The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:





The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:

Dott. Riccardo Carbonetti PT, BsC, DO
Mail: riccardo.carbonetti@opbg.net
Neuroscience and Neurorehabilitation Area; Service of Functional Rehabilitation
Bambino Ges˘ Children Hospital, IRCCS, Roma, Italy
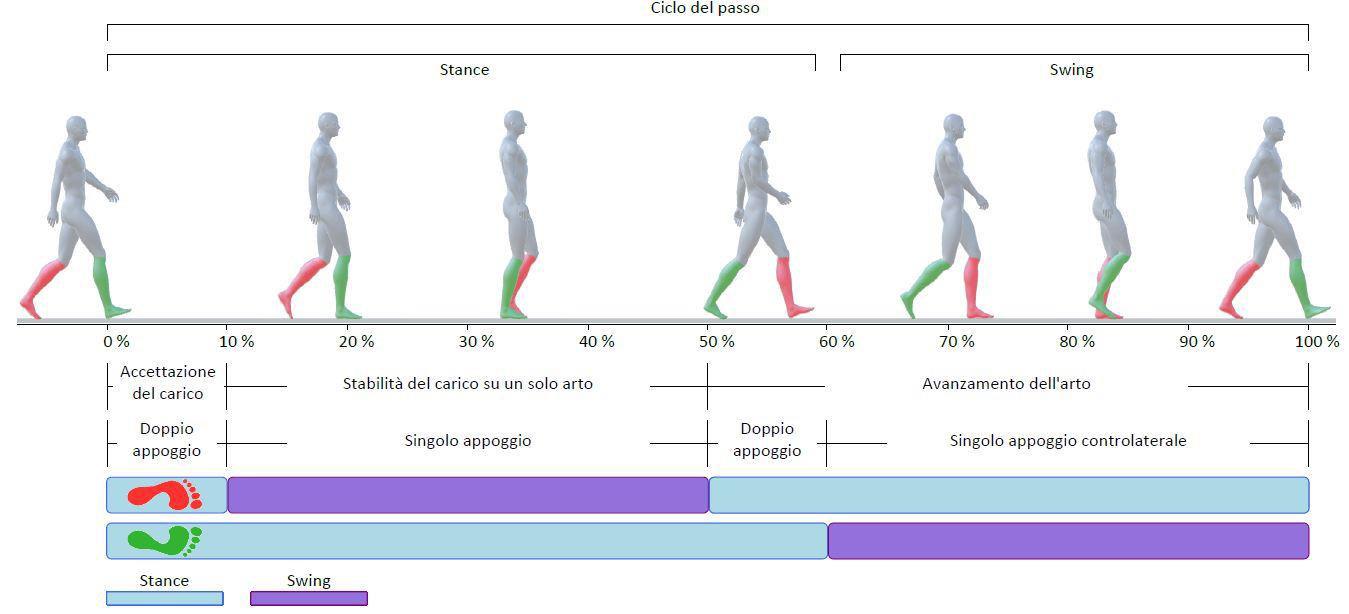
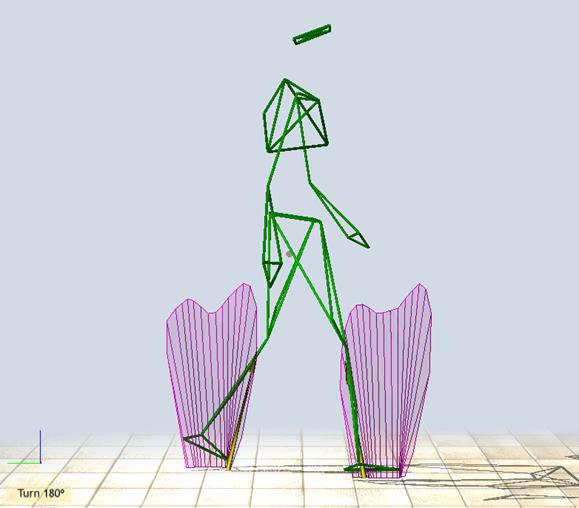
Represents the functional unit of gait
It refers to the mechanical and kinetic actions of a single limb, and its duration is defined as the interval between two consecutive initial contacts of the same foot. It includes two step phases: the interval between the initial contacts of both feet.
It is divided into two phases, whose duration varies depending on the individual's walking speed.
Stance phase: divided into three sub-phases: initial double support / single limb support / terminal double support.
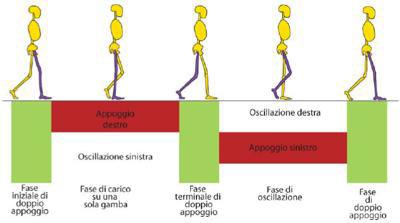
Swing phase: begins with toe-off and corresponds to the period during which the foot is off the ground.
Dipartimento di Neuroscienze e Neuro-riabilitazione
Propulsion
Stability during stance
Impact absorption
Energy conservation

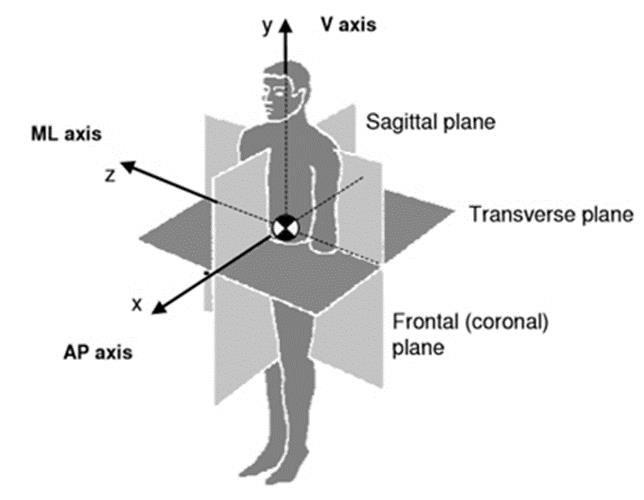
Each phase reflects a complex interplay between body mass and the segments of both lower limbs, which coordinate during gait to produce a cohesive three-dimensional movement pattern.
Based on correlation studies regarding the interrelationships between the movement patterns of the hip, knee, and ankle—which adaptively vary to maintain body alignment—and the different functional demands associated with gait, the gait cycle is divided into eight phases.
The sequential combination of these phases enables the limb to perform three fundamental tasks:
1) Initial load acceptance
2) Single limb support phase
3) Swing limb advancement
Dipartimento di Neuroscienze e Neuro-riabilitazione
This phase involves the greatest number of functional demands within the gait cycle: impact absorption, initial limb stabilization, and maintenance of forward progression.
To achieve this, the first two phases of the gait cycle are engaged:
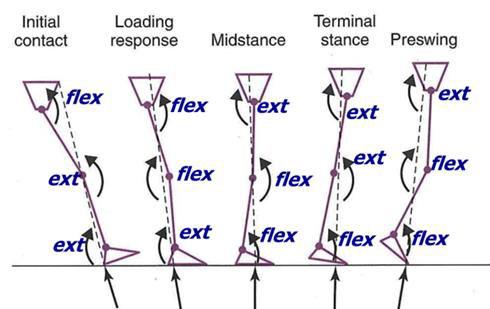
1_Initial contact (0–2%): The hip is flexed, the knee extended, and the ankle positioned in neutral dorsiflexion. The joint configuration at this moment determines how the limb responds to loading.
2_Loading response (0–10%): This corresponds to the initial period of double support, during which body weight is transferred while maintaining load stability.
• The knee flexes slightly to absorb the impact.
• Heel rolling is controlled by plantarflexion of the ankle joint, facilitated by forefoot contact with the ground.
• The contralateral limb is in the pre-swing phase.
Preservation of forward progression
Dipartimento di Neuroscienze e Neuro-riabilitazione
Begins with the lift-off of the contralateral foot and ends when it contacts the ground again (final double support phase). During this interval, the reference limb bears the entire body weight in both the sagittal and frontal planes, while simultaneously enabling forward progression. This segment involves the third and fourth phases of the gait cycle.
3 - Mid stance (10–30%): This phase begins with the lift-off of the contralateral foot and continues until the body weight is aligned over the forefoot. The functional objective of this phase is to allow forward progression over the supporting foot while maintaining stability of the trunk and the stance limb.
4 - Terminal stance (30–50%): This phase begins with heel rise of the reference foot and e with initial contact of the contralateral foot. During this interval, body weight is transferred beyond the forefoot.
The heel rises from the ground as the limb advances by rolling over the forefoot.
The knee continues to extend, then flexes slightly, concurrently with increasing hip extension.
The contralateral limb is in the terminal swing phase.
The final four phases of the gait cycle are involved:
5 – Pre-swing (50–60%): this represents the second period of double support in the gait cycle. It begins with initial contact of the contralateral foot and ends with toe-off of the reference limb. During this phase, weight is transferred, and the functional goal is to prepare the limb for the swing phase.
6 – Initial swing (60–73%): starts with the foot leaving the ground and ends when the swinging limb is aligned with the stance limb. Functionally, the limb is lifted and begins to advance, with hip flexion, pronounced knee flexion, and partial ankle dorsiflexion.
7 – Mid swing (73–87%): this phase begins when the swinging limb is opposite the stance limb and ends when the advancing limb’s hip and knee reach equivalent flexion. The limb moves forward beyond the body’s center of mass.
8 – Terminal swing (87–100%): this phase concludes when the foot contacts the ground.
The physiological task is to maintain stability during stance through control of the center of mass descent and limb advancement. The amount of muscular work required during these actions determines the energy cost.
The lower the energy cost, the higher the quality of the motor task.
Agait cycle includes two mechanisms of energy conservation:
Modulation of gravitational alignment
Selective muscular control

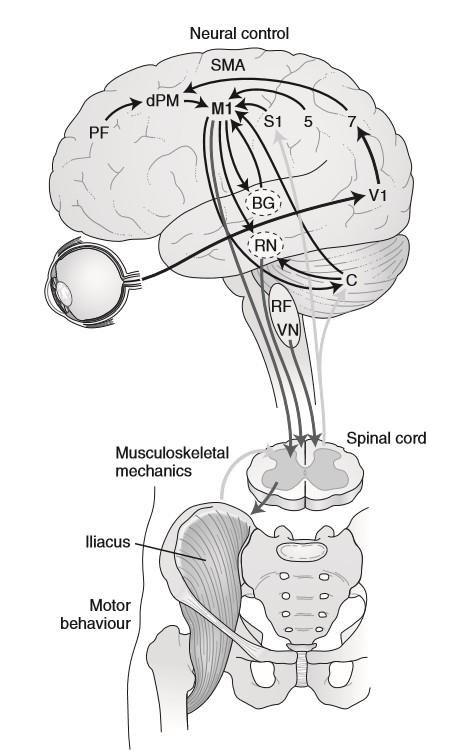
Beyond the biomechanical, physical, and neurological variables that regulate movement, the anatomy and structural design of the human body reflect an optimized and highly adaptable system for gait function.

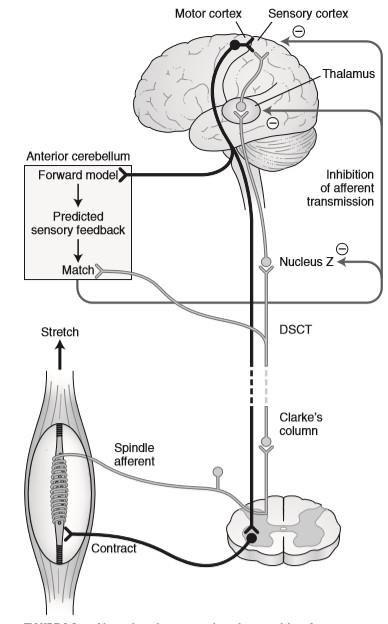
obtained through strategies that are:
Anticipatory
Predictive
Reactive
Patla AE. Understanding the roles of vision in the control of human locomotion. Gait Posture 1997;5:54-69.
The forces are in dynamic equilibrium with each other in accordance with the laws of physical mechanics.
External Forces
The body is subjected to gravitational force and moments of inertia.
Internal Forces
The combined actions of muscles, soft tissues, and ligaments acting on the joints generate an internal joint moment.
The ground reaction force (GRF) changes its point of application and varies in magnitude and direction; at the joint level, it generates external moments: flexor or extensor depending on the phase of the gait cycle.
Internal moments in response to external forces that generate external moments.
Articular or skeletal deformities can alter the point and direction of the ground reaction force (GRF), generating abnormal external moments that are difficult to balance.
If muscles or neuromuscular control are impaired, the ability to generate compensatory internal moments may be compromised.
The difference between the required moment and the one produced causes evident gait abnormalities.
When the system is unable to compensate, gait becomes less efficient, even from an energetic standpoint.
The assessment of biomechanical deviations informs the selection of the most appropriate orthotic and bracing strategies for targeted therapeutic intervention.
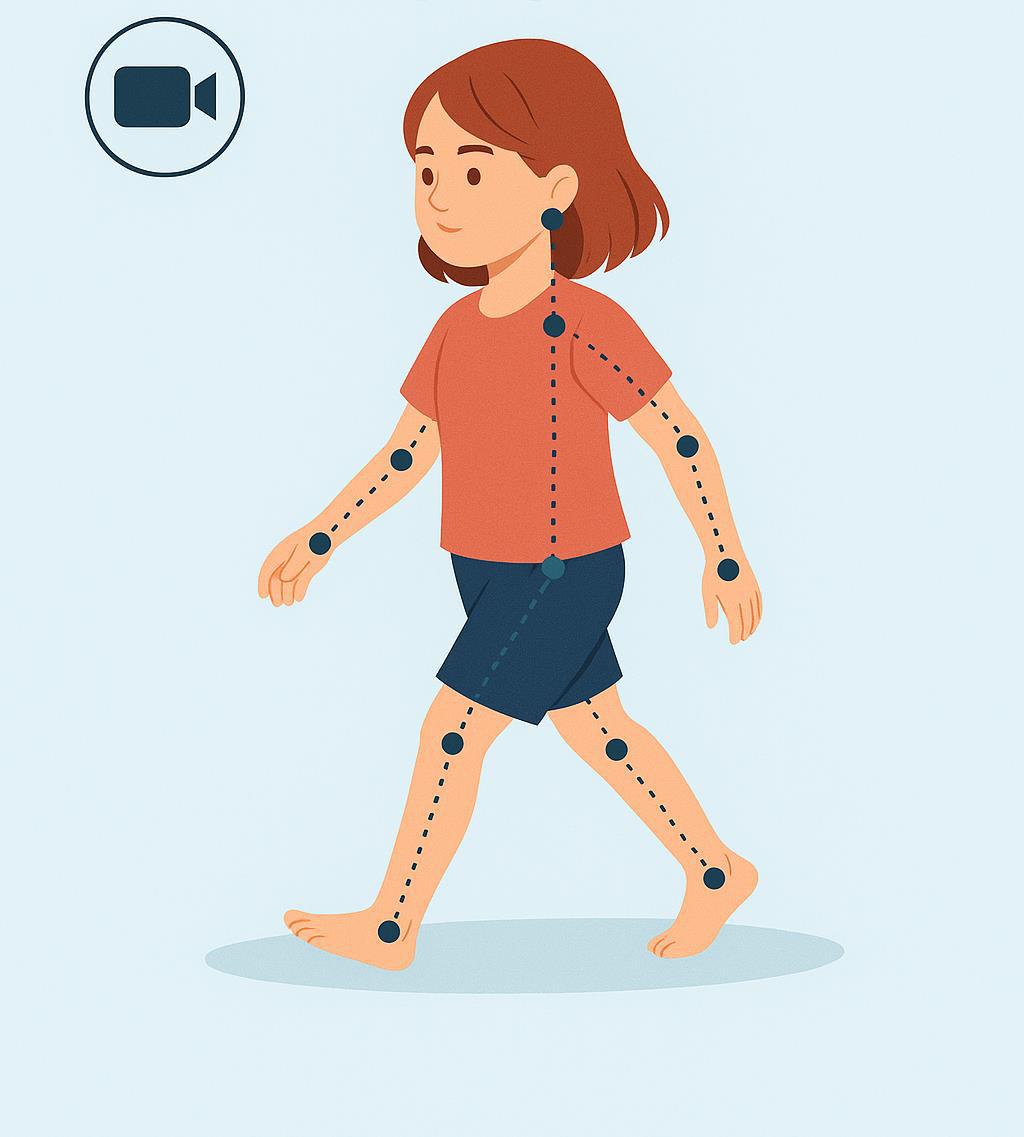
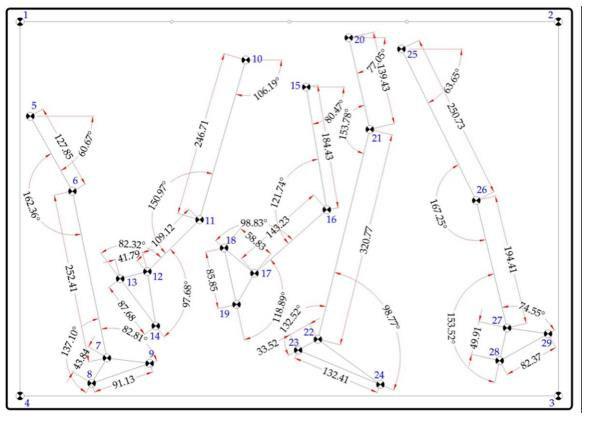
• Video recording of gait offers an accessible and non-invasive tool to observe and analyze walking more objectively than clinical examination alone.
• It allows capturing the motor act in its entirety, observing repeatable patterns, and documenting the evolution of gait over time, especially in children with neuromotor disorders.
• Video analysis does not replace clinical observation—it enhances it.
• It helps us capture subtle details, analyze changes over time, and improve the quality of rehabilitation planning.
• Allows objective assessment of pathological gait patterns
• Facilitates temporal comparison (follow-up)
• Supports shared clinical reasoning among professionals
• Complements visual observation with more systematic analysis (e.g., joint angles, foot contact)
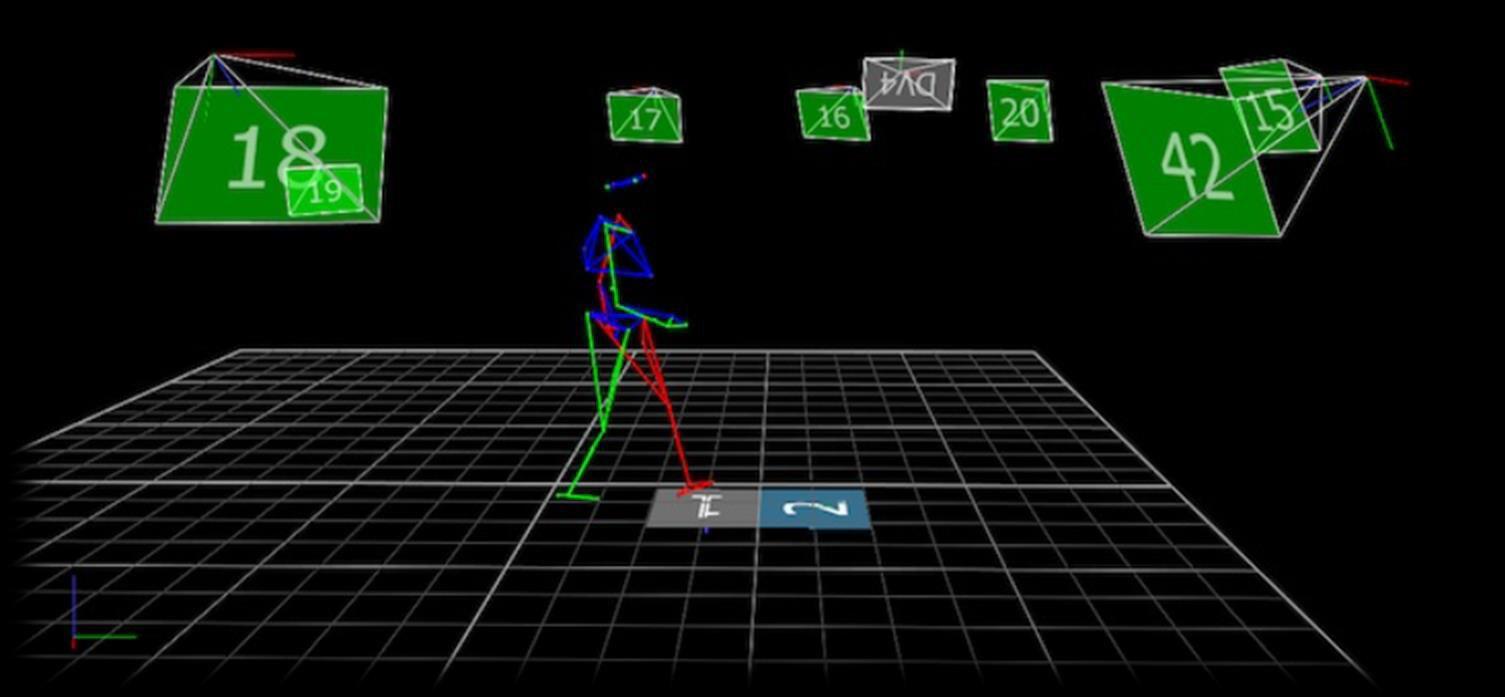
• Compatible with open-access motion analysis tools (e.g., Kinovea, Dartfish)
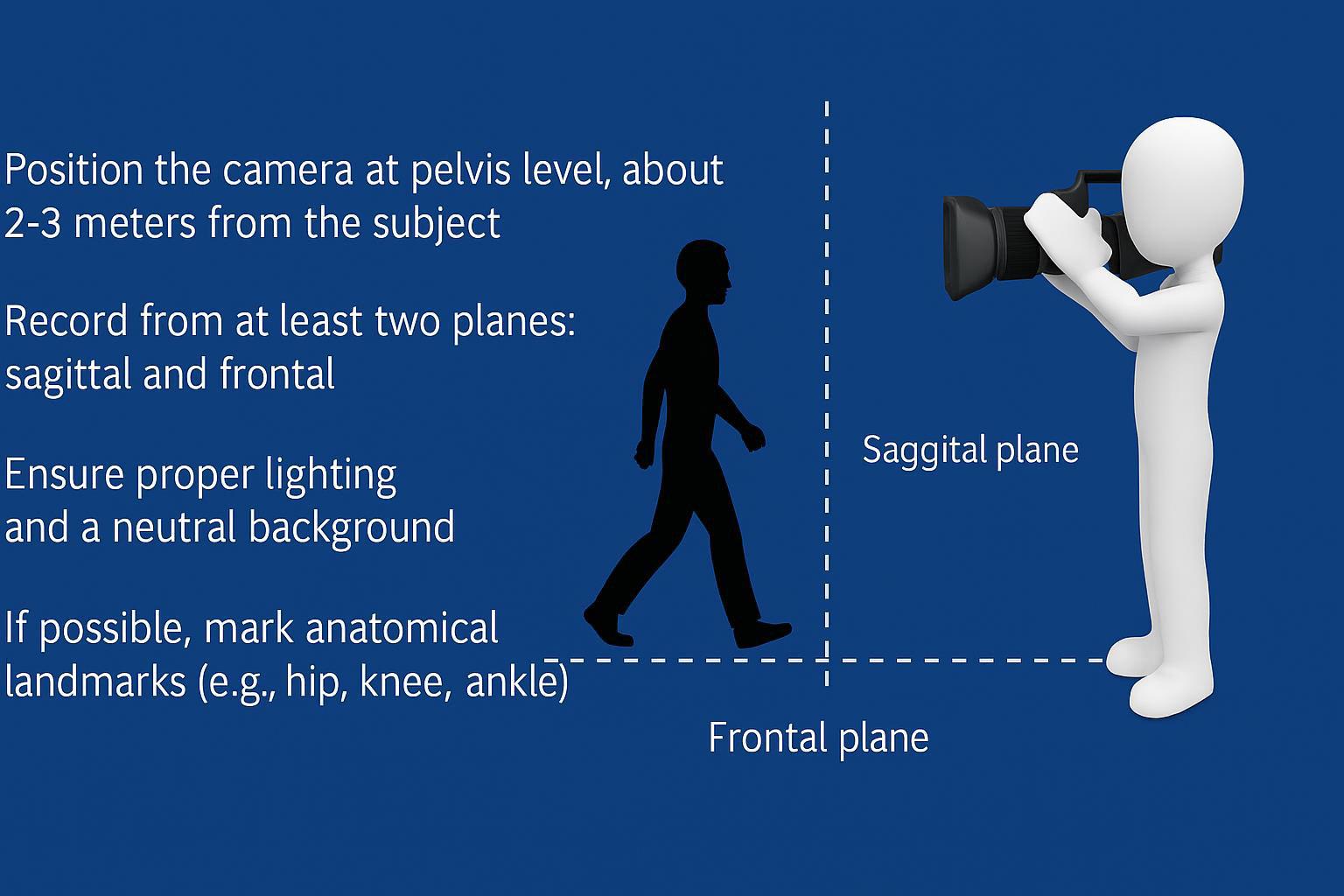
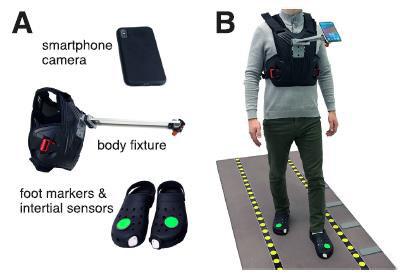
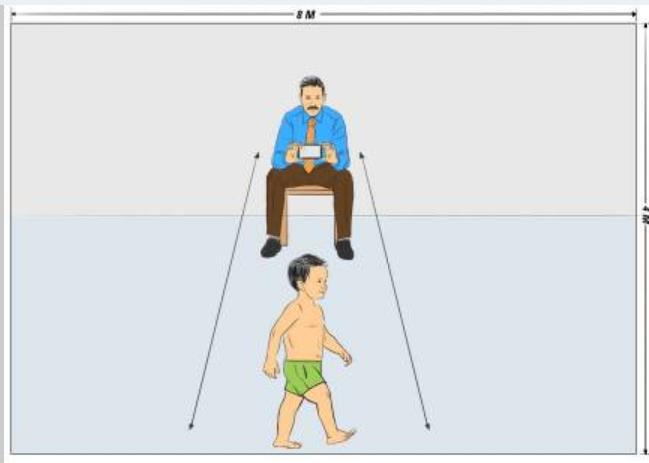
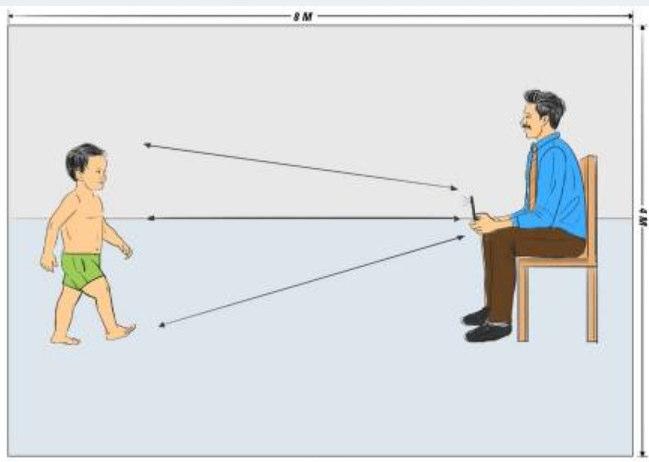
• Position the camera at pelvis level, about 2–3 meters from the subject
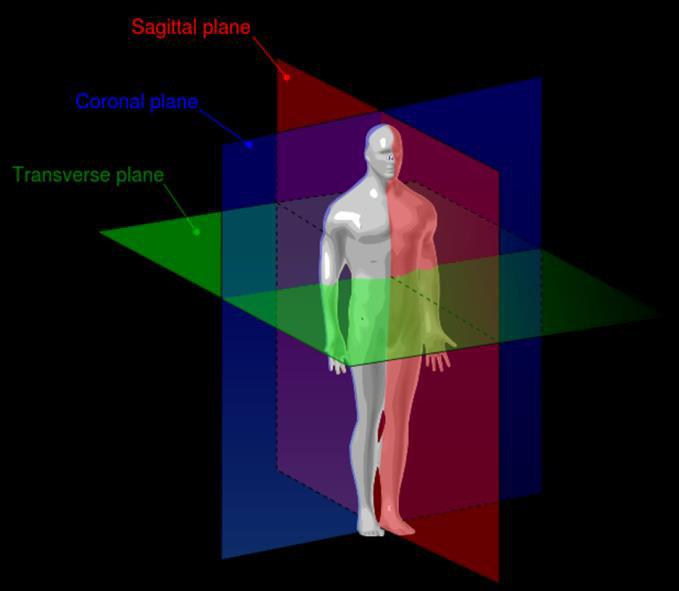
• Record from at least two planes: sagittal and frontal
• Ensure proper lighting and a neutral background
• If possible, mark anatomical landmarks (e.g., hip, knee, ankle)
•Structured and repeatable recording setting.
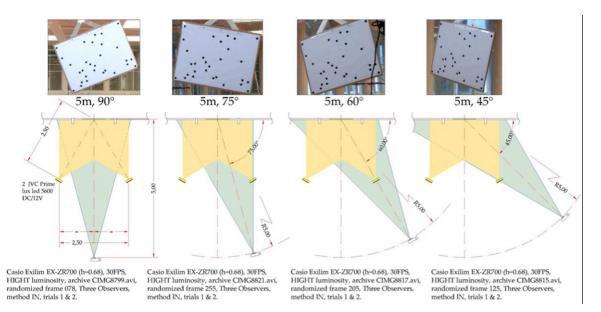
•Camera positioning in space with a defined angle.
•Recording from different spatial planes (frontal–sagittal).
•Record 3–5 sequences of interest.
•Use reference targets to facilitate video evaluation.
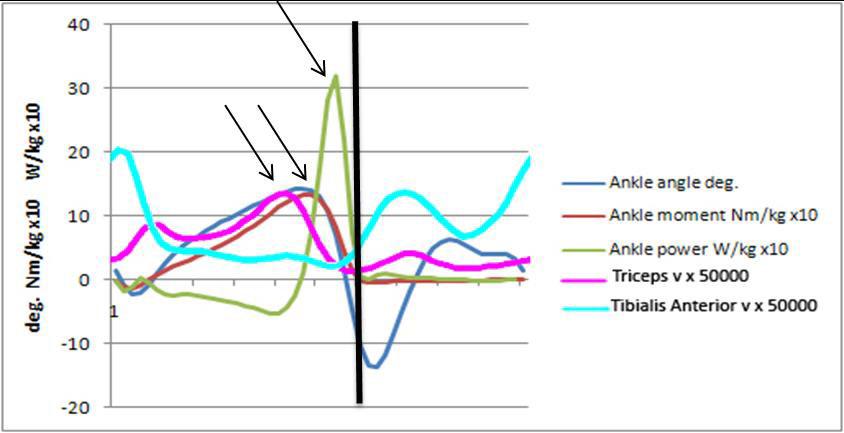
Can we extract objective information?

What does the scientific literature tell us?

Can we organize a more detailed video analysis?



• Clinical tool to assess gait in neurological patients (e.g., CP, stroke)
• Modified from the Physician’s Rating Scale (PRS)
• Evaluates 8 domains via video observation (frontal & lateral views)
• Scoring: each domain to 3 points, max 22 per limb
https://assesschild.com/observational-gait-scale
1. Knee position at mid-stance
2. Initial foot contact
3. Foot contact at mid-stance
4. Timing of heel rise
5. Hindfoot alignment
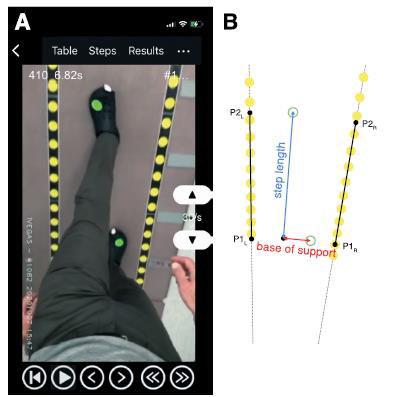
6. Base of support width
7. Use of walking aids
8. Change compared to prior assessment
Validity, Reliability & Clinical Use
• Good inter- and intra-rater reliability (κ = 0.4–0.9)
• Strong correlation with 3D gait analysis (esp. knee & foot)
• Best applied to barefoot walking with short clothing
• Ideal for monitoring therapeutic outcomes over time

VIDEO ANALYSIS SOFTWARE:
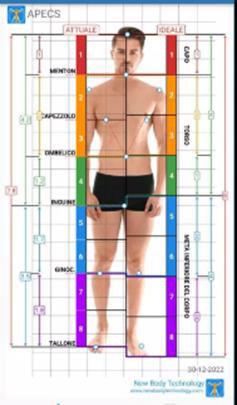
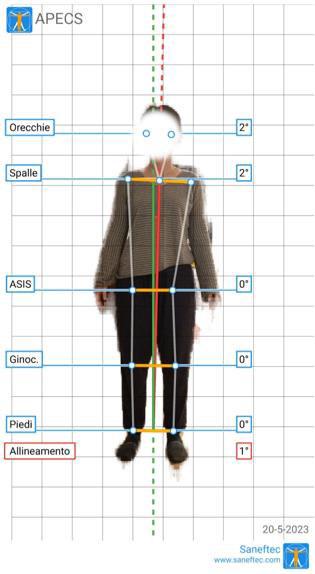
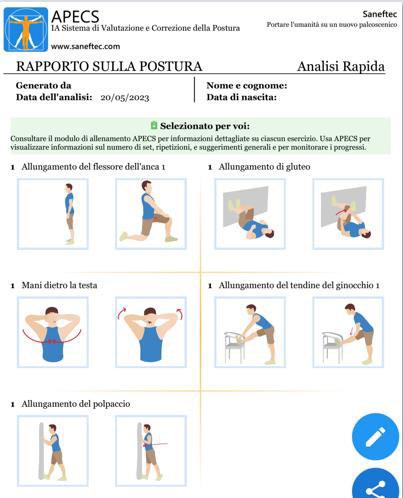
APECS Pro
VIDEO EDITING:
•Pinnacle Studio
•DaVinci Resolve Studio
•Vegas Pro
KINOVEA
Muscle&motion posture
Dartfish
Tracker


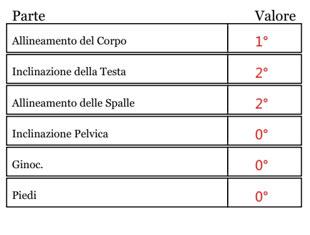
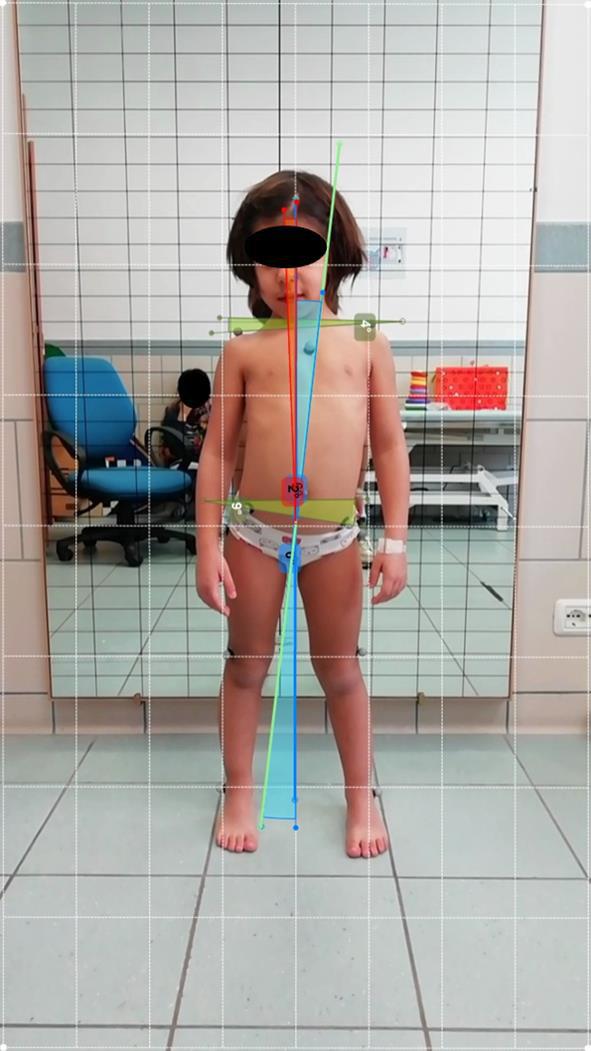
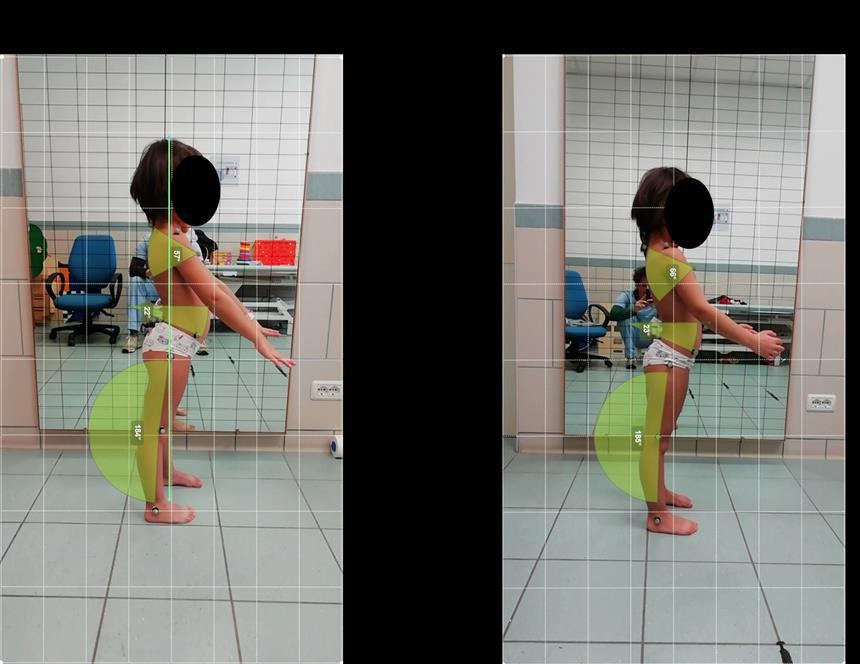
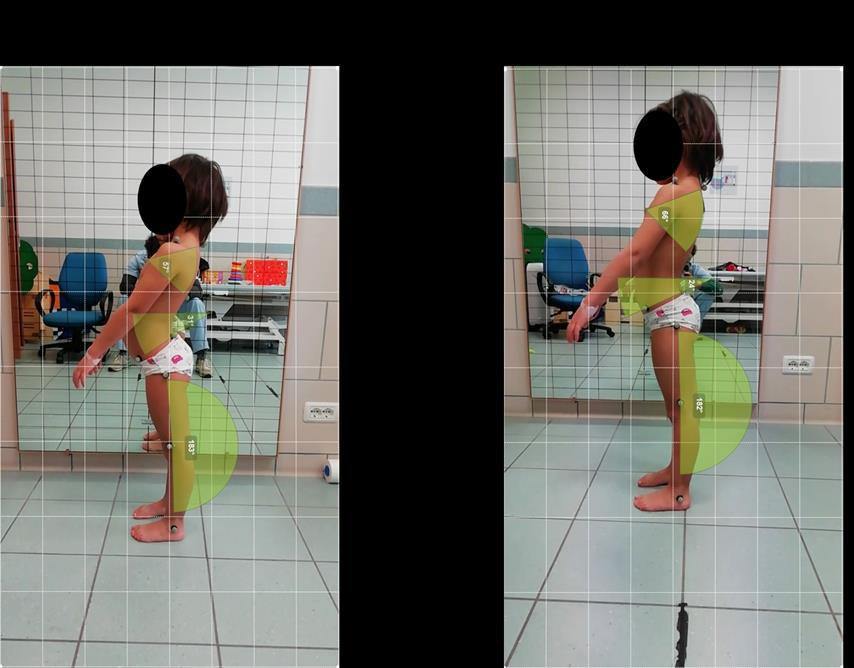
•Postural assessment
•Golden ratio analysis
•Range of motion evaluation
•Postural recommendations with specific exercises
•Postural observation through video during movement (in development)






RECORDING METHODOLOGY AND PROTOCOL
SOFTWARE FOR VIDEO PROCESSING AND ANALYSIS
SPECIFIC SMARTPHONE APPS
Monitoring motor patterns over time
Structuring observation in a more objective way
Supporting personalized clinical reasoning Building shared and communicable documentation

This document was prepared in 31 slides by the Bambino Ges˘ Children's Hospital on 20/06/2025. Its contents are strictly confidential; reproduction or distribution, even partial, is prohibited without the written consent of Bambino Ges˘ Children's Hospital.
