1 - Cerchiari-Giordani_Feeding and Swallowing Disorders in Infant with neuronal Damage
The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:
Feeding and Swallowing Disorders
in Infant, Children and Young People with Neuronal Damage.
Antonella Cerchiari
Speech Language Pathologist
Program Coordinator Feeding and Swallowing Services
U.O.C. Day Hospital Neuroriabilitazione e attivit‡ sportiva
adattata
Carolina Giordani
Speech Language Therapist
U.O.C. Oncoematologia, trapianto emopoietico e terapie cellulari trial
Material provided by Antonella erchiari
Overview
Introduction: feeding and swallowing disorders in neurological damage
Definition and terminology
Common signs and symptoms of dysphagia in neurologically impaired children
An assessment and management protocol:
Interdisciplinary feeding/swallowing team approach
Assessment process:
– Family, developmental and feeding history
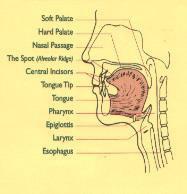
– Physical examination of oral structure
– Development milestones
– Upper airway and Cardiopulmonary features
– Feeding observation
Instrumental evaluation:
– Fiberoptic Endoscopic Evaluation
– Videofluoroscopic swallowing study
Treatment principles and perspectives: needs and objectives
Prevention of complications due to aspiration: tube feeding
Material provided by Antonella erchiari
INTRODUCTION
Feeding problems and disorders swallowing are very common in infant and children with neurological damage.
About 80% of pediatric population with neurological disabilities has these difficulties
Cerebral palsy is the most common type of neurologic problem associated with swallowing problems
Material provided by Antonella erchiari
Introduction : Feeding and swallowing disorders in children with brain demage
Swallowing feeding disorders are often diagnosed after multiple hospitalisations for breathing infections.
Feeding and swallowing disorders have enormous consequences for the health of the child and the quality of life of the whole family. It is important to make an early diagnosis.
Feeding and swallowing disorders are the principal cause of death in severely disabled children.
More than 90% of children with cerebral palsy die from pneumonia.
Material provided by Antonella erchiari
Introduction : Feeding and swallowing disorders in children with brain demage
Feeding and swallowing disorders are the principal cause of death in severely disabled children.
More than 90% of children with cerebral palsy die from pneumonia.
Swallowing feeding disorders are often diagnosed after multiple hospitalisations for breathing infections.
Feeding and swallowing disorders have enormous consequences for the health of the child and the quality of life of the whole family. It is important to make an early diagnosis.
Material provided by Antonella erchiari
Introduction : Feeding and
swallowing
disorders in children with brain demage
Extent of the Problem
✓ improved survival rates
✓ development of diagnostic techniques
✓ more understanding of the issue
✓ increased life expectancy in children with neuromotor disabilities
Material provided by Antonella erchiari
Definition and Terminology:
Feeding disorders:
Problems in a broad range of feeding activities that may or may not be accompanied by a difficulty with swallowing food or/and liquid.
J.C. Arvedson 2008
Material provided by Antonella erchiari
Definition and Terminology:
Swallowing disorders:
Dysphagia in one or more phases of swallowing.
Dysphagia: a swallowing disorders.
(J.C. Arvedson 2008)
Oral phase
Pharyngeal Phase
pharyngeal/e sophageal phases
Esophageal phase
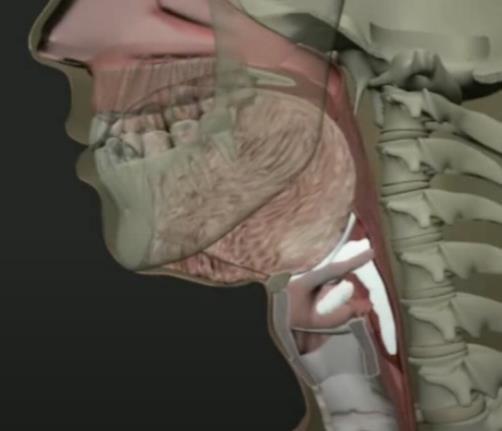
Definition and Terminology
Swallowing disorders - Dysphagia
Penetration
The bolus and/or oral secretion goes into the laryngeal vestibule but remains above the vocal cords
Material provided by Antonella erchiari
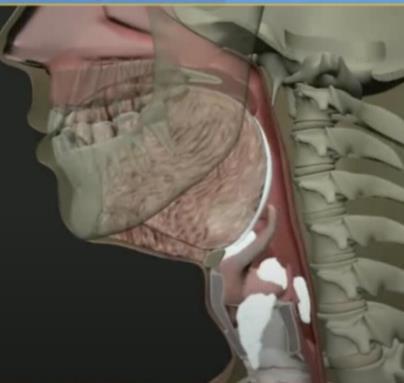
Definition and Terminology
Swallowing disorders - Dysphagia
Aspiration
The bolus and/or oral secretion goes into the larynx, passes through the vocal cords and goes down in to the lungs
Material provided by Antonella erchiari
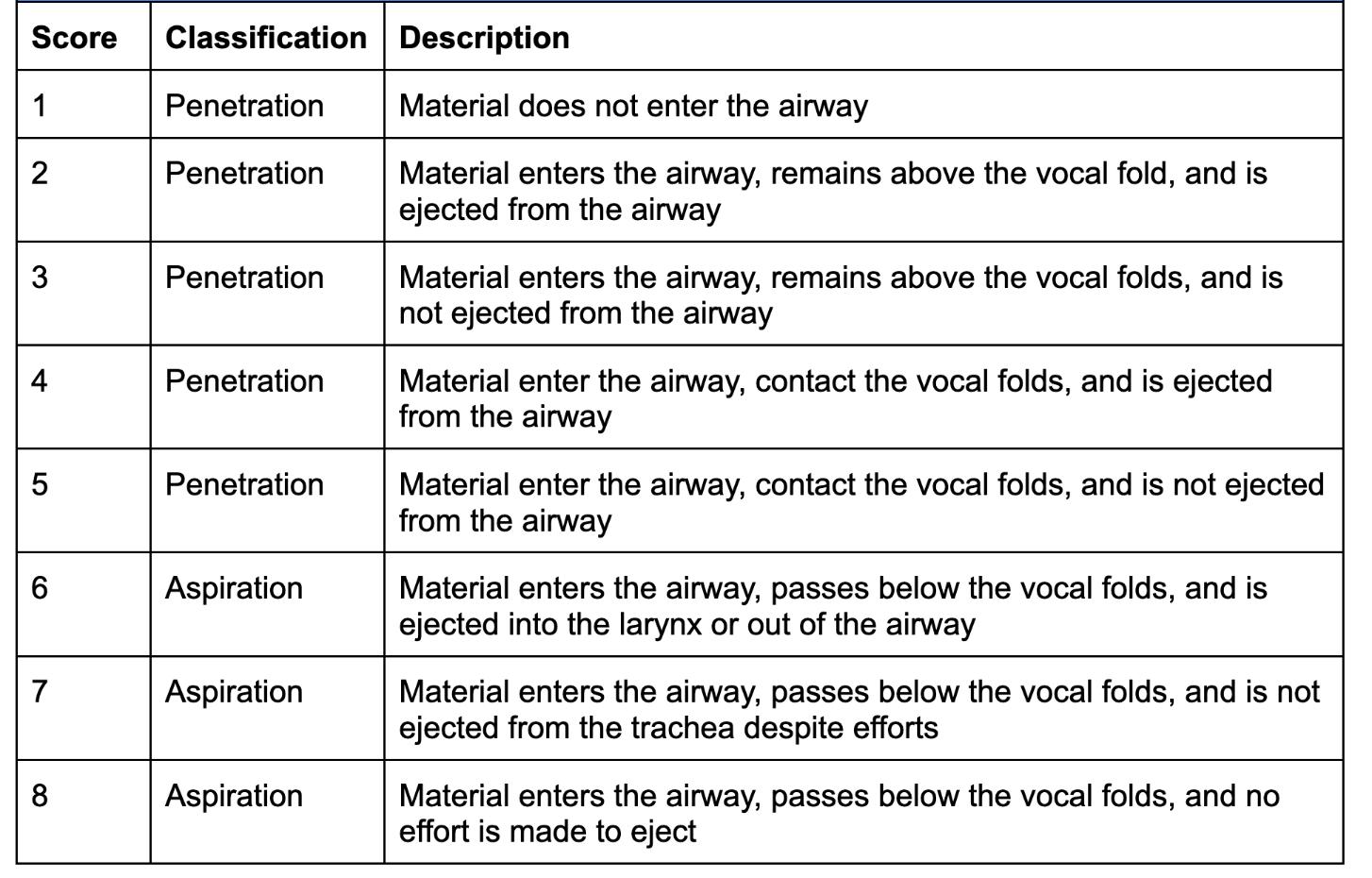
Penetration Aspiration Scale
Material provided by Antonella erchiari
Aspiration:
Definition and Terminology
Unintentional movement of liquid, food or oral secretion that enters the airways and goes to the trachea moving belove the vocal cords.
Anterograde Aspiration:
Happens during swallowing
pre-swallowing aspiration
intra-swallowing aspiration
post-swallowing aspiration
Aspiration Retrograde: Happens during gastro-oesophageal reflux and oesophageal reflux
(S. R. Jadcherla 2010)
Material provided by Antonella erchiari
Prerequisites for the development of feeding and swallowing skills and comparison with NEUROLOGICAL DAMAGE
Normo-typical Brain development
Anatomical integrity of structures
Stability and postural control
Impaired conduction of neuronal signals and (sometime) epilepsy medications
Anatomical integrity of structures
Adequate food experiences
Lack of motor control, instability Hypotonia
Oro-facial Dyskinesia
Limited food sensory development
Material provided by Antonella erchiari
Signs and Symptoms of Dysphagia
Swallowing
is the ability to swallow food and liquids without functional deficits, manage oral secretions and satisfy nutritional needs through oral feeding.
Material provided by Antonella erchiari
Signs and Symptoms of Dysphagia
✓ Choking
✓ Aspiration and pneumonia
✓ Prolonged mealtime
✓ Posterior drooling
✓ Malnutrition and/or dysidratation
✓ Poor growth
✓ Feeding with consistency and unsuitable food for the child’s development stage
✓ Feeding tube
✓ Anatomical changes
Material provided by Antonella erchiari
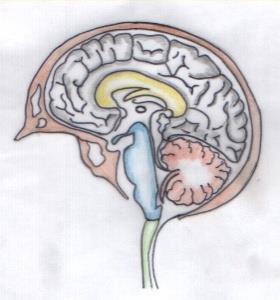
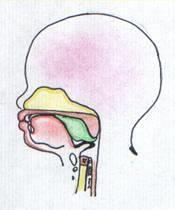
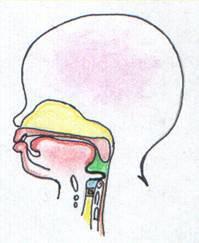
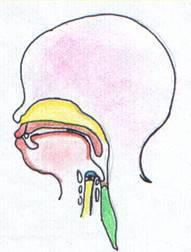
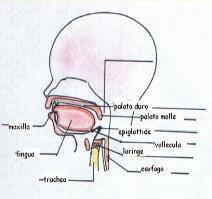
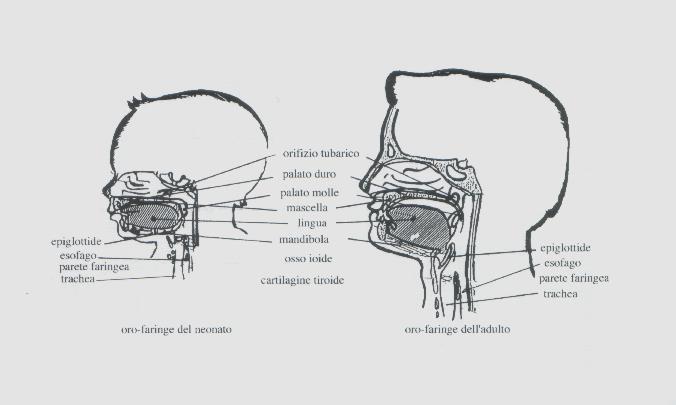
Anatomical & Functional Differences in Swallowing: Children vs. Adults
Material provided by Antonella erchiari
antonella.cerchiari@opbg.net
Development of feeding abilities
The development of feeding and swallowing skills begins in the womb.
At the twelfth week of gestation, the baby starts to swallow amniotic fluid.
The baby is an active part of intrauterine life.
During intrauterine life, the first motor and sensory experiences are started.
Sensory experiences Motor experiences
Feeding ability development
Gastrointestinal
Otorinholaryngological
Cognitive-behavioural
Maxillofacial
neurological
Clinical conditions
Material provided by Antonella erchiari
Feeding ability development
Red Flags
✓ Low-Stimulation Environment
✓ Non-Developmental Situations.
✓ Absence of Daily Routines
✓ Negative Experiences
Environmental condition
Material provided by Antonella erchiari
Feeding ability development
Specifications
Size and form
Sensory difficulties: hyper- or hyposensitivity
Upper limbs: does not touch, does not bring to the mouth, does not get their hands dirty
Does not eat independently
Perioral region: does not want the mouth to be dirty, cleans quickly, gags, cries, turns the face away
Remains with a dirty mouth
Leaves food residues in the mouth
Overfills the mouth excessively
Feeding ability development
Weaning block
Texture
Specifications
Taste
Temperature
Size and form
•Holds food in the mouth
•Refuses food
•Eats only a few types of food
•Frequently gags
•Often coughs
•Continues using infant feeding and non-feeding aids for too long
•Does not eat independently
•Difficulty articulating sounds
Material provided by Antonella erchiari
provided by Antonella erchiari
Material
Interdisciplinary Feeding/swallowing team
Material provided by Antonella erchiari
Interdisciplinary Feeding/swallowing team
Collaboration is Crucial in Pediatric Dysphagia
Cannot, efficiently treat feeding and swallowing disorders in vacum
Material provided by Antonella erchiari
Overview
Introduction: feeding and swallowing disorders in neurological damage
Definition and terminology
Common signs and symptoms of dysphagia in neurologically impaired children
An assessment and management protocol:
Interdisciplinary feeding/swallowing team approach
Assessment process:
– Family, developmental and feeding history
– Physical examination of oral structure
– Development milestones
– Upper airway and Cardiopulmonary features
– Feeding observation
Instrumental evaluation:
– Fiberoptic Endoscopic Evaluation
– Videofluoroscopic swallowing study
Treatment principles and perspectives: needs and objectives
Prevention of complications due to aspiration: tube feeding
Material provided by Antonella erchiari
The assessment of paediatric feeding and swallowing abilities often represents an activity that cannot be postponed due to the complexity of pathologies and the presence of associated conditions. In the paediatric age, early intervention on swallowing and feeding aspects is fundamental to the child's health status. Failure to address swallowing disorders could create sequelae for the rest of the child's and family's life in terms of health, growth and quality of life.
The aim of the assessment is to establish the anatomical integrity of the structures and the correct action of the districts involved in the feeding and swallowing functions.
Material provided by Antonella erchiari
Useful concepts for assessment
The assessment of feeding and swallowing disorders consists of two phases:
• Clinical assessment
- General and feeding history
- General physical and orofacial structure evaluation
- Meal-time evaluation
• Instrumental assessment – to be performed only if necessary
✓Infants , children and young people with feeding and swallowing disorders are increasing significantly.
PEDIATRIC POPULATION WITH FEEDING AND SWALLOWING DISORDERS IS:
✓numerous
✓eterogeneous
✓complex conditions
• Greatersensitivityto de issue
• Improvementin medicalcare and tchnologicaldevelopment
• Highesurvival rate for childrenwith serioushealth conditions
INCREASED INCIDENCE OF DYSPHAGIA IN THE PEDIATRIC POPULATION
LONGER HOSPITAL STAY
FREQUENT HOSPITAL ADMISSIONS
INCREASED COSTS
CLINICAL NEEDS: PEDIATRIC DYSPHAGIA Screening
Material provided by Antonella erchiari
Goal of Screening
Identify children at risk of dysphagia
Material provided by Antonella erchiari
Priority Screening- Paediatric
Two levels of risk for dysphagia (low and at-risk) were identified according to PS–PED scores.
The PS–PED allows prioritization of dysphagia management and
according to the level of risk.
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Data collection
Medical history and feeding and swallowing iter, are important for the understanding of the problem
The medical history contains all the information, news and sensations that can help clinicians to lead to a diagnosis.
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Data collection
Medical history is the first step to form a relationship of trust and cooperation between the clinician and the parent
The medical history emphasizes the psychological and social aspects of the parent to the child's problem.
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Data collection
The data, collected through the narration of the parent, should be monitored and controlled through the study of medical records
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Medical and Feeding History
➢ GENERALITY: name, surname, …….
➢ PREGNANCY INFORMATION: physiologic, gestosis,…… ➢ CHILDBIRTH INFORMATION: natural o caesarean, …. etc. ➢ INFANT CONDITION AT BIRTH AND AFTER : umbilican cord, weight, cranial circumference, APGAR I and V min. , etc….
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Medical and Feeding History
➢ INFANT CARE AFTER BIRTH: ducted, incubator, respiratory support etc
➢ INSIGHIS ABOUT PRIME PATHOLOGY: Heat Disease, Cerebral palsy, respiratory disease, genetic syndromes, epilepsy etc.
➢ INFORMATION ABOUT SECONDARY PATHOLOGY: Respiratory diseas , Gastroesophageal reflux, constipation etc.
➢ INFORMATION ABOUT DRUGS: antiepileptics, antacids medication,…. etc.
FEEDING AND SWALLOWING PROTOCOL
Medical and Feeding History
➢ INSTRUMENTAL EXAMINATION: cerebral ultrasonography, cerebral MRI , etc.
➢ SPECIFIC INSTRUMENTAL EXAMINATION: VFSS, EASF, digestive RX , PH testing etc.
Material provided by Antonella erchiari
FEEDING AND SWALLOWING PROTOCOL
Medical and Feeding History
➢ FEEDING HISTORY: parenteral nutrition, enteral feeding, gavage, tube feeding, oral feeding, breastfeeding, use bottle, use spoon…
➢ CURRENT NUTRITION: breakfast, lunch and dinner, (oral or tube feeding).
Material provided by Antonella erchiari
FEEDING AND SWALLOWING
PROTOCOL
Medical and Feeding History
➢ USE OF NUTRICIONAL AIDS : bottle, glass for child, pacifier.
➢ USE OF AIDS: aspirator (number of aspiration), etc…
NUTRITIONAL AIDS: silicon spoon, hard plastic spoon, metal spoon, bottle, short or long teast, glass, cup, etc.
Time of the meal (from 30 to 45 mins)
FEEDING AND SWALLOWING
PROTOCOL
functional assessment
Observation during mealtime
Level of oral motor ability: sucking, chewing, chewing stile,use of glass for drinking ,use of straw, food loss from the mouth…. etc.
Child Reactions : cough, vomiting, refusal, crying, anger, etc.
Caregivers’ Reaction: anxiety, fear, refusal, anger… etc.
QUANTITY OF FOOD : adapted to needs of the child, fluid intake
FEEDING AND SWALLOWING PROTOCOL
functional assessment
Observation during mealtime:
BREATHING AUSCULTATION: in different moment of the meal
SWOLLOWING AUSCULTATION : in different moment of the meal
OXIMETRY MEASUREMENT
Overview
Introduction: feeding and swallowing disorders in neurological damage
Definition and terminology
Common signs and symptoms of dysphagia in neurologically impaired children
An assessment and management protocol:
Interdisciplinary feeding/swallowing team approach
Assessment process:
– Family, developmental and feeding history
– Physical examination of oral structure
– Development milestones
– Upper airway and Cardiopulmonary features
– Feeding observation
Instrumental evaluation:
– Fiberoptic Endoscopic Evaluation
– Videofluoroscopic swallowing study
Treatment principles and perspectives: needs and objectives
Prevention of complications due to aspiration: tube feeding
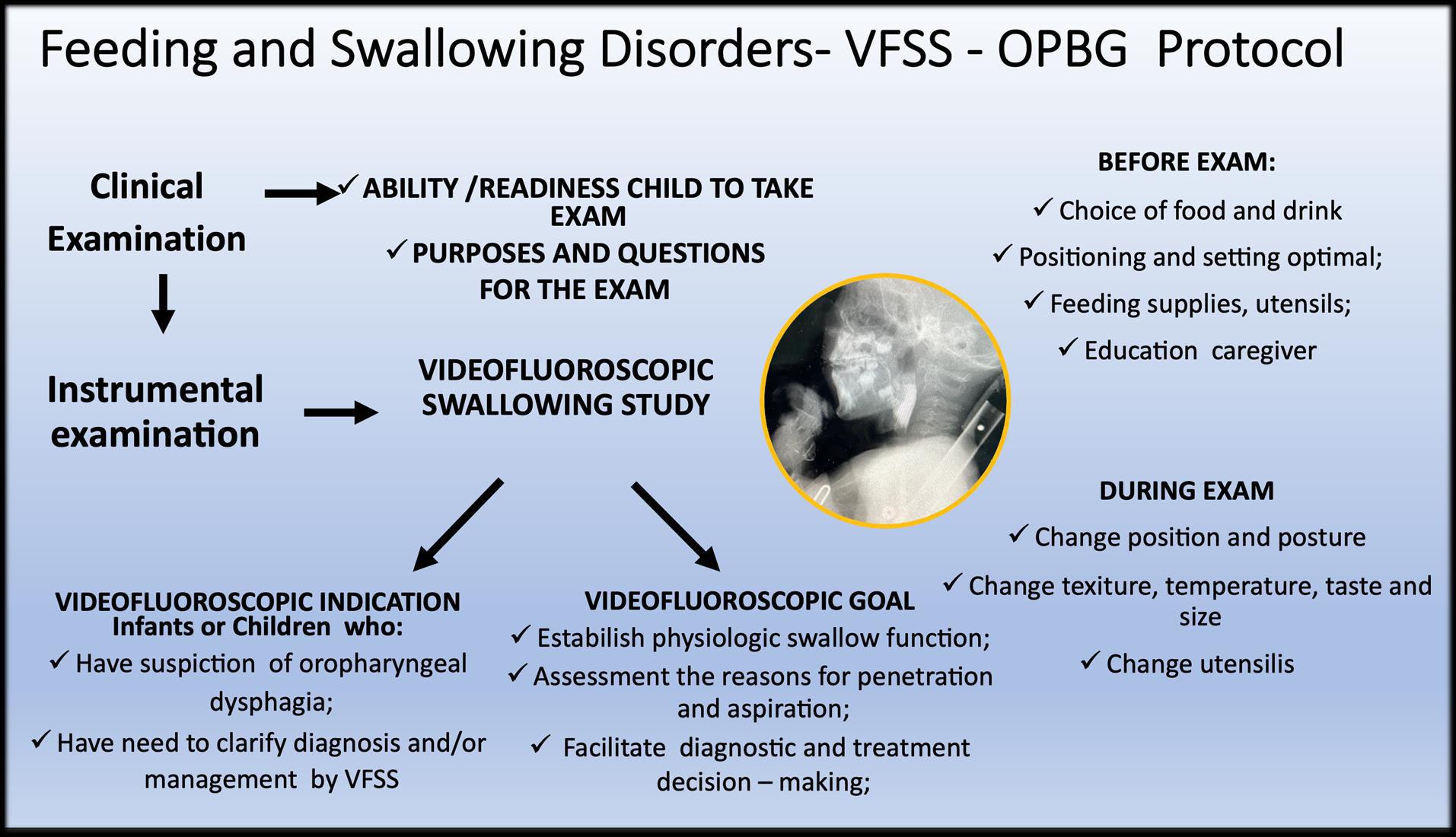
Instrumental techniques used to evaluate oral, pharyngeal, laryngeal, upper esophageal, and respiratory function may include: VFFSS, Endoscopic assessment of swallowing function.
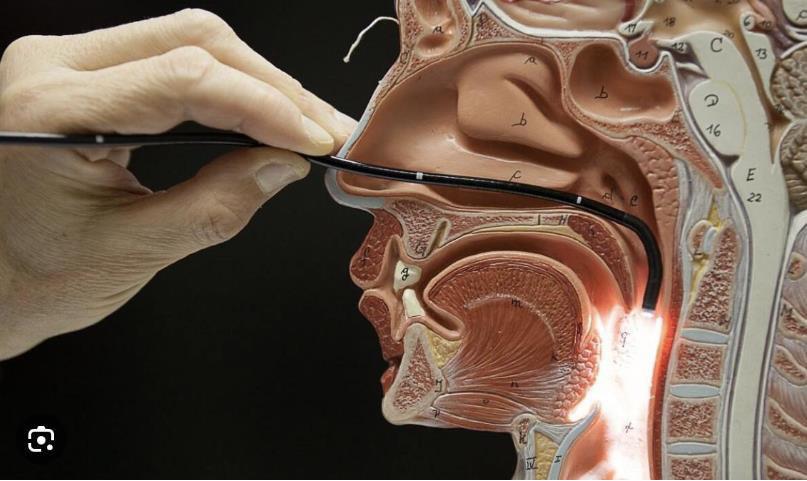
Fiberoptic endoscopic evaluation of swallowing
ADVANTAGES:
1) no radiation exposure;
2) position of patient is flexible;
3) observation of structures;
4) sensory component;
5) can be repeat frequently.
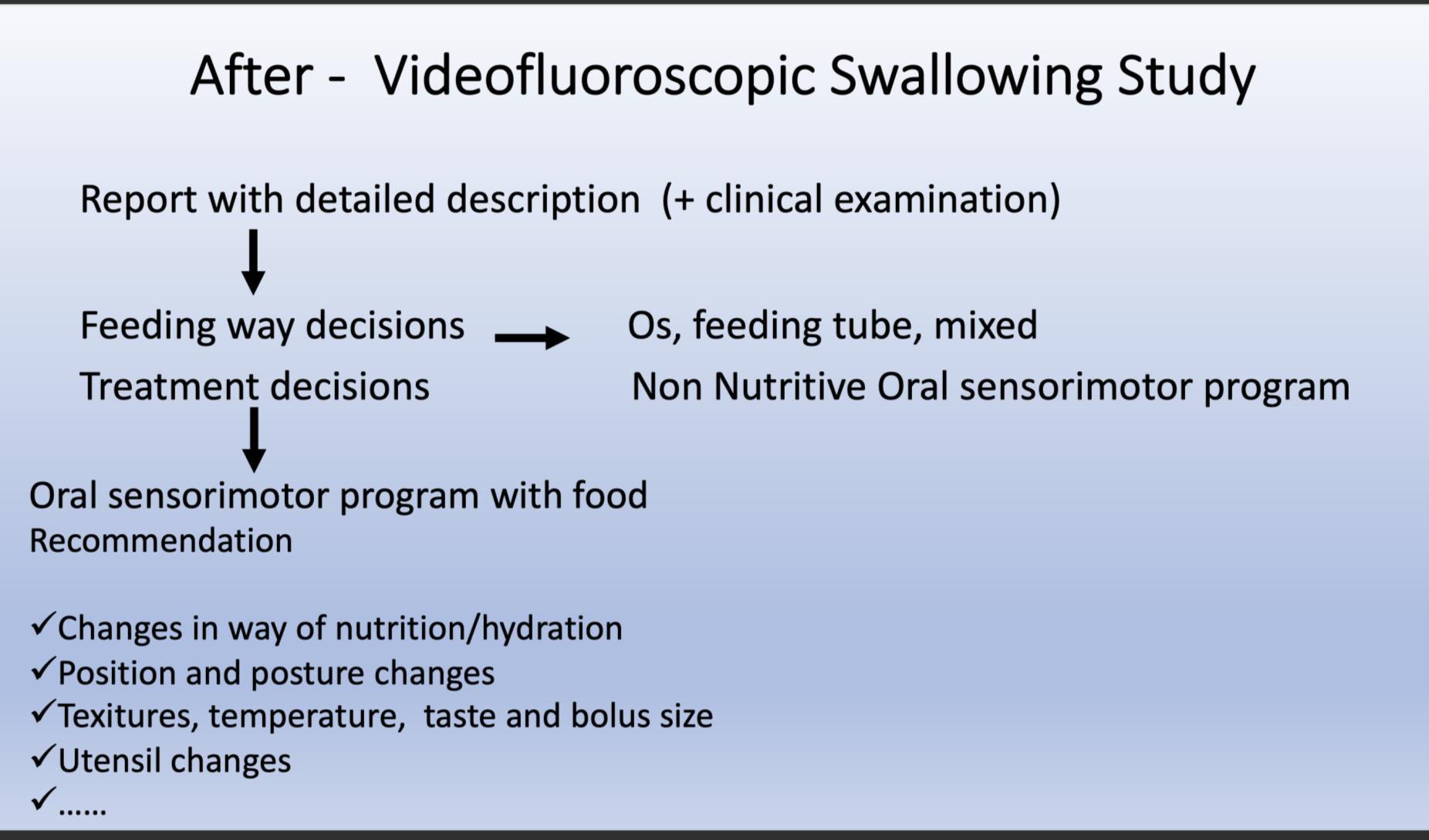
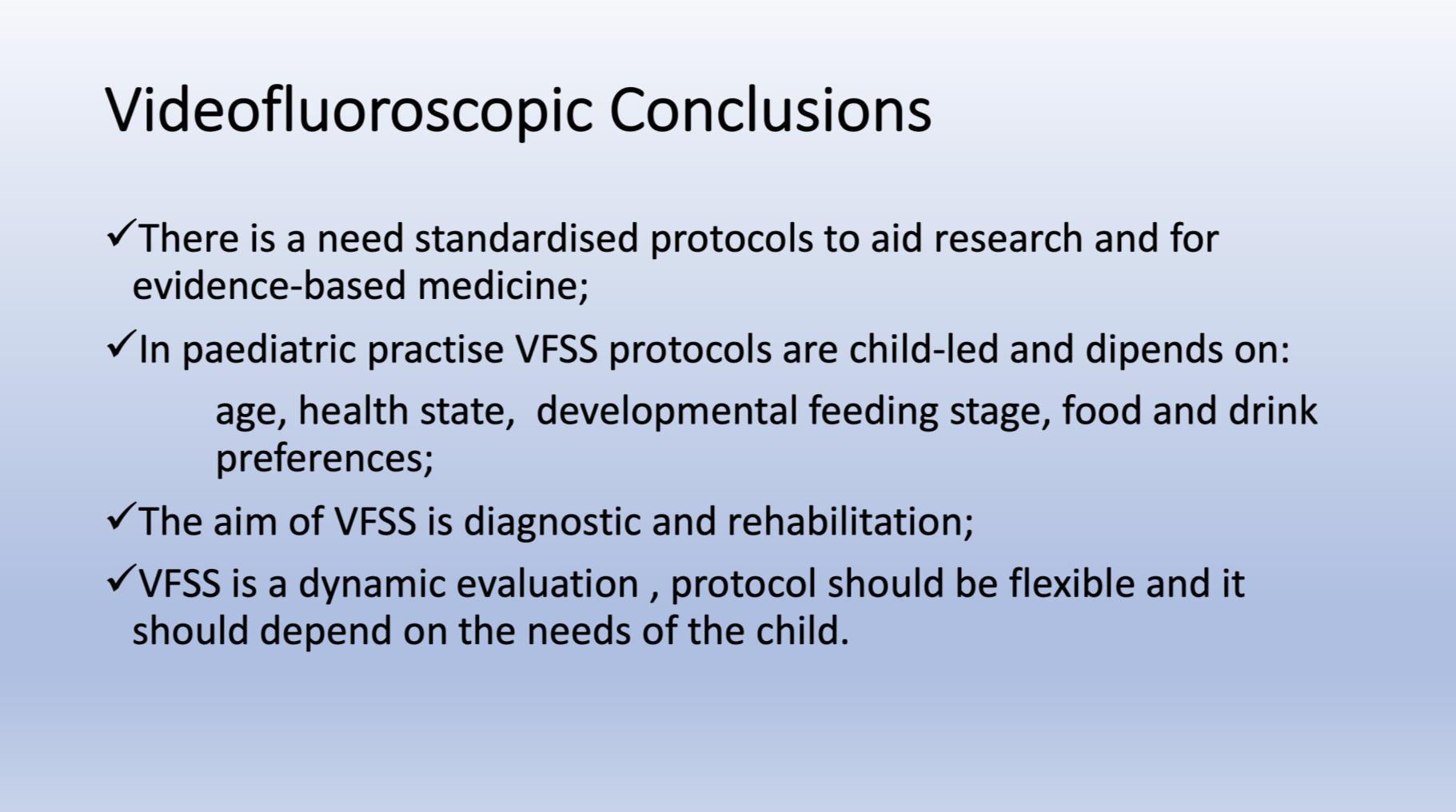
Videofluoroscopy
Videofluoroscopy
ORAL PREPARATORY PHASE IN EATING SOLID FOOD
✓ Loss of food out mouth, pushed out with tounge
✓ Food in anterior sulcus
✓ Limited tongue movement
✓ Problem about turning the food into bolus formation
✓ Food in valleculae and pharynx,
pre swallow
✓ Jaw grading inappropriate
ORAL PREPARATORY PHASE IN DRINKING LIQUID FOOD
✓ Loss of food out mouth
✓ Liquid in anterior sulcus
✓ Limited tongue movement
✓ Food pushed out with tounge
✓ Food in valleculae and pharynx, pre swallow
✓ Jaw grading inappropriate
ORAL PROPULSIVE. PHASE:
✓ Food or liquid remains in anterior and/or lateral sulcus
✓ Food or liquid remains on floor of mouth
✓ Limited posterior tongue movement
✓ Reduced base of tongue action
✓ Tongue-soft palate contact incomplete
✓ Multiple swallows per bolus
✓ Delayed oral transit time
Videofluoroscopy
PHARYNGEAL PHASE
✓ Nasopharyngeal regurgitation
✓ Slow bolus passage through Pharynx
✓ Reduced pharyngeal contraction/motility
✓ Residue cleared with next swallow
✓ Residue not cleared
✓ Reduced hyolaryngeal execursion
✓ Penetration to underside of epiglottis
✓ Penetration to laryngeal vestibule
✓ Aspiration before, during and after swallow
✓ Aspiration respons: not effective cough, no cough – silent aspiration