Thank you for your interest in advancing diversity, health equity and inclusion (DHEI)! This playbook was created by a group of champions who work in a variety of areas within the University of Colorado Department of Pediatrics. As people who have initiated and led DHEI efforts within our own spaces, we understand how daunting the first (and second and third) steps can be. We also understand just how critical DHEI work is and firmly believe we will be most effective when sections can partner with the organization to work at multiple levels.
Each of our teams differs in size, focus, leadership and readiness; yours is also unique. We recognize there is no one-size-fits-all approach to DHEI initiatives and your approach will be shaped by all of those factors and more. In this document we have pulled together our ideas of practices and resources that helped us, as well as some of our own lessons learned. We hope you can take from it what you need and please reach out to any of us with questions; our contact information can be found at the end of the document. Cheers to the journey ahead!
Who is this playbook for?
This playbook is for anyone participating in or thinking about starting a group focusing on DHEI topics or initiatives. Those earlier in group formation or in their own personal journey may benefit most from the content, and we hope there are useful ideas, activities and resources for those further along their DHEI journey, too.
We have written this from different levels of experience and from perspectives with the goal to teach, provide resources and coach each reader on their path. We hope this guide will be helpful at any stage of your DHEI journey.
Curious about what diversity, health equity and inclusion is
On any part of the DHEI journey
Looking to lead activities and/or develop a DHEI program in your section
Aspiring to be a DHEI champion in your group and community
Interested in starting on your own DHEI journey
Looking to further your own DHEI engagement
Recognizing a need for DHEI progress in your group
Definitions of Common DEI-related Terms and Concepts
Everyone is on a different point in their DHEI journey. To ensure a commonality in language and understanding, we have included a short list of terms and definitions from the Experience Difference Program at CHCO as well as the Office of Health Equity in the Colorado Department of Public Health and Environment.
• ally: Someone who acts in support of non-dominant group members and who does not identify as part of that non-dominant group. Allies practice genuine allyship. That is, they take action, reflect on their own thinking and beliefs, seek out learning opportunities, take initiative in interpersonal relations, and work to create systems of equity. (Office of Health Equity in the CDPHE)
• anti-racism: Some form of focused and sustained action, which includes inter-cultural, inter-faith, multi-lingual and inter-abled (i.e., differently abled) communities with the intent to change a system or an institutional policy, practice or procedure which has racist effects. *Adapted from the Anti-Racism Digital Library. (Office of Health Equity in the CDPHE)
• BIPOC (Black, Indigenous, and people of color): Specific to the United States and intended to center the experiences of Black and Indigenous communities by recognizing that not all people of color face equal levels of injustice and that Black and Indigenous people are severely impacted by systemic racial injustices.
• cisgender: A person whose gender identity matches their sex assigned at birth. (Office of Health Equity in the CDPHE)
• disparities: Measurable differences among groups of people. Inequities cause disparities. (Office of Health Equity in the CDPHE)
• diversity: Diversity is all the ways we are different. The differences we are born with and the differences we have acquired. The broad dimensions of diversity include but are not limited to creed, ethnicity, religion, language, race, physical and intellectual ability, neurodiversity, gender expression and identity, culture, sexual orientation, geographic location, socio economic status, veteran status, professional background and age. (Experience Different CHCO)
• equity: When everyone, regardless of who they are or where they come from, has the opportunity to thrive. This requires eliminating barriers like poverty and repairing injustices in systems such as education, health, criminal justice and transportation. (Office of Health Equity in the CDPHE)
• ethnicity: a large group of people with a shared culture, language, history, set of traditions, etc., or the fact of belonging to one of these groups (Cambridge Dictionary online)
• implicit bias: Attitudes or stereotypes that affect our understanding, actions and decisions. People are usually unaware of their own biases because biases operate at the subconscious level. (Office of Health Equity in the CDPHE)
• inclusion: Inclusion is the active process of inviting, engaging and involving the broad community, where the inherent worth and dignity of all people are recognized. An inclusive organization promotes and sustains a sense of belonging for all its members; it values and practices respect for the unique intersection of identities found in each person and community. (Experience Different CHCO)
• health equity: Health equity is achieved when everyone has access to the resources and opportunities they need to attain their highest level of health. Fostering health
equity requires intentionally engaging in the process of removing obstacles to health such as poverty and discrimination. Achieving health equity is linked to access to good jobs, quality education, healthcare and safe housing. (Experience Different CHCO)
• LGBTQIA+: lesbian, gay, bisexual, transgender, queer or questioning, intersex, asexual and more, plus people who use different language to describe identity; see Common Identity Definitions from The Center
• microaggressions: Brief or casual comments/exchanges, verbal and nonverbal, that send degrading messages to individuals because of their membership in any marginalized or oppressed group. (Office of Health Equity in the CDPHE)
• minority tax aka diversity tax: The expectation (from leadership, colleagues, society) that those who have marginalized identities lead or participate in DEI-related efforts, without time, monetary or promotional compensation and often without regard for the availability, interest or wellbeing of those expected to participate
• preferred gender pronouns or personal gender pronouns: A set of pronouns that an individual wants others to use in order to reflect that person’s gender identity.
• race: A social construct that artificially groups people by skin tone and other physical traits. The concept – which has no genetic or scientific basis – was created and used to justify social and economic oppression of people of color by white people. *Adapted from Luna Jiménez Institute for Social Transformation. (Office of Health Equity in the CDPHE)
• social determinants of health: The social and economic factors that determine where we live, work, play and pray. These factors demonstrate that one’s health is not merely a result of individual behavior, but largely due to barriers in systems and institutions that prevent oppressed groups from thriving. (Office of Health Equity in the CDPHE)
• SOGI (Sexual Orientation and Gender Identity): An inclusive term that applies to everyone, whether they identify as lesbian, gay, bisexual, transgender, queer, two-spirit, heterosexual or cisgender (identifying with the same gender that one was assigned at birth).
• structural racism: When our institutions, such as housing, education and transportation, collectively create systems and policies that work better for white people than for people of color. Structural racism limits opportunities for some, and contributes to poor outcomes for all. Other forms of structural discrimination may relate to classicism, ableism, heterosexism, etc. (Office of Health Equity in the CDPHE)
• URIM (underrepresented in medicine): Racial and ethnic populations that are underrepresented in the medical profession relative to their numbers in the general population.
DHEI Needs in a Group: Baseline Assessments and Information Gathering
There is a wide spectrum of how DHEI groups begin, from informal grassroots ideas and gatherings to formally structured official initiatives. The goals of the group and who is involved will impact what approaches will be more effective in supporting the group’s success. A group of team members who are treated as outsiders and who are getting together to support each other and to bring joy into their experiences may define success and, maybe more so, how they get there differently than would a group of formal physician leaders meeting to assess and improve the outcomes of a particular patient population. (As a tangent and to whet your appetite for topics covered later, it is interesting to consider if these two groups are likely to be comprised of the same individuals and why that might be.)
In the paragraph above, we share that how a group approaches DHEI work may differ group to group more so than what each is trying to accomplish. This is because, in the context of this playbook, we are all defining success as achieving DHEI. Since that is an enormous goal, however, the work of particular DHEI groups tends to focus on goals that are achievable in a reasonable timeframe For this work to be sustainable, at some point relatively early in group formation, members should identify the shared focus(es) of the group and related outcomes hoped for
In more structured initiatives, information-gathering and evaluation tools can be helpful when starting and cultivating DHEI efforts. Assessments reinforce a process and offer important measurable information to define an activity or movement. They help set the context and assist in establishing a common language for the expression of needs and goals. Although the author of the quote, “what gets measured gets done,” can be attributed to many different people, from Rheticus in the 1500s to Lord Kelvin in 1883, the message is clear: “To measure is to know.” That said, who is determining what to measure, who does the measuring, what is measured and who interprets the measurements are all variables that can impact whether the group moves toward equity or unintentionally undermines that goal.
When using formal assessments, it is important to communicate their purpose, how the information will be used to create a more inclusive community, and to evaluate how the information gathering might be experienced by your section and community. Gaps identified, processes and outcomes should also be transparently disseminated as available. For initiating and following progress in diversity, health equity and inclusion efforts in a group, we organize assessments into two broad categories:
(1) Assessment of DHEI awareness, which is a broad perspective assessment of a group and (2) Assessment of availability and accessibility of DHEI resources. Some surveys distributed institutionally (e.g., AHRQ climate survey, Children’s Hospital Colorado Team Member and Medical Staff surveys, etc.) may have questions that address both of these categories.
Alternatively, before or instead of performing formal assessments, seeds are sown more organically for DHEI efforts through conversations and shared experiences. We encourage anyone interested in DHEI efforts to use any combination of these approaches that they feel will support their group’s success.
Assessments of DHEI Awareness
Key Questions to Ask:
- Do the group's associated staff surveys include questions about DHEI?
- Does this group respect individuals and their differences?
- Do individuals of different backgrounds feel they belong and are meaningfully included within this group?
- Are all group members actively working to dismantle barriers to DHEI that exist in the group?
- How can DHEI efforts be improved upon in this group?
- What are examples of inequalities that exist in this group and community?
- Can further understanding of different backgrounds improve teamwork and communication in this group?
Assessing DHEI needs in a group
Assessment of DHEI Resource Availability and Accesssibility
Individual/Group assessments of awareness:
- Individual assessments of implicit bias
- "Examining our wiring" lecture
- Intercultural Development Inventory (IDI)
Key Questions to Ask:
- Is there a known process for individuals within the group to escalate concerns of discrimination as they occur, are concerns submitted regularly to indicate use of system, and are those who submit concerns satisfied with the response received/actions taken?
- Are there members of the group who are motivated to do more work to support DHEI?
- Do members participate in courses, activities and/or training to become more knowledgeable,involved and effective in DHEI?
Assessments of availability and accessibility:
- Culture and Climate Surveys (see examples from the Breathing Institute in the appendix)
To Start, You Need Champions
One of the earliest elements that needs to be put in place for a new DHEI effort is finding champions. The champions will keep the body of work moving forward when momentum stalls, be primary contacts for concerns from team members, and be connections for formal leaders who are interested in incorporating DHEI into all of the team’s priorities and work
Below we share accounts from three of the champions who created this playbook on how they started this work and where it has led.
Marcy Mendenhall, MD (Emergency Medicine)
As the daughter of a Mexican immigrant, I spoke both English and Spanish in the home. When my family visited, I served as interpreter and, when I eventually learned to read and write, as translator I grew up spending several weeks each year in Mexico under the watchful eyes of my aunts and uncles, blissfully playing with my cousins, and over the years, grew keenly aware of the differences in health care access and health outcomes between the two countries, all of which sparked my journey into the field of medicine. Fast forward many years and I am now a mid-career pediatric emergency medicine physician in the largest section in the Department of Pediatrics. I am certified as QBS (qualified bilingual staff). My commitment to health equity remains steadfast.
The Emergency Department is the front door to the hospital and directly impacts the health and livelihood of over 200,000 children and their families each year. Historically, health equity work was siloed in our section. That all changed when George Floyd was murdered, inspiring many within our section to cohesive action. With the support of our section head, including funded time for myself as our leader, we organized and created a novel, multidisciplinary group: PEM GUIDE (Pediatric Emergency Medicine Group for Unity, Inclusion, Diversity and Health Equity). PEM GUIDE meets monthly and welcomes all team members who walk through the ED, in whatever capacity, to share stories (clinically and non-clinically), grow comfortable having uncomfortable conversations, and learn about DHEI through structured lectures, journal clubs and invited speakers. Through PEM GUIDE, we engage in advocacy in action. For example, during the COVID pandemic, we created specific discharge instructions targeting COVID vaccine misinformation and hesitancy. We created a shared DHEI vocabulary, including person first language, that we engage in our daily interactions. We added a DHEI lens to each clinical case review. We work with the hospital and the Department of Pediatrics on projects, including clinical pathways which aim to minimize bias and standardize care for all children. We now have dedicated ED Spanish interpretation. Through PEM GUIDE, we foster a culture of inclusivity and belonging, celebrating the diversity of our group and the patients and families we serve
Michele Loi, MD (Critical Care)
Encouragement of DEI principles and progress within a division must all start somewhere and it usually starts with a champion – someone who believes in the necessity of DEI and is willing to obtain DEI training for themselves and then foster other interested people within the group to also undergo education and training. It is very important that we can speak the same terminology when it comes to DEI and learn from others (like the other champions in this section) and what has been successful so far. The same format may not work for all groups, however, and may need to be adapted to each group. Hospital collaborative DEI efforts, like the DEI task force is also helpful for guidance as each group of champions work within their division.
My division is in the earlier stages of recognizing the importance of DEI principles in any high functioning team and how formal efforts in DEI ultimately improve patient care. Implicit bias training has been given at our mandatory faculty meetings and opened our eyes to issues many were not aware of. We are giving our morbidity and mortality case reviews a DEI lens and are identifying where we can do better. We hope that this will lead to concerted quality improvement efforts to provide better patient care. We are finding ways to make fellowship recruitment more equitable, and our leadership are working on doing the same for faculty recruitment. These are all initial small efforts that will hopefully turn into more polished program development like my colleagues above. Being a champion may seem like a daunting task at first, but everyone starts somewhere, and this change takes thoughtfulness and time.
Kate Johnston, MPH (Pulmonary Medicine)
In 2020, conversations about racial justice were happening everywhere and our section was no exception. Work was already underway to create a more equitable fellowship recruitment process and to address social determinants of health for our patients; new DEI initiatives, like a Social Justice Book Club, began that summer. Unfortunately, as a large section (almost 200 members), these efforts were siloed. As those involved connected more, we recognized the need for a formal DEI structure that could provide increased visibility and support for these and future efforts.
We presented a request to the section leadership team; they not only agreed to the need but named two formal leaders and provided funding for dedicated time. Having such strong leadership support has been invaluable, from providing time to focus on this work to working with hospital leaders when needed. At the same time, everyone involved is incredibly busy and asks of their time must be both reasonable and valuable. Two years in, the champions still do most of the heavy lifting and rely on the larger DEI team for guidance and feedback. We have collected data from our section on diversity, belonging and experiences of discrimination and have created a three-year strategic plan. I believe as we continue to develop, there are opportunities for increased power sharing as our DEI efforts become more deeply embedded in our section.
Beginning Issues and Conversations
There is a historical, societal, organizational and department/section context for any group trying to set and achieve goals. Aspects of these contexts may be known or hidden, and group members may have widely varying levels of awareness of these contexts. Based on our different experiences, we each also have different perspectives on how we experience, understand and function within these contexts, whether we're aware of it or not. The topics below are some ideas to support your group in increasing awareness of:
• your own and others' lived experiences and perspectives;
• how those experiences and perspectives may impact the dynamics of your group; and
• how these differences bring a variety of strengths, creativity and resources that will support your group achieving, as a team, what you hope to. These topics, information and activities are geared toward establishing yourselves as a working group and taking part in reflection, learning, development and collaboration that will be helpful to you as individuals and as an effective team. These issues are critical to building and fostering a diverse and inclusive working group, and they will likely show up repeatedly throughout your activities and efforts.
Zone of proximal development
If you aren’t making mistakes, you likely aren’t making much progress. When it comes to DEI work, many of us are building the plane as we fly it. Our efforts to establish and expand the edge of our knowledge and skills in DEI is where and how we learn and grow, as individuals and as a group. In DEI groups, we can strive to offer spaces where we can put aside some of our fears of saying the wrong thing or not knowing the “right” answer, both of which can hinder advancement in this work. Growing more comfortable in an uncomfortable space is where growth happens!
Lev Vygotsky, a psychologist, offered a framework for thinking about this “edge” of our knowledge and skills, dividing it into three levels:
1. what we can do on our own,
2. what we can do with guidance, and 3. what we cannot do.
As those of us writing this playbook understand it, the experience of learning from others who are more knowledgeable and skilled is integral to efficiently expanding the edge of our own abilities. This is the zone of proximal development. This is what we offer each other in our DEI spaces – for all of us to be both learners and teachers, and, together, grow more knowledgeable and skilled.
Awareness of our “edges” is important to our development, and DEI committees often strive to be spaces to test those boundaries and practice new skills within our zones of proximal development. However, when we step into areas of knowledge and skills we simply don’t have, even with others’ support, no matter how well-intentioned we are, we are at significantly greater risk of causing harm. Before taking that risk, consider other approaches. For example, have a one-on-one conversation with someone who has insight into the topic or skill before bringing it to a larger group As a rule of thumb, those 1:1s should be with individuals whose marginalized identities don’t overlap with the area you are exploring.
In addition to our own DEI groups, there are opportunities to work with others at various stages of learning to explore and grow together. The nature of collaboration involves the introduction of multiple perspectives and styles and offers the opportunity to learn from one another through successes and failures. Some ideas are to join a DEI-focused group in another section or department, apply to the Children’s Colorado Captains of Inclusion program, or seek out the myriad of opportunities waiting for you. For those leading a group on their DEI journey, you serve as a learning guide. No section, department or even DEI group is the same, thus you help make your group’s dive into DEI salient to their needs, intellectually, emotionally and contextually.
As a group, consider doing an inventory of current DEI knowledge – some kind of level-setting so individuals have an idea of areas they’re more apt to lead and other areas in which they’re better positioned to approach as a learner. And remember: If you’re not making mistakes and experiencing discomfort, you’re probably not making much change, progress or impact (on self, others, institution)
Identities
Our identities are how we see ourselves. They are aspects of what make us who we are. They also influence which groups we feel part of. When thinking about your identities and sharing them with others, consider focusing on those that have been most impactful in your life and that are most relevant to the particular context.
We are not always immediately aware of how our different identities impact our experiences. Especially if our identities are common among those with whom we surround ourselves, we tend to see our identities as "normal" and the standard by which we view the world. At the same time, what we think is normal might be completely foreign and new to someone else. For example, we may not consciously recognize being housed as one of our identities, whereas if we are currently experiencing or have experienced homelessness, that status might be an identity very much in the front of our minds and be a significant part of how we identify.
It can be challenging to not think of different perspectives as right or wrong, better or worse. While who we are, how we see things, and how we make choices can be very different, they are just that – different. Others also put identities on us that we may not choose ourselves. This might be based on societal stereotypes, assumptions and endless other ways we're each – often unintentionally – guided in how we think things are or should be. Some examples that may influence how people identify: race, ethnicity, gender identity, ability, sexual orientation, language(s) spoken, homeland or nationality, familial relationships (parent, child, sibling, partner, spouse), employment status, wealth bracket, religiosity, education level, political affiliations, etc.
Intersectionality
Looking at the examples of some identity categories above, it is clear we each encompass a variety of identities, and that those identities may change over time. Intersectionality is the concept that our identities overlap and interact. Kimberlé Crenshaw coined the term and says intersectionality is “…a lens, a prism, for seeing the way in which various forms of inequality often operate together and exacerbate each other. We tend to talk about race inequality as separate from inequality based on gender, class, sexuality or immigrant status. What’s often missing is how some people are subject to all of these...” (from Time article, 2020)
Power and Privilege
Thinking about our identities and intersectionalities, we see that we each bring different experiences and perspectives to any situation. Often, we're unaware of these differences and/or how they impact our experiences with others and others' experiences with us. This diversity of experience and perspective is an amazing resource in and of itself and can lead to insights, innovation and success that wouldn't be possible otherwise. Like any resource, we have to learn how to embrace and tap the power of diversity. At the same time, we have to make sure we don't misuse or deplete it. Now that we have explored our identities, it's time to consider how our identities give us power and privilege (P&P), what we can do to keep from causing harm with our P&P, and how we can use our P&P to achieve to our diversity, equity, inclusion and justice goals.
Power is the ability to affect change, for yourself or others (or things, like the environment). Power can be achieved (i e., a job promotion or winning an election) or received based on cultural values (i.e., men's ideas valued more than women's because of gender stereotypes). Privilege is unearned resources or attributes that allow for power to be relatively easier to achieve. Privilege can come from something you have or experience that others don't (an inherited house), or it can be the absence of something that others have or experience (being able-bodied). Power and privilege are:
• experienced relative to others (i.e., more or less than someone else),
• context dependent, and
• possessed and experienced in one way or another by everyone. The P&Ps we have and how much are often based on our identities (both how we self-identify and how others perceive and categorize us) and how identities have been and are valued historically and systemically.
The balance or imbalance of P&P and how they are used impact the levels of DEI experienced by individuals and within teams, organizations, communities and societies. It is because of this that awareness of and conversations about P&P are important for a DEI committee to be effective. Because the end does not justify the means, it is important that your committee strives for DEI to exist in all your structures and processes, including in your initiatives and outcomes.
Myth of Meritocracy
Meritocracy – A system that rewards merit (ability + effort) with success, like wealth, power and privileges; success determined by individual achievement and not based on one’s inherited social status (Boston Medical Center glossary for cultural transformation link)
• Meritocracy is often considered a myth in the U S because it ignores the multiple factors that contribute to one’s achievements and status in society 1. people do not start on equal footing, 2. it is not because of individual lack of will, effort or intelligence, rather there are systems of oppression that inhibit marginalized populations from accessing resources that lead to health, wealth, power and privileges. (Boston Medical Center glossary for cultural transformation link)
• An illustration of this is origin of “pull yourself up by the bootstraps” (from the Samuel DuBois Cook Center on Social Equity at Duke Univ.): In 1834, the first-known appearance in a text of the phrase “pulling oneself up by the bootstraps” was supposed to be satirical. It was intended as a metaphor for something that was absurdly impossible: In this case, the image of a man trying to haul himself across a river simply by tugging on his bootstraps. Yet, over time, the phrase has come to be the driving force behind the notion that anyone who works hard can become prosperous.
Being Effective in DEI Work
How to work toward positive change effectively – not too little, not too much, not too slow, not too fast
Ideas for How to Get Started
Section-level DEI efforts can look like many different things and can have a variety of starting places. We have listed a few of the most common here, but they are certainly not the only options. When choosing where to start, you will want to keep in mind how many people are likely to participate and who those people are (what identities do they hold?). Are your initial goals to educate, promote conversation, or make measurable change to policies and practices? These questions will help determine your starting point.
Assemble a team to start initiatives that will impact practice and policy changes
Individual enrichment – Raising self-awareness
• Attend DEI/equity rounds (link if present)
• Journal articles
• Ted Talks
• Books
• Attend lectures and training on DHEI topics
• Attend Celebrate Difference Week
• Attend a section/department-based DEI meeting (link to recurrent meeting calendar with zoom link)
Embark on individual journey toward learning more about DHEI
Gather a group of people to engage in learning and conversation
Group gathering and learning – Raising awareness in a group
• Incorporate and share a DHEI moment at the beginning of meetings, similar to a target zero safety moment
• Invite guest speakers on topics of interest to the group
• Journal club
• Monthly spotlight on different cultures
• Celebrating your kickoff with a multicultural potluck
• Facilitate a movie and discussion session
• Attend Celebrate Difference Week
Assembling a team to impact practice and policy changes
• Ask for guidance from guest leaders with experience leading similar discussions or committees
• Perform a DEI climate assessment on your group to assess for areas of need
• Hold a Kaizen or brainstorming session with interested parties to generate ideas for projects and initiatives
• Develop mission, vision and values statements to align group and drive work forward
Building Blocks of a DHEI Team
As you begin establishing a DEI structure in your section, you need to build a team around you. Not only is there too much work for one or two people, but diversity within the team will make the work you do more inclusive, more effective and more sustainable. To understand who you need on the team, you should define your scope of influence. Will your work focus on a specific team within your section (e.g., providers, nurses, leaders)? Or will it encompass everyone within your section, regardless of role or employer (e.g., CHCO, CUSOM)? Since all of our work here – and especially patient care – is multidisciplinary in nature, we recommend your DEI efforts seek to serve everyone in your section.
All the teams represented in this playbook began by asking for volunteers. While this is a great way to start, you may miss people who are interested but don’t feel like they have time, aren’t able to control their own schedule, don’t feel it is their place to participate based on their identity, or don’t feel safe participating based on their identity. We recommend your first task be identifying who is NOT at the table. Are there specific identities not represented (e.g., black women, people with disabilities, LGBTQIA+ team members)? Are most of the roles in your section represented? As you identify gaps in your participation, you can do targeted recruitment to address those gaps and ensure you have as many perspectives at the table as possible.
Also based on our experience, it is important to consider sustainability and participants’ wellness. Much of DHEI work is currently done on a voluntary basis, with many of the same people participating in an overlapping array of groups and initiatives that seem to be constantly multiplying. Ideally, those contributing significant time to DEI work would be compensated with
protected time and/or additional pay and/or formal recognition in evaluations. We encourage you to discuss this with your leadership, and we also acknowledge that this support is not currently common. This is particularly disturbing for those who are already marginalized by our society and organizations and who are often expected to do the most work in these areas. This is referred to as the minority tax (definition in glossary above) In addition to seeking some sort of compensation (or offering it, if you’re in a position to do so!) some suggestions are:
• clearly define the expectations of members or particular roles;
• rotate leadership responsibilities regularly, and
• openly discuss this issue and check in with your group members about what they’re experiencing with their own time commitments and how your contributions are viewed
Once your team is established, it is helpful to ensure you’re using common language and working toward the same goals. You can take the definitions offered earlier in this playbook and review them together, making any adjustments that are important to your group. Establishing a mission and vision for your DEI efforts is also valuable; these serve as a north star for your team as well as a communication tool when presenting your work to others. Below we have included examples from within the organization. There are many processes you can use to create these as a team. We recommend getting specific words/phrases from all team members and then having 1–2 people use those to create a few choices for each that members can then vote on. This can be done in person (using sticky notes, poster board) or virtually (using surveys, word cloud tools).
Leadership of the group is something else to consider. A formal leader or group of leaders can help maintain the momentum of the group. Leaders might rotate over time, both for practical reasons of how much time and energy it takes to lead a group, and to respond to different dynamics and goals the group may develop over time.
From What is the difference between mission, vision and values statements? by SHRM:
• mission statement – a concise explanation of the group’s reason for existence
• vision statement – forward looking, creates a mental image of the ideal state the group organization wishes to achieve
• values statement – lists the core principles that guide and direct the group and its culture
Experience Different Vision: We aspire to be leaders, building an inviting, engaging, inclusive environment for EVERY team member, patient, family and community member.
Pediatric Emergency Medicine Group on Unity Inclusion Diversity and health Equity (PEM GUIDE) Vision: We lead with our commitment to health care equity for all children and promote an inclusive and diverse work environment through education, advocacy, research and outreach.
Pediatric Emergency Medicine Group on Unity Inclusion Diversity and health Equity (PEM GUIDE) Mission:
Return to Table of Contents
• Ensure health equity to all children at CHCO by recognizing and mitigating the impact of structural racism and socioeconomic disparities within our hospital and community.
• Cultivate a diverse environment by prioritizing the recruitment, retention, and support of staff, trainees, and faculty from underrepresented groups, striving for pluralism in race, ethnicity, sexual orientation, gender identity, physical disability, and religion.
• Promote a culture of inclusion within the Section of Emergency Medicine as we learn about and acknowledge our implicit and explicit biases in order to transform our behavior in everyday interactions.
Breathing Institute Equity Council Vision: Creating a culture that centers equity and justice
Breathing Institute Equity Council Mission: Centering equity, inclusion and diversity in all aspects of pediatric pulmonary and sleep medicine care, research, education and advocacy
Diversity in Pediatrics Committee: Our mission is to foster a residency program that supports its diverse residents, reflects the patients we care for, understands the way in which systemic inequalities impact our patients and families, and commits to working towards equity and justice through recruitment, education, mentorship, and community engagement.
Department of Surgery Diversity Mission: The Department of Surgery is committed to ensuring diversity among our faculty, staff and learners. We will maintain an environment that is free of discrimination and harassment, reflects the diversity of the communities we serve, and brings to life the department’s vision of Improve Every Life.
Department of Surgery Equity Mission: We are steadfast in ensuring that our faculty, staff and learners can thrive in an equitable environment. This commitment ensures unbiased care and eliminates discrimination in all forms and at all levels. This is essential to our success. It will be achieved by aligning our policies, practices and resources so that people of all races, cultures, genders, sexual orientations and socioeconomic statuses have opportunities to thrive.
Department of Surgery Inclusion Mission: The Department of Surgery is dedicated to maintaining an environment of inclusivity where all members of our community feel valued and appreciated. We embrace the collective and individual talents, skills and perspectives of our faculty, staff and learners to foster a culture of excellence and innovation.
Recommended Training
Please note: Different trainings will be more effective for different people, below are some suggestions to get you started
Training from Children’s Hospital Colorado
• Dixon Focused Health Initiative Simulation Series Offered each year through CHCO Continuing Education
Return to Table of Contents
• Captains of Inclusion Development Program
This extensive, in-person series through CHCO Diversity, Health Equity and Inclusion encourages participants to challenge their mental models, inspires behavioral change and provides actionable steps toward building an inclusive culture.
• Destination Equity
Required for all CHCO team members including medical staff and faculty. A multi-part training and development series designed to advance our efforts to improve patient care and achieve health equity to provide team members with the knowledge and skills they need to address healthcare disparities and improve outcomes for patient families. Sessions include Identity & Bias, Relationships, Systems and Our Shared Commitment to Advancing Health Equity; CHCO team members can search “Destination Equity” in Cornerstone and register for in-person or virtual sessions.
Training from University of Colorado Anschutz Medical Campus
• Health Equity in Action Lab (HEAL) Trainings and Workshops
This extensive, in-person series encourages participants to challenge their mental models, inspires behavioral change and provides actionable steps toward building an inclusive culture.
• LinkedIn Learning
Log in to the CU Anschutz Employee Portal and select Training from the CU Resources Home menu to access LinkedIn Learning. Enter DEI in the search field to find thousands of DEI training courses and videos.
External Training
• Right to Be (formerly Hollaback!)
Provide free trainings to the public and customized training experiences for businesses, organizations, schools and colleges that are oriented to empower you to make a change and channel attention into simple, creative and effective action. Find tools to learn how to respond, intervene and heal from harassment.
Challenges Experienced and Lessons Learned
DHEI-dedicated groups are relatively new at CHCO. Without a template or structure to follow, engaging in this work may seem daunting. As DHEI champions in our sections, we have learned a few lessons and challenges along the way.
The first challenge is, if possible, gathering support of your leadership team. Leadership support and sponsorship can remove barriers as DHEI efforts develop. Visibility of leaders and champion support may also motivate others to be interested and engaged in your DHEI vision and efforts. Collaborate with interested team members and delegate work and roles. A team with members who build a structure together will be less likely to let it be torn down.
The second challenge is developing metrics to know when you have made a difference. What will success of the DHEI group look like? Although metrics can seem arduous and not directly
relevant to DEI overall goals, they provide the facts and oomph to show how you have impacted change. These metrics will help additionally show leadership and your team why this work is important. Please see the next section “Goals and Outcomes” for additional ideas about measures.
The third challenge is maintaining momentum and engagement. During the initial phase of creating your group, you may find interest and enthusiasm are high. After several months, this momentum may slow down. Do not give up hope. DEI work is on-going. Consider doing a check-in with your group to better assess the decline in engagement. Perhaps the group needs to meet less often or would benefit from a speaker or training session from the Experience Difference team. Consider the bandwidth of those involved and invite others to join your group. These considerations take time and if you are the champion for these efforts in your group, consider meeting with leadership to ask for dedicated time.
Dedicated funding and recognition for leading section-based DEI work is helpful to success and is the fourth challenge we’ll mention Meet with leadership in your section to start the conversation about how this work will be further supported and what resources are available to build DEI programs We also recommend reaching out to other section-based DEI champions to learn from their experiences.
Goals and Outcomes
As you progress on your DEI journey, keep both short- and long-term goals and outcomes in mind.
Your goals and outcome measures will be different depending on what your intentions are on your DEI journey. Some quantifiable sources of data include results from the medical staff survey, follow up surveys on workplace climate, patient outcome measures. The number and quality of projects that develop from the start of a DEI program can represent the success of a group’s engagement. Surveys, from patients/families and staff can also be both quantitative and qualitative.
Culture change, which DEI efforts are inevitably impacting, takes time and is hard to measure in short intervals. Also, do not discount the impact of individual stories and experiences from your colleagues, your teams and the patients you care for. These stories can be incredibly powerful.
“The work of DEI is never done. Without continued vigilance, even an organization that has designed systems and structures to remain sustainable through change can easily slide backward. True commitment to DEI requires continuous improvement by reassessing strategies and initiatives as the organization grows and as the world changes. For example, if you open your first-ever office in India, you will have new DEI challenges to solve. The same is true if some event in the world shines a bright light on inequity that you hadn’t known was there.
Regardless of which stage you’re in, knowing where you are on your DEI journey can help you focus on the right questions to keep moving forward.”
(Washington 2020, Harvard Business Review “The Five Stages of DEI Maturity”)
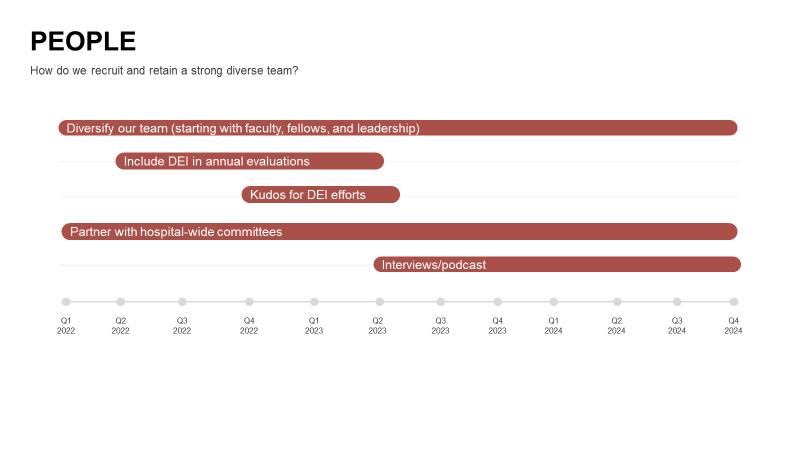
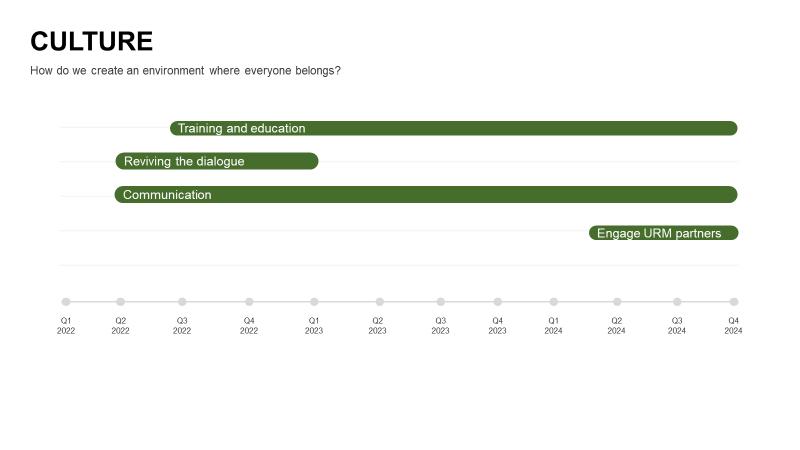
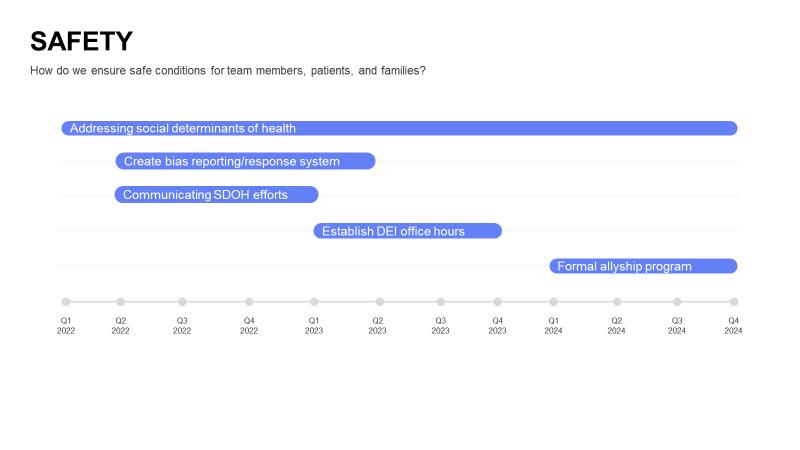
Strategic Planning, Overview
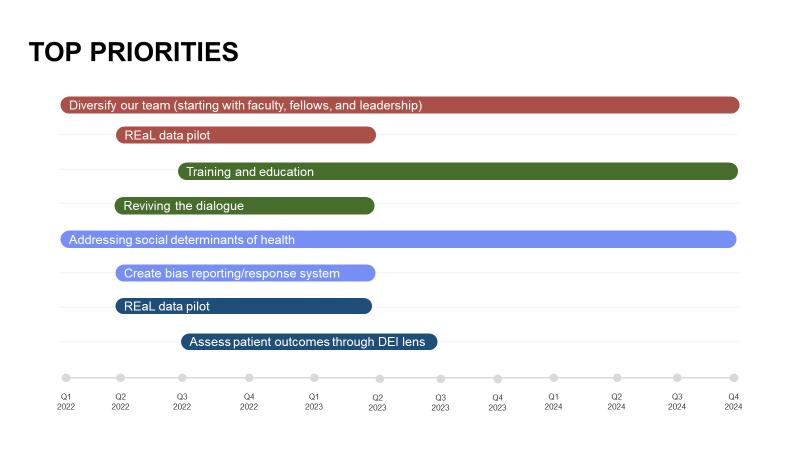
Strategic planning is an incredibly helpful exercise to prioritize and communicate DEI efforts within your section. However, it is not likely to be one of your first steps when establishing DEI infrastructure in your section. For one section that completed a DEI strategic plan (available in the Resources section), formal DEI efforts had been in place for 18 months before the plan was drafted. This allowed the section time to take many of the steps outlined earlier in this playbook, including establishing a committee, agreeing on a vision and mission and collecting data to inform the plan. The creation and approval of a strategic plan at this juncture also helped institutionalize DEI work in the section and galvanize team members.
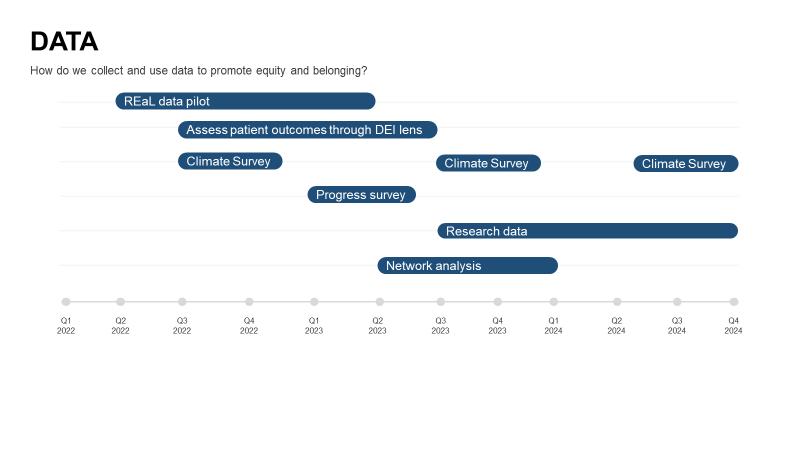
Your section’s strategic plan should be guided by section-specific data, if at all possible. The assessment section of this playbook has great recommendations for options your team can explore. The example strategic plan used two years of Climate Survey data as well as a progress survey. The Climate Survey was administered to the entire section (CUSOM and CHCO employed team members); the progress survey was completed by members of the DEI committee. These helped leaders understand what the section’s needs were as well as what mattered most to team members.
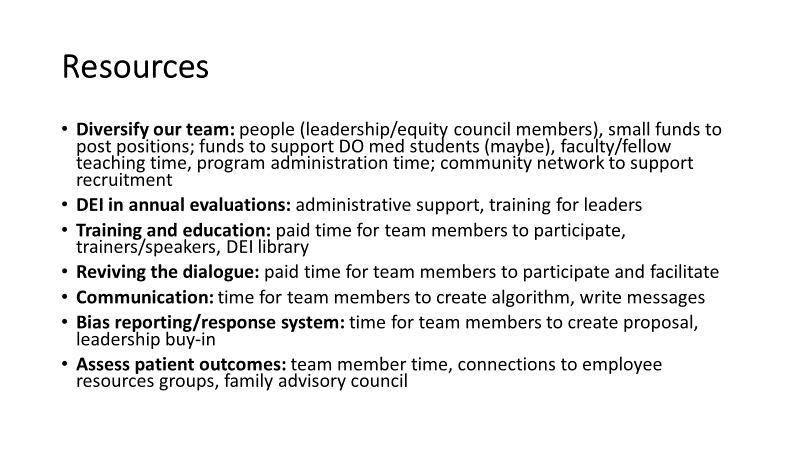
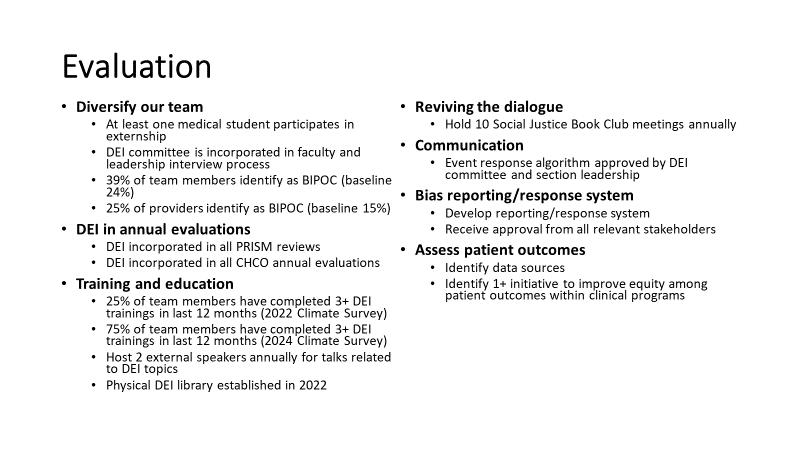
As we all know, change takes time. Your strategic plan should last for at least one year, to give your team time to accomplish the goals you set out. Five or more years may be too long, as your section’s needs will likely change over that time as your DEI work progresses. We recommend a time frame of two to three years to balance the pace of change and the need for adaptability. Whatever time frame you choose, measuring metrics will likely extend beyond the end of your official strategic plan. We recommend identifying process, short-term and longterm outcome measures to assess progress on your strategic plan. These measures should be named when the plan is created and can be updated over time as needed. It will also be important to identify resources needed to accomplish each activity on the strategic plan. Leaders will want to understand the personnel and resource needs prior to approving the plan.
Shepherding a strategic plan from creation to implementation involves several steps. We recommend drafting the plan in a small group of stakeholders, likely two to four people. These people will use data from the larger section to inform the plan. If your section has a DEI committee or other structure in place, that team should be your first step for review and approval. These team members will best understand current state and what is needed to move forward DEI efforts in your section. The plan should then be presented to the section leadership team. Once leadership approval is received, the plan should be presented as broadly as possible to the full section. This allows everyone to understand the work that will occur as well as provide opportunities to involve team members who are not already part of the DEI infrastructure. Periodic updates should also be presented to the full department.
Conclusion
We hope this playbook provides helpful guidance as you launch DEI efforts within your section. Our goal in this work has been to be reformers and revolutionaries, but not to be reckless. We would not be doing our jobs if we didn’t warn you that there will be challenges ahead. While we can’t address every challenge in this document, we will hold occasional roundtable discussions where we can share our experiences in more detail and help you brainstorm solutions. We encourage you to come to those or to reach out to us for individual support. Our contact information is below. We’d like to leave you with successes we have experienced to help bolster you when the hard days come.
• Contact authors for individual support:
o DOP DEI Committee, Community Culture & Equity Subcommittee (those who initially drafted this playbook)
▪ Brandi Freeman (DOP DEI Committee Lead): Brandi.Freeman@childrenscolorado.org
Resources
• Children’s Hospital Colorado DHEI team intranet site
• University of Colorado Diversity, Equity, Inclusion and Community Engagement site
• CU SOM Office of Diversity and Inclusion, training request form
• Books
o See “ExD Learning List Books” on the CHCO DHE&I intranet site here
• Articles, Chapters
o The Five Stages of DEI Maturity (Harvard Business Review, Nov-Dec 2022)
o From Elena Aguilar
▪ Free tools from Coaching for Equity (including an the activity “Exploring Identity Markers”
▪ Chapter 3 from Elena Aguilar’s book, Coaching for Equity: How to Understand Race, Racism, and White Supremacy
• Activities for a group
o The Shape of Trust - Principles To Cultivate A Community Of Practice, from the Race and Social Justice Initiative
▪ “An interactive drawing and discussion activity to explore cultivating principles. Principles are ways of being and relating that help us nurture and maintain a community of practice. A community of practice is a group learning environment oriented toward relationship, health and wellbeing, adaptivity, authentic presence with difficult content, and space for personal and collective growth. This activity can be adapted for live, virtual learning.”
o 21-Day Racial Equity Habit Building Challenge, by Food Solutions New England
▪ An annual live experience usually in the spring; lots of related info here, organized by topic
• To watch and listen to
o Addressing Unconscious Bias as a Leader (LinkedIn)
▪ “Dismantling unhealthy workplaces requires action. Although it's increasingly common for companies to recognize the importance of diversity and inclusion in the workplace, many are unaware of bias in the cultures they've unwittingly created. Others might know there's a problem, but don't know how to properly address it. In this course, Stacey Gordon, CEO of Rework Work and an expert in helping companies move from awareness to action, teaches you how to identify bias and leverage proven tools for actively removing barriers and ensuring equity throughout your organization.”
o Translators – The Untold Story of Children Who Give A Voice to Generations (a film)
▪ “Every kid needs their parents. But for 11 year-old Densel, 13 year-old Harye, 16 year-old Virginia, and the over 11 million children across the U.S. who are the only English speakers in their family, sometimes that relationship gets flipped. This is the untold story of kids who act as their family's translators on matters that are sometimes more adult than they are.”
o Select episodes from Elena Aguilar’s Brightmorning Podcast – easy to peruse titles for particular topics
▪ Most of Elana’s work is focused on coaching, particular in the grade school arena. Many offer amazing insights that are explicitly focused on DEI topics and apply to a much broader context than education.
Return to Table of Contents
o Don’t Call Me Resilient, a podcast about race and racism
• Climate Survey (please see appendix)
• Strategic Plan example (please see appendix)
• Connections! Who else can help?
o CHCO Captains of Inclusion (list of graduates on CHCO intranet site)
o Committee members and leaders of other DEI groups/committees (list to be gathered)
o CHCO Team Member Resource Groups (TMRGs)
o DOP DEI Committee, Community Culture & Equity Subcommittee (those who initially drafted this playbook)
▪ Brandi Freeman (DOP DEI Committee Lead): Brandi.Freeman@childrenscolorado.org
APPENDIX
Sample DEI Climate Survey
Welcome to the annual [section] Diversity, Equity, and Inclusion climate survey. This important survey is to 1) understand who we are as a department, 2) measure our current climate regarding diversity, equity, and inclusion, and 3) target areas for improvement. All responses are anonymous. If you have any questions or concerns, please reach out to [contact name and email].
Please complete the following demographic information. The purpose of this section is to better understand the demographic makeup of the [section] team and to inform future policies, training, recruitment, and department practices.
1. What is your primary current role in the [section]?
a. Administrative staff
b. Clinical (nursing, MA, RT)
c. Community-based
d. Provider (MD/DO, Advanced Practice Providers, Psychologist)
e. Research
f. Supervisor/Manager/Director
g. I prefer not to answer
2. What is your racial or ethnic identity? (select one)
a. Black/African American
b. East Asian
c. Middle Eastern
d. Native American/Indigenous/Alaskan Native
e. Pacific Islander, including Native Hawaiian
f. Spanish, Hispanic or Latino/a/x/e
g. South Asian
h. Southeast Asian
i. White
j. Multiracial, please specify
k. Prefer to self-describe, please specify
l. I prefer not to answer
3. Is English your first language?
a. Yes
b. No
c. I prefer not to answer
4. What language(s) do you speak at home?
5. What is your gender identity? (Select all that apply)
a. Agender
b. Genderqueer/Gender fluid/Non-binary
c. Man
d. Pangender
e. Questioning or unsure
f. Two-Spirit
g. Woman
h. Prefer to self-describe, please specify
i. I prefer not to answer
6. Do you identify as transgender?
a. Yes
b. No
c. I prefer not to answer
7. What is your sexual orientation? (select all that apply)
a. Asexual
b. Bisexual
c. Gay
d. Heterosexual/straight
e. Lesbian
f. Omnisexual
g. Pansexual
h. Queer
i. Questioning or unsure
j. refer to self-describe, please specify
k. I prefer not to answer
8. Do you identify with any of the following religions? (select all that apply.)
a. Agnostic
b. Atheist
c. Buddhism
d. Christianity
e. Confucianism
f. Hinduism
g. Islam
h. Judaism
i. Native American/Indigenous Spiritualism
j. No religion
k. Shinto
l. Sikhism
m. Spiritual
n. Taoism
o. Prefer to self-describe, please specify
p. I prefer not to answer
9. How old are you? (Say N/A if you prefer not to answer.)
10.Do you identify as neurodiverse?
a. Yes
b. No
c. I prefer not to answer
11.Are you a person living with a disability?
a. Yes
b. No
c. I prefer not to answer
12.Are you a current or former member of the U.S. Armed Forces (includes Reserves or National Guard)?
a. Yes
b. No
c. I prefer not to answer
13.Are you a caretaker of a child(ren)?
a. Yes
b. No
c. I prefer not to answer
14.Are you a caretaker of an adult(s)?
a. Yes
b. No
c. I prefer not to answer
15.What is your highest level of education completed?
a. Less than high school
b. High school diploma or equivalent
c. Some college, no degree
d. Associate degree
e. Bachelor’s degree
f. Master’s degree
g. Professional degree
h. Doctoral degree
i. I prefer not to answer
16.Do you consider yourself a first-generation college graduate?
a. Yes
b. No
c. I prefer not to answer
17.What is your current annual salary?
a. Less than $10,000
b. $10,000 to $14,999
c. $15,000 to $24,999
d. $25,000 to $34,999
e. $35,000 to $49,999
f. $50,000 to $74,999
g. $75,000 to $99,999
h. $100,000 to $149,999
i. $150,000 to $199,999
j. $200,000 or more
k. I prefer not to answer
The remainder of this survey looks at the [section]’s culture around inclusion and its related policies and practices. Please read each statement and rate your level of agreement or disagreement. Please answer these questions based on how you feel things currently are in the [section] (even if that’s different from how you think they should be). Strong ly disagr ee Disagr ee Neither agree nor disagre e Agr ee Strongly Agree
Return to Table of Contents
People fit into the [section] when they are similar to our already existing workforce.
Qualification matters in the [section], not background.
Promotion is dependent upon employee performance, not on someone’s background.
Everybody is welcome as long as they meet the necessary requirements. We regard it as important to give employees from disadvantaged groups specific support for their further development.
Matching employees’ cultural background with that of our clients/customers fosters the quality of the [section].
Cultural diversity brings new ideas and different knowledge to the [section] for various business units.
Cultural diversity helps the [section] to become more innovative.
Please answer these questions based on what you think would be ideal state in the [section] (even if that’s different from how they are now). Strongly disagree Disagree Neither agree nor disagree Agree Strongly Agree
People fit into the [section] when they are similar to our already existing workforce.
Qualification matters in the [section], not background.
Promotion is dependent upon employee performance, not on someone’s background.
Everybody is welcome as long as they meet the necessary requirements. We regard it as important to give employees from disadvantaged groups specific support for their further development.
Matching employees’ cultural background with that of our
Return to Table of Contents
clients/customers fosters the quality of the [section].
Cultural diversity brings new ideas and different knowledge to the [section] for various business units.
Cultural diversity helps the [section] to become more innovative.
How many times during the last year while working in the [section] have you been discriminated against in each of the following ways because of such things as your race, ethnicity, gender, age, religion, physical appearance, sexual orientation, or other characteristics? Please read each question and indicate the appropriate response: Never Rarely Sometimes Often Very Often
I have been passed over for a work role/task.
My contributions are not valued as much. I have been given fewer opportunities to express my ideas.
I have unfairly been evaluated less favorably.
I receive less social support.
I have been treated as though I am less capable.
I have been treated with less respect. Someone has delayed or ignored my requests.
Someone has blamed me for failures or problems.
Have there ever been times in the past 12 months that you felt you’ve been treated differently from either your colleagues or your supervisors when working at CHCO because of an aspect of your identity (race, ethnicity, gender, sexual orientation, age, beliefs, physical disability, etc.)?
a. Yes
b. No
How much do you agree or disagree with each of the following statements?
Strongly agree Agree Neither agree nor disagree
Disagree Strongly disagree
I feel like I belong in the [section]. I can voice a contrary opinion without fear of negative consequences. I feel that my compensation is fair, relative to similar roles in the [section].
I feel like I can be my authentic self at work
I feel like my colleagues understand who I really am.
The [section] hires people from diverse backgrounds.
How important is diversity to you, yourself?
How much of a priority is diversity to your direct manager?
How much of a priority is diversity to senior leaders in the [section]?
In the past year, how frequently did the [section] acknowledge diversity or difference within our team?
In the past year, how frequently have you witnessed discrimination toward a team member in the [section]?
In the past year, how frequently have you witnessed discrimination toward a patient or family member in the [section]?
1. Do you know how to report an instance of discrimination or bias against yourself or another team member?
a. Yes
b. No
2. Do you know how to report an instance of discrimination or bias against a patient or family member?
a. Yes
b. No
3. If you witness discrimination or bias toward a team member, patient or family member, how comfortable would you feel reporting this event?
a. Not comfortable
b. Slightly comfortable
c. Somewhat comfortable
d. Mostly comfortable
e. Completely comfortable
f. I do not know/Unsure
4. In the past year, have you reported an instance of discrimination toward a team member, patient or family member within the [section]?
a. Yes
b. No
5. In the past year, have you recognized how a specific law or policy has been or still is harmful to a patient or family we serve?
a. Yes
b. No
c. I’m not sure
6. Is there anything else you would like to share with us regarding diversity, equity, and inclusion in the [section]?
7. Please feel free to share any thoughts you have about this survey.