The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.

Implemented by: Partner:





The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:
U.D.G.E.E. and D.H. Neurorehabilitation

Task
Goal
• Definition of treatment goals on the child’s profile of functioning (motor, cognitive, sensorial, relational, emotional aspects).
• Sharing treatment’s goals and strategies with families.
ORIENTED APPROACH
Context
• Definition of learning methods appropriate to age and cognitive level of the child (imitation, problemsolving, trial and error, verbal instructions).
• Importance of motivational aspects
“GUIDED MEANINGFUL EXPERIENCES”.
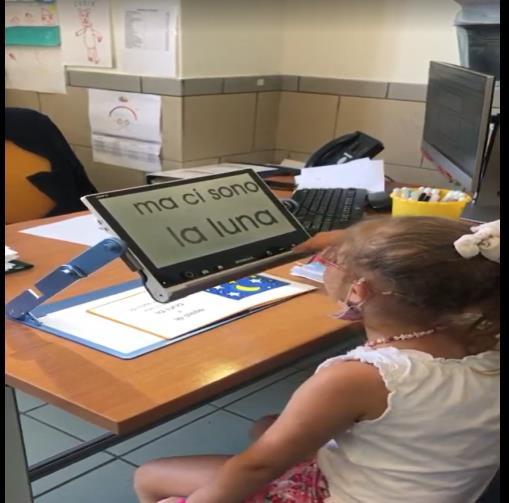
Perceptual facilitations

Therapist’s role





• Physical space (personal, peripersonal, extrapersonal).
• Perceptual facilitations (auditory, visual, tactile, vestibular, proprioceptive, multimodal).
• Objects (size, shape, weight, texture, spatial orientation, silent or sound-producing, colored or neutral, fixed or moving, function).
• Therapist (modeling, physical or verbal facilitation, feedback, relationship).



Sensory stimulation strategies:
• Environmental enrichment;
• Intensification of incoming stimuli;
• Receptor activation;
• Focused attention.
The lower the level of consciousness, the simpler the setting should be!!!
To avoid overstimulation:
• Control of stimuli (e.g., dimming the lights);
• Presentation of stimuli at scheduled intervals (habituation);
• Ritualization of actions performed (anticipation);
• Use of protective measures (e.g., dark glasses, noise-canceling headphones).



- Lighting (well-lit environment/directed artificial light on the target/darkened environment with illuminated target);
- Target (type/size/color/distance);
- High contrast on the working surface (contrast between target and background);
- Minimal visual clutter;
- Positioning of objects within the child's preserved field of vision;
- Spatial and tactile reference points;
- Supporting visuo-motor integration and visual recognition.

SUB-ACUTE PHASE: It is the period directly after the acute treatment phase, when a child or adolescent is medically stable and admitted to an inpatient or outpatient rehabilitation programme.
In this period the rehabilitation aims to:
- facilitate the recovery of impairments and to promote compensation for residual difficulties, - to improve the awareness of the surrounding environment and to promote participation in daily activities.
Which factors should we consider when designing intensive physical rehabilitation interventions for children and adolescents with TBI during the subacute phase?
Expert consensus to guide Physical Rehabilitation in pABI (JRM, 2023)
Health condition/injury-related variables Body Functions
• Severity of injury
• Time since injury
• Stage of recovery
• Comorbidities
• Level of consciousness
• Fatigue
• Medical and pharmacological managment
• Cardiovascular functions
• Respiratory functions
• Nutritional status
• Quality of sleep
• Mental functions (cognitive, behavioral, emotional)
• Sensory functions
• Neuromusculoskeletal and movement-related functions
Expert consensus to guide Physical Rehabilitation in pABI (JRM, 2023)
Activity and participation Contextual factors
• Relevant in community and daily life
• Focused on participation
Related to the child’s ability to:
• learn and apply knowledge
• Communicate
• Move
• Interact
• Knowledge of facilitators and barriers
• Family involvement in goal settings and in therapeutic activities to stimulate transfers of skills to a variety of context
• Peer interaction
• Housing adaptations
• Attitudes and norms held by family and friends
• Pre-injury developmental stage
• Age at injury
• Personality
• Internal motivation
• Personal perseverance and resilience
Consequences of TBI Complex pattern of deficits and needs
- Acute and long term effects
- Severity from mild to severe
Developmental context
The rehabilitation should target:
- The effects of the TBI supporting progress towards normative developmental milestones
- The changing needs of the individual providing ongoing support during transition periods
Communication between teem members
Scheduled meetings, Cross-disciplinary report, Managing plans.
Autonomy in daily life
Tone control
ROM improvement
Upper limb recovery
Head and trunk control
Manual therapy and stretching
Neuro-functional tape
Positional splints
Cognitive Functional Therapy
Vibratory, tactile and proprioceptive stimulation
1. Reduction of muscle tone through muscle inhibition techniques (MET and Reciprocal Inhibition).
2. Increase in joint ROM using manual joint techniques (Graded Oscillation and Sustained Hold).
3. Pain Modulation (Joint Oscillations).
4. Treatment of peripheral nerve deficits through neurodynamic therapy techniques (Sliding and Tensioning).
5. Scar mobilization (Cross-friction Massage and Skin Stretching).
6. Enhancing therapeutic alliance through manual physical contact.

Neuro-tape can be applied using two techniques, depending on the needs:
1) Decompressive technique: promotes drainage, reduces muscle tone, improves dermal trophism and fluid drainageof under the skin. It can also serve as a sensory stimulus (both perceptual and visual
2) Compressive technique: facilitates muscle movement, stimulates muscle tone, provides joint stabilization. Both techniques can be combined and applied to the same body area in multiple applications.

They can vary in length depending on the body part that needs protection:
• Ankle-foot splints
• Knee-foot splints
• Thigh-foot splints
• Thigh-mid tibia splints (with an abduction bar between the legs)
They can be made of :
• Plaster (exclusively for the acute post-surgical phase): they can be full-length for surgical correction procedures (e.g., equinus) or open at the top but covered with a layer of gauze for fibrotomy and tenotomy.
• Thermoplastic materials with internal padding.
Proprioceptive input can be increased to stimulate the patient by:
1. Varying the load by adding weights.
2. Reducing the base of support.
3. Introducing destabilizing perturbations.
4. Bringing attention to compensatory movements and posture.
5. Using visual references and feedbacks.
6. Challenging the Comfort Zone


Autonomy in daily life
Tone control
Upper limb recovery
ROM improvement
Head and trunk control
Is a fundamental milestone in gross motor recovery since it allows to: explore the environment, reach for objects, interacts with others, tranist between different positions.
- Required abilities: proper postural alignment and stability + balance and parachute reactions.
- Progression strategies: the therapist stands behind the patient if control is partial and posterior support is needed (from shoulder to pelvis) or in front if control is more efficient.
- Functional tasks: destabilizing objects such as proprioceptive cushions, targets to reach and transport, or external forces to balance can be introduced.
They can:
- Be customized for the patient (Frame, shape and control system);

- Includes modifiable postural accessories (headrests, containment cushions, and straps);
- Be electronic or manual;
- Be tiltable and/or reclinable;
- Can be raised or lowered (Only postural systems) to allow patients to be at the same level as their peers or to reach tables of different heights.
It is crucial to carefully evaluate all features with the physician and orthopedic technician, as the patient will spend most of their day using it and it will allow the patient to achieve maximum autonomy.


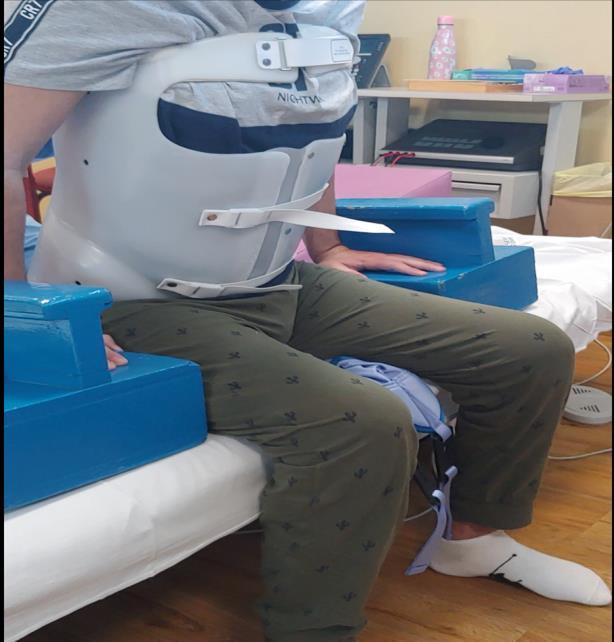
When trunk control in not sufficient! They can:
- Be available in various materials, ranging from rigid to flexible;
- Provide spinal protection;
- Be integrated with KAFO braces to improve trunk control;
- Have neck support;
- Be elastic-compressive suits to support trunk control.
Autonomy in daily life
Tone control
Upper limb recovery
ROM improvement
Head and trunk control
It is recommended for all clinically stable patients, following approval from specialist doctors, primarily to promote:
- Axial and lower limb strengthening;
- Restoration of upright posture.
- Visceral functions
- Respiratory function.


Monitor vital signs as pressure, saturation and heart rate during verticalization!!!
They can:
- Be customized for the patient in terms of frame, shape and control system;
- Be used to upright the patient who requires support;
- Be progressive in weight-bearing (Tilt-Table) or immediate and total (Vertical Standing).
- Be prone or supine, depending on the patient’s trunk control and pathological movement patterns triggered by loading.
- Have postural correction accessories.
- Include hip abduction features for subluxation prevention or correction.
- Facilitate manual activities when combined with a table.

They can:
- Have posterior plastic braces with internal padding and a front rigid fabric strap for leg support and containment.
- Be extended from below the hip to the foot (Knee-Ankle-Foot Orthosis
- KAFO).
- Be designed to verticalize the patient, supporting weight-bearing while allowing pelvic mobility training.
- Be associated with single or combined platforms to ensure proper foot contact with the ground.

Autonomy in daily life
Tone control
Upper limb recovery
ROM improvement
Head and trunk control
Restoring gait is always a major milestone for the patient, their family, and the rehabilitation team.
However, it is not always possible or advisable, as all aspects of the patient must be evaluated, including their cognitive level, tolerance, and intentionality.
For some patients, walking may be too exhausting and difficult, making it preferable to introduce a self-propelled or electronic wheelchair and teach them how to use it.
In general, walking rehabilitation is conducted using:
- assistive devices appropriate to the patient’s posture and residual/acquired functions, - with therapist support, which should only be a temporary aid towards independent walking.
Working on a proper gait pattern is essential to restore an harmonious walking cycle, avoiding compensatory movements or unnecessary energy consumption.

They can:
- be customized for the patient in terms of frame, shape and control system;
- Include upper limb, trunk, or pelvic supports;
- Have an anterior or posterior movement system;
- Have wheels that can be locked or adjusted according to the patient’s needs.
Compared to tripods or crutches, walkers reduce weight-bearing stress and offer greater stability.

They can:
- Have plastic braces with internal padding.
- Be extended from below the knee to the foot (Ankle - Foot Orthosis - AFO).
- Be used to protect joints, support weight-bearing and maintain correct positioning of the foot and knee.
- Be paired with reinforced orthopedic shoes.

- Enclosing AFOs: Feature a posterior and lateral plastic shell to fully support the leg, reducing knee hyperextension (genu recurvatum) while preventing any foot movement (used for advanced standing and early walking phases).
- Posterior-bar AFOs: Open laterally to allow dorsiflexion during walking.
- Anterior-shell AFOs: Provide anterior tibial support to help reduce knee flexion contractures (flexum).
- Dynamic AFOs with tension bands: Include foot-to-tibia straps to assist dorsiflexion.
STANDING
Poor or no head-trunk control
Modest upper body control
Full head and trunk control acquisition
No orthosis
Any state of consciousness
Trunk-pelvis training
Preparatory for walking
Proper lower limb posture
No hypertonia
Autonomy in daily life
Tone control
Upper limb recovery
ROM improvement
Head and trunk control
Physical Therapy (PT)
Constraint Induced Movement Therapy (CIMT)
Robot Mediated Therapy (RMT)
Splint/Orthoses
Neuro-tape
Manual fucntion
Orientation (head-trunk)
Targeting (shoulder)
Reaching (upper limb)
Grasping (hand)
Manipulation
Release
Variables in Setting Arrangement
Postural care/Visual cues
Object’s position and orientation
Object’s position and orientation
Object’s features
Actions with the object
Relationship between objects
GRASP (Power grip): Global/ Digito – palmar grasp/release task varying object sizes and weights
PINCH (Precision grip): Bi-digital/ Three-digital /Lateral/ Interdigital intrinsic hand movement control task.

AUXILIARY GRIPS
• Mouth
• Chin
• Axilla
• Arm against thorax
• Forearm against abdomen
COMPENSATORY STRATEGIES

• Wrist flexion
FACILITATION STRATEGIES
• Sensory cues
• Synergic movements
• Trunk compensations
• Passive loading
• Grips
• Postural care
• Positioning of proximal joints
• Verbal and tactile prompts
Evaluation criteria:
• Child’s manipulative strategy
• Developmental stage of the function
• Positions that facilitate or inhibit motor synergies
• Primary clinical issue
• Functional purpose of the orthosis




STATIC
Fractures, ligament and tendon lesions (plastic)
STATICPROGRESSIVE
DINAMIC
FUNCTIONAL
ROM improvement (nylon)
Tone control (elastic tissue)
Grasping and manipulation improvement
Autonomy in daily life
Tone control
Upper limb recovery
ROM improvement
Head and trunk control
Restoring the child indipendence in daily life trough:
- Fine motor training (strength and reliability of grip and fingers individuation)
- Upper limb training in functional gestures and daily activities (dressing/undressing, washing, toileting, writing and using tools);
- Activity organization (planning, sequencing, controlling);
- Wheelchair training in different settings (indoor, outdoor, electronic wheelchair, peripersonal space management);
- Postural transitions.



• Supine – lateral decubitus – prone position,
• Supine to sitting,
• Sit to stand,
• Bed to wheelchair transfer.
Achieved through :
- Muscle strengthening, - Transfer exercises,
- Use of assistive devices (e.g., sliding sheet, turning disc, lift system)
- Environmental adaptations (e.g., light modulation, removal of physical obstacles, positioning of handrail)


If the patient is in a state of coma, vegetative state or severe minimally conscious state the training focuses on:
- Tone control and maintenance of ROM;
- Multisensory stimulation to facilitate emergence of consciousness;
- Postural changes and use of a postural system to prevent bed-rest complications and ensure proper positioning (eye-level alignment, even with closed eyes);
- Gradual return to upright positioning using a standing table or postural system;
- Dysphagia management;
- Visual stimulation.
Long-term goals are defined to be achieved after hospital discharge.
- They vary based on the type of residual injury from the trauma and the patient’s level of consciousness.
- They should be established at discharge in agreement with the entire team but may change over time according to the patient’s needs and progress.
- For the multidisciplinary team, it is crucial to coordinate with local healthcare services to ensure continuity in medical and rehabilitative treatment.
- Additional hospital stays or follow-up Day Hospital visits may be planned to monitor the patient's progress. These can be scheduled at discharge or arranged later.
Rehabilitation primarily at the patient’s home (due to mobility difficulties and frequent respiratory infections).
- Maintenance of muscle length and joint ROM;
- Frequent postural changes combined with positioning in a postural system and possible standing (excluding red flags);
- Respiratory physiotherapy, also teached to parents;
- Multisensory stimulation (tactile, visual, auditory, oral);
- Short-term hospitalizations are preferred to reduce the risk of nosocomial infections.
Home or facility - based rehabilitation.
- Maintenance of muscle length and range of motion;
- Frequent use of the postural system and standing support system;
- Training on re-acquired fine and gross motor skills;
- Neuro-cognitive-motor training;
- Training for activities of daily living;
- Gradual return to school with reduced hours and support teacher;
- A follow-up hospitalization is typically scheduled shortly after discharge to monitor progress and adjust the treatment plan.
Rehabilitation in a specialized facility.
- Maintenance of muscle length and range of motion.
- Use of a postural system or the most suitable assistive device to maximize autonomy (if needed).
- Training on acquired fine and gross motor skills and muscle strengthening.
- Training for autonomy in different settings (home, school, work).
- Neuro-cognitive-motor training.
- Gradual return to school with progressively adapted schedules and programs.
- Recreational, sports, and social activities adapted to the patient’s condition in terms of timing and intensity.
- Day Hospital treatment is generally preferred
1. Teach how to recognize the evolution of clinical phases and needs
2. Provide emotional and psychological support
3. Anticipate child’s needs, guiding their management, and share a discharge plan
4. Facilitate direct contact between services, school, and the rehabilitation facility
5. Teach family members how to solve problems, manage stress, and intervene in behavioral disorders
6. Emphasize the importance of community integration.
As the patient returns to everyday life, both the achievable goals and the challenges they may face evolve, depending on their level of consciousness and the type of residual injury.
The greatest uncertainties arise in patients with a consciousness level ranging from "moderate disability" to "good recovery," as they regain more cognitive functions and expand their social network.
Furthermore, once the perilesional cerebral inflammatory phase has ended, the remaining damaged areas will play a crucial role in shaping the patient's ability to manage daily life.
Depending on their age, neuroplasticity will enable the patient to adapt to daily challenges.
Some difficulties the patient may encounter include:
- Behavioral dysregulation and lack of inhibition due to damage to the frontal and prefrontal circuits, which can affect social interactions.
- Attention deficits, visuospatial disorders, memory, and language impairments (expressive/receptive), which may impact academic progress.
- Motor, sensory (paresis), and praxis deficits, which can hinder activities of daily living.
- Movement and coordination disorders, which may interfere with returning to recreational and sports activities.
- Cognitive impairments.
- Epileptic seizures.
- Tracheostomy management.
