62, 32 Finally, there is, in general, a lack of clinical trial data in non-Caucasian populations or low-income countries and this remains a very important issue to address in future clinical trials.
CONCLUSION
There have been many advances in treatments for PD over the last 5 years, which have allowed for a finer, personalized approach to symptomatic management of symptoms. On demand, dopaminergic medications can now be delivered via oral, nasal, subcutaneous, and sublingual routes. There are four different forms of continuous infusion available via subcutaneous or intra-jejunal route, all offering “on demand” bolus medications. In addition, advances in DBS devices have led to new methods
of modulating the abnormal network oscillations that are now recognized to be a key biomarker of bradykinesia. While there are still no commercially available diseasemodifying therapies, the presence of a new CSF biomarker of PD, α-synuclein, has allowed for more accurate diagnosis of both PD and prodromal disease. Innovations in
References
1. Postuma RB et al. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord. 2015;30(12):1591-601.
2. Feigin VL et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459-80.
3. Hacker ML et al. Deep brain stimulation in early-stage Parkinson disease: five-year outcomes. Neurology. 2020;95(4):e393-401.
4. McFarthing K et al. Parkinson’s disease drug therapies in the clinical trial pipeline: 2024 update. J Parkinsons Dis. 2024;14(5):899-912.
5. Fox SH et al. International Parkinson and movement disorder society evidencebased medicine review: update on treatments for the motor symptoms of Parkinson's disease. Mov Disord. 2018;33(8):1248-66.
6. Stewart CB et al. The longitudinal progression of autonomic dysfunction in Parkinson's disease: a 7-year study. Front Neurol. 2023;14:1155669. Corrected and republished from: Front Neurol. 2023;14:1218633.
7. Shi Y et al. Association of baseline depression and anxiety with longitudinal health outcomes in Parkinson's sisease. Mov Disord Clin Pract. 2024;11(9):1103-12.
8. Hemphill L et al. Synergistic associations of depressive symptoms and aging on cognitive decline in early Parkinson’s disease. Clin Park Relat Disord. 2023;8:100192.
9. Gandhi SE et al. Dopa responsiveness in Parkinson's Disease. Mov Disord Clin Pract. 2024;11(9):1113-24.
10. Hauser RA et al. Efficacy of istradefylline, an adenosine A2A receptor antagonist, as adjunctive therapy to levodopa in Parkinson's disease: a pooled analysis of 8 phase 2b/3 trials. J Parkinsons Dis. 2021;11(4):1663-75.
the way that the drug trials are conducted have the potential to increase the efficiency, whereby new medications can be investigated and may be well utilized to explore a new focus of treatment, preventing or at least prolonging the time to onset of PD.
11. LeWitt PA et al. Safety and efficacy of CVT-301 (levodopa inhalation powder) on motor function during off periods in patients with Parkinson's disease: a randomised, double-blind, placebocontrolled phase 3 trial. Lancet Neurol. 2019;18(2):145-54.
12. Olanow CW et al. Apomorphine sublingual film for off episodes in Parkinson's disease: a randomised, double-blind, placebo-controlled phase 3 study. Lancet Neurol. 2020;19(2):135-44.
13. Postuma RB et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study. Brain. 2019;142(3):744-59.
14. Heinzel S et al. Update of the MDS research criteria for prodromal Parkinson's disease. Mov Disord. 2019;34(10):1464-70.
15. Marek K et al. Evidence for alphasynuclein aggregation in older individuals with hyposmia: a crosssectional study. EBioMedicine. 2025;112:105567.
16. Parkinson Progression Marker Initiative. The Parkinson Progression Marker Initiative (PPMI). Prog Neurobiol. 2011;95(4):629-35.
17. Jan A et al. The prion-like spreading of alpha-synuclein in Parkinson's disease: update on models and hypotheses. Int J Mol Sci. 2021;22(15):8338.
18. Pagano G et al. Trial of prasinezumab in early-stage Parkinson’s disease. N Engl J Med. 2022;387(5):421-32.
19. Pagano G et al. Sustained effect of prasinezumab on Parkinson’s disease motor progression in the open-label extension of the PASADENA trial. Nat Med. 2024;30(12):3669-75.
20. Pagano G et al. Prasinezumab slows motor progression in rapidly progressing early-stage Parkinson’s disease. Nat Med. 2024;30(4):1096-103.
21. Kang UJ et al. Comparative study of cerebrospinal fluid α-synuclein seeding aggregation assays for diagnosis of Parkinson's disease.
Mov Disord. 2019;34(4):536-44.
22. Russo MJ et al. High diagnostic performance of independent alphasynuclein seed amplification assays for detection of early Parkinson's disease. Acta Neuropathol Commun. 2021;9(1):179.
23. Rossi M et al. Ultrasensitive RTQuIC assay with high sensitivity and specificity for Lewy body-associated synucleinopathies. Acta Neuropathol. 2020;140(1):49-62.
24. Grossauer A et al. α-Synuclein seed amplification assays in the diagnosis of synucleinopathies using cerebrospinal fluid—a systematic review and metaanalysis. Mov Disord Clin Pract. 2023;10(5):737-47.
25. Jack Jr CR et al. NIA-AA research framework: toward a biological definition of Alzheimer's disease. Alzheimers Dement. 2018;14(4):535-62.
26. Simuni T et al. A biological definition of neuronal α-synuclein disease: towards an integrated staging system for research. Lancet Neurol. 2024;23(2):178-90.
27. Höglinger GU et al. A biological classification of Parkinson's disease: the SynNeurGe research diagnostic criteria. Lancet Neurol. 2024;23(2):191-204.
28. Bargar C et al. Streamlined alphasynuclein RT-QuIC assay for various biospecimens in Parkinson's disease and dementia with Lewy bodies. Acta Neuropathol Commun. 2021;9(1):62.
29. Siderowf A et al. Assessment of heterogeneity among participants in the Parkinson's Progression Markers Initiative cohort using α-synuclein seed amplification: a cross-sectional study. Lancet Neurol. 2023;22(5):407-17.
30. Espay AJ et al. Revisiting protein aggregation as pathogenic in sporadic Parkinson and Alzheimer diseases. Neurology. 2019;92(7):329-37.
31. Espay AJ, McFarthing K. Alphasynuclein and the Parkinson's disease drug pipeline. Parkinsonism Relat
Disord. 2023;111:105432.
32. Westenberger A et al. Relevance of genetic testing in the gene-targeted trial era: the Rostock Parkinson’s disease study. Brain. 2024;147(8):2652-67.
33. Schneider SA, Alcalay RN. Neuropathology of genetic synucleinopathies with parkinsonism: review of the literature. Mov Disord. 2017;32(11):1504-23.
34. The Michael J. Fox Foundation for Parkinson’s Research. LRRK2 Investigative Therapeutics Exchange (LITE). Available at: https://www. michaeljfox.org/grant/lrrk2investigative-therapeutics-exchangelite. Last accessed: April 10, 2025.
35. Vijiaratnam N et al. Progress towards therapies for disease modification in Parkinson's disease. Lancet Neurol. 2021;20(7):559-72.
36. Kim HJ et al. Motor complications in Parkinson's disease: 13-year follow-up of the CamPaIGN cohort. Mov Disord. 2020;35(1):185-90.
37. Katzenschlager R et al. Apomorphine subcutaneous infusion in patients with Parkinson's disease with persistent motor fluctuations (TOLEDO): a multicentre, double-blind, randomised, placebo-controlled trial. Lancet Neurol. 2018;17(9):749-59.
38. Soileau MJ et al. Safety and efficacy of continuous subcutaneous foslevodopa-foscarbidopa in patients with advanced Parkinson's disease: a randomised, double-blind, activecontrolled, phase 3 trial. Lancet Neurol. 2022;21(12):1099-109.
39. Olanow CW et al. Continuous intrajejunal infusion of levodopa-carbidopa intestinal gel for patients with advanced Parkinson's disease: a randomised, controlled, double-blind, double-dummy study. Lancet Neurol. 2014;13(2):141-9.
40. Nyholm D, Jost WH. Levodopa–entacapone–carbidopa intestinal gel infusion in advanced Parkinson’s disease: real-world experience and practical guidance. Ther Adv Neurol Disord. 2022;15:17562864221108018.
41. Deuschl G et al. A randomized trial of deep-brain stimulation for Parkinson's disease. N Engl J Med.
2006;355(9):896-908.
42. deSouza RM et al. Timing of deep brain stimulation in Parkinson disease: a need for reappraisal? Ann Neurol. 2013;73(5):565-75.
43. Kleiner-Fisman G et al. Subthalamic nucleus deep brain stimulation: summary and meta-analysis of outcomes. Mov Disord. 2006;21 Suppl 14:S290-304.
44. Esper CD et al. Necessity and feasibility of remote tele-programming of deep brain stimulation systems in Parkinson's disease. Parkinsonism Relat Disord. 2022;96:38-42.
45. Herreras O. Local field potentials: myths and misunderstandings. Front Neural Circuits. 2016;10:101.
46. Neumann WJ et al. Subthalamic synchronized oscillatory activity correlates with motor impairment in patients with Parkinson's disease. Mov Disord. 2016;31(11):1748-51.
47. Barow E et al. Deep brain stimulation suppresses pallidal low frequency activity in patients with phasic dystonic movements. Brain. 2014;137(Pt 11):3012-24.
48. Mathiopoulou V et al. Modulation of subthalamic beta oscillations by movement, dopamine, and deep brain stimulation in Parkinson’s disease. NPJ Parkinson’s Dis. 2024;10(1):77.
49. Stanslaski S et al. Sensing data and methodology from the Adaptive DBS Algorithm for Personalized Therapy in Parkinson’s Disease (ADAPT-PD) clinical trial. NPJ Parkinson’s Dis. 2024;10(1):174.
50. Bronte-Stewart H et al. Chronic adaptive DBS provides similar “on” time with trend of improvement compared to continuous DBS in Parkinson’s disease and 98% of participants chose to remain on aDBS (S2.008). Neurology. 2024;102(17_supplement_1):2824.
51. van Rheede JJ et al. Diurnal modulation of subthalamic beta oscillatory power in Parkinson's disease patients during deep brain stimulation. NPJ Parkinson’s Dis. 2022;8(1):88.
52. Feldmann LK et al. Christmas-related reduction in beta activity in Parkinson's disease. Mov Disord. 2023;38(4):692-7.
53. Pasquini J et al. The clinical profile of tremor in Parkinson's disease. Mov Disord Clin Pract. 2023;10(10):1496-506.
54. Hauser RA et al. Burden of tremor in Parkinson's disease: a survey study. J Parkinson’s Dis. 2025;DOI:10.1177/1877 718X251329328.
55. Mittal SO et al. Botulinum toxin in Parkinson disease tremor: a randomized, double-blind, placebocontrolled study with a customized injection approach. Mayo Clin Proc. 2017;92(9):1359-67.
56. Mittal SO et al. Novel botulinum toxin injection protocols for Parkinson tremor and essential tremor - the Yale technique and sensor-based kinematics procedure for safe and effective treatment. Tremor Other Hyperkinet Mov (N Y). 2020;10:61.
57. Bond AE et al. Safety and efficacy of focused ultrasound thalamotomy for patients with medication-refractory, tremor-dominant Parkinson disease: a randomized clinical trial. JAMA Neurol. 2017;74(12):1412-18.
58. Martínez-Fernández R et al. Prospective long-term follow-up of focused ultrasound unilateral subthalamotomy for Parkinson disease. Neurology. 2023;100(13):e1395-405.
59. Möhrle JJ. How long does it take to develop a new drug? Lancet Reg Health Eur. 2024;43:100998.
60. Foltynie T et al. Towards a multi-arm multi-stage platform trial of disease modifying approaches in Parkinson’s disease. Brain. 2023;146(7):2717-22.
61. Medical Research Council. Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE). NCT00268476. https://clinicaltrials.gov/study/ NCT00268476.
62. Berg D et al. Path to Parkinson disease prevention. Neurology 2022;99(7_Supplement_1):76-83.
63. Parkinson's Progression Markers Initiative. Path to Prevention Platform Trial. Available at: https://www. ppmi-info.org/study-design/pathto-prevention-platform-trial. Last accessed: May 7, 2025.
MRI Markers and Vascular Cognitive Impairment: A Systematic Review of Randomized Controlled Trials from the Last 10 Years and Implications for Future Interventions
Authors: Pedro Henrique Rodrigues da Silva,1 Beatriz Araújo Cavendish,1
Renata Ferranti Leoni2
1. Departamento e Instituto de Psiquiatria, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, Brazil
2. Faculdade de Filosofia Ciências e Letras de Ribeirão Preto da Universidade de São Paulo, Ribeirão Preto, Brazil
*Correspondence to pedrojoanabrit@usp.br
Disclosure: da Silva is a recipient of the FAPESP grant 2022/03266–0. Cavendish is a recipient of the FAPESP grant 2021/10827-6. Leoni has received meeting support from the University of São Paulo. The authors have declared no conflicts of interest.
Acknowledgements da Silva contributed to the concept and design of the study, analysis, and interpretation of data, and drafting of a significant portion of the manuscript and figures. Cavendish contributed to manuscript drafting and review. Leoni contributed to the concept and design of the study, analysis, and interpretation of data, and manuscript review.
Received: 01.17.2025
Accepted: 04.22.2025
Keywords: MRI, randomized controlled trials (RCT), vascular cognitive impairment (VCI).
Citation: Neurol AMJ. 2025;2[1]:83-95. https://doi.org/10.33590/neurolamj/OTPI1708
Abstract
Vascular cognitive impairment (VCI) is characterized by cognitive deficits arising from cerebrovascular diseases, and ranks as one of the primary contributors to dementia, following Alzheimer's disease. Currently, there is no single treatment that universally addresses VCI. Accurate diagnosis relies heavily on MRI. We systematically reviewed randomized controlled trials from the past decade to identify gaps in the application of MRI in understanding therapeutic mechanisms in VCI, and to propose future research directions. We included eight studies focusing on various interventions, such as cognitive training, aerobic exercise, electroacupuncture, the Chinese therapy Dengzhan Shengmai, and the Naoxin’an capsule. Our findings highlighted significant heterogeneity in both MRI methods and cognitive assessments used across these studies. This variability complicates the comparison of results and may affect the overall understanding of how different interventions impact cognitive function. The authors also discussed the implications of their findings for future research, suggesting a need for standardized protocols and comprehensive methodologies to better assess the brain mechanisms underlying treatment efficacy in VCI.
Key Points
1. Vascular cognitive impairment (VCI) refers to cognitive deficits caused by cerebrovascular diseases and is one of the leading causes of dementia after Alzheimer's disease. MRI can be a crucial tool in randomized clinical trials to assess the mechanisms underlying treatment effectiveness in VCI.
2. A systematic review of randomized controlled trials from the past decade to identify gaps in the application of MRI for understanding therapeutic mechanisms in VCI and to propose future research directions.
3. Different interventions with varying underlying mechanisms can effectively mitigate the cognitive deficits associated with VCI. However, there is heterogeneity in both the MRI methods and cognitive assessments used across the included studies, which necessitates the implementation of standardized MRI protocols and cognitive evaluation to better assess the brain mechanisms underlying treatment efficacy in VCI.
INTRODUCTION
Vascular cognitive impairment (VCI) refers to cognitive deficits caused by cerebrovascular diseases and is one of the leading causes of dementia after Alzheimer’s disease.1 This impairment results from alterations in cerebral blood circulation, such as lesions in small and large vessels.2 VCI encompasses a range of presentations, from mild VCI, which involves subtle changes like slow information processing and difficulties in executive functions, to major VCI or vascular dementia, where deficits in at least one cognitive domain will compromise independence in daily activities, often resulting in dementia, which is associated with cerebrovascular diseases with evidence on neuroimaging, primarily through MRI.3 With an aging population and a lack of effective treatments, a dementia epidemic is expected, and it is estimated to affect 150 million people by 2050, at the cost of more than two trillion USD,4 imposing national plans and efforts to the establishment of effective therapeutic strategies.
The absence of a single, universally effective treatment for VCI is due to several factors, including the high heterogeneity of VCI in terms of underlying mechanisms and clinical presentation.5,6 It can result from different cerebrovascular processes, such as lacunar infarcts and white matter hyperintensities (WMH), among others, with each type of lesion potentially impacting cognitive functions in distinct ways, making
standardization of treatments complex. Another factor to consider is VCI’s generally progressive nature, which is often linked to multiple vascular risk factors such as hypertension, diabetes, and a sedentary lifestyle, indicating that treatment should address not only cognitive impairment but also underlying risk factors and cerebrovascular events that may worsen the condition.6 The frequent comorbidities of VCI with other neurodegenerative conditions, such as Alzheimer’s disease, should also be considered, as it can lead to mixed dementia, making it challenging to identify which pathology is primarily responsible for the symptoms and which should be the main focus of treatment.7 Brain imaging is critical to identify the nature and severity of vascular brain lesion types, including WMH, cortical and subcortical infarcts, lacunes of presumed vascular origin, microbleeds, and perivascular spaces, which are among the most established MRI markers of vascular brain lesions.8 Furthermore, the analysis of brain networks using functional MRI (fMRI) and diffusion tensor imaging has proven to be another vital element in understanding how these focal lesions relate to symptom heterogeneity through their impact on brain circuitry.9-16 In this context, neuroimaging techniques, especially MRI, and their markers can be crucial tools in randomized clinical trials (RCT) to assess the mechanisms underlying treatment effectiveness in VCI. They can enable the detailed diagnosis and characterization of patients, the monitoring
of the progression of markers and their association with clinical outcomes, the identification of early response markers, and the use of a multidimensional approach, combining structural and functional MRI findings with clinical outcomes to provide a more comprehensive view of the mechanisms underlying treatment efficacy.17-22 However, as previously mentioned, the complex presentation of VCI has limited the establishment of effective treatments,3,23 and the inconsistent correlation between MRI findings and clinical results, along with the lack of validated biomarkers and variability in MRI protocols across studies, reinforces the need to reassess the methodologies and MRI protocols used in clinical trials.
Therefore, this systematic review of RCTs conducted in the last 10 years aimed to identify gaps in the use of MRI to evaluate the mechanisms underlying therapeutic efficacy in VCI, and to propose a discussion on future perspectives for the development of more effective treatments, focusing on the validation of specific biomarkers and improving the integration between MRI and clinical outcomes.
METHODS
Review Protocol
This study followed a structured methodology to identify and evaluate relevant literature on MRI-based evaluations of interventions aimed at mitigating VCI. The research question was developed using the Population, Intervention, Comparison, and Outcome (PICO) framework.24 The population of interest consisted of patients with (VCI). The authors included any type of intervention, with comparisons between these two groups. The primary outcomes assessed were cognitive performance and neuroimaging markers obtained through MRI. The research question guiding the study was: “What are the MRI findings underlying the effects of interventions aiming to mitigate cognitive deficits in VCI?”
Eligibility Criteria
To ensure a comprehensive and systematic search, the authors used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.25 The databases searched included PubMed and Scopus. Two of the authors (Pedro Henrique Rodrigues da Silva and Renata Ferranti Leoni) independently screened the titles and abstracts to identify the eligible trials. Any disagreements were discussed with the coauthors and resolved through consensus.
The following key search terms were used: “vascular cognitive impairment”, “magnetic resonance imaging”, and “randomized controlled trial”. The authors focused on the broader term “vascular cognitive impairment”, because they aimed to capture a broader range of relevant literature that may address multiple forms of cognitive decline associated with cerebrovascular disease, including those represented by vascular dementia and VCI with dementia.16 In this way, they ensured that the search remained comprehensive without unnecessarily narrowing the focus to specific subcategories. The search was limited to studies published in English and within the last 10 years. The authors included articles published within the last decade, starting from 2014, as this period follows the publication of key references on MRI in cerebral small vessel disease, the most common cause of VCI.16 These include the position paper,26 which provided the STandards for ReportIng Vascular changes on nEuroimaging (STRIVE), and its recent update, STRIVE-2,27 which uses, as in the authors' review, 2014 as the starting point for literature searches. While focused on small vessel disease (SVD), they also provide information related to other vascular lesions, such as ischemic or haemorrhagic stroke, which can also contribute to VCI. This effort is important for clinical trials, because standardizing the definitions and imaging markers ensures consistency in participant selection, outcome measures, and interpretation of imaging findings across studies. Additionally, by applying consistent criteria across various pathologies associated with the development of VCI, researchers
can better differentiate between overlapping mechanisms, improve diagnostic accuracy, and identify shared or distinct imaging biomarkers. This not only strengthens the design and comparability of clinical trials across a spectrum of neurovascular conditions, but also facilitates more personalized and precise therapeutic strategies.
The authors exclusively focused on RCTs, as they provide the highest level of evidence for evaluating the efficacy of interventions. Articles were excluded if they met the following criteria: they were duplicates, there was a potential sample and analysis overlap, or they used other study designs rather than RCT.
Quality Assessment
Two researchers (PHRS and RFL) assessed the risk of bias and applicability of selected studies using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2).28 The tool comprises four key domains: patient selection, index test, reference standard, and flow and timing. Each domain contributes to an overall assessment of the risk of bias and applicability (except flow and timing) concerns, categorized as low, unclear, or high risk.
Data Extraction
After duplicate removal, two researchers (da Silva and Leoni) independently screened the results, considering titles and abstracts, and resolved conflicts with consensus when needed. The remaining articles were fully read by PHRS, who independently extracted eligible studies.
The following data were extracted: basic study data (authors’ last name and year of publication), VCI presentation form, intervention, control condition, sample size, MRI analysis performed, and cognitive and MRI findings.
RESULTS
Studies Screening
The flow diagram is shown in Figure 1. A total of 66 articles were retrieved based on the search strategy. Eleven duplicate records were removed. After reading the abstract and title, three articles were excluded because they were systematic reviews, leaving 52 for preliminary screening. The two raters disagreed on 19 articles, but all disagreements were discussed and resolved through consensus. Finally, after a thorough examination of the complete text, eight articles were included. The others were excluded because there was no VCI (n=15), no cognitive assessment (n=5), no intervention (n=4), no MRI assessment (n=4), use of a different study protocol (n=10), use of an animal model (n=1), or they involved other diseases (n=3).
Quality Assessment
Seven studies presented an overall low risk of bias, whereas one indicated some concerns (Figure 2). The main problems that were noted referred to the flow and timing domain, since no study reported the MRI acquisition interval between the start and end of treatments, nor did they report the blinding of the person responsible for performing the MRI analyses. In the patient selection domain, two studies presented some concerns due to the VCI presentation form, and two presented high concerns about applicability, also due to the VCI presentation form.
Characteristics of Included Studies
The essential characteristics of the eight studies are shown in Table 1. Regarding the VCI presentation form, they focused on distinct patient populations with varying risks of progression to vascular dementia, including MCI patients with SVD,29 mild subcortical ischemic VCI (without dementia),30,31 VCI due to subcortical ischemic SVD,32 subcortical VCI without dementia,33,34 and VCI without dementia.35,36 The interventions conducted in
Identification of studies via databases and registers
Records identified from:
• PubMed(n=37)
• Scopus (n=29)
• Registers (n=0)
Records Screened (n=55)
Records sought for retrieval (n=52)
Records removed before screening:
• Duplicate records removed (n=11)
• Records marked as ineligable by automation tools (n=0)
• Records removed for other reasons (n=0)
Records excluded (n=3)
Records not retrieved (n=0)
Records assessed for eligibility (n=52)
Records excluded:
• No vascular cognitive impairment (n=15)
• Study protocol (n=10)
• No cognitive assessments (n=5)
• No intervention (n=4)
• No MRI assessment (n=4)
• Only baseline results (n=2)
• Rats (n=1)
• Alzheimer's disease (n=1)
• Parkinson's disease (n=1)
• Schizophrenia (n=1)
Studies included in review (n=8)
Reports of included studies (n=8)
Figure 1: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the literature search.
Figure 2: Summary of the risk of bias and applicability concerns across the included studies.
Risk of bias domains
Pantoni L et al.,29 2017
ten Brinke LF et al.,30 2018
Hsu CL et al.,31 2018
Tang Y et al.,32 2019
Lu H et al.,33 2023
Lu H et al.,34 2020
Lin R et al.,35 2024
Li QG et al.,36 2024
Domains:
D1: Patient selection.
D2: Index test.
D3: Reference standard.
D4: Flow & timing.
Pantoni L et al.,29 2017
ten Brinke LF et al.,30 2018
Hsu CL et al.,31 2018
Tang Y et al.,32 2019
Lu H et al.,33 2023
Lu H et al.,34 2020
Lin R et al.,35 2024
Li QG et al.,36 2024
Domains:
D1: Patient selection.
D2: Index test.
D3: Reference standard.
Applicability Concerns
Judgement
Some concerns
the included studies encompassed cognitive training (n=3),29,32,36 aerobic training (n=2),30,31 electroacupuncture (n=1),35 the Chinese therapy Dengzhan Shengmai (n=1),34 and the herbal remedy Naoxin’an capsule (n=1).33 Only one study did not report significant, nor within or between groups, cognitive changes.30
MRI evaluation in the studies ranged from analysis of WMH and gray matter volumes, through functional connectivity analysis at rest or task, regional homogeneity (ReHo), amplitude of low-frequency fluctuation (ALFF), and fractional ALFF (fALFF), to analysis of white matter tracts with machine learning algorithms or through the application of network topological analysis. Several studies included multimodal approaches.32,33,35 MRI findings also showed great heterogeneity, with most studies reporting significant MRI changes and significant associations of MRI findings with cognitive outcomes after the interventions. Details of MRI findings and their associations with cognitive outcomes are described in Table 1
DISCUSSION
In this systematic review of RCTs conducted over the last decade, we observed that interventions aimed at mitigating the effects of VCI employed a diverse array of treatments that effectively reduced cognitive deficits. The findings indicate significant improvements in cognitive function and changes in MRI markers following these treatments, including cognitive training, physical exercises, and alternative therapies, highlighting relevant associations between cognitive enhancements and neurobiological alterations.
A critical aspect of understanding VCI is the diverse presentations it can manifest, ranging from mild cognitive impairment to severe dementia-like symptoms.3 This heterogeneity is a challenge when comparing outcomes across studies. Thus, exploring which interventions are most effective for each specific form of VCI and their corresponding
markers is essential. Cognitive training was shown to improve cognition and alter brain function in patients with mild cognitive impairment and SVD,29 VCI without dementia caused by subcortical ischemic small vessel disease,32 and VCI in general.36 The aerobic training intervention conducted by ten Brinke et al.30 failed to produce improvements in executive functions in patients with mild subcortical ischemic VCI without dementia. Additionally, no difference in cortical thickness was revealed after the intervention. However, the study by Hsu et al.31 involving patients with the same VCI presentation improved attention and brain function in the group who performed aerobic training. The traditional Chinese medicine therapy conducted by Lu et al.34 and Lu et al.,33 both in patients with subcortical VCI without dementia, were successful in improving cognition, with related brain microstructural and functional changes, respectively. Finally, electroacupuncture35 in patients with VCI without dementia improved cognition and brain functional connectivity.
Collectively, these studies provide evidence that different interventions can effectively mitigate the cognitive deficits associated with different VCI severities, although they do not clarify which ones are most effective for a given severity. Future research should focus on elucidating the interactions between different treatment modalities, their time course effects, and how best to personalize these interventions based on individual patient profiles, including the severity and specific type of VCI. Other considerations include comorbidities and risk factors that can influence intervention responses.3,7,20,23,37 Understanding the interplay between VCI and these comorbidities and risk factors is vital for developing comprehensive treatment strategies that address both cognitive deficits, and the broader health challenges patients face.38
Moreover, the variety of MRI approaches in the included studies is noteworthy, as they incorporate structural, microstructural, and functional analyses. Regarding
Table 1: Details of the eight studies included in the analysis.
Author (Year of publication)
Pantoni et al.,29 2017 MCI patients with SVD, no dementia
ten Brinke et al.,30 2018
Mild subcortical ischemic VCI, no dementia
Hsu et al.,31 2018 Mild subcortical ischemic VCI, no dementia
group (n=21) and standard care group (n=22) ReHo Analysis
group (n=14) and control group (n=14) Cortical thickness
AT group (n=10) and control group (n=11)
Task-based fMRI
Tang et al.,32 2019 VCI, no dementia caused by subcortical ischemic SVD Cognitive training
Training group (n=27) and control group (n=27)
Hippocampal GM volume, WM integrity, and functional connectivity
Lu et al.,34 2020
Subcortical VCI, no dementia Chinese medicine DZSM treatment DZSM group (n=45) and placebo group (n=37) WM connectivity and Machine Learning
Lu et al.,33 2023
Subcortical VCI, no dementia
Li et al.,36 2024 VCI, no dementia
NXA capsules group (n=50) and the ginkgo biloba capsules control group (n=50). GM density, WMH total volume, ALFF, fALFF, ReHo, and DC
Computerized cognitive training Training group (n=30) and control group (n=30)
Resting-state functional connectivity
Lin et al.35 2024 VCI, no dementia
group (n=70) and control group (n=70). VBM and resting-state functional connectivity
Table 1: Continued.
Author (Year of publication)
Pantoni et al.,29 2017
Cognitive findings
The APT-II program did not induce positive effects on functional status and quality of life. The APT-II group showed significant improvement in the Rey Auditory-Verbal Learning Test immediate recall.
ten Brinke et al.,30 2018 Any significant between- or within-group was found for the executive function domain evaluated by Stroop 3–2, TMT B-A, and DSST.
Hsu et al.,31 2018 The aerobic training group presented significantly improved flanker task reaction times.
Tang et al.,32 2019 The training group showed significant improvement in the MoCA compared to the control group.
Lu et al.,34 2020 The drug groups showed significantly improved performance in ADAS-cog scores.
Lu et al.,33 2023
Compared to the control group, the NXA group significantly improved overall cognitive ability, memory, and executive function performance after treatment.
Li et al.,36 2024 In the training group, significant improvements were found in the MoCA and BNT after Week 7, but not after Month 6.
Lin et al.35 2024 EA intervention increased the MoCA and improved the neutral and consistency response of the STROOP test.
MRI findings and associations with cognitive findings
The cerebellar areas’ ReHo changes were significantly greater in the APT-II group compared to the standard care group (p<0.05).
There were no significant overall cortical thickness differences when comparing the groups after treatment. Maintenance of cortical thickness was associated with improved processing speed performance (p=0.014). Change in DSST performance was positively associated with change in right superior frontal thickness (p=0.002).
The AT group presented reduced activation in the left lateral occipital cortex (p <0.03) and right superior temporal gyrus (p=0.03), associated with improved flanker task performance (p<0.05). No significant correlations were found between conflict resolution and percent signal change in the areas of interest.
No significant changes in hippocampus volume and WM integrity were observed. There was a significant increase in functional connectivity between the left dorsolateral prefrontal cortex and medial prefrontal cortex (p<0.05), which significantly and positively correlated with MoCA changes (p 0.017).
It was observed that increased streamlines connected the left thalamus and right hippocampus in the DZSM group (p<0.001 uncorrected), and the lower nodal efficiency of the right olfactory was associated with a slower decline in general cognition (p=0.048). Support vector machine classification analyses also indicated significant alterations in the WM network of the DZSM group after the treatment (accuracy: 68.18%).
Significant brain function changes evaluated with DC and fALFF, in addition to structural changes in GM density, were observed in the NXA group after treatment (p<0.001 at the voxel level combined with p<0.05 at the cluster level, GRF-corrected). No significant change in total WMH was observed (p>0.05). It was also observed that the changes in brain functions were related to the improvement in executive function in the NXA group (p<0.05).
Significant increased connectivity between the DMN and SMN (p=0.01), and between the LN and ECN (p<0.001) were observed in the training group at month 6. Additionally, it was observed that significant connectivity changes within LN regions (p=0.049), and these changes were associated with improvements in neuropsychological measures (p<0.05).
The EA group presented a GM volume increase after treatment (p<0.05). The functional connectivity of the DMN was significantly modulated by the EA intervention. Furthermore, connectivity between the posterior cingulate gyrus with the left middle frontal gyrus and the right superior temporal gyrus was associated with cognitive function (p<0.05).
ADAS-Cog: Alzheimer's Disease Assessment Scale-Cognitive subscale; ALFF: amplitude of low-frequency fluctuation; APT-II: Attention Process Training-II; AT: aerobic training; BNT: Boston Naming Test; DC: degree centrality; DMN: default mode network; DSST: Digit Symbol Substitution Test; DZSM: Dengzhan Shengmai; EA: electroacupuncture; ECN: executive control network; fALFF: fractional ALFF; fMRI: functional magnetic resonance imaging; GM: gray matter; GRF: Gaussian random field; LN: language network; MCI: mild cognitive impairment; MoCA: Montreal Cognitive Assessment; NXA: Naoxin’an capsule; ReHo: regional homogeneity; SMN: somatomotor network; SVD: small vessel disease; TMT: Trail Making Test; VBM: voxel-based morphometry; VCI: vascular cognitive impairment; WM: white matter; WMH: white matter hyperintensities.
structural findings, a significant increase in gray matter volume was found after treatment with Naoxin’an capsules33 and electroacupuncture,35 although changes in cortical thickness were not reported after aerobic training.30 Assessment of structural connectivity indicated an increased streamline between the thalamus and hippocampus after Chinese medicine Dengzhan Shengmai treatment,34 with significant associations regarding cognitive outcome. Most studies reported functional changes, including greater ReHo changes after attention process trainingII intervention;29reduced activation in the occipital cortex and superior temporal gyrus, associated with improved flanker task performance after aerobic training;31 and increased functional connectivity between the left dorsolateral prefrontal cortex and medial prefrontal cortex, which was significantly and positively correlated with Montreal Cognitive Assessment (MoCA) changes.32 They also reported increased functional connectivity between the default mode network and somatomotor network, and between the language network and executive control network after computerized cognitive training;36 increased fALFF in precentral and superior parietal gyrus, while reduced fALFF was observed in parahippocampal and inferior temporal gyrus;33 and significant modulation of the default mode network after electroacupuncture therapy.35 Such findings corroborate the importance of multimodal neuroimaging analyses.
Some studies also explored multimodal protocols,32,33,35 emphasizing functional findings, suggesting that such an approach may be the most appropriate to detect the effects of treatments. However, the wide range of possibilities involving functional data analysis, such as task-based, resting functional connectivity, ReHo, ALFF, and fALFF, among others, can make it challenging to summarize the results. Therefore, future studies may benefit from combined fMRI analytic methods and neuropsychological assessments, with the aim of observing an
overlap of findings that ultimately indicates a robust marker.39 Therefore, the multimodal MRI approach must be analyzed in an integrated and standardized approach, as proposed by the Harmonizing Brain Imaging Methods for Vascular Contributions to Neurodegeneration (HARNESS) initiative,40 and built on the work of STRIVE and the Biomarkers for Vascular Contributions to Cognitive Impairment and Dementia (MarkVCID) consortium,21 ultimately contributing to a better understanding of brain alterations.11,41 It is noteworthy that the authors included articles published after the STRIVE-1 guidelines publication. This international effort is key to ensuring consistency in how SVD and other VCIrelated conditions are defined and assessed in research. Standardized imaging criteria improve participant selection, outcome measurement, and help distinguish overlapping mechanisms, leading to more accurate diagnoses and the clearer identification of biomarkers. However, none of the included studies reported the use of guidelines such as STRIVE regarding the use of neuroimaging, making it difficult to synthesize the findings and compare them. This issue is raised as a limitation by the most recent study included, which mentions the need to improve the diagnosis of SVD as a cause of dementia using standardized MRI.35 The authors note the increase in sample size over the years, with all included studies consisting of at least 30 patients in each intervention arm as of 2020. Bigger sample sizes produce more reliable results, increasing the statistical power to identify significant effects.42,43 However, the authors note that challenges regarding the acquisition of neuroimaging data remain present: the oldest study included was considered a pilot study, once a subgroup of the included patients underwent fMRI acquisition,29 while the newest study included, consisting of 70 patients per intervention group, managed to include only 20 patients per group in the neuroimaging analysis.35 In this context, pre-study power calculations that specify effect sizes are required for future trials.43 Another reported limitation refers to the
liberal cluster threshold applied,31 justified based on the use of the same threshold in previous studies, but which can inflate false positives. This is a still common practice, as reported in a survey of fMRI studies published in 2017, which indicated that almost 53% of the studies applied more liberal thresholds for the cluster-defining primary threshold, mitigating reproducibility.44 Other challenges that were noted include: the prolonged acquisition time of longer MRI protocols, which may pose difficulties for patients with more severe cognitive impairment;30 the thresholding strategy in matrices in light of newer methods;33 and the focus on a single brain network, which may obscure significant findings in other critical networks.35 Furthermore, there is the mention of improving the diagnosis of SVD as a cause of dementia using standardized MRI,35 as discussed previously.
Furthermore, studies may benefit from incorporating other advanced MRI techniques not considered in the studies included in this review, such as arterial spin labeling,45 cerebrovascular reactivity MRI,46 and intravoxel incoherent motion.47 These methodologies can provide insights into cerebral blood flow and microstructural changes that may be associated with treatment effects.48-50 By integrating these advanced imaging approaches with the multimodal traditional ones and neuropsychological assessments, future studies can aid in uncovering the underlying neurobiological therapeutic mechanisms and their associations with cognitive outcomes.20 Another source of heterogeneity between the included studies was the cognitive assessments. Establishing standardized evaluation criteria is crucial in enhancing the comparability of research efforts. Such standardization would facilitate the identification of effective interventions and ensure that cognitive outcomes can be meaningfully compared, regardless of the VCI presentation or the type of intervention employed. To address this challenge, researchers have developed consensus guidelines aligned with the Fifth Edition of the Diagnostic and Statistical
Manual of Mental Disorders (DSM-5) for cognitive and neuroimaging assessments, and standardized terminology for evaluating patients with VCI. A notable contribution is the second phase of the VICCCS-2.3 This international consensus is based on the Delphi methodology, and builds upon the foundational work of VICCCS-1 for establishing severity criteria and subtypes of VCI associated with different etiologies. In its second phase, VICCCS-2 delineates the core cognitive domains to be assessed during VCI evaluations and recommends specific tests for evaluating cognitive dysfunctions related to the disorder. Additionally, the guideline provides imaging recommendations, identifying key neuroimaging protocols and markers considered reliable and robust for characterizing the underlying brain pathology in VCI. Therefore, it is strongly recommended that future studies adopt these guidelines as the foundation for their cognitive and neuroimaging assessment protocols. Doing so will ensure the use of consistent metrics, facilitate comparability between different types of interventions, and account for the heterogeneity of VCI presentations.
CONCLUSION
In conclusion, this systematic review highlights the efficacy of cognitive training, aerobic training, traditional Chinese medicine therapy, and electroacupuncture in altering brain structure and function, and mitigating the cognitive deficits associated with VCI. It also underscores the complexity involved in evaluating and treating this condition. Future research should focus on exploring the different VCI manifestations, standardized multimodal MRI and neuropsychological assessments, and interactions with comorbidities, risk factors, cognitive dysfunction, and MRI markers. Additionally, utilizing other advanced MRI techniques can be helpful in advancing our understanding of VCI and treatment underlying mechanisms, leading to more targeted and effective treatment strategies for individuals affected by this multifaceted condition.
References
1. Smith EE. Clinical presentations and epidemiology of vascular dementia. Clin Sci (Lond). 2017;131(11):1059-68.
2. GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7(2):e105-25.
3. Skrobot OA et al. Progress toward standardized diagnosis of vascular cognitive impairment: Guidelines from the Vascular Impairment of Cognition Classification Consensus Study. Alzheimers Dement. 2018;14(3):280-92.
4. Velandia PP et al. Global and regional spending on dementia care from 2000-2019 and expected future health spending scenarios from 2020-2050: An economic modelling exercise. EClinicalMedicine. 2022;45:101337.
5. Biessels GJ. Diagnosis and treatment of vascular damage in dementia. Biochim Biophys Acta. 2016;1862(5):869-77.
6. Biesbroek JM, Biessels GJ. Diagnosing vascular cognitive impairment: current challenges and future perspectives. Int J Stroke. 2023;18(1):36-43.
7. Schneider JA, Bennett DA. Where vascular meets neurodegenerative disease. Stroke. 2010;41(Suppl 10):S144-6.
8. Clancy U et al. Imaging biomarkers of VCI: a focused update. Stroke. 2024;55(4):791-800.
9. Schulz M et al. Functional connectivity changes in cerebral small vessel disease - a systematic review of the resting-state MRI literature. BMC Med. 2021;19(1):103.
10. Ter Telgte A et al. Cerebral small vessel disease: from a focal to a global perspective. Nat Rev Neurol. 2018;14(7):387–98.
11. Zhang Q et al. Multimodal magnetic resonance imaging on brain structure and function changes in vascular cognitive impairment without dementia. Front Aging Neurosci. 2023;15:1278390.
12. da Silva PHR et al. Contrast agent-free state-of-the-art magnetic resonance imaging on cerebral small vessel disease - Part 2: diffusion tensor imaging and functional magnetic resonance imaging. NMR Biomed. 2022;35(8):e4743.
13. Du J, Xu Q. Neuroimaging studies on cognitive impairment due to cerebral
small vessel disease. Stroke Vasc Neurol. 2019;4(2):99-101.
14. Elahi FM et al. Cerebral small vessel disease-related dementia: more questions than answers. Stroke. 2023;54(3):648-60.
15. Pan C et al. Incremental value of stroke-induced structural disconnection in predicting global cognitive impairment after stroke. Stroke. 2023;54(5): 1257-67.
16. Dichgans M, Leys D. Vascular cognitive impairment. Circ Res. 2017;120(3):573-91.
17. Tap L et al. New horizons in cognitive and functional impairment as a consequence of cerebral small vessel disease. Age Ageing. 2023;52(8):afad148.
18. Ye Q, Bai F. Contribution of diffusion, perfusion and functional MRI to the disconnection hypothesis in subcortical vascular cognitive impairment. Stroke Vasc Neurol. 2018;3(3):131-9.
19. Wei Z et al. A mini-review on functional magnetic resonance imaging on brain structure of vascular cognitive impairment. Front Neurol. 2023;14:1249147.
20. Iadecola C et al. Vascular cognitive impairment and dementia: JACC scientific expert panel. J Am Coll Cardiol. 2019;73(25):3326-44.
21. Lu H et al.; MarkVCID Consortium. MarkVCID cerebral small vessel consortium: II. Neuroimaging protocols. Alzheimers Dement. 2021;17(4):716-25.
22. Silva NCBS et al. Vascular cognitive impairment and dementia: An early career researcher perspective. Alzheimers Dement (Amst). 2022;14(1):e12310.
23. Ji L, Zhang J. Complex interactions and composite burden of risk factors in vascular cognitive impairment. J Neurol Sci. 2025;468:123367.
24. Schardt C et al. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7:16.
25. Knobloch K et al. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J Craniomaxillofac Surg. 2011;39(2):91–2.
26. Wardlaw JM et al.; STandards for ReportIng Vascular changes on nEuroimaging (STRIVE v1). Neuroimaging standards for research into small vessel disease and its contribution to ageing and
neurodegeneration. Lancet Neurol. 2013;12(8):822-38.
27. Duering M et al. Neuroimaging standards for research into small vessel disease-advances since 2013. Lancet Neurol. 2023;22(7):602-18.
28. Whiting PF et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-36.
29. Pantoni L et al. Effect of attention training in mild cognitive impairment patients with subcortical vascular changes: the RehAtt study. J Alzheimers Dis. 2017;60(2):615-24.
30. ten Brinke LF et al. Increased aerobic fitness is associated with cortical thickness in older adults with mild vascular cognitive impairment. Journal of Cognitive Enhancement. 2018;2:157-69.
31. Hsu CL et al. Aerobic exercise promotes executive functions and impacts functional neural activity among older adults with vascular cognitive impairment. Br J Sports Med. 2018;52(3):184-91.
32. Tang Y et al. The effects of 7-week cognitive training in patients with vascular cognitive impairment, no dementia (the Cog-VACCINE study): a randomized controlled trial. Alzheimers Dement. 2019;15(5):605-14.
33. Lu H et al. Naoxin’an capsules protect brain function and structure in patients with vascular cognitive impairment. Front Pharmacol. 2023;14:1129125.
34. Lu H et al. Network topology and machine learning analyses reveal microstructural white matter changes underlying Chinese medicine Dengzhan Shengmai treatment on patients with vascular cognitive impairment. Pharmacol Res. 2020;156:104773.
35. Lin R et al. Electroacupuncture improves vascular cognitive impairment no dementia: a randomized clinical trial. J Stroke Cerebrovasc Dis. 2024;33(8):107788.
36. Li QG et al. Effects of computerized cognitive training on functional brain networks in patients with vascular cognitive impairment and no dementia. CNS Neurosci Ther. 2024;30(6):e14779.
37. Zhu Z, Liao H. Impact of cognitive impairment and systemic vascular comorbidities on risk of all-cause and cardiovascular mortality: National Health and Nutrition Examination Survey 1999 to 2002. Int J Cardiol. 2020;300:255-61.
38. Badji A et al. Vascular cognitive impairment - past, present, and future challenges. Ageing Res Rev. 2023;90:102042.
39. Wang R et al. The application of rs-fMRI in vascular cognitive impairment. Front Neurol. 2020;11:951.
40. Smith EE et al. Harmonizing brain magnetic resonance imaging methods for vascular contributions to neurodegeneration. Alzheimers Dement (Amst). 2019;11:191–204.
41. Liu Q, Zhang X. Multimodality neuroimaging in vascular mild cognitive impairment: A narrative review of current evidence. Front Aging Neurosci. 2023;15:1073039.
42. Marek S et al. Reproducible brain-wide association studies
require thousands of individuals. Nature. 2022;603(7902):654-60.
43. Szucs D, Ioannidis JP. Sample size evolution in neuroimaging research: An evaluation of highly-cited studies (1990-2012) and of latest practices (2017-2018) in high-impact journals. Neuroimage. 2020;221:117164.
44. Yeung AWK. An updated survey on statistical thresholding and sample size of fMRI studies. Front Hum Neurosci. 2018;12:16.
45. Petcharunpaisan S et al. Arterial spin labeling in neuroimaging. World J Radiol. 2010;2(10):384-98.
46. Liu P et al. Cerebrovascular reactivity (CVR) MRI with CO2 challenge: A technical review. Neuroimage. 2019;187:104-15.
47. Paschoal AM et al. Intravoxel incoherent motion MRI in neurological and cerebrovascular diseases. Neuroimage Clin. 2018;20:705-14.
48. Huang D et al. Recent advances in arterial spin labeling perfusion MRI in patients with vascular cognitive impairment. J Cereb Blood Flow Metab. 2023;43(2):173-84.
49. Sleight E et al. Cerebrovascular reactivity in patients with small vessel disease: A cross-sectional study. Stroke. 2023;54(11):2776-84.
50. Paschoal AM et al. Contrast-agent-free state-of-the-art MRI on cerebral small vessel disease-part 1. ASL, IVIM, and CVR. NMR Biomed. 2022;35(8):e4742.
Seizure Disorders: Clinical Insights and Review of the Major Clinical Topics Impacting the
Reproductive Lifespan
Author: Joel Oster1
1. Tufts University School of Medicine, Boston, Massachusetts, USA *Correspondence to joel.oster@tuftsmedicine.org
Disclosure: The author has declared no conflicts of interest.
Acknowledgements The author would like to dedicate this work to his patients, their children, and families who have entrusted him with their neurological care during pregnancy. Words cannot express what an honor and privilege this has represented. He is also appreciative of the mentors and colleagues who have been instrumental in his education and ongoing understanding of the nuances of this important field within clinical medicine and epileptology.
Received: 04.01.25
Accepted: 04.28.25
Keywords: Bone health, oral contraception, pregnancy, reproductive lifespan, seizure disorder, teratogenicity, women with epilepsy.
Citation: Neurol AMJ. 2025;2[1]:96-111. https://doi.org/10.33590/neurolamj/YDNP3298.
Abstract
The medical management of women with epilepsy is an evolving specialization within neurology and epileptology. This article highlights the major topics and key challenges, providing clinical insights regarding best current practices alongside associated clinical rationales and recommendations within this emerging field. Additionally, this article identifies opportunities for further study and outlines current gaps and limitations in understanding.
Key Points
1. The comprehensive evaluation and management of women with epilepsy is an evolving specialization within neurology and epileptology that clinically assesses issues that impact the entire reproductive lifespan. Such adjunctive management assists patients planning for and going through pregnancy in collaboration with other healthcare providers.
2. This article highlights major clinical topics and summarizes the current understanding of best practices and recommendations relevant to specialized consultations. While it emphasizes pregnancy-related care, it also covers other issues that affect patients throughout their lifespan.
3. Several important issues remain unresolved, and this article outlines these gaps, emphasizing the need for further research to optimize the adjunctive role of emerging therapies and future developments.
INTRODUCTION AND OVERVIEW OF SEIZURES
This work highlights seizure disorders and summarizes the major topics, key challenges, and clinical insights into how seizure disorders impact women across the reproductive lifespan. It highlights and summarizes the current understandings of many topics such as hormonal influences on the menstrual cycle, catamenial epilepsy (CE), and the impact of seizure disorders on contraception and fertility, alongside issues surrounding bone health and menopause in patients with seizure disorders and sexual dysfunction, and the current understanding of genetic and inheritance risks of seizure disorders. Additionally, the article highlights the evolving practice of pre-pregnancy planning and issues surrounding pregnancy, including anti-seizure medication (ASM) management, teratogenicity, and postpartum care, including breastfeeding and ASM tapering. This review notes some issues affecting males, concluding with an overview of some potential future directions, gaps in the literature, and where further study might be indicated.
WHAT IS A SEIZURE?
A seizure is a pathological disturbance of the normal or baseline electrocorticography or electrical rhythm of the brain that may result in abnormal clinical manifestations, although some seizures may be subclinical without readily observable signs.1-4 The location of the seizure discharges may cause motor signs and clinical manifestations, depending on what cortico-functional anatomy or networking is activated, and signs and symptoms depend on the particular anatomical localization, spread, and termination of such abnormal electrical activities within specific brain regions.5,6 Seizures that occur in response to provocative factors, for example, metabolic derangements, may not be indicative of epilepsy, which refers to a condition where there are continuous risks of unprovoked seizures. In contrast, a seizure occurring
in the appropriate physiological context may be expected and not pathological, whereas epilepsy involves a persistently increased probability of seizures.1-6 Seizures, and especially uncontrolled or repetitive seizures, may result from and alter brain function and cortical functional anatomy over time, potentially triggering seizures in other brain regions through a process known as kindling.7-10 Seizure disorders can significantly impact neurocognition and quality of life, both due to the seizures themselves and associated treatments.11 Seizures may be associated with injury, loss of independence, and decreased self-esteem. They have also been linked to mood disorders, sudden unexplained death in epilepsy, and other injuries, especially when poorly controlled.12,13 The major etiologies of seizures include idiopathic ones, or unknown origins, which account for approximately two-thirds of cases. Other etiologies of epilepsy include syndromes such as mesial temporal sclerosis, head trauma, intracranial tumors, strokes, hemorrhages, neurovascular lesions, neuronal migration disorders, metabolic abnormalities, genetic causes, and any other condition that disrupts functional cortical anatomy, thereby chronically lowering the seizure threshold.14-20
How the relevant issues concerning women and the reproductive lifespan impact and influence the occurrence of seizures and vice versa will be reviewed within the framework of the various subtopics that follow in this review.
HORMONAL INFLUENCES AND THE MENSTRUAL CYCLE
Both estrogen and progesterone levels exert hormonal control on the menstrual cycle, and the relative balance of estrogen to progesterone is considered the key factor.21 Ovulation is caused by a relative surge in estrogen, and for menstruation to occur, this surge must be followed by progesterone levels falling lower than those of estrogen.21 During anovulatory cycles, in which more seizures might occur, estrogen levels remain relatively high compared to levels
of progesterone.21-23 Higher estrogen or an increased estrogen-to-progesterone (E/P) ratio can potentiate glutamate receptors, leading to increased neuronal excitability and a higher risk of seizures. In contrast, a higher progesterone-to-estrogen ratio may facilitate gamma-aminobutyric acid (GABA) and chloride receptors, which have inhibitory effects on seizure activity.22,23
Estrogens are thought to be epileptogenic through several mechanisms, including those noted above, as well as their effects on the cycling of GABAA and GABAB receptors.21-23 Estrogen and progesterone ratios are also linked to effects mediated by calcium and chloride influx at GABAA receptors. These hormones modulate hippocampal glutamate receptors with estrogens acting as agonists, while estrogens may also increase both dendritic arborization and sprouting, and excitability in such neuronal networks, causing the CA1 region of the hippocampus to be more susceptible to glutamate-induced excitation.21-23 Progesterone is generally thought to be protective, as noted above, with promotion of enhanced synthesis of GABAA and GABAB receptors promoting increased chloride influx, potentially reducing glutaminergic activity.21-23
During puberty and menarche, it is common to experience the onset or worsening of seizures due to a relatively increased E/P ratio. Hormone replacement may have corresponding effects, generally increasing seizure frequency when the E/P ratio is high, and decreasing seizures when the ratio is lower, according to the literature.21-23
Self-reported sexual dysfunction is a common complaint, as approximately 40% of people with epilepsy report complaints including decreased sexual desire, increased dysmenorrhea, increased anxiety and impaired social functioning, and negative effects on self-esteem.23 These issues are related to seizure frequency, drug exposure, central nervous system effects or dysfunction, and altered impacts on central molecular substrates such as serotonin and
prolactin. The levels of these substrates may be reduced and influenced by ASMs.22-24
Birth rates in general are reduced in women with epilepsy due to an increased incidence of irregular menses and anovulatory cycles. An estimated 25–40% of menstrual cycles in women with epilepsy may be anovulatory, compared to about 10% in women without epilepsy.22-24 Additionally, there is an increased incidence of polycystic ovaries and reproductive endocrine disorders in women with epilepsy, with some effects potentially due to the ASMs. For example, enzymeinducing ASMs might reduce estradiol, have effects on androgens, and contribute to complex effects on steroid metabolism.22-24
Polycystic ovaries have been noted in approximately 15% of women without epilepsy, but occur in approximately 30% of women with epilepsy, especially those who are taking /valproate. 22-25 However, not all women with polycystic ovaries exhibit polycystic ovarian syndrome, a condition associated with an abnormality in insulin receptors leading to insulin resistance, obesity, acne, hirsutism, elevated luteinizing hormone, abnormal effects on androgens, abnormal lipids, and anovulation.22-25 The consequences of polycystic ovarian syndrome include infertility, dyslipidemia, diabetes mellitus, and endometrial cancer.25
In rare cases, hormonal effects, predominantly estrogen or progesterone ratio increases, might enhance the growth of an arteriovenous malformation or make such lesions symptomatic due to growth mediated at the receptor level. This stems from impacts on the E/P ratios, angiogenesis or blood flow effects, including volume of distribution, and renal and liver metabolism of these hormones.22-26
A Brief Summation of Hormonal Influences on the Occurrence of Seizures
• Estrogen or increased E/P ratio: increased seizures due to activation of glutaminergic mechanisms, which are excitatory.
• Progesterone or decreased E/P ratio: decreased seizures due to the modulation of GABA receptors, which are inhibitory.
• Estrogen has effects on the promotion of kindling, impacting the modulation of hippocampal CA1 pyramidal cells and increasing sensitivity to excitatory input.
A Brief Summation of Seizure Disorders and Sexual Functioning
• Decreased sexual desire: increased dysmenorrhea with anovulatory cycles and impact on gonadotropin-releasing hormone (GnRH) and association with early menopause.
• Increased anxiety.
• Impaired social functioning with negative effects on self-esteem.
• Association with polycystic ovary syndrome.
• Lower birth rate in males, as well as decreased libido and testosterone, and impaired spermatozoa; however, this could be due to confounding issues of medications.
CATAMENIAL EPILEPSY AND HORMONAL TREATMENT STRATEGIES FOR EPILEPSY IN WOMEN
CE occurs in up to approximately 70% of women with epilepsy and is defined in the current literature as seizures that occur at up to twice the baseline frequency during specific phases of the menstrual cycle. Due to the previously noted hormonal influences, CE is thought to result from elevated estrogen levels or an increased E/P ratio, which promote glutamatergic excitation, facilitate kindling, and lower the seizure threshold. In contrast, progesterone has anticonvulsant properties, enhancing allosteric modulation of GABA
receptors.21,22,27-29 In patients with CE, there may be either regular or irregular menstrual cycles, and seizures may occur around ovulation, just prior to menses or within approximately 3 days before to 3 days after ovulation. There is a significant association with anovulatory cycles (approximately 35% of patients with epilepsy as opposed to about 8% of controls).27-31 Stress, sleep deprivation, and reduced serum concentration of ASMs from non-compliance may enhance the occurrence of catamenial seizures.27-31
The mainstay of treatment of patients with irregular menses is intramuscular (IM) medroxyprogesterone or oral contraceptive pills (OCP) with withdrawal weeks.27-31
Seizures in women with epilepsy typically occur just before or during menstruation, when there is an increase in the E/P ratio or a drop in progesterone. Seizures are also more likely to occur mid-cycle during ovulation, when estrogen levels surge. In anovulatory cycles, seizures tend to occur more frequently during the second half of the menstrual cycle.27-31
Progesterone can be used as a mainstay of treatment, particularly in patients with catamenial seizures and regular menstrual cycles. It is typically administered as 100–200 mg lozenges or capsules up to three times a day during Days 14–25 of the menstrual cycle, with withdrawal occurring on Days 26–28. This regimen targets the luteal phase of the menstrual cycle, which includes the peri-ovulatory period.27 Side effects may include weight gain, acne, breast tenderness, irritability, and weight gain, and such treatment may induce perimenopause or menopause in some patients.27-31
The most specific treatment for patients is based on identifying the specific patterns of seizure occurrences that might occur with the menstrual cycle. Herzog et al.29 proposed three designations, including a C1 pattern, which is perimenstrual, C2, periovulatory, and C3, which is associated with an inadequate luteal phase. The C1 pattern involves seizures that occur from Days 0–3 of the menstrual cycle, prior to the ovarian follicular phase.29-31
The C2 pattern of CE involves seizures that occur from approximately Days 10–14, or the pre- or periovulatory phase, of the menstrual cycle.29-31 The C3 pattern occurs subsequently to the C2 designation at the latter stages of the periovulatory phase, and extends through the luteal phase and menstrual phases, while the C3 pattern is highly associated with anovulation.29-31 Treatment of patients with regular cycles includes natural progesterone lozenges during the luteal phase (from approximately Days 14–25).29-31 The treatment protocols for patients with irregular menses (C2 and C3 patterns, or failed treatment with progesterone lozenges during the luteal phase of the C1 type) include increasing baseline ASMs for several days, using or adding benzodiazepines, clobazam, or implementing acetazolamide for a number of days during the menstrual cycle.29-31
CONTRACEPTION AND FERTILITY
ASMs may be affected by OCPs and vice versa.27-31 The effectiveness of the OCPs may be significantly reduced, especially those that are metabolized by the cytochrome p450 system and impacted by ASMs.27-31ASMs may cause reduced binding of OCPs to receptors and may enhance metabolism of OCPs, making the OCPs less effective.27-31 Subdermal or progesterone levels may fall due to enhanced metabolism, which can result in mid-cycle spotting and an increased risk of pregnancy. Low-dose OCPs containing approximately 30–33 mcg of estrogen, with around 50 mcg of estrogen, may help mitigate these effects.27-31 Knowledge about such interactions is critical for the optimal management of these patients.
Current standards indicate that for patients on enzyme-inducing agents, the first line of contraception would be depot medroxyprogesterone acetate 150 mg, administered with a dosing interval of 10–12 weeks. The second-line option would be an intrauterine device that is either copper-based or progestin-based.27-31 It is noteworthy that for emergency contraception, levonorgestrel
might require a second dose due to metabolic effects from the enzyme-inducing ASMs.27-31
For patients not taking enzymeinducing agents, there are no absolute restrictions on OCPs; however, medications should be monitored for potential serum changes. For example, lamotrigine may require dose adjustments when initiating or terminating treatments.
PRE-PREGNANCY PLANNING AND CONSULTATION
Pre-pregnancy planning and consultation, with and having an expert input focused on epilepsy and the female reproductive lifespan, is an evolving field. It is becoming increasingly available in epilepsy centers as a comprehensive way to ascertain and manage medical care for seizure disorders, particularly in relation to an upcoming pregnancy.11,32-35 Recent literature and studies, such as the WEPOD study by French et al.,36 indicate that female patients with epilepsy seeking pregnancy had a comparable likelihood of achieving pregnancy, time to achieve pregnancy, and pregnancy outcomes compared to a group of healthy controls, when their care needs are addressed. These findings should reassure both patients and clinicians during counseling for these women who are planning a pregnancy.36
Preconception management of pregnancy in women with epilepsy involves counseling, establishing baseline seizure frequency, and determining the necessary ASM blood levels. It also includes assessing whether monotherapy or polytherapy is indicated. Folic acid supplementation, up to 4 mg/ day, is encouraged, and counseling should caution patients against the abrupt withdrawal of ASMs, which could be associated with a significant amount of breakthrough seizures (occurring in approximately 50% of patients). In general, ASMs should be prescribed at the lowest possible dose and thereby minimize the teratogenic risk.31-35 Compared with monotherapy, polytherapy
increases risk of intrauterine death, cesarean section, low birth weight, premature birth, risk of poor neural development, and major malformations.31-35 Folate should be started according to recent practice guidelines within 3 months of pregnancy to reduce the risk of neural tube defects and to improve IQ and neurodevelopmental outcomes, as some research has indicated that folate might reduce autistic traits.31-35,37-43 While the American College of Obstetrics and Gynecology (ACOG) guidelines include recommending high-dose folate up to 4 mg/day starting during the month prior to conception, the UK and European guidelines are considering recommending up to 5 mg/day.37-43
ASMs and their relevant side effects, with a focus on women with epilepsy, should be highlighted. Phenytoin is associated with dysmorphisms and coarsening of features with chronic use, and significant weight gain is associated with valproic acid and carbamazepine.6,28,31-35,41-42 Weight loss is associated with zonisamide and topiramate, while enzyme-inducing ASMs, especially valproic acid, might contribute to polycystic ovaries as well as hair thinning, or hirsutism, depending on the specific metabolism.6,28,41,42
MANAGEMENT OF SEIZURES DURING PREGNANCY: AN OVERVIEW OF CURRENT PRACTICE STANDARDS
Anti-Seizure Medication Management, Teratogenicity, and Complications
As previously mentioned, effective seizure management during pregnancy is essential for optimal outcomes in this evolving specialization. ASM monitoring should be encouraged every 4 weeks during pregnancy. Baseline doses may need to be increased by approximately 35% from preconception levels, whether based on dosage or serum levels, due to physiological changes such as enhanced hepatic metabolism, increased renal blood flow and clearance, altered protein binding, and increased volume of distribution. These changes generally lead
to decreased serum levels of ASMs as pregnancy progresses.31-35 ASM monitoring should be done more frequently, weekly if possible, during the last trimester and final month of pregnancy, as seizures, particularly generalized tonic–clonic seizures (GTCS), are associated with placental abruption and significant utero-placental insufficiency. These events could lead to potentially significant effects such as hypoxemia or hypoperfusion, potentially resulting in fetal organ damage.31-35 Ultrasonography to identify neural tube defects, such as anencephaly and myelomeningocele, may be performed at Week 13 of gestational age.31-35,43-46 Orofacial clefts and cardiac defects are detectable at approximately 20 weeks. The literature does not currently recommend any preferred methods of delivery, such as an electively planned cesarean section as opposed to a normal and spontaneous vaginal delivery.31-35,43-45 Vitamin K should be given for the final month of pregnancy if hepaticinducing ASMs are being used.31-35,43-47
Observations and older literature, largely unchanged since the 1980s, indicated that newborns of mothers treated with enzymeinducing ASMs are at risk of hemorrhagic disease of the newborn. This is likely due to increased turnover of vitamin K due to hepatic enzyme induction affecting the vitamin K-dependent clotting factors II, VII, IX, and X.46,47 A prior, well-known, pivotal study in1985 by Motohara K et al.,46 identified cohorts of babies born given vitamin K compared to those that were untreated with vitamin K. The untreated group had a higher number of PIVKA II-positive babies, particularly those born to mothers on enzyme-inducing ASMs, in a study of fetal cord blood, supporting the idea that vitamin K deficiency was a factor.47 The study by Motohara K et al.46 indicated that the risks of hemorrhagic complications in newborns could be predicted by PIVKA II proteins as a biomarker. The presence of these proteins supports the recommendation of administering 10 mg of vitamin K daily during the last month of pregnancy for women taking enzyme-inducing ASMs, which is effective in preventing hemorrhagic disease of the newborn.47
Practice Guidelines: Women with Epilepsy
• Pre-pregnancy planning is recommended to establish a risk assessment, determine whether monotherapy or polytherapy is indicated, include baseline ASM levels, and note dosing for the overall strategy to prevent GTCS, with monthly levels monitored until the last trimester/month, when levels might be done weekly or biweekly.
• Folate 1 mg/day for women with epilepsy generally, but 4 mg/day within 3 months of conception.
• European Countries and UK recommend 5 mg/day.
• Vitamin K supplementation during the last month of pregnancy to prevent hemorrhagic disease of the newborn for mothers taking enzyme-inducing ASMs.
• Breastfeeding should be generally encouraged.
• The risk of major fetal malformations are highest with valproate.
• Neural Tube defects may be screened at 13 weeks (for anencephaly and myelomeningocele) and 20 weeks (for orofacial clefts and cardiac defects) with high-level ultrasounds.
• Consideration of dose adjustment of medications during pregnancy, due to changes in volume of distribution, hepatic and renal clearance, and metabolism, and after post-partum to prevent toxicity, with lamotrigine requiring rapid taper of a few days and most other ASMs within 3 weeks.
• Consider bone health screening and calcium and vitamin D supplementation in women with epilepsy who are on enzymeinducing ASMs, with calcium 1000–1500 mg/day and vitamin D 400–800 IU/day.
ANTI-SEIZURE MEDICATIONS AND NEUROCOGNITIVE RISKS IN OFFSPRING
Current Practice and Evolving Literature
Seizure medications are associated with major congenital malformations, dysmorphism, preterm birth, intrauterine growth retardation, and potentially neurocognitive and neurodevelopmental adverse effects.32-43
The NEAD study enrolled pregnant women with epilepsy who were taking a single antiepileptic agent (carbamazepine, lamotrigine, phenytoin, or valproate) in a prospective, observational, multicenter study in the USA and the UK to determine whether, and the extent to which, ASMs had neurocognitive effects.48 The primary analysis reviewed neurodevelopmental outcomes at 6 years of age, after exposure to different antiepileptic drugs in utero. The report focused on a planned interim analysis of cognitive outcomes in 309 children at 3 years of age and noted that in utero exposure to valproate, compared to other commonly used antiepileptic drugs, was associated with an increased risk of impaired cognitive function at 3 years of age.48 The 2013 publication regarding the NEAD study, by Meador et al.,49 also identified that fetal valproate exposure had dose-dependent associations with reduced cognitive abilities across a range of domains at 6 years of age. Additionally, reduced right-handedness and verbal (versus non-verbal) abilities may be attributed to changes in cerebral lateralization induced by exposure to antiepileptic drugs. The positive association of periconceptional folate with IQ was consistent with other studies.49 Additional reports, such as in both a follow-up 2019 and 2020 analysis, illustrate further benefits of folate with improved neurocognitive outcomes when combined with ASM exposure.50,51
POST-PARTUM ISSUES AND BREASTFEEDING
Generally, ASM concentration in breast milk is about one-third or less of that in serum, and is further reduced depending on the drug’s protein binding. These levels are significantly lower than those seen with in utero exposure.52,53 The author suggests that if breast milk is relatively safe, the presence of ASMs may not significantly influence organogenesis, as that process is already complete by the time breastfeeding is considered or initiated.52,53 While there may be significant benefits to maternal–fetal bonding and the development of appropriate immune mechanisms, and while literature cited above notes benefits of breastfeeding in women with epilepsy, poor feeding, irritability, or lethargy may indicate that such an infant might be intolerant of the ASMs.52,53 Drugs with high protein binding, such as phenytoin, carbamazepine and derived compounds, valproic acid, and other enzyme inducers might offer lower levels in breast milk compared to medications with low protein binding. This may lead to relatively higher levels in breast milk for drugs such as levetiracetam, gabapentin, ethosuximide, topiramate, and zonisamide.42-45
Generally, most ASMs are classified as pregnancy category C or worse, primarily due to their association with neural tube defects.42-45 Of note, there may not be exhaustive studies in humans, and such a categorization indicates that some pregnant animals treated with such medications had babies with medical issues or malformations, although the medication might still be helpful and a risk–benefit analysis would be required for use and full recommendations in clinical settings.44,45
Tapering of ASMs should generally occur within a few weeks of delivery as maternal physiologyreturns to baseline pre-pregnancy status; however, due to stressors and sleep deprivation, some relatively higher dosing than baseline might be considered (approximately at 125% of baseline values).33-35 Strategies to
allow for sleep and stress mitigation should be sought to minimize the risk of seizures, with encouragement of a good diet, hygiene, and a survey for mood changes and post-partum depression.4,14,28,33-35,44,45 For some medications, maternal metabolic changes after delivery, such as reduced drug clearance due to the absence of fetal liver and kidney function, and a decreased volume of distribution, may warrant tapering the dose by 50% within 3 days postpartum, with lamotrigine, in particular, often requiring the most rapid tapering.11,28,33-35,43-45
Current literature has indicated that, generally, breastfeeding should be encouraged regardless of ASM exposure, as breastfeeding facilitates maternal–fetal bonding and also allows colostrum to supplement the baby’s developing immunity.11,28,33-35,43-45 ASMs are divided into three categories: “safe,” “moderately safe,” and “may be hazardous.” ASM levels in breast milk are significantly lower than concentrations or exposure in utero, and are more variable, with approximately half of all ASMs concentrations lower than detectable limits.11,28,33-35,43-45 As alluded to above, monitoring for baby irritability and sedation would be advised if benzodiazepines or barbiturates are used.33-35,43,52-58
Numerous articles have cited the benefits of breastfeeding and indicate that no significant overall adverse effects of ASM exposure via breast milk appear to have been observed. Furthermore, in the Meador et al.53 study, breastfed children exhibited higher IQ and enhanced verbal abilities.52-58 The exact mechanisms for the findings, while encouraging, however, are not yet known.
TERATOGENESIS AND WOMEN WITH EPILEPSY
The literature indicates that the risk of birth defects in babies from mothers not taking ASMs is approximately 2–4 %. In contrast, babies born to mothers who take ASMs have a risk of approximately 4–8%, with increased
risks associated with polypharmacy and higher medication doses.59-61 Major abnormalities include facial clefts, congenital heart disease, and neural tube defects, which can be diagnosed with approximately 95% accuracy by Week 16 of gestation with ultrasound and alpha-fetoprotein screening.59-61 Minor abnormalities, such as ocular hypertelorism and nail hypoplasia, among others, occur at twice the baseline rate, and the incidence is estimated to be approximately 5–20 % in babies born to mothers taking ASMs, according to the literature.59-61
The ACOG has recommended folic acid to mitigate the incidence of neural tube defects (such as encephalocele, meningoencephalocele, and other major malformations). Based on the literature, women of childbearing age without a diagnosis of epilepsy are recommended to take a minimum of 400 mcg of folate daily when not on ASMs. For those taking ASMs, the recommended daily dose is 1 mg of folic acid. Furthermore, when actively planning a pregnancy while on ASMs, the folate dose should be increased to 4 mg daily approximately 3 months prior to pregnancy. European guidelines recommend up to 5 mg of folate per day.12-14,37-43
Folate metabolism may be affected by ASMs, and vice versa. ASMs such as phenytoin can lower folate concentrations, and in cases of malabsorption, approximately 1% of patients may be at risk of megaloblastic anemia.48 Folate may lower phenytoin concentration, at least transiently, so breakthrough seizures may occur in patients who suddenly start taking folate, which is added to their regimen after well-intentioned prenatal counseling.37-43
Folate metabolism is involved in the cytochrome p450 enzyme-mediated conversion or hydroxylation of phenytoin. Adding folate seems to increase phenytoin metabolites, leading to reduced serum levels. Similar effects may occur with carbamazepine.37-43 Gabapentin, lamotrigine, and other medications, however, have minimal effects on folate metabolism.32-35,37-43
See Table 1 for an overview of important drug characteristics in women with epilepsy.
BONE HEALTH AND MENOPAUSE
Osteoporosis
Osteoporosis is defined when bone mineral density is less than 2.5 standard deviations below compared to what would be expected.62-64 Osteopenia occurs when bone mineral density is between 1.0 and 2.5 standard deviations below the expected norm.62-64 Decreased bone mass or bones with an abnormal matrix or architecture are more prone to fracture. ASMs that contribute to bone turnover or relative osteoclastic activity (osteoclasts break down bone, while osteoblasts build bone and may become less active with aging and other factors) pose a risk of reducing bone mass or density, particularly in women who take these medications chronically.62-64
Women have less peak bone mass by age 20 compared to men. Approximately 40% of White women will have a fracture related to decreased bone mass as they age. Risk factors include low body weight, lack of weight-bearing exercise, and the hormonal changes of perimenopause. Over their lifespan, women have a threefold higher risk of osteoporotic fractures compared to men, and may lose about 4% of their bone mass each year.62-64 It is estimated that up to 10% of the skeleton may be undergoing remodeling at any given time, with osteoblast activity decreasing with age.62-64 Therefore, due to these noted factors, women generally have lower bone mass and a higher risk of developing osteoporosis and osteopenia. This risk is potentially greater in women with epilepsy, as ASMs commonly increase vitamin D metabolism. As a result, there may be decreased calcium absorption and reduced cellular responsiveness, which can lead to a relative increase in parathyroid hormone, promoting osteoclastic activation and bone resorption.62-64 Therefore, the biochemical and metabolic changes in women with epilepsy, due to ASMs and the chronic
Table 1: Important drug characteristics in women with epilepsy.
nature of treatment, are associated with risks such as hypocalcemia, hypophosphatemia, low vitamin D levels, elevated alkaline phosphatase, and increased parathyroid hormone levels, as noted above.62-64
Screening for osteoporosis in high-risk individuals is recommended, and treatment with weight-bearing exercise, calcium 1000–1500 mg/day, and vitamin D 400–800 IU/day would be recommended, particularly for women taking ASMs that induce liver metabolism. These medications may lead to the above metabolic cascade, posing the risk of bone loss.62-64
GENETICS AND INHERITANCE
Risks of Seizures in Children Born to People with Epilepsy
Patients often inquire about the risk of epilepsy in their children, yet a large amount is still unknown about this expanding field. The inheritance of epilepsy is incompletely understood and complex, with the greatest risk observed in individuals with known genetic syndromes.65-70
The literature indicates that such risks are greater compared with the general population, and could be up to twofold when the parent with epilepsy is the mother. These risks are most pronounced in idiopathic epilepsies, where a genetic mechanism is present or suspected, rather than in symptomatic epilepsies.65-70
In primary generalized epilepsy syndromes, where thalamocortical circuits may be impacted most significantly, there is an estimated 15–40% risk of relatives having childhood absence epilepsy.65-70 Juvenile myoclonic epilepsy may be associated with multiple chromosomal abnormalities.65-70 Familial temporal lobe epilepsy may be, in some cases, autosomal dominantly inherited with 60% penetrance, and in autosomal dominant nocturnal frontal lobe epilepsy, there may be up to 75% penetrance, from a review of the literature.65-70
SEXUAL DYSFUNCTION AND SEIZURES
Literature indicates that overall, there is decreased sexual desire, increased dysmenorrhea with anovulatory cycles, an impact on GnRH, association with seizures, early menopause, and the association of polycystic ovary syndrome.71,72 Other associated risks involving seizure disorders include mood disorders, increased anxiety, and impaired social functioning with negative effects on self-esteem.71,72 In males, lower birth rate and decreased libido and testosterone impaired spermatozoa; however, this could be due to confounding medication issues.73
MENOPAUSE
Literature suggests that seizures may affect GnRH release in the hypothalamus, which may account for women with epilepsy having lower fertility, a higher frequency of anovulatory cycles, and earlier menopause.74,75 Catamenial seizures tend to increase in the perimenopausal period, but
reduce post menopause and, in general, since estrogens (or an increased E/P ratio) might induce seizures, non-estrogen-based supplementation may be recommended.74,75
SPECIAL CONSIDERATIONS IN MALES WITH EPILEPSY
Males with epilepsy are less likely to father a child compared to controls, and this may be due to decreased potency and libido, decreased testosterone, or decreased sperm count and motility due to reduced effects of testosterone, or possibly direct effects of medications such as valproate or carbamazepine.73
FUTURE DIRECTIONS AND CURRENT GAPS IN UNDERSTANDING
Although there are currently multiple medications available, and there may be imminent newer medications, technology such as responsive neurostimulation is an available option to treat intractable epilepsy. Responsive neurostimulation was approved by the FDA in 2013, and real-world experience in post-marketing retrospective observational studies has indicated that there are women who have become pregnant after implantation.76,77 The small and limited studies available so far indicate that there does not appear to be any increased risk of malformation or significant impact on the fetus.77 Whether such technology might, in some cases, lead to significant medication reduction, and therefore reduce the risks associated with polypharmacy in pregnancy, such as fetal malformations and challenges with seizure control, remains to be seen, as this was not studied in the pivotal trials that were conducted for authoritative approval. Similarly, future precision medicine might be able to provide specific, effective, and targeted treatment options with the potential to incrementally enhance the diagnosis path, treatment trajectories, and outcomes for patients.78 Exactly which genetic
analyses, panels, or tests are indicated for comprehensive risk assessment and therapeutic decision-making in a given patient remains uncertain. In the United States, such testing is often not reimbursed by healthcare insurance providers, particularly since, even when genetic profiling is performed, it may not yield definitive therapeutic options beyond initiating conventional ASMs. The author speculates that testing is currently highly variable among epilepsy centers.
There is little research on new-onset seizures during pregnancy, although limited literature exists, and popular beliefs are noted on the internet.79-82 There may be conflicting evidence regarding the incidence of seizures during labor and parturition. It has been believed or speculated that parturition itself is generally associated with rare or well-controlled seizures, although seizures can occur during labor and delivery by an unknown mechanism. Conditions such as eclampsia or vasoconstriction syndromes, which have a proclivity to occur during this time, are also associated with significant comorbidities and mortality.79-83 Further studies could clarify risks and best practices, potentially having practical implications on, for example, whether or not to proceed with an evolving labor versus planning, or converting to, a cesarean section when risks surrounding labor and parturition and seizures are better understood.
Studies cited above note that seizure risks during pregnancy and the postpartum period may increase or decrease due to significant fluctuations in drug levels. These fluctuations can be influenced by changes in volume of distribution, metabolism, and pharmacokinetics, with both maternal and fetal systems contributing individually and collectively to these factors.32-35 The binding of ASMs to albumin and proteins impacts ASM blood levels. Therefore, measuring free levels may be useful in managing select patients on ASMs that are highly proteinbound. Further literature may help clarify when such measurements are most beneficial.32-35
Furthermore, ASMs may impact levels of sex hormone-binding globulin, which could influence libido and fertility, and this could be a subject for significant further study.32-35,82,83,84
A small amount of literature exists that documents patient-centered fears that antiseizure medications themselves may confer the risk of seizures.85 The authors of this study speculated that, while genetic factors likely play a significant role in the development of epilepsy, prenatal ASMs exposure might exhibit a causative role, and further research would be useful in this regard.85
Significant confounding sleep disorders that occur concurrently may impact the occurrence of seizures in relation to the reproductive lifespan, and this connection is becoming increasingly accepted.86-89 Nonrestorative sleep increases risks of seizures, although the exact biological mechanism is unknown.87-89 Processes that increase nonrestorative sleep, or fragment sleep, are caused by various issues and diagnoses.86-89 Such issues and diagnoses may include weight gain, which can cause or contribute to obstructive sleep apnea and seizures, as well as restless leg syndrome, periodic limb movements in sleep, and nocturnal seizures, which might also further fragment sleep and increase seizures.86-89
The optimal timing for assessing a pregnant patient for obstructive sleep apnea and determining the appropriate treatment, such as continuous positive airway pressure titration, which may result in a fixed prescription based on airway resistance, weight, and the size of the gravid uterus, has not yet been clearly defined in clinical practice. Additionally, the use of automatic, adjustable continuous positive airway pressure devices, which adjust depending on detected flow limitation, may also be considered. However, due to the changes in airway resistance caused by increased weight and the growing uterus, as well as the effects on respiratory mechanics and airway collapse during pregnancy, further studies are needed to optimize these approaches.87-89
There may be non-pharmacological options of significant utility for the management of patients and their babies when the patient has a seizure disorder. Newborn safety is a significantly understudied issue.81 The author suggests that it may be beneficial to advise changing the height and location of the baby’s feeding and care area, keeping it low to the ground. This precaution would reduce the risk of injury to the baby in the event of a maternal seizure during activities such as diaper changing, dressing, or feeding, as it would help prevent the baby from falling and sustaining a traumatic injury. The author also advocates for general awareness and assessment of safety in the home to be considered from the vantage point of how to best keep the mother and baby safe in case the patient experiences altered awareness. Exactly how wearable, or other portable technologies in the home, might be useful is yet unknown; however, the author shares an example of a patient in which a case of parasomnia, rather than a seizure, was identified and detected using a home security camera system. This allowed for further evaluation and helped clarify the situation. Additionally, the author has advised involving the patient’s partner to help facilitate continuous sleep to mitigate the risk of seizures. The author has also recommended maternal milk harvesting and storage as a strategy, allowing the partner to assist in feeding, which could help women with epilepsy achieve uninterrupted sleep during the night. This approach may reduce overall seizure occurrences and support breastfeeding, ensuring the infant can still consume breast milk during the night if needed. However, comprehensive studies on these practices remain relatively anecdotal.
Although there is scarce literature, the author advises that, in appropriate cases, excluding psychogenic nonepileptic seizure disorders may be useful and should potentially be pursued in an epilepsy monitoring unit stay to eliminate or minimize the risk of ASMmediated teratogenicity. Evaluation should be undertaken in a timely manner, before conception, to prevent unnecessary ASM
exposure to a developing fetus. However, there is limited literature and guidance currently available on this important topic, and the incidence of ASM exposure in psychogenic nonepileptic seizure patients and their fetuses is unknown, even among those practicing in epilepsy centers.90
Although there is an extensive understanding of the hormonal influences of menstruation and CE, the full extent of the evaluation and management of increased seizures with in vitro fertilization is not known, although the literature is evolving and could be a practical course of study.91
Generally, the current literature advocates for mitigating GTCSs, as they may carry the highest comorbidities and potential effects on uteroplacental insufficiency and the risk of abruption by the third trimester of pregnancy. However, it remains unknown how or to what extent other seizure types might impact maternal-fetal insufficiency and maternalfetal physiology, requiring further management and investigation.32-35
There are no guidelines regarding whether medication reduction or down-titration strategies to mitigate exposure during the first trimester might reasonably be undertaken in certain, well-defined circumstances. From the author’s experience, some patients often insist on or request such maneuvers, even when seizures have occurred very remotely, sometimes decades ago. However, the current practice rationale does not specify what to do in these circumstances. The general tendency seems to be to continue ASMs anyway, aiming to achieve the best seizure control possible despite the potential risk of ASM exposure to the fetus.32-35 Currently, although there is a consensus in aiming not to have risks of generalized seizures by the third trimester, to prevent placental abruption and/or placental fetal insufficiency, the issue of whether or not to taper medication in those with what might be considered an “outgrown” seizure disorder as part of preconception counselling is not fully clarified in the literature.32-35
Finally, there are no comprehensive consensus guidelines on how to optimally manage patients with intractable seizures having uncontrolled seizures during pregnancy. This applies to patients who are not seizure-free and require medication changes or additional adjunctive medications, or those who have already transitioned to second-line therapy but continue to experience seizures due to conditions like idiopathic generalized epilepsy. While there are evolving articles on managing
References
1. Kammerman S, Wasserman L. Seizure disorders: part 1. Classification and diagnosis. West J Med. 2001;175(2):99-103.
2. Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. 2015;5(6):a022426.
3. Sarmast ST et al. Current classification of seizures and epilepsies: scope, limitations and recommendations for future action. Cureus. 2020;12(9):e10549.
4. Fisher RS et al. Epileptic seizures and epilepsy: definitions proposed by the international league against epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia. 2005;46(4):470.
5. Maganti RK, Rutecki P. EEG and epilepsy monitoring. Continuum (Minneap Minn). 2013;19(3 Epilepsy):598-622.
6. Jones HR (ed.), Epilepsy and Syncope. (2013) 2nd edition, Philadelphia: Elsevier.
7. Ben-Ari Y et al. Seizures beget seizures in temporal lobe epilepsies: the boomerang effects of newly formed aberrant kainatergic synapses. Epilepsy Curr. 2008;8(3):68-72.
8. Sculier C et al. Long-term outcomes of status epilepticus: a critical assessment. Epilepsia. 2018;59(Suppl 2):155-69.
9. Scott RC. What are the effects of prolonged seizures in the brain?. Epileptic Disord. 2014;16 Spec No 1(Spec No 1):S6-11.
10. Gunawardane N, Fields M. Acute symptomatic seizures and provoked seizures: to treat or not to treat?. Curr Treat Options Neurol. 2018;20(10):41.
11. Milligan TA. Epilepsy: a clinical overview. Am J Med. 2021;134(7):840-7.
these “second-line treatment” options or adjunctive ASM management for seizure control, newer non-hepatic enzyme inducers such as levetiracetam and lamotrigine show promise. Among non-valproic acid add-on regimens, the combination of levetiracetam and lamotrigine may demonstrate superior effectiveness compared with other ASM combinations in certain cohorts of women.32-35,92 Significantly more studies and treatment options are needed for this specific cohort of patients.
12. Jayalakshmi S et al. Anxiety, depression, and psychosocial adjustment in people with epilepsy. J Neurosci Rural Pract. 2023;14(1):111-8.
13. Nguyen R, Téllez Zenteno JF. Injuries in epilepsy: a review of its prevalence, risk factors, type of injuries and prevention. Neurol Int. 2009;1(1):e20.
14. Villamizar-Torres D et al. Mesial temporal sclerosis and epilepsy: a narrative review. Acta Epileptologica. 2024;6:28.
15. Beghi E. The epidemiology of epilepsy. Neuroepidemiology. 2020;54(2):185-91.
16. Yang LZ et al. A populationbased analysis of the global burden of epilepsy across all age groups (1990-2021): utilizing the Global Burden of Disease 2021 data. Front Neurol. 2024;15:1448596.
17. Barbour K et al. Population-based study of rare epilepsy incidence in a US urban population. Epilepsia. 2024;65(8):2341-53.
18. Chen Z et al. Editorial: epidemiology of epilepsy and seizures. Front Epidemiol. 2023;3:1273163.
19. Sander JW, Shorvon SD. Epidemiology of the epilepsies. J Neurol Neurosurg Psychiatry. 1996;61(5):433-43. Erratum in: J Neurol Neurosurg Psychiatry. 1997;62(6):679.
20. Annegers JF. Epidemiology and Genetics of Epilepsy. Neurol Clin. 2001;19(1):1530.
21. Hawkins SM, Matzuk MM. The menstrual cycle: basic biology. Ann N Y Acad Sci. 2008;1135:10-8.
22. Taubøll E et al. Interactions between hormones and epilepsy. Seizure. 2015;28:3-11.
23. Ejigu AK et al. Sexual dysfunction and associated factors among patients with epilepsy at Amanuel Mental Specialty Hospital, Addis Ababa, Ethiopia. BMC Neurol. 2019;19(1):255.
24. Farmen AH et al. Age-specific birth rates in women with epilepsy: a population-based study. Brain Behav. 2016 Jun 14;6(8):e00492.
25. Witchel SF et al. Polycystic ovary syndrome: pathophysiology, presentation, and treatment with emphasis on adolescent girls. J Endocr Soc. 2019;3(8):1545-73.
26. Mekaru K et al. Spontaneous regression of uterine arteriovenous malformations with conservative management. Case Rep Obstet Gynecol. 2017;2017:6437670.
27. Herzog AG. Hormonal therapies: progesterone. Neurotherapeutics. 2009;6(2):383-91.
28. Patel T, Grindrod KA. Antiseizure drugs and women: challenges with contraception and pregnancy. Can Pharm J (Ott). 2020;153(6):357-60.
29. Herzog AG et al. Three patterns of catamenial epilepsy. Epilepsia. 1997;38(10):1082-8.
30. Frank S, Tyson NA. A clinical approach to catamenial epilepsy: a review. Perm J. 2020;24:1-3.
31. Navis A, Harden C. A treatment approach to catamenial epilepsy. Curr Treat Options Neurol. 2016;18(7):30.
32. Pegg EJ et al. Preconception counselling in women with epilepsy. Pract Neurol. 2024;24(6):478-84.
33. Putta S, Pennell PB. Management of epilepsy during pregnancy: evidence-based strategies. Future Neurol. 2015;10(2):161-76.
34. Nucera B et al. Treatment and care of women with epilepsy before, during, and after pregnancy: a practical guide. Ther Adv Neurol Disord. 2022;15:17562864221101687.
35. Li Y, Meador KJ. Epilepsy and pregnancy. Continuum (Minneap Minn). 2022;28(1):34-54.
36. French J et al. A prospective study of pregnancy in women with epilepsy seeking conception (The WEPOD Study). Neurology. 2016;86(Suppl 16):I5.001.
37. The American College of Obstetricians and Gynecologists. Prepregnancy counseling. 2019. Available at: https:// www.acog.org/clinical/clinical-guidance/ committee-opinion/articles/2019/01/ prepregnancy-counseling. Last accessed April 24 2025.
38. Loperfido F et al. Folic acid supplementation in European women of reproductive age and during pregnancy with excessive weight: a systematic review. Reprod Health. 2025;22(1):13.
39. Cawley S et al. A review of European guidelines on periconceptional folic acid supplementation. Eur J Clin Nutr. 2016;70(2):143-54.
40. Mutanana N et al. General side effects and challenges associated with antiepilepsy medication: A review of related literature. Afr J Prim Health Care Fam Med. 2020 Jun 30;12(1):e1-e5.
41. U.S Food & Drug Administration. FDA online label repository. Available at: https://labels.fda.gov/. Last accessed April 26 2025.
42. The Daily Journal of the United States Government: Federal Register. Pregnancy, lactation, and reproductive potential: labeling for human prescription drug and biological products-content and format; draft guidance for industry; availability. 2014. Available at: https://www.federalregister.gov/ documents/2014/12/04/2014-28242/ pregnancy-lactation-and-reproductivepotential-labeling-for-humanprescription-drug-and-biological. Last accessed: March 27 2025.
43. Borgelt LM et al. Epilepsy during pregnancy: focus on management strategies. Int J Womens Health. 2016;8:505-517.
44. Khan M et al. Epilepsy and issues related to reproductive health. Cureus. 2023;15(11):e48201.
45. Ng E, Loewy AD. Guidelines for vitamin K prophylaxis in newborns. Paediatr Child Health. 2018;23(6):394-402.
46. Motohara K et al. Effect of vitamin K administration on acarboxy prothrombin (PIVKA-II) levels in newborns. Lancet. 1985;326(8449):242-4.
47. Meador KJ et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs. N Engl J Med. 2009;360:1597-05.
48. Meador KJ et al. Fetal antiepileptic drug exposure and cognitive outcomes at age 6 years (NEAD study): a prospective observational study. Lancet Neurol. 2013;12(3):244-52.
49. Meador KJ et al. Effects of periconceptional folate on cognition in children of women with epilepsy: NEAD study. Neurology. 2020;94(7):e729-40.
50. Meador KJ et al. Two-year-old cognitive outcomes in children of pregnant women with epilepsy in the maternal outcomes and neurodevelopmental effects of antiepileptic drugs study. JAMA Neurol. 2021;78(8):927-36.
51. Yan R et al. Management of antiseizure medications in lactating women with epilepsy. Front Neurol. 2022;13:1005890.
52. Shawahna R, Zaid L. Concentrations of antiseizure medications in breast milk of lactating women with epilepsy: A systematic review with qualitative synthesis. Seizure. 2022;98:57-70.
53. Meador KJ et al. Neurodevelopmental Effects of Antiepileptic Drugs (NEAD) study group. Breastfeeding in children of women taking antiepileptic drugs: cognitive outcomes at age 6 years. JAMA Pediatr. 2014;168(8):729-36.
54. Karceski S, Quinn H. Breastfeeding and mothers with epilepsy. Neurology. 2023;101(22):e2341-4.
55. Haunt S. Antiepileptic medications and breastfeeding: better news than expected?. Epilepsy Curr. 2016;16(2):84-6.
56. Birnbaum AK et al. Antiepileptic drug exposure in infants of breastfeeding mothers with epilepsy. JAMA Neurol. 2020;77(4):441-50.
57. Harden CL et al. Practice parameter update: management issues for women with epilepsy--focus on pregnancy (an evidence-based review): vitamin K, folic acid, blood levels, and breastfeeding: report of the quality standards subcommittee and therapeutics and technology assessment subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology. 2009;73(2):142-9.
58. Etemad L et al. Epilepsy drugs and effects on fetal development: potential mechanisms. J Res Med Sci. 2012;17(9):876-81.
59. Meador KJ. Effects of maternal use of antiseizure medications on child development. Neurol Clin. 2022;40(4):755-68.
60. Wiggs KK, Rickert ME, Quinn PD et al. Specific birth defects following antiseizure medications used by pregnant women with epilepsy. Neurology. 2024;64(3):14.
61. Sözen T et al. An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46-56.
62. Föger-Samwald U et al. Osteoporosis: pathophysiology and therapeutic options. EXCLI J. 2020;19:1017-37.
63. Gross RA et al. Antiseizure drugs and reduced bone density. Neurology. 2004;62(11):E24-5.
64. Lindquist BE et al. Thalamocortical circuits in generalized epilepsy: pathophysiologic mechanisms and therapeutic targets. Neurobiol Dis. 2023;181:106094.
65. Stiriano P, Pasquale C. The genetic basis of juvenile myoclonic epilepsy. Lancet Neurol. 2018;17(6):493-5.
66. Berkovic SF et al. Familial temporal lobe epilepsy: a common disorder identified in twins. Ann Neurol. 1996;40(2):227-35.
67. Gambardella A et al. Familial temporal lobe epilepsy autosomal dominant inheritance in a large pedigree from southern Italy. Epilepsy Res. 2000;38 (2-3):127-32.
68. Berkovic SF, Scheffer IE. Genetics of the epilepsies. Epilepsia. 2001;42 Suppl 5:16-23.
69. Dreier JW et al. Epilepsy risk in offspring of affected parents; a cohort study of the "maternal effect" in epilepsy. Ann Clin Transl Neurol. 2021;8(1):153-62.
70. Atif M et al. The relationship between epilepsy and sexual dysfunction: a review of the literature. Springerplus. 2016;5(1):2070.
71. Chaturbhuj R et al. Sexual dysfunction in people with epilepsy. Epilepsy Behav. 2019;100(Pt A):106495.
72. Montouris G et al. Reproductive and sexual dysfunction in men with epilepsy. Epilepsy Behav. 2005;7(1):7-14.
73. Gerard EE et al, “Change in Seizure Pattern and Menopause,” Sazgar M, Harden C (eds.), Controversies in Caring for Women with Epilepsy (2016), Cham: Springer, pp 141-52.
74. Abbasi F et al. Effects of menopause on seizures in women with epilepsy. Epilepsia. 1999;40(2):205-10.
75. Avachat C et al. Management of antiseizure medications during pregnancy: advancements in the past decade. Pharmaceutics. 2022;14(12):2733.
76. Li Y et al. Pregnancy outcomes of refractory epilepsy patients treated with brain-responsive neurostimulation. Epilepsy Res. 2021;(169):106532.
77. McGinn RJ et al. Precision medicine in epilepsy. Prog Mol Biol Transl Sci. 2022;190(1):147-88.
78. Li W et al. Clinical characteristics and pregnancy outcomes of new onset epilepsy during pregnancy. Medicine (Baltimore). 2019;98(27):e16156.
79. Aya AG et al. Seizures in the peripartum period: epidemiology, diagnosis and management. Anaesth Crit Care Pain Med. 2016;35 Suppl 1:S13-21.
80. Klein A. The postpartum period in women with epilepsy. Neurol Clin. 2012;30(3):867-75.
81. The Defeating Epilepsy Foundation. Epilepsy and childbirth. Available at: http://defeatingepilepsy.org/livingwith-epilepsy-series/epilepsy-andchildbirth/. Last accessed April 27 2025.
82. Goulopoulou S. Maternal vascular physiology in preeclampsia. Hypertension. 2017;70(6):1066-73.
83. Herman S. Sex hormones and epilepsy: no longer just for women. Epilepsy Curr. 2008;8(1):6-8.
84. Calabrò RS, Cerasa A. Drug-induced sexual dysfunction in individuals with epilepsy: beyond antiepileptic compounds. Medicines (Basel). 2022;9(3):23.
85. Voinescu PE, Bui E. Do my children have a higher risk of epilepsy because of my epilepsy or seizure medications?. JAMA Netw Open. 2024;7(2):e2356379.
86. Maniaci A et al. Obstructive sleep apnea in pregnancy: a comprehensive review of maternal and fetal implications. Neurol Int. 2024;16(3):522-32.
87. Tayade S, Toshniwal S. Obstructive sleep apnea in pregnancy: a narrative review. Cureus. 2022;14(10):e30387.
88. Moore JL et al. Sleep and epilepsy: a focused review of pathophysiology, clinical syndromes, co-morbidities, and therapy. Neurotherapeutics. 2021;18(1):170-80. Erratum in: Neurotherapeutics. 2021;18(1):655.
89. DeToledo JC et al. Nonepileptic seizures in pregnancy. Neurology. 2000;55(1):120-1.
90. Mostacci B et al. Estrogenrelated seizure exacerbation following hormone therapy for assisted reproduction in women with epilepsy. Seizure. 2018;61:200-2.
91. Irelli EC et al. Second-line medications for women aged 10 to 50 years with idiopathic generalized epilepsy. JAMA Netw Open. 2025;8(3):e250354.
92. Kiiski R et al. Treatment outcomes in women with idiopathic generalized epilepsy. Acta Neurol Scand. 2022;145(4):423-33.
Reversible Cerebral Vasoconstriction Syndrome Presenting with Multifocal Infarcts: A Case Report
Authors: Ibrahim Kaleel,1 Leyan Abu Hasan,1 *Abdel Salam Kaleel1
1. Department of Neurology, Grand River Hospital, McMaster University/Michael De Groote School of Medicine, Ontario, Canada. *Correspondence to kaleela@mcmaster.ca
Disclosure: The authors have declared no conflicts of interest. Written informed consent was obtained from the patient in accordance with AMJ policy.
Received: 01.26.2025
Accepted: 04.22.2025
Keywords: Multifocal infarcts, neurological diagnosis, nimodipine therapy, reversible cerebral vasoconstriction syndrome (RCVS).
Citation: Neurol AMJ. 2025;2[1]:112-116. https://doi.org/10.33590/neurolamj/ZLUS4806
Abstract
Introduction: Reversible cerebral vasoconstriction syndrome (RCVS) is a rare and underdiagnosed cause of multifocal infarcts, characterized by transient segmental narrowing of cerebral arteries. This case highlights the diagnostic challenges, as well as the therapeutic response to nimodipine and intra-arterial therapy.
Main Symptoms and Clinical Findings: A 54-year-old female presented with a month-long history of confusion, headaches, and weakness. MRI findings revealed multifocal infarcts across multiple vascular territories.
Main Diagnoses, Therapeutic Interventions, and Outcomes: RCVS was diagnosed following a diagnostic cerebral angiography, which demonstrated the reversibility of vasospasm with intraarterial milrinone and verapamil. Treatment with nimodipine resulted in symptom stabilization, and rehabilitation services were initiated.
Conclusion: This case underscores the need to consider RCVS early in the diagnostic process for multifocal infarcts. Rapid identification through angiography and prompt initiation of nimodipine therapy can prevent unnecessary interventions and support meaningful neurological recovery.
Key Points
1. Reversible cerebral vasoconstriction syndrome can mimic more common pathologies like central nervous system vasculitis or infection, and is often underrecognized.
2. Accurate diagnosis of reversible cerebral vasoconstriction syndrome relies on imaging techniques such as cerebral angiography, which can demonstrate reversible vasospasm, a key diagnostic hallmark.
3. Prompt treatment with calcium channel blockers, such as nimodipine, is essential to both prevent further neurological damage and improve outcomes. Early diagnosis reduces the risk of overtreatment with immunosuppressants and improves functional outcomes.
INTRODUCTION
Reversible cerebral vasoconstriction syndrome (RCVS) is a rare, but critical diagnosis in patients presenting with recurrent, thunderclap headaches, and multifocal infarctions.1,2 Misdiagnosed as central nervous system vasculitis or infection, RCVS is typified by segmental cerebral arterial vasoconstriction that resolves spontaneously or with targeted therapeutic regimens.3 The diagnostic and therapeutic pathway of a 54-year-old female patient with RCVS, and the utmost significance of proper diagnosis and management of this condition, are both demonstrated in this article.
PATIENT INFORMATION
The patient is a 54-year-old woman living in Ontario. She is independent in daily activities, with occasional support from her daughter.
Primary Concerns and Symptoms
The patient was admitted to the hospital with a history of confusion, progressive headaches, and a weakness in the legs that had started 1 month prior. The symptoms evolved into expressive aphasia and right hemianopsia.
Medical, Family, and Psychosocial History
The patient had generalized anxiety disorder and bipolar disorder in her medical history. She also had a 20+ pack-per-year smoking history with a current daily use of cannabis and a recent smoking cessation.
Relevant Past Interventions
Past interventions included recent treatment with psychotropic medications for her mental
health conditions, and two prior emergency department visits for similar symptoms, where initial investigations were inconclusive.
CLINICAL FINDINGS
The physical exam was notable for detecting expressive aphasia, right hemianopsia, and difficulty with word finding. The neuro exam was otherwise unremarkable. Vital signs were stable without any apparent cardiovascular or pulmonary disease.
TIMELINE
In September 2024, the patient initially presented with weakness and confusion, and a CT scan of the head was negative for any acute process (Figure 1). By late September 2024, MRI imaging demonstrated multifocal infarcts, leading to the initiation of antibiotic therapy for a presumed central nervous system infection. In October 2024, a diagnostic cerebral angiogram confirmed RCVS, and the patient was started on nimodipine.
DIAGNOSTIC ASSESSMENT
The patient’s MRI imaging revealed multifocal infarcts with evolving features (Figure 2A/2B). A cerebral angiography thereafter confirmed the presence of segmental vasospasm and demonstrated reversibility following intra-arterial administration of milrinone and verapamil. Extensive infectious and autoimmune panels were negative.
The main diagnostic challenge was the resemblance of RCVS to vasculitis and central nervous system infections, which led to an initial misdiagnosis and delays in targeted therapy. Additionally, access to advanced
An axial, non-contrast CT of the brain performed at initial presentation demonstrates no evidence of acute hemorrhage, mass effect, or ischemia. The ventricular system and sulci are preserved, with no signs of raised intracranial pressure or midline shift. These findings contributed to a delay in diagnosis, emphasizing the limitation of an early CT scan in reversible cerebral vasoconstriction syndrome evaluation.
2B: MRI fluid-attenuated inversion recovery sequence.
Axial fluid-attenuated inversion recovery (FLAIR) MRI sequence shows symmetric, hyperintense lesions in the bilateral frontal lobes, representing subacute infarcts in watershed territories. These findings prompted further investigation for vasculopathy and supported the diagnosis of reversible cerebral vasoconstriction syndrome.
Figure 2A: Non-contrast magnetic resonance angiography of the head.

Time-of-flight magnetic resonance angiography of the circle of Willis reveals diffuse, multifocal segmental narrowing of the circle of Willis involving the anterior cerebral arteries, middle cerebral arteries, and posterior circulation. This is consistent with severe cerebral vasospasm.
Figure 3: Digital subtraction angiography showing anterior and middle cerebral arteries.
A digital subtraction angiography performed after an intra-arterial administration of milrinone and verapamil. It shows a near-complete resolution of prior segmental vasoconstriction in the anterior and middle cerebral arteries. These findings confirm the reversible nature of the vasospasm, supporting the diagnosis of reversible cerebral vasoconstriction syndrome and ruling out fixed stenotic processes such as vasculitis.
Figure 1: Non-contrast head CT.
Figure
neurointerventional studies was limited. The final diagnosis was RCVS with multifocal infarcts secondary to cerebral vasospasm. The patient's prognosis was stable upon discharge with continued nimodipine therapy and multidisciplinary rehabilitation support.
THERAPEUTIC INTERVENTION
The patient was treated with intra-arterial milrinone and verapamil during the cerebral angiography (Figure 3). Pharmacologic therapy was initiated with nimodipine at a dose of 30 mg, four times a day, titrated as needed. In addition, she received supportive therapy, including physiotherapy, occupational therapy, and speech-language pathology services. Corticosteroids were discontinued upon confirmation of RCVS, as they are ineffective for this condition and may lead to worse outcomes in some people.
FOLLOW-UP AND OUTCOMES
Following treatment, the patient’s symptoms stabilized, and she showed improvement in cognitive function with the resolution of acute neurological deficits. Rehabilitation services were initiated to address residual deficits. Repeated neuroimaging was planned to monitor vascular status. Given the incidental finding of thyromegaly, thyroid function tests were also performed and were to be followed up as an outpatient in this regard.
The patient demonstrated good adherence to nimodipine therapy, with no significant side effects reported. One notable adverse event was an acute rise in creatinine induced by acyclovir, which was resolved with hydration.
TIMELINE OF CLINICAL EVENTS IN 2024
• Early September: Initial symptoms of confusion and leg weakness.
• Mid-September: Head CT unremarkable.
• Late September: MRI shows multifocal infarcts; empiric antibiotics are given for presumed infection.
• Early October: Cerebral angiography confirms reversible cerebral vasoconstriction syndrome; intra-arterial therapy given.
• Mid-October: Initiation of nimodipine and rehabilitation services.
• Late October: Clinical stabilization; discharged with outpatient follow-up.
DISCUSSION
This case highlights the value of a cerebral angiography in differentiating RCVS from similar conditions.4,5 Limitations included the delayed access to neurointerventional studies, and psychosocial barriers.6,7 Cannabis use has been associated with RCVS in several case series and reviews, potentially through the modulation of cerebral vascular tone. Given the patient’s daily cannabis use, it may have been a precipitating or exacerbating factor in this case.8
RCVS is often underdiagnosed as it masquerades as vasculitis and other cerebrovascular disorders.9,10 Acute management with calcium channel blockers has been shown to be useful, as demonstrated in the present case, as the reversibility of vasospasm that is evidenced by intra-arterial therapy is diagnostic of RCVS and warrants targeted treatment with nimodipine.11-14 Although calcium channel blockers such as nimodipine are the mainstay of treatment, other agents like magnesium sulfate have been trialed with varying success.15 However, evidence remains limited. Patients with RCVS typically have a good long-term prognosis with the resolution of vasoconstriction, though some may develop residual deficits or recurrent events. It is advised to monitor for complications such as seizures, posterior reversible encephalopathy syndrome, and stroke recurrence.16
PRIMARY TAKEAWAY
RCVS must be included in the differential diagnosis of patients with multifocal infarcts of unclear etiology, as early diagnosis and treatment can greatly influence outcomes.17
References
1. Ribas MZ et al. Reversible cerebral vasoconstriction syndrome: literature review. Egypt J Neurol Psychiatry Neurosurg. 2023;59:5.
2. Slivka A, Philbrook B. Clinical and angiographic features of thunderclap headache. Headache. 1995;35(1):1-6.
3. Singhal AB. Cerebral vasoconstriction syndromes. Top Stroke Rehabil. 2004;11:1-6.
4. Crowley RW et al. Angiographic vasospasm is strongly correlated with cerebral infarction after subarachnoid hemorrhage. Stroke. 2011;42(4):919-23.
5. Chen SP et al. Magnetic resonance angiography in reversible cerebral vasoconstriction syndromes. Ann Neurol. 2010;67(5):648-56.
6. White PM et al. Can noninvasive imaging accurately depict intracranial aneurysms? A systematic review.
Radiology. 2000;217(2):361-70.
7. Ducros A et al. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome: a prospective series of 67 patients. Brain 2007;130:3091-101.
8. Uhegwu N et al. Marijuana induced reversible cerebral vasoconstriction syndrome. J Vasc Interv Neurol. 2015;8(1):36-8.
9. Hajj-Ali RA et al. Benign angiopathy of the central nervous system: cohort of 16 patients with clinical course and long-term follow-up. Arthritis Rheum. 2002;47(3):662-9.
10. Oz O et al. Reversible cerebral vasoconstriction syndrome: case report. J Headache Pain. 2009;10(4):295-8.
11. Cho S et al. Effect of nimodipine treatment on the clinical course of reversible cerebral vasoconstriction syndrome. Front Neurol. 2019;10:644.
12. Dodick DW. Reversible segmental cerebral vasoconstriction (CallFleming syndrome): The role of calcium antagonists. Cephalalgia. 2003;23(3):163-5.
13. Lu SR et al. Nimodipine for treatment of primary thunderclap headache. Neurology. 2004;62(8):1414-6.
14. Bouchard M et al. Intra-arterial milrinone for reversible cerebral vasoconstriction syndrome. Headache. 2009;49(1):142-5.
15. Mijalski C et al. Magnesium for treatment of reversible cerebral vasoconstriction syndrome: case series. Neurohospitalist. 2016;6(3):111-3.
16. Lange KS et al. Complications of reversible cerebral vasoconstriction syndrome in relation to age. J Neurol. 2023 Jul;270(7):3584-94.
17. Breville G et al. Case report and review of the literature: fatal reversible cerebral vasoconstriction syndrome. Front Neurol. 2021;12:589062.
Cocaine-Induced Leukoencephalopathy: A Case Report
Authors: Miranda Montion,¹ Wyatt Ferrelle,¹ Srusty Patel,² Jonathan Quinonez,³ Samir Ruxmohan⁴
1. Ross University School of Medicine, Saint Michael, Barbados
2. St. George’s University, London, UK
3. HCA Brandon Regional Hospital Department of Pain and Addiction Medicine, Florida, USA
4. University of Texas Southwestern Medical Center, Dallas, USA
*Correspondence to mirandamontion@mail.rossmed.edu
Disclosure: The authors have declared no conflicts of interest. Consent was obtained or waived by all participants in this study.
Received: 01.06.25
Accepted: 05.22.25
Keywords: Adulterated cocaine, drug-induced, leukoencephalopathy, polysubstance abuse.
Citation: Neurol AMJ. 2025;2[1]:117-123. https://doi.org/10.33590/neurolamj/BWLF8260
Abstract
Cocaine-induced leukoencephalopathy is a rare neurological condition usually associated with substances used to adulterate cocaine. A common adulterant of cocaine includes levamisole, an anti-helminthic agent, causing pathologies including vasculitis, agranulocytosis, and, in rare cases, leukoencephalopathy when ingested. Here, the authors present a comprehensive analysis of a cocaine-induced leukoencephalopathy case with the likely presence of levamisole. The patient, a 31-year-old male with an unknown past medical history, presented to the emergency department with seizure-like activity, stiffness, and posturing. Signal abnormalities found in imaging can be seen in the setting of acute cocaine-induced leukoencephalopathy and other metabolic etiologies. The patient was admitted to the neurocritical care unit for management of toxic leukoencephalopathy, acute respiratory failure with hypoxia, non-traumatic rhabdomyolysis, aspiration pneumonia, acute renal failure, and hypertensive emergency. After a 12-day hospitalization, the patient improved towards baseline and continued follow-up for further management. The case study exhibits the importance of early recognition and treatment of cocaine-induced leukoencephalopathy, the possible impacts of adulterated cocaine, the clinical outcomes of induced leukoencephalopathy, and the poor clinical outcomes without prompt intervention. Also included is the argument for levamisole testing when suspected and the use of intravenous methylprednisolone in these cases versus previously described management with methylprednisolone.
Key Points
1. Cocaine-induced leukoencephalopathy is a rare and potentially lethal adverse outcome of cocaine ingestion. This article discusses the use of high-dose IV methylprednisolone and its success in this case, adulterant considerations with testing and treatment, and future indications regarding testing and treatment of suspected cocaine-induced leukoencephalopathy.
2. A case study of a patient diagnosed with cocaine-induced leukoencephalopathy, its unique management, and considerations for similar cases.
3. Methylprednisolone has had mixed results in the treatment of cocaine-induced leukoencephalopathy in other case reports. Clarifying the dosing of intravenous methylprednisolone may be of benefit to patients in the future, especially if suspicion of Levamisole adulteration is present.
INTRODUCTION
Cocaine-induced leukoencephalopathy is a rare neurological condition usually associated with substances used to adulterate cocaine. A common adulterant of cocaine includes levamisole, an anti-helminthic agent causing pathologies including vasculitis and agranulocytosis when ingested .1 Levamisole is thought to be used to add weight and volume, with possible potentiation of the effects of cocaine.2 With over five million Americans using cocaine and an estimated 70% of cocaine in the United States being adulterated with levamisole, this poses a serious health burden.1 Other known adulterants of cocaine include the historical use of local anesthetics, and more recently phenacetin, amphetamines, methamphetamines, and psychoactive substances.3 These substances commonly amplify the toxic effects of cocaine, creating more serious health risks.
Patients with toxic leukoencephalopathy usually present with confusion, behavior changes, extrapyramidal symptoms, generalized motor deficits, and unresponsiveness, which can result in death. The case studies published detailing cocaineinduced leukoencephalopathy usually result in the patient making a full recovery when identified and treated promptly.4-6 This pathology has been compared to spongiform encephalopathies, with fluid
entrapment within vacuoles within the myelin lamellae that surround the axons and are represented on imaging by the expansion of brain involvement, though clinical improvement is being made.4 Below is a detailed report of a patient’s hospital course after the use of suspected adulterated cocaine and its 12-day management.
CASE
We present a case of suspected cocaineinduced leukoencephalopathy. The patient, a 31-year-old male with an unknown past medical history, presented to the Emergency Department (ED) after being found with altered mental status in his vehicle. On arrival to the ED, the patient was ill-appearing and could not protect his airway and was therefore given naloxone and intubated, with seizure-like activity occurring, with stiffness, posturing, and incontinence. On admission, his vitals included a heart rate of 56 beats per minute, temperature of 98.1 °F (36.7 °C), respiratory rate of 16 per minute, oxygen saturation of 97%, and blood pressure of 210/110 mmHg, indicative of hypertensive emergency.
His neurological exam yielded a Glasgow Coma Scale (GCS) score of four. There were roving eye movements with no gaze deviation, which improved throughout his hospital stay. The cough reflex was intact when elicited. Brachioradialis deep tendon
reflexes included a 3+ response bilaterally, with a positive Hoffman sign bilaterally. The left lower extremity deep tendon reflex was 3+, with a crossed adductor reflex present. The patellar reflex in the right lower extremity was 2+. An upgoing Babinski reflex was present in the left lower extremity and absent in the right lower extremity. The general sensory response included intermittent grimacing to proximal painful stimuli to the face and trapezius muscle.
The patient was admitted to the neurocritical care unit for management of an initial working problem list, including toxic leukoencephalopathy as the primary problem, acute respiratory failure with hypoxia, status epilepticus (resolved in ED), non-traumatic rhabdomyolysis, aspiration pneumonia, hypertensive emergency, and acute renal failure. The ED review of symptoms for this patient was not received, but was negative for signs of trauma, with normal heart and abdominal sounds. The patient’s girlfriend denied observation of fever, chills, nausea, and vomiting.
Additional history taken from her was consistent with the patient likely experiencing a seizure in his car after ingestion of cocaine. A previous stay of the patient revealed no history of seizures. His serum CK level was later found to be elevated at 26,369 with concern for rhabdomyolysis, another sign that is associated with seizures. The patient’s status epilepticus resolved after Lorazepam and a Levetiracetam load of 4.5 g, followed by 750 mg twice daily during stay.
Labs ordered for the patient included a urine drug screen (UDS), metabolic and blood panels, and inflammatory markers, with the UDS positive for cocaine and negative for other illicit drugs tested on a basic UDS. Cardiac exam included auscultation negative for rubs, murmurs, or gallops. A transthoracic echocardiogram revealed a normal ejection fraction of 52%, with no wall motion abnormalities and normal systolic function.
CT-Angiography (CTA) of the chest was obtained on day one of admission and resulted in bilateral upper and lower lobe-dependent opacities concerning for aspiration. Based on these findings, periodic chest X-rays were ordered to monitor progression. CTA of the abdomen was suggestive of an indeterminate left renal lower pole <1 cm lesion. CTA of the head, neck, and pelvis reported no acute abnormalities. Chest X-ray from day five demonstrated a small left pleural effusion with mild interval improvement in hazy opacities in the right lower lung field and ideal endotracheal tube placement.
An MRI of the head conducted on Day 2 revealed bilateral hemispheric diffusion restriction predominantly involving the subcortical and deep white matter, sparing the subcortical U fibers. Signal abnormalities, diffusion restriction within the cerebellar hemispheres, and a single small nodular focus of diffusion restriction in the left cingulate gyrus were also found. These signal abnormalities would not usually present in status epilepticus and would be highly atypical in infectious etiology, further narrowing the authors' differential diagnosis towards cocaine-induced leukoencephalopathy and other metabolic etiologies.
An MRI of the head conducted on Day 5 is shown below in Figure 1 A–B, demonstrating an interval increase in the extent of white matter signal abnormality, likely representing the evolution of toxic leukoencephalopathy. Evolving small late-acute to early subacute infarcts in the left cingulate gyrus and bilateral cerebellar hemispheres are thought to be due to cocaine-induced vasospasms. Hypoxic ischemic injury could have contributed to these findings, but is less likely due to the lack of additional cortical and gray matter involvement.
Management of this patient’s cocaineinduced leukoencephalopathy included empiric intravenous (IV) methylprednisolone with a ketamine drip due to clinical suspicion and lack of convincing alternative diagnoses.
A B
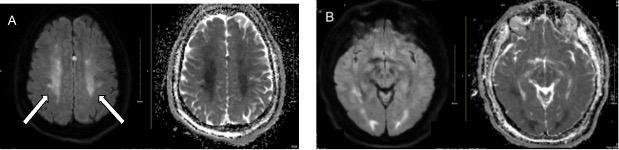
Figure 1A and B show bilateral hemispheric diffusion restriction predominantly involving the subcortical and deep white matter with sparing of the subcortical U fibers, as well as signal abnormality and diffusion restriction within the cerebellar hemispheres. A single small nodular focus of diffusion restriction in the left cingulate gyrus is also shown.
The patient’s systolic blood pressure goal was <140 mmHg, and oxygen saturation was stable, being above 95% while intubated and status-post intubation on Day 10.
The patient’s hypertensive emergency was managed with amlodipine and hydrochlorothiazide given daily during a hospital stay. Management of aspiration pneumonia due to positive findings on chest CT, chest x-ray, and CBC with leukocytosis was managed with vancomycin and piperacillin/tazobactam injection on Days 1-2, ampicillin sodium/sulbactam sodium on Days 2-6, and piperacillin/tazobactam injection on Day 12 through the discharge course. His acute renal failure and rhabdomyolysis improved during stay with a fluid goal of 100 mL/hour, and CK and creatinine levels returned to normal values by the end of stay.
The patient’s acute respiratory failure with hypoxia was managed with intubation upon admission for airway protection and placed on continuous positive airway pressure. Sedation was controlled with midazolam and ketamine, with ketamine boluses administered for agitation episodes. Nicardipine was given as needed for blood pressure control due to previously prescribed amlodipine and hydrochlorothiazide for hypertension management that was continued through
his hospital stay. Additional medications for acute altered mental status management and agitation were as needed: lorazepam, IV thiamine, and 50 mg of quetiapine twice daily. For pain management, the patient was given oxycodone, gabapentin, and fentanyl.
FOLLOW-UP AND OUTCOMES
On Day 10, the patient was extubated and placed on bilevel positive airway pressure, continuing to show improvement in his respiratory status. He experienced no additional seizure activity after his initial event. After a 12-day hospitalization, the patient improved towards baseline, being alert and oriented, ambulatory without assistance, and without complaints of pain or shortness of breath. The patient returned for follow-up for further management of baseline hypertension and post-hospital assessment.
DISCUSSION
Clinical Course
The neurologic complications of cocaine overuse are many, with the most common being strokes, seizures, and cognitive deficits.7 However, cocaine-induced
Figure 1A–B: MRI head with and without contrast on Day 5.
leukoencephalopathy is a rare problem occurring most likely due to adulterated cocaine, namely levamisole. Common MRI findings are diffuse white matter involvement with sparing of the subcortical U fibers, T2 signal abnormalities, and diffusion restriction; in this case, it was present in the left cingulate gyrus. Subcortical U fibers are also called short association fibers and connect adjacent gyri, located either within the cortex or immediately deep in the subcortical white matter.8 Due to their myelination and good blood supply, they tend to be affected last in chronic ischemic disease unless in the setting of a direct attack on oligodendrocytes, such as leukoencephalopathy.8
Repeated MRI brain imaging was performed to compare white matter evolution, which is important in monitoring the progression of hyperintensities. Other differential MRI findings of brainstem or cerebellar involvement point more toward leukoencephalopathy due to heroin use.9 Aside from MRI findings, complications of cocaine-induced leukoencephalopathy include confusion, behavior changes, extrapyramidal symptoms, generalized motor deficits, and unresponsiveness, which can result in death.
Comparing Management
While the patient was in the Neuro-ICU, empiric IV methylprednisolone was initiated to reduce inflammation, and levetiracetam was initiated for status epilepticus present upon arrival. Discontinuation of the offending agent is also important for the progression of treatment. In this case, a 12-day hospital stay resulted in this patient’s return to baseline due to medical stabilization and treatment with removal of the offending agent. One similar case of cocaine-induced leukoencephalopathy from 2015 reported that the patient, after stabilizing from initial treatment, was readmitted because of further cocaine use, and an MRI showed prominent worsening of the patient’s lesions.9
One controversial aspect of cocaine-induced leukoencephalopathy is the management of
the clinical disease due to uncertainty on what management is best for patients undergoing this disease course. The authors' patient received a daily IV of methylprednisolone 1 g for 5 days. Other cases with similar presentations, however, have shown patients receiving different doses of steroids or different treatments altogether. For instance, some professionals suggest higher doses of steroids, such as methylprednisolone 1 g, can result in the death of these patients,10 with possible benefit of lower doses of 250 mg to allow recovery. Two similar cases of cocaine-induced leukoencephalopathy in a 31-year-old female and a 19-year-old male sadly resulted in their deaths despite undergoing treatment with boluses of 1g methylprednisolone.11 This may suggest dosing changes based on clinical parameters to be advantageous for patient recovery, with these parameters not yet established.
An alternative route is a more conservative approach. One case presented with a 58-yearold male who received supportive care once the infectious etiology was ruled out.12 This approach showed symptom resolution with a hospital length of stay like our patient. Another conservative approach for a 55-year-old male did not end in recovery. His treatment consisted of CoQ10, vitamins E and C, and levetiracetam for seizure prophylaxis.13 While this patient partially recovered, he did not regain full cognitive function, which may allude to more aggressive treatment with steroids, as with our patient, as is the treatment of choice. This would be especially true if Levamisole is detected.
Management and Diagnostic Considerations
Due to the rarity and inconsistent clinical presentation of cocaine-induced leukoencephalopathy, it is essential to consider the factors potentially causing the wide array of symptoms. Cocaine used by patients is often adulterated with substances such as levamisole, diltiazem, local anesthetics, and hydroxyzine.14
Levamisole causes central nervous system vasculitis and reversible leukoencephalopathy by interfering with mitochondrial function and oxidative stress pathways, exacerbating neuronal damage.14 The combination of levamisole and cocaine can result in the formation of aminorex, an amphetamine-like drug, leading to synergistic effects. This combination can have irreversible effects on neuronal receptors, eliciting a stronger response than if either drug were used alone.14 As a result, the composition ratio heavily influences the symptoms experienced by the user.
In any suspected case of cocaine-induced leukoencephalopathy, further testing to evaluate the concentration of levamisole may be necessary to guide treatment regimens, typically including pulsed IV methylprednisolone. This case is notable because the patient was treated with high-dose methylprednisolone, which in combination with removal of substance exposure is aligned with treating primary levamisole intoxication. The patient’s rapid improvement toward baseline may be an indication that the cocaine ingested by the patient had a higher concentration of levamisole, making the treatment effective.
In a similar case presentation, a patient was being treated with only supportive care and was not improving.15 After the use of methylprednisolone, the patient’s mental status improved, and was subsequently extubated 10 days later, similarly to the authors' patient. These scenarios underscore the potential benefit of levamisole testing, which uses sulfate or glucuronide levels in the urine to determine the appropriate treatment approach. Further research would benefit from clarifying whether levamisoleinduced leukoencephalopathy responds to dose-based methylprednisolone, and if identifying levamisole amounts would steer clinical decision making regarding these treatment options.
Differential Considerations
Though negative in the authors' patient, in patients with heroin-induced leukoencephalopathy, similar MRI findings can be noted when compared to cocaineinduced leukoencephalopathy. A case study analyzed the MRI findings of three patients abusing heroin, cocaine, and cannabis, and a symmetrically increased T2 and T2FLAIR signal intensity of the cerebellar and posterior cerebral white matter and sparing of subcortical U fibers.16 Although imaging and lab findings are similar in both diagnoses, they significantly differ in pathophysiological disease progression. Patients with heroininduced leukoencephalopathy typically present with a more progressive spongiform type of encephalopathy with the presence of intracytoplasmic vacuoles. Those affected by cocaine-induced leukoencephalopathy have a more demyelinating pattern.17 These patterns could influence disease progression and prognosis, respectively. Many factors must be taken into consideration when deciphering between polysubstance abuse leukoencephalopathy and purely cocaineinduced leukoencephalopathy, for reasons including increased adulterant use in illicit drugs, drug–drug interactions competing for common neuron receptors, and the method of use, since inhalation versus intravenous intake causes neuronal receptor concentration discrepancies.
Another differential to consider in this patient’s hospital course is hypertensive leukoencephalopathy. Hypertensive leukoencephalopathy primarily affects the white matter of the brain, which is usually due to a sudden and severe elevation in blood pressure. It’s often part of a hypertensive emergency and can be reversible when treated promptly. Similar signs present in this case that were present in our patient were his altered mental status and seizure activity. As explained in the case presentation, however, this was less likely due to imaging findings. Regardless, blood pressure goals were maintained as a part of the patient’s treatment protocol.
Limitations
This case study is inherently limited by its observational and anecdotal nature, which restricts the generalizability of its findings. The treatment approach used, while clinically guided, requires further investigation to establish broader applicability and efficacy. Although levamisole was strongly suspected as the adulterant in the patient’s cocaine use, this was not confirmed through toxicological testing, leaving room for uncertainty regarding the specific causative agent. Additionally, the absence of certain clinical data limits the authors' ability to fully understand the underlying pathophysiology and clinical trajectory in this case. Regardless, we believe the novel treatment and the need for additional, more specific testing would be of benefit in future cases.
CONCLUSIONS AND RECOMMENDATIONS
The case study exhibits the importance of early recognition and treatment of cocaineinduced leukoencephalopathy, the impact of levamisole-adulterated cocaine, the clinical outcomes of induced leukoencephalopathy, and the poor clinical outcomes without
References
1. El Khoury et al. Cutaneous Necrotizing Vasculitis and Leukopenia in a Cocaine User: Is Levamisole the Culprit? Case Rep Rheumatol. 2016;2016:2685267.
2. Buchanan JA et al. Prevalence of levamisole in urine toxicology screens positive for cocaine in an inner-city hospital. JAMA. 2011;305(16):1657-8.
3. UNOD.C, Cocaine: A – a spectrum of products. , Cocaine Insights 2. 2021. Available at: , UNODC, Vienna, October 2021.chrome extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.unodc. org/documents/data-and-analysis/cocaine/Cocaine_Insights_2021_2.pdf. Last accessed: 19 April 2025.
4. González-Duarte A, Williams R. Cocaine-induced recurrent leukoencephalopathy. Neuroradiol J. 2013;26(5):511-3.
5. Abdilla Y et al. Cocaine-induced toxic leucoencephalopathy with complete clinical recovery. BMJ Case Reports CP. 2019;12:e229134.
6. Mader EC Jr et al. Full recovery from cocaine-induced toxic leukoencepha-
prompt intervention. This patient presented with altered mental status and diagnoses of cocaine-induced leukoencephalopathy, hypertensive emergency, and acute respiratory failure. The combination of intubation with IV methylprednisolone and levetiracetam and discontinuation of the offending agent offered a swift recovery to baseline for this patient. Had the recognition of cocaine-induced leukoencephalopathy not been so expeditious, this patient’s prognosis would likely be more severe. Therefore, early diagnosis and recognition are vital in treating this condition.
A larger understanding of adulterated cocaine complications will not only advantage treatment and management protocol but will help the general population through a greater appreciation of the negative outcomes of illicit cocaine use. There is still more information needed to determine the best course of action for the treatment of suspected cocaine-induced leukoencephalopathy, but this study highlights possible benefits of IV methylprednisolon along with supportive care, along with the potential benefit of levamisole testing. Additional reports comparing treatment options will greatly benefit the medical care for this condition.
lopathy: emphasizing the role of neuroinflammation and brain edema. J Investig Med High Impact Case Rep. 2019;7:2324709619868266.
7. Casas Parera I et al. Complicaciones neurológicas por abuso de cocáina [Neurologic complications by cocaine abuse]. Medicina (B Aires). 1994;54(1):35-41.
8. Vosoughi R, Schmidt BJ. Multifocal leukoencephalopathy in cocaine users: a report of two cases and review of the literature. BMC Neurol. 2015;15:208.
9. Wu VC et al. Levamisole-induced multifocal inflammatory leukoencephalopathy: clinical characteristics, outcome, and impact of treatment in 31 patients. Medicine. 2006;85(4):203-13.
10. Gaillard F et al. Subcortical U-fibers. Available at: https://radiopaedia.org/articles/subcortical-u-fibres-3?lang=us Last accessed: 22 May 2024.
11. Maingard J et al. Cingulate gyrus. Available at: https://radiopaedia.org/articles/ cingulate-gyrus?lang=us.Last accessed: 22 May 2024.
12. Eshan S et al. Cocaine-induced toxic leukoencephalopathy: a case report. Cureus. 2024;16(2):e54574.
13. Cartier R et al. Fatal toxic leukoencephalopathy associated with consumption of pasta base of cocaine: Report of three cases. Revista médica de Chile. 2015;143(11):1484-9.
14. Gartz A et al. Effects of cocaine and levamisole (as adulterant) on the isolated perfused Langendorff heart. Int J Legal Med. 2020;134:1741-52.
15. Burger C et al. Toxic Leukoencephalopathy due to presumed levamisole exposure treated with methylprednisolone in an elderly male with illicit cocaine use. CHEST. 2024;166(4):A2874-5
16. Achamallah N et al. Chasing the wrong dragon: a new presentation of heroin-induced toxic leukoencephalopathy mimicking anoxic brain injury. J Intensive Care Soc. 2019;20(1):80-5.
17. Alshamam MS et al. Heroin-Induced Leukoencephalopathy. Cureus. 2021;13(2):e13093.
If you like it,why not share it...

Share with a colleague today