


Welcome to the second issue of the Arbona Health Hub’s Newsletter. We are so happy you are here!

Welcome to the second issue of the Arbona Health Hub’s Newsletter. We are so happy you are here!

Arbona Health Hub began one afternoon when Alejandro and I were brainstorming ways to make science more accessible. We envisioned a platform that could bridge the gap between complex research and everyday understanding. For me, this mission resonates deeply, coming from a public health background. I am passionate about increasing health education, particularly around health policy, which plays a pivotal role in our lives and healthcare.
Avery R. Arsenault
This edition, is a testament to the dedication of our writers and peer reviewers, leadership of our Board of Directors, and the engagement of you, our readers. Your support and curiosity fuel our passions for fostering a community where science knowledge is shared and accessible to all. Thank you!!
Vice-chair







Research Breakdown
1. Educational Articles Impact of Video Games on the Development of Carpal Tunnel Syndrome by Adrián A Almodóvar Díaz - p. 6
Assessing the Impact of Paraben- and Phthalate-Free Products on Breast Cancer Risk by Sofía I Malavé Ortiz - p. 4
1. Breastfeeding’s Role in Reducing Breast Cancer Risk by Jan Paul Villanueva Medina, MPH - p. 9
2. Why Do We Die of Cancer? A Brief Overview of the Pathophysiology of Cancer by Ángel R Ocasio-Gracia - p. 12
3. Understanding the Role of AGEs and sRAGE in Diabetes: Insights from Recent Research by Marcel A de Jesús Vega - p. 15
4. Understanding Congenital Aural Atresia: Causes and Treatments by Roberto A. Oliveras Meléndez - p. 19
6.
5. A Look into America’s Struggle with Healthcare Access and Insurance Coverage by Avery R. Arsenault - p. 22

Writtenby:SofíaI.MalavéOrtiz
PublishedonlineonOctober31,2024
This article is a research breakdown of the study Reduction of daily-use parabens and phthalates reverses accumulation of cancerassociated phenotypes within disease-free breast tissue of study subjects by Darike et al, 2023
An estrogenic compound is a substance that can mimic or interfere with the action of estrogen (estradiol), the primary female reproductive hormone, binding to its receptors and triggering similar effects to those of natural estrogen (Souza et al, 2024) This interference can disrupt hormonal balance and contributing to women’s health issues (eg breast cancer, reproductive problems) (National Institute of Environmental Health Sciences, 2024)
It important to understand how estrogenic chemicals, also known as xenoestrogens (XEs) (Tolu, 2007), affect healthy breast tissue, regarding their role in breast cancer development Parabens and phthalates are estrogenic compounds that can be found in common consumer products and can be absorbed even at low doses, raising health concerns These chemicals are used in common everyday personal care products (PCPs) ¾ shampoos, lotions, fragrances, make up, skin care, and deodorants, with higher usage linked to increased urinary levels of parabens (Dairkee et al, 2023)
Studies suggest that significant amounts of these chemicals can penetrate breast tissue and higher urinary phthalate levels have been linked with an increased risk of breast cancer (Wu et al, 2021)
This research aims to evaluate the impact of parabens and phthalates on healthy breast tissue, determine if the reduction of PCPs containing these chemicals can reverse accumulation in cancer-related changes in breast tissue, and finally analyze these molecular and phenotypic changes in breast tissue before and after reducing PCPs exposure Overall, seeking to provide insights into the potential health benefits of minimizing exposure of these compounds
Participants were recruited and consented from Breast Cancer Over Time (BCOT), a communitybased organization of breast cancer survivors and their supporters Eligible individuals were included if they regularly used PCPs, had no personal cancer diagnosis and had a regular menstrual cycle; and those who were pregnant, breastfeeding, had breast augmentation, kidney disease or heart disease, were excluded
For the intervention, these individuals were assigned to either REDUXE group which replaced their usual products with parabenand phthalate-free alternatives for a three-day period, or control group which had no XEs reduction To assess the impact of this reduction, breast tissue samples were collected from participants before and after each intervention, for researchers to compare cancerassociated characteristics Additionally, urine samples were analyzed to measure levels of parabens and phthalates, confirming the effectiveness of reducing their exposure. The collected tissue samples underwent pathwaybased functional analysis to evaluate changes in molecular markers linked to cancer
The study found that reducing daily exposure to parabens and phthalates led to significant changes in breast tissue characteristics After the three-day intervention, participants showed a decrease in cancer-associated features in their breast tissue samples. Urine analyses confirmed reduced levels of these chemicals, indicating successful exposure reduction Molecular assessments revealed that the intervention positively impacted key pathways linked to breast cancer risk, suggesting that lowering exposure to these estrogenic compounds may help reverse certain cancer-related changes in healthy breast tissue Overall, the results highlight the potential health benefits of minimizing exposure to parabens and phthalates
The findings of this study suggest that even short-term substitution of personal care products containing these chemicals may lead to beneficial changes on a molecular level, potentially lowering the risk of breast cancer risk and improving health outcomes This highlights the importance of minimizing exposure to estrogenic compounds and supports the need for further research and public awareness regarding the safety of personal care products
1
Souza DN, Mounteer AH, Arcanjo GS
Estrogenic compounds in drinking water: A systematic review and risk analysis. Chemosphere 2024 Jul;360:142463 doi: 10 1016/j chemosphere 2024 142463 Epub 2024 May 29 PMID: 38821126
U.S. Department of Health and Human Services (n d -a) Endocrine disruptors National Institute of Environmental Health Sciences https://www.niehs.nih.gov/health/topics/age nts/endocrine 2.
3
Tolu Oyelowo, Chapter 2 – Estrogen Concepts, Editor(s): Tolu Oyelowo, Mosby’s Guide to Women’s Health, Mosby, 2007, Pages 8-10, ISBN 9780323046015, https://doi org/10 1016/B978-0323046015 50003-4
4.
Dairkee SH, Moore DH, Luciani MG, Anderle N, Gerona R, Ky K, Torres SM, Marshall PV, Goodson Iii WH Reduction of daily-use parabens and phthalates reverses accumulation of cancer-associated phenotypes within disease-free breast tissue of study subjects Chemosphere 2023 May;322:138014 doi: 10.1016/j.chemosphere.2023.138014. Epub 2023 Feb 4 PMID: 36746253
5
Wu AH, Franke AA, Wilkens LR, Tseng C, Conroy SM, Li Y, Polfus LM, De Rouen M, Caberto C, Haiman C, Stram DO, Le Marchand L, Cheng I Urinary phthalate exposures and risk of breast cancer: the Multiethnic Cohort study Breast Cancer Res 2021 Apr 6;23(1):44 doi: 10 1186/s13058-02101419-6 PMID: 33823904; PMCID: PMC8025373

Writtenby:AdriánA.AlmodóvarDíaz
PublishedonlineonNovember12,2024
People of all ages, from children to adults, have engaged in video games in one way or another. The wide range of genres offers something for every preference, from classic board games to immersive battlefield simulations Video games have become a regular part of daily life for nearly all children and adolescents, with 97% in the United States playing for at least an hour each day (Granic et al., 2014). During the COVID-19 lockdown, children spent approximately 12 hours per week playing videos games (Donati et al, 2021)
The high prevalence of video games usage is alarming and raises concerns about the potential health effects it may impose Particularly concerning is the development of addiction and its potential effects on the musculoskeletal system Addiction to social networks and online games has a prevalence of 328% among university students and may increase the risk of neck disorders (Heidarimoghadam et al, 2020) A study done among 665 university students reported that social network and online game addiction can increase the risk of wrist pain (Babamiri et al, 2018) Both findings highlight the importance of understanding how video game sessions can impact an individual’s health. Video games that involve constant wrist pressure and repetitive movements can cause entrapment neuropathies, such as Carpal Tunnel Syndrome.
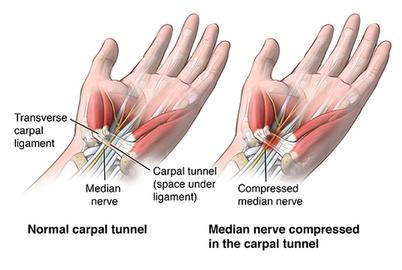
The carpal tunnel refers to a canal between the transverse carpal ligament and the carpal bones of the wrist (Figure 1) Lesions or hypertrophy in this area can compromise the median nerve found within the canal causing pain, paresthesia, hypoesthesia, and anesthesia The pathophysiology is not fully understood, but it is believed that the increase in interstitial pressure causes ischemia and demyelination of the median nerve (Osiak et al, 2022) Recognizing the significant strain placed on the wrist during video game play, I set out to explore the current understanding of the relationship between video game usage and the development of Carpal Tunnel Syndrome.
Carpal Tunnel Syndrome can be elicited by constant pressure and repetitive movement, often associated with electronic device usage University students who used electronic devices for more than 5 hours per day exhibited notably higher positive results in Phalen’s and Durkan’s tests, a larger median nerve cross-sectional area, and reported increased wrist pain (Woo, White & Lai, 2017) Phalen’s and Durkan’s tests are used to evaluate median nerve compression and aid in the diagnosis of Carpal Tunnel Syndrome A larger median nerve crosssectional area may suggest nerve compression and inflammation, both being a plausible cause of Carpal Tunnel Syndrome development
Electronic sports, commonly known as esports, athletes are the most susceptible to the consequences of video games usage As their job involves playing video games, they devote more time to gaming than the average person In a study consisting of 95 esports athletes and a control group of 103, those who had been esports athletes for longer periods experienced a higher score in the Boston Carpal Tunnel Questionnaire Symptom Severity Scale (BCTQSSS) (Basuodan et al , 2023) A higher BCTQ-SSS score suggests that players with more prolonged gaming involvement experienced more symptoms related to Carpal Tunnel Syndrome, such as pain and numbness. In addition, there was a positive correlation between functional severity symptoms and hours of play The authors also concluded that the method of play influenced the BCTQ score. Especially, the use of armrest and controllers resulted in a lower BCTQ score compared to PC gamers with keyboard/mouse
Kendal et al (2022) found that as game addiction score increased, esports players experienced a higher risk of musculoskeletal system discomfort and mental toughness decreased Due to the high prevalence of Carpal Tunnel Symptoms in video game players, it is important to address which treatment options are available. Osiak et al. (2022) recommends non-surgical methods in cases of mild symptoms, however, surgical treatment is indicated in moderate to severe cases after confirmation of axonal injury. Self-myofascial stretching of the carpal ligament showed improvements in numbness, tingling, pinch strength, and symptom severity in participants diagnosed with median mononeuropathy across the wrist (Shem, Wong & Dirlikov, 2020)
This approach would be more accessible for gamers since it can be done without a therapist Implementing rehabilitation practices can be essential to prevent and reduce the development of Carpal Tunnel Syndrome
The constant pressure and repetitive movements of the wrist seen while playing video games can result in the development of Carpal Tunnel Syndrome Carpal Tunnel Syndrome has a positive correlation with hours spent playing video games Mild symptoms of Carpal Tunnel Syndrome can be treated with stretching of the carpal tunnel, however, moderate to severe symptoms may require surgery There is a need for more longitudinal studies as the prevalence of video games keeps rising For future research, it will be crucial to explore how a video game’s genre influences the likelihood of developing Carpal Tunnel Syndrome, particularly among PC gamers, as those using a keyboard and mouse have been found to be the most prone to this condition
References
1
Granic, I , Lobel, A , & Engels, R C (2014) The benefits of playing video games The American psychologist, 69(1), 66–78 https://doi.org/10.1037/a0034857)
2
Donati MA, Guido CA, De Meo G, Spalice A, Sanson F, Beccari C, Primi C Gaming among Children and Adolescents during the COVID19 Lockdown: The Role of Parents in Time Spent on Video Games and Gaming Disorder Symptoms International Journal of Environmental Research and Public Health 2021; 18(12):6642. https://doi org/10 3390/ijerph18126642
Heidarimoghadam, R , Mortezapour, A , Ghasemi, F , Ghaffari, M E , Babamiri, M , Razie, M., & Bandehelahi, K. (2020). Musculoskeletal Consequences in CyberAddicted Students – Is It Really A Matter of Health? A ROC Curve Analysis for Prioritizing Risk Factors. J Res Health Sci, 20(2), e00475–e00475 doi:10 34172/jrhs 2020 10 3
Babamiri, M , Haidari Moghaddam, R , Ghasemi, F , Ghaffari, M , Razee, M , Bandeh Ellahi, K., & Mortezapour, A. (2018). Addiction to Social Networks and Online Games: A Wrists’ Pain Survey in Students Journal of Ergonomics, 6(3) doi:10 30699/jergon 6 3 4 4
5 Osiak, K, Elnazir, P, Walocha, J A, & Pasternak, A (2022) Carpal tunnel syndrome: state-of-theart review Folia morphologica, 81(4), 851–862 https://doiorg/105603/FMa20210121
6 Woo, E H C, White, P, & Lai, C W K (2017) Effects of electronic device overuse by university students in relation to clinical status and anatomical variations of the median nerve and transverse carpal ligament Muscle & nerve, 56(5), 873–880 https://doiorg/101002/mus25697
7 Basuodan, R M, Aljebreen, A W, Sobih, H A, Majrashi, K A, Almutairi, N H, Alhaqbani, S S, Alanazy, M H (2023) The impact of electronic gaming on upper-limb neuropathies among esports athletes Med Pr Work Health Saf, 74(4), 279-287 https://doiorg/1013075/mp589301421
8 Kendal, K, Ataç, A, & Köse, İ T (2022) Effects of game addiction on musculoskeletal system discomfort and mental toughness in e-sport players Addicta: The Turkish Journal on Addictions, 9(2), 212-217
9. Shem, K., Wong, J., & Dirlikov, B. (2020). Effective self-stretching of carpal ligament for the treatment of carpal tunnel syndrome: A double-blinded randomized controlled study. Journal of hand therapy : official journal of the American Society of Hand Therapists, 33(3), 272–280 https://doiorg/101016/jjht201912002
Figure 1 Normal carpal tunnel versus Carpal tunnel Syndrome Retrieved from https://wwwhopkinsmedicineorg/health/conditions-and-diseases/carpal-tunnel-syndrome

Writtenby:JanPaulVillanuevaMedina,MPH
PublishedonlineonNov20,2024
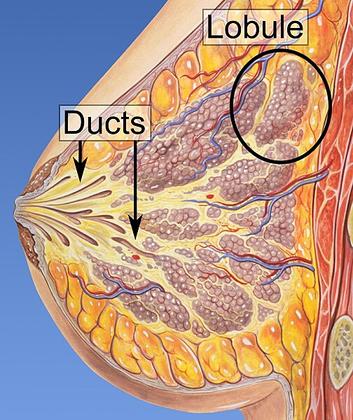
Breast feeding is vital for the nutrition and immune system development of the newborn To fulfill this function, breast tissue undergoes processes of differentiation or “activation” at the histological level to begin the production of breast milk and develop the necessary structures for its expulsion.
Four stages of differentiation of this tissue have been described: Proliferative, in which there is extensive growth in the number and size of epithelial cells during conception and pregnancy; Secretory, characterized by an increase in adipose tissue in the form of large droplets, biochemical changes prior to lactation, and inhibition of milk secretion by progesterone; Secretory Activation, in which progesterone levels drop and prolactin levels rise, allowing for the active secretion of milk along with the expression of milk protein genes; and lactation, which is the continuous production of milk, divided into colostrum stage (high immunoglobulin content) and mature secretion stage (high milk volume for neonatal support), a process dependent on the presence of adipose tissue (Anderson et al, 2007)
It has been observed that this reorganization and proliferation of tissue, followed by apoptosis and immune response at the end of lactation, has the potential to cause pregnancy-associated breast cancer, given that adipose tissue secretes growth factors that can promote tumorigenesis by increasing vasculogenesis and angiogenesis, in addition to serving as a source of energy, fatty acids, and cholesterol (Kothari et al., 2020).
Given this information, it is important to determine if the breastfeeding process after childbirth represents a risk factor for developing breast cancer
The data found indicated that to explain the association between breastfeeding and breast cancer, it is necessary to involve the parity factor, physical activity, diet and the subtype of breast cancer The subtypes of this disease can be separated into positive (+) or negative (-) for Estrogen or Progesterone receptor, that is, +ER/-ER or +PR/-PR and the triple negative (ER/-PR) which is also negative for the type 2 receptor of the human epidermal growth factor (HER2) A study found that breastfeeding is a protective factor against negative hormone receptors (-ER/-PR/-HER2) However, no association was found with the subtypes of hormone receptor-positive (+ER/+PR) Additionally, it was found that breastfeeding for more than 12 months represented a 4% decrease in breast cancer incidence, and parity provided an additional 7% (Islami et al, 2015) Regarding the triple-negative subtype, it was observed that breastfeeding not only served as a protective factor, but the duration is another factor to consider, given that mothers who breastfed for more than 6 months had an 82% reduction in risk (Ma et al, 2017) Although these percentages are different in both studies, both assert that breastfeeding reduces the risk of incidence
Additionally, another study of 7,663 women in Malaysia found that, along with breastfeeding, consuming soy foods and engaging in physical activity are other protective factors, with breastfeeding being the strongest predictor for breast cancer It is worth noting that this study also found that consuming alcohol and having a high BMI are risk factors, again highlighting the importance of adipose tissue, both in the breasts and throughout the body, in the cancer development process (Tan et al, 2018)
On the other hand, it was found that just as breastfeeding can affect the incidence of breast cancer, the breastfeeding process can be interrupted in patients who have survived the disease and its treatment Due to the irradiation or removal of tissue when treating this disease, the burden of breastfeeding may fall on only one breast, causing pain to the mother, a decrease in milk production and duration of breastfeeding, and psychological insecurity about the viability of breastfeeding and the quality of the milk (Ogg et al, 2020; Azim et al, 2010; Gorman et al, 2009) However, studies have confirmed that it is possible to breastfeed if the psychological aspect is addressed through counseling and the help of multidisciplinary teams, given that it has been observed that the
doctors handling these patients’ cases have erroneously recommended that they abstain from breastfeeding This support would provide mothers with the necessary and vital tools to obtain the protective benefits of breastfeeding against the recurrence of cancer (Bhurosy et al, 2021; Azim et al, 2010)
It is worth noting the lack of studies conducted in the field of survivor patients with aspirations to become mothers or pregnant women who wish to breastfeed their children. Most, if not all, of the aforementioned studies highlighted the lack of research on breastfeeding experiences once breast cancer treatments are completed and how this could eliminate their protection. This is why greater attention should be paid not only to treatment during the illness but also after it, to ensure the quality of life for these patients who have already gone through a highly stressful stage in their lives This would allow for the creation of treatments and preventive measures with a better approach and, in turn, increase the efficiency of those already in place
It can be observed that the process of breastfeeding and its duration have an inverse relationship with breast cancer for the negative subtypes (-ER/-PR) and triple-negative (-ER/PR/-HER2), but no significant association was found with the positive subtypes (+ER/+PR) In other words, a longer duration of breastfeeding reduces the risk of the negative subtypes of breast cancer (-ER, -PR and -ER/-PR/-HER2) Parity, physical activity, and the consumption of soy in foods along with breastfeeding are other protective factors against the incidence of this disease Likewise, this disease can interrupt the breastfeeding process in survivor mothers if they are not treated with counseling and support from multidisciplinary teams during this process This shows a reciprocal relation in which breastfeeding protects against negative subtype breast cancers, but the disease can also affect or eliminate said protection if it causes the mother to stop breastfeeding Finally, it is urgent to study the experiences and difficulties that patients who aspire to be or are already mothers may face once they have overcome the disease, in order to determine better treatment and prevention measures to maximize their efficiency.
References:
1. Anderson, S. M., Rudolph, M. C., McManaman, J. L., & Neville, M. C. (2007). Key stages in mammary gland development Secretory activation in the mammary gland: ¡it's not just about milk protein synthesis! Breast cancer research: BCR, 9(1), 204 https://doi org/10 1186/bcr1653
Bhurosy, T., Niu, Z., & Heckman, C. J. (2021). Breastfeeding is possible: A Systematic Review on the Feasibility and Challenges of Breastfeeding Among Breast Cancer Survivors of Reproductive Age Annals of Surgical Oncology, 28(7), 3723-3735 https://doi org/10 1245/s10434-020-09094-1
2. Kothari, C., Diorio, C., & Durocher, F. (2020). The Importance of Breast Adipose Tissue in Breast Cancer International Journal of Molecular Sciences, 21(16), 5760 https://doi org/10 3390/ijms21165760
3. Islami, F , Liu, Y , Jemal, A , Zhou, J , Weiderpass, E , Colditz, G , Boffetta, P , & Weiss, M (2015) Breastfeeding and breast cancer risk by receptor status--a systematic review and metaanalysis Annals of Oncology : official journal of the European Society for Medical Oncology, 26(12), 2398-2407 https://doi org/10 1093/annonc/mdv379
4 Ma, H , Ursin, G , Xu, X , Lee, E , Togawa, K , Duan, L , Lu, Y , Malone, K E , Marchbanks, P A , McDonald, J. A., Simon, M. S., Folger, S. G., Sullivan-Halley, J., Deapen, D. M., Press, M. F., & Bernstein, L (2017) Reproductive factors and the risk of triple-negative breast cancer in white women and African-American women: a pooled analysis Breast cancer research : BCR, 19(1), 6 https://doi org/10 1186/s13058-016-0799-9
5 Tan, M. M., Ho, W. K., Yoon, S. Y., Mariapun, S., Hasan, S. N., Lee, D. S., Hassan, T., Lee, S. Y., Phuah, S Y , Sivanandan, K , Ng, P P , Rajaram, N , Jaganathan, M , Jamaris, S , Islam, T , Rahmat, K , Fadzli, F , Vijayananthan, A , Rajadurai, P , See, M H , Teo, S H (2018) A casecontrol study of breast cancer risk factors in 7,663 women in Malaysia PloS One, 13(9), e0203469 https://doi org/10 1371/journal pone 0203469
6. Ogg, S , Klosky, J L , Chemaitilly, W , Srivastava, D K , Wang, M , Carney, G , Ojha, R , Robison, L L , Cox, C L , & Hudson, M M (2020) Breastfeeding practices among childhood cancer survivors Journal of cancer survivorship : research and practice, 14(4), 586-599 https://doi org/10 1007/s11764-020-00882-y
7 Azim, H A , Jr , Bellettini, G , Liptrott, S J , Armeni, M E , Dell'Acqua, V , Torti, F , Di Nubila, B , Galimberti, V , & Peccatori, F (2010) Breastfeeding in breast cancer survivors: pattern, behaviour and effect on breast cancer outcome Breast (Edinburgh, Scotland), 19(6), 527-531 https://doi org/10 1016/j breast 2010 05 018
9
8 Gorman, J R , Usita, P M , Madlensky, L , & Pierce, J P (2009) A qualitative investigation of breast cancer survivors' experiences with breastfeeding Journal of cancer survivorship : research and practice, 3(3), 181-191 https://doi org/10 1007/s11764-009-0089-y
Figure 1 https://commons wikimedia org/wiki/File:Lobules and ducts of the breast jpg

Writtenby:ÁngelR.Ocasio-Gracia
PublishedonlineonNov26,2024
People often talk about cancer and the ruthless, painful, and terrifying disease it can be With incidences in the USA of 4405 per 100,000 men and women per year (National Institute of Cancer, 2017-2021) According to the World Health Organization, “in 2022, there were 20 million new cases and 97 million deaths from cancer worldwide,” making it one of the leading causes of death worldwide (World Health Organization, 2022)
Many wonder, even I did until almost halfway through my undergraduate degree, about what makes cancer so bad Why does it end life as we know it? All these questions deserve an explanation that science attempts to offer This article aims to describe, in a general and easy-tounderstand manner, the different elements associated with death from cancer I must clarify that this article does not intend to represent an exhaustive analysis of the cellular, molecular and biochemical mechanisms of death from cancer, but rather a general summary of the elements involved in the collapse of life and the development of cancer
First, it is important to define cancer This disease is understood as an uncontrolled proliferation of cells caused by DNA damage of different genes involved in cell replication Following multiple mutations, this initial localized irregular division of cells can transform into a mass (i.e. tumor) and extend to other organs The arrival of these abnormal cells to fundamental parts of the human body, such as the brain, the lungs, among others, is the problem
The masses that form can be benign or malignant A benign tumor is a localized cancer that is nonmigrating to other parts of the body A malignant cancer can occur when abnormal cells reach the lymphatic or vascular vessels and travel to other parts of the body, continuing their uncontrolled proliferation This is better known as metastases and is considered a more complicated health scenario since the cancer can virtually reach any part of the body, compromising essential structures and processes for human life
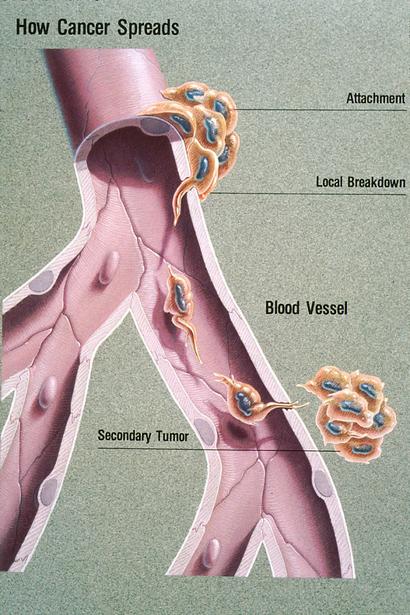
Figure 1. This illustration titled “How Cancer Spreads” explains the process of metastasis Once metastatic cells are attached to the basement membrane (a physical barrier that seperates tissue components), they break through with the help of an enzyme called type IV collagenase. Cancer cells then move through the blood stream enabling them to spread to other parts of the body A secondary tumor may form at another site in the body
According to various sources, the mechanisms involved in death from cancer are complex and multifactorial These include a series of structural and chemical changes that cause the deterioration of vital structures In some cases, cancer can compress vascular structures causing tissue hypoxia, or in other words lack oxygen supply It can also include the destruction of organ parenchyma causing serious cascades of inflammation and tissue damage, among many others In other cases, cancer can cause severe external or internal bleeding due to tumor invasion of blood vessels This hemorrhage can cause rapid blood loss, leading to a decrease in blood pressure and the development of hypovolemic shock If not properly controlled, this can be life-threatening due to organ hypoxia
Depending on the location and extent of the tumor, local complications may arise such as hormone imbalances, urinary, respiratory or intestinal tract obstruction, severe bleeding and others These abnormalities can affect vital signs, such as blood pressure, heart rate, breathing, and body temperature, and eventually lead to multiple organ failure and death According to Sonoda, as cancer progresses and invades tissues, there is an increasing risk of failure of major organs, including the liver, lungs, kidneys and heart, which could lead to organism collapse (Sonoda, 2016)
In addition to the natural effects of cancer itself, side effects of prescribed treatments, such as radiotherapy, chemotherapy or surgery, can also contribute to the weakening of the body and increase the risk of serious complications. For example, patients could be at risk of serious infections and severe systemic inflammatory responses that could be fatal, especially if the immune system is compromised due to the treatment (Lier, 2018)
In closing, it is understood that death from cancer is a multivariable and composite event precipitated by an uncontrolled proliferation of cells Numerous DNA mutations can eventually lead to a cancer that could potentially disrupt and destroy the integrity of surrounding organs and structures These damages, sometimes irreparable, are the phenomena responsible for the death of a person Today, it is known that the prolonged exposure of substances that are proven harmful, combined along with genetic and environmental factors, can predispose a person to cancer It remains urgent that policymakers worldwide consider the scientific findings on the etiology of the different diseases in a population to better promote a good quality of life
1. Centers for Disease Control and Prevention. (2018) Uterine cancer incidence and mortality –United States, 1999–2016 Centers for Disease Control and Prevention https://wwwcdcgov/mmwr/volumes/67/wr/mm 6748a1htm
2. Dvoretsky, P.M., Richards, K.A., Angel, C., Rabinowitz, L, Beecham, JB, & Bonfiglio, TA (1988). Survival time, causes of death, and tumor/treatment-related morbidity in 100 women with ovarian cancer Human pathology, 19(11), 1273–1279 https://doiorg/101016/s0046-8177(88)80281-8
3 Estadísticas del cáncer Comprehensive Cancer Information – NCI – NIH (2024) https://www.cancer.gov/espanol/cancer/naturaleza/estadisticas#:~:text=La%20tasa%20de%20c asos%20nuevos,muertes%20de%202018%20a%202022)
4 Lier, H , Bernhard, M , & Hossfeld, B (2018) Hypovolämisch-hämorrhagischer Schock [Hypovolemic and hemorrhagic shock] Der Anaesthesist, 67(3), 225–244 https://doi.org/10.1007/s00101-018-0411-z
5 Sonoda K (2016) Molecular biology of gynecological cancer Oncology letters, 11(1), 16–22 https://doi org/10 3892/ol 2015 3862
Uterine sarcoma treatment Robert H Lurie Comprehensive Cancer Center of Northwestern University: Feinberg School of Medicine (n d ) https://www cancer northwestern edu/types-ofcancer/gynecologic/uterine-sarcoma html
6 World Health Organization (n d ) Cáncer World Health Organization https://www who int/es/news-room/fact-sheets/detail/cancer
7 Yale Medicine (2022, February 4) Small cell lung cancer Yale Medicine https://www yalemedicine org/conditions/small-cell-lungcancer#: :text=Due%20to%20how%20quickly%20it,bones%2C%20adrenal%20glands%20and%2 0brain
8 Yue, X , Pruemer, JM, Hincapie, AL, Almalki, ZS, & Guo, JJ (2020) Economic burden and treatment patterns of gynecologic cancers in the United States: evidence from the Medical Expenditure Panel Survey 2007-2014 Journal of gynecologic oncology, 31(4), e52 https://doi org/10 3802/jgo 2020 31 e52
Figure 1 This image was released by the National Cancer Institute, an agency part of the National Institutes of Health, with the ID 2446 (image) (next)
Writtenby:MarcelA.deJesúsVega
Hello! Welcome back to the AGEs series This is the third entry for this series, where we focus on understanding what are Advanced Glycation End Products (AGEs) and discuss novel research findings on this topic. If you have missed our past two entries or would like to refresh your memory on the topic, I suggest you go back and read these articles:

Part 1

Part 2
Aim and conclusion from the main article of reference
During my most recent literature search I came across a systematic review conducted by Chen et al. (2024) that aimed to clarify inconsistent findings regarding levels of the soluble receptor for advanced glycation end products (sRAGE) in both type 1 diabetes (T1DM) and type 2 diabetes (T2DM). The article concluded that sRAGE levels increased in T1DM patients and T2DM patients with complications, while decrease in newly diagnosed T2DM patients Results indicated that changes in sRAGE levels in patients with T1DM or T2DM depend on the different types and stages of the disease I believe you will make better sense of this information after you have read this entry.
This article was very insightful and went into detail to explain from a molecular level how diabetes and AGEs are related through some of the disease’s chronic complications In this entry I will focus on explaining how AGEs are involved in one of the major mechanisms underlying the development and progression of complications associated with diabetes Let’s dive in!
Diabetes is a chronic condition characterized by the body’s inability to properly regulate blood sugar levels, either due to insufficient insulin production (T1DM) or insulin resistance (T2DM) Complications from diabetes arise when high blood sugar levels persist over time, leading to damage in blood vessels and nerves. This can result in conditions such as heart disease, kidney failure, nerve damage, vision loss, and poor wound healing, significantly impacting overall health and quality of life (1) (2). It is known that AGEs and their associated molecular pathways play a role in exacerbating some of these complications in patients
From our past entries in this series, you should remember that AGEs formation is accelerated in hyperglycemia, due to increased availability of glucose Hence, in a patient with diabetes we should except to encounter a higher quantity of AGEs AGEs can directly capture and crosslink proteins or bind to advanced glycation end product receptor (RAGE) and activate signaling pathways that lead to inflammation and oxidative stress (like we have discussed in the past)
AGEs may bind to RAGE in different forms: fulllength RAGE (fl-RAGE) and soluble RAGE (sRAGE) Here are the differences between them:
This is the membrane-bound form of the receptor
It is expressed on the surface of various cell types and plays a crucial role in mediating the effects of AGEs and other ligands
Activation of fl-RAGE triggers intracellular signaling pathways that can lead to inflammation, oxidative stress, and cellular dysfunction
Soluble RAGE (sRAGE):
This term generally refers to all soluble forms of RAGE that are released into the circulation.
Soluble RAGE acts as a decoy receptor, binding to AGEs and preventing them from interacting with fl-RAGE, thereby potentially mitigating the harmful effects associated with AGEs
It includes both esRAGE and cRAGE
Endogenous Secretory RAGE (esRAGE):
esRAGE is a splice variant of RAGE that is secreted by cells
It is produced through alternative splicing of the RAGE gene and is found in the bloodstream
Like sRAGE, esRAGE can bind to AGEs and other ligands, helping to modulate their effects and reduce inflammation
Cleaved RAGE (cRAGE):
cRAGE is generated through the proteolytic cleavage of full-length RAGE by matrix metalloproteinases (MMPs) This form is also soluble and can circulate in the blood
Similar to esRAGE, cRAGE can bind to AGEs, acting as a decoy receptor and potentially reducing the activation of fl-RAGE
In summary, while full-length RAGE is the active receptor on cell membranes, soluble RAGE forms (esRAGE and cRAGE) are released into circulation and serve to modulate the effects of AGEs by preventing their interaction with flRAGE sRAGE are recognized as protective receptors
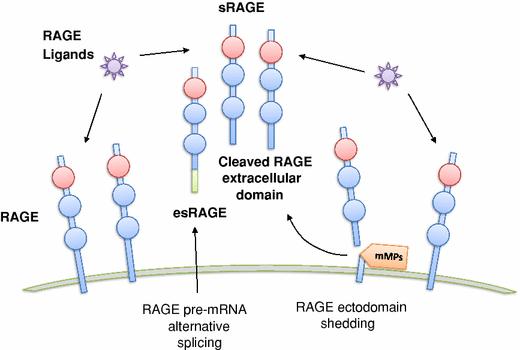
Figure 1. RAGE Forms and Functions This diagram illustrates how full-length RAGE triggers inflammation, while soluble forms (sRAGE, esRAGE, cRAGE) act as decoys to reduce harmful effects, playing a role in diabetes and inflammation.
The meta-analysis provides clarity to inconsistent findings concerning sRAGE levels in T1DM and T2DM, showing that sRAGE levels are elevated in T1DM patients and in T2DM patients with complications, while a decrease is observed in newly diagnosed T2DM patients
The increase in sRAGE levels is suggested to be a compensatory response to the chronic hyperglycemia, inflammation, and oxidative stress associated with diabetes As advanced glycation end products (AGEs) accumulate, they exacerbate these conditions, leading to increased expression of RAGE and subsequent shedding of its extracellular domains, which contributes to higher sRAGE levels
The authors also note that certain medications, such as insulin and oral hypoglycemic agents, can influence sRAGE levels Clinical studies have shown that sRAGE levels can rise significantly after treatment with these medications, indicating that pharmacological interventions may play a role in modulating sRAGE This suggests that managing diabetes through medication not only helps control blood glucose levels but may also impact sRAGE levels, potentially affecting the progression of diabetesrelated complications
If medications, such as insulin and oral hypoglycemic agents, lead to increased sRAGE levels, this could be a protective mechanism Higher sRAGE levels may help mitigate the harmful effects of AGEs and reduce inflammation, potentially leading to better management of diabetes-related complications In this scenario, effective medication management could help slow down or prevent the progression of complications, such as neuropathy, retinopathy, and cardiovascular issues

Conversely, if the management of diabetes does not adequately control blood glucose levels or if it leads to decreased sRAGE levels, this could result in a more aggressive progression of complications Lower sRAGE levels may be associated with increased inflammation and oxidative stress, which can exacerbate tissue damage and lead to a higher risk of complications The relationship is complex and underscores the importance of tailored treatment strategies in diabetes care
Furthermore, the discussion emphasizes that the presence of complications in T2DM patients is a significant factor affecting sRAGE levels The authors suggest that damage to target organs may be linked to the observed elevations in sRAGE, highlighting the need for further research to understand these mechanisms The article also mentions that genetic factors can significantly affect sRAGE levels and, consequently, the progression of diabetesrelated complications. Understanding these genetic influences can help tailor treatment strategies to improve outcomes for individuals with diabetes.
The authors call for more experimental studies to elucidate the specific mechanisms behind the changes in sRAGE levels in diabetes, as well as the potential implications for treatment strategies aimed at managing AGEs and their effects on diabetic complications Overall, the discussion underscores the complexity of the relationship between AGEs, sRAGE, and diabetes, emphasizing the importance of understanding these interactions for better management of the disease and its complications
3
References:
1 Caballero, E. (n.d.). Prevention and Management of Diabetes Complications Cmecataloghmsharvardedu https://cmecatalog.hms.harvard.edu/preventi on-management-diabetes-complications
Complications Diabetes Education Online (2011, September 22) https://dtcucsfedu/living-withdiabetes/complications/
2. Chen, Q, Liu, L, Ke, W, Li, X, Xiao, H, & Li, Y (2024). Association between the soluble receptor for advanced glycation end products and diabetes mellitus: systematic review and meta-analysis BMC endocrine disorders, 24(1), 232 https://doi.org/10.1186/s12902-02401759-2
Vazzana, N, Santilli, F, Cuccurullo, C et al Soluble forms of RAGE in internal medicine Intern Emerg Med 4, 389–401 (2009) https://doi.org/10.1007/s11739-009-0300-1
4 Cover image was generated using AI It is not meant to represent the actual appearance of the AGEs.
Figure 1 Vazzana, N, Santilli, F, Cuccurullo, C et al Soluble forms of RAGE in internal medicine Intern Emerg Med 4, 389–401 (2009) https://doiorg/101007/s11739-009-0300-1
Figure 2
https://wwwflickrcom/photos/sriram/221988684 4
Thank you for taking the time to explore the connections between AGEs, sRAGE, and diabetes with me. I hope you found this discussion insightful and engaging. If you’re curious to learn more, I encourage you to dive deeper into the subject and share your thoughts, questions, or suggestions for future topics in the comments. Your feedback and ideas are always welcome!

Writtenby:RobertoA.OliverasMeléndez
PublishedonlineonDecember13,2024
The external acoustic meatus, also known as the external auditory canal, is a structure found in the external part of the ear that serves to connect the outside world to the middle ear and acts as a passageway for sound waves heading towards the tympanic membrane Due to the presence of this canal, and the funneling action of the auricle, sound waves are able to initiate the vibratory mechanism of sound conduction
Atresia (Greek for ‘absence of an opening’) of this canal can lead to a partial or total loss of hearing capability Congenital aural atresia is a condition characterized by the atresia, or narrowing, of the external auditory canal and often presents with various associated ear anomalies, such as microtia (Greek for ‘micro’ and ‘otia’, meaning ‘little ear’) and malformations affecting the middle and inner ears (Abdel – Aziz, 2013). It is imperative to diagnose and promptly treat newborns with this condition to ensure adequate language development (Lim et al, 2023) Treatment options for congenital aural atresia vary and include the implementation of bone-anchored hearing aids and the surgical creation of an ear canal, a procedure known as atresiaplasty (Pellinen et al., 2018)
Classical air–conducting hearing aids are inadequate for use in this condition, because they rely on the existence of a canal in order to amplify sound waves, which is why bone–conducting hearing aids are preferred Bone–anchored
hearing aids (BAHA) are a special type of bone–conducting hearing aids that are commonly used in patients living with conductive hearing loss, such as those with congenital auricular atresia (Hagr, 2007). These bone–anchored hearing aids consist of a titanium screw, implanted directly into the skull, that holds a bone–conducting hearing aid; vibrations are carried by the screw to the skull and vestibulocochlear nerve (CN VIII), allowing the transmission of auditory information (Farnoosh et al, 2014) You can view a video explaining how these devices work here.

BAHA have several advantages over other bone–conducting aids, which are not permanently attached to the skull For example, they tend to be more comfortable and provide higher sound quality, since the structures that overlay the skull, such as the skin, do not interfere with the vibrations (Hagr, 2007) As with all procedures, complications related to BAHA implantations exist, including infections and the inadequate integration of the device into the bone (Farnoosh et al 2014)
Atresiaplasty is another common way to remedy congenital aural atresia According to Li et al (2014), atresiaplasty is a surgical technique that involves the creation of a cavity reaching the area of the tympanic membrane, so that an artificial external ear canal may be created Skin grafts are then inserted into the ear, in order to cover the newly–made canal (Abdel – Aziz, 2013) As mentioned previously, congenital aural atresia may involve a variety of malformations to other parts of the ear, which is why this correctional surgery is oftentimes coupled with other procedures, such as ossicular replacements and tympanic membrane reconstruction (Li, 2014)
Several complications related to the atresiaplasty surgery are known and may negatively affect the patient’s hearing Closure of the artificial canal, infections due to problematic skin grafts, and lateralization of the tympanic membrane, which causes it to separate from the ossicles, are possible complications of this procedure (Abdel–Aziz, 2013) Due to its proximity to the surgical area, the facial nerve (CN VII) may be damaged, resulting in partial or complete unilateral facial paralysis, which is why extreme care must be taken during this procedure (Abdel–Aziz, 2013) Even in the absence of these complications, the procedure may not completely or adequately restore hearing, necessitating the continued use of hearing aids (Farnoosh et al , 2014)
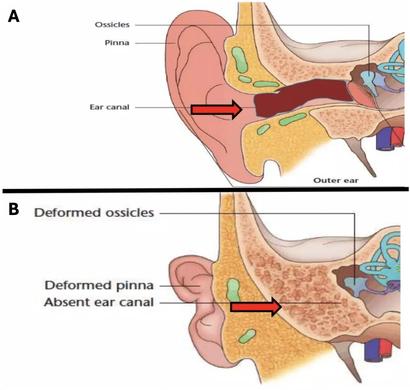
Figure 1. Anatomical comparison of normal ear anatomy (A) and congenital aural atresia (B) Panel A depicts a normal outer ear with a fully developed ear canal, ossicles, and pinna. Panel B illustrates congenital aural atresia, characterized by an absent ear canal, a deformed pinna, and deformed ossicles, which contribute to conductive hearing loss. The red arrows highlight the ear canal’s presence in A and its absence in B, demonstrating the structural differences between normal anatomy and congenital aural atresia.
The use of BAHAs and the atresiaplasty technique are common treatments for congenital aural atresia, and several studies have attempted to compare the effectiveness of these remedies According to Farnoosh et al (2014), people who underwent atresiaplasties had “poorer audiological outcomes when compared to the BAHA group,” and experienced “a mild deterioration over time in hearing gain ” These conclusions are based on data that found that the BAHA group had a 44 3 ± 14.3 dB hearing gain in the short-term and a 44 5 ± 11 3 dB hearing gain in the long-term, while the atresiaplasty group experienced a gain of 20 0 ± 18 9 dB in the short-term and 15 3 ± 19.9 dB in the long-term (Farnoosh et al., 2014).
Another study states that patients in the BAHA group experienced a postoperative hearing gain of 46 9 ± 7 0 dB at 6 months and 39 8 ± 7 2 dB at 1 year, compared to the atresiaplasty group, which led them to conclude that atresiaplasty is as efficient as BAHA only when used in conjunction with hearing aids (Bouhabel et al , 2011) However, Bouhabel et al did not provide explicit hearing gain data for atresiaplasty without hearing aids Their conclusion hinges on the complementary use of hearing aids with atresiaplasty, which may explain the discrepancy with Farnoosh et al ’s findings Despite atresiaplasty seemingly correcting the underlying defect, several studies have suggested that BAHAs tend to offer better and more consistent outcomes overall
Congenital aural atresia results in the total or partial loss of the external auditory canal and, therefore, can lead to varying degrees of auditory problems in affected patients. Bone–anchored hearing aids allow the direct transmission of vibratory information and provide high sound quality, while surgical atresiaplasty creates an artificial canal in order to substitute the incomplete or absent external auditory meatus BAHAs tend to be safer and provide more complete hearing outcomes, compared to surgical atresiaplasty.
1
Abdel – Aziz, M (2013) Congenital Aural Atresia The Journal of Craniofacial Surgery, 24(4), e418 – e422 10 1097/SCS 0b013e3182942d11
2
Lim R , Abdullah, A , Hashmin, W F H , & Goh, B S (2023) Hearing rehabilitation in patients with congenital aural atresia: an observational study in a tertiary center The Egyptian Journal of Otolaryngology, 39(90) https://doi.org/10.1186/s43163-02300436-w
3
Pellinen, J , Vasama, J P , & Kivekas, I (2018) Long – term results of atresiaplasty in patients with congenital aural atresia Acta Oto – Laryngologica, 138(7), 521 – 624 http://dx.doi.org/10.1080/00016489.2018.14 31402
4
Hagr, A (2007) BAHA: Bone – Anchored Hearing Aid International Journal of Health Sciences, 1(2), 265 – 276 https://www.ncbi.nlm.nih.gov/pmc/articles /PMC3068630/#:~:text=The%20BAHA%20sy stem%20uses%20an,the%20skin%20and%2 0subcutaneous%20tissues
5
Farnoosh, S , Mitsinikos, F T , Maceri, D , & Don, D. M. (2014). Bone – Anchored Hearing Aid vs Reconstruction of the External Auditory Canal in Children and Adolescents with Congenital Aural Atresia: A Comparison Study of Outcomes. Frontiers in Pediatrics, 2(5) https://doi.org/10.3389%2Ffped.2014.00005
7.
Li, C , Zhang, T , Fu, Y , Qing, F , & Lu, F (2014) Congenital aural atresia and stenosis: Surgery and long – term results International Journal of Audiology, 53, 476 –481 10 3109/14992027 2014 890295
6 Bouhabel, S., Arcand, P., & Saliba, I. (2012). Congenital aural atresia: Bone – anchored hearing aid vs external auditory canal reconstruction International Journal of Pediatric Otorhinolaryngology, 76(2), 272 –277 https://doi.org/10.1016/j.ijporl.2011.11.020
Figure 1 image credit: https://microtiaatresia.com.au/hearing-loss/

Writtenby:AveryR.Arsenault
I thought it would be interesting to dive into the current state of insurance practices in the United States and the resounding negative sentiments toward the US healthcare system With the United States spending the most per capita on healthcare and being a world leader in healthcare innovation, there are still 30 million Americans with no health insurance and many more underinsured (Alpert, 2023). Due to the complexities of the insurance system, Americans are eligible for different types of coverage depending on whether their employer offers it or not, income level, age, and healthcare needs These categories fall into employersponsored insurance, private coverage, Medicare and Medicaid, all of which have complexities in how much coverage is offered and how much someone has to pay out of pocket (Collins, 2022)
Because the United States does not have any autoenrollment mechanisms for insurance, Americans who are not under employersponsored insurance must figure out what programs they are eligible for and then go through the enrollment process, which can be lengthy and complex (Collins, 2022) This is where other problems also sink in, as US health literacy is very poor The Milken Institute has found that at least 88% of adults in the US have inadequate health literacy to navigate the healthcare system, with 14% of adults with below basic proficiency. This leads to complications in understanding how to enroll in insurance coverage and lack of understanding in following medical advice,
leading to worsening health outcomes (Alpert, 2023).
American families have trouble affording healthcare costs, with high deductibles, copays, out-of-pocket costs, unexpected bills and prescription drugs In today’s landscape, about half of US adults say that it is “very or somewhat difficult” for them to afford their healthcare costs (47%), and this percentage rises among adults unor underinsured, older, or Black and Hispanic At least 60% of Black and 65% of Hispanic adults report difficulty affording health care costs compared to 39% of White adults Particularly, affording healthcare is a problem for those who need it most, as those who describe their health as “fair” or “poor” say they or a family member had problems paying for healthcare in the last year, with 51% of uninsured adults saying they are in fair or poor health (Lopes, 2024).
Lack of good health insurance, and high cost of care is leading to adults skipping or delaying seeking services One-quarter of adults say they have skipped or postponed healthcare because of the cost, with the number rising to 36% of adults skipping or delaying care among those uninsured. Even those with insurance, 21% still reported not getting healthcare needed due to cost (Lopes, 2024)
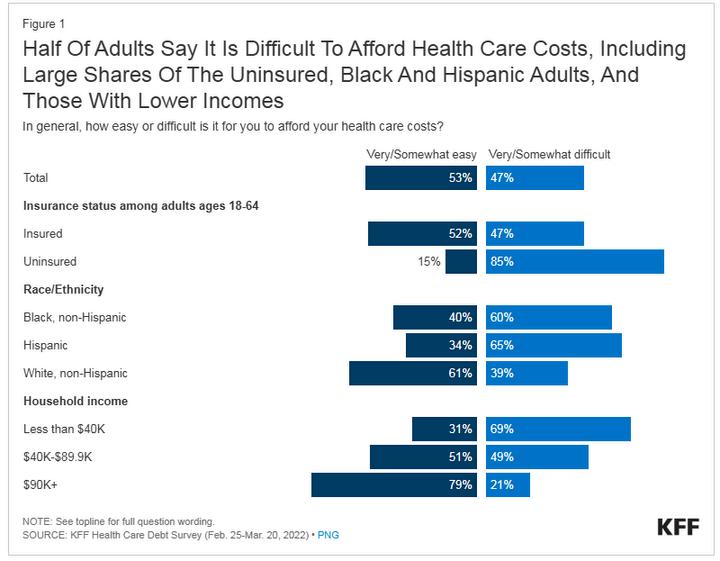
Source: https://wwwkfforg/health-costs/issue-brief/americans-challenges-with-health-care-costs/
In a report by the Commonwealth fund, as much as 25% of people with chronic health problems, like diabetes, said that out-of-pocket costs for prescription drugs to treat their illnesses had caused them to skip doses or not fill a prescription for their conditions (Collins, 2022) This is worrisome and it highlights the compounding effects of cost barriers on longterm health outcomes Skipping necessary treatments or medications, especially for chronic conditions, can lead to worsening health, increased and unnecessary hospitalizations, lifethreatening complications and further adds to avoidable healthcare costs. This cycle not only exacerbates the individual’s health challenges but also places a heavier financial burden on the healthcare system overall by costing billions of dollarsforemergencytreatments(Rohatgi,2021).
About half (48%) of insured adults worry about affordingtheirmonthlyinsurancepremiums,and many with employee-sponsored or marketplace coverage rate it “fair” or “poor” in terms of the costs still associated with seeing a medical professional This goes to show that all Americans’nomatterhavingcoverageornot,are not immune to burdens of the healthcare insurancesystem.
Healthcare debt is a wide reaching problem for US adults, with 41% having some sort of debt due to medical or dental bills past due or unable to pay. These staggering statistics illuminate the growing and ever-present hardships for American adults in dealing with the healthcare system and the fear surrounding the possibility of not being able to pay off medical costs (Lopes, 2024) These issues are disproportionately affecting low income and marginalizedpopulationsacrosstheUS.
Even with these high costs, this does not indicate better administrative efficiency, therefore US physicians and patients are most likely to face hurdles related to insurance rules, billing disputes, and paperwork (Blumenthal, 2024) In this context, administrative efficiency focuses on the challenges doctors have in dealing with insurance or medical claim issues, reportingandcharting,andpatients’timespent disputing medical bills Due to the US’s complex system of different public and private insurances, there are thousands of health plans that all have different requirements Therefore, physiciansandprovidersintheUSspendthe
most amount of time and effort billing the different insurance systems compared to other countries
On top of this, denials of services are common, requiring more time and effort from all parties on appealing the decisions, with many not challenging the denial and not getting care their doctor recommends (Blumenthal, 2024)
Claim denials take a toll on patients’ health and delay or prevent care This not only causes worry and anxiety about getting the care they need, but their health problems worsen in the interim or delay diagnosis to get the proper treatment (Commonwealth Fund, 2024)
“Serious health and financial consequences arise as a direct result of insurance problems, and consumers whose problems include denied claims are far more likely to have needed care delayed or denied, to experience a decline in health status, and to face higher out-of-pocket costs,” according to a report on the KFF survey. Source: Pollitz, 2023
These statistics underscore the urgent need for systemic policy changes that address affordability and proper insurance coverage. No one should have to choose between financial stability and their health. Policymakers and healthcare executives must explore strategies to lower out-of-pocket costs, improve prescription drug affordability, and expand insurance coverage to reduce the barriers preventing individuals from accessing necessary care Programs like Medicaid expansion under the Affordable Care Act have demonstrated success in improving access for vulnerable populations, but gaps remain, particularly in states that have not adopted these measures
Addressing this issue requires a multilayered approach at all levels starting from congressional legislation, how insurance network systems are run, and school systems teaching health Systematic changes at these points will contribute to changes all the way down, from business meetings, to the exam room between a provider and a patient. Patient education is a high priority as surveys show there is considerable consumer confusion among patients and their families about their right to appeal and who to contact in insurance denial cases Equitable transparency, education and standardization is needed to ensure
providers and patients know their rights on denial decisions and how to get the care they need– reducing these barriers is a step in the right direction Additionally, customer assistance programs would benefit patients in submitting an appeal as the process can be complex (Commonwealth Fund, 2024)
By creating a system that prioritizes preventive care, the U.S. could reduce the long-term costs associated with avoidable hospitalizations and poor health outcomes, benefiting both individuals and the healthcare system as a whole Such reforms could shift the focus of the US healthcare system from reactive, high-cost interventions to a proactive, patient-centered model one where seeking care is not a luxury but a fundamental right
2
3
4
Alpert J S (2023) Twenty-First Century Health Care Challenges in the United States The American journal of medicine, 136(7), 609–610 https://doiorg/101016/jamjmed202301002
1 Collins, S, Haynes, L, & Masitha, R (2022, September 29) The state of US health insurance in 2022 Commonwealth Fund https://wwwcommonwealthfundorg/publicati ons/issue-briefs/2022/sep/state-us-healthinsurance-2022-biennial-survey
Lopes, L, Montero, A, Presiado, M, & Hamel, L (2024, March 1) Americans’ Challenges with Health Care Costs Kaiser Family Foundation https://www.kff.org/health-costs/issuebrief/americans-challenges-with-health-carecosts/
Rohatgi, K W, Humble, S, McQueen, A, Hunleth, J M, Chang, S H, Herrick, C J, & James, A S (2021) Medication Adherence and Characteristics of Patients Who Spend Less on Basic Needs to Afford Medications Journal of the American Board of Family Medicine : JABFM, 34(3), 561–570 https://doiorg/103122/jabfm202103200361
5 Unforeseen Health Care Bills and Coverage Denials by Health Insurers in the U.S. (2024). Commonwealthfundorg https://doiorg/1026099/jqpw-jz55
7
Blumenthal, D, Gumas, E D, Shah, A, Gunja, M Z, & Williams II, R D (2024) Mirror, Mirror 2024: A Portrait of the Failing US Health System The Commonwealth Fund https://doi.org/10.26099/ta0g-zp66
6 Pollitz, K, Pestaina, K, Lopes, L, Wallace, R, & Published, J L (2023, September 29) Consumer Survey Highlights Problems with Denied Health Insurance Claims KFF https://wwwkfforg/affordable-care-act/issuebrief/consumer-survey-highlights-problemswith-denied-health-insurance-claims/

University of Puerto Rico School of Medicine

University
University of Puerto Rico School of Medicine

Arbona Health Hub Invites Premeds, Medical Students, Residents, and Healthcare Professionals to Contribute!
We are extending an open invitation for these groups to submit their articles for consideration.
Why Contribute?
Showcase Expertise: Share your knowledge with our engaged audience.
Impactful Insights: Contribute to vital health discussions, making a positive impact.
Networking Opportunities:
Connect with a community of healthcare professionals and enthusiasts.
Profile Elevation: Boost your online presence and credibility in healthcare.
Volume 1. Issue 2. October-December 2024

The Arbona Health Hub Newsletter is published quarterly by the Arbona Health Hub team. Email: arbonahealthhub@gmail.com
Publisher: Arbona Health Hub INC. Caguas, Puerto Rico
Newsletter Editors: Alejandro Arbona-Lampaya, Avery R. Arsenault
Peer Reviewers: Alejandro Arbona-Lampaya, Avery R. Arsenault, Héctor Cancel Asencio, Marcel De Jesús Vega, Sofía I. Malavé Ortiz, Christian G. Correa García, Alejandro R. Gonazalez-Barreto, Jan P. Villanueva Medina, MPH
Contributing Writers: Sofía I Malavé Ortiz, Adrián A Almodóvar Díaz, Jan P Villanueva Medina, MPH, Ángel R Ocasio-Gracia, Marcel A de Jesús Vega, Roberto A Oliveras Meléndez, Avery R Arsenault
Cover Art Credit: Bruce Wetzel and Harry Schaefer, National Cancer Institute, National Institutes of Health
