The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:
Tnpee Giulia Giorgi: giulia.giorgi@opbg.net
Neuroscience and Neurorehabilitation Area
Bambino Ges˘ Pediatric Hospital
OUR SERVICE
•Hospital stay (UOC of Neurorehabilitation)
•Day hospital (DH Neurorehabilitation and Adapted Sports Activity)
• Evaluation
• NEUROREHABILITATION TREATMENT
DEVELOPMENT OF THE THERAPEUTIC PROGRAM
Decision-making process (Shumway-Cook, Woollacott, 1995)
Essential process to develop a treatment plan adequate for the child's disorders
Child evaluation
Analysis and interpretation of evaluation
Definition of short and long-term goals
Development of a treatment plan
Implementation of the treatment plan
Child re-evaluation and outcome
GENERAL CONSIDERATIONS
Rehabilitation intervention must be personalized and individualized for each child.
It must consider the child's clinical conditions (comorbidities, any secondary disorders such as epilepsy, colics, altered sleep-wake rhythm, response times, signs of stress and avoidance, etc.).
It must consider the family compliance.
It must be shared with a multidisciplinary team.
GOAL OF EARLY INTERVENTION
Journal "Pediatrics and Child Health", 2024; Symposium of American neonatologists
´Promote child health and wellbeing, enhance emerging competencies, minimise developmental delays, remediate existing or emerging disabilities, prevent functional deterioration, and promote adaptive parenting and overall family functionª
Promote the child's harmonious development
Support and involve the parent in the child's rehabilitation journey
MAIN AREAS OF INTERVENTION
What does the literature tell us?
Review "Developmental medicine & child neurology" , 2019
•Self-initiated motor activity
•Self-regulation
•Early communication skills
•Responsive parenting
"Components to include in early intervention programmes are: (1) promotion of self-initiated, appropriate motor activity; (2) supporting infant self-regulation and the development of positive parent-infant self-regulation and the development of positive parent-infant relationships; and (3) promotion of early communication skills, parent coaching, responsive parenting, and supporting parental mental well-being.”
Review "Journal of clinical medicine", 2021
• Family: key people to impact development
• Interventions adapted to the family, the child, and their relationship
“During the last decades it has become crystal clear that the family is the cornerstone of early intervention. Families are the pivotal environment of children, and family members are the key people who may impact child development through daily interaction during caregiving and play. “
“The available evidence suggests that skills improve, when they are practiced intensively in a playful daily care giving setting. This suggests that interventions in which families are coached on the nature of the skills emerging and the ways in which the child may explore and perform these skills are most promising. In other words, interventions that are tailored to the family, the child and their interaction, may be most successful.”
´FAMILY CENTERED INTEGRATE CAREª
INVOLVEMENT OF PARENTS
PROMOTORS AND AMPLIFIERS NOT CO-THERAPISTS
Therapist:
Therapeutic role
Parents: Educational role
Choose functional activities with GUIDING FUNCTION: adapting rehabilitation strategies in caregiving practices and daily life.
AREAS OF INTERVENTION
EMOTIONAL, RELATIONAL AND COMMUNICATIVE AREA
MANIPOLATION AND FINE MOTOR AREA
ADAPTATION AND ENVIRONMENTAL INTERACTION
TARGETED, MOTIVATING AND VARIABLE PROPOSAL PLAY BASED
CENTRAL ROLE OF THE FAMILY
GROSS MOTOR AREA
SENSORY AREA
REHABILITATION SETTING: THE ENVIRONMENT
´Defining the characteristics of the object and the space in which the object is placed and amplifying these characteristics allows the extraction of perceptually relevant informations useful for planning and performing the action."
(M.M.Pierro)
ENRICHED ENVIRONMENT
The characteristics of the physical environment and perceptual elements make it more easily readable to the child and facilitate and expand the developmental paths.
ENVIRONMENT
Definition of the action space
• Personal, peripersonal and extrapersonal space
• Lighting, setup and structuring of the setting
Perceptual facilitation
• Acoustic, visual, tactile, proprioceptive, or multimodaldosed and introduced gradually
Qualitative variables of objects:
•Dimension
•Shape
•Weight
•Consistency
•Spatial orientation
•Fixed or in motion
AFFORDANCE
(Ecological theory of perception - Gibson, 1979)
Physical characteristics of an object or space that evoke "action possibilities" for the user.
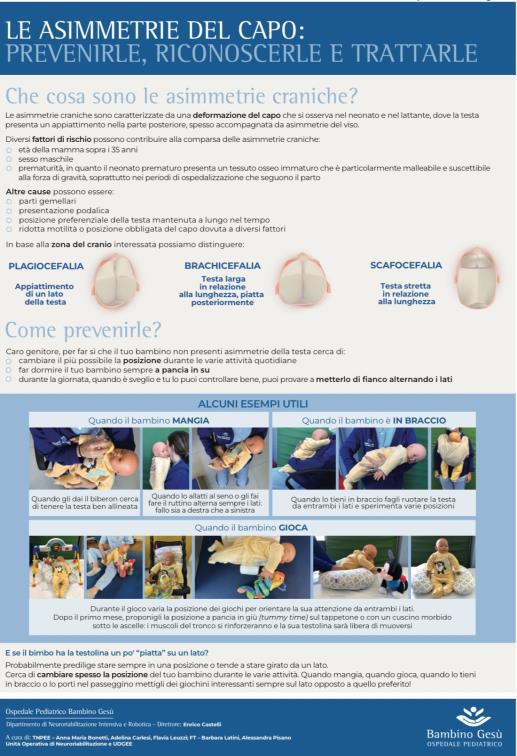
POSTURE
Postural Care
• Facilitating and contained postures (to limit the emergence of reflexive and/or pathological patterns)
• Postures that facilitate the use of the visual channel and allow the integration of sensory channels (motor, praxic and cognitive abilities).
POSTURE
Parent comfort
• Sharing and guiding the parent on postures to adopt (good containment, consolation methods, good relational contact, postural variations during the day as child in arms, in the crib, in the bouncer....)
EMOTIONAL, RELATIONAL, AND COMMUNICATIVE AREA
Promote, within all activities, emotional, relational, and interactive-communicative skills.
Modalities/strategies:
• Use collected positions and close proximity during the interactions.
• Use of language with voice intonation and emphasized facial expressions.
• Interact through all sensory channels (use of gaze, mimic, voice, touch...).
• Propose progressive and gradual consolation methods: use face and voice, use touch by holding hands and feet, pick up, rock...
• Propose and support the first communicative signals (YES, NO, AGAIN, ENOUGH).
EMOTIONAL, RELATIONAL, AND COMMUNICATIVE AREA
AREA OF ADAPTATION AND ENVIRONMENTAL INTERACTION
Set up an environment proactive to the child's development and adapt it on emerging functions.
Modalities/strategies:
•Advices on positioning and postural situations that facilitate the motor component and improve the relationship and exploration of the surrounding environment.
•Setup of living contexts: the stroller, the crib space, the play space...
•Choice and adaptation of the type and method of proposing games and activities.
•Create daily routines by associating objects, music, scents linked to that moment.
•Promote autonomy in these contexts.
AREA OF ADAPTATION AND ENVIRONMENTAL INTERACTION
Too much?....... An opportunity to remodel!!
SENSORY AREA
Promote the development of visual, auditory, tactile, proprioceptive skills and encourage multisensory integration.
Modalities/strategies:
• Care of the environment and context: setting up the pace of work (inclined plane, use of background panel or spatial screening, monochrome or patterned or use of sensory panels).
• Evaluations of perceptual facilitations (visual, auditory, tactile...), starting from unimodal to integrate.
• Use objects meaningful for the child, known objects that capture their interest.
• Seek environmental stability (await response).
• Consultation/collaboration with the orthoptist.
SENSORY AREA
GROSS MOTOR AREA
Promote postures and the development of emerging motor skills.
Modalities/strategies:
•Use a facilitating setting: initially identify the tools and support strategies for the execution of motor patterns (inclined plane, stairs…) and then gradually decrease the facilitations to make the child more autonomous.
•Support body schema knowledge: use of sensory gloves and socks.
•Observe and support the child's motor initiative and spontaneous postural transitions: increase/contain motor patterns, organization and variability.
•Anticipate and verbally guide the proposed movement.
•Goal-directed and purposeful activities: use a motivating target to reach.
•Promote the achievement and maintenance of anti-gravity postures.
•Postural stability, muscle tone, and prevention of any asymmetries and altered motor patterns.
GROSS MOTOR AREA
GROSS MOTOR AREA
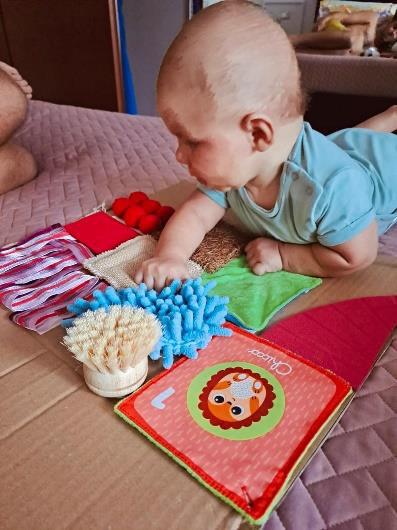
FINE MOTOR AREA
Promote skills of reaching, grasping, and manipulating objects.
Modalities/strategies:
•Encourage the child's interest by proposing objects he know/like.
•Propose objects of various shapes, textures and sizes that allow for hand adaptation.
•Use facilitations: postural hygiene of the child, who must be well stabilized and contained to encourage maximum integration of sensory skills; objects fixed on non-slip surfaces, with velcro or suction cups, and clearly visible.
•Variability of play proposals to experiment with different action schemes on the object.
FINE MOTOR AREA
TAKE HOME MESSAGE
material
CONCLUSIONS FUTURE PROJECTS
Greater sharing of information with the territorial network
“I disordini dello sviluppo motorio”-Ermellina Fedrizzi
“Early intervention programmes for infants at high risk of atypical neurodevelopmental outcome”Developmental medicine & Child neurology, Review 2019
“Early intervention to improve neurodevelopmental outcomes for high-risk infants”-Pediatrics and child health, Symposium: social pediatrics, 2023
“Early Diagnostic and Early Intervention in Neurodevelopmental disorders-Age-Dependent Charleston and Opportunities” -Journal of clinical medicine, Review 2021