Centre for Medical Microbiology, University College London, UK
Richard Barton
Mycology Reference Centre, Leeds General Infirmary, UK
Neil A.R. Gow
Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Susan Howell
Mycology Laboratory, St John’s Institute of Dermatology, Viapath, London, UK
Donna M. MacCallum
Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Rohini J. Manuel
Public Health Laboratory, National Infection Service, Public Health England, London, UK
1
Great Clarendon Street, Oxford, OX2 6DP, United Kingdom
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and in certain other countries
The moral rights of the authors have been asserted
First Edition published in 2018
Impression: 1
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by licence or under terms agreed with the appropriate reprographics rights organization. Enquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above
You must not circulate this work in any other form and you must impose this same condition on any acquirer
Published in the United States of America by Oxford University Press
198 Madison Avenue, New York, NY 10016, United States of America
British Library Cataloguing in Publication Data
Data available
Library of Congress Control Number: 2017943525
ISBN 978–0–19–875538–8
Printed in Great Britain by Bell & Bain Ltd., Glasgow
Oxford University Press makes no representation, express or implied, that the drug dosages in this book are correct. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulations. The authors and the publishers do not accept responsibility or legal liability for any errors in the text or for the misuse or misapplication of material in this work. Except where otherwise stated, drug dosages and recommendations are for the non-pregnant adult who is not breast-feeding
Links to third party websites are provided by Oxford in good faith and for information only. Oxford disclaims any responsibility for the materials contained in any third party website referenced in this work.
Foreword
I have a fondness for mycology because I have worked all my life on the fungus fission yeast, trying to uncover the mechanisms underlying the control of the eukaryotic cell cycle. Medical mycology is a specialty which has made great strides in recent years and is having increasing influence on the clinical outcomes of individuals with immunocompromising diseases such as leukaemia and AIDS. The mortality of some of their infections is still well over 70%. For example, there are around a million cases of cryptococcosis a year, of which more than 600,000 will result in death. Overall, infections due to fungi occur on a scale similar to malaria, and to many bacterial and viral diseases.
This is a timely comprehensive text on the subject, which has its roots in the British Society for Medical Mycology (BSMM) global Master’s programme, and is aimed at both scientists and clinicians. Advances in targeted chemotherapy can be marred by invasive fungal infections, and there is a real need to encourage young scientists and clinicians to fully engage with this specialty. In the last 50 years, we have gone from a time when there was just one broad-spectrum antifungal agent for the treatment of serious invasive disease, to one
when there are around 20. Diagnostic methods have been refined and studied in clinical trials, antifungal susceptibility assays are internationally defined and tested, and our understanding of fungal taxonomy and epidemiology has been transformed by molecular biology. There is much to be optimistic about and there is a significant body of knowledge to be assimilated by those working in this area. I think that this Oxford Textbook will go a long way towards achieving this last aspiration.
The editors have recruited international experts to produce upto-date and detailed chapters aimed at a postgraduate readership. The scope of the book is broad and is divided into six sections, dealing in turn with the basics of mycology, the causative organisms, a systems approach to the mycoses, infections in special populations, diagnostics, and therapy. This book should be a companion for mycology courses and for many scientists and healthcare workers looking to further their knowledge of these topics.
Professor Sir Paul Nurse Director, The Francis Crick Institute, London
Preface
This book had its genesis in the British Society for Medical Mycology (BSMM) Master’s programme. The editors are tutors on this programme and came together with the express idea of producing a suitable textbook to accompany the courses. Hence, the structure of the book is loosely based on the course structure, expanding content in areas of focused study and bringing together recently acquired knowledge in one place.
However, it was apparent that such a book could be a companion for other courses and, indeed, for scientists and clinicians looking to further their knowledge of medical mycology in topics as diverse as cell function, epidemiology, and advanced diagnostics, through to therapeutic drug monitoring in the management of mycoses. As a consequence, the scope of the book is broader and deeper than originally planned and its readership is expected to be much wider. We have, therefore, divided the book into more sections than originally considered, dealing in turn with the basics of mycology (cell function, taxonomy, pathogenesis, immunology, and so on), the causative organisms, a systems approach to the mycoses, infections
in special populations, diagnostics, and therapy. To take advantage of this broad remit, the reader should make use of all the different sections. For example, whilst the general principles of therapy are dealt with in the clinical sections, the reader will find more details of the individual drugs and strategies in the therapy section, and more about the causative fungi in the mycology section.
We have recruited a faculty of international experts, many of whom are lecturers on the BSMM programme, to produce up-todate and detailed chapters aimed at a postgraduate readership, and we are very grateful to them for the time and care they have put into their efforts on your behalf. In addition, I would like to thank my fellow editors and everyone who has been involved with the BSMM course. This Oxford Textbook of Medical Mycology is dedicated to them and to the current and former students scattered around the world.
Professor Chris Kibbler London, January 2018
List of Abbreviations xi
List of Contributors xv
SECTION 1
The principles of medical mycology 1
1 Introduction to medical mycology 3
David W. Warnock
2 Fungal taxonomy and nomenclature 8
Andrew M. Borman
3 Physiology and metabolism of fungal pathogens 17
Neil A.R. Gow and Alistair J.P. Brown
4 Fungal cell structure and organization 23
Nick D. Read
5 Fungal genetics 35
Paul S. Dyer, Carol A. Munro, and Rosie E. Bradshaw
6 Fungal genomics and transcriptomics 43
Carol A. Munro and Duncan Wilson
7 Epidemiology of fungal disease 50
Rajal K. Mody, Angela Ahlquist Cleveland, Shawn R. Lockhart, and Mary E. Brandt
8 Pathogenesis of fungal disease 56
Frank C. Odds
9 Immunology of fungal disease 62
Ivy M. Dambuza, Jeanette Wagener, Gordon D. Brown, and Neil A.R. Gow
SECTION 2
Medically important fungi 71
10 Aspergillus species 73
Stephanie J. Smith, Rohini J. Manuel, and Christopher C. Kibbler
11 Candida species 77
Bernhard Hube and Oliver Kurzai
12 Cryptococcus species 80
Catriona L. Halliday and Sarah E. Kidd
13 Other yeasts 83
Chris Linton and Susan Howell
14 Dematiaceous fungi 88
Sarah E. Kidd and Catriona L. Halliday
15 The dermatophytes 93
Susan Howell
16 Endemic dimorphic fungi 98
Angela Restrepo, Angel González, and Beatriz L. Gómez
17 Hyaline moulds 107
Elizabeth M. Johnson
18 Mucoraceous moulds 111
Thomas R. Rogers and Elizabeth M. Johnson
19 Pneumocystis jirovecii 116
Stuart Flanagan
SECTION 3
Fungal diseases 119
20 Fungal bone and joint infections 121
Damien Mack, Simon Warren, Shara Palanivel, and Christopher P. Conlon
21 Fungal cardiovascular infections 128
Sarah Drake and Jonathan Sandoe
22 Fungal central nervous system infections 135
Tihana Bicanic and Thomas S. Harrison
23 Fungal infections of the skin and subcutaneous tissue 145
Roderick J. Hay
24 Fungal diseases of the ear, nose, and throat 154
Arunaloke Chakrabarti
25 Fungaemia and disseminated infection 163
Rebecca Lester and John H. Rex
26 Fungal diseases of the gastrointestinal tract 171
Silke Schelenz
27 Genito-urinary fungal infections 177
Jack D. Sobel
28 Fungal eye infections 183
Heather L. Clark and Eric Pearlman
29 Fungal infections of the kidney and those associated with renal failure, dialysis, and renal transplantation 190
Eileen K. Maziarz and John R. Perfect
30 Fungal diseases of the respiratory tract 205
Samantha E. Jacobs, Catherine B. Small, and Thomas J. Walsh
31 Fungal toxin-mediated disease 215
Christopher C. Kibbler
SECTION 4
Fungal infections in specific patient groups 223
32 Fungal infections in haemato-oncology 225
Philipp Koehler and Oliver A. Cornely
33 Fungal infections among patients with AIDS 235
Blandine Denis, Fanny Lanternier, and Olivier Lortholary
34 Fungal infections in solid organ transplantation 243
Darius Armstrong James, Anand Shah, and Anna Reed
35 Fungal infections in neonates 251
Adilia Warris
36 Fungal infections in intensive therapy units 258
Rosemary A. Barnes and Matthijs Backx
37 Fungal disease in cystic fibrosis and chronic respiratory disorders 266
Chris Kosmidis, David W. Denning, and Eavan G. Muldoon
SECTION 5
Diagnosis 275
38 Biosafety and quality assurance in the mycology laboratory 277
Michael D. Palmer and Shila Seaton
39 Microscopy and culture of fungal disease 283
Gillian S. Shankland
40 Histopathology of fungal disease 289
Sebastian B. Lucas
41 The imaging of fungal disease 298
Joanne Cleverley
42 Serology of fungal disease 307
Richard Barton
43 Molecular diagnosis of fungal disease 313
P. Lewis White and Rosemary A. Barnes
44 Guidelines for the diagnosis of fungal disease 327
Manuel Cuenca-Estrella
SECTION 6
Antifungal therapy 335
45 Principles of antifungal therapy 337
Russell E. Lewis
46 Antifungal agents 343
Donna M. MacCallum
47 Antifungal susceptibility testing and resistance 350
Elizabeth M. Johnson
48 Antifungal therapeutic drug monitoring 355
H. Ruth Ashbee
49 Antifungal treatment guidelines 360
Laura Cottom and Brian L. Jones
Index 373
List of Abbreviations
AAPCC American Association of Poison Control Centres
ABLC amphotericin B lipid complex
ABPA allergic bronchopulmonary aspergillosis
ABPM allergic bronchopulmonary mycosis
AFLP amplified fragment length polymorphism
AFRS allergic fungal rhinosinusitis
ADI AIDS-defining illness
AGREE II Appraisal of guidelines research & evaluation II (system)
AIDS acquired immune deficiency syndrome
AmB-D amphotericin B-deoxycholate
APACHE Acute Physiology and Chronic Health Evaluation (system)
APECED autoimmune polyendocrinopathy with candidiasis and ectodermal dystrophy
APPH acute primary pulmonary histoplasmosis
ART antiretroviral therapy
ATCC American Type Culture Collection
ATP adenosine triphosphate
AUC area under the concentration curve
BAL bronchoalveolar lavage
BCR B-cell receptor
BCSH British Committee for Standards in Haematology
BDG (1→3) β-D-glucan
bp base pair
BSMM British Society for Medical Mycology
cART combination antiretroviral therapy
CATs conidial anastomosis tubes
CCPA chronic cavitary pulmonary aspergillosis
CDC Centers for Disease Control and Prevention
CFP cyan fluorescent protein
CFT complement fixation test
CFTR cystic fibrosis transmembrane regulator
ChIP-Seq chromatin immunoprecipitation sequencing
CGB canavanine-glycine-bromothymol blue (agar)
CGD chronic granulomatous disease
CLRs C-type lectin receptors
CMI cell-mediated immunity
CMV cytomegalovirus
CNPA chronic necrotizing pulmonary aspergillosis
CNS central nervous system
CONSORT Consolidated Standards of Reporting Trials
COPD chronic obstructive pulmonary disease
CPA chronic pulmonary aspergillosis
CRAG cryptococcal antigen
CRBSI catheter-related bloodstream infection
CSF cerebrospinal fluid
CT computed tomography
CT-PET CT–positron emission tomography
CVC central venous catheter
DALI Defining Antibiotic Levels in Intensive care unit patients (study)
DAPI 4′, 6-diamidino-2-phenylindole (stain)
DCs dendritic cells
DD double diffusion (test)
ds double-stranded
EAPCRI European Aspergillus PCR Initiative
ECIL European Conference on Infections in Leukaemia
ECOFF epidemiological cut-off
EDTA ethylenediaminetetraacetic acid
ECMM European Confederation of Medical Mycology
EFRS eosinophilic fungal rhinosinusitis
EIA enzyme immunoassay
ELBW extremely low birth weight
ELISA enzyme-linked immunosorbent assay
EMA European Medicines Agency
EMRS eosinophilic mucin rhinosinusitis
ENT ear, nose & throat services
EORTC European Organisation for Research and Treatment of Cancer
EQAS external quality assurance schemes
ESCMID European Society of Clinical Microbiology and Infectious Diseases
H. Ruth Ashbee, School of Molecular and Cellular Biology, University of Leeds, UK
Matthijs Backx, Public Health Wales Microbiology Division, University Hospital of Wales, Cardiff, UK
Rosemary A. Barnes, Infection and Immunity, School of Medicine, Cardiff University, University Hospital of Wales, Cardiff, UK
Richard Barton, Mycology Reference Centre, Leeds General Infirmary, Leeds, UK
Tihana Bicanic, Institute for Infection and Immunity, St George’s, University of London, UK
Andrew M. Borman, Public Health England National UK Mycology Reference Laboratory, Bristol, UK
Rosie E. Bradshaw, Institute of Fundamental Sciences, Massey University, Palmerston North, New Zealand
Mary E. Brandt, Mycotic Diseases Branch, Centers for Disease Control and Prevention, Atlanta, GA, USA
Alistair J.P. Brown, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Gordon D. Brown, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Arunaloke Chakrabarti, Postgraduate Institute of Medical Education and Research, Chandigarh, India
Heather L. Clark, University of California, Irvine, CA, USA
Angela Ahlquist Cleveland, Mycotic Diseases Branch, Centers for Disease Control and Prevention, Atlanta, GA, USA
Joanne Cleverley, Department of Radiology, Royal Free Hospital, London, UK
Christopher P. Conlon, Nuffield Department of Medicine, University of Oxford, UK
Oliver A. Cornely, Department I of Internal Medicine, University Hospital of Cologne, Germany, Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), and Clinical Trials Centre Cologne, ZKS Köln,
University of Cologne, Germany, German Centre for Infection Research, Partner Site Bonn-Cologne, Germany
Laura Cottom, NHS Greater Glasgow and Clyde Health Board, Glasgow, UK
Manuel Cuenca-Estrella, Instituto de Salud Carlos III, Madrid, Spain
Ivy M. Dambuza, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Blandine Denis, Service des maladies infectieuses et tropicales, Hôpital Saint Louis, AP-HP Paris, France UMR S 1136, INSERM et Sorbonne Universités, UPMC Univ Paris 06, Paris, France
David W. Denning, University Hospital of South Manchester NHS Foundation Trust, Manchester, UK
Sarah Drake, University of Leeds and Leeds Teaching Hospitals NHS Trust, Leeds, UK
Paul S. Dyer, School of Life Sciences, University of Nottingham, Nottingham, UK
Stuart Flanagan, Department of Infection and Immunology, Royal London Hospital, London, UK
Beatriz L. Gómez, School of Medicine and Health Sciences, Universidad del Rosario, Bogotá, Colombia
Angel González, Basic and Applied Microbiology Research Group (MICROBA), School of Microbiology, Universidad de Antioquia, Medellín, Colombia
Neil A.R. Gow, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Catriona L. Halliday, Clinical Mycology Reference Laboratory, Centre for Infectious Diseases and Microbiology Laboratory Services, NSW Pathology, ICPMR, Westmead Hospital, Westmead, NSW, Australia
Thomas S. Harrison, Institute for Infection and Immunity, St George’s, University of London, UK
Roderick J. Hay, Skin Infection Clinic, King’s College Hospital NHS Trust, Denmark Hill, London, UK
Susan Howell, Mycology Laboratory, St John’s Institute of Dermatology, Viapath, London, UK
Bernhard Hube, Department of Microbial Pathogenicity Mechanisms, Leibniz Institute for Natural Product Research and Infection Biology – Hans Knöll Institute (HKI), Jena, Germany
Samantha E. Jacobs, Transplantation-Oncology Infectious Diseases Program, Division of Infectious Diseases, Weill Cornell Medical Center, New York, NY, USA
Darius Armstrong James, National Heart and Lung Institute, Imperial College London, UK
Elizabeth M. Johnson, Public Health England National UK Mycology Reference Laboratory, Bristol, UK
Brian L. Jones, NHS Greater Glasgow and Clyde Health Board, Glasgow, UK
Christopher C. Kibbler, Centre for Medical Microbiology, University College London, UK
Sarah E. Kidd, National Mycology Reference Centre, SA Pathology, Adelaide, SA, Australia
Philipp Koehler, Department I of Internal Medicine, University Hospital of Cologne, Germany Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), and Clinical Trials Centre Cologne, ZKS Köln, University of Cologne, Germany
Chris Kosmidis, University Hospital of South Manchester NHS Foundation Trust, Manchester, UK
Oliver Kurzai, National Reference Center for Invasive Fungal Infections, Leibniz Institute for Natural Product Research and Infection Biology – Hans Knöll Institute (HKI), Jena, Germany
Fanny Lanternier, Université Paris-Descartes, Centre d’Infectiologie Necker-Pasteur, Hôpital Necker-Enfants Malades, Paris, France Centre National de Référence Mycoses Invasives et Antifongiques, Unité de Mycologie Moléculaire, Institut Pasteur, Paris, France
Rebecca Lester, University of Liverpool, Liverpool, UK
Russell E. Lewis, Infectious Diseases Unit, S. Orsola-Malpighi Hospital, Department of Medical and Surgical Sciences, University of Bologna, Bologna, IT
Chris Linton, Public Health England National UK Mycology Reference Laboratory, Bristol, UK
Shawn R. Lockhart, Mycotic Diseases Branch, Centers for Disease Control and Prevention, Atlanta, GA, USA
Olivier Lortholary, Université Paris-Descartes, Centre d’Infectiologie Necker-Pasteur, Hôpital Necker-Enfants Malades, Paris, France Centre National de Référence Mycoses Invasives et Antifongiques, Unité de Mycologie Moléculaire, Institut Pasteur, Paris, France
Sebastian B. Lucas, Department of Histopathology, St Thomas’ Hospital, London, UK
Donna M. MacCallum, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Damien Mack, Division of Infection and Immunity, University College London, UK
Rohini J. Manuel, Public Health Laboratory, National Infection Service, Public Health England, UK
Eileen K. Maziarz, Department of Medicine, Duke University School of Medicine, Durham, NC, USA
Rajal K. Mody, Mycotic Diseases Branch, Centers for Disease Control and Prevention, Atlanta, GA, USA
Eavan G. Muldoon, Mater Misericordiae University Hospital, Dublin, Ireland
Carol A. Munro, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Frank C. Odds, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Shara Palanivel, Royal Free London NHS Foundation Trust, and Royal National Orthopaedic Hospital, Stanmore, London, UK
Michael D. Palmer, Public Health England (PHE) National Mycology Reference Laboratory, Bristol, UK
Eric Pearlman, Case Western Reserve University, Cleveland, OH, USA
John R. Perfect, Department of Medicine, Duke University School of Medicine, Durham, NC, USA
Nick D. Read, Manchester Fungal Infection Group, Division of Infection, Immunity and Respiratory Medicine, University of Manchester, UK
Anna Reed, Royal Brompton and Harefield NHS Trust, London, UK
Angela Restrepo, Corporación para Investigaciones Biológicas (CIB), Medellín, Colombia
John H. Rex, F2G, Ltd., Eccles, UK; CARB-X, Boston, MA; Rex Life Sciences LLC, Wellesley, MA
Thomas R. Rogers, Department of Clinical Microbiology, Trinity College Dublin, St James’s Hospital Campus, Dublin 8, Ireland
Jonathan Sandoe, University of Leeds and Leeds Teaching Hospitals NHS Trust, Leeds, UK
Silke Schelenz, Department of Microbiology, Royal Brompton Hospital, London, UK
Shila Seaton, National External Quality Assessment Service (NEQAS), National Infection Service, Public Health England, Colindale, London, UK
Anand Shah, Fungal Disease Immunobiology, Imperial College London, UK
Gillian S. Shankland, School of Medicine, Dentistry and Nursing, University of Glasgow, UK
Catherine B. Small, Transplantation-Oncology Infectious Diseases Program, Division of Infectious Diseases, Weill Cornell Medical Center, New York, NY, USA
Stephanie J. Smith, Barts Health National Health Service Trust, London, UK
Jack D. Sobel, Wayne State University, School of Medicine, Detroit, MI, USA
Jeanette Wagener, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
Thomas J. Walsh, Transplantation-Oncology Infectious Diseases Program, Division of Infectious Diseases, Weill Cornell Medical Center, New York, NY, USA
David W. Warnock, Faculty of Biology, Medicine and Health, University of Manchester, UK
Simon Warren, Royal Free London NHS Foundation Trust, London, UK
Adilia Warris, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
P. Lewis White, Public Health Wales, Microbiology, Cardiff, University Hospital of Wales, Cardiff, UK
Duncan Wilson, Aberdeen Fungal Group, MRC Centre for Medical Mycology at the University of Aberdeen, UK
The principles of medical mycology
1 Introduction to medical mycology 3
David W. Warnock
2 Fungal taxonomy and nomenclature 8
Andrew M. Borman
3 Physiology and metabolism of fungal pathogens 17
Neil A.R. Gow and Alistair J.P. Brown
4 Fungal cell structure and organization 23
Nick D. Read
5 Fungal genetics 35
Paul S. Dyer, Carol A. Munro, and Rosie E. Bradshaw
6 Fungal genomics and transcriptomics 43
Carol A. Munro and Duncan Wilson
7 Epidemiology of fungal disease 50
Rajal K. Mody, Angela Ahlquist Cleveland, Shawn R. Lockhart, and Mary E. Brandt
8 Pathogenesis of fungal disease 56
Frank C. Odds
9 Immunology of fungal disease 62
Ivy M. Dambuza, Jeanette Wagener, Gordon D. Brown, and Neil A.R. Gow
CHAPTER 1
Introduction to medical mycology
David W. Warnock
Changing patterns of fungal diseases
Over the last four decades, the spectrum of fungal disease has evolved, to the extent that a medical mycologist who retired in the 1970s would find the discipline today almost unrecognizable. Until that time, few groups of fungi were regarded as pathogenic for humans or animals. These few included the aetiologic agents of the common superficial diseases, dermatophytosis and mucosal candidiasis, but these were not seen as serious. There were also several well-recognized subcutaneous mycoses, including chromoblastomycosis, mycetoma, and sporotrichosis, but these were largely a problem in the tropics and subtropics. The principal systemic mycoses—aspergillosis, candidiasis, and cryptococcosis—were largely untreatable and usually fatal. However, these diseases were regarded as uncommon. Furthermore, Pneumocystis jirovecii infection was not even recognized to be a fungal disease.
Many factors have contributed to the emergence of fungal diseases as an increasingly important problem. As with other microbial infections, these have included: medical progress and changes in healthcare practices; changes in the environment; increased international travel and commerce; and the development of antimicrobial drug resistance (Institute of Medicine 1992). This chapter will highlight the importance of fungi as human pathogens and discuss the challenges they pose for global public health and for healthcare.
The biggest single change in the pattern of fungal disease since the 1970s has been the emergence of opportunistic mycoses, such as aspergillosis and candidiasis, as major causes of life-threatening infection in immunocompromised individuals. These diseases now constitute the predominant group of fungal infections seen in healthcare settings, and a number of them have emerged as problems of global significance. However, the impact of these infections on human health is not widely recognized, and deaths resulting from these diseases are often overlooked (Brown et al. 2012).
For all of its benefits, medical progress has led to an expanding population of susceptible hosts with impaired immune defences against infection. These individuals are at heightened risk for many serious fungal diseases, including aspergillosis, candidiasis, cryptococcosis, mucormycosis, and pneumocystosis. The most significant emergence of opportunistic fungal infections worldwide has occurred in people living with human immunodeficiency virus (HIV) infection. Before the widespread usage of anti-retroviral therapy, up to 80% of HIV-infected individuals developed mucosal candidiasis, while many were diagnosed with cryptococcosis,
histoplasmosis, pneumocystosis, or other lethal fungal diseases including Talaromyces (Penicillium) marneffei infection. While the numbers have diminished significantly in the developed world since the late 1990s, many countries in sub-Saharan Africa and Asia remain highly affected by the AIDS (acquired immune deficiency syndrome) pandemic, and there are few signs of a decline in the importance of the mycoses.
Other emerging populations at risk for serious fungal diseases have included those who have received immunosuppressive medications or invasive medical interventions. These groups include patients receiving critical care and those who are undergoing organ or stem cell transplantation. With new developments in the management of the underlying disorders, the populations at risk for fungal disease are constantly evolving. For example, in the endemic regions of the United States, histoplasmosis has become one of the most frequent life-threatening infections in patients being treated with tumour necrosis factor (TNF)-alpha blockers for diseases such as rheumatoid arthritis, inflammatory bowel disease, and various dermatological conditions (Hage et al. 2010).
In addition to infections acquired in hospitals and other healthcare settings, there has also been a marked increase in the incidence of several of the community-acquired systemic mycoses that are endemic in the Americas, particularly coccidioidomycosis. Thousands of cases of this disease, caused by two closely related soil-dwelling fungi—Coccidioides immitis and Coccidioides posadasii are now reported each year in the endemic regions of the south-western United States, mostly from Arizona and California. Massive population growth, urban development, and consequent changes in land-use patterns have contributed to this trend, as has the seasonal migration of increasing numbers of previously unexposed persons from non-endemic areas of the United States (Park et al. 2005). Many of these individuals are older, with underlying chronic illnesses and debilitation, and consequently are at greater risk of developing the more serious forms of coccidioidomycosis.
Our current understanding of the geographic distribution of coccidioidomycosis in the United States is largely based on the results of skin testing conducted in the 1950s. However, since 2010, unrelated cases of the disease have been recognized in growing numbers of eastern Washington State residents, far to the north of the known geographic range (Marsden-Haug et al. 2013). Epidemiological and microbiological findings, including whole-genome sequencing analysis, indicate that these infections were acquired in Washington State, exposure likely having occurred during soil disruption
(Litvintseva et al. 2015). The reasons for this recent emergence of coccidioidomycosis are not clear, but possible explanations for the presence of Coccidioides include recent extreme weather events and/or climate change. The extensive drought that has affected California may have resulted in the production of contaminated dust that spread fungal spores to the North. It is also possible that Coccidioides has been established in Washington for some time, but infrequent human exposure and/or lack of awareness among physicians delayed its recognition. The retrospective detection of cases of the disease among animals lends support to this hypothesis (Marsden-Haug et al. 2013). Nonetheless, whatever the precise cause, it is clear that factors such as anthropogenic dispersal, animal host movement, and climatic changes conducive to colonization may influence the endemic ranges of fungal pathogens.
While coccidioidomycosis remains a regional problem, cryptococcosis is an emerging fungal disease of global importance. Virtually all cases of cryptococcosis are caused by Cryptococcus neoformans and the closely related species Cryptococcus gattii. The former has a worldwide distribution, particularly in soil and avian habitats. In contrast, C. gattii is found in association with trees, and until recently, its geographic range was thought to be limited to the tropics and subtropics. However, since 1999, human and animal cases of C. gattii infection have been reported with increasing frequency on Vancouver Island in western Canada, and the outbreak has since spread to mainland British Columbia and to the adjacent states of Washington, Oregon, Idaho, and California in the United States. The outbreak has been associated with significant ill-health and high rates of death among those infected (Harris et al. 2011).
The recent emergence of C. gattii in a temperate region suggests that the pathogen may have adapted to a new climatic niche, or that climatic warming may be creating a more hospitable environment for its development. However, the possibility that environmental conditions supportive of C. gattii are broader than previously suspected cannot be discounted. Nonetheless, the rapid geographic expansion of this fungal pathogen has raised concerns that C. gattii infections could emerge as an even greater threat to public health. This is underscored by evidence that human activity has contributed to the dispersal of the outbreak (Kidd et al. 2007).
International travel and tourism is another factor that has affected the pattern of fungal diseases. The number of reported outbreaks and sporadic cases of histoplasmosis and coccidioidomycosis has increased among individuals who normally reside in places far distant from the areas where these diseases are endemic. The largest number of travel-related mycoses has been reported from US residents, many of whom have acquired an infection while visiting an endemic area within North or Central America or, less commonly, in South America, Africa, or Asia (Panackal et al. 2002). Travel-related infections have also been reported among European visitors to the United States and Latin America (Buitrago et al. 2011). With increasing numbers of visitors and immigrants to the United States from Asia, reports of travel- and migration-related mycoses are beginning to emerge from India and China. Healthcare providers increasingly need to consider these diseases in their differential diagnosis when treating returning travellers with a febrile respiratory illness.
Estimating the burden of fungal diseases
Despite general agreement that the mycoses are becoming more important, our understanding of the true magnitude of the burden
posed by these diseases and their socioeconomic impact remains largely incomplete. Understanding the burden of different fungal diseases is important because it will allow meaningful comparisons to be made between these infections and other important diseases. Only then will it be possible to persuade policy makers of the benefits to be derived from allocating resources to diagnosing, treating, and preventing the mycoses.
The first step in developing estimates of the burden of any disease is to obtain epidemiological surveillance data regarding its incidence and prevalence. In the case of fungal diseases, our efforts have been undermined by the limited amounts of data available, and in many instances, by the ways in which these data were acquired. Most public health agencies, with the exception of the US Centers for Disease Control and Prevention (CDC), do not conduct any active epidemiological surveillance for fungal diseases. Usually, this is because these diseases are seen as low priorities, and because active surveillance is labour-intensive and expensive to perform. The CDC has conducted active population-based surveillance for Candida bloodstream infections (Cleveland et al. 2015) and cryptococcosis (Mirza et al. 2003), and performed prospective surveillance for invasive fungal infections among haematopoietic stem cell and solid-organ transplant recipients (Kontoyiannis et al. 2010; Pappas et al. 2010). Similar active surveillance programmes have been reported from other countries, mostly in Europe, but few have been sustainable in the long term.
Passive surveillance, which relies on healthcare providers and laboratories to submit information to public health agencies, is less expensive to conduct than active surveillance, but is not ideal in relation to fungal diseases. Because these infections are not usually transmissible from person to person, there is minimal incentive for healthcare providers to report cases since no immediate public health action needs to be taken. In the United States, only coccidioidomycosis is a notifiable disease, and reporting is only required in states where it is endemic (Arizona, California, Nevada, New Mexico, Texas, and Utah) and about 15 others. In other developed countries, such as the United Kingdom and France, there are ongoing, informal reporting schemes for some fungal infections, but these are limited in scope. There are no data from many parts of the developing world.
Even when all diagnosed cases of a disease are reported, most surveillance systems do not capture the total burden of that disease in a population. This is because some of those affected do not seek medical care, or because specimens are not obtained from all cases, or because the appropriate tests are not performed. Given the limitations of current tests, it seems probable that invasive fungal infections are under-diagnosed. If these infections are also underreported, it must be assumed that the existing surveillance data underestimate the incidence and prevalence of these diseases.
Numerous studies have been conducted to measure the global burden of infectious diseases, but few have focused on the mycoses. Among the first to do so was one from the CDC that estimated the yearly global burden of cryptococcal meningitis in persons with HIV infection to be nearly one million cases (Park et al. 2009). The region with the greatest number of cases was sub-Saharan Africa, with 720,000 cases, followed by South and Southeast Asia with 120,000 cases. In addition, almost 625,000 deaths were estimated to occur globally, mostly occurring in sub-Saharan Africa, with over 500,000 deaths annually. These estimates of the global burden of cryptococcosis involved major extrapolations from the available
epidemiological data. Nonetheless, they are important because they showed that the disease was one of the leading causes of death among people with HIV infection. In sub-Saharan Africa, cryptococcosis was estimated to cause more deaths than tuberculosis.
Much effort is currently being devoted to developing similar global burden of disease estimates for other mycoses. This work has served to highlight the many gaps in current surveillance data and the methodological limitations involved. Until additional data and more refined methods become available, it will be essential to exercise caution when reviewing published estimates of the burden of ill health and death caused by fungal diseases.
Improving the diagnosis of fungal diseases
Determining the infectious agent responsible for a patient’s illness remains fundamental to evidence-based treatment and care decisions. Among the challenges in dealing with opportunistic invasive fungal diseases—with many caused by unusual environmental fungi—none is more critical than early diagnosis of these infections. Improved laboratory diagnostic tools that allow earlier implementation of appropriate therapy have the potential to affect healthcare decisions to a degree well out of proportion to their cost (Institute of Medicine 2000).
In the developed world, new diagnostic approaches, such as fungal antigen tests and fungal nucleic acid detection, offer great promise for diseases such as aspergillosis, candidiasis, and pneumocystosis. However, even as more of these tools become commercially available, interpreting the test findings still calls for a high level of mycological competence. The new diagnostic procedures that have been developed have not yet had a significant impact in many clinical laboratories, largely because they have not been standardized and validated, and because there remains a lack of consensus on their performance characteristics. These complexities, combined with subtle clinical presentations, continue to result in delayed diagnosis and may compromise clinical care (Brown et al. 2012).
In the under-developed and developing countries, where the burden of fungal disease is highest, many clinical laboratories are small and poorly equipped, and may be staffed by individuals with minimal training. Furthermore, they are often inaccessible to many patients. In these settings, inexpensive but dependable point-of-care (POC) diagnostic tests can make a tremendous difference to the cost and quality of healthcare. A new POC dipstick test for detection of cryptococcal antigen in urine or blood has improved the capacity for diagnosis of cryptococcal meningitis in sub-Saharan Africa (Kabanda et al. 2014), and a similar approach could transform the diagnosis and management of AIDS-associated histoplasmosis throughout South America (Nacher et al. 2013). Setting priorities and ensuring that these tests are developed and implemented in the most efficient way will be challenging. With widened access to improved diagnostics, it may be possible to reduce the burden of these and other fungal diseases to the lower levels seen in the developed world.
Improving the therapy of fungal diseases
Just as improved diagnostics may help to reduce the morbidity and mortality associated with fungal diseases, so may better therapeutics. The rising incidence of serious opportunistic fungal infections
has brought about an increased use of existing antifungal agents and has stimulated the search for new ones. The last two decades have seen the introduction of an important new class of antifungal agents (the echinocandins), the expansion of an established class of agents (the azoles), and the development of novel methods for delivering established agents (lipid-based formulations of amphotericin B).
In the developed world, the new drugs that have been introduced have changed the standards of care for the treatment of many invasive fungal diseases, particularly aspergillosis and candidiasis, yet patient outcomes remain disappointing (Ostrosky-Zeichner et al. 2010). This is due, in large part, to the lack of early antifungal therapy resulting from delays in disease diagnosis and fungal identification. The available drugs also suffer from restrictions in spectrum of activity, in bioavailability in target tissues, and in routes of administration. Further complications include toxicity, undesirable drug interactions, and the emergence of drug resistance. Unfortunately, few antifungal drugs are currently in active development. This is because fewer companies are now developing antimicrobials of any type, and because the global market for antifungal drugs is not predicted to give a sufficiently large financial return to attract the needed investment.
In the developing world, many antifungal drugs are either unavailable or simply unaffordable. While fluconazole is available in almost all countries, amphotericin B is not. This is despite the older drug often being life-saving in the management of cryptococcal meningitis and disseminated histoplasmosis. Moreover, while there is mounting evidence for the benefit of flucytosine (5-fluorocytosine)-containing combination therapy for cryptococcosis, access to the drug in sub-Saharan Africa and Asia, where disease burden is greatest, is inadequate at present (Loyse et al. 2013). Coordinated efforts from governmental and international stakeholders are needed to develop, disseminate, and implement antifungal treatment guidelines, to encourage generic drug production and facilitate registration, and to widen access to these agents.
Evolving problems of drug resistance
In general, acquired resistance to antifungal drugs has been a much less common problem than antibacterial drug resistance. In the 1990s, long-term use of fluconazole to treat oral candidiasis in people with HIV infection led to the widespread emergence of resistant strains of Candida albicans, which were associated with treatment failure and relapse. However, with the advent of more effective antiretroviral therapy, a dramatic decline occurred in the rates of oral colonization and symptomatic infection, and this was accompanied by falling rates of azole drug resistance (Martins et al. 1998).
First described in 2009, Candida auris has since been reported from at least 12 countries across four continents (Vallabhaneni et al. 2016). This emerging pathogen has caused large outbreaks of invasive infection following transmission in healthcare settings (Schelenz et al. 2016) and it appears to be increasing in prevalence, at least in some countries such as India, where it now accounts for almost 5% of Candida bloodstream infections among patients receiving intensive care (Chakrabarti et al. 2015).
Candida auris is of concern because it is often resistant to multiple antifungal drugs. In one recent report, 50 of 54 isolates (93%) from South Asia, South Africa, and South America were found to be resistant to fluconazole, while 54% were resistant to voriconazole,
35% to amphotericin B, 7% to echinocandins, and 6% to flucytosine (Lockhart et al. 2017). Moreover, 41% of isolates were resistant to two or more classes of antifungal agents, a feature not seen in other clinically important Candida species. Whole genome sequencing analysis has demonstrated that isolates became grouped into unique clades by geographic region, suggesting nearly simultaneous and recent, independent emergence of C. auris on three continents, rather than spread from a single geographic source (Lockhart et al. 2017). Although data on antifungal prescribing practices are difficult to obtain, anecdotal evidence suggests that empirical and prophylactic use of antifungal agents has been increasing, and this supports the hypothesis that antifungal selection pressure may, in part at least, be responsible for the emergence of C. auris
More recently, azole resistance in Aspergillus fumigatus has emerged as a potential global public health concern. Many of these resistant isolates appear to have been acquired as such from the environment as an unintended consequence of agricultural fungicide use (Vermeulen et al. 2013). Others have been recovered from patients with chronic lung disease during long-term azole treatment (Howard et al. 2009; Mortensen et al. 2011). Although evidence for a causal role of agricultural triazole use in resistance development is accumulating, definitive proof is lacking. Putative azole-resistant environmental strains of A. fumigatus have been recovered from patients across Europe and are now also being reported from Asia, the Middle East, Africa, and Australia. Similar strains have recently been identified among A. fumigatus isolates collected in US institutions (Wiederhold et al. 2016).
Taken as a whole, these developments have potentially serious consequences for patient management. In the case of Candida auris, treatment options may be limited. Implementation of strict infection control measures and rapid detection of cases may be the best options to contain hospital-acquired transmission (Schelenz et al. 2016). However, when traditional biochemical methods are used, C. auris is often misidentified, most commonly as C. haemulonii Specialized methods, such as MALDI-TOF MS (matrix-assisted laser desorption/ionization–time-of-flight mass spectrometry) or molecular identification, are required and these may not be immediately available in countries where resources are limited, and where access to antifungals other than fluconazole may also be restricted.
For azole-resistant Aspergillus fumigatus, dose-escalation of mould-active azoles, such as voriconazole and posaconazole, will be inadequate, and the outcome of azole–echinocandin combination treatment at best uncertain. New molecular diagnostic tools are urgently needed to allow rapid detection of resistance mechanisms in both culture-positive and -negative patients. Ongoing investment in surveillance programmes, such as the Surveillance Collaboration on Aspergillus Resistance in Europe (SCARE) network (van der Linden et al. 2015), will be critical for monitoring trends in the incidence and prevalence of azole resistance and for detecting the emergence of new resistance mechanisms.
Improving the prevention of fungal diseases
Antifungal chemoprophylaxis is currently one of the most promising prevention strategies for the prevention of fungal infections. It can provide protection to susceptible individuals, such as transplant recipients and patients receiving intensive care, although this is not always economically or medically justified, especially if the cost is high and the perceived benefit does not outweigh the risk of
adverse drug interactions or selection for resistance. Expert guidelines, based on evidence from well-designed clinical trials, support the use of targeted prophylaxis in various high-risk patient groups (Maertens et al. 2011). There is, however, an almost complete lack of genetic and other prognostic biomarkers that would allow identification of those individuals at greatest risk.
Cryptococcosis is among the most common causes of meningitis in sub-Saharan Africa, and is a leading cause of death among people with HIV infection. Although prophylaxis is not a cost-effective means of preventing infection, targeted pre-emptive treatment with fluconazole has emerged as a highly promising approach to managing the disease (Meya et al. 2015). This has become feasible with the advent of a simple POC dipstick test that can detect cryptococcal antigen several weeks before overt signs of meningitis develop. The substantial public-health benefits of screening people with HIV for cryptococcal infection when they access healthcare have recently been confirmed in a large clinical trial in Tanzania and Zambia (Mfinanga et al. 2015). Broader implementation of this ‘screen and treat’ approach in countries with a high burden of cryptococcosis could save thousands of lives each year.
Vaccination is the ultimate tool for the prevention and control of infectious disease. Unfortunately, there are no vaccines in clinical use for any fungal disease. This is despite the development of vaccines against a number of fungal pathogens, including several that have proven effective in animal models. Few have been translated to human clinical trials because the target market is perceived to be too small to justify the costs of manufacturing and testing a vaccine in today’s rigorously controlled clinical research environment.
Conclusion
Fungal diseases exact a tremendous toll in terms of human life and healthcare costs in both the developed and the developing world. This chapter has outlined several areas that require attention if we are to improve this dismal situation. Firstly, ongoing surveillance programmes need to be established for a range of fungal diseases, both on a national basis and within individual sentinel medical centres, if we are to determine the true magnitude of the burden posed by these mycoses. Until more precise estimates become available, it will be difficult to convince policy makers that fungal diseases are common and that the burden they impose on public health and medical care is large and rising. Only then will it become possible to obtain the investment needed to stimulate scientific interest in combating and preventing these diseases.
Secondly, better and more rapid diagnostics need to be developed to allow earlier implementation of appropriate antifungal therapy. Development of such tools would also facilitate the gathering of accurate epidemiological surveillance data. Although better diagnostics may not prevent fungal diseases, simpler and easier diagnosis may lead to increased numbers of patients being successfully treated for mycoses, and this may in turn reduce the burdens of ill health and death. If access to affordable diagnostics can be increased in the developing world, it may be possible to reduce the fungal disease burden to levels seen in the developed world.
Thirdly, there is an ongoing need for safer and more effective antifungal drugs, and to translate the growing understanding of fungal immunopathogenesis into novel immunotherapeutic strategies, especially for the treatment of opportunistic fungal infections in susceptible individuals. In under-developed and developing
countries, improved access to low-cost antifungal drugs is a critically important issue. Wider availability may ultimately be of benefit not only for invasive infections, such as cryptococcosis and histoplasmosis, but also for diseases such as mycetoma and fungal keratitis, which can have devastating economic consequences for those affected. Finally, new strategies are needed to slow the emergence of antifungal drug resistance.
References
Brown GD, Denning DW, Gow NAR, Levitz SM, Netea MG and White TC (2012) Hidden killers: human fungal infections. Sci Transl Med 4: 165rv13.
Buitrago MJ, Bernal-Martinez L, Castelli MV, Rodriguez-Tudela JL and Cuenca-Estrella M (2011) Histoplasmosis and paracoccidioidomycosis in a non-endemic area: a review of cases and diagnosis. J Travel Med 18: 26–33.
Chakrabarti A, Sood P, Rudramurthy SM, et al. (2015) Incidence, characteristics and outcome of ICU-acquired candidemia in India. Intensive Care Med 41: 285–95.
Cleveland AA, Harrison LH, Farley MM, et al. (2015) Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008-2013: results from populationbased surveillance. PLoS ONE 10: e120452. doi:10.1371/journal. pone.0120452
Hage CA, Bowyer S, Tarvin SE, Helper D, Kleiman MB and Wheat LJ (2010) Recognition, diagnosis, and treatment of histoplasmosis complicating tumor necrosis factor blocker therapy. Clin Infect Dis 50: 85–92.
Harris JR, Lockhart SR, Debess E, et al. (2011) Cryptococcus gattii in the United States: clinical aspects of infection with an emerging pathogen. Clin Infect Dis 53: 1188–95.
Howard SJ, Cerar D, Anderson MJ, et al. (2009) Frequency and evolution of azole resistance in Aspergillus fumigatus associated with treatment failure. Emerg Infect Dis 15: 1068–76.
Institute of Medicine (1992) Emerging Infections: Microbial Threats to Health in the United States (Washington, DC: National Academy Press).
Institute of Medicine (2000) Medicare Laboratory Payment Policy: Now and in the future (Washington, DC: National Academy Press).
Kabanda T, Siedner MJ, Klausner JD, Muzoora C and Boulware RR (2014) Point-of-care diagnosis and prognostication of cryptococcal meningitis with the cryptococcal antigen lateral flow assay on cerebrospinal fluid. Clin Infect Dis 58: 113–16.
Kidd SE, Bach PJ, Hingston AO, et al. (2007) Cryptococcus gattii dispersal mechanisms, British Columbia, Canada. Emerg Infect Dis 13: 51–7.
Kontoyiannis DP, Marr KA, Park BJ, et al. (2010) Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001-2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) database. Clin Infect Dis 50: 1091–100.
Litvintseva AP, Marsden-Haug N, Hurst S, et al. (2015) Valley fever: finding new places for an old disease: Coccidioides immitis found in Washington State soil associated with recent human infection. Clin Infect Dis 60: e1–3.
Lockhart SR, Etienne K, Vallabhaneni S, et al. (2017) Simultaneous emergence of multidrug resistant Candida auris on 3 continents confirmed by whole genome sequencing and epidemiological analyses. Clin Infect Dis 64: 134–40.
Loyse A, Dromer F, Day J, Lortholary O and Harrison TS (2013) Flucytosine and cryptococcosis: time to urgently address the worldwide accessibility of a 50-year-old antifungal. J Antimicrob Chemother 68: 2435–44.
Maertens J, Marchetti O, Herbrecht R, et al. (2011) European guidelines for antifungal management in leukemia and hematopoietic stem cell transplant recipients: summary of the ECIL 3–2009 update. Bone Marrow Transplant 46: 709–18.
Marsden-Haug, N, Goldoft M, Ralston, C, et al. (2013) Coccidioidomycosis acquired in Washington State. Clin Infect Dis 56: 847–50.
Martins MD, Lozano-Chiu M and Rex JH (1998) Declining rates of oropharyngeal candidiasis and carriage of Candida albicans associated with trends towards reduced rates of carriage of fluconazole-resistant C. albicans in human immunodeficiency virus-infected patients. Clin Infect Dis 27: 1291–4.
Meya DB, Rajasingham R, Nalintya E, Tenforde M and Jarvis JN (2015) Preventing cryptococcosis: shifting the paradigm in the era of highly active antiretroviral therapy. Curr Trop Med Rep 2: 81–9.
Mfinanga S, Chanda D, Kivuyo SL, et al. (2015) Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: an open-label, randomized controlled trial. Lancet 385: 2173–82. doi: 10.1016/S0140-6736(15)60164–7
Mirza SA, Phelan M, Rimland D, et al. (2003) The changing epidemiology of cryptococcosis: an update from population-based active surveillance in 2 large metropolitan areas, 1992-2000. Clin Infect Dis 36: 789–94.
Mortensen KL, Jensen RH, Johansen HK, et al. (2011) Aspergillus species and other molds in respiratory samples from patients with cystic fibrosis: a laboratory-based study with focus on Aspergillus fumigatus azole resistance. J Clin Microbiol 49: 2243–51.
Nacher N, Adenis A, McDonald S, et al. (2013) Disseminated histoplasmosis in HIV-infected patients in South America: a neglected killer continues on its rampage. PLoS Negl Trop Dis 7: e2319.
Ostrosky-Zeichner L, Casadevall A, Galgiani JN, Odds FC and Rex JH (2010) An insight into the antifungal pipeline: selected new molecules and beyond. Nat Rev Drug Discov 9: 719–27.
Panackal AA, Hajjeh RA, Cetron MS and Warnock DW (2002) Fungal infections among returning travelers. Clin Infect Dis 35: 1088–95.
Pappas PG, Alexander BA, Andes DR, et al. (2010) Invasive fungal infections among organ transplant recipients: results of the TransplantAssociated Infection Surveillance Network (TRANSNET). Clin Infect Dis 50: 1101–11.
Park BJ, Sigel K, Vaz V, et al. (2005) An epidemic of coccidioidomycosis in Arizona associated with climatic changes, 1998-2001. J Infect Dis 191: 1981–7.
Park BJ, Wannemuehler KA, Marston BJ, et al. (2009) Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 23: 525–30.
Schelenz S, Hagen F, Rhodes JL, et al. (2016) First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control 5: 35. doi: 10.1186/s13756-016-0132-5
Vallabhaneni S, Kallen A, Tsay S, et al. (2016) Investigation of the first seven reported cases of Candida auris, a globally emerging invasive, multidrug-resistant fungus—United States, May 2013-August 2016. MMWR Morb Mortal Wkly Rep 65: 1234–7.
van der Linden JW, Arendrup MC, Warris A, et al. (2015) Prospective multicenter international surveillance of azole resistance in Aspergillus fumigatus. Emerg Infect Dis 21: 1041–4.
Vermeulen E, Lagrou K and Verweij PE (2013) Azole resistance in Aspergillus fumigatus: a growing public health concern. Curr Opin Infect Dis 26: 493–500.
Wiederhold NP, Gil VG, Gutierrez F, et al. (2016) First detection of TR34 L98H and TR46 Y121F T289A Cyp51 mutations in Aspergillus fumigatus isolates in the United States. J Clin Microbiol 54: 168–71.
CHAPTER 2
Fungal taxonomy and nomenclature
Andrew M. Borman
Introduction to fungal taxonomy and nomenclature
Fungi can be uni- or multicellular. Unicellular organisms which divide by budding have traditionally been referred to as yeasts, whereas multicellular fungi (moulds) exist as filament-like hyphae which grow via apical extension to form a mycelial mat. However, moulds and yeasts are not taxonomically valid divisions, and many medically important endemic fungi exhibit thermal or nutritional dimorphism allowing them to interconvert between morphologically distinct yeast (or spherule) and mould forms. The fungal kingdom is vast and ancient. Of the estimated 1–10 million species (Cannon 1997; Blackwell 2011; Hawksworth 2001), only approximately 1% has been formally described and named. Of the small proportion of fungi that have been named, less than a thousand are commonly reported as the agents of animal and human infections, with only a small proportion of these being capable of eliciting disease in immunocompetent hosts (Guarro et al. 1999).
Classical, phenotype-based taxonomy
Fungal reproduction can be asexual (mitosis), resulting in the production of usually large numbers of asexual spores (conidia) that are essentially identical to the parent and permit spread to, and colonization of, new geographic niches, or sexual (resulting from hyphal and nuclear fusion followed by meiosis) (Alexopoulos et al. 1996). Historically, the identification and hierarchical classification of filamentous fungi have been based on examination of their microscopic morphology, and in particular their reproductive structures (Ainsworth et al. 1973; Sutton 1973; Kendrick 1979; Weresub and Hennebert 1979; Sutton 1980; Subramanian 1983; Sugiyama 1987; Hennebert 1991; Reynolds and Taylor 1993; Hawksworth 1994; Guarro et al. 1999). On the basis of the types of sexual structures that fungi can be induced to form, the kingdom was divided into a limited number of distinct phyla—the Ascomycota, Zygomycota, and Basidiomycota—for fungi with recognized sexual (teleomorph) forms (Figures 2.1 and 2.2). The sexual spores of Ascomycota (ascospores) are typically produced in sacs (asci) contained in large, thick-walled structures called ascocarps (although some species produce single, solitary ascospores). Basidiomycota species produce sexual basidiospores borne on basidia which are often contained within macroscopic fruiting bodies (basidiomata) typical of mushrooms, toadstools, smuts, and bracket fungi. Conversely,
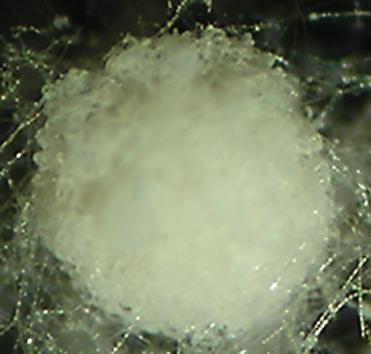
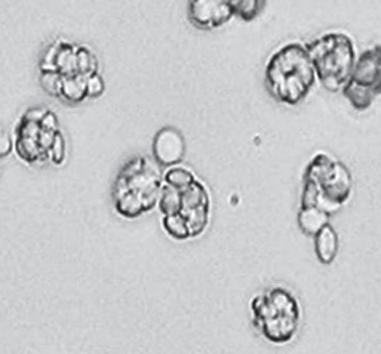
fungi classified in the phylum Zygomycota produce single, thickwalled, sexual zygospores which are often highly ornamented. However, with a few notable exceptions, most fungi are heterothallic and will only undergo sexual reproduction when two independent, compatible isolates are present (Figure 2.2), and often in unique environmental conditions. Thus a fourth form-division, the Deuteromycota (or Fungi Imperfecti), was created to encompass all those fungi for which a sexual form (teleomorph) had not been described or could not be induced (Figure 2.2) (reviewed in Talbot 1971; Kendrick 1981; Seifert 1993). A similar classification into Ascomycota, Zygomycota, and Basidiomycota could be achieved on the basis of examination of the anamorph (asexual) forms of the fungi, including the presence of specific hyphal structures (septa, clamp connections) and the types of asexual spores formed and their method of production (conidiogenesis) in laboratory cultures (Figure 2.1) (Hughes 1953;. The hyphae of Zygomycota species are hyaline (colourless), broad, and ribbon-like and possess few to no septa (pauci-septate), and asexual conidia (termed sporangiospores) are typically produced inside large sac-like structures (sporangia). Conversely, the hyphae of filamentous Ascomycota species (many medically important Ascomycota species are yeasts) are narrow and highly septate, and may be either hyaline or dematiaceous (brown). Ascomycota species typically produce large numbers of conidia in culture on appropriate media, although the precise mechanism of conidiogenesis varies dramatically. Finally, species of the filamentous Basidiomycota, whilst producing hyphae similar to those of the Ascomycota, rarely produce conidia in culture, and most often present as rapidly growing floccose (fluffy) white colonies. However, upon careful examination, the hyphae can be distinguished from those of the Ascomycota by the presence of clamp connections (Alexopoulos et al. 1996; Figure 2.1) and, occasionally, delicate lateral projections termed spicules. It should, however, be noted that most medically important Basidiomycota species have anamorph states that are spherule (yeasts) rather than hyphal in form.
Although there is a staggering diversity in conidial forms and mechanisms of production, especially amongst the Ascomycota, different fungi have undergone either convergent or divergent evolution, with the result that many genetically unrelated species have very similar conidial characteristics, while other genetically similar species have vastly different morphological appearances. To further complicate matters, since fungi are of interest to a wide range of scientists (medical mycologists, geneticists, phytopathologists,
Figure 2.1 Approaches to fungal identification and taxonomy. Common features of the sexual cycles (left-hand side) and asexual cycles (right-hand side) of Basidiomycota, Ascomycota, and ‘Zygomycota’. Reproduced courtesy of Andrew M. Borman.
ASCOMYCOTA
BASIDIOMYCOTA
FUNGI
ZYGOMYCOTA
DEUTEROMYCOTA “Fungi imperfecti”
Figure 2.2 Traditional separation of the fungal kingdom into three phyla (Ascomycota, Basidiomycota, Zygomycota) and the form-division Deuteromycota for those fungi without a known sexual stage.
the biotechnology industry, and so on) and the sexual and asexual forms of fungi often develop independently of each other with little obvious morphological relatedness, a single genetic entity may have been described and named independently several times (Weresub and Pirozynski 1979).
Molecular approaches to identification and taxonomy
Since it is well established that different fungal species have dramatically varied antifungal susceptibility profiles (see, for example, Pfaller et al. 1998), the accurate identification of the agents of human infections is essential for appropriate patient management. However, many fungal isolates from deep and chronic infections do not produce conidia in the laboratory, rendering their conventional identification impossible. The advent of rapid and costeffective approaches for extracting and analyzing fungal DNA has vastly facilitated the accurate identification of clinically important isolates, and has also permitted a greater taxonomic understanding of the fungal kingdom. Molecular analyses involving PCR (polymerase chain reaction) amplification and sequencing of conserved regions of the fungal genome encoding the rRNA (ribosomal ribonucleic acid) genes have permitted pan-fungal approaches to fungal identification (reviewed in Borman et al. 2008), and indeed the internal transcribed spacer region 1 (ITS1) has been proposed and accepted as an excellent candidate for fungal DNA barcoding (Balajee et al. 2009; Schoch et al. 2012). More sophisticated
approaches examining additional protein-coding gene loci have permitted the development of multi-locus sequence typing and fungal strain typing (reviewed in Peterson 2012). However, a more immediate impact of such approaches has been the radical and continual revision of the fungal tree of life based on a phylogenetic approach to species recognition (see Hawksworth 2006 for review) where DNA sequence similarity is used to define species boundaries.
On the basis of such approaches, the fungal kingdom is now known to comprise at least seven phyla (Glomeromycota, Blastocladiomycota, Chytridiomycota, Neocallimastigomycota, and Microsporidia—with the retention of Ascomycota and Basidiomycota, which now constitute the sub-kingdom Dikarya (Figure 2.3; Hibbett et al. 2007). Organisms previously ascribed to the Deuteromycota can now be sequenced and their correct positions in the fungal kingdom ascertained. More dramatically, the phylum Zygomycota has been disbanded, after molecular approaches demonstrated unequivocally that it was polyphyletic. The fungi previously classified in the phylum Zygomycota are now spread between the phylum
KingdomSub-kingdom Phylum
ASCOMYCOTA (see Figure 2.4)
DIKARYA
FUNGI
Glomeromycota, and four subphyla incertae sedis (of uncertain position): the Mucoromycotina, Entomophthoromycotina, Kickxellomycotina, and Zoopagomycotina, with most of the medically important members contained in the order Mucorales within Mucoromycotina (Hoffmann et al. 2013; Figure 2.3).
The phylum Ascomycota has now been divided into three subphyla, which comprise at least 14 classes and 60 orders (Figure 2.4). The subphylum Taphrinomycotina to date contains only one medically important fungal genus, Pneumocystis, which is formally located within the fungal kingdom. The subphylum Saccharomycotina contains a single medically important order, Saccharomycetales, which encompasses most pathogenic ascomycetous yeasts. The remainder of the medically important ascomycete genera are classed within the subphylum Pezizomycotina, and are divided between at least 14 orders, including: the Capnodiales (Cladosporium and related genera); the Pleosporales (Alternaria, Bipolaris, Curvularia, Exserohilum, Ulocladium, and many of the agents of dark-grain eumycetoma); the Chaetothyriales (Cladophialophora, Exophiala, Fonsecaea, Phialophora, Ramichloridium, and Rhinocladiella); the Eurotiales (Aspergillus, Penicillium, Paecilomyces, Rasamsonia,
Figure 2.3 Recent taxonomy of the fungal kingdom. Organisms previously accommodated in the phylum ‘Zygomycota’ are highlighted in the blue-shaded lozenge. The positions of the more common, medically important mould genera are shown.
Source: data from Hibbett D. M. et al., ‘A Higher-Level Phylogenetic Classification of the Fungi’, Mycological Research Volume 111, pp. 509–47. Published by Elsevier Ltd, http://www.sciencedirect. com/science/article/pii/S0953756207000615
Figure 2.4 Revised taxonomy of the Ascomycota. The position of medically relevant genera is shown.
Talaromyces, and Thermoascus); the Onygenales (the dermatophytes [Trichophyton, Microsporum, Epidermophyton, and fungi with Arthroderma teleomorphs], the thermally dimorphic fungi with Ajellomyces teleomorphs [Blastomyces, Coccidioides, Emmonsia, Histoplasma, and Paracoccidioides], Chrysosporium, Lacazia, Myceliophthora, and Nannizziopsis); the Hypocreales (Acremonium and allied genera, Fusarium and allied genera, Purpureocillium, and Stachybotrys); the Microascales (Lomentospora, Scedosporium, and Scopulariopsis); the Sordariales (Chaetomium, Madurella, and Phialemonium); the Dothideales (Aureobasidium); the Patellariales (Rhytidhysteron); the Coniochaetales (Lecythophora); the Diaporthales (Phaeoacremonium); the Ophiostomatales (Sporothrix); and the Calosphaeriales (Pleurostomophora). Even
Sub-Phylum
with this greatly revised taxonomy, some medically important ascomycete genera (Neoscytalidium, Geomyces, Pseudogymnoascus) remain incertae sedis, pending molecular analyses of more of the fungal kingdom (Figure 2.4).
Finally, the phylum Basidiomycota contains three subphyla (Pucciniomycotina, Ustilaginomycotina, and Agaricomycotina) and at least 46 orders (Figure 2.5). To date, only around a dozen basidiomycete genera have been formally associated with human infections (Figure 2.5), and these are restricted to five orders. Order Sporidiales (Pucciniomycotina) contains the basidiomycete yeast genera Rhodotorula and Sporobolomyces; Trichosporon and Cryptococcus are classified in the order Tremellales (Agaricomycotina); Bjerkandera, Coprinus, Irpex, Hormographiella,
Figure 2.5 Revised taxonomy of the Basidiomycota. The position of medically relevant genera is shown.
Entorrhizales
Perenniporia, Schizophyllum, and Sporotrichum reside within the order Agaricales (Agaricomycotina); and Tilletiopsis is classified within the order Georgefischeriales (Ustilaginomycotina). The fifth order, the Malasseziales (Malassezia spp.), is also a member of the subphylum Ustilaginomycotina, but its exact position remains to be determined (Figure 2.5).
A further repercussion of the widespread adoption of molecular approaches to fungal identification and classification is the discovery of cryptic species (species which can only be distinguished by DNA sequencing) within many medically important morphospecies (reviewed in Hawksworth 2006). It is now accepted that Aspergillus fumigatus is a species complex that encompasses in excess of 40 cryptic species (reviewed in Johnson and Borman 2009), and a similar number of cryptic species have been discovered in the Fusarium solani species complex (see, for example, Short et al. 2013). In some cases, certain cryptic species have been reported to have altered antifungal susceptibility profiles (Balajee et al. 2005; Borman et al. 2008), whereas in others discrimination to species level within a species complex appears to be less medically important (Borman et al. 2013). Nevertheless, regardless of the medical relevance, the demonstration of cryptic species in most
medically important genera has further added to the complexity of fungal taxonomy and nomenclature (see below).
Impact of molecular approaches on fungal nomenclature
Fungal nomenclature is governed by strict rules established by the International Code of Nomenclature (ICN) for algae, plants, and fungi. Under the ICN dictates, a name for a fungal species is only valid if it is in Latin binomial form, has been submitted to the MycoBank database, and has a living culture (usually of the type strain) permanently preserved in an accepted culture collection. Fungal name changes have always been permitted, and historically concerned the most commonly encountered fungal species which had been described and named independently many times by different authorities, only for those isolates later to be demonstrated to be identical and thus the names synonymous (Figure 2.6). Under such circumstances, the earliest valid name was usually retained. Molecular approaches to fungal identification have, to some extent, facilitated this process, as fungi which are genetically indistinguishable should, in theory, be synonymous. However, there are
(a) (b) Rhizopus umbellatus A.L. Sm , J. Roy. Microscop. S oc.1: 193 (1901)
Mucor corymbifer Cohn, 1884 in Lichtheim, Z. klin. Med 7: 149
Lichtheimia sartor yi A. Bailly & Sartor y, Champ. paras. homme anim 2: 5 (1927)
Lichtheimia ucrainica Naumov, Opred. Muko r., Edn 2: 80 (1935)
Absidia ginsan Komin., Kobayasi & Tubaki, Mycol. J. Na gao Inst. 2: 56 (1952)
Figure 2.6 The taxonomic (a) and nomenclatural (b) ‘merry-go-round’.
a The principal taxonomic revisions of Lichtheimia corymbifera; dashed arrows indicate temporary changes, and the solid arrow indicates the final (hopefully) taxonomic position.
b Some of the various nomenclatural synonyms of L. corymbifera over the past century.
Source: data from Index Fungorum, accessible at http://www.indexfungorum.org/