- Intramedullary metal fixation of the right humerus with brace (17/07).
NEUROLOGICAL EXAMINATION
- Stuporous state;
- No seizures;
- Anisocoria with left mydriasis;
- Spontaneous eye opening, no ocular motility;
RED AREA AND NEUROSURGERY
NEUROMOTOR PHYSIOTHERAPY
CONSULTATION
- Global hypotonia (with later hypertonia onset, major on the left side);
Therapy:
Baclofen and positioning orthoses for the lower limbs.
- Altered consciousness with chaotic environmental participation;
- Reducible distal hypertonia in the lower limbs with tonic-clonic jerks;
- Bilateral plantar flexion;
- Hyperactive deep tendon reflexes in the lower limbs, bilateral clonus;
- Spontaneous disorganized movements of the left upper limb.
Improvement in Consciousness and Motor Function:
- Periods of alertness;
- Ocular motility;
- Spontaneous motor activity on the right side.
RESPIRATORY PHYSIOTHERAPY
CONSULTATION
Tracheostomized patient with spontaneous breathing but dense secretions.
Parental educational training: Management of upper airway secretions, aspiration, and drainage.
Therapy:
- Passive mobilization and sensory stimulation as tolerated.
Parental educational training: Positioning and pressure ulcer prevention.
SEVERE LEFT-SIDED HEMIPARESIS.
RED AREA AND NEUROSURGERY
PSYCHOLOGICAL CONSULTATION
Supporting parents to:
- The mother is deeply distressed (feelings of guilt), struggling to understand healthcare staff communication;
- The father is lucid and stable.
Therapy: Weekly supportive counseling for both parents.
- Express their emotions and find resources to cope with uncertainty regarding N.’s condition;
- Approach the child and convey emotional closeness.
- Address communication difficulties.
Parental Adaptation Over Time:
The father improves in handling N.'s needs (aspiration, mobilization);
The mother remains in shock (anxiety, hyper-alertness);
Both parents regain hope through their child’s small improvements; They support each other.
SUB-ICU ADMISSION
Supine in bed Left hemiparesis
Left side Neglect
Nasogastric tube and tracheostomy;
Marked hypovision, but some ocular movements present; No verbalization
REHABILITATIVE ASSESSMENT
State of consciousness
Family
Residual functions
Side effects management (medicaltherapeuticalnursing)
Assistive devices/Orthoses
Pre-existing abilities
CONSCIUOUSNESS ASSESSMENT SCALES
Coma Recovery Scale – Revised (CRSR):
MINIMAL CONSCIOUS STATE
Musculoskeletal System
Supine in bed:
- Generalized hypotonia, with emerging left hypertonia;
- Initially preserved ROM (later restricted in left foot and hand due to severe progressive hypertonia).
Medical Research Council Scale (MRC) for muscle strength:
- Right upper limb: MRC 2 (active movement in the absence of gravity);
- Rest of the body: MRC 0 (no contraction).
Gross Motor Abilities
• No control of head or trunk movements;
• No autonomous postural transitions;
• Rare voluntary movements under tactile and verbal stimulation (right side);
• Left-sided neglect.
Gross Motor Function Measure-88 (GMFM-88): Non assessable
Visual abilities
Assessment performed at the patient's bedside
• reduced facial expressiveness , head, and gaze turned rightward;
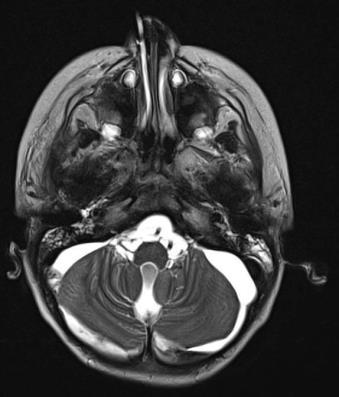
• Right-sided, third cranial nerve deficit, ptosis, exotropia and mild nystagmus in leftward gaze;
• Refusal of monocular vision in the left eye;
• In binocular vision, tracks objects only in the right visual field;
• Marked field restriction in the left visual field.
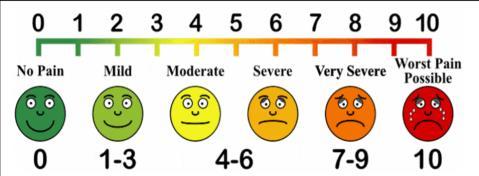
Sensibility and Pain
• No evident areas of altered sensitivity
• No evident pain
• No scars to evaluate or burns
Visual Analog Scale (VAS) for pain = 0 (genitore)
Upper Limb Abilities
• Severe left upper limb distal hypertonia, clenched fist, functionally excluded;
• Latent but possible activation of the right side;
• Reduced spontaneous motor initiative;
• Grasping only with passive object placement by an operator;
• Global grip with strength and adaptation deficits;
• Basic cause-effect interaction with simple activation schemes (shaking/agitating);
• Movement facilitation through compensatory strategies: supine position, shoulder/elbow fixed on a support surface, proximal movements;Absent eye-hand coordination.
Melbourne Assessment Scale – 2 (MA-2) Non assessable
Autonomic reflex functions
• Spontaneous breathing;
• Frequent aspiration needed due to secretion management difficulties;
• No oro-buccal movements;
• Feeding via naso-gastric tube.
Communication and Language
• Possible unsupported eye contact
• Rarely chosen through the gaze with target in the right hemifield
• Amimic
• No verbalization
• If guided and supported, orients the right upper limb in the direction of an interesting game
• AFO positioning splints (prescribed in NCH) for:
• Preventing bilateral equinus foot deformity
• Preventing excessive external rotation of the lower limbs through lateral supports
• Nasogastric tube
• Tracheostomy
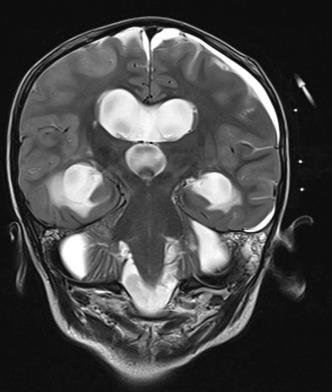
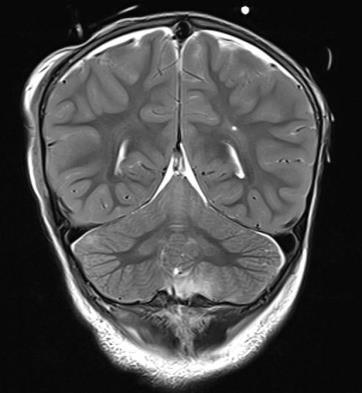
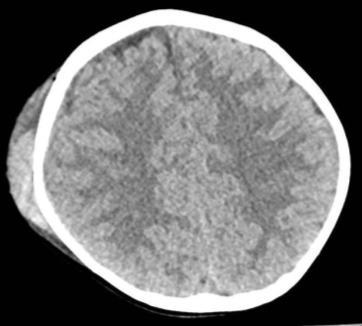
• Presence of a ventriculoperitoneal shunt
• Presence of a subcutaneous cannula and central venous catheter on the left side
Perinatal history: Normal pregnancy, full-term eutocic delivery.
• Visual stimulation: human face, lighted targets in darkened environment .
• Proprioceptive stimulation: Assisted sitting on the bed (perception of weight-bearing through pelvis and lower limbs).
• Updates on N.’s current condition.
• Recommendations for optimizing the patient’s room environment. Empathic Communication with Family
• Guidance on caregiving techniques.
↑ ↑ Visual-motor coordination and goaldirected movement
↑ ↑ Postural-motor and praxis-manual abilities
• Neuroplasticity stimulation
IMPROVING LEVEL OF CONSCIOUSNESS
↑ ↑ Cognitive abilities
↑ ↑ Social-relational and communication skills
• Restoration of age-appropriate functional skills
• Potential return to independent living and age-appropriate activities
Head and Trunk
Control
Horizontal Postural Transitions
Functional Use of Vision
MEDIUM-TERM GOALS
• Maintaining assisted sitting position
• Weight-bearing perception
• Upper limb support for postural stability
Right Upper Limb
Functionality
• Facilitated rolling to both sides
Left-Sided Perception
• Left visual field exploration with lightened or high-contrast targets in tasks of fixation and tracking from the midline towards the left peripheral visual field, following variable trajectories.
• In supine or seated position using a postural system.
• Orientation and facilitated reaching.
• Global grip strength and precision (gesture simplification, physical guidance, use of adapted objects in terms of shape, weight, and position).
• Eye-hand coordination.
• Functional use of familiar objects/gestures in social play.